Part two of a series: So you want to marry a surgeon?
9 PAD
Textbook outcomes are ‘very rare’ after revascularization for CLTI, new study finds
By Bryan Kay
10 SVS year in review
A message from the executive director
30 SAVS 2025
First woman president of Southern Association for Vascular Surgery takes reins
www.vascularspecialistonline.com
INTERVIEW
DEEP VEIN
ARTERIALIZATION: MUCH REMAINS TO BE LEARNED BUT USE POISED TO EXPAND IN PATIENTS WITH LESS SEVERE ISCHEMIA
By Bryan Kay
THESE REMAIN EARLY DAYS for transcatheter arterialization of the deep veins (TADV) in the setting of patients with severe chronic limb-threatening ischemia (CLTI), says Daniel Clair, MD, one of the principal investigators in key clinical trials of the procedure, but the learning-curve process promises that “we are going to continue to see slow but not insignificant improvement in results” with the technique.
“Even within all of the PROMISE trials, you’re talking about only 250 patients that have been assessed, published and looked at carefully,” says the professor and chair of the Department of Vascular Surgery at Vanderbilt University Medical Center in Nashville, Tennessee. “There is still a lot to learn.”
Late last year, Clair presented two-year outcomes from the prospective, multicenter, singlearm PROMISE II trial of the LimFlow system (Inari Medical) for TADV in so-called no-option CLTI patients at the 2024 edition of Vascular Interventional Advances (VIVA) in Las Vegas (Nov. 3–6), demonstrating sustained limb salvage and wound healing.
See page 9
Medical Editor Malachi Sheahan III, MD
Associate Medical Editors
Bernadette Aulivola, MD | O. William Brown, MD | Elliot L. Chaikof, MD, PhD
| Carlo Dall’Olmo, MD | Alan M. Dietzek MD, RPVI, FACS | John F. Eidt, MD | Robert Fitridge, MD | Dennis R. Gable, MD | Linda Harris, MD | Krishna Jain, MD | Larry Kraiss, MD | Joann Lohr, MD
| James McKinsey, MD | Joseph Mills, MD | Erica L. Mitchell, MD, MEd, FACS | Leila Mureebe, MD | Frank Pomposelli, MD | David Rigberg, MD | Clifford Sales, MD | Bhagwan Satiani, MD | Larry Scher, MD | Marc Schermerhorn, MD | Murray L. Shames, MD | Niten Singh, MD | Frank J. Veith, MD | Robert Eugene Zierler, MD
Resident/Fellow Editor
Saranya Sundaram, MD
Executive Director SVS
Kenneth M. Slaw, PhD
Senior Director for Public Affairs and Advocacy
Megan Marcinko, MPS
Manager of Marketing
Kristin Spencer
Communications Specialist
Marlén Gomez
SVS Consultant
Beth Bales
Published by BIBA News, which is a subsidiary of BIBA Medical Ltd.
Publisher Stephen Greenhalgh
Content Director Urmila Kerslake
Managing Editor Bryan Kay bryan@bibamedical.com
Editorial contribution
Jocelyn Hudson, Will Date, Jamie Bell and Éva Malpass
Design
Josh Lyon and Terry Hawes
Advertising Nicole Schmitz nicole@bibamedical.com
Letters to the editor vascularspecialist@vascularsociety.org
BIBA Medical, Europe
526 Fulham Road, London SW6 5NR, United Kingdom
BIBA Medical, North America
155 North Wacker Drive – Suite 4250, Chicago, IL 60606, USA
In the second of a two-part series of editorials, Vascular Specialist Medical editor Malachi Sheahan III, MD, offers further insight into the world of surgeon-surgeon marriages with a little help from a few friends.
Welcome to the first Vascular Specialist editorial of 2025. If your spouse did not learn from social media that you wrote an article about your marriage, your year is already off to a better start than mine. As promised, here is the second part of our series, examining surgeon-surgeon marriages. I have assembled an all-star cast of married surgeons to offer advice, counsel and condolences. Participating were vascular surgeons Sunita Srivastava, MD, and Matthew Eagleton, MD; vascular surgeon London Guidry, MD, and surgical oncologist John Lyons, MD; vascular surgeon Kelli Summers, MD, and plastic surgeon Michael Borrero, MD; vascular surgeon Marie Unruh, MD, and plastic surgeon Adam Hauch, MD; pediatric surgeons Fabienne Gray, MD, and Jenny Stevens, MD; and a few others who learned from my misadventures and requested anonymity. I have presented their guidance unattributed, loosely categorized under a few broad topics.
❤ Selecting a spouse
- It’s important to identify a spouse who understands the urgency and the unpredictability of surgery as a job. Surgery requires the doctor to leave planned family gatherings unexpectedly when duty requires. This can be very frustrating for a non-medical spouse, therefore it is vital to select a spouse who is understanding and tolerant of this unpredictability.
- We met in training and early career. We both wish we’d had the opportunity to meet each other in “normal lives.” There is a whole experience of “normal dating” that just didn’t happen for us (or for anyone in medicine, in particular surgery). It wouldn’t have changed anything, but sometimes we feel like we missed out on the fun aspect of courtship.
- I have observed that having a spouse in healthcare is helpful for my female surgeon colleagues, and another surgeon is preferable. Non-MD/healthcare husbands don’t seem to understand the obligations of their spouses.
- I think we both wish we’d met outside of the hospital and could’ve gotten to know each other in a more natural habitat, as was previously said. But it’s really hard to meet people when you’re mired in this world. I met so many fascinating people as I moved from city to city for research, and residency and fellowship, but it was always hard to find someone who understood/had time for/could handle the significance of the job (time constraints, emotional toil, prolonged schooling). That said, I am so frankly impressed (with myself) by the person I found to share it all with. Being at different points in our careers certainly made it harder. Conflicts between supportive partner, “back in my day” historical narratives, and mentoring opportunities were confusing and not always handled correctly (by me). As we all
know, the muted highs from a case that went well and the devastating lows of any complication are simply not fully grasped by those who don’t do this.
- I think it’s very different if you’re asking a male surgeon versus a female surgeon. I think female surgeons have a narrower criteria than males (and no, not because we are “picky”). I think there are still societal norms in place for male versus female roles in the house, and being a female surgeon breaks a lot of those rules. We have to find someone who understands and accepts a busy work and call schedule, is willing to work as a team (cannot have a breadwinner mentality), and is OK with picking up our slack. Also, we have to physically find someone, which can be challenging when we are working all the time. If you don’t find a spouse before med school, I think it’s probably more likely that a woman will find a male physician as her partner (no, I don’t have data). Another physician automatically meets most of the criteria.
- We met while I was still early in training and there was an instant connection that was beautiful. However, we knew that the next 5–10 years of making a relationship work while one of us was moving across the country trying to accomplish the goal of becoming a pediatric surgeon would be very challenging. There are advantages and disadvantages of having a spouse in surgery. One thing that I think has been wonderful for us is having someone to talk through difficult cases with, to bounce ideas off of, to work through a bad outcome, etc. We have a deep understanding of the intricacies of this job and how it impacts us as humans, and it has been nice to have a partner to walk through that with. It is fun to learn things about surgery from each other and to celebrate our wins, and also to grieve our losses together. I am thankful for that.
Your heart will choose who your heart will choose. Then your brain will have to spend the rest of your life trying to figure out how the hell to make it work
- Your heart will choose who your heart will choose. Then your brain will have to spend the rest of your life trying to figure out how the hell to make it work. (Editor’s note: OK, some of these are mine. You’ll have to find the rest.)
❤ Balancing work obligations
- If you operate together, pick who will be in charge and who will assist. There are no cosurgeons in marriage.
- I still don’t think we’re doing this right, but she is the person I trust completely. And it is really nice that she has a handle on most of the players in the script. We both have really worked on learning to step out of ourselves and listen to each other without our personal opinions playing too much
I think it’s important to try to get work done on the fringes of family time—early in the morning/late in the evening. One has to be smart about their schedule, penciling in and protecting family time in order to balance both. You have to make best use of down time when the family is less likely to miss you.
- We were once told by a vascular leader: “You both cannot be successful. Choose which of the two of you that should be, and the other just shouldn’t plan on having a successful career, especially in academics.” I think this was a motivating statement for us. This is completely false.
continued on page 28
Malachi Sheahan III
PULMONARY EMBOLISM
NEW ANALYSIS DETAILS LEARNING CURVE EFFECT BEHIND
‘SIGNIFICANT IMPROVEMENT’ IN PERFORMANCE OF PE MECHANICAL THROMBECTOMY OVER TIME
By Bryan Kay
A MULTISITE HOSPITAL SYSTEM
analysis of the safety and procedural learning curve behind the performance of percutaneous mechanical thrombectomy for pulmonary embolism (PE) shows significant reductions in both fluoroscopy and procedure times alongside contrast volume over time.
The data, the senior author behind the study says, lend weight to the argument that vascular surgeons need to become more involved in performing this type of procedure in this part of the vasculature.
“Vascular surgeons can do this, we can do it safely, and, with practice, we can do it even better,” explains Jason Chin, MD, a vascular surgeon at Cleveland Clinic Abu Dhabi, the United Arab Emirates, and previously with MedStar Health in Baltimore, Maryland, where the study was carried out. “And
CAROTID DISEASE
this is a conversation vascular surgeons need to get involved in now or get left behind.”
The MedStar analysis—presented during the 2025 Southern Association for Vascular Surgery (SAVS) annual meeting in St. Thomas, the U.S. Virgin Islands (Jan. 22–25)— involved 420 patients undergoing PE mechanical thrombectomy from January 2020 to July 2024.
In addition to detecting statistically significant falls in fluoroscopy and procedure times and contrast volume, the researchers identified institutional plateaus for improvement of 55 and 138 cases for fluoroscopy time and procedure time, respectively.
Averaged across the number of surgeons participating, it would take an individual surgeon 3.4 cases to become proficient in imaging-related efficiency and 8.6 cases to
become proficient in broader procedural efficiency. Additionally, presenting author Perry Diaz, a medical student at Georgetown University School of Medicine, told SAVS 2025, they found no statistically significant differences between the first and last 50 cases in hospital or intensive care unit (ICU) length of stay or complications. The overall mortality rate was 4.49%.
“Importantly, we also saw that, with the first 50 cases and the last 50 cases out of the 400 we did, we still had good results for both, which I think says good things about being able to start a program, and still do it safely,” Chin details in an interview with Vascular Specialist. “But I think that as we gather more data, within our system and among PE interventionalists at large, we’ll certainly see that improvement in ICU and hospital length of stay, and in some of these outcomes that we saw trends in.”
this part of the vasculature, Chin says. “Certainly, putting a 24F sheath through multiple chambers of the heart can be a little bit nerve racking the first time you do it,” he says, “but when I look at vascular surgeons compared to other interventionalists, in our field we work with these wires, these sized devices, at least as much if not more than any of those other fields.
“Maybe we haven’t always crossed the right atrium and the right ventricle with them, but I think our skillset and the natural anxiety we might have about some of the complications we might have to deal with from related procedures, it does make us safe in that section of the vasculature, and it’s a natural extension of a lot of the deep venous work we do.”
Navigating the heart is not an area in which vascular surgeons are traditionally trained but the data—which represent different types of practice settings and operators—illustrate they can perform the PE procedure safely and with good results in
Chin also drew reference to the scale of venous disease circulating among the population at large. “Venous thromboembolic disease—and venous disease in general—is at least as common, if not a lot more common than arterial disease. And maybe it isn’t as limb or necessarily life threatening compared to arterial disease, but it’s still out there and still affects a lot of people,” he adds.
FFRCT diagnosis of coronary ischemia with ischemia-targeted coronary revascularization more than halves five-year risk of cardiac death and MI following CEA
By Bryan Kay
PREOPERATIVE DIAGNOSIS OF LESION-SPECIFIC ischemia using coronary computed tomography (CT)-derived fractional flow reserve (FFRCT) and ischemia-targeted coronary revascularization after carotid endarterectomy (CEA) can reduce the five-year risk of cardiac death and myocardial infarction (MI) by more than 50% and improve long-term-survival, new data show.
The findings, from a single-center observational study, represent the latest results from Dainis Krievins, MD, and colleagues from Pauls Stradins Clinical University Hospital in Riga, Latvia, on the use of FFRCT in patients undergoing vascular procedures. The data were presented at the 2025 Southern Association for Vascular Surgery (SAVS) annual meeting in St. Thomas, the U.S. Virgin Islands (Jan. 22–25). Fundamentally, Krievins et al sought to determine whether FFRCT-guided coronary revascularization improves longterm survival of CEA patients, under the theory that if coronary CT angiography identifies coronary stenosis, FFRCT more precisely shows functional significance of lesions.
The cohort study included 200 patients with no cardiac history or coronary symptoms undergoing elective CEA from 2017–2019, Krievins outlined. Half received preoperative cardiac evaluation with FFRCT to identify asymptomatic ischemia-producing coronary stenoses with ischemia-targeted coronary revascularization following CEA, compared to matched controls with standard preoperative cardiac evaluation and no elective coronary revascularization. In the FFRCT cohort, lesion-specific ischemia was defined as FFRCT ≤0.80 distal to >30% stenosis, and severe ischemia as FFRCT ≤0.75. Endpoints included all-cause death, cardiac death, MI, stroke and major adverse cardiovascular events (MACE) at five-year follow-up.
Of those patients in the FFRCT cohort, coronary CT revealed ≥50% stenosis in 48 patients, with lesion-specific coronary ischemia present in 57 FFRCT patients, severe ischemia in 44, multivessel ischemia in 28, and left main ischemia in seven patients. Forty-three patients had no coronary ischemia (FFRCT >0.80). The status of coronary ischemia in the control cohort was unknown, Krievins noted.
Elective coronary revascularization was performed one to three months following CEA in 33 patients: 27 patients underwent percutaneous coronary intervention (PCI) and six coronary artery bypass grafting (CABG).
Krievins revealed that, at five years, there was a two-fold reduction in all-cause death in the FFRCT group compared to controls—24% vs. 11%. Annual mortality in the control group was 4.8% compared to 2.3% among the FFRCT cohort. Further, there was a four-fold reduction in risk of cardiac death, seven-fold reduction in the risk of MI, and three-fold reduction in MACE, he added. There was no difference in stroke rate.
A subgroup analysis of patients with significant ischemia who underwent coronary revascularization showed that allcause mortality was similar to those who had no ischemia, Krievins continued. Further, among those with significant ischemia but who did not undergo coronary revascularization, all-cause mortality was similar to the control group.
Five-year survival was 76% in the control group and 89% among the FFRCT cohort. “Improved survival is associated with diagnosed treatment of asymptomatic ischemic-producing coronary stenosis,” Krievins said, concluding: “Patients with no known coronary artery disease undergoing CEA have a high prevalence of silent, or asymptomatic, coronary ischemia, which is a marker for high risk of death and MIs. This single center study showed that preoperative diagnosis of lesion-specific ischemia using coronary CT-derived FFR together with ischemia-targeted coronary revascularization following CEA can improve five-year risk of cardiac death and MI by more than half and improve long-term survival.” Validation of the results require multicenter randomized trials, one of which, SCORECAD, is currently underway, Krievins added.
“Preoperative diagnosis of lesionspecific ischemia using coronary CT-derived FFR together with ischemia-targeted coronary revascularization following CEA can improve five-year risk of cardiac death and MI by more than half ”
DAINIS
KRIEVINS
Dainis Krievins
Perry Diaz
The future of vascular surgery (and the role a hybrid OR plays in it)
Two leaders in vascular surgery preview the future of interventional imaging and consider the emergence of the hybrid operating room (OR) as a future model for success.
The hybrid OR is emerging as a cornerstone development in the future of interventional imaging. With seamless integration of advanced imaging technologies with traditional surgical tools, hybrid ORs will deliver real-time, high-resolution visuals during new and complex interventional procedures. The expected result will be greater precision, faster decision making coupled with improved patient outcomes.
As minimally invasive techniques continue to evolve, hybrid ORs will enable multidisciplinary teams to collaborate in new ways to enhance the safety and efficiency of treatments.
The continued development and adoption of hybrid ORs will undoubtedly transform the landscape of modern medicine, pushing the boundaries of what can be achieved in surgical and interventional care.
The future of vascular surgery and the role a hybrid OR plays in the space took center stage at the 2024 edition of the VEITHsymposium in New York City (Nov. 19–23).
Daniel Clair, MD, chair of the Department of Vascular Surgery at Vanderbilt University Medical Center in Nashville, Tennessee, and Alan Lumsden, MD, the Walter W. Fondren III presidential distinguished chair, at DeBakey Heart & Vascular Center, Houston Methodist Hospital, in Houston, Texas, weighed in on how new advances and changing concepts in interventional imaging will transform tomorrow’s interventional imaging suite.
What does the future of vascular surgery look like for you, and how does medical imaging play a role in that future?
DC: As I think about the future of vascular surgery, we’re already seeing indications of what’s to come with a move towards less invasive procedures, more outpatient procedures, and the combination of open and interventional procedures. Almost all of it involves imaging in one way or another.
I do think that as we move forward, mechanisms to reduce radiation dosing for physicians and for patients is going to be a critical aspect of imaging and its integration with imaging as well.
AL: We’re an imaging-dependent specialty. Again, let’s talk about what imaging is to us. It’s ultrasound, and obviously Siemens Healthineers is a big player in the ultrasound space.
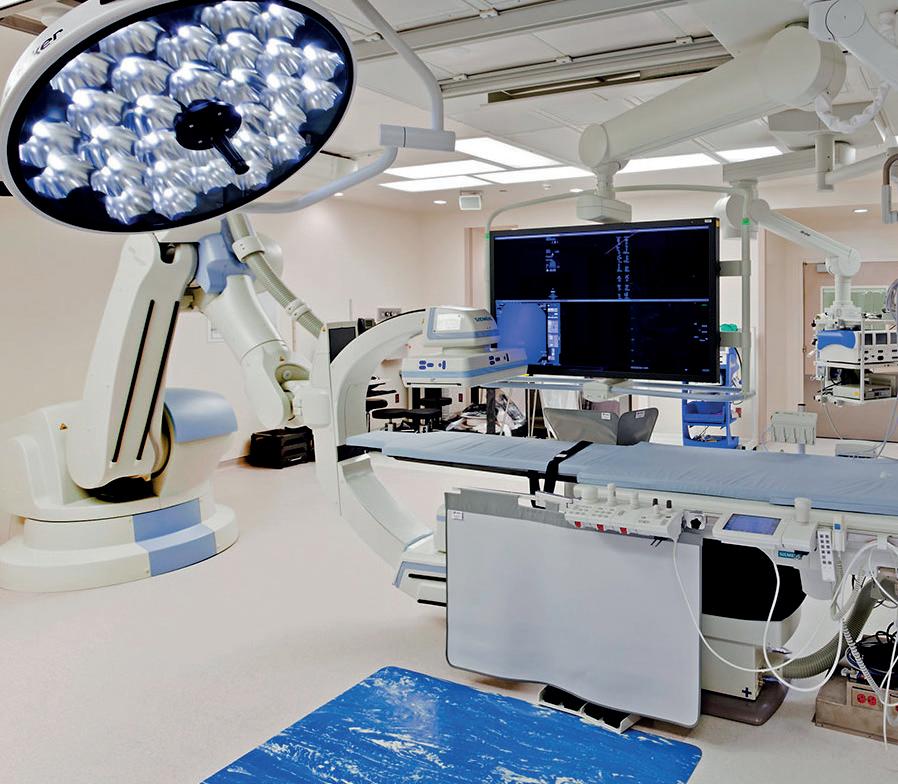
A hybrid OR is a surgical space that combines traditional operating equipment with imaging technology. This allows surgeons to perform both open and minimally invasive procedures in the same room, without moving the patient. Houston Methodist Hospital and Vanderbilt University Medical Center both leverage the features of ARTIS pheno from Siemens Healthineers.
