SINGLE SHORT IMPLANT IN MAXILLARY SECOND MOLAR
NYU COLLEGE OF DENTISTRY
LEBANESE ORTHODONTIC SOCIETY
2024 SIDC 2024
AEEDC








Don’t just go with the flow. Pick the right flow!

FLOWABLE YET STABLE RESTORATIVE MATERIAL
You have the choice:
• Light Flow – low viscosity
Precise application thanks to the very fine cannula and therefore optimally suitable for hard-to-reach areas and small cavities
• Flow – medium viscosity
Outstanding flow behaviour, universal and precise application
• Heavy Flow – high viscosity Increased stability, i. e. universal application and no undesirable runoff
*Filler content by weight
76 %* 81 %*
83 %*
Flowables

Also available as Caps
VOCO GmbH · Anton-Flettner-Straße 1-3 · 27472 Cuxhaven · Germany · Freecall 00 800 44 444 555 · www.voco.dental

SWISS PROFESSIONAL OR AL C ARE Follow us on Social Media
www.wild-pharma.com #wildredesign






















18 ml 25 ml 18 ml 25 ml 75 ml 400 ml 400 ml 75 ml 400 ml 250 ml Redesign Tebodont Packaging 75 ml 75 ml 75 ml 75 ml 75 ml 75 ml 75 ml 75 ml 85 ml 85 ml 85 ml 85 ml
packaging
Oral
Redesign Emoform Packaging
Experience the new
design of Dr. Wild
Care












Based on the close and fruitful cooperation with dental institutes and practicing dentists since the 1940s, we have a uniquely broad portfolio of specially developed, innovative toothpastes, gels, sprays, mouthwashes and mouth baths. These products, which are marketed under the brands Tebodont®, Emofluor®, Emoform®, Depurdent® and Emofresh® are sold exclusively in pharmacies in Switzerland and in more than 40 other countries outside Switzerland, their various innovative formulations and compositions offer excellent solutions for daily dental care, addressing specific needs and problems (e.g. caries prevention, sensitive teeth, gum problems) and general oral health.
With the REDESIGN we have clarified the positioning of the oral care products: every toothpaste and every mouthwash now has a clear application area. At the same time, our new packaging is "digitalized": each product has a QR code that allows detailed information to be downloaded directly to the mobile phone. The redesign of the products should make the Wild brand tangible and perceptible.
• WILD will be used as umbrella brand on all products, which results in an easier promotion among the whole product range
• Same design for all brands leads to recognition and synergy effects across product range
• Clear unique main indication on the packaging avoids confusion among dental profession, pharmacists and end consumers due to overlapping benefits
• New design underscores clinical benefits and professionalism of the products which leads to cross-brand and cross-portfolio products awareness and helps to create trust among the dental profession, pharmacists and end consumers
• Unifying of the packaging system - all toothpastes in the same size and shape of tubes, all mouthwashes in the same size and packaging - leads to a uniform, eye-catching and space-saving shelf-impact
• Product portfolio becomes fresh, easy to recommend and attractive for the POS
75 ml 400 ml 50 ml 500 ml 75 ml 75 ml 75 ml 75 ml 400 ml 75 ml 75 ml 500 / 250 ml Redesign Emofluor Packaging Redesign Depurdent Packaging
SWISS PROFESSIONAL OR AL C ARE Follow us on Social Media
EDITORIAL TEAM
Alfred Naaman, Nada Naaman, Khalil Aleisa, Jihad Fakhoury, Dona Raad, Antoine Saadé, Lina Chamseddine, Tarek Kotob, Mohammed Rifai, Bilal Koleilat, Mohammad H. Al-Jammaz
INTERNATIONAL CALENDAR

COORDINATOR
ART DEPARTMENT
SUBSCRIPTION
ADVERTISING
Suha Nader
Marc Salloum
Micheline Assaf, Nariman Nehmeh
Josiane Younes
Albert Saykali
Gisèle Wakim
Tony Dib
1026-261X

Lebanese Dental Association-Tripoli 2024
IDEX 2024

EDSIC 2024

BIDM 2024

ATREO 2024

37th CAPP International Dental ConfEx
April 25 – 27, 2024
BAU campus | Tripoli, LEBANON
www.ldatripoli.org
May 8 – 11, 2024
EXPO Center | Istanbul, TURKEY www.idex.org.tr
September 4 – 6, 2024
Intercontinental Citystars, Cairo, EGYPT www.edsic.org
October 3 – 5, 2024
Seaside Arena | Beirut, LEBANON www.lda.org.lb
Association Tunisienne de Recherches et d'Etudes en Orthodontie
October 4 – 5, 2024
Hotel Hilton Skanes | Monastir, TUNISIA association.atreo@gmail.com
November 15 – 16, 2024
Madinat Jumeirah | Dubai, UAE www.cappmea.com

SIDC 2025
AEEDC 2025
January 16 - 18, 2025
Riyadh International Convention & Exhibition Center | Riyadh, KSA www.sidc.org.sa
February 4 – 6, 2025
World Trade Center, Dubai, U.A.E. www.aeedc.com
6 Dental News Quarter II - 2024 This magazine is printed on FSC – certified paper. WWW.DENTALNEWS.COM DENTAL NEWS – Sami Solh Ave., G. Younis Bldg. POB: 116-5515 Beirut, Lebanon. Tel: 961-3-30 30 48 Fax: 961-1-38 46 57 Email: info@dentalnews.com Website: www.dentalnews.com www.instagram.com/dentalnews Statements and opinions expressed in the articles and communications herein are those of the author(s) and not necessarily those of the Editor(s) or publisher. No part of this magazine may be reproduced in any form, either electronic or mechanical, without the express written permission of the publisher. DENTAL NEWS IS A QUARTERLY MAGAZINE DISTRIBUTED MAINLY IN THE MIDDLE EAST & NORTH AFRICA IN COLLABORATION WITH THE COUNCIL OF DENTAL SOCIETIES FOR THE GCC.
Volume XXXI, Number I, 2024 This magazine is printed on FSC – certified paper. www.facebook.com/dentalnews1 twitter.com/dentalnews
PHOTOGRAPHY TRANSLATION DIRECTOR ISSN





January

January

February

7 Dental News Quarter II - 2024
A. CONGRESSES ARTICLES Single Short Implant in Maxillary Second Molar in Areas of Low Density Experiences with VistaCam iX HD Smart NYU College of Dentistry No Spittoon Interview 8 20 32 56 Acteon 11 A-dec 23 Belmont 9 DMP 1 DURR 15 FKG 21 HU-FRIEDY 42-43 Hyperloupe 25 MESA 40-41 Mani 17 NSK C2 Promedica 37 Rekita 35 Rolence 31 Scheu 29 Shining 3D 27 SDI Pola 19 Septodont 84 Trident C4 Ultradent 19 VOCO C3 VOCO 2 Wild Pharma 3-4-5 58 Emerging Horizons in Pediatric Dentistry
12, 2024 - BAU - LEBANON Lebanese Orthodontic Society
Oleg O. Yanushevich, Igor V. Maev, Natella I. Krikheli, Dmitrii N. Andreev , Svetlana V. Lyamina ,Filipp S. Sokolov, Marina N. Bychkova, Petr
January
26-27, 2024AEEDC
6-8, 2024 - DUBAI, UAE SIDC 2024 The Saudi International Dental Conference
18-20, 2024 RIYAH - KSA 62 66 74 ADVERTISING INDEX Mövenpick Hotel, BEIRUT

SINGLE SHORT IMPLANT
IN MAXILLARY SECOND MOLAR IN AREAS OF LOW DENSITY. RETROSPECTIVE STUDY.
Eduardo Anitua DDS, MD, PhD1,2,3
1. Private practice in oral implantology, Eduardo Anitua Institute, Vitoria, Spain.
2. Clinical researcher, Eduardo Anitua Foundation, Vitoria, Spain.
3. University Institute for Regenerative Medicine and Oral ImplantologyUIRMI (UPV/EHUFundación Eduardo Anitua), Vitoria, Spain.
Corresponding author : Dr. Eduardo Anitua, Eduardo Anitua Foundation; C/ Jose Maria Cagigal 19, 01007 Vitoria, Spain; Phone: +34 945160653, e-mail: eduardo@ acioneduardoanitua.org.
Summary
Introduction
The replacement of maxillary second molars with implants is always a complex task due to the fact that there is usually less residual bone height at this level and also the density of the posterior maxillary area close to the tuberosity is usually low. When these molars are also replaced in a single unit, the situation is even more complex. In this article we present a series of clinical cases of maxillary second molars replaced with unitary implants.
Material and methods
A retrospective study was carried out selecting patients with short, extra-short implants located in maxillary posterior sectors, with a bone density between 200 and 300 Hu objectified in the planning tac using the software (BTI-Scan III), in a private clinic in Vitoria, Spain, during the period from January 2017 to December 2018. Statistical data collection and analysis was performed by two different researchers. A Shapiro-Wilk test was performed on the data obtained to verify the normal distribution of the sample. The main variable evaluated was implant survival followed by crestal bone loss. Qualitative variables were described by frequency analysis. Quantitative variables were described by mean and standard deviation. Implant survival was calculated using the Kaplan method.
Results
Thirty patients were recruited and 40 single implants with lengths of 5.5 and 6.5 mm were inserted in upper second molar positions that fulfilled the inclusion criteria. The length of the implants was mostly 6.5 mm (60% of cases) followed by 7.5 mm (30%) and finally 10% were 5.5 mm long implants. The mean densitometry of the implant insertion sites was 240 Hu (+/- 54; range 200-300 Hu). The mean insertion torque achieved for the implants studied was 40 Ncm (+/14.7; range 20-65 Ncm). The mean bone loss of the implants studied measured mesial to the implants was 0.5 mm (+/- 0.6) and measured distally was 0.3 mm (+/- 0.5).The mean follow-up of the implants studied was 60 months (+/- 34). None of the implants failed during the follow-up period.
Conclusions.
In the position of upper second molars, even with bone atrophy and low density we can use single implants. It is important that the rehabilitation follows an adequate surgical and prosthetic sequence that guarantees the success of the treatment, so all the steps from the beginning to the completion and placement of the crown are important.
8 Dental News Quarter II



EURUS
Embodies our belief of bringing highly reliable Japan-quality products to dentists in the world.

Instagram Facebook Follow Us Touch Panel
Legrest Chair (option) Wireless Foot Controller (option)
Folding
New Flushing tray (option)
TAKARA BELMONT CORPORATION Osaka, Japan https://dental.takarabelmont.co.jp/
EURUS S3 / S 4 B uil t - i n X- r a y D e b u t !
Introduction.
The loss of residual bone height in maxillary posterior edentulism is a very common occurrence. Teeth in direct contact with the maxillary sinus, or antral teeth, when they have to be extracted, leave an alveolus which, when healing, undergoes partial healing that generates less available bone height. This, together with the excessive pneumatization that is generated from the sinus located just above the area, especially when edentulism is of long evolution, makes the placement of implants at this level sometimes difficult, or it is necessary to resort previously or concomitantly to the insertion of the implant. In order to avoid more complex regenerative processes such as sinus lift, short implants have been developed. Today, these implants are one of the rehabilitation techniques for the atrophic maxilla that can be considered «routine», being a minimally invasive option and with survival rates of around 99%1,2. Many of the short and extra-short implants are rehabilitated as part of bridges or complete rehabilitations, with a smaller percentage being used for single crowns. The position in which these implants are inserted is also a fact to be taken into account, as the posterior maxillary areas have a lower bone density and therefore a worse situation to stabilise a short or extra-short implant and allow its correct posterior integration without micro-movement. Many of the short and extra-short implants are rehabilitated as part of bridges or complete rehabilitations, with a smaller percentage being used for single crowns. The position in which these implants are inserted is also a fact to be taken into account, as the posterior maxillary areas have less bone density and therefore a worse situation for stabilising a short or extra-short implant and allowing its correct posterior integration without micromovements, especially when we replace a second upper molar, a fact which sometimes means that this molar is not even restored in some patients.7 Furthermore, this area in particular (posterior maxilla) usually has a lower bone density, so that rehabilitation with dental implants in these sectors is complicated when the residual bone volume in height is very low and the bone density is also very low. In these cases, controlling all factors to achieve implant insertion with predictability is key. The protocol described by our study group highlights the importance of prior diagnosis of
the residual bone (height, width, density and bone type) and the planning of the drilling to achieve three-dimensional stability of the implant and avoid micromovement in the initial phase of osseointegration9-10. In this sense, the use of implants of different diameters and lengths can provide us with a larger contact surface for osseointegration and different anchorage points that guarantee greater primary stability7,11-13 The factors that influence the achievement of primary stability in general and in these cases in particular are: geometry, length and macrodesign of the implant, drilling pattern and bone density, mainly16-18. In the present work, we show a series of cases of short (7.5 mm) and extra-short (5.5 and 6.5 mm) single-tooth implants placed in the maxillary second molar position (17 and 27), rehabilitated in a single-tooth fashion with low bone density.
Material and methods.
A retrospective study was carried out selecting patients with short, extra-short implants located in maxillary posterior sectors, with a bone density between 200 and 300 Hu, as measured in the planning tac using the software (BTI-Scan III), in a private clinic in Vitoria, Spain, during the period from January 2017 to December 2018.
Surgical and rehabilitation protocol.
In all cases, an accurate diagnosis of residual bone volume (height, width and bone density) was performed, measured using the specific software BTI-Scan III (Biotechnology Institute, Vitoria, Alava, Spain). Prior to implant insertion, antibiotic premedication consisted of amoxicillin 2g orally one hour before surgery and paracetamol 1g orally (as an analgesic). Subsequently, patients were treated with amoxicillin 500-750 mg orally every 8 hours (according to weight) for 5 days and the necessary analgesia based on paracetamol on demand with a maximum of 3 grams daily. All implants were inserted by the same surgeon using the biological drilling technique, at low revolutions14 , described by our study group, where the neoalveolus is widened using incremental drills in diameter. Subsequently, patients underwent control panoramic radiographs every 6 months and the necessary measurements were taken on these radiographs to check bone stability. Easily reproducible periapical radiographs with
10 Dental News Quarter II Single Short Implant in Maxillary Second Molar in Areas of Low Density.


Caring People. Improving Lives










The key philosophies of ACTEON
Being a human centric organization focused on the needs of patients and care providers.
Providing tailored workflow solutions that maximize the total effectiveness, efficiency, and economics of achieving desired clinical outcomes.
Providing innovative and integrated healthcare solutions that address the continuous healthcare needs over patients’ lifetimes.






