The emergency department as a place of opportunity for helping vulnerable patients
8-11
Cracks in the system
Why the NHS must be better prepared for cyberattacks
12-15
Here to help
Doctors who desperately want to work, in a country that desperately needs doctors
16-19
Emergency measures
The doctors taking direct action against climate change
20-21
Comfort and joy
A GP visit lights up a patient’s life
22-23
Your BMA
How The Doctor magazine raises awareness of the issues facing the profession
Welcome
Phil Banfield, BMA council chair
I would like to take this opportunity to wish a peaceful festive period – and a happy New Year – to all friends, colleagues and peers reading this column. Being BMA council chair is an incredible privilege for me for so many reasons. It’s been an honour to lead the medical profession through unprecedented industrial action but it has been your organised commitment to our shared goals that has delivered real improvements for doctors. With this unity we are becoming a stronger fighting trade union while our expertise as a professional association navigates scientific, ethical and controversial matters important to you as our members.
I’ve enjoyed introducing the magazine to you each month. Our publication has put doctors at the absolute heart of everything we have done – it has represented our members, advocated for our members, and amplified the voices of our members.
This issue of the magazine – the 74th – is most likely the final in print as we move to our new online home at thedoctor.bma.org.uk to enable us to bring you more content. There are no measures of success by which the print magazine hasn’t succeeded – its writers have won numerous national awards, competing against national news organisations with huge budgets and large staff rosters. It has increased the external influence of the BMA, too, with our investigations often featured across the wider media and having significant influence across the health landscape, and even in Parliament.
We are tremendously proud of our achievements and we will continue to invest in high-quality journalism online to ensure we can tell the stories of our members and our profession and keep investigating the issues which affect doctors, the NHS and society, with the same commitment and dedication as the digital transformation of the BMA takes place.
This month we hear from doctors working in emergency departments in some of the most deprived areas of the country, speak to refugee doctors hoping to work in Northern Ireland, and find out about the staff fighting back against cyber threats such as ransomware attacks.
This festive season we also tell the story of a GP making a home visit to a lonely, older patient and transforming her Christmas. Small kindnesses can have a big effect, so I hope we can all do something to make it a better festive season for everyone.
Keep in touch with the BMA online at instagram.com/thebma twitter.com/TheBMA
AT A GLANCE
DOCTOR AND PATIENT: Protections sought for both parties
BMA sets out doctors’ priorities for assisted dying legislation
The national debate on assisted dying took another decisive step last month, as MPs voted to allow the Terminally Ill Adults (End of Life) bill to proceed to committee stage.
Put forward as a private members’ bill by the Labour MP for Spen Valley Kim Leadbeater, the proposed law could eventually see England and Wales adopt a new legal framework, which would enable those terminally ill adults who were expected to die within six months and who wished to end their lives to seek medical assistance in doing so.
By its very nature, the issue of assisted dying is one which often evokes deeply held as well as divided opinions among the public and members of the medical profession. In recognition of the diversity of thought among doctors, the BMA has, since 2021, held a position of neutrality on the issue of whether PAD (physician-assisted dying) should be legalised.
While this position remains unchanged, the association has not stayed silent during the continuing political debate, spelling out in exacting terms what it believes would be the concerns and requirements of doctors should Parliament ultimately seek to change the law.
In a detailed briefing submitted to all MPs, and in constructive dialogue with Ms Leadbeater in advance of the debate, the BMA emphasised that any future model of assisted dying must be explicitly ‘opt-in’ in nature, with doctors able to determine precisely if, when and how they participate in that process.
For those doctors either opposed to assisted dying
or to their personal involvement in it, the bill must enshrine a provision giving doctors a general right to refuse to participate for any reason, which is distinct from the existing conscientious objection clause for procedures such as termination of pregnancies.
The BMA has also made clear that prospective legislation must also seek to protect doctors and patients. While the association has welcomed a specific provision in the bill making it illegal for employers to subject doctors on either side of the debate to detriment, it wants to see a commitment to creating safe PAD access zones, should the need arise to protect staff and patients from harassment and/or abuse, a feature absent from the bill’s current draft.
The current iteration of the bill would not impose a duty on doctors but rather allow them to use their professional judgement when deciding whether to broach the issue of assisted dying with a terminally ill patient who meets the criteria. While this is welcomed by the BMA, the association has insisted that there must be more clarity on how an assisted dying service might be delivered and funded, areas that the draft law provides little to no detail on.
The BMA has also said should PAD be legalised it would strongly support the creation of an independent and transparent system of oversight and monitoring to regulate it, and a patient information service to be provided by an official, legally accountable body.
For more detail on the BMA’s position on PAD and the assisted dying bill, go to https://tinyurl.com/ ewzds86h
URGENT: Doctors say there is an urgent need to deal with the underlying causes of many ED attendances
Inequality is an emergency too
It might be hard to see a chaotic emergency department as presenting ‘opportunities’, but a group of doctors committed to tackling health inequalities say they can be places where meaningful interventions can be made which benefit patients – and reduce pressure on emergency medicine. Peter Blackburn reports
‘Your chances of ending up in an emergency department are not equal across society’
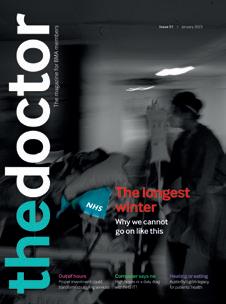
Ask Joanna Quinn why she does what she does and she only has to think back to the previous weekend of night shifts working in an emergency department in Glasgow’s East End.
‘I saw a guy who had just spent 10 years in prison and was struggling to readjust. Prison just hadn’t prepared him at all. He was suffering with abdominal pain, he had been
an IV drug user and he was absolutely terrified to come to hospital – he had been putting it off and eventually turned up in the middle of the night.
‘Here was this big, tough lad who was sobbing and in pain and scared and I just despaired thinking about his life chances. He just hadn’t had the opportunities others have had, he was only in his 50s but his health was pretty poor – physiologically he was
much older.’
Later that weekend
Dr Quinn, who was born and raised in Yorkshire and came to Glasgow via London and a range of roles overseas, saw a homeless patient who had come out of prison and been left to live on the streets –back in the embrace of drug use, which likely started while inside. Both doctor and patient felt ‘hopeless’.
These aren’t unusual cases.
That weekend was full of such stories, each a damning indictment of the state of society – each acting as motivation for someone with a burning sense of injustice in their core.
As Dr Quinn says: ‘Nearly every patient has an element of poor life chances.’
Or, as one of Dr Quinn’s peers, a consultant called David Chung who also works in emergency medicine, more brutally describes things: ‘This is shit life syndrome.’
Recent patient stories stand out for Dr Chung, too. One patient had been brought to the emergency department by police and was suicidal. After spending some time trying to understand, it became clear the man was a prisoner in his own flat, which had been taken over and used as a drug den and party venue.
Dr Chung says: ‘Wouldn’t you be expressing extreme despair and possibly suicidal ideation if that was you? What this man needed was some police support and a locksmith. He may not really have had a mental health issue at all. We were able to effect those changes and help. That needs to be a more mainstream solution.’
Disease burden
For Dr Quinn, who had come into medicine hoping to work for Médecins Sans Frontières to help the poorest and most vulnerable and has also worked in refugee camps, with street homeless people in Greece, and trying to improve care in rural Myanmar, there has been a stark realisation: ‘You don’t have to fly halfway across the world to make a difference in disadvantaged populations.’
It is exactly these sorts of experiences which led to a group of doctors, including Dr Quinn, in Scotland to found the Emergency Medicine at the Deep End group – a project which aims to bring doctors together to try to intervene to mitigate these inequalities in emergency care.
The group aims to make the case that people experiencing socio-economic disadvantages have higher rates of emergency attendance – that the disease burden is significantly higher in deprived groups, with resultant high levels of premature and excess mortality and that patients from these areas are more likely to die from critical illness, regardless of severity. The group believes these issues are not niche, not areas of special interest, but fundamental to the work of emergency medicine and that addressing health inequality is a pursuit of social justice and an ameliorating prospect for emergency departments under huge pressure.
