This is only a brief summary of important information about BIKTARVY® and does not replace talking to your healthcare provider about your condition and your treatment.
MOST IMPORTANT INFORMATION ABOUT BIKTARVY
BIKTARVY may cause serious side e ects, including:
` Worsening of hepatitis B (HBV) infection. Your healthcare provider will test you for HBV. If you have both HIV-1 and HBV, your HBV may suddenly get worse if you stop taking BIKTARVY. Do not stop taking BIKTARVY without fi rst talking to your healthcare provider, as they will need to check your health regularly for several months, and may give you HBV medicine.
ABOUT BIKTARVY
BIKTARVY is a complete, 1-pill, once-a-day prescription medicine used to treat HIV-1 in adults and children who weigh at least 55 pounds. It can either be used in people who have never taken HIV-1 medicines before, or people who are replacing their current HIV-1 medicines and whose healthcare provider determines they meet certain requirements.
BIKTARVY does not cure HIV-1 or AIDS. HIV-1 is the virus that causes AIDS.
Do NOT take BIKTARVY if you also take a medicine that contains:
` dofetilide
` rifampin
` any other medicines to treat HIV-1
BEFORE TAKING BIKTARVY
Tell your healthcare provider if you:
` Have or have had any kidney or liver problems, including hepatitis infection.
` Have any other health problems.
` Are pregnant or plan to become pregnant. Tell your healthcare provider if you become pregnant while taking BIKTARVY.
` Are breastfeeding (nursing) or plan to breastfeed. Talk to your healthcare provider about the risks of breastfeeding during treatment with BIKTARVY. Tell your healthcare provider about all the medicines you take:
` Keep a list that includes all prescription and over-thecounter medicines, antacids, laxatives, vitamins, and herbal supplements, and show it to your healthcare provider and pharmacist.
` BIKTARVY and other medicines may a ect each other. Ask your healthcare provider and pharmacist about medicines that interact with BIKTARVY, and ask if it is safe to take BIKTARVY with all your other medicines.
POSSIBLE SIDE EFFECTS OF BIKTARVY
BIKTARVY may cause serious side e ects, including:
` Those in the “Most Important Information About BIKTARVY” section.
` Changes in your immune system. Your immune system may get stronger and begin to fight infections that may have been hidden in your body. Tell your healthcare provider if you have any new symptoms after you start taking BIKTARVY.
` Kidney problems, including kidney failure. Your healthcare provider should do blood and urine tests to check your kidneys. If you develop new or worse kidney problems, they may tell you to stop taking BIKTARVY.
` Too much lactic acid in your blood (lactic acidosis), which is a serious but rare medical emergency that can lead to death. Tell your healthcare provider right away if you get these symptoms: weakness or being more tired than usual, unusual muscle pain, being short of breath or fast breathing, stomach pain with nausea and vomiting, cold or blue hands and feet, feel dizzy or lightheaded, or a fast or abnormal heartbeat.
` Severe liver problems , which in rare cases can lead to death. Tell your healthcare provider right away if you get these symptoms: skin or the white part of your eyes turns yellow, dark “tea-colored” urine, light-colored stools, loss of appetite for several days or longer, nausea, or stomach-area pain.
` The most common side e ects of BIKTARVY in clinical studies were diarrhea (6%), nausea (6%), and headache (5%).
These are not all the possible side e ects of BIKTARVY. Tell your healthcare provider right away if you have any new symptoms while taking BIKTARVY.
You are encouraged to report negative side e ects of prescription drugs to the FDA. Visit www.FDA.gov/medwatch or call 1-800-FDA-1088.
Your healthcare provider will need to do tests to monitor your health before and during treatment with BIKTARVY.
HOW TO TAKE BIKTARVY
Take BIKTARVY 1 time each day with or without food.
GET MORE INFORMATION
` This is only a brief summary of important information about BIKTARVY. Talk to your healthcare provider or pharmacist to learn more.
` Go to BIKTARVY.com or call 1-800-GILEAD-5.
` If you need help paying for your medicine, visit BIKTARVY.com for program information.
#ADVOCACY
Fighting against HIV and AIDS has always been a struggle. Much work remains to end the epidemic. POZ encourages you to get involved in advocacy. Go to poz.com/ advocacy to find the latest news and learn how you can make a difference in the fight. D #CRIMINALIZATION
Advocates around the world are working to change laws that criminalize HIV, which harm people living with the virus. For more information and to learn how to get involved in reform efforts to make such laws reflect current science, go to poz.com/criminalization
D #UNDETECTABLE
The science is clear: People who have an undetectable viral load don’t transmit HIV sexually. In addition to keeping people healthy, effective HIV treatment also means HIV prevention. Go to poz.com/undetectable for more.
D
POZ DIGITAL
Scan the QR code (le ) with your smartphone camera or go to poz.com/digital to view the current and past issues online.
22 CHANGING THE HIV NARRATIVE Straight men living with the virus are speaking up. BY ALICIA GREEN
28 WHAT’S IN A NAME? The debate over who qualifies as a long-term survivor is in the spotlight. BY VICTORIA NOE
the
Ball
There is more to Thomas Dobbs, MD, a beloved HIV doctor, than the abortion ruling that bears his name.
6 POZ PLANET
R.I.P. Cornelius Baker, an esteemed HIV policy expert • health insurers must cover all pre-exposure prophylaxis (PrEP) • smoking and HIV in Black adults • the HIV Medicine Association honors HIV clinical education and research • Camp Heartland is closing • POZ Stories: Tom Fikiri Masarara • Everyday: HIV milestones 10
In a post titled “How to Be an Advocate for Yourself and Others,” The Well Project shares how you can make a difference on an individual or community level.
NOTES
Three-month vaginal ring offers longer protection • two-drug regimen for advanced HIV • metformin shrinks viral reservoir • heart and liver health
18 CARE & TREATMENT
Weekly oral HIV medications look promising • PrEP need remains unmet • loneliness linked to frailty in older people with HIV • first U.S. report of Clade 1 mpox
20
Feds uses
about HIV.
EDITOR-IN-CHIEF
ORIOL R. GUTIERREZ JR.
MANAGING EDITOR
JENNIFER MORTON
DEPUTY EDITOR
TRENT STRAUBE
SCIENCE EDITOR
LIZ HIGHLEYMAN
COPY CHIEF
JOE MEJÍA
EDITORIAL ASSISTANT
LAURA SCHMIDT
ART DIRECTOR
DORIOT KIM
ART PRODUCTION MANAGER
MICHAEL HALLIDAY
CONTRIBUTING WRITERS
SHAWN DECKER, OLIVIA G. FORD, ALICIA GREEN, MARK S. KING, TIM MURPHY, MATHEW RODRIGUEZ, CHARLES SANCHEZ
CONTRIBUTING ARTISTS
JOAN LOBIS BROWN, LIZ DEFRAIN, ARI MICHELSON, JONATHAN TIMMES, BILL WADMAN
FOUNDER
SEAN STRUB
LEGACY ADVISER MEGAN STRUB
ADVISORY BOARD
GUILLERMO CHACÓN, SABINA
HIRSHFIELD, PHD, KATHIE HIERS, TIM HORN, PAUL KAWATA, NAINA KHANNA, DANIEL TIETZ, MITCHELL WARREN
PRESS REQUESTS NEWS@POZ.COM
SUBSCRIPTIONS HTTP://ORDER.POZ.COM
UNITED STATES: 212-242-2163
SUBSCRIPTION@POZ.COM
FEEDBACK
EMAIL WEBSITE@POZ.COM OR EDITOR-IN-CHIEF@POZ.COM
SMART + STRONG
PRESIDENT AND COO
IAN E. ANDERSON
EDITORIAL DIRECTOR
ORIOL R. GUTIERREZ JR.
CHIEF TECHNOLOGY OFFICER
CHRISTIAN EVANS
VICE PRESIDENT, INTEGRATED SALES DIANE ANDERSON
INTEGRATED ADVERTISING MANAGER
JONATHAN GASKELL
INTEGRATED ADVERTISING COORDINATOR
SARAH PURSELL
SALES OFFICE
212-938-2051; SALES@POZ.COM
CDM PUBLISHING, LLC
CEO
JEREMY GRAYZEL
CONTROLLER
JOEL KAPLAN
Whenever I Call You Friend
IFULLY EMBRACE BEING called a long-term survivor and calling myself one. That wasn’t always true. For the longest time, I refused to adopt the phrase. After three decades of living with HIV, I have finally given myself permission to do so.
I tested HIV positive in 1992; I was 22 years old. I thought I would be dead by 30, so it took me many years to get my head above water enough to actually appreciate what surviving meant. Nonetheless, the phrase “long-term survivor” held a particular status that I associated with those who were living with HIV since the early days.
I wasn’t alone in that thinking. I’m sure that some folks still think that way. We’re all entitled to our opinions. That said, as people with HIV get older, more of them will be living with the virus for decades. If they’re not long-term survivors, then what should they be called?
To complicate matters, a new wrinkle to this conversation has emerged in the past few years. There are people who experienced the trauma of the early epidemic but remained HIV negative. Some long-term survivors are encouraging them to also identify as long-term survivors. Victoria Noe, one of these allies, has some thoughts on the subject. Go to page 28 for more.
Another group in the HIV community that doesn’t often get discussed is straight men, especially straight Black men. They constitute a larger share of the community than many folks realize. Andy Feds, our cover subject, among other advocates such as Larry Bryant and Derrick Robinson, want to change the narrative about straight men with HIV. Go to page 22 to learn more.
This special issue focuses on African Americans and highlights contributions of other Black advocates, including Tom Fikiri Masarara and Joanna Robinson.
Masarara is an HIV activist originally from the Republic of Burundi who now resides in South Africa with his wife and three children. He fled violence, seeking refuge in many countries before starting a new life in South Africa, where he tested HIV positive in 2002. Go to page 8 to read about his advocacy.
Robinson is a longtime HIV advocate in Miami. As a transgender Black woman living with the virus, she knows firsthand what it’s like to live on the margins. She now uses that experience to help others with HIV, including people newly diagnosed with the virus. Go to page 32 to read more about her contributions.
As we were closing this print issue of POZ, we learned about the passing of Cornelius Baker. He died unexpectedly of natural causes. He was a beloved HIV policy expert and a longtime activist for gay Black men. His career spanned decades working for federal and national organizations. He was also a member of the POZ Advisory Board. Go to page 6 to read more about his legacy.
Many people with HIV occasionally experience anxiety or depression. However, if you’re having persistent anxiety or depression, it may be time to seek assistance. Psychotherapy and medications can help. Go to page 16 for more.
ORIOL R. GUTIERREZ JR. EDITOR-IN-CHIEF editor-in-chief@poz.com
Want to read more from Oriol? Follow him on X @oriolgutierrez and check out blogs.poz.com/oriol.
MEET THOMAS DOBBS
There is more to this beloved HIV doctor than an abortion ruling.
THE NAME DOBBS IS NOW SHORTHAND FOR DOBBS V. JACKSON
Women’s Health Organization (JWHO), the 2022 ruling by the Supreme Court of the United States (SCOTUS) that overturned Roe v. Wade, which had since 1973 guaranteed the right to an abortion nationwide.
Dobbs refers to Thomas Dobbs, MD, whose name ended up on the case because he was the head of the Mississippi State Department of Health while the case was being brought by JWHO, Mississippi’s only abortion clinic, in protest of a 2018 state law banning abortions after 15 weeks of pregnancy. The case eventually made its way to a then newly conservative-majority SCOTUS, landing the final blow to Roe
When a draft of the SCOTUS ruling on Dobbs leaked in May 2022, Dobbs took to X (at the time Twitter) to write that he “had no direct involvement in any component of this legal action.” Shortly after, on a Zoom meeting with the Mississippi State Medical Association, he said, “I personally, and the health department specifically, have had no active role in this legal action. It’s just a quirk of how the naming convention works.... And we want to just keep on doing our good work and stay out of the crosshairs.”