17, avenue Gustave Eiffel Zone Industrielle du Phare 33700 MERIGNAC FRANCE Tel. +33 (0) 556 340 607 Fax. +33 (0) 556 349 292 info@acteongroup.com
a positioner were used to establish bone loss. At each of the visits, periapical radiographs are taken with a parallelisation device to estimate the crestal bone loss. Marginal bone loss was measured on the last periapical radiograph taken with a follow-up positioner. Once the X-ray was obtained in digital format, it was calibrated using specific software (Digora for Windows, SOREDEX Digital Imaging systems) through a known length in the X-ray, such as the dental implant. Once the calibration measurement has been entered, the software performs a calculation based on this measurement to eliminate the magnification, allowing linear measurements to be made free of this error. The crestal bone loss was measured at two points: mesial and distal to each implant.
Statistical analysis
Statistical data collection and analysis was carried out by two different researchers. A Shapiro-Wilk test was performed on the data obtained to verify the normal distribution of the sample. The main variable evaluated was implant survival followed by crestal bone loss. Qualitative variables were described by frequency analysis. Quantitative variables were described by mean and standard deviation. Implant survival was calculated using the Kaplan-Meier method. Data were analysed with SPSS v15.0 for windows (SPSS Inc., Chicago, IL, USA).
Results
Thirty patients were recruited and 40 single implants with lengths of 5.5 and 6.5 mm were inserted in upper second molar positions that fulfilled the inclusion criteria. Thirty percent of the patients included in the study were male and 70% female, with a mean age of 62 (+/- 3.5) years. Implant position was 50% for tooth 17 and 50% for tooth 27. The diameter of the inserted implants was mostly 5 mm (56.42% of cases), followed by 5.5 mm (23.58%) and 4.5 mm in 20% of cases. The length of the implants was mostly 6.5 mm (60% of cases) followed by 7.5 mm (30%) and finally 10% were 5.5 mm long implants. The mean densitometry of the implant insertion sites was 240 Hu (+/- 54; range 200-300 Hu). The mean insertion torque achieved for the implants studied was 40 Ncm (+/- 14.7; range 20-65 Ncm). The mean bone loss of the studied implants measured mesial to the implants was 0.5 mm (+/- 0.6) and
measured distally was 0.3 mm (+/- 0.5). The mean follow-up of the studied implants was 60 months (+/- 34).
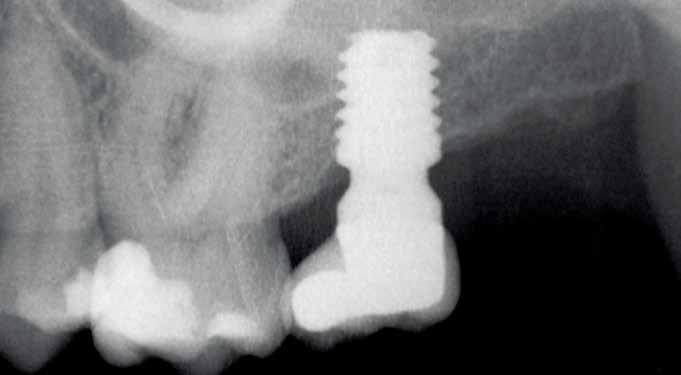
None of the implants failed during the follow-up period, resulting in 100% survival and no adverse surgical or prosthetic events were recorded. Images 1-7 show one of the cases included in the study.
Discussion
Rehabilitation with dental implants is one of the most widely used techniques in dentistry. These implants, with the modifications they have undergone in recent years, adapt to most bone atrophies, whether vertical, horizontal or mixed. Short and extra-short implants are safe and predictable alternatives for vertical atrophy, as in the cases of second molars discussed in this article, presenting fewer biological complications, lower economic cost and fewer surgical sessions for patients than the accessory techniques of bone augmentation or regeneration that would be used in the case of wanting to initially recover the lost bone volume.15-17. Long-term survival rates of these implants are reported to be 98.9%, so they have a similar survival to longer implants placed without bone augmentation or to those inserted in augmented bone by different procedures18-19
One of the main drawbacks reported in the literature is the lower predictability of these short implants when inserted in the posterior maxilla is the achievement of correct primary stability. This primary stability ensures that the newly inserted implant does not undergo micromovements during the integration phase and that the treatment is successful. To achieve this, the three-dimensional images of the cone-beam in its sectional slices allow us to choose the point of greatest density where to strategically place our anchorage zone and to individualise the drilling sequence 8-10 .
If we achieve the desired stability, even if the torque is low, we can achieve treatment success if the implant is inserted conservatively without damaging the bone bed. Systematic reviews and prospective studies on the insertion torque of dental implants at different torques do not find statistically significant differences between high and low insertion torques in implant survival or crestal bone loss20-23. Another point to bear in mind in this type of restoration is the use of a prosthesis that transmits the load effectively and generates a seal that avoids implant-prosthesis microleakage, such as the single transepithelial
12 Dental News Quarter II Single Short Implant in Maxillary Second Molar in Areas of Low Density.
Restorations with JUST ONE SHADE
Transcend universal composite provides unprecedented shade matching with just one Universal Body shade due to its patented Resin Particle Match™ technology that eliminates the need for a blocker.
If you prefer a layering technique Transcend composite also includes four dentin shades and two enamel shades.
Before After


Deep amalgam staining presents one of the most difficult restoration situations to clinicians. In this case only the Transcend composite Universal Body shade was used to replace the amalgam no blocker needed. Note the excellent color blending of the preserved oblique ridge.


Scan the QR code to learn more about Transcend Universal Composite or go to ultradent.eu/transcend
800.552.5512 | ULTRADENT.COM
prostheses used in the cases studied. In addition, the way this transepithelial works in the prosthesis laboratory through the interfaces allows us to make a screwed or cemented crown, avoiding the machined connection portion having to undergo excessive heating processes by entering the ceramic furnace several times. All the work can be fabricated on the burn-out portion of the interface and then cemented to it once all the finishing and adjustments have been made.
Conclusions
In the position of upper second molars, even with bone atrophy and low density, we can use single implants. It is important that the rehabilitation follows an adequate surgical and prosthetic sequence that guarantees the success of the treatment, so all the steps from the beginning to the completion and placement of the crown are important.



Figure 1. Initial X-ray of the case, where we can see in the second quadrant an edentulous section corresponding to tooth 27 that will be rehabilitated using dental implants.
Figure 2. Planning of the implant to be placed.
Figure 3. Post-surgical panoramic X-ray with the recently placed implant.
Figure 4. Placement of the unitary transepithelial after the second phase at 5 months for progressive loading of the implant.
14 Dental News Quarter II Single Short Implant in Maxillary Second Molar in Areas of Low Density.
Figure 2
Figure 3
Figure 4
Figure 1
Flexibility during treatment Nozzles compatible withMyLunos® Reliable service
The new MyLunos Duo® table-top device
▪ Supra- and subgingival prophylactic treatment with ultrasound and powder jet
▪ Constant air flow to protect against blockage
▪ Two chambers for quick powder changes
▪ Nozzles compatible with the MyLunos® powder jet handpiece
Find out more at www.lunos-dental.com


Video MyLunos Duo®
Any questions? Please contact: Dürr Dental Middle East, Phone: +968 7194 6652, Mail: middle.east@duerrdental.com
NEW!
ALL-ROUNDER


References
1. Anitua E, Orive G. Short implants in maxillae and mandibles: a retrospective study with 1 to 8 years of follow-up. J Periodontol 2010;81:819-826.
2. Atieh MA, Zadeh H, Stanford CM, Cooper LF. Survival of short dental implants for treatment of posterior partial edentulism: a systematic review. Int J Oral Maxillofac Implants 2012; 27: 1323-1331.
3. Tutak M, Smektala T, Schneider K, Golebiewska E, Sporniak-Tutak K. Short dental implants in reduced alveolar bone height: a review of the literature. Med Sci Monit. 2013;19:1037–1042.
4. Queiroz TP, Aguiar SC, Margonar R, de Souza Faloni AP, Gruber R, Luvizuto ER. Clinical study on survival rate of short implants placed in the posterior mandibular region: resonance frequency analysis. Clin Oral Implants Res. 2015;26:1036–1042
16 Dental News Quarter II Single Short Implant in Maxillary Second Molar in Areas of Low Density.
.
Figures 5-6 Clinical images of the patient at the time of crown placement.
Figure 7. Radiographic image at 4 years of follow-up showing the bone stability of the implant and the rehabilitation.



MADE IN JAPAN CONTACT US FOR MORE INFORMATION: WWW.MANI.CO.JP/EN/PRODUCT/JIZAI/ DENTAL.EXP@MS.MANI.CO.JP
5. Feldman S, Boitel N, Weng D, Kohles SS, Stach RM. Five-year survival distributions of shortlength (10 mm or less) machined-surfaced and osseotite implants. Clin Implant Dent Relat Res. 2004;6:16–23.
6. Gastaldi G, Felice P, Pistilli R, Barausse C, Trullenque-Eriksson A, Esposito M. Short implants as an alternative to crestal sinus lift: a 3-year multicentre randomised controlled trial. Eur J Oral Implantol. 2017;10(4):391-400.
7. Anitua E, Alkhraisat MH. Single-unit short dental implants. Would they survive a long period of service? Br J Oral Maxillofac Surg. 2019 May;57(4):387-388.
8. Anitua E, Flores C, Fernández-de-Retana S, Anitua B, Alkhraisat MH. Performance of Immediately Loaded Short Implants Using Low-Speed Drilling Protocol and Plasma Rich in Growth Factors: A Controlled Retrospective Observational Study. Int J Periodontics Restorative Dent. 2023;43:232-239b.
9. Anitua E, Carda C, Andia I. A novel drilling procedure and subsequent bone autograft preparation: a technical note. Int J Oral Maxillofac Implants. 2007;22:138-45. Erratum in: Int J Oral Maxillofac Implants. 2007 Mar-Apr;22:309.
10. Anitua E, Alkhraisat MH, Piñas L, Orive G. Efficacy of biologically guided implant site preparation to obtain adequate primary implant stability. Ann Anat. 2015;199:9-15.
11. Esposito M, Grusovin MG, Coulthard P, Worthington HV. The efficacy of various bone augmentation procedures for dental implants: a Cochrane systematic review of randomized controlled clinical trials. Int J Oral Maxillofac Implants. 2006;21:696-710.
12. Bernardello F, Righi D, Cosci F, Bozzoli P, Soardi CM, Spinato S. Crestal sinus lift with sequential drills and simultaneous implant placement in sites with <5 mm of native bone: a multicenter retrospective study. Implant Dent. 2011;20:43944.
13. Tsai CF, Pan WL, Pan YP, Chan CP, Ju YR, Wang YM, Lin CY, Chang CC. Comparison of 4 sinus augmentation techniques for implant placement with residual alveolar bone height ≤3 mm. Medicine (Baltimore). 2020;13;99:e23180.
14. Anitua E, Carda C, Andia I. A novel drilling procedure and subsequent bone autograft preparation: a technical note. Int J Oral Maxillofac Implants. 2007 Jan-Feb;22(1):138-45. Erratum
in: Int J Oral Maxillofac Implants. 2007 MarApr;22(2):309.
15. Kim YH, Choi NR, Kim YD. The factors that influence postoperative stability of the dental implants in posterior edentulous maxilla. Maxillofac Plast Reconstr Surg. 2017;39(1):2. Published 2017 Jan 5.
16. Anitua E, Alkhraisat MH. 15-year follow-up of short dental implants placed in the partially edentulous patient: Mandible Vs maxilla. Ann Anat. 2019;222:88-93.
17. Thoma DS, Haas R, Sporniak-Tutak K, Garcia A, Taylor TD, Hämmerle CHF. Randomized controlled multicentre study comparing short dental implants (6 mm) versus longer dental implants (11-15 mm) in combination with sinus floor elevation procedures: 5-Year data. J Clin Periodontol. 2018;45(12):1465-1474.
18. Altaib FH, Alqutaibi AY, Al-Fahd A, Eid S. Short dental implant as alternative to long implant with bone augmentation of the atrophic posterior ridge: a systematic review and meta-analysis of RCTs. Quintessence Int. 2019;50(8):636-650.
19. Cruz RS, Lemos CAA, Batista VES, Oliveira HFFE, Gomes JML, Pellizzer EP, Verri FR. Short implants versus longer implants with maxillary sinus lift. A systematic review and meta-analysis. Braz Oral Res. 2018;32:e86.
20. Verrastro Neto A, Andrade R, Corrêa MG, Casarin RCV, Casati MZ, Pimentel SP, Ribeiro FV, Cirano FR. The impact of different torques for the insertion of immediately loaded implants on the peri-implant levels of angiogenesis- and bone-related markers. Int J Oral Maxillofac Surg. 2018;47:651-657.
21. Norton MR. The Influence of Low Insertion Torque on Primary Stability, Implant Survival, and Maintenance of Marginal Bone Levels: A ClosedCohort Prospective Study. Int J Oral Maxillofac Implants. 2017;32:849-857.
22. Berardini M, Trisi P, Sinjari B, Rutjes AW, Caputi S. The Effects of High Insertion Torque Versus Low Insertion Torque on Marginal Bone Resorption and Implant Failure Rates: A Systematic Review With Meta-Analyses. Implant Dent. 2016;25:532-40.
23. Wang TM, Lee MS, Wang JS, Lin LD. The effect of implant design and bone quality on insertion torque, resonance frequency analysis, and insertion energy during implant placement in low or low- to medium-density bone. Int J Prosthodont. 2015;28:40-7.
18 Dental News Quarter II
Single Short Implant in Maxillary Second Molar in Areas of Low Density.

