How CBCT is becoming an essential tool in decision making?
EDSIC 2021
2021
DECEMBER 2021
YEARBOOK 2022
APEC


























How CBCT is becoming an essential tool in decision making?
EDSIC 2021
2021

• Unbeatably durable: Fully withstands masticatory forces, excellent physical properties1
• Unbeatably simple: Universal shade with chameleon effect, 4 mm bulk fill
• Unbeatably quick: Exposure time of only 10 seconds (x-tra fil), applied in one layer – only 35 seconds total working time (Futurabond M+)
1 Tiba A et al., Journal of American Dental Association, 144(10), 1182-1183,2013.
2 based on sales figures
More than 13 million restorations worldwide!2























Based on the close and fruitful cooperation with dental institutes and practicing dentists since the 1940s, we have a uniquely broad portfolio of specially developed, innovative toothpastes, gels, sprays, mouthwashes and mouth baths. These products, which are marketed under the brands Tebodont®, Emofluor®, Emoform®, Depurdent® and Emofresh® are sold exclusively in pharmacies in Switzerland and in more than 40 other countries outside Switzerland, their various innovative formulations and compositions offer excellent solutions for daily dental care, addressing specific needs and problems (e.g. caries prevention, sensitive teeth, gum problems) and general oral health.
With the REDESIGN we have clarified the positioning of the oral care products: every toothpaste and every mouthwash now has a clear application area. At the same time, our new packaging is "digitalized": each product has a QR code that allows detailed information to be downloaded directly to the mobile phone. The redesign of the products should make the Wild brand tangible and perceptible.
• WILD will be used as umbrella brand on all products, which results in an easier promotion among the whole product range
• Same design for all brands leads to recognition and synergy effects across product range
• Clear unique main indication on the packaging avoids confusion among dental profession, pharmacists and end consumers due to overlapping benefits
• New design underscores clinical benefits and professionalism of the products which leads to cross-brand and cross-portfolio products awareness and helps to create trust among the dental profession, pharmacists and end consumers
• Unifying of the packaging system - all toothpastes in the same size and shape of tubes, all mouthwashes in the same size and packaging - leads to a uniform, eye-catching and space-saving shelf-impact
• Product portfolio becomes fresh, easy to recommend and attractive for the POS
Volume XXVIII, Number IV, 2021
EDITORIAL TEAM
Alfred Naaman, Nada Naaman, Khalil Aleisa, Jihad Fakhoury, Dona Raad, Antoine Saadé, Lina Chamseddine, Tarek Kotob, Mohammed Rifai, Bilal Koleilat, Mohammad H. Al-Jammaz
Suha Nader
Marc Salloum
Micheline Assaf, Nariman Nehmeh
Josiane Younes
Albert Saykali
Gisèle Wakim
Tony Dib 1026-261X
DENTAL NEWS IS A QUARTERLY MAGAZINE DISTRIBUTED MAINLY IN THE MIDDLE EAST & NORTH AFRICA IN COLLABORATION WITH THE COUNCIL OF DENTAL SOCIETIES FOR THE GCC.
Statements and opinions expressed in the articles and communications herein are those of the author(s) and not necessarily those of the Editor(s) or publisher. No part of this magazine may be reproduced in any form, either electronic or mechanical, without the express written permission of the publisher.
DENTAL NEWS – Sami Solh Ave., G. Younis Bldg. POB: 116-5515 Beirut, Lebanon.
Tel: 961-3-30 30 48
Fax: 961-1-38 46 57
Email: info@dentalnews.com Website: www.dentalnews.com www.instagram.com/dentalnews

January 20 - 22, 2022 Riyadh, KSA www.sidc.org.sa





February 1 - 3, 2022 Dubai, UAE www.aeedc.com
March 9 - 11, 2022
Cairo, EGYPT www.idexegy.com
March 22 - 24, 2022 Amman, JORDAN www.confjda26.com
May 19 - 21, 2022 Rimini, ITALY www.expodental.it

September 29 - October 2, 2022 Mumbai, INDIA www.fdiworlddental.org Saudi International Dental Conference
June 9 - 11, 2022
Chia Laguna, Sardinia, ITALY www.congressaio.it

October 12 - 14, 2022 Almaty, KAZAKHSTAN www.cadex.kz/en
8. P Dhanrajani, Tony Rynberg, Gabriel Hajjar
How CBCT is becoming an essential tool in decision making

How Often Are Dental Care Workers Exposed to Occupational Characteristics that Put Them at Higher Risk of Exposure and Transmission of COVID-19?

28. The material of the future for all kind of indications
Nicolás Gutiérrez Robledo

September 1 - 3, 2021 Cairo, Egypt

September 9 - 11, 2021 Beirut, Lebanon

3SHAPE 56
BELMONT 58
BISCO 60
CAVEX 62
CENTRIX 64
DENMAT 66
DENTSPLY SIRONA 68
DMP 70
MANI 72
RENFERT 74
ULTRADENT 76
WHITESMILE 78
3SHAPE 13
A-DEC 17
ACE SURGICAL 9
BA INTERNATIONAL 41
BELMONT 15
BISCO 11
COLTENE 33
DENTAURUM 12
DENTSPLY SIRONA C3
DMP 1
DXP 35
DURR 19
EDGE ENDO 49
FKG 39
HENRY SCHEIN 53
NSK C2
PROMEDICA 25
ROLENCE 20
SCHEU 32,
SEPTODONT 80
TRIDENT C4
ULTRADENT USA 27
VOCO 2, 29
WILD 3, 4, 5

Dr P Dhanrajani BDS, MDS, MSc, MSC, FRACDS, FDSRCS, FFDRCSI Oral Surgeon
dan.dhanrajani@gmail.com
Dr Tony Rynberg, BDS Senior Dentist
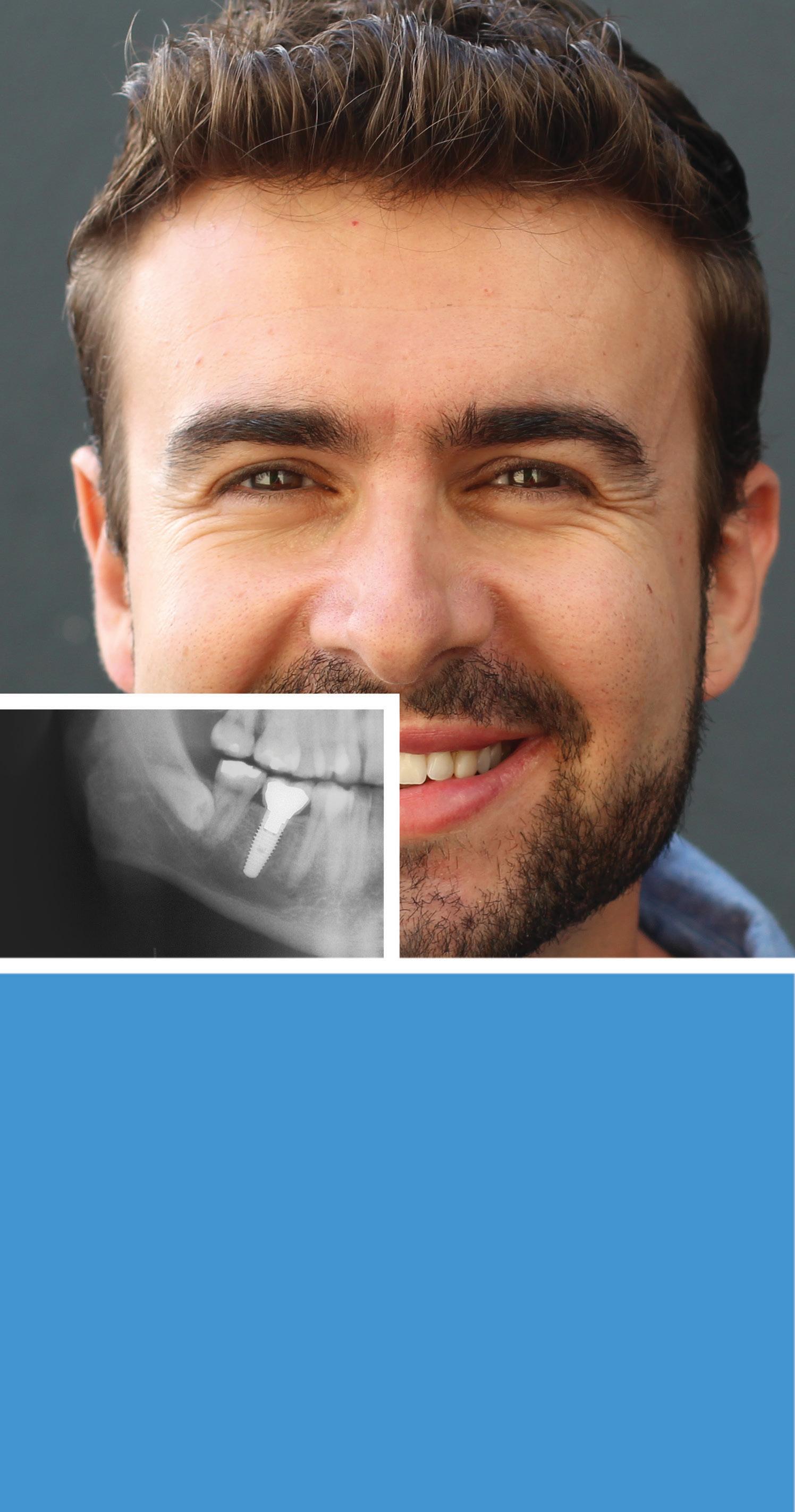
Radiographic signs, detectable on an orthopantomogram (OPG) indicating the presence of close relationship between the inferior alveolar nerve (IAN) and lower third molar requires further investigation to better understand its relevant course. Cone beam computed tomography (CBCT) is an essential radiographic investigation for understanding the accurate course of the IAN in high risk mandibular third molars. This has become a standard preoperative risk assessment for lower third molar procedures1,2,3
becoming the standard of care to assess its applicability during the development of the treatment plan and to explain the advantages and disadvantages during the consultation4,5
Dr Gabriel Hajjar, BDS HCF Dental Centre Network Clinical Manager
Coronectomy has been proposed as a valid treatment option to reduce the risk of inferior alveolar nerve (IAN) injury in selected cases. It is increasingly
The technique of coronectomy as described by Pogrel6, where the tooth is sectioned at the CEJ is being used more widely within the profession since then. The modified coronectomy is a variation of the technique where the crown is sectioned at or below the furcation with further reduction of the height of the roots. This aims to allow a good skirt of alveolar bone around the roots and the advancement of the buccal flap to achieve primary closure for good postoperative bone and soft tissue healing.
This paper supports the routine use of CBCT as a preoperative decision-making tool for the removal of lower third molars to prevent IAN nerve injuries. The traditional state of the art imaging, orthopantomogram (OPG), may be sufficient in most cases, however CBCT is essential, when one or more signs of close contact between the tooth and mandibular canal are seen on standard panoramic radiography.
Imaging investigation is undoubtably an essential protocol required to achieve proper diagnosis and to executing treatment plan. The traditional method and state of art is panoramic imaging. There are some limitations of this two-dimensional imaging which
Solid solutions for maintaining and promoting healthy bone. Backed by years of documented and proven success, our products have been engineered to meet your specific surgical needs.
lacks in high diagnostic accuracies when it comes to assessment of the risk in surgical extractions of lower third molars. Extractions of lower third molars carry risk to the inferior alveolar nerve (IAN), varying from 0.42% to 7.8%. Risk varies between the operating skills of individuals. The cost of medicolegal litigation settlement in these cases have been sky rocketing1,2
Increasing use of cone beam computed tomography (CBCT) aids assessment of the relationship of the IAN and roots in providing treatment planning to reduce the risk of nerve trauma. Coronectomy is an alternative procedure increasingly accepted world-wide to reduce the risk of nerve injuries3,4,5
This paper presents and highlights the shortcoming of panoramic imaging and elaborates the importance of cone beam CT as an important tool in visualising the course of inferior alveolar nerve in relation to lower third molars. Nowadays the CBCT technology is available in most of the chairside clinics and clinical situation like this can get advantage in achieving proper diagnosis and executing appropriate treatment plan.
A 23-year-old girl presented to the oral and maxillofacial clinic referred by her general dental practitioner as an emergency. She had history of recurrent pain and discomfort associated with her lower wisdom teeth. The dentist attempted to remove her lower right wisdom tooth (RL8) under local anaesthetic to alleviate pain but was not able to anaesthetise and decided to refer her to a maxillofacial surgeon.
She was fit and well and a regular visitor to her dentist. During the consultation visit, the patient described having pain on the right lower side. Clinical examination revealed that RL8 was partially erupted showing mild pericoronitis with soft tissue lacerations, suggesting a recent attempted extraction. LL8 was impacted, UR8 was buccally inclined and UL8 partially erupted and buccally inclined and traumatising cheek mucosa.
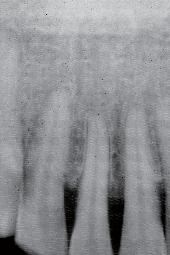
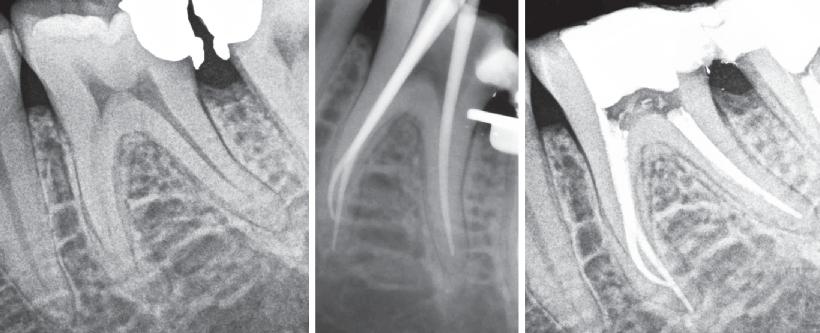
An orthopantomogram (OPG) revealed RL8 and LL8 were mesioangularly impacted and their roots were crossing both upper and lower white lines of the inferior alveolar canal (IAC). LL8 roots showed darkening of root at the level of IAC (Fig 1).

It was decided to request a Cone Beam CT to substantiate findings of the routine OPG in relation to the IAN.
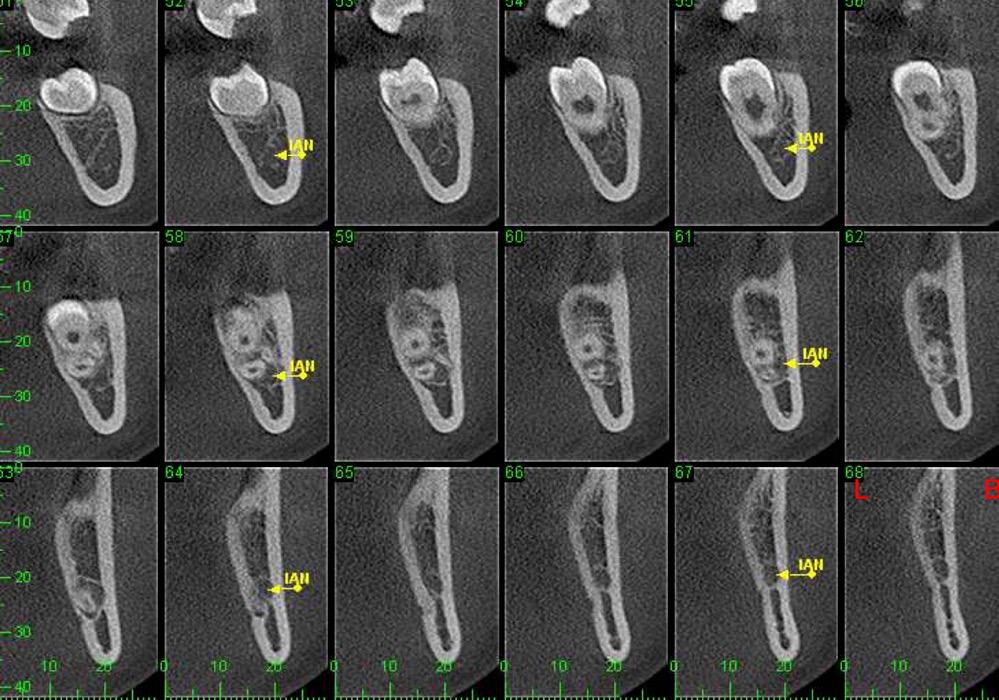
CBCT revealed the following findings:
LL8: IAC was running buccal to roots of LL8 which had 3 roots (Fig 2).
RL8: IAC was seen running between the buccal root which was hooked mesially and lingual roots at its apex, vulnerable to surgical injury (Fig 3).

















On discussion with the patient, keeping in mind the clinical and CBCT findings, the option of coronectomy was suggested for LL8 and RL8. If roots become loose during the procedure, then complete removal. The patient consented to have her wisdom teeth removed and coronectomies for the lower wisdom teeth under general anaesthesia.



























A standard coronectomy technique for removal of RL8 tooth was carried out. Lingual periosteum was not reflected to avoid lingual nerve injury. Following sectioning and trimming of the tooth until the cementoenamel junction (CEJ), there was insufficient soft tissue to achieve primary closure of the socket.
The decision on which abutment is best for your patient – conical or platform – is yours.

To achieve good primary closure, it was decided to modify the procedure and trim the roots up to the furcation to ensure a sound collar of alveolar bone and advance the buccal flap. This modification helped significantly during primary closure of the socket. LL8 tooth was removed completely as the roots became loose as well as UR8 and LU8. The post-operative phase was uneventful, and she recovered well (Fig 4).
Radiographic examination precedes and contributes to the treatment planning and decision making of removal of lower wisdom teeth and aims to reduce post-operative complications. OPG will often be the first gold standard imaging method of choice for evaluation of mandibular third molars.
An OPG finding undoubtably provides valuable information about state of impaction, tooth position, morphology of roots and most importantly the relation between tooth/roots and the mandibular canal3,4,5


Introducing 3Shape Unite. An open platform that brings together world-leading dental companies, solutions and labs. Manage all your cases with choice and ease, from TRIOS scan to treatment completion.

