Inventing for Life
MSD Ireland is one of the country’s leading healthcare companies, having first established here over 50 years ago. We have a dynamic and diverse team of over 2,800 employees across six sites in Ballydine, Co Tipperary, Brinny, Co Cork, Dunboyne, Co Meath, Carlow and Dublin, and, in addition, operate substantial Human Health and Animal Health businesses.
At MSD Ireland, we work at the forefront of science and technology to advance manufacturing excellence and R&D across our Irish sites and global company network. Our Irish sites manufacture approximately half of MSD’s top twenty products, saving and enhancing lives in over sixty countries around the world.

At MSD, we have and always will be Inventing for Life. These three powerful words reflect our commitment to inventing new medicines and vaccines that save lives by preventing and fighting disease. MSD has dedicated researchers trained in many different scientific disciplines who work tirelessly to find solutions for significant health challenges that still afflict millions around the world.

As a team, we firmly believe that the most important thing we make is a difference – to patients, to our employees, to our communities and to the Irish healthcare landscape generally. We are 100% committed to putting the patient at the heart of everything we do.
To find out more about our people and our work, visit www.msd.ie
ADULTS AGED
ABBREVIATED PRESCRIBING INFORMATION
Prevenar 13* Suspension for Injection



Pneumococcal polysaccharide conjugate vaccine (13-valent, adsorbed)
Presentation: Each 0.5ml dose of Prevenar 13 contains 2.2 micrograms of each of the following pneumococcal polysaccharide serotypes: 1, 3, 4, 5, 6A, 7F, 9V, 14, 18C, 19A, 19F, 23F and 4.4 micrograms of pneumococcal polysaccharide serotype 6B. Each pneumococcal polysaccharide is conjugated to CRM197 carrier protein and adsorbed on aluminium phosphate. 1 dose (0.5 ml) contains approximately 32 µg CRM197carrier protein and 0.125 mg aluminium. Indications: Active immunisation for the prevention of invasive disease, pneumonia and acute otitis media caused by Streptococcus pneumoniae in infants, children and adolescents from 6 weeks to 17 years of age. Active immunisation for the prevention of invasive disease and pneumonia caused by Streptococcus pneumoniae in adults ≥18 years of age and the elderly. Dosage and Administration: The immunisation schedules for Prevenar 13 should be based on official recommendations. It is recommended that infants who receive a first dose of Prevenar 13 complete the vaccination course with Prevenar 13. For intramuscular injection. Infants aged 6 weeks-6 months: Three dose primary series: The recommended immunisation series consists of four doses, each of 0.5ml. The primary infant series consists of three doses, with the first dose usually given at 2 months of age and with an interval of at least 1 month between doses. The first dose may be given as early as six weeks of age. The fourth (booster) dose is recommended between 11 and 15 months of age. Two dose primary series: Alternatively, when Prevenar 13 is given as part of a routine infant immunisation programme, a series consisting of three doses, each of 0.5ml, may be given. The first dose may be administered from the age of 2 months, with a second dose 2 months later. The third (booster) dose is recommended between 11 and 15 months of age. Preterm infants (< 37 weeks gestation): In preterm infants, the recommended immunisation series consists of four doses, each of 0.5 ml. The primary infant series consists of three doses, with the first dose given at 2 months of age and with an interval of at least 1 month between doses. The first dose may be given as early as six weeks of age. The fourth (booster) dose is recommended between 11 and 15 months of age. Unvaccinated infants and children ≥ 7 months of age: Infants 7-11 months: Two doses, each of 0.5 ml, with at least a 1 month interval between doses. A third dose is recommended in the second year of life. Children aged 12-23 months: Two doses, each of 0.5 ml, with at least a 2 month interval between doses. Children and adolescents aged 2-17 years: one single dose of 0.5 ml. Prevenar 13 vaccine schedule for infants and children previously vaccinated with Prevenar (7-valent) (Streptococcus pneumoniae serotypes 4, 6B, 9V, 14, 18C, 19F, and 23F): Infants and children who have begun immunisation with Prevenar may switch to Prevenar 13 at any point in the schedule. Children aged 12-59 months: Children who are considered completely immunised with Prevenar (7-valent) should receive one dose of 0.5 ml of Prevenar 13 to elicit immune responses to the 6 additional serotypes. This dose of Prevenar 13 should be administered at least 8 weeks after the final dose of Prevenar (7-valent). Children and adolescents aged 5-17 years: One single dose of Prevenar 13 if they have been previously vaccinated with one or more doses of Prevenar. This dose of Prevenar 13 should be administered at least 8 weeks after the final dose of Prevenar (7-valent). Adults ≥18 years of age and the elderly: One single dose. The need for revaccination with a subsequent dose of Prevenar 13 has not been established. Regardless of prior pneumococcal vaccination status, if the use of 23 valent polysaccharide vaccine is considered appropriate, Prevenar 13 should be given first. Special Populations: Individuals who have underlying conditions predisposing them to invasive pneumococcal disease (such as sickle cell disease or HIV infection) including those previously vaccinated with one or more doses of 23-valent pneumococcal polysaccharide vaccine may receive at least one dose of Prevenar 13. In individuals with an haematopoietic stem cell transplant (HSCT), the recommended immunisation series consists of four doses of Prevenar 13, each of 0.5 ml. The primary series consists of three doses, with the first dose given at 3 to 6 months after HSCT and with an interval of at least 1 month
between doses. A fourth (booster) dose is recommended 6 months after the third dose. Contra-indications: Hypersensitivity to any component of the vaccine or to diphtheria toxoid. As with other vaccines, the administration of Prevenar 13 should be postponed in subjects suffering from acute, severe febrile illness. However, the presence of a minor infection, such as a cold, should not result in the deferral of vaccination. Warnings and Precautions: Do not administer intravascularly. Appropriate medical treatment and supervision must be readily available in case of a rare anaphylactic event. This vaccine should not be given as an intramuscular injection to individuals with thrombocytopenia or any coagulation disorder that would contraindicate intramuscular injection, but may be given subcutaneously if the potential benefit clearly outweighs the risks of administration. Prevenar 13 will only protect against Streptococcus pneumoniae serotypes included in the vaccine, and will not protect against other microorganisms that cause invasive disease, pneumonia, or otitis media. As with any vaccine, Prevenar 13 may not protect all individuals receiving the vaccine from pneumococcal disease. Individuals with impaired immune responsiveness, whether due to the use of immuno-suppressive therapy, a genetic defect, human immunodeficiency virus (HIV) infection, or other causes, may have reduced antibody response to active immunization. Safety and immunogenicity data are available for a limited number of individuals with sickle cell disease, HIV infection, or with an HSCT. Safety and immunogenicity data for Prevenar 13 are not available for individuals in other specific immuno-compromised groups (e.g., malignancy or nephrotic syndrome) and vaccination should be considered on an individual basis. Infants and children aged 6 weeks to 5 years: Prevenar 13 does not replace the use of 23-valent pneumococcal polysaccharide vaccine in at risk children ≥ 24 months of age. Children ≥ 24 months of age at high risk, previously immunised with Prevenar 13 should receive 23-valent pneumococcal polysaccharide vaccine whenever recommended. The potential risk of apnoea and the need for respiratory monitoring for 48-72 hours should be considered when administering the primary immunisation series to very premature infants (born ≥ 28 weeks of gestation) and particularly for those with a previous history of respiratory immaturity. When Prevenar 13 is administered concomitantly with Infanrix hexa (DTPa-HBV-IPV/Hib), the rates of febrile reactions are similar to those seen with concomitant administration of Prevenar (7-valent) and Infanrix hexa. Increased reporting rates of convulsions (with or without fever) and hypotonic hyporesponsive episode (HHE) were observed with concomitant administration of Prevenar 13 and Infanrixhexa. Antipyretic treatment should be initiated according to local guidelines for children with seizure disorders or with a history of febrile seizures and for all children receiving Prevenar 13 simultaneously with vaccines containing whole cell pertussis. Adults aged 50 years and older: When Prevenar 13 was given concomitantly with trivalent inactivated influenza vaccine (TIV), the immune responses to Prevenar 13 were lower compared to when Prevenar 13 was given alone, however, there was no long-term impact on circulating antibody levels. The immune responses to Prevenar 13 were noninferior when Prevenar 13 was given concomitantly with quadrivalent inactivated influenza vaccine (QIV) compared to when Prevenar 13 was given alone. As with concomitant administration with trivalent vaccines, immune responses to some pneumococcal serotypes were lower when both vaccines were given concomitantly. Fertility, Pregnancy & Lactation: There are no data from the use of pneumococcal 13-valent conjugate in pregnant women. It is unknown whether pneumococcal 13-valent conjugate is excreted in human milk. Animal studies do not indicate direct or indirect harmful effects with respect to reproductive toxicity. Side Effects: Analysis of postmarketing reporting rates suggests a potential increased risk ofconvulsions, with or without fever, and HHE when comparing groups which reported use of Prevenar 13 with Infanrix hexa to those which reported use of Prevenar 13 alone. Adverse reactions reported in clinical studies or from the post-marketing experience for all age groups are listed in this section per system organ class,in decreasing order of frequency and seriousness. The frequency is defined as follows: very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1,000 to < 1/100), rare (≥ 1/10,000 to < 1/1,000), very rare (≤ 1/10,000), not

Alcoholism
Current smokers

Diabetes
known (cannot be estimated from available data). Infants and children aged 6 weeks to 5 years: Very common (≥ 1/10): Decreased appetite, fever, pyrexia, irritability, any vaccination-site erythema, induration/swelling or pain/tenderness, somnolence, poor quality sleep. Vaccination-site erythema or induration/swelling 2.5cm – 7.0 cm (after the booster dose and in older children [age 2-5 years]. Common (≥ 1/100 to < 1/10): Vomiting, diarrhoea, rash, pyrexia >39 °C, vaccination-site movement impairment (due to pain), vaccination-site erythema or induration/swelling 2.5cm – 7.0cm (after infant series). Uncommon (≥ 1/1,000 to < 1/100): Convulsions (including febrile convulsions), urticaria or urticaria-like rash, vaccination-site erythema, induration/swelling >7.0cm, crying. Rare: Hypersensitivity reaction including face oedema, dyspnoea, bronchospasm, hypotonic-hyporesponsive episode. Not known: Lymphadenopathy (localised to the region of the vaccination site), anaphylactic/anaphylactoid reaction including shock, angioedema, erythema multiforme, vaccination site urticaria, vaccination-site dermatitis, vaccination-site pruritus, flushing. In clinical studies infants vaccinated at 2, 3 and 4 months of age, fever ≥ 38°C was reported at higher rates among infants who received Prevenar (7-valent) concomitantly with Infanrix hexa than in infants receiving Infanrix hexa alone. After a booster dose at 12 and 15 months of age, the rate of fever ≥ 38°C was greater in infants who received Prevenar (7 valent) and Infanrix hexa at the same time compared to infants receiving Infanrix hexa alone. These reactions were mostly moderate (less than or equal to 39°C) and transient. Additional information in special populations: Apnoea in very premature infants (≤ 28 weeks of gestation). Children and adolescents aged 6 to 17 years of age: Very common (≥ 1/10): Decreased appetite, irritability, any vaccination-site erythema, induration/swelling or pain/ tenderness, somnolence, poor quality sleep, vaccination-site tenderness (including impaired movement). Common (≥ 1/100 to < 1/10): Headaches, vomiting, diarrhoea, rash, urticaria or urticaria-like rash, pyrexia. Additional information in special populations: Children and adolescents with sickle cell disease, HIV infection or an HSCT transplant have similar frequencies of adverse reactions, except that headaches, vomiting, diarrhoea, pyrexia, fatigue, arthralgia, and myalgia were very common. Adults ≥18 years of age, and the elderly: Very common (≥ 1/10): Decreased appetite, headaches, diarrhoea, vomiting,(in adults aged 18 to 49 years), rash, chills; fatigue; vaccination-site erythema; vaccination-site induration/swelling; vaccination-site pain/tenderness (severe vaccination-site pain/ tenderness very common in adults aged 18 to 39 years); limitation of arm movement (severe limitation of arm movements very common in adults aged 18 to 39 years), arthralgia; myalgia.

Common (≥ 1/100 to < 1/10): Vomiting (in adults aged 50 years and over), pyrexia(very common in adults aged 18 to 29 years). Uncommon (≥ 1/1,000 to < 1/100): Nausea, hypersensitivity reaction including face oedema, dyspnoea, bronchospasm, lymphadenopathy localized to the region of the vaccination site. Additional information in special populations: Adults with HIV infection have similar frequencies of adverse reactions, except that pyrexia and vomiting were very common and nausea common. Adults with an HSCT have similar frequencies of adverse reactions, except that pyrexia and vomiting were very common.
For full prescribing information see the Summary of Product Characteristics.

Legal Category: S1A. Package Quantities: Pack of 1 single-dose prefilled syringe (with separate needle) or pack of 10 single- dose pre-filled syringes. Marketing






Authorisation Numbers: Single-dose pre-filled syringe (with separate needle) pack of 1: EU/1/09/590/002, single-dose pre-filled syringe pack of 10: EU/1/09/590/003. Marketing
Authorisation Holder: Pfizer Europe MA EEIG, Boulevard de la Plaine 17, 1050 Bruxelles, Belgium. For further information on this medicine please contact: Pfizer Medical Information on 1800 633 363 or at EUMEDINFO@pfizer.com. For queries regarding product availability please contact: Pfizer Healthcare Ireland, Pfizer Building 9, Riverwalk, National Digital Park, Citywest Business Campus, Dublin 24 + 353 1 4676500.
Date of preparation: 11/2018.
mark. Ref: PN 11_0 IE.
*Trade
References: 1. Prevenar 13 Suspension for Injection. Summary of Product Characteristics. 2. Shea K, Edelsberg J, Weycker D, et al. Rates of Pneumococcal Disease in Adults with Chronic Medical Conditions. Open Forum Infectious Disease. 2014;1-9. 3. Bonten M.J.M., Huijts S.M, Bolkenbaas M, et al. Polysaccharide Conjugate Vaccine Against Pneumococcal Pneumonia in Adults. The New England Journal of Medicine. 2015;372:1114-25. 4. Pfizer Inc. Press Release Mar 18, 2015. INDICATED FOR THE PREVENTION OF PNEUMOCOCCAL PNEUMONIA IN ADULTS1 IN
≥ 65 YEARS With each additional comorbid condition, the risk for pneumococcal pneumonia multiplies compared to healthy adults of the same age Proven to reduce the risk of community-acquired pneumonia: Results from the Community-Acquired Pneumonia Immunisation Trial in Adults (CAPiTA) – one of the largest vaccine efficacy trials ever conducted in older adults.3,4
Asthma Chronic cardivascular disease Chronic liver disease Chronic pulmonary disease
These underlying conditions included2: Date of Preparation: February 2021 | PP-PNA-IRL-0006 Help prevent pneumococcal pneumonia with the proven protection of Prevenar 131,3 4.2x increased risk 2 underlying conditions 2.1x increased risk 1 underlying condition 9.2x increased risk >3 underlying conditions



















Celebrate the future. Celebrate life. Join the story: celebratelife.roche.com

1www.ihca.ie






Advanced Medicine Exceptional Carebonsecours.ie Organization Accredited by Joint Commission International C O R K | D U B L I N | G A LWA Y | L I M E R I C K | T R A L E E > 300k Patients 5 JCI Accreditations > 490 Consultants > 3,000 Employees Advanced Medicine Exceptional Carebonsecours.ie Organization Accredited > 300k Patients 5 JCI Accreditations > 490 Consultants > 3,000 Employees Advanced Medicine Exceptional Care | G A LWA Y | L I M E R I C K | T R A L E E 5 Accreditations > 490 Consultants > 3,000 Employees Advanced Medicine Exceptional Carebonsecours.ie Organization Accredited by Joint Commission International C O R K | D U B L I N | G A LWA Y | L I M E R I C K | T R A L E E > 300,000 Patients 5 JCI Accreditations > 490 Consultants > 3,000 Employees
Yearbook & Diary
Heritage House, Dundrum Office Park, Main Street, Dundrum, D14 C2R2 Telephone: +353 1 298 9123 Fax: +353 1 298 9395 Email: info@ihca.ie Web: www.ihca.ie
2023























PERSONAL DETAILS
Name: Hospital: Address: Tel: Fax: Email: Medical Council Reg. No.:
MPS/Challenge/MDU/Medisec-MedPro Reg. No.: Vhi Dr No.: Laya Healthcare Dr No.: Irish Life Health Dr No.:
5www.ihca.ie




6 www.ihca.ie Contents 9 End of Year Checklist 10 President’s Address 13 Members’ Handbook Contents 30 Consultants’ Common Contract 2008 – Enabling Circular 33 Consultants’ Common Contract 2008 68 Professional Directory 68 Medical Indemnity Organisations 69 Health Insurers & Medical Council 72 IHCA National Council 2022-2023 73 IHCA Officer Board 2022-2023 74 Voluntary & Support Organisations 78 Charts & Tables Published on behalf of The Irish Hospital Consultants Association by Ashville Media Group • Tel: (01) 432 2200 • www.ashville.com Errors and Omissions Disclaimer: While every effort has been made to ensure that all information contained in this yearbook is accurate and correct at time of publication, errors, omissions, or discrepancies may have occurred in preparation of the manuscript. Ashville Media Group and the Irish Hospital Consultants Association cannot accept any liability for loss, distress or damage resulting from errors or omissions. © 2022/2023
Delivering value in Ireland across the entire lifecycle of new medicines.


The task of turning possibilities into reality for doctors and their patients is constant. More than 2,700 AbbVie employees support this goal at nine locations in Ireland including Cork, Dublin, Sligo and Westport. AbbVie has 135+ potential medicines under investigation. More than 75% are first in kind. An innovative medicine is created in four stages and AbbVie adds value in Ireland at each point in this journey. Learn more at abbvie.ie
Supporting Discovery
• Creating treatment possibilities.
• Partnering with Science Foundation Ireland to fund research in university and hospital laboratories.
Clinical Trials and Data Generation
• 76 Irish clinical trial sites have tested the safety and efficacy of potential AbbVie medicines.

People. Passion. Possibilities.®

Public Access to New Medicines
• The ultimate value of innovation is to ensure those in medical need have new treatment options.
• Offers patients new hope and allows doctors advance the standard of care.
World-Leading Manufacturing





• Our industry works with IDA Ireland to ensure Ireland is an international medicines powerhouse.
• Irish plants are playing a key role in supporting AbbVie’s global supply of treatments.












Date of preparation: January 2022 | IE-ABBV-220003
diet, during treatment with Suvezen. Suvezen is not suitable for initial therapy. Treatment initiation or dose adjustment, if necessary, should only be done with the monocomponents and after setting the appropriate doses the switch to the fixed dose combination of the appropriate strength is possible. Patient should use the strength corresponding to their previous treatment. The recommended dose is one Suvezen tablet daily. To be administered at any time of the day, with or without food. The tablet should be swallowed whole with a drink of water. If co-administered with bile acid sequestrant (BAS), administration of Suvezen should occur either ≥2 hours before or ≥4 hours after administration of a BAS. Special populations: Paediatric (<18 years): Safety and efficacy has not been established. Elderly (>70 years): Starting dose of 5 mg rosuvastatin is recommended. The combination is not suitable for initial therapy. Hepatic impairment: Mild: No dosage adjustment is required. Moderate/Severe: Treatment with Suvezen is not recommended. Renal impairment: Mild: No dose adjustment is necessary. Moderate (creatinine clearance <60 ml/min): The recommended start dose is rosuvastatin 5mg. Race: The recommended start dose is rosuvastatin 5 mg for patients of Asian ancestry due to increased systemic exposure. The fixed dose combination is not suitable for initial therapy. Monocomponent preparations should be used to start the treatment or to modify the dose. Suvezen 40 mg/10 mg tablets are contraindicated in these patients. Genetic polymorphisms: In patients who are known to have specific types of genetic polymorphisms that can lead to increased rosuvastatin exposure, a lower daily dose of Suvezen is recommended. Dosage in patients with pre-disposing factors to myopathy: The recommended start dose is rosuvastatin 5mg in patients with pre-disposing factors to myopathy. Suvezen 40 mg/10 mg tablets are contraindicated in some of these patients. Concomitant therapy: The risk of myopathy (including rhabdomyolysis) is increased when Suvezen is administered concomitantly with certain medicinal products that may increase the plasma concentration of rosuvastatin (e.g. ciclosporin and certain protease inhibitors including combinations of ritonavir with atazanavir, lopinavir, and/or tipranavir). Whenever possible, alternative medications should be considered, and, if necessary, consider temporarily discontinuing Suvezen therapy. In situations where co-administration of these medicinal products with Suvezen is unavoidable, the benefit and the risk of concurrent treatment and rosuvastatin dosing adjustments should be carefully considered. Contraindications: Hypersensitivity to the active substances or excipients. Pregnancy, breast-feeding and in women of childbearing potential not using appropriate contraceptive measures. Active liver disease or any serum transaminase elevations which are unexplained, persistent or exceeding 3x the upper limit of normal (ULN). Severe renal impairment (creatinine clearance <30ml/min); myopathy or receiving concomitant ciclosporin. 40mg/10mg dose contraindicated in patients with predisposing factors for myopathy/rhabdomyolysis; such factors include: Moderate renal impairment (creatinine clearance <60ml/min), hypothyroidism, personal or family history of hereditary muscular disorders, previous history of muscular toxicity with another HMG-CoA reductase inhibitor or fibrate, alcohol abuse, situations where an










or progressive renal disease. An assessment of renal function should be considered during routine follow-up of patients treated with a dose of 40mg. Diabetes mellitus: Some evidence suggests that statins raise blood glucose and in some patients, at high risk of future diabetes, may produce a level of hyperglycaemia where formal diabetes care is appropriate. This risk, however, is outweighed by the reduction in vascular risk with statins and therefore should not be a reason for stopping statin treatment. Patients at risk (fasting glucose 5.6 – 6.9mmol/l, BMI >30kg/m2, raised triglycerides, hypertension) should be monitored both clinically and biochemically according to national guidelines. Interstitial lung disease: Exceptional cases have been reported with some statins, especially with long term therapy. Presenting features can include dyspnoea, non-productive cough and deterioration in general health (fatigue, weight loss and fever). If it is suspected, statin therapy should be discontinued. Severe cutaneous adverse reactions: Stevens-Johnson syndrome (SJS) and drug reaction with eosinophilia and systemic symptoms (DRESS), which could be life-threatening or fatal, have been reported with rosuvastatin. If signs and symptoms suggestive of this reaction appears, Suvezen must be discontinued immediately and an alternative treatment should be considered. Treatment with Suvezen must not be restarted at any time. Protease inhibitors: Increased systemic exposure to rosuvastatin has been observed in subjects receiving rosuvastatin concomitantly with various protease inhibitors in combination with ritonavir. Consideration should be given both to the benefit of lipid lowering by use of Suvezen in HIV patients receiving protease inhibitors and the potential for increased rosuvastatin plasma concentrations when initiating and up titrating rosuvastatin doses in patients treated with protease inhibitors. The concomitant use with certain protease inhibitors is not recommended unless the dose of rosuvastatin is adjusted. Fibrates: The safety and efficacy of ezetimibe administered with fibrates have not been established. If cholelithiasis is suspected in a patient receiving Suvezen and fenofibrate, gallbladder investigations are indicated and therapy should be discontinued. Anticoagulants: If Suvezen is added to warfarin, another coumarin anticoagulant, or fluindione, the International Normalised Ratio (INR) should be appropriately monitored. Fusidic acid: Suvezen must not be co-administered with systemic formulations of fusidic acid or within 7 days of stopping fusidic acid treatment. In patients where the use of systemic fusidic acid is considered essential, statin treatment should be discontinued throughout the duration of fusidic acid treatment. There have been reports of rhabdomyolysis (including some fatalities) in patients receiving fusidic acid and statins in combination. The patient should be advised to seek medical advice immediately if they experience any symptoms of muscle weakness, pain or tenderness. Statin therapy may be reintroduced seven days after the last dose of fusidic acid. In exceptional circumstances, where prolonged systemic fusidic acid is needed, e.g., for the treatment of severe infections, the need for co-administration of Suvezen and fusidic acid should only be considered on a case by case basis and under close medical supervision. Suvezen contains lactose monohydrate and sodium: Patients with rare hereditary problems of galactose intolerance, total lactase deficiency or glucose-galactose malabsorption should not take this medicine. This medicinal product contains less than 1 mmol sodium (23 mg) per tablet, that is to say essentially ‘sodiumfree’. Interactions: Contraindicated combinations: Ciclosporin. Not-recommended combinations: Fibrates and other lipid-lowering products, protease inhibitors, transporter protein inhibitors and fusidic acid. Other possible interactions: Cytochrome P450 enzymes, antacids, colestyramine,

a confirmatory test should be carried out within 5 – 7 days. If the repeat test confirms a baseline CK >5x ULN, treatment should not be started. Patients with pre-disposing factors for myopathy/rhabdomyolysis: Caution should be exercised in these patients. Risk: benefit of treatment should be considered and clinical monitoring is recommended. CK levels should be measured in these patients. Therapy should be discontinued if CK levels are markedly elevated (>5x ULN) or if muscular symptoms are severe and cause daily discomfort. If symptoms resolve and CK levels return to normal, then consideration should be given to re-introducing treatment at the lowest dose. Immune-mediated necrotising myopathy (IMNM): Clinically characterised by proximal muscle weakness and elevated serum CK, has been reported very rarely during or after treatment with statins, including rosuvastatin, despite discontinuation of statin treatment. In clinical trials an increase in the incidence of myositis and myopathy has been seen in patients receiving other HMG-CoA reductase inhibitors together with fibric acid derivatives. Suvezen should not be used in any patient with an acute, serious condition suggestive of myopathy or predisposing to the development of renal failure secondary to rhabdomyolysis (e.g. sepsis, hypotension, major surgery, trauma, severe metabolic, endocrine and electrolyte disorders; or uncontrolled seizures). Liver effects: In controlled coadministration trials in patients receiving ezetimibe with statin, consecutive transaminase elevations ≥3x ULN have been observed. It is recommended that liver function tests be carried out prior to, and 3 months following, the initiation of treatment. Rosuvastatin should be discontinued or the dose reduced if the level of serum transaminases is >3x ULN. The reporting rate for serious events is higher at the 40mg dose. In patients with secondary hypercholesterolaemia caused by hypothyroidism or nephrotic syndrome, the underlying disease should be treated prior to initiating therapy with rosuvastatin. Liver disease and alcohol: As with other HMG-CoA reductase inhibitors, rosuvastatin should be used with caution in patients who consume excessive quantities of alcohol and/or have a history of liver disease. Renal effects: Proteinuria has been observed in patients treated with higher doses of rosuvastatin and was transient or intermittent in most cases. Proteinuria has not been shown to be predictive of acute
diabetes mellitus, headache, dizziness, constipation, nausea, abdominal pain, diarrhoea, flatulence, myalgia, ALT and/or AST increased, asthenia and fatigue. Uncommon (≥1/1,000 to <1/100): decreased appetite, paraesthesia, hot flush, hypertension, cough, dyspepsia, gastroesophageal reflux disease, nausea, dry mouth, gastritis, pruritus, rash, urticaria, arthralgia, muscle spasms, neck pain, back pain, muscular weakness, pain in extremity, ALT and/or AST increased, blood CPK increased, gamma-glutamyltransferase increased, liver function test abnormal, chest pain, pain, asthenia, oedema peripheral. Rare (≥1/10,000 to <1/1,000): thrombocytopenia, hypersensitivity reactions including angioedema, pancreatitis, increased hepatic transaminases, myopathy (including myositis), rhabdomyolysis, lupus-like syndrome and muscle rupture. Very rare (<1/10,000): polyneuropathy,



















20 mg /10 mg Rosuvastatin + Ezetimibe 10 mg /10 mg Rosuvastatin + Ezetimibe 40 mg /10 mg Rosuvastatin + Ezetimibe Suvezen is indicated for substitution therapy in adult patients who are adequately controlled with rosuvastatin and ezetimibe given concurrently at the same dose level as in the fixed combination, but as separate products, as adjunct to diet for treatment of primary hypercholesterolaemia (heterozygous familial and nonfamilial) or homozygous familial hypercholesterolaemia1 MAT-IE-2101261 (v2.0) | April 2022 Reference: 1. Suvezen Summary of Product Characteristics * LDL-C: Low-density lipoprotein Cholesterol ** Suvezen is available in 3 doses in Ireland. Suvezen 10mg/10mg, 20mg/10mg and 40mg/10mg: Each film-coated tablet contains 10mg; 20mg or 40mg of rosuvastatin (as rosuvastatin calcium) respectively, and 10mg ezetimibe. Prescribing Information: Suvezen (rosuvastatin/ ezetimibe) film-coated tablets Please refer to the Summary of Product Characteristics (SmPC) for full prescribing details. Presentations: Suvezen 10mg/10mg, 20mg/10mg and 40mg/10mg: Each film-coated tablet contains 10mg; 20mg or 40mg of rosuvastatin (as rosuvastatin calcium) respectively, and 10mg ezetimibe. Indication: Suvezen is indicated for substitution therapy in adult patients who are adequately controlled with rosuvastatin and ezetimibe given concurrently at the same dose level as in the fixed combination, but as separate products, as adjunct to diet for treatment of primary hypercholesterolaemia (heterozygous familial and non-familial) or homozygous familial hypercholesterolaemia. Dosage and Administration: The patient should be on and continue, an appropriate lipid-lowering
increase in plasma levels of rosuvastatin may occur, Asian patients, concomitant use of fibrates. Precautions and Warnings: Skeletal muscle effects: have been reported in rosuvastatin-treated patients with all doses and in particular with doses >20mg. As with other HMG-CoA reductase inhibitors, reporting rate for rhabdomyolysis is associated with use at doses >40mg. Post-marketing experience with ezetimibe, cases of myopathy and rhabdomyolysis have been reported. If myopathy is suspected based on muscle symptoms or is confirmed by a creatine phosphokinase (CPK) level, Suvezen and any of these other agents that the patient is taking concomitantly should be immediately discontinued. All patients starting therapy with Suvezen should be advised of the risk of myopathy and told to report promptly any unexplained muscle pain, tenderness or weakness, particularly if associated with malaise or fever. Creatine kinase (CK) measurement: CK should not be measured following strenuous exercise or in the presence of a plausible alternative cause of CK increase. If CK levels are significantly elevated at baseline (>5x ULN)
anticoagulants, Vitamin K antagonists, erythromycin, oral contraceptive/hormone replacement therapy. When coadministering rosuvastatin with other medicinal products known to increase exposure to rosuvastatin, doses should be adjusted (see SmPC for full details). The maximum daily dose should be adjusted so that the expected rosuvastatin exposure would not likely exceed that of a 40mg daily dose of rosuvastatin taken without interacting medicinal products. Fertility, Pregnancy and Breastfeeding: No clinical data are available on the use of ezetimibe during pregnancy. Potential risk from inhibition of HMG-CoA reductase outweighs the advantage of treatment during pregnancy. If a patient becomes pregnant during use of Suvezen, treatment should be discontinued immediately. Animal studies have shown excretion of medicinal product through breast milk. However, there are no data in humans. No clinical trial data on the effects of fertility in humans. Adverse Reactions: Adverse drug reactions previously reported with one of the individual components (ezetimibe or rosuvastatin) may be potential undesirable effects with Suvezen. Common (≥1/100 to <1/10):
memory loss, jaundice, hepatitis, arthralgia, haematuria, gynaecomastia. Not known: thrombocytopenia, hypersensitivity (including rash, urticaria, anaphylaxis and angioedema), depression, peripheral neuropathy, sleep disturbances (including insomnia and nightmares), dizziness, paraesthesia, cough, dyspnoea, diarrhoea, pancreatitis, constipation, hepatitis, cholelithiasis, cholecystitis, Stevens Johnson syndrome, erythema multiforme, drug reaction with eosinophilia and systemic symptoms, immune-mediated necrotising myopathy, tendon disorders (sometimes complicated by rupture), myalgia, myopathy/ rhabdomyolysis, oedema, asthenia. Prescribers should consult the SmPC in relation to other adverse reactions. Legal Category: POM. Marketing Authorisation Numbers: 10mg/10mg: PA0540/193/001; 20mg/10mg: PA0540/193/002; 40mg/10mg: PA0540/193/003. Marketing Authorisation Holder: Sanofi-Aventis Ireland Ltd. T/A SANOFI, Citywest Business Campus, Dublin 24, Ireland. Further information is available from: Sanofi, 18 Riverwalk, Citywest Business Campus, Dublin 24 or contact IEmedinfo@sanofi.com Date of Preparation: February 2022 (MAT-IE-2200101 v1.0) Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie; email: medsafety@hpra.ie Adverse events should also be reported to Sanofi Ireland Ltd. Tel: 01 403 5600. Alternatively, send via email to IEPharmacovigilance@sanofi.com Single-pill combination of rosuvastatin and ezetimibe available in 3 doses** COMBINING POWER AND CONFIDENCE AGAINST LDL-C* IN THE TREATMENT OF HYPERCHOLESTEROLAEMIA
End of Year Checklist
Item Check
Medical Council Requirements Ensure you adhere to all Medical Council registration requirements.
Medical Indemnity & Direct Debit Payments
Basic Salary
B Factor
Structured Weekend Attendance and C Factor
Rest Days
Annual Leave
Ensure that any payment made by Direct Debit is actually processed by your bank. This is particularly important in the case of medical indemnity and Medical Council registration fees.
Check that your annualised salary corresponds with the latest Salary Scale for your contract type.
Check that you are receiving the appropriate B Factor for your on-call rota and rate of call out. Note for those on 1:1, 1:2 and 1:3 rotas, higher allowances are payable.
Check that all structured weekend attendance and C Factor claims have been submitted and paid. Where claims have not been paid send a reminder to your employer.
Check that you have claimed and been paid for your rest day entitlements where not taken as leave.
Notify your employer of any untaken annual leave for current year. Payment should be sought for any untaken leave not rolled over. Earlier this year the HSE confirmed flexibility in the carryover of annual leave due to service needs during the pandemic.
Travel & Subsistence
CME Allowance
Ensure all outstanding claims for travel and subsistence have been submitted and paid. Note: travel expense is claimable for C Factor calls in the hospital.
Members are advised to claim their CME Allowance before the end of the year. Your College and CPD fees are eligible costs. Those who have accrued unutilised CME funding should write to their employer to carry it over to 2023. Consultants can utilise part of their 2021 and 2022 CME funds for the purchase of ICT equipment (up to €1,000 from 2021 and €1,000 from 2022). This arrangement terminates on 31st December 2022. Members should make enquires with local payroll regarding the tax implications or Benefit-in-Kind liability that may arise from one’s purchase.
Phone
Flat-Rate Expense Allowance
Statement of Interest under the Ethics Act
Tax Clearance Cert
Health Insurers’ Schedules
Health Insurer Payments
Ensure that rental on mobile or landline is claimed and paid by employer when due.
Check that you are benefiting from the 695 flat-rate expense allowance in your tax credits each year. You can claim a tax rebate for the previous four years.
Interests that could materially influence you in the performance of your contract must be declared under Ethics in Public Office Legislation.
All Consultants must within nine months of their date of appointment provide a Tax Clearance Certificate and Statutory Declaration to the Standards in Public Office Commission.
Review the three main insurers’ schedules and the procedures codes that you claim regularly.
Reconcile all outstanding claims and payments with private health insurers, paying particular attention to pended claims. Check F45 forms supplied by health insurers to ensure that the Professional Services Withholding Tax amounts are consistent with own accounts.
HSE and Private Hospitals Engagement
Medico Legal Fees
Private Practice Consultants are advised to maintain regular contact with their private hospital CEOs in this regard.
Review medico-legal fees and notify requesting solicitors accordingly – see Pro Forma letter on page 23.
9www.ihca.ie
President’s Address



Dear Colleagues, It gives me great pleasure to introduce the 26th edition of the IHCA Yearbook and Diary.
The Association continues to highlight the deteriorating capacity deficits in our public hospitals to Government and the need for practical, sustainable solutions that will address the record waiting lists. The priority actions the Government must address urgently are the 900 permanent Consultant posts that are not filled as needed and the severe shortage of hospital beds, theatres, diagnostic and other facilities to provide timely care to those who need it and the almost 1 million on waiting lists.
Unfortunately, motivation to fix the problems in Ireland’s health system is waning, at a time when energy should be firmly behind implementing the practical solutions. We know what the problems are, and we know what is required to fix them. We need the beds and the Consultants to treat patients in a timely manner.
The consistent failure of Government to deliver on its undertakings in successive plans, budgets and Ministerial unambiguous commitments is leading to the continued exodus of medical and surgical talent abroad and increased waiting times.
Despite the immense pressures placed on those on the frontline at the height of Covid, there was a semblance of hope that its impact would be a catalyst to finally tackle the obvious problems. Instead, another year and momentum has been lost, resulting in worsening patient wait times.
The solution is obvious: we must recruit and appoint additional Consultants without delay. Addressing the Consultant recruitment and retention crisis and making our public hospitals sufficiently attractive in an era of increased international competition is essential to attract the number and calibre of specialists they need. This can be achieved if the Government ends the discrimination imposed on Hospital Consultants appointed since October 2012.
The Consultant contract negotiations need to result in a contract that will work in practice. Those negotiations must restore trust by honouring the ‘unambiguous commitment’ made by the Minister for Health Stephen Donnelly to end the 2012 pay discrimination.
The onus is now on the Government to provide attractive working conditions in our health service, for our existing Consultants, our Consultants in training and the new medical talent we want to attract into permanent posts. If the opportunity is not availed of it will be lost to the detriment of the population that depends on public hospital services.
The health service is at a critical juncture, with decisions made around both the Cabinet and the negotiation table pointing it in one of two directions. One direction involves implementing the practical, sustainable solutions as proposed by the Association; the other ignores the practical, workable solutions resulting in unacceptable waiting times and poorer patient outcomes.
The Association’s Pre-Budget Submission for Budget 2023 provides the reasons and recommendations. Give us the essential resources, the capacity and the Consultants to treat our patients on time. The ask has not changed over the past number of years. The response must realistically provide the resources we need, or public hospital care will deteriorate. A focus of my presidency is to ensure that the response is the right one.
Similarly, the Association is actively engaged in addressing issues and problems with the HSE, employers, clinical indemnifiers, health insurers and a host of other organisations.
On behalf of my National Council colleagues and the staff of the Association, I would like to take this opportunity to thank you for your continued support. We look forward to successfully addressing the concerns of our members in the year ahead.
Finally, I wish you and your families a happy and successful 2023.
Prof Robert Landers, President

www.ihca.ie


10
We’re growing our healthcare network












Vhi Healthcare DAC trading as Vhi Healthcare is regulated by the Central Bank of Ireland. Ad 1597
Our latest Vhi 360 Health Centre, Dublin is now open
Maven Financial Planning
Maven Financial Planning is one of Ireland’s leading financial planning and advisory firms. Maven provides impartial financial advice on pensions, savings, investments and protection including estate planning for clients. The team at Maven Financial planning are both professional and experienced who are committed to gathering relevant information and recommending the most suitable products to clients.
Life Journey
Padraig is a Chartered Accountant with over 20 years’ experience working in the professional services area. Areas of expertise include Financial Planning, Wealth creation, Wealth preservation, Public sector pensions, Group pensions. Padraig is a fellow of the Institute of Chartered
and a Qualified Financial Advisor. He also holds the internationally recognised CFP® accreditation which is the highest qualification an individual working in this area can attain.
Our Solutions Your Financial
Key Contact; Padraig Kelly, Director of Maven Financial Planning
Accountants
MAVEN FINANCIAL PLANNING LTD T/A MAVEN FINANCIAL PLANNING IS REGULATED BY THE CENTRAL BANK OF IRELAND reception@mavenfinancial.ie 091 769566 087 2030913 Block 3 Galway Financial Services Centre, Moneenageisha Road, Galway CONTACT US Financial Protection Investment Planning Lifelong Financial Planning Retirement Planning Changing PrioritiesThe Prime of LifeGetting Started Living the Dream
Members’ Handbook Contents
INTRODUCTION
Brief History
Basic Rules
Retired Consultants
Services Offered
Public Appointments
Consultants’ Common Contract
Probation
Joint Appointments
Pension Arrangements
Existing Superannuation Scheme Members
Single Public Service Pension Scheme Members
Standard Fund & Personal Fund Thresholds
Early Retirement
Travel & Subsistence Expenses
Continuing Medical Education (CME)
Out of Hours Service
PRIVATE PRACTICE
INDEMNITY
MATTERS
LIMITATIONS
PROTECTION & PATIENT CONFIDENTIALITY


& INQUESTS
ASSISTANCE FOR CONSULTANTS
IRELAND FRAMEWORK
HEALTH POLICY
13www.ihca.ie
PAGE NO. 14
IHCA -
-
15 -
16 -
-
-
-
-
18 -
-
-
19 -
-
-
20 -
-
21 - Rest Days 21
22 MEDICAL
22 MEDICO-LEGAL
24 RESOURCE
25 DATA
26 POST-MORTEMS
26 REPRESENTATIONAL
26 HEALTHY
27 GOVERNMENT
Members’ Handbook
INTRODUCTION
The Members’ Handbook is provided to all members of the Irish Hospital Consultants Association. It is a useful resource which will assist members to quickly identify key features and entitlements arising from their appointments, whether public or private.
It also provides an outline of the services that the Association offers to its members. Members are encouraged to avail of these services by contacting the Secretariat as and when necessary.
IRISH HOSPITAL CONSULTANTS ASSOCIATION
Brief History
Initial steps to establish the Irish Hospital Consultants Association were taken in 1988. Hospital Consultants at that time felt that their needs were not being adequately represented by existing representative bodies and so formed their own Association.
Since then the organisation has thrived, representing members’ interests in contractual and broader medico-political matters. It is also steadfast in its advocacy of patients’ interests.
The Association currently represents more than 3,300 Hospital Consultants, around 95% of the total in the Irish health service. It is the only representative body in Ireland that speaks solely for hospital consultants.
Basic Rules
There are different classes of membership with varying rights and entitlements. Membership of the Association is open to the following:
(a) The members of the Association shall either:
(aa) Hold a current enrolment on the Irish Medical Register or Irish Dental Register and be: (i) Hospital Consultants who have subscribed to and paid in full the annual membership fee to the Association at the date of adoption of these Rules; or (ii) Consultants who are holders of the Common Contract; or (iii) Medically qualified Consultants in hospital practice who though not holding the Common Contract, are eligible to hold a Comhairle na n-Ospidéal/Health Service Executive structured public appointment; or (iv) Academic Dental Consultants referred to in Paragraph 8.8 of Report Number 36 of the Review Body on Higher Remuneration in the Public Sector; or (v) Consultant Orthodontists and Consultant Oral Surgeons in public hospital practice; or
(ab) be Top-Grade Bio-Chemists of Consultant status as defined in correspondence from the Department of Health of January 17th 1972 (reference A155-42) and who hold posts structured by Comhairle na n-Ospidéal/the Health Service Executive. or
(ac) be life members appointed by the National Council pursuant to Rule 3(e).
(b) In addition to the above, no person shall be eligible for membership of the Association unless they are either registered on, or eligible to be registered on, the Specialist Division of the Register of Medical Practitioners or the Register of Medical Specialists as maintained by the Irish Medical Council, save for the following groups of persons who are exempt from this requirement:
(i) Top-Grade Bio-Chemists of Consultant status as defined in correspondence from the Department of Health of January 17th 1972 (reference A155-42) and who hold posts structured by Comhairle na n-Ospidéal/the Health Services Executive; (ii) Academic Dental Consultants referred to in Paragraph 8.8 of Report Number 36 of the Review Body on Higher Remuneration in the Public Sector; (iii) Consultant Orthodontists and Consultant Oral Surgeons in public hospital practice; and (iv) Existing fully paid up members of the Association who were accepted as members by the Association prior to Oct 4th 2008.
(c) Associate Members
(ca) Doctors who have not yet been appointed to a Consultant post and who meet the requirements outlined in this subsection will be eligible to apply for Associate Membership of the Association in which case none of the requirements outlined above in Sections (a) or (b) will apply. An Associate Member is required to: (i) Hold or have previously held enrolment on the Irish Medical Register or Irish Dental Register; and (ii) Have commenced in or completed the final two years of his or her specialist training; or
(iii) Have received a Certificate of Satisfactory Completion of Specialist Training from an Irish Postgraduate Training Body.
(cb) An Associate Member will be eligible to receive such advice, representation and other services from the Association as may be determined by the National Council at its absolute and sole discretion from time to time. The National Council will determine the annual membership fee, if any, to be charged for Associate Membership and the nature of voting rights, if any, attached to such membership.
14 www.ihca.ie
Members’ Handbook
(cc) A person shall ipso facto cease to be an Associate Member of the Association with immediate effect upon the happening of any of the following: (a) upon resignation in writing; or (b) upon death; or (c) upon failure to pay the annual membership fee, if any, for the time being in force to the Association in the manner prescribed by the National Council; or (d) upon expulsion pursuant to Rule 5 hereof; or (e) upon a decision by the National Council to cease his or her Associate Membership for such reason or reasons as it may at its absolute and sole discretion consider appropriate.
(cd) The procedure for the expulsion of an Associate Member will operate in accordance with Rule 5 save that an Associate Member will not have any voting rights.
(ce) For the avoidance of doubt, with the exception of Rule 5 as referenced in subparagraph (cd) above and Rule 12(a), all other references in these Rules to a member will be read and construed as a reference to a member who satisfies the requirements outlined in Section (a) and (b).
(d) No person shall, for the purposes of these Rules, be deemed to be a member of the Association or be entitled to exercise or receive any of the benefits or privileges of membership (including the right to be present and vote at any general meeting of the Association) unless and until he has paid in full the annual membership fee as determined from time to time by the National Council in such manner as is determined by the National Council.
(e) The amount of annual membership fee and the manner of payment thereof for Hospital Consultants who have reached retirement age under the Common Contract or who had they held such Contract would be deemed to have reached retirement age thereunder or academic Dental Consultants referred to in Rule 3(a) (aa)(iv) who have either reached or deemed to have reached retirement age shall be determined from time to time by the National Council. The National Council shall have power to grant such members who have reached retirement age as outlined in this Rule and who have been members of the Association for each of the five years immediately prior to reaching such retirement age life membership upon payment of a lump sum and upon satisfying such conditions as the National Council may in its discretion impose and such life members shall not be liable for annual membership fee of whatever nature thereafter.
RETIRED CONSULTANTS
Members who reach retirement age under the Common Contract or who, had they held such a Contract, would be deemed to have reached retirement age thereunder, may become life members of the Association on payment of a once-off fee, provided they were fully paid up members during the preceding five years.
Life members are entitled to the same rights and privileges of membership as full members, including the right to vote at general meetings and in elections to National Council.
The National Council is obliged to co-opt a life member to membership of the National Council with effect from June 2000.
Termination of Membership
A person shall ipso facto cease to be a member of the Association with immediate effect upon the happening of any of the following events: (a) upon resignation in writing; or (b) upon death; or (c) upon failure to pay the annual membership fee for the time being in force to the Association in the manner prescribed by the National Council; or (d) upon removal for whatever reason from the Irish Medical Register (other than pursuant to an order granted under the Medical Practitioners Act, 1978, or the Medical Practitioners Act, 2007); or the Irish Dental Register (other than pursuant to an application pursuant to Section 44 of the Dentist’s Act, 1985) where the decision of the Medical Council or the Dental Board (as appropriate) to remove the member from such register is not the subject of an appeal by such member to the High Court, prosecuted with due diligence; or (e) upon expulsion pursuant to Rule 5 hereof; or (f) upon ceasing to qualify for membership of the Association pursuant to Rule 3(a) or life membership referred to in Rule 3(d) of these Rules.
www.ihca.ie 15
National Council
The National Council manages the affairs of the Association.
The Council consists of 30 members; 25 members are directly elected and the remaining five are co-opted. Members of Council hold office for a period of four years. They may be re-elected for a further period of four years after which they must resign. The members of Council are representative of eight regions whose functional areas coincide with the corresponding former Health Board functional areas.
The co-opted members are appointed so that there is representation on Council from the following specialties:
• Anaesthesiology
• Surgery
• Obstetrics/Gynaecology
• Paediatrics
• Psychiatry
• Medicine
• Radiology
• Pathology
One of the co-opted members must be a life member of the Association.
In addition to the Council, a full-time Secretariat is employed. The Secretary General, Assistant Secretary General, Senior Executive Officer and Senior Policy & Research Executive are supported by an administrator and secretary.
Services Offered
The Association provides a broad range of services to members, including:
Contract negotiations with health service employers and other bodies; High level representation and advice to members on contract, employment and industrial relations issues;
• Local negotiations with health service employers in the context of resourcing issues, workplace disputes and grievances; Representation of members’ views through the Association’s advocacy and communications function including publication of policy submissions, national circulars, press statements and member surveys; Detailed guidance for members on a range of issues including private practice, health insurance, superannuation, taxation, GDPR and medico-legal concerns; A range of financial products and services are provided by Lyons Financial Services.
The Association represents the views of Consultants through the formulation of policy documents and position papers on a wide range of issues affecting acute hospital services, mental health services, and patient care.
PUBLIC APPOINTMENTS
Health Service Executive
The number and range of Consultant appointments in the public sector in Ireland are regulated by the Health Service Executive. As of May 2022 there were 3,671 WTE Consultants employed in the public health system under public contract and a total of 3,930 approved Consultant posts. There are an estimated 550 Consultants in full-time private practice in Ireland. The granting of admitting rights and/or practice privileges to Consultants in private hospitals is a matter for each individual hospital.
Consultants’ Common Contract
Each Consultant with a public appointment works under the Consultants’ Common Contract. The terms of the 2008 Consultant Contract were agreed between the Health Service Executive, on behalf of all employers, and the Irish Hospital Consultants Association on behalf of Consultants. The terms and conditions of this contract apply to all new appointees with effect from 1 June 2008.
Each Consultant and his/her employer sign a copy of the contract. Sections 2(a), 5 and 8(a) along with the HSE letter of approval (Appendix I) are unique to each individual Consultant. These should be carefully checked prior to signing to ensure accuracy. The Association will assist in this process.
Section 2 identifies the employer’s name and address, the Consultant’s name and address, the title of the post and the agreed start date.
Section 5 identifies the type of contract being offered.
Section 8(a) identifies the employer and the location(s) in which the Consultant will work. The location(s) should be a physical location and not the name of a service.
Probation
Public sector appointments are permanent and pensionable. Appointees are, however, subject to a 12-month probationary period. This may be extended at the employer’s discretion. At the end of your probationary period the employer shall certify that your service has been satisfactory and confirm your appointment or give stated reasons why it has not and you will cease to hold the appointment. In the event of a Consultant moving from one public appointment to another, he or she will not be required to serve more than 12 months’ probation in the aggregate. The probation period may not have to be completed if a Consultant has been in the post on a locum basis pending the permanent appointment.
Joint Appointments
A number of posts in Ireland are structured as joint appointments.
Consultants holding such posts have two employers with the commitment to be devolved to each employer being decided by the HSE. This will be indicated by way of sessional split in the letter structuring the post.
If you hold a joint appointment, e.g. with a University and a hospital, your holding of one part of the post is contingent on you holding the other part also.
Members’ Handbook 16 www.ihca.ie
Membership means...









