FROM THE EDITORS-IN-CHIEF
Dear Reader,
As we emerge from the COVID-19 Pandemic, we must consider its far-reaching impact on our society’s well-being, barriers to resource access, and mental health. For this reason, our Winter 2022 issue emphasizes mental health and human behavior as it relates to healthcare and medicine. Our hope is that you can both appreciate and absorb something meaningful from the issue so that we can continue to collectively grow as a society with greater perceptivity.
We are happy to present nine articles that encapsulate these themes as we look on to a brighter future. Covering everything from nanoparticle-based therapeutics to the tenets of intermittent fasting, each piece contributes to an overarching story of mental health solidarity in a post-pandemic world.
We want to recognize the work of the writers, editors, and layout and cover design team for their invaluable efforts and contributions to this quarter’s issue. As new Editors-in-Chief, we hope that this issue leads you to gain new perspective on the fields of public health and medicine as you understand them. Thank you for contributing to our continued success of the magazine, and we look forward to working with you in the future. We hope that you enjoy the issue as much as we do.
All the Best, Jack & EJ
EDITORS WRITERS

Meagan Johnson
Miles Kaufman
Neeharika V
Caroline Kellogg
Rahul Barra

Ayman Lone
Sanaa Imami
Chris Cardenas
Eva McCord
Marissa McCollum
Riley Hurr
Eve Tanios
Rachel Zhang
Ashley Chen
Ruka Adachi
Sophie Hu
Michelle Ma
Teresa Nam
LAYOUT COVER DESIGN
Katrina Schmitt Sam Goslin
pulse - winter 2022
CONTENTS ASKING FOR JANE: AT-HOME, HERBAL ABORTIONS IN AMERICA 2 THE RIGHT TO DIE 6 THE TRUTHS AND ILLUSIONS SURROUNDING INTERMITTENT FASTING 8 MENTAL HEALTH RESOURCES ON COLLEGE CAMPUSES 10 table of contents 1 NANOPARTICLE-BASED VACCINE DESIGN 12 EPIDEMIOLOGY: THE BEDROCK OF PUBLIC HEALTH 16 A DANGEROUS ADDICTION 18 ANTIBIOTIC-RESISTANT BACTERIA: A MODERN PUBLIC HEALTH PHENOMENA 20 “PUT ME BACK IN COACH”: THE DANGER OF THE REPEAT CONCUSSION 23
ASKING FOR JANE
AT-HOME, HERBAL ABORTIONS IN AMERICA


 By Meagan Johnson and Marissa McCollum
By Meagan Johnson and Marissa McCollum
On a winter morning, Anna* walked the aisles of an herbal-medicine store, picked up a bottle each of blue cohosh and black cohosh, along with a plastic bag of pennyroyal tea, and drove to the topless bar on the edge of town where she worked. There, she met Jules*, another dancer. The women, both in their 20s, then drove to the Motel 6 where Jules lived and entered her dim room on the second floor, which smelled of grape cigars. Anna pulled out the tinctures and tea and explained the plan. She was going to help Jules try to have an abortion. Anna had found the herbal recipe online. She’d read other tips as well: frequent hot baths, vigorous exercise, lots of gin. Women have relied on herbal abortion for thousands of years, and though specific regimens were hard to come by, anecdotal accounts littered the internet. Anna didn’t know how long it would take, so she moved in with Jules at the motel, dancing at the club each night. She set an alarm every four hours, keeping Jules to a schedule of 20 tincture droplets under the tongue and a cup of brewed tea. She drew baths for Jules, listened as she ran the stairs, and watched as she gulped Tanqueray. Anna repeatedly took her temperature and handed her glasses of water.
pulse 2
Given the recent and controversial abortion ban in Texas, it is now harder for women to receive an abortion than it was in 1650 Puritan New England. In fact, Texas’six-week abortion ban is a stark constrast to early abortion law in the 1600s, which dictated the legality of the procedure until “quickening”—the first time the mother feels the fetus kick, which can happen anywhere between fourteen and twenty-six weeks into pregnancy. If a woman living in 17th and 18th century New England wanted an abortion, there were no religious, legal, or social constraints placed on her. By 1860, abortion until “quickening” became illegal after the first official abortion laws were put on the books in 1821. Unfortunately, today, even if a women has the legal right to abortion in her state, she is often faced with a sea of hostile protesters outside of abor-
tion clinics. Already making one of the most private and sensitive decisions of their lives, women are burdened by death threats, guilt, and moral judgements. In fact, national anti-abortion organizations such as the National Right to Life have spun an incorrect narrative to suggest that legal abortion is a historical anomaly, a direct reflection of America’s increasingly loose moral standards and strong Biblical adherence. Meanwhile, Americans United for Life have an affinity for misquoting the infamous Thomas Jefferson quote as a maxim for anti-abortion sentiment: “The care for human life and happiness, and not their destruction, is the first and only legitimate form of government.” In reality, the first waves of anti-abortion arguments were based on economics and gender-inequality. Given that homeopaths and midwives had the ability to perform safe and
successful abortions, American physicans felt the need to reinforce the authority and legitimacy of the male-dominated field of medicine. White physicians were also concerned that low-birth rates among White women would lead to racial inferiority and immigrants from overrunning the country. By the turn of the 19th century, women’s choices over their bodies were incredibly limited; it wasn’t until Roe v. Wade in 1973 that America saw a reversal in female autonomy.
However, since the 70s, abortion has become synonymous with sexual promisciousity, poor contraceptive choices (despite an uneven access to birth control), and anti-Christian practices. An unwillingness to reframe abortion as an act of feminist science and a right to one’s body has caused a rise in at-home, herbal abortions over the last two decades.

pulse 3
With the accessibility of Google, links to herbal recipes that can evacuate a fetus from the womb can be found in about 1.8 seconds. Suction devices, such as a Del-Em, only require a mason jar, tube, and syringe—all of which can be purchased at a local drugstore. At-home abortions are placing scientific knowlege and procedures back in the hands of women, but a secret coalitaton of abortionists have taken this one step further: at-home, herbal abortions are viewed to be more comfortable and personable than most abortion clinics throughout the U.S. Anna*, a stripper and at-home abortionist, is a part of this secret society For her, it all started when after finding herself pregnant by an abusive partner and unable to afford the cost of a clinic procedure, she stumbled upon an online posting that suggested that consuming 10,000 mg of Vitamin C every day could induce a miscarriage. On the second day, she started vomiting and ran a fever. Not knowing what to do, she relented and went into a clinic. She vividly remembers her physicians walking into the poorly-lit room wearing acid-washed jeans, without uttering a word. The procedure lasted thirty minutes, after which she was ushered into a univiting observational room, surrounded by women hysterically crying or staring off blankly at