Experiences with VistaCam iX HD Smart, Dürr Dental
Dr. Frank Döpper, Remshalden, Germany
Contact:
Michael.koll@ duerrdental.com
“Patients believe what they can see with their own eyes”
Exploiting the potential of digital imaging in day-to-day working practice
It is safe to say that anyone who is not yet working with visualization tools as part of their patient communication processes is probably not keeping up with the times. This is more than apparent now that intraoral cameras have been used on a daily basis for nearly 15 years. But this modern camera technology has not only proved itself invaluable in terms of how it makes consultations with patients much easier – users also benefit from the options for seamless documentation, e.g. for forensic backup or as an instrument for quality control and monitoring the quality of their own work.
Explaining a marginal gap to a patient, along with the indicated treatment measures, can in some cases be hard work for both sides, but thanks to modern technology this can be reduced or eliminated altogether. As someone who has been using intraoral camera technology ever since it was first launched, over the years it has become clear to me that patients believe what they can see with their own eyes. Even the gentlest and most careful of explanations are often followed up by challenging, critical questions –
or, in some cases, even a complete lack of understanding. But if patients can be shown the pressure point or aphthous ulcer in real time in their mouth, particularly if the facility for zooming in is used, then there is almost no need for further explanations.
Using images to visualize technical explanations
Most patients are quite surprised when they get to see inside their own mouth for the first time. And it is not only the tech-savvy ones among them that find the state-ofthe-art digital equipment exciting. Even small children get really excited – and often rather impatient – about seeing images from inside their mouth.
Experience has shown that, whatever the situation, a visualization of what is going on in the patient’s mouth always helps a great deal in discussions with the patient to make the more detailed technical explanations of a diagnosis much easier to understand. This has also been confirmed by scientific research, which has shown that people only take in 11 percent of audio information, with only two percent actually being stored. The averages are much better if the information is provided visually: here, 80 percent of the information
20 Dental News Quarter II





S W ISS Q UALI T Y F KG
THE SAFEST * SIMPLY. RECIPROCATION Smooth to use, minimally invasive. Why choose anything else? *Based on internal laboratory results compared with equivalent competitors' instruments www.fkg.ch/r-motion
Experiences with VistaCam iX HD Smart
is picked up via the eyes, with around 40 percent also being stored1
If patients feel that they have a clear overview of the situation, they will generally also be much more open to a conversation e.g. about treatment proposals. The use of a camera also strengthens the credibility of the treating dentist and encourages patient compliance. A recent study documented the positive impact of the camera technology on the outcome of a periodontitis treatment, with patients displaying significant improvements in terms of clinical, psychological, and behavior-based factors and in terms of their periodontal health even months after the treatment. 2
Visualization does more than just boost patient communication
At the dental practice in Remshalden, the digital intraoral camera VistaCam iX HD Smart from Dürr Dental is now well established not only as a fixed part of patient communication, but also as an integral element in the day-to-day practice routine. Right from the first appointment with the patient, image data helps with diagnostics and documentation. If different forms of treatment, such as the treatment of dental caries in a tooth or a root canal treatment, are backed up with images, this makes it possible not only to deal with billing questions from private health insurance providers (Did you really fill four root canals?) or queries from the patient, but also to demonstrate various steps in the treatment.
In addition, the image documentation can also be used for quality control of your own work, e.g. in prosthetics. On average, around four to five images are taken for these purposes during each patient treatment. Since the handling of the Vista Cam iX HD Smart used here is incredibly straightforward, anyone can use it competently after brief training. Depending on the situation and the requirements, image acquisition can also be performed by the dental assistant. The direct connection to the computer and therefore also to the practice software makes it much easier to work with the patient images and then archive them.
Tried and tested: use of cameras right from the first appointment
In this author’s practice, VistaCam iX HD Smart is now used as a matter of course during the first appointment with a new patient and has now become indispensable. In the process, after recording the clinical status and medical history, intraoral images are routinely taken of every tooth. With the aid of the interchangeable heads, the camera serves as a type of “early warning system” with which the dentist can gain a very detailed image of even small, incipient enamel lesions – and, of course, the results can be presented to the patient straight away.
Immediately afterward, the condition of the teeth and any existing prosthetic treatments can be discussed using the images, along with oral hygiene etc. With the aid of macro images, it is possible not only to highlight details, but also to place markers in the image via the imaging software VistaSoft. In this way, one or two areas can be marked for subsequent monitoring. What this means is that the camera has established itself as more than just a tool for taking snapshots of the current state of a patient’s oral health –it is now also a valuable instrument for tracking progress and monitoring developments.
Images can be displayed side by side in the imaging software VistaSoft for direct comparisons between them, allowing the success of a treatment to be clearly demonstrated, whether during the course of a periodontitis treatment or with before/after images for a session with a dental hygienist. This approach is also perfect for monitoring initial caries lesions – has the site become remineralized over time, or is the caries infection progressing? When doing this, it is possible to accurately measure the extent of the lesion. In addition to the visual image, this also provides comparison data for the next checkup.
Interchangeable attachments for maximum flexibility
When intraoral camera technology was in its infancy, separate cameras were required for each indication, e.g. for intraoral images or fluorescence images, but nowadays the VistaCam iX HD Smart
22 Dental News Quarter II
- Dr Megan Nevills, Murrayhill Dental


EXPERIENCE REDUCED RESISTANCE & FATIGUE

With no handpiece pull-back and longer instrument tubing, even electric handpieces feel light. Longer instrument tubing makes it easy to retrieve and return handpieces and other instruments, which means you can focus on what matters most: your patients.
The A-dec 500 Continental delivery moves effortlessly and feels weightless in my hand.
© 2023 A-dec Inc. All rights reserved. For complete trademark information, visit a-dec.com/legal/trademarks.
a-dec.co.uk/500EXPERIENCE
your local A-dec Territory Manager for more: T: +971 (0) 585 93 1983 | E: nick.olive@a-dec.com
Scan the QR code to book your showroom appointment Contact
combines all the different solutions in a single unit. Thanks to its special design with interchangeable heads, a single camera can be used for a range of indications, making this a particularly userfriendly, cost-effective, and time-saving solution. The device includes:
A Cam head, which has been developed for intraoral images and videos and delivers HD quality images with the aid of an autofocus (intraoral, extraoral, macro). This supports additional dental diagnostics and creates the perfect basis for consultations with the patient and for good documentation.
The Proof head, is designed for specialist diagnosis of occlusal and fissure caries but can also be used to visualize calculus and dental plaque with the aid of the fluorescence method. The surface of teeth is displayed in different colours depending on the caries activity. Green indicates healthy tooth enamel, while carious regions are shown in blue, red, orange or yellow depending on the level of activity. This range of colours makes it very easy for the patient to follow the dentist’s explanations and better understand the next treatment steps that need to be taken. The Proxi head for diagnosis of proximal surface caries. Because this system uses infrared technology, unlike with X-ray diagnostic imaging there is no radiation exposure for the patient. Depending on translucence, the brightness of the displayed dental structures varies, and changes caused by caries bacteria are visible as bright, opaque regions. As a result, the extent of any enamel caries can be clearly defined.
Is this the end of the line for conventional X-ray imaging?
In future, will we be able to completely do without conventional X-ray imaging in the diagnosis of caries? The answer is perhaps yes and no. In cases where the findings are unclear, or in children, pregnant women or for patients who are otherwise unwell, radiation-free imaging with an intraoral camera can be called upon as the first diagnostic option. It is extremely convenient here that the patient can remain in the treatment room while the images are taken. This procedure is very comfortable for both the therapist and the patient.
If critical regions in the proximal region are highlighted by the camera, then (at the moment) additional bitewing images are still taken in the dental practice in Remshalden – this is particularly as a safeguard for legal/forensic reasons, because X-ray images are legally considered the state-ofthe-art. However, from a diagnostic perspective, this is only necessary in isolated cases since –for a trained user – the extent of the caries can normally be identified very clearly with the aid of the camera. The images only ever confirm the clinical impression, and there have never been any false positives to date.
KEY CONCLUSIONS FOR DAY-TO-DAY USE IN DENTAL PRACTICES
At the dental practice in Remshalden, the use of the intraoral camera VistaCam iX HD Smart is seen as a service that forms part of the overall package that is provided to the patients. Its use really pays for itself – the potential of the technology can be exploited right from the very first appointment with a patient, where it can be used for an initial visual snapshot to provide patients with a clear overview of their dental health. For further treatments or as part of follow-up checkups, the camera serves as a monitoring and documentation instrument, but it also makes a dependable contribution to safeguarding the quality of treatments and for quality management.
It is likely though that intraoral cameras will be used most commonly in treatment discussions with patients. Here, not only does the visualization of diagnostic findings save time during explanations and consultations, but the process also makes for closer, more intensive contact between patient and therapist, strengthening trust in the process. Experience has also shown that visualization increases patient acceptance of necessary treatments.
Based on observations, patients feel well looked after when they are taken care of under a modern treatment concept – and this of course completely without the health burden of ionising radiation. VistaCam iX HD Smart is easy to use and links up directly with the computer system of the practice. This means that there is no need
24 Dental News Quarter II
Experiences with VistaCam iX HD Smart
for complicated processes for copying data from external image files or converting the files from one format to another in the way we know from SLR cameras – which of course has a huge positive impact on workflows in this area. As a
result, I can thoroughly recommend intraoral cameras as an integral part of day-to-day work in dental practices to any colleagues who might be interested.

Dr. Frank Döpper, Remshalden
Dentist
Dr. Frank Döpper has been running a modern dental practice in RemshaldenGrunbach near Stuttgart/Germany since 2011, where he uses state-of-the-art technologies such as a surgical microscope, a digital X-ray system/ intraoral camera and CAD/CAM in the day-to-day treatment of his patients. He was one of the very first dentists to adopt digital intraoral camera technology. He and his team regularly attend professional training courses in all fields of dental, oral, and maxillofacial medicine with the aim of
being able to offer his patients responsible and highly-qualified consultations and treatments. Dr. Döpper is a graduate of the comprehensive dentistry curriculum of Deutsche Gesellschaft für Umwelt-ZahnMedizin, which he is also a member of, and he also holds memberships of Gnathologischer Arbeitskreis Stuttgart and the Swiss Society for Endodontology. In addition to his work as a practicing dentist, he also lectures on a regular basis.
26 Dental News Quarter II
Experiences with VistaCam iX HD Smart

SHINING3DDENTAL.COM

Fig. 1: The use of VistaCam iX HD Smart during the first appointment of a new patient is part of the standard treatment and has now become indispensable for initial diagnosis.
(Image: Practice Dr. Frank Döpper)

Fig. 3: Intraoral images of a mucosal lesion (image: Practice Dr. Frank Döpper)


Figs. 2a and b: Use of the intraoral camera to check failing fillings. During the consultation, the visualisation of the situation in the patient’s mouth makes the detailed technical explanations much more tangible for the patient and helps provide motivation for the further treatment required.
(Images: Dürr Dental)

Fig. 4: Intraoral images of a pressure point in an edentulous lower jaw. (Image: Practice Dr. Frank Döpper)
28 Dental News Quarter II
Experiences
VistaCam iX HD Smart
with
Treatment Options
The patient was presented with the following options to address her chief complaint.
Option 1: Space Opening
Real-time data sharing and collaboration have revolutionized modern dental technology, making it easier for dental professionals to access patient data and engage with each other.



work seamlessly in the background to help scale the business. This means that once staff members have set up the technology correctly, they can rely on it to handle many routine administrative tasks automatically. As a result, staff and providers can spend less time on manual tasks and more time to devote to diagnosis, treatment planning, and patient education.
Cloud-based systems, for example, can handle the additional workload and data that comes with increased patient volume. They are an efficient way to store, process, and share patient data, helping to ensure the dental practice is prepared for growth and equipped to deliver the best possible care at scale.
With the power of modern technology, dental practices can position themselves for success in today’s fast-paced healthcare landscape, staying ahead of the curve and providing higher-quality care and, ultimately, better outcomes for all.
Wet & dry trial was done to check the marginal fit. Veneers were prepared for final bonding.
Fig. 11: Chairside Armamentarium for Bonding the Prosthesis9%HF by Angelus, Silane coupling agent(Angelus), Single bond Univeral bonding agent (3M), Relyx veneer light cured adhesive cement (3M)to lute the veneers.
Rubber dam isolation was carried out. The veneers were cleaned thoroughly & stabilised using a putty bed. This was followed by etching the intaglio surface of the veneer with 9%HF for 10-15 secs followed by rinsing & air drying. This was followed by applying a coat of the silane coupling agent.
After a tooth extraction, approximately 30% of the alveolar ridge is lost because of resorption¹. Using a membrane improves the amount, quality, and contour of the desired bone.
Thanks to years of research leading to a patented technology, R.T.R.+ Membrane is the first resorbable membrane composed of 100% vegetalbased polymer, making it effective and easy to handle. It is the perfect addition to the bone graft R.T.R.+ for a successful, synthetic procedure.
● With a resorption time of 4 to 6 months and a bilayer structure, R.T.R.+ Membrane is highly effective within an appropriate time frame for bone regeneration.
● R.T.R.+ Membrane has a great resistance to exposure. In case of suture rupture, it can be left in place to guide tissues to heal properly.
As the prosthesis was now ready for bonding the intraoral steps for bonding were carried out. 37% phosphoric acid was applied to the tooth surfaces of the central incisors for 20 secs. followed by rinsing thoroughly & the surface was air dried. Universal bonding agent (Single bond universal 3M) was applied & air dried to a thin uniform layer.
● R.T.R.+ Membrane is compatible with every bone graft and available in 4 sizes.
1 Hsi Kuei Lin, Yu Hwa Pan, Eisner Salamanca, Yu Te Lin 5 and Wei Jen Chang. Int. J. Environ. Res. Public Health 2019, 16, 4616; Prevention of Bone Resorption by HA/β-TCP + Collagen Composite after Tooth Extraction: A Case Series
For more information, please visit www.septodont.com
Mini screw Assisted Limited Orthodontic Tooth Movement: About 2 Cases Reports
Dental Care in the Network Age R.T.R.+ Membrane
Fig. 10 - (L-R): Veneers received from the lab. Lab credits: Precision Dental Lab, Thane, Mumbai
Fig. 12: (L-R):1. HF application, 2.Frosty appearance of the intaglio surface, 3.Application of silane-coupling agent.
Age-defining Principles of Smile Design

Fig. 5: Intraoral image taken with the Cam interchangeable head of VistaCam iX HD Smart to visualise an occlusal caries lesion. (Image: Practice Dr. Frank Döpper)
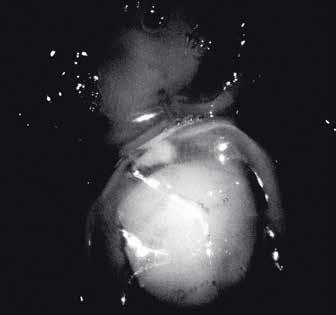
Fig. 7: Translucence image taken with the VistaCam Proxi interchangeable head for caries detection (distal caries lesion on tooth 45).
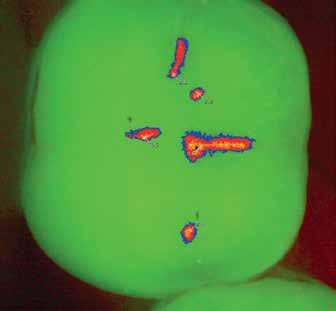

Fig. 6: Caries detection with the VistaCam Proof interchangeable head. The left of the image shows the representation in the caries filter with different colours used to highlight the development of the caries, while the right shows the numerical values for the caries activity. (Left-hand image: Practice Dr. Frank Döpper; right-hand image: Dürr Dental)
Bibliography
[1] Kraft, Ina Sophie. Einsatz der Intraoralkamera als Instrument zur Qualitätssicherung in der zahnmedizinischen Prothetik (Use of intraoral cameras as an instrument for quality assurance in dental prosthetics). Master thesis, University of Greifswald (2021)
[2] Araújo MR, Alvarez MJ, Godinho CA, Pereira C. Psychological, behavioral, and clinical effects of intra-oral camera: a randomized control trial on adults with gingivitis. Community Dent Oral Epidemiol
30 Dental News Quarter II
Experiences with VistaCam iX HD Smart