The project was conceived around clinical research fellow Ryan McHenry’s kitchen table. Dr McHenry, an emergency, pre-hospital and retrieval medicine registrar in Glasgow, who also researches deprivation, isolation and emergency care, had been wanting to raise awareness
of the social determinants of health since his first experiences on a Glasgow hospital respiratory ward.
The son of two parents who met working with kids excluded from school in innercity Belfast, Dr McHenry – who trained in Dundee and has been in Scotland’s biggest city ever since – says: ‘It was the East End of Glasgow, with the worst social deprivation in Western Europe on our doorstep, and the thing that became very quickly clear was that every single person who was on that ward was there because of a disease that you could say had been inflicted on them by society – people were suffering the effects of asbestos from Glasgow’s industrial past, or from smoking or drugs. And moving into emergency medicine that just became increasingly clear. The truth is that your chances of ending up in an emergency department are not equal across society.’
Ask a layperson on the street and they may well believe the chances of ending up in a hospital emergency
‘Every single person was there because of a disease that you could say had been inflicted on them by society’
QUINN: Profoundly affected by seeing patients in ‘hopeless’ situations
DOUGLAS ROBERTSON
department, or needing hospital care, are largely equal from one person to the next. In reality this could hardly be further from the truth.
‘The last thing we want is to put more burden of work on to the emergency departments to try to solve society’s health problems’
And Dr McHenry spells out the reality: ‘If you experience social deprivation, you’re more likely to have an emergency illness, you’re around three times more likely to require intensive care. If you’re in the most deprived 10 per cent versus the most affluent 10 per cent you’re also more likely to have a bad experience in your emergency department – the work that we have done shows you’re more likely to wait for more than 12 hours for a bed if you’re in the most socially deprived groups.
‘This is fundamentally unjust, and we can’t stop feeling that that’s unjust.’
For Dr Chung, the motivations are similar, but having worked in emergency medicine in Glasgow since the 1990s, history also brings a sense that change is possible. Dr Chung saw the ‘immense power’ of a concerted publichealth approach to knife crime
and violence, previously just seen as a criminal justice issue. ‘It needs all of us to start thinking like that – working out what the real problem is – and feed into it,’ he says.
The group follows the now long-established Scottish Deep End project, which is made up of a group of GPs from the 100 most socio-economically deprived practices in Scotland. It has had significant success in raising awareness of health inequalities and affecting public policy. Their model has been adopted internationally, with 16 Deep End groups operating in seven countries and the entire project is founded around a relentless drive to overturn the inverse-care law.
Dr McHenry says: ‘We need to recognise we do not have one of the big tools GPs have to make a difference in this area – continuity. But we do have, we think, a reachable moment for people who might not otherwise actually usually present to the GP – I firmly believe there is nowhere else in society where people turn to whenever they have lost
all hope or they’ve nowhere else to go like they do in our department. We have to accept both those things.’
Whereas in general practice the Deep End group has a long-established presence – their narrative understood and their influence consistent from grassroots to national policymakers – these are early days for this new project. As things stand the NHS often sees language like ‘frequent flyers’ or ‘high-volume service users’ and hospital philosophies grounded in principles of moving people on quickly and reducing numbers coming through the door. Success for this group of doctors would be moving from those narratives to seeing the emergency department attendance as an opportunity – as a moment of intervention, which could have a significant effect.
‘We all know emergency departments are in crisis at the moment, and the last thing we want is to put more burden of work on to the emergency departments to try to solve society’s health problems. That is absolutely not what this is about,’ says Dr McHenry. ‘I suppose what we want, what ultimately we think is maybe useful, is to say, we do have a reachable moment for some people to be able to try to change some part of whatever has brought them to the emergency department at that time. And that doesn’t necessarily need to be delivered by emergency clinicians.’
If common sense or morals don’t drive the approach, then perhaps the evidence can. Dr McHenry cites a study, which shows the positive effects of putting
CHUNG: History gives a sense that change is possible
DOUGLAS ROBERTSON
smoking-cessation workers into emergency department waiting rooms – providing cost-effective services. And, as we speak, he’s also preparing to tell delegates at a Royal College of Emergency Medicine conference that emergency attendances dropped by 29 per cent, and scheduled care increased, following the introduction of a navigator programme intervention in an emergency department.
He says: ‘This is hard to do when our emergency departments are overflowing as it is, and people are really coming to harm. It’s not about all emergency physicians becoming social workers or us trying to somehow undo the continuities that the GPs have by stepping into that place. We know that intervention to try to improve people’s lives actually has the ability to reduce use of emergency care, and therefore it’s worthwhile doing whether there’s an emergency care crisis or not.’
Unmet need
Doctors working in Deep End projects frequently speak of the comfort and positivity they get from being part of a collective – from fostering a sense that together, big issues can seem a little less insurmountable. In an environment where doctors have been on the front line through permacrisis and so many are burned out or dealing with moral injury, could this sort of project present an aid to those serious issues, if not a solution?
Dr Quinn says: ‘There’s definitely an element of compassion fatigue and moral injury and I see it in a lot of colleagues. I think this is giving me hope. It doesn’t change the
fact that sometimes things can feel pretty bleak – when the department is full to bursting and you’re struggling. But I have a renewed sense of purpose and hopefully we will see some changes eventually.’
There are many challenges ahead for the group. Winning hearts and minds can be a long process and even then influencing policy decisions and driving real change remains a major challenge.
A first step is to make a convincing case for a move away from demand management and promoting an understanding of ‘unmet need’.
This, the group says, ‘better represents the reality of people who don’t choose to be in hospital, but attend because their needs aren’t met elsewhere’. The group hopes to crystallise the benefits of social interventions in emergency departments such as the care navigators programme in Scotland and to advocate for a sustainable integration of similar schemes everywhere. The project will be driven by
new research, often led by Dr McHenry, and strong advocacy, following the GPs at the Deep End project, for recognition of the effects of social deprivation on the delivery of emergency medicine.
Many of these arguments need to be won broadly, but also in emergency departments where not all staff are likeminded. The group will look to campaign for a much greater focus on inclusion health –particularly health equity, the social determinants of disease and training in trauma-informed care – in education and training at all levels.
‘It’s a daunting prospect to take on,’ Dr Chung says. ‘But to ignore it is just going to lead to more despair … To really get to the heart of what is wrong and what is bringing people into emergency medicine we need to accept that there is a social element, an economic element and a political element. If you don’t start to think about these things then perhaps you’re not doing as much for your patients as you could.’
