
Beyond the Referral Developing True Partnerships with Physicians philanthropyHEALTHCARE Journal of the Association for Healthcare Philanthropy | www.AHP.org | Spring 2023 Benchmarking Success: Overcoming the Challenges of Continuous Improvement Is Conventional Wisdom Still Holding Fundraising Hostage? The Moment I Realized I was a Terrible Leader and What Happened Next 36 17 31 Also in this Issue FORWARD THINKING SPONSOR


Integrated Marketing for Planned Gifts 800-858-9154 crescendointeractive.com ROCK-SOLID — Linda Spuck Gift Planning Officer Sharp HealthCare Foundation Crescendo’s multi-faceted marketing tools have been transformational for Sharp HealthCare Foundation’s legacy giving efforts. We have seen year-over-year increases of nearly 50% in bequest commitments from our donors. Crescendo Interactive offers an integrated marketing system that helps you: Build donor relationships Reach fundraising goals Close more gifts Fundraising
CONTENTS
5 6 8 10 17 23
By Arthur J. (Art) Ochoa, JD
Letter from the Chair CEO Corner
By Alice Ayres, MBA
Letter from the Journal Chair
By Bob Nolan, FAHP, CFRE
By Lora Croley, MBA, CFRE and Erin Stitzel, FAHP, CFRE
The team at Baptist Health has worked to engage physicians in all aspects of the donor cycle, building meaningful partnerships and driving healthcare advancement in the community. Their key to success? Treat physicians as you would a valued donor.
Is
By Steven A. Reed
Fundraising in 2023 is all about engagement, but the challenge is to harness the power of engagement from all of the players in the process—not just the donor. This article explores the tools and tactics to bring healthcare fundraising into the present.


Community
By Amy Dorrill, FAHP
Healthcare organizations are increasingly taking on the role of addressing community health and well-being, so where does healthcare philanthropy fit in? Whether community health should be a philanthropic case for support depends on several key factors.
AHP Healthcare Philanthropy Journal|Spring 2023| 3
Beyond the Referral: Developing True Partnerships with Physicians
Conventional Wisdom Still Holding Fundraising Hostage?
Health and Well-Being: Is it Healthcare Organization’s Lane? And, if so, Can Healthcare Philanthropy Make the Case for Support?
SPRING 2023 | VOL. 51 NO. 1
The Moment I Realized I was a Terrible Leader and What Happened Next
By Adam P. Blanchard, MS, CFRE
From stage to page: This article was adapted from a live presentation given at AHP’s 2022 International Conference.
/ FORWARD THINKING
Benchmarking Success: Overcoming the Challenges of Continuous Improvement
By Jenny Love
Benchmarking is an essential tool for healthcare philanthropy organizations that want to improve their performance. Learn to overcome the challenges that can get in the way.
FORWARD THINKING SPONSOR
President and Chief Executive Officer: Alice Ayres, MBA
2023 AHP Journal Advisory Council

Chair: Robert Nolan, FAHP, CFRE
Members:
Murray Ancell, MS, CFRE
Mendal Bouknight
Michelle J. Collins
Sarah Fawcett-Lee, CFRE
Jolene Francis, FAHP, CFRE
Matthew Lang, CFRE
Ben Mohler, MA, CFRE, ACFRE
Andrea Page, FAHP, CFRE
Harrison Porter, CAP, CFRE
Elizabeth Rottman, CFRE
AHP Board of Directors:
Chair: Arthur J. (Art) Ochoa, JD
Vice Chair: Tammy Morison, CFRE
Secretary/Treasurer: Shawn A. Fincher
Immediate Past Chair: Randy A. Varju, MBA, FAHP, CFRE
Directors:
Julie E. Cox, FAHP, CFRE
Jeanne Jachim, MBA
Crystal Hinson Miller
Preston Walton
Published by: Association for Healthcare Philanthropy, 2550 South Clark Street, Suite 810, Arlington, VA 22202
Managing Editor: Olivia Hairfield
Business Manager: Michelle Gilbert
By Jeremy Riley, MA
Grants are a fundamental part of a healthcare philanthropy professional’s knowledge set. This philanthropy 101 article evaluates the steps needed to make grant writing successful.

Creating Programmatic Change Through Grant Development Campaign Goal Setting with Limited Data: A case study
By Heather Perdue, MA, FAHP
Every year, candidates for the Fellow of the Association for Healthcare Philanthropy designation submit a case study for consideration as part of their applications. Read 2022 FAHP recipient Heather Perdue’s submission.

About Us: The Association for Healthcare Philanthropy (AHP) is the healthcare development professionals’ definitive source of thought leadership, connections to facilitate innovation, and tools to advance knowledge and elevate philanthropy. As the world’s largest association for healthcare fundraising professionals, AHP represents 7,000 members who raise more than $11 billion each year for community health services. Our mission is to inspire, educate, and serve those transforming healthcare through philanthropy.
The Journal’s Mission: Healthcare Philanthropy will be an authoritative resource for healthcare development professionals by providing a timely, informative, and insightful collection of literature that will raise the standard of individual and organizational performance. Serving as the premier forum for healthcare philanthropy literature, the Healthcare Philanthropy journal will educate, empower, and inspire development professionals and, thereby, help strengthen the case for philanthropic support and the mission of AHP.
AHP Healthcare Philanthropy Journal|Spring 2023| 4 36 43 46
31
Letter from the Chair

It is my great pleasure to welcome you to the latest edition of the AHP journal, Healthcare Philanthropy. As the Chair of the Board, I am honored to introduce this publication that embodies our mission of advancing knowledge and research in support of healthcare philanthropy.
I invite you to explore this latest edition and engage with the rich content presented by our authors. This new edition covers topics that are most important to you—from cultivating clinician partnerships to benchmarking to health equity fundraising. We’re grateful for the thought leaders and practitioners who have shared their knowledge and insights through these articles. We know you will walk away inspired.
Beyond these pages, AHP has many upcoming educational opportunities. You can find additional resources online in the On-Demand Learning Hub or participate in one of our virtual webinars Immerse yourself in learning by attending our educational intensive, the AHP Madison Institute, from July 16 through 21. Looking ahead to the fall, you can join hundreds of your peers for the annual AHP International Conference in Orlando this September.
Thank you for your continued support of AHP and the journal.
Best,
Art
AHP Healthcare Philanthropy Journal|Spring 2023| 5
Arthur J. (Art) Ochoa, JD
CEO Corner
At the end of March, I had the privilege of participating in the conversation at the Leading Forward Health Equity Summit. As is always the case when I attend an AHP conference, I came away invigorated by the energy, ideas, and results that AHP members are achieving toward bettering our profession, our organizations, and the health of our communities.
Achieving health equity faces many obstacles, including income inequality, lack of access to education, housing, and employment opportunities, discrimination, and bias in healthcare systems. These obstacles extend beyond our hospital walls, but not beyond our ability to impact them if we stop and give them the attention they deserve.
Alice Ayres, MBA President and Chief Executive Officer of

At the summit, we saw example after example of healthcare foundations that have partnered successfully with community and government organizations to effect positive change on the health, not just the healthcare, of the communities they serve. Here are just a few examples from around the United States:
• BElovedBIRTH Black Centering, which is creating an entirely new birthing experience for Black folks in California.
• The West Lakes Early Learning Center, which offers combined early childhood education and comprehensive health services to underserved families in Florida.
• The Inova Pride Clinic, which provides primary care for the LGBTQ+ community in Virginia.
• The IU Health Fellowship at Crispus Attucks High School, which offers Black high school students in Indiana a path to an economically stable future in a healthcare career.
Our philanthropy teams are uniquely qualified to contribute to these types of projects. We know the communities we
AHP Healthcare Philanthropy Journal|Spring 2023| 6
AHP
“There’s this power dynamic that exists in any position, and the bigger voice, the bigger pockets, the bigger chair at the table shifts the power dynamic when decisions are being made. In this partnership, we know when to shift our power. We know when to give our power away, and we know when we need to hold that power.”
Felicia DeHaney Director of Program and Strategy at W.K. Kellogg Foundation
serve better than anyone else at the hospital. We understand which philanthropic partners are most likely to want to support health equity work and secure its sustainability, and we have the necessary relationships with our c-suite partners to ensure that this work is prioritized.
It’s worth the effort. Studies have shown that community-based health programs that aim to improve access to medical and other care for underserved populations can significantly improve health outcomes for these individuals and reduce disparities for underserved populations. Moreover, investing in health equity projects can help our organizations achieve their mission of promoting good health for all individuals, regardless of their background.
It’s valuable work, but it’s also hard work, especially during the single biggest financial crisis in our history, when there is pressure to allocate philanthropic dollars to our core business. Some of you are struggling to keep commitments made in your communities because the dollars simply aren’t there. Others are struggling to convince the board and leadership to stay committed to health equity and health justice in the face of negative margins.
I hope that by seeing what is possible, it will give you renewed motivation to keep moving forward. If we all make even a small difference in health equity in our own communities, together we can make a big difference for the health of all Americans.
At the end of the day, it’s simply the right thing to do.
As Gary Cates, chief philanthropy officer at ProMedica, said at his session at the summit, “I understand the urgency as an industry we face right now, and I know the adage ‘no margin, no mission. But God help us if we ever arrive having restored margin but lost our mission.”
In gratitude for all you do, Alice

AHP Healthcare Philanthropy Journal|Spring 2023| 7
Letter from the Journal Chair
How often do you, as a philanthropic development professional, talk about the concept of investment? Do you talk about it with your donors when encouraging them to give to your institution? Do you talk about it with your leadership team to grow and build a successful fundraising organization? Do you talk about it with your staff and their professional development?
We all do that to one degree or another, even if we don’t use the word “investment” specifically. I’d like you to consider one more question. How do you invest in yourself and the profession of healthcare philanthropy? I’ll ask the question and offer this suggestion. Write an article for Healthcare Philanthropy, the Journal of the Association for Healthcare Philanthropy.
Bob Nolan, FAHP, CFRE Chair–AHP Journal Advisory Council Executive Director of Development Indiana University School of Public Health

You have unique experiences and perspectives on the subject of healthcare philanthropy. Your work in an academic medical center, large hospital system, rural hospital, or in any of a dozen other settings presents challenges and opportunities that are shared by your colleagues in AHP. Documenting those challenges and opportunities through an article submitted to Healthcare Philanthropy can advance the body of knowledge in our profession, and help your colleagues to be more efficient, raise more support, and build better fundraisers and teams.
We’ve been gratified by the increasing numbers of AHP members who have written and submitted articles for the journal. That’s results in a better journal and a more useful resource for our members.
One last question…what do you need to get started authoring an article on an aspect of your fundraising experience? The AHP Journal Advisory Council, made up of your colleagues in the profession, are available to assist you in the process. Please reach out to us through the communications team at AHP for more information. We’re looking forward to working with you!
AHP Healthcare Philanthropy Journal|Spring 2023| 8




Purpose-Built
for
to help high-impact healthcare organizations
the world
and increase
revenue.
Solutions
Healthcare Organizations You change the world. We provide the tools. We’re proud
around
drive success
philanthropic
blackbaud.com
Beyond the Referral: Developing
True Partnerships with Physicians
By Lora Croley, MBA, CFRE, System Director of Donor Relations for Baptist Health | Kentucky & Southern Indiana and Erin Stitzel, FAHP, CFRE, Principal Consultant at Accordant

This is not a paid advertisement,” said Justin Leighty, Baptist Health Louisville foundation executive, following an impromptu story shared by grateful patient Mike Cronin. Mike, along with more than 100 fellow donors, was at a gathering to hear three Baptist Health neurosurgeons speak about advancements in their service line, and how philanthropy supports their work. This in and of itself was enough to garner applause and excitement from the crowd–but then Mike spoke unprompted. Mike shared his profound gratitude for Dr. Nathan Todnem, who performed surgery on him less than a year ago.
On that same evening in Lexington, Kentucky, two neurologists were teaching a group of donors about the ways their giving can advance stroke care at Baptist Health Lexington. The duo of doctors educated, engaged, and graciously thanked donors, many of whom chose to support the hospital because of their patient experience.
These are not rare occurrences throughout the Baptist Healthcare system in Kentucky and southern Indiana. Many physicians are key partners in engaging at all levels of the donor cycle–from identification, to cultivation, all the way through stewardship–and the
AHP Healthcare Philanthropy Journal|Spring 2023| 10
number of those involved continues to grow. Grateful engagement is now engrained in the organizational culture. Physicians and philanthropy teams are developing true partnerships to move healthcare forward in the communities they serve.
In healthcare philanthropy, it is widely touted that most gifts are provided by grateful patients and families. Our sector relies on an abundance of affinity for our organizations, our missions, and the incredible ways innovative, quality healthcare touches our lives. That affinity is almost always rooted in gratitude, an emotion that drives action.
The ways we identify and connect with grateful patients have become more sophisticated, targeted, and strategic through the years. Thanks to the article “Major gift officers: A valuable commodity—are we using them well?” published by the Association for Healthcare Philanthropy’s Fall 2010 journal1, we know the profound effects our physicians have on driving these relationships. The period of cultivation from the donor’s point of view began with their patient experience, making the physician a key part of the continuation of the philanthropic relationship.
Today’s doctors are busier than ever, so how does partnership with philanthropy teams become a priority? In a word: relationships. Philanthropy professionals must treat our physicians just as we would our valued donors and build meaningful relationships over time. As trust is established and values become more aligned, physician partnership will occur. This is not an overnight change. At Baptist Health, the physician and philanthropy team relationships have evolved across a three-year period of intentional engagement.
Where to Start?
Our organizations are filled with many beloved physicians who are known for their clinical expertise or their compassionate bedside manner, making it tempting to seek out physician allies in mass. However, it’s vital to
remain targeted on service lines that best align with your fundraising initiatives. This ensures a deeper appreciation by the physician for why to partner with philanthropy if they have a clear understanding of how the dollars they are helping raise benefit their patients, families, and the work that they do. It also ensures that the philanthropy team has viable projects to talk about with to prospective patient donors surfaced through these efforts. Once the appropriate service line is identified, key partners such as the service line department leaders or executive leaders can help identify potential physician partners.
Once potential partners have been identified, authentic relationship building can begin. Philanthropy teams can learn the physician’s passions, preferences, and aspirations and become a meaningful partner in their work. Deliberate time must be spent prioritizing the relationship as rushing this process may derail any future efforts. The philanthropy team must put forth the same time, focus, and energy in building relationships with physician partners as they would with any traditional major gift prospect.
Passion Projects and Partnership
Many physicians went into their professions because they want to make a difference–to save lives, heal, cure, and treat. That passion does not wane over time and often, continues to fuel them forward. It should be noted that in today, physician burnout is at an all-time high. Many physicians today have burdensome administrative commitments and must spend hours logging information in electronic medical record systems. The COVID-19 pandemic only exasperated physician burnout. Philanthropy has the opportunity to help physicians reignite their passion by partnering with them in a way that is desired by the physician. Over the past decade, the practice of working with physicians to encourage the physician to make introductions of their grateful patients and families to philanthropy officers has become widely utilized.
AHP Healthcare Philanthropy Journal|Spring 2023| 11
Many times, this type of relationship becomes one-sided and does not take into account the unique talents or the wishes of the physician for how they might want to partner with philanthropy. Philanthropy professionals can be creative in helping our physicians demonstrate their passions beyond practice and beyond just making grateful patient referrals, all while raising the profile for philanthropy.
One of the most effective ways to do this is through the creative implementation of physician feature events. By inviting physician partners to share their expertise in small, intimate gathering with prospective grateful patients and families, the philanthropy program is positioned to raise awareness about the impact of the physician’s work and the organization, but also to receive referrals for potential prospect follow up. Most importantly, the physician’s passion is ignited through speaking at these events about how their work is making an impact for their patients and communities served.
Celebrating Gratitude is a Two-Way Street
Centering our work on gratitude is about more than just asking our physicians to identify and refer it, it is imperative that we remind our physician partners of the impact that can be generated through it.
There are varieties of ways to ensure your physician partners receive meaningful stewardship in addition to the grateful patients. Invite your physicians to attend stewardship events with no expectations–let them see their grateful patients and donors in an informal setting where they can get to know one another on a more personal level. This fosters a deeper sense of community while providing an atmosphere for gratitude to be freely expressed. Creative storytelling of the patient experience can create a culture in which gratitude is the conduit to numerous shared, meaningful experiences.
Physicians and philanthropy teams are both working toward shared goals: to make their communities healthier, better places. When working together, the impact that can be achieved is immeasurable.

