STUDY OFFERS INSIGHTS ON VALUE-BASED CARE AND O&P’S OPPORTUNITY P.24
Anchored In Innovation
As U.S. patients undergo osseointegration, clinical care evolves P.16
THE PREMIER MEETING FOR ORTHOTIC, PROSTHETIC, AND PEDORTHIC
September 3–6, 2025, for an ideal combination of top-notch education and entertainment at the 108th AOPA National Assembly in Orlando, FL, at the Orange County Convention Center (OCCC).
EARN CE CREDITS
EXHIBITS EDUCATION NETWORKING
AOPAASSEMBLY.ORG
Hundreds of Americans have already undergone osseointegration (OI) to achieve direct skeletal attachment of a prosthesis, so it’s time for prosthetists to learn more about implants, recent advances in OI, and associated risks. Meet clinicians who have
and find out
By CHRISTINE UMBRELL
The O&P profession can become a vital part of the emerging value-based healthcare system, improving patient care while reducing healthcare costs. Learn more about this opportunity and the basics of value-based care in this primer, based on a new whitepaper by Avalere and funded by AOPA.
By JOSEPHINE ROSSI
Kris Kail, CP, proves age is just a number in providing a
AOPA Contacts
A world where orthotic and prosthetic care transforms lives.
Board of Directors OFFICERS
President
Rick Riley
O&P Boost, Bakersfield, CA
President-Elect
Kimberly Hanson, CPRH Ottobock, Austin, TX
Vice President
Matt Swiggum Proteor, Tempe, AZ
Treasurer
Chris Nolan Össur, Foothills Ranch, CA
Immediate Past President Mitchell Dobson, CPO Hanger Clinic, Austin, TX
Executive Director/Secretary Eve Lee, MBA, CAE AOPA, Alexandria, VA
DIRECTORS
Jeff Erenstone, CPO Mountain Orthotic and Prosthetic Services, Lake Placid, NY
Catherine Marinoff, art director, 786-252-1667, catherine@marinoffdesign.com
Bob Heiman, director of sales, 856-520-9632, bob.rhmedia@comcast.net
Christine Umbrell, editorial/production associate and contributing writer, 703-662-5828, cumbrell@contentcommunicators.com
PUBLISHER EVE LEE, MBA, CAE
EDITORIAL MANAGEMENT CONTENT
COMMUNICATORS LLC
ADVERTISING SALES RH MEDIA LLC
DESIGN & PRODUCTION MARINOFF DESIGN LLC
PRINTING SHERIDAN
SUBSCRIBE
O&P Almanac (ISSN: 1061-4621) is published monthly, except for combined issues in June/July and November/ December, by the American Orthotic & Prosthetic Association, 330 John Carlyle St., Ste. 200, Alexandria, VA 22314. To subscribe, contact 571-431-0876, fax 571-431-0899, or email info@aopanet.org. Yearly subscription rates: $59 domestic, $99 foreign. All foreign subscriptions must be prepaid in U.S. currency, and payment should come from a U.S. affiliate bank. A $35 processing fee must be added for non-affiliate bank checks. O&P Almanac does not issue refunds. Periodical postage paid at Alexandria, VA, and additional mailing offices.
ADDRESS CHANGES
Postmaster: Send address changes to: O&P Almanac, 330 John Carlyle St., Ste. 200, Alexandria, VA 22314.
Share your message with AOPA membership— approximately 9,000 orthotic and prosthetic professionals, facility owners, and industry personnel. Contact Bob Heiman at 856-520-9632 or email bob.rhmedia@comcast.net. Learn more at bit.ly/AlmanacMediaKit25
Discover Meracus®
100% composite design for a seamless gait experience
AOPA Board of Directors Launches 2025 Agenda
As AOPA prepares for a new year, the association’s leadership team is off and running, leveraging their experience and dedication to the profession to advocate for AOPA members and advance AOPA’s vision: a world where orthotic and prosthetic care transforms lives. Elected by the membership, the AOPA Board of Directors is representative of the membership and serves as the governing body, responsible for the supervision and direction of its mission. The members of the 2024-2025 Board of Directors took office Dec. 1, 2024, and will serve through Nov. 30, 2025.
Elected during the AOPA National Assembly in September, Rick Riley, who has been a member of AOPA’s Board of Directors for the past eight years, will serve as president of AOPA for the coming year. Riley is a long-time participant in AOPA’s Policy Forum and a vocal advocate for women in the O&P profession; he was honored with AOPA’s Legislative Advocacy Award in 2015. Riley has spent his 41-year career in the healthcare sector, including 30 years on the supplier side of O&P. He founded O&P Boost in 2020 and currently provides management, marketing, and sales consulting services to O&P suppliers.
Kimberly Hanson, CPRH, has assumed the president-elect position. Hanson is director of reimbursement, North America, for Otto Bock HealthCare, and an enthusiastic advocate for O&P in the states of Texas and Minnesota and on the federal level.
Elected as AOPA vice president for the new term is Matt Swiggum, who has worked in the field of prosthetics since 1997. A dedicated O&P advocate, Swiggum believes that having access to care is critical for the long-term success of people with limb loss and limb differences. He brings decades of experience in executive leadership, sales, and marketing.
Chris Nolan serves as treasurer for the upcoming year. He has worked in the O&P profession for more than 25 years, for some of the largest and most respected names in the industry. Currently, Nolan is vice president of upper-limb prosthetics at Össur for the company’s combined Naked Prosthetics, Touch Solutions, and Livingskin business.
Rounding out the 2024-2025 officer roster are Mitchell Dobson, CPO, who serves as immediate past president, and Eve Lee, MBA, CAE, who is AOPA’s executive director and serves as secretary (nonvoting) until she steps down as executive director on January 22, 2025, and a named interim director assumes the role.
Four individuals are new to the AOPA Board of Directors this year: Jeff Erenstone, CPO, is head clinician and chief researcher for Mountain Orthotic and Prosthetic Services and founder of Operation Namaste. Deanna Fish, MS, CPO, is a clinician who currently serves as clinical outreach manager for Orthomerica Products Inc. Shane Kelly is chief executive officer of Thuasne North America. Andrew Steele, MBA, CPO, LPO, is an owner/managing partner of Clark & Associates Prosthetics and Orthotics, based in Waterloo, Iowa.
To the right is the full list of 2024-2025 AOPA Board of Directors members.
2025 AOPA Officers
2025 AOPA Board Members
Special Thanks To Departing Members
AOPA appreciates the significant work of these individuals, who concluded their terms as AOPA board members Nov. 30, 2024.
Rick Riley, President
Chris Nolan, Treasurer
Kimberly Hanson, CPRH, President-Elect
Mitchell Dobson, CPO, FAAOP, Immediate Past President
Matt Swiggum Vice President
Eve Lee, MBA, CAE, Secretary (Nonvoting)
Deanna Fish, MS, CPO
Jeff Erenstone, CPO
Jim Kingsley
John “Mo” Kenney, CPO, LPO, FAAOP
Teri Kuffel, JD
Linda Wise
Arlene Gillis, MEd, CP, LPO
Lesleigh Sisson, CFo, CFm
Andrew L. Steele, MBA, CPO, LPO
Adrienne Hill, MHA, CPO, LPO, FAAOP
Shane Wurdeman, PhD, CP, FAAOP(D)
Shane Kelly
RESEARCH ROUNDUP
Attitude and Behavioral Control Help Predict AFO Use in Stroke Survivors
A research team from the United Kingdom sought to identify predictors of ankle-foot orthosis (AFO) adherence among stroke survivors using the theory of planned behavior (TPB), an established theoretical framework that predicts how a person’s intentions, or self-control, influence their behavior.
Forty-two individuals who experienced strokes completed a TPB questionnaire upon being prescribed an AFO, then again one month later. The researchers leveraged regression analyses to evaluate predictors of intention and AFO adherence behavior.
The researchers found that 63% of participants adhered to prescribed AFO use, with TPB accounting for 61% of the variance
Decision-Making Tool May Aid New Prosthesis Users
Recognizing that prosthesis design decisions do not always reflect a prosthesis user’s needs, values, and preferences, a team of researchers from the University of Colorado’s Department of Physical Medicine and Rehabilitation and others developed a patient decision aid (PDA) prototype.
The team examined a qualitative needs assessment and referenced the International Patient Decision Aid Standards to develop the PDA. Steering groups of experienced prosthesis users, prosthetists, and researchers tested usability, accuracy, and comprehensibility via focus groups, individual interviews, and a Likert scale ranging from 1 to 10.
The final prototype PDA features six sections: amputation and early recovery; communication; values; prosthesis design; preferences; and prosthetic journey. Early testing by prosthesis users gave high scores to usability, accuracy, and comprehensibility of the tool. Details were published in October in Prosthetics and Orthotics International
in intentions and 43% of the variance in AFO adherence behavior. They concluded that TPB is a useful model for explaining adherence to AFOs in people with stroke: “The current study found that attitude and perceived behavioral control were significant predictors of intention to adhere to AFOs. In turn, intention was a significant predictor of adherence,” they reported. They recommended that interventions be designed to increase intentions to use an AFO as prescribed “by promoting positive attitudes toward, and perceived behavioral control of, AFO adherence.”
The study was published in Prosthetics and Orthotics International in September.
ABC Donates $1.5 Million to O&P Foundation, Pledges To Match Additional Donations
The American Board for Certification in Orthotics, Prosthetics, and Pedorthics (ABC) recently donated $1.5 million to the Orthotics and Prosthetics Foundation for Education and Research (O&P Foundation). In addition, ABC has announced it will build on its unrestricted $1.5 million donation by pledging to match every donation made to the O&P Foundation through November 2025, up to $1 million. Potential donors are encouraged to consider giving to help advance the O&P Foundation’s mission of advancing orthotic and prosthetic rehabilitation through scholarships, research grants, and professional training awards.
“In any new endeavor, someone must always be the first,” said Chris Fairman, CPO, chair of the O&P Foundation. “The O&P Foundation will be eternally grateful to ABC and its Board of Directors, who decided to commit substantial resources and be the first major donor to the O&P Foundation. This donation will catalyze efforts to transition to a sustainable endowment model and allow the O&P Foundation to raise levels of awareness beyond that of the O&P community.
“Through the O&P Foundation’s education, research, and professional awards programs, this donation not only strengthens the future of our profession but empowers the next generation of practitioners and researchers to contribute to the highest quality of practice in orthotic and prosthetic rehabilitation,” said Fairman.