the sterile walls.
A few months after the procedure, still strapped for cash, Anna began work at a local topless bar. Quickly, she found a niche community among the group of strippers and soon turned the dressing room into a forum for the women to speak freely about family planning. Often, these women complained about receiving poor sexual education during their school years, an inability to receive birth control, the dread they would feel if someone recognized them at a clinic, and the coldness felt while recieving a clinic procedure Outside of work, Anna filled her reading anatomy textbooks and participating in online chatrooms within herbal abortion and midwife communities. By March of 2015, Anna found herself in a unassuming suburban home, which served as a meeting place for secret society members (who refer to themselves as Jane Collective) to take workshop classes—this included watching a pregnant women receive an abortion with a Del-Em, how to mix herbal teas, and how to make the patient feel at ease with their decision. Most importantly, Anna learned how to dose Misoprostol—a hormone typically used to treat stomach ulcers, also known as the “abortion pill.”
Anna found a community in the Jane Collective, who mostly consisted of
low-income individuals like herself frustrated by their experiences with family planning. Many are doulas or midwives. Some have had only a few months of training. Despite these statistics, the Jane Collective has reported their success rate somewhere between 80 and 85 percent with minimal risk. Numbers amongst the Jane Collective have increased from 45 to over 2,000 women over the last few years. As of today, there are only 1,671 licensed abortion clinics in the U.S. In recent years, there has been a global trend to expand abortion access by training midwives and community health workers; in the U.S. this has been restricted by dozens of laws. The women of the Jane Collective are risking their lives and families to improve abortion access, often committing crimes that, if prosecuted, could carry life sentences. These women are breaking roughly 40 national and state laws, which include: unauthorized mailing of abortion pills, practicing medicine without a license, and abuse of a corpse (by burying fetuses). Members of the Jane Collective are acting in place of physicians and take this role seriously. In order to practice, members must be well-versed in monitoring blood-flow, prescribing medication regimens, and monitoring blood pressure. To protect their anonymity, the Jane Collective has not
pulse 4
produced any official reporting on the number of women serviced, exact success rates, an accurate member count, nor the demographics of its patients. With the rise of organizations such as the Jane Collective, it is worth questioning the future of abortion clinics. Even if we soon see a direct reversal of Roe v. Wade, women around the United States will continue to perform these practices without extensive medical knowledge.

Misoprostol is safe and affordable and miscarriage-inducing teas carry an out of pocket cost of around $35. Jane Collective hopes to revolutionize abortion as a procedure “for women, by women.”They hope to support, guide, and encourage marganalized women who face structural barriers (both economic and social) to abortion clinics. The organization is a metaphor for the need to embrace female-centered care and represents the lengths women will happily go to express their bodily freedoms. The Jane Collective is an honest and progressive place to to speak about abortion and birth control, but also challenges a plethora of issues with our
current health care system.
Although the U.S. Food and Drug Administration recently began allowing abortion pills to be sent by mail, stipulations made by lawmakers require these pills to be administered by telemedicine. In over nineteen conservative states hoping to limit the access of abortion pills, administration through telemedicine has been banned. Although women living within these states are not required to visit the clinic to receive telemedicine, these women are often forced to drive to more liberal states, sit in a parking lot, and log on to their virtual appointments. These meetings are impersonal and require the need for an inconvenient car or bus ride to the nearest state allowing telemedicine access, creating medical service deserts. Despite the Jane Collective directly addressing these disparities, some providers may feel this is not the safest or most effective step towards patient-centered care. But given America’s increasingly polarized political climate, remedies to ensure female autonomy may rely on less
conventional means. Lawmakers, elected to uphold constitutional and human rights laws for all, may have to deal with the “necessary evil” organizations like the Jane Collective bring to the abortion conversation. Although work remains, we must not forget these conversations are finally being had— finally, being voiced loudly by the previously voiceless.
After some time, Anna decided to have a child with her boyfriend, whom she’d moved in with. He saw how little she liked stripping and how absorbed she was helping women with their abortions, so he of ered to cover more of the bills if she chose to leave the club. She did, and she provided home abortions throughout her pregnancy Anna knew the optics might be hard for clients, so she talked about it in their initial phone calls. “I’m pregnant. This is a wanted pregnancy, a planned pregnancy, and just as much as I support and respect people’s right to have children, I also respect people’s right to not have children,” she told them. “Just because it’s my time doesn’t mean it’s yours.”
Presser, Lizzie. “‘Whatever’s Your Darkest Question, You Can Ask Me.” .” The California Sunday Magazine, 28 Mar. 2018, https://story.californiasunday.com/ abortion-providers/.
Dine, Ranana. “Scarlet Letters: Getting the History of Abortion and ...” American Progress, 8 Aug. 2013, https://www.americanprogress.org/article/ scarlet-letters-getting-the-history-of-abortion-and-contraception-right/.
Preidt, Robert, and Robin Foster. “FDAAllows Abortion Pill to Stay Available by Mail.” WebMD, WebMD, 17 Dec.
2021,https://www.webmd.com/baby/
pulse 5
THE RIGHT TO DIE
By Caroline Kellogg and Rachel Zhang
Among all the personal freedoms honored in constitutions, governments, and politics, one which is not often discussed but critical to our understanding of human rights is the right to die. While one might easily advocate for freedom of expression or freedom to own property, an individual’s right to die is a freedom met with much more resistance. The right to die is further complicated by the fundamental moral and ethical issues surrounding the loss of life of an individual when so much of human existence is defined by trying to stay alive. This dilemma can be summarized as follows: who has the right to
choose who can die – the people most directly affected by their death, or the person themselves?
Currently, the right to die is reserved for only the most terminally ill in the U.S. The reasons that drive these patients to assisted suicide are ones that many face as they age: an inability to particiapte in activites that make life enjoyable, a loss of autonomy, and a loss of dignity. As one of the central aims of medicine is to maintain and preserve the quality of life, assisted suicide acts as a treatment to improve a patient’s quality of life by ending it. Only recently has the right to die been extended to chronically ill patients; the
first person with a non-terminal illness was legally euthanized just this past January. However, there have long been moral reservations concerning the right to die. In the most current version of the American Medical Association’s code of ethics, assisted suicide is prohibited as it is, “fundamentally incompatible with the physician’s role as healer”. The Hippocratic Oath, an oath central to medicine for centuries, is yet another argument against assisted suicide: “I will not give a lethal drug to anyone if I am asked, nor will I advise such a plan.” It is in direct opposition to the use of lethal drugs in assisted suicide.
In addition to the reservations against assisted suicide by the ethical code of physicians, there are also religious arguments against assisted suicide. In both Christianianity and Islam, life is viewed as a gift from God that humans should not interfere with. A similar perspective is seen in Buddhism, where it is considered immoral “to embark on any course of action whose aim is to destroy human life, irrespective of the quality of the individual’s motive.” Hinduism also shares similar beliefs as voluntary euthansisa disrupts the cycle of death and rebirth; those who assist in suicide then recieve the karma of the euthanized. There is

