LEADER BUILT A STRUGGLING SPINOFF INTO A STRUCTURAL HEART POWERHOUSE WITH PATIENTS AS THE PRIMARY PURPOSE.
MEDTECH’S BIGGEST PERSONNEL MOVES
Resonetics fosters an ecosystem of innovation— combining industry-leading nitinol processing capabilities, dedicated resources, and unmatched material expertise, enabling medtech leaders to deliver the next generation of groundbreaking devices.
THE POWER OF SMOOTH FLOW
ORDER A TEST PUMP: knf com/shop
KNF further expands its Smooth Flow series, with the introduction of FP 7 and FP 25. These new liquid pumps
KNF further expands its Smooth Flow series, with the introduction of FP 7 and FP 25. These new liquid pumps
Self-priming
•
Learn more at knf.com/en/us/stories-events/news/article/fp7-fp25
Learn more at knf.com/en/us/stories-events/news/article/fp7-fp25
LEADERSHIP IN MEDTECH
EDITORIAL
CREATIVE SERVICES
DIGITAL MARKETING
US HONOR
Editor in Chief Chris Newmarker cnewmarker@wtwhmedia.com
Managing Editor Jim Hammerand jhammerand@wtwhmedia.com
VP, Creative Director Matthew Claney mclaney@wtwhmedia.com
AUDIENCE DEVELOPMENT
VP, Operations Virginia Goulding vgoulding@wtwhmedia.com
Digital Marketing Manager Taylor Meade tmeade@wtwhmedia.com
Ryan Ashdown 216.316.6691 rashdown@wtwhmedia.com
Jami Brownlee 224.760.1055 jbrownlee@wtwhmedia.com
Senior Editor Danielle Kirsh dkirsh@wtwhmedia.com
Director, Audience Growth Rick Ellis rellis@wtwhmedia.com
Digital Marketing Coordinator Matthew Kulkin mkulkin@wtwhmedia.com
The medical device industry just wrapped up another year with more blockbuster mergers grabbing headlines around the world and new, innovative technologies emerging seemingly every day.
Associate Editor Sean Whooley swhooley@wtwhmedia.com
This level of success wouldn’t be possible without the innovation, ingenuity and determination of the people who drive it: leaders. These individuals and companies are working for the growth of the entire medical device industry.
Editorial DirectorDeviceTalks Tom Salemi tsalemi@wtwhmedia.com
LEADERSHIP TEAM
Customer Service Manager Stephanie Hulett shulett@wtwhmedia.com
The future of medtech will build on the foundation of today’s efforts and Medical Design & Outsourcing would like to acknowledge such achievements.
We think they deserve recognition from you, too. Vote online for one or more of the companies listed through October.
Managing EditorDeviceTalks Kayleen Brown kbrown@wtwhmedia.com
Editor in Chief -
bbuntz@wtwhmedia.com
CEO & Co-Founder Scott McCafferty smccafferty@wtwhmedia.com 310.279.3844
Senior Vice President Courtney Nagle cseel@wtwhmedia.com 440.523.1685
Customer Service Rep Tracy Powers tpowers@wtwhmedia.com
Customer Service Rep JoAnn Martin jmartin@wtwhmedia.com
Customer Service Rep Renee Massey-Linston renee@wtwhmedia.com
vgrespan@wtwhmedia.com Jim Powers 312.925.7793 jpowers@wtwhmedia.com Brian Toole 267.290.2386 btoole@wtwhmedia.com
4 AXIS SERVO
- brushed or bldc motors - 5 amps per axis - 16 analog inputs - 16 on/off drivers - home and limit in - live tech support - made in the USA
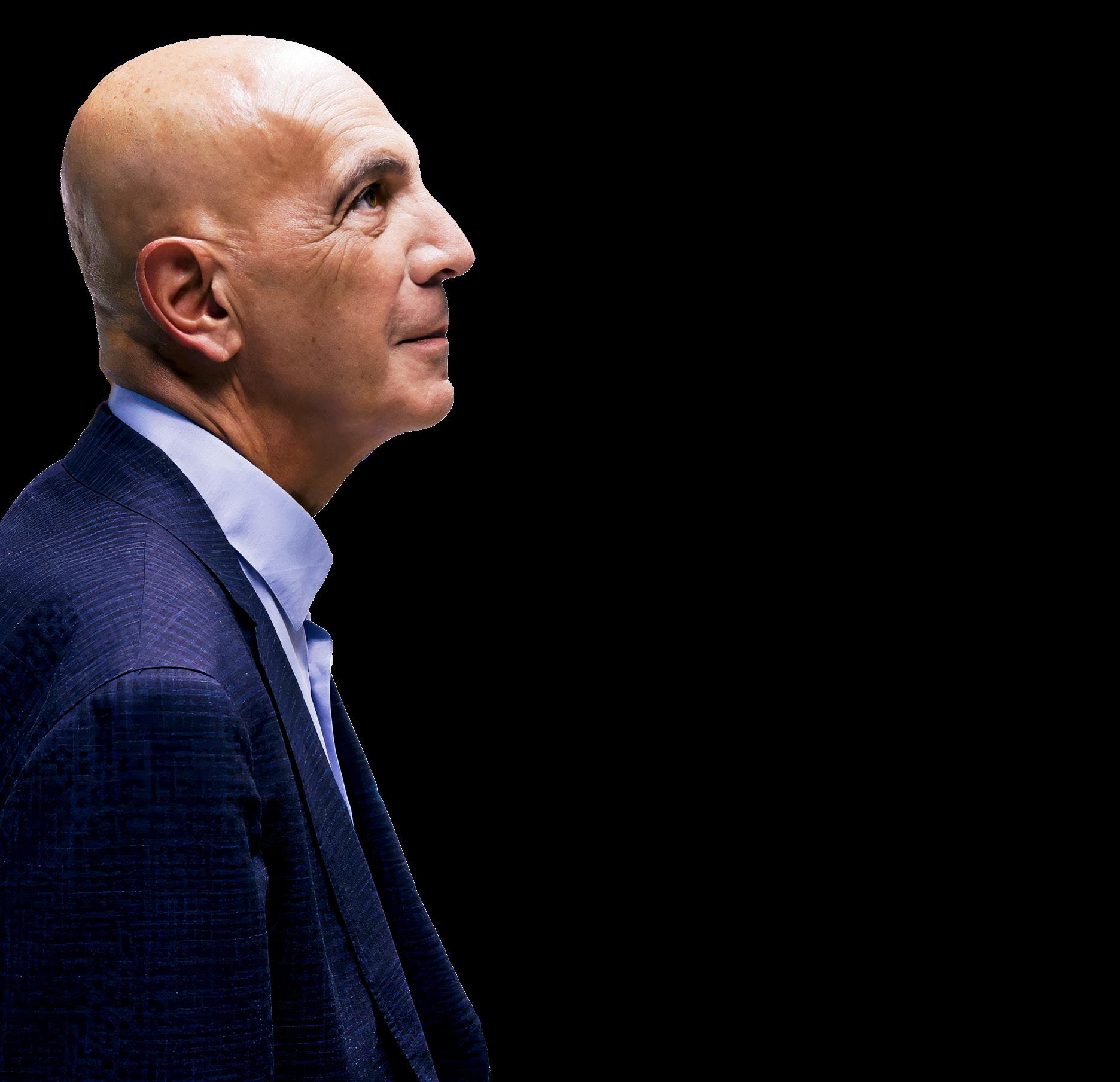
The opportunity — and obligation — of leadership
Mike Mussallem has earned his place among the greatest medtech leaders ever.
Mussallem took Baxter’s struggling cardiovascular business public as Edwards Lifesciences, serving as CEO and chair for more than two decades as the company developed and commercialized revolutionary structural heart procedures like transcatheter aortic valve replacement (TAVR).
For our latest Leadership in Medtech issue, we interviewed Mussallem and some of his Edwards contemporaries for their insights on leadership and innovation. Medical Design & Outsourcing readers already know how important it is for device developers to focus on patients and listen to clinicians when searching for opportunities to innovate. But the story of TAVR at Edwards shows what’s possible when medtech leaders feel obligated to develop new options for patients even when their surgeon customers say they’re not needed — or possible.
And Mussallem’s career should cause medtech professionals to reconsider their own opportunities to lead. When he joined Baxter in 1979, his first engineering project wasn’t glamorous but gave him an opportunity to prove himself. It was the same situation when he moved from manufacturing to R&D and when he later took over the underperforming cardiovascular unit that he and his team would grow into Edwards Lifesciences.
“It became a theme for me,
because it was a chance for a young guy to get a lot of responsibility,” he said. “And if you put your head down and you put a team around it, you can make some progress — and we made some things happen.”
This issue of Medical Design & Outsourcing also features an interview with Dr. Michelle Tarver, the new director of the FDA’s Center for Devices and Radiological Health. She says she wants to improve collaboration with device developers to support innovation while ensuring devices are effective and safe.
She’ll need the medtech industry’s help, especially as Donald Trump returns to the White House with a slate of nominees to lead the U.S. Department of Health and Human Services, the FDA and other federal agencies. Speaking shortly after the election, FDA Commissioner Dr. Robert Califf said industry support will be the biggest factor in keeping talented employees and their expertise at the FDA.
“It’s pretty clear that the gist of this administration from everything that’s been said is to change a lot of things, and how it gets changed depends on who gets appointed to key positions and how the various policies play out — and also, I think as FDA is concerned, how the broader regulated industries see things and play into this. … In times of change and chaos, there’s also opportunity.”
As always, I hope you enjoy this edition of Medical Design & Outsourcing — and thanks for reading.
ᘩ 11,000+ standard parts
ᘩ Customizable with No-Tooling-Charges™
ᘩ
ᘩ Trusted performance in 25,000+ applications
ᘩ Trusted performance in 25,000+ applications
ᘩ
ᘩ
ᘩ
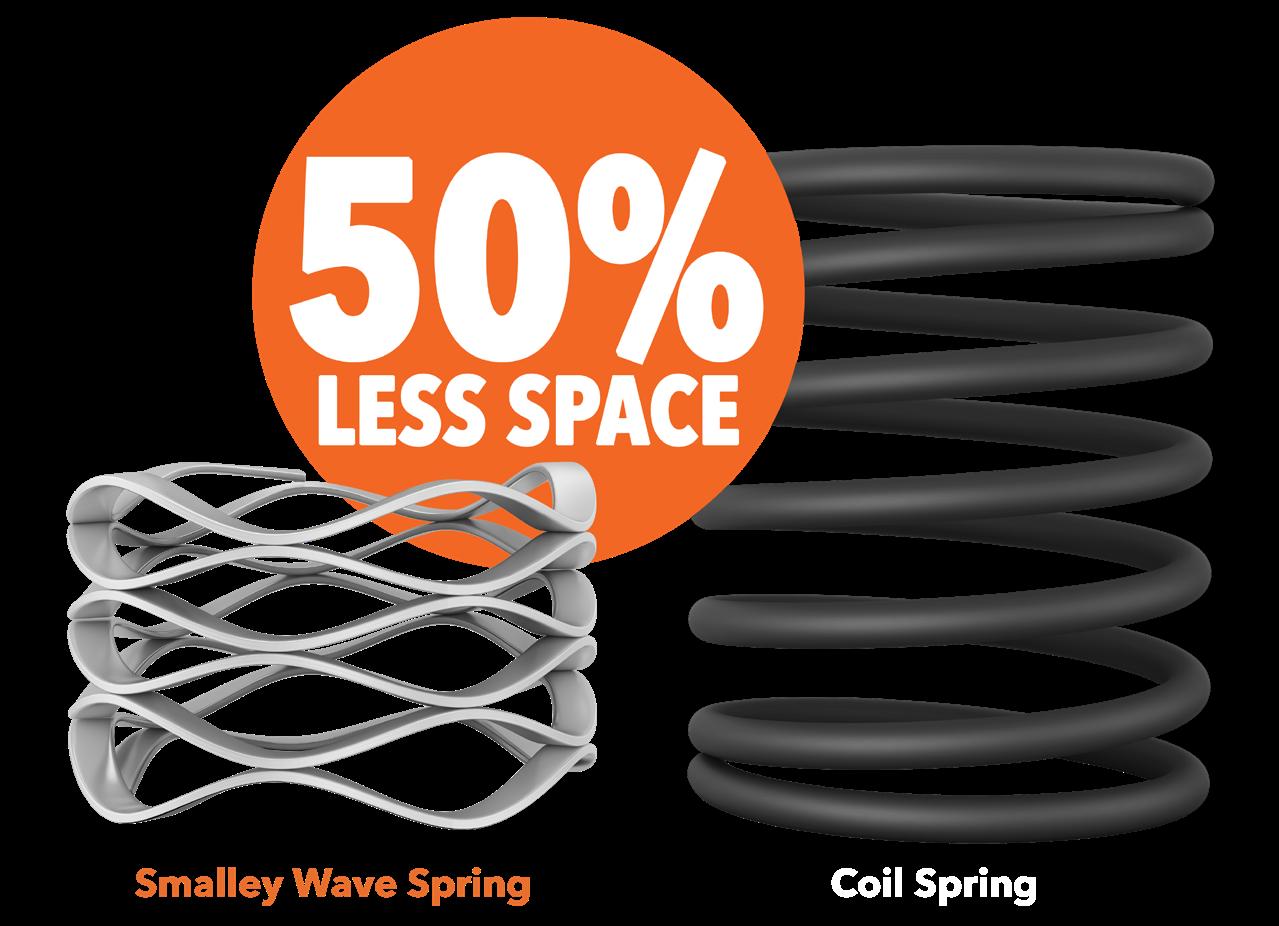
Smalley Wave Springs
Smalley Wave Springs
Smalley Wave Springs
ᘩ Same Force, Same Travel as a coil spring
ᘩ Same Force, Same Travel as a coil spring
ᘩ Same Force, Same Travel as a coil spring
ᘩ Lightweight and compact
ᘩ Lightweight and compact
ᘩ Lightweight and compact
ᘩ Diameters from .118” to 120” in 40+ materials
ᘩ Diameters from .118” to 120” in 40+ materials As
ᘩ Diameters from .118” to 120” in 40+ materials
DEPARTMENTS
HERE’S WHAT WE SEE:
The opportunity — and obligation — of leadership
MATERIALS:
InBrain Neuroelectronics CEO on graphene’s ‘phenomenal’ advantages for medtech
MOLDING:
How sensors enable shot-toshot data control for highvolume injection molding
ONCOLOGY:
5 technologies that are key to bringing CAR T-cell therapy closer to cancer patients
REGULATORY:
A surgical robotics co-founder offers lessons from the de novo pathway
REIMBURSEMENT:
5 design and development tips for AI medtech reimbursement
ROBOTICS:
Overcoming latency and jitter to expand telerobotic surgical procedures
TUBING:
VISION CHECK WITH FDA CDRH DIRECTOR DR. MICHELLE TARVER
Medtronic Endoscopy’s leader on smart tech versus analog, R&D, tuck-ins and quick wins
DEVICETALKS: Inclusive
design is no longer optional
In an interview, the leader of FDA’s Center for Devices and Radiological Health discusses medtech regulation, safety, innovation and health equity.