Baptist Health Foundation Case Study2
In order to prepare for and accelerate success for Baptist Health’s comprehensive $100 million campaign, Baptist Health Foundation partnered with Accordant to develop and implement a comprehensive grateful patient and clinician engagement strategy across eight Baptist Health markets to identify a new pool of prospective grateful patient and family donors.
About Baptist Health | Kentucky & southern Indiana Healthcare
• 9 markets
• 2,770 licensed beds
• 400+ points of care in KY and IN
• 94K inpatients
• 2.1 million outpatients
About Baptist Health Foundation
• 36 FTEs across system office and 9 market foundations
• $25 million raised in FY22
AHP Healthcare Philanthropy Journal|Spring 2023| 12
• System office founded in 2019
Following a rigorous campaign planning process across all markets, Baptist Health Foundation worked with Accordant and market leadership to identify, recruit, and train clinician partners that practice within clinical service lines aligned with campaign funding priorities.
Initial efforts over the six months following clinician training saw some success with the following results:
• 175 leaders, physician, clinician, and nursing partners engaged
• 100+ physicians, clinicians, and nurses trained in gratitude
• 130 1:1 meetings between Baptist Health Philanthropy Officers and physician and clinician partners
• 78 grateful patient referrals
• 10 gifts
Commencing grateful engagement at Baptist Health helped Baptist Health Foundation engage leaders, physicians, and clinicians across the system, align with and support the campaign and begin embedding philanthropy into the culture at Baptist Health. However, several factors provided Baptist Health the opportunity to find deeper success with grateful engagement. COVID-19 made it difficult for Baptist Health market leadership to participate in a meaningful way, which made it difficult to engage some key, influential physician leaders. Some recruited physician partners lost interest due to a lack of a real relationship with their assigned philanthropy officer and lack of true understanding of philanthropy at Baptist Health. Ultimately, Baptist Health Foundation knew that to build true, lasting, mutually beneficial partnerships with physicians and clinicians, an enhanced strategy and approach would be needed.
Building True Partnerships
Several strategies were employed to build deeper grateful engagement clinician partnerships.
Leadership activation | Baptist Health Foundation activated leadership through recruiting Grateful Engagement Executive Sponsors in larger Baptist Health markets to champion grateful engagement and partnered with system service line vice presidents to personally invite key physician leaders to participate through hosting dinners and staying involved until the foundation built strong relationships with the physicians.
Coaching and mentorship for philanthropy officers | Conversation guides, progress report templates, and extensive bi-weekly, 1:1 coaching and support were provided to philanthropy officers managing clinician relationships to help guide their efforts to build true partnerships with service line leaders and clinician partners in their assigned service lines. Philanthropy officers were encouraged to take time to build relationships first with clinician partners before asking for referrals.
Physician feature events | In a switch from solely focusing on receiving grateful patient referrals from clinician partners, philanthropy leaders and officers invited physician partners to share their expertise and experience to small groups of prospective grateful patients and family donors at physician feature events. This highly effective strategy exponentially boosted referrals through physician’s collaborating with the foundation to personally invite their own grateful patients to the events, and the physician’s embraced the opportunity to passionately speak about the impact their work has on the community. This garnered significant interest for philanthropic investment to Baptist Health from many patients and families who had never engaged before.
AHP Healthcare Philanthropy Journal|Spring 2023| 13
The Critical Importance of Strategic Internal Ally Engagement
An internal study examining two years of solicitations from Baptist Health’s highest producing philanthropy officers proved that when allies like board members, C-Suite, or clinicians support the philanthropy officer through introducing the prospect or participating in the cultivation, solicitation, or stewardship of the donor, the solicitation and gift amount of the prospect is exponentially higher than when the philanthropy officer works alone.
This data, coupled with increasingly complex circumstances for navigating hospitals due to COVID-19 and the fact that many Baptist Health Foundation philanthropy officers started their roles working from home during the pandemic, made building important relationships with internal allies challenging for many Baptist Health Foundation philanthropy officers.
This data represents Baptist Health Foundation solicitations that equaled $10,000 or more from six high performing Baptist Health Foundation philanthropy officers between July 1, 2020, through March 1, 2022. Any solicitation where a board member, C-Suite, or clinician ally introduced the prospect to the philanthropy officer and supported the cultivation, solicitation, and/or stewardship of the donor is counted as having ally support.
This study also proved that involving the ally directly in the philanthropic process proves more impactful than receiving the referral alone.
data represents Baptist Health Foundation solicitations equaled $10,000 or more from six high performing Health Foundation philanthropy officers between July through March 1, 2022. Any solicitation where a board member, C-Suite, or clinician ally introduced the prospect to philanthropy officer and supported the cultivation, solicitation, and/or stewardship of the donor is counted as ally support.
AVERAGE GIFT WITH NO REFERRAL OR ALLY SUPPORT $20,029
AVERAGE GIFT WITH A REFERRAL $95,584
AVERAGE GIFT WITH ALLY SUPPORT $143,902
This data represents the average gift for gifts $1,000+ closed by nine high performing Baptist Health philanthropy officers between July 1, 2020, through August 31, 2022.
To encourage philanthropy officers to embrace the strategic engagement of internal allies within the hospital, training and parameters were provided to encourage philanthropy officers to engage internal allies on a formal and informal basis. Philanthropy officers were encouraged to informally engage allies within their assigned service lines on a weekly basis through rounding, attending huddles, and department meetings. Philanthropy officers were encouraged to conduct formal ally engagement on a monthly and quarterly basis with service line leaders and clinician partners through 1:1 interactions and strategy meetings.
General relationship
INFORMAL ALLY ENGAGEMENT
Can be in a group setting 1 per week
Must be strategic/within assigned service lines/ clinical areas
Find a rounding partner/ guide
1:1 engagement
1 touch per month; 1 meeting per quarter
FORMAL ALLY ENGAGEMENT
INFORMAL ALLY ENGAGEMENT
General relationship building
Primary goal is to elicit
Can be in a group setting 1 per week
Approach with a “moves management” mindset donor cultivation
Must be strategic/within assigned service lines/ clinical areas
All activity should “move” the relationship along and elicit action
Find a rounding partner/ guide
1:1 engagement
1 touch per month; 1 meeting per quarter
FORMAL ALLY ENGAGEMENT
Primary goal is to elicit action Approach with a “moves management” mindset in donor cultivation
All activity should “move” the relationship along and elicit action
AHP Healthcare Philanthropy Journal|Spring 2023| 14
SUPPORT FOR SOLICITATIONS $10,000+
ALLY
$20M $25M $15M $10M $5M 0 ALLY SUPPORT $23,722,500 $8,156,500 NON-ALLY SUPPORT
GIVING WITH ALLY SUPPORT $8M $6M $4M $2M 0 FY 2021 $2,548,400 $6,058,765 FY 2022 TOTAL CLINICIAN REFERRALS 160 120 80 40 0 YEAR 1 78 133 YEAR 2
TOTAL
SUPPORT FOR SOLICITATIONS $10,000+
ALLY SUPPORT $23,722,500
NON-ALLY
$8,156,500
SUPPORT
TOTAL GIVING WITH ALLY SUPPORT TOTAL CLINICIAN REFERRALS
General relationship building
Can be in a group setting
1 per week
Must be strategic/within assigned service lines/ clinical areas
Steadfast focus on the engagement of internal allies and involving allies in the philanthropic process proved to be impactful. Total giving with ally support increased from over $2.5 million in FY 2021 to over $6 million in FY 2022.
Find a rounding partner/ guide
INFORMAL ALLY ENGAGEMENT
1 per week
Must be strategic/within assigned service clinical areas
Overall, through advancing grateful engagement at Baptist Health, giving from grateful patients and families increased exponentially by 1,160% at Baptist Health from $188,250 in FY 2021 to $2,375,211 in FY 2022.
Lessons Learned
Find a rounding guide
1:1 engagement
1 touch per month; 1 meeting per quarter
1:1 engagement
1 touch per month;
1 meeting per quarter
Primary goal is to elicit action
Approach with a “moves management” mindset in donor cultivation
All activity should “move” the relationship along and elicit action
Clinician referrals increased 70% from 78 in year one to 133 in year two.
This data represents Baptist Health Foundation solicitations that equaled $10,000 or more from six high performing Baptist Health Foundation philanthropy officers between July 1, 2020, through March 1, 2022. Any solicitation where a board member, C-Suite, or clinician ally introduced the prospect to the philanthropy officer and supported the cultivation, solicitation, and/or stewardship of the donor is counted as having ally support. TOTAL
Active leadership participation
FORMAL ALLY ENGAGEMENT
Verbal support from leadership is not enough. The active participation of leadership in inviting physician and clinician partners must occur to encourage clinician partners to meaningfully participate.
Primary goal is to Approach with a management” mindset donor cultivation
All activity should the relationship and elicit action
Relationships come first
Relationships must be built with clinician partners first before ever asking for a referral to build true partnerships.
Find the physician’s passion
There are many ways for clinician partners to engage with the foundation beyond just making referrals. Asking the physician to speak on behalf of the foundation about their work, knowledge, and experiences can ignite the physician’s passion for partnering with the foundation.
Focusing on internal Ally Engagement is a must
Do not assume that philanthropy officers who started with the organization during the COVID-19 pandemic know the importance of or know how to navigate the hospital to build important internal relationships. Ample training, guidance, and parameters are needed to help support philanthropy officers in building relationships with strategic internal partners to strengthen the philanthropic process.
When an organization prioritizes building relationships first with physician partners and sees value in the partnership beyond asking for grateful patient and family referrals, transformational culture change occurs that results in more dollars raised. Doing this at Baptist Health has transformed the way that
AHP Healthcare Philanthropy Journal|Spring 2023| 15
ENGAGEMENT 1, 2020, through March 1, 2022. Any solicitation where a
TOTAL GIVING WITH ALLY SUPPORT $8M $6M $4M $2M 0 FY 2021 $2,548,400 $6,058,765 FY 2022
$2M $2.5M $1.5M $1M $500,000 0 FY 2021 $188,250 $2,375,711 FY 2022 TOTAL CLINICIAN REFERRALS 160 120 80 40 0 YEAR 1 78 133 YEAR 2 management” mindset donor cultivation
board member,
C-Suite, or clinician ally introduced the prospect to the philanthropy officer and supported the cultivation, solicitation, and/or stewardship of the donor is counted as having ally support.
TOTAL GIVING FROM GRATEFUL PATIENTS
“move”
ENGAGEMENT FORMAL ALLY ENGAGEMENT TOTAL CLINICIAN REFERRALS 160 120 80 40 0 YEAR 1 78 133 YEAR 2
All activity should
the relationship along and elicit action INFORMAL ALLY
$25M $15M $10M $5M 0 ALLY SUPPORT
SUPPORT
$20M
$23,722,500 $8,156,500 NON-ALLY
GIVING WITH ALLY SUPPORT $8M $6M $4M $2M 0 FY 2021 $2,548,400 $6,058,765 FY 2022 TOTAL GIVING FROM GRATEFUL PATIENTS $2M $2.5M $1.5M $1M $500,000 0 FY 2021 $188,250 $2,375,711 FY 2022 TOTAL CLINICIAN REFERRALS 160 120 80 40 0 YEAR 1 78 133 YEAR
physicians participate in the philanthropy process, resulting in elevated status of the foundation across the system and in the communities we serve, and has exponentially increased the number of patients and families the foundation has been able to engage to support our mission of expanding healthcare in our communities.
Lora Croley, MBA, CFRE Lora serves as the System Director of Donor Relations for Baptist Health system in Kentucky and southern Indiana. She leads annual giving, communications, stewardship, and grateful patient engagement strategies for the ninehospital system philanthropy program.
In recent years, Lora has demonstrated success in leading annual and major gift programs as well as capital campaign efforts in healthcare philanthropy. With nearly 20 years of healthcare experience, she specializes in developing and executing strategic initiatives that focus on building market awareness and acquiring philanthropic support.
Erin Stitzel, FAHP, CFRE
Endnotes
1 https://www.ahp.org/docs/default-source/ resource-center/healthcare-philanthropy-journal/fall2010ahpjournalfinal.pdf?sfvrsn=15960673_2
2 https://www.accordanthealth.com/post/ beyond-the-referral-developing-true-partnerships-with-physicians-at-baptist-healtha-case-study
Erin is a leader in creating and implementing grateful patient and clinician partnership strategies. She has worked in over 65 hospitals across the United States, Canada, and the United Kingdom to implement comprehensive grateful patient engagement and clinician partnership strategies including partnering with hundreds of physicians, clinicians, and nurses in philanthropy. She has a proven track record of success in helping organizations substantially increase giving from grateful patients and families and building robust, service-line based clinician partnerships to increase grateful patient referrals. Erin is a Fellow of the Association for Healthcare Philanthropy (FAHP), the highest level of certification that can be obtained in healthcare philanthropy and a member of the Association for Healthcare Philanthropy’s inaugural 40 Under 40 class. She is a frequent speaker at local and international healthcare philanthropy conferences and webinars and has published numerous papers on grateful patient engagement and clinician partnership strategies, including being published by the American Hospital Association, the Association for Healthcare Philanthropy, and Blackbaud.
AHP Healthcare Philanthropy Journal|Spring 2023| 16
Is Conventional Wisdom Still Holding Fundraising Hostage?
By Steven A. Reed, Chairman and Chief Executive Officer of Marketing Partners, Inc.
Consider the state of healthcare philanthropy today.
Most fundraising shops are structured and managed the same way they were two or three decades ago. The typical modality mix is the same. Advances like KPI metrics are mostly measuring the same old ways of thinking and doing.
There’s still a distance—maybe more so— between donors and the organizations they support. Annual campaign retention rates are still abysmal. Few major donors (who aren’t board members) are truly engaged with either the fundraising effort, or the organization itself.
The 2021 “Tipping Point” study commissioned by the Blackbaud Institute noted the speed at which the fundraising environment has been changing but also noted little change in how
fundraising is conducted 1 The report, based on surveys of 1,168 professionals at nonprofit organizations and 1,024 donors, pointed out that the fundraising models still widely used today were created by and for the generation that preceded the Baby Boomers.
It is amazing how little fundraising has changed. Is it possible conventional wisdom is holding fundraising hostage?
Total giving has been stuck at 2% of GDP for decades. In June of 2022, Giving USA reported total charitable giving, while increased in current dollars over 2020, remained flat (-0.7%) in 2021 after adjusting for inflation.2 One month later, the July 2022 Chronicle of Philanthropy cover story—titled The Giving Crisis—said fundraising can bring Americans back to charity, but only if fundraising changes (italics mine).3 Fewer than half of American households are giving—a big
AHP Healthcare Philanthropy Journal|Spring 2023| 17
contrast to the two-thirds who made donations in the early 2000s. Annual campaigns and events are diminishing in both real dollars, and as a percentage of funds raised.
Generational differences, broad societal changes, and long-term deficiencies in fundraising practice are all part of the problem. Indications are today’s donors are less engaged, which decreases their likelihood of giving again. This creates a revolving door of donors that must be constantly replenished. The traditional emphasis on transactional fundraising modalities depersonalizes giving, letting the chase for dollars dominate relationships with donors.
The Blackbaud report highlighted a conclusion: “For nonprofits, this moment may be remembered as the time when conventional wisdom came crashing down—a conventional wisdom based in part on oversights and risk aversion, and a refusal to really believe that tomorrow is not going to look like yesterday.”4
The “truths” cited in fundraising practice, training, and education need to be challenged.
Hope is still not a strategy. We suggest radical change to achieve three goals:
• Engaged Fundraisers working within structures and policies that give people the maximum freedom to excel;
• Engaged Donors welcomed as full participants in the mission and endeavor; and
• Engaged Partners who understand the potential of philanthropy, invest in it, and personally participate as integral parts of the process.
Engaging Fundraisers
In Gallup’s November 2022 employee engagement survey, the Q12®, which measures employees’ perspectives on the most crucial elements of workplace culture, only about a
third of employees strongly agreed with the statement: “I have the opportunity to do what I do best every day.”5
Gary Hamel, in his 2020 book, Humanocracy, argues that organizations burden themselves with what is, in essence, a tax on human effort.6 His book and Frederic Laloux’s earlier (2014) book, Reinventing Organizations, advocate a radical leap to a whole different set of management principles and practices.7 Both cite success stories that have inspired thousands of organizations throughout the world.
This isn’t about motivating employees. That’s a manipulative fallacy. From Douglas McGregor’s The Human Side of Enterprise 8 to Dan Pink’s Drive9, the formula for engagement hasn’t changed in sixty years: purpose, autonomy, collegiality, and an opportunity to gain experience. Unfortunately, as Hamel notes, engagement levels haven’t changed much either. “It seems that every generation rediscovers the essential elements of human engagement and then does nothing,” he says.10
How do you think you or your fundraisers would feel at work if…
• They had the tools and the right to track and manage their own performance?
• They were allowed, without career or compensation penalty, to focus on what they love to do and do best?
• They felt trusted to make decisions using their best judgment?
• They were primarily accountable to their metrics and coworkers rather than a boss?
• They were encouraged to grow their skills and take on new challenges?
• They never felt encumbered by pointless rules and red tape?
• Their influence and compensation depended on their abilities and impact, not their rank?
AHP Healthcare Philanthropy Journal|Spring 2023| 18
Do you think you would enjoy a significant increase in fundraising production?
Engaging Donors
Consider a meta-finding from the Blackbaud institute study: Many organizations appear to be out of touch with the attitudes of their donors … donors are rarely asked their opinions and feelings. “That is increasingly risky given the speed at which the fundraising environment has been changing,” notes the report.11
According to the latest Fundraising Effectiveness Project report (Q3 2022), fewer than one-in-five new donors give again after their first gift.12 Year-over-year, the number of newly acquired donors is down by 19.2%. And retention of those new donors is down by 24.7%. Overall donor count decreases are driven by weaker acquisition rates as well as less retention of new donors. And the retention rate of even those repeat donors categorized as “loyal” is falling.
How loyal do you think your donors would be if…
• They didn’t receive communications from you only when you were asking for money?
• They realized you know why and in what ways they prefer to give?
• They were asked for their opinions and their answers mattered?
• They felt your organization was accountable because you shared performance metrics with them?
• They were encouraged to ask questions and even challenge pending decisions?
• They truly felt they were part of a real community?
• They understood in depth the impact of the work they made possible?
• Investment-level donors were welcomed to the organization’s strategy table, were asked for their opinions, and their answers mattered?
Do you think you would enjoy a significant increase in fundraising production?
Engaging Partners
Partnerships with executives, program leaders, physicians, other clinicians, and established donors are vital ways to connect with and engage potential major donors. But more fundamentally important are those internal partnerships with senior leaders that lead to an organization-wide culture for philanthropy.
Much has been written about the need for a “culture of philanthropy.” This has sparked many an employee giving campaign in hopes that employee giving will somehow orient the organization as a whole towards involvement and support for the fundraising operation.
What’s really needed is not a culture of philanthropy but a culture for philanthropy. What’s too-often missing in healthcare is an understanding of the investment and the freedom needed to achieve the potential for philanthropy. (Unfortunately, past performance is usually considered predictive.)
What would fundraising be like if …
AHP Healthcare Philanthropy Journal|Spring 2023| 19
• You had the financial, human, and organizational resources and freedoms to break the “glass ceiling” between you and your fundraising potential?
• Internal partners shared accountability for fundraising performance metrics with you?
• You were allowed complete freedom to use internal services or to contract for external capabilities as best met fundraising’s unique needs?
• You could organize your work and your team in a structure that meets fundraising’s unique needs without forcing people into the boxes mandated by formal hierarchy and HR policies?
• Your periodic and annual financial reports were cast as comprehensive accrual-based operating statements? And cost-perdollar-raised was replaced with net margin and return-on-investment as financial accountabilities?
• Your annual budget was an update of an evergreen three-year rolling proforma forecast where investment and production were immutably linked?
Do you think you would enjoy a significant increase in fundraising production?
Focus on Engagement
The above are three distinct areas of opportunity, each with its own mix of strategic and tactical elements. What they have in common is a need for an intertwined and different way of thinking about fundraising at both the frontline and organizational levels.
The challenge is to harness the power of engagement—not just donor engagement (as vital as that is), but full engagement of all of the players in the process.
Minimize Hierarchy
Formal hierarchies assume a need for somebody other than the worker to manage the work. This is so pervasive it is rarely questioned. The solution to every problem is “put someone in charge.” This pushes decision-making up, disempowering and disengaging the people who do the work. And, to make it worse, the root of the problem usually is an absence of clear specifications and expectations for the work, compounded by no leading metrics to objectively measure progress. (There is little if anything of value that cannot be objectively measured.)
The solution is to make day-to-day management unnecessary through quantitative feedback along with process-based coaching to facilitate self-management. This alleviates the span-ofcontrol issue that was the impetus for the tiered management structure that dates back to the Roman legions.
Catalyze Culture Change
Streamlining your organizational structure can be a powerful catalyst for the organizational engagement that drives performance improvement. Minimizing hierarchy and silos is a powerful catalyst for organizational engagement because frontline and operations employees alike benefit from a structure that describes and quantifies success while providing the means and feedback to empower the people who do the work.
But ongoing culture change will derail fundraising performance. Do it once. Do it right with a critical path model, no silos and real-time leading-metric performance feedback.
Invest in the Frontline
One of the ways you can raise more money is by achieving a 75% direct staffing ratio that will keep more of your salary budget, and your best fundraisers, on or directly supporting the front line. (Management functions do not meet the definition of direct support.) One of the key benefits of such a radical reorganization
AHP Healthcare Philanthropy Journal|Spring 2023| 20
is significant reduction of the amount of time and expense associated with supervision, management, and bureaucracy. You put more resources into direct fundraising work and less into indirect activities. Michael Porter, the Harvard Business School strategy guru, rightly points out the real essence of strategy is what you decide not to do.13
Elevate Philanthropy Within the Organization
The definition of a culture for philanthropy within an organization is a top leadership commitment to, and top-to-bottom understanding of, the importance of philanthropy to the organization’s mission. For that to happen, the organization needs to understand the nature of support and amount of investment required to achieve its fundraising potential. This requires an ongoing C-suite effort—and sometimes crucial conversations—by the CDO.
The organization’s leadership needs to make investments of both time and money— which requires them to have confidence in the fundraising team’s ability to make those investments worthwhile. This means applying the same kind of attention and professional relationship management internally as to the development of external relationships. You don’t need a separate critical path model to do this. Just have your frontline relate to internal partners with the same model and intensity as with major donors.
Embrace Donors and Partners Alike
Investment-level donors today are thinking more like investors and favor those organizations willing to treat them as such. Hospital executives, physicians, clinical managers, and other internal partners are more likely to make fundraising part of their responsibilities if they are not relegated to programs that train and treat them simply as referral sources. Today’s healthcare philanthropy frontline needs both an external and internal focus.
Savvy fundraisers today understand that the nature of giving is changing and one of the major changes is that support is shifting away from the organization itself, to the mission of the organization. This is subtle but significant.
That shift is a reflection of societal change toward lower trust levels of institutions in general. Larger donors often are interested in making significant philanthropic investments not to support the organization, but to effect what they perceive as positive change to enhance mission achievement.
As one example, Design Forums—structured and professionally facilitated ideation sessions— can be a powerful donor engagement tool to bring key executives, clinicians, board members, and potential major donors together. The role of fundraising as a conduit to valuable input of external expertise into the management and strategic direction of the organization—as well as a source of capital and operational support—is becoming increasingly important.
Tools like this can bring the “voice of the customer” to the organization, as well as significant operating and capital support through subsequently successful major gift solicitations.14
A Huge Opportunity
Over 20 years of process improvement work in fundraising have led us to two key observations:
1. Many healthcare fundraising organizations are overstaffed relative to the amount of money they are raising; but,
2. Most are understaffed relative to their fundraising potential.
Given the resources and freedom to do so, most healthcare fundraising shops could dramatically increase revenue, typically at least doubling production. But to do so, organizations will
AHP Healthcare Philanthropy Journal|Spring 2023| 21
need to change the way they raise money, with emphasis on personalized individual giving strategies. Fundraisers need to adopt tools, processes, and technology that create highperformance development organizations. And—most important—we need to challenge the ways we think about, talk about, lead, and manage fundraising.
Steve Reed is chairman of Engaged Donors , a Marketing Partners, Inc. company focused solely on fundraising performance improvement. He also is a partner in Engaged Donors Canada. He has authored several articles for Healthcare Philanthropy since “Hope is Not a Strategy,” his 2012 first appearance in this publication. Reed spent the early years of his career working in the for-profit marketing and market research arena. He later became active in healthcare business development, fundraising and performance improvement. Along the way he combined the latter two to focus on improvements in the philanthropy sector. He may be reached at sareed@ mpicompanies.com.
Endnotes
1 Blackbaud Institute and Edge Research, “Tipping Point: Aligning with Supporters in a Changing World,” (Report released November 2, 2021).
2 Indiana University Lilly Family School of Philanthropy at IUPUI., “Giving USA 2022: The Annual Report on Philanthropy for the Year 2021,” Giving USA Foundation, (June 21, 2022).
3 Drew Lindsay, “How Fundraising Can Help Reignite Giving in America — if It Changes,” The Chronicle of Philanthropy, Volume 34, Issue 9 (July 2022).
4 Blackbaud, “Tipping Point.”
5 https://www.gallup.com/394373/indicator-employee-engagement.aspx
6 Gary Hamel, Michele Zanini, et al., Humanocracy: Creating Organizations as Amazing as the People Inside Them, Harvard Business Review Press, Boston (2020).
7 Frederic Laloux, Reinventing Organizations: A Guide to Creating Organizations Inspired by the Next Stage of Human Consciousness, Nelson Parker, Brussels (2014).
8 Douglas McGregor, The Human Side of Enterprise, McGraw-Hill (1960).
9 Danial H, Pink, Drive: The Surprising Truth About What Motivates Us, Canongate Books (2011).
10 Hamel, Humanocracy
11 Blackbaud, “Tipping Point.”
12 AFP Foundation Fundraising Effectiveness Project, https://afpglobal.org/FundraisingEffectivenessProject
13 Joan Magretta, Understanding Michael Porter: The Essential Guide to Competition and Strategy, Harvard Business Review Press, Boston (2012).
14 For more on Voice of the Customer, see https://onlinelibrary.wiley.com/doi/10.1002/9781444316568.wiem05020
AHP Healthcare Philanthropy Journal|Spring 2023| 22
Community Health and Well-Being:
Is it Healthcare Organization’s Lane?
And, if so, can Healthcare Philanthropy Make the Case for Support?
By Amy Dorrill, FAHP, Community Health and Well-Being Practice Lead and Principal Consultant at Accordant
It has been a common topic of discussion. Whose lane is community health and well-being? And, more specifically, should community health and well-being actually be a healthcare organization’s lane?
For many, these questions prompt a visual–a picture of a pool, possibly an Olympic-sized pool with rows of swimming lanes. The pool lanes are divided neatly by racing lanes with all swimmers starting, swimming, and ending in “their lanes,” with no crossover of swimmers interfering with the path of other swimmers. Each lane is well defined, and each swimmer engages independently.