pulse 6
therefore a common theme against voluntary euthanasia among these four religions: the natural course of life should never be disturbed. A final consideration in this argument is that legalization of assisted suicide results in a “slippery slope” of morality where society permits increasingly immoral actions if it allows assisted suicide. Assisted suicide might also be abused in order to “kill” people legally. Take the case of Terri Shiavo. Following cardiac arrest and the subsequent deprivation of oxygen to her brain, Terri was reduced to a vegetative state and relied on life support to stay alive. Terri could not talk, walk, move, eat, or do anything at all–the most she could do was breathe. While the family could petition to remove her feeding tube, there was one problem: Terri never left an advance directive about what her family should do if she was in such a state. While Terri’s husband supported euthanasia, Terri’s family
argued that she showed some signs of consciousness and therefore should remain alive. This case epitomizes a central concern of voluntary euthanasia–who has the power to decide if someone should die? Is it the person themselves? Their family, religion, or their doctor? The court sided with Terri’s husband, and her feeding tube was removed March 18th, 2005.
Considering how life is the most essential part of being human, is it even possible to make a “correct” decision when it comes to ending life? Religious and moral codes attempt to address this argument via assisted suicide’s interference with higher beings, human life, and unintended effects on other peoplee. Nevertheless, it’s also important to consider the personal freedom which one should have to end their own life. If one has freedom of expression, freedom to own property, freedom of asso-
ciation, freedom of religion, and countless others, why shouldn’t one have the freedom to choose how to die? This issue speaks to a larger philosophical debate in communities, governments, and individuals: how much freedom should we grant ourselves and the people around us, and is it dangerous to grant an individual too much freedom?
Credits:
https://worldpopulationreview. com/state-rankings/right-to-diestates
2: https://www.ama-assn.org/delivering-care/ethics/physician-assisted-suicide

3: http://www.euthanasia.com/ oathtext.html
pulse 7
THE TRUTHS AND ILLUSIONS SURROUNDING INTERMITTENT FASTING
By Miles Kaufman and Riley Hurr
As with every fad diet that quickly gains popularity, the science behind intermittent fasting is shrouded in myths. Despite much scientific research, most people do not have an accurate perception of both the merits and downfalls of this diet. Many people believe that intermittent fasting is the key to easy weight loss or that it will prevent them from developing diabetes, but as with most health advice, nothing is that straight forward. Intermittent fasting takes many forms. Some people only eat within an 8 hour window during the day, while others only eat on certain days of the week. Regardless of these specifics, the main principle behind intermittent fasting is to increase the amount of time your body spends in a postabsorptive state — a state during which your body is not absorbing nutrients and relying on its energy reserves instead. Many nutritionists have argued that intermittent fasting promotes weight loss and lowers one’s risk of developing heart disease and diabetes, but how effective is this method compared to other eating patterns?
When it comes to intermittent fasting, some of the most promising results are seen with regards to diabetes prevention. Type 2 diabetes is caused by insulin resistance, which, simply put, is caused by elevated blood sugar over a long period of time. Therefore, many scientists have theorized that instilling a fasting period could lower a patient’s exposure to elevated blood sugar and prevent insulin resistance from developing. In mice, intermittent fasting has been shown to both prevent and cure type 2 diabetes, but in humans the data is less straightforward. It appears that intermittent fasting can be effective at preventing type 2 diabetes, but it is unclear whether intermittent fasting is better at preventing type 2 diabetes compared to other low calorie diets. These mixed results could suggest poor study designs or they could suggest that the metabolic benefits of fasting are related to reducing caloric consumption instead of reducing exposure to high blood sugar.
There is also some data that suggests that intermittent fasting may
be more effective than other weight loss methods because it adjusts an individual’s eating window to a more ideal time-period. Our circadian rhythm is designed such that hunger suppressing hormones are secreted at night, allowing us to get a full night’s sleep. Since hormones that boost your metabolism tend to be secreted during the day, some theories suggest that eating during daylight hours improves metabolic health and promotes weight loss. Studies conducted in rodents suggest that synching the feeding window to the circadian rhythm improves metabolic health, but the data that has been collected in humans is inconsistent at best.
In addition to diabetes prevention and circadian realignment, many studies have examined the relationship between intermittent fasting and cardiac health. The metabolic factors associated with fasting are also associated with low cholesterol and inflammation. Therefore, some scientists have theorized that intermittent fasting reduces cholesterol and plaque build-up which
pulse 8
prevents heart attacks and other cardiac issues. But yet again, it seems unclear whether the driver of these health benefits is weight loss or fasting. It seems that many of the metabolic benefits of intermittent fasting are due to weight loss, but how effective is intermittent fasting at promoting weight loss? The human body was designed to store energy very effectively, because humans evolved under conditions of nutritional scarcity. Therefore, there are many biological mechanisms devoted to ensuring we do not lose weight. As fad diets come and go, people have come to realize that when it comes to weight loss, there are no proven short-cuts and no easy fixes. Most data suggests that the only way for a metabolically healthy individual to lose weight is by expending more energy than they consume, which is a difficult task considering that our bodies are hardwired to prevent energy deficits at all costs. The question remains of whether intermittent fasting is an effective weight loss strategy, and most data suggests that intermittent fasting results in weight
loss because people eat less when they do not eat all day long. Most reviews of the scientific literature agree that intermittent fasting is not a more effective weight loss strategy than caloric restriction. It is also important to note that weight loss is not ideal for many people, and there are many people for whom intermittent fasting is not recommended. Athletic performance is often impaired by intermittent fasting due to the reduced energy intake. Additionally many people’s energetic needs would not be met through fasting, so it is not recommended for pregnant and breastfeeding patients, diabetic individuals or those with existing eating disorders.
Not only is intermittent fasting not ideal for everyone, in some ways fasting has been shown to promote weight gain. Fasts have been known to promote binging. During the month of Ramadan, many muslims fast from sunrise to sunset. Surprisingly, many Ramadan observers report gaining weight during the holiday, which is likely due to changes in energy expenditure