MEDTECH’S TOP LEADERSHIP CHANGES OF 2024: HIRINGS, FIRINGS, PROMOTIONS AND RETIREMENTS
Our annual recap of the medical device industry’s biggest personnel changes includes leaders moving up, over and out.
Precision Control Solutions
Designing efficient systems involves much more than simply understanding a few basic principles. There is a true art to balancing the specific requirements of an application in order to achieve the desired goals in the best possible way. Help us understand the unique needs of your application and together, we’ll develop something that surpasses what any of us could have done alone.
Contact your distributor to learn more, or visit clippard.com to request a free catalog and capabilities brochure.
THE PERFECT PARTNERSHIP
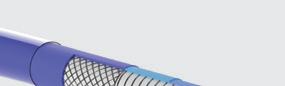
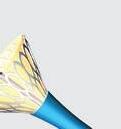
The experts in design, development, and large-scale manufacturing of interventional catheter-based devices and implants.
PARTNERING WITH YOU EVERY STEP OF THE WAY
Learn more about our offerings at www.confluentmedical.com or email sales@confluentmedical.com for a custom quote. NITINOL
TUBING
COMPONENTS BALLON CATHETERS BIOMEDICAL TEXTILES
InBrain Neuroelectronics CEO
on graphene’s ‘phenomenal’ advantages for medtech
By Jim Hammerand Managing Editor
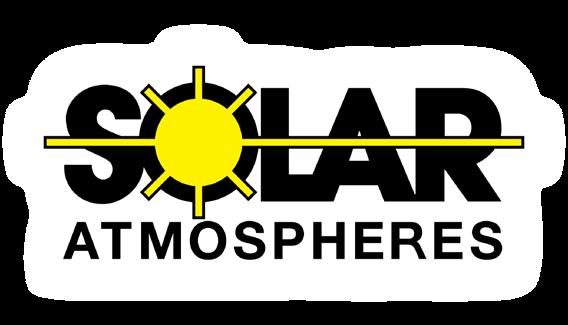
Graphene is the novel material behind the brain-computer interface (BCI) technology developed by InBrain Neuroelectronics.
In 2020, Barcelona, Spain-based InBrain Neuroelectronics spun out of the Graphene Flagship, an EU research and innovation initiative focused on advancing graphene technology.
InBrain Neuroelectronics secured FDA breakthrough device designation for its system in 2023, with the goal of providing adjunctive therapy for Parkinson’s disease. In September 2024, the device developer launched a first-in-human study, which was the first time graphene has been implanted in a patient’s brain.
“We have a combination of a BCI cortical module [and] a highdensity subcortical module that come together in a skull-mounted device that actually decodes — in very high resolution — brain networks, and then can stimulate in micrometric resolution as well,” InBrain Neuroelectronics co-founder and CEO Carolina
Aguilar said in a Medical Design & Outsourcing interview. “We call this BCI therapeutics (BCI-Tx), the fact that we can read and write — so decode and modulate — in high-density and micrometric resolution.”
We asked Aguilar to share some of what she and her team have learned about graphene and its medtech applications. (We’ve lightly edited her responses for clarity and length.)
Graphene’s medtech advantages
Graphene’s “phenomenal” advantages are that it offers micrometric precision for sensing and stimulation, as well as biocompatibility and long-term stability, she said.
The reduced graphene oxide (rGO) that InBrain uses is essentially a stack of flakes, making it a very porous material.
“That porosity also makes the impedance quite low, and therefore the signal-to-noise ratio very, very high,” she said. “And on top of that, you can induce 200 times more charge density compared to metals.” >>
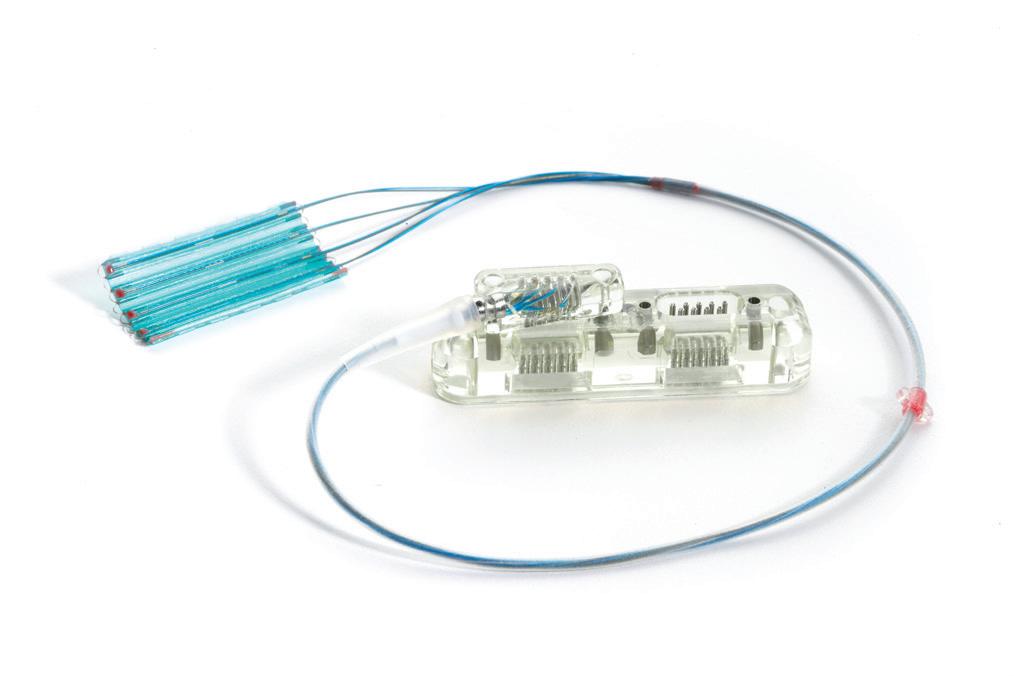
The InBrain Neuroelectronics cortical brain-computer interface system uses graphene to sense brain signals and deliver therapeutic energy.
Photo courtesy of InBrain Neuroelectronics
Harness our leading-edge vacuum technology . . . because lives depend on it.
Medical Vacuum Heat Treating Services
Your high-value medical parts need special treatment. Solar’s leading-edge vacuum heat treating technology produces clean, bright, consistent results. From annealing to age hardening, rest assured knowing your life-critical parts were vacuum heat treated to your exact specs.
For your prosthetics, guide wires, stents, surgical tools, device and battery cases, hypodermics and hypodermic tubing, brazements for analytical devices...and more, trust Solar Atmospheres to provide you with uncompromising quality.
“That is a great advantage in our field, because, you can miniaturize … from 10 micrometers to maybe 1 mm — in our case, so far we use 25 micrometer ‘dots,’ we call them — and that gives you that sensitivity, that resolution, but also that density,” she said.
Graphene contact spacing as little as millimeters or micrometers yields more precise sensing and energy delivery than metals, where those contacts need at least 1 cm of space between them.
“That precision or that resolution gives you a lot of information of [certain] biomarkers, and understanding those biomarkers allows you to modulate them,” she said. “And on the modulation side, because it’s a non-metal, you don’t have these faradaic reactions that you have in metals, and it becomes a very, very stable material [for] stimulation or modulation. … It’s a critical factor to ensure stability and long-term reliability on the brain of someone for many, many years, 10 or 20 years.”
The technology has “endless applications” beyond neural sensors, including catheter technology and retinal implants.
“It allows you to not only find these biomarkers that sometimes with metals you cannot even see,” Aguilar said. “… Also, to modulate these fibers or these nuclei of the brain at that micrometric precision allows us to get a greater effectiveness, but also reduce side effects, because you are not spreading current around tissues [that] could actually generate different side effects. It is very important to understand which network of the brain you are really targeting and not to cause a lot of other side effects or stimulation in the non-targeted networks or areas.”
Another advantage of working with a material as thin as graphene is conformity. InBrain’s working with thicknesses of 10 to 12 micrometers, which “perfectly adapts to the tissue … like a second skin,” she said, without the stiffness of materials like silicon.
“And then, we have technology that allow us to multiplex so we can get 1,024 contacts with very few wires, which has been one of the one of the challenges in neurotechnology,” she said.
But it’s less about maximizing the number of contacts a device developer can put into a brain and more about the right number and placement of contacts for safe and effective treatment.
“In this field, there is a race to put as many contacts as you want or you think you need,” Aguilar said. “... But I think it’s not about who can put more contacts on the surface of the brain. It’s more about what those contacts can do clinically in a relevant and meaningful way for the patient. We can not forget about that, because this is not a technology race.”
Medical graphene challenges
The most challenging part of working with graphene is sorting through the various types, configurations and suppliers.
“To make it biocompatible and stable for our application has been the target and the focus,” Aguilar said.
“So making sure that the graphene we wanted was in the conditions and specifications we wanted, that it will be absolutely biocompatible, and that on top of that we could keep those properties that make it an ideal BCI interface — that required time. Before InBrain was founded, there were eight years of development for that.”
The Graphene Flagship (founded in 2013) conducted studies on biocompatibility before InBrain launched its preclinical testing for the U.K.’s Medicines and Healthcare products Regulatory Agency (MHRA), the FDA and ISO 13485.
“We got very good results from the very beginning, which reassured us big time,” she said.
Studies on graphene have even looked into the potential risks for people who inhaled graphene oxide nanosheets, including a first-in-human controlled study.
As research continues, graphene will one day become as accepted in medical devices as silicon or platinumiridium is now, Aguilar said.
“This is something that is a long-term effort, and we will continue,” she said.
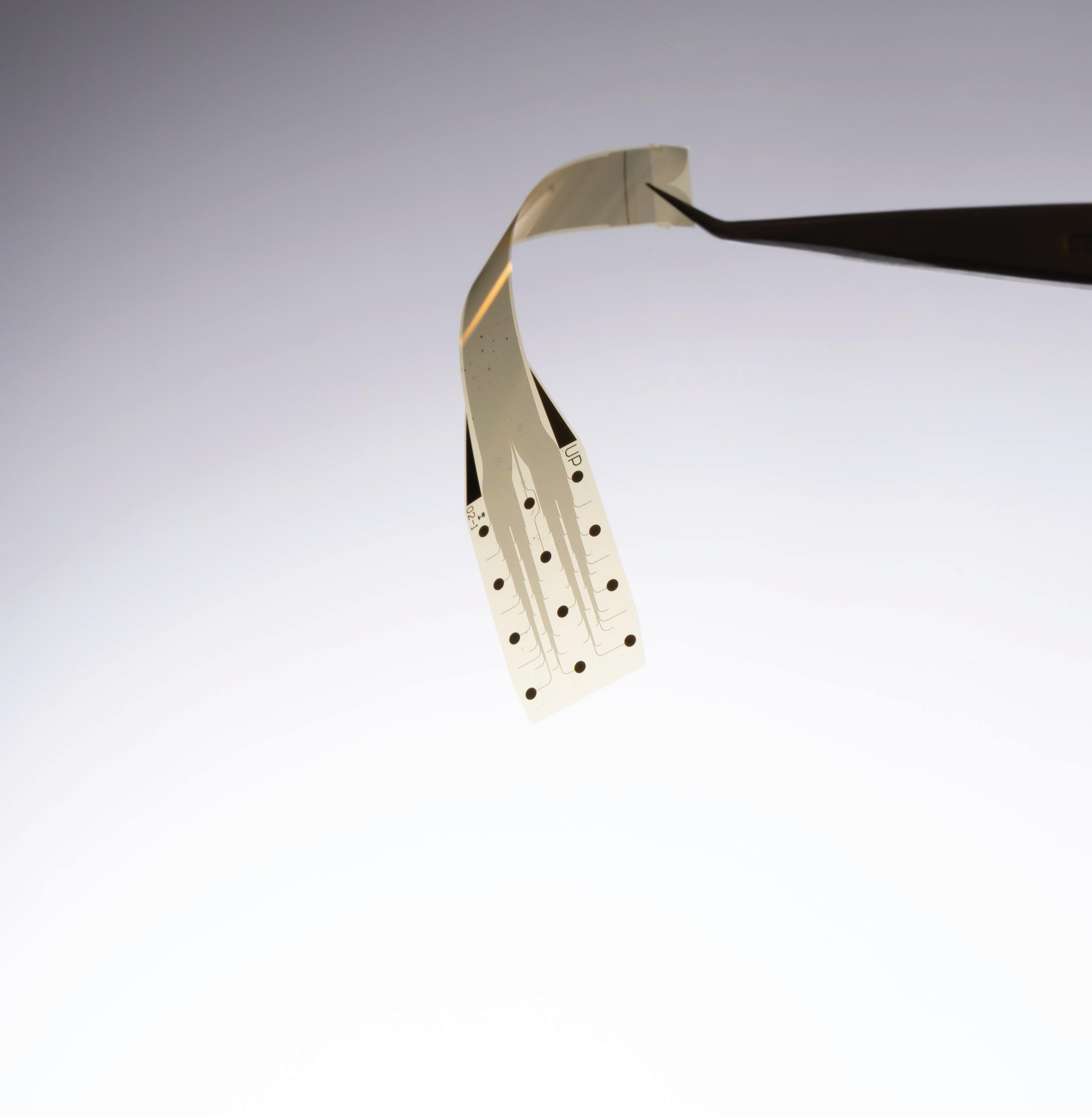
This image shows InBrain Neuroelectronics' graphene electrodes set in a silicon wafer. Photo courtesy of InBrain Neuroelectronics
relentless.
How sensors enable shot-to-shot data control for high-volume injection molding
Injection molding sensors that go beyond a machine’s standard equipment improve product quality and production efficiency.
For medical devices used in and on sensitive areas of the body, the part quality must be high to guarantee the patient’s comfort. Small adjustments can prevent defects like sharp edges on a parting line when doing a long run.
So much time and energy goes into designing and developing products — even single-use disposables — that tracking shot-to-shot data ensures that investment pays off with the maximum number of quality pieces per run.
Injection molding heats polymers to a molten state and forces them into a mold where the polymer solidifies to form Class I, II, and III components and devices. Controlling temperature, position, and pressure are among the factors that help meet the particularly high requirements for manufacturing medical devices. Advanced sensors like thermocouples are some of the measurement tools. With a combination of direct and indirect sensors (whether in direct contact with the melt or positioned behind an ejector),
manufacturers can detect deviations from an ideal molded part.