In reality, addressing community health and wellbeing is less like siloed lanes in a pool and more similar to a vast ocean, an ecosystem made up of
many organisms including fish, plants, and coral along with factors such as weather and pollution that are deeply interconnected. Each “wave” impacts another, and each organism depends on others.
Community health–and a person’s health–is influenced by many factors including social, economic, and environmental. Negative health is attributed to multidimensional factors from the location of someone’s home, access to quality healthcare, access to healthy food, housing, transportation, and more throughout the lifetime of a person. To address community health, communities must operate within an ecosystem, engaging a holistic and inclusive solution. It will take policy, environmental changes, removal of existing barriers, equitable treatment, and more to move the needle. Who is best to lead this charge?
AHP Healthcare Philanthropy Journal|Spring 2023| 23
It is very rare for one organization to tackle this alone. For something this complex, it takes many organizations coming together. Community health requires representation from many aspects such as healthcare and public health, housing, transportation, government agencies (including parks and recreation), faith-based organizations, education (early childhood, primary, secondary, and colleges/universities), financial institutions, food banks, restaurants, and more. Additionally, civic organizations, trade agencies, community foundations, and other philanthropic agencies and even the media must be involved. Health equity, community health, and overall well-being must look beyond singular interventions to long-term, more systemic changes. It is multi-sectoral and demands multilevel collaborations with diverse approaches.
Expertise and resources are needed to identify the most important need(s) of the community, establish data collection systems to gauge a baseline and track progress, select the right strategies, execute on each strategy, fund each step, maintain marketing, and report out to provide transparency and accountability. It is a lot, and it is challenging; but it is not impossible.
Why are healthcare organizations stepping into this role? Healthcare organizations are seen by many as a significant contributor to address community health. Many even see healthcare organizations serving as the anchor institution of the community and the most logical to lead this charge. However, the healthcare industry is always shifting. Whether the future will deliver the exact value-based, population health fee structure that is presently on the table or will morph into something different, it is apparent a new healthcare model will continue to evolve. Why? First and foremost, the existing healthcare model is failing. The US continues to underperform other high-income countries on measures of healthcare outcomes, access to care, equity, and administrative efficiency even though it outspends other nations on healthcare by almost double.1 Based on this, it
has become apparent our nation’s current model is ineffective.
Beyond the ongoing need to deliver better healthcare outcomes, the financial landscape and the shift in consumer expectations for a more holistic experience is forcing healthcare organizations to continually move beyond their walls for care. They must provide care and services that focus more on social determinants of health and prevention instead of the current methods of treating illness.
Let’s consider factors that place healthcare organizations as the most likely leaders in community health and well-being initiatives:
1. One of the largest employers: Hospitals are generally one of the largest employers in a community. This provides a general strength in numbers as well as having the ability to impact health equity through hiring and purchasing goods and services from local businesses.
2. Financial resources: Many healthcare organizations have one of the largest operating budgets in a community.
3. Data collection: Hospitals are already identifying health needs through a community health needs assessment (CHNA), a regulatory requirement of nonprofit hospitals participating in Medicare.
4. Expertise: Hospital physicians, nurses, and other clinicians have a history of providing preventative and curative care to patients and the community.
5. History of community outreach: Most hospitals have spent decades serving the community with a focus of promoting healthy behaviors and disease prevention through health fairs, health screenings, mobile clinics, and more.
AHP Healthcare Philanthropy Journal|Spring 2023| 24
6. Existing community partnerships: As of 2018, 74% of hospitals have entered into at least one type of community partnership.2
7. Mission-aligned: Hospitals’ mission statements are trending to more inclusive statements beyond just patient population. Four of the 2022 U.S. News & World Report top ten hospitals in the United States extend beyond patients.3 One example is New YorkPresbyterian Hospital, whose mission is, “It must be known, owned, and energized by all.” The New York-Presbyterian Westchester mission is, “To provide caring, high quality, fiscally responsible healthcare services that meet the needs and expectations of the communities we serve.”
8. Government regulations: The Affordable Care Act (ACA) expanded the responsibilities of healthcare organizations beyond clinical care to address the upstream social determinants of health.4
9. Financial pressure: Five percent of the population accounts for 50% of a healthcare organization’s total expenditures. Preventing diseases by addressing social determinants can reduce the cost of delivering more costly emergency care and hospitalizations for chronic diseases.5
These are all valid reasons for health organizations to take the lead role in community health and well-being; however, let’s remember hospitals and other care agencies cannot tackle it alone. The mere fact cutting healthcare costs through prevention and well-being could help health organizations with prevalently negative margins experienced since the pandemic. Investing in the creation of well-being initiatives could not only help reduce and even prevent high-cost treatment within their walls but also enhance the quality of life across communities they serve.
Community health is not healthcare’s lane to claim alone, but it does have an essential part to
play with much engagement, involvement, and commitment. Health organizations can claim a leading role in these initiatives and invest in care outside of their walls that can result in a favorable return on investment. But, this is not just a numbers game. It’s the game of life, health, quality, and care. It’s time to get started.
So, if we can agree that it makes sense for health organizations to take a lead—or the lane—in community health and well-being, then consider the next question…is community health and well-being worthy of being a philanthropic case for support for healthcare foundations.
Determining if community health and wellbeing is the right philanthropic case for support for a healthcare foundation starts by asking three questions:
1. Is the proposed community health focus a strategic priority of the organization?
2. Is the organization positioned to lead the community health initiative?
3. Is the community health case aligned with donor interest?
Is the proposed community health focus a strategic priority of the organization?
Financial pressures, along with the desire to meet patient expectations and deliver better health outcomes, are moving healthcare organizations beyond their facilities to identify risks and provide preventive care and strategies. Government regulations and new payment models are supporting these new models. In fact, addressing health disparities and improving health equity is the top priority identified by Deloitte in a 2021 survey Deloitte Center for Health Solutions Survey of CEOs on health equity.6 It is time to provide not only health fairs, mobile units, and onsite pop-up health clinics but also to identify and address the social determinants of health underlining the health issues presented at the hospital. Of
AHP Healthcare Philanthropy Journal|Spring 2023| 25
reporting hospitals, 84.2% screen their patients for the social determinants of health (SDOH), and 72% of hospitals report having at least one program or strategy to address the identified SDOH.7 As hospitals lead the community health charge, these numbers will continue to increase.
Is the organization positioned to lead the community health initiative?
The case must be made that your particular organization is one of the best organizations to execute the chosen strategies. Does the organization have the ability to execute and accomplish the community health goals? Does the community have trust and faith in the organization’s role to advance the chosen case? What resources and partnerships are available to help?
Is the community health case aligned with donor interest?

