



MARCH 2023 rcsed.ac.uk BRITISH ASSOCIATION OF BLACK SURGEONS HOSTS INAUGURAL CONFERENCE MEMBERS AND FELLOWS RECOGNISED IN NEW YEAR HONOURS 2023 22 05 Celebrating International Women’s Day and the pursuit of equity #EmbraceEquity #'> Q 9 Q p Q
ality everytimest time
The world’s leading surgeons and healthcare professionals can always rely on the consistent quality, precision and performance of surgical blades, handles and scalpels from Swann-Morton.
The world's leading surgeons and healthcare professionals can always rely on the consistent quality, precision and performance of surgical blades, handles and scalpels from Swann-Morton.
For more information on the complete range of surgical blades, handles, scalpels, disposable, fine and retractable scalpels please go to our website.
For more information on the complete range of surgical blades, handles, scalpels, disposable, fine and retractable scalpels please go to our website.

Our extensive range includes over 70 blade shapes and a selection of 27 handles. Used in various disciplines for both general and specialist surgery, all our products are subject to the strictest quality control procedures and are guaranteed never to let you down.
Our extensive range includes over 70 blade shapes and a selection of 27 handles. Used in various disciplines for both general and specialist surgery, all our products are subject to the strictest quality control procedures and are guaranteed never to let you down.

Where only Swann-Morton will do.
Where only Swann-Morton will do.
Owlerton Green, Sheffield S6 2BJ Telephone: 0114 2344231, Sales: 0114 2344223
Owlerton Green, Sheffield 56 2BJ Telephone: 0114 2344231, Sales: 0114 2344223
uksales@swann-morton com, exportsales@swann-morton.com
uksales@swann-morton.com, exportsales@swann-morton.com.. , [!] • .


www.swann-morton.com
www.swann-morton.com
‘Swann-Morton’ and the ‘Ring Pattern Logo’ are the registered trade marks of Swann-Morton Limited and related companies.
2797 FM 73368 EMS 633531 CE EMS 633531 2797 FM 73368
'Swann-Morton' and the 'Ring Pattern Logo' are the registered trade marks of Swann-Morton Limited and related companies.
SPRINGHERALDSRETURN TOA‘NEW’NORMALITY
Despite two new COVID variants in circulation, the healthcare system is rallying, says Roger
Iam writing this after returning from the Council development session in Edinburgh, the first under the presidency of Professor Rowan Parks.
On my trip back, I reflected that this is the seventh President who I have been fortunate enough to support through my various College roles. It was also clear from discussions that our Council is modern, sleek and keen to engage with all related individuals to improve the provision and standards of patient care, not only in the UK, but worldwide –most notably with the exciting new developments in the Faculty of Remote, Rural and Humanitarian Healthcare led by Professor Angus Watson.
As I write this I have just spent the weekend on call for our regional service, and have operated in and completed ward rounds in two hospitals in two different boards. My feeling is that we are getting back to a ‘new’ normality.
As we move into spring there is some evidence that the winter crisis is starting to abate. We are seeing fewer ambulance waits, but still high demand. COVID-19 numbers are fairly static, but thankfully not causing significant mortality. We know two new variants are in circulation and must learn and adapt to work around these ongoing challenges.
Focus on surgical waiting lists is, rightly, very high both with politicians and the public. It has been gratifying to see colleagues rise to challenges with innovations, including high-impact lists, increased day surgery, modified length of stays, maximal prehabilitation, digital pre-op and hospital at home. Using a combination of these in our health board we have managed a 10% increase in surgical flow between
Currie
issues of Surgeons’ News. Again, this effort is not surgical alone and we must acknowledge our anaesthetist colleagues, nurses, surgical care practitioners and all the other healthcare practitioners who support the surgical team.
I hope this edition of Surgeon’s News provides something for everyone. We celebrate International Women’s Day, and feature updates on surgical care practitioners and excellent articles on training, Fellowships and tackling burnout. We also have a sign-off from our longstanding contributor and Past Vice-President, Graham Layer, with a very fitting food column. We thank him for all his efforts and contributions over the years.
Just prior to Christmas, we received word that Surgeons’ News had been selected as Business Publication of the Year at the PPA Scotland Awards. I must congratulate both the in-house team and our colleagues at Think Publishing for all the hard work over the last few years, which has been recognised by peers in the publishing industry.
While recognition is good, this is at heart a magazine by Members and Fellows for Members and Fellows. In these pages we strive to reflect our membership accurately and appropriately, sharing different opinions, ideas and experiences. In order to do so, your feedback is important. Occasionally we get things wrong, and we appreciate feedback from our readership when we do. As editor, I take that responsibility and challenge very seriously and endeavour to edit a magazine suitable for all.
Finally, I wish all our readers a happy and peaceful period as we move in the northern hemisphere from winter to spring and, hopefully, some sunshine.
Roger Currie surgeonsnews@rcsed.ac.uk

rcsed.ac.uk | 1
Aswemoveintospringtime, thereissomeevidencethatthe wintercrisisisstartingtoabate
EDITOR’S WELCOME ''
THE ROYAL COLLEGE OF SURGEONS OF EDINBURGH
EDITOR
EDITOR Roger Currie
DENTAL EDITOR Carole Ann Boyle
DENTALEDITOR
CHANNELS PLANNING MANAGER
CHANNELS PLANNING MANAGER

Aaron Mackie
SOCIAL AND CONTENT OFFICER
SOCIALAND CONTENTOFFICER



Terri Borthwick
PUBLISHED BY
PUBLISHEDBY
The Royal College of Surgeons of Edinburgh, Nicolson Street, Edinburgh EH8 9DW
Registered Charity No. SC005317 contributions@surgeonsnews.com
Tel: +44 (0)131 527 1600
For editorial enquiries contact surgeonsnews@rcsed.ac.uk
04 AGENDA
The latest news from the College, including the NHS memorial unveiling and College election results

08 PRESIDENT WRITES
30 THE PATH TO EQUITY
Four personal experiences to mark International Women’s Day
32 GREEN CHECKS
Find out more about our new sustainable surgery checklist
DESIGN AND PRODUCTION
DESIGNAND PRODUCTION T H I N K I MEMBERSHIP& BRANDEDCONTENT
Think Publishing Ltd, 20 Mortimer Street, London W1T 3JW
Tel: +44 (0)20 3771 7200 www.thinkpublishing.co.uk
ACCOUNT MANAGER Indira Mann
DESIGNER, Juanita Adu, Alistair McGown
SUB EDITOR Kirsty Fortune
MEDICAL SUB EDITOR Dr Arshad Makhdum
GROUP ACCOUNT DIRECTOR John Innes john.innes@thinkpublishing.co.uk
12
14
16
Professor Rowan Parks on enhanced training and international links
PUZZLE SOLVER
A useful terminology buster for trainers and trainees alike
INITIATIVES IN INDIA Forum debates the challenges of providing pre-hospital care
36 TRAINEES AND STUDENTS
Championing careers and the dos and dont’s of post-CCT pathways
40 SURGICAL EDUCATION

Alex Philips charts the achievements of a joint training initiative
42 FELLOW TRAVELLERS

Two new Dental Fellows share their route to Fellowship with Carole Boyle
PRINTED BY
PRINTEDBY
Acorn Web Offset Ltd, Yorkshire, UK
ISSN 1750-7995


The views expressed in Surgeons’Newsare not necessarily those of the editorial team or the Royal College of Surgeons of Edinburgh. Information printed in this edition of Surgeons’Newsis believed to be correct at the time of going to press. The Royal College of Surgeons of Edinburgh permits single copying of individual articles for private study or research. Multiple copying of individual articles for teaching purposes is permitted without specific permission. For copying or reproduction for any other purpose, written permission must be sought from the Royal College of Surgeons of Edinburgh. Exceptions to the above are those institutions and non-publishing organisations that have an agreement or licence with the UK Copyright Licensing Agency or the US Copyright Clearance Center. Access to the magazine is available on the College website rcsed.ac.uk
Cover: RCSEd
18
THE CARE CURRICULUM Colleges join forces to develop SCP curriculum and register

SAFE PASSAGE
Claire Morgan on the development and necessity of the National Patient Safety Syllabus
20
22
26
NEW FACES
Meet your new Council and Office-Bearers
BRINGING BALANCE
The inaugural conference of the British Association of Black Surgeons

44 POSITIVE CHANGE
Zahra Shehabi on dental practices with a lower carbon footprint
46 BEATING BURNOUT
Combating the impact of burnout on patient safety and staff wellbeing

48 COLLEGE INFORMATION
Awards and grants, diploma ceremony listings and obituaries
56 LIFESTYLE
48 hours in Malta; Graham Layer’s concluding tour; chardonnay revisited; and two inspiring sculptors
PIONEER AND VISIONARY The life and times of Robert Liston BLACK SURGEONS HOSTS INAUGURAL CONFERENCE RECOGNISED IN NEW YEAR HONOURS 2023 22 05 Celebrating International Women’s Day and the pursuit of equity #EmbraceEquity
2 | Surgeons’News | March2023
Contents March 2023
22 08 62
JOURNAL OF THE ROYAL COLLEGES OF SURGEONS OF EDINBURGH AND IRELAND

Get
10 extrajournalswhen you opt for online only access
RCSEd and RSCI Fellows and Members can sign up to read TheSurgeonon line only and receive unlimited access to 10 additional titles at no extra cost:
• Surgery
• International Journal of Cardiology
• Surgical Oncology
• Clinical Neurology and Neurosurgery
• Injury
• Journal of Dentistry
• International Journal of Surgery
• Best Practice and Research: Clinical Gastroenterology
• Current Anaesthesia and Critical Care
• Seminars in Fetal and Neonatal Medicine
Fellows and Members can sign up for this by contacting:
RCSEd: membership@rcsed.ac.uk / +44 (o) 1315271654
RCSI: fellows@rcsi.ie / +353 (o) 1 402 2116
Pleasequote your RCS/ Constituent ID in all correspondence.
Receive an update when the latest issues in TheSurgeonare published. Sign in to set up alerts at:
'kjournalCitationReports"' (ClarivateAnalytics,2019) ;:,:;-:,,,:a,-*
1.874
------illc;::::=:;==::=::;;~ • RCSI
Volumel7,hsuc5
El
ELSEVIER www.thesurgeon.net .thcsurgeon.nct RCSI
The latest news from the College and profession

Warm reception for MRCS course and exam in Pakistan
RCSEd extended its presence to Pakistan in 2022 by arranging two events. The Edinburgh International MRCS OSCE Preparation Course took place at the Shaukat Khanum Memorial Cancer Hospital & Research Centre in Lahore on 24 and 25 September.


This was the RCSEd’s first international preparation course after a three-year break due to the COVID-19 pandemic.
Zahid Raza, the College’s Examinations Convener, directed the course in person. A Faculty of examiners from Pakistan and other countries carried out coaching during the two-day state-of-the-art course. The candidates had a good learning experience, as shown by their
enthusiastic participation and excellent feedback.
Two months later the College’s MRCS Part B Clinical Examination took place at the same venue.
Eighty candidates were examined over two days. RCSEd Immediate Past President Professor Michael Griffin, Vice-President Tim Graham and a team of senior
examiners travelled to Lahore to conduct the examination.
The feedback from candidates and examiners was exceptional. In particular, the candidates said they were extremely grateful for the presence of the College in Pakistan.
The host for both events was RCSEd International Surgical Ambassador Muhammad Asad Parvaiz, who works as a consultant oncoplastic breast surgeon in Lahore. The facilities provided to the examiners and candidates were considered on par with international standards.
Despite their busy schedule, the examiners were able to visit the culture and architecture of the historic city of Lahore, and enjoy Lahori cuisine.
It was Raza’s vision that paved the way for developing both of these events. The examinations team, headed by Kirsten Anderson and Anna Bielnik, played a pivotal role in realising this vision and in the smooth running of the examination.
The College plans to run many more academic activities and exams in Pakistan in the coming years.
4 | Surgeons’News | March2023 Agenda
EVENTS
The candidates had a good learning experience, as shown by enthusiastic participation and excellent feedback
Faculty and candidates at the Edinburgh International MRCS OSCE Preparation Course in Lahore
''
From left: Zeeshan Khan, Mike Griffin, Muhammad Asad Parvaiz and Shahid Khattak
New Year Honours
2023: Members and Fellows
recognised
The 2023 New Year Honours list recognises the achievements and service of extraordinary people across the UK, and we’re incredibly proud that some of our Members and Fellows were included in this historic list.
Andrew Kent, Deputy Chair of our Faculty of Remote, Rural and Humanitarian Healthcare, was awarded an OBE for services to UK health support overseas, particularly in Ukraine, and during the COVID-19 pandemic. Kent is a Trauma and Orthopaedic Surgeon at Raigmore Hospital in Inverness, Surgical Director at UK-Med and Medical Adviser at Halo Trust.
Ewen M Harrison, Member of RCSEd Global Surgery Committee and Professor of Surgery and Data Science at the University of Edinburgh, received an OBE for services to the COVID-19 response.
Ross Hemingway, Member of RCSEd’s Faculty of Pre-Hospital Care and Civilian Medical Practitioner, Commando Training Centre Royal Marines, was awarded an OBE For services to the Royal Marines.

Helen Margaret Sweetland, RCSEd Fellow and Emeritus Clinical Professor at Cardiff University’s School of Medicine, received an OBE for services to Patient Care and Medical Education.
Faculty nets charitable status
We are pleased to announce that, following a successful application to the Office of the Scottish Charity Regulator, the Faculty of Sport and Exercise Medicine UK has now been awarded charitable status as an independent organisation.

The Faculty was formed as an intercollegiate Faculty of the Royal College of Physicians and RCSEd, and works to develop and promote the medical specialty of Sport and Exercise Medicine (SEM). Find out more at www.fsem.ac.uk
Jacqueline Taylor, Honorary Surgical Fellow of the RCSEd, was awarded an MBE for services to Medical Education and to Health. Professor Taylor dedicated 38 years of service to the NHS, spending over 25 years as a consultant physician, and was President of the Royal College of Physicians and Surgeons of Glasgow until 2021. The College would like to congratulate all those recognised
with these deserved accolades and thank them for their incredible efforts and service.
Correction
In the December 2022 issue of Surgeons’ News, Clare Gerada’s name was spelled incorrectly on page 23 of the article ‘Safe team, safe patient’.
rcsed.ac.uk | 5
SPORT HONOURS
We’re incredibly proud that some of our Members and Fellows were included in the New Year Honours List
The Faculty of Sport and Exercise Medicine is now an independent charity
Order of the British Empire (OBE) medal
Alamy/Shutterstock
''.. I -• •
College announces first Women in Leadership event
The College has collaborated with the Royal College of Physicians of Edinburgh to bring you the inaugural Academy of Medical Royal Colleges (AoMRC) Women in Leadership Conference.
Taking place on 27–28 April 2023, the event will bring together expert speakers from across healthcare, financial services and government to discuss how we can enhance opportunities for women in leadership.
It will tackle key issues such as the gender pay gap and how to widen participation to drive continued growth and diversity for those looking to break into leadership and management roles.
The event will appeal to women in leadership positions, those aspiring to develop leadership skills
COURT OF REGENTS
Lord McConnell joins the Court
The College is delighted to welcome The Rt Hon. the Lord McConnell of Glenscorrodale, former First Minister of Scotland and Chancellor of the University of Stirling, as the latest Member to join our Court of Regents.
Lord McConnell was formally installed into the Court of Regents at the first RCSEd diploma ceremony of 2023 on 3 February.
He said: “Thank you to the RCSEd for this honour … I am looking forward to joining the RCSEd Court of Regents and supporting one of our top professional organisations in their important work across the world.”Scan the QR code (right) to read the full story.
or roles, NHS employers and educators, and allies to women in the workplace.
Key speakers confirmed for the conference include Dame Sally Davies, former CMO and Chief Scientific Adviser to the UK Government; Dame Anne Richards, Chief Investment Officer for Fidelity International; and Nadine Heggie, Vice-President, Media Sales & Brand Partnerships, National Geographic, at The Walt Disney Company. Opportunities for both in-person and virtual participation are available.
There will also be a an opportunity to network over drinks and canapés on 27 April.
AWARD
Follow the QR code (left) for further details or visit events.rcpe. ac.uk/rcpe-rcsedassociation-aomrcwomen-leadership



ANNIVERSARY WMSS hits 70
The West Midlands Surgical Society (WMSS) celebrated its 70th anniversary in 2022. WMSS Core Committee member Omar Mostafa and Honorary Secretary Sriram Rajagopalan have written an article highlighting its achievements.
Scan the QR code (right) to read the piece.
AWARD
Council seeks nominations
Nominations for three upcoming vacancies on the RCSEd Council will close on 19 May. Details have been sent to Fellows via email in relation to this.
Farquharson Award open for key contributors to surgical teaching

Nominations are now requested for the 2023 Farquharson Award, which is offered on a biannual basis.

The award is made in memory of Eric Farquharson, surgeon and Fellow of the College, and a previous RCSEd Vice-President, who wrote Farquharson’s Textbook of Operative Surgery
In keeping with the original bequest, the award is offered to anyone who has made significant contributions to surgical teaching or surgical anatomy at either undergraduate or postgraduate level.
Although it was traditionally reserved for those who taught at the bedside, in theatre, in the dissecting room, or through lectures or textbooks, the award
has broadened to incorporate new methods of teaching through simulators, wet laboratories, operative videos and distancelearning programmes.
Nominations are open not only to junior and senior surgeons, but also to those in allied professions who have contributed to surgical and anatomy teaching. Recipients do not have to be Fellows or Members of the RCSEd, nor do they have to be medically qualified.
The closing date for the 2021 Farquharson Award is Friday 26 May.
A proforma for the citation can be obtained from Irene MacDonald-Kennedy by emailing i.macdonald-kennedy@rcsed.ac.uk
6 | Surgeons’News | March2023
EVENT
Theawardhasbroadenedto incorporatenewmethodsofteaching
Dame Sally Davies will be speaking at the conference
Alamy--.,._ £!1. .• :· !'I • • . . . l!i. i• . THEROYAL COLLEGE OF SURGEONSt'llfrlOFEDINBURGH ''
Previous RCSEd Vice-President Eric Farquharson
IN BRIEF
The latest guidance, articles and studies
The Operating Room Black Box: understanding adherence to surgical checklists
This retrospective study looked at the use of the Operating Room Black Box (ORBB) – a data capture system for identifying intraoperative errors, events, and distractions – to track checklist compliance, engagement and quality. After a hospital policy change, the debrief scores improved significantly to 85%, P<0.001 for compliance; 88%; P<0.001 for engagement; and 71%; P<0.001 for quality. The authors concluded that the ORBB provides the unprecedented ability to assess compliance with surgical safety checklists and also engagement and quality.
Al Abbas A, Sankaranarayanan G, Polanco P et al. Ann Surg 2022; 276(6): 995–1001
Planned caesarean births have doubled in 20 years in Scotland The number of planned caesarean births in Scotland has more than doubled in the past 20 years. Public Health Scotland said there were 8,884 elective C-sections last year, up from 4,285 in 2001. The number of emergency C-sections also rose, from 7,526 to 9,359, despite the total number of births falling. Experts have attributed the rise to higher obesity rates and older mothers.

BBC Scotland News, November 2022. www.bbc.co.uk/news/ukscotland-62926167
Factors associated with postprocedure opioid prescribing and persistent opioid use among opioidnaive patients
This observational study determined factors associated with post-procedure opioid receipt and persistent opioid use among opioid-naive patients. Younger age, certain locations, in-patient procedures and musculoskeletal diagnosis were associated with increased
Higher rates of caesarean sections in Scotland may be due to higher rates of obesity and older mothers
opioids. Persistent opioid use was associated with certain locations, musculoskeletal diagnosis, public insurance and a positive depression screener. Authors concluded this information should be used to inform national guidelines for opioid prescribing and post-procedure pain management.
Parikh MA, Fabiyi C, Mistry K. Ann Surg 2022; 276(6): e706–e713
Effect of oral antimicrobial prophylaxis on surgical-site infection after elective colorectal surgery
This randomised trial evaluated the addition of 1g oral ornidazole to standard intravenous prophylaxis in 926 patients undergoing elective colorectal surgery. Surgical site
Updated guideline for closure of abdominal-wall incisions from the European and American Hernia Societies
These updated guidelines are intended to help surgeons in selecting the optimal approach and location of abdominal-wall incisions. Laparoscopic surgery and non-midline incisions are preferred when safe and feasible. In laparoscopic surgery, suturing the fascial defect of trocar sites of 10mm and larger is advised, especially after
infection within 30 days after surgery occurred in 13% in the oral prophylaxis group and 22% in the placebo group. The proportion of patients with deep infections was 4.8% in the oral prophylaxis group and 8% in the placebo group. Authors concluded that the addition of ornidazole (1g, p.o.) significantly reduced surgical site infections.
Futier E, Jaber M, Garot M et al on behalf of the COMBINE group. BMJ 2022; 379: e071476
Surgery or endovascular therapy for chronic limb-threatening ischemia
A randomised trial of 1830 patients with chronic limbthreatening ischemia contained two parallel-cohort trials. Patients with suitable great saphenous vein were cohort 1; those needing an alternative bypass conduit were cohort 2. In cohort 1, a major adverse limb event or death from any cause occured in 43% in the surgical group and 57.4% in the endovascular group. In cohort 2 it occured in 43% in the surgical group and 48% in the endovascular group. Authors concluded that surgical revascularisation had lower adverse events than endovascular treatment if saphenous vein was available; in the absence of saphenous vein, results were similar.
Farber A, Menard MT, Conte MS et al. N Engl J Med 2022, DOI: 10.1056/
NEJMoa2207899
single-incision laparoscopic surgery and at the umbilicus.

For closure of an elective midline laparotomy, a continuous small-bites suturing technique with a slowly absorbable suture is suggested. Prophylactic mesh augmentation after elective midline laparotomy can be considered.
Deerenberg EB, Henriksen NA, Antoniou GA et al. Br J Surg 2022; 109(12): 1239–1250
rcsed.ac.uk |7 Shutterstock
Getting off to a flying start
New College President Professor Rowan Parks on his commitment to ‘Making it Better’, enhancing training opportunities and strengthening international links

The passing of the reins from one President to the next can be seen as a flawless transition from one leader to another and, while it can be a traumatic time, I must thank our Past President, Mike Griffin, for making this a comfortable handover.

