2 Guest editorial The CLTI conundrum: My spirited journey through the CLTI saga
9 Membership SVS announces merger that creates the new Section on Ambulatory Vascular Care
11 Training
APDVS launches vascular surgery curriculum e-book for medical students
12 Executive Board
SVS president champions continuity and unified future
www.vascularspecialistonline.com
STUDY SHEDS LIGHT ON VASCULAR-SPECIFIC ADVANCED PRACTICE PROVIDER EXPERIENCE
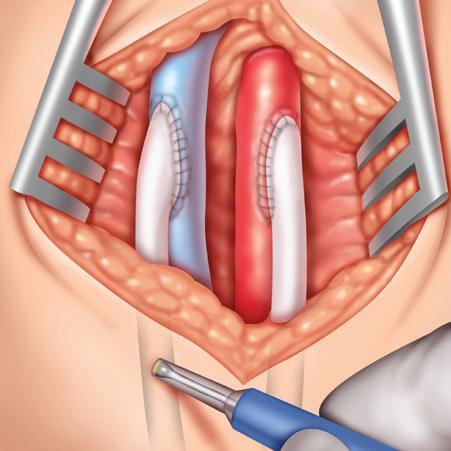
‘Select CLTI patients may be safely treated in the office-based lab’
Single-center analysis finds outpatient setting met SVS objective performance goals
By Bryan Kay
retrospective analysis of endovascular interventions performed for chronic limb-threatening ischemia (CLTI) in an office-based lab (OBL) associated with a large New York City medical center across seven years determined that carefully selected patients may be treated safely in the outpatient setting.
Researchers from NYU Langone Medical Center report that 44.8% of the 230 patients included in the study required ipsilateral reintervention, with 30.4% warranting inpatient reintervention; and 20.4% required ipsilateral amputation, with 9.1% undergoing major amputation. All-cause mortality was 16.5% at three-year follow-up. This is set against Society for
Vascular Surgery (SVS) objective performance goals for revascularization carried out for CLTI of 55% freedom from reintervention, 84% limb salvage and 80% survival at one year.
The data, from September 2016–February 2023, are to be presented at the 2024 annual meeting of the Eastern Vascular Society (EVS) in Charleston, South Carolina (Sept. 19–22), by Moira McGevna, a medical student at Rutgers Robert Wood Johnson Medical School in New Brunswick, New Jersey, who worked on the project during a research year at NYU under
By Jocelyn Hudson
IN A RECENTLY CONDUCTED survey, over 200 U.S. advanced practice providers (APPs) in vascular surgery cited performing at the top of their license as the most important determinant of job satisfaction. This and other key findings are set to be presented at the Midwestern Vascular Surgical Society (MVSS) annual meeting (Sept. 12–14) in Chicago.
The research—conducted by author Saideep Bose, MD, and colleagues—investigated scope of practice, workplace satisfaction and burnout among vascular-specific APPs who practice in the U.S. Bose, a vascular surgeon and assistant professor at Saint Louis University in Missouri, told Vascular Specialist ahead of his MVSS presentation that there is a “strong contingent” of APPs in vascular practice. “The main issue is that we don’t know how people in these APP positions feel about their careers or their jobs and if they feel like they are being utilized effectively or just being asked to do tasks that no one else wants to do,” he said, highlighting the genesis for the research.
In order to illuminate the experience of vascularspecific APPs, the researchers conducted a survey of 50 questions. The main component was the Mini Z survey—a
Medical Editor Malachi Sheahan III, MD
Associate Medical Editors
Bernadette Aulivola, MD | O. William Brown, MD | Elliot L. Chaikof, MD, PhD
| Carlo Dall’Olmo, MD | Alan M. Dietzek MD, RPVI, FACS | John F. Eidt, MD | Robert Fitridge, MD | Dennis R. Gable, MD | Linda Harris, MD | Krishna Jain, MD | Larry Kraiss, MD | Joann Lohr, MD
| James McKinsey, MD | Joseph Mills, MD | Erica L. Mitchell, MD, MEd, FACS | Leila Mureebe, MD | Frank Pomposelli, MD | David Rigberg, MD | Clifford Sales, MD | Bhagwan Satiani, MD | Larry Scher, MD | Marc Schermerhorn, MD | Murray L. Shames, MD | Niten Singh, MD | Frank J. Veith, MD | Robert Eugene Zierler, MD
Resident/Fellow Editor
Saranya Sundaram, MD
Executive Director SVS
Kenneth M. Slaw, PhD
Senior Director for Public Affairs and Advocacy
Megan Marcinko, MPS
Manager of Marketing
Kristin Spencer
Communications Specialist
Marlén Gomez
Published by BIBA News, which is a subsidiary of BIBA Medical Ltd.
Publisher Stephen Greenhalgh
Content Director Urmila Kerslake
Global Sales Director
Sean Langer
Managing Editor Bryan Kay bryan@bibamedical.com
Editorial contribution Jocelyn Hudson, Will Date, Jamie Bell, Éva Malpass and George Barker
Design Terry Hawes
Advertising Nicole Schmitz nicole@bibamedical.com
Letters to the editor vascularspecialist@vascularsociety.org
BIBA Medical, Europe
526 Fulham Road, London SW6 5NR, United Kingdom
BIBA Medical, North America
155 North Wacker Drive – Suite 4250, Chicago, IL 60606, USA
The CLTI conundrum: My spirited journey through the CLTI saga
By Omid Jazaeri, MD
Welcome to the CLTI Chronicles, a saga of mystery, medicine and misadventures in limb salvage unfolding weekly in my office, where the drama of threatened limbs rivals any Latin telenovela. My clinic has become a crossroads for the second opinion seekers, the exclusive club of the limb-threatened, each bearing the mysterious mark of CLTI—critical or chronic limb-threatening ischemia, who can say?—a definition that looms like a shadow and is as elusive as a politician’s promise. Imagine this: A parade of patients, each with a medical history reading like a travelogue through the land of “100% successful interventions.” They’ve journeyed through the valleys of endovascular treatments, scaled the mountains of open surgeries, and been guided by a motley crew of vascular magicians and interventionalist du jour. Yet, here they are, in my office, still sporting their troublesome limbs like unwelcome souvenirs from a trip gone wrong. After a forensic dive into their histories, imaging and procedures, the twist emerges—the majority did not have CLTI as their opening act.