“The decision to sunset two well-established foundations in the pursuit of new opportunities through the creation of a singular O&P Foundation could have raised some concerns. ABC’s generous donation gives rise to a new horizon, one in which the vision for the O&P Foundation comes into focus with the same clarity as held by the founders,” said Shane Wurdeman, PhD, CP, FAAOP(D), immediate past chair of the O&P Foundation and past chair of Center for O&P Learning. “We could not be more thrilled and invite all members of the O&P community to be a part of our vision.” To learn more, visit oandpfoundation.org
DIABETES DOWNLOAD
MEDICARE MATTERS
Beneficiaries With Amputation
Experience Adverse Health Outcomes
PREVALENCE RATES ON THE RISE
“The prevalence of diabetes in the United States increased by 18.6% from 2012 to 2022, with notably higher rates among racial and ethnic minorities, men, older adults, and socioeconomically disadvantaged populations.” SOURCE:
A newly released report from the Government Accountability Office (GAO) examines trends in limb loss in the United States, studying amputation among beneficiaries enrolled in traditional Medicare in 2016. The researchers found that two thirds of the 50,202 traditional fee-for-service Medicare beneficiaries who lost a limb that year were male (66%).
Medicare Beneficiaries Who Lost a Limb in 2016 Who Received a Prosthesis
Nearly half of the Medicare beneficiaries who lost a limb suffered a “minor” lower-limb amputation: loss of a toe or toes or part of a foot (48%). Another 39% suffered a “major” lower-limb amputation, or loss of an entire foot or all or part of a leg. Almost one out of 10 experienced both major and minor lower-limb amputation (9%). Just 4% experienced major or minor upper-limb amputation.
Among the traditional Medicare beneficiaries who lost a limb in 2016 and received at least some sort
ACCESSIBILITY
of rehabilitative services and/or prostheses postamputation, 96% underwent physical therapy, 41% were treated by physical medicine and rehabilitation physician services, and 30% received a prosthetic limb.
“Most beneficiaries in traditional Medicare with limb loss in 2016 experienced adverse health outcomes within four years,” noted the researchers. For example, 61% of beneficiaries who lost a limb died within four years. “Underlying health conditions in individuals living with limb loss—e.g., diabetes and vascular disease—contribute to a beneficiary’s overall health and could lead to fatal events such as heart attacks.”
Details were published in GAO’s “Limb Loss: Rehabilitation Services and Outcomes for Medicare Beneficiaries” in October.
Utah, Nevada Named States With Least Accessible Healthcare
A new survey from Gallup and West Health found that only 55% of U.S. adults can access and afford quality healthcare when needed. Researchers from Forbes Advisor examined these results and conducted a state-by-state analysis to determine where healthcare is “least accessible.” Fourteen key health metrics were used to determine the least accessible states, including hospital beds per 1,000 residents; number of primary care physicians per 10,000 residents; number of specialist physicians per 10,000 residents; percentage of residents who lack health insurance coverage; and a variety of related factors.
Utah offers the least accessible healthcare, according to the study, due to its lack of resources, including qualified healthcare professionals and hospital beds. Nevada, Texas, Arizona, Georgia, South Carolina, Indiana, Wyoming, Idaho, and North Carolina rounded out the list of top 10 states with least accessible healthcare.
“Accessing affordable healthcare is a challenge for many Americans nationwide,” Zoi Galarraga, senior digital PR manager at Forbes Advisor, said in an article in Newsweek. “In some states, accessing healthcare may be more challenging due to high costs, a lack of health insurance coverage, and a shortage of healthcare providers.”
TRUST THE INNOVATORS
By the Numbers
How Does Your Company Compare?
Newly published AOPA reports offer key business insights, select financial measures for O&P facilities
People & Places
PEOPLE
Visit the AOPA Hub To Purchase the Full Reports
For details and comprehensive findings on key performance metrics and data-driven insights, purchase AOPA’s “2024 O&P Operating Performance Report” and “2024 Compensation and Benefits Report.” Visit the AOPA Hub, or contact Betty Leppin with questions, bleppin@aopanet.org.
VGM & Associates has announced two leadership updates: Cindi Petito has joined as director of clinical networks, and Nikki Grace has joined as director of the Orthotic and Prosthetic Group of America (OPGA).
Petito has more than 29 years of experience in multiple healthcare settings, including complex rehabilitation. She has more than 20 years of experience working with Medicare and Medicaid, commercial insurance companies, and workers’ compensation programs. In her new role, Petito will support U.S. Rehab and VGM Live at Home, both divisions of VGM & Associates, and will build out a network of occupational therapists that will allow VGM to increase referrals to members, among other initiatives, to better align mutual efforts and support market growth. “I am incredibly grateful for the opportunity to
contribute to this outstanding organization, support VGM’s members and vendor partners, and the industries to which I have devoted my career,” said Petito.
Grace, an advocate and leader in osseointegration education, will support VGM’s OPGA community and continue advancing the O&P profession for OPGA’s members and supplier partners. Grace previously served as director of North American operations for Osseointegration International, and established Central Illinois Amputees, a nonprofit organization that raises awareness and addresses challenges faced by amputees in rural areas. “I am thrilled to join OPGA and honored to contribute to its legacy during such exciting times for the O&P profession,” said Grace.
“We are extremely excited for Cindi and Nikki to join VGM & Associates and expand our team of experts to strengthen the programs we offer to our members and the entire industry,” said Lindy Tentinger, president, VGM & Associates.
Cindi Petito
Nikki Grace
Wendy Miller, BOCO, LO, CDME, has been honored with the Board of Certification/Accreditation’s (BOC’s) 2024 Jim Newberry Award for Extraordinary Service.
Miller has played important roles at BOC for the past 30 years. She helped develop the organization’s orthotist clinical simulation and multiple-choice exam teams. She accepted a role on the Board of Directors in 1995, then served on the BOC board for six years, including one year as secretary. She played a pivotal role in creating BOC’s orthotic fitter (COF) and mastectomy fitter (CMF) certifications in 2000 and 2001.
In 2007, Miller joined BOC’s team as facility accreditation manager, advanced to chief credentialing officer in 2015, and later served as special assistant to the chief executive officer. She helped enhance BOC’s accreditation process, assisted in creating the durable medical equipment specialist (CDME) certification, and served as an ambassador for BOC at many conferences.
Miller also contributed numerous articles to industry publications and met with members of Congress to advocate for O&P advancements, which resulted in actionable change. Miller professionally retired from BOC in December 2023.
IN MEMORIAM
Ron Cheney, CPO
Ron Cheney, CPO, president of American Prosthetics & Orthotics Inc. (APO), passed away Oct. 14 at the age of 84. Cheney advanced the field of O&P over a five-decade career span and built a facility that served as the cornerstone of the Iowa healthcare industry. He consistently advocated for continuous learning and the adoption of new technologies to enhance patient care.
Cheney completed his training at both Northwestern University and New York University. He began his career in 1958 at Winkley Artificial Limb Co. and co-purchased the spinoff American Prosthetics Inc. in 1972. His acquisition of the company in 1988 led to its growth and expansion, establishing eight offices in Iowa and one in Illinois. The company was renamed American Prosthetics & Orthotics in the 1990s to reflect its comprehensive services.
Cheney supported the Iowa Amputee Golf Association, Iowa Prosthetics and Orthotics Association, and a rehabilitation facility called On With Life. He also was a past supporter of AOPA’s O&P PAC.
“There are few people who have served BOC for so many years and in so many capacities,” said Cameron Stewart, BOCO, BOCP, chair of BOC’s Board of Directors. “Wendy is very deserving to be among the ranks of BOC’s Newberry recipients. It is one of BOC’s highest honors, and our Board of Directors is proud to recognize Wendy for her many accomplishments and contributions.”
BUSINESSES
The Board of Certification/Accreditation (BOC) announced the launch of a new accreditation product for pharmacies. The product is the result of a new partnership with the Long-Term Care at Home Pharmacy Quality Commission (LTC@HQC). With this collaboration, BOC is one of the qualified accrediting organizations in the United States to offer customers LTC@Home Pharmacy Accreditation. The accreditation validates the quality standards established by LTC@HQC and supports pharmacies in delivering high-quality, patient-centered care for individuals with long-term healthcare needs who qualify to receive care in their homes.
Several O&P providers were honored with a 2024 Freedom Award by the Orthotic and Prosthetic Group of America (OPGA) in recognition of their high-quality care of military personnel. “We’re proud to recognize these O&P providers for the exceptional care they provide to those who have sacrificed for our freedoms,” said Nikki Grace, director of OPGA. “The Freedom Award highlights their dedication to the distinguished veterans they treat and to our nation’s armed forces.”
The following AOPA member companies were honored with 2024 Freedom Awards:
• Restorative Health Services, Murfreesboro, Tennessee
• Sierra Prosthetics-Orthotics, Grass Valley, California
• Total Care Orthotics and Prosthetics, Tulsa, Oklahoma.
Wendy Miller, BOCO, LO, CDME
BY DEVON BERNARD
Closing Out 2024
Review recent policy changes and refused/returned item guidelines
As the end of the year approaches, it’s time to look at policy and billing changes impacting O&P facilities. This month’s Reimbursement Page reviews recent changes in policy that are causing some denials; previews an upcoming billing and coding change; and examines the handling of returned and refused items.
Policy Changes
The O&P community is well aware of the major shift that occurred when the LowerLimb Prosthesis Policy was updated earlier this year, which expanded Medicare
coverage of microprocessor knees, pneumatic and hydraulic knees, and compatible prosthetic feet to include patients that are classified as K2 functional-level ambulators when certain specific conditions are met—detailed in the February 2024 O&P Almanac Reimbursement Page
What some may have forgotten are the new rules for required modifiers. This oversight is causing many claims to be denied for “the procedure code is inconsistent with the modifier used” (Reason 4) and “invalid combination of Health Code Common Procedure Coding System (HCPCS) modifiers” (Remark Code N519).
As of Sept. 1, 2024, all claim lines for lower-limb prostheses must include one of the following modifiers: KX, GA, GY, or GZ. This is true not just for the claim lines for knees, ankles, and feet, but for all claim lines. So, if all policy criteria have been met and you have the proper documentation, place the KX on each claim line. If you don’t believe coverage and policy criteria have been met and you had the patient sign an Advanced Beneficiary Notice (ABN), then use the GA modifier. If you did not have an ABN signed and you believe the policy criteria have not been met, use the GZ modifier.