included as standard








Because we believe prevention is better than cure, we do all we can to help our members learn. With over 60 hours of verified CPD included in your membership, you can continually build your skills and reduce your risk through: • training days • live webinars • extensive online learning resources. Over 60 hours of CPD
Comfort in protection that’s right for you: medicalprotection.org/ireland The Medical Protection Society Limited (“MPS”) is a company limited by guarantee registered in England with company number 00036142 at Level 19, The Shard, 32 London Bridge Street, London, SE1 9SG. MPS is not an insurance company. All the benefits of membership of MPS are discretionary as set out in the Memorandum and Articles of Association. MPS® and Medical Protection® are registered trademarks. 2201242981 03/22
Members’ Handbook
Pension Arrangements
All Consultant posts in the Public Health Sector are pensionable.
Existing Superannuation Scheme Members
Consultants who are not new entrants, e.g. Consultants who took up their public appointments before 1 January 2013, are deemed to be superannuated under the pre-existing schemes. There are three main schemes in place, namely:
The Voluntary Hospitals Superannuation Scheme;
• The HSE/Local Government Superannuation Scheme; and The Nominated Health Agency Superannuation Scheme.
There is interchangeability between each scheme. The scheme under which a member is superannuated is contingent on the employer’s status.
Consultants who were recruited before 1 April 2004 who previously had a mandatory retirement age of 65 can now remain in employment up to age 70 if they wish.
The pension payable on retirement is based on years of reckonable service. 1/80th of the final pensionable remuneration is payable for every completed year of reckonable service up to a maximum of 40/80th. A pro rata adjustment is made for parts of years. The schemes make allowance for the late entry age of consultants into public sector employment by the discretionary award of ‘Professional Added Years’, which can result in an award of additional service calculated as 1/3 of actual service up to a maximum of 10 years at no cost to the member. For new entrants recruited on or after 1 April 2005 an award of up to five years may be granted. Members must purchase all reckonable service e.g. temporary service, for which refunds/gratuity was authorised before granting an award for professional added years. Following the death of a retired Consultant, a pension of 50% of the member’s pension is payable to the spouse. One sixth of the member’s pension is payable to each dependent child up to a maximum of three children. All service in a pensionable position, including that served during training, counts in arriving at the length of service. NCHDs who leave with less than five years’ service after completion of training may be given a refund of their superannuation contributions if they do not avail of the career break scheme to pursue their training. It is possible to “buy back” this service at a later stage. The Department of Finance issues tables under which credits for these years and appropriate contributions are calculated.
A lump sum is payable on retirement. It is calculated at the rate of 3/80th of the final pensionable remuneration for each year of reckonable service up to a maximum of 120/80th. This may be subject to abatement in respect of any period during which the Consultant was not contributing to the Spouse and Child element of the scheme. The first e200,000 of pension lump sum payable on retirement is tax-free. This is a total lifetime limit even if lump sums are taken at different times and from different pension arrangements. Lump sums between e200,001 and e500,000 are taxed at 20%, with any balance over this amount taxed at the marginal rate of income tax and subject to the Universal Social Charge.
Single Public Service Pension Scheme Members
Consultants deemed to be new entrants taking up public appointments after 1 January 2013 are superannuated under the Single Public Service Pension Scheme. Those who are not deemed new entrants continue to be superannuated under their pre-existing scheme (see above).
Main features of the Single Public Service Pension Scheme: career average earnings are used to calculate benefits (a pension and lump sum amount accrue each year and are up-rated each year by reference to CPI) minimum pension age for most members is linked to the current State Pension age of 66. (The State pension age and minimum retirement age was due to rise to 67 from January 2021, but this was deferred and a Pensions Commission was established to consider the matter. In October 2021, the Commission recommended a gradual incremental increase in the State Pension age by three months each year commencing in 2028, reaching 67 in 2031, with further increases of three months every second year reaching 68 in 2039. This recommendation has not been accepted by Government.) • compulsory retirement age of 70 applies for most members post retirement pension increases are linked to CPI there is no provision for the award of professional added years. Pension and lump sum are separately accrued each year using the following formulae:
Pension:
Accruing rate of 0.58% pensionable remuneration up to a ceiling of 3.74 x State Pension Contributory (SPC) (currently e49,432) plus (where applicable) 1.25% of pensionable remuneration above that level.
Lump Sum: 3.75% of pensionable remuneration. Contributions to the scheme are deducted at 3.5% of net pensionable remuneration i.e. pensionable remuneration less twice the rate of the State Pension, plus 3% of
18 www.ihca.ie
Members’
pensionable remuneration. During the scheme membership, the amounts accrued each year will be increased to reflect the CPI increase between that year and retirement. The annual pension and lump sum payable at retirement will equal the total of these CPI adjusted amounts. The minimum retirement age under this scheme is currently 66 years and retirement becomes compulsory at 70. Members required to retire on medical grounds with less than two years' service will receive a gratuity of 8.5% of pensionable remuneration per year of service. Those with more than 2 years' service will receive an immediate payment of retirement benefits accrued to the point of retirement (with no actuarial reduction). Where a member superannuated under the Scheme dies in service, a lump sum becomes payable to the estate of the deceased member equal to twice the annual pensionable remuneration in the 12 months prior to the date of death. In those circumstances the spouse/civil partner will receive a pension equal to 50% of the member's pension that would have been awarded had the Single Scheme member retired on medical grounds on the date of death. Also, children's benefits is calculated at the rate of one sixth (1/6th) of the member’s pension per eligible surviving child up to three children; and where there are four or more eligible children, a child’s pension, calculated at the rate of one half (1/2) of the member’s pension divided by the number of eligible children, is payable per child. Following retirement, pension increases will be based on increases in the CPI.
Standard Fund Thresholds & Personal Fund Thresholds
In 2014, budgetary measures were introduced to reduce the Standard Fund Threshold (SFT) for the capital value of pension funds from e2.3m to e2.0m with effect from 1 January 2014. The reduction in the SFT means that an increased number of hospital consultants could potentially incur a tax liability in respect of the capital value of their superannuation and other pension entitlements at point of retirement.
Up until July 2015, a mechanism existed whereby members affected by the SFT reduction could apply for a Personal Fund Threshold (PFT) to protect superannuation entitlements in excess of the SFT, up to a maximum of e2.3m as at 1 January 2014. While the deadline to apply for a PFT has now passed, members may still be eligible to apply for a PFT at point of retirement on a ‘look back’ basis. The ‘look back’ arrangements are relevant for Consultants who receive Professional Added Years as part of their reckonable service at point of retirement. Consultants who have already been issued with a PFT as at either 7 December 2010 or 1 January 2014 may be eligible on foot of the High Court Settlement Agreement (HC-SA) to apply on a ‘look back’
basis for a revised PFT. Those who were not previously eligible to apply for a PFT in either 2010 or 2014 may now be eligible on foot of the HC-SA to apply on a ‘look back’ basis. Members are advised to contact the Secretariat for further information in this regard.
Early Retirement
A Consultant, who commenced employment in the public health service prior to April 2004, may take retirement from age 60 onwards when in normal health. Retirement benefits are based on the salary at retirement and the length of completed service plus added years. There are provisions in all superannuation schemes, including the Single Public Service Scheme, for Consultants to retire on an actuarially reduced pension from age 50 or 55 depending on date of entry.
Where a Consultant retires on grounds of ill health and has more than five years’ service, their pension and gratuity is based on completed reckonable service. Further years may be added to reckonable service as follows:
A Consultant with between 5 and 10 years of service may add the equivalent amount of service actually served to a limit of their potential service at age 65.
A Consultant with between 10 and 20 years of reckonable service may add the more favourable of:
(a) The difference between actual service and 20 years subject to a limit of potential service at age 65; or (b) 6.67 years subject to a limit of potential service at age 60.
A Consultant with more than 20 years’ service may add 6.67 years to a limit of his/her potential service at age 65.
A Consultant with less than five years’ service retiring on ill health grounds will receive a gratuity of 1/12th of salary for each year of service. In addition, if he/she completed service of more than two years, a further 3/80th of salary for every year of service is paid. No pension is payable in these circumstances. Note: There are slightly different arrangements applying in respect of Consultant Psychiatrists working in certain registered mental hospitals. Reckonable service in excess of 20 years may be counted as double and they may retire from age 55 onwards.
Travel & Subsistence Expenses
Travelling and subsistence expenses necessarily incurred in the course of a Consultant’s work are paid according to the public sector rates for senior staff. Travel expenses are payable in respect of each emergency call-out and in respect of travel between locations when a Consultant is scheduled to work away from his or her base.
Handbook www.ihca.ie 19
Members’ Handbook
Details of the most recent motor travel rates applying domestically from 1st September 2022 are available in HSE HR Circular 26/2022 and DOH Circular 05/2022 which are available on request from the Assocciation, on the IHCA website or from your Human Resources department.
Subsistence Allowance (Domestic)
Members should note that claims may be made for periods in excess of five hours when a Consultant is absent from his/ her base as part of his/her contractual obligation or when representing his/her employing authority hospital (day allowance).
HSE HR Circular 27/2022 outlines revised arrangements for overnight allowances in Dublin. Full details can be found on the IHCA website or from your Human Resources department.
Subsistence Allowance (Overseas)
Members should be aware of the specific rates of subsistence which are payable for international travel. Details applicable since April 2017 are available in the members section of the website - www.ihca.ie.
Continuing Medical Education
In April 2014, the HSE issued a revised CME Guidance document with the following proposals:
Continuation of the existing e3,000 CME annual allowance, with provision for the relevant Clinical Director to apply for funding in excess of that amount on an exceptional basis.
Eligible costs would include registration fees for courses/conferences, associated travel, e-learning courses, certain medical journals and text books, computer software that has a CME/CPD component, annual registration fees for enrolment on a recognised Professional Competence Scheme in Ireland or outside Ireland where it is not possible for the Consultant to register on a professional competence scheme in Ireland for their specialty or subspecialty and the annual registration fee for professional memberships. In relation to computer hardware such as laptops, tablets and iPads, the Guidance provides that “HSE MET reserves the right to directly fund site purchase of computer hardware for CME/CPD purposes. Such funding will be in line with national medical education and training policy and final decision on allocation rests with MET.”
“In very exceptional circumstances” a Clinical Director may apply prospectively for funding in excess of the e3,000 per annum figure or may apply for approval for an individual Consultant’s fund to roll over for a maximum period of three years.
Refusals to provide funding may be appealed initially to hospital management and subsequently under the Grievance and Dispute procedure provided for in Consultant Contracts.
The Association subsequently wrote to the HSE highlighting that the contract CME entitlements must be honoured. This includes the provision for the carryover of unused CME for up to five years, indexation of the e3,000 annual CME allowance, recognition of a wider range of CME activities, the extension of coverage of course types and the funding of a more extensive range of software and hardware.
The Association has secured agreement from the HSE that Consultants can utilise part of their 2021 and 2022 CME funds for the purchase of ICT equipment (up to €1,000 from 2021 and €1,000 from 2022). It is envisaged this arrangement will terminate on 31st December 2022. Members should make enquires with local payroll regarding the tax implications or Benefit-in-Kind liability that may arise from one’s purchase.
The Association’s advice to its members is that the CME entitlements contained in their contracts cannot be diminished or restricted by unilateral communications from the HSE HR office. Members are advised to claim their CME Allowance before the end of the year.
Out of Hours Service
Employers are responsible for arranging clinical cover for emergencies that arise within the hospital or for patients brought to the hospital for emergency treatment. The employers are responsible for arranging suitable rosters to provide this cover.
An allowance is payable in respect of this availability for duty. This Allowance (B Factor) is part of the pensionable remuneration.
The rotas used for this are those that have been formally ratified by the hospital management. Consultants who wish to operate a sub roster within a general specialty, e.g. vascular surgery within general surgery, need to have management approval in order to attract the additional allowance.
Consultants are paid an additional allowance (C Factor) in respect of instances where they are called to the hospital for emergencies. To qualify for these additional payments, a Consultant must be: • Rostered for on-call duty and contacted by another hospital doctor, by a senior nurse or other member of the hospital staff specifically designated for the purpose and attends at the hospital; or
• Rostered for on-call duty and in the exercise of his professional judgement (EPJ) attends at the hospital and performs clinical work of an urgent nature or carries out urgent diagnostic or therapeutic procedures.
20 www.ihca.ie
Details of the relevant B Factor, C Factor and other allowances are outlined in the Consolidated Salary Scales, which are available on request from the Association. B Factor allowance should be paid together with salary payments.
Members are reminded of the HSE circular to hospitals requiring that claims for emergency call outs (C Factor claims) must be made no later than three months from the earliest date of the on-call liability to which they relate in default of which they will be forfeited. While this is not a contract requirement, members are advised to submit their claims for emergency call outs (C Factor claims) without delay to ensure that claims are not deemed ineligible. If necessary, please contact the Secretariat for advice on the issue.
In addition, travelling expenses to and from the hospital are payable. Income tax should not be levied on emergency call-out (C Factor) travel when claimed in respect of a named patient (See Revenue Statement of Practice - SP - IT/2/07 - Tax treatment of the reimbursement of Expenses of Travel and Subsistence to Office Holders and Employees (Revised July 2015)).
Rest Days
In April 2014, the HSE unilaterally circulated proposals for Consultants on 1:3 and 1:4 on-call rotas which can be summarised as follows:
Under the proposed arrangements, regardless of the rest assigned for each category of on-call incident, there will be a minimum of 15 rest days for Consultants on a 1:3 on-call rota and a minimum of 10 days for those on a 1:4.
For attendance on site on weekdays, the amount of rest assigned with each on-call incident will be two hours where the callout occurs before midnight and three hours after midnight, or the actual time if exceeded. In addition, travel time will be allowed to and from the location.
For telephone consultations, the amount of rest assigned with each call will be 30 minutes before midnight and 60 minutes after midnight, or the actual time if exceeded.
The amounts of rest assigned above will be doubled in circumstances where the on-call incident occurs on a Saturday, Sunday or bank holiday.
Each Consultant will be responsible for recording each incidence of call-out and submitting the claim to the Clinical Director by a defined date.
Rest will be taken where possible by the end of the next following month or, at the latest, within eight weeks.
When for operational reasons, a Consultant cannot take all or any of their compensatory rest within eight weeks, the hours outstanding will be paid at the relevant hourly rate.
Clinical Directors will have authority to assign additional rest to Consultants, where time spent providing on-call services consistently exceeds three call-outs per month. In such circumstances, the Clinical Director will assign up to 150% additional rest.
Payment of B Factor and C Factor will continue as per existing contracts.
The Association’s advice to its members is that the rest day entitlements provided in their contracts cannot be diminished or restricted by unilateral communications from the HSE HR office. Accordingly, members should continue to claim their rest day entitlements without any of the restrictions or reductions proposed by the HSE which have not been agreed.
Rest Day Entitlement*
lieu
HISTORIC REST DAYS
Consultants who have an entitlement to accrued Historic Rest Days as part of a legacy entitlement dating back to 1997 should note that the deadline for the taking of historic rest days was extended to the end of December 2023. The Association has sought a further extension from the HSE to 31st December 2024.
PRIVATE PRACTICE
It is estimated that there are around 550 Consultants in full-time private practice.
Consultants wishing to establish admitting rights to a private hospital should apply, in the first instance, to the hospital management. The medical board normally considers the application and a recommendation is put forward for consideration by the hospital directors.
The terms and conditions under which Consultants work in private hospitals vary from institution to institution.
Members’ Handbook www.ihca.ie 21
Roster
1:1 5 1:2 3 1:3 2 1:4 1 * Days in
per four-week period
Consultants considering such a move should satisfy themselves in relation to these matters with the hospital directly.
Consultants who propose treating patients privately should register with the health insurers at an early date. Insurers will recognise Consultants who hold posts approved by the HSE. They will also recognise Consultants in private practice who are eligible to hold permanent posts. Each health insurer publishes a schedule of benefits for professional fees in respect of procedures and treatments provided by Consultants.
There are three main health insurers operating in the Irish market: VHI Healthcare, Laya Healthcare, and Irish Life Health. In August 2016, Irish Life Group completed its acquisition of Aviva and GloHealth.
Other private health insurance schemes operating in Ireland include:
ESB Staff Medical Provident Fund
• Irish Life Assurance Plc Outdoor Staff Benevolent Fund
• Irish Life Medical Aid Society
• New Ireland/Irish National Staff Benevolent Fund
• Prison Officers Medical Aid Society
• St Paul’s Garda Medical Aid Society
• The Goulding Voluntary Medical Scheme
Membership of these schemes is restricted to employees of the relevant organisations only and their families. In addition, serving Officers of the Permanent Defence Forces are covered for private health insurance by the military authorities. Those of the rank of Lieutenant and Captain, or equivalent, are entitled to semi-private cover whilst officers of higher ranks are entitled to private cover. Non-commissioned officers of the Permanent Defence Forces are not covered for private health care by the military authorities.
MEDICAL INDEMNITY
All Consultants are obliged to indemnify themselves against claims arising from malpractice and negligence. The Clinical Indemnity Scheme (CIS) provides cover in respect of practice in public hospitals.
The Medical Practitioners (Amendment) Act 2017 introduced a mandatory legal requirement for all medical practitioners currently registered or applying to register with the Irish Medical Council (IMC) to have the required level of professional medical indemnity. If evidence of adequate indemnity is not provided to the IMC on
registration or renewal, via a Professional Indemnity Declaration Form, the doctor will not be placed on the medical register.
The CIS covers all Consultants working in public hospitals and mental health services and is deemed to be sufficient for the purpose of the Act. For those working in private hospitals, evidence of the relevant minimum level of indemnity will have to be provided by way of a certificate from your insurer/broker or indemnity provider. Under the caps on professional indemnity for Consultants in private practice, the CIS covers claims in excess of minimum levels provided that such Consultants purchase indemnity up to the relevant cap applying to his or her specialty.
It is the unequivocal advice of the Association that Consultants maintain membership of a medical defence body, such as the Medical Protection Society, Medisec/MedPro or other provider, for those aspects of practice not covered by the CIS (i.e. legal costs that could potentially be incurred in the context of appearing before the Coroner’s Court or defending one’s self before the Medical Council).
As a Consultant undertakes full clinical responsibility for his or her patients, he or she could be held personally liable in the event of an adverse event occurring. Indemnity may provide cover against such an eventuality, details of which may not materialise until many years after the incident that gave rise to the injury.
MEDICO-LEGAL MATTERS
Consultants are regularly called upon to provide opinions in medico-legal matters. This can vary from providing an examination and report in respect of an insurance policy application, to acting as an expert witness in a court action arising from an accident. The Medical Council, in agreement with the Law Society, states that a doctor has a moral and professional responsibility to supply a medico-legal report on request from a patient’s solicitor as failure to comply may lead to a patient being deprived of benefits to which he/she may be entitled.
The Medical Council has also indicated that, under ordinary circumstances, medico-legal reports should be provided within two months after the examination or receipt of the request, whichever occurred last.
Consultants are entitled to charge fees in respect of this work. The fee charged by a Consultant in this regard is a matter entirely at his or her own discretion. As a result of competition law provisions, the Association does not provide a scale of medico-legal fees.
Members’ Handbook 22 www.ihca.ie
Members’ Handbook
In 2012, the Revenue Commissioners issued guidance to the effect that medico-legal work may be liable for VAT. Members are advised to contact the Association and to consult with their financial advisors with regard to the appropriate treatment of such income and whether they are required to register with Revenue for VAT purposes. You are strongly advised to respond to requests for medico-legal opinions using the pro-forma letter on this page. By so doing you will avoid any confusion or disagreement later in the matter of fees.
PRO FORMA LETTER
Re: Medico-Legal Fees: Terms & Conditions Dear Sir/Madam
I write to you in response to your request to examine and prepare a medical report on behalf of your client, …………………….. I detail hereunder my fees for the following items for medico-legal work.
• Examination and First Report e
• Follow up Report e
Note: Reports will be dispatched on receipt of the appropriate fee Attendance at Court
• Half Day e
• Full Day e
• Travelling expenses at public service rate of e
• Consultation with Solicitor or Counsel (other than at Court Hearing) e
Consultation with other party’s medical advisor
• By telephone e
• By correspondence e
• By attendance at examination e
Cancellations - Courts
• Standby for any reason, with less than 1 working day e
• Standby for any reason, with less than 3 working days e
• Attendance for any reason, with less than 1 working day e
• Attendance for any reason, with less than 3 working days e
I would be grateful if you would provide me with your written undertaking that your firm will be responsible for the above fees, irrespective of the outcome of the Court case or the decision of any third party.
Yours faithfully,
www.ihca.ie 23
Members’ Handbook
RESOURCE LIMITATIONS
It is acknowledged that Consultants are currently working in underresourced hospitals and attending to increased demand for patient care. Recognising your professional, ethical and contractual obligation to advocate on behalf of the patient and the services you provide, see below and right a draft wording that may be used in these circumstances and addressed to Management. Please contact the Secretariat for further advice as it relates to the specific circumstances.
Private & Confidential
PRO FORMA LETTER
Re: Early Discharge/Bed Shortages/Resource Restrictions
Dear,
I wish to advise you that I had to discharge _______________ at ___________ to provide a bed for _______________ who required emergency/urgent admission on _________. I am not satisfied that ______________ was sufficiently well to be discharged and I would not have discharged him/her at this time except, as I have stated, the demand for beds from patients requiring emergency/urgent admission had to take precedence.
I do not regard this practice as in the interest of patients and I am not satisfied that best standards are being observed as I am not allowed to exercise my clinical judgement in an independent manner and in the best interest of my patients.
I am obliged to inform you that should anything untoward devolve on (name) due to lack of resources or should anything untoward devolve on any patient who is discharged prematurely due to a shortage of beds, responsibility for same will rest with (name of board/hospital).
Note: You should quote the relevant extracts below from the Contract that you personally hold in the above letter.
2008 Consultant Contracts
10 (b) “The Consultant is clinically independent in relation to decisions on the diagnosis, treatment and care of individual patients. This clinical independence derives from the specific
relationship between the patient and the Consultant in which the patient places trust in the Consultant personally involved in his/her care to make clinical decisions and to take continuing responsibility for their consequences.”
4 (c) “Services not provided as a consequence of a resource limit are the responsibility of the Employer and not the Consultant.”
4 (d) “The Employer recognises the Consultant’s obligations regarding the application of the Medical Council’s (or Dental Council, as appropriate) ethical and professional conduct guidance to the clinical and professional situations in which (s)he works.”
1997 ‘Buckley’ Consultant Contract
6.3.2 “Being a consultant involves taking responsibility in his own name for the diagnosis and treatment of his patients, or that aspect of care appropriate to him when consulted, without supervision of his clinical judgement. This is the essence of clinical independence.”
6.3.3 “Clinical independence derives from the concept of the specific relationship between the patient and the doctor in which the patient authorises and trusts the doctor(s) personally involved in his care to make clinical decisions in the patient’s best interest and to take continuing responsibility for their consequences.”
6.3.5 “The contract must, therefore, recognise and expressly protect the right of the patient to the independent judgement of his personal consultant except where appropriately transferred by that consultant.”
6.5.4 “Services not provided as a consequence of a resource limit are the responsibility of the Employing Authority and not the consultant”.
Medical Council, Guide to Professional Conduct and Ethics, 8th Edition 2019, Section 24* Healthcare Resources
24.1 “Your duty is to act in the best interests of patients and you have a responsibility to engage and advocate with the relevant authorities to promote the provision of suitable healthcare resources and facilities. If you work in a facility that is not suitable for patients or for the treatment provided, you have a responsibility to advocate on behalf of your patients for better facilities.”
Yours sincerely,
* Please note, the Medical Council has commenced a review in preparation for a new 9th Edition of the Guide to Professional Conduct and Ethics.
www.ihca.ie
24
Members’
DATA PROTECTION AND PATIENT CONFIDENTIALITY
Consultants and their colleagues are subject to Irish Data Protection legislation and the EU General Data Protection Regulation (GDPR) along with the obligations required of them in respect of patient data. The Association has prepared a Guideline document, with expert input from Ward Solutions Ltd, to ensure that affected Consultants are aware of the actions they need to take to meet their obligations under the new GDPR data protection regime. The Guideline is available in the Members’ section of the Association’s website.
It is strongly recommended that you read the Guideline and ensure that appropriate actions are taken, as may be required depending on your specific circumstances, to adhere to GDPR requirements.
Consultants who satisfy the GDPR definition of a ‘Data Controller’ or ‘Data Processor’ should note that GDPR compliance is not discretionary. Enforcement actions for non-compliance include the imposition of significant fines. The Guideline document will help you to determine your status and whether you are affected.
The Guideline is comprised of:
• An overview of the legal basis for processing by Consultants
• A series of practical action points
• Frequently asked questions
• A suite of template policies and procedures (available in MS Word Format for adaptation).
The above suite of policy documents can be downloaded in MS Word Format from the Association’s website.
The integrity of the health system relies upon defined and adhered rules regarding patient confidentiality. Depending on the circumstances, the following draft letter may be relied upon in corresponding with Management on issues of patient data and confidentiality. Please contact the Secretariat for further advice as it relates to the specific circumstances.
Private & Confidential PRO FORMA LETTER

Copying of Charts/Medical Notes
Dear,
It has come to my attention that the charts/medical notes belonging to (patient’s name) have been photocopied without my prior knowledge and I having had an opportunity to express an opinion. You will be aware that all patients are entitled to the maximum possible confidentiality in all matters concerning their medical management. This requirement applies particularly to patients who attend the psychiatric services. Consultants are obliged by their contract, the Medical Council’s Ethical Guidelines and their binding contract with their patients to observe the strictest confidence regarding their treatment.
(1) I am extremely concerned that patients’ charts/notes are not always securely deposited so as to eliminate the possibility of their being perused by unauthorised personnel.
(2) I have equal concerns that patients’ charts/notes have been copied by personnel who may not be fully briefed on the need for adherence to strict confidentiality.
(3) I also wish to place on record my concerns that copying of charts/ notes of patients under my care has taken place without any reference to me. I acknowledge that these charts/notes are the property of the patient and I am aware that the final decision on the release of information under, for example the Freedom of Information Act, is a matter for the CEO and not the managing consultant. However, I wish to emphasise that it is prudent that the managing consultant should be advised that charts are to be copied and the consultant should be allowed the opportunity to study the chart/notes in order to advise on whether or not it is appropriate to provide copies of any or all documents in a chart, depending on the nature of the request.
I wish to advise that I cannot be held responsible for any action that may be taken by a patient/next of kin in the event of sensitive patient information falling into the possession of any inappropriate or unauthorised persons. This responsibility must lie with (name of employer).
Yours sincerely,
Handbook www.ihca.ie 25
Members’
POST-MORTEMS & INQUESTS
Consultants are, on occasion, asked to perform post-mortems or to appear as witnesses at inquests. The revised scale of fees (SI 155 of 2009) has been published by the Department of Justice. Consultants wishing to acquaint themselves with the current scale may contact the Association.
REPRESENTATIONAL ASSISTANCE FOR CONSULTANTS
The Association is always available to provide representational assistance to Consultants in their dealings with employers and other service providers.
If you require such assistance please contact a member of the Secretariat in writing, by email or by telephone. Please provide as much information as possible about the issue concerned together with any relevant documentation.
The provision of legal advice may be facilitated for members on request. In general, if a Consultant decides to pursue legal action following the provision of such advice, the action will be taken by the Consultant in his or her own right and he or she will assume responsibility for the associated legal costs. Finally, members may be assured that any request for assistance is treated in the utmost confidence.
HEALTHY IRELAND — A FRAMEWORK FOR IMPROVED HEALTH AND WELLBEING
The Government published Healthy Ireland – A Framework for Improved Health and Wellbeing 2013-2025 in March
2013. It described four high level goals and 64 actions that were to work together to help achieve these goals.
The four high level goals are:
1. Increase the proportion of people who are healthy at all stages of life
2. Reduce health inequalities
3. Protect the public from threats to health and wellbeing
4. Create an environment where every individual and sector of society can play their part in achieving a healthy Ireland.
These goals were to be delivered through a series of 64 separate actions grouped into six themes. The themes cover the following broad areas.
Theme 1 – Governance and Policy
A Cabinet Subcommittee on Social Policy was to oversee the implementation of the plan and oversee, monitor and address common Government policy, agenda, targets and action plans to improve health and wellbeing.
All public sector organisations were to be required to promote and protect the health and wellbeing of their workforce, their clients and the community they serve.
Theme 2 – Partnerships and Cross Sectoral Work
This set out a series of fourteen actions designed to ensure that health and wellbeing be devolved to local areas for implementation.
Theme 3 – Empowering People and Communities
Action points within this theme were directed at supporting, linking and improving existing partnerships so that various sectors of society could improve their health and wellbeing.
Theme 4 – Health and Health Reform
The most concrete action within this theme was one to establish multi-disciplinary national teams that will lead and take responsibility for policy areas. There was to be the development of a health and wellbeing human resource plan with a view to building capacity for health and wellbeing activities.
Theme 5 – Research and Evidence
The development of a Healthy Ireland research plan was at the core of this theme. It was also planned to work with the Health Research Board to implement a plan to build research capacity.

Handbook 26 www.ihca.ie
Theme 6 – Monitoring Reporting and Evaluating
A series of nine actions were set out to ensure that the capacity and systems were in place to report and evaluate the success of Healthy Ireland.
The Healthy Ireland Strategic Action Plan 2021-2025, published in May 2021, focuses on the remaining years of the Healthy Ireland Framework.
Building on the first seven to eight years of the Framework, the Action Plan provided a roadmap for the remaining five years and built on the cross-society approach that is central to Healthy Ireland by involving Government Departments, local authorities, public bodies, schools and education institutions, businesses and employers, sports, cultural, creative and voluntary groups, communities, families and individuals.
The ongoing implementation of Healthy Ireland is a key action under the Sláintecare Report and the Sláintecare Implementation Strategy and Action Plan 2021-23, through Sláintecare’s Healthy Living workstream.
GOVERNMENT HEALTH POLICY Patient Safety Bill
The Patient Safety (Notifiable Patient Safety Incidents) Bill 2019 was approved by Government on 3 December 2019. When enacted, it will establish a framework for mandatory open disclosure.
The legislation will require notification of serious patient safety incidents externally to the Health Information and Quality Authority (HIQA), the Chief Inspector of Social Services (CISS) and the Mental Health Commission (MHC) to contribute to national patient safety learning and improvement.
Mandatory open disclosure and the notification system for these ‘notifiable patient safety incidents’ will apply to both public and private health services.
Regional Health Areas
The Government announced in 2019 plans to establish six new regional health areas (RHA). The Government Decision on RHA Implementation, approved on 5 April 2022, provides further policy direction and a mandate for the RHA work programme. However, the Cabinet decided that the RHAs will be organised on an administrative rather than on a legal basis. The detailed system and RHA design and associated implementation plan is currently being developed between the HSE and Department of Health and is due to be finalised by the end of 2022. Area A takes in the northeast of the country, including Dublin North, Meath, Louth, Cavan and Monaghan. Area B takes in Longford, Westmeath, Offaly, Laois,
Kildare and parts of Dublin and Wicklow. Area C focuses on the south and southeast, including Tipperary South, Waterford, Kilkenny, Carlow, Wexford, Wicklow and part of South Dublin. Counties Kerry and Cork account for Area D, while Area E is made up of Limerick, Clare and Tipperary North. Area F includes Donegal, Sligo, Leitrim, Roscommon, Mayo and Galway. The regional bodies will have clearly defined populations and will plan, resource and deliver health and social care services for the needs of its population. The restructuring is in line with the Sláintecare Report, which recommended that regional bodies should be responsible for the planning and delivery of integrated health and social care services. The HSE will continue to be the central executive with responsibility for overall planning and strategy.
HSE Board
The Health Service Executive (Governance) Act 2019 was signed into law on 5 June 2019 and the newly established Board of the HSE, under the Chairmanship of Ciarán Devane, met for the first time on 28 June 2019. The legislation provides for an independent Board for the HSE, as opposed to a directorate, aimed at strengthening the management, governance and accountability of the organisation. The Board is accountable to the Minister for the performance of its functions and is responsible for the appointment of a CEO. The CEO is responsible to the Board and the Board takes responsibility for assessing the CEO’s performance. The Act provides for a 10 person non-executive board together with the Chairperson and the Deputy Chairperson.
National Development Plan
The Government published its revised National Development Plan (NDP) 2021-2030 in October 2021. Regrettably the NDP does not deliver any additional acute public hospital bed capacity over and above previous commitments. In a submission to the Department of Public Expenditure and Reform in February 2021, ahead of the revised NDP, the Association recommended that a minimum of 6,000 additional public hospital beds must be funded to reduce bed occupancy rates, operate within appropriate infection control measures including single occupancy rooms and deliver more timely, safe care. This is in contrast with the increase of 2,600 acute beds referenced in the 2021 NDP. The Association also indicated that dedicated theatre and bed capacity to deliver elective scheduled care must be expanded across our acute hospital base, as opposed to in just three locations. Overall, the pace of implementing the recommendations in the 2018 Capacity Review and the provisions in the 2018 and 2021 NDPs has been far too slow. This reality became shockingly apparent during the Covid-19 pandemic, which exposed the existing acute hospital capacity deficits. The Government’s NDP 2018-2027
Members’ Handbook www.ihca.ie 27
Members’ Handbook
published in February 2018 pledged e10.9 billion in capital funding for the health services, to include the planned addition of a minimum of 2,600 acute hospital beds and new dedicated elective-only hospitals in Dublin, Cork and Galway to tackle waiting lists and provide access to diagnostic services. An additional 4,500 long term and short term residential beds in Community Nursing Homes in the public system were also proposed in the 2018 NDP. Between 2017 and 2022 public hospital inpatient and day case bed capacity increased by 874 beds, significantly less than the additional 1,300 beds provided for on average in the 2018 NDP. The increase in bed capacity in the five-year period has been more than offset by the population and demographic changes and therefore public hospital capacity deficits continue to increase as do the number of patients on waiting lists. Furthermore, there is an urgent need to double the ICU capacity to a minimum 579 beds as recommended in an HSE commissioned report a decade ago, and further increase critical care capacity to over 640 beds to reach the EU average number of ICU beds on a population basis. This is essential because the existing public hospital capacity is far too low and has over the years created significant problems in providing timely care. This must be addressed on a sustainable basis.
Health Service Capacity Review 2018
The previous NDP 2018 followed the publication in January 2018 of the Health Service Capacity Review 2018 by the Department of Health, which outlines projections of demand and capacity requirements for a range of health services to 2031.
If key reforms and productivity measures are implemented, the following additional capacity will be required by 2031: nearly 2,600 extra acute hospital beds 48% increase in primary care workforce 13,000 extra residential care beds (older persons services) and; 120% increase in homecare.
Without reform, the Capacity Review estimates that more than 7,000 extra acute hospital beds will be required to meet projected demand.
Sláintecare
The Oireachtas Committee on the Future of Healthcare published the Sláintecare Report in May 2017 – its proposals for a 10 year strategy for healthcare and health policy in Ireland. The proposed new model envisages a universal single-tier health and social care system, the shifting of care out of hospitals and into the primary and community setting, waiting time guarantees for hospital care, expanded hospital capacity and the phased elimination of private care in public hospitals. A separate independent group chaired by Donal de Búitléir was set up to examine the impact of removing private practice from public hospitals and reported in August 2019. The IHCA welcomed the fact that the Review Group acknowledged the current consultant recruitment and retention crisis and the need to end the existing pay inequity for consultants appointed after 2012. However, the proposal to remove
private practice from public hospitals will have the effect of removing 6.5bn in private health insurance income over a 10-year period, from already severely underfunded acute public hospitals. Adjusted for inflation, the estimated loss will be closer to 8bn or 800m per year. The IHCA has no confidence that the loss in private health insurance income to public hospitals will be replaced by the Exchequer. The proposal to remove private practice from what is perceived as an inequitable system will perpetuate the delays in accessing care because public hospitals will be even more under-resourced. It will result in an extreme two-tier system with functioning and adequately resourced private hospitals operating separately in parallel with an under-resourced and overcrowded public hospital system. The cost of implementing the proposals in the Sláintecare Report has been understated and will actually cost the taxpayer e30bn, based on Irish Fiscal Advisory Council (IFAC) estimates, if implemented over 10 years, compared with e2.8bn stated in the Report. The IFAC in a recent Fiscal Assessment Report (May 2022) noted that the Sláintecare reforms are not costed properly, nor are they budgeted for beyond this year. The Council said that while total costs were estimated at €2.8bn per annum in 2017, these are highly outdated and do not include subsequent price and wage pressures. The IFAC said it appears that some €2.1bn of recurrent spending has been allocated to the reforms to end-2022. A mechanical estimate, using wage and price pressures in the interim, would suggest that costs could prove to be upwards of €3.5bn by 2027 to implement the reforms, with recent price pressures and capacity constraints in the economy likely to raise such estimates.
May 2022 marked 5 years since the Government launched Sláintecare, yet at the halfway point of the 10-year plan, we are faced with a health service, staff and patients who are suffering more than ever. There has been a 56% increase in people waiting on some form of hospital list since the plan was launched in 2017 – with around 910,000 adults and children across the country now on waiting lists for hospital care. We are also decades away from achieving the Sláintecare targets that no-one should wait more than 12 weeks for an inpatient procedure, 10 weeks for an outpatient appointment and 10 days for a diagnostic test.
The negotiations between the Association and the health service management on a proposed new consultants’ contract is a critical element in ensuring that we can recruit the number and the calibre of Consultants who are required urgently. The Consultant Contract negotiations need to result in a contract that will work in practice.
It should be noted that a Type A contract was offered with very limited success to consultants in 2008 and again in March 2011, when the then HSE Director for Human Resources issued a circular stating that all future hospital consultant contracts would be Type A except in exceptional circumstances. The consequences of the circular were that it led to a failure to recruit
www.ihca.ie
28
Members’ Handbook
consultants for most of 2011 until the circular ceased to apply. Countries such as the UK, Australia, New Zealand and Canada, do not impose such prohibitions on hospital consultants providing specialist consultant care to people off-site. On the contrary, they take the view that such restrictions are retrograde steps for the public given the need for Consultants to maintain a skill set, and to provide a specialist service that is clearly a scarce and valuable resource. Provision of such services should be optimised in the public’s best interests.
The recruitment and retention of hospital consultants remains the overwhelming blockage to the provision of timely patient care. The disastrous consequences of the 2012 decision to impose inequity on consultants taking up contracts since then remain. Growing pressures day-after-day are pushing consultants and public hospitals to breaking point. Global advancements in medical and surgical treatment cannot be matched here at home, meaning patients and those that care for them lose out. The Contract negotiations provide an opportunity to tackle these long-standing challenges. If all the parties do not grasp this opportunity at this crucial juncture, the experiences, sacrifices, and learnings during the pandemic will have been squandered.
Future Health
Future Health: A Strategic Framework for Reform of the Health Service 2012-2015 set out the Government’s intention to deliver major reshaping of the health system by restructuring service delivery and improving organisational, financial, governance and accountability systems across the primary, community and hospital sectors.
1. The Approach to Reform – Four Pillars
1.1 Health and Wellbeing
There was to be a new focus on the need to move away from simply treating ill people to a new concentration on keeping people healthy. Future Health committed to the development of a comprehensive Health and Wellbeing Policy Framework and the establishment of a Health and Wellbeing Agency.
1.2 Service Reform
Future Health supported a move away from hospital centric care to a new model of integrated care. It was the intention of Future Health that people be treated at the lowest level of complexity that was safe, timely, efficient and as close to home as possible. This was to support the reduction of costs, improve access and move towards a model of preventative and planned care.
1.3 Structural Reform
Future Health committed to the structural reform of the health service and indicated that this would be critical in the journey towards Universal Health Insurance. The key concerns of structural reform included good governance, avoiding duplication and ensuring a
strong regional focus in managing performance and delivering value for money. This reform included the abolition of the HSE board, the establishment of a Directorate and a new management structure in the HSE. This included the establishment of Hospital Groups, with Group CEOs having budgetary responsibility for both the HSE and voluntary hospitals within their group.
1.4 Financial Reform
Future Health committed to introducing measures aimed at addressing the financial control issues within the HSE which included the return of the Vote to the Department of Health from the HSE; the introduction of programme based budgeting; implementation of the recommendations of the 2012 Review of Financial Management Systems in the Irish Health Service; and the development and roll-out of a comprehensive financial management system as a matter of priority.
A new ‘Money Follows the Patient’ (MFTP) funding model was to be introduced in order to create incentives that encourage treatment at the lowest level of complexity. This was in order to reduce costs and achieve key quality and safety objectives.
2016 was the year in which hospitals began migrating from the historic block budget approach to a model of ‘Activity Based Funding’ (ABF) for public hospital care covering inpatients and day-cases. ABF involves a ‘revenue’ stream being given to each group/hospital for specified inpatient and day-case activity, together with a block grant for other work. The combined total can be referred to as the budget, but with a very different underlying construction — if the specified work is not delivered, the ABF revenue will not be paid.
The HSE National Service Plan 2022 committed to the further development of activity based funding for hospitals and community.
Service Planning in 2023 Service planning for 2023 is again likely to be undertaken in a context which includes the need to resume health services, prepare for the expected pressures associated with winter and deliver services in the context of the potential continuing prevalence of Covid-19. Planning in 2022 attempted to address the backlog of care following the unprecedented interruption of routine services during the pandemic. There were almost 380,000 fewer inpatient/day case procedures carried out over the period 2020 and 2021 compared with 2019 activity, and 483,000 less outpatient hospital appointments over those two years combined. While the health service may not have to catch up on all of these missed appointments and procedures, such a volume suggests it could take decades to clear this backlog of deferred care which has yet to present and bring our already unacceptable waiting lists under control.
29www.ihca.ie
Consultants’ Common Contract 2008 Enabling Circular - 25th July 2008
To: Hospital Network Managers, Assistant National Directors (PCCC), Health Agencies
Please forward this circular and attached document to all HSE agencies, voluntary hospitals, relevant corporate bodies and other non-HSE agencies under your remit.
Please ensure the required form is completed in respect of each Consultant in your employment (i.e. hospital/agency).
1) General
a) The purpose of this circular is to convey approval to the introduction with effect from 1 June 2008, of a revised contract for Consultant medical staff providing services under the Health Acts and to notify arrangements for the implementation of the provisions of the revised contract. A copy of the new contract is enclosed. The contract is hereafter referred to as ‘Consultant Contract 2008’.
b) The terms of Consultant Contract 2008 follow negotiations with the representative bodies of the medical profession.
c) Agencies should ensure that the name of the employer is inserted in the locations indicated in the document and that the appropriate deletions are made where indicated.
2) Consultants to be offered the Contract
The Contract consists of the documentation specified in the preamble to the Consultant Contract 2008 document. The terms and conditions of Consultant Contract 2008 shall be offered to the following:
a) Consultants currently in your employment holding permanent posts.
b) Consultants currently in your employment holding fixed term (temporary) posts. The expiry date of their existing fixed-term (temporary) contract and/or its specified purpose must be incorporated into their new contract.
c) Consultants currently in your employment holding locum posts. The structure, time and attendance arrangements of their contract must be incorporated into their new contract.
3) Options for Existing Consultants
Subject to Section 2 above:
a) Category I Consultants may opt for a Type A or Type B contract.
b) Category I Consultants in Emergency Medicine may also opt for a Type B* contract.
c) Category II Consultants may opt for a Type A, Type B or Type B* contract.
d) Geographical wholetime without fees Consultants may opt for a Type A or Type B contract.
e) Consultants holding the Academic Consultant Contract 1998 on a Category 1 basis may opt for a Type A or Type B Contract. Section 15 of Consultant Contract 2008 will apply to such individuals.
f) Consultants holding the Academic Consultant Contract 1998 on a Category 2 basis may opt for a Type A, Type B or Type B* Contract. Section 15 of Consultant Contract 2008 will apply to such individuals.
g) Regional Consultant Orthodontists may opt for a Type A, Type B or Type B* Contract on a pro-rata basis. Should such Consultants opt for a Type B or Type B* their entitlement to retained private practice is as described at Section 21 of the Consultant Contract 2008.
h) Consultants (including Regional Consultant Orthodontists) holding Temporary or Locum appointments may opt for a Type A, Type B or Type B* Contract on a Temporary or Locum basis commensurate with their current Temporary or Locum post.
i) Consultants who are not encompassed by the above should apply to the HSE Consultant Appointments Unit via the relevant Hospital Network Manager/Assistant National Director PCCC to be offered Consultant Contract 2008.
4) Atypical Work Arrangements
a) Consultants who are currently engaged in atypical working (e.g. flexible working, job sharing, etc.) will be offered Consultant Contract 2008 on a pro-rata basis to their current working arrangements. Should such Consultants wish to restructure their commitments such restructuring shall be subject to approval from the HSE Consultant Appointments Unit in line with the provisions of the Consultant Contract.
b) Consultants who opt for Consultant Contract 2008 and who wish to avail of atypical work arrangements (e.g. flexible working, job sharing, etc.) may do so with the prior agreement of the employer.
5) Joint Appointments
a) The following wording should be used where the Consultant has a joint appointment at Section 2 of Consultant Contract:
i) “This Contract is a contract of employment between (name(s) and address(es) of employer(s) for __ hours per week) and (name and address of employee)”
or
ii) “This Contract is a contract of employment between (name and address of employer) for __ hours per week and for __ hours per week with (name and address of other agency/agencies) and (name and address of employee)”
30 www.ihca.ie
Consultants’ Common Contract 2008 Enabling Circular - 25th July 2008
b) Employers who are the contract holders for joint appointments should ensure at all times, and in respect of all aspects of the appointment, that they keep each other fully informed of any matter likely to affect the appointment. Particular attention should be paid to matters affecting probation and the confirmation or termination of appointments.
6) Making the Offer
a) Employers should take great care in drawing up and issuing the contract documents. All of the bracketed spaces in the contract documentation should be filled by the employer before a contract is offered.
b) Signed acceptances of the offer of Consultant Contract 2008 must be received by the employer on or before 31 August 2008. Only Consultants who accept the offer before 1 September 2008 will benefit from retrospective salary arrangements.
c) Should the Consultant accept the offer of the Contract, the employer and the Consultant must sign the contract simultaneously. Under no circumstances should an employer issue signed blank forms of contract to Consultants. Where it is not possible to have the
contract signed simultaneously, the Consultant must sign the Contract prior to the employer. The returned signed contract should be checked carefully to ensure that it is identical to that issued for signature. Any corrections, alterations, etc., should be made by the employer and fresh documents issued for signature.
7) Working Hours
Consultant Contract 2008 provides – inter alia – for the following:

a) The Consultant is required to undertake such duties/ provide such services as are set out in the contract in the manner specified for 37 hours per week. This 37 hour commitment will normally be delivered across a span of 12 hours between the hours of 8am and 8pm Monday to Friday. The Consultant will not be obliged to work more than eight hours in any one day.
b) The Consultant may be required to participate in the on-call roster as determined by the Employer.
c) The Consultant rostered on-call may be required to provide an additional structured commitment on-site of up to five hours on a Saturday and/or five hours on a Sunday and/or five hours on a public holiday.
www.ihca.ie 31
Consultants’ Common Contract 2008
Enabling Circular - 25th July 2008
8) Private Practice
The private practice arrangements (where applicable) for the different contract types are set out in Sections 20 and 21 of Consultant Contract 2008. A joint management/ union committee is currently devising a measurement system to support the new private practice arrangements.
9) Salary and Other Payments
a) The remuneration provisions of Consultant Contract 2008 are outlined in Section 23 of the contract document.
b) A schedule setting out the updated salaries and other payments (i.e. current) for the various contract types is attached to this circular.
c) Serving Consultants who opt for Consultant Contract 2008 by 31 August 2008 shall be paid the applicable revised rate at the maximum point with effect from 1st June 2008 and 1 June 2009, as set out in the attached schedule.
d) Serving Consultants who exercise their option to take the revised contract between 1 September 2008 and 31 December 2008 will be assimilated onto the applicable new salary scale, at the maximum point, from the date of their signing of Consultant Contract 2008.
e) Applications for the offer of the Consultant Contract 2008 after 31 December 2008 should be made to the HSE Consultant Appointments Unit.
10) Superannuation
a) The Consultant will be covered by the terms of the HSE/VHSS/NHSS (as appropriate) Superannuation Scheme and the contributory associated spouses and children superannuation schemes. Appropriate deductions will be made from his/her salary in respect of his/her contributions to the scheme. In general, 65 is the minimum age at which pension is payable; however, for appointees who are deemed not to be ‘new entrants’ as defined in the Public Service Superannuation Miscellaneous Provisions Act 2004 an earlier minimum pension age may apply.
b) Should:
i) the Consultant be deemed to be a new entrant (as defined in the Public Service Superannuation [Miscellaneous Provisions] Act 2004), there is no specified retirement age in respect of his/her appointment to this position.
or
ii) the Consultant be deemed not to be a new entrant (as defined in the Public Service Superannuation [Miscellaneous Provisions] Act 2004), retirement is compulsory on reaching 65 years of age.
11) Clinical Directors
Consultant Contract 2008 provides at Appendix IV for the appointment and selection of Clinical Directors. Information on how these appointments and selections will be made will issue separately.
12) Rest Days
a) Consultants with an on-call liability shall have an entitlement to avail of rest days on the following basis:
i) 1 : 1 on-call roster entitles the Consultant to five days in lieu per four week period; ii) 1 : 2 on-call roster entitles the Consultant to three days in lieu per four week period; iii) 1 : 3 on-call roster entitles the Consultant to two days in lieu per four week period; iv) 1 : 4 on-call roster entitles the Consultant to one day in lieu per four week period.
b) Rest days should be taken as soon as possible following the on-call liability to which they relate. Where service demands do not permit them to be taken immediately, rest days may be accumulated: i) for a maximum of six months from the earliest date of the on-call liability to which they relate and at that point they must be availed of or forfeited. or ii) for a maximum of three months from the earliest date of the on-call liability to which they relate. If it is not possible to avail of them at the end of the three month period the Consultant may seek to be compensated for them at a rate equivalent to the daily rate for the type of post which (s)he occupies.
c) A Consultant who established an entitlement to historic rest days which was recognised under the 1997 Consultant Contract retains such entitlement.
13) Record of Transition to Consultant Contract 2008
The HSE Consultant Appointments Unit will forward letters to the Employer for issue to each Consultant who opts for the Consultant Contract 2008 noting his/ her move to this contract and relevant terms.
32 www.ihca.ie
Consultants’ Common Contract 2008
Section B – Appendices
33www.ihca.ie Preamble 34 Section A Terms and Conditions 1) Core Principles 34 2) Appointment and Tenure 35 3) Probation 36 4) Mutual Obligations 36 5) Contract Designation 36 6) Reporting Relationship 36 7) Hours of Work 37 8) Location and Residence 37 9) Scope of Post 37 10) Role of Consultant 39 11) Professional Competence 39 12) Standard Duties and Responsibilities 39 13) Intellectual Property 40 14) Medical Education, Training and Research 40 15) Provisions Specific to Academic Consultants 41 16) Advocacy 41 17) Consultative Structures 42 18) Leave, Holidays and Rest Days 42 19) Locum Cover 43 20) Regulation of Private Practice 43 21) Contract Type 43 22) Change in Contract Type 47 23) Salary and Other Payments 47 24) Superannuation 48 25) Confidentiality 48 26) Records/Property 48 27) Clinical Indemnity 48 28) Grievance and Disputes Procedure 49 29) Role of Review Body on Higher Remuneration 50 30) Conflict of Interest/Ethics in Public Office 50 31) Review by Employers and Medical Organisations 50 32) Acceptance of Contract 50
Appendix I – HSE Letter of Approval 51 Appendix II – Disciplinary Procedure 51 Appendix III – Clinical Directorate Service Plan 56 Appendix IV – Clinical Director Appointment and Profile 58 Appendix V – Extracts from Consultants Contract 1997 62 Appendix VI – Granting of Sick Leave 63 Appendix VII – Correspondence Between the Parties 64 Appendix VIII – Special Leave Provisions for Consultants in Non-HSE Employment 65 Appendix IX – Committees to Advise HSE on Consultant Applications 66 Page No.
Consultants’ Common Contract 2008
PREAMBLE
This document is comprised of the following:
a) Terms and Conditions;
b) Appendices;
c) Correspondence exchanged between the parties as set out at Appendix VII; d) Terms expressly incorporated.
The foregoing, constituting the contract documents, shall be read together and embody the entire understanding of the parties in respect of the matters contained therein.
Note 1: Throughout this document the use of the masculine pronoun is intended to also denote the feminine gender, save where the context does not admit of such meaning.
Note 2: Job descriptions for new appointees will form part of the Consultants’ Contract.
SECTION A - TERMS AND CONDITIONS
1) Core Principles
The core principles of this Contract are:
a) That both the Consultant and the Employer recognise that the relationship must be founded upon mutual trust and respect for each other and that any differences under the agreement should be processed expeditiously through the grievance and disputes procedure or such other procedures provided for herein;
b) Recognition of the importance of the role of Clinical Director, which places Consultants within the leadership structure in the management of the health service;

c) Recognition of clinical independence and the unique nature of the relationship between each Consultant and his/her patients;
d) Recognition by the Consultant that (s)he must operate within a system in which policy and procedures are determined through the corporate entity in which staff at all levels must be accountable;
e) Recognition of the Consultant’s role as an advocate and the concomitant responsibility, in the first instance, to express any concerns within the employment context;
34 www.ihca.ie
Consultants’ Common Contract 2008
f) Recognition of the Consultant’s role in the delivery of education and training and research.
2) Appointment and Tenure
a) This Contract is a contract of employment between (name and address of Employer) and (name and address of employee). (name of appointee)* is appointed to a post of ___________ and accepts the appointment from (insert date). The Contract is: i) permanent, subject to the completion of probation (as set out in Section 2);
ii) for a fixed term/purpose; or
iii) a locum appointment.
In the case of Consultants appointed on a fixed term / locum basis in accordance with Sections 2 a) ii) or 2 a) iii) above, Section 3 of this Contract (entitled ‘Probation’), other than paragraph 3 (f) thereof, does not apply.
*Hereafter referred to as ‘The Consultant’
b) A candidate for and any person holding the office must be in a state of health such as would indicate a reasonable prospect of ability to render regular and efficient service.
c) The qualifications required for this post are set out in the Health Service Executive’s Letter of Approval as attached at Appendix I.
d) Should the Consultant be required by the terms of the offer of appointment to comply with specified requirements or conditions (including a requirement or condition that (s)he shall acquire a specified qualification) before the expiration of a specified period the employment shall be terminated unless within that period the Consultant has complied with such requirements or conditions.
e) With regard to resignation or retirement, the holder of a joint appointment* must act similarly in relation to each of his/her component commitments, e.g. (s)he cannot retire or resign from one participating Employer and not from the other(s).
*A joint appointment is one which involves a commitment by the Consultant to two or more employing authorities.
Consultants appointed on such a basis are entitled to a single contract or interdependent contracts (with reciprocal clauses).