and eating excess calories after sunset as overcompensation for the caloric deficit they experienced during the day.
On the other hand, many people report that they are able to restrict their caloric intake more effectively through intermittent fasting than they are through other diets. For these individuals, the current research suggests that intermittent fasting may be a valid alternative to caloric restriction. One of the main barriers to weight loss is the difficulty individuals have maintaining a caloric deficit, so any method that could possibly make that easier is worth looking into.
Credits:
Mattson, Mark P., Valter D. Longo, and Michelle Harvie. “Impact of intermittent fasting on health and disease processes.” Ageing research reviews 39 (2017): 46-58.
2. Antoni, R., Johnston, K., Collins, A., & Robertson, M. (2017). Effects of intermittent fasting on glucose and lipid metabolism. Proceedings of the Nutrition Society, 76(3), 361-368. doi:10.1017/S0029665116002986
3. Hatori, Megumi, et al. “Time-restricted feeding without reducing caloric intake prevents metabolic diseases in mice fed a high-fat diet.”
pulse 9
MENTAL HEALTH RESOURCES ON COLLEGE CAMPUSES
 By Neeharika Venuturupalli and Eve Tanios
By Neeharika Venuturupalli and Eve Tanios
Content warning: discussion of themes such as suicide, substance abuse, and sexual assault
In a 2010 study conducted in various American universities, researchers attempted to compare students’ need for mental health services with their knowledge about the resources offered at their school. The results of the survey, which was distributed to undergraduate students, displayed a trend often echoed among conversations between college students: approximately 30% of the respondents did not know that the mental health services existed, and of the 70% who did know, they either did not have adequate enough information to be able to use them or simply did not want to. Some of the common reasons listed for not
having used the resources included (1) not having enough time to use them (2) being embarrassed about seeking help or (3) believing that the resources would not help them feel better. This study raises some questions on what measures a university could take to increase knowledge about mental health resources. One of the first major efforts made towards mental health outreach in American colleges was the on-call system, which acted as a bridge between university students and mental health professionals. In a 1993 study conducted on an unnamed university campus, it was found that the university crisis on-call services
were most commonly used in extreme scenarios such as suicidial thoughts, panic attacks, anxiety attacks, substance abuse, and sexual assault. 76% of these calls led to out-patient counseling and most of the calls took approximately 1.5 hours. Considering many students’ embarrassment at seeking help, it makes sense that they tend to wait until the height of a mental health issue before they seek help for it. However, one of the most common complaints about the current on-call system is the wait time associated with the services, often discouraging students from further usage of university mental health services.
pulse 10
While crisis on-call services are extremely beneficial at universities, it is important for them to also raise awareness of other mental health resources offered at their schools. Outreach in universities should be improved so that not only do more people know of the resources, but they also know exactly how to use them and how to access them. It is also important to address why students have not wanted to use the resources in the past.
As mentioned earlier, one of the biggest reasons for why students hesitate about using mental health resources is because they feel like they don’t have enough time to properly address a mental health issue. Students often worry about the burden of catching up on lectures and making up assignments, which makes it harder for them to take some time off to address mental health issues. Possible solutions to this could include making it easier for students to ask their professors
for a mental health break without worrying about the consequences of lost time. Recently, the Illinois public school board released a statement saying that students can take up to five days off for mental health reasons. This should be implemented in universities as well, with professors providing multiple sick days that students can use for either physical or mental health reasons. Students should also not feel embarrassed about using mental health resources. There are several de-stigmatization efforts being done across American university campuses which has led to significant change in the way mental illness and treatment is viewed. Destigmatization efforts also aim to show that the services are worth using because they are able to help students improve their mental health and wellbeing. The study about crisis on-call services also suggests that most of the time when students do use mental health resources, it is when they are
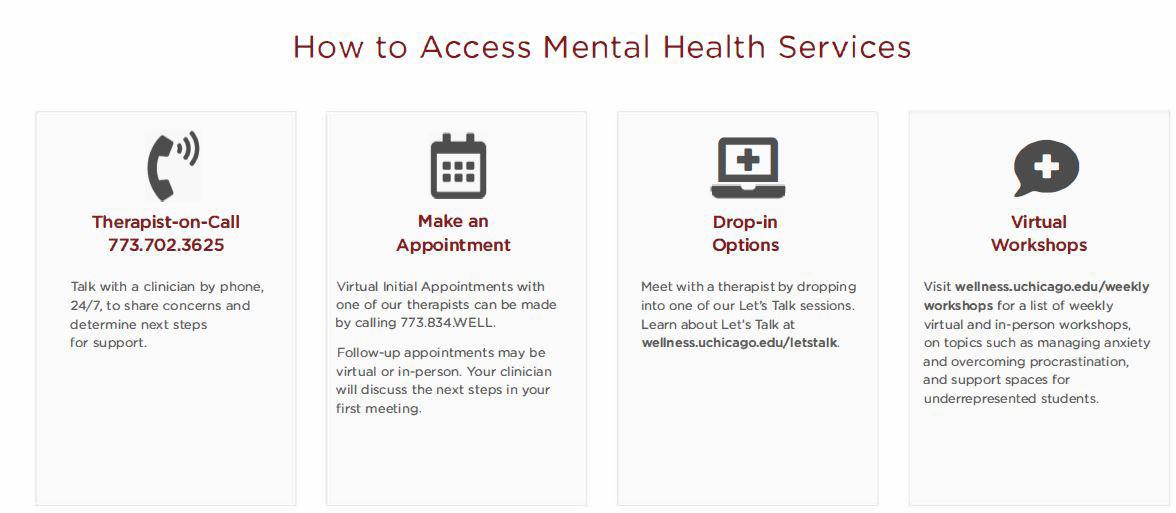
facing the worst part of their mental health journey. On the flip side, however, it is important to encourage students to use these resources even if they would consider themselves to be mentally stable. Consistent usage of mental health services allows for better mental health stability and could even potentially prevent extremely poor mental health circumstances. At our school, the University of Chicago, some mental health resources include a therapist on-call (773-702-3625), initial therapy appointments which can be set up through the Wellness portal, anonymous drop-in therapy sessions with licensed therapists (wellness.uchicago.edu/letstalk). There are also several mental health services offered to help students with different needs. Students struggling with their academics can use the Academic Skills Assessment Program which helps students by coaching them to develop techniques to improve their academic
pulse 11
performance. Students concerned with substance abuse can contact a therapist through the Wellness portal to evaluate their situation. The university also offers Brief Alcohol Screening and Intervention for College (and Graduate) Students (BASICS) to help evaluate students’ alcohol usage and come up with a plan to help them. There are many different options for therapy including individualized therapy, couples therapy, and even welcoming therapy groups. Student Wellness can also refer students to various psychiatrists, psychologists, and therapists with whom they could continue a long term plan. The abundance of mental health resources at universities are a step forward from when the only available resource was the crisis on-call services. However, most students still don’t seem to use these resources until they are in a crisis or are actively looking for help. Schools should work with faculty members and residential
leaders to encourage all students to use mental health resources to uplift and help maintain students’ mental wellbeing. While many schools are moving in the right direction with destigmatization efforts and offering more resources, there is still a lot of work to be done. All students must feel comfortable using the mental health resources and no student should have to feel confused about how to receive help.