Funding is by far the limiting factor to advance community health. There is a substantial need for philanthropy in this space. In a survey
conducted by ReThink Health, 82% state that, “Not enough funding for our services, programs, or policies,” is a barrier contributing to equitable community well-being. The next largest barrier was, “Short-term results matter more than longterm gains,” at 27%, which in itself has a financial implication.8
Philanthropy can be used to leverage a healthcare organization’s community health and well-being initiatives by simply providing seed funding–allowing the initiative to be ignited by philanthropy prior to becoming financially sustainable, while testing new and innovative opportunities with the ability to become a best practice model.
Even if an organization “needs” money, it doesn’t make it the ideal case for philanthropic support. Parking lots, replacement of machinery, and advancement of technology are all very important to the patient experience, but they are not usually the best cases for philanthropic support. The question comes down to is the community health case aligned with donor interest.
AHP Healthcare Philanthropy Journal|Spring 2023| 26
Many healthcare foundations have begun the journey beyond typical capital investments as they discover donors have the passion and capability to make positive impact in their communities beyond buildings and other projects. Community health has become increasingly more appealing and understandable to donors, especially after COVID-19. In fact, it has likely been a donor passion; however, there has often been little or no opportunity, or even request, for donors to consider gifts specific to the areas of well-being.
The fear has been that healthcare donors will not support non-traditional, non-capital community health initiatives. On the surface, it would appear that historical data would justify those fears. The 2022 Association of Healthcare Philanthropy Report on Giving Survey 9 identified the top three healthcare areas supported by philanthropy were: 55% other programs, 31% capital, 5% grants to outside organizations, 5% education, 3% charity care/patient assistance, and 1% employee relief/caregiver assistance. In 2019, the same AHP survey broke down the gifts in more specific categories with the top three listed as 20.5% construction and renovation, 19.6% patient care program support, and capital equipment at 14.6%, while community aligned initiatives represented a much smaller portion such as community support/advocacy at only 4.2%.10 The reality is that many healthcare organizations are not asking donors to support community health initiatives. While donors ultimately drive where their gift is allocated, donors do not usually give to projects not presented to them. Sixty-three percent of Fidelity Charitable donors designated their gifts to the highest need, following the direction of the trusted organizations.11
The sector with the second largest increase in philanthropic support in 2021 was publicsociety benefit with an increase of 23.5% equaling $55.85 billion. (Public-society benefit includes community improvement, civil rights and liberties, etc.)12 The same year, the health
sector experienced an increase in 2022 by 7.7% after experiencing a reduction the previous year. While some nonprofit organizations have experienced a reduction in philanthropic support, other nonprofits saw a rise especially in social services/community-based initiatives. For example, Feeding America received 47% increase in charitable gifts taking over the top charity rankings by Forbes. Another dozen food banks moved into Forbes top 100 nonprofit list. Philanthropists saw the need and the impact making an upstream investment could have on more major, downstream issues such as a chronic disease.13
Corporations are increasingly focused on social/community impact as part of their Environmental, Social, and Governance (ESG) obligation. Corporations are moving further away from marketing/branding relationships with nonprofits as a golf or gala sponsor and more as a partner in addressing community health disparities. Seventy-eight percent believe it is no longer acceptable for companies to just make money. Corporations are defining their purpose and alignment to community impact to appease their stakeholders: employees, consumers, and investors.14 Community improvement and capacity building was ranked #6 for top causes receiving corporate grants in 2021.15
The question is not, “Are philanthropists giving to community health/well-being,” but “Where are philanthropists making gifts to advance community health?”
Now is the time to connect philanthropists with healthcare organizations that are leading the way to advance community health and well-being. Philanthropy officers specialize in connecting healthcare organization priorities with donors who have a passion for making transformational change. What better way for donors to make a wide-spread, positive impact than through identifying, addressing, and caring for the health needs of the community?
AHP Healthcare Philanthropy Journal|Spring 2023| 27
Getting Started
Philanthropy teams can start the process by expanding engagements and inquiries with current and potential donors. Ask broad, inclusive questions focused beyond the organization to identify what each donor cares about. Ask what other organizations they support and why (to determine passion, purpose, and intentions). Once well-being or other community health issues are surfaced, present the case in simple terms, sharing why healthcare organizations are adding community health, health equity, and well-being on top of core service lines. Connect the strategy with a familiar scope. For example, how does insufficient housing impact asthma? How will a positive change in housing have a positive change in asthma? How can their gift in this area impact the well-being of their communities and reduce the repeat patients visiting the emergency room with recurring asthma problems? Are they interested in talking with other organizations and partners who have joined in this effort?
While this is just a start to identifying and engaging donors, it IS the place to start. Including donors in the organization’s goals, mission, and impact can result in a long-time donor and partner in community health.
Health organizations are primed to take the lead role in community health and wellbeing. Healthcare philanthropy is primed to be a major funding source when community priorities are aligned with the healthcare organization’s priorities and the donor passion. The foundation’s philanthropic mission is to help support the parent organization while meeting the needs of its constituents. Therefore, foundations are increasingly pivoting to adjust their case for philanthropic support to align with new organizational priorities such as community health/health equity/well-being. The benefits are numerous. Investing in the creation of well-being initiatives could not only help reduce and even prevent high-cost treatment within the hospital walls but also enhance the quality of life for the
communities they serve. Involving philanthropy–engaging and cultivating donors who want to advance and elevate the overall health of the people around them–is an ideal way to help fund a long-underserved need.
Amy Dorrill has 25+ years of front-line, leadership, and consulting experience at rural, community, system, and academic healthcare organizations. Her expertise includes securing community health and well-being (along with more traditional capital and clinical specialty care programming) philanthropic and strategic partnerships, leveraging governing and foundation board leadership, assessing and elevating philanthropy programs, working with organizations to identify the right strategic priority that aligns with philanthropic interest, and designing a case for support that inspires and engages philanthropic partners (grateful patients, community members, corporations, etc.)
Amy is the Community Health and WellBeing Practice Leader for Accordant, a consulting firm solely dedicated to healthcare. Accordant elevates health and well-being through philanthropy and partnership. Accordant delivers value in three key areas: elevating charitable giving, forging partnerships to promote healthy communities, and strengthening healthcare governance. Amy has previously served as Adventist Health’s Philanthropy Executive for Well Being, Blue Zones Project Philanthropy Executive, and has held other leadership positions at Emory University’s Nell Hodgson Woodruff School of Nursing and University Health Care System. Amy is a Fellow of Association of Healthcare Professionals (FAHP), and she holds a masters degree from the University of Georgia.
AHP Healthcare Philanthropy Journal|Spring 2023| 28
Endnotes
1 Commonwealth Fund, August 201
2 American Hospital Association, 2018.
3 US News, July 26, 2022.
4 New York Presbyterian, 2023.
5 JAMA Network Open, 2018.
6 Deloitte Center for Health Solutions Survey, 2021.
7 American Hospital Association Annual Survey 2021.
8 Rippel Foundation, 2022.
9 Association of Healthcare Philanthropy Report on Giving Survey, 2022.
10 Association of Healthcare Philanthropy Report on Giving Survey, 2019.
11 Fidelity, 2023.
12 Giving USA, 2023.
13 Forbes, 2022.
14 Cone/Porter Novelli Purpose study, 2018.
15 National Center for Charitable Statistics, 2021.
AHP Healthcare Philanthropy Journal|Spring 2023| 29
The Moment I Realized I was a Terrible Leader and What Happened Next
By Adam P. Blanchard, MS, CFRE, Director of Donor Engagement at Dayton Children’s
In today’s world, a solid reputation seems to be in short supply. From those who are caught up in controversy, either by their own doing or as a victim of circumstance, to others who are getting “canceled” for any number of reasons that play out in the court of public opinion.
The reality is people who are highly visible and who have some degree of authority, including leaders at all levels, are regularly scrutinized. It’s no wonder there’s an absence of authenticity from those in positions of influence, as often, the ones who are willing to allow space for
FROM STAGE TO PAGE:
This article was adapted from a live presentation given at AHP’s International Conference in October 2022.
vulnerability and transparency are subject to criticism and blame.
The result is leaders who shut themselves off from the humanity of their job and focus strictly on the production, not the people. I used to believe this was normal; after all, the research

