

ISSN 1026 261X www.dentalnews.comVolumeXVII,NumberIV,2010 Beirut International Dental Meeting 2010 SOCIALMEDIA ANDDENTISTRY Self adhering flowable composite resin Gulf Dental Association Conference “Find” us on www.facebook.com/dentalnews1


Theexceptionalsinteringfurnace
•SinteringZrO2 single-toothcrownsinjust90minutes
•Verycompactdesign(correspondingtoapressfurnace)
•Easy,language-independentoperation
•Lowenergyconsumption(PowerSavingTechnology)
•Lowweightofjust27kg
Foradditionalinformation,pleaserequestthecorrespondingbrochures.
Engineeredfor performanceandefficiency Programat® S1 Programat® ASTORYOFSUCCESS www.ivoclarvivadent.com IvoclarVivadentAG Bendererstr.2 | FL-9494Schaan | PrincipalityofLiechtenstein | Tel.:+423/2353535 | Fax:+423/2353360
Volume XVII, Number IV, 2010
EDITORIAL TEAM
Alfred Naaman, Nada Naaman, Jihad Fakhoury,
Dona Raad, Antoine Saadé, Lina Chamseddine, Tarek Kotob, Mohammed Rifai, Bilal Koleilat, Mohammad H. Al-Jammaz
COORDINATOR
Vanessa Abdelahad
Krystel Kouyoumdjis
Micheline Assaf, Nariman Nehmeh
Josiane Younes
Albert Saykali
Gisèle Wakim, Marielle Khoury
Tony Dib
1026-261X
DENTAL NEWS – Sami Solh Ave., G. Younis Bldg.
POB: 116-5515 Beirut, Lebanon.
Tel: 961-3-30 30 48
Fax: 961-1-38 46 57
Email: info@dentalnews.com
Website: www.dentalnews.com www.facebook.com/dentalnews1
INTERNATIONAL REVIEW BOARD
Pr. M.A. Bassiouny BDS, DMD, MSc, Ph.D. Director International Program, Temple University, Philadelphia, USA.
Pr. N.F. Bissada D.D.S., M.S.D Professor and Chairman, Department of Periodontics, Case Western Reserve University, USA.
Pr. Jean-Louis Brouillet D.C.D, D.S.O. Chairman, Department of Restorative Dentistry, Aix-Marseille II, France. Pierre Colon D.C.D., D.S.O. Maître de conférence des universités, Paris, France.
Dr. Jean-Claude Franquin, Directeur de l’Unité de Recherche ER116, Marseille, France.
Pr. Gilles Koubi D.C.D., D.S.O. Department of Restorative Dentistry, Aix-Marseille II, France.
Pr. Guido Goracci. University LA SAPIENZA, School of Medicine & Dentistry, Roma, Italia.
Dr. Olivier Hue, Faculté de chirurgie dentaire de Paris VII, rue Garancière, Paris, France.
Brian J. Millar BDS, FDSRCS, Ph.D. Guy’s, King’s, and St. Thomas’ College School of Medecine & Dentistry, London, UK.
Pr. Dr. Klaus Ott, Director of the Clinics of Westfälischen Wilhelms-University, Münster, Germany. Wilhelm-Joseph Pertot DEA, Maître de conférence, Aix-Marseille II, France.
Pr. James L. Gutmann, Professor and Director, Graduate Endodontics, Baylor College of Dentistry, Dallas, Texas, USA.
Pr. Dr. Alfred Renk, Bayerische Julius-Maximilians-University, Würzburg, Germany.
Dr. Philippe Roche-Poggi DEA. Maître de conférence des universités, Aix-Marseille II, France. Michel Sixou D.C.D., D.E.A. Department of Priodontology, Toulouse, France.
Pr. M. Sharawy B.D.S., Ph.D. Professor and Director, Department of Oral biology, Medical College of Georgia, Augusta, Georgia, USA.
DENTAL NEWS IS A QUARTERLY MAGAZINE DISTRIBUTED MAINLY IN THE MIDDLE EAST & NORTH AFRICA IN COLLABORATION WITH THE COUNCIL OF DENTAL SOCIETIES FOR THE GCC.
Statements and opinions expressed in the articles and communications herein are those of the author(s) and not necessarily those of the Editor(s) or publisher. No part of this magazine may be reproduced in any form, either electronic or mechanical, without the express written permission of the publisher.
Social media and dentistry
Lucy Abillama, Samer Nadim Karam

Case Report:Endodontic Retreatment of a Tooth with a Large Periapical Lesion
Jamal M. BouJbara
Clinical study of the self-adhering flowable composite resin Vertise Flow in Class I restorations: six-month follow-up Alessandro Vichi, Cecilia Goracci, Marco Ferrari
Mandibular first molars with five canals Report of cases among Kuwait population
Milind P. Gaidhane, Ahmed A. Abdul Rahem, Arun Gopinath, Mansour F. Al Ajmi
Beirut International Dental Meeting

Gulf Dental Association Conference
Dental - Facial Cosmetic International Conference
Lebanese Society of Pediatric Dentistry
Lebanese Society of Prosthodontics
52 62 69 76
13 16 19 36 42
ART DEPARTMENT SUBSCRIPTION ADVERTISING PHOTOGRAPHY TRANSLATION DIRECTOR ISSN
Contents 3 CONTENTS


CompothixoTM Improved Quality Restorations

Smart Vibrations
Compothixo™ is a unique generation in composite placing and modelling instrument suitable for all class restorations.
The new Compothixo™ technology optimizes the thixotropic properties of composites by changing viscosity only, without altering the chemical and mechanical characteristics of the material.
•Better wettability
•Superior adaptation of composite to cavity walls
•Reduction of air bubbles
•Precise application
•Layer thickness control
•Improved sculptability
•Reduced stickiness
Your practice is our inspiration.™ KerrHawe SA P.O. Box 2726934 Bioggio Switzerland Freephone: 00800 41 05 05 05 Fax: ++41 91 610 05 14 www.kerrdental.eu

Naturally sterilisers





We build them silent, fast and practical.


Our guarantee: your safety.




























We ensure performance and efficiency.


Drop by drop: the best water treatment.









Millennium B 17 litres, B+ 22 litres. B2 Quality System certified by: 9120.MOOM9124.MOOM Mocom Srl Via delle Azalee, 1 • 20090 Buccinasco (MI) Italy • Tel. (+39) 0245701505 r.a. • Fax (+39) 0248840514 mocomcom@mocom.it • www.mocom.it
We focus solely on sterilisation. That’s why we are so good at it. Naturally. new Millennium We offer different programs to suit different sterilisation loads. ams 22litres.
th tr We focus on Protection of your data. Different dimensions, the same high quality.
pe and D

instruments
With the Hu-Friedy XTS product line, the processing of differing composite materials has been completely revolutionised. The result: XTS instruments with a black aluminium and titanium nitrate coating are especially hard, smooth and scratch-resistant - various composites can be processed better and more simply.

Smooth surface can be cleaned easily and is corrosion-proof
Lighter grip makes fatigue-free working possible
Working end of flexible immunity steel with aluminium and titanium nitrate coating
Hard, non-adhesive and scratch-resistant surface
Larger diameter for more relaxed gripping
Matt Satin Steel grip makes dazzle-free work possible
Black working end for a better contrast between instrument, tooth and composite

Gentle, conical transition from handle to working end makes control easier

IM12DIN108
1/2 DIN cassette for 10 instruments. Dimensions: 152 x 184 x 34 mm.
Manufacturer: Hu-Friedy Mfg. Co., LLC I 3232 N. Rockwell Street I Chicago, IL 60618 IUSA European Headquarters & Customer Care Department: Hu-Friedy Mfg. B.V. I P.O. Box 29025 I NL-3001 GA Rotterdam Tel. +800 HUFRIEDY (00800 48 37 43 39) I Fax 00800 48 37 43 40 E-Mail: info@hu-friedy.eu I www.hu-friedy.eu Hu-Friedy Middle East: zqwaider@hu-friedy.com I Mobile : 00 962 79 50 45 700
THE BEST SYSTEM FOR YOUR INSTRUMENT AND INFECTION CONTROL !
December 15 – 16, 2010
5th Riyadh International Dental Meeting and Exhibition
RIDM entitled New Era in Esthetic Dentistry at the Intercontinental Hotel, Riyadh, Kingdom of Saudi Arabia Tel: 966 533336151
E-mail: meeting@riyadh.edu.sa www.riyadh.edu.sa/meeting
January 12 – 14, 2011
Yemeni Dental Association
The second scientific conference for the Yemeni Dental Association and international exhibition will be held in Sanaa city in the police officer club, 1-3 December 2010. Contact Dr. Mohamed ben Hafeed president Yemeni Dental Association
Email: y_d_a_ry@yahoo.com
January 21 – 23, 2011
International Meeting of the Egyptian Orthodontic Society Sheraton Montazah Hotel, Alexandria, Egypt. Contact: Dr. Abbas Zaher E-mail: azaher@idsc.net.eg
January 24 – 26, 2011
22nd Saudi Dental Society International Dental Conference entitled Promoting Excellence in Dental Care. At the Riyadh International Exhibition Center Email: esamson@ksu.edu.sa www.sdssa.org
February 1 – 3, 2011
AEEDC DUBAI 2011
The 15th edition of the UAE International Dental Conference & Arab Dental Exhibition _ AEEDC Dubai will take place at the state of the art Dubai International Convention & Exhibition Centre (DICEC) from 1st - 3rd February 2011
E-mail: vaneza.santos@index.ae www.aeedc.com
INTERNATIONAL CALENDAR
March 22 – 26, 2011
IDS 2011 34th International Dental Show
The leading trade fair for the dental sector, to be held in Cologne, Germany http://english.ids-cologne.de/en/ids
April 6 – 7, 2011
The 7th Jordanian Orthodontic Congress
The Scientific Committee of the Jordanian Orthodontic Society invites colleagues to submit their abstracts for consideration into the scientific program for the upcoming 7th Jordanian orthodontic Congress, to be held in Amman between April 6th-7th 2011. Email: info@jos.org.jo www.jos.org.jo
May 12 – 13, 2011
5th CAD/CAM & Computerized Dentistry Int'l Conference
The Address Hotel Dubai Marina, UAE Email: info@cappmea.com www.cappmea.com/cadcam5
June 2 – 4, 2011
12th Lebanese University convention at the Rafic Hariri campus, Hadath, Lebanon entitled “Facing Challenges in Dental Practice”
Contact Dr. Elie Maalouf: congresul@ul.edu.lb
October 26 – 28, 2011
The Egyptian Dental Association In collaboration with Future University will organize the 15th International Dental Congress from the 25th to 28th October 2011 at Cairo City Stars Hotel. For More Inquiries Please contact Prof. Tarek Abbas Hassan - President of the Congress E-mail: drtabbas@gmail.com www.eda-egypt.org
ADVERTISING INDEX
ACTEON 53 - A-DEC 27 - ALTURKI 34 - BELMONT 57 - BEYOND 39 - BIEN AIR 31 - BLUE X 47 - CASTELLINI 23 - CAVEX 79 - COLTENE WHALEDENT 59DISCUS DENTAL 61 - DR. WILD 4, 5 - DUERR 18 - GC 33 - GSK C3, 55 - HU-FRIEDY 10 - INTENSIV 51 - IVOCLAR – VIVADENT 1, C4 - KAVO C2 - GENDEX 7KERR 6, 73 - KETTENBACH 30 - KOMET 28 - MECTRON 41 - MEDESY 58 - METASYS 75 - MICRO MEGA 25 - MOCOM 9 - MORITA 37 - NISSIN 12 - NOBEL BIOCARE 35 - NSK 80 - SiCan 45 - SIRONA 21 - SOREDEX 29 - SULTAN 71 - Sybron Endo 49 - VITA 77 - VOCO 63 - W&H 8 - ZHERMACK 2 - ZIMMER 44

DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010 11
www.dentalnews.com Tel: 961-3-30 30 48 Fax: 961-1-38 46 57 Email: info@dentalnews.com Volume XVII, Number IV, 2010 www.facebook.com/dentalnews1 www.dentalnews.com GETYOURISSUEONLINE



















































