1 2
KalandiSingh,Dr.PrasannaKumarPatra1Ph.DScholar(NFHEFellow),PGDepartmentofAnthropology,UtkalUniversity,VaniVihar-751004,Odisha,India.

2 AssociateProfessor,PGDepartmentofAnthropology,UtkalUniversity,VaniVihar-751004,Odisha,India.

1 2
KalandiSingh,Dr.PrasannaKumarPatra1Ph.DScholar(NFHEFellow),PGDepartmentofAnthropology,UtkalUniversity,VaniVihar-751004,Odisha,India.
2 AssociateProfessor,PGDepartmentofAnthropology,UtkalUniversity,VaniVihar-751004,Odisha,India.
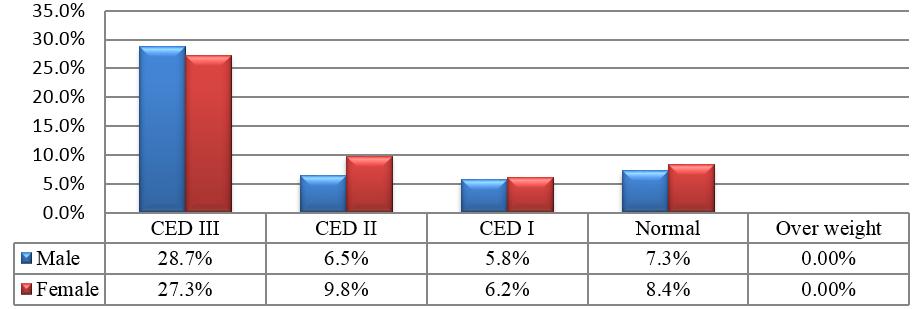
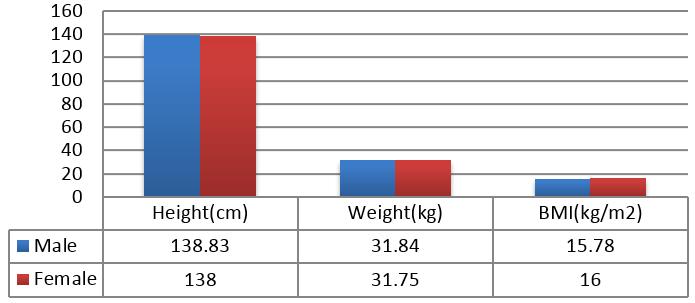
Introduction:ThepresentstudyattemptstoexaminetherelationshipbetweenadultBhumija'sBMIandCEDinMayurbhanjDistrict,Odisha,India.Methods:For thestudytotal275respondents(men-133andwomen-142)wereselectedfromthreevillagesthosewereovertheageof18-49wasinvestigated.Results:Themale respondentsaveragemeanbodymassindex(BMI)were138.8(19.4)cm,31.84(12.1)kg,18.14(3.3)cm,and15.7(2.3)kg/m2,respectively Femalesaveragemean BMIwere138.0(19.2)cm,31.7(11.4)kg,18.1(3.2)cm,and16.0(2.3)kg/m2respectively Amongmalesbelongedtotheunder-nutritiongroup,79(28.7%)wereCED III,18(6.5%)wereCEDII,16(5.8%)wereCEDI,and23(8.4%)werenormal.Ontheotherhandamongfemales75(27.3%)wereCEDIII,27(9.8%)wereCEDII, 17(6.2%)wereCEDI,and23(8.4%)werenormal.AspertheguidelinesoftheWorldHealthOrganization(WHO),therateofundernutritionbasedonBMIandCED washigh(≥40%),indicatingaseriousnutritionalcondition.Conclusion:Thestudysuggeststhatneed-basedandculturallyappropriatesocio-economic,educational andpublichealthprogramsshouldbeinitiatedamongtheBhumijainordertoreducetheprevalenceofhealthconditionamongtheBhumija.
KEYWORDS:Bhumija,CED,BMI,Adult,Odisha.
