page 14


page 14







































NSW Nurses and Midwives’ Association
For all membership enquiries and assistance, including The Lamp subscriptions and change of address, contact our Sydney office.
Sydney Office
50 O’Dea Avenue, Waterloo NSW 2017 (all correspondence)
T 8595 1234 (metro) 1300 367 962 (non-metro)
F 9662 1414 E gensec@nswnma.asn.au
W www.nswnma.asn.au
Hunter Office
8–14 Telford Street, Newcastle East NSW 2300
NSWNMA Communications Manager
Danielle Blasutto
T 02 8595 1234 (metro) T 1300 367 962 (regional)
For all editorial enquiries, letters and diary dates
T 8595 1234 E lamp@nswnma.asn.au
50 O’Dea Avenue, Waterloo NSW 2017
Produced by
Hester Communications T 0414 550 376
Press Releases
Send your press releases to: F 9662 1414 E gensec@nswnma.asn.au
Editorial Committee
Shaye Candish, NSWNMA General Secretary
Michael Whaites, NSWNMA Assistant General Secretary O’Bray Smith, NSWNMA President
Michelle Cashman, Long Jetty Continuing Care
Richard Noort, Justice Health
Michelle Cutler, Tweed Hospital
Diane Lang, South East Regional Hospital, Bega Valley
Karen Hart, Wagga Wagga Base Hospital
Printed by
Printed by IVE Group Sydney
Advertising
Danielle Nicholson T 8595 2139 or 0429 269 750 F 9662 1414 E dnicholson@nswnma.asn.au
Information & Records Management Centre
To find archived articles from The Lamp, or to borrow from the NSWNMA nursing and health collection, contact: Adrian Hayward, Coordinator. T 8595 2175 E gensec@nswnma.asn.au
The Lamp ISSN: 0047-3936
General Disclaimer
The Lamp is the official magazine of the NSWNMA. Views expressed in articles are contributors’ own and not necessarily those of the NSWNMA. Statements of fact are believed to be true, but no legal responsibility is accepted for them. All material appearing in The Lamp is covered by copyright and may not be reproduced without prior written permission. The NSWNMA takes no responsibility for the advertising appearing herein and it does not necessarily endorse any products advertised.
Authorised by S. Candish, General Secretary, NSW Nurses and Midwives’ Association, 50 O’Dea Avenue Waterloo NSW 2017
Privacy Statement
The NSWNMA collects personal information from members in order to perform our role of representing their industrial and professional interests. We place great emphasis on maintaining and enhancing the privacy and security of your personal information. Personal information is protected under law and can only be released to someone else where the law requires or where you give permission. If you have concerns about your personal information, please contact the NSWNMA office. If you are still not satisfied that your privacy is being maintained, you can contact the Privacy Commission.
Subscriptions for 2024
Free to all Association members. Professional members can subscribe to the magazine at a reduced rate of $30. Individuals $84, Institutions $140, Overseas $150


14
PRIVATE HOSPITALS
Healthscope forces nurses into industrial action
Healthscope is owned by a hugely profitable corporate giant but its NSW nurses and midwives must fight to get the same pay as the company’s Queensland nursing staff.
16
PRIVATE HOSPITALS
Strike highlights Northern Beaches staffing gap
Industrial action throws spotlight on understaffing of public healthcare services under private ownership.
18 PACIFIC HEALTH
Fiji is losing its nurses
Tough working conditions and the lure of better-paid jobs abroad have shrunk Fiji’s nursing workforce.
20 FIRST NATIONS HEALTH
An innovative solution improves child referral
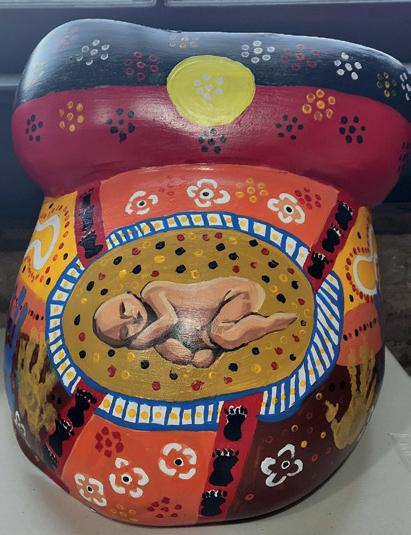
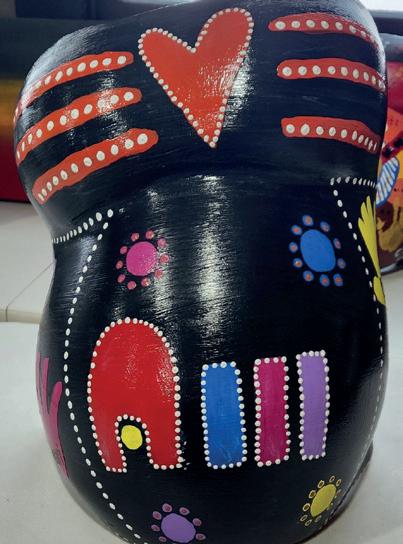
A program offering First Nations women in two regional NSW communities a plaster cast of their bellies towards the end of their pregnancies has transformed health outcomes for children and mothers who take part.
22 AFFORDABLE HOUSING
Living on the edge
Nurses and other essential workers face an affordable housing crisis that governments are only now beginning to respond to.


GENERAL SECRETARY
Good on the police for their historic pay outcome but what does it say about this NSW government when it tells nurses and midwives they should be grateful for what they are offered.
Hypocrisy is on full show when we compare the recent decision by the Minns Government to grant police officers (72 per cent male workforce) pay increases of up to 39 per cent while offering nurses and midwives (86.7 per cent female workforce) a fraction of that amount.
Teachers, paramedics and now police have all received historic pay increases, while the state’s largest femaledominated workforce is, once again, left behind and forgotten.
We can’t make the trade-offs or find the savings to fund our pay rise like other unions have. They simply aren’t there. The health budget is already stretched beyond its limits. We need more money to be put into health.
The government is in denial about the state of the NSW public health system.
Recent wage agreements with other unions will further exacerbate the gender pay gap in NSW which has now risen three years in a row to 6.2 per cent, the highest in the last decade, and in contradiction to the government’s professed objectives.
This blatant undervaluing of our professions is not only profoundly unjust, it is also driving a dangerous staffing crisis that jeopardises the safety and quality of healthcare across New South Wales.
The government is in denial about the state of the NSW public health system (PHS). This denial of reality leads to a wilful neglect which is running our public health system into the ground. Drastic measures need to be made to stop the loss of nurses and midwives out of the PHS. The recruitment and retention needed to fulfil the government’s own objectives of
introducing ratios cannot be funded by savings. The government needs to find more money for health.
Rather than address workloads and burnout in our hospitals through improved working conditions, we have officials from the Ministry of Health denigrating ratios, telling the Special Commission of Healthcare Funding that the system is locked into “ratios of high cost, high scope practitioners and rigid turf wars”.
What we need is new money to put into the health budget. This is why we commissioned the Deloitte report, which pointed to extra money that could be claimed from federal funding and initiatives that improved patient care and generated cost efficiencies. These initiatives were intended to generate real dollars to support a pay rise for nurses and midwives, yet the NSW Government rejected it.
Both the Queensland and Victoria Labor governments found the money to fund ratios and a significant pay rise for nurses and midwives. NSW can do the same.
Recent independent reports reinforce our analysis of the dire state of the public health system.
The national workforce report on midwifery warned of the increasing numbers of midwives looking to exit the sector due to work-related issues including burnout, understaffing, not feeling valued and poor skill mix.
The report makes it clear that to secure the required workforce, we need to encourage midwives to work more hours than they currently do. They won’t do that unless we fix the structural issues of pay, workloads and support.
The federal government inquiry into the response to COVID-19 also highlighted the large backlogs in elective surgery from the pandemic period which inflates demand coupled
with the workforce shortages from burnout that have impeded any semblance of “recovery to business as usual”.
Other actors see clearly that what we are arguing is transparently true.
The Sydney Morning Herald recognised that nurses and midwives “bravely pushed for better nurse-to-patient ratios as their number one priority to ensure improved service delivery and stop the flight interstate caused by high levels of exhaustion and lower wages”.
The SMH slammed Premier Minns who had “chosen to conflate their demands for better ratios and more money and said they could not have both. But they are separate issues. The government sees the sense of rewarding police to attract recruits and retain experience but is blind to the same plight facing nurses and midwives, instead penalising them for wanting better care for patients”.
The figures are increasingly dire. Eight in 10 nurses and midwives in NSW are considering moving interstate in the next five years, according to the 2024 Unions NSW survey.
This is hardly surprising. In other states like Victoria and Queensland wages are 18 per cent higher and conditions are better.
The actual number of nurses and midwives in the state dropped by 412 with even more moving interstate, in the year to 30 June. This simply cannot continue.
The government keeps banging on about delivering ratios, but it cannot and will not fulfil its ratio commitment without delivering competitive and attractive rates of pay to recruit the nurses and midwives needed to fulfil safe staffing levels.n
Imagine bringing new life into the world under conditions that make you feel like you're failing before you've even begun.
As an early-career midwife in a critically understaffed rural maternity unit, I often find myself in-charge as well, despite having only a few years of experience.
Most of my colleagues are junior also, and without senior midwives around for guidance, I’m constantly navigating situations I’ve never faced before, alone. While we are trying to operate with a more than 60 per cent staffing deficit, we also have to accept transfers from other outlying hospitals who are on bypass due to poor staffing, sometimes even when we are on bypass ourselves!
Having to transfer women to other hospitals for care, purely due to a lack of midwifery staff, is heartbreaking and is contributing to a breakdown in trust between the local community and the healthcare system.
Most days I come home from work feeling broken, unable to give women and babies the care they deserve and exhausted from doing unplanned overtime.
Attracting and retaining midwives in regional NSW is an uphill battle. Many nurses come to places like Tamworth to complete their midwifery training but leave when it's done, disheartened by low pay, lack of staffing ratios, and upper management’s expectation of mandatory overtime to keep the unit safely staffed. And why wouldn’t they leave? Midwives across the border in
Queensland earn significantly more, have safer staffing ratios, and access to real incentives for rural work. Directentry midwives suffer too, with many walking away from the profession altogether. After three years of university, enduring 24/7 on-call requirements, and leaving with a huge HECS debt, they step into a field that is poorly staffed, underpaid and undervalued.
Of the 110 people I started university with, only 30 graduated, and many of them aren’t even midwives anymore. Most who remain have moved to Queensland, where the pay, conditions, and support are better. NSW’s midwifery profession is in crisis – this is not just a call for change, but a cry for help. As we lose more midwives to other states, agency work, or burnout, it’s clear the current conditions make this career unsustainable. If I’d known how dire things would be, I would have chosen differently. A 15 per cent pay rise, safe staffing ratios, and proper incentives are not luxuries – they’re necessities. Without them, we’re at risk of losing even more dedicated midwives and leaving rural communities like ours without the care they deserve. The NSW government says they can’t afford to give nurses and midwives a 15 per cent pay rise, but the real question is, can they afford not to?
Zoe Sattler, Midwife
Editor’s note: Zoe’s experiences are consistent with a recently released report: Midwifery Futures: The Australian Midwifery Workforce Project. To read more visit: https:// www.nursingmidwiferyboard.gov.au/ News/Midwifery-Futures.aspx
Advertise in The Lamp and reach more than 75,000 nurses and midwives.
To advertise contact Danielle Nicholson 02 8595 2139 / 0429 269 750 dnicholson@nswnma.asn.au
NSW Health’s Clinical Resource Unit (CRU) and agency staff working in rural and remote hospitals provide an essential service. NSW Health employs CRU and agency staff as casuals under the public health system award, and as such, they are not entitled to overtime.
As these rural and remote sites are critically short of nurses and midwives, CRU and agency staff are regularly asked to work in excess of 76 hours a fortnight, yet NSW Health is unable to pay overtime. This anomaly needs to be corrected.
Interstate jurisdictions employ agency staff on contracts and classify those as full time and pay overtime. The employment as casuals in NSW public hospitals needs to change to ensure CRU and agency staff are paid appropriately, and rural and remote sites are staffed accordingly.
Michael Clarke, RN
When I went into nursing 30 something years ago, I never expected to become wealthy, what I did expect was that I would be able to support my family.
With the closure of two public hospitals, we were promised a private operator that would provide all the bells and whistles and “state of the art equipment” our public system couldn’t afford. But the working conditions and pay at Northern Beaches Hospital are far from a dream situation.
As a member representative in negotiations with Healthscope, I was naïve to what these processes were like. I was shocked by how quickly my passion for my profession, turned into a fight for us to be valued for the work we do.
I was emboldened for us to be seen as more than a commodity attached to some corporate, profit driven business plan.
Negotiations have been fierce: Our heartfelt stories of being stretched
beyond what is humanly possible, of leaving work in tears because we had to sacrifice the quality of care we provide to our patients, has fallen on deaf ears. I’m part of an extraordinary team of member negotiators, from Healthscope hospitals across the state. We have been supported by amazing NSWNMA organisers and staff, but we are now at an impasse. We know what we’re worth. Our local community knows our value. When we took historic industrial action, they didn’t know what hit them, they weren’t ready for us. They underestimated the strength we have collectively.
We have been pushed to the point of taking industrial action and will continue our fight. We have just started. A couple of Healthscope strikes in, and the feeling of unity has ignited our members to fight back.
I am extremely proud to be a voice for my colleagues in this fight.
Sheridan Brady, RN
Premier, you’re not picking between rent and food each week I bet. That must be nice.
My name is Emma, and I am a third-year registered nurse, and I like many of my colleagues I am struggling to make ends meet. This is why I need a real pay rise. Before the pandemic, a salary of $70,000 was considered reasonable and comfortable for a single person. Today, it is not.
As a nurse earning $70,000, I have a take-home pay of approximately $2,100 per fortnight after tax and salary packaging. However, after accounting for basic living expenses, I cannot afford to live in NSW.
The average rent in Sydney is $627 per week, or $1,254 per fortnight. This leaves me with just $846 to cover all other expenses. My commute to work, including parking, costs me an additional $180 per fortnight, reducing my available funds to $666. The average cost of groceries for a single person is $193 per week, or $386 per fortnight. This leaves me with just $140 per week to pay for expenses like car registration, utilities, medical expenses, internet.
If there’s something on your mind, send us a letter and have your say. You could
You do the maths Premier Minns and Treasurer Moohkey - $140 a week doesn’t cover this. So, I’m left each week with less than nothing. Recently, Chris Minns said the government would not entertain our request for a wage increase, because we had “chosen” safe ratios over a pay rise. The reality is that we are being asked to choose between our own survival and the survival of our patients. We are not being paid enough to make ends meet, and we are not being given the resources necessary to provide safe care.I love my job so much. I worked so hard for years to get here. I am deeply committed to my patients and the nursing profession. However,
I am now faced with a harsh reality: I cannot afford to continue working in a system that undervalues my contributions. If I am forced to leave the workforce, it will not be because of my dedication to patient care, but because the government has failed to adequately support the healthcare system and the people who work within it.
So, pay us more. We deserve it. Of course, we deserve it. It’s a human right to be able to live. We clearly have the money. The average politician makes $211,250. You’re not picking between rent and food each week I bet. That must be nice.
Emma, RN

