19 Deep venous stening: “Safe” with low complication rate
Has interventional radiology reached its global tipping point?
Co-published in the journal CardioVascular and Interventional Radiology (CVIR) and Journal of Interventional Radiology (JVIR), a new global statement produced by the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) and the Society of Interventional Radiology (SIR) queries: Have we reached the tipping point? It aims to set forth the essential elements of interventional radiology (IR) and the continuing challenges facing the specialty.
Quality over quantity? The growing focus on QoL in interventional oncology
A focus session dedicated to quality-of-life (QoL) outcomes in interventional oncology (IO) at this year’s Cardiovascular and Interventional Radiological Society of Europe (CIRSE) annual congress (14–18 September, Lisbon, Portugal) saw experts study the critical importance of patient-reported outcome measures (PROMs) and the growing recognition of these data as key indicators of procedural success in cancer care.
In conversation with Interventional News, Roberto Iezzi (Policlinico Universitario Fondazione Agostino Gemelli, Rome, Italy) extracted key points from his presentation. “The journey is becoming more important than the destination,” he stated, praising the range of effective interventions that have been developed in IO today. “The good news is that we have so many treatment options—the bad news is that we have so many treatment options,” Iezzi deliberated. “Tailored to each patient’s disease and comorbidities, approach to treatment can be more dynamic and the right selection is the most important part of our job”, he added.
Iezzi explained that, today, precision cancer care has come so far as to cure 50% of metastatic cancer cases and extend the life expectancy of the other 50%. He referenced a study published earlier this year by Wörns et al, in which the investigators interviewed patients with hepatocellular carcinoma (HCC) on their treatment goals. Patients described extending overall survival as their most important goal in early-stage HCC, whereas for advanced/unresectable disease, QoL and managing side effects became their key priority.
“Undeniable connection” between QoL and survival
In treating advanced disease, Iezzi described the creation of a new subgroup of ‘chronic’ cancer patients, in whom lifeextending treatment is achieved, but quality of life is maintained in careful balance. “This is a future concept,” said Iezzi, teasing new research to be published this year in which he and his
Roberto Iezzi
CIRSE AND SIR FIRST published a joint statement which sought to define IR in 2010, following the Royal College of Physicians and Surgeons of Canada’s denial of the Canadian Interventional Radiology Association’s request for official recognition. The motivation for the 2024 document was both to reflect on how far IR has come as a discipline and where it needs to go next. This updated statement was first presented during the Global IR Summit at the CIRSE annual congress (14–18 September, Lisbon, Portugal), and sparked talks over the desynchronised development of international IR. The central tenet of the updated document is the uptake of clinical practice and longitudinal care in IR over the 14-year interim, as presented in the session by Parag Patel (Froedtert Hospital, Milwaukee, USA) and Robert Morgan (St George’s NHS Trust, London, UK). They outlined the areas that necessitated an update, which included increased clinical practice, recognition of longitudinal care of patients provided by IR in some countries, the need to promote subspeciality or specialty
SIR/CIRSE
Interventional radiology: A play in three acts
I became an interventional radiologist by accident. As a resident in cardiology, I had an unusual chief: he belonged to a new breed of cardiologists who did cardiac catheterisations and coronary angioplasties. When I expressed an interest in doing the same, he said: “This work is usually done by radiologists. I am the exception to the rule. Go to the Hammersmith Hospital and ask Robert Steiner, the professor of radiology, to train you.” Steiner said: “If you want me to teach you, you have to become a radiologist.” “Thank you, Professor,” I said. “You start on the first of October.” That was my job interview. How times have changed…
Act I: Interventional cardiology
During my basic training in radiology, I went to the cardiac lab, within the department of radiology, just to observe the work, in preparation for what I thought would be my future career. Steiner allowed cardiologists as well as radiologists to be trained in cardiac catheterisation and intervention. Although the radiologists had excellent technical skills, it was obvious to me that their role in this new discipline was destined to disappear. Why? Because they were interested mainly in the catheters and the pictures. They were happy for the cardiologists to monitor the electrophysiological parameters and, most importantly, to look after the patients. That battle was lost before it even started.
Act II: Peripheral vascular interventions
Hammersmith Hospital was the home of the emerging discipline of interventional radiology (IR). It was an exciting time, with such a dizzying number of developments in all organ systems that it was difficult to choose a focus. Some of the things we did would be illegal today, like drawing the shape of a plastic spiral biliary stent on the silver paper in a cigarette packet (no, not mine), having the device in my hand a week later, and implanting it across a malignant hilar stricture the following day. What one could do was limited only by the anatomy of the human body and imagination. There was no challenge to IR from any other discipline. But, having witnessed the loss of cardiac intervention, I was certain that Charles Dotter’s exhortation to ‘accept clinical responsibility’ was wise. When I was appointed to the university chair of IR by the Senate of the University of London in 1992, I approached the Royal College of Radiologists (RCR) to encourage them to create a new method of training, distinct from that of diagnostic radiology (DR), that would allow future interventional radiologists to look after their own patients. A historic meeting of the three governing bodies of the college—the faculties of radiation oncology and radiology, and the RCR council—was convened by the president of the college, who was a radiation oncologist. I told them that devices called ‘aortic stent grafts’ would change the way peripheral vascular disease was managed and that radiologists had an opportunity to play a major role in this field, provided they were trained as clinicians rather than as imagers. The radiation oncologists understood and agreed. The radiologists didn’t. I was told that ‘teamwork is the way forward’, which was code for ‘others can look after the patients of interventional radiologists’. I allowed my frustration to show and said, ‘teamwork is the kiss of death’.
What I meant was that ‘shared’ clinical responsibility is an illusion; either you are a fully-fledged clinician, or you are not. My retort was inelegant and ungracious, but it was correct. Much of vascular IR is now in the hands of vascular surgeons.
Act III: Interventional oncology (IO)
The encroachment on IO by other specialties is still patchy because, until recently, it has focused on palliation and the treatment of small tumours in patients who are not candidates for surgery. This is changing fast, as solid scientific evidence now supports the use of ablation as a primary treatment of small tumours in the kidney and the liver. As IO expands, surgeons will want to use its techniques to replace major surgery.
Several countries are trying to establish IR as a specialty separate from DR, following the example of the American Board of Radiology (ABR). This is necessary, but not sufficient. If IR is to thrive as an independent discipline, rather than just tick along as an optional extra to surgery and radiation therapy, its practitioners must be full-time clinicians. They must stop spending time reading diagnostic images other than those concerning the patients they treat. Even those studies must be formally reported by diagnostic radiologists rather than by interventional radiologists. This will not happen without radical changes to training and recruitment.
The future of IR will be decided by institutions such as the RCR, and its counterparts in other countries, which define the pattern of training and practice of their members. If such professional bodies want to retain IR, they must create a specialty that focuses on clinical and procedural training. Although the intimate understanding of radiological imaging is a vital aspect of the skillset of interventional radiologists, they should be able to use that knowledge to guide their interventions and to assess the results. True, full-time clinical practice in IR can become a reality only if dual certification stops. Such a specialty would attract trainees with a surgical mindset, who are understandably reluctant to spend several years away from clinical practice in diagnostic radiology learning to be imagers. Will this happen? Well…anything is possible. But betting more than half a pint of beer on it might be a little too optimistic.
ANDREAS ADAM is emeritus professor of interventional radiology at King’s College London, UK and joint editor-in-chief of Interventional News.
Editors-in-chief: Professor Robert Morgan, Professor Andy Adam, Professor Brian Stainken
NEWS IN BRIEF THE LATEST STORIES FROM THE INTERVENTIONAL WORLD
n UK IR WORKFORCE
ANALYSIS:
An analysis of data collected on interventional radiology (IR) practice in the UK has shown an increasing trend in the number and complexity of procedures between 2017 and 2021, despite an imbalance in provision and demand of IR services, as well as a “striking” lack of records regarding safety and service-cost data.
For more on this story go to page 8.
n TWO-YEAR GAE RESULTS:
Published in the Journal of Vascular and Interventional Radiology during Pain Awareness Month, a new study shows that a minimally invasive treatment for knee osteoarthritis (KOA) may have a lasting benefit of at least two years. The study of genicular artery embolization (GAE) followed 40 patients with moderate-to-severe KOA after their GAE treatment and measured pain scores up to 24 months.
For more on this story go to page 16.
n EXERCISE AND VTE RISK:
Published in the Journal of Thrombosis and Thrombolysis, new research with a follow-up of 27 years has found an association between high levels of physical activity (PA) and an elevated risk of venous thromboembolism (VTE).
The research, led by Per Wändell (Karolinska Institutet, Huddinge, Sweden) and colleagues, was drawn from the Uppsala Longitudinal Study of Adult Men (ULSAM).
For more on this story go to page 19.
Publisher: Stephen Greenhalgh | Content director: Urmila Kerslake | Global sales director: Sean Langer
Editor: Éva Malpass | Editorial contribution: Jocelyn Hudson, Jamie Bell, and George Barker
Design: Terry Hawes, Josh Lyon and David Reekie
Advertising: Michael Broughton michael@bibamedical.com
Subscriptions: subscriptions@bibamedical.com
Published by: BIBA News, which is a subsidiary of BIBA Medical Ltd
If you have comments on this issue or suggestions for upcoming editions write to eva@bibamedical.com Subscribe
higher risk of VTE in men regularly engaging in strenuous exercise 2X
Andreas Adam
Quality over quantity?
The growing focus on QoL in interventional oncology
Continued from page 1
colleagues will investigate how much life is sacrificed by cancer patients due to life-extending treatments.
Recent research attempted to evaluate the effect of QoL improvement on patient outcome. Earlier this year, Balitsky et al’s systematic review and metaanalysis of PROMs across Medline and Embase databases suggested that integration of PROMs into treatment improved health-related quality of life (HRQoL) and the overall risk of mortality at 12 weeks. In their report, however, the authors note that improvements in HRQoL dropped off at the 24-week mark and showed no association at 48 weeks.
Their results suggest that QoL improvements could benefit patients in the early phase of treatment. Vlasios Sotirchos (Memorial Sloan Kettering Cancer Center, New York, USA), who presented on the immediate QoL impact that IO treatments have for liver cancer patients, stated that there is an “undeniable connection” between QoL and overall survival in general. He told Interventional News that this could be due to the development of patient-centred treatment plans adapted to individual patient needs reported via PROMs data collection at each patient visit, rather than taking a one-size-fits-all approach. By placing focus on the physical, emotional and social effects of cancer and its treatments, interventionists can help dispel distress and elevate QoL, which Sotirchos stated can be “extremely meaningful” in patients with with cancer at any stage.
A dynamic approach to QoL
Placing QoL at the centre of the algorithm, treatment takes customisable form in Iezzi’s view. “We can select the best multimodality approach—we know that ablation is better than surgery when considering quality of life, and that chemoembolization and radioembolization are better than systemic chemotherapy. This way, we can provide dynamic systemic and locoregional treatment and achieve quality-of-life improving strategies such as chemoholidays, and then restart treatment with appropriate systemic intensification,” he stated.
Iezzi made clear that setting a well-planned, dynamic treatment plan in motion is all well and good, but without clear communication to manage patient expectations, the overall success of said procedures can be limited. He went on to expand on what defines curative or palliative treatment and the flexibility of these concepts.
“If a 50-year-old man is given 10 years, this is not a curative approach, but, if an 85-year-old man is also given 10 years, this would be considered curative despite the treatment modality. The term palliative has completely changed over the last ten years,” Iezzi said. “Previously, palliation was akin to ‘waiting for death’ whereas today, all treatments are considered palliative due to the dual goal of extending-life years and maintaining good quality of life.”
Addressing the psychological impact of a cancer diagnosis and subsequent treatment on the patient, Iezzi suggested that a psychoncologist should be inducted into the multidisciplinary team. He noted that discussion during the session at CIRSE turned to cultural differences in communication with cancer patients, noting that in Italy patient-physican communication styles are more indirect than those of Canadan interventionists—to which session moderator and native Canadian, Riad Salem (Northwestern University, Evanston, USA) agreed. Providing emotional support throughout the therapeutic process, the implementation of a psychoncologist in routine cancer care could help to standardise PROMs from country to country.
Disparities between countries worldwide are well-documented, Sotirchos added, stating that many patients have limited access to this level of treatment or can experience significant delays in receiving care. “Treatment access inequities impact QoL and addressing this issue should be a priority for healthcare systems,” he said.
Barriers to collecting QoL data
Although research conducted by Basch et al found that obtaining PROMs data has a positive impact on the patient and therapy outcomes, the collection of said data has been shown to be burdensome for both patients and centres.
Presenting on why this is during the CIRSE session, Nathalie Kaufmann—chief operating officer and procurator at Next Research—highlighted that, in 10 years of experience conducting CIRSE research, limited staffing, logistical centre issues, and patient refusal and incapacity were detrimental to the collection of PROMs. While about 86% of hospitals participating in CIRSE research projects returned PROMs data overall, most of the questionnaires were completed at baseline visits before treatments and return rates declined thereafter.
She detailed their plan of launching an electronic PROMs questionnaire in 2017–2018 in the hope of improving questionnaire return rates. Despite a lengthy development process improving language functionalities and browser compatibility, no hospital
Treatment access inequities impact QoL and addressing this issue should be a priority for healthcare systems”
Vlasios Sotirchos
used the online questionnaire throughout the time period.
Centres attributed this to average patient age, which was mid-60s—“this may have created a challenge”, Kaufmann said, however, looking back now, the electronic PROMs tool might not have simplified the data collection process sufficiently.
Today, Kaufmann added that technology and patients’ ability to navigate it has improved, and they intend on conducting a similar study in the near future. Irrespective of how QoL data will be collected in future, it will remain an essential part of research in IR. In an ideal world, Kaufmann states that PROMs data would be used in routine clinical practice outside of research as well. Demonstrating the value of collecting QoL data during research projects is an important step in this direction.
“Through our research projects we’re sometimes working with centres that are collecting quality-oflife data for the first time and we are then helping to establish processes, such as, if they think their patient might be experiencing depression, how do they communicate with the patient and where can they refer them,” Kaufmann said. “Collecting this data is valuable to the patient and healthcare professional to improve communication between the two,” she added.