The other policy change to remember is specific to two HCPCS codes:
• L1843—Knee orthosis, single upright, thigh and calf, with adjustable flexion and extension joint (unicentric or polycentric), medial-lateral and rotation control, with or without varus/valgus adjustment, prefabricated item that has been trimmed, bent, molded, assembled, or otherwise customized to fit a specific patient by an individual with expertise • L1951—Ankle-foot orthosis, spiral, (Institute of Rehabilitative Medicine type), plastic or other material, prefabricated, includes fitting and adjustment.
These two codes were added to the list of codes that require prior authorization as a condition of payment. The durable medical equipment Medicare administrative contractors and Pricing, Data Analysis, and Coding (PDAC) contractor issued a coding verification requirement for L1843 and L1951 for all claims with dates of service on or after Dec. 1, 2024. Under this requirement, any item you deliver and bill to Medicare using L1951 or L1843 must be reviewed and cleared by the PDAC by Dec. 1, 2024.
Remember that L1951 is considered a custom-fitted code, so you must document the fitting that was required at the time of delivery and, most importantly, the medical necessity for why the adjustment was needed. A new code for an off-the-shelf version of the L1951 may be introduced in 2025. A code application was submitted for this purpose, and it is currently under review by CMS.
Returned Items & the Supplier Standards
The handling of returned items—items that a patient brings back to you after delivery— must be guided by the Supplier Standards for Durable Medical Equipment, Prosthetics, Orthotics, and Supplies. Supplier Standard 15 states: “A supplier must accept returns of substandard (less than full quality for the particular item) or unsuitable items (inappropriate for the beneficiary at the time it was fitted and rented or sold) from beneficiaries.”
If a patient returns an item, you must accept it, within reason, and it will be up to you to show that the item was not substandard and was suitable for the patient. This can be accomplished by having patients acknowledge their satisfaction at the time of delivery. If a patient expresses concerns, document those concerns and what you did to address them. In addition, document all subsequent encounters with the patient, including all attempts that you made to make the device satisfactory to the patient’s requests.
If a patient returns an item, you must accept it, within reason, and it will be up to you to show that the item was not substandard and was suitable for the patient.
To ensure you are documenting the suitability of the item, your final standard written order or written order prior to delivery should clearly indicate what item was ordered as this will help to demonstrate— along with your documentation and the referring physician’s documentation—that the item provided was “appropriate” for the patient at the time it was ordered and delivered. In other words, you can show that you provided exactly what the physician ordered, meaning it was suitable.
In some cases, returned items may involve an overpayment or recoupment request. If the item could not be adjusted to satisfy the patient and the patient returns the item, and you have already billed for the item and received payment, you are under no direct obligation to make a refund to the patient at the time they make the return. However, be sure that you have documented that the patient returned the item, and consider providing the patient with a
statement indicating that they returned the item.
The only time you must make a refund is when Medicare sends you an official overpayment request. At this point, you may appeal the refund request, as you would any other overpayment request, and demonstrate that you provided what was ordered and made good faith attempts to satisfy the patient. This is where documentation of how you tried to satisfy the patient, and that you delivered what was ordered, will come into play.
When handling returns, pay attention to Supplier Standards 13 and 20, which relate to patient complaints. Standard 13 states: “A supplier must answer questions and respond to complaints of beneficiaries and maintain documentation of such contacts.” Standard 20 states: “Complaint records must include the name, address, telephone number, the health insurance claim number of the beneficiary, a summary of the complaint, and any actions taken to resolve it.” So, be sure to complete your complaint log—even if it means that the resolved actions were accepting the return and issuing a refund.
Billing for Refused Items
When processing and billing for refused items, note that “refused” can have different meanings. Refused may mean that the patient voluntarily decides not to come in for delivery. An item also may be considered refused if the patient makes an involuntary choice not to accept delivery of the item because the item is no longer medically necessary, or due to a change in condition that no longer makes the item required.
Once you have established that a patient has refused an item, either by their own choice or by the fact that the item is no longer medically necessary, you must determine what you may be able to bill to Medicare and what to use as your date of service. To accomplish these two tasks, you must establish what type of item was going to be delivered: Was it prefabricated or custom fabricated, and when did you learn of the refusal?
’Tis the Season: Review the Rules for Gift Giving
If your facility is considering purchasing gifts for patients or referral sources, be sure to abide by the rules.
Referral Source Gifts
Patient Gifts
The giving of gifts to Medicare patients is acceptable and allowed; however, you must adhere to three main guidelines: Gifts cannot be cash or eligible for cash equivalents; gifts must be inexpensive or of nominal value; and you may not give a gift with the purpose of securing your services to a patient. Gifts of cash or cash equivalents, such as gift certificates or gift cards, are prohibited. The use of nonmonetary gifts is acceptable if they are of nominal value and do not exceed $15 per gift, with a $75 aggregate per calendar year. Finally, there may not be terms or strings associated with a gift, such as requiring that the patient come in for an evaluation first.
The giving of gifts to referral sources is acceptable; however, as with gifts to beneficiaries, gifts of cash or cash equivalents of any kind—gift certificates, gift cards, PayPal, Zelle, and even free samples of products—are prohibited. Nonmonetary gifts are allowed, under very limited circumstances.
First, the value of the gift may not be tied to the volume of referrals received from a physician’s office. Second, gifts may not be directly solicited by referral sources. Finally, there is a limit to the amount of money that may be spent on gifts for referral sources. This gift limit is not a fixed sum, and it fluctuates from year to year as the limit is set and adjusted according to the increase in the Consumer Pricing Index. For 2024, there is an aggregate limit of $507, so any gift or gifts provided to a referral source in 2024 may not exceed $507. The annual $507 aggregate is a limit, not an entitlement.
The date you learned about the refusal, or the date you learned the item was no longer medically necessary, will become your date of service for billing purposes. If the patient has voluntarily refused the item—did not respond to your attempts to schedule a final delivery—your date of service would be the last day you attempted to deliver the item. If the patient has passed away, your date of service is the date of the patient’s passing and not the date you
learned of their passing, because most likely it will be after they have passed. If you use a date of service that is after the date of the patient’s death, your claim will be denied.
If the item to be delivered is custom fabricated, was the fabrication completed, or were you still fabricating the item when you learned of the refusal? If you have completed fabrication, you may bill for the complete item, except for any components
that may be salvaged and reused or returned to the manufacturer for a refund. For example, if you are fabricating a below-knee prosthesis and fabrication was completed when you learned of the refusal, but you can return the foot to the manufacturer for a refund, then you may bill for everything except the foot because the foot is salvageable. If the custom fabrication process was not completed when you learned of the refusal, you may only bill for the work that you have completed up to the point you learned of the refusal. Once again, you may not bill for any parts and components that may be salvaged and reused. If the item to be delivered is prefabricated, you may not have the ability to bill Medicare because you may have the option to return the item to your stock and reuse it for a different patient, or you may have the ability to return it the manufacturer for a refund. If the item has been modified/ altered and cannot be returned to stock to be used with a different patient, you may consider it like a custom-fabricated item for billing purposes.
Once you have determined that the item has been refused and you have the ability to submit a claim to Medicare, submit your claim as you normally would. This would include using any of the modifiers (KX, LT, RT, GA, K1, K2, etc.) that are required by policy. There is not a special modifier to indicate that the claim is being billed as a refused item, so you must include a detailed statement in the narrative field of the claim indicating that you are billing for a refused item and why the item is considered refused—for example, patient passed away, condition changed, etc.
May these tips, reminders, and updates help you with understanding the latest policies and handling your returned and refused items properly during and after the holiday season.
Devon Bernard is AOPA’s assistant director of coding and reimbursement services, education, and programming. Reach him at dbernard@AOPAnet.org
FABRICATED WITH ACCURACY & PRECISION
CUSTOM: FOOT ORTHOTICS • AFO’S • RICHIES
At Hersco, we pride ourselves on being on the leading edge of technology. We have mastered the art of accepting scans and 3D printing to bring you precise orthotics every time. Our team works to deliver custom orthotics tailored to each individual’s needs and specifications. We also keep an exact digital record of each patient’s foot orthotics for ease of reproduction.
Cover Story COVER STORY
BY CHRISTINE UMBRELL
ANCHORED IN INNOVATION
As more limb loss patients receive implants, the responsibilities of modern clinical care become more defined
After 10 years of relying on crutches and a wheelchair for mobility— unable to wear a prosthesis due to an extremely short above-knee residual limb—a veteran under the care of Jon Holmes, PT, CP, LP, finally achieved his goal of walking with a prosthesis. Thanks to osseointegration (OI) surgery and prosthetic care from Holmes, the active veteran—who has always exercised regularly on a handcycle— now wears a prosthesis comfortably.
NEED TO KNOW:
f With approximately 2,200 to 2,300 individuals having undergone osseointegration (OI) internationally, and up to 500 in the United States, more American limb loss patients are viewing OI as an accessible and acceptable option.
f Implants used for anchoring prostheses directly to the bone may be particularly beneficial to lowerlimb patients who have been unable to wear a prosthesis due to socket or skin issues, short residual limbs, or lingering traumatic injuries.
“He just couldn’t wear a leg full-time,” recalls Holmes, owner of Holmes Prosthetic Center in Houston. “After 10 years of not wearing a prosthesis, he underwent OI through the Veterans Health Administration in Houston,” achieving direct skeletal attachment of a prosthesis to his residual limb via implant. Now, the patient walks every day and continues to handcycle; his quality of life has vastly improved.
f Some individuals with upperlimb loss have undergone OI in recent years and experienced impressive benefits, although the procedure is not yet FDA-approved for this patient population.
f Many patients experience profound transformations post-OI, but prosthetists should understand the risks and potential adverse events associated with the procedure before speaking with and selecting components for patients with implants.
f OI prosthetic care involves some nuances compared to socket care, including understanding the different surgical techniques, OI implants, and connector types, and recognizing the importance of proper and precise alignment.
f New OI-related techniques, and new ways to don prostheses post-OI surgery, are on the horizon, so prosthetists should do their homework and stay up-to-date on advances.
OI has become a game-changer for similar patients. Individuals with limb loss who cannot comfortably wear a socket—due to skin irritation, injured or short residual limbs, lingering traumatic injuries, burns, or other reasons—are benefiting from OI, and more clinicians are learning to provide optimal care for these patients.