pulse 12
NANOPARTICLE-BASED VACCINE DESIGN
 By Eva McCord and Teresa Nam
By Eva McCord and Teresa Nam
In the realm of biosynthetic pathways, as well as within the underlying mechanisms that govern molecular interactions, much of the complexity that determines successful signaling can be reduced to one trait: shape. Ranging from the weaving alpha helix to the microtubule lattice to the seemingly simple formation of a dimer from two compatible monomers, a molecule’s shape and structure doesn’t just provide researchers insight into the molecule’s behavior. Experimenters and scientists can capitalize on these molecular attributes and make crucial inferences regarding how the molecule plays a role in its greater cellular
environment. By extension, this same principle of shape itself determining the nature of a molecule can be applied to engineering-centric solutions for some of the greatest battles in healthcare, namely the use of nanoparticles as anticancer drug delivery systems. Based on recent findings from Xu et al., shape—with specific emphasis on chirality—can be capitalized upon in order to create “nanoparticle enantiomers,” or otherwise identically-structured nanoparticles that yield vastly different immune responses. But amidst other experimental, design-driven approaches to the ever-present demands of modern
healthcare, it is important to recognize and disseminate knowledge regarding the importance of developments in nanoparticle technology. In doing so, more and more individuals may contribute to conversations pertaining to the socioeconomic tapestry of healthcare and medicine itself, and how these miniscule structures may enable advances in patient care previously thought impossible. In order to properly understand the impact of the Xu team’s discovery, a clear definition of what nanoparticles even are must be established. With the rapidly-evolving and ever-expanding realm of biotechnology already a somewhat nebulous
pulse 13
field in the minds of the general public, simultaneously introducing the nanoscale may prove daunting, as well as cause understandable confusion. How are nanoparticles created? How do nanoparticles work? What makes nanoparticles distinct and separate from other therapeutic methods already employed in both clinical and research settings? Nanoparticles can be succinctly summarized by two key components: size and shell (and now shape, of course!). These devices operate on the very same scale as the actin and tubulin monomers that assist your cells through mitosis, the DNA helicase and ligase that oversee DNA repair, and the hemoglobin carrying oxygen throughout your body. However, the most interesting aspect to nanoparticles is not necessarily their size—which is implied in their name—but their shell-like structure. Often designed in the shape of a sphere, the outer surface of the hollow “nanoball” is coated in a specially-chosen biological coating; this coating allows for the nanoparticle to interact with both its general environment and specific molecular

targets, and ultimately facilitates the particle’s overall biocompatibility. This shell houses the “core particle,” which in medical applications is often the drug the nanoparticle had been created to deliver. A helpful analogy to better visualizing nanoparticle structure would be to liken the nanoparticle to a biological Trojan Horse; the outer shell of the nanoparticle allows the particle to freely interact and associate with its target tissues, only for the inner core to pack a surprise, nano-scale punch. And while the answer may be intriguing to some, yet dissatisfactory to others, nanoparticles can be applied to an incredibly vast array of medical challenges and pursuits, ranging from the aforementioned drug and gene delivery to full-scale tissue engineering and tumor destruction (Salata). Within these interdisciplinary applications that the genuine beauty of nanoparticles is revealed, along with the overarching motivations to fuel and support innovation within bionanotech.
Pivoting back towards the work of Xu et al., while bioengineers
have long understood the aforementioned importance of size and structure, the shape of nanoparticles—and the degree to which this shape influences a nanoparticle’s efficiency—had been only vaguely understood. Through the creation of a tunable system using circularly polarized light, Xu et al. was able to directly control and adjust the asymmetry of left- and right-handed enantiomers of gold nanoparticles (Xu). In doing so, the chirality of the nanoparticle could be directly linked to the strength of immune cells in mice, with left-handed enantiomers found to produce an immune response twice as strong as their right-handed counterparts (Hooftman). This significant deviation in performance was found to be due to the left-handed nanoparticles exhibiting a greater binding affinity for specific receptors within the immune cells themselves, suggesting that the enantiomers of gold nanoparticles at large could be used as immune system stimuli (Hooftman). This additional stimuli, thus, may improve the efficacy of a vaccine. This was later proven by Xu’s
pulse 14
team after they discovered that the left-handed enantiomer was more effective at triggering antibodies against the influenza virus than not just the right-handed enantiomer, but alum—the conventional substance utilized to enhance the body’s immune response to the influenza virus.
While these results seem alltoo good to be true for biomedical researchers and bioengineers alike, seizing on this moment of promise also provides a crucial window for researchers to discuss not just how they can improve the quality of treatment, but the quality of care delivered to patients. In other words, questions such as: How do nanoparticles play a role in the socioeconomic design of healthcare and medicine? How do advancements in learning how to make them more efficient and effective impact patients and care accessibility? There is no time more relevant or pressing than today, following a period of rapid vaccine development and subsequent discourse regarding the ethical and moral faces of vaccinology, to discuss the future of clinically-applied nanoparticles. There emerges a distinct “fork” in the
conversation of nanoparticle-driven global healthcare, split between the creation of life-saving, non-invasive treatments for the world’s most in-need and vulnerable populations and the threat of a “nano-divide” (Salamanca-Buentello and Daar). This nano-divide, in which wealthier nations could isolate and restrict access to nanoparticle treatment from nations lacking the same financial and medical means, would simply serve to further aggravate and amplify the already-present fragility and power imbalances that define these global relationships. In saying all of this, it is important to keep an eye to the future of nanoparticle-driven care, particularly as it runs parallel to the future of medicine at large. By identifying what qualities and characteristics are most indicative of nanoparticle effectiveness—and by deducing how these characteristics can be made tunable—engineers and healthcare workers alike will be able to collectively reduce the toxicity burden faced by patients undergoing intensive immunotherapy. Likewise, with nanoparticles being comparatively non-invasive alternatives to surgery, supporting advances in
nanomedicine are directly conducive to making necessary, life-saving opportunities accessible to more patients than ever. Ultimately, while Xu et al.’s findings stand as just one of many critical junctures on the path to sparking dialogues around nanomedicine, these efforts assist in making nanoparticles “seen” in the eyes of both healthcare workers and the general public—no electron microscope necessary.

