Cardiovascular News - Issue 76 - February 2025 OUS
3 STS 2025 New data on aortic valve selection
13 SCOT-HEART
Ten-year results of landmark CCTA trial
Profile Bruno Scheller
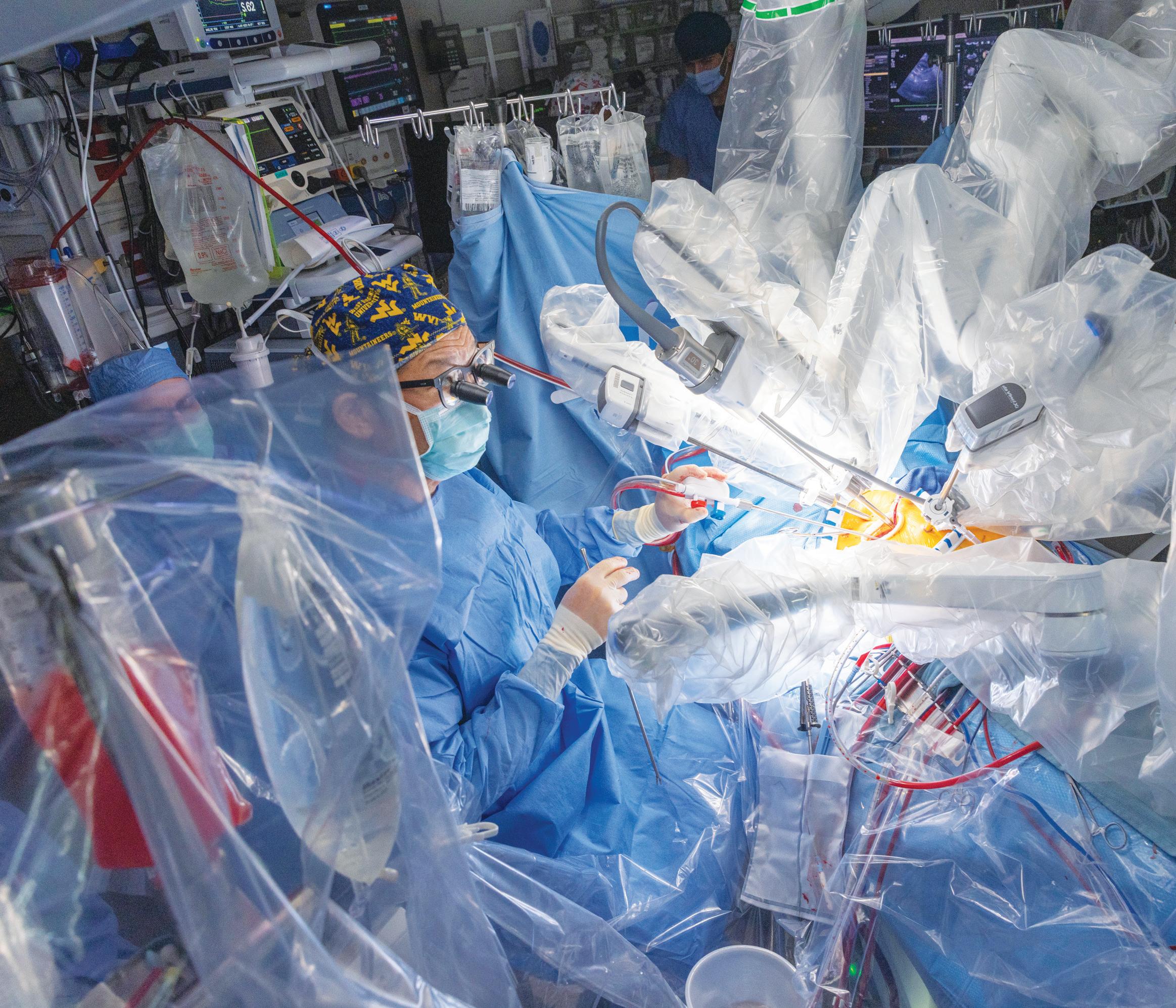
Pioneering procedures promise new era for robotic cardiac surgery
A series of world-first robotic procedures performed in recent months have pushed the boundaries of possibility for robotics in the cardiac surgery arena and demonstrate the potential to broaden the availability of these procedures worldwide, experts in robotic surgery have said.
Recent advancements include the first ever fully robotic heart transplant, performed by surgeons at the King Faisal Specialist Hospital and Research Centre (KFSHRC, Riyadh, Saudi Arabia), whilst surgeons at West Virginia University (WVU, Morgantown, USA) have claimed their own milestone with a pioneering fully robotic procedure combining aortic valve replacement with coronary bypass grafting.
Cardiac surgeon Feras Khaliel, the head of cardiac surgery and director of the Robotics and Minimally Invasive Surgery programme at KFSHRC led the heart transplant procedure in September 2024, which involved a 16-year-old patient suffering from end-stage heart failure.
KFSHRC has gone on to claim a subsequent milestone by performing the first robotic-assisted implantation of a HeartMate 3 (Abbott) artificial heart pump, which was offered to a 35-year-old man who had been hospitalised for 120 days due to advanced heart failure in January 2025.
Khaliel says that the use of robotic technology facilitates a minimally invasive approach that should theoretically shorten recovery time and improve quality of life for patients. Following the implantation of the HeartMate 3 heart pump, for example, the patient spent four days in the intensive care unit, in contrast to the 26-day average for similar procedures performed
with traditional surgical methods.
“Robotic cardiac surgery has transformed patient outcomes through its minimally invasive techniques, which reduce trauma, pain, and recovery times,” Khaliel tells Cardiovascular News. “Hospital stays are shortened by over 50%, and patients experience fewer complications and reduced reliance on blood transfusions. Procedures like robotic heart transplants take just two and a half hours, compared to six–12 hours with traditional methods.”
KFSHRC is looking to position itself as world leader in robotic cardiac surgery and in 2024 performed over 1,127
Robotic cardiac surgery has transformed patient outcomes through its minimaly invasive techniques.”
Studies add fuel to debate over choice of surgical or transcatheter strategies in dual treatment of aortic and coronary disease
A LARGE-SCALE ANALYSIS of data from the US Centers for Medicare and Medicaid Services (CMS) inpatient database, including over 37,000 patients with significant coronary artery disease requiring aortic valve replacement and coronary revascularisation, has found that patients fared better in the long term when they were treated with a surgical approach compared to transcatheter techniques.
The analysis, presented by J Hunter Mehaffey (West Virginia University, Morgantown, USA) at the Society of Thoracic Surgeons’ (STS) 2025 annual meeting (25–27 January, Los Angeles, USA) is the latest in a series of studies attempting to establish the optimal approach for the treatment of patients presenting with concomitant aortic and coronary disease, with contrasting results—prompting calls for more randomised data to settle the question.
“Very frequently during our structural heart conference we’re faced with patients who are low-risk candidates by STS risk score, who are being presented for severe aortic stenosis needing an aortic valve replacement. Based on the current data many of us believe there is equipoise about what approach is best in a low-risk patient,” Mehaffey tells Cardiovascular News, outlining the rationale for the research. “If they have concomitant disease that plays a role because there are treatment options that we can provide surgically in patients who have coronary disease.”
The analysis by Mehaffey and colleagues evaluated patients aged 65 years and older with a diagnosis of coronary artery disease present on admission undergoing coronary artery
Continued on page 2
STS 2025
Studies add fuel to debate over choice of surgical or transcatheter strategies in dual treatment of aortic and coronary disease
Continued from page 1
bypass graft (CABG) surgery and surgical aortic valve replacement (SAVR) using a tissue valve only compared to transcatheter aortic valve implantation (TAVI) with elective percutaneous coronary intervention (PCI) within three months before or after between January 2018 and December 2022.
A total of 37,822 beneficiaries underwent PCI/TAVI (n=17,413) or CABG/SAVR (n=20,409). The PCI/TAVI cohort consisted of 14,500 (83.3%) patients receiving elective PCI three months before elective TAVI and 2,337 (13.4%) patients receiving non-emergent PCI during their index TAVI admission with only 576 (3.3%) patients requiring elective PCI within three months after TAVI.
SAVR/CABG, with the trial ultimately showing that the transcatheter approach elicited more favourable results against a primary endpoint of all-cause mortality, myocardial infarction, disabling stroke, clinically driven target-vessel revascularisation, valve reintervention, and life-threatening or disabling bleeding at one year post-treatment.
Kedhi and colleagues reported that FFR-guided PCI plus TAVI resulted in favourable outcomes for the primary endpoint (four of 91 patients) versus SAVR plus CABG (17 of 77 patients), which was below the study’s 15% prespecified non-inferiority margin. FFRguided PCI plus TAVI was superior to SAVR plus CABG, which was driven mainly by allcause mortality and life-threatening bleeding.
“I was a little surprised by the strength of the conclusions based on sample sizes of less than 100 patients in each arm, and a one-year endpoint,” Mehaffey comments in response to these findings, adding that he believed the rate of mortality seen in the surgical arm of the trial stood higher than figures seen in real-world practice or in clinical trial settings.
NEWS IN BRIEF
THE LATEST STORIES FROM THE CARDIOVASCULAR WORLD
Following their analysis Mehaffey and colleagues found that the index admission PCI/TAVI was associated with lower rates of major bleeding, acute kidney injury and in-hospital mortality, with no difference in stroke, but a higher rate of new pacemaker and surgical repair of the femoral artery compared to CABG/SAVR.
In this five-year study, risk-adjusted longitudinal analysis, demonstrated PCI/TAVI treatment was associated with significantly higher readmission for stroke, myocardial infarction, all-cause mortality and the primary composite outcome of stroke, myocardial infarction, valve reintervention or death.
“You have to make a decision with the patient,” says Mehaffey, reflecting on the findings. “They have to understand the recovery is going to be more significant with surgery, but it’s important to make sure that patients make an informed decision and know what they’re going to feel like five years from now or what their adverse event rate is going to be over the next 10 or 15 years, especially when we’re talking about younger lower risk patients.”
Whilst Mehaffey et al’s analysis points to a benefit for the surgical approach, research published in The Lancet in January points towards a different conclusion. The TCW trial represents the only randomised trial to compare TAVI and fractional flow reserve (FFR)-guided PCI versus conventional surgical valve replacement and CABG for the treatment of patients with aortic valve stenosis and complex or multivessel coronary disease.
Investigators, led by Elvin Kedhi (McGill University Health Center, Montreal, Canada), enrolled 172 patients, 91 randomised to transcatheter therapy and 81 to
Speaking to Cardiovascular News, Kedhi acknowledges the limitations of the TCW trial relating to length of follow-up and the number of patients, but pointed to the findings of a recent multicentre retrospective analysis of patients enrolled in 14 centres in Spain, published in JACC: Cardiovascular Interventions, in which
Based on the current data many of us believe there is equipoise about what approach is best in a low-risk patient.”
CABG and SAVR were associated with a higher rate of death and stroke compared to PCI and TAVI. The authors of the study, Ignacio Amat-Santos (Hospital Clínico Universitario, Valladolid, Spain) and colleagues, acknowledge that the findings highlight the need for more randomised data in this area. “I truly believe that we really need a large, randomised trial to answer this question,” says Kedhi, endorsing this recommendation.
Responding to this point, Mehaffey says that a trial “wouldn’t be the easiest to design” but suggests “it needs to have a pragmatic design and with surgeons and interventionalists at the table during trial design”.
“I do think it’s going to have to be a fairly large trial, and most importantly, I think it’s going to have to have longitudinal outcomes far beyond one year, because especially as we start to roll these out in younger, low-risk patients that may have a 10-, 15-, 25-year life expectancy, it is critical to understand implications of treatment,” he comments.
Editor-in-chief: Simon Redwood | Publisher: Stephen Greenhalgh
Content Director: Urmila Kerslake
Senior editor: Will Date will@bibamedical.com | Editorial contribution: Jamie Bell, Jocelyn Hudson
n EACTS: European Association for Cardio-Thoracic Surgery (EACTS) immediate past president Franca Melfi (Pisa, Italy) speaks to Cardiovascular News about the organisation's work to encourage a culture of innovation within the field of cardiothoracic surgery, and explains why this is important to attracting a younger, more diverse workforce to shape the future of the specialty.
For more on this story go to page 8.
n EARLY AORTIC INTERVENTION:
Following the release of the results of the EARLY TAVR and EVOLVED trials, heart teams now have more evidence to potentially consider an early intervention in patients with severe, asymptomatic aortic stenosis. Cardiovascular News unpacks some of the details of the trials, examines what these add to our existing dataset, and looks ahead to future studies that are set to provide more knowledge in this arena.
For more on this story go to page 14.
n PCR LONDON VALVES 2024:
Catch up on highlights from PCR London Valves 2024 (24–26 November, London, UK) which include late-breaking data from a new analysis of the LANDMARK trial, detailing the performance of a novel balloon-expandable transcatheter aortic valve implantation (TAVI) system, compared to one of the most widely used commercially available devices; as well as findings from the CLASP IID trial investigating the use of two transcatheter edge-to-edge repair (TEER) for the treatment of degenerative mitral regurgitation (MR).
For more on this story go to page 21.
Scan the QR code to subscribe
If you have comments on this issue or suggestions for upcoming editions write to will@bibamedical.com
J Hunter Mehaffey
Mechanical valves offer a survival advantage in younger patients undergoing SAVR
Use of mechanical valves in patients aged 60 or younger who are undergoing surgical aortic valve replacement (SAVR) yields a significant long-term survival benefit when weighed against the use of bioprosthetic valves, research presented at the 2025 Society of Thoracic Surgeons (STS) annual meeting (25–27 January, Los Angeles, USA) has shown.
THE STUDY LEVERAGING DATA from the STS Adult Cardiac Surgery Database (ACSD), encompassing over 100,000 patients, seeks to show how age and valve type influence outcomes for patients undergoing SAVR.
The authors of the study, led by Michael Bowdish (Cedars-Sinai Medical Center, Los Angeles, USA), assert in their full publication of the research in the Journal of the American College of Cardiology (JACC) that the findings of the study should “make us pause” when considering treatment strategies in younger patients, increasing numbers of whom are receiving bioprosthetic valves or undergoing transcatheter aortic valve implantation (TAVI).
“Controversy persists over both provider recommendations and individual patient selection of a bioprosthetic or mechanical prosthesis at the time of SAVR, particularly in younger patients,” Bowdish and colleagues write in their paper, adding that the relevance of this challenge has increased with the rapid expansion of TAVI, which may be partly based on an acceptance of bioprosthetic valve replacement in young patients and a continuum of lifetime management that would include future valve-in-valve therapy or reoperation.
Mechanical valves have been shown to be more durable than bioprosthetic valves but are more thrombogenic, requiring lifelong anticoagulation.
Recent trends have shown a move toward the use of more bioprosthetic valves across the age spectrum, even though it is recommended that younger patients receive a mechanical valve— and the study highlights a decreasing proportion of mechanical valve use over its 12-year lifespan, from 20% in 2008 to less than 10% in 2019.
Bowdish and colleagues aimed to evaluate the relationship between bioprosthetic and mechanical SAVR and longitudinal survival in patients between the ages of 40 and 75, hypothesising that there is an age cut-off at which mechanical SAVR would have a risk adjusted survival benefit compared to bioprosthetic SAVR.
The researchers identified all patients undergoing isolated first-time SAVR in the STS database between July 2008 and March 2019, capturing a total of 109,842 individuals, 94,125 (85.7%) having undergone SAVR with a bioprosthetic valve, and 15,717 (14.3%) with a mechanical valve. At baseline, patients had similar characteristics except for mean age, which stood at 65.2 years for bioprosthetic valves and 55.7 years for mechanical valves.
After risk adjustment, freedom from all-cause mortality favoured mechanical valves to age 60, whilst freedom from all-cause mortality or valve reoperation favoured mechanical valves to age 65. Age group-specific analyses demonstrated mechanical valves to be
associated with lower all-cause mortality in all age groups ≤60 years, with the results remaining consistent across all sensitivity analyses.
“The decision between a bioprosthetic and mechanical valve is one of the most consequential for patients requiring aortic valve replacement,” said Bowdish. “Our research underscores that for patients with an age threshold of 60 years, mechanical valves confer a significant survival advantage. This data will help patients and providers make more informed choices about their care.”
Reflecting on the results for Cardiovascular News, interventional cardiologist and trialist David Cohen (St Francis Hospital and Heart Center, Roslyn, USA), comments that the results of the study did not appear surprising, and that the results “serve as a reminder” of the durability of mechanical valves.
for many younger patients that provides greater durability than any current bioprosthetic aortic valve replacement— either surgical or transcatheter—at the ‘cost’ of a substantial increase in bleeding, since patients who receive a mechanical valve require lifelong anticoagulation.
“We should inform young patients with aortic stenosis about this additional option when they are weighing the choice between TAVI and SAVR and help them to understand these potential trade-offs. Individual patients may value these attributes differently, and we should respect and attempt to honour their preferences whenever feasible.”
“The results of this observational study provide evidence to suggest that, in contemporary practice, patients under the age of 60 who undergo aortic valve replacement with a mechanical valve live longer than patients who receive a bioprosthetic valve. There was no such survival advantage for patients over the age of 60—who constitute the majority of patients who undergo aortic valve replacement in the USA.”
These concur with other observational studies conducted over the last 10 years, according to Cohen, who said that, with the coming from a large surgical database, the data allowed the authors to account for many additional differences between patients undergoing mechanical versus bioprosthetic AVR, which he described as “reassuring”.
“While the observational nature of the study limits our ability to be certain about this benefit, the study does serve as a reminder that a mechanical aortic valve replacement is a very good option
Shortlist for second ever Global Cardiovascular Awards revealed
The shortlist for the second Global Cardiovascular Awards—which will recognise the important work of individuals, teams and organisations to improve the life of those impacted by cardiovascular disease—has been revealed.
JUDGES HAVE HAND-PICKED FINALISTS across 12 categories, with the winners to be announced in-person at an exclusive event at the Sheraton Grand Hotel in central London on the evening of 13 March. Visit globalcardiovascularawards.com to find out how you can attend. Support for the event comes from Boston Scientific and Cardialysis.
Awards categories touch on the work of clinicians, researchers, healthcare providers, industry, innovators and institutions. Across several industry-led categories, the awards will honour major advances in technologies in areas such as interventional cardiology, patient and operator safety, and cardiac imaging. Medtronic has received two nominations
in the Best Cardiovascular Product Launch category for its Aurora extravascular implantable cardiodefibrillator system and the Symplicity Spyral renal denervation system, alongside the Rampart Guardian and Rampart Sentry from Rampart IC. Siemens Healthineers and ORSIF are vying for the Best Education Campaign, whilst the Best Prevention Campaign category includes entries from the British Heart Foundation, Global Heart Hub and ORSIF.
Among the industry categories, Egg Medical and Syndeo Medical are finalists for the Best New Startup, whilst Ahmed Elmouelhi of TriCares, Athanasios Justin Lampropoulos of Syndeo Medical and Gaurav Agarwal of Innvolution have been selected for the CEO of the Year Award.
Cardiac surgeon Tirone David (Toronto General Hospital, Toronto, Canada), renowned for his research into aortic disease, describes the publication as an “important paper on the choices of heart valve for aortic valve replacement”.
“I have never understood the trend towards bioprosthetic valve replacement in patients younger than 65 years of age,” he tells Cardiovascular News, adding that this trend appears to have preceded the advance of TAVI, and that the present paper could lead to more mechanical valves being implanted.
“Although I believe that mechanical valves confer a survival benefit in patients younger than 65 years of age, there may be confounding factors that affected the surgeons’ choice of valve in this study based on the STS database. Certain variables such as patients’ education, geographic location, concomitant disease or previous cancer treatment may have interfered in the decision making. In other words, only ‘healthy patients’ had mechanical valves, and the sicker ones got a bioprosthetic valve because, in the surgeon’s estimate of lifespan, the first ones would have had a survival benefit.”