What many people outside of Mississippi do not know is that Dobbs has been caring for people living with HIV since the mid-’90s. In the mid-’00s, he became the in-house infectious diseases specialist at a Ryan White–funded clinic in Hattiesburg. He also started a Ryan White clinic in underserved rural McComb that operated for seven years until, according to Dobbs, a federal funding complication shut it down. Dobbs left the state health department in 2022 after getting it through the early years of the COVID-19 pandemic and went on to helm the John D. Bower School of
Population Health at the University of Mississippi Medical Center (UMMC) in Jackson, where he continues to see thousands of folks living with HIV at UMMC’s Adult Special Care Clinic.
“He’s one of our greatest HIV doctor champions in Mississippi and has been since before the Roe overturn tragedy,” says Robin Webb, a longtime Mississippi activist living with HIV, who urged POZ to interview Dobbs. “He’s very progressive, gay-friendly, reproductive justice–friendly. All of us in the HIV world here in Mississippi know an entirely different man than what is implied. He’s saved many a gay man’s life over all these years and others, of course.”
Dobbs agreed to talk with POZ about his career as an HIV doctor.
How did you first get into HIV care? It was when I was a medical resident at
Clockwise from left: Thomas Dobbs (left) and colleagues representing the University of Mississippi Medical Center at an outreach event; Dobbs and colleagues at a free clinic event in Jackson; colleagues at a Jackson event
the University of Alabama in 1996 and we had a patient with advanced HIV disease. That was a great year to start working in HIV because protease inhibitors started coming on. [Those medications marked the beginning of effective HIV treatment.]
I started him on [the now outdated protease inhibitor] Crixivan, which was the inflection point where he went from despair to exuberance and optimism. From 2005 to 2015, I worked at a Ryan White–funded HIV clinic in Hattiesburg.
What was it like back then at that clinic? It was, and still is, a fantastic community health center with a huge cohort of folks. At that time, we didn’t have quite as many single-pill regimens as we do now, and we were still seeing a lot of resistance [to older HIV meds], so we had to concoct these complicated non-standardized regimens. That’s changed a lot.
Also, our work overlapped with what I would say was the worst of the opioid epidemic. What lagged behind the HIV science were the mechanisms to make sure that people had stable housing and food security. In places where we didn’t have certain components of Ryan White services, especially rural areas, resources were limited. Since then, the clinic’s support network team has been spectacular.
Tell us about the rural McComb clinic. I founded the McComb clinic, which we kept open for about seven years. It got tangled up with HRSA [Health Resources and Services Administration, a federal health agency], and they shut us down because you were not supposed to use HRSA funds to support STI [sexually transmitted infection] testing.
What I saw mostly at that clinic was severe HIV disease—really atrocious. I saw a bunch of cases of Kaposi sarcoma, lymphoma and MAC [Mycobacterium avium complex, a bacterial infection most commonly seen in people with advanced HIV disease]. Those are things we really shouldn’t see anymore.
But also, if you live hours away from a Ryan White provider, you’re not going to be getting care with regularity. This was all before telehealth. But while that clinic lasted, we drew people from all over the
southwest part of the state. They loved the clinic because it was in a sequestered, private spot, so they didn’t have to go somewhere in their hometown.
In small-town rural areas, [HIV] stigma is magnified. We did a great job at that clinic taking care of folks. We never charged people.
What was it like at the less rural Hattiesburg clinic?
We saw a lot of the same stuff despite those patients having more access to care. We saw tuberculosis, cryptococcal meningitis, tertiary syphilis. Mississippi as a state didn’t expand Medicaid, so a lot of people with HIV don’t have access
prenatal care. We know that the biggest problem is getting women into prenatal care earlier and making doctors understand that they must screen them and, if necessary, treat them for syphilis.
We’ve also seen a massive divestment in public health here and in other southeastern states. We now have only a third of the disease investigation workforce that we had in the ’90s—the people who track STIs and make sure that patients get treated and their partners get tested. That’s a task of public health that cannot be recreated by the private sector. There’s no local funding here for public health, essentially. We only have federal funding.
“Since then, we’ve made progress in the state.”
to care [beyond their HIV needs]. I saw people with gallbladder disease, and all we could do was tell them to go to the ER when they got sick enough and maybe the ER would give them surgery. Since then, we’ve made progress in the state [using Ryan White services to cover more non-HIV-related issues].
Tell us about the school of public health. We’re trying to bring about the next generation of public health researchers. We have a PhD program and programs in advanced data science, stats and AI. We also have master’s level training for people on the ground making things happen. I teach a few classes. And we also do research.
We’ve got implementation projects to combat congenital syphilis, which is a real tragedy. In the past six years, we’ve had a more than 1,000% increase in such cases. It’s a nationwide problem, but, like a lot of things, it’s worse here because of the lack of health care and delays in
As a result of SCOTUS overturning Roe in the ruling that bears your name, you posted on social media to let people know you had nothing to do with it, but you refrained from sharing your personal opinion about the ruling or about abortion access. Why?
I inquired about getting my name removed from the case once it was referred to the Supreme Court, but I was unable to. As you can imagine, it’s kind of a big deal, so I’ve wanted to lay low [on that issue] to continue to do the work I’m doing around HIV and STIs and public health. I honestly try not to think about it—and folks leave me alone about it.
Thank you for talking with POZ. To end on a positive note, what do you do for self-care and joy outside of work?
My wife and I are big cyclists and sailors. Primarily on the Gulf Coast, but we also have a nice little lake in town where we can sail. Q
Thomas Dobbs, MD
He was an esteemed HIV policy expert. R.I.P. Cornelius Baker, Longtime HIV Advocate
Cornelius Baker, a beloved HIV policy expert and longtime activist for Black gay men, died unexpectedly of natural causes at his home on November 9, reports the Washington Blade. His career encompassed a who’s who of federal and national organizations, including the President’s Emergency Plan for AIDS Relief (PEPFAR), the National Institutes of Health, the Whitman-Walker Clinic, the Rollins School of Public Health, the National Association of People with AIDS and The Elizabeth Taylor AIDS Foundation (ETAF). He was also a member of the POZ Advisory Board.
“A. Cornelius Baker stood with our founder, Elizabeth Taylor, at the beginning of the HIV/AIDS movement and throughout her legacy,” wrote ETAF.
“The ETAF officers and staff team join his family, friends and community as
we mourn his loss together. We find comfort in knowing that his spirit, along with Elizabeth’s, will continue to guide and inspire us and the entire HIV/AIDS movement in our ongoing work.”
Cornelius Baker
“Cornelius was a fierce fighter and educator whose influence was felt worldwide,” wrote Harold Phillips, the deputy director of programs at NMAC.
“He used his lived experience as a Black gay man living with HIV and his knowledge to make the world a better place for people with HIV across the world. His work reflected faith in action. He saw our humanity and the potential in many of us. Cornelius pushed us to be better and act on behalf of those often cast aside. He also spent many nights making us laugh and smile while developing strategy, policy and actions to
influence everything from the HIV research to Ryan White Reauthorization, to PEPFAR implementation and reauthorization. He met with federal officials and community members. He marched and testified before the city council to the halls of Congress.
“A friend put it best, ‘Cornelius was like a river that ran through many lands.’ Just like a river, he helped shape so many of us and left us changed. We are grateful and will continue his legacy and the work. Rest In Power.”
—Trent Straube
HEALTH INSURERS MUST COVER ALL PrEP
The three FDA-approved versions are included.
The federal government now requires health insurers to cover the three forms of pre-exposure prophylaxis (PrEP) to prevent HIV—including two daily tablet regimens and a long-acting injectable. What’s more, the health plans must cover related PrEP services without cost-sharing and cannot force patients to choose one form of PrEP over another.
The updated guidance was issued October 21 via an FAQs about the Affordable Care Act released jointly by the depart-
ments of Labor, Health and Human Services, and Treasury.
Earlier in 2024, over 60 HIV advocacy groups had requested that federal health leadership offer clarity on PrEP coverage. Many HIV advocates issued statements praising the guidance.
“With low uptake of PrEP among the communities most impacted by HIV, this insurance coverage requirement with zero cost-sharing will help jump-start the use of more effective forms of PrEP and lead to fewer HIV transmissions,” says Carl Schmid, executive director of HIV+Hepatitis Policy Institute. “We are grateful to the Biden-Harris administration for responding to our request to issue this guidance. Without it, we feel some insurers would continue to only cover daily oral PrEP and not provide PrEP users with the choice they need. With up to a third of privately insured PrEP users still being charged cost-sharing, we must ensure that both federal and state regulators vigorously enforce PrEP coverage requirements.”
To date, the Food and Drug Administration (FDA) has approved three forms of PrEP: Truvada and Descovy are daily pills; Apretude is a shot given every two months. Generic (and much cheaper) versions of Truvada are available.
A twice-yearly injectable, lenacapavir as PrEP may be added to prevention options in the near future, as clinical trial results have shown it to be highly effective in women, gay men and gender-diverse populations.
It remains unclear whether insurers must cover forms of PrEP that receive approval in the future. —TS
SMOKING AND HIV IN BLACK ADULTS
A $4.7
million
grant will help test a mobile app.
Can a mobile health app help Black adults living with HIV quit smoking and manage their stress? Scientists from the University of Houston (UH) Health Research Institute are using a $4.7 million grant to test just such an app, according to a UH news release.
The National Institute on Minority Health and Health Disparities grant will support a randomized control trial with more than 300 Black smokers with HIV to test the benefits of a mobile health app developed to help users quit smoking and better manage their stress and chronic diseases.
“Our results will fuel the expansion of culturally tailored mobile health interventions, offering innovative, accessible support for those most in need,” says grant recipient Lorra Garey, PhD, a research associate professor in the Department of Psychology at the university and an affiliate of the UH Health Research Institute.
As of 2022, nearly 105,400 people were living with HIV in Texas, according to AIDSVu.org, an interactive site that maps and visualizes national HIV data. By race, Black folks account for almost 30% of new HIV diagnoses in the state.
Even with good treatment, people living with HIV have higher rates of certain lung diseases, such as chronic obstructive pulmonary disease (COPD). COPD, including emphysema and chronic bronchitis, causes blockage of airflow and makes breathing more difficult. COPD risk increases with age, and cases are rising among HIV-positive people as they live longer. Chronic inflammation and a higher smoking rate contribute to the elevated risk.
In 2018, about 19.2% of the Texas population smoked cigarettes, and 25% of those smokers were Black, according to a study published in the National Library of Medicine. What’s more, although the smoking rate of Black Americans in Texas is high, they represented only about 18% of the calls to the Texas Tobacco Quitline.
Black smokers with HIV struggle to quit and manage their HIV because of issues pertaining to HIV stigma, discrimination and racism-related stress, note the UH researchers. —Laura Schmidt
Honoring HIV Clinical Education and Research
HIV Medicine Association recognizes three experts.
The Transformative Leader Award recognizes members of the HIV Medicine Association (HIVMA) who have transformed the field through significant achievement in HIV clinical care, provider education, research or advocacy. The 2024 honoree is Daniel R. Kuritzkes, MD, FIDSA.
Kuritzkes, the Harriet Ryan Albee Professor of Medicine at Harvard Medical School, is a trailblazer in advancing knowledge of drug-resistant HIV. He has had a transformative impact on the understanding and care of people with HIV and on countless trainees and colleagues.
