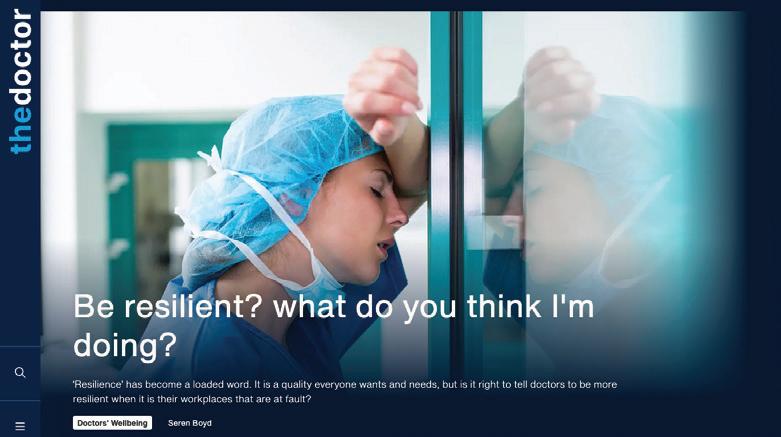
Huge demands on primary care, yet GPs can’t find work
‘Duty-bound’ GP climate campaigner gets suspended
Resident doctors
The new name for juniors
In this issue
3
At a glance
Goodbye juniors, hello resident doctors
4-7
Right to care
Overcoming barriers to registering refugees and asylum seekers
8-11
‘Ridiculous situation’
Locum GPs can’t find work despite intense demands on primary care
12-13
‘Duty-bound’ to act
Doctor has licence to practise suspended after climate-change activism
14-17
Taking a stand
A GP paid a heavy price for taking on bullies at work
18-19
Life in colour
How art therapy can help patients overcome trauma
20-21
‘An NHS on its knees’
Interview with NHS
Confederation chair Lord Victor Adebowale
22
BMA wins legal challenge
Disabled doctor backed in challenging RCGP policy on exam attempts
23 Your BMA
How the BMA reaches decisions on key issues
Welcome
Phil Banfield, BMA council chair
As The Doctor went to press, the BMA resident doctors (formerly junior doctors) committee was receiving the results of the pay ballot from our members in England. They have worked tirelessly to campaign for better pay for doctors during a period of unprecedented industrial action. Whatever the outcome of the vote, this is not the end of our fight but marks a significant step toward full pay restoration. We have begun our climb and set up base camp on our mountain; in stages, it is onwards and upwards from here.
In this edition of The Doctor we find out the effects being a whistle-blower can have on a doctor – with Scottish GP and BMA Scotland chair Iain Kennedy explaining the trauma he went through and the ‘shame’ and ‘embarrassment’ he felt being ‘terrified’ of one particular member of NHS leadership in his area. It is an issue close to my heart and one of the priorities of the remainder of my time in post is to ensure whistle-blowers have better and earlier support from the BMA as well as working towards a patient-safety focused no-blame culture in workplaces and addressing bias and discrimination across the health service.
Elsewhere in the magazine, we investigate access to primary care for asylum seekers, speaking to humanitarian charity Doctors of the World, doctors who advocate for better care for asylum seekers, and a patient, Cat, who came to London for sanctuary from violence in her country but found herself facing repeated demands for documentation and proof of address, even when her child was ill and needed a doctor. The BMA website has a toolkit explaining refugee and asylum-seeker entitlement to NHS care. As one GP said: ‘It’s only by identifying and understanding the most vulnerable in a community that we’re able to advocate for them effectively.’
We assess the ‘ridiculous situation’ of GP practices being unable to hire doctors, despite a BMA survey revealing 84 per cent of locum GPs are struggling to find work, and report on a fitness-to-practise process suspending a doctor who blocked traffic on the M25 as part of environmental action – finding her actions amounted to misconduct. We also feature an interview with NHS Confederation chair Lord Victor Adebowale and hear about the effect art therapy can have on patients and staff. It is critical for the NHS we stop the exodus of doctors, and looking after health and well-being would seem a nobrainer. But until pay and deteriorating conditions are addressed, discontent will remain bubbling just under the surface.
AT A GLANCE
The name they deserve
Sometimes it is the smallest of changes which can make the biggest difference.
After many years of discourse and deliberation, the popularly demanded and democratically endorsed call to dispense with the term ‘junior doctor’ has, at last, been realised.
As of 18 September, this misleading and in many ways demeaning term has offi cially been replaced with ‘resident doctor’, a title which will now be used by the BMA in all its communications, and which the association will be encouraging the health service and public to adopt.
The cynical or casual observer might dismiss the decision to revise a long-standing title applied to tens of thousands of hard-working and highly skilled doctors, perhaps invoking a Shakespearean perspective of ‘what’s in a name?’
This attitude, however, ignores the strong conviction held by those doctors who, in recent years, put themselves in harm’s way to save lives during a pandemic and who have fought tirelessly for fairness and restoration of pay and respectful working conditions.
A 2022 investigation and report produced by consultant orthopaedic surgeon Scarlett McNally found more than three-quarters of the doctors she surveyed considered the term ‘junior’ as inappropriate, with around half feeling similarly about the title of ‘trainee’.
A NEW CHAPTER
We’ve launched the first dedicated website for our content, at thedoctor.bma.org.uk . We are encouraging members to opt out of receiving the printed magazine by logging into the BMA website and adjusting your preferences. At the end of this year, for cost and environmental reasons, The Doctor will be fully digital, and the print edition will no longer be sent.
This groundswell in disaffection led to a motion at the BMA’s 2023 annual representative meeting, in which members overwhelmingly backed a call to adopt the name of resident doctor, formally.
On that day, Sai Ram Pillarisetti, who delivered the case for renaming, emphasised the thoughts and feelings of thousands of doctors throughout the UK when he explained there was nothing junior about the responsibilities placed on doctors like him.
‘Every day these so-called junior doctors act as the fi rst point of contact for sick and unwell patients on the ward,’ he told the conference.
‘They’re in theatre operating on your loved ones, and they’re leading teams across various specialties in our health service.’
Going forward, the resident doctor title will apply to all medical professionals from foundation year 1 onwards through to achieving the certifi cate of completion of training, with the historic renaming just part of wider change.
By Tim Tonkin
– Results of the vote by resident doctors in England on the pay offer from the Government were expected as The Doctor went to press. Leaders of the BMA resident doctors committee were due to discuss the results and next steps. For the latest information and updates, see the BMA website.
RIGHT TO CARE
Refugees and asylum seekers are often wrongly turned away from primary care because they lack proof of ID and address. Seren Boyd reports on a scheme which makes it easier for them to register
Cat waited for as long as she could. She had not slept, worried her feverish baby might die in the night.
The receptionist at the local GP surgery was adamant, though, despite her pleas: they couldn’t register her or her eight-month-old daughter without proof of ID or address. No, she couldn’t see a doctor. Cat left in tears.
They had not needed a doctor before, not even after armed men attacked their village back home, forcing them to flee the country and seek sanctuary in London.
‘I was seeing people dying to my front, to my left,’ recalls Cat. More than a decade on, the memories are still suffocating. ‘I ran but kept falling: I don’t know how I managed to keep hold of my daughter. I still haven’t heard from my sister.’
Cat used to pray she and
‘If people are refused access to healthcare once, they often don’t try again’
her daughter wouldn’t get sick while their asylum claim in the UK was being processed: she didn’t want to ask for help, for fear of being sent back.
When her baby did fall ill, and she was refused GP registration, she turned to the church who had supported her. Her minister wrote to the surgery, confirming Cat’s asylum status and her temporary address: for a long time, she relied on different friends for accommodation.