CI managed to mutter something about the looming threat of limb loss, avoiding the gory details of wounds, arterial blockages, and the like. That encounter sparked in me a quest through the vascular literature and the abundance of expert forums including SVSConnect, searching for that Holy Grail: a definition of CLTI. A definition that would be as easy to recite as ordering an iced latte at Starbucks. What I uncovered was a labyrinth of conflicting viewpoints, a chaotic battleground of Current Procedural Terminology (CPT) codes and ambulatory surgery centers, along with squabbles over interventional integrity, all leaving me still craving that elusive clarity. By the end, I found myself more tangled than a season finale of the Bachelorette.
In the world of vascular disease, we have a lexicon to define just about everything, except, it seems, for CLTI. It’s like trying to nail jelly to the wall. Guideline-directed therapies? Sure, we’ve got those—a veritable buffet of evidence-based options, from interventional routines, to limb salvage approach, to cardiovascular risk reduction. But where’s the meat of the matter? My commentary is not about the mechanics of arterial repair (stents, balloons and atherectomies), but about the missing clarity in the definition, a gap leading to fragmented and variable care for our characters in distress, turning CLTI recommendations into a kind of medical chooseyour-own-adventure.
But wait, there’s more to this plot. It seems there’s a CLTI epidemic sweeping the nation, and it’s not just confined to the realms of vascular journals or my office; it’s trending on social media as well. You’ve seen the angiograms, those before-and-after images where you can’t help but wonder: “Really? Was that truly CLTI?” It’s a diagnosis in vogue and it appears my community has become the unofficial epicenter of CLTI, defying statistical probabilities where CLTI represents 10% of patients with peripheral arterial disease (PAD). But beneath the surface lies a narrative steeped in gravity: amputation risk as high at 40% in six months and an all-cause mortality rate of 70% in five years that overshadow colorectal cancer, breast cancer, stroke and coronary artery disease. CLTI is not just a hashtag; it’s a killer outshining the darkest plots of a Stephen King novel. Then came that moment of reckoning. A patient asked me an innocent question: “What is CLTI?” I was dumbstruck, my mind a vortex of nothingness. Eventually,
The backstory takes us to the 1980s European effort to define not just questionable fashion but this elusive antagonist, focusing on rest pain, tissue loss and hemodynamic parameters. But like all great plots, it’s riddled with twists— subsequent studies showed a broader spectrum of patients with ulcers and normal hemodynamics who benefited from early interventions, despite the initial definitions of CLTI. Fast-forward through decades of academic adventures and classification crusades—from TASC-I followed by TASC-II to the University of Texas classification to PEDIS to the SVS Lower Extremity Threatened Limb Classification better known as WIfI (Wound, ischemia and foot infection)— each a chapter in the never-ending saga of CLTI. Yet, despite all these classifications, the true essence of CLTI remains as elusive.
In the world of vascular disease, we have a lexicon to define just about everything, except, it seems, for CLTI. It’s like trying to nail jelly to the wall
Omid Jazaeri
PILOT STUDY LOOKS AT UNDIAGNOSED VASCULAR DISEASE IN HOMELESS
By Bryan Kay
A PILOT STUDY IN CANADIAN capital Ottawa aimed at uncovering the extent of undiagnosed vascular disease among the city’s homeless population detected a subset of the population who may be in need of treatment for venous disease.
The work was carried out by a team from The Ottawa Hospital Division of Vascular Surgery. The group’s findings are being presented at the 2024 annual meeting of the Canadian Society for Vascular Surgery (CSVS) being held in St. John’s, Newfoundland and Labrador (Sept. 13–14) by Ian Malnis, MD, a vascular surgery resident at the institution. The pilot is set to give way to a survey-based study aimed at establishing what are the barriers to obtaining wound care from vascular-trained providers.
The study grew out of Ottawa inner-city health authority’s review of the area’s growing homeless population, with the
hospital identifying that they did not see a great deal of this demographic unless members presented with a big vascular problem.
“Ottawa inner city health has been operating there for a long,” explained Malnis.
“They run a clinic downtown in Ottawa. Their mandate is for people with no fixed address or who are housing insecure. We partnered with them to run a monthly clinic there just to see what kinds of wounds they were seeing and whether or not those wounds were related to vascular disease or other traumatic injuries or infections that aren’t related to perfusion.”
Malnis, previously a nurse in Vancouver, has previous experience working with the homeless in the Canadian west coast city where there is a greater homeless problem. Among their findings while conducting the monthly clinics, Malnis and colleagues found that the nurse practitioners who as-
sess patients reported a vascular knowledge gap. “They said ‘We’d really benefit from having some extra education targeted specifically at how to refer, when to refer, how to properly assess people that we think have vascular disease,’” Malnis said. That led to afternoon classes, with more referrals from the downtown area now landing with the hospital’s vascular surgery division. “The nurse practitioners are accurately diagnosing people as not being in vascular disease. Most of the people that we saw who had any vascular problem was for venous disease. I think we saw one person with an arterial problem, and it was CLTI [chronic limb-threatening ischemia].”
Novel AI-assisted DVT diagnostic pathway aims to ‘democratize’ point-of-care ultrasound
By Jocelyn Hudson
A NEW DEEP VEIN THROMBOSIS (DVT) diagnostic pathway incorporating non-expert artificial intelligence (AI)-guided compression ultrasound could reduce workload and costs for healthcare systems while providing a quicker diagnosis and improving patient care.
Efthymios (Makis) Avgerinos, MD, is set to share this key conclusion from a pilot study of the ThinkSono guidance system (ThinkSono) at the upcoming European Society for Vascular Surgery (ESVS) annual meeting (Sept. 24–27).
“The diagnosis of DVT in a tertiary setting is part of a complicated clinical pathway including clinical probability scoring, D-dimer testing and a full duplex scan, often leading to long waiting times,” Avgerinos—who is co-director of the Clinic of Vascular and Endovascular Surgery at Athens Medical Group and visiting professor of vascular surgery at the University of Athens in Greece—told Vascular Specialist ahead of the Kraków, Poland, gathering. He added that the need to have trained radiologists or sonographers available 24/7 incurs high costs and represents a “suboptimal use of resources.”
The ThinkSono system, Avgerinos explained, is based on the point-of-care ultrasound concept and eliminates the need for an expert operator and the absolute need to perform a standard duplex. “It is an AI-based software that you can install on your cell phone or tablet and will guide a non-expert on how to perform a compression ultrasound using a wireless probe,” he continued.