AHP Healthcare Philanthropy Journal|Spring 2023| 31
Hospital Foundation
supports it. “For many years leaders of all respects have embraced that sentiment, doing everything they could to come more across as powerful, strong, and flawless.”1
When you’re brought up as a leader in a certain way, recognizing how things are done, it becomes easy to go overboard on the bravado and fall into an imposter syndrome, holding relationships at arm’s length.
It’s taken a while, but I feel like I’m finally moving in the right direction, and I’m not alone. In their January 2023 Harvard Business Review article, Li Jiang, Maryam Kouchaki, and Leslie K. John noted that “recent research has found that effective leadership isn’t about always being perfect, but about being genuine.”2
Learning I Was a Terrible Leader
With that in mind, I’d like to share my story... it’s about the day I learned I was a terrible leader and what’s happened since. It’s a tale of relationships made, relationships damaged, and relationships recovered. It’s a snapshot of my leadership journey so far.
Hopefully you’ll leave having read this with some nugget or a new a-ha. Or perhaps, you’ll even become a bit more confident in your own leadership practice. But before we dive in, let me provide a little background.
I’m a husband, father, son, brother, and child of God. I’m also the Director of Donor Engagement at Dayton Children’s Hospital Foundation in Ohio. I’m a two-time college graduate, earning my bachelor’s degree at the University of Cincinnati, and then my masters at St. Joseph’s University in Philly. I’m an unapologetic Cincinnati Bengals fan—long before they were good! And I’ve been in the same fantasy football league for over a decade, winning it just once.
I serve on boards and committees, have earned my CFRE, presented at conferences, and was previously published in this very journal. I’ve
helped drive significant philanthropy during my career for some incredible organizations.
But at face value, none of this really matters.
You see, the good things in life, the positive outcomes, only come from the strength of our relationships and how we maintain them. We know this as leaders, but sometimes we can become defensive or distracted, and lose our way. We’re all trying to navigate a challenging and ever-changing world; I hope my experience can provide some perspective.
Allow me to set the scene. The annual giving team had been four people; the previous director left the role abruptly after nine years and another manager resigned shortly thereafter to be a stay-at-home mom. What remained was a junior staff member who was still relatively new, a longtime volunteer auxiliary liaison, and me. In this moment of relative desperation, it was the first time I recognized that our greatest resource as fundraising leaders is the human resource. More on that later!
Once I was in the position, I immediately began to think about how to assemble the team. I reimagined what our purpose and goals should be and what types of roles and people should play a part. Within six months, we had backfilled a critical program manager role, hired a brandnew digital fundraising specialist, and promoted another member from the major giving team to our staff to work in donor engagement.
Everything seemed to really start clicking from where I sat. But as I would soon learn, I had some blind spots…three years of blind spots!
Fast forward to early 2020 and I felt like I was on top of the world. We were hitting our metrics, performance evaluations were solid, and we were growing. I was cruising, but at the same time, becoming somewhat of a box-checker–we were working hard, but I was operating with blinders.
AHP Healthcare Philanthropy Journal|Spring 2023| 32
People were successful, but not necessarily happy. And it took a complete shock to my system to wake up and understand what was really happening around me.
Have you ever had a time when you realize something is obvious to everyone except you? Yeah, me too. I had thought things were just fine, but others felt different. And when the opportunity came for our staff to share anonymous feedback through a 360-degree evaluation, this fact became painfully clear.
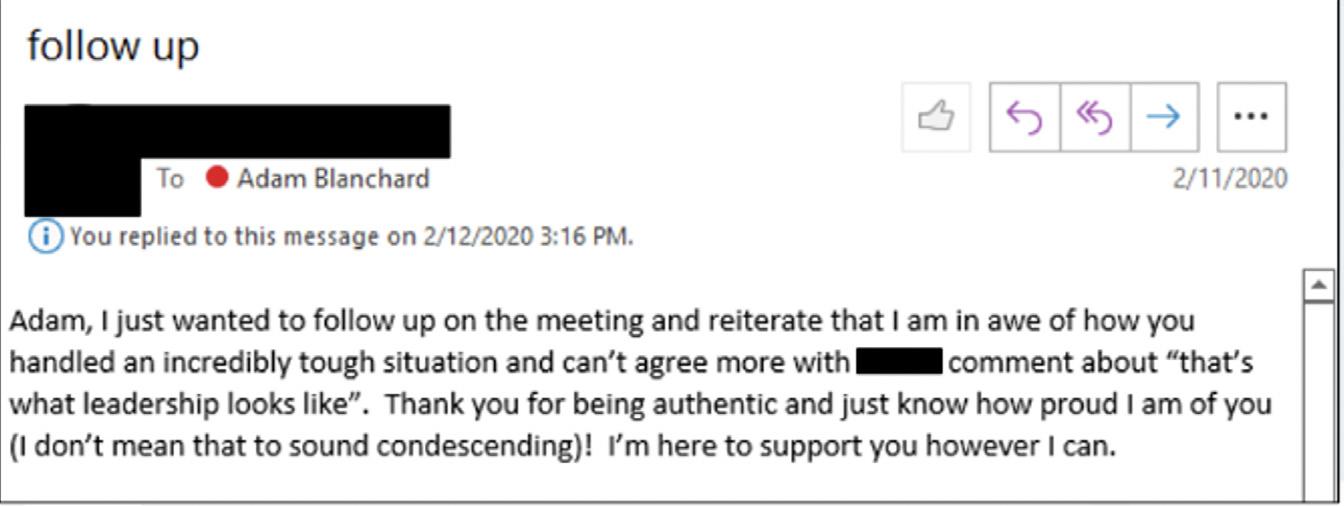
Really, for the first time in my career, I began to question out loud whether I was cut out for this whole leadership thing. I was spinning and catastrophizing and had to figure out where to go and what to do, and what should happen next.
After some tears, some yelling, and some cursing, and after some very intentional conversations with several trusted individuals, I began to recover and try focusing on how to learn from this. I had to figure out how to move ahead productively.
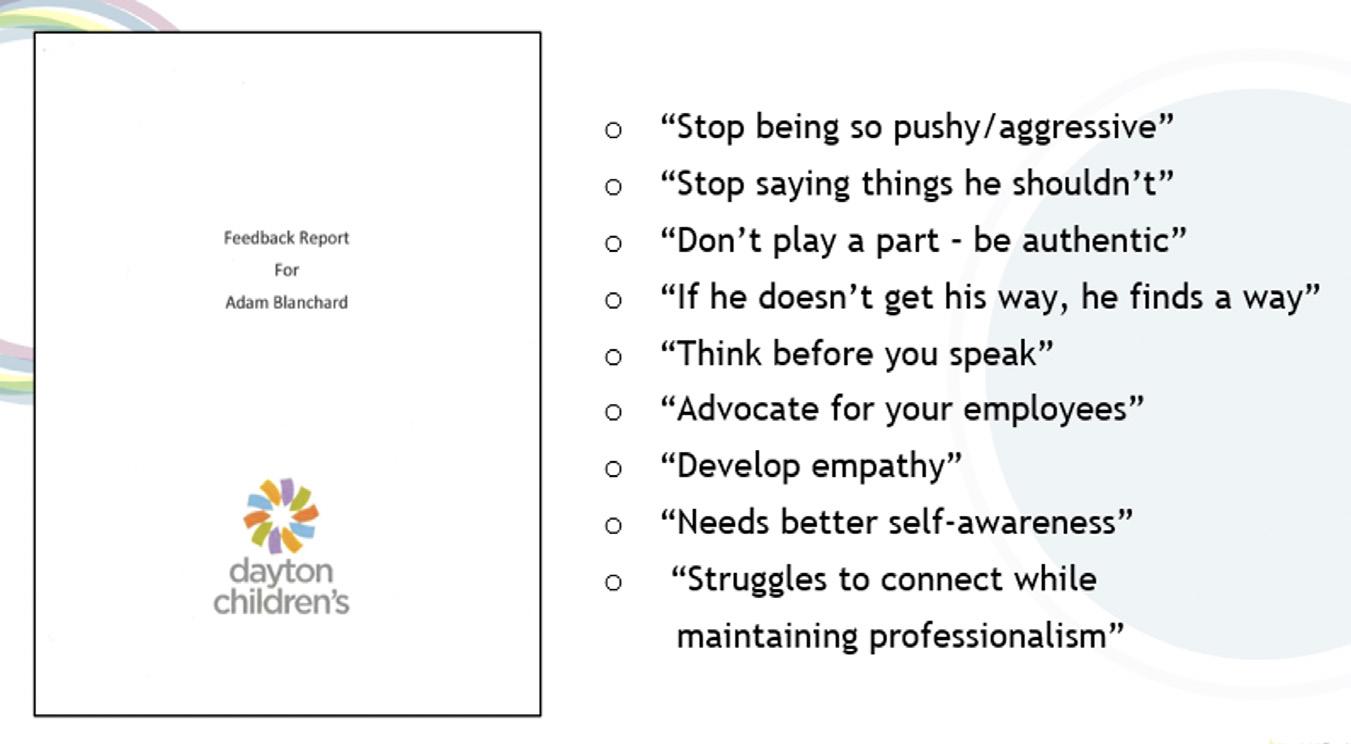
I was quickly reminded that truth is in the eye of the beholder and perception is reality. The 360-degree evaluation allowed our staff to be radically candid about their feelings toward leaders, including everything from strengths and weaknesses to management style, from the culture within our foundation to suggestions for growth, and so forth.
To say the least, I was blown away and completely caught off guard by the feedback. I vividly remember asking myself “How could they think that about me?”
When reviewing the report with my staff leader and the hospital’s head of human resources, I experienced a whole new level of self-awareness, but also some significant self-doubt. I was angry, and I was hurt. I was perplexed and confused.
With the help of my staff leader and the HR leader, I put together a 90-day action plan to spark some immediate change. I identified the top things I wanted to achieve and what I need to be successful. Through this work, I began to journal weekly about my trials and errors, recording very honestly what worked and what didn’t. I made sure to celebrate the successes and recognize the failures so I could continue to learn.
When I started doing this, my behaviors began to change. And so did the perspectives of others. I quickly learned that vulnerability is a strength, not a weakness.
In fact, as the research suggests, there’s strong evidence to support this approach. “Leaders’ selfdisclosure of weaknesses can foster perceptions of authenticity, meaning that many leaders miss an opportunity to develop rapport [with
AHP Healthcare Philanthropy Journal|Spring 2023| 33
their teams].”3 If I was willing to look at things differently, recognize, and apologize where I had come up short, it would provide a level of genuine transparency and help strengthen my relationships. That it did.
I also identified available resources and sought advice from trusted individuals, including executive coaches. Over the past three years, I have leaned into better understanding emotional intelligence (EQ) and how to leverage it in my leadership practice.
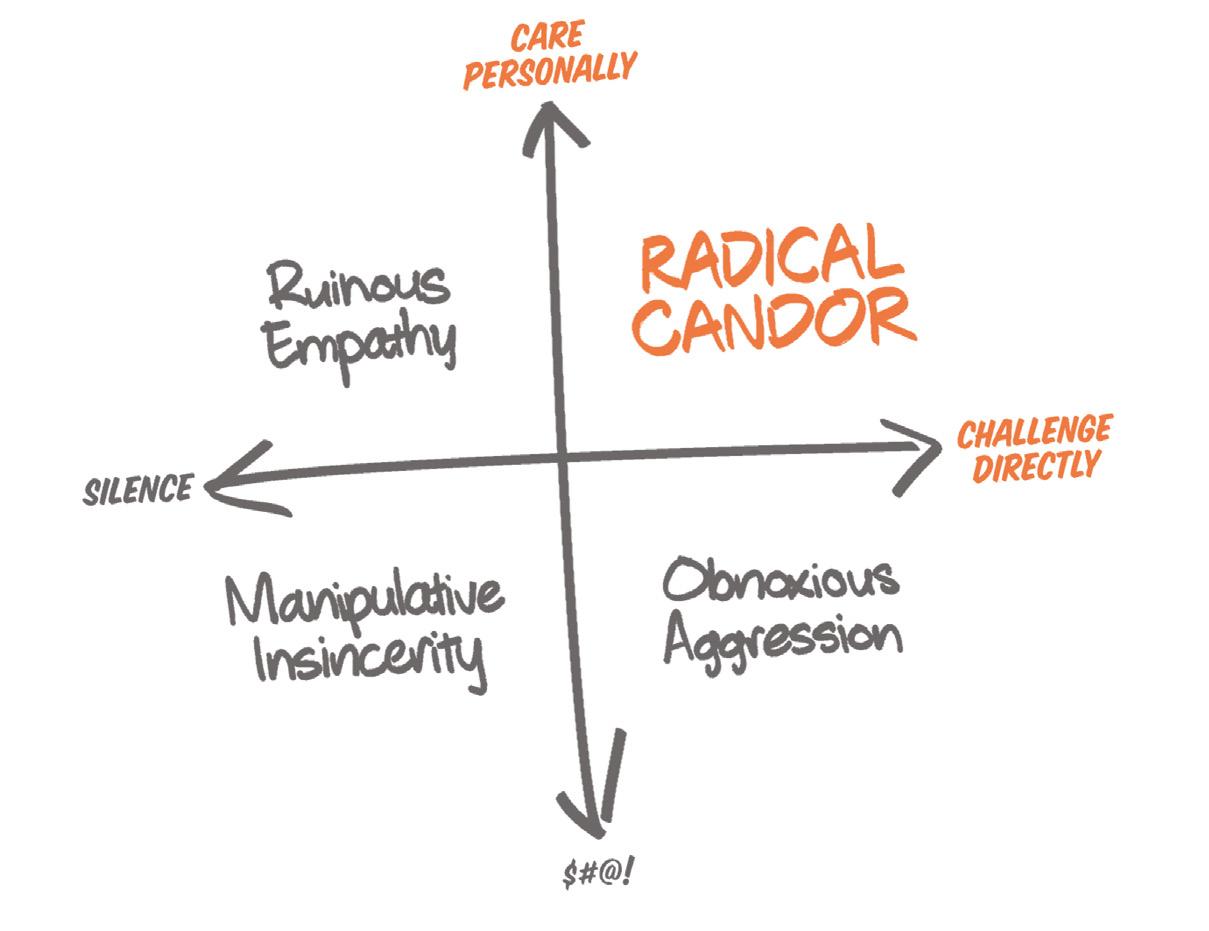
The BlueEQ assessment and training was conducted with our staff about a year after the initial 360-degree feedback exercise. This provided a great introspective look at my emotional intelligence and a safe space to discuss and learn how to keep improving. Shortly thereafter, Crucial Conversations training was provided to all hospital leaders to teach us how to effectively carry difficult situations forward. It helped me learn how to get unstuck with some of my staff and address challenging issues in a very respectful and productive way–clear is kind! Finally, I read the book, Radical Candor, by Kim Scott. Of the many takeaways, my main insight was that I can challenge people directly and care for them personally, all at the same time.
It’s been said before and I’ll say it here again: education is power. When I developed new skills
and added new tools for a different approach, my relationships improved. In his book, Partnership is the New Leadership, Ty Bennett notes, “taking time to create an atmosphere that develops relationships, builds trust, and strengthens the team is invaluable to fashioning the environment you desire.”4
It’s critical to put people first and regularly invest time inviting them to be part of a psychologically safe culture.
For fundraising leaders, the business of our work can quickly become all about the numbers. If you find yourself exclusively focused on the outcomes, and not on who is best positioned to help deliver them, and how you foster an environment of trust and authenticity, fear not! The trajectory for leadership isn’t simply a straight line from Point A to Point B.
Understanding this truth is the first step to owning where you’ve been and declaring where you want to be. Be open to always learning, recognize that feedback is a gift, and remember that the greatest resource is the human resource. Self-awareness of your own shortcomings is the foundation for building greater strengths.
Paying it Forward from My Lessons Learned
I don’t presume to have all the answers. I’m an imperfect human on a journey to try and help create better humans to impact our little corner of the world. But my hope is that some of the things I’ve picked up through my experiences will resonate and allow you to improve your own leadership today, tomorrow, and into the future.
Always talk less and listen more. Don’t be afraid to learn about yourself. READ every day! Your head is a scary place; it’s therapeutic to clean it out from time to time.
Identify your sounding board of trusted advisors and regularly seek their advice. Take a genuine interest in those entrusted to your guidance. Oh, and by the way, this all works with donors too!
AHP Healthcare Philanthropy Journal|Spring 2023| 34
I challenge you to take just two minutes and make a single commitment to yourself today. What will you do different? What one change can you make to realize a different outcome? Write it down and revisit it frequently.
Regardless of your position, you are a leader who is visible to many and who will be judged. How you’re seen depends entirely on whether you value relationships ahead of results. As Simon Sinek says, ensure your time, effort, and decisions go into the people you lead.5 Take an opportunity to invest in YOU so that others may benefit.
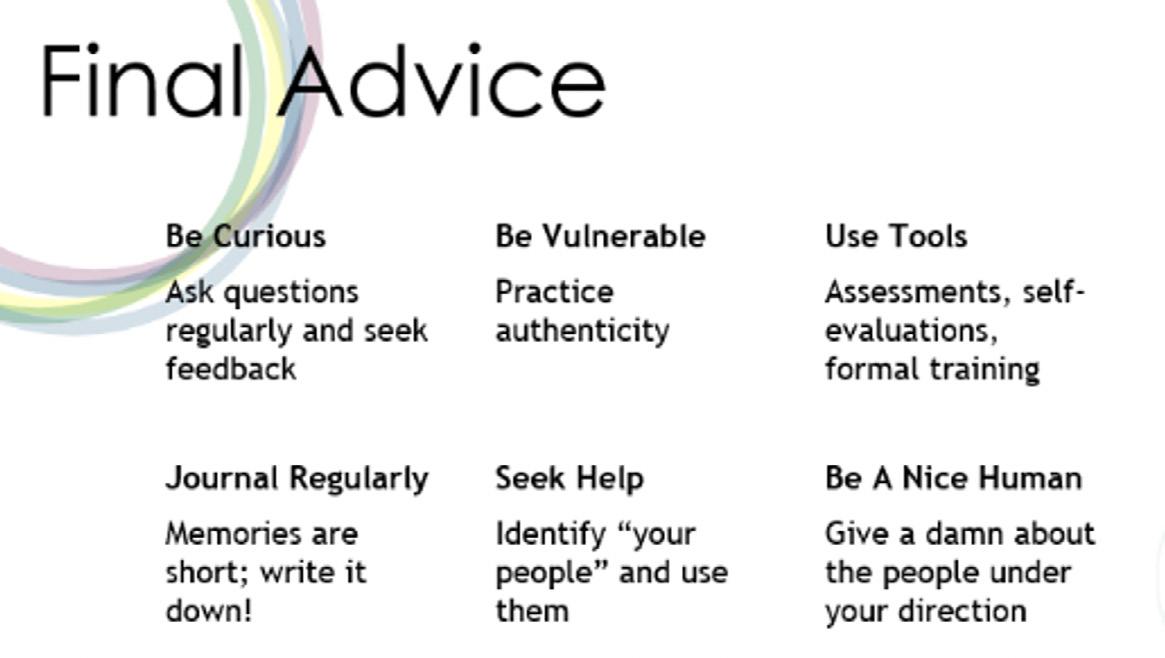
Endnotes
1 Li Jiang, Maryam Kouchaki, and Leslie K. John, “Research: Why Leaders Should Be Open About Their Flaws,” Harvard Business Review (2023).
2 Li Jiang, Maryam Kouchaki, and Leslie K. John, “Research: Why Leaders Should Be Open About Their Flaws,” Harvard Business Review (2023).
3 Bennett, Ty, Partnership is the new Leadership (United Graphics, LLC., 2016.), 101.
4 Sinek, Simon., The Infinite Game (Penguin Random House, LLC., 2019), 42 .
Adam Blanchard serves as the Director of Donor Engagement at Dayton Children’s Hospital Foundation. He joined Dayton Children’s in 2015 after spending nearly eight years with the Boy Scouts of America in Cincinnati, Ohio in various fundraising and leadership capacities. Blanchard has over 18 years of professional fundraising experience.
Throughout his career, he has been engaged in fund development and strategic leadership. While studying as an undergraduate at the University of Cincinnati, he gained interest in fundraising and philanthropy as a student caller for the university foundation and developed a strong passion for the work. Blanchard also places high value on professional development and the mentorship of young people in the workforce. He has translated these passions into a career that matches his affinity for fundraising with his desire to cultivate talent.
In addition to his professional accomplishments, Adam has a strong record of community service. He is a member of both the Association of Fundraising Professionals and the Association for Healthcare Philanthropy, where he was recognized as a member of the 40 under 40 class in 2022. He is also a member of the board of directors for Miami Valley Council, Boy Scouts, serving as Vice President of Membership, and Discover Classical.
AHP Healthcare Philanthropy Journal|Spring 2023| 35
Benchmarking Success: Overcoming the Challenges of Continuous Improvement
 By Jenny Love, Chief Content and Marketing Officer, Association for Healthcare Philanthropy
By Jenny Love, Chief Content and Marketing Officer, Association for Healthcare Philanthropy
Benchmarking is the process of comparing the performance of an organization to that of other organizations in its industry or sector. It involves analyzing the processes and practices of these other organizations, with the goal of finding best practices and ways to improve the organization’s performance being benchmarked.