As the injection molding process and part develops, facility managers can tap into sensors to pull data into a central monitor. This allows shot-toshot visualization of the device-making process. While molding and assembly firms can measure an array of variables, the primary ones they monitor are temperature, position, and pressure.
Gathering shot-to-shot data requires placing independent sensors on a molding machine as well as ancillary production machines and the diagnostic components in a cell. With independent sensors (those beyond what the machine calls for) placed across the manufacturing process, a firm can control the parameters within an upper and lower specification limit. If a limit goes out of specification, the machine will reject the part and notify a robot to remove that part for that condition. This ensures the customer and patient receive a product made to specification vis-à-vis the initial validation protocol. >>
A monitor like this collects sensor data from across an injection molding machine to set and monitor parameters for temperature, position and pressure.
Photo courtesy of Polymer Medical
To gather this data, contract manufacturers and their partners can install sensors on resin hoppers, dryers, and inside and outside molds as well as on other locations like barrels. Sensors such as resistance temperature detectors (RTDs) and thermocouples monitor the temperature of water, dryers and the melted plastic throughout the inject and hold phase.
Manufacturers use linear transducers and encoders to monitor the important positions of the molding machine’s screw as it travels during injection. Monitoring the “shot size” is a critical way to prevent injecting too little or too much material, which can cause defects. Pressure sensors track the pressure of the plastic melt as it makes its way from the barrel into the cavity. The goal is not filling the mold, but stopping the injection velocity and applying pressure to pack out the cavity geometry while adjusting the pressure to meet the dimensions.
While the manufacturers of injection molding machines already install sensors that provide a look into the injection molded process, auxiliary equipment sensors are critical to monitoring other key properties of the plastic resin. For example, if you have a hygroscopic material that readily absorbs moisture, sensors will monitor the drying process at different temperatures and times along with how much humidity the material pulls from the air drying the part. There is also a temperature control unit for the water flowing through a mold to manage the shrink rate so the part is solid when ejected.
Sensors for better maintenance and better products
Sensors also shine a light on how a contract manufacturer’s equipment is performing. The data that advanced sensors gather can help a contract manufacturing and assembly firm determine which machines consistently deliver the best part.
In fact, process monitoring techniques available via Industry 4.0 solutions enable contract manufacturers to pull in machine information and monitor it from shot to shot. With sensors, engineering teams can establish tight bands (or tolerances) for, say, 10 to 15 characteristics critical to the part they’re producing. They can then monitor production to ensure they stay within those bands.
With sensor data, operators and owners can see the machine changing its ability to mold parts over time. With that data and an eye on trends, engineers can plan preventive maintenance and even know when to begin the process of buying a new machine — or a different brand.
Independent sensors: The checks and balances for a superior part
A contract manufacturer can rely on up to 40 or 50 independent sensors connected to their injection molding machines to collect shot-to-shot data. And to properly manage any process, there should be about 10 to 15 sensors in place. Managers, engineers, and operators collaborate to decide where an independent sensor is critical for making a part and archiving data about the piece. Contract manufacturers can also pull in signals and log data for other elements to measure and store the DNA of an injection molded part.
Since sensors track every shot’s temperature, pressure and position, a firm may choose to chart and catalog this over time for all the parts they make.
(continued on page 21)
Polyvinylidene fluoride pellets like these go into an injection molding machine’s resin hopper, which includes sensors for detecting material levels.
Photo courtesy of Polymer Medical
The original manufacturer of this injection molding machine installed this sensor on the resin hopper to detect the pellet level, but device manufacturers and CMOs can install additional auxiliary sensors when needed
Photo courtesy of Polymer Medical
(continued from page 18)
If a run of parts for a splitter or clamp doesn’t look identical to the last set, a manager can look at sensor data with a time stamp and see why there’s an anomaly. While the parts may not have a rejectable anomaly, the sensor data can pinpoint this variance and allow a manager to correct the process before there is a problem.
Installing independent sensors on injection molding equipment also ensures the machine’s sensors are accurate. Independent sensors supply the trend data over time to tell you if a machine component might be out of calibration. By contrast, relying solely on the machine’s built-in sensors and an annual calibration means potentially producing inconsistent parts. Independent sensors on auxiliary equipment can report if a machine requires calibration more frequently. Independent sensors also help monitor temperature and pressure separately for tighter tolerances.
Asahi_2023-MDO_printer.pdf
Final
thoughts
As the adage goes, “Whatever is worth doing at all, is worth doing well; and nothing can be done well without attention.” By paying attention to each step of manufacturing medical devices, firms can achieve consistency through tighter tolerances. Machine and auxiliary sensors are a tag-team approach. Tightly monitoring and controlling the process benefits OEMs and delivers a safe, quality product for patients.
Ben Harp, president and co-founder of Polymer Medical, has 30 years of materials science and process engineering experience and is president of the board of directors of Healthy Manufacturers of New York State (HMNYS) and the Manufacturers Association of Plastic Partners (MAPP). He earned his MBA and bachelor’s degree in mathematics from Canisius University.
The Sigmatek industrial personal computer at the bottom of this photo is the nexus for collecting sensor data from across the injection molding machine and supplying it to the central monitor for technicians to read.
courtesy of Polymer Medical
Best in Class, High Performing Components for Your Medical Devices
Drawing
CDMO / CMO Services
Minimally Invasive Device Solutions
Co-development Opportunities
Access, Delivery, & Retrieval Systems
Wire & Catheter Based Devices
Contract Manufacturing
Vascular Access Devices
Guidewires, Therapeutic & Diagnostic
Braided & Coiled Catheter Shafts
Class 8 Clean Room
Photo
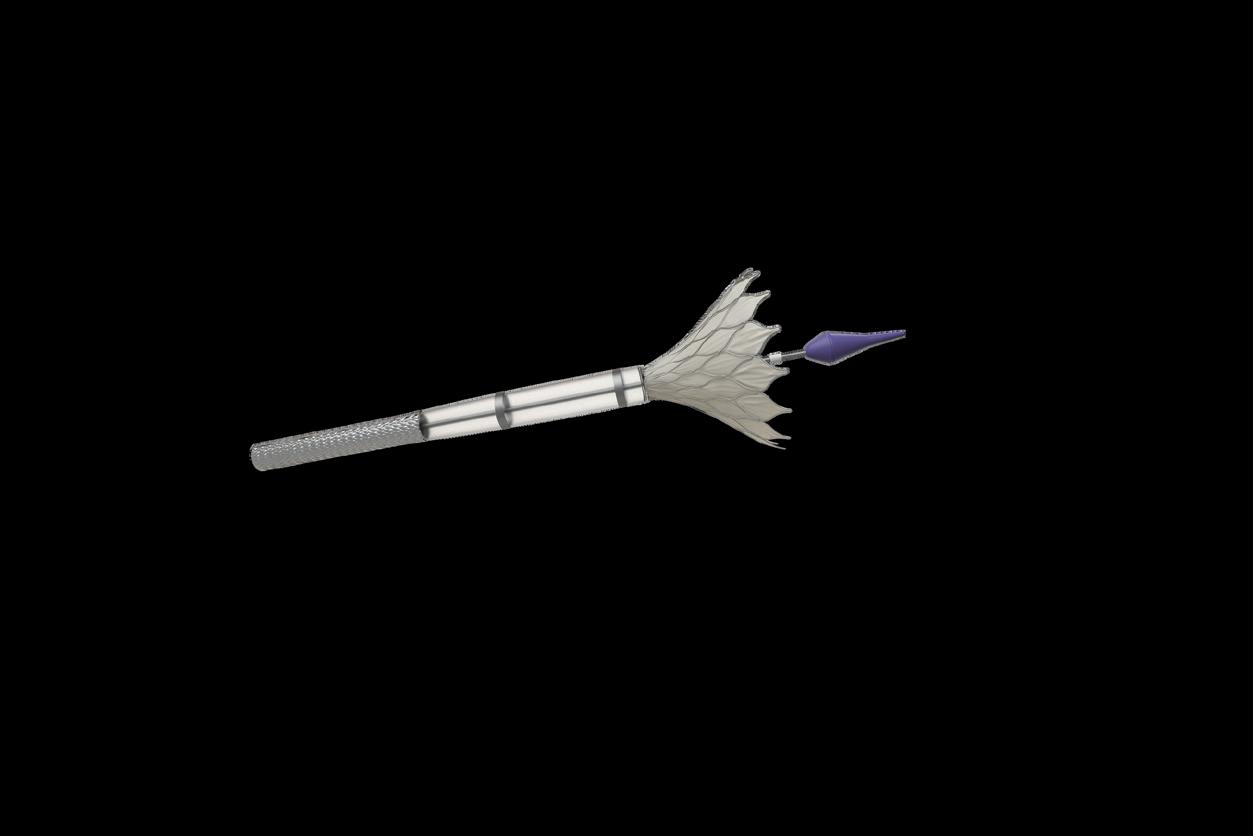
5 technologies that are key to bringing CAR T-cell therapy closer to cancer patients
Manufacturing
automation, machine learning, instrumentation standardization, consolidation/miniaturization and connectivity can bring the unique potential of CAR T-cell therapies closer to patients — but also present regulatory challenges.
CART-cell therapy has emerged as a revolutionary approach to combat cancer, holding immense promise in its ability to target cancerous cells while leaving healthy ones untouched.
This innovative approach harnesses the body’s immune system to fight cancer, offering remarkable precision and efficacy. However, the widespread adoption of CAR T-cell therapy has been hindered by accessibility and cost challenges.
The shift from centralized manufacturing of CAR T-cell therapy to point-of-care (POC) manufacturing is a significant leap forward in cancer treatment. Closed-system automation leverages advanced technologies to enable onsite production at the POC, reducing logistical complexities and costs.
The development and commercialization of POC closedsystem automation for fabricating CAR T-cells is made possible by five key technologies — and faces significant regulatory challenges that could also be considered opportunities.
1. Manufacturing automation
Manufacturing automation is the backbone of closed-system CAR T-cell production. By automating the entire fabrication process — from T-cell extraction to genetic modification and expansion — the system minimizes human intervention and the associated risks of contamination and errors. Automation ensures consistent quality and scalability, enabling the production of CAR T-cells in high volume. This is crucial for meeting the growing demand of CAR T-cell
therapy and making it more accessible to patients who need it urgently.
2. Machine learning
Machine learning plays a pivotal role in controlling the fabrication process of CAR T-cells. By analyzing data from various stages of production, machine learning algorithms optimize the process parameters, ensuring the highest quality and efficiency. For instance, machine learning can predict the optimal conditions for T-cell activation and expansion, leading to better yields and more effective therapies. Additionally, it can detect anomalies in real-time, preventing potential issues before they impact the final product. This level of control and precision is essential for maintaining the efficacy and safety of CAR T-cell therapy.
3. Instrumentation standardization
Standardizing instrumentation across different POC settings is critical for ensuring uniformity in CAR T-cell production. This involves using standardized equipment, disposables and reagents, which simplifies the biopharma manufacturing process and reduces variability. Standardization also facilitates regulatory compliance, as consistent methods and tools make it easier to demonstrate adherence to stringent FDA guidelines. Moreover, it enables interoperability between different systems and sites, enhancing the scalability and flexibility of CAR T-cell therapy production.
4. Consolidation/miniaturization
Consolidation and miniaturization are key to transforming the traditionally complex
By Chris Montalbano, MIDI Medical Product Development
and bulky CAR T-cell production setup into a single, compact instrument suitable for POC use. This involves integrating the functionality of multiple off-the-shelf instruments into one bespoke device that can perform all necessary functions within a closed system. Miniaturization reduces the physical footprint of the equipment, making it feasible to install in a variety of healthcare settings, including smaller clinics and hospitals. Consolidation streamlines the workflow, reducing the time and labor required for CAR T-cell production and ultimately lowering costs.
5. Connectivity/cybersecurity
Connectivity is vital for integrating the closed system automation into existing hospital information systems (HIS) and laboratory information systems (LIS). This integration allows for seamless data flow and coordination, improving efficiency and accuracy in patient care. Connectivity also enables remote monitoring and management of the CAR T-cell production process, providing real-time insights and support. (continued on page 25)
Engineering Services
Testing Laboratory
& Material Processing
COMPREHENSIVE EXPERTISE: From early-stage product development to biocompatibility testing, we provide a full spectrum of services under one roof, ensuring a seamless process and faster time-to-market.
CUTTING-EDGE CAPABILITIES: With advanced equipment and industry know-how, we offer specialized testing in drug stability, device verification, and biocompatibility.
TAILORED SOLUTIONS: Whether you're a new startup or an established pharmaceutical company, we offer customized support, guiding your product through its entire lifecycle with precision and care.
Biocompatibility & Toxicology
(continued from page 23)
However, increased connectivity requires robust cybersecurity measures to protect sensitive patient data and ensure the integrity of the production process. Implementing advanced cybersecurity protocols safeguards against potential threats and ensures compliance with regulatory standards.
CAR T-cell closed-system automation regulatory challenges and opportunities There are significant regulatory challenges in the development and commercialization of closed-system automation for CAR T-cell therapy production. The FDA, often regarded as “the big gorilla in the room,” has only provided draft guidance for POC CAR T-cell fabrication. This lack of established guidelines and predicates presents both hurdles and opportunities for instrument manufacturers.
The draft guidance from the FDA outlines the expectations for manufacturing CAR T-cells at POC, emphasizing the need for consistent quality and safety across different sites. However, without finalized regulations and established predicates, manufacturers must tread carefully to ensure compliance while innovating. This uncertainty can slow development and increase costs, but it also offers a unique opportunity for companies to shape the standards and become leaders in this emerging field.
Instrument manufacturers can leverage their expertise to develop systems that meet the FDA’s evolving requirements, setting benchmarks for quality and safety. By engaging with regulatory bodies and participating in the development of guidelines, manufacturers can help pave the way for widespread adoption of POC CAR
T-cell therapy, making this life-saving treatment more accessible to patients worldwide and taking a big step forward in the fight against cancer.
Chris Montalbano is co-founder and CEO of MIDI Medical Product Development, an advisory board member at Stony Brook University’s Center for Biotechnology, judge and advisor at Columbia’s BioMedX, and an innovation advisor for JLABS & Texas Medical Center (TMCx). He holds a bachelor’s degree in mechanical engineering from Rensselaer Polytechnic Institute and an MBA from Hofstra University.
Streamline Medical Device Development
Uncover New Possibilities in Medical Device Design with Porex Custom Solutions
Precisely engineered porous components that deliver critical functionality for your toughest design challenges.