His most significant contributions include his work to establish the significance of resistant mutations against nucleoside reverse transcriptase inhibitors and his insight that certain drug resistance mutations reduce viral fitness.
The inaugural Ada Adimora Citation Award honors the late Ada Adimora, MD, MPH, FIDSA, a past chair of HIVMA. The award recognizes exemplary contributions or service to HIVMA as well as advancing efforts to end HIV as an epidemic. The inaugural award goes to Oni Blackstock, MD, MHS. Blackstock—a primary care and HIV physician, researcher and public health practitioner—has spent her career in the relentless pursuit of equity and justice in health care. She has conducted transformative research and championed policies that prioritize the needs of Black and Latinx people with HIV.
As founder and executive director of Health Justice, a consulting firm that helps health care organizations center antiracism and equity in the workplace, she serves as an expert consultant on HIV clinical research projects.
The Innovator Award recognizes early or midcareer HIVMA members who have made outstanding and original contributions to HIV medicine in clinical care, provider education, research or advocacy. The 2024 recipient is Onyema Ogbuagu, MD, FACP, FIDSA.
Ogbuagu, an associate professor of infectious diseases at Yale School of Medicine, is a prolific researcher who has conducted groundbreaking investigator-initiated clinical trials and other research on HIV and COVID-19. —HIVMA
Breaking the Silence
Tom Fikiri Masarara has experienced a journey of survival and hope.
I’m a 51-year-old man who is blessed to have a lovely wife and three beautiful children. We are originally from the French-speaking Republic of Burundi, which is situated in East-Central Africa, bordered by the Democratic Republic of the Congo, Tanzania and Rwanda. Currently, we live in the township of Lehae, a suburb of Johannesburg in the Republic of South Africa. For 17 years, we have lived as asylum seekers.
I am a living testimony of survival and that there is hope beyond an HIV-positive diagnosis. Most people in the world no longer consider HIV a death sentence, but we in Africa often still do.
I fled to the Congo from violence and war between the ethnic groups of Hutus and Tutsis in Burundi in April 1993. I was married in August 1994, when I was 21. After living in several other countries, we finally landed in South Africa in 2009. We can identify with so many other people on this planet who must leave their homeland to seek life elsewhere.
In early 2002, I decided to take an HIV test. I wasn’t sick, but I wanted to know my status. I was confident I was negative. Before taking the test, I went through counseling and remember I was asked questions like: “Are you single or married?” “What results are you expecting?” “Are you going to reveal your positive result to your wife if so?” etc.
Some were not easy questions to answer. But I felt like I would be fine with God by my side if I received a positive result.
I tested positive. I was shocked! I didn’t know what to do and had a lot of questions and no clear answers. Fearing death was around the corner, I thought of the future of my children. It was a heavy weight on my shoulders. I was only 29 years old. My daughter Rebecca, the eldest, was only 8 years old. My future did not seem promising. My prayers and passion for my children to grow up with both parents is what kept me going.
I began reading everything concerning HIV. I remember one of my colleagues asked me, “Are you now a new researcher on HIV and AIDS? Why are all the books you take from the library about HIV and AIDS? Are you infected by the virus? Tell us early so that we can start preparing for your burial.”
After discovering that nondisclosure
can be a “silent killer,” I decided to break my silence. The first person I revealed my status to was my friend Pascal. He told me there is still life inside me, but it still seemed like I was smelling death. I revealed my status to my mother. She couldn’t believe it and just cried, knowing it might be the end of me soon.
I finally had the courage to tell my wife, and we all went together to get tested. She tested positive as well. Our children all tested negative—praise God!
I became an HIV activist after educating myself and being led by God. I attended many seminars, conferences and training programs, some offered by the World Health Organization. I became a beacon of hope for those living with the virus, also to those who have loved ones who are HIV positive. I always encouraged people to get tested and stressed there is life beyond an HIV diagnosis.
Today I work with the organization the Power of Women and Children (POFWC). We have an orphanage that cares for children infected and affected by HIV and AIDS. For four years, I have been a caregiver for these children and have provided home-based care as well.
POFWC provides food for many people on antiretroviral treatment through donations from other organizations and individuals.
I came to South Africa seeking asylum in 2007. My family joined me in 2009. My daughter finished primary school in Burundi, while the two boys finished primary and secondary education in South Africa. But none of them can access the university because we have been denied proper documentation.
In South Africa, the asylum seeker visa permits are difficult to get renewed. So besides the challenges of living with HIV, we are also stateless citizens of no country. We cannot get passports or visas.
I resisted taking HIV treatment for 17 years, until June 2019, when my health started deteriorating. I was afraid to take treatment due to issues of documentation and fear of deportation as a refugee. Today marks five years on treatment, and I am still strong and aging well.
Breaking the silence is a strategy I use to conquer HIV. Understanding and accepting myself, being positive and trusting God are among the others.
I have learned to have hope, live life
and always have faith and perseverance. God wasn’t finished with me even when I thought I was finished.
We are still facing stigmatization, discrimination and rejection, but we are still called to be strong.
What three adjectives describe you? Hopeful, strong and resourceful.
What is your greatest achievement? Staying alive and being with family in a safe place.
What is your greatest regret? Not disclosing my HIV status to my loved ones sooner. Keeping it to myself almost killed me.
What keeps you up at night? Reliving the war in Burundi and being afraid for my life. You could say I have posttraumatic stress.
If you could change one thing about living with HIV, what would it be? Have better health care and meds available. As asylum seekers and refugees, we cannot get jobs or afford private health care and therefore can’t get certain medications. I need to rely on donations.
What drives you to do what you do? Service to others less fortunate than myself.
What is the best advice you’ve received? Trust in God, and be grateful for every day!
If you had to evacuate your house immediately, what is the one thing you would grab on the way out?
My antiretroviral medications.
Read other POZ Stories or share your own at poz.com/stories.
Tom Fikiri Masarara
Camp Heartland Is Closing
The longtime retreat served youth living with HIV.
Since 1993, Camp Heartland has offered a much-needed respite and joy to youth living with and affected by HIV. But the beloved Minnesota camp is closing because the facility is for sale. It has served over 6,000 youth affected by HIV and AIDS during its threedecade run.
“My Dear One Heartland Friends, I have a range of emotions today as I have bittersweet news to share,” announced camp founder Neil Willenson in an October 29 Facebook post. “I was informed recently that the Board of Directors of One Heartland has made the very hard decision to place the beautiful One Heartland Center up for sale. The ‘sweet’ is that mother-to
child-transmission of HIV has virtually been eliminated in the United States in recent years. The number of children now born with HIV is in the handfuls versus the estimated 1,630 babies born with HIV during our founding year in 1993. One never could [have] imagined this incredible progress in three decades.”
Located in Willow River, Minnesota, about 90 minutes from the Twin Cities, the One Heartland facilities include cabins, lakes, a health center, a swimming pool and more spread across 93 acres. One Heartland has operated several camps targeted to different youth populations. For example, Camp Heartland served
EVERYDAY
January
United Nations Secretary-General Kofi Annan announces the launch of the GLOBAL MEDIA AIDS INITIATIVE, which aims to get media organizations to expand public knowledge and understanding about HIV and AIDS. (2004)
youth living with and affected by HIV, while Camp True Colors was open to LGBTQ and gender-expansive youth. One Heartland has offered camping experiences for young people facing other serious health issues, such as diabetes, as well as for unhoused youth and children facing other hardships.
In his Facebook announcement, Willenson continued:
“When we were founded 31 years ago, we had the goal of providing children affected by HIV/AIDS with a one-time, weeklong experience of
unconditional love and acceptance.
Through the tireless and unwavering support of tens of thousands of donors, camp volunteers, staff, board members and more, the program lasted 30 more years than my original intention. Along with moments of great joy and inspiration, there have been painful and profound losses of at least 150 prior campers. We cherish the time we had with them and remember them always.”
—Trent
Straube
These dates represent milestones in the HIV epidemic. Visit poz.com/aidsiseveryday to learn more about the history of HIV and AIDS. BY JENNIFER MORTON
15 24 February 13 28
Model and jewelry designer TINA CHOW dies of AIDS-related complications at age 41. Chow spoke publicly about living with HIV and worked with many AIDS organizations, including Project Angel Food in Los Angeles. (1992)
3 7
PRINCESS DIANA visits the pediatric AIDS unit at Harlem Hospital in New York City. (1989)
NATIONAL BLACK HIV/AIDS AWARENESS DAY
AIDS Healthcare Foundation launches INTERNATIONAL CONDOM DAY to remind people that wearing a condom can prevent pregnancy and sexually transmitted infections, including HIV. (2009) HIV IS NOT A CRIME AWARENESS DAY
Camp Heartland
Margaret Heagarty, MD, and Princess Diana
SPEAK UP
In a blog post titled “How to Be an Advocate for Yourself and Others,” The Well Project shares how you can make a difference on an individual or community level. Below is an edited excerpt.
WHAT IS AN ADVOCATE?
By definition, an advocate is a person who publicly supports or recommends a particular cause or policy. However, if the thought of being an HIV advocate in public makes you nervous, other types of advocacy might be a first step.
SELF-ADVOCACY
You might not think of yourself as an advocate, but in many ways, you already are. Every time you speak up for yourself or others, you are an advocate. It may be as simple as letting the cashier at the grocery store know she overcharged you for an item or telling your children not to speak to you disrespectfully. It can also be more di cult, like fighting for disability status or filing a complaint with human resources at your job for discrimination or harassment. In one way or another, you are likely an advocate for yourself or someone else every day.
SELF-ADVOCACY IN HEALTH CARE
Much of your advocacy as a person living with HIV may revolve around your health
and the health care you receive. To get the best care possible, it is important to speak up for and support yourself. Below are some ways you can advocate for yourself with your health care team:
• Learn as much as you can about HIV, your health and your treatment options.
• Make a list of questions for your health care provider before your appointment.
• Ask questions about the medications you are taking or new medications you have heard about.
• Ask your health care provider for an explanation anytime you do not understand something they say.
• Take notes during or immediately a er your visit to help you remember the important points when you get home, or invite a friend or family member to the visit to take notes for you.
• Discuss with your provider any health issues that are on your mind, even if they do not seem like a big deal.
• Ask for copies of all your medical records, such as lab results.
• Get a second opinion about any important health issue.
• Offer your health care team
suggestions and feedback about ways to improve services for people with HIV.
INDIVIDUAL ADVOCACY FOR OTHERS AND PEER ADVOCACY
Individual advocacy refers to supporting someone when they need help or trying to find a solution when someone has a problem. You likely advocate for other people o en in your daily life, yet you may not think of it as advocacy.
Examples of being an individual advocate for others:
• Helping an elderly neighbor figure out local shuttle and bus schedules so they can continue to live independently without driving;
• Contacting school o cials a er learning a child was bullied at school;
• Practicing or role-playing a di cult conversation that a friend expects to have with her boss;
• Writing or calling city o cials to improve or address an issue in your community.
Examples of being an HIV peer advocate:
continued on page 12
continued from page 10
• Helping someone in your support group who is having trouble understanding HIV treatment materials;
• Linking a friend to a better health care provider a er hearing that her questions were not being answered or she was not getting the care she needed;
• Volunteering at an AIDS service organization (ASO) as a resource/peer advocate for newly diagnosed people;
• Helping people in prison or jail obtain their HIV medications, either by advocating for someone you know or by volunteering for an organization involved in this work.
COMMUNITY ADVOCACY
It can be wonderful to advocate for yourself or on someone else’s behalf. It can also be very empowering to work together with a group of people. When more than one person speaks up, the message can be even stronger.