The robotic C-arm will play an important role in future interventional imaging solutions, where high-quality imaging must be met with robust flexibility to satisfy the demand for mixed, multi-modality solutions.
DC: The integration of imaging in fluoroscopy rooms, and in rooms with imaging that is based on them—combining different modalities of imaging and using them virtually in the OR—is increasingly going to be something we do.
It is something we will need to have the capacity to do. That’s certainly true for interventional procedures, and I actually think it’s true for open procedures as well. It’s kind of a mixed reality assessment of the patient.
AL: Here’s an example. When we want to
anatomy. As we explore robotics, this can be valuable in planning open and robotic procedures.
You’re starting to use robotics and navigation with no radiation. Where do you see these two capabilities coming into play in the future?
DC: I do think that robotics are going to be a significant part of how we evolve [as a specialty]. There are portions of what we do in vascular surgery that are not going to
Vascular surgery always plays a major role in vascular ultrasound, but it’s also about computed tomography (CT), magnetic resonance (MR) and intravascular ultrasound (IVUS) and all the other imaging modalities.
Our specialty uses what I call applied imaging. What we really try to do is figure out how to use the imaging modalities to better treat the patients.
In the past, you got a CT scan and then you diagnosed an aneurysm. It’s not like that anymore. Now, we take that CT scan, we diagnose the aneurysm, we fuse that on top of the patient, and we deploy complex devices based upon the CT scan.
So, the CT scans must be good. That really was one of the things that pushed us into getting involved in the preoperative CT scan.
The nice thing is that the CT scans are generic, but not completely. So, understanding how that CT scan is acquired and the timing of the contrast is important for us.
We’re fortunate at Methodist because the DeBakey Heart and Vascular Center owns the cardiovascular movement. It’s all done by clinicians. I think that’s a big advantage in helping me understand what I need to know to execute all of these complex procedures.
do a case, we don’t access a blood vessel without using ultrasound—and that’s transformed our ability to utilize many different blood vessels to perform ever more complex interactions safely.
So, we use ultrasound to get access. We use a CT scan to fuse with our pheno image. And we use fluoroscopy to monitor the procedure. The hybrid OR is the forum by which we can mix these different imaging technologies.
We spend a long time planning endovascular procedures, and then we just go and do an open operation without having looked at the CT scan. All that information is still there.
Increasingly, I think we need to educate residents so that they know there is a retroaortic renal vein because it’s on the CT scan. If we go to type II endoleaks, we ought to know where the lumbar arteries are and how we’re going to localize them, because they are all right there on a high-quality CT scan.
Using cinematic rendering, we can make the CT scan look ever more like surgical
“Now,
we take the CT scan, we diagnose the aneurysm, we fuse that on top of the patient, and we deploy complex devices based upon the CT scan”
ALAN LUMSDEN
convert over to interventional or endovascular therapies. There is no question that if you look at recovery times and impairment and morbidity from larger vascular procedures—or larger procedures of any kind—these variables are reduced with the use of robotics. That’s number one. Number two, if you are just looking at non-fluoroscopy or virtual imaging as a
Alan Lumsden
Daniel Clair
method of doing interventions, there is no question that it provides better guidance with good imaging and reduces the time and radiation exposure for the patients, staff and physicians.
All of that will be a significant part of what we do in the future.
AL: We must parse this out into endovascular robotics and surgical robotics. I know endovascular robotics has had its challenges. [But]I still think it’s going to come back. Look at the relationship you have with Intuitive or on the Ion [Robotic Bronchos-
copy] platform. Most people here do not even know what the Ion is. And that’s an example of how, if it is not happening within your own specialty, you have no direct line of sight to it.
I think about the bronchi as long thin tubes, just like blood vessels. What Intuitive has done—and part of it is partnering with Siemens Healthineers—is you’ve got a preoperative CT scan, and you see a lung nodule. You bring your C-arm in and allow fusion to occur. You then diagram a path for the endobronchial robot, through those long thin tubes, to a peripheral target using fused imaging.
So, I think robotics can take you to one level. And then I think imaging can take you to another level. The power is going to be in putting these two things together, so now the imaging is space-specific and driving the robots. It is saying that either, “No, you cannot go in that area,” or, “This is the path that you are going to take to get there.”
If it can be done in the bronchi, I see no reason why it can’t be done in the blood vessel.
We’ve discussed a lot of technologies. How can they be used together in a hybrid OR?
AL: We need to have someone who translates the imaging capability and understands what the physician needs and helps make that bridge. That’s the physician at the moment, but there is a real need for imaging specialists who bridge the gap between what the imaging can provide and what we need. How you find those people is a challenge. That is the difference between creating a CT scan and creating an imaging modality that we can actively engage with.
DC: As clinicians there is a lot that we want in terms of imaging and its integration through multiple modalities. That interaction between engineers who design the systems and physicians who use them is what is going to drive the changes we need to see. That interaction will help us bridge the gap between what we need and what is actually possible.
All of us need to be involved. Without that interaction, it is difficult. That interaction allows us to be able to say, “I’d like this to do endobronchial, but what if we combined it with a thoracoscopic intervention done by a robot at the same time so that we can divide the blood vessels directed to that area?” This is the integration and the interaction that improve what we’re doing.
Hybrid ORs in interventional imaging integrate multiple imaging modalities to provide more accurate, real-time and comprehensive guidance during minimally invasive procedures. They are equipped with imaging systems and robotic equipment that combine the strengths of the different imaging technologies to improve diagnostic accuracy, procedural precision and patient outcomes.
Nationally ranked Houston Methodist DeBakey Heart & Vascular Center is home to four such operating rooms within its Texas Medical Center campus, bringing highly advanced care to patients in the Houston area. The rooms combine advanced medical imaging devices and an operating room. In short, these new hybrid ORs will allow for more minimally invasive procedures for both cardiovascular surgery and neurosurgery.
Cardiovascular surgeons, cardiologists, neurosurgeons and neurologists from these centers believe that the advanced technology in this building will transform clinical care for the future and will serve as the new standard for similar facilities around the country.
In 2022, Vanderbilt University Medical Center opened two of the latest generation of hybrid ORs, and each combine a traditional operating room with the latest advanced imaging equipment, simplifying procedures and allowing them to be more efficient and safer for patients.
Though Vanderbilt has built a handful
of such rooms in recent years, these are the medical center’s first that will be shared by a multidisciplinary cohort. Teams performing cardiology and electrophysiology
“ That interaction between engineers who design the systems and physicians who use them is what is going to drive the changes we need to see”
DANIEL CLAIR
procedures as well as cardiac and vascular surgery will benefit from the sophisticated technology in the room—and from each other.
Both medical centers leverage the advanced robotic imaging capabilities of the ARTIS pheno from Siemens Healthineers. ARTIS pheno significantly improves precision and workflow during complex procedures. It delivers high-definition, 3D imaging with a level of detail that helps
surgical teams visualize anatomical structures in real time, facilitating more accurate interventions.
The robotic design enables flexible and precise positioning, ensuring optimal imaging angles without the need for time-consuming manual adjustments. This efficiency not only accelerates the procedure but also reduces radiation exposure for both patients and medical staff.
With its ability to seamlessly integrate into the hybrid OR environment, ARTIS pheno supports a wide range of minimally invasive surgeries, ultimately enhancing the overall success of interventional procedures and improving patient outcomes.
The robotic imaging system was built to expand a hybrid OR’s ability to perform multiple surgical and interventional procedures. More than 1,350 hybrid operating rooms and interventional radiology suites worldwide are using the versatility of ARTIS pheno in order to advance their case mix and better facilitate more complex procedures.
To learn more about the role of the robotic ARTIS pheno in hybrid ORs, visit www.siemenshealthineers.com/en-us/clinical-specialties/ surgery/surgery-product-portfolio/hybrid-or/ artis-pheno
(1) Houston Methodist’s hybrid OR; (2) Vanderbilt University’s hybrid OR endovascular angiography suite; and (3) Siemens Healthineers ARTIS pheno
Ketamine reduces postoperative opiate use and pain scores as part of spinal cord protection protocol for TAAA repair
By Bryan Kay
THE INTRODUCTION OF KETAMINE into a spinal cord ischemia (SCI) protection protocol used during thoracoabdominal aortic aneurysm (TAAA) repairs led to significant reductions in postoperative opiate administration and patient-reported pain scores, a randomized-controlled trial (RCT) performed by a team of researchers at the University of Kentucky in Lexington, Kentucky, demonstrated.
The 20-patient doubled-blind RCT showed that among the 10-patient cohort who received ketamine as part of their SCI protection bundle, estimated mean six-hour oral morphine-equivalent use over the first 48 hours was 49mcg (95% confidence interval
[CI] 28.7–69.3) vs. 110mcg (95% CI 89.8–130.3) in the saline placebo cohort (p=0.019).
The estimated six-hour mean pain score for the cohort given ketamine, meanwhile, was 1.9 (95% CI 0.4–3.4) vs. 4.2 (95% CI 2.6–5.8) for those who received the placebo.
The data were delivered during the 2025 Southern Association for Vascular Surgery (SAVS) annual meeting in St. Thomas, the U.S. Virgin Islands (Jan. 22–25) by senior investigator Sam Tyagi, MD, an assistant professor of surgery at the University of Kentucky. Tyagi received the prestigious SAVS Founders’ Award for the paper.
Tyagi and colleagues sought to address the specter of low-dose naloxone, a component
UNCOVERS
of the SCI protection bundle, in worsening perioperative pain scores and increasing the need for postoperative opiate administration.
The study grew out of a previous multidisciplinary retrospective analysis aimed at identifying a pain management strategy to alleviate perioperative pain and reduce opiate reliance alongside, later, an informal conversation in which the potential for the use of ketamine in the mix emerged, Tyagi explained.
That study demonstrated that patients who received a continuous infusion of naloxone with their SCI protection bundle recorded pain scores that were statistically significantly higher and were receiving more morphine-equivalent pain medications when compared to patients who had similar operations but were under no SCI protection protocol.
“So, not only were we giving them much higher doses of opiates, we were also poorly controlling their pain on top of that,” Tyagi explained.
That’s when the suggestion to incorporate ketamine emerged during a holiday season chat with his physician brother. After some
investigation, the project was set in motion.
The RCT saw patients randomized by the University of Kentucky pharmacy team before arriving in the operating room for their TAAA procedure, where ketamine administration—or the placebo—was initiated and continued during the time they were on the SCI protection protocol. “Nothing else was changed,” Tyagi said.
Results showed that no patients had adverse outcomes related to the ketamine, though one died from procedural-related complications. Another enrollee withdrew from the study several hours after randomization.
“The amount of morphine equivalents [administered] was essentially half in the ketamine group versus the placebo saline group,” Tyagi told SAVS, with pain scores showing “a 2.3 [point] difference in the ketamine vs. placebo group.”
Among future directions of study, the researchers aim to quantify the impact of incisions on pain scores, explore excitatory amino acids in cerebrospinal fluid in the setting of ketamine, as well as expand on the 20-patient RCT itself.
DECREASE IN USE OF PROPHYLACTIC SPINAL DRAINS AT SAME TIME AS SPINAL CORD ISCHEMIA STEEPLY DECLINES
continued from page 1
Despite a “dramatic” decrease in the use of prophylactic cerebrospinal fluid drains (CSFD) for the prevention of spinal cord ischemia (SCI) in patients undergoing fenestrated and branched endovascular aortic repair (F/BEVAR), the rate of SCI has tracked a similarly dramatic decrease, according to the senior author of a new analysis of U.S. Aortic Research Consortium (ARC) data from 2011–2024.
Adam Beck, MD, the Holt A. McDowell Jr., MD, endowed chair of vascular surgery at the University of Alabama at Birmingham (UAB), described the data as likely practice-changing for many specialists who carry out complex repairs of thoracoabdominal aortic aneurysms (TAAAs) ahead of their presentation at the 2025 annual meeting of the Southern Association for Vascular Surgery (SAVS) in St. Thomas, the U.S. Virgin Islands (Jan. 22–25).
The retrospective analysis of the ARC registry— which encompasses 10 major medical centers with individual investigational device exemption (IDE) studies for complex aortic repairs—included 2,585 patients undergoing elective F/BEVAR.
Eras of repair were divided into early (2011–2013), mid (2014–2021) and late (2022–2024) based on the publication of influential papers which changed ARC practices. Patient cohorts were separated by prophylactic (n=949), therapeutic (n=27) and no CSFD (n=1609) use.
A composite variable consisting of any SCI, major CSFD complication or intracerebral hemorrhage was designated as the primary outcome. The ARC data showed that 196 patients (7.6%) experienced the primary composite outcome and 160 (6.2%) experienced SCI. Presenting the data, Angela Sickels, MD, an integrated vascular surgery resident at UAB, told SAVS 2025: “The yearly incidence of the primary composite outcome and any SCI gradually declined over time, from a maximum of 25% [for both primary composite and SCI] in 2011 to
2.8% and 2.3%, respectively, in 2023.”
Meanwhile, the use of prophylactic CSFD declined from “being essentially universally done” in 2011 down to just 10.9% in 2023 “without any substantial increase in therapeutic CSFD use, which reached a maximum of just 3.5%.”
In high-risk patients (n=1,026), 12.9% (n=132) and 10.6% (n=109) experienced the primary composite outcome or any SCI event, respectively, the data revealed. Rates of the primary composite outcome declined from 38.5% in 2013 to 3% in 2023.
Prophylactic CSFD use in high-risk patients—while nearly universal (92.9–100%) until 2016—has also since been on a continuous decline, reaching a minimum of 22.6% in 2023, the research shows. “This subset of patients also saw no increase in therapeutic drain use, reaching a maximum of 5.9%,” Sickels added.
Speaking to Vascular Specialist about the significance of the findings, Beck noted how, as experience of endovascular long-segment coverage of TAAAs over the last decade has expanded, discussion and education
“Now, the SCI rate is in that 5–10% range, so essentially the risk of SCI is almost equivalent to—or is equivalent to—the risk of putting a drain in, so there is clinical equipoise there” ADAM BECK
around SCI prevention protocols, too, have broadened at most large medical centers.
The ARC data, Beck said, show a “rapid drop, especially over the last eight years or so, in the rate of SCI.
In addition, interestingly people have been using less and less prophylactic spinal drains, and we think that that’s probably because the rate of SCI has dropped with the use of SCI prevention protocols and is almost equivalent to the risk of the placement of spinal drains.”
Beck continues: “Most of the surgeons who have been doing these procedures will have stories about complications associated with the drains, which can be anywhere from 5–10%. Now, the SCI rate is in that 5–10% range, so essentially the risk of SCI is almost equivalent to—or is equivalent to—the risk of putting a drain in, so there is clinical equipoise there.”
One question remains, added Beck. “If you were to randomize patients with an especially high risk of SCI to prophylactic drains or not, whether prophylactic drains would actually prevent SCI—we still do not know the answer to that question.”
Beck believes the education that the ARC research has yielded has led to better outcomes. “There is a learning curve to this and there has been a regression to the mean with how everyone is managing these patients,” Beck explained.
“Early on, some of us had well-defined SCI prevention protocols, and some of us were doing things that we thought reduced the risk but didn’t necessarily have a well-formed protocol for it. There has been a lot of conversation around this complication in our monthly ARC meetings and at national/international educational meetings, and I think the dissemination of information and everyone learning from each other has led to this decrease in SCI.”
Angela Sickels
Adam Beck
48% fewer patients require reinterventions through 2 years.1,2 Go above expectations with the only device that does it all for CLTI.*
1. Reintervention defined as CD-TLR. 2. Brian G. DeRubertis et al., Two-Year Outcomes of the LIFE-BTK Randomized Controlled Trial Evaluating the Esprit™ BTK Drug-eluting Resorbable Scaffold for Treatment of Infrapopliteal Lesions, VIVA 2024. Now Proven With 2-Year RCT Data
INDICATIONS
The Esprit™ BTK Everolimus Eluting Resorbable Scaffold System is indicated for improving luminal diameter in infrapopliteal lesions in patients with chronic limb-threatening ischemia (CLTI) and total scaffolding length up to 170 mm with a reference vessel diameter of ≥ 2.5 mm and ≤ 4.00 mm.
Esprit™ BTK Everolimus Eluting Resorbable Scaffold System
INDICATIONS
The Esprit™ BTK Everolimus Eluting Resorbable Scaffold System is indicated for improving luminal diameter in infrapopliteal lesions in patients with chronic limb-threatening ischemia (CLTI) and total scaffolding length up to 170 mm with a reference vessel diameter of ≥ 2.5 mm and ≤ 4.00 mm.
CONTRAINDICATIONS
The Esprit™ BTK Everolimus Eluting Resorbable Scaffold System is contraindicated for use in:
• Patients who cannot tolerate, including allergy or hypersensitivity to, procedural anticoagulation or the post-procedural antiplatelet regimen.
• Patients with hypersensitivity or contraindication to everolimus or structurally related compounds or known hypersensitivity to scaffold components poly(L-lactide), poly(D, L-lactide), and platinum.
WARNINGS
• This device is intended for single use only. Do not reuse, reprocess, or re-sterilize. Note the product “Use-by” date on the package. Reuse, reprocessing, or re-sterilization may compromise the structural integrity of the device and / or delivery system and / or lead to device failure, which may result in patient injury, illness, or death. Reuse, reprocessing, or resterilization may also create a risk of contamination of the device and / or cause patient infection or cross-infection, including, but not limited to, the transmission of infectious disease(s) from one patient to another. Contamination of the device and / or delivery system may lead to injury, illness, or death of the patient.
• The Esprit™ BTK System is intended to perform as a system. The scaffold should not be removed for use with other dilatation catheters.
• The Esprit™ BTK System should not be used in conjunction with other non-everolimus drug eluting devices in the same vessel as the Esprit™ BTK Scaffold.
• It is not recommended to use this scaffold to treat lesions located at any joint or other hinge points, such as the knee or ankle. The recommended region for below-the-knee (BTK) treatment with the Esprit™ BTK Scaffold is the infrapopliteal arteries at a location ≥ 10 cm above the proximal margin of the ankle mortise. The Esprit™ BTK Scaffold has not been tested for use outside the recommended implant locations.
• This product should not be used in patients with aneurysms immediately adjacent to the scaffold implantation site.
• Insertion of the Esprit™ BTK System and implantation of the scaffold should be performed only under fluoroscopic observation with radiographic equipment providing high resolution images.
• Quantitative imaging is strongly recommended to accurately measure and confirm appropriate vessel sizing (reference vessel diameter ≥ 2.5 mm). If quantitative imaging determines a vessel size < 2.5 mm, do not implant the Esprit™ BTK Scaffold.