Scan to request porous polymer concept samples or to schedule a consultation with a Porex Engineer.
ust more than a decade after CMR Surgical‘s founding, the surgical robotics developer won FDA de novo authorization for its multi-port, soft tissue Versius platform in October 2024.
A surgical robotics co-founder offers lessons from the de novo pathway
When announcing the regulatory milestone, CMR Surgical said Versius (which had a CE mark since 2019) was already the world’s second-most-utilized surgical robotic system, with more than 26,000 procedures completed. CMR Surgical sought marketing authorization in the U.S. after conducting clinical trials in Poland and India.
“It’s a great relief as you can imagine, and a lot of work — my goodness,” CMR co-founder Dr. Mark Slack said in an interview with Medical Design & Outsourcing.
We asked Slack for advice that could help other device developers
navigate the FDA de novo pathway, meet new cybersecurity standards and successfully launch their own products. The following has been lightly edited for clarity and length.
MDO: What did you learn taking your Versius surgical robotics system through the de novo platform that you and your team wish you knew when you started on that journey?
Slack: “Pick very carefully who you work with, and you have to pick very carefully somebody who’s got the right background to do it. And then you need to absolutely match it with in-house capability as well. You cannot just go out to consultants and leave out a real skill in your internal, because otherwise you just get caught. >>
CMR Surgical won FDA de novo authorization for its Versius surgical robotics system in October 2024.
Photo courtesy of CMR Surgical
REGULATORY
To me, the biggest problem with regulation at the moment is that they are trying to prevent things that occurred due to criminality rather than things that occurred just by chance. Theranos is a good example. They were lying, making it up. Regulation’s not going to catch that. We have the same with the doctors. If you have a bad doctor who maims and kills people, then they change the appraisal process and they change the paperwork, but that won’t catch them. We are at the very critical point where regulation expenses are becoming an issue, and it is an issue for us in medtech, because Medtronic — they make $30 billion a year, they’ve got 800 products. An average drug [maker might bring in] $20-$30 billion a year for the blockbusters. They can afford the regulatory process, and I think we can’t. So one, you’ve got to pick your person really, really well. Number two, you must not self-complicate. I have a line with my team: ‘We’re not here to set the standards. We’re here to meet them.’ … We have absolute chaos in Europe with the MDR. It is not fit for purpose. It is harming the industry more than you can imagine. At the moment, it is easier to work with FDA than with Europe and a lot of companies in Europe will be making a decision to go to the FDA.”
MDO: What are the advantages you would note of working with the FDA?
Slack: “I can do a Q-Sub (Q-Submission), I can get to know the team. I can get meetings, I can ask questions, I get answers. The Q-Sub process is a very good one … but you’ve got to be very careful to make sure that you create Q-Subs correctly, because otherwise you waste a hell of a lot of time. Sometimes you also have to take some risk as well and just do it, depending on the size of it or what that particular issue is. The de novo process is so big, it was scary.”
MDO: What about cybersecurity standards and regulations?
CMR Surgical co-founder and Chief Medical Officer
Dr. Mark Slack
house, using external test houses as well. You’ve got to get the people to come and try and hack you. But our software people largely did our cyber themselves, which was really good. We did very well. We got a very high score and it’s just such a delight to see.”
MDO: Do you have tips for finding a cybersecurity partner? How would you vet somebody to hack into your systems?
Slack: “We went through legitimate companies, and there are plenty springing up at the moment. I would be very scared of using a hacker. I wouldn’t know where they would be coming from, or
that the patient population was similar to the U.S. And that’s a very difficult one, because what is the normal American in 2024? I think the white population is going to be in the minority relatively soon. You’ve got people of Indian origin, people of Far Eastern origin, you’ve got your traditional Black Americans, you’ve got your traditional white Caucasian. It’s not dissimilar to Europe. But we definitely got pushed quite hard on matching. They are not keen on OUS (outside of the U.S.) data still. So I think going into the U.S. you need — depending on the depth of your pocket — to think very carefully about doing U.S. studies.”
MDO: If you had to do it over again, would you have paid to do trials in the U.S.?
Slack: “Yeah, 100%. An even bigger question — it depends on your depth of pocket, you know — would it not be better to from the outset do an IDE? I think the U.S. finds that very comforting. I suspect it’s congressional pressure to make people do de novos and so on. But you know, if you can afford it and you come and you do an IDE, well you’ve got all the same questions. You’re getting the data. You’re getting it in the right place. You’re getting it with the right surgeons. I think that would solve, for many people, quite a lot of problems.”
“To me, the biggest problem with regulation at the moment is that they are trying to prevent things that occurred due to criminality rather than things that occurred just by chance. Theranos is a good example. They were lying, making it up. Regulation’s not going to catch that.”
where they’d be going and so on. … The software team went up pretty quickly. We got one or two involved. They came in with their teams. It was a very set process for cyber, but anything cyber is money. It’s how many hours can you afford.”
MDO: Any other advice for navigating the regulatory process?
Slack: “The other area that I think probably we weren’t anticipating was cybersecurity, but we did do that very, very well, and have learned a lot, and are now very well prepared going into the future for that. And we did that largely in-
Slack: “The other bit of advice I’ll give with the FDA is working out how much they will tolerate outside of the U.S., and that remains a problem. FDA want U.S. data, and it cost us quite a lot of effort trying to justify that our surgical population was similar to the U.S. one and
MDO: What are your thoughts on real-world data?
Slack: “It’s frustrating, and I’m not sure what the way forward is. At the moment, people mustn’t be fooled. If you go into the FDA and you get to use the term real-world data, make absolutely certain that your real-world data matches the criteria stipulated in the FDA document from around 2018. It’s out of date, it’s not accurate, but if you don’t use that they will argue with you about your real-world data as well.
(continued on page 30)
(continued from page 28)
The FDA is very concerned about clinical acceptance criteria. And when you go to real-world data rather than a curated trial, the chance that you will get to those conversion rates and so on are quite small. The fact that instead of dealing with 50 people you have a data set of 12,000 doesn’t seem to impact them. I’m a great believer that the future is real world data, but you have to curate your real world data particularly well. You have to have auditable standards.”
MDO: Any other advice you’d like to share with device developers?
Slack: “When you start a company like this, be very careful not to over commercialize too quickly. Get yourself solid, get your basics done. And if I did it again, I’d probably sell 50 systems and then stop, and then work those 50 systems to massively improve, get it to as strong as you can, and then go back out commercially. I think that’s a sensible move. Unfortunately, you get pressure from investors and so on. And we’ve basically done that now. We’ve matured the system and it’s giving performance to doctors that are coming back saying, ‘This is as good as, if not better than.’ That’s what I’ve always wanted. Cofounder Luke Hares used to say to me, ‘Mark, you’re always whinging, you’re always moaning. You always want things better. So when are you going to be happy?’ I said, ‘It’s got nothing to do with me. It’s when the surgeons tell me they’re happy.’”
“When you start a company like this, be very careful not to over commercialize too quickly. Get yourself solid, get your basics done.”
Staying Ahead of Polymer Regulatory Changes
In the medical device industry, maintaining compliance with evolving regulations and ensuring supply chain stability are critical concerns. Recent regulatory developments have highlighted risks associated with a certain chemical substance, NMP (n-Methyl-2-pyrrolidone), commonly used in the manufacturing of polyimide tubing and thermoplastic polyurethane (TPU) outerjackets produced using a filmcast or dipcoat process. Both materials play pivotal roles in catheter and other medical device applications.
Filmcasting Polyimide and TPUs have traditionally relied on the use of NMP (n-Methyl-2-pyrrolidone) as a solvent in the manufacturing process. NMP, however, is on the EU’s REACH restricted substance list. NMP is restricted to 0.1% by weight for products sold or used within Europe. Through traditional processing of polyimide tubing, the residual NMP does not meet the 0.1% maximum threshold. One option that suppliers of polyimide tubing may utilize is to bake out any residual solvents. This adds an additional process which adds cost. There is also significant concern that lot-to-lot variability could lead to non-compliance if the additional processes are not validated or if each lot is not tested as part of the lot release.
In addition, a recent finding by the EPA could have ramifications in the medical device industry. The EPA has identified NMP as presenting “unreasonable risks of injury to human health when evaluated under its conditions of use”. It poses risks from both Acute and Chronic exposures through inhalation and dermal exposure. This includes developmental, reproductive, liver, and kidney toxicity concerns.
The EPA’s findings have placed significant scrutiny on NMP which puts the established filmcast polyimide and TPU supply chain in question due to the uncertainty of final restrictions or bans.
To mitigate this risk to the medical industry’s supply chain, Confluent has developed a completely NMPFree option for filmcast polyimide and TPU materials. By eliminating this REACH restricted solvent, Confluent’s offers a solution to OEMs and Contract Manufacturers (CMs) that is a greener option, streamlines compliance, and minimizes risk.
The medical device industry is at a critical juncture where compliance, safety, and supply chain stability must align. Confluent Medical's REACH Compliant Polyimide and TPU solutions offer pathways to meet stringent regulatory requirements while maintaining product performance. By proactively adopting safer and compliant alternatives, manufacturers can safeguard their operations against future disruptions and ensure continued innovation in medical device technology.
For more information and consultation, please visit www. confluentmedical.com or email fastpolymertubing@ confluentmedical.com
5 design and development tips for AI medtech reimbursement
Device designers and engineers of AI-enabled medical technology must focus on reimbursement early in the development process for widespread adoption.
By Tim Fonte HeartFlow
Artificial intelligence (AI) has been increasingly adopted in healthcare. Many of these improvements are related to medical transcription, digital communications and diagnostics. Despite innovation, few AI enhancements and offerings receive additional reimbursements from federal or private insurance payors.
Some AI improvements add incremental value or efficiency to existing medical products or services. That’s a useful benefit for the facility and staff, but does not correlate to higher reimbursement like a distinctly new product or service would. For example, an algorithm that helps a physician more efficiently perform an existing service like interpreting an X-ray can be valuable, but would most likely require payment from a hospital budget and not be eligible for independent reimbursement.
If AI-enabled medical technologies that offer new products and services are to be widely adopted, they need to achieve broad coverage and reimbursement. Product designers and developers should consider reimbursement at each stage of the development process.
Design plays a pivotal role in reimbursement from the start Bringing new AI-enabled medical technology to market is not a matter of launching a new product and expecting immediate commercial viability, even for compelling products. Pursuing the reimbursement process and ensuring broad access and payment for patients is a multi-year journey that requires patience and grit.
Don’t wait for a new technology to be cleared by the FDA before
addressing how it fits existing reimbursement codes or if new codes need to be developed. How the clinical value of a new technology is studied and how the indication is submitted to the FDA have implications for achieving reimbursement.
Here are tips to help guide new AI-enabled medical technology through development while positioning it well to achieve reimbursement.
1. Determine what problem the new technology solves
In order to be reimbursed, the new technology must offer independent clinical value, such as informing diagnosis or treatment decisions for patients in a way not possible with existing methods. Creating a distinctly new product or service that generates useful information can change how physicians or staff care for patients. Ideally, the new technology should offer operational or financial value as well. During the development process, it’s important to ask what unmet need the technology addresses, and is the impact compelling enough that it could be demonstrated?
2. Bring in reimbursement advisors early on
Once there is proof-of-concept for the new technology, ask for the help of reimbursement or market access advisors. These experts can help assess how the new technology could be used and how it could be classified and paid for under the existing reimbursement system — or if new reimbursement codes need to be developed. Later on, these experts can help payers understand the technology and how it benefits patients. (continued on page 34)
and Cara Santillo HeartFlow
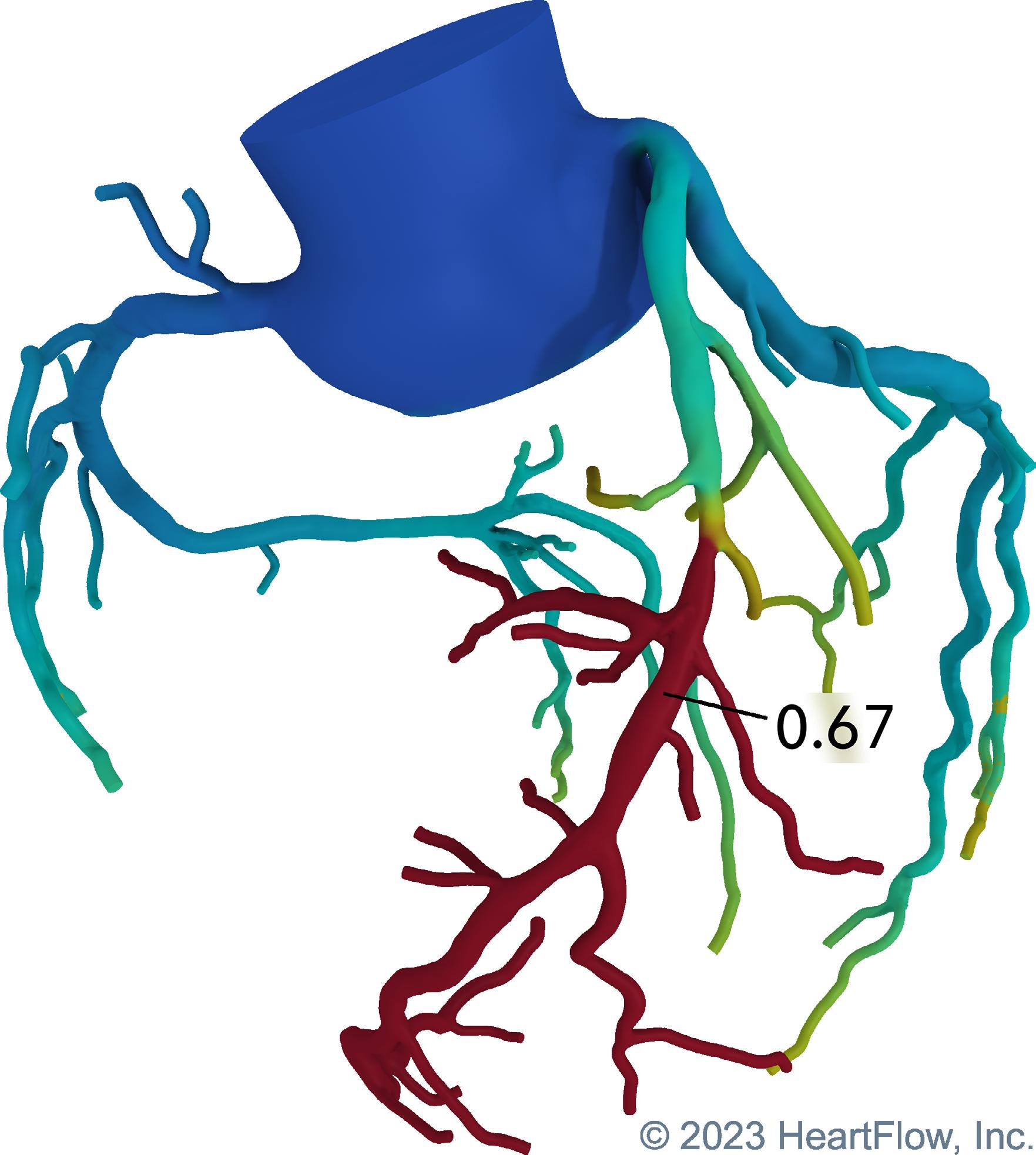
Analysis is a noninvasive procedure that provides a 3D model of a patient’s coronary arteries to identify
(continued from page 32)
3. Commit to getting clinical data to show the technology provides a benefit
All too often, AI-enabled medical technologies do not have the clinical data to back up their claims, or the data only answers some of the key clinical questions. For example, demonstrating the accuracy of a diagnostic test is important, but you need a plan for evidence to also show how it impacts decision-making and patient care. Defining these needs early is important because it could affect the design of the product or regulatory claims, and many studies take significant time to enroll and complete, sometimes as long or longer than the development process itself. Consider clinical evidence jointly with your overall technology development plans.