35www.ihca.ie
or
Consultants’ Common Contract 2008
The Consultant’s total commitments should not exceed that which is expected from Consultants in the same specialty who have a full-time commitment to one employer.
f) If the Consultant wishes to terminate this employment (s)he shall provide the Employer(s) with three months notice of his/her proposed termination date.
g) Except in cases of serious misconduct, the Employer will provide the Consultant with three months notice of the intention to terminate his or her employment.
3) Probation
a) Appointment to a Consultant post (under Section 2 a) i) above) is dependent upon the satisfactory completion of a probationary period of 12 months. The probationary period may be extended at the discretion of the Employer for a period of not more than 6 months. In such event the specific reasons for the extension shall be furnished in writing to the probationary Consultant.
b) At the end of the probationary period, the Employer shall either: i) certify that the Consultant’s service has been satisfactory and confirm the appointment on a permanent basis; or
ii) certify, with stated specified reasons, that the Consultant’s service has not been satisfactory, in which case the Consultant will cease to hold his/her appointment.
c) If the Employer should fail to certify in accordance with (b) above, the Consultant shall be deemed to have been appointed on a permanent basis.
d) The Employer undertakes to advise the probationary Consultant on a timely basis of issues likely to result in the termination or extension of the probationary period.
e) A Consultant who currently holds a permanent Consultant appointment in the Irish public health service will not be required to complete a probationary period should (s)he have done so already.
f) A Consultant will not be required to complete the probationary period where (s)he has for a period of not less than 12 months acted in the post pending its filling on a permanent basis.
g) During the probationary period, the probationary Consultant will be subject to ongoing review and a formal review will take place not more than six months after the date of first appointment on a probationary basis.
h) In cases where an allegation of serious misconduct is made against a probationary Consultant, the matter will be dealt with in accordance with Stage 4 of the Disciplinary Procedure (attached at Appendix II). This does not affect
the Consultant’s statutory rights under the Industrial Relations Acts, 1946-2004 or any other statute.
i) In the case of joint appointments, the holding of any one part of the post is contingent on continuing to hold the other part or parts of the post.
j) Employment may be terminated by either party during the probationary period. Should employment be terminated by the Employer, the Employer shall set out in writing the specific reasons for such termination.
4) Mutual Obligations
a) Both the Consultant and the Employer recognise the need for mutual trust, confidence and respect in giving effect to the terms of this contract.
b) Both the Consultant and the Employer shall co-operate in giving effect to such arrangements as are put into place to verify the delivery of the Consultant’s contractual commitments.
c) The determination of the range, volume and type of services to be provided and responsibility for the provision of same within available resources rests with the Employer. Services not provided as a consequence of a resource limit are the responsibility of the Employer and not the Consultant.
d) The Employer recognises the Consultant’s obligations regarding the application of the Medical Council's (or Dental Council, as appropriate) ethical and professional conduct guidance to the clinical and professional situations in which (s)he works.
5) Contract Designation
This contract is designated as a Type ___ (insert in line with HSE Letter of Approval) Contract as set out in the HSE Letter of Approval for this post attached at Appendix I. Details regarding Type of Contract and change of Type of Contract are set out at Sections 21 and 22.
6) Reporting Relationship
The Consultant’s reporting relationship and accountability for the discharge of his/her contract is:
i) to the Chief Executive Officer/General Manager/Master of the hospital (or other employing institution) through his/her Clinical Director* (where such is in place). The Hospital Network Manager or Assistant National Director HSE PCCC Directorate may require the Consultant to report to him/her from time to time.
or
ii) in the case of Consultant Psychiatrists, to the Clinical Director and the Local Health Office Manager PCCC Directorate
36 www.ihca.ie
Consultants’ Common Contract 2008
(where the Consultant is employed by the HSE)/Chief Executive Officer (where the Consultant is not employed by the HSE).
*Details of the Appointment and Profile of the Clinical Director are contained in Appendix IV
7) Hours of Work
a) The Consultant is contracted to undertake such duties/ provide such services as are set out in this Contract in the manner specified for 37 hours per week. This 37 hour commitment will normally be delivered across a span of 12 hours between the hours of 8am and 8pm Monday to Friday. The Consultant will not be obliged to work more than eight hours in any one day. This will be structured as a single continuous episode. Scheduling arrangements may be changed from time to time within the 8am to 8pm period in line with clinical and/or service need as determined by the Clinical Director/Employer in consultation with the Consultant.
b) The aggregation of the Consultant’s commitments in a given time period shall be on a cumulative basis of 37 hours per week. This does not imply that the Consultant’s work is organised in equal periods of time. If the time worked consistently and significantly varies from the scheduled commitment, there will be a review of the commitment to ensure that the Consultant is not working regularly in excess of or less than the 37 hour weekly commitment. Where the commitment is being unavoidably exceeded for reasons of a temporary nature, local arrangements will be made to compensate the Consultant concerned.
c) In addition to the contracted commitment per week specified at Section 7 (a) above:
i) the Consultant may be required to participate in the on-call roster as determined by the Clinical Director/Employer.
Payment arrangements for on-call liability are set out at Section 23 (i) and for the provision of call-out services when on-call outside scheduled commitments at Section 23 (j).
ii) the Consultant rostered on-call may be required to provide a structured commitment on-site of up to five hours on a Saturday and/or five hours overtime on a Sunday and/or five hours on a public holiday. Consultants on onerous on-call rosters* shall not be expected to deliver the upper end of this requirement as determined by the Clinical Director. The Consultant’s liability for on-call outside such structured or other scheduled overtime hours will continue to apply.
*Only on-call rosters of 1:4, 1:3, 1:2 or 1:1 are regarded as onerous
d) As a senior professional employee, the Consultant may be required, from time to time, to work beyond his/her rostered period in line with the exigencies of the service. The Employer will endeavour to ensure that this will be an exceptional rather than a standard requirement.
e) Where there is local agreement to implement different work patterns, (including any arrangements providing for up to 24/7 hour working) the involvement of any individual Consultant in any such arrangement(s) shall be subject to his/her agreement.
8) Location and Residence
a) The Consultant’s appointment shall be to ___________________ (name HSE area/HSE-funded Hospital/Agency as set out in the HSE Letter of Approval). The Consultant’s employment location(s) is ____________ (as per HSE Letter of Approval for the post if relevant).
b) The Consultant’s employment location may be changed within the functional area and service range applicable to his/her Employer. In the first instance, this will be within the Hospital Network area/remit of the HSE-funded Hospital/ Agency. The Consultant shall be consulted should (s)he be required to change to an employment location outside the (Hospital Network Area/ HSE-funded Hospital/ Agency). In circumstances where a change of location is required, (e.g. hospital closures or major changes taking place in the character of the work being carried out there) the Consultant will be offered an appropriate alternative appointment without competition and consideration will be given to any request from the Consultant to change Contract Type or title of post. Subject to the provisions of the removal expenses scheme for the Health Service Executive, removal expenses shall be payable, if claimed.
c) The Consultant shall be available to respond readily to clinical or service needs at the location(s) specified above. This will require the Consultant to reside convenient to the hospital/agency in which (s)he holds his/her appointment.
9) Scope of Post
a) The scope of this post is as set out in the HSE letter of approval for this position at Appendix I and the Job Description as issued by the Employer. These describe the Consultant’s service commitments, accountabilities and specific duties.
b) The Consultant’s annual Clinical Directorate Service Plan will detail how these are to be implemented and will be validated by a series of performance monitoring arrangements.
37www.ihca.ie
BRAIN HEALTH

TIRELESSLY DEDICATED TO RESTORING
SO EVERY PERSON CAN BE THEIR BEST The patient is at the heart of everything we do PUSHING THE BOUNDARIES OF NEUROSCIENCE FOR OVER 70 YEARS A Specialist in Psychiatric & Neurological Disorders Neurology Migraine Alzheimer’s Disease Parkinson’s Disease Psychiatry Depression Generalised Anxiety Disorder Schizophrenia Alcohol Dependence Panic Disorder Social Anxiety Disorder Obsessive-Compulsive Disorder Lundbeck Ireland Ltd 4045 Kingswood Road Citywest Business Park Co. Dublin, Ireland Tel: +353 1 468 9800 Date of preparation: March 2022 Job Code: IE-NOTPR-0138 Focused • Passionate • Responsible
Consultants’ Common Contract 2008
c) Certain decision-making functions and commensurate responsibilities may be delegated to the Consultant by the Employer. These will be documented in the Clinical Directorate Service Plan.
d) The Consultant may apply through the Employer to the Health Service Executive to change the structure of this post as set out in the HSE Letter of Approval. Any change in the structure of the post is subject to the determination of the HSE.
e) The Consultant may apply for atypical working arrangements under the relevant health service scheme.
10) Role of Consultant
a) For the purposes of this contract, a Consultant is defined as a registered medical or dental practitioner who by reason of his/her training, skill and expertise in a designated specialty, is consulted by other registered medical practitioners and who has a continuing clinical and professional responsibility for patients under his/her care, or that aspect of care on which (s)he has been consulted.
b) The Consultant is clinically independent in relation to decisions on the diagnosis, treatment and care of individual patients. This clinical independence derives from the specific relationship between the patient and the Consultant in which the patient places trust in the Consultant personally involved in his/her care to make clinical decisions in the patient’s best interests and to take continuing responsibility for their consequences.
c) The Consultant acknowledges that (s)he is subject to statutory and regulatory requirements and corporate policies and procedures.
d) The Consultant has a substantial and direct involvement in the medical diagnosis, treatment and delivery of care to patients. Each patient will have a named Consultant who has continuing responsibility for his/her diagnosis, treatment and care.
e) The Consultant may discharge his/her responsibilities through: i) a direct personal relationship with the patient;
ii) shared responsibility with other Consultants who contribute significantly to patient management;
iii) delegation of aspects of the patient’s care to another appropriate staff member. Delegation of responsibility to other doctors or staff by a Consultant is subject to: (1) the Consultant being satisfied that the relevant staff member has the necessary professional capability and (2) the continued provision of a commensurate level of diagnosis, treatment and care to the patient.
The Consultant shall retain a continuing overall responsibility for the care of the patient.
f) The Consultant will generally work as part of a Consultant team. The primary purpose of Consultant teams is to ensure Consultant provided services to patients on a frequent and continuing basis. In effect this requires that the Consultant provides diagnosis, treatment and care to patients under the care of other Consultants on his/her Consultant team and vice versa. This may include discharge and further treatment arrangements, as appropriate.
g) The membership of the Consultant team will be determined in the context of the local working environment. The team may be defined at specialty/ sub-speciality level or under a more broadly based categorisation, e.g. general medicine, general surgery.
11) Professional Competence
The Consultant shall maintain his/her professional competence on an ongoing basis pursuant to any Medical Council/Dental Council professional competence scheme applicable to the Consultant as a medical/dental practitioner. The Employer shall facilitate the maintenance of the Consultant’s professional competence pursuant to any Medical Council/Dental Council professional competence scheme applicable to the Consultant as a registered medical practitioner. Commitments in this regard will be reflected in the Clinical Directorate Service Plan.
12) Standard Duties and Responsibilities
a) To participate in development of and undertake all duties and functions pertinent to the Consultant’s area of competence, as set out within the Clinical Directorate Service Plan* and in line with policies as specified by the Employer.
*A sample Clinical Directorate Service Plan is attached at Appendix III. Appendix VII also refers.
b) To ensure that duties and functions are undertaken in a manner that minimises delays for patients and possible disruption of services.
c) To work within the framework of the hospital/agency’s service plan and/or levels of service (volume, types etc.) as determined by the Employer. Service planning for individual clinical services will be progressed through the Clinical Directorate structure or other arrangements as apply.
d) To co-operate with the expeditious implementation of the Disciplinary Procedure (attached at Appendix II).
39www.ihca.ie
Consultants’ Common Contract 2008
e) To formally review the execution of the Clinical Directorate Service Plan with the Clinical Director/ Employer periodically. The Clinical Directorate Service Plan shall be reviewed periodically at the request of the Consultant or Clinical Director/Employer. The Consultant may initially seek internal review of the determinations of the Clinical Director regarding the Service Plan.
f) To participate in the development and operation of the Clinical Directorate structure and in such management or representative structures as are in place or being developed. The Consultant shall receive training and support to enable him/her to participate fully in such structures.
g) To provide, as appropriate, consultation in the Consultant’s area of designated expertise in respect of patients of other Consultants at their request.
h) To ensure in consultation with the Clinical Director that appropriate medical cover is available at all times having due regard to the implementation of the European Working Time Directive as it relates to doctors in training.
i) To supervise and be responsible for diagnosis, treatment and care provided by non-Consultant Hospital Doctors (NCHDs) treating patients under the Consultant’s care.
j) To participate as a right and obligation in selection processes for non-Consultant Hospital Doctors and other staff as appropriate. The Employer will provide training as required. The Employer shall ensure that a Consultant representative of the relevant specialty/sub-specialty is involved in the selection process.
k) To participate in clinical audit and proactive risk management and facilitate production of all data/ information required for same in accordance with regulatory, statutory and corporate policies and procedures.
l) To participate in and facilitate production of all data/information required to validate delivery of duties and functions and inform planning and management of service delivery.
13) Intellectual Property
Intellectual property generated by the Consultant in the course of his/her employment shall be in the ownership of the relevant health sector/academic Employer(s). Due regard shall be given to national policy and national codes of practice*.
*e.g. the National Code of Practice for Managing Intellectual Property from Publicly Funded Research (ICSTI, April 2004) and National Code of Practice for Managing and Commercialising Intellectual Property from Public-Private Collaborative Research (ASC, November 2005).
14) Medical Education, Training and Research
a) The Consultant shall, as part of his/her standard contractual commitment, contribute to the education, training and supervision of students, non-Consultant Hospital Doctors and trainee professionals including members of the multi-disciplinary team.
b) The Consultant shall, as part of his/her standard contractual commitment, contribute to the advancement of knowledge by facilitating and supporting research.
c) Where the Consultant is employed by an Academic Teaching Hospital/Agency, the Employer(s) shall, through the Clinical Director, ensure that the Clinical Directorate Service Plan takes account of the academic schedule and related delivery of academic commitments.
d) The Employer shall liaise with:
i) The relevant University/Universities regarding local arrangements for the provision of undergraduate medical education and training, and research; and
ii) The relevant University/Universities and the relevant recognised Postgraduate Training Body(ies) regarding local arrangements for the provision of postgraduate medical education and training
e) The Consultant may, with the agreement of the Employer, within the 37 hour commitment, make an explicit further structured and scheduled commitment to educational activities commensurate with his/her role in conjunction with (i) the relevant affiliated Medical/Dental School(s) and (ii) training bodies for postgraduate medical education and training. Such structured and scheduled commitment, responsibility and accountability for same will be agreed with the relevant Medical/Dental School or training body and will be consistent with the agreed training principles for postgraduate medical education and training*. These structured commitments shall be set out in the Clinical Directorate Service Plan.
*‘Training Principles to be incorporated into new working arrangements for doctors in training’, published by the Medical Education and Training Group, July 2004.
f) The Consultant may, in line with Section 9, have the opportunity to restructure his/her commitments to facilitate structured research or educational programme development for a defined period, subject to the agreement of the relevant Employer; funding being identified to support such activity for that period and such research being subject to appropriate research governance and ethics.
40 www.ihca.ie
Consultants’ Common Contract 2008
15) Provisions Specific to Academic Consultants
a) All terms of this contract are applicable to the holders of Academic Consultant posts which have been approved through the established HSE/HEA process in response to agreed submissions from the relevant University(ies) and clinical Employer(s). The provisions set out in this section are confined to holders of Academic Consultant posts approved by the HSE/HEA* and are additional and particular to Academic Consultants.
*And previously Comhairle na nOspidéal.
b) Academic Consultant posts are joint appointments between Universities* and the HSE or its funded agencies. They are structured to ensure a minimum 50 per cent commitment to the academic institution.
*For the purposes of this document the term ‘University’ shall include the Royal College of Surgeons in Ireland.
c) The HSE (or HEA, as appropriate), may, following consultation and agreement with the Employer(s), structure Academic Consultant posts at Senior Lecturer and Associate Professor level to reflect a lower commitment*, where:
i) the nature of the clinical sub-specialty associated with the Academic Consultant post is such that a commitment to clinical duties in excess of 50 per cent is required for the appointee to maintain the required skills and competencies and/or
ii) the academic department does not require an individual structured commitment of 50 per cent to deliver its teaching and research programmes.
*Structured Academic Consultant posts will have a minimum 30 per cent commitment to the Academic Institution.
d) Academic Consultants are graded as follows:
i) Professor/Consultant; ii) Associate Professor/Consultant; iii) Senior Lecturer/Consultant.
The Professor/Consultant, where appointed pursuant to the relevant statutes and regulations of the University, will act as head of the Academic Department or other relevant academic unit, with responsibility for the academic curriculum and administration of the Academic Department or unit*.
*The academic governance and management structures in universities are subject to ongoing reform and change and the Academic Departments may no longer be the fundamental organisational unit within these structures.
e) The Academic Consultant is accountable for the delivery of the clinical component of the post as provided for in the body of this Contract.
f) The Academic Consultant is accountable via the management and governance structures in place in the University in relation to the delivery of their academic commitment.
g) The Academic Consultant’s role in teaching and training on the University campus extends to the relevant clinical site(s) for both undergraduates and postgraduates and shall, where required, include responsibility for relevant University students, teaching, training, assessment, modules and courses.
h) Management and governance structures in respect of academic activities will be described in a framework developed by the Employer(s) which shall, inter alia, set out the relationship between academic and clinical activities; roles and responsibilities within these structures, including the respective roles of the Clinical Director and the Academic Head of Department(s) and/or other relevant academic unit; have regard to national policy on medical education and training, and standards of medical education and training for basic and specialist medical qualifications set and published by the Medical Council.
i) The Academic Consultant will fully commit to and play a key role in the development and reform of medical education and training and research in alignment with Government policy. This may include a requirement to participate in and collaborate across University and clinical sites and with postgraduate bodies and the Medical Council on international, national and regional initiatives in academic and related activities.
j) The rights and obligations implied in the exercise of academic independence are recognised.
16) Advocacy
a) The Consultant may advocate on behalf of patients/ service users or persons awaiting access to service.
b) In the first instance such advocacy should take place within the employment context through the relevant Clinical Director or other line manager.
c) Information given to the public should be expressed in clear and factual terms. It must never cause unnecessary public concern or personal distress nor should it raise unrealistic expectations.
41www.ihca.ie
Consultants’ Common Contract 2008
17) Consultative Structures
It is recognised that Consultants organise themselves in groupings within hospitals/health agencies in order to deal with collegiate or non-executive matters. This representative system provides a mechanism to complement and inform the work of corporate management structures including Clinical Directorates. Where these representative structures do not exist, Employers will encourage and support their establishment, provide appropriate administrative support and encourage the fullest participation by all Consultants in the arrangements. The appropriate representative head (Chairperson or Secretary) of such a structure, e.g. Medical Board, Medical Advisory Board, Medical Committee will be accorded a consultative status regarding issues which have a significant effect on the delivery of clinical services within the hospital/health agency commensurate with their important representative function.
18) Leave, Holidays and Rest Days
a) All leave or planned absences, other than those described under (e) and (f), must have prior approval from the Clinical Director/Employer.
b) Leave and absences from work will normally be planned and scheduled in advance in conjunction with the Clinical Director/Employer. Leave will be approved by the Clinical Director/line manager in line with agreed rota and service requirements and notice is required in accordance with the Employer’s policy.
c) Annual Leave: The Consultant’s annual leave entitlement is 31 working days per annum and as determined by the Organisation of Working Time Act 1997.
d) Public Holidays Entitlement:
Public holidays shall be granted in accordance with the Organisation of Working Time Act 1997 as follows:
(i) In respect of each public holiday, an employee’s entitlement is as follows:
(1) a paid day off on the public holiday; or (2) a paid day off within the month; or (3) an extra day’s annual leave; or (4) an extra day’s pay as the Employer may decide.
e) Sick Leave:
The Consultant may be paid under the Sick Pay Scheme for absences due to illness or injury. Granting of sick pay is subject to a requirement to comply with the Employer’s sick leave policy. Details of the scheme are set out at Appendix VI.
f) Other Leave:
Details regarding Maternity, Adoptive, Paternity, Parental, Force Majeure, Compassionate and other leave in accordance with procedures can be obtained from the Employer.
g) Sabbatical Leave/Career Breaks:
The Consultant may apply for Sabbatical Leave or Career breaks in accordance with the terms of the relevant circulars.
The Employer has the right to approve or refuse such leave.
h) Leave to provide services abroad:
The Consultant may apply for special leave to provide services in countries where health services are underdeveloped in accordance with the relevant circular.
The Employer may grant or refuse such leave.
i) Special Leave:
(i) Leave for special circumstances shall be available to the Consultant in accordance with the relevant circulars and subject to the agreement of the Employer.
(ii) In addition and unless otherwise addressed by circular, for Consultants employed by the HSE, the provisions below and those set out in the HSE Employee Handbook apply. For Consultants employed by non-HSE agencies, the provisions below and those set out at Appendix VIII apply.
The Employer may grant leave with pay for:
(1) continuing education or attendance at clinical meetings of societies appropriate to the Consultant’s specialty of not more than seven days in any one year excluding travel time.
(2) attendance at courses, conferences, etc. approved by the Minister for Health and Children and which the Employer is satisfied are relevant to the work on which the Consultant is engaged.
(3) World Health Organisation or Council of Europe Fellowships.
j) Rest Days:
Consultants with an on-call liability shall have an entitlement to avail of rest days on the following basis:
(1) 1 : 1 on-call roster entitles the Consultant to five days in lieu per four week period;
(2) 1 : 2 on-call roster entitles the Consultant to three days in lieu per four week period;
(3) 1 : 3 on-call roster entitles the Consultant to two days in lieu per four week period;
(4) 1 : 4 on-call roster entitles the Consultant to one day in lieu per four week period.
Rest days should be taken as soon as possible following the
42 www.ihca.ie
Consultants’ Common Contract 2008
on-call liability to which they relate. Where service demands do not permit them to be taken immediately, rest days may be accumulated:
For a maximum of six months from the earliest date of the on-call liability to which they relate and at that point they must be availed of or forfeited; or
For a maximum of three months from the earliest date of the on-call liability to which they relate. If it is not possible to avail of them at the end of the three-month period the Consultant may seek to be compensated for them at a rate equivalent to the daily rate for the type of post which (s)he occupies.
k) Historic Rest Days:
A Consultant who established an entitlement to historic rest days under the Consultant Contract 1997 (i.e. by 30th June 1998) retains such entitlement.
l) Other HR Policies:
All other generally applicable human resource policies, e.g. Flexible Working, Trust in Care, Dignity at Work, etc. shall apply to the Consultant.
m) Travel and Subsistence:
Travelling and subsistence expenses necessarily incurred in the course of a Consultant’s duties shall be met on the basis applicable to persons of appropriate senior status in the public sector. Consultants holding joint appointments or appointments involving a commitment at more than one location will be reimbursed expenses in respect of travel between locations specified in the Clinical Directorate Service Plan and agreed with the Employer(s).
19) Locum Cover
a) In the event of the Consultant being absent on a scheduled or unscheduled basis, the Clinical Director/ Employer will determine the requirement for locum cover and make necessary arrangements.
b) The Clinical Director/Employer will work with the Consultant in the development and execution of such arrangements as required.
c) In exceptional circumstances where either sufficient cover cannot be provided or appropriate locum cover obtained, the Clinical Director/Employer may request the existing Consultants to undertake the routine work of an absent colleague in addition to their scheduled commitment. In such circumstances, appropriate compensation will be agreed with the Clinical Director.
20) Regulation of Private Practice
a) Subject to the provisions of this section, the Consultant may engage in privately remunerated professional medical/dental practice as determined by his or her Contract Type as described at Section 21 below.
b) The volume of private practice may not exceed 20 per cent of the Consultant’s workload in any of his or her clinical activities, including in-patient, day-patient and out-patient.
c) The volume of practice shall refer to patient throughput adjusted for complexity through the medium of the Casemix system.
d) The 80:20 ratio of public to private practice will be implemented through the Clinical Directorate structure. The Employer has full authority to take all necessary steps to ensure that for each element of a Consultant’s practice, s(he) shall not exceed the agreed ratio.
e) The Consultant will be advised on a timely basis if his or her practice is in excess of the 80:20 ratio of public to private practice in any of his or her clinical activities. An initial period of six months will be allowed to bring practice back into line but, if within a further period of three months the appropriate ratio is not established, (s)he will be required to remit private practice fees in excess of this ratio to the research and study fund under the control of the Clinical Director.
f) The Clinical Director may exercise some discretion in dealing with the implementation of the ratio either for an individual or a group of Consultants once the overall ratio in relation to the particular clinical activity is satisfied.
g) The implementation of the 80:20 ratio of public to private practice shall be the subject of an audit, including an audit by the Department of Health and Children.
21) Contract Type
Consultant Contract Type A
a) A Consultant holding Contract Type A may engage in professional medical/dental practice exclusively for the public Employer(s) or as provided for at (c) below.
b) A Consultant holding Contract Type A shall not engage in privately remunerated professional medical/dental practice. (S)he can only be remunerated for professional medical practice by way of salary as an employee under this contract or as provided for in (c) below.
c) Professional medical/dental practice carried out for or on behalf of the Mental Health Commission, the Coroner, other Irish statutory bodies*, medical/dental education and training
43www.ihca.ie
Consultants’ Common Contract
bodies shall not be regarded as private practice. In addition, the provision of expert medical/dental opinion relating to insurance claims, preparation of reports for the Courts and Court attendance shall not be regarded as private practice.
The HSE may specify additional bodies* dealing with public patients or aspects of the public health system to which this provision will also apply. The use of public facilities for all such activities is subject to the prior agreement of the Employer.
*An indicative list of such bodies is available from the HSE Employers Agency, 63-64 Adelaide Road, Dublin 2, Tel: 01 6626966, Web: www.hseea.ie.
Consultant Contract Type B
a) A Consultant holding Contract Type B may engage in privately remunerated professional medical/dental practice only in hospitals or facilities operated by the Employer, as part of such activities that arise as part of the employment contract (e.g. home visits), colocated private hospitals on public hospital campuses and as described at (b) below.
b) A Consultant holding Contract Type B who previously held a Category I or Category II Contract under the Consultants Contract 1997 may continue to hold the right to engage in privately remunerated professional medical/dental practice in locations outside the public hospital campus, subject to the Consultant fully discharging his/her aggregate 37-hour weekly standard commitment as required by the Employer and such private practice being commensurate with the entitlement to off-site private practice held by a Category I Consultant under the Consultants Contract 1997*; *Sections 2.9.4 to 2.9.7 inclusive of the Memorandum of Agreement attached to the Consultants Contract 1997 refer. These are attached at Appendix V.
c) Where a Consultant holding Contract Type B cannot be provided with facilities on the hospital campus for outpatient private practice the Employer shall make provision for such facilities off-campus, on an interim basis, pending provision of on-campus facilities.
d) The volume of private practice as described at (a) and (c) may not exceed 20 per cent of the Consultant’s clinical workload in any of his or her clinical activities, including in-patient, day-patient and out-patient.
e) With respect to Emergency and Outpatient Departments specifically, the Consultant shall not charge private fees in respect of: i) patients attending Emergency Departments in public hospitals;
or
ii) patients attending Public Outpatient Services in public hospitals.
f) A common waiting list operated by the public hospital will apply to both public and private patients undergoing diagnostic investigations, tests and procedures (including radiology and laboratory procedures) on an out-patient basis in public hospitals (including referrals from General Practitioners).
Status on the common waiting list will be determined by clinical need only. The list will be subject to clinical validation by the relevant Clinical Director.
The Consultant may charge private fees in relation to private patients undergoing diagnostic investigations, tests and procedures on an outpatient basis subject to: i) the common waiting list provisions described above;
ii) all billing being processed by the Consultant in a manner that is satisfactory to the hospital and in the event that insufficient information is available for verification purposes recourse may be had to the measures provided for at Section 20 (d) and (e);
iii) the volume of such private practice not exceeding 20 per cent.
g) The Consultant may charge private fees in relation to diagnostic investigations, tests and procedures (including radiology and laboratory procedures) referred to the public hospital by private hospitals, private clinics or other sources outside of the public health system but only where all arrangements for such referrals are effected through the Employer.
h) Professional medical/dental practice carried out for or on behalf of the Mental Health Commission, the Coroner, other Irish statutory bodies or medical education and training bodies shall not be regarded as private practice. In addition, the provision of expert medical opinion relating to insurance claims, preparation of reports for the Courts and Court attendance shall not be regarded as private practice.
The HSE may specify additional bodies dealing with public patients or aspects of the public health system to which this provision will also apply. The use of public facilities for all such activities is subject to the prior agreement of the Employer.
Consultant Contract Type B*
a) Contract Type B* is immediately available to:
i) A Consultant who held a Category II Contract under the Consultants Contract 1997; subject to the Consultant fully discharging his/her aggregate 37-hour weekly standard commitment as required by the Employer.
2008 44 www.ihca.ie
Consultants’ Common Contract 2008
ii) A Consultant who held a Category I or II Contract as a Consultant in Emergency Medicine under the Consultants Contract 1997, subject to the Consultant fully discharging his/her aggregate 37-hour weekly standard commitment as required by the Employer.
b) A Consultant who held a Category I Contract under the Consultants Contract 1997 may apply to change Contract Type to Contract Type B* two years after taking up Contract Type A or B.
c) A Consultant holding Contract Type B* may engage in privately remunerated professional medical/dental practice in: i) hospitals or facilities operated by the Employer; ii) as part of such activities that arise as part of the employment contract (e.g. home visits), and/or in colocated private hospitals on public hospital campuses; iii) in locations outside the public hospital campus, subject to such private practice being: (1) commensurate with the entitlement to off-site private practice of a Category II Consultant under the Consultants Contract 1997; and (2) confined to periods outside the aggregate 37 hour weekly commitment and other scheduled commitments to the public service.
d) The volume of private practice as described at (c) (i) and (ii) may not exceed 20 per cent of the Consultant’s clinical workload in any of his or her clinical activities, including in-patient, day-patient and out-patient.
e) With respect to Emergency and Out-patient Departments specifically, the Consultant shall not charge private fees in respect of: i) patients attending Emergency Departments in public hospitals, or ii) patients attending Public Out-patient Services in public hospitals.
f) A common waiting list operated by the public hospital will apply to both public and private patients undergoing diagnostic investigations, tests and procedures (including radiology and laboratory procedures) on an out-patient basis in public hospitals (including referrals from General Practitioners). Status on the common waiting list will be determined by clinical need only. The list will be subject to clinical validation by the relevant Clinical Director. The Consultant may charge private fees in relation to private patients undergoing diagnostic investigations, tests and procedures on an out-patient basis subject to: i) the common waiting list provisions described above;
ii) all billing being processed by the Consultant in a manner that is satisfactory to the hospital and in the event that insufficient information is available for verification purposes recourse may be had to the measures provided for at Section 20 (d) and (e); iii) the volume of such private practice not exceeding 20 per cent.
g) The Consultant may charge private fees in relation to diagnostic investigations, tests and procedures (including radiology and laboratory procedures) referred to the public hospital by private hospitals, private clinics or other sources outside of the public health system but only where all arrangements for such referrals are effected through the Employer.
h) Professional medical/dental practice carried out for or on behalf of the Mental Health Commission, the Coroner, other Irish statutory bodies or medical education and training bodies shall not be regarded as private practice. In addition, the provision of expert medical opinion relating to insurance claims, preparation of reports for the Courts and Court attendance shall not be regarded as private practice.
The HSE may specify additional bodies dealing with public patients or aspects of the public health system to which this provision will also apply.
The use of public facilities for all such activities is subject to the prior agreement of the Employer.
Consultant Contract Type C
a) A Consultant holding Contract Type C may engage in privately remunerated professional medical/dental practice in: (i) hospitals or facilities operated by the Employer; (ii) as part of such activities that arise as part of the employment contract (e.g. home visits), in colocated private hospitals on public hospital campuses; (iii) in locations outside the public hospital campus, subject to the Consultant fully discharging his/her aggregate 37-hour weekly standard commitment as required by the Employer.
b) The volume of private practice as described at (a) (i) and (ii) may not exceed 20 per cent of the Consultant’s clinical workload in any of his or her clinical activities, including in-patient, day-patient and out-patient.
c) With respect to Emergency and Outpatient Departments specifically, the Consultant shall not charge private fees in respect of: (i) patients attending Emergency Departments in public hospitals;
45www.ihca.ie
Consultants’ Common Contract 2008
or
(ii) patients attending Public Outpatient Services in public hospitals.
d) A common waiting list operated by the public hospital will apply to both public and private patients undergoing diagnostic investigations, tests and procedures (including radiology and laboratory procedures) on an out-patient basis in public hospitals (including referrals from General Practitioners). Status on the common waiting list will be determined by clinical need only. The list will be subject to clinical validation by the relevant Clinical Director. The Consultant may charge private fees in relation to private patients undergoing diagnostic investigations, tests and procedures on an outpatient basis subject to:
i) the common waiting list provisions described above;
ii) all billing being processed by the Consultant in a manner that is satisfactory to the hospital and in the event that insufficient information is available for verification purposes recourse may be had to the measures provided for at Section 20 (d) and (e);