•
A GLOBAL LEADER, AT THE FOREFRONT OF DENTISTRY: An overview of NYU College of Dentistry
Located along the NYU health sciences corridor on First Avenue in Manhattan, NYU College of Dentistry offers a unique, exceptional experience for students pursuing careers in oral health care.
Our students benefit from the largest and most diverse patient population in the U.S., expert faculty, innovative learning technologies, a wealth of research and outreach opportunities, exciting new leadership initiatives, and a commitment to fostering a deep understanding of dentistry’s integral role in overall health.
We’re focused on the future –advancing oral health, researching new treatments and methodologies, and preparing students to become exceptional providers and to lead the profession, with ample opportunities to “think big.”
In just the past few years, NYU Dentistry has opened the Oral Health Center for People with Disabilities; NYU Dentistry Brooklyn Patient Care; Metro Community Health Centers at NYU Dentistry, a federally qualified health center located on the first floor of the NYU Dental Center in Manhattan, providing DDS students with experience in the medical management of dental patients; and the NYU Dentistry Center for Oral
Health Policy and Management, an interdisciplinary action lab that is working to develop and promote a national agenda for oral health policy and management that recognizes the fundamental relationship between oral health and overall health and the responsibilities that the dental professions have for the overall well-being of the public. And NYU Dentistry’s WHO Collaborating Center for Quality-improvement, Evidence-based Dentistry – one of only ten Collaborating Centers worldwide and the only one in the Americas – is focused on achieving oral health equity globally.
EDUCATIONAL PROGRAMS:
• Doctor of Dental Surgery (DDS) program
• Dental Hygiene programs
• Master’s degree programs: Biomaterials, Clinical Research, Dual MS
• Advanced Education: Endodontics, Oral & Maxillofacial Surgery, Orthodontics, Pediatric Dentistry, Periodontics, Prosthodontics
• Advanced Clinical Fellowship Programs: Apa Advanced Clinical Fellowship in Aesthetic Dentistry, Operative and Digital Dentistry, Implant Dentistry, Oral Surgery
• Fast Facts:
• NYU Dentistry is the 3rd oldest
32 Dental News Quarter II
Only in New York, Only @NYU: NYU Dentistry Imagines a World Where Everyone Smiles®
and the largest dental school in the U.S.
• 300,000 patient visits annually ensure superb clinical training for students
• Nearly 10% of dentists in the U.S have been educated at NYU Dentistry
• NYU Dentistry is ranked 5th in the U.S. in National Institutes of Health research funding
• 21,000+ alumni network practicing worldwide
• 1,959 students across all academic programs
• 93 NIH-funded and other funded researchers advance science every day
• 14 Academic Societies, each led by a Senior Mentor, promote a strong sense of community and afford DDS students small-group learning and mentoring experiences while still having access to the vast resources of a large university
• An average of 27 students per class year in each Academic Society, supported by its own Student Success Network, which connects every DDS student with a network of academic advisors, peer tutors, and peer and faculty mentors who provide one-on-one guidance and support to promote success from the moment students enter at Orientation


MOVING THE NEEDLE: NYU Dentistry’s Center for Oral Health Policy and Management Addresses Advocacy and Leadership Issues
The NYU Dentistry Center for Oral Health Policy and Management, an interdepartmental, interdisciplinary action laboratory, was founded in 2021 on the premise that the current oral health policy and management environment in the U.S. requires a holistic approach to the situation — one that has been lacking.
“While tremendous strides have been made in improving the oral health status of Americans through scientific breakthroughs, many are left without access to basic dental care,” notes Dean Charles Bertolami. “Dental benefits remain separated from other health care coverage and out of reach for many individuals and families,” he added.
In addition, the rigorous curriculum for dental students focuses predominantly on basic sciences and clinical care, but most learn little about the complexity of the dental and general health care systems of which they will soon be a part. The center aims to change this through new programming and academic offerings on oral health policy and leadership.
ACCESS TO CARE AND ADVOCACY INITIATIVES
“NYU Dentistry is uniquely well positioned to undertake these challenges,” said Richard Valachovic, DMD, MPH, a clinical professor at NYU Dentistry and president emeritus of the American Dental Education Association, who serves as founding director of the center.
Several of the College’s access to care and advocacy initiatives align with critical issues related to oral health policy and management.
DEVELOPING ADAPTIVE LEADERS FOR THE FUTURE
Another priority for the NYU Dentistry for Oral Health Management and Policy is to develop the next generation of policy-oriented leaders for the dental and related health care professions through creating new leadership programming and courses.
“The major reason given by dental school deans and independent search firms for not filling vacancies
33 Dental News Quarter II
Only in New York, Only @NYU: NYU Dentistry Imagines a World Where Everyone Smiles®
Charles Bertolami Michael O Connor
for faculty and dental leadership positions is a lack of qualified candidates,” said Michael P. O’Connor, EdD, MPA, executive vice dean at NYU Dentistry, who serves as co-director of the center. “The center strives to develop adaptive leaders who are prepared to perform in uncertain environments in the future using a differentiating character-based model of leadership, one that develops leadership habits and attitudes that aim for human flourishing in organizations, communities, and society.”
These concerns propelled NYU Dentistry to create a portfolio of leadership opportunities for students at the College. These include:
• The NYU Dentistry Leadership Track. This program is open to all students throughout the academic year. In 2022, this offering was enhanced by formalizing it as a twice-monthly lecture series focused on character-based leadership, and also opened it to all administrators, staff, and faculty along with students.
• Student Leadership Mock Congressional Hearing. Each spring, students are invited to apply for this competitive program, which trains students in leadership advocacy and public speaking. Participants prepare and deliver testimony on a health policy topic before a mock congressional committee panel.
• The NYU Dentistry Dental Student Leadership Institute (DDSLI). Each year, up to 35 D1 students are selected to take part in the DDSLI. Over the next three years, participants are given access to seminars, workshops, internships, mentoring, and other opportunities designed to prepare them to manage the complex challenges of advancing oral health in the 21st century.
• Global Health Care Leaders: Washington, DC Students from across the College of Dentistry, including advanced standing international students and dental hygiene program students, are eligible to apply for this professional development experience, which takes students to NYU’s DC campus to hear from oral health advocates and meet with federal lawmakers.



34 Dental News Quarter II
Only in New York, Only @NYU: NYU Dentistry Imagines a World Where Everyone Smiles®
Community outreach
WhiteCoat Ceremony,Lincoln Center
WhiteCoat Ceremony,Lincoln Center
Only in New York, Only @NYU: NYU Dentistry Imagines a World Where Everyone Smiles®



• Global Health Care Leaders: NYU Global Academic Centers D4 students are eligible to apply for this international experience. Selected students travel to one of NYU’s Global Campuses each year to explore complex policy issues with leaders in government and oral health advocacy. In fall 2023, the experience took place at NYU’s Villa LaPietra in Florence, Italy.
The process of leadership development differs significantly from most other experiences in dental education. Leadership is an art; it is creative and experiential rather than scientific. To foster leaders who will ensure a healthy future for dentistry, a different kind of education must be available. Despite the familiar adage, leaders are made, not born. While certain leadership qualities are native or part of a personality, leadership also requires specific knowledge and skills. Fortunately for all of us, these can be learned and cultivated.
NYU Dentistry is committed to cultivating students who can carry on the work begun by today’s oral health care leaders. Our first cohort of students has been engaged in the new DDSLI curriculum for just over two years, and already they are demonstrating an understanding of what leadership is all about.
Advocacy and Access-to-Care Initiatives
1. The NYU Dentistry Oral Health Center for People with Disabilities (OHCPD)
The OHCPD provides care based on a deep commitment to assuring disabled patients, their families, and caregivers that they aren’t just cared for, but cared about. Our dental care providers have the specialized skillsets needed to provide sensitive, essential care for individuals whose disability or disabilities prevent them from being treated in a conventional dental setting. Every component of the center has been designed to accommodate the physical and support needs of our patients, their families, and/or caregivers. And because it provides dental care across the lifespan, the center offers a dental home for disabled patients on an ongoing basis.
Special accommodations available for patients with intellectual and/or developmental (I/DD) include:
• Multisensory room: Designed to reduce patients’ agitation and anxiety, help them relax,
36 Dental News Quarter II
graduation caps
Student Leadership Retreat cropped
Welcome Week

Light-curing Glass Ionomer Filling Material
(immediately packable after placement in the cavity)
• Excellent working time and the setting time is individually adjustable by light-curing
• No varnish required- fill, polymerise and finish
• No need to condition the dental hard tissue
• Does not stick to the instrument
• Easy to model
• Suitable for large cavities
If you are interested in our entire product range and detailed product information please visit our website or contact us directly...

Dental Material GmbH - phone: +49 4321 / 5 41 73 - Email: inf PROMEDICA
and engage their senses. Amenities include a bubble tube; noise-cancelling headphones; soothing, adjustable, multi-colored lighting; weighted blankets; body socks; and a projection screen.
• Wheelchair tilt: Designed to accommodate patients receiving dental treatment in their own wheelchairs, without the need to transfer to a dental chair.
• Bariatric chairs: Designed to accommodate patients up to 650 pounds.
• Spacious, private treatment rooms: Designed to offer privacy and comfort, with soothing, adjustable, multi-colored lighting; noisecancelling headphones; and personal entertainment tablets.
• Sedation: A complete team meets all the needs of physically and intellectually disabled patients who require varying levels of pain and anxiety control, including the use of conscious and deep sedation, and general anesthesia techniques.
Advocacy Initiatives, as part of its advocacy initiatives on behalf of access to care for people with disabilities, the OHCPD:
• conducts a continuing education program, Unit Zero, to train dentists and their staff to provide care for people with disabilities.
• Members of the OHCPD team regularly appear before the New York City Council, the State Legislature in Albany, New York, and Congress in Washington, DC, to advocate for funds on behalf of the OHCPD.
• The OHCPD also sponsors an annual AHEAD (Achieving Health Equity through Access for All with Disabilities) Symposium. The annual symposium brings together experts in the areas of health care advocacy, access, and funding at the state and federal levels for people with disabilities.
In addition, The NYU Dentistry Center for Oral Health Policy and Management has presented an inaugural PROHmotion Symposium (Policy & Research in Oral Health: Moving Forward). The symposium brought together experts in the fields of health policy, education, research, leadership, and advocacy to discuss how these fields intersect



38 Dental News Quarter II Only in New York, Only @NYU: NYU Dentistry Imagines a World Where Everyone Smiles®
Veterans care
MARTTI translator
New Dental Van
Only
and explored actions to advance the profession’s ability to fulfill the responsibilities it has for the overall well-being of the public. A second PROHmotion Symposium is being planned.
2. Serving Those Who Served: NYU Dentistry’s VOCARE Program
NYU College of Dentistry is celebrating the second anniversary of the Veterans Oral Care Access Resource (VOCARE), part of the U.S. Department of Veterans Affairs’ VETSmile program, a pilot program designed to improve dental care access for veterans who are not eligible for dental care through the VA by partnering with community providers like NYU.
During the second year of VETSmile/VOCARE, 2,245 veterans received dental care over a total of 16,825 encounters. Nearly 32,000 procedures were completed.
VETSmile/VOCARE is a partnership between NYU Dentistry and the VA New York Harbor Healthcare System, which includes campuses in Manhattan, Brooklyn, Queens, and Staten Island, and the VA Bronx Health Care/Veterans Affairs. Through the program, the VA New York Harbor Healthcare System and the Bronx VA refer veterans who are not eligible to receive dental services at the VA to NYU for comprehensive care at no out-of-pocket cost to the veteran.
Veterans are seen at NYU College of Dentistry in Manhattan and at NYU Dentistry Brooklyn Patient Care. Some veterans, including those with a history of post-traumatic stress disorder, are seen at the NYU Dentistry Oral Health Center for People with Disabilities, where the staff are trained with special skill sets to ensure quality treatment and holistic care for people with disabilities and complex medical conditions.
3. Community-based Programs
A major component of the NYU College of Dentistry mission is extensive community outreach. Faculty from many departments lead NYU dental, dental hygiene, and postgraduate students in a wide range of patient care initiatives, traveling throughout the five boroughs of New York City to provide care to underserved populations.
The College’s mobile dental van, Smiling Faces, Going Places, is a unique program that brings comprehensive dental care to underserved children in New York City at public schools and
Head Start facilities.
Part of NYU’s teaching mission consists of preparing students for lives in a diverse world, and our faculty believe that such preparation is most effective through collaboration. Our relationship to New York City — the diversity of thought represented by all our schools, colleges, and programs, and our internationally connected and collaborative faculty — enable students and faculty alike to broaden the scope and vision of knowledge through interdisciplinary and interprofessional learning to make a real difference in the world. Dentist shortages are widespread: In 25 states and the District of Columbia, at least 10 percent of residents do not have adequate access to a dentist.
There are volunteer opportunities for all four years. In the D3 and D4 year, participation in communitybased outreach programs is required. Some of the long-standing NYU Dentistry health education and treatment initiatives provided to underserved children in New York City by the NYU Department of Pediatric Dentistry include:
• Screenings and education to over 1,000 children in public schools and childcare centers.
• Exams and fluoride varnish for 4,000 preschool-aged children at 80 different centers (Head Start).
• School-based sealant program at four public schools with over 400 sealants placed.
• Parent & staff workshops on children’s oral health given at childcare centers and public schools.
• Graham Windham partnership providing comprehensive care to children and adolescents in foster care, with over 1600 patient visits since 2011.
• Participating in over a dozen health fairs and community events, including two Special Olympics events.
• “Playing It Safe” Mouth Guard Program, providing preventive services at community centers and schools.
• A community outreach program with a special emphasis on meeting the dental needs of older New Yorkers brings care to people at
39 Dental News Quarter II
in New York, Only @NYU: NYU Dentistry Imagines a World Where Everyone Smiles®

The Best In Practice
We are a combination of companies that have come together under one roof to deliver the products, services, and solutions you need to be The Best In Practice.
With our passion for infection prevention solutions, premium instrumentation, and service and support programs, HuFriedyGroup will help you perfect your craft and continue to deliver the highest level of care to each patient.
HuFriedyGroup Mfg. Co., LLC. • European Headquarters • Lyoner Str. 9 • 60528 Frankfurt am Main, Germany • HuFriedyGroup.eu All company and product names are trademarks of HuFriedyGroup Mfg. Co., LLC, its affiliates or related companies, unless otherwise noted. ©2024 HuFriedyGroup Mfg. Co., LLC. All rights reserved. HFL-896GB/0324
Total Dental Solution

Ensuring safe, efficient and organized chairside management.




Instrument Management System
IMS™ standardizes and combines transportation, cleaning, sterilization and storage during the instrument reprocessing.

Procedural Sets
Infection prevention disposables assembled in Procedural Sets.