In their pilot study of the ThinkSono system, Avgerinos and colleagues set out to evaluate its clinical utilization in real-world practice—having previously demonstrated its ability to generate valid images—hoping to show that the system could spare the need for standard venous duplex.
The researchers prospectively enrolled 53 patients who were suspected to have a DVT. These patients underwent a ThinkSono scan, performed by a nurse or resident in
the emergency room, with the resulting images then reviewed remotely by the on-call radiologist. D-dimer testing was also performed as a safety measure.
Avgerinos shared that all 53 scans generated were of appropriate quality to be read by the radiologist.
“This is a great milestone for an AI technology in the hands of non-experts,” he said, going on to reveal that 89% of the scans were negative for DVT. The team managed to discharge one-third of the patients without performing any standard duplex scan, which Avgerinos commented represents significant cost and time savings.
Six out of eight suspected DVTs were confirmed on standard duplex to be real, with the ThinkSono technology not missing a diagnosis. “Interestingly enough,” Avgerinos added, “all positive D-dimer testing patients who had a negative ThinkSono scan were also eventually negative, indicating D-dimer has a very low specificity and is not really a powerful testing method to rule in DVT.”
Avgerinos continued that it took on average six and a half minutes in total for scan and review. The median length of
“A nurse at the community hospital, a nurse at the GP’s office or at the ambulatory center could perform the scan and an expert could review it remotely from the main hospital”
EFTHYMIOS
(MAKIS) AVGERINOS
DAY OF SERVICE DURING 2024 EVS ANNUAL MEETING
THE EASTERN VASCULAR SOCIETY (EVS) has incorporated a day of service into its 2024 annual meeting, being held in Charleston, South Carolina (Sept. 19–22).
Leading vascular surgeons, alongside nurse practitioners and advanced practice partners, will educate local residents about their peripheral vascular health under an initiative entitled, “From A to V: Completing the Circuit. The Truth About Arteries and Veins.”
The event, which takes place at. St. Julian Devine Community Center in downtown Charleston on Friday, Sept. 20, from 6:30–8:30 p.m., includes a free screening and compression stockings for attendees.
A multidisciplinary panel will provide expert advice about both arterial and venous disease, including on the most common signs and symptoms of venous insufficiency. A question-and-answer session will also form part of the event. The event is taking place in partnership with the American Venous Forum, with collaboration from MUSC.— Bryan Kay
time between scan and review was 30 minutes, although there was a wide variation in this figure. According to Avgerinos, this “reflects unoptimized hospital logistics—mainly the availability of the qualified clinician to review the data.” He clarified that the expert clinicians who took part in the pilot study were volunteers who had various other clinical lab duties, going on to suggest that careful resource planning or the use of dedicated reviewers could help to maximize the efficiency of the AI-assisted pathway.
Avgerinos summarized: “Our study demonstrated that in DVT diagnostic workflow, using AI and remote expert review could safely decrease the need for a full duplex ultrasound and even D-dimer testing for a significant proportion of the patients who are suspected to have a DVT in the emergency room.”
Looking ahead, he noted that a large trial is needed to validate the results of this pilot study, and that clinical commercialization will soon launch in the United Kingdom and Germany, while a Food and Drug Administration (FDA) trial is underway in the U.S..
Finally, Avgerinos considered the wider application of this technology. While the pilot study focused on tertiary centers, he hinted at its potential future use in community hospitals and ambulatory centers. “Not a lot of hospitals have radiologists who can perform standard duplex scans 24/7,” he said.
“With this technology, patients would not need to travel to the reference centers. A nurse at the community hospital, a nurse at the GP’s office or at the ambulatory cen ter could perform the scan and an remotely from the main hospital. The applica tion eventually expands to any remote or rural underserved area, essen tially democratizing ul trasound—anybody can do it, anywhere.”
Efthymios (Makis) Avgerinos
Ian Malnis helps conduct an Ottawa downtown clinic as part of a pilot study
SVS TASK FORCE ASSESSES PROGRESS MADE, REMAINING GAPS IN OPTIMAL
BOARD CERTIFICATION FOR VASCULAR SURGERY
Examining the key forces and factors shaping vascular surgery and how they may interact to create different environments.
By Kenneth M. Slaw, PhD
The Society for Vascular Surgery (SVS) Strategic Board of Directors (SBOD), at its January 2024 meeting, reached a consensus to form and launch a special task force appointed by Immediate Past President Joseph Mills, MD, to assess the significant progress made by vascular surgery as an independent medical specialty over the past two decades and looking forward, analyze and identify strategic gaps, if any, that must be addressed for vascular surgery to reach its “optimal state.”
The process began before there were talks of the recent submission to the American Board of Medical Specialties (ABMS) of the planned American Board of Cardiovascular Medicine (ABCVM). The goal of this task force—called the SVS Task Force on Free-Standing or Federated Board Certification—is to help the vascular surgery community fully understand the implications to individual diplomats, trainees and our organizations regarding forming an independent board versus maintaining the status quo.
“While many have a visceral reaction to what they think would be preferable, the SVS will make a well-informed decision after genuinely understanding all the ramifications,” said Michael Dalsing, MD, task force chair.
A membership call for action resulted in 30 volunteers for the task force. The SVS Executive Board (EB) approved the appointees and overarching objective of the task force: to examine the two primary existing models of board certification, free-standing or federated, and complete an objective, concise analysis of their strengths and weaknesses, which may provide an optimal path forward. The composition of the task force intentionally provides a representative cross-section of the SVS membership from practice type to time in practice, as well as including those who support the formation of an independent board and those who lean against its formation. Michael Dalsing, MD, serves as chair of the task force and members include the following: James Black,
FROM THE COVER ‘SELECT CLTI PATIENTS MAY BE SAFELY TREATED IN THE OFFICE-BASED LAB’
continued from page 1
MD; Karan Chawla, MD; R. Clement Darling III, MD; Alan Dietzek, MD; Dennis Gable, MD; Elizabeth Genovese, MD; Tom Huber, MD; Vikram Kashyap, MD; Elina Quiroga, MD; Matthew Sideman, MD; Natalie Sridharan, MD; and Gabriela Velazquez, MD. Matthew Eagleton, MD, SVS president; Keith Calligaro, MD, president-elect; Linda Harris, MD, vice-president; and Joseph Mills, MD, immediate past president, are ex-officio members.
tics and differences in free-standing models within the ABMS and federated models within the American Board of Surgery (ABS)/ABMS: an opportunity analysis; detailed review of the ABS and the Vascular Surgery Board (VSB); financial variables and cost considerations; training/workforce impacts; and branding the specialty and board certification.