The GP who eventually saw the child apologised for the wait.
Later, when Cat moved area and had to register with a different GP, she was asked again for proof of ID and proof of address.
Cat delayed seeking a GP appointment for herself for much longer. By then, her blood pressure was sky-high.
‘The doctor’s mouth was open. “Madam, where have you
been? Why haven’t you been to the doctor?” If my daughter didn’t fall sick, I wouldn’t have gone. Maybe I would have been dead by now.’
She has been in the UK for years now but has yet to be granted indefinite leave to remain. Cat is not her real name.
Proof of address
NHS England guidance is clear that immigration status has no bearing on a patient’s entitlement to register with a GP surgery and access primary care services without charge. It explicitly states that lack of proof of identity and address are not ‘reasonable grounds’ for refusing to register a patient.
Yet, many surgeries in England still refuse registration and make proof of address and ID a prerequisite for sign-up, according to humanitarian charity DOTW (Doctors of the World).
The Bureau of Investigative Journalism found 62 per cent of GP surgeries they surveyed in 2021 in 10 locations across the UK would not register a patient without proof of address, proof of ID or legal immigration status.
Part of the problem may be confusion on reception desks with NHS guidance and differences in policy between primary and secondary care. In England, patients who are not classified as ‘ordinarily resident’ may be charged for secondary care services, unless they are refugees or asylum seekers with an active application or appeal (or if other exemptions apply). Entitlement differs in other parts of the UK too (see BMA website, details on page 7).
LANGFORD: Encourages practices in her borough to sign up to the Safe Surgeries initiative
DOTW insists there are many other barriers which undermine people’s ability and confidence to access healthcare they have a right to, and not all of them are obvious.
‘Many living in the UK fall through the cracks of our NHS systems’
This summer’s antiimmigration riots – purloining the previous Government’s ‘Stop the boats’ slogan – have reinforced many people’s fear and sense of insecurity, says Marina Davidson, DOTW primary care lead.
‘If people are refused access to healthcare once, they often don’t try again, or they’re too afraid to try at all,’ she says. ‘Either way, it has a profound effect on their mental health and they may end up with serious health issues or in A&E, all of which could have been prevented.
‘Many living in the UK fall through the cracks of our NHS systems, struggle with their health alone, and do not show up in public health and service data.’
Newham in East London is one of the UK’s most diverse and deprived boroughs, with
a high population turnover. It’s still waiting for its Olympic legacy, despite hosting London 2012.
The borough has been home to several asylumseeker hotels since COVID and has a great deal of dispersal accommodation.
Last month, Newham Council said spending on temporary accommodation for homeless households was pushing it towards the brink of bankruptcy.
Lucy Langford is a local GP and, in her capacity as health equity fellow for the Newham Training Hub, has encouraged all 46 general practices in the borough to join the Safe Surgeries initiative run by DOTW, which the BMA also endorses.
This means practices not only comply with NHS policy on patient registration but also commit to proactively dismantling barriers that prevent access. To this end, Safe Surgeries provides training for practice teams, a toolkit of resources – from at-a-glance guidance for
DOCTORS OF THE WORLD
reception staff to patientfacing information in different languages – and a readymade community of inclusion champions.
In Newham, fruitful partnerships with public health, DOTW and the voluntary sector, consolidated during the pandemic, are helping primary care teams identify and reach out to those as yet unregistered with a GP.
Dr Langford is passionate about this work and insists that GP surgeries have no excuse for not registering local people, including vulnerable migrants. But she understands why some may baulk.
Some asylum seekers and refugees often have complex needs, she says: they may need double appointments, interpreters and specialist services for trauma, unmonitored conditions or interrupted care. The housing crisis in Newham is also taking a particular toll on health and GPs’ workload. Dr Langford’s training did not prepare her for this work.
‘We tried having one of my
WELCOME: One practice that has become a Safe Surgery
clinics just to see new hotel residents but we could have filled it 10 times over and it was very challenging,’ she says.
‘We might be emailing housing, the Home Office or trying to chase up outpatient stuff – and often being ignored. The resources for GP teams and our patients just aren’t there.’
‘The resources for GP teams and our patients just aren’t there’
Dr Langford feels intensely the pressure of trying to contain patients’ care within the primary setting, to protect them from bills they cannot afford. Debts to the NHS in secondary care are reported to the Home Office and can affect immigration applications, something DOTW is still campaigning against. Yet, sometimes patients’ clinical needs are such that Dr Langford has no option but to refer.
‘Someone with a complex condition which hasn’t been monitored for several years, I’d normally refer to the specialty team, but then they might get charged. These are the patients I go to bed
thinking about.’
While her practice received some LES (local enhanced service) funding for registering patients from asylum seeker hotels, it wasn’t enough to cover thorough initial health checks and screening, Dr Langford says. Thankfully, North-East London ICB (integrated care board) is now introducing an outreach service to provide these checks.
‘Most GPs want to help disadvantaged patients like these but the current funding equation and support available for primary care just aren’t enough,’ she says.
Spreading the word
Recently, DOTW passed a significant milestone, registering its 2,000th Safe Surgery in England.
The heat map of sign-ups shows high concentrations in London, Manchester, Birmingham and West Yorkshire, areas where it has worked with champions such as Dr Langford.
For example, West
Yorkshire ICB has been promoting Safe Surgeries to general practice for some time now and this year it is asking all GP surgeries in Leeds to sign up as part of its ‘Resilient practice’ scheme.
The scheme is part of the ICB’s local investment: practices receive funding as an incentive and the ICB provides follow-up support.
Yet, Safe Surgeries’ 2,000 sign-ups represent only about a third of general practices in England. Marina feels it should not fall to a charity such as DOTW to ensure surgeries are complying with NHS England guidance – just as health professionals should not be made to feel responsible for charging for care or information-sharing.
The new ‘Register with a GP surgery’ online service being rolled out by NHS Digital –taking patient registration online and clarifying who can register – may help break down barriers, although it won’t help the many with limited internet access or IT literacy.
Something as simple as a poster in reception, a clear statement on the website, telling people in different languages ‘Don’t have documents? Don’t worry…’ can make a sizeable difference, says Marina.
‘Registering them with a GP is part of welcoming people, connecting them to the system and community. It’s a very basic thing with a huge impact.’
Summer riots
The background hum of anti-migrant narratives has been unsettling for many. But it has made others even
CONSULTING: A Doctors of the World clinic in east London
‘If we don’t have proper, inclusive registration, we can’t know what people’s needs are’
more determined to stand up for health inclusion. Marina has had emails from primary care staff saying the riots this summer have spurred them on to register as Safe Surgeries and ‘take a stand’ against intolerance.
Laura Dinsley, manager of primary care integration for Leeds, West Yorkshire ICB, feels the same: ‘We felt this was important given Leeds’ population and with the recent issues we’ve seen up and down the country, including in Leeds, we feel even more so now that it’s so important not to have barriers to healthcare.’
Cat now works alongside DOTW as an advocate for her community. ‘Before, when I couldn’t register, I felt like I wasn’t recognised
as a human being,’ she says. ‘Now, the doctor I’ve been seeing speaks to me calmly, doesn’t rush me. He takes my health seriously, just like everyone’s should be.’
Despite all the pressures, Dr Langford is still committed to promoting inclusive patient registration. It’s the only way of identifying and understanding the needs of the most vulnerable in a community – and being able to advocate for them effectively, she says.
‘If we don’t have proper, inclusive registration, we can’t know what people’s needs are. How do we hear their voices? If everyone was registered, the insights we would get, the political power, would be huge.’
