December - January 2023
 Mr Frank Aviles
Wound Care Clinical Coordinator, Natchitoches Regional Medical Center
Natchitoches LA, United States
Mr Frank Aviles
Wound Care Clinical Coordinator, Natchitoches Regional Medical Center
Natchitoches LA, United States

December - January 2023
Mr Frank Aviles
Wound Care Clinical Coordinator, Natchitoches Regional Medical Center
Natchitoches LA, United States
In healthcare, skin color presents its own set of challenges where inequity is evident. Studies have indicated that black and brown people are twice as likely to die from diabetes than white people,3 black and brown people account for 12.1% of people with diabetes, compared to 7.4% of non-hispanic white people,4 darker pigment skin have a higher occurrence of pressure injuries (PI) 5,6,75.5% of black men and 75.7% of black women developed hypertension by the age of 55 compared to 54.5% of white men and 40% of white women,7 and blacks had 1.5 to 2 times higher risk of hypertension.7 This article outlines how these issues can be addressed.
Health disparity in the United States has been defined as differences that exist among specific population groups in the attainment of full health potential that can be measured by differences in incidence, prevalence, mortality, burden of disease, and other adverse health conditions.1 These disparities can negatively impact outcomes on a specific group of people creating a downward spiral in their health, their quality of life and burden the health system affecting future generations.
In healthcare, skin color presents its own set of challenges where inequity is evident. Studies have indicated that black and brown people are twice as likely to die from diabetes than white people,3 black and brown people account for 12.1% of people with diabetes, compared to 7.4% of non-hispanic white people,4 darker pigment skin have a higher occurrence of pressure injuries (PI),5,6 75.5% of black men and 75.7% of black women developed hypertension by the age of 55 compared to 54.5% of white men and 40% of white women,7 and blacks had 1.5 to 2 times higher risk of hypertension.7

In the wound care field, especially in the outpatient clinics, our chronic wounds are typically stuck in the inflammatory phase and our aim is to progress them along the healing cascade. While in the inpatient settings, patients are at risk of developing pressure injuries, admitted for management of a diabetic foot ulcer infection, and surgical site infections or dehiscence. The common denominator in both settings is the fact that the
wound/ periwound tissue may be in the proverbial prolonged inflammatory stage.
Skin has been an indicator of our health. As healthcare workers, we assess each individual patient’s skin to unfold the untold story. Do they have scars to determine history of prior wounds and/ or surgeries, any healed or unhealed areas over bony prominences, visual and tactile changes assessing signs of inflammatory abnormalities, eliciting a blanchable response, presence of callouses, and diabetic foot ulcer complications. These signs can be helpful in preventative and treatment programs.
A key successful element to any pressure injury prevention program is a skin assessment. The National Pressure Injury Advisory Panel (NPIAP) recommends that an assessment should include noting localized heat, edema or induration. The visual skin assessment may be easier to observe on a light pigmented individual, but it becomes a challenge and a disadvantage on darker pigmented skin. Baumgarten et al.8 and then Rosen et al.9 found darker pigmented residents were more likely to have a grade 2 - 4 ulcers than lighter counterparts suggesting failure to identify early signs based on skin pigmentation.
In 1995, the National Pressure Ulcer Advisory Panel (NPUAP. Currently known as the National Pressure Injury Advisory Panel –NPIAP) developed a task force to determine the best method to detect early signs of pressure damage on dark pigmented skin.10,11
“We can harness the power of technology to help improve our skin assessment. Long wave infrared thermography (LWIT) is a powerful assessment tool to aid our visual assessments where skin pigmentation is not a factor.”
Their recommendations were as follows: Then in 2016, the NPIAP stated that pain and temperature changes often precede skin color changes in deep tissue injury (DTPI) and that discoloration could appear differently in darker pigmented skin.12 The NPIAP clinical practice guideline recommends considering skin temperature as an adjunct assessment strategy for patients with darker pigment skin.13
• The color of intact dark pigmented skin may remain unchanged (does not blanch) when pressure is applied over a bony prominence
• Localized skin color changes can occur where pressure is applied. These changes may differ from the individual’s usual skin color.
• Local areas of intact skin subject to pressure may feel either warm or cool when touched. This assessment should be performed without gloves to make it easier to distinguish differences in temperature. It is important to clean the skin of any body fluids before this direct contact.
• If patients have had a previous pressure ulcer, the healed area may be lighter in color.
• Areas of skin subjected to pressure may be purplish/ bluish/violet in color. This can be compared with the erythema seen in people with lighter skin tones.
• Edema may occur with an induration (area of skin hardness) more than 15mm in diameter. The skin may be taut and shiny.
• Patients may complain of or indicate current or recent pain or discomfort at body sites where pressure has been applied.
The utilization of specialized cameras to determine patients at risk of deep tissue injuries, surgical dehiscence, high levels of inflammation disturbing the wound healing progression, infection, and levels of hypoperfusion continues to benefit patients especially darker pigmented patients. Our visual assessments when looking for deep tissue injuries and the classic signs of inflammation are difficult to assess on our patients with a higher level of melanin.
Sprigle et al. utilized technology to identify early skin changes on darker pigmented patients with a 90% accurate rate for identifying erythema for light and dark pigmented volunteers.14
We can harness the power of technology to help improve our skin assessment. Long wave infrared thermography (LWIT) is a powerful assessment tool to aid our visual assessments where skin pigmentation is not a factor. LWIT does not discriminate skin color, and it is useful in pressure injury preventative programs. This author has utilized this technology for approximately the past 36 months and has found many applications such as in a preventative fashion, assessment assistance, intervention selection, assessing interventions, just to name a few. I will highlight this technology in the following case studies to understand the usefulness of this technology.
LWIT’s specialized cameras capture the amount of radiation (thermal energy) that a body is emitting in the nonvisible range of the electromagnetic spectrum. This thermal energy is not viewed by the human eye and
and once captured, it is translated into a relative temperature pattern viewed on a device. The viewed pattern is not related to core temperature but rather about the thermal energy being produced due to an abnormal metabolic or physiological process occurring in the site being inspected. An increase of thermal energy or increased temperature indicates an inflammatory response, an infectious process, or results from increased circulation to the area. A decrease in thermal energy or decrease in relative temperature could indicate hypoperfusion, edema, or an ischemic response. Below you will find images to describe normal and abnormal responses on both light and dark skin pigmented individuals. After seeing the images below, one will note how this technology can be our assistance in various applications especially when assessing dark pigmented skin. I do admit that more research is needed, but seeing is truly believing.