The task force has conducted five Zoom calls and most recently held a meeting on July 25 at SVS Headquarters. The foundation for the task force’s work was identifying key guiding research questions solicited from the SVS EB, the SBOD and task force members, which helped with discovery and discussion during each call/meeting. Questions focused on the following areas: the role, function and relationships of key organizations involved in Vascular Board Certification; characteris-
“While many have a visceral reaction to what they think would be preferable, the SVS will make a well-informed decision after genuinely understanding all the ramifications”
MICHAEL DALSING
To answer these questions, interviews were conducted with the executive staff and leadership of the ABS, VSB, the Accreditation Council for Graduate Medical Education (ACGME), ABMS, the American Board of Thoracic Surgery (ABTS) and the American Board of Colon and Rectal Surgery (ABCRS). At the in-person meeting on July 25, a panel of representatives from the organizations interviewed was convened for a two-hour Q&A session. Follow-up questions based on the interviews were asked of the participants. The task force members also engaged in a “scenario planning” exercise to examine key forces and factors shaping vascular surgery and how they may interact to create different environments, as well as an analysis of how to best prepare for those conditions. The task force will finish its analysis in September and prepare a final summary report for review by the SVS EB in November. Upon review, the SVS will share an executive summary with members for comment. SVS leadership will present the final report to the SBOD at the January 2025 meeting. The SVS EB will then process the feedback from the SBOD.
the senior authorship of Thomas Maldonado, MD, NYU Langone professor of surgery.
Acknowledging the controversy that often surrounds the role of the OBL in the treatment of vascular disease, Maldonado notes in an interview with Vascular Specialist ahead of EVS 2024, “we found that despite not being adjoined or adjacent to a hospital, the OBL plays an important role, even in patients with critical limb ischemia [or CLTI].”
surgery, patient selection and good judgment are paramount. Despite the OBL being a setting that is not in the context of a hospital with all its support, I still believe it has an important role, even with patients with critical limb ischemia who have higher comorbidities.”
The tendency with CLTI patients, often bearing the risk of limb loss, is to treat them “in-house,” he says. “When we looked at our experience of 230 patients over seven years who had a minimum of one year of follow up—we had a mean follow up of 3.1 years—in these patients we found really very favorable outcomes with respect to major amputation, for instance, of only 9.1%. This compares very favorably to the SVS performance goals, which suggest limb salvage at 84, 85%.”
The key, Maldonado says, is in patient selection. “I think what we’re taking from this is that the OBL has a role to play even in patients who have more advanced comorbidities, with higher risk of limb loss, and may be an appropriate place to treat these patients, understanding that we only have a 9.1% risk of major amputation in this cohort. We feel that the OBL may be an appropriate setting in select patients with critical limb ischemia. Like anything we do in vascular
To this end, the analysis showed that patients who underwent amputation were more likely to have diabetes (79.2% vs. 58.2%). “When we looked at comorbidities, diabetic patients in particular were more likely to have amputation after out patient endovascular procedures for CLTI—not particularly surprising for this higher-risk cohort of patients is at increased susceptibility to infection, wound complications, etc.,” says Maldonado.
“But again, that speaks to proper patient selection and understanding that these patients need to be vetted and properly worked up to make sure that their comorbidities have been optimized and well managed before attempting something like this in the outpatient setting.”
Future research directions will look at cost implications of OBL use for CLTI patients, Maldonado continues. “Anytime you use the hospital infrastructure for taking care of these sick patients, there is an associated cost. Future studies should examine the health economics associated with caring for a patient with critical limb ischemia in the inpatient versus outpatient setting.
“Our present study has shown that over 70% of these
patients do not require inpatient reinterventions. We can keep them out of the hospital and that may be beneficial, not just for the patient but it also may be economic from a cost-savings standpoint.”
Maldonado also points toward likely gains in terms of patient quality of life and overall satisfaction.
“There’s no doubt that patients coming into the hospital, often resulting in an overnight stay or longer, can result in decreased patient satisfaction and negatively impact their quality of life,” he adds.
New OBL column to launch in October issue
Vascular Specialist is launching a new column in the October issue of the newspaper dedicated to issues important to—and involving—the OBL setting. Entitled “The Outpatient,” it will run bimonthly (or six times per year) and be edited by Anil Hingorani, MD, who was chair of the SVS Section on Outpatient and Office Vascular Care (SOOVC) until it was recently merged with the Community Practice Section (CPS) to form the new Section on Ambulatory Vascular Care (SAVC), which he will also chair.
Hingorani, a clinical professor of surgery at NYU Langone Hospital-Brooklyn and a vascular surgeon at the Vascular Institute of New York, also in Brooklyn, will write the maiden column.
KENNETH M. SLAW is SVS executive director.
Kenneth M. Slaw
Moira McGevna
Thomas Maldonado
The Doppler Designed for the Modern OR
It’s the next generation of our Trans-Q-taneous Intraoperative (TQI) Doppler System, combining the reliability and cost effectiveness of the original TQI Doppler with new, user-friendly features.
RELIABLE
VTI’s single-use surgical Doppler probes provide a higher degree of performance reliability since probe failure due to reprocessing is eliminated. You’ll reach for your Doppler with confidence!
COST EFFECTIVE
Single-use surgical Doppler probes eliminate reprocessing costs as well as the hidden expenses associated with the malfunctioning of reusable probes such as lost OR time.
EASIER TO USE
Increased Portability
In addition to its smaller size, the TQI 2.0 Doppler now features an IV pole mount and a handle for easy transport.
Greater Control
The modern design of the TQI 2.0 Doppler allows for a foot pedal for increased control from the surgical field.
Improved Sound
The TQI 2.0 Doppler System is optimized for clear audio signals for both intraoperative and transcutaneous use.
To request more information on
FROM
THE COVER STUDY SHEDS LIGHT ON VASCULAR-SPECIFIC ADVANCED PRACTICE PROVIDER EXPERIENCE
continued from page 1
validated questionnaire that was created by the Institute for Professional Worklife to look specifically at clinical burnout.
Bose shared that, of the 280 survey respondents, 47% were nurse practitioners, 31% were physician assistants and 21% were registered nurses.
One of the key questions on the survey probed the predictors of a joyful workplace. “Interestingly, there were only two things that were strongly predictive of a joyful workplace,” Bose revealed, “the ability for an APP to practice at the top of their license and a shorter shift length.”