“It’s extremely important for prosthetists to start learning about OI,” says Haris Kafedzic, MPO, CPO. “It’s part of our future as prosthetists.” Kafedzic, director of prosthetics at Eschen Prosthetic and Orthotic Laboratories, has fitted 170 OI patients with prostheses as part of the limb replacement team at the Hospital for Special Surgery in New York City. Prosthetists should recognize that a lot of the decision-making regarding whether to undergo OI surgery is patientdriven or surgeon-driven, he says, “so these patients will get OI. Prosthetists need to be able to follow up and help treat these patients.”
Know the Recent Developments
Approximately 2,200 to 2,300 individuals have undergone OI internationally, and between 400 and 500 in the United States, according to experts. “More patients are seeing OI as an option, and more patients are having successful outcomes,” says Jason Stoneback, MD, chief of the Orthopedic Trauma and Fracture Surgery Service and director of the University of Colorado Hospital Limb Restoration Program.
Stoneback has performed more than 90 primary OI surgeries plus hundreds of related surgeries as part of a multidisciplinary team at the University of Colorado over the past seven years, and he has watched most patients return to a more natural gait—using
a prosthesis but without a socket. Stoneback believes recent OI patients have benefited from greater implant selection, improved rehabilitation protocols, and more fine-tuned alignment compared to patients who underwent the procedure in the early years.
OI “has begun to open up as a more accessible and acceptable option for prosthetic treatment of amputees,” says Dan Milius, CPO, a prosthetist for the University of Colorado who works with Stoneback’s limb restoration team. He predicts OI will gradually gain in popularity. “I’m impressed at the growth of empirical evidence and research that is ongoing in the U.S. involving OI and care of patients.”
Perhaps even more promising is the expansion of OI to upperlimb prosthesis users. Though not many upper-limb OI surgeries have been performed in the United States—between 10 and 20, according to experts—some patients have experienced impressive benefits. Stoneback predicts transhumeral implants will improve outcomes for upper-limb prosthesis users. Current myoelectric prostheses can be heavy and difficult to wear, he says—but direct attachment of the prosthesis reduces the overall weight of the device and will allow more individuals to use advanced technologies.
Kafedzic’s group has worked with five patients who have undergone upper-limb OI: three transhumeral and two transulnar patients. For transhumeral OI patients, undergoing OI gives them full range of motion of their shoulder and better control of their prosthesis, he says.
Kafedzic also notes that the individuals that he has treated with a transulnar amputation have had a very short ulna and no radius, “so if they did not undergo OI, the only other option to wear a prosthesis would be to amputate above their elbow, and turn them into a transhumeral patient,” he says. “With OI, transulnar patients have very good control of their prosthetic hand and, more importantly, full range of motion of their natural elbow joint.”
Upper-limb osseointegration still faces many roadblocks: More trials are needed (see sidebar on page 20), and insurers often do not want to pay for high-end prostheses. Despite the obstacles, Stoneback believes it will one day become a mainstay in OI treatment for transhumeral amputation. “It will be offered in limited numbers until an Investigational Device Exemption (IDE) trial is
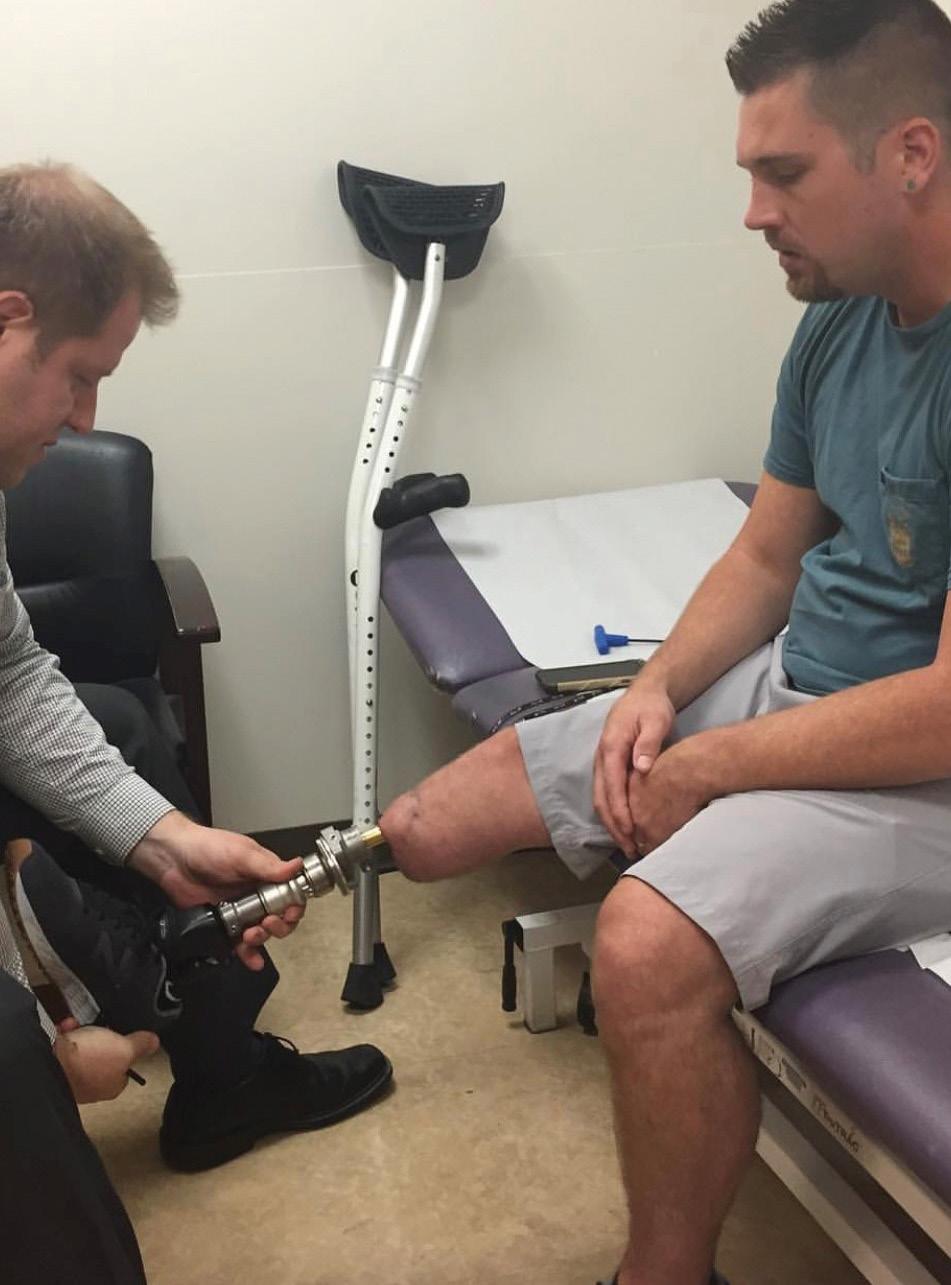
Christopher Hoyt, CP, works with an above-knee patient with an implant.
Jon Holmes, PT, CP, LP
Jason Stoneback, MD
Holmes, top center, traveled with three patients several years ago when they underwent OI at Osseointegration Group of Australia.
Not just a 3.0
Redefining the Ankle Experience
It actually feels like you have a leg. Feels a lot lighter, very comfortable. When I stand still, I balance very easily. It’s like a part of you and you’re not scared.”
For the first time in all the different prostheses and feet I have tried, and I have tried so many, it felt like I had my leg back again. The Kinterra is life changing. It has inspired me.”
Retired Car Salesman Francisco M.
Behavioral Therapist Tarsha N.
Osseointegration Shows Promise for Patients With Transhumeral Limb Loss
While not yet approved in the United States by the Food and Drug Administration, implants for use with transhumeral amputation offer significant improvements in functional outcomes, according to a study published in Plastic and Reconstructive Surgery— Global Open in May. An international research team comprising surgeons and doctors at multiple institutions, including Massachusetts General Hospital and Harvard Medical School, conducted a systematic review of eight articles focusing on upper-limb osseointegration (OI). Most study subjects had been fit with an Osseointegrated Prostheses for the Rehabilitation of Amputees implant in conjunction with myoelectric systems.
The researchers concluded that “most of the studies showed participants demonstrating an enhanced range of motion and improved performance of activities compared with traditional socket-based prostheses.” They also noted that quality-of-life measures consistently showed positive outcomes, “with individuals reporting better physical and psychosocial well-being following OI.”
completed,” he says. “IDE studies take many years to complete … so in the next five years, we will probably see more patients getting this treatment.”
Understand Prescreening and Implant Options
OI surgery is not without its risks, with the five most impactful adverse events being failure of biological fixation, deep infection, aseptic loosening, no mechanical fixation, or implant breakage, according to a study published in October in Prosthesis
Holmes says that healthcare professionals have gotten better at the prescreening process prior to OI surgery. “We’re doing more scans and studying the bone that will be implanted—anticipating problems before they occur,” he says. Postsurgery, “we’re better at recognizing symptoms” of infection, and “treating it quickly—we’re monitoring things better.”
Prosthetists with patients who have, or are considering, implants should do their homework on the procedure. Holmes was able to successfully treat his veteran handcycle patient because he has treated 35 OI patients in the past decade. Holmes also traveled to Australia when the procedure was new to learn about it at the Osseointegration Group of Australia, then became team prosthetist at an OI surgical clinic in Texas.
While Holmes embraces his responsibilities as an OI prosthetist, not all clinicians are eager to treat this patient population. “Many prosthetists are afraid to get involved because they either lack knowledge of the intricacies associated with prosthetic care, are concerned about liability, or simply realize the coding system does not reimburse for the time, intensity, and skill to care for boneanchored individuals,” says Christopher Hoyt, CP, an OI educator who previously served as the lead prosthetist on a collaborative OI team. Hoyt, who offers guidance, education, and problemsolving to prosthetists working directly with clients, believes O&P professionals should understand which patients will benefit from OI and how prosthetists can support patients with implants.
The implant market is constantly evolving, so prosthetists should recognize the different types available. Screw-fixation implants utilize a threaded cylindrical design and are applied through a two-stage surgery. Press-fit implants are similar to common artificial knee and hip joints and can be performed in a two-stage or single-stage surgery. Other implants are currently in development and awaiting approvals for use in the United States.
The only implant that has received approval by the U.S. Food and Drug Administration is the Osseointegrated Prosthesis for the Rehabilitation of Amputees (OPRA) Implant System, a screw-fit device. In late 2020, the FDA approved the OPRA for some individuals with above-knee amputation.
