May
- June 2022


May
This Masterclass Guide is a concise overview aimed at exploring the technique of a mechanical debridement device and how to incorporate this into your clinical practice.
Debridement is the technique by which non-viable devitalized tissue is removed from the wound bed and periwound.
The first step of the wound healing process begins with adequate preparation of the wound bed, and this is a vital step.
Depending on the clinical setting, wound types, and patient factors, different methods of debridement will be required; these include mechanical, chemical, autolytic, and biological.
■ A sterile, single-use debridement device for adults and paediatric wounds, the Debrisoft® monofilament pad and ‘lolly’ utlize patented technology (figure 1), composed of monofilament polyester fibres cut with angled tips
■ Designed for acute or chronic wound care in the community and hospital, the Debrisoft® family group of products has added versatility
■ Debris, slough, bacteria and biofilm are lifted, bound and removed by millions of soft, polyester, monofilament fibres

■ Debrisoft® effectively removes barriers to healing
■ This is an innovative, evidence based alternative to inappropriate debridement methods such as the wet-to-dry technique, which have the potential of damaging healthy tissue and causing discomfort to the patient
■ Available as a pad (figure 3) in two sizes: Debrisoft® pad 10x10cm, for debriding shallow wounds and accessible areas of skin, and Debrisoft® pad 13x20cm, for larger wounds or areas of hyperkeratosis
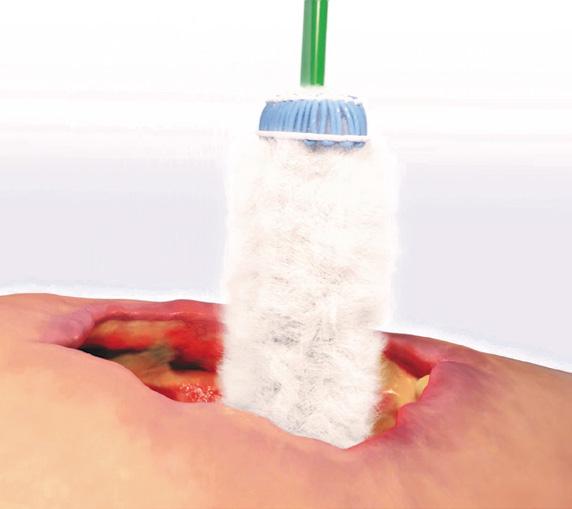
■ Available as a ‘Lolly’ (figure 4), specially developed to debride hard to reach areas of wound and skin, including deep surgical wounds and for cavity wounds
■ Patented monofilament fibre technology™ aids mechanical debridement (figure 1)
■ The best evidenced tool for mechanical debridement, and the only method recommended by The National Institute for Health and Care Excellence (NICE)1
■ The Medical Technologies Advisory Committee concluded that the Debrisoft® monofilament debridement pad was likely to completely debride appropriate wounds more quickly than gauze or hydrogel and may give earlier visibility of the wound bed1
■ Debrisoft® was considered convenient, easy to use, well tolerated by patients and had a significant reduction in pain immediately after treatment1
Keywords
■ Debridement
■ Monofilament
■ Debrisoft®
■ Wound
■ Wounds
■ Wound debridement
■ Chronic wounds
1 Choose a patient with the appropriate wound type. In wounds with hard necrotic tissue, softening by means of autolysis may be necessary before using Debrisoft®2
2 Debrisoft® products can be easily and safely used by any healthcare practitioner in a healthcare environment, with minimal preparation
3 Specialised training is not required for the use of this product
4 The patient can also comfortably self-administer
5 Ensure all emollients are removed. Using only water to moisten the pad, wipe the surface of the wound with the soft fleecy layer
6 Gently wipe over the wound in a circular motion for 2 to 4 minutes, or use soft, sweeping strokes on the surrounding skin
7 Devitalized tissue will bind with the fibres and be removed from the wound bed, benefiting exudate production, maintaining moisture balance, preventing infection and aiding wound healing3
8 Cellular debris, slough, exudates and hyperkeratotic tissues will collect on the soft fleecy layer and be removed from the wound
9 One or more pads are needed for each wound, or surrounding skin, to achieve the level of debridement needed
10 Use appropriate dressing to cover wound



What Types of Wounds Are Suitable?
■ Superficial, acute and chronic wounds

■ Diabetic ulcers
■ Arterial and venous ulcers
■ Decubitus ulcers (Pressure injury)

■ Postoperative wounds
What Types of Wounds Are Not Suitable?