His support during this time has been invaluable. The College and I
thank him for his stewardship over these last four years, guiding us through one of the most difficult healthcare challenges of our age. My first two months as RCSEd President have gone by in a whirlwind as I delved head first into a diary full of College activities and events from the outset. Following the College’s annual general meeting, when I took office,
I travelled down to London to attend the Future Surgery Show on 15 and 16 November. One of the largest surgical conferences of the year, this was an excellent event, with expert speakers discussing the challenges facing our workforce as well as celebrating new advancements and surgical innovations.
During the conference I also had the opportunity to discuss the College’s focus on ‘Making It Better’, a term coined for the College’s 2022 Triennial/ICOSET Conference, which perfectly summarises what we, the College, are working towards as we aim to improve the working lives of surgeons and the wider healthcare community.
GOING GLOBAL
My next commitment was to bolster our bonds with the international healthcare community. Along with Professor Mike Griffin and Past Honorary Secretary Dr Judy Evans, I journeyed to the College of Surgeons of Sri Lanka to support our existing partnership, train examiners and contribute to the scientific programme. It was a great honour to be awarded their Honorary Fellowship, presented to me by Past President of the Sri Lankan College Dr Jayindra Fernando.
Shortly thereafter, Past VicePresident Pala Rajesh joined Mike and I to visit the College of Surgeons of East, Central and Southern Africa (COSECSA), where we engaged with our partners, including the Royal College of Surgeons in Ireland and the American College of Surgeons. The visit gave us the opportunity to support the evolution of COSECSA’s assessment and examination processes while celebrating 148 new graduates, including a number from our own Edinburgh Surgery Online courses, a partnered Master’s programme with the University of Edinburgh.
A true highlight at the end of this year was the RCSEd’s annual Festive President’s Drinks Reception in the Fellows’ Library. This offered the opportunity to thank friends of the College for their ongoing support over the past year and discuss areas of collaboration for the year ahead for the benefit of our Members and the healthcare
THE PRESIDENT WRITES 8 | Surgeons’ News | March 2023
Rowan Parks with outgoing Faculty of Perioperative Care Lead Charlie Auld at a ceremony marking his vital contribution to the Faculty
community. This was a moment of celebration with friends and colleagues that has been greatly missed over the past few years.
Finally, I spent a tremendous few days with the Association of Surgeons of India (ASI) in Mumbai, having the honour of being awarded an Honorary Fellowship. During this visit I also had the opportunity to deliver a talk on management of biliary complications following HPB surgery at ASICON 2022. It was great to meet and congratulate the new Fellows at the conference, hear the experiences of healthcare conditions in India, and continue to foster the bonds of collaboration and knowledge sharing with our international peers.
The new year started with a visit to the College of Physicians and
Surgeons Pakistan conference in Karachi, where I delivered a talk on ‘Changing Paradigms in Postgraduate Medical Education’, was chief guest at their 55th convocation ceremony and was awarded their Honorary Fellowship.
I have just returned from Dumfries House having seen the incredible work of the Prince’s Foundation. This included visiting its wellbeing centre and getting an introduction to the innovative and inspiring education programmes that range from traditional arts and crafts to horticulture and farming.
The purpose of these education and training programmes is to support learners of all ages with experiential, hands-on activities and provides many parallels to core functions of the College in terms
of offering opportunities for the development of skills and knowledge. The day ended with a private dinner with His Majesty the King, our Patron.
FUTURE AMBITIONS
As we’ve now entered a new year, my key focus will be to continue making it better for healthcare workers and patients, particularly as we continue to face challenges in staff retention and workforce planning. We will continue to work across the College and through our Policy team to lobby government and push for change to do all we can to support a workforce that is still in recovery from the pandemic. We will also work with key partners to enhance training opportunities for those progressing in their surgical career. One such example is our work with the maker of the Da Vinci robots, Intuitive, to start a robotics training programme in Scotland for surgical trainees in selected specialties. This builds on the previous training already having taken place in the clinical skills laboratories within the College, and demonstrates our commitment to continued innovation in surgical practice and training.
I believe that with a superb team and Council behind me the College can and will carry on the fabulous work of the last administration and truly make a difference for young doctors, surgeons and our patients.
Professor Rowan Parks president@ rcsed.ac.uk

rcsed.ac.uk |
We will continue to work across the College and through our Policy team to lobby government and push for change
Left (from left): Honorary Secretary Robin Patton, Professor Rowan Parks and Vice-President Clare McNaught Below: RCSEd President Professor Rowan Parks
''
SURGICAL SAFETY UPDATE
Cases from the Confidential Reporting System for Surgery (CORESS)

PEG feeding tube resistant to removal
A 49-year-old woman underwent a Roux-En-Y gastric bypass for obesity. This resulted in good weight loss, but unfortunately the patient later developed recurrent attacks of hyperinsulinaemic hypoglycaemia. Other methods to try to control the reactive hypoglycaemia were attempted without success and so bypass reversal was considered.
The patient then had a 16Fr percutaneous endoscopic gastrostomy (PEG) feeding tube inserted laparoscopically. This helped to control the hypoglycaemia, enabling the surgeon to plan conversion to sleeve gastrectomy. However, in the interim the patient was not able to tolerate the tube due to pain and asked for its removal after three months.
The surgical registrar on call was tasked with removing the PEG tube, on a day-case list, under local anaesthesia. He attempted to do so, having checked that the tube rotated freely, but found the tube resistant to attempts to dislodge it. Rather than risk injuring the patient, he contacted the PEG team, who had not been involved with the placement of the tube. The PEG team explained that, with this particular device, it was necessary to deflate an internal balloon prior to device removal, a facet of the device that the registrar was unfamiliar with (Figure 1). The tube was subsequently removed with only minor discomfort to the patient. The case was discussed at a joint educational session between the PEG service and surgical team involved.
Reporter’s comments:

PEG tubes have various securing mechanisms preventing inadvertent dislodgement. In this hospital, the majority of PEG tubes are placed in situ by a dedicated PEG service. However, in this case the tube had been placed by the upper GI/bariatric team as a surgical procedure. The registrar who was asked to remove the tube was not provided with information necessary for the safe conduct of the procedure and had no access to information about the device employed. In the event he made the sensible decision to desist from attempting removal against resistance and sought the advice of the PEG team.
CORESS comments:
This case has several learning points. The registrar knew his limitations and made a sensible decision not to persist with tube removal when he was unfamiliar with the equipment and the procedure. The supervising consultant should not have delegated an unfamiliar procedure to a trainee without ensuring either that he was either confident to undertake this or providing adequate supervision. A record describing the type of PEG and implications for removal should have been included in the patient’s notes, facilitating eventual removal.
Airway obstruction by haemostatic gauze
A patient was admitted to the cardiothoracic intensive care unit (CTICU) from their local hospital with retroperitoneal bleeding following anticoagulation for pulmonary emboli secondary to COVID-19 pneumonitis. To facilitate longerterm ventilation the patient was taken to theatre for insertion of a tracheostomy. At the end of the procedure absorbable haemostatic gauze was placed around the tracheostomy tube wound to stem skin-edge bleeding and the tube was secured. The patient returned to CTICU following the procedure.
Twenty-four hours later the patient desaturated following routine repositioning and there were difficulties passing a suction catheter down the tracheostomy. An airway emergency was declared. The tracheostomy tube was removed. Attempts were made to ventilate the patient, but these were unsuccessful and the patient lost output.
CPR was commenced. The patient was re-intubated with an endotracheal tube and return of spontaneous circulation was achieved. A bronchoscopy was then performed, revealing an obstruction at the base of the trachea. Saline flushes revealed a woven synthetic material (likely the absorbable haemostatic gauze), which had entered the airway during the resuscitation. Ventilation and oxygenation were compromised as a result. The material was successfully removed under anaesthesia and a further tracheostomy tube inserted.
Frank CT Smith Programme Director on behalf of the CORESS Advisory Board coress.org.uk
AGENDA 10 | Surgeons’News | March 2023
CORESS & reporter’s comments:
Tracheostomy tubes are susceptible to potential complications including obstruction and displacement. Equipment facilitating tube replacement should always be kept at the bedside. Endoscopy to check tube siting and potential obstruction may help in planning further action. Various teams may be involved in tracheostomy tube siting and maintenance, including otolaryngology, maxillofacial surgery, anaesthetics and intensive care. Standardised procedures within an individual unit may reduce risk of complications arising from error. Use of the haemostatic gauze employed in this case, around the tracheostomy, was not indicated and posed a potential risk of aspiration.

Problems with drains
1. A 62-year-old man underwent elective sigmoid colectomy and defunctioning ileostomy. A corrugated drain was left in place in the left iliac fossa and brought out through the abdominal wall into a stoma bag. Two days postoperatively, an entry in nursing notes recorded that the drain was shortened and cut and the stoma bag removed because it was irritating the patient, who had mild dementia. There was no mention of drain removal. There was no mention in either the operation note or nursing notes of use of a safety pin or suture to secure the drain and prevent retraction into the abdomen. When assessed by the surgical team, the wound had been dressed and there was no sign of the drain. It was later noticed as an incidental finding on follow-up CT abdomen scan that a piece of the drain had been retained in the left iliac fossa. Patient and relatives were informed and the retained portion of drain was subsequently removed at re-look laparotomy.
2. A 72-year-old woman underwent laparotomy for colonic perforation due to diverticular disease. There was a sizeable
We are grateful to those who have provided the material for these reports.
The online reporting form is on our website, coress.org. uk, which also includes previous Feedback Reports. Published cases will be acknowledged by a Certificate of Contribution, which may be included in the contributor’s record of continuing professional development.


CORESS is an independent charity supported by AXA Health, the MDU and the Kirby Laing Foundation.
pelvic collection and on completion of surgery a tube drain was placed in the pelvis and secured to the skin with a suture by the surgeon. Nursing staff on the ward cut and bagged the drain. No safety pin was employed. On the ward round on the third postoperative day the drain was noted to be absent. The retaining suture was still in the skin, but had come undone. Radiography confirmed the drain to be lying loose in the peritoneal cavity. Further laparotomy was required to remove this.
3. A 26-year-old woman underwent appendicectomy and drainage of an appendix abscess. On completion of the operation a Robinson tube drain was placed to the appendix bed and brought out though the abdominal wall. It was secured with a spiral suture wrapped around the drain and sutured to the skin next to the drain exit wound. The drain was left on free drainage and a stoma bag placed over it. On the second postoperative day, when the bag was changed, the drain was not visible, although the silk ‘retaining’ suture was apparent, loosely coiled at its point of attachment to the skin. Drain removal from the abdominal cavity necessitated laparotomy.
Reporter’s comments:
NHS England Improvement undertook a review of the National Reporting and Learning System in 2021, identifying nine reports of intra-abdominal wound-drain shortening for closed drainage systems – ‘cutting and bagging’ – in which the drain had retracted into the abdomen. Suggested critical steps in the procedure, relevant to patient safety, include:
• Cut the drain approximately 7–10cm from the patient’s skin, allowing adequate protrusion.



• Place a sterile safety pin through the drain as close as possible to the skin (to prevent drain retraction), but not under tension against the skin, where it could cause an abrasion or pressure injury.
• Document in the patient’s notes that the drain has been cut and bagged. State clearly the drain length from skin exit site to drain end and the intra-abdominal site of drainage.
• On routine dressing change, observe the site for signs of drain retraction, withdrawal or infection. Report any unusual signs or complications and record in appropriate documentation.
CORESS comments:

The Advisory Board agreed with the comments above. The operation note should clearly state where the drain is sited and should include a drain-management plan, which should be communicated at handover to recovery staff and subsequently to ward staff. If multiple abdominal drains are used, each should be labelled.

rcsed.ac.uk | 11
Figure 1: Before removing the percutaneous endoscopic gastrostomy feeding tube, an internal balloon must be deflated
c.oress FOR A SAFER SURGICAL FUTURI
Puzzle solver
JCIE
Postgraduate medical education in general, and surgical education in particular, can be confusing. There are many different bodies and acronyms in use across the UK, which can make it difficult to understand who to speak to or who is responsible for an aspect of training.
The Joint Committee on Intercollegiate Examinations oversees the appointment of examiners and assessors, and the regulation and organisation of the FRCS exams for surgical specialties covered by the JCST.
This article outlines the role of each and explains the responsibility of each body and professional in an attempt to simplify the terminology. A useful summary of the roles of the TPD, AES, CS, other assessors and the trainee are outlined at ow.ly/v0i250MBcEL.
RoT
Recognition of Training was introduced by the General Medical Council (GMC) in August 2016. Trainers must be recognised if they are in named educational roles, such as educational and clinical supervisors. In secondary care it is the DoME that gives evidence to the GMC demonstrating that trainers meet the requirements to be recognised for training. The collection of this evidence may be carried out through the appraisal process.
The educational supervisor or assigned educational supervisor (AES) in all JCST documentation is a consultant surgeon responsible for ensuring trainees have clinical supervision, helping
them with their professional development and providing induction to a new department. They also need to ensure that trainees maintain their portfolio of evidence in Intercollegiate Surgical Curriculum Programme (ISCP) and document meetings with trainees in ISCP.
The clinical supervisor (CS) will also be a consultant surgeon. They work directly with the trainee to observe clinical practice and to complete work-based assessments (WBAs).
The supervising clinician also has day-to-day contact with a trainee and observes their clinical practice. They are not required to be on the RoT list or to complete formal documents on ISCP, but they may complete WBAs and MSFs. They do not have to be a consultant.
JCST
Stephen Jones, Consultant ENT Surgeon, Deputy DME, NHS Tayside, FST Committee
Russell
Duncan, Consultant in Emergency Medicine, NHS Tayside, Postgraduate Dean, NES
Haroon Rehman, Consultant Trauma and Orthopaedic Surgeon, Victoria Hospital, Kirkcaldy
The Joint Committee on Surgical Training is the body that makes the strategic decisions on the structure of surgical training in core surgery, general surgery, trauma and orthopaedics, vascular surgery, urology, paediatric surgery, otolaryngology, plastic surgery, neurosurgery, cardiothoracic surgery, and oral and maxillofacial surgery. The JCST is also responsible for the ISCP website and eLogbook.
TRAINING
We sift through the acronyms and terminology to ensure both trainees and trainers know where to turn with any questions relating to training
TPDs
Deaneries
There is a statutory health education authority for each of the four UK countries. They are NHS Education Scotland (NES), Health Education England (HEE), Health Education and Improvement Wales and the Northern Ireland Medical & Dental Training Agency (NIMDTA). These authorities are ultimately accountable for managing the delivery of postgraduate medical training to the standards required by the regulatory body, the GMC. The structure of each differs. As HEE is so large, it is divided into seven regions. Some of them still refer to themselves as deaneries, but the term is no longer used in many. Each one will have a Lead Dean or equivalent for surgical training who is responsible for the day-to-day management of specialty training and quality management of specialty training
SACs
programmes. They are accountable to their Medical Director.
Each Dean is responsible for one or more of the specialty groupings and works with Associate Deans, GP Associate Advisors, Training and Quality Managers and their teams to ensure the delivery of postgraduate medical training.
Within NES, Associate Postgraduate Deans provide a local deputy for the Lead Dean in the relevant deanery workstreams of specialty training, quality assurance, less-than-full-time working, and trainee development, wellbeing and support. They support local training teams, TPDs and trainees. If there are concerns about the quality of training, they are responsible for visiting departments to review them and make recommendations about improvements.
There are specialty advisory committees for each of the surgical specialties covered by the JCST. One member of the SAC will be the liaison member for each region, which is not generally the region they work in, and will attend Annual Review of Competency Progression (ARCP) and Specialty Training Committee meetings in that region. The committee includes members whose responsibilities include quality, curriculum, Certificate of Eligibility for Specialist Registration (CESR) and simulation for the relevant specialty. It will also include representatives from trainees, the intercollegiate exam board for that specialty and national specialty committees.
The principal roles of the SACs include advising trainees and trainers, Surgical Royal Colleges and the JCST, and national selection and assessment of applications for the Certificate of Completion of Training (CCT). Visit www.jcst.org for a more complete summary.
LEP
You may come across this acronym, which means local education provider and refers to organisations offering training. In general it refers to Trusts and Health Boards, depending on the area of the country it is located.
Training Programme Directors are responsible for overseeing the trainees and their progression in a given specialty and region. They are appointed by Deaneries and are usually consultants in that specialty. They may be responsible for trainees in a single LEP or across multiple sites, where trainees rotate within a region. They will chair ARCP and Specialty Training Committee meetings, and are responsible for the outcomes of ARCP, including recommendation for CCT.
DoME
Otherwise known as the Directorate of Medical Education. Every Health Board or Trust is required to have a Director of Medical Education (DME). They will have a team of deputies, associates and administration staff, but the exact structure of the DME varies from one LEP to another. The DME’s role is to oversee the undergraduate and postgraduate learning environment in their LEP. This involves liaison with the deanery and any universities with medical students on placement in the LEP. The DoME is also responsible for the assessment of consultants and SAS doctors’ trainer status and recommendation for recognition of trainer status. The DoME will usually organise induction to the LEP for new members of medical staff. A member of the DoME team will help clinical departments with preparation for scheduled or triggered quality assurance visits to a department from deaneries. The department is also responsible for responses to training surveys on behalf of the LEP. They will investigate and report to the local deanery if any concerns are raised.
In this brief article we have tried to explain the role of the various bodies and people involved in surgical training and some of the confusing terms you may come across. You will find a host of useful information on the following websites:
• www.jcst.org
• www.iscp.ac.uk
• www.hee.nhs.uk
• www.nes.scot.nhs.uk
• www.heiw.nhs.wales
• www.nimdta.gov.uk
rcsed.ac.uk | 13
Initiatives in India
be met,
The development of pre-hospital care (PHC) in India was the focus of a joint workshop held alongside the RCSEd International Conference in Chennai last October. It was delivered by the Faculty of Pre-Hospital Care (FPHC) International Development Lead, David Bruce, and other speakers.

FPHC were invited to support developments in India via the Faculty of Disaster Medicine – India and Nepal (FDMIN), supported by the charity Saving Lives.
India has a mixed healthcare delivery system. Policy recommendations in the 1940s laid the foundation for a governmentfunded, three-tiered public health system to deliver preventive and curative health services. By the 1980s the private sector’s role in health began to gain prominence. Currently almost 70% of all outpatient visits and about 58% of inpatient episodes are provided by either for-profit or not-for-profit
private providers1. Central Government coordinates the work of state health authorities, but health is a state responsibility. Each one operates its own facilities and determines how government aims and policies are delivered. This has led to variation in levels of care between states, amplified by variations in geography, population density and access to care.
JOINED-UP APPROACH
Emergency medical services (EMS) are a relatively new concept in India2 and are evolving to reflect a change from a simple transportation system to one in which medical care and resuscitation occur in transit. There are numerous models for EMS capabilities, and systems in India have been described as “fragmented with no uniformity”. An emergency referral transport system was introduced under the National Health Mission and is available in 31 states and union territories. This system is accessed through toll-free numbers 108 (a public-private
David Bruce OBE International Development Lead, Faculty of Pre-Hospital Care

partnership) and 102 (a separate programme aimed at transporting pregnant women and children).
In 2021 there were 19,290 ambulances operating under these schemes, but most do not provide advanced life support, and there are limited data on the quality of care and response times. There are also private ambulance companies and ambulances may be despatched from hospitals. In terms of trauma workload, there were over 155,000 road-traffic deaths in India in 20213 – clearly there are many more serious and life-changing injuries.
TAKING THE INITIATIVE
Above: Speakers and delegates at the joint FPHC workshop in Chennai, India
It was against this backdrop that the FPHC decided to take advantage of UK speakers being in Chennai for the RCSEd International Conference to cooperate with the FDMIN and the Sri Ramachandra Institute of Higher Education and Research (SRIHER) to deliver a workshop on developing PHC in India.
Peter Patel of the FDMIN and Professor TV Ramakrishnan of
14 | Surgeons’ News | March 2023 INTERNATIONAL
The recent international College gathering in Chennai provided the perfect opportunity to discuss the provision of pre-hospital care in India and how challenges can
writes David Bruce
SRIHER invited key speakers from India and Nepal to the event, which was held on 7–8 October. I constructed a timetable with the aims of sharing current PHC initiatives in India, discussing the applicability of UK capabilities, identifying capability gaps, introducing the FPHC Pre-Hospital Trauma Course (PHTC) and providing networking opportunities.
THE STATE OF PLAY
We had 10 speakers from different Indian states, five from the UK, and one from the Nepal Disaster and Emergency Medicine Centre in Kathmandu. A second morning was added to the workshop for further discussions and the launch of the first edition of the Emergency Services First Aid Drills Aide Memoire. The workshop opened with a remote presentation by FPHC Chair Pam Hardy. Professor P V Vijayaraghavan, Vice-Chancellor of SRIHER, then highlighted the importance of early resuscitative care to survival rates and its impact on longer-term outcomes. Tausif Thangalvadi, former Head of Emergency Medicine and Director of Premier Hospital Hyderabad, gave an overview of ambulance systems and pointed out that India’s first public-service ambulances – 15 vehicles – were only established in Mumbai as recently as 1985. Prior to that, patients were taken to hospital in auto-rickshaws or ambulances sent from the hospital; outcomes were poor. Subroto Das of the Lifeline Foundation spoke about the
Highway Rescue Project he established in 2002 to reduce the number of deaths on state highways. This was after his wife sustained very serious injuries and took 5.5 hours to reach hospital. More recently he has focused his efforts on training the population to provide high-quality CPR in India’s techno-cities and using alternative healthcare practitioners, who are already established in communities. He stated that studies of private ambulance services revealed that there was no regulation, crew training was variable and equipment was either not working or staff had not been trained in its use in 20–70% of cases.
Professor Aruna Ramesh of Ramaiah Medical College, Bengaluru, highlighted that 50% of patients with acute coronary syndrome aged 30–70 years died before reaching hospital. This had prompted her to set up a hub-andspoke system and ECG telemedicine capability to reduce time to thrombolysis. She has also introduced an awareness campaign for stroke and chest pain, allied with CPR training for communities.
Further initiatives were introduced by Professor Vijaysankar of the Government Kilpauk Medical College & Hospital, including a trauma registry, and speedier thrombolysis and triage tools to aid junior clinicians.
Rod Mackenzie, from the UK, described the evolution of PHC, trauma systems and the introduction of the Pre-Hospital Emergency
References
1. Selvaraj S, Karan KA, Srivastava S, Bhan N, Mukhopadhyay I. India health system review. New Delhi: World Health Organization, Regional Office for South-East Asia; (2022).
2. Emergency Medical Service in India: a Concept Paper by National Health Systems Resource Centre (Undated).
3. Accidental deaths and suicides in India from National Crime Records Bureau (2021).
Medicine sub-specialty in the UK. He handed over to Professor Mark Wilson, who outlined technological developments that could aid effective PHC. Pragya Mallick, who trained in Chennai and is a pre-hospital emergency medicine (PHEM) trainee in the East of England, then gave a unique insight into her career. I also introduced the PHTC, which we plan to run at SRIHER in 2023 allied with a Train the Trainers course, with the intention of the course rippling out across India.
AIMS AND AMBITIONS
Day One was rounded off by our host, Professor Ramakrishnan, describing the variations in ambulance personnel training and how SRIHER had introduced a four-year degree course, but that most graduates left India as their status and remuneration was much greater in the Middle East. We agreed that a system of paramedic registration and defined scope of practice were important topics for development, but were long-term goals.
Below: Dr David Bruce, left, making presentation to Professor T V Ramakrishnan of SRIHER

On Day Two Rashmisha Maharjan from the Nepal Disaster and Emergency Medicine Centre outlined the nation’s ambulance capability. Two regions have a toll-free 102 service but crew training and equipment are variable. To address this, the Centre has produced a first-aid handbook in Nepali and delivered advanced, community and maternal health first-aid courses to more than 12,000 civilians.
Our Emergency Services First Aid Drills Aide Memoire is based, with permission, on a publication by Major General Tim Hodgetts and had been updated by FPHC and Indian contributors. An initial print run of 500 has been funded by Saving Lives for distribution to trained personnel in India.
In summary, the workshop achieved its aims, and a number of work strands are being taken forward by the FPHC and colleagues in India.
rcsed.ac.uk | 15
India’s first public service ambulances – 15 vehicles – were only established in Mumbai as recently as 1985
''
The care curriculum
The RCSEd and RCSEng have developed the SCP curriculum and register, as Bill Allum and Charles Auld explain

The development of multidisciplinary team working is essential to delivering high-quality and safe patient care. Medical associate professionals (MAPs) are nonmedically qualified practitioners who work within multi-professional teams, and the group encompasses physician associates (PAs), anaesthesia associates (AAs) and surgical care practitioners (SCPs).
The regulation of these professional groups was set out by the Department of Health and Social Care in its publication entitled The regulation of medical associate professionals in the UK in 20191 Although statutory regulation was granted for PAs and AAs, with the General Medical Council (GMC) as the regulatory body, the UK Government stated that it would only consider statutory regulation for SCPs if recruitment to SCP training posts was open to a direct-entry route – that is, for those SCPs not from a healthcare background. In response, the options for this route are actively being explored by the SCP National Advisory Committee at Health Education England (HEE).
In a previous edition of Surgeons’ News2, we addressed the need for better recognition and improved regulation of SCPs. This included the need to develop a voluntary yet formal register of SCPs similar to the Physician Associate Managed Voluntary Register (PAMVR), implemented by the Faculty of Physician Associates for PAs, which has been crucial to the approval of statutory regulation
(see www.fparcp.co.uk for more information). More recently, the Royal College of Anaesthetists (RCoA) has set up a voluntary register of AAs (see www.rcoa.ac.uk).
WORKING TOGETHER
To support this case for statutory regulation and to demonstrate a commitment to SCPs, the Royal College of Surgeons Edinburgh (RCSEd) and the Royal College of Surgeons of England (RCSEng) agreed to work together on a bi-collegiate basis and as equal partners. As the surgical bodies currently championing and supporting the work of the extended surgical team (EST), they formed the joint EST Project Board with two principal aims:

To revise and update the SCP curriculum, previously owned by the RCSEng, for the MSc in Surgical Care Practice to support the postgraduate training for SCPs and provide a future route to facilitate direct entry to SCP roles.
To develop a managed voluntary register (MVR) for SCPs.
The two work streams had representatives from both surgical colleges, HEE, SCPs from different surgical specialties and programme directors from higher education institutes running the MSc programme, as well as representatives from governance and the legal profession.
CURRICULUM FRAMEWORK
SCPs have become well established in healthcare organisations and this has been shown to enhance the capability of the surgical team to
develop professionally. They support and enhance training opportunities for surgical trainees and provide surgical services that complement the medically trained workforce.

The educational governance of SCPs has expanded since the first SCP curriculum was published in 2006. In addition, there have been significant changes to curricula following the GMC publication of Excellence by design (GMC 2017)3 , which sets the standard for postgraduate medical curricula, with inclusion of practice-based outcomes, as well as defined evidence of practising professionally.
The 2022 SCP curriculum revision incorporates the principles of Excellence by design by using workbased assessments to provide evidence of capability in practice. The revision has built on the 2014 version, providing generic and specialty-specific knowledge, and clinical and technical skills. A key component of this curriculum revision is the inclusion of those capabilities that define the professional role of an SCP alongside the clinical and technical training.
These are based on the four pillars of advanced practice defined in the
SURGICAL CARE PRACTITIONERS
16 | Surgeons’ News | March 2023
Charles Auld Former Lead for Faculty of Perioperative Care, past Council member RCSEd
Bill Allum RCS England Council Member and Chair, Workforce and Training Committee. Chair, SCP National Advisory Committee
-t-• •
The new curriculum and MVR will ensure SCPs are well qualified and will be a great asset to the surgical team
HEE’s Multi-professional framework for advanced clinical practice in England4:
Management and leadership
Professional values and behaviour
Education and training
Audit and research
The curriculum is designed to be taught over two phases (phase one: generic; and phase two: specialtyspecific topics) and usually to be completed in three years. This design allows flexibility of entry to enable recognition of previously gained knowledge, skills and experience. This complements the option of direct entry from a non-healthcare background or from an established non-medically qualified background.
The components of the assessments have been designed to meet the requirements of the higher education institutes that offer the MSc in Surgical Care Practice. It is expected that SCPs will advance their career with appropriate professional development to work independently within the surgical team. The pluri-professional skill set learnt from the course will prepare them for pursuing more advanced practice should they so wish.
The RCSEng and RCSEd wish to ensure that a qualified SCP is educated to a standard approved by the colleges.
The combination of a full curriculum revision to meet the current GMC standards and the development of an MVR are consistent with ensuring a highquality, well-qualified practitioner who can work within the surgical team and gain great job satisfaction in their professional role.
REGISTER BENEFITS
References
1. The regulation of medical associate professions in the UK. www.gov.uk, 2019.
2. Surgeons’ News, Mar 2020: 32–33.