Credits:
https://www.nature.com/articles/ d41586-021-03806-7
https://www.nature.com/articles/ d41586-021-03806-7
https://jnanobiotechnology. biomedcentral.com/track/ pdf/10.1186/1477-3155-2-3.pdf
https://www.nature.com/articles/ s41565-021-00899-z
pulse 15
EPIDEMIOLOGY
THE BED ROCK OF PUBLIC HEALTH
By Sanaa Imami and Sophie Hu
The field of epidemiology has a storied yet underappreciated history in the US. Epidemiology is the study of identifying the cause of disease and other various outcomes in specific populations. Epidemiology focuses on both the community and the patient or individual. The field is incredibly broad; studies can be scientific, systematic, and data-driven. The focus of these studies include the distribution and determinants of various health-related events in all ranges of populations from schools and small events to whole nations. The intrinsic value of epidemiology lies in its applicability for future events. Information learned from one health event can be applied in numerous others, which further emphasizes the versatility and importance of the field.
While epidemiology arose as a commonplace practice around the time of World War II, the inherent principles of the discipline can be traced back thousands of years. The first time these concepts were proposed was around 400 B.C., when Hippocrates, a physician and an incredibly profound figure in the history of medicine, proposed in his
essay “On Airs, Waters, and Places” that illnesses could be influenced by environmental and host factors as opposed to supernatural forces, which was a radical idea at the time. The idea that disease and illness were not due to divine interference was an incredibly unpopular idea, but this concept was expanded upon throughout the following centuries. Similar to Hippocrates, John Snow also made groundbreaking contributions to the field. The anesthesiologist was later deemed “the father of field epidemiology” for his work in the 1800s. One of Snow’s most significant cases centered around the height of London’s cholera outbreak in 1854, when he proposed that the spread of disease could be linked to the city’s water supply. Snow identified a correlation to one of the pumps in the city, and confirmed his hypothesis by interviewing residents and determining that almost all of the cholera patients were getting their water supply from the same pump. After the pump was removed, the outbreak predictably ended. As the years went on, the study of epidemiology has grown and expanded to resemble the modern-day field
that’s more well-known today. Following John Snow’s findings about the London cholera outbreak, various epidemiological practices were first implemented while investigating disease outbreaks and epidemics. In the mid-1900s, the definition of epidemiology expanded from solely the study of acute infectious disease to include noninfectious disease as well as violence, injury, and various other health-related illnesses and outcomes. Epidemiologists broadened their studies to focus on pressing health matters, like cancer and inheritable diseases. One notable study on cancer was conducted by Richard Doll and Bradford Hill in the UK in 1948. During the mid-1900s, lung cancer was a rapidly increasing health issue for both the British and Americans. Doll and Hill interviewed British lung cancer patients about their smoking use and compared the responses to that of a control group to see if there were any environmental factors that could be causing heightened levels of disease. Surely enough, Doll and Hill found a correlation between smoking and lung cancer levels. Patients with lung
pulse 16
cancer levels. Patients with lung cancer were both more frequent and heavier smokers than those in the control group. This study was radical - until then, there were no assumed risks between smoking and cancer, and this link has remained incredibly significant today. In addition, the use of a control group in epidemiological studies was a practice that became frequently adopted after the publishing of Doll and Hill’s smoking study. This has vastly changed the way case studies are performed today. With the inclusion of a control group, researchers have been able to more conclusively establish causal relationships in case studies while further validating their hypotheses.
A significant part of epidemiological study is implementing preventative measures to eradicate disease. An example of this subfield of epidemiology put into practice was during the measles endemic. Before the creation of a measles vaccine, almost all children contracted the disease before they turned 15. In the 1950s and 60s, researchers developed several formulations of measles vaccines, some of which
proved to be incredibly effective at preventing the contraction of measles. With the help of epidemiologists and government organizations like WHO and CDC, these vaccines were promoted and distributed to communities worldwide. These campaigns proved themselves to be extremely successful - by 2000, the US declared that measles had been eradicated on the national level, and measles outbreaks have greatly reduced since the inception of the vaccine, meaning that the disease only occurs in sporadic outbreaks. Campaigns and messaging like those implemented for the measles vaccine has since been utilized for other vaccinations and immunizations like the HPV and Meningitis B vaccines.
In recent years, the practice of epidemiology has been integral in managing the COVID-19 pandemic. As the pandemic began, epidemiologists have worked to trace the disease to its origin, looking for both the first reported patient and the source of the disease. Since then, epidemiologists have worked with the government to reduce transmission with public health policy
and community-specific messaging. Most recently, with the development of several COVID vaccines, the CDC and other epidemiology-related organizations have focused on the distribution of these vaccines, ensuring that all communities have access to them. In the midst of the pandemic, the epidemiological field has been paramount in all fronts, whether through determining the source to fighting the spread of infection to working on prevention and distribution. The field of epidemiology is incredibly versatile and has grown immensely since the age of Hippocrates - as such, it has become synonymous with clinical practice while serving an integral role in the development of comprehensive, holistic views of disease and treatment.
Credits:
Centers for Disease Control and Prevention. (2012, May 18). Principles of Epidemiology | CDC. Centers for Disease Control and Prevention. Retrieved February 27, 2022, from https://www.cdc.gov/csels/ dsepd/ss1978/index.html

Prevention. (2020, November 5).
pulse 17
A DANGEROUS ADDICTION
By Christopher Cardenas and Michelle Ma
From synthetic drugs to slot machines to sugar-packed snacks, our modern world’s constant stream of stimuli and stressors has produced a plethora of addictions familiar to us all. However, one concerning tendency has seemingly slipped under the radar – porn usage. With the rise and expansion of the global internet over the last 30 years, porn consumption has skyrocketed.
Videos, pictures, webcams, chats are now all accessible with the click of a button. Contrary to the popular belief that porn is harmless, new research suggests that chronic porn consumption is linked to addictive tendencies in men, which negatively impact various aspects of their lives and the lives

of the women around them.
Drug addiction affects the brain by mimicking naturally occurring neurotransmitters in our bodies. A 2016 publication asserts that dopamine is directly involved in the “reward system” of the brain. In response to pleasurable or positive sensations, dopamine transmission increases. Contrary to popular belief, dopamine itself is not a “pleasure chemical” (like serotonin or oxytocin); however, it plays a motivating role, driving us to repeat the same actions later (and often in response to the same stimuli).
Arias Carrión found in 2010 that some substances cause addiction by affecting this reward system. For instance, cocaine inhibits the uptake of dopamine”,
creating an artificial “overabundance”. Such dopamine surges motivate one to continue pursuing those massive levels of dopamine release – the “high” – thus creating a dependency on the substance. . Even as the drug’s pleasurable effects fade, the pursuit of a dopamine “high” keeps addicts locked in the cycle.
Through this dopamine-driven reward system, the instant gratification produced by pornography usage can result in addiction as well. Some have rallied against the idea of having a “porn addiction”, portraying it as a remnant of outdated beliefs such as purity culture. New research, however, however, has shown that the neural processes underlying internet addic-
pulse 18
tion.
Moreover, when examining the neuroscientific effects of internet pornography addiction, researchers found “strong evidence for considering addictive internet behaviors sas behavioral addiction.” In contrast to naturally-occuring positive stimuli, “supranormal stimuli” was coined by Nikiolaas Tinbergen to describe the rise of “fake” stimuli such as junk food, TV, and unsurpisingly: pornography. Porn use is not restricted to any particular gender, but men are significantly more likely to use it and use it often. This gap can be quite dramatic, as the Institute for Family Studies finds that casually dating men are “42 times more likely” to view pornography at least weekly than casually dating women. Although there is much more to investigate concerning porn’s effect on the mind, preliminary studies indicate that porn addiction has negative physical, behavioral, emotional, and interpersonal impacts on men, the consequences of which impact women as well.
Excessive porn usage desensitizes men, leading to physical problems with intimacy and behavioral changes. Prestige Men’s Medical Center writes that “pornography is fantastical by nature” – it involves scripted actors putting on an unrealistic performance, often engaging in extreme or degrading sexual acts. According to Tim Jacobs, MD at the University of Antwerp, men who watch excessive amounts of porn men who watch excessive amounts of porn are more likely to suffer from erectile dysfunction because the “arousal level that porn induces through extreme content is often not matched in real life intercourse”. In fact, a study presented at the 35th
Annual EAU Congress found that “roughly 30-40% of men who watched 40 minutes of porn per day had ED, compared with 10% of men who watched less than 30 minutes per week”. Moreover, because porn often contains verbal and/or physical abuse, it has been found that, “Men look at women in a degrading fashion more often after viewing pornography”. PMMC furthers that men who regularly consume large amounts of pornography demonstrate a markedly higher tolerance of abnormal behaviors such as aggression, promiscuity, and violence. Sadly, this behavioral change has alarming implications for women. Fouberti finds in “Pornography Viewing among Fraternity Men: Effects on Bystander Intervention, Rape Myth Acceptance and Behavioral Intent to Commit Sexual Assault” that men who view pornography are less likely to intervene as a bystander, report rape, and deny rape myths. Although the direct cause of these results are unknown, the link between these measured effects display a correlation between consumption of pornography and indifference towards rape. This desensitization combined with the addictive nature of pornography also damages men’s relationships and emotional health. PMMC finds that men with porn addictions often find themselves choosing porn over people or social events, prioritizing their next “hit” over their goals and valuable experiences. Undoubtedly, this is one major reason why “more than 85 studies [...] suggest a link between poor mental and emotional health, and porn use.” Maddox further elabrate further elaborates on how porn use affects marriage.
Particularly, “Men tend to judge partners by comparing them to those he sees on the pornographic websites, and their sexual performance might give the man the idea that his partner cannot perform as she should.” This leads to dissatisfaction in the relationship due to the imposition of unrealistic expectations on the woman by the fantastical portrayal of women in pornography. These unrealistic standards are ultimately both created and perpetuated by the pornographic industry, solidifying the link between sexual dissatisfaction in relationships and porn consumption. Ultimately, a 2018 survey found that men who began watching porn regularly after their marriage were twice as likely to divorce than men who did not, demonstrating the important of sexual satisfaction in healthy and long-lasting relationships.
With effects ranging from increased rates of divorce to desensitization to sexual assault, the harmful nature of porn addiction cannot be overstated.. Alarmingly, as unrestricted internet access among children increases, boys as young as twelve are beginning to use pornography. For these boys, the physical and emotional impacts of addiction could potentially stunt their development, causing damage that will affect their relationships, mental health, and the women around them for a lifetime. As difficult as it may be in our hypersexualized culture, increasing public awareness of the dangers of pornography is essental to preventing this. For the sake of our children, and the men and women they will become, we can no longer afford to turn a blind eye.
pulse 19
ANTIBIOTIC-RESISTANT BACTERIA A MODERN PUBLIC HEALTH PHENOMENA
By Ayman Lone and Ruka Adichi
Ricky Lanetti was a 21-year-old star football player for Lycoming college in Pennsylvania, at the pinnacle of his health. In December of 2003, after a week of having flu-like symptoms, the soon-to-be All-American was taken to the hospital the night before the NCAA quarterfinal. Twelve hours after he checked in, Ricky died the morning of the game. His cause of death was ruled as MRSA – methicillin-resistant Staphylococcus aureus – bacteria that entered his body through a small pimple. In half a day, a fully healthy individual succumbed to a seemingly trivial bacterial infection.
Ricky’s tragic death is a warning of a modern public health phenomena – antibiotic-resistant bacteria. Antibiotic resistance refers to certain bacteria becoming resistant to antibiotics that normally kill the strain. ake the MRSA mentioned above: since its discovery in 1961,
it has become immune to penicillin, methicillin, amoxicillin, penicillin, oxacillin, and many other common treatments. Other notable resistant bacteria include C. difficile and N. gonorrhoeae, AKA super gonorrhea. Where do these superbugs come from?