For more information on refugees’ and asylum seekers’ entitlement to NHS care, visit: bma.org.uk/refugeesNHScare
To learn more about Safe Surgeries, visit: www.doctorsoftheworld.org.uk/safesurgeries
Jobless GPs –just when they’re needed most
General practice is under intense pressure and yet many locum GPs are unable to find enough work. They tell Ben Ireland that the funding crisis and perverse incentives to hire anyone but GPs must be urgently resolved
In GP-land, there is something of an absurd paradox taking place.
On the one hand, patients complain about a lack of access to family doctors. At the same time, there is an army of GPs desperate for work, but practices are unable to hire them.
This ‘ridiculous situation’, as BMA GPs committee chair Katie Bramall-Stainer describes it, comes from practices – already starved of cash after huge real-terms cuts to their funding – being incentivised to hire anyone for their multidisciplinary teams except for GPs.
The knock-on effect? A staggering 84 per cent of locum GPs, according to a recent BMA survey, are struggling to find enough suitable work. Locums are now working an average of three sessions a week, down from 5.8 in 2022, a
difference of a full additional day a week per person.
Some 91 per cent of respondents said availability of locum GP roles had decreased and 84 per cent said suitability had reduced where jobs were available, and 83 per cent of those who can find work did not feel they had enough time in sessions to provide patients with safe and thorough care. Nearly a third (31 per cent) reported having to work beyond their agreed session contracts to meet these standards.
The Royal College of GPs conducted a similar survey in June, which provided similar findings. Of its respondents, 61 per cent who had looked for an NHS GP role in the past year found it ‘difficult’ to find an appropriate vacancy, rising to 72 per cent among GPs in training.
NHS Digital data shows a drop in the number of
‘The number has reduced, and the competition has increased’
locum GPs employed across England. In July, 1,498 ad-hoc locums (those employed for short periods in a practice, perhaps a single session) were employed, down by 400 in a month and down 43 per cent (from 2,624) since July 2023. However, the number employed in July 2024 is likely to rise due to a reporting lag.
The number of regular locums is also slightly down, by 2.1 per cent. Meanwhile, there has been an 18 per cent rise in the number of physician associates in the year to July 2024, to 819.
West Midlands locum GP Aaliya Goyal told The Doctor how the number of sessions offered – via purpose-built apps, WhatsApp groups and direct contacts with practices – have dried up, from a combination of fewer sessions offered and more doctors competing for them.
Dr Goyal explains how, on
GOYAL: Scarce job offers are pounced upon immediately
one leading app, it is typical for as many as 25 locum GPs to register interest in a single session when it used to be more like one or two – and how job offers on WhatsApp are ‘pounced’ upon almost immediately.
‘The number has reduced, and the competition has increased,’ she says. ‘You have to be glued to your phone 24/7 [to secure a session] because there will always be someone who will reply within minutes.’
This competition-based GP market has resulted in lower rates of pay for locums, who have additional outgoings compared with salaried GPs such as indemnity costs and their own study leave. This has resulted in a significant loss of earnings amid a cost-of-living crisis.
‘You hear stories of doctors becoming Uber drivers to make up the difference,’ says Dr Goyal. ‘If it wasn’t for my specialist interest in occupational health, I would have really struggled. That has kept me afloat. Lots of GPs with specialist interests are in the same position.’
Dr Goyal resigned from a salaried role because the employing practice would not accommodate her request for a reduction in hours based on her personal circumstances. Other GPs make the choice for reasons such as combating burnout, health issues, caring responsibilities and seeking work/life flexibility.
Dr Goyal accepts that locum GPs should expect that a level of ‘entrepreneurship’ is required, and that by their nature as expert generalists GPs typically ‘thrive in chaos’ but says the current landscape has created a
BRAMALLSTAINER: A ‘ridiculous situation’
fastest-fingers-first mentality.
‘You hear stories of doctors becoming Uber drivers to make up the difference’
The situation, as it stands, has led many doctors to seek alternate work, with the risk that once they leave the profession they may not return. Some 33 per cent of survey respondents told the BMA they had already made definite plans to change career paths, with 31 per cent of those saying the lack of suitable shifts was forcing them to leave the NHS entirely.
The result? The number of GPs per patient continues to be stretched. NHS data released in August shows a record average of 10,113 registered patients per practice. Each full-time equivalent GP is now responsible for an average of 2,293 patients, an increase of 355 patients per GP, or 18 per cent, since 2015.
Dr Goyal notes how GPs who struggle to obtain locum sessions, and as a result don’t complete enough sessions a year, could lose their place on the national performers list, which is required to work as a GP.
‘I’ve had conversations with GP trainers who have put their heart and soul into training doctors to become GPs but see them leaving once qualified because
there isn’t enough work,’ she adds. ‘Locum GPs are an undervalued and underutilised section of the workforce who have been neglected. If this continues, more and more will start drifting away.’
Dr Goyal has considered returning to a salaried role, for extra job security, but says the opportunities available come with too great a supervision responsibility – with some practices asking salaried GPs to supervise multiple members of the team such as GP registrars, nurses and ‘additional’ roles such as physician associates.
‘That is a level of risk I’m not prepared to take,’ she says. ‘Even if it’s the right setting, the right number of sessions and the right pay. I don’t feel comfortable taking responsibility for the interpretation of patient presentations by multiple members of the team in the same session time even if others may be happy to.’
One of the reasons given for the crunch in locum roles, in England, is ARRS (additional roles reimbursement scheme). Introduced in 2019, ARRS allows PCNs (primary care networks) to claim reimbursement for the salaries (and some
costs) of 17 roles within the multidisciplinary team.
Life or death
Clare Bannon, a GP partner and the BMA’s GPs committee England lead for clinical and interface policy, says the ring-fencing of those funds has essentially ‘blocked us from employing GPs’.
Dr Bannon explains that, as expert generalists, GPs are able to differentiate between routine conditions and serious illnesses where non-GPs are not. So, reducing access to GPs is ‘potentially a matter of life and death’.
Royal College of GPs chair Professor Kamila Hawthorne agrees. She says: ‘Schemes like this are now proving counterproductive and leaving GPs without jobs and, in some cases forcing them to leave the profession altogether or look for opportunities overseas.
‘Members of the wider practice team are valuable and can help to expand the services available to patients, but they aren’t substitutes for the key specialist skills and expertise GPs provide and they can’t be used to plug gaps in the GP workforce.’
The new Labour Government sought to relieve
STEGGLES: GPs are becoming locums almost by default
RATWATTE: Long-term solution needed for general practice
this pressure by ‘removing red tape’ and allowing newly qualified GPs to be hired through ARRS money by the end of this year. Health secretary Wes Streeting said this would mean 1,000 more GPs could be recruited.
for patients and better job satisfaction for doctors.
‘The opportunities for GPs entering the NHS workforce are fewer and fewer’
But this does not appease either existing and experienced locum GPs seeking work, or the practices that want to hire them. Even GP registrars who are due to take advantage of the change as they qualify as GPs are not satisfied – for the good of their patients and their careers.
Because funding is allocated at PCN, not practice level, some newly qualified GPs may even be forced to move across the country at short notice, uprooting their families. And the BMA is pushing for more clarity on pay, job plans and mentoring for newly qualified GPs hired through ARRS. Many, before and since the update, are being targeted by overseas recruiters.
Malinga Ratwatte, chair of the BMA’s GP registrars committee, says: ‘Newly qualified GPs want to develop long-term relationships with their patients in order to provide continuity of care, leading to better outcomes
‘Newly qualified GPs need to be part of a practice team to get the mentorship needed for fully independent practice. While this [amendment to the scheme] will alleviate short-term unemployment concerns, we still need a long-term solution for general practice.’