A lively crowd assembled in Sydney’s Hyde Park and marched to Parliament House in support of the NSWNMA’s 15 per cent pay claim on 13 November.
The rally coincided with a second 24-hour statewide strike by 10,671 nurses and midwives.
Outside Sydney, rallies were held in Armidale, Broken Hill, Coffs Harbour, Crookwell, Lismore, Moruya, Port Macquarie, Taree and Tweed.
The strike followed eight months of talks with the government including four weeks of intensive negotiations.
Premier Chris Minns told the Sydney Morning Herald the government could not afford to fund safe nurse-to-patient ratios and a pay rise above 10.5 per cent over three years.
However, on the eve of the nurses’ strike the government granted police a massive wage increase of up to 39 per cent over four years, with the stated aim of attracting recruits and retaining experienced officers.

NSWNMA General Secretary, Shaye Candish, slammed the Minns government’s decision to grant police officers, a 72 per cent male workforce, pay rises of up to 39 per cent while offering nurses and midwives, who are 86.7 per cent women, only a quarter of that amount.
The decision “highlights a stark and troubling disparity” Shaye told the nurses’ Sydney rally.
“Good on the police for getting their historic outcome, but it is clear there is one reality here for maledominated workforces and another for female- dominated workforces.
“The white-hot rage of the biggest female dominated workforce in this state is bearing down on this government right now.
“The government is making the gender gap worse not better.
“This government, and every government before it is taking the gender wage gap to the bank – every budget surplus and every minimised
deficit has been built on the fact that women in this state have taken lower wages to make that happen.
“Government after government has traded on the goodwill of nurses and midwives to sacrifice their pay for the care of their patients, and we aren't going to stand for it anymore.”
Shaye said the gender pay gap in the NSW public sector had risen three years in a row to 6.2 per cent – the highest gender pay gap in the last decade.
“This is directly attributable to the wages of nurses and midwives stagnating while male dominated workforces continue to receive pay rises around us.” n
“This government, and every government before it is taking the gender wage gap to the bank.”
— Shaye Candish
‘We won’t pay for better staffing out of our own pockets’

The state government expects that nurses and midwives will remain low paid in order to staff the hospitals via ratios, said NSWNMA Assistant General Secretary Michael Whaites.
“It is abhorrent to argue that nurses and midwives in NSW should pay for better staffing out of their own pockets. That’s what the Liberals used to say,” Michael told the Sydney rally.
He said that before the 2023 state election the union prioritised safer patient care through mandatory minimum staffing.
“We didn't ask for higher than average wage rises because the cost-of-living crisis hadn't hit at that time.”
He said that not even the Reserve Bank had seen the cost-of-living crisis coming.
“In NSW we have the highest cost of living – upward of 12 per cent higher than nearby states.
“We have the highest housing prices in the country – 1.5 times nearby states.
“Meanwhile, NSW has the lowest wages for AiNs and ENs of any state.
“And once you add in the (recently granted) 3 per cent (interim) wage rise the only state lower than NSW for most RN classifications is South Australia.” n
“It is abhorrent to argue that nurses and midwives in NSW should pay for better staffing out of their own pockets.”
— Michael Whaites

‘I won’t work for less than my interstate colleagues’
Three years ago, NSWNMA member and theatre RN Nanette Nowakowski from Kempsey Hospital returned to NSW after working in Queensland hospitals – public and private, city and rural – for eight years.
Speaking at the Sydney rally, she sharply contrasted working conditions in the two states.
“Everywhere I worked (in Queensland) the staff were working to ACORN standards and I was surrounded by medical and nursing professionals who valued the standards that should guide our practice,” she said.
“We always had the required staff, and staff were never expected to push beyond a reasonable workload.
“It’s not that every day was a perfect day but I definitely felt valued by every hospital I worked in. I was never made to feel bad if I couldn't work an extra hour or extra shift.

“In Queensland… nurses are valued with education, supervision and guidance. Nurse educators educate 100 per cent of the time. Nurses are encouraged to know the standards and implement them in their practice.
“When I got to NSW, I was shocked by the pay difference and by the expectation that I will do overtime and sometimes be expected to not claim it.”

She said the NSW government “has money for other essential services but not enough money to properly resource the healthcare system and definitely no money for nurses.”
“It’s time for us to say I'm not afraid anymore, I deserve to earn the same amount as my interstate colleagues and I won't work for less.” n
Regional, rural and remote area midwives face “staff deficits, outdated facilities and equipment, outdated ratios and outdated pay”, Tamworth midwife and NSWNMA member Nami Munikwa told the Sydney rally. She said midwives just four hours away in Queensland are earning 18 per cent more than her and her NSW colleagues.
“We're working for a government that encourages our colleagues to move to interstate, retire early or change profession,” she said. n

he NSW Labor government is out of step with Labor governments in Queensland, Victoria and federally that have acted to support majorityfemale workforces in public sector nursing, aged care and childcare, said NSWNMA President O’Bray Smith.
“This (NSW Labor) government got elected on the platform of supporting essential workers. What they meant were just the male dominated workforce,” O’Bray, a midwifery manager told the Sydney rally. She contrasted the Minns government’s hardline stance against NSW nurses with federal
Labor’s support for nurses and other workers in aged care.
“They have also supported early childhood educators in another female dominated industry to get an historic pay rise, recognising gender inequity,” she said.
“Victorian Labor has recognised the undervaluing of nurses and midwives by giving them a once in a generation pay rise.
“The Queensland Labor government implemented proper gender assessment tools that resulted in night shift penalties, overtime rates and pay rates that recognise the gender pay gap and fixed it.” n
‘Disrespect will only make us fight harder’
The state Labor government has widened the gender pay gap for nurses and midwives, NSWNMA member Belinda Renshaw, Macarthur Branch, told the Sydney rally.
“I stand here today as a single mother and registered nurse and midwife of 21 years,” she said.
“To make ends meet I work full time 12-hour night shifts, one or two overtime shifts a fortnight and babysit two days a week – all of it possible with the help of my retired mother.
“I tell my daughter every day that she is amazing and can be whatever she wants to be when she grows up, but the reality is that's not true, is it?
“The state government proves it by perpetuating the gender gap and making it harder for women to reach their full potential.
“Why will you not pay us what we are worth? Your counterparts across the border are doing the right thing.
“Your disrespect will only make us fight harder.” n


A key finding of the Commonwealth Government inquiry into the COVID-19 response is that pandemic preparation requires a robust and resilient health system.
Almost five years after the COVID-19 pandemic broke out “there is much to learn from our collective experiences”, the inquiry found.
While emphasising that “there was much to be proud of as a nation” from the country’s response to the crisis, the inquiry acknowledged it took its toll on the health system and its workforce and there was some loss of community trust in public health orders.
“We heard from many individuals across government and in the community about the toll the pandemic response had taken,” it said.
“People worked beyond normal limits, and many of the public health professionals, frontline community service and health staff, political leaders, health experts and public servants we relied on to get through the pandemic are no longer in their positions.
“This poses risks to our resilience to face another crisis. Trust has also been eroded, and many of the measures taken during COVID -19 are unlikely to be accepted by the population again. That means there is a job to be done to rebuild trust.”
These consequences of COVID-19 continue and are still impeding the delivery of patient care today, the report said.
“Workforce shortages across the system, burnout, ongoing sickness and the furloughing of staff have impeded health services in their recovery to business as usual, let alone enabling them to find the additional capacity needed to address substantial backlogs.

‘The stronger the existing health systems are the greater the resilience Australia will have in a future pandemic.’
“These system - wide issues are having an ongoing impact on Australians in need of health care.”
The report points out that almost five years after the pandemic began, large backlogs in elective surgery remain due to its suspension during the pandemic.
The focus on controlling the spread of COVID -19 meant broader health issues were often given a lower priority. These issues included increased poor mental health due to the negative impacts of social isolation and increased anxiety, and reduced access to usual health care, such as cancer and other disease screening, non- emergency surgery and chronic disease management. A key lesson to be learnt from the crisis is “the stronger the existing health systems are the greater the resilience Australia will have in a future pandemic” the report emphasised.
The lack of preparedness for the pandemic was most clearly seen in aged care, the report says.
Inadequate staffing and precarious employment among aged care staff exacerbated the sector’s existing vulnerabilities.
A lack of staff and agency and surge workforce was repeatedly mentioned as the most significant challenge faced by aged care workers when dealing with COVID -19 and was a fundamental contributor to the degree of crisis faced by the sector.
Notwithstanding the early success in containing the spread of the virus, the majority of the approximately 900 COVID -19 associated deaths in 2020 were among older Australians. While outbreaks impacted only a small number of residential aged care facilities, they accounted for 75 per cent of all COVID -19 deaths.
Pre - existing vulnerability in the aged care system, including insecure employment arrangements and workers operating across multiple facilities; a lack of planning and preparation; cases of weak leadership at the provider level; inadequate infection prevention and control; and a lack of mechanisms to share learnings and experiences were all contributing factors.
The panel that conducted the inquiry warned that another global health crisis will happen, even if it is hard to predict when.
“Human history tells us that it will occur, and it will once again test us in ways that are hard to imagine. Acting today will ensure in the future we are better prepared, benefiting from our learnings of what worked well and what didn’t during the COVID -19 pandemic,” the panel said in its conclusion.
The inquiry said it consistently heard in submissions that throughout the pandemic, ‘the plane was being built while it was flying’, and this meant there was little ability to think ahead and anticipate the next challenges as the crisis unfolded.
The lesson for the future is that, in a pandemic, the unimaginable can quickly become necessary and planning should cover the full suite of possible responses.
“Preparedness involves building the strength and resilience of systems to efficiently respond to and manage an emergency. Specific actions governments can take include strengthening the healthcare system.
“The capacity of systems to respond to a pandemic is an important part of preparedness and cannot be built at sufficient speed during a crisis. Australian governments need to ensure their collective resources, capabilities, services and workforce are ready ahead of time.”
‘Throughout the pandemic the plane was being built while it was flying.’
The inquiry report made special mention of the “continuing failure of the healthcare system to utilise nurses and midwives to their full scope of practice”.
“(It) is limiting consumer access to evidence -based, cost- efficient nurse and midwife -led models of care.”
It recommended as an immediate action: nationally consistent reforms to allow health professionals to work to their full training and experience. n