Simply connect to the right partners with app-based efficiency and make digital dentistry easier than ever with 3Shape Unite.
Studies6,7 suggest that seven specific signs observed on OPG:
a. darkening of roots b. deflection of roots c. narrowing of roots d. bifid root apex e. diversion of canal f. narrowing of canal g. interruption of white lines of canal
are a reliable way to assess the relationship between third molars and the mandibular canal. From the above seven signs, interruption of radio-opaque white lines of the canal, diversion of canal and darkening of the roots are the most valid to predict a close contact which guides the clinician to investigate the relation further by requesting a CBCT8 In recent years, coronectomy has been put forward as a valid treatment modality where the risk of injury to IAN is imminent. The technique is gaining popularity worldwide but still remains controversial.
Salzma et al9 did a study comparing high risk signs identified on OPG in impacted third molars and CBCT and their effect on treatment decisions. The result showed surgeons confidence in treatment decisions increased after CBCT imaging resulting in fewer coronectomies.
The population of this study was specialist oral and maxillofacial surgeons. Another study by Baqain et al10 reported use of CBCT provides a better understanding of the anatomic relationship between IAN and roots of lower third molars. However, they found that for experienced surgeons dealing with impacted lower wisdom teeth with evidence of proximity to IAC, an OPG alone could decide on the treatment modality without CBCT. This is contradictory to our presentation. The case presented was successfully managed by a modified coronectomy and achieved good primary closure and subsequent healing.
This case also raises the limitation of the traditional method of imaging with an OPG and shows the importance of CBCT in deciding on the treatment plan. The patient initially visited her dentist in pain with the RL8 and the dentist attempted to remove the tooth to alleviate pain based only on her OPG finding which showed the root apex crossing the upper white line of IAC. Only after referring to a specialist, where CBCT revealed the course of IAC running between the roots of RL8, was the risk of nerve injury avoided.
It is becoming the standard of care for both general dentists interested in removal of third molar, as well as oral and maxillofacial surgeons, to request and assess a CBCT where the proximity of the roots to the IAN is in
question. Coronectomy offers a safe alternative where extraction of lower third molars has an established high risk of IAN injury. The evidence that is emerging so far is quite encouraging and in general shows good outcomes.
Two lessons to be learnt from this case are:
1. If the dentist had removed the tooth without the CBCT finding, IAN injury was highly likely.
2. A modified coronectomy is sometimes required to achieve primary closure and avoid a gap in the wound and post op healing issues.
SC: Standard coronectomy MC: Modified coronectomy
IAC/N: Inferior Alveolar canal/Nerve LN: Lingual Nerve
OPG: Orthopantomogram CBCT: Cone Beam CT scan
1. Matzen L, Wenzel A. Efficacy of CBCT for assessment of impacted third molars: a review-based on hierarchical model of evidence Dentomaxillofacial Radiology 2015; 44: 20140189.
2. Neves F, Souza T, Ameilda S, Haiter-Neto F, Freitas D and Boscolo F. Correlation of panoramic radiography and cone beam CT findings in the assessment of the relationship between impacted third molars and the mandibular canal. Dentomaxillofacial Radiology 2012; 41: 553-557.
3. Martzen L, Christensen J, Hintze H, Schou S, Wenzel A. Influence of cone beam CT on treatment plan before surgical intervention of mandibular third molars and impact of radiographic factors on deciding on coronectomy vs surgical removal. Dentomaxillofacial Radiology 2113; 42: 98870341: 2-8.
4. Dhanrajani PJ, Smith M. Coronectomy: A recognised procedure? Oral Surg 2018;11:4:273-282.
5. Dhanrajani PJ, Smith M. Coronectomy Patients with comorbidities, carious teeth and associated cyst, 10 years’ experience. Dentalnews; 2021, 8-22.
6. Pogrel MA, Lee JJ, Muff DF. Coronectomy: A technique to protect the inferior alveolar nerve. Journal of Oral and Maxillofacial Surgery 2004; 62; (12): 1447-1452.
7. Rood J, Shehab B. The radiological prediction of inferior alveolar nerve injury during third molar surgery. Br J Oral Maxillofac Surg 1990;28:20-25.
8. Renton T. Update on coronectomy. A safer way to remove high-risk mandibular third molars. Dental Update 2013; 40: 362-368.
9. Szalma J, Vajta L, Lovasz B, Kiss C, Soos B, Lempel E. Identification of specific high-risk signs in impacted third molar cases in which cone beam computed tomography changes the treatment decision. J Oral Maxillof Surg 2020;78:1061-1070.
10. Baqain Z, AlHadidi A, AbuKaraky A, Khader Y. Does the use of ConeBeam Computed Tomography before mandibular third molar surgery impact treatment planning? J Oral Maxillofac Surg 2020;78:1071-1077.







Community Dentistry
Abstract
Sonica Singhal, BDS, MPH, PhD, FRCD(C) public health dentistsonica.singhal@mail.utoronto.ca
Christine Warren, MPH epidemiologist
Introduction: Occupational characteristics of dental care — including closed environment, proximity to staff and patients and the use of aerosol-generating procedures — put workers at high risk of COVID-19 exposure and transmission. We describe the frequency of workplace situations that potentially increase the risk of exposure to COVID-19 in dental care compared with other occupations including health care.
Erin Hobin, PhD scientist
Brendan Smith, PhD scientist
Methods: We conducted a cross-sectional study using sociodemographic and occupational data from the 2016 Canadian census linked to workplace characteristics from the Occupational Information Network (O*NET) dataset. We assessed frequency of workplace indicators using an intensity score from 0 (low) to 100 (high) from O*NET on exposure to infection or disease, physical proximity to others, indoor controlled environments, standard protective equipment and specialized protective equipment.
Results: In 2016, 87 815 Canadians worked in the 5 dentistry occupations of interest: dentists; denturists; dental hygienists and dental therapists; dental technologists, technicians and laboratory assistants; and dental assistants. These occupations were routinely ranked in the top 10 of all occupations examined in terms of exposure to workplace indicators that increase the risk of exposure to COVID-19. Dental hygienists and dental therapists, dental assistants, dentists and denturists, rank as the top 4 occupations, in that order, with the highest exposure to disease or infection and physical proximity to others combined.
Conclusions: Compared with other occupations, dental care workers are at a higher risk of occupational exposure to COVID-19. These results support the development of workplace guidance to reduce the risk of COVID-19 transmission and enhance the well-being of the dental care workforce.
Occupational risk assessment is a method “for estimating health risks from exposure to various levels of a workplace hazard.”1 As workplace transmission was observed early in the COVID 19 pandemic,2 characterizing the role of the workplace in COVID-19 exposure and transmission became an important public health consideration.
Agencies, including the World Health Organization,3 the Canadian Centre for Occupational Health and Safety4 and the Centers for Disease Control and Prevention (CDC),5 emphasize the importance of understanding the risk of exposure to and transmission of COVID-19 associated with varying occupations and implementing workplace safety or mitigation strategies accordingly. Republished from


Current evidence indicates that COVID-19 spreads primarily among people who come into close contact (≤ 2 m); transmission is via respiratory droplets generated when an infected person coughs, sneezes or talks.5 There is increasing evidence that transmission also occurs through aerosols and less evidence that surface transmission is a major route.6 Health care workers are considered to be at a higher risk of exposure to infectious diseases compared with other occupations. Their increased COVID-19 risk results from the provision of treatment, performing “essential” and other routine services for patients with COVID-19 and regular communication with staff and the public in a typical work day.7 In Canada, as of 23 July 2020, 19% (21 842) of all COVID-19 cases were among health care workers.8
A CDC data from 13 locations in the United States between 1 March and 31 May 2020 showed that health care workers accounted for 6% of adults admitted to hospital with COVID-19.9 Dental care workers face unique challenges in mitigating COVID-19 transmission when delivering care as they work in closed environments in close proximity to staff and patients and they conduct aerosol-generating procedures.10,11 COVID-19 outbreaks have been reported in dental offices in Canada,12-17 although none included provider-to-patient or patient-to-provider transmission.
However, any time an outbreak is reported, it creates panic among dental workers, regulators and associations, and queries related to the nature and extent of the outbreak arise. This raises an important question: what is the risk of occupational exposure to COVID-19 in the dental care workforce compared with other occupations including health care? Understanding the occupational characteristics that increase the risk of COVID-19 exposure and transmission would support the development of upstream prevention measures for the profession, both at the workplace (e.g., developing workplace policies, training dental staff about infection prevention) and regulatory levels (e.g., paid sick leave, compensation for exposure to hazard during a pandemic).7
We conducted a cross-sectional study of employed people aged 15 and over who completed the longform 2016 Canadian Census of Population. The longform 2016 Census was completed by 25% of Canadian households and includes detailed information related to demographic, social and economic characteristics.18 For this study, Statistics Canada provided customized aggregate-level tables of data from the 2016 Canadian
census, which included 18,497,145 labour force participants.18 The 2016 census classified occupation using the hierarchical National Occupational Classification (NOC) 2016 system. We identified occupations using the NOC 2016 4-digit unit group codes, representing the most specific occupational description available (n = 500).
Occupational characteristics of interest were provided by the publicly available Occupational Information Network (O*NET) database (v. 24.3; updated May 2020) developed by the United States Department of Labor/ Employment and Training Administration.19 O*NET is a comprehensive database20 that includes characteristics (e.g., skills, knowledge and abilities) on 974 Standard Occupational Classification (SOC) occupations in the United States.21
Occupational characteristics from O*NET were mapped to occupations in the 2016 census using a publicly available “crosswalk” between occupational classifications systems from the United States (SOC)21 and Canada (NOC 2016), described elsewhere.22 This data linkage combines a rich set of population-representative occupation and sociodemographic data in Canada with comprehensive data on workplace indicators that increase risk of exposure to and transmission of COVID-19. Complete O*NET information was available for 485 of 500 NOC 2016 4-digit occupations.
O*NET gathers information on occupational indicators through self-reported Likert-scale ratings in questionnaires administered to about 25 people in each SOC occupation.23 For each indicator, occupationspecific continuous weighted-average intensity scores, ranging from 0 to 100, are calculated.23 Recently, O*NET indicators have been used to describe occupational characteristics related to COVID-19 risk in the United States and the United Kingdom.24-27 Based on the existing literature and established COVID-19 risk factors, such as close physical contact, aerosol transmission in indoor settings and accessibility of personal protective equipment (PPE),10,11,24-28 5 O*NET indicators were selected for this study. For each of these, the specific questions asked and derived continuous weightedaverage intensity scores were as follows.
• Frequency by which workers are exposed to diseases or infections: Based on the question “How often does this job require exposure to disease/infections?” intensity scores were: 0 = never exposed, 25 = once a year, 50 = once a month, 75 = once a week, 100 = every day.




The VistaPano S Ceph is the efficient X-ray solution for jaw orthopaedics and more. It supplies fast Ceph shots (4.1 seconds) with outstanding image quality and low exposure to radiation. At the same time, thanks to S-Pan technology, its 2-D panorama shots provide excellent definition. More at www.duerrdental.com



• Physical proximity to other workers in a typical workday: Based on the question “How physically close to other people are you when you perform your current job?” intensity scores were: 0 = do not work near people, 25 = work with others, but not closely, 50 = slightly close, e.g., shared office, 75 = moderately close, e.g., arm’s length, 100 = very close, e.g., near touching.
• Indoors, environmentally controlled: Based on the question “How often does this job require working indoors in environmentally controlled conditions?” intensity scores were: 0 = never, 25 = once a year, 50 = once a month, 75 = once a week, 100 = every day.
• Wear common protective or safety equipment: Based on the question “How much does this job require wearing common protective or safety equipment?” intensity scores were: 0 = never, 25 = once a year, 50 = once a month, 75 = once a week, 100 = every day.
• Wear specialized protective or safety equipment: Based on the question “How much does this job require wearing specialized protective or safety equipment, such as breathing apparatus, safety harness, full protection suits or radiation protection?” intensity scores were: 0 = never, 25 = once a year, 50 = once a month, 75 = once a week,
100 = every day. In addition, ability to work from home (yes/no) was assessed given its potential for reducing an occupation’s risk of COVID-19 infection transmission. Ability to work from home was derived for SOC occupations from Dingel & Nieman’s white paper,29 by applying cut-offs to ordinal responses for 17 O*NET indicators related to work context and activities.

Huge Panasonic ba�ery capacity 2900mAh. Up to 1500 exposures a�er fully charge.

Latest Canon X-Ray D-045 tube. Extremely low dose under the double sca�er shield.