Community advocacy is a larger version of the individual advocacy you may already practice in your daily life. The difference is that community advocacy involves groups of people acting together to bring about positive change. Before becoming involved, decide how comfortable you are about disclosing your HIV status. This personal decision requires careful thought and discussion with people close to you. Whether or not you decide to go public with your status, you can still be a community advocate.
You can advocate in a number of ways. For example, you can speak about the needs of people living with HIV or about HIV prevention at a house of worship or at an organization. You can raise HIV awareness and funds for an organization by participating in a local AIDS walk or other event. You can join a patient advisory group at an HIV research site, an ASO or an HIV planning council. You can also advocate on behalf of your community through the media, including social media.
POLITICAL/PUBLIC ADVOCACY
If you are interested in politics and policy, you may want to help a group make a difference on a local, national or international level. In that type of advocacy role, you would focus on policies that, for example, affect HIV treatment, funding, gender equality, women- centered health care or crimi-
nalization. You might be asked to call, visit or write letters to government o cials. If this interests you, most groups will provide training to help people learn how to become public or political advocates.
A er the recent U.S. Supreme Court decision against abortion rights and the passage of local laws limiting gender-a rming care, advocacy for reproductive rights and justice has become even more important.
Many amazing advocacy organizations are fighting for the rights of people living with HIV:
GLOBAL ADVOCACY GROUPS: ATHENA Network, CARE, CHANGE, Frontline AIDS, the Global Coalition on Women and AIDS, International Community of Women Living with HIV; U.S.-BASED ADVOCACY GROUPS: Advocates for Youth, AIDS United, Black AIDS Institute, Housing Works, Iris House, National Women and AIDS Collective, NMAC, Positive Women’s
“CONSIDER YOUR OPTIONS AND FIND THE BEST FIT FOR YOU.”
Network—USA, SisterLove, Treatment Action Group;
PROVIDER-BASED ADVOCACY GROUPS: While these groups are primarily for medical professionals, you can join them as a patient advocate: American Academy of HIV Medicine, HIV Medicine Association, Ryan White Medical Providers Coalition.
SERVING FROM A FULL CUP: SELF-CARE FOR ADVOCATES
Serving as an HIV advocate can be very rewarding, especially when you see the difference you are making in people’s lives. However, if you are constantly giving and not taking time to refill yourself, you’ll be at risk for burnout. Burnout is a state of physical and/or emotional exhaustion o en accompanied by a loss of passion or a sense of detachment from your advocacy work. If you are burned out, you may feel cynical about your advocacy or doubt your effectiveness. You may also feel overwhelmed, numb, frustrated, bored or unappreciated. If you find yourself
also feeling hopeless, lacking interest in many activities (not just work), having trouble sleeping or concentrating or not taking your HIV drugs, you may be depressed. Unlike burnout, depression is a medical condition. If you think you may be depressed, talk with your health care provider.
Exhaustion is a normal reaction to high levels of stress and not necessarily a sign of illness. HIV advocacy can be particularly stressful because there are so many areas and people in need of advocacy, and people’s lives are at stake. But denying yourself proper rest and replenishment, even when others are in need and the cause is worthy, can have serious negative effects on your mental and physical health.
Self-care (caring for yourself)— which may include taking some of the very advice you are sharing with others— can break the stress cycle that leads to burnout and help you recover your energy and passion. It is important to pay attention not only to what drains you but also to what reenergizes you. This differs for each person. Do you need more sleep? Time outdoors? A good laugh? Some time to journal? To connect with friends? All of these are opportunities to reenergize. Consider what it would look like for you to take care of yourself before serving others. Imagine how much more you will have to share—with both others and with yourself.
MANY POSSIBILITIES
There are many ways to be an advocate. Some are larger and require a lot of time and commitment. Some are more public and may seem confrontational. However, being an advocate does not necessarily mean speaking to the media, meeting with politicians or participating in rallies and demonstrations. Many other forms of advocacy are just as valuable. Take time to consider your options and find the best fit for you. Becoming an advocate for yourself, another person or large numbers of people can be very rewarding and empowering. Q
The Well Project is a nonprofit organization whose mission is to change the course of the HIV and AIDS pandemic through a unique and comprehensive focus on women and girls across the gender spectrum. For more information, go to thewellproject.org.
•A daily resource for people living with and a ected by HIV and AIDS
• Clear, comprehensive prevention and treatment information
•News, personal stories, blogs, HIV-speci c resources and more
•Sign up for free email newsletters
BALL TO END AIDS 2024
On September 26, 2024, The Elizabeth Taylor AIDS Foundation (ETAF) hosted its fifth annual Ball to End AIDS at the Beverly Hills Hotel. Actress Dominique Jackson, best known for her portrayal of Elektra Abundance on the FX series Pose, hosted the gala fundraiser, which this year honored Emmy-, Grammy-, Oscar- and Tony-winning actress Jennifer Hudson and Gap Inc. CEO Richard Dickson. Hudson received the first-ever Elizabeth Taylor Rowdy Activist Award, while Dickson received the Elizabeth Taylor Commitment to End AIDS Award. The event featured an auction held in partnership with Christie’s, a performance by top-selling singer Natasha Bedingfield and a display of select items from the personal archive of ETAF’s Academy Award–winning namesake.
Taylor founded ETAF in 1991 to provide direct care— along with love and moral support—to the most vulnerable people living with HIV and AIDS at the peak of the AIDS epidemic and paid for the nonprofit’s overhead costs herself. Since her death in 2011, her estate has continued to fund ETAF’s work and donates 25% of royalties from the use of her image and likeness to the foundation. Over more than 30 years, ETAF has raised millions of dollars and continues to draw attention to the ongoing HIV crisis via star-studded events.
1. As chairman and CEO of Gilead Sciences, which sponsored the ball, Daniel O’ Day oversees the pharmaceutical company responsible for Truvada, the first pre-exposure prophylaxis for HIV. Gilead helps support more than 2,000 nonprofits fighting HIV and racial and health disparities. 2. A longtime advocate for the LGBTQ and HIV communities, Jennifer Hudson counts a 2024 GLAAD Excellence in Media Award among her many accolades. On World AIDS Day 2023, Hudson’s eponymous daily talk show featured a special segment on HIV advocates in the South. 3. Grammy-nominated artist Natasha Bedingfield performed her uplifting Billboard hit song “Pocketful of Sunshine” at the fundraiser.
4. Victoria Ortega , national president of FLUX, a network of trans leaders, serves on ETAF’s advisory board. 5. Dressed in “Vogue,” San Francisco AIDS Foundation CEO Tyler TerMeer, PhD, serves a glam look while posing with HIV decriminalization advocates Robert Suttle and Lashinda Salinas , both of whom made remarks at the gala. 6. Gap creative director Zac Posen celebrates his boss—and honoree— Richard Dickson , who was recognized for his longtime support of people living with HIV, particularly his work with the Children Affected by AIDS Foundation. 7. Attorney Moorisha Bey-Taylor was happy to see Toni Newman , director of the Coalition for Justice and Equality Across Movements at NMAC, who described the gala as a “fabulous evening of love and celebration.”
HIV AND MENTAL HEALTH
Psychotherapy and medications can help manage anxiety and depression.
MANY PEOPLE LIVING WITH HIV experience anxiety or depression—either temporary or long-term—but you can take steps to ease your mind and elevate your mood.
While occasional worry and sadness are normal, living with HIV can lead to persistent changes in mental well-being. Fear of worsening illness or death, loss of loved ones, survivor’s guilt, concerns about disclosure, worry about transmitting the virus, stigma, financial stress, chronic pain and di culty performing daily activities can all contribute to anxiety and depression.
Anxiety can range from mild apprehension to a disabling sense of dread that interferes with daily life. Depression, likewise, can range from feeling down to persistent depressive disorder (dysthymia) to more severe major depressive disorder. Clinical depression is distinct from temporary grief related to an event such as the death of a loved one.
People living with chronic illnesses— including HIV—are more likely to experience anxiety and depression compared with the general population. Feelings of hopelessness or low self-esteem can lead to poor treatment adherence and worse disease outcomes. What’s more, some people with anxiety or depression seek relief through excessive use of alcohol, recreational drugs or risky sex,
which can have detrimental effects on mental and overall health.
On the other hand, starting antiretroviral treatment, achieving good adherence and maintaining an undetectable viral load can help alleviate concerns about disease progression and HIV transmission.
Symptoms of anxiety may include restlessness or agitation, a racing heart, chest pain, muscle tension, di culty concentrating and trouble falling or staying asleep. Symptoms of depression can include irritability, inability to find pleasure in most activities, loss of interest in sex, changes in appetite, fatigue, brain fog, insomnia and recurrent thoughts about death or suicide.
If you’re experiencing persistent anxiety or depression, it may be time to seek help. Start by talking with your primary care provider or HIV doctor. You may be referred to a psychiatrist, psychologist, clinical social worker or other mental health specialist.
Diagnosing anxiety or depression involves ruling out physical problems that can affect mood—for example, a low testosterone level or an underactive thyroid gland. Uncontrolled HIV and opportunistic infections that attack the brain can lead to changes in mood and behavior. Medication side effects may also play a role.
Talking with a psychologist or other
trained therapist may be enough to improve your mood. Evidence-based approaches include cognitive behavioral therapy and interpersonal therapy. Many people find group therapy or peer support groups to be helpful.
Various medications are used to treat anxiety and depression. These conditions are o en related to chemical imbalances in the brain, and many of these drugs affect neurotransmitters that neurons use to communicate.
Antidepressants can take several weeks to start working, and they are not equally effective for everyone. But many people who don’t respond to one drug will do well on another. It may take trial and error to find the right regimen, but in most cases, anxiety and depression can be successfully treated.
Combining talk therapy and medications may offer the best results. Other steps to relieve anxiety and improve your mood include exercise, meditation or prayer, eating a healthy diet, getting enough sleep, engaging in enjoyable activities and spending time with others. Studies show that people with HIV who have little social support are more prone to anxiety and depression, and these, in turn, can worsen social isolation. Q
If you have thoughts about self-harm or suicide, dial 988 for the national Suicide and Crisis Lifeline, available 24 hours.
RESEARCH NOTES
BY LIZ HIGHLEYMAN
PREVENTION
3-Month Vaginal Ring
A vaginal ring worn for three months may prevent HIV as well as the existing onemonth ring, offering greater convenience at a lower cost. The flexible silicone ring slowly releases dapivirine, a non-nucleoside reverse transcriptase inhibitor. A one-month ring is authorized in 11 African countries, but it is not yet approved in the United States. The one-month ring is moderately effective. In one trial, it reduced the risk of HIV acquisition by 27% overall, rising to 56% for older women. A real-world study in Zimbabwe showed that HIV incidence was similar for women who used the ring or daily pre-exposure prophylaxis (PrEP) pills. In a Phase I trial of 124 women in South Africa, a three-month ring containing four times as much dapivirine led to higher drug levels in blood plasma and vaginal fluid. Both versions of the ring were safe and well tolerated. Surveys have shown that when offered a choice of prevention methods, a substantial number of women prefer a vaginal ring over daily oral or long-acting injectable PrEP, and some research suggests that rings may encourage better adherence than pills.
TREATMENT
Treating Advanced HIV
Dovato, a single-tablet regimen containing dolutegravir and lamivudine, can be a good option for people with advanced HIV who are starting antiretroviral therapy for the first time. The Phase IV DOLCE trial assessed the e cacy of Dovato for previously untreated adults with a CD4 count below 200, meaning they meet the criteria for AIDS. The 230 participants were randomized to receive Dovato or dolutegravir plus tenofovir disoproxil fumarate/emtricitabine or tenofovir alafenamide/ emtricitabine. The regimens were comparably effective at 48 weeks: 82% of people on Dovato and 80% of those on a three-drug regimen had an undetectable viral load. Among people with a high baseline viral load, 74% and 67%, respectively, achieved viral suppression. Time to viral suppression and CD4 cell gains were also similar. Dovato is currently approved for people with no history of treatment failure and no known viral mutations associated with resistance to dolutegravir or lamivudine, but another Phase IV trial found that Dovato is also a feasible option when drug resistance testing is unavailable.