That long-term solution, he suggests, should be to provide adequate funding for GPs at practice level, rather than via PCNs.
It is a view endorsed by the RCGP and the BMA GPs committee for England, which is taking collective action over the ‘underfunded and overstretched GMS contract’. The BMA calculates that core funding to the GP contract in England (general medical services) has fallen by £659m (or 6.6 per cent) in real terms since 2018/19. An 11 per cent uplift in funding would be required to restore funding to 2018/19 levels.
Financial restraints
Mark Steggles, chair of the BMA’s sessional GPs committee, says: ‘Practices’ costs are going up, and funding isn’t keeping up. So, they’re
having to look at how they can make savings to keep their doors open, making really tough financial decisions. Some would love to have more locums on board, but that’s becoming less possible.’
He says the disincentives to employ GPs, combined with the erosion of funding, has led to a decrease in the number of GP partnership opportunities and salaried roles – which means those who do end up with jobs face an even higher risk of burnout.
Dr Steggles became a locum GP after four and a half years in a salaried role owing to ‘escalating workloads’, and ‘so I could continue to do what I did, rather than leave [the profession] altogether’.
He says: ‘The opportunities for GPs entering the NHS workforce are fewer and fewer. GPs can’t find salaried roles, the ones that exist are less manageable and there’s a real lack of funding to employ locum GPs.’
With some 58,000 doctors on the GMC’s GPs register in England, and about 38,500 GPs working for the NHS in England, Dr Steggles points out that about a third are not working.
He said that while the new Government has made some ‘encouraging’ noises around its promise to ‘bring back the family doctor’, which offer ‘hope’, he stresses: ‘We need to see actions’.
‘Patients want to be seeing GPs, and the GPs who are working are overwhelmed, having to supervise more staff as well as doing their own regular clinics. We need to take the pressure off GPs who are in practices already, and make sure the fully qualified
Plummeting job opportunities
In July, 1,498 ad hoc locums were employed, down by 400 in a month and down 43 per cent (from 2,624) since July 2023
Source: NHS Digital, figures
refer to England
‘There are talented GPs ready and able to work but practices can’t afford to hire them’
The number of regular locums is also slightly down, by 2.1 per cent
GPs looking for work in the NHS have opportunities.
‘In the current situation, many GPs don’t have much choice [than to become a locum]. You’re almost becoming a locum by default. All GPs are working beyond what is safe, and with increased competition, locums are having to compromise on safe working to get the roles.
‘The situation is desperate for all GPs, but when you’re faced with unemployment and you have mortgages, bills and families to support, you make decisions based on that. People can see this is not sustainable, so many are choosing to leave.’
Diverting the £1.4bn ARRS funding to practices and opening it up to spending on experienced locums as well would be a welcome step, says Dr Steggles. But he would prefer to see practices’ core funding increased overall so they can make their own choices based on which roles they feel are required for their patients rather than being led by incentives.
Meanwhile, there has been an 18 per cent rise in the number of physician associates in the year to July 2024, to 819
His assessment: ‘General practice is on its knees and needs more investment.’
The BMA GPs committee for England has begun its dispute with Government, with GPs urged to ‘work-torule’ as part of collective action until an adequate contract is agreed.
All the while, practices face soaring energy costs, higher wages for other staff and are still catching up with prices following years of double-digit inflation.
Labour’s tweaks are ‘nowhere near enough to save general practice’, Dr Steggles and Dr Bramall-Stainer said after its announcement. They insist fixing the contract at its very roots by improving core funding is the only solution.
‘We need to see the core GP contract funding increased so that practices have full control over who they recruit, without the need to go via bolt-on schemes.
‘There are experienced and talented GPs, ready and able to work, but practices can’t afford to hire them.’
DUTY-BOUND TO ACT
Diana Warner, whose licence to practise was suspended following her environmental activism, told a tribunal that it was part of her vocation as a doctor. Ben Ireland reports
Adoctor who blocked traffic on the M25 as part of environmental action for Insulate Britain has been suspended for three months after a tribunal found her fitness to practise impaired.
Diana Warner, a GP since 1989, admitted sitting down on the carriageway, holding a banner and gluing herself to the road on 27 October 2021 to an MPTS (Medical Practitioners Tribunal Service) hearing – this was in breach of an injunction made by the High Court preventing such behaviour.
Dr Warner, who retired from clinical practice in 2019, admitted ‘blocking, endangering, slowing down, preventing, or obstructing the free flow of traffic on to or along or off the M25 for the purposes of protesting’ on 29 October 2021 and ‘refusing to leave the area of the M25 when asked’ by police.
Her non-violent direct action was considered by a criminal court to be deliberate and in contempt of court. She was sentenced to two months and 30 days in prison, respectively.
In May 2022, Dr Warner was sentenced to a further 12 weeks in prison after being convicted of ‘damaging furniture’ at Stratford Magistrates Court by gluing herself to it during a hearing in which she was charged with causing a public nuisance on the M25 near Heathrow
Airport on 27 September 2021. She also admitted this to the August MPTS hearing.
The hearing last month, which was triggered because GMC rules stipulate all convictions resulting in a custodial sentence are referred to a tribunal, found Dr Warner’s fitness to practise had been impaired by her criminal convictions.
The tribunal found Dr Warner’s action amounted to misconduct and chose to suspend her licence to practise for three months. The GMC submitted it was not in the public interest to strike her from the register altogether. The tribunal said a lengthier suspension would have been ‘disproportionate’.
‘Responsibility’ to act
The tribunal heard there have been no previous concerns raised about Dr Warner’s fitness to practise, and of her long-standing environmental activism – she twice stood as a Parliamentary candidate for the Green Party.
Dr Warner stated she tried to set up a dialogue with the GMC around doctors’ responsibility to safeguard the public’s health from the ‘existential threat’ of climate change and ecological emergencies in 2019. She said the GMC should do more to bring doctors and organisations together to safeguard population health.
WARNER: (Pictured second from left) outside the High Court with fellow activists in Ferbruary 2022
DENISE
In the hearing, Dr Warner said work being done to halt climate change was not enough and that this was analogous to treating a patient for just part of their illness despite the other part being potentially fatal.
She said it was ‘incumbent’ on the healthcare system and professionals to work with scientists and the Government to make sure societies keep within planetary boundaries so all key earth systems can recover.
Dr Warner told the hearing of her ‘strong conviction’ that the only way to force this agenda was through disruption.
Suffragettes and ANC.
Dr Warner told the hearing she intended to continue protesting to draw attention to the climate emergency and that she had thought ‘long and hard’ about her actions in advance.
‘Serious departure’ from guidelines
The GMC submitted that Dr Warner’s committals to prison amounted to misconduct, and that her fitness to practise is impaired ‘by reason of misconduct and conviction’.
‘Climate change is the biggest public health crisis in the UK and globally’
She argued the aims of the Insulate Britain campaign were ‘uncontroversial’ and ‘evidence-based’. She accepted the peaceful protests were unlawful in that they breached a civil injunction and caused inconvenience to road users, noting that was ‘the essence of the protest’.
Dr Warner – who self-referred to the GMC in April 2022 – argued that criminal convictions for matters of social conscience should not automatically be subject to regulatory action, ‘otherwise there would be a de facto blanket restriction on the ability of doctors to participate in acts of civil disobedience without risking their careers’.
She submitted that the nature of the protest, its relationship with the medical profession, and a doctor’s cooperation with the justice system and GMC should be taken into consideration.