PRACTICE MANAGEMENT
SOCIAL MEDIA & DENTISTRY




 Lucy Abillama*, Samer Nadim Karam**
Lucy Abillama*, Samer Nadim Karam**
*Social Media Marketeer - lucy@seeqnce.com
**Seeqnce Consultant – Social Media - samer@seeqnce.com
Social media is still somewhat new, and its definition and history are a bit subjective. According to Wikipedia, social media uses web-based technologies to turn communication into interactive dialogues; it can include text, video, audio, images, podcasts, and other multimedia communications. Some businesses refer to social media as consumer-generated media (CGM). Social media expedites conversation between the readers, viewers, or listeners, allowing them to shape and evolve brands. Social media’s main goals are developing and managing reputation, showing that you are up-to-date, in the sense of not using antiquated marketing techniques, increasing customer engagement or mobilizing advocates to drive Word of Mouth, and achieving brand loyalty.
Whereas some say social media started during the Stone Age, when sending messages consisted of drawing pictures on walls that were meant to reach the next generation, others say it started with Phreaking (cracking phone networks, making free calls, and getting access to the experimental back end of the telephone system). Personally, I like to believe that social media started when mass media became social. What I mean by this is that people exposed to mass media had very limited, if any opportunity to interact with it, whereas today, people using social media define, shape, and evolve brands. The public, which was once named the audience, is now entitled user, because he is reusing the information and is certainly taking part in it. Users crave information about the latest news, products, technologies, services…
There are several tools used in social media, but the ones that we will be covering are: Facebook, LinkedIn, Twitter, blogs, and Youtube
2010 Social Media Statistics:
• According to Facebook, there are more than 500 million active users, and 50% of these users log on to Facebook everyday. People spend over 700 billion minutes on Facebook per day, including 46.2 years of videos watched, also per day.
• According to cleancutmedia.com, Youtube has more than 2 billion videos that are viewed per day, and each minute, there is an average of 24 hours video uploaded on Youtube. It has also
been noted that an average person spends 15 minutes a day on Youtube. It is the largest worldwide video-sharing community.
• As for Twitter, it currently has more than 175 million users, as a result of a growth rate of 15 million users per month. Twitter is often considered the SMS of the Internet.
• LinkedIn has over 50 million members worldwide, resulting from an increase of 1 million users per month since July 2009.
• Over 3 million people are connected and auto-sharing to at least one social network.
Today, as a marketing tool, social media is replacing word-ofmouth and tell-a-friend, methods that were previously used to increase awareness and shape people’s ideas about a certain product, idea or service.
To succeed when using social media marketing, one has to keep an open mind, and be willing to adjust the marketing strategies according to what’s effective and what isn’t, because social media is forever changing. A few years ago, everyone had a Myspace account whereas today, Myspace is slowly being replaced with Facebook. Some of the reasons for Myspace’s downturn are, its initial target, which was teenagers, and spam.
Another key to success would be to emphasize that social media is not just about Return on Investment. Relatively to dentistry, it is about establishing with your patients a mutually beneficial relationship. For example, a dentist with a Twitter account will post tips on his account for his (potential) patients to see, once these patients become aware of the dentist’s expertise and his way of going, they will most likely follow him, and maybe even visit him one day.
Social media will keep you, as a doctor, out in the community of potential patients or acquired patients. It will keep you interacted with this community, and it creates an up-to-date, patient driven image. Although conventional media is more expensive, in my opinion, it is not more effective. Social media enhances your relationship with your patients, which will give them a sense of security, promising you their trust.
DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010 13 SOCIAL MEDIA & DENTISTRY
PRACTICE MANAGEMENT
The tools that are most used nowadays in the Arab world are, as previously stated, Facebook, Twitter, LinkedIn, Youtube, and personal blogs.
Facebook is a social network through which people can share their thoughts, pictures, videos, music, links… One of Facebook’s essential roles in the social media plan is that it helps build brand awareness. It can also focus on audiences based on demographics (age, gender, location…), and based on networks that can be geographic or even corporate. What you can also do is create a fan page. Facebook provides you with tips on how to effectively promote your fan page using Facebook advertising.
Twitter allows people to “Tweet” or write about whatever they like in 140 characters or less while tagging people, brands, groups, interests… This allows you to target people by specific words that they might look up. For example, if you write something about toothaches and place a hash tag before toothaches (#toothaches), if someone looks up toothaches, your Tweet will appear in the list of results. You can also use Twitter to share deals and promotions after you’ve found and connected with your target audience.
LinkedIn is a professional network where you expose your education and work experience to colleagues, people you know, companies… You can also follow groups or companies that interest you. LinkedIn allows you, as a dentist, to present your (potential) patients to your degree of expertise (i.e. your certificates, your innovations, your work experience…). Once you complete your profile, you should find groups that are compatible with your profession, and be frequently active in the discussions.
Youtube allows you to upload, view, rate, and comment on videos. What dentists could and should do is upload videos showing a tour of their clinic to the viewers. This creates a feeling of comfort for patients, and it raises your credibility and expertise for patients and referring dentists.
Personal Blogs can establish you as an expert and thought leader in your industry. By sharing your thoughts and views, or unique knowledge, you can be perceived as an expert in your area. People will trust you and see you as knowledgeable, hence they will more likely join your practice. For example, you can share patient success stories or new procedures offered exclusivelyat your practice, as well as some tips about oral hygiene.
You should make sure that you have a consistent profile picture on each of these websites to ensure recognition, status, and last but not least, credibility.
To use social media marketing effectively, businesses have to be perceived as members of the social media community, willing to


14 SOCIAL MEDIA & DENTISTRY DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010
PRACTICE MANAGEMENT
How to create your Facebook page
Are you ready to put your dental clinic on Facebook? Here are a few tips to get you started on creating your very own page
1. 2. 3. 4. 5.
visit www.facebook.com/pages/create.php
Choose local business under Create a Page
Pick your page name
Choose the name of your clinic
Fill in basic information like location, business hours and contact information
Start telling your patients to “Like” your page (formerly known as becoming a fan) via word of mouth, e-mails to them or on paperwork they might receive in your office
Benefits of social media
Patients can stay current with the latest services their dentists provide
Dentists can show patients what continuing education courses they have attended
The office can introduce new products as special offers
Social media offers dentists a non-intrusive way to maintain constant communication with patients that have signed up to “Like” their Facebook pages
It’s a great way to go green in the office and use less direct mail
interact with other members on a regular basis; which is why it is very important to sacrifice time to interact, network, and talk with people in your community through these websites. Businesses need to make sure they are always present and active. If you do not have time to do so, you should consider hiring someone to take care of this task, since it is very time consuming.
All of these tools will guarantee you a long-term profitable growth, which is why I believe it is essential for dental practices to have social media plans.
A good example of a successful dental social marketing campaign would be Dr. Irena Vaksman, a San Francisco dentist. She activated a Twitter account, a Facebook account, a LinkedIn profile, a Youtube channel, and a dynamic website.
Her website links to some of the most popular social marketing sites and offers a newsletter. Her website includes a photo tour of her sophisticated office, and testimonials of her current patients encouraging potential patients to choose her practices. New patients can schedule an appointment right on the site or shoot a quick email by clicking the email address on the site. Also available on her site is a map to get to her office.
Her Facebook page provides updates for her clients about promotions, articles, and tips, not to mention the personal testimonials and thank you notes posted on her wall by her patients.
On Twitter, she informs her followers of her upcoming newsletter by linking to it and informs her patients about new promotions and dental techniques.
On her Youtube channel, she explains the various procedures she offers.
In October 2009, Dr. Vaksman received 320 new patients by offering promotions on her social media sites; this was a reflection of the five-month-old plan implemented in the right direction. Her retention rates are also remarkable compared to dental practices that depend on traditional marketing.
According to Dr. Jason Lipscomb, a Virginia dentist who is the co-author of the book, “Social Media for Dentists”, “Social media is here, it's not a fad, and 96% of generation Y is already heavily involved in it… Social media is instant word of mouth to thousands of people at once, and it's a fundamental shift in the way we communicate. Your patients and prospects are already there. Are you?” Social media is a very powerful tool, if used right, especially for dentists. I think everyone in dental practices should start exploring what is out there, social media wise, in order to attract patients, businesses, and even referring dentists.
DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010 15 SOCIAL MEDIA & DENTISTRY
• • • • •
Endodontic Retreatment of a Tooth with a Large Periapical Lesion Case Report:
Jamal M. BouJbara, DDS, MDS boujbara@gmail.com
INTRODUCTION:
The predictability of endodontic treatment has definitely improved with research into the endodontic niche, advancement in treatment techniques, improved materials and the introduction of rotary endodontics7. A multiple sitting procedure has been reduced to a single visit endodontic treatment in most of the lesions. However the unpredictability of large lesions has been documented. As yet a non-surgical approach for its resolution has been far from realized. Even those cases which had been treated non-surgically, it had involved the placement of a drain into the lesion surgically which had to be removed at a later date as the lesion resolved4. Also the retreatment cases have a questionable prognosis. Thus the prognosis of a large lesion be it a periapical cyst or a periapical granuloma, in a tooth already treated endodontically can best be described as questionable. Here a case is presented which has been retreated endodontically havinga large lesion extending into the palate without the use of any surgical procedures including the use of a surgical drain.
CASE REPORT:
A 47 year old patient reported to our endodontic department in April of 2008 with pain and swelling in the upper left side for the past three months. During this period she had undergone root canal treatment twice. However, the swelling and symptom did not subside so she reported to the center for a second opinion. Clinical examination of the patient showed the presence of a huge diffuse linear swelling on the palate with the maximum width near the midpoint of the swelling extending from the anterior region on the palate near the marginal gingiva extending


posteriorly on the left palate till the posterior vibrating line. There was no pointing of the lesion. IOPA and occlussal radiographs were taken (Fig1a & b). The IOPA revealed a huge radiolucent lesion with diffuse margins in relation to the periapical region of the upper left lateral which had a root canal filling and a separate smaller radioluscent periapically to the adjacent central incisor also. The occlussal radiograph showeda large radiolucent lesion on the palatal aspect in relation to the upper left lateral. It was decided to retreat the case and the patient was advised of the poor prognosis of the tooth.
The central incisor was opened and the canal was dry with no pus discharge. And the canal was instrumented using rotary endodontics and the canal closed for a period of 7-10 days for observation. The root canal filling of the left lateral was removed and the canal instrumented beyond the apex. Pus discharge was seen through the canal. Irrigation was done using sodium hypochlorite and hydrogen peroxide. The palatal swelling was massaged using a mild force in an anterior direction to facilitate drainage through the canal. The patient was recalled after 7 days for review. At the next visit the patient reported marked changes in the level of pain and reduction in the swelling. The canal was seen to have a reduced amount of pus discharge. Again the canal was copiously irrigated with sodium hypochlorite and hydrogen peroxide. Again an open dressing was given and the patient recalled after 2 days. The next visit saw the patient with minimal pain and a further reduction in swelling. The canal was seen to be quite dry at this stage. The Periapical radiograph at this stage still showed the large radioluscent lesion. The canals were irrigated with sodium


ENDODONTICS 16 ENDODONTIC RETREATMENT OF A TOOTH WITH A LARGE PERIAPICAL LESION DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010
Fig 1a: First visit (IOPA) Fig 1b: first visit (occlussal) Fig 2a: Pre obturation 14 months (IOPA) Fig 2b: Pre obturation 14 months (occlussal)

hypochlorite and hydrogen peroxide and then washed with saline. A closed dressing with calcium hydroxide was given and patient recalled after one month. Thereafter, periodic monthly appointments were given where the canal was irrigatedand closed irrigation with calcium hydroxide was given. After around 14 months after the first visit the swelling was completely absent and patient reported no pain. The periapical radioluscency was still present though localized to the periapical and reduced to around 5mm in diameter (Fig2a & b). This time the canals were obturated using lateral condensation technique (Fig 3). And the patient recalled after six months for a review. Six months after obturation it was seen that the periapical radioluscencywas almost absent with a mild crescent shaped radioluscent around the apex (Fig 4a & b). The patient had no symptoms to report. During the intervening six months the patient had crowns made to correct the discoloration. The patient was recalled after a period of six months to further review the healing.
One year after obturation the patient had absolutely no signs and no symptoms. The occlussal radiograph and periapical radiograph showed a very thin crescent shaped radioluscency at the apex (Fig 5).
DISCUSSION:
Dumsha et al 1988 had stated that the establishment of drainageis important for the resolution of large lesions this is supported by histological studies conducted by Fuji & Machida (1991)5. Thus in this case drainage was established by over-instrumentation. It had been stated by Bender (1972)2 that over-instrumentation would establish drainage of the lesion and relieve the pressure which would facilitate extrusion of the lesional fluid through the canal. As root canal treatment is based on the removal of microbial flora from the complex root canal system irrigation of the canal plays an important role in reaching all the inaccessible areas of accessory and secondary canals present, those areas which would normally be inaccessible for instrumentation7. Thus in this case sodium hypochlorite and hydrogen peroxide was used. Sodium hypochlorite is the most commonly used irrigant in