Beyond FDA-approved procedures, many U.S. patients obtain a Compassionate Use Exemption (CUE) or Custom Device Exemption (CDE) that allows medical devices that are not otherwise FDA-approved for marketing to be used in limited circumstances without requiring evidence of effectiveness. Some Americans who have used CUE to undergo OI have received a press-fit implant that is completed in one surgery, rather than the OPRA implant, which requires two surgeries. The type of implant a patient receives
depends on several factors, including their insurance, their anatomy, their overall clinical condition, and their overall capacity for rehabilitation, says Stoneback. “All OI, including OPRA, is heavily dependent on the patient’s insurance and our ability to provide the proper documentation” to the payor, Stoneback says. “That’s why it’s important to go to an experienced OI clinic” for the surgery. Stoneback’s team also is involved in clinical trials for new procedures, using new implants.
Hoyt notes that “we’re expecting to see a redesigned Compress implant—which is neither screw-fit nor press-fit—soon.” This implant has been designed to prevent bone resorption by allowing stress sharing via the implant and bone while providing a motion-free environment suitable for biologic fixation, according to the manufacturer’s website.
Patients with above-knee amputation continue to be the most likely to undergo OI in the United States, says Stoneback. However, some U.S. patients with transtibial or upper-limb amputation also have received implants using compassionate use or custom use exemptions, he says.
At the Hospital for Special Surgery in New York, most patients receive press-fit implants through compassionate use exemptions or under approval as part of an ongoing research study under the FDA, says Kafedzic
Recognize the Benefits—and Limitations—of OI
Kafedzic adjusts a prosthesis for a patient with a short transtibial residual limb who had been unsuccessful with a socket prior to OI.
For upper-extremity patients who undergo OI, “they often gain what we consider a larger working envelope—that is, a larger amount of space around their body that they are successfully able to operate and use a prosthesis,” says Milius
Most OI patients experience “really profound” transformations after the surgery, says Stoneback. The majority feel relief from socket-related symptoms, such as poor fit, chafing, discomfort sitting on the socket, and volume changes; gain osseoperception, or the unconscious perception of the position of the body, movement, and spatial orientation; and report feeling as if they’re less disabled than prior to surgery, according to Stoneback OI is best suited for those who “have had a difficult experience using sockets,” says Milius. “This could be related to chronic skin issues, such as fragile skin, from burns; a consistent incidence of pain in using a socket, which could be an unresolved neuroma; or simply a difficult limb shape to fit comfortably in a socket.
Dan Milius, CPO
“Often, I see OI patients going from very sedentary lives to much more active lives in terms of mobility and use of a prosthesis,” Milius says. Many such patients then experience the health benefits— both physical and psychological—that come with mobility and activity, and “are able to complete activities that they [were unable to perform as] socket users either because of restrictions of socket comfort or because they felt they couldn’t with their current prosthetic use—for example, a socket made them feel unbalanced.”
Despite the benefits, “OI is not for everyone,” cautions Holmes, and should be an option only for those patients experiencing significant socket challenges. Three of his 35 OI patients have had their implants removed, and others have suffered infections. Patients need to “consider the risk versus the reward” when making the decision.
Embrace Your Role as a Prosthetist
As clinicians who are highly trained and knowledgeable in alignment, proper biomechanics, material properties, and component selection, prosthetists play key roles in returning OI patients to mobility, says Milius
Preoperatively, a prosthetist can serve as part of a multidisciplinary team and assist in evaluations to determine suitability for OI surgery, says Kafedzic. Postoperatively, the prosthetist can take patient measurements and help explain the process to patients. Once the patient is approved for full weight-bearing, the prosthetist can evaluate the implant and prosthetic quality, including torque, implant position, static alignment, bench alignment, and initial dynamic alignment.
Haris Kafedzic, MPO, CPO
OI prosthetic care involves some “nuances” compared to socket care, says Milius—namely, understanding different OI connectors, maintenance, and troubleshooting, and field servicing these parts; recognizing the different implant types, surgical techniques, and corresponding rehab protocols; and knowing the rules and regulations for OI care related to the O&P scope of practice, “all of which are important for proper management of these patients.”
Selecting the proper prosthesis and components is a critical aspect of treating OI patients, adds Kafedzic. Because OI prostheses are connected directly to the bone and do not involve the use of liners and socks, “it’s very important that we have the correct components that have vertical shock absorption units and axial rotation units, in order to keep their leg safe.”
Osseoperception also plays a role in prosthetic care; because some patients experience increased tactile sensation, “changes being made either to alignment or componentry are at a more microlevel, as opposed to the macrolevel of socket users,” Milius says. Whereas a socket user might require a full turn of an alignment screw to effect change, “a quarter turn might be more appropriate with OI patients.”
Prosthetists cannot provide an OI prosthesis according to the principles appropriate for socket prostheses, says Kafedzic. “Doing so could leave an OI patient improperly aligned and provoke maladaptive accommodations,” he says. “OI patients generally have complete and ultimate skeletal control of their prosthesis. Therefore, little changes can make big differences.”
Hoyt recommends researching the transcutaneous connectors that attach the prosthetic limb to the metal implant that has been inserted into the bone. These connectors have specific nuances, and using the connector recommended by the manufacturer is critical, says Hoyt, as mismatched connectors may cause premature wear and breakage issues. “Alignment of componentry inferior to the implant can more easily be obtained now that we can eliminate the variables associated with a prosthetic socket.
“Repeatedly, we have seen that prosthetists play a huge role in pain management,” Hoyt adds. He suggests that prosthetists can help eliminate some types of pain by optimizing alignment and implementing shock-attenuating componentry, without the need for more invasive treatments, such as steroid injections.
Weigh the Pros and Cons
Hoyt and Holmes say the risk of infection or even removal of the implant continue to be factors in decision making when determining whether to pursue OI. Hoyt notes that females, patients with high BMI scores, and individuals who smoke experience the highest rates of infection.
Stoneback believes that risk of infection is decreasing as healthcare professionals come to understand how implant-related infections occur. “Not everything that is thought to be an infection is actually an infection,” he says, noting that some “infections” are actually rashes or alignment-related issues. In addition, “Management of the soft tissue envelope—which requires involving a plastic surgeon on the OI team—is critical,” he says.
Because the technology is relatively new, Hoyt says more data on implant outcomes is needed. “We need to see which implants, and which OI teams and protocols, have fewer adverse events,” he says. “We need to begin separating out who is successful and why.”
Patients who are appropriate candidates for OI, according to Holmes, should be healthy; have not experienced previous infection; have strong bones that have not gotten brittle; and have a penchant for taking care of themselves. “OI is really designed for someone who has had consistent socket problems for a considerable amount of time—persistent, consistent socket issues,” Holmes says, including individuals who have skin problems or physical issues from a trauma that make it difficult or painful to wear a socket.
Kafedzic works with patients with transulnar amputation who benefit from implants due to short below-elbow residual limbs.
Christopher Hoyt, CP
Prosthetists also should make sure their patients understand the long rehabilitation process and the limitations that will persist after surgery. Patients must rely on crutches or a wheelchair and won’t be able to use a prosthesis for several months, says Holmes. “For those who were already prosthesis users, it takes between six months and a year to get back to where they were before” in using a prosthesis, he says—so patience is a key factor in post-op rehabilitation.
In addition, candidates must be educated that high-impact activities are not recommended for patients with implants. “We don’t know yet how active patients can be,” says Stoneback. “There are restrictions based on connector types.” This is why he recommends that patients who are very active and who tolerate a traditional socket well avoid osseointegration.
Prepare To See More Patients With Implants
As more patients undergo OI, and as more research becomes available, Stoneback predicts that patient outcomes will continue to improve, and “we’ll do a better job of preventing negative outcomes.”
More U.S. institutions will increasingly look to OI as an option for treatment of amputees, according to Milius: “This will create more trained individuals for all positions of stakeholders,” including surgeons, physical therapists and rehabilitation specialists, and, of course, prosthetists.
Kafedzic believes that new OI-related techniques, and new ways to don prostheses following surgery, are on the horizon. “Manufacturers are designing products with safety in mind, to integrate breakaway systems and fail-safes,” he says.
With this growth will come a heightened need for education. “I anticipate [OI] being touched upon more in-depth in schools— specifically, O&P schools,” says Milius
Education will improve prosthetists’ confidence to treat OI patients, says Hoyt. He encourages new prosthetists to learn the intricacies of selecting and fitting appropriate componentry and aligning prostheses for OI patients, and to contact experts in the field if they have questions.
“Though we’re working with an implant integrated into a bone, it should not detract you from caring for these patients,” Milius says. “Prosthetists are one of the only, if not the only, trained healthcare providers that can understand all aspects related to care for amputees, whether it is socket- or OI-related. And though no socket is involved, prosthetists will be highly sought after to be involved in the clinical picture for OI. We are still very much involved in the process, and these patients will need us to help them get to the level of functionality they desire.”
Christine Umbrell is a contributing writer to O&P Almanac Reach her at cumbrell@contentcommunicators.com
VBC
THE QUEST FOR QUALITY
How value-based payment models are reshaping primary to prosthetic care—and why outcomes matter
BY JOSEPHINE ROSSI
In medical offices across America, physicians are no longer only counting patient visits or procedures performed. They also are examining new metrics, such as prevention rates, patient outcomes, and most notably, the total cost of care for their patient populations.
This shift represents an attempt to solve one of America’s most persistent policy challenges: a healthcare system that consistently delivers worse results at higher costs than those of other developed nations.
While technologically advanced, the American healthcare system has patterns of overutilization and fragmented care delivery. A system of traditional fee-for-service (FFS) provider reimbursements has fostered innovation but also created problems. While the system compensates providers for services delivered, it offers no incentive for achieving better patient outcomes. CMS established its Center for Medicare and Medicaid Innovation (CMMI) to test new healthcare payment and delivery models on their ability to improve care quality, reduce costs, and promote patient-centered practices throughout Medicare, Medicaid, and the Children’s Health Insurance Program.
In 2021, CMS announced the goal to use value-based care (VBC), a payment model that links payment to quality and outcomes, for all Medicare beneficiaries’ healthcare by 2030. Some commercial insurers are also aligning their contracts to the model. Initial VBC models targeted primary care providers and high-cost specialty areas such as cardiology, oncology, and nephrology. With the focus
of O&P on functional improvement, the profession is well-positioned to be included in future VBC models, according to a new whitepaper by Avalere and commissioned by AOPA.
The following is a primer based on that whitepaper focusing on the different aspects of VBC and the role that the O&P field can play. Here’s what O&P professionals need to know.