The term “benchmarking” was first coined in the 1980s by Dr. Robert Camp, a management consultant and researcher, after a surveyor’s mark used as a reference point in measuring altitudes.1 Though it dates to the early days of computing, benchmarking has become increasingly important as technology has advanced and become more integral to our
daily lives. The growth of the Internet and the increasing reliance on technology in businesses and other organizations led to the development of more sophisticated benchmarking tools and techniques. These tools made it possible to evaluate the performance of systems and products in a more comprehensive and accurate way.
AHP Healthcare Philanthropy Journal|Spring 2023| 36
/ FORWARD THINKING
Forward Thinking article sponsored by
Today, benchmarking is used in a wide range of industries, including computing, manufacturing, finance, and healthcare. It is an essential tool for healthcare philanthropy organizations that want to improve their performance.
“There’s a lot of work that gets done by the gut, but if you really want to become a more efficient and effective fundraiser, use benchmarking,” says Jared Langkilde, MBA, CFRE, president and CEO of HonorHealth Foundation in Scottsdale, Arizona. “The shortest distance between two points is a straight line, and that’s what benchmarking gives you. It shows you what you should be doing, and whether what you are doing is making a difference.”
Benchmarking can also help fundraising organizations build credibility.
“Numbers are the most effective way to show relevance,” says Julie Cox, vice president of development for Life Bridge Health in Baltimore, Maryland, who has been benchmarking for several years. “Benchmarking gives my foundation credibility and helps me articulate the business of fundraising to our donors, our staff and our C-suite.”2
Elizabeth Gross, interim vice president at Luminis Health Anne Arundel Medical Center in Annapolis, Maryland, agrees.
“People think the foundation is just parties and pearls,” she says. “Being able to show how datadriven we are and how we measure up helps our profile in the organization.”
Benchmarking can be a powerful tool, but it is not without its challenges. Here are tips from organizations with established benchmarking programs for overcoming those challenges and reaping the benefits of regularly assessing performance against peers.
Challenge #1: Identifying Appropriate Benchmarks
One of the first challenges of benchmarking is finding the organizations or practices that will serve as benchmarks. It is important to select benchmarks that are relevant and meaningful to your organization, and that represent the best practices in the industry or sector.
Identify the specific areas you want to benchmark.
The first step in finding good benchmarks is to find the specific areas of your organization that you want to benchmark. This will help you to focus your search and ensure that you are comparing your organization to others that are relevant and meaningful. It’s ok to start small.
“The biggest mistake I made at the beginning was trying to look at everything,” says Keith Curtis, CFRE, executive director of Grande Prairie Regional Hospital Foundation in Grande Prairie, Alberta. “And I couldn’t. I had to break it down.”
Dzenan Berberovic, Chief Philanthropy Officer at Avera Health in Sioux Falls, South Dakota, recommends a similar approach.
“What gets measured gets managed. When you embark, you’re going to feel there are many measures that can be implemented to establish as your goals,” he says. “Select a few that will lead you to where you want to go. Maybe it’s only three in that first year. Focus on them, and you’ll start to see results. It’s invigorating when you realize you are on the right track—or you’re not and you need to keep iterating.”
Healthcare philanthropy experts recommend starting with the following metrics, all of which are benchmarked in the AHP Report on Giving and defined in the AHP Standards Manual:3
• Return on investment (overall and by activity type—e.g., major gifts, events)
AHP Healthcare Philanthropy Journal|Spring 2023| 37
• Cost to raise a dollar, and
• Net fundraising revenue (overall and per fulltime employee).
Seek out organizations with similar characteristics.
Look for organizations that are like your own to find benchmarks that are more directly comparable to your organization.
“We look for organizations that are similar to our size from an employee base, overall patient revenue, number of hospitals or that are in the same part of the country,” says Berberovic. When choosing the right foundations to compare to, Curtis looks for organizations with a similar size and structure and that are specific to healthcare.
“We stay away from broad philanthropy benchmarks,” he says. “A university foundation has a low cost to raise a dollar, but they have no labor, because it’s all paid for by the university. They have multiple buildings and multiple wings that they can use for naming rights. Whereas in our hospital, that’s impossible. It’s hard to benchmark against that.”
Use external benchmarking resources
Your own internal data can be a valuable source of information and can help you to benchmark your organization’s performance against its own past performance, which can be a great place
to start the process of becoming more data oriented. However, you will get the most insight from benchmarking yourself against others.
There are many external benchmarking resources available to help you compare your organization’s performance to that of other healthcare foundations, such as industry associations, consulting firms, and donor management system databases, which can be a valuable source of benchmarking data and information. Participating in AHP’s annual Report on Giving is a good place to start out.
“The Report on Giving is a light version of benchmarking, and it’s also a lot easier to understand the data. Don’t be afraid of the numbers, stick your toe in, and learn from it,” Jory Pritchard-Kerr, FAHP, executive director at Collingwood General and Marine Hospital Foundation in Collingwood, Ont. “You don’t know what’s effective until you find your starting point. How do you know whether you’re improving if you’re not measuring the same thing year over year over year?”4
Align your organization with industry standards
One considerable hurdle to beginning external benchmarking is that the way your organization tracks processes and results can differ from the way it is done at the organizations you want to compare yourself to. For example, let’s say your organization holds a large fundraising gala, which