endodontic for its gross debridement, lubrication, destruction of microbes and dissolution of the tissues. It is commonly used in conjunction with hydrogen peroxide which has an effervescent action by the release of nascent oxygen which dislodges and extrudes the loose debris through the access opening7
Souza et al (1989)6 had stated that the action of the calcium hydroxide is fourfold: a) anti-inflammatory, b) neutralization of acid products, c) activation of the alkaline phosphatase, d) antibacterial action. Various studies conducted by different authors have established the fact the use of calcium hydroxide with the resolution of large periapical lesions. It was seen that overinstrumentation with the use of copious irrigation and the use of closed dressing brought about a favorable result in this case.
Bender and associates1 1966 defined the criteria for success:
1) Absence of pain or swelling
2) Disappearance of fistula
3) No loss of function
4) No evidence of tissue destruction
5) Radiographic evidence of an eliminated or arrested area of rarefaction after 6-24 months.
Thus based on this criteria it can be concluded that the lesion in the present case has healed based on the lack of symptomsor signs and the radiographic evidence of increasing radio-opacity.
SUMMARY:
The results obtained in this single case indicate that single visit endodontics is not the answer in each and every single case. However further studies have to be done before it can be accepted and the conservative treatment protocol in this case be established. Cases with large lesions heal better when they are allowed to drain and the lesion is allowed dry out on its own. The drainage established by instrumenting the apex to facilitate drainage is an accepted procedure. That along with the calcium hydroxide with its antibacterial action is thought to have brought about the resolution in this case.
REFERENCES
1) Bender I B, Seltzer & Soltawf W; Endodontic success; a reappraisal of criteria I and II. Oral Surgery (1966) 22: 780.
2) Bender I B; A commentary on General Bhaskar’s hypothesis. Oral surgery, Oral Medicine and Oral Pathology (1972) 34, 469 – 476.
3) Dumsha TC, GutMann JL; Problem solving in endodontics, Year Book Medical Publishers Inc (1988) 123-137.
4) Eugene Natkin et al; The relationship of lesion size to diagnosis, incidence, and treatment of periapical cysts and granulomas; oral surg; (1984);57; 8294.
5) Fuji H & Machida Y; Histologic study of therapy for infected nonvital permanent teeth with incompletely formed apices. Bulletin of the Tokyo Dental College; (1991); 32; 35-45.
6) Souza V, Bernabe PFE, Holland R, Nery MJ, Mello W, Otoboni Fiho JA; tratamento nao curugico de dentis com lesos periapicais. Revista Brasileira de Odontologia (1989) 46; 46-46.
7) Stephen cohen & Richard c Burns ; Pathways of the Pulp; 7th edition.
DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010 17 ENDODONTIC RETREATMENT OF A TOOTH WITH A LARGE PERIAPICAL LESION
ENDODONTICS
Fig 3: Obturation (IOPA)
Fig 5: Post Obturation 1 year (IOPA)
Fig 4a: Post Obturation 6 months (IOPA)
Fig 4b: Post Obturation 6 months (IOPA)
Clinical study of the self-adhering flowable composite resin Vertise Flow in Class I restorations: six-month follow-up
ABSTRACT
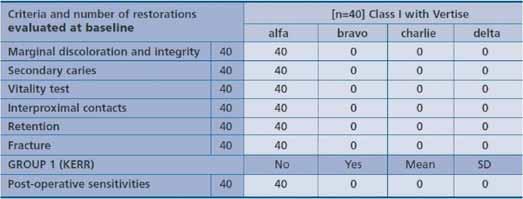
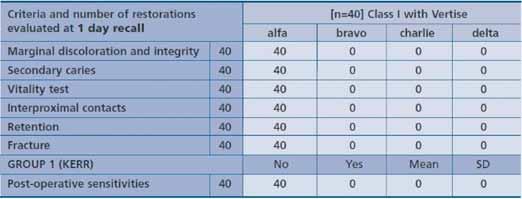
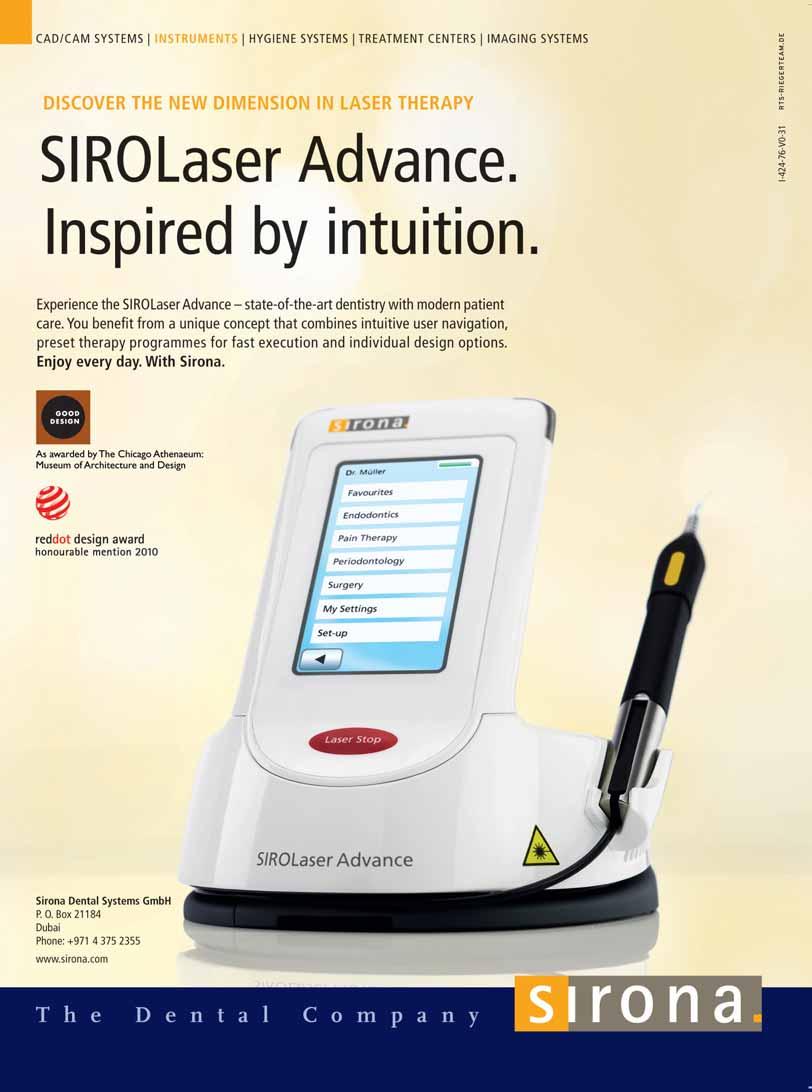
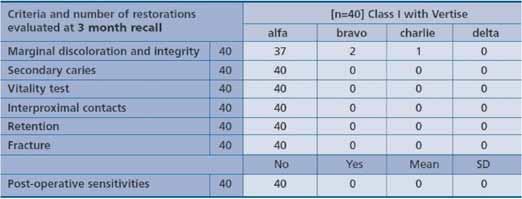
Purpose: The aim of this study was to evaluate over a 6-month follow-up period the clinical outcome of restorations performed with a new self-adhering flowable composite resin. Materials and methods: Forty Class I restorations were placed between January and March 2009 using a self-adhering flowable composite resin (Vertise Flow, Kerr, Orange, CA, USA). Restorative procedures were performed following manufacturers’ instructions. The restorations were assessed for post-operative sensitivity, marginal discoloration, marginal integrity, secondary caries, maintenance of interproximal contact and fracture at baseline, as well as after 1 day, 1 week, 1 month, 3 months and 6 months of clinical service. Results: No restoration was affected by post-operative sensitivity at any recall. At the 6-month clinical evaluation, all the 40 restorations scored “alfa” for secondary caries, vitality test, interproximal contacts integrity, retention and fracture. About marginal discoloration/marginal integrity, 37 of the 40 restorations scored “alfa” at the six-month recall. Two restorations showed minimal discoloration and a minimal defect of the marginal integrity, thus receiving a ‘bravo’ score. One restoration received a ‘charlie’ score for marginal discoloration and integrity.
Conclusions: All the evaluated restorations remained in place and in acceptable conditions over the 6-month follow-up period. No post-operative sensitivity was recorded at any evaluation. Key Words: Adhesive systems, Flowable composite resin, Class I restoration
INTRODUCTION
The use of composite resins has considerably increased in recent years, concurrently with the improvement of their performances.1-3 Despite such constant improvement; polymerization contraction stress remains a challenge. Post-operative sensitivity, marginal discoloration, secondary caries, and loss of restoration may be associated with curing shrinkage and stress derived from shrinkage.4 The cavity configuration (C-factor), i.e. the ratio of bonded surface area to the un-bonded or free surface area, plays a determinant role in stress development.5 C-factor is particularly unfavorable in Class I cavities, exhibiting a ratio of 5 bonded walls to one free surface5-7 The use of a bonding agent is therefore generally indicated in order to resist the stress that develops during curing.
Unfortunately, the adhesive systems may not be completely effective at counteracting the curing stress of the restorative composite resin, thereby micro leakage and gap formation at composite/tooth interface have been observed in clinical conditions.8-10
The negative effect of polymerization shrinkage can be reduced using appropriate layering technique11-13 and incremental curing.13-14 another factor possibly influencing stress development is the elastic behavior of the composite resin. In stiffer materials, the forming polymer chains have restricted relative mobility during the polymerization process, leading to the development of higher stress. For this reason, the use of a less rigid resin has been proposed for the restoration of cavities with unfavorable C-factor.7 Composite resins with a reduced filler load and a lower modulus of elasticity marketed as “flowable” composites have been used for this purpose.15-18
In addition to the development of a lower stress, flowable composite resins offer the advantage of favorable handling properties. Their viscosity is such that material placement is eased and adaptationto cavity walls is improved.
Flowable materials have been proposed as liners under a hybrid composite resin, with the function of stress absorbing layer,19-23 or for stand-alone use. Flowable composite resins have also found applications in pit and fissure sealing,24 orthodontic brackets bonding,25 and restoration of small-sized class I cavity.26
As flowable composite resins do not have adhesive properties per se, the combined use of a dental bonding system is necessary. Among dental adhesive systems, all-in- one adhesive system are gaining popularity mainly due to their simplified handling. These single-bottle systems are chemically based on a complex mixture of hydrophilic and hydrophobic monomers in water and organic solvents. Their adhesion process is based on the self-etch approach and combines etching, priming and bonding into a single applications step.4,27-30 The exclusion of rinsing and drying steps is indeed an attractive clinical advantage of all-in-one systems, since the contamination risk is reduced and the bonding procedure is less sensitive to possible over-drying or over-wetting mistakes.31,32 Despite the attractiveness of their simplified handling, single-step adhesives are still matter of research, in order to further evaluate relevant aspects of their bonding mechanism, such as the etching potential in various clinical situations and bond durability.33-35 Recently, an innovative resin-based material, combining the
RESTORATIVE DENTISTRY
DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010 19 CLINICAL STUDY OF VERTISE FLOW IN CLASS I RESTORATIONS
Alessandro Vichi, Cecilia Goracci, Marco Ferrari
RESTORATIVE DENTISTRY
properties of self-adhesion and flowability was developed (Vertise Flow, Kerr, Orange, CA, USA), introducing a new category of restorative materials defined as “self-adhering composite resins”. These materials are claimed to eliminate the need for a separate bonding application step, thus simplifying the direct restorative procedure. For this reason, Vertise Flow may be considered to start the 8th generation of dental adhesive systems or to representa cross-link between all-in-one adhesive systems and flowable composite resins.
The aim of the present prospective 6-month clinical trial was to evaluate in vivo the clinical behavior of small-sized Class I restorations made with Vertise Flow.
MATERIALS AND METHODS
Approval to the clinical study was preliminarily given by the Ethical Committee of the University of Siena. A consecutive sample of 40 patients in need of a Class I restoration was selected from the pool of patients accessing the department of Restorative Dentistry of the University of Siena. Patients’ written consent to the trial was obtained after having provided a complete explanation of the aim of the study.
Inclusion criteria
Males and females aged 18-60 years in good general and periodontal health were included.
Exclusion criteria
Patients with the following factors were excluded from the clinical trial:
1. Age < 18 years;
2. Known pregnancy;
3. Disabilities;
4. Potential prosthodontic restoration of teeth;
5. Pulpitic, non-vital or endodontically treated teeth;
6. (Profound, chronic) periodontitis;
7. Deep carious defects (close to pulp, < 1mm distance) or pulp
7. capping;
8. Heavy occlusal contacts or history of bruxism;
9. Systemic disease or severe medical complications;
10. Allergic history concerning methacrylates;
11. Rampant caries;
12. Xerostomia;
13. Lack of compliance;
14. Language barriers.
TEST STIMULI AND ASSESSMENT
Before restoring the tooth, a pain measurement was performed utilizing a simple pain scale based on the response method. Response was determined by a 1-second application of air from a dental unit syringe (at 40-65 p.s.i. and approximately 20°C), directed perpendicularly to the root surface at a distance of 2 cm and by tactile stimuli with a sharp #5 explorer. The patient was asked to rate the perception of the sensitivity experienced during this thermal/evaporative stimulation by placing a mark on a 0-10 visual analog scale, in which 0 indicated absence of pain and 10 excruciating pain. In order to translate these rating into easily understood pain levels, a score system was developed. Score 0 was defined as no pain, scores 1-4 as mild sensitivity (which was provoked by the dentist air blast), and scores 5-10 as strong sensitivity (which was spontaneously reported by the patient during drinking and eating). Only patients scoring low on the visual analog scale were included in the study, whereas high score cases were excluded by the assumption that irreversible pulp inflammation might be sustaining the high
20 CLINICAL STUDY OF VERTISE FLOW IN CLASS I RESTORATIONS DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010
Table 1: Performance criteria according to Ryge. For post-operative sensitivities, mean value and standard deviationism provided (1 = lowest sensitivity, 10 = highest sensitivity).
Table 2: Performance criteria according to Ryge. For post-operative sensitivities, mean value and standard deviation is provided (1 = lowest sensitivity, 10 = highest sensitivity)
RESTORATIVE DENTISTRY
Table 3: Performance criteria according to Ryge. For post-operative sensitivities, mean value and standard deviation is provided (1 = lowest sensitivity, 10 = highest sensitivity)
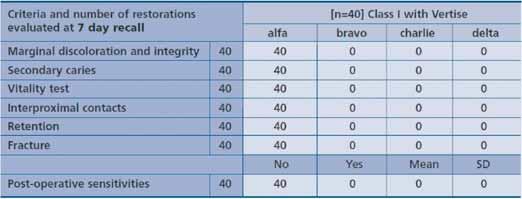
Table 4: Performance criteria according to Ryge. For post-operative sensitivities, mean value and standard deviation is provided (1 = lowest sensitivity, 10 = highest sensitivity)
sensitivity. The status of the gingival tissues adjacent to the test sites was observed at baseline and at each recall. Patients were recalled to the department for testing post-operative sensitivity at baseline, after 1 week, 1month, 3 months and 6 months.
CLINICAL PROCEDURE
Two different operators performed the clinical procedures. Class I restorations were of small dimensions and did not have to involve functional areas. Only if a preliminary occlusion check excluded that the cavity preparation would extend to functional areas was the patient included in the study. Following anesthesia, rubber dam was placed, all carious structures were excavated, and any restorative material was removed. Preparation was performedusing conventional diamond burs in a highspeed hand piece, with no bevel on margins. The preparation design was dictated by the extent of decay. After the complete excavation of the carious lesion, and before applying the restoration, the occlusion was again checked in order to definitively exclude the possibility that the restoration could be placed in direct functional areas. The teeth were restored following manufacturer’s instructions. A small amount of Vertise Flow was applied into the cavity with the included dispenser tip. This first thin layer (no more than 0.5mm in thickness) was brushed on the cavity surfaces for 1520s. After brushing, a 20s polymerization was performed with a DEMI LED light curing unit (Kerr, Orange, CA, USA). Then, the
cavity was filled in bulk unless the thickness of the single increment would exceed the limit for effective polymerization. In the latter case the cavity two layers had to be stratified and singularly cured to fill the cavity. Following an additional 20s polymerization, the filling was contoured using 12- Blade Carbide Burs and 40μm-grit Diamond Burs. Then, the restoration surface was finished with Carbide Burs at 30 Blades and 20μm-grit Diamond Burs. Final polishing was performed with Opti1Step Polisher (KerrHawe, Bioggio, Switzerland). The restorations were placed in the time period between January and March 2009, and examined at baseline, after 1 day, 1 week, 1 month, 3 months, and 6 months by a different operator who had been blinded with regard to the restorative material used. At each recall, data regarding post-operative sensitivity, stability and longevity were collected with reference to the Ryge criteria.36 Postoperative sensitivity, was assessed as the patient comfort with the restoration under function, cold and warm stimuli, and a gentle air stream. Sensitivity was defined by a scale from 0-10, as described above. The other evaluated clinical parameters were: marginal discoloration and integrity, secondary caries, fracture, vitality test, retention and interproximal contacts.
RESULTS
The results at each recall are shown in Tables 1-6. After 6 months of clinical service, all the 40 restorations made with Vertise Flow were scored “alfa” for secondary caries, vitality test, interproximal contacts integrity, retention and fracture. Of the 40 restorations, 37 scored alfa, 2 bravo and 1 charlie for marginal discoloration and integrity. In particular, 1 bravo and 1 charlie score were assigned after 1 month, while another restoration was scored Bravo at the 3-month recall. In accordance with Ryge criteria, the restoration scored Charlie for marginal discoloration/ marginal integrity was a candidate for replacement at the 1-year control. No restored tooth showed post-operative sensitivity at any recall.
DISCUSSION
Despite their large use, the data available in the literature regarding the use of flowable composite resins for posterior restorations
22 CLINICAL STUDY OF VERTISE FLOW IN CLASS I RESTORATIONS DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010
RESTORATIVE DENTISTRY
do not provide a conclusive evidence. The reason why the issue remains controversial is also that the clinical outcome of flowable composite restorations can not merely be ascribed to the intrinsic


material properties, but should also be related to other factors, suchas cavity extension, layering technique, and curing dynamic.11,37-39 The discordant research findingson flowable composite resins may also be explained by the large variability of products in this category, that may lead to different experimental results. The lower filler content leads to a lower modulus of elasticity,thus reducing curing stress. Yet, the lightly filled resin undergoesa greater polymerization shrinkage.16-18 The higher matrix content may also contribute to increased water solubility, possibly affecting the restorations long-term performance. The reduced filler load may also impair the resistance to deformation of the restorations duringf unction. Due to their inferior mechanical properties, flowablecomposite resins are generally not recommended as stand-alone restorative materials especially in cavities with high-stress occlusal function.7,16,1
In such cavities, the use of a flowable material is recommended