Another question considered factors
NURSING
Being a vascular nurse: Notes from SVN president ahead of Vascular Nurses Week
By Kristin Spencer
Saideep Bose
that predict being comfortable in taking care of vascular patients. “Again, the number one thing was practicing at the top of the license,”
Bose reported, also citing number of years practicing as an APP taking care of vascular patients and being a member of the Society for Vascular Surgery (SVS) Physician Assistant Section or the Society for Vascular Nursing (SVN).
Bose et al subsequently investigated the defining factors of practicing at the top of one’s license, which they identified as seeing new patients in the outpatient clinic, a salaried pay structure and working with specific physicians. On the latter, Bose shared: “In my personal experience, I have seen that, because oftentimes a physician will have a particular specialty—for example aortic work or peripheral work—and so a physician nurse practitioner or a physician assistant who works specifically with them will become a master of that specialty as well. I think everyone benefits when there’s
that pairing with specific physicians.”
Bose commented that the significance of these findings comes from the fact that “some of these are factors that we can change.” He elaborated: “We can make sure our APPs are paired with a particular
“The main issue is that we don’t know how people in these APP positions feel about their careers or their jobs and if they feel like they are being utilized effectively or just being asked to do tasks that no one else wants to do”
SAIDEEP BOSE
LEADERSHIP
IN RECOGNITION OF VASCULAR NURSES WEEK (Sept. 8-14), Vascular Specialist spoke with Society for Vascular Nursing (SVN) President Karen Bauer, DNP. Bauer is a clinical assistant professor, lead vascular and wound surgery advanced practice provider (APP) and director of Vascular and Wound Services at the University of Toledo Physicians.
What does being a vascular nurse mean to you?
I am honored to be among such a diverse group of high-quality clinicians. Vascular nursing allows so many touchpoints with patients and provides opportunities to not only manage their vascular diseases, but to impact their lifestyles and overall happiness and well-being. As a vascular nurse/advanced practice nurse (APN), I get to engage with such a broad range of other professionals and, while vascular nursing can be mastered, there is always more to learn. I love the challenge!
Why do you think it is important that Vascular Nurses Week is celebrated?
Vascular nurses are crucial members of healthcare teams across so many different roles, which unfortunately is something that is often overlooked. We are positioned perfectly to positively affect the health and well-being of our patients and our teams, and that deserves some recognition. To recognize vascular nurses is to recognize great patient care.
How long have you been in the vascular field?
My first love was wound care, which integrates organically with the vascular field. I have been doing wound care for over 16 years, discovered my passion for limb salvage about eight years ago, and expanded my knowledge and skill set in vascular surgery about five years ago.
Why are you passionate about vascular care?
Small victories make for big wins in our field. I love the challenge and joy of figuring out how to meet my patients where they are and help them better understand both their disease process and how to prevent additional disease or other sequelae of it. The sheer happiness and pride I get to see on the faces of patients when they close a wound, or have improved leg pain, or successfully navigate new diets and exercises regimens, is endlessly fulfilling.
During Vascular Nurses Week, SVN invites Society for Vascular Surgery (SVS) members to give the gift of membership to their nurses and nurse practitioners. SVN membership offers valuable benefits, including a journal subscription, educational resources and leadership opportunities. Learn more at svnnet.org/page/ VascularNursesWeek
Tell us about a specific patient story that stands out when you think of a favorite vascular nursing memory. All patients are special to me, but one patient that stands out was an older gentleman with a severe diabetic foot ulcer and concurrent peripheral arterial disease (PAD) who was told he would end in amputation after his initial emergent debridement/revascularization. I love a good challenge. He trusted our team, and while it took almost a year total of countless visits, diagnostics and surgeries, his ulcer closed, and he was able to dance at his granddaughter’s wedding. What was most striking throughout our journey together, still, was his willingness to be vulnerable and share with us his life stories as well as his family, who always attended visits with him. He is my constant reminder that our patients are human first and deserve our undivided attention.
physician, we can make sure they see new patients and we can make sure that they are salaried.”
On some of the key strengths of the survey, Bose highlighted that this is “one of the largest surveys that asks APPs about their experiences, their feelings and their work patterns.” What’s more, he noted that no studies to date have looked at vascularspecific APPs.
He did, however, recognize the limitations associated with this being a survey, including recall bias. “People that have very strong opinions one way or the other are more likely to respond to a survey,” he remarked.
Overall, he described the survey as a “good overview” of APPs’ experience, stressing that the next step should be to study this more systematically—to “really go into the programs where APPs are happy and ones where they are unhappy and try to tease out factors that explain that.”
“Our ultimate goal is not just to explain what’s going on, but to try to figure out management factors, practice factors that we can implement to increase the job satisfaction of these APPs.”
FORMER SVS PRESIDENT NAMED CHAIR OF AAMC BOARD OF DIRECTORS
THE ASSOCIATION OF AMERICAN MEDICAL COLLEGES (AAMC) has elected Julie A. Freischlag, MD, as chair of its 2024–25 board of directors. Her term will commence on Nov. 12 and extend through the conclusion of the AAMC’s “Learn Serve Lead” annual meeting in November 2025.
Freischlag, a prominent vascular surgeon and healthcare leader, currently serves as chief academic officer and executive vice president of Advocate Health, chief executive officer and academic officer of Atrium Health Wake Forest Baptist and executive vice president for health affairs at Wake Forest University. She is also the previous dean of Wake Forest University School of Medicine.
Throughout her career, Freischlag has broken new ground in academic medicine. She was the first female surgeon-in-chief at The Johns Hopkins Hospital and the first female chief of vascular surgery at the University of California in Los Angeles (UCLA). Her previous roles include vice chancellor for Human Health Sciences and dean of the School of Medicine at UC Davis.
Beyond her administrative and academic roles, Freischlag is an accomplished vascular surgeon specializing in thoracic outlet syndrome. She is a past president of the American College of Surgeons and was elected to the National Academy of Medicine in 2015. In 2021, she was inducted into the Academy of Master Surgeon Educators.
As a member of the Society for Vascular Surgery (SVS), Freischlag has made significant contributions to the field. She served as 2013-2014 SVS president and received the 2023 SVS Lifetime Achievement Award, the Society’s highest honor. Freischlag also holds the distinction of being the sixth woman in the U.S. to receive board certification in vascular surgery.
“It is an honor to lead the AAMC at such a pivotal time in healthcare. I look forward to working alongside my colleagues to advance academic medicine and ensure that we continue to educate the next generation of physicians and healthcare professionals,” said Freischlag.