Healthscope is owned by a hugely profitable corporate giant but its NSW nurses and midwives must fight to get the same pay as the company’s Queensland nursing staff.
Nurses and midwives working for Healthscope in NSW have stopped work and held rallies in support of improved pay and conditions and safer staffing.
During November NSWNMA members staged strikes at several of the company’s hospitals, including Northern Beaches, Norwest Private, Nepean Private and Campbelltown Private, Sydney Southwest Private, Hunter Valley Private Hospital and Newcastle Private Hospital.
NSWNMA Healthscope members voted in a secret ballot to approve industrial action.
More than 77 per cent of members voted in the ballot, and over 95 per cent of those who participated voted ‘Yes’.
Healthscope is Australia’s second biggest private hospital operator with 38 hospitals in all states and territories including 12 in NSW. However, its NSW nursing and midwifery staff are paid less than their Queensland colleagues and experience heavy workloads while the company refuses to even discuss
‘How does Healthscope think it is acceptable to pay its NSW nurses and midwives up to 16 per cent less than their colleagues in Queensland?’
— Shaye Candish


MEMBERS FROM NORWEST PRIVATE HOSPITAL (TOP) AND NORTHERN BEACHES HOSPITAL (BOTTOM)
nurse to patient ratios such as those in the public health system.
“It is clear that our members are tired and fed up with the pay and conditions at Healthscope,” said NSWNMA General Secretary Shaye Candish.
“How does Healthscope think it is acceptable to pay its NSW nurses and midwives up to 16 per cent less than their colleagues in Queenslandbased Healthscope hospitals for the same work?”
She said Healthscope could afford to fund a decent pay rise and increases to staffing levels.
The company is owned by Brookfield, a global asset management company that distributed US$2.2 billion (A$3.4 billion) to shareholders in the 12 months to August 2024.
“Our members have been negotiating with Healthscope for almost six months now with little progress on our pay and conditions claim,” Shaye said in November.
“Members feel they have no choice but to take industrial action, after being undervalued and receiving inadequate recognition for their incredible contribution to patients and workplaces.”
Since May, the NSWNMA has held 15 bargaining meetings with Healthscope to negotiate a new enterprise agreement, but the company has refused to budge on the union’s main claims.
They include mandated nurse/ midwife-to-patient ratios and a 15 per cent one-year pay increase from 1 July 2024, with ongoing increases over the life of the agreement to maintain pay rates above those in the public health system.
Healthscope’s pay offer was 13 per cent over three years when this edition of The Lamp went to press. n
Bella Vista,
led the hospital’s first-ever nurses’ strike in November.

SARAH KNEEVES, NORWEST PRIVATE BRANCH SECRETARY
‘Now that we have a branch, there is a lot more discussion about the issues and far greater support for the industrial action we are taking.’ — Sarah Keevers
About 200 nurses and midwives from Norwest Private and another Healthscope hospital, Nepean Private, held a roadside rally to alert the community to their claims for safer staffing and improved conditions.
“We got a great reception from the public, with all the passing cars and trucks beeping their horns in support,” said the Association’s Norwest Private branch secretary Sarah Keevers, who is a theatre nurse.
“It was reassuring to see so many nurses and midwives walk out the door and gather on the side of Old Windsor Road with their placards.
“There was a real sense of camaraderie between nurses and midwives from the various departments getting together to fight for the same things.”
The NSWNMA’s push for an improved Healthscope enterprise agreement (EA) led to the formation of Norwest Private’s first Association branch in March.
Sarah said the branch resulted in members being better informed about, and more involved in, the EA campaign.
“If we didn’t have a branch, no one would know what was going on, which is what members said about previous EBAs.
“Now that we have a branch, there is a lot more discussion about the issues and far greater support for the industrial action we are taking.”
Formation of the branch has led to the appointment of Association representatives or stewards on most wards. They serve as a point of contact between branch officials (secretary, president, assistant secretary and vice-president) and members in each ward or unit.
Sarah is one of eight rank and file members on the NSWNMA bargaining team that has held 15 meetings with Healthscope management (at time of writing).
She said members were struck by the poor attitude and lack of manners shown by some management reps during meetings.
“While our reps were talking about our personal experiences on the wards and the importance of ratios, management were doing other work on their computers and answering their phones,” she said.
“To have management reps completely ignoring the proceedings while a midwife is breaking down in tears telling her story is utterly disrespectful.”
Sarah said Healthscope management conduct improved when Fair Work Commissioner Alana Matheson began attending meetings as a mediator. n
Industrial action throws spotlight on understaffing of public healthcare services under private ownership.
All patients in New South Wales deserve the same standard of care regardless of who owns the treating hospital.
During November NSWNMA members staged strikes at several of Healthscope’s hospitals, including Northern Beaches, Norwest Private, Nepean Private and Campbelltown Private, Sydney Southwest Private, Hunter Valley Private Hospital and Newcastle Private Hospital.
ICU nurse Sheridan Brady, president of the NSWNMA branch at Northern Beaches, said the rally was a “brilliant response” to the union’s call for strike action in support of a new enterprise agreement.
“All patients, public or private, whether they can afford private health insurance or not, and regardless of who owns the treating hospital, deserve the same standard of care,” Sheridan said.
Northern Beaches is the only privately owned hospital in NSW that offers public health services.
This came about through a privatisation scheme implemented by the former NSW Coalition government to replace Manly and Mona Vale public hospitals with the new Healthscope facility.
Public hospital nurse-to-patient ratios do not apply to Northern Beaches nurses even though they treat public patients.
“Our patients deserve the same level of nursing care that they would receive from the other two major hospitals in our LHD – Royal North Shore and Hornsby,” Sheridan said.

‘Healthscope is a for-profit organisation. As nurses and midwives, we struggle to justify that good patient care should be balanced against profit for shareholders.’
— Sheridan Brady
She said the annual leave dispute “has come down to the interpretation of a single clause in our EBA”.
“Healthscope is trying to restrict access to additional annual leave for 7 day shift workers.
“Also, we are entitled to less maternity leave (10 weeks) than the public sector (up to 16 weeks).
“We have no separate entitlement to family and carer leave; this instead comes out of our sick leave balance.
“It is not hard to see why we are losing staff to the public sector, including Royal North Shore which is 20 minutes away.
“However, we are excluded from the safe staffing ratios being rolled out in the public health system.
“We get less take-home pay with no access to salary packaging and our annual leave is in dispute before the Fair Work Commission.”
“Healthscope is a for-profit organisation. As nurses and midwives, we struggle to justify that good patient care should be balanced against profit for shareholders.
“We have a big public emergency department where members have openly disclosed that it is not

uncommon for a single RN to be responsible for caring for 20 to 30 patients and beyond.
“This is simply not safe and is unsustainable.”
Sheridan said, “unmanageable workloads, unsafe ratios and a junior-heavy skill mix on wards are commonplace and are taking a toll.”
“ACORN and ACCCN standards should not be guidelines or a suggestion. They should be mandatory.”
She pointed out that government departments issue licences to private hospitals “with no mandated rules around how to staff these facilities”.
Sheridan said local state and federal politicians attended the NSWNMA rally and “they are in strong support of us as a profession and for the members of our community that we provide care for.”
She said support for industrial action was growing among younger nurses.
“I thought younger members may be a little more timid but they’ve got a fair bit of fire in their bellies.
“Junior nurses and midwives have become increasingly aware that their conditions are vastly below that of their peers in the public health sector. They know they deserve better.
“As an RN with 30 years of experience, I frequently hear of nurses and midwives of my vintage leaving Northern Beaches Hospital, the state or the entire profession.
“We need to have some means to retain all that experience, to entice us old girls to stay and pass that knowledge onto the next generation of nurses and midwives.
“It has become a very hard sell when you don’t have to look far to find a better deal.
“We are not bargaining for an agreement better than the public sector. We just want parity.” n
Healthscope is owned by Brookfield, a giant Canadian company which owns $1.5 trillion in assets worldwide.
These include private equity investments (meaning businesses that are not publicly traded on stock markets) such as Healthscope.
Brookfield borrowed $1.6 billion to buy Healthscope for $4.1 billion in 2019. Brookfield also sold many hospital properties and then leased them back with new owners.
“Brookfield has been asking insurers, its landlords, lenders and the even government for help,” the Australian Financial Review reported in September.
In a report titled “Is private equity unhealthy for our hospitals?” the AFR’s health editor, Michael Smith, wrote, “There is little sympathy for private equity, which has a reputation for saddling targets up
with debt, slashing costs and jobs, and selling out at a big profit.”
“Brookfield’s leverage is the threat of unprofitable hospital closures, putting more pressure on the country’s public healthcare system,” he added.
“This has not gone down well in Canberra, where Health Minister Mark Butler is trying to come up with ways to help private hospitals without a government injection.
“There is little to no appetite to bail out a private equity firm, but the government also needs to avoid mass hospital closures, particularly in the bush.”
Labor MP Mike Freelander, who chairs a parliamentary committee on health policy, told the AFR, “My view, and I’m pretty sure the government’s view as well, is that investment in the health system should be long term and should not be one of asset stripping and walking away.”n

‘Brookfield’s leverage is the threat of unprofitable hospital closures, putting more pressure on the country’s public healthcare system.’— Australian Financial Review
Tough working conditions and the lure of better-paid jobs abroad have shrunk Fiji’s nursing workforce.
Fiji’s nurses go to extraordinary lengths to care for remote communities across 100 inhabited islands.
Filomena Talawadua, general secretary of the Fiji Nursing Association (FNA), provided a snapshot of the challenges her members face when she addressed NSWNMA annual conference.
She said 98 of Fiji’s 223 government health facilities are in very remote locations.
Via a series of slides, Filomena showed her members walking along rough tracks, riding horses and wading and rafting across rivers in order to reach their patients.
“Even if you're not familiar with [horses] you have to find a way to be able to get on that horse. I've been there, I’ve done it and I tell you it's an experience you wouldn’t want to talk about,” she said.
Showing a photo of a nurse wading a river, Filomena said, “To reach one of his villages he has to cross that same river 28 times with the depth of the river varying from ankle height to up to his neck.”
Another picture showed a nurse’s husband carrying a baby in a sling carrier and a box of medical supplies while accompanying his wife on her rounds.
A third photo showed two nurses ferrying vaccines across a river on a bamboo raft.

‘We have allowed our systems to bully us and to undervalue us.’
984 nursing positions are currently vacant, Filomena said.
The country’s sole psychiatric hospital, St Giles, has only 53 nurses instead of the required 178, she added.
“Right now, we have a skill drain. We have even had lecturers who have left Fiji to come to Australia to work as caregivers.
“We now have a population of nurses who are very young because most of our senior nurses and middle managers have left.
“If the system undervalues them, we cannot blame them. If they are happy to be here, we are happy that they are here. But we would be happier if they could work [in Fiji] as RNs sometime soon.
“The exodus [of nurses] has completely depleted the system in so many ways.”
She said the skill drain had weakened child health services resulting in an increase in morbidity among children under five.
Fiji has to meet such challenges with a fast-diminishing nursing workforce.
Nurse numbers fell by 807 or 23 per cent between 2022 and 2023 after steep declines in previous years.
Ministry of Health figures show the number of nurses “actually on the ground now” is only 1826, indicating
The FNA is urging the government to declare a national nursing crisis.
“When [the government] declares something as reaching a stage of national crisis they have reserve funds for it and they need to pull out those funds and address the situation.