New technologies from Innvolution, Elixir Medical, Biotronik, Medtronic and TriCares are competing for the Innovation in Interventional Cardiology award, whilst the Innovation in Patient and Operator Safety award includes entries from Egg Medical and Rampart IC, whilst entries from Arineta, Acarix, Caristo, HeartFlow and Vista.Ai make up the Innovation in Cardiac Imaging category. Efforts to improve cath lab safety are recognised in the Innovation in Patient and Operator Safety Award with entries from Egg Medical and Rampart IC.
In the Digital Innovation category, entries include the Breakthrough Collaboration’s Redo TAV APP, the CADScor system from Acarix, HeartFlow ONE and Megi-Mum. Projects from Boston Scientific and the University of Glasgow are recognised for their contribution to improving equity and diversity in cardiovascular care. Waqas Akhtar (Guys & St Thomas NHS Trust, London, UK), Simone Fezzi (University of Verona, Verona, Italy), and Monica Mittal (Kings College Hospital, London, UK) are vying to be named Future Leader. Other awards, including the vaunted Lifetime Achievement category, will be announced on the night.
Michael Bowdish
Challenges of 21st century aortic education, innovation and evidence get top billing at CX 2025
Critical challenges in open and endovascular treatment of aortic disease will be brought into focus when world leaders in cardiac, aortic, and vascular therapies return to London this spring for the 47th annual Charing Cross (CX) Symposium 2025 (23–25 April, London, UK).
CX, the world’s largest vascular meeting, has a three-year cycle of raising vascular and endovascular controversies to challenge the available evidence and reach a consensus after discussion with an expert audience.
“The highlight this year is challenges, and we have challenges in clinical practice in aortic care every day,” CX co-chair Dittmar Böckler (University Hospital Heidelberg, Heidelberg, Germany) tells Cardiovascular News, looking ahead to the highlights on the aortic programme in 2025. “We need evidence, we need teaching, we need technical skills and tips and tricks, [and] all this will be provided by a really outstanding programme with key opinion leaders in the field of aortic disease and aortic care.”
The CX 2025 programme has sessions touching upon all vascular domains, spanning aortic, peripheral, venous, acute stroke and vascular access. The aortic pillar of the programme offers attendees insights from 119 presentations, augmented by 11 edited cases, with new data set to be brought to light in 12 podium first presentations, alongside debates on five hotly contested issues. There will also be opportunities for attendees to translate theory into practice through a series of handson workshops running throughout the three days.
Aortic techniques and technologies will be the focus on day one, with Böckler highlighting a case involving the treatment of a thoracoabdominal aneurysm using a four-inner-branched device as one to look out for.
“We need off-the-shelf devices to treat these emergent and urgent patients, as customised devices are not available. How to handle those devices, how to implant them, [and] what the evidence is so far is the focus,” he says of the case.
Turning to the highlights among the many podium first presentations featuring at CX 2025—with more
than 50 across the full programme—Böckler mentions the SUNDAY trial, a randomised trial looking at treatment options for uncomplicated type B aortic dissection (TBAD), as being of particular importance. “We have a lack of evidence there, and we are going to have the first insight into early outcomes of this trial,” he comments. Other podium first presentations include data on the impact of blood pressure on abdominal aortic aneurysm (AAA) growth rates, risk stratification after endovascular aneurysm repair (EVAR), a multicentre study on physician-modified endografts for very large and urgent complex AAA, and more.
The use of artificial intelligence (AI) in patient evaluation is among the “disruptive” technologies featuring alongside topics that impact daily clinical practice such as sarcopenia, the risk of abdominal cancer after EVAR, the use of proteomics to predict sac shrinkage after EVAR and quality-of-life assessment following vascular care.
“Something we have really neglected for years, in my mind, is quality-of-life assessment after vascular care, specifically in TBAD,” explains Böckler. “Many patients get conservative treatment, but we didn’t pay attention to their psychological status, how they behave, how they feel, so quality of life is something very new. And that’s in the programme of the aortic sessions this year.”
Among other highlights, Gustavo Oderich (University of Texas Health Science Center at Houston, Houston, USA) will deliver the inaugural Roger M Greenhalgh memorial lecture, speaking on the challenges of 21st century aortic
education, innovation and evidence. Citing this as one of the event’s must-attend presentations, Böckler says that the talk will continue CX founding chair Roger Greenhalgh’s legacy of advocating for the best medical education for the optimal care of patients with vascular disease.
“The unique and special thing about Charing Cross is the style of discussion,” Böckler adds, paying tribute to another of Greenhalgh’s CX legacies. “We have a one-to-one relationship between presentations and discussions. I love the discussion culture at Charing Cross. This makes it unique and special. We have a
I love the discussion culture at Charing Cross. This makes it unique and special.”
Dittmar Böckler
special style, a special atmosphere. Everybody can go to the microphone, ask questions, and you will get excellent answers from the leading physicians of the world.”
AT A GLANCE
● The largest vascular meeting in the world
● 50+ podium firsts
● Inaugural Roger M Greenhalgh memorial lecture
Attendees can join world-leading experts in the management and treatment of aortic disease from the cardiovascular, vascular and endovascular worlds who are participating in 2025 including CX aortic executive board members Oderich, Tilo Kölbel (University Heart Center Hamburg, Hamburg, Germany), Joseph Bavaria (University of Pennsylvania, Philadelphia, USA), Alexander Zimmermann (University Hospital Zürich, Zürich, Switzerland), Aung Oo (St Bartholomew’s Hospital, London, UK). Registration and programme details for CX 2025 can be found online at cxsymposium.com.
Full IDE dataset from AMDS PRESERVE trial presented at STS 2025
DATA FROM THE ASCYRUS medical dissection stent (AMDS) PERSEVERE clinical trial were presented in a late-breaking science presentation at the Society of Thoracic Surgeons (STS) 2025 annual meeting (25–27 January, Los Angeles, USA). The data include clinical outcomes across the full investigational device exemption (IDE) cohort at one year following AMDS implantation.
The trial is a prospective, multicentre, non-randomised clinical trial to determine if patients with acute DeBakey type I aortic dissection can be treated safely and effectively using the AMDS hybrid prosthesis (Artivion), designed to support Artivion’s application to the US Food and Drug Administration (FDA) for premarket approval of the AMDS.
The trial consists of 93 participants in the USA who have experienced an acute DeBakey type I aortic dissection complicated by malperfusion.
Shinichi Fukuhara (University of Michigan, Ann Arbor, USA) presented the data from the PERSEVERE US IDE trial, demonstrating a sustained benefit of AMDS out to one year, showing minimal new occurrence of stroke, renal failure requiring dialysis, or myocardial infarction. Eighty percent of patients survived through one year with mortality after 30 days attributed to comorbidities and dissection-related complications.
Core lab analysis of follow-up computed tomography (CT) scans suggests AMDS prevents the occurrence of distal anastomotic new entry (DANE) tears which compares favourably to expected rates of early reintervention and DANE tears in this population, Artivion states in a press release. DANE tears occur in up to 70% of patients following hemiarch repair without AMDS, allowing continued blood flow into the false lumen created by the dissection.
The presence of DANE is associated with enlargement of the aorta, reoperation, and increased mortality. DANE has not been detected in any patients in the PERSEVERE study and it was not reported in the DARTS study through five years of follow-up. The need for unanticipated aortic reoperations was low at 4.3%.
Fukuhara commented: “Patient outcomes following AMDS treatment of acute DeBakey type I aortic dissection with malperfusion remain impressive through one year after operation. AMDS is an important tool for cardiovascular surgeons in treating this devasting disease.”
Analysis sheds light on impact of surgeon preference in choice of multiversus single-arterial grafting in CABG
In patients undergoing coronary artery bypass grafting (CABG), a novel analysis evaluating surgeon preference for multi- versus singlearterial grafting may explain the differing results between prior retrospective analyses and randomised controlled trials regarding longterm survival, researchers have claimed.
Astudy presented at The Society of Thoracic Surgeons (STS) 2025 annual meeting (25–27 January, Los Angeles, USA) explores findings in more than a million US Medicare beneficiaries who underwent CABG from 2001 to 2019.
The researchers found that patients who received multiarterial grafting (MAG) had improved survival over those who received single-arterial grafting (SAG), supporting findings from prior retrospective studies.
They also found that MAG recipients tended to be younger, from neighbourhoods with more community resources, with fewer comorbidities. However, when they re-analysed the data, substituting surgeon preference as an instrumental variable to account for unmeasured confounding variables, they noted no difference in long-term survival.
“Our analysis provides new insights on an important clinical question—whether CABG with multiple arteries used as a conduit, rather than one artery and veins from the leg, may benefit patients by improving their long-term survival,” said lead study author Justin Schaffer (Baylor Scott & White Healt, Plano, USA).
Retrospective studies, including a landmark study published last year that employed the STS National Database, have suggested that MAG may improve long-term survival over SAG. However, the Arterial Revascularization Trial (ART), a randomised controlled trial by David Taggart (University of Oxford, John Radcliffe Hospital, Oxford, UK) and colleagues, found no significant difference in 10-year survival among the two patient cohorts.
“ART is difficult to interpret in terms of MAG broadly, because a substantial number of patients, about 20% in each arm, also received radial artery conduit, and about 17% of patients randomised to bilateral internal mammary arteries received only a single mammary artery graft,” Schaffer said. “These factors have led to controversy in its interpretation, but ART remains the highest level of evidence regarding MAG that is currently available.”
Schaffer’s team used surgeons’ preference for performing MAG or SAG as an instrumental variable instead of a traditional as-treated analysis comparing patients who received MAG or SAG:
The team’s application of surgeon-preference as an instrumental variable requires several assumptions, including that certain surgeons prefer MAG, while others prefer SAG; patient-to-surgeon assignment is unrelated to the surgeon’s treatment preference, and that a surgeon’s use of MAG or SAG is independent of additional treatments that may affect outcomes.
Several variables may influence a surgeon’s decision, said Schaffer, but those variables aren’t or can’t be measured in clinical or administrative databases. One broad category includes conduit availability “Allen’s test,” or previous lower-extremity vein stripping procedures—unmeasured factors that may bias surgeons for or against MAG.
“Another important variable is what is termed the ‘surgeon eyeball test,’” Schaffer added. “If a surgeon ‘eyeballs’ a patient and does not expect them to live for many years after CABG, they may elect SAG over MAG because the purported benefits of MAG may only manifest over the long term.”
Although their traditional “as-treated” analysis supported the findings of the STS National Database analysis published last year by Saadat and colleagues in The Annals of Thoracic Surgery, the research team’s “surgeon-preference” analysis
If a surgeon ‘eyeballs’ a patient and does not expect them to live for many years after CABG, they may elect SAG over MAG”
noted no difference in outcomes between patients who underwent CABG by frequent MAG compared to frequent SAG surgeons. Schaffer’s team was “somewhat surprised by the results of our surgeon-preference analysis.” However, they added, the results “perhaps explain the discordance between current ‘as-treated’ retrospective analyses and data from the ART trial.”
The researchers emphasised that understanding the survival benefit of MAG over SAG requires randomised data, and it remains an important and open clinical question. They also noted that the Randomization of Single vs Multiple Arterial Grafts (ROMA) trial randomised 4,300 patients to receive either MAG or SAG, and the results from this trial (when available) will perhaps help answer this important clinical question.
They noted that because their analysis was focused on the Medicare population, the cohort was limited to older patients.
“We do not believe our findings suggest that MAG should be performed less frequently,” he said. “Both surgeons who frequently perform MAG and those who rarely perform MAG can be justified in using their clinical acumen to decide on an optimal conduit strategy for each individual.”
Justin Schaffer
EACTS past president puts innovation and inclusivity at the top of the agenda
The immediate past president of the European Association for Cardio-Thoracic Surgery (EACTS) speaks to Cardiovascular News about the organisation’s work to encourage a culture of innovation within the field and to support efforts to improve diversity among the cardiothoracic surgery workforce. Franca Melfi, the first woman president at EACTS, comments that both agendas are closely linked, given their importance in attracting new talent.
MELFI IS A THORACIC SURGEON, AND IT IS through her pioneering work in robotic surgery—having performed the first robotic procedure for lung tumour removal in 2001 at University Hospital Pisa (Pisa, Italy)— that she has gained a unique insight into the advent of new technologies in the surgical realm, as well as familiarity with the research and training needs that these novel solutions bring. Melfi drew on this experience during her recent Presidential Address at the EACTS 2024 annual meeting (9–12 October, Lisbon, Portugal), where she told delegates: “Innovation requires courage to challenge established norms and to open doors for new insights, techniques and technology.”
“When we talk about innovation, people think of robotic surgery, but in many ways, this is almost the past. I started with robotic surgery almost 23 years ago, at that time it was an unbelievable, unexpected and experimental field,” Melfi tells Cardiovascular News. Robotic techniques are continuing to advance in the cardiac arena, which she identifies as a fertile ground for innovation, alongside areas such as artificial intelligence (AI) and machine learning, which she says have potential to influence how treatments are delivered.
EACTS’ commitment to innovation has included the establishment of an Innovation Hub, launched at the organisation’s second annual Innovation Summit (19–20 April, Paris, France) this spring, which is intended to attract investment to support the development of cardiothoracic surgical treatments and improve outcomes for patients. Through the Innovation Hub, EACTS members can apply for grant funding to support research and advance innovation in cardiothoracic surgery, with grants to be awarded via a recently established fund through a competitive process over a five-year period.
“I believe that we can consider the Innovation Hub as a dynamic platform for new ideas, for testing and implementing new technologies, and for facilitating
partnerships between academia, healthcare providers and industry,” says Melfi. “This is very important. The EACTS Innovation Hub has many tasks, including supporting young innovators and researchers.”
Supporting innovation and pioneering new techniques and technologies are at the centre of efforts to attract a new generation of cardiothoracic surgeons, alongside the Association’s work to improve the representation of underrepresented groups—such as women and minorities— within the field.
“EACTS is strongly committed to promoting an inclusive and diverse membership,” comments Melfi, who highlights the work of EACTS’ Women in Cardio-Thoracic Surgery Committee (WiCTS) to promote diversity and equality within the Association and spread awareness of the importance of gender equality more widely across the specialty.
“This is clear evidence that our Association has changed a lot and plays a key role in promoting gender equality, as well as also trying to address some challenges that women face in specific countries, especially in low- and lower-middle income countries,” she comments.
“EACTS tries to support and give an equal opportunity for leadership and development, and I believe it has a very important role in this context, especially to ensure the representation of women surgeons from underrepresented regions and also to guarantee the presence of women during the scientific sessions in our annual meeting and other events.”
On a personal level, Melfi has recently taken up a post as a full professor at the University of Calabria (Cosenza, Italy) to ensure robotic surgery is more widely available in southern Italy. The new role will focus on opportunities afforded by digital technologies and AI, underlining her passion for innovation. Melfi will also retain her professorship at Pisa and continue to guide the team she has established there.
Cardiac surgery societies endorse ESC coronary revascularisation recommendations
FOUR CARDIAC SURGERY
societies have endorsed recommendations of the European Society of Cardiology’s (ESC) chronic coronary syndromes (CCS) guidelines on coronary revascularisation.
The American Association for Thoracic Surgery (AATS), Society of Thoracic Surgeons (STS), Latin American Association of Cardiac and Endovascular Surgery (LACES) and Asian Society for Cardiovascular and Thoracic Surgery (ASCVTS) released a multi-society paper, endorsing the statements from ESC.
ESC’s guidelines were published in 2024, and among a series of broad recommendations include a review of the indications for and selection of the optimal revascularisation modality based on findings from large randomised controlled trials and individual patient data analyses.
The latest ESC guidelines state that in CCS patients with left ventricular ejection fraction >35%, myocardial revascularisation is recommended, “in addition to guideline-directed medical therapy, for patients with functionally significant three-vessel disease to improve long-term cardiovascular mortality and the risk of spontaneous myocardial infarction”, which carries a class I recommendation.
CABG and optimal medical therapy are recommended over percutaneous coronary intervention (PCI) and optimal medical therapy alone in patients with diabetes, whilst in non-diabetic patients, CABG is recommended over optimal medical therapy to improve survival, symptoms and major cardiovascular events.
PCI is recommended alongside CABG in patients with intermediate or low coronary complexity if similar completeness in revascularisation can be achieved. When PCI and CABG have equal weighting, a heart team discussion is needed, and ad hoc PCI should not be performed.
“Until new evidence changes our current assessment, the surgical societies represented in this statement support the recommendations of the 2024 ESC guidelines for the management of chronic coronary syndromes,” the statement published in the European Journal of Cardio-Thoracic Surgery and the Journal of Thoracic and Cardiovascular Surgery reads. “The consensus is that in patients with complex, three-vessel coronary artery disease on optimal medical therapy, CABG is recommended to improve survival and decrease major adverse cardiovascular events and symptoms (compared with optimal medical therapy alone or PCI), irrespective of left ventricular ejection fraction.”
Franca Melfi
Edoxaban an “effective alternative” to warfarin following valve replacement surgery
Edoxaban may be an effective alternative to warfarin—the current standard of care— for patients undergoing bioprosthetic valve surgery, new research has shown.
CHISATO IZUMI (NATIONAL CEREBRAL AND Cardiovascular Center, Suita, Japan) presented findings of the ENBALV trial, in which researchers compared edoxaban to warfarin in 410 patients undergoing aortic or mitral valve replacement surgery at 24 centres in Japan, at the American Heart Association (AHA) 2024 Scientific Session (16–18 November, Chicago, USA).
Embolic events such as stroke are high after bioprosthetic valve surgery, Izumi noted in her presentation, especially among patients without anticoagulation therapy, and is typically caused by thrombus formation around the valve, perioperative atrial fibrillation (AF) and cardiac dysfunction shortly after the procedure.
Warfarin, a vitamin K antagonist, is presently the only recommended anticoagulant for this group of patients, but comes with several disadvantages, including a narrow therapeutic range which requires frequent blood tests for dose adjustment, as well as interactions with various other drugs and foods.
“These are burdens on patients and medical staff,” commented Izumi, noting that, by contrast, direct oral anticoagulants (DOACs) can be used with a constant dose, without the need for frequent blood tests for monitoring anticoagulation activity. “If DOACs were
available for this group of patients, it could simplify the care process and reduce the burden on patients and medical staff,” she said.
The ENBALV trial evaluated the effectiveness and safety of edoxaban, which was approved by the US Food and Drug Administration (FDA) in 2015 for patients with non-valvular AF, compared to warfarin within three months after bioprosthetic valve surgery. Researchers randomised the participants into two equal groups to receive either edoxaban or warfarin for 12 weeks after their surgery.
Reporting on an analysis among 389 of the 410 enrolled patients, the investigators found edoxaban was equally or more effective than warfarin at preventing stroke and systemic embolism, with 0.5% of patients receiving edoxaban having a stroke or systemic embolism, compared to 1.5% of patients receiving warfarin.
Major bleeding was higher among patients receiving edoxaban, occurring in 4.1% of the edoxaban group and in 1% of the warfarin group, though no fatal bleeding or intracranial haemorrhage was observed in patients treated with edoxaban, whereas one fatal cerebral haemorrhage occurred in the warfarin group. Intracardiac thrombus did not occur in any of the patients in the edoxaban group, but did occur in 1% of patients in the warfarin group. Additionally, patients who received edoxaban did experience higher instances of gastrointestinal bleeding compared to patients who received warfarin
Humacyte files investigational drug application for use of tissue
engineered vessel in CABG
(2.1% vs. 0%, respectively).