AHP Healthcare Philanthropy Journal|Spring 2023| 38
has the potential to raise gifts of $10,000 or more. While some development programs might categorize these donations under “events,” others might track them under “major gifts.”5
Aligning definitions for the metrics you choose to track is important to avoid confusion and promote apples-to-apples comparisons. AHP’s Standards Manual is a good place to start to understand best practice methods for tracking metrics specific to healthcare philanthropy.
If your organization is larger and many different people are involved in entering gifts, it may be necessary to coordinate among everyone to ensure the same definitions are used throughout the organization. At Avera Health, a crossfunctional group of philanthropy staff have been leading a 24-month database hygiene initiative. The database governance committee has created standards, operating procedures, and logic documents to ensure that entries into the database are consistent and support Avera’s philanthropic growth agenda and strategic plan. As a result, their data is easier to benchmark.
“We’re all trying to pull together in the same direction for the same purpose,” says Dan Cook, Operations Officer at Avera Health. “That’s really key.”
Elizabeth Gross, who works with her database administrator, Elizabeth Foley, to fill out the AHP Report on Giving benchmarking survey for her organization annually, is intimately familiar with the complexities of ensuring that her organization’s numbers align well with the organizations she benchmarks against. When Foley pulls data to report against benchmarks, she notes areas that do not align for future process changes. She keeps as close as possible to the definitions in the standards manual, but she also tries not to get too hung up on perfection. Both Elizabeths believe that a close comparison is better than no comparison at all. “I would give the advice to go into this with the spirit of ‘I’m going to answer this as best I
can,’” Gross says. “If you take too long getting everything correct it won’t be sustainable.”
Use benchmarking software.
There are many software tools available that can help you to gather and analyze benchmarking data. These tools can automate the data collection process and make it easier to compare your organization’s performance to that of other organizations. For example, Report on Giving participants get access to AHP’s benchmarking platform with predefined comparison data sets for community hospitals, academic organizations, health systems, children’s hospitals, and more to enable you to analyze performance against similar organizations with the click of a mouse.
Challenge #2: Maintaining Momentum
Another significant challenge of benchmarking is maintaining momentum and staying committed to continuous improvement. It can be easy for organizations to lose sight of their benchmarking goals and to fall back into old habits. In organizations that have historically not used data to drive decision making, team members can be reluctant to embrace it. Culture is notoriously difficult to change, but there are a few steps you can take to increase your organization’s comfort with using data in operations and strategic planning and to help you stay committed to continuous improvement.
Set clear, measurable goals
One of the best ways to stay committed to continuous improvement is to set clear, measurable goals for your organization. This will help you to focus your efforts, track your progress over time, and ensure that everyone understands what they are working for and how data can help achieve these goals. Having clearly stated goals also helps you take corrective actions more easily before you get too far off course.
“If a gift officer’s performance is struggling, and it’s showing up in the data, it’s a great opportunity for a leader to come to the rescue
AHP Healthcare Philanthropy Journal|Spring 2023| 39
before the officer even knows that they are in need of support,” says Langkilde.
Involve your team—and senior leadership
Involving your team in the continuous improvement process can help to build buy-in and commitment to the process. People are more likely to be committed to initiatives they are personally invested in. Encourage open communication and collaboration and involve your team, your C suite, and your board in setting goals and finding areas for improvement.
“Hospital leadership is so data driven. They are looking at clinical data and length of stay and case mix index all day long,” says Gross. “To be able to put your own points in there is critical when advocating for resources and explaining challenges and needs.”
It can be scary to bring underperformance to light, but it’s a necessary part of the process. “One of the things that I hear a lot from people who aren’t [benchmarking] is they’re afraid of the information that their board will find out. You can’t be afraid to have that conversation with your C-suite or with your board and tell them that this is all about improving,” says Pritchard-Kerr.
Pritchard-Kerr shares 10 years of benchmarking data with her board annually.
“It’s something to make them understand how revenues can fluctuate, especially during campaign cycles, and we want them to have a long-term look at what’s going on,” PritchardKerr says. “By using the benchmarking data, we can validate to our board what is happening across the industry and use it as a tool for them to determine whether the investments we’re asking for are valid and will pay off in the end.”vi
Berberovic also finds value sharing benchmarking data with his system board.
“We take a look at the data and highlight three or four key measures that are most important for
a board member to understand,” he says. “The figure that our board has started to look closely at is overall return on investment.”
Measure your progress
Regularly measuring your progress and tracking your progress towards your goals will help you to stay motivated and focused on continuous improvement.
Berberovic, for example, has created dashboards that the individual giving team can see at any point to track goals, progress and key performance indicators. The dashboards are used as much as daily for one-on-one meetings and in meetings with their prospect and strategy officer. Transparency allows the team to see and celebrate early wins and to observe growth in philanthropic giving on a regular basis.
“You have to make it part of your everyday life,” says Curtis. “If you wait until the last Friday of the month, you’re not going to keep up with it. Take the time to set up ongoing reports, and work with other people to run their reports that you need.”
It’s also important to make the reports you create easily accessible to everyone involved, either through a business intelligence tool or even a spreadsheet on a shared drive. Berberovic’s team will soon be able to access their dashboards live via a hyperlink.
“Coming up with the report and then shelving it doesn’t do anyone any good,” Landkilde says. “You have to review it on a regular basis.”
If your staff is not used to working with data, it might be necessary to supply training in understanding data, analytics, and how to use the data to drive decision making, so that they can benefit from the progress reports you create.
Be open to new ideas
Be open to innovative ideas and approaches and encourage your team to think creatively and
AHP Healthcare Philanthropy Journal|Spring 2023| 40
challenge the status quo. Encourage data-driven decision-making by promoting a culture of experimentation and hypothesis testing. This can be achieved by rewarding employees who use data to inform their decisions and by promoting an open dialogue about the insights that emerge from data analysis.
“Beneath each benchmark is a best practice,” says Langkilde. “If you identify that best practice and start doing the work with intentionality and integrity, you’re going to see results. [For example], our donor count had been declining for years. We’ve stabilized and are now growing the donor pool by doing categorical work identified in AHP benchmark reports, such as direct mail, phone-a-thon, and email campaigns.”
Engage with other organizations
Don’t be afraid to reach out to other organizations and ask them about their processes and practices. Many organizations are willing to share information and best practices, and this can be a valuable source of benchmarking data and process improvement advice.
“I often look at other high performers in the industry and try to learn who is running those programs,” says Cox. “We work in a profession where we all want to learn and share best practices, so I’ve found my peers are always open to meeting and learning from one another.”7
There’s a Chinese proverb that says, “The best time to plant a tree was 20 years ago. The second-best time is now.” So it is with benchmarking.
“You’ve got to start somewhere,” says Langkilde. “The world is not going to improve overnight, so the sooner you start benchmarking and develop a baseline for your performance, the sooner your efforts will yield fruit and provide a positive story that can be shared. Benchmarking is a means of helping you and your organization to become your best.”
Jenny Love is a highly skilled marketing professional with a strong focus on content marketing. She has more than 20 years of experience in the industry and currently serves as the chief content and marketing officer at the Association for Healthcare Philanthropy. In this role, Jenny oversees marketing and communications and is responsible for creating and publicizing thought leadership content on healthcare philanthropy topics in a variety of media.
Prior to her current role, Jenny held senior marketing positions at several healthcare organizations, including CAQH and the Advisory Board Company. She has written extensively about the business of healthcare and has led several successful product launches and customer acquisition campaigns.
Jenny holds a bachelor’s degree in international economics from Georgetown University and a master’s degree in healthcare administration from the Johns Hopkins University Bloomberg School of Public Health.
Endnotes
1 HotStats. “The Story of Benchmarking: History, Processes and Practice,” November 17, 2018. Accessed January 27, 2023. https://www.hotstats.com/hotel-industry-resources/the-story-of-benchmarking-history-processes-and-practice
2 Momberg Lawver, Alissa. “Using Benchmarking to Improve Performance, Show Value.” www.ahp.org, n.d.
3 “Philanthropy KPIs and Why You Need Them,” May 11, 2018. Accessed January 27, 2023. https://www.ahp.org/ resources-and-tools/ahp-connect/ahp-connect-details/ philanthropy-kpis-and-why-you-need-them
4 Jones, Jasmine and Jacqueline Walsh. “5 Common Misconceptions About Benchmarking Data,” December 5, 2018. Accessed January 27, 2023. https://www.ahp. org/resources-and-tools/ahp-connect/ahp-connect-details/5-common-misconceptions-about-benchmarking-data.
AHP Healthcare Philanthropy Journal|Spring 2023| 41
Three vital signs for checking the health of your fundraising plan
Donor retention is critical for building a robust fundraising growth plan. Ignoring your leadership annual fund or mid-level donors can lead to missed opportunities and decreased revenue. To keep your donor pipeline healthy, monitor these three vital signs:
1. Keep taking the temperature of your donors; conduct advanced prospect profiling and data modeling.
“Don’t just diagnose your donors one time. Use advanced prospect profiling and data modeling to keep uncovering hidden giving potential,” says Graham-Pelton’s Senior Vice President of Data Analytics Jim Rude, CFRE, bCRE-Pro. “Regularly review your data analytics models to identify donors whose giving potential has increased and develop strategies to move them to major gifts or planned giving prospect pools. Use prospect profiling techniques to identify other donors who exhibit similar giving patterns and may also be inclined to give at higher levels.”
2. Quicken your donor’s pulse through personalized communications.

“Effective communication with leadership annual and mid-level donors should use an increasingly personalized approach,” says Brian O’Leary, Graham-Pelton’s Senior Vice President of Fundraising Communications. “Use data analytics to identify a donor’s areas of interest, such as a program or project they’ve supported in the past. In your communications, create a link between giving and the direct impact it has on the causes they care about most.”
3. Keep breathing life into your clinician and healthcare provider engagement.
“Many of your donors were introduced to your organization as grateful patients or family members, and their gratitude doesn’t have to end with their first gift,” says Bridget Murphy, CFRE, Graham-Pelton’s Chief Growth Officer and Healthcare Practice Group Leader. “Graham-Pelton is known for helping fundraisers coach healthcare professionals to find their own voice when talking about philanthropy, and regular coaching allows them to keep development in mind when continuing meaningful relationships with their patients. It’s a prescription for a healthier fundraising pipeline!”
To learn more, visit www.grahampelton.com/healthcare

Spring 2022
Creating Programmatic Change Through Grant Development
How grants can lead the way to programmatic change
 By Jeremy Riley, MA, Grants Development Coordinator at CHI Memorial Hospital
By Jeremy Riley, MA, Grants Development Coordinator at CHI Memorial Hospital
Productivity guru Stephen R. Covey made famous the concept that we ought to “begin with the end in mind.” Meaning, prior to the launch of any day, task, or project, we ought to relay a clear vision for our desired outcome. In healthcare philanthropy, stewarding the trust of donors and serving the patients who benefit from philanthropic giving is our end in mind. In philanthropy in general, the intentions and desires of the donor rightfully take center stage. Grant writing is certainly no different from the stewardship of annual or major gifts. The process of how to effectively pursue grant funding is what separates this vital fundraising resource from other avenues of funding.
Ask any grant professional, and they will likely have a story to share where a programmatic leader generally asks for grant funding for a project. Whether it is new carpet, new equipment, or funding to cover an operational deficit, grants are often little understood tools within the toolbox of philanthropy. As someone who entered into the grant writing role closer to serendipity than purpose, I wish to share a roadmap that ought to help provide a bit of clarity on the grantwriters’ role within the fundraising team.
As finances tighten across industries like nonprofit healthcare, resourcefulness allows
AHP Healthcare Philanthropy Journal|Spring 2023| 43
HEALTHCARE PHILANTHROPY FUNDAMENTALS
for programs to move beyond stabilization to effectiveness. Grant funding is an excellent avenue to begin the process of advancing new and innovative programs and projects through a few practical manners. Grants can elevate a program, moving a particular program or service from ordinary to extraordinary. They can cover the operational cost of a vital, new staff member or pay for the expansion of a new medical procedure. Before the dreams of an overworked and underfunded philanthropy staff can be made reality, it’s best to begin with the end in mind—your long-term goal—and then plan for it.
Develop a Plan
When an opportunity presents itself in a government or private foundation grant solicitation, it requires philanthropy and program leadership to meet together and process a pathway for a project. Just as in any relationship, setting boundaries is healthy and good for both parties. Similarly, having this important conversation with curiosity and a copy of the request for proposal will certainly help as you aim to set forth clear expectations, assignments, and a workable timeline. Ensuring the project fits within the scope of the mission and is indeed a priority of the organization will save a tremendous amount of frustration down the road. Seeking funding for a major pediatric project when there is no operational support to sustain the project after the end of the grant lifecycle will lead to the project’s inevitable demise. Grant funding helps to move an organization in the direction they want to go as the icing on the proverbial cake, instead of the only driver and sustainer of a project.
When developing a grant proposal, it is important to get the right people involved. This includes relevant leadership in administration, finance, legal and compliance, and subject matter experts in the field. Having the right people will allow multifaceted perspectives to consider the full scope of the proposal and the inevitable reporting requirements. Some private or corporate foundations might
require minimal reporting while other grantor organizations might require more detailed reports. Looking at the reporting requirements ahead of a submission will sometimes warrant a broader discussion within the organization to discuss whether it is worth pursuing a large funding opportunity. I can personally attest that sometimes it’s just not worth the pursuit of funding when there are meticulous demands tied to a grant. We all make mistakes; however, the returning of grant money is not a pleasant one to make.
Stay Organized to Avoid Last Minute Stress
As every hero has a nemesis and every sports team has a main rival, the potential foe for anyone who pursues a grant is the looming deadline. While major gift solicitations and annual gift appeals might have more flexible deadlines, a June 15 deadline comes to a close at 5 pm whether you have an itemized budget or not. For many organizations, a sprint to the finish can become a likely scenario.
In order to minimize the risk of the preventable mad rush to the end, allowing for enough time to develop a cohesive strategy, a compelling case statement, thoughtful logic model, and a viable budget, it is necessary to identify your team who will help bring you over the finish line.
Submit Well-Written, Data-Driven Proposals
Within my work in healthcare fundraising, my organization has compelling projects that are effective in its scope of work complete with knowledgeable project leads. Not every project or nonprofit has this on demand, that is why it is important to create case statements for your project(s). This particular tactic will help inform the strategy to further the effectiveness of a nonprofit’s reach, as all the necessary pieces for soliciting gifts can be housed in one central document. This includes demographics for a program, budget, implementation timelines, logic models, and other vital pieces of information that can be readily used for grant applications. The benefit of this approach is that
AHP Healthcare Philanthropy Journal|Spring 2023| 44
most grant application questions will require information that has already been considered, thus reducing one less barrier for grant submissions. Not only will grant writers benefit, but major gift officers, annual fund coordinators, and planned giving staff will all benefit from a case statement with stats, thought out needs, and plenty of information for most donor related questions.
Pursuing and securing grants is best for an organization when it is considered as an avenue for furthering the expansion of a program. In my experience, grant funds can be viewed as offsetting the cost of the effort, whether it is a small purchase of diapers for the parents of NICU patients or the enormous reimbursement of a mobile screening bus. Grant funding can take the organization to where it wants to be with well-timed proposals that provide clear direction for the program. It also can provide an opportunity for stakeholders to plan out the future direction of the organization or program, large or small.
Beginning with the end in mind is a good place to start in a grant proposal. Envisioning what can best assist your clients, patients, participants, or demographics you serve and then moving backwards with your programmatic activities. With enough deliberate thought and crucial conversation followed with action, an effective grant program can bring lasting change to an organization and truly elevate a program.
Jeremy Riley is the Grants Development Coordinator at CHI Memorial in Chattanooga, TN. In his role he oversees the pre- and post-award management for governmental and private foundations, working with clinical leaders to advance health equity in the greater Chattanooga region. He has been with CommonSpirit Health, CHI Memorial’s parent company for more than seven years, with five years overseeing the grant portfolio for Dignity Health hospitals for the California Central Coast, including Arroyo Grande Community Hospital Foundation, French Hospital Medical Center Foundation, Marian Regional Medical Center Foundation, and St. John’s Healthcare Foundation. Prior to joining Dignity Health, Jeremy was the founding Area Director for Fellowship of Christians in Universities and Schools (FOCUS) in San Francisco where he worked with high school and middle school students in private, independent boarding and day schools. He was also a District Representative for (retired) US Representative John Campbell where he assisted and advocated for immigrants and veterans in Orange County, CA. He holds a BA in Political Science and History from Vanguard University of Southern California and an MA in Theology from Fuller Theological Seminary. He is an avid runner, reader, painter, and a suffering San Diego sports fan.
AHP Healthcare Philanthropy Journal|Spring 2023| 45
Campaign Goal Setting with Limited Data: A Case Study
 By Heather Perdue, MA, FAHP, Vice President, Campaigns and Philanthropy at Indiana University Health Foundation
By Heather Perdue, MA, FAHP, Vice President, Campaigns and Philanthropy at Indiana University Health Foundation
Campaigns are powerful tools to rally donors and key stakeholders around a common goal and accelerate fundraising performance.
IU Health Foundation’s current and firstever statewide comprehensive campaign serves our mission, jump starts critical fundraising performance as part of a longrange financial commitment to the health system, and positions us as a top-performing healthcare philanthropy organization using the Association of Healthcare Philanthropy’s national performance metrics. The campaign also benefits our person-to-person connections by fostering positive donor engagement, partnership with hospital leaders, and meaningful volunteerism.
However, because this campaign is a firsttime effort, we had no data tail or history from previous statewide campaigns to use in goal setting. This case study focuses on how I successfully set a comprehensive campaign goal by relying on other predictors. And it’s working: IU Health Foundation has reached over 50% of its campaign goal ahead of schedule for a campaign running from 2020 through 2026.
Every year, candidates for the Fellow of the Association for Healthcare Philanthropy designation submit a case study for consideration as part of their applications. This case study was submitted by Heather Perdue, MA, FAHP for her application to the AHP Fellows program in July 2022.