The device used is the Scout by WoundVision (Indianapolis, In) which offers a digital camera to capture the picture of the area in question and an infrared camera capturing thermal images that are at the invisible end of the electromagnetic spectrum. The software system converts the image into a color scale of relative degrees Celsius found in between the picture and thermal image. Temperatures above 0 degrees indicate an increased thermal response whereas below 0 degrees indicates a decreased thermal response.
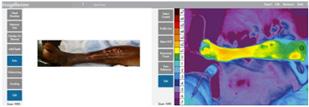
1a: Normal thermal image on light skin.
1b: Abnormal thermal image on light skin (note the presence of periwound redness on picture and infection).
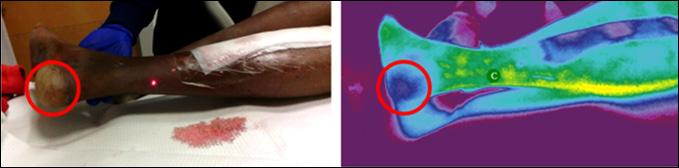
1c: Normal thermal image on dark pigmented skin.
1d: Deep Tissue Injury on dark pigmented skin.
Institutionalized elderly patient at risk for pressure injuries was imaged with LWIT device. Image review revealed no abnormal thermal findings-within normal limits.



“A decrease in thermal energy or decrease in relative temperature could indicate hypoperfusion, edema, or an ischemic response.”Figure 1: Case 1: Normal Visual and Thermographic Images
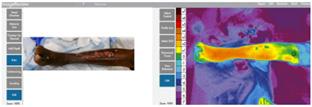
Case 2: Atypical and Infection
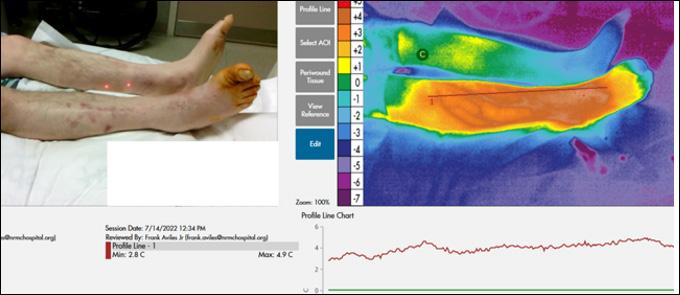
49-year old patient with type 1 Diabetes Mellitus (DM), a hard-to-heal wound, LWIT showed increased thermal energy/ pattern which led to additional testing including a positive culture biopsy which resulted in an atypical vascular ulcer diagnosis.