24 CLINICAL STUDY OF VERTISE FLOW IN CLASS I RESTORATIONS DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010
Table 5: Performance criteria according to Ryge. For post-operative sensitivities, mean value and standard deviation is provided (1 = lowest sensitivity, 10 = highest sensitivity)
Pre-operative view.First layer placement.Brushing for 20s.
20s polymerization of the first layer.Cavity fill-up.First layer placement of the second restoration.
Table6: Performance criteria according to Ryge. For post-operative sensitivities, mean value and standard deviation is provided (1 = lowest sensitivity, 10 = highest sensitivity)
Class I restoration performed with Vertise Flow.
RESTORATIVE DENTISTRY






Opti1Step PolisherRestorations after contouring-finishing-polishing.6 months follow
instead for lining, in order to produce a stress absorbing layer.38,40 When used as an intermediatelayer between adhesive system and hybrid composite, the flowableprovides the elasticity to absorb the stress generated by the overlaying, more rigid composite.20-23,4143 Conversely, in small-sizedcavities, the use of a flowable composite as a stand-alone restorative material has been proposed.15 In a small-sized cavity no heavy functional stress is expected to occur, as most of the occlusal forces are resisted by the residual tooth structure. A point of criticism that has been raised toward the use of a flowablecomposite as a stand-alone material regards its lack of sculptabilitythat would make layering difficult. In small Class I restorations, however, this issue is not critical as a layering technique is not mandatory. The main advantage of incremental technique is in fact that the volume reduction of each increment is compensatedby the next increment, thus the polymerization shrinkage of the last layer only may effectively damage the bond.7 Loguercio et al.44 reported that the layering technique did not significantly improve the bond strength in small cavities. Similarly, Tjan et al.45 revealed that, in comparison with the one-bulk technique, incremental placement could not substantially improve adaptationto cavity walls in small cavities. He et al38 stated that the incrementaltechnique may be effective only when the cavity size is large.
In the present study, an innovative, recently formulated material was tested. Vertise Flow is a flowable resin with adhesive properties, not requiring any additional adhesive step. According to the manufacturer the bonding mechanism is primarily based on the chemical bond between the phosphate functional group of GPDM monomer and calcium ions of the tooth. A micromechanical bond resulting from an interpenetrating network between Vertise Flow polymerized monomers and dentin collagen fibers also contributes to adhesion (Vertise Flow Product Manual, November 2009).
It was the specific objective of this study to verify clinically whether the new self-adhesive flowable composite is able to establish an effective seal, thus avoiding post-operative sensitivity phenomena. The manufacturer recommends a great attention to some of the steps that the clinician has to perform in the clinical use. Differently from traditional flowable systems, the material does not have an underlying bonding agent. For this reason, for proper handling of the material the manufacturer indicates as crucial the achievement of a proper contact of the material with the tooth substrate, as well as an appropriate brushing motion. A brushing motion of 15-20s is required with a thin layer of material (0.5mm). As the accuracy of the brushing motion is of great importance, specific applicators are supplied for adequately dispensing the material. Brushes with bristles of proper elasticity are also supplied by the manufacturer. After brushing, the material has to be cured for 20s. The reason why Vertise Flow requires a longer polymerization time in comparison with conventional adhesives or other marketed flowable composites is that adhesive monomers tend to have a slower response to light curing than non-adhesive monomers. The less efficient curing mechanism could be attributed to the mono-functionality of Vertise Flow adhesive monomers in comparison with di-functional monomers of traditional composites or to the hydrophilicity of the adhesive monomers. Beside post-operative sensitivity, other clinical aspects related to improper marginal sealing, such as recurrent caries, marginal discoloration,and loss of retention were also evaluated in time. Based on the collected data, the new material gave proof of a satisfactory clinical behavior. At the 6-month recall, no postoperative sensitivity was reported. Of the 40 performed restorations, only 3 showed limited marginal discoloration and a minor defect in marginal integrity. Therefore, at this stage of the prospective clinical trial, the claimed ability of Vertise Flow to achieve an effective sealing at the tooth-restoration interface was confirmed.
26 DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010 CLINICAL STUDY OF VERTISE FLOW IN CLASS I RESTORATIONS
Brushing for 20s.20s final polymerization.Diamond bur 20μ.
up.

As for any new material, longer-term studies are needed in order to validate this initial promising behavior. Further investigations are also advised to assess whether the encouraging performance of the new material finds confirmation in other clinical applications, such as the use as a liner in larger Class I, Class II, and Class V cavities. In vitro and in vivo tests are currently being performed with these objectives.
CONCLUSION
Over a 6-month follow-up period, Class I restorations performed with Vertise Flow exhibited a satisfactory clinical performance. In particular, no post-operative sensitivity was reported at any time. Clinical relevance: The results of this 6-month study demonstrated a successful clinical outcome of the self-adhering flowable composite resin Vertise Flow when used to restore small Class I cavities.
ACKNOWLEDGEMENT
This research was granted by Kerr Company, Orange, CA, USA.
REFERENCES
1. Christensen GJ. Amalgam vs. composite resin. J Am Dent Assoc 1998;129:1757-1759
2. Baratieri LN, Ritter AV. Four-year clinical evaluation of posterior resin-based composite restorations placed using the total-etch technique. J Esthet Restor Dent 2001;13:50-57
3. Wilson NH. Conference report. Direct adhesive materials: current perceptions and evidence – future solutions. J Dent 2001;29:307-316
4. De Munck J, Van Landuyt K, Peumans M, Poitevin A, Lambrechts P, Braem M, Van Meerbeek B. A critical review of the durability of adhesion to tooth tissue: methods and results. J Dent Res 2005;84:118-132
5. Feilzer AJ, de Gee AJ, Davidson CL. Setting stress in composite resin in relation to configuration of the restoration. J Dent Res 1987;66:1636-1639
6. Choi KK, Ryu GJ, Choi SM, Lee MJ, Park SJ, Ferracane JL. Effects of cavity configuration on composite restoration. Oper Dent 2004;29:462-469
7. Yoshikawa T, Sano H, BurrowMF, Tagami J, Pashley DH. Effects of dentin depth and cavity configuration on bond strength. J Dent Res 1999;78:898-905
8. Hilton TJ. Can modern restorative procedures and materials reliably seal cavities ? In vitro investigation. Part 1. Am J Dent 2002;15:198-210
9. Irie M, Suzuki K, Watts DC. Marginal gap formation of lightactivated restorative materials: effects of immediate setting shrinkage and bond strength. Dent Mater 2002;18:203-210.
10. Lutz F, Krejci I, Barbakow F. Quality and durability of marginal adaptation in bonded composite restorations. Dent Mater 1991;7:107-113
11. Nikolaenko SA, Lohbauer U, Roggendorf M, Petschelt A, Dasch W, Frankenberger R. Influence of C-factor and layering technique on microtensile bond strength to dentin. Dent Mater 2004;20:579-585.
12. Tsai PCL, Meyers IA, Walsh LJ. Depth of cure and surface microhardness of composite resin cured with blue LED curing units. Dent Mater 2004;20:364-369
13. Ferracane JL. Developing a more complete understanding of stresses produced in dental composites during polymerization. Dent Mater 2005;21:36-42
14. Hannig M, Friedrichs C. Comparative in vivo and in vitro investigation of interfacial bond variability. Oper Dent 2001;26:3-11.
15. Helvatjoglu-Antoniades M, Papadogiannis Y, Lakes RS, Dionysopoulos P, Papadogiannis D. Dynamic and static elastic moduli of packable and flowable composite resins and their development after initial photo curing. Dent Mater 2006;22:450–9.
16. Bayne SC, Thompson JY, Swift Jr EJ, Stamatiades P,Wilkerson M. A characterization of first-generation flowable composites. J Am Dent Assoc 1998;129:567–77
17. Baroudi K, Silikas N, Watts DC. Time-dependent viscoelastic creep and recovery of flowable composites. Eur J Oral Sci 2007;115:517–21.
18. Labella R, Lambrechts P, Van Meerbeek B, Vanherle G. Polymerization shrinkage and elasticity of flowable composites and filled adhesives. Dent Mater 1999;15:128–37.
19. Leevailoj C, Cochran MA, Matis BA, Moore BK, Platt JA. Microleakage of posterior packable resin composites with and without flowable liners. Oper Dent 2001;26:302–7.
20. Unterbrink GL, Liebenberg WH. Flowable resin composites as filled adhesives: literature review and clinical recommendations. Quintessence Int
RESTORATIVE DENTISTRY
1999;30:249–57.
21. Alomari QD, Reinhardt JW, Boyer DB. Effect of liners on cusp deflection and gap formation in composite restorations. Oper Dent 2001;26:406–11.
22. Kemp-Scholte CM, Davidson CL. Complete marginal seal of Class V resin composite restorations effected by increased flexibility. J Dent Res 1990;69:1240–3.
23. Van Meerbeek B, Willems G, Celis JP, Roos JR, Braem M, Lambrechts P, Vanherle G. Assessment by nano-indentation of the hardness and elasticity of the resin–dentin bonding area. J Dent Res 1993;72:1434–42.
24. Francescut P, Lussi A. Performance of a conventional sealant and a flowable composite on minimally invasive prepared fissures. Oper Dent 2006;31(5):543550
25. Park SB, Son WS, Ko CC, Garcia-Godoy F, Park MG, Kim HI, Kwon YH. Influence of flowable resins on the shear bond strength of orthodontic brackets. Dental Materials Journal 2009; 28(6): 730–734
26. Helvatjoglu-Antoniades M, Papadogiannis Y, Lakes RS, Dionysopoulos P, Papadogiannis D. Dynamic and static elastic moduli of packable and flowable composite resins and their development after initial photo curing. Dent Mater 2006;22:450–9.
27. Kugel G, Ferrari M. The science of bonding: from first to sixth generation. J Am Dent Assoc, 2000. 131 Suppl: p. 20S-25S.
28. Moszner N,Salz U, Zimmermann J. Chemical aspects of self-etching enameldentin adhesives: a systematic review. Dent Mater, 2005. 21(10): p. 895-910.
29. Van Landuyt KL, De Munck J, Snauwaert J, Coutinho E, Poitevin A, Yoshida Y, Inoue S, Peumans M, Suzuki K, Lambrechts P, Van Meerbeek B. Monomer-solvent phase separation in onestep self-etch adhesives. J Dent Res, 2005. 84(2): p. 183-8.
30. Van Landuyt KL, Peumans M, De Munck J, Lambrechts P, Van Meerbeek B. Extension of a one-step self-etch adhesive into a multi-step adhesive. Dent Mater, 2006. 22(6): p. 533-44.
31. Tay FR, Gwinnett AJ, Pang KM, Wei SH. Resin permeation into acid-conditioned, moist, and dry dentin: a paradigm using water-free adhesive primers. J Dent Res, 1996. 75(4): p. 1034-44.
32. Tay FR,Gwinnett JA, Wei SH. Micromorphological spectrum from overdrying to overwetting acid-conditioned dentin in waterfree aceton-based, single-bottle primer/adhesives. Dent Mater, 1996. 12(4): p. 236-44.
33. Pashley DH, Tay FR. Aggressiveness of contemporary selfetching adhesives. Part II: etching effects on unground enamel. Dent Mater, 2001. 17(5): p. 430-44.
34. Breschi L, Mazzoni A, Ruggeri A, Cadenaro M, Di Lenarda R, De Stefano Dorigo E. Dental adhesion review: aging and stability of the bonded interface. Dent Mater, 2008. 24(1): p. 90-101.
35. Kubo S., Kawasaki K, Yokota H, Hayashi Y. Five-year clinical evaluation of two adhesive systems in non-carious cervical lesions. J Dent, 2006. 34(2): p. 97105.
36. Bayne SC, Schmalz G. Reprinting the classic article on USPHS evaluation methods for measuring the clinical research performance of restorative materials. Clin Oral Invest 2005;9:209-214
37. Cadenaro M, Marchesi G, Antoniolli F, Davidson CL, De Stefano Dorigo E, Breschi L. Flowability of composites is no guarantee for contraction stress reduction. Dent Mater 2009;25(5):649-54.
38. He Z, Shimada Y, Sadr A, Ikeda M, Tagami J. The effects of cavity size and filling method on the bonding to Class I cavities. J Adhes Dent 2008;10:447-453
39. Reis AF, Giannini M, Anbrosano GMB, Chan DCN. The effects of filling techniques and low-viscosity composite liner on bond strength to Class II cavities. J Dent 2003;31:59-66.
40. Chuang SF, Liu JK, Chao CC, Liao FP, Chen YH. Effects of flowable composite lining and operator experience on microleakage and internal voids in class II composite restorations. J Prosthet Dent 2001;85:177–83, 24.
41. Cadenaro M, Biasotto M, Scuor N, Breschi L, Davidson CL, Di Lenarda R. Assessment of polymerization contraction stress of three composite resins. Dent Mater 2008; 24(5):681-685.
42. Davidson CL, Feilzer AJ. Polymerization shrinkage and polymerization shrinkage stress in polymer-based restoratives. J Dent Res 1997;25:435–40.
43. Braga RR, Hilton TJ, Ferracane JL. Contraction stress of flowable composite materials and their efficacy as stress-relieving layers. J Am Dent Ass 2003;134:721–8.
44. Loguercio AD, Reis A, Ballester RY. Polymerization shrinkage: effects of constraint and filling technique in composite restorations. Dental Mater 2004;20:236–243
45. Tjan AH, Bergh BH, Lidner C. Effect of various incremental techniques on marginal adaptation of Class II composite resin restorations. J Prosthet Dent 1992; 67:62-66
Panasil® initial contact. Precise, even in extreme situations.