‘To ignore [the issue] is just going to lead to more despair’
MCHENRY: A ‘reachable moment’ for people who might not usually present to their GP
DOUGLAS ROBERTSON
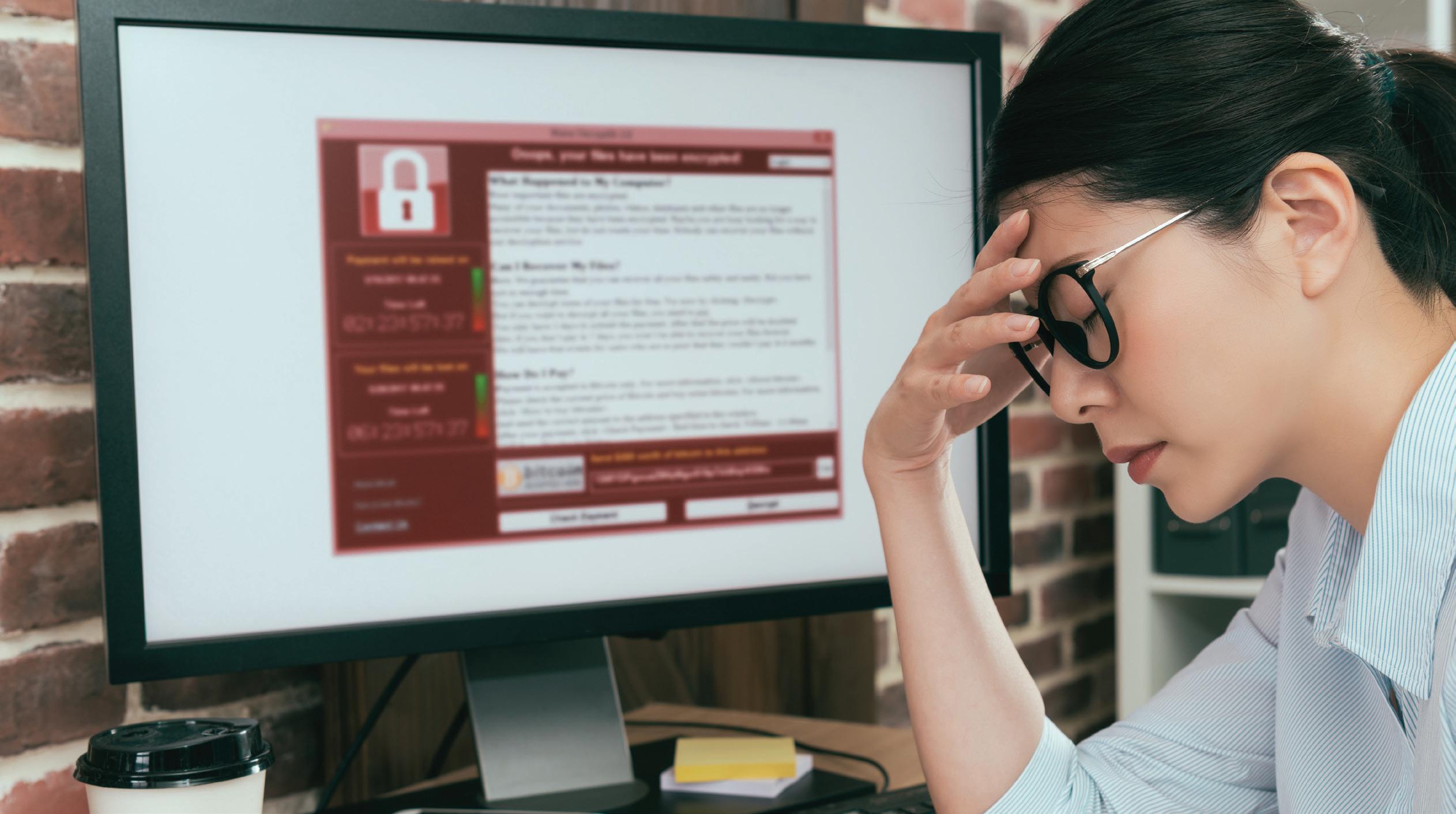
Cracks in the system
A ransomware onslaught on a hospital in London this year has exposed the vulnerability of online patient data, which has compromised care and breached privacy. Doctors tell Tim Tonkin of the urgent need for the NHS to be better prepared and protected
Synnovis, a partnership organisation providing pathology services to NHS trusts in south-east London, became the victim of a ransomware cyberattack launched by an overseas criminal enterprise in June this year.
incident that it took more than three months for normal services to be largely restored, with NHS England confirming the disruption during this time period caused 10,152 acute outpatient appointments and 1,710 elective procedures to be postponed.
‘We know cyberattacks on the NHS, and on all critical national infrastructure, are increasing year on year’
Responsible for processing blood tests for five foundation trusts, Synnovis suffered the theft of patient data, including names, NHS numbers and test codes and lost access to its medical records through the attack on its IT systems, leaving hospitals unable to crossmatch patients’ blood types.
The cascading chaos saw hospitals declare critical incidents and resident doctors, who at that time were still engaged in industrial action around pay restoration, step off from picket lines to manage the fallout.
Such was the scale and severity of the
With trusts unable to verify patients’ blood types safely, the attack also necessitated desperate appeals for O-negative blood, which in turn contributed to a national shortage – an occurrence arguably without precedent in the history of cyberattacks on health services.
‘I think health systems globally are much further behind other critical sectors in terms of shoring up cyber services, very much so if you compare it to industries like fintech, transport and energy,’ warns Saira Ghafur, consultant in respiratory medicine and digital health lead at Imperial College.
‘The Synnovis attack saw a third-party supplier of pathology services, a small piece of the NHS in London, targeted but I think it’s probably one of the biggest cyberattacks to hit the NHS in the UK because of the amount of disruption.
‘We have no idea really what the impact has been, the cost of all the tests that were cancelled or delayed, the economic costs or the cost to patient outcomes.’
Indeed, as serious as the Synnovis attack was, it is far from unique when it comes to the recent history of cybersecurity and the NHS.
In 2017, the health service was one of many victims targeted by the global WannaCry ransomware attack, which saw the theft and encryption of data and which ultimately cost the NHS £92m in lost output and IT support.
Meanwhile, this year alone has seen multiple cybersecurity breaches involving staff or patient data, not including the attack on Synnovis, with incidents reported by the NHS Dumfries and Galloway health board and the Norfolk and Norwich University Hospitals NHS foundation trust.
‘We know cyberattacks on the NHS, and on all critical national infrastructure, are increasing year on year,’ warns Isabel Straw, an emergency medicine doctor and researcher in AI and cybersecurity in healthcare.
‘We’re seeing this in the finance sector and all kind of other areas, but we know healthcare as well is becoming increasingly targeted.’
Dr Straw is based at the UCSD (University of California San Diego) Center for Healthcare Cybersecurity, with her work giving explicit focus to the threats posed by ransomware to health services.
She says that there are several factors which make healthcare systems worldwide a vulnerable target, such as the reliance on digital services provided by third parties and the challenges around implementing system updates.
In addition to these, Dr Straw adds there are issues more specific to the NHS connected to long-running underfunding of IT infrastructure, which has led to healthcare staff relying on outdated or inadequate technology.
Ageing IT
‘Healthcare [in particular] relies on this huge landscape of interacting vendors and servers, different technologies,’ explains Dr Straw.
‘When a cyberattack hits, even if it might not have initially been targeting healthcare, healthcare services can end up being taken down as a result. Additionally, the lack of IT investment in the NHS creates specific vulnerabilities, as we’re using very old IT systems.
‘There’s also the global issue in healthcare in that it’s very difficult to update systems because you can’t just turn something off.
‘If the emergency department relies on a particular IT system, and you need to do a software patch to update it, you can’t just turn off the [emergency] department [so] every time you want to make that kind of update and improvement, you have to weigh it up against the clinical impact and patient care.’
As well as being hamstrung by its patchwork of increasingly archaic IT systems, the NHS is made further vulnerable to cyber-based attacks as an indirect consequence of the enormous day-to-day pressures facing health service staff.
With doctors and other healthcare professionals focused on caring for patients in a woefully under-staffed and under-resourced NHS, and amid an unprecedented backlog of unmet care, this high-pressure, time-poor working environment is often not conducive to good cyber-hygiene practices such as the use of multifactor authentication.
‘We know there are lots of technological issues in the NHS that present risks such as outdated technologies and legacy systems but the other vulnerability is human behaviour ... but a lot of that is related to the conditions staff are working under,’ says Dr Straw.
‘With all the pressures that exist in the NHS in terms of staffing and volume of patients, cyber hygiene is the last thing on your mind.
GHAFUR: Health systems lag behind other critical sectors in cybersecurity
‘With all the pressures that exist in the NHS, cyber hygiene is the last thing on your mind’
STRAW: ‘It’s very difficult to update systems because you can’t just turn something off’
That might mean that you share logins or you leave computers logged in, as you don’t have that capacity to be doing things that are really secure.
‘With something like MFA [multi-factor authentication] there’s a challenge of how you balance these security practices with the capacity that doctors, who are already working under such intense pressures, have.
themselves unable to access patients’ records, Dr Molodynski says they were forced to resort to creating temporary records by collating any existing data with records requested from GP practices.