“Mandatory” QoL outcome measures in clinical trials
Later in his presentation, Iezzi drew attention to the European Society for Medical Oncology-Magnitude of Clinical Benefit Scale (ESMO-MCBS) grading system to assess the robustness for QoL research. In the introduction to the scale, the authors asserted that QoL—assessed with a validated tool—must be at least a secondary endpoint in future IO trials. Advocating for mandatory QoL questionnaires, Iezzi underlined that particularly in a non-curative setting, these assessments can aid multidisciplinary teams in selecting effective interventions. “It’s important we make patients aware of the real purpose, aim and outcomes of the procedures we are performing,” Iezzi added, so that patient and procedural goals align.
Sotirchos reflected that obtaining QoL metrics has a two-fold benefit for patients and interventionists, and will help to improve outcomes and healthcare policy decisions.
“Due to the multidimensional nature of QoL assessments, including several generic and diseasespecific instruments, comparisons across studies can be very challenging,” he said. Yet, Sotirchos averred that, through the development of new technologies and the demonstrated value of recording PROMs to exemplify the benefit of IO procedures, the collection of this data must be prioritised in both clinical trials and routine
Left to right: Roberto Cazzato, Vlasios Sotirchos, Nathalie Kaufmann, Riad Salem, Roberto Iezzi
Has interventional radiology reached its global tipping point?
Continued from page 1
recognition, and the developments in certification over the last decade, particularly via the European Board of Interventional Radiology (EBIR). The increased commitment to diversity amongst interventional radiologists and overarching workforce developments, such as their increased presence on interdisciplinary boards, and the importance of IR-led clinical studies, were also covered.
The project for this updated global statement was launched during CIRSE 2022 and spearheaded by lead authors Morgan, Patel, Alda Tam (MD Anderson Cancer Center, Houston, USA), and Christoph Binkert (Medizinisch Radiologisches Institut, Zürich, Switzerland). At the time of print, the document has been circulated and endorsed by 47 national IR societies.
Morgan indicated that the statement is essentially a call to action to promote IR, especially in countries where interventional radiologists have limited resources to endorse their services. “Our global IR societies must collaborate closely to advance common strategic
goals and must continue to promote the field of IR and the treatments we provide as first options for patients whenever appropriate.” Informing their understanding of geographical disparities across international IR training and practice, Morgan referenced a global survey of IR status carried out by the international division of the SIR, presented earlier in the session by Constantinos T Sofocleous (Memorial Sloan Kettering Cancer Center, New York, USA).
Sofocleous stated that “the world is not equal, and IR services throughout are extremely different with many disparities”. The anonymous survey was distributed to members of global IR societies and investigated demographics, local/regional practice characteristics, and professional challenges and practice needs.
“Of our responders, 92% agreed that there is a great need to establish unified global IR training standards”, Sofocleous said. He described the shortage in dedicated IR training programmes in “most” regions worldwide, as well as a “pronounced” shortage in IR exposure in Africa, Asia and South America. He also highlighted the lack of IR teaching responsibilities in Africa, noting, however that, “interestingly”, they were more prevalent in Europe when compared to the USA. Regarding IR practice, the investigators found that
public awareness of IR services was a universal issue, showing “no difference” between Africa and the USA—the geographies at either end of the spectrum concerning IR infrastructure.
“Public awareness is our greatest universal need, and this should drive our future investments. Establishing training programmes, providing access to online education and organising local IR conferences in Asia, South America and Africa are all key takeaways [from the survey],” said Sofocleous.
With the information gained through the survey, the subsequent Global IR Statement concludes that a ‘tipping point’ may in fact be reached in the next two decades, initiating the formal designation of IR as a distinct sub- or primary specialty worldwide. However, this goal can only be achieved through “close collaboration”, the authors write, between societies to promote IR as the first option for patients when appropriate.
The talk then turned to monitoring and measuring the progress of IR, and how development can be captured worldwide. Sofocleous
stated that attention should be paid to marketing IR, shifting focus from imaging-oriented to disease-oriented messaging—“to show what our field has to offer each disease type”. However, “we don’t have enough boots on the ground”, he added, explaining that, if this were not the case, the installation of an interventional radiologist among every panel that dictates disease-specific guidelines would be an ideal metric to mark IR’s international growth in the coming years.
Patel inserted that: “As a specialty that has organised ourselves, we need to take responsibility for the promotion of IR services. We must be more vocal as a field, enrol in more clinical trials, and be at the table when multidisciplinary guidelines are being brought about.”
Closing the session, Morgan stated that raising the profile of IR worldwide is a question that has “taxed people better than us for many, many years”. He stated that through continual ideasharing in forums such as the Global IR Summit, headway can be made, and a feasible method of monitoring IR’s development can be established.
We must be more vocal as a field, enrol in more clinical trials and be at the table”
Parag Patel
WAVE trial reports Wrapsody superiority over standard PTA
Six-month results of the Wrapsody Arteriovenous Access Efficacy (WAVE) pivotal trial have reported superior target lesion primary patency (TLPP) with the Wrapsody (Merit Medical) cell-impermeable endoprosthesis (CIE) when compared to percutaneous transluminal angioplasty (PTA). These data were presented by Mahmood Razavi (St Joseph Heart & Vascular Center, Orange, USA) during a FIRST@CIRSE session at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) annual congress (14–18 September, Lisbon, Portugal).
WRAPSODY WAS DEVELOPED TO AID physicians in treating patients with stenosis/occlusion in the vessels used for haemodialysis. Creation and maintenance of an arteriovenous fistula or graft (AVF/ AVG) to achieve long-term vascular access is required for patients undergoing haemodialysis, although progressive stenosis or occlusion can pose lifethreatening consequences.
In 2021, clinical outcomes from the first-in-human trial of Wrapsody showed a 12-month TLPP rate of 84.6% and an access circuit primary patency (ACPP) of 65.9%. Building on these results, the WAVE trial was created to determine Wrapsody’s superiority to PTA. The prospective, multicentre study enrolled 245 patients with AVF peripheral venous circuit outflow lesions requiring intervention from 43 international centres. Of this cohort, 122 patients were randomised to PTA and 123 to Wrapsody.
Their results showed that six-month patency was “significantly” higher for both TLPP (89.8% vs. 62.8%, p<0.0001) and ACPP (72.6% vs. 57.9%, p<0.015) in patients treated with Wrapsody when compared with patients randomised to PTA. Additionally, in a summary of safety events through to 30 days post treatment, only one device-related event was reported against Wrapsody, compared with nine in patients treated with standard PTA. Four procedure-related events including bleeding, erroneous stent placement and haematoma were reported using Wrapsody, versus PTA’s 12 which included death, dissection and infection.
Speaking to Interventional News following his presentation, Razavi noted that Wrapsody’s superiority over PTA concerning ACPP is crucial, as this is a “critical” metric for physicians and patients when
identifying the magnitude of an intervention’s benefit.
Razavi stated that: “While covered stents and drugcoated balloons have improved lesion patency in these patients, ACPP still remains a challenge. Results of this trial not only showed superiority of Wrapsody over angioplasty but also numerical improvement over prior technologies. This six-month analysis provides insight regarding Wrapsody’s anticipated long-term performance.”
Results of this trial not only showed superiority of Wrapsody over angioplasty but also numerical improvement over prior technologies”
Mahmood Razavi
In a roundtable following the presentation of the WAVE trial results, Razavi, alongside the WAVE trial’s co-principal investigator Robert Jones (Queen Elizabeth Hospital Birmingham, Birmingham, UK) and Wrap Global Registry principal investigators Dheeraj Rajan (University of Toronto, Toronto, Canada) and Panagiotis Kitrou (Patras University Hospital, Patras, Greece) discussed the findings.
Razavi pointed out that, numerically, the six-month trial results are “better than anything else we have seen” which he determined is due to performance characteristics imbued in the device which can overcome typical “mechanisms of failure” such as
The first report of six-month results from the SUCCESS PTA trial evaluating the Selution SLR (Cordis) drug-eluting balloon has shown that consistent haemodynamic, functional and clinical improvements were observed, associated with a 97.7% freedom from clinically driven target lesion revascularisation (CD-TLR), which was reported as 97% for the chronic limbthreatening ischaemia (CLTI) subgroup.
PRESENTER MICHAEL Lichtenberg (Vascular Center Clinic, Arnsberg, Germany) shared these data during the FIRST@CIRSE session at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) annual congress (14–18 September, Lisbon, Portugal).
The SUCCESS PTA trial enrolled
723 patients from 27 sites across Europe, Asia, and South America, primarily evaluating CD-TLR. Lichtenberg described the cohort’s Rutherford classification at baseline, noting that 74.2% of patients had claudication and 25.8% were identified as having CLTI. Describing lesion characteristics of
negative remodelling, recoil or tissue proliferation.
Jones commented that the engineering process for the Wrapsody device focused on limiting edge stenosis—the ‘Achilles’ heel’ of covered stents. The Wrapsody device is designed with a scalloped and softened edge to exhibit less force at the interface with the normal adjacent vein where stenosis typically develops.
Sticking with Greek mythology, Kitrou described a “Sisyphean struggle” with stenosis and restenosis in these patients. “This data shows that not only for de novo, but also restenotic lesions, the Wrapsody device had a tremendous effect even for fistulas at dedicated lesions sites,” Kitrou added, underlining the significance of the ACPP finding in the WAVE data. “I was optimistic with the initial trial outcomes involving fistulas, but these results further strengthen my opinion that covered stents could be the first option.”
The speakers then discussed the prospective, observational Wrap Global Registry, which seeks to evaluate TLPP and safety outcomes at six months in international centres which are using the Wrapsody device. Rajan and Kitrou stated that 309 patients of their 500-patient target have currently been enrolled, a third of whom have provided six-month follow-up. “The first-in-human [WAVE] trial gives you an indication of what the outcomes of this registry will look like,” Rajan said. “The hope is that we get a better understanding of how the device performs in a real-world setting,” he stated, adding that preliminary results should be released in the near future.
the full cohort, Lichtenberg pointed to the percentage of grade 3 and 4 lesions, which were 20% and 16.3%, respectively. He stated that bail-out stenting occurred in 32% of patients— the reasons for this being residual stenosis (47.5%), flow-limiting dissection (45.6%), and other factors (11.4%).
In the full cohort, the identified procedural and device success rate was 97.9% and 99%. In the claudication subgroup, device and procedural success was 99.2% and 98.3%, and 98.6% and 96.8% in the CLTI subgroup, respectively. Using a Kaplan-Meier curve, freedom from CD-TLR at 180 days was 97.7% across the full cohort—97.9% for the claudication subgroup and 97% for the CLTI subgroup.
The study’s major
adverse limb event (MALE) rate composite endpoint—including severe limb ischaemia leading to an intervention on target limb or major vascular amputation—was 5.9% in the full cohort at six months, which translated to 4% and 12.2% in the claudication and CLTI subgroups, respectively. Overall, 85.4% of patients improved by least one Rutherford classification category.
In conversation with Interventional News at CIRSE 2024, Lichtenberg stated these results are “game changing” in the treatment of peripheral arterial disease (PAD) in patients with claudication and CLTI. He commented that these six-month results are encouraging and show a consistent improvement across a range of associated disease processes.
Michael Lichtenberg
Mahmood Razavi presents at CIRSE 2024
CIRSE Clinical Practice Survey: Patient safety and quality improvement in IR
Andreas Mahnken
Andreas Mahnken (University Hospital Marburg, Marburg, Germany), distinguished interventional oncologist, educator and advocator for interventional radiology (IR) standardisation, dives into the most salient outcomes from the recent Cardiovascular and Interventional Radiological Society of Europe (CIRSE) Clinical Practice Survey.
Interventional radiology—IR—has become a clinical discipline, with interventional radiologists ideally taking care of the entire patient pathway, from initial multidisciplinary tumour board (MDT) assessment to discharge and follow-up.1 The implementation of continuous quality improvement (QI) activities represents a major factor for high-quality provision of clinical care as well as patient safety.
1-3 To what extent such activities as well as the use of patient safety checklists are currently undertaken by interventional radiologists was part of the recent CIRSE Clinical Practice Survey, conducted by the CIRSE Clinical Services in IR Task Force from November 2023 to January 2024.4-5 The findings of the survey will further
feed into CIRSE’s activities supporting clinical practice building, quality management and patient safety in IR.
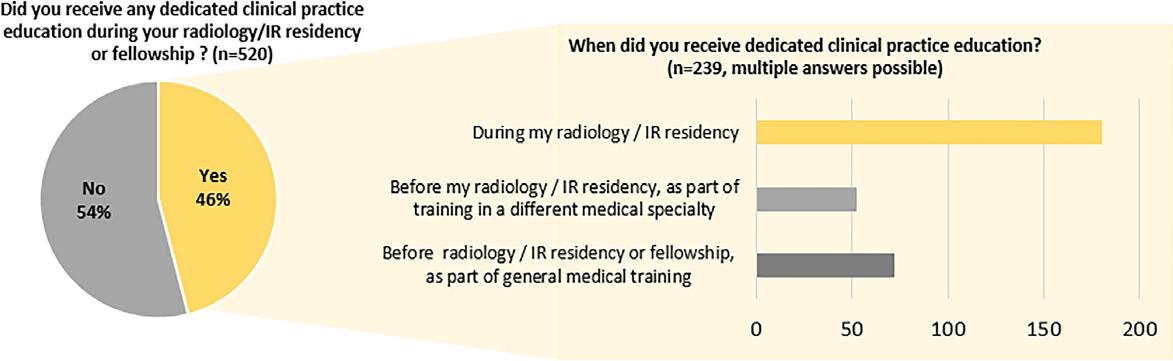
The CIRSE Clinical Practice Survey included 63 structured items addressing the areas of clinical practice training, infrastructure and personal experience as well as patient safety and continuous quality improvement. Eight items were dedicated to the latter two topics. The survey collected a total of 520 responses and was closed in January 2024.
The member survey, which was answered by interventional radiologists from Europe and beyond, showed encouraging results with over half of the respondents having an established clinical practice as well as direct patient access, taking primary responsibility for patient care. A total of 77.3% of
respondents indicated the regular use of patient safety checklists (Figure 1), which is strongly encouraged by CIRSE, with a checklist dedicated to IR being available in multiple languages. In terms of continuous quality improvement, 68.1% indicated that they perform dedicated quality improvement activities. These included recording morbidity and mortality data (70.9%), daily case discussion (68.1%) and MDT outcome (56.5%).
In the open responses, respondents to this question indicated most frequently case discussions, education and certification, quality assurance registries or programmes, audits, checklists and team teachings as regular activities in their departments.