020903_4009 www.kettenbach.com

CHIROPRO L ERGONOMICS REDEFINED
With the 20:1 contra-angle of the Chiropro L system, you'll rediscover the meaning of the word ergonomics. This Swiss Made instrument has an internal irrigation system unique to Bien-Air, which leaves the handling area completely free. The irrigant is directed at the base of the drill, running along it precisely. It offers perfect irrigation, especially for fitting implants using surgical guides. With the smallest head on the market and a very light weight, this instrument is as easy to handle as it is precise. Its LED lighting with two glass rods diffuses a natural white light and its power can be adjusted to suit your requirements. With so much comfort, you could almost forget that the 20:1 contra-angle of the Chiropro L is driven by the most powerful micromotor in the world, the extraordinary MX-LED.
CHIROPRO L - increase your expectations.
Bien-Air Dental SA Länggasse 60 P.O. Box 2500 Bienne 6, Switzerland Phone +41 (0)32 344 64 64 Fax +41 (0)32 344 64 91 dental@bienair.com www.bienair.com
Program ME training GC Europe
Beirut, 10 & 11 June 2010
Thursday, June 10, 2010
The first dealer meeting started with a welcoming speech by Dr. Mohamad Fayad, Sales Manager for the Middle East Territory. During the speech he addressed the importance of this first meeting as it forms an excellent platform for sharing product knowledge between GC and the customers, but also business knowledge amongst the customers.
The training session started with the GC Europe Company presentation by Mr. Ward Gerets. The presentation highlights the rich history of the family owned company and shows the development of the company which will celebrate it 90th anniversary next year. During the presentation an overview was given of the wide assortment of products GC is offering and ended with a more detailed part on the important luting products. Focus was on the most recent addition of this versatile portfolio, nl. G-Cem Automix, the self adhesive resin cement which offers many advantages and is probably the best solution for modern metal free restorations such as zirconium. After the break Dr. Brigitte Douaihy took over and gave an overview of the different glass ionomer based restoratives GC is offering. The most of the time was spent on EQUIA, the latest restorative system GC developed and which offers new opportunities for restorative treatments. EQUIA is considered as the alternative to amalgam and compomers since it is fast, easy and aesthetic.
Friday, June 11, 2010

The second day of the meeting was focussing on GC’s portfolio of composites and related products. The presentations concentrate firstly on the newly introduced composite restoratives Kalore and G-ænial. Kalore features a special monomer developed by Du Pont and promises high end restorations that will last longer, whilst being compatible with all current bonding system. G-ænial is the successor of the successful Gradia Direct system and offers an extremely easy to use shade system with age related enamel shades. On top the material offers high radiopacity without compromising the aesthetic possibilities. During the presentation information was given as well on upcoming new releases in the field of composites. Closely related to the composites is the Gradia Core and Fiber Post system, that allows to lute and build-up any core restoration with the same material. This principle was further presented in detail with many clinical tip & tricks by Dr. Elie Farès. As a KOL of GC he was sharing his experience with the latest products with the entire group. The meeting was concludedby a presentation on the Minimum Intervention approach GC is pushing forward. The new concept encompasses the identification of the caries risk, the preventive measure a patient should take and when needed new approaches to the restorative treatment.
All together this was a very successful meeting with exchange of information, knowledge and experience on various levels. GC promises that meeting like this will take place every year in order to strengthen the relation with dealers and partners even more.


DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010


GC Kalore™:







Kalore™ is the composite restauration of the future. A perfectly mouldable filling material based on the revolutionary monomer technology from DuPont. Kalore™ hardens with extremely low shrinkage, is easy to polish and has a natural sheen. This guarantees highly aesthetic results.



Are readyfor the future?
Are you ready for the future?





















Experience the dental composite of the future: http://www.gceurope.com
encethedentalcompositeofthefuture:
composite material
unique monomer technology
DuPont. GC EUROPE N.V. Head Office Tel. +32.16.74.10.00 info@gceurope.com http://www.gceurope.com
The
of the future. Thanks to the
from

Thank you for subscribing at the dentalnews.com website. The winner of the W&H LED Contra - Angle Handpiece (ALEGRA WE - 56LED G) is Dr. Marwan Qasem from al Bireh.
The results will be posted on the Dentalnews Facebook Page (www.facebook.com/dentalnews1) and also on www.dentalnews.com

by
WIN a
subscribing to
newsletter on www.dentalnews.com LED Contra - Angle handpiece
FREE
our
ALEGRA WE - 56LED G
ENDODONTICS Mandibular first molars with five canals
Report of cases among Kuwait population
Milind P. Gaidhane MDS*, Ahmed A. Abdul Rahem MS** , Arun Gopinath MDS* , Mansour F. Al Ajmi MS***
*Endodontist, Jahra Dental Speciality Centre
**Endodontist, Director, Jahra Dental Speciality Centre
*** Farwaniya Dental Speciality Centre
Email – agmolar@gmail.com
ABSTRACT
Mandibular first molar with five root canals have been previously reported mainly among Hispanics, Latin Americans and North Americans. This case report presents Mandibular first molar with five root canals among the Kuwait population. Each tooth had three independent canals in the mesial root with separate orifices and two canals in the distal root. One should be aware of the distribution of anomalies to anticipate and treat the tooth successfully. Key Words: Root canal, Root morphology, Anomalies, Extra canal, Mandibular molar.
INTRODUCTION
Successful endodontic treatment depends on complete debridement and obturation of root canal system. In order to achieve complete debridement, it is necessary to be familiar with the root canal morphology and its variations. It is well established that the pulpal remnants can lead to infection in endodontically treated cases and subsequently leading to failure. Understanding the morphology of root canals will help in achieving complete debridement and satisfactory obturation of the root canals, thereby enhancing the success rate of endodontic therapy.
The majority of first molars are two rooted with two mesial and onedistal canal. Occurrence of an extra canal is a common morphological variation. These extra canals may begin from the pulpal floor with separate orifices or with a common orifice, proceedingto end at the apex separately or in a single foramen. Sometimes, an extra root may be present, in which case, the canal orifice is usually located wide apart from the main canal.
The number of root canals to be anticipated in any case is usually based on the data from root canal morphological studies that have evaluated the frequency and distribution. Multiple canals in mandibular first molar have been documented1-9. It is common to find four canals in lower first molars and usually, the extra
canal is seen in the distal root. In vitro studies by Pedro Bandelli et al1 have shown that four canals are present in 30-50% of mandibular first molars.
Mandibular first molars with five canals, with three canals in either mesial or distal root have been documented in the literature. Studies of the internal anatomy of extracted molars using dyes, elastomers or by cross section through the roots, Barker et al2, Diaz3, Kerekes and Tronstad4 showed existence of a third canal in the mesial root. Pomeranz et al5, Weine6, and Vande Voorde7, reported cases of three independent canals in the mesial root of mandibular first molar. Fabra Campos10, in a study of 760 mandibular first molars showed that 2.6% had three canals in the mesial root.
Fabra Campos11,12, Stroner et al13, reported several cases of five root canals in mandibular first molar with three canals in the distal root and two in the mesial root. Earlier reports have found the mandibular first molars with five canals mainly in Hispanics, Latin Americans and North Americans. The purpose of this clinical report is to emphasize the presence of five root canals in mandibular first molar from individuals belonging to the Kuwait population. The following are the case reports in which three canals were located in mesial root and two canals in distal root and all of which were successfully treated.
CASE REPORTS
Case 1:
A 40-year-old male patient presented with a complaint of pain in the posterior right mandibular region for two weeks. He gave a history of intermittent pain in the same region for the past two months. His past medical history was found to be non-contributory, clinical exam revealed a carious right mandibular first molar. The clinical and radiographic findings led to a diagnosis of chronic
36 MANDIBULAR FIRST MOLARS WITH FIVE CANALS DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010
ENDODONTICS




Case 2:
A 20 year old male was referred to Endodontic Department of Jahra Dental Speciality Centre for root canal treatment of lower right first mandibular molar. The referring dentist had done pulpotomy of the tooth. On examination, the tooth was slightly tender on percussion. Patient had no other symptoms and medical history was non contributory. Preoperative radiograph showed mandibular molar with one mesial and two distal roots. The distal root was with additional distolingual root. (Figure 5). Endodontic procedure was carried out under local anesthesia and rubber dam isolation. Initially two mesial and two distal canals were detected. The distal canal orifice was wide and opened to two separate canals. In mesial root after initial debridement of two canals, a bleeding spot remained in between the two canals which led to further exploration with a K file #08 and subsequently an intermediate canal was located. (Figure 6). Working length radiograph with distal angulation showed three mesial canals and two distal canals. (Figure 7). All the five canals were negotiated, working length determined, biomechanical preparation was carried out followed by obturation. (Figure 8). The patient was followed up.
irreversible pulpitis of the right mandibular first molar which requires endodontic therapy.
Radiographic evaluation of the involved tooth indicated a normal canal configurations of canals. (Figure 1)
Endodontic access was carried out under local anesthesia and rubber dam isolation. Four canals were detected following access preparation, two each in distal and mesial root. After debridement of the pulp chamber, some pulp tissue remained at the isthmus of mesial orifices. Further, careful probing in the isthmus area with an endodontic explorer revealed an intermediate canal. (Figure 2). Distal angulation working length radiograph showed three distinct canals mesially and two canals distally joiningat the apex. (Figure 3). All the five canals were negotiated and working length was determined. Cleaning and shaping was performed using crown down preparation with Profile nickel titanium rotary instrument (Maillefer, Dentsply), along with copiousirrigation of sodium hypochlorite and RC Prep (Premier,USA). On the second visit, master cone selection was made and obturated by lateral condensation procedure. The patient was recalled for check up and after a week, the tooth was restored with a permanent restoration. (Figure 4). The patient was followed up for two years.




38 MANDIBULAR FIRST MOLARS WITH FIVE CANALS DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010
Figure 1- Pre operative radiograph showing distal caries.
Figure 2- Pulp chamber floor showing three independant mesial and two distal orifices.
Figure 5- Pre operative radiograph showing mesial root and a distal root with an additional indistinct distolingual root.
Figure 6- Pulp chamber showing three mesial and two distal canal orifices.
Figure 7- Working length radiograph taken with distal shift technique.
Figure 8- Post operative obturation radiograph showing three mesial and two separate distal roots.
Figure 3 - Working length radiograph reveals three canals in the mesial root and two canals in the distal root.
Figure 4- Post operative obturation radiograph.

ENDODONTICS
Case 3:
A 19 year old girl was referred to Endodontic Department of Jahra Dental Speciality Centre for root canal treatment of lower right first mandibular molar. Pulpotomy of the tooth had already been carried out. On examination the tooth was asymptomatic and medical history was non contributory. Radiograph revealed two separate roots. (Figure 9). Endodontic procedure was carried out under local anesthesia and rubber dam isolation. Access opening showed four canal orifices, two mesially and two distally. The orifices of mesial canals were placed slightly apart and after initial debridement, the orifices appeared unclean. Further exploration revealed a third orifice located more towards the mesiolingual canal. Working length radiograph with a distal angulation presented with three separate canals in mesial root and two in distal root. (Figure 10). Working length of all the five canals were determined followed by biomechanical preparation and obturation. (Figure 11). After one week the tooth was restored with permanent restoration and patient was followed up.


Figure 9- Pre operative radiograph.Figure 10- Working length radiograph showing three mesial and two distal canals.

Figure 11- Post obturation radiograph showing five canals.
DISCUSSION
It has already been demonstrated that mandibular molars may manifest variations of root canal morphology. The root canal system consists of multiple canals occasionally interconnected by transverse anastomoses. The possibility of variation in root canal morphology and its distribution should be considered before the root canal
treatment is undertaken. The present case report describes the treatment of the first mandibular molar with five canals.
Earlier studies and case reports by Pomeranz et al5, Weine6, Martinez Berna and Bandelli14, Fabra Campos8,10,11,12, found intermediate canals in the mesial root, more frequently in younger patients. The present case report suggests that it is commonly seen more in younger age group. As the age advances, root canals may get obliterated, therefore it is rarely found in elderly patients.
Studies by Seelig and Gills15, Hasselgren and Tronstal16, and Roberstont17, Baugh18, showed presence of pulpal remnants between two main canals in the mesial root of mandibular first molar. Hence, long term success of root canal therapy requires exploration and treatment of intermediary canals.
Diagnostic measures such as multiple preoperative radiographs, examination of the pulp chamber floor with a sharp explorer, troughing of the grooves with ultrasonic tips, staining the chamber floor with 1% methylene blue dye, performing the sodium hypochlorite “champagne bubble test” and visualizing canal bleeding points, use of magnifying loops and fiber optic illumination, surgical operating microscope are all important aides in locating root canal orifices.
Detecting extra canals invariably offers a sense of accomplishment and is a key factor for boosting the professional morale of clinicians in endodontics.
REFERENCES
1. Bandelli P, Martinez-Berna A. Preparacion quirurgica de los conductos radiculares. Rev Esp Endod 1983; 1:61-77.
2. Barker DCW, Parson KC, Mills PR, Williams GL. Anatomy of root canals III permanent mandibular molars. Aust Dent J 1974; 19: 408 – 13.
3. Diaz JV. Comparacion de hallazgos radiologicos y de transparentacion en la anatomia de conductos radiculares ( cuadro de resultados No.6 ). Caracas Imprenta Universitaria de la Universidad Central de Venezuela,1977.
4. Kerekes K, Tronstad L. Morphometric observations on the root canals of human molars. J Endodon 1977; 3:114-8.
5. Pomeranz HH, Edelman DL, Goldberg MG. Treatment considerations of the middle mesial canal of the mandibular first and second molars., J Endodon 1981; 7: 565-8.
6. Weine FS. Case reports: three canals in the mesial root of a mandibular first molar. J Endodon 1982; 8: 517-20.
7. Vande Voorde HE, Odendahl D, Davis J. Molar 4th canals: frequent cause of endodontic failure, Illinos Dent J 1975; 44: 779-86.
8. Fabra–Campos H. An unusual root anatomy of the human mandibular first molar. J Endodon 1985; 11: 568-72.
9. Richard G Beatty, Keith Krell. Mandibular molar with five canals: report of two cases. J Am Dent Assoc 1987; 114:802-4.
10. Fabra–Campos H. Three canals in mesial root of mandibular first permanent molars: a clinical study. Int Endo J 1989; 22: 39-43.
11. Fabra-Campos H. La probelematica de los primeros molars inferiores en el tratamiento endodontico. Rev Esp Endo 1983; 1: 135-53.
12. Fabra-Campos H. Tres conductos en la raiz distal de dos primeros molars inferiors. Rev Esp Endo 1984; 2: 1.
13. Stroner WF, Remeikis NA and Carr GB. Mandibular molar with three distal canals. Oral Surg 1984; 57: 554-57.
14. Martinez Berna A, Badanelli P. Investigacion clinica de molars inferiors con cinco conductos. Bol Inf Dent 1983; 10:27-41.
15. Seeling A, Gillis R. Preparation of cleared specimens for pulp cavity studies. J Dent Res 1973; 52: 1154.
16. Hasselgren G, Tronstad L. The use of transparent teeth in the teaching of pre clinical endodontics. J Endodon 1975; 1: 278-80.
17. Robertson D, Leeb IJ, Mckee M, Brewer E. A clearing technique for the study of root canal systems. J Endodon 1980; 6: 421-24.
18. Baug D, Wallace J. Middle mesial canal of the mandibular first molar. A case report and literature review. J Endod 2004; 30: 185-6.
40 MANDIBULAR FIRST MOLARS WITH FIVE CANALS DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010














































mectron s.p.a., via Loreto 15/A, 16042 Carasco (Ge), Italia, tel +39 0185 35361, fax +39 0185 351374, www.mectron.com, mectron@mectron.com Û SINUS PHYSIOLIFT® – MICROMETRIC DETACHMENT OF THE SCHNEIDERIAN MEMBRANE THANKS TO THE HYDRODYNAMIC PRESSURE Û BY MECTRON CRESTAL SINUS LIFT – SAFE, SIMPLE AND FAST!