• Adequate lesion preparation prior to scaffold implantation is required to ensure safe delivery of the scaffold across the target lesion. It is not recommended to treat patients having a lesion that prevents complete inflation of an angioplasty balloon.
• Successful pre-dilatation with residual diameter stenosis of < 30% by visual estimation is required for treatment of the target lesion; < 20% by visual estimation is preferred.
• Ensure the scaffold is not post-dilated beyond the allowable expansion limits.
• Use of appropriate anticoagulant and / or antiplatelet therapy per standard of care is recommended for use of this scaffold system.
• This product should not be used in patients who are not likely to comply with the recommended antiplatelet therapy.
• Judicious selection of patients is necessary, since the use of this device carries the associated risk of
scaffold thrombosis, vascular complications, and / or bleeding events.
PRECAUTIONS
• Scaffold placement should not be performed in patients with known allergies to contrast agent that cannot be medically managed.
• It is not recommended to treat patients having a lesion with excessive tortuosity proximal to or within the lesion.
• When multiple scaffolds are required, only combinations of Esprit™ BTK Scaffolds must be used. Any potential interaction with other drugeluting or coated devices has not been evaluated.
• The delivery system is intended for deployment of the scaffold only and should not be used to dilate other locations.
• I mplantation of the scaffold should be performed only by physicians who have received appropriate training.
• A s with all catheter-based procedures, scaffold placement should be performed at facilities where patient can be prepared for necessary intervention and / or surgical removal of the device and vessel repair as per facility protocol.
• P re-dilatation should be performed with an angioplasty balloon. Cutting or scoring balloons can be used per physician discretion, if the lesion appears to be mildly calcified.
• Failure to pre-dilate the vessel may impair nominal / optimal scaffold delivery.
• I mplanting a scaffold may lead to dissection of the vessel distal and / or proximal to the scaffold, requiring additional intervention.
Note: In cases of bailouts, bailout treatment of the target lesion can be done using the Esprit™ BTK Scaffold of the appropriate length. If an appropriate length Esprit™ BTK Scaffold is not available, physicians should use standard of care.
• A n unexpanded scaffold may be retracted into the introducer sheath one time only. An unexpanded scaffold should not be reintroduced into the artery once it has been pulled back into the introducer sheath.
• Post-dilatation is strongly recommended for optimal scaffold apposition. When performed, postdilatation should be performed at high pressure (> 16 atm) with a non-compliant balloon up to 0.5 mm larger than the nominal scaffold diameter.
• Use an appropriately sized non-drug coated balloon to pre-dilate the lesion. When treating a long lesion, scaffold the distal portion of the lesion prior to scaffolding the proximal portion of the lesion.
• Ensure that the scaffolded area covers the entire lesion / dissection site and that no gaps exist between scaffolds.
• The extent of the patient’s exposure to drug and polymer is directly related to the number of scaffolds implanted. The safety of everolimus, polymer, and polymer breakdown products was evaluated in preclinical studies and the biocompatibility assessment of the Esprit™ BTK Scaffold.
• The safety and effectiveness of the Esprit™ BTK Scaffold in patients with prior brachytherapy of the target lesion or the use of brachytherapy for treatedsite restenosis in the Esprit™ BTK Scaffold have not been established. Both vascular brachytherapy and the Esprit™ BTK Scaffold alter arterial modeling. The potential combined effect on arterial remodeling by these two treatments is not known.
• The safety and effectiveness of the Esprit™ BTK System have not been established in clinical trials with the use of either mechanical atherectomy devices (directional atherectomy catheters, rotational atherectomy catheters) or laser atherectomy catheters.
• Formal drug interaction studies have not been performed with the Esprit™ BTK Scaffold because of limited exposure to everolimus eluted from the scaffold.
• Everolimus, the Esprit™ BTK Scaffold’s active pharmaceutical ingredient, is an immunosuppressive agent. Therefore, consideration should be given to patients taking other immunosuppressive agents or who are at risk for immune suppression.
• Oral everolimus use in renal transplant and advanced renal cell carcinoma patients was associated with increased serum cholesterol and triglyceride levels, which in some cases required treatment.
• Non-clinical testing has demonstrated the Esprit™ BTK Scaffold is MR Conditional. A person with the Esprit™ BTK Scaffold may be safely scanned under the following conditions. Failure to follow these conditions may result in injury.
• Static magnetic field strength of 7 Tesla or less
• The Esprit™ BTK Scaffold should not migrate in this MRI environment. MRI at 7 Tesla or less may be performed immediately following the implantation of the Esprit™ BTK Scaffold.
POTENTIAL ADVERSE EVENTS
Potential adverse events include, but are not limited to: Allergic reaction or hypersensitivity to contrast agent, anesthesia, scaffold materials (poly[L-lactide] [PLLA], poly[D, L-lactide] [PDLLA], platinum, or everolimus), and drug reactions to anticoagulation or antiplatelet drugs
• Vascular access complications which may require transfusion or vessel repair, including:
CAUTION: This product is intended for use by or under the direction of a physician. Prior to use, reference the Instructions for Use, inside the product carton (when available) or at manuals.eifu.abbott for more detailed information on Indications, Contraindications, Warnings, Precautions and Adverse Events. This material is intended for use with healthcare professionals only.
Illustrations are artist’s representations only and should not be considered as engineering drawings or photographs. Photo on file at Abbott.
Information contained herein for DISTRIBUTION in the U.S. ONLY.
Abbott
3200 Lakeside Dr., Santa Clara, CA 95054 USA, Tel: 1.800.227.9902
™ Indicates a trademark of the Abbott Group of Companies. www.cardiovascular.abbott
The risks described below include the anticipated adverse events referenced in the contraindications, warnings, and precautions sections of the everolimus labels / SmPCs and / or observed at incidences ≥ 10% in clinical trials with oral everolimus for different indications. Refer to the drug SmPCs and labels for more detailed information and less frequent adverse events.
• A bdominal pain
• A nemia
• A ngioedema (increased risk with concomitant angiotensin-converting enzyme [ACE] inhibitor use)
• A rterial thrombotic events
• Bleeding and coagulopathy (including hemolytic uremic syndrome [HUS], thrombotic thrombocytopenic purpura [TTP], and thrombotic microangiopathy; increased risk with concomitant cyclosporine use)
• Constipation
• Cough
• Diabetes mellitus
• Diarrhea
• D yspnea
• Embryo-fetal toxicity
• Erythema
• Erythroderma
• Headache
• Hepatic artery thrombosis (HAT)
• Hepatic disorders (including hepatitis and jaundice)
• Hypersensitivity to everolimus active substance, or to other rapamycin derivates
• Hypertension
• I nfections (bacterial, viral, fungal, or protozoan infections, including infections with opportunistic pathogens). Polyoma virus-associated nephropathy (PVAN), JC virus-associated progressive multiple leukoencephalopathy (PML), fatal infections and sepsis have been reported in patients treated with oral everolimus.
• K idney arterial and venous thrombosis
• Laboratory test alterations (elevations of serum creatinine, proteinuria, hypokalemia, hyperkalemia; hyperglycemia, dyslipidemia including hypercholesterolemia and hypertriglyceridemia; abnormal liver function tests; decreases in hemoglobin, lymphocytes, neutrophils, and platelets)
• Lymphoma and skin cancer
• Male infertility
• Menstrual irregularities
• Nausea
• Nephrotoxicity (in combination with cyclosporine)
• Wound healing complications (including wound infections and lymphocele)
There may be other potential adverse events that are unforeseen at this time.
Study demonstrates textbook outcomes after CLTI revascularization occur less than
a quarter of the time
By Bryan Kay
TEXTBOOK OUTCOMES
remain “very rare” after revascularization for chronic limb-threatening ischemia (CLTI), with the main driver being an enduring inability to attain complete wound healing and return patients to their preoperative ambulatory
FROM THE COVER DEEP
status, according to the lead researcher behind a new study looking into a version of the performance outcome metric.
Jayer Chung, MD, an associate professor in the Division of Vascular Surgery and Endovascular Therapy at the Michael E. DeBakey Department of Surgery, Baylor College of Medicine, in Houston, Texas, was speaking to Vascular Specialist shortly after presenting data at the 2025 Southern Association for Vascular Surgery (SAVS) annual meeting in St. Thomas, the U.S. Virgin Islands (Jan. 22–25).
“Textbook outcomes at one year were rare,” Chung told SAVS 2025. “They occurred in less than quarter of our population. And what is significant is when you split the composite, we see that the traditional metrics used to measure clinical success, such as survival, limb salvage and freedom from 30-day complications, were met,” he continued. “Yet, many of
VEIN ARTERIALIZATION: MUCH REMAINS TO BE LEARNED BUT USE POISED TO EXPAND IN PATIENTS WITH LESS SEVERE ISCHEMIA
continued from page 1
All patients enrolled in the trial had Rutherford class 5/6 disease, with a total of 105 CLTI patients undergoing the procedure between 2018 and 2022. At VIVA, Clair reported a limb salvage rate of 65% and improvement in Rutherford classification: 65.8% of patients had class 4 or below and 54.3% had class 0. Wounds were completely healed/healing in 82% of patients and the mean pain score was 1.2 out of 10. When combined with the PROMISE I trial, the two-year limb salvage rate was 68%, with no differences observed based on age, sex, race, baseline Rutherford classification, diabetes or dialysis, Clair had added.
Those type of data are likely to be built upon, with the future portending wider use of TADV, Clair reflects in a recent interview with Vascular Specialist
“What is likely is that you are going to see an expansion in the use of this technology in patients who perhaps are not as far down the path of ischemia as we have seen,” he explains. “I also think that there will likely be some complementary role in terms of arterial revascularization in people who have very bad distal disease.”
The data show that 25–30% continue to lose their limbs even when TADV is used, so opportunities to enhance benefits from the procedure require exploration, Clair continues. “The use of deep vein arterialization with
the patient-centric metrics, such as wound healing, ambulation and freedom from wound-related procedures, were not met. Complete wound healing and a return to ambulatory status were achieved in approximately two thirds, almost half of our patients underwent another revascularization at one year, and only two thirds of our patients were able to get by with one or less wound-related procedure.”
Chung and colleagues performed a nineyear retrospective, single-center analysis of consecutive CLTI patients undergoing revascularization (open, endovascular or hybrid). Textbook outcome was defined as a composite of survival, limb-salvage, no reinterventions (wound or vascular), freedom from major complications, less than one wound-related procedure, and complete wound-healing at one year.
“Patients with WIfI [wound ischemia and foot infection] stage 1 had more than 2.5-fold odds of achieving a textbook outcome compared to all of the other WIfI stages, whereas taking anticoagulants at baseline, diabetes at baseline or residing in an assisted living facility were independently less likely to achieve a textbook outcome,” Chung added during SAVS 2025. “In our opinion, current performance metrics overlook the true procedural burden of revascularization, therefore we feel that our definition of textbook outcomes should be factored into future patient education and treatment selections, in outcome evaluations, in clinical trials and quality assessments.”
vascular growth factors to enhance angiogenesis in the foot might be ideal. Right now, we are trying to understand how to optimize the venous flow in the foot to enhance, expedite and speed up the arterialization and delivery of oxygen to the tissues in the foot so we don’t lose the forefoot or toes, but we get them this delivery of oxygenated blood so they can heal the wounds that they have. Part of what we’re doing is trying to look at the angiographic and duplex data from PROMISE I and II patients to see if we can identify who are the patients who did really well and the patients who did not do well, and can we identify differences between them.”
Clair is clear on this direction of travel. The patient population who informed the clinical trials typify the necessity of the procedure, he says. “In the past, essentially everyone I have enrolled in these trials is a patient who likely would have had an amputation, and I can say that because I have watched them worsen before enrolling them, having tried other measures to help get them through. In the PROMISE trials, we carried this out in what I call the sickest of this group of patients, because they had to be externally validated as having no option; they had to be more than a month out from any previous angiogram or attempted intervention; and they had to have a wound on their foot in order to allow them to qualify. One of the critical issues now is, while that was what the trial was, in the community this technology is being used more in patients who don’t have good options, but who get an angiogram, can’t have percutaneous intervention, and the next day they are going for this venous arterialization.”
Chung later expanded on why he believes the textbook outcome metric better elucidates CLTI care. “Our current outcome metrics fail to capture the full depth and scope of the patient experience,” he told Vascular Specialist. “It misses particular functional outcomes like ambulation and domiciliary status, as well as fails to truly capture the impact of wound care and the progress that patients have on their journey to try and salvage their limb. The current metrics that are used to track performance across clinical trials or quality assessments, for instance, overestimate the quality of care that is being given. It causes us to misappropriate resources to some extent, as well as misjudge the true quality when we are comparing two different therapies.”
Chung added: “I think utilizing a comprehensive metric like textbook outcome to adjudicate and help educate our patients ahead of time is going to be critical going forward as we try to improve the care of our patients overall.”
“In our opinion, current performance metrics overlook the true procedural burden of revascularization”
JAYER CHUNG
believers in the technology start to embrace it and make referrals. His previous involvement in angiogenesis trials underscore how sick the PROMISE patients are, he says: in those, patients who had rest pain, severe claudication, and no foot wound could be enrolled. “[PROMISE trial participants] are patients who have not been studied in any previous trial because, frankly, they are sicker than any company was willing to look at, particularly in interventional trials.”
Some form of forefoot amputation is not unusual in the first two to three months after TADV, nor is an increase in pain in the first month, PROMISE data reveal.
“It’s unusual for these patients to keep everything because they have such severe disease in the foot by the time they present for treatment with this therapy,” Clair points out.
“Intriguingly, in PROMISE I, with every patient who kept their limb, if they made it three months with their limb on, they were going to keep their limb for the long term. In PROMISE II, there were very few patients who lost their limb beyond that first three-to-four-month period. If you get a good venous arterialization, and you see a response through six to 10 weeks, these people are likely going to keep their limb.”
In his own practice, Clair has seen previous non-
Meanwhile, PROMISE III will take another extended look at the same group of patients “in a little more real-world applications,” Clair adds. “So many of these patients have bilateral limb ischemia, so we included patients in whom you could do the procedure on both sides. We did not mandate an independent review committee; we did not mandate a 30-day waiting period between a previous angiogram or attempted intervention and moving on to venous arterialization.”
Daniel Clair
Jaye Chung
2024 in review: Message from the SVS executive director
The Society for Vascular Surgery (SVS) takes a moment to recognize the dedication, achievements and progress made over the past year. In a letter to members, SVS Executive Director Kenneth M. Slaw, PhD, highlights the Society’s unwavering focus on quality, advocacy and education while celebrating the collective efforts that have shaped the year’s successes.
vascular surgeons who qualify for the CMS MIPS Value Pathways (MVP) payment program. Many thanks to Evan Lipsitz, MD, and an incredible Quality and Performance Measures Committee and staff for a wonderful achievement.
Leadership education commonly states that leaders must not just “talk the talk” but “walk the walk.” If SVS members truly believe in quality, they need to engage in quality improvement, and a fantastic way to walk the walk is to encourage health systems to become verified as a Vascular Center of Excellence by the American College of Surgeons (ACS)-SVS Vascular Verification Program (VVP). Launched in 2023, the VVP added eight new practices in 2024. The focus in 2025 will be support for the Outpatient Standards Program. All SVS members are encouraged to practice through the program.”
Thank you for your relentless commitment to quality and safety in the care of patients with vascular disease, as well as your commitment and dedication to vascular surgery and the SVS. Last year was another fast-paced 12-month period, filled with challenges, opportunities and milestone achievements, none of which would be possible without the leadership and efforts of more than 560 member volunteers serving on over 40 committees, task forces and writers groups, and an incredible professional staff. I am delighted to refresh your memory regarding a few highlights.
Hello America, we are vascular surgery
Under the leadership of the Executive Board and Strategic Board, led by William Shutze, MD, and the Communications and Branding Committee, and an implementation team led by Megan Marcinko, the SVS launched its national branding initiative “Highway to Health.” In just the first three months, the media airways were flooded with video, social media and media interviews, reaching 452 million media impressions, close to 1,000 media placements and what soon will be over 40 live media interviews. It has been a very successful launch with our public relations firm partner, BRG, and this is just the beginning. Phase one of the launch introduced vascular surgery to the public, including SVS’s new Your Vascular Health patient website. In 2025, the focus will shift to referring providers and the healthcare system C-suite. Please watch your social media apps for SVS Highway to Health messaging.
Back to the future on health policy and advocacy
It was another year of struggle, challenge and intensive advocacy to protect and preserve physician payment and numerous pieces of legislation protecting both physicians and patients, including Centers for Medicare & Medicaid Services (CMS) fee schedules, budget neutrality, inflation adjustments, pre-authorization, wellness and many more issues. The SVS is front and center at the
table for key discussions and is a highly respected source of expertise on Capitol Hill. With the return of the Trump administration, it will never be more important for the voice of vascular surgery to be unified and strong and show strength through its political action committee (PAC) and face-to-face advocacy efforts. New in September 2025 will be the SVS’s first Advocacy Leadership Summit and Hill visit. We hope you will join us in September to become a trained leader in health policy and advocacy, and march up to the Hill to educate members of Congress and their staff to make our case loud and clear.
Media coverage in the vascular arena became a national issue in 2023, focusing on the appropriateness of vascular care across practice settings. Due to a strong response and leadership from the SVS, building relationships and educating medical journalists and the launch of the branding/ PR initiative, the headlines and stories in 2024 have slowly shifted attention from a small number of outliers in practice to the standards, guidelines, and quality improvement initiatives that define the vast majority of vascular surgeons’ practices.
Translation to transformation in clinical practice
Quality and quality improvement define our core
The core of the SVS’s reputation and expertise is derived from its focus on best science and quality improvement. The SVS Patient Safety Organization Vascular Quality Initiative (PSO VQI) is second to none among medical specialty registries in moving the needs on quality. The PSO VQI achieved its landmark one-millionth entry in 2024 and has over 1,200 subscribing institutions contributing data. The 17 regional meetings are focused on moving the quality improvement bar on selected procedures and disease states. This year’s true milestone was the launch of the Na tional Smoking Cessation Initiative, making the PSO/VQI among the first data registries to mobilize around prevention and preventive factors in vascular disease.
The SVS membership continues to grow and diversify, with total membership now closing in on 6,400 members
To address a major gap in credible data, the SVS organized a national compensation study and program for vascular surgery in 2023 to answer a long-standing query and need from SVS members and address a major gap in credible data. Having worked hard to achieve the requisite 20% of eligible SVS members to privately and confidentially input their financial data, under the leadership of Keith Calligaro, MD, and Compensation Task Force, the first aggregate report of vascular surgery compensation data was accepted for publication in the Journal of Vascular Surgery (JVS) in 2024. It was a busy year for developing and publishing clinical practice guidelines, and in 2024, the SVS continued its popular “Translating Guidelines into Practice” webinar series, focusing on varicose veins.
tional efforts and support the inclusion of patient perspectives.
Coming in 2025? An update on the SVS claudication guidelines! Emphasizing its ongoing commitment to office and outpatient care in the community, the SVS Section on Outpatient and Office-Based Care (SOOVC), now named the Section on Ambulatory Vascular Care (SAVC), developed an outstanding OBL Handbook released to SVS members in 2024. The SVS recognizes the value and importance of research and promotes data collection, analysis and new research in the outpatient space. This helps with safety and cost-effectiveness and expands patients’ access to care.