“Our findings show that edoxaban could help prevent blood clots and stroke as effectively as warfarin, indicating that it is a viable post-surgery treatment alternative to consider for patients who have received a bioprosthetic heart valve replacement,” Izumi said. “Edoxaban could make life easier for patients recovering from heart valve surgery. Since this medication does not require regular blood tests to monitor anticoagulation activity and can be taken in a fixed dose, without fears of interaction with food or other medications, it reduces the burden on patients and improves their quality of life, especially in those crucial first few months after surgery.”
Researchers have said that future research is needed to understand which patients have the highest risk of bleeding with the use of edoxaban and how to mitigate this risk while still offering effective treatment options
Edoxaban could make life easier for patients recovering from heart valve surgery.”
in post-surgery treatment and recovery.
“Edoxaban can be considered for this indication,” commented Manesh Patel (Duke University School of Medicine, Durham, USA) who summarised the implications of the findings following Izumi’s presentation. “I would say this area of our practice has to importantly improve the stratification of patients undergoing valvular surgery, specifically those that are undergoing bioprosthetic valvular surgery without known atrial fibrillation to see who is at risk for stroke and systemic embolism in that short-
was observed to sustain patency (blood flow), recellularised with the animals’ host cells, and remodelled to effectively reduce the initial mismatch between the sdATEV and the native artery.
Humacyte has announced that it plans to file an investigational new drug (IND) application with the US Food and Drug Administration (FDA) to allow first-in-human clinical testing of the small-diameter (3.5mm) acellular tissue engineered vessel (sdATEV) in coronary artery bypass grafting (CABG).
The company’s current plans for filing an IND are based on the outcome of a meeting with the FDA, including agreements reached with the agency. To date only the 6mm configuration of the ATEV has been studied in human trials, specifically in studies conducted in vascular trauma repair, arteriovenous (AV) access for haemodialysis, and
peripheral artery disease (PAD).
To enable the IND filing, the sdATEV has been studied in multiple preclinical CABG models. The results of a sixmonth preclinical study in primates were presented in November 2024 at the American Heart Association’s scientific sessions 2024 meeting (16–18 November, Chicago, USA). In the
“CABG surgery can be lifesaving in appropriately selected patients with coronary artery disease,” said John H Alexander (Duke Clinical Research Institute at Duke University, Durham, USA). “A long-standing, major limitation of CABG surgery has been the availability of ideal conduits to use as bypass grafts. If clinical trials are successful, this tissue-engineered graft could have the potential to transform CABG surgery by providing an unlimited supply of an off-the-shelf conduit to use in patients undergoing CABG surgery. We look forward to helping to advance this technology into human studies.”
The ATEV is a first-in-class bioengineered human tissue that is designed to be a universally implantable vascular conduit for use in arterial replacement and repair. Harvesting vein from a CABG patient may lead to complications and may not be feasible due to missing or diseased veins, ATEV is designed to be available off-the-shelf, and does not require further injuring the patient to obtain arterial replacement material.
The FDA granted a full approval for the ATEV (Symvess) on 19 December 2024 for use in adults as a vascular conduit for extremity arterial injury when urgent revascularisation is needed to avoid imminent limb loss, and when autologous vein graft is not feasible.
For uses other than the FDA approval, the ATEV is an investigational product and has not been approved for sale by the FDA or any regulatory agency.
World-first procedures promise new era for robotic cardiac surgery
Continued from page 1
robotic surgical procedures. The KFSHRC robotic programme is organised around eight centres of excellence (CoEs) spanning different specialities which are unified under a multidisciplinary framework. Within the Heart CoE, surgeons, anaesthesiologists, robotic specialists, and nursing teams, collaborate on the planning and delivery of cases.
“KFSHRC’s multidisciplinary teams collaborate to align patient-specific needs with robotic technology’s capabilities, ensuring precision, safety, and optimal outcomes in every case,” Khaliel comments. Patients are deemed suitable for robotic cardiac surgery through a comprehensive evaluation process, based upon factors including the patient’s overall health, the complexity of their condition, and the anticipated benefits of minimally invasive techniques, such as recovery time and complications.
“For example, in the world’s first fully robotic heart transplant, the decision to proceed robotically was guided by the patient’s specific request for a minimally invasive approach,” explains Khaliel. “This reflected not only the clinical feasibility, but also the patient’s preferences, ensuring a personalised care plan. Similarly, robotic procedures have been successfully performed in high-risk groups, such as patients with morbid obesity, where the minimally invasive method significantly reduced procedural risks.”
According to Khaliel, KFSHRC’s goal is to broaden the scope of its robotic procedures and integrate artificial intelligence (AI) to enhance precision.
“Globally,” he says, “robotics is poised to become a standard for complex surgeries, transforming healthcare delivery by reducing invasiveness and improving recovery times. KFSHRC’s leadership in this field ensures it will continue to drive these advancements here in Saudi Arabia and globally.”
In December, the multidisciplinary team at the WVU Heart and Vascular Institute in Morgantown, USA announced the completion of its first operation combining valve replacement and coronary artery bypass operations for the first time.
Involving a 73-year-old female patient with previous stroke, brain surgery and ongoing weight loss, it was feared that she may not tolerate conventional openheart surgery when it was discovered that she had severe aortic valve disease and a significant blockage in her coronary artery. The patient was referred to Vinay Badhwar, executive chair of the WVU Heart and Vascular Institute and professor and chairman of the Department of Cardiovascular and Thoracic Surgery, who first broached the possibility of a robotic procedure after discussing the risks with the patient and her family. The procedure was a technical success, and the patient’s heart function improved after the operation.
“While we are still in the early days of this latest innovation, the ability to perform valve surgery and coronary artery bypass surgery fully robotically through a single incision has the potential to open up a new era of robotic heart surgery,” said Badhwar. “We must always keep quality outcomes at the forefront of all innovation. However, if surgeons adopt and gain experience with techniques such as this one, they will tackle this last frontier that previously limited a robotic approach. One day in the near future, this may serve as a platform to perform nearly all types of heart surgery.”
Since 2017 the WVU team has been at the forefront of the development of the robotic aortic valve replacement (RAVR) procedure with access via a 3cm
Robotics is poised to become a standard for complex surgeries.”
transaxillary right lateral mini thoracotomy, which they now routinely use alongside traditional surgical aortic valve replacement (SAVR) and transcatheter aortic valve implantation (TAVI) to treat symptomatic aortic stenosis.
The rapid growth of TAVI has been the story of the last two decades in the treatment of aortic valve disease. Favourable results from major trials covering a broad population of patients have widened access to a minimally invasive treatment option which has now overtaken surgery as the predominant treatment strategy for many aortic stenosis patients, for whom previously only surgery may have been considered. However, Badhwar believes that the emergence of RAVR could provide an additional minimally invasive option for patients alongside the establishment modes of treatment.
“While I remain an ardent supporter of TAVI and its role in the management of aortic valve disease, there are times when surgery may be more appropriate for anatomic or durability reasons. We live in an environment that is consumer based, and despite the recent literature—from which there are signals that all-TAVI all the time may not be ideal—patients, consumers and providers are seeking alternatives to an anterior chest approach surgical option,” Badhwar tells Cardiovascular News, discussing the treatment of aortic stenosis within his institution.
The robotic platform for the RAVR procedure is performed via a similar approach used for robotic mitral valve surgery, a well-established technique performed in many centres worldwide. RAVR uses traditional biologic or mechanical valves rather than a sutureless prosthesis and, in addition, allows for concomitant mitral or tricuspid valve procedures, as well as arrhythmia therapies such as the maze procedure or left atrial appendage closure.
After honing the technique through cadaver experiments, Badhwar and the WVU team performed the first-in-human RAVR case in January 2020 and are now well into the hundreds of cases.
Many centres around the world have adopted the WVU RAVR platform and integrated this as a heart team option. Initial results have been promising. At the recent European Association of Cardio-Thoracic
Surgery (EACTS) 2024 annual meeting (9–12 October, Lisbon, Portugal)
Badhwar presented longitudinal outcomes from the first 300 consecutive patients undergoing RAVR across 10 established robotic cardiac surgery programmes at centres in the USA, Europe, Saudi Arabia, Brazil, Taiwan and Australia, reporting low rates of operative mortality (0.7%), stroke (1%), and pacemaker implantation (2.3%), following the procedure.
These early results have prompted optimism that RAVR could emerge as a viable alternative to TAVI, and indeed at WVU, Badhwar says that the development of RAVR has created a new pathway for care. “Our team philosophy is to always do the right thing for the right patient at the right time,” he comments, noting that the choice of therapy goes beyond simply determining which procedure is most appropriate based upon the age of the patient. “Our programme looks at the anatomy, the patient comorbidities and condition, as well as age, to determine treatment. Our heart teams, which are led by our cardiologists, have followed the short-term and long-term results of RAVR as compared to TAVI. Instead of many centres approaching patients with aortic stenosis with a TAVI-first strategy—here it is RAVR first. Our cardiologists have flipped that management philosophy.”
Alongside developing the procedure, Badhwar and his colleagues have worked on training pathways that have helped to seed the technique in other centres across the USA and globally, with around 20 sites now proficient in the approach and many
more in development. “Our goal was to transparently develop this in such a way to make it reproducible and standardisable,” he says. “One of the challenges with the implementation of any new technology or technique is that while it’s great to do one or two cases, in order to make it sustainable and reproducible in multiple centres with a minimal learning curve, one must make it somewhat standardised.”
As well as disseminating guidance and best practice on how to learn the robotic aortic procedure, WVU recently hosted a two-day international RAVR symposium (14–15 November, Morgantown, USA) to bring together innovators and practitioners to look at the challenges and opportunities in growing this approach further.
“When some see these new things via edited videos or brief presentations, they think it is impossible, or it is going to take all day. This is not the case. These are operations that can be done in only a few hours, efficiently and, most importantly, very safely. That was one of the most important things we wanted to share,” says Badhwar reflecting on the take-home messages from the event. “We consistently receive feedback from other surgeons and cardiologists around the world as to where RAVR now fits in their armamentarium, so I think we are entering a potentially exciting next chapter for both cardiologists and surgeons where a healthy equipoise of therapy exists within multidisciplinary heart teams.”
What of the future for the technique, and its prospects for becoming a widely used alternative to TAVI and SAVR? Badhwar says it is reasonable to expect that centres that are already established in performing robotic mitral surgery procedures can learn the RAVR technique, with experience from his own centre pointing to a learning curve of between five and 10 cases. However, he is cautious about predicting an explosion in sites adopting this technique.
“The excitement is significant, but it must be realistic and tempered. We have to do this in a diligent and transparent way, always keeping quality first. It is technically a little bit more demanding than robotic mitral surgery, largely because we are dealing with the aorta. However, once the learning curve is crested, particularly in experienced robotic teams, then it becomes more and more routine just like any other robotic operation.”
Instead of many centres approaching patients with aortic stenosis with a TAVI-first strategy— here it is RAVR first.”
ROBOTICS IN CARDIAC SURGERY:
KEY MILESTONES
The first robotic mitral repair was performed by Alain Carpentier in 1998, using an early prototype of the Intuitive Medical da Vinci surgical system.
A team at Leipzig Heart Centre also experiments with early mitral valve repairs using the same prototype.
2002:
Intuitive Surgical’s da Vinci system receives the first US Food and Drug Administration (FDA) approval for use in mitral valve repair surgery.
W Randolph Chitwood, a leader in the use of robotics in cardiac surgery, completes his 400th robotassisted mitral valve repair.
The first robotic coronary bypass grafting procedures are performed at Hôpital Broussais in Paris.
2000:
Intuitive Surgical’s da Vinci system receives the first US Food and Drug Administration (FDA) approval for use in mitral valve repair surgery.
The first robotic coronary bypass surgery in the USA was performed at NewYorkPresbyterian's Columbia Presbyterian Medical Center. The surgery was performed without a chest incision.
2020:
Vinay Badhwar and the WVU team perform the first-inhuman RAVR case. A first in the world fully robotic heart transplant procedure is performed at the King Faisal Specialist Hospital and Research Centre in Ryadh, Saudi Arabia led by Firas Khaliel.
2024:
The WVU team performs the first procedure using a robotic system to combine aortic valve replacement with coronary artery bypass grafting.
Left: Feras Khaliel, head of cardiac surgery at KFSHRC. Above: The WVU team performs a robotic aortic valve replacement procedure. Above right: Vinay Badhwar
“Myth-busting” radiation safety campaign aims to encourage women into interventional cardiology field
In a bid to encourage more women into the field of interventional cardiology, a recently launched campaign from the Society for Cardiovascular Angiography and Interventions (SCAI) Women in Innovation (WIN) committee aims to put a focus on some of the myths and realities around radiation exposure in the cath lab. SCAI WIN Chair Nadia Sutton (Vanderbilt University Medical Center, Nashville, USA) speaks to Cardiovascular News about why radiation exposure is a particular area of concern for women in the field, and how technology may play a role in improving protection for cath lab operatives.
What is the current gender mix in interventional cardiology and are trends shifting in either direction?
It’s always a little bit tricky to come up with the exact numbers, but a study published in JAMA Cardiology last year by Sarah Snow (Duke University School of Medicine, Durham, USA) reported that the number of women in cardiovascular medicine rose from 18% in 2008 up to 26% in 2022.1 In interventional cardiology specifically, the percentage of women in training rose from 6% in 2008 to 20% in 2022 suggesting that incredible progress has been made to more than triple the number of women in training. That said, the number of women who are actually practising interventional cardiologists hovers around the 5% range. Certainly, there is still a lot of room for growth.
Why is it important to improve gender parity in interventional cardiology?
From my perspective, I don’t think that having gender parity is an absolute goal. What’s more important is that women have the opportunity to follow this career path if they would like to. Ultimately, I don’t think that every field has to be exactly balanced in terms men and women. I was fortunate to have had mentors at my training institution, the University of Michigan (Ann Arbor, USA), who encouraged me to pursue this path. I don’t know if, without having that encouragement, I would have chosen this path.
As far as patient outcomes, the data that we have would suggest that women in general take as good care of patients as men. In 2017, a study in JAMA Internal Medicine comparing in-hospital mortality and readmission rates for Medicare patients treated by male versus female physicians showed that patients who were treated by female internists had a lower mortality and readmission rate compared to those cared for by male internists, and
there were some slight differences in potential practice patterns in terms of alignment of practices with guidelines.2
Separately, there was a study published in 2020 by colleagues at the University of Michigan—the DISCO study—that was more specific to interventional cardiologists, finding that there was no difference in the procedural outcomes of patients treated by male versus female interventional cardiologists.3 That study included interventional cardiologists from Michigan and there were only 18 were women physicians in that study versus 385 men. You can see how the numbers still are so small that it’s hard to make big representative assessments of the outcomes.
I definitely have patients who seek me out because I’m a female, as they feel more comfortable with a female provider for one reason or another. Presumably those patients would have still sought care even if they didn’t have the opportunity for a female provider, so I don’t know that necessarily having more women is going to be something that we can point to as providing more access for patients, but I do think that patients do sometimes have a preference.
To what extent do concerns about radiation exposure in the cath lab deter women from entering the field?
First of all, I do think it’s very important that there’s a push in our field for radiation safety, but there are multiple factors that potentially might dissuade a woman from pursuing a career in this field. A 2019 study in JACC: Cardiovascular Interventions by Celina Yong (Stanford University School of Medicine, Palo Alto, USA) and colleagues gave us more granular information about why women are choosing this specialty versus our male colleagues.4 Some of the things that potentially dissuaded women were that they were interested in another field, they were concerned about not having job flexibility or the demanding nature
of the job, and concern about radiation during child-bearing was certainly one of the key things, alongside concern about the culture and the lack of female role models, as well as potential sex discrimination. Both men and women were concerned about radiation exposure, and that was a deterrent in both groups. But, for women it was also radiation during child-bearing that was a consideration. A lot of these issues— the concern about job flexibility, the demanding nature of the job, and the radiation exposure around childbearing—are intertwined and related to family obligations.
What are the safety requirements for physicians during pregnancy?
In the USA if a woman thinks they may be pregnant, are early in pregnancy, or potentially trying to become pregnant, they would selfreport to their institution and they would be provided with a foetal monitoring badge to be worn under their lead to ensure that they don’t exceed a specific volume of radiation. In general, it’s very safe for a foetus that’s protected by lead to be in the cath lab and there’s no limitation on the individual working for any specific amount of time as long as they don’t exceed the limit of radiation exposure, but it’s very rare for somebody to even come close to what that amount is.
can help women with—to provide the appropriate information that we can safely have children alongside working in the cath lab. This is not just something for physicians either, this is something that affects nurses, technicians, or anyone who might be working in or around the cath lab.
What are the technologies and techniques that can help with radiation protection?
The first stop should be maximising the existing options, which means appropriately positioning our equipment, reducing frame rates, and making sure we’re wearing the appropriate equipment, including eye protection. That’s the ground layer. Then we have another layer, with some other easy things we can do like using disposable radiation drapes to add some additional protection and using some of the advanced features that come with our equipment.
I’ve never been pregnant myself in the cath lab as I had my children before I trained, but I’ve seen colleagues go through it and it does look fairly uncomfortable, especially during those later months.
We can safely have children alongside working in the cath lab.”
What are some of the messages that the SCAI WIN radiation protection campaign hopes to get across?
The biggest things that we want to convey in our campaign is that, number one, it is a great field where there are many women and the number is rising. We think this is fantastic and we think people should really give this strong consideration. Another aspect is that we do have ways of reducing our radiation exposure and making the cath lab safer. The third message is that we really don’t have data to suggest that it’s unsafe for pregnant women to be in the cath lab. That might be one of the lowest hanging fruits for us to try to dispel that myth because that is something we do know that we
There are several different categories of types of devices including those that essentially block radiation by providing an additional shield. Some of them enable us to remove our lead entirely so we’re not subject to the orthopaedic problems related to radiation exposure, which is probably the most common injury that people get. Other devices can attach to the C-arm and almost act like a form of radiation bubble, preventing us from being exposed and that particular type of device is being advocated to be used with light lead because it’s regulated in a different way. Light lead feels like you’re wearing a sweatshirt and means it would be much easier for us not to be exposed to the orthopaedic risk.
Probably less than 5% of cath labs have this type of equipment, but I think that is where SCAI as a professional society is key in being an advocacy group for us as physicians. It’s really challenging as an individual physician to go to the administrative body at your hospital to say that you need this equipment which may be rather expensive and the hospital doesn’t derive any revenue from it.
What resources can people access through the campaign?
The SCAI WIN radiation safety campaign has a toolkit which includes a video as well as other resources for women who may be interested in doing more reading around this. SCAI has made it a priority to discuss some of these issues and James Hermiller (Ohio State University College of Medicine, Columbus, USA), the current SCAI President, has really championed this as a concern for our profession.
Coronary CT angiographyguided management of stable chest pains shows benefit out to 10 years
Coronary computed tomography angiography (CCTA)-guided management of patients with stable chest pain was associated with a sustained reduction of deaths related to coronary artery disease or non-fatal myocardial infarction (MI), long-term results of the SCOT-HEART trial have shown.
THIS IS THE HEADLINE 10-YEAR finding of the study, an open-label, multicentre trial involving more than 4,000 patients treated at 12 outpatient cardiology chest pain clinics across Scotland, results of which were published in The Lancet authored by Michelle Williams (University of Edinburgh, Edinburgh, UK) alongside other SCOT-HEART investigators. During the trial, the study team assigned patients aged 18–75 years with symptoms of suspected stable angina 1:1 to undergo standard treatment either with or without the guidance of CCTA. The study has previously shown that
the use of CCTA led to a change in diagnosis in 27% of patients, a change in investigations in 15% of patients and a change in treatment in 23% of patients. At five years, this led to a reduction in the composite endpoint of coronary heart disease-related death or MI, with similar rates of coronary revascularisation and an increase in the use of preventive therapies when compared with standard care delivered without the aid of CCTA. The latest prespecified analysis sought to assess the impact of CCTA on the long-term management and outcomes for patients.