For example, HeartFlow’s Fractional Flow Reserve – Computed Tomography (FFRCT) Analysis is a noninvasive procedure that provides a 3D model of a patient’s coronary arteries to identify potential blockages. We wanted to show from the outset that it creates novel information and addresses a need. To do this, we obtained clinical data throughout the development process to build,
validate and prove the new technology. This clinical evidence showed that the product was accurate, helped physicians make decisions, improved patient outcomes, and was of economic benefit to the healthcare providers. All of these elements are essential for reimbursement.
We are continuing to leverage this expertise and proven success to create new AI reimbursement categories in the development of additional products like HeartFlow Plaque Analysis, a product that quantifies and characterizes plaque type and volume enabling physicians to accurately assess a patient’s risk and optimize treatment for coronary artery disease.
4. Prove the new technology’s value with physician advocates
It is important to show from the start that the new technology addresses an unmet need. It is also important to identify physician advocates for the new innovation. This is key as new technologies rarely achieve reimbursement without physicians standing behind them.
Designers and marketing teams should work together to summarize what the new technology will do in a
simple, compelling way for physicians. Once physicians use the new technology, develop the experience and data to show it creates value for them and that they need it for patient care.
Keep in mind that the new technology should not require physicians to perform additional work for which they are not paid. First, design the new technology to be as accessible, interpretable and as efficient as possible. Second, ensure physicians get reimbursed for additional time spent using the new information.
5. Establish pricing
A particular challenge for AI-enabled technology is that, unlike most healthcare products, it doesn’t often fit existing codes. Medicare has not often valued or priced AI technologies, and there are varying perceptions about what AI does. While some AI simply runs one algorithm alone, other products like HeartFlow use multiple algorithms on large datasets incorporated in a service that includes human quality review and verification on every patient’s analysis. It is important to look at healthcare economics and consider the overall net savings to the healthcare system, including savings for patients, providers and insurers. Additionally, benchmarking your technology against other technologies can help you to better understand the market. Product and technology design can play a pivotal role in achieving reimbursement for AI-enabled medical technology. By keeping reimbursement in mind as an end goal from the start, designers and developers can ensure adoption of breakthrough technologies that help physicians care for their patients.
Tim Fonte is chief technology officer at HeartFlow Inc., a leader in noninvasive integrated AI heart care solutions. Fonte has 18 years of experience leading the development and market introduction of innovative healthcare technologies.
Cara Santillo, HeartFlow SVP of market access and reimbursement, is responsible for reimbursement strategy across the device developer’s product portfolio and pipeline. Most recently, Santillo helped establish a reimbursement pathway for the HeartFlow Fractional Flow Reserve –Computed Tomography (FFRCT) Analysis.
Overcoming latency and jitter to expand telerobotic surgical procedures
Latency and jitter are the final telecommunications challenges for telerobotics developers working to advance remote procedures as mainstream treatment options.
When Dr. Jacques Marescaux and his team of surgeons in New York City completed the world’s first remote-controlled robotic surgery on a patient in France in 2001, they set the stage for remote-controlled robotic surgery to fundamentally revolutionize medical interventions.
More than two decades after that breakthrough gallbladder removal (known as the Lindbergh Operation), telerobotics — treating emergent conditions through remote controlled robotics — is still in the labs of a small number of pioneering surgeons. Yet
advancements in telerobotic capability have positioned the technology to uniquely impact specific areas of medicine — most notably, stroke treatment. Every year, 15 million people around the world suffer a stroke, and the patient risk of mortality or morbidity depends on how quickly they receive treatment.
With telerobotics, care providers can dramatically decrease time to treatment and increase access to the highest standard of stroke care — mechanical thrombectomy — particularly among rural and underserved patient populations. >>
Physicians training on robotic surgery systems at the Institute for Research into Cancer of the Digestive System (IRCAD) in France.
Photo courtesy of IRCAD
ROBOTICS
Rather than wasting time transporting patients to centralized stroke treatment centers, telerobotics platforms could bring high-quality care to any location with an internet connection. Given the multitude of costs, applying telerobotics within stroke treatment is both a humanitarian and an economic imperative.
Logistical obstacles remain for remote-operated surgeries, such as how to reconcile insurance coverage and legal responsibilities for a patient who is in a different location than the operating physician. But the two main technical challenges for telerobotics developers are latency and jitter.
Clinical impact: Latency versus jitter
Latency refers to the time between an input command and the robotic platform’s response to that command. Studies have shown existing network connections (including 5G wireless, dedicated fiber, and commercial public internet networks) can support remote medical procedures, with network latency that was either imperceptible or so low that it did not affect the procedure.
When moving medical devices within the vasculature, latency rates can make the difference between a properly or improperly placed stent or balloon. Challenges in overcoming latency include light speed delays from geographical distance, lack of control in the signal routing direction, and congestion in bandwidth variation. These affect the round trip time (RTT), or the duration in milliseconds from sending the initial browser request to receiving a response from the server.
Remote surgeon consoles, patientfacing surgical systems and additional auxiliary systems will most likely utilize a direct fiber optic connection at the onset of a telerobotic treatment program. These programs will require signal redundancy as a failsafe for potential network fluctuations or failures, and emerging 5G wireless networks
could serve as an ideal backup. Highspeed, high-bandwidth 5G networks have already shown the ability to have download speeds up to 10 times faster than incumbent 4G networks. They might also offer a safer connection for medical procedures because they can leverage multiple connections between two points, creating a “safety net” connection in case the primary (presumably direct fiber optic) connection fails.
A more dangerous hurdle, jitter, occurs when the bandwidth of a network connection fluctuates and compromises the quality of the signal. Fluctuations in network quality have been shown to increase surgeon fatigue and can lengthen the time of a procedure. In neurovascular procedures the surgeon must navigate tortuous vessels, an unstable environment that becomes exponentially more difficult to maneuver when network fluctuations add a new layer of instability. When placing a stent inside a brain, for instance, a fraction of a millimeter can make the difference between proper or improper placement. Surgeons need a consistent signal to move medical devices through the brain’s vasculature and place them as accurately as possible.
Several tactics to minimize the potential for jitter have already shown effectiveness. Packet prioritization creates an order of priority within the network so the most critical applications have the bandwidth they
Dr. Jacques Marescaux of the Institute for Research into Cancer of the Digestive System (IRCAD)
Photo courtesy of IRCAD
Dr. Jacques Marescaux of the Institute for Research into Cancer of the Digestive System (IRCAD) during the Lindbergh Operation in 2001.
Photo courtesy of IRCAD
need. Similarly, it’s possible to reserve the amount of bandwidth needed for a specific application ahead of time, and enhancing the network buffer can mitigate fluctuations. Protocols and standards including real-time transport protocol (RTP), quality of service (QoS), or traffic engineering (TE) mechanisms can also play a part in combatting jitter.
Realizing the potential of remote procedures
Solving these telecommunications challenges has the potential to reimagine the treatment paradigm for stroke care, which has an urgent need for that level of disruption.
Currently, the U.S. has only about 300 facilities that offer comprehensive stroke treatment for a population of more than 300 million people. By connecting those facilities to skilled physicians, they can exponentially expand the number of patients they can reach and create access to high-level treatment where no options currently exist. Networkconnected care facilities also elevate the standard of care, as the most accomplished physicians can reach patients anytime, anywhere.
Ever since Marescaux introduced the potential of telerobotic procedures, our communications networks have increased in speed, bandwidth and capability, offering the infrastructure for telerobotics. With the birth of 5G and an array of tactics to mitigate challenges such as latency and jitter, our health system is on the verge of fully realizing the disruptive humanitarian and economic potential of robotic-powered remote procedures.
Eduardo Fonseca is the CEO of XCath, an early-stage medical device company dedicated to expanding endovascular treatment modalities through its robotic systems and steerable guidewires.
Advanced Manufacturing for Every Generation
As medical devices have evolved, we have advanced our capabilities to meet your increasingly complex design requirements. Backed by 80 years of proven manufacturing expertise and a laser focus on minimally invasive surgical instruments, MICRO delivers the highest quality components and complete devices, whether hand-held, rigid, articulating or robot-assisted.
Evolving our capabilities to help your devices excel
Our full suite of through prototyping and full-scale production – plus our comprehensive machining, welding and laser capabilities assure that our components help your devices excel.
Medtronic Endoscopy’s leader on smart tech versus analog, R&D, tuck-ins and quick wins
Raj Thomas — previously GM of Mechanical Circulatory Support at Medtronic — shares what he’s learned about the endoscopy operating unit since taking charge in 2024.
By Jim Hammerand Managing Editor
Afew months after Raj Thomas became president of Medtronic Endoscopy in 2024, he spoke with Medical Design & Outsourcing about the operating unit’s place within the world’s largest medical device company, the technology that will drive it and how he’ll fight for a share of the world’s largest medical device R&D budget. (The following has been lightly edited for clarity and space.)
MDO: At Medtronic, there’s always a fierce competition for R&D spend. How is endo making the case?
Thomas: “We have to think about the value we provide and the opportunity. We’re not renal denervation (RDN) — we’re not Jason Weidman who’s got this huge investment that’s gone and got this billion-dollar market that’s sitting out there, and this is one of the bets that we’ve made — or diabetes, or Hugo the robot. So we have to look at our asks in the framework of what the company can afford to do in the present, but also then get the return a little bit faster than Hugo, diabetes and RDN. Those have been long-term investments. We need to show quicker wins, and that’s where we’re going to have to do the investment. In one to five years, I think it is about market development with the products we have. And then it might be tuck-in investments — but they have to be accretive pretty quickly, because we’ve got enough dilutive things going on at the moment.”
Medtronic Endoscopy
President Raj Thomas
MDO: How does Medtronic Endoscopy fit within the larger enterprise framework, and have you found a common theme among all the business units?
Thomas: “There’s about 15, 16 revenuegenerating operating units right now within Medtronic — we still call it 20, but I think it’s 16. We all have roles within the portfolio. We are a portfolio of companies. For us, I think it is taking advantage of the greenfield space and growth. While we’re not the largest — we fit within the Medical Surgical portfolio — our ability to grow and grow not only to access more patients, but grow through a technology that is not well adopted or maybe really well understood to apply in medical devices and healthcare, I think that’s our opportunity. I think that’s where you see [Medtronic CEO Geoff Martha and Chief Technology and Innovation Officer] Ken Washington spending >>
Medtronic announced the successful first ingestion of its new PillCam Genius SB Kit in December 2024.
Photo courtesy of Medtronic
TUBING
a lot of their time with AI: What can we be doing, what can endoscopy do? So we’ll do our part from the financial piece — but from the innovation and technology push piece, that’s how the company is looking at us at the moment.”
MDO: Are you prioritizing smart technology over analog technology, and how does that impact those tuckin acquisitions or R&D, market share and AI development?
Thomas: “Growing from the base that we are would be great, but can we be a larger player and offer more? Frankly, it’s going to take a combination of those kinds of things. There is a spot right now that is ours within endoscopy for the most part: AI. And there are certain technologies that we have that others don’t play in that aren’t with AI yet, but can — so this is Barrx and EndoFLIP. But then there is how do you play with endoscopic retrograde cholangiopancreatography (ERCP) and other markets that Boston Scientific frankly dominates and how do we get after that? And that is one of the questions that we have to answer for ourselves and then work with our Executive Committee — Geoff and team — and say, ‘This is
the strategy. Is this where you want to put your capital?’ And that’s really not up to me. Our job is to offer up the capital investments that may grow and they fit that into the portfolio of companies.”
MDO: How do you think about market development for Medtronic Endoscopy?
Thomas: “AI is one place, the third space might be five years after this one, endoluminal robotics (ELR) is another spot that is being investigated. Those are the spaces where you do technology development and then market development. AI, though, at the moment for endoscopy — at least for us — is a lot of market development.”
MDO: Strategically, are you thinking deeper or wider, and how does that influence your approach to customer discovery?
Thomas: “In order to take up more mindshare of the gastroenterologist, do we have to offer more? The question you balance that with is how does that fit in the overall financial and overall strategy of Medtronic? You’ve talked to other executives — a lot of talk about margin expansion, growth, growing at 5% at the top line or 8% in our earnings, etc. So how do we fit while trying to be broader in, frankly, some products that have lower margins? That’s where you
“Growing from the base that we are would be great, but can we be a larger player and offer more? Frankly, it’s going to take a combination of those kinds of things. There is a spot right now that is ours within endoscopy for the most part: AI.”
probably used to pivot to depth — where can we go deeper? And that’s where I keep going back to AI. Some physicians I’ve talked to say, ‘Don’t forget that there’s actual hardware that has to go in, we actually have to do something, it’s not just about the AI.’ So I think it’s going to be a balance. And it’s an interesting challenge, where you can’t just go and say, ‘We’re an independent company, this is what we’re going to go do. And we’re going to go broad and deep.’ We have to fit within the paradigm of Medtronic to grow the overall company.”