Further, she argued the GMC’s Good Medical Practice guidance says ‘we don’t wish to prevent doctors from practising in line with their beliefs and values’.
Public health crisis
Dr Warner said she saw her activism as a continuation of her vocation as a doctor and it would enhance, not reduce, trust in the profession.
‘Direct
The regulator has ‘no concerns about Dr Warner’s clinical capabilities’ but argued her actions were a ‘serious departure’ from its Good Medical Practice guidelines.
Its representative argued Dr Warner’s actions had risked harm to others or damage to property and involved repeated breaches of the law.
It submitted that a finding of impairment was required to ‘promote and maintain public confidence in the medical profession’.
The tribunal panel noted Dr Warner’s conduct had not occurred in her professional life, and she had a ‘previously unblemished career’.
But it found her actions were a departure from the GMC’s guidelines and could affect public trust in the profession. The tribunal concluded that, while some members of the public would agree with Dr Warner’s decision to engage in peaceful protests, ‘a portion’ would be ‘extremely concerned by a medical practitioner deciding to put the public at risk, no matter the motivation’. The tribunal found a ‘significant risk’ of repetition as Dr Warner has not ruled out acting again.
action has been effective throughout history, from the woman’s suffrage movement to the ANC’
She told the tribunal her grandmother was killed by the Nazis in the Second World War and this meant she ‘grew up with the conviction government cannot be relied on to keep you safe’.
‘Climate change is the biggest public health crisis in the UK and globally,’ she said, comparing the lack of action with a ‘missed diagnosis’.
Dr Warner said evidence shows direct action has been effective throughout history, from the women’s suffrage movement to Nelson Mandela’s African National Congress fighting against apartheid, adding that Insulate Britain has been entirely non-violent – unlike the
Previous hearing
Dr Warner’s hearing followed the tribunal of Sarah Benn, a retired GP who had her GMC licence suspended for five months having breached a court order preventing her from protesting by an oil terminal. The BMA is supporting Dr Benn with an appeal.
The decision to suspend Dr Benn is to be reviewed, at which point she will either have her licence revoked, extended or her registration erased.
Dr Warner will not face a review. The tribunal concluded that her position, ‘that her misconduct was justified’, was ‘unlikely to change’.
Members at this year’s BMA annual representative meeting backed a motion calling for the union to advocate for protections against punitive actions for doctors participating in activism ‘lawfully’.
KENNEDY: Workplace bullying left him feeling ‘terrified’
TAKING STAND
TAKING A STAND
GP Iain Kennedy stood up to bullies at work. He was able to help other victims and eventually get the Government to take action, but only at great personal cost. Jennifer Trueland reports
Even today, Iain Kennedy sounds as though he can’t quite believe he was a whistleblower.
As a respected senior GP in Inverness, holding regional and national roles, he had nevertheless felt so bullied, so threatened, so isolated, so ill – and so worried about patient care – that he decided he had no choice but to raise concerns.
The decision took an enormous personal toll. After blowing the whistle about a bullying culture in his local health board, NHS Highland, he was personally and professionally vilified –and left with complex PTSD (post-traumatic stress disorder).
Now, however, he can look back relatively calmly on the situation, which came to a head in 2018, although it had been brewing for a number of years before that. Speaking to The Doctor as he published his own research into whistle-blowing, he reflects on the experience –and calls for action to ensure others do not face similar trauma.
‘There was an overt culture of bullying in NHS Highland and it was coming from the very top of the organisation,’ says Dr Kennedy, now chair of BMA Scotland. ‘There was a lot of talk about person-centred care, quality, and compassionate leadership, but what we were witnessing didn’t fit with that. We were seeing and working in a very toxic culture. There was lots of fear, there were subliminal threats of job loss or disinvestment in your department or medical practice – and when healthcare workers are working in a toxic environment, that ultimately affects patient care.’
NHS Highland is one of 14 geographical or territorial health boards in Scotland. It covers a huge swath of northern Scotland in terms of
square miles, but a relatively small population of around 320,000 people, many in some of the most remote areas of the UK. Employing more than 10,000 people, it is a major economic force in the region, and essentially is the purchaser and provider of most health services, answerable to the Scottish Government. Like all health bodies, it has faced years of financial pressure, as well as increased demand and – even pre-COVID – lengthy waiting lists.
Undermined
‘There was an overt culture of bullying in NHS Highland and it was coming from the very top of the organisation’
things I wasn’t responsible for, and making it clear that the improvements could easily be undermined by withdrawal of funding and support. It was a lot of subtle behaviours, and there was a strong sense if you didn’t appease one particular person at the top of the organisation, that you’d be criticised and marginalised.’
At the time he was bewildered – and tired. Working full time as a GP and taking on additional roles, he didn’t understand what was going on. Hindsight has brought some clarity, laced with additional confusion.
As GP clinical lead in Inverness around 2009, Dr Kennedy was keen to get involved in tackling these pressures and improving services for patients. But the more successful his efforts, the more he began to feel undermined by senior management of the health board.
‘Like
‘I set up a federation of GP practices and basically worked very hard to deliver what the health board was wanting, but the harder we worked, the more success we achieved –and we did deliver on some significant areas, including anticipatory care planning and reducing polypharmacy – it seemed the health board felt threatened by our success and I would just hear negative comments about GPs in general and about my own motives. I had various one-to-one conversations where I was spoken to in a very sinister way – the person speaking to me would change the tone of their voice, speak very slowly, trying to hold me accountable for
many victims of bullying, I was in a state of confusion’
‘Looking back, I was terrified of one individual; there’s no doubt I was terrified,’ he says. ‘When I say that, that makes me feel embarrassed, shameful, because people would regard me as quite a confident, experienced individual, and the thought that I’d be terrified of somebody – and terrified of a female – was quite difficult, and I was probably personally suppressing that fear. Like many victims of bullying, I was in a state of confusion.’
Front-page news
Fast forward to 2018 and the situation had become untenable – and its effect on Dr Kennedy was strong. But then he realised he wasn’t alone. ‘I was personally being bullied by the senior leadership [of the health board]. I was being undermined, marginalised within my peer group, and like all victims of bullying, I was very isolated –I thought it was only me.’
IMPACT: Dr Kennedy experienced complex PTSD
Eventually he was handed a dossier of five very senior employees within NHS Highland who had been severely bullied by the same people and suffered serious ill health and job loss. ‘It was at that point that I realised there were potentially many others experiencing what I was experiencing, and I felt we should be raising concerns,’ he says.
Having exhausted formal avenues to do this, he and three colleagues wrote a letter to The Herald newspaper complaining of the bullying and toxic culture – and NHS Highland became front-page news.
‘Whistle-blowing
All four suffered insomnia and psychological reactions after blowing the whistle, says Dr Kennedy, including flashbacks, intrusive thoughts and hypervigilance.
most victims of bullying get, and it was quite severe. But I went through treatment and I’ve managed to process a lot of the suppressed trauma that I had, and I actually struggle to recall some of the events, and I know others have had the same benefit and that’s been good.’
is not without risk. But it’s also extremely rewarding when you take the right ethical decision’
‘I had a lot of people contacting me, sharing their experiences, and I was a lot more emotional listening to their stories than I would normally have been –these were often mutually tearful conversations… I was taking on a lot of people’s trauma, and in some ways that was important in itself, because it affirmed what we had assessed was true and confirmed that there were potentially hundreds of victims.’
The whistle-blowers also had support from other doctors from across the country, and from the BMA, but not everyone backed them. He was also ‘ostracised’ in public by some colleagues who would be supportive in private, but would avoid being seen with him to avoid being tainted by association. ‘That ostracism was particularly difficult to cope with.’