Meeting member needs and challenges
Each month of the year brings new ideas, energy and opportunities, as well as new challenges and threats that make strategy and change a universal constant for the SVS. The pace of change is accelerating and has become its own unique challenge. The SVS leadership remains committed to continue evolving the Society to address new opportunities and challenges, which is a challenge in itself, given the need to prioritize finite resources. Members contribute every dollar through dues, donations or program support, an essential lifeline to help the SVS continue to embrace new opportunities. The SVS is very fortunate to have a diverse revenue portfolio, relying on member dues for only 14% of its revenue, but each of those dollars is vitally important.
The SVS membership continues to grow and diversify, with total membership now closing in on 6,400 members.
The 2022 establishment of the Young Surgeons Section (YSS) has fostered and accelerated value and engagement for Early Career members, and, in 2024, the SVS approved a new Senior Section to maintain membership, value and engagement amongst later-career members. Many thanks to Enrico Ascher, MD, for his leadership in this.
The value and strength of SVS Affiliate membership is substantial—with over 500 vascular physician assistants (PAs), nurse practitioners and nurses—and essential as the SVS sculpts the future of vascular care delivery. In 2024, the SVS convened an Advanced Practice Provider (APP) Task Force to discuss future models for integrating the engagement of all APPs working with vascular surgeons.
Another milestone in 2024 was the development and acceptance by CMS of a new vascular quality measure now up for public comment. If accepted, this will be a new measure developed by vascular surgeons for
In 2023–2024, hundreds of SVS members heard about the translation of the global chronic limb-threatening ischemia (CLTI) guidelines, Best Endovascular vs. Best Surgical Therapy in Patients with Critical Limb Ischemia (BEST-CLI) trial results, as well as updated varicose veins clinical practice guidelines. To further this work, the SVS was awarded a $100,000 educational grant from the Council of Medical Specialty Societies (CMSS) to further these transla-
Some five years ago, the SVS embarked on a series of assessments and potential governance changes to increase the diversity of perspectives. In 2024, the last of these governance changes—a change to the structure of the SVS Executive Board—was ratified by the voting membership and implemented. Congratulations to new EB members Chelsea Dorsey, MD, Yazan Duwayri, MD, Katherine Gallagher, MD, Vikram Kashyap, MD, and Robert Molnar, MD, who now join the SVS officers.
If quality is the core of the SVS, education is its cornerstone By all accounts and perspectives, the Vascular Annual Meeting (VAM) 2024 in Chicago
Kenneth M. Slaw
(1) President Joseph Mills, MD, at VAM 2024; (2) Highway to Health; (3) Congress beckons; (4) Keith Calligaro, the driver behind the compensation survey; (5) The OBL Handbook
was superb and groundbreaking, thanks to Andres Schanzer, MD, who finished his term as VAM Program chair. More than 92% of VAM 2024 attendees rated the educational programming as excellent or good; international attendance doubled in size from 2023 to 2024; and a track specifically designed for the early career surgeon was piloted, leading to the highest participation from young surgeons of any VAM to date. VAM also introduced a track specifically designed for medical students/general surgery residents, specific educational programming and networking opportunities, and a Residency Fair with over 150 residency programs represented. We hope to see you all in New Orleans!
Beyond VAM, the Education Council, led by Kellie Brown, MD, has continued to develop innovative education opportunities for members.
The third Annual Complex Peripheral Vascular Interventions (CPVI) Hands-On Skills Course had another successful year, featuring 20 trainees able to attend with scholarship support.
The SVS launched its new and updated VascuLEARN learning management system (LMS), which is now the home for accessible webinars, micro-learning and short videos. This creates a one-stop online hub for educational content. Over the past three years, 1,365 vascular experts and trainees have taken advantage of these resources.
The SVS launched the sixth edition of the Vascular Education and Self-Assessment Program (VESAP6), with over 700 users
burning through the questions and testing their knowledge.
Coding and reimbursement remains one of the top non-clinical content areas requested in the 2021 and 2024 education needs assessments. In addition to the live Coding Course, the SVS launched three new on-demand foundational videos and created a forum for submitting monthly questions, ensuring your questions are answered. The Coding Course will likely sell out quickly, with the potential of new lower extremity codes coming in 2025, so watch for registration in late spring.
The SVS held its fifth successful Leadership Development Program, with 96% of cohort five participants reporting they intended to incorporate changes into their practice following the course. Over the past five cohorts, the SVS has trained over 140 vascular surgeons in leadership skills. Registration for Cohort 6 will launch in April.
vascular surgeons, vascu lar nurses, vascular PAs and podiatrists. The curriculum consists of on-demand videos and in-person hands-on workshops held in conjunction with VAM 2025, 2026 and 2027.
Another milestone was hit in our scholarly journal publishing. Thanks to the leadership of Alan Dardik, MD, staff member Tyler Cosgrove, and our publisher Elsevier, the Journal of Vascular Surgery-Vascular Science (JVS-VS) has been indexed and will now have an impact factor, helping to establish it as the premier journal for vascular basic science research.
Coding and reimbursement remains one of the top nonclinical content areas requested in the 2021 and 2024 education needs assessments
Finally, the SVS launched a new Wound Care Curriculum in February 2025. This collaborative effort between the SVS, the Society for Vascular Nursing (SVN), and the American Podiatric Medical Association (APMA) includes faculty members who are
Our SVS Foundation, led by Joseph Mills, MD, and staff members Catherine Lampi and Sarah Murphy, is evolving, thriving,and garnering renewed attention through a “lights out” 2024 Gala at the Museum of Science and Industry at VAM, where the new James S. T. Yao Lectureship was announced. Whether they attended our annual gala, walked for PAD awareness during the annual Vascular Health Step Challenge, shared their story during the Voices of Vascular campaign or made a charitable contribution, their support has been invaluable in advancing
our mission. The Voices of Vascular campaign highlighted the accomplishments of 17 SVS members; Step Challenge donors came together to fund a new Vascular Care for the Underserved grant that will support an innovative project that addresses the unique challenges faced by underserved populations affected by PAD; SVS donors stepped up during Giving Tuesday, smashing our fundraising goal, raising more than $34k in 24 hours.
Finally, SVS member volunteers have pressed forward to sculpt the future with numerous new task forces in 2024, including in pediatric vascular care, patient engagement, innovation in vascular care, and clinical trials. The Vascular Board Certification Task Force is completing an assessment of progress made over the past 20 years, looking toward a future that strengthens the specialty.
Alignment to ‘True North’
Last year was one of significant achievements for the SVS, its Foundation, PSO and PAC. We hope you are as proud of these accomplishments as we as your staff are.
As we look down the lens of 2025 and the year ahead, the SVS remains steadfast in its commitment to championing quality and safety in patient care, the best science in the field, and advancing vascular surgery through meaningful collaboration, innovation, and letting the world know how special you are as vascular surgeons. I extend my sincere gratitude to each member for their invaluable contributions.
‘It needs to no longer be seen as late-stage therapy’
Two prominent vascular surgeons discuss a rising tide of evidence pointing toward benefits of adjunct use of cyclically pressurized Topical Wound Oxygen (TWO2) therapy in the treatment of vascular ulceration.
The best way to think about modern-day limb salvage, says Anahita Dua, MD, is through the analogy of what would constitute a fully functioning car. Underpinning the chassis, you might have the perfect set of tires, that never puncture, to enable motion, she relates, but without a multitude of other vital components—an operational engine, safe, working seatbelts—the vehicle is going nowhere. Without them, “that is not a car,” Dua explains.
Substitute in limb salvage for the car, and a similar picture emerges, the associate professor of surgery at Harvard Medical School in Boston and a vascular surgeon at the Massachusetts General Hospital continues. “The approach to limb salvage has historically been very much, ‘What is my silo? I’m a vascular surgeon. I am good with blood flow. I am going to increase your blood flow.’ That’s great, but if someone is not doing good wound care, and someone is not putting you on antibiotics, and you, as the patient, are not stopping smoking, your leg is going to get amputated.”
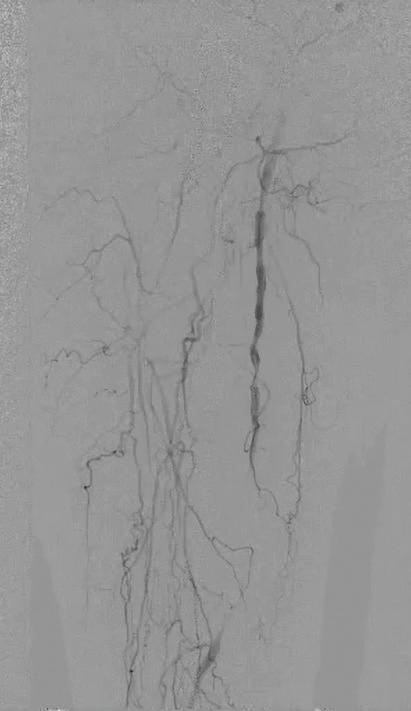
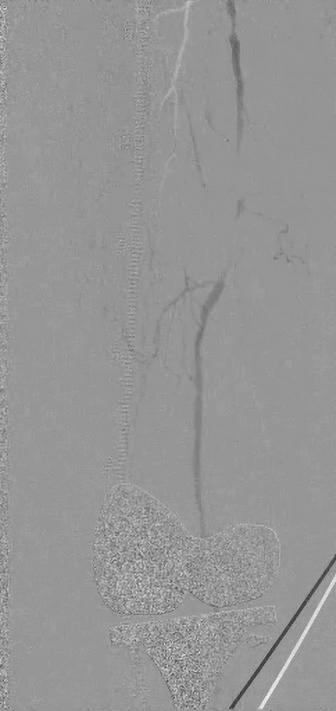
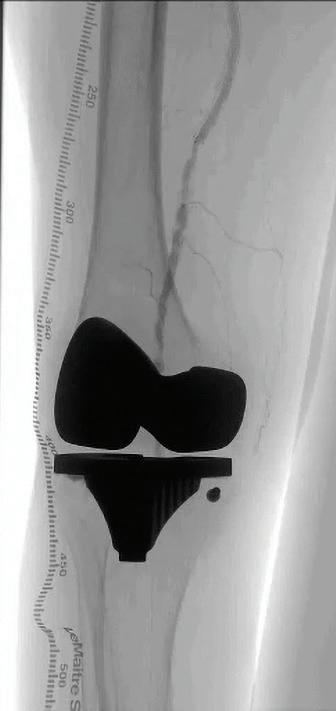
In the case of the car, an operational vehicle is more than the sum of its parts. In the case of limb salvage, the contributions of a multidisciplinary team yield better results than individual specialties operating in isolation. Fitting squarely into the heart of this picture is the role of patient-applied at home TWO2 therapy (AOTI) in aiding ulcer healing following revascularization. Dua points to a classic case to demonstrate how crucial the therapy is to successful wound salvage (see figures 1–4).
“This patient, a 68-year-old male with diabetes and end-stage kidney disease [ESKD], is absolutely someone who would have been amputated, but on whom we carried out a deep-vein arterialization [DVA] procedure, allowing blood flow to get to the foot,” she says. “That process takes time, and, during that time, you don’t want the wound to disintegrate, get infected and the person end up getting amputated. This being a patient with diabetes and ESKD, we are talking about the worst of the worst type of blood vessels. In spite of that, we healed this wound with, of course, great wound care: good blood flow was formed from the DVA, and then came TWO2 therapy.”
David Dexter, MD, an assistant professor of clinical surgery at Eastern Virginia Medical School and a vascular surgeon at Sentara Vascular Specialists in Norfolk, Vir-
ginia, sees the role of multimodality TWO2 therapy in a similar way. In the setting of arterial disease, he explains, both macroand microvascular problems need to be tackled. An array of major technologies exists for the former while therapies for the latter remain in their infancy, Dexter says, but there is also the issue of ischemic skin changes—and these “need to be addressed in order that continued ongoing tissue loss be reversed and healed.”
“We have the ability to revascularize a limb that’s functionally dead, but without the ability to heal the wound after we’ve removed necrotic tissue after we’ve fixed the macrovascular problems, we’re at a loss,” he explains.
That’s where Dexter sees TWO 2 performing a crucial role, not only in tackling the totality of the disease process but also in returning patients to normal, everyday life.
“First, I would say it needs to no longer be seen as late-stage therapy to bring wound care adjuncts like TWO2 in,” he continues. “There must be a plan: that when somebody comes in with CLTI [chronic limb-threatening ischemia] and ulceration, or with gangrene that will lead to tissue loss, we say, ‘How do I get this patient back to a functional foot that they can walk on?’ If you have a wound that you’re going to create, do you have the ability to surgically close this wound, or will advanced local, topical therapy assist me in that? Because the longer the wound is open, the longer the patient is off their extremity floor and non-ambulatory, the worse they are going to do from a protoplasmic standpoint.”
have made a difference? The studies show that when you randomize patients to two groups, the ones who got TWO2 therapy did better.”
“It needs to no longer to be seen as late-stage therapy to bring wound care adjuncts like TWO2 in”
Both Dua and Dexter are unequivocal in how TWO2 functions to help heal wounds. Referencing the same case involving the 68-year-old diabetic ESKD patient who underwent DVA and then received TWO2 therapy, Dua tackles the counterargument of the same patient receiving the same treatment plan, minus TWO2
DAVID DEXTER
An international randomized controlled trial [RCT], conducted by Robert G. Frykberg, DPM, and colleagues, showed that cyclical pressurized topical oxygen therapy adjunctive to optimal standard of care is significantly superior to standard care alone in healing diabetic foot ulcers (DFUs) at 12 weeks and one year. For Dexter, the venous side, on the other hand, reveals what he describes as the flip side of the coin. “The number is debatable, but 15% of all venous ulcers do not heal, have not healed and likely will not heal, and they become a chronic health problem for these patients,” he says. “They don’t lead to amputation, they are ambulatory, they are at their normal state of health but still have this wound that changes their everyday function and everyday life,” he continues, adding, “that’s where the increased oxygenation uptake of giving local topical hyperbaric oxygen therapy with some moisture directly to a wound comes in. If you can heal half of that 15%, that’s a huge magnitude of patients we have helped.”
“What if you did everything that you did, but you didn’t do the cyclical compression oxygen therapy?” she explains. “Would it
Dexter tackles the subject of how oxygen therapy is traditionally viewed: full-body hyperbaric oxygen delivered in dive tanks. “I don’t think any of the skeptics argue with the math,” he says. “There is very clear ev-
(1) Wagner Grade 4 s/p transmetatarsal amputation with osteomyelitis and cellulitis; (2) Negative pressure wound therapy discontinued and topical oxygen therapy initiated; (3) Topical wound oxygen therapy continues, with demonstrated reduction in wound size and appearance of healthier wound bed and reduced edema; and (4) Wound continues to progress in preparation for wound closure
idence you can hypersaturate with hyperbaric pressure oxygen and deliver more to wounds both intravascularly and directly through the skin surface. From a cost standpoint, it becomes prohibitively expensive to dive, or pressure chamber, the number of patients we have. We have restricted that resource across the world for three generations. So the reason we don’t have data is it’s impossible to get enough people into trials doing things like this.
“TWO2 therapy allows at-home application for a fraction of the cost, both to the payor and to the patient. We are in a position where we are ready for an appropriately powered randomized controlled trial in venous leg ulcers [VLUs], to support existing published observational cohort studies, looking at wound healing rates and wound healing percentages.”
Fundamentally, says Dua, returning to her earlier argument, the types of wounds in question here are not those that “would have healed anyway.” These are vascular patients who see marked wound healing through the use of TWO2 therapy in the setting of severe vascular disease, she explains.
“If I told you the wound would heal seven days faster than if you didn’t use it, but it costs a million dollars, you’re going to say, ‘You know what, I’m just going to wait the week and heal it.’ Why would I spend a million dollars, right? That’s the whole point about cost effectiveness, but all of those situations are about wounds that are ‘going to heal anyway.’ These wounds I’m talking about would have probably progressed and the patient may have become an amputee.”
The therapy won’t work for every patient, every time, Dua adds. Like the tires on a car, “this is an adjunct, a piece of the puzzle that is going to help you save legs” and obviate wound complications down the road before they get the chance to develop.
Anahita Dua
David Dexter
Open surgery, endovascular intervention and robotics: The coming ‘third revolution’ in vascular surgery
The 2025 Southern Association for Vascular Surgery (SAVS) presidential address featured the hashtag phrase #OnlyUs, a allusion to the specialty’s “unique” differentiator. By Bryan Kay
SAVS 2024–25 President Alan Lumsden, MD, returned to a familiar recent theme for his address to the 49th annual meeting of SAVS in St. Thomas, the U.S. Virgin Islands (Jan. 22–25): the topic of robotics in vascular surgery.
The twist this time around was that it was his SAVS presidential address, and he carved his pitch for robotic vascular surgery in bolder terms: digital surgery and robotics will form the third revolution in the specialty in the coming years. Only vascular surgeons are capable of being positioned at the epicenter of open surgery (the first vascular revolution), endovascular intervention (the second) and robotics, he said, “working in that space where we can integrate these things, which I think is going to allow us to be branded differently, to market us differently and will fundamentally differentiate us.”
Lumsden, the medical director of Methodist DeBakey Heart and Vascular Center at Houston Methodist in Houston, Texas, said robotics were the epitome of digital surgery and are “going to change the way we practice.” Referencing the long-running Pumps & Pipes collaboration between Houston industries sparked by a conversation between Lumsden and an oilfield engineer, he told SAVS 2025 that a lot of the solutions to vascular surgery’s problems “exist in somebody else’s toolkit.”
He said, “I submit to you that you’re going to see in the next few years digital surgery and robotics as the third revolution, and I think you’re eminently capable of managing that,” coining the social media phrase #OnlyUs in suggesting only vascular is poised to pull off the feat.
In the case of the endovascular revolution, the empowering technology was real-time imaging, Lumsden explained. “There were headwinds, so the message to younger people is, ‘Don’t always listen to your seniors, they don’t always know exactly what is going on in the future. So challenge what the dogma is.”
Right now, vascular surgery has two products: open surgery and endovascular intervention, the latter of which is not unique to the vascular specialty, Lumsden said. “Have we gone too far with this?” he asked. Open case volumes are diminishing, with advances in technology “that we have been good at embracing having a knock-on effect on our volumes.”
Then there is the competition. Interventional radiologists and, crucially, cardiologists, who are “bigger, better organized—and they can control the patients.”
heart of it are the 100–120 fellows per year who join the specialty with a certificate in robotic surgery. “People like me have traditionally said, ‘Waste of time, I’m never going to use that again.’ We are in the endo world—but so are many others.” Robotic surgery, Lumsden said, offers the prospect of combining the “best long-term therapeutic intervention” of open surgery with a superior delivery system in the form of endovascular intervention. “What if we could actually go back to using some of those principles and apply both, and can we do this?” Lumsden tackled the difficulty factor. “How hard is this going to be? Not nearly as hard as going from open to endo: we had no pre-existing skillsets [then]; a lot of headwinds from other people who didn’t really want us to do it; the cost for participation was massive; we didn’t have catheters, we didn’t have wires, we didn’t have imaging.” On the other hand, the robots exist, though there are credentialing challenges and costs to consider.