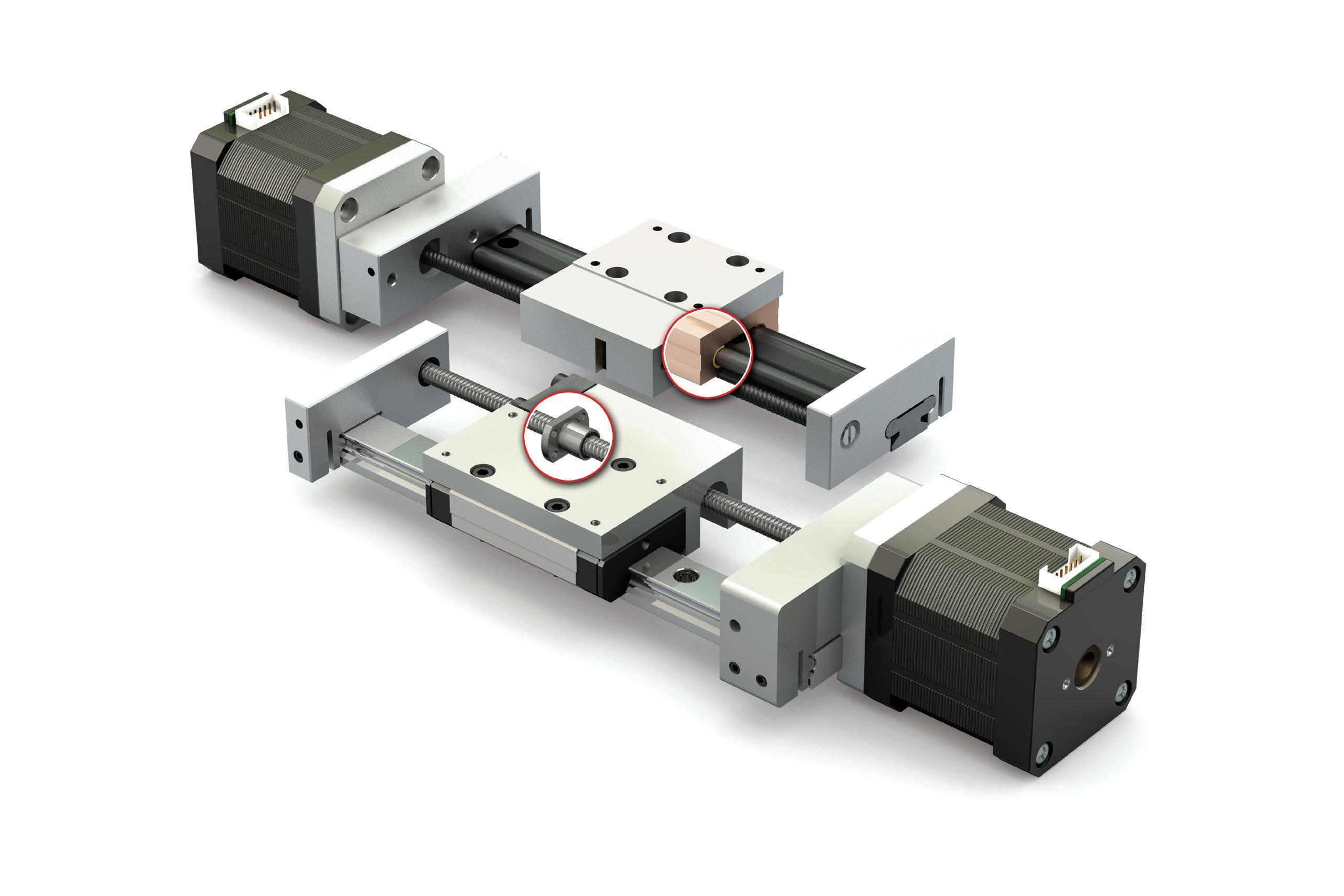
Compact Series Actuators
• 6 & 10 mm lead screw and 8 mm ball screw options
• MAX stroke length up to 1000 mm
• Integrated NEMA 17 or 23 motor
Miniature Ball Screws
• Metric sizes: 6 x 1, 6 x 2, 8 x 1, 8 x 2, 8 x 2.5, & 10 x 2
• Grades 5, 7, & 10
• Flanged and cylindrical nut configurations
• Lengths up to 1,650 mm
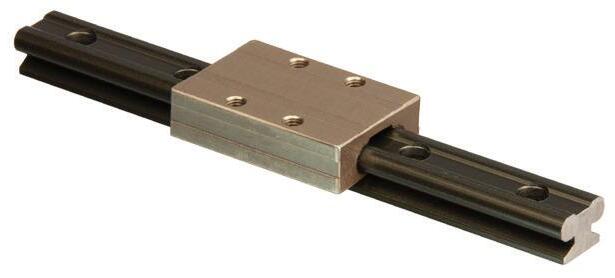
Mini-Rail Linear Guides
• 5 sizes: 7, 9, 12, 15, & 20 mm
• Self lubricating FreelonGold®
• Withstands vibration & shock
• Rail lengths up to 3,600 mm
• Corrosion resistant
After more than two decades leading Edwards Lifesciences as it developed minimally invasive technologies for replacing and repairing heart valves, retired chair and CEO Mike Mussallem now has his name on the Stanford University biodesign program that was so crucial to his company’s innovation.
But success wasn’t a sure thing for Edwards Lifesciences when it spun out out of Baxter in 2000.
“The securities analysts didn’t love us, let’s put it that way,” he said. “We needed a lot of improvement. … It wasn’t apparent that we were destined for greatness. It was a slow road. You have to be tough enough and courageous enough to come in every day … and say, ‘We’re going to make this happen.'” >>
Go to wtwh.me/ mussallem for more from this interview.
MIKE MUSSALLEM | EDWARDS LIFESCIENCES
In an interview with Medical Design & Outsourcing, Mussallem shared some of the lessons he’s learned about innovation and leadership as he starts his next chapter: advancing medtech through the Linda and Mike Mussallem Foundation and the Stanford Mussallem Center for Biodesign.
“People think of it as kind of a light switch, but the innovation process is a long, arduous one that takes a lot of commitment and carries with it a ton of failure,” he said. “You’re going to be disappointed on a regular basis, but [it’s about] trying to fail fast, pick yourself up, learn from what just happened, make an adjustment, and create a culture that encourages that.”
kind of palpable feeling was something that really resonated for me personally, and I fell in love with the business.”
Founded in 1958 by the developers of the Starr-Edwards mitral valve, Edwards was purchased by Baxter in 1985. But in the 1990s it was Baxter’s poorest-performing business, while cardiovascular competitors like Medtronic, Guidant, Boston Scientific and St. Jude were excelling. Something needed to change.
“When you analyze it — and it didn’t take a lot of analyzing — what [we were] missing was innovation,” he said.
Well before the spinoff, Mussallem started studying what separated the best innovators from the worst. What
Spinning off to innovate Mussallem’s first job after earning his chemical engineering degree was at a plant that made and filled antifreeze bottles, where he was a production supervisor for about 30 people on the line.
“Most of them were women my mother’s age,” he said. “Being the supervisor taught me a good lesson. I thought bosses told people what to do, and I found out right away that’s not the way it works. You ask people if they would like to join you on the journey.”
Seeking a more fulfilling career in medtech, he joined Baxter in 1979. After working with different units that made high-volume products like IV bags, he took charge of the cardiovascular business in 1994.
“It became personal,” he said. “A patient would lay down multiple times each day and have a successful outcome — or not. That kind of feedback, that
Irvine, California-based Edwards is now the world’s 23rd-largest medical device manufacturer, with more than $6 billion sales in 2023, compared to $804 million in 2000.
For the first few years as an independent company, Edwards divested products and got smaller as it searched for the best path forward. They considered peripheral vascular diseases, atrial fibrillation, transmyocardial revascularization and even becoming a biotech focused on angiogenesis to grow new coronary arteries. Over time, they realized they should stay close to home with structural heart.
“For Edwards to be good at what it did, it needed to be an innovator,” Mussallem said. “We purposely chose a focused strategy [on] only structural heart disease. The thought was to understand it really deeply, to innovate in that space, and to innovate to make our current technologies better, but also — what else could be? Truly innovating from scratch was an element of our strategy.”
he learned from Stanford Biodesign’s focused approach to innovation and others would influence the course he and his team set for Edwards.
Stanford Biodesign’s “needsdriven process wasn’t about the ‘a-ha’ moment where somebody had a great idea,” he said. “It was more doing a deep dive into really understanding what the needs were, looking at multiple approaches, and then from that trying to identify the best approach for the deep need.”
Mussallem struggled to put his new innovation know-how to work within Baxter, which ran its businesses for efficiency and cash flow over R&D.
“We developed a strategy plan that said we either need to invest a lot in this business or exit,” Mussallem said.
Baxter had a history of successful spinoffs, so it was an easy call. Mussellem asked to lead the way.
Mussallem’s successor, Edwards CEO Bernard Zovighian, described Mussallem as an empathetic, humble leader, and said one of his greatest strengths is his ability to foster innovation.
“Mike’s vision was to pioneer big innovations and breakthrough technologies, underpinned by highquality science,” Zovighian told MDO “Today, we continue to build on Mike’s vision by defining new categories, leading these categories and ultimately delivering sustainable and long-term growth for our company.”
Building a culture for innovation
Edwards brought more products to market in 2003 than ever before, but it was the 2004 acquisition of Percutaneous Valve Technologies (PVT) that made Edwards what it is today. PVT pioneered the minimally invasive transcatheter aortic valve replacement (TAVR) procedure as a more inclusive alternative to open-heart surgery. (continued on page 48)
Mike Mussallem with patients and families during Edwards Lifesciences patient days
Photo courtesy of Edwards Lifesciences
(continued from page 46)
“Being able to replace a heart valve in under an hour all over the world and have great success with patients going home in a day or so, that’s stunning. It’s still mind-boggling to me,” Mussallem said.
Like the founders of Edwards — Dr. Albert Starr and engineer Miles “Lowell” Edwards — PVT’s founders were also doctors and technical experts. That sort of collaboration “is where the magic happens” in medtech, Mussallem said.
“When the technologists — whether they’re engineers or scientists or whatever — are exposed to the problem as opposed to exposed to the solution, that’s where the ideas come from,” he said. “… That exposure to the problem is often missing because it’s tough for technology people to get experience directly with patients and really see what’s going on with them and do a deep study of their condition. It’s when you really understand it from the patient’s perspective and that clinical perspective, that deep introspection, that’s where the ideas come from and that’s when you start dreaming about what could be.”
“You have to decide purposely that you’re going to make that happen,” he later continued, “and it doesn’t happen without real leadership from above to make the time to do that, to devote a chunk of time and resources to running down some alleys that might be dark.”
Let Argon Medical Custom Product Solutions team up with you today.
PVT co-founder and CEO Stan Rowe — who later became chief scientific officer at Edwards — said Mussallem was committed to making TAVR available for patients, despite overwhelmingly negative feedback from surgeons who felt it wasn’t technically feasible or even necessary.
“There were many times Edwards could have bailed out,” Rowe told MDO. “… You’ve got to give Mike and the team huge credit for saying, ‘I’m going to look beyond my key customer and work to adopt something that is disruptive to my key customer.’”
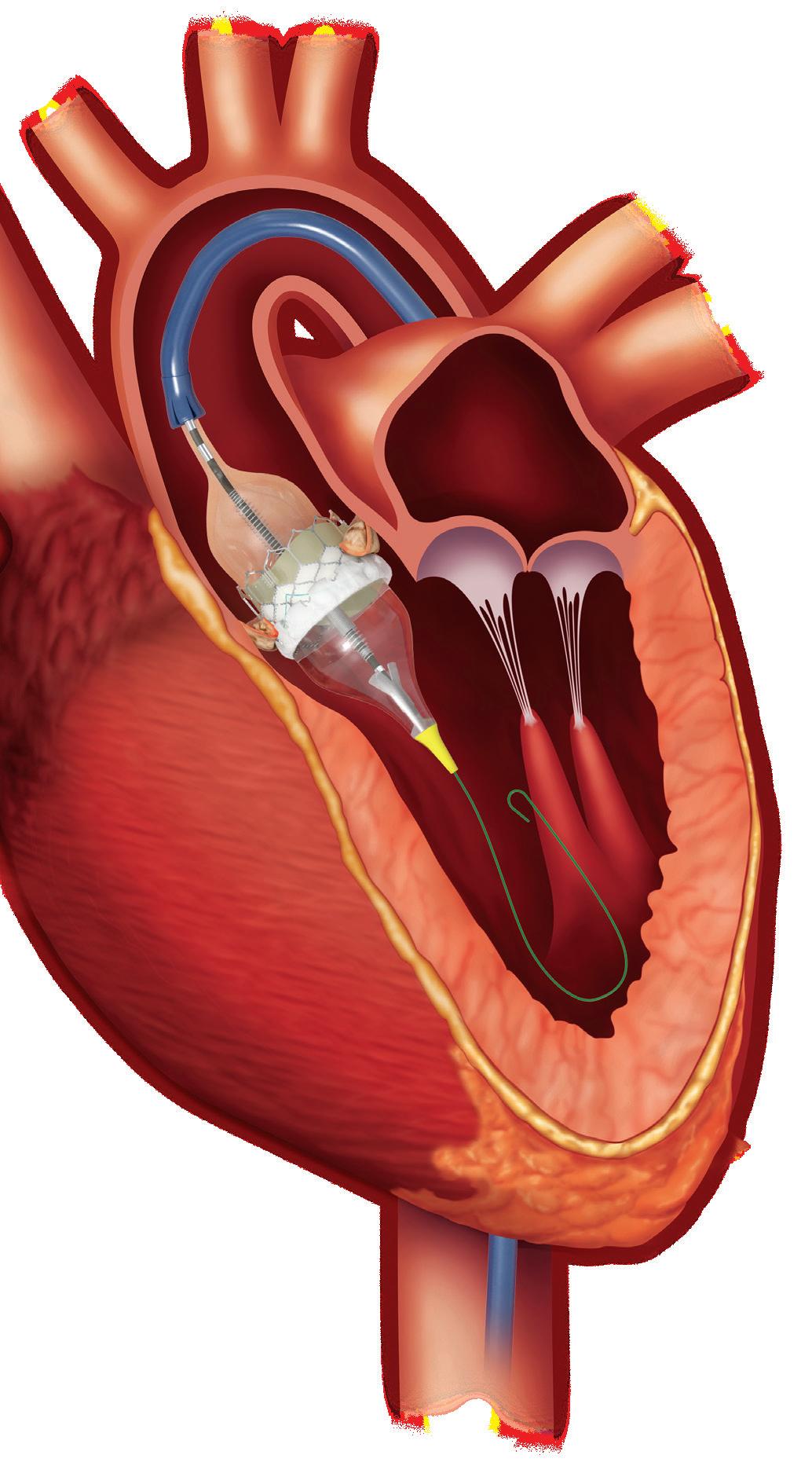
This illustration shows how the Edwards Sapien 3 transcatheter heart valve is implanted inside a patient’s heart.
Illustration courtesy Edwards Lifescienes
Instead, Mussallem and Edwards focused on the patients who could benefit from TAVR because they were not candidates for open surgery or who had a high risk of complications, knowing that TAVR could take off — and take business from those surgeon customers.