Theimportanceofhealthisanessentialindicatorofbothfinancialdevelopment andgrowth.Thehealthsignificanceofspecifiedresidentsisabsolutelyorharmfully partial to the nation's financial increase. Dependent health factors like incomepercapita,socialinfrastructure,diet,sanitation,medicalcarefacilities, secureintakewater,poverty,employmentstatus,etc.,changethehealthofeach person and there is a link between development and health (Sharma; 2012). Higherrisksofunder-nutritioninthetribalpopulationareduetothecultural,ecological,andsocio-economicfactors.Nutritionalstatusisanessentialtooltolearn abouthealthanddependsontheuseoffoodstuffsrelativetotherequirementsand necessities.Somestudieshaverevealedarelationshipbetweentheethnicgroup's dietary and economic status (Tiwari 2007; Rao & Rao 1994) and health outcomes.Thenutritionalandhealthstatusofthehumaninhabitantsofanynationis determinedthroughthevalueofeconomicgrowth.Usually,atthefamilycircle level, cultural norms, socioeconomic factors and practice resolve the level of health issues in tribal people. The causes of diseases, poverty, illiteracy, unfriendlysurroundings,lackofdrinkingwater,poorsanitation,unsightedbelief systems, etc. are consider as miseries among the tribal communities. The Bhumija are one of the Hindu tribes and are found largely in the district of Mayurbhanj.Etymologically,theterm"Bhumija"means"onewhoisbornfrom the soil." Dalton classifies the Bhumijas as Kolarians on linguistic grounds. Racially, they belong to the proto-australoids. Rishsley says that the Bhumijas are nothing more than a branch of the Munda, which has spread to the east (Goswamietal2009;Behera2021).
The present study focused on two villages in the Khunta block of Mayurbhanj District, Odisha. With a landmass of 10418 square kilometres, Mayurbhanj is Orissa'slargestdistrict.Thedistrictishometothestandardizedbiosphereandis richinbiodiversity Thedistrictwasplaced9thinhumandevelopmentandhas madesignificantimprovementinliteracyandotherhumandevelopmentindicatorsinrecentyears.(DHDR,2011).

Forthestudy,primarydatahasbeencollectedbyadoptingfieldsurveymethod forcollectingthedata.Indepthinterviewsandindividualquestionnairewereprepared for collection the data. The participant observations were conducted in threevillagesforverifythedatainKhuntablockofMayurbhanjDistrict,Odisha. The paper based on the secondary data obtained from various books, articles, journals,reports,researcharticlesandunpublishedreportssoon.Fieldnotewere made by researcher to analysis the data.Audio records were done after getting permissionfromrespondents.
MeasurementsofAnthropometricTraits: Anthropometricmeasurementsofeachsubject'sheight(cm),MUAC(cm),and weight(kg)usingLohmanetal.'smethodology(1988)weretaken.Weightand circumference were measured to the nearest 500 g, while circumference and heightweremeasuredtothenearest1mm.
MeasurementofNutritionalStatus: Nutritional status was calculated by globally acknowledged Body Mass Index (WHO,1995)guidelines:
2
CEDIII:BMI<16.00kg/m 2 CEDII:BMI=16.0-16.9kg/m 2 CEDI:BMI=17.0-18.4kg/m 2 Normal:BMI=18.5-24.9kg/m 2
Overweight:BMI=25.0-29.9kg/m
WeusedtheclassificationofWorldHealthOrganization's(1995)lowBMIofthe communityphysicalconditiondilemmainadultpopulationsallabovetheworld. Thisclassificationdividesfrequencyintopercentagesofthepopulationswitha BMI(<18.5kg/m2).
Low(5-9%):warningsign,monitoringrequired.
Medium(10-19%):poorsituation.
High(20-39%):serioussituation.
Veryhigh(≥40%):criticalsituation.