3. Excellence by design. GMC; 2017.
4. Multi-professional framework for advanced clinical practice in England. 2017. www.hee.nhs.uk
Although an MVR is not a compulsory requirement for SCPs, it is the official register of SCPs held jointly by the two surgical colleges. Appearing on the register is an asset to individual practitioners as it demonstrates to their peers, employers and patients that they are appropriately qualified and working to the standards expected by the two surgical colleges.
The register will set the standards for postgraduate education and training, enhance the credibility of the SCP among their peers, employers and patients, and advance the case for statutory regulation by the GMC.
Inclusion on the register is based on three entry points (see ‘MVR routes of entry’, below) reflecting
MVR routes of entry
1 An SCP with a qualification aligned with the SCP Curriculum Framework 2022, that is, an MSc/PGDip in Surgical Care Practice that is aligned with the SCP Curriculum Framework.
2 An SCP-in-training, who is enrolled in an SCP Programme aligned with the SCP Curriculum Framework 2022.
3 An established SCP fulfilling a relevant academic, clinical or training role who does not hold the approved qualification, but can provide evidence of working as an SCP.
the various levels of academic qualification and experience, as well as the inclusion of SCPs in training. The eligibility criteria and application process are set out on the MVR website at www. scpregister.org
SCPs must also remain in good standing with their regulatory body and commit to meeting the ongoing CPD requirements.
In time, the information held on the MVR will allow the colleges to provide the necessary guidance for the SCP community to support appropriate job plans and structured CPD in order to enable SCPs to perform their duties to the highest standard.
LAUNCHING THE MVR
Early access to the Curriculum Framework and MVR was available from October 2022 to higher education institutes that deliver the MSc in Surgical Care Practice and those affiliated to the RCSEd Faculty of Perioperative Care, Associate Members of RCSEng, and members of the Association of SCPs (AoSCP) and the Association of Cardiothoracic SCPs (ACTSCP).
As a member benefit, those affiliated to RCSEng or RCSEd through either the RCS Associate Membership or the Faculty of Perioperative Care can join the MVR at no cost. For all others, an annual fee of £25 applies.
To find out more visit: www. scpregister.org or contact scpmvr@rcsed.ac.uk
The EST Project Board, which will continue to work together on further projects for the benefit of SCPs, would like to thank all those who contributed to the development of the curriculum and MVR. In particular, they would like to thank HEE for its financial support towards the MVR development costs.
rcsed.ac.uk | 17
• • • •
The register will set the standards for postgraduate education and training, and enhance the credibility of the SCP
,,
Safe passage
In 2002 the World Health Organization (WHO) declared patient safety a priority. Globally, one in 20 patients experiences preventable harm as a result of medical care, of which 12% of these events result in permanent disability or death (Panagioti et al, 2019). The WHO developed International Patient Safety Curricula for medical schools (2009) and multidisciplinary teams (2011), the uptake of which are unknown. As a global issue, although patient safety principles are transferable, healthcare systems and delivery are very different.
Supporting the concept of education and training in patient safety, Health Education England (HEE) commissioned a review of stakeholders’ opinions through Imperial College’s Centre for Health Policy in 2015. And in 2018 the Care
Quality Commission stated that “with so many different bodies having a role in education, the importance of patient safety training is slipping through the cracks at undergraduate level and throughout careers”.
In the UK the first NHS Patient Safety Strategy was published in 2019 with one of its three strategic aims, ‘involvement’, supporting the creation of a National Patient Safety Syllabus (NPSS) that would provide a framework for all NHS staff. It was stated this would be applicable “across a variety of competence levels and address the different learning needs of 1.3 million staff in 350 different careers”.
One size does not fit all, although the potential benefit of a single syllabus of standardised patient safety education and shared terminology for all NHS staff is huge. HEE, working with a team from the

PATIENT SAFETY
Claire Morgan on the development and importance of the National Patient Safety Syllabus, which provides an NHS-wide safety framework
18 | Surgeons’ News | March 2023
______ ! _______
Academy of Medical Royal Colleges, wrote the first NPSS, published in 2020. Following widespread consultation, it was republished the following year with updated content as version 2. It is planned that the NPSS is reviewed every three years.
FIVE-WAY CONTENT
The syllabus covers five domains: a systems approach to patient safety, learning from incidents, human factors, creating safe systems and being sure about safety. There are four cross themes based on systems thinking, human factors, risk expertise and safety culture.
The syllabus has tools for incident reporting and investigation, including systems to prevent harm reflecting those used within other safety-critical industries. It also encompasses national safety initiatives, including national
alerts, key safety regulations and safety campaigns. Updated content in version 2 includes competencies in Safety-II, medico-legal education, and the value of patient, carer and public involvement in patient safety. Some terminology was changed to reflect less of a blame approach, describing ‘human error’ as a ‘systems-induced error’ or ‘human performance variation’.
DELIVERING THE SYLLABUS
While some use the terms ‘syllabus’ and ‘curricula’ synonymously, the NPSS authors inform that some content not included will be more appropriately delivered through curricula. Research has shown patient safety curricula should be adapted to the needs of the learners, with different groups of healthcare professionals having different clinical and regulatory priorities.
Education in patient safety requires practical application with experiential examples and team training. Some stress the value of patient involvement in patient safety education, with delivery by experts. In addition, the introduction at undergraduate level or the start of clinical practice is considered important, with ‘spiral’ curricula revisiting themes iteratively to foster lifelong patient safety learning.
Curricula for the first two levels of the NPSS are now accessible to NHS and care workers on the national e-Learning for Healthcare platform. Delivery is animated, with written interactive content supported by regular quizzes/questions, including those for self-reflection. There are references to seminal research papers that can be accessed through the portal, and links to reports and policies through relevant web pages.
‘Level 1: Essentials of Patient Safety’ is aimed at all staff and includes an additional session for leaders. The content is at a basic level and includes purpose of patient safety education and impacts of harm; in the leaders session their role is described along with key behaviours. ‘Level 2: Access to Practice’ is aimed at clinicians and those with an interest or need for more in-depth knowledge. It expands on systems, risks, human factors and cultures. Levels 3, 4 and 5 have just been published in a
curriculum guidance document aimed at patient safety experts and those working in the patient safety field.
DIFFERENT SOURCES
With the appointment of patient safety specialists in organisations to lead safety improvement across the system, the NPSS will provide an excellent resource. While it was developed to be applicable nationally, due to differences in NHS systems it may be appropriate for development of additional nationspecific, as well as specialty-specific, educational modules to be added.
There are numerous education and learning platforms, and courses, to complement and expand on the NPSS to support curricula. Many of these can be found through the charity Patient Safety Learning, with information found on its hub. Patient safety improvement programmes also provide resources through national NHS websites, as do many regular UK patient safety conferences.
The RCSEd runs non-technical skills training courses for surgeons, perioperative care practitioners and dentists, with similar programmes elsewhere. Specific courses have recently been launched by the Healthcare Safety Investigation Branch, providing extensive training for systematic incident investigation.
A more academic approach can be undertaken on university-approved courses such as the College’s MSc in patient safety and clinical human factors run in partnership with the University of Edinburgh.

Echoing the 2013 Berwick Report on patient safety in the NHS, by looking after NHS staff and providing them with the tools and education they need, patient safety can be a priority for all. By moving forward with the development of open and learning cultures with patients at the centre, improvements in care will be realised.
This article is written with acknowledgement to all those who contributed to the NPSS. To find out more visit www.hee.nhs.uk/ our-work/patient-safety
Shutterstock
rcsed.ac.uk | 19
Claire Morgan Consultant in Restorative Dentistry, and member of Dental Council and RCSEd Patient Safety Group
Education in patient safety requires practical application with experiential examples ,,
Your new Council and Office-Bearers

COLLEGE 20 | Surgeons’ News | March 2023
the people elected to represent the College
Meet
The Council is the governing body of the RCSEd and represents the professional interests of the College’s membership. As the College is a charitable organisation, the Council Members are also Trustees of the College. The Council comprises five OfficeBearers, 15 elected members, one trainee member and the Dean of the Faculty of Dental Surgery. For more about our Office-Bearers, visit www.rcsed.ac.uk/the-college/office-bearers
 Back row from left to right: Stuart Clark, Alistair Mountain, Nirmal Kumar, Philip Turner, Christopher Caddy, Ahmed Nassef, Zahid Raza, Angus Watson, Majid Mukadam, Ian Hawthorn. Front row from left to right: Amanda McCabe, Anna Paisley, Robin Paton (Honorary Secretary), Timothy Graham (VicePresident), Rowan Parks (President), Clare McNaught (Vice-President), Siong Liau (Honorary Treasurer), Philip Taylor (Dean of the Faculty of Dental Surgery), Claire Edwards. Not pictured: Katie Hurst, Krishnakumar Madhavan, Sai Krishna Vittal, Michael Silva
Back row from left to right: Stuart Clark, Alistair Mountain, Nirmal Kumar, Philip Turner, Christopher Caddy, Ahmed Nassef, Zahid Raza, Angus Watson, Majid Mukadam, Ian Hawthorn. Front row from left to right: Amanda McCabe, Anna Paisley, Robin Paton (Honorary Secretary), Timothy Graham (VicePresident), Rowan Parks (President), Clare McNaught (Vice-President), Siong Liau (Honorary Treasurer), Philip Taylor (Dean of the Faculty of Dental Surgery), Claire Edwards. Not pictured: Katie Hurst, Krishnakumar Madhavan, Sai Krishna Vittal, Michael Silva
Bringing balance
The British Association of Black Surgeons (BABS), the UK’s largest collaboration of Black surgical professionals, was launched in October 2021. They aim to promote diversity and inclusivity across the surgical field, widen participation in surgical leadership and promote long-term career development. BABS strive for professional excellence in patient care, education, and research. They encourage students and trainees to be involved in audits, quality improvement and collaborative research. Furthermore, they recognise that early mentorship can have a huge impact on future generations.


BABS held their inaugural conference at the Royal College of Surgeons of England in November last year. It was a memorable day for all, honouring surgeons of the past, present, and future, whilst recognising the journey that must be continued to ensure equity and inclusivity for all. The platinum sponsor for the conference was the Royal College of Surgeons of
Edinburgh (RCSEd). BABS is an organisation that strives for professional excellence in patient care, education and research. It encourages students and trainees to be involved in audits, quality improvement and collaborative research. Furthermore, it recognises that early mentorship can have a huge impact on future generations.
RECOGNISE THE CHALLENGES
Sarah Itam, Consultant Urological Surgeon, BABS CEO and Chair, kicked off the day highlighting some of the proven surgical challenges faced by Black individuals. These range from difficulty entering medical school (despite having equivalent grades), through to entering positions of leadership as a consultant.


After an honest and wholesome introduction in relation to these challenges, and the importance of associations such as BABS, one could sense heartfelt movement within the crowd, who were simultaneously filled with anticipation and high expectations for the rest of the day. In Itam’s words: “If the surgical
landscape fails to include everyone, everyone in the surgical landscape has failed [and therefore] ultimately, we have failed our patients.”
Lord Victor Adebowale CBE and Patron of BABS then gave an address. He shared with us his mother’s experiences of racism and the lack of opportunities she faced as a nurse within the NHS. The NHS is celebrating 75 years of service and, although steps have been taken to improve the racial disparity in health outcomes and the lack of diversity in leadership, these issues persist. Offering his personal support, Lord Adebowale engaged an audience of current and future surgeons with his words of encouragement and fervent support.
Professor Michael Griffin OBE, Immediate Past President of the RCSEd, led a factual discussion that provided the audience with hard-hitting statistics regarding the poor representation of Black surgeons in the College and the wider surgical community. The reality being that the Royal Colleges of Surgeons in the UK, the NHS and its supportive collaborators need to

22 | Surgeons’News | March 2023
Sabrina Samuels, CT2 Burns and Plastic Surgery, Nottingham University Hospitals
Ofuchi Egbuji CT3 Otolaryngology, Norfolk and Norwich University Hospitals
BABS CONFERENCE
Sabrina Samuels and Ofuchi Egbuji report on the inaugural conference of the British Association of Black Surgeons, and its mission to achieve diversity and inclusivity across the surgical field
“work together to put it right”.
Tim Mitchell, Senior VicePresident of RCS England, further highlighted the important role the Royal Colleges will play in the coming years, emphasising that this is a “wake-up call” for them.


Differential attainment is a hot topic at present. Samantha Tross, the first female of African-Caribbean descent to become a trauma and orthopaedic surgeon, explained some of the multiple problems in this area and offered solutions to help close the gap in attainment –for example, grassroots projects, mentorship schemes, zero tolerance against discrimination and minority support groups such as BABS.


Consultant Oncoplastic Breast
Surgeon Louise Alder then went on to lead the delegates in a lively digital quiz that focused on the different characteristics of the surgical specialties.

LISTEN AND BELIEVE
Referring to the themes in Maslach and colleagues’ paper, Richard Jones from Practitioner Health stated that “burnout only happens in
rcsed.ac.uk | 23
If the surgical landscape fails to include everyone, everyone in the surgical landscape has failed
''Above, clockwise from top left: Sarah Itam, CEO and Chair of BABS starts proceedings; Lord Victor Adebowale CBE and Patron of BABS; Samantha Tross discusses differential attainment; Louise Alder leading the lively digital quiz; speakers’ group shot; from left: Tim Mitchell, Christopher Sanderson, Shireen McKenzie, Sarah Itam and Professor Michael Griffin OBE; debate on the MCR
Left: Lord Simon Woolley Kt, founding Director of Operation Black Vote delivers his keynote address
Photos courtesy of BABS/Ian Kiffin
organisations that are on fire”. He explored the causes of this fire, including the onus being placed on individuals to improve the situation in which they work. So how can we change the culture within healthcare? He believes we need to want to listen to each other, believe in our colleagues and want them to succeed. We also need to establish safe pathways for raising concerns.
Consultant Urological and Robotic Surgeon Professor Kingsley
Ekwueme interviewed Consultant Urological Surgeon Professor Frank Chinegwundoh MBE. Professor Chinegwundoh discussed his gateway into research and why he was so invested.

The discussion highlighted a popular paper published in BJU International entitled ‘Risk and presenting features of prostate cancer amongst African-Caribbean, South Asian and European men in north-east London’ – research that has greatly helped to improve equity of treatment of prostate cancer.
Above: Andrew F Alalade makes the case for the MCR
Above right: Professor Frank Chinegwundoh MBE (left) being interviewed by Professor Kingsley

Ekwueme
Below: Georgette Oni taking part in afternoon panel debate on the multiple consultant report
MCR DEBATE
In the early afternoon, we entered a panel debate around the topic of the multiple consultant report (MCR). Andrew F Alalade, Consultant Neurosurgeon, on the team arguing for the MCR, commented that having multiple assessors, being able to choose your clinical supervisor and a national selection programme have helped break down racial barriers.
become financially healthy, with tips and tricks on how to invest for future generations.
After a coffee break and networking session, there was a vibrant buzz among delegates.
References Montgomery A, Panagopoulou E, Esmail A, Richards T, Maslach C. Burnout in healthcare: the case for organisational change.
BMJ. 2019 Jul 30;366:l4774. doi: 10.1136/bmj.l4774.
PMID: 31362957.10.1136/ bmj.l4774
Georgette Oni, Consultant Plastic Reconstructive and Oncoplastic Breast Surgeon, argued against the MCR, suggesting that the MCR can be a subjective process and that work-based assessments may be heavily weighted based on your relationship with the assessor.
Burnout only happens in organisations that are on fire
Deepa Bose, consultant orthopaedic, trauma and limb-reconstructive surgeon, humbled attendees with her experiences in global and humanitarian surgery. She emphasised that a lack of diversity is life-threatening on a local and global scale. She stated, “investment is affordable and can save lives” and highlighted areas to be invested in, including clinical care, advocacy, education and research.
After this, Consultant Urological Surgeon Graham Watson gave an inspiring talk about the work he is doing with Medi Tech Trust and invited delegates to get involved.
ALLYSHIP AND RESPECT
Martin Griffiths CBE DL, consultant trauma and vascular surgeon, shared his experiences of working with schools and the community to build compassion and help prevent violent attacks that lead to many unnecessary deaths. He is a firm supporter of allyship and working together to achieve a safe community for all.
This was followed by a presentation from Olamide Dada, founder and CEO of Melanin Medics, a non-profit organisation that supports African-Caribbean medical students to get into medical school, and a key advocate in moulding the future generation.

Jerran D Whyte, Managing Partner at Belvedere Wealth Management, offered his knowledge on how to
For the investment to be a success, being prepared to learn from others, and having patience and respect, is integral.
RESOUNDING SUCCESS
To improve equity and diversity within healthcare, Lord Simon Woolley Kt, founding Director of Operation Black Vote, gave an empowering keynote speech. He invited everyone to look around the conference hall to take in this historic occasion. He stated that we need to own our voice, demand change, keep hope alive and inspire a generation to help one another succeed.
The BABS inaugural conference, held on the 15th November 2022, was a momentous day for all. One that exceeded all expectations. Sarah Itam thanked those who attended and supported the event. BABS certainly went above and beyond to show the next generation what Black excellence looks like: a mirror image of themselves.
Photos courtesy of BABS/Ian Kiffin
''
Cultivating the surgical community
The British Association of Black Surgeons welcomes members at all levels

The vision of the British Association of Black Surgeons (BABS) is to enrich patient care through diverse and inclusive leadership promoting equality, diversity and inclusion across the surgical field.
BABS has both the tools and the team to enable it to develop and enhance surgical excellence among all of its members, and would like you to be a part of this. No matter your background or experience, it welcomes everyone from medical students to consultants.
By joining you will have access to a large community of surgeons from

multiple specialties who will support and enrich your surgical journey. You will also be the first to know of any upcoming events, seminars, conferences and courses, with discounts available to members.
The association is currently recruiting for various roles in BABS. There will also be opportunities throughout the year to help facilitate events and join the BABS leadership and management teams. Find out more about becoming a member or joining the leadership team by following the links and QR codes shown (right).
To sign up please use the weblink babs-uk.org/ membership or this QR code


To apply for a role please use the weblink babs-uk. org/jobs or this QR code
More information can be found on the official social media platforms @babsuk_org babs-uk.org
rcsed.ac.uk | 25
ROBERT LISTON Pioneer and visionary
History often reduces pre-anaesthesia surgery to a ‘butchering art’. While the horror of surgery before the discovery of ether and antisepsis can only be imagined, the skill shown by many surgeons operating at this time cannot be understated.


Perhaps the greatest myth from this period is Robert Liston’s 300% mortality rate. Best known for being the first to operate using ether in the UK, Liston (1794–1847) is often reduced to a surgical showman.
It is claimed he walked into the surgical theatre declaring: “Time me, gentlemen”, giving him the accolade ‘the fastest knife in the west end’ – and, of course that he killed three people during one surgery.
Born in Linlithgowshire in 1794, he studied at the University of Edinburgh from the age of 14 covering a range of topics before focusing on medicine. He did not, however, graduate MD and instead took extramural anatomy lessons, becoming an assistant to Dr John Barclay. With a focus on surgery, he became a surgeon’s clerk at the
Edinburgh Royal Infirmary before completing his surgical training in London. He became a Fellow of both the RCSEd and the Royal College of Surgeons of England.

He returned to Edinburgh and started his own anatomical teaching school with his distant cousin, James Syme (1799–1870), although after around four years Liston withdrew from anatomy and focused on a full-time surgical career. In Edinburgh he had a private surgical practice and worked at the Edinburgh Royal Infirmary but, after numerous fallouts, he left for London in 1834, where he spent the remainder of his career, passing away at the age of 53 in 1847.
DISPELLING THE MYTH
The 300% mortality story has become apocryphal and is widely replicated. The tale goes that during an amputation of the leg, in his desire for showmanship and speed, he cut off two of his assistant’s fingers and sliced the coat tail of an audience member. All three are supposed to have succumbed, the patient to blood loss, the assistant to gangrene and the audience member to a heart attack caused by the
shock. However, recent research has found the apparent origin of this story lacking in historical fact and accuracy. In my own research, I have found no primary sources relating to this event and it is hard to believe that someone of his stature could have avoided the public scrutiny of such an occurrence.
A rare instance when Liston did fail, resulting in negative publicity, highlights this point. In 1841 a child of 12 was admitted to University College Hospital, London. The house surgeon examined the boy and presented the case to Mr Liston as a suspected aneurysm. However, on seeing the boy and examining his neck, Liston claimed the boy was too young for an aneurysm and diagnosed the swelling as a tumour and proceeded to cut to prove his diagnosis. The incision was followed
26 | Surgeons’ News | March 2023
Louise Wilkie dispels the myths surrounding the 19th-century surgeon whose innovation, skill and compassion enhanced the lives of many
FROM THE ARCHIVES
Above inset: Portrait of Robert Liston
Louise Wilkie Curator Surgeons’ Hall Museums
instantly by excessive bleeding and Liston closed the incision and returned later to operate. Despite tying the artery, the boy unfortunately died from haemorrhage a few days later. Liston published his account of this case and immediately received criticism, particularly from his house surgeon, who published his own account in the Provincial Medical Journal.
He criticised Liston’s write-up and his conduct, arguing he had made a mistake in his assumption and covered it up. Liston received a sustained barrage of criticism about this case for the remainder of his career. This case alone significantly highlights that if Liston had indeed gained a 300% mortality for a single surgery, there would have been ample discussion of that failure in contemporary medical literature
(and no doubt a similar publication of his own defence).
At a time where the mortality rate for surgery was extremely high, Liston had remarkably low mortality statistics. There are numerous reasons for this, including his noted speed. This speed was arguably not a mark of showmanship, but instead a skill that was enabled out of a unique combination of proficiency, precision and dexterity, which qualified Liston as one of the most technically competent of his era. His amputations were measured in
seconds and were often performed solo, and his lithotomy procedures were performed in two minutes, which with no anaesthesia most likely reduced the two main causes of operative mortality – blood loss and shock.
His speed can also be attributed to a real concern for the patient’s experience. He advised to always take into consideration the mental state of the patient, only operating on those who believed in a positive outcome. With this attitude it is hardly surprising that he was the first surgeon in the UK to undertake an operation using anaesthesia in 1846, merely a year after it was discovered by dentists in America. It is regrettable that Liston passed away only a year after his most famous surgery – it would have been very interesting to see what developments he could have made with anaesthesia in his arsenal.
PIONEERING SURGEON
A case that embodies Robert Liston’s skill and confidence as a surgeon, as well as his patient advocacy, is a tumour removal, the cast of which resides in the museum. In 1834 a Mrs Fraser had a facial tumour removed at the Edinburgh Royal Infirmary by Liston. This tumour obstructed the entire left side of her face and Liston could see numerous veins in the tumour through the skin and feel arteries beating within. With the help of an assistant he removed the tumour while the patient was in a seated position, before lying her down to secure the bleeding vessels after the tumour was removed. This tumour was nine inches long and, of course, this was pre-anaesthesia.