“What it takes to succeed, sometimes, is to endorse a disruptive technology,” Rowe said. “If it works, it can be hugely profitable for you, and if it doesn’t, at least you’ve been in control of it. That, I think, was a lot of Mike’s perspective on this. He didn’t want a Boston Scientific or Medtronic to develop this and then disrupt the surgical side.”
Innovation also requires a culture that encourages curiosity and learning, where employees don’t fear punishment for honest mistakes.
“Culture is one of the most important elements of a successful company,” Mussallem said. “Of course, you have to have a great strategy, you have to have a great team and a business plan and all that, but if your culture is not aligned, it doesn’t work very well. Finding the element to glue everybody together and for people to broadly rally around was something that I became obsessed about.”
“There were many times Edwards could have bailed out … You’ve got to give Mike and the team huge credit for saying, ‘I’m going to look beyond my key customer and work to adopt something that is disruptive to my key customer.’”
He made it clear with a sign on his desk: “It’s the patient, stupid,” modeled after the message that helped Bill Clinton win his first run for president.
“There are a lot of competing factors when you’re working inside a company: schedules to hit, budgets to hit, regulators to keep happy, key opinion leaders to keep happy,” he said. “We have a lot of people to keep happy, but let’s never lose focus of the patient, because that’s ultimately our customer’s customer, and if we get that right, we’re probably going to be OK.” >>
Mussallem’s vision for a patient-first culture was clear from the start, Zovighian said.
“He believed that by putting patients at the center of everything we do, we could achieve remarkable outcomes,” he said. “This philosophy became the cornerstone of our company, guiding our decisions and actions. Mike’s unwavering commitment to this principle inspires all of us to strive for excellence in our work, knowing that our efforts ultimately benefit patients around the world.”
First, the company started sporadically inviting patients to meet the employees who hand-sewed their heart valves or inspected the implants for defects.
“We would watch these unbelievable reunions between patients and the people that made the valve,” Mussallem said. “The patients would put their arms around our people and say, ‘Thank you for saving my life.’ … It inspired the patients, and it inspired our people. So you say, ‘OK, how do we bottle that?’”
Edwards then created short videos featuring patients for company meetings and started bringing patients in more frequently to meet with employees, which led to regularly scheduled days with dozens of patients.
“It was inside our people all the time,” Mussallem said of the patient-first culture. “It was just unlocking it.”
Mussallem encouraged medtech professionals to search for meaning in their own work to bring out their best selves.
“You might surprise yourself in terms of what you can accomplish. … It’s unique to each of us in terms of what matters,” he said. “We might stumble around for a while, and it’s OK to not have the perfect job or the perfect boss, but you owe it to yourself to find fulfillment.”
Mussallem’s next chapter
Stanford Biodesign co-founder and Director Dr. Josh Makower described Mussallem as an “inspirational leader.”
“Mike demonstrates all the courage, grit and determination needed to transform medicine and surgery, and through that vision has saved and extended thousands of lives,” Makower told MDO. “Mike persevered through many challenges as he transformed Edwards Lifesciences into the innovation powerhouse it is today. He invested in science, technology and clinical studies to bring percutaneous valve replacement into reality against many odds, all [while] Edwards was a relatively small public company. Almost an impossible task, but the outcome has been transformative for the treatment of valve disease worldwide.”
Makower declined to disclose the size of Mussallem’s financial commitment to the program, but called it “a meaningful start to our endowment campaign to secure the future of Biodesign for generations to come” as the program expands its offerings.
Mussallem and his wife, Linda, have launched a charitable foundation to support healthcare innovation, whole-person health and two underserved populations: pediatric heart defect patients and people born with Down syndrome. (Mike and Linda both had older brothers with Down syndrome.)
“The idea here is to really transform care, and I believe it’s very much possible. I think innovation will be a key part of that,” Mussallem said. “… We never would have imagined we’d have the privilege of having a foundation. For my wife, Linda, and I to be in a position to be able to give back is something that we take very seriously.”
Linda and Mike Mussallem have been married since 1976.
Photo courtesy of the Linda and Mike Mussallem Foundation
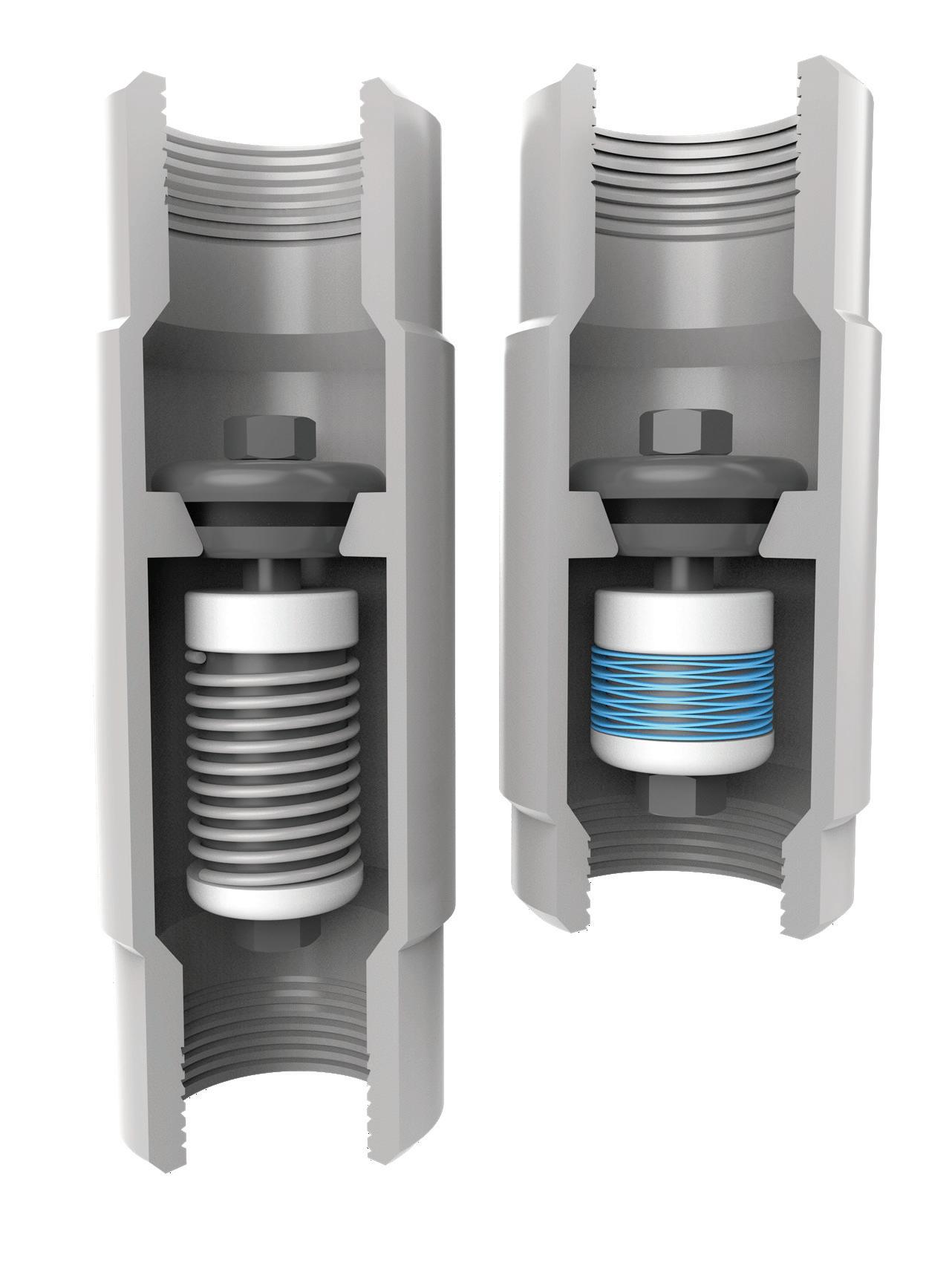
Rotor Clip Wave Springs are engineered to save space and weight by reducing spring heights up to 50%. Our experienced engineering team is ready to assist you in specifying a standard spring or developing a custom design in the material and size you require. From prototype to production, we'll provide you with the perfect spring solution for your application.
Coil Spring
Rotor Clip Wave Spring
with FDA CDRH Director
Dr. Michelle Tarver
IN AN INTERVIEW, THE LEADER OF FDA’S CENTER FOR DEVICES AND RADIOLOGICAL HEALTH DISCUSSES MEDTECH REGULATION, SAFETY, INNOVATION AND HEALTH EQUITY.
BY DANIELLE KIRSH SENIOR EDITOR
DR.
Michelle Tarver, a veteran leader at the FDA, has become director of the Center for Devices and Radiological Health at a pivotal time in medtech.
Tarver has spent over 15 years as a medical device regulator within the FDA and has extensive policy experience in regulation, crafting guidance and conducting premarket and postmarket reviews. Her appointment — which became permanent in October 2024 — comes as emerging technologies like artificial intelligence and the growing demand for equitable healthcare solutions challenge medtech companies and regulators.
“It’s definitely an honor to be able to serve with so many people who are so connected to the mission of ensuring that the U.S. public has access to safe and effective medical devices,” Tarver said
in an interview with Medical Design & Outsourcing. Tarver said she’ll balance device innovation, safety, equity, and usability. Her vision for CDRH includes supporting device developers with tailored resources, collaboration, and addressing regulatory challenges that arise with emerging technologies.
“It’s an exciting time for medical devices, where we’re increasingly seeing new technology like artificial intelligence and machine learning, as well as new diagnostic approaches [and] new therapeutic options coming onto the market, and patients also being able to utilize more of those technologies within the walls of their own home. It really has fostered greater empowerment by patients to be true agents in their own healthcare solutions,” Tarver said. >>
Dr. Michelle Tarver, FDA CDRH director and a practicing ophthalmologist, spoke at the AdvaMed Medtech Conference in October.
Photo courtesy of AdvaMed
DR. MICHELLE TARVER | FDA
More collaboration and FDA resources for developers
One of Tarver’s main goals is to improve collaboration between the FDA and device developers. Programs like the FDA’s collaborative communities initiative allow manufacturers, regulators, and patient advocates to address shared challenges.
The FDA also plans to expand other resources built for device developers, like the Total Product Life Cycle Advisory Program (TAP), which supports companies in developing and approving breakthrough devices. The
access and outcomes. Tarver highlighted the importance of designing technologies that empower patients and integrate seamlessly into their lives.
“If we understand the lived environment for people who have the least amount of resources, we can understand better how those devices may need to nestle into those homes in a way that is going to promote people wanting to engage with those devices as well as nestle seamlessly in the background, so they don’t overtake the home,” Tarver said. “Home is where we like to be with our family and our friends and where we relax. We don’t want to transform homes into little clinics. So how do we imagine an environment that allows the smallest footprint to experience the biggest benefit from those devices moving into the home?”
program accelerates the development and market access of innovative devices that are deemed critical to public health. It was initially launched as part of the FDA’s MDUFA V commitments and focuses on fostering early, frequent, and strategic communication between medical device companies and the FDA.
“This program is specifically geared for those devices that meet the breakthrough designation criteria,” Tarver said. “And they will get a TAP advisor that helps connect them to the different offices … giving them helpful insights as they navigate the process.”
Tarver also emphasized that engaging with the FDA early in the development process can help companies avoid setbacks and accelerate the time it takes to get to market.
The role of digital health
Digital health technology gives opportunities for improved healthcare
By leveraging virtual realityenabled prototypes, the FDA is working with device developers to simulate how their products might fit into a variety of living spaces for effectiveness with minimal disruption to patients’ daily lives.
Balancing
innovation and oversight
Tarver has a unique perspective on the needs of medical device developers.
“Having had a foot both in the postmarket and the premarket arena at various points of my career, I have an appreciation for the importance of both,” Tarver said. “Both the innovation that fuels and catalyzes a lot of the premarket submissions that we see come through our doors, as well as the importance of having responsible oversight of those devices when they’re in the U.S. marketplace to ensure they continue to perform as expected and they remain safe and effective.”
For device makers, this means keeping up with evolving regulatory expectations, particularly for emerging technologies like AI. AI and
machine learning are powering new diagnostics, treatments, and patient monitoring systems.
“Artificial intelligence is an algorithm that is trained on a particular data set and validated in a certain context. But when it’s in real-world use, there can be challenges,” she said. “And so I think at each point along that node, meaning the data that’s used to train the algorithm, does it reflect the intended use population, and is it appropriately vetted to ensure that it performs as expected?”
Focusing on diversity in clinical trials
Tarver has been an advocate for diversity in clinical trials, emphasizing the importance of designing device studies that reflect their intended populations.The FDA’s diversity action plans encourage manufacturers to include underrepresented groups, such as racial and ethnic minorities, women, and older adults, in their trials.
“In 2022 through 2025, we put forward a strategic priority that no person should be left behind in healthcare and that we were going to take deliberate actions to help advance health equity for those who live in various geographic locations, across the age spectrum, people of different sex, people with different racial and ethnic groups, [and] physical limitations,” Tarver said.
Digital health technologies can help overcome barriers to participation, such as geographic distance and various caregiver responsibilities. Remote data collection and virtual trial designs are also emerging as tools to increase trial inclusivity.
In addition to support for digital solutions, the FDA’s diversity action plans encourage manufacturers to actively engage with communities historically excluded from clinical trials. This includes partnering with local organizations to build trust and developing logistical support to enable participation.
“Ensuring that the evidence generated in a clinical trial reflects the people who will use the device … is how we can foster trust and improve health outcomes for everyone,” she said.
Transparency measures such as the FDA’s Device Trial Participation Snapshots pilot, which publicly displays demographic data from clinical trials, help patients and providers better understand who was represented in studies supporting device approvals. (continued on page 56)
Dr. Michelle Tarver replaced Jeff Shuren as acting director of the FDA’s Center for Devices and Radiological Health (CDRH) in July 2024 and was named permanent director in October.
Photo courtesy of the FDA
• CATHETERS
• TUBING & SYSTEMS
• MOLDED COMPONENTS
• CONDUCTIVE MATERIALS
• HYPOTUBES
• COATINGS
(continued from page 54)
Tarver has been “instrumental” in getting the FDA to make age, sex and demographic data available for adverse events, said DeviceEvents founder and CEO Madris Kinard, an advocate for better transparency between the FDA and patients.
“There has been progress in which the FDA is recommending that clinical trials be expanded to women and minorities,” she said. “It will be difficult to know for a while if that is successful. Many devices are also used primarily in the Medicare population (typically 65-plus), but the devices were tested in younger individuals.”