iii) the volume of such private practice not exceeding 20 per cent.
e) The Consultant may charge private fees in relation to diagnostic investigations, tests and procedures (including radiology and laboratory procedures) referred to the public hospital by private hospitals, private clinics or other sources outside of the public health system but only where all arrangements for such referrals are effected through the Employer.
f) Professional medical/dental practice carried out for or on behalf of the Mental Health Commission, the Coroner, other Irish statutory bodies or medical education and training bodies shall not be regarded as private practice. In addition, the provision of expert medical opinion relating to insurance claims, preparation of reports for the Courts and Court attendance shall not be regarded as private practice. The HSE may specify additional bodies dealing with public patients or aspects of the public health system to which this provision will also apply. The use of public facilities for all such activities is subject to the prior agreement of the Employer.
46 www.ihca.ie
Consultants’ Common Contract 2008
22) Change in Contract Type
a) Consultants may apply to change Contract Type to Type A, B or C at five-yearly intervals. An appeals process is set out at Section 22 (d) below.
b) Those Consultants who previously held a Category I or Category II Contract under the Consultants Contract 1997 may, two years after accepting the Consultant Contract 2008 and thereafter at five yearly intervals, make application to the Health Service Executive Consultant Applications Advisory Committee* to transfer to Contract Type B*. A decision on such application will be made by the HSE following the advice of the Committee. Applicants must demonstrate that the change in Contract Type is consistent with the public interest and that there is a demonstrable benefit to the public health system.
*Please refer to Appendix IX.
c) Where significant changes occur in a particular area in the delivery of acute hospital care (e.g. hospital closures or major changes taking place in the character of the work being carried out there*) or where the volume of private practice is significantly below 20 per cent of total clinical workload, the Consultant shall be entitled to have his/her Contract Type reviewed by the Health Service Executive Consultant Applications Advisory Committee/ Type C Committee within the five year period.
*Please refer to Section 8.
d) Applications for change of Contract Type A, B or B* will be considered by the Health Service Executive Consultant Applications Advisory Committee together with the Employer’s views on the application. A decision on such application will be made by the HSE following the advice of the Committee. Applications for change of Contract Type to Contract Type B* will be considered subject to the condition that the total number of Consultants holding B*, Type C and Category 2 Contracts will be subject to an upper limit of such posts within the system. In the event that the HSE does not accede to the request, the Consultant may refer the matter to the Independent Appeals Panel for a recommendation. The Independent Appeals Panel shall be composed of: i) an Independent Chairperson, ii) a representative of the Consultant (e.g. from the relevant medical organisation), and iii) an Employer representative.
e) Appointments for reclassification to a Type C post will be considered by the Health Service Executive Type C Committee*. A decision on such application will be made by the HSE following the advice of the Committee. Applications
for change of Contract Type to Type C will be considered with reference to the total number of Consultants holding Type B*, Type C and Category II Contracts not exceeding the specified limit. In the event that the Type C Committee does not accede to the request, the matter will be referred to Chief Executive Officer of the Health Service Executive for a final decision.
*Please refer to Appendix IX.
23) Salary and Other Payments
a) The Consultant’s annual salary shall be as follows (in June 2007 terms) and shall be implemented on a phased basis as set out at d) below:
i) for Type a Contracts a salary scale in four points as follows will apply: e222,000, e228,000, e234,000, e240,000; ii) for Type B Contracts a salary scale in four points as follows will apply: e205,000, e210,000, e215,000, e220,000; iii) for Type B* Contracts a salary rate of e190,000 will apply.
iv) for Type C Contracts a salary scale in four points as follows will apply: e160,000, e165,000, e170,000, e175,000.
b) The annual salary for Consultant Academics shall be as follows:
i) For a Professor (Type A Contract) a salary scale in four points as follows will apply: e272,860, e280,240, e287,620, e295,000.
ii) For a Professor (Type B Contract) a salary scale in four points as follows will apply: e265,650, e272,100, e278,550, e285,000
iii) For a Professor (Type B* Contract) a salary of e255,000 will apply.
iv) For a Professor (Type C Contract) a salary scale in four points as follows will apply: e219,450, e226,300, e233,150, e240,000
c) All serving Consultants who take up the offer of the Consultant Contract 2008 by 31 August 2008 will be assimilated to the maximum point of the applicable new salary scale.
d) The salary scales at a) and b) above will be phased on the following basis:
i) a five per cent increase on the Consultant’s existing (June 2007) rate from 14 September 2007; ii) half the balance* from 1 June 2008; iii) the remaining balance from 1 June 2009.
*The term ‘half the balance’ refers to the difference between the 14 September 2007 rate and the fully implemented salary scale.
These rates will attract a 2.5 per cent Towards 2016 general round increase from the 1st March 2008 and a further 2.5 per cent
Towards 2016 general round increase from 1 September 2008.
47www.ihca.ie
Consultants’ Common Contract 2008
e) An allowance of e50,000 per annum will be paid to those Consultants appointed as Clinical Directors.
f) Saturday, Sunday and Public Holidays:
Structured on-site attendance at weekends and on public holidays will be subject to the following premium payments:
i) Time + ½ on Saturdays.
ii) Double time on Sundays and Public Holidays.
g) Continuing Medical Education:
The CME allowance will be increased to e3,000 with effect from the 1 June 2008. Payment will continue to be on a vouched basis, to be adjusted in line with the Consumer Price Index (CPI). This allowance may be carried over annually for a maximum of five years.
h) Telecommunications:
The Consultant shall be reimbursed either the cost of home or mobile phone rental.
i) B Factor (On-Call) Payments:
An increase in the flat annual payment to e6,000 will take effect from 1 June 2008. The payments for more onerous rosters will increase by five per cent from the same date.
j) C Factor (Call-Out) Payments:
The Consultant will be eligible for payment on a per call-out basis for the provision of on-site services when:
i) rostered for on-call duty and is contacted by another medical practitioner in the hospital, by a senior nurse or other member of staff specifically designated for that purpose and attends on-site to provide emergency services;
ii) rostered for on-call duty and who, in the exercise of his/her professional judgment, attends on-site and performs clinical work of an urgent nature or carries out urgent diagnostic or therapeutic procedures;
iii) requested by another Consultant to provide on-site services in public hospital/agency to which the Consultant does not have a scheduled commitment and where such services cannot be provided within the Consultant’s scheduled commitment as adjusted by the Clinical Director/Employer. This payment shall be on the basis of the equivalent payment per call-out.
24) Superannuation
a) The Consultant will be covered by the terms of the HSE/VHSS/ NHSS Superannuation Scheme and the contributory associated spouses and children superannuation schemes. Appropriate deductions will be made from his/her salary in respect of his/ her contributions to the scheme. In general, 65 is the minimum age at which pension is payable. However, for appointees
who are deemed not to be ‘new entrants,’ as defined in the Public Service Superannuation Miscellaneous Provisions Act 2004, an earlier minimum pension age may apply.
b) Should:
i) the Consultant be deemed to be a new entrant (as defined in the Public Service Superannuation (Miscellaneous Provisions) Act 2004), there is no specified retirement age in respect of his/her appointment to this position.
or
ii) the Consultant be deemed not to be a new entrant (as defined in the Public Service Superannuation (Miscellaneous Provisions) Act 2004), retirement is compulsory on reaching 65 years of age.
25) Confidentiality
a) In the course of the Consultant’s employment (s)he may have access to, or hear information concerning the medical or personal affairs of patients and/or staff. Such records and information are strictly confidential and in whatever format and wherever kept, must be safeguarded.
26) Records/Property
a) The Consultant should take all reasonable measures to ensure that records are stored in such a manner that ensures confidentiality, security and ready accessibility for clinical staff when required for patient management.
b) The Consultant shall not remove from the employment location any records in any format, electronic or otherwise, belonging to the Employer/Health Service Executive at any time without having authorisation. Such authorisation will be issued in advance of the first instance and apply thereafter.
c) The Consultant will return to the Employer/Health Service Executive upon request, and, in any event, upon the termination of his/her employment, all records and property and equipment belonging to the Employer/Health Service Executive which are in his/her possession or control.
27) Clinical Indemnity
a) The Consultant will be provided with an indemnity against the cost of meeting claims for personal injury arising out of bona fide actions taken in the course of his/her employment.
b) This indemnity is in addition to the Employer’s(s’) Public Liability/Professional Indemnity/Employer’s(s’) Liability in respect of the Consultant’s nonclinical duties arising under this contract.
c) Notwithstanding (a) above, the Consultant is strongly advised and encouraged to take out supplementary membership
48 www.ihca.ie
Consultants’
with a defence organisation or insurer of his/her choice, so that (s)he has adequate cover for matters not covered by this indemnity such as representation at disciplinary and fitness to practise hearings or Good Samaritan acts outside of the jurisdiction of the Republic of Ireland.
d) Under the terms of this indemnity the Consultant is required to report to an officer designated by the Employer in such form which may be prescribed, all adverse incidents which might give rise to a claim and to otherwise participate in the Employer’s risk management programme as may be required from time to time. In the event that an adverse incident is first reported by a third party, the Consultant/ Head of Department should be notified as soon as practicable.
28) Grievance and Disputes Procedure
a) In the case of a dispute arising regarding these terms and conditions, the Employer and Consultant will have recourse to and, as necessary, complete the Grievance and Disputes Procedure below.
b) The purpose of this procedure is to deal with problems arising under the Contract. To the greatest extent possible, such problems should be addressed and resolved within the normal structures of the employing authority and at the earliest possible point. The parties recognize the finite nature of resources and agree that issues involving the resourcing of services, roles of hospitals and other general service issues are not amenable to the Grievance and Disputes Procedure. However, the parties further agree that disputes may arise, which although touching on or concerning such issues, are essentially concerned with the operation of the individual contract and are therefore amenable to the procedure.
c) Stage 1:
Local level discussions must be undertaken and completed within three months from the date on which each party to a dispute indicates in writing that it wishes to avail of this procedure. Where individual issues of an urgent nature arise, such as difficulties in obtaining locum cover, the Consultant shall have the right to process the matter up to the level of the Chief Executive or his nominated representative/deputy.
d) Stage 2 – Mediation/Adjudication:
In exceptional cases where resolution at local level does not prove possible, the matter may be referred by way of written submission to the Mediator/Adjudicator by either party. The said submission shall be transmitted in the first instance to the Secretariat who shall immediately forward the
complaint to the Mediator/Adjudicator. It is prerequisite to the invocation of this procedure that local discussions have taken place prior to referral to the Mediator/Adjudicator. The Mediator/Adjudicator shall decide whether all avenues at local level have been adequately explored and exhausted and further whether the matter is appropriate for his/ her consideration. The respondent will have a period of six weeks within which to prepare and lodge a counter statement with the Secretariat and shall forward a copy of same immediately to the complainant. Mediation/ Adjudication shall commence within two weeks of the expiry of the aforesaid time limit. Should the dispute not be resolved by mediation the Mediator/Adjudicator shall proceed to issue a recommendation within four weeks of the completion of the adjudication hearing or such further time as might be agreed between parties. i) disputes about the admissibility of particular cases shall be decided by the mediator/adjudicator; ii) hearings before the Mediators/ Adjudicators shall be held in private; iii) both parties shall be entitled to representation at their own expense; iv) decisions of the Mediator/Adjudicator shall be non-binding but the parties agree that such decisions shall be afforded the status of a Labour Court Recommendation; v) the costs of the mediator/adjudicator process shall be borne by the employing authority; vi) the HSE Employers Agency shall provide the Secretariat;
e) List of Mediators/Adjudicators:
A list of Mediators/Adjudicators have been agreed between the parties as suitable nominees for appointment in any individual case*. It shall be for the Secretariat, in conjunction with the parties, to determine the precise Mediator/ Adjudicator to be employed in any given case. The Secretariat will have due regard in the appointment of Mediators/ Adjudicators from the panel to any possible conflict that might arise.
* These are available from the HSE Employers Agency at 63-64, Adelaide Road, Dublin 2, Tel: (01) 662 696, Web: www.hseea.ie.
f) Review:
The parties agree that the Grievance and Disputes procedure shall be reviewed within two years of date of implementation i.e. not later than 2010. However, in the event that difficulties arise concerning individual
Common Contract 2008 49www.ihca.ie
Consultants’ Common Contract 2008
issues of an urgent nature, then an earlier review may take place in respect of such matters at the election of any of the parties hereto not earlier than the end of June 2009.
29) Role of Review Body on Higher Remuneration
The parties to this agreement accept that Consultants' remuneration and terms and conditions of employment should be reviewed on a regular basis. Accordingly, the Review Body on Higher Remuneration in the Public Sector should undertake such reviews as part of the general reviews undertaken by the Review Body from time to time.
30) Conflict of Interest/Ethics in Public Office
a) Each Consultant should refrain from knowingly engaging in any outside matter that might give rise to a conflict of interest.
b) If in doubt (s)he should consult the relevant Clinical Director/ Employer and, subject to a right of appeal, any direction given must be followed.
The term ‘you’ is used in the remainder of this section to refer to the Consultant.
c) Should you occupy a designated position of employment* under the Ethics in Public Office Acts 1995 and 2001, you are required, in accordance with Section 18 of the Ethics in Public Office Act 1995, to prepare and furnish an annual statement of any interests which could materially influence you in the performance of your official functions:
• by Consultants employed by the Health Service Executive to the Chief Executive Officer Health Service Executive; • by Consultants employed by HSE funded agencies to the Chief Executive of the agency; not later than 31 January in the following year.
* Applicable to those employees in public service whose remuneration is not less than the lowest remuneration for a Deputy Secretary in the Civil Service, i.e. e168,992 as at 14 September 2007.
d) In addition to the annual statement, you must whenever you are performing a function as an employee and you have actual knowledge that you, or a connected person, has a material interest in a matter to which the function relates, provide at the time a statement of the facts of that interest. You should provide such statement to the Chief Executive Officer. The function in question cannot be performed unless there are compelling reasons to do so and, if this is the case, those compelling reasons must be stated in writing and must be provided to the Chief Executive Officer.
e) Under the Standards in Public Office Act 2001, you must within nine months of the date of your appointment provide the following documents to the Standards in Public Office Commission at 18 Lower Lesson Street, Dublin 2: i) A Statutory Declaration, which has been made by you not more than one month before or after the date of your appointment, attesting to compliance with the tax obligations set out in section 25(1) of the Standards in Public Office Act and declaring that nothing in section 25(2) prevents the issue to you of a tax clearance certificate and either:
i) a Tax Clearance Certificate issued by the CollectorGeneral not more than nine months before or after the date of your appointment; or
ii) an Application Statement issued by the CollectorGeneral not more than nine months before or after the date of your appointment.
f) You are required under the Ethics in Public Office Acts 1995 and 2001 to act in accordance with any guidelines or advice published or given by the Standards in Public Office Commission. Guidelines for public servants on compliance with the provisions of the Ethics in Public Office Acts 1995 and 2001 are available on the Standards Commission’s website www.sipo.gov.ie.
31) Review by Employers and Medical Organisations
The terms and conditions of employment as set out in this contract will be reviewed in 2013 by the representatives of the Employers and the medical organisations.
32 Acceptance of Contract
a) This Contract, the associated Terms and Conditions and Appendices and terms expressly incorporated by reference or by statute contain the terms of the Consultant’s employment with _____ (insert name of Employer).
b) The Consultant confirms his/her agreement to the following declaration by signing below:
i) I declare that I am not the subject of any investigation by a medical registration or licensing body or authority in any jurisdiction with regard to my medical practice or conduct as a practitioner. I have not been suspended from registration nor had my registration or licence cancelled or revoked by any medical registration or licensing body or authority in any jurisdiction in the last ten years nor am I the subject of any current suspension
50 www.ihca.ie
or any restrictions on practise. Also, I confirm that I am not aware that I am the subject of any criminal investigation by the police in any jurisdiction.
ii) I am aware of the qualifications and particulars of this position and I hereby declare that all the particulars furnished by me are true. I hereby declare that to the best of my knowledge there is nothing that would adversely affect the position of trust in which I would be placed by virtue of this appointment.
iii) I understand that any false or misleading information submitted by me will render me liable to automatic disqualification or termination of employment if already employed. I understand that this appointment is subject to the receipt of appropriate registration with the Medical Council/ Dental Council, satisfactory references, Garda/Police Clearance and Occupational Health clearance.
Name (Block Capitals):
Signature of Consultant:
Date:
iv) I have read and understood the Medical Council's 'Guide to Ethical Conduct and Behaviour'/Dental Council guidance on ethical conduct and behaviour and any other relevant guidance provided by the relevant Council in relation to ethical or professional conduct.
I undertake to apply the relevant Council's ethical and professional conduct guidance to the clinical and professional situations in which I may work.
v) I have read this document and I hereby accept the post of in accordance with the terms and conditions specified and I undertake to commence duty on:
Name (Block Capitals):
Signature of Consultant:
Date:
Employer (Block Capitals):
Signature on behalf of Employer:
Date:
SECTION B – APPENDICES
APPENDIX I – HSE LETTER OF APPROVAL
The HSE Letter of Approval is individual to each post and will be inserted at this section of each contract.
APPENDIX II – DISCIPLINARY PROCEDURE
Guidance Notes
Guidance notes on the practical operation of this disciplinary procedure are set out below. These guidelines form part of the Disciplinary Procedure:
i) Where it is proposed to bypass Stages 1 or 2 of the Procedure in any case not involving an allegation of serious misconduct, the Consultant shall be advised why it is so proposed.
ii) With respect to the right to confront one’s accuser and to introduce witnesses, dealt with more particularly under Stage 4 and the Appendix to the Procedure, there should be consideration in each case of the most effective manner in which disputed facts might be determined, respecting principles of natural and constitutional justice, the right of a Consultant to his/ her good name and the relevant provisions of any Code of Practice issued by the Labour Relations Commission.
iii) Review of a decision to continue a Consultant on administrative leave, dealt with more particularly under the heading Protective Measures, should refer specifically to the reason(s) why continuation of the administrative leave is proposed.
iv) In any investigation conducted under Stage 4 of the Procedure there should be close scrutiny of all of the evidence in arriving at any decision, having regard to the potentially serious consequences for the Consultant of a finding of misconduct.
v) Disciplinary Proceedings should be confidential save where disclosure is required by law. All parties to such proceedings shall be advised that breach of such duty could itself give rise to disciplinary proceedings.
Consultants’ Common Contract 2008 51www.ihca.ie
Consultants’ Common Contract 2008
1. Purpose
The delivery of a high quality health service is dependent on all staff meeting the highest standards of performance and conduct. Where possible, and as appropriate, the Clinical Director/Line Manager or such person(s) as is/are determined by the Employer will deal with individual shortcomings through discussion, counselling and appropriate assistance. The key objective is to assist the Consultant to meet the required standards. If, however, the Consultant continues to fail to meet the required standards then the disciplinary procedure will be invoked.
The principles of natural and constitutional justice apply and the Consultant will be afforded the right of representation at all stages of the disciplinary process.
Where the issue(s) of concern are of a clinical nature, appropriate clinical input will be obtained by the Employer in advance of any steps of the Procedure being undertaken.
Where it is alleged that a Consultant’s capability, competence or conduct does not meet the required standards, the matter will be dealt with under the following procedure.
2. Scope
This procedure covers all Consultants.
3. Procedure in Operation
While the disciplinary procedure will normally be operated on a progressive basis, in cases of apparent serious misconducts Stages 1, 2 and 3 of the procedure may be bypassed and in other cases Stage 1 and/or Stage 2 may be bypassed if appropriate.
In each instance where it is intended to invoke the Disciplinary Procedure, the Consultant shall be advised in writing of the specific grounds of the complaint(s) made against him/her and afforded an adequate opportunity to respond before any disciplinary action is imposed.
Stage 1: Oral Warning
The Consultant will normally be issued with a formal oral warning by the Clinical Director/Line Manager. This shall follow prior notification of the purpose of the meeting at which the Oral Warning may be delivered. The Oral Warning will give details of the precise nature of the matter, the improvements required and the timescale for improvement. S/he will be advised that the Oral Warning constitutes the first stage of the disciplinary procedure and failure to improve within the agreed timescale may result in further disciplinary action under Stage 2 of the disciplinary procedure. A record of the warning will be kept on the Consultant’s personnel file and will be removed after six months, subject to satisfactory improvement during this period.
The Consultant will have a right to appeal the Oral Warning to a more senior level of management*.
Appeals must be made in writing setting out the grounds for appeal within 14 working days of the Consultant being notified of the decision.
*Appeals will be to the Assistant National Director, NHO/National Director PCCC/CEO of the HSE-funded Agency, as appropriate.
Stage 2: Written Warning
If the Consultant fails to make the necessary improvements, s/he will normally be issued with a formal written warning by the Clinical Director/Line Manager. The written warning will give details of the matter, the improvements required and the timescale for improvement. The Consultant will also be advised that failure to improve within the agreed timescale may result in the issuing of a final written warning under Stage 3 of the disciplinary procedure. The warning will be removed after 9 months, subject to satisfactory improvement during the specified period.
The Consultant will have a right to appeal the written warning to a more senior level of management*. Appeals must be made in writing setting out the grounds for appeal within 14 days of the Consultant being informed of the decision.
*Appeals will be to the Assistant National Director, NHO/National Director PCCC/CEO of the HSE-funded Agency, as appropriate.
Stage 3: Final Written Warning
If the Consultant fails to make the necessary improvements, s/ he will normally be issued with a final written warning by the Clinical Director/appropriate Line Manager. The warning will give details of the matter, the improvements required and the timescale for improvement. The Consultant will be advised that failure to improve within the agreed timescale may lead to dismissal or some other sanction short of dismissal under Stage 4 of the disciplinary procedure. The warning will be removed after a specified period, usually 12 months, subject to satisfactory improvement during this period. Where the warning relates to clinical practice there will be a peer review.
The Consultant will have a right to appeal the written warning to a more senior level of management*. Appeals must be made in writing setting out the grounds for appeal within 14 days of the Consultant being notified of the decision.
*Appeals will be to the Assistant National Director, NHO/National Director PCCC/CEO of the HSE-funded Agency, as appropriate.
52 www.ihca.ie
Consultants’
Stage 4: Dismissal or Action Short of Dismissal
Failure to meet the required standards of performance/ conduct following the issuing of a final written warning will lead to a disciplinary hearing under Stage 4. The decisionmaker will be the relevant National Director, HSE or CEO/ General Manager in other health agencies. The outcome of the disciplinary hearing may be dismissal or action short of dismissal. The delegation of such a decision should take place only in the most exceptional circumstances.
i) Serious Misconduct:
The following are some examples of serious misconduct which will be dealt with from the outset under Stage 4:
Serious negligence/serious dereliction of duties;
• Incapacity to perform duties due to being under the influence of alcohol, prescribed drugs or unprescribed medication; Serious breach of the Employer’s policy(ies) on electronic equipment;
Serious bullying, sexual harassment or harassment (This would only arise where a complaint has been upheld following an investigation under the Dignity at Work policy); Abuse of patients or clients (intellectual disability service users, relatives, etc.)*.
Note: The above list is not exhaustive.
*This would only arise where a complaint has been upheld following an investigation under the Trust in Care policy.
ii) Capability and Competence:
Where possible, as made clear at ‘Purpose’ above and subject to the relevant provisions of the Medical Practitioners Act 2007, issues of capability and competence (including clinical competence and health) will be resolved through ongoing review and support and, where necessary, through the progressive stages of the Disciplinary Procedure. However, it is acknowledged that there may be exceptional cases where there has been an apparent serious failure on the part of a Consultant to deliver the required standard of care due to some lack of capability on his/her part. In such cases of apparent serious failure, the matter will be investigated and dealt with under this stage. The investigation will include appropriate clinical input.
iii) Mechanism for dealing with complaints under (i) and (ii) above: Complaints under (i) and (ii) above will be dealt with as follows:
a) Notifying the Consultant of the allegation:
Upon being made aware of any instance of apparent serious misconduct, senior management/the Clinical Director/Line Manager will arrange for the gathering of preliminary facts relating to the issue in order for the precise allegation to be formulated. The Consultant
against whom the allegation is made will be advised in writing of the precise details of the allegation and invited to make an initial response. When dealing with the allegation, management will ensure, insofar as possible, that confidentiality is maintained and the Consultant against whom the allegation is made is fully protected throughout the process.
b) Protective Measures:
Where it appears to the Hospital General Manager/Chief Executive, HSE Network Manager, Assistant National Director PCCC that by reason of the conduct of a Consultant there may be an immediate and serious risk to the safety, health or welfare of patients or staff the Consultant may apply for or may be required to and shall, if so required, take immediate administrative leave with pay for such time as may reasonably be necessary for the completion of any investigation into the conduct of the Consultant in accordance with this procedure. This investigation should take place with all practicable speed.
Placing the Consultant on paid administrative leave pending the outcome of the investigation will be reserved for only the most exceptional of circumstances. The Chair of the Medical Board or his/her deputy shall be consulted and his or her opinion considered before a decision is taken to place the Consultant on administrative leave. A review of the decision to place the Consultant on administrative leave shall be taken within two weeks of the decision and fortnightly thereafter until the matter is concluded. Where a review is sought by or on behalf of the Consultant, and the grounds for the review are stated, the review should take place immediately (the above two week limit is therefore an outer limit). The Consultant will be advised that the decision to place him/her on administrative leave is a precautionary measure designed to ensure his or her personal safety and well-being/the safety and well-being of patients and staff and not as a disciplinary sanction nor an indication of guilt. Alternative protective measures may include:
• Providing an appropriate level of additional supervision.
• Amendment or restriction of certain clinical duties.
• Other appropriate action.
The views of the Consultant and his or her response will be taken into consideration when determining the appropriate protective measures to take in the circumstances but the final decision rests with the Hospital General Manager/Chief Executive, HSE Network Manager, Assistant National Director PCCC or another equivalent person. This would also include the Masters of Maternity Hospitals, Chief Executives/General Managers of Intellectual Disability Agencies and Chief Executives of specific agencies.
Common Contract 2008 53www.ihca.ie
Patients with type 2 diabetes should expect more after metformin
REALISE THE POTENTIAL
Ozempic®
Once-weekly type 2 diabetes treatment with CV benefits† and superior efficacy1-9*
SUPERIOR GLYCAEMIC CONTROL1-9

• Ozempic® -1.8% vs dulaglutide -1.4%1,2,§
• Up to 79% achieved ADA target of HbA1c <7% (53 mmol/mol) vs other diabetes treatments1-10
SUPERIOR AND SUSTAINED WEIGHT LOSS
• More than double the weight loss vs dulaglutide (-6.5 kg vs -3.0 kg)1,2,§

• Weight loss sustained over 2 years1,3
PROVEN CV BENEFITS
• 26% CV risk reduction in patients with type 2 diabetes and high CV risk,compared to placebo in addition to standard treatment
t This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information.
Ozempic® is indicated for the treatment of adults with insufficiently controlled type 2 diabetes mellitus as an adjunct to diet and exercise • as monotherapy when metformin is considered inappropriate due to intolerance or contraindications • in addition to other medicinal products for the treatment of diabetes. For study results with respect to combinations, effects on glycaemic control and cardiovascular events and the populations studied, see sections 4.4, 4.5 and 5.1. of the summary of product characteristics.1 CV=cardiovascular. SUSTAIN = Semaglutide Unabated Sustainability in treatment of Type 2 Diabetes.


*Results apply to Ozempic® across SUSTAIN trials, which included placebo, sitagliptin, dulaglutide, canagliflozin, exenatide PR and glargine U100.1-9 †In SUSTAIN 6, Ozempic® reduced CV risk (CV death, nonfatal myocardial infarction [MI] or nonfatal stroke) versus placebo in patients with type 2 diabetes at high CV risk treated with standard of care.1,3 ‡When added to standard of care, which included oral antidiabetic treatments, insulin, antihypertensives, diuretics and lipid-lowering therapies.



ABBREVIATED PRESCRIBING INFORMATION
Ozempic®t semaglutide. Please refer to the Summary of Product Characteristics (SmPC) before prescribing. Ozempic® 0.25 mg solution for injection in pre-filled pen. Ozempic® 0.5 mg solution for injection in pre-filled pen. Ozempic® 1 mg solution for injection in pre-filled pen. One ml of solution contains 1.34 mg of semaglutide (human glucagon-like peptide-1 (GLP-1) analogue). Indication: Ozempic® is indicated for the treatment of adults with insufficiently controlled type 2 diabetes mellitus as an adjunct to diet and exercise • as monotherapy when metformin is considered inappropriate due to intolerance or contraindications • in addition to other medicinal products for the treatment of diabetes. For trial results with respect to combinations, effects on glycaemic control and cardiovascular events, and the populations studied, see sections 4.4, 4.5 and 5.1 of the Ozempic® SmPC. Posology and administration: Administered once weekly at any time of the day, with or without meals. Injected subcutaneously in the abdomen, thigh or upper arm. Starting dose: 0.25 mg once weekly. After 4 weeks the dose should be increased to 0.5 mg once weekly. After at least 4 weeks with a dose of 0.5 mg once weekly, the dose can be increased to 1 mg once weekly to further improve glycaemic control. If a dose is missed: administer as soon as possible and within 5 days after the missed dose. If more than 5 days have passed, the missed dose should be skipped, and the next dose should be administered on the regularly scheduled day. In each case, patients can then resume their regular once weekly dosing schedule. The day of weekly administration can be changed, as long as the time between two doses is at least 3 days. After selecting a new dosing day, once-weekly dosing should be continued. When Ozempic® is added to existing metformin and/or thiazolidinedione therapy or to a sodium-glucose co-transporter-2 inhibitor (SGLT2) inhibitor, the current dose of metformin and/or thiazolidinedione or SGLT2 inhibitor can be continued unchanged. When Ozempic® is added to a sulfonylurea (SU) or insulin, a reduction in dose of SU or insulin should be considered to reduce the risk of hypoglycaemia. Blood glucose self-monitoring is necessary to adjust the dose of SU and insulin, particularly when Ozempic® is started and insulin is reduced. A stepwise approach to insulin reduction is recommended. Children: No data available. Elderly: No dose adjustment required, therapeutic experience in patients age ≥75 is limited. Renal impairment: No dose adjustment is required for patients with mild, moderate or severe renal impairment. Experience in severe renal impairment is limited. Not recommended for use in patients with end-stage renal disease. Hepatic impairment: No dose adjustment is required for patients with hepatic impairment. Experience with severe hepatic impairment is limited. Caution should be exercised when treating these patients with semaglutide. Contraindications: Hypersensitivity to the active substance or to any of the excipients. Special warnings and precautions for use: Should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis (DKA). Not a substitute for insulin. DKA has been reported in insulin-dependent patients whom had rapid discontinuation or dose reduction of insulin. There is no experience in patients with congestive heart failure NYHA class IV and is therefore not recommended in these patients. Use of GLP-1 receptor agonists (RAs) may be associated with gastrointestinal adverse reactions. This should be considered when treating patients with
§SUSTAIN 7, Ozempic® 1.0 mg vs. dulaglutide 1.5 mg.







impaired renal function as nausea, vomiting, and diarrhoea may cause dehydration which could cause a deterioration of renal function. Acute pancreatitis has been observed with the use of GLP-1 RAs. Patients should be informed of the characteristic symptoms of acute pancreatitis. If pancreatitis is suspected, semaglutide should be discontinued; if confirmed, semaglutide should not be restarted. Exercise caution in patients with a history of pancreatitis. Use of semaglutide in combination with a SU or insulin may have an increased risk of hypoglycaemia; consider reducing the dose of SU or insulin when initiating treatment with Ozempic®. In patients with diabetic retinopathy treated with insulin and semaglutide, an increased risk of developing diabetic retinopathy complications has been observed. Exercise caution when using semaglutide in patients with diabetic retinopathy treated with insulin, monitor such patients closely and treat according to clinical guidelines. Rapid improvement in glucose control has been associated with a temporary worsening of diabetic retinopathy, but other mechanisms cannot be excluded. When semaglutide is used in combination with a SU or insulin, patients should be advised to take precautions to avoid hypoglycaemia while driving and using machines. Fertility, pregnancy and lactation: Women of childbearing potential are recommended to use contraception when treated with semaglutide. Should not be used during pregnancy or breast-feeding. Discontinue at least 2 months before a planned pregnancy. Effect on fertility unknown. Undesirable effects: Very common (≥1/10): Hypoglycaemia when used with insulin or sulfonylurea, nausea, diarrhoea. Common (≥1/100 to <1/10): Hypoglycaemia when used with other oral antidiabetic medications, decreased appetite, dizziness, diabetic retinopathy complications, vomiting, abdominal pain, abdominal distension, constipation, dyspepsia, gastritis, gastro-oesophageal reflux disease, eructation, flatulence, cholelithiasis, fatigue, increased lipase, increased amylase, weight decreased. Uncommon (≥1/1 000 to <1/100): Hypersensitivity, dysgeusia, increased heart rate, acute pancreatitis, injection site reactions. Rare (≥1/10 000 to <1/1 000): Anaphylactic reaction. Not known (cannot be estimated from available data): Angioedema. The SmPC should be consulted for a full list of side effects. MA numbers: Ozempic® 0.25 mg pre-filled pen EU/1/17/1251/002. Ozempic® 0.5 mg pre-filled pen EU/1/17/1251/003. Ozempic® 1 mg pre-filled pen EU/1/17/1251/005. Each pre-filled pen delivers 4 doses and includes 4 disposable NovoFine® Plus needles. Legal Category: POM. For complete prescribing information, please refer to the SmPC which is available on www.medicines.ie or by email from infoireland@novonordisk.com or from the Clinical, Medical and Regulatory Department, Novo Nordisk Limited, 1st Floor, Block A, The Crescent Building, Northwood Business Park, Santry, Dublin 9. Date last revised: January 2022
tThis medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Adverse events should be reported to the Health Products Regulatory Authority. Information about adverse event reporting is available at www.hpra.ie. Adverse events should also be reported to Novo Nordisk on Tel: 1850 665 665 or complaintireland@novonordisk.com.
www.medicines.ie 2. Pratley RE et al. Semaglutide versus dulaglutide once-weekly in patients with type 2 diabetes (SUSTAIN 7): a randomised, open-label, phase 3b trial. Lancet Diabetes Endocrinol. 2018; 6: 275 - 286. 3. Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375:1834-1844. 4. Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375(suppl1):S1-S108. 5.Lingvay I, Catarig AM, Frias JP, et al. Efficacy and safety of once-weekly semaglutide versus daily canagliflozin as add-on to metformin in patients with type 2 diabetes (SUSTAIN 8): a double-blind, phase 3b, randomised controlled trial. Lancet Diabetes Endocrinol. 2019;7(11):834-844. 6. Ahmann AJ et al. Efficacy and safety of once-weekly semaglutide versus exenatide ER in subjects with type 2 diabetes (SUSTAIN 3): A 56-Week, Open-Label, Randomized Clinical Trial. Diabetes Care 2018;41:258-266. 7. Aroda VR et al. Efficacy and safety of once-weekly semaglutide versus once-daily insulin glargine as add-on to metformin (with or without sulfonylureas) in insulin-naive patients with type 2 diabetes (SUSTAIN 4): a randomised, open-label, parallel-group, multicentre, multinational, phase 3a trial. Lancet Diabetes Endocrinol. 2017;5: 355–66. 8. Sorli C et al. Efficacy and safety of once-weekly semaglutide monotherapy versus placebo in patients with type 2 diabetes (SUSTAIN 1): a double-blind, randomised, placebo-controlled, parallel-group, multinational, multicentre phase 3a trial. Lancet Diabetes Endocrinol 2017; 5: 251–60. 9. Ahrén B et al. Efficacy and safety of once-weekly semaglutide versus once-daily sitagliptin as an add-on to metformin, thiazolidinediones, or both, in patients with type 2 diabetes (SUSTAIN 2): a 56-week, double-blind, phase 3a, randomised trial. Lancet Diabetes Endocrinol. 2017; 5: 341–54. 10. Buse JB et al. 2019 update to: Management of hyperglycaemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2020 Feb; 43(2): 487-493.

References: 1. Ozempic®
Novo Nordisk Limited, First Floor, Block A, The Crescent Building, Northwood Business Park Santry, Dublin 9, D09 X8W3, Ireland. Tel: 01 8629 700, Fax: 01 8629 725, Lo call: 1 850 665665 infoireland@novonordisk.com www.novonordisk.ie
Ozempic®, NovoFine® and the Apis bull logo are registered trademarks owned by Novo Nordisk A/S Date of preparation: June 2022. IE22OZM00103


Summary of Product Characteristics
*
1-9*
1,3†‡
1,3,4,†
Consultants’
Contract
c) Investigation:
An investigation will be conducted by person(s) who is/are acceptable to both parties.
The principles governing the conduct of the investigation and the steps in conducting the investigation are set out in Appendix 1.
If the findings of the investigation uphold the allegation of serious misconduct, a disciplinary hearing will be held as at Stage 4. Both the Consultant and the employing authority shall co-operate with the investigation team to ensure that any investigation is conducted as expeditiously as possible.
Investigations should normally be completed within one month of the commencement date. Both parties agree to full co-operation with the investigation process in order to ensure that it can be conducted expeditiously. The timescale may be extended in exceptional circumstances and the Consultant will be advised of the reasons for the proposed extension and given the opportunity to comment.
Where an allegation is not upheld the Consultant is considered to be exonerated.
d) Disciplinary Hearing:
The decision maker will be the relevant National Director, HSE or the Hospital Chief Executive/General Manager as appropriate.
The Consultant will be provided with a copy of the investigation report and all relevant documentation and will be informed of the following in writing in advance of the disciplinary hearing:
• The status of the hearing, i.e. that it is a formal disciplinary hearing under Stage 4 (Dismissal or Action Short of Dismissal) of the Disciplinary Procedure;
• The purpose of the hearing, i.e. to consider representations on the Consultant’s behalf and to decide if disciplinary action is appropriate and the nature of the sanction if any;
• The possible outcome of the hearing, i.e. it may result in a decision to terminate his or her employment; and
• The right to be accompanied by a representative or work colleague.
The disciplinary hearing will be conducted as follows:
• The Consultant will be informed of the purpose of the disciplinary hearing, the nature of the allegation and the findings of the investigation.
The Consultant and his/her representative will have the opportunity to present his/her case in response to the findings of the investigation.
• The disciplinary hearing will allow the Consultant to raise any concerns regarding the investigation process if s/he feels that these
concerns were not given due consideration by the investigation team. The hearing will be adjourned to allow the decision maker to carefully consider the representations made on the Consultant's behalf.
• The hearing will be reconvened and the Consultant will be advised of the outcome.
The outcome of the disciplinary hearing will be confirmed to the Consultant in writing and copied to his/her representative. The decision may be that the allegation was not upheld, to take no further action, to dismiss the Consultant or to take disciplinary action short of dismissal which may include final written warning, suspension without pay or such other lesser sanction as is deemed appropriate.
The Consultant will be advised of his/ her right to appeal the decision.
iv) Appeals under Stage 4: a) Appeals against Disciplinary Sanctions Short of Dismissal:
Appeals against Stage 4 disciplinary sanctions short of dismissal will be heard by an independent adjudicator who is acceptable to the Consultant. The Consultant will be required to submit the grounds for the appeal in writing within 14 days of being notified of the original decision
b) Appeal against Dismissal Decisions:
If the outcome of the disciplinary hearing is a decision to dismiss, the Consultant may appeal the decision to a committee of three persons.
The Consultant will be required to submit the grounds for the appeal in writing within 14 days of being notified of the original dismissal decision.
An appeal against dismissal decisions will be heard by a committee comprising persons selected from a nominated panel which has been agreed between the HSE and the Consultant’s representative body. Membership of the panel will consist of:
• An Independent Chairperson;
• An Employee representative; and
• An Employer representative.
Membership of the panel will be reviewed every three years. The Chair will be selected from an agreed panel of appropriately qualified legal practitioners or other appropriate persons that may be agreed between the parties. The Committee will adopt its own procedures and may conduct such enquiries as it deems appropriate.
The Committee will decide whether to confirm or vary the original dismissal decision. If the original decision is confirmed, the Consultant will be removed from the payroll.
Common
2008 55www.ihca.ie
Consultants’ Common Contract 2008
c) Ad Misericordium Appeal:
In the event of an appeal against the decision to dismiss being unsuccessful, the Consultant may make a final “mercy appeal” to the Hospital Chief Executive Officer, HSE, or other appropriate persons in the case of non-HSE agencies. The grounds for this appeal must be submitted in writing within 21 days of the employee being notified of the Committee’s decision. Nothing in this Procedure affects the Consultant’s legal rights.
Appendix to Disciplinary Procedure – Investigation
The investigation into allegations of serious misconduct will be carried out in accordance with the following principles:
• The investigation will be conducted as expeditiously as possible and without inordinate delay;
• The investigation will be carried out in strict accordance with the terms of reference and with due respect for the right of the Consultant who is the subject of the allegation to be treated in accordance with the principles of natural justice, including a presumption of innocence;
• Allegations of serious misconduct or allegations that there has been a breach of discipline sufficient to invoke Stage 4 of the Disciplinary Procedure should be made in writing so that there is clarity as to the allegation(s) faced by the Consultant;
• Where an allegation of serious misconduct is denied the facts supporting an allegation must be proved and an opportunity afforded to the Consultant to confront any accuser(s);
• The investigation team will have the necessary expertise to conduct an investigation impartially and expeditiously;
• Confidentiality will be maintained throughout the investigation to the greatest extent possible, consistent with the requirements of a fair investigation. It is not possible, however, to guarantee the anonymity of the complainant or any person who participates in the investigation;
• A written record will be kept of all meetings and treated in the strictest confidence;
• The investigation team may interview any person who they feel can assist with the investigation. All employees are obliged to co-operate fully with the investigation process;
• Employees who participate in the investigation process will be required to respect the privacy of the parties involved by refraining from inappropriately discussing the matter with other work colleagues or persons outside the organisation; and
• It will be considered a disciplinary offence to intimidate or exert pressure, directly or indirectly, on any person who may be required to attend as a witness or to attempt to obstruct the investigation process in any way.
Steps in conducting the Investigation:
• The investigation will be conducted by person(s) nominated by senior management and acceptable to both parties.
• The investigation will be governed by predetermined terms of reference based on the alleged misconduct (which will be set out in writing) and any other matters relevant to the allegation. The terms of reference shall specify the following:
The timescale within which the investigation will be completed; and
The scope of the investigation.
The Consultant against whom the allegation is made will be advised of the right to representation and given copies of all documentation prior to and during the investigation process, e.g:
Details of alleged misconduct.
Witness statements (if any).
Minutes of any interviews held with witnesses.
Any other evidence of relevance.
• The investigation team will interview any witnesses and other relevant persons. Confidentiality will be maintained as far as practicable.
• Persons may be required to attend further meetings to respond to new evidence or provide clarification on any of the issues raised.
• The investigation team will form preliminary conclusions based on the evidence gathered in the course of the investigation and invite the Consultant concerned to provide additional information or challenge any aspect of the evidence.
• On completion of the investigation, the investigation team will form its final conclusions and submit a written report of its findings to the Hospital General Manager/Chief Executive/HSE Network Manager/Director PCCC/ Assistant Director PCCC, as appropriate.
• The Consultant against whom the allegation is made will be given a copy of the investigation report.
• On completion of the investigation, the investigation team will submit a written report in accordance with its terms of reference. However, no decision regarding disciplinary sanction should be decided upon until the decision maker has held a disciplinary hearing with the Consultant.
APPENDIX III – CLINICAL DIRECTORATE SERVICE PLAN
Clinical Directorate Service Plans – Consultant
Schedules
1. Introduction
Provisions for organisation and delivery of services at the front-line at operational level are set out primarily in Directorate Service Plans.
56 www.ihca.ie
Assignment/Work
Consultants’ Common Contract 2008
The Plan is concerned, inter alia, with specifying resources/ funding available (including workforce, facilities, etc.) and how these are deployed in delivering services. The plan specifies quantity of services to be delivered and quality/outcomes parameters to apply thereto.

The Consultant is simultaneously the key directorate resource with respect to service delivery and the core decision-maker regarding utilisation of resources of the Directorate and the organisation generally. It is accordingly centrally important that the Consultant’s contribution at individual level is scheduled into the Directorate Service Plan over designated parameters (i.e. assignments, services, etc.)
This paper sets out high level provisions to apply in this regard. These provisions are likely to develop considerably over time. Further development of these issues will also be required at local level.
2. Directorate Service Plan
The Directorate Service Plan is developed and executed at two levels as follows:
Corporate level: As part of the overall Service Plan of the organisation. Set at high level. Progressed and reported on quarterly.
Directorate level: As part of the operations provisions of the Directorate. Set at directorate level. Developed, progressed and reported on monthly.
57www.ihca.ie
Consultants’
Individual Consultant assignment/work schedules are incorporated as part of the latter. Responsibility for development and execution of the Directorate Service Plan lies with the Clinical Director. This is effected with the full participation of Directorate personnel. In developing the Directorate Service Plan the Clinical Director, inter alia,
Quantifies the total resources available to the Directorate for the forthcoming year/month;
Specifies services to be delivered through these resources in quantity and qualitative terms by the Directorate on an annual/ monthly basis;
Explores and determines with key Directorate personnel (including Consultants) how to deploy resources in a manner which optimises service delivery, quantity and quality in the context of requirements set out in the Corporate Service Plan;
Determines the monthly assignment/work schedule for Consultants and how each Consultant’s commitment will be discharged in achievement of the planned level of service determined for the Directorate.
3. Consultant Assignment/Work Schedules
The Directorate Service Plan incorporates, inter alia, Consultant assignment and work schedules set at both Directorate and personal levels monthly. Sample assignment/work schedule documentation is found on the following pages.
4. Reporting on Directorate/Consultant Performance against Service Plans
Reports on Directorate/Consultant performance against targets set in the Service Plan are produced on a monthly basis. Typically, these are provided at the following levels:
Directorate; • Specialty; and • Consultant.
A sample outline of a performance report can be found on page 61.
5. General
This document addresses Directorate Service Plans at a high framework level. Detailed provisions in this respect will be developed at local level within the parameters set out herein.
APPENDIX IV – CLINICAL DIRECTOR APPOINTMENT AND PROFILE
Appointment of Clinical Directors
1) The post of Clinical Director is an Executive position, appointed by the Employer.
2) It is recognised that for an appointee to function effectively as a Clinical Director (s)he would require the general confidence and support of Consultant colleagues and management.
3) The normal appointment process for a Clinical Director is a follows:
a) Applications are invited in a formal manner from all Consultants in the eligible Consultant grouping
b) All applicants are interviewed
c) Interview panel to comprise:
i) Chair
ii) Two management/board representatives
iii) Two Consultant representatives of whom one will be a member of the directorate grouping and the other, a non-directorate grouping member.
In the case of academic appointments the interview board will include a Consultant Academic attached to the relevant Academic School.
4) In recognition of the importance of securing confidence of all parties in these new provisions, appointment in the first instance will be for two years, made on the following basis:
a) Applications are invited in a formal manner from all Consultants in the eligible Consultant grouping.
b) The body of Consultants within the Directorate may nominate a candidate agreed by all members of the group for the post to the Employer. In the event of an agreed nomination being secured and submitted in writing, signed by all members of the grouping, the nominee, if acceptable to the Employer, will be appointed to the post.
c) In the event that no such agreed candidate emerges, the normal process will apply.
Clinical Director Profile
1) A Clinical Director may cover one speciality area or a range of specialities. Each Directorate is headed by a Clinical Director, generally supported by a Nurse Manager and a Business Manager.
2) A Clinical Director will be a Medical/Dental Consultant Contract holder of the relevant Clinical Directorate, appointed by the employing authority.
Common Contract 2008 58 www.ihca.ie
•
Consultants’ Common Contract 2008
Clinical Directorate Plan
Consultant Assignment Schedule:
Month:
Clinical Directorate Work Schedule - Location and Activity
Service Commitment Absence/ leave OPD
Day of month
1st Am Pm
Am Pm
Am Pm
Am Pm
Am Pm
Am Pm
Am Pm
Am Pm
Am Pm
Am Pm
Am Pm
Am Pm
Ward Rounds / Inpatient care
Theatre / Day Theatre On-call Quality & Risk (incl. Audit)
Medical Education Training and Research
Statutory Commitment
CME / CPD (protected time)
59www.ihca.ie
2nd
3rd
4th
5th
6th
7th
8th
9th
10th
11th
Etc
Consultants’ Common Contract 2008
Consultant Work Schedule - Month
Service Commitment Absence/ leave OPD
Day of month
1st Am Pm
Am Pm
Am Pm
Am Pm
Am Pm
Am Pm
Am Pm
Am Pm
Am Pm
Am Pm
Am Pm
Am Pm
Ward Rounds / Inpatient care
Theatre / Day Theatre On-call Quality & Risk (incl. Audit)
Medical Education Training and Research
Statutory Commitment
CME / CPD (protected time)
60 www.ihca.ie
2nd
3rd
4th
5th
6th
7th
8th
9th
10th
11th
Etc
Performance Report - at Directorate, speciality / sub-speciality and Consultant level Planned vs. Actual (month)
of Focus
Consultants’ Common Contract 2008 61www.ihca.ie
Areas
Planned Actual Public Private Total Public Private Total In-patient Measures ............... Day Patient Measures ............... Out Patient Measures Ed Measures ............... ............... Other Measures Quality Performance Indicators • Corporate ............... • Management ............... • Operational ............... • Clinical (including outcomes)
Consultants’ Common Contract 2008
3) The primary role of a Clinical Director is to deploy and manage Consultants and other resources, plan how services are delivered, contribute to the process of strategic planning and influence and respond to organisational priorities. This will involve responsibility for agreeing an annual Directorate Service Plan, identifying service development priorities and aligning Directorate Service Plans with Hospital or Network Plans.
4) Executive power, authority and accountability for planning and developing services for and managing available resources (direct or indirect) by the Clinical Directorate are delegated from the Employer.
5) Clinical Directors report to a voluntary hospital or agency: the Chief Executive; under the Health Service Executive: Hospital Manager, the Hospital Network Manager, the Local Health Manager or the Assistant National Director, HSE PCCC Directorate, as appropriate.
6) The Clinical Director is accountable for resources used, directly and indirectly, by the Directorate and the transformation of these resource inputs into pre-planned and commensurate levels of service output in line with clinical need and as defined in patient service or other relevant terms and agreed with the Employer.
7) Each member of staff in the Directorate has a reporting relationship, through their line manager, to the Clinical Director. Each Consultant reports to the Clinical Director.
8) The role of the Clinical Director is exercised within the framework of prevailing corporate policy in areas including clinical assurance and effectiveness, quality assurance, Personnel, Finance, ICT, Estates and subject to budgetary and allocation constraints.
9) The principal duties and responsibilities of the Clinical Director include:
a) Provision of strategic input and clinical advice;
Leading the development and execution of a Service Plan for the Directorate.
c) Monitoring and controlling actual performance of the Directorate against planned clinical, business and budgetary performance indicators.
d) Identifying service development priorities and annual budget bids.
e) Implementing the clinical audit function within the Directorate.
f) Developing Practice Plans with individual Consultants and monitoring implementation.
g) Fostering and implementing teamworking within the Directorate.
h) Implementing the measures required to meet accreditation requirements
i) Implementing and compliance with risk management policy and provisions.
j) Participating in the grievance and disciplinary procedures in line with corporate policy.
k) Ensuring a consistency of approach across the Directorate in relation to application of corporate and ethical standards/ clinical protocols in accordance with best practice.
l) Contributing to effective communications within the Directorate, across the hospital/ service and with external stakeholders.
m) Supporting clinical training and continuing professional development throughout the Directorate.
n) Fostering a culture of teaching and research within the Directorate.
o) Participating in the recruitment of permanent, temporary and locum staff as required.
p) Engaging with Service Users and Representatives and actively including the Service User perspective in Service Management.
q) Clinical Directors in Psychiatry have specific duties pursuant to the Mental Health Act, 2001.
Appendix V – Extracts from Consultants Contract 1997
Sections 2.9.4 to 2.9.7 of the Memorandum of Agreement attached to the Consultants Contract 1997: “2.9.4 Each Consultant will be entitled to engage in private practice within the hospital or hospitals in which he is employed. The extent to which a Consultant is entitled to engage in private practice outside the hospital or hospitals in which he is employed is determined by the category of post which he holds (see Section 3 of the Memorandum of Agreement) and subject to him satisfying the employing authority that he is fulfilling his contractual commitment to the public hospital(s).
2.9.5 Where a Consultant is engaged in private practice within institution(s) financed from public funds, and with which he has a contract, then that private practice will be considered as on-site.
2.9.6 Conversely, where a Consultant is engaged in private practice within institution(s) where the managing authority is separate from the public hospital and/or the hospital is financed from private funds, then that private practice will be considered as off-site.
2.9.7 Notwithstanding the provisions of paragraphs 2.9.4 and 2.9.5 above, a Category 1 Consultant who, by definition, devotes substantially the whole of his professional time to a public hospital cannot treat patients in a private hospital or clinic. He may, however, see private patients in consulting rooms which are not on the site of the public hospital. The nature and extent of the activities pursued in consulting rooms should not extend beyond
62 www.ihca.ie
b)
Consultants’
consultation, examination of patients and the performance of minor treatments, i.e. activities normally carried out in out-patient clinics. It does not encompass day-ward procedures involving anaesthesia. The principal criterion to be employed in assessing whether any particular activity falls within the permitted limits is the effect which it has on a Consultant's ready availability to the public hospital. The long-term objective is to provide consulting rooms in the public hospital(s) which may be availed of by Category 1 Consultants to see fee paying patients. Occasional consultations at the request of another Consultant are not precluded by the above provisions.”
APPENDIX VI – GRANTING OF SICK LEAVE
a) Sick leave may be granted to the Consultant if (s)he is incapable of performing their duties owing to illness or physical injury by the Chief Executive Officer/General Manager/Master of the hospital (or other employing institution) or in the case of Consultant Psychiatrists, the Local Health Office Manager PCCC Directorate (where the Consultant is employed by the HSE)/Chief Executive Officer (where the Consultant is not employed by the HSE) only if he/she is satisfied that there is a reasonable expectation that the Consultant will be able to resume the performance of his/her duties and in the case of a fixed-term Consultant will be able to resume during his/her period of office.
b) The Consultant may be required to submit him/ herself to independent medical examination before (s) he is granted sick leave and at any time during the continuance of sick leave granted to him/her.
c) The Chief Executive Officer/General Manager/Master of the hospital (or other employing institution) or in the case of Consultant Psychiatrists, the Local Health Office Manager PCCC Directorate (where the Consultant is employed by the HSE)/Chief Executive Officer (where the Consultant is not employed by the HSE) may pay salary during sick leave to permanent officers in accordance with the following provisions.
i) Except in the case mentioned at (c) (iv) below no salary shall be paid to a Consultant when the sick leave granted to such a Consultant during any continuous period of four years exceeds in the aggregate 365 days.
ii) Subject to limitation mentioned in at (c) (i) above, salary may be paid to a Consultant at the full rate in respect of any days sick leave unless, by reason of
such payment the period of sick leave during which such Consultant has been paid full salary would exceed 183 days during the twelve months ending on such day.
iii) Subject to the limitation mentioned at (c) (i) above, salary may be paid at half the full rate after salary has ceased by reason of the provision at (c) (ii) above to be paid at the full rate.
iv) If before the payment of salary ceases by reason of the provision at (c) (i) and the Chief Executive of the HSE (where the Consultant is employed by the HSE)/Chief Executive Officer/Master of the hospital or other employing institution (where the Consultant is not employed by the HSE) so consents; salary may be paid to a pensionable officer with not less than 10 years service notwithstanding (c) (i) at either half the full rate or at a rate estimated to be the rate of pension to which such officer would be entitled on retirement, whichever of such rates shall be the lesser.
d) For the purposes of these provisions every day occurring within a continuous period of sick leave shall be reckoned as part of such period. From the salary paid during sick leave to a Consultant who is an insured person within the meaning of the Social Welfare Acts, 1952 to 1968, there shall be deducted the amount of any payments to which such officer has become entitled under those Acts during the period of such sick leave.
e) The Chief Executive Officer/General Manager/Master of the hospital (or other employing institution) or in the case of Consultant Psychiatrists, the Local Health Office Manager PCCC Directorate (where the Consultant is employed by the HSE)/Chief Executive Officer (where the Consultant is not employed by the HSE) may make appropriate salary payments during sick leave to a fixed term/locum Consultant if (s)he considers that having regard to all the circumstances of the case, such payment is reasonable.
f) Where a Consultant is suffering from tuberculosis and is undergoing treatment, the Chief Executive Officer/General Manager/Master of the hospital (or other employing institution) or in the case of Consultant Psychiatrists, the Local Health Office Manager PCCC Directorate (where the Consultant is employed by the HSE) or Chief Executive Officer (where the Consultant is not employed by the HSE) may extend the foregoing provisions to allow the payment of salary at three quarters the full rate to the Consultant for the second six months of his/her illness and at half the full rate during the third six months of his/her illness.
Common Contract 2008 63www.ihca.ie
Consultants’ Common Contract 2008
APPENDIX VII – CORRESPONDENCE BETWEEN THE PARTIES
The following correspondence is incorporated into this contract as noted in the preamble: Irish Hospital Consultants Association & Irish Medical Organisation 25 July 2008
I write to you in response to your request for written confirmation of our position on the following issues which have arisen during the negotiations on the proposed terms and conditions for a contract for Consultants employed in the public health service. This letter now supersedes my earlier letter of 16 May 2008 in this regard.
Co-location
In accordance with Mark Connaughton’s letter of 1 February 2008, discussions will take place on the practical issues arising from co-location, when appropriate.
Working Hours
The normal span of the working day will be between the hours of 8am to 8pm, Monday through Friday (Section 7A of the contract refers). However some scheduled variations outside these hours will be permitted where this is demonstrably in the best interest of patient care. With respect to local agreements provided for under section 7 (e), any issues which arise around the implementation of this provision will be referred to the Contract Implementation Group. With respect to the more onerous requirements of the on-call arrangements provided for under the contract, and particularly late night working, it is agreed that consideration will be given to the position of older Consultants, having regard to the provisions of equality legislation.
Flexible Working
Consultants are eligible to apply for flexible working under the “Health Service Flexible Working Scheme” which is designed to facilitate the retention and recruitment of staff and the maintenance of the workforce at the levels required to deliver and develop services into the future, while seeking to accommodate their work life balance.
Membership of Specialist Register
New appointees to Consultant posts must be either eligible for entry in the Register of Medical Specialists maintained by the Medical Council pursuant to the Medical Practitioners Act 1978, or be already entered in that Register. Once the relevant sections
of the Medical Practitioners Act 2007 are commenced, new appointees to Consultant posts must be either eligible for registration, or be already registered in the Specialist Division of the register of medical practitioners to be established and maintained by the Medical Council under that Act.
Letter of Appointment
Letters of appointment will stipulate that contracts to be offered to each individual Consultant will be consistent with the nationally agreed contract.
1997 Contract Holders – Pension Adjustments
Retired Consultants will, in addition to the standard national pay round increases, have special increases applied to their pensions on the same basis as their serving counterparts who opt to remain on the 1997 contract.
Public Private Ratio – Serving Consultants
Serving Consultants whose public to private ratio in 2006 was greater than 20 per cent will be permitted to retain this higher ratio, subject to an overriding maximum ratio of 70:30, and this will endure for the lifetime of the agreement.
Separation vs. Aggregation of Clinical Activity
While the HSE’s position is that the 80:20 ratio should apply to in-patient, day case and out-patient activity (i.e. the same ratio will apply in all cases but will be calculated separately for each type of activity), the Public Private Mix Measurement Group shall consider whether such activities can be aggregated to form a single 80:20 public:private ratio. However, this is subject to the implementation of Clause 20(b) with effect from 1 September 2008, in the absence of any agreed alternative measurement arrangement by that date.
Contract Implementation Committee
A Contract Implementation Committee, comprising representatives of the HSE and the medical organisations, will be established. The Committee will be chaired by Mr Mark Connaughton, SC.
Deadline Date for Contract Acceptance
Consultants who sign for the new contract by 31 August 2008 will benefit from the enhanced pay rates with effect from 1 June 2008. However, consultants who sign up for the new contract between 1 September 2008 and 31 December 2008 will only benefit from the improved pay rates from the date of sign up.
64 www.ihca.ie
Consultants’ Common Contract 2008
Eligibility Regulations
I refer to Section 11.6 (Private Practice) of Mark Connaughton’s report of 4 October 2007 and again confirm our acceptance of the totality of Mr Connaughton’s Report.
Clinical Indemnity/Scope of Practice Document