‘Our admin team were amazing and put in a huge shift creating temporary folders just using Word documents for all our patients and putting into those folders whatever they could because by then, it was becoming obvious that no one knew how long [the situation] was going to go on for,’ he says.
‘It was a bit like going back in time to preelectronic records and when people were being seen in [emergency departments] as an emergency when staff wouldn’t have had their notes.
‘There was obviously a gap there for some of the very acute stuff, which we felt created an increased risk and made looking after people more difficult.’
Dr Molodynski says his experience of trying to care for patients while having no access to records has been difficult at times and unsettling.
‘We don’t have much of a conversation about cyber security because there is not a direct connection as to how this is going to impact patient care’
‘This is made harder especially when we don’t have much of a conversation about cyber security and medicine and when there is not a direct connection in people’s heads to how this is going to impact patient care.’
Impact of attack
The human cost of a cyberattack on healthcare to doctors and patients is something consultant psychiatrist Andrew Molodynski unfortunately knows only too well.
Dr Molodynski’s workplace, Oxford Health NHS Foundation Trust, was one of a dozen trusts affected by a ransomware attack in August 2022.
The incident saw CareNotes, a patientrecords system supplied to the NHS by software provider Advanced, compromised and doctors and other healthcare staff unable to access vital clinical information.
More than two years on, Dr Molodynski can still recall the chaos and confusion generated by the incident which, like this year’s attack on Synnovis, took months to rectify fully.
‘Initially we all just heard basically that the system was down but without knowing why or for how long,’ he says.
‘It then became apparent over the next few days that there was a fairly major problem.’
With he and his colleagues suddenly finding
He adds that, while he was not aware of the cyberattack which affected his trust having led directly to serious negative consequences for his patients, the incident overall would have undoubtedly resulted in ‘situations where the outcome was not as good as it could have been’.
‘When you’re seeing a patient, you want to be absolutely certain what treatment they’re on, because usually you’re thinking of making changes to that treatment,’ he says.
‘If you don’t know exactly what someone’s taking, it’s hard to make changes, and we don’t do it from memory for a very good reason, because it’s not very safe.’
Theft risk
As well as the disruption to day-to-day services that attacks on IT and other electronic systems can have, the theft of sensitive personal information, as seen in ransomware attacks, also presents data-protection risks.
Nineteen days after the attack on its systems on 3 June, Synnovis confirmed some patient data stolen during the attack had subsequently been published online.
Dr Molodynski says the prospect of patient data being leaked as the result of a cyberattack poses serious concerns and threatens to undermine patient confidence in health services and the doctor/patient relationship.
ADRIAN
DE LEON
‘Patients come and see psychiatrists, they tell us the most personal and most difficult things about their lives,’ he says.
‘They do that with trust and with an expectation of privacy and that’s the only way it can work. If that were to be blown apart by repeated incidents like this, it would be a big thing and pretty scary.’
In August this year the Information Commissioner’s Office imposed a provisional fine of £6m on Advanced Ltd on the grounds that the provider had ‘failed to implement measures to protect the personal information of 82,946 people’ during the 2022 attack.
Despite the apparent vulnerabilities when it comes to cybersecurity, the NHS is poised to embrace more deeply digitisation, through the rise of AI in healthcare and new plans to give patients full access to their medical records via the NHS app.
Dr Ghafur says that while she welcomes the principle of democratised healthcare through greater sharing of data with patients, she believes there was a danger of rushing ahead with changes without ensuring these were secure.
‘I think it’s a great idea to open up patient records to patients – at the end of the day it’s their data – but I don’t think the security challenges have been fully considered,’ she says.
‘At the end of the day we’re data controllers in the NHS; any kind of healthcare professional has that duty of care to make sure that you are, whether it’s paper records or digitised health records, to do your utmost to protect that patient data.
‘There is a huge element of trust that takes years to build up and just a second to wipe out.’
The growing cyber-security threat posed by bad actors, state and criminal, to institutions including the NHS, is being increasingly recognised, with NHS England beefing up its approach to security in September this year by adopting the National Cyber Security Centre’s CAF (cyber assessment framework).
Clinical guidelines
Meanwhile, the Government is pressing ahead with its Cyber Security and Resilience Bill, proposed legislation which will bring the UK’s cybersecurity laws in line with those which exist in the EU, and which will expand regulation to digital services and supply chains and mandate the reporting of cyberattacks.
Dr Straw welcomes the bill and adoption of the CAF and believes one area which remains underdeveloped is that of doctors and healthcare professionals being part of the conversation and contingency planning for cyber incidents.
As part of her work at UCSD, she and her colleagues are also seeking to develop the first ever set of clinical guidelines to assist doctors in responding to cyberattacks on their workplaces – guidance she hopes will ultimately be adopted on both sides of the Atlantic.
Alongside her work at UCSD, Dr Straw runs non-profit organisation bleepDigital, which aims to educate healthcare professionals around the risks of cyberattacks to health services and how to respond to such attacks when they occur.
‘The more dependent you are on digital systems, the more vulnerable you will be to digital attacks and one thing that is really lacking at the moment, is orienting our response plans in terms of the clinical impact,’ she says.
‘There are specific medical conditions that we know are more likely to be impacted by ransomware attacks, such as strokes and other time-critical conditions.
‘These guidelines are clinically orientated for doctors to read, as opposed to for the IT team. I haven’t seen [them] in the UK or a lot of Europe at all, it’s definitely something we want to integrate and bring to hospitals so there is an immediate response plan when those things occur.
‘If you’re going to connect something to the internet or to a network, that connection has to be secure,’ Dr Straw warns.
‘At the moment, we’re connecting everything before we’re securing everything, and as a result creating this Wild West where we’re playing catch up on the cybersecurity front.’
Forced to create temporary records
‘There is a huge element of trust [with patient data] that takes years to build up and just a second to wipe out’
MOLODYNSKI:
Here to help
Doctors who desperately want to work, in a country that desperately needs doctors – but it’s far from simple for those leaving war-torn countries to practise in the UK. Jennifer Trueland meets two who are benefiting from a scheme to help their language skills, while Tim Tonkin hears about an initiative which offers continuing medical education
When paediatric consultant Yasmeen Elrashib Ibrahim Ahmed was arrested and imprisoned in her native Sudan, she knew she had to get out. Her ‘crime’ – along with medical colleagues – had been to campaign for peace in the revolution-torn country.
It meant giving up everything: her home, her family (particularly her mother), a job she loved, and finding USD3,000 (£2,400) to pay a people smuggler to bring her to safety – a risky prospect given that she was a young woman travelling on her own.
and verify their qualifications and prepare for advanced English tests and medical exams to ensure they are qualified to practise medicine in the UK.
‘The Government fought us with guns and tear gas’
It’s a programme that should bring benefits to the doctors themselves and to the health service in Northern Ireland, which suffers from acute workforce shortages and has the longest waiting times in the UK.
Dr Ahmed, 34, is now living in Belfast, and is one of the first cohort to take part in an English Language Support Academy for medics, the first of its kind in Northern Ireland.
The Belfast City Council programme aims to help experienced doctors to navigate the process to register
Dr Ahmed arrived in Belfast last year having been forced to flee her homeland in 2019. ‘There was revolution and there were problems against doctors,’ she explains. ‘We, the people, mostly doctors, were asking about justice and peace and equality and freedom, and the Government fought us with guns and tear gas. I was arrested in 2019 and held for three days, but 10 days after that, I managed to get out to Egypt.’
AHMED: Arrested in Sudan after campaigning for peace and equality
People smugglers
Once in Egypt, she took the difficult decision to pay a people smuggler USD3,000 (£2,400) to get her safely to the UK. This was frightening as a single woman, she says, because she essentially had to trust that a stranger would keep his word. It was also a lot of money but she received help from friends. ‘It was hard, but I had no option,’ she says simply.