Driving quality and reliability in manufacturing Tarver’s leadership builds on FDA initiatives to support device developers like the Case for Quality program, which encourages manufacturers to implement quality-focused processes beyond basic compliance to improve device reliability, reduce risk and expedite patient access.
“We’ve matured that program, looking at ways in which we can encourage
“It’s an exciting time for medical devices, where we’re increasingly seeing new technology like artificial intelligence and machine learning, as well as new diagnostic approaches [and] new therapeutic options coming onto the market, and patients also being able to utilize more of those technologies within the walls of their own home. It really has fostered greater empowerment by patients to be true agents in their own healthcare solutions.”
companies to inculcate quality across their entire organization,” Tarver said.
The program also recognizes and shares successful manufacturing practices that can serve as benchmarks for the device industry, including thirdparty assessments through initiatives like the Voluntary Improvement Program, which helps manufacturers identify areas for improvement while reducing regulatory burdens.
“Companies who invest in quality not only improve their manufacturing outcomes but also experience fewer product complaints and higher customer satisfaction,” Tarver said.
Additionally, the FDA continues to refine its postmarket surveillance strategies to ensure devices remain safe and effective once they enter the market. Efforts to enhance transparency in recalls, improve manufacturing quality, and streamline regulatory processes are a part of these initiatives.
“It’s about fostering a culture of continuous improvement,” Tarver said. “When manufacturers prioritize quality, it benefits everyone — from the developers and regulators to the providers and patients who rely on these devices every day.”
BY SEAN WHOOLEY ASSOCIATE EDITOR
Hirings, firings, promotions and retirements in
2024
OUR ANNUAL RECAP OF THE MEDICAL DEVICE INDUSTRY’S BIGGEST PERSONNEL CHANGES INCLUDES LEADERS MOVING UP, OVER AND OUT.
Some of 2024’s biggest medtech personnel moves were at the biggest company in the industry: Medtronic. It started in February with CEO Geoff Martha sharing that EVP and Medical Surgical President Bob White was leaving as part of a reorganization with the device maker exiting the ventilator market. He spent 14 years at Medtronic, where he led its integration with Covidien. Medtronic EVP Mike Marinaro added the medical surgical
portfolio to his role when White left. In March, two business unit leaders — Respiratory Interventions President Ariel Mactavish and Gastrointestinal President Gio Di Napoli — announced their own departures, with Endoscopy President Raj Thomas taking on Di Napoli’s responsibilities. EVP and Global Regions President Rob ten Hoedt announced his retirement in June. Shortly after, CFO Karen Parkhill said she was leaving after eight years with Medtronic to join HP. >>
Former Medtronic CFO Karen Parkhill
LEADERSHIP CHANGES
In August, Acute Care & Monitoring Chief Medical Officer Dr. Sam Ajizian announced that he was leaving after nearly 10 years with the company.
In September, Medtronic announced the retirement of Structural Heart Chief Medical Officer Dr. Jeffrey Popma, replaced by Dr. Kendra Grubb.
Investors oust Masimo founder and CEO
In September, Masimo founder Joe Kiani resigned as CEO after activist investor Politan Capital Management ousted him as board chair.
Michelle Brennan stepped in as interim CEO. The former Johnson & Johnson executive won a Masimo board seat in 2023 along with Politan Managing Partner and Chief Investment Officer Quentin Koffey. In 2024, Politan’s successful proxy battle added former Stryker President and Chief Operating Officer Tim Scannell and private equity investor Wendy Lane to the expanded, eight-member board.
Under its new management, Masimo filed a lawsuit against Kiani and investment firm RTW Investments, accusing them of illegally manipulating a recent shareholder vote, while Kiani filed his own lawsuit seeking a payout under his employment contract.
Olympus sacks CEO
Olympus terminated CEO Stefan Kaufmann in October following an allegation that he purchased illegal drugs. Kaufmann had been at Olympus for more than 20 years and became CEO in April 2023, taking over for Yasuo Takeuchi, who stepped back in as CEO after Kaufmann’s departure. Kaufmann pleaded guilty in December as Olympus continued its search for a new CEO.
Changes at BD
In February, BD announced the retirement of longtime EVP and Life Sciences President Dave Hickey, replaced by Mike Feld, who was previously president of Hatch at Danaher spinoff Veralto.
In April, BD promoted Rian Seger to president of surgery, replacing Brooke Story. Story stepped down to care for her sister, and is now leading the integration of the Edwards Lifesciences Critical Care business it bought and renamed Advanced Patient Monitoring.
J&J vet becomes LivaNova CEO
LivaNova hired Vladimir Makatsaria as CEO in February to succeed Bill Kozy, who took over on an interim basis when Damien McDonald resigned in 2023. Makatsaria spent nearly 30 years at Johnson & Johnson MedTech, ultimately leading the Ethicon surgery business as group chair. He joined LivaNova as it planned to wind down its advanced circulatory support business to focus on the cardiopulmonary and neuromodulation units.
CVRx hires CEO from Augmedics Augmedics President and CEO Kevin Hykes left the spine tech developer to take the same position at CVRx, replacing retiring CEO Nadim Yared. Hykes had already served on the neurostimulation technology developer’s board since 2022.
ZimVie spine unit names CEO under new owner
After ZimVie sold the spine business that Rebecca Whitney led as president, she was named CEO of the newly independent company. The buyer, HIG Capital, calls it Highridge Medical, and it also includes ZimVie’s EBI Bone Healing business, led by EBI CEO Glen Kashuba. With $409 million in annual revenue, Highridge Medical made its debut on Medical Design & Outsourcing’s 2024 Medtech Big 100 ranking of the world’s largest medical device companies at No. 97.
CMR Surgical CEO steps down
CMR Surgical CEO Supratim Bose stepped down for personal reasons in October, but remains on the board as vice chair. The surgical robotics developer named Chief Commercial Officer Massimiliano Colella as interim CEO. Two days later, the FDA officially granted de novo clearance for CMR’s Versius platform.
Former CMR Surgical CEO Supratim Bose
Stryker promotes longtime leader to lead medical unit
In July, Stryker promoted VP and Acute Care GM Jessica Mathieson to serve as president of the medical business. Mathieson joined the orthopedic giant in 2008 as an account manager.
Integra LifeSciences CEO retires
In November, Integra announced President and CEO Jan De Witte would retire on Jan. 6, 2025, with former 3M Health Care President Mojdeh Poul replacing him at the tissue regeneration and neurologicaltreatment technology company.
President and CEO Mojdeh Poul
A TRUSTED PARTNER TO
AMPLIFY YOUR INNOVATION
NEUROMODULATION
From components and finished devices to the next generation of medical technologies, now more than ever, you can count on us.
Implantable Pulse Generator Systems
Strengthen your innovation with our rapid prototyping and clinical know-how to take you seamlessly from concept to production
Introducers Guidewires
Delivery & Retrieval
Get to market faster by utilizing our platform technologies and market-ready products that provide differentiated performance and portfolio expansion
Extend your reach through our global R&D and manufacturing capabilities to consistently achieve design requirements, quality standards, and on-time delivery
Suppor t Catheters Cardiac Leads Batteries & Capacitors
Imaging & Sensing
Delivery Systems Electrophysiology Catheters
or too long, the medical device industry has taken a one-size-fitsall approach to innovation, often neglecting the anatomical and physiological nuances of women and other underrepresented groups.
Inclusive medical device design is no longer optional
Tailored solutions can bridge critical gaps in clinical research and medical device design, driving equity for women and diverse populations.
One of the many roots of this disparity runs back to the thalidomide tragedy of the 1960s, in which a morning sickness drug was linked to birth defects. Following public outcry, the FDA excluded women of childbearing age from clinical trials. This exclusion lingered for two decades, during which the majority of clinical research was conducted on male subjects, creating a systemic gap in data and understanding of women’s unique health needs
Against this backdrop, leaders from across the medical device industry gathered at DeviceTalks West 2024 to discuss how the industry is tackling these inequities head-on.
Panelists included Dr. Jennifer Jones-McMeans, divisional VP of global clinical affairs at Abbott Vascular, who has pioneered efforts to enhance diversity in clinical trials; Hexagon Health CEO Dr. Shirin Towfigh, one of the few female hernia surgeons in the U.S., whose patented innovations are reshaping hernia repair; and Frontline Medical Technologies co-founder and CEO Dr. Asha Parekh, whose engineering
expertise has driven the development of devices for critical care applications with specific focus on women’s anatomies.
Overcoming historical oversights in clinical trials
The historical lack of women in clinical trials has far-reaching consequences and has led to missed opportunities for improving care across all populations.
“Women present differently with cardiovascular disease symptoms. Their arteries are smaller, and their needs are often overlooked in design,” said JonesMcMeans.
Towfigh shared a particularly egregious example from her field. In hernia research, women were almost entirely excluded.
“There’s been about seven prospective randomized clinical trials for inguinal hernias. Over 10,000 patients enrolled, a total of 17 women. Only one of those trials had women. All the rest had zero,” she said. “That alone skews industry standards, skews what industry sees as how to design.”
This imbalance not only skews device performance data but also outcomes.
“The female pelvis is different, yet female patients are often misdiagnosed or underserved because the designs don’t reflect their needs,” Towfigh said. (continued on page 62)
(From left) Hexagon Health
CEO Dr. Shirin Towfigh, Abbott Vascular Divisional VP Dr. Jennifer Jones-McMeans and DeviceTalks
Managing Editor Kayleen Brown
Photo courtesy of DeviceTalks
Italian machine builders are set to showcase their cutting-edge ‘Breaking Necks’ solutions and technologies
Italian machine builders are the key to unlocking your strategic business potential.
How are end users leveraging Italian machinery to advance their operational goals and address significant industry trends? Machines Italia’s Spring 2025 issue will explore key trends across various sectors utilizing Italian machinery, including advancements in automation, environmental sustainability, and the increasing demand for flexible and adaptable machinery. For more details, visit machinesitalia.org
Abbott Global Clinical Affairs Divisional VP
Jennifer Jones-McMeans
(continued from page 60)
Her patented hernia mesh aims to bridge this gap, reducing complications like chronic pain and dysfunction.
Parekh noted that while addressing the unique needs of women often highlights critical gaps in clinical trials, these innovations can ultimately benefit all patients.
“Our device is an aortic occlusion device, used specifically for postpartum hemorrhage,” she said. “Women have smaller arteries and pregnant women are susceptible to being hypercoagulable, so thrombosis is an issue. [But] it’s not just women in these emergency scenarios — men come into the emergency room too.”
To address these challenges, Parekh designed with these considerations in mind from the very beginning, prioritizing a smaller, minimally invasive device.
“We’re all trying to miniaturize minimally invasive [devices], everything as small and unobstructed as possible,” she said.
Starting with a focus on specific populations like women ensures that devices are better suited for all patients in the long run.
The role of representation in medical device design
Inclusive medical device design begins with diverse voices at the table. As one of the few female hernia surgeons, Towfigh said her practice sees a disproportionate number of female patients. This exposure gives her a unique lens to identify trends and unmet needs in her field.
“If I wasn’t here, who would notice these patterns?” she asked.
Parekh echoed the sentiment, saying, “Whether it’s engineers, clinicians, or trial participants, representation matters at every stage of development. You can’t design for a population you don’t truly understand.”
Abbott’s approach, as described by Jones-McMeans, involves both topdown and grassroots strategies. Abbott is intentionally recruiting more women for leadership roles in clinical trials and as investigators at clinical sites, and made a concerted effort to ensure gender parity among study participants.
“We’ve partnered with organizations like Women as One to support female physicians and MedtechWomen to promote inclusivity,” she said. “Internally, we created a diversity and research office to ensure these priorities are embedded across our clinical trials.”
Investment in inclusive innovation
Funding remains a significant barrier to advancing gender-sensitive medical device design. Historically, investors have hesitated to fund devices tailored to smaller patient populations, often viewing them as niche markets. But this mindset is shifting.
”Many investors are simply unaware of the market opportunity until you present the data,” Parekh said, emphasizing the importance of using clinical and market data to build a compelling case during funding pitches.
Towfigh’s solution has been to self-fund her innovations, which isn’t always an option.
CEO
Frontline Medical Technologies co-founder and
Dr. Asha Parekh
“It’s tough because you have to convince industry to invest money in a niche product … for a small proportion” of the population, she said.
Beyond gender and toward truly inclusive innovation
While much of the discussion focused on women, the broader goal is designing for diverse anatomies.
“Whether it’s pediatric patients, underserved ethnic groups, or individuals with unique physiological needs, personalized medicine is the future,” Parekh said.
Inclusive innovation — whether addressing women’s cardiovascular needs or designing for pediatric patients — has far-reaching benefits. But it won’t be achieved overnight, as systemic change takes sustained effort and collaboration.
“It’s a long game,” JonesMcMeans said. “The efforts we’re putting in now may not bear fruit until decades down the line. But maybe in 30 years, there’s a different group of women sitting here talking about the fruits of the work we’re doing today.”
Parekh was optimistic, given the growing momentum behind inclusive medical device design.
”I think we have come such a long way in terms of moving things forward for not just women but for diverse anatomies,” she said.
Towfigh shared in the optimism, emphasizing that progress comes through persistence and building a solid foundation of data. “You just have to keep pushing,” she said. “It takes time. People need to start hearing it over and over and over again, and you have to persist.”
YOUR CUSTOM SOLUTIONS ARE CGI STANDARD PRODUCTS
Advanced Products for Medical Applications
CGI Motion standard products are designed with customization in mind. Our team of experts will work with you on selecting the optimal base product and craft a unique solution to help di erentiate your product or application. So when you think customization, think standard CGI assemblies.
Connect with us today to explore what CGI Motion can do for you.
NEMA & International Hospital-Grade Cords in 1 Week!
Robust Interpower® hospital-grade cords are manufactured beyond minimum agency standards. Interpower NEMA and international hospital-grade cords provide correct amperages and voltages for medical devices—portable CT scanners, X-ray machines, medical-grade treadmills, and ECMO machines—essential machines demanding essential power. Interpower cords are hospital-grade torture tested!
When designing, manufacturing, and maintaining hospital-grade products used worldwide, it is vital to know the medical requirements of the country of export—select hospitals in Australia, Canada, Denmark, Japan, and the United States have proprietary requirements. Interpower hospital-grade cords surpass UL 817 (18.2.4.1) requirements, and the C22.2 No. 21-14 requirements for hospital-grade cords and cord sets through rigorous testing.
Our testing facility in Ames, Iowa, was designed to meet or exceed many of the testing criteria used at various test agencies worldwide. Also, every cord and component made in Oskaloosa and Lamoni is subjected to in-house testing and inspection after each phase of production via Interpower ’s strict quality control procedures and tortuous testing.