In his write-up, he talks of the patient numerous times: “She had firmly made up her mind to undergo the operation” and had “borne all this with the utmost courage and without a murmur”. After Liston left Edinburgh for London only months after this surgery, Mrs Fraser’s local surgeon wrote to Liston to report on her condition ending: “In a word she is one of the most happy women I am acquainted with.”
Aside from his operating skill, Liston displayed great innovation in his advocacy on cleanliness both pre-surgery and post-surgery. He
rcsed.ac.uk | 27
Wellcome Collection
His noted speed was arguably a unique combination of proficiency, precision and dexterity
''
Postoperative plaster cast of Mrs Fraser’s face and a wax cast of the removed tumour
insisted on a clean apron, clean instruments and clean sponges for each surgical case (bearing in mind this was the era where a bloody washing bowl and apron represented the success of the surgeon). Wounds and limbs would be cleaned before operating and even – and this is quite remarkable – the limb shaved (this was only discovered in the 20th century as a means to eliminate potential bacteria on hairs).
This indicates that Liston linked cleanliness and postoperative inflammation long before most. These innovative procedures most likely assisted in his low mortality rate after amputation between 1835 and 1840, being around 15%, which is remarkable during this time. It would take Joseph Lister’s fascination with inflammation some 20 years later to discover the cause of infection and invent the aseptic surgery we know today (incidentally, Lister was present during Liston’s 1846 ether surgery).
Liston’s contributions to surgical development are endless, including improving amputations by championing the importance of the amputation flap and eliminating the circular cut previously used. He was one of the first to attempt and advocate lithotrity (one of the first minimally invasive surgical procedures) and advanced surgical treatment of aneurysms. He also invented numerous medical instruments, some in collaboration with Edinburgh instrument maker Alexander Young. Liston thought surgical instruments should be simpler and felt that some of these instruments’ complexities seemed “to be chiefly intended to compensate for want of tact and manual dexterity”.
FREQUENT FALLOUTS
His flaws seem to centre on his character: confident, argumentative, critical and outspoken. His career is littered with public fallouts with fellow surgeons and medical institutions. Perhaps the most unfortunate of these was with his distant cousin and fellow surgeon, James Syme.
Syme and Liston’s disagreement stemmed from growing competition for surgical posts in Edinburgh during the 1820s. This fallout is
MR. YEARSLEY':::; LET'lEI S TO THE PRESIDENT AND COUNCIL OF THE ROYAL COLLEGE OF SURGEONS IN LONDON, ON THE UNPROFESSIONAL CONDL'CT OF MR. LISTON.
1\fR. PRESIDENT AND GENTLEMEN, MosT reluctantly I come before you in the character of a complainant, more especially as the gentleman whose conduct I must arraign is a member of your honourable Council.
It may still be in your recollection that, in the month of March 1841, I addressed a note to many of the leading members of the profession, inviting them to witness and investigate the effects of extirpation of enlarged tonsils, and also of the uvula, in certain cases of Stammer and defective speech. In the course of my professional practice, I had frequently performed the former of these operations for the cure of deafness. For this I claim no merit. It had frequently been done with the same intention. Neither was the latter operation novel. Both, in short, had long been recognised as minor surgical operations. The only novelty consisted in their application to the treatment of Stammer, and that I freely own was the result of accident.
In some cases in which Deafness and Stammer were associated with enlarged tonsils, and an elongated or thickened uvula, I found that on the removal of these morbid conditions, not only the deafness, but the defective speech was cured or relieved. The observation of this fact led me to direct my attention to Stammer ;and after the treatment of numerous cases, with more or less success; I gave the result of my researches to the profession ; and in selecting the mode of doing this, I consulted the feelings of the profession, my own duty as a member of the College, and altogether waived my personal interest.
Among others whom I invited to be present were Sir Benjamin Brodie and Mr. Robert Liston. I have preserved the replies of these gentlemen. The first, from Sir Benjamin Brodie, is remark.able for its gentlemanly and candid tone. It is as follows:-
" DEAR Sm, "14, Saville-row, March 8, lll41. " I tbank yon for your invitation, and nm sorry that I cannot avail myself" of it. It will give me grcnt pleasure to learn •that your efforts to cure so great a. calamity prove successful. "Your faithful ~en•ant, "B. C. Bnoon:."
particularly frustrating as they had assisted each other on some remarkable surgeries in their early careers. Syme actually used one of Liston’s own surgical developments to defend his own risky amputation (amputation at the hip joint), which many said could not be done.
Syme wrote: “When Mr Liston, two years ago, tied the subclavian artery with success for the first
time in Great Britain, that operation was looked upon as desperate as amputation at the hip-joint is now. But, since then, instances of its success have become quite common in the records of surgery.”
It would have been interesting to see what else they might have achieved together, but it would seem Edinburgh was not big
FROM THE ARCHIVES
28 | Surgeons’ News | March 2023
Right: Yearsley’s stammer argument against Liston
enough for these two giants. They did nevertheless resolve their differences shortly before Liston’s early death.
One of the more infamous public fallouts was with the Edinburgh Royal Infirmary in 1822, when Liston’s fellow surgeons accused him of poaching hospital patients for his own private practice. The hospital board dismissed and barred Liston from practising on the wards. Liston published letters to the hospital in efforts to clear his name, signing off his last with: “Your much injured, but not yet extinguished humble servant, Robert Liston.”
In his many letters, Liston asked the Infirmary managers, should he really refuse to help a patient just because they happened to have been previously seen at the hospital? He asked the RCSEd to review the matter, but the College declined to become involved.
CRITICAL VOICE
Liston was prone to publish surgical cases and new procedures, in which he would criticise previous methods and note failures by other surgeons. In addition, as an ambitious, confident and gifted young surgeon, he willingly attempted surgeries that his peers dared not. Therefore, situations often arose where patients would either have undergone unsuccessful surgeries at the hospital or be told their condition was not operable, only for that patient to be discharged and treated successfully at Liston’s private practice.
This all caused great embarrassment, resentment and perhaps a little jealousy from his fellow surgeons. Nevertheless, six years later, Liston seems to realise that the error of his ways lay in his conduct rather than his actions and apologised to the board of managers for his behaviour towards his fellow surgeons. He was welcomed back on the wards in 1828.
While Liston’s criticism of fellow surgeons or practices was rarely gracious, one might argue that occasionally it assisted in the development of medicine. A great example is represented in a pamphlet, written by a Mr Yearsley in 1842, attacking Liston for his comments on the treatment of
stammers. Yearsley had been advertising his surgical work as a cure for patients presenting with deafness and stammers. In one of his published articles on the subject, the editor, clearly in disagreement, used Liston’s review of an alternative therapy to denounce the surgical option offered by Yearsley. The publishers stated: “We refer for confirmation of our opinion to as high an authority as lives” before quoting the following letter from Liston:
“I have … witnessed Mr Hunt’s process for the removal of stammering. It is founded on correct physiological principles … and unattended by pain ... Several young persons have, in my presence, been brought to him … some of them could not utter a sentence … by following Mr Hunt’s instructions, they have been able to speak and to read, continuously … without difficulty. Some of these individuals had previously been subjected to painful and
Above: The face of Mrs Fraser showing a large fibroma, captured by a preoperative wax cast
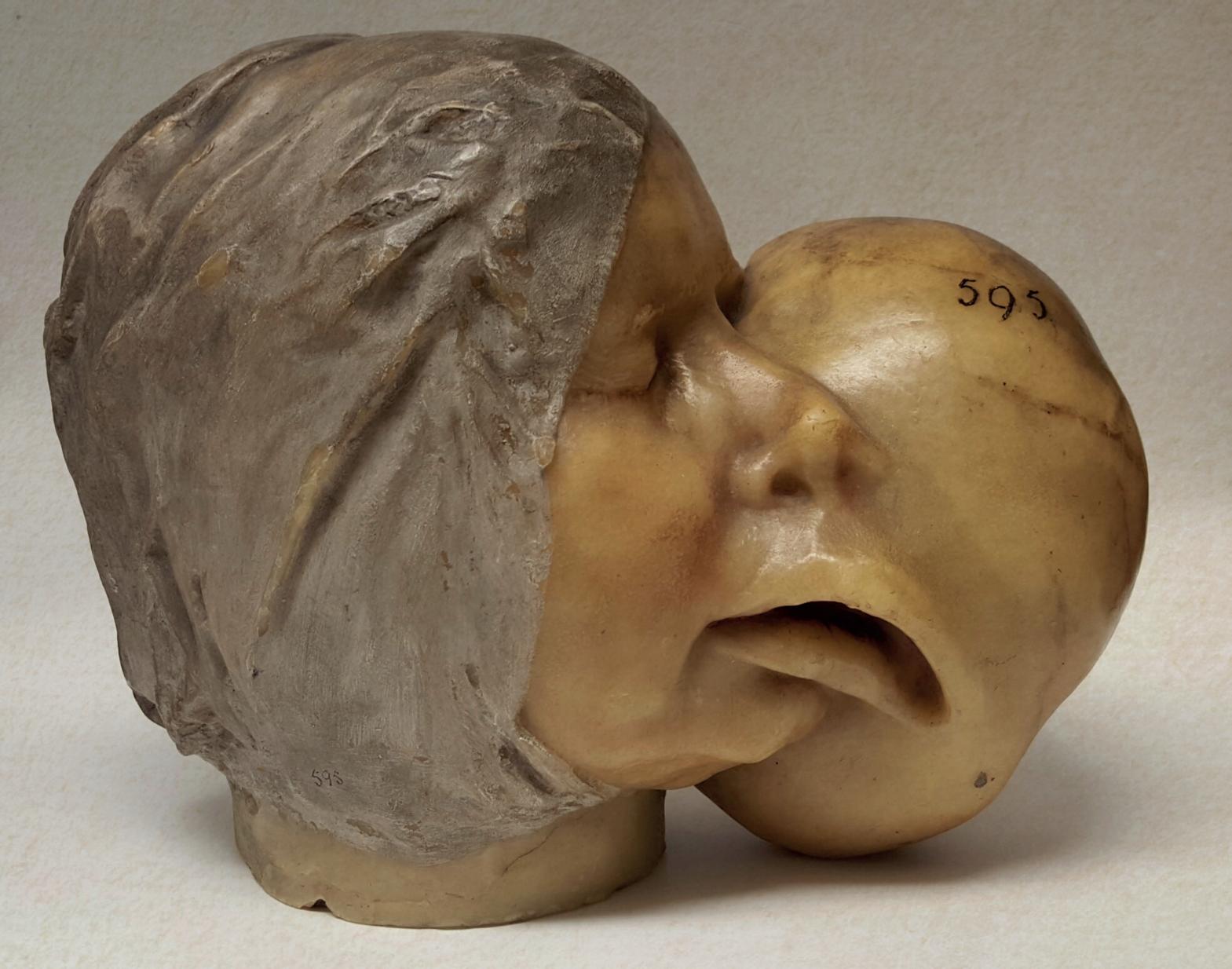
unwarrantable incisions … left with their palates horribly mutilated, hesitating in their speech, and stuttering as before.”
Liston was able to accept that ‘cutting’ was not always the answer. Yearsley took great offence, with the pamphlet designed to publicly ask the English Surgical College to intervene and sanction Liston’s conduct (which they declined). Yearsley called this letter from Liston an ‘attack’ aimed to do him professional injury and a clear indication of Liston’s support of ‘quackery’ and of a treatment that only offered ‘temporary service’. A treatment that, of course, we know now as speech therapy.
It is clear Liston had his flaws – some might even call him arrogant, particularly in his early career – but what is also evident is that his skills made him one of the most innovative surgeons of his day, and he deserves more from history than the apocryphal stories that dominate and perhaps even foil his legacy.
rcsed.ac.uk | 29
Wounds and limbs would be cleaned before operating and even – and this is quite remarkable – the limb shaved ''
The path
to equity
International Women’s Day, a global celebration of the achievements of women and a driver for change, takes place on Wednesday 8 March. The campaign’s theme for this year, #EmbraceEquity, highlights the individuality of each person’s circumstances and calls for a targeted approach to allocating “the exact resources and opportunities needed to reach an equal outcome”.
The College strives to be an engaged and welcoming organisation, but recognises that more needs to be done in this area. In celebration of this important date in the calendar, and to help open the dialogue on this subject, we invited women from across the medical profession and at different stages of their careers to share their experiences as a woman in their field.
As well as reflecting on their experiences to date, they share what they would like to see happen in the profession going forward in the pursuit of true equity.
Smita Vittal Praveen, Director, Academics, Medical Research Foundation, Chennai

At the very outset, ladies, let’s get one thing clear: work-life balance is a myth. Once we accept this, our lives become that much simper. I am an ophthalmologist at a tertiary eye-care centre. For the past 20 years I have held a variety of positions ranging from Head of the Community Ophthalmology Wing to practising neuroophthalmology and a post as Director of Academics. Being a woman allows me the freedom to frequently re-invent my role at work, enabling me to feel relevant. Often this means giving up some of the visible signs of success or choosing to focus on family over work at certain points, even remaining on the fringes of the organisation rather than being
mainstream. I am lucky that my organisation values me enough to let me be flexible with work hours, take on additional responsibility and give up some responsibility. Having children helped me manage these scenarios, as it increased my capacity for patience.
Weighing the pros and cons of decisions made has helped me move from a position of success to one of significance – professionally and personally. I have taken the road less travelled and it has benefited me in unimaginable ways. As women in the medical field, we have a tremendous capacity to handle pressures at work and home with skill, dignity and patience. I firmly believe that the future is bright and it is female.
30 | Surgeons’ News | March 2023
INTERNATIONAL WOMEN’S DAY
To mark International Women’s Day, four women from across the medical field share their experiences and their hopes for a more inclusive future
‘Let’s get one thing clear: work-life balance is a myth’
i INTERNATIONAL WOMEN'S DAY ------'-----------------------
I was fortunate to study dentistry at the London Hospital Medical College, and graduated in 1992 alongside many amazing women, who supported and empowered one another.

There have long since been equal numbers of men and women entering dentistry, but on reflection there were pitifully few female consultants and professors who taught me.
Did this ‘glass ceiling’ affect my career progression? I was once overlooked for an StR post in favour of a male candidate who was less qualified than I was. As frustrating as that was, the experience only served to make me more determined, and I went on to do a self-funded clinical Master’s degree and was subsequently successful on my next StR application. To this day I believe I am a better clinician for having done that and so I do not regret it.
The next StR interview panel comprised six men and no women. I was asked if, as a married woman, I was planning on taking any career breaks during the five-year training programme. There was no mistaking the feeling that it would not be encouraged.
Fortunately, attitudes towards gender diversity have gradually evolved in the last 19 years that I have been an NHS consultant. Recruitment and flexible training opportunities have developed.
I am proud that I played an active part in these improved processes as a Training Programme Director for 10 years. Now, as Director of Dental Education, I work with a great many fabulously talented female dental consultants and professors.
We have made great strides, but the journey will only be complete when there are equal numbers of men and women at all levels of the profession.
Jun Wei Lim, ST5 Trauma and Orthopaedic in North of Scotland, RCSEd Trainees’ Committee Member

My reasons for entering the surgical field are not any more unique than those of my male colleagues. When I was a second-year medical student I was able to go to theatre to observe a total hip replacement and I knew I wanted to be a surgeon as I wished to have an immediate effect on individuals’ quality of life. There were no female consultant orthopaedic surgeons at that time, but I have been very fortunate to have highly supportive male mentors throughout medical school and surgical training. When I was on-call on Christmas Day 2022 it was a predominantly female surgical team, which is a reflection of the changing landscape in surgery.
Despite women now comprising more than half of medical school admissions, they still face significant hurdles, particularly in surgery. We are still being subjected to gendered expectations of
child-rearing responsibility, and female surgeons who have had children are still on the receiving end of the double-standard culture in medicine. With the lack of role models, women are less likely to pursue an academic surgical career as well. The truth is we can have accomplished surgical careers, but we can also be great mothers and wives – and ultimately be ourselves. Of course, we cannot progress effectively without a suitable workplace environment. Supporting women in surgery can be done by expanding the number of women in surgical training, allowing greater autonomy in rota scheduling and more room for job-sharing. Having mentors who understand the challenges and colleagues who appreciate you are equally important. Sometimes you have to create your own path to ‘have it all’. It may not be the easiest thing to do, but it’s possible.
Clare McNaught, RCSEd Vice-President
As you get older and further into your surgical career you’re often faced with additional pressures in life, such as children going into higher education, greater levels of responsibility at work and your body can take a little longer to recover from such a physically demanding job.
Of course, these things don’t just affect women – they are relevant to everyone getting to that stage of their life and career. However, the menopause is a unique challenge for women, which has a huge impact on mental and physical health. There seems to be a taboo around discussing the menopause, but considering
Find out more
Learn more about the RCSEd’s approach to equality, diversity and inclusion by following this QR code to our website.

www.rcsed.ac.uk/professional-supportdevelopment-resources/equality-diversity-andinclusion
there are roughly 30,000 doctors across the UK going through it at any given time it’s vital that we open the dialogue.
If we make it better for women, we make it better for everyone in surgery, which is exactly what we want.
As a surgical college, we will continue to work with both government and employers to ensure our Members are supported, allowing them to have happy, full and productive lives.
rcsed.ac.uk | 31
‘The experience only served to make me more determined’
Lochana Nanayakkara, Convener of Dental Education, Faculty of Dental Surgery, RCSEd
‘It’s vital that we open the dialogue’
‘It may not be the easiest thing to do, but it’s possible’
Green checks
Climate and ecological crises represent the biggest threat to health that humanity has ever faced, the World Health Organization has warned. As healthcare professionals, it is important for us to play our part in looking after our planet and its ecosystems, which support all life on Earth.
Surgery is a significant contributor to the environmental impact of healthcare globally, so it is absolutely vital for us to identify and tackle areas to focus on as we try to limit the environmental and ecological damage caused by our profession.

Over the last year the RCSEd’s Sustainability Champions have worked to unite surgical colleges in the UK and Ireland in an attempt to combine efforts and improve outcomes in sustainable surgery.
As part of our intercollegiate approach, we have created a new checklist, which includes a range of changes – both small and hospitalwide – that will help us make a significant difference across the field. For example, using local anaesthetic where possible, or switching to reusable equipment when it is safe to do so.
The checklist is divided into four sections: the first is dedicated to anaesthetic care, whereas the other three focus on preparation for surgery, intraoperative practice and postoperative measures. Initially the checklist can be used at the daily brief, at the start of an operating list, to remind the team of more sustainable practices that could be adopted.
Once these interventions have been embedded into practice, then the checklist may be used less frequently – for example, to monitor
adherence and long-term improvement. It can also act as a scorecard to record progress.
At present, some theatres will lack the infrastructure required to enact all the suggested interventions, and so the different sections can serve as a roadmap for discussion with management, or at departmental meetings, to guide the required changes.
However you choose to use the checklist, we hope that it will be a valuable tool for you to identify and understand interventions and considerations to decrease the environmental impact of your work.
Alongside the checklist, we have compiled a compendium of peerreviewed evidence, guidelines and policies that inform the interventions suggested. The compendium should support our Members and Fellows to introduce change in their own operating departments.
32 | Surgeons’ News | March 2023 SUSTAINABILITY
We’re taking the lead on sustainability in the operating theatre and our new intercollegiate Green Theatre Checklist shows how you can play a part
GREEN THEATRE CHECKLIST
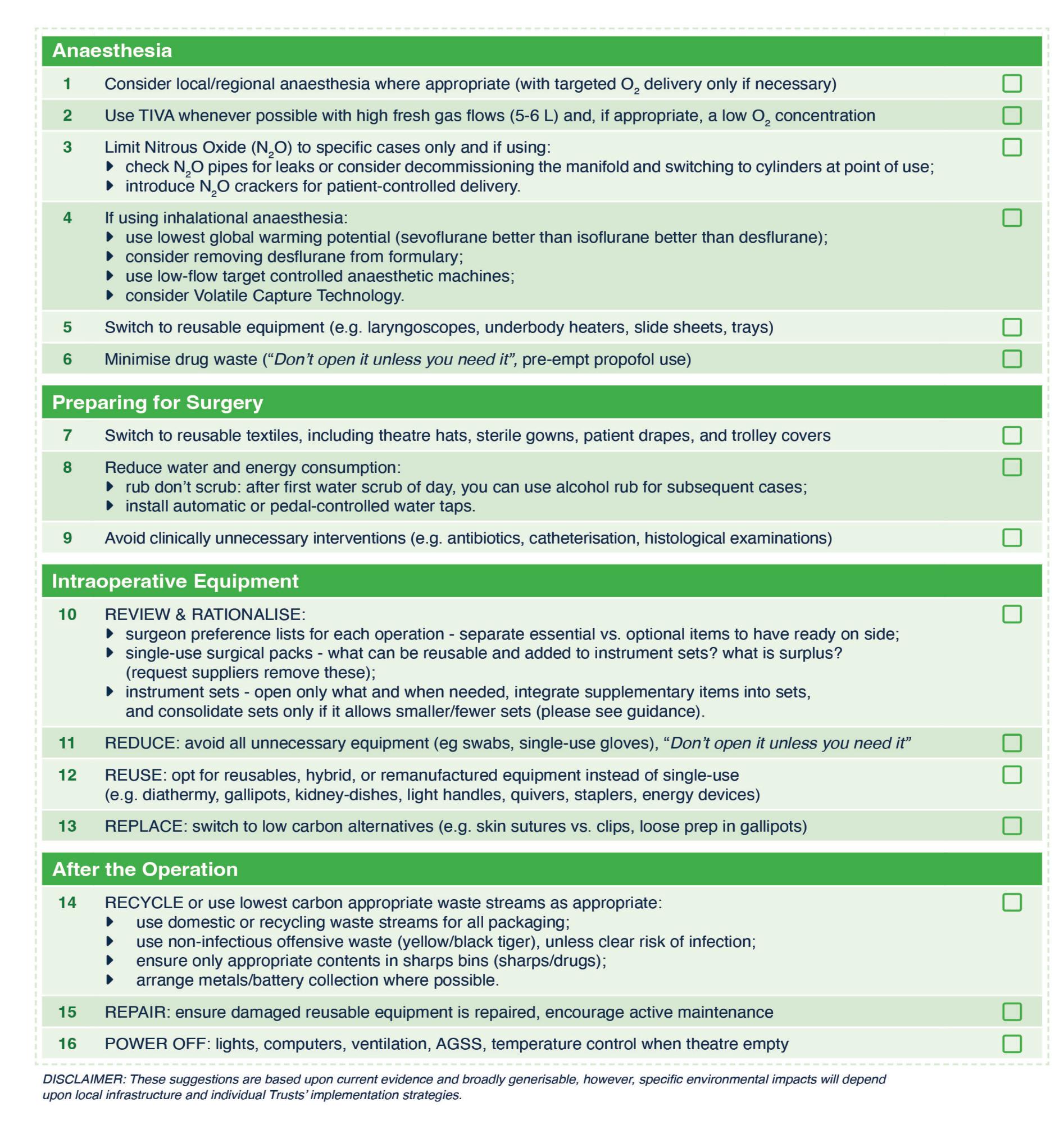
Recommendations to reduce the environmental impact of operating theatres



Anaesthesia
RoyalCollege of Surgeons
ROYAL COLLEGE OF PHYSICIANS AND SURGEONS OF GLASGOW
SURGEONS Ill OF EDINBURGH
~g=~c.
Consider local/regional anaesthesia where appropriate (with targeted 0 2 delivery only if necessary)
2 Use TIVA whenever possible with high fresh gas flows (5-6 L) and, if appropriate, a low 0 2 concentration
3 Limit Nitrous Oxide (N,O) to specific cases only and if using: check N,O pipes for leaks or consider decommissioning the manifold and switching to cylinders at point of use; introduce N2 0 crackers for patient-controlled delivery.
4 If using inhalational anaesthesia: use lowest global warming potential (sevoflurane better than isoflurane better than desflurane); consider removing desflurane from formulary; use low-flow target controlled anaesthetic machines; consider Volatile Capture Technology.
s Switch to reusable equipment (e.g. laryngoscopes, underbody heaters, slide sheets, trays)
6 Minimise drug waste ("Don1 open it unless you need it", pre-empt propofol use)
Preparing for Surgery
7 Switch to reusable textiles, including theatre hats, sterile gowns, patient drapes, and trolley covers

8 Reduce water and energy consumption: rub don't scrub: after first water scrub of day, you can use alcohol rub for subsequent cases; install automatic or pedal-controlled water taps.
9 Avoid clinically unnecessary interventions (e.g. antibiotics, catheterisation, histological examinations)
lntraoperative Equipment
10 REVIEW & RATIONALISE:
surgeon preference lists for each operation -separate essential vs. optional items to have ready on side; single-use surgical packs -what can be reusable and added to instrument sets? what is surplus? (request suppliers remove these); instrument sets -open only what and when needed, integrate supplementary items into sets, and consolidate sets only if it allows smaller/fewer sets (please see guidance).
REDUCE: avoid all unnecessary equipment (eg swabs, single-use gloves), "Don1 open it unless you need it"
REUSE: opt for reusables, hybrid, or remanufactured equipment instead of single-use (e.g. diathermy, gallipots, kidney-dishes, light handles, quivers, staplers, energy devices)
REPLACE: switch to low carbon alternatives (e.g. skin sutures vs. clips, loose prep in gallipots)
RECYCLE or use lowest carbon appropriate waste streams as appropriate: use domestic or recycling waste streams for all packaging; use non-infectious offensive waste (yellow/black tiger), unless clear risk of infection; ensure only appropriate contents in sharps bins (sharps/drugs); arrange metals/battery collection where possible.
REPAIR: ensure damaged reusable equipment is repaired, encourage active maintenance
POWER OFF: lights, computers, ventilation, AGSS, temperature control when theatre empty
DISCLAIMER: These suggestions are based upon current evidence and broadly generisable, however, specific environmental impacts will depend upon local infrastructure and individual Trusts' implementation strategies.

DECLARATION OF CLIMATE EMERGENCY
The Royal College of Surgeons of Edinburgh, the Royal College of Surgeons of England, the Royal College of Physicians and Surgeons of Glasgow and the Royal College of Surgeons in Ireland acknowledge that climate change and anthropogenic environmental degradation pose a major threat to both human and planetary health. We have reached and overstepped several planetary boundaries within which humanity can survive and thrive, and this calls for decisive, collaborative and urgent action.
Our colleges strive to promote patient health

and wellbeing, and climate change poses a direct and indirect threat to this. As such, it is within our charge to protect patients’ health by urgently minimising the environmental impact of everything we do within our institutions and among our membership activities.
With this declaration, the colleges accept their duty to provide leadership and guidance among the surgical community in tackling the environmental impact of surgical care, and commit to do so urgently at local, regional and national levels.