How Does VBC Work?
Value-based care fundamentally restructures healthcare reimbursement by connecting payment to patient outcomes rather than service volume. This approach shifts the focus from treating illness reactively to promoting wellness proactively through preventive care and chronic disease management. By aligning financial incentives with improved health outcomes, VBC models encourage healthcare providers and payors to deliver higher quality care while managing costs more effectively. The goal is to create a healthcare system where financial success depends on keeping patients healthy rather than simply delivering more services.
More specifically, key financial features distinguish VBC models from traditional FFS payment systems. First is the risk amount: VBC shifts financial responsibility from insurance companies to healthcare providers. The amount of risk that providers take on varies among contracts, but the basic principle is that providers become responsible for the healthcare costs of their patient population.
Risk structure also varies. Contracts can be either “one-sided” with only upside risk or “two-sided” with both upside and downside risks. In one-sided contracts, providers receive bonuses for better outcomes, whereas in two-sided contracts, providers can either earn bonuses or be penalized based on outcomes. Providers may receive payments either before care is delivered or retrospectively, with many models combining both approaches.
To ensure goals are being met consistently, VBC payment models incorporate mechanisms that focus on either quality processes and reporting requirements or financial incentives and penalties. All VBC models require providers to report specific data that demonstrates care quality and health outcomes. Some models also mandate providers to implement quality-improving processes, such as care coordination services, clinical decision support tools, or shared decision-making frameworks. In more sophisticated models, a provider’s performance on quality measures directly affects their revenue. This can take several forms, including direct performance-based payment bonuses and penalties, quality thresholds for shared savings, or public quality ratings that influence patient enrollment and provider selection.
Several different approaches to VBC payment models exist. The most basic is the pay-for-performance model, which incorporates a small degree of quality measure performance assessment, such as outcomes, efficiency, or cost, to supplement payment decision. On the other end of the spectrum is full capitation, in which a provider is given a single fixed payment for management of the patient’s care. Under this arrangement, providers assume complete financial responsibility for the costs of delivering care throughout the covered period. This creates a strong incentive for efficiency and cost management. All other VBC payment models fall somewhere between these two models (see sidebar on page 26).
Growth and Adoption
By late 2023, nearly half (48.9%) of traditional Medicare spending flowed through value-based payment programs. Medicare Advantage—also known as “Part C,” Medicare-approved plans from private companies that offer an alternative to original Medicare— had 57.2% of spending in value-based models. This growth is particularly evident in Medicare Advantage’s population-level programs, which saw spending surge from $88.2 billion in 2017 to $219.3 billion in 2022, according to Avalere.
ONE-OF-A-KIND CUSTOM ORTHOTICS
Types of Value-Based Payment Models
The healthcare system has developed several different approaches to value-based payment:
• Pay-for-Performance: Adds quality metrics to fee-for-service, with potential bonuses or penalties. (Examples: hospital value-based purchasing and MeritBased Incentive Payment System.)
• Pro Fee Capitation: Upfront payments for overhead costs like care coordination, typically for specialists. (Example: Kidney Care First model.)
• Surgical Bundles: Fixed payment covering procedure and related services in a short timeframe. (Example: bundled payment for care improvement model.)
• Condition-Based Bundles: Longer-term bundled payments for specific conditions, encouraging preventive care. (Example: ESRD Treatment Choices model.)
• Population Health: Providers manage costs for entire patient populations against benchmarks, focusing on prevention. (Example: accountable care organizations, or ACOs.)
• Full Capitation: Maximum risk model with payments based on historical trends and risk scores. Requires sophisticated cost modeling and care coordination. (Example: ACO REACH Global Track.)
SOURCE: “AVALERE WHITE PAPER: VALUE-BASED CARE AND ORTHOTICS AND PROSTHETICS,” DECEMBER 2024
Adoption among private payors has been slower. The frequent turnover in commercial insurance makes it difficult to realize returns on long-term preventive health investments, as members often change plans before the benefits materialize. Additionally, commercial populations tend to be younger and healthier, creating fewer opportunities for cost reduction through care management. As a result, commercial insurers typically use shorter-term, episode-based payment models that align with their population dynamics, according to the whitepaper.
The implementation of VBC also depends heavily on provider capabilities, particularly as risk levels increase. Organizations taking on substantial financial risk must demonstrate sophisticated clinical and operational capabilities, supported by robust technology infrastructure. However, many healthcare providers currently lack the advanced data capture and analytics capabilities
to be successful with VBC implementation. As tech vendors bolster the sophistication of their solutions, Avalere predicts that provider adoption of VBC will likely accelerate across the healthcare landscape.
The O&P Opportunity
The case for including O&P care in value-based models is compelling, says Avalere. More than 5.7 million Americans live with limb loss or limb difference—a number expected to double by 2050. The demand for orthoses continues to rise with an aging population and increasing chronic disease burden, with orthopedic devices projected to see 3.36% annual growth over the next four years.
Research has demonstrated both improved outcomes and reduced costs because of O&P interventions. For instance, a comprehensive 2013 Medicare population study found that patients who received orthotic or prosthetic devices had lower total care costs and better quality of life compared to those who did not receive these devices. Further, a 2017 RAND study showed that advanced microprocessor-equipped lower-limb prostheses not only improved quality-adjusted life years but also reduced fall-related injuries, highlighting how O&P devices and patient care can directly impact patient safety and wellbeing.
The shift to value-based payments also offers an opportunity to correct ongoing misconceptions about O&P professionals as device suppliers rather than clinicians providing healthcare services, Avalere asserts. While O&P providers might not serve as primary participants in value-based care models, they are well-positioned as affiliates to model participants, contributing to better patient outcomes and lower total care costs.
For O&P to realize its full potential in value-based care, Avalere analysts strongly encourage the profession to continue to ramp up its coordinated outcomes data collections and research efforts. It also suggests the profession actively pursue partnerships with model developers, payors, and integrated delivery networks to create innovative value-based arrangements that include O&P services. The success of these partnerships depends heavily on evidence showing that including O&P professionals on care teams leads to better outcomes and lower costs. This evidence will not only attract potential partners but also help design optimal partnership structures. Integrated delivery networks and payors should view these partnerships as opportunities to both enhance current O&P care and identify new patient populations that could benefit from O&P services.
As healthcare continues to evolve toward value-based models, O&P has an unprecedented opportunity to demonstrate its crucial role in improving patient care while reducing overall healthcare costs. The path forward for VBC will depend not only on primary care transformation, but on the integration of specialized services that significantly impact patient outcomes, such as O&P. In value-based care models, it is an important step toward a more comprehensive, patient-centered healthcare system.
Josephine Rossi is editor of O&P Almanac. Reach her at jrossi@contentcommunicators.com
PATENT: US9119735 B2 SmartPuck
Internal Vacuum for Superior Hold
No more leaky valves and tubing
Smart App and Manual Control
YOUNG AT HEART
Indiana clinician looks past age in creating solutions for a bilateral limb loss patient
The Transformations column features the success story of an O&P clinician who has worked with an inspiring or challenging patient. This month, we speak with Kris Kail, CPO, an Indiana facility owner who provided a comfortable and practical solution for a patient with bilateral transtibial limb loss.
Age is just a number—a number that shouldn’t limit treatment options for patients with limb loss, according to Kris Kail, CPO, owner of Prevail Prosthetics & Orthotics, a facility with six locations in Indiana. Over the course of his 25-year career, Kail has learned to get to know patients as individuals before determining the best prosthetic solution. That’s how he came to design comfortable and functional devices for bilateral patient Mary Ippel.
Ippel has not been defined by her disability. At 72, she is a mother to 10 children, a grandmother to 16 children, a master gardener at Purdue University, an active hiker and cyclist, and a longtime volunteer at Muncie Mission, a homeless center and rehabilitation clinic for men who have addiction. All of that activity temporarily ended nine years ago, when she lost both legs below the knee as well as several fingertips due to a medical emergency.
Sudden Illness
Ippel was visiting her daughter in Williamsburg, Virginia, on May 28, 2015, when she awoke in the middle of the night with excruciating abdominal pain, thinking she was going to die. She was rushed to an emergency room where she was diagnosed with hemorrhagic pancreatitis, or the disruption of pancreatic microcirculation, which results in necrotizing pancreatitis. “My pancreas had started dumping all of the toxic fluid into my abdomen, and burned my colon to my abdominal wall,” she says.
Ippel coded twice and suffered a heart attack. For the next two-and-a-half months, she was under such heavy sedation that
Kris Kail, CPO
Kail and patient Mary Ippel
she has no memory of the time. When she awoke Aug. 3, both of her legs had been amputated below the knee, and she would soon undergo amputation of six fingertips. She suffered hearing loss from several days of fevers, had broken teeth, and experienced severe weight and muscle loss.
When she became conscious and aware of her condition, Ippel chose to adopt a positive attitude and stay thankful. She was fit with prosthetic legs in the hospital—a requirement to be transferred to a rehab facility rather than a nursing home. “The hospital prosthetist told me he had never fit anyone who was in such bad shape with prosthetic legs—but I had to be able to stand for two minutes” to avoid the nursing home.
Ippel spent three weeks in the rehab facility. “By the end, I was able to walk down a hallway,” she recalls, although it was painful. Then she went home to Indiana and began working with another prosthetist. Unfortunately, for the next several years, Ippel experienced significant problems using prostheses: “I felt like my legs weren’t really working for me,” she recalls. “It was causing me a lot of pain,” so she decided
to try another prosthetist—that’s when she went to Prevail P&O and met Kail.
Return to Action
Kail, as a practitioner, was a great match for Ippel. Kail has worked at Prevail P&O since 2000. He eventually became lead practitioner for the Muncie and Anderson, Indiana, offices, and helped facilitate the opening of the Indianapolis location. He purchased the facility in 2018 and became sole owner. “I got into this field to help people,” Kail says. “Patients come to see us so we can return them back to their lives.”
Kail recalls that Ippel was experiencing several complications with her prostheses during her first appointment at Prevail P&O three years ago. “She was having a lot of pain; she felt her legs were loose; the prostheses were too heavy and hard for her to pull up; and they were giving her sores on her legs,” he says.
He quickly learned that Ippel was not the average 69-year-old. In addition to gardening, volunteering, parenting, and home projects, she had done cross-fit prior to amputation, and she still rode a recumbent bike. But she needed more appropriate
prostheses to accomplish her daily goals. “She didn’t feel secure” in her old prostheses, which would fill up with sweat and give her the feeling that they might fall off.