Once she arrived in Belfast as an asylum seeker she immediately started the process of becoming qualified to practise medicine in the UK. ‘I didn’t want to waste time waiting, so I started to study for the [medical] royal college exam for paediatrics – I’ve done the first part.’
She was, she says, ‘struggling’ to improve her English enough to pass the OET (occupational English test) exam, a crucial step towards being able to practise in the UK. That’s where the Belfast City Council English Language Support Academy for medics has been invaluable.
‘It’s been very helpful with English in general,’ she says. ‘They helped with speaking, listening and writing, and an especially lovely teacher has been helping us in engagement with the community, with [local] culture, with speaking in general, and correcting us with many things we have no idea about.’
Ready to work
Having failed to pass the OET English language test, Dr Daher, who travelled to Belfast with his wife and children, switched tack and made three attempts to pass the member of the Royal College of Surgeons exam – in the last try, he missed a pass mark by five points.
‘I was a bit depressed, I was thinking “why, why why?”. But then I heard that Belfast City Council would like to help refugee doctors, and now I am preparing for OET and PLAB [Professional and Linguistic Assessments Board].’
Having worked as an orthopaedic surgeon for many years – first in Syria, then in Lebanon and Saudi Arabia – he is keen to push forward and practise in the UK. It’s been difficult, however. ‘Every time I try to get a clinical attachment here, there’s nothing,’ he says.
‘But every day, I get messages from friends in Syria, sending me X-rays and pictures to get my opinion about it. Maybe 10 times a day.’
He and his wife, an English teacher, left Syria in 2013. ‘It was impossible to stay. If I wanted to protect my life, and my family, it was impossible.
‘I have knowledge, and it’s hard to be here doing nothing’
‘If you stay in Syria people come to you and say, “you are a doctor, you are rich, give me money, give me everything”. A colleague refused to give them any money, and that meant a gunshot – he died.’
Everything Dr Daher owned in Syria – including his house –was destroyed.
She has personal experience of difficulties in the Northern Ireland health service, which makes it all the more frustrating she cannot yet work as a doctor and help get local services back on their feet.
‘There are delays everywhere – in appointments with GPs, and specialists. I’ve been waiting since I came here one year and a half ago [to see a specialist]. In my country or the Middle East, you wait a maximum of seven or 10 days to meet a specialist.
Feeling welcome
‘It was impossible to stay. If I wanted to protect my life, and my family, it was impossible’
‘I really want to pass OET and start practising, initially as a GP until I complete the full membership of the royal college, and after that, I can resume my previous career as a paediatric specialist to help people and communities.
‘I have knowledge, and it’s hard to be here doing nothing. I hope to pass exams and work here – and the next interview [with The Doctor ] will be as doctors, as real doctors working here.’
Ghaleb Daher, 51, an orthopaedic surgeon from Syria, came to Belfast as a refugee in 2019. He has welcomed the opportunity to take part in the Belfast City Council programme as he too is desperate to put his surgical skills to good use.
Speaking before the recent deposition of the Syrian dictator Bashar al-Assad, Dr Daher said doctors were told to go to the war zone, but as well as the dangers of conflict, they could be punished for acting in accordance with medical values. He knows a former colleague who performed an operation on a soldier on the opposing side to the Government and who died in prison. Another is still in prison 10 years later.
‘This is from the two “sides” – the Government will do this to you, and those against the Government will also do it to you.’
Belfast is a nice city, he says – although arriving just before the COVID lockdowns did make settling in quite challenging. ‘Everything is good. There’s a good school, there are nice people, quiet people, and anyone you meet is ready to give you support.’
The English Language Support Academy is funded by Belfast City Council and the Belfast Labour Market Partnership. It is also supported by other organisations including the Belfast Trust, Department
of Health, Queen’s University Belfast and REACHE Project Manchester.
Belfast Lord Mayor Councillor Micky Murray expressed gratitude to the other agencies. ‘I hope
these talented medical professionals feel well supported and welcomed as they study and work to become much-needed members of Belfast’s healthcare workforce.’
Support at hand
International medical graduates need to undergo rigorous assessments before they can practise in the UK, but aid is available
While not all doctors taking shelter in this country necessarily hold refugee status, requirements for obtaining a licence to practise medicine are the same for all.
Before any international medical graduate doctor can hope to resume their clinical duties in the UK, they must undertake a series of rigorous assessments.
These include passing evaluations of English-language skills encompassing speaking, writing, reading and listening abilities and completing a two-stage assessment of clinical skills known as the Professional and Linguistic Assessments Board. Doctors must also undertake an unpaid clinical attachment in the NHS usually lasting four to eight weeks, to familiarise themselves with UK medical practice.
These requirements, while understandable in their necessity, can sometimes seem insurmountable to those who find themselves in new and uncertain surroundings often arriving with only the traumatic memories of the homelands they had to leave.
Fortunately, there are a variety of sources of support available to doctors.
Through its refugee doctor initiative, the BMA provides measures including support through its international department, free access to the BMJ and to the association’s 24-hour phone-counselling service, with around 900 refugee doctors being supported by the initiative.
The GMC meanwhile will aid doctors granted refugee status by helping them get primary and postgraduate medical qualifications independently verified, and by providing financial assistance with registration fees.
DAHER: House destroyed in Syria
JENNIFER
Restoring hope
The Crisis Rescue Foundation seeks to support medical students and doctors whose education has been disrupted
Having to leave your home and normal life behind and start again in a new and unfamiliar land owing to conflict or crisis is an enormously daunting prospect for any human being. For doctors who seek refuge in the UK after fleeing from overseas, the process of restarting their career is often onerous and far from straightforward.
Ukrainian paediatrician Olena* arrived in the UK in late 2022, having had to flee her home country owing to the devastation wrought by the Russian invasion. Having departed Ukraine when heavily pregnant, she fled initially to Poland before coming to the UK where she and her newborn son were joined by her husband. Despite having been in the country for two years and eager to put her clinical skills to good use, Olena is yet to secure a licence to practise.
‘We thought we would spend our entire lives in Ukraine, but one day [the date of the Russian invasion] changed everything,’ she says. ‘When the war started, I was nine months pregnant, so it was a very difficult decision for our family to move on abroad. I’m not working right now because it’s not allowed here to work without registration, but I’m continuing my studying because I want to stay up to date. It is difficult because I don’t know what happens next or how long I will be here. I’m always thinking about my friends from university who are still living in Kyiv or in the eastern parts of Ukraine.’
There is also a raft of voluntary and charitable organisations that provide assistance to refugees in general but specifically to doctors and healthcare professionals who have sought asylum in the UK.
The Crisis Rescue Foundation is one such group and has been helping medical students and doctors in countries disrupted by war or other crises to continue their education through its medical school elective programme, a free-to-access series of online lectures.
The programme, which was set up in 2022 partly in response to the war in Ukraine, has also sought to support medical professionals who have relocated to the UK through in-person events focusing on Professional and Linguistic Assessments Board exams and UK medical practice.
‘I have received countless, at times, heartbreaking communications from refugee medics from various countries affected by war and national crisis who have struggled to reach the UK, access medical education, support and eventually work as a doctor here,’ says programme founder and GP Sharon Raymond.
‘These challenging experiences prompted
RAYMOND: Support doctors on the ‘often arduous’ journey to eventually achieving work in the NHS
the establishment of the CRF medical school UK elective programme. For more than two and a half years, we have had the privilege of supporting refugee doctors from the start of their often arduous journey to finally achieving work as doctors in the NHS; whilst still overseas, they have joined our online medical lectures, peer support and wellbeing sessions as refugees in the UK [and] they have participated in our in-person PLAB/ UKMLA training days.’ Dr Raymond says the CRF has also helped the doctors arrange more than 60 clinical placements, and it has provided guidance to help them secure work as a doctor in the UK, online and at events supported by organisations such as the GMC, BMA and MDU.