FILOMENA TALAWADUA, GENERAL SECRETARY OF THE FIJI NURSING ASSOCIATION
‘ We have even had lecturers who have left Fiji to come to Australia to work as caregivers.’
“However, they continue to say we are managing, so for us it's been hard. But we say, OK we'll see how long you will wait.
“That is what we've been doing since 2022. We feel that there needs to be policy intervention. We need to have workforce retention strategies that we are part of.
“But when it comes to top level government policymaking we are shunned as an organisation.”
Filomena said nurses sometimes forgot the importance of their role and “we have allowed our systems to bully us and to undervalue us”.
She said experienced nurses were educated and trained at Fiji’s expense “and then we lose them through the lucrative offers that other countries offer them”.
She said Australia and New Zealand were “top of the list” of receiving countries.
She called for collaboration between Fijian and Australian nursing unions to lobby governments to find ways of encouraging nurses to remain in Fiji.
On a positive note, Filomena said more than 80 per cent of public sector nurses had joined the FNA, which recently won pay increases ranging from 15 per cent to 41 per cent.
Nurses achieved the increases after voting for industrial action in a secret ballot in November 2023 and following a series of mediation sessions.
“There were times when I really just wanted to throw in the towel. But I'm a nurse – a community health nurse for that matter and a nurse educator for 15 years before I retired.
“I’ve been there when you're not appreciated, when you're undervalued, when they take you for granted.”
Eventually, the union achieved big wage increases thanks to “commitment, courage, teamwork, patience and perseverance” and she hoped these gains would attract nurses back to Fiji’s healthcare system. n
A program offering First Nations women in two regional NSW communities a plaster cast of their bellies towards the end of their pregnancies has transformed health outcomes for children and mothers who take part.

NICKI CALLAN (THIRD FROM RIGHT) AND MARY SMALL (FOURTH FROM LEFT) CELEBRATING THE FIRST YEAR ANNIVERSARY OF DOLLY PARTON IMAGINATION LIBRARY WITH MOTHER MARIE EHNERT (HOLDING BABY MCARTHUR) AND STAFF FROM WARREN SHIRE LIBRARY AND WARREN SHIRE COUNCIL.
When Child and Family Health Nurse Nicki Callan began working in the central NSW communities of Warren and Trangie, she found they had been without a child and family nurse for 12 months and 18 months respectively.
“A child family health nurse in a rural and remote community is often the first point of call for assessment and appropriate referral pathways,” says Nicki.
However, she noticed many families were not accessing services and many children were falling behind on immunisation schedules and other health measures.
To help build a positive relationship with new mothers, and create trust in health services, Nicki and her colleagues came up with the creative idea to offer mothers in their final weeks of pregnancy a session taking a plaster cast of their pregnant belly.
Working closely with Mary Small, an Aboriginal Health Worker, and Emma Howard, an outreach midwife, Nicki began meeting with mothers who took up the offer of a belly cast in their final trimester.
Making the belly cast takes around half an hour, explains Nicki, who would normally only see mothers and babies after birth. “It’s a really amazing positive tool where you can engage with the mother, who now feels more comfortable and supported to come back to you and use our services.”
The first group of women who took part in the program were led by Wayilwan elders in painting classes.
The mothers-to-be decorated their casts with stories that are meaningful to them. “While they painted their casts, they were discussing women's health and traditional women’s health knowledge and women’s business,” Nicki explains.
The first group met over a two-month period, and the project culminated in an exhibition of casts at Warren Art Gallery and Museum that was launched with Indigenous dancers and celebration in language.
“Mothers and the families are coming back to use our services, and they are bringing their babies to be immunised,” Nicki says. “And they are reaching out with concerns they may have about their little ones.”



In mid-2023 the Warren LGA achieved a 100 per cent immunisation rate. When new mothers return to use her service, Nicki will talk to them about any health concerns and make GP referrals for issues such as post birth infections in mum and baby or poor baby weight gain.
However, Nicki still faces an uphill battle working in a regional area that lacks services and specialists who can work with children who need extra support.
When she began working in the Warren area, the local paediatric unit told her due to staffing levels, they were unable to see any child with a developmental or behavioural delay. Nicki contacted two local preschools to identify children with speech delays and any other needs for extra supports. And working with the local NDIS provider and other funders, she has been since been able to access speech and occupational therapy for children that had previously not received any services.
She is now working with the Royal Flying Doctor Service on a plan she hopes will see a paediatrician servicing the Warren community each month.
When she saw many children in the community who needed support to improve their reading and literacy levels, Nicki came up with another creative solution: bringing the Dolly Parton Imagination Program to the community.
‘Working within a team, we are strong. Working within a community, we are stronger. And working in partnerships is where magic happens.’
— Child and Family Health nurse Nicki Callan
“It’s an amazing program where children get a book every month of their life until they turn five, and it’s a great initiative to get kids reading,” explains Nicki.
Nicki, working with Mary and with her manager’s approval, contacted the local council and the local library to establish a branch of Dolly Parton Imagination Library in Warren.
Children in the community now receive books from the program, and any child that comes into the hospital for any reason are offered a book.
“In October 2024 we celebrate our first-year anniversary of the program.”
Nicki and Mary didn’t stop there. Working with the Indigenous Literacy Foundation, they have also organised book deliveries to all children 0 to 18 years that access the Warren Multi-Purpose Services (MPS).
“Working in a rural and remote community we constantly need to look outside the box to provide a referral pathway for a child. We do not have the services of the big cities, but all children should have the right to access health care, no matter where they live.”
The Bellies and New Life project was recognised as a finalist in the Western NSW Local Health District Awards 2023, but Nicki is quick to emphasise that she is not working alone.
“Working within a team, we are strong”, she says. “Working within a community, we are stronger. And working in partnerships is where magic happens.” n
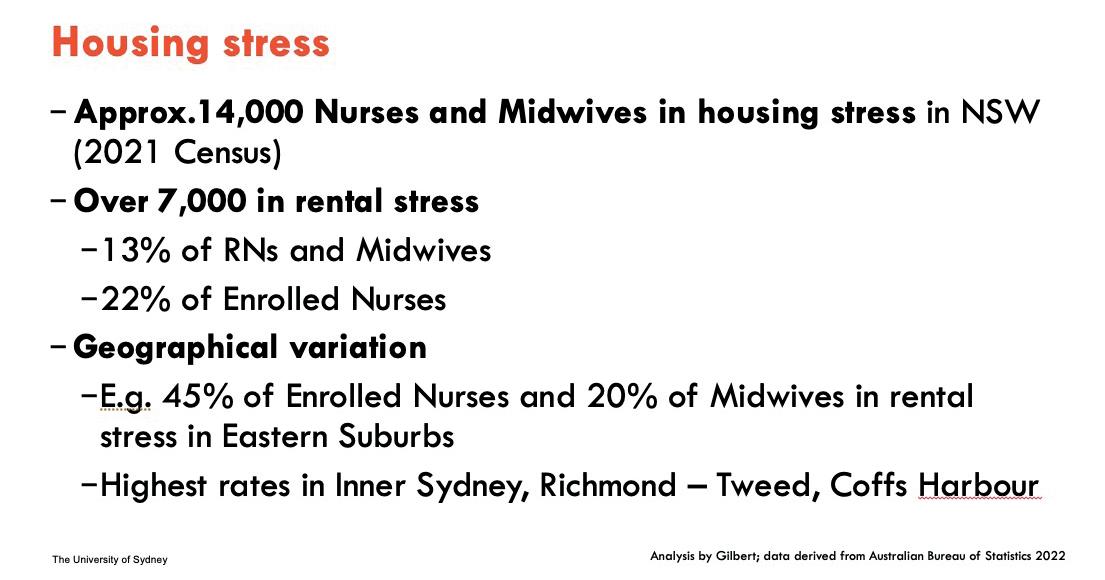
Nurses and other essential workers face an affordable housing crisis that governments are only now beginning to respond to.
The average nurse/midwife is battling to buy or rent a home in large parts of Sydney and coastal New South Wales, an expert on housing affordability told the NSWNMA’s 2024 annual conference.
Dr Catherine Gilbert from Sydney University’s School of Architecture, Design and Planning blamed the “affordable housing crisis” on housing costs accelerating faster than wages and failure to provide enough housing for essential workers.
The result is a “growing spatial mismatch between where low- and moderate-income workers can afford to live and where jobs are located,” Dr Gilbert said.
She and fellow researchers looked at housing affordability for 21 occupation groups including RNs, midwives, enrolled nurses, nursing support workers and hospital cleaners.
These occupations fell into the category of key workers who provide important public services.
Typically, they are required to be physically present to perform work and need to live close to their workplace to be on call.
Dr Gilbert’s study found that the inner and northern sub-regions of Sydney has suffered a net loss of key-worker residents over several census periods.
On the other hand, areas such as the Hunter, Illawarra and some outer suburbs of Sydney experienced a net gain – indicating essential workers are being forced out of Sydney to the fringes.
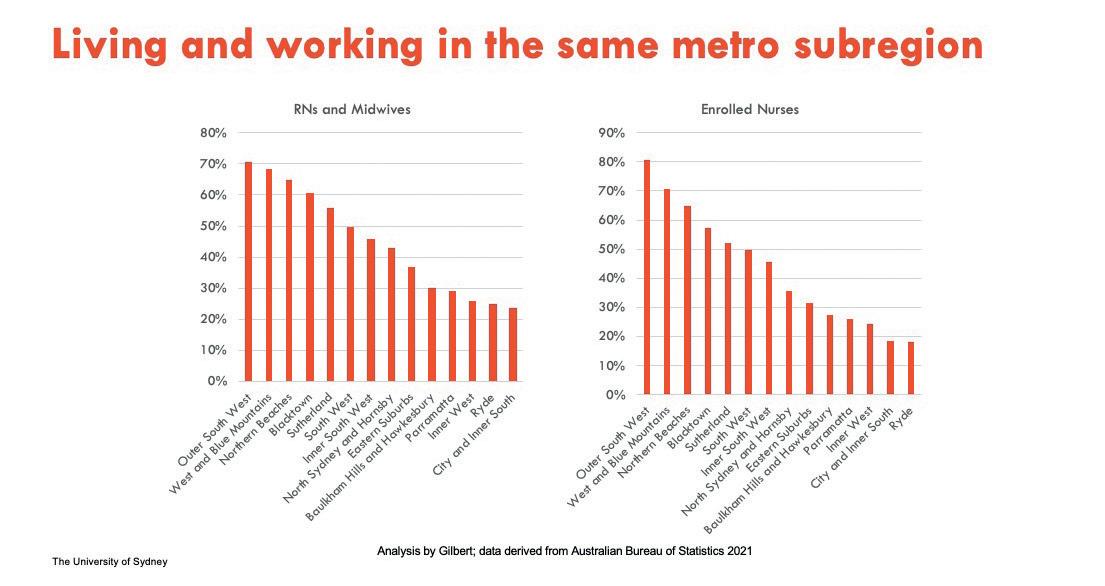
In local government areas such as Ryde, City of Sydney and Inner West, only 20–30 per cent of nurses working in those areas also live in them.