Fundamentally, he said, this is “uniquely differentiating for the vascular surgery community if we can embrace it.” Integrating imaging gave vascular surgery high volume and low risk, with the patient “actually benefiting from the [endovascular] procedure. You need the same thing from robotics in order to be able to scale it up,” he added.
Lumsden’s “ah-ha moments” over the role played by robotics in vascular procedures, only at the hands of other specialists, are well-documented. In that vein, he alluded to the vascular “firemen” concept, in which vascular surgeons come to the aid of other specialties. “Increasingly you and I are not going to have to deal with problems that are being generated unless we learn how to do this,” he said. “A lot of the procedures that we need to incorporate into these robotic training programs already exist. And we have to focus on how we bring this together. The gynecologists are using it; the urologists, the thoracic surgeons are using it; the cardiac surgeons are using it. Need I say more?”
“The gynecologists are using it; the urologists, the thoracic surgeons are using it; the cardiac surgeons are using it. Need I say more?”
ALAN LUMSDEN
Displaying a Venn diagram showing the intersecting realms of open surgery, endovascular intervention and robotics, Lumsden stated that “only you and I can play in this pace.” The “secret weapon” at the
Key to developing a robotic surgery program is identifying who on the team has the largest skillset, and case volume needs to be pushed on to that individual who is able to perform the procedures safely, Lumsden said.
“There needs to be graded risk.” A mistake in the robotic world “is leaping to the aorta too early,” he observed. “Gradually increase the skillset,” he said.
The challenge remains that there is no indication for vascular on the existing robot, Lumsden pointed out, citing the need for a database to collect cases with a view to achieving Food and Drug Administration (FDA) approval.
“There are a lot of different tools that we are completely oblivious to but your fellows coming into your programs are well aware of, and that’s the advantage we’ve got,” he added.
MAIDEN ROGER M GREENHALGH LECTURE BRINGS ROBOTICS INTO GLOBAL FOCUS
THE WORLD FEDERATION OF Vascular Societies (WFVS) late last year staged its inaugural Roger M. Greenhalgh Lecture in honor of his work as pioneer in the field of vascular surgery.
The memorial lecture took place during the 31st Annual Meeting of the Vascular Society of India in Jaipur, India (Oct. 17–19), and was presented by Alan Lumsden.
Fittingly, the talk focused on the frontier-pushing topic that was also the subject of the SAVS 2025 presidential address: robotic vascular surgery and artificial intelligence (see opposite).
Like Greenhalgh, Lumsden hails from the United Kingdom and is known for pushing the envelope in the field of vascular surgery.
Lumsden’s team at Houston Methodist DeBakey Heart & Vascular Center is at the vanguard of efforts to bring robotics into the vascular surgical space.
In the lecture, entitled “Robotics and AI: Next revolution in vascular surgery,” the chair of cardiovascular surgery outlined a roadmap for bringing robotic vascular surgery into the fold of clinical practice.
Lumsden referenced his moment of clarity around the concept, how he realized major vascular operations were being handled robotically by other specialties, and how vascular surgery must not miss the boat.
He looked at ways of evaluating feasibility; selecting faculty with the necessary skillset to carry out robotic procedures; mitigating risk in getting teams up to speed; identifying high-frequency, low-risk procedures; expanding the pool of procedures that can be performed; using training resources to test in cadavers; and obtaining Food and Drug Administration (FDA) approval in order to obtain a vascular indication.
Lumsden cast robotic vascular surgery against the current treatment landscape of open surgery versus endovascular intervention. With open surgery, he said, the core therapeutic component is both “excellent and proven”, while the delivery system—via open exposure—is “unacceptable.” Endovascular treatment, on the other hand, bears an “excellent”, minimally invasive delivery system, but a “less durable” core therapeutic component. The question becomes, he said, whether robotics can provide an excellent delivery system while retaining an excellent core therapeutic component.
Bryan Kay
Alan Lumsden
How likely are your surgical patients to have disruptive bleeding?
COMMENT& ANALYSIS
The torrid number of hospital mergers and integrations do not create value for our healthcare system
By Bhagwan Satiani, MD
It is now common to see headlines like “When hospital prices go up, local economies take a hit” (Wall Street Journal), “Hidden hospital prices harm patients: Can this new pricing tool make a difference?”(USA Today ) or “Hospital mergers and health care price increases: A primer for reporters” (from the Association of Healthcare Journalists). And yet, large mergers and acquisitions (M&A) have continued at a torrid pace. Robert Pearl calls it a “conglomerate of monopolies” pointing out that “the 40 largest health systems own 2,073 hospitals, roughly one-third of all emergency and acute-care facilities in the United States.”
Let me summarize our recent publication in the Journal of the American College of Surgeons 1 My co-authors are David Way, David Hoyt and Chris Ellison. I will be using the term M&A as a proxy for hospital and health system consolidation/integration, and for simplicity will include horizontal (two or more hospitals joined) or vertical integration (hospital and physicians merged) within M&A.
We systematically reviewed 384 of
the 1,297 articles discussing healthcare M&A from 1990–2024. We then selected 37 studies, which measured at least one of three measures of value: quality, price and cost/spending. Some 77% of studies measuring quality of care showed either no change or lower quality of care after M&A. Of the six showing improvement, five showed better care management processes (CMPs) (for instance health screenings, patient satisfaction or more nurse clinicians), and only one showed improved mortality. Some 93% of studies demonstrated increased prices, and 81% focusing on healthcare spending showed either higher cost or no change.
Hospital and health system M&A has continued to trend upwards, purportedly to create operational, strategic and financial value. While the concept of M&A can be traced back to the Mayo Clinic in 1892, “corporatization” has now advanced even in states where it is banned by law due to weak enforcement efforts. Health systems now own about 68% of all hospitals in the U.S., and the
some cases, system ownership may have reduced the care quality. An interesting question is whether the quality of care improves after “vertical integration” (physicians becoming hospital employees). One such study compared 803 “switching hospitals” (hospitals changed to employing physicians) to 2,084 non-switching hospitals, looking at common measures such as riskadjusted hospital-level mortality rates, 30-day readmission rates, length of stay, etc. Matched for year and regions, two years later no improvement was identified between the two groups in four quality metrics.4 Where there has been improvement in “quality,” this has been almost entirely due to process measures, not true outcome metrics that surgeons are used to.
largest health systems own one-third of all hospitals in the U.S. Furthermore, hospitals now employ 55% of U.S. physicians and another 23% are employed by other corporate entities.2
The premise of M&A in healthcare includes: cost savings (economy of scale, elimination of redundancies, better asset leverage), better quality of care (expertise due to access to talent, innovation and best practices, better care coordination and continuum of care, improved outcomes), financial benefits (greater revenue, value chain integration, access to capital and new markets), intellectual capital (health and technology workforce) and stronger branding.
We report that the premise that M&A would result in cost savings by relieving competitive pressure and improving pricecost margins has not been convincingly demonstrated. Furthermore, increased market share, particularly in concentrated markets, has not led to significant and consistent cost savings. When M&A has shown savings partly because of strong negotiating positions with insurers, the savings have reportedly not been passed to commercially insured patients, resulting in higher premiums for the patient and employers. In one study, the average Affordable Care Act (ACA) marketplace premiums increased from 5% to 12% because of higher concentrations of healthcare organizations competing for the same patients.3
Similarly, M&A largely failed to show consistent and significant relationships between M&A and improved quality of care. In most studies we reviewed there was no change after M&A and, in
A recent study by the National Bureau of Economic Research also concluded, after reviewing 304 hospital mergers between 2010 and 2015, that hospital mergers led to higher inpatient and outpatient prices for patients, with 40% of hospitals involved in mergers increasing prices by 5% or more. The American Hospital Association disputed their findings. While we did not measure the extent of price increases, a 20–40% increase in prices following horizontal integration and a 15–33.5% increase after vertical integration have been reported. The Urban Institute tied hospital concentration to debt on household financial well-being and health across the U.S. They report that medical debt as indicated by credit card reports in 2022 has been a major burden for almost 27 million U.S. consumers.
Of concern is the deluge of hospital M&A leaving markets susceptible to
In most studies we reviewed there was no change after M&A and, in some cases, system ownership may have reduced the care quality
antitrust scrutiny by state and federal regulators for monopolistic behavior. One study by Zack Cooper pointed out that only 1% (13 of 1,164) of mergers of acute-care hospitals between 2002 and 2020 had enforcement actions taken by the Federal Trade Commission (FTC). The lax antitrust enforcement has not gone unnoticed. There has been a recent backlash against hospital mega-mergers. The FTC and Department of Justice (DOJ) have started more enforcement
actions by asking for a request for information (RFI) to collect more information about corporate and private equity control over healthcare services. However, their success so far with litigation efforts is mixed at best.
Our study has several limitations detailed in the manuscript, chiefly the fact that most studies do not have consistent definitions for cost/spending, price and quality of care, making it difficult to arrive at valid comparisons or definitive conclusions. This is because the true cost is either not known or not shared, and prices are misleading. Despite efforts at transparency, our healthcare system remains opaque. Hospital care accounts for close to $1.6 trillion, or almost a third, of our total healthcare expense of roughly $4.9 trillion. However, not many hospitals or service lines know or disclose how much they spend (not billed or charged amount) on each patient. Do we have national, consensus-based true quality measures, regardless of payor, which every hospital, ambulatory surgery center (ASC) or office-based lab (OBL) should be required to disclose? Only a single study in our systematic review showed improved mortality, whereas even CMPs, which are essentially payor incentive measures, were improved in six, but either worse or showed no change after M&A in 20 of 26 studies.
Some but not most M&As in our review have indeed demonstrated value. Can hospital M&A achieve value for our healthcare system and patients given the right combination of changes? Yes. An example may be to rescue failing hospitals in “hospital deserts” in poor areas or rural hospitals that need financing for upgrades, new technology, or physician coverage. However, although the evidence is mixed, we do not find that the past 20 years of M&A have achieved significant and consistent value in terms of improved quality, reduced cost/ spending, or price. It appears that M&A alone is insufficient to lead the U.S. to a value-based (quality/cost) healthcare system and “cannot be achieved through mergers alone without the infrastructure, methodology, and discipline to achieve this state of value.”1
Can physicians make a difference in leading our healthcare system to value? I believe so. There is enough evidence to support physician executives successfully leading healthcare organizations. We laid out some necessary skillsets to lead healthcare systems almost 15 years ago.5 There are recent examples of successful physician CEOs of large health systems.
Joon Sup Lee, MD, CEO of Atlantabased Emory Healthcare has achieved a “16% revenue spike after a leadership reboot” within two years. Neurosurgeon
Steven Kalkanis went from chair to chief academic officer and senior vice president, then CEO of the medical group before he was appointed CEO of Henry Ford Hospital. These are good examples of the path to CEO roles.
The increasing complexity of healthcare “requires leadership and management competencies encompassing systems thinking, self-awareness, selfmanagement, social awareness, and relationship management domains.”1
The scope of learning and experience required for a CEO role is broader than obtaining an MBA degree. There is no requirement to be a financial wizard. A good understanding of budgets and financial statements is enough. Leadership and soft skills are much more important.
The leadership pipeline can be facilitated by fast-tracking physicians interested in a leadership track. My most meaningful professional endeavor has been to start the Faculty Leadership Institute and help train faculty interested in the leadership track. In younger hands now, our medical center is in its 13th year of training faculty in leadership skills.6 In a senior executive dyad structure, wellrounded physicians trained in leadership skills should be given hands-on experience and the independent authority to commit to a patient-centered quality and safety
culture, and change processes to allow evidence-based care. Physician leaders need to be able to get back to our roots of being able to effect change and ensure that the patient comes first. Physicians and other clinical leaders leading qualityof-care efforts should be at par with senior executives and reporting to health system boards directly, whose job it is to monitor quality. It seems to me a much better return on investment when artificial intelligence can be realized to arrive at cost, spending and price transparency in our massive healthcare system. Someone please send a tweet to Elon Musk (@ elonmusk) and see if he has time with his numerous other interests! Be sure to copy me, @SatianiBhagwan
BHAGWAN SATIANI is an associate editor for Vascular Specialist
SAME RELIABILITY AND COST EFFECTIVENESS OF THE ORIGINAL TQI
VTI’s single-use surgical Doppler probes eliminate reprocessing, providing a higher degree of performance reliability and reduced costs. Scan the QR code to learn more.
NEW PORTABILITY FEATURES
Smaller size, an IV pole mount and a handle allow for easy transport
NEW FOOT PEDAL
The modern design allows for a foot pedal to provide increased control from the surgical field
COMMENT& ANALYSIS
CONTINUED FROM PAGE 17
CORNER STITCH
BECOMING A COMMUNITY-ENGAGED VASCULAR SURGEON
By Lindsey Olivere, MD
At the end of my intern year, I was tired. It had been a long year of rounding, placing orders, seeing consults and refining basic suturing skills on primarily general surgery rotations—an experience not dissimilar from many of my fellow integrated trainees. I was looking forward to attending the 2022 Vascular Annual Meeting (VAM), not only as a reprieve from intern responsibilities, but also as a mental reset and reminder of why I chose to become a vascular surgeon. I stuck around until the end of the meeting for one of the final Saturday sessions, which I had been eagerly anticipating: “Improving Vascular Care in Underserved Communities.” In this small conference room, I heard about truly amazing community engagement and outreach projects in Oklahoma, Sacramento, Houston, San Antonio and Morgantown (among others). I was incredibly inspired by the passion and perseverance of the men and women who shared their successes and failures, in building these programs and initiatives, primarily with the goal of improving limb salvage in the highest-risk communities.
It was the first time I had ever considered what it truly meant to be a community-engaged vascular surgeon. I had spent four years learning about healthcare disparities as a medical student, another year experiencing them as a bright-eyed intern, and I
was preparing for a lifetime of justifying to family and medical colleagues why I chose a field where I was seemingly fighting a losing battle against amputations. It was beyond exciting to know that mentors in the field were also ready to do something to challenge and change the status quo.
In the years since I was so impacted as an audience member, I have continued to follow the progress of the growing number of programs and outreach initiatives aimed at improving awareness of vascular disease and promoting limb salvage. It continues to inspire me that we, as surgeons, can become leaders, not only in the operating room, but also in the community and in guiding multidisciplinary teams to make a real difference in patient care.
A growing number of publications and general publicity and financial support from the SVS, and organizations like the Foundation to Advance Vascular Cures and the American Limb Preservation Society, continue to promote patient-engagement programming aimed at limb salvage.1,2 The community engagement sessions were well incorporated into last year’s VAM. There is consistent buzz about efforts like community diabetic foot screenings, outreach to patients experiencing homelessness,3,4 rural
Senate scrutiny of HHS nominees poses key moment for vascular surgery advocacy GOVERNMENT GRAND ROUNDS
By Dylan Lopez
WHEN IT COMES TO A PRESIDENTIAL administration’s impact on our healthcare system, personnel is policy. So, a presidential transition is always a critical juncture for the direction of our federal government’s healthcare policy. That is especially the case for a transition like this one, where the incoming administration differs from the outgoing administration on so many fundamental issues.
The makeup of the incoming administration’s healthcare policy team, from the top down, will be largely dependent on the Senate’s advice and consent power. So, it will be important for the SVS and its members to advocate and inform senators proactively
cardiovascular education initiatives 5—the list, excitingly, goes on. Even the front page of the November issue of Vascular Specialist touted the novel “Days of Service” at the most recent American Venous Forum and Eastern Vascular Society meetings—a testament to the ever-growing visibility and recognition of building this cadre of community-engaged vascular surgeons.
I am proud that I am now using my academic time to do what I can to learn the necessary skills to engage with my local Pittsburgh community and join forces with existing programming to build awareness of PAD and diabetic foot care. I am collaborating with a multidisciplinary team to improve amputation care at my institution. I am lucky to have mentors who paved the way in establishing programming to provide foot exams and cardiovascular disease education to patients experiencing homelessness that I am now excited to continue and expand. There are, without a doubt, a growing number of patients with diabetes and advanced cardiovascular disease manifestations like chronic limb-threatening ischemia (CLTI). Despite improved therapies and novel interventions, the incidence of amputations remains high, particularly in the most socioeconomically disadvantaged communities.6 While this admittedly feels particularly daunting, especially as many of my fellow trainees and I are on the precipice of our careers, it is not the time to be tired. I am so thankful for all those that have paved the way in establishing a precedence for community engagement and continue
about the potential effects of presidential nominations on the practice.
The secretary of health and human services (HHS) nominee is likely to be the subject of much public attention in this space. To the extent that he has any relevant experience for the job, Robert F. Kennedy, Jr., can be described as an advocate around issues that fall more into the Food and Drug Administration (FDA) jurisdiction than issues directly affecting doctors. Kennedy “has been met with mixed feelings on Capitol Hill.” His nomination will draw national attention, and the final vote should be closely contested, as Senate Republicans have been reluctant to express support thus far.
to bring awareness to the role vascular surgeons can play in outreach and beyond.2
References
1. Minc SD, Powell C, Drudi LM, et al Community-engaged research in vascular surgery: An approach to decrease amputation disparities and effect population-level change. Seminars in Vascular Surgery. 2023/03/01/ 2023;36(1):100-113. doi:https://doi. org/10.1053/j.semvascsurg.2022.12.001
2. Kempe K. Vascular surgeons are positioned to fight healthcare disparities. Journal of Vascular Surgery: Venous and Lymphatic Disorders. 2024;12(1) doi:10.1016/j.jvsv.2023.08.013
3. Boelitz KM, Lee J, Pepin MD, et al Utilizing Multidisciplinary Mobile Outreach Clinics To Provide Comprehensive Diabetic Foot Care To Patients Experiencing Homelessness. JVS-Vascular Insights: An Open Access Publication from the Society for Vascular Surgery. doi:10.1016/j. jvsvi.2024.100183
4. Benadda I, Lozano-Franco R, Coutu F-A, et al. A Preliminary Assessment of Barriers and Facilitators to Accessing Foot Care in Homeless Shelters: A Scoping Review. Annals of Vascular Surgery. 2025;111:279289. doi:10.1016/j.avsg.2024.10.026
6. Creager MA, Matsushita K, Arya S, et al Reducing Nontraumatic Lower-Extremity Amputations by 20% by 2030: Time to Get to Our Feet: A Policy Statement From the American Heart Association. Circulation 2021;143(17):e875-e891. doi:doi:10.1161/ CIR.0000000000000967
LINDSEY OLIVERE, MD is a vascular surgery resident at the University of Pittsburgh Medical Center (UPMC) in Pittsburgh, Pennsylvania.
Outside of Kennedy, the next-most senior nominee to watch for vascular surgeons will be Dr. Mehmet Oz, the expected nominee to lead the Centers for Medicare & Medicaid Services (CMS). Oz similarly lacks relevant experience for this job. However, he does have more relevant publicly stated opinions, having made a serious run for the Senate in Pennsylvania in 2022. He has touted his support for Medicare Advantage and has generally
talked about running the service more like a business. Oz’s nomination will also be closely contested, though he has some solid support among key Senate Republicans and even has been met with open minds among some Senate Democrats.
Whether it’s Kennedy, Oz or any of the other incoming Senate confirmation fights at HHS, vascular surgeons have a voice and should be heard. SVS members and supporters can get involved in the SVS’s formal advocacy efforts and reach out to their Senators via constituent feedback, letters to the editor, and staying informed and active.