After some brainstorming, Kail designed a prosthesis featuring hybrid suspension that utilizes a pin system and vacuum. He selected feet that are lightweight and that adapt easily to uneven terrain. As with all of the prostheses provided at Prevail P&O, Kail fabricated Ippel’s devices in-house. She tested them shortly thereafter.
“We went through one set of check sockets, then fit her with the definitives—and she’s still wearing them three years later,” Kail says. “They help her legs feel lighter, and she has the sensation that her legs are part of her.” The pin system provides a sense of security, so Ippel doesn’t worry about the prostheses falling off.
Ippel, who chooses not to wear any devices on her fingers because only the distal tips are missing, says she loves her lower-limb prostheses, which help her feel “less clumsy” compared to her old devices.
Today, she spends her days gardening, riding her recumbent bicycle, and volunteering at the Muncie House—she has even encouraged some wheelchair-bound residents to consider prostheses of their own. Each January, Ippel walks a mile in a Muncie House charity walk to raise funds— then walks another mile back to amplify her support. She also takes care of her own house, and recently washed 36 lowerstory windows by herself, easily navigating a stepladder.
Kail adjusts Ippel’s prosthesis.
Ippel relies on her prostheses for her work as a gardener.
On top of her day-to-day responsibilities, Ippel has become a peer mentor at Prevail P&O, as part of the facility’s Patient Advocate Group to help new patients navigate the nuances that come with new prosthesis use. “I have an opportunity to tell others my story,” she says. “I try to practice thankfulness.”
Appearances Deceive
Kail has thoroughly enjoyed meeting Ippel and fabricating well-fitting prostheses to keep her mobile. In addition to seeing her for regular appointments and providing new sleeves as needed, he has shared his private cell phone number with Ippel “so she can text me if something comes up.”
He cautions other practitioners to “never write a patient off based on their appearance, or what they think a patient ‘should’ be doing.” He also encourages clinicians to listen to patients’ needs, then design a prosthesis according to those needs. “Pay attention to the details.”
“Kris listens, smiles, and takes the time to talk to me” during appointments, notes Ippel. “He’s very fast, and he keeps on task—but when he’s with me, he stops, sits down, and really listens to me.”
With Kail’s assistance, Ippel has returned to activities she enjoys.
PHOTOS: KRIS KAIL, CPO/MARY IPPEL
Turbomed’s premium foot drop or thosis sits on the outside of the shoe to facilitate maximized ankle movement while reducing the risk of injury
New MONOCORE TechnologyTM for a drill-less, one-piece design
New height-adjustable calf culf with pressure screws
FACILITY:
Boland Prosthetic & Orthotic Center
Why Am I an AOPA Member?
“If we didn’t have AOPA, who would we have to advocate for us, to help with reimbursement, and to assist with all the business issues that arise? We frequently call and always appreciate their answering our questions. And AOPA’s meetings are outstanding!”
—Paul
Boland, CPO
OWNER:
Paul Boland, CPO
ILOCATIONS:
Warner Robins and Macon, Georgia
HISTORY: 26 years
O&P on the Run
Georgia facility owner sponsors annual 5K and fun run for patients
n 1998, Paul Boland, CPO, opened Boland Prosthetic & Orthotic Center in Warner Robins, Georgia. His mother offered to babysit so that Paul and his wife, Lis, could work together on their new business venture. Since then, the facility has grown, expanding to a second location in Macon and employing a team of 12, including Darrell Hallman, CPO, and Will Ruark, a prosthetic-orthotic resident.
Boland, originally from Macon, and Lis, have fostered a friendly atmosphere in the facility, embracing both patients and employees as family. “There wasn’t much of a medical community here when we started,” Boland recalls. “We developed and grew as the area became home to more doctors and medical facilities.”
Because Boland P&O was the only O&P provider in town when it first opened, the facility started off providing a full range of orthotic and prosthetic services. Today, the facility faces a little more competition, but Boland feels his business handles it well. His team sees a large pediatric orthotic population and treats many veterans and patients with traumatic injuries.
“We are independent and extremely persistent in making sure patients are happy,” Boland says. “For example, we offer patients a double-wall prosthetic socket. It requires a lot of fabrication time, but it provides unmatched suspension, and we think the extra time and effort are worth it.”
All prostheses are fabricated in-house. While Boland likes hand-casting, he does use 3D printing to create some of the tools used in casting techniques. “Curtis Doster, our lab manager and prosthetic artist, owns about 40 3D printers” and has printed several tools for the facility, he says. Boland’s team uses central fabrication for most pediatric lower-extremity orthoses, scoliosis braces, and cranial remolding helmets.
Boland’s dedication to patients extends to community activities. The facility supports veteran patients through activities like skeet shooting and shrimp boils on Veterans Day. And each year, Boland P&O sponsors the Cantrell 5K and 1-mile fun run/walk for amputees, an event designed to encourage physical activity and inspire individuals with recent limb loss. Many patients
have made strides in their recovery through this supportive environment.
“We use that event all year to inspire our patients,” Boland explains. “When we have new patients who have recently been fit for a prosthesis, or others who have decided to become more active, we encourage them to come to the race and fun run. They can just cheer for the others or walk 30 yards over the finish line—whatever they can do.”
Boland likes to recount the story of one patient—a “cautious ambulator.” Boland encouraged him to try the 1-mile walk, and he completed it. “He was so excited he vowed to do the 5K walk the next year, and he did it—and did it again the next five years. Because his activity level improved so much, he was able to get a new job. It really changed his life!”
Another patient stands out for Boland: a veteran who lost his leg below the knee to an IED in Iraq. After being fitted with a prosthesis, he went back to the military and was deployed to Afghanistan, where he injured his prosthetic leg. Today, he is a state trooper, and he has participated in the 5K run, winning one of the prizes Boland P&O hands out to the fastest participants.
Looking to the future, Boland envisions expanding the Warner Robins facility to include an outdoor gait pavilion with parallel bars, ramps, and steps set in a garden atmosphere, providing a natural and empowering setting for patient rehabilitation. He says, “We remain committed to patient-centered care, innovation, and fostering a sense of family for staff and patients alike.”
Deborah Conn is a contributing writer to O&P Almanac. Reach her at deborahconn@verizon.net
Boland P&O sponsors an annual fun run.
Paul Boland, CPO, with a fun run participant
Staff at Boland Prosthetic & Orthotic Center
BY DEBORAH CONN
ALOCATION:
HISTORY: Two years
Facilitating Foot Care
Startup simplifies the process of scanning and ordering insoles and shoes
mit Bhanti has been in the O&P industry for decades. He launched Comprehensive Orthotics & Prosthetics in 2008; the facility has 40 locations today. Over the course of his career, Bhanti has seen many patients who needed diabetic shoes and orthotic inserts when many facilities stopped offering them.
“We can’t ignore this patient population,” he says. “We have a lot of rural practices where patients couldn’t get appropriate care. They either didn’t have access or couldn’t afford it, often resorting to overthe-counter insoles.” He decided to find a way to serve these patients that was efficient, streamlined, and still profitable.
Why Am I an AOPA Member?
“We are part of AOPA as it’s the best way to engage with the broader O&P community. The clinical resources, member education, and events are all top tier, and allow us to tell our story with others who care about restoring mobility and quality of life for patients. Additionally, the political advocacy is a major driver for our membership.”
“In the face of medical problems, reimbursement pressures, and regulatory headwinds, we looked to technology to approach the problem,” Bhanti explains. “We also wanted to reach more people on the preventive side, because by the time we see them, pathology is present.”
Bhanti’s son, Aadi, recognized that the most common technological approach involved scanning apps, but he wanted to build a solution that didn’t require an app or an iPhone. Working with a team of engineers from such companies as Amazon, Google, and SpaceX, he developed a web-based program that not only addresses scanning the foot and 3D printing the insole, but also automatically generates Medicare-compliant notes.
“This changed the paradigm of how we take care of patients,” says Bhanti. “Our artificial intelligence (AI) is so smart, that if the foot isn’t scanned properly, it can even reconstruct part of it.” The platform includes pathology detection, so as clinicians develop the models, the AI will tag wounds, ulcers, hammertoes, bunions, and other deformities and include them in the Medicare documentation.
After successfully testing the technology among patients of Comprehensive O&P, Bhanti, his son, and
another partner, Steven Chacko, launched insoles.ai in January 2023. The company, located in Peoria, Illinois, has 15 employees. The startup works with orthotists, pedorthists, chiropractors, and podiatrists.
To get started, potential clients can book an online demo. Scanning the foot requires a device with a camera; an iPhone or iPad is not required. A sevenminute digital evaluation yields a Medicare-compliant note that is entered into the clinician’s electronic medical records system, according to Bhanti.
The company offers clinicians the opportunity to order shoes as well as insoles. “The whole thing is integrated,” says Aadi Bhanti. “We work with major orthopedic shoe brands, whose products appear on our website. Everything comes in one package.”
As technology continues to advance, Aadi Bhanti sees artificial intelligence as less a tool than a co-pilot. He predicts, “It will feel more like an assistant, helping clinicians with their day-to-day activities. The idea is that it is actually taking actions for providers, leaving them to focus on taking care of their patients.”
Aadi Bhanti says his wife, a certified orthotic fitter, “used to see two to three patients an hour for foot orthotics and then spend her spend evenings writing up notes,” but now she is able to see and interact with many more patients. “People keep thinking that AI will replace us,” he says, but he believes AI will augment the work of O&P clinicians so they can focus on patient care.
Amit Bhanti was initially reluctant to spend money on developing a whole new technology. “But Aadi wanted to make it accessible, and we pretty much created this new thing. We can take any video and our algorithms and create a 3D model—super scalable and accessible,” he says. “I am so excited this idea came to fruition.”
Deborah Conn is a contributing writer to O&P Almanac. Reach her at deborahconn@verizon.net
OWNERS: Amit Bhanti, Aadi Bhanti, and Steven Chacko
Peoria, Illinois
—Amit Bhanti
Original founders Aadi Bhanti and Steven Chacko
The insoles.ai booth at the 2024 AOPA National Assembly in Charlotte, North Carolina
PROFESSIONALS.
Save the Date for the Next AOPA National Assembly
Meet up in Orlando
Mark your calendar now for the 108th AOPA National Assembly, which will take place Sept. 3-6, 2025, in Orlando.
The Call for Presentations Is Now Open! Submit your proposal by March 12, 2025. Visit bit.ly/3ZxhJnH or email assembly@aopanet.org for details.