While the vast majority of responding interventional radiologists actively engage in continuous QI activities and the use of patient safety checklists, there is still room for improvement and the European IR community will take advantage of the survey results to further design tools that will help interventional radiologists engage in clinical practice activities and encourage dedicated IR quality improvement. As part of this process a clinical practice manual was developed and CIRSE actively supports qualitydriven accreditation measures, such as
Figure 1: Exemplary results from the clinical practice survey reporting the level of quality improvement activities throughout the European IR community.
the International Accreditation System for Interventional Oncology Services (IASIOS).1
The full results of the survey have been published in the journal CardioVascular and Interventional Radiology (CVIR) with Anthony Ryan (University Hospital Waterford, Waterford, Ireland) as lead author.4 A presentation on the results relating to quality improvement and patient safety was held at the CIRSE 2024 annual congress (14–18 September, Lisbon, Portugal) and is available in the CIRSE Library.5
References:
1. Mahnken, A.H., Boullosa Seoane, E., et al. CIRSE Clinical Practice Manual. Cardiovasc Intervent Radiol 44, 1323–1353 (2021). https://doi.org/10.1007/ s00270-021-02904-3.
2. Binkert, C.A. Fostering clinical practice in IR regardless of (sub) specialty status. CVIR Endovasc 6, 23 (2023). https://doi.org/10.1186/s42155-02300370-1.
3. Morgan, R., Haslam, P., et al. Provision of Interventional Radiology Services 2023. Cardiovasc Intervent Radiol 47, 3–25 (2024). https://doi. org/10.1007/s00270-023-03600-0.
4. Ryan, A.G., Slijepcevic, B., et al. Developing a Clinical Service in Interventional Radiology: Results from the 2024 CIRSE Clinical Practice Survey. Cardiovasc Intervent Radiol (2024), https://doi.org/10.1007/ s00270-024-03858-y.
5. CIRSE 2024 Book of Abstracts. Cardiovasc Intervent Radiol 47 (Suppl 7), 441–1880 (2024). https://doi. org/10.1007/s00270-024-03850-6.
Andreas Mahnken is an interventional radiologist and oncologist at the University of Marburg, Marburg, Germany.
Roadsaver CAS subanalysis by country finds positive correlation between post-dilatation and major adverse event rate
In a comparative analysis of carotid artery stenting (CAS) practice trends and peri-procedural outcomes by country using data from the European multicentre ROADSAVER trial, found the observed difference in major adverse event (MAE) rate between geographies may be attributed to post-dilatation practices and the number of patients per site.
USING THE ROADSAVER (TERUMO) DUALlayer micromesh carotid artery stent, 1,967 patients with non-occlusive and non-thrombotic carotid artery stenosis were enrolled across 13 countries at 52 sites, speaker Stefan Müller-Hülsbeck (Hospital Flensburg, Flensburg, Germany) stated. The heterogeneous cohort presented with multiple comorbidities and risk factors across the included countries.
Concerning procedural characteristics, Hungary reported a high radial access usage rate; Poland identified a higher use rate of embolic protection
devices; Portugal and the Czech Republic reported higher rates of pre-dilatation, and the Netherlands an elevated rate of post-dilatation.
Müller-Hülsbeck reported that there was a low rate of 30-day major adverse event rates in this realworld elective CAS setting in both asymptomatic and symptomatic patients.
Speaking to Interventional News following his presentation, Müller-Hülsbeck commented that, of their key findings, “post-dilatation after stenting procedures is of utmost importance, but post-dilatation
should be performed with the greatest of care”.
He continued: “The second finding of this subanalysis is that patient volume at each respective centre is a certain issue—the more patients you treat, the more experience you have. In summary, operator experience and adequate postdilatation are predictors of a good outcome, meaning a low 30-day major adverse event rate, and this is what we identified in the Roadsaver subanalysis.”
Post-dilatation after stenting procedures is of utmost importance, but post-dilatation should be performed with the greatest of care”
Point of View
Stefan MüllerHülsbeck
IR in the UK: What we know
Raghu Lakshminarayan
Point of View
Sharing an update with Interventional News, consultant vascular radiologist Raghu Lakshminarayan (Hull University Teaching Hospital, Hull, UK) describes where interventional radiology (IR) stands within UK healthcare today.
THE ROLE OF INTERVENTIONAL radiology (IR) in patient care pathways and care delivery is gaining prominence in healthcare leadership across hospital trusts and primary care in the National Health Service (NHS). The speciality demonstrated its key role especially with an increase in day unit procedures benefitting patient care during the COVID-19 pandemic. The evolving nature of IR jobs, with greater emphasis
on clinical responsibilities and patient involvement, highlights the challenges of operating solely within a diagnostic radiology environment. There is an increasing recognition of the need to establish IR as a distinct faculty within radiology to promote patient care. Dual certification in diagnostic radiology will enable interventional radiologists to integrate imaging expertise with clinical skills. Additionally, the interdisciplinary
Analysis of UK IR
shows “major” discrepancy between workforce and service demand
An analysis of data collected on interventional radiology (IR) practice in the UK has shown an increasing trend in the number and complexity of procedures between 2017 and 2021, despite an imbalance in provision and demand of IR services, as well as a “striking” lack of records regarding safety and service-cost data.
In their introduction in the journal Clinical Radiology, researchers led by Mo Hamady (Imperial College London, London, UK) state that demand for IR services has been driven by the evolution of technology and clinical knowledge as well as an expanding range of treatments. However, the Royal College of Radiologists (RCR) commented that the expansion of IR has not met anticipated rates due to a shortage in consultants, nurse and radiographer support, as well as inpatient and day beds.
“To help improve the future provision of IR services, we need to understand the current demand as well as a shortfall in the resources dedicated to provide 24/7 IR services nationally and regional variations in IR provision,” the authors write. Currently, there is no comprehensive data collection protocol to outline the number and type of IR
collaboration will provide opportunities to influence government policy for the Royal College of Radiologists (RCR).
Establishing a dedicated faculty of IR would enhance leadership allowing for establishment of IR clinical leads who can address budgetary concerns, equipment needs, and staffing requirements. This would reflect positively in the job plans of IR consultants with adequate time for clinic and inpatient responsibilities. Addressing the shortage of qualified IR professionals is essential to support any new training and faculty structures. Healthcare system constraints make it difficult to support dedicated IR training programmes with its own clinical responsibilities and on-call training. Developing a comprehensive IR curriculum would attract trainees to apply from a broader pool of medical graduates providing a structured dedicated run through programme which emphasises the clinical and patient management issues of IR.
Current awareness of IR is low amongst stakeholders, patients and the public in the UK. This creates challenges and barriers in ensuring consistency in the availability of, and access to, minimally invasive imageguided treatments across the healthcare landscape. The only way of changing
procedures carried out in the UK, and limited data are available on IR facilities and workforce within National Health Service (NHS) trusts.
To remedy this, Hamady et al used the 2000 Freedom of Information Act to obtain data regarding IR procedures carried out in radiology departments only at NHS trusts in England and Wales between 2017 and 2021. This included IR workforce and facility information, number of IR consultants, nurses, trainees, angiographic suites and day-case units; analyses of procedure complexity, and frequency by region.
Vascular procedures included those for which the basis of the procedure was mainly endovascular, such as angiogram, angioplasty, vascular stents, embolization, and thrombolysis. Non-vascular procedures included those for which an endovascular approach was not necessary, including ultrasound-guided biopsies and aspirations, nephrostomy, tumour ablation and vertebroplasty.
A total of 1,340,352 IR procedures were analysed from 116 NHS trusts between 2017 and 2021. Throughout this period, the number of IR procedures increased from 256,592 to 292,030 procedures per year, respectively. A decrease in procedure numbers was observed in 2020—falling to 232,202 in correlation with the COVID-19 pandemic—but rose by 20.5% in 2021.
Over the five-year period, there were significantly more intermediate and complex IR procedures performed. Intermediate procedures were defined as a day or inpatient case of up to one hour using local anaesthetic with or without moderate sedation. The procedure must involve more than one type of equipment with an average cost of up to £500 and postoperative monitoring of at least two hours must be carried out.
this is to enable key decisions of IR to be taken by interventional radiologists. At local, regional and national levels, having interventional radiologists represent the speciality at NHS and government level is necessary to provide the right leadership framework to advance the speciality and optimise patient care. The ideal way to achieve progression would be for IR in the UK to have a faculty status within the RCR, which is a current matter of debate.
Raghu Lakshminarayan is a consultant vascular radiologist at Hull University Teaching Hospital, Hull, UK.
The ideal way to achieve progression would be for IR in the UK to have a faculty status within the RCR, which is a current matter of debate”
Between 2017 to 2021, a total of 423,235 vascular and 917,117 non-vascular procedures were performed across the trusts. In 2021, across 118 trusts, there were a total of 561 IR consultants, 982 IR nurses, and 103 IR trainees. The authors comment that, in this analysis, they confirm the demand and utilisation of IR services has increased despite a “major” shortage in workforce, which no doubt has caused widespread burnout among UK interventional radiologists.
The authors add that a “postcode lottery” became clear in their analysis of IR procedures and number of consultants per region, highlighting the difficulty in maintaining IR services in certain areas of the UK.
“The main way to understand the need to achieve a standard level of IR service provision across the UK, monitor the quality of care and identify areas of cost saving is through a robust and centralised data registry,” the authors state. Previously, there has been “useful but limited” efforts to collect data on IR applications by the British Society of Interventional Radiology (BSIR) inferior vena cava registry and iliac angioplasty and stent registry, Hamady et al state.
Hamady and colleagues assert that a revision of services is needed and should include on-call provision and a broader national registry by the RCR. They note that their analysis, although a start, was limited by NHS trusts’ limited resource to capture data and the subjectivity of criteria for the complexity of procedures. The research team state that “centralised and harmonised data collection of IR procedures is key to better understand the scope of IR services”, and to better understand pitfalls and assess training opportunities.
Mo Hamady
US interventional radiology: 12 years of primary specialty status
Interventional radiology (IR) was officially recognised as a primary medical specialty in the USA by the American Board of Medical Specialties (ABMS) in 2012. This marked a significant milestone for the field, which had previously been considered a subspecialty of diagnostic radiology (DR). With 12 years of specialty distinction, Interventional News spoke to Parag Patel (Medical College of Wisconsin, Milwaukee, USA) who debriefed on their progress so far.
IN THE DECADE THAT FOLLOWED THE ABMS distinction, the crucial development of new training pathways in the USA dedicated to both DR and IR was a highlight for Patel. In 2014, the Accreditation Council for Graduate Medical Education (ACGME) followed the ABMS distinction by approving a dedicated training pathway—the integrated IR residency—which replaced the traditional model of completing a DR residency followed by an IR fellowship. “This is a further commitment to clinical care for our patients as this was mandated within the training programmes,” Patel said.
match announced via the National Residency Matching Program (NRMP) found that that IR-integrated spaces were the fifth-highest percentage (91.4%) among positions filled with US seniors. Although falling short of the 100% match rate that was achieved in 2022 and 2023, nearly all available resident positions for DR (97.9%) and IR (98%) were filled in 2024.
Similarly, with the recognition of IR as a distinct specialty, Patel stated that it would hold that the specialty should be provided its own representation at these discussions when appropriate.
“For example, interventional radiology should not rely on diagnostic radiology colleagues to support therapeutic interventions within National Comprehensive Cancer Network [NCCN] guideline development. Interventional radiology is best suited to voice the role of minimally-invasive interventional therapies for patients that are most suitable.”
“We now recruit the best and brightest senior medical students into IR. The talent pool is extraordinary and these will be our future leaders in the field.” In 2024, the results of the main residency
“Furthermore, we have seen increased opportunities for specialty representation that would have otherwise been relinquished to DR alone. The American College of Radiology (ACR) and Radiological Society of North America (RSNA) represent DR, radiation oncology, and IR. However, it is highly unusual for DR to be asked to represent radiation oncology for any clinical committees or guideline development.”
Clinical IR practice often goes unseen due to lack of distinct performance metrics in Australia
Published last month in the journal CardioVascular and Interventional Radiology (CVIR), Matthew Lukies and colleagues from Alfred Health in Melbourne, Australia have released data collected from their institution giving visibility to the clinical interventional radiology (IR) service that they state has gone largely unnoticed. As IR has not yet achieved formal distinct speciality status in Australia or New Zealand, the authors sought to show IR’s increasing self-governance independent from diagnostic radiology (DR).
THE AUTHORS WRITE THAT providing optimal care for patients in IR is dependent on interventional radiologists’ adoption of clinical responsibility—from referral and clinical assessment, through to treatment, and follow-up care. Lukies et al state that clinical practice in IR enables the provision of a comprehensive service, helping to develop a “robust referral pathway” and provide optimal care for patients. They believe this keeps IR “relevant and competitive” among other interventional specialties who are performing endovascular and minimally invasive procedures.
Lukies and colleagues detail that the strategic direction of IR and DR have “diverged” in the recent past and note that the output of DR is increasingly benchmarked via relative value units and other metrics. Without distinct specialty status away from DR, IR sits within these datasets, they state,
operating via an ancillary ‘service provision’ structure which has created “inherent problems for interventional radiologists”. This is partly due to the fact that the clinical aspects of IR work, which include ward rounds, ward consultations, preadmission assessments, and outpatient appointments, are not captured in traditional DR key performance metrics.
This has led to a perceived “imbalance” in work output between IR and DR, Lukies and colleague state, resulting in interventional radiologists feeling “pressured” to achieve particular levels of diagnostic output to the detriment of clinical IR practice.
To capture their own data to measure clinical IR output, Lukies et al created a searchable tag within their inpatient ward round and electronic medical record consultation notes. This tag could then be measured over a given time period and collated as a ‘clinical IR’ key performance indicator.
In 2023, Patel concluded his term as president of the Society of Interventional Radiology (SIR), having progressed along the four-year pathway through secretary, president-elect, president and past president roles. He commented that the growth of IR in the USA has informed the direction of the SIR, with distinct primary specialty recognition allowing the society to advocate for board certified interventional radiologists. “In doing so, we are able to support interventional radiologists to pursue credentialing and hospital privileges specifically for procedures that would have otherwise not been available to them.”
We now recruit the best and brightest senior medical students into IR”
A ward consultation constituted a face-to-face, bedside review of an inpatient by one or more members of the IR team (consultant, fellow, and intern) including ward rounds and consultation referrals. Excluded from this data collection were outpatient clinic reviews, phone consults to patients or family members and discussions with other specialities regarding patients.