Dental Water Management
DentaPure™ cartridge for 365 days* of safe and compliant dental unit water.
* Up to 240L of water.
Visit HuFriedyGroup.eu/IMS
community-based facilities, including food pantries, homeless shelters, centers for abused women, foreign missions, senior centers, and foster care agencies.
4. Migrant Families Outreach Program
The newest addition to the Community-based programs is an initiative to enable migrant children and their families to receive dental care. More than 110,000 people seeking asylum have arrived in New York City since last spring—many of them families with young children. These children are facing a range of challenges, from the trauma of a difficult journey to the United States to unstable housing and language barriers in their new schools. One little-discussed challenge: poor oral health and a high prevalence of dental caries.
Research shows that refugee children experience many barriers to receiving dental care, including cost, different cultural norms and beliefs about oral health, difficulty navigating the healthcare system, and language barriers. NYU Dentistry’s Department of Pediatric Dentistry has been working to remove these obstacles to provide a range of services to meet the oral health needs of children from migrant and asylum-seeking families in New York City—often where they already are. Their approach is three-fold:
• Outreach events - NYU dental professionals and students take part in outreach events to provide oral health education, toothbrushes, dental exams, and apply fluoride varnish to children’s teeth. Thus far, they’ve provided dental exams and fluoride varnish to approximately 300 children and have shared oral health information and resources with approximately 1,200 families at Open Arms Resource Fairs at The Shed, a community event organized by the Department of Education to provide resources to families living in NYC’s temporary housing.
• School-based care - NYU Dentistry provides dental screenings and care in New York City public schools and Head Start centers. School-based care has been shown to lower the barriers to dental care by bringing care to children. In several high-need schools— including those with large numbers of migrant children—students are seen twice a year for cleanings, fluoride, sealants, x-rays and even restorations and extractions, serving as the children’s “dental home.” An estimated 200
children from asylum-seeking families are receiving ongoing dental care in NYC schools.
• Follow-up care at NYU Dentistry - Children who are screened at outreach events and those who are seen in schools but need more in-depth care that is best provided in a dental office are invited to schedule appointments at NYU Dentistry. Care is provided at no cost to families, with funding from New York City Council covering the cost of basic oral health care for children who are uninsured. A grant from the Mother Cabrini Health Foundation provides additional funds for dental care, as well as transportation to and from NYU, as getting children to appointments is a significant barrier to care.
5. Let’s GO! Student Service, Education, and Research Around the World
For over 20 years, NYU Dentistry’s Global Outreach program has built an exemplary global outreach model that provides participants with a unique service-learning experience, opportunities to conduct critically-needed research, and an increased awareness of access to care issues, while fostering a passion for volunteerism and social responsibility.
The program has become the largest, voluntary, university-based dental outreach program in the world. Participants on these outreaches—who included dental students, postgraduate students, dental hygiene students, and international students--speak of being challenged to re-think their roles as health care providers and describe their experiences as “transformative.” Equally important, the communities served by these programs are empowered by NYU Dentistry’s outreach model as sustainable oral health services become a reality. Outreach sites have included Phnom Penh, Cambodia; Pokhara and Surkhet, Nepal; Granada, Nicaragua; and Cape Town, South Africa. Within the United States, students have provided care and conducted research in Hudson, Plattsburgh, and Poughkeepsie, New York; Machias, Maine; and several villages in Alaska.
This year, the Global Outreach Program team will travel to the following locations:
• Machias, Maine, USA
• Monticello, New York, USA
• Eleuthera, Bahamas
44 Dental News Quarter II
Imagines
Only in New York, Only @NYU: NYU Dentistry
a World Where Everyone Smiles®
• La Romana, Dominican Republic
• Punta Cana, Dominican Republic
• Santiago, Chile
SIGNALING HOPE: NYU DENTISTRY OPENS
THE NYU PAIN RESEARCH CENTER
A Conversation with Dr. Brian Schmidt
Adapted and reprinted with permission from Global Health Nexus, the flagship publication of NYU Dentistry.
On January 1, 2022, NYU Dentistry opened the NYU Pain Research Center. The new Center brings together a cadre of investigators with interest and experience in the neurobiology of pain, provides mentorship, recruits and trains the next generation of basic science and clinical pain investigators, and facilitates clinical trials of new non-opioid pain therapies.
The Center has been in the planning stage for several years by Brian Schmidt, DDS, MD, PhD, and Nigel Bunnett, PhD. Dr. Schmidt is the senior vice dean for research development and academic affairs and the director of the NYU Oral Cancer Center and the NYU Dentistry Translational Research Center and a professor of oral and maxillofacial surgery. Dr. Bunnett is professor and chair of the Department of Molecular Pathobiology and assistant dean for research development. We spoke with Dr. Schmidt recently about the NYU Pain Research Center’s project to provide alternatives to opioids to treat chronic pain.
Why is research into chronic pain so important?
Dr. Schmidt: The National Institutes of Health estimates that 100 million people in the U.S. suffer from chronic pain. According to the National Institute on Drug Abuse, over 20% of patients prescribed opioids for chronic pain misuse them and 8-12% of people using an opioid for chronic pain develop an opioid use disorder. Opioid abuse leads to lost productivity, reduced quality of life, and rising health care costs. Since 2000, opioids have caused half a million deaths in the United States. The toll of these pointless deaths on friends, families, and communities is impossible to overstate.
What makes this the right time to
establish a pain research center at NYU Dentistry?
Dr. Schmidt: Pain research falls squarely within the mission of the College of Dentistry. Our faculty and students serve a large population of patients who endure acute and/or chronic pain, and there is a persuasive case to be made for founding a pain center within NYU Dentistry. Our school already employs numerous investigators with expertise in basic science pain research as well as clinical pain research, and our facilities can easily accommodate additional pain studies. Eight investigators within four departments currently undertake federally funded pain research related to oral cancer pain, colitis pain, headache, and itch. And through collaboration with investigators from NYU Langone Health, NYU College of Arts and Science, NYU Tandon School of Engineering, and NYU Meyers College of Nursing, as well as extramural investigators, the work of the NYU Pain Research Center transcends traditional disciplinary boundaries.
Are there plans to recruit additional pain researchers?
Dr. Schmidt: Definitely. We have been given the green light to hire about three new pain research faculty each year for the next several years. Ultimately, about 15 faculty members will be associated with the Center. The recruitment of additional pain researchers with a focus on facilitating clinical trials of new non-opioid pain therapies will set us apart from other dental schools. More federally funded research will be undertaken, collaborative opportunities for investigators will be expanded, and we will cement our reputation as a preeminent research institution.
How is the Center being funded?
Dr. Schmidt: The Center launched with more than $37 million in NIH and Department of Defense grants. In addition, the Japanese pharmaceutical company Takeda has committed to some seed funding.
It is our intention to submit an NIH Program Project Grant application to support the core facilities that will underpin the Center. The formal structure and explicit purpose of the Center could help researchers garner federal resources to address the vexatious problem of pain. Indeed, the former NIH Director Francis S. Collins recently launched
45 Dental News Quarter II
Only in New York, Only @NYU: NYU Dentistry Imagines a World Where Everyone Smiles®
the HEAL (Helping to End Addiction Long-term) Initiative to accelerate new approaches to pain treatment to combat the opioid crisis. The NYU Pain Research Center aligns our research efforts more closely with federally established priorities and our structured approach will improve our competitiveness with related federal grant opportunities.
What is your long-term vision for the NYU Pain Research Center?
Dr. Schmidt: NYU Dentistry is already a leader in clinical research; the Translational Research Center is the most tangible product of institutional support for clinical and translational research at any dental school in the country. The NYU Pain Research Center will play to the strengths of our clinical research facilities and expertise and will maximize the utility of resources already in play. It will be an incubator where basic scientists, clinician scientists, and clinicians learn from each other and collaborate. Basic scientists will have the unique opportunity to interact directly with patients and gain firsthand knowledge of the clinical challenges in treating pain. Ultimately, patients will benefit from the knowledge gleaned from work facilitated by the Center.
TOMORROW’S DENTISTRY TODAY: VIRTUAL REALITY AND ROBOTICS
Dentistry is undergoing one of the most remarkable transitions in its history. The use of digital imaging technology in daily practice is being further enhanced by the introduction of artificial intelligence. Meanwhile, progress is being made in the quest to reduce radiation exposure. Magnetic resonance imaging and robotics may soon be routinely used to plan implant or orthodontic treatments while ultrasound transducers monitor periodontal inflammation and bone graft healing.
Virtual reality and augmented reality (VR/AR) are becoming established technologies with a wide range of possibilities. 3-D imaging, computer-aided design, and manufacturing technologies such as 3-D printing are also transforming the materials and processes dentists use to restore teeth. Most notably, long-lasting dental implants are rapidly supplanting older restorative techniques in many dentists’ treatment plans for their patients.
The following provides an overview of the current use of some of these technologies in dental education, and at NYU in particular, explores their
impact on teaching and learning, and envisages their potential in this field.
What is VR and AR . . . and MR?
Broadly, VR can be thought of as immersion into a computer-generated environment. By contrast, AR can be thought of as superimposition of a computer-generated environment on reality. In short, VR replaces reality while AR supplements it. And merged reality can be thought of as interaction with and manipulation of both the physical and virtual environment.
The following are some examples of augmented reality (AR) vs. Virtual Reality (VR)
Augmented Reality (AR)
• Overlays computer generated 3D content on the real world.
• Users can interact with the real world and the virtual world.
• Users can clearly distinguish between both worlds.
• AR is achieved by smartphones, tablets, and/or AR wearables.
VS
Virtual Reality (VR)
• Visually immerses the user with simulated objects and environment.
• Completely shuts down the real world and makes user think that they are really in the virtual world.
• Users find it hard to differentiate between virtual and real world.
• Achieved by VT headsets.
Currently, AR ad VR are being developed, researched, and used in dental education at various institutions in the US and abroad for all kinds of dental disciplines.
Educational Goals/Objectives for Using VR in Dentistry include:
• Building foundational knowledge and skills
• Providing more opportunities to practice and learn
46 Dental News Quarter II
Only in New York, Only @NYU: NYU Dentistry Imagines a World Where Everyone Smiles®
• Address educational gaps (e.g., plastic manikin vs virtual reality)
• Streamline administrative work (e.g., feedback, scoring)
• Remediation/standardization
• Student and instructor satisfaction
• Patient satisfaction
At NYU, VR techniques are being used in several programs, including haptic feedback in dental hygiene and virtual reality surgery, as well as in the examples below.
VR for Surgery: Haptic Feedback for Local Anesthesia Training
NYU Dentistry, in collaboration with NYU Abu Dhabi, is developing and evaluating haptic feedback in a virtual reality (VR) local anesthesia training simulation, specifically for the inferior alveolar nerve block (IANB). This VR-based training program is currently in use by all secondyear students at NYU Dentistry as part of their preclinical training.
In addition to an immersive visual experience, this project enables dental students to experience the tactile sensation of inserting a real needle in a patient by using a haptic interface designed specifically for this purpose. A 3D printed carpule syringe has been designed and attached to the Geomagic haptic interface to provide a realistic grip experience in addition to providing force feedback during the anesthesia procedure.
Haptic data, such as position, orientation, force, speed, etc., is recorded to provide a quantitative measure of the quality of performance. The ability of haptic feedback to improve learning outcomes is being evaluated using an experimental study with dental professors and students from NYU Dentistry. The results from the quantitative evaluation will be cross-validated using subjective feedback from dental professors and students.
Robotic technology enhances dental education and clinical practice
In 2022, dental students at NYU became the first in the U.S. to perform dental implant surgery using state-of-the-art robotic technology.
NYU Dentistry is one of only three dental schools in the nation with a robotic system for dental implant surgery. While NYU faculty and postdoctoral
students have completed approximately 150 dental implant cases since acquiring robotic technology the previous year, this surgery marked the first time that dental students led the procedure from start to finish.
Three students performed robot-assisted dental implant surgery under faculty supervision. The students, who were completing their third year of dental school, had already been observers and surgical assistants for approximately 20 facultyled implant procedures using robotic technology.
On the day of the surgery, imaging was conducted using both a handheld intraoral scanner and cone beam computed tomography (CBCT) to create detailed 3D images of the patient’s oral cavity. The team used the imaging to plan for the precise placement of the dental implant to replace a single tooth.
The students then used the robotic system to guide them in implementing the plan. The system uses haptic technology to provide real-time, physical cues, augmenting a provider’s “feel” and assisting them in the accurate placement of the dental implant. While the robotic arm acts as a guide and can adjust to a patient’s movement in real time to maintain the proper alignment of the implant, the provider always maintains control of the dental handpiece.
At NYU, robotic technology is now an elective for all interested DDS students and part of the curriculum for all postgraduate students.
CONCLUSION
While Augmented Reality (AR) in dental education offers enhanced learning experiences to cost effectiveness, challenges like technical limitations, content development, and a learning curve need to be considered when integrating AR into dental curricula. In short, the actual significance of VR simulation on dental education outcomes is not entirely clear. VR significantly enhanced the acquisition of dental manual skills even in short periods of training. However, few studies report longer periods of follow up and insignificant differences between virtual and traditional groups. The actual significance of VR simulation on dental education outcomes is not entirely clear. Also, challenges like cost, technical issues, and ethical considerations need to be addressed to fully harness its potential for educating the next generation of dental professionals.
48 Dental News Quarter II
Only in New York, Only @NYU: NYU Dentistry Imagines a World Where Everyone Smiles®
BELLISSIMA! NYU DENTISTRY ADVANCES AESTHETIC DENTISTRY PROGRAMS WITH ALUMNUS MICHAEL APA
Internationally renowned education program and new clinical suite will honor leader in aesthetic dentistry
“Make the most out of what you worked so hard to obtain.”
This inspirational advice in NYU College of Dentistry’s Class of 2003 yearbook came from Michael Apa, DDS, then a newly minted dentist with a passion for aesthetics. In the 20 years since his graduation from NYU, Dr. Apa has helped to transform the evolving field of aesthetic dentistry and distinguished himself as one of its leaders.
Now, Dr. Apa is “making the most” of his achievements by investing in the dentists of tomorrow and enhancing the College’s programs in aesthetic dentistry.
In recognition of Dr. Apa and his contributions to the field, NYU Dentistry will rename its education program in aesthetic dentistry the Apa Advanced Clinical Fellowship in Aesthetics. The College is also establishing the Apa Aesthetic Suite at the College, a state-of-the-art clinical space and the first permanent home for aesthetic dentistry education at NYU. These advances are made possible by a transformational gift from Dr. Apa.
“We are so grateful that Dr. Apa has chosen to support NYU College of Dentistry, the institution that shaped him as a dentist and set him on his path to success,” said Dean Bertolami. “Dr. Apa is recognized internationally as a leader and innovator in aesthetic dentistry, and we are eager to incorporate his experience and vision to further strengthen our programs.”
“Having found a home at NYU during my time as a student, it is my hope that the next generation of dentists will share that experience, and they too will set out to have an impact on our profession and the world around them,” said Dr. Apa.
Dr. Apa will collaborate with Anabella Oquendo, DDS, director of the renamed Apa Advanced Clinical Fellowship in Aesthetics, to provide input on bringing international and U.S. dentists state-ofthe-art training that restores and enhances natural smiles. The renowned, one-year program has attracted practicing dentists from 47 countries to study the latest techniques in aesthetic dentistry.
“Channeling Dr. Apa’s expertise and enthusiasm into our clinical fellowship program will bring new vitality to our training in aesthetic dentistry, a field that goes beyond appearances, intertwining beauty, health, and function. As we enhance smiles, we elevate confidence and promote overall oral health, which contribute to improved wellbeing,” said Dr. Oquendo, the assistant dean for international programs at NYU Dentistry.
The new Apa Aesthetic Suite, designed in collaboration with Dr. Apa, will be located on the first floor of NYU Dentistry. Planning for renovations to the existing clinical space will begin this fall, and the suite will open in fall 2024.
“As dentists, we work at the intersection of health and art. I look forward to helping to transform this space into a suite that reflects the design and energy of our craft and inspires both patients and clinicians,” added Dr. Apa.
As one of the world’s most sought-after aesthetic dentists, with practices in New York, Los Angeles, and Dubai, Dr. Apa has maintained his connection to NYU Dentistry as a lecturer and mentor to dental students. His passion for aesthetic dentistry blossomed while at NYU, where he founded NYU Dentistry’s Aesthetics Society and was part of the College’s Aesthetics Honors Program.
Honors Program in Aesthetic Dentistry named for Dr. Apa
The naming of the Apa Honors Program in Aesthetic Dentistry, an elective course for fourth-year dental students, recognizes Dr. Apa’s excellence in and contributions to the field of aesthetic dentistry. Beginning in the fall of 2024, the honors program will be housed in the new Apa Aesthetic Suite, a state-of-the-art clinical space on the first floor of NYU Dentistry and the College’s first permanent home for aesthetic dentistry education.
The honors program in aesthetic dentistry was founded in 2000 and since directed by John Calamia, DMD, the co-developer of Bonded Porcelain Veneer Technology. Dr. Calamia was Dr. Apa’s professor at NYU Dentistry and Dr. Apa credits him with being an influential figure and mentor in his interest and early development in aesthetic dentistry.
“Dr. Michael Apa is one of our most prominent alumni members of the Honors Program in Aesthetics family. I am truly grateful to Michael for providing a permanent home for this program to
49 Dental News Quarter II Only in New York, Only @NYU: NYU Dentistry Imagines a World Where Everyone Smiles®
be housed in the soon-to-be-constructed, stateof-the-art Apa Aesthetic Suite. He has stepped up to the plate and showed his commitment to the continuance of a program that has started him and many others on their journey to provide responsible aesthetic restoration as the focus in their careers,” said Dr. Calamia.
In the Apa Honors Program in Aesthetic Dentistry, students will continue to receive didactic and clinical experience, participating in lectures, seminars, literature reviews, and case presentations as well as dedicated weekly clinical sessions to treat advanced aesthetic cases. The clinical sessions enable students to develop treatment plans and complete aesthetic restorations using a range of cutting-edge materials and methods for inlays, onlays, crowns, porcelain veneers, and ceramic bridges. Students learn to use high-tech equipment for planning and restoration, including CAD/CAM and lasers, as adjuncts to traditional restorative treatment.
Students enter the honors program through a competitive application and interview process; eight to 12 DDS students are accepted to this D4 program.
“At NYU Dentistry, we truly value Dr. Apa’s ongoing dedication, vision, and commitment to advancing aesthetic dentistry, making a lasting impact. His pursuit of excellence serves as a source of inspiration to our students,” said Anabella Oquendo, DDS, assistant dean for international programs and director of the Apa Advanced Clinical Fellowship in Aesthetics.
ON THE HORIZON: EXPLORING NEW DEGREE OPPORTUNITIES INTEGRATED WITH ADVANCED CLINICAL TRAINING
Propelled by our collaborative and entrepreneurial mindset, and recognizing that the need for qualified dental faculty is a global challenge, the College is currently exploring the creation of a new degree program, a Doctor of Science in Dentistry (DScDent) degree, which is envisioned as a professional degree program suitable for outstanding dental health professionals seeking additional education in one of five thematic areas: Research (basic or applied); Public Health; Leadership; Educational Technology or Sub-specialization in Clinical Fields such as implantology, care for people with disabilities, and aesthetic dentistry. Successful applicants to the DScDent program would exhibit a career interest
in one of these five thematic areas, evidence of excellent scholarship, and research potential.
While the program is still in the planning stages, the College anticipates that the DScDent program would appeal to international dental school faculty and those who aspire to become faculty. International students may be attracted to our DScDent program because of its relatively short duration and because it could be efficiently combined with specialty or other clinical programs via separate degree tracks.
Dental faculty with education and credentials in teaching and learning, clinical research, and leadership are relatively rare and yet are a critical aspect of improving oral health globally. We invite you to contact us and learn more about our plans for this program and other exciting new initiatives on the horizon at NYU Dentistry. Our tradition of innovative thinking – all in service of improving public health – provides the headwind needed to continue to advance programs, partnerships, and people who are energized to join NYU Dentistry and imagine a world where everyone smiles.®