SPSSsoftwarewasusedtoanalysisthedataafterthefigureswereassembled(V20.00).Descriptivestatisticsisusedtoexaminethemean,maximum,minimum, standarddeviation,andpercentiles.Thesexdifferenceinmeanweight,height, BMI,andCEDwasdeterminedusingtheStudent'st-test.TheChisquaretestwas usedtodeterminetheassociationbetweentwovariables.Theimpactlevelwas setat0.05.
Table.1 shows the participants of sex wise the mean (SD) values of weight, height,andBMIforeachparticipant.Males31.8(12.1)kg,138.8(19.4)cm,and
15.7 (2.3) kg/m2 had a higher average height, weight and BMI than females 138.0 (19.2) cm, 31.7(11.4) cm and 16.0 (2.3) kg/m2. The gender disparities werestatisticallysignificant(p0.001).
Variables
Male(n=133) Female(n=142) Mean SD Mean SD
Sabar 19.4 18.0 52.0 65.0 WestBengal Bhandarietal. 2019
Bhumij 18.6 52.3 WestBengal Ghosh&Bose 2015
Munda 19.35 35.8 WestBengal Das&Bose 2010
Oraon 19.46 37.5 WestBengal Boseetal. 2011
Oraon 18.0 53.1 Jharkhand Chakraborty& Bose,2008
Tangkhul Naga 21.2 16.2 Manipur Mungreiphy,et al,2012
Bhotias 19.5 45.3 Uttarakhand Kapooretal, 2012
Sabar 19.4 18.0 52.0 65.0 WestBengal Bhandariet al.2019
Table.2 revealed the participants of the nutritional status, In case of males, 79 (28.7%)wereclassifiedasCEDIII,18(6.5%)CEDII,16(5.8%)CEDIand20 (7.3%) were normal. In case of females 75 (27.3%) were CED III, 27 (9.8%) CEDII,17(6.2%)CEDI,and23(8.4%)werenormal. Table2:NutritionalStatusoftheBhumijaMalesandFemales
ThenutritionalhealthconcernsofIndia'svasttribalpopulationarecausedbyethnic groupings that are close to conflating socioeconomic, social, and malnutritiondiversity,whichiswidespreadamongthetribalpeople(Deka,2011).Many studiesontheirsocioeconomicandnutritionalstatushavebeenundertakeninthe past. The studies revealed a significant relationship between them. In the Mymensingh district, the Garo people's nutritional situation is dire.Underweight,normalweight,overweight,andobesepeoplemadeup30%, 46percent,16percent,and8%ofthepopulation,respectively Duetoalackof resources and ignorance (Naser, 2015), owing to their traditional customs and poorliteracylevels,asectionoftribalpeopleisparticularlyvulnerabletomalnutrition. According to a separate study, Saharia's low socioeconomic status is reflected in their low educational and income status. The higher prevalence of CEDandoverweightinguyscomparedtofemalesreflectstheirsuperiorunderstanding of BMI in relation to their environment. It was also discovered that SahariafemaleshadagreaterrateofundernutritionbasedonMUAC.Inthepresent study, we discovered a link between nutritional status and socioeconomic levelaswell.Menweremostlyworkinginagriculture(39.3%),whereaswomen (30.9%).Therewasalargegenderdivide.Wealsodiscoveredthatmalnourished femaleshadagreaterrateofmalnutritionthanmalesinthisstudy
The above table reveals that the higher prevalence of CED and overweight in males as compared to females reflects their superior understanding of BMI in relationtotheirenvironment.Inthepresentstudy,werevealedthattherelation betweenBMIandCEDlevelaswell.TheprevalenceofCED(%)andmeanBMI kg/m2 in India's major tribal populations are shown in Table 8. In the case of males,themeanBMIwaslargerinSantals,andBirhorsofWestBengal,asseen in the table. Females had a higher mean BMI thanWest Bengal Birhors. In the case of males, WHO guidelines indicate that CED is prevalent among Santals (Mukhopadhyay2010),Birhor(Dasetal.2013),Mahalis(Ghosh&Bose2017) ofWestBengal,Oraons(Beck&Mishra,2010)ofOrissa,Savar(Bisai&Bose, 2012)ofOdisha.Ontheotherhand,haveaveryhighfrequencyofCED(40%). Accordingtothesecriteria,Sabars(Bhandarietal.2019)fromWestBengal,as wellasBhumijafromthepresentstudy,wereinacatastrophicstate.Asaresultof this research, it was found out that the CED percentage in females was higher thaninmalesamongtheBhumijatribeofMayurbhanjdistrict,Odisha.