The mechanisms behind these superbugs developing resistance revolve around population and evolutionary biology, or selective pressure. Consider a few fundamental traits of bacteria: their extremely high replication rates and subsequently high mutation rates. When encountering an antibiotic, the majority of a bacterial population will die, minus a small few that carry adaptive mutations that allow them to survive the effects of the drug. These adaptations may include limiting the number of entryways on the membrane for a drug to enter or having enzymes that break down a drug. The small population with such abilities will quickly replicate and evolve into a new strain that the antibiotic can not eradicate as effectively. Rinse and repeat with multiple strains against multiple drugs, and now you have a whole new generation of bacteria resistance to our antibiotics. This process is a microscopic example of natural selection and an inescapable fact of biology, which is impossible to override. This is why it is equally
important to consider what’s happening with drugs and bacteria on a macroscopic level.
Over the years, society has misused antibiotics, allowing bacterial resistance to emerge rapidly. Ironically enough, some of the issues have stemmed from inside the hospitals. Having sicker patients in such close quarters in a hospital provides the perfect breeding grounds for new bacterial strains, especially if many of them are on a number of drugs. In other cases, doctors and other health workers may inappropriately prescribe antibiotics, particularly in cases of imperfect diagnoses or succumbing to a persistent and uninformed patient. In countries without proper public health guidelines, certain drugs may be acquired even without a prescription. The other major brewing grounds of antibiotic resistance are the animal and crop industries. Over half of all antibiotics in the US are used by this sector of the economy to cultivate healthier crops and livestock. The issue is that the use of antibiotics may not be required with other methods such as vaccination and proper hygiene of animals and farmers,. In comparison, those treatments do not promote bacterial evolution to the level that antibiotic overuse does. This applies to the misuse of antibiotics everywhere, as ideally, they are used as a last resort or only
pulse 20
or only when absolutely needed. However, our society’s overuse of antibiotics has propagated drug-resistant bacteria faster than they should have emerged.
Because of this trend of antibiotic misuse yielding resistant bacteria, we are now facing a point in our public health history dubbed the “post-antibiotic era.” This era is exactly what it sounds like: a time in which “common infections and minor injuries can kill…a very real possibility for the twenty-first century,” due to even the most simple of bacterial infections being untreatable by traditional methods, says Keiji Fukuda of the WHO. Furthermore, many scientists believe we are fully in the post-antibiotic era right now. For some facts, the WHO reports, “in some areas of the world, more than half the infections caused by one major category of bacteria — Gram-negative, which includes Escherichia coli and Klebsiella pneumoniae — involve species
resistant to carbapenem drugs,” the most powerful kind of antibiotic. Vox reports that the deaths per year from bacterial resistance may go up from 700,000 today to 10 million by 2050 if our antibiotic use trends don’t change.The research and development of newer antibiotics are facing difficulty as well, as they are antithetical to a firm’s interests. Unlike a traditional product that is meant to be sold and consumed as much as possible, antibiotics are ideally regulated in their consumption. On top of that, producing successful antibiotics takes many years and trials. The time, money, and resources invested would likely outweigh the sales, meaning a company would If the bacteria that the bacteriophage binds to is not present, the phage will not replicate. The specificity of phages also means that they won’t disturb the beneficial bacteria in our bodies, a potential side effect of antibiotics. A 2020 study from the Iran University of Medical Sciences found phages to be effective in treat-
ing infections from multidrug-resistant, extensively-drug-resistant, and pan-drug-resistant bacteria, even calling phages “one of the biggest hopes in the future for the treatment of resistant bacteria.” The same study still mentioned a need for more research and development. Although they seem like a perfect successor to antibiotics, phage therapy has not been researched yet and is still not approved for humans in the US or Europe. However, bacteriophages are beginning to be used in the farming industry, which may alleviate the issue of superbugs coming from livestock and crops. However, the biggest kicker is that bacteria may still develop resistance to phages due to the inescapable fact of evolution and natural selection.
With this knowledge, scientists and doctors will likely be more cautious in issuing bacteriophages for patients for a while, and we may not see the treatments in hospitals for years.