Between April and July 2024, the authors write that their IR service provided a total of 394 inpatient consultations—a mean of 4.7 ward consultations per day. They describe that their service is typically comprised of two to four interventional radiologists and one advanced training fellow each day. They utilise three angiography suites, and deal with admissions, discharges, referrals and consultations, as well as twice weekly outpatient clinics.
The authors presented these data to their DR colleagues—including direct managers—who were unaware that this work takes place. They stated, however, that they were appreciative of its “value in audit and role in governance changes for optimal patient care”.
Demonstrable of the importance of measuring clinical care in IR, Lukies et al that giving visibility to the day-to-day workload of interventional radiologists outside of DR’s metrics is “critical” in
providing optimal care and initiating workforce planning for the future. They state that the promotion of their clinical work through distinct performance indicators is an important component in assessing and thereby resourcing IR services.
“Clinical practice is the cornerstone of modern IR, and we must be provided with sufficient time, resources and workforce to ensure safe and highquality clinical care for our patients,” Lukies and the research team add.
Clinical practice is the cornerstone of modern IR, and we must be provided with sufficient time, resources and workforce to ensure safe and high-quality clinical care”
Parag Patel
ASPCVIR president-elect provides a glimpse into IR in the Asia-Pacific region
Born and raised in Singapore, interventional radiologist Tay Kiang Hiong is professor and head of the department of vascular and interventional radiology at Singapore General Hospital and and president-elect of the Asia-Pacific Society of Interventional Radiology (ASPCVIR). After completing his medical and diagnostic radiological training in Singapore, Kiang Hiong trained at the University of British Columbia in Vancouver, Canada under the mentorship of Lindsay Machan. Reflecting on his training and career in conversation with Interventional News, Kiang Hiong talks about the past, the present and the future of interventional radiology (IR) in the Asia-Pacific region, imparting advice for trainees starting out.
How was it starting a career in IR in Singapore?
Starting a career in IR in Singapore has been both exhilarating and challenging. Exhilarating because I started in the 1990s and 2000s where IR was experiencing rapid evolution and growth in Singapore. We had new devices or techniques emerge every few months and it was very gratifying to see IR procedures replacing traditional surgical treatments as the new standard of care. In many patients with dire conditions who are unfit for surgery, IR often is the last bastion that can save their lives. To this day, I feel very privileged to be an interventional radiologist.
However, it was also challenging as we are short of manpower. Especially in the early days, where the work hours were long, it was extremely hard to balance work and spending time with the family, not to mention research and teaching commitments limiting this quality time as well. As IR gained success, it attracted other specialists, leading to exhausting “turf wars”. Additionally, IR’s lack of public and physician awareness has limited referrals, though this is gradually improving through public campaigns and medical school education on IR.
What are the key differences in IR practice between the Asia Pacific region and Europe?
It is not surprising that the IR practice is different in Asia Pacific and Europe due to differences and variations in healthcare infrastructure, patient demographics and disease prevalence, economic status and regulatory frameworks.
Healthcare infrastructure in the Asia-Pacific region varies greatly, from advanced systems (e.g. Japan, Singapore, South Korea, Australia) to developing countries with no access to advanced medical technologies. As a result, IR services and technologies differ significantly, with some countries having no IR presence. In less developed economies, IR is limited to basic procedures like biopsies and drainages due to cost constraints, while well-developed countries offer a full range of IR procedures, often reimbursable. Interventional oncology (IO) is common due to high rates of hepatocellular carcinoma (HCC), but endovascular interventions for peripheral vascular and aortic diseases are diminishing and limited to a few centres of excellence in our region as they are mostly handled by cardiologists or vascular surgeons currently. With respect to IR training, the Asia Pacific region has fewer formalised and standardised IR training programmes. Some countries have established formal IR fellowships and specialised training pathways, but in many parts of our region, training is much less structured, with trainees often having to go abroad for fellowship training, often times in Europe or
North America. In the future, the ASPCVIR aspire to implement a vehicle for IR training much like
Kiang Hiong
In many patients with dire conditions who are unfit for surgery, IR often is the last bastion that can save their lives. To this day, I feel very privileged to be an interventional radiologist”
the European Board of Interventional Radiology (EBIR) certification, to standardise IR training and certification in our region.
As president-elect of APSCVIR, what do you hope to achieve in your term?
I have been involved with the APSCVIR for many years. Before 2016, I sat in the executive committee for several years. After 2016, I was the secretary general for three terms under the newly registered society, and now I am the president elect. I have been in a very privileged position for many years now, with the ability to influence and shape some of the strategic directions for APSCVIR.
We formerly registered the society in 2016 because we wanted to do more than just organising a scientific meeting. IR education has always been the main focus of APSCVIR and we do this through our annual scientific meeting and outreach programme.
The outreach programme is a signature programme of our society. Led by Bien Soo Tan (Singapore General Hospital, Singapore) it is comprised of onsite lectures, workshops and live case demonstrations supplemented by webinars every two to three months. The faculty of the outreach programme are all volunteers who fund their own travel to do so, and faculty from the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) and the Society of Interventional Radiology (SIR) are regularly invited to help out in these programmes. We are poised to expand this initiative to more countries. The Japanese Society of Interventional Radiology (JSIR) recently offered their online journal InterVentional Radiology (IVR) to be the official journal of JSIR and APSCVIR. This opens up another avenue for IR education and research for our members which I hope to actively promote in the coming years.
Strengthening international collaboration with other IR organisations around the world, especially SIR and CIRSE remains our top priority. Other than knowledge and skills exchange at our respective annual meetings, we hope to collaborate in other areas like journal publishing, IR certification exams, advocacy for IR, online education platforms etc. Through these efforts, my colleagues and I in the executive board of APSCVIR hope to leave a lasting impact on the growth, accessibility, and quality of IR across the Asia-Pacific region.
What advice can you give to interventional radiologists starting out in the Asia-Pacific region?
Starting out as an interventional radiologist in the Asia-Pacific region offers both exciting opportunities and unique challenges. The region’s diversity in healthcare systems, patient populations, and access to technology means that your path might vary depending on where you’re based. I have the following tips for new interventional radiologists in this dynamic environment:
● Build a strong foundation in diagnostic radiology
Proficiency in imaging interpretation ensures precise planning and execution, while knowledge of cross-sectional anatomy is key for guiding complex interventions.
● Prioritise hands-on training
Hands-on experience across various IR subspecialties is crucial for working in diverse clinical settings.
● Adapt to local healthcare realities
Adapt to local healthcare infrastructure and get involved in expanding IR services.
● Stay current with technological advances
IR is closely linked to advances in imaging and device technology. Stay updated on innovations like robotic interventions and new embolization or ablation devices.
● Focus on research and evidence-based practice
Research is critical to advancing the field of IR, and there is great potential for original research in the Asia-Pacific region.
● Focus on patient-centred care
Many patients in the Asia-Pacific region may be unfamiliar with IR. Spend time educating patients about how IR can help them, the risks involved, and what to expect during recovery.
● Advocate for policy and reimbursement changes
Advocate for improved reimbursement models and integration of IR into the national healthcare system.
Tay
VQI comparison shows higher mortality in Asian CLTI population, despite similar success rates
A study which benchmarked results from prospectively collected Vascular Quality Initiative (VQI) data for patients who have undergone peripheral vascular interventions (PVI) for chronic limb-threatening ischaemia (CLTI) has found that patients in Singapore “fared worse” than patients in the USA, despite comparable technical success rates. These results were published in the Journal of Vascular Surgery (JVS).
THE RETROSPECTIVE
review conducted by Joel Jia Yi
Soon (Singapore General Hospital, Singapore) et al, used the Society for Vascular Surgery (SVS) VQI registry database from the first, and at present only, VQI centre in Asia. The researchers reviewed the database to identify patients with CLTI who underwent endovascular revascularisation between July 2019 and April 2024, comparing these data with those collected from participating centres in the USA.
A total of 2,862 procedures were identified from Singapore General Hospital (SGH) and were benchmarked against 129,347 procedures from 406 centres in the USA and Canada. The researchers note that the average age of patients in their cohort was younger than those in the USA, reported as 68.8 years versus 69.6 years. Their patient cohort also had significantly lower body mass index (BMI) and a lower
proportion of patients with a history of smoking.
Soon et al state that their cohort had a higher burden of comorbidities,
including diabetes mellitus, end-stage renal disease, and cardiac disease, and presented with advanced Wound, Ischemia, and Foot Infection (WIfI) stages. The investigators add that their patients had more heavily calcified and longer (14.8cm vs 6cm) diseased vessels with higher prevalence of multilevel (87% vs 54.6%), infrapopliteal (52.6% vs 38.9%) and inframalleolar (9.6% vs 2.4%) disease.
amputation rates (13.3% vs. 7.8%) were significantly higher in the Singapore cohort.
Technical success and symptom improvement between the SGH VQI centre and those in the USA were comparable, reported as 92.7% versus 93%, and 39.1% versus 40.4%, respectively. However, one-year mortality (28.9% vs. 25.1%) and major
Social support associated with improved health outcomes for patients with PAD, Yale-led study reports
Social support is thought to bolster cardiovascular health by facilitating healthpromoting behaviours and acting as a buffer against the impacts of stress on the heart. A team led by Santiago Callegari of the Yale Department of Internal Medicine (Yale University, New Haven, USA) used questionnaires to assess perceived social support (ENRICHD Social Support Inventory), PAD-specific health status (Peripheral Artery Disease Questionnaire), and general health status (EuroQOL Visual Analog Scale) for 949 patients at baseline and 12 months later.
FOR THE 18.2% OF RESPONDENTS THAT reported low social support, the incidence of financial constraints as well as mental health symptoms including depression, stress and anxiety were higher. These patients also reported a lower disease-specific and generic health status at baseline and at 12 months. Most patients included were from the USA (64.9%), followed by The Netherlands (27.9%), and Australia (7.2%). Patients with low social support were less likely to be married or living with someone (77.5% vs 50%) and have a higher financial reserve at the end of the month. In the group that reported low social support, the
researchers found scores more than seven points lower on average on both the Peripheral Artery Disease Questionnaire and the EuroQOL Visual Analog Scale, indicating significantly poorer outcomes in PAD-specific and general health metrics. The association between low social support and poorer outcomes remained strong even when adjusting for factors including stress,
The authors note that although their patients had improved shortterm outcomes despite more advanced disease and comorbidities, they experienced worse long-term outcomes. They call for further research to investigate the underlying causes of these discrepancies. The study highlights that since 2019 when SGH was enrolled in the PVI registry, they remain as the only VQI centre outside of North America. The authors emphasise that the majority of VQI data on CLTI is based on North American patients, limiting the generalisability of findings to Asian populations.
“Enrolment of our centre in the VQI registry has been tremendously helpful in improving our understanding and management of our patients with CLTI via the standardisation of data collection, reporting of post-procedural outcomes and allowing for benchmarking against centres from the rest of the world,” the investigators write.
They hypothesise that differences in patient characteristics, disease morphology, and treatment approaches may explain the varying clinical outcomes between Asian and North American patients with CLTI undergoing endovascular revascularisation. The authors conclude that their findings offer valuable insights into improving treatment outcomes for Asian patients with CLTI.
depression, and socioeconomic status.
The team say their work highlights the importance of psychosocial factors, like social support and depression, in the treatment of cardiovascular disease. One in five patients with PAD report low social support, the authors report. They state the importance of addressing this issue noting that “social support should be promoted as an element of biopsychosocial PAD management” and could lead to better outcomes.
“The focus has been on specific devices to open blockages or do bypasses,” says corresponding author Carlos Mena-Hurtado, associate professor of medicine (cardiology) at Yale. “This study shows that it is time to see patients with PAD in a multidimensional way, such that a multidisciplinary team needs to get involved in their management.”
of PAD patients report low social support 18.2%
Social support should be promoted as an element of biopsychosocial PAD management”
Joel Jia Yi Soon
29 JANUARY – 3 FEBRUARY
PARIS LAS VEGAS HOTEL & CASINO
Interventional liquid biopsy shows what you have been missing
Point of View
Where is liquid biopsy today? Bruno Damascelli, Vladimira Tichà, Giancarlo Beltramo, Alberto Gramaglia and Gianluigi Patelli write on the complexities and challenges of the procedure as it gains ground among select interventional radiologists.
Liquid biopsy is gaining momentum on its path toward clinical utility, but the current role of this important advance in oncology is difficult to pinpoint. While it is easy to obtain a blood sample, molecular analysis of tumour biomarkers is still remarkably complex. The aim is to identify the genetic mutations of cancer in the biological markers it releases into blood. The most widely used of these is circulating tumour DNA (ctDNA) which is released into circulation primarily through apoptosis and cell necrosis. In the blood, ctDNA is mixed with cell-free DNA (cfDNA) which is produced in larger quantities because of cell turnover in normal tissues. This means ctDNA must be separated by an extraction process, which is followed by genetic sequencing—known as next generation sequencing (NGS)—covering a variable number of genes chosen according to their frequency in tumours. The cases presented here used Guardant360 (Guardant Health) comprehensive genetic profiling which reports the amount of ctDNA as a percentage of cfDNA.
The greatest difficulty in molecular analysis is the scarcity of ctDNA detectable in the general circulation, which has given rise to various methods of obtaining a significant amount of
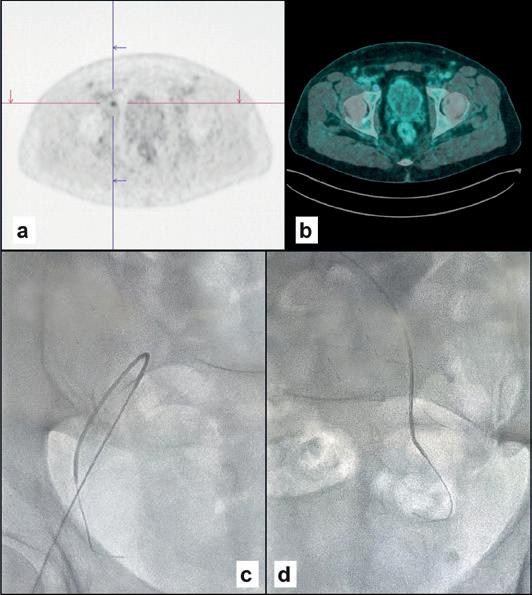
CASE ONE
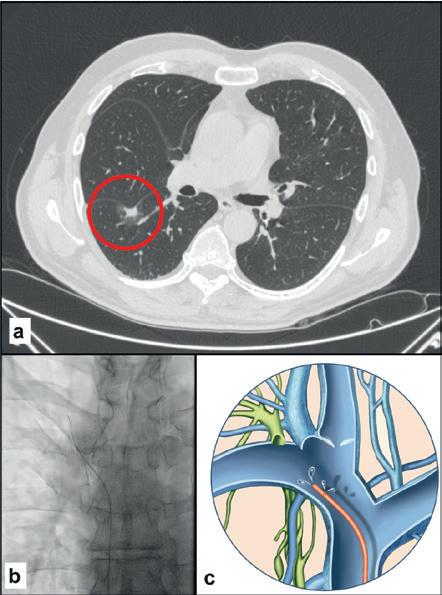
Male, 76 years old
Spiculated lung nodule, 14mm (A) in the right lower lobe, ischaemic heart disease, respiratory failure. Liquid biopsy from the right subclavian vein (B, C) with a finding of pathogenic mutation CDH1. Surgical histological confirmation of minimally invasive adenocarcinoma.
this biomarker. The simplest method, investigated by us and confirmed by another research group, is to draw venous blood in proximity to the tumour site. Percutaneous venous catheterisation is part of the armamentarium of interventional radiologists and relies on their familiarity with navigating the vascular system under fluoroscopic guidance. Sampling sites can be chosen as dictated by the natural history of the disease, which includes both primary and metastatic sites.