50 Dental News Quarter II
Only in New York, Only @NYU: NYU Dentistry Imagines a World Where Everyone Smiles®
trident View Gold
I-View Gold Intraoral sensor
Thanks to the advanced calibration tool, the I-View Gold captures high-definition images without any filters. Calibration files are used to remove any imperfections during acquisition, reducing noise and enhancing detail. As a result, the images captured by the I-View Gold require no further processing, ensuring reliable images, accurate diagnosis and time efficiency.
- DICOM compatibility
- Bridge feature for connecting to other dental management software.
- TWAIN option
- Multiuser connection
THE SAFEST


Tests show the superiority of the latest reciprocation technology from FKG R Motion®
Swiss precision and quality triumph with the launch of the R-Motion® range as the safest reciprocation solution, eclipsing old files systems. The minimally invasive philosophy from endodontics experts FKG is now available for reciprocation users, offering an affordable treatment with the ultimate simplicity for most clinical cases. While FKG stands for Swiss quality in minimally invasive endodontics, R-Motion® continues its legacy of advanced endodontic instruments that challenge existing norms by setting new standards in reciprocation. Test results highlight its superiority in mechanical design, with uncompromising safety and simplicity. R-Motion®. Reciprocation Redefined. Minimally invasive with no compromise on performance, the R-Motion® range is a novel solution in reciprocation. R-Motion® combines cutting efficiency, flexibility, and resistance to cyclic fatigue with a design that respects the anatomy of the root canal at all times. Due to extremely precise engineering, R-Motion® is up to times more flexible and up to 3.6 times more resistant to cyclic fatigue. With 60% less transportation than standard reciprocating NiTi systems, R-Motion® delivers better centering and up to a 40% less dentinal stress than other providers.
COMPREHENSIVE WHEN YOU NEED IT: SIMPLE WHEN YOU DON’T
For the majority of cases, R-Motion® delivers results

with just two files. To cover all possible cases, R-Motion® offers one of the largest lines of instruments.
With the new R-Motion Glider C glide path file and R-Motion 20 shaping file there are in total seven files:
• R-Motion Glider
• R-Motion 20
• R-Motion 30
• R-Motion 50
• R-Motion Glider C
• R-Motion 25
• R-Motion 40
With the addition of two new instruments in the range, R-Motion® is pursuing FKG’ tradition of excellence in minimally invasive endodontics. www.fkg.ch
52 Dental News

Ultradent Unveils New Universal Shade Composite
Ultradent Products, Inc., a leading developer and manufacturer of high-tech dental materials, is announcing the launch of Transcend™ universal composite, a new composite material providing unmatched esthetics and handling properties. Transcend composite is designed to simplify the restorative process by allowing dentists to complete most restorations with just one shade of composite.
Thanks to Ultradent’s Resin Particle Match™ technology, Transcend™ composite offers high levels of translucency, allowing for ideal pigmentation and opacification to match the surrounding dentition. The Universal Body shade also has optimal opacity to help block the underlying tooth color, eliminating the need for a blocker shade.
“Transcend™ composite enables dentists to achieve excellent esthetic results with ease,” says Ultradent Sr. VP of Research & Development, Neil Jessop. “Its unique formulation offers the perfect balance of flexibility, strength, and gloss retention to ensure the long-lasting results patients are seeking.”
Transcend™ composite is a nanohybrid formula that combines high strength and easy sculptability, making it ideal for both posterior and anterior composite restorations. The handling properties of Transcend™ composite have been finely tuned to be firm but
VOCO Retraction Paste
VOCO Retraction Paste – a must-have for every practice
The basis for a perfect impression is an exposed and dry sulcus. With VOCO Retraction Paste, which is applied directly from the cap into the sulcus, VOCO is introducing a product for the effective, temporary opening of the sulcus and its isolation from moisture. This product is also the ideal complement to the V-Posil precision impression material. VOCO Retraction Paste offers the prerequisites for successful classic or digital precision impressions, as well as for cavity preparation of class II or V restorations, but also as preparation for either permanent or temporary cementing of restorations.
The retraction paste impresses users not just through its results, but also through its handling: For example, the shade contrasts well against the gingiva, facilitating in particular the work in hard-to-see areas. Thanks to the very slender and slightly flexible cannula, the material can be easily dosed and applied, whereby the paste is easy to press out and subsequently scores points with very good flow viscosity, coupled with uniform stability for opening of the sulcus. During application, the aluminium chloride paste with astringent effect temporarily fills the sulcus, stops any bleeding and eliminates moisture. VOCO Retraction Paste only requires a short exposure time, it has a neutral taste and can be easily and fully rinsed off.
The paste can be used as an alternative to, or in combination with a retraction thread, for example. It can be used in the classic way or digitally, with an intraoral scanner. Soft tissue

malleable, allowing it to stay in place without drooping or slumping during manipulation. The material is highly wear-resistant, but also less abrasive to opposing dentition than other composites on the market.
In addition to the Universal Body shade, Transcend™ composite features four dentin shades and two enamel shades for cases when a layering technique is appropriate. These layering shades were handpicked to include only the most popular shades from Ultradent’s esthetic composite lines to ensure dentists have the shades needed to accomplish restorative work done on a regular basis.
www.ultradent.com

management is often the key to success for the resulting class II and V fillings as well as for permanent or temporary cementation of restorations, especially when using the adhesive technique with not very moisture-tolerant products.
Hygienic SingleDose VOCO Retraction Paste can be applied directly into the sulcus easily and hygienically from the SingleDose Cap, developed in-house by VOCO. The SingleDose Cap is compatible with commercially available composite dispensers such as the VOCO Caps Dispenser, and is sufficient for up to 3 sulci.
Advantages of the SingleDose: each patient receives their very own product, an easy way to avoid the risk of crosscontamination as well as other potential for contamination.
54 Dental News Quarter II
www.voco.dental

Since the Covid-19 pandemic here at Dental News we have been hearing more about clinics choosing equipment without dental spittoons to improve hygiene and reduce cross infection risk. We visited Dr Michel Souccar in Beirut to understand why he chooses to work in this way.
No Spittoon Interview
Dr. Michel Souccar
Dental News:
‘Dr. Michel Souccar, good morning, we are now in your clinic in Beirut where you have been practicing dentistry for 47 years, since 1977. What brought me to your dental office is my curiosity to hear from you your experience practicing dentistry on a dental chair without spittoon. I understand that both you and your wife Dr Aimée practice in this way.’
Dr. Michel Souccar:
‘When we first began work as fresh graduates we quickly abandoned using spittoons. We did not like the view of the saliva mixed with blood spinning in the spittoon. To us we always felt that this was unhygienic and unpleasant for patients. Particularly when the patient is anesthetized, he may not have full control over his lips and consequently he will lose some liquids while spitting that will drip and contaminate the floor and the chair, etc…’
Dental News:
‘So how do you help patients who need to clean their mouths due to a bad taste or debris from treatment?’
Dr. Michel Souccar:
‘When a patient needs to spit and empty his mouth, he closes his mouth on the suction canula and this simple procedure empties his mouth from any liquid and non liquid residue. We can also use the 3:1 syringe to help clean the mouth for the patient. We have a saliva ejector and high volume suction on our chairs. This is much more efficient that using a spittoon’ ‘We find that patients are very happy with this process. Sometimes after scaling or powder jet a patient may rinse at the end of the treatment in the lavatory room. This allows us to
prepare for the next treatment and saves any embarrassment of the patient by spitting in the spittoon.’
‘I must say that simply washing the mouth with the 3:1 syringe and using suction in enough to clean the mouth after the dental work for nearly all patients.’
Dental News:
‘Did you ever regret not having a spittoon?’
Dr. Michel Souccar:
‘I never felt the need to use the spittoon or the cuspidor in my office. On the contrary, I removed the spittoon to improve hygiene. The act of spitting in the cuspidor creates cross contamination risks, especially when the saliva mixed with blood splashes over the surfaces.’
‘I also feel that patients can use a spittoon to ‘escape’ treatment or ‘la fuite au crachoir’ in French. This unnecessarily extends and delays treatment. When the spittoon is removed so is the temptation for patients to use it to interrupt treatment. This makes our treatments much more efficient!’
Dental News:
Are your patients satisfied without a spittoon?
Dr. Michel Souccar:
Until now, we have more than 10,000 patient files/records, not a single patient has complained. If a patient asks to spit, we guide them to use the suction. It really is as simple as that. We have very happy and satisfied patients and a more hygienic office.
56 Dental News Quarter II

Nick Olive is the A-dec Territory Manager for the Middle East and Egypt. Nick has written about this way of working for Dental News previously so we asked him how he sees the adoption of this way of working in the region.
‘Working without a cuspidor is already the predominant way of working for our customers in the markets such as the USA and France. Since the Covid-19 pandemic we have seen a big increase in other markets such as the UK where this way of working has become very popular. The standard way to equip Dental Universities in the USA and France for example is without spittoons. The number one reason we hear for this is to improve hygiene in the clinics’.
‘More locally we have recently seen two new clinics in Dubai chose to equip their chair packages without spittoons as a way to improve hygiene and efficiency. We also have some exciting projects in the pipeline including dental universities who are looking to move towards this spittoon free USA style of working. I was recently talking to a prestigious clinic in Saudi Arabia who have kept their spittoons covered and out of use since the pandemic as a way to improve hygiene. The feedback from dentists in this clinic has been
really positive. I certainly expect the trend to equip dental chairs without spittoons to continue to grow in the region as it has in other European and American markets.’