Enrolling from November 2010 to September 2014, SCOT-HEART recruited 4,146 patients, who had a mean age of 57 years, half (2,073) of whom were assigned to standard care with CCTA and half (2,073) standard care without CCTA. After 10 years, the investigators report that coronary disease-related death or non-fatal MI were less frequent in the CCTA group (6.6%) versus standard care (8.2%).
“In patients with stable chest pain, management guided by CCTA was associated with a sustained reduction in death from coronary heart disease or non-fatal myocardial infarction at 10 years, which appeared to be due to the prevention of non-fatal myocardial infarction,” the study’s authors write in their paper in The Lancet “These differences occurred despite no difference in the use of invasive coronary angiography or coronary revascularisation, although the use of preventive therapies remained higher in those with CCTA-guided management
Spironolactone misses primary endpoints in CLEAR SYNERGY trial
Routine use of the blood pressure medication spironolactone among patients who have undergone percutaneous coronary intervention following acute myocardial infarction (MI) may reduce heart failure, but is not likely to reduce mortality, recurrent MI or stroke.
THESE ARE AMONG THE LATEST FINDINGS of the CLEAR SYNERGY (OASIS 9) trial, presented by Sanjit S Jolly (McMaster University and Hamilton Health Sciences, Hamilton, Canada) at the American Heart Association (AHA) 2024 Scientific Session (16–18 November, Chicago, USA) and published simultaneously in The New England Journal of Medicine
CLEAR SYNERGY was a randomised, doubleblind, 2×2 factorial design, placebo-controlled clinical trial, which randomised 7,062 patients between February 2018 and November 2022 into four groups receiving either spironolactone and the antiinflammatory medicine colchicine; spironolactone and a placebo; colchicine and a placebo; or two placebos. Patients were aged an average of 60 years old, and 20% were women. Among them, 95% had ST elevation myocardial infarction (STEMI), and 18% had type 1 or 2 diabetes.
Jolly presented findings from the analysis of the effect of colchicine within the trial at TCT 2024 (27–30 October, Washington, DC, USA), where he reported that the use of the medication after acute MI did not reduce cardiovascular death, MI, stroke or ischaemiadriven revascularisation compared to placebo. Spironolactone is a mineralocorticoid receptor antagonist medication that blocks certain hormones.
The trial’s focus was to determine whether the routine use of spironolactone after acute MI—regardless of whether the person had heart failure—could provide broader benefits in reducing the incidence of heart failure and death.
Reporting on the spironolactone arm of the trial at AHA 2024, Jolly detailed that the overall rates of death from heart-related issues were similar between the spironolactone groups and the placebo groups (3.2% vs. 3.3%, respectively), and that participants taking spironolactone (with or without colchicine) had a 31% lower risk of new or worsening heart failure than people taking colchicine with placebo or two placebos (1.6% vs. 2.4%, respectively).
High potassium levels occurred at twice the rate within the spironolactone group compared to the placebo group (1.1% vs. 0.05%, respectively), leading to more participants discontinuing medication use.
“While spironolactone didn’t reduce deaths or other major heart complications after a heart attack, it did reduce the likelihood of
even after 10 years of follow-up.”
The findings could have important implications for the diagnosis and long-term prevention of coronary artery disease and MI, the study team suggests.
There are some limitations to the study, the authors acknowledge, including that outcomes and medication use were defined based on nationally coded data, and there was no independent clinical endpoint adjudication. Additionally, the investigators state that the diagnosis of coronary artery disease was higher in patients allocated to CCTA, which they suggest would lead to overestimation of coronary events in this group.
Alongside this, a small number of patients were lost to follow-up and subsequent crossover of clinical evaluations and investigations may have influenced patient management during the subsequent 10 years.
Changing practice relating to the management of stable coronary disease and the evolution of CT technology and techniques may also have had a bearing over the length of the long-term followup, they note.
“We have shown that CCTA-guided management is associated with a beneficial long-term impact on patient care,” the SCOT-HEART investigators write in their concluding remarks.
“After 10 years of follow-up, CCTAguided management continued to be associated with reduction in the rates of coronary heart disease death or non-fatal myocardial infarction and sustained increases in the use of preventive therapies.”
heart failure, which is an important finding for patients and healthcare professionals,” said Jolly. “Participants fared much better in this trial than in previous ones. This reflects the advances in angioplasty techniques in the overall care for heart attacks. Modern treatment approaches, including medication, stent technology and more timely interventions, have positively impacted patient outcomes.”
The research group highlighted several key study limitations, noting that women and people of different races and ethnicities were underrepresented in the participant pool, therefore making it difficult to generalise the results to the larger population.
The side-effects of colchicine could have influenced a participant’s decision to stop taking spironolactone, they note, which may partly explain the higher-thanexpected rate (28%) of people who discontinued using spironolactone and likely reduced the study’s statistical power.
Sanjit S Jolly
While spironolactone didn’t reduce deaths or other major heart complications after a heart attack, it did reduce the likelihood of heart failure”
Heart teams digest role of early aortic intervention following EARLY TAVR and EVOLVED trials
Two trials delivered in late 2024 have offered fresh evidence on the potential role that early intervention could play in the treatment of aortic stenosis, as well as shedding new light on the progression of the disease that investigators say could provide important insights for heart teams when considering treatment strategies.
Garnering many headlines at the time of their release in late October, EARLY TAVR and EVOLVED both investigated a strategy of preemptive treatment for asymptomatic aortic stenosis. However, diverging results seen across the two trials have fuelled discussion over whether watchful waiting should continue to be the favoured approach among those patients who are at high risk—albeit yet to develop symptoms of aortic valve disease—or if heart teams have the necessary evidence to buy in to the preventive strategy.
EARLY TAVR, which enrolled more than 900 patients who were deemed to be eligible through the use of a treadmill stress test, compared early intervention with transcatheter aortic valve implantation (TAVI) to clinical surveillance—meeting its endpoint of a reduction in a composite of death, stroke or unplanned cardiovascular hospitalisation between the two arms out to two years, driven largely by a reduction in hospitalisations in the TAVI group. EVOLVED, meanwhile, involved more than 200 patients with asymptomatic severe aortic stenosis and mid-wall myocardial fibrosis, assessed via cardiac magnetic resonance (CMR) imaging, who underwent either early intervention with TAVI or surgical aortic valve replacement (SAVR) or received guideline-directed conservative management. Unlike the EARLY TAVR trial, EVOLVED ultimately fell short in demonstrating a clinically meaningful difference in outcomes for patients undergoing the early intervention strategy against a primary endpoint of all-cause death or unplanned aortic stenosisrelated hospitalisation.
Trials in surgical valve replacement
This sentiment was echoed by Rebecca Hahn (Columbia University Irving Medical Center, New York, USA), who, speaking during a spotlight session on the implications of the latest data for heart teams at PCR London Valves 2024 (24–26 November, London, UK), said: “The trials give us a justification for speaking to our patients about the safety of early intervention and give us a better timeline of when symptoms will occur and how short it [the timeline] is.”
One important talking point to have emerged from the latest round of trials is the speed at which symptoms appear to develop among patients who had previously been considered asymptomatic.
Philippe Généreux
Prior to these latest studies, two smaller scale trials— AVATAR and RECOVERY—had investigated the potential benefit of early surgical valve replacement among patients with severe, asymptomatic aortic stenosis, with both indicating that initiating surgery early could lead to better clinical outcomes compared to conservative management. Marko Banovic (University of Belgrade Medical School, Belgrade, Serbia), principal investigator in the AVATAR trial, tells Cardiovascular News that the two latest trials are “landmark trials that deliver an additional degree of evidence supporting the consideration of early aortic valve replacement” on top of the existing evidence.
“As a cardiologist seeing these patients in daily clinical practice and following the evolution within the randomised controlled trials [including EARLY TAVR and EVOLVED], I would say that the totality of available randomised data supports the option for offering the patient pre-emptive treatment in shared decision making, tailoring the choice for the intervention to the patient’s risk profile,” he comments.
“In the current guidelines it is suggested that the development of symptoms may take years, but it was less than a year mean time—[in EARLY TAVR]—the median time was 11 months to develop symptoms, so it is actually much shorter. That helps patients to decide whether or not they go early, or they wait,” commented Hahn.
According to Banovic, the timing of adverse events is an important common thread seen in both the AVATAR and EARLY TAVR trials. “It is of note that event rates start to increase rather early from the time of diagnosis of significant aortic stenosis, on average 11 months in EARLY TAVR and 15 months in the AVATAR trial. Here, the adverse events in the watchful strategy arm remained higher after valve replacement as compared to those undergoing early valve replacement,” he comments. “Thus, these data provide me with a greater confidence to discuss the pre-emptive intervention in the setting of severe asymptomatic aortic stenosis and normal left ventricular function and overall low risk profile.
“Re-establishing the natural history”
EARLY TAVR principal investigator Philippe Généreux (Morristown Medical Center, Morristown, USA) tells Cardiovascular News that one of the important legacies of the research will be in “reestablishing the natural history of the progression of aortic stenosis”, pointing out that as many as 26% of patients in his trial’s clinical surveillance arm developed symptoms at six months, and 47% at one year, all of whom ultimately required TAVI.
Some critics have questioned whether the rapid rate of crossover between the surveillance and TAVI arms seen in EARLY TAVR could be attributed to patients essentially convincing themselves of the presence of symptoms due to their enrolment in the trial, a point that was highlighted by Davide Capodanno (University of Catania and G Rodolico-San Marco, Catania, Italy) in his appraisal of the research at PCR London Valves.
“The question is: you had a negative exercise test and you are totally asymptomatic, then you
Heart teams are deciding whether to treat aortic stenosis early
It is time to elevate aortic stenosis to the level of cancer— when you have it, treat it. We need to have a sense of urgency around aortic stenosis.”
are randomised and you rapidly start developing symptoms. Something is strange there. If I imagine myself in that situation, I believe I would be thinking, thinking and thinking, that this disease is deadly, that I have been randomised to the unlucky arm, because I will not receive any intervention, and of course start to develop anxiety,” he said. However, regardless of the rate at which symptoms occur, many, including Capodanno, acknowledge that the progressive nature of aortic stenosis means that waiting will only delay the inevitable need for an intervention.
“The vast majority of patients with moderate aortic stenosis are going to go through this phase of mildto-moderate stenosis, and then moderate stenosis, and then severe stenosis [with] no symptoms, and eventually severe aortic stenosis with symptoms,” Généreux comments on this point. “To wait a very long time it is going to [become] severe aortic stenosis with depressed cardiac function, and then death.
“From a philosophical point of view, all patients with aortic stenosis will at some point reach this zone
of moderate-to-severe aortic stenosis with no symptoms. Now we are entering an era of preventive valve therapy we are more proactive and less reactive, we don't wait until it is too late, we don't wait until the patient has severe or critical aortic stenosis with symptoms.”
Timing is key
Initial trials including AVATAR and RECOVERY have demonstrated that early intervention with surgical aortic valve replacement (SAVR) may benefit asymptomatic patients
Généreux also notes that the results of the two latest trials bring into stark focus the importance of the timing of the intervention, pointing out the significant differences in the initiation of “early” treatment seen in both the EARLY TAVR and EVOLVED trials. Though patients randomised to the early intervention group in EVOLVED were treated on average 15 months before those undergoing conservative treatment, they still faced vastly greater waiting times than patients undergoing early treatment in the EARLY TAVR trial, who were typically treated within two weeks of their assignment to a treatment group.
“The EVOLVED trial showed, without a doubt, that waiting for symptoms kills,” he comments, pointing out that in the EVOLVED trial, some deaths occurred in the early intervention arm whilst patients were waiting to undergo their treatment. This point touches upon one of the major areas of contention regarding the two trials—whether an early intervention approach is practical in a real-world setting, given the waiting times faced within many healthcare systems, including the UK’s National Health Service (NHS) where most of the patients for EVOLVED were recruited.
“This is important for me to discuss,”
Généreux says in response to this point.
“People say that this is the system they are living in, well they need to change the system, because patients are dying because of that. It is time to elevate aortic stenosis to the level of cancer—when you have it, treat it. We need to have a sense of urgency around aortic stenosis. A lot of people are complacent, and the mentality of waiting for symptoms has been ingrained for 50 years. So, I think it is going to take time before we change people's perceptions of the disease.”
Trial pipeline
Pooling data from the four available trials is likely to offer further insight on any potential beneficial impact of early intervention, and Généreux confirms that investigators
are conducting a meta-analysis of the four trials to bring together the insights from across the datasets. Additionally, he singles out the ongoing PROGRESS trial, looking at TAVI or clinical surveillance in patients with moderate aortic stenosis as being a further important trial to watch in this arena, as it will add some fresh data on whether the presence of cardiac damage puts patients at higher risk for more rapid disease progression.
EARLY TAVR and EVOLVED are the first trials to include a transcatheter approach to treat severe asymptomatic aortic stenosis, though results were not entirely consistent
For Banovic, research into the field of preventive treatment for aortic stenosis remains an important live topic—whilst he hopes to see more focus on the question of where SAVR or TAVI should be favoured in this scenario.
“This is a very dynamic field of clinical research,” he comments. “There are still a few ongoing trials in the setting of asymptomatic severe aortic stenosis, in particular EASY AS which is planned to include more than 2,500 patients. These trials will shed further light on this important question.
“An additional, highly important question to address is the choice of optimal treatment strategy: either transcatheter or surgical. This question is of paramount importance in the current times with increasing, often uncontrolled use of TAVI in younger patients with consequences for lifetime management. The direct randomised comparison of the surgical versus the transcatheter approach in patients younger than those included in the EARLY TAVR trial is, in my view, important and very timely to consider.”
TRIALS TO WATCH
DANAVR
● 1,700 patients with asymptomatic severe aortic stenosis
● SAVR or TAVI versus watchful waiting
A further trial in this space, DANAVR, will also compare SAVR and TAVI in asymptomatic severe aortic stenosis, enrolling more than 1,700 patients, although results from either this trial or EASY AS are not anticipated until the latter half of the decade. Though the evidence to date has yet to conclusively show that pre-emptive intervention should be considered in all cases, many are reassured that the safety of early aortic replacement seen across the four trials should mean it is on the table for a greater number of patients in future.
● Primary endpoint: All-cause death
● Follow-up: Five years
EASY AS
● 2,844 patients with asymptomatic severe aortic stenosis
● Aortic valve replacement versus expectant management
● Primary endpoint: Cardiovascular death or hospitalisation for heart failure
● Event-driven
PROGRESS
● 2,250 patients with moderate, calcific aortic stenosis
● TAVI with Sapien 3 (Edwards Lifesciences) or clinical surveillance
● Primary endpoint: Death, heart failure hospitalisation or adverse events
● Follow-up: Two years
“What we can say is that early aortic valve replacement does not harm, that is an important piece of information, and that sooner or later treatment is needed,” Capodanno said in summing up his view of the new evidence at PCR London Valves. “What we cannot say is that early AVR is a strict necessity, because patients may base their choices on personal preferences and their own philosophy to risk.
“My take is that we have to explain to our patients the pros and cons of earlier intervention versus watchful waiting and now we have data in order to do so. Also, we have to consider the quality of the clinical surveillance in our centre. If we can deliver prompt aortic valve replacement when symptoms arise is one matter—if not—it is probably better to go earlier.”
BRUNO SCHELLER
Despite a complicated early path into medicine, which was shaped by a major tragedy, Bruno Scheller (University of Saarland, Saarland, Germany) realised early on that interventional cardiology was his calling. As one of the foremost figures in research of drug-coated balloon (DCB) therapy for the treatment of coronary artery disease, he tells Cardiovascular News about how his interest in this technology came about, and what its arrival means for the future of percutaneous coronary intervention (PCI).
Why did you initially choose to become a doctor, and what was it that made you decide to specialise in cardiology?
I was born into a working-class family. My father, a coal miner, taught me manual skills, which I still benefit from every day in the cath lab. At secondary school, my strengths were in maths and physics, though my Abitur grade wasn’t good enough for me to fulfil the requirements for studying medicine. From a practical standpoint, it made sense to apply to study engineering or, even better, to learn a good trade. At that time, it was possible to obtain one of the desired places to study medicine in Germany by taking a test focusing on pattern recognition. This test really suited my mathematical talents, and I got a place to study medicine. However, my family had limited financial resources to support my studies, so, at the age of 19, I was faced with several challenges.
I was working part-time in an industrial plant to co-finance my education. I tried to decide which subject to study by doing internships. In the late summer of 1988, the area I was living in was shaken by the Ramstein aviation disaster. Our university hospital was one of the hospitals that had to care for the most civilian casualties. My nursing internship was in the intensive care unit, which had to bear the main burden. The professional attitude of the nursing staff made a deep impression on me and ultimately led to my decision to study medicine.
However, doubts remained. At that time, there was an oversupply of medical students in Germany, and you were only allowed to work as a junior doctor—Arzt im Praktikum—for around 700 Deutschmarks in the first year, if at all. There was no way I could afford to be unemployed or finance my life with this amount of money, meaning that in the summer of 1990 I was faced with exmatriculating from medicine and instead enrolling in a degree in electrical engineering, which would leave me with no formal way back into medical school. In my case, there was an older member of staff at the University of Saarland who apparently recognised my inner turmoil and didn’t proceed with my de-registration. I am deeply indebted to this person, as he made it possible for me to continue studying medicine. The decision to specialise in cardiology, on the other hand, was very simple and straightforward. During an internal medicine lecture in the winter of 1990, our cardiologists proudly demonstrated how they could reopen a vessel in an ST-segment elevation myocardial infarction (STEMI) patient at night. At that time, primary percutaneous coronary intervention (PCI) was still considered
experimental. It was immediately clear to me that interventional cardiology was my destiny.
Who were the biggest influences on your early career?
As a young student, I was able to join the cardiology working group of a senior physician at Saarland University Hospital. Here, I was given the opportunity to work as a student assistant and was able to learn how to plan, conduct and analyse clinical trials.
The topic of my dissertation was the influence of X-ray contrast media on the microcirculation. This work was supported by Ulrich Speck, who was then the head of the research and development (R&D) department for contrast media at Schering AG in Berlin. In addition to X-ray contrast agents, his group developed gadolinium for magnetic resonance imaging (MRI). I started my training in internal medicine and cardiology at the end of 1994 at the age of 25. Among other topics, we published data in the European Heart Journal on the influence of X-ray contrast media on outcomes after PCI.
This led to an invitation to Berlin from Schering in December 1999. Shortly before that I attended the TCT Congress in Washington, DC, where. I was impressed by preclinical data on drug-eluting stents (DESs).
In Berlin, together with Prof Speck, we discussed options for modifying the properties of contrast media. One idea was to use them as carriers for antiproliferative agents.
You have been instrumental in the development of coronary DCB therapy— how did this come about?
In 2000, Prof Speck moved to the Radiology Department at Charité Hospital, Berlin, for a professorship under the direction of Bernd Hamm. We established a porcine stent restenosis model and conducted the first investigations into contrast agent-taxane formulations. We were able to show that a short-term contact of antiproliferative drugs, such as paclitaxel, with the vessel wall can lead to a dose-dependent, long-lasting biological effect.
However, it was difficult to control which dose was applied in which vascular territory. It therefore made sense to use a more lesionspecific technique such as balloon catheters, which were necessary anyway for local drug application. Surprisingly, a coating of the contrast agent iopromide and paclitaxel led to a significant inhibition of neointimal formation after experimental stent implantation. When we presented those preclinical results on DCBs in the early 2000s, the typical reaction was that, even if it worked in pigs it wouldn’t work
in humans, and even if it did, nobody would need such a technology, let alone use it. We discussed several options for a first-inman study. At that time, it was not possible to predict from the animal data whether efficacy could be clinically proven at all or, on the contrary, whether patients could be harmed by an excessive effect. My proposal was to start with a safe indication that also represented an unmet clinical need, namely coronary in-stent restenosis (ISR), as a stent is already in place with a lot of tissue protecting it. Our first clinical study in the ISR indication was successful and paved the way for the indication of DCB for coronary ISR. Meanwhile, our Paccocath ISR trial is seen as one of the milestones in interventional cardiology.