CURE
Viral Reservoir
Metformin, a medication used to treat type 2 diabetes, may help the immune system recognize HIV and reduce the viral reservoir. Antiretrovirals can keep HIV replication suppressed, but the virus inserts its genetic blueprints into human cells and establishes a long-lasting reservoir that the drugs can’t reach. Metformin, an mTOR inhibitor, promotes insulin activity, decreases glucose production in the liver and helps control blood sugar. Researchers in Montreal previously showed that metformin reduced HIV transcription in CD4 cells and decreased inflammation in nondiabetic people with HIV. In the new study, they used a viral outgrowth assay to analyze CD4 cells from 13 HIV-positive people on antiretroviral therapy. When the cells were exposed to HIV in the laboratory, metformin increased the number of productively infected CD4 cells, but it also inhibited the release of new viral particles from these cells and led to improved recognition by broadly neutralizing antibodies. This suggests that metformin might be used as part of a “shock and kill” strategy for a functional cure.
CONCERNS
Heart and Liver Health
People living with HIV who have fat accumulation around the heart have poorer metabolic health and are more likely to develop liver fibrosis than people without HIV, according to a recent study. As they age, people with HIV are more prone to comorbidities, including cardiovascular and liver disease. Italian researchers evaluated the link between increased epicardial fat thickness (the amount of fat surrounding the heart) and liver stiffness, a measure of liver fibrosis, in 91 people on effective antiretroviral therapy. They found that 30% of those with epicardial fat thickness above the median had a liver stiffness measurement suggesting clinically relevant liver fibrosis, compared with 11% of those with less fat around their heart. Worse insulin resistance predicted increased epicardial fat and liver stiffness, while greater liver stiffness also correlated with current and nadir (lowestever) CD4 T-cell counts. The researchers concluded that people with greater epicardial fat thickness have a worse metabolic profile and are more likely to have clinically relevant fibrosis even with normal liver function tests.
Weekly Oral HIV Meds Look Promising
A once-weekly oral regimen of lenacapavir and islatravir can keep HIV suppressed for a year, researchers reported at IDWeek 2024. Gilead Sciences’ lenacapavir, an HIV capsid inhibitor, remains active against highly resistant virus. Injectable lenacapavir (Sunlenca) is approved as a twiceyearly treatment for people with multidrug-resistant HIV. Merck’s Islatravir is an experimental nucleoside reverse transcriptase translocation inhibitor.
Amy Colson, MD, MPH, of the Community Resource Initiative in Boston, and colleagues conducted a Phase II trial to test an oral version of lenacapavir plus islatravir pills administered once weekly as a switch option for people on daily Biktarvy pills (bictegravir/tenofovir alafenamide/emtricitabine). The study enrolled 104 adults with an undetectable viral load and no history of virological failure.
Earlier this year, Colson reported that switching to the weekly regimen worked as well as staying on daily pills at 24 weeks. At IDWeek, she reported that the experimental combination remains effective at 48 weeks. The viral suppression rate was 94.2% in the lenacapavir plus islatravir group versus 92.3% in the Biktarvy group. Both regimens were safe and generally well tolerated. Islatravir was put on a clinical hold in 2021 a er higher doses led to CD4 cell
and overall lymphocyte declines in earlier clinical trials, but this was no longer the case using the lower dose in this study.
Gilead and Merck are developing a combination pill containing lenacapavir and islatravir, which could become the longest-acting regimen without injections. “The future of HIV treatment is person-centered, with long-acting options tailored to help meet the needs and preferences of people affected by HIV,” says Gilead senior vice president Jared Baeten, MD, PhD.
NEED FOR PrEP REMAINS UNMET
Use of pre-exposure prophylaxis (PrEP) is rising overall, but disparities in need and lack of equitable access remain a challenge.
Using a metric called the PrEP-to-need ratio—defined as the number of individuals using PrEP each year divided by the number of new HIV diagnoses the previous year—one recent analysis showed that men living in predominantly white neighborhoods or covered by commercial insurance have ready access to PrEP and low unmet need. In contrast, despite moderate increases in PrEP use from 2019 to 2023, men living in mainly Black or Latino neighborhoods and those covered by Medicaid still have a high level of unmet need.
Targeted interventions can help improve PrEP access for specific populations. In another study, researchers from the HIV Prevention Trials Network assessed an integrated strategy to increase daily oral PrEP use among transgender women in four U.S. cities and Rio de Janeiro. Women in one group were offered gender-a rming hormone therapy, PrEP pills and peer health navigation sessions at a single site, while the other group received case management and referrals for hormone therapy. In both groups, PrEP uptake rose from 11% at the start of the study to nearly 90%, and half achieved good adherence.
“Transgender women have one of the highest HIV prevalence of any population yet continue to struggle to access and adhere to PrEP,” says study investigator Wafaa El-Sadr, MD, MPH, of Columbia University. “Tailoring strategies to address the unique needs of this population is critical to addressing this challenge.”
LONELINESS LINKED TO FRAILTY IN OLDER PEOPLE WITH HIV
Nearly one in five older people living with HIV showed signs of frailty in a recent Canadian study, and being single or lonely increased the odds. Frailty is a common syndrome among older adults that carries an increased risk for poor health outcomes, including falls, cognitive impairment, disability, hospitalization and death.
Alice Zhabokritsky, MD, of the University Health Network in Toronto, and colleagues assessed the prevalence of frailty and associated risk factors among 439 HIV-positive people ages 65 and older who were on effective antiretroviral therapy. In particular, they looked at the link between frailty and nadir (lowest-ever) CD4 T-cell count, noting that persistent immune dysregulation and chronic inflammation seem to play an important role in the development of frailty.
Frailty was assessed using a metric that includes unintentional weight loss, exhaustion, poor grip strength, slow walking speed and low physical activity. The overall prevalence of frailty was 16.6%—more than double the rate seen in a previous study of HIV-negative Canadians in the same age group. The likelihood of frailty increased with age, and women had a slightly higher prevalence than men.
Contrary to their hypothesis, the researchers did not see an increase in frailty among people with a lower nadir CD4 count. However, people who had higher scores on a loneliness scale had a 25% greater likelihood of frailty, and those who were not married or partnered had about double the risk.
“While nadir CD4 count did not correlate with frailty, being single and lonely did, highlighting the importance of recognizing and addressing these social vulnerabilities among people aging with HIV,” the study authors concluded.
First Report of Clade I Mpox in U.S.
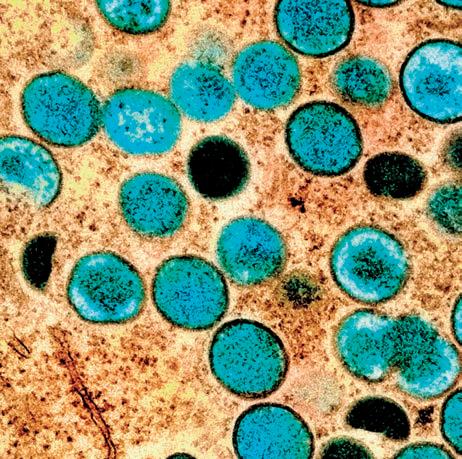
The first U.S. case of a potentially more severe type of mpox (formerly monkeypox), known as Clade I, was reported near San Francisco in November. The patient had recently traveled from eastern Africa, where there is an ongoing Clade I mpox outbreak. The individual, who had mild illness, was treated at a local medical facility and isolated at home while recovering.
There are two major strains of mpox, Clade I and Clade II. The latter was responsible for the global outbreak in 2022, which mainly affected gay and bisexual men. This strain continues to circulate at a low level in the United States. Concurrent Clade I mpox outbreaks are underway in the Democratic Republic of the Congo and nearby countries. One (due to Clade Ia) mainly affects children via household transmission and contact with wild animals, while the other (due to Clade Ib) appears to be largely driven by sexual transmission. Clade I mpox has historically had a higher fatality rate than Clade II, but mortality depends on access to medical care.
Health o cials consider the risk of a Clade I mpox outbreak in the United States to be low, but they’re urging people at higher risk to get vaccinated. These include men who have sex with men, transgender and nonbinary individuals, people living with HIV, those using or eligible for HIV pre-exposure prophylaxis (PrEP), sex workers and others in their sexual networks. Two doses of the Jynneos vaccine should be given at least four weeks apart. Booster doses are not recommended for those who have completed the two-dose series, and people who have already had mpox do not need to be vaccinated. Evidence indicates that the vaccine protects against both Clade I and Clade II mpox.
HOMEMADE
GRANOLA
Store-bought granola is more like candy.
MAKING GRANOLA AT HOME IS EASY. The ingredients in a lot of store-bought granola are more like those of a candy bar than breakfast. Granola from the store is often loaded with sugar and contains a lot of oil and preservatives with long names. Homemade granola is more nutritious and can include your choice of dried fruits and nuts.
SERVINGS: 12 / INGREDIENTS: 10 / PREP: 15 MINUTES
INGREDIENTS
2 cups rolled oats
1⁄3 cup whole wheat pastry flour
¼ cup almonds, sliced
¼ cup walnuts, chopped
DIRECTIONS
¼ cup unsweetened coconut flakes
Pinch of salt
1 teaspoon cinnamon (optional)
1⁄3 cup maple syrup (optional)
1. Preheat the oven to 375°F. Line a baking sheet with parchment paper or lightly butter it. Set aside.
2. In a medium bowl, stir together oats, flour, almonds, walnuts, coconut flakes, salt and cinnamon, if using. Stir in maple syrup and melted butter until the oats are completely coated. Transfer to the prepared baking sheet.
3. Bake for 30 minutes, turning the oats often for even browning. Granola can burn quickly, so keep a close eye on it! Once golden, allow to cool completely, then stir in dried fruit. Eat with milk or over yogurt. Store in an airtight container for up to two weeks.
NUTRITION FACTS (per serving)
¼ cup vegetable oil or melted butter
½ cup unsweetened dried cherries, raisins and chopped apricot or any combination of dried fruit
SUPERFOODS: MISCELLANEOUS
By Craig Ramsay
What if you could lower your cholesterol, reduce your risk for heart disease and cancer and improve your state of mind with food? Turns out, you can! Superfoods contain a high level of nutrients and are a great way to boost your health.
Toss these miscellaneous items into your grocery cart:
Craig Ramsay is a fitness expert, an author and a winner of season 8 of The Amazing Race Canada
Follow him on Instagram at @craigramsayfit.
Basil
Dark chocolate
Staying in HIV care is the most important part to becoming undetectable.
“In my journey as a transgender man, the first time I was able to become undetectable was the year after I transitioned. There were a few things that happened there. I felt comfortable with who I was. I had a great provider. I had stability.”
— JA’MEL FROM ATLANTA, GEORGIA
BE
cdc.gov/HIVTreatmentWorks
Andy Feds was born with HIV.
STRAIGHT MEN LIVING WITH THE VIRUS ARE SPEAKING UP.
BY ALICIA GREEN
IN JULY 2024, SIX STRAIGHT MEN SERVED AS panelists on a Zoom webinar hosted by The Reunion Project, a nonprofit founded by and for long-term survivors. They shared their journey of living with HIV, specifically as straight men with the virus who have felt forgotten and unheard.
“[The webinar] was a space we wanted just for us to share our experiences on a virtual platform where others could join in,” says Larry Bryant, senior program manager at The Reunion Project, who was one of the panelists.