I can confirm that the revised Scope of Practice document, which is currently being finalised by the State Claims Agency will, when completed, be appended to the Consultant contract.
Psychiatry/Clinical Directors
The practice whereby Clinical Directors were appointed for up to seven years and the method associated with such appointment may continue under the new contract. However, it’s important to understand that this arrangement is quite separate from the transitional arrangement under the new Consultants contract (i.e. two year appointments).
The number of Category 2/Type B*/Type C appointments With reference to the number of Category 2/Type B*/Type C appointments, the approach to be adopted will be in line with Mark Connaughton’s document of 2 May 2008 in which he expected “an upper limit in the order of approximately 700 appointments of Category 2/Type B*/Type C appointments within the system”.
Practice Plans/Service Plans
Consistent with Mark Connaughton’s letter dated 2 May 2008, it is agreed that further discussions shall take place on this subject at the Contract Implementation Committee, informed by the general principles already agreed between the parties.
Yours sincerely, Gerard Barry Chief Executive
APPENDIX VIII – SPECIAL LEAVE PROVISIONS FOR CONSULTANTS IN NON-HSE EMPLOYMENT
These provisions are in addition to those set out in Section 18 (i).
The Employer may grant leave with pay:
g) To a Consultant appointed by a Minister of State to be a member of any Commission, Committee of Statutory Board or a Director of a Company to enable him/ her to attend meetings of the body in question.
h) To a Consultant invited by the Public Appointments Service, a Government Department, the HSE, or a
local or other public authority, to act on a selection board to enable him/her to serve on the Board.
i) For annual training with the Defence Forces/Reserves for one week. Subsequent leave is without pay.
j) For up to three days on the serious illness or death of a near relative.
k) When the Consultant is a candidate for a post, advertised by the Public Appointments Service, a Government Department, the HSE, or a local or other public authority for a maximum of six days with pay in any one year, to enable him/her to appear before such selection board.
l) To the Consultant for the purpose of attending clinical meetings of societies appropriate to his/her specialty of not more than seven days with pay, in any one year (exclusive of travel time).
65www.ihca.ie
Consultants’ Common Contract 2008
APPENDIX IX – COMMITTEES TO ADVISE HSE ON CONSULTANT APPLICATIONS
Health Service Executive
Terms of Reference
Establishment The Consultant Applications Advisory Committee (CAAC) will be established by the CEO of the HSE.
Purpose The purpose of the CAAC is to provide independent and objective advice to the HSE on applications for medical Consultants and qualifications for Consultant posts. The CAAC provides a significant opportunity for Consultants to contribute their expertise and professional knowledge to the decision-making process for the development of Consultant services throughout the country.
Membership Membership will comprise:
(i) An independent Chair;
(ii) Senior HSE planning officials from relevant Directorates (i.e. NHO, PCCC, Population Health, HR and Finance). The METR Unit band the Nursing Services Director will also be represented;
(iii) Consultant representatives covering the nine relevant medical specialties (anaesthesia, emergency medicine, medicine, pathology, paediatrics, psychiatry, obstetrics & gynaecology, radiology, surgery). These members will be selected by the CEO from a pool comprising the Chairs of the Expert Advisory Groups and proposed nominees of the training bodies such as the Chairpersons and Honorary Secretaries;
(iv) Patient advocacy groups;
(v) Voluntary hospital CEO;
(vi) Two representatives of each of the Irish Hospital Consultants Association and Irish Medical Organisation Members will be appointed by the CEO. Factors such as gender mix and geographic spread will be taken into account in the selection of members.
Modus Operandi
It is envisaged that the CAAC will meet every two months, or more often as required. The members of the CAAC will consider applications (new and replacement) submitted to it which have been processed by the Consultant Appointments Unit. All posts presented to the CAAC will have received financial clearance from the relevant service Directorate (NHO/PCCC).The officials of the Consultant Appointments Unit (CAU) will prepare background information on and initial analysis of each application and will present this to the CAAC. The CAAC will consider each application in the context of information received from the officials of the CAU, published policy, workload statistics, precedent, literature review, professional advice and knowledge, developments in medical education and training, relevant local information, demography, workload statistics and any other relevant advice (e.g from Expert Advisory Groups). The CAAC will provide advice in relation to each individual application. Advice could include:
(i) Recommendation to approve the post.
(ii) Recommendation to seek clarification of aspects of the post or aspects of policy not already clarified by the CAU.
(iii) Recommendation to amend the structure, sessional commitment, etc.
(iv) Recommendation to refuse approval to the post.
The CAAC will also provide advice to the HSE on the appropriate qualifications for Consultant posts. Other functions may be assigned by the National Director, Human Resources, following discussion with the Committee. Advice provided by the CAAC will be forwarded by the Head of the CAU to the National Director, Human Resources, to whom responsibility for the regulation of Consultant posts has been delegated by the CEO of the HSE. The National Director will in turn regulate each post taking into account the advice provided. The recruitment and appointment of Consultants and related staff is approved by the National Employment Monitoring Unit (NEMU) in accordance with the Employment Control Framework approved by the Board of the HSE.The National Director, Human Resources, provides regular updates to the Board of the HSE on the Consultant posts recommended for approval.
Executive Support The CAAC will be supported by the officials of the Consultant Appointments Unit (CAU).
Term The CAAC will be
for an initial period of one year.
66 www.ihca.ie
appointed
Consultants’
Consultant Applications Advisory Committee Type C Consultant Posts
Establishment process
1. Introduction
• The proposal with respect to Type C Consultant posts is set out in the report of the Independent Chairman of the Consultant Contract negotiations – Mark Connaughton SC – dated 4 October 2007. The report was fully adopted by the HSE and DoHC. The requirement to be more specific with respect to how such posts might be established and be somewhat less rigid in its application than envisaged in the Chairman’s report and associated discussion was also recognised.
• This paper sets out, at a high level, the process to be pursued in establishing such posts.
2. Establishment process
2.1 Application process
• Applications for Consultant posts are generated through the pertinent hospital/network/PCCC agency/area in the prescribed format.
• The applicant organisation is required to specify its proposed post type (A, B or C) in its related submission.
• Where a Type C post is recommended, the applicant organisation will be required to satisfy a number of criteria pertinent thereto, which would include, but not be limited to, the following:
A clear indication as to why the post requirements cannot be met through a Type A or B arrangement;
A clear demonstration as to the added patient, service and public system benefits and values to be achieved through establishment of the post as a Type C rather than a Type A or B position.

2.2 Decision process
• The application will be submitted to the HSE Consultant Appointments Unit (CAU) for initial review. This review will be undertaken with input from NHO/PCCC Corporate. Where, following internal review, the CAU considers that the case for a Type C designation is not adequately made, by reference to the specified criteria, the proposal will be returned to the applicant source for further development and resubmission. Where the CAU considers that the proposal meets the specified criteria, the submission will be furnished to a Type C Consultant Committee for consideration and recommendation.
• Recommendations from the Type C Consultant Committee will be forwarded to the CEO of the HSE for approval/final decision.
3. Type C Consultant Committee
• The Committee will be established by the CEO of the HSE.
• Appointments to the Committee will be made by the CEO of the HSE.
• Representation on the Committee will include:
Chairperson;
HSE Corporate;
DoHC;
Public voluntary agencies;
Members of the public;
representative of the Irish Hospital Consultants Association;
representative of the Irish Medical Organisation.
Common Contract 2008 67www.ihca.ie
One
One
Professional Directory Medical Indemnity Organisations


Medical Protection Society
Victoria House, 2 Victoria Place, Leeds LS11 5AE, UK.
Medicolegal advice: 1800 936 077*
Membership information: 1800 932 916
Fax: (0044) (113) 241 0500
Email: member.help@medicalprotection.org
*Freephone number from Republic of Ireland
Challenge Unit 11 Burnell Square, Malahide Road, D17 VY04.
Tel: (01) 839 5942
Fax: (01) 832 4254
Email: insurance@challenge.ie
Medisec/MedPro
7 Hatch Street Lower, Dublin, D02 AW92.
Freephone: 1800-460-400
Tel: (01) 611 0504
Email: info@medisec.ie
Medical Defence Union (MDU)
One Canada Square, London E14 5GS, UK.
Tel: (0044) 20 7202 1500
Tel Ireland Medico-legal Queries: 1800 535 935
Tel Ireland Membership: 1800 509 132
Fax: (0044) 20 7202 1696
Email: advisory@themdu.com or membership@themdu.com
Healthlink

St. Vincent’s Private Hospital handles complex and high-acuity patients who benefit from over 250 consultants across over 50 specialties on a multi-hospital campus in Elm Park, Dublin 4.
St. Vincent’s Private
Elm Park, Dublin 4, Ireland.
+353 1 263 8000
info@svph.ie www.svph.ie
www.ihca.ie
68
E-Referrals • All SVPH consultants • MRI service • Endoscopy service Healthlink now open for e-referrals to:
Hospital
T
E
• Sleep studies • Cardiology (echos and ECGs) • Bariatric service
Irish Life Health
Irish Life Centre, Abbey Street Lower, Dublin 1.
Tel: (01) 562 5100 or
Participating Consultants can call (01) 562 5162 or
Email: partnersupport@irishlifehealth.ie
Head of Provider Affairs: Mr Brian Scollard
ESB Staff Medical Provident Fund
PO Box 384, Rosbrien, Limerick.
Tel: (061) 430561 or Ext 55361
Fax: (061) 430500
Email: mpf@esb.ie
Programme Leader: Mr John Conneely
Professional Directory Health Insurers
Vhi Healthcare
IDA Business Park, Purcellsinch, Dublin Road, Kilkenny, R95 WKK6.
Vhi House, Lower Abbey Street, Dublin 1, D01 DX77.
Tel: 1890 444 444
Tel: (Kilkenny): (056) 444 4444
Vhi Corporate
Tel: (01) 799 4120 Fax: (01) 619 7453
Email: info@vhi.ie
Medical Director: Dr Bernadette Carr
Head of Provider Affairs (Acting): Ms Aoife de Paor
HSF Health Plan
5 Westgate Business Park, Kilrush Road, Ennis, Co. Clare, V95 TR66.
Tel: 0818 451 451/00 353 65 6862 500
(if outside Ireland)
e-mail: customer@hsf.ie
Professional Directory Medical Council
Laya Healthcare Eastgate Road, Eastgate Business Park, Little Island, Co Cork, T45 E181.
Tel: (021) 202 2000
Email: info@layahealthcare.ie Medical Practice Manager: Ms Noreen Quinlan
Prison Officers’ Medical Aid Society
397e North Circular Road, Dublin 7, D07 TAC9.
Tel: (01) 830 8963
Email: info@pomas.ie Secretary: Mr PJ Dunne
MEDICAL COUNCIL
The Medical Council was established under the Medical Practitioners Act, 1978 as amended by the Medical Practitioners Act of 2007. It is the guardian of the public’s interest in relation to the Medical profession and protects the public by promoting and better ensuring high standards of professional conduct and professional education, training and competence among doctors.
The principal functions of the Council are:
• To prepare and establish a register of medical practitioners that is known as the Register of Medical Practitioners;
• To satisfy itself as to the suitability of medical education and training, the standards of theoretical and practical knowledge for primary qualifications, the clinical training and experience required for the granting of a certificate of experience, and the adequacy and suitability of postgraduate education and training;
• To enquire into the conduct of registered medical practitioners for alleged professional misconduct or fitness to engage in the practice of medicine by reason of physical or mental disability
• To promote good medical practice and oversee doctors’ continuing professional development.
The Council has 25 members including elected and appointed members. Under the provisions of the Medical Practitioners Act, 2007, the Council is comprised of 13 non-medical members and
12 medical members representing a range of medical specialties, teaching bodies and members of the public and stakeholders, all of whose appointments have been approved by the Minister for Health. The current Council’s period of office is 2018 to 2023.
Consultants are advised to be registered in the Specialist Division of the Medical Register. Details of this are to be found overleaf.
The Medical Council published an amended 8th Edition of its Guide to Professional Conduct and Ethics in 2019. This was updated in light of the Health (Regulation of Termination of Pregnancy) Act 2018. The Council is in the process of revising its Guide in preparation for the publication of a new 9th Edition. Consultants are strongly advised to acquaint themselves with the contents of the Guide. It lays out information on the operation of the Registers, on ethical conduct and behaviour, and on the operation of the fitness to practise process.
The Medical Council
Upper Ground Floor & 5th Floor, Block 9 (Europa House), Harcourt Centre, Harcourt Street, Dublin 2, D02 WR20.* Tel: (01) 498 3100 Email: medicalcouncil@mcirl.ie www.medicalcouncil.ie
* The Medical Council has temporarily moved office location from Kingram House, Kingram Place, Dublin 2.
www.ihca.ie 69
MEMBERSHIP
Dr Suzanne Crowe (President)
Professional Directory Medical Council
Medical Member
Dr Tom Crotty (Vice President) Medical Member
Ms Vicky Blomfield
Non-Medical Member/HIQA Nominee
Dr Anthony Breslin Medical Member
Ms Teresa Bulfin
Ms Marie Culliton
Non-Medical/HSE Nominee
Non-Medical Member
Mr Ian Drennan Non-Medical /Ministerial Nominee
Mr John Gleeson
Mr Paul Harkin
Non-Medical /Ministerial Nominee
Non-Medical / Ministerial Nominee
Prof John Hyland Medical Member /Med School RCSI Nominee
Prof Marina Lynch Non-Medical /Royal Irish Academy Nominee
Mr Bill Maher
Non-Medical/Private Hospital Association Nominee
Dr Michael McGloin Medical Member
Prof Joe McMenamin Medical Member/Joint Nominee of the Medical Schools
Dr Aoife Mullally Medical Member
Mr John Murray
Non-Medical/NMBI Nominee
Mr Jim O’Sullivan Non-Medical/HSE Nominee
Prof Mary O’Sullivan
Non-Medical/Minister for Education Nominee
Dr Margaret O’Riordan Medical/ ICGP Nominee
Dr Orla Kelly Medical Member/Co-opted
Ms Jill Long
Non-Medical/ Ministerial Nominee
Prof Edna Roche Medical/ NUI Medical School Nominee
Dr Mary Davoran Medical Member/ College of Psychiatrists of Ireland Nominee
Mr Ronan Quirke
Non-Medical/ Ministerial Nominee
Prof Paul Finucane Medical Member/ RCPI Nominee
REGISTER OF MEDICAL PRACTIONERS
The Medical Council maintains this Register in which every practising doctor must be registered. It is an offence to practise medicine, except in some strictly defined exceptions, if you are not registered.
Every doctor is responsible for ensuring that their registration is current within one of the following categories:
(a) General Division, which shall include the names of those medical practitioners registered in that division pursuant to Section 46 and such other identifying particulars of those practitioners as the Council considers appropriate. Doctors with general registration may practise independently without supervision but may not represent themselves as being specialists;
(b) Specialist Division, which shall include the names of those medical practitioners registered in that division pursuant to Section 47 and such other identifying particulars of those practitioners as the Council considers appropriate. Doctors with specialist registration may practise independently, without supervision, and may represent themselves as specialists;
(c) Trainee Specialist Division, which shall include the names of those medical practitioners registered in that division pursuant to Section 48 or 49 and such other identifying
particulars of those practitioners as the Council considers appropriate. Doctors with trainee specialist registration are on recognised training programmes and practise solely within the confines of posts allocated by the HSE, in conjunction with the national postgraduate training bodies; and (d) Visiting EEA Practitioners Division, which shall include the names of those medical practitioners registered in that division pursuant to Section 50 and such other identifying particulars of those practitioners as the Council considers appropriate. This allows EU citizens who are fully established to practise medicine in another EU member state to practise medicine in Ireland on a temporary and occasional basis without having to take out registration. (e) Internship Registration allows a doctor to carry out internship training in a hospital recognised by the Medical Council. Internship registration is open to both graduates of Irish and EU/EEA member State Medical Schools.
(f) Supervised Division
For doctors to be considered for registration within the Supervised Division they must have been offered a post with the HSE that has been approved by the HSE as an individually numbered, identifiable post, which has specific supervisory arrangements.
www.ihca.ie
70
SPECIALIST DIVISION
The following specialties are recognised in the Specialist Division of the Register:
Anaesthesiology
• Anaesthesiology
• Intensive Care Medicine
• Pain Medicine
Emergency Medicine
• Emergency Medicine
General Practice
• General Practice
• Military Medicine
Medicine
• Cardiology
• Clinical Genetics
• Clinical Neurophysiology
• Clinical Pharmacology & Therapeutics
• Dermatology
• Endocrinology & Diabetes Mellitus
• Gastroenterology
• General (Internal) Medicine
• Genito-Urinary Medicine
• Geriatric Medicine
• Infectious Diseases
• Medical Oncology
• Nephrology
• Neurology
• Palliative Medicine
• Pharmaceutical Medicine
• Rehabilitation Medicine
• Respiratory Medicine
• Rheumatology
• Tropical Medicine
Obstetrics & Gynaecology
• Obstetrics & Gynaecology
Occupational Medicine
• Occupational Medicine
Professional Directory Medical Council
Ophthalmology
• Ophthalmology
Paediatrics
• Paediatrics
• Paediatric Cardiology
• Neonatology
Pathology
• Chemical Pathology
• Haematology (Clinical & Laboratory)
• Histopathology
• Immunology (Clinical & Laboratory)
• Microbiology
• Neuropathology
Psychiatry
• Child & Adolescent Psychiatry
• Psychiatry
• Psychiatry of Learning Disability
• Psychiatry of Old Age
Public Health Medicine
• Public Health Medicine
Radiology
• Diagnostic Radiology
• Radiation Oncology
Sports & Exercise Medicine
• Sports & Exercise Medicine
Surgery
• Cardiothoracic Surgery
• General Surgery
• Neurosurgery
• Ophthalmic Surgery
• Oral & Maxillo-Facial Surgery
• Otolaryngology
• Paediatric Surgery
• Plastic, Reconstructive & Aesthetic Surgery
• Trauma & Orthopaedic Surgery
• Urology
• Vascular Surgery
www.ihca.ie 71
NAME
Eastern Region
Prof Gabrielle Colleran
Professional Directory
IHCA National Council 2022-2023
HOSPITAL/REGION
CHI at Temple Street/NMH
SPECIALITY
Radiology
Prof Anne Doherty Mater Hospital Psychiatry
Dr David Kevans St James’s Hospital Gastroenterology
Mr Rustom Manecksha Tallaght University Hospital Urological Surgery
Mr Timothy Martin Murphy Tallaght University Hospital Orthopaedics
Dr Patricia Walsh Naas General Hospital Psychiatry
South Eastern Region
Dr Carmel Ann Daly University Hospital Waterford Radiology
Prof Robert Landers University Hospital Waterford Histopathology
Dr Conor O’Riordan St Luke’s Hospital, Kilkenny Radiology
Midland Region
Prof Clare Fallon
Midland Regional Hospital, Mullingar
Geriatric Medicine
Dr Conor Meehan Midland Regional Hospital, Tullamore Radiology
North Eastern Region
Dr Rachel Cullivan
Cavan General Hospital Psychiatry
Dr Mike Staunton Our Lady of Lourdes, Drogheda Anaesthesiology
North Western Region
Dr Áine Burke
Sligo University Hospital
Haematology
Dr John Scully Letterkenny University Hospital Anaesthesiology
Western Region
Dr Brian Egan Mayo University Hospital
Gastroenterology
Dr Jan Steiner Galway Clinic Anaesthesiology
Mid Western Region
Mr Colin Peirce University Hospital Limerick General Surgery
Prof Clodagh O’Gorman University Hospital Limerick Paediatrics
Southern Region
Ms Eimear Conroy University Hospital Kerry Orthopaedic Surgery
Mr Greg Fulton Cork University Hospital Vascular Surgery
Dr Sinead Harney Cork University Hospital Rheumatology
Dr Nóirín Russell Cork University Maternity Hospital Obstetrics & Gynaecology
Co-Options
Prof Elizabeth Barrett
CHI Temple Street
Psychiatry
Dr Gerard O’Connor Mater Hospital Emergency Medicine
Dr Ikechukwu Okafor CHI Temple Street Paediatrics
72 www.ihca.ie
President
Prof Robert Landers
Consultant Histopathologist, University Hospital Waterford, Waterford.
Vice President
Prof Gabrielle Colleran
Consultant Paediatric Radiologist, National Maternity Hospital, Holles Street, Dublin 2 and CHI at Temple Street, Dublin 1.
Vice President
Prof Anne Doherty
Consultant Liaison Psychiatrists, Mater Hospital, Dublin 7.
Professional Directory
IHCA Officer Board 2022-2023
Membership Secretary
Dr Conor O’Riordan
Consultant Radiologist, St Luke’s Hospital, Kilkenny.
Treasurer
Prof Clare Fallon
Consultant in Geriatric Medicine, Midland Regional Hospital, Mullingar.
Immediate Past President
Prof Alan Irvine
Consultant Dermatologist, Children’s Health Ireland at Crumlin, Dublin 12.
SECRETARY GENERAL: Martin Varley Tel: 087 2274099
Email: m.varley@ihca.ie
SENIOR EXECUTIVE OFFICER: Aidan O’Reilly Tel: 086 1590733
Email: a.oreilly@ihca.ie
IHCA Secretariat
ASSISTANT SECRETARY GENERAL: Alice McGarvey Tel: 086 803 2707
Email: a.mcgarvey@ihca.ie
SENIOR POLICY AND RESEARCH EXECUTIVE: Dara Gantly Tel: 087 803 3336
Email: d.gantly@ihca.ie
www.ihca.ie 73
A Little Lifetime Foundation - for bereaved parents and their families

18 Orion Business Campus, Rosemount Business Park, Ballycoolin, Blanchardstown, D15 HD91.
Tel: (01) 882 9030
Email: info@alittlelifetime.ie Web: www.alittlelifetime.ie
Alcoholics Anonymous Ireland General Service Office, Unit 2, Block C, Santry Business Park, Swords Road, Dublin 9, D09 H584.
Tel: (01) 842 0700, Mobile for the deaf and Hard of Hearing: (087) 146 0387
Email: gso@alcoholicsanonymous.ie Web: www.alcoholicsanonymous.ie
Alone
Olympic House, Pleasants Street, Dublin 8.
Tel: (01) 679 1032
Helpline: 0818 222 024
Email: hello@alone.ie Web: www.alone.ie
Alzheimer Society of Ireland Temple Road, Blackrock, Co. Dublin. Tel: (01) 207 3800
Fax: (01) 210 3772
Helpline: 1800 341 341 / helpline@alzheimer.ie
Email: info@alzheimer.ie Web: www.alzheimer.ie
Professional Directory Voluntary & Support Organisations
Arc Cancer Support Centres
65 Eccles St, Dublin 7, D07 TD35
Tel/Support Line: (01) 215 0250 Email: info@arccancersupport.ie Web: www.arccancersupport.ie
Arthritis Ireland
1 Clanwilliam Square, Grand Canal Quay, Dublin 2, D02 DH77.
Tel: 0818 252 846 / (01) 661 8188
Email: helpline@arthritisireland.ie Web: www.arthritisireland.ie
Asthma Society of Ireland
42-43 Amiens Street, Dublin 1.
Tel: (01) 817 8886
Helpline: 1800 44 54 64 WhatsApp 086 059 0132
Email: reception@asthmasociety.ie Web: www.asthma.ie
Aware
9 Upper Leeson Street, Dublin 4, D04 KD80.
Tel: (01) 661 7211
Helpline: 1800 804 848/ supportmail@aware.ie
Email: info@aware.ie Web: www.aware.ie
Bodywhys – The Eating Disorders
Association of Ireland
PO Box 105, Blackrock, Co. Dublin.
Tel: (01) 283 4963
Helpline: (01) 210 7906
Email: info@bodywhys.ie
Email Support Service: alex@bodywhys.ie Web: www.bodywhys.ie
Cheshire Ireland
1st Floor, Block 4, Bracken Business Park, Bracken Road, Sandyford Business Park, Dublin 18, D18 VOYO.
Tel: (01) 297 4100
Fax: (01) 205 2060
Email: info@cheshire.ie Web: www.cheshire.ie
Children in Hospital Ireland Suite 113, 4-5 Burton Hall Road, Sandyford, Dublin 18.
Tel: (01) 290 3510
Email: info@childreninhospital.ie Web: childreninhospital.ie
Chime - National Charity for Deafness and Hearing Loss
35 North Frederick Street, Dublin 1.
Tel: (01) 817 5700/ 1800 256 257
Text: (087) 922 1046
Email: info@chime.ie
Skype: Chime NFS Web: www.chime.ie
www.ihca.ie
74
CLAPAI - Cleft Lip and Palate Association of Ireland
c/o 36 Woodlands Avenue, Glenageary, Co. Dublin, A96 R2F4.
Tel: 087 131 9803
Email: info@cleft.ie Web: www.cleft.ie
Coeliac Society of Ireland
Dolcan House, 78/80 Tower Road, Clondalkin, Dublin 22, D22 N6F6.
Tel: (01) 872 1471
Email: info@coeliac.ie Web: www.coeliac.ie
Coolmine Therapeutic Community