Long commutes have serious health, environmental and economic implications, and threatened the quality and functioning of critical public services, Dr Gilbert said.
Key workers’ inability to live close to work presented operational challenges such as capacity to be on call and to respond to spikes in service demand and emergencies.
Long commutes also pose recruitment and retention challenges.
Dr Gilbert and colleagues studied housing stress, which is defined as having to pay 30 per cent or more of income on rental or owned housing.
The 2021 census data indicated at least 13 per cent of RNs/RMs and 22 per cent of ENs were in housing stress across NSW on average.
The percentages were probably an underestimate due to a lack of data for some areas, she said.
‘Some
local governments are acquiring affordable key-worker housing through planning agreements with developers, which is good to see.’
The highest rates of housing stress were in inner Sydney and some coastal areas such Richmond/ Tweed and Coffs Harbour.
Dr Gilbert said both the United States and United Kingdom have longstanding policies and programs to try to provide more housing for essential workers.
Both the US and UK have planning or zoning requirements for affordable housing, she said.
‘There is essentially no post code area in greater Sydney where an enrolled nurse could afford a one-bedroom apartment.’
“In a lot of renewal precincts and developments around major hospital sites … there are statutory legal requirements for developers to include a proportion of housing that's affordable including for the local workforce.
“There are capital grants to affordable housing providers as well as access to low-cost finance for developers who provide purpose built rental housing that is affordable to essential workers.”
On the demand side, US authorities provide financial help to essential workers to purchase a home.
Dr Gilbert said that in NSW, increasing concern about the housing needs of essential workers has led to some initiatives, including an attempt to use the planning system to deliver affordable housing.
“It is now legal for local governments to have affordable housing contribution schemes,” she said.
“Some local governments are acquiring affordable key-worker housing through planning agreements with developers, which is good to see.”
She said government responses to the housing crisis must take into account the huge regional variation in the nature of the housing crisis.
For example, in regional areas one of the biggest issues is a lack of smaller homes and a shortage of homes to rent.
Dr Gilbert noted that the NSW government had made budgetary commitments for key-worker housing in regional areas. n
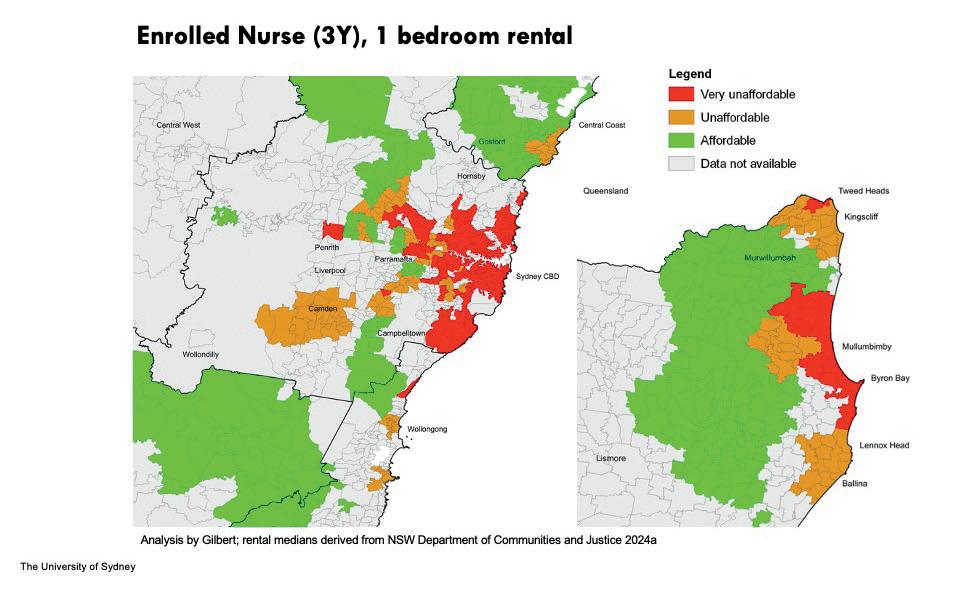
Nurses struggle to afford to rent even small apartments in large chunks of Sydney and the NSW north coast, as shown by the above map. “There is essentially no post code area in greater Sydney where an enrolled nurse could afford a one-bedroom apartment,” Dr Gilbert said.
The situation is almost as bleak for a higher earner such as a Year 4 RN/midwife seeking to rent a one-bedroom flat. Dr Gilbert said they would face a weekly rental deficit of over $240 in the Randwick or Royal Prince Alfred hospital precincts (eastern and inner Sydney) and $200 in St Leonards (Sydney’s lower north shore).
housing costs growing much faster than wages, nurses are forced to live far from their places of work.
A
new report by respected economist Saul
Eslake says it
is “incontrovertible”
that allowing prospective
homebuyers
to access their super will result in house prices rising at a faster rate.
The report says there is a growing sense in Australia of a “housing crisis”.
Housing costs have been a major contributor to the rise in inflation since the end of the COVID19 pandemic, with rents rising by 16.4 per cent and new dwelling purchase costs by 36.2 per cent over the two years to the June quarter of 2024, compared to a 10.7 per cent increase in wages.
Almost 122,500 people were estimated to be experiencing homelessness at the time of the last Census, in August 2021, a 50 per cent increase from 2001.
The proportion of low-income rental households (those in the bottom 40 per cent of the income distribution) spending more than 30 per cent of their income on housing rose from 21.6 per cent in 2009-10 to 46.7 per cent in 2019-20.
The proportion of low-income owner-occupier households with a mortgage spending more than 40 per cent of their income on housing rose from 21.6 per cent to 37.4 per cent over the same period.
There has been a long-term decline in home ownership. This is not surprising, the report says, when we see the relationship between housing prices and the cost of housing. The ratio of house prices to household income rose from 4.5 times to 13 times between 1980 and 2024.
This has had two highly detrimental consequences for aspiring home buyers. First, they need to accumulate much larger deposits in order to qualify for a mortgage. Second, first time buyers are required to take out and service much bigger mortgages.
Eslake says there is now almost six decades of evidence pointing unambiguously to the conclusion that, policies which enable Australians to pay more for housing than they would otherwise be able to do result in more expensive housing rather than in a higher proportion of the population owning housing.
In the light of that evidence, he says, it is incontrovertible that allowing prospective homebuyers to access some proportion of their superannuation, as proposed by the Liberal and National Parties during the 2022 election, and subsequently, will result in residential property prices rising at a faster rate than they would otherwise.
“In practice, the scheme proposed by the Liberal and National Parties would be of little benefit to people in the

five-figure increases in the median property price. Aside from Adelaide, in all other cities, the resulting price increases and extra property taxes could approach the amount of super withdrawn, which maxes out at $100,000 per couple. First home buyers would lose most if not all of their super withdrawal through price
The scheme also comes with considerable long-term costs in the form of
Age Pension payments and lower superannuation tax receipts. SMC analysis finds that a 30-year old couple who withdraws $35,000 each from their super, could retire with around $195,000 less in today’s dollars and have around $125,000 less in disposable income during their retirement.
Table 1: Estimated price impact from allowing first home
‘traditional’ first-home buyer age cohort of 25-34 years, because their accumulated superannuation savings are typically too small for withdrawing even the stipulated maximum of 40 per cent to make a material difference to their prospects for attaining home ownership.
Also, most people who would be likely to take up such a scheme would end up having lower disposable income after housing costs and much lower incomes in retirement.

Branch Beat with NSWNMA Assistant General Secretary Michael Whaites
Clause 44 of the Nurses’ and Midwives’ (State) Award 2023 says you should not have to undertake duties carried out by health workers who belong to other classifications.
NSW Health is increasingly asking our members to carry out tasks that are not the responsibility of nurses and midwives.
Management needs to fill vacancies and hire sufficient staff instead of increasing nurses and midwives' workloads, taking you away from your role providing patient care.
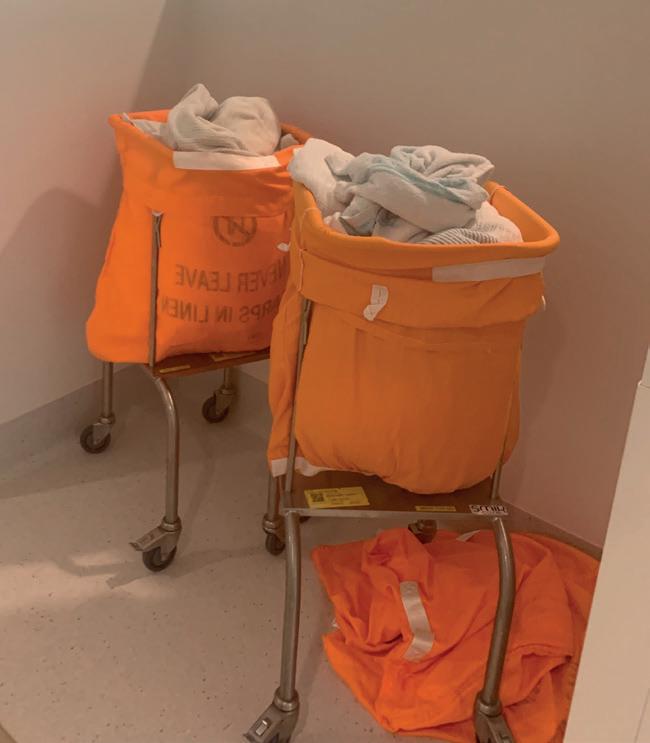
At the new Tweed Valley Hospital members were expected to take on cleaning responsibilities impacting on their care for patients,
They used clause 44 to force management to act. It was not industrial action, just invoking the award clause.
When staff and patients moved into the brand-new $723 million Tweed Valley Hospital development in May, it was a matter of days before the pristine Mental Health Unit looked like a rubbish tip.
“We had no designated cleaners on our ward. Rubbish piled up all day, so we had to beg, borrow and steal from other wards,” says Donna Chambers, a CN specialist in the acute mental health ward.
“Empty food trays, dressings, and anything that couldn’t fit into overflowing rubbish bins was piling up in corridors and patient common areas.”
In their previous Tweed Hospital location, there had been cleaners every day. At the new site, a Health and Security Assistant could theoretically be assigned to cleaning duties.
“But after doing security work and transporting patients to and from theatre and ED, he had no time.”
Mental health nurse and Tweed Hospital branch member Neralee

Jeffrey said she initially “picked up a broom and the mop. I didn’t think patients should live in that kind of condition. But I shouldn’t have to work in that kind of environment either.”
Members held a meeting to discuss the issue and decided to work to rule. They also escalated their concerns to workplace health and safety as an infection control issue, and wrote to management seeking an
undertaking that a cleaner would be allocated to the unit.
“Our nurse unit manager was extremely supportive of staff, but we had to take a stand to force hospital management to deal with the problem,” Donna says.
“Patients were trying to help by piling the rubbish up and making their kitchen area as clean as possible. Younger nurses were trying to clean up, but we had to ask them to stop so that it didn’t become our responsibility.”
Branch members also invoked section 44 of the state award, which says nursing staff should not be carrying out duties performed by health workers in other classifications.
After the branch’s strong stance, management employed a full-time cleaner to the day shift. Meanwhile, HSA staff contribute to cleaning during afternoon and night shifts when they are rostered on. n








Wishing our members a holiday season full of peace, joy, and happiness. We invite you to be part of this year's giveaway.

endota exists to help you care for your wellbeing with professionally developed products & treatments made with a sustainable focus.
endota spas offer the rejuvenating benefits of relaxing, targeted massage and high-performance facials, while the same COSMOS Certified Organic and results-driven skincare used in their treatments are available to purchase to continue the benefits at home.
endota is here to help you nourish and nurture your mind, body and skin. Discover the limitededition Christmas range at endotaspa.com.au
Thanks to endota you could win a 12 Days of endota gift pack, valued at $266
25% off endota products* use code NSWNMA25 at checkout
10% off endota gift cards^ use code NSWNMA10 at checkout

Sistasaidso+ is the go-to brand for modern nurses and midwives, offering stylish and functional accessories and apparel, designed by nurses who get it. From their best-selling, highperformance compression socks to a curated selection of stylish essentials, you’re covered from head-to-toe. Discover how they’re making every shift more comfortable and stylish!
Sistasaidso+ is giving away an exclusive Christmas bundle packed with compression socks, a sleep mask, reusable cutlery, earrings, and so much more, valued at $343
10% OFF* all online orders at Sistasaidso+! Simply use code NSWNMA10 at checkout www.sistasaidso.com


Fluidform at Home (FFAH) is your very own personalised, online Pilates and wellness app. Gain unlimited access to a library of 300+ on-demand workouts, motivational challenges, recipes, and meal plans.
Experience Kirsten King's specialised and effective programming designed to transform your body in just 20 minutes a day. Fluidform doesn’t just change bodies, it transforms lives.
Thanks to Fluidform you could win a 12-month FFAH subscription and Ultimate FFAH Equipment Set, valued at $310

Go-To is Australia's go-to brand for effective, quality and results-driven skincare. They've spent the last decade developing simple, clinically proven and 5-star-rated skincare right here in Australia.
The Lamp has partnered with Go-To and is offering you the chance to win a $350 gift pack comprising customer favourites, new launches and the iconic Face Hero.
Face Hero balances oily skin, hydrates dry skin, and creates a bright, bouncy canvas for makeup. It’s your all-in-one daily skin guardian, and quite frankly, just the hero we've been waiting for.

Have a great Aussie Christmas from the eNurse team – Australia’s one stop nurse shop!
The Lamp and eNurse are offering you the chance to win a $250 voucher – imagine yourself in new scrubs, new shoes and accessories!
10% off* all your online purchases exclusive to nswnma members. Simply use code NSWNMA10OFF at checkout www.enurse.com.au
You could win a $100 WISH eGift Card thanks to the NSWNMA. We have four to giveaway!

Shop at a wide range of stores including Woolworths, BIG W, BWS, Dan Murphy’s and participating EG Ampol fuel sites. With no expiry date, you can shop at any time.

*Conditions apply. Scan the QR code for full t&c’s and to enter.