‘AOPA Hub’ Goes Live
Hot Off the Press: O&P Compensation, Benefits, and Operations Reports
Purchase your copies now
How does your organization stack up against other O&P businesses?
Find out by purchasing AOPA’s brand new “2024 O&P Operating Performance Report” and “2024 Compensation and Benefits Report.” These timely, in-depth reports provide up-to-date insights and data, empowering you to make informed decisions, drive growth, and stay ahead in a rapidly evolving landscape.
The reports feature key performance metrics; information on trends and opportunities; and data-driven insights. Executives and leadership teams, operations and finance professionals, marketing and sales team, and clinic managers will gain a strategic advantage from accessing these reports.
Purchase the full reports on the AOPA Hub, aopahub.aopanet.org, and contact Betty Leppin with questions, bleppin@aopanet.org
The AOPA Hub, aopahub.aopanet.org, AOPA’s new member portal, went live Sept. 30. AOPA Hub has been designed to improve the AOPA member experience and provide more convenient access to key resources and tools.
AOPA Hub offers a range of features that will make managing your membership and access to AOPA benefits easier than ever:
1. User-friendly app-based dashboard: Navigate through your account with ease, accessing your membership information, event registrations, education, and more, all in one place
2. Enhanced capabilities: Quickly find the resources, contacts, and information you need in the app-based structure
3. Secure access: As always, your data is protected with security features, ensuring that your information is safe and secure
4. Improved experience: Enjoy the ability to easily access all of your member benefits and AOPA resources in one place.
Be assured your information from the former member portal has been transferred to the AOPA Hub. You can access your account and
AOPAversity on AOPA Hub now. AOPA will be rolling out additional updates over the next few weeks.
Visit AOPA’s website and go to the AOPA Hub to access your account. If you have any questions or need assistance, email info@aopanet.org or call 571-431-0876.
For Job Seekers:
Job searching is easy with the pane-view job search page. Set up job alerts, upload your resume or create an anonymous career profile that leads employers to you.
For Employers:
Reach 4,500+ O&P professionals through the Job Flash™ email. Ensure high visibility for your open positions through this highly engaging email.
For
Statement of Ownership, Management and Circulation
(required by U.S.P.S. Form 3526)
1. Publication Title: O&P Almanac 2. Publication No.: 1061-4621 3. Filing Date: 10/1/24 4. Issue Frequency: Monthly, except for combined issues printed June/July and November/ December 5. No. of Issues Published Annually: 10 6. Annual Subscription Price: $59 domestic/$99 foreign 7. Complete Mailing Address of Known Office of Publication (Not Printer): American Orthotic & Prosthetic Association, 330 John Carlyle St., Suite 200, Alexandria, VA 22314 8. Complete Mailing Address of Headquarters or General Business Office of Publisher (Not Printer): Same as #7 9. Full Names and Complete Mailing Addresses of Publisher, Editor, and Managing Editor: Publisher: Eve Lee, address same as #7. Editor: Josephine Rossi, Content Communicators LLC, PO Box 938, Purcellville, VA 20132. 10. Owner (Full Name and Complete Mailing Address): American Orthotic & Prosthetic Association, same as #7 11. Known Bondholders, Mortgagees, and Other Security Holders Owning 1 Percent or More of Total Amount of Bonds, Mortgages, or Other Securities: None. 12. The purpose, function, and nonprofit status of this organization and the exempt status for federal income tax purposes: Has Not Changed During the Preceding 12 Months. 13. Publication Name: O&P Almanac 14. Issue Date for Circulation Data Below: August 2024
Allard’s Meracus® Prosthetic Foot
Discover pure motion through pure composite.
• Composite Rivet Technology: This patent pending, bold innovation connects the heel and keel together where the toe-lift begins to remove “dead spots.”
• Extended Heel Lever: Provides a stable base and a more functional transition into mid-stance.
• Full split heel and keel: More closely mimics the natural movement of a human foot.
For more information, contact customer service at 888-678-6548 or email sales@allardusa.com
Precision Fit With Mt Emey® Custom Shoes
Embrace the comfort of custom-fit with Mt Emey®’s Custom Shoe (Medical) Program.
Our precise 3D scanning captures your unique foot contours, promising a perfect fit without the wait or waste. From stylish athletics to roomy comfort designs, our handcrafted shoes adapt to your needs. Satisfaction guaranteed before payment. Plus, qualified wholesale accounts receive a free 3D scanner. Step into the Mt Emey difference— where every shoe is made for you.
Limited
Time Offer: Coyote Is Having Our 20% Off Lab
Equipment Sale.
Upgrade your O&P Lab with our advanced air purification systems and more:
• Kleenaire & Mini Kleenaire—Our industrial dual-filter air purifiers recycle the air, eliminate odors, and filter airborne particles. Easy to install, and plugs directly into a standard outlet.
• Socket Extractor & Silent Air Compressors—Also 20% Off!
• Hurry—Sale ends Dec. 31, 2024!
Don’t miss out on improving air quality and efficiency in your lab. Order today and save! Contact Coyote at 208-429-0026 or visit coyote.us
For more information, call 1-888-937-2747 or visit emeys.com
Hersco 3D Printing
Hersco is delighted to offer HP’s advanced 3D-printing technology for custom orthotics. 3D printing has unique design capabilities not possible with other methods—reducing landfill waste by 90%! The accuracy of 3D is unparalleled, specs exceed direct-milled polypro, and manual plaster fabrication. Among the benefits: a 90% reduction in landfill waste, many new design possibilities for posting, and the ability to vary thickness and flexibility across the shell. The PA-11 polymer is a biobased renewable material that has been tested and proven in research and industry. Call today, 800-301-8275, for a free sample.
Finger and Partial-Hand Amputee Peer + Support Group
Join a dynamic online support group specifically for finger and partial-hand loss.
EVAQ8
The same elevated vacuum system that amputees already love in the RUSH EVAQ8 collection by PROTEOR is now available in our carbon fiber feet, providing more choices and greater versatility. The EVAQ8 Collection provides an optimal design with no added build height, high durability rubber that is built to last, and responds automatically to pull vacuum with every step. Try the expanded EVAQ8 Collection by PROTEOR today. More Materials, More Choices, Now More EVAQ8. Visit us.proteorusa.com
Turbomed Foot Drop AFOs
Turbomed’s leading line of foot drop ankle-foot orthoses sit completely outside the shoe for an invisible, painless support that will follow you as long and as far as you want. Their unique design acts as an exoskeleton to the impaired limb, keeps the foot at 90 degrees, and provides the user with unparalleled levels of function. Each model takes minutes to assemble and is easily transferrable to most shoes, boots, and sandals through an innovative lace clip design.
The Xtern Summit is the lightest model, has the most dorsiflexion power, and features a see-through design. The Xtern Frontier was designed for patients with reduced hand dexterity and requiring front leg support. Visit turbomedusa.com, and think outside the shoe!
Contact
December 1–31
ABC: Application Deadlines, Exams Dates, O&P Conferences, and More! Check out ABC’s Calendar of Events at abcop.org/calendar for the latest dates and event details, so you can plan ahead and be in the know. Questions? Contact us at info@abcop.org; abcop.org/contact-us
March 12
Deadline to Submit Proposal for 2025 AOPA National Assembly. Visit aopanet.org or email assembly@aopanet.org
June 13–14
27th Annual PrimeFare East—NEW VENUE! Downtown Marriott Hotel and Convention Center, Chattanooga, TN. Contact Cathie Pruitt at 901-359-3936, primecarepruitt@gmail.com, or visit primecareop.com
September 3–6
AOPA National Assembly. Orlando. For more information, visit aopanet.org
Live and Online/On Demand
CEs
The Pedorthic Footcare Association: Diabetic Wound Prevention, Management, and Healing Program. 10-session online education program series. Approved CEs by ABC and BOC, monthly classes are 1.5 hours each. For more information and to register, visit pedorthics.org/page/.Diabetic_Series_LMS_List
A large number of O&P Almanac readers view the digital issue— If you’re missing out, visit issuu.com/americanoandp to view your trusted source of everything O&P. Scan the QR to start advertising in the O&P Almanac or visit https://bit.ly/AlmanacMediaKit25
Learn & Earn
Share Your Calendar Event
Advertise O&P events for maximum exposure with O&P Almanac. Contact Bob Heiman at bob.rhmedia@comcast.net or learn more at bit.ly/AlmanacMediaKit25. Announcement and payment may also be sent to O&P Almanac, Calendar, P.O. Box 34711, Alexandria, VA 22334-0711 or emailed to jklapp@AOPAnet.org along with VISA or MasterCard number, cardholder name, and expiration date. Make checks payable in U.S. currency to AOPA. Note: AOPA reserves the right to edit calendar listings for space and style considerations.
A ballot measure called Proposition 35 passed in California after being included in the state ballot on Election Day. This proposition protects funds intended for healthcare purposes, such as rate increases for MediCal providers, from being used for other purposes without resulting in tax increases. This law may help expand patient access to care across specialties.
Colorado
Rates for prosthetics, orthotics, and disposable supplies are scheduled to be reviewed under the
Medicaid Provider Rate Review Advisory Committee (MPRRAC) process in Colorado in 2025. The state’s Department of Health Care Policy and Financing works alongside MPRRAC during these reviews. The sufficiency of fee-for-service provider reimbursements is reviewed every three years to ensure that adequate access remains available in compliance with regulatory guidelines. MPRRAC will hold public, quarterly meetings in 2025, where stakeholder feedback will be solicited. For more information or to find out how to get involved, contact AOPA’s Joe McTernan, jmcternan@aopanet.org, or Morgan Fabber, mfabber@aopanet.org
The Latest From So Every BODY Can Move
In five states—Colorado, Illinois, Maryland, Minnesota, and New Hampshire—So Every BODY Can Move (SEBCM) laws are scheduled to take effect Jan. 1, 2025. These states join three others—Arkansas, Maine, and New Mexico—in having enacted legislation. AOPA and its partners in the SEBCM initiative continue to provide support in assisting states with implementation and help support states preparing to pursue legislation.
New York
In October, the New York State Office of the Medicaid Inspector General (OMIG) asked AOPA for feedback on its audit protocols for durable medical equipment. AOPA experts and members collaborated to provide feedback on the audit protocols to OMIG.
NEW! Genium X4. Redefining human potential.
The new X4 is the next revolutionary step in advanced knee technology. Its unmatched functionality and cutting-edge digital ecosystem provide a whole new mobility experience for users.