Check it out
For further details about the RCSEd declaration, checklist and compendium visit bit.ly/sustainablesurgery or use the QR code.

rcsed.ac.uk | 33
Alamy
RCSEd Sustainability Champions Group
Jasmine Winter Beatty
Katherine Hurst
James Chu
Nathan Stephens
Haroon Rehman
11
13
12
After the Operation 14 15 16
D D D D D D D D D D D D D D D D
Dates for your diary
The latest surgical and dental events, seminars and courses
MARCH
1–3 Edinburgh Head and Neck Module 2 Course (Edinburgh)
2 & 3 RAPID (Birmingham)
3 MOrth Process Course (online)
6 Thyroid and Parathyroid Masterclass (Edinburgh)
11 Surgical Anatomy of the Limbs (online)
11 & 12 Basic Surgical Skills (Cardiff)
14 & 15 Basic Surgical Skills Course (QE Birmingham)
15 NOTSS Course (Birmingham)
16 & 17 Complete Ear Surgery (Edinburgh)
20 The Edinburgh Hand Course (Edinburgh)
22 Non-Technical Skills for Surgeons Course (Edinburgh)
23 & 24 Basic Surgical Skills (Edinburgh)
24 MRCS Part B Surgical Anatomy Revision Day (Online)
25 & 26 Future Surgeons Key Skills (Birmingham)
30 & 31 Training the Trainers (Edinburgh)
APRIL
1 & 2 Edinburgh MRCS OSCE Preparation Course (Edinburgh)
3 Basic Microsurgical Skills Course (Edinburgh)
13 & 14 Non-Technical Skills for Surgeons Course (Leeds)
14 Plastering Techniques for Fracture Treatment (Edinburgh)
20 & 21 Basic Surgical Skills (Edinburgh)