The whistle-blowers managed to keep the story in the media – losing some of their protections under the Public Interest Disclosure Act as a result – and faced a backlash from NHS Highland, who tried to shut the issue down, in part by turning other doctors against them.
But the Scottish Government commissioned a review which essentially backed what the whistle-blowers had said. Key individuals left the organisation and a ‘healing process’ was inaugurated to try to right the wrongs.
‘Almost 200 victims of bullying engaged with that healing process and had the opportunity to tell their stories to a panel. Many of them received written apologies from the subsequent chief executives of NHS Highland, some were redeployed, many received psychological therapy and also financial settlements approaching £3m.’
PTSD
As for Dr Kennedy, some six years on, he would say he is ‘95 per cent cured’ of the trauma he suffered. ‘I’m honest enough to say that I did have complex PTSD, as
He used the money he received as a financial settlement to do an MBA, and his thesis focused on whistle-blowing in Scotland. A survey of BMA Scotland members painted a picture of a medical workforce still afraid to blow the whistle, and where those who had raised concerns experienced being marginalised, blacklisted, bullied, and reported to the GMC. He hopes the findings will help prompt greater awareness and culture change across the NHS.
Despite everything, he doesn’t regret his actions. ‘Whistle-blowing is not without risk. But it’s also extremely rewarding when you take the right ethical decision – and actually follow the duties of a doctor in Good Medical Practice [GMC] to speak up.
‘As well as being rewarding, it can also remove the burden of holding on to knowledge that you know, if it was revealed, could prevent ongoing harm or new harm being caused to others.’
Advice for potential whistle-blowers from Iain Kennedy
– Don’t go it alone – do it as a group if at all possible
– Follow whistle-blowing procedures to the letter, or risk losing the protections given under whistle-blowing legislation
– Involve politicians to get support
– If necessary, make judicious and skilled use of the media – we had support from a former NHS communications expert
– Prepare to get ill: you will suffer psychological sequelae; you’re likely to have some form of adjustment reaction, possibly elements of post-traumatic stress disorder, so make sure you have support around you in the workplace and the home
– Involve your family and let them know the likely impacts so that they can support you and you get the love and care you need, and to make sure you are able to continue to provide that love and care to your family.
The use of art therapy to aid recovery or treat trauma has helped patients and doctors alike to the extent that many professionals now advocate offering it more widely on the NHS. Tim Tonkin reports
Life in colour
Art therapy can sometimes be described in loose and ill-defined terms; it means more than just the notion that art can be therapeutic.
While engaging in creative activities, such as joining an art class or choir, can form part of social prescribing, art therapy uses creation as a form of treatment in its own right or in addition to other elements, such as CBT and talking therapies.
The British Association of Art Therapists describes art therapy as ‘a form of psychotherapy that uses visual and tactile media as a means of self-expression and communication’.
Delivered by accredited art psychotherapists, art therapy has been used in conjunction with a wide range of illnesses and medical conditions and can centre around a variety of media from visual art to dance, drama and music.
As a form of treatment, however, art therapy is not without its detractors, with some criticising the historic lack of an evidence base as to the efficacy of using art therapeutically when compared with more traditional forms of treatment.
Consultant child and adolescent psychiatrist Sabina Dosani has a professional and personal appreciation of
the benefits art therapy can yield.
As a medical student, Dr Dosani was for a time hospitalised with depression at Guy’s Hospital in London. During her stay she received group-based art therapy alongside talking therapies as part of her treatment.
‘I just thought that was a normal part of treatment, I didn’t realise how unusual that was,’ she explains.
‘It really helped me put certain things into a form of communication that I hadn’t been able to articulate, and it helped me to form a sense of identity.
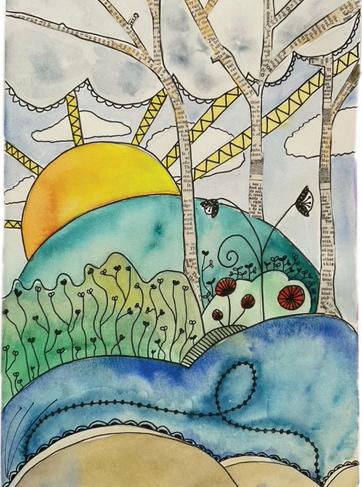
‘When I looked at the paintings, when I was discharged, I realised how my life had increasingly become more colourful, and I really attribute a lot of my recovery to the creative therapies that I had access to.’
Engagement tool
After gaining her medical qualification, Dr Dosani again found herself finding success with art therapy after being diagnosed with postnatal depression.
Dr Dosani’s experiences led her to undertake a master’s degree in medical humanities and to begin considering what role arts-based interventions could play with some of her own patients.
ART WORK: Pictures of houses and sunrise by Sabina Dosani, the doctor and patient by Gehan Soosaipillai, and, top right, a collaborative work by healthcare staff in a project organsed by Megan Tjasink
A consultant child and adolescent psychiatrist, Dr Dosani is also involved in medico-legal work and serves as an expert witness to the family courts and to asylum cases involving children and young people.
‘When I’m assessing children, I don’t think of that as art therapy, but as using arts basically as tools to help with engaging with assessment,’ she says.
‘I see a lot of young people who’ve crossed in small boats or had trauma from coming from conflict. We often don’t have language in common, but there’ll be an interpreter, [and I] invite them to draw whatever is in their minds.
‘They very typically will draw very detailed scenes of the kinds of difficulties and adversities they’ve experienced, they might draw pictures of abuse, graphic representations of war or pictures of the camps that they’ve been in.
Dr Tjasink, who aims to publish the fi ndings of her research later this year, says she hopes art therapy can become an established and more accessible form of treatment within the health service.
She says: ‘I wanted to create an intervention [for healthcare professionals] that fi t around their work schedule and so developed a six-session art therapy intervention based on themes pertinent to burnout and using the Maslach Burnout Inventory.
‘I attribute a lot of my recovery to the creative therapies that I had access to’
‘That feels like a much richer description than asking open-ended questions as a stranger through an interpreter,’ explains Dr Dosani.
‘It breaks down one of the communication barriers, and those pictures do become part of your clinical record, they help to evidence things like post-traumatic stress disorder when these cases go to immigration and asylum courts.
‘It’s a really useful way of getting clinical information, but for some children those assessments are [also] therapeutic, as it’s the first time they’ve been able to put down something on paper and have an adult witness it and care.’
Wider access
Clinical research fellow Megan Tjasink is hoping her work, examining the use of art therapy as a means of addressing burnout among healthcare professionals in secondary care settings, will further bolster the case for art therapy.
‘There’s something about art making and creative expression that gets to the sort of heart of things. You’re connecting with feelings on a deeper level than you would if you were just using sort of your intellect or cognition.’
Anaesthetic registrar Denise Gomez is one of about 50 doctors who participated in Dr Tjasink’s study.
Even though she went in with an open mind, Dr Gomez says she was genuinely surprised by the effect creating art had for her and those around her and would now love to see art therapy offered more widely across the NHS.
‘I think whether we call it stress, burnout, depression, any other clinical names, I just feel like, nearly everyone in the NHS is struggling in some way or another and it’s not something that’s going to go away anytime soon,’ says Dr Gomez.
‘There’s something about art making that gets to the heart of things’
Having served as the lead art psychotherapist at Barts Health NHS Trust’s cancer and palliative psychological services departments, Dr Tjasink has been leading the CHArt group art therapy intervention as part of a randomised control study at Queen Mary University of London.
The study, which grew out of an earlier project delivering art therapy to staff in Barts’ oncology teams almost a decade ago, involved getting different healthcare professionals together, including doctors, to participate in making art and encouraging discussion.