Workers comp for COVID-19related illness
I have been diagnosed with COVID-19 and am unsure of how or where I caught it. I’ve heard that I can claim workers compensation because I’m a health worker.
Yes, if you are a nurse or midwife and contract COVID-19, there is a legal presumption that you contracted it in the workplace, unless it can be proven otherwise. You are therefore eligible to claim workers compensation for any hours of work missed, as per s19B of the Workers Compensation Act 1987 (NSW).
If you have COVID-19:
1. keep a record of your positive test result, including the date and time
2. if you’ve taken a RAT, take a photo of the result
3. then consult your general practitioner and request a SIRA Certificate of Capacity
4. submit the certificate, along with evidence of your positive test result, to your employer as soon as possible.
Your employer is legally obliged to pass the claim on to its insurer to decide about the claim.
Please contact the NSWNMA should you have any questions or require further information on lodging a claim for workers compensation. You should also contact us if your claim is declined.
I’m a full-time nurse at a workplace that does not have an Enterprise Agreement. My employment contract says that I get 4 weeks of annual leave per year. Is this correct?
As a nurse in the private sector without an Enterprise Agreement, your employment is covered by the Nurses Award 2020
Clause 22.2 of the Nurses Award 2020 says that a nurse who is not a shift worker is entitled to 5 weeks of paid annual leave for each year of service with their employer, and an employee who is a shift worker is
When it comes to your rights and entitlements at work, NSWNMA General Secretary Shaye Candish has the answers.
entitled to 6 weeks of paid annual leave for each year of service with their employer.
A shift worker is someone who is regularly rostered over 7 days of the week and regularly works on weekends.
This means you should be getting at least 5 weeks of annual leave per year, or 6 weeks if you are a shift worker, whatever your employment contract says.
Please contact NSWNMA if you believe you are not receiving the correct amount of annual leave.
Redeployment or redundancy?
My job is being deleted and my employer has offered me another position at the facility. Do I have to accept this, or can I get a redundancy?
If your position is being deleted, your employer must offer you reasonable redeployment if it’s available. If your employer cannot find you reasonable redeployment, they may be required to pay you a redundancy.
Redeployment is reasonable if you either have the skill and experience to undertake the role, or if you would reasonably have the skill and experience to undertake the role if training was provided by your employer. Other factors may also determine whether a role being offered is reasonable including any change to the location, salary, grade or shift pattern.
If you believe the role you are being offered is not reasonable then you should contact NSWNMA for assistance as you may be entitled to a redundancy.
In the event the role being offered is reasonable, you may still enquire as to whether your employer is willing to offer you a voluntary redundancy.
The amount of your redundancy payment and the notice period required will depend on your employer.
For public health system employees, please review the NSW Health Managing Excess Employees’ Policy PD2012_021 for redundancy entitlements and other useful information.
For private employees, first determine whether your workplace has an Enterprise Agreement as this will contain your redundancy entitlement and other useful information.
If there is no Enterprise Agreement covering your workplace, please review the National Employment Standards redundancy provisions at: https://www.fwc.gov.au/documents/ resources/nes-redundancy-pay.pdf
Casual to permanent conversion
I am employed as a casual RN at a private facility and have worked every Thursday and Friday morning shift for the past 12 months. Am I able to request to become a permanent employee?
As you have worked a regular pattern you may request to become a permanent employee if you’ve been employed for at least 6 months (or 12 months if you work for a small business). This is referred to as casual conversion
You should put this request in writing and make it clear you are asking to change to permanent employment. Your employer must respond in writing within 21 days of receiving your letter. They must also consult with you about what your new employment status will be, your new hours of work and when the change will take effect. Your permanent employment status applies from the first full pay period after the employer’s response, unless you and your employer agree to another day.
If your employer does not accept the change, they will need to tell you the reasons why within 21 days of your letter. An employer can only refuse the request if they do not believe you have been working a regular pattern, or on reasonable business grounds or if it would be unlawful. Their reasoning must be explained to you.
If there is an Enterprise Agreement that covers your workplace, you can check to see if there are further provisions for casual conversion in the agreement.
Please contact NSWNMA if you need assistance with making a request for permanency.






Face-to-face education sessions to the end of June 2025!
Go online to register for these education sessions and our free range of live webinars. Use the dropdown search fields to search by topic (Professional Courses, WHS Courses and Webinars), suburb or month
We’re still adding sessions so keep an eye out for our education emails and the next edition of the Lamp!
The Diabetes eduKate Workshop
Monday 17 March, 9am-4pm 6 CPD Hours
Cost: members $95 / non-members $190
CaLD Seminar: Connect, Challenge and Change
Friday 21 March, 9am-4pm, 6 CPD Hours
Cost: members $75 / non-members $150
Clinical Communication and Documentation
Tuesday 25 March, 9am-4pm 6 CPD Hours
Cost: members $95 / non-members $190
Student and Early Career Midwifery Forum
Thursday 10 April, 9am-4pm 6 CPD Hours
Cost: B.Mids students $50 / members $75 / non-members $150
The Deteriorating Patient
Tuesday 15 April, 9am-4pm 6 CPD Hours
Cost: members $95 / non-members $190
Midwifery Seminar
Friday 9 May, 9am-4pm 6 CPD Hours
Cost: members $75 / non-members $150
Understanding Your Annual CPD Obligations
Friday 16 May, 9am-1pm, 3.5 CPD Hours
Cost: members $50 / non-members $100
Environmental Health and Sustainability Seminar
Friday 13 June, 9am-4pm, 6 CPD Hours
Cost: members $75 / non-members $150

Supporting People Living with Dementia
Tuesday 8 April, 9am-4.30pm, 6 CPD Hours
Cost: members $95 / non-members $190
Medications: How we do it better
Thursday 6 March, 9am-4pm, 6 CPD Hours
Cost: members $95 / non-members $190
Griffith
Medications: How we do it better
Tuesday 29 April, 9am-4pm, 6 CPD Hours
Cost: members $95 / non-members $190
Newcastle
Perinatal Loss and Bereavement Workshop
Friday 4 April, 9am-4.30pm, 6 CPD Hours
Cost: members $95 / non-members $190
SAVE THE DATE
Rural Regional & Remote Nurses & Midwives
Professional Development Conference
Partnership between NSWNMA and CSU
Thursday 8 May, 9am-5.00pm, 7 CPD Hours
Cost: members $50 / non-members $100 / nursing and midwifery undergrad students $25
Clinical Communication & Documentation
Thu 5 Jun, 9am-4pm, 6 CPD Hours
Cost: members $95 / non-members $190


REGISTER NOW
Join the NSW Nurses and Midwives’ Association (NSWNMA) as we help to prepare you to transition from being a nursing or midwifery student to becoming a new graduate. There will be plenty of time to ask questions of the presenters throughout each session.
International Day for the Elimination of Racial Discrimination – 21 March 2025 9am to 4pm, 6 CPD Hours NSWNMA, 50 O’Dea Avenue, Waterloo NSW 2017
Join us for an impactful day dedicated to tackling workplace racism and advocating for change. This seminar will bring together experts, community leaders, and advocates to explore strategies for fostering diversity, inclusion, and equity in the workplace.
COUNT TOWARDS CPD HOURS
This webinar series will be held across 3 x Thursdays, 1 – 3pm:
Part 1: Thurs 23 Jan, 1–3pm
• About the NSWNMA
• What does transitioning mean
• Know your award and how to read your payslip
Part 2: Thurs 30 Jan, 1–3pm
• Professional Obligations
• Law and Ethics
Part 3: Thurs 6 Feb, 1–3pm
• Documentation
• Annual CPD Obligations
• Reflective Practice
Can’t attend on the day? These sessions will be recorded and made available following in Member Central and the Student Portal. Register and we will notify you when the series is online and ready to be viewed.
REGISTER NOW

Keynote Speaker:
Dr. Virginia Mapedzagama
Dr. Mapedzagama, a critical race academic and Black feminist theorist, is the Member Education Director at Diversity Council Australia. Her research explores race, migration, ethnicity, and gendered violence, focusing on the experiences of Black African migrants and diaspora communities in Australia.

This seminar covers:
• Workplace Racism Survey Report Findings
• Advocacy Strategies
• Visa & Immigration Information
• Workshops & Panel Discussion
Why Attend? This seminar is a unique opportunity to learn, network, and engage with leaders committed to challenging racial discrimination and promoting workplace equity.
Cost: members $75 / non-members $150
After an incident at work several nurses and carers were reported to the Aged Care Quality and Safety Commission (ACQSC). I have been invited to an interview and the letter says it is voluntary. Do I have to attend?
Call us if you are a member of the NSWNMA so we can help you navigate the complex and difficult process of an ACQSC investigation. We have an in-house team of lawyers and paralegals who can assist.
If you receive a letter from the ACQSC inviting you to a voluntary interview you can turn down the invitation and choose not to attend.
• If you choose to attend, please know the interview is video and audio recorded and the questions that will be asked and documents (policies, records CCTV) are not provided in advance. An investigation can be extended to include you as the subject of the investigation. Banning orders are a possibility in some cases.
• If you choose not to attend the ACQSC, the investigation will either be finalised without your participation or the ACQSC may issue a notice compelling you to attend an interview.
The NSWNMA can assist you in some instances to provide a written response or support you at any interview (whether voluntary or involuntary.
What does the new Health Legislation Amendment mean for nurse practitioners (NPs) and endorsed midwives starting 1 November 2024?
The new legislation removes the outdated requirement for a 'collaborative arrangement' with a medical practitioner. This means NPs and endorsed midwives can now prescribe medicines under the Pharmaceutical Benefits Scheme (PBS) and provide services under Medicare autonomously. This change empowers NPs and endorsed midwives to work to their full scope of practice, allowing them to deliver high-quality healthcare directly to their patients without the need for additional GP visits, which is especially beneficial in underserved communities and rural areas.
You can find out more here: https://www.mbsonline.gov.au/ internet/mbsonline/publishing. nsf/Content/FactsheetRemoval%20of%20legislated%20 collaborative%20arrangements
I am a student and did not pass a subject linked to a 4-week placement. My educational provider is now saying that I must take the whole subject again, including the 4-week placement. Can they make me do the whole subject again?
Unfortunately, the Association does not have jurisdiction over educational providers regarding outcomes of courses. However, your educational provider has an obligation to have a grievance/ complaints procedure for academic and non-academic complaints.
As a first action, we recommend that you go through your providers course coordinator or student administration to try to resolve the issue. If this is unsuccessful you can lodge a grievance/ complaint through your provider. We recommend that you keep a written record of your complaint as evidence should you require it later.
If you are not satisfied in the outcome with your educational provider, you can contact the NSW Ombudsman. The role of the Ombudsman is not to make a new decision, but rather to review if the educational provider followed the relevant policies in making their decision. They will then make a recommendation on how the decision or process can be improved.
But if the clinical placement is an element of the subject that you need to repeat, you will need to redo the whole subject including all assessment items – one of which may be placement. You may not be eligible for a recognition of prior learning as all elements of this subject will need to be repeated, based on the subject containing clinical learning that needs to be connected to theory.
I’m working on an employersponsored visa but I’m having some problems with my employer and want to find another job. Where can I seek advice on my rights?
As a financial member of the NSWNMA you can access free visa assistance through the Immigration Advice and Rights Centre in NSW. For any visa assistance contact the NSWNMA for support, and we will refer you to this service if required.
I had a Christmas function on the weekend and was stopped by the police for a random breath test. I have been issued a notice to attend court for a midrange drink driving offence. Do I need to tell AHPRA?
If you are unsure of your obligations and you receive a charge or court outcome, please contact the NSWNMA immediately. Our in-house team of lawyers can provide you with advice and support.
Section 130 of the Health Practitioner Regulation Law (National Law) requires you to notify AHPRA of a charge with a possible term of imprisonment of over 12 months. This applies to students and registered health practitioners.
You can do this by completing a Notice of Certain Events form and posting or e-mailing it to AHPPRA notifications. The failure to notify the National Board is considered noncompliance and may result in disciplinary action.
Section 130 requires you to notify AHPRA again if there is a conviction or, even if there is no conviction, if there is a ‘finding of guilt’. This can all be very confusing so please seek advice from the NSWNMA early. You should also check the code of conduct for your employer to see if you need to report to them.
This article is for information only and does not constitute legal advice.
More information:
On Section 130: https://legislation.nsw.gov.au/ view/html/inforce/current/ act-2009-86a#sec.130
Notice of Certain Events Form: https://www.ahpra.gov.au/ documents/default.
The Association’s professional team answers your questions about professional issues, your rights and responsibilities.
I am a midwife. I am pregnant and starting a blog about my pregnancy and birth journey –are there any professional considerations I need to know about?
As a Midwife you have professional obligations under the NMBA codes and guides. You must be aware of your standards for practice, code of conduct and code of ethics to meet your professional obligations if you are going to start a blog about your pregnancy and birth journey.
You may also wish to clearly distinguish the professional boundary between when you are providing education and care as a midwife and sharing you experiences as a pregnant person. Any blogging, website or videos would fall under the umbrella of social media. While you may be using social media in a private capacity, as a midwife and especially if the private group know you are a midwife you must make it clear when you are giving a personal opinion rather than a professional opinion.
In addition to the NMBA and NMC guides to social media and your employer’s code of conduct would also apply to you. If you are going to give a professional opinion, ensure that it is evidence-based practice and provide avenues for referral so that you do not inadvertently present information that could be false, misleading, or deceptive including advertising claims that are not supported by an objective evidence base. Inappropriate use of social media can result in harm to the profession and may be reported to AHPRA.
I am a single qualified midwife and am being asked to care for general patients on the maternity ward, am I allowed to do this?
As a midwife you should always be working within your scope of practice referring to the Midwives' Standards for Practice if you are unsure. The Decision-Making Framework published by the NMBA gives clear instructions on how to define if something is within your scope. There is a quick reference, midwifery flow chart which is easy to read and follow to assist with this.
Within the framework it also mentions that under the National Law, midwives must not be directed to work outside of their professional standard, guidelines, or code of conduct/ethics so if you are put into a situation, you feel is outside of your scope, you must escalate and can refer to the framework for support. There may be occasions where caring for nonmaternity patients is within the scope of a midwife’s practice. The Midwife standards for practice state that a midwife's role may extend to include women’s health, reproductive and sexual health, but if you still determine it to be outside of your individual scope you must escalate to your manager, preferably in writing, and request further educational support and supervision to be able to adopt the practice into your scope.
Nurse & Midwife Support o ers free, confidential and 24/7 health and wellbeing support to nurses, midwives and students across Australia.