For Bryant, this was a long time coming. As a straight man living with HIV, he’d never felt a sense of community like this. “It was amazing,” he says. “But in my 20-plus years working in this field, I could count on one hand—and not use all my fingers—the number of times that I’ve been in such a space.”
According to the Centers for Disease Control and Prevention, in 2022, an estimated 31,800 people were newly diagnosed with HIV in the United States. Men who acquired the virus through heterosexual contact accounted for 6% of these cases.
When straight men who became HIV positive through other modes of transmission are included, the proportion of heterosexual men living with the virus is larger than many people realize.
Bryant and other straight men with HIV are hoping to change the narrative and bring awareness to this group, which has often felt neglected or misunderstood within the HIV community.
WHEN BRYANT TESTED POSITIVE FOR HIV IN
1986, it was a common misconception that only gay men got the virus. But Bryant was a 19-year-old straight man from Washington, DC, who had just been told he had HIV and only eight years to live.
“I thought I was going to die, but I didn’t know how to tell anyone,” says Bryant, now 58 and living in New York City. “So I just kept it a secret for the next five years.”
His diagnosis and presumed death sentence took a large toll on him. Bryant dropped out of college, ending his dream of someday making it to the NFL.
“I went from being a freshman all-American with NFL scouts already talking to me to dropping out of school,” he says.
He experienced homelessness and attempted to take his own life several times. But his loved ones still knew nothing.
Below: Larry Bryant on the cover of POZ in 2007; right: Bryant today with his dog, Button
By 1991, Bryant had reached his breaking point. After being rejected from the Army, he broke down and shared his status with his family.
“This is right after Magic Johnson disclosed his status, and he had to leave basketball,” Bryant says. “That was the first time I saw someone who I could kind of connect with as a heterosexual Black male athlete.”
Of course, before Johnson, there had been tennis legend Arthur Ashe. But he acquired HIV through a blood transfusion.
AT
THE
TIME, PEOPLE QUESTIONED WHETHER
Johnson was gay or bisexual despite his denials that he was neither.
“The whole idea of a heterosexual man living with HIV was just not something we talked about or something we acknowledged, and I was one,” Bryant says.
Bryant hadn’t ever considered himself to be at risk for HIV. He wasn’t gay and didn’t use drugs. His main concerns were
“I THOUGHT I WAS GOING TO DIE, BUT I DIDN’T KNOW HOW TO TELL ANYONE.”
—LARRY BRYANT
getting someone pregnant or acquiring some other sexually transmitted infection.
“All these teen movies were about how there was always a guy who had an itch or scratch,” he recalls. “You get a shot, and you’ll be fine, but you’re a man now. So that’s how we talked as young guys or how men talked to teenage guys growing up.”
encounter many other straight Black men living with HIV.
“It was a lost community,” he says. “It’s only because of the silence with people just being afraid to talk about it. So it was [nice] being able to see that empowerment of not only straight men but also Black men together.”
Conversations about straight men with HIV seemed nonexistent to Bryant. That remained the case as he engaged in HIV advocacy in the mid-’90s and even later.
Indeed, as a straight man living with HIV, Bryant was such a rarity that when he introduced himself as such at a peer group, people called him a unicorn.
That spurred him to appear on the May 2007 cover of POZ and share his story of living with HIV as a straight man.
ANDY FEDS, A STAND-UP
comedian, emceed that Reunion Project webinar and was also a panelist. The 31-year-old from Las Vegas calls himself the first-ever openly HIV-positive stand-up comedian born with the virus.
Since 2017, Feds has used comedy to share his story and raise awareness
Derrick Robinson
Feds aims to challenge the societal misconception that HIV affects only gay men by normalizing conversations about HIV for straight men living with the virus via his Keeping It Positive movement.
“That [myth] has been debunked for like 40 years now,” Feds says. “However, people aren’t getting that education because we don’t want to talk about sexual health at all, whether it be to our partners, our doctors, whatever the case.”
As part of Keeping It Positive, Feds posts engaging videos on various platforms—sometimes including his girlfriend, who is HIV negative— about living with HIV.
“The concept of being straight with HIV is foreign to people, and I think the reason is stigma,” Fed says.
BRYANT AGREES THAT MORE conversations about straight men with HIV are needed. But they aren’t taking place in the spaces where they should be.
“THE CONVERSATION NOW IS BEYOND HIV, BECAUSE MOST OF US LIVING WITH HIV ARE OVER THE AGE OF 50.” —DERRICK ROBINSON
about the virus. Comedy has been like therapy for him, he says, as he navigates his journey with HIV.
Feds had grown up seeing and hearing how negatively people reacted to HIV. As a result, he didn’t disclose his status publicly until he was 24.
“I always heard the HIV jokes,” Feds says. “Somebody talking about ‘Oh, you got HIV’ or ‘Oh, you got AIDS.’ I heard people say HIV is just for gay people. It hurt. I think that’s why I didn’t date as a teenager.”
Feds had always feared that girls would reject him if they knew his status.
“I was like, Are they going to label me these misconceptions that they heard from people that have no idea what they’re talking about?” he says.
IT WAS IMPORTANT FOR FEDS
TO PARTICIPATE in the Reunion Project webinar. For a long time, he didn’t
“We need more stats on heterosexual men,” Bryant says, referring to the dearth of studies on straight men with HIV.
If you wanted to know about the few stats that are available, there is no one to ask, Bryant explains. That’s because most providers and health professionals lack knowledge on straight men with HIV.
“There is no go-to person at the Centers for Disease Control and Prevention, the Office of National AIDS Policy or on the Presidential Advisory Council on HIV/AIDS that has an expertise or, dare I say, interest in adding that as a topic or priority,” Bryant says.
Bryant also notes that HIV organizations don’t do their part to foster dialogue about or create programs aimed at the lived experiences of straight men with HIV. Nor do they center HIV prevention for straight men.
“We have the elevation of groups saying that women, particularly women of color, are significantly affected by HIV,” he
COURTESY OF DERRICK ROBINSON
says. “Yet we haven’t seen any direct messaging to outreach to just men in general regardless of their HIV status.”
As Bryant points out, because HIV is often transmitted through sex, prevention messaging should be targeting straight men too.
“The same environment that existed when I was graduating high school is that community right now,” he says. “We have an opportunity to engage young men in a way that at least lets them know to protect themselves and know they are at risk.”
“THE CONCEPT OF BEING STRAIGHT WITH HIV IS FOREIGN TO PEOPLE, AND I THINK THE REASON IS STIGMA.”
—ANDY FEDS
ONE WAY BRYANT HOPES TO REACH STRAIGHT
men living with or at risk for HIV is via a special awareness day.
“With all of the awareness days that we have for HIV that you could find on HIV.gov, why not a heterosexual men and HIV awareness day?” Bryant says.
It would give organizations the opportunity to enter the conversation or give communities the opportunity when organizations don’t want to step up.
“When you put up an awareness day, it gives the template and the space to have these events that raise awareness on heterosexual men who are living with HIV,” he says.
“It invites young men and boys to be a part of that conversation, especially as it involves prevention, education and sexuality.”
Until such a day is on the calendar, though, Bryant and other straight men living with HIV are doing their part to nurture community and raise HIV awareness on their own.
TAKE DERRICK ROBINSON, FOR EXAMPLE. THE
61-year-old from Panama City, Florida, also participated in the Reunion Project webinar. Robinson has a private support group on Facebook for Black straight men with HIV called Straight and Positive; the group meets every Tuesday via Zoom.
“We’re not asking you to show your face or anything,” he says. “But we want you to be empowered and feel some positive energy.”
Robinson, who tested positive for HIV in 1991, turned to social media to look for other straight men with HIV but couldn’t find anyone. When he finally met someone, the COVID-19 pandemic struck, and everything shut down. That’s when he created the Facebook group.
“It was four of us,” he says. “We met every Tuesday for a whole year, and we made it through the pandemic together.”
About five years later, the group has over 90 members from across the United States.
“The conversation now is beyond HIV, because most of us living with HIV are over the age of 50,” Robinson says. “We have other comorbidities. We try to hit all the health and social issues that affect Black men, whether you’re coming out of prison with a diagnosis or you gotta deal with the virus stigma.”
BRYANT
EXPLAINS THAT STIGMA AND FEAR ARE largely to blame for why straight men living with HIV, particularly Black men, sometimes don’t show up to certain spaces. He believes straight men need more HIV representation.
“I think heterosexual men who are living with HIV would like to see some prioritization and some real connection with any level of program or interventions,” Bryant says. “We want to see ourselves represented in leadership in an organization.”
That could be a program director or manager or outreach specialist. And Bryant believes such men don’t necessarily need to be living with HIV.
“There are a lot of male-identified leaders and gatekeepers in our communities who aren’t living with HIV who can be invited to these spaces to help broaden this conversation,” Bryant says.
But he urges HIV organizations to do their part too.
WHILE
BRYANT ACKNOWLEDGES THE STRIDES that the HIV community has made since the beginning of the epidemic, he knows that the work is not yet done.
“We are light years better and beyond where we were as a collective community in 1986, but we still have so much to do, particularly among heterosexual men and our role in the entire conversation,” he says.
It’s not just about lowering infection rates and prevention, Bryant explains. It’s also about men actively owning their role in safer sex, domestic and sexual violence and reproductive rights.
Men shouldn’t just be in the room nodding their heads in agreement with their female partners.
“We need to be active leaders in this community so that we are not just forgotten as part of the equation of protecting, assisting and collaborating within all of our communities,” Bryant says.
His advice to other Black straight men living with HIV is to step up and show up for the entire Black community. That means Black women, Black youth and Black LGBTQ people.
“We need to be present,” he says. “We need to be purposeful. If you’re living with HIV, ask for help. Once we break through that whole inability to speak or share, we build trust and connection. The rest will follow.” Q
THE DEBATE OVER WHO QUALIFIES AS A LONG-TERM SURVIVOR IS IN THE SPOTLIGHT.
BY VICTORIA NOE
IN 2015, I LEARNED THAT LONG-TERM SURVIVOR JEFF BERRY was forming The Reunion Project to address the needs of long-term survivors. A lot of my friends and women I was writing about, particularly in my book Fag Hags, Divas and Moms: The Legacy of Straight Women in the AIDS Community, are HIV-positive long-term survivors, so I asked whether I could attend the group’s first gathering and observe. He said I was welcome— not to observe but to participate.
I argued that I’m not living with HIV or AIDS, so I’m not a long-term survivor. But he insisted that I was. Of the early days of the epidemic, he said: “You were there.”
At that time, the needs of long-term survivors were only beginning to be addressed. The death in 2012 of ACT UP New York’s Spencer Cox due to AIDS-related illness after he stopped taking his medications is cited as a wake-up call, one that revived ACT UP. His death showed that the complacency in the community since the 1996 advent of effective treatment had consequences. Those who had lived through so much had been forgotten, neglected and even dismissed, inconvenient reminders of those dark, early days. That community was now mobilized.
It took me years to embrace Berry’s definition, though I can’t say I’m comfortable with it. I’m an ally, a title I wear proudly. A straight, cisgender woman who is HIV negative. I’m just not sure I have the right to consider myself a long-term survivor.
Over the years, I did many of the same things my friends living with HIV did: marched; advocated for funding and policies on the local, state and federal levels; raised money; made hospital visits; attended memorial services; raged; grieved.
The conversations on this topic ramped up as I worked on my book. One of the women I reference in it, Terri Wilder, told me something I saw in myself and others: “We are all damaged.”
But what are we? And does it matter how we identify?