■ Burns and scalds
■ Lymphoedema
■ Wounds with dark necrotic tissue1

■ Wounds with hard eschar1

Debrisoft® a monofilament fibre debridement pad has been found to be a rapid and effective mechanical method of debriding acute and chronic wounds4. This mechanical debridement tool is recommended by NICE for use in the community setting based on the most evidence for effectiveness and predicted cost savings. It is the most well evidenced method of mechanical debridement1 .
■ The success of the Debrisoft® product family in terms of patient comfort and compliance in treatment has been unprecedented
■ Non-invasive Debrisoft® tools are a less painful and safer option compared to potentially destructive debridement techniques in treating wounds in patients with epidermolysis bullosa and pyoderma gangrenosum5
■ Denyer also notes that Debrisoft® could aid in the early diagnosis of certain skin cancers, as these can go undetected when hidden beneath devitalised tissue and debris in the wound area6
■ Can be used by any health care professional
■ Ease of use when self-administered by a patient
■ Avoids travelling to a secondary or tertiary healthcare facility or hospitalization saving time and money
■ Significant savings were shown when Debrisoft® was used in a community and a home setting medical technologies guidance report on Debrisoft®1
■ Before the introduction of Debrisoft® in an audited dataset, the average cost per patient was £64. The cost per patient after Debrisoft® was introduced reduced significantly, to just £204
■ Total cost of wound care products prescribing fell by 14%, in the large audited patient dataset of 4644
■ The use of monofilament fibre debridement pad could reduce wound care products prescribing costs and the subsequent use of costly antimicrobial and negative pressure therapies4
■ “In all patients, almost pain-free and almost complete removal of the fibrin slough was possible by a single application of the debrider without further analgesic procedures... debridement using the debrider represents a non-invasive and therefore safe, almost pain-free alternative, particularly in patients with very painful chronic wounds... This new therapy option can be performed in an out-patient setting without major expenditure in terms of time or materials.” Weindorf & Dissemond, 2014
■ “Most wound debridement requires the skills of specialist practitioners which can be both time consuming and expensive... the new system was found to be a fast and effective method of debridement causing minimal pain to the patients. This new approach to wound debridement could potentially have far reaching benefits to the patient, the nurse and the organisation.” Johnson et at., 2012
■ “When used by a nurse in a community clinic, there were cost savings per patient of £99 for the Debrisoft pad compared with hydrogel, £152 compared with gauze and £484 compared with bagged larvae. When used by a nurse in the home, there were cost savings per patient of £222 for the Debrisoft pad compared with hydrogel, £347 compared with gauze and £469 compared with bagged larvae.” NICE Guidance, 2014
■ Overall cost saving of 20% (included antimicrobial dressings, negative pressure dressings and nonmedicated dressings) using this mechanical debridement device illustrated a 20% cost saving4
■ Compared to other methods of debridement, Debrisoft® may reduce patient consultations with an overall cost savings7
■ Avoiding the inherent costs associated with delayed wound healing is another aspect of cost saving in the use of this product family1
■ Simple and effective to use
■ Is not user-specific; a variety of healthcare professionals can use it early as an effective and immediate method of debridement
■ Well tolerated technique by patients
■ Debrisoft® can be used alone or as an adjunct to other treatment modalities


■ Debrisoft® is the only mechanical debridement method recommended by NICE1
1. National Institute for Health and Care Excellence. The Debrisoft monofilament debridement pad for use in acute or chronic wounds. NICE Medical technologies guidance 17. Last updated March 2019 [Internet]. 2014. www.nice.org.uk/ guidance/mtg17 [accessed 05/03/2021]