To discover more about how to work without a spittoon and explore equipment options in more detail you can contact Nick Olive.
Nick Olive Territory Manager Middle East & Egypt
A-dec
+971 585931983
nick.olive@a-dec.com
57 Dental News Quarter II Dr Michel Souccar – No Spittoon Interview
Dr. Michel Souccar Operatory

Emerging Horizons in Pediatric Dentistry
12 th January 2024 - BAU - Lebanon
Dr. Marlene Khoury, Prof. roula abiaD, Dr. Janine azar, Dean MagueD fahMi, Prof. aly Sharaf, Dr. SanDra Dagher, Dr bourane aMbriSS


58 Dental News Quarter II
. ءازعلأا ءلامزلاو تلايمزلا ةيبرعلا تايعملجا ءاسؤرو ءادمعلاو ءابقنلا ةيبرعلا ةعمالجا سيئر ةداعس ،لافتحلاا يعار ةضرح ،تويرب في نانسلأا ءابطأ ةباقنل ةميركلا ةياعرلا تتح 28 لا يملعلا مويلاب ،لافطلأا نانسأ بطل ةينانبللا ةيعملجا مسابو يمساب مكب بحرن .ةيبرعلا تويرب ةعمالج ةميركلا ةفاضتسلاا و لافطلأا نانسأ بطل ةيبرعلا ةيعملجا عم نواعتلاب انعم مويلا مكروضح . ءاقللا اذه دقع لىع نيصرم انك ،يرضحتلل تقولا قيض مغرو ،نانبل اننطوو انتقطنم ابه رتم ليلا ةبعصلا فورظلا مغر .ةميركلا ةكراشلما هذه ايرثك ردقن و انل يربك عفاد ناك مفلا ةحص ينمأتل ةيربك ةيلوؤسم انيدل ،لاجلمابه ينثحابو نيضرامحو ينيئاصخأك انحن ليلق لضب ونع انيكح ام دق لافطلأا نانسأ بط ةيهمأ اذبه مايقلاب انراصراب حضاو ،حضاو ةيضقلا هذبه انمازتلا .ةايلحا ىدلم ةيحص ةكحض نلنمأنم ةقيرطلابهو ةماعلا مهتحص لياتلابو انلافطأ دنع نانسأ ةحصب ةيانعلل تاروطتلا ديدج شرنو تابرلخا لدابتب حضاو ىطعت فوس ليلا تاضراحلماب يربكلا عونتلاو ىوتسلما في حضاو .رتمؤلما .انلصفت يتلا تافاسلماو دودلحا مغر ةيبرع تايعمجك اننيب نواعتلاب حضاو ،انلافطأ .اهجراخو انتقطنمب لافطلأا نانسأ بط ةسرامم ىوتسم عفرل سياسا مازتللاا اذه انعم مهتكراشمو مهروضح لىع لافطلأا نانسأ بطل ةيبرعلا ةيعملجا ركذلاب صخاو يملعلا مويلا اذه حاجناب مهاس نم لك ركشأ نأ دوأ اذه حاجناب ةيساسا مهتهماسم ليي sponsors لاو moderator لاو نيضراحلما ركشا يدب ،ةميركلا اهتفاضتسا لىع ةيبرعلا ةعمالجاو مويلا Executive Board لل صاخ ركشو مويلا .نانبل اننطوو بيرعلا لماعلا ملاسلا معي نأ ىنتما ايرخأو ، هحاجنلا ةلاعفلا ةكراشملل مكوعدبو رمثم يملع موي مكلانمتب لافطلأا نانسأ بطل ةينانبللا ةيعملجا ةسيئر ، رغاد اردناس ةروتكدلا
Dr. SanDra Dagher, PreSiDent of the lebaneSe Society of PeDiatric DentiStry Prof aMr abDelaziz, PreSiDent of the arab Society of PeDiatric DentiStry






59 Dental News Quarter II
Prof aly Sharaf, PreSiDent of the egyPtian PeDiatric DentiStry aSSociation
l to r. DrS elySe JaD, SanDra Dagher, bourane aMbriSS, ahaMaD tarabay
l to r. DrS. SanDra Dagher, Prof ronalD youneS, Dean MagueD fahMi, Dr ahMaD tarabay
l to r. DrS bechara aSMar, bourane aMbriSS, aMr abDelaziz, fatMa abDel MonieM, Dean MagueD fahMi, aly Sharaf
PictureS froM the exhibition
PictureS froM the exhibition














Accutron™ Digital Ultra™ Flowmeters
The Accutron Digital Ultra™ Flowmeter offers user-friendly, advanced technology and includes enhanced safety features. It allows clinicians to work in a digital environment with color-coded, fingertip controls, while displaying critical parameters both numerically and as electronic flow tubes. Its sealed flush surface makes it easy to disinfect or barrier-protect. The unit‘s design complements aseptic, contemporary operatory environments.
• Automatic compensation to easily adjust total flow or gas ratio while the other stays constant.
• Both digital and electronic flowtube displays for ease of use.
• Maximum nitrous oxide ratio at 70% for patient safety.
• Audible and visual alarms to notify of low oxygen.
• Oxygen fail-safe and flush for additional safety.
• Emergency oxygen resuscitation connector.
• Sealed flush surface makes it easy to disinfect or barrier protect.
There are two options for portable Digital Ultra solutions that can seamlessly move between operatories – the 4-cylinder stand package and the Newport™, which is fully enclosed.
HuFriedyGroup Mfg. Co., LLC. • European Headquarters • Lyoner Str. 9 • 60528 Frankfurt am Main, Germany • HuFriedyGroup.eu All company and product names are trademarks of HuFriedyGroup Mfg. Co., LLC, its affiliates or related companies, unless otherwise noted. Accutron™ Flowmeters and Nasal Masks are made in Phoenix, Arizona, USA ©2023 HuFriedyGroup Mfg. Co., LLC. All rights reserved. 1223
Advanced Conscious Sedation Systems
Accutron™, a proud member of HuFriedyGroup, is a leading manufacturer of innovative nitrous oxide/oxygen sedation equipment and accessories. For over forty-five years, our focus has been to design and manufacture the highest quality sedation products that assist dental practitioners in relaxing their patients and making their dental visit a comfortable experience.
Accutron™ products are proudly made in the USA, in Phoenix, Arizona.
Accutron™ ClearView Nasal Masks
Accutron™ ClearView™ Nasal Masks feature a mask-in-mask design to minimize ambient nitrous oxide in the operatory. This design eliminates the need for a “scavenging hub” on the scavenging circuit in older designs such as the Accutron™ PIP+ Nasal Mask and others. The clear outer mask allows you to monitor patient breathing, as condensation appears when the patient is properly breathing through their nose. The colorful, soft inner mask design creates an improved facial seal.
Additional Features:
• Lower profile than original designs to expand clinical field of view
• Single-use minimizes cross-contamination; saves staff time
• Appealing colors and scents engage and relax patients
• Can be used with other brands of scavenging circuits
• 12 individually wrapped nasal masks/box
Not made with natural rubber latex.

For more information, contact Piro Trading International +1-209-667-7204
• caroline@pirotrading.com
Accutron is now a proud member of

SIDC 2024
The Saudi International Dental Conference 18-20 January 2024
During the SIDC 2024, a series of academic and clinically oriented comprehensive and focused scientific sessions and workshops took place. We have 127 expert speakers, 150 lectures and 35 hands-on workshops so that general dental practitioners, specialists, and dental students can gain knowledge about dentistry through well-known speakers from all over the world. The organization of SIDC 2024 was a great experience in planning, execution and resulted as a well-coordinated event. My sincere gratitude is owed to the great support from the scientific committee and the able Boards members and of the Saudi Dental Society who approached professional speakers and forums around the world. The primary focus of our team was to update the dental fraternity of Saudi Arabia with current and advanced technologies and management techniques in par excellence. Dates and topics were confirmed; speakers were finalized and thus started our journey! SIDC is changing Saudi Arabia’s outlook of global dentistry by their technology and creativity. Congratulations to each member of the Scientific committee for their excellent contributions and performance. We are really happy with the fantastic results! The SIDC event turned out to be an enormous success because of you all!
A successful event results from creativity, hard work, and effort from all the Deans and administrative heads of the premier institutions in Saudi Arabia. A lot of preparation, time, and planning goes into ensuring a smooth drive of such a huge international event. So, we owe
the memorable time spent in SIDC to all the kind hearts who supported us in every single endeavor of SIDC.
Thank you once again, and hope you enjoy SIDC 2024.
Ziyad Allahem President SIDC 2024

62 Dental News Quarter II






63 Dental News Quarter II
Opening
phOtO frOm the Audience during the Opening ceremOny
trOphy tO prOf. AbdullAh Al sAlmAn, Vice president Of King sAud uniVersity
ribbOn cutting Of the exhibitiOn flOOr
grOup phOtO Of delegAtes frOm KAu with deAn AbdulghAni mirA
inAugurAtiOn Of the exhibitiOn
Opening ceremOny






64 Dental News Quarter II
Al turKi And hufriedy bOOth
cAre And trident bOOth
belmOnt bOOth
l tO r
KAu dentistry bOOth with deAn AbdulghAni mirA
drs hussAm Al fAwAz, KhAlid sAif, AbdulrAhmAn AlsArhAn, KhAled hAmdAn, sultAn sudAis
mps bOOth
exhibitiOn






65 Dental News Quarter II
neOss bOOth
sAudi OrthOdOntic sOciety with dr mOhAmed elhArbi, pr. KhAlil AleisA, dr reem AlAnsAri
nsK bOOth
septOdOnt bOOth VOcO bOOth
sAudi prOsthOdOntic sOciety with prOf mAnsOur Assery And dr KhOlOOd AlAli, dr. fOutOun eteibi And dr mOhAmed AlAsmAry
exhibitiOn


66 Dental News Quarter II
في نانــسلأا بــط بــيقن ةرــح ،لاــفتحلاا يــعار ســنوي دــلانور روــسفوبرلا ةرــح ،لاــشلا ،طباورلاو تايعملجا ءاسؤر تارح ،تاعمالجا ءادمع ليثممو ءادمع تارح ،نانسلأا ميوقتل ةيبرعلا تايعملجا ليثمم تارح ،ميركلا روضلحا ايها ،ءازعلأا يئلامز يــتلا ةــلمؤلماو ةــنهارلا فورــظلا لــظ في موــيلا مــكروضح نــمثأو ركــشأ نا لاا ينعــسي لا في اررــقم ناك يذــلا اــنرتمؤم لــيجأت ىــع اــنتبرجأ يــتلا فورــظلا هذــه ،ةــقطنلما اــبه رــم دوــمصلا ةدارا ىــع دــيكأتلل موــيلا هــميظنت ىــع انتعجــش اــتهاذ يــه ،ضياــلما نياــثلا نــيشرت تــناك ناو ،راكنتــساو نــماضت ةــفقو نــع نــلعنلو لــصيح اــم لك مــغر رارمتــسلااو ناــنبل بوــنج في وا ةزــغ في ناك نا ةيناــسنلاا دــض بــكترت يــتلا مــئارلجا لكــل ،ةــعضاوتم نــع روــملأا جرــتخ لاا نــلما ملاــسلا لوــلح ىــنمتنف ،ءاــسنلاو لاــفطلأل يــجملها لــتقلاو .ةرطيــسلا قاــطن عاــضولأا ةــهجاوم في اــتهردق ىــع اــئاد تــنهرب دــق نانــسلأا مــيوقتل ةــينانبللا ةــيعملجا نا مــغرف .دــعاصتلما يداــصتقلاا عــضولا راــينها عــم نــتيضالما نتنــسلا للاــخ ةــصاخ ةــبعصلا نا ،ناــنبل في نانــسلأا مــيوقت بــط مــعد في ةــيعملجا ترمتــسا ،ةيــشيعلما تاــمزلأا مــقافت يــتباقن اــهمظنت يــتلا تارــتمؤلما في ةكراــشلماو مــيظنتلا للاــخ نــم يــملعلا دــيعصلا ىــع ناك للاــخ نــم اــضيأو رمتــسلما مــيلعتلا تارود فيو ةــينانبللا تاــعمالجاو ناــنبل في نانــسلأا )40( نــعبرأ نــم رــثكأ باــستنا نــمأت في اــنحجن دــقف .اــهيلا نبــستنلما ءاــضعلأا ناــضتحا عــفري اــمم اوــضع )60( نتــس نــم رــثكلأ ةــميدق تاكارــشا لــيعفت ةداــعاو ادــيدج اوــضع اوــضع )180( نــناثو ةــئم نــم رــثكأ لىا ةــيعملجا في نــلعافلاو نبــستنلما ءاــضعلاا ددــع لاــمج في ناك نا تاراــهم تاــبثا نــم مــهنكمتل اــنئابطأب يرــخف نــع برــعأ نا لاا ينعــسي لا اــك .ةقباــسلا ننــسلا في ةــنراقم %150 ةبــسنب عاــفترا يا .ةــيلودلاو ةــيلحلما ،ةــيملعلا تارــتمؤلما مــهأ في نــيضراحمك ةــلعفلا تاكاراــشلما للاــخ نــم يــملعلا لاــجلما في وا لودــلا فــلتمخ في لــمعلا كــلذ لكــشيف نــيزيمتم نــيضرامح نــم ةــبكوك هــيف عــمتتج ثــيح ،رــخا يــملع ءاــقلل ةبــسانم ةــينانبللا نانــسلاا مــيوقت ةــيعملج نــيشرعلا رــتمؤلما تيأــيو في مهاــس نــم لك لىا ركــشلا لــيزج هــيجوت دــيرأ اــنه نــمو .يــعمالجا مــهصصتخ ةــلحر في ةــمهم ةــطمح اــنبلاطلو مــتهامولعم رــيوطتل ءلاــمزلل ةــصرف ةكراــشملل مــهتقوب اوــلخبي لم نــيذلا نــيضراحلما لىا اــضياو لودــلا فــلتمخ نــمو ناــنبل نــم اوــمدق نــيذلا ءازــعلأا ءلاــمزلاب أدــبأ ،رــتمؤلما اذــه حاــجن اــنرتمؤم نــم أزــجتي لا اءزــج تــتاب ذا ةــيعمجلل ةــمئادلا ةــمعادلاو ةــيفولا تاكشرــلا لك لىا صاــلخا ركــشلاب هــجوتأ اــعبطو ،مــتهبرخب رــتمؤلما اوــنغأف .يونسلا ةــيميظنتلاو ةــيملعلا نــتنجللا لــبق نــم لذــب يذــلا راــبلجا دوــهجلماب هوــنأو ةــيعملجا ناــلج فــلتمخ في يــئاقدصأو يــئلامزل نياــنتما نــع برــعأ ارــخأو .لياوــتلا ىــع لوــبحد يداــف روــتكدلاو هداعــس اــيرام ةروــتكدلا ةداــيقب ،ءازعلأا يئلامز ببــسب رــتمؤلما ءاــغلا ةــيضرفل ناــيحلأا ضــعب في هــجوتلاو قبــس يذــلا في وا رــتمؤلما اذــه في ناك نا ،اــنتهجاو يــتلا تاــبوعصلا لك مــغر ىرــخأ ةرــم قوــتيو ةاــيلحا بــيح ،رــكني لا بعــش اــننا دــيدج نــم تــبثنل اــعم موــيلا فــقن اــنهه ،دلاــبلا اــبه رــتم تــلاز اــمو تــناك يــتلا ةــقيقدلا فورــظلا .اــنب قــينفلا رــئاط هيبــشت ىدــجلاا لــب قــينفلا رــئاطب انهيبــشت ادــعاصف نلاا نــم زوــيج لاــف ةرــم لك في داــمرلا تــتح نــم ثــعبني ،ملاــسلل .ةمداقلا ةنسلا في ءاقللا لما ىع مكتقوب اوعتمتست نا ىنتماو اددمج مكب بحرا ،رتمؤملل هتياعرل سنوي دلانور روسفوبرلا ركشأ نانسلأا ميوقتل ةينانبللا ةيعملجا سيئر - دادح يزمر روتكدلا
Lebanese Orthodontic Society 26-27 January 2024, Mövenpick Hotel, Beirut