pulse 21
The bottom line, the responsibility falls on us. Once new treatments like bacteriophages become approved for use, society must make the right decisions to avoid the catastrophe that is phage-resistant bacteria. In the meantime, we still have the power to fight these invisible killers. As they say, prevention is the best cure; maintain good hygiene in all parts of life, be responsible in the prescription and use of antibiotics, stay up to date on current events in infectious diseases and treatments. We, humans, are a resilient species, and we have what it takes to prevent tragedies such as Ricky’s in the future.
Credits:
https://www.who.int/news-room/factsheets/detail/antibiotic-resistance
https://www.vox.com/future-perfect/2019/11/14/20963824/drug-resistance-antibiotics-cdc-report

https://www.niaid.nih.gov/research/ antimicrobial-resistance-causes
https://www.idsociety.org/public-health/patient-stories/patient-stories/
https://www.healthline.com/health/ phage-therapy#:~:text=Phage%20therapy%20(PT)%20is%20also,the%20natural%20enemies%20of%20bacteria.
https://www.cdc.gov/drugresistance/ about/how-resistance-happens.html
https://www.ncbi.nlm.nih.gov/pmc/
pulse 22
“PUT ME BACK IN COACH” THE DANGER OF THE REPEAT CONCUSSION
By Rahul Barra and Ashley Chen
Incidence rates of mild traumatic brain injury (mTBI) — namely concussions — remain severely underreported within exclusive reliance on emergency department statistics, due to a litany of factors ranging from poor pediatric diagnosis and delayed symptom onset to medical hesitancy in cases of abuse and occupational injury. Even so, it is estimated that over 2 million mild TBI’s occur annually in the United States alone. With studies increasingly implicating activities with greater frequency or severity of concussions as a significant risk factor for neurodegenerative pathologies, efforts to mitigate the long-term burden of concussions now increasingly center on one particular facet: the timecourse of recovery and potential for re-injury within it.
A concussion describes the phenomenon wherein an external impact or rapid deceleration of the skull results in slight movement of the brain within the surrounding calvaria. Not only can this cause focal bruising of the brain, but the shearing forces produced from this internal rotation is capable of tearing axons from nerve cell bodies, releasing toxic concentrations of neurotransmitters and reactive oxygen species that leave surrounding brain tissue vulnerable to further damage. Symptoms associated with a concussion can vary significantly
in degree and type: including such things as acute loss of consciousness, persistent headaches, nausea, light sensitivity, sleep disruption, and balance issues. Accordingly, concussions are generally classified into categories of severity ranging from grade 1 to 3 based on symptom presentation and duration. Importantly, concussions are considered a separate designation from the more acutely dangerous moderate and severe TBI, which often present with abnormal CT structural imaging and significant swelling in the brain. In contrast, concussions are characteristically undetectable by standard CT imaging, with microscopic white matter tract lesions only occasionally picked up by advanced MRI. This is a fact that contributes significantly to the high levels of under-diagnosis associated with the injury, as patients who are relatively symptom-free or have delayed symptom onset underestimate their condition and may re-engage with activities capable of inducing a second, more harmful concussion.
By age group, children and adolescents aged 5 to 24 maintain the largest burden of concussions in the U.S. by a significant margin, and annual concussion rates for adolescents have shown a substantial rise over the last 20 years. This age stratification is partially a result of recreation and sports being among
the largest contributing factors for initial and repeat mild TBI at the amateur, collegiate, and pro level. It is estimated that anywhere between 300,000 and 3 million sports-related concussions occur in the U.S. annually, with bicycling, football, basketball, and soccer accounting for the largest percentage of these brain injuries. The potential for repeat concussions is not solely a risk factor associated with athletics, however. Military service, domestic violence, compounding diseases with associated fall risks, and substance abuse have all also shown significant correlation with repeat head injury. However, particular focus has been placed on brain injuries in athletics for its outsized role in re-injury potential and seemingly greater capacity for substantial reform.
While an initial concussion can be dangerous by itself in potentially contributing to prolonged issues with cognition and focus past the typical recovery period of 16-29 days, subsequent follow-up concussions have been linked to significantly worse prognosis in both the short and long-term — particularly when a second concussion occurs before the prior recovery period is finished. Multiple studies have now shown that athletes and other individuals with a history of past concussions present more symptoms and have longer recovery times
pulse 23
following each new concussion, regardless of time since prior injury. For even minor second head injuries sustained before symptoms from a previous concussion subside, a generally fatal condition known as Second Impact Syndrome (SIS) can occasionally occur due to rapid brain swelling. In the long-term, suffering multiple concussions in early life has increasingly been shown to be associated with persistent deficits in memory, concentration, balance, and chronic traumatic encephalopathy (CTE). It should be noted that the evidence is still not definitive on the role of repetitive sub-concussive events (impacts that do not meet the criteria of a full concus-
sion) in long-term issues like CTE. Nonetheless, the comparative danger of multiple concussions over a single concussive event in life is now largely irrefutable - with particular concern in situations where initial concussions may go undiagnosed and untreated. Efforts to improve brain injury safety among athletes have shifted to focus largely on two specific areas in recent years: more robust prevention protocols and more rapid diagnostic abilities. From a preventative standpoint, programs like the Center for Disease Control’s HEADS UP initiative, in conjunction with schools and professional leagues, have focused on improvements in such things as protective equipment design, player-to-player contact protocols, and education of coaches and players. Moreover, all 50 states have now passed concussion legislation focusing on head injury education, removing athletes from same-day play following head impacts, and requiring clearance from a healthcare professional trained in concussion
management for players to return. From the diagnostic point of view, one particularly exciting new advancement in the field has been the development of hand-held, rapid blood tests for detecting TBI on-site. Such tests rely on detection of specific protein markers associated with TBI in the blood, and have shown surprisingly few false negative results in clinical trials. Used in tandem with more traditional systems of diagnosis like patient questioning and visual exam, these advancements have the potential to dramatically increase rates of identifying concussions in a player that otherwise would have gone undiagnosed. In doing so, the long-term and acute risks associated with repeat concussions can be partially mitigated by ensuring athletes do not return to play while recovering from even a mild prior concussion.
An at-times simultaneously controversial, widely prevalent, and under-discussed issue, continuing to confront mild traumatic brain injuries - and specifically, unnecessary cases of
repeat concussion - in the areas of daily life where they most occur via new preventative, diagnostic, and therapeutic techniques, is thus an effort both littered with many hurdles and replete with extraordinary necessity.

Credits:
Finally, A Blood Test for Traumatic Brain Injury. (n.d.). Abbott. from https://www.abbott.com/corpnewsroom/products-and-innovation/finally-a-blood-test-for-traumatic-braininjury.html
What does concussion do to the brain? (1525844700). https://qbi.uq.edu.au/ blog/2018/05/what-does-concussiondo-brain
What happens to the brain during a concussion? (n.d.). Scientific American. from https://www.scientificamerican.com/article/what-happens-to-thebrain/
Albano, A. W., Jr, Senter, C., Adler, R. H., Herring, S. A., & Asif, I. M. (2016). The Legal Landscape of Concussion Sports Medicine Providers.
pulse 24
pulse 25