¢ù«d ÉÑjôZ ¿G ó≤©æj ô“ƒe »ª∏Y √ò¡H ᫪g’G Gò¡Hh ºé◊G ‘
øWh Qó°U ±ô◊G ¿Éch ádƒãeG ¢ûjÉ©àd äGQÉ°†◊G äÉfÉjódGh øëf
AÉæHG øWh ádÉ°SQ ‘ óM ,É¡JGP ºZôdÉÑa øe πc Ée …ôéj ’ ™LGÎf ’h Ö©àf òNÉfh øe ÜÉ©°üdG GôNR Qƒ£à∏d ƒëf π°†a’G
±ƒ«°†∏d ,Üô©dG ÓgG Ó¡°Sh ºμH ‘ ºμæWh ÊÉãdG .¿ÉæÑd
Éæà«°†b ,IóMGh Éæeƒªg IóMGh , πc Ée ƒÑ°üf ¬«dG ¿G Qƒ£f ÌcG ÌcÉa
ÉfƒcQÉ°ûàd
¿hÉ©àdG Éææ«H øjô°VÉëª∏d ,ÖfÉL’G ”óÑμJ AÉæY ôØ°ùdG Ωhó≤∏d ¤G ¿ÉæÑd
ºμJGÈN Éfƒ©∏£Jh ≈∏Y çóMG äÉ«æ≤àdG , øëf ºμd øe ,øjôcÉ°ûdG
øμdh OhG ¿G õ¡àfG √òg áÑ°SÉæŸG ≈æ“’ ºμ«∏Y Ωhó≤dG Iôe á«fÉK ¤G
¿ÉæÑd øμdh √òg IôŸG áMÉ«°ù∏d ´ÓWÓd ≈∏Y ∫ɪL »bQh Gòg ó∏ÑdG , ºZôdÉÑa øe ä’ƒ÷G á«MÉ«°ùdG »àdG É¡ª¶ææ°S ,ºμd Ée ∫GR ∑Éæg ÒãμdG .¬àjhôd Ég »g áæ°ùdG ¤h’G »eÓà°S’ »eÉ¡e Ö«≤æc AÉÑW’ ¿Éæ°S’G ób âaQÉ°T ≈∏Y É¡àjÉ¡f , óbh âdòH πc Ée â«JhG øe ábÉW ôjƒ£àd πª©dG .»HÉ≤ædG äÉHPÉŒ á«°SÉ«°S IÒãc ∞°ü©J ÉææWƒH øμdh ¬∏dh óª◊G ’ ôKG É¡d ‘ ÉæàHÉ≤f áaÉ°V’ÉÑa ¤G Oƒ¡L ¢ù∏› áHÉ≤ædG ∑Éæg áæ÷ πã“ πc äÉfƒμe º°ù÷G »HÉ≤ædG ¢Uô– ≈∏Y áÑcGƒe á°SGQOh πc ™jQÉ°ûŸG á«∏Ñ≤à°ùŸG áæ÷h ájÉbƒdG øe QGó°UG OMS Éæ©£à°SG É°†jG ¿hÉ©àdÉHh ™e IQGRh áë°üdG äÉ°TÓØdGh á«fÓYG õØ– ≈∏Y AÉæàY’G .¿Éæ°S’ÉH áMÉ«°ùdG á«Ñ£dG ÉgÉæ«dhG ÉeɪàgG É°UÉN ÉfQó°UÉa ¿hÉ©àdÉHh ™e IQGRh áMÉ«°ùdG ÉfÓYG É«FÉYO ≥∏©àj Gò¡H ™°VƒŸG ” ¬ãH ≈∏Y πc
äÉ°TÉ°T .IõØ∏àdG OhG ¿G ¬LhG AGóf øe Ö∏≤dG ¤G πc äÉÄ«¡dG áæeÉ°†dG ‘ ¿ÉæÑd øe IQGRh áë°U ¿Éª°Vh »YɪàLG ‹ƒàd áHÉÑW ¿Éæ°S’G ÉeɪàgG ÈcG PG ¿G áë°U ºØdG øe áë°U ¿É°ùf’G
Ö«≤f AÉÑWG ¿Éæ°S’G ‘ ¿ÉæÑd - ähÒH
¿É°ùZQƒàcódG OQÉj


during the live transmission of the aesthetic procedure

42 BIDM 2010 DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010
Dr. Stephan Koubi lecturing on dental bonding agents
Dr. Ghassan Yared, President of the Lebanese Dental Association
Dr. Ronald Younis, President of the Scientific Committee
Dr. Carole Yared






DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010 43 BIDM 2010
Picture of the members of the Lebanese Dental Association during the dinner at Mounir Restaurant in Broummana
and Mrs.
MORE PICTURES AVAILABLE ON www.facebook.com/dentalnews1
Dr. and Mrs. Aouni IssaDr. and Mrs. Jean Moussa Dr.
and Mrs. Joseph El ChaerDr.
Ammar Al Ekri
HemCon ® – Stops bleeding.
HemCon Dental Dressing is self-adhesive and self-dissolving.
After one minute – the bleeding has stopped.
After 48 hours – dressing has dissolved*.

NE NEWW!



• Faster hemostasis
Bleeding is controlled in less than 1 minute**, compared to 9.53 minutes for conventional dressings.
• Effective pain relief
Creates a physical barrier to protect the wound from irritation.
• How it works
Attracts red blood cells and platelets to the dressing, forming a coagulum that seals the wound.

* The dressing usually dissolves within 48 hours. In some cases this may take up to seven days.
** Malmquist JP, Clemens SC, Oien HJ, Wilson SL. Hemostasis of oral surgery wounds with HemCon Dental Dressing. Journal of Maxillofacial Surg. 2008:66:1177-1183.
©2010 Zimmer Dental Inc. 2346, Rev. 7/10. HemCon is a registered trademark of HemCon Medical Technologies, Inc. HemCon Dental Dressing is manufactured by HemCon Medical Technologies and distributed by Zimmer Dental Inc. Please note that not all products and regenerative materials are registered or available in every country. Please check with a Zimmer Dental representative for availability and additional information.
HemCon Dental Dressing
Coagulum is formed
www.zimmerdental.com

99.9999% deadly. Just




Virucidal. Bactericidal. Tuberculocidal. Just not harmful to you or your patients. disinfecting wipes kill germs on surfaces fast – up to10 times cleans supreme using a patented formulation based on Hydrogen Peroxide that has virtually no odor. Also, the solution readily biodegrades into water and oxygen after disinfection. So OPTIM is eco-friendly and people friendly. In fact, it’s really only germs that aren’t too fond of it. Take control, because the stakes are too high.™
For further information on SciCan products please contact your local SciCan dealer or Dr. Ashraf Suleiman (Middle East Area Manager) at asuleiman@scican.com or by phone at +20 12 3267870. www.scican.com
OPT IM is a registered trademark and “Because the stakes are too high” and “Your Infection Control Specialist” are trademarks of SciC an Ltd.
to you.
It’s
not

TROPHYDISTRIBUTION






46 BIDM 2010 DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010
Dr. Barakat Al Jaabari from JordanDr. Rajaa Kadhem from BahrainDr. Ahmad Al Kahtani from Saudi Arabia
Picture from the dinner in a restaurant facing the Saida CitadelDr. and Mrs. Mohammad Kalash
Various pictures of the delegates during the dinner in Saida
Pr. Tarek Abbas from EgyptDr. Mohammad Bin Hafeedh from YemenPr. Nada Naaman, Dean of USJ Dental School
MORE PICTURES AVAILABLE ON www.facebook.com/dentalnews1



Thick volume digital panoramic imaging
Pan Volume OPT PantOs
PantOs ART Plus is simple and a compact panoramic system combining the best digital imaging technologies patented
The high resolution CdTe sensor, featuring high sensitivity at high speed, is the only one for direct conversion of X-rays to electrical signals, thus the most efficient: clear and bright images delivered
A new acquisition methodology performs image reconstruction into a panoramic volume 30 mm thick, along the dental arch. This always allows for optimal adaptation of the image to the anatomy of the patient, through autofocus or manual focus within the thick panoramic volume
OrisWin DG Suite is the imaging software with optional module to access CT DICOM files for 3D reconstruction and extraction of panorex and cross section views
panoramic imaging for implants



a company Blue X Imaging Srl Via Idiomi 1/8-33 • 20090 Assago • Italy Tel. +39 02 45712171 • Fax +39 02 45703385 e-mail: bluex@bluex.it • www.bluex.it
ART Plus









48 BIDM 2010
Dr. Ibrahim Taki from KuwaitDr. Mourad Abdul Salam from EgyptPr. Nour Habib from Egypt
MORE PICTURES AVAILABLE ON www.facebook.com/dentalnews1
Dr. Safouh Al Bunni from SyriaDr. Hamad Al Harthy from the Sultanate of OmanDr. Mohammad Darwish from Qatar
PICTURESFROMTHEEXHIBITIONFLOOR
EndoInnovations III
SybronEndooffersyouadvancedtechnologyforsafer, moreefficientprocedures.


TF–Faster,Safer,Stronger
TF™ istwisted,notground–unlikeother nickeltitanium files–makingitmore durable.Endodonticfilesaremadeby grindingtheflutes,weakeningthemetal’s molecularstructurewhichcanleadtoseparation. Ouruniquemanufacturingprocess producesa filewithoptimalsharpness, strengthandflexibility.TFallowsyouto workindifficultsituationsfaster,saferand withastrongerfile.
REALSEAL1Warm-Bonded Obturator
AllthecomponentsofRealSeal1™ –sealer,fillerandcore–areresinbasedmaterialsthatchemicallybond witheachothertoforma superior seal.Asanadded benefit, thissystem’scoreisengineeredtobeeasily seenonaradiograph.

SybronEndoEurope,Basicweg20,3821BRAmersfoort,TheNetherlands tel:+31334536159fax:+31334536153email:Endo@SybronDental.com SybronEndo,1717WestCollinsAvenue,Orange,CA92867 800.346.ENDO714.516.7979Fax714.516.7911SybronEndo.com
©2009SybronEndo










50 BIDM 2010 DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010 MORE PICTURES AVAILABLE ON www.facebook.com/dentalnews1

“FACING CHALLENGES IN DENTAL PRACTICE”
Venue: Lebanese University, Rafic Hariri Campus, Hadath, Lebanon
Date: June 2, 3 and 4, 2011
Scientific program: formal lectures, hands-on workshops, specialized seminars, research and poster sessions, live transmissions of clinical procedures.
Official languages of the convention: English and French
Registration fees: For dentists: 75,000 LP. For residents and students: 50.000 LP. (Workshops not included).
Contact Person:
Dr. Elie Azar Maalouf, Scientific Chairperson E-mail: congresul@ul.edu.lb
Deadline for abstracts:
December 31, 2010
Submit electronically 100-200 words abstract in English with recent photograph and diplomas/ degrees and present clinical and / or academic position.

Intensiv ProxoStrip
A unique diamond-coated metal strip for the final polishing of proximal surfaces. Practical,
Dear colleagues, On behalf of Lebanese University School of Dentistry, it is our utmost pleasure to invite you to join us for the 12th Annual convention of our School that will be held in our campus, in Hadath, Beirut, from June 2 to 4, 2011.
Our scientific program will include formal lectures as well as hand-on workshops, seminars, research and poster sessions and live transmissions, featuring skilled dental practitioners and gifted scientists.
Lebanon is the ideal vacation with special programs for everyone: Tyr, Baalbeck, Sidon, Jbeil, Faqra, Aanjar, Beiteddine, Tripoli, Jeita and other historical sites. Memorable learning adventures are awaiting you, with your family members and colleagues.
On behalf of our dental faculty, headed by Dean and Professor Mounir Doumit, we look forward to welcoming you personally during our convention.
Dr. Elie Azar Maalouf, Scientific Chairperson Prof. Mounir Doumit, President

Ask for your ProxoStrip free sample: i.assy@intensiv.ch

Intensiv UniglossPaste
Clinically tested and scientifically approved by the University of Zurich
One step universal extra fine grit diamond paste with uniquely surface adapted micro grain for high gloss shining of all aesthetical restorations.