Unlike tissue molecular diagnosis, which is inevitably restricted to a few sections, liquid biopsy provides a wider reflection of the tumour’s epigenetic heterogeneity. Other advantages of selective sampling compared with conventional peripheral sampling are that it avoids the ctDNA dilution that occurs in the general circulation, and it exploits the topographical contribution of lymphatic drainage, a leading route of cancer spread. Lymph from the left hemithorax, the entire abdomen and the lower limbs drains into the thoracic duct, which empties into the left venous angle. Sampling from this site can provide information about intra- and extra-peritoneal cancers. Lymph from the right hemithorax and part of the head and neck drains into lymphatic trunks that empty into the right venous angle,
TWO
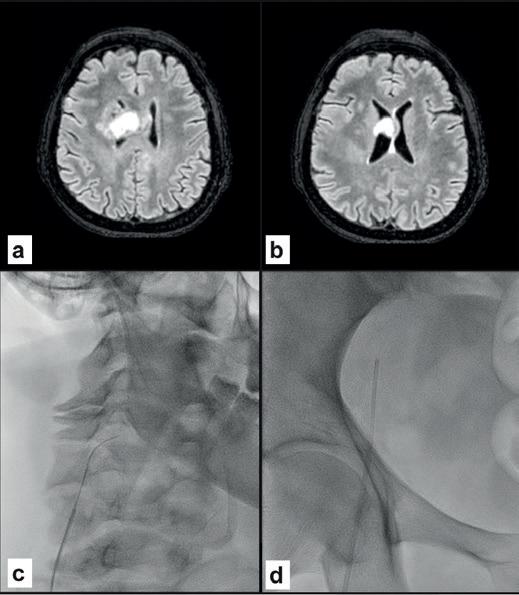
Female 60 years old
High-grade right frontal glioblastoma extending to the corpus callosum (A, B). Surgical histological confirmation but with negative tissue-based molecular testing. Pre-operative liquid biopsy from the right jugular vein (C) showing BRAF and PIK3CA mutations. Negative peripheral sample (D).
where venous sampling provides more effective molecular characterisation than peripheral sampling.
Liquid biopsy is beginning to be considered for use in diagnosis of lung nodules (Case one) for which no convenient solution is offered by imaging methods or percutaneous biopsy, which can prove inconclusive or unfeasible because of the associated risks.
Radiosurgery is increasingly used in cancer treatment, sometimes as the only option, with a consensus for its use in the absence of histological examination. Liquid biopsy can confirm the diagnosis and assess treatment response or resistance during follow-up. A liquid biopsy showing a mutation consistent with glial neoplasm (Case two) is decisive not only when histological diagnosis is not possible but also for monitoring treatment in the event of recurrence or progression. Molecular diagnosis has a higher success rate on cerebrospinal fluid than on peripheral blood but repeated lumbar puncture is not without risk for the patient. Retrograde percutaneous catheterisation of the jugular veins is an outpatient procedure known since its use in the diagnosis of pituitary tumours.
Another application of selective venous sampling is in ocular cancers. Uveal melanoma (Case three) can express mutations predicting disease evolution. Follow-up relies on abdominal ultrasound to detect hepatic metastases, which are invariably detected too late for effective treatment. Sampling from the jugular vein on the melanoma side allows molecular characterisation of the tumour, predicting its behaviour and guiding the use of new drugs with recent, promising results. Until now, this tumour has been treated with radiotherapy based on a diagnosis made with physical and radiological means applied to the intact eye.
Prostate adenocarcinoma (Case four) affects 16% of the male population. Early diagnosis of this cancer has
ASE THREE
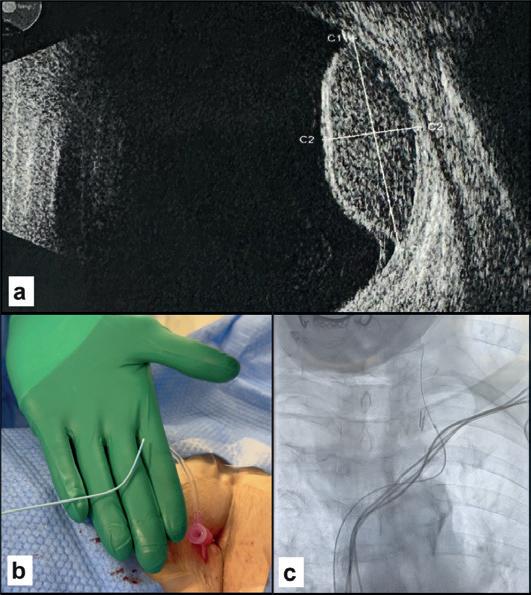
Female, 83 years old
Uveal melanoma, left eye (A). Right transfemoral catheterisation of the left jugular vein (B, C) with finding of HNF1A mutation indicating a poor prognosis.
had a positive effect on survival but metastatic spread leads to a longlasting deterioration in quality of life. Peripheral sampling or selective sampling from the hypogastric veins can provide timely detection of the somatic mutations involved in resistance to radiotherapy or androgen suppression, guiding appropriate personalised treatments.
Liquid biopsy is not yet recognised for its diagnostic accuracy, clinical utility and patient benefit, and few molecular tests are approved by regulatory bodies. While it is unrealistic to imagine that liquid biopsy could replace histological examination, it is nonetheless true that in monitoring the evolution of a tumour and its sensitivity or resistance to treatment, blood sampling is always possible, whereas tissue biopsy often is not.
References: Tichà V., Patelli G., Basso G. et al, Case Report: Potential role of selective venous sampling for liquid biopsy in complex clinical settings: Three case presentations, Frontiers, https://doi:10.3389/fgene.2023.1065537. Tamrazi A., Sundaresan S., Gulati A. et al, Endovascular image-guided sampling of tumour-draining veins provides an enriched source of oncological biomarkers, Frontiers, https://doi:10.3389/fonc.2023.916196.
Saife N. Lone, Sabah Nisar, Masoodi T. et al., Liquid biopsy: a step closer to transform diagnosis, prognosis and future of cancer treatments, Molecular Cancer, https://doi:10.1186/s12943-022-01543-7.
Bruno Damascelli is an interventional radiologist at Fondazione Falciani ONLUS, Milan, Italy.
Vladimira Tichà is an interventional radiologist at Fondazione Falciani ONLUS, Milan, Italy
Giancarlo Beltramo is head of radiosurgery at Centro Diagnostico Italiano, Milan, Italy.
Alberto Gramaglia is head of radiotherapy at Monza General Hospital, Monza, Italy.
Gianluigi Patelli is head of radiology at Casa di Cura San Francesco, Bergamo, Italy.
FOUR
Male, 63 years old
Operated prostate adenocarcinoma, Gleason grade 7 (3+4), PSA increase to 0.26 six years after surgery. PET PSMA (A, B) positive for right pelvic adenopathy. In the right hypogastric vein (C) we found ESR1, FGFR2 and MAP2K1 mutations. In the left (D) vein, mutations were FGFR2, MAP2K1 and RET. Pelvic radiotherapy is indicated.
CASE
C
CASE
MUNEEB AHMED
Tracing back his line to interventional radiology (IR), Muneeb Ahmed, interventional radiologist and the current president of the Society of Interventional Oncology (SIO), told Interventional News of how he followed in the footsteps of his father, Rashid Ahmed, an influential interventional radiologist who propelled the field in Pakistan. Guided to IR, Ahmed’s career has driven research and innovation, and, throuought his presidency, Ahmed has sought the global expansion of the interventional oncology (IO) community and furthered clinical discovery via SIO-led clinical trials. As his term concludes, he reflects on these accomplishments and his continued commitment to advancing the field of IO.
What attracted you to a career in IR?
I have known IR as a field from a young age, both with regards to its impact on patients, and to its novelty and innovation. My father, Rashid Ahmed, was an interventional radiologist who trained in the USA before moving back to Pakistan, his home country, to develop both diagnostic and interventional radiology as fields within that country. Throughout his 35-year career there, he introduced a multitude of new procedures and types of imaging studies in the country, established new training programmes, started a national radiology society and journal, trained several generations of diagnostic and interventional radiologists, and was ultimately recognised by the government for his service with one of the highest national civilian awards. All this while, he was passionate for learning new techniques, and happiest when he had performed a life-saving procedure on a patient. I remember watching him perform angiography and embolization, talking with him about his cases, and meeting his grateful patients. This passion for continuous learning in IR left a significant impression on me. When I had the chance to work within IR, and more specifically interventional oncology (IO), I understood his excitement for the field. There were so many different procedures to learn, a wide range of diseases to understand, and the technological advances seemed endless. By the time I was deciding on fellowship, IR was the clear and only choice, and I haven’t looked back since. IR has fulfilled that promise, as I continue to be excited about where the field is going, and all of the new and innovative treatments that are being developed.
Who were your mentors throughout your career?
I have been fortunate to have had several important mentors who have provided very important opportunities, guidance, and support at critical steps in my career-to-date. The earliest was Melvin Clouse, a worldrenowned interventional radiologist at Beth Israel Deaconess Medical Center (BIDMC) in Boston, USA, who involved me in summer research programmes as a medical student from Pakistan, and encouraged my interests in scientific research, and ultimately in radiology. One of the key introductions he made was to a young Nahum Goldberg, who was just starting out as an attending consultant at BIDMC and doing innovative research in percutaneous tumour ablation with radiofrequency energy. From that point onwards, through a three-year post-doctoral research fellowship, and in the over 25 years
since, we continued to work together on our shared research to advance the field of imageguided tumour ablation. Nahum has been my key mentor throughout this time, instilling a passion for research, providing advice at critical career decision points, and serving as a role model for how to build an academic career.
More recently, I have also benefited from mentors that I have met later in my career. Fred Lee shared his insights in leadership and entrepreneurship during my time as a division chief. Through my volunteerism with the SIO, I have also been able to follow amazing examples of societal leaders in Matt Callstrom and Bill Rilling, both of whom have provided me with valuable mentorship.
I have appreciated each of these mentors, and sought to emulate and honour their generosity by providing similar opportunities, support, and guidance to younger interventional radiologists who are trying to develop successful careers in IR.
Is there a memorable case that stands out to you?
Many years ago, I started treating a patient with metastatic renal cell cancer who had already survived six years following a nephrectomy and various immunotherapies. He stood out at the time for his positivity and enthusiasm for life, his desire to find the right balance between his quality of life and longevity, and his faith in and excitement for new and emerging therapies (he received interleukin therapy as part of early clinical trials in renal cell carcinoma). When I first met him, he had developed isolated metastases in his single kidney—for which I performed a successful cryoablation. Over the next eight years, I treated additional metastasis in his liver, lung, and adrenal gland—and we were able to keep his cancer at bay through intermittent IO therapies, including repeated ablation and embolization. He ultimately succumbed to his disease, but after living his life to the fullest and with happiness and excitement. When his family reflected on his experiences after he passed away, the thing that they were most thankful for from the various minimally-invasive treatment options that he received over the years, was that he always had hope. Hope, even near the end of life, is an important thing that IR often offers even when patients receive news that their cancer has progressed through other therapies. When I think about him, I remember that it’s important to appreciate what we can do for people’s happiness—the importance of kindness and empathy, and the value of IR done well on a patient’s life.
FACT FILE
CURRENT APPOINTMENTS
2022–present: Professor of radiology, Harvard Medical School, Boston, USA
2014–present: Chief, vascular and interventional radiology, Beth Israel Deaconess Medical Center, Boston, USA
PREVIOUS APPOINTMENTS (SELECTED)
2020–2022: Founding co-director, Multidisciplinary Portal Vein Thrombosis Clinic, Beth Isreal Deaconess Medical Center, Boston, USA
2019–2021: Director of radiology research, Beth Isreal Deaconess Medical Center, Boston, USA
RESEARCH GRANTS (SELECTED)
Principal investigator, Extent of radiofrequency ablation-induced cell growth, Radioloigcal Society of North America (RSNA) Foundation Research Seed Grant
Principal investigator, Modifying radiofrequency ablation-induced upregulation of interleukin-6, National Cancer Institute Center for Cancer Nanotechnology Excellence Grant
You have published several research papers in 2024. Which of your recent endeavours has been the most insightful? I firmly believe that we need to advance IR through a multi-pronged research approach, developing early ideas, proving their clinical efficacy (starting with proof-of-concept studies and progressing through to robust prospective clinical trials), and then tackling barriers to widespread clinical implementation such as cost-effectiveness and utilization research, and then training the next generation of interventional radiologists. I am excited about all of the research projects coming out of the BIDMC IR team in recent years— tackling questions at each of the various phases I mentioned. If I had to pick, the work that my partner Jeff Weinstein and I are doing on studying an operator’s hand motion while doing IR procedures is very interesting, as it provides us with insight into how interventional radiologists learn. This work will hopefully provide objective measures to assess technical skill acquisition and design better training methods in IR.
Similarly, I am also excited about our recent study with percutaneous cryoablation for locally recurrent prostate cancer—Vijay Ramalingam et al in the Journal of Vascular and Interventional Radiology (JVIR) 2024—as this incorporates a computed-tomography (CT) guided approach to treating focal prostate bed cancer recurrences that can be expanded and used at many centres overcoming resourcelimitations that are associated with previously reported magnetic resonance imaging (MRI) guidance based techniques. Focusing on ways to make IO therapies accessible to a wider range of patients is something that I am very passionate about.