Our collective strength is in our numbers – the larger the membership, the louder our voice. You can help build the NSWNMA by recruiting a member.
Once you have recruited 4 new members you will be entitled to an $80 e-gift card. For every new member you sign up after that, you will receive a $20 e-gift card.
Digital gift cards are emailed to recruiters at the end of financial year and valid for 3 years. Gift cards are not deemed to be income for the purposes of taxation.

Did you know, if you’re going on parental leave, paid or unpaid, we’ll waive your Association fees until you return to work? You’ll still be entitled to access advice and receive The Lamp. Contact the Association and let us know when you plan to take parental leave so we can set up your waiver. Call 1300 367 962 or email gensec@nswnma.asn.au www.nswnma.asn.au

“The
entire population of northern Gaza is at risk of dying”
– UN
The UN, WHO and Israeli human rights organisations are urgently warning of an unfolding catastrophe in Northern Gaza.
Hundreds of thousands of people ae enduring starvation, disease without access to medical care and incessant bombardments and gunfire since Israel began its current operation in the northern Gaza strip on 5 October, according to the Israeli human rights organisation B’Tselem.
B’Tselem says testimonies out of northern Gaza describe “dead bodies lining the streets, hunger, drinking water nowhere to be found, and civilians being killed as bombs are dropped on their homes without warning or as they flee for their lives”.
The World Health Organization says “hospitals have been almost entirely cut off from supplies and have come under attack, killing patients, destroying vital equipment, and disrupting life-saving services. Health workers and patients have been taken into custody. Fighting has also reportedly taken place inside hospitals”.
“Rescue teams have been deliberately attacked and thwarted in their attempts to pull people buried under the rubble of their homes.
“The situation unfolding in northern Gaza is apocalyptic. The entire Palestinian population in North Gaza is at imminent risk of dying from disease, famine and violence.”
The WHO Director-General Tedros Adhanom Ghebreyesus said:
“Intensive military operations unfolding around and within healthcare facilities and a critical shortage of medical supplies, compounded by severely limited access, are depriving people of life saving care.”
Testimonies out of northern Gaza describe “dead bodies lining the streets, hunger, drinking water nowhere to be found, and civilians being killed”
Israeli human rights organisation B’Tselem
UNRWA, the United Nations Relief and Works Agency for Palestinian Refugees is the organisation that provides schooling, health services and food distribution for Palestinian refugees. Israel has declared it a terrorist group and banned it.
UN officials say humanitarian efforts for 2.3 million people in Gaza are “completely dependent” on UNRWA staff, facilities and logistical capabilities. Another 900,000 Palestinians in the West Bank rely on the organisation for basic services.
From an initial focus on relief, UNRWA now also provides resources into education, healthcare and social services. The total regional budget in 2023 was about $1.6 billion.
“I have studied UNRWA for many years; I can emphatically say there is no alternative. It is not like other UN agencies in terms of the scope and scale of what the international community and Israel has asked it to provide while there is no solution to the conflict,” Dr Maya Rosenfeld, a sociologist and anthropologist at the Hebrew University of Jerusalem told the Guardian . “Emergency providers can step in for a short time, but they cannot replace what UNRWA does long-term. It is too big to fail,” she said.
Legislation to ban UNRWA passed by a 92–10 vote in the Israeli parliament, the Knesset. It is being challenged in Israel’s supreme court by human rights groups.
If the ban is enforced aid to the Gaza Strip would effectively be blocked.
“Hundreds of thousands of people will slip from acute food insecurity into mass starvation,” said Chris Gunness, who was a UNRWA spokesperson from 2007 to 2020.
If the ban is enforced aid to the Gaza Strip would effectively be blocked.
Qantas and Virgin among 1200 major companies that paid no income tax last financial year.
A major streaming service, media outlets, big airlines and a pizza chain are among more than 1200 large companies that paid no income tax in 2022–23, a new ATO report reveals, as many businesses deducted losses and used offsets to dial their tax bills down to zero.

Documents show Netflix’s Australian operations generated more than $1.15 billion in income in the 2023 financial year, but had no tax payable, reported The Guardian Airlines Qantas Airways and Virgin Australia also paid no tax in 2022–23 after they were able to carry forward losses accumulated early in the pandemic. Tech company Canva also had a zero-tax bill.
News Australia Holdings – part of News Corp – generated $1.88 billion in income in 2022–23 but had no tax payable.
Other large businesses also have multiple entities that use transfer agreements to charge other divisions, which can reduce the amount of tax they pay in the jurisdiction where the money is earned.
New protections introduced by the federal government have been lauded as a step towards improving migrant worker rights in Australia.
Two pilots have been launched recently – a Workplace Justice Visa and regulations to strengthen protections against visa cancellations for workers who report exploitation.
The Workplace Justice Visa will allow eligible migrant workers to remain in Australia while they take action against an employer, if their rights have been breached.
And under the new reporting protections, the Department of Home Affairs must consider if exploitation has occurred when deciding whether to cancel a person’s visa where a breach of visa conditions has occurred.
Joshua Strutt, CEO and Principal Solicitor at the Immigration Advice and Rights Centre welcomed the pilots as being key to fighting the exploitation of migrant workers.
“The migration system can effectively trap visa holders and give power to employers to exploit workers and let them get away with it. These reforms are a crucial step towards giving that power back to migrant workers,” he said.
To access the new visa, applicants will follow certain eligibility criteria and have their claim certified by an eligible organisation.
More info:
NSWNMA members needing legal advice on immigration or visa problems can access the Association’s free Visa Assist scheme:
https://www.nswnma.asn.au/membership/ visa-assist/


Shadow Treasurer Angus Taylor has voiced his preference for an Americanised superannuation system for Australia.
The ACTU says the Coalition has given its strongest signal yet that it would dismantle and Americanise Australia’s compulsory superannuation system if it were returned to office.
In a speech at Sydney University, Shadow Treasurer Angus Taylor stated the Coalition’s ambition included “aligning superannuation with other global retirement schemes – like [America’s] 401k”.
The ACTU condemned the comments as further evidence that the Coalition’s dream of dismantling super is alive and well.
This policy, it said, would lead to the effective dismantling of Australia’s compulsory superannuation system in favour of a voluntary approach to retirement savings, in which “bosses can choose to offer a retirement plan as a work ‘perk’, but they do not have to”.
In the Australian system every worker has a workplace right to superannuation paid on their wages, preserved until retirement. In the United States, 401Ks are optional, not preserved for retirement, often plagued with issues like high fees, low returns, and are regularly subject to misuse by employers using the money for corporate purposes.
ACTU Assistant Secretary Joseph Mitchell said Australia’s superannuation system is consistently rated as one of the best in the world.
“Angus Taylor’s pronouncement he wants Australia’s super system to be Americanised should send shivers down the spines of Aussies.
“Every worker in Australia has the right to be paid superannuation and have that entitlement preserved for retirement.”
“Every worker in Australia has the right to be paid superannuation and have that entitlement preserved for retirement.” ACTU Assistant
Secretary Joseph Mitchell
Business and employer groups want to shred workers’ rights. Again.
An industrial relations ‘blueprint’ paper from the HR Nicholls Society – a think tank closely aligned with the Liberal Party – outlines a radical employers’ agenda designed to tear up protections for workers and deliver big business large scale wage cuts.
The paper calls for the scrapping of awards, the abolition of unfair dismissal rights for workers in businesses with up to 50 employees and preventing any worker earning over $125,000 from being covered by a collective agreement.
If adopted, the policy wish list would result in more than 3.3 million Australians being kicked off awards and collective agreements and, in many cases, pushed onto a single lower minimum wage resulting in huge wage reductions.
The agenda has support among business leaders.
Australian Resources and Energy Employer
Association Chief Executive Steve Knott told the HR Nicholls Society that the Howard-era WorkChoices agenda “did not go far enough”.
“The awards system must be abolished,” he said in his address.
“Employers should have the right to make decisions about who to employ or not to employ and who to keep in their business and who not.”
ACTU Secretary Sally McManus said the business lobby was looking for the green light to shred workers’ rights.
“Already the Coalition has promised to abolish the right to disconnect, multi-employer bargaining, rights for casual workers and higher wages for labour hire employees.
“The last thing any working person needs is less rights at work, less pay and less job security.”
“Already the Coalition has promised to abolish the right to disconnect, multiemployer bargaining, rights for casual workers and higher wages for labour hire employees.”

A new report commissioned by the Nursing and Midwifery Board Australia (NMBA) highlights a crisis in the midwifery workforce.
The Midwifery Futures Report highlights the current state of midwifery in Australia, with more than a third of midwives surveyed considering leaving the industry due to poor working conditions.
New South Wales has the lowest number of midwives per capita in the country, with only 104 midwives per 100,000 population. There are 6,600 practicing midwives in the state.
NSWNMA Assistant General Secretary Michael Whaites said the recruitment and retention issues in midwifery required the urgent attention of federal and state governments, and employers in NSW.
“This national workforce report reinforces what we already knew – increasing numbers of midwives are looking to exit the industry due to work-related issues including burnout, understaffing, not feeling valued and poor skill mix,” he said.
“The report makes it clear that to secure the required workforce, we need to encourage midwives to work more hours than they currently do. They won’t do that unless we fix the structural issues of pay, workloads and support.
“In NSW, we urgently need to see midwifery-related ratios implemented in all postnatal wards.
Michael also acknowledged the need for greater investment in continuity of care models such as Midwifery Group Practice (MGP).
“It’s clear from this national survey that more and more midwives want to work in MGP,” said Mr Whaites.
“We know continuity of care is an increasingly preferred option for midwives.
Read more:
Midwifery Futures: The Australian Midwifery Workforce Project
https://www.nursingmidwiferyboard.gov.au/News/ Midwifery-Futures.aspx
From just 700 members in 1924, the ANMF has grown to stand as Australia’s largest union, boasting a membership of more than 326,000 nurses, midwives, personal carers and students.
ANMF Federal Secretary Annie Butler said the centenary was a time to stop and reflect on the long list of ANMF’s achievements, from fair wages and better working conditions to promoting safer healthcare practices and improved patient care.
“We have worked together in making transformative strides that have improved working conditions for nurses and midwives, while enhancing the health and aged care we’ve provided to all Australians across the country.
“The ANMF’s many, many accomplishments span decades –from establishing nursing and midwifery schools in the 1920s to the transition into university education during the 1970s and early 80s.
“Importantly, we’ve fought hard for, and won vital nurse-topatient ratios, penalty rates, and better pay and conditions for our members. We have been instrumental in lobbying for and supporting national registration.
“While this centennial year gives us an opportunity to reflect on our significant progress, it is also a time to look forward to the work we have ahead of us, such as advancing workforce reforms, particularly strategies addressing workforce shortages, continuing to strengthen Medicare so there is equitable access to healthcare for all Australians, ensuring nurses and midwives can work to their full scope of practice, and advocating for gender pay equity.”
‘We have worked together in making transformative strides that have improved working conditions for nurses and midwives.’
ANMF Federal secretary Annie Butler
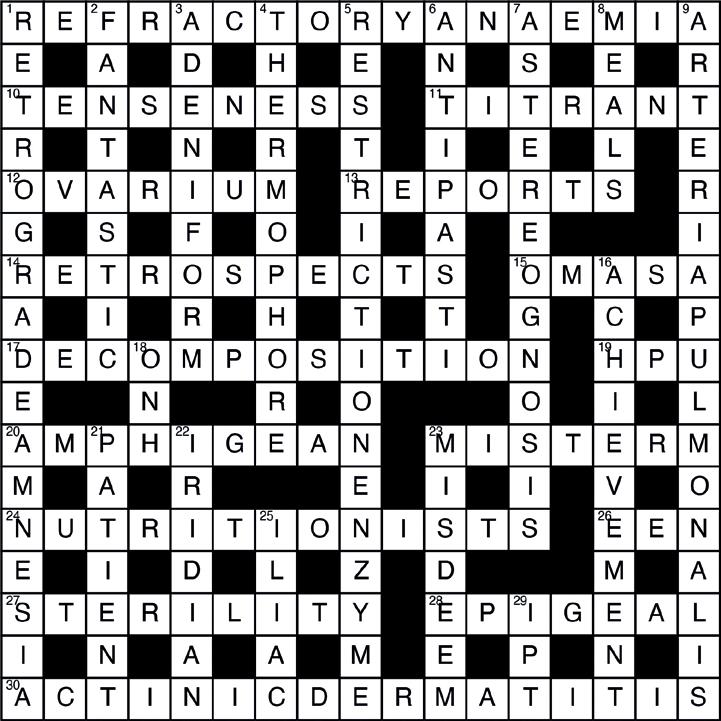
