AHP Healthcare Philanthropy Journal|Spring 2023| 46
Background
IU Health Foundation was founded on January 1, 2018, by integrating disparate fundraising entities supporting IU Health hospitals and programs statewide. These independent foundations were all governed, operated, and managed differently. The integration respected the intentions of the original donors but brought more power to each philanthropic dollar invested in IU Health. It ensured parity in the donor experience across the health system, facilitated a grateful patient program, aligned with system strategy, and ensured standardized operations.
Prior to integration, each independent fundraising operation tracked gifts and metrics differently. Some were tracked as income to a nonprofit system hospital and not as a function of a fundraising organization. System and hospital leaders ran the gamut on their work with–and even awareness of–philanthropy. Fundraising priorities were identified but not necessarily vetted with key stakeholders.
In 2019, IU Health Foundation began the early planning stages for a statewide fundraising campaign. This was an aspirational timeline given the very recent 2018 integration and absence of available data and shared fundraising practice standards. However, IU Health was planning significant capital investments across the state beginning in 2020 (including a new $1.6 billion academic medical center in Indianapolis scheduled to open in 2026). Philanthropy had an important role to play in driving system strategy implementation through meaningful gift opportunities presented in cases for support.
Evaluation of the Case
Lacking consistently tracked data and giving histories, I knew that the pre-campaign analysis and preparation required thoughtful problemsolving and careful strategy to ensure successful goal and timeline setting. I relied on several key practices to inform the campaign goal:
• A quantitative analysis based on past performance and rated capacity
• A qualitative analysis based on the missionbased needs and donor input
• National peer benchmarks and a long-range planning financial goal
• A gift range chart populated by donor and prospect information.
The cumulative annual fundraising total for the pre-integration foundations was around $5 million. Statewide fundraising results accelerated substantially post-integration, quickly demonstrating that more robust fundraising performance was possible. The following chart (on the top of page 2), “Historical Cumulative Giving,” shows the prior fundraising performance leading up to and two years past the integration in 2018. It’s clear that fundraising performance accelerated quickly post integration in 2018 and 2019, with peak fundraising performance hitting just over $6 million.1
CUMULATIVE GIVING FUNDRAISING RESULTS
Thus, considering a campaign goal with a campaign counting start date in 2020 required thoughtful analysis about what was possible given the new organization structure, new projects coming online through capital growth, a growing donor base, and a desire to be a national leader in fundraising performance.
What became more important was understanding fundraising potential post-
AHP Healthcare Philanthropy Journal|Spring 2023| 47
SINCE
$20M $15M $10M $5M 0 FY 10 FY 11 FY 12 FY 13 FY 14 FY 15 FY 16 FY 17 FY 18 FY 19 $20M $25M $30M $15M
HISTORICAL
INTEGRATION
integration and aligned with meaningful campaign needs. If 2018 and 2019 were any indication of future performance, then a larger campaign goal might be possible.
Best practice in fundraising and campaign strategy involves engaging external counsel to assist with unbiased pre-campaign analysis and goal setting.2 IU Health Foundation enlisted two consulting firms to develop key analyses to help inform campaign goal setting for a campaign running from 2020 through 2026: a quantitative analysis conducted by BWF and a qualitative analysis by Accordant Philanthropy.
The Quantitative Analysis
BWF3 conducted a database analysis of fundraising performance coupled with national trends in fundraising. Key findings noted that IU Health Foundation’s major gifts program was outpacing national averages. As part of the quantitative analysis, IU Health Foundation requested several analyses—conservative (logarithmic), aggressive (exponential), and linear. Based on its analysis, BWF recommended a logarithmic goal of $64.4 million and exponential goal of $97.9 million for a campaign spanning seven years (2020-2026).
BWF’s analysis didn’t include government grants with philanthropic impact, but through my analysis of the 2015 through 2020 Schedule of Expenditures of Federal Awards (SEFA), I found that an average of about $5 million of government grants could be captured toward the campaign goal. I knew that if I could find a way to capture these totals through the Foundation toward the impact to the mission, then the campaign goal could increase by at least 25%.
and my analysis, the quantitative data seemed to suggest a $125 million campaign goal.
The Qualitative Analysis
Accordant’s4 analysis used internal and external interviews and focus groups, coupled with highlevel reporting from the database. I worked closely with Accordant to ensure a balanced and representative sample of interviews. I also included the nuance of the size and influence of an organization like IU Health with $6 billion in total assets, knowing that a statewide campaign goal needed to make an important statement on our organizational position and influence.
Accordant recommended a $100 million internal working campaign goal5 over the span of seven years (2020-2026). Accordant’s analysis also did not include my SEFA analysis. Thus, this qualitative analysis seemed to suggest a $125 million campaign goal as well.
National Peer Benchmarks
Considering national benchmarks became an important part of my goal-setting process. The 2019 AHP Report on Giving indicated to me that a system the size of IU Health should have a return on investment (ROI) of $5.80 for every $1.00 invested in philanthropy, meaning IU Health Foundation, with an average annual budget of $7.5 million, was underperforming the benchmark and would set an annual fundraising target closer to $43.6 million, which is above past performance.
The chart on page 49 reflects cost per dollar raised (CPDR) and return on investment (ROI) for similar organizations.6 This analysis revealed important work that needed to take place not only in fundraising but also through controlled and decreased operating expenses.
Given data and pipeline information that I reviewed, I felt strongly that the $97.9 million exponential goal was challenging yet achievable. Furthermore, that goal would be key to align IU Health Foundation to national peer benchmarks (which is further detailed in this case). Given BWF
Campaigns are powerful tools to help fundraising organizations improve performance. As part of the campaign strategy and fundraising work that I lead, I’m working with IU Health Foundation executive leaders to improve
AHP Healthcare Philanthropy Journal|Spring 2023| 48
performance within national peer benchmarks by increasing dollars raised and driving down the operating expenses through the life of the campaign.
The Gift Range Chart
Fundraising organizations have long used the gift range chart to calculate fundraising goals. However, I’ve found that a typical critical omission in gift chart creation is the analysis of not only the number of prospects needed –but the actual number of prospects identified
To help set the campaign goal for IU Health Foundation, I led work with the prospect management and data teams to analyze the number of donors, number of prospects, and number of prospects identified at each gift level.
This work is demonstrated in the gift range chart below. I observed from this analysis key gaps in many of the gift levels, signaling important prospect identification and qualification work that needed to take place during the campaign planning and early campaign phases.
This analysis quickly demonstrated areas of risk within the campaign pipeline, especially at the major gift level. This finding aligned with my observations in reviewing national peer benchmarks. So the campaign plan called for a specific focus on building the major gift pipeline, including grateful patient fundraising.
Case Study Results: Board Approved Goal Setting
Using data and analysis from the qualitative study, quantitative analysis, peer benchmarking, and gift range chart, I proposed and received board approval of a seven-year 2020-2026 baseline $125 million campaign goal. This goal takes into account the maturing fundraising program, with ambition to incrementally improve performance. Using my approach to campaign goal setting in the absence of key historical data, I was also able to deliver a
AHP Healthcare Philanthropy Journal|Spring 2023| 49
GIFT RANGE CHART (BASED ON 2020 DATA PULL) GIFT LEVEL NUMBER OF DONORS NUMBER OF PROSPECTS NEEDED TOTAL RAISED NUMBER OF PROSPECTS IDENTIFIED $15,000,000 1 4 $15,000,000 1 $10,000,000 1 4 $10,000,000 1 $5,000,000 4 12 $20,000,000 1 $2,500,000 8 24 $20,000,000 0 $1,000,000 12 20 $12,000,000 7 $500,000 24 48 $12,000,000 12 $250,000 45 80 $5,000,000 43 $100,000 35 140 $3,500,000 209 $50,000 50 200 $2,500,000 127 $25,000 100 400 $2,500,000 204 $10,000 200 800 $2,000,000 Data gap Annual Fund Many Many $1,000,000 TOTAL 437 1748 $85,000,000 GIFT RANGE CHART — 3-YEAR AVERAGE (2019-2021) 25TH PERCENTILE 50TH PERCENTILE 75TH PERCENTILE CPDR $0.26 $0.14 $0.12 ROI $4.50 $7.27 $9.50
FUNDRAISING RESULTS SINCE INTEGRATION
increase its campaign goal through performance. This has been a particularly helpful tool as I’ve worked closely with system and board leadership to explain the role of the campaign in long-range fundraising performance and health system financial planning.
Art and Science
campaign plan that addressed key areas of risk and implementation plans to address those. If the 2021 fundraising performance is any indication of future growth, IU Health Foundation is well on its way to exceed the campaign goal and reach key national peer metrics. The following chart demonstrates that IU Health Foundation is consistently outperforming its goal year-over-year. This is promising performance to move closer to national peer benchmarks.
With campaign goal approval and campaign goal planning analysis in hand, IU Health Foundation also solidified a 10-year long-range financial plan. This plan incorporates the seven-year campaign goal toward a 10-year long-range goal, signaling the likelihood that IU Health Foundation will
I’ve found that campaigns are powerful tools to fulfill donors’ visions, propel and advance key programs and initiatives, and improve fundraising performance. In the absence of key historical performance data, setting a challenging and meaningful campaign goal was an important exercise that required my thoughtful analysis utilizing all tools available to me, including:
• A quantitative analysis based on past performance and rated capacity
• A qualitative analysis based on the missionbased needs and donor input
• National peer benchmarks and a long-range planning financial goal
• A gift range chart populated by donor and prospect information.
Many people approach fundraising as an art— the art of relating to people and persuading them to give. As this case study shows, science is just as important in predicting and measuring the effectiveness of healthcare philanthropy.
Endnotes
1 “Insight Analysis,” August 2020. Prepared by © BWF.
2 “Principles and Techniques of Fundraising,” The Fund Raising School curriculum guide. © 2004.
3 www.bwf.com
4 www.accordantphilanthropy.com
5 “Campaign Planning Study Report.” Prepared by © Accordant, 2021.
6 Data from Association of Healthcare Philanthropy. www.ahp.org
AHP Healthcare Philanthropy Journal|Spring 2023| 50
$20M $25M $30M $15M $10M $5M 0 2018 MONEY RAISED 2019 2020 2021 GOAL
Heather Perdue, MA, FAHP is the Vice President, Campaigns and Philanthropy at Indiana University Health Foundation. In her role, Heather works alongside donors who are thinking intentionally about their giving and what it can do to change the landscape of healthcare and communities in Indiana. She also leads IU Health’s first multi-year, system-wide philanthropic campaign.
In previous roles at the Lilly Family School of Philanthropy at Indiana University, she worked with national donors who care deeply about philanthropy and the role that it plays in our society, funding projects like the Million Dollar list, summits on International Disaster Philanthropy, and the largest longitudinal study on American giving by household. She also worked in fundraising and program management for Riley Children’s Foundation. She received her Master of Arts in Philanthropic Studies from Indiana University and doublemajored in Communication Studies and Journalism with a concentration in Public Relations at Butler University. She became a Certified Fund Raising Executive in 2009 and received her Certificate in Fund Raising Management in 2007.
AHP Healthcare Philanthropy Journal|Spring 2023| 51
the grateful patient fundraising methodology backed by physicians

Beyond Gratitude™ is the only grateful patient model developed from individual coaching sessions with more than 2,000 doctors, nurses, and clinical professionals. grahampelton.com/

beyond gratitude ™
beyond