As your presidency of the SIO comes to a close, what have been your greatest achievements?
Two years as SIO president has flown by! The society team, including all of the volunteers and the staff (under Jena Stack’s extremely capable leadership) continues to accomplish so much. I am very excited that we have gotten the ACCLAIM trial off the ground and well on its way to completion, and are now planning additional trials. We have expanded our society membership through key global partnerships and are continuing to build collaborations with other societies on joint projects. We have continued to develop and offer the highest calibre of meeting content— last year’s SIO 2024 annual meeting having been one of our most successful meetings yet, and we have an exciting programme planned for 2025. Our most recent SIO Masterclass in musculoskeletal IO, a unique hands-on immersion-style programme that we recently held here at BIDMC, was also exciting and very successful.
At the beginning of my presidency, a priority was to strengthen IO’s global voice. We have made a lot of progress towards this goal. One of our key objectives has been to implement a ‘big-tent’ philosophy within the SIO, and specifically that anyone involved in the IO space—whether performing IO or wanting to learn more about IO—has a place in our society. To this end, we have created global SIO chapters through partnerships with different societies around the world, including the Middle East, creation of our Asia-Oceanic
chapter and most recently with creation of our Latin American chapter. This has led to closer collaboration in these regions, and a growth in the SIO’s membership to over 1,300 members worldwide.
Overall, I am most proud of the extremely energetic and growing group of volunteers that we are attracting to the SIO—without whom we would not be able to continue to advance the IO space on many fronts. Success begets success.
How is the ACCLAIM trial progressing?
I am very excited about the ACCLAIM trial— we are making great progress! Thanks goes to Constantinos T Sofocleous, the trial’s global principal investigator, all of the volunteers who are involved in the trial, and the SIO staff team that is overseeing trial operations. We have opened 10 international sites, and have already recruited over half of the necessary patients, ahead of our original schedule, and look to close out patient recruitment by the fall of 2025. This is a pivotal prospective study that incorporates formal ablation
margin confirmation as the technical endpoint to performing ablation for colorectal liver metastases, and the successful completion will provide necessary evidence to help us establish use of margin confirmation as the standard of care when performing liver ablation. This is the first multi-industry supported trial in our space, and the first that the SIO has developed and initiated, so I am particularly proud that we have been able to execute this so well.
Have any recent research papers caught your attention in the last 12 months?
I am very excited about the recent presentation of the COLLISION trial—a phase three randomised multicentre study comparing surgical resection and percutaneous thermal ablation for small liver-only colorectal cancer metastases led by Martjin Meijerink and colleagues from Amsterdam University Medical Center. This study stands out to me for how well it was designed and executed, how it incorporated many of the lessons that we have learned about thermal ablation over the years,
“It’s important to appreciate what we can do for people’s happiness— the importance of kindness and empathy, and the value of IR done well on a patient’s life”
including the importance of achieving a documented appropriate ablation margin (>1cm for colorectal metastases), use of contrast-enhanced margin assessment, and re-ablating patients where an adequate ablative margin was not achieved. To me, this underscores how the IO community has grown in the field—implementing highquality studies that prove that our therapies offer patients excellent outcomes in a safer and better tolerated manner. The study team is to be commended, and I look forward to reading the full published manuscript when it becomes available.
What are your hobbies and interests outside of medicine?
As I am originally from Karachi, Pakistan, I enjoy travelling to new places around the world. Some of my most enjoyable trips have been to the Mediterranean, Mallorca, and the Maldives. I enjoy reading and spending time with my family, including my wife, Susan, my two children, Saif and Sofia, and our two snowshoe cats.
New study shows durability of minimally invasive procedure to combat knee pain
A new study shows that a minimally invasive treatment for osteoarthritis (OA) in the knees may have a lasting benefit of at least two years.
PUBLISHED IN THE
Journal of Vascular and Interventional Radiology (JVIR) during Pain Awareness Month, the study of genicular artery embolization (GAE) followed 40 patients with moderate-to-severe symptomatic knee OA after their GAE treatment and measured pain scores throughout the 24-month study period. The patients were not candidates for total knee replacement.
“Knee osteoarthritis is a leading cause of adult disability and, until now, most minimally invasive treatment options have been proven to provide only short-term relief, measured in weeks or months,” said Siddharth A Padia (UCLA Health, Los Angeles, USA), the lead author of the study. “For patients who are not candidates for knee replacement surgery, our study shows that GAE provides durable benefit to many patients, measurable for up to two years, a great leap forward in offering this cohort lasting relief.”
OA was once considered just a “wear and tear” process, but there is increasing evidence that the growth of new, abnormal synovial blood vessels causes painful inflammation, greatly contributing to OA symptoms throughout the body. GAE targets this abnormal blood flow to reduce inflammation, quickly improving patients’ pain.
To deliver treatment, interventional radiologists create a pinhole-sized incision in the hip and insert a small catheter into the arteries in the arthritic knee. They, then, inject tiny particles to normalise the blood supply to inflamed and painful areas of the knee. The outpatient procedure takes approximately one to two hours, followed by a twohour recovery period.
For this prospective,
Analysis finds GAE more cost-effective than RFA for symptomatic knee osteoarthritis
A cost-effectiveness analysis of genicular artery embolization (GAE), radiofrequency ablation (RFA) and corticosteroid therapy for knee osteoarthritis (KOA) has identified GAE as the most cost-effective treatment option, although clinical success rates, attrition rates, and utility values impact its cost-effectiveness. These results were published in the American Journal of Roentgenology (AJR).
LED BY DANIEL H KWAK
(The University of Chicago Medical Center, Chicago, USA), the researchers conducted the comparison using a Markov model based on a de novo network meta-analysis (NMA) of randomised controlled trials (RCTs) for the treatment of KOA. The cost-effectiveness analysis for each procedure was conducted from the perspective of the US Medicare and Medicaid payer’s perspective over a four-year time period.
Treatment success, attrition rate, cost and utility benefit were included in Kwak and colleagues’ evaluation. Utility benefit values were derived at short-term (0.5–3 months) and long-term (6–12 months) post-treatment follow-up from a NMA of published RCTs using an outcome of improved knee pain and/or function. The authors note
that analyses were also conducted via a willingness-to-pay threshold of US$100,000 per quality-adjusted life year.
Their results show that RFA demonstrated larger treatment affect than GAE, which was more pronounced at short-term follow-up.
Kwak et al note that incremental cost-effectiveness ratios were between US$561–1,563 per quality-adjusted life year for corticosteroid therapy, compared to US$76–429 quality-adjusted life year for GAE.
GAE demonstrated a higher cost-effectiveness probability compared to RFA—41.6–54.8% vs. 18.4–29.2%, respectively. When noting clinical success rates, GAE was more costeffective than RFA, and showed a post-GAE utility value which exceeded 32.1–51.0% and 0.562–
single-arm study, researchers defined clinical success as a greater than 50% reduction in OA symptoms using the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). A previous study of this cohort found that 25 of the patients (66%) reported improvement at one year. Of those 25, 18 patients (72%) have since reported continued relief of symptoms at two years. Overall, 18 of the original 38 patients (47%) who remained in the study throughout the two-year follow-up period reported a greater than 50% reduction in OA symptoms over the two years. No long-term adverse effects were reported.
“GAE is a promising therapeutic option for patients with osteoarthritis in the knee, allowing patients to return to their normal activities without lengthy recovery times,” said Padia. “We believe further investigation with larger cohorts and randomised controls should be conducted so we can validate these findings, refine patient selection and optimise the management of OA-related knee pain.”
For patients who are not candidates for knee replacement surgery, our study shows that GAE provides durable benefit”
0.617, respectively. The quarterly attrition rate for GAE was identified as less than 8.8–17.4%. RFA was more cost-effective when baseline pre-treatment utility values exceeded 0.695–0.713.
GAE is an emerging minimally invasive treatment which can a provide a cost-effective alternative”
In their discussion, Kwak and colleagues state that many patients with symptomatic KOA are refractory to traditional non-surgical treatments, such as intraarticular corticosteroid injection, but are not yet eligible for or decline surgery. They state that “GAE is an emerging minimally invasive procedure which can a provide cost-effective alternative for the treatment of KOA”.
Siddharth A Padia
Daniel H Kwak
VENOS-1 FIH trial oneyear results demonstrate advantages of the nextgeneration Velocity percutaneous AVF system
Presenting at the Controversies in Dialysis Access (CiDA) 2024 meeting (3–5 October, Washington D.C., USA), Robert Shahverdyan (Hamburg, Germany) shared the one-year results of the VENOS-1 first-in-human study, which examined the Velocity (Venova Medical) percutaneous arteriovenous fistula (pAVF) system.
BEGINNING BY OUTLINING THE background of pAVFs, Shahverdyan pointed out that, whilst there are currently two US Food and Drug Administration (FDA)-approved devices available—WavelinQ (BD) and Ellipsys (Medtronic)—the lack of worldwide adoption was, in his opinion, a “missed opportunity” that has led to decreased usage of pAVFs over the past couple of years. After outlining his algorithm for the use of pAVFs and sharing some of his own experiences and results with their use from the last six years, Shahverdyan conceded that the main challenges with pAVFs are the issues with cannulation
and a high rate of reinterventions (such as flow directing procedures and/or juxtaanastomotic stenosis angioplasties), which consecutively increase the costs for pAVFs.
Following on from this, he stated that what was needed from the next generation of pAVFs was a revaluation of cost-effectiveness, fewer interventions after pAVF creation, and an improved procedural efficiency without compromising on efficacy.
A device that he feels fulfils this brief is Velocity—the “generation 2.0 pAVF”. Shahverdyan stated that it is able to replicate surgical AVF anatomy, via its optimal geometry that allows
DCB versus plain balloon AV access angioplasty: More investigation is needed, study concludes
At the recent Cardiovascular and Interventional Radiological Society of Europe (CIRSE) annual meeting (14–18 September, Lisbon, Portugal), Kate Steiner (East and North Herts NHS Trust, Stevenage, UK) presented the results of a study comparing intimal hyperplasia measurements on ultrasound of preand post-percutaneous transluminal angioplasty (PTA) of arteriovenous (AV) access stenoses with both paclitaxelcoated balloons and plain balloon angioplasty.
AFTER OUTLINING THE BENEFITS OF drug-coated balloons (DCBs) for use in PTA, as well as some of the “mixed” trial results, Steiner shared the aims and methods of the trial with the CIRSE audience. The two aims of the trial were, as she stated, to examine intimal hyperplasia measured on B-mode ultrasound pre- and post-PTA procedures quantified as %-intimal–media thickness (%IMT), and to determine whether there is a significant decrease in intimal hyperplasia post angioplasty
for ideal flow conditions to support fast maturation, and a low incidence of anastomotic stenosis thanks to the endothelium being shielded from turbulence, inflammation or thermal injury.
The first-in-human (FIH) trial for this device, VENOS-1, commenced in 2023, with enrolment being completed by October of the same year. It consisted of two cohorts; with the last cohort of 10 patients treated by the updated and final design, and now completed the final one-year follow-up visits. All 10 procedures were technically successful, with all of them being performed under regional anaesthesia. There were no serious adverse events at six weeks, as well as no instances of hand ischaemia.
The ultrasound findings showed that there was a 1:1 relationship between arterial flow and superficial venous flow, confirming a targeted AVF
The Velocity pAVF system demonstrates the least inflammatory way of creating an AVF”
comparing DCB angioplasty with plain balloon angioplasty.
To meet these aims, Steiner and colleagues performed a pre-procedural duplex ultrasound for the investigation of dialysis fistula dysfunction—“as is standard practice at our institution,” Steiner stated. Once the procedure was complete, patients were then followed up with a duplex ultrasound and clinical review six to 12 weeks post-intervention. A total of 191 consecutive PTA procedures for AV access dysfunction were screened retrospectively for inclusion, with those procedures where there was an ultrasound prior to and following PTA, with measurements of IMT, included. The two DCBs that were used were Lutonix (BD) and Ranger (Boston Scientific).
Eighty-seven patients were included in the study, with a total of 99 stenotic lesions. Twenty-six of the 99 lesions were treated using DCB angioplasty, and 83 were treated using plain balloon angioplasty. All duplex examinations were within 180 days pre- and postprocedure. The average pre-PTA duplex in days was 45, with the average post-PTA duplex being 65. What the researchers found was that there was a greater difference in %IMT post-PTA in the DCB group, with a minimal decrease in IMT in the plain balloon group.
flow, and that 100% of the pAVFs matured within six weeks, with no re-interventions needed to reach this endpoint. The trial results also demonstrated 80% of primary patency years at one year, with only two re-interventions for the entire cohort in the first year, including a single angioplasty for a juxtaanastomotic stenosis at day 242.
With that, Shahverdyan concluded that “the Velocity pAVF system demonstrates the least inflammatory way of creating an AVF” with the implant shielding the juxtaanastomotic segment from turbulence and developing a stenosis, improving maturation rates, adding that a VENOS-2 US-based early feasibility study is planned to start end of 2024.
DCBs. Drawing her presentation to a close, she said that further investigation examining lesion response to antiproliferative therapy is warranted.
Sharing her thoughts on the results from this study with Interventional News, Steiner said: “As well as using patency rates as outcome measures in clinical studies, we can also examine lesion morphology as a response to antiproliferative therapy. The %IMT measurements we have made are easily reproducible.” Adding some context to the results, she stated: “We did not see a decrease in %IMT translate into improved patency rates because we primarily used the DCBs in a higher risk group. Lesions had a higher baseline %IMT and had had a higher number of previous angioplasties.”
She also detailed that selected centres in the PAVE 2 clinical study, which has recently started recruiting in the UK, will be examining lesion morphology using b-mode ultrasound pre- and post-PTA procedures. “The study is a three-armed prospective randomised controlled trials,” she stated, “comparing plain balloon angioplasty with paclitaxel coated balloon angioplasty and sirolimus coated balloon angioplasty.
Results show:
Steiner then concluded her presentation, stating that she and the other researchers saw a significant decrease in %IMT post-PTA using a DCB, when compared to the plain balloon angioplasty group. This, she argued, demonstrates an antiproliferative drug effect on lesion intimal hyperplasia. She also highlighted, however, that this did not translate into a sustained difference in target lesion primary patency, despite the more positive outcomes with use of
A greater difference in %IMT post-PTA in the DCB group
A minimal decrease in IMT in the plain balloon group
Kate Steiner
Robert Shahverdyan
Leading Innovation in Endovascular Therapy
Since its inception, the International Symposium on Endovascular Therapy (ISET) has been instrumental in fostering interdisciplinary dialogue and showcasing groundbreaking research that enhances patient care and outcomes. With a focus on practical application and scientific rigor, ISET continues to set the standard for excellence in endovascular therapy.