Inconclusion,thepresentstudyvisiblydemonstratedthenecessitytorecognize, alter, and restructure assets for the indigenous community according to their needs.Theintendedimprovementinitiativesandthehealthneedsofethnicpopulationsmustbedeterminedwhilemaintainingtheirsocio-culturaltraditionsand habitatinmind.TheprevalenceofundernutritionbasedonCEDandBMIwas high,indicatingacriticalnutritionalstate,accordingtoWorldHealthOrganization (WHO) guidelines. To alleviate this ethnic group's nutritional stress, an immediate and appropriate nutritional participation programme must be established.To improve their health conditions, a need-based socio-economic interventionprogrammeshouldbeinitiated.
Asaresult,werecommendthatcomparableresearchbeconductedtofindoutthe frequencyofundernutritionamongBhumijasfromotherregions,particularlyin ruralareas.Thisresearchwillaidinthegenerationoffreshdatathatmaybeused toanalysetheprevalenceofmalnutritiononalocal.
TheauthorswouldliketothankalltheresearchparticipantsfromBhumijacommunitywhovolunteeredtoparticipateinthestudy Thefirstauthorwouldliketo thanktheUGC-NFHE(NationalFellowshipforHigherEducation)forgranting DoctoralFellowship,basedonwhichthisresearchhasbeencarriedout.
REFERENCES:
I. Basu,S.K.,Jindal,A.Kshatriya,G.K.1990.‘Thedeterminantsofhealthseeking behaviour among tribal population of Bastar district’, Madhya Pradesh. South
AsianAnthropologist,1:1-6
II. Beck,P andMishra,B.K.2010:Socio-EconomicProfileandQualityofLifeof Selected OraonTribal Living in andAround SambalpurTown, Orissa. Current ResearchJournalofSocialSciences,2(6),340–349.
III. Behera,G.2017.“ImpactofliteracystatusonParticipationofTribalWomenin Panchayati Raj – A case study of Nilgiri ITDA Block of Balasore district in Odisha”.IOSR.22(6):14-23
IV Bisai, S, Bose, K. 2012. “Critical nutritional stress among adult tribal populationsofWestBengalandOrissa,India”.NaturePreceding:2012.7068.1
V Bhattacharya, K.K., Haque, M., Biswas,T.K., 2006.” Nutritional status of two primitivetribesofeasternIndia:AnthropologyofPrimitiveTribesofIndia.323
VI. Bose,K.,Debsharma,B.,andDas,S.2011.‘Isbodyadiposityindexagoodmeasureofnutritionalstatus:AstudyamongtwoadulttribalpopulationsofPaschim Medinipur’, West Bengal, India. Science Journal of Sociology andAnthropology.1,1–7
VII. Bhandari,S.,Ghosh,M.andBoseK.,2019.’Socio-DemographicCharacteristics And Prevalence Of Under NutritionAmongAdult Sabars Of Bankura District, West Bengal, India.International Journal of Advancement in Life Sciences Research,2(1),pp.1-10.