One of those assisted by the programme is Samira* who came to the UK from Sudan 18 months ago. As a UK-born dual Sudanese and British national, Samira is not a refugee but had no prior experience of training or practising in the UK until her arrival last year. Having completed her medical training in Sudan during years in which the country was riven by revolution and then civil war, she says that she has found the transition to the UK far from straightforward.
‘I would say that the experience of being a Sudanese doctor has, you know, has been quite difficult,’ she explains. ‘With the revolution, there were a lot of pauses when it came to education and a lot of struggles, that took a toll on the whole country.’
Since coming to the UK and with support from organisations such as the CRF, Samira has undertaken her English language and PLAB assessments and recently completed a clinical attachment. Despite making progress with the support of the CRF, she feels that too little is done at a national level to help refugee doctors navigate UK medical systems and into the medical workforce.
‘I’ve been here for a year and a half now and completed all my exams but I’m still looking for work,’ Samira explains. ‘There’s no guidance really on how to achieve that – no one really tells you how you find work to begin with. I think there could be a lot more support, especially after registration.’ * Some names have been changed
EMERGENCY MEASURES
July 2022 was the hottest day ever recorded in the UK, reaching 40.3°C in Coningsby, Lincolnshire.
‘Climate change is making us sick, and urgent action is a matter of life and death’
Two days earlier, six medical professionals – including four doctors – broke glass windows at the Canary Wharf offices of banking giant and major fossil-fuel financier JP Morgan as they saw forecasts of a record heatwave.
After they ‘carefully
cracked’ the windows, they put up posters saying, ‘IN CASE OF MEDICAL EMERGENCY BREAK GLASS’.
They say the climate emergency is also a health emergency and point to evidence-based studies, which show direct action is the most effective way to affect change –in this case ending the burning of fossil fuels.
Two years on from breaking the glass, which JP Morgan
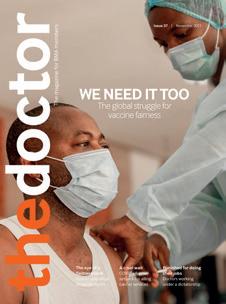
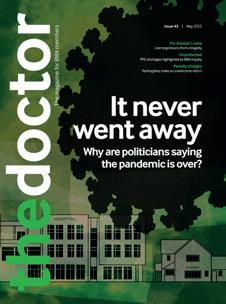
says cost nearly £200,000 to replace, the six – consultant psychiatrist Juliette Brown, GPs David McKelvey and Patrick Hart, consultant in obstetrics and gynaecology Alice Clack, dementia specialist nurse Maggie Fay and child and adolescent mental health specialist Ali Rowe – went on trial accused of criminal damage. They pleaded not guilty at Snaresbrook Crown Court, London, in June.
HAND IN HAND: (left to right) Maggie Fay, Alice Clack, Patrick Hart, Ali Rowe, David McKelvey and Juliette Brown
Shortly before the trial began, the judge ruled that the defences the defendants had planned to use were not available to them. These defences included that of belief in consent, which is where those alleged to have committed the offence believe the persons they understand to be entitled to consent to the destruction or damage of the property had so consented, or would have consented, if they
Global warming is considered a threat to health by many doctors, some of whom are prepared to take direct action to make their voices
heard. Ben Ireland reports
had known of the damage and its circumstances.
The judge said the defence was not available as the factors upon which it was based ‘do not include the political or philosophical beliefs of the person causing the damage’ and consent ‘was not intended to afford a defence to protesters based on the merits, urgency or importance of their cause’.
But he did allow them to speak on their motivations for taking action, namely that they believed it was their obligation as health professionals to do what they could to prevent the damage to people’s health they said would be caused by the continued burning of fossil fuels that JP Morgan helps facilitate – the bank has financed US$432bn (£341bn) of fossil fuel deals since the UN’s 2016 Paris Agreement, a treaty aimed at limiting the global average temperature rise to 1.5°C.
At the end of the trial, the jury did not reach a verdict. A retrial is slated for 2026.
No regrets
The impasse has left the four doctors in limbo, their careers potentially in jeopardy if a retrial finds them guilty of criminal damage.
Their case follows that of GP
Sarah Benn, who received a fivemonth suspension from a MPTS (Medical Practitioners Tribunal Service) hearing, which found that her environmental activism and resulting convictions amounted to misconduct. The BMA is supporting Dr Benn, who retired from clinical practice in 2022, with an appeal.
Still working, and with legal bills to pay, the effect on the JP Morgan doctors’ lives could be momentous. Speaking to The Doctor, Drs Clack, Brown and McKelvey say they have no regrets.
As medical professionals, they are keen to point out that their reasons for taking non-violent direct action over the climate emergency are evidence-based.
The term ‘climate emergency’ is recognised by the UN and many leading global organisations agree it is a health emergency, too.
The Lancet, in 2021, said: ‘Health is already being harmed by global temperature increases and the destruction of the natural world,’ noting: ‘The science is unequivocal.’
This year’s Lancet Countdown urged a divestment from fossil fuels on health grounds, saying: ‘Climate change is the greatest health
‘It’s been a journey about health justice and how we frame health in general as a profession’
IMAGES BY GARETH MORRIS
CLACK:
‘Somebody has to take responsibility’
threat facing the world in the 21st century.’
A World Health Organization special report for this year’s COP29 declared: ‘Health is the argument for climate action,’ noting: ‘Climate change is making us sick, and urgent action is a matter of life and death.’ Director general Tedros Adhanom Ghebreyesus said in the foreword: ‘The climate crisis is a health crisis.’
‘We did the right thing’
In the month the four doctors were involved in the action at JP Morgan there were 3,898 excess deaths in the UK. The Office for National Statistics said some were associated with the ‘exceptionally hot weather’.
This August, a study published in Nature Medicine showed that heat ‘fuelled by heat-trapping greenhouse gases’ killed nearly 50,000 people in Europe in 2023.
‘We have an existential crisis unravelling and we’re not doing anywhere near enough to stop it,’ Dr Clack tells The Doctor. ‘It’s a massive health issue. And the response is completely inadequate.
needs to change.
‘As health workers we have even more responsibility, not just because we have a code of conduct to protect public health but because we have a trusted voice within society.’
The doctors point to studies which prove how direct-action campaigners throughout history have effectively driven change, such as Australian doctor Arthur ChesterfieldEvans, who was convicted of ‘wilfully marking premises with paint’ when taking on big tobacco advertising by ‘refacing’ billboards in the 1980s (his sentence was remitted on appeal).
‘Somebody has to take responsibility,’ says Dr Clack. ‘And it’s potentially very powerful to have people with trusted voices doing that. We have a professional responsibility to follow the evidence and we’re well-placed to do that because we’re trained scientifically – and are communicators.’
The Government’s own guidance can be interpreted to support the argument, too. Its document on climate and health says: ‘Health and care professionals should recognise the climate crisis as a health crisis, and therefore climate action as a core part of their professional responsibilities.’
for their individual health and we don’t look at it in the context of social and political decisions that are being made constantly which undermine people’s health and limit their access to health justice.’
Asked how she felt sitting in a courtroom for, in her view, doing her duty as a doctor, Dr Brown says: ‘If anything I was feeling more certain we did the right thing.
‘There are hundreds of thousands of people worldwide who want change to happen quickly and it feels like, as medics, we need to stand alongside those people who are taking enormous risks, here and overseas. We have the credibility, the reputation and we have a lot of security where we are, not just in the UK but as [medical] professionals.’
‘Health and care professionals should recognise the climate crisis as a health crisis’
‘As health workers, we have a responsibility to stand up, make clear what’s happening and draw the public’s attention to the fact that this is a huge public health catastrophe, that the establishment is not protecting health and something radical
For change to happen, Dr Clack believes ‘it needs people who are in a position to actually change things to recognise what’s going on and risk what they’ve invested in – which is a system that is going to destroy us.’