FACT FILE
CURRENT APPOINTMENTS
2017–present: Full professor for clinical and experimental interventional cardiology, Saarland University (Homburg/ Saar, Germany)
2019–present: Head of the DGK Center for Training in Interventional Cardiology, Saarland University (Homburg/ Saar, Germany)
2019–present: Head of the DGK TAVI Center (TAVI Zentrum), Saarland University Hospital (Homburg/Saar, Germany)
2024–present: Deputy director, Internal Medicine, Saarland University Hospital (Homburg/ Saar, Germany)
EDITORIAL BOARDS)
Clinical Research in Cardiology EuroIntervention Cardiovascular Revascularization Medicine
Journal of the Society for Cardiovascular Angiography & Interventions (JSCAI)
AWARDS
Award of Excellence and Innovation in Interventional Radiology, Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2021
Clinical Research Excellence Award, Global Cardiovascular Awards 2024
What role will DCBs play in the future treatment of coronary artery disease?
DESs have the best outcomes in non-complex coronary artery disease. However, we are well aware that permanent implants are associated with a device-related event rate of 2–3% per year. The more and the longer stents are implanted, the higher the event rate. Nevertheless, the treatment of ISR is actually the worst DCB indication. The real advantage of DCB therapy lies in avoiding unnecessary stent implantations and thus reducing the long-term risk for patients. The greatest advantages are in the treatment of complex lesions (long diffusely diseased, often small vessels, or bifurcations) or complex patients (diabetes mellitus, high-bleeding risk, impaired renal function, acute coronary syndrome). In the treatment of multivessel disease, especially, it is often a blended approach with a combination of DES and DCB. Current forecasts predict that around half of all coronary lesions worldwide will be treated with DCBs by the end of the decade.
How should interventionalists weigh up the choice between different DCB drug coatings?
It is important that there is corresponding clinical evidence for a specific coating. Unfortunately, if this criterion is taken into account, the DCB choice is very limited. Personally, I usually review experimental data on tissue concentration and drug persistence over time. A long persistence of the drug is crucial for antirestenotic efficacy. Here you can see very surprising things, which in most cases are also consistent with clinical data. For example, there are big differences even for the paclitaxel-iopromide coating. A crystalline formulation with medium-sized crystals shows very good tissue persistence, while amorphous or formulations with very small crystals show a rapid decline in tissue levels. This explains, for example, the poor effectiveness in the REC-CAGEFREE 1 trial investigating a coating associated with a sharp dose decline already at 28 days. In contrast, the paclitaxel-urea coating in the same animal model shows therapeutic tissue levels still at six months. In the case of sirolimus, tissue persistence is even more critical. Here, too, we see very different data with different technologies.
Which are the studies to watch in the DCB space?
Larger trials with sirolimus DCBs are currently underway. The issue here is that larger
randomised trials in de novo vessels have been started either without angiographic data (Selution, Cordis) or with negative efficacy data (MagicTouch, Concept Medical). In my view, the direct lesion-related comparison of DCB with DES is also not appropriate, as the combination of both technologies to reduce the number of permanent implants makes more sense clinically. The ongoing REVERSE study in Asia and the planned European Bifurcation Club DCB, as well as the BASKET B-ALL study will provide important data here.
What are the key unanswered questions you would like to see prioritised in future research?
For lesion preparation, the definition of quality criteria based on intravascular imaging is of great importance. Further technological improvements are possible in the field of DCB. Here, the topics of loss in the blood, transfer rate into the tissue, persistence of the drug in the vessel wall, and the reduction of distal embolisation are the goals. New drugs or combinations of drugs are also of interest.
Finally, the question remains as to what we can do if we need to scaffold the lesion despite optimal preparation. Here, too, new concepts are being developed that are based on the fixation of dissections and the temporary overcoming of elastic recoil (resorbable repair device).
We are also investigating new indications for local drug delivery beyond restenosis. Topics here include the local regression of atherosclerosis, the stabilisation of unstable plaques and aneurysms, or the neurohumoral regulation to influence cardiovascular risk factors.
DCB therapy for the treatment and prevention of restenosis was the first step into a completely new medical discipline for the prevention and treatment of cardiovascular diseases.
What is your advice to young cardiologists entering the field today?
Interventional cardiology is one of the exciting specialties in medicine. It is innovative and includes the opportunity to help patients
“When we presented preclinical results on DCBs in the early 2000s, the typical reaction was that, even if it worked in pigs, it wouldn't work in humans”
directly. It offers many temptations, especially for young ambitious cardiologists. At the same time, this is also the greatest risk for the young cardiologist themself, but even more so for the patient.
Therefore, training in interventional cardiology requires the unconditional ability for critical self-reflection, the willingness to accept criticism from more experienced colleagues, and, above all, to understand that it is always only about the wellbeing of the patient.
Once you understand these basic principles, you will also understand why my most memorable cases were not the successes, but the cases that didn’t go so well, from which you can learn to avoid failures in the future.
Outside of medicine what are your hobbies and interests?
I used to do a lot of sports and play music, mainly keyboard instruments. Now, any remaining time has become precious, so I reserve it exclusively for my wife, my son and our puppy.
Precision in every branch
Elevate bifurcation procedures with Onyx Frontier™ DES
Precisely engineered to meet the needs of bifurcation and left main PCI.1
1. Data on file at Medtronic.
The most relevant data addressing critical questions in bifurcation and left main PCI.2-4
2. Hildick-Smith D, Egred M, Banning A, et al. The European bifurcation club Left Main Coronary Stent study: a randomized comparison of stepwise provisional vs. systematic dual stenting strategies (EBC MAIN). Eur Heart J. October 1, 2021;42(37):3829–3839.
3. Tarantini G, Fovino LN, Varbella F, et al. A large, prospective, multicentre study of left main PCI using a latest-generation zotarolimuseluting stent: the ROLEX study. EuroIntervention. February 6, 2023;18(13):e1108–e1119.
4. Chevalier B, et al. KISS: provisional stenting in bifurcation lesion: benefit of side branch intervention? Presented at PCR 2023.
This material should not be considered the exclusive source of information, it does not replace or supersede information contained in the device manual(s). Please note that the intended use of a product may vary depending on geographical approvals. See the device manual(s) for detailed information regarding the intended use, the implant procedure, indications, contraindications, warnings, precautions, and potential adverse events. For a MRI compatible device(s), consult the MRI information in the device manual(s) before performing a MRI. If a device is eligible for eIFU usage, instructions for use can be found at Medtronic’s website manuals.medtronic.com. Manuals can be viewed using a current version of any major internet browser. For best results, use Adobe Acrobat® Reader with the browser. Medtronic products placed on European markets bear the CE mark and the UKCA mark (if applicable). For any further information, contact your local Medtronic representative and/or consult Medtronic’s websites.
Advancing bifurcation education through meaningful collaborations. See clinical evidence Europe Medtronic
For distribution only in markets where the Resolute Onyx and Onyx Frontier coronary stent systems have been approved. Not for distribution in the US, Canada, Japan, or France.
Structural Heart Interventions
ACURATE IDE results put spotlight on impact of valve underexpansion after TAVI
“Disappointed is an understatement,” Michael Reardon (Houston Methodist DeBakey Heart & Vascular Center, Houston, USA) said of the results of the ACURATE IDE trial comparing Acurate neo2 (Boston Scientific) transcatheter aortic valve implantation (TAVI) to two contemporary systems.
RESULTS OF THE TRIAL, A PROSPECTIVE, multicentre, randomised study, were presented by Reardon at TCT 2024 (27–30 October, Washington, DC, USA). There, Reardon reported that Acurate neo2 failed to meet noninferiority against two competitor valves—Evolut (Medtronic) or Sapien 3 (Edwards Lifesciences)—across an endpoint of allcause mortality, stroke or rehospitalisation at one year.
Investigators have stated that the comparison was “complicated” by a challenging trial environment, with much of the enrolment occurring during the COVID-19 pandemic. Sites were also relatively inexperienced in using the investigational device, Reardon said, with only 10% of enrolling physicians at the trial’s 70 sites throughout the USA having carried out more than 10 cases with Acurate neo2.
“We started this several months before the first COVID-19 wave and it took us 47 months to complete,” said Reardon. “The average time between Acurate implants was three months, and only three sites did one a month, so there was not much experience with this valve, while we were continuing to do control valves multiple times every week.”
Despite limited operator experience with the Acurate neo2 platform, Reardon reported that early outcomes with the device were “encouraging”, with periprocedural outcomes in line with those seen in the control arm, no anomalies in echocardiography outcomes such as mean valve gradient and paravalvular regurgitation, and no acute safety signals.
However, one-year composite rates of all-cause mortality, stroke or rehospitalisation stood at 16.16% in the Acurate neo2 arm and 9.53% in the control arm, meaning that Acurate neo2 did not meet the prespecified 8% margin for non-inferiority. The disparity between 30-day and one-year outcomes prompted Reardon and the study team to probe the potential mechanisms underlying the findings. What they found was a clear signal that under-expansion of the implanted valve may have been linked to the negative outcomes.
“We went back and looked at these and saw some of the valves did not look fully expanded, by looking at the posts not being parallel. We had engineers blinded out, go back and look at every case, and they found about 20% of these were underexpanded,” Reardon explained.
“Under-expanded valves had higher flows, turbulent flow and
reduced washout. That is a very plausible reason for platelet activation and clumping possible micro-emboli which could affect later strokes and later myocardial ischaemia. When we look at time to event, what we saw with under-expanded valves was that you had double the risk of all-cause mortality and triple the risk of stroke.”
Speaking to Cardiovascular News, Reardon said that despite operator inexperience with the Acurate neo2, it proved to be an easy and reliable valve to implant with early results in line with the commercially tested valves.
“Operator inexperience was manifest as lack of recognition of under expansion. Under expanded valves had twice the risk of mortality and three times the risk of stroke compared to expanded valves,” he said. Reardon hopes that the ability to recognise and treat under expansion will lead to better outcomes going forward.
The significance of valve under-expansion was picked up by Ole De Backer (Rigshospitalet, Copenhagen, Denmark) at PCR London Valves (24–27 November, London, UK) where he discussed analysis of outcomes amongst patients receiving Acurate neo2 in Europe.
“We identified, not in 20% as in the US trial, but in 9% of our patients who had an Acurate neo2 implanted, valve underexpansion. And, indeed, we confirmed that in this 9% of patients with an under-expanded Acurate neo2 valve, there were higher events of mortality and stroke,” De Backer revealed. “We could repeat this ACURATE IDE trial, which makes it clear that valve under-expansion is the root-cause of the clinical issues seen between 30 days and one year.”
De Backer echoed the comment that TAVI operators should be aware of the potential impact of transcatheter aortic valve under-expansion on outcomes regardless of the platform that they are using, and advised that performing post-dilatation can eliminate this valve under-expansion and clinical complications.
“For me as a TAVI implanter using a lot of different platforms, this is not only important for this particular platform. What we see in ACURATE IDE and in our European cohort is the understanding that we should not only consider valve post-dilatation in case of paravalvular leak or residual high trans-prosthetic gradients, but also in case of important valve under-expansion, whether it is a balloon-expandable valve, or any self-expanding platform,” he said. “I think we have to become better at detecting this during our case, and if we see valve under-expansion, to address it.”
ALERT study to use AI to identify underserved patients eligible for valve therapies
A randomised study—ALERT—aims to address the undertreatment of severe aortic stenosis or moderate-to-severe or severe mitral regurgitation, whilst evaluating racial, ethnic, gender, and geographic disparities associated with guideline recommended treatments such as transcatheter aortic valve implantation (TAVI).
The study is sponsored by Tempus, a technology company seeking to lead the adoption of artificial intelligence (AI) to advance precision medicine and patient care, in collaboration with Medtronic.
Investigators will use the Tempus Next platform to identify severe aortic stenosis or moderate-tosevere mitral regurgitation patients who meet guideline indicated therapy criteria, but do not have a treatment plan in place.
The study will evaluate the impact of electronic health record notifications generated by Tempus Next on treatment with valve therapies such as TAVI and clinical visits with heart valve centres. Tempus Next provides a suite of software including a cloudbased, automated patient identification and care pathway management for cardiovascular disease based on practice guidelines, as well as a patient communication and data collection/ analysis platform.
Data suggest white patients represent the majority (91%) of all TAVI procedures. Conversely, patients who are Black, Hispanic, Asian, or part of other racial groups are not being treated with TAVI at the same rates as white patients. Existing evidence suggests that this minimally invasive option could result in less time in the hospital and a quicker recovery compared to open heart surgery.
“Undertreatment of symptomatic severe aortic stenosis can be devastating for patients’ recovery and potentially fatal within two years if intervention does not happen. The goal of this study is to move towards better solutions for more equitable and timely care and eliminate barriers to treatment,” said Wayne Batchelor (Inova Health System, Fairfax, USA), steering committee chair of the ALERT study.
“We are excited to be one of the first sites activated in this critically important study. We look forward to working to address health disparities to bring more equitable and timely care to patients with valvular heart disease in our community. I am encouraged by the potential impact of this initiative as additional sites are activated around the country,” said Brian R Lindman (Vanderbilt University Medical Center, Nashville, USA)
TAVI
Michael Reardon
Below inset: Acurate neo2
First experience of novel transseptal puncture device shared at STS 2025
First-in-human results of a novel transseptal puncture device from Protaryx Medical were presented at the 2025 Society of Thoracic Surgeons (STS) annual meeting (25–27 January, Los Angeles, USA).
THE DEVICE IS A NOVEL catheter system designed to improve the safety, accuracy and ease of transseptal puncture to facilitate access to the left atrium for procedures such as left atrial appendage closure (LAAC), transcatheter mitral valve procedures, and atrial fibrillation (AF) ablation. The device features an atraumatic, echogenic retractable nitinol mesh, as well as an extendable distal catheter, which are intended to enhance imaging visibility and aid deployment.
Results of the first-in-human study, which included five cases conducted on 3 December 2024 at Sanatorio Italiano de Asunción (Asunción, Paraguay) under approval from the Research Ethics Committee of the Paraguayan Institute of Social Studies, were presented at STS 2025 by Rachael Quinn (Johns Hopkins Health System, Baltimore, USA).
“We spent a lot of time analysing clinical needs. The result is a device designed to simplify workflow, enhance precision, and provide excellent echocardiographic visibility. Our goal was not just to develop another transseptal system, but to rethink the approach—ensuring greater predictability and ease of use for physicians while prioritizing patient safety. We’re excited to provide a solution that truly aligns with what
Two-year CLASP IID trial results “reinforce” value of mitral TEER
clinicians have been asking for.” Quinn tells Cardiovascular News. “A major finding from our research was that poor device visibility under echocardiography was a key factor contributing to procedural challenges, safety concerns, workflow inefficiencies, and increased radiation exposure. With the Protaryx device, we’ve changed that. Our system is highly visible under echo, making transseptal puncture a simpler and faster procedure.”
Patients enrolled in the study averaged 46 years old (23–60 years), and four were female. In all, five transseptal puncture procedures were conducted to facilitate the delivery of essential left heart therapies. Two of the cases involved balloon mitral valvuloplasty were guided by transoesophageal echocardiography (TEE) and three were patent foramen ovale (PFO) closures guided by intracardiac echocardiography (ICE). The Protaryx device was highly visible under both echocardiographic modalities.
All transseptal punctures were successful at the targeted locations without adverse events, Quinn reported, and median transseptal puncture time, defined as the time elapsed between placement of the guidewire in the femoral vein to removal of the wire and dilator from the left atrium, was
Two-year results of the CLASP IID trial, comparing two transcatheter edge-toedge repair (TEER) devices, “reinforce TEER as a valuable treatment option” amongst patients with degenerative mitral regurgitation (MR).
RAJ MAKKAR (CEDARS-SINAI, LOS Angeles, USA) presented the latest findings from the CLASP IID randomised pivotal trial and registry— comparing the Pascal (Edwards Lifesciences) and Mitraclip (Abbott) mitral TEER systems—at PCR London Valves (24–26 November, London, UK).
The randomised trial enrolled patients with significant symptomatic degenerative MR who were at high risk for surgery at 57 sites across North America. Patients were assigned 2:1 to receive either Pascal or Mitraclip, and those ineligible for the randomised trial were enrolled in the Clasp IID registry.
On the 294 patients treated in the randomised trial, Makkar reported that there was a median age of 81 years, more than half had MR severity class
10 minutes. Median fluoroscopy time during transseptal puncture was nine seconds. Puncture time was favourable compared to previously reported values within the literature, and fluoro time was ten-fold less than those previously reported. The device catheter and distal extendable end-effector were very visible on both ultrasound modalities, allowing the operating physician to precisely pick the crossing point
We believe that this will slash the learning curve and facilitate surgeons’ involvement in left heart catheter-based procedures.”
III or IV severity, and there was high prevalence of comorbidities including pulmonary hypertension and atrial fibrillation (AF).
Echocardiographic data indicate that there was a significant and sustained MR reducion at two years, with both devices, with moderate or less MR present in 94.9% of Pascal cases, compared to 93.2% with Mitraclip. Mild or less MR was recorded in 78.8% of Pascal patients and 68.5% of Mitraclip patients.
“The benefits that were accrued per year were actually sustained in both groups and there was no significant statistically significant difference between the groups,” Makkar said.
Transmitral gradients were sustained at the same level up to two years at a mean below 5mmHg, Makkar stated, reported that these gradients were not different between the two devices. Evidence of left ventricular (LV) remodelling was also seen with both devices, and beneficial effects that were seen at 30 days and one year also persisted out to two years.
“The initial beneficial effects are sustained, both in terms of end diastolic volume and end diastolic diameter, and the same holds true for the functional and quality of life outcomes—the benefits were sustained up to two years, with 88% of the patients being New York Heart Association (NYHA) class I or II in the Pascal and Mitraclip groups,” Makkar said.
On quality of life measures, Makkar reported that there was no statistically
applicable to the subsequent therapeutic device.
None of the patients required more than one transseptal puncture attempt, and there were no incidences of perioperative or postoperative mortality, stroke, renal failure, AF, cardiac tamponade, or pericardial effusion. All patients were discharged within 12 hours in good condition.
Protaryx Medical anticipates a 510(k) submission to the US Food and Drug Administration (FDA) for the device in late 2025.
“There are more than half a million transseptal punctures done every year in the USA, and we believe that this will slash the learning curve and facilitate surgeons’ involvement in left heart catheter-based procedures,”
James Gammie, Protaryx co-founder and system chief of cardiac surgery at Johns Hopkins Health System, tells Cardiovascular News. “We think it will make it safer for patients and it will enable operators to precisely pick where they cross the fossa.”
significant difference in Kansas City Cardiomyopathy
Questionnaire (KCCQ) scores, which stood at 16.9 in the Pascal group and 12.7 in the Mitraclip group. Harder endpoints, all-cause mortality, cardiovascular mortality, heart failure hospitalisation rates and freedom from mitral valve reintervention, were similar in the two groups.
Makkar described the 98 patients enrolled in the registry portion of the study as being sicker than those in the randomised trial, with more in NYHA class III, and a greater prevalence or renal insufficiency.