Deep venous stenting determined “safe” with low rates of major complications
A recent analysis of deep venous stent placement has determined that the procedure is safe with low rates of major complications. Published in the journal CardioVascular and Interventional Radiology (CVIR), the researcher team, led by Doireann P Joyce (Galway University Hospital, Galway, Ireland), state that responsibility is placed on the operator to be aware of the risks associated with deep venous stenting, although rare, so that fully informed consent can be obtained from the patient.
IN THEIR INTRODUCTION, THE AUTHORS describe the development of deep venous stenting into a primary treatment modality for venous obstruction across recent decades. Largely, reported complications rates are low, and are typically based on patient case reports and single-centre cohorts, which limits the broader applicability of collected data.
Aimed to determine the incidence of major complications associated with iliocaval and iliofemoral stent placement, Joyce et al collected data from three tertiary deep venous referral centres between January 2014 and September 2023. Their focus was on major complications which included: death, major bleeding requiring transfusion, massive pulmonary embolism, any complication that required endovascular or open surgical intervention, vessel rupture, acute kidney injury requiring dialysis, stent crushing, fracture, migration, involution or erosion.
stent crushing (29.5%), followed by stent fracture (16.4%) and erosion of the stent through the vessel wall (13.1%). The authors note that death was a rare event (0.2%).
Doireann P Joyce
Within the nine-year study period, 1,814 patients were treated for acute or chronic deep venous pathology. Concerning the venous pathology of their cohort, 44 patients were identified as having post-thrombotic syndrome; nine with acute deep vein thrombosis (DVT); six with May-Thurner lesions with DVT; and two with phlegmasia cerulea dolens. Among these patients, 61—3.3%—experienced a major stent-related complication, the most frequent of which was reported to be
“Interventionists performing these procedures must be aware of the occurrence of complications associated with stent placement to counsel patients adequately and promote avoidance through optimal procedural approach,” Joyce and colleagues write.
Speaking to Interventional News, Joyce commented that: “This paper, highlighting the low rate of major complications associated with deep venous stenting, is timely given the increasing number of these procedures being performed worldwide. It is essential that interventionalists remain cognisant of potential risks and audit their own outcomes at regular intervals in order to ensure compliance with international best practice.”
Interventionists performing these procedures must be aware of the occurrence of complications associated with stent placement”
Research suggests potential link between strenuous physical activity and increased VTE risk in men
Published in the Journal of Thrombosis and Thrombolysis, new research with a follow-up of 27 years has found an association between high levels of physical activity (PA) and an elevated risk of venous thromboembolism (VTE).
THE RESEARCH, LED BY PER Wändell (Karolinska Institutet, Huddinge, Sweden) and colleagues, was drawn from the Uppsala Longitudinal Study of Adult Men (ULSAM). Their team followed a cohort of 2,294 patients in Uppsala, Sweden who were initially examined at age 50, with data on their PA levels collected over four follow-up periods at ages 60, 70, and 77. After a median follow-up time of 33 years, 186 cases of first-time VTE were recorded, with a total of 68,263 person-years at risk.
Wändell and his team defined activity levels by grade 1–4:
2. Walking or cycling (for pleasure walking, cycling)
3. Recreational sports or heavy gardening for at least three hours every week
4. Regularly engage in hard physical training (hard training or participation in competitive sports, regularly and several times a week)
Results from the study showed that men with the highest levels of physical activity—defined by the authors as engaging in regular strenuous exercise—had a more than doubled risk of developing VTE (adjusted hazard ratio [HR] of 2.22; 95% confidence interval [CI] 1.05–4.67) compared to those who reported the lowest PA levels. The findings suggest that, while moderate exercise has welldocumented health benefits, there may
Pilot study looks at undiagnosed vascular disease in homeless
A PILOT STUDY CARRIED out by a team from The Ottawa Hospital Division of Vascular Surgery, Ottawa, Canada, aimed at uncovering the extent of undiagnosed vascular disease among the city’s homeless population, detected a subset who may be in need of treatment for venous disease.The pilot grew out of Ottawa inner-city health authority’s review of the area’s growing homeless population, with the hospital identifying that they did not see a great deal of this demographic unless members presented with a big vascular problem.
Malnis and his team partnered with Ottawa’s inner-city health clinic to run monthly assessments of wounds among the homeless, aiming to determine if they were vascularrelated or due to other causes like trauma or infection. Malnis, with prior experience working with the homeless in Vancouver, noted that nurse practitioners identified a knowledge gap in recognising vascular issues. This has led to targeted training sessions to enhance their ability to assess and refer vascular cases accurately.
be a point at which intense physical activity could increase VTE risk.
Using Cox regression analysis, Wändell et al adjusted for cardiovascular risk factors such as blood pressure, cholesterol levels, body mass index, diabetes, and smoking. Despite these adjustments, the elevated risk remained significant in the highest PA group.
In their subsequent commentary, the authors write that VTE is the third most common type of cardiovascular disease in Sweden, with a marked increased risk with age. Although low levels of exercise are associated with higher cardiovascular disease and VTE risk, there have been documented cases of cardiovascular events occurring after strenuous exercise, such as sudden cardiac death in longdistance running.
with an imbalance between prothrombotic and fibrinolytic factors, thus causing hypercoagulability together with a weakened fibrinolysis, Wandell et al state.
higher risk of VTE in men regularly engaging in strenuous exercise 2X
In men, the increased risk of VTE may be due to exercise sessions including long and vigorous exertion
The study authors acknowledge limitations of their study, including the relatively small sample size and the use of self-reported physical activity data, which may have led to misclassification of activity levels. They state that their variables do not provide absolute predictors of VTE due to the potential for unaccounted factors, yet they contend that their lengthy follow-up period and careful patient examination bolster their results.
The researchers emphasise that clinicians should be aware of the possible risk of VTE in patients engaging in high levels of strenuous exercise on a regular basis, as to not delay diagnosis and treatment. Further, for individuals taking part in marathons or ultra competitions, they add that spreading awareness of the early signs of VTE is crucial.
Why attend?
• 4 plenary sessions
• 12+ technology showcases
• 40+ scientific sessions with over 400 oral presentations
• 200+ poster and educational exhibit presentations
• 125+ exhibiting companies
• Brand-new networking opportunities
• Much, much more!
Endovascular BCI technology achieves positive results in US COMMAND study
Synchron has announced positive results from the COMMAND study evaluating the safety and efficacy of the company’s Stentrode brain-computer interface (BCI) device in six patients over a 12-month period.
THE STUDY RESULTS WERE presented yesterday at the 2024 Congress of Neurological Surgeons (CNS) annual meeting (28 September–2 October, Houston, USA) by Elad Levy (Jacobs Institute/University at Buffalo, Buffalo, USA). Levy is a co-principal investigator for the COMMAND study alongside David Lacomis (University of Pittsburgh, Pittsburgh, USA) and David Putrino (Mount Sinai Health System, New York, USA).
“The COMMAND study results represent a major medical milestone, confirming the safety of the Stentrode BCI with no neurologic safety events reported during the 12-month study period,” said Levy. “This minimally invasive approach has the potential to unlock BCI technology at scale for the
millions of patients with paralysis and other mobility challenges.”
With support from the National Institutes of Health (NIH) BRAIN initiative, COMMAND was conducted at three US clinical sites and enrolled six patients with severe chronic bilateral upper-limb paralysis who were unresponsive to therapy, all of whom received the BCI implant.
All six patients successfully met COMMAND’s primary endpoint of no device-related serious adverse events resulting in death or permanent increased disability during the oneyear post-implant evaluation period. Additionally, the results have reported that patients had no serious adverse events (SAEs) related to the brain or vasculature during the 12-month study
period.
As stated in a press release from Synchron, the study also demonstrated that brain signals related to motor intent can be consistently captured and transformed into digital motor outputs (DMOs)—allowing participants to successfully perform a range of digital tasks. In 100% of cases, the Stentrode device was accurately deployed, demonstrating a median deployment time of 20 minutes and achieving target motor cortex coverage in the brain for all six patients.
“The users were able to generate DMOs with the BCI. These are simple, thought-derived expressions of intent, converted into digital actions on computers,” said Tom Oxley, Synchron’s chief executive officer and founder. “Making the DMOs easy to
use, stable over time, and generalisable across technology platforms, will unlock layers of independence and autonomy for patients.”
The COMMAND study is the first US Food and Drug Administration (FDA)-approved investigational device exemption (IDE) trial of a permanently implanted BCI, according to Synchron. The company’s BCI is implanted in the blood vessel on the surface of the brain’s motor cortex via the jugular vein, utilising a minimally invasive endovascular procedure. Once implanted, it is designed to detect and wirelessly transmit motor intent out of the brain with the goal to restore the capability for severely paralysed people to control personal devices through hands-free, ‘point-and-click’ techniques.
Carotid intervention linked to improved survival versus medical management in symptomatic patients
New study data suggest that the interventional treatment of symptomatic carotid artery disease may result in an improved rate of age-adjusted overall survival compared to medical management. However, the same study—presented at this year’s ESVS annual meeting—also indicates a relatively low future ipsilateral stroke risk among patients who were not offered carotid intervention, highlighting medical management’s importance as a standalone strategy in patients deemed to be ‘high risk’ if treated via intervention.
FINDINGS FROM THE STUDY IN QUESTION were delivered by Eric T A Lim (Waikato Hospital, Hamilton, New Zealand), on behalf of Manar Khashram (Waikato Hospital, Hamilton, New Zealand) and other investigators at ESVS 2024. “There is Level 1 evidence around the management of symptomatic carotid artery stenosis, with superiority of intervention compared to medical therapy for stroke prevention,” Lim and colleagues state in their abstract. “While, long term, the efficacy of carotid intervention has been clearly documented, the natural history on symptomatic patients with ipsilateral carotid stenosis has not been well described in the contemporary era—when best medical therapy has evolved.”
On this basis, Lim et al’s prospective, observational study— undertaken in a single vascular tertiary referral centre in New Zealand—aimed to assess the outcomes of symptomatic carotid artery stenosis cases that were managed non-operatively. The study was carried out from June 2019 to January 2024. Lim and colleagues performed Kaplan-Meier analyses to
assess ipsilateral stroke-free and age-adjusted Cox proportional hazard models, and ultimately determine all-cause survival.
During the study period, a total of 280 patients were referred with symptomatic carotid disease.
The majority of these patients (63.7%) underwent carotid endarterectomy, while 1.3% underwent carotid artery stenting and 35% were managed medically. In the 84 patients managed medically—or ‘conservatively’—the median age was 73.6 years. Lim et al found that the three most common reasons for selecting conservative management were the patient being below the threshold for the consideration of intervention (43.2%); internal carotid artery (ICA) occlusion/near occlusion (25%); and poor neurological recovery post-stroke (11.4%).
Out of the 10 patients with poor neurological recovery post-stroke, only two went on to receive a delayed carotid intervention, the investigators report. However, there were five patients (6%) who developed a further ipsilateral stroke or transient ischaemic attack (TIA) following conservative
management during the follow-up period. The majority of patients (65.5%) were commonly managed with dual antiplatelet therapy (DAPT) and statins, Lim et al relay.
According to the investigators, patients who underwent carotid intervention had a 0.25 (0.17–0.5) hazard ratio of survival compared to patients managed conservatively—when adjusted for age. The overall survival rates at one and four years were 88% and 57%, respectively, and corresponding ipsilateral stroke-free survival rates at both one and four years were 97% in the medically managed patient group.
“These data support [the finding] that patients who were not offered intervention for symptomatic carotid artery disease, and were managed medically, had lower age-adjusted overall survival compared to patients undergoing carotid intervention,” Lim and colleagues conclude. “However, the risk of future ipsilateral stroke was relatively low compared to the landmark trials, highlighting the importance of medical therapy as a standalone strategy for those patients deemed high risk for carotid intervention.”
These data support [the finding] that patients who were not offered intervention for symptomatic carotid artery disease, and were managed medically, had lower age-adjusted overall survival compared to patients undergoing carotid intervention”
View exclusive video interviews and industry-sponsored content online
Get daily updates on the latest device approvals, clinical data and company news
Stay up to date with real-time coverage of key neurovascular conferences
CIRSE is the world’s largest community of healthcare professionals specializing in minimally invasive image-guided treatments. It is the ideal platform for your career, every step of the way.
Share your work by submitting your abstract!
European Conference on Interventional Oncology
ECIO 2025
April 13-16 | Rotterdam, NL
SUBMISSION OPEN: October - January 9
International Conference on Complications in Interventional Radiology ICCIR 2025
May 22-24 | Pörtschach, AT
SUBMISSION OPEN: November - February 6
European Conference on Embolotherapy ET 2025
June 11-14 | Porto, PT
SUBMISSION OPEN: December - February 27
ecio.org etconference.org
CIRSE Annual Congress CIRSE 2025
September 13-17 | Barcelona, ES
SUBMISSION OPEN: January - March 20
cirsecongress.cirse.org cirse.org/iccir
Cardiovascular and Interventional Radiological Society of Europe
FlowPhysix announces partnership with 3comma for global distribution of thrombectomy device FlowPhysix, formerly known as Expanse ICE, has announced a strategic partnership with 3comma Medical who will serve as their international commercial partner for their FlowRunner aspiration thrombectomy system.
This partnership between FlowPhysix and 3comma will provide physicians outside of the USA access to new standards in thrombectomy technology, enabling FlowPhysix to focus on US commercialisation.
3comma managing partner and former vice president of Penumbra, Marc Paris, believes the FlowRunner system will make an immediate impact in the peripheral thrombectomy segment. “We can rapidly activate our established international commercial infrastructure to accelerate adoption of the FlowRunner system. We are confident that FlowPhysix will be the next major disruptor in the global thrombectomy market and we are excited to be part of this endeavour,” Paris said.
“Our game-changing technology has the potential to alter the current standard of care for thrombectomy. This partnership provides FlowPhysix expanded reach in delivering our unique solutions to patients worldwide. We strongly believe that 3comma’s proven leadership and deep expertise will drive commercial success internationally and increase shareholder value for the company,” said Jeff Hopkins, chief executive officer of FlowPhysix.