She says participating in art therapy as part of a group felt individually liberating while also fostering a sense of solidarity with colleagues.
‘At a time when so many of us are already overwhelmed with the demands of our work, “maintaining wellbeing” and “developing resilience” often feel like initiatives that just burden us with yet more tasks or responsibilities,’ Dr Gomez says.
‘Art therapy is the reverse. It doesn’t feel top down because you’re actually being allowed to express yourself as an individual. You’re given this opportunity to create and to feel a sense of self that often gets lost in a very big institution such as the health service.
‘Staff often feel like numbers, and I think when that happens it’s easy for them to treat patients like numbers. Having that opportunity to do something truly for your own wellbeing really distinguishes art therapy from any of the other initiatives I’ve seen in hospitals.’
DOSANI: Pictures help evidence things such as posttraumatic stress disorder
‘AN NHS ON ITS KNEES’
In a health service ravaged by COVID and years of funding cuts, the NHS Confederation chair sets out his priorities.
Interview by Tim Tonkin
If a week ‘is a long time in politics’, as Harold Wilson once wryly observed, for those involved in healthcare the past few years must often feel like a lifetime.
In the almost four-and-a-half years since he was appointed chair of the NHS Confederation, Lord Victor Adebowale has seen the health service endure a period of unprecedented challenges and change.
Chief among these were the huge pressures and service demands imposed by the pandemic and the bitter disputes between doctors and other healthcare professionals and the Government over improvements to pay and working conditions.
These more recent phenomena came on top of entrenched and long-standing problems in the NHS concerning staffing shortages, year-on-year underfunding and underinvestment in infrastructure, and amid growing levels of inequality and standards of health in society.
In apparent recognition of the scale of these challenges, the new Government commissioned an independent review of NHS performance in England to be overseen by Lord Darzi. His report, published last week, concludes that the NHS is in a critical condition having been battered by a decade of austerity and the demands of the pandemic, and left ‘chronically
weakened by a lack of capital investment’ and a demoralised and exhausted workforce.
‘On its knees’
Speaking to The Doctor before publication of the review, Lord Adebowale says he and the Confed welcome it, but stresses he is under no illusions as to the scale of the challenges it is likely to identify.
‘I think the Government has inherited an NHS on its knees no question [and] we need to be honest with the public about what that means,’ he says.
‘We have had year on year of effectively flat cash, which means cuts, [and] that has affected everything and everybody. We had COVID which caused a lot of pain and anguish and moral harm.
‘We have a waiting list, which is historically large, we have staff at all levels that are stressed and overworked and we have clinicians who feel that they are at the end of their tether. All this is underlined by an increasing demand [for services], our aging population, multiple morbidities and the gap between rich and poor going in the wrong direction.’
It is perhaps no coincidence that many of the challenges facing the NHS and the health of those it serves were among Lord Adebowale’s priorities when
assuming his role as chair, notably tackling inequality in healthcare and improving access to services.
Stressing that while there is no single solution that will solve the current shortcomings, Lord Adebowale’s belief is that moving towards a preventive model of care through greater integration of services should be the ultimate goal, with government collaboration with ICSs (integrated care systems) critical to this.
To this end he says he feels there has been encouraging early signs from health secretary Wes Streeting, but that actions rather than words will ultimately be what matter. ‘We have to attack this challenge at both ends [and] see it as a system challenge within which no one solution but a series of interventions which move the NHS into a more efficient position where we are preventing the illness,’ he says. ‘To do that we need structures which enable us to understand population health, so we can commission services will move the needle away from the inverse care law and bend the demand curve. I can’t imagine there are structures that can do that better than ICSs and ICBs [integrated care boards].
Vulnerable tech
The issue of data in healthcare, particularly regarding expanding digitisation of services and patient records, and the increasing role of artificial intelligence, is something which is gaining prominence in discussions around the future delivery of care.
‘We have staff at all levels that are stressed and overworked’
While there is considerable excitement around the potential benefits of these emerging technologies, there is also concern with risks to the safety and integrity of patient data, something which was starkly illustrated earlier this year following a ransomware cyber-attack on NHS services in South London.
As the co-founder of a digital company which seeks to provide connectivity across healthcare, Lord Adebowale says ensuring digital services are prioritised to meet the needs of patients rather than companies designing them is vital. He would ultimately like to see the formation of a ‘NICE-type body’ tasked with registering and overseeing the apps and algorithms ‘used within the context of NHS applications’.
‘If you look at places like West Yorkshire, there are already green shoots there with the Prevention Agenda, which we should be watering, nurturing, fertilising and encouraging.’
Unacceptable outcomes
Inequality in health outcomes in the NHS and the role racism plays in this, is something which has been a focus for Lord Adebowale even before taking on his role as chair at the Confed.
Together with colleagues he helped establish the NHS WRES (Workforce Race Equality Standard) and the RHO (Race and Health Observatory) and was the keynote speaker at the BMA patient liaison group symposium, which this year focused on inclusivity and intersectionality in health policy.
‘How we manage digital in such a way that it is meeting our needs, as opposed to the needs of investors, I think is a really big challenge and I don’t think we’ve got there yet,’ he says.
‘We need to build the public’s trust in the use of their data and people need to see that data, their personal data, is actually benefiting them and not just being used to make some person who believes in breaking things and getting rich richer.’
‘We have had year on year of effectively flat cash, which means cuts’
The issue of money and specifically NHS capital funding, which the Confed believes needs to ultimately be increased to £14bn a year, is perhaps the biggest obstacle to the improvements those such as Lord Adebowale would wish to see realised.
Lord Adebowale says that, while he believes the WRES and RHO have and will continue to make a positive difference, he has often felt frustrated at the slow pace at which progress is being made.
‘The fact that pain medicine is likely to be administered poorly if you’re black, or the fact that, if you are a black woman, you have a greater chance of dying in childbirth, these are utterly unacceptable and yet have been accepted and been part of the norm in healthcare for many, many years,’ he says. ‘What the RHO does is hold up a mirror to the NHS and say: “Hang on a minute, you know this is happening you can’t just ignore it.”’
One change he would like to see, however, is a reversal of the narrative borne out of the many years of austerity during the Cameron Conservative Government, that a strong economy must precede a strong NHS.
‘There is no wealth without health,’ he says.
‘[As a nation] we have a significant productivity challenge caused by the fact that we’ve got people who are ill and on the waiting list and usually require someone to look after them who also can’t work.
‘For every one pound we spend on health, we get three pounds back to the economy. So, this is investment, this isn’t burning money, which is, I think, a quite erroneous notion that somehow spending on health is wasted. I consider it’s probably the best value that government, society can spend.’
BMA WINS LEGAL CHALLENGE FOR DISABLED DOCTOR
An RCGP policy affecting some disabled doctors was found to be unlawful. Ben Ireland reports
The High Court has ruled the Royal College of GPs’ refusal to grant additional exam attempts to disabled doctors was ‘irrational’ and unlawful.
The RCGP had a policy of not allowing additional attempts or resits to GP registrars who were diagnosed with disabilities after one or more unsuccessful exam attempts, without the reasonable adjustments they would have been entitled to if they had known about their disabilities before.
The BMA supported a GP candidate in bringing legal action, in this case specifically challenging the college’s policy on the AKT (applied knowledge test). The GP candidate successfully argued the college was acting unlawfully and putting disabled trainees receiving a late diagnosis at a significant disadvantage.
The court ruled ‘the college has failed entirely to provide a coherent justification for its policy’ and that the legal grounds underpinning its ruling are ‘applicable in principle to the generality of candidates for membership of the college’.