Similar results in MR reduction were noted amongst these patients, he reported, sustained out to two years, albeit at a slightly lower level, with 91.7% having moderate or less MR. Functional and quality of life outcomes were also “significant and sustained”, Makkar added, noting that cardiovascular mortality, heart failure hospitalisations and reintervention rates were favourable in the type of patients
“This is the longest follow up, randomised comparison that is clinical events committee and core lab adjudicated looking at contemporary mitral-
“TEER is a valuable treatment option and this trial reinforces that,”
Protaryx transseptal puncture
Raj Makkar
Five-year Amulet IDE data show similar outcomes with Amplatzer and Watchman devices
Latest data from the Amulet investigational device exemption (IDE) trial, comparing the Amplatzer Amulet (Abbott) left atrial appendage occluder (LAAO) to the first-generation Watchman 2.5 (Boston Scientific) in patients with non-valvular atrial fibrillation (AF) at increased risk of stroke, demonstrate similar clinical outcomes with the two devices out to five years.
RESULTS OF THE TRIAL WERE PRESENTED at the American Heart Association (AHA) 2024 Scientific Session (16–18 November, Chicago, USA) by the trial’s principal investigator, Dhanunjaya Lakkireddy (Kansas City Heart Rhythm Institute at HCA Midwest Health, Kansas City, USA), and published in the Journal of the American College of Cardiology (JACC)
LAAO works by preventing blood from entering the left atrial appendage, a pouch-like sac connected to the left atrium, to prevent blood clot formation and theoretically reduce the risk of stroke. Abbott’s Amulet device features dual-seal technology—a lobe to fill the body of the LAA and a disc to close off the opening into the LAA—which, according to the device manufacturer, offers immediate closure of the LAA, reducing the risk of stroke and immediately eliminating the need for anticoagulation post-implant.
To assess the safety and efficacy of the device, investigators in the trial enrolled 1,878 patients at sites internationally, with device implants attempted in 917 patients for the Amulet, and 916 for Watchman.
Three-year findings from the Amulet IDE were reported at the 2022 Transcatheter Cardiovascular Therapeutics (TCT) meeting, where Lakkireddy reported that more patients receiving Watchman (7%) were placed on oral anticoagulation than those receiving Amulet (4%), whilst rates of cardiovascular death (6.6% vs. 8.5%) and all-cause death (14.6% vs. 17.9%) trended lower with Amulet than Watchman, while stroke and major bleeding where comparable between the two groups.
At five years, Lakkireddy detailed that clinical outcomes were similar between the Amulet and Watchman devices, including the composite of ischaemic stroke or systemic embolism (7.4% vs. 7.1%), the composite of stroke, systemic embolism, or cardiovascular death (20.3% vs. 20.7%), major bleeding (20.1% vs. 20%), cardiovascular death (14.3% vs 15.4%), and all-cause death (28.7% vs 31.1%).
Annualised ischaemic stroke rates at five years were low and the same for Amulet (1.6%/year) and Watchman (1.6%/year) devices, the study investigators have found.
Additionally, they report that stroke in patients with the Amulet occluder were less severe (38 non-disabling, 11 disabling, 11 fatal, 12 unknown) than stroke in patients with the Watchman device (19 non-disabling, 22 disabling, 17 fatal, 10 unknown).
Abbott’s Amulet IDE study, doctors can even more confidently offer AF patients the minimally invasive Amulet device that not only closes the LAA and reduces their risk of stroke, but can also keep them off blood-thinning medication long term.”
The five-year results from the Amulet IDE study provide “important information that informs the field of LAAO broadly and helps to guide clinical decisionmaking,” write Daniel Friedman (Duke University Hospital, Durham, USA) and James Freeman (Yale School of Medicine, New Haven, USA) in an editorial comment accompanying the paper in JACC
Device-related thrombus or peri-device leak of 3mm or greater preceded stroke events and cardiovascular deaths more frequently in patients with the Watchman device (63) compared with patients with the Amulet
These findings emphasise the importance of de-escalation antithrombotics to optimise the net clinical benefit of LAAO.”
occluder (31), the investigators found. A significantly higher percentage of patients were free of oral anticoagulation in the Amulet occluder group at each follow-up visit, with 94% and 90.9% free of oral anticoagulation at the last five-year follow-up visit in the Amulet and Watchman device groups, respectively, the investigators report in their JACC paper.
“Because blood thinners may cause excessive bleeding and side effects like nausea or dizziness, we as physicians want to avoid these medications for our patients following an LAA closure procedure,” Lakkireddy was quoted as saying in a press release issued by Abbott. “With the five-year findings from
COMPARE-TAVI shows noninferiority of Myval TAVI system to established device
NEW ANALYSIS OF THE MYVAL transcatheter aortic valve implantation (TAVI) system (Meril Life Sciences), presented as late-breaking data at PCR London Valves (24–26 November, London, UK), have demonstrated the non-inferiority of the device for a composite of death, stroke, moderate or severe aortic regurgitation and valve deterioration at one year compared to Sapien (Edwards Lifesciences).
Results of the COMPARE-TAVI study were presented by Henrik Nissen (Odense University Hospital, Odense, Denmark) and include outcomes among patients treated at centres in Aarhus, Odense and Aalborg, all in Denmark.
Alongside meeting non-inferiority against the trial’s composite primary endpoint (13.8% for Myval versus 13% for Sapien), Myval also exhibited a lower incidence of patient-prosthesis mismatch (17.5% vs. 28.6%).
A differentiating feature of the balloon-expandable valve is its availability in a wider range of prosthesis sizes than the comparator valves, with intermediate valve sizing making it possible for physicians to avoid over- or under-sizing the prosthesis based on patient anatomy. Previously, results of the LANDMARK multicentre trial, which compared Myval to both Sapien and
The comparable performance of the two devices in rates of stroke, embolism, cardiovascular death and all-cause death demonstrate the “remarkable consistency” in the effectiveness of percutaneous LAAO.
Of note, they highlight that although there was nearly four times more use of postimplant oral anticoagulation with Watchman, the annualised rate of major bleeding for the first six months was numerically lower with Watchman compared to Amulet (18.7% vs. 22.2%).
For both arms, the annualised rate of major bleeding dropped precipitously after the transition to aspirin monotherapy (3.8% with Amulet, 4% with Watchman).
“These findings emphasise the importance of deescalation antithrombotics to optimise the net clinical benefit of LAAO and challenge the dogma that dual antiplatelet therapy (DAPT) is associated with lower risk of bleeding than oral anticoagulation which has previously been called into question by a large registry analysis.”
The Amplatzer Amulet LAAO has been approved for use in countries in Europe, the USA, Canada and Australia, since its initial CE mark approval in 2013 and US food and Drug Administration (FDA) approval in 2021.
Evolut (Medtronic) valves, presented by Patrick Serruys (National University of Ireland, Galway, Ireland) at EuroPCR 2024 (13–17 May, Paris, France) showed that the performance of the Myval device in terms of safety and effectiveness was non-inferior to the contemporary devices for the occurrence of a primary composite endpoint of death, stroke, major bleeding, acute kidney injury, major vascular complications, moderate or severe
valve regurgitation, and the need for new permanent pacemaker implantation (24.7% vs. 27%).
Further analysis from LANDMARK, presented at PCR London Valves and published in EuroIntervention have confirmed Myval’s non-inferiority to both Sapien and Evolut valve series at 30 days post-implantation. The results highlighted comparable safety and effectiveness outcomes between Myval and Sapien (24.7% vs. 24.1%), with Myval demonstrating a lower rate of permanent pacemaker implantation (15% vs. 17.3%) and superior haemodynamic performance. Myval matched Evolut in composite endpoints (24.7% vs. 30%), showing benefits in reducing pacemaker implantation rates and moderate/severe valve regurgitation. Effective orifice areas were comparable between 26mm and 29mm Myval and Evolut devices.
Dhanunjaya Lakkireddy
Watchman LAAO
AmplatzerAmulet
Henrik Nissen at PCR London Valves 2024
Research weighs up discordance between bleeding risk calculation tools
A study assessing the performance of two commonly used definitions for determining which patients are at high risk of bleeding after percutaneous coronary intervention (PCI) has found a “substantial discordance” in categorisation between the two tools.
WRITING IN A PAPER IN JACC: Cardiovascular Interventions, CarlEmil Lim (Karolinska Institutet, Stockholm, Sweden) and colleagues outline their analysis of the ARC-HBR and PRECISE-DAPT score definitions for high bleeding risk, which are two methodologies that can be used by clinicians to help determine if patients would benefit from shorter or less intensive antiplatelet therapy after coronary stenting.
ARC-HBR—the Academic Research Consortium for High Bleeding Risk— is based upon expert opinion and bleeding rates from clinical trials of dual antiplatelet therapy (DAPT) after PCI, taking in criteria such as prior stroke and severe kidney disease.
PRECISE-DAPT—Predicting
Study finds adverse outcomes after decreased use of paclitaxelcoated devices
bleeding complications in patients undergoing stent implantation and subsequent dual antiplatelet therapy— on the other hand, is based upon pooled data from eight randomised trials and includes variables such as age, creatinine clearance, haemoglobin count and previous bleeding.
Lim and colleagues used data from several Swedish registries, including SWEDEHEART, the national registry recording outcomes of patients hospitalised for acute coronary syndrome or undergoing coronary or valvular intervention, to assess all patients who were discharged after coronary stenting with DAPT between January 2013 and July 2018. The study’s primary outcome was bleeding type predicted by each risk tool: BARC
type 3 to 5 bleeding in the analyses of the ARC-HBR definition and TIMI major or minor bleeding in the analyses of the PRECISEDAPT score.
Of the 7,562 patients, 27% (2,004) were categorised as high bleeding risk using the ARC-HBR definition, whereas 38% (1,696) were classified as being high bleeding risk when using the PRECISE-DAPT score. Overall, the numbers indicate a discordance in 22% of patients—1,696 of those included in the study.
Additionally, the study noted that patients at high bleeding risk were also at increased ischaemic risk and that observed risks for bleeding risk were higher than those predicted by the PRECISE-DAPT score.
“Our analyses indicate a need for the refinement of tools to guide personalised antiplatelet therapy after coronary stenting,” Lim and colleagues write in
Kim and colleagues detail that their study included all Medicare fee-for-service beneficiaries aged ≥66 years who underwent femoropopliteal revascularisation by International Classification of Diseases-10th Revision codes between 1 January 2016 and 31 December 2023.
their report of the results in JACC: Cardiovascular Interventions. “Instead of attempts to predict the absolute risks under the assumption that the impact of DAPT on bleeding is a function of the patient’s risk, using clinical trial data to directly model heterogenous treatment effects may be possible.
“Specifically, if a score can identify patients who experience no ischaemic benefit or no bleeding harm from longer DAPT duration (regardless of their absolute risk for the outcomes), calibration would not be crucial when it is applied in new populations.”
The authors go on to state that their study highlights the uncertain generalisability of guideline-recommended high bleeding risk definitions and decision rules across patient populations seen in routine clinical practice, indicating a need for “more refined” scoring systems.
COVID-19. “By the time of the FDA’s reversal of its warning against routine use of drug-coated devices in 2023,” the authors continue, “DCB use had reached 23.46%.” They go on to note that the use of uncoated PTA stabilised at a proportion higher than was seen before the safety concern.
A recent analysis of over 270,000 Medicare fee-for-service beneficiaries has found an increase in adverse outcomes and death after a US Food and Drug Administration (FDA) warning led to decreased use of paclitaxel-coated devices for peripheral revascularisation procedures.
WRITING IN THE JOURNAL OF THE American College of Cardiology (JACC), a team of researchers from the Richard A and Susan F Smith Center for Outcomes Research at the Beth Israel Deaconess Medical Center (Boston, USA) begin by stating that peripheral revascularisation has faced “intense scrutiny” in the past decade.
The authors—Joseph M Kim and colleagues—first cite the impact of a 2018 meta-analysis associating paclitaxel-coated devices with increased mortality when used for peripheral revascularisation. The paper led the FDA to warn against routine use of such devices. It was not until 2023, the authors add, that the FDA reversed its warning following the publication of several further studies showing no mortality signal.
COVID-19 also impacted peripheral revascularisation, Kim et al continue, noting that the pandemic “complicated peripheral arterial disease (PAD) management by reducing access to patient care”.
To assess the impact of these events, the researchers conducted a study to evaluate trends in femoropopliteal revascularisation from 2016 to 2023 and to analyse safety outcomes during three key time periods: 1) before the paclitaxel safety concern; 2) after the onset of the paclitaxel safety concern; and 3) during and after the COVID-19 pandemic.
Regarding statistical analysis, the authors state that they examined trends of femoropopliteal artery revascularisation procedures by quarter year across the eight-year study period. Endovascular revascularisation procedures were stratified by percutaneous transluminal angioplasty (PTA) alone, drug-coated balloon (DCB) alone, bare metal stent (BMS) alone, or drug-eluting stent (DES) alone. The study’s primary outcome was the composite of major amputation and all-cause mortality.
“During the study period, the number of endovascular revascularisation procedures declined 38.2%; the number of surgical revascularisation procedures declined 59.7%,” Kim et al report in JACC
The authors share that PTA was the primary method (27.72%) used for endovascular revascularisation
The paclitaxel safety concern sparked a rapid shift away from the use of paclitaxel-coated devices and toward the use of uncoated devices.”
before the onset of the paclitaxel-coated device safety concern, followed closely by DCB (24.91%). After the paclitaxel safety concern, the use of DCBs declined to a low of 17.89% by 2019, with a proportional increase in the use of uncoated PTA (34.52%).
In addition, Kim and colleagues write that the proportion of DCB use increased after the onset of
Furthermore, Kim et al reveal that revascularisations performed between the paclitaxel safety concern and the COVID-19 pandemic were associated with a higher rate of the primary outcome compared with procedures before the paclitaxel safety concern. They note that this was driven by increased risk of all-cause mortality. “By contrast,” Kim and colleagues report, “there were lower rates of major amputation after the paclitaxel safety concern.”
“The paclitaxel safety concern sparked a rapid shift away from the use of paclitaxelcoated devices and toward the use of uncoated devices, particularly PTA,” the authors write. “The use of DCBs has only recently regained some ground since its nadir in 2019, but their use remains remarkably low relative to PTA despite evidence supporting their superior efficacy and the FDA’s reversal of its warning against their routine use.”
Regarding limitations to their study, Kim et al recognise that claims data lack detailed anatomical and procedural information, and that the Medicare population “may not represent the US population at large, including those who are younger, are of minority background, or are privately insured”.
Eric Secemksy, senior author of the study, remarks on the significance of the findings: “This analysis is critical in informing how external events impact patient care. Between device safety concerns and the COVID-19 pandemic, treatment approaches changed dramatically for lower extremity interventions and patient outcomes were negatively impacted. How we approach existential threats to peripheral vascular care will require thought and caution, as informed by these novel data that were generously supported by the SCAI [Society for Cardiovascular Angiography and Interventions] Early Career Research Grant.”
Eric Secemksy
DCB Days showcases new momentum in drugcoated balloon PCI
Drug-coated balloons (DCBs) are building towards a new momentum in percutaneous coronary intervention (PCI) with increased interest in the potential advantages that these devices can offer over drug-eluting stents (DES) in a range of settings for the treatment of coronary artery disease (CAD). This growing understanding of the role of DCBs was brought into focus at DCB Days (8–9 October, Berlin, Germany), a two-day advanced training course hosted by B Braun at the prestigious Aesculap Academy in the German capital. The event saw experts in DCB-PCI from across the world sharing the latest data, insights and experience to underscore how DCBs—in particular the SeQuent DCB (B Braun) family of devices—have become an essential tool in the modern PCI toolkit.
“Leaving nothing behind” in the coronary vessels is not a new concept, attendees of the event heard—with roots back to the firstin-man coronary angioplasties performed in Zürich, Switzerland, by the godfather of interventional medicine Andreas Grüntzig. PCI practice has moved away from this idea in subsequent decades as the DES has become the dominant technology for interventional cardiologists to reopen coronary arteries. But, the “leave nothing behind” concept is experiencing a modern renaissance with the latest generation of cath lab operators waking up to the benefits that DCBs can bring to their practice, and more clinical evidence being gathered to support this approach in a wide range of clinical scenarios.
“I remember when this room was not packed out,” said DCB Days course director Raban Jeger (Triemli Hospital Zürich, Zürich, Switzerland) in his opening to a busy auditorium at the 2024 event, reflecting on how interest in this area of cardiology continues to gather pace. “This is important because DCBs have now become a real tool for the treatment of CAD. In the beginning it was really a technique that not many people adopted. Today, we have lots of believers.”
Jeger spoke alongside his fellow course directors, Fernando Alfonso (La Princesa University Hospital, Madrid, Spain) and Victor Jiménez (Hospital Álvaro Cunqueiro, Vigo, Spain), all three of whom are among Europe’s leading proponents of DCB therapy. The group worked together to craft a programme that encompassed the fundamentals of DCB angioplasty, touching on topics that range from the important role of lesion preparation, the use of imaging tools to optimise outcomes, emerging data on the expanding
clinical indications for DCB usage, understanding the different properties of the available drug coatings and how these could confer benefits in different scenarios, and the fundamentals to establishing a DCB programme. Talks were punctuated by both live and recorded cases to demonstrate DCB-PCI in action and to illustrate key learning points. An engaged audience of around 150 attendees from more than 10 countries joined the course to understand how DCBs can play a greater role in their practice.
preparation, enhancing initial lumen gain to address residual stenosis and vascular recoil. Later, vessel thrombosis was addressed through advances in antithrombotic therapies and dual antiplatelet therapy (DAPT). DES then emerged as a solution to the challenge of overcoming restenosis due to neointimal proliferation or neoatherosclerosis. Additional technologies, including bioabsorbable scaffolds, have been geared towards vascular restoration, facilitating local drug delivery without the need for a permanent implant, and this has ultimately paved the way for DCBs as the next step for optimising PCI, providing a way of delivering anti-stenotic drugs to the vessel wall whilst leaving no permanent metallic structure behind.
Overcoming DES limitations
“The fact that stents have limitations in certain clinical and anatomic conditions led to the need to develop some other techniques,” said Jeger, detailing the 2020 international consensus statement from the International DCB Consensus Group, which sets out best practice for DCB-PCI. “These recommendations were based on the fact that, at the time, implants in CAD did have big problems. An event rate of more than 2% per year is quite cumbersome.”
The consensus document, which, despite being four years old, still remains relevant to present-day practice, according to Jeger, contains various sections that include technical considerations about the choice of DCB, lesion preparation, the role of functional measurements and intravascular imaging, delivery of the DCB, as well as the angiographic and clinical indications that are best suited for DCB-PCI, and future perspectives on DCBs.
“In the consensus group recommendations, we discussed a couple of indications; of course in-stent restenosis (ISR) has been examined in depth, this is a clear indication, then high bleeding risk, small vessels, bifurcations—these are the classical indications for DCBs,” said Jeger, commenting on some of the situations in which DCB-PCI has been considered to be an advantageous approach, and in which evidence and experience is growing. “We can't say for all instances that this is the way to go, but in these indications, we have the best results. We think that in special situations where stents are not really working well, DCBs could
Attendees were taken “behind the scenes” at the drivers pushing forward the current global momentum for DCB-PCI, learning about the evolution of PCI and how technological developments over the years have been shaped by clinical need. Stents were first used to prevent early vessel closure caused by flow-limiting dissection, aiming to restore blood flow. Later, new techniques and tools were developed to improve lesion
Today, we have lots of believers in this”
Presentations offered a deep dive into the specific indications that may favour DCBs, focusing on ISR, bifurcation lesions, chronic total occlusion (CTO) and diffuse disease, examining present data and probing where further research is needed.
Alfonso argued in favour of DCBs as the gold standard for the treatment of ISR, commenting that in patients who have already been implanted with multiple layers of metal, further stent implantation is not an “elegant” solution to the problem.
Delegates learned that evidence to date has established DCBs as a first-line option for the treatment of ISR, with 2018 guidelines from the European Society of Cardiology (ESC) and the European Association of Cardio-Thoracic Surgery (EACTS) on myocardial revascularisation bestowing a class I recommendation—with the level of evidence A—for the use of DCBs in this setting. This recommendation is based largely on studies performed with the SeQuent paclitaxel and iopromide coating, including the PACCOATH ISR I and II and PEPCAD trials, with the guidelines noting “a class effect for all
DCB Days delivered two days of education on drug-coated balloon PCI
SeQuent® Please Neo
DCBs cannot be assumed”.