Coolmine House, 19 Lord Edward Street, Dublin 2.
Tel: (01) 679 4822 / 087 122 9307
Email: info@coolminetc.ie or admissions@coolminetc.ie Web: www.coolmine.ie
COPE Foundation
1st Floor, 1D - 1F, The Atrium, Blackpool Retail Park, Blackpool, Cork, T23 T2VY.
Tel: (021) 464 3100
Fax: (021) 450 7580
Email: headoffice@cope-foundation.ie Web: www.cope-foundation.ie
Professional Directory Voluntary & Support Organisations
Cuidiú
Carmichael Centre, 4 North Brunswick Street, Dublin 7.
Email: info@cuidiu.ie Web: www.cuidiu.ie
Cystic Fibrosis Ireland
CF House, 24 Lower Rathmines Road, Dublin 6, D06 A9P3.
Tel: (01) 496 2433
Tel: 1800 832 022
Fax: (01) 496 2201
Email: info@cfireland.ie Web: www.cfireland.ie
Diabetes Ireland
19 Northwood House,
Northwood Business Campus, Santry, Dublin 9, D09 DH30.
Tel: (01) 842 8118
Email: info@diabetes.ie Web: www.diabetes.ie
Down Syndrome Ireland Unit 3, Park Way House, Western Parkway Business Park, Ballymount Drive, Dublin 12, D12 HP70.
Tel: (01) 426 6500
Email: info@downsyndrome.ie Web: www.downsyndrome.ie
Enable Ireland
32F Rosemount Park Drive, Rosemount Business Park, Ballycoolin Road, Dublin 11
Tel: (01) 872 7155
Fax: (01) 866 5222
Email: hello@enableireland.ie Web: www.enableireland.ie
Epilepsy Ireland
249 Crumlin Road, Crumlin, Dublin 12, D12 RW92.
Tel: (01) 455 7500
Email: info@epilepsy.ie Web: www.epilepsy.ie
Fighting Blindness
3rd Floor, 7 Ely Place, Dublin 2, DO2 TW98.
Tel: (01) 678 9004
Email: info@fightingblindness.ie Web: www.fightingblindness.ie
GROW – Mental Health Recovery
National Support Office, Apartment 5, Forrest Mews, Forrest Road, Swords, Co. Dublin, K67 XR96.
Tel: (01) 840 8236 Infoline: 0818 474 474
Email: info@grow.ie Web: www.grow.ie
www.ihca.ie
75
Health Protection Surveillance Centre
25-27 Middle Gardiner Street, Dublin 1, D01 A4A3.
Tel: (01) 876 5300,
Fax: (01) 856 1299
Email: hpsc@hse.ie Web: www.hpsc.ie
Headway - Brain Injury Services & Support
Blackhall Green, off Blackhall Place, Dublin 7. Tel: (01) 604 0800
Fax: (01) 604 1700
Freephone: 1800 400 478
Email: helpline@headway.ie Web: headway.ie
HIV Ireland
70 Eccles Street, Dublin 7.
Tel: (01) 873 3799
Fax: (01) 873 3174
Email: info@hivireland.ie Web: www.hivireland.ie
Huntington’s Disease Association of Ireland
Carmichael House, 4 North Brunswick Street, Dublin 7. Tel: (01) 872 1303
Helpline: 1800 393939
Email: info@huntingtons.ie Web: www.huntingtons.ie
Irish Cancer Society
43/45 Northumberland Road, Dublin 4, D04 VX65.
Tel: (01) 231 0500
Fax: (01) 231 0555
Freephone: 1800 200 700
Email: info@irishcancer.ie Web: www.cancer.ie
Irish Deaf Society
Deaf Village Ireland, Ratoath Road, Cabra, Dublin 7, D07 W94H.
Tel: (01) 860 1878
Text: (086) 380 7033
Skype: Call IDS
Email: info@irishdeafsociety.ie Web: www.irishdeafsociety.ie
Professional Directory Voluntary & Support Organisations
Irish Family Planning Association
Solomons House, 42a Pearse Street, Dublin 2.
Tel: (01) 607 4456
IFPA Appointment Line: 0818 49 50 51
Email: reception@ifpa.ie Web: www.ifpa.ie
Irish Haemochromatosis Association
The Carmichael Centre, North Brunswick Street, Dublin 7.
Tel: (01) 8735911
Email: info@haemochromatosis-ir.com Web: haemochromatosis-ir.com
Irish Haemophilia Society
First Floor, Cathedral Court, New Street, Dublin 8, D08 VH64.
Tel: (01) 657 9900
Fax: (01) 657 9901
Email: info@haemophilia.ie Web: www.haemophilia.ie
Irish Heart Foundation
17-19 Rathmines Road Lower, Dublin 6, D06 C780. Tel: (01) 668 5001
Fax: (01) 668 5896
Email: info@irishheart.ie Web: www.irishheart.ie
Irish Hospice Foundation
4th Floor, Morrison Chambers, 32 Nassau Street, Dublin 2, D02 YE06.
Tel: (01) 679 3188
Bereavement Support Line: 1800 80 70 77
Email: info@hospicefoundation.ie Web: www.hospicefoundation.ie
Irish Kidney Association
Head Office, Donor House, Block 43A, Park West, Dublin 12, D12 P5V6.
Tel: (01) 620 5306
Email: info@ika.ie Web: www.ika.ie
Irish Motor Neurone Disease Association Unit 3, Ground Floor, Marshalsea Court, 22/23 Merchant’s Quay, Dublin 8, D08 N8VC.
Tel: (01) 670 5942
Helpline: 1800 403 403
Email: info@imnda.ie / services@imnda.ie Web: www.imnda.ie
Irish Multiple Births Association
Carmichael Centre, North Brunswick Street, Dublin 7.
Tel: (01) 874 9056
Email: info@imba.ie/services@imnda.ie Web: www.imba.ie
Irish Osteoporosis Society 1B Clonskeagh Square, Clonskeagh, Dublin 14, D14 A0K8.
Tel/Helpline:(01) 637 5050
Email: info@irishosteoporosis.ie Web: www.irishosteoporosis.ie
Irish Patients’ Association Email: info@irishpatients.ie Web: www.irishpatients.ie
The Irish Sleep Society P.O. Box 11850, Dublin 1. Email: theirishsleepsociety@gmail.com Web: www.irishsleepsociety.org
Irish Society for Autism Unity Building, 16/17 Lower O’Connell Street, Dublin 1, D01 E9WO. Tel: (01) 874 4684
Email: admin@autism.ie Web: www.autism.ie
Crohn’s & Colitis Ireland
Carmichael Centre, North Brunswick Street, Dublin 7, D07 RHA8.
Tel: (01) 872 1416
Support Line: (01) 531 2983
Email: info@iscc.ie Web: iscc.ie
www.ihca.ie
76
Irish Wheelchair Association
Áras Cúchulainn, Blackheath Drive, Clontarf, Dublin 3, D03 AW62.
Tel: (01) 818 6400
Email: info@iwa.ie Web: www.iwa.ie
LGBT Ireland
80 Dame Street, Dublin 2.
Tel: (01) 6859280
Helpline: 1800 929 539
Email: info@lgbt.ie Web: www.lgbt.ie
Meningitis Research Foundation
Suite 204, Park House, 10 Park St, Bristol BS1 5HX, UK.
Helpline: 1800 41 33 44
Email: helpline@meningitis.org Web: www.meningitis.org
Mental Health Ireland
Second Floor, Marina House, 11-13 Clarence Street, Dun Laoghaire, Co. Dublin, A96 E289.
Tel: (01) 284 1166
Email: info@mentalhealth.ie Web: www.mentalhealthireland.ie
Miscarriage Association of Ireland
Carmichael Centre, North Brunswick Street, Dublin 7.
Tel: (01) 873 5702
Helpline: 087 365 6887 / 086 3324040/ 087 9239217
Email: info@miscarriage.ie Web: www.miscarriage.ie
MS Ireland
National Office, 80 Northumberland Road, Dublin 4, D04 T856.
Tel: (01) 678 1600
Helpline: 0818 233 233
Fax: (01) 678 1601
Email: info@ms-society.ie Web: www.ms-society.ie
Muscular Dystrophy Ireland
75 Lucan Road, Chapelizod, Dublin D20 DR77.
Tel: (01) 623 6414
Fax: (01) 620 8663
Email: mdiinfo@mdi.ie Web: www.mdi.ie
www.ihca.ie
Professional Directory Voluntary & Support Organisations
My Options - HSE Sexual Health & Crisis Pregnancy Programme
Freephone: 1800 828 010
Web: www2.hse.ie/unplanned-pregnancy/
National Council for the Blind Head Office, Whitworth Road, Drumcondra, Dublin 9.
Tel: (01) 830 7033
InfoLine: 1800 911 250
Email: info@ncbi.ie Web: www.ncbi.ie
National Infertility Support
& Information Group
P.O. Box 131, Togher, Cork, T12 C825.
Tel: (087) 797 5058.
Email: contact@nisig.com Web: nisig.com
Pact – Adoption Agency
Arabella House, 18D Nutgrove Office Park, Rathfarnham, Dublin 14, D14 FC03.
Tel: (01) 296 2200
Email: info@pact.ie Web: www.pact.ie
Parkinson’s Association of Ireland
Carmichael House, North Brunswick Street, Dublin 7.
Tel: (01) 872 2234
Fax: (01) 872 5540
Helpline: 1800 359 359
Email: nationaloffice@parkinsons.ie Web: www.parkinsons.ie
Dublin Rape Crisis Centre
McGonnell House, 70 Lower Leeson Street, Dublin 2, D02 VW13.
Tel: (01) 661 4911
Email: info@rcc.ie
24-Hour Helpline: 1800 77 88 88 Web: www.drcc.ie
Rape Crisis Network Ireland
Carmichael Centre, North Brunswick Street, Dublin 7, D07 RHA8.
Email: admin@rcni.ie Web: www.rcni.ie
Rehab Group
10D Beckett Way, Park West Business Park, Park West, Dublin 12.
Tel: (01) 205 7200
Fax: (01) 205 7211
Email: info@rehab.ie Web: www.rehab.ie
Samaritans Ireland
4-5 Usher’s Court, Usher’s Quay, Dublin 8. Tel: (01) 671 0071
Helpline: 116 123
Email: jo@samaritans.ie Web: www.samaritans.org
Scoliosis Ireland Web: www.facebook.com/ ScoliosisAdvocacyNetwork/ Twitter: @scolionetwork
Shine – Supporting People Affected by Mental Ill Health Block B, Maynooth Business Campus, Straffan Road, Maynooth, Co Kildare, W23 W5X7.
Tel: (01) 541 3715
Email: info@shine.ie Web: www.shine.ie
Spina Bifida Hydrocephalus Ireland
National Resource Centre, Old Nangor Road, Clondalkin, Dublin 22, D22 W5C1. Tel: (01) 457 2329
Email: info@sbhi.ie Web: www.sbhi.ie
St Michael’s House
Ballymun Road, Ballymun, Dublin 9, D09 DX37.
Tel: (01) 884 0200
Email: info@smh.ie Web: www.smh.ie
Women’s Aid
5 Wilton Place, Dublin 2, D02 RR27. Tel: (01) 678 8858
24-Hour Helpline: 1800 341 900
Email: info@womensaid.ie or helpline@womensaid.ie Web: www.womensaid.ie
77
Tables
%
146,396 139,696 147,926
2.9% 35.7% 37.3% 34.5%
% DC 63.2% 62.1% 1.8% 64.3% 62.7% 65.5%
Emergency IP discharges 383,643 381,500 0.6% 362,667 5.2% 36,446 36,346 35,966
Elective IP discharges 74,866 68,042 9.1% 63,735 6.8% 7,273 6,907 6,918
Maternity IP discharges 83,270 92,322 10.9% 89,894 2.7% 8,515 8,784 8,220
Inpatient
110,599 105,504 4.8% 10,778 10,144 10,119
180,442 158,122 14.1% 18,506 17,143 18,921
(33.3%),
(57.8%),
(62.5%)
Nenagh 70.6%.
(72.8%)
(33.3%),
(33.3%),
(66.7%),
(66.7%)
(68.2%)
Croom (50%),
(61.4%), RVEEH (72.7%)
RVEEH (43%),
(47.1%), Ennis (50.3%)
Charts &
(as of December 2021) 78 www.ihca.ie Source: Health Service Performance ProfileOctober - December 2021 Quarterly Report Performance Profile October December 2021 55 Acute Hospital Services Overview of Key Acute Hospital Activity Activity Area Expected Activity YTD % Var YTD Revised Expected Activity YTD Result YTD 2021 Revised % Var YTD Result YTD 2020 SPLY % Var Current ( 2) Current ( 1) Current Emergency Presentations 1,409,846 2.8% 1,449,987 1,278,170 13.4% 139,675 129,073 123,223 New ED Attendances 1,166,404 2.7% 1,168,414 1,198,356 2.6% 1,063,727 12.7% 115,427 104,949 102,955 OPD Attendances 3,165,163 2.5% 3,235,143 3,243,277 0.3% 3,007,047 7.9% 277,824 312,975 228,644 Activity Area (HIPE data month in arrears) Expected Activity YTD Revised Expected Activity YTD Result YTD 2021 Revised % Var YTD Result YTD 2020 SPLY % Var Current ( 2) Current ( 1) Current Inpatient discharges 541,781 541,864 0% 516,296 5% 52,234 52,037 51,104 Inpatient weight units 533,005 533,479 0.1% 50,659 49,424 48,033 Day case (includes dialysis) 931,679 929,734 0.2% 844,974 10% 94,162 87,659 96,822 Day case weight units (includes dialysis) 895,877 810,571 10.5% 91,818 81,236 88,218 IP & DC Discharges 1,473,461 1,471,598 0.1% 1,361,270 8.1%
IP 36.8% 37.9%
discharges >75 years
Day case discharges >75 years
Performance Profile October December 2021 56 Inpatient, Day case and Outpatient Waiting Lists Performance area Target/ Expected Activity Freq Revised Target/ Expected Activity YTD Current Period YTD SPLY YTD SPLY Change Current ( 2) Current ( 1) Current Best performance (in month) Outliers (in month) Inpatient adult waiting list within 15 months 85% M 80% 77.5% 76.9% 0.6% 74.6% 75.7% 77.5% 20 out of 36 hospitals reached target RUH
GUH
SJH
Day case adult waiting list within 15 months 95% M 85% 85.9% 85.4% 0.5% 83.2% 84.5% 85.9% 29 out of 42 hospitals reached target
LUH 70.7%), St John’s
Inpatient children waiting list within 15 months 95% M 85% 75.1% 79.6% 4.5% 71.9% 73.8% 75.1% 10 out of 18 hospitals reached target LUH
Croom
CUH
Mercy
UHL
Day case children waiting list within 15 months 90% M 85% 82.3% 81.4% 0.9% 77.7% 79.7% 82.3% 19 out of 26 hospitals reached target
LUH
Outpatient waiting list within 52 weeks 75% M 65% 62.9% 57.8% +5.1% 61.4% 62.0% 62.9% 22 out of 42 hospitals reached target
UHL
Inpatient & Day Case Waiting List Inpatient & Day Case Waiting Outpatient Waiting List Outpatient Waiting List Total Waiting List Numbers Total Total SPLY SPLY Change >12 Mths >15 Mths Adult IP 17,383 17,614 231 4,863 3,911 Adult DC 50,136 47,713 2,423 9,832 7,087 Adult IPDC 67,519 65,327 2,192 14,695 10,998 Child IP 3,670 3,429 241 1,191 915 Child DC 4,274 4,087 187 1,012 758 Child IPDC 7,944 7,516 428 2,203 1,673 OPD 617,448 612,576 4,872 229,254 185,285 12,432 12,671 8,691 10,369 0 10,000 20,000 Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec 15m+ 18m+ 72,475 75,463 60,000 70,000 80,000 90,000 Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total 200,263 185,285 157,162 153,372 0 50,000 100,000 150,000 200,000 250,000 Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec 15m+ 18m+ 606,230 617,448 550,000 600,000 650,000 700,000 Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
Charts & Tables (as of December
Performance
Michaels (83.9%),
(71.3%), Navan (53.3%)
Tallaght Adults (33.6%),
(19.3%), Naas (20.4%),
(37%), Beaumont (40.4%)
(23.3%)
Naas (85.9%), Mercy, Tallaght Adults (89.1%)
Tallaght Adults (19.3%), Naas (20.4%), UHK (23.3%)
Naas (85.9%), Mercy, Tallaght Adults (89.1%)
Naas (67.6%), Mercy (68.9%), Tallaght Adults (75.3%)
(67.6%),
(68.9%),
(75.3%)
2021) 79www.ihca.ie Source: Health Service Performance ProfileOctober - December 2021 Quarterly Report Performance Profile October December 2021 57 ED
Performance area Target/ Expected Activity Freq Current Period YTD SPLY YTD SPLY Change Current ( 2) Current ( 1) Current Best performance (in month) Outliers (in month) % within 6 hours 70% M 62.8% 69.3% 6.5% 60.2% 60.3% 60% 5 out of 28 hospitals achieved target
Naas
75 years or older within 6 hours 95% M 42.7% 50.5% 7.8% 38.3% 38.5% 38.6% St
SLK
% in ED within 24 hours 97% M 97.4% 98% 0.6% 96.4% 96.6% 96.7% 16 out of 28 hospitals achieved target
% 75 years within 24 hours 99% M 94.1% 95.3% 1.2% 91.3% 91.5% 91.9% 6 out of 27 hospitals achieved target Naas
Mercy
Tallaght Adults
% patients admitted or discharged within 6 hours % 75 years within 6 hours ED over 24 hours % in ED within 24 hours % 75 years within 24 hours 66.5% 60% 70% 50% 60% 70% 80% Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month 20/21 46.8% 38.6% 95% 30% 50% 70% 90% Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month 20/21 557 1,228 1,851 3,563 00 5,000 Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Patients 75+ >24 hrs All patients > 24 hrs 98.1% 96.7% 97% 80% 90% 100% Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month 20/21 96.1% 91.9% 99% 80% 90% 100% Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month 20/21 Performance Profile October December 2021 57 ED Performance Performance area Target/ Expected Activity Freq Current Period YTD SPLY YTD SPLY Change Current ( 2) Current ( 1) Current Best performance (in month) Outliers (in month) % within 6 hours 70% M 62.8% 69.3% 6.5% 60.2% 60.3% 60% 5 out of 28 hospitals achieved target Tallaght Adults (33.6%), Naas (37%), Beaumont (40.4%) 75 years or older within 6 hours 95% M 42.7% 50.5% 7.8% 38.3% 38.5% 38.6% St Michaels (83.9%), SLK (71.3%), Navan (53.3%) Tallaght Adults
UHK
% in ED within 24 hours 97% M 97.4% 98% 0.6% 96.4% 96.6% 96.7% 16 out of 28 hospitals achieved target
% 75 years within 24 hours 99% M 94.1% 95.3% 1.2% 91.3% 91.5% 91.9% 6 out of 27 hospitals achieved target
% patients admitted or discharged within 6 hours % 75 years within 6 hours ED over 24 hours % in ED within 24 hours % 75 years within 24 hours 66.5% 60% 70% 50% 60% 70% 80% Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month 20/21 46.8% 38.6% 95% 30% 50% 70% 90% Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month 20/21 557 1,228 1,851 3,563 00 5,000 Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Patients 75+ >24 hrs All patients > 24 hrs 98.1% 96.7% 97% 80% 90% 100% Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month 20/21 96.1% 91.9% 99% 80% 90% 100% Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month 20/21 Performance Profile October December 2021 58 Colonoscopy / Gastrointestinal Service Performance area Target/ Expected Activity Freq Revised Target/ Expected Activity Current Period YTD SPLY YTD SPLY Change Current ( 2) Current ( 1) Current Best performance (in month) Outliers (in month) Urgent Colonoscopy no. of new people waiting > 4 weeks 0 M 3,933 6,475 2,542 513 323 385 25 out of 38 hospitals achieved target LUH (250), MUH (64), UHL (26) Bowelscreen no. colonoscopies scheduled > 20 working days M 262 212 +50 35 44 38 6 out of 14 hospitals achieved target Wexford (17), RGH (8), Ennis (4) Colonoscopy and OGD <13 weeks 65% M 50% 48.3% 39.2% +9.1% 43.1% 46.2% 48.3% 20 out of 37 hospitals achieved target MMUH (20.3%), MUH (20.6%), Nenagh (21.9%) Urgent Colonoscopy no. of new people waiting Total No. on waiting list for Colonoscopy and OGD BowelScreen Urgent Colonoscopies No. on waiting list for Colonoscopy and OGD 365 385 0 0 300 600 900 Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month 20/21 32,539 27,145 0 20,000 40,000 Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total 12,478 13,112 20,061 14,033 8,000 11,000 14,000 17,000 20,000 23,000 26,000 Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec <13 weeks > 13 week breaches Current ( 2) Current ( 1) Current Number deemed suitable for colonoscopy 198 203 262 Number scheduled over 20 working days 35 44 38
HCAI Performance
Rate
Rate
Services Update
Staph.
commentary of hospital performance for Year to date a comparison with equivalent reporting periods
Delayed Transfers of Care
factors to note when considering the analysis of
activity in Quarter 1. As a result of the surge, elective ensure that our hospitals had adequate capacity time dependent care. We also saw a significant As a result, comparisons with Quarter 1 2020 /
significant and sustained effect on the HSE in terms treat patients in all settings. With specific reference particular challenges on reporting activity. Accordingly, as meaningful analysis of activity and trends is
Attendances
Delayed Transfers of Care (DTOC)
Department attendances: The total number of ED was up 146,553 (13%) compared with 2020 but For the month of December, the total number of higher than 2020 (14,405) but 5 % lower than 2019. Presentations. The number of emergency presentations increased by 16% compared with the same period than 4.5% (5745) compared with 2019 the full year 2021 have increased by 13.4% 2020 but are lower than 2019 by 3.7% contributing to the increase in ED attendances participation in vaccination programmes,
There was 453 Delayed Transfers of Care at the end of December 2021 which is an increase of 24.8% on the same month last year (363); but a decrease of (16.9%) from the number of DTOCs in December 2019 (545).
The 453 reported in December 2021 included 92 patients waiting to go home and 196 waiting on long term residential care. The DTOC categories are listed in Table 1 opposite:
Charts & Tables (as of December
Bantry
(5.4),
(3.4)
RUH (7.1),
(7.0), Nenagh (7.0)
hospital didn't achieve the target.3 hospitals didn’t submit data.
Requirements for screening with CPE Guidelines
o Gradual return of patients to EDs as lockdown measures are eased and vaccination levels increase. Similar trends have been observed in other jurisdictions during the Pandemic.
• Patient Experience Time: 96.7% of all patients attending ED were seen within 24 hours in Decem ber 2021 which is marginally below the NSP target of 97%. This compares with 98.1% in Decem ber 2020 and is an improvement on 95.8% in Decem ber 2019.
• ED Patient Experience Time less than 24 hours for patients aged 75+ was 91.9% in Decem ber 2021, this is below the NSP target of 99.0%. This compares with 96.1% in Decem ber 2020 and is an improvement on Decem ber 2019 which was at 88.8%.
Delayed Transfers of Care (DTOC)
• There was 453 Delayed Transfers of Care at the end of Decem ber 2021 which is an increase of 24.8% on the same month last year (363); but a decrease of (16.9%) from the number of DTOCs in Decem ber 2019 (545).
• The 453 reported in Decem ber 2021 included 92 patients waiting to go home and 196 waiting on long term residential care. The DTOC categories are listed in Table 1 below:
1
Transfer of Care Categories:
Care
80 www.ihca.ie
2021) Source: Health Service Performance ProfileOctober - December 2021 Quarterly Report Performance Profile October December 2021 59
Performance area Target/ Expected Activity Freq Current Period YTD SPLY YTD SPLY Change Current ( 2) Current ( 1) Current Best performance (in month) Outliers (in month)
of new cases of Staph. Aureus infection <0.8 M 0.8 0.9 0.1 0.9 1.0 0.8 35 out of 47 hospitals achieved target
(6.9), St. Michael's
TUH
Rate of new cases of C Difficile infection <2 M 2.3 2.2 +0.1 1.9 2.3 2.3 30 out of 47 hospitals achieved target
Naas
% of hospitals implementing the requirements for screening with CPE Guidelines 100% Q 91.7% 83% +8.7% 87.5% 93.8% 91.7% 44 out of 48 hospitals achieved target 1
of
Aureus bloodstream infections Rate of new cases of C Difficile associated diarrhoea
Performance area Target/ Expected Activity Freq Revised Target/ Expected Activity Current Period YTD SPLY YTD SPLY Change Current ( 2) Current ( 1) Current Best performance (in month) Outliers (in month) Number of beds subject to delayed transfers of care ≤480 M ≤371 453 363 +90 476 499 453 3 hospitals have (0), 3 hospital has (1) Tallaght Adults (51), OLOL (49), SJH (49), SVUH (32) Delayed Transfers of Care7 Delayed Transfers of Care by Category Over 65 Under 65 Total Total % Home 78 14 92 20.3% Residential Care 169 27 196 43.3% Rehab 21 19 40 8.8% Complex Needs 28 12 40 8.8% Over 65 Under 65 Total Total % Housing/Homeless 9 18 27 6.0% Legal complexity 26 10 36 7.9% Non compliance 14 1 15 3.3% COVID 19 7 0 7 1.5% Total 352 101 453 100% 7 DTOC data not available for May July due to cyber attack 1.0 1.1 <0.9 0.8 <0.8 0.5 1.0 1.5 Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month 19/20 Month 20/21 2.6 2.1 2.3 <21.7 2.0 2.3 2.6 2.9 3.2 Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month 19/20 Month 20/21 53.2% 83% 91.7% 100% 0% 50% 100% Q1 Q2 Q3 Q4 2020 2021 545 363 453 ≤480 ≤371 200 300 400 500 600 700 Dec Jan Feb Mar Apr Aug Sep Oct Nov Dec Month 19/20 Month 20/21 Revised Target '21 2021 64
Table
Delayed
End December 2021 Home 92 Residential
196 Rehab 40 Complex Needs 40 Housing/Homeless 27 Legal complexity 36 Non compliance 15 COVID 19 7 Total 453
Surgery and Medical Performance
Surgery and Medical Performance
Emergency
Performance area
admissions
30 days of discharge
Activity
Charts & Tables (as of December 2021)
Outliers
(17.8%),
Emergency re admissions within 30 days of discharge
Procedure conducted on day of admission (DOSA)
Laparoscopic Cholecystectomy day case rate
≤11.1% M 1M 11.4% 11.7% 0.3% 10.3% 10.3% 10.4% 22 out of 34 hospitals achieved target
hospitals achieved target
Procedure conducted on day of admission (DOSA) 82.4% M 1M 75.4% 73.8% +1.6% 79.4% 75.8% 79.3% 17 out of 32 hospitals achieved target
(0%), TUH (20%),
Ennis (17.8%), Wexford (15.4%), TUH (15%)
(28.1%)
25 hospitals achieved target 5 Hospitals (0%)
Navan (0%), TUH (20%), Croom (28.1%)
Laparoscopic Cholecystectomy day case rate 60% M 1M 43.8% 43.6% +0.2% 45.8% 43.4% 51.2% 12 out of 25 hospitals achieved target 5 Hospitals (0%)
Surgical re admissions within 30 days of discharge
out of 38 hospitals achieved target Croom (0.9%), SIVUH (0.7%), Portlaoise (4.9%)
Surgical re admissions within 30 days of discharge ≤2% M 1M 1.9% 2.1% 0.2% 1.6% 1.6% 1.5% 29 out of 38 hospitals achieved target
Hip fracture surgery within 48 hours of initial assessment
Emergency re admissions within 30 days
Emergency re admissions within 30 days
Procedure conducted on day of admissions
Procedure conducted on
2 out of 16 hospitals achieved target CUH (57.9%), Connolly (58.1%), UHW (60.6%)
Croom (0.9%), SIVUH (0.7%), Portlaoise (4.9%)
Hip fracture surgery within 48 hours of initial assessment 85% Q 1Q 75.9% 75% +0.9% 81.1% 74.8% 71.2% 2 out of 16 hospitals achieved target CUH (57.9%), Connolly (58.1%), UHW (60.6%)
Laparoscopic Cholecystectomy
Laparoscopic
Surgical
Hip fracture surgery within 48 hours
Hip fracture surgery within 48 hours
Beaumont,
(96.7%) CUH (14.5%), SVUH (22.4%), MMUH (24.7%)
(100%), UHW (97.5%),
(100%) UHW (1.3%), GUH (11.3%), LUH (14.3%)
6 hospitals reached target UHL (62.3%), CUH (65.5%)
MMUH, Beaumont, UHW (100%), SVUH (97.1%) CUH (13%), GUH (73.4%), SJH (78.6%),
UHL (100%) SLRON (71.7%), GUH (77%), UHW (86.8%)
81www.ihca.ie Source: Health Service Performance ProfileOctober - December 2021 Quarterly Report Performance Profile October December 2021 60
Target/ Expected
Freq Current Period YTD SPLY YTD SPLY Change Current ( 2) Current ( 1) Current Best performance (in month)
(in month)
Cholecystectomy day case rate
day of admissions
re admissions within 30 days
9.9% 10.6% 10.4% ≤11.1% 0% 5% 10% 15% 20% Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Month 19/20 Month 20/21 41.2% 40.4% 51.2% 60% 0% 10% 20% 30% 40% 50% 60% Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Month 19/20 Month 20/21 78.4% 77.% 79.3% 82% 55% 65% 75% 85% Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Month 19/20 Month 20/21 1.7% 1.8% 1.5% ≤2% 0% 1% 2% 3% 4% Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Month 19/20 Month 20/21 76.8% 72.7% 71.2% 85% 50% 60% 70% 80% 90% Q1 Q2 Q3 Q4 2020 2021 Performance Profile October December 2021 60
Performance area Target/ Expected Activity Freq Current Period YTD SPLY YTD SPLY Change Current ( 2) Current ( 1) Current Best performance (in month) Outliers (in month)
re
within
≤11.1% M 1M 11.4% 11.7% 0.3% 10.3% 10.3% 10.4% 22 out of 34 hospitals achieved target Ennis
Wexford (15.4%), TUH (15%)
82.4% M 1M 75.4% 73.8% +1.6% 79.4% 75.8% 79.3% 17 out of 32
Navan
Croom
60% M 1M 43.8% 43.6% +0.2% 45.8% 43.4% 51.2% 12 out of
≤2% M 1M 1.9% 2.1% 0.2% 1.6% 1.6% 1.5% 29
85% Q 1Q 75.9% 75% +0.9% 81.1% 74.8% 71.2%
day case rate
Surgical re admissions within 30 days
9.9% 10.6% 10.4% ≤11.1% 0% 5% 10% 15% 20% Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Month 19/20 Month 20/21 41.2% 40.4% 51.2% 60% 0% 20% 30% 40% 50% 60% Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Month 19/20 Month 20/21 78.4% 77.% 79.3% 82% 55% 65% 75% 85% Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Month 19/20 Month 20/21 1.7% 1.8% 1.5% ≤2% 0% 1% 2% 3% 4% Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Month 19/20 Month 20/21 76.8% 72.7% 71.2% 85% 50% 60% 70% 80% 90% Q1 Q2 Q3 Q4 2020 2021 Performance Profile October December 2021 61 Cancer Services Performance area Target/ Expected Activity Freq Current Period YTD SPLY YTD SPLY Change Current ( 2) Current ( 1) Current Best performance (in month) Outliers (in month) % of new patients attending Rapid Access Breast, Lung and Prostate Clinics within recommended timeframe 95% M 60.8% 70.3% 9.5% 57.9% 57.2% 65.7% LUH (100%),Beaumont (99.6%), UHW (98.4%) CUH (20.1%), GUH (41.1%), SVUH (41.9%) Urgent breast cancer within 2 weeks 95% M 55.8% 70.4% 14.6% 52% 49.9% 58.9%
LUH
UHL
Non urgent breast within 12 weeks 95% M 41.4% 57% 15.6% 39.9% 45.6% 47.8% Beaumont, MMUH
Lung Cancer within 10 working days 95% M 89.6% 86.4% +3.2% 87.8% 90.5% 87%
Prostate cancer within 20 working days 90% M 66.4% 52% +14.4% 68.6% 70% 82.1%
Radiotherapy within 15 working days 90% M 75.4% 82.2% 6.8% 76.6% 75.4% 77.3%
Rapid Access within recommended timeframe Lung Cancer within 10 working days Breast Cancer within 2 weeks Prostate Cancer within 20 working days Non urgent breast within 12 weeks Radiotherapy within 15 working days 68.2% 69% 65.7% 95% 30% 80% Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month 19/20 Month 20/21 87.2% 92%87% 95% 65% 85% Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month 19/20 Month 20/21 67% 67.3% 58.9% 95% 0% 50% 100% Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month 19/20 Month 20/21 54.7% 48% 82.1% 90% 30% 45% 60% 75% 90% Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month 19/20 Month 20/21 75.0% 60.7% 47.8% 95% 0% 50% 100% Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month 19/20 Month 20/21 74.9% 77.7% 77.3% 90% 50% 70% 90% Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month 19/20 Month 20/21
Ambulance Turnaround
Charts & Tables (as of December
Pre Hospital Emergency Care Services
Dublin Fire Brigade (77.5%), North Leinster (74.2%), South (65.5%), West (71.4%)
Dublin Fire Brigade (24.0%), North Leinster (43.0%), South (34.9%, West (43.1%)
2021) 82 www.ihca.ie Source: Health Service Performance ProfileOctober - December 2021 Quarterly Report Performance Profile October December 2021 62
Performance area Target/ Expected Activity Freq Current Period YTD SPLY YTD SPLY Change Current ( 2) Current ( 1) Current Best performance (in month) Outliers (in month) % of ambulances that have a time interval ≤ 30 minutes 80% M 27.5% 36.4% 8.9% 23.6% 24.2% 23.4% Rotunda (77,8%), CHI (67.9%), NMH (59.4%) CUH (5%), Mercy (6.2%), SUH (6.5%) Ambulance Turnaround % delays escalated within 30 minutes 85% M 72.7% 82.2% 9.5% 66.4% 69.2% 62.1% Ambulance Turnaround % delays escalated within 60 minutes 98% M 95.9% 97.2% 1.3% 95.2% 95.4% 94.9% Ambulance Turnaround within 30 minutes Delays Escalated within 30 minutes Delays Escalated within 60 minutes 34.0% 31.6% 23.4% 80% 0% 20% 40% 60% 80% 100% Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month 19/20 Month 20/21 58.1% 80.9% 62.1% 85% 45% 55% 65% 75% 85% 95% Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month19/20 Month 20/21 96.2% 96.8% 94.9% 98% 90% 92% 94% 96% 98% 100% Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month19/20 Month 20/21 Performance Profile October December 2021 63
Performance area Target/ Expected Activity Freq Current Period YTD SPLY YTD SPLY Change Current ( 2) Current ( 1) Current Best performance (in month) Outliers (in month) Response Times ECHO 80% M 74.6% 79.5% 4.9% 71.0% 70.6% 72.3%
Response Times DELTA 70% M 44.0% 54.0% 10.0% 40.5% 39.5% 37.1%
Return of spontaneous circulation (ROSC) 40% Q 1Q 38.4% 42.4% 4.0% 36.6% 39.3% 39.0% Response Times ECHO Return of spontaneous circulation (ROSC) Response Times DELTA Call Volumes (arrived at scene) 75.9% 76.3%72.3% 80% 45% 55% 65% 75% 85% 95% Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month19/20 Month 20/21 45.0% 40.5% 39.0% 40% 35% 45% 55% Q3 Q4 Q1 Q2 Q3 Q 19/20 Q 20/21 48.9% 47.4% 37.1% 70% 20% 40% 60% 80% 100% Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month19/20 Month 20/21 Target/ Expected Activity Current Period YTD % Var YTD SPLY YTD SPLY change ECHO 4,940 5,857 18.6% 5,088 769 DELTA 125,000 126,828 1.5% 110,050 16778
Mental Health Services
Charts & Tables (as of
CAMHs
CAMHs
CHO1,
CHO2 (33), CHO7 (99), CHO5 (294)
CHO3 (90%) CHO4 (90%)
CHO4 (702), CHO8 (599), CHO6 (510)
CHO2 (0), CHO7 (0) CHO4 (105), CHO3 (91), CHO8 (28)
(47.8%), CHO5 (84.2%)
Source: Health Service Performance ProfileOctober - December 2021 Quarterly Report
December 2021) 83www.ihca.ie Performance Profile October December 2021 30
Child and Adolescent Community Mental Health Teams Performance Area Target/ Expected Activity Freq Current Period YTD SPLY YTD SPLY Change Current ( 2) Current ( 1) Current Best Performance (in month) Outliers (in month) Admission of Children to CAMHs 85% M 92.5% 100% CAMHs Bed Days Used 95% M 99.6% 98.8% +0.8% 99.5% 99.9% 100% All CHO’s reached target
first appointment within 12 months 95% M 95.9% 95.7% +0.2% 98.2% 97.6% 96.7%
2, 5, 6, 7 & 8 reached target
waiting list 2,308 M 2,973 2,755 +218 3,073 3,357 2,973
CAMHs waiting list > 12 months 0 M 249 266 17 202 221 249
No of referrals received 14,895 YTD 14,895 FYT M 22,613 17,436 +5,177 2,050 2,378 1,272 Number of new seen 9,338 YTD 9,338 FYT M 12,376 10,456 +1,920 1,075 1,166 657 % of urgent referrals to CAMHs Teams responded to within three working days >90% M 93.7% 89.1% +4.6% 93% 90.9% 90.9% CHO1, 2, 3, 6, 7 & 8 reached target CHO4
% offered an appointment and seen within 12 weeks % of urgent referrals responded to within 3 working days Waiting list > 12 months 83.4% 82.8% 72.8% 72% 55% 65% 75% 85% Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month 19/20 Month 20/21 86.5% 97.6% 90.9% 90% 60% 64% 68% 72% 76% 80% 84% 88% 92% 96% 100% Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month 19/20 Month 20/21 212 266 249 0 50 100 150 200 250 300 350 400 Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month 19/20 Month 20/21 Performance Profile October December 2021 31 General Adult Mental Health Performance Area Target/ Expected Activity Freq Current Period YTD SPLY YTD SPLY Change Current ( 2) Current ( 1) Current Best Performance (in month) Outliers (in month) Number of referrals received 36,962 YTD 36,962 FYT M 41,886 39,537 +2,349 3,536 3,745 2,771 Number of referrals seen 23,042 YTD 23,042 FYT M 25,202 23,883 +1,319 1,983 2,319 1,635 % seen within 12 weeks 75% M 74.8% 75.1% 0.3% 71.1% 71.5% 72.2% CHO1, 2, 5 & 6 reached target CHO9 (59.2%), CHO8 (59.2%), CHO4 (70.3%) Psychiatry of Later Life Performance Area Target/ Expected Activity Freq Current Period YTD SPLY YTD SPLY Change Current ( 2) Current ( 1) Current Best Performance (in month) Outliers (in month) Number of referrals received 10,340 YTD 10,340 FYT M 11,037 11,406 369 906 954 718 Number of referrals seen 7,388 YTD 7,388 FYT M 7,623 7,643 20 613 663 516 % seen within 12 weeks 95% M 93.4% 95% 1.6% 90.4% 92.3% 93.2% CHO1, 2, 3, & 5 reached target CHO8 (83.3%), CHO9 (84%), CHO4 (85%) Adult Mental Health % offered an appointment and seen within 12 weeks Psychiatry of Later Life % offered an appointment and seen within 12 weeks 72.3% 75% 72.2% 75% 69% 73% 77% Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month 19/20 Month 20/21 93.3% 93.8% 93.2% 95% 90% 93% 96% 99% Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month 19/20 Month 20/21
Charts & Tables (as of December 2021)
Health Sector Workforce
Health Sector Workforce: December 2021
Headlines
Health Sector Workforce
Health Sector Workforce: December 2021 Headlines
Employment levels at the end of December 2021, show there were 132,323 WTE (equating to 150,903 personnel) directly employed in the provision of Health & Social Care Services by the HSE and the various Section 38 hospitals & agencies.
Employment levels at the end of December 2021, show there were 132,323 WTE (equating to 150,903 personnel) directly employed in the provision of Health & Social Care Services by the HSE and the various Section 38 hospitals & agencies.
• The change is +1,059 WTE this month and +6,149 WTE year-to-date. The employment increase this month shows significantly strong growth in comparison to recent years (the five-year average is +570 WTE).
• The change is +1,059 WTE this month and +6,149 WTE year to date. The employment increase this month shows significantly strong growth in comparison to recent years (the five year average is +570 WTE).
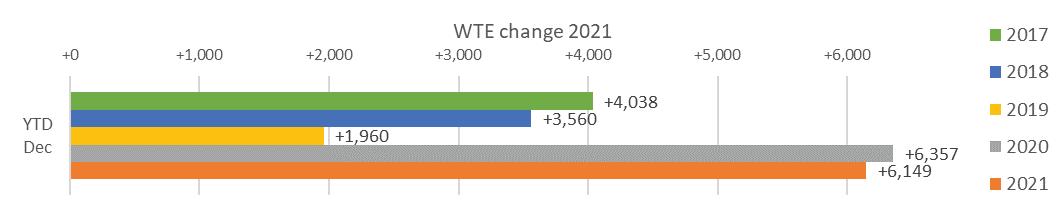
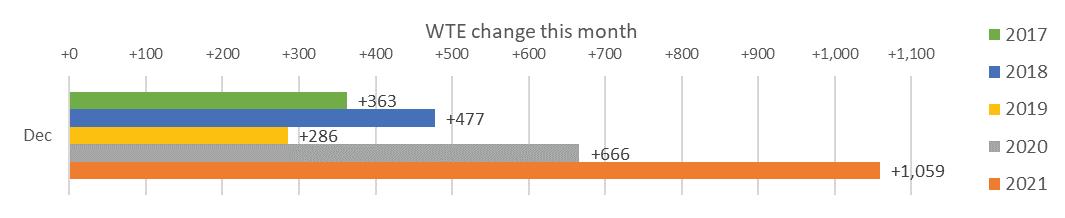
Key findings by Staff Category & Staff Group
• The largest increase was in Management & Administrative (+311 WTE) including +143 WTE Clerical (III & IV), +133 WTE Administrative/Supervisory (V to VII) and +35 WTE Management (VIII & above)
Nurses and Midwives also reporting the greatest WTE increase at +2,157 WTE followed by Health Care Assistants at +1,930 WTE. All staff categories over the period have shown significant growth within each category ranging from 13% 14% in H&SCPs and Management and Adminisration to 8% 10% across Nursing and Midwifery, Medical and Dental and Patient and Client Care. The lowest percentage growth was seen in General Support at +6.3%.
• Acute Services shows the largest WTE increase since December 2019 at +7,592 WTE with Community Operations up by +4,282 WTE followed by H&WB Corporate and National up by +632 WTE.
• Patient & Client Care showed the second highest growth with a +223 WTE increase. Health Care Assistants +163 WTE, Home Help +37 WTE, Care Other + 22 WTE and Ambulance Staff +1 WTE.
Key findings by Staff Category & Staff Group
• The largest increase was in Management & Administrative (+311 WTE) including +143 WTE Clerical (III & IV), +133 WTE Administrative/Supervisory (V to VII) and +35 WTE Management (VIII & above)
• Nursing & Midwifery also increased by +274 WTE overall; including +327 WTE Staff Nurse/Staff Midwife (driven by the registration of new graduates), + 44 WTE Nurse/Midwife Manager, +31 WTE Nurse/Midwife Specialists & AN/MP and +4 WTE Nursing/ Midwifery other.
• Patient & Client Care showed the second highest growth with a +223 WTE increase. Health Care Assistants +163 WTE, Home Help +37 WTE, Care Other +22 WTE and Ambulance Staff +1 WTE.
• Health & Social Care Professionals increased by +172 WTE overall. There was a +57 WTE increase in Therapy Professions, +50 WTE H&SC other, +19 WTE in Pharmacy, +18 WTE Social Care, +10 WTE Health Science/Diagnostics, +10 WTE Social Workers and +7 WTE Psychologists .
• Nursing & Midwifery also increased by +274 WTE overall; including +327 WTE Staff Nurse/Staff Midwife (driven by the registration of new graduates), +44 WTE Nurse/Midwife Manager, +31 WTE Nurse/Midwife Specialists & AN/MP and +4 WTE Nursing/ Midwifery other.
• Health & Social Care Professionals increased by +172 WTE overall. There was a +57 WTE increase in Therapy Professions, +50 WTE H&SC other, +19 WTE in Pharmacy, +18 WTE Social Care, +10 WTE Health Science/ Diagnostics, +10 WTE Social Workers and +7 WTE Psychologists .
• General Support increased by +42 WTE; distributed as follows, +40 WTE Support (portering & catering) and +1 WTE Maintenance/Technical.
• General Support increased by +42 WTE; distributed as follows, +40 WTE Support (portering & catering) and +1 WTE Maintenance/Technical.
• The latest employment figure represents a 10.4% (+12,506 WTE) increase over December 2019. This figure however, excludes non direct HSE employees such as externally contracted Contact Management Programme contact tracers and vaccination staff that add an additional minimum +2,200 staff.
• Overall since December 2019, the staff category with the greatest WTE increase is Nursing and Midwifery at +3,372 WTE, with the grade group
• The latest employment figure represents a 10.4% (+12,506 WTE) increase over December 2019. This figure however, excludes non-direct HSE employees such as externally contracted Contact Management Programme contact tracers and vaccination staff that add an additional minimum +2,200 staff.
• Overall since December 2019, the staff category with the greatest WTE increase is Nursing and Midwifery at +3,372 WTE, with the grade group Nurses and Midwives also reporting the greatest WTE increase at +2,157 WTE followed by Health Care Assistants at +1,930 WTE. All staff categories over the period have shown significant growth within each category ranging from 13%-14% in H&SCPs and Management and Adminisration to 8%-10% across Nursing and Midwifery, Medical and Dental and Patient and Client Care. The lowest percentage growth was seen in General Support at +6.3%.
• Acute Services shows the largest WTE increase since December 2019 at +7,592 WTE with Community Operations up by +4,282 WTE followed by H&WB Corporate and National up by +632 WTE.
• Medical & Dental increased by +37 WTE; distributed as follows, +18 WTE Consultants, +12 WTE Medical/Dental, other, +6 WTE Registrars and SHO/Intern WTE remained the same from the previous month.
• Further details are shown in the charts & tables below:
• Medical & Dental increased by +37 WTE; distributed as follows, +18 WTE Consultants, +12 WTE Medical/Dental, other, +6 WTE Registrars and SHO/Intern WTE remained the same from the previous month.
• Further details are shown in the charts & tables below:
Performance Profile October December 2021 98
Source: Health Service Performance ProfileOctober - December 2021 Quarterly Report
84 www.ihca.ie
Charts & Tables (as of December 2021)
Ambulance Services
Acute Hospital Services
Acute Services
Community Health & Wellbeing
+507 +3,620 +5.6% +7,465 +12.3%
+510 +3,690 +5.6% +7,592 +12.1%
+11 +37 +25.9% +181
Mental Health 9,954 10,301 10,289 10,362 +73 +61 +0.6% +408 +4.1%
Primary Care 10,599 11,572 12,395 12,582 +187 +1,009 +8.7% +1,982 +18.7%
Disabilities 18,303 18,944 19,507 19,623 +116 +678 +3.6% +1,320 +7.2%