The BMA said: ‘This plainly supports the BMA’s longstanding conviction that the RCGP’s relevant policy on exam attempts was unlawful and unfair to disabled trainees.’
The policy for the AKT has been quashed as a result of the High Court judgment and must now be replaced. The court did not, however, find the policy to be discriminatory under the Equality Act 2010, which had been argued by lawyers for the BMA and the candidate.
The BMA says the judgment has ‘vindicated’ its legal challenges, which followed long-standing efforts by the association to persuade the RCGP to revise its exam attempt policies as they relate to disabled doctors who receive a late diagnosis.
Following BMA lobbying, the AoMRC (Academy of
Medical Royal Colleges) produced new guidance in 2023, which states medical royal colleges should consider granting additional attempts to candidates for whom a later diagnosis of disability was ‘likely to have affected all previous [examination] attempts’.
The BMA then urged medical royal colleges, faculties and exam bodies to implement policies which provided fair opportunities for all candidates, in line with that guidance. However, the RCGP did not change its stance.
In August last year, the college changed part of its rules on exam attempts by increasing the maximum number of attempts available to doctors entering GP training on or after 2 August 2023 from four to six on the AKT and simulated consultation assessment.
In December last year, the BMA GP registrars committee wrote an open letter to RCGP chair Kamila Hawthorne urging her to amend the college’s policies in line with the AoMRC’s recommendations.
In presenting its case to the High Court, the association’s legal team labelled the RCGP’s ‘point-blank refusal’ to cancel out previous unsuccessful exam attempts as ‘unreasonable and perverse’ and a ‘deliberate decision not to treat disabled candidates fairly’.
After the judgment, a BMA spokesperson said: ‘The BMA is delighted the court has vindicated our efforts to stand up for disabled doctors who have been treated unfairly by the RCGP.’
The spokesperson added: ‘While today’s judgment is welcome and will pave the way for disabled trainee GPs to receive much fairer treatment over examinations, it is hugely disappointing that legal action was necessary to achieve this outcome.’
A spokesperson for the Royal College of GPs said: ‘We will be considering the finer detail of today’s judgment before deciding on our course of action.’
Your BMA
How the BMA arrives at its big policy decisions
The BMA announced it would undertake an evaluation of the Cass review last month – the independent report on gender identity services for children and young people in the UK.
The review will be chaired by BMA board of science chair Professor David Strain. It includes looking at the methodology used to underpin the report’s recommendations.
Perhaps unsurprisingly, this news led to a great deal of member engagement – with some people incredibly supportive and some hugely critical of the announcement and our plans.
One thing we know, from existing policy, is that our members care about these issues and about providing high-quality healthcare to transgender patients. The BMA believes transgender and gender-diverse patients should have access to specialist healthcare. The association has argued that clinicians, patients and families should make decisions about treatment on the best available evidence, not politicians. This is a group that has poorer outcomes owing to a lack of equality of care.
In the light of these developments – and with so many members engaging with this news – I thought now would be a good time to discuss how big policy decisions are made outside of our major annual meetings and conferences, which are generally the primary way we decide on the association’s work.
For instance, between the resident doctors (formerly junior doctors) conference, which took place in May, and their meeting next year, resident doctor representatives are likely to make policy decisions
The Doctor BMA House, Tavistock Square, London, WC1H 9JP. Tel: (020) 7387 4499
Email thedoctor@bma.org.uk
@TheDrMagazine @theBMA
The Doctor is published by the British Medical Association. The views expressed in it are not necessarily those of the BMA. It is available on subscription at £170 (UK) or £235 (non-UK) a year from the subscriptions department. All rights reserved. Except as permitted under current legislation, no part of this work may be photocopied, stored in a retrieval system or transmitted in any form or by any means, electronic, mechanical or otherwise without the written permission of the editor. Printed by Warners Midlands. A copy may be obtained from the publishers on written request. The Doctor is a supplement of The BMJ. Vol: 386 issue no: 8444 ISSN 2631-6412
on behalf of resident doctors. The same applies with our biggest policy-making platform, the BMA annual representative meeting. Lots of issues arise between those set-piece events and we have to be able to react. Our primary method of doing that is through our principal executive committee, BMA council. Council is made up of democratically elected members from across the UK who represent all 199,000 of our members. Sometimes these meetings are held in closed, private, sessions for understandable reasons. But there has been a move, under the current leadership of Phil Banfield and Emma Runswick, to increase transparency of all council meetings, which has been well received.
Council meetings feature robust debate followed by a fair and free vote where everyone is able to have their say. That is the best process we have for making these decisions and while not everyone will agree with decisions – it is perhaps a strength and a weakness of having such a large membership that viewpoints are diverse – I think this is the right way to do things. If you disagree with the decisions we come to, all I can say is that there is, in my experience, a deep, unrelenting, commitment from elected representatives and staff to do the right thing by our profession, our patients and our society.
That is the case when we are commenting on public health measures such as vaccinations or vaping and it is the case here. For those who suggest we shouldn’t comment on the actions of Government or national NHS leaders, what else would you have us do? This is our everyday work. We are a trade union and a professional association and we will give our members a voice.
I would like to address everyone commenting on the decisions we have taken. To those who have considered our policies helpful and to those who have criticised constructively, thank you for engaging with us.
We are always listening. To anyone who has taken this opportunity to abuse members, elected representatives or staff – shame on you. This behaviour is unacceptable.
Your voice can still be heard even if you disagree with the decisions we make. We are always listening.
You can contact me on RBChair@bma.org.uk or @DrLatifaPatel. Dr Latifa Patel is chair of the BMA representative body
Editor: Neil Hallows (020) 7383 6321
Chief sub-editor: Chris Patterson
Senior staff writer: Peter Blackburn (020) 7874 7398
Staff writers: Tim Tonkin (020) 7383 6753 and Ben Ireland (020) 7383 6066
Scotland correspondent: Jennifer Trueland
Feature writer: Seren Boyd
Senior production editor: Lisa Bott-Hansson
Design: BMA creative services
Cover photograph: Ed Moss
Read more from The Doctor online at thedoctor.bma.org.uk
HARLEY ACADEMY
HIGHER EDUCATION IN AESTHETIC MEDICINE
“I REALISED THAT I COULD DO OTHER THINGS AS WELL AS BEING A GP” -
DR NADIA TAHA
NHS GP & COSMETIC DOCTOR
We offer healthcare professionals like you the opportunity to expand and take control of your career, flex your creativity and enhance your job satisfaction, with no night shifts!
“I did three years of plastics and reconstructive surgery... I ended up training as a GP,” says Dr Nadia who then went on to take her Ofqual-regulated Level 7 in Botox & Dermal Fillers with Harley Academy.
“I really enjoyed it, I found it really, really thorough. They were all very helpful and very supportive throughout - I loved it.
“The courses were on days that you could pick. If you did your mentorship, for example, you can pick what days and what times would suit you.
Harley Academy is the UK’s leading provider of postgraduate higher education in aesthetic medicine, with more graduates than any other.
“I was more confident because I was shown and taught how to do the injectables. I had no idea before then. That's important, to have a course where you can learn properly.
“But being at Harley Academy helped.
“You learn the anatomy, the physiology, you learn all the injection points and the different techniques. As well as all the tips and types of fillers and toxins.
“A lot of people get quite scared and afraid that they're going to do something, make a mistake, don’t know enough or are just not confident and secure enough.
“And the good thing is, you can always come back. It's like a continuing relationship.”
As innovators of the Level 7 in injectables, we are at the forefront of driving up patient safety standards through training cohorts of medical professionals using evidence-based techniques.