IN HIS SEPTEMBER 2024
“WHO ‘counts’ as a long-term HIV survivor?” essay on the San Francisco AIDS Foundation (SFAF) website, long-term survivor
Hank Trout enumerates various definitions. For the first time, Trout notes, the federal government this year defined some key populations through the HIV/AIDS Bureau of the Health Resources and Services Administration to identify Ryan White HIV/AIDS Program recipients:
fer the same PTSD [posttraumatic stress disorder], especially those caregivers and activists who rushed to the front lines of the fight against AIDS.”
I took a very unscientific poll, in person and on social media, to find out where people in the HIV community stand on this topic. Their perspectives varied as much as their locations:
“My brother buried his partner of 13 years and cared for him during the last horrific two years of his life. Please don’t tell me that my brother, who is HIV negative, doesn’t know what it is like to live with AIDS. My brother survived, as we all have, and is just as haunted by those years as most long-term HIV survivors.” —Mark S. King, Atlanta
“BUT WHAT ARE WE? AND DOES IT MATTER HOW WE IDENTIFY?”
“I do not consider myself to be a long-term survivor, not because I haven’t been impacted by HIV and AIDS, because of course I have, but because I feel it would be disrespectful of me to presume that the challenges of people who aren’t HIV positive are in any way identical to the challenges of those who are…. I am not going to be in a situation where, like Spencer Cox, I will be so deep in the depths of despair that I choose to just stop taking my meds and allow immune deficiency to take me…. Unless I walk in those shoes for decades, I can’t in any way rank myself as someone who deserves the respect due to them for having lived the life experience of truly being a ‘long-term survivor’ of an HIV-positive status. That is a term that deserves great respect. It is a kind of respect that someone like me simply does not merit.” —Tony Arena, New York City
• Older adults are people with HIV ages 50 and older.
• Long-term survivors are adults who acquired HIV prior to the availability of antiretroviral treatment.
• Lifetime survivors are adults who acquired HIV at birth or as young children.
The Ryan White Program’s mission demands that its definitions include only those living with HIV. At the same time, it makes a clear distinction between people who have lived with the virus for decades and those who have acquired HIV more recently. But for programming at SFAF, the nonprofit considers anyone who lived through the height of the AIDS epidemic a long-term survivor. SFAF recognizes that HIVnegative long-term survivors experienced the same loss and grief as those living with HIV. Indeed, we are included in the landmark San Francisco Principles:
“We embrace in our definition of ‘long-term survivors’ our HIV-negative sisters and brothers who faced the same fears, suffered the same losses, and endured the same grief as we HIV-positive survivors. And to this day, they continue to suf-
“I’d say HIV-negative long-timers have important roles and perspectives but probably should use a different term.” —Liz Highleyman, San Francisco
“I could see how people with HIV would want us to use a different term and not co-opt theirs. We’re all long-term survivors of the HIV and AIDS crisis, if not AIDS itself.” —David Hamburger, Boston
“The same term? Def no, though definitely worth a suitable descriptive moniker. One that honors your trauma, contributions and life of ‘living alongside and contemporaneously with HIV and AIDS.’” —Patrick Smith, Palm Springs, California
“I consider myself incredibly lucky to be HIV negative and do not consider myself a survivor, but having not experienced the reality of living with HIV, I don’t think I could publicly call myself that. I really do think, though, that as witnesses to the microbiological disaster, we have a place but would never want to belittle the life experiences of someone living with HIV.” —Ian Johns, London
“As an HIV-negative man, I absolutely believe that I, along with
any other HIV-negative person who struggled to end the AIDS crisis, should be included as a long-term survivor.” —Jeffrey Griglak, New York City
“I sometimes take issue with the term ‘survivor.’ I’m not quite sure that reflects our experience. But I believe there must be some acknowledgement of what we experienced. We were there, in the midst of it all. We saw friends and family die; we were at funeral homes making arrangements; we were at the hospitals negotiating care. We acted as power of attorney for many, some of whom did not have other family members or friends to advocate on their behalf. We advocated for benefits and proper medical care. How can this go unacknowledged? So if ‘survivor’ is not an acceptable term, there must be another term to identify those of us who, while being HIV negative, still were impacted by the HIV epidemic.” —Rosa E.
Martinez-Colón, Chicago
RECENTLY, I AGAIN DISCUSSED THIS TOPIC WITH Jeff Berry and was surprised to learn that our 2015 conversation had partially sparked his decision to include people like me in the long-term survivor definition. But the question remained: Do we deserve to be included? I looked to the military community, oddly enough, for guidance.
My father and his older brother both served in the Navy in the 1940s. My uncle was in Normandy for D-Day operations; my father signed up several months after V-J Day and never left the coast of California. Normandy saw intense combat; California saw none. The federal government classified them both as World War II veterans. They enlisted, underwent basic training, gave up their lives at home and served their country. Their service ribbons, like their experiences, were not the same. But as far as the government is concerned, they were both WWII veterans, deserving of all the perks of that title.
It’s technically true. But is it fair?
Trauma and grief are all too real for those who are HIV negative. Psychotherapy was not an option for most people in the 1980s and early ’90s. Those of us who were not living with the virus, often straight, could not find people outside the HIV or LGBTQ communities sympathetic to our experience. Subjects were changed; no words of support were offered. We kept our trauma to ourselves, only to have it present in ways that often made no sense.
It took me a couple of decades to recognize how my trauma most often manifests. Those of us who were around during those first 15 years of the epidemic remember the pages of obituaries in the weekly LGBTQ papers. Unless you were close enough friends to be part of a phone chain, you often did not know someone was gravely ill until reading their obituary, because so much of the suffering happened behind closed doors.
Nowadays, I freak out if I don’t hear from my friends, if they don’t respond to my texts or emails within a few days. I immediately assume they’re dead or dying, when the reason for the silence is almost always quite benign. A few years before the COVID-19 pandemic, I asked my closest friends whether they would tell me if they were sick: not with a cold or flu but something life-threatening. One who initially said
no opened up to me in unexpected ways when she was dying. The most common response was “Why wouldn’t I?” But I’d seen too much in the early days of AIDS to make any assumptions about them or their families.
That means, for good or bad, I know a lot about my friends’ health. They know, based on what I’ve been through, that I will listen without judgment, that I will keep our conversations to ourselves and respect their desire for privacy, that I will have the hard conversations with them that they cannot face having with their families. I think living through those awful early days made me a better friend.
This is not a trauma competition between long-term survivors living with HIV and those who are not. When fellow HIVnegative long-term survivor Gene Fedorko first told me about documenting the names of those he knew who died of AIDS, I was stunned that there were over 1,100 names in what he has titled The Book of the Dead—Bearing Witness. He explains:
“I started keeping this list in the late ’80s, and I just kept adding to it. I didn’t want to forget any of these people that were acquaintances, but I might’ve forgotten them years later was my thinking. It’s actually a work of art now. I’m leaving it to the New York Public Library when I die; it’s a historic document. Tabboo! [the New York City–based visual artist] did the cover. And it’s in the Museum of Modern Art here in New York. It’s a narrative, if you will, of my journey through the epidemic. At Dr. Paul Bellman’s office [a practice in Manhattan where Bellman treated people with AIDS starting in 1988], where I worked for 26 years, we were at the epicenter of inner-city HIV and AIDS, and we were at the front lines. It’s been quite a process for me—all kinds of emotions, severe emotions. It gives me comfort to know that I was able to help so many people. Lots of palliative memories. The survivor’s guilt was intense for a long time, but that has mostly dissipated by now. I was very surprised, and I’m glad I’m alive. Also, it’s a way of putting people to rest with dignity.”
Long-term survivor support groups, like those held at GMHC, do not include us, and I don’t disagree with that. But we need our own “I was there too” groups. Maybe we got lucky; maybe we weren’t truly at risk. But as Jeff insisted, we were there. And that experience has shaped our lives.
BACK TO A NAME FOR US. I THREW OUT A COUPLE of suggestions to the people who responded to my inquiry. For those uncomfortable being called a long-term survivor, “witness” was deemed too passive. “Ally” was a possibility. Maybe “long-term survivor ally”? That’s a mouthful.
Part of me wants to insist that people like me don’t need a name or title. We know all too well what we endured. We’re not looking for awards or applause. But it would be nice to be acknowledged. Q
Victoria Noe is an award-winning author, speaker and activist. Her HIV and AIDS activism inspired her to write Fag Hags, Divas and Moms: The Legacy of Straight Women in the AIDS Community, the first book to honor the ways women changed the course of the epidemic.
Joanna Robinson is a longtime HIV advocate in Miami.
Stigma Warrior
Joanna Robinson took a long, winding path to become one of Miami’s highest-profile and most influential HIV activists. A er 40 years of living with HIV, much of that time spent battling drugs and alcohol, she has committed the past decade to ending HIV and the accompanying stigma.
“I started activism to break through my own HIV stigma and also to help others break through theirs,” she says.
Robinson is a patient representative at the Miami Dade HIV/AIDS Partnership, where she also serves on the planning council. From that perch, she helps to ensure an effective and equitable distribution of Ryan White funds to prevent and treat HIV in Miami Dade County, which is home to 3.5 million residents.
Robinson is also a longtime volunteer at Empower U Community Health Center, where she counsels people newly diagnosed with HIV. As a Black transgender woman who previously performed sex work to survive, Robinson knows firsthand what it’s like to live on the margins. Now, she’s using that experience to help stigmatized populations at risk for HIV.
“I was diagnosed in 1983,” Robinson says. “And it was a lot of years of not practicing acceptance. My decision at that time was to get high for the rest of my life, not coping with the diagnosis. I spent 35 years in active addiction.”
Her life changed when she stopped using in June 2014 and turned her attention to activism, which she says gave her life meaning. Service to others, she discovered, was therapeutic for her as well.
“I began my activism to be that person to step in and help with a newly diagnosed person or somebody struggling to manage their HIV,” she says. “I’m glad that I can build a solution for that person, because there are so many young people, especially transgender women and sex workers, who need the support.”
Robinson notes the nexus between survival sex, addiction and HIV among LGBTQ youth rejected by their families, circumstances she relates to. “That’s how I became positive,” she adds. “I was a sex worker, and I was in active addiction.”
“I started my HIV treatment by taking AZT in the early days. Talking about my miraculous longevity, meds nowadays are the miracles,” Robinson says. “Even with the long-acting injectables now available to treat HIV, all the current meds are a miracle, because I remember taking 15 pills at one time. Now I’m on a one-pill regimen, and I look forward to eventually being on long-acting injectables.”
Robinson is living proof that HIV treatment and prevention have come a long way. But all these years later, HIV-related stigma stubbornly persists.
“For most of us, we’re not dying from HIV today— we’re living,” she says. “But the stigma is thriving, and that’s the roadblock keeping a lot of people from getting to an undetectable viral load.” Q
If your test result is positive (reactive)
Today, it’s recommended that people living with HIV start treatment as soon as possible. Starting and staying on today’s treatment can help you get to and stay at an undetectable status and prevent transmission of HIV to others through sex. Here are some steps you can take for yourself and your sexual partner(s):
1
Talk to your healthcare provider
Ask what your test results mean for you and find out about HIV treatments that could best fit your personal routine.
2
Find out everything you can
The more you know about HIV, the better. You can discover resources by scanning the QR codes, or even find helpful information on your own.
3
Maintain your sexual health
Use condoms, practice safer sex, and start and stay on the treatment discussed with your healthcare provider.
Helpful terms to know
TasP
Treatment as Prevention
If you’re living with HIV, current research shows that taking HIV treatment as prescribed and getting to and staying undetectable prevents transmitting HIV to others through sex. This is also known as U=U (undetectable=untransmittable).