Dental care workers were defined as those working in the following NOC 2016 4-digit occupations: 3113 dentists; 3221 denturists; 3222 dental hygienists and dental therapists; 3223 dental technologists, technicians and laboratory assistants; and 3411 dental assistants. In total, 87 815 individuals worked in dentistry occupations of interest.
Characteristics for each dentistry NOC 2016 4-digit occupation included median employment income (2015 Canadian dollars [CAD]) and aggregate counts for the total number of workers and across sociodemographic information, including age (15–24, 25–34, 35–44, 45–54, 55–64, 65+ years); sex (male/female); immigrant status (non-immigrant, immigrant, nonpermanent residents); household income adequacy quintiles; and visible minority status as proxy for race/ethnicity (Visible minority total, South Asian, East Asian, Black, Southeast Asian, Middle Eastern, Latin American, Visible minority included elsewhere, Multiple visible minorities, Nonvisible minority).
Demographic characteristics of the 5 dental occupations (n = 87 815) were assessed descriptively using univariate analysis. For each O*NET indicator, we identified the top 10 occupations (n = 485) based on their respective scores. The O*NET scores of all dental occupations, irrespective of representing the top 10 occupations for the O*NET indicator, were assessed and presented. A cross-tabulation for the 2 most relevant indicators — exposure to infection/ disease and physical proximity to others — was conducted to calculate an average
score to assess which occupations are at the highest risk of exposure to COVID-19 because of the nature of the occupation.
Occupational exposure and sociodemographic information about the 5 dental occupations are presented in Table 1. In 2016, of the 87 815 Canadians who worked in the 5 dentistry occupations of interest, most identified as dental assistants (n = 34 160), dental hygienists/therapists (n = 26 645) and dentists (n = 18 930). Compared with other dentistry occupations, a higher proportion of workers age ≥ 65 years were found among dentists (10%) and denturists (11%). Women were overrepresented in dental hygienist/therapist (98%) and dental assistant occupations (99%), but underrepresented in the other dentistry occupations, e.g., dentists (39%). The representation of immigrants in dental occupations varied from 16% among dental hygienists/therapists to 52% among dental technologists, technicians and laboratory assistants. Moreover, the proportion of people in dental occupations who were in the lowest household income quintile varied from 4% of dentists to 21% of dental technologists, technicians and laboratory assistants. Based on 2015 figures, dentists had the highest median income of the 5 occupations. Visible minority groups were prominent among dental technologists, technicians and laboratory assistants (37%) as well as dentists (35%). Workers who identified as East Asian, South Asian, Southeast Asian, and Middle
Eastern were the most prominent visible minority groups in all dentistry occupations.
None of the 5 dental occupations allow the ability to work from home. Apart from dental technologists, technicians and laboratory assistants, dentistry occupations ranked high for all O*NET indicators except for “Wear specialized protective or safety equipment.” Dental technologists, technicians and laboratory assistants ranked high for 2 indicators: “Wear common protective or safety equipment” and “Indoors, environmentally controlled.”
O*NET scores for the top 10 occupations in terms of risk of exposure to COVID-19 at work for each relevant indicator are presented in Table 2.
• Frequency with which workers are exposed to diseases or infections: O*NET scores for the 10 most exposed occupations ranged from 89 to 100; these were all in health care including 4 dental occupations. The only dental occupation not in the top 10 was dental technologists, technicians and laboratory assistants, which scored 72. These scores are interpreted to mean that dental hygienists/therapists, dental assistants, dentists and denturists are all exposed to disease or infection almost every day, whereas dental technologists, technicians and laboratory assistants are exposed at least once a week.
• Physical proximity to other workers in a typical workday: Of the top 10 occupations that require working in close physical proximity to others, 8 were in health care, including 4 dental occupations. O*NET scores were
Note: Counts, proportions and income information are from the 2016 Canadian census. The Brookfield crosswalk23 was used to map O*NET indicators to National Occupational Classification codes used in the 2016 census.
Table 1: Sociodemographics and Occupational Information Network (O*NET) indicator scores for 5 dental occupations.96–100 for the top 10; dental technologists, technicians and laboratory assistants, who were not in the top 10, scored 52. Therefore, dentists, dental hygienists/ therapists, dental assistants and denturists nearly touch other individuals during their routine work, and dental technologists, technicians and laboratory assistants work only slightly close to others as they share office space.
• Indoors, environmentally controlled: The top 10 occupations who work indoors in a controlled environment include only 2 in health care (pharmacists and chiropractors) and none in a dental occupation. The O*NET scores for these occupations were 99–100; dental occupations scored 97 for dental hygienists/ therapists and for dental technologists, technicians and laboratory assistants; 94 for dentists and denturists; and 92 for dental assistants. From the frequency perspective, the O*NET scores indicate that dental occupations work in environmentally controlled indoors almost all (if not all) days.
• Wear common protective or safety equipment: Because 21 occupations reported wearing common protective equipment at all times in the workplace, an O*NET score of 100, all have been included in the table. Dental hygienists/therapists and dental assistants were the only 2 dental occupations among them. Dental technologists, technicians and laboratory assistants scored 93, and dentists and denturists both scored 91. These scores indicate that dental technologists, technicians and laboratory assistants, dentists and denturists wear common protective or safety equipment at almost all (if not all) times.
• Wear specialized protective or safety equipment: Among the top 10 occupations, the only health care workers who wear specialized protective safety equipment are medical radiation technologists. O*NET scores for the top 10 ranged from 74 to 91. The 5 dental occupations scored 52 for dentists and denturists, 38 for dental assistants, 16 for dental technologists, technicians and laboratory assistants and 14 for dental hygienists/ therapists. This means that dentists and denturists wear specialized protective equipment almost once a month, dental assistants a few times in a year and dental technologists, technicians and laboratory assistants and dental hygienists/therapists very rarely.
A bubble plot of all occupations (Figure 1) shows average O*NET scores for the 2 most prominent indicators: exposure to disease or infection and physical proximity to others in a typical workday. Of the 10 occupations with high scores for both indicators (upper right of the graph), all are in the health care sector, and dental hygienists/ therapists (100), dental assistants (97.5), dentists (96.5) and denturists (96.5) rank as the top 4.
This is the first study to attempt to assess the occupational characteristics that increase risk of exposure and transmission of COVID-19 in the dental care workforce compared with other occupations including health care. Based on O*NET indicators, our study suggests that dental care workers have potentially high occupational risk of such exposure and transmission. In particular, this risk relates to working in close physical proximity to others and a high frequency of exposure to disease or infection. Dental care workers had similar occupational risk of exposure to COVID-19 as some other health care occupations and, on average, higher risk compared with non-health care occupations in Canada.
Although no patient-to-provider or provider-to-patient infection transmission cases have been reported in dental settings in Canada, it is important to acknowledge the potential for underreporting of patient acquisition of COVID-19 infection in dental offices; because symptoms may present only 2–14 days later, patients could have multiple exposures during that time making it difficult to identify specific sources. As such, the high O*NET scores observed among dental care workers for indicators, such as working in close proximity to others and exposure to infection/disease are, in a way, validated through multiple dental office outbreaks reported in the media, which were mainly among staff.12-17
Overall, our purpose is not to scare the dental community but rather provide data to allow better understanding of workplace characteristics that can increase risk of infection transmission. Attention has focused on how to prevent infection transmission during aerosol generating procedures, but only limited information is available on how staff communicate during off hours or in a staff room. This study will support dental professionals in targeting COVID-19 infection transmission prevention in their offices more comprehensively.
In general, dental care workers do take utmost precautions during dental care delivery to prevent infection. This is evident from our findings that dental workers report using standard protection almost every day to at all times. None of the dental professions was in the top 10 occupations for wearing specialized protective equipment; this is understandable, as specialized protective gear is not required when providing standard care. Currently, specialized protective equipment in dental care occupations is only recommended under special circumstances, for example, when providing care to a patient with a highly infectious disease, such as COVID-19.
Table 2: Top 10 National Occupational Classification (NOC) 2016 occupations, based on relevant Occupational Information Network (O*NET) indicators and associated scores.
Note: Where >10 occupations had similar scores, all occupations are listed.
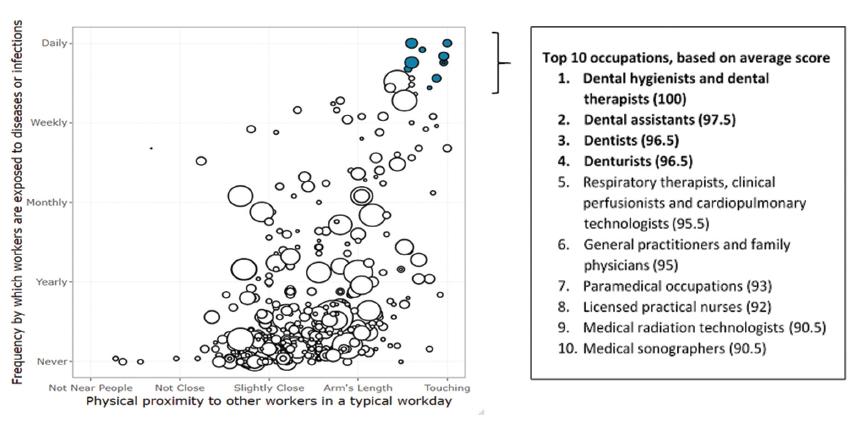
Figure 1: Average Occupational Information Network scores for National Occupational Classification (NOC) 2016 occupations (n = 485) by physical proximity to others in a typical workday versus frequency with which workers are exposed to diseases or infections. The size of each “bubble” reflects the number of individuals working in that occupation (2016 census). Filled bubbles highlight occupations with the highest average score, and these are listed in descending order below.
Throughout the COVID-19 pandemic, the use of nonroutine protective equipment, such as N95 respirators, American Society for Testing and Materials level 3 face masks, face shields, safety goggles and protective gowns, has been recommended, based on point-of-care risk assessment, while providing dental care.11 Familiarity with specialized protective equipment may have reduced COVID-19 outbreaks in dental care settings despite the increased occupational risk of exposure to COVID-19.
Throughout the COVID-19 pandemic, the importance of heating, ventilation and air conditioning (HVAC) systems in dental care settings has been boldly underscored. Efficient HVAC systems in a dental operatory are directly linked to the time required to remove aerosol from the area after a procedure.
With understanding that dental professionals are at the highest risk of exposure to COVID-19, not only because of conducting aerosol-generating procedures, but also because of other factors identified in this study (i.e., high exposure to disease or infections and working in close proximity to others), it becomes all the more important that they always work in controlled environments.
However, results show that dental workers do work in a controlled environment almost every day; thus, inbuilt HVAC systems may not be sufficient to provide the desired
indoor environment, especially in older constructions, and supplementary means, such as portable filters, might have to be employed.30
We found that dental technologists, technicians and laboratory assistants do not share the same high level of risk exposure as other dental workers. This may be because technicians work in laboratory settings and, therefore, have no physical contact with patients, have fewer interactions with other staff and are not exposed to infection directly. That said, a systematic review of crossinfection control in dental laboratories highlighted flaws in cross-infection control procedures and disinfection strategies and recommended improved training in disinfection in such settings.31 Another factor that is crucial in terms of controlling infection transmission is “presenteeism,” where employees are present at work despite having a sickness that justifies their absence and, as a result, are working under suboptimal conditions, which can be harmful to themselves and others.32
Our results show that no workers in the 5 dental occupations have the ability to work from home. Health care workers, including those in dentistry, are essential skilled workers. The limited availability of substitute workers is exacerbated during COVID-19; therefore, one may expect more presenteeism and, thus, more transmission
of infection. This observation calls for costeffective workplace interventions to reduce dental care worker presenteeism while maintaining a sustainable workforce.33 Some limitations identified in this work include acknowledgement that risk of exposure to COVID-19 at work measured through O*NET scores is based on typical job characteristics and activities within occupations, not a measure of association based on COVID-19 cases or COVID-19 transmission. Also, workplace exposure indicators were assessed before the COVID-19 pandemic and do not account for changes in workplace policies and/or infection mitigating strategies instituted during the pandemic, e.g., additional environmental controls, specialized personal protective equipment, maintaining physical distance.
In addition, the O*NET database is designed and maintained in the United States. Although, it is a common assumption that job characteristics, such as skills, knowledge and abilities, are generalizable to the Canadian workforce, practices such as frequency of wearing common protective or safety equipment might differ. A similar survey among Canadian dental workers would be useful for making more certain assessments. In addition, the O*NET scores are based on self-reported data, which can be subject to response bias. Misclassification of occupations can also occur for those who are engaged in more than 1 occupation, but we assume that such numbers would be very low.
This analysis has several strengths. It was the first to specifically quantify the intensity of occupational characteristics that potentially increase the risk of exposure and transmission of COVID-19 in dental care workers and objectively compare them with other occupations. These indicators fill an important information gap regarding the lack of COVID-19 data by occupation in Ontario. The study includes the latest census data from Statistics Canada, which provide reliable and comprehensive populationbased Canadian information on specific
occupations. In terms of assessing occupational risk indicators, O*NET scores were used, which cover working conditions that are derived from survey responses from large, representative samples of workers.
Overall, the results of this study suggest that dental care workers are at a higher risk of exposure to COVID-19 at work than those in other occupations. In addition, the study also identifies opportunities where dental care workers have the potential to improve their work practices to further mitigate the risk of infectious disease transmission. The results of this study will be helpful to administrators and regulators in developing workplace guidance to not only reduce infection transmission but also ensure well-being of the dental care workforce.
Full article with references available on www.dentalnews.com

• Excellent working time and the setting time is individually adjustable by light-curing
• Immediately packable after placement in the cavity
• No varnish required- fill, polymerise and finish
• No need to condition the dental hard tissue
• Does not stick to the instrument and is easy to model
• Suitable for large cavities
Are you interested in our entire product range and detailed product information? Visit our website or contact us directly!


Workplace environment and culture are so often touted in job postings, recruiter messages, and ‘about us’ pages—but they can often be shallow houses built of cards, ready to topple with the slightest breeze of inquisition into their deeper meaning.
Recognized as one of Fortune Magazine’s Best Large Workplaces in Manufacturing and Production for 2021, Ultradent’s claims to a caring work environment and engaging culture have been carefully curated since the company was formed in 1978. “This recognition is joyous for the whole Ultradent community,” says Ultradent Founder and CEO Emeritus, Dr. Dan Fischer. “I’m so proud of our team members and the inspirational accomplishments they’re able to achieve together.” Walking through the sprawling halls of Ultradent’s Salt Lake City area headquarters, you will eventually come across a long, curved hallway adorned with dozens upon dozens of smiling photos of longtime employees. Some recognized for 10 years of dedication, others for 20. New employees may wonder what keeps all of them around so long—could it simply be a paycheck and a few perks that would spur the kind commitment showcased in this hallway?
It won’t take them long to figure out what it is: abundant care for employees combined with widespread trust in our mission of improving oral health globally. Ultradent colleagues take interest in each other in ways that are unique from the common workplace, reflected in Fortune’s top-10 recognition as a premier manufacturer to work for. “Culture is rooted to the core of this company, that’s evident from the first day you start here,” says Ultradent President and CEO Dirk Jeffs. “Our core values are as prominent in our actions as they are in our words, and that’s not always common.” Those core values of care, integrity, quality, innovation, and hard work are found in numerous locations around Ultradent HQ and are used to guide Ultradent’s action plans and decision-making processes.

“More than four decades ago when I first started Ultradent in our home, it was my family, my children helping me,” Fischer says. “As we grew, we brought in more family members, then friends. Eventually, we had to start hiring from outside our immediate circle, and we wanted to ensure the same family environment remained throughout our various expansions.”
“By adhering to these core values, we’ve been able to create a consistent culture despite growing to more than 1,600 global employees with offices on 5 continents. It’s really remarkable, and it’s a credit to the amazing people we’ve been lucky enough to call colleagues over the past four-plus decades,” Fischer adds. Ultradent invests in a progressive Human Resources team whose purpose is to constantly find the ideal balance between human experience and profitable outcomes. «Not every company can find the balance for culture and profitability,” says Ultradent VP of Human Resources David Alsop.
That is one of the unique and extraordinary elements of working for this company. We invest in the development of leaders and employees who partner to find maximum success here, as well as at home. We do everything we can to support the financial, physical, and mental wellness of our people. As an example, we’re now able to offer profit bonuses for team members worldwide as we achieve profit goals. The profit bonus is just one example of how we invest in our people as they invest in our shared company success. Our benefits and development programs go above and beyond to ensure the best quality of life for everyone here at Ultradent.»
Recognition as a Fortune Magazine Best Workplace in Manufacturing and Technology doesn’t come easy—the culture and environment acknowledged by Fortune have been meticulously crafted over more than 40 years. Dr. Fischer often says “Companies are not made of concrete, glass, and steel, they’re made of people serving people.”


 Dr. Nicolás Gutiérrez Robledo DOA Dental Clinic
Dr. Nicolás Gutiérrez Robledo DOA Dental Clinic
www.doadental.com

Implant prosthetics and dental prosthetics differ considerably, with the absence of periodontal ligament in the implant/ prosthesis complex. This situation causes mechanical problems to the implants, especially to the implant prosthetic material, due the lack of stress absorption resulting from the normal impact during chewing (1) (2). Among the problems we face in daily practice is the unscrewing and fracturing of veneering material of the implant crown and fracturing of implant/ abutment components.
It is very important to consider that resin based blocks give us the missing part from ceramic materials to solve the problem of anterior exposure. It is also necessary to consider the importance of reliable bonding/union between the resin block and the abutment component of the

implant, because the right transmission of occlusal load depends on the reliability of this bonding interface. One of the biggest advantages of BRILLIANT Crios blocks is the combination with ONE COAT 7 UNIVERSAL, the best bonding system for the resin based blocks according to the scientific literature (3) (4) and also tested in my own practice over the last five years of use.
Another very important feature is the size and distribution of ceramic fillers. We have learned from the past that bigger size fillers are better for the strength but, at the same time, are more prone to detach from the surface creating craters iniciating the material degradation. A homogeneous filler size and distribution is much better for the material’s wear, luster, aesthetics and strength over long term.


Excellent material properties and terrific handling characteristics!
• High filler degree (> 83 % w/w), minimal shrinkage (< 1,8 %)
• Outstanding abrasion resistance
Developed to make the day-to-day running easier
• Universal application
• Easy handling, won’t stick to instrument

During daily practice, it is very common to face situations where the implant has to be placed lingually due to normal resorption (Fig. 1) of the buccal plate after the extraction. But, at the same time, it is not necessary to perform bone grafting procedures. The result of this scenario is to increase the stress on the implant-bone complex when we use rigid materials like conventional ceramics (Fig. 2).
For this daily practice situation, the combination of rigid and resilient materials against the antagonist, allows the stress to the implant-bone complex to be reduced (Fig. 3,4).



Oblique loads have been reported to increase stress values in peripheral bone and prosthetic components also generating high stress in the crown, implant, abutment, and cortical bone. The Young’s modulus, also known as elastic modulus, is one of the important factors determining a material’s behaviour. (5)
Another common situation is a full mouth restoration over implant. It is well known that the big issue is chipping and delimitation of the ceramics, due to the high forces applied in the patient with dental implants.
In regards to this problem, the combination of rigid materials to support the connectors and resilient materials to absorb the shock and, at the same time, allow easy fixation, make the use of resin based blocks the logical choice for this kind of restoration. (Fig. 6,7 and 8)

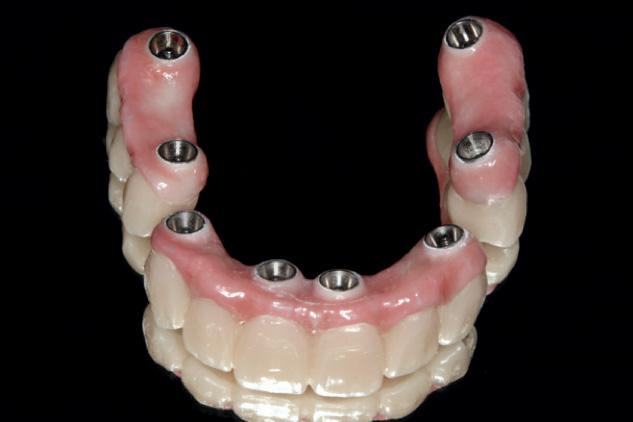




A combination of a rigid metal structure over the telescopic bar and a thimble structure made of PEEK (Fig. 13,14) works as base for the final restorations.
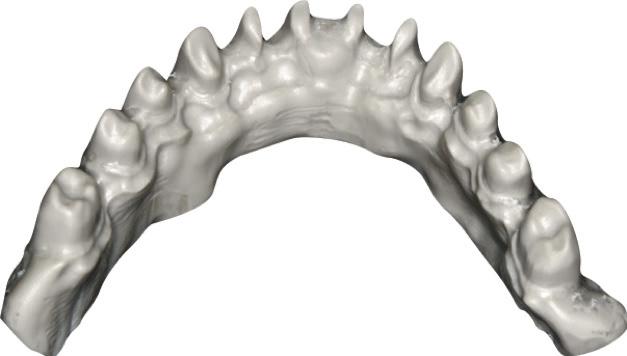

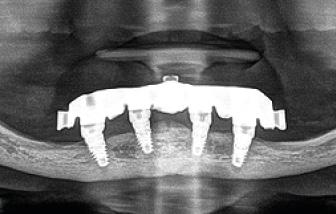
In this case, a patient presented with extremely atrophic bone in the mandible, with four short implants placed between the dental nerve foramen (Fig, 10a,10b). These were milled out of a BRILLIANT Crios disc either as single tooth units or bridges and cemented on the thimble struc-ture (Fig. 15-17). Using BRILLIANT Crios instead of prefabricated teeth, we can increase the strength of the restoration, have good aesthetics and keep the weight low for this kind of prosthesis.

After some time, patients wearing this kind of restoration with prefabricated teeth, their muscle activity increase considerably, which very often leads to fracture or debonding of the prefab-ricated teeth (Fig. 12).

 Fig. 7: Zirconia bridges ready to be screwed.
Fig. 10a and 10b : Patient with extremely atrophic bone in the mandible with four short implants placed between the dental nerve foramen
Fig. 12: Debonding of prefabricated tooth is very common on overdentures.
Fig. 8: Upper and lower bridges in the mouth.
Fig. 14: Secondary metal structure
Fig. 9: Panoramic view of the finished case.
Fig. 13: PEEK thimble structure
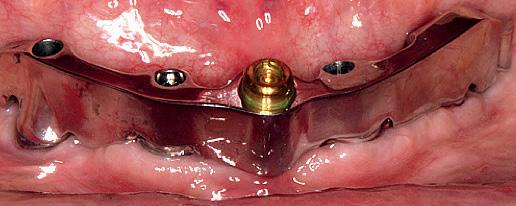
Fig. 11: Telescopic bar with retentions for the secondary structure
Fig. 15 and 16: Telescopic prosthesis with BRILLIANT Crios restorations. Occlusal and bottom view.
Fig. 7: Zirconia bridges ready to be screwed.
Fig. 10a and 10b : Patient with extremely atrophic bone in the mandible with four short implants placed between the dental nerve foramen
Fig. 12: Debonding of prefabricated tooth is very common on overdentures.
Fig. 8: Upper and lower bridges in the mouth.
Fig. 14: Secondary metal structure
Fig. 9: Panoramic view of the finished case.
Fig. 13: PEEK thimble structure
Fig. 11: Telescopic bar with retentions for the secondary structure
Fig. 15 and 16: Telescopic prosthesis with BRILLIANT Crios restorations. Occlusal and bottom view.
Innovative double shell construction.