67 Dental News Quarter II
Dr. AhmeD Zribi Lecturing on SmiLe trAnSformAtion with tADS
Prof ronALD YouneS, PreSiDent of the LebAneSe DentAL ASSociAtion
Prof. mAriA SAADeh hADDAD chAir Scientific committee
L. to r. DrS fADi ghAith, mAriA hADDAD, fADi DAhbouL, SAmer rifAi, rAmZi hADDAD, ALi fAhS, mAuricio bALut, AhmAD Zribi, mAriA hAiDAr
Prof. monA ghoSSoub receiving the certificAte for her Lecture on mAxiLLArY exPAnSion






68 Dental News Quarter II
Dr. JoSePh ghAfAri Lecturing on comPLimentArY inteLLigence in orthoDonticS
DrS. ALY oSmAn receiving the certificAte for hiS Lecture on three DimenSionAL APProAch in orthoDonticS
L. to r. DrS. _ roLA KhALAf, eLie hAYecK, ALine riZK, monA ghoSSoub, DeAn george Aoun, mAriA hAiDAr, mAriA hADDAD
L. to r. DrS. AhmeD Zribi, rAmZi hADDAD, AKim benAttiA
L. to r. DrS. fADi DAhbouL, ronALD YouneS, rouLA AbiAD, DeAn mAgeD fAhmi, SAmer rifAi, nAZem hAffAr, biLAL bArAKe






69 Dental News Quarter II
L. to r. DrS roY SAbri, mAuricio gonZALeZ bALut, LinA meDAwAr
Prof. JoSePh bouSerhAL receiving the certificAte for hiS Lecture on SmiLe eStheticS AnD verticAL DimenSion
Picture from the exhibition
Lumi SmiLe booth
Picture from the exhibition orthoLeADer booth

Tony Dib Interview with Rajender Kumar, General Manager,DS - Middle East & North Africa
What are the advantages that Dentsply Sirona brings to the Dental Office and to the Dental Laboratory?
As more and more dental professionals add digital capabilities to their practices and labs, they need a true partner to help them advance confidently and fully leverage new technologies. We are committed to providing a distinctive customer experience, emphasizing education, innovation, and support for practice growth.
Our digital solutions are designed to simplify treatment, ensuring it is easy, safe, and achieves excellence in terms of accuracy and patient satisfaction. Recent launches, particularly the DS Core platform, exemplify our dedication to this philosophy. DS Core serves as a comprehensive solution, connecting products, services, and technology through a cloudbased platform, fostering efficient
work processes and collaboration among colleagues and partners. Primeprint Solution, our medicalgrade 3D printing system for dental practices and labs, stands out as another exceptional product, offering a multitude of benefits.
The shift to digital dentistry is likened to an investment in digital workflows, where each component seamlessly interacts to yield repeatable, reliable results. This approach to standardization not only mitigates errors but also elevates the overall patient experience and helps to create efficiency for both dental offices and labs.
Our vision is to reinforce our position as a leading digital solutions provider, and continue to grow our already loyal customer base.
70 Dental News Quarter II - 2024
What is the focus or the directions in which DS is leading the dental market to?
Dentsply Sirona has a vision to transform dentistry to improve oral health globally. We believe that the age of digital dentistry has arrived and also represents the future of care. We see the value and importance of digital technologies in dental workflows. That’s why we are focused on delivering the digital dental solutions that meet the needs of dental professionals and of course, their patients – this is how we move dentistry forward collaboratively.
Digitalization is also an enabler for dental professionals to increase their offering and set their practices apart in the eyes of patients. It is important that we keep asking how can we make it easier for the dentist? How can we help them to increase patient acceptance of treatment and to remain in treatment through its completion?
We are doing this by building a digital ecosystem of connected technologies. Together these create a single source for professionals to utilize that helps them to confidently communicate with their patients, improve outcomes, and also gain efficiency to bring more people into dental practices.
DS was the pioneer in CAD/CAM technology, is it still leading the way?
As pioneers in the field of digital dentistry, our unwavering commitment to leadership in this area is a cornerstone of our business strategy. To fuel continuous progress, we allocate over $180 million annually towards advancing dentistry, supported by a robust research and development team comprising more than 650 scientists and engineers. As a customer-centric organization, we collaborate closely with our customers and dental experts, ensuring a holistic understanding of their practice needs and fostering the development of cutting-edge solutions for the future.
In our relentless pursuit of innovation, we recognize the pivotal role technology plays in shaping our offerings. With a focus on maintaining the highest standards of research, we are dedicated to refining the technology that underpins our innovative solutions. Additionally, we strive to provide dental professionals with up-to-date resources, enabling them to expand their clinical knowledge and digital skills in tandem with the evolving landscape of dentistry.
A prime example of this commitment is evident in our 3D printing technology. Already a transformative force in the dental industry, 3D printing is actively contributing to the production of surgical guides and aligners, with vast potential to become a key technology for this part of dentistry. Recognizing the significance of 3D printing, we developed Primeprint Solution to be fully automated and the process is incredibly streamlined. And we continue working to enhance its efficiency and productivity and increase its indications of use.
In essence, our dedication to leadership, innovation, and technological excellence positions us at the forefront of digital dentistry, driving the evolution of solutions that not only meet current needs but anticipate and address the challenges of tomorrow.
How are you helping the dental offices in the digital migration?
I mentioned that we want to be a true partner, helping our customers to give their patients the best possible care to achieve healthy smiles, and to achieve their professional goals. In that spirit of partnership, we can guide dental professionals on their journey into the digital practice and laboratory. Regardless of where a dental office is on its journey into digital dentistry, Dentsply Sirona offers the right solutions and the clinical education –both online and in-person – to integrate new technology into the workflow and take the next
71 Dental News Quarter II Interview with Rajender Kumar
steps in that journey.
Our Dentsply Sirona Academy offers both live and on-demand educational programs. Each year, we engage approximately 490,000 dental professionals through the DS Academy’s educational courses.
Is DS striving to offer the dental market quality products and services?
We strive to deliver great products and solutions with an uncompromising focus on quality in everything we do. That’s something that we have recommitted to as a company. And to help ensure that, we maintain strong relationships with many leading dental professionals worldwide. We listen to their needs and integrate their feedback into our development processes.
Dentsply Sirona has a proven track record
in terms of innovation and bringing quality solutions to market. Our aim is not to digitalize analogue procedures, but to develop digital dentistry that advances dentistry as a whole. In other words, we don’t want to be known just for digital dentistry; we want digital to be synonymous with better.
Managing a broad portfolio is not new to us and we are focused on connecting this product portfolio intelligently. We have developed a range of signature workflows designed to help dental professionals seamlessly integrate products and equipment from our end-to-end portfolio to optimize efficiency and ensure confidence at every step of the patient journey. This has the added benefit of improving the patient experience while also being able to handle more cases in less time – key factors for growing a practice.

72 Dental News Quarter II - 2024
Interview with Rajender Kumar


AEEDC Dubai, 6-8
February 2024, WTC Dubai

The 28th UAE International Dental Conference and Arab Dental Exhibition (AEEDC Dubai 2024) concluded with unprecedented success, boasting a groundbreaking record of business deals totaling AED 19 billion and a remarkable attendance of 70,000 participants from 180 countries.
The event drew a diverse audience, showcasing 5,328 brands represented by 3,924 international companies specializing in oral health supplies and dental technology. A highlight of the conference was the hosting of the 21st annual meeting of the Global Scientific Dental Alliance (GSDA) on its third day, which attracted 383 members from around the world. These delegates, representing 184 international medical organizations, hospitals, academic institutions, dental associations, global health ministries, and various governmental and private sectors, included esteemed representatives from universities and dental colleges worldwide.
During the meeting, the Global Dental Alliance unveiled the “GSDA 2024 Declaration,” a collaborative initiative serving as a strategic framework with essential guidelines, recommendations, and solutions aimed at driving future innovations and enhancements across the dental field. Comprising eight main
pillars, this declaration covers leadership in dentistry, dental operational efficiency, dental innovation advancement, dental education, patient-centric dental care, dental community engagement, sustainable dental practices, and dental procedure guidelines and policy excellence.
His Excellency Amb. Dr. Abdulsalam AlMadani, PAM Roving Ambassador for the GCC Region, Executive Chairman for AEEDC Dubai, and the Global Scientific Dental Alliance (GSDA), commended the tremendous success of the annual meeting, emphasizing the importance of continuous education and scientific research in advancing the field of dental and oral health. He stated, “There is no limit to the development of the dental and oral health sector.”
Furthermore, H.E. Amb. Dr. Abdulsalam AlMadani underscored the sector’s commitment to maintaining its position as the most advanced among medical sectors and invited scientific bodies and organizations specializing in dentistry to actively participate in and contribute to the annual global forum, thus furthering the dissemination of scientific knowledge and innovation in dentistry.
74 Dental News Quarter II







75 Dental News Quarter II
PeriOPtix BOOth
PrOMeDiCA BOOth
SDi Booth NSK Booth
AEEDC opENiNg CErEmoNy
SChEU Booth








76 Dental News Quarter II
ACtEoN Booth
A-DEC Booth Dmp Booth
DUrr Booth
BElmoNt Booth
ArAB DElEgAtES At thE itAliAN pAvilioN
CUrAproX Booth
DENtAUrUm Booth exhibition





77 Dental News Quarter II
hU FrieDY BOOth
mESA implANt Booth FKg Booth
NEoSS Booth itAliAN pAvilioN exhibition


vOCO BOOth




78 Dental News Quarter II
UltrADENt Booth
exhibition
SEptoDoNt Booth
GerMAn PAviliOn in the COnCOUrse
EmS Booth







80 Dental News Quarter II
ChristiAn COAChMAM tAlkinG On the Present AnD FUtUre OF DentistrY
Dr. riCCArDO tOnini leCtUre On enDOPeriODOntAl lesiOns AnD PerFOrAtiOns
Dr. DinA DBAYBO ChAirinG the PeDiAtriC DentistrY sYMPOsiUM
Dr nOrA AlhAzMi leCtUre ABOUt GenetiCs AnD OrthODOntiCs
Dr. zUhAir nAttO leCtUrinG On DesiGn AnD stAtistiCAl AnAlYsis in DentAl reseArCh
PrOF. AlAin rOMAnOs sheDDinG liGht On hOw tO DeAl with MAlPOsitiOneD PlACeD iMPlAnts





81 Dental News Quarter II
Drs. AlessAnDrO AnD AnDreA AGnini reCeivinG the CertiFCAtes FOr their leCtUre On the MAnAGeMent OF the PeriiMPlAnt PAPillA
l
PrOF. AlY shArAF reCeivinG the CertiFiCAte FOr his leCtUre On esthetiC restOrAtiOns in PresChOOlers
tO
r. PrOF nOUr hABiB, tArek ABBAs, AhMAD GAMAl
PrOF. AMr MOUrsi reCeivinG his CertiFiCAte AFter his leCtUre On MiniMAllY invAsive CAries MAnAGeMent FOr PeDiAtriC PAtients
PrOF. FABiO GOrni leCtUre ABOUt rOAD tO exCellenCe in enDODOntiCs MiCrOsUrGerY


l to r. Prof. tAreK AbbAs, nAhAwAnD thAbet, sAmeer reDwAn, hetAf reDwAn, tony Dib

l. to r. Drs. AysAr KAbbAch, ZuhAir nAtto, sArA AlAnqAri, leilA bAhAmAm, KholouD AlAli, sArA AlsubAit

l. to r. Drs. mohAmeD AlhArbi, linA meDAwAr, chArbel AllAm, tony Dib

l. to r. Drs. tony Dib, fAten benAmor, ADel benAmor, AKim benAtiA
82 Dental News Quarter II
ArAb DelegAtes with Prof. AbDullAh AlshAmmery At the DentAl news booth



DrS. toNy DiB, tArEK ABBAS, mUShirA SAlAhUDiN, grEg ChADwiCK-prESiDENt oF thE FDi


l. to r. roDNy ABDAllAh, tArEK ABBAS, mAyA NohrA, JoSiANE DiB, piErrE
83 Dental News Quarter II
Dr. roBErt EDwAB, proF. KhAlil AlEiSA
KhoUry, NoUr hABiB, ANtoiNE ChoUFANi, toNy DiB
DrS. Ali ZAhrANi, ABDElAZiZ JEhANi, toNy DiB, roBErt EDwAB, mEShAri AlotAiBi, pAUl wilSoN, KhAlil AlEiSA
l to r mohAmED ElghAK, FoUAD FArhAt, EiD KhAlil, ABoUBAKr rAwi, mohAmED oBEiDA, BASEm mAAtAr, ZiAD EllAhEm, hANi SAlAm

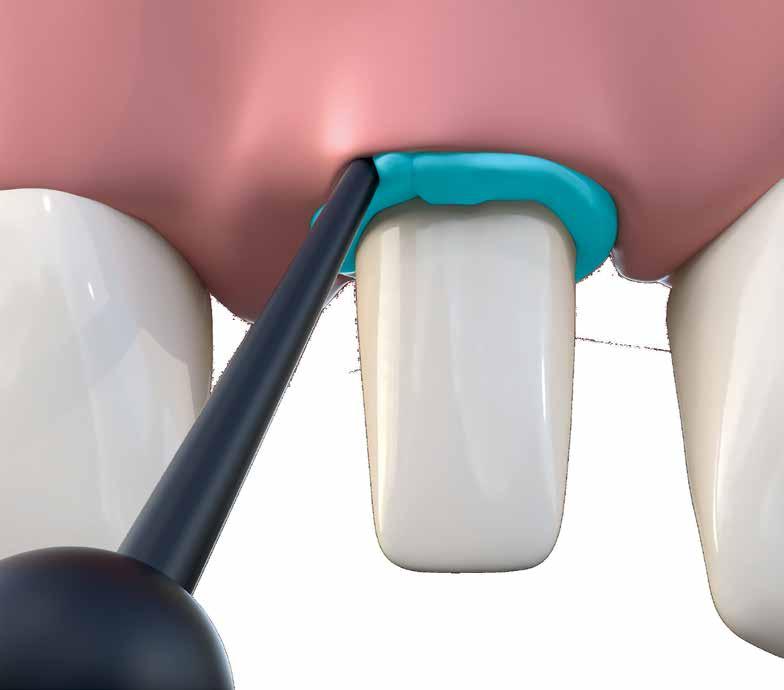
THE CORD FROM THE CAPSULE
• Thin cannula with flexible tip – easy and pinpoint application into the sulcus
• Viscosity Change – paste consistency varies during application and sulcus widening
• Good visibility – contrasty to the gingiva
• A clean product – quick and easy to spray off Easy application into the sulcus
VOCO Retraction Paste
For more information please contact VOCO‘s Business Development in Middle East/Northern Africa, Mohamad El Fil (+961-3-805758 / m.elfil@voco.com).

VOCO GmbH · Anton-Flettner-Straße 1-3 · 27472 Cuxhaven · Germany · Tel. +49 4721 719-0 · www.voco.com
King of Less Radiation and Extended FOV in a Compact Unit

Our 11 x 14 FOV is sufficiently large to extend up to the condyles. Reverse the trend and explore the field of view that enables you to cover all your scanning requirements with reduced patient exposure. Join us and experience the difference!
X-VIEW, YOUR BEST CHOICE
trident-dental.com
Discover a world of images
X-VIEW 3D CBCT