New!
Intensiv UniglossPaste
Single Patient Use
Blister of 0,2 g, Ref. 2520/E

Ref. 2500 syringe of 2.5 g
Ask for your free sample: i.assy@intensiv.ch

Pat. 699 819
Intensiv SA 6926 Montagnola Switzerland Intensiv representative for Gulf and Middle East: Mr. Imad Assy: i.assy@intensiv.ch Tel. 00961 3 288367 Tel.+ 41 91 986 50 50 Fax+ 41 91 986 50 59 info@intensiv.ch www.intensiv.ch Scientifically tested by the University of Ancona, Italy 40 μm15 μm 1:1 Ref.
Strips Ref.
4015/12 Package of 12 Strips
rapid, ergonomic, sterilizable!
PX 4015/6 Package of 6
PX


Dr. Hamad Al Harthy president of the Oman Dental Society and Chairman of the 7th Gulf Dental Association Conference
á∏eÉ°ûdG ºK ¥ô£J ¤G åjó◊G øY á£HGôdG á«fɪ©dG Ö£d ¿Éæ°S’G Éë°Vƒe É¡fG òæe É¡FÉ°ûfG âªàgG áªgÉ°ùŸÉH ‘ ôjƒ£J áæ¡e ÖW ¿Éæ°S’G ‘ áæ£∏°ùdG ™aQh äGAÉØμdG π≤°Uh ÖgGƒe Ú∏eÉ©dG ÚYÉ£≤dÉH ΩÉ©dG ¢UÉÿGh ‘ ∞∏àfl ä’É› äÉ°ü°üîJh ÖW ¿Éæ°S’G
øY ≥jôW áeÉbG äGô“ƒŸG äGhóædGh äÉ≤∏Mh πª©dG ,Iôªà°ùŸG
¤G L ÖfÉ ã“ « π ¡ŸG æ á ‘ aÉÙG π ∏ÿG « é « á b’Gh ∏ « ª « á á«dhódGh
Égó©H §∏°S ¢ù«FQ á£HGôdG á«fɪ©dG Ö£d ¿Éæ°S’G Aƒ°†dG ≈∏Y ô“ƒŸG ™HÉ°ùdG á«©ªé∏d á«é«∏ÿG Ö£d ¿Éæ°S’G Éæ«Ñe ¬fG »JÉj c ã ª Iô e ø K ª QÉ ¡÷G Oƒ °†àŸG aÉ Iô àŸGh °UGƒ ∏ á e ø b Ñ π ª÷G © « äÉ HGhQh § ÖW °S’G æ ¿É ∏ÿG « é « á M å« °†j º ô“ƒŸG ¢Vô©ŸGh ÖMÉ°üŸG ¬d áÑîf øe IòJÉ°S’G ÚjQÉ°ûà°S’Gh AÉÑWGh ¿Éæ°S’G Ú°ü°üîàŸG øe ∞∏àfl äÉ©eÉ÷G äÉ°ù°SƒŸGh ᫪∏©dG ‘ ∫hO ∏ÿG « è dG © Hô » dG jò ø j ≤ eó ¿ƒ ¥GQhG Y ª π e ¡ ª á ‘ àfl ∏ ∞ J °ü°üî äÉ ÖW °S’G æ ¿É H °V’É á˘aÉ ¤G ¥GQhG π˘ª˘Y á«∏fi É¡eó≤j áÑîf øe ÚjQÉ°ûà°S’G AÉÑWGh ¿Éæ°S’G Ú«fɪ©dG ,Ú°ü°üîàŸG å«M ºàj ‘ ô“ƒŸG ∫OÉÑJ äGÈÿG äGAÉØμdGh øª°V ∞∏àfl äÉ°ü°üîàdG ÖW ¿Éæ°S’G e ø L fÉ Ñ ¬ dG ≤ ≈ ÚeG Y ΩÉ ª÷G © « á ∏ÿG « é « á d Ö£ °S’G æ ¿É óªfi.O øH π¶«æM Rɪ÷G áª∏c ¢Vô©à°SG øe É¡dÓN IÒ°ùe

a’G à à ìÉ H μ ∏ ª á FQ ¢ù« dG HGô £ á dG á«fɪ©
æŸG ¶ ª á d ∏ ª ô“ƒ O M ª ó KQÉ◊G » °TG QÉ ‘ H jGó à ¡ É ¤G dG Yó º »î°ùdG …òdG »¶M ¬H ô“ƒŸG øe ΩÉ≤ŸG »eÉ°ùdG Iô°†◊ ÖMÉ°U ádÓ÷G ¿É£∏°ùdG ¢SƒHÉb øH ó«©°S º¶©ŸG - ¬¶ØM ¬∏dG √ÉYQhÉe ¿Éc ¬d ≠dÉH ôK’G ≈∏Y ™«ªL Úª¶æŸG ÚcQÉ°ûŸGh Gò¡d
ô“ƒŸG ‘ aQ ™ dG ¡ ª º Jh μ ã « ∞ ¡÷G Oƒ ‘ ìÉ‚G a © dÉ « äÉ
ô“ƒŸG
ócGh »KQÉ◊G ‘ ¬àª∏c ≈∏Y ΩɪàgG IQGRh áë°üdG áæ¡Ã ÖW °S’G æ ¿É îà à ∏ ∞ a Yhô ¡ É Jh °ü°üî JÉ ¡ É c é Aõ ’ j à

52 7 TH GULF DENTAL ASSOCIATION CONFERENCEMUSCATSULTANATE OF OMAN DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010
Dr. Mohammad Al Jammaz Secretary General of the Gulf Dental Association
Picture from the audience during the opening ceremony
eÉ
H Gó H fô
è
Ö£d ¿Éæ°S’G ¢ù«FQ á«©ª÷G á«é«∏ÿG Ö£d ¿Éæ°S’G ¢ù«FQ áæé∏dG
é Gõ e ø ájÉYôdG á«Ñ£dG
á«©ª÷G
πeÉ°T äGóH ¬Jôμa øe áμ∏‡ øjôëÑdG ΩÉ©dG 1998 äGô“ƒŸGh »àdG É¡Jó≤Y á«©ª÷G ‘ ∫hO ¢ù∏› ¿hÉ©àdG ’ƒ°Uh ¤G OÉ≤©fG ô“ƒŸG ‹É◊G ‘ áæ£∏°ùdG ó©H ∂dP ΩÉb ôjRh áë°üdG ‹É©e óªMG.O øHG óªfi øH ó«ÑY …ó«©°ùdG ìÉààaÉH ¢Vô©ŸG »ª∏©dG ÖMÉ°üŸG .ô“ƒª∏d
á«é«∏ÿG Ö£d ¿Éæ°S’G òæe IGƒf É¡FÉ°ûfG ™ªéàc »é«∏N

ThenewPiezotome2andImplantCenter2combinedunitsfor bonesurgerydonotjustofferthebestofSatelec ® knowhow... Theyarethreetimesmorepowerfulthanthepreviousgeneration!The extrapowerofPiezotome2,togetherwithanexcellentsurgicalmotor, willguaranteeyoushorter,betterorganizedtreatmentsintotalsafety andcomfortforthepatientthankstotheprecisionandselectivecut procuredbyultrasonics.
17av.GustaveEiffel•BP30216•33708MERIGNACcedex•FRANCE•Tel+33(0)556340607•Fax+33(0)556349292•E-mail:info@piezotome.com•www.piezot ome.com MiddleEastOffice•POBox468•Amman11953•JORDAN•Tel+96265534401•Fax+96265537833•E-mail:info@jo.acteongroup.com
www.piezotome.com Satelec® surgicaltips. Perfectlyintune. 1 6881








54 7 TH GULF DENTAL ASSOCIATION CONFERENCEMUSCATSULTANATE OF OMAN DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010
Dr. Hamad Al Harthy with the Minister of Health H. E. Dr. Ahmed Al Saidi at the Inauguration of the Technical Exhibit
Dr. Mohamad Darwish from Qatar receiving his trophy
The board members of the Oman Dental Society Dr. Abdulaziz Bakathir and Dr. Jassim Al-Saidi
Dr. Barakat Al Jaabary from Jordan receiving his trophyDr. Mohammad Al Jammaz from Saudi Arabia during the trophy ceremony
MORE PICTURES AVAILABLE ON www.facebook.com/dentalnews1
Mr. Abdul Salam Al Madany from Dubai rewarded for his contributionDr. Aisha Sultan from Dubai receiving the trophy






56 7 TH GULF DENTAL ASSOCIATION CONFERENCEMUSCATSULTANATE OF OMAN DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010
Picture of the representatives of the Arab Dental Societies INAUGURATIONOFTHETECHNICALEXHIBITIONFLOOR MORE PICTURES AVAILABLE ON www.facebook.com/dentalnews1
Dr. Abdulaziz Bakathir during his poster presentation





PICTURESFROMTHEBOATEXCURSIONONTHE SEAOF OMAN MORE PICTURES AVAILABLE ON www.facebook.com/dentalnews1






AESTHETIC DENTISTRY MENA AWARDS

Lebanon,

his awardDr.
The 2nd Dental - Facial Cosmetic International Conference on November 5th-6th 2010 was another great success, accomplishing record attendance and further establishing itself as a leading international event in Aesthetic Dentistry in the Middle East. Hosted at Jumeirah Beach Hotel Dubai and organized by CAPP (Centre for Advanced Professional Practices) and Emirates Medical Association Dental Society, the conference was supported by the UAE Ministry of Health and Saudi Dental Association.
For the second time, Dubai gathered the world experts in Aesthetic Dentistry. Renowned speakers and specialists in the

different fields of dental and facial cosmetics shared their experience. More than 600 participants from 25 countries and dental professionals, industry players, business and government visitors got together for the event and. Participants soaked up the latest opinions, trends, and insights from the industry leaders, shared experience with colleagues, and honed their ideas and knowledge.
Dentists came from; UAE, Syria, Iraq, Iran, Kurdistan, Lebanon, KSA, India, Sudan, Jordan, Pakistan, Palestine, Egypt, Bahrain, Qatar, Kuwait, Oman, Germany, Italy, Austria, Denmark, Netherlands, Romania, Switzerland , Norway and UK.

62 DENTALFACIAL COSMETIC INTERNATIONAL CONFERENCE DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010
Dr. Hani Tohme from
receiving
Dina Dbaybo from Dubai, receiving her awardDr. Michael Ziegler from Dubai, receiving his award
Photographs by Elements Vision Filmingvision@elementsvision.com
The jury panel: Dr. Nadim Aboujaoude, Dr. Ali Emamgholipour, Dr. Mazen Tamimi, Pr. Yousef Talic, Dr. Roy Sabri, Dr. Ninette Banday, Dr. Aisha Sultan, Dr. Mohammed Abdullah, Dr. Adel Alhadlaq

E MDULUS ABRASIN CNSISTENCY


RÉટG âjRƒÑeƒμdG
äGôŸG ÚjÓe √QÉÑàNGh ¬ÑjôŒ ” …òdG âjRƒÑeƒμdG .¬∏c ⁄É©dG ‘ íLÉf
® - Grandio
äGPh áæ«àe äɪ«eôJ ≥«≤ëàd πcÉà∏d á≤FÉØdG áehÉ≤ŸÉHh êÉ©∏d ¬HÉ°ûe áfhôe πeÉ©H õ«ªàj
ΩɶæH á°UÉÿG ᫪∏©dG Iô°ûædG Ö∏£H Gƒ∏°†ØJ .Grandio®
âjRƒÑeƒc íª°ùj ≥°UÓdG ÒZ …ô£dG øjƒμàdG .πjƒW ôªY Grandio® íjôe πμ°ûH πª©dÉH .ôØ◊G ±Éæ°UG πc ‘ …OÉ°üàbGh









DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010 65 DENTALFACIAL COSMETIC INTERNATIONAL CONFERENCE
Dr Roy Sabri, Lecturing on Facial AnalysisDr. Nadim Abou Jaoude Lecturing about the Smile Management
Dr. Luca Dalloca Lecturing about the Fusion of Beauty and ArtDr. Ramesh Sabhlok receiving the Trophy from Dr. Mounir Selwadi
The audience at the invisible aligner seminar organized by 3D Ortholine Dr. Barakat Al Jaabari president of the Jordanian Dental Society offering a Shield to Dr. Aisha Sultan, president of the Emirate Dental Society
Picture of the Sponsors in front of the Jumeirah Beach Hotel











DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010 67 DENTALFACIAL COSMETIC INTERNATIONAL CONFERENCE
Exhibition Floor MORE PICTURES AVAILABLE ON www.facebook.com/dentalnews1
Picture of the delegates from the Arab countries
Join us in Beirut, Lebanon for the ITI
First Middle East Congress May 6-7, 2011


Setting the Trends in Implant Dentistry Over 30 Years.
The ITI Middle East Section has the pleasure of on May 6-7, 2011 at the Palais des Congrès, Dbayeh. This event promises to combine excellence and
towards diversifying treatment approaches and varying degrees of case complexity, accompanied by higher patient expectations, the ITI Middle East Section
It will be a great opportunity to see top international and local university professors as well as expert practitioners present, debate, and discuss current trends in implant dentistry.
Don’t pass up the chance to participate:
More than 600 visitors from all Middle East countries
Informed audience of medical dental practitioners
Ideal event to reach a dedicated audience of decision-makers
Focus on implant dentistry, its methodologies and tools
International Guest Speakers:


ITI International Team for Implantology | www.iti.org/congressMiddleEast
Prof. Daniel Buser ITI President Bern, Switzerland
Prof. Urs Belser Geneva, Switzerland
Dr. Stephen Chen
Dr. Will Martin


The Lebanese Society of Pediatric Dentistry
International Congress of Mediterranean and Arab Societies of Pediatric Dentistry
On October 28, 2010, the founding of the Mediterranean Association of Pediatric Dentistry was declared at the Bristol Hotel – Beirut, Lebanon
The Assembly incorporated the following Mediterranean countries: Lebanon, Syria, Egypt, Tunisia, Greece, Turkey, France and Italy.
The elected officials for the next 4 years are:
President: Dr. Mohamed Ezzeddine (Lebanon).
Secretary: Professor Giomelli Falcolini (Italy)
Treasurer: Dr. Bechara Al Asmar (Lebanon)

¢†«H’G §°SƒàŸG øe øª°V äÉ«dÉ©a á«©ª÷G á«fÉæÑ∏dG Ö£d ¿Éæ°SG ∫ÉØW’G h ” ¿ÓY’G øY ¢ù«°SÉJ á«©ªL ÖW ¿Éæ°SG ∫ÉØW’G ∫hód ôëÑdG ¢†«H’G §°SƒàŸG ‘ 2010/10/28 ‘ π«JhG ∫ƒà°ùjÈdG - ^ähÒH ¿ÉæÑd óbh
⪰V √òg á«©ª÷G ,¿ÉæÑd ,ÉjQƒ°S ,ô°üe ,¢ùfƒJ ,¿Éfƒ«dG ,É«côJ É°ùfôa É«dÉ£jGh
ºK ” ÜÉîàfG h IóŸ ™HQG :äGƒæ°S :É°ù«FQ QƒàcódG óªfi øjódGõY (¿ÉæÑd)
Éæ«eG :ô°ù∏d Qƒ°ùahÈdG »∏«eƒ«L »æ«dƒμdÉa (É«dÉ£jG)
ÚeG :¥hóæ°ü∏d QƒàcódG √QÉ°ûH ôª°S’G (¿ÉæÑd)

DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010 69 LEBANESE SOCIETY OF PEDIATRIC DENTISTRY
Dr. Mohamed Ezzeddine President of the Lebanese Society of Pediatric Dentistry
á«©ª÷G
Ö£d
∫ÉØW’G ó≤©fG ô“ƒe äÉ«©ªL ÖW ¿Éæ°SG ∫ÉØW’G ∫hó∏d á«Hô©dG ∫hOh ôëÑdG
Picture from the opening ceremony
á«fÉæÑ∏dG
¿Éæ°SG









70 LEBANESE SOCIETY OF PEDIATRIC DENTISTRY DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010
Dr. Alice Harfouche from Canada
Dr. Stephan Moss from the US during his lectureDr. Badiaa Jemmali from Tunisia receiving the trophy from Dr. Bechara Al Asmar
Dr. Elias Berdouses from Greece receiving the trophy from Dr. Bechara Al Asmar
Dr. Walid Al Saadi from Syria receiving the trophy from Dr. Mohamed Ezzeddine
Professor Giomelli Falcolini from Italy receiving the trophy from Dr. Bechara Al Asmar
MORE PICTURES AVAILABLE ON www.facebook.com/dentalnews1
Dr. Ahmad Abdellah from Egypt receiving the trophy from Dr. Mohamed Ezzeddine
® BETTER TASTE GUARANTEE!