Fig. 17: BRILLIANT Crios restorations used for removable telescopic implant prosthesis.

Fig. 18: Final case in the mouth of the patient. Wearing a complete denture on top and tele-scopic BRILLIANT Crios on the
Magne P, Silva M, Oderich E, Boff LL, Enciso R. Damping behavior of implantsupported restorations. Clinical Oral Implants Research. 2013;24(2):143–8.
Liebig J. Energy Dissipation and Damping Behavior of Commonly Used CAD / CAM Materials. 2018;35392.
3. Reymus M, Roos M, Eichberger M, Edelhoff D, Hickel R, Stawarczyk B. Bonding to new CAD/CAM resin composites: influence of air abrasion and conditioning agents as pretreat-ment strategy. Clinical Oral Investigations. 2019;23(2):529–38.
4. Emsermann I, Eggmann F, Krastl G, Weiger R, Amato J. Influence of Pretreatment Methods on the Adhesion of Composite and Polymer Infiltrated Ceramic CAD-CAM Blocks. The journal of adhesive dentistry. 2019;21(5):1–11.
High elasticity and break resistance thanks to the double shell construction with flexible elastomer core.
constant force level less initial force continuous force transmisson high wearing comfort
5. Kaleli N, Sarac D, Külünk S, Öztürk Ö. Effect of different restorative crown and customized abutment materials on stress distribution in single implants and peripheral bone: A three-dimensional finite element analysis study. Journal of Prosthetic Dentistry [Internet]. 2017;1–9. Available from: http:// dx.doi.org/10.1016/j. prosdent.2017.03.008

DOA Dental Clinic
Dr. Nicolás Gutiérrez Robledo Calle Alcala 199 28028 Madrid Spain
www.doadental.com

›
›
›
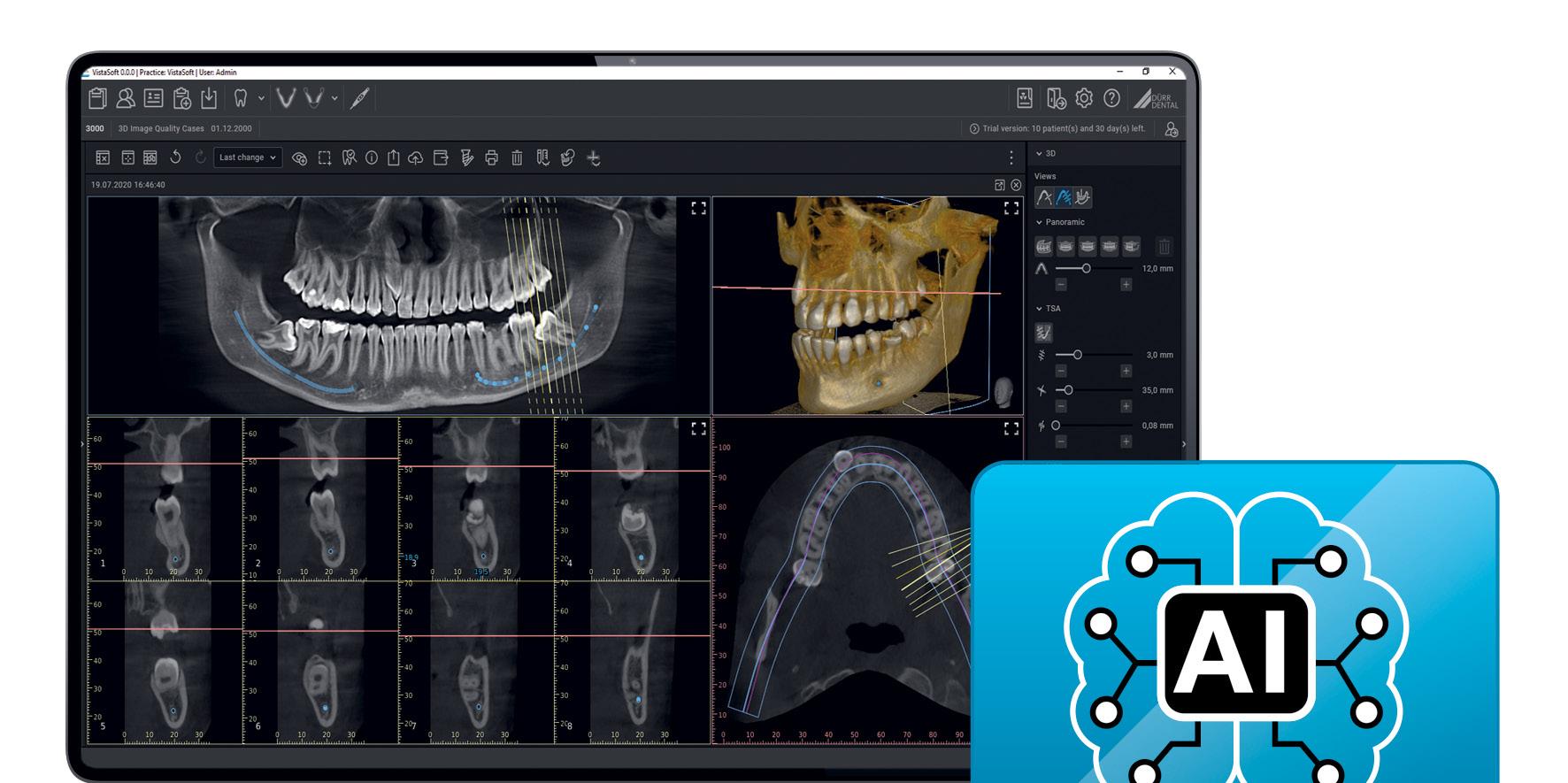
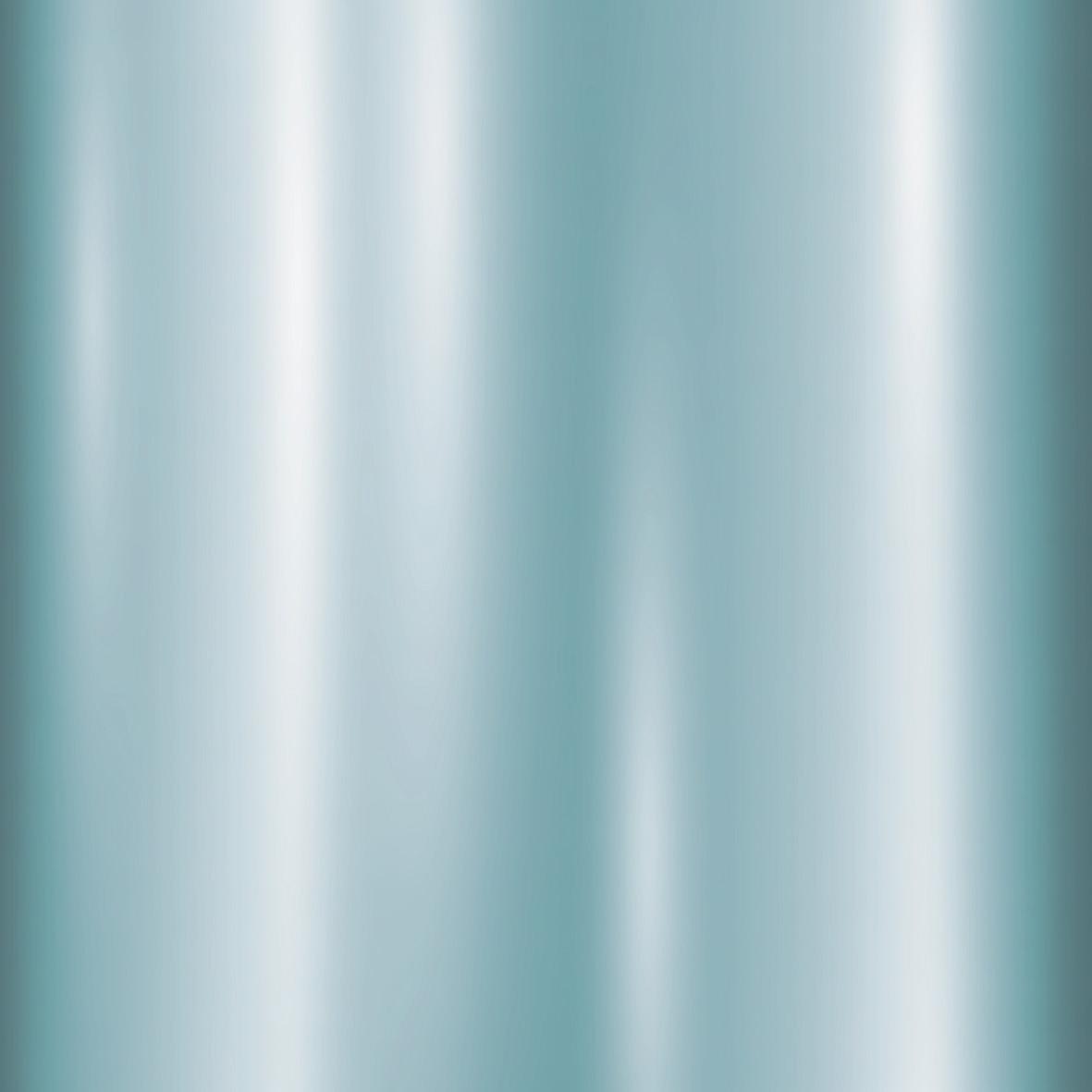
Version 3.0 of the imaging software VistaSoft from Dürr Dental gives you access to powerful AI features that will make your day-to-day work in the practice noticeably more efficient.
With VistaSoft 3.0, Dürr Dental has managed to bring pioneering AI technology into dental practices, where it offers efficient help with day-to-day tasks. Routine work is taken care of, mistakes are identified at an early stage, and timeintensive work is accelerated, allowing the practice team to focus on the most important thing – their patients.
As part of its image plate quality checking, VistaSoft automatically detects whether or not an IQ image plate still meets the required high quality standards even after frequent use, and if not it recommends replacement of the image plate. Another intelligent algorithm detects the orientation of intraoral X-ray images with the aid of anatomical features shown and corrects the rotation of the image automatically if needed. The advantage of this is that a
work step that would be performed many times by hand now takes place completely automatically.
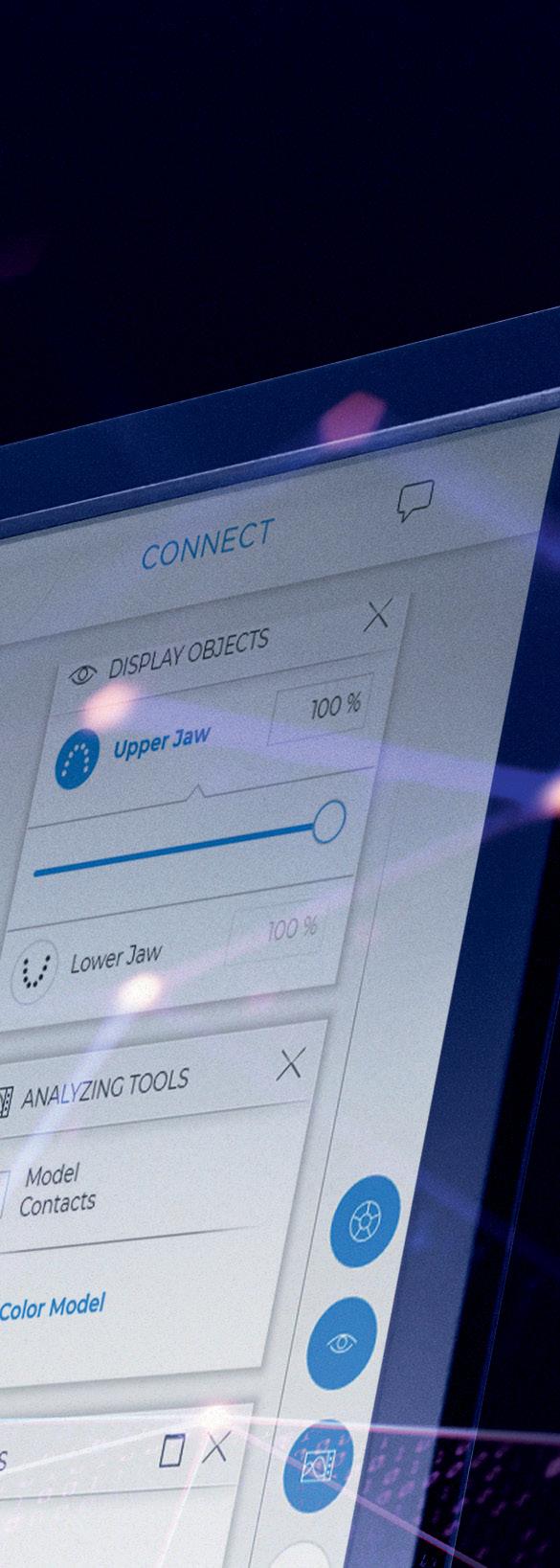
The AI-assisted mandibular canal detection system calculates the position of the nerve canal in three-dimensional X-ray images in just a few seconds. The diagnostician merely needs to check the proposed position, whereas even as an experienced user of CBCT software he or she would have needed several minutes to plot the location by hand. With the aid of artificial intelligence, the calculated panoramic view for 3D images is also matched to the anatomy of the patient for a significantly improved OPG image.
For orthodontists VistaSoft Trace is a new software model for cephalometric analyses in a matter of seconds. The user-friendly software add-on identifies reference points and soft tissue silhouettes automatically for the simulation of treatments.
The visualisation of the successful treatment offers huge time savings for therapists.




Innovation
 Nick Olive CEAS Territory Manager Middle East & Egypt, A-dec
Nick Olive CEAS Territory Manager Middle East & Egypt, A-dec
nick.olive@a-dec.com
An astounding 87% of dentists suffer from back pain while working (Ball, 2015).
As dental professionals it isn’t just our backs we need to worry about - musculoskeletal disorders including back, neck and shoulder pain, as well as fatigue are all commonplace within the industry.
We all know that we should consider ergonomics and proper posture while working, but what do we mean by ‘good ergonomics’ and ‘good posture’ and what are the route causes of the issues so many of us face while working as dentists?
The word ergonomics is derived from the Greek works ‘ergon’ (work or labor) and ‘nomos’ (natural laws). Ergonomics is the study of people efficiency in their working environment (Oxford, 2021).
To work with good ergonomics is to be efficient in our working environment and expend the least amount of energy to achieve the same result. In dentistry this means reducing the strain on our bodies while working.

The topic of ergonomics in dentistry is wide and varied. Here we discuss one of the primary causes of pain experienced by dental professions.
Managing your head can help
The average human head weights 5kg
(GW Osteopathy, 2021). When delivering an ergonomic assessment, we undertake exercises using a 5kg medicine ball. Try to find one, or a similar item weighing 5kg and experience how heavy this weight feels. When you have this weight in your hands it is hard to imagine that we walk around all day with this weight on top of our shoulders. Notice when you hold this weight the natural position you adapt to hold the weight. You will hold the weight close to your body. You probably wouldn’t be comfortable holding 5kg outstretched from your core or indeed holding this weight anywhere for a prolonged period.
Now try resting the 5kg weight on your shoulders and standing in a neutral position. With the weight now going through your body into your feet. You will probably feel like you could hold the weight there for much longer.
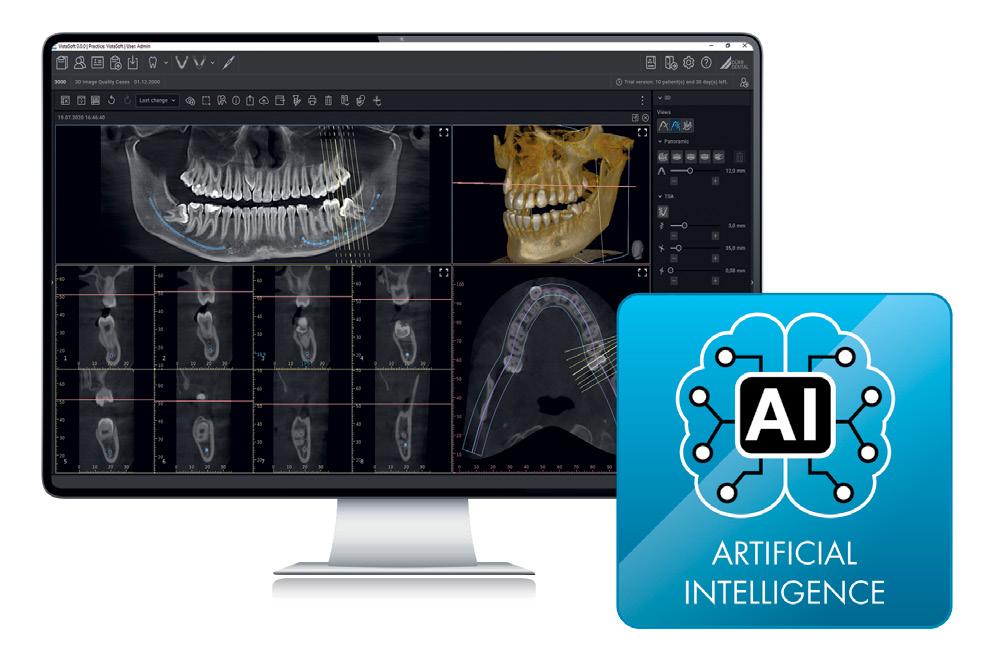
Our bodies are designed to cope with the weight of our head and the best way for us to manage this is to support the weight through our core, into our legs and feet and into the ground below us.
When the weight of our head is held away from the center of our body in front of us we will experience pain in our neck and upper back. Where the weight of our head is transferred through our body but not into our legs and feet, we will begin to experience pain in our lower pack.
The pressure from the weight on our spine and supporting neck and back muscles increases exponentially as our head is tilted away from our body.
We can help to reduce this tendency to tilt our heads forward by wearing loupes and correctly positioning our stool with legs under the patients head which encourages a more upright head position.
It is important to correctly position patients by fully utilizing a dual articulating head rest on your patient chair.