Alfonso also outlined some of the occasions where operators may choose to elect for DCB-PCI, citing cases where there is evidence of resistant underexpansion or optimal initial angiographic results. In the first instance of ISR, he commented, many operators may feel that using a DCB could be a suitable strategy, as they can return to use a DES if they are not satisfied with the result.
A perceived advantage of the DCB-PCI approach is that patients may only require a shorter duration of DAPT following their procedure, and Tuomas Rissanen (North Karelia Central Hospital, Joensuu, Finland) touched on how the use of DCBs can reduce the risk of bleeding in patients seen to be at high bleeding risk (HBR).
Typically, patients would require up to six months of DAPT after a PCI procedure with a DES, but Rissanen offered examples of investigations that have pointed to the utility of a shorter duration DAPT strategy after DCB implantation. Occasions where this may be a useful approach include in the primary prevention of bleeding, or as a means of “secondary prevention” through early cessation of antiplatelets if bleeding occurs post-PCI, he said. Other strategies may include a single antiplatelet therapy (SAPT)-only approach, he added, something that may be necessary in patients requiring imminent urgent surgery.
More data on this topic are coming, and Rissanen later offered delegates details of the ongoing DEBATE study, comparing the use of SeQuent Please NEO or DES in the HBR patient population, as well as different antiplatelet treatment regimens. Investigators hypothesise that the DCB strategy coupled with a shorter regimen of antiplatelets will be non-inferior to DES treatment with a longer DAPT duration against a primary endpoint of major adverse cardiovascular events (MACE) and bleeding at 12 months in patients with stable or acute coronary disease. Currently, the multicentre, international trial has enrolled around 30% of patients, Rissanen revealed.
Complex lesions, bifurcations and more For bifurcation lesions, Bimmer Claessen (Amsterdam UMC, Amsterdam, The Netherlands) argued that DCBs have been shown to lead to angiographically superior results in side branches compared to plain balloon angioplasty, commenting that it may be a suitable therapy where the operator is keen not to compromise the main branch. “DCBs are also great in small side branches,” he said, adding: “we need more evidence of an all-DCB approach in true bifurcation lesions and left main bifurcations”.
“In our daily life, we know that DCBs can work. We have very good experience with DCBs in complex lesions,” argued Florim Cuculi (Heart Centre Lucerne, Lucerne, Switzerland) in his presentation ‘Redefining indications for DCBs in CTO PCI’. Jiménez, meanwhile, put forward the case for the use of DCBs in the setting of diffuse disease. “Most of the current worldwide population does not die after the first ischaemic event, they survive, and they develop more complex and diffuse CAD over the years. We are going to have to deal with this in the cath lab,” Jiménez said. He pointed out that, presently, there are a lack of randomised trial data to underpin this approach, but said that DCBs alone, or alongside DES as a part of a hybrid strategy, are a safe and effective option in diffuse disease.
Robert Byrne (Royal College of Surgeons in Ireland University of Medicine and Health Sciences, Dublin, Ireland) offered insight into some of the key data shaping practice, demonstrating the performance of current technologies, and stressing that, as the most widely studied device to date, SeQuent Please NEO is positioned as the “gold standard” by investigators as the comparator device when studying DCB-PCI. Among the early studies highlighted by Byrne was
ISAR-DESIRE 3, which pitted the SeQuent Please against paclitaxel-eluting stents or balloon angioplasty alone. This showed that the paclitaxel-coated balloon has a similar revascularisation rate as the stent, but lower than balloon angioplasty. Ten-year results of the study, published in 2023, show that the results are sustained out to the long term.
More data on DCB outcomes and safety are anticipated in the coming years, with devices from several companies under investigation. At present, however, SeQuent DCBs remain the most-studied devices in use—with no evidence of a class effect across the available technologies.
Byrne picked out studies comparing SeQuent Please to competitor devices that include the recently-US Food and Drug Administration (FDA)-approved Agent DCB (Boston Scientific). In both the AGENT ISR trial from 2020 and the ISAR-DESIRE 3A trial from 2022 the SeQuent Please was shown to perform favourably in comparison to Agent.
Data from the TRANSFORM I trial were also shown, a trial that compared the SeQuent Please NEO to the MagicTouch (Concept Medical) sirolimuscoated balloon in the setting of de novo small vessel
disease, with the investigational MagicTouch device failing to meet non-inferiority for the endpoint of angiographic net gain at six months in comparison to SeQuent Please NEO.
A further study of note is REFORM, comparing the Biolimus A9-coated balloon (Biosensors) to SeQuent Please, in which it was shown that the percentage in-segment diameter stenosis at six months was 41.8% with the Biolimus-coated balloon versus 31.2% for SeQuent Please, meaning that the Biolimus A9 balloon did not meet non-inferiority versus SeQuent Please.
“Large trials are needed to move the field along,” commented Byrne, singling out the REVERSE study as one that has “captured the imagination” among followers of DCB research. REVERSE, a randomised, open-label multicentre trial is enrolling 1,436 patients at centres in South Korea, Malaysia, Taiwan and Singapore, comparing SeQuent Please NEO to a current-generation DES for the treatment of large CAD with de novo culprit lesions—which is indicative of the move to establish DCBs in a wider range of indications, beyond ISR, where the therapy has typically been positioned. Enrolment in the trial is slightly ahead of expectation, Byrne noted, with more than 520 patients recruited as of August 2024. Delegates heard how new data are shaping approaches to PCI in Europe and further afield. Claessen opened the session with an introduction to the DEBuT LRP trial, a study looking at changes in plaque characteristics after DCB usage in patients with acute coronary syndrome as measured by intravascular
ultrasound (IVUS)-near-infrared spectroscopy (NIRS). The trial sought to assess the impact of paclitaxelcoated balloon treatment of lipid-rich plaques on the reduction of maxLCBI4mm—the maximum lipid-core burden index in a 4mm segment.
“Our goal is to achieve plaque stabilisation in a therapy where the benefits outweigh the risks,” said Claessen. DCBs may provide the best strategy in this setting compared to a permanent implant, Claessen said, as they can provide local delivery of the drug with minimal injury to the vessel, homogenously across the vessel.
The first-in-human, proof-of-concept study showed that use of the SeQuent Please NEO resulted in a significant reduction of maxLCBI4mm without eliciting any safety concerns. The concept will be explored further in the DELETE-LRP study, a randomised trial comparing the paclitaxel treatment of lipid-rich plaque versus control.
Takashi Ashikaga (Japanese Red Cross Musashino Hospital, Tokyo, Japan) shared insights from Japan, where he explained that DCBs have been in use for over a decade and detailed that around 20% of PCIs currently involve the use of DCB technology.
Controversies: Guidelines and trials
Though the field of DCB-PCI is rapidly evolving, it is not without controversies. Byrne offered an analysis on two developments from the recent 2024 ESC congress (30 August–2 September, London, UK), focusing on two areas: the release of new guidelines on the management of chronic coronary syndromes (CCS) prioritising DES over DCB for the treatment of ISR following PCI; as well as results of the RECCAGEFREE 1 trial, in which DCB was found to be less effective than DES for previously untreated non-complex coronary lesions. “It’s fair to say that both of these came as a bit of a surprise,” Byrne said, reflecting the view of many proponents of DCB-PCI. Byrne questioned whether the studies cited within the CCS guidelines reflected the best available evidence to elicit a change to recommendations for DCBs as a first-line treatment for ISR and commented that more evidence from investigational device exemption (IDE) trials taking place in the USA could help to change this picture.
Offering his critique of the randomised RECCAGEFREE 1 trial, which compared the Swide (Shenqi Medical) DCB to the Firebird 2 (Microport) among 2,272 patients at 42 sites in China, Byrne expressed surprise at the outcome, and highlighted some of the limitations of the trial.
REC-CAGEFREE 1 did not meet its primary
In our daily life, we know that DCBs can work”
endpoint of reducing combined rates of cardiovascular events: cardiac death, target vessel myocardial infarction, and clinically and physiologically indicated target lesion revascularisation. And, patients who received the DCB were significantly more likely to experience a cardiovascular event after two years. Byrne said that the most important limitation of the study is a lack of knowledge of the relative performance of the investigational device, commenting: “the clinical performance of the study device remains somewhat unclear”.
Lesion preparation: Techniques and tools Sessions also homed in on optimising the use of DCBs, with a focus on the role of imaging and physiology techniques and technologies, new devices
Continued on page 26
Left to right: Bimmer Claessen, Fernando Alfonso, Florim Cuculi, Klaus Bonaventura, Takashi Ashikaga, Raban Jeger, Simon Eccleshall, Tuomas Rissanen and Victor Jimenez
Continued from page 25
in lesion preparation and antithrombotic regimens after DCB therapy.
“Lesion preparation is key for success,” Rissanen said. “In the past we have used angiographically based methods and maybe FFR [fractional flow reserve] in some cases, but now we are using more imaging, and this will be very important for the assessment of DCB cases in the future.”
Klaus Bonaventura (Ernst von Bergmann Klinikum, Potsdam, Germany) expanded on this point, explaining how lesion preparation is a key step for any PCI procedure—whether that involves the use of a DCB or other available devices—and considering the criteria for optimal lesion preparation. Cardiologists should consider all contemporary available tools in the cath lab when deciding on their approach, Bonaventura said, in a presentation in which he also considered the occurrence of intimal dissection, describing this as an outcome that should not be feared when adopting a DCB-PCI approach. The acceptable outcome of lesion dissection for DCB use should be a non-flow-limiting dissection with a residual stenosis of ≤30%.
Though not necessarily new, according to Jeger, tools including semi-compliant balloons, noncompliant balloons, scoring or cutting balloons, intravascular lithotripsy (IVL) or atherectomy all have a role in lesion preparation, depending on lesion characteristics and plaque composition.
“The plaques we encounter are not all similar. We have some soft plaques, some persistent plaques, there are sometimes some fibrotic lesions and some calcified lesions,” he said. “Depending on the enemy, you have to use different weapons.”
Non-compliant balloons might be deployed in uncomplicated lesions, for example, and these devices exhibit higher rates of angiographic success with lower rates of residual stenosis and high-grade expansions, Jeger detailed. Scoring and cutting balloons produce a controlled dissection and facilitate radially concentric vessel expansion.
Rotational or orbital atherectomy may reduce the rate of high-grade dissection, whilst IVL is used to modify softer plaque and shows similar vessel expansion in calcified lesions as compared to either atherectomy approach. “Stepwise escalation using different tools is the way to success,” Jeger commented.
Claessen, meanwhile, offered an overview of the latest advances in imaging guidance and physiology and their use in DCB-PCI. “We are in an era now where we have a lot of techniques that allow the use of physiology,” he said, touching on the growing number of physiology indices, which include computed tomography (CT)-derived FFR,
angiography-derived FFR and wire-based methods including hyperaemic pressure ratio and nonhyperaemic wire-derived pressure ratios. All of these tools can aid lesion preparation by measuring flow status and predicting late lumen enlargement (LLE), he detailed.
Intravascular imaging, which includes technologies such as IVUS, optical coherence tomography (OCT), IVUS-OCT and NIRS-IVUS, meanwhile, can serve as useful options for lesion severity assessment, as well as providing anatomical guidance pre-, during, and post-PCI. “Contemporary PCI mandates the use of physiology and imaging, particularly in selected clinical scenarios,” Claessen told attendees in summing up his talk.
Coatings: Paclitaxel and sirolimus Presenters also looked at technology and innovation in the DCB arena, with a focus on the differences in the drug coatings currently available in the market. Attendees heard how different coatings, dosage, excipients and coating procedures play a role in drug release, crystallinity and particle size, and how these factors influence drug bioavailability and persistence.
B Braun is presently the only provider with both paclitaxel- and sirolimus-coated balloons in its range, attendees heard—SeQuent Please NEO (paclitaxel) and SeQuent SCB (sirolimus). Both anti-stenotic drugs have been used extensively in the treatment of CAD since the beginning of the 21st century, though paclitaxel remains the most widely used drug for coronary DCBs, with balloons using sirolimus the most prevalent coating for DES technologies. The
The DCB is here to stay, and we know it will be an important add-on to current interventional techniques.”
evidence base for the efficacy of sirolimus-coated balloons remains some way behind paclitaxel, though studies are ongoing. Taking the SeQuent DCB family of devices as an example; to date, there are more than 110 studies, including 35 randomised controlled trials, with a total of more than 25,000 patients having received the SeQuent Please NEO, as well as five randomised trials with 500 patients enrolled investigating the SeQuent SCB.
DCB Days attendees heard how both drugs elicit different properties, with paclitaxel taking less time to administer at the vessel wall. Additionally, paclitaxel
is more lipophilic than sirolimus and has been shown to have a lower solubility in aqueous solutions (0.3µg/mL vs. sirolimus 2.6µg/mL). The mechanism of action between the two drugs also differs, as paclitaxel binds irreversibly to microtubule structures, whereas sirolimus binds reversibly to the mTORenzyme, making paclitaxel more persistent and able to remain in-situ for a longer duration.
As Alfonso commented, the availability of two different DCB coatings—paclitaxel and limus derivatives—may mean that “there is opportunity to be specific on using different drugs for different patient and anatomic subsets”.
Coatings: Data, drug delivery and physician preference
Bonaventura considered the relative merits of paclitaxel and sirolimus and the question of the ideal drug—highlighting the current disparity in data between the two agents. Due to the wide usage of sirolimus in DES platforms, and historic safety concerns over the use of paclitaxel-coated devices in the peripheral arteries—since allayed—there may be a “psychological” preference for this drug amongst some operators, he suggested, but more data will be crucial to determining its role alongside the established paclitaxel in DCBs.
Jiménez highlighted the concerns regarding the challenge posed by sirolimus-coated balloon technology in effectively delivering sirolimus to the vessel wall and ensuring its sustained presence over time. He addressed these doubts with a series of documented cases with sequential OCT imaging, demonstrating the presence of the drug in the arterial wall after DCB-PCI with SeQuent SCB, as well as its persistence weeks later. These findings were accompanied by excellent angiographic and clinical outcomes. “These are results we consistently observe in cases where we use SeQuent SCB alongside intracoronary imaging,” Jiménez stated. These are very intruiging data, and we are progressing with a study in this direction to better understand these findings and establish their relationship with optimal long-term patient outcomes.”
Cuculi offered insights into the use of the SeQuent SCB—“the new kid on the block”—in a real-world setting, summarising some of the cases and published data for the device from his centre. “Classic” cases for using the SCB might include a CTO, where the presence of diffuse disease means there is no option to use a stent, calcified lesions, or instances where a reduction in antithrombotic therapy may be appealing.
Though there are promising signs for the safety and efficacy of some sirolimus-coated balloons, including the SeQuent SCB, at present, there are very limited clinical data, Bonaventura went on to note, with no indication of a clinical advantage of sirolimus over paclitaxel, which has proven safety and efficacy. More data and experience of the efficacy of the available sirolimus-coated devices are needed, he said, commenting that many interventionalists will need this to build up trust in the use of these devices.
“For those who already have trust in sirolimuscoated balloons, this may be an alternative to work implant-free if data on selected sirolimus-coated balloons confirm at least non-inferiority to established paclitaxel-coated balloons,” he concluded.
“It is great to see that the DCB technique is gaining momentum,” Jeger told Cardiovascular News, reflecting on the outcomes of the event. “We know from lots of trials and lots of experience in clinics that the technique works, and we want to show how you can use these devices and how you can trust in the technique. The DCB is here to stay, and we know it will be an important add-on to current interventional techniques.”
Product News
Harmony transcatheter pulmonary valve gains CE mark
Medtronic has received CE mark for the Harmony transcatheter pulmonary valve (TPV) system, a minimally invasive alternative to open-heart surgery for congenital heart disease patients with native or surgically repaired right ventricular outflow tract (RVOT).
The Harmony TPV system is designed to treat patients with RVOT anomalies with severe pulmonary valve regurgitation (PR)
“The expansion of the Harmony TPV system enables a critical new solution, ensuring that more patients can have access to cutting-edge transcatheter technology and potentially lessen the need for multiple surgeries,” said Nina Goodheart, senior vice president and president of the Structural Heart & Aortic business, which is part of the Cardiovascular Portfolio at Medtronic.
The current standard of care is openheart surgery or other interventions early in life to address these malformations. For the 80% of CHD patients who require a native or surgically repaired RVOT at birth, many will need a pulmonary valve replacement later in life, which often requires another openheart surgery.
with symptomatic acute decompensated heart failure (ADHF) and cardiogenic shock.
Johnson & Johnson MedTech has partnered with the Advanced Cardiac Therapies Improving Outcomes Network (ACTION) to provide the real-world data necessary to support on-label use of Impella 5.5 and Impella CP, both left-sided heart pumps, for paediatric patients with symptomatic ADHF and cardiogenic shock.
ACTION is a global healthcare network comprised of patients, families, clinicians, researchers and industry representatives that collaborate with ACTION leadership to improve outcomes for patients.
“Receiving CE mark for the Harmony TPV system helps advance options for minimally invasive solutions for physicians to treat this vulnerable patient population and optimise their outcomes,” said Peter Ewert, director of the Department of Congenital Heart Defects and Pediatric Cardiology at the German Heart Center in Munich, Germany. “Clinicians across Europe are in need of solutions to fill this gap, and this milestone will be a potential turning point for patients who want to avoid multiple surgeries and minimise medical disruptions in their daily lives.”
CE Mark follows US Food and Drug Administration approval of the system in 2021. Harmony TPV US mid-term (three-year) data results demonstrated superior patient outcomes with positive sustained RV remodeling, effective valve function, and a strong safety profile, all contributing to significant improvement in patient quality of life. The device is expected to be commercially available across Europe later this month.
Impella heart pump approved for use in paediatric patients
The US Food and Drug Administration (FDA) has expanded the indications for the Impella 5.5 with SmartAssist and Impella CP with SmartAssist heart pumps (Johnson & Johnson Medtech), granting premarket approval (PMA) for use in specific paediatric patients
represents a meaningful advancement in transseptal access,” said Lee Geist, president and chief executive officer (CEO) at Circa. “The system is designed to offer consistent performance while enhancing control, visibility, procedural efficiency and potential cost savings for physicians.”
“This marks a monumental achievement for children with heart failure as, historically, this area of paediatric care has been underfunded and understudied,” said Angela Lorts and David Rosenthal, cofounders of ACTION.
“We are proud to have worked with Johnson & Johnson MedTech on this crucial approval and look forward to further collaborations that will enhance care for these vulnerable patients.”
Impella CP and Impella 5.5 heart pumps unload the heart’s left ventricle, allowing the heart to rest while also ensuring delivery of oxygenated blood throughout the body. The PMA amendment expands the usage of left-sided Impella devices to specific paediatric patients weighing ≥52kg for Impella CP and ≥30kg for Impella 5.5.
Circa announces first procedures with Crosswise RF transseptal access system
Circa Scientific has announced the launch of its innovative Crosswise radiofrequency (RF) transseptal access system, which is designed to provide precise puncture of the septal wall with a streamlined, zero-exchange workflow.
The Crosswise system delivers RF energy directly to the tip of a shapeable, radiopaque cannula, enabling precise navigation and controlled crossing during procedures requiring left heart access, such as atrial fibrillation (AF) ablations, left atrial appendage occlusions (LAAOs), and mitral valve interventions. That is according to a Circa press release.
The release also notes that the device’s zero-exchange design allows clinicians to maintain guidewire accessibility throughout, enhancing procedural efficiency by eliminating additional steps and reducing the need for extra consumables.