28 21st QI and Audit Symposium (Edinburgh)
26–28 Women in Leadership
(Edinburgh)
MAY
3 Basic Skills in Paediatric Surgery (Edinburgh)
4 Non-Technical Skills for Surgeons Course (Great Yarmouth)
11 & 12 Basic Surgical Skills (Edinburgh)
15–17 ATLS (Edinburgh)
19 Advanced Laparoscopic Suturing Course (Edinburgh)
22 & 23 Training the Trainers (Edinburgh)
22–24 Core Skills in Orthopaedic Surgery (Edinburgh)
30 May – 1 June Surgical Approaches to the Spine (Edinburgh)
Formoreinformation,visitrcsed.ac.uk/events-courses emaileducation@rcsed.ac.ukortelephone+44(0)1315271600
34 | Surgeons’News | March2023 34 | Surgeons’News | March2023
~~~az:~F SURGEONS ail OF EDINBURGH
The path to publishing
Karthikeyan Parthasarathy Iyengar’s own journey highlights the benefits of publications and research in professional development
member for the Société Internationale de Chirurgie Orthopédique et de Traumatologie. Nationally, these roles have helped me become a Fellow of RCSEd’s Faculty of Surgical Trainers, a member of the Academy of Medical Educators, and a board member of the British Indian Orthopaedic Society.
Academic and research scholarship are the fundamental pillars of providing evidencebased medicine at the heart of patient care. SAS surgeons and physicians have a high level of specialist knowledge and diverse skills to share.
However, traditional barriers to scientific publishing include lack of time, resources or effective articulation of the English language1. The art of effective scientific writing and publishing can be cultured. It can support professional development and career promotion, and fulfil the aspirations of all SAS doctors.
Academic publishing in indexed, peer-reviewed journals has several benefits. It is a portal to share knowledge, enhance patient care, enrich clinical confidence, provide supportive evidence for career development and, crucially, earn peer recognition. These attributes also demonstrate the requirements for a scholarship framework for good-medical-practice research set by the GMC, as well as professional standards set by Health Education England and Academy of Medical Educators (AoME) professional standards, while supporting the appraisal and revalidation process for all clinicians.
OPPORTUNITIES
Although my editorial journey began in 2005, it accelerated during COVID-19 and has offered unique learning opportunities2
This period enabled me to undertake collaborative research with clinicians across the globe and develop collective writing, enhancing my editorial entrepreneurship. Consequently, my h-index increased significantly.
The h-index is a measure of the number of publications published and how often they are cited. My h-index increased from a low 2 to 26 (and 50 on Google Scholar’s i-10 index) on citation databases with more than 2,500 citations (see Figure 1: h-index).
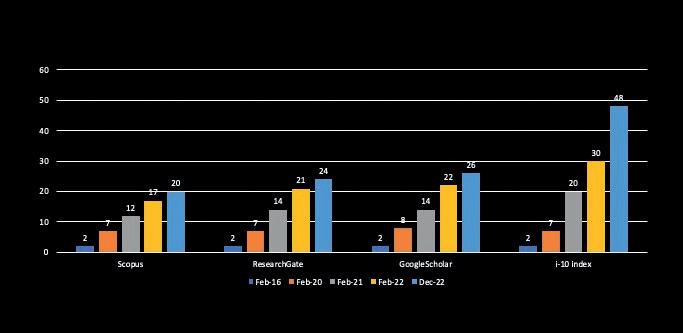
This has provided supportive testimony for my current professional, editorial and university appointments.
At an international level, I have been conferred the title of Honorary Professor at Apollo Hospitals Educational & Research Foundation and selected as an Education Day Committee
MENTORSHIP
The rise in my h-index has also elevated me on the editorialboard hierarchy to become Deputy Editor for the Journal of Clinical Orthopaedics &Trauma and Associate Editor at the Journal of Orthopaedics, both of which are PubMed-indexed journals. I promote academic mentorship, empowering my junior colleagues and senior colleagues as coauthors to demonstrate evidence for their appraisal portfolios.
I have also had three eponymous articles published, including a new anatomical description of structures on the medial side of the knee3 .
Academic publishing and research scholarship can be tough but rewarding endeavours. These pursuits need not be the realm of academic scholars.
To paraphrase Robert Frost’s famous poem, The Road Not Taken, I would encourage all my SAS colleagues and LEDs to take the path of academic publishing. Believe me, the results will be there for all to see.
Karthikeyan
Parthasarathy

Iyengar Fellow, RCSEd Faculty of Surgical Trainers, Fellow of AoME, and member of SASL Committee, Southport & Ormskirk NHS Trust, Merseyside
References
1 Jain VK, Iyengar KP, Vaishya R. Is the English language a barrier to the non-Englishspeaking authors in academic publishing? Postgrad Med J 2022; 98(1157): 234–235. doi: 10.1136/postgradmedj2020-139243. Epub 2020 Nov 6. PMID: 33158939.
2. Iyengar K, Mabrouk A, Jain VK, Venkatesan A, Vaishya R. Learning opportunities from COVID-19 and future effects on healthcare system. Diabetes Metab Syndr. 2020; 14(5): 943–946. doi: 10.1016/j. dsx.2020.06.036. Epub 2020 Jun 20. PMID: 32599533; PMCID: PMC7305503.
3 Iyengar KP, Jain VK, Gupta H, Azzopardi C, Botchu R. IyengarBotchu (IB) confluence of the medial kneeanatomy and clinico-radiological review. J Clin Orthop Trauma 2021;22: 101591. doi: 10.1016/j. jcot.2021.101591. PMID: 34567973; PMCID: PMC8447233.
Ipromoteacademicmentorshipand empowermyjuniorandseniorcolleagues asco-authors
rcsed.ac.uk | 35 SAS UPDATE
Figure 1: h-index Citation databases
''
Number of citations
Growing stronger
The FTSS celebrate their successes in championing surgical careers
in numerous specialties. Several have also run revision courses for the MRCS Part A examination, with the Oxford and Cambridge FTSS collaborating to run an online MRCS course through the College’s e-learning platform, which had an international audience of more than 2,000 across its 12 episodes. This content remains online for College Associate and full Members to access free of charge.
A big thank you
The Foundation Trainees Surgical Societies (FTSS) are part of the College’s ongoing commitments to excellence in surgical education, maximising access to surgical careers and supporting trainees at all stages.
Closely aligned with the College’s Regional Surgical Ambassador (RSA) network, the FTSS initiative offers a platform for foundation doctors and medical students considering surgical careers to attend educational events, develop their understanding of surgical training pathways and interact with the College prior to membership.
The first of the FTSS originated in Oxford in 2014 under the supervision of Consultant HPB Surgeon Michael Silva (currently on the RCSEd Council) and Katie Hurst (then a foundation doctor,
now Specialty Registrar in General Surgery, RCSEd Trainee Representative on Council and RCSEd Sustainability Champions Chair). In 2020 the FTSS became a national initiative, with 15 societies covering the breadth of England, Wales, Scotland and Northern Ireland.



NURTURING SURGEONS
Each regional FTSS is supported by the College’s RSAs, consultant surgeons who act as mentors and conduits between the College and trainees in their region. The College is pleased to point to the blossoming success of the FTSS as a testament to the commitment of developing and nurturing the next generation of surgeons.
In the past two years the FTSS have run surgical skills events, careers advice evenings, taster sessions and mentorship schemes
Following the overwhelmingly positive feedback from the FTSS National Conferences, the FTSS UK Committee hopes next year’s event will be bigger and better. Local FTSS across the UK have a host of plans for events to raise the profile of College among the next generation of surgeons and continue the highest standard of surgical training.

The FTSS Committees across the UK would like to express their sincerest thanks to the College and Conference sponsors. They would also like to thank Barnaby Green (Consultant Vascular Surgeon, Director of the RSA network) for his ongoing support of the initiative and help on the day.
As ever, the FTSS thanks Michael Silva for his tireless work in championing education in general – for which he was recently awarded the College’s Faculty of Surgical Trainers’ Medal – and the whole FTSS initiative in particular. Last but never least, the FTSS would like to thank Una Curran and Stacey Warner of the College’s Marketing/ Outreach team –their enthusiasm, energy and hard work over the past two years have made the FTSS Conferences possible.
36 | Surgeons’ News | March 2023
TRAINEES AND STUDENTS
The online MRCS course had an international audience of more than 2,000 across its 12 episodes
Sirat Lodhi Academic FY2 Doctor at the Manchester University NHS Foundation Trust
From left: Alex Ribbits, Rory Thompson, Sirat Lodhi, Michael Silva, Alexander Barclay, Corey Chan and Dave Fellows
Dave Fellows Junior Clinical Fellow, Oxford University Hospitals NHS Foundation Trust
Max Stewart Clinical Research Training Fellow, Nuffield Department of Orthopaedics, Rheumatology and Musculoskeletal Sciences, University of Oxford
Do or do not … there is no ‘try’?
Three trauma and orthopaedic surgeons illustrate through their personal experiences the benefits and pitfalls of postCCT pathways to a consultant position
 HAROON REHMAN
ORTHOPAEDIC SURGEON, NATIONAL TREATMENT CENTRE, FIFE ORTHOPAEDICS
HAROON REHMAN
ORTHOPAEDIC SURGEON, NATIONAL TREATMENT CENTRE, FIFE ORTHOPAEDICS
There are very good arguments for following the traditional route of obtaining CCT and then working a Fellowship or two prior to beginning consultant practice. Even if you have received exceptional basic and advanced training, a Fellowship is a well-recognised path to take.

Most established and traditional Fellowships will deliver a higher volume of cases than standard training schools. They run like well-oiled machines and, although some of the typical NHS challenges do creep in, they are often mitigated by an enthusiastic training Faculty and staff who appreciate training is part of the culture.
Surgery is a craft specialty. Complex cases require hands-on experience and most decent Fellowship centres will deliver the volume of disease to facilitate future specialist practice. Surgery is also a perishable skill and, in the current dry training environment, Fellowships providing a high-volume, low-complexity workload may also be right for some surgeons.
Fellowship centres are accustomed to supporting the growth of surgeons at this stage of their career. Alternate learning models are often used without the stresses of formal training assessments. Traditional units will provide mentorship and will work hard to develop your professional identity. Opportunities to engage with high-profile experts in your field may not present themselves to you in a similar fashion again.
In this sense Fellowships are invaluable in self development and professional
networking, which will go on to benefit your patients, colleagues and trainees. Fellowship trainers are often exceptionally experienced individuals who have influenced surgical practice. Contemporary Fellows are peers who you may turn to if you experience difficulty in your own practice.
The specialist nature of Fellowship centres tends to mean that there are also opportunities to conduct top-level research. This will be of greater appeal to academic surgeons but is also useful in developing your CV for conventional roles.
I recommend Fellowships to surgeons finishing training. For me it was important this year wasn’t simply a repeat of training. My plan in my final years’ training was to develop surgical and decision-making skills in revision hip and knee surgery. Reduced operating opportunities due to COVID-19 limited exposure to this aspect of reconstructive surgery. This period of training can be a struggle socially and financially for a surgeon and their family. Yet any financial sacrifice made during this year can be compensated for quite quickly on starting a consultant post.
Unfortunately, most prestigious Fellowships are known only by word of mouth. I feel it is the duty of the profession to formally assess UK and international Fellowships and set benchmarks. Despite being a strong supporter of Fellowship training, I would add – as one of my mentors said to me – that the real learning does in fact start when you are a consultant.
THOMAS HOWARD CONSULTANT ORTHOPAEDIC SURGEON, NATIONAL TREATMENT CENTRE, FIFE ORTHOPAEDICS

A Fellowship in trauma or in the subspecialist area is usually a ‘desired’ rather than ‘required’ characteristic for the job application. How, then, might attending interview without a Fellowship penalise you, and might there be cases where there is advantage to going without?
I knew where I wanted to work.
I was lucky enough that there was a high-performing department with an excellent team with whom I had worked in my training years – and in the location where my family wanted to settle, the grass is pretty green here. Jobs were being advertised six months prior to my due CCT date. My post was based on a business case for a retiring senior colleague. In the current climate I couldn’t be 100% confident the business case would still exist on my return had I gone on a Fellowship. I have a wife,
38 | Surgeons’ News | March 2023 TRAINEES’ COMMITTEE
DO NOT DO
CONSULTANT
“Fellowships are invaluable in developing yourself and your professional networks”
and young children that need schooling. Another year of travelling and being unsettled might have been good for my CV, but at what detriment to my family? You can obtain a forever job that you desire without a Fellowship – why pay the cost to family, children’s education, reduced salary and the expense of moving an extra time?
If I was not successful at interview, I’d have lost nothing: I would have gained interview experience and could go on a Fellowship at that point. The cost of not going for that interview, however, might emphasise the negatives of a Fellowship if unemployment is lined up afterwards.
A Fellow is an attractive colleague in a department as they have usually secured the job through a competitive application and have the skills to reflect this. They have completed training and can usually be left autonomously at consultant level.
The downside to having a Fellow, however, is the very same reason:
they are attractive colleagues, another department may want them, and they may decide to cut their Fellowship short to start a career post.
COVID-19 has had a huge impact on orthopaedic delivery in the NHS. Some units have been affected more than others. Within the same units, elective and trauma work are sometimes disproportionately affected – the benefits of a Fellowship might not be so clear if you end up in a unit where clinical performance has been impacted by the pandemic.
In the end, what do you truly gain?
Is the Fellowship required for private practice? Where did your mentors say they learned the trade? It goes without saying that equipment and techniques used in routine practice aren’t necessarily those learned and used on a Fellowship. Surgeons unanimously agree that real experience is gained on the actual job as a consultant, rather than on a Fellowship.
THERE IS NO ‘TRY’
PHIL WALMSLEY
CONSULTANT ORTHOPAEDIC SURGEON, NATIONAL TREATMENT CENTRE, FIFE ORTHOPAEDICS; CHAIR, SCOTTISH ARTHROPLASTY PROJECT (SAP); ASSOCIATE POSTGRADUATE DEAN (QUALITY LEAD), NES; HONORARY SENIOR LECTURER, UNIVERSITY OF ST ANDREWS MEDICAL SCHOOL

Fellowships after the end of surgical training have become commonplace and might be viewed by some quarters as an orthopaedic ‘gap year’, which misses the original aims of undertaking a Fellowship. The word ‘Fellowship’ means sharing a community of interest, with the motivations and aims of trainees undertaking them naturally varying.
While for some subspecialist areas of practice Fellowships are a prerequisite, the skills required for broad consultant practice should be achieved within a specialist training programme and attainment of CCT.
The choice of whether to undertake a Fellowship will largely be determined by personal circumstances, financial position, career aspirations and opportunity.
Overseas Fellowships are perceived in some quarters to be more prestigious than those within the UK, but this is not necessarily the case. When I’m interviewing a prospective consultant colleague, if they have completed a Fellowship I am less interested by location and more in what knowledge and skills they gained.
It’s worth noting that unnecessary pressure for trainees to undertake a Fellowship isn’t helpful unless there are clear benefits in return for additional burden of doing so and appropriate support is available.
One issue for those seeking a Fellowship post is the lack of benchmarking, raising the question of whether units offering these posts should have regular external reviews of the quality of training provided.
There should now be multiple options for trainees to gain additional experience during the final stages of training. It is important that there is flexibility in how additional training is achieved during the final years of training and the immediate post-CCT period. Advice from mentors, training programme directors, specialty organisations and those who carry out an area of practice are all worth seeking.
I was fortunate to complete two Fellowships at the end of my specialist training: one within the UK and one overseas. While I enjoyed and benefitted from these posts, they wouldn’t automatically be good for every trainee. Fellowships can enhance training, but be clear on the aims and costs of undertaking one, as well as keeping in mind that there are multiple ways in which training could be achieved.
rcsed.ac.uk | 39
“The real experience is gained on the actual job as a consultant”
“Unnecessary pressure for trainees to undertake a Fellowship isn’t helpful”
Research in surgical education
Alex Phillips charts the achievements of a joint initiative aimed at developing our understanding of surgical training with a look to future needs
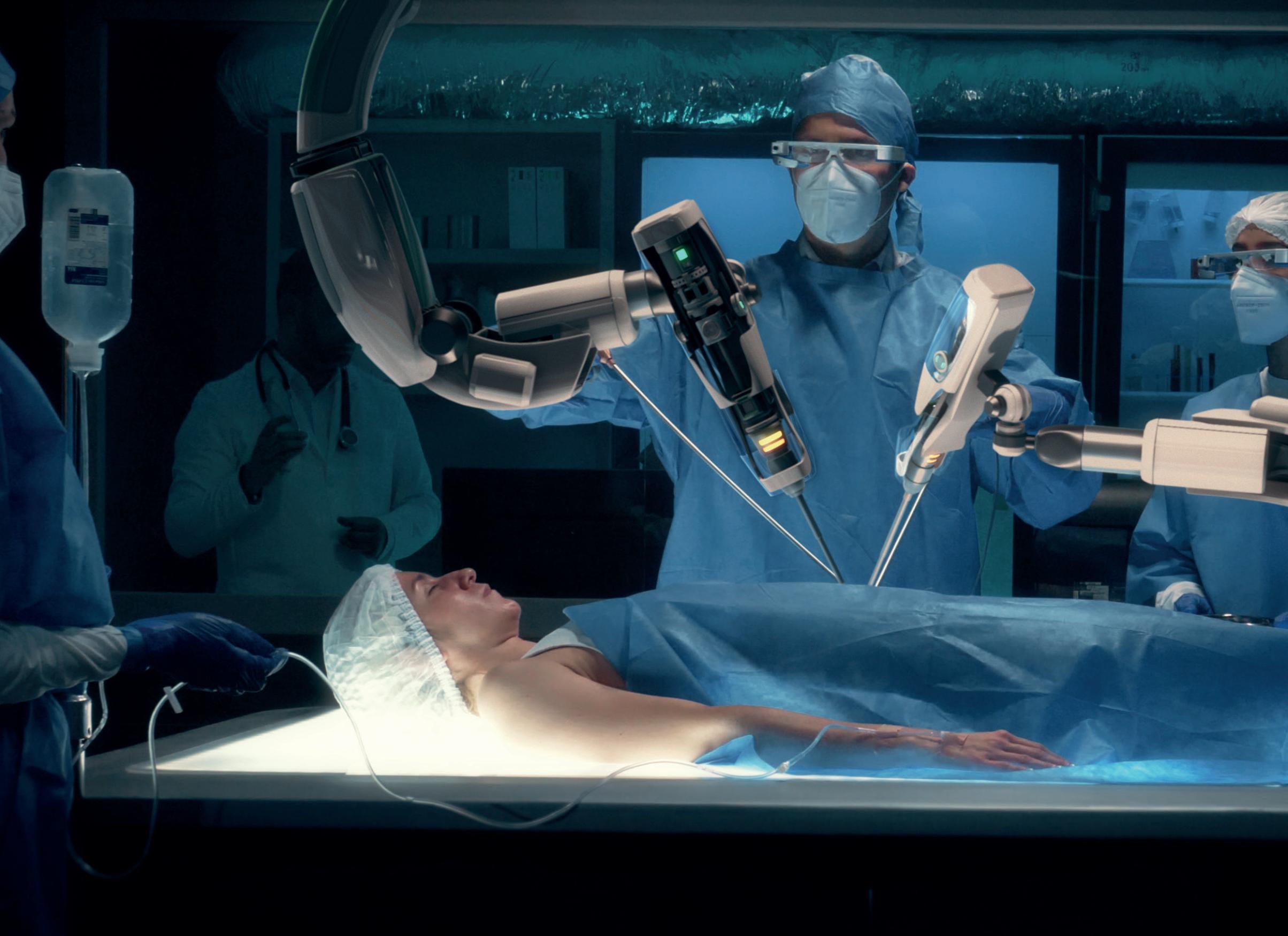
Ajoint FST/ASME (Faculty of Surgical Trainers/Association for the Study of Medical Education) initiative was set up in 2016 as a way for the two organisations to work together to promote and stimulate research into surgical education. Such research is poorly funded, with major challenges for those keen to pursue work in this area to secure funding and develop their ideas.
With a very real understanding that evidence-based medicine helps enhance patient outcomes, it is now also important that we extend this to evidence-based training.
Since it was first initiated, the FST/ ASME grant has awarded more than £20,000 in funding to nine research
40 | Surgeons’ News | March 2023
SURGICAL TRAINING ______ ! __________________________________ _
projects on a range of topics. Projects have included randomised trials, assessment of technical skills and non-technical skills, and have employed both quantitative and qualitative research methods.
UNDERSTANDING SKILLS
The first grant winners back in 2016 were Paul Sutton, who sought to explore clinical decision-making in trainees in a simulated environment, and Sotiris Papaspyros, who looked at surgical skill acquisition in a low-fidelity model.
Thus, right from the start these grants have permitted study into practical applications for developing our understanding of surgical training and have ensured that the focus is not simply on operating skills and hand-eye coordination, but also

on the other skills and components that make up surgical training.
Joshil Lodhia (in 2017) and Matyas Fehervari (in 2021) both looked at learning surgical skills but with very different approaches. Lodhia, a cardiothoracic trainee at the time, used magnetic sensors to assess fine movements of the surgeon, whereas Fehervari sought to validate online laparoscopic surgical training – perhaps a timely proposal in the middle of the COVID-19 pandemic.
Although we learn much of our craft in the operating theatre, James Ashcroft (in 2021) explored the participation of surgical trainees in this environment. We now recognise that there is more to the making of a surgeon than simply operating.
ASSESSMENTS
Work-based assessments are now embedded into the surgical curriculum so how do we learn from them? This question was posed by Arpan Tahim (in 2018) as part of his research project and evaluated by Aimee Charnell (in 2020), who learned from outpatient clinics – a vital place of learning for all surgeons. Furthermore, how do we assess our trainees – can we use real-life procedural videos (asked Professor Karin Baatjes, in 2020), which is
 Alex Phillips Consultant Oesophagogastric Surgeon and Surgical Director of the FST
Alex Phillips Consultant Oesophagogastric Surgeon and Surgical Director of the FST
something that might make life simpler for assessment?
The use of technology in surgical training has become even more important as a consequence of COVID-19. Virtual reality simulators can help individuals perfect skills, but could training the team together using VR improve performance?

Kartik Logishetty used his research grant to explore this (in 2019).
FUTURE RESEARCH
So what should we focus on next? There is no right answer to this question. Yes, we must strive to learn how to best maximise training opportunities so that learning curves can be passed as quickly as possible, but we have all learned that surgical skill is not just about what we do with our hands in the operating theatre.
Decision-making, non-technical skills and the knowledge we impart on the ward and in clinics are every bit as important at influencing patient outcomes. Maximising these opportunities is what is required to ensure we produce well-rounded surgeons who can deal with the demands of modern medicine.
Left and below: As welcome as they are, advances in technology can make this a challenging time for surgical trainees
Technology can no doubt assist with this and there is still much to learn about how technology can facilitate training and support the surgeon to excel at their trade. With robotic surgery increasingly used, how do we ensure our current trainees do not lose out while established surgeons attempt to learn a new surgical skill? The rise in technology and the recovery from COVID-19 make for challenging times for trainees and trainers. It is important that we continue our drive to research novel, efficient ways of training that will have a positive impact on outcomes for both the trainee and patients.
rcsed.ac.uk | 41
Shutterstock
With robotic surgery increasingly used, how do we ensure our current trainees do not lose out while established surgeons attempt to learn a new surgical skill?
''
Fellow travellers
Carole A Boyle asks two new Fellows about their route to a Fellowship without examination
Carole A Boyle Dental Editor, Surgeons’ News



Recently the routes to an RCSEd Fellowship have been streamlined and the process made more straightforward. Route 1 is for those Dental Fellows of sister colleges, who can apply in writing to the Faculty for consideration. Applications are processed by the College’s Membership Department.
Route 2 is for dental practitioners in a post equivalent to a consultant dental surgeon or experienced registered specialist. Proposals must be supported by five Fellows. Applications are assessed against eight criteria by a panel who make recommendations to Dental Council.
Route 3 is for those who have passed a recognised dental specialty membership examination of a Royal Surgical College and who have held membership of the Faculty of Dental Surgery for a minimum of five consecutive years. Applications are assessed in the same way as Route 2. So, have you got what it takes to become a Fellow? Contact dental@ rcsed.ac.uk for more information.
Fellowship criteria
To find out more about the eight criteria used to assess Route 2 and 3 applications scan the QR code.

Professional standing
Clinical experience
Research
CPD
Dental education and training
Management and leadership
Commitment to the Faculty
Probity
FEES: Fellowship without examination fees are: UK £554 / Rest of World £207/Low Income Countries £88 www.rcsed.ac.uk/faculties/faculty-of-dental-surgery/ fellowship-in-dental-surgery-without-examination
TAMEEZA TEJANI Specialist Prosthodontist Dental Studio, Dubai Science Park, Dubai, UAE
It was a great pleasure to be elected recently as an RCSEd Fellow in Dental Surgery without examination by the College.
I applied for the Fellowship for a variety of reasons. Its significance is well recognised in universities within the Middle East, in particular the UAE. The Fellowship will distinguish my CV from other applicants if I apply for an adjunctive academic position alongside my private practice role.
Moreover, in the competitive worldwide job market the Fellowship represents a significant achievement for any clinician, which is attractive to prospective employers.

The application process was straightforward and I found the paperwork easy to complete.
Personally, the Fellowship and my recent appointment as examiner for the Membership in Prosthodontics has given me the opportunity to network with various specialist and consultants, offering me access to potential research and career opportunities worldwide. I plan to continue contributing to the College as an examiner and in any other areas that open up to me as a Fellow.
CLAIRE CURTIN
Specialist in Special Care Dentistry at Cork Dental Hospital and Senior Dental Surgeon with the HSE Dental Service in Cork, Ireland
Being a Fellow of the RCSEd is a recognised global marker of professional excellence. In my specialty I don’t have the opportunity to sit an ISFE to become a Fellow of the College.
I feel strongly that it is important to be a Fellow to show equivalence with colleagues in other specialties, promote my specialty and develop as a leader in the College’s Dental Faculty. I have worked hard to further my career and I feel this award recognises my achievements. When applying I contacted the College requesting information about the process and I promptly received documentation with comprehensive detail on the application and regulations. Once I submitted the documentation I was kept up-to-date on the progress of my application, including guidance on when I could expect a decision.
I have been involved in many aspects of the RCSEd over the last nine years in both the education and examination departments. I hope that as a Fellow I will be able to strengthen my role within the College as both an examiner and educator.
42 | Surgeons’News | March2023
DENTAL
• • • • • • • [!I •
This year, The RCSEd Faculty of Dental Surgery is introducing a new suite of open access Dental Diploma examination qualifications, set at level two of the published speciality guidelines (which translates to Tier 2 in England and Wales).

The following sub-specialist Diplomas will be introduced:
آ Endodontics
آ Dental Sedation
آ Implant Dentistry
آ Oral Medicine
آ Oral Surgery
آ Paediatric Dentistry
آ Periodontology
آ Prosthodontics
آ Special Care Dentistry
Find out more at rcsed.ac.uk/NewDentalDiplomas
If you’re a General Dental Practitioner with an interest in the dental specialties, this could be for you.
Positive change
The narrative in recent years regarding the climate crisis has shifted from planetary health to human health. The health impacts (see Table 1) hit home when The Lancet described the climate emergency as the largest existential threat to human health of the 21st century1 . Healthcare is the largest public sector industry2 and so by default becomes a hefty carbon emitter, contributing to 4% of the UK’s carbon footprint.
As a high-turnover surgical specialty, dentistry is resourceintensive in its use of materials and waste generation. Carbon footprinting has been attempted and the annual 675 kilotonnes of carbon dioxide equivalent (CO2eq) produced in primary dental care is likely to be underestimated, as data is NHS-specific3
The growing demands of aesthetic dentistry will inevitably contribute to the increase in the carbon burden, but further work is required to capture the true picture. Nevertheless, rethinking the way dental care is delivered is essential in addressing dentistry’s environmental challenges, which may be achieved in the following ways.

IDENTIFYING CARBON HOTSPOTS
Carbon hotspots can be identified by taking into account carbon
emissions of the patient pathway. This differs from medicine, as the major source of carbon emissions in dentistry is thought to be staff/ patient travel and energy use (see Figure 1).
Energy consumption is one of the biggest financial pressures the nation is facing and so energy efficiency has a two-fold benefit. Both financial and environmental energy savings can be achieved by good insulation
to help maintain heat, switching to LED lighting and turning devices off when not in use. Switching to a green energy supplier that invests in renewable energy sources is a simple yet effective way of committing to sustainable purchasing practices.
REDUCING WASTE
Segregation of waste can affect energy utilisation and where waste ends up. Unfortunately, due to local contracts many dental practices use infectious waste bags (orange, intended for known infectious patients only) even though the majority of clinical waste could be placed in the offensive waste stream (yellow tiger bag for non-infectious clinical waste), which is less carbon-emitting.
Ensuring that clean packaging is discarded in domestic or recycling bags avoids the need to treat at higher temperatures. However, emphasis should be placed on reducing waste overall as the recycling process has its flaws.
The number of disposable instruments and products available for dental use is growing, creating significant waste. When choosing alternatives to disposable items, life cycle assessments (LCAs) can establish whether switching to reusable items is a ‘greener’ option. The LCA takes into account the embodied emissions of items from raw-material extraction, manufacturing, shipping over long distances and disposal. Reusing autoclavable instruments, however, is generally the preferred option4 Since the COVID-19 pandemic, at least 19.8 billion items of PPE have been distributed to Health and Social Care services5, contributing to microplastic pollution6 While PPE is important in protecting patients and

44 | Surgeons’ News | March 2023
Zahra Shehabi explores some changes to dentistry practices to address our carbon footprint while caring for patients
DENTAL
Zahra Shehabi, Consultant in Special Care Dentistry, Green at Barts Health Organiser, The Royal London Dental Hospital, Barts Health NHS Trust
8% 19% 30% 31%
0.9% 8% 19% GAS
References
1. Watts N et al. Health and climate change: Policy responses to protect public health. Lancet. 2015; 386(10006): 1861–1914
2. Tomson C. Reducing the carbon footprint of hospital-based care. Future Hosp J. 2015; 2(1): 57–62.
3. Public Health England. Carbon modelling within dentistry: Towards a sustainable future. London: Crown; 2018.
4. Rizan C et al. Plastics in healthcare: Time for a re-evaluation. J R Soc Med. 2020 February 7; 13(2) 49–53.
5. Department of Health and Social Care.
Official Statistics
staff, its use must be appropriate to ensure minimal waste. An example of this is using sterile gloves (which have a much higher carbon footprint7) for non-sterile procedures such as extractions. Reusable textiles such as gowns, Type IIR masks and surgical hats are available and offer a cost-efficient alternative to single-use disposable PPE. This change can be implemented relatively quickly in general dental practice. For those who work in NHS Trusts and organisations, liaison with infection control and estates teams would be required.
The use of digital technology also helps to reduce waste associated with paper, films, materials and transportation of goods (see Figure 2) and should be considered to improve patient workflow.
ENCOURAGING ACTIVE TRAVEL AND PREVENTION
A large proportion of the dental carbon footprint is linked to staff and patient transport. Therefore, the promotion of active travel can help mitigate travel-related emissions, contribute to better air quality and encourage public health though physical activity.
This may not be as practical in rural areas, where car use is the most feasible option, so exploring electric vehicle use or car-sharing within the team could be considered. Preventing poor dental health reduces the reliance on dental resources and travel to clinics.
Empowering patients to take control of their oral health as part of social prescribing is a powerful tool. As a trusted voice, dental care
professionals can be highly influential, especially on social media platforms. Committing to dental environmental sustainability sends a clear message to peers, patients and the public that climate change is a real health threat that everyone needs to take seriously. Acting locally or nationally by working with Royal Colleges and dental networks to influence change can help create a sustainably savvy dental workforce.
MEDICINE MANAGEMENT
Medicines and anaesthetic cases make up around 25% of the NHS carbon footprint. Nitrous oxide is 298 times more potent as a greenhouse gas than CO2, so its use has gained widespread attention. Most dental clinics that provide inhalation sedation use nitrous oxide supplied in cylinders, which eliminates the problem of pipe-leaking associated with gas manifolds in larger Trusts. Ensuring cylinders are almost empty before return reduces unnecessary expulsion into the atmosphere.
Experimental statistics – personal protective equipment distributed for use by health and social care services in England: 1 March to 31 March 2022. Updated 13 October 2022. www. gov.uk.
6. Adyel TM. Accumulation of plastic waste during COVID-19. Science. 2020; 369 (6509): 1314–1315.
7. Journal of Hospital
Infection
Jamal H et al. Non-sterile examination gloves and sterile surgical gloves: which are more sustainable? 2021; 118: 87–95.
1. Virtual appointments
Where intra-oral assessment is not essential/possible (e.g. results/uncooperative patient). They also reduce staff/patient travel
2. Digital notes and radiographs
These reduce the need for paper,chemicals and films. Can facilitate communication
3 Digital scanners
These improve accuracy and eliminate the need for impression/lab materials and lab transplant
4. digital communication
Encrypted email communication facilitates patient care and avoids paper and postage
5. Virtual CPD
This reduces the need to travel. Also has financial and social added value.
Unused and expired medicines enter water and food streams if they are not discarded properly. Reducing prescription days could help avoid this and regularly checking expiry dates of medicines in the surgery may ensure efficient use of stock.
DENTISTRY WITHOUT HARM
The interplay of health provision and disease prevention is a complex one in relation to sustainability. While global action is required to secure a liveable and viable future, we owe it to our patients and communities to reduce the environmental burden by providing dentistry without harm.
Worsening of infectious diseases by 58%
Warm conditions
Cholera in water from multiplying algae
Disease-carrying mosquitoes, e.g. malaria, Dengue fever
Water-borne diseases
Floods
Migration of animals
Air pollution
Migration of populations and spreading of diseases
Virus transmission from animal reservoir to human populations amplifying to epidemics/pandemics
Cardiorespiratory disease
rcsed.ac.uk | 45 Shutterstock\Getty
STAFF PATIENT GAS & ELECTRICITY PROCUREMENT NITROUS OXIDE TRAVEL CONSULTATION & ASSESSMENT TREATMENT
Table 1: Health impacts of climate change
Figure 1: Carbon emissions associated with the patient pathway
PROCUREMENT
Figure 2: Sustainable workflows
mo Hill & [IT~ 0 O-G;';)-O G'-;)@G'-;) LO I> OJ G'-;) G'-;)
Beating burnout
says Liz Price
No one would dispute that NHS staff are under growing pressure due to multiple factors, from understaffing to rising patient demand. Research by a range of organisations is consistently finding increased rates of burnout across all areas of healthcare.
Burnout can be defined as a state of physical, mental and emotional exhaustion, usually occurring when someone experiences a lot of stress over a long period of time.