Dr Brown adds: ‘For me it’s been a journey about health justice and how we frame health in general as a profession. We put this responsibility on people
Dr Clack also felt ‘very certain’ the doctors had done the right thing. ‘It’s been a rollercoaster,’ she says. ‘Working in a very conventional profession, you’re often trying to explain why you did something like break a bank’s window to people who are fully embedded in this system where everyone is acting like it’s fine and there have been periods where it felt bizarre. You have to keep reminding yourself of the facts of the situation, what the science says and that this sort of action is necessary.’
Greater purpose
Dr McKelvey says: ‘It was the right thing, but at the time you go in there and you’re stepping up to the threshold from being a “good citizen”, stepping across a boundary where you are potentially going to be found guilty of causing criminal damage. That was a moment of feeling very nervous and
BROWN:
unsettled. But while you’re going into a place of potential personal difficulty, you’re doing it for the motivation of something bigger than yourself. That’s why we could go into the courtroom and stand tall.’
With the retrial listed for 2026, the doctors face a long wait for a decision and feel a continued sense of not knowing what lies ahead.
This year, some climate activists were jailed for record terms of four and five years for non-violent direct action, being found guilty of conspiracy to cause a public nuisance for their roles in planning to block traffic on the M25 motorway. The sentences were longer than many handed to people found guilty of violent disorder in recent far-right riots.
The UN’s special rapporteur on environmental defenders, Michel Forst, said the climate activists’ sentences represented ‘a dark day for peaceful environmental protest’ in the UK and ‘set a very dangerous precedent’.
In that case, defendants including Just Stop Oil cofounder Roger Hallam had their evidence discontinued when defying the judge’s ruling not to discuss their motivations on the basis they did not amount to a defence, but rather a ‘political or philosophical belief’ – as upheld by the Court of Appeal.
In the JP Morgan case, the judge told the defendants, and the jury, that concerns about the climate emergency were not a defence for criminal damage, but he did allow the doctors to speak about their motivations in court.
‘That he let us speak meant all the information was there
[for the jury],’ says Dr Clack. ‘Some of them felt that we had a valid reason for doing what we did, regardless of the written law.’
She adds: ‘The law changes all the time. Two years ago, we would have had a number of legal defences. That was all withdrawn, so we had to defend ourselves outside of the written law.’
Dr Brown says: ‘We made the moral case, and the jury clearly had a lot to think about around the question of intent.’
Dr McKelvey said the financial cost was his biggest concern, with the group having already racked up legal bills in excess of £80,000. ‘If we go to a retrial we would have another tranche of costs,’ he explains. ‘And if we’re found guilty then of course we’ve got more problems.’
The group has launched a fundraising page, which has so far raised more than £50,000 towards the £85,000 target.
For Dr Clack, the main concern is being referred to the GMC.
All criminal convictions, whether they result in immediate imprisonment or not, are automatically referred to the regulator, as was the case for Dr Benn who earlier this year had her licence to practise suspended for five months after being found in contempt of court for breaching an injunction by ‘spreading out and sitting down across the road’ at Kingsbury Oil Terminal holding a placard saying ‘stop new oil’.
The BMA is supporting Dr Benn with her appeal against the MPTS finding that her actions amounted to misconduct despite ‘no clinical concerns’.
Another retired GP, Diana
Warner, had her licence suspended for three months following an MPTS hearing in August. She was found in contempt of court for breaching an injunction by protesting on the M25 motorway in October 2021.
‘Given the fitness-topractise tribunal appears to have been a tick-box exercise, [conviction] would probably mean we would lose our jobs,’ says Dr Clack. ‘I would be scared to go to prison, but I would be more worried about my potential to work and my livelihood.’
Supporting activists
A motion was passed at this year’s BMA annual representative meeting urging the association to lobby to safeguard the rights of healthcare workers and medical students engaged in activism. The motion calls for the BMA to work with the GMC to develop guidelines that protect doctors’ rights to protest and express themselves lawfully, ‘especially in relevant contexts such as climate change’.
For the doctors facing a retrial, the word ‘lawfully’ potentially confuses the level of support, and they believe the motion should have gone further.
Dr Brown says: ‘Every individual should take whatever decision is right for them.
‘There are thousands of people taking these kinds of actions because they recognise what’s at stake. Once you grasp what’s at stake, it’s difficult to sit back and do nothing.’
‘You have to keep reminding yourself that this sort of action is necessary’
MC KELVEY: Financial strain greatest concern
COMFORT AND JOY
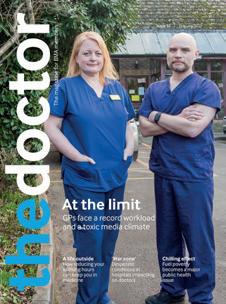
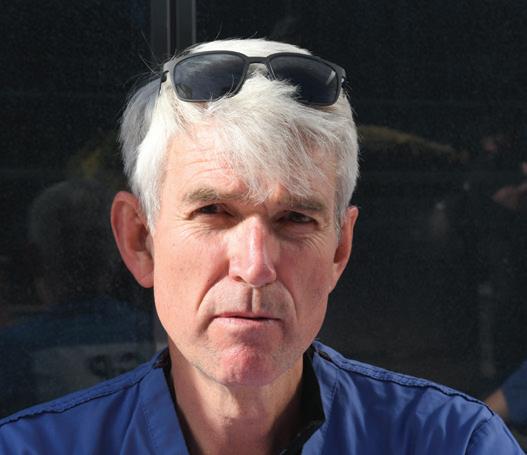
A home visit to a lonely and dignified patient left GP Adam Simon determined that she wasn’t going to miss out on Christmas
She was more than 100 years old and a typical older lady from Oldham. She had married and had children quite early, and her husband and children had all died: she had outlived them all.
She didn’t really have friends, so she was quite lonely. But there’s a lot of pride in that generation: the feeling of, ‘I don’t want to cause bother, I’ll manage’.
It was a basic terraced home in Chadderton, a suburb of Oldham, with a steep, narrow staircase that she went up and down each day. She kept the place very clean, and in a state that would have been lovely if people
‘It really hit me how alone she was’
had come to visit. I can’t remember the reason for my visit that day. It might have been a chest infection or something relatively minor, she wasn’t too unwell.
But what struck me was that there were no decorations up; no cards, no tinsel, no decorations, no tree, nothing. I’m Jewish and don’t celebrate Christmas myself but it was all very stark and made me feel very sad.
Christmas was going to be like any other day for her: she was going to spend it by herself. She had all the food she needed but it really hit me how alone she was.
I had looked after her for many years, and she always made me a cup of coffee. From the very first time I met her, when she was in her early 90s, she said: ‘You know, I wish I could just go to sleep and not wake up.’ She was never depressed, she just felt it was a little bit cruel that she kept waking up each morning.
Making a difference
I just wanted to cheer her up that day. I would normally have had to go straight back for the afternoon clinic but we closed at lunchtime on Christmas Eve so staff could get off early.
So, I went to the local supermarket and I bought some cards, tinsel, whatever decorations they had, some Sellotape. I didn’t tell her what I was going to do; if I had, she would have been angry with me and told me I wasn’t to do that.
When I reappeared, she was a bit overwhelmed. She had a parlour, a smarter room, but she lived in the kitchen, so I put the decorations up there. I spent maybe an hour with her. We sat talking about previous Christmases when she was a child, how different it was. And she was so happy. I felt 20 feet tall when I left.
I spoke to her a couple of days later and she was still happy. It was so simple and wasn’t a lot of time out of my day, but it made such a difference to her.
I have had other memorable things happen at Christmas. Situations where I have inadvertently been given a tea or coffee laced with rum or some other spirit – thankfully, only a small amount – and been worried about being fit to drive home or do my afternoon clinic. I’ve had some amazing and some really bad mince pies. And lots and lots of Quality Street.
But that one was special. It made me
very aware how lucky I was that I had people around me.