This diary does more than help organise our lives, it’s packed with expert health advice important to every woman. Plus you’ll be helping identify new treatments that save and improve the lives of people with breast cancer.

$ 19.99 from Newsagents, Woolworths, Participating Post Offices & womenshealthdiary.com.au









Recruit a new member and you could win a 4-night wellness retreat at Billabong Retreat. You and a friend will stay in a Treehouse Ensuite Cabin with the following inclusions:
All meals, drinks and snacks
Daily yoga and meditation
Access to retreat program during stay
Two x spa treatments per person (per stay)
One x infrared sauna session per person.
Every member you sign up over the year gives you an entry in the draw!
Award winning Billabong Retreat was founded and opened in 2010. The 26 room eco retreat is located on 12 acres of natural bushland in Maraylya, just 45 minutes from the Sydney CBD. The wellness haven delivers day retreats as well as overnight retreats that include delicious wholefoods, daily yoga, evening meditation and education workshops to empower and inspire. For more information visit billabongretreat.com.au
RECRUITERS NOTE: Join online at www.nswnma.asn.au
If you refer a member to join online, make sure you ask them to put your name and workplace on the online application form, so you will be entered in the draw.
Nurses, midwives and students are exposed to professional demands that may make them vulnerable to health issues, including addiction.
Early intervention provides the best outcomes for people experiencing an addiction. As with any health issue, addiction is treatable with the right support.
Workplace demands and selfimposed personal and professional expectations may result in nurses, midwives and students resorting to harmful behaviours in an attempt to self-manage health issues. These health issues, including addiction, can affect a health professional's ability to perform competently at work, putting the public at risk of harm.
You may be reluctant to access support and treatment for an addiction or mental health issue because you fear it may lead to:
• loss of employment or ability to continue with studies
• being deregistered as a nurse or midwife
• the inability to work and consequent loss of income
• professional and social isolation
• stigma and judgment from colleagues within the team
• legal ramifications especially if diverting drugs from the workplace for own use
• loss of respect and trust between colleagues and the wider community, or
• a threat to career advancement and promotion opportunities.

You may have not asked for support or treatment because you:
• believe that you should have the expertise to be able to manage the issues on your own
• are too unwell or unaware of the direct effect and severity of your health issue and resulting risk to others
• feel ashamed and guilty about your behaviour or actions
• have a sense of failure, personal and professional, causing an internal conflict in accessing support
• have feelings of loss of control and guilt about not coping
• are unaware of treatment pathways/support available
• are unsure where to access support or navigate your way through treatment.
Nurse and Midwife Support provides free and confidential support 24/7, to nurses, midwives and students Australia wide. If you would like to speak to someone call 1800 667 877, or you can request support via email (https://www. nmsupport.org.au/support).
If you would like to find out more about a particular substance the Australian Drug Foundation (ADF) has fact sheets that may be of assistance.
https://adf.org.au/drug-facts/
Gambling Help Online
Information and support for anyone affected by gambling 24/7, free and confidential. https://www. gamblinghelponline.org.au/
Counselling Online
Information and support for anyone affected by alcohol or other drugs 24/7, free and confidential.
https://www.counsellingonline. org.au/
Kate Adams, a professional officer with the Association, was recently acknowledged at a gala ceremony for her lifetime support of CATSINaM, the Congress of Aboriginal and Torres Strait Islander Nurses and Midwives.
Kate’s award, the 2024 Lifetime Ally Award, was presented by CATSINaM president Vanessa Browne.
The award recognises Kate’s “lifelong support and leadership in advocating for and leading systemic changes within the nursing, midwifery and broader health and education sector for the benefit of Aboriginal and Torres Strait Islander nurses, midwives, students and care recipients.”
When CATSINaM was being established in the mid1990s, Kate sent emails to NSWNMA members asking any Aboriginal and Torres Strait Islander members to contact her about a new organisation being established to represent them.
“We were lucky to get 25 people to come to the first meeting. I’m very proud that I was involved in that very first meeting,” says Kate, who was a nurse specialising in women’s health before joining the Association.
The Indigenous leader and nurse, the late Lowitja O'Donoghue AC CBE DSG, was an early supporter and spoke to the first gathering, later becoming a CATSINaM patron.
When CATSINaM was being established the NSWNMA did not have any record of ATSI membership, but Kate says the Association’s “engagement with ATSI members has improved” over the intervening years. NSWNMA members who identify as Aboriginal and/or Torres Strait Islander are now automatically members of the Aboriginal and Torres Strait Islander Member Circle.
“The greatest thing is there are now a lot of ATSI nurses and midwives who are engaged in all nursing unions across Australia.”
CATSINaM and NSWNMA still have much work to do to, says Kate. “There are Indigenous health practitioners out there who are absolutely outraged at the equipment they can’t get, and that ATSI people are suffering diseases that have been eradicated in the rest of the population.”
As part of her award, Kate was presented with a custom designed two-toned brooch, designed by Jawoyn and Kala Lagaw Ya man Thomas Coen, that incorporates elements of the CATSINaM logo. n

‘The
greatest thing is there are now a lot of ATSI nurses and midwives who are engaged in all nursing unions across Australia.’
— Kate Adams
(4/5/1961- 4/7/2024)
Cathy undertook her general training at Canterbury Hospital from 1982 to 1985 and went on to do midwifery at Blacktown. She then worked as a midwife at Auburn Hospital before completing the Child and Family Certificate.
She moved to the south coast and while living in the Illawarra, worked as a community midwife at Shellharbour Hospital and then in child and family both as an early childhood nurse and a manager. During Cathy’s time as community midwife at Shellharbour, she became very active in the branch taking on both branch president and delegate positions. It was during her time at Shellharbour that the maternity services came under threat of closure and Cathy, as the union delegate, along with the other midwives, fought a hard campaign resulting in the reopening of the maternity unit in 2000.
Although it was a tough campaign, midwives versus the Area Health Service, strong friendships and bonds were formed. We also had lots of fun, laughing at management’s ridiculous proposals and excuses and leaking information to the press, not to mention dressing up in op shop clothes for the Midwives Ball. Cathy was in the thick of it all, fighting injustices and advocating for women in the area.
At the same time, Cathy completed a Master of Business Administration. Later, after becoming completely disillusioned with the bureaucracy of the Area Health Service, she left the Illawarra to fulfill a dream she held, of working in many different locations across Australia including Western Australia, Tasmania, Queensland and King Island as Director of Nursing, and also as Health Services Manager with International Health and Medical Services in detention centres in Darwin, Hobart and Christmas Island.
In 2010, Cathy moved to Lennox Head with her daughter, and she held nursing management positions at Mt Isa, Charters Towers and Murwullimbah. Cathy certainly managed to fulfill her dream to work in a variety of places around Australia.
Cathy was a member of the ANMF/ NSWNMA for all of her nursing career and actively participated in many union campaigns, such as What’s a Nurse Worth? And ‘Your Rights at Work’ and of course the fight to save Shellharbour Maternity.
After some years of deteriorating health, she was sadly diagnosed with a rare degenerative neurological disorder, and eventually became wheelchair bound. Despite her deteriorating condition for the last five years of her life, Cathy never lost

her sense of humour and remained politically aware and engaged. She fought a courageous battle to remain independent and stay at home, right to the end and it was fitting that she passed away peacefully surrounded by her family and carers on 4th July, aged 63.
Cathy was a compassionate midwife, an understanding and caring manager and a fun and loyal friend. She formed lifelong friendships with the nurses she trained with and with many of the nurses she met and worked with throughout her varied career. We will miss her wicked sense of humour, her political astuteness, her friendship and her caring personality.
She is survived by her daughter Tara and granddaughter Tully, Mum Eileen, and siblings Julie and Anthony.
Submitted by her midwifery and early childhood colleagues from Shellharbour. n
ACROSS
1. Blood disorder resistant to treatment (10.7)
10. Feeling of nervousness (9)
11. Chemical used to determine concentration (7)
12. Egg-producing organ (7)
13. Summaries of findings (7)
14. Looks back (11)
15. Swelling of the abdomen (5)
17. Breakdown of organic matter (13)
19. Haemopyrrollactamuria (1.1.1)
20. An organism that is native to both old and new worlds (9)
23. To label wrongly (7)
24. Dietary experts (13)
26. A nurse classification (1.1.1)
27. Inability to reproduce (9)
28. Growing above ground (7)
30. Skin inflammation caused by exposure to sunlight (7.10)
DOWN
1. Loss of memory for events before a traumatic incident (10.7)
2. Extraordinarily great (9)
3. Having a glandular shape (9)
4. An instrument for estimating heat sensibility (11)
5. DNA-cutting enzyme (11.6)
6. Italian appetizers (9)
7. Inability to recognise objects by touch (13)
8. Daily food servings (5)
9. Blood vessel to the lungs (7.10)
16. Something accomplished (11)
18. Optic Nerve Hypoplasia (1.1.1)
21. Recipient of medical treatment (9)
22. Relating to the iris of the eye (7)
23. Incorrectly judge (7)
25. Related to the pelvis (5)
29. Insulin potentiation therapy (1.1.1)
Access to online CPD
FREE for NSWNMA members and student members
Hundreds of hours of FREE CPD online
Meeting your Continuing Professional Development (CPD) obligations is now even easier with this great benefit for NSWNMA members. As a financial member you have access to over 200 CPD modules – all part of your Association membership.
FREE access to over 200 CPD modules online
Highly visual and interactive modules you can do at your own pace
New modules added regularly
Your own personalised ePortfolio and CPD tracker so you can provide evidence to the Nursing and Midwifery Board of Australia (NMBA) of participation in CPD annually.



The NSWNMA is committed to protecting the interests of nurses and midwives by purchasing a range of insurances to cover members.
Journey Accident Insurance
provides cover for members who are injured as a result of an accident while travelling between their home and their regular place of employment.
Professional Indemnity Insurance*
provides legal representation and protection for members when required.
Make sure your membership remains financial at all times in order to access the insurance and other benefits provided by the NSWNMA.




Update your details using our online portal during 1 April 2024 - 30 March 2025 and you will automatically be entered in the draw to win.
We are giving away two gift card bundles, each prize valued at $350.
Winner may choose one gift card valued at $350 or a selection* of gift cards to the value of $350.




1 Scan or go to nswnma.info/mc
Update your details 3 Go into the draw to WIN one of two gift card bundles
* Up to a maximum of three different gift cards, to the total value of $350 per prize. **Winner must be a financial member of the NSWNMA. The Association will contact winners, ascertaining preferred gift cards. Gift cards are subject to availability and supplier t&c’s apply. Keeping your membership details up to date is very important. If you’re a dualqualified nurse/midwife, you can now update your role at