There is a well-established causal relationship between reduced clinician wellbeing and increased patient safety incidents. The rise in the incidence and severity of reported burnout is concerning for clinicians themselves and for the potential impact on their patients and colleagues.
CONSEQUENCES
New evidence has revealed several groups of clinicians who are at high risk of burnout, that is those: working in remote areas or isolated roles; those with disabilities; those with care-giving responsibilities; and those working in specialties where there is an extreme backlog of work associated with the COVID-19 pandemic.
Furthermore, it is becoming clear that clinicians can experience burnout at any stage of their career, and that the personal consequences include a reduction in work satisfaction, a deterioration in health, and difficulty in empathising with and demonstrating compassion to colleagues.
Consequences at the team or organisational level for clinical and non-clinical leads include increased numbers of errors, reduced productivity and efficiency, and a reduction in measures of patient satisfaction. There may also be a
reduction in the quality of care delivered and an increase in unprofessional behaviours, which is directly associated with the inability to empathise and demonstrate compassion. This also reduces the levels of both supportive and help-seeking behaviours, which are essential to ensure safe practice.


Individuals can adopt protective strategies against burnout on a personal level (see some tips below), but it is now evident that systems and organisational factors within healthcare settings are increasingly contributing to the reduced wellbeing and diminished resilience of clinicians.
Such factors include heavy workloads, challenging working environments – even at the level of basic needs, such as adequate hydration, rest and personal safety – normalisation of aberrant behaviour within teams and ineffective leadership styles.

Right: Burnout is on the increase throughout the healthcare sector
Below: Make sure you are supportive of your team
This is an extremely worrying trend. Clinical leaders may feel that there are some major factors beyond their ability to control or influence – for example, funding or staffing –but the following may be helpful.
CHECK-INS
Ask yourself: “Do I understand how my team members are doing?” Can you incorporate check-ins across their mental, physical and emotional wellbeing? These can be formalised at briefings or debriefings, or as straightforward as asking “How are you?” and really listening to the reply.
This can be daunting, as we often worry about opening a Pandora’s box. However, I often find that people will say: “I’m fine, thanks”, but non-verbal cues and delving a little deeper will reveal that things are not quite that fine.
You may need to consider the level of psychological safety you have in play if the team are not letting you know that things are challenging at times. People who don’t feel supported or properly listened to are less likely to raise concerns about themselves or others, and again this is problematic for patient safety and demonstration of professional responsibilities.
POSITIVE ENERGY MANAGEMENT
There is growing evidence to support the concept of positive energy management – making sure that, as a leader, you always bring your best self to the team. Being able to step aside from the stuff that negatively drains your emotional capacity and convert it to a positive is important when leading others. It’s still important to recognise the negatives and their effect (particularly in front of the team), but being able to demonstrate you can move forward through anything in a positive way helps the team feel supported and provides reassurance.
Can you incorporate check-ins across your team’s mental, physical and emotional wellbeing?
46 | Surgeons’ News | March 2023
The impact of burnout on staff wellbeing and patient safety has been well documented, but there are ways to combat it,
Liz Price, Head of Training, CPD and Risk Advisory Services at MDDUS
WELLBEING
------r----,,_
BEING SELF-AWARE
My key tip here for all clinicians (including leaders) is to work on self-awareness. Starting to notice early warning signals is an important first step in managing your response. These are different for different people, but can frequently include:
• feeling tired or drained
• frequent illness (lowered immunity)
• lack of motivation
• memory loss
• changes in your attention span
• feelings of failure or self-doubt
• feeling detached or isolated.
You may also notice a reduction in the quality of your interactions with colleagues or experience increased negative emotions towards patients and/or colleagues. This requires increased levels of self-management and control: are they getting annoyed with you, are you getting more annoyed than usual with them, are you avoiding some colleagues as you don’t have the energy and are you cutting encounters short for that very reason?
PROACTIVE WELLNESS
It can be helpful to reflect on things you can do proactively to manage your own wellness. For example, write down a wellness ‘plan on a page’ that includes activities that you could incorporate into daily life to support your own wellness across mind, body and spirit.
For me, these headings would include: mind – listening to music or reading; body – doing a mini strength workout twice a week, switching off my phone earlier before I try to get to sleep; spirit – walking the dog, making sure I connect with friends more often.
CHALLENGING ENCOUNTERS
Practise self-compassion when reflecting on challenging interactions with colleagues. It may be that your approach or response to a situation contributed to a negative outcome. However, just
because you got one interaction wrong doesn’t make you a bad person. Just take the opportunity to be honest and apologetic the next time you see them.
Of course, if there is a pattern developing, it’s worth delving a little deeper to see whether there are actions you need to take to break the cycle.
TAKE ACTION
Take time to understand your own lived experience in relation to burnout. Ask for support if you are experiencing signs of burnout. Patient safety can be impacted and all clinical colleagues have a professional responsibility to provide a supportive response in these circumstances. Remember that clinicians in leadership roles
have additional professional responsibilities in relation to creating safe, inclusive and health-promoting work environments.
NO EASY SOLUTION
It is important to acknowledge that all these issues present a complex challenge for health service organisations and individual clinicians, and there is much more to say on the topic of burnout.

At MDDUS, we have been lobbying UK governments on addressing workforce health and wellbeing issues.
We have also developed different courses for leaders on how to build conditions that support resilience and support for individual members to develop strategies to maintain wellness.
rcsed.ac.uk | 47
AWARDS & GRANTS
All the latest grants, Fellowships and bursaries that are available from the RCSEd
The Dundas Medal
The medal is in commemoration of Dr Charles Robert Dundas FFARCS FRCP Glasgow, a senior lecturer in the Department of Surgery (Anaesthetics) in Aberdeen and honorary consultant anaesthetist from 1975 to 1995. In recognition of Dr Dundas’ lifelong enthusiasm for teaching, research and innovation, an annual award recognises efforts to improve the provision of palliative care for patients when they are in hospital. The award is open to individuals or teams (medical, nursing or
paramedical) working in any hospital in the UK. It is not essential that the applicant should be an FRCSEd. The term hospital applies to both acute and community hospitals.
The closing date for applications is Wednesday 12 April 2023
Jane Goodman Memorial Scholarship in Paediatric Dentistry
Jane Goodman (1948–2019) was a consultant in paediatric dentistry who made a significant
contribution to the speciality. A former Vice-Dean of the College, she had an abiding interest in training, education and supporting the next generation of dentists. The scholarship is a recognition and memorial to the support Goodman offered. The College is deeply indebted to the Trustees of the Jane Goodman Charitable Trust for making this scholarship possible.
Applications are invited from those studying paediatric dentistry in the UK. The Dental Faculty is pleased to offer Affiliates, Members
48 | Surgeons’ News | March 2023
COLLEGE INFORMATION
'1t \\ • •
and Fellows of the Faculty and/or the Faculty of Dental Trainers the opportunity to apply for financial support to help them pursue an educational qualification at Diploma, Master’s or Clinical Doctorate level in paediatric dentistry. Funding of up to £10,000 will be awarded.
The closing date for applications is Wednesday 3 May 2022
Small Research Pump
Priming Grants
Applications are invited from surgical trainees and recently appointed consultants who are Fellows/Members of the College in good standing. Grants are awarded for pump priming projects for a period of one year only. Please note that requests for running
costs to support established projects will be less favourably reviewed than those for pilot work that has the potential to facilitate applications for more substantial funding in the future.
Research project submissions should satisfy one or more of the College’s four priority areas for research, as listed below. Up to £10,000 may be awarded and may only cover one year of the project.
Surgical/dental translational research.
Surgical/dental health services research. Research into surgical/dental aspects of patient safety, simulation and non-operative technical skills.
Cancer research of demonstrable direct clinical relevance to the management of solid tumours.
The closing date for applications is Wednesday 14 June 2023
King James IV Professorship



Applications are invited from practitioners of surgery or dental surgery who have made a significant contribution to the clinical and/or scientific basis of surgery.
The successful applicant will receive an honorarium of £500 towards any expenses incurred in travelling to a meeting/conference to give the lecture. The awardee may also use the courtesy title of ‘King James IV Professor’ for the duration of the College year in which their lecture is delivered. The successful applicant will also receive a plaque and certificate. Applications are invited from Fellows/Members of the College in good standing.
The closing date for applications is Wednesday 14 June 2023
Syme Medal
James Syme (1799–1870) was a leading surgeon of his day and an enthusiastic teacher and surgical innovator. He was also the mentor of Joseph Lister. The Syme Medal is a prestigious mark of excellence awarded by the College to a Fellow or Member of the College in good standing, based on a recently submitted thesis (MD or PhD), published body of research or educational development. Research should have been published in high-quality, peerreviewed journals. Consideration will be given to the impact of the work on future research or clinical practice.
The Medal is awarded to surgeons in training or recently appointed consultants, and is often based on work leading to a doctoral thesis. This award is distinct from the







King James IV Professorship. All applicants should be a Member or Fellow of the College in good standing.
The closing date for applications is Wednesday 14 June 2023
The Cutner Travelling Fellowship in Orthopaedics
This Fellowship provides funding for travel abroad for either of the folllowing: Trainee orthopaedic surgeons around the time of their appointment to a



























IN MEMORY
HONORARY FELLOWS
Sir Peter John MORRIS, FRCSEd1995
SURGICALFELLOWADHOMINEM



Jack L GLUCKMAN, FRCSEd(ad hominem) 2000
SURGICAL FELLOWS AND MEMBERS
David John AUSTIN, FRCSEd1974
lndrajit BASU, FRCSEd1965
Leslie Harold BLUMGART, FRCSEd1976
Robert Keith CARRUTHERS, FRCSEd 1966
Benjamin Coplan COHNEY, FRCSEd1960
Robertson Lindsay DOIG, FRCSEd1967
Arthur Rudolph EDGHILL, FRCSEd1967
Gwyn Amman EVANS, FRCSEd1980
John Millie Dow GALLOWAY, FRCSEd 1964
Roger Spencer HOLE, FRCSEd1960
Alfred William HUSBAND, FRCSEd1967
Angus Martin JAMIESON, FRCSEd1971
John LOUDON, FRCSEd1954
Michael EC MCFARLANE, FRCSEd1985
John Winton MCNAB, FRCSEd1973
John Bower MORTON, FRCSEd1969
John Nelson NORMAN, FRCSEd1967
Jeremy John POWER, FRCSEd1966
Sankar PRASAD, FRCSEd1966.
Clive Anthony Livingston THOMAS, FRCSEd1989
John William TURNER, FRCSEd1962.
DENTAL FELLOWS AND MEMBERS
William Dennis MCHUGH, FDSRCSEd1970
rcsed.ac.uk | 49
• • • • •
consultant post, to enable them to study in centres with particular expertise relating to the responsibilities of their new appointment.
Surgeons making short visits to learn new orthopaedic techniques or to work in other centres to develop orthopaedic surgery.
The award may provide up to £3,000 towards gaining experience/training in the field of orthopaedic surgery abroad. Applications are invited from Fellows/Members of the College in good standing.
The closing date for applications is Wednesday 14 June 2023
The Alban Barros D’Sa Memorial Travelling Fellowship in General Surgery
The Alban Barros D’Sa Travelling Fellowship enables those starting out in their surgical careers to attend educational events. The
scholarship was generously donated by the family of the late Alban Barros D’Sa, Fellow and Examiner at the RCSEd. The funding for this Fellowship contributes in part, or in whole, to the cost of one period of study/attachment.
The award may provide up to £1,000 towards attending international education meetings or conferences, or to gain further experience or training abroad. Applications are invited from Members or Fellows of the College in good standing who are higher surgical trainees who have not yet attained consultant grade.
The closing date for applications is Wednesday 14 June 2023 11.59pm BST
Tom Bereznicki Dental Education Grant
The Faculty of Dental Surgery of the Royal College of Surgeons of Edinburgh supports educational endeavours for individuals who are
Affiliates, Members and Fellows of the Dental Faculty and/or the Faculty of Dental Trainers. Grants (up to £3,000) will be available to defray expenses for those undertaking an appropriate educational qualification.
The closing date for applications is Wednesday 7 June 2023
For more information about the College's awards and grants contact: Researchand Grants Coordinator, Development and Partnerships Office, Royal College of Surgeons of Edinburgh, Nicolson Street, Edinburgh EH8 9DW Tel: +44 (0)131 5271616 • Email:awards@ rcsed.ac.uk • Web: bit.ly/2wKpRTr
The RCSEdcollects personal data lrom application process for awards and this information with any third used solely for


TO THE FOLLOWING AWARDS AND GRANTS RECIPIENTS
CONGRATULATIONS TO THE FOLLOWING AWARDS AND GRANTS RECIPIENTS
OPHTHALMOLOGY MAJOR GRANT
RobertEdwardMaclaren, professor of ophthalmology and honorary consultant. 'Development of a CRISPRtreatment for USH2A-associated retinitis pigmentosa.'
Manjit Singh Mehat, consultant ophthalmologist and National Research Scotland Fellow. 'Profiling the proliferative vitreoretinopathy niche at the single cell transcriptional level to identify potential theraputic targets for adjunctive therapy in retinal detachment surgery.'
RolyMegaw, clinical lecturer and consultant ophthalmologist, 'Determining genetic causes of previously unsolved inherited retinal dystrophies.'
FST·ASMEGRANT














LauraAwad,core training year 2 (CT2) doctor in plastic surgery. 'A pilot study on the application of mixed-reality simulation of hand fracture anatomy and percutaneous fixation in higher surgical training.'
RUSSELLTRUSTBURSARY
Mohammad Ashraf, University of Glasgow. Visiting the Department of Neurosurgery,
Allama Iqbal Medical College, Jinnah Hospital Lahore, Punjab, Pakistan.
Vratko Himic,University of Oxford. Visiting the University of Iowa Carver College of Medicine, US.
George PaulTeng-HauLiu,Anglia Ruskin University. Visiting Kindai University Nara Hospital, Japan.
Hari McGrath, King's College London. Visiting Johns Hopkins University School of Medicine and Yale University School of Medicine, US.
AziziSheik-Ali,University of Exeter. Visiting Massachusetts General Hospital, US.
HermesManos,University of St Andrews/ University of Dundee. Visiting Western Isles Hospital, Stornoway, Isle of Lewis.
LINDSAY STEWART PRIZE
Faraja M Magwesela, 'Experiences of Women with Breast Cancer in Sub-Saharan Africa: A Systematic Review'




























RalphObure, 'Determining the prognostic value of peripheral blood derived
inflammatory markers in predicting diseasefree survival in early breast cancer.'
THE FRRHH FELLOWSHIP
AshutoshKumarSingh,'Oral health status in remote and rural Nepal: A systematic review and thematic analysis.'



MuhammadZeeshanAslam,'Surgical training and primary healthcare services in post-conflict Liberia.'
RichardMiti, 'Taking surgery there -rural surgical camps.'
Nigel Rossiter,'Trauma outcomes study after simulation training in Burundi (TOAST B).'
Michael Mwachiro,'Basic and advanced endoscopy for surgeons training (BEST).'
TracernMugodo,'Improving tenotomy skills in medical doctors working at hospitals with clubfoot clinics.'
BarnabasAlayande,'Baselining surgical access in rural north-central Nigeria.'
50 | Surgeons’News | March2023
COLLEGE INFORMATION
•
REGIONAL AMBASSADORS IN YOUR AREA
The
Council Member with responsibility for RSAs
1 Mike Silva, Churchill Hospital, Oxford
Director
2 Barnabas (Barney) Green, James Cook Hospital, Middlesbrough
Deputy Director
3 Replacement TBC
SCOTLAND
EAST
4 Jaiganesh Manickavasagam, Ninewells Hospital, Dundee
4 Andrew Martindale, Ninewells Hospital, Dundee
4 Stephen Jones, Ninewells Hospital, Dundee
NORTH
5 Malcolm Nicol Raigmore Hospital, Inverness
6 Pragnesh Bhatt, Aberdeen Royal Infirmary, Aberdeen
6 Manoj Kumar, Aberdeen Royal Infirmary, Aberdeen
6 Bhaskar Ram, Aberdeen Royal Infirmary, Aberdeen
WEST
7 William Andrew Clement, South Glasgow University Hospitals, Glasgow
7 Maria Coats, Glasgow Royal Infirmary, Glasgow
SOUTH EAST
8 Robyn Webber, Victoria Hospital, Kirkcaldy
8 Peter Driscoll, Victoria Hospital, Kirkcaldy
2 Andrew Tambyraja, Royal Infirmary of Edinburgh
ENGLAND
EAST OF ENGLAND
9 Anita Balakrishnan, Cambridge University Hospitals, NHS Foundation Trust, Cambridge
10 Stuart Irving, Norfolk and Norwich University Hospital, Norwich
11 Roshan Lal, James Paget University Hospital NHS Trust, Great Yarmouth
EAST MIDLANDS
12 Hazem Khout, City Hospital, Nottingham
13 Paul Lee, Grantham and District Hospital, Grantham
14 Aravind Desi Syamarao, Diana, Princess of Wales Hospital, Grimsby
KENT, SURREY AND SUSSEX
15 Mike Williams, Eastbourne District General Hospital, Eastbourne
LONDON
16 Cynthia-Michelle Borg, University Hospital, Lewisham
16 Jihene El Kafsi, Frimley Park Hospital, Wexham
16 Nagarajan Muthialu, Great Ormond Street Hospital
16 Michael Saunders, The Royal Free London (NHS Foundation Trust)
MERSEY
17 Ravi Pydisetty, St Helens and Knowsley Teaching Hospitals
NHS Trust, Whiston
18 Janardhan Rao, Countess of Chester Hospital, Chester
19 John Taylor, University Hospital, Aintree
NORTH WESTERN
20 Richard Graham, North Manchester General Hospital, Manchester
20 Aiman Khunda, Salford Royal Hospital, Manchester
20 Nadeem Khwaja, Wythenshawe Hospital, Manchester
21 Jayadeep Jayachandran Saraswathy, Cumberland Infirmary, Carlisle
NORTHERN
22 Paul Gallagher, Northumbria Healthcare NHS Foundation Trust
23 Sanjay Pandanoboyana, Newcastle Freeman Hospital, Newcastle upon Tyne
23 Alex Phillips, Royal Victoria Infirmary, Newcastle upon Tyne
23 Dan Saleh, Royal Victoria Infirmary, Newcastle upon Tyne
3 Peng Wong, James Cook Hospital, Middlesbrough
3 Sarah Healy, James Cook University Hospital, Middlesbrough
OXFORD
1 Giles Bond-Smith, Oxford University Hospitals NHS Trust, Oxford
1 Stephen Boyce, Oxford University Hospitals NHS Trust, Oxford
24 Niteen Tapuira, Milton Keynes University Hospital, Milton Keynes
SEVERN
25 Jamshed Shabbir, University Hospitals, Bristol
SOUTH EAST
26 Jeremy Rodriguez, Stoke Mandeville Hospital, Buckinghamshire
SOUTH WEST PENINSULA
27 Ashok Sridhara Subramanian, Musgrove Park Hospital, Somerset
WESSEX
28 Hunter MacLean, Queen Alexandra Hospital, Portsmouth
29 Aiman Alzetani, University Hospital Southampton, Southampton
29 Arjun Takhar, University Hospital Southampton, Southampton
29 Nandita Pal, Southampton General Hospital, Southampton
WEST MIDLANDS
30 Yuvraj Agrawal, The Royal Orthopaedic Hospital NHS Trust, Birmingham
31 Sriram Rajagopalan, Royal Stoke University Hospital, Stoke-on-Trent
31 Vittal Rao, Royal Stoke University Hospital, Stoke-on-Trent
32 Ramanan Vadvivelu, Royal Wolverhampton Hospital NHS Trust, Wolverhampton
33 Devaraj Srinivasamurthy, University Hospital, Coventry
YORKSHIRE AND HUMBER
34 Nathan Chidambaram, Northern General Hospital (Sheffield Teaching Hospitals NHS Foundation Trust), Sheffield
35 Amaran Krishnan, York Teaching Hospital, NHS Foundation Trust, York
36 Mark Peter, Calderdale and Huddersfield NHS Foundation Trust, Huddersfield
36 Shireen McKenzie, Leeds Teaching Hospital, Leeds
NORTHERN IRELAND
37 Mano Shanmuganathan, Royal Victoria Hospital, Belfast
37 Andrew Diver Royal London Hospital
WALES
38 Raymond Delicata, Nevill Hall Hospital, Abergavenny
39 Keshav Swarnkar,Royal Gwent Hospital, Newport
40 David Owens, University Hospital of Wales, Cardiff
41 Konstantinos Serafeimidis, Singleton Hospital, Swansea
College’s support and advice network throughout the country
7 8 4 6 5 27 15 19 24 34 35 2 30 33 32 16 38 40 39 41 28 29 18 10 1 26 13 17 25 23 21 22 31 37 20 12 11 36 14 9 3 rcsed.ac.uk | 51
If you are interested in applying for a Regional Adviser role please email outreach@ rcsed.ac.uk
DIPLOMA LISTINGS
Congratulations to all our Fellows and Members who were presented with diplomas and awards in Edinburgh and Chennai in October and November
SATURDAY 8 OCTOBER 2022, ITC GRAND CHOLA, CHENNAI, INDIA
Admission to Fellowship ad hominem
Professor Bhagavan C Balagopal, MBBS, MS, FMAS, Vice-Principal, Professor and Head of Unit, Department of General Surgery, Kempegowda Institute of Medical Sciences and Research Centre, VV Puram, Bengaluru, India
Associate Professor Warwick Jonathan Teague, FRACS, Director, Trauma Service; Clinical Lead, Burns Service; Paediatric Surgeon, The Royal Children’s Hospital, Melbourne; Associate Professor, Department of Paediatrics, University of Melbourne, Australia
The College International Medal 2020
Sai Krishna Vittal, MS, DNB, FRCSEd, FRCS(Eng), Consultant Endocrine Surgeon, Chennai; Adjunct Professor of the Tamil Nadu Dr MGR Medical University, Chennai, India
Award of Fellowship in Surgery (Without Examination)
Shweta Agarwal, Senior Consultant, Cornea and Ocular Surface Disorders, Sankara Nethralaya, Chennai
Kaushik Bhattacharya, Specialist (Surgery), CAPFs Composite Hospital, Border Security Force, Siliguri
Professor Utpal De, MS, FAIS, FRCPS (Glasg), Professor and Unit Chief, Department of Surgery, Nil Ratan Sircar Medical College, Kolkata
Rajendra Prasad Kathula, Professor of Surgery, Great Eastern Medical School and Hospital, Srikakulam
Professor Dattatraya P Muzumdar, FRCSI, FACS, Professor, Department of Neurosurgery, Seth G.S. Medical College and KEM Hospital, Mumbai
Professor Harshavardhan K Reddi, FRCPS(Glasg), Senior Consultant
Cardiothoracic Surgeon, Venkateswara Hospital, Chennai
Professor Gouthaman
Shanmugasundaram, Professor of Surgical
Oncology and Senior Consultant, Surgical Oncologist, SRIHER, Chennai
Professor Rauf A Wani, FACS, Professor, General and Minimally Invasive Surgery, Sher-I-Kashmir Institute of Medical Sciences, Srinagar
Diploma of Fellowship in the Specialty of Cardiothoracic Surgery
Neeraj Aravind Kamat, Maharashtra University of Health Sciences
Diplomas of Fellowship in the Specialty of Trauma and Orthopaedic Surgery
Pardha Saradhi Davuluri, Dr NTR University of Health Sciences
Rajeev Srinivasa Rao Ghat, University of Mysore
Diploma of Joint Surgical Colleges’ Fellowship in General Surgery
Hemanth Kumar Kimavat, Rajiv Gandhi University of Health Sciences
Diploma of Joint Surgical Colleges’ Fellowship in Trauma and Orthopaedic Surgery
Mahesh Karthik Ragavan, Tamil Nadu Dr MGR Medical University
Diploma of Fellowship in Surgery (Without Examination – By Application)
Vinitha Nair, University of Kerala
Diplomas of Fellowship of the Faculty of Surgical Trainers
Vishal Kumar, University of Calcutta
Pawanindra Lal, University of Delhi
Intercollegiate Diplomas of Membership in Ophthalmology – ICO
Marushka Aguiar, Goa University
Tudymol Devasia, Mahatma Gandhi
University
Saranya DV, Bharath University
UM Vara Prasad Gajula, Dr NTR University of Health Sciences
Subathra Gnanavelu, Mahatma Gandhi University
Bharat Gurnani, Maharashtra University of Health Sciences
Kirandeep Kaur, Baba Farid University of Health Sciences
Sharika Erikapatil Mangad, Calicut University
Arthi Mohankumar, Pondicherry University
Reni Philip, University of Kerala
Harsha Pradyumnan, Calicut University
Anjana Ramanathan, All India Institute of Medical Sciences
Rokhsanda Rehnuma, Kumudini Women’s Medical College, Bangladesh
Pragya Saini, University of Delhi
Zainu Shams, Tamil Nadu Dr MGR Medical University
Shabnam Singh, Assam University
Sruthi R, Calicut University
Rekha Sravya M, Rajiv Gandhi University of Health Sciences
Juliana Rositta Stephen, Tamil Nadu
Dr MGR Medical University
Sivaviganesh Subramanian, Tamil Nadu
Dr MGR Medical University
Nagalekshmi SV, Tamil Nadu Dr MGR Medical University
Prithvi Vishwanath, Manipal University
Intercollegiate Diplomas of Membership in Otolaryngology
Gayathri Bhaskaran, Tamil Nadu Dr MGR Medical University
Catrin Sian Evans, University of Liverpool, UK
Srinivasan Venkataraman, Sri Ramachandra University
Intercollegiate Diplomas of Membership in Surgery in General
PM Abdul Gafoor, Calicut University
Kaustubh Ahuja, University of Delhi
Nasrin Aktar, Sylhet MAG Osmani Medical College, Bangladesh
Ashok Kumar Baskar, Tamil Nadu Dr MGR Medical University
Pradeep Baskaran, Tamil Nadu Dr MGR Medical University
Sharika Chandran, Cochin University of Science & Technology
Sanjay Kanth Dayanandan, Tamil Nadu
Dr MGR Medical University
52 | Surgeons’ News | March 2023
Kunal Fadte, Goa University
Giri Babu Gattupalli, Dr NTR University of Health Sciences
Rajeshwar Jotheeswaran, Tamil
Nadu Dr MGR Medical University
Azim Khan, University of Kerala
Nida Khan, Pravara Institute of Medical Sciences
Suha Meher, University of Dhaka, Bangladesh
Anand Mohan, Pondicherry University
Anushka Nair, Kasturba Medical College, Manipal
Progga Parmita Pondit, Sylhet MAG
Osmani Medical College, Bangladesh
Deerush Kannan Sakthivel, Tamil Nadu Dr MGR Medical University
Priyanka Sharma, Kathmandu University School of Medical Sciences, Nepal
Nagesh Sherikar, Rajiv Gandhi University of Health Sciences
Amarjeet Singh, Kasturba Medical College Manipal
Kartik Sridhar, Babasaheb Bhimrao
Ambedkar Bihar University
Siddarth Sridhar, Chettinad University
Chithra Thomas, Cochin University of Science & Technology
Diplomas of Membership of the International Postgraduate Deanery
Shekar Mudramaiah, Rajiv Gandhi University of Health Sciences
Anjan Prabhakara, Rajiv Gandhi University of Health Sciences
Diploma of Membership in Endodontics
Vinay Shivagange, University of Mysore
Diploma of Membership in Oral and Maxillofacial Surgery
Hussein Ali Mohammed Abdulnabi, University of Baghdad, College of Dentistry, Iraq
Diploma of Membership in Orthodontics
Arun Vels Shailendran, Tamil Nadu Dr MGR Medical University
Diploma of Membership of the Faculty of Dental Surgery
Sabarni Arshaj Gaikwad, Saveetha University
FRIDAY 14 OCTOBER 2022, ROYAL COLLEGE OF SURGEONS OF EDINBURGH
Installation to the Court of Regents
Eric Macfie Young, Director, Archangels, Edinburgh
Conferment of Honorary Fellowship
Shaf Keshavjee, MD MSc FRCSC FACS, Chief of Innovation, University Health
Network, Toronto; Director, Toronto Lung Transplant Program; Director, Latner Thoracic Research Laboratories; Professor, Thoracic Surgery and Biomedical Engineering, Sprott Department of Surgery; Vice-Chair for Innovation, Department of Surgery, University of Toronto, Canada
Admission to Fellowship ad hominem
Professor Andrew Graham Hill, MBCHB, MD, FACS, FISS, FRACS, FRNZ, Professor of Surgery, Assistant Dean, Faculty of Medical and Health Sciences, University of Auckland; Consultant Colorectal Surgeon, Middlemore Hospital, Auckland, New Zealand
Professor Derek M Steinbacher, DMD, MD, MA, Professor, Plastic and Reconstructive Surgery, Yale School of Medicine; Professor and Chief, Oral and Maxillofacial Surgery; Director of the Cleft and Craniofacial Program, Yale New Haven Health, US
The President’s Gold Medal Charles D Auld, MD DA FRCSEd, former Member of RCSEd Council and retired Consultant General Surgeon

Award of Fellowship in Surgery (Without Examination)
Professor Rajiv Jha, MD, MS, M Ch, IFAANS, Professor and Senior Consultant Neurosurgeon; Chief, Department of Neurosurgery, National Academy of Medical Sciences, Bir Hospital; Chief, Department of Neurosurgery, Norvic International Hospital, Kathmandu, Nepal Benjamin Woodham, BMedSc(Hons) MBBS
FRACS, Clinical Academic Consultant
Surgeon, Western Sydney Local Health District/Western Sydney University, Australia
Award of Fellowship in Dental Surgery (Without Examination)
Professor Mona Fayed, BDS, MSc, PhD, DrMedDent, Professor of Orthodontics, Head of Quality Assurance Unit, Faculty of Dentistry, Cairo University, Egypt
Diploma of Fellowship in the Specialty of Cardiothoracic Surgery
Gentjan Jakaj, Ege University, Turkey
Diploma of Joint Surgical Colleges’ Fellowship in Cardiothoracic Surgery
Varun Shetty, Rajiv Gandhi University of Health Sciences, India
Diploma of Fellowship in the Specialty of General Surgery
Salman Ahmed Abdul Jabbar, University of Dundee
Diplomas of Fellowship in the Specialty of Neurosurgery
Mikhail Antonio De Santos, University of Guyana
Rathijit Mitra, Ravishankar University, India
Stuart Alexander Gordon Roberts, University of Dundee
Diploma of Fellowship in the Specialty of Plastic Surgery
Lucie J Wright, University of Edinburgh
Diplomas of Fellowship in the Specialty of Trauma and Orthopaedic Surgery
Carl Fenton, Hull York Medical School
rcsed.ac.uk | 53 COLLEGE INFORMATION
Niak Puei Koh, National University of Ireland
Nishant Singh, Maharashtra University of Health Sciences, India
Diplomas of Fellowship in the Specialty of Urology
Flora Elizabeth Rodger, University of Edinburgh
Yogit Deepak Wagh, Maharashtra University of Health Sciences, India
Diplomas of Fellowship in Surgery (without Examination – by Application)
Dave James Cloke, Newcastle University
Mohend Abbass Nori Alshalah, Al-Mustansiriya University, Iraq
Senthur K Sahathevan, University of London
Diploma of Fellowship of the Faculty of Surgical Trainers
Dave James Cloke, Newcastle University
Sukri Rahman, Andalas University, Indonesia
Intercollegiate Diplomas of Membership in Ophthalmology
Ruksana Aboobaker, Rajiv Gandhi University of Health Sciences, India
Raghda Reda Ibrahim Alramady, Misr University for Science and Technology, Egypt
Sujit Kumar Biswas, University of Dhaka, Bangladesh
Nehal Elfarouk, Cairo University, Egypt
Omar Samir El-Mulki, Jordan University of Science & Technology, Jordan
Elshimaa Mosalam, Zagazig University, Egypt
Andrew Ross, Assiut University, Egypt
Soma Rani Roy, University of Dhaka, Bangladesh
Anirudh Singh, Savitribai Phule Pune University, India
Intercollegiate Diplomas of Membership in Otolaryngology
Fateh Almohammad Alsalem, University of Aleppo, Syria
Syed Zohaib Maroof Hussain, Dow University of Health Sciences, Pakistan
Kah Heng Lim, Queen’s University Belfast
Intercollegiate Diplomas of Membership in Surgery in General
Sumera Ashfaq, University of the Punjab, Pakistan
Calum Blacklock, University of Edinburgh
Julian Camilleri-Brennan, University of Edinburgh
Adeel Qamar Ghumman, University of Health Sciences Lahore, Pakistan
Muhammad Adeel Kaiser, University of Health Sciences Lahore, Pakistan
Ketki Kaushal, University of Dhaka, Bangladesh
Naomi Mercieca, University of Malta
Karim Moawad, Alexandria University, Egypt
Farah Nobi, University of Dhaka, Bangladesh
Joshua Owiti, University of Nairobi, Kenya
Lilia Hebia Ragad, University Ferhat Abbas de Setif, Algeria
Prashanth Ramaraj, Imperial College London
Shenol Sasankan, University of Kerala, India
Henry Searle, University of Edinburgh
Ahmed Salah Mahmoud Ahmed Shehata, Ain Shams University, Egypt
Sadaf Sohrabi Sedeh, University of Glasgow
Akhil Taneja, Guru Gobind Singh
Indraprastha University, India
Adithya Varma, University of Liverpool
Rebecca Windle, University of Manchester
Diplomas of Membership of the Faculty of Surgical Trainers
Niamh Mary Haughey, University of London
Pratik Roy, University of London
Diplomas in Immediate Medical Care
Markus Arnold, University of Manchester
Timothy Austin, Staffordshire University
Liam Sands, University of East Anglia
Diploma in Remote and Offshore Medicine
Robert Etall, Birmingham City University
The Sir David Brewster Medal 2018/19 Awarded to the highest-placed graduate of the MSc in Primary Care Ophthalmology programme during an academic year.
Fadi Ghazala, University of St Andrews
Diplomas of Fellowship of the Faculty of Dental Trainers
Derek John Maguire, Queen’s University
Belfast
Leonard John Maguire, Queen’s University Belfast
Diploma of Membership in Oral Surgery
Robert Gareth Michael Williams, Newcastle University
Diplomas of Membership in Orthodontics
Hans Antov, University of Leeds
Alison Comerford, National University of Ireland
Dima Mobarak, University of Birmingham
Sara Mohammed Saed, University of Manchester
William Samuel Maguire, Queen’s University Belfast
Abdallah Sharafeldin, Ain Shams University, Egypt
Diploma of Membership in Primary Dental Care
Deena Abawi, Jordan University of Science and Technology, Jordan
Diploma of Membership in Prosthodontics
Konstantinos Roumpeas, The National and Kapodistrian University of Athens, Greece
Diplomas of Membership of the Faculty of Dental Surgery
Ruba Basim Hasan Al-Zuhairi, University of Baghdad, College of Dentistry, Iraq
Simrat Dhanjal, University of Bristol
Nur Farhana Mohd Fikri, Universiti Teknologi
MARA, Malaysia
Andreas Flouri, The National and Kapodistrian University of Athens, Greece
Madiha Habib, University of Health Sciences
Lahore, Pakistan
Benveer Singh Kaley, Queen Mary University of London
Mahwesh Naaz Khan, Dr NTR University of Health Sciences, India
Haris Naseer, Liaquat University of Medical Health Sciences, Pakistan
Roshni Anupriya Sanikop, King’s College London
Sharmila Raghuji Thorat, Rajiv Gandhi University of Health Sciences, India
James Wege, University of Sheffield
Alizeh Zaffar, National University of Ireland
Diplomas in Orthodontic Therapy
Shauna Gill, University of Central Lancashire
Carmel Mary Taylor, University Dental Hospital of Manchester
The William Houston Medal 2019/20
Awarded for an outstanding performance in the Membership in Orthodontics Examination in an academic year.
Alison Comerford, National University of Ireland
FRIDAY 11 NOVEMBER 2022, ROYAL COLLEGE OF SURGEONS OF EDINBURGH
Honorary Fellowship
Professor Francis A Frizelle, FRACS, FACS, FASCRS, FNZMA, FRCSI (Hon), Professor of Colorectal Surgery, Department of Surgery, University of Otago, New Zealand
Admission to Fellowship ad hominem
Carl Davis, FRCSI, FRCPSGlasg, Consultant Paediatric Surgeon and Honorary Clinical Senior Lecturer, University of Glasgow
William B Kleinman, MD, Clinical Professor of Orthopaedic Surgery, Indiana University
School of Medicine; Senior Attending Surgeon, the Indiana Hand to Shoulder Center, Indianapolis, US
Fellowship in Surgery (Without Examination)
Safdar Alam, MD, MSc, FRCPS(Glasg), Consultant Ophthalmologist, North West Anglia NHS Foundation Trust, Peterborough City Hospital
Professor Subhash Khanna, MS, FALS, FAGIE, FIAGES, Chief Department of Minimal Access,
54 | Surgeons’ News | March 2023
GI and Robotic Surgery, Swagat Super Speciality Surgical Institute, Guwahati, India
The Council Medal 2022
Mariette Naud-Betteridge, Head of International Engagement, RCSEd