It is important to remember that it’s not just about the yes-or-no vote to confirm, though that does matter. The Senate’s advice and consent role is also about asking tough questions of these nominees, putting them on the record, probing them, educating them, and fostering a transparent policy-driven process. Senate offices consider their constituents’ opinions, so vascular surgeons need to be engaged now more than ever.
DYLAN LOPEZ is the SVS advocacy and public affairs manager.
Lindsey Olivere
U.S. Congress
POWER AND PRECISION:
INDICATIONS FOR USE
Caution: Federal (USA) law restricts the use of the system by or on the order of a physician. Refer to Directions for Use and/or User Manual provided with the product for complete Instructions, Warnings, Precautions, Possible Adverse Effects and Contraindications prior to
BURNOUT
‘BATTLEFIELD FIRST AID’: A PEER-TO-PEER PRESCRIPTION FOR DEALING WITH ADVERSE SURGICAL OUTCOMES
By Bryan Kay
“BATTLEFIELD FIRST AID” AFTER a colleague has a bad case as the cornerstone of peer-to-peer support in vascular surgery was the feature of the recent Jesse E. Thompson, MD, Distinguished Guest Lecture at the 2025 Southern Association for Vascular Surgery (SAVS) annual meeting in St. Thomas, the U.S. Virgin Islands (Jan. 22–25).
John Eidt, MD, the chief of vascular surgery at Baylor, Scott & White Heart and Vascular Hospital in Dallas and a former SAVS president, asked attendees to consider what they do in response to an adverse outcome during the course of their clinical care; how they treat their colleagues after they have a bad case; whether they have sought professional counseling after an adverse surgical event; and how they teach trainees to deal with these adverse events.
“We all have patients who have left an indelible mark on us,” Eidt told those gathered. “The asymptomatic carotid that has a stroke in the recovery room. The routine EVAR that goes bad. The claudicant that winds up with an amputation.”
He highlighted the importance of peer support and not suffering in silence. “In vascular surgery, our actions and inactions have immediate consequences,” he said. “There is no delay like a recurrent hernia. There is no shifting blame. Our memories may be vivid and precise and filled with details like patients’ middle names, and children’s faces
CAREER
and spouses’ occupations. Sometimes we can see the operations like it was yesterday, but, in other cases, we just see fragments, those that haunt our memories and invade our dreams, though we never fully forget.”
Eidt raised the specter of the “second victim” concept, which describes the doctor who makes a mistake and needs help too. Under this definition, he described how in the absence of mechanisms for healing, physicians find dysfunctional ways to protect themselves. They respond to their own mistakes with anger, projection of blame and may act defensively or callously, and blame or scold the patient or other members of the healthcare team, Eidt said. “Distress escalates in the face of a malpractice suit. In the long run, some physicians are deeply wounded.” They may lose their nerve, burn out, or seek solace in alcohol or drugs, he added.
“I think that’s an unfortunately accurate picture of how sometimes we do respond to these situations.”
But “second victim” is an ill-fitting term in this arena, Eidt continued. “Victim” most commonly refers to those who experience devastating loss at the hands of others, he pointed out. “Placing both clinicians and patients in this category after medical error seems erroneous given the degree of intentionality and violent harm that the word victim connotes,” Eidt said. “It’s not really a good illustration of how we all experience these events.”
The potential consequences from bad outcomes for physicians are well reported: for instance, the literature documents that more than 90% of surgeons reported an emotional impact from adverse surgical outcomes. These included anger, anxiety, guilt, shame— “all the stuff you know you’ve felt after a bad case,” Eidt said. “It can mess up your sleep, how you’re thinking, even how you relax. And it can change practice patterns if you stop doing evidence-based medicine and start doing anecdote-based medicine.”
Women and minorities might carry added burdens, he considered. “It’s bad enough for a White guy, but if you have extra scrutiny, it may even be harder.”
In light of all of this, the question becomes how surgeons deal with the reality of facing up to bad outcomes, Eidt continued. “The most common way surgeons want to deal with these things is to talk to each other. We have a lot of evidence that adverse clinical events have a significant bad impact on you,
but we tend not to seek professional help. We know the reasons why: there is so much stigma, all kinds of negative connotations.” What surgeons do like is peer-to-peer support, he said. “It’s got to be confidential, available 24/7. They are almost inevitably, though, not point of care.” Surgeons also prefer something longitudinal, as well as thoughtful critique, with questions like, “What would you have done? How can I do better?” Eidt added.
There are four tiers of peer support, with “self” peer support, hospital-level structured support and professional counseling among them. But it is the second tier where the greatest value might be yielded, Eidt argued: that is, battlefield first aid. At the base of this approach, he said, is “reaching out to each other, listening, offering support, providing acceptance, offering trust, confidentiality, providing a safe space, normalizing talking about feelings.”
There are also don’ts, he pointed out. That means don’t isolate, pry, place blame, try to fix it, minimize it or give false reassurance, Eidt reasoned. “What we tend to do is pretend it didn’t happen. Everyone knows it went south, but no one is talking about it, and that creates more paranoia.”
“We all have patients who have left an indelible mark on us. The routine EVAR that goes bad. The claudicant that winds up with an amputation”
JOHN EIDT
Vascular surgery trainee autonomy driven by well-being, study finds
A NEW CROSS-SECTIONAL ANALYSIS AS PART OF the SECOND trial found that most vascular surgery trainees are satisfied with their operative and clinical autonomy but that those who are not had increased odds of professional dissatisfaction, personal life dissatisfaction, burnout, thoughts of attrition and suicidal ideation.
The findings were presented during the 2025 Southern Association for Vascular Surgery (SAVS) annual meeting held in St. Thomas, the U.S. Virgin Islands (Jan. 22–25), by Margaret Reilly, MD, a vascular surgery resident at Northwestern Medicine in Chicago.
The research team sought to address concerns around the graduated autonomy of trainees as training paradigms shift and increasing comorbidities among vascular disease patients. They analyzed trainee perceptions of autonomy and evaluated associations with wellness metrics in a voluntary survey performed after participants took the Vascular Surgery In-Training Exam (VSITE) from 2020–2024.
In assessing learning environment domains, the analysis looked at efficiency and resources, organizational control, mistreatment and faculty engagement.
The primary outcome measure was burnout, with secondary measures including suicidal ideation, thoughts of attrition, professional satisfaction and personal satisfaction.
Autonomy was evaluated around whether trainees have appropriate amounts of time in the operating room and participation in clinical decision making, as well as level of operative autonomy. The survey involved the Likert rating scale, dichotomizing between “disagree” and “agree.”
The analysis did not find any differences in satisfaction of autonomy based on postgraduate year, Reilly reported, “and this was also the case when we grouped trainees based on seniority.”
She continued, “We did find significant differences in gender, where male trainees were more likely to be satisfied with their autonomy as compared to female trainees. And this was also true when comparing community and academic programs, where trainees at community programs were more likely to be satisfied with their autonomy as well.”
Bivariable analysis of learning environment factors and their associations with satisfaction with autonomy revealed significant differences for all learning environment factors, Reilly told SAVS 2025. Among them, the results showed that trainees who felt that their educational time was protected, who felt belonging and cooperation among trainees and
support staff, and who felt they had adequate and appropriate attending mentorship were all more likely to be satisfied with their autonomy.
Multivariable logistic regression of predictors of training autonomy showed that satisfaction with faculty engagement was associated with 4.8 times more odds of being satisfied with the level of autonomy, while being satisfied with efficiency and resources in a training program was associated with 10 times more odds of being satisfied.
“We then evaluated wellness metrics and their associations with satisfaction with autonomy,” Reilly said. “We found that trainees who were satisfied with their autonomy were less likely to report suicidal ideation, less likely to report thoughts of attrition, and also less likely to have weekly symptoms of burnout.
“When looking at work-life integration factors, we found that trainees who were satisfied with their autonomy were more likely to be happy with their decision to pursue vascular surgery and with their personal life, and also more likely to be satisfied with their ability to perform personal health maintenance tasks.”
Future analysis of surgical milestones and Entrustable Professional Activities (EPAs) “will ultimately help to contextualize the possible interventions that will help improve trainee perception of autonomy,” Reilly concluded.—Bryan Kay
John Eidt
Margaret Reilly
CAROTID STENOSIS
ROADSTER 3 provides
key evidence that ‘goes beyond registry data’ on TCAR-related stroke rates
By Jamie Bell
THIRTY-DAY RESULTS FROM THE ROADSTER 3 study have demonstrated that transcarotid artery revascularization (TCAR) is a safe and effective approach in patients who are deemed to be standard risk for experiencing adverse events related to carotid endarterectomy (CEA)—part of findings presented at the 2024 Vascular Interventional Advances (VIVA) conference (Nov. 3–6) in Las Vegas by Meghan Dermody, MD, chief in the Division of Vascular Surgery at Penn Medicine Lancaster General Health, in Lancaster, Pennsylvania.
Recently speaking to Vascular Specialist, she emphasized the importance of being able to “quote stroke rates that go beyond registry data” for this patient population.
“Since we are unable to conduct an adequately powered randomized controlled trial to study TCAR against other modalities to treat severe carotid stenosis, and especially without a TCAR arm in the forthcoming CREST-2 trial, it is imperative that we study TCAR in a standard-risk population—ideally in a prospective fashion,” Dermody said. “ROADSTER 3 is an FDA [Food and Drug Administration]-required, post-approval study, but it allowed us the opportunity to acquire data from across the U.S. with multiple generations of surgeons performing the procedure.”
Touted by Silk Road Medical (Boston Scientific) as the first-ever prospective, multicenter trial evaluating the safety
LARGE DATABASE STUDY FINDS NO DIFFERENCE IN OUTCOMES BETWEEN THREE CAROTID SHUNTING STRATEGIES
By Jocelyn Hudson
A NEW VASCULAR QUALITY
Initiative (VQI) data analysis, recently published in the European Journal of Vascular and Endovascular Surgery (EJVES), has found no statistically significant differences between three carotid endarterectomy (CEA) shunting strategies regarding in-hospital stroke and death rate, including in patients with contralateral carotid occlusion or recent stroke.
In the journal’s editor’s choice paper, Xavier Hommery-Boucher, MD, a vascular surgery resident at Centre Hospitalier de l’Université de Montréal [CHUM] in Montreal, Canada, and colleagues outline that the study aimed to evaluate in-hospital outcomes after CEA according to shunt usage, particularly in high-risk groups of
and effectiveness of TCAR using the company’s Enroute transcarotid stent system (TSS) in conjunction with its Enroute transcarotid neuroprotection system (NPS) for the treatment of carotid stenosis in standard surgical risk patients, ROADSTER 3 enrolled a total of 344 patients across 53 U.S. sites for intention-to-treat (ITT) analyses. The single-arm study’s primary endpoint is a composite of major adverse events (stroke, death or myocardial infarction [MI]) through 30 days post-procedure, plus ipsilateral stroke from day 31 to day 365 post-procedure, while incidence of cranial nerve injury (CNI) within 30 days post-procedure is described by the authors as a key secondary endpoint.
In ROADSTER 3’s ITT population, 75.3% of patients were younger than 75 years of age, 42.7% were female, and 16.3% had symptomatic carotid stenosis, with a quarter of these symptomatic patients experiencing a neurologic event within the two weeks preceding their TCAR procedure. Dermody and colleagues report that the mean lesion length was 23.3mm, while 47.4% of patients presented with a Type II or Type III aortic arch, and 17.2% of lesions had severe calcification.
lation of standard surgical risk patients treated via carotid revascularization. The company also claims that, in line with the previous ROADSTER and ROADSTER 2 registry studies, ROADSTER 3 demonstrates consistently low adverse event rates across all risk levels.
“Given TCAR is less invasive than CEA and has similar stroke rates with less nerve injury risk, if a patient is able to take dual antiplatelet and statin therapy, and their anatomy is amenable, there is no reason why TCAR shouldn’t be your first-choice modality,” Dermody told Vascular Specialist, outlining how the minimally invasive procedure may fit within existing carotid revascularization paradigms. “But, given the anatomic and physiologic requirements needed for a successful TCAR, naturally, not all patients will be good candidates for this approach.”
“There aren’t enough data regarding surveillance of carotid stents, how or when to treat recurrent carotid stenosis within a stent, or long-term outcomes from TCAR yet” MEGHAN DERMODY
The rate of stroke/death/MI at 30 days in the study’s ITT population was 0.9%—a figure that decreased to 0.6% within per-protocol analyses involving 320 patients. The researchers found that 30-day stroke rates specifically were the sole contributor to these numbers, with no deaths or MIs being reported through the 30-day follow-up. They further relay that the incidence of CNI within 30 days was 0.6% in both the ITT and per-protocol analyses, and that all cases in both of these populations were resolved within six months.
According to Silk Road, this constitutes—to date—the lowest reported rate of adverse event outcomes in a popu-
patients, such as those with contralateral carotid occlusion or recent stroke.
Considering the context for their study, the authors underline a lack of data on the topic of carotid shunting. They note that systematic reviews comparing the three shunting strategies have concluded the evidence is too limited to support one over the others, and that there are no randomized data available on the subject.
She continued: “Personally, I believe the treatment of carotid stenosis needs to be more focused on the lesion morphology rather than the degree of stenosis alone. The amount of calcification within or around the lesion; the amount of irregularity or ulceration to the atheroma; any thrombus burden within the plaque; arterial wall inflammation; and a slew of other anatomic features, should truly be what we base our shared decision-making on in the future. This requires thorough scrutiny of preoperative imaging, specifically an adequately thin-sliced and well-windowed CT [computed tomography] angiogram.”
Dermody and colleagues also note that symptomatic status did not appear to have a statistically significant bearing on the 30-day incidence of stroke/death/MI, which occurred at a rate of 1% in asymptomatic patients (n=3) versus 0% in symptomatic patients in ROADSTER 3’s ITT population, and 0.7% (n=2) versus 0% in its per-protocol analysis.
the study criteria. Of this total, 31,147 were asymptomatic, while a majority of 82,055 were asymptomatic.
Hommery-Boucher et al set out to perform a registry-based analysis. Specifically, they analyzed data from CEAs registered in the VQI database between 2012 and 2020, excluding surgeons with fewer than 10 CEAs registered in the database, concomitant procedures, reinterventions and incomplete data.
The authors note that participating surgeons were divided into three groups based on their rate of shunt use: nonshunters (<5%); selective shunters (5–95%), and routine shunters (>95%). They analyzed primary outcomes of in-hospital stroke, death, and stroke and death rate in both symptomatic and asymptomatic patients.
Hommery-Boucher and colleagues share that, in total, 113,202 patients met
Writing in EJVES, the authors report that 12.1% of the 1,645 surgeons included in the study were non-shunters, while 63.6% were selective and the remaining 24.3% were routine shunters.
The number of procedures in each group was 10,557, 71,160 and 31,579, respectively.
Hommery-Boucher et al reveal that, in the symptomatic cohort, in-hospital stroke, death, and the combined stroke and death rate were not statistically different among the three groups, based on univariable analysis. Similarly, they note that the asymptomatic group also did not show a statistically significant difference for any of the three primary outcome measures.
The authors go on to state that a multivariable model did not show a statistically significant difference for the primary outcomes between the three shunting cohorts and that, on subgroup analysis, the stroke and death rates were not statistically significantly different for patients with contralateral carotid occlusion and those presenting with a
recent stroke. “This paper adds new data collected from a large registry regarding postoperative outcomes related to shunt use during [CEA],” HommeryBoucher and colleagues write in EJVES, remarking that the design of the study enabled comparison between three shunting strategies.
The authors summarize that the results of their study “demonstrated that there was a two-fold increase in the percentage of surgeons using the non-shunting strategy between 2012 and 2020, with no significant difference in outcomes compared with the other two strategies.”
In the discussion of their findings, Hommery-Boucher et al recognize some limitations of their research, including those “intrinsic” to the use of a large database like the VQI.
The researchers conclude that, despite its limitations, their study “could not define a preferential shunting strategy,” leading them to advise that the strategy “should be mainly based on a surgeon’s preference and skillset.” They go on to stress that their study has “provided quality data on the impact of a surgeon’s shunting pattern on postoperative stroke and death rate, particularly for the most at-risk groups.”
Xavier Hommery-Boucher
THE MOST COMPLETE ONE-DAY ENDOVASCULAR CONFERENCE
The 2025 Pacific Northwest Endovascular Conference will offer its signature interactive learning format, 80+ key opinion leaders on faculty, focused breakout sessions, resident competition and Simulation Summit live in Seattle.
PROGRAM HIGHLIGHTS:
• One-day Powerhouse Program
• 9 CME Credit Hours
• Three Focused Breakout Sessions
MAIN SESSIONS
• Aortic – Modern Management
• Lower Extremity
• Venous
• Physician Practice
• Technical Pearls and Tips
• Simulation Summit for Vascular Trainees
• Resident Competition
• Exhibit Hall and Networking
• Industry Satellite Sessions
CONCURRENT SESSIONS
• Updates on Vascular Surgery for Advanced Practice Providers
• Limb Preservation & Wound Care
• The Business of Vascular Surgery
MAY 22, 2025 SIMULATION SUMMIT FOR VASCULAR TRAINEES
Scholarship includes:
• Registration to Summit & PNEC
• Lodging at the Westin Seattle
• Travel reimbursement (U.S.-based)
CHRONIC KIDNEY DISEASE
BEST-CLI TRIAL SPLINE MODEL ANALYSIS BREAKS NEW GROUND IN ASSESSING THE IMPACT OF CKD SEVERITY ON CLTI OUTCOMES
surgery Mahmoud Malas, MD, were delivered during the 2025 Southern Association for Vascular Surgery (SAVS) annual meeting in St. Thomas, the U.S. Virgin Island (Jan. 22–25) and simultaneously published by the Journal of Vascular Surgery (JVS).
SVS FOUNDATION
“We identified GFR of less than 30 as the inflection point that is associated with double the risk of MALE [major adverse limb events] or death and triple the risk of cardiovascular events and all-cause mortality,” presenting author Mohammed Hamouda, MD, a postdoctoral fellow at UC San Diego in San Diego, California, told SAVS 2025.
“We also see that, in the BEST-CLI trial, that those patients on dialysis had very poor longterm survival, which raises many questions of if we need to treat every single patient on dialysis or revascularize them.”
A total of 1,797 patients were included in the analysis, which categorized patients into three groups according to CKD stage: group A includes non-CKD and CKD stages 1 and 2 patients; group B stages 3 and 4; and group C stage 5 and dialysis-dependent patients. Three-quarters of the patients belonged to group A, and 14.7% and 11.5% were in group B and group C, respectively.
Malas and colleagues established that the group C patients had double the risk of amputation with a hazard ratio [HR] of 2.13 (p<0.001), MALE or all-cause mortality (HR, 2.05; p<0.001), and more than triple the risk of all-cause mortality with an HR of 3.40 (p<0.001), compared with group A. In dialysis-dependent patients, endovascular therapy was associated with slightly better survival, but twice the risk of reintervention compared with open surgical bypass, they found.
But, Hamouda elaborated, this National Kidney Foundation staging system of CKD is not designed to investigate surgical outcomes, which then led the research team to carry out a spline analysis in order to establish the significant cutoff at which surgical outcomes in CLTI patients hit statistical significance.