Unfortunately, I’ve lost my parents recently. So, I’m very aware of how important family is. You must not lose touch with the older generation, the stories they can tell you, their wisdom.
Whatever the holiday, whether it be Ramadan, Diwali, the Jewish festivals, or Christmas or Easter, these are times when people are a little more vulnerable, especially if they are isolated. Christmas TV always talks about family and togetherness, and that can really accentuate people’s loneliness.
Home visits
I was an NHS GP for just under 20 years – 17 as a GP partner – before I left to do private general practice. Now we have clinics across Greater Manchester, Lancashire and Cheshire, and demand is rising at quite a frightening rate. And the majority of patients we’re seeing are people who are struggling to get to see their NHS GPs or feel they’re not getting enough time with them.
The reason we are all doing this is because we don’t feel we can do our job properly in the NHS system. None of us are in it for money; it is about having more time with people, making them feel valued. A lot of the GPs who work with us are NHS GPs as well; working in the private environment is almost therapy for them.
If we are going to maintain the caring side of general practice, we need to take the pressure off GPs. And we need more GPs. I don’t do home visits now because we are so busy – and it does trouble me because I am aware there are people who are becoming increasingly immobile. We do try to mobilise as many services as we can to help them, including other GP services who do house calls.
But I miss home visits. You can glean a lot from seeing someone in their home environment, about how well they’re eating, how well they’re looking after themselves. That social aspect of the GP role, that social awareness, is so important, especially at holiday times.
Adam Simon is a private GP based in Cheshire and clinical director of AJ Primus Healthcare Interview by Seren Boyd
‘She was so happy. I felt 20 feet tall when I left’
Your BMA
The Doctor has achieved so much in print but the story doesn’t end here
This is the final issue of The Doctor magazine in its current format. Having first landed on doorsteps in September, 2018, the team has been proud to investigate the issues which matter most to our profession in great detail, placing doctors at the heart of that storytelling and the debate, for 74 editions now.
As I said in last month’s column, we’ll now be moving to our new online home at thedoctor.bma.org.uk . While it will be sad to see the print edition of the magazine cease, I am tremendously proud of everything the team has achieved in that medium and I know they will go on telling the stories of our members and our profession –and investigating the issues which affect our lives – with the same commitment and dedication.
In last month’s column I wrote about how I have often been most proud of the magazine for offering an outlet where doctors can speak about the most difficult of issues – often these are things we find it incredibly hard to talk about across society or where it doesn’t always feel there is another safe space, and this magazine has been that place. These features included the story of a GP’s dogged attempt to find answers over the death of her consultant husband, the colleagues of a GP speaking about her suicide, sexism in surgery and a litany of pieces
The Doctor BMA House, Tavistock Square, London, WC1H 9JP. Tel: (020) 7387 4499
Email thedoctor@bma.org.uk
a BMA adviser 0300 123 1233
@theBMA
lobbying for better support for doctors under NHS and GMC investigation, among others.
In this month’s final column I would like to reflect on some of the magazine’s most impressive investigations and campaigns to date.
When the pay restoration campaign first kicked off in late 2022, the team set about telling the human stories of the junior (now resident) doctors at the heart of the campaign. These in-depth interviews gave the doctors in question the space and time to share their experiences of how poor pay and conditions had affected their lives and their own health.
The Doctor magazine covered doctors with different stories, from being forced to sit on bins when working and fi nancial worries owing to taking on insurmountable levels of debt, to how international medical graduates have been exploited over pay and conditions and what it feels like through the eyes of a more senior doctor who has seen the erosion fi rst hand throughout their career.
At the very beginning of the magazine’s existence the team campaigned to tell the positive stories of overseas doctors coming to this country – and the massive benefit immigration brings to the NHS. The series, called, They
Editor: Neil Hallows (020) 7383 6321
Chief sub-editor: Chris Patterson
Senior staff writer: Peter Blackburn (020) 7874 7398
Staff writers: Tim Tonkin (020) 7383 6753 and Ben Ireland (020) 7383 6066
Scotland correspondent: Jennifer Trueland
Feature writer: Seren Boyd
Senior production editor: Lisa Bott-Hansson
Design: BMA creative services
Cover photograph: Andrew Bainbridge
Read more from The Doctor online at thedoctor.bma.org.uk
Come Here told some incredibly powerful stories over the course of many months.
Over recent years we have regularly shone a spotlight on the parlous state of mental health services – culminating in our recent, ongoing, campaign called Paucity of Esteem for which our writers Ben Ireland and Peter Blackburn won a British Journalism Award last year. In that campaign they uncovered the state of mental health services, the scandal of patients being sent further than ever to out-of-area placements and a rapid rise in detentions under the Mental Health Act –highlighting a system so broken it simply ‘stores’ people up until they are in absolute crisis.
For another piece in the series Ben Ireland spent a week in Bristol covering the inquest into the death of young artist Evie Wilson, whose GP father and mother, who has worked in healthcare roles, spoke poignantly about how she was passed from pillar to post in a mental health system which was not listening to her concerns. Evie’s experiences came across in her own artwork, through which she explained how she was told she was ‘too sick’ for some services yet ‘not sick enough’ for others, treatment which only added to her feelings of being left behind and ‘othered’. The evidence heard in the inquest pointed to some of the findings of a BMA report which concluded the mental healthcare system in England is ‘broken’ and ‘dysfunctional’.
The magazine has also been recognised by national awards schemes for investigative pieces looking at poverty and health, homelessness, and, recently, an indepth exposé of failings at the mental health trust which treated Nottingham attacks perpetrator Valdo Calocane.
These are just a few examples from an enormous catalogue of campaigning and investigative journalism which has sought to place doctors at its very heart. I am beyond proud of the work the team is doing and delighted the BMA will continue to invest in this highquality journalism.
I would like to extend my thanks, on behalf of the association and our members, to Neil Hallows – who has been a peerless editor of this magazine from its inception – and the rest of the team for their brilliant, tireless, work.
I look forward to the many more stories the team will bring to our membership in their new home online. Please do make those few clicks and join us online. The success of The Doctor magazine has always been its dialogue with our members, its readers – you.
As ever, I am always happy to hear from you and any questions you might have. To get in touch please write to me at RBChair@bma.org.uk or @DrLatifaPatel
Dr Latifa Patel is chair of the BMA representative body
Tired eyes as the evenings draw in?
If you wear glasses or are increasingly frustrated by blurred vision, better light will transform your view. Your optician will con rm. This is because everything you see is light. Better light gives your eyes more of a ghting chance. It is why we have spent nearly 40 years building the best lights we possibly can. Others cut corners. Fall back in love with detail.
A Serious Light has one job; to help you see detail and colour as clearly as you possibly can when you need it the most. We use specialist technology to mimic the natural light spectrum, bringing out the ner details in everything you see. Building every light takes 224 speci cally designed individual components. Manufacturing the hi-tech parts employs 24 di erent machines in 5 di erent countries. Each light build involves 85 assembly engineers and technicians working in 82 di erent workstations. This is no ordinary light.
● Up to TWELVE TIMES more light on your page than a traditional 60W bulb
● Recommended by over 500 opticians
● Available as a Floor or Table Light
wheel Allows you to precisely adjust the light output.
Dimmer
Timber windows
Naturally beautiful, our award-winning timber windows and doors are the logical choice. Constructed from engineered timber slow grown in cold climates, their strength, stability and beauty are guaranteed.
Whether your home is a country cottage, a Victorian semi, a modern townhouse or a converted barn, we have a range of traditional and contemporary timber windows and doors that will complement it perfectly.
Our collection has been carefully and sensitively tailored to complement the English home. Unlike timber windows of old, our products will not twist, will not rot and require very little maintenance. High levels of insulation and security ensure there is no need to sacrifice beauty for comfort.
With a15% discount off all windows & doors in our Winter Sale, explore the range in 50 showrooms nationwide. T: 0800 030 2000 timberwindows.com/dr