Diplomas of Fellowship in the Specialty of General Surgery
David Lewis Bowden, University of Liverpool
Madhu Srinivasan Durairaj, Dr MGR Medical University, India
Ahmed Mohammed Adam Mohammed, University of Khartoum, Sudan
Diploma of Fellowship in the Specialty of Otolaryngology
Mark Robert Williams, University of Manchester
Diplomas of Fellowship in the Specialty of Trauma and Orthopaedic Surgery
Daniel Dawson, Queen’s University Belfast
Girish Gopinath, Calicut University, India
Kohila Vani Sigamoney, University of Leicester
Diplomas of Fellowship in the Specialty of Urology
Stephanie Marie Guillaumier, University of Malta
Alice Elizabeth Hartley, University of London
Debashis Nandi, Kuvempu University, India
Amit Patel, Maharashtra University of Health Sciences, India
Diplomas of Fellowship in the Specialty of Vascular Surgery
Mukesh Kumar Garg, Guru Gobind Singh
Indraprastha University, India
David Michael Riding, University of Manchester
Diplomas of Fellowship of the Faculty of Surgical Trainers
Nishan Fernando, University of Aberdeen
Intercollegiate Diplomas of Membership in Ophthalmology
Noor Hussain Abady, Al-Mustansiriya University, Iraq
Rameear Abdullah Abubaker, Hawler Medical University, Iraq
Rawya Abdelhadi Gadallah Diab, University of Khartoum, Sudan
Achraf Mohamad Hejazi, Jordan University of Science and Technology, Jordan
Ahmed Mohamed Lotfi Khattab, Alexandria University, Egypt
Udayaditya Mukhopadhyay, University of Calcutta, India
Sagnik Sen, University of Delhi, India
Chaw Hsu Win, Yangon University, Myanmar
Intercollegiate Diploma of Membership in Otolaryngology
Haatsari Kujeke, University of the Witwatersrand, South Africa
Intercollegiate Diplomas of Membership in Surgery in General
Eleftherios Orestis Argyriou, University of Ioannina, Greece
Sujit Gnanakumar, University of Cambridge
Jing Xian Lee, Newcastle University
Rebecca Lefroy, University of Manchester
Maaz Ahmad Maghazi, Shifa Tameer-e-Millat University, Pakistan
Nichola Manu, University of Liverpool
Richard Adam Robert McLellan, Newcastle University
Wendy Minks, University of Leeds
Arjun Charles Paramasivan, University of Leeds
Ganan Thambiah Radhakrishnan, University of Leeds
Ganeshan Ramsamy, University of London
Anish Singh, University of the West Indies
Ifeanyi Charles Umoke, Ebonyi State University, Nigeria
Diploma of Membership of the Faculty of Surgical Trainers
Andrew James Diver, Queen’s University, Belfast
Diploma in Immediate Medical Care
Jamie Short, Coventry University
Diploma in Retrieval and Transfer Medicine
David George, University of Leeds
Diplomas of Membership of the International Postgraduate Deanery
Avinash Ranganagouda Odugoudar, Rajiv Gandhi University of Health Sciences, India
Sharjil Wahid, Islamia University, Pakistan
The Dundas Medal 2022
SPOT – The Safer Prescription of Opioids Tool
Roger Flint, Scott Jamieson, Professor Jacob George, Deans Buchanan
The GB Ong Medal 2019
David Lewis Bowden, University of Liverpool
The GB Ong Medal 2022
Ahmed Mohammed Adam Mohammed, University of Khartoum, Sudan
The Sir David Brewster Medal 2020/2021
Sarah Donaldson, University of Edinburgh
The Sir David Brewster Medal 2021/2022
Wanok Godfrey, University of Edinburgh
Diploma of Fellowship in the Specialty of Restorative Dentistry
Martin James, University of Sheffield
Diplomas of Membership in Endodontics
Praveen Rajesh, Rajiv Gandhi University of Health Sciences, India
Maria De Los Angeles Vallina, University of Birmingham
Diplomas of Membership in Oral Surgery
Elpida Samara, The Aristotle University of Thessaloniki, Greece
Andrew Travers, University of Liverpool
Diplomas of Membership in Orthodontics
Saarah Nisa Juman, University of the West Indies
Camilla Ellie Miles-Hobbs, University of Bristol
Diploma of Membership in Periodontics
Martin James, University of Sheffield
Diplomas of Membership of the Faculty of Dental Surgery
Raveena Kaur Juttla, Cardiff University
Sadia Sajid, Bahria University, Pakistan
Diplomas in Paediatric Dentistry
Clare Margaret Burton, Leeds Dental Institute
Diplomas in Orthodontic Therapy
Heather Joan Bannon, Edinburgh Dental Institute
Malgorzata Elzbieta Bednarz, Manchester Dental Hospital
Moreya Begum, University of Central Lancashire
Sophie Bicknell, University of Bristol Dental School
Lucy Anne Dewane, University of Central Lancashire
Laura Jane Hall, University of Central Lancashire
Sarah Rose Hartley, University of Bristol Dental School
Emily Jane Hunt, Manchester Dental Hospital
Samiya Mahamed, University of Bristol Dental School
Pamela Malczuk, Edinburgh Dental Institute
Lisa Marie Morris, University of Bristol Dental School
Arlene Ormsby, University of Central Lancashire
Amy Thomson, Edinburgh Dental Institute
Asta Ulinskaite, Edinburgh Dental Institute
Paige Eleanor Zubiena, University of Central Lancashire
rcsed.ac.uk | 55
COLLEGE INFORMATION
HOURSIN...

MALTA
Whether you want to explore UNESCO ruins or sample Maltese cuisine in the sun, two days is enough to get a taste of this Mediterranean isle, says Sarah Riches
Tantalising glimpses of fishing villages and hilltop towns in buttermilk hues peek between cirrus clouds as you land on Malta, 80km south of Sicily.
A trio of islands – Malta, Gozo and Comino – the Maltese archipelago has been inhabited since the Neolithic period, 6,000 years ago.
Conquered by the Arabs in AD 870, the region fell under Sicilian then French rule, before the British took control in the 1800s.
Malta gained independence in 1964 and while it’s now part of the EU, its chequered history is palpable – from its Arab-inspired language to its Sicilian-style kannoli pastries. As for the British influence? Well, if you hire a car, remember to drive on the left.
DAY 1
Small but mighty, it only takes 20 minutes to stroll around the capital, Valletta, but when it comes to ambience and historical attractions the city packs a punch.


Prized for its 320 monuments, the walled city is a UNESCO World Heritage Site. A 42m dome crowns the Basilica of Our Lady of Mount Carmel, which is perched on a hill, making it the city’s tallest building – and a good place to begin your self-guided tour.
The Grandmaster’s Palace is nearby. Once the home of the Knights of St John – a community of monks who defended Malta against Ottoman Turks in the 1500s – it is now the Maltese president’s
residence. Its state rooms and marble hallways are lined with fine art, armour and trompe l’œil paintings. After a pitstop in the courtyard, continue one street west to St John’s Cathedral. This 16th-century place of worship is valued for its ornate Baroque interiors, which feature three-dimensional frescoes, limestone carvings and marble tombs.
56 | Surgeons’ News | March 2023
HERITAGE
HIGHLIGHTS
Above: The impressive city skyline of Malta’s capital, Valletta
Right: Explore colourful streets in historic Valletta
-----l--
Its ambience and historical attractions pack a punch
,,
Ready for lunch?
Then pop into Is-Suq Tal-Belt, a grand food hall in a restored Victorian building, to sample Malta’s national dish: stewed rabbit.
After your meal make time to see two UNESCO World Heritage Sites on Valletta’s outskirts. The Hal Saflieni Hypogeum catacombs in Paola, carved into limestone around 2,500 BC, house 7,000 bodies, so it’s hard to believe they were only discovered in 1902. The nearby Tarxien Temples, unearthed in 1913, may be older – it’s thought that their bas-relief sculptures date back to 3,600 BC.
If you want a break from history, sign up to a tile workshop with Art Classes Malta in Marsa. Learn about Maltese tiles as you design a coaster made from plaster or cement, apply it to a mould then paint it with acrylic.
Once you’ve finished your masterpiece, celebrate with a glass of white, red and rose on a tasting tour of Marsovin Cellars, also in Marsa.
Cheese and olives won’t fill you up, so return to Valletta for dinner at
DAY 2
The Harbour Club, a fine-dining Mediterranean restaurant in a converted ice warehouse. After your meal, meander through Upper Barrakka Gardens to the waterfront, which is lined with alfresco restaurants.
On your second day on the island, hop on the 51 bus from Valletta and wind through terraced fields blooming with poppies, anemones and borage to Mdina, in the middle of the island.
Above: Palazzo Falson Historic House Museum in Mdina is a treasure trove of antiques and art

Left: Try one of Malta’s delicious kannoli pastries

Below: Stroll through Upper Barrakka Gardens

Another UNESCO World Heritage Site, Mdina existed in the Bronze Age, although much of it was constructed in the 1600s.
A Baroque gate grants access to the fortified hilltop town. Once inside, spend a morning ambling around its winding streets, which are flanked by grand buildings, including the 18th-century Vilhena Palace, a former hospital housing a natural history museum.
However, it’s St Paul’s Cathedral that most visitors come to see. Founded in the 12th century, the current building – with its twin clock towers – was constructed in the early 1700s. Along with frescoes and marble columns, a painting of a shipwreck tells the tale of how the saint allegedly arrived on the island.
If you like fine art, visit Palazzo Falson Historic House Museum next for a glimpse into the life of an aristocrat. Once you’ve explored this former private residence, amble around the courtyard and stop for a spot of lunch in its rooftop café. If that’s full, you can request a table upstairs at Fontanella Tea Garden, which has countryside views.
From Mdina you can stroll to Rabat, a tangle of limestone alleyways bursting with bougainvillea. While away an afternoon dipping in and out of historic sites and discover Roman mosaics in Domus Romana and antique furniture in Casa Bernard, a 16th-century family home inside a mediaeval watchtower. Don’t miss St Paul’s Catacombs, a vast underground network of Roman tombs used between AD 200 and AD 700.
Alternatively, after lunch return to Valletta and treat yourself to a sunset cruise with Malta Sailing Experiences and paddleboard as the sky turns rose pink. Take your own food and wine or request Maltese dishes such as stuffed artichokes, lampuka (fish) and octopus stew to enjoy as you sail from Marsamxett Harbour to the fortified cities of Cospicua, Vittoriosa and Senglea – a memorable way to end your time on Malta.
Sarah Riches Twitter: @healthy_holiday
For more information about Malta visit www.visitmalta.com/en
rcsed.ac.uk | 57
Shutterstock
From Mdina you can stroll to Rabat, a tangle of limestone alleyways bursting with bougainvillea
The terminal episode
Graham Layer concludes his tour de force of culinary features for Surgeons’ News with a smörgåsbord of fine European dining

With the relaxation of most of the restrictions introduced during the pandemic, but with shortages still overt in the hospitality industry, I am fortunate to have visited a large number of restaurants in the last few weeks – and my taste buds have recovered.
I have noticed that prices are higher everywhere and staffing is a major problem – not just in the UK, but in the US, Canada and Europe – resulting in some frenzied service from often newly trained staff members who are willing but overwhelmed and underpaid. Can you think of any parallels closer to home?
Anna Haugh, the new BBC MasterChef: The Professionals presenter who has taken over from Monica Galetti, is the chef at Myrtle, an Irish restaurant on a side street in Fulham in London. Chef-owner Haugh started out at L’Ecrivain in Dublin and has worked at Elystan Street in London and Gordon Ramsay’s restaurant London House among others.
We had an outstanding lunch with eight tasting plates of Gaelic morsels, all supposedly originating from the various counties to provide “a taste of Ireland”. Black pudding bites wrapped in a delicate potato filo were a worthy extra to go with our drinks while we interpreted the menu. Attractive root vegetables followed, then a crunchy cheese mousse, pig’s head in a sort of sausage roll with cheese, outstanding poached thick fillet of sea bass with smoked potatoes, magnificent pink slices of lamb loin served with a tiny lamb pie, a novel tart lemon posset with cardamon and a Guinness cake with a honeycomb mousse, all finished off with multiple petits fours. An entirely memorable gustatory experience.
The new concept Ivy Asia brand has arrived on some high streets. A spicy mix of Far Eastern dishes as interpreted in the UK with a stylish flair, and the fantastic décor and staff uniforms create a real piece of theatre. The food was all round rather good, but left me clutching for omeprazole.
A version of Peking duck came adorning an enormous pewter duck placed in the middle of the table, and the
dumplings of all sorts were mouth-watering. For the main courses, straightforward teriyaki salmon, a good curry and a generous pork belly bathed in a variant of chilli sauce. The place in Chelsea was packed out with everyone in the world seemingly celebrating their birthdays and having a great time.
Menu Gordon Jones in Bath appears to be a rather ordinary establishment on a road junction, which is not easy to navigate. However, it is extraordinarily innovative and the chef-owner originates from Buckie in Scotland. Jones trained at the iconic Restaurant Martin Wishart in Edinburgh. He is larger than life and always present. The food is a surprise every day and is a multiple-course tasting menu, including local produce, particularly vegetables. Our surprises included a bao bun, a creamy mushroom soup, a crispy fish course and a glorious beef fillet surmounting a mixture of vegetables with a béarnaisestyle sauce followed by a number of sweet delicacies.
I visit Malta often. Our College has a good relationship with the excellent Maltese surgical teams and undoubtedly this will flourish over the years to come. I recently discovered a great restaurant, Terrazzo, a short walk along the cliff edge from the village of Xlendi in the south-west of the island of Gozo. It is affordable and in a delightful modern glass building with fabulous views of the village and the sea from the terrace. The young chef there produces superb fish dishes in true Maltese style with foraged accompaniments.
58 | Surgeons’ News | March 2023
Graham Layer Past VicePresident, RCSEd
OUT OF HOURS
Customers can choose their preferred method of cooking and preparation of whole fish, which are on display on ice. Rabbit was prominent on the menu, as were various types of unusual and delicious pasta. Of course, sunset was wonderful and could not but improve the flavours of the food.

I was a tourist in Florence and was aware of the late chef Fabio Picchi’s Cibrèo, the famous Tuscan restaurant to the east of the Duomo. Expensive. Fortunately similar food, prepared by the same kitchen, is also available and affordable at the Cibrèo Trattoria next door and in the Cibrèo Caffè of the Helvetia & Bristol Hotel.
I was tempted by the cheaper brands, which are excellent in all respects: food, service and surroundings. Here we could have the classics: lasagne with a beef ragout, parmigiana di melanzane, the most outstanding tagliolini with cacio and butter sauce, stunning salt cod with leeks and potatoes au gratin, finishing with pannacotta or, the highlight, cheesecake with a bitter marmalade topping.
I stayed at Villa Neri, in Linguaglossa, Sicily. This bizarre hotel in a vineyard on the eastern slopes of Mount Etna looks like a contemporary crematorium without an entrance or exit. The in-house restaurant, Twelve Fountains, has a stunning, fashionable but captivating design and serves brilliant food full of intense flavours courtesy of the excellent soil on the fertile Etna slopes.
I chose individual items from the menu, but found they came interspersed with so many other nibbles that it felt very much like a tasting menu – Villa Neri residents enjoy this display at a considerable discount. The magnificent meal consisted of Japanese-style beef tataki, baked potato slices in cream with burrata, saffron ravioli stuffed with pork, followed by the most tender buttery sirloin of veal coated with cherries, aubergines and truffle. Gorgeous sweet desserts then petits fours on an exquisite ‘tree-oflife’ stand finished off the evening.
I commemorated Remembrance weekend in Flanders, Belgium. Despite being close to our shores, its culinary heritage is very different. Two restaurants stood out. I cannot speak highly enough of Découverte close to the Menin Gate in Ieper, which focuses on unusual concoctions. Our menu of smoked fillet of venison followed by salmon and then fillet of hare, finishing with a rhubarb dish, was welcomingly different, but also really interesting and tasty.
in Zonnebeke near Passchendaele is a few miles away in misty countryside, where our ancestors fought and died during grim First World War battles. The restaurant features superb local food. Our first course at lunch was various presentations of home-made pseudo-foie gras followed by pheasant with all the trimmings, then a plate of local cheeses. Belgian wines accompanied the menu. All perfect, uplifting and with charming service.
Beef done two ways: Japanesestyle beef tataki at the Twelve Fountains restaurant in Linguaglossa; inset, beef with vegetables and sauce in a French style at Menu Gordon Jones, Bath
a mention Le in Springs, California, which I visited the San Diego ACS meeting. This is part of the cool Soho House Group based in the UK, which caters for piring young The restaurant
o e s refined gourmet fare on a




I conclude my final column with a brief mention of Le Vallauris in Palm Springs, California, which I visited following the San Diego ACS meeting. This is part of the famously cool Soho House Group based in the UK, which caters for “aspiring young professionals”. The restaurant offers French-style refined gourmet fare on a stunning outdoor tree-lined patio. It is outstanding with no-nonsense service. It could not have been more professional and the team looking after me earned that 25%+ optional service charge that appears on your bill.
The meal began with perfect espresso martinis. Lobster ravioli followed and was in a velvety sauce, bursting with fishiness. The cold lobster salad was also superb, as was the sesame-encrusted tuna. The rack of lamb was generous and to die for, and all four of us concluded with fabulous emphysematous Grand Marnier soufflés.
I will not be reporting on my imminent stay and the tasting menu at Le Manoir Aux Quat’ Saisons. Like the November announcement that Gary Jones, the two-starred Michelin executive head chef of Raymond Blanc’s famous Oxfordshire icon, “I am stepping down to pursue new opportunities” as Surgeons’ News now transitions. This is my terminal episode of 54 since 2009 and I really hope you have enjoyed our culinary adventures.
rcsed.ac.uk | 59
\ s " r f
CHARDONNAY REVISITED
Carole A Boyle DipWSET Dental Editor, Surgeons’ News
 Richard Lane DipWSET DipWSET wine educator, journalist and podcaster The Wine List
Richard Lane DipWSET DipWSET wine educator, journalist and podcaster The Wine List
Your reaction to the name chardonnay may well depend on your age: those of us old enough to remember the heavy oak style of the 1990s may have less happy memories of the grape. It was everywhere then, becoming the shorthand for easy drinking, fruity white wines with toasty oaky flavours. It even became a popular first name for girls. This ubiquity became its downfall when New World producers – especially in Australia and California –began overdoing the oak – not just from barrels, but using staves or chips, or even adding essence. These were all much cheaper and quicker to lend the required oak aromas of smoke, toast and vanilla.
The negative reaction to the buttery, rich and fat chardonnays 25 years ago led to the term ‘ABC’ –Anything But Chardonnay. However, many of those drinkers who rejected the grape variety would also have happily accepted a glass or two of chablis, not realising that they would be drinking chardonnay, albeit made in a more restrained, mineral and usually oak-free style reflecting the fossil-rich soils of northern Burgundy.
Other classic white burgundies include those produced in celebrated villages including Meursault and Montrachet, but with the French custom of not naming the grape on the label, consumers can perhaps be forgiven for the confusion.

OUT OF HOURS 60 | Surgeons’ News | March2023
COOL CONTENDER
Chardonnay grapes are easy to grow in a wide range of climates. The vines produce high yields, and therefore profits, in both cool and hot conditions. Winemakers use a variety of techniques to produce a wide range of styles, including the use of oak vessels. They can age the wine on the dead yeast cells (known as sur lie ageing) after fermentation, a process that increases mouth feel and complexity of flavour. Chardonnay can also can be blended with cheaper and less-fashionable varieties, including sémillon and chenin blanc.

While France maybe the heartland for chardonnay, its ease of growing means it is found in winemaking regions across the world. Notable examples include Margaret River in Western Australia, where small quantities are produced of high-quality wines with characteristic ripe stone and tropical fruit flavours; Hemel en Aarde, in South Africa, where the cool breezes from Walker Bay help produce wines with high acidity; and California, the home of chardonnay in the US. Fine expressions are also found in neighbouring Oregon, although small production output leads to higher prices.
Left: It may have been a mainstay of the 1990s wine scene, but chardonnay has a lot to offer, with styles to suit all tastes
Tasting notes
From blossom to bread and butter
Rustenberg Chardonnay 2021
Available from Waitrose (£14.99)
A lightly oaked chardonnay from Stellenbosch where the climate is warmer, resulting in tropical fruits. The wine has eight months in new French oak barrels, but these are large, which reduces the oak influence. Suitable to drink now, but does have potential for ageing.
Chablis Premier Cru ‘Les Vaillons’ 2020, Louis Moreau

Available from Vinatis (£27)
Chile, too, makes quality chardonnay, notably in regions exposed to cooling ocean breezes, which slows grape ripening in the warm climate to enable more nuanced grape flavours to develop. Even New Zealand, best known for sauvignon blanc, makes great chardonnay, especially in the Hawkes Bay region of the north island, where it is the most widely planted white variety. The wines are full bodied with high acidity and peach flavours.
BUBBLY PERSONALITY
Chardonnay is also one of the three classic grapes of champagne, alongside pinot noir and meunier. Look for blanc de blanc on the label to indicate a 100% chardonnay with fresh green apple aromas when young, leading to the development of toasty bread characteristics with age. Many regard blanc de blanc as the most elegant of champagne styles, with great ageing potential. Chardonnay also grows well on English chalk soils, similar in character to those found in Chablis and Champagne
Chardonnay should be a grape for all white wine drinkers, be it an easy-drinking, food-friendly Aussie ‘chard’ with lots of oak, or something more angular, mineral and austere from Chablis. It is more a case of identifying a style of chardonnay that fits your palate and pocket, rather than pursuing the now-outmoded views of the ABC movement a quarter of a century ago. Rather than asking yourself whether you like chardonnay or not, consider which style of chardonnay suits from this hugely versatile and widely planted grape variety.
Push the boat out a touch with a premier cru chablis, from better positioned vineyards giving light blossom, ripe apple and peach flavours with characteristic chablis poise and minerality.
The Society’s Exhibition English Blanc de Blancs 2018 , Ridgeview, ABV 12% Available from www.thewinesociety.com (£28) This shows typically English high acidity with restrained fruit lemon and peach and just a hint of toast from four years spent on the lees. This wine is made by Ridgeview in Sussex and compares well both on price and complexity with blanc de blanc champagnes.
Bread & Butter Chardonnay 2019/20, California, ABV 13.50%
Available from Majestic (£15.99)
This bold chardonnay is made to taste of bread and butter by combining grapes from two areas: fresh. Monterey, known for its big chardonnays; and cool Carneros, resulting in more refined flavours. Understated, it has fresh notes of citrus, stone fruit with vanilla and almond. Worth trying if you like full-bodied wine with lots of oak and want to relive those heady nights of the 1990s.
It is a grape for all white wine drinkers, be it an easy-drinking Aussie ‘chard’ with lots of oak, or something more angular, mineral and austere from Chablis
rcsed.ac.uk | 61
--•-,,_
Statement pieces
RCSEd has recently commissioned two significant works of art and in this article Ann Shearer speaks to the artists

roles. When he has a good understanding of the background he starts to develop 3D models to share with the client and have further negotiations before coming to an agreed plan for the work.
The RCSEd commissioned Hunter to create a COVID-19 memorial sculpture. As part of its development he interviewed several surgeons at his studio and it was when he looked at the transcripts that four words surfaced: resilience, reflection, empathy and exhaustion. These words helped him focus his ideas and develop the sculpture of four figures in the act of removing PPE kit, losing their anonymity and revealing their humanity. This piece of public sculpture has galvanised collective memory and articulated a social moment in a way that only art can.

The College has been acquiring art for centuries, from portraits of notable individuals to large sculptures. This art could be said to reflect the changing identity and values of the College over time, but it is not only of historical interest: the collecting of art has benefits for both the people who view it and those who create it.
Kenny Hunter
Kenny Hunter’s obsession with sculpture started as a child when an art teacher handed him some clay. The joy of manipulating materials has been part of his life ever since. After art school he completed a residency in Athens, where he undertook an intense period of research and developed new ideas for a gallery show. He began to get small commissions and these led to his first public sculpture for the outside walls of the Tron Theatre in Glasgow: a two-piece sculpture of a cherub and a skull, referring to the time between childhood and growing old.
For commissioned work, Hunter starts the process with a period of research followed by conversations with the client. He believes that this dialogue is essential to get inside the world of the client and to discover more about their history and
Hunter relishes the challenges that making public art present: researching, developing ideas, taking risks, interacting with clients and a being part of the debate around public art, as well as creating the sculptures themselves. His life-size elephant sculpture on the site of the 1938 British Empire Exhibition in Bellahouston Park, Glasgow, was cast at an industrial foundry from 11 tonnes of iron, some of which was from recycled, redundant or scrap parts of Glasgowbuilt locomotives sourced from India and South Africa.
The original model was made in resin and this elephant formed part of Hunter’s recent exhibition, titled Sculpture Court, at Aberdeen Art Gallery. Having a gallery profile is important to Hunter because it allows him to display his own ideas and reflect his personality in the pieces.
The title of his show at Aberdeen was chosen to suggest review or trial. Sculpture does not always have positive connotations: it has a long history of being defaced or toppled, and for Hunter this poses the question of what are monuments, what are they for, who decides where they go and what do they represent? Hunter’s work is part of this civic discourse and shows us that the true value of art is not in the object, it’s in the message.
More of Kenny Hunter’s work can be seen at www.kennyhunter.com
62 | Surgeons’ News | March 2023
IN THE STUDIO
Ann Shearer Former Vice Dean of Dental Faculty, now designing and making jewellery in Edinburgh
(
Four words surfaced: resilience, reflection, empathy and exhaustion
''
Keith Breeden
Keith Breeden’s work will be familiar to any Fellow or Member who has visited the College, as his portraits of four College presidents hang on the walls of the Playfair building. John Smith, John Temple, Ian Ritchie and Michael Griffin have all selected Breeden to capture their image for posterity.

Becoming a painter took Breeden many years of hard work, but by painting the things around him he gradually improved his technique, established his own language of mark making and started winning prizes, including the BP Portrait Award 1996 Visitors’ Choice for an oil painting of his neighbours.

Breeden begins a portrait commission by having conversations with the sitter and exploring expectations. He makes sketches in pencil and oil paint and takes some photographs. This is followed by a period of thinking about what he wants to achieve in the portrait. For Breeden, portrait painting is a balance between what comes from the sitter and what comes from the artist. He tries to capture a presence of the person in the painting. His conversations with sitters help him to get to know the person he wants to see in the final painting.
For his portrait of Griffin, a small number of sittings took place in the Playfair Hall of the College with the rest at Breeden’s
studio in Wales. Being in the College gave Breeden further insight into Griffin’s personality, his job as a surgeon and his role as College President during the pandemic.
Breeden’s decision to include the pandemic memorial came relatively late and he believes it makes a strong patient-centred statement. He visited the sculptor, Kenny Hunter, at his studio in Edinburgh and borrowed the maquettes of the statues.
Portraits can take him up to a year or more depending on the number and timing of sittings, but equally can be done within three months.
Breeden prefers to work from life, but uses photographs in support of this, and has undertaken posthumous work entirely from photographs.
For his poignant portrait of the late Charles Kennedy MP, he had only completed one sitting before Charles’ early death. The portrait reflects Charles’ decency and strong principles, but also the forlorn end of his career. Breeden describes himself as a perfectionist, which drives him on but can also inhibit his painting. He realises the painting is just enough when the sitter starts looking back at him from the canvas. This can feel intrusive as he senses a life, a person in the painting. For Breeden, sitters become a part of his life; he never forgets them and they remain in his head forever.
See more of Keith Breeden’s work at www.keithbreeden.com; email: baldini55555@gmail.com
rcsed.ac.uk | 63
Above: Michael Griffin beside his portrait, which hangs in the Playfair Building; inset, Keith Breeden
Opposite page: Kenny Hunter works on the COVID-19 memorial sculptures
Theartofsurgery
Danielle Dray on a project that aims to set the records straight on the valuable role of modern medical illustration

The ‘Rehoming Schetky’ project aims to catalogue, digitise and rehome our historic art collections. As such, we have had a fantastic opportunity to get to grips with an area of our collections that can sometimes be overlooked.
Medical illustrations are a valuable tool in teaching and demonstrating pathologies and techniques that surgeons may have few opportunities to observe. Detailed depictions of disease, injuries and operations became an important area of medical teaching that developed in both style and function.
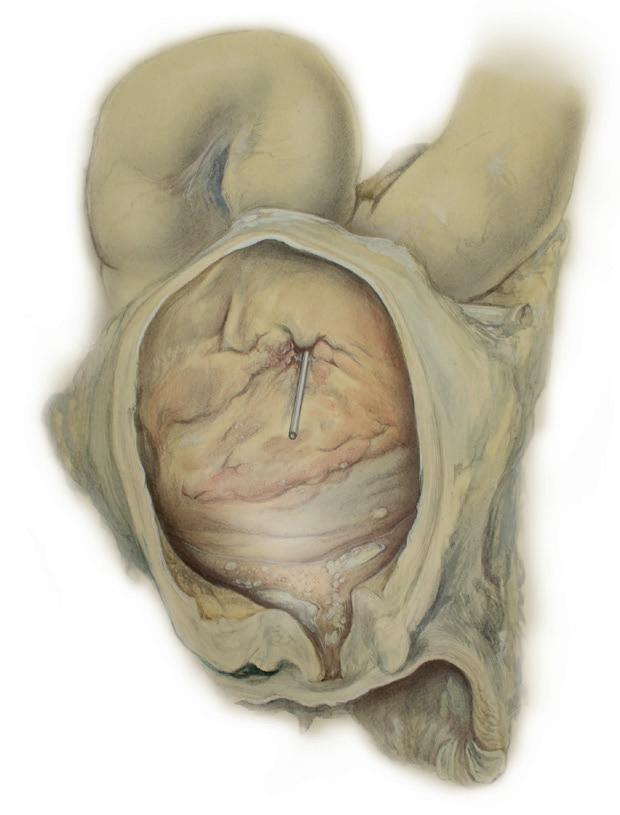
Throughout history many outstanding surgeons were also talented artists. Charles Bell, Joseph Lister and John Alexander Schetky all illustrated interesting and rare cases they came across during their practice. These illustrations all relied on traditional artistic techniques and styles. However, in the early 20thcentury new styles and techniques were developed that changed the face of medical illustration.
Max Brödel (1870–1941) was a German immigrant living and working in the US. He arrived in Baltimore in 1894 to accept a post at Johns Hopkins Hospital illustrating pioneering abdominal surgeries undertaken by Dr Howard Kelly. However, he had not originally trained to draw operations and organs, and felt unable to capture the complex textures of living tissue with traditional techniques. He therefore developed a new technique using Ross board and carbon dust.
The technique involved outlining an image on tracing paper and using this to leave an imprint on a heavy board covered with either chalk or china clay. Carbon dust would then be slowly layered onto the outline to give a sense of depth. Precise details were etched in afterwards.
In 1910 Brödel became Associate Professor of the Department of Art as Applied to Medicine and established the world’s first medical illustration programme. In his 30 years of teaching Brödel taught his methods to over 200. Audrey Arnott (1901–1974) is recognised as the only British student he taught. She returned to the UK and shared what she had learned with three professional associates, Dorothy Davison (1889–1984), Margaret McLarty (1908–1996) and Clifford Shepley (1908–1980).
The group were concerned with the standards of UK medical illustrators. Both world wars had highlighted the need for skilled artists who could accurately convey the disease or injury shown. For example, AK Maxwell (1884–1975) was highly regarded for capturing, in a more aesthetic style, the injuries from First World War trench warfare. Shepley, who valued realism, said he had “never much cared” for Maxwell’s work.
Davison proposed the formation of a professional association to ensure a high standard of work and provide accreditation. The Medical Artists Association of Great Britain was established in 1949 and with it the recognition of medical illustration as a professional practice.
Professional medical art thereafter tended to follow a more standardised form; clear, straightforward illustrations that demonstrated the technique or disease being shown. Shepley, Davison and Arnott continued to favour the Ross board method, and the technique became something of a 'gold standard' in British medical illustration. However, across the Atlantic, medical art was again moving in a different direction. American Frank Netter (1906–1991), who trained in both art and medicine, worked with pharmaceutical companies to produce illustrations advertising their products. Netter’s bold, eye-catching style was markedly different from Brödel’s. Throughout the 1940s wartime propaganda posters successfully utilised a similar style. The broad influence of Netter’s work led to a more visually appealing style of medical illustration.
The fact that relatively few early medical illustrations survive today is a testament to how undervalued they have been. Some were unfortunate losses: a huge portion of Maxwell’s work was lost when the Royal College of Surgeons of England was bombed during the Second World War. Others were discarded and even within our own collection it is not uncommon to find notes on the reverse of drawings that read “keep until cast is found”.
We have in our care several hundred illustrations from the early 19th to the late 20th century. Our project has provided an insight into a field that bridges the gap between art and science, and elicited an opportunity to bring these fantastic artworks back into the limelight.
64 | Surgeons’News | March2023
FROM THE COLLECTIONS
Danielle Dray Project Assistant, RCSEd
Above left, black-and-white drawing by C Shepley of a portion of a jejunum with multiple diverticula; right, watercolour drawing by A K Maxwell of a urinary bladder with a portion of the bowel showing tuberculosis
RCSEDLET'STALK SURGERYPODCAST

BRINGINGYOUTHELATESTNEWSFROMTHECOLLEGE.
LISTENONPOPULARSTREAMING SERVICESORVIATHERCSEDAPP:
RCSEd


