Freischlag earned her medical degree from Rush Medical College and completed her residency at Ronald Reagan UCLA Medical Center. Her election as chair of the AAMC Board of Directors adds another significant chapter to a career marked by leadership, innovation and service.—Marlén Gomez
Karen Bauer
VQI ANALYSIS OF CLTI PRACTICE FOLLOWING BEST-CLI FINDS NO PICK UP IN BYPASS RATE
A Vascular Quality Initiative (VQI) analysis of evolving practice in the wake of the BEST-CLI trial demonstrated no increase in the rate of surgical bypass in the year afterwards.
By Bryan Kay
MORE ANALYSIS NEEDS TO BE DONE comparing the data pre- and post-publication of BEST-CLI in the New England Journal of Medicine (NEJM) in November 2022, explains lead author Marc Schermerhorn, MD, “but I still think it’s surprising that there has been essentially no increase whatsoever about a year later. There wasn’t really a trend.”
Among 29,000 patients, overall use of bypass was 15%, the chief of vascular surgery at Beth Israel Deaconess Medical Center in
Boston continues. “When we compared the time period before the publication and the time period afterwards, it really didn’t change: it went from 14% to 15%; in men it went from 16% to 14%; and women from 11% to 16%—but none of those are anything close to anything significant.”
Broken down by segment, there was still no change, Schermerhorn added of the data, which will be presented at the New England Society for Vascular Surgery (NESVS) annual meeting in Portland, Maine (Oct. 25–27).
BEST-CLI demonstrated that surgical bypass with adequate single-segment great saphenous vein (GSV) is a more effective revascularization strategy for patients with chronic limb-threatening ischemia (CLTI) who are deemed to be suitable for either an open or endovascular approach.
Speaking with Vascular Specialist ahead of the NESVS meeting, Schermerhorn points to several possibilities to explain why the needle hasn’t shifted.
“It always takes time after new data comes out for it to diffuse out broadly,” he says. “I suspect that that’s the main thing. Sometimes practice doesn’t change until a guideline comes out.” As chair of the Society for Vascular Surgery (SVS) Document Oversight Committee, he points out an update of the CLTI guidelines is in the works. “That will certainly incorporate [the BEST-CLI trail data],” Schermerhorn adds, explaining that that too remains more than a year down the road owing to the guideline development process. “We will re-evaluate this after that to see if
there is a change after the guidelines are published … I think we need to get the word out to more people, to the New England community, to the SVS and internationally—that people with a good single-segment saphenous vein should at least be considered for bypass more so that they were in the past.”
Schermerhorn acknowledges that there may be differing interpretations of the BEST-CLI results between specialties to a certain extent but says even among vascular surgeons there may be a hesitancy to do more bypasses. “People have gotten so used to doing peripheral interventions, and their volume of bypass grafts have gone way down,” he explains. “It’s possible that surgeons are less comfortable with bypass than they used to be, or that they’re more fearful of the potential complications and feel that the patients are too frail for bypass. And that may well be the case for many patients.”
The Harvard University professor of surgery also concedes that the BASIL-2 trial
results, though based on a slightly different patient population, may be “holding things back.” As a result, he believes those data should likewise be “considered differently” and underscores his belief that bypasses should nevertheless be performed more often. “[BEST-CLI] certainly changed my practice and that of our group,” says Schermerhorn. “We always check to see if someone has got saphenous vein before we do an angio, which is something we started doing when we participated in the trial. We hadn’t done that previously. We’re much more likely now in a patient with extensive multi-level disease—and significant ischemia and significant foot lesions—to recommend bypass.”
He finishes by referencing an analysis conducted by a partner that looked at graduating vascular surgery trainees’ facility with infrapopliteal bypasses. “It showed that when they graduate, they have done very, very few during their training period—I think the average is well below 10,” Schermerhorn says. “The last time we looked at that was probably eight or 10 years ago. It’s an area where people are not being trained adequately because we have made such a switch to peripheral intervention.”
“When we compared the time period before the publication and the time period afterwards, it really didn’t change”
MARC SCHERMERHORN
Marc Schermerhorn
CORNER STITCH COMMENT& ANALYSIS
OUR PATIENTS NEED MORE SPANISH-SPEAKING VASCULAR SURGEONS: AN ARGUMENT FOR MEDICAL SPANISH IN VASCULAR RESIDENCY
By Melissa D’Andrea, MD
Since there are more than 40 million Spanish speakers in the United States, training more bilingual physicians could potentially improve equitable care in Latino communities, according to an article published on July 18, 2023, by the Association of American Medical Colleges (AAMC).1
To provide better care to Spanish-speaking patients, there is a call for medical schools and residencies to recruit and retain more Hispanic, Latino and multilingual doctors, and to provide medical Spanish language training and proficiency testing to medical students and physicians to enhance their ability to communicate with and relate to their patients.
Patients without language-concordant healthcare providers are more likely to experience miscommunication and adverse events, are less likely to comply with medications and medical advice, and are less likely to come to follow-up appointments, according to a case study published in February 2023.2
Moreover, only 2% of physicians speak Spanish, according to AAMC diversity facts and figures from 2019, which is a very low number compared to the demand that exists among Spanish-speaking patients in the U.S. According to a more specific poll conducted by the Society for Vascular Surgery (SVS) that was published in 2012, only 3.7% of vascular surgeons are Hispanic. It is unknown how many speak Spanish.3
So, how can we address this issue as a specialty? By implementing Spanish-language competency programs—
A
call to action for the 119th
Congress GOVERNMENT GRAND ROUNDS
By Andrew Kenney
A FOUNDATIONAL ELEMENT FOR effective advocacy is understanding the profound impact that legislative decisions have on the practice of medicine and the health of our patients. The retirement announcements of several key members of Congress from the “Doc Caucus” present both a challenge and an opportunity as we approach the 119th Congress.
The Doc Caucus, a group of Republican physician-legislators, brought firsthand experience to Capitol Hill. This group has also established a mechanism for
especially in training regions with large Spanishspeaking populations during the course of surgical training—we could significantly improve patient care.
The goal of medical Spanish proficiency classes is not to create perfect Spanish interpreters or bilingual fluency geniuses, but to have enough Spanish knowledge to get your point across to a patient in basic medical terms in order to gain patient trust. The classes can be implemented for those trainees practicing in areas where most of the patient population speaks Spanish and has limited English proficiency, and ideally students enrolled have at least intermediate Spanish skills and an interest in working in the Hispanic-Latino community.