“The idea is that we use GFR as a continuous variable, and against it we plot the hazard of MALE or death,” he explained. “We wanted to see where the GFR hits statistical significance, or where is the inflection point at which the hazard of MALE or death be-
SVS leadership and membership integral to ‘far-reaching’
BEST-CLI trial
By Beth Bales
SUPPORT FROM THE SOCIETY FOR VASCULAR Surgery (SVS) and, later, funding from the SVS Foundation were integral to the BEST-CLI trial, said one of the landmark trial’s leaders.
BEST-CLI sought to determine the best revascularization treatment strategy—surgical or endovascular—for patients with chronic limb-threatening ischemia (CLTI). The trial was initially funded by the federal National Heart, Lung and Blood Institute at the National Institutes of Health (NIH). The Society for Vascular Surgery (SVS), the Society for Clinical Vascular Surgery (SCVS) and a host of other regional and national vascular societies contributed funds toward BESTCLI. The SVS Foundation provided a $100,000 bridge grant at a critical juncture to ensure the trial could run through to its conclusion.
In late 2022, Novo Nordisk Foundation contributed $3.9 million to further fund the investigators to undertake a full analysis of the wealth of data the trial produced.
SVS members Matthew Menard, MD, and Alik Farber, MD, were two of the trial’s principal investigators. They first conceived of the idea in 2007, began preparations in 2009 and received funding in 2013. The trial randomized and followed 1,830 patients between 2014 and 2021, and the headline results were announced in late 2022. BEST-CLI found that surgical bypass with adequate single-segment great saphenous vein (GSV) is a more effective initial revascularization strategy for patients with CLTI who are deemed to be suitable for either an open or endovascular approach. The principal investigators also found that both strategies can be accomplished safely and are generally a very effective treatment for CLTI.
“The work of analyzing the large volume of data we have is ongoing,” said Farber. Many articles have been written
about the trial since the initial publication of data. Vascular Specialist alone has published more than 20 follow-up articles on various facets of the BEST-CLI data. The interest, said Farber, indicates the trial’s significant impact and also highlights the SVS Foundation’s role in funding such critical research.
Menard indicated that “all of the things we have been able to achieve with regard to completion of the trial, as well as analysis and dissemination of the results directly stem from the funding we received during the early phase of our critical need. The SVS Foundation support represented the first contribution at a national society level. Its critical endorsement set the stage for other national societies to follow suit, and then for our industry partners to additionally champion our efforts. It is impossible to underestimate the impact of this critical initial sponsorship.”
Farber said that up to 40 supplemental secondary analyses have either been completed and published or are underway to bring additional important key findings to light.
“ These supplemental studies will help all of us better understand and interpret the results, and be better able to formulate treatment plans that are most suitable to individual CLTI patients”
ALIK FARBER
comes statistically significant.” That then established a GFR of under 30 as statistically positive for increased hazard of MALE or death. “But we wanted to see if there was any confounding by treatment type,” Hamouda continued. Comparing those patients receiving open bypass and endovascular intervention, “we found similar results: as long as the GFR is below 30, there is no difference in the treatment modality when it comes to the hazard of MALE or death,” he added. Those hazard ratios for eGFR <30 vs. ≥60 were 2.03 (95% confidence interval [CI], 1.68–2.43; p<0.001) and 3.46 (95% CI, 2.80–4.27; p<0.001) for MALE and mortality, respectively.
“One concerning but not surprising point we found during this study was that BESTCLI was designed to include only patients who have more than two years of expected survival after the procedure, but, with those patients on dialysis in the trial, it doesn’t matter whether they are getting an open bypass or endovascular intervention: as long as they hit the three-year mark, survival was below 50%, which was very sobering.”
These secondary analyses are helping to put the trial into appropriate context, by elucidating the results of the trial in different patient subgroups of interest. Farber and Menard are hoping the additional analyses will further help surgeons and other vascular care providers better understand the relevance of the trial to their own patients.
“These supplemental studies will help all of us better understand and interpret the results, and be better able to formulate treatment plans that are most suitable to individual CLTI patients,” Farber said.
SVS Foundation grants are meant to stimulate innovative research and thinking, said Menard. “It was always part of our goal to inspire the next generation of scientific investigators, and for them to build on the foundation established by BEST-CLI.”
They noted that high-quality research within the vascular surgical community is increasing. While judging BEST-CLI’s impact on this trend is difficult, Farber said, “we do think it was very important to demonstrate that vascular surgeons can lead high-quality trials and research. A number of trials that are currently works-in-progress are, in some ways, direct descendants of BEST.” He added that a great many SVS members are leading the secondary analyses of the BEST-CLI dataset. “It’s a very far-reaching effort,” he said.
What is one way of measuring Menard’s regard for the SVS Foundation? He’s now on the Foundation’s board of directors, and, as such, helped the body in its efforts to reach its fundraising goal before the year’s end. “There is no question that the support of the Society has been incredibly important to Alik and me as we journeyed through this trial experience. We have always been very aware that we would not have been able to achieve what we did without the incredible encouragement and assistance of both the Society leadership and its membership,” Menard said.
“The trial was completed because of the collective efforts of so many dedicated members of the Society, who, along with the wider vascular community, believed in what we were trying to do and, through their hard work and unwavering endorsement, brought it across the finish line.”
From top: Mahmoud Malas and Mohammed Hamouda
SYMPOSIUM FEATURES
• Comprehensive and Practical Programming
• Practice Management Essentials
• Clinical Case Reviews
• New Methods, Early Results, Clinical Trials and Innovation
• International Call for Abstracts and E-Poster Presentations
• Latin Session in Collaboration with CADECI
• Extensive Exhibition Hall
• Social Networking Events
LIVE PATIENT SESSIONS
• Live Patient Consultations, Examinations
• Ultrasound Protocols
• Interactive Discussions on The Evaluation, Diagnosis, Treatment and Follow Up of The Patients
Researchers develop machine learning models to predict IVC filter complications
By Jocelyn Hudson
RESEARCHERS IN CANADA HAVE DEVELOPED
machine learning (ML) models that they claim, “can accurately predict one-year IVC [inferior vena cava] filter complications, performing better than logistic regression”.
Writing in the Journal of Vascular Surgery: Venous and Lymphatic Disorders (JVS-VL), Ben Li, a vascular surgery resident at the University of Toronto in Toronto, Canada, and colleagues highlight that IVC filter placement is associated with long-term complications and posit that predictive models for filter-related issues “may help guide clinical decision-making.” The authors state that it was their objective to develop ML algorithms that predict one-year IVC filter complications using preoperative data.
Li et al write that they used the Vascular Quality Initiative (VQI) database to identify patients who underwent IVC filter
VENOUS REFLUX
ONE-YEAR
placement between 2013 and 2024. They identified 77 preoperative demographic and clinical features from the index hospitalization when the filter was placed.
The authors note that the primary outcome of the study was one-year filter-related complications, specifically a composite of filter thrombosis, migration, angulation, fracture and embolization or fragmentation, vein perforation, new caval or iliac vein thrombosis, new pulmonary embolism, access site thrombosis, or failed retrieval.
Going into more detail regarding their study methods, Li and colleagues share that the data were divided into training (70%) and test (30%) sets, and that six ML models were trained using preoperative features with 10fold cross-validation. These were Extreme Gradient Boosting, random forest, Naïve Bayes classifier, support vector machine, artificial neural network, and logistic regression. The primary model evaluation metric was area under the receiver operating characteristic curve (AUROC).
period, of whom 584 (4%) experienced one-year filter-related complications.
“Patients with a primary outcome were younger and more likely to have thrombotic risk factors including thrombophilia, prior venous thromboembolism (VTE), and family history of VTE,” the authors detail.
Furthermore, Li and colleagues reveal that the best prediction model was Extreme Gradient Boosting, achieving an AUROC of 0.93. Comparatively, they continue, logistic regression had an AUROC of 0.63.
The authors state that calibration plot showed “good agreement” between predicted and observed event probabilities with a Brier score of 0.07.
“Model performance remained robust across all subgroups”
The researchers also assessed model robustness, detailing that they used calibration plot and Brier score to do so, and evaluated performance across subgroups based on age, sex, race, ethnicity, rurality, median Area Deprivation Index, planned duration of filter, landing site of filter, and presence of prior IVC filter placement.
Li et al report in JVS-VL that 14,476 patients underwent IVC filter placement over the course of the 11-year study
SAVVE TRIAL RESULTS ARE ‘MOST ENCOURAGING DATA EVER PRODUCED FOR A BIOPROSTHETIC VEIN VALVE’
By Bryan Kay
THE ONE-YEAR DATA FROM the SAVVE trial represent the “most encouraging clinical data that have ever been produced for a bioprosthetic deep vein valve” in more than half a century of attempts at developing such a device, according to one leading venous disease specialist.
Manj Gohel, MD, from Cambridge University Hospitals in Cambridge, England, cautiously welcomed what he described as an outstanding set of one-year results for the VenoValve device (enVVeno Medical) but also reflected on patient selection, durability and health economics challenges to come. “There have been efforts to treat deep venous reflux for at least 50 years,” says the Cambridge University Hospitals consultant. “A native valve—a healthy normal valve—is a thing of beauty: it is incredibly flexible, mobile, is not thrombogenic at all, and is also really strong. So that is a tough ask for anything prosthetic. And, for half a century, people
have been trying to do this and have generally failed.”
Case selection will pose the greatest challenge, Gohel explains. “Deep reflux is very common. Of all the patients I see, probably a third, if not a half, of them will have deep venous reflux. The potential population is enormous, but we need to be very selective of the people we put through this procedure because it is still going to be experimental, expensive and invasive.” As such, for Gohel, VenoValve implantation is a third-line treatment option after superficial vein procedures and deep venous stenting “for those people who have still not responded.”
Further, Gohel says he will be closely following the durability of the device as longer-term data emerge. “The one-year
In addition, Li et al report that top 10 predictors of one-year filter-related complications were, in order, thrombophilia, prior VTE, antiphospholipid antibodies, factor V Leiden mutation, family history of VTE, planned duration of IVC filter (temporary), unable to maintain therapeutic anticoagulation, malignancy, recent or active bleeding, and age. “Model performance remained robust across all subgroups,” the researchers share.
In their conclusion, Li and colleagues posit that the ML algorithms assessed in the present study “have potential to guide patient selection for filter placement, counseling, perioperative management, and follow-up to mitigate filter-related complications and improve outcomes.”
data are nice, but one year is nothing in the grand scheme of things when it comes to venous disease. The problem is, if you get device failure, then the risk is you might get thrombosis of this prosthesis,
and that is effectively a DVT [deep vein thrombosis].”
Gohel says he will also be following the price at which the VenoValve device enters the market in light of health economics considerations.
“Venous ulceration is extremely expensive, but even with the very best treatments, the best they do is improve the ulceration rate and reduce recurrence rates by 50%—you
don’t cure the problem,” he points out. “Even then, cost effectiveness is only just demonstrated, because the treatments that you are carrying out—dressing the ulcers—cost money, but they are still relatively cheap next to a very expensive procedure. So, you’ve got to get a lot of ulcer healing benefit in order to demonstrate cost effectiveness.”
Ultimately, says Gohel, reducing the level of invasiveness of the procedure will be key. “At the moment, the procedure is an open surgery and has to be performed by a vascular surgeon,” he adds. “A lot of these patients are quite elderly and frail. You may not want to be putting many of them through relatively major surgery, so the percutaneous valve—which I know [enVVeno Medical] are working on—is going to be a really important next step.”
Recent years have brought other efforts to produce innovative technology that treats deep venous reflux, adding to the 50-year canon of vein valve replacement attempts.
“There was one valve called the Sail [flow regulator] valve, that there was a lot of interest in, and that had some first-in-man data, but that has disappeared,” recalled Gohel. “There was the endovenous, percutaneous valve called Blueleaf, which also disappeared. So we don’t want to get too excited, but [Food and Drug Administration] approval is a big thing.”
Manj Gohel
FROM THE EDITOR SO YOU WANT TO MARRY A SURGEON?
continued from page 2
- We are often viewed as one employee or partner, and there are a lot of issues with this. People think we share practices and should be responsible for each other’s patients (NOT!). We share benefits and salaries, so we should be compensated less. Benefits available to other surgeons should only be available to us as a couple and not as individual surgeons. We take too much time away at the same time, which makes more work for the rest of the team. People think we will use our “power couple” dynamic to influence the department’s direction. The truth is we frequently do not agree on programmatic issues.
- This has been hard as I have been in training for the entirety of our relationship up to this point. My hours and flexibility have not been great. Additionally, I have spent a lot of time over the last few years living in another city or even state. At the same time, my wife is a fulltime pediatric surgeon with a demanding schedule and career goals of her own. I think we have tried to value both of our dreams and goals, and support each other in accomplishing those. When we live together, we try to schedule our calls in a way that allows time off together, or that supports the other one during a difficult week/ month.
❤ Balancing home obligations
- Have a “call” bedroom.
- You’ve got to pick your battles. Especially as a mom. You aren’t going to be able to have it all so you have to
prioritize. If your kids or spouse are getting antsy about you being gone too much, then you have to give up some stuff that you might want to do at work or for yourself (i.e. morning workouts or journal clubs).
- Call schedules done a year in advance are always helpful, so at least you have some idea of holidays and weekends.
learnedhow makethosepeskystemcellsstick totheendothelium.Withherresearchtimedwindling,Claudie needed get fewprojects thefinishline.So, PubMedcanattest,ourrelationshipbeganstudyingminoramputations bypasses transplantpatients.Whoneedsromance?Theprospectof marryinganotherphysicianwasterrifying. Howwouldthisallwork?Atthetime,thereweren’tevenmany women vascularsurgery,nevermindmarriedcouples.Claudieneverseemedhesitant,though.
incredibly brightandseemsalwaystohave plan;shemusthavethought beenthisthrough.Wellreader,shehadnot.Twentyyearslater,ithas lifeof complications. of extremes.And,primarily
chosenspouse,
despitemydecadesof experience, amdefinitivelynotexpertinphysicianmarriages.Myinsightismoreakin one mypatientswith 9.5cmaneurysm. don’treallyknowwhathappening,butit’sprobablygoingtokillme. fewmonthsago,myfriendandSVSPresidentMattEagleton
- When one spouse is on call, the other spouse just keeps the routine. Don’t wait to eat! The routine works so much better, especially when the kids are in school.
- Committees work well for some decisions but not for running a home. Make sure every responsibility is clearly assigned to one of you.
- Both spouses need to be OK with the fact that the division of labor will sometimes be uneven due to forces that are out of your control.
- We outsource everything we can (house cleaning, drivers to take our kids to sports practice, etc.).
- With one of us being a trainee traveling between cities and then living long-distance for research (during COVID!), and now for fellowship, we’ve mostly had to maintain separate homes. It’s been hard when we do share a living space as it takes a minute to figure out life together (you should also bring a glass of water to bed if you are going to want some water in the middle of the night) and chore responsibilities. Sometimes, amidst these difficult times, work is the common denominator that we can always agree on and more easily navigate.
The American Irish Medical Summit
Outsourcing is extremely helpful, and also educational.
- We split chores. I like doing the laundry, and I hate grocery shopping. My spouse cooks, and I only do that if it is a special occasion; otherwise, I’m an Uber Eats person.
- At home, we work as a team. The person who is not as busy picks up the slack. He does the trash and I do the laundry. I guess we still have some traditional roles.
- This is a tricky one for us, as we have not lived together for the majority of our relationship due to surgical training. We also added a child into the mix 15 months ago and that drastically changed the “responsibilities and obligations” at home. We try to have certain chores that are split in order to offload some of the mental load of those things for the other person. Admittedly, I think we are still in the process of figuring this one out. Understanding that we can’t do this alone and having help (nannies, cleaning services, etc.) have been helpful, I think. Right now, we live in separate states and each have our own home and home responsibilities. I think this is a challenge but will hopefully help us learn the best way to divide labor once we live together again.
- We “outsource” many things. I now have the nanny do our child’s laundry and the housekeeper does most of our laundry. We have the meal delivery service for our baby. The housekeeper comes once a week. The nanny does our dishes and does some food prep/meals for us.
us in Chicago for the Annual American-Irish Medical Summit, held at the Northwestern University College of Medicine! The AIMS Summit has established itself as a premier, pivotal platform fostering transatlantic collaboration between
AIMS
AIMS
❤ Time for your spouse
- Scheduling time for each other is mandatory, and unfortunately the first to get cut when there are work needs.
I think all marriages have ups and downs, and this is amplified for those with dual-surgeon families. Currently, we are both working harder and more hours than we have ever worked, including residency (we are not accomplishing more though). I think we are learning that children are a great grounding force for the family. We are empty nesters and had high aspirations of dating each other again, traveling, getting to know each other as individuals all over again—and hoping we still liked each other (we do). That’s not happening on the timeframe we had hoped, as work sucks the life out of us.
- One day, I hope to have this. I think we have to wait until the baby is about 5 years old. I will then be old, but she’ll still be younger than I am now. So, maybe they can bond over visiting me in the nursing home.
- We are always prioritizing, and the first person to fall off the list of priorities is our spouses. We just assume they’ll understand (and they do, but it gets old sometimes. No, it gets old all of the time). This is in both directions.
- The advantage is that my partner is everything to me and the person I most want to hang out with. Making your partner the priority is hard with competing needs and work. You always regret not choosing your partner.
- One of the things I love about my wife is her love for community and life outside of the hospital. She has always been involved in so many aspects of life in New Orleans, and one of the things I think we do really well is prioritize time outside of the hospital for fun (Mardi Gras, going out to dinner, Saints games, Jazz Fest, travel). As we have added a child into the family, we are in a new phase of figuring out what time for the two of us together looks like.
- You have to get a good nanny if you are a two-surgeon family. Period. It’s not gonna happen any other way. You have to be OK with the fact that, at least once, your kids are going to call that person “Mom” if the nanny is female. It’s awful, but it’s going to happen.
- We try to always do vacations with our kids, which is not true for a lot of our non-medical friends. People definitely think we are crazy for having taken our kids to Iceland when they were one and three, but they loved it, and they still talk about it to this day. So, I guess I try to take the time I’m with them and be really present and focused on them so they feel special whenever I’m around.
- Our children used to get annoyed when we would talk work at home, especially during dinner. We ultimately set a timer—10 minutes each to vent/ talk/question when we were all together. Timer goes off, and you’re done.
We are often viewed as one employee or partner, and there are a lot of issues with this. People think we share practices and should be responsible for each other’s patients (NOT!)
- My biggest piece of advice is to maintain and cherish common interests and each other.
❤ Children
- Our kids are all exactly three years apart. That’s how long it takes to realize that you will never have life under control, so you might as well have another kid.
- Building a network of other parents is my saving grace. You will be underwater, and these people will throw you a lifeline. Let them into your world of chaos, and you will be surprised by how many will be there to help you. A pro tip: you do not need to do in-person, 10-minute parent-teacher conferences, but you can definitely be available by phone, and so can your husband. On that note, if you have a good school from pre-K to 12th grade and multiple children, life is way easier with one drop-off and pick-up point.
- There was some time consideration as a woman who had completed training at the tender age of 38. Female surgeons have a 50% serious complication rate. It was hard to be the birthing parent and pause my job, while my partner was still working so hard to finish her training. We have a long way to go with him, and our nannies are arguably the best thing that ever happened to our household. But our village is strong, and I hope we continue to provide the time and loving home for him that he needs and deserves.