“The introduction of Crosswise
Gregory Feld (Sulpizio Cardiovascular Center, University of California San Diego [UCSD], San Diego, USA), who participated in the early clinical experience with the system, commented: “Crosswise is a valuable addition to our EP [electrophysiology] lab, offering significant benefits for the many procedures requiring transseptal access. Its seamless integration with our existing tools and techniques ensures it adapts effortlessly to our established workflow.”
Biotronik nets short DAPT and calcified lesion indications for Orsiro Mission DES
Biotronik has announced CE mark approval of two new indications for the Orsiro Mission drug-eluting stent (DES).
These include one-month dual antiplatelet therapy (DAPT) for high bleeding risk (HBR) patients, allowing practitioners to offer personalised, shorter DAPT durations to their patients at high risk of bleeding events, in accordance with the most recent guidelines.
Additionally, the Orsiro Mission DES has been approved for calcified lesion treatment, allowing practitioners to target more complex lesions with moderate or severe calcification. These new indications complement the recent global regulatory approval of the Orsiro Mission DES for an increased maximum allowed diameter (MAD) post-dilation (2.25–3mm, MAD: 4mm, 3.5–4mm, MAD: 5mm).
Following these approvals, labelling including adapted Instructions for Use will become effective in the coming months, pending further national regulatory approvals.
First patient procedures performed with Abbott’s balloonexpandable TAVI system
Abbott has announced the first patient procedures with its investigational transcatheter aortic valve implantation (TAVI) balloon-expandable system for treating symptomatic severe aortic stenosis.
This investigational Abbott TAVI system is the first step toward Abbott’s software-guided balloon-expandable TAVI system and is designed to build a foundation for artificial intelligence (AI)-guided procedures, the company says in a press release. Once the investigational balloon-expandable system completes clinical development and is approved by regulatory authorities, Abbott’s structural heart portfolio will offer physicians another
TAVI management option along with the company’s Navitor TAVI system, which is already commercially available.
“Transcatheter aortic valve implantation treatment has benefitted both physicians and patients over the years, but physicians have come to understand one device does not fit all their patients with aortic stenosis,” said Azeem Latib (Montefiore Health System, New York, USA) who conducted the first procedures with the device alongside cardiac surgeon, Vinayak Bapat (Minneapolis Heart Institute, Minneapolis, USA). “We, and hospitals worldwide, remain focused on helping this growing patient population by investigating and providing expanded treatment options that adapt to the unique needs and anatomies of patients.”
The first-in-human procedures were successfully conducted at the Republican Centre of Emergency Medicine in Tashkent, Uzbekistan, in collaboration with site principal investigator, interventional cardiologist, Saidamir Djafarov.
Caranx Medical makes US FDA submission for AI TAVI guidance software
Caranx Medical has announced that it has made a submission to the US Food and Drug Admnistration (FDA) for its artificial intelligence (AI) software for real-time intraoperative guidance of transcatheter aortic valve implantation (TAVI)—Tavipilot.
The FDA submission marks a significant milestone in the company’s strategy towards planned market introduction of the software by the end of 2025, Caranx Medical says in a press release.
“The team at Caranx has achieved an important milestone in the submission to the FDA. This extremely promising step paves the way to early commercialisation of the Tavipilot Soft by end 2025. I am very excited about the real-time guidance of TAVI, a key to accurate and precise positioning of the heart valve as well as the promotion of potentially more predictable and controlled valve deployment,” says CEO of Caranx, Jorgen Hansen.
Tavipilot Soft is an AI-driven intra-operative software which tracks real-time anatomical and instrument landmarks. It is compatible with all cardiac imaging systems and will be compatible with principal TAVI heart valves on the market, the company press release adds.
“This first release of our Tavipilot software marks an important step toward AI-augmented procedures. Our software is designed to be userfriendly, ensuring that cardiologists and surgeons can integrate it seamlessly into their usual practice. Tavipilot Soft allows clinicians to position a prosthetic valve easily and with high precision, ensuring that more patients could benefit from a high quality of care,” says Caranx co-founder Pierre Berthet-Rayne.
Harmony TPV
Impella heart pump
First patients treated in TRICURE EFS study of Topaz tricuspid heart valve replacement system TRiCares has announced that the first patients have been successfully implanted with Topaz, its transcatheter tricuspid heart valve replacement (TTVR) system, in an early feasibility study (EFS) in the USA.
The TRICURE EFS, a prospective, multicentre, single-arm study approved under a US Food and Drug Administration (FDA) investigational device exemption (IDE), will assess the safety and performance of TRiCares’ Topaz TTVR system in adult patients
with severe tricuspid regurgitation (TR) who are identified with increased operative risk. The study is taking place in up to eight sites across the USA and Canada, aiming to enrol 15 patients.
The first two implantations in the TRICURE EFS were carried out by the experienced teams at Piedmont Heart Institute in Atlanta and the Medical University of South Carolina (MUSC) in Charleston.
Susheel Kodali, director of the Structural Heart and Valve Center at Columbia University/New York Presbyterian Hospital (New York, USA) and principal investigator of the TRICURE EFS study, stated: “I am pleased to oversee this important TTVR study. In the months ahead, I’ll work with the study participants and organisers to investigate how Topaz might improve long-term outcomes for TR patients. Physicians are certainly in need of new solutions that address adverse events and simplify the implantation procedure.”
Pradeep Yadav, director of Structural Interventions at the Marcus Heart and Vascular Center, Piedmont Heart Institute (Atlanta, USA), commented: “Our first implant of the Topaz valve was successful with the patient’s TR eliminated and the patient discharged in good condition shortly thereafter. The simple Topaz procedure was completed in less than an hour and it was less demanding of our imaging specialists than other TR therapies.”
Yadav performed the procedure with Vinod Thourani, Marcus chief of cardiovascular surgery, Piedmont Heart Institute.
CAPTURE-1 study of EmStop embolic protection system concludes EmStop has announced the completion of the CAPTURE-1 early feasibility clinical trial assessing the safety and
performance of the EmStop embolic protection system.
The device is currently being investigated for use as an embolic protection device to capture and remove thrombus during transcatheter aortic valve implantation (TAVI) procedures. This investigatory study was a prospective, multicentre, singlearmed clinical trial.
A total of 15 subjects underwent treatment with a currently marketed TAVI device and the EmStop system and were evaluated under the approved clinical protocol.
“The successful completion of the CAPTURE-1 clinical trial marks yet another important milestone in the development and clinical understanding of this novel embolic protection technology,” said Phil Ebeling, EmStop president and CEO. “I am thankful for the many healthcare professionals and the entire EmStop team who have supported the advancement of this platform technology.”
In addition to submitting the CAPTURE-1 results for regulatory review, EmStop is looking ahead toward future data publication and the initiation of additional clinical trials based on the totality of these results, the company says in a press release.
“Stroke is a well-known and feared complication of TAVI,” said Michael Chenier (Mission Hospital, Asheville, USA), CAPTURE-I primary investigator. “EmStop offers patients a potential alternative to reduce the likelihood of stroke and other embolic events. Due to the novel integrated filter design, physicians can perform TAVI, and potentially other procedures, while providing patients complete embolic protection and without loss of procedural efficiency or requiring additional vascular access.”
EmStop, currently under active clinical investigation, is designed to provide full cerebral protection for lefthearted catheterisation procedures.
Enrolment completed in ALLRISE trial of FFRangio coronary physiology assessment
CathWorks has announced the successful completion of enrolment of the Advancing Cath Lab Results with FFRangio Coronary Physiology Assessment (ALL-RISE) randomised controlled trial (RCT), evaluating the clinical and economic benefits of the CathWorks FFRangio system in
diagnosing and treating coronary artery disease (CAD).
The ALL-RISE Study included over 1,924 patients across 59 sites in North America, Asia, Europe and the Middle East. Participants presenting with coronary stenoses of intermediate significance and requiring physiology assessment were randomised to receive either FFRangio-guided treatment or invasive pressure wire-guided treatment. Notably, this was the firstever randomised controlled trial in the USA to assess clinical outcomes using an angiography-based tool for physiologic lesion assessment, CathWorks said in a press release.
In a joint statement, the ALL-RISE study chair, Ajay Kirtane (NewYorkPresbyterian/Columbia University Irving Medical Center, New York, USA) and principal investigators, William Fearon (Stanford University, Stanford, USA) and Allen Jeremias (St. Francis Hospital & Heart Center, Roslyn, USA), stated: “On behalf of the study executive committee, we would like to congratulate and thank all the global investigators, study coordinators and patients who collectively enabled this incredible accomplishment. The high level of engagement and record speed of enrolment parallel the growing adoption of FFRangio globally. We look forward to sharing the results of this landmark study after clinical follow-up is completed.”
APEX-AV trial results of AlphaVac PE system published in JSCAI AngioDynamics has announced the publication of the results from the Acute Pulmonary Embolism Extraction Trial with the AlphaVac system—APEX-AV—in the Journal of the Society for Cardiovascular Angiography & Interventions (JSCAI).
The primary efficacy endpoint of the APEX-AV trial was the reduction in right ventricle to left ventricle (RV/LV) ratio between baseline and 48 hours post-procedure. The primary safety endpoint was the rate of major adverse events (MAEs), including events such as major bleeding and serious device-related clinical deterioration, pulmonary vascular injury, and cardiac injury within the first 48 hours. Patients were followed for 30 days post-index procedure. The results demonstrated the device as a safe and effective treatment for acute intermediate-risk PE with a significant reduction in RV/ LV ratio and clot burden with a low rate of adverse events.
The APEX-AV trial demonstrated a 35.5% reduction in clot burden (via the Modified Miller index score), comparing favourably to other mechanical aspiration devices on the market. The unique design features of the device, including its funnel tip, optional wireless navigation, and blood loss mitigation, contributed to clinically significant improvements in both safety and efficacy.
The APEX-AV trial was initiated in partnership with the Pulmonary Embolism Response Team (PERT)
Consortium and was led by co-principal investigators William Brent Keeling, associate professor at the Emory School of Medicine (Atlanta, USA), and Mona Ranade, assistant professor, interventional radiology, at the David Geffen School of Medicine at University of California, Los Angeles (UCLA, Los Angeles, USA). The trial results were presented at The Society for Cardiovascular Angiography & Interventions (SCAI) 2024 Scientific Sessions (2–4 May, Long Beach, USA).
“The results from the APEX-AV trial demonstrate the significant impact of the AlphaVac F1885 technology in treating pulmonary embolism,” said Ranade, assistant professor, interventional radiology at the David Geffen School of Medicine at UCLA. “We observed a significant reduction in clot burden pre- and post-treatment, and saw a notable improvement in pulmonary artery pressures, underscoring the efficacy of this innovative approach.”
First patients enrolled in JENAVAD registry
JenaValve Technology has announced the completion of the first patient procedure for inclusion in the JENAVAD registry.
The JENA-VAD registry is a prospective, multicentre, single-arm clinical registry nested within the ALIGN-AR study evaluating the ability of the JenaValve Trilogy heart valve system device to treat severe symptomatic aortic regurgitation safely and effectively in patients with a continuous flow left ventricular assist device (cfLVAD). The first case was completed at Cedars-Sinai Medical Center in Los Angeles, USA.
“We are excited for the initiation of the JENA-VAD registry and this meaningful step in exploring treatments for the large population of LVAD patients suffering from AR,” said Raj Makkar, Cedars-Sinai Medical Center, who performed the case. “The positive results of the ALIGN-AR study provide a strong base and justification for moving forward with this registry studying whether transcatheter aortic valve implantation (TAVI) with a dedicated device may be a solution for these patients with significant AR. We look forward to the results of this registry.”
The JenaValve Trilogy device is used to treat symptomatic severe AR commercially in the EU under CE mark and is being evaluated in the ALIGNAR IDE study and ALIGN-AR CAP protocol for high-risk patients.
In these situations, patients with LVAD are excluded because of left ventricular fraction (LVEF) <25% and other exclusions. As such, patients with LVAD have been treated under compassionate use consideration in the USA and off-label in the EU. The registry protocol will ensure consistency in performing the procedure, patient management, and documentation of results in this population.
FFRangio
Topaz TTVR system
Boston Scientific to acquire IVL developer Bolt Medical Boston Scientific has announced it has entered into a definitive agreement to acquire Bolt Medical, the developer of an intravascular lithotripsy (IVL) advanced laser-based platform for the treatment of coronary and peripheral artery disease.
“Representing one of the fastest growing medical device segments, intravascular lithotripsy therapy addresses a significant unmet need for patients with complex calcified arterial disease through a minimally invasive approach,” said Lance Bates, senior vice president and president, Interventional Cardiology Therapies, Boston Scientific. “Bolt Medical is developing a nextgeneration technology that is highly complementary to our existing portfolio.
The addition of this system to our offerings can help us better serve physicians and their patients and provides a platform for future innovation.”
Lithotripsy is a procedure in which a physician breaks up hardened masses such as calcium to help restore blood flow. The Bolt IVL system is designed with a novel application of lithotripsy to fracture calcium by creating acoustic pressure waves inside of a balloon catheter. The system also includes visible, directional emitters for consistent energy delivery in the treatment of the calcified lesions.
Boston Scientific initially developed the concept for the Bolt IVL system which helped establish Bolt Medical in 2019. As a strategic investor in Bolt Medical, Boston Scientific has an equity stake of approximately 26%.
Conference calendar
As a result, the transaction consists of an upfront payment of approximately US$443 million for the 74% stake not yet owned and up to US$221 million upon achievement of certain regulatory milestones.
Bolt Medical recently announced the completion and results of the RESTORE ATK and RESTORE BTK pivotal clinical trials investigating the Bolt IVL above-the-knee (ATK) and below-the-knee (BTK) systems for the treatment of peripheral arterial disease in patients with moderate to severely calcified lesions. The data from both studies will be used to support US Food and Drug Administration (FDA) and CE mark regulatory submissions for the devices. In December 2024, Bolt Medical received FDA approval to commence the global FRACTURE investigational device exemption IDE clinical trial in the USA, which is investigating the use of the Bolt IVL coronary system for the treatment of coronary arterial disease with severely calcified lesions.
Boston Scientific anticipates the transaction to be completed in the first half of 2025.
Relief Cardiovascular closes financing round to fund first-inhuman study
Relief Cardiovascular has announced the closing of a US$12 million series A financing.
The funding round was co-led by Broadview Ventures and Advent Life Sciences, with participation from Pacific Health Investment, Heartwork Capital, and an undisclosed multinational strategic.
The funds will support further product development and the initiation of the company’s first-in-human feasibility study, designed to evaluate the safety and efficacy of the Relief system—a transcatheter smart implant designed to monitor and modulate renal vein pressures, offering a novel approach to fluid management in heart failure.
The Relief system employs a transcatheter implant to reduce renal vein pressure using an innovative “puller” mechanism, paired with integrated sensors that autonomously
29–31 March
American College of Cardiology (ACC) 2025 Scientific Session Chicago, USA expo.acc.org/acc25/public
23–25 April
Charing Cross (CX) Symposium 2025 London, UK cxsymposium.com/
capture renal vein pressures and multiparametric data. The system provides physicians with actionable data for optimising fluid management and offers tailored therapeutic devicedriven intervention.
“The Relief system’s ability to integrate monitoring and therapeutic modulation of renal pressures represents a promising advance in volume management in heart failure,” said William T Abraham, professor of medicine at The Ohio State University Wexner Medical Center (Columbus, USA).
Alex Rothman, professor of cardiology at the University of Sheffield (Sheffield, UK), added: “By enabling data-driven adjustments, the Relief system empowers more personalised and effective care for patients, particularly those with diuretic resistance.”
CMS launches review of coverage for renal denervation
The Centers for Medicare & Medicaid Services (CMS) has opened a national coverage analysis (NCA) on renal denervation, with a view to reviewing and developing a national Medicare coverage policy for the therapy for patients with hypertension.
The expected completion date for the NCA is 11 October 2025. Until a national coverage determination (NCD) is put into effect, renal denervation procedures will continue to be evaluated for coverage based on medical necessity for individual Medicare patients.
This latest news follows the announcement in late 2024 that CMS had granted transitional pass-through (TPT) payment for Medtronic’s Symplicity Spyral renal denervation (RDN) catheter and Recor Medical’s Paradise ultrasound RDN (uRDN) system.
TPT payment, which is effective for
up to three years beginning 1 January 2025, aims to support patient access to new and innovative technology. Both the Medtronic and Recor Medical renal denervation systems gained US Food and Drug Administration approval in November 2023. Medtronic‘s Symplicity Spyral system is a minimally invasive procedure that delivers radiofrequency energy to nerves near the kidneys that can become overactive and contribute to high blood pressure, whilst the Paradise system is an ultrasoundbased technology.
In a press release, Medtronic says that the national coverage analysis was initiated by CMS in response to its request to support Medicare beneficiary access to the Symplicity Spyral system.
Recor Medical has similarly welcomed the commencement of the analysis, describing it as the first step in the National Coverage Determination (NCD) process towards the potential expansion of coverage of the Paradise system among Medicare beneficiaries.
Terumo and Medis partner on coronary imaging technology
Terumo Health Outcomes (THO) and Medis Medical Imaging have entered into a strategic partnership in the USA to drive utilisation of Terumo’s proprietary clinical decision support platform ePRISM and Medis’ quantitative flow ratio (QFR) technology.
The use of ePRISM and Medis QFR will be piloted at selected clinical sites, leveraging real-time data from electronic health records to provide prospective insights to help enhance patient care, the companies have said in a press release.
The press release adds that the partnership represents a significant step forward in enhancing clinical decision support capabilities, streamlining workflows and improving patient outcomes by providing interventional cardiologists with precise anatomical and physiological assessments of coronary artery disease QFR is an angiographic image-based approach that replacing the more invasive wire-based approach in assessing coronary physiology. It is also capable of evaluating multiple areas from the same images versus the wire-based approach which is vessel- and often lesion-specific.
1–3 May
Society for Cardiovascular Angiography & Interventions (SCAI) Scientific Sessions Washington, DC, USA scai.org/scai-scientific-sessions
19–23 May EuroPCR Paris, France pcronline.com
12–13 June Actif 2025 Paris, France actif-cardio.com 25–27 June New York Valves, The Structural Heart Summit New York, USA nyvalvesconference.com
29 August – 1 September
European Society of Cardiology (ESC) Congress Madrid, Spain escardio.org/congresses-events/ esc-congress
8–11 October
European Association for Cardio-Thoracic Surgery (EACTS) annual meeting Copenhagen, Denmark eacts.org/39th-annual-meeting/
Blood pressure reading
Boston Scientific Global headquarters
Onyx Frontier™ DES
Great just got better
Onyx Frontier DES inherits the same stent platform, clinical data, and indications you’ve come to rely on with Resolute Onyx™ DES. What makes it even better is its delivery system resulting in best-in-class with a lower crossing profile.2
See more at medtronic.com/ OnyxFrontierGlobal
†Stent delivery system updates were implemented on the 2.0–4.0 mm Onyx Frontier DES diameters.
1 Based on bench test data on file at Medtronic. May not be indicative of clinical performance. N = 7 DES of each tested: Onyx Frontier DES, Resolute Onyx DES, Orsiro®* Mission DES, XIENCE Sierra™* DES, XIENCE Skypoint™* DES, SYNERGY™* DES, SYNERGY™* XD DES, Ultimaster™* Tansei™* DES.
2 Based on bench test data on file at Medtronic. May not be indicative of clinical performance. N = 5 DES of each tested: Onyx Frontier DES, Orsiro Mission DES, Resolute Onyx DES, XIENCE Skypoint DES, SYNERGY DES, Ultimaster Tansei DES.
Europe Medtronic Intl. Trading SARL Tel: 41.21.802.7000
Asia Pacific Medtronic Intl. Ltd. Tel: 65.6436.5000
Latin America Medtronic USA, Inc. Tel: 786.709.4200