2. Benbow M. Using Debrisoft for Wound Debridement. Journal of Community Nursing, Vol.25(5), Sept/Oct 2011
3. Kirshen C, Woo K, Ayello EA, Sibbald RG. Debridement: a vital component of wound bed preparation. Adv Skin Wound Care. 2006 Nov-Dec;19(9):506-17; quiz 517-9. doi: 10.1097/00129334-200611000-00011. PMID: 17132956.
4. Burnett J, Kerr A, Morrison M, Ruston A. An audit to assess the impact of prescribing a monofilament fibre debridement pad for patients with unhealed wounds after six months. J Wound Care. 2021 May 2;30(5):381-388. doi: 10.12968/ jowc.2021.30.5.381. PMID: 33979215.
5. Weindorf M, Dissemond J. Wound debridement with a new debrider: A case report series about dermatological patients with chronic painful ulcerations of differing aetiology. EWMA conference, Vienna, Austria 2012
6. Denyer J. The use of debridement pads in the management of children with severe Epidermolysis Bullosa. Poster presentation. EWMA conference, Copenhagen, Denmark 2013
7. Pietroletti R, Capriotti I, Di Nardo R, Mascioli P, Gonzales M, Ermolli R. Economical comparison between three different types of debridement (autolytic and enzymatic vs mechanical debridement with polyester fibres) [poster]. Wounds UK Conference, November 2012, Harrogate, UK
8. Johnson S et al. A multi-centre observational study examining the effects of a mechanical debridement system. Journal of Community Nursing 2012. 26(6):43-46
9. Meads C, Lovato E, Longworth L. The Debrisoft® Monofilament Debridement Pad for Use in Acute or Chronic Wounds: A NICE Medical Technology Guidance. Appl Health Econ Health Policy. 2015 Dec;13(6):583-94. doi:
10.1007/s40258-0150195-0. PMID: 26315567; PMCID: PMC4661219.
10. Strohal R, Dissemond J, Jordan O’Brien J, Piaggesi A, Rimdeika R, Young T, et al. EWMA Document: Debridement. An updated overview and clarification of the principle role of debridement. J Wound Care. 2013;22:S1–52
11. Murphy C, Atkin L, Swanson T, Tachi M, Tan YK, de Ceniga MV, et al. Defying hard-to-heal wounds with an early antibiofilm intervention strategy: wound hygiene. J Wound Care. 2020;29(Sup3b):S1–26.
12. Edmunds B. Wound debridement in the community. Journal of Community Nursing. 2018;32(4 Sup) L&R, Debrisoft. https://lohmann-rauscher.co.uk/woundcare/debrisoft/debrisoft [accessed 05/03/2021]
13. Bahr S, Mustafi N, Hättig P, Piatkowski A, Mosti G, Reimann K, et al. Clinical efficacy of a new monoflament fibre-containing wound debridement product. J Wound Care. 2011;20(5):242–8
14. Dissemond J, Eberlein T, Bültemann A, Riepe G, Stoffels I, Stephen-Haynes J, et al. A purpose-designed monofilament-fibre pad for debridement of hard-to-reach wounds: experience in clinical practice. J Wound Care. 2018;27(7):421–5
15. Madhok BM, Vowden K, Vowden P. New techniques for wound debridement. Int Wound J. 2013;10(3):247–51
16, Meads C, Lovato E, Longworth L. The Debrisoft Monofilament Debridement Pad for Use in Acute or Chronic Wounds: A NICE Medical Technology Guidance. Appl Health Econ Health Policy. 2015;13(6):583–94.
17. Haemmerle G, Duelli H, Abel M, Strohal R. The wound debrider: a new monofilament fibre technology. Br J Nurs. 2011;20(Sup2):S35–42

18. Johnson S, Collarte A, Lara L, Alberto A. A multi-centre observational study examining the effects of a mechanical debridement system. Journal of Community Nursing. 2012;26(6):43–7
19. Callaghan R, Stephen-Haynes J. Changing the face of debridement in pressure ulcers [poster]. Wounds UK Conference, November 2012, Harrogate, UK
20. Guest JF, Fuller GW, Vowden P. Cohort study evaluating the burden of wounds to the UK’s National Health Service in 2017/2018: update from 2012/2013. BMJ Open. 2020;10(12):e045253
21. Goodridge D, Trepman E, Sloan J, Guse L, Strain LA, McIntyre J, et al. Quality of life of adults with unhealed and healed diabetic foot ulcers. Foot Ankle Int. 2006;27(4):274–80
22. Olsson M, Järbrink K, Divakar U, Bajpai R, Upton Z, Schmidtchen A, et al. The humanistic and economic burden of chronic wounds: A systematic review. Wound Repair Regen. 2019;27(1):114–25
23. Wounds UK. Best practice statement: improving holistic assessment of chronic wounds. 2018. https://www.wounds-uk.com/resources/details/best-practice-statement-improving-holistic-assessment-chronicwounds [accessed 05/03/2021]
24. Vowden KR, Vowden P. Wound debridement, Part 1: non-sharp techniques. J Wound Care. 1999;8(5):237–40
25. Roes C, Calladine L, Morris C. Rapid debridement with monofilament fibre debridement technology: clinical outcomes and practitioner satisfaction. J Wound Care 2019; 28(8):534–541. https://doi.org/10.12968/jowc.2019.28.8.534
26. Atkin L, Bućko Z, Montero EC, Cutting K, Moffatt C, Probst A, et al.Implementing TIMERS: the race against hard-to-heal wounds. J Wound Care. 2019;28(Sup3a):S1–50
27. Schultz GS, Woo K, Weir D, Yang Q. Effectiveness of a monofilament wound debridement pad at removing biofilm and slough: ex vivo and clinical performance’, J Wound Care 2018; 27(2):80–90. https://doi.org/10.12968/jowc.2018.27.2.80
28. Roes C, Calladine L, Morris C. Biofilm management using monofilament fibre debridement technology: outcomes and clinician andpatient satisfaction. J Wound Care 2019; 28(9):608–622. https://doi.org/10.12968/jowc.2019.28.9.608