Adjusting the position of a patient’s head can offer increased patient comfort by properly supporting the weight of the head, whilst opening the oral cavity and providing the best possible view to your working area. Your patient should be seated fully back against the back rest of your dental chair before moving into a treatment position, to make adjustments easier. You can encourage patients to adapt this position by presenting the headrest in the fully up position before they enter.
A properly adjusted dental stool offering a positive tilt, to transfer some of the weight from your head and body through your legs and feet to the ground can make a huge difference to your health. This will also give you the optimum working height to clearly see your working area without tilting your head excessively.
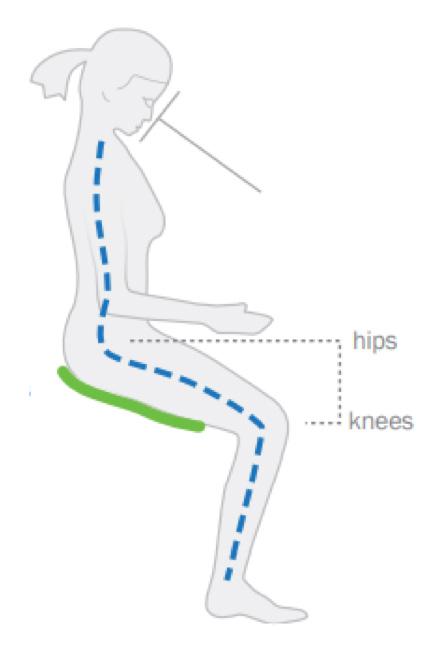
In a healthy, dynamic seated position your hips will be positioned above your knees with a tilted seat encouraging weight transfer into your feet.
From a dynamic seated position which may be higher than you are used to working, you can adjust your patient chair to allow you to get as close as possible to your patient. Ideally your patient chair will have a thin backrest to allow you to position your legs under the patient and keep your head above your shoulders.
With your head positioned above your body, weight transferred to your feet by seating correctly and positioning your patient to allow direct vision into the oral cavity, you can effectively reduce strain on your neck, shoulders and back.
Nick has a passion for dental ergonomics and is certified by The Back School in the USA. Nick offers free dental ergonomic workshops both in person and online.
Graphic Reference: The Guardian / Source: Surgical Technology International
 FKG Dentaire SA
FKG Dentaire SA
Switzerland
www.fkg.ch
A cordless endodontic motor, which can reach high speeds.
FKG Dentaire SA presents the Rooter® X3000, redefining endodontic standards. This novel cordless endo-motor combines technology, functionality, and adaptability in a 20-centimeter unit. It stands out for the fastest speed on the market (3000 rpm), 10 programmable memories, and preset programs for different types of FKG files.
Its ergonomic design, light weight, and 360° rotatable extra-slim contra-angle head ensure perfect handling and visibility.
Every new FKG product responds to the most exacting needs of endodontists with leading-edge technology and uncompromising quality. The Rooter® X3000 advances endodontics with a new cordless, brushless endo-motor with integrated apex locator achieving a speed of 3000 rpm.

Adaptability as technical keyword
Benchmark speed coupled with guaranteed stability and precision are only the tip of the iceberg of Rooter® X3000 features. Adaptability reflects its core, starting with the four FKG presets: XP-endo® Treatment, XP-endo® Retreatment, RACE® EVO, and R-Motion®.
This saves time for endodontists, who can rely on manufacturer’s predefined recommendations for each file type.
The endo motor also provides 10 userprogrammable memories for all modes (EAL, CW, CCW, REC, or ATR), more than 60 speeds, and—of course—a highprecision built-in apex locator and a range of automatic apical functions.
Agility as practical credo
As with any device, practice validates innovation. With its ergonomic handpiece weighing only 157 grams, perfect balance, and fully rotatable ultra-slim contraangle head, the Rooter® X3000 ensures a comfortable grip, agile handling, and excellent visibility of the operating field.
FKG has designed and developed all details to provide maximum freedom of use to the practitioner, optimizing both speed and efficiency.
Features include complete adaptability of the device and its display for both left- and right-handed users, a broad range of usercontrolled settings, extensive file brand compatibility, wireless charging stand, and volume control.


September 1 - 3, 2021
International City Stars, Cairo - Egypt

 HEIkAL, PRESIDENT EGYPTIAN DENTAL SYNDICATE
HEIkAL, PRESIDENT EGYPTIAN DENTAL SYNDICATE

The president of the Egyptian Dental Syndicate, Dr Ehab Heikal, welcomed the guests, then went through the various achievements of the syndicate in one year since the election of the current board, as well as the ongoing activities. He also expressed his thanks to the board that created those achievements.
The EDSIC was preceded by a three days specialized Congress, EDSIC Ortho that attracted many orthodontists from Egypt and 12 other European and Asian countries. The President announced that every year the EDSIC will be preceded by a different specialized congress, while the success of EDSIC Ortho resulted in the decision of holding it bi annually as a separate specialized congress.
The next EDSIC will take place on 7-9 September 2022.


• Plug and play micromotor, easy to install
• Connects to your chair’s air supply
• Cost-efficient conversion to electric
• Perfect for speed increasing handpieces
• Internal spray and LED
• 1:1 blue band contra-angle
• Push button
• No light or spray
• Autoclavable & thermodisinfectable


• 1:5 red band contra-angle
• Anti-retraction valve
• Less aerosol generation
• Ceramic bearings
• Fibre-optics and quadruple spray
• Titanium body with PVD coating




TO

Trophy Distribution


TO DR. MOHAMED EID ELkHALIL FROM LEBANON



TO DR. NAWAL RABI FROM MOROCCO
Cairo, Egypt
September 1 - 3

PROF. ABDULSALAM ALASkARY

(L TO R) PROF. MOHAMMED MURSHED ALHARBI (SAUDI ARABIA), PROF. kLEBER MEIRELES (BRAZIL), PROF. MONA SAYEGH GHOSSOUB (LEBANON), PROF. AkRAM ALHUWAIZI (IRAQ), PROF. HANAN ISMAEL (EGYPT), PROF. PETER BUSCHANG (USA) AND DR. ABDALHADI kAWAIAH




September 9 - 11, 2021
Hilton Habtoor, Beirut - Lebanon View

On top of the pandemic that hit the world very hard and set its clock to COVID timing; Our beloved country experienced the worst crisis in history from the Harbor blast to the Economic meltdown. Nevertheless, we decided to take up the challenge and organize the first in person meeting. The Lebanese Society of Endodontology Organized the APEC 2021; The 21st Scientific congress of Asian Pacific Endodontic Confederation on 9-11 September 2021 in Beirut, Lebanon at the Hilton Beirut Habtoor.
For more than thirty-three years, the biannual APEC congresses have brought together leading experts to help address different aspects of Endodontology. The event provided the researchers and the Endodontic community the opportunity to share expertise, help identify emerging trends and engaged in lively debates that positively impacted our Specialty.
APEC 2021 presents exciting knowledge platforms and prominent speakers on Endodontics best practices. The scientific program covered science and research, technological and technique updates, clinical matters as well as educational innovations.

 ROGER RBEIZ, PRESIDENT OF THE LEBANESE DENTAL ASSOCIATION
ROGER RBEIZ, PRESIDENT OF THE LEBANESE DENTAL ASSOCIATION

 CHAIRMAN ORGANIZING COMMITTEE
CHAIRMAN ORGANIZING COMMITTEE



TO

Trophy Distribution

TO

TO DR. FREDERIC BUkIET FROM FRANCE










1. How is technology changing endodontics?
In recent decades, technology has improved dentistry and endodontics significantly, providing useful tools for better diagnosis and root canal treatment. In the 2000’s, microscopy has been the game changer in endodontics, while in the decade after, threedimensional radiography has played this role. CBCT has proved to be clinically useful not only by improving diagnosis and treatment planning (especially in the most difficult cases), but also in the clinical visualization and understanding of anatomic complexities. In addition, CBCT is a fundamental device providing images for guided endodontics.
Static guides and dynamic navigation are proving to be effective in the treatment of calcified canals, and also helpful in more conservative access cavities both in non-surgical and surgical endodontics. Moreover, in the last decade, two other new manufacturing technologies have changed root canal instrumentation and obturation: the heat-treatment of nickel-titanium rotary instruments, and the introduction of new bioceramic endodontic sealers, both aiming to improve the performance, safety, and simplicity of endodontic treatments.
2. How important is clinical understanding of root canal anatomy?
Endodontics has been a “2-dimensional” specialty for nearly 100 years due to the fact that traditional 2D radiographs only allowed a partial visualization of anatomy and canal trajectories. This was related to the buccal-lingual direction of the X-rays and the superimposition of different structures. Using CBCT (and ideally using dedicated software for 3D reconstruction), the REAL anatomy of each case can be visualized by the endodontist, including hidden curvatures, hidden confluences,
calcifications, etc. This is a huge advantage not only in terms of proper diagnosis and treatment planning, but also to reduce iatrogenic errors during instrumentation procedures. Hidden curvatures (which always lead to increased instrumentation stress), if not properly recognized, may easily result in intracanal separation.
For more than 25 years endodontists have been fearing sudden, unexpected breakage of nickel-titanium rotary instruments. Nowadays, we can tell that the great majority of those failures were related to poor clinical understanding of anatomy, and consequently, improper choice and use of the instruments in very stressful (usually hidden) complexities.
Clinical understanding of anatomy in three dimensions, commonly defined as “3d endodontics”, is therefore a breakthrough in the clinical approach to improve safety and simplicity of instrumentation procedures. In surgical endodontics a 3d approach does the same, allowing a less invasive procedure and reducing risks of iatrogenic errors.




3. How does the anatomy dictate improved properties on NiTi files?
Three-dimensional analysis of root canal trajectories and shapes have clearly shown that root canals are more complex in 3D compared to tradition 2D visualization, and consequently, these findings affect properties of the NiTi files allowing:
a) More flexibility to properly negotiate curvatures, avoiding iatrogenic errors
b) More mechanical resistance to avoid intracanal breakage
c) Changes in design or in clinical use to increase performance in oval canals (which can be more easily visualized in 3D) which improve cleaning (by touching more canal walls) and debris removal. Cleaning is obviously related to proper use of irrigants and irrigation techniques, but instruments also play a significant role in creating more debris or removing debris properly, dispersing the solutions, and disrupting biofilm.


Improvement of NiTi files can be done mainly in three different ways:
1. Improving design, which has been the primary direction during the first 20 years after NiTi was introduced.
2. Improving motors and motions, to make them less stressful than continuous rotation.
3. Improving alloy and manufacturing processes, including heat treatments. This last option has recently become the most important feature to significantly improve flexibility and fracture resistance of the NiTi files.
4. Which is the clinical difference between austenitic and martensitic files?
In the first 20 years after the introduction of NiTi, all instruments have been super-elastic, austenitic files. The superior properties of the alloy, compared to traditional stainless steel, was considered a huge advantage, and allowed the clinical use of files with greater tapers in continuous rotation. However, this increase of instrument dimensions and the greater stress induced by the motion resulted in quite rigid instruments which increased risk of failure, especially in complex curvatures and the larger sizes and tapers. NiTi is a “delicate” alloy, very sensitive to heat, and during the manufacturing process the alloy is weakened by the grinding wheels that create the flutes and the geometry of the file, both externally and internally.
External defects can be partially adjusted by electropolishing, while internal defects can be partially adjusted by specific heat treatments after the manufacturing process. Heat treatments can vary drastically, and each manufacturer has its own proprietary, undisclosed treatment process. Generally speaking, all heat treatments can improve flexibility and fracture resistance to a certain degree, but there are huge differences on how they are performed and the resulting effects. Some companies, i.e., EdgeEndo, have invested a lot in research to produce better heat treatments, which have recently become, perhaps, the most important manufacturing treatment to improve mechanical properties of the instruments.
For instance, changes in design could increase flexibility and resistance by 20-30%, while in our research, FireWire heat treatment by EdgeEndo has shown to increase flexibility up to 3 times (300%) and even more for fatigue resistance. These new heat-treated files can also exhibit different shape memory effects, and therefore are defined as martensitic NiTi files: they can be pre-bent, if needed, and produce less bounce back, allowing easier negotiation and less canal transportation.
These improvements have significantly changed our clinical procedures, because such a difference between austenitic and martensitic files (some manufacturers provide the same file in the two versions, i.e., EdgeTaper and EdgeTaper Platinum) has modified our clinical approach to instrumentation, depending on which type of instruments are we using.
5. Is minimally invasive the current trend in endodontics?
Minimally invasive is obviously a trend, since we know that any endodontic treatment (to a certain extent) can weaken a tooth, and tooth fracture is the main cause for long term failures (even if it depends a bit more on the quality and type of post-endodontic restorations).
However, when treating complex root canals, we should always make some compromise between the tendency to be more conservative and the risk of poor access cavity design or coronal flaring, which may create interferences that lead to iatrogenic errors, including ledges, transportation, or intracanal breakage. This is why I prefer to use the term: RATIONALLY INVASIVE endodontics.
Because we cannot modify the apical curvature, the only way to improve efficacy and safety (providing that we are using very flexible and resistant martensitic files, with proper motions and techniques) is to slightly modify the coronal and middle curvatures, reducing the overall instrumentation stress. Therefore, how invasive a shaping procedure can be, is mainly determined by the anatomical complexities: the easier the canal, the less coronal flaring we need, and we could also create a smaller access cavity.
A martensitic file is more suitable for this approach because it can be pre-bent, and having less bounce-back slightly reduces influence from interferences. In complex canals the strategy is opposite; we have to reduce instrumentation stress because high stress is already present due to the anatomy.
3D understanding of anatomy is crucial in these cases because it clarifies the need for different strategies which will significantly improve a less-invasive approach. More specifically, coronal flaring must be “selective”, avoiding unnecessary enlargement of canals and reduction of cervical dentine. Depending on trajectories, canals should be flared by only one or two sides to make the curvatures easier. Such a rationally invasive approach based on 3D understanding of anatomy, is my preferred method.
6. Which is your opinion about simplified techniques and single file reciprocation?
Once again, we should be rational in our choice. Most of the canals are quite easy to negotiate and shape (the main difficulty in these cases is proper cleaning and disinfection); therefore, I am in favor of simplified techniques. Can they work in more difficult canals?
In my opinion, yes, but only if the proper instruments, strategies, and motions are used. I am currently using two techniques in my practice:
A) A simplified technique using only two martensitic NiTi rotary files: X7 17.04 and 25.04
B) A single file reciprocation technique using EdgeOne Fire (EOF).
Actually, I like both, but I use the single file reciprocation technique in the majority of simple, medium, mediumdifficult, and molar cases. I use this technique because it is simple, rapid, and easy to perform. EOF are martensitic NiTi files that are designed to be used in a reciprocating (30° clockwise - 150° counter-clockwise) motion.
Compared to competitors’ files, EOF are more flexible and fatigue resistant due to EOF’s fire-wire heat treatments. Through research I conducted in Differences in cyclic fatigue lifespans between two different heat treated NiTi endodontic rotary instruments: WaveOne Gold vs. EdgeOne Fire my findings showed EOF has twice the cyclic fatigue compared to WaveOne Gold. The flexibility of EOF allows me to also use them in moderately curved canals in a very safe way. The reciprocating motion itself contributes to reducing instrumentation stress.
I often perform a manual glide-path up to size 15, but not in all cases because in easy canals a glide-path already exists. The EOF has excellent properties, and it usually negotiates canals very easily; however, if needed, I can increase cutting efficiency by slightly increasing the speed. This is also very useful when I do brushing with EOF because this increases its ability to remove debris which is slightly more prevalent with reciprocating techniques.
The EOF is an instrument of greater (variable) taper and easily and quickly creates a proper tapered preparation; nevertheless, I always brush to increase the capability of touching (please pay attention…it is touching, NOT CUTTING) more canal walls and improve cleaning and disinfection, especially in oval, elongated canals.
Since I am using only one instrument, if it does not progress easily (i.e., in a hidden curvature) I can slightly increase the glide path or, more frequently, I flare the canal a bit more before progressing apically. I define this last approach as “crown-down with the same instruments”.
7. Which instruments would you recommend in complex cases?
In very complex cases my preferred choice is a simplified technique using only two martensitic NiTi rotary files: X7 17.04 and 25.04 at a speed of 300 to 500 rpm, torque settings 250 to 410 g/cm. Due to their excellent properties (flexibility, fatigue resistance, less bounce back) these files are excellent in the management of complex apical curvatures. The X7s have a maximum flute diameter of 1 mm which can be considered “minimally invasive instruments”.
The X7 instruments are available in different sizes and two (constant) tapers: .04 and .06., but I like to use a simplified technique with .04. If I want more tapered preparation (but I tend to be less invasive in my initial approach) I can brush more and create more taper. This is much safer in a very complex curvature than using an instrument with bigger taper.
Similarly, in most cases I don’t need an orifice opener or a glide-path (they can be optional files in very peculiar cases), because the 17.04 can do the work of both.
Following a manual glide-path up to size 10 or 15, the 17.04 can pre-enlarge the canal, thus creating a better glidepath and easier progression for the shaping file (.04 25).
If I need to flare the canal more in the coronal and middle part, I can brush with this file, eliminating interference where needed (selective flaring) and create more room for the shaping file.
This is the technique I usually adopt for my “rationally invasive approach”; it is simple, predictable, easy to perform, and can be adapted to many different complexities. If I need more “prepared space” for my final irrigation technique, I sometimes brush a little bit more to increase penetration of irrigants.
I no longer choose this strategy for obturation because single-cone cold bioceramic obturation allows me to be less invasive since I don’t need to create space for pluggers, obturators, etc.
The martensitic X7 files are excellent for this approach because their superior mechanical properties allow me to use only two instruments without compromising quality and safety. I only need to understand anatomy and select the proper strategy for each case.
• Full-time Professor; Head of Endodontic and Restorative, University of Rome, La Sapienza, Dental School; Director of Master of Endodontics in Sapienza.
• International lecturer and researcher, He is author of more than 480 scientific articles, He has lectured all over the world (more than 500 presentations) as a main speaker in the most important international congresses and many Universities worldwide.
• During his academic career he gained many awards and recognition, and was responsible of many scientific projects with national and international grants.
• He has focused his interests on endodontic materials and clinical endodontics. He is also actively cooperating as a consultant to develop new technologies, operative procedures and materials for root canal treatment. He has many patents concerning endodontic technologies.
• He is member of the Executive Board of ESE and Chairman of Clinical Practice Committee.
• He still maintains a private practice limited to Endodontics in Rome, Italy




www.trident-dental.com
Trident presents the most complete model of the X-VIEW family: X-VIEW 3D PAN CEPH. Along with its exceptional 3D imaging capabilities this unit features 2D digital panoramic imaging and cephalometric analysis.
X-VIEW 3D PAN adopts the most advanced image acquisition technology:
Two CMOS Detectors
• CMOS Flat panel sensor for 2D and 3D images
The following FOVs are available:
- Single FOV 9x9 cm
- Single FOV 11x11 cm
- MultiFOVs 11x11, 9x9, 6x11, 5x5 cm
• DR CMOS flat panel sensor with single shot technology for Cephalograms
Modern acquisition software
X-VIEW 3D PAN includes functional and versatile software tools that allow to acquire, filter, store and manage thousands of images in less time and with the best possible result.
Specific tools are useful to diagnose and analyze several pathologies; plan and perform dental treatments and surgeries and, follow up the results.
MAR algorithm
Pulsed mode DC X-Ray generator