Boston Scientific completes acquisition of Silk Road Medical Boston Scientific announced the close of its acquisition of Silk Road Medical, the company behind transcarotid artery revascularisation (TCAR).
“The integration of the TCAR platform into our portfolio means we can offer a treatment option for patients suffering from carotid artery disease that can reduce the risk of stroke and lead to improved patient outcomes,” said Cat Jennings, president of vascular peripheral interventions at Boston Scientific.
Boston Scientific revealed on 18 June that it had entered into a definitive agreement to acquire Silk Road.
GE HealthCare acquire Intelligent Ultrasound’s clinical AI software GE HealthCare has agreed to acquire the British medical device company Intelligent Ultrasound Group’s clinical artificial intelligence (AI) software unit for up to US$51m.
GE HealthCare intends to integrate Intelligent’s solutions into its ultrasound portfolio. The deal follows GE HealthCare’s acquisition of Caption
Health last year and is expected to be closed in quarter four of 2024.
GE HealthCare president and ultrasound and image-guided therapies chief executive officer Phil Rackliffe said: “We are pleased to bring
innovative technology from Intelligent Ultrasound into GE HealthCare’s ultrasound portfolio, allowing us to fully integrate these solutions into our systems. This technology and the experts who developed it will help enhance our portfolio of AI-enabled devices and accelerate our pace of development of next-generation AI tools.”
Intelligent Ultrasound has developed the ScanNav Assist AI technology, which powers its SonoLystlive and SonoLyst X/IR solutions. Both solutions are available on GE HealthCare’s Voluson Expert and Voluson Signature ultrasound devices, while SonoLyst is also featured on its Voluson SWIFT.
Intelligent Ultrasound chief operating officer Nick Sleep said: “I really believe that we are at the start of a wave of AI making a profound difference to medical imaging, and especially ultrasound. “Becoming part of the GE HealthCare family will help speed the adoption of this technology and make ultrasound even easier for customers to use.”
Sonio announce acquisition by Samsung Medison Sonio has announced the official approval by the French Ministry of the Economy and Finance of the complete acquisition of shares by Samsung.
The deal closes following the company’s second wave of US Food and Drug Administration (FDA) clearance in 2024 and with Sonio reporting and workflow solution operating in multiple sites across the USA.
“Alongside Samsung Medison, we are excited to make significant strides in the maternal care industry. In addition, Sonio plans to continue to advance medical reporting technology and diagnostic software globally, including for underserved areas in healthcare” says Cecile Brosset, chief executive officer (CEO) and co-founder of Sonio.
Samsung Medison CEO Kyu Tae Yoo said: “With the workforce shortages affecting the global healthcare industry, the real-time ultrasound exam guidance and quality assurance developed by Sonio is becoming more relevant to ensure high quality care. We look forward to combining Sonio’s and Samsung’s advanced engineering to enhance our ultrasound roadmap.”
Product News
Medinol announces first-inhuman implantation of drugeluting peripheral stent in Australia
Medinol has announced the successful first-in-human implantation of the ChampioNIR drug-eluting peripheral stent by Gerard S Goh and Thodur Vasudevan of the Alfred Hospital in Melbourne, Australia.
“We were impressed with ChampioNIR’s deliverability and its straightforward deployment”, said Goh, head of interventional radiology at The Alfred Hospital. “The frictionless deployment mechanism made the precise positioning of the stent very straightforward.”
Yoram Richter, chief executive officer of Medinol, added: “Medinol is excited to bring to clinical practice the culmination of years of research and development into novel stent designs, tailor-made for unmet clinical challenges in vascular interventions,”
The CHAMPIONSHIP study will enrol a total of 30 patients across seven sites in Australia and the USA.
Radiology, Greensboro, USA).
The TLAB transvenous liver biopsy system is an expansion of Argon Medical’s TLAB transjugular liver biopsy system, adding US Food and Drug Administration (FDA)-clearance for a unique approach for collecting biopsy samples from the liver via access in the femoral vein.
First cases completed in SPIRARE I trial with Vertex system
Jupiter Endovascular has announced that the first two patients have been treated in SPIRARE I, a multicentre study of the Vertex pulmonary embolectomy system using the company’s Endoportal Control platform technology.
The Vertex system is designed to treat acute pulmonary embolism (PE) in an endovascular procedure.
Sahil Parikh (Columbia University Irving Medical Center, New York, USA) principal investigator of the CHAMPIONSHIP study commented: “The ChampioNIR stent represents a breakthrough in treatment for superficial femoral artery (SFA) lesions. I am excited to see this device come to life after years of development.”
Argon Medical announces expansion of liver management portfolio Argon Medical has announced the launch of the Intara introducer sheath and the TLAB transvenous liver biopsy system.
The Intara introducer sheath is intended to maintain access to a patient’s peripheral or central vasculature (excluding coronary and neuro vasculature) to facilitate the introduction of therapeutic or diagnostic devices. The 10Fr sheath is resistant to kinking and it offers enhanced visibility to assist with the introduction, navigation, and delivery of devices for a variety of vascular procedures. Argon Medical anticipates the Intara introducer sheath will help facilitate the use of the company’s TLAB transvenous liver biopsy system and the Scorpion and Traveler portal vein access sets, as well as stents for the transjugular intrahepatic portosystemic shunt (TIPS) procedure, a recent press release states.
“The Intara introducer sheath is an upgrade to the current market options. It provides more resilience, ease of use, and safety throughout the TIPS procedure and stent placement,” said Dylan Suttle (Greensboro
The successful first two cases were performed at St John Paul II Hospital in Krakow, Poland, a cardiothoracic specialist centre affiliated with the Jagiellonian University, by study investigators Grzegorz Kopec, Jakub Stepniewski and Krzysztof Bartus.
“In these first cases, the Vertex system was successful in safely navigating through the right heart and into the pulmonary vasculature, facilitating an efficient and effective pulmonary embolectomy with no safety issues,” said Kopec, who is the head of the team for the diagnosis and treatment of pulmonary circulatory diseases at St John Paul II Hospital. “The patients’ clinical condition and haemodynamics improved on the table during the procedure, and postoperative imaging showed noticeable improvements in right heart function.”
“Controlling interventional devices within the pulmonary arterial tree when treating patients with intermediate-risk and high-risk PE can be challenging with today’s commercially available technology,” said Stepniewski, the Pulmonary Embolism Response Team (PERT) coordinator at St John Paul II Hospital.
“The endoportal technology enabled the large-bore Vertex system to remain stable in tachypneic patients, allowing us to quickly access and revascularise multiple areas of the pulmonary vasculature in a controlled manner when facing a high degree of cardiorespiratory movement.”
“I was pleasantly surprised that the endoportal technology provided a level of control similar to what I experience in an open surgical embolectomy, with the added ability to directly access a much wider range of vessels,” said Bartus, professor of medicine at the Jagiellonian University.
Vertex PE system
Clinical News
Penumbra announces completion of enrolment in THUNDER IDE study
Penumbra has announced the completion of enrolment in its THUNDER investigational device exemption (IDE) clinical study for patients with acute ischaemic stroke.
THUNDER is evaluating the safety and efficacy of the company’s latest computer-assisted vacuum thrombectomy (CAVT) technology— the Penumbra system with Thunderbolt aspiration tubing—for the removal of blood clots in the brain. This multicentre, single-arm study is evaluating patients with acute ischaemic stroke secondary to intracranial large vessel occlusion (LVO) who are eligible for mechanical thrombectomy, and its primary efficacy endpoint includes revascularisation of the occluded target vessel immediately post-procedure.
“This critical milestone brings us another step closer to providing physicians with the latest technology for stroke management,” said Adam Elsesser, president and chief executive officer of Penumbra. “The THUNDER study will provide the dataset needed to evaluate Penumbra’s Thunderbolt technology and I am optimistic that we are at the dawn of a new era in stroke treatment.”
As stated in a press release, the Penumbra system with Thunderbolt aspiration tubing uses an advanced CAVT software algorithm to generate proprietary, modulated aspiration, reducing friction between the clot and reperfusion catheter, and facilitating a more rapid and complete removal of blood clots in the brain.
InspireMD receives IDE approval from US FDA for CGUARDIANS II pivotal trial InspireMD has announced that the
Conference calendar
6–8 November
British Society of Interventional Radiology (BSIR) 2024 Brighton, UK https://www.bsirmeeting.org/
16–18 January SPECTRUM 2025 Miami, USA https://thespectrumconference.org/
US Food and Drug Administration (FDA) approval of the company’s investigational device exemption (IDE) application to initiate the CGUARDIANS II pivotal study of its CGuard Prime 80cm carotid stent system during transcarotid artery revascularisation (TCAR) procedures.
In February 2024, InspireMD announced that professor of surgery and radiology Patrick Geraghty (Washington University School of Medicine, St. Louis, USA) and programme director and chief of vascular surgery Patrick Muck (Good Samaritan Hospital, Cincinnati, USA) have agreed to act as lead investigators for the trial.
Marvin Slosman, chief executive officer of InspireMD, stated: “The approval of our CGUARDIANS II IDE is an important milestone and a significant step forward in our mission to serve the broadest range of physician and patient needs with a comprehensive set of tools that can deliver our best-in-class carotid stent system, CGuard Prime, for both carotid artery stenting and TCAR procedures. The CGUARDIANS II study is intended to facilitate approval of the use of CGuard Prime in an optimised TCAR version and indication.”
“In parallel, we continue to advance development of our comprehensive next generation TCAR Neuroprotection System, SwitchGuard NPS. Each of these initiatives helps pave the way, once approved, for us to initiate commercial sales and strive for market leadership in the USA. Our mission to improve stroke prevention and carotid disease management with our CGuard platforms continues as we build our company toward US expansion and global success. Additionally, as we previously announced, we are thrilled to have Geraghty and Muck as coprincipal investigators for the study, as well as a world class group of investigators committed to the trial’s success,” Slosman concluded.
30 January–03 February Society of Interventional Oncology (SIO) 2025 Las Vegas, USA https://www.sio-central.org/
2–5 February
International Symposium on Endovascular Therapy (ISET) 2025 Florida, USA https://www.hmpglobalevents. com/iset
Contego Medical’s Neuroguard IEP system receives US FDA approval for carotid revascularisation Contego Medical has announced the US Food and Drug Administration’s (FDA) premarket approval (PMA) of the Neuroguard IEP system for carotid revascularisation.
The company shares in a press release that clinical studies of the Neuroguard IEP system, including the PERFORMANCE I trial and PERFORMANCE II investigational device exemption (IDE) trial, have recorded low event rates—zero major strokes, zero neurologic deaths, and zero stent thrombosis at 30 days and one year.
William Gray, system chief of the Division of Cardiovascular Diseases at Main Line Health, Wynnewood, USA and co-national principal investigator of the PERFORMANCE II trial, said in the press release: “FDA approval confirms the results of the clinical studies.
The innovative Neuroguard IEP system performs exceptionally well with the lowest oneyear stroke rates ever shown for any type of carotid revascularisation, thereby establishing a new standard of care for meaningfully reducing the risk of procedural and long-term stroke in patients with carotid artery disease.”
for patient care. The Neuroguard IEP system transforms how we approach patients with carotid artery disease by addressing the specific threats of microembolisation while simultaneously reducing procedural steps, ensuring patients receive the highest level of protection throughout the procedure,” said Ravish Sachar, Contego Medical’s chief executive officer and founder.
Argon Medical announces launch of peripheral venous thrombectomy system
Argon Medical has announced the launch of the CLEANER Vac thrombectomy system for the removal of blood clot from the peripheral venous vasculature.
The Cleaner Vac thrombectomy system is a disposable, large-bore aspiration system designed to quickly and effectively remove blood clot, also known as thrombus, from vessels with restricted blood flow. In a recent press release, the company states that the device enables physicians to manually control powered aspiration, enabling procedures with precise clot removal that may minimise vessel damage and reduce blood loss.
The Neuroguard IEP system utilises Contego Medical’s Integrated Embolic Protection (IEP) technology, featuring a 40-micron filter integrated on a 6 French delivery catheter. The size of the integrated filter can be adjusted by the operator to custom fit each patient’s unique anatomy, and the pores on the filter are three to four times smaller than those on traditional filters, the company claims, improving protection against stroke and cognitive impairment. According to Conteo Medical, the newest generation closed cell stent is highly conformable and shows remarkable short- and longterm durability, with no thromboses, no clinically driven target lesion revascularisation, and very low restenosis rates at one year.
“This FDA approval is a huge step forward for Contego and
“Removing thrombus from the venous anatomy can be very challenging depending on the patient’s condition. Interventionalists need a simple and intuitive tool that allows them to easily navigate through the vasculature to the treatment area and control the removal of any obstructive thrombus. The streamlined design of the Cleaner Vac enables easy assembly, quick navigation, and efficient treatment, making it a welcomed treatment option for patients with this disease state.” said Fakhir Elmasri (Lakeland Vascular Institute in Lakeland, USA). Elmasri was the first physician in the USA to treat a patient with the Cleaner Vac system.
“We are excited to deliver the newest thrombectomy solution to interventionalists who prioritise efficient, successful outcomes for their patients,” said George Leondis, president and chief executive officer at Argon Medical.
13–15 February
6th Symposium on Vascular and Endovascular Access 2025 São Paulo, Brazil https://www.ecio.org/
20–22 February
International Multidisciplinary Endovascular (IM Endo) Forum 2025 Florence, Italy www.imendoforum.com
29 March–3 April Society of Interventional Radiology (SIR) 2025 Nashville, USA https://www.sirmeeting.org/
9–12 April
Pan Arab Interventional Radiology Society (PAIRS) 2025 Dubai, United Arab Emirates https://www.pairscongress.com/
13–16 April
European Conference on Interventional Oncology (ECIO) 2025 Rotterdam, The Netherlands https://www.ecio.org/
23–25 April
Charing Cross (CX) Symposium 2025 London, UK https://www.cxsymposium.com/
Neuroguard IEP system
Conventional Side-notch Biopsy Instrument
Side Notch BioPince Ultra
Join us as our guest speakers share their findings of studying targeted tumour sample quality with BioPince Ultra and its impact on diagnosis, tumour cell content and genomic sequencing. Side Notch
Webinar Guest Speakers
Professor Jon Bell Consultant Interventional Radiologist, The Christie Foundation NHS Trust
A., Brisson, M.L., Kwan, J., and Proulx, F.,
Dr Pedro Manuel Lino Soares de Oliveira Consultant in Histopathology, The Christie Foundation NHS Trust
Up to 58% more tissue volume by scanning the QR code below