VIII. Chakrabarty, S., Pal, M., Bharati, S., Bharati, P., 2008. Chronic Energy DeficiencyamongTribalCommunitiesof Orissa,India.Tribes&Tribals.2,95–101
IX. Chakraborty,R.,and Bose,K.,2008.Anthropometriccharacteristicsandnutritional status of adult Oraon men of Gumla District, Jharkhand, India : The InternetJournalofBiologicalAnthropology.2-1
X. Das,K.(2012).Healthasaneconomicindicator,Kurukshetra60(10),6
XI. Das, S. and Bose, K., 2010. Body Mass Index and Chronic Energy Deficiency among adult Santal of Purulia , West Bengal, India : International Journal of HumanSciences.7(2)
XII. Das, S. Mahata, M. and Bose, K., 2013. Nutritional profile of adult Birhors of Purulia:AparticularlyvulnerabletribalgroupofWestBengal,India:AsianAcademicResearchJournalofMultidisciplinary;1(5):262-275
XIII. Deka,S.2011.HealthandNutritionalStatusoftheIndianTribesofTripuraand EffectsonEducation,StudentPulse,3(03)
XIV DistrictHumanDevelopmentReport-Mayurbhanj(Odisha),2011
XV Ghosh, M. & Bose, K. 2015. Assessment of Nutritional Status among male BhumijofWest Bengal,India:Acomparisonofbodymassindexand mid-upperarmcircumference.Human BiologyReview,4(2)
XVI. Ghosh,M.&Bose,K.,2017.PrevalenceofundernutritionamongadultMahalis of Bankura district., West Bengal. National Seminar on tribal development in WestBengal,atCulturalResearchInstitute;Abstractpageno.28
XVII. Hamid, T and Vaida, N. 2017.Astudy on nutritional status of scheduled tribe (Gujjar and Bakerwal) women of Kashmir International Journal of Home Science.,3(3)203-205
XVIII. James,W.P.T.,Mascie-Taylor,C.G.N.,Norgan,N.G.,Bristrian,B.R.,Shetty,P., Ferro-Luzzi,A.1994.ThevalueofarmcircumferencemeasurementsinassessingchronicenergydeficiencyinThirdWorldadults.EuropeanJournalofClinicalNutrition.48,883-894
XIX. John,P.,andRamadas,S.2008.Bodymassindex:AnindicatorofnutritionalstatusamongadultMannantribesofidukkiDistrict,Kerela:AcademicReview15(1 &2),60–65
XX. Kapoor,A.K., Saluja, K.,Verma, D., Kapoor, S. 2012. Predictors of HypertensionamongAdultTribalMalesof India :InternationalJournalofTropicalDisease&Health.2(4),241–256
XXI. Mukhopadhyay, A. 2010.Anthropometric characteristics and undernutrition amongadultsantaltribeofBirbhumDistrict,WestBengal,India,AnthropologicalScience.118(1),57-60
XXII. Mungreiphy,N.K.,Kapoor,S.,Sinha,R.2012.Relationshipbetweennutritional status,respiratoryperformanceandage:studyamongTangkhulNagafemalesof NortheastIndia.ActaBiologicaSzegediensis.,56(1),31–36
XXIII. Naser,M.A.2015.SocioeconomicProfileandNutritionalStatusofAgedGaro EthnicPeople,EuropeanAcademicResearch.III(7),8045-8051
XXIV Rao,K.M.,Kumar,R.H.,Krishna,S.R.,Bhaskar,V.,Laxmaiah,A.2015.Diet& nutrition profile of Chenchu population -A vulnerable tribe in Telangana & AndhraPradesh,India.IndianJMedRes.141(8),688-96
XXV Sarkar,R.2016.AStudyontheHealthandNutritionalStatusofTribalWomenin Godam Line Village of Phansidewa Block, Darjeeling, District. IOSR.21 (11),15-18
XXVI. Singh,H.S.,Ghritlahre,M.,Das,S.2014.NutritionalStatusamongFemalesof BhainaTribeofBilaspur,ChhattisgarhIndia:AnAnthropologicalinsight.JournalofAnthropology
XXVII. SharmaPal,A.2012.RuralHealthScenarioinIndia,Kurukshetra.60(10),9
XXVIII. Shinde,D.N.,Patil,C.L.2016.MalnutritionandDrinkingwaterofthechildren’s intribalareainIndia,Review NewMan.3(1),52-55
XXIX. WorldHealthOrganization,1995.PhysicalStatus:TheUseandInterpretationof Anthropometry,TechnicalReportSeriesNo.856