Melissa D’Andrea
period. This schedule is ideal for the first couple of years of surgical residency when residents are doing more floor work, intensive care unit (ICU), and night shifts so that attendance can be optimized prior to busy operative senior years. The classes are built such that if you miss the first Thursday of the month class (for Main campus), you can still make it to the third Thursday class (for South campus). This allows flexibility in the schedule.
Medical schools with higher Spanish-speaking populated cities such as Texas Tech University Health Sciences Center in El Paso, Texas, and Loyola University Chicago Stritch School of Medicine in Chicago, where I went to medical school, teach medical Spanish as a part of the pre-clerkship curriculum for students. However, few residency programs offer medical Spanish courses, most likely due to pre-existing, busy service obligations.
Here in Tucson where I am a resident, one hour from the U.S.-Mexico border, there is a large Spanish-speaking and Sonoran Mexican population. At the University of Arizona College of Medicine-Tucson, there is a weekly medical Spanish class for advanced speakers to learn medical terminology offered through the Diversity Equity and Inclusion Department that takes place every Thursday. The course is to be completed over a two-year
“Implementing Spanishlanguage competency programs, especially in training regions with large Spanish-speaking populations during surgical training, could significantly improve patient care”
lawmakers to directly educate their peers on the real-life impact of health-related policies. The Doc Caucus has been a vital voice in Congress, ensuring that the perspectives of healthcare providers are considered in legislative decisions. These physician-legislators understood the unique challenges of balancing patient care with the regulatory and financial constraints imposed by federal policies. The Doc Caucus has been at the forefront of efforts to address the unsustainable Medicare payment system, advocating for reforms that ensure fair reimbursement for physicians while maintaining access to care for seniors.
With the retirement of several of these influential members, there is a risk that the voice of physicians in Congress could be diminished. However, this is not a time for retreat—it is a call to action. As we
Then, there is an ALTA Language Services exam at the end of the year to show competency. If graduates attain >80% proficiency on the oral exam, they receive a badge confirming they can speak with patients in Spanish and even consent them for procedures without the need for an interpreter. This can potentially allow for more efficiency, better patient-physician relationships and fewer miscommunications.
As a fellow champion of the argument for increased medical Spanish training, I plan to develop a booklet that can be carried around in providers’ white coats or in a phone app. These will contain key medical and surgical terminology in Spanish to help describe common pathology and interventions relevant to vascular surgery, so those trainees who don’t have access to classes can utilize this platform to make connections with their Spanish-speaking patients more feasible.
Please reach out to be involved in this future project via LinkedIn or Twitter (@MelissaDAndrea4).
2. Lopez Vera A, Thomas K, Trinh C, Nausheen F. A case study of the impact of language concordance on patient care, satisfaction, and comfort with sharing sensitive information during medical care. J Immigr Minor Health. 2023 Dec;25(6):1261–1269.
3. Woo K, Kalata EA, Hingorani AP. Society for Vascular Surgery Diversity, Equity and Inclusion Committee. Diversity in vascular surgery. J Vasc Surg. 2012; 56: 1710–1716
MELISSA D’ANDREA is a fourth-year integrated vascular surgery resident at the University of Arizona-Tuscon.
look ahead to the 119th Congress, it is imperative that the Society for Vascular Surgery (SVS) and the broader medical community remain actively engaged in the legislative process. We must ensure that the needs and concerns of our profession continue to be heard. We must build relationships with new members of Congress, particularly those who may not have a healthcare background. It is essential to educate them on the challenges we face and the impact of their decisions on patient care. Our input is crucial to crafting policies that support both physicians and patients. We also need to become more aggressive in identifying and supporting candidates with health-related backgrounds. As we look toward the January 2025 start of the 119th Congress, we must mobilize members
to be active participants in the political process. Whether through letter-writing campaigns, or visits to Capitol Hill, every effort counts. Collective action can drive significant change.
The departure of crucial Doc Caucus members may initially be viewed as a challenge to overcome, but it also opens the door for new opportunities. By staying engaged, informed, and active, we can continue to advocate for the policies that protect patients and the profession. Let us recommit to our role as advocates for vascular surgery and the broader medical community. The future of healthcare depends on our continued involvement and leadership.
ANDREW KENNEY is a member of the SVS advocacy staff, representing the Society in Washington, D.C.
SVS announces merger creating Section on Ambulatory Vascular Care
By Marlén Gomez
THE SOCIETY FOR VASCULAR Surgery (SVS) announced the merger of its Section on Outpatient and Office Vascular Care (SOOVC) and the Community Practice Section (CPS), marking the creation of the new Section on Ambulatory Vascular Care (SAVC), which is set to launch in early fall. In a bid to advance outpatient vascular care, the SVS established SOOVC in 2019 and, then, in 2021, the CPS.
The decision to merge these two sections comes as the traditional boundaries of vascular care continue to blur as the vascular surgical specialty evolves.
According to SVS leadership, increasing overlap between community practices, outpatient labs, vein clinics and other outpatient settings has highlighted the need for a more unified approach.
Recognizing this, Anil Hingorani, MD, of Total Vascular Care in New York, and Robert Molnar, MD, of Michigan Vascular
GUEST EDITORIAL
Center, in collaboration with SVS staff, proposed the merger to bring together resources and expertise under one umbrella. Hingorani previously held the role of chair of the SOOVC Steering Committee, while Molnar chaired the CPS Steering Committee.
SAVC will encompass a broad range of outpatient vascular care settings, includ ing community practices, office-based labs (OBLs), ambulatory surgery centers (ASCs) and hospital-affiliated outpatient facilities.
With this new section, the SVS aims to enhance its efforts in education, advocacy, quality, ethics, research and overall member value within the burgeoning landscape of outpatient vascular care.
“All current members of the CPS and SOOVC
will automatically become members of the new section,” said Hingorani, who will serve as the chair of the SAVC. “We are excited about the contributions this section will make to the field of vascular care.”
Hingorani will be joined on SAVC by Geetha Jeyabalan, MD, of MedStar Health and Vascular Institute in Annapolis, Maryland, who will perform the role of vice chair.
nations are now open for the 2024–25 SVS awards. The Excellence in Community Practice Award will retain its name, continuing to honor outstanding contributions in this area.