Ifyou like Topex® Fluoride Foam, you’ll love these Sultan products…
Topex® APF Fluoride Gel
Thixotropic formulation remains in the tray, reducing fluoride ingestion. Fast, 60-second application. Available in five great Topex flavors.
DuraShield® 5% Fluoride Varnish
Unit dose application with an UltraBrush™ prevents separation of fluoride. Sets on contact with saliva, lasts up to eight hours.
Topex® Topical Anesthetic
Themost flavorfulway tofight cavities.
It’s a fluoride taste sensation! Topex® APF Fluoride Foam comes in five, delicious Topex® flavors* —strawberry, spearmint, grape, Bubble Fun®, and Orange Dream™
And with its 60-second application, Topex Fluoride Foam is a breeze to use. Its dense consistency provides excellent coverage, yet stays in the tray under bite pressure… so it won’t gag patients or clog your suction system.
Best of all, fluoride foam works… 1.23% acidulated phosphate fluoride with a 3.5pH enhances fluoride uptake in enamel. And at about 110 applications per can, Topex Fluoride Foam is a great value, too—costing only pennies per treatment.
To learn more visit www.sultanhealthcare.com.
*For patients with ceramic restorations, neutral mixed berry is also available.


Quick onset delivers maximum strength 20% benzocaine for fast, temporary relief of pain. Reduces salivation, keeping gel active longer. Seven great flavors!
Topex® Dual Arch Fluoride Trays
Its natural arch and more defined occlusal anatomy helps force fluoride onto all biting and interproximal tooth surfaces. Locking handles allow for easy placement and removal. Available in four sizes.
Topex®
Foam’s dense consistency provides better overall coverage. Competitor Foam Fluoride Foam
Fluoride
Topex

BOOK REVIEW BOOK REVIEW
Launching of the Arabic Translation of FDI Dental Ethics Manual

The Arabic translation of the FDI Dental Ethics manual was launched during the scientific events of the 22nd annual conference of the Jordanian Dental Association and the 39th conference of Arab Dental Association held in AmmanJordan from 19-22 October 2010
The manual was translated by Dr Ziad AL-Dwairi and Dr Hayder AL-Waeli from faculty of Dentistry-Jordan University of Science and Technology on behalf of the Jordanian Dental Association
Dr AL-Dwairi said that the manual is published in a practical pocket size format and it is hoped that it will become an invaluable aid to the work routine of dental practices and dental schools in the Arab World in order to give all involved in dental education and care the opportunity to benefit from the principles conveyed in this book.
Dr AL-Dwairi added: The manual provides a concise introduction to the basic concepts of ethics and their application to the most common issues encountered by dentists in their daily practice. In addition to its emphasis on the practical application of ethical principles, the Manual focuses on the relationship among ethics, professionalism and human rights.
It is worthy to mention that Dr AL-Dwairi was a member of the international advisory group formed for the publication of the manual in its English language. Email: ziadd@just.edu.jo


72 BOOK REVIEW DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010
MORE PICTURES AVAILABLE ON www.facebook.com/dentalnews1
All·in·One Matrix System



The easiest solution for creating a perfect contact point
•Integrated tensioning and opening device
•Easy creation of contact point
•No additional tools needed
MetaFix™
Your practice is our inspiration.™ KerrHawe SA P.O. Box 2686934 Bioggio Switzerland Freephone: 00800 41 05 05 05 Fax: ++41 91 610 05 14 www.KerrHawe.com
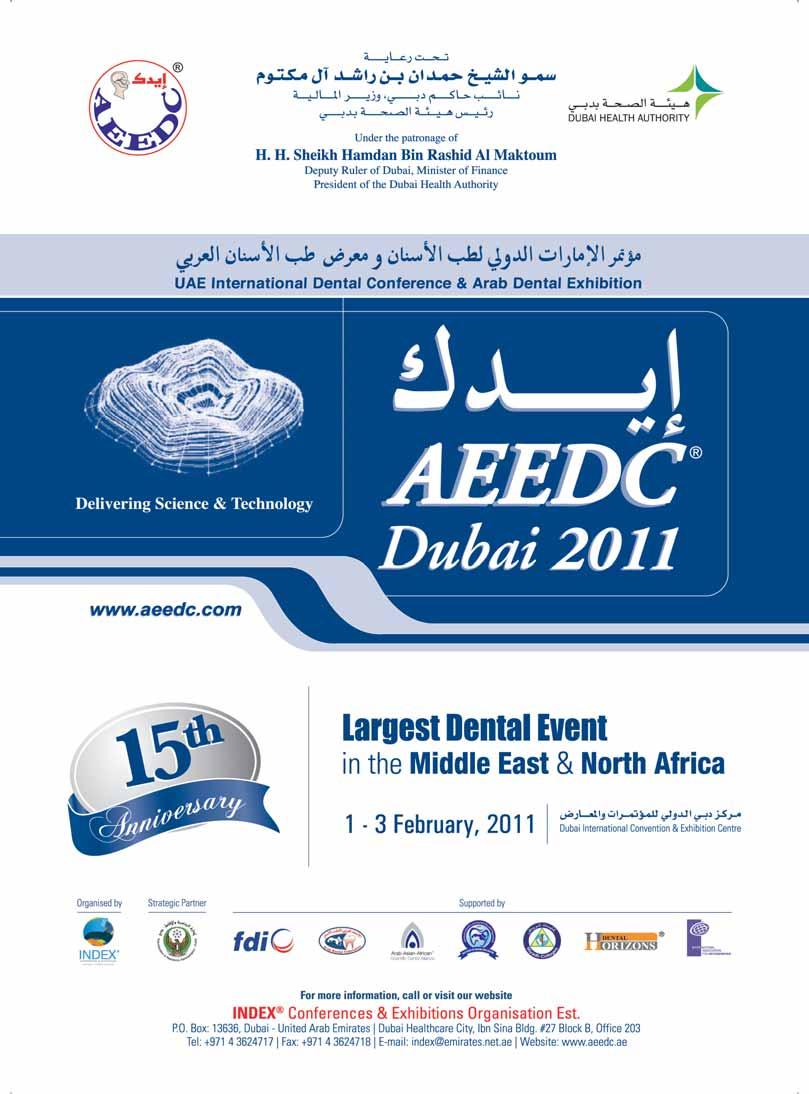
EXCOM Central Suction



u Reliable function, even with large amounts of water
u High, constant suction power
u For 1 up to 15 dental units
u Optional amalgam separation module



www.metasys.com METASYS Medizintechnik GmbH Florianistrasse 3 A-6063 Rum bei Innsbruck
EXCOM
EXCOM hybrid 2 EXCOM hybrid A2-ECO II from 1 up to 15 dental units
Z-ECO Light

WxtÜ vÉÄÄxtzâxá?
It is with great pleasure that we celebrate, through this first scientificevent, the launch of the Lebanese Society of Prosthodontics.
We have seized the opportunity of this day-long conference, chaired by our friend—and a friend of Lebanon—Dr. Antonio Patti, to meet all together for the first time.
Ever since Professor André Sacy first uttered mention of the idea to his entourage, ten years ago already—and having shared his plans with me, the idea has never ceased to imbue the minds of all the pioneers in the area of prosthetics, but also the minds of specialists from across the board, of practitioners, and of residents of the various postgraduate programs.
But the idea, great as it was, would have never materialized were it not for the enthusiasm of Prof. José Chidiac, who took it upon himself to collect the signatures of three representatives from each of the Lebanese dental schools. After receiving approval from the LDA, the executive committee was declared operational end 2008, and was constituted of the following colleagues, whether professors or doctors: Nohad Rizk, Khaldoun Rifai, José Chidiac, Elie Zbouni, Lévon Naltchian, later replaced by Joseph Makhzoumi, Georges Téhini, Nazem Assaad, Ahmad Mekkawi and myself.
Our first major decision was to organize a one-day event dedicated as much to science as to PR. And here we are. Nevertheless, we are already planning, for next May, a two-day seminar on Hybrid Implant Dentures and Implant Overdentures. We have been told that we are setting the bar too high, but this is true only if we choose to ignore the distinguished role that prosthodontics societies play in the developed world, due in part to the central position of prosthetics in modern dentistry, especially when implementing an interdisciplinary approach but also as a result of the increasing demand for aesthetic.
All dental disciplines converge towards our own and thereby make our knowledge and skills a crucial element in the coordination of treatment, from start to finish.
Mastering our specialty requires in-depth knowledge, but also a high level of manual dexterity and corresponding clinical experience. Herein lies the mission of the Society of Prosthodontics: we aim to sharpen the proficiency of our colleagues through various professional development programs.
The demand is high for our professional services and will

Dr. André Assaf President of the Lebanese Society of Prosthodontics
doubtlessly continue to grow. The science of prosthodontics is vast and, believe me, the topics we can present to the public are many!
To conclude, I invite you all to be involved in the Society not merely as Observers, but also as Actors. On our hand, we will do whatever it takes to engage you and keep you interested.
To our Society, I wish a great start, a great continuation, but more importantly great progress, under our administration and beyond.
And thank you to all of you here today, Members, Orthodontists and Generalists.
Dr. André ASSAF
76 LSPFIRST SCIENTIFIC DAY DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010
VITAVACUMAT ® NewGeneration
Productivitytothepoweroffour!
Operateuptofourfiringunitswithasingleoperatingpanel.

Whenitcomestoperformance–themorethebetter.Nowis yourchancetobenefitfrommaximumperformanceand efficiencywiththeVITAVACUMATNewGeneration.Operate uptofourpremiumfurnacesoftheVACUMAT6000Mseries and/orthecombinationpressingfurnacesoftheVACUMAT 6000MPserieswithasinglevPadcontrolpanelandsetnew
standardsforoptimizedworkflowinyourlaboratory.Thanksto itsmodularstructure,thefiringsystemcanbecustomized tomeetyourrequirements.Plus,youcanaddfurtherfiring units,operatingpanelsandaccessoriesatanytime.Youwill hardlyfindamoreefficientwaytomeetfuturerequirements.
www.myvacumat.com
NEW!Combinationfurnace VITAVACUMAT®6000MP
3389_3E







78 LSPFIRST SCIENTIFIC DAY DENTAL NEWS, VOLUME XVII, NUMBER IV, 2010
Dr. Ahmad MekkawiDr. Ghassan Yared president of the Lebanese Dental Association
Dr. Antonio PattiDr. Joseph Makhzoumi chairing the session with Dr. André Assaf
Picture from the audiencePicture from the presentation
Pictures from the exhibit floor













Introducing new Sensodyne Rapid Action –relief from the pain of dentine hypersensitivity



How does Sensodyne Rapid Action work?



The strontium acetate formulation forms a deep occlusive plug within the dentinal tubules






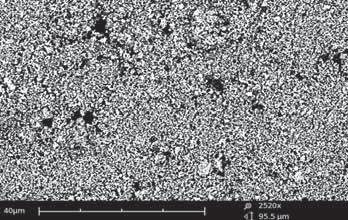


The robust occlusion formed by Sensodyne Rapid Action is still maintained after an acid challenge










Sensodyne Rapid Action
–
Clinically proven relief. Works in just 60 seconds*



Proven long-lasting relief with twice-daily brushing 4

instant and long-lasting relief from sensitivity




Creates deep, acid-resistant occlusion 1,2 Contains fluoride


*When used as directed on pack 1. Banfield N and Addy M. J Clin Periodontol 2004; 31: 325–335. 2. Parkinson C and Willson R. J Clin Dent 2010. Accepted for publication. . J Clin Dent 2010. Accepted for publication. . J Clin Dent 2010. Accepted for publication.










dentineAfter treatment and After treatment
a 10-minute acid challenge
Unoccluded
and
study of dentinal tubule patency following an acid challenge (immersion in grapefruit juice, pH 3.3) applied after dabbing and massaging for 60 seconds with Sensodyne Rapid Action. Adapted from Parkinson and Willson 2010.

www.ivoclarvivadent.com IvoclarVivadentAG Bendererstr.2 | FL-9494Schaan | Liechtenstein | Tel.:+423/2353535 | Fax:+423/2353360 Significantlyimproved adhesiontoenamel Nowfeaturinga fill-levelindicator Economical–around 120applicationsperVivaPen AdheSE
Click&Bond® withtheVivaPen® Fluoride-releasing,selfetchingall-in-oneadhesive
® OneF