Case 6: Pyoderma Gangrenosum (PG)
78-year-old patient with non-healing leg wound, history of type 2 DM, end stage renal disease (ESRD), and PAD referred for revascularization. LWIT showed increased thermal energy/ pattern in combination with clinical and objective testing led to a diagnosis of PG with subsequent prednisone therapy.
57-year-old patient with Type 2 DM, nonhealing foot wound complicated by infection. LWIT showed increased thermal energy/ pattern resulting in additional diagnostic tests which revealed gas gangrene.



Patient imaged one-week post-prednisone treatment showed a decrease in thermal energy/ pattern.
Case 7: Infection and Dehisced Incision
45-year-old patient with a dehisced abdominal wound that became infected. Readmitted to hospital for Incision & Drainage (I & D) and antibiotics. LWIT demonstrated increased thermal energy/ pattern. Extensive induration palpated.
Patient reimaged 6 days later noting a decrease in thermal pattern. Induration decreased noted by palpation.


This technology continues to prove beneficial in multiple areas in addition to detecting patterns of early inflammation/infection and pressure injury prevention on dark pigmented skin. There are various applications in both the inpatient and outpatient settings but since this is beyond the scope of this article, be in the lookout for upcoming articles as well as published research using this device.
Figure 2:
2a: This is a patient with an autoimmune condition on IV antibiotics for an infected wound on medial mid distal leg to ankle. Appreciate the absence of visual signs of inflammation on the picture and the intense level of inflammation on the thermal image. This image led to the selection of immediate advanced treatments to control the level of inflammation/ infection. (Right great toe does not have redness but was painted with betadine at time of picture).
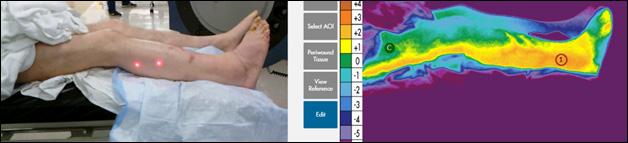
2b: Serial image at 4 weeks with significant resolution of abnormal physiological inflammation.
LWIT is proving useful in preventative programs to detect early signs of skin damage, providing us with real time point of care objective assessment validation for treatment decision making, intervention validation, earlier recognition of inflammatory/ infectious conditions, decrease overutilization of antibiotics, amongst other applications. It is a powerful objective tool allowing us to advocate for patients, especially ones with darker skin.
1. NIH (National Institutes of Health). Health disparities. 2014. [November 2, 2016]. http:// www.nhlbi.nih.gov/health/educational/healthdisp.
2. 3. U.S. Department of Health and Human Services Office of Minority Health. Diabetes and African Americans.
4.
5.
6.
7. Thomas S J et al. Cumulative Incidence of Hypertension by 55 Years of Age in Blacks and Whites: The CARDIA Study. J Am Heart Assoc. 2018;7:e007988.
8. Baumgarten M et al (2004) Black/white differences in pressure ulcer incidence in nursing home residents. Journal of the American GeriatricsSociety; 52: 8, 1293-8.
9. Rosen J et al (2006) Pressure ulcer prevention in black and white nursing home residents: A QI initiative of enhanced ability, incentives and management feedback. Advances in Skin and Wound Care; 19: 5, 262-8.

10. Bennett MA (1995) Report of the task force on the implications for darkly pigmented intact skin in the prediction and prevention of pressure ulcers. Advances in Wound Care; 8:
6, 34-35.
11. Clark M (2010) Skin assessment in dark pigmented skin: a challenge in pressure ulcer prevention. Nursing Times; 106: 30, early online publication

12. National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel. NPUAP Announces a change in terminology from pressure ulcer to pressure injury and updates the stages of pressure injury. 2016. Available online: www.woundsource.com/blog/nationalpressure-ulcer-advisory-panel-npuap-announces-change-in-terminology-pressure-ulcer
13. Kottner J, Cuddigan J, Carville K, Haesler E. A closer look at the 2019 international guideline on the prevention and treatment of pressure ulcers/injuries. J Tissue Viability. 2020;29(4):225–6.
14. Sprigle S et al (2009) Detection of skin erythema in darkly pigmented skin using multispectral images. Advances in Skin and Wound Care; 22: 4, 172-79.