Company name: 3Shape
Country of origin: Denmark
Website: www.3shape.com
3Shape is changing dentistry together with dental professionals across the world by developing innovations that provide superior dental care for patients. Our portfolio of 3D scanners and CAD/CAM software solutions includes the multiple award-winning 3Shape TRIOS intraoral scanner, as well as marketleading scanning and design software solutions for both dental practices and labs.

Two graduate students founded 3Shape in Denmark’s capital in the year 2000. Today, 3Shape has over 1,600 employees serving customers in over 100 countries from an ever-growing number of 3Shape offices around the world. 3Shape’s products and innovations continue to challenge traditional methods, enabling dental professionals to treat more patients more effectively.
We’re on a mission to change dentistry together. We believe that there is always a better and more efficient way to provide care and dialogue around dental treatment. We also believe that none of this can be done alone, which is why we collaborate with a network of dental professionals, industry leaders and resellers.
MENA DISTRIBUTORS
ALGERIA
ORODENT Algérie
EGYPT
Dentixx for Dental Equipment & Turnkey Solutions
IRAQ
Al-Shara’a Dental Supplies
FIA Group
JORDAN
Manshore Medical Supplies LLC
KUWAIT
Noon Medical Supply Company
LEBANON
Prodent
MOROCCO
Exelle Medic
QATAR
Shine Tech (under Henry Schein Middle East)
Masar Medical Establishment
SAUDI ARABIA
MELAT TRADING
STATE OF PALESTINE
The Embassy Dental Supply Co.
TUNISIA
Newmed - Al Hayat Group
UNITED ARAB EMIRATES
Henry Schein Middle East Regional Office
Bio Link Medical (under Henry Schein Middle East)
Al Hayat Pharmaceuticals
Our most powerful intraoral scanner, the wireless 3Shape TRIOS® 4 comes with smart tips that heat faster so you’re ready to scan in seconds, and it includes all the same app integrations as TRIOS 3.
Wired and wireless in one
No more need to choose. TRIOS 4 now comes as a flexible two-in-one solution that combines wired and wireless with a simple plug-in cord for that moment when you want to switch to wired.
• Realistic colors & proven accuracy
• Artificial Intelligence scanning
• Best in class shade measurement utilizing Vita Classic, Vita 3D Master and Ivoclar Shade Guide
• Standalone HD camera & zoom feature
• Connect with over 20,000 labs
• Work with over 80 Implant companies
• Work with over 40 clear aligner providers
• Wireless
• Smart Tips
• Longer Battery Life

20% faster is just the beginning
The 3Shape E1, E2, and E3 lab scanners have been upgraded to the same next-generation scanning platform as E4.
The E4 lab scanner is our fastest and most accurate scanner ever. Its superior speed and accuracy reduce scanning steps, save you time, and powers up your productivity.
You will recognize them all by their red ring and speedy performance – at the same great price!
For those seeking the speed and accuracy to drive lab productivity and growth, look no further.
The E4 boasts double the speed, double the accuracy, and double as many cameras as its predecessor the E3, delivering improved efficiency and consistency with every scan.
From small labs seeking the best-of-the-best, to high-volume, full-service labs striving for a leaner workflow, our E4 lab scanner is the right choice for you.

Company name: Takara Belmont Corporation
Country of origin: Japan
Website: www.takarabelmont.co.jp/global/dental/
Takara Belmont has been contributing to people’s wish to stay healthy and beautiful through a century of our history. Founded in Japan in 1921, and we drew on our hydraulic technology and began manufacturing dental chairs in 1960s.
Committing to the healthy life not only for patients, but also for dentists & staff, our products are designed and developed to support dentist, forging a bond of trust with their patients. Based on the spirit of Japanese manufacturing, each belmont chair is the result of more than 50 years of product research and development, meticulous engineering expertise and innovative production methods.

Through our worldwide network of offices and subsidiaries, Belmont continually monitors current industry and market needs as we strive to design and introduce high quality, creative products that help increase work efficiency and productivity.
ALGERIA EXPERT DENTAL INDUSTRY
R. Ben Aissa Madani-Ain Azel-Setif
Phone: +213 36 83 47 02 edi-setif@hotmail.fr
BAHRAIN
MEDICAL & PHARMACEUTICAL SERVICES CO. W.L.L.
Building 1877 Office 4 Road 2124 Bl. 321
Phone: +973 37 77 18 67 mahmoud-akil@bashirco.com.sa
EGYPT
SAFWAN EGYPT
10 Lebanon St., Mohandessen, Giza
Phone: +20 2 33 02 27 92 info@safwa negypt .com
IRAN
ARDIN CO.
App.#12,#64, Next to the Mehrshad Alley, Saiedi St. Africa Blvd., Tehran
Phone: +98 21 22 65 59 53 info@vivanvesta.com
TASVIR TEB HUMERS
199, Zafar St, Modares Highway, Tehran
Phone: +98 21 22 22 9155 ashkan.yousefi@gmail.com
IRAQ
NASEEM BAGHDAD COMPANY FOR MEDICAL & LABORATORY EQUIPMENT TRADING LTD.
AI-Mansoor, Hay Dragh, Block No.603, Street No.17, Building No.11, Baghdad
Phone: +964 l 54 81 25 dental@naseem-baghdad.com
JORDAN
SALBASHIAN TRADING CO.
Arar Mustafa Wahbi Al Tai St 128, Amman 11118 Ammam
Phone: +962 64 64 58 45 mohammad.m@salbashiangroup.com
KENYA
DENTMED (K) LTD 3rd Floor, Darshan Towers, Woodvale Grove, Westlands, P.O. Box 43873, Nairobi, 00100
Phone: +254 2 04 44 53 07 infinity@iconnect.co.ke
KUWAIT
AL-SAYAFE MEDICAL & PHARMACEUTICAL SUPPLIES CO. W.L.L Al-Arabia Tower, 18th Floor Jaber Mubarak Street, Sharq, Kuwai Phone: +965 22 25 59 09 bdm@alsayafemedical.com
LEBANON
FIMALCO DENTAL Mazraa-Mar Elias Street-Hariri Center 1st Floor, Beirut
Phone: +961 1 30 24 32 fimalco@hotmail.com
MOROCCO SOGEDENT
13500 Casa-Principal, Casablanca Phone: +212 5 22 89 30 14 info@sogedent.ma
OMAN
MEDICAL& PHARMACEUTICAL SERVICES CO. L.L.C Qurum - A-Harty Complex Sultan Centre Bldg. 2nd Floor Mina’ AI-Fahal - Muscat Phone: + 968 92 61 63 43 mahmoud-akil@bashirco.com.sa
SAUDI ARABIA
MEDICAL & PHARMACEUTICAL SERVICES BASHIR SHAKIB AL JABRI & CO. LTD Rehab District, Palestine Street, Jeddah
Phone: +966 l 26 70 04 30
mahmoud-akil@bashirco.com.sa
SUDAN
RASD Medicines & Medical Equipment Import No.761, Block 22, Alta if, Khartoum
Phone: +249 1 83 52 79 m.eisa@rasdtec.com 21
RADMED MEDICAL COMPANY
No.344 Block 1, Al sitteen street, al jureif west khartoum
Phone: +249 l 23 16 99 09 mohamed.osman@radmedco.com
TUNISIA MED PRO TUNISIA
Building lntegram Ang street Mexico & Argentina street 4et office No. 4 1002 Tunis Belvedere
Phone: +216 71 89 16 60 med-pro@outlook.com
TURKEY
LIDER DIS
Fevzi Cakmak Sokak No: 11 /5 Kizilay Ankara Phone: +90 31 22 31 64 85 lider@liderdis.com.tr
UNITED ARAB EMIRATES
CITY PHARMACY CO.
P.O. Box 2098 Airport Rd., Abu Dhabi
Phone: +971 26 73 29 54
headoffice@citypharmacyco.ae
YEMEN YEMEN STORES FOR DRUGS & MEDICAL SUPPLIES
P.O.Box 1465 Alzybairy Street, Y.R.
Sana’a Amman St.
Phone: +967 l 44 54 79 info@yemenstores.com

The hydraulic mechanism of the chair ensures smooth and quiet movement of the joints and provides a comfortable feeling for patients. One of the characteristics, touch screen interface has been designed to improve efficiency and reduce stress during treatment. When a handpiece is chosen and picked up, the screen displays only necessary information, helping the dentist concentrate on the treatment.
EURUS is shown in AEEDC Dubai 2022, so we welcome your visit at our Belmont booth.


Our new product, CLESTA elll SWING, is an ambidextrous dental unit and provides practical functions to use.
Basic
• Easy changeover to right/left handed use
• Compact space
Light
• Base-mount doctor table can be moved lightly and smoothly
• Reducing fatigue for arms of dentists and assistants
Flexible
• Making comfortable operating space
• Providing a variety of operating styles and preparation zones as you like




Company name: BISCO, INC.
Country of origin: United States of America
Website: www.bisco.com
BISCO, a global leader in aesthetic dentistry continues to develop innovative products for contemporary dentistry. At BISCO “Adhesion is our passion” and we dedicate our lives to understanding and improving the bond. We understand the importance of the supporting layer of the restoration. Whether you are working with implants, zirconium, ceramics/lithium disilicate, or porcelain fused to metal we focus on dentistry from the bottom up so your patients can enjoy top down esthetics.

BISCO proudly manufactures its materials in the United States and markets its products through highly trained, focused distributors outside the United States. At BISCO, we understand that product quality, consistency and freshness are of great importance. BISCO Dental Products are available worldwide with award winning brand names such as ALL-BOND UNIVERSAL®, AELITE ™, DUO-LINK UNIVERSAL™, TheraCal LC ®, TheraCem® and Z-PRIME ™ Plus.
BAHRAIN
GLOBAL MEDICAL ESTABLISHMENT
Block 644, road 4433
Building 627, flat 3, Nuwaidrat
Contact: dr. Abdullah nasser
Phone: 973- 172 17093
Email: admin@gme-bh.Com
EGYPT
ALEX DENT
31 El Rashidi St., Kasr EL Ainy Shaheen Medical Mall, Cairo
Phone & Fax: (20100) 140-6378 heshamelsheikh79@yahoo.com
IRAN
DONYAYE KALAYE SINA (DKS) CO.
#1, No.9 Vernous St. Keshavarz Blvd. Tehran 1415953131
Phone: 98-21-88998248 farazbehzadi@gmail.com
IRAQ
MZK DENTAL PRODUCTS Bloomfield Township, MI. 48302
Contact: Dr. Nizar Mansour
Phone: (248) 423-4644
JORDAN
BASAMAT MEDICAL SUPPLIES
125 Al-Razi Street
Jabal Al-Hussein, Abdali Area, Amman
Phone: 962-6-5605395 ziad@basamat.com
KUWAIT
ALPHA MEDICAL
Shareq, Ahmed Al Jaber St. Dasman Complex, Block 1 9th Floor, Office 22 Code: 35153, Dasmah Phone: 965-2-2478611 georgesaba@alphamedicale.com
LEBANON
DENTAL MEDICAL SUPPLIES - DMS Lebanon - Sed el Bouchreih Imad el Hachem Center, 2nd Floor, Beirut Phone: (961) 124-0444 dms@dms-leb.com
LIBYA
AL RADWAN GROUP
Dat Elmad complex, tower NO 5, H7 first floor, Tripoli Phone: (21891) 900-1106 muataz@alradwangroup.org
MOROCCO
DENTAL EXPERT
Rue Ibnou Katir Lot 7, Maarif Extension, Casablanca Phone: (21262) 350-5758 dentalexpert1@gmail.com
OMAN
DELTA NEW VISION
S.I. Building No. 93, 2nd Floor
Preah Sihanouk Blvd Muscat, Sultanate of Oman Contact: Mr. SAMI KANAAN sami@odontoprimegroup.com
QATAR
NASSER TRADING & CONTRACTING Salwa Rd, Midmac Roundabout, Nawar Building, Doha Phone: (9744) 466-5409 ntc@qatar.net.qa
SAUDI ARABIA
CIGALAH BIO MEDICAL
5th. Floor, Al-Ma’moun Tower, Ali Bin Abi Taleb Street, Al-Sharafiyah District, Jeddah Phone: (96612) 231-6194 ifarra@cigalah.com.sa
TUNISIA
L’EXCELLENCE MEDICALE Avenue des Martyres, IMB Palmaruim 4 B71, Sfax 3000, Tunisia Phone: (2163) 153-8072 import@excellencemedicale.tn
UNITED ARAB EMIRATES BIO LINK MEDICAL AND SURGICAL TRADING Office 301& 302, 3rd Floor Jumeirah Terrace Building, 2nd December St., Jumeirah 1, Dubai Phone: 971-4-3596242 info@biolinkdubai.com
YEMEN
EZ DENTAL MATERIALS & SUPPLIES
Mujahid St. Sana’a Phone: (96777) 022-2319 ezzaden.m@gmail.com
Dual-Cured Resin Modified Calcium Silicate Pulpotomy Treatment
TheraCal PT is a biocompatible, dual-cured, resinmodified calcium silicate designed for pulpotomy treatment. TheraCal PT maintains tooth vitality by performing as a barrier and protectant of the dental pulpal complex.
TheraCal PT’s chemical formulation consists of synthetic Portland Cement calcium silicate particles in a unique hydrophilic matrix which facilitates calcium release. TheraCal PT is radiopaque allowing for easy identification and differentiation
from recurrent decay and other restorative materials. TheraCal PT’s physical properties resist breakdown and degradation leading to a durable seal. TheraCal PT is also indicated for direct and indirect pulp capping (liner) and as a base.
BISCO’s THERA brand includes TheraCal LC, TheraCem, TheraCal PT and now TheraBase. BISCO believes that better dentistry can be achieved when practicing the THERA way.

TheraBase is a dual-cure, calcium and fluoride releasing, self-adhesive base/liner. Utilizing the THERA technology, TheraBase chemically bonds to tooth structure, and releases and recharges calcium and fluoride ions.1
TheraBase’s calcium release generates an alkaline pH which promotes pulp vitality. 2
It is a dual-cured material that will polymerize even in deep restorations where light cannot reach.
TheraBase is stronger and more durable than other base materials, glass ionomers and resin-modified glass ionomers.* Additionally, it is radiopaque allowing for easy identification on radiographs, providing a quick and effective diagnosis.
TheraBase has the strength, durability, and THERA technology to provide the best foundation for each restoration.
Base and Liner. The THERA way.

*Data on file, BISCO Inc.
1. Gleave CM, Chen L, Suh BI. Calcium & fluoride recharge of resin cements. Dent Mater. 2016 (32S):e26
2. T. Okabe, M. Sakamoto, H. Takeuchi, K. Matsushima. Effects of pH on Mineralization Ability of Human Dental Pulp Cells.Journal of Endodontics. Volume 32, Number 3, March 2006

Company name: Cavex Holland BV
Country of origin: The Netherlands Website: www.cavex.nl
Since 1908, Cavex has been developing and manufacturing premium solutions for the dental industry. Right from the start, all the company’s operations have been performed in-house in Haarlem, The Netherlands.
Every new Cavex product is a result of intensive collaboration between R&D, Regulatory, Production, Marketing, Sales and Logistics. This enables Cavex to develop, produce and distribute high-quality products all over the world.