PrEP
Pre-Exposure Prophylaxis
Undetectable
A major goal of HIV treatment is getting your viral load to undetectable. Undetectable means that there is so little virus in the blood that a lab test can’t measure it. If you have questions about your lab results and what it means to be undetectable, talk with your healthcare provider.
PrEP (pre-exposure prophylaxis) means routinely taking prescription medicine before you’re exposed to HIV to help reduce your chances of getting it. There are different PrEP options available, some of which are 99% effective. Just remember, PrEP doesn’t protect against other STIs, so be sure to use condoms and other healthy sex practices.
If your test result is negative (non-reactive)
When it comes to HIV prevention, the Centers for Disease Control and Prevention (CDC) recommends that ALL sexually active adults and adolescents be informed about PrEP (pre-exposure prophylaxis). PrEP means routinely taking prescription medicine before you’re exposed to HIV to help reduce your chances of getting it. Here are some steps you can take for yourself and your sexual partner(s):
Talk to your healthcare provider
Have a conversation with your healthcare provider about all of your HIV prevention options, including PrEP.
Find out everything you can
Maintain your sexual health
Regularly test for HIV and other sexually transmitted infections (STIs), use condoms, and communicate honestly with your partner(s). If you have been prescribed PrEP, continue to take it exactly as prescribed. 1 3 2
Scan the QR codes and explore resources on your own to get tips on how to be proactive about protecting your sexual health, including understanding your HIV prevention options, like PrEP medications.
Whatever your results may be...
Speak with a healthcare provider:
1.How can I help protect myself and others?
2.How often should I get tested and retested?
3.How can I talk to my partner(s) about my status and theirs?
Share your status with partner(s)
It may not be easy, but having a conversation with your partner(s) about your HIV status can help:
•Normalize the conversation around status, sexual health, and testing
•Empower others to make informed decisions about their sexual health
• Encourage all people to have conversations and stay engaged with their healthcare providers
If your test result (reactive)
Today, it’s recommended that people living with Starting and staying on today’s treatment can help status and prevent transmission of HIV to others take for yourself and your sexual partner(s):
Talk to your healthcare provider
Ask what your test results mean for you and find out about HIV treatments that could best fit your personal routine.
Find out everything you can
The more you know HIV, the better. discover resources scanning the QR even find helpful on your own.
Helpful terms
Treatment as Prevention
If you’re living with HIV, current research shows that taking HIV treatment as prescribed and getting to and staying undetectable prevents transmitting HIV to others through sex. This is also known as U=U (undetectable=untransmittable).
PrEP
Pre-Exposure Prophylaxis
PrEP (pre-exposure prophylaxis) means routinely taking medicine before you’re exposed to HIV to help reduce of getting it. There are different PrEP options available, are 99% effective. Just remember, PrEP doesn’t protect STIs, so be sure to use condoms and other healthy sex
HIV start treatment as soon as possible. help you get to and stay at an undetectable through sex. Here are some steps you can
everything can know about better. You can resources by QR codes, or information own.
Maintain your sexual health
Use condoms, practice safer sex, and start and stay on the treatment discussed with your healthcare provider.
A major goal of HIV treatment is getting your viral load to undetectable. Undetectable means that there is so little virus in the blood that a lab test can’t measure it. If you have questions about your lab results and what it means to be undetectable, talk with your healthcare provider.
taking prescription reduce your chances available, some of which protect against other sex practices.
2025 HIV AND AIDS AWARENESS DAYS
Awareness days help educate the general public and specific communities about HIV and AIDS. Display this poster as a reminder of upcoming awareness days, and use the hashtags provided to spread the message on social media.
FEBRUARY
7
National Black HIV/AIDS Awareness Day
#NBHAAD
According to the Centers for Disease Control and Prevention (CDC), Black people account for 37% of new HIV cases, even though they make up only 12% of the U.S. population. NBHAAD helps raise awareness of HIV testing, prevention and treatment in communities of color.
28
HIV Is Not a Crime Awareness Day
#HIVisNotaCrime
HIV-specific laws are outdated, they punish people living with HIV and they disproportionately impact Black, Latino and LGBTQ people and individuals who engage in sex work. This awareness day aims to educate people about HIV criminalization laws in the country and amplify the work of those trying to reform them.
observed in 2014, this
MARCH 20
National Women and Girls
HIV/AIDS Awareness Day
#NWGHAAD
Women are less likely to be screened for HIV, in part because of the perception that they are not at risk. This awareness day emphasizes the need for further prevention efforts aimed at women and girls and promotes equity in HIV care and treatment.
Observed on the first day of spring, this day aims to combat HIV-related stigma in Indigenous communities. It also encourages American Indians, Alaska Natives and Native Hawaiians to get tested and promote awareness of HIV in their communities. 10
National Native HIV/AIDS Awareness Day
#NNHAAD
APRIL
National Youth HIV & AIDS Awareness Day
#NYHAAD
MAY
18
HIV Vaccine Awareness Day
#HVAD
Led by the National Institute of Allergy and Infectious Diseases, HVAD showcases the progress made in the search for a safe and effective HIV vaccine. It also marks an opportunity to educate communities about the importance of vaccine research.
19
National Asian & Pacific Islander
HIV/AIDS Awareness Day #APIMay19
This awareness day presents an opportunity to highlight how HIV uniquely affects Asians and Pacific Islanders. The goal is to promote HIV testing and treatment and encourage conversations about HIV in these communities.
Southern HIV/AIDS Awareness Day
#SHAAD
In 2022, nearly half of new HIV diagnoses were in the South. SHAAD raises awareness of the HIV crisis in the region and
19
Hepatitis Testing Day
#HepTestingDay
Approximately 20% of people living with HIV nationwide also have hepatitis C, and around 10% of people with HIV are also living with hepatitis B. Hepatitis Testing Day aims to raise awareness of hep B and C and encourage testing.
According to the CDC, people ages 13 to 34 accounted for 60% of estimated new HIV infections in 2022. This awareness day was launched to encourage young people to talk about HIV and AIDS.
18
National Transgender HIV Testing Day #NTHTD HIV disproportionately affects the transgender community. NTHTD recognizes the importance of routine testing and a continued focus on HIV prevention and treatment among people who are transgender, gender-nonconforming and nonbinary.
National Faith HIV/AIDS Awareness Day #NFHAAD HIV affects people of all
who engage in sex work. This awareness day aims to educate people about HIV criminalization laws in the country and amplify the work of those trying to reform them.
This awareness day aims to educate people about HIV criminalization laws in the country and amplify the work of those trying to reform them.
The goal is to promote HIV testing and treatment and encourage conversations about HIV in these communities.
The goal is to promote HIV testing and treatment and encourage conversations about HIV in these communities.
hepatitis B. Hepatitis Testing Day aims to raise awareness of hep B and C and encourage testing.
Hepatitis Testing Day aims to raise awareness of hep B and C and encourage testing.
who are transgender, gender-nonconforming and nonbinary.
who are transgender, gender-nonconforming and nonbinary.
HIV Long-Term Survivors Awareness Day #HLTSAD
HIV Long-Term Survivors Awareness Day #HLTSAD
First observed in 2014, this awareness day honors long-term survivors of HIV, highlights the challenges they face and provides an opportunity to advocate for resources to meet their particular needs.
First observed in 2014, this awareness day honors long-term survivors of HIV, highlights the challenges they face and provides an opportunity to advocate for resources to meet their particular needs.
27
27
National HIV Testing Day #HIVTestingDay
National HIV Testing Day #HIVTestingDay
According to the CDC, approximately 13% of people living with HIV don’t know they have the virus. This awareness day serves as a reminder to people of all ages to learn the facts about HIV and get tested for the virus.
According to the CDC, approximately 13% of people living with HIV don’t know they have the virus. This awareness day serves as a reminder to people of all ages to learn the facts about HIV and get tested for the virus.
JULY
JULY
21
Zero HIV Stigma Day #ZeroHIVStigmaDay
Zero HIV Stigma Day #ZeroHIVStigmaDay
This awareness day spearheads a movement that highlights the detrimental impacts of HIV-related stigma around the world and promotes ways to take action against it.
This awareness day spearheads a movement that highlights the detrimental impacts of HIV-related stigma around the world and promotes ways to take action against it.
Southern HIV/AIDS Awareness Day #SHAAD
Southern HIV/AIDS Awareness Day #SHAAD
In 2022, nearly half of new HIV diagnoses were in the South. SHAAD raises awareness of the HIV crisis in the region and marks an opportunity to advocate for resources to address it.
In 2022, nearly half of new HIV diagnoses were in the South. SHAAD raises awareness of the HIV crisis in the region and marks an opportunity to advocate for resources to address it.
National Faith HIV/AIDS Awareness Day
National Faith HIV/AIDS Awareness Day #NFHAAD HIV affects people of all faiths across the United States. The goal of NFHAAD, which is observed on the last Sunday in August, is to bring together Muslims, Christians, Jews, Buddhists, Hindus and members of other religions to raise awareness and fight the virus.
#NFHAAD HIV affects people of all faiths across the United States. The goal of NFHAAD, which is observed on the last Sunday in August, is to bring together Muslims, Christians, Jews, Buddhists, Hindus and members of other religions to raise awareness and fight the virus.
SEPTEMBER
National African Immigrants and Refugee HIV/AIDS and Hepatitis Awareness Day #NAIRHHADay
National African Immigrants and Refugee HIV/AIDS and Hepatitis Awareness Day #NAIRHHADay
This awareness day draws national and local attention to the HIV and viral hepatitis needs of African immigrants living in the United States through awareness, education and resources. The goal is to address some of the unique issues that African immigrants face.
This awareness day draws national and local attention to the HIV and viral hepatitis needs of African immigrants living in the United States through awareness, education and resources. The goal is to address some of the unique issues that African immigrants face.
9 18 15
National HIV/AIDS and Aging Awareness Day #HIVandAging
National HIV/AIDS and Aging Awareness Day #HIVandAging
According to the CDC, more than 50% of people living with HIV in the United States are ages 50 and older. This awareness day promotes education around HIV and encourages HIV testing for all older adults.
According to the CDC, more than 50% of people living with HIV in the United States are ages 50 and older. This awareness day promotes education around HIV and encourages HIV testing for all older adults.
OCTOBER
OCTOBER
National Latinx AIDS Awareness Day #NLAAD
National Latinx AIDS Awareness Day
#NLAAD
According to the CDC, Latinos accounted for 33% of new HIV infections in 2022. NLAAD’s objective is to unite and mobilize the community to promote HIV testing and education.
According to the CDC, Latinos accounted for 33% of new HIV infections in 2022. NLAAD’s objective is to unite and mobilize the community to promote HIV testing and education.
27
National Gay Men’s HIV/AIDS Awareness Day #NGMHAAD
National Gay Men’s HIV/AIDS Awareness Day #NGMHAAD
According to the CDC, gay and bisexual men accounted for 71% of new HIV infections in the United States in 2022. NGMHAAD is a time to promote HIV testing and raise awareness about HIV prevention and treatment and the unique needs of gay and bi men.
According to the CDC, gay and bisexual men accounted for 71% of new HIV infections in the United States in 2022. NGMHAAD is a time to promote HIV testing and raise awareness about HIV prevention and treatment and the unique needs of gay and bi men.
DECEMBER
1
World AIDS Day #WorldAIDSDay
World AIDS Day #WorldAIDSDay
Nearly 40 million people across the globe were living with HIV in 2023, according to UNAIDS. On this awareness day, the world comes together to show solidarity in the fight against HIV, express support for those living with the virus and remember those lost to the epidemic.
Nearly 40 million people across the globe were living with HIV in 2023, according to UNAIDS. On this awareness day, the world comes together to show solidarity in the fight against HIV, express support for those living with the virus and remember those lost to the epidemic.