Older People 13,233 13,415 13,538 13,623 +84 +208 +1.6% +390 +3.0%
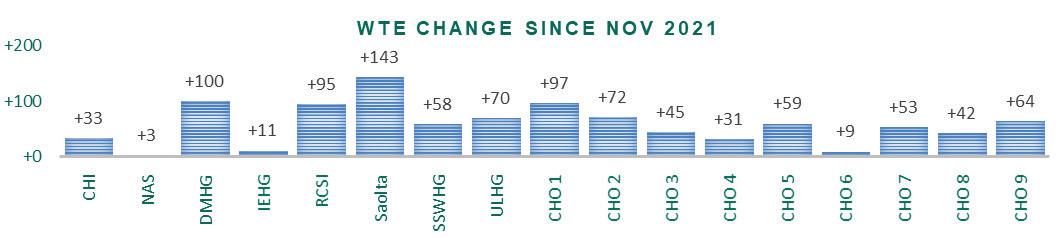
Services
+471 +1,993 +3.7% +4,282 +8.2%
+11 +129 +25.2% +67 +11.7%
+51 +601 +18.7% +782 +25.8%
This
85www.ihca.ie Source: Health Service Performance ProfileOctober - Decemberr 2021 Quarterly Report Performance Profile October December 2021 103 2019 2020 2021 2021 since Nov 2021 since Dec 2020 2020 since Dec 2019 2019 CHO 6 3,378 3,465 3,552 3,561 +9 +96 +2.8% +183 +5.4% CHO 7 6,515 6,783 7,020 7,073 +53 +290 +4.3% +559 +8.6% CHO 8 6,135 6,337 6,407 6,449 +42 +112 +1.8% +314 +5.1% CHO 9 6,582 6,950 7,101 7,165 +64 +216 +3.1% +583 +8.9% other Community Services 638 709 741 740 +0 +31 +4.4% +102 +16.0% Community Services 52,089 54,377 55,899 56,370 +471 +1,993 +3.7% +4,282 +8.2% Health & Wellbeing 574 511 629 641 +11 +129 +25.2% +67 +11.7% Corporate 3,035 3,216 3,765 3,816 +51 +601 +18.7% +782 +25.8% Health Business Services 1,583 1,631 1,351 1,367 +15 265 16.2% 216 13.7% H&WB Corporate & National Services 5,191 5,358 5,746 5,824 +77 +465 +8.7% +632 +12.2% By Division/ Care Group: December 2021 Division/ Care Group WTE Dec 2019 WTE Dec 2020 WTE Nov 2021 WTE Dec 2021 WTE chance since Nov 2021 WTE chance since Dec 2020 % chance since Dec 2020 WTE chance since Dec 2019 % chance since Dec 2019 Total Health Service 119,817 126,174 131,265 132,323 +1,059 +6,149 +4.9% +12,506 +10.4%
1,933 1,990 2,057 2,060 +3 +70 +3.5% +127 +6.6%
60,604 64,449 67,562 68,069
62,537 66,439 69,620 70,129
144 170 181
Community
52,089 54,377 55,899 56,370
Health & Well being 574 511 629 641
Corporate Functions 3,035 3,216 3,765 3,816
104 Division/ Care Group WTE Dec 2019 WTE Dec 2020 WTE Nov 2021 WTE Dec 2021 WTE chance since Nov 2021 WTE chance since Dec 2020 % chance since Dec 2020 WTE chance since Dec 2019 % chance since Dec 2019 Health Business Service 1,583 1,631 1,351 1,367 +15 265 16.2% 216 13.7% H&WB Corporate & National Services 5,191 5,358 5,746 5,824 +77 +465 +8.7% +632 +12.2% Health Service Absence Rates: December 2021 This report provides the overview of the reported National Health Sector Absence Rates for December 2021 The reported absence rate for December 2021 stands at 7.9%. This compares to 5.9% reported for the same month in 2020, however these figures notably include COVID 19 related absence for both periods. Excluding COVID 19 the current months absence rate is 4.9% compared to 4.25% in 2020.
months’ absence rate is higher than that reported for the previous month, reported at 7.7% (including COVID 19). Notwithstanding the fact that the overall absence referral when someone has Covid 19 symptoms, SLWP will apply in certain circumstances as set out in HR Circular 038/2021. • All agencies with the exception of St John’s Hospital Limerick provided a national absence return for December. Due to a cyber attack, the Coombe Hospital provided a partial return with the following categories missing: Medical & Dental, Nursing & Midwifery and General Support Performance Profile October December 2021 101 • Saolta University Hospital Care (+143 WTE), Dublin Midlands Hospital Group (+100 WTE) and University of Limerick
Hospital
Group (+70 WTE)
show the largest
increases over this period in Acute with CHOs 1 (+97 WTE), 2 (+72 WTE) and 9 (+64 WTE) showing the largest increases in Community. • There were no Hospital Groups or Community Hospital Organisations that showed a WTE decrease this month All care groups also showed increases this month with the greatest increase (+507 WTE) in acute hospital services. However, each community services care group, led by primary care, also showed increases
Charts & Tables (as of December 2021)
Health Service Absence Rates: December 2021
Health Service Absence Rates: December 2021
This report provides the overview of the reported National Health Sector Absence Rates for December 2021
The reported absence rate for December 2021 stands at 7.9%. This compares to 5.9% reported for the same month in 2020, however these figures notably include COVID 19 related absence for both periods. Excluding COVID 19 the current months absence rate is 4.9% compared to 4.25% in 2020.
This months’ absence rate is higher than that reported for the previous month, reported at 7.7% (including COVID 19). Notwithstanding the fact that the overall absence rate continues to be impacted by COVID 19 related absence, excluding COVID 19 absence, this months’ absence rate is 4.9% which is 0.4% lower than the rate reported last month. It is important to note that this month’s data, is occurring at a time of increased COVID 19 case reports.
This report provides the overview of the reported National Health Sector Absence Rates for December 2021. The reported absence rate for December 2021 stands at 7.9%. This compares to 5.9% reported for the same month in 2020, however these figures notably include COVID-19 related absence for both periods. Excluding COVID-19 the current months absence rate is 4.9% compared to 4.25% in 2020. This months’ absence rate is higher than that reported for the previous month, reported at 7.7% (including COVID-19). Notwithstanding the fact that the overall absence rate continues to be impacted by COVID-19 related absence, excluding COVID-19 absence, this months’ absence rate is 4.9% which is 0.4% lower than the rate reported last month. It is important to note that this month’s data, is occurring at a time of increased COVID-19 case reports. These figures are reflected in the attached National Absence Report.
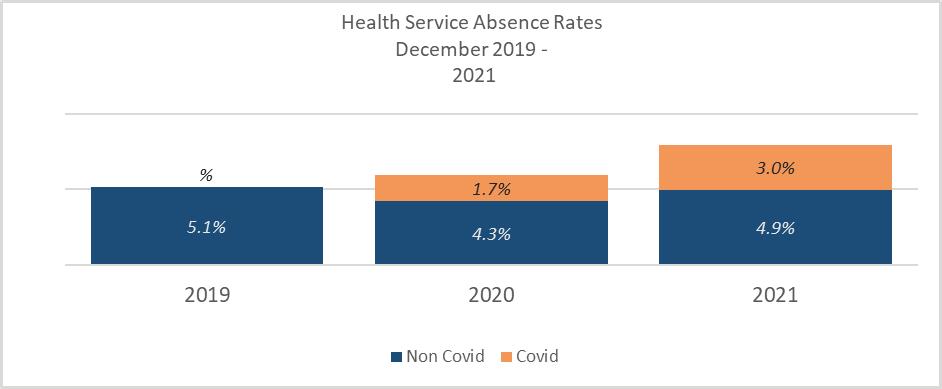
These figures are reflected in the attached National Absence Report.
www.ihca.ie
-
86
Source: Health Service Performance
Profile
October - December 2021 Quarterly Report
104 Division/ Care Group WTE Dec 2019 WTE Dec 2020 WTE Nov 2021 WTE Dec 2021 WTE chance since Nov 2021 WTE chance since Dec 2020 % chance since Dec 2020 WTE chance since Dec 2019 % chance since Dec 2019 Health Business Service 1,583 1,631 1,351 1,367 +15 265 16.2% 216 13.7% H&WB Corporate & National Services 5,191 5,358 5,746 5,824 +77 +465 +8.7% +632 +12.2%
Benchmark Target Nov 21 Certified Absence December 2021 Self Certified Absence December 2021 COVID 19 December 2021 Dec 21 Full Year 2020 Year to date 2021 3.5% 7.7% 4.38% 0.55% 2.98% 7.9% 6.1% 6.1% Note: • COVID 19 will only apply when an employee is advised to self isolate and is displaying symptoms of COVID 19, or had a positive test. Public health advice now allows for self referral when someone has Covid 19 symptoms, SLWP will apply in certain circumstances as set out in HR Circular 038/2021. • All agencies with the exception of St John’s Hospital Limerick provided a national absence return for December. Due to a cyber attack, the Coombe Hospital provided a partial return with the following categories missing: Medical & Dental, Nursing & Midwifery and General Support Performance Profile October December 2021 105 Latest monthly figures (December 2021) December 2021 absence rate stands at 7.9% of which 4.4% is certified, 0.6% Self Certified with 3% (or 37.7% of all absence) relating to COVID 19. • Excluding COVID 19 related absence, the December 2021 absence rate of 4.9% is higher than the same period last year however is lower than 2019. Based on 2019 data, this months’ data is showing a 0.2% decrease i.e. 5.1% (2019), 4.8% (2018) and 4.8% (2017). • For Acute Services the absence rate is 8.1% of which 3.3% (40.3% of the total) is COVID 19 related. Community Services stands at 8.0% of which 2.8% (34.7% of the total) is also COVID 19 related. Health & Wellbeing, Corporate & National Services rate is 4.6% of which 1.3% (28.5% of the total) is COVID 19 related. Details are as follows:
Charts & Tables (as of December 2021)
Latest monthly figures (December 2021)
December 2021 absence rate stands at 7.9% of which 4.4% is certified, 0.6% Self-Certified with 3% (or 37.7% of all absence) relating to COVID-19. • Excluding COVID-19 related absence, the December 2021 absence rate of 4.9% is higher than the same period last year however is lower than 2019. Based on 2019 data, this months’ data is showing a 0.2% decrease i.e. 5.1% (2019), 4.8% (2018) and 4.8% (2017).
• For Acute Services the absence rate is 8.1% of which 3.3% (40.3% of the total) is COVID-19 related. Community Services stands at 8.0% of which 2.8% (34.7% of the total) is also COVID-19 related. Health & Wellbeing, Corporate & National Services rate is 4.6% of which 1.3% (28.5% of the total) is COVID-19 related. Details are as follows:
December 2021
Total
Health
Ambulance Services 6.8% 0.7%
25.2%
2.5% 10.0%
Acute Hospital Services 4.1% 0.6% 4.8% 3.3% 8.1% 59.0% 41.0%
Acute Services 4.2% 0.6% 4.9% 3.3% 8.1% 59.7% 40.3%
Ambulance Services
Community Health & Wellbeing 2.3% 0.1% 2.4% 1.6% 4.0% 60.3% 39.7%
8.1% 59.0% 41.0%
Mental Health 4.3% 0.4% 4.8% 2.9% 7.7% 62.1% 37.9%
Acute Hospital Services
Acute Services 4.2% 0.6%
Primary Care 4.4% 0.3% 4.7% 2.1% 6.8% 68.8% 31.2%
Disabilities 4.6% 0.7% 5.3% 2.8% 8.1% 65.7% 34.3%
Older People 5.6% 0.6% 6.1% 3.4% 9.5% 64.6% 35.4%
Community Services 4.7% 0.5% 5.2% 2.8% 8.0% 65.3% 34.7%
3.3% 8.1% 59.7% 40.3% Community Health & Wellbeing Mental Health Primary Care 0.3%
Disabilities
Health & Wellbeing 3.5% 0.2% 3.7% 1.3% 5.0% 73.9% 26.1%
Corporate 3.3% 0.2% 3.5% 1.4% 4.9% 72.1% 27.9%
Health Business Services 1.7% 0.2% 1.9% 1.1% 3.0% 64.2% 35.8% HWB, Corporate & National 3.1% 0.2% 3.3% 1.3% 4.6% 71.5% 28.5%
Older People Community Services 4.7% 0.5% 5.2% 2.8% 8.0% 65.3% 34.7% Health & Wellbeing 0.2%
Corporate 3.3% 0.2% 3.5% 1.4% 4.9% 72.1% 27.9% Health Business Services 1.7% 0.2% 1.9% 1.1% 3.0% 64.2% 35.8%
• At Staff Category Patient & Client Care reports the highest total absence rate at 9.7% followed by General Support (9.5 %) and Nursing and Midwifery (9.2 %). Notably, these increases are impacted by COVID 19, with 35.2% of all absence related to COVID 19 in General Support, 39% in Nursing and Midwifery and 33.7% in Patient & Client Care. Medical and Dental reported the lowest absence rate at 2.6% in December, however reported the highest COVID 19 related absence, at 51.4%. Details as follows: December 2021
• At Staff Category Patient & Client Care reports the highest total absence rate at 9.7% followed by General Support (9.5 %) and Nursing and Midwifery (9.2 %). Notably, these increases are impacted by COVID-19, with 35.2% of all absence related to COVID-19 in General Support, 39% in Nursing and Midwifery and 33.7% in Patient & Client Care.
HWB, Corporate & National 3.1% 0.2% 3.3% 1.3% 4.6% 71.5% 28.5%
• At Staff Category Patient & Client Care reports the highest total absence rate at 9.7% followed by General Support (9.5 %) and Nursing and Midwifery (9.2 %). Notably, these increases are impacted by COVID 19, with 35.2% of all absence related to COVID 19 in General Support, 39% in Nursing and Midwifery and 33.7% in Patient & Client Care. Medical and Dental reported the lowest absence rate at 2.6% in December, however reported the highest COVID 19 related absence, at 51.4%. Details as
Health Service Absence Rate by Staff Category: Decv 2021 Certified absence
Total
87www.ihca.ie Source: Health Service Performance ProfileOctober - December 2021 Quarterly Report
Performance Profile October December 2021 106 December 2021 Health Service Absence Rate by Care Group: Dec 2021 Certified absence Self certified absence Non Covid 19 absence Covid 19 absence Total absence rate % Non Covid 19 absence % Covid 19 absence
4.4% 0.6% 4.9% 3.0% 7.9% 62.3% 37.7%
7.5%
74.8%
Self certified absence Non Covid 19 absence Covid 19 absence Total absence rate % Non Covid 19 absence % Covid 19 absence
4.4% 0.6% 4.9% 3.0% 7.9% 62.3% 37.7% Medical & Dental 1.1% 0.1% 1.2% 1.3% 2.6% 48.6% 51.4% Nursing & Midwifery 4.8% 0.8% 5.6% 3.6% 9.2% 61.0% 39.0% Health & Social Care Professionals 3.5% 0.3% 3.9% 2.9% 6.8% 56.9% 43.1% Management & Administrative 3.9% 0.3% 4.3% 2.2% 6.5% 65.5% 34.5% General Support 5.7% 0.5% 6.2% 3.4% 9.5% 64.8% 35.2% Patient & Client Care 5.7% 0.7% 6.4% 3.3% 9.7% 66.3% 33.7% Performance Profile October December 2021 106
Service Absence Rate by Care Group: Dec 2021 Certified absence Self certified absence Non Covid 19 absence Covid 19 absence Total absence rate % Non Covid 19 absence % Covid 19 absence Total 4.4% 0.6% 4.9% 3.0% 7.9% 62.3% 37.7%
6.8% 0.7% 7.5% 2.5% 10.0% 74.8% 25.2%
4.1% 0.6% 4.8% 3.3%
4.9%
follows: December 2021 Health Service Absence Rate by Staff Category: Decv 2021 Certified absence Self certified absence Non Covid 19 absence Covid 19 absence Total absence rate % Non Covid 19 absence % Covid 19 absence Total 4.4% 0.6% 4.9% 3.0% 7.9% 62.3% 37.7% Medical & Dental 1.1% 0.1% 1.2% 1.3% 2.6% 48.6% 51.4% Nursing & Midwifery 4.8% 0.8% 5.6% 3.6% 9.2% 61.0% 39.0% Health & Social Care Professionals 3.5% 0.3% 3.9% 2.9% 6.8% 56.9% 43.1% Management & Administrative 3.9% 0.3% 4.3% 2.2% 6.5% 65.5% 34.5% General Support 5.7% 0.5% 6.2% 3.4% 9.5% 64.8% 35.2% Patient & Client Care 5.7% 0.7% 6.4% 3.3% 9.7% 66.3% 33.7%
Charts & Tables
Medical/ Dental, other
Medical & Dental
SHO/ Interns
Medical/ Dental, other
812 804 +21 19 10 8 1,131
Medical & Dental 10,857 11,762 12,113 12,188 12,237 +904 +352 +124 +49 13,185
Nurse/ Midwife Manager 7,984 8,344 8,852 9,007 9,039 +360 +508 +187 +32 9,916 Nurse/ Midwife Specialist & AN/MP 1,996 2,299 2,481 2,569 2,617 +302 +183 +136 +48 2,922
Staff Nurse/ Staff Midwife 25,693 26,763 27,850 27,762 27,841 +1,070 +1,087 9 +78 31,904
Nurse/ Midwife Manager 7,984 8,344 8,852 9,007 9,039 +360 +508 +187 +32 9,916
Public Health Nurse 1,537 1,557 1,523 1,499 1,495 +20 34 28 3 1,782
Nurse/ Midwife Specialist & AN/MP 1,996 2,299 2,481 2,569 2,617 +302 +183 +136 +48 2,922
Nursing/ Midwifery Student 644 592 526 1,176 1,150 52 65 +624 26 1,929
Staff Nurse/ Staff Midwife 25,693 26,763 27,850 27,762 27,841 +1,070 +1,087 9 +78 31,904
Nursing/ Midwifery other 350 362 344 323 324 +12 18 20 +1 371
Public Health Nurse 1,537 1,557 1,523 1,499 1,495 +20 34 28 3 1,782
Nursing & Midwifery 38,205 39,917 41,576 42,336 42,467 +1,712 +1,660 +890 +130 48,824
Nursing/ Midwifery Student 644 592 526 1,176 1,150 52 65 +624 26 1,929
Therapy Professions 5,234 5,565 5,947 6,081 6,109 +331 +382 +162 +28 7,025
Nursing/ Midwifery other 350 362 344 323 324 +12 18 20 +1 371
Health Science/ Diagnostics 4,500 4,731 4,918 4,926 4,927 +230 +188 +9 +1 5,472
Nursing & Midwifery 38,205 39,917 41,576 42,336 42,467 +1,712 +1,660 +890 +130 48,824
Social Care 2,710 2,909 3,127 3,106 3,102 +199 +219 25 4 3,634
Therapy Professions 5,234 5,565 5,947 6,081 6,109 +331 +382 +162 +28 7,025
Social Workers 1,165 1,238 1,296 1,318 1,331 +74 +58 +35 +13 1,490
Health Science/ Diagnostics 4,500 4,731 4,918 4,926 4,927 +230 +188 +9 +1 5,472
Social Care 2,710 2,909 3,127 3,106 3,102 +199 +219 25 4 3,634
Psychologists 1,004 1,066 1,095 1,111 1,109 +62 +29 +14 1 1,255
Social Workers 1,165 1,238 1,296 1,318 1,331 +74 +58 +35 +13 1,490
Pharmacy 1,038 1,164 1,292 1,285 1,294 +126 +128 +3 +9 1,449 H&SC, Other 1,123 1,134 1,324 1,311 1,282 +12 +189 41 29 1,554
Psychologists 1,004 1,066 1,095 1,111 1,109 +62 +29 +14 1 1,255
Pharmacy 1,038 1,164 1,292 1,285 1,294 +126 +128 +3 +9 1,449 H&SC, Other 1,123 1,134 1,324 1,311 1,282 +12 +189 41 29 1,554
Health & Social Care Professionals 16,774 17,807 18,999 19,138 19,156 +1,033 +1,192 +157 +18 21,879 Management (VIII & above) 1,842 1,969 2,216 2,305 2,332 +128 +246 +117 +27 2,401
Health & Social Care Professionals 16,774 17,807 18,999 19,138 19,156 +1,033 +1,192 +157 +18 21,879 Management (VIII & above) 1,842 1,969 2,216 2,305 2,332 +128 +246 +117 +27 2,401 Administrative/ Supervisory (V to VII) 5,199 5,821 6,705 6,951 7,010 +622 +884 +304 +59 7,443 Clerical (III & IV) 11,805 12,038 12,661 12,827 12,833 +233 +623 +171 +6 14,611
Administrative/ Supervisory (V to VII) 5,199 5,821 6,705 6,951 7,010 +622 +884 +304 +59 7,443 Clerical (III & IV) 11,805 12,038 12,661 12,827 12,833 +233 +623 +171 +6 14,611
Management & Administrative 18,846 19,829 21,583 22,083 22,175 +982 +1,754 +592 +92 24,455 Support 8,234 8,676 8,813 8,877 8,925 +442 +137 +112 +48 10,337 Maintenance/ Technical 1,182 1,200 1,197 1,196 1,185 +17 3 12 11 1,229
Management & Administrative 18,846 19,829 21,583 22,083 22,175 +982 +1,754 +592 +92 24,455 Support 8,234 8,676 8,813 8,877 8,925 +442 +137 +112 +48 10,337 Maintenance/ Technical 1,182 1,200 1,197 1,196 1,185 +17 3 12 11 1,229
General Support 9,416 9,876 10,010 10,073 10,111 +459 +135 +100 +37 11,566 Health Care Assistants 17,396 18,554 19,326 19,546 19,588 +1,157 +772 +262 +42 22,478 Home Help 3,569 3,543 3,546 3,531 3,630 26 +2 +85 +99 5,240 Ambulance Staff 1,828 1,877 1,936 1,917 1,903 +49 +59 32 14 1,966 Care, other 2,925 3,011 3,234 3,287 3,305 +85 +224 +71 +18 3,902
25,719 26,985 28,042 28,282 28,427 +1,266 +1,057 +385 +145 33,586
9,416 9,876 10,010 10,073 10,111 +459 +135 +100 +37 11,566 Health Care Assistants 17,396 18,554 19,326 19,546 19,588 +1,157 +772 +262 +42 22,478 Home Help 3,569 3,543 3,546 3,531 3,630 26 +2 +85 +99 5,240 Ambulance Staff 1,828 1,877 1,936 1,917 1,903 +49 +59 32 14 1,966
2,925 3,011 3,234 3,287 3,305 +85 +224 +71 +18 3,902
26,985 28,042 28,282 28,427 +1,266 +1,057 +385 +145 33,586
88 www.ihca.ie Source: Health Service Employment Report: April 2022
(as of April 2022) Health Service Employment Report: April 2022 Employment by Staff Group Staff Category /Staff Group WTE Dec 2019 WTE Dec 2020 WTE Dec 2021 WTE Mar 2022 WTE Apr 2022 Change Dec 2019 to Dec 20 Change Dec 2020 to Dec 21 Change Dec 2021 to Apr 22 Change Mar 2022 to Apr 22 Headcount [No.] Apr 2022 Overall 119,817 126,174 132,323 134,101 134,573 +6,357 +6,149 +2,249 +472 153,495 Consultants 3,250 3,458 3,608 3,656 3,667 +208 +150 +58 +11 4,011 Registrars 3,679 3,876 4,104 4,167 4,170 +196 +229 +66 +3 4,298 SHO/ Interns 3,116 3,594 3,587 3,553 3,596 +478 8 +10 +44 3,745
812 833 814 812 804 +21 19 10 8 1,131
10,857 11,762 12,113 12,188 12,237 +904 +352 +124 +49 13,185
Patient & Client Care
+1,712 +1,660 +890 +982 +1,754 +592 +459 +135 +100 +904 +352 +124 +1,266 +1,057 +385 +1,033 +1,192 +157 0 200 400 600 800 1,000 1,200 1,400 1,600 1,800 Nursing Man/ Admin Support Medical PCC HSCP WTE change 2020, 2021, 2022 Health Service Employment Report: April 2022 Employment by Staff Group Staff Category /Staff Group WTE Dec 2019 WTE Dec 2020 WTE Dec 2021 WTE Mar 2022 WTE Apr 2022 Change Dec 2019 to Dec 20 Change Dec 2020 to Dec 21 Change Dec 2021 to Apr 22 Change Mar 2022 to Apr 22 Headcount [No.] Apr 2022 Overall 119,817 126,174 132,323 134,101 134,573 +6,357 +6,149 +2,249 +472 153,495 Consultants 3,250 3,458 3,608 3,656 3,667 +208 +150 +58 +11 4,011 Registrars 3,679 3,876 4,104 4,167 4,170 +196 +229 +66 +3 4,298
3,116 3,594 3,587 3,553 3,596 +478 8 +10 +44 3,745
812 833 814
General Support
Care, other
Patient & Client Care 25,719
+1,712 +1,660 +890 +982 +1,754 +592 +459 +135 +100 +904 +352 +124 +1,266 +1,057 +385 +1,033 +1,192 +157 0 200 400 600 800 1,000 1,200 1,400 1,600 1,800 Nursing Man/ Admin Support Medical PCC HSCP WTE change 2020, 2021, 2022
Charts & Tables
Consultant Dentistry
Consultant Emergency Medicine
Consultant Intensive Care Medicine
Consultant Medicine
Consultant Obstetrics & Gynaecology
Consultant Paediatrics
Consultant Pathology
272 285 288 288 +14 +13 +3 +0 312
Consultant Psychiatry 407 422 438 439 439 +16 +16 +1 +0 485
Consultant Radiology 295 301 309 311 310 +5 +9 +0 1 332
Consultant Surgery 553 575 602 608 606 +22 +27 +4 2 673
Consultant, Other 1 1 1 1 +1 0 +1 2
Consultants 3,250 3,458 3,608 3,656 3,667 +208 +150 +58 +11 4,011
Registrar 2,271 2,378 2,451 2,527 2,540 +107 +72 +89 +13 2,623
Senior Registrar 211 238 249 254 257 +27 +11 +8 +3 266
Specialist Registrar 1,197 1,260 1,405 1,386 1,373 +63 +145 32 13 1,409
Registrars 3,679 3,876 4,104 4,168 4,170 +196 +229 +66 +3 4,298
Interns 726 971 867 839 836 +245 104 32 4 890
Senior House Officer 2,390 2,623 2,719 2,713 2,760 +233 +96 +41 +47 2,855
SHO/ Interns 3,116 3,594 3,587 3,553 3,596 +478 8 +10 +44 3,745
Dentists 311 313 315 309 308 +2 +2 7 1 413
Other Medical 501 520 499 503 496 +19 21 3 7 718
Medical/ Dental, other 812 833 814 812 804 +21 19 10 8 1,131
Medical & Dental 10,857 11,762 12,113 12,188 12,237 +904 +352 +124 +49 13,185
Clinical Nurse/ Midwife Manager 6,746 7,038 7,443 7,561 7,593 +292 +404 +150 +32 8,384
Director Nursing/Midwifery, Assistant 941 1,000 1,077 1,114 1,108 +59 +77 +30 6 1,184
Director of Nursing/Midwifery 298 306 332 332 339 +8 +27 +6 +6 348
Nurse/ Midwife Manager 7,984 8,344 8,852 9,007 9,039 +360 +508 +187 +32 9,916
Advanced Nurse/ Midwife Practitioner 385 519 597 628 645 +134 +78 +48 +16 677
Clinical Nurse/ Midwife Specialist 1,612 1,780 1,885 1,941 1,972 +168 +105 +88 +32 2,245
Nurse/ Midwife Specialist & AN/MP 1,996 2,299 2,481 2,569 2,617 +302 +183 +136 +48 2,922
Nursing Bank 31 23 13 11 9 8 10 4 2 22
Staff Midwives 1,465 1,486 1,466 1,421 1,398 +21 20 68 23 1,686
Staff Nurse [Intellectual Disability] 1,602 1,866 1,824 1,636 1,655 +264 42 168 +19 1,905
Staff Nurse [Psychiatric] 3,018 3,067 3,204 3,110 3,082 +49 +137 123 29 3,359
Staff Nurses [General/ Children's] 19,577 20,321 21,342 21,584 21,697 +744 +1,022 +355 +113 24,932
Staff Nurse/ Staff Midwife 25,693 26,763 27,850 27,762 27,841 +1,070 +1,087 9 +78 31,904
Public Health Nurse 1,537 1,557 1,523 1,499 1,495
Preregistration Nurse/ Midwife Intern 138 28
Preregistration Nurse Intern (C0VID19)
Postregistration Nurse/ Midwife Student
Nursing/ Midwifery awaiting registration
Nursing/ Midwifery Student
Nursing Education/Clinical
Other Nursing/ Midwifery
Nursing/ Midwifery other
28 3 1,782
1,499
1,929
89www.ihca.ie Source: Health Service Employment Report: April 2022
(as of April 2022) Health Service Employment Report: April 2022 Employment by Grade Group April 2022 WTE Dec 2019 WTE Dec 2020 WTE Dec 2021 WTE Mar 2022 WTE Apr 2022 Change Dec 2019 to Dec 20 Change Dec 2020 to Dec 21 Change Dec 2021 to Apr 22 Change Mar 2022 to Apr 22 Headcount [No.] Apr 2022 Overall 119,817 126,174 132,323 134,101 134,573 +6,357 +6,149 +2,249 +472 153,495 Consultant Anaesthesia 407 431 437 444 445 +24 +6 +8 +1 474
17 16 16 19 19 1 0 +3 +0 23
108 121 131 137 139 +13 +10 +8 +3 150
16 18 21 20 20 +2 +3 0 0 22
828 914 978 997 1,003 +86 +64 +25 +5 1,102
161 170 170 176 176 +9 1 +6 +0 192
197 216 221 218 221 +19 +5 1 +3 244
259
+20 34
124 725 742 110 +96 +618 +17
230 1 +230 229 1
293 258 277 274 271 35 +19 6 3 284
213 76 124 177 137 137 +49 +12 40 146
644 592 526 1,176 1,150 52 65 +624 26
300 315 297 299 301 +16 18 +4 +2 347
50 47 47 24 23 3 0 24 1 24
350 362 344 323 324 +12 18 20 +1 371 Page 1 of 3
Charts
Tables
+10 +3 128
Speech & Language Therapists 1,103 1,150 1,186 1,219 1,216 +47 +36 +30 3 1,403 Therapy Professions 5,234 5,565 5,947 6,081 6,109 +331 +382 +162 +28 7,025
Audiology 72 82 92 95 94 +11 +9 +2 2 108
Biochemists 79 84 77 72 74 +4 7 3 +2 78
Cardiac Physiologists 227 243 254 254 256 +16 +11 +2 +2 277
Clinical Engineering 164 171 181 185 185 +7 +10 +4 +1 190
Dosimetrists 13 14 15 15 13 +1 +0 1 1 16 E.C.G. Technicians 10 11 7 8 8 +1 4 +1 +0 10
Gastrointestinal Physiologists 2 2 4 4 4 0 +2 0 0 5
Medical Science 1,977 2,045 2,088 2,085 2,074 +69 +42 13 11 2,280
Perfusionists 22 22 19 19 21 0 2 +2 +2 23
Phlebotomists 173 184 198 202 198 +11 +13 0 4 277
Physicists 188 178 183 185 189 10 +5 +7 +4 205 NeuroPhysiologists 50 56 54 54 55 +7 2 +0 +1 59
Radiation Therapists 199 212 199 203 207 +13 13 +7 +4 227
Radiographers 1,229 1,325 1,441 1,443 1,446 +95 +117 +5 +3 1,605
Respiratory Physiologists 66 73 74 70 71 +7 +2 3 +1 75
Vascular Physiologists 29 28 32 32 33 1 +4 +1 +1 37
Health Science/ Diagnostics 4,500 4,731 4,918 4,926 4,927 +230 +188 +9 +1 5,472
Social Care 2,710 2,909 3,127 3,106 3,102 +199 +219 25 4 3,634
Social Workers 1,165 1,238 1,296 1,318 1,331 +74 +58 +35 +13 1,490
Psychologists 1,004 1,066 1,095 1,111 1,109 +62 +29 +14 1 1,255 Pharmacists
802 +75 +89 7 +2 889 Pharmacy Technicians
+50 +39 +9 +7 560 Pharmacy 1,038 1,164 1,292 1,285 1,294 +126 +128 +3 +9 1,449 Counsellor Therapists
+6 +30 +13 +0
90 www.ihca.ie Source: Health Service Employment Report: April 2022
&
(as of April 2022) Health Service Employment Report: April 2022 Employment by Grade Group April 2022 WTE Dec 2019 WTE Dec 2020 WTE Dec 2021 WTE Mar 2022 WTE Apr 2022 Change Dec 2019 to Dec 20 Change Dec 2020 to Dec 21 Change Dec 2021 to Apr 22 Change Mar 2022 to Apr 22 Headcount [No.] Apr 2022 Overall 119,817 126,174 132,323 134,101 134,573 +6,357 +6,149 +2,249 +472 153,495 Nursing & Midwifery 38,205 39,917 41,576 42,336 42,467 +1,712 +1,660 +890 +130 48,824 Dietitians 574 638 696 708 707 +63 +58 +11 0 823 Occupational Therapists 1,599 1,702 1,840 1,866 1,873 +103 +138 +34 +7 2,114 Orthoptists 35 38 40 39 39 +3 +2 1 0 51 Physiotherapists 1,851 1,958 2,091 2,147 2,169 +107 +133 +78 +22 2,506 Podiatrists & Chiropodists 72 80 95 102 104 +8 +15
645 721 809 801
393 443 482 484 492
238 244 274 286 287
321 Dental Hygienists 58 62 60 61 59 +4 3 1 1 77 Environmental Health Officers 528 541 550 546 544 +13 +9 6 2 592 HSCP Trainees/ Students 70 56 68 92 91 14 +13 +22 2 102 Other Health & Social Care 183 189 192 189 184 +6 +3 8 5 217 Play Therapists/ Specialists 46 43 43 46 44 3 +0 +1 2 55 Vaccinators 136 91 74 +136 62 17 190 H&SC, Other 1,123 1,134 1,324 1,311 1,282 +12 +189 41 29 1,554 HSCP 16,774 17,807 18,999 19,138 19,156 +1,033 +1,192 +157 +18 21,879 Executive Management 331 373 388 389 395 +42 +15 +7 +7 404 Senior Management (VIII & GM) 1,511 1,596 1,828 1,917 1,937 +85 +231 +109 +20 1,997 Management (VIII & above) 1,842 1,969 2,216 2,305 2,332 +128 +246 +117 +27 2,401 Middle Management (VVII) 5,163 5,786 6,671 6,906 6,963 +624 +885 +292 +57 7,395 Other Administrative 37 35 34 45 47 2 1 +12 +2 48 Administrative/ Supervisory (V to VII) 5,199 5,821 6,705 6,951 7,010 +622 +884 +304 +59 7,443 Clerical (III & IV) 11,805 12,038 12,661 12,827 12,833 +233 +623 +171 +6 14,611 Management Admin 18,846 19,829 21,583 22,083 22,175 +982 +1,754 +592 +92 24,455 Catering 877 887 875 882 884 +11 12 +9 +2 971 Page 2 of 3
Charts & Tables
Portering 1,639 1,669 1,715
Support
8 7 1,083 Technical Services 117 129 149 148 145 +13 +19 4 4 146
1,066 1,070 1,049 1,048 1,041
8,234 8,676 8,813 8,877 8,925 +442 +137 +112 +48 10,337
Maintenance/ Technical 1,182 1,200 1,197 1,196 1,185 +17 3 12 11 1,229
Maintenance 1,066 1,070 1,049 1,048 1,041 +5 22 8 7 1,083
Support 9,416 9,876 10,010 10,073 10,111 +459 +135 +100 +37 11,566
Technical Services 117 129 149 148 145 +13 +19 4 4 146
Attendant/ Aide 4,753 4,556 3,881 3,749 3,722 197 674 159 27 4,230
Maintenance/ Technical 1,182 1,200 1,197 1,196 1,185 +17 3 12 11 1,229
Health Care Assistant/ Care Assistant 12,405 13,617 15,123 15,465 15,531 +1,212 +1,506 +408 +66 17,870
Support 9,416 9,876 10,010 10,073 10,111 +459 +135 +100 +37 11,566
Health & Social Care Assistants 238 308 320 332 335 +70 +13 +15 +3 378
Attendant/ Aide 4,753 4,556 3,881 3,749 3,722 197 674 159 27 4,230
HCA (Student Nurse/Midwife COVID19) 73 2 1 +73 71 2 1
Health Care Assistant/ Care Assistant 12,405 13,617 15,123 15,465 15,531 +1,212 +1,506 +408 +66 17,870
Health Care Assistants 17,396 18,554 19,326 19,546 19,588 +1,157 +772 +262 +42 22,478
Health & Social Care Assistants 238 308 320 332 335 +70 +13 +15 +3 378
Home Help 3,569 3,543 3,546 3,531 3,630 26 +2 +85 +99 5,240
HCA (Student Nurse/Midwife COVID19) 73 2 1 +73 71 2 1
Ambulance Control 180 181 163 159 162 +2 19 1 +2 169
Health Care Assistants 17,396 18,554 19,326 19,546 19,588 +1,157 +772 +262 +42 22,478
Ambulance Education 162 138 253 215 190 24 +115 63 25 191
Home Help 3,569 3,543 3,546 3,531 3,630 26 +2 +85 +99 5,240
Ambulance Officers 78 85 86 95 97 +7 +2 +10 +2 99
Ambulance Control 180 181 163 159 162 +2 19 1 +2 169
PreHospital Care (Ambulance) 1,408 1,473 1,434 1,448 1,455 +65 40 +22 +7 1,507
Ambulance Education 162 138 253 215 190 24 +115 63 25 191
Ambulance Officers 78 85 86 95 97 +7 +2 +10 +2 99
Ambulance Staff 1,828 1,877 1,936 1,917 1,903 +49 +59 32 14 1,966 Health Promotion 31 32 35 65 79 +2 +3 +44 +14 91
PreHospital Care (Ambulance) 1,408 1,473 1,434 1,448 1,455 +65 40 +22 +7 1,507
Home Care Services 135 136 167 161 162 +1 +30 4 +2 186
Ambulance Staff 1,828 1,877 1,936 1,917 1,903 +49 +59 32 14 1,966
Other Care Grades 1,017 1,091 1,250 1,293 1,306 +74 +159 +57 +13 1,543
Health Promotion 31 32 35 65 79 +2 +3 +44 +14 91
Pastoral Care 145 136 128 128 127 9 8 1 2 187
Home Care Services 135 136 167 161 162 +1 +30 4 +2 186
Other Care Grades 1,017 1,091 1,250 1,293 1,306 +74 +159 +57 +13 1,543
Workshop Services 1,597 1,616 1,656 1,640 1,631 +19 +40 25 9 1,895 Care, other 2,925 3,011 3,234 3,287 3,305 +85 +224 +71 +18 3,902
Pastoral Care 145 136 128 128 127 9 8 1 2 187
28,042 28,282 28,427 +1,266 +1,057 +385 +145
3,011 3,234 3,287 3,305 +85 +224 +71 +18 3,902
Workshop Services 1,597 1,616 1,656 1,640 1,631 +19 +40 25 9 1,895 Care, other
91www.ihca.ie Source: Health Service Employment Report: April 2022
(as of April 2022) Health Service Employment Report: April 2022 Employment by Grade Group April 2022 WTE Dec 2019 WTE Dec 2020 WTE Dec 2021 WTE Mar 2022 WTE Apr 2022 Change Dec 2019 to Dec 20 Change Dec 2020 to Dec 21 Change Dec 2021 to Apr 22 Change Mar 2022 to Apr 22 Headcount [No.] Apr 2022 Overall 119,817 126,174 132,323 134,101 134,573 +6,357 +6,149 +2,249 +472 153,495 Household Services 4,198 4,571 4,602 4,638 4,648 +374 +30 +46 +10 5,510 Other Labs & Associated 385 448 525 548 567 +63 +77 +42 +19 621 Other Support 1,136 1,100 1,097 1,102 1,098 36 3 +1 3 1,407
1,707 1,728 +31 +45 +14 +22 1,828
8,234 8,676 8,813 8,877 8,925 +442 +137 +112 +48 10,337 Maintenance
+5 22
PCC 25,719 26,985
33,586 +208+150+58 +196+229+66 +478 8+10 +21 1910 +360+508+187 +302+183+136 +20 3428 5265 +624 +121820 +230+188 +9 +62+29+14 +126+128 +3 +12 +189 41 +128+246+117 +199+219 25 +442 +137+112 +1,157 +772 +262 26 +2+85 +49+59 32 +74+57+35 +1,070+1,087 9 +331+382+162 +85+224+71 +233 +623 +171 +17312 +622 +884 +304 200 0 200 400 600 800 1,000 1,200 Consultants Registrars SHO/ Interns Medical other Nurse Manager CNMS/ ANMP PHN Nurse Student Nurse other Science &Diag Psychologists Pharmacy H&SC, Other VIII+ Social Care Support HCAs Home Help Ambulance Social Workers Staff Nurse Therapists Care, other Clerical (III & IV) Mainten/Tech Grade VVII WTE change 2020, 2021, 2022 Page 3 of 3 Health Service Employment Report: April 2022 Employment by Grade Group April 2022 WTE Dec 2019 WTE Dec 2020 WTE Dec 2021 WTE Mar 2022 WTE Apr 2022 Change Dec 2019 to Dec 20 Change Dec 2020 to Dec 21 Change Dec 2021 to Apr 22 Change Mar 2022 to Apr 22 Headcount [No.] Apr 2022 Overall 119,817 126,174 132,323 134,101 134,573 +6,357 +6,149 +2,249 +472 153,495 Household Services 4,198 4,571 4,602 4,638 4,648 +374 +30 +46 +10 5,510 Other Labs & Associated 385 448 525 548 567 +63 +77 +42 +19 621 Other Support 1,136 1,100 1,097 1,102 1,098 36 3 +1 3 1,407 Portering 1,639 1,669 1,715 1,707 1,728 +31 +45 +14 +22 1,828 Support
2,925
PCC 25,719 26,985 28,042 28,282 28,427 +1,266 +1,057 +385 +145 33,586 +208+150+58 +196+229+66 +478 8+10 +21 1910 +360+508+187 +302+183+136 +20 3428 5265 +624 +121820 +230+188 +9 +62+29+14 +126+128 +3 +12 +189 41 +128+246+117 +199+219 25 +442 +137+112 +1,157 +772 +262 26 +2+85 +49+59 32 +74+57+35 +1,070+1,087 9 +331+382+162 +85+224+71 +233 +623 +171 +17312 +622 +884 +304 200 0 200 400 600 800 1,000 1,200 Consultants Registrars SHO/ Interns Medical other Nurse Manager CNMS/ ANMP PHN Nurse Student Nurse other Science &Diag Psychologists Pharmacy H&SC, Other VIII+ Social Care Support HCAs Home Help Ambulance Social Workers Staff Nurse Therapists Care, other Clerical (III & IV) Mainten/Tech Grade VVII WTE change 2020, 2021, 2022 Page 3 of 3
Charts
Tables
1: The HSE
of €173.3m
for
HSE
Adjs =
• Within this deficit of €173.3m, acute operations have a YTD surplus of (€7.3m), community services a surplus of (€273.1m), pensions and demand led services a deficit of €104.2m and other operations/services are showing a deficit of €349.6m (mainly COVID-19 related).
The
Within this deficit of €173.3m, acute operations have a YTD surplus of (€7.3m), community services a surplus of (€273.1m), pensions and demand led services a deficit of €104.2m and other operations/services are showing a deficit of €349.6m (mainly COVID 19 related).
The COVID 19 deficit of €784.1m to the end of December comprises a surplus of (€5.3m) in acute operations, deficit of €179.9m in community services, deficit of €166.0m (of which PCRS has a deficit of €161.9m) in Pensions & Demand Led Areas and a deficit of €443.5m in other operations/services.
• The COVID-19 deficit of €784.1m to the end of December comprises a surplus of (€5.3m) in acute operations, deficit of €179.9m in community services, deficit of €166.0m (of which PCRS has a deficit of €161.9m) in Pensions & Demand Led Areas and a deficit of €443.5m in other operations/services.
The COVID 19 related deficit of €443.5m in other operations/services comprises of: a deficit of €278.0m in the Testing & Tracing Programme, a surplus of (€9.5m) in regional services relating to COVID 19 support funding, and a deficit of €110.2m in health and wellbeing mainly relating to the COVID 19 Vaccination Programme.
• The COVID-19 related deficit of €443.5m in other operations/services comprises of: a deficit of €278.0m in the Testing & Tracing Programme, a surplus of (€9.5m) in regional services relating to COVID-19 support funding, and a deficit of €110.2m in health and wellbeing mainly relating to the COVID-19 Vaccination Programme.
Acute
(5.3) (2.8) National Ambulance Service 201.9 202.7 201.9 0.8 0.4% (0.0) 0.8 Private Hospitals 151.0 151.0 151.0 Access to Care 150.9 150.9 (150.9) 100.0% (150.9)
Acute Operations Total 7,062.9 7,055.5 7,062.9 (7.3) 0.1% (5.3) (2.0)
Acute operations incl. Ambulance Services, Private Hospitals & Access to Care has full year expenditure of €7,055.5m against a budget of €7,062.9m, leading to a year end surplus of (€7.3m) or (0.1%), of which (€5.3m) surplus has been categorised as being directly attributable to COVID 19 expenditure and a surplus of (€2.0m) attributable to core service expenditure. The national ambulance service (NAS) has a year end deficit of €0.8m. The performance by hospital group is illustrated in table 2 above.
Acute hospital services aim to improve the health of the population by providing health services ranging from self management support, brief intervention and early diagnosis to specialist tertiary services. These services are provided for adults and children within six hospital groups, Children’s Health Ireland and the National Ambulance Service (NAS). The six hospital groups provide the structure to deliver an integrated hospital network of acute care to the population in each geographic area. Children’s Health Ireland provides paediatric services in the greater Dublin area and incorporates the National Paediatric Hospital Development Board which is responsible for overseeing the building of the new children’s hospital.
These services include scheduled care (planned care), unscheduled care (unplanned / emergency care), diagnostic services, specialist services (specific rare conditions or highly specialised areas such as critical care and organ transplant services), cancer services, trauma services, maternity and children’s services, as well as the pre hospital emergency and intermediate care provided by NAS. These services are provided in response to population need and are consistent with wider health policies and objectives, including those of Sláintecare. Hospitals continually work to improve access to healthcare, whilst ensuring quality and patient safety initiatives are prioritised within allocated budgets, including the management of COVID 19 and other infections.
Acute operations incl. Ambulance Services, Private Hospitals & Access to Care has full year expenditure of €7,055.5m against a budget of €7,062.9m, leading to a year-end surplus of (€7.3m) or (0.1%), of which (€5.3m) surplus has been categorised as being directly attributable to COVID-19 expenditure and a surplus of (€2.0m) attributable to core service expenditure. The national ambulance service (NAS) has a year-end deficit of €0.8m. The performance by hospital group is illustrated in table 2 above. Acute hospital services aim to improve the health of the population by providing health services ranging from self-management support, brief intervention and early diagnosis to specialist tertiary services. These services are provided for adults and children within six hospital groups, Children’s Health Ireland and the National Ambulance Service (NAS). The six hospital groups provide the structure to deliver an integrated hospital network of acute care to the population in each geographic area. Children’s Health Ireland provides paediatric services in the greater Dublin area and incorporates the National Paediatric Hospital Development Board which is responsible for overseeing the building of the new children’s hospital. These services include scheduled care (planned care), unscheduled care (unplanned / emergency care), diagnostic services, specialist services (specific rare conditions or highly specialised areas such as critical care and organ transplant services), cancer services, trauma services, maternity and children’s services, as well as the pre-hospital emergency and intermediate care provided by NAS. These services are provided in response to population need and are consistent with wider health policies and objectives, including those of Sláintecare. Hospitals continually work to improve access to healthcare, whilst ensuring quality and patient safety initiatives are prioritised within allocated budgets, including the management of COVID-19 and other infections.
Source: Health Service Performance ProfileOctober - December 2021 Quarterly Report
&
(as of December 2021) 92 www.ihca.ie Performance Profile October December 2021 87 Table 1 Net Expenditure by Division YTD December 2021 Detailed analysis of the divisional performances is provided in the relevant sections below. December 2021 YTD Actual Spend vrs YTD Budget YTD Variance Analysed As: Approved Allocation YTD Actual YTD Budget YTD Variance YTD Variance Covid 19 Related Variance Core related variance €m €m €m €m % €m €m Acute Operations 7,062.9 7,055.5 7,062.9 (7.3) 0.1% (5.3) (2.0) Community Services 7,280.9 7,007.8 7,280.9 (273.1) 3.8% 179.9 (453.0) Other Operations/Services 1,669.1 2,018.7 1,669.1 349.6 20.9% 443.5 (94.0) Total Operational Service Areas 16,012.9 16,082.0 16,012.9 69.1 0.4% 618.1 (549.0) Total Pensions & Demand Led Services 4,629.7 4,734.0 4,629.7 104.2 2.3% 166.0 (61.8) Overall Total 20,642.6 20,816.0 20,642.6 173.3 0.8% 784.1 (610.8) Note
Annual Report incorporates the HSE Annual Financial Statements (AFS) and provides a final audited financial position
2021 for the HSE’s directly provided services.
deficit
in table 1 can be related to the 2021 final AFS figure of €195m as follows; €173.3m + €6.0m s.38 voluntary surplus + €15.7m Balance Sheet
€195.0m
AFS deficit.
Performance Profile October December 2021 88 Acute Operations Table 2 Acute Operations December YTD December 2021 Acute Operations Approved Allocation YTD Actual YTD Budget YTD Variance YTD Variance YTD Variance Attributable to Covid 19 Expenditure Attributable to Core Expenditure €m €m €m €m % €m €m RCSI Hospital Group 1,007.3 1,006.1 1,007.3 (1.2) 0.1% 0.4 (1.6) Dublin Midlands Hospital Group 1,183.0 1,182.7 1,183.0 (0.3) 0.0% (0.1) (0.2) Ireland East Hospital Group 1,329.3 1,329.3 1,329.3 (0.0) 0.0% 1.1 (1.1) South South West Hospital Group 1,158.1 1,156.0 1,158.1 (2.1) 0.2% 0.1 (2.2) Saolta University Health Care Group 1,064.7 1,064.3 1,064.7 (0.4) 0.0% 0.0 (0.4) University of Limerick Hospital Group 485.8 485.3 485.8 (0.5) 0.1% 1.1 (1.6) Children's Health Ireland 411.0 411.2 411.0 0.2 0.1% 0.4 (0.2) Regional & National Services 70.9 67.0 70.9 (3.9) 5.5% (8.3) 4.4
Hospital Care 6,710.0 6,701.9 6,710.0 (8.2) 0.1%
Yearbook & Diary
2023
INTERNATIONAL INFORMATION
COUNTRY CAPITAL GMT DIAL CODE MONETARY UNIT
Argentina Buenos Aires -3 54
Argentine Peso/Centavo
Australia (Sydney) Canberra +10 61 Australian Dollar/Cent
Austria Vienna +1 43 Euro/Cent
Belgium Brussels +1 32 Euro/Cent
Brazil Brasilia -3 55 Real/Centavo
Canada (Toronto) Ottawa -5 1 Canadian Dollar/Cent
China Beijing +8 86 Yuan/Jiao
Denmark Copenhagen +1 45 Krone/Ore
Egypt Cairo +2 20 Egyptian Pound/Piastre
Finland Helsinki +2 358 Euro/Cent
France Paris +1 33 Euro/Cent
Germany Berlin +1 49 Euro/Cent
Ghana Accra GMT 233 Cedi/Pesewa
Greece Athens +2 30 Euro/Cent
Hong Kong SAR Victoria City +8 852 Hong Kong Dollar/Cent
India New Delhi +5.5 91 Rupee/Paise
Indonesia Jakarta +7 62 Rupiah/Sen
Ireland Dublin GMT 353 Euro/Cent
Israel Jerusalem +2 972 New Shekel/Agora Italy Rome +1 39 Euro/Cent
Japan Tokyo +9 81 Yen
Luxembourg Luxembourg +1 352 Euro/Cent Malaysia Kuala Lumpur +8 60 Ringgit/Sen
Mexico Mexico City -6 52 Mexican Peso/Centavo
Netherlands Amsterdam +1 31 Euro/Cent
New Zealand Wellington +12 64 New Zealand Dollar/Cent
Nigeria Abuja +1 234 Naira/Kobo
Philippines Manila +8 63 Philippine Peso/Sentimo
Portugal Lisbon GMT 351 Euro/Cent
Russia (Moscow) Moscow +3 7 Rouble/Kopeck
Saudi Arabia Riyadh +3 966 Riyal/Halala Singapore Singapore +8 65 Singapore Dollar/Cent
South Africa Pretoria +2 27 Rand/Cent
Spain Madrid +1 34 Euro/Cent
Sweden Stockholm +1 46 Krona/Ore
Switzerland Berne +1 41 Franc/Centime
Taiwan Taipei +8 886 New Taiwan Dollar/Cent
United Kingdom London GMT 44 British Pound/Pence USA (New York) Washington DC -5 1 US Dollar/Cent
Zimbabwe Harare +2 263 US Dollar/Cent
The information in this
is
carefully at the time of printing. No responsibility can be accepted if any errors occur.
publication
checked
JANUARY
MARCH APRIL MAY JUNE
FEBRUARY
Mon. 1 ❋ Tue. 2 Wed. 1 1 3 Thur. 2 2 4 1 Fri. 3 3 5 2 Sat. 4 4 1 6 3 Sun. 1 5 5 2 7 4 Mon. 2 ❋ 6 ❋ 6 3 8 5 ❋ Tue. 3 7 7 4 9 6 Wed. 4 8 8 5 10 7 Thur. 5 9 9 6 11 8 Fri. 6 10 10 7 12 9 Sat. 7 11 11 8 13 10 Sun. 8 12 12 9 14 11 Mon. 9 13 13 10 ❋ 15 12 Tue. 10 14 14 11 16 13 Wed. 11 15 15 12 17 14 Thur. 12 16 16 13 18 15 Fri. 13 17 17 ❋ 14 19 16 Sat. 14 18 18 15 20 17 Sun. 15 19 19 16 21 18 Mon. 16 20 29 17 22 19 Tue. 17 21 21 18 23 20 Wed. 18 22 22 19 24 21 Thur. 19 23 23 20 25 22 Fri. 20 24 24 21 26 23 Sat. 21 25 25 22 27 24 Sun. 22 26 26 23 28 25 Mon. 23 27 27 24 29 26 Tue. 24 28 28 25 30 27 Wed 25 29 26 31 28 Thur. 26 30 27 29 Fri. 27 31 28 30 Sat. 28 29 Sun. 29 30 Mon. 30 Tue. 31 1 RoI & UK 17 St.Patrick’s Day Observed. RoI (B.Hol. NI) 18 RoI & UK 2 RoI & UK 31 UK 2-3 UK 6 RoI ❋ Holidays Week 53 Week 5 Week 10 Week 14 Week 19 Week 23 Week 1 Week 6 Week 11 Week 15 Week 20 Week 24 Week 2 Week 7 Week 12 Week 16 Week 21 Week 25 Week 3 Week 8 Week 13 Week 17 Week 22 Week 26 Week 4 Week 9 Week 14 Week 18 Week 23 Week 27 Week 5 Week 23 YEAR PLANNER 202 3
Holidays
AUGUST SEPTEMBER OCTOBER NOVEMBER DECEMBER
YEAR PLANNER 2023 ❋
1 RoI & Scot. 29 UK 24 RoI 30 Scot. 25 RoI & UK 26 RoI & UK JULY
Mon. Week 27 Week 32 Week 36 Week 40 Week 45 Week 49 Tue. 1 Wed. 2 1 Thur. 3 2 Fri. 4 1 3 1 Sat. 1 5 2 4 2 Sun. 2 6 3 1 5 3 Mon. 3 Week 28 7 ❋ Week 33 4 Week 37 2 Week 41 6 Week 46 4 Week 50 Tue. 4 8 5 3 7 5 Wed. 5 9 6 4 8 6 Thur. 6 10 7 5 9 7 Fri. 7 11 8 6 10 8 Sat. 8 12 9 7 11 9 Sun. 9 13 10 8 12 10 Mon. 10 Week 29 14 Week 34 11 Week 38 9 Week 42 13 Week 47 11 Week 51 Tue. 11 15 12 10 14 12 Wed. 12 16 13 11 15 13 Thur. 13 17 14 12 16 14 Fri. 14 18 15 13 17 15 Sat. 15 19 16 14 18 16 Sun. 16 20 17 15 19 17 Mon. 17 Week 30 21 Week 35 18 Week 39 16 Week 43 20 Week 48 18 Week 51 Tue. 18 22 19 17 21 19 Wed. 19 23 20 18 22 20 Thur. 20 24 21 19 23 21 Fri. 21 25 22 20 24 22 Sat. 22 26 23 21 25 23 Sun. 23 27 24 22 26 24 Mon. 24 Week 31 28 Week 36 25 Week 49 23 Week 44 27 Week 49 25 ❋ Week 52 Tue. 25 29 26 24 28 26 ❋ Wed. 26 30 27 25 29 27 Thur. 27 31 28 26 30 28 Fri. 28 29 27 29 Sat. 29 30 28 30 Sun. 30 29 31 Mon. 31 Week 32 30 ❋ Week 45 Tue. 31
JANUARY
Wk M T W T F S S
1 1 2
2 3 4 5 6 7 8 9
3 10 11 12 13 14 15 16
4 17 18 19 20 21 22 23
5 24/31 25 26 27 28 29 30
MAY
Wk M T W T F S S 18 1 19 2 3 4 5 6 7 8
20 9 10 11 12 13 14 15
21 16 17 18 19 20 21 22 22 23/30 24/31 25 26 27 28 29
SEPTEMBER
Wk M T W T F S S 36 1 2 3 4 37 5 6 7 8 9 10 11 38 12 13 14 15 16 17 18 39 19 20 21 22 23 24 25 40 26 27 28 29 30
JANUARY
Wk M T W T F S S
52 1
1 2 3 4 5 6 7 8
2 9 10 11 12 13 14 15
3 16 17 18 19 20 21 22
4 23/30 24/31 25 26 27 28 29
MAY
Wk M T W T F S S
18 1 2 3 4 5 6 7
19 8 9 10 11 12 13 14
20 15 16 17 18 19 20 21 21 22 23 24 25 26 27 28 22 29 30 31
SEPTEMBER
Wk M T W T F S S
35 1 2 3 36 4 5 6 7 8 9 10
11 12 13 14 15 16 17 38 18 19 20 21 22 23 24
25 26 27 28 29 30
JANUARY
Wk M T W T F S S
1 1 2 3 4 5 6 7
2 8 9 10 11 12 13 14
3 15 16 17 18 19 20 21
4 22 23 24 25 26 27 28 5 29 30 31
MAY
Wk M T W T F S S
18 1 2 3 4 5
19 6 7 8 9 10 11 12
20 13 14 15 16 17 18 19
21 20 21 22 23 24 25 26 22 27 28 29 30 31
SEPTEMBER
Wk M T W T F S S
THREE YEAR CALENDAR