ALGERIA
PROMODENTA SARL.
21, Rue Boumenir Mouloud 26000 Medea
Phone: +213 25 596277 promodenta@gmail.com
BAHRAIN
AL NOOR EST. FOR MEDICAL MATERIALS
PO Box 21538, Manama
Phone: +973 17 592 291 alnoor99@batelco.com.bh
CYPRUS
CYPRUS PHARMACEUTICAL ORGANIZATION LTD.
P.O. Box 21005
1500 Nicosia
Phone: +357.22.863.100 www.papaellinas.com
EGYPT
ERZING DENTAL SUPPLY
13, 26th July Street, Cairo
Phone: +20 2 24192946 kevork@erzingdentalsupply.com
IRAQ
WAZIN DENTAL & MEDICAL LTD
EDC Building Bakhiyarie Street 66, Erbil Phone: +964 751 721 1227 wazin.erbil@yahoo.com
JORDAN BURGAN DRUGSTORES
P.O. Box 773, 11118 Amman Phone: +962 6 533 7910 www.burgan.com.jo
KUWAIT
MEDICALS INTERNATIONAL WLL Abd Al-Latif Al-Sarraf Tower 5th floor Ahmed Al Jaber Street Block 1, Sharq Phone: +96522250228 www.medicalsintl.com
LEBANON DIÉTI-PHARM
P.O. Box 16-6680, 1100 2140 Beirut Phone: +961.1.500.991 www.dietipharm.com
QATAR
ACCROS TRADING COMPANY
P.O. Box 23006, Doha Phone: +974 44 81 65 11 www.accros.org
SAUDI ARABIA
BATTERJEE NATIONAL PHARMACEUTICAL
P.O. Box 2, 21411 Jeddah
Phone: +966126602933 www.battererjeenat.com
TUNISIA
MSI EQUIPMENTS MEDICO-DENTAIRES
R6, Rue Abdelkader Mhalla 5000 Monastir
Phone: +21673449401 commercial@ims.com.tn
INTER MEDICAL SERVICE
40, rue Dr. Burnet, 1082 Tunis Phone: +21671799344
msi.bouzgarrou@@topnet.tn
UNITED ARAB EMIRATES
MEDICALS INTERNATIONAL WLL
Suite 3103, 31st floor
Plaza Tower 1, Emaar Blvd
Dubai downtown Area, Dubai Phone: +971 44479796 www.medicalsintl.com
























YOUR IMPRESSION IS OUR SPECIALTY



Company name: DenMat
Country of origin: United States of America Website: www.denmat.com
Since 1974, DenMat has been a leader in high-quality dental products for dental professionals in more than 60 countries around the world. DenMat makes and assembles most of its products at its world headquarters on the Central Coast of California. DenMat offers three main product categories: Consumables, Small Equipment, and a full-service Dental Laboratory. DenMat’s consumables include the brands known and trusted: Geristore®, Core Paste®, Tenure®, Ultra-Bond®, Infinity®, Splash®, Precision®, Perfectemp®, and LumiBrite® and infection control.
DenMat’s small equipment includes a broad suite of products, including NV® PRO3™, and SOL™ soft-tissue diode lasers, Rotadent®, PeriOptix™ magnification loupes and lights, Flashlite™ curing lights, & VizilitePRO for oral lesion screening. DenMat is the home of the world’s #1 patient-requested thin veneer, Lumineers®. Now better than ever and backed by

Thinnovation®: DenMat’s fresh multi-disciplinary approach to anterior esthetics using the latest generation of Lumineers, all hand-finished by skilled lab artisans in California. DenMat also features Snap-On Smile®, the ultimate provisional appliance.
Each of DenMat’s more than 400 employees is focused on assuring that you—our dental customers—love our products and love your customer experience.
We’re building one of the world’s great dental companies—one happy dentist at a time!
www.denmat.com
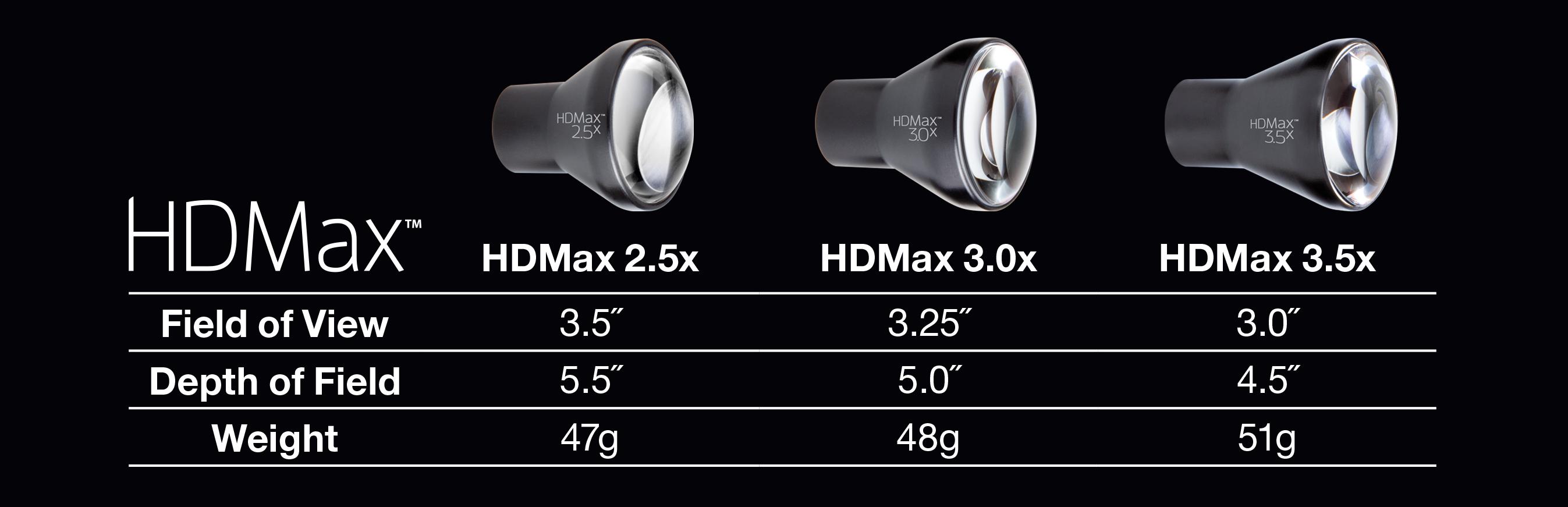



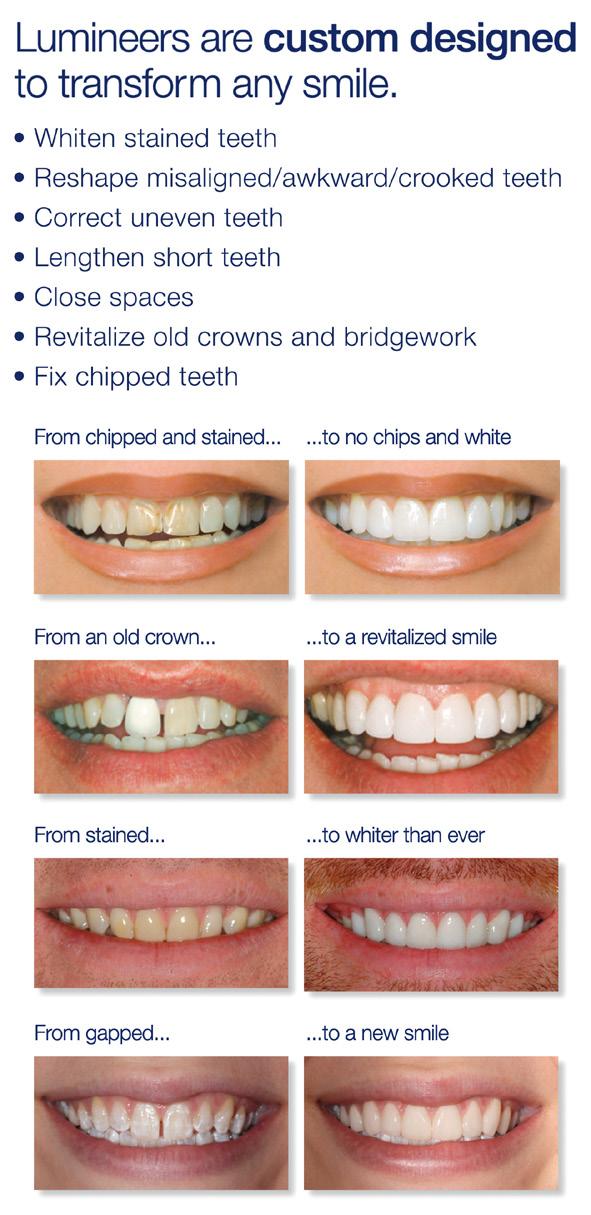


Company name: Dentsply Sirona E-mail: MEA-Marketing@dentsplysirona.com Website: dentsplysirona.com
Dentsply Sirona is the world’s largest manufacturer of professional dental products and technologies, with a history of innovation and service to the dental industry and patients worldwide. Dentsply Sirona develops, manufactures, and markets a comprehensive solutions offering including dental and oral health products as well as other consumable medical devices under a strong portfolio of world class brands. As The Dental Solutions Company™, Dentsply Sirona’s products provide innovative, high-quality and effective solutions to advance patient care and deliver better, safer and faster dentistry. With a sales presence in more than 120 countries, patients and practitioners virtually everywhere in the world rely on Dentsply Sirona.

For a full list of Dentsply Sirona authorized distributors in the Middle East & North Africa please visit bit.ly/DSMENA-Distributors or scan the QR code

Our decades of innovation in composite materials taught us what matters most to dentists. Neo Spectra™ ST is the successor of ceram.x® SphereTEC™ one, now a complete portfolio covering the full range of handling preferences and aesthetic needs with a single product line. SphereTEC® filler technology offers optimised performance in the areas that matter most, helping clinicians to achieve reliable, aesthetic results efficiently.
Neo Spectra™ ST composite offers optimised handling in a creamy and spreadable Low-Viscosity (LV) or a firm and packable High-Viscosity (HV) to accommodate your preference and technique for placement efficiency.

Features and Benefits
• Novel SphereTEC™ filler technology.
• Exceptional handling comfort! Easy to adapt to cavity walls, margins and surfaces, no stock to the hand instrument, precise to sculpt, slump resistant and easy to extrude.
• Extremely simple Cloud shade concept.
• Exciting clinical results made easy.
• Fast and easy polishing.
• Extra glossy.
• Great mechanical properties.
• Excellent choice for long-lasting restorations.
Primescan and Omnicam
The basis for best treatment results is the precise depiction of reality in a virtual model. With Primescan, intraoral scanning delivers excellent results like never before. It opens a world of possibilities for you - decide for yourself which way you want to take. Simply scan and send with a click - to whom you want. Work as usual with your lab and the partners of your choice - with open data formats or in a validated, secure workflow. Whether in prosthetics, implantology, orthodontics or other areas - stay flexible. Take the first step and let us accompany you on your individual path to digital dentistry. Make your workflows better, faster, and safer with digital impressions by Dentsply Sirona.
Primescan AC
Redefine your standards of outstanding accuracy and speed: Primescan enables all kinds of treatment, from single tooth to full arch. With Primescan intraoral scanning is now more accurate, faster and easier than ever before.
Omnicam AC
In addition to the new superstar Primescan, the proven Omnicam is a real alternative. Omnicam is still one of the smallest scanners available. It is therefore particularly easy to handle, scans powder-free and in colour. For more than seven years, it has impressed users worldwide and is always up to date thanks to continuous software updates.
Omnicam AF
New to the MENA region the Omnicam AF comprises the individual components of Omnicam including camera tray and PC. With more than 7 million scans per year, Omnicam is one of the most widely used scanners on the market – now with the option of the Acquisition Center (AC) and the flexible tabletop unit (AF).
For more information visit: dentsplysirona.com/digital-impression


Company name: DMP
Country of origin: Greece
Website: www.dmpdental.com
With more than 35 years of experience in dental material manufacturing DMP successfully supplies the dental market worldwide. Certified with ISO 9001, 13485 and MDSAP, DMP’s products carry the CE mark and have U.S. FDA clearance. DMP creates bright smiles achieving excellence and reliability through integrity, passion and commitment which are ingrained in DMP’s culture.

DMP specializes in three main groups of dental materials. The largest group of products are the precision silicone impression materials both for the dentist and the dental laboratory. The second major group of products are the composites for aesthetic dentistry, including bonding and etching materials. They are primarily resin-based materials and are available in light, self or dual cure varieties. The last group is the amalgams which were launched with the establishment of DMP and consist of various types for every need.
DMP aims to create BRIGHT smiles and to provide the highest level of satisfaction, by closely cooperating with its customers and maintaining a high degree of flexibility for individual market needs.
EGYPT
AL WARDANY FOR IMPORT & COMMERCIAL AGENCIES
5 Alsraya Street - Fl. No.2 Office 14, Almnyal, Cairo Phone: +20 23654 322 alwardany@link.net
IRAN
PARSEH ETTEKAL Co.
Miremad St, Motahari Ave, Suite 4, Building 12, 13th Alley, Tehran Phone: +98 (21) 88545400 vaheh@parsehettekal.com
IRAQ
DANA AMIN ABDALRAHMAN COMPANY FOR GENERAL TRADING Medicine Street _40m, 44001, Erbil Phone: +964 751 2383432 dana.amin.arch@gmail.com
JORDAN
BADAWNEH MEDICAL SERVICE
Almallab Albalady Str., Irbid, P.O. Box 2873, Jordan Phone: +96227261901 badawneh@hotmail.com
KUWAIT
M&H MEDICAL COMPANY TO IMPORT MEDICINES & MEDICAL SUPPLIES
Salem Al Mubarak St., KIB Bldg, Reem Mall, Flr-2, Office No-8, Block-2, Salmiya Phone: +96551719517 sanjay@mh-kw.com
LEBANON
D-VARD
Principal St, Bld. Botros EL Achkar, Area Maten, Ground Floor – Next To Champville School Main Gate, Deek El Mehdi Phone: +961 78 942 468 khalil.achkar@gmail.com
LIBYA
AL BASMA DENTAL CENTER
310 Mizran St., Tripoli, Libya Phone: +218 213615043 basmacenter.ly@gmail.com
MOROCCO
MIADENT
5 Rue Jabal Bouiblane, App1, Agdal, Rabat, Phone: + 212537671145 ihssan.b@amed.ma
OMAN
GLOBAL GULF ELITE
Nuzha Street 3152 - Flat Number 22, Wadi Kabir, Muscat, Oman Phone: + 96891718373 info@globalgulfelite.com
QATAR
ABM4 TRADING AND CONTRACTING
Building No:9, Office No: 39, Barwa Village, Al Wakara, Cr No.113157, Doha Phone: +97444365531 drazeem@abm4trades.qa
GHAYDAA HOSPITALITY & BIOMEDICAL TRADE
Building No 06, st. No 873, Zone No 54, Muraick, Doha, Qatar Phone: +97444365531 imthath@ghaydaa.org
SAUDI ARABIA
ASNAN EST. FOR MEDICAL SERVICES
Buraida Street, Building no 40, P.O.Box 26316, Al-Rayyan, Riyadh, Phone: +966(11)4451075 anis@asnan.net.sa
AFIA AL KHALEEJ TRADING EST Batha Quraish, Jabal Thawr Rd, Makkah, 23343, Saudi Arabia Phone: +966 567373720
afiaa.m.s.info@gmail.com
SYRIA
OMAR ALKASHTO FOR DENTAL SUPPLIES Almazzeh - Alalam St. 9/5519, Damascus Phone: + 963992722111
omar.alkashto@dentacham.com
TUNISIA
DENTAL ATLAS S.R.L
1st floor- Rouached Medical Center, Sidi Ahmed Zarroug, Gafsa, 2112, Tunisia Phone: +216 76211720
dental.atlas.tn@gmail.com
NEW VISION LE SERVICE
MEDICO–DENTAIRE
12 Rue Jawhara Cite El Mouna, Boumhel, 2097, Tunisia
Phone: + 216 71 905065
beji.bennsib@newvision-tn.com
UNITED ARAB EMIRATES ADVANCED HEALTHCARE MEDICAL EQUIPMENT AND DRUG TRADING LLC
1903 Lake Central Tower, Marasi Drive, Business Bay, P.O. BOX: 234923 Phone: + 97144547730 alaay@advanced-hc.com
DMP expands its BRIGHT Temporary Crown & Bridge family with the 10:1 and 4:1 delivery systems.
Exceptional aesthetic results, combined with optimal mechanical and physical properties, make them ideal products to fabricate provisional restorations.
The unique and highly advanced technology of BRIGHT Temporary C&B also offers:
• Natural tooth-looking aesthetics due to the perfect combination of shade opacity and fluorescence
• Very low temperature during intra-oral setting which protects against damage of the dental pulp
• Very high compressive and flexural strength for long lasting provisionals
• Colour stability
• Easy polishing due to low oxygen inhibition layer
• Optimum elastic properties
• Easy to cut and trim


Leading the BRIGHT range of composites is NANOCERAM-BRIGHT, a strongly radiopaque nanohybrid composite with exceptional aesthetic results. its creamy consistency and ease of sculpting make it the ideal composite for both anterior and posterior restorations.
Moreover, the high filler loading combined with fine particle size distribution, leads to low polymerization shrinkage, yielding high marginal integrity and minimized post-operative sensitivity. Its benefits include:
• Outstanding aesthetic results with chameleon effect
• Excellent handling characteristics with no slumping
• Extremely high polishability
• High resistance to wear
• Universal composite
Company name: MANI, INC.
Country of origin: Japan
Website: www.mani.co.jp/en
MANI, INC. is a manufacturer of medical devices and dental instruments. Ever since we started manufacturing surgical needles in 1956, we have contributed to society as a medical device manufacturer supplying surgical and dental instruments. Our products, which are safe and high-quality medical devices that satisfy the needs of doctors and patients, have also passed the strict standards of countries overseas.
DENTAL WORLD & MEDICAL SUPPLIES
Manama
Phone: +97317896322 dwms.bh@gmail.com
EGYPT
GENERAL EGYPTIAN TRADING
Giza
Phone: +2025729368 getegypt@yahoo.com
IRAN
DOUSTKAM CO, INC.
Tehran
Phone: +982177534652 doustkamco@gmail.com
IRAQ
ZUHAIR BUREAU
Baghdad
Phone : +96407903760781 zuhair@zuhairbureau.iq
JORDAN
MATEST COMPANY
Amman
Phone: +96265690807 matest1@orange.jo