- I think if you have two physician parents, it is very difficult to have the children in every single extracurricular activity. That is very challenging in today’s climate of travel sports and over-scheduled children. Additionally, it’s important to make time to be present at the children’s extracurricular programs. It is unreasonable to think that you can make every one, but you should attempt to make some of them (prioritize the big ones).
- Children forced at least one of us to be available somehow. And that meant the other pitched in more in the hospital or with other obligations. We scrutinized our travel more rigorously. And we said no more. We really relied on each other to make it work. I trust no one in the world more than my spouse—and she has never let me down. Our children specifically are not choosing medicine because they do not want to live the chaotic, uncontrolled lives we have. They are not bitter towards us, they are just potentially prioritizing things differently. I don’t think they feel like they have missed out on anything, but I do think they feel for us for not getting to relax more.
- We had our son 15 months ago, and he is an absolute joy and the love of our lives. Having said that, the process of getting pregnant, having the baby and the first year of life has been one of the hardest experiences for us. Having kids is so hard. And as a same-sex couple, there were additional challenges for us. We went through IVF (part of which we did while I was still away for my research years) and had to balance that process while both still practicing as surgeons. The pregnancy was not easy, but as many female surgeons experienced, there were difficulties. I was in my chief year of residency when our son was born, and then left for fellowship for two years. Being away has been really hard, and my wife is now doing the bulk of the work at home. We have been saved by having an amazing nanny who is basically a part of our family now. I hope that we can show our son that a life in medicine and as a surgeon is hard but is also extremely rewarding. My father is a physician and the reason that I went into medicine, and I hope that I can pass the joy of medicine down.
- With our initial nanny difficulties we really had to balance work obligations because we were unexpectedly without childcare multiple times. We constantly
compared schedules to see how long each person’s day would be and who could go in a little later or come home earlier to avoid paying overtime. We had to make sure our operating room days weren’t the same and we were never on call at the same time. Another strategy for some people is having a live-in nanny.
- When your kids are young, they don’t recognize that you have made a choice, but when they are older, they do. So they may grow to resent your jobs and time away.
❤ Miscellaneous
- I’ll throw a couple of trite phrases in here: the hours were long, but the years were short; and enjoy the journey—there is no destination
- Sometimes I wish I could quit it all and just hang out with my spouse. We see each other less now than we ever have. Working in the same hospital does not ensure you will have time together.
- I will offer a few things I would tell my younger self! Take out loans, borrow from family and friends, use credit cards, beg, borrow or steal to make your life as easy as possible. Hire a cleaning service, get childcare for a few hours on the weekends you are off and work out or sleep, have a delivery food service, always have childcare backup no matter the cost, and stop worrying because you will make the money to pay it back.
- You continually grow together. There are so many stages of adulthood and surgery life, and it’s fascinating to do it with another person, as we all learn things at different times and in different ways. The things I’ve learned from my wife about surgery, from her perspective and work habits and thought processes, and the “how does that staff do it?” are innumerable. I learn about her from her responses and about myself from mine. Adaptability and resourcefulness are things we develop as surgeons, and things that I depend upon in myself and my spouse.
- It also feels really cool to have a partner who is doing something they love and care about as much as I love and care about my job, basically because it’s the same damn job and it’s the best job (for us).
- As two surgeons, understand your spouse’s aspirations and be supportive. Make sure each of you has friends you can lean on in your respective fields.
- We are a same-sex couple in surgery and I think that is an even more rare thing. There are not a lot of examples to look up to as mentors or as a guide of how to navigate life in this unique space. One of the challenges of that has been that there are no true “gender roles” at home or at work. That is unique when it comes to raising children and obligations at home, etc. We are working through all of that and learning a lot about each other in the process, and I hope that we can be a resource for others that find themselves in this unique space in the surgery community.
- Overall, it’s amazing that my spouse is a surgeon too. Our main topics of conversation are how amazing our son is and cases. I love that he truly understands what I deal with, and I find that helps me immensely with the emotional toll this job can sometimes take.
- Some final tips: try and leave work frustrations at work, but also recognize that’s not always possible, so give your partner some grace.
- Make sure you keep hospital communication and home communication styles separate. Your partner is not a resident or PA, etc., that you are dictating orders to. Be a team. It will never be equal so don’t try and make it 50/50.
MALACHI SHEAHAN III is the Claude C. Craighead Jr. professor and chair in the division of vascular and endovascular surgery at LSU in New Orleans. He is Vascular Specialist medical editor.
SOCIETY BRIEFS
Compiled by Marlén Gomez and Beth Bales
Foundation grant projects
HERE’S A CLOSER LOOK AT A PROJECT funded partially through grants from the Society for Vascular Surgery (SVS) Foundation.
Samantha Minc, MD, received a Clinical Research Seed Grant in 2018 and a National Institute of Diabetes and Digestive and Kidney Diseases-funded K-23 award in 2022 (with additional funding by the SVS Foundation and the American College of Surgeons) to help with her project to implement interventions and amputation prevention in underserved areas across the country.
Her seed grant started her on intense mapping in the highly rural, very underserved community in West Virginia where she worked to understand and identify “amputation” hotspots, followed by qualitative work with focus groups with people dealing with amputations and amputation prevention. She has since relocated to Duke University in North Carolina.
“Funding helped me engage and empower stakeholders in those areas to work together with me to build our actual amputation prevention intervention,” she said.
“The seed grant funding got me the preliminary information I needed to help empower the communities being disproportionately affected by amputation.”
Inaugural visiting professorship to advance careers of young surgeons
A NEW SVS YOUNG SURGEON
Section (YSS) visiting professorship is set to provide mentorship opportunities, foster professional development and introduce young vascular surgeons to diverse clinical and research environments.
Each year, the YSS Award Selection Committee will award one recipient within the first 10 years of their practice a $1,000 travel stipend and a $1,500 honorarium to support their role as a visiting professor.
“We’ve left the topic for this visiting professorship open-ended. We want to hear from you, young vascular surgeons, what you’re currently interested in,” said YSS Steering Committee Chair Ted Gifford, MD.
This professorship program was the brainchild of the inaugural YSS chair, Chelsea Dorsey, MD, who will host the first visiting professorship at the University of Chicago.
For more information on joining the YSS and accessing the application form, visit vascular.org/YSS.
SVS CALLS FOR COMMENTS ON VASCULAR SURGERY MIPS VALUE PATHWAY
THE SOCIETY FOR VASCULAR Surgery (SVS) announced that the Vascular Surgery MIPS Value Pathway (MVP) was posted for public comment by the Centers for Medicare & Medicaid Services (CMS). Developed by the SVS Quality and Performance Measure Committee (QPMC), the pathway is designed to reflect the care of vascular patients across all practice types and locations while minimizing the burden of data submission.
The Vascular Surgery MVP is the first step toward creating specialty-specific quality metrics that improve vascular care. While awaiting CMS approval, the QPMC continued to develop additional measures for potential use in other CMS payment programs.
“This is a significant milestone in our ongoing efforts to improve the quality of care for vascular patients while meeting CMS reporting requirements,” said Dennis Gable, MD, chair of the SVS Quality Council. “The proposed MVP design offers non-burdensome quality metrics that elevate care for multiple vascular procedures.”
MVPs, or MIPS Value Pathways, are part of the Merit-based Incentive Payment System. They focus on measures and activities tied to specific specialties or medical conditions. Compared to traditional MIPS, MVPs require fewer but more targeted measures, easing the reporting burden
for physicians. As part of the 2025 Medicare Physician Fee Schedule Final Rule, CMS has committed to transitioning entirely to MVP reporting by 2028. This shift is a cornerstone of CMS’ move toward value-based care models.
The SVS has engaged in productive discussions with CMS during the MVP development phase and will continue to work with the agency to finalize and maintain the pathway.
“There arise certain times when a medical specialty must unify and act to bring voice and change,” said Kenneth M. Slaw, PhD, SVS executive director.
“This is such a time for members of the SVS to support our vascular surgery MVP and lead the way in developing vascular measures that CMS adopts.”
“This is a significant milestone in our ongoing efforts to improve the quality of care for vascular patients while meeting CMS reporting requirements”
DENNIS GABLE
The public comment period for the Vascular Surgery MVP was open from Dec. 11, 2024, to Jan. 24, 2025. The SVS encouraged members and stakeholders to contribute comments. Visit vascular.com/MVP.
Tracci assumes presidency of Southern Vascular
MARGARET (MEGAN) TRACCI, MD, has become the firstever woman president of the Southern Association for Vascular Surgery (SAVS). The University of Virginia professor of surgery assumed the role at the close of the 2025 SAVS annual meeting in St. Thomas, the U.S. Virgin Islands (Jan. 22–25).
Tracci took over from Alan Lumsden, MD, medical director of Methodist
DeBakey Heart and Vascular Center at Houston Methodist.
Mark Farber, MD, chief of the Division of Vascular Surgery at the University of North Carolina at Chapel Hill, is the new president-elect. Dennis Gable, MD, chief of vascular and endovascular surgery at Baylor Scott & White, The Heart Hospital BaylorPlano, Texas, became a councilor-at-large.
Countdown to New Orleans: VAM 2025 set to explore innovation,
impact
THE 2025 VASCULAR ANNUAL Meeting (VAM) will take place in New Orleans, Louisiana, from June 4–7 with a particular focus this year on innovation. Key program highlights coming up this year include case-based learning sessions entitled “Optimal Management of the ‘No Option’ CLTI Patient” and “Spinal Cord Ischemia,” as well as interactive courses with topics like “Carrying the Weight: Parenthood in Vascular Surgery.”
“With VAM 2025 set in New Orleans, attendees can look forward to enriching their professional knowledge through discussions on complex cases, advancements in vascular care, and skill enhancing activities,” said Program Committee Chair Jason T. Lee, MD.
Visit vascular.org/VAM for updates on sessions, keynote speakers and special events.
Take advantage of Mentor Match
(SVS) MEMBERS HAVE THE opportunity to give—and receive— career guidance as part of the SVS Mentor Match program.
The SVS has expanded the program— originally designed for medical students and general surgery residents—to include all SVS members in good standing. Mentors help mentees explore the specialty, grow in their careers and achieve professional goals.
The program is run on the online, members-only SVSConnect platform. Currently, approximately 35 mentees have the attention of nearly 20 mentors. Christine Shokrzadeh, MD, regards the program as one of the top benefits of SVS membership. Now an attending vascular surgeon at the University of Texas Medical Branch in Galveston, Texas, when she was still a trainee a more senior member helped her with a query into academic medicine. Now, she said in a video, “I’m able to pay it forward by helping medical students and residents who are interested in a career in vascular surgery.”
Learn more and sign up at svsconnect.vascular.org
Margaret (Megan) Tracci
CLINICAL&DEVICENEWS
Compiled by Jocelyn Hudson and Bryan Kay
New data support role of F/BEVAR for treatment of thoracoabdominal aortic aneurysms
A RECENT PROSPECTIVE, MULTICENTER cohort study provides insights into early and late aortic-related mortality and rupture after fenestrated and branched endovascular aneurysm repair (F/ BEVAR) of thoracoabdominal aortic aneurysms (TAAAs). Researchers claim these are likely to represent the most comprehensive data on the topic for the foreseeable future, citing the unworkable nature of a randomized study.
Gustavo Oderich, MD, until recently chief of vascular and endovascular surgery, Ying Huang, MD, assistant director of the Advanced Endovascular Aortic Research Program at University of Texas Health Science Center at Houston-McGovern Medical School in Houston, Texas, and colleagues, on behalf of the U.S. Aortic Research Consortium (ARC), write in Circulation that F/BEVAR has been used as a minimally invasive alternative to open surgical repair to treat patients with TAAAs.
The authors explain that, despite the widespread use of fenestrated and branched aortic devices worldwide, they are not currently commercially approved by the Food and Drug Administration (FDA).
Access to these devices, they continue, is limited to those centers with ongoing physician-sponsored investigational
ESVS publishes 2025 vascular trauma guidelines
THE EUROPEAN SOCIETY FOR Vascular Surgery (ESVS) has developed new guidelines for the care of patients with vascular trauma. The 2025 clinical practice guideline document was recently published as an open-access article in press in the European Journal of Vascular and Endovascular Surgery (EJVES).
A writing committee consisting of first author Carl Magnus Wahlgren, MD, a vascular surgeon at Karolinska University Hospital in Stockholm, Sweden, and colleagues from across Europe has outlined a total of 105 recommendations.
The guidelines cover several topics, namely technical skillsets, bleeding control and restoration of perfusion, graft materials, and imaging; management of vascular trauma in the neck, thoracic aorta and thoracic outlet, abdomen, and upper and lower extremities; postoperative considerations after vascular trauma; and pediatric vascular trauma. Unresolved vascular trauma issues and patients’ perspectives are also discussed.
FDA approves Humacyte’s Symvess for vascular trauma
HUMACYTE RECENTLY SHARED THAT the Food and Drug Administration (FDA) has granted a full approval for the Symvess acellular tissue-engineered vessel.
A company press release notes that Symvess is indicated for use in adults as a
device exemption (PS-IDE) studies. The researchers detail that the ARC has been collecting prospective data from these studies since 2018.
The aim of the present study, the authors note, was to evaluate aortic-related mortality and aortic aneurysm rupture after F/BEVAR of TAAAs. In order to do so, the research team analyzed patients enrolled in eight prospective, non-randomized, PS-IDE studies between 2005 and 2020 who underwent elective F/BEVAR of asymptomatic intact TAAAs.
The primary endpoints of the study, Oderich, Huang et al detail, were aortic-related mortality, defined as any early mortality (30-day or in-hospital) or late mortality from aortic rupture, dissection, organ or limb malperfusion attributable to aortic disease, complications of reinterventions, or aortic rupture. Secondary endpoints were early major adverse events, TAAA life-altering events—defined as death, permanent spinal cord injury, permanent dialysis, or stroke— all-cause mortality, and secondary interventions.
Oderich, Huang and colleagues share in Circulation that 1,109 patients were analyzed in the study, noting that 589 (53.1%) had extent I–III and 520 (46.9%) had extent IV TAAAs. The patients had a median age of 73.4 years and just under one-third were women.
The investigators report that early mortality was 2.7% and that congestive heart failure was associated with early mortality. Furthermore, they reveal that the incidence of early aortic rupture was 0.4% and that the incidence of early major adverse events and TAAA life-altering events was 20.4% and 7.7%, respectively.
Oderich, Huang et al continue that there were 30 late aortic-related mortalities; the five-year cumulative incidence was 3.8%; and older age and extent I–III TAAAs were
01: 4.5” x 5.625”
vascular conduit for extremity arterial injury when urgent revascularization is needed to avoid imminent limb loss, and when autologous vein graft is not feasible.
Gore receives CE mark for lower profile Viabahn VBX endoprosthesis
GORE HAS ANNOUNCED THE RECENT CE mark approval of a lower profile Viabahn VBX balloon expandable endoprosthesis. No changes to the stent graft design were made to achieve the lower profile, the company stated in a press release. By focusing on improvements to the delivery system only, the characteristics and performance of the stent graft itself remain, Gore states.
Boston Scientific to acquire IVL developer
Bolt Medical
BOSTON SCIENTIFIC HAS ANNOUNCED it has entered into a definitive agreement to acquire Bolt Medical, the developer of an intravascular lithotripsy (IVL) advanced laser-based platform for the treatment of coronary and peripheral artery disease.
The Bolt IVL system is designed with a novel application of lithotripsy to fracture calcium by creating acoustic pressure waves inside a balloon catheter.
The system also includes visible, directional emitters for consistent energy delivery in the treatment of the calcified lesions.
independently associated with late aortic-related mortality. Furthermore, the authors report that 14 late aortic ruptures occurred; the five-year cumulative incidence was 2.7%; extent I–III TAAAs were associated with late aortic rupture; five-year all-cause mortality was 45.7%; and five-year cumulative incidence of secondary intervention was 40.3%.
In the conclusion of their findings, Oderich, Huang and colleagues write that aortic-related mortality and aortic rupture are “uncommon” after elective F/BEVAR of asymptomatic intact TAAAs. They add that half of the aorticrelated mortalities within the study occurred early, and that most of the late deaths were not aortic related.
Oderich, Huang et al reiterate that five-year all-cause mortality was high—45.7%—mostly due to non-aorticrelated causes, “likely reflecting selection of higher-risk subgroups compared with historical reports of [open surgical repair].”
The final conclusion the authors make is that secondary interventions were needed in one in four patients. They stress, however, that three-quarters of these were minor procedures.
The authors recognize several limitations of their study, including possible patient selection bias due to a need to adhere to PS-IDE inclusion and exclusion criteria, the frequency of cause of death being unknown, and the reason for aortic rupture and the aortic diameter at the time of rupture not being available for all patients, among others.
Despite these limitations, the authors underline the significance of the present study. “Given a perceived lack of clinical equipoise to justify a randomized controlled trial,” they comment, “these data are likely to be the most reliable and obtainable to validate the role of F/BEVAR for the treatment of TAAA.”
GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface*
Consult Instructions for Use eifu.goremedical.com
INDICATIONS FOR USE IN THE U.S.: The GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface is indicated for improving blood flow in patients with symptomatic peripheral arterial disease in superficial femoral artery de novo and restenotic lesions up to 270 mm in length with reference vessel diameters ranging from 4.0 – 7.5 mm. The GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface is indicated for improving blood flow in patients with symptomatic peripheral arterial disease in superficial femoral artery in-stent restenotic lesions up to 270 mm in length with reference vessel diameters ranging from 4.0 – 6.5 mm. The GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface is indicated for improving blood flow in patients with symptomatic peripheral arterial disease in iliac artery lesions up to 80 mm in length with reference vessel diameters ranging from 4.0 – 12 mm. The GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface is also indicated for the treatment of stenosis or thrombotic occlusion at the venous anastomosis of synthetic arteriovenous (AV) access grafts. CONTRAINDICATIONS: The GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface is contraindicated for non-compliant lesions where full expansion of an angioplasty balloon catheter was not achieved during pre-dilatation, or where lesions cannot be dilated sufficiently to allow passage of the delivery system. Do not use the GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface in patients with known hypersensitivity to heparin, including those patients who have had a previous incident of Heparin-Induced Thrombocytopenia (HIT) type II. Refer to Instructions for Use at eifu.goremedical.com for a complete description of all applicable indications, warnings, precautions and contraindications for the markets where this product is available.
5-YEAR PATENCY IN COMPLEX, REAL-WORLD SFA LESIONS.
The VIABAHN® Device demonstrated 85% primary patency at 1 year and 62% at 5 years.1
Patent VIABAHN® Device at 6-year follow-up
Images courtesy of Osamu Iida, M.D. Used with permission.
* As used by Gore, Heparin Bioactive Surface refers to Gore’s proprietary CBAS® Heparin Surface.
1. Iida O, Ohki T, Soga Y, et al. Five-Year outcomes of the GORE VIABAHN Endoprosthesis for the treatment of complex femoropopliteal lesions from a Japanese post-market surveillance study. Vascular Medicine 2024;29(4):416-423. W. L. Gore & Associates, Inc. Flagstaff, Arizona 86004 goremedical.com
Please see accompanying prescribing information in this journal.
Products listed may not be available in all markets.