2022
FEBRUARY
Wk M T W T F S S
6 1 2 3 4 5 6
7 7 8 9 10 11 12 13
8 14 15 16 17 18 19 20
9 21 22 23 24 25 26 27 10 28
JUNE
Wk M T W T F S S 23 1 2 3 4 5 24 6 7 8 9 10 11 12 25 13 14 15 16 17 18 19 26 20 21 22 23 24 25 26 27 27 28 29 30
OCTOBER
Wk M T W T F S S 40 1 2 41 3 4 5 6 7 8 9 42 10 11 12 13 14 15 16 43 17 18 19 20 21 22 23 44 24/31 25 26 27 28 29 30
FEBRUARY
Wk M T W T F S S
5 1 2 3 4 5 6 6 7 8 9 10 11 12
7 13 14 15 16 17 18 19
8 20 21 22 23 24 25 26 9 27 28
JUNE
Wk M T W T F S S 22 1 2 3 4 23 5 6 7 8 9 10 11 24 12 13 14 15 16 17 18 25 19 20 21 22 23 24 25 26 26 27 28 29 30
OCTOBER
Wk M T W T F S S 39 1 40 2 3 4 5 6 7 8 41 9 10 11 12 13 14 15 42 16 17 18 19 20 21 22 43 23/30 24/31 25 26 27 28 29
2023 2024
MARCH
Wk M T W T F S S
10 1 2 3 4 5 6 11 7 8 9 10 11 12 13 12 14 15 16 17 18 19 20 13 21 22 23 24 25 26 27 14 28 29 30 31
JULY
Wk M T W T F S S 27 1 2 3 28 4 5 6 7 8 9 10 29 11 12 13 14 15 16 17 30 18 19 20 21 22 23 24 31 25 26 27 28 29 30 31
NOVEMBER
Wk M T W T F S S 45 1 2 3 4 5 6
7 8 9 10 11 12 13
14 15 16 17 18 19 20
21 22 23 24 25 26 27
28 29 30
MARCH
Wk M T W T F S S
9 1 2 3 4 5
10 6 7 8 9 10 11 12 11 13 14 15 16 17 18 19 12 20 21 22 23 24 25 26 13 27 28 29 30 31
JULY
Wk M T W T F S S 26 1 2 27 3 4 5 6 7 8 9 28 10 11 12 13 14 15 16 29 17 18 19 20 21 22 23 30 24/31 25 26 27 28 29 30
NOVEMBER
Wk M T W T F S S 44 1 2 3 4 5 45 6 7 8 9 10 11 12 46 13 14 15 16 17 18 19 47 20 21 22 23 24 25 26 48 27 28 29 30
FEBRUARY
Wk M T W T F S S 5 1 2 3 4
6 5 6 7 8 9 10 11
7 12 13 14 15 16 17 18
8 19 20 21 22 23 24 25 9 26 27 28 29
JUNE
Wk M T W T F S S 22 1 2 23 3 4 5 6 7 8 9 24 10 11 12 13 14 15 16 25 17 18 19 20 21 22 23 26 24 25 26 27 28 29 30
OCTOBER
APRIL
Wk M T W T F S S 14 1 2 3
15 4 5 6 7 8 9 10 16 11 12 13 14 15 16 17 17 18 19 20 21 22 23 24 18 25 26 27 28 29 30
AUGUST
Wk M T W T F S S
32 1 2 3 4 5 6 7 33 8 9 10 11 12 13 14 34 15 16 17 18 19 20 21 35 22 23 24 25 26 27 28 36 29 30 31
DECEMBER
Wk M T W T F S S 49 1 2 3 4 50 5 6 7 8 9 10 11 51 12 13 14 15 16 17 18 52 19 20 21 22 23 24 25 53 26 27 28 28 30 31
APRIL
Wk M T W T F S S 13 1 2 14 3 4 5 6 7 8 9 15 10 11 12 13 14 15 16 16 17 18 19 20 21 22 23 17 24 25 26 27 28 29 30
AUGUST
Wk M T W T F S S
31 1 2 3 4 5 6 32 7 8 9 10 11 12 13 33 14 15 16 17 18 19 20 34 21 22 23 24 25 26 27 35 28 29 30 31
DECEMBER
Wk M T W T F S S
48 1 2 3 49 4 5 6 7 8 9 10 50 11 12 13 14 15 16 17 52 18 19 20 21 22 23 24 52 25 26 27 28 29 30 31
MARCH
Wk M T W T F S S
9 1 2 3 10 4 5 6 7 8 9 10 11 11 12 13 14 15 16 17 12 18 19 20 21 22 23 24 13 25 26 27 28 29 30 31
JULY
Wk M T W T F S S
27 1 2 3 4 5 6 7 28 8 9 10 11 12 13 14 29 15 16 17 18 19 20 21 30 22 23 24 25 26 27 28 31 29 30 31
NOVEMBER
1
2 3 4 5 6 7 8
9 10 11 12 13 14 15
16 17 18 20 21 23 22
23/30 24 25 26 27 28 29
Wk M T W T F S S 40 1 2 3 4 5 6 41 7 8 9 10 11 12 13
42 14 15 16 17 18 19 20 43 21 22 23 24 25 26 27 44 28 29 30 31
Wk M T W T F S S
1 2 3 45 4 5 6 7 8 9 10
11 12 13 14 15 16 17 47 18 19 20 21 22 23 24 48 25 26 27 28 29 30
APRIL
Wk M T W T F S S
14 1 2 3 4 5 6 7 15 8 9 10 11 12 13 14 16 15 16 17 18 19 20 21 17 22 23 24 25 26 27 28 18 29 30
AUGUST
Wk M T W T F S S
31 1 2 3 4
32 5 6 7 8 9 10 11 33 12 13 14 15 16 17 18 34 19 20 21 22 23 24 25 35 26 27 28 29 30 31
DECEMBER
Wk M T W T F S S 48 1 49 2 3 4 5 6 7 8 50 9 10 11 12 13 14 15 51 16 17 18 19 20 21 22 52 23/31 24/31 25 26 27 28 29
44
46
37
39
35
36
37
38
39
46
47
48
49
IRELAND
New Year’s Day:
WORLD HOLIDAYS FOR 2023
UNITED KINGDOM
2 Jan
St Brigid’s Day: 6 Feb
St Patrick’s Day Observed: 17 Mar
Easter Mon: 10 Apr
May Bank Hol: 1 May
June Bank Hol: 5 Jun
Aug Bank Hol: 7 Aug
Oct Bank Hol: 30 Oct
Christmas Day: 25 Dec
St Stephen’s Day: 26 Dec
USA
New Year’s Day: 6 Jan
Martin Luther King Day: 16 Jan
Presidents’ Day: 20 Feb
Memorial Day: 29 May
Independence Day: 4 Jul Labor Day: 4 Sep
Columbus Day: 9 Oct
Veterans Day: 10 Nov
Thanksgiving Day: 23 Nov Christmas Day: 25 Dec
New Year’s Day: 2 Jan St Patrick’s Day Observed (NI): 17 Mar
Good Fri: 7 Apr
Easter Mon (except SCO): 10 Apr
Early May Bank Hol: 1 May Spring Bank Hol: 29 May
The Twelfth/Orangemen’s Day (NI): 12 Jul Summer Bank Hol (SCO): 7 Aug Summer Bank Hol (UK, except SCO): 28 Aug St Andrew’s Day (SCO): 30 Nov
Christmas Day: 25 Dec Boxing Day: 26 Dec
CANADA
New Year’s Day: 2 Jan Family Day (BC): 20 Feb
Family Day (AB, ON, SK, MA, NB, NS): 20Feb
Good Fri: 7 Apr
Easter Mon: 10 Apr Victoria Day (except NB/NS/PE): 22 May
National Patriots’ Day (QC): 22 May
AUSTRALIA
New Year’s Day: 1 Jan
Australia Day Observed: 26 Jan Labour Day (WA): 6 Mar
Good Fri: 7 Apr
Easter Mon: 10 Apr
ANZAC Day: 25 Apr May Day (NT): 1 May
Western Australia Day (WA): 5 Jun Queen’s B’Day (except WA): 12 Jun Labour Day (NSW/ACT/SA/QLD): 2 Oct Christmas Day: 25 Dec Boxing Day: 26 Dec
National Aboriginal Day (NT): 21 Jun St Jean Baptiste Day, Quebec 24 Jun Canada Day: 1 Jul Public Hol (BC, SK, MB, ON, NB, NU, PE): 7 Aug Labour Day: 4 Sep Thanksgiving Day (BC, AB, SK, MB, ON, QC, YT, NT, NU): 9 Oct
Remembrance Day (except ON/QC): 11 Nov
Christmas Day: 25 Dec Boxing Day (except AB/BC/NU): 26 Dec
JAPAN
New Year’s Day: 2 Jan Coming-of-Age Day: 9 Jan
National Foundation Day: 11 Feb Spring Equinox: 21 Mar Shõwa Day: 29 Apr
Constitution Memorial Day: 3 May
CHINA
New Year’s Day: 1 Jan
Spring Festival Golden Week/Chinese NY: 21-27 Feb Qing Ming Jie: 5 Apr
Labour Day: 1 May
Dragon Boat Festival: 22-24 Jun
Mid-Autumn Festival: 29 Sep
National Day: 1 Oct Golden Week: 1 Oct - 7 Oct
Greenery Day: 4 May
Children’s Day: 5 May Marine Day: 17 Jul
Mountain Day: 11 Aug
Respect for the Aged Day: 18 Sep Autumn Equinox: 23 Sep Health & Sports Day: 9 Oct Culture Day: 3 Nov Labour Thanksgiving Day: 23 Nov
CONVERSION FORMULAE
From To Multiply by
Inches Centimetres 2.54
Centimetres Inches 0.3937
Feet Metres 0.3048
Metres Feet 3.281
Yards Metres 0.9144
Metres Yards 1.094 Miles Kilometres 1.609
Kilometres Miles 0.6214
Sq Inches Sq Centimetres 6.452
Sq Centimetres Sq Inches 0.155
Sq Metres Sq Feet 10.76
Sq Feet Sq Metres 0.0929
Sq Yards Sq Metres 0.8361
Sq Metres Sq Yards 1.196
Sq Miles Sq Kilometres 2.59
Sq Kilometres Sq Miles 0.3861
Acres Hectares 0.4047
Hectares Acres 2.471
Cubic Inches Cubic Centimetres 16.39
Cubic Centimetres Cubic Inches 0.06102
Cubic Feet Cubic Metres 0.02832
Cubic Metres Cubic Feet 35.31
Cubic Yards Cubic Metres 0.7646
Cubic Metres Cubic Yards 1.308
Cubic Inches Litres 0.01639
Litres Cubic Inches 61.03
Gallons Litres 4.546
Litres Gallons 0.22
Grains Grams 0.0648
Grams Grains 15.43
Ounces Grams 28.35
Grams Ounces 0.03527
Pounds Grams 453.6
Grams Pounds 0.002205
Pounds Kilograms 0.4536
Kilograms Pounds 2.205
Tons Kilograms 1016.0 Kilograms Tons 0.000984
Distance
Athlone
Ballymena
Bantry
Cavan
Coleraine
Cork
Derry
Donegal
Bantry Cavan Coleraine
METRIC CONVERSION
The bold figures in the central columns can be read as either the Metric measure or the Imperial measure. For example: 1 metre=1.09 yards; or 1 yard=0.91 metres
LITRES
PINTS METRES YARDS 0.28 0.50 0.88 0.91 1 1.09 0.43 0.75 1.32 1.83 2 2.1 0.57 1.00 1.76 2.74 3 3.28 0.71 1.25 2.20 3.66 4 4.28 0.85 1.50 2.64 4.57 5 5.47 0.99 1.75 3.08 1.14 2.00 3.52
KILOMETRES MILES 1.42 2.50 4.40 1.61 1 0.62 1.70 3.00 5.28 3.22 2 1.24 1.99 3.50 6.16 4.83 3 1.86 2.27 4.00 7.04 6.44 4 2.48 2.84 5.00 8.80 8.05 5 3.11 9.66 6 3.7
LITRES
GALLONS 11.26 7 4.25 4.55 1.00 0.22 12.87 8 4.97 6.82 1.50 0.33 14.48 9 5.59 9.09 2.00 0.44 11.36 2.50 0.55
CENTIGRADE FARENHEIT 13.64 3.00 0.66 -18 0 32 15.91 3.50 0.77 -15 5 41 18.18 4.00 0.88 -12 10 50 20.46 4.50 0.99 -9 15 59 22.73 5.00 1.10 -7 20 68 27.28 6.00 1.32 -4 25 77 31.82 7.00 1.54 -1 30 86 36.37 8.00 1.76 2 35 95 40.91 9.00 1.98 4 40 104 7 45 113
KILOGRAMS POUNDS 10 50 122 0.11 0.25 0.55 13 55 131 0.23 0.50 1.10 16 60 140 0.45 1.00 2.20 18 65 149 0.68 1.50 3.31 21 70 158 0.91 2.00 4.41 24 75 167 2.27 5.00 11.02 27 80 176 2.27 6.00 13.23 32 90 194 3.18 7.00 15.43 38 100 212
IRELAND DISTANCE CHART
Distances in kilometres between principal towns
Drogheda
90 192 304 196 192 Dundalk 84 85 53 150 129 105 431 79 151 338 159 179 39 Ennis 338 230 269 111 362 359 225 195 391 137 343 272 245 262
Enniskillen 138 175 87 142 135 159 443 53 148 360 98 61 132 103 245
Galway 306 212 237 93 336 327 293 177 323 209 272 204 227 245 68 183
Kilkenny 285 114 264 116 309 306 243 175 346 148 335 309 167 201 150 232 172 Killarney 436 304 389 232 481 457 77 315 488 87 441 407 352 386 145 364 193 198 Larne 34 204 93 261 34 60 547 166 76 451 114 229 158 117 372 172 330 319 470
Letterkenny 150 237 122 230 122 171 533 156 82 449 32 48 198 161 322 101 251 333 455 146
Limerick 323 193 278 121 372 344 188 204 377 105 328 296 243 278 37 262 105 113 111 357 351
Longford 183 127 126 43 220 204 354 53 224 262 183 146 119 132 154 85 111 156 275 217 187 164
Monaghan 87 126 27 129 122 108 438 45 126 348 108 121 87 51 240 60 222 220 360 121 113 249 90
Mullingar 177 87 143 47 229 198 196 61 232 245 212 190 79 92 158 114 140 117 278 211 217 150 43 106
Navan 137 48 106 101 183 158 394 68 204 275 201 182 27 58 203 121 169 146 323 171 188 195 89 93 45
Newry 61 105 31 163 108 82 452 87 129 351 140 158 61 21 278 111 264 219 402 95 153 266 140 51 116 76
Omagh 117 174 222 185 90 135 486 97 105 404 55 68 142 105 288 43 227 275 407 119 60 306 129 53 158 146 93
Portlaoise 251 85 212 71 280 272 303 130 301 175 282 254 130 166 151 183 151 51 225 285 286 114 113 175 69 100 190 227
Roscommon 224 156 156 32 251 245 343 84 254 251 211 151 151 164 126 119 80 158 264 249 198 150 31 129 64 109 171 163 103
Rosslare 330 153 285 201 348 351 295 267 391 208 398 391 204 240 245 312 274 98 275 364 391 211 241 280 198 203 259 333 135 241
Sligo 206 214 150 117 200 227 428 121 185 336 135 66 201 169 206 68 138 245 343 240 113 233 106 126 135 188 177 111 188 85 327
Tipperary 346 177 307 137 375 367 185 225 230 103 346 320 227 261 79 278 145 76 132 380 367 40 180 270 166 192 285 322 95 169 124 254
Tralee 425 298 380 222 473 446 109 306 480 119 430 398 346 380 138 364 206 214 32 459 452 101 266 351 251 296 367 407 216 251 291 335 11
Waterford 333 163 298 164 357 354 216 224 394 126 383 357 211 246 166 280 220 48 193 367 381 129 204 269 164 195 267 322 100 208 79 293 82 212
Westport 303 257 253 150 303 325 377 188 288 293 238 169 254 267 151 171 84 256 277 338 216 180 146 225 179 224 275 214 220 114 352 103 220 282 309
Wexford 309 135 264 183 330 330 277 256 372 187 378 372 190 225 227 295 253 80 254 344 372 190 224 261 180 183 240 314 116 222 19 307 143 272 61 333
Wicklow 219 51 145 177 145 266 233 113 137 251 288 275 98 134 209 129 270 124 335 209 217 277 161 153 121 89 89 185 124 198 116 261 169 257 142 233 90
in Kilometres From: Belfast Dublin Armagh Athlone Ballymena Bangor
Cork
Derry Donegal Drogheda Dundalk Ennis Enniskillen Galway Killkenny Killarney
Larne Letterkenny Limerick Longford Monaghan
Mullingar
Navan
Newry Omagh Portlaoise Roscommon Rosslare Sligo Tipperary Tralee Waterford
Westport
Wexford Wicklow
Belfast
Dublin 166 Armagh 60 129
227 127 158
45 195 82 253 Bangor 21 187 85 246 68
513 346 468 311 560 534
132 114 72 84 167 153 393
87 237 98 254 43 109 566 171
417 254 383 219 476 438 90 303 481
117 232 109 209 82 138 541 151 50 428
180 233 127 183 146 201 484 114 119 402 69
122 50 92 132 167 143 396
NOLLAIG
8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
DECEMBER 2022 Wk Mo Tu We Th Fr Sa Su 49 1 2 3 4 50 5 6 7 8 9 10 11 51 12 13 14 15 16 17 18 52 19 20 21 22 23 24 25 53 26 27 28 29 30 31 November 2022 28 Monday | Luain 29 Tuesday | Máirt 30 Wednesday | Céadaoin WEEK 49
NOLLAIG
Satharn
December 2022 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
JANUARY 2023 Wk Mo Tu We Th Fr Sa Su 53 1 1 2 3 4 5 6 7 8 2 9 10 11 12 13 14 15 3 16 17 18 29 20 21 22 4 23 24 25 26 27 28 29 5 30 31 01 Thursday | Déardaoin 02 Friday | Aoine 04 Sunday | Domhnach03 Saturday |
WEEK 49
NOLLAIG
Máirt
Céadaoin
December 2022 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
DECEMBER 2022 Wk Mo Tu We Th Fr Sa Su 49 1 2 3 4 50 5 6 7 8 9 10 11 51 12 13 14 15 16 17 18 52 19 20 21 22 23 24 25 53 26 27 28 29 30 3105 Monday | Luain 06 Tuesday |
07 Wednesday |
WEEK 50
NOLLAIG
December 2022 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
JANUARY 2023 Wk Mo Tu We Th Fr Sa Su 53 1 1 2 3 4 5 6 7 8 2 9 10 11 12 13 14 15 3 16 17 18 29 20 21 22 4 23 24 25 26 27 28 29 5 30 31 08 Thursday | Déardaoin 09 Friday | Aoine 11 Sunday | Domhnach10 Saturday | Satharn WEEK 50
NOLLAIG
December 2022 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
DECEMBER 2022 Wk Mo Tu We Th Fr Sa Su 49 1 2 3 4 50 5 6 7 8 9 10 11 51 12 13 14 15 16 17 18 52 19 20 21 22 23 24 25 53 26 27 28 29 30 3112 Monday | Luain 13 Tuesday | Máirt 14 Wednesday | Céadaoin WEEK 51
NOLLAIG
Déardaoin
Friday
Aoine
December 2022 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
JANUARY 2023 Wk Mo Tu We Th Fr Sa Su 53 1 1 2 3 4 5 6 7 8 2 9 10 11 12 13 14 15 3 16 17 18 29 20 21 22 4 23 24 25 26 27 28 29 5 30 31 15 Thursday |
16
|
18 Sunday | Domhnach17 Saturday | Satharn WEEK 51
NOLLAIG
Máirt
December 2022 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
DECEMBER 2022 Wk Mo Tu We Th Fr Sa Su 49 1 2 3 4 50 5 6 7 8 9 10 11 51 12 13 14 15 16 17 18 52 19 20 21 22 23 24 25 53 26 27 28 29 30 3119 Monday | Luain 20 Tuesday |
21 Wednesday | Céadaoin WEEK 52
NOLLAIG
Day
December 2022 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
JANUARY 2023 Wk Mo Tu We Th Fr Sa Su 53 1 1 2 3 4 5 6 7 8 2 9 10 11 12 13 14 15 3 16 17 18 29 20 21 22 4 23 24 25 26 27 28 29 5 30 31 22 Thursday | Déardaoin 23 Friday | Aoine Christmas
25 Sunday | Domhnach24 Saturday | Satharn Christmas Eve WEEK 52
NOLLAIG
Máirt
8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
DECEMBER 2022 Wk Mo Tu We Th Fr Sa Su 49 1 2 3 4 50 5 6 7 8 9 10 11 51 12 13 14 15 16 17 18 52 19 20 21 22 23 24 25 53 26 27 28 29 30 31 December 2022 26 Monday | Luain St.Stephen’s Day 27 Tuesday |
28 Wednesday | Céadaoin WEEK 53
Year’s Eve
EANÁIR
Thursday
Déardaoin
Friday | Aoine
Year’s Day 01 Sunday | Domhnach
January 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
FEBRUARY 2023 Wk Mo Tu We Th Fr Sa Su 5 1 2 3 4 5 6 6 7 8 9 10 11 12 7 13 14 15 16 17 18 19 8 20 21 22 23 24 25 26 9 27 28 29
|
30
New
31 Saturday | Satharn New
WEEK 53
EANÁIR
Máirt
January 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
JANUARY 2023 Wk Mo Tu We Th Fr Sa Su 53 1 1 2 3 4 5 6 7 8 2 9 10 11 12 13 14 15 3 16 17 18 29 20 21 22 4 23 24 25 26 27 28 29 5 30 31 02 Monday | Luain 03 Tuesday |
04 Wednesday | Céadaoin WEEK 1
EANÁIR
Aoine
Satharn
Domhnach
January 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
FEBRUARY 2023 Wk Mo Tu We Th Fr Sa Su 5 1 2 3 4 5 6 6 7 8 9 10 11 12 7 13 14 15 16 17 18 19 8 20 21 22 23 24 25 26 9 27 28 05 Thursday | Déardaoin 06 Friday |
08 Sunday |
07 Saturday |
WEEK 1
EANÁIR
January 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
JANUARY 2023 Wk Mo Tu We Th Fr Sa Su 53 1 1 2 3 4 5 6 7 8 2 9 10 11 12 13 14 15 3 16 17 18 29 20 21 22 4 23 24 25 26 27 28 29 5 30 31 09 Monday | Luain 10 Tuesday | Máirt 11 Wednesday | Céadaoin WEEK 2
EANÁIR
Satharn
January 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
FEBRUARY 2023 Wk Mo Tu We Th Fr Sa Su 5 1 2 3 4 5 6 6 7 8 9 10 11 12 7 13 14 15 16 17 18 19 8 20 21 22 23 24 25 26 9 27 28 12 Thursday | Déardaoin 13 Friday | Aoine 15 Sunday | Domhnach14 Saturday |
WEEK 2
EANÁIR
Máirt
January 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
JANUARY 2023 Wk Mo Tu We Th Fr Sa Su 53 1 1 2 3 4 5 6 7 8 2 9 10 11 12 13 14 15 3 16 17 18 29 20 21 22 4 23 24 25 26 27 28 29 5 30 31 16 Monday | Luain 17 Tuesday |
18 Wednesday | Céadaoin WEEK 3
EANÁIR
Aoine
January 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
FEBRUARY 2023 Wk Mo Tu We Th Fr Sa Su 5 1 2 3 4 5 6 6 7 8 9 10 11 12 7 13 14 15 16 17 18 19 8 20 21 22 23 24 25 26 9 27 28 19 Thursday | Déardaoin 20 Friday |
22 Sunday | Domhnach21 Saturday | Satharn WEEK 3
EANÁIR
January 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
JANUARY 2023 Wk Mo Tu We Th Fr Sa Su 53 1 1 2 3 4 5 6 7 8 2 9 10 11 12 13 14 15 3 16 17 18 29 20 21 22 4 23 24 25 26 27 28 29 5 30 31 23 Monday | Luain 24 Tuesday | Máirt 25 Wednesday | Céadaoin WEEK 4
FEABHRA
Satharn
Déardaoin
Friday
Aoine
February 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
MARCH 2023 Wk Mo Tu We Th Fr Sa Su 9 1 2 3 4 5 10 6 7 8 9 10 11 12 11 13 14 15 16 17 18 19 12 20 21 22 23 24 25 26 13 27 28 29 30 31 26 Thursday |
27
|
29 Sunday | Domhnach28 Saturday |
WEEK 4 FEBRUARY 2022 Wk Tu We Th Su 5 1 4 5 6 6 7 8 10 13 7 14 15 16 17 18 19 20 8 21 22 23 24 25 26 27 9
February 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes FEABHRA FEBRUARY 2023 Wk Mo Tu We Th Fr Sa Su 5 1 2 3 4 5 6 6 7 8 9 10 11 12 7 13 14 15 16 17 18 19 8 20 21 22 23 24 25 26 9 27 2830 Monday | Luain 31Tuesday | Máirt 01 Wednesday | Céadaoin WEEK 5
Satharn
February 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes FEABHRA MARCH 2023 Wk Mo Tu We Th Fr Sa Su 9 1 2 3 4 5 10 6 7 8 9 10 11 12 11 13 14 15 16 17 18 19 12 20 21 22 23 24 25 26 13 27 28 29 30 31 02 Thursday | Déardaoin 03 Friday | Aoine 05 Sunday | Domhnach04 Saturday |
WEEK 5
FEABHRA
Máirt
February 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
FEBRUARY 2023 Wk Mo Tu We Th Fr Sa Su 5 1 2 3 4 5 6 6 7 8 9 10 11 12 7 13 14 15 16 17 18 19 8 20 21 22 23 24 25 26 9 27 2806 Monday | Luain St.Brigid’s Day 07 Tuesday |
08 Wednesday | Céadaoin WEEK 6
FEABHRA
Satharn
Thursday
Déardaoin
Friday
Aoine
February 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
MARCH 2023 Wk Mo Tu We Th Fr Sa Su 9 1 2 3 4 5 10 6 7 8 9 10 11 12 11 13 14 15 16 17 18 19 12 20 21 22 23 24 25 26 13 27 28 29 30 31 09
|
10
|
12 Sunday | Domhnach11 Saturday |
WEEK 6
Tuesday
Máirt St.Valentine’s Day
FEABHRA
Céadaoin
February 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
FEBRUARY 2023 Wk Mo Tu We Th Fr Sa Su 5 1 2 3 4 5 6 6 7 8 9 10 11 12 7 13 14 15 16 17 18 19 8 20 21 22 23 24 25 26 9 27 2813 Monday | Luain 14
|
15 Wednesday |
WEEK 7
Thursday
Déardaoin
Friday
Aoine
Satharn
Domhnach
February 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes FEABHRA MARCH 2023 Wk Mo Tu We Th Fr Sa Su 9 1 2 3 4 5 10 6 7 8 9 10 11 12 11 13 14 15 16 17 18 19 12 20 21 22 23 24 25 26 13 27 28 29 30 31 16
|
17
|
19 Sunday |
18 Saturday |
WEEK 7
Máirt
February 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes FEABHRA FEBRUARY 2023 Wk Mo Tu We Th Fr Sa Su 5 1 2 3 4 5 6 6 7 8 9 10 11 12 7 13 14 15 16 17 18 19 8 20 21 22 23 24 25 26 9 27 2820 Monday | Luain 21 Tuesday |
22 Wednesday | Céadaoin WEEK 8
FEABHRA
Friday
Aoine
February 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
MARCH 2023 Wk Mo Tu We Th Fr Sa Su 9 1 2 3 4 5 10 6 7 8 9 10 11 12 11 13 14 15 16 17 18 19 12 20 21 22 23 24 25 26 13 27 28 29 30 31 23 Thursday | Déardaoin 24
|
26 Sunday | Domhnach25 Saturday | Satharn WEEK 8
MÁRTA
March 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
MARCH 2023 Wk Mo Tu We Th Fr Sa Su 9 1 2 3 4 5 10 6 7 8 9 10 11 12 11 13 14 15 16 17 18 19 12 20 21 22 23 24 25 26 13 27 28 29 30 3127 Monday | Luain 28 Tuesday | Máirt 01 Wednesday | Céadaoin WEEK 9
MÁRTA
Aoine
Satharn
Domhnach
March 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
APRIL 2023 Wk Mo Tu We Th Fr Sa Su 13 1 2 14 3 4 5 6 7 8 9 15 10 11 12 13 14 15 16 16 17 18 19 20 21 22 23 17 24 25 26 27 28 29 30 02 Thursday | Déardaoin 03 Friday |
05 Sunday |
04 Saturday |
WEEK 9
MÁRTA
Máirt
March 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
MARCH 2023 Wk Mo Tu We Th Fr Sa Su 9 1 2 3 4 5 10 6 7 8 9 10 11 12 11 13 14 15 16 17 18 19 12 20 21 22 23 24 25 26 13 27 28 29 30 3106 Monday | Luain 07 Tuesday |
08 Wednesday | Céadaoin WEEK 10
MÁRTA
Thursday
Déardaoin
Friday | Aoine
Satharn
Domhnach
March 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
APRIL 2023 Wk Mo Tu We Th Fr Sa Su 13 1 2 14 3 4 5 6 7 8 9 15 10 11 12 13 14 15 16 16 17 18 19 20 21 22 23 17 24 25 26 27 28 29 30 09
|
10
12 Sunday |
11 Saturday |
WEEK 10
MÁRTA
Máirt
March 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
MARCH 2023 Wk Mo Tu We Th Fr Sa Su 9 1 2 3 4 5 10 6 7 8 9 10 11 12 11 13 14 15 16 17 18 19 12 20 21 22 23 24 25 26 13 27 28 29 30 3113 Monday | Luain 14 Tuesday |
15 Wednesday | Céadaoin WEEK 11
MÁRTA
Saturday
Satharn
16 Thursday | Déardaoin
St.Patrick’s Day 17 Friday | Aoine
Sunday | Domhnach
March 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
APRIL 2023 Wk Mo Tu We Th Fr Sa Su 13 1 2 14 3 4 5 6 7 8 9 15 10 11 12 13 14 15 16 16 17 18 19 20 21 22 23 17 24 25 26 27 28 29 30
19
18
|
WEEK 11
MÁRTA
Máirt
March 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
MARCH 2023 Wk Mo Tu We Th Fr Sa Su 9 1 2 3 4 5 10 6 7 8 9 10 11 12 11 13 14 15 16 17 18 19 12 20 21 22 23 24 25 26 13 27 28 29 30 3120 Monday | Luain 21 Tuesday |
22 Wednesday | Céadaoin WEEK 12
MÁRTA
Friday
Aoine
Satharn
Domhnach
March 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
APRIL 2023 Wk Mo Tu We Th Fr Sa Su 13 1 2 14 3 4 5 6 7 8 9 15 10 11 12 13 14 15 16 16 17 18 19 20 21 22 23 17 24 25 26 27 28 29 30 23 Thursday | Déardaoin 24
|
26 Sunday |
25 Saturday |
WEEK 12
MÁRTA
March 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
MARCH 2023 Wk Mo Tu We Th Fr Sa Su 9 1 2 3 4 5 10 6 7 8 9 10 11 12 11 13 14 15 16 17 18 19 12 20 21 22 23 24 25 26 13 27 28 29 30 3127 Monday | Luain 28 Tuesday | Máirt 29 Wednesday | Céadaoin WEEK 13
MÁRTA
Satharn
March 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
APRIL 2023 Wk Mo Tu We Th Fr Sa Su 13 1 2 14 3 4 5 6 7 8 9 15 10 11 12 13 14 15 16 16 17 18 19 20 21 22 23 17 24 25 26 27 28 29 30 30 Thursday | Déardaoin 31 Friday | Aoine 02 Sunday | Domhnach01 Saturday |
WEEK 13
AIBREÁN
Máirt
April 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
APRIL 2023 Wk Mo Tu We Th Fr Sa Su 13 1 2 14 3 4 5 6 7 8 9 15 10 11 12 13 14 15 16 16 17 18 19 20 21 22 23 17 24 25 26 27 28 29 3003 Monday | Luain 04 Tuesday |
05 Wednesday | Céadaoin WEEK 14
AIBREÁN
Déardaoin
Friday
Aoine
Satharn
Domhnach
April 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
MAY 2023 Wk Mo Tu We Th Fr Sa Su 18 1 2 3 4 5 6 7 19 8 9 10 11 12 13 14 20 15 16 17 18 19 20 21 21 22 23 24 25 26 27 28 22 30 31 06 Thursday |
07
|
09 Sunday |
08 Saturday |
WEEK 14
April 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes AIBREÁN APRIL 2023 Wk Mo Tu We Th Fr Sa Su 13 1 2 14 3 4 5 6 7 8 9 15 10 11 12 13 14 15 16 16 17 18 19 20 21 22 23 17 24 25 26 27 28 29 3010 Monday | Luain Easter Monday 11 Tuesday | Máirt 12 Wednesday | Céadaoin WEEK 15
AIBREÁN
Friday
Aoine
Satharn
April 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
MAY 2023 Wk Mo Tu We Th Fr Sa Su 18 1 2 3 4 5 6 7 19 8 9 10 11 12 13 14 20 15 16 17 18 19 20 21 21 22 23 24 25 26 27 28 22 30 31 13 Thursday | Déardaoin 14
|
16 Sunday | Domhnach15 Saturday |
WEEK 15
Máirt
April 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes AIBREÁN APRIL 2023 Wk Mo Tu We Th Fr Sa Su 13 1 2 14 3 4 5 6 7 8 9 15 10 11 12 13 14 15 16 16 17 18 19 20 21 22 23 17 24 25 26 27 28 29 3017 Monday | Luain 18 Tuesday |
19 Wednesday | Céadaoin WEEK 16
Friday
Aoine
April 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes AIBREÁN MAY 2023 Wk Mo Tu We Th Fr Sa Su 18 1 2 3 4 5 6 7 19 8 9 10 11 12 13 14 20 15 16 17 18 19 20 21 21 22 23 24 25 26 27 28 22 30 31 20 Thursday | Déardaoin 21
|
23 Sunday | Domhnach22 Saturday | Satharn WEEK 16
April 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes AIBREÁN APRIL 2023 Wk Mo Tu We Th Fr Sa Su 13 1 2 14 3 4 5 6 7 8 9 15 10 11 12 13 14 15 16 16 17 18 19 20 21 22 23 17 24 25 26 27 28 29 3024 Monday | Luain 25 Tuesday | Máirt 26 Wednesday | Céadaoin WEEK 17
April 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes AIBREÁN MAY 2023 Wk Mo Tu We Th Fr Sa Su 18 1 2 3 4 5 6 7 19 8 9 10 11 12 13 14 20 15 16 17 18 19 20 21 21 22 23 24 25 26 27 28 22 30 31 27 Thursday | Déardaoin 28 Friday | Aoine 30 Sunday | Domhnach29 Saturday | Satharn WEEK 17
May 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes BEALTAINE MAY 2023 Wk Mo Tu We Th Fr Sa Su 18 1 2 3 4 5 6 7 19 8 9 10 11 12 13 14 20 15 16 17 18 19 20 21 21 22 23 24 25 26 27 28 22 30 3101 Monday | Luain May Day 02 Tuesday | Máirt 03 Wednesday | Céadaoin WEEK 18
BEALTAINE
Déardaoin
Friday
Aoine
Satharn
Domhnach
May 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
JUNE 2023 Wk Mo Tu We Th Fr Sa Su 22 1 2 3 4 23 5 6 7 8 9 10 11 24 12 13 14 15 16 17 18 25 19 20 21 22 23 24 25 26 26 27 28 29 30 04 Thursday |
05
|
07 Sunday |
06 Saturday |
WEEK 18
Máirt
May 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes BEALTAINE MAY 2023 Wk Mo Tu We Th Fr Sa Su 18 1 2 3 4 5 6 7 19 8 9 10 11 12 13 14 20 15 16 17 18 19 20 21 21 22 23 24 25 26 27 28 22 30 3108 Monday | Luain 09 Tuesday |
10 Wednesday | Céadaoin WEEK 19
Aoine
May 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes BEALTAINE JUNE 2023 Wk Mo Tu We Th Fr Sa Su 22 1 2 3 4 23 5 6 7 8 9 10 11 24 12 13 14 15 16 17 18 25 19 20 21 22 23 24 25 26 26 27 28 29 30 11 Thursday | Déardaoin 12 Friday |
14 Sunday | Domhnach13 Saturday | Satharn WEEK 19
Máirt
May 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes BEALTAINE MAY 2023 Wk Mo Tu We Th Fr Sa Su 18 1 2 3 4 5 6 7 19 8 9 10 11 12 13 14 20 15 16 17 18 19 20 21 21 22 23 24 25 26 27 28 22 30 3115 Monday | Luain 16 Tuesday |
17 Wednesday | Céadaoin WEEK 20
BEALTAINE
Thursday
Déardaoin
Friday | Aoine
Satharn
Sunday
Domhnach
May 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
JUNE 2023 Wk Mo Tu We Th Fr Sa Su 22 1 2 3 4 23 5 6 7 8 9 10 11 24 12 13 14 15 16 17 18 25 19 20 21 22 23 24 25 26 26 27 28 29 30 18
|
19
21
|
20 Saturday |
WEEK 20
Máirt
May 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes BEALTAINE MAY 2023 Wk Mo Tu We Th Fr Sa Su 18 1 2 3 4 5 6 7 19 8 9 10 11 12 13 14 20 15 16 17 18 19 20 21 21 22 23 24 25 26 27 28 22 30 3122 Monday | Luain 23 Tuesday |
24 Wednesday | Céadaoin WEEK 21
May 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes BEALTAINE JUNE 2023 Wk Mo Tu We Th Fr Sa Su 22 1 2 3 4 23 5 6 7 8 9 10 11 24 12 13 14 15 16 17 18 25 19 20 21 22 23 24 25 26 26 27 28 29 30 25 Thursday | Déardaoin 26 Friday | Aoine 28 Sunday | Domhnach27 Saturday | Satharn WEEK 21
May 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes BEALTAINE MAY 2023 Wk Mo Tu We Th Fr Sa Su 18 1 2 3 4 5 6 7 19 8 9 10 11 12 13 14 20 15 16 17 18 19 20 21 21 22 23 24 25 26 27 28 22 30 3129 Monday | Luain 30 Tuesday | Máirt 31 Wednesday | Céadaoin WEEK 22
MEITHEAMH
Satharn
June 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
JULY 2023 Wk Mo Tu We Th Fr Sa Su 26 1 2 27 3 4 5 6 7 8 9 28 10 11 12 13 14 15 16 29 17 18 19 20 21 22 23 30 24 25 26 27 28 29 30 31 31 01 Thursday | Déardaoin 02 Friday | Aoine 04 Sunday | Domhnach03 Saturday |
WEEK 22
MEITHEAMH
Máirt
Céadaoin
June 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
JUNE 2023 Wk Mo Tu We Th Fr Sa Su 22 1 2 3 4 23 5 6 7 8 9 10 11 24 12 13 14 15 16 17 18 25 19 20 21 22 23 24 25 26 26 27 28 29 3005 Monday | Luain June Bank Holiday 06 Tuesday |
07 Wednesday |
WEEK 23
MEITHEAMH
Aoine
Satharn
June 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
JULY 2023 Wk Mo Tu We Th Fr Sa Su 26 1 2 27 3 4 5 6 7 8 9 28 10 11 12 13 14 15 16 29 17 18 19 20 21 22 23 30 24 25 26 27 28 29 30 31 31 08 Thursday | Déardaoin 09 Friday |
11 Sunday | Domhnach10 Saturday |
WEEK 23
June 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes MEITHEAMH JUNE 2023 Wk Mo Tu We Th Fr Sa Su 22 1 2 3 4 23 5 6 7 8 9 10 11 24 12 13 14 15 16 17 18 25 19 20 21 22 23 24 25 26 26 27 28 29 3012 Monday | Luain 13 Tuesday | Máirt 14 Wednesday | Céadaoin WEEK 24
MEITHEAMH
Thursday
Déardaoin
Friday | Aoine
Satharn
Sunday
Domhnach
June 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
JULY 2023 Wk Mo Tu We Th Fr Sa Su 26 1 2 27 3 4 5 6 7 8 9 28 10 11 12 13 14 15 16 29 17 18 19 20 21 22 23 30 24 25 26 27 28 29 30 31 31 15
|
16
18
|
17 Saturday |
WEEK 24
Máirt
June 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes MEITHEAMH JUNE 2023 Wk Mo Tu We Th Fr Sa Su 22 1 2 3 4 23 5 6 7 8 9 10 11 24 12 13 14 15 16 17 18 25 19 20 21 22 23 24 25 26 26 27 28 29 3019 Monday | Luain 20 Tuesday |
21 Wednesday | Céadaoin WEEK 25
MEITHEAMH
Thursday
Déardaoin
Friday
Aoine
Satharn
Sunday
Domhnach
June 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
JULY 2023 Wk Mo Tu We Th Fr Sa Su 26 1 2 27 3 4 5 6 7 8 9 28 10 11 12 13 14 15 16 29 17 18 19 20 21 22 23 30 24 25 26 27 28 29 30 31 31 22
|
23
|
25
|
24 Saturday |
WEEK 25
June 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes MEITHEAMH JUNE 2023 Wk Mo Tu We Th Fr Sa Su 22 1 2 3 4 23 5 6 7 8 9 10 11 24 12 13 14 15 16 17 18 25 19 20 21 22 23 24 25 26 26 27 28 29 3026 Monday | Luain 27 Tuesday | Máirt 28 Wednesday | Céadaoin WEEK 26
MEITHEAMH
Satharn
June 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
JULY 2023 Wk Mo Tu We Th Fr Sa Su 26 1 2 27 3 4 5 6 7 8 9 28 10 11 12 13 14 15 16 29 17 18 19 20 21 22 23 30 24 25 26 27 28 29 30 31 31 29 Thursday | Déardaoin 30 Friday | Aoine 02 Sunday | Domhnach01 Saturday |
WEEK 26
IÚIL
Máirt
July 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
JULY 2023 Wk Mo Tu We Th Fr Sa Su 26 1 2 27 3 4 5 6 7 8 9 28 10 11 12 13 14 15 16 29 17 18 19 20 21 22 23 30 24 25 26 27 28 29 30 31 31 03 Monday | Luain 04 Tuesday |
05 Wednesday | Céadaoin WEEK 27
IÚIL
Aoine
Satharn
Domhnach
July 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
AUGUST 2023 Wk Mo Tu We Th Fr Sa Su 31 1 2 3 4 5 6 32 7 8 9 10 11 12 13 33 14 15 16 17 18 19 20 34 21 22 23 24 25 26 27 35 28 29 30 31 06 Thursday | Déardaoin 07 Friday |
09 Sunday |
08 Saturday |
WEEK 27
IÚIL
July 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
JULY 2023 Wk Mo Tu We Th Fr Sa Su 26 1 2 27 3 4 5 6 7 8 9 28 10 11 12 13 14 15 16 29 17 18 19 20 21 22 23 30 24 25 26 27 28 29 30 31 31 10 Monday | Luain 11 Tuesday | Máirt 12 Wednesday | Céadaoin WEEK 28
IÚIL
Aoine
Satharn
July 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
AUGUST 2023 Wk Mo Tu We Th Fr Sa Su 31 1 2 3 4 5 6 32 7 8 9 10 11 12 13 33 14 15 16 17 18 19 20 34 21 22 23 24 25 26 27 35 28 29 30 31 13 Thursday | Déardaoin 14 Friday |
16 Sunday | Domhnach15 Saturday |
WEEK 28
IÚIL
Máirt
July 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
JULY 2023 Wk Mo Tu We Th Fr Sa Su 26 1 2 27 3 4 5 6 7 8 9 28 10 11 12 13 14 15 16 29 17 18 19 20 21 22 23 30 24 25 26 27 28 29 30 31 31 17 Monday | Luain 18 Tuesday |
19 Wednesday | Céadaoin WEEK 29
IÚIL
Friday
Aoine
July 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
AUGUST 2023 Wk Mo Tu We Th Fr Sa Su 31 1 2 3 4 5 6 32 7 8 9 10 11 12 13 33 14 15 16 17 18 19 20 34 21 22 23 24 25 26 27 35 28 29 30 31 20 Thursday | Déardaoin 21
|
23 Sunday | Domhnach22 Saturday | Satharn WEEK 29
IÚIL
July 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
JULY 2023 Wk Mo Tu We Th Fr Sa Su 26 1 2 27 3 4 5 6 7 8 9 28 10 11 12 13 14 15 16 29 17 18 19 20 21 22 23 30 24 25 26 27 28 29 30 31 31 24 Monday | Luain 25 Tuesday | Máirt 26 Wednesday | Céadaoin WEEK 30
IÚIL
July 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
AUGUST 2023 Wk Mo Tu We Th Fr Sa Su 31 1 2 3 4 5 6 32 7 8 9 10 11 12 13 33 14 15 16 17 18 19 20 34 21 22 23 24 25 26 27 35 28 29 30 31 27 Thursday | Déardaoin 28 Friday | Aoine 30 Sunday | Domhnach29 Saturday | Satharn WEEK 30
August 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes LÚNASA AUGUST 2023 Wk Mo Tu We Th Fr Sa Su 31 1 2 3 4 5 6 32 7 8 9 10 11 12 13 33 14 15 16 17 18 19 20 34 21 22 23 24 25 26 27 35 28 29 30 3131 Monday | Luain 01 Tuesday | Máirt 02 Wednesday | Céadaoin WEEK 31
LÚNASA
Déardaoin
Friday
Aoine
Satharn
Domhnach
August 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
SEPTEMBER 2023 Wk Mo Tu We Th Fr Sa Su 35 1 2 3 36 4 5 6 7 8 9 10 37 11 12 13 14 15 16 17 38 18 19 20 21 22 23 24 39 25 26 27 28 29 30 03 Thursday |
04
|
06 Sunday |
05 Saturday |
WEEK 31
LÚNASA
Máirt
Céadaoin
August 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
AUGUST 2023 Wk Mo Tu We Th Fr Sa Su 31 1 2 3 4 5 6 32 7 8 9 10 11 12 13 33 14 15 16 17 18 19 20 34 21 22 23 24 25 26 27 35 28 29 30 3107 Monday | Luain August Bank Holiday 08 Tuesday |
09 Wednesday |
WEEK 32
LÚNASA
Déardaoin
Aoine
August 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
SEPTEMBER 2023 Wk Mo Tu We Th Fr Sa Su 35 1 2 3 36 4 5 6 7 8 9 10 37 11 12 13 14 15 16 17 38 18 19 20 21 22 23 24 39 25 26 27 28 29 30 10 Thursday |
11 Friday |
13 Sunday | Domhnach12 Saturday | Satharn WEEK 32
August 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes LÚNASA AUGUST 2023 Wk Mo Tu We Th Fr Sa Su 31 1 2 3 4 5 6 32 7 8 9 10 11 12 13 33 14 15 16 17 18 19 20 34 21 22 23 24 25 26 27 35 28 29 30 3114 Monday | Luain 15 Tuesday | Máirt 16 Wednesday | Céadaoin WEEK 33
LÚNASA
Thursday | Déardaoin
18 Friday | Aoine
Saturday | Satharn
Sunday | Domhnach
August 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
SEPTEMBER 2023 Wk Mo Tu We Th Fr Sa Su 35 1 2 3 36 4 5 6 7 8 9 10 37 11 12 13 14 15 16 17 38 18 19 20 21 22 23 24 39 25 26 27 28 29 30 17
20
19
WEEK 33
LÚNASA
Máirt
August 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
AUGUST 2023 Wk Mo Tu We Th Fr Sa Su 31 1 2 3 4 5 6 32 7 8 9 10 11 12 13 33 14 15 16 17 18 19 20 34 21 22 23 24 25 26 27 35 28 29 30 3121 Monday | Luain 22 Tuesday |
23 Wednesday | Céadaoin WEEK 34
LÚNASA
Aoine
August 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
SEPTEMBER 2023 Wk Mo Tu We Th Fr Sa Su 35 1 2 3 36 4 5 6 7 8 9 10 37 11 12 13 14 15 16 17 38 18 19 20 21 22 23 24 39 25 26 27 28 29 30 24 Thursday | Déardaoin 25 Friday |
27 Sunday | Domhnach26 Saturday | Satharn WEEK 34
August 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes LÚNASA AUGUST 2023 Wk Mo Tu We Th Fr Sa Su 31 1 2 3 4 5 6 32 7 8 9 10 11 12 13 33 14 15 16 17 18 19 20 34 21 22 23 24 25 26 27 35 28 29 30 3128 Monday | Luain 29 Tuesday | Máirt 30 Wednesday | Céadaoin WEEK 35
MEÁN FÓMHAIR
September 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
OCTOBER 2023 Wk Mo Tu We Th Fr Sa Su 39 1 40 2 3 4 5 6 7 8 41 9 10 11 12 13 14 15 42 16 17 18 19 20 21 22 43 23 24 25 26 27 28 29 44 30 31 31 Thursday | Déardaoin 01 Friday | Aoine 03 Sunday | Domhnach02 Saturday | Satharn WEEK 35
MEÁN FÓMHAIR
Máirt
September 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
SEPTEMBER 2023 Wk Mo Tu We Th Fr Sa Su 35 1 2 3 36 4 5 6 7 8 9 10 37 11 12 13 14 15 16 17 38 18 19 20 21 22 23 24 39 25 26 27 28 29 3004 Monday | Luain 05 Tuesday |
06 Wednesday | Céadaoin WEEK 36
MEÁN FÓMHAIR
Thursday
Déardaoin
Friday | Aoine
Satharn
Domhnach
September 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
OCTOBER 2023 Wk Mo Tu We Th Fr Sa Su 39 1 40 2 3 4 5 6 7 8 41 9 10 11 12 13 14 15 42 16 17 18 19 20 21 22 43 23 24 25 26 27 28 29 44 30 31 07
|
08
10 Sunday |
09 Saturday |
WEEK 36
MEÁN FÓMHAIR
September 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
SEPTEMBER 2023 Wk Mo Tu We Th Fr Sa Su 35 1 2 3 36 4 5 6 7 8 9 10 37 11 12 13 14 15 16 17 38 18 19 20 21 22 23 24 39 25 26 27 28 29 3011 Monday | Luain 12 Tuesday | Máirt 13 Wednesday | Céadaoin WEEK 37
MEÁN FÓMHAIR
Aoine
September 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
OCTOBER 2023 Wk Mo Tu We Th Fr Sa Su 39 1 40 2 3 4 5 6 7 8 41 9 10 11 12 13 14 15 42 16 17 18 19 20 21 22 43 23 24 25 26 27 28 29 44 30 31 14 Thursday | Déardaoin 15 Friday |
17 Sunday | Domhnach16 Saturday | Satharn WEEK 37
MEÁN FÓMHAIR
Máirt
September 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
SEPTEMBER 2023 Wk Mo Tu We Th Fr Sa Su 35 1 2 3 36 4 5 6 7 8 9 10 37 11 12 13 14 15 16 17 38 18 19 20 21 22 23 24 39 25 26 27 28 29 3018 Monday | Luain 19 Tuesday |
20 Wednesday | Céadaoin WEEK 38
MEÁN FÓMHAIR
Thursday
Déardaoin
Friday | Aoine
Satharn
Sunday
Domhnach
September 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
OCTOBER 2023 Wk Mo Tu We Th Fr Sa Su 39 1 40 2 3 4 5 6 7 8 41 9 10 11 12 13 14 15 42 16 17 18 19 20 21 22 43 23 24 25 26 27 28 29 44 30 31 21
|
22
24
|
23 Saturday |
WEEK 38
MEÁN FÓMHAIR
September 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
SEPTEMBER 2023 Wk Mo Tu We Th Fr Sa Su 35 1 2 3 36 4 5 6 7 8 9 10 37 11 12 13 14 15 16 17 38 18 19 20 21 22 23 24 39 25 26 27 28 29 3025 Monday | Luain 26 Tuesday | Máirt 27 Wednesday | Céadaoin WEEK 39
MEÁN FÓMHAIR
September 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
OCTOBER 2023 Wk Mo Tu We Th Fr Sa Su 39 1 40 2 3 4 5 6 7 8 41 9 10 11 12 13 14 15 42 16 17 18 19 20 21 22 43 23 24 25 26 27 28 29 44 30 31 28 Thursday | Déardaoin 29 Friday | Aoine 01 Sunday | Domhnach30 Saturday | Satharn WEEK 39
DEIREADH FÓMHAIR
October 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
OCTOBER 2023 Wk Mo Tu We Th Fr Sa Su 39 1 40 2 3 4 5 6 7 8 41 9 10 11 12 13 14 15 42 16 17 18 19 20 21 22 43 23 24 25 26 27 28 29 44 30 31 02 Monday | Luain 03 Tuesday | Máirt 04 Wednesday | Céadaoin WEEK 40
DEIREADH FÓMHAIR
Thursday
Déardaoin
Friday
Aoine
Satharn
Domhnach
October 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
NOVEMBER 2023 Wk Mo Tu We Th Fr Sa Su 44 1 2 3 4 5 45 6 7 8 9 10 11 12 46 13 14 15 16 17 18 19 47 20 21 22 23 24 25 26 48 27 28 29 30 05
|
06
|
08 Sunday |
07 Saturday |
WEEK 40
DEIREADH FÓMHAIR
October 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
OCTOBER 2023 Wk Mo Tu We Th Fr Sa Su 39 1 40 2 3 4 5 6 7 8 41 9 10 11 12 13 14 15 42 16 17 18 19 20 21 22 43 23 24 25 26 27 28 29 44 30 31 09 Monday | Luain 10 Tuesday | Máirt 11 Wednesday | Céadaoin WEEK 41
DEIREADH FÓMHAIR
October 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
NOVEMBER 2023 Wk Mo Tu We Th Fr Sa Su 44 1 2 3 4 5 45 6 7 8 9 10 11 12 46 13 14 15 16 17 18 19 47 20 21 22 23 24 25 26 48 27 28 29 30 12 Thursday | Déardaoin 13 Friday | Aoine 15 Sunday | Domhnach14 Saturday | Satharn WEEK 41
DEIREADH FÓMHAIR
October 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
OCTOBER 2023 Wk Mo Tu We Th Fr Sa Su 39 1 40 2 3 4 5 6 7 8 41 9 10 11 12 13 14 15 42 16 17 18 19 20 21 22 43 23 24 25 26 27 28 29 44 30 31 16 Monday | Luain 17 Tuesday | Máirt 18 Wednesday | Céadaoin WEEK 42
DEIREADH FÓMHAIR
October 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
NOVEMBER 2023 Wk Mo Tu We Th Fr Sa Su 44 1 2 3 4 5 45 6 7 8 9 10 11 12 46 13 14 15 16 17 18 19 47 20 21 22 23 24 25 26 48 27 28 29 30 19 Thursday | Déardaoin 20 Friday | Aoine 22 Sunday | Domhnach21 Saturday | Satharn WEEK 42
DEIREADH FÓMHAIR
October 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
OCTOBER 2023 Wk Mo Tu We Th Fr Sa Su 39 1 40 2 3 4 5 6 7 8 41 9 10 11 12 13 14 15 42 16 17 18 19 20 21 22 43 23 24 25 26 27 28 29 44 30 31 23 Monday | Luain 24 Tuesday | Máirt 25 Wednesday | Céadaoin WEEK 43
DEIREADH FÓMHAIR
October 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
NOVEMBER 2023 Wk Mo Tu We Th Fr Sa Su 44 1 2 3 4 5 45 6 7 8 9 10 11 12 46 13 14 15 16 17 18 19 47 20 21 22 23 24 25 26 48 27 28 29 30 26 Thursday | Déardaoin 27 Friday | Aoine 29 Sunday | Domhnach28 Saturday | Satharn WEEK 43
November 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes SAMHAIN NOVEMBER 2023 Wk Mo Tu We Th Fr Sa Su 44 1 2 3 4 5 45 6 7 8 9 10 11 12 46 13 14 15 16 17 18 19 47 20 21 22 23 24 25 26 48 27 28 29 3030 Monday | Luain October Bank Holiday 31 Tuesday | Máirt Halloween 01 Wednesday | Céadaoin WEEK 44 OCTOBER 2022 4 7 8 9 41 11 18 25 28 29 30 44 31
SAMHAIN
Aoine
Satharn
November 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
DECEMBER 2023 Wk Mo Tu We Th Fr Sa Su 48 1 2 3 49 4 5 6 7 8 9 10 50 11 12 13 14 15 16 17 51 18 19 20 21 22 23 24 52 25 26 27 28 29 30 31 02 Thursday | Déardaoin 03 Friday |
05 Sunday | Domhnach04 Saturday |
WEEK 44
Máirt
November 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes SAMHAIN NOVEMBER 2023 Wk Mo Tu We Th Fr Sa Su 44 1 2 3 4 5 45 6 7 8 9 10 11 12 46 13 14 15 16 17 18 19 47 20 21 22 23 24 25 26 48 27 28 29 3006 Monday | Luain 07 Tuesday |
08 Wednesday | Céadaoin WEEK 45
SAMHAIN
Satharn
Thursday
Déardaoin
Friday | Aoine
November 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
DECEMBER 2023 Wk Mo Tu We Th Fr Sa Su 48 1 2 3 49 4 5 6 7 8 9 10 50 11 12 13 14 15 16 17 51 18 19 20 21 22 23 24 52 25 26 27 28 29 30 31 09
|
10
12 Sunday | Domhnach11 Saturday |
WEEK 45
Máirt
November 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes SAMHAIN NOVEMBER 2023 Wk Mo Tu We Th Fr Sa Su 44 1 2 3 4 5 45 6 7 8 9 10 11 12 46 13 14 15 16 17 18 19 47 20 21 22 23 24 25 26 48 27 28 29 3013 Monday | Luain 14 Tuesday |
15 Wednesday | Céadaoin WEEK 46
SAMHAIN
Thursday
Déardaoin
Friday | Aoine
Satharn
Sunday
Domhnach
November 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
DECEMBER 2023 Wk Mo Tu We Th Fr Sa Su 48 1 2 3 49 4 5 6 7 8 9 10 50 11 12 13 14 15 16 17 51 18 19 20 21 22 23 24 52 25 26 27 28 29 30 31 16
|
17
19
|
18 Saturday |
WEEK 46
Máirt
November 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes SAMHAIN NOVEMBER 2023 Wk Mo Tu We Th Fr Sa Su 44 1 2 3 4 5 45 6 7 8 9 10 11 12 46 13 14 15 16 17 18 19 47 20 21 22 23 24 25 26 48 27 28 29 3020 Monday | Luain 21 Tuesday |
22 Wednesday | Céadaoin WEEK 47
SAMHAIN
Satharn
Thursday
Déardaoin
Friday
Aoine
November 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
DECEMBER 2023 Wk Mo Tu We Th Fr Sa Su 48 1 2 3 49 4 5 6 7 8 9 10 50 11 12 13 14 15 16 17 51 18 19 20 21 22 23 24 52 25 26 27 28 29 30 31 23
|
24
|
26 Sunday | Domhnach25 Saturday |
WEEK 47
November 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes SAMHAIN NOVEMBER 2023 Wk Mo Tu We Th Fr Sa Su 44 1 2 3 4 5 45 6 7 8 9 10 11 12 46 13 14 15 16 17 18 19 47 20 21 22 23 24 25 26 48 27 28 29 3027 Monday | Luain 28 Tuesday | Máirt 29 Wednesday | Céadaoin WEEK 48
SAMHAIN
November 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
DECEMBER 2023 Wk Mo Tu We Th Fr Sa Su 48 1 2 3 49 4 5 6 7 8 9 10 50 11 12 13 14 15 16 17 51 18 19 20 21 22 23 24 52 25 26 27 28 29 30 31 30 Thursday | Déardaoin 01 Friday | Aoine 03 Sunday | Domhnach02 Saturday | Satharn WEEK 48
NOLLAIG
Máirt
December 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
DECEMBER 2023 Wk Mo Tu We Th Fr Sa Su 48 1 2 3 49 4 5 6 7 8 9 10 50 11 12 13 14 15 16 17 51 18 19 20 21 22 23 24 52 25 26 27 28 29 30 3104 Monday | Luain 05 Tuesday |
06 Wednesday | Céadaoin WEEK 49
NOLLAIG
Friday
Aoine
Satharn
Domhnach
December 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
JANUARY 2024 Wk Mo Tu We Th Fr Sa Su 1 1 2 3 4 5 6 7 2 8 9 10 11 12 13 14 3 15 16 17 18 19 20 21 4 22 23 24 25 26 27 28 5 29 30 31 07 Thursday | Déardaoin 08
|
10 Sunday |
09 Saturday |
WEEK 49
NOLLAIG
December 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
DECEMBER 2023 Wk Mo Tu We Th Fr Sa Su 48 1 2 3 49 4 5 6 7 8 9 10 50 11 12 13 14 15 16 17 51 18 19 20 21 22 23 24 52 25 26 27 28 29 30 3111 Monday | Luain 12 Tuesday | Máirt 13 Wednesday | Céadaoin WEEK 50
NOLLAIG
Friday
Aoine
Satharn
December 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
JANUARY 2024 Wk Mo Tu We Th Fr Sa Su 1 1 2 3 4 5 6 7 2 8 9 10 11 12 13 14 3 15 16 17 18 19 20 21 4 22 23 24 25 26 27 28 5 29 30 31 14 Thursday | Déardaoin 15
|
17 Sunday | Domhnach16 Saturday |
WEEK 50
NOLLAIG
Máirt
December 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
DECEMBER 2023 Wk Mo Tu We Th Fr Sa Su 48 1 2 3 49 4 5 6 7 8 9 10 50 11 12 13 14 15 16 17 51 18 19 20 21 22 23 24 52 25 26 27 28 29 30 3118 Monday | Luain 19 Tuesday |
20 Wednesday | Céadaoin WEEK 51
NOLLAIG
Thursday
Déardaoin
22 Friday | Aoine
Christmas Eve 24 Sunday | Domhnach
December 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
JANUARY 2024 Wk Mo Tu We Th Fr Sa Su 1 1 2 3 4 5 6 7 2 8 9 10 11 12 13 14 3 15 16 17 18 19 20 21 4 22 23 24 25 26 27 28 5 29 30 31 21
|
23 Saturday | Satharn WEEK 51
NOLLAIG
Luain Christmas Day
Tuesday | Máirt St. Stephen’s Day
Wednesday | Céadaoin
December 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
DECEMBER 2023 Wk Mo Tu We Th Fr Sa Su 48 1 2 3 49 4 5 6 7 8 9 10 50 11 12 13 14 15 16 17 51 18 19 20 21 22 23 24 52 25 26 27 28 29 30 3125 Monday |
26
27
WEEK 52
NOLLAIG
Thursday
Déardaoin
Friday
Aoine
Satharn
Years Eve 31 Sunday
Domhnach
December 2023 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
JANUARY 2024 Wk Mo Tu We Th Fr Sa Su 1 1 2 3 4 5 6 7 2 8 9 10 11 12 13 14 3 15 16 17 18 19 20 21 4 22 23 24 25 26 27 28 5 29 30 31 18
|
29
|
New
|
30 Saturday |
WEEK 52 52 3 4 5 6 7 8 9 10 17 25 26 27 28 29 5 30 31
EANÁIR
January 2024 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
JANUARY 2024 Wk Mo Tu We Th Fr Sa Su 1 1 2 3 4 5 6 7 2 8 9 10 11 12 13 14 3 15 16 17 18 19 20 21 4 22 23 24 25 26 27 28 5 29 30 3101 Monday | Luain New Years Day 02 Tuesday | Máirt 03 Wednesday | Céadaoin WEEK 01
EANÁIR
Déardaoin
Friday
Aoine
Satharn
Domhnach
January 2024 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
FEBRUARY 2024 Wk Mo Tu We Th Fr Sa Su 5 1 2 3 4 6 5 6 7 8 9 10 11 7 12 13 14 15 16 17 18 8 19 20 21 22 23 24 25 9 26 27 28 04 Thursday |
05
|
07 Sunday |
06 Saturday |
WEEK 01
EANÁIR
January 2024 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes 8 9 10 11 12 13 14 15 16 17 Notes
JANUARY 2024 Wk Mo Tu We Th Fr Sa Su 1 1 2 3 4 5 6 7 2 8 9 10 11 12 13 14 3 15 16 17 18 19 20 21 4 22 23 24 25 26 27 28 5 29 30 3108 Monday | Luain 09 Tuesday | Máirt 10 Wednesday | Céadaoin WEEK 02