We employ more than 3,000 people worldwide and use our own channels of distribution to deliver products to more than 120 countries. MANI offers a wide range of dental instruments, including burs, sutures, root canal instruments, polishing instruments, posts and dental accessories.
GLOBALMED TECHNOLOGY
Kuwait Phone: +96522431647 ab@globalmedtechnology.org
DIETI PHARM DENTAL PRODUCTS
Beirut Phone: +9611500991 dietipha@inco.com.lb
LIBYA
AL BYAN CENTER
Tripoli Phone: +218213333021 albyan_almotagaded@yahoo.com
BEST MADE
Casablanca Phone: +212522834482 best.made@yahoo.fr
OMAN
SALA MEDICAL COMPLEX
Muscat Phone: +96824485159 salamedical@yahoo.com
AL MANARA
Ramallah
Phone: +97222953718 kshatara@p-ol.com
SHARQ MEDICAL SUPPLIES
Doha Phone: +97444566100 samer@sharq.qa
SAUDI ARABIA
AL RAZI MEDICAL SUPPLIES
Jeddah
Phone: +966126520132 alrazimed@yahoo.com
SYRIA
SALLOUM DENTAL CO
Damascus
Phone: +963112248772 psalloum@scs-net.org
UNITED ARAB EMIRATES
SAWHNEY TRADING LLC
Dubai
Phone: +97143597756 sawbros@eim.ae
YEMEN
YEMEN STORES
Sana’a
Phone: +9671444622 s.radman@yemenstores.com



Company name: Renfert
Country of origin: Germany Website: www.renfert.com


We at Renfert have been developing intelligent solutions and reliable service for technology and products since 1925, enabling dental technicians and dentists worldwide to put their passion for detail into practice.
Around 200 employees work in our owner-managed, medium-sized German company. The main headquarters is located in Hilzingen in the Lake Constance region.
ALGERIA
EQUIPEMENT MEDICO DENTAIRE SARL Fréres Bekkouche Villa n° 126
Cité El Mouna 25000 CONSTANTINE
Phone: +213(31)667021 odontomedicadz@yahoo.fr
ODONTOMEDICA SARL
Zone d’activité Ain smara tranche I n° 26 - A 25140 CONSTANTINE
Phone: +213 31 60 15 86 87 odontomedicadz@yahoo.fr
BAHRAIN
SEEF DENTAL HOSPITAL
Bldg. 1029, 3rd Floor, Road 3621
436 SEEF AREA
Phone: +(0973) 17587991
Seefdental@info.com
EGYPT
MIDDLE EAST INTERNATIONAL TRADING CO. LTD.
7 Amin Al-Kholy Str. 5240 Heliopolis West
Phone: +20(2) 22419296 meit@meit.com.eg
MODERN TRADING CO.
15 Al Adib Ali Adham Sheraton
Phone: +20222683882 info@mtchealthcare.net
IRAQ
EBDA-DENT
Karrada - Sharqia - Attar st., Q. 905 st. 11 bldg. no. 84 - 1st floor
Phone: +964(7810) 785511 ebda.dent@gmail.com
HIGH TECHNOLOGY FOR DENTAL SUPPLIES
Al-Sarrafiya, near Al-Sarrafiya Bridge beside Althakira Librar, 10053 BAGHDAD
Phone: +964 770 348 59 73 iraqidigitaldentistry@gmail.com
All our products are made in Germany. From here we deliver through qualified retailers to more than 120 countries.
Our products are renowned for their operational reliability, functionality, and longevity. Modern, efficient development and manufacturing technologies allow us to produce high quality competitively for best price-performance ratio.
PACOTECH COMPANY
Al Qassab bulding no 155/1/140 str 18 section 204 mustaufi or Phone: +964 750 448 1485 office@pacotech.info
JORDAN
MADINA DENTAL SUPPLIES
Sport City, Lauozi Building No. 11, P.O. Box 19070, 11196 AMMAN Phone: +962 651 665 64 bilaldent@hotmail.com
KUWAIT
HEALTHCARE DYNAMICS
Salem Al Mubarak Street, Zahra Complex, 2nd Floor Office No. 9, P.O. Box 7811, 22089 SALMIYA Phone: +965 222 841 22 info@hcdynamics.com
LEBANON
DENTALTECH S.A.R.L.
Brazilia Str. - Hikmeh Bldg, 1st Basement Phone: +961(5) 950707 accounting@dentaltechsarl.com
MOROCCO
D.E.M.I. SARL 11, Rue El Wahda Boulevard du 11 Janvier 20000 CASABLANCA
Phone: +212(522) 441414 demi@demi.ma
OMAN
AL FARSI NATIONAL
ENTERPRISES L.L.C
Flat No: 4, Wy No: 3521, Building No: 1992, Block No: 235, Post Box: 158, Al Khuwair Phone: +96824485625 director@alfarsi.me
SALA MEDICAL COMPLEX
P.O.Box 780 Postal Code: 131 Phone: +968(24)485159 salamedical@yahoo.com
QATAR
ALI BIN ALI MEDICAL W.L.L. ABA Tower, Airport Road, P.O. Box 75 Phone: +974 44799000 Dergam.AlLakood@alibinali.com
SHINE TECHNOLOGY COMPANY 01, 2nd floor, Above Oman Air, Beside takeaway, Al Sadd Phone: +974 444 244 23 medical@qatar.net.qa
SAUDI ARABIA CIGALAH BIO MEDICAL MEDICAL & PHARMACEUTICAL SERVICES BASHIR SHAKIB AL-JABRI & CO. LTD. P.O. Box 9584, 21423 JEDDAH Phone: +966 12 670 04 30 bashirco@bashirco.com.sa
SYRIA FARZAT CHATTA
P.O. Box 4588
Phone: +963(11)2220211 chatta.d.s@gmail.com
TUNISIA PROMOSCIENCES
Rue n° 7 ZI La Charguia I 2035 TUNIS Phone: 0021671772 promosciences@planet.tn
UNITED ARAB EMIRATES NOOR ALHUDA TRADING Office 107, Al Muhairi Plaza, Al Khabaisi Area, Deira Phone: +971 50 6330 575 info@nht-hightec.com
YEMEN NOORDENT FOR DENTAL SUPPLY Hadda St. Next to Al-Ghrasi Phone: +9671208827 noordent@gmail.com
3D filament printer system
Dental filament printing - intuitive and simple. With its unique advantages, the SIMPLEX stands out from other filament printers.
With the dental slicer software, you can reliably print models that meet processing requirements and do not pose a risk either to health or to the environment.
making work easy -
This is what makes work easier:
• Reliable and easy to use thanks to the ‘Plug and Print’ concept.
• High precision thanks to a level resolution of up to 50 µm.
• Extremly quiet (≤ 49 dB).
• Process reliability thanks to a filament monitoring system.
• Easy to use thanks to the dental slicer software.
• No post-processing (no cleaning, no curing).
• Low printing and material costs.






See it, share it, work it - digital and simple. The digital solution for case discussions between technicians and dentists.
Two options available for purchase: with a 3D ready screen included (EASY view+ 3D) or without screen (EASY view+).
making work easy -
This is what makes work easier:
• Saves time and simplifies communication with dentists.
• Easy documentation and communication of the patient situation using the Renfert CONNECT app.
• Fast download and upload via Wi-Fi with the Renfert CONNECT stick.
• Detailed views and complete model representations through 4x, 15x and 20x magnification.
• Simplifies everyday work, quality control and demonstrations.

Company name: Ultradent Products Inc.
Country of origin: Salt Lake City, UT (USA) Website: www.ultradent.com
Ultradent Products Inc. was founded in 1978 in Salt Lake City by Dr. Fischer dentist, researcher and university professor (now Founder & CEO Emeritus of Ultradent Products, Inc.) with the aim of improving the techniques and products used by dentists in the entire world, in order to solve patient problems faster and without invasive methods.
Now, marking its 44th year as a family-owned, international dental supply and manufacturing company, Ultradent has continued its vision to improve oral health globally by creating better dental products that continue to set new industry standards.
MUHAMMAD AHMAD SABAWOON LTD
Khushal khan, mina block 32, muqabil sello, Kabul
Phone: (00) 788775555 chughtai1@hotmail.com
BAHRAIN
DENTAL WORLD & MEDICAL SUPPLIES
Office 11, bldg 932
Road 632 , block 706, salmabad
Phone: (00)973 (178) 96322 dwms.bh@gmail.com
CYPRUS
PM DENTAL
11A KORITSAS, Nicosia Phone: (00)35722594050 p.m.dental@cytanet.com.cy
EGYPT
ELWAN DENTAL SUPPLIES
70 Merghani street 10th floor Managger, Cairo
Phone: (00)202.33873883 elwanyegypt@yahoo.com
IRAN
GOLNAR NIKAN DANDAN
Unit 9, #64 Building, Opp Bahar St, Enghelab Ave P.O. Box: 1148836873, Tehran Phone: (00)9821 77533716 kavehgolnar@yahoo.com
IRAQ
SMART DENT
Almansoor street, beside zain

Ultradent currently researches, designs, manufactures, and distributes more than 500 materials, devices, and instruments used by dentists around the world, has subsidiaries in 9 countries and sells products in over 125 countries. Ultradent also works to improve the quality of life and health of individuals through financial and charitable programs.
communication bldg
Bldg no. 3 Floor 2, Baghdad Phone: (00)7810775922 smartdent79@yahoo.com
MALEK DENTAL & MEDICAL SUPPLY
jo 75 Al Buhturi Street, 2nd Circle, Jabal Amman, P.O. Box 7067, Amman Phone: (00)7810775922 mhdentamed@go.com.jo
KUWAIT
ADVANCED TECHNOLOGIES Hawali 32060, P.O.Box 44558
Kuwait City Phone: (00)962795533513 ali@atc.com.kw
LIBYA
ALBYAN ALMOTAGADED FOR IMPORTING OF EQUIP & MEDICAL SUPPLIES CO LTD
Mohd Fkini St., Bldg No. 20, PO Box 82525, Tripoli Phone: (21) 333-3021 albyan_centre@hotmail.com
MOROCCO
A.M.E.D.
47, Rue de bruxelles, Casablanca Phone: (00)212.522823134 ihssan.b@amed.ma
OMAN
PIONEER TRADE & MEDICAL SUPPLY
Khalid Al Said Investment Co. PO Box 77 PC 103, Muscat Phone: (00)68 9780 4272 raed@pioneersoman.com
PAKISTAN
PAK-MED DENTAL SUPPLIES
pmdsupplies@gmail.com
Phone: (00)92 52 325 722
BILAL ENTERPRISES
Chughtai1@hotmail.com
QATAR
CEDARS DENTAL CENTER
P.O. Box 47684
Al Hilal, Doha Phone: (00)974.44864088 chaanine@cedars-dental.com
SAUDI ARABIA
DENTAL ERA
Al-Abdel Latif Plaza, King Fahd Rd, 3RD Floor, Office # 306 P.O. Box 126122, Jeddah Phone: +966 12 2752 382 ashraf.mubarak@dentalera.com
SYRIA
BADRIG AYDENIAN
Shouhada street, Damascus Phone: (00)963 (11) 444 6429 aydbaco@gmail.com
TUNISIA
DISTRI MED
Av. De Madrid, Tunis Phone: (+216) 71 334 812 distri-med@planet.tn
UNITED ARAB EMIRATES
ELWAN TECHNICAL SUPPLIES
P.O. Box 43305, Abu Dhabi Phone: (00)97126393292 etselwan@emirates.net.ae
When you want to give your patients the best results, your only choice is Opalescence™ teeth whitening!
Opalescence™ PF whitening | The most customizable of our whitening options. Use Opalescence PF whitening with custom trays made by your dentist for a personalized whitening solution day or night.
Opalescence Go™ whitening | It’s a portable, quick application. You pop in the UltraFit™ tray for the directed time and then brush afterwards. The tray gets thrown away and you pop in a new one next time! You can keep it anywhere there’s a fridge and a toothbrush.
Opalescence™ Boost™ in-office whitening | This miraculous product is so potent, it still needs to be applied by your dentist. It’s worth mentioning here because it’s an excellent option for fast, powerful teeth whitening. Think of it as a boost to start your whitening experience. Complete your whitening treatment with an Opalescence whitening take-home option.
Opalescence™ Whitening Toothpaste | Did you know that foods and other factors can cause surface stains on your teeth? A safe, everyday whitening toothpaste gently scrubs away surface stains and helps maintain a healthy smile. Achieve the best results by using toothpaste in tandem with our other whitening products which work to whiten below the surface.




All VALO LED curing lights to use a custom, multiwavelength light-emitting diode (LED) for producing high-intensity light at 385–515 nm, which is capable of polymerizing all light-cured dental materials. This intensity will also penetrate porcelain and is capable of curing underlying resin cements similar to a quality halogen light. Every VALO™ LED curing light starts as a single bar of tempered, high-grade aerospace aluminium, which is CNC precision milled at Ultradent’s facility in Utah, USA and ends as the most advanced curing light in the world.
• Ultra-high-energy broadband LEDs cure all dental materials
• Optimally collimated beam delivers consistent, uniform power
• Three curing modes accommodate your preferences
• Extremely durable, slim, ergonomic shape allows unprecedented access to all restoration sites
• Unique unibody design is both extremely durable and lightweight
• Highly efficient LEDs and aerospace unibody aluminium keep the wand body cool to the touch
• 5 years Warranty

Company name: WHITEsmile GmbH
Country of origin: Germany
Website: www.whitesmile.com
In 1994 WHITEsmile was one of the first companies in Europe to specialize in the production of tooth-whitening products. Our “Made in Germany” materials and whitening lamps are the result of constant consultation with dentists and users in over 60 countries. WHITEsmile materials are clinically tested, certified medical products and devices.
Tooth whitening is becoming more and more a central point of dental treatments. For aligner, implant, and restorative patients only the white smile at the end fulfills the desired result. And here a reliable result is key for success.
SARL THE ABOU SAMRA BROTHERS
Cité Abdouni N° 24, Dar El Beida 16100 Alger
Phone: +213-21-506 578 arcco.algeria@yahoo.fr
EGYPT
GET, GENERAL EGYPTIAN TRADING 446, El – Ahram St., 4th Bld., Floor 12, Giza 12111
Phone: +(202) 37765001/2/3 get.egypt@yahoo.com
IRAQ
(for fläsh products)
CAPITAL Y FZCO / PAZI PHARMA
Phone: +964 750 332 1390, +971 56 344 1936 management@capitalyholding.com
(for WS products)
BAYATI COMPANY
University District, Musul Phone: +964 7725404952
JORDAN
BASAMAT MEDICAL SUPPLIES (PHARMADENT)
P.O. Box: 141375, Amman 11814
Phone: + 962 79 50 45 700 info@basamat.com

fläsh is the innovative new brand from WHITEsmile for the most reliable whitening for every patient. Based on over 25 years of tooth-whitening experience, our cutting-edge, “Made in Germany” fläsh device light optimizes in-office whitening. Our extensive experience makes WHITEsmile a partner you can trust for tooth whitening.
For all MENA inquiries:
WHITEsmile GmbH mena@whitesmile.de
KUWAIT
NOON MEDICAL SUPPLY CO.
Al Derwaza tower, st 65, block 3 building 6, floor 1, flat 2 Bnied al qar, Kuwait Phone: +965 22423 600 info@noonmedical.com
LEBANON DMS
Bauchrieh, Imad Hashem Center 2nd Floor, Beirut Tel.: +961-1- 240 444 dms@dms-lb.com www.dms-leb.com
MOROCCO
CLAIRE DENT
Siège Social : 6, Rue Ghandi Appt. N°3, Rabat Phone: +212-37-72-62-64 clairedent@menara.ma
SAUDI ARABIA
MASAR MEDICAL COMPANY
Al Ha`ir Road , Al Lolo`a Stores Store #56, Al-Riyadh Phone: +966-1-2930598 info@masarmedical.com
SYRIA
KASSAB DENTAL
Damascus, Syria
Phone: +96311-2313288 kassabdent@yahoo.com
OMAN AL MAZROUI MEDICAL & CHEMICAL SUPPLIES
P.O. Box 1259 PC 112
Muscat Phone: +968 24 595 670 nasser@almaz.com.om
QATAR GERMINMED
Building 82
P.O. Box 11755
Doha, Qatar
Tel.: +974 44272 148 info@germinmed.com.qa sales@germinmed.com.qa www.germinmed.com.qa
TUNISIA SEM
L’EXCELLENCE MEDICALE
Avenue des Martyres immb Palmaruim 4 B71
3000 Sfax Phone: +216-31-538 072 contact@excellencemedicale.tn
UNITED ARAB EMIRATES NEW AL FARWANIYA SURGICALS P.O.Box 47837
Abu Dhabi
Phone: +97126775447 farwania@emirates.net.ae

1994 - 2019
1994 - 2019
WHITEsmile is proud to celebrate the 25th company anniversary 2019. We thank all of our customers and partners for the trust shown in the past years and look forward to an even brighter future.

Proven “Made in Germany” products for in-office and at-home whitening: WHITEsmile LIGHT Whitening, POWER Whitening, HOME Whitening. WHITEsmile provides all varieties of tooth whitening offerings for your dental clinic.











Enjoy the scan. With the connectivity options of Primescan. Scan and connect digitally. Or treat it in a single visit. Either way, it‘s prime.