SOOVC CPS
Anil
Hingorani
The merger’s call for volunteers to join the SAVC Steering Committee closed in August. Members interested in leadership roles will find opportunities to shape the direction of the new section as it begins to
They are encouraged to keep an eye out for upcoming SVS communications for more information and to stay updated on SAVC’s progress, including within the pages of Vascular Specialist
Awards update
Under their current section names, nomi-
THE CLTI CONUNDRUM: MY SPIRITED JOURNEY THROUGH THE CLTI SAGA continued from page 2
Then, in a sudden plot twist, 65 years after Fontaine first attempted to classify this process, enter the GLASS investigators, the latest heroes in our tale, attempting to demystify CLTI with a blend of PAD, rest pain, tissue loss present for greater than two weeks, and a sprinkle of hemodynamic intrigue including ABIs, toe pressures and transcutaneous oxygen measurements. But wait, there’s more! Embedded within CLTI are definitions within definitions layering our CLTI mystery novel—PAD, rest pain, gangrene and ulcer, each a subplot within the grand narrative of CLTI. Does one have PAD based on anatomy, hemodynamics or symptoms? Many patients with PAD are sedentary (obesity, shortness of breath, lumbar disc disease, diabetic neuropathy, frailty) and do not experience symptoms. What if the patient describes burning, tingling or numbness, is that considered rest pain?
In the latest chapter of the ongoing saga that is CLTI, definitions have taken a dark turn, becoming less about medical precision and more about wielding the grim reaper’s scythe over the heads of our protagonists. It’s as if some Dickensian villain has whispered into the collective ear of the vulnerable, “Beware, an amputation awaits those with rest pain,” turning a choice into a tale of certain dread.
Now enters our reluctant hero, the every-patient, who earns his living from his motor skills and finds himself at a crossroads. Offered the devil’s bargain: a “low-risk” procedure pitched with the same persuasive charm as Clark Stanley, aka the Rattlesnake King, versus the foreboding loss of a limb—a phantom limb, haunting his future. The narrative escalates, becoming a weapon that doesn’t just threaten physical loss but launches a calculated strike at the patient’s dignity and self-worth. The looming threat of amputation casting a long shadow in the corridors of his mind is compounded by the barking of the black dog of depression causing our
character to turn to a form of self-flagellation.
“Well, if my leg’s going to be tossed out like bad leftovers, why not call the shots on my way down,” he suggests as the cigarette smoke swirls like the fog in a San Francisco sunrise. Unfortunately, following a “100% successful procedure” and now post amputation, he is only a shadow of his former self—a poignant reminder that our medical decisions are not just clinical; they’re deeply personal. We forget and overlook the human element in return for technical success and financial gain.
The tale of CLTI cannot be told without the pioneers who in the early- to mid-20th century outlined the early principles of vascular occlusive disease and oversaw both clinical and experimental techniques in revascularization.
Perhaps the answer lies in simplicity—a return to the basics, where critical limb threat encompasses not just a focus on what can be intervened upon anatomically but a larger story about the human element
We tip our hats to the trailblazers—Carrel, Leriche, Jaboulay, Kunlin, DeBakey, Dotter and Grüntzig—who, with the verve of pioneers and the audacity of explorers, sketched the early maps of vascular wilderness. Yet, here we are, nearly a century later still caught in the whirlwind of defining and redefining CLTI. Despite the cash tsunami funneled into research and development, we’re somewhat akin to hamsters on a wheel—spirited but spinning in place.
Starting in 2025, the awards previously associated with SOOVC will be rebranded under the new SAVC. This includes the SOOVC Presentation Award and the Research Seed Grant, which will carry the new SAVC acronym moving forward.
SVS members are encouraged to apply for the current awards, and nominations are due by Tuesday, Oct. 15.
For more information and to submit your nominations for any of the awards, visit vascular.org/Awards
“All current members of the CPS and SOOVC will automatically become members of the new section”
ANIL HINGORANI
We’ve also now ventured into new territories, from infrapopliteal to inframalleolar, with the same zeal and optimism as a toddler’s first steps—eager, if not a tad wobbly. Over the last century, through the thick tome of literature, with acronyms that could double as the latest tech start-ups, we’ve showcased our unwavering commitment to tackling PAD and limb salvage. But the gold standard? It’s still Kunlin’s single-segment GSV bypass from 1948—vintage, classic, yet undefeated. And so, I lament, perched upon decades of innovation and introspection: “Have we truly advanced in our quest against CLTI, or are we just marching to the nostalgic rhythm of past triumphs?”
Our final chapter calls for unity—a rallying cry for a collaborative, evidence-based definition of CLTI that stands the test of time and scrutiny. A definition that’s not a mere classification of the severity of a disease process but a clear and concise answer to the question, “What is CLTI?” We can all conclude that CLTI is not localized and segmental, as our interventions suggest. The complexity of CLTI, influenced by a kaleidoscope of patient factors, poses a formidable challenge and we should start to look to the future where advanced molecular, genomic and imaging techniques is what helps define CLTI. After all, rest pain, multi-level occlusions, wounds and hemodynamic derangements are simply downstream consequences of CLTI and we should get away from the circularity of using these constructs to define CLTI. Perhaps the answer lies in simplicity—a return to the basics, where critical limb threat encompasses not just a focus on what can be intervened upon anatomically, but a larger story about the human element: the people attached to the limbs, their stories, their risk factors and paths through the intricate world of vascular health.
OMID JAZAERI is a medical director of vascular services at AdventHealth in Denver, Colorado.
REGISTER TODAY
REGISTER BY SEPTEMBER 10 TO SECURE PRIME TUITION RATES viva-foundation.org/register
• 2 days of venous education featuring sessions on medical management, cases & complications, DVT, and more
• The 5th Annual Blue Sky Breakfast providing a first look at the future of venous care
• Late-Breaking Clinical Trials session featuring first-on-podium data
• PE Summit open to all VIVA and The VEINS attendees offering a foundational understanding of the current state of PE, high-value RCT results, and strategies to improve patient outcomes
22nd Annual V ascular I nter V entional A dvances
NOVEMBER 3 - 6, 2024 • WYNN LAS VEGAS
• 5 Pre-Courses: CLTI, Aortic, Dialysis, PharmacoRx, and PE Summit
• The Global Theater featuring international live cases, groundbreaking clinical trials, great debates, and disruptive tech sessions
• Dynamic case discussions in Strategies on the Frontline
• Roundtable forums on AI/robotics, carotid intervention, and renal denervation
• Case presentations by the next generation of vascular leaders in the Face-Off Competition
• Simulator Showcase and Hands-on Cadaver Lab
Learn more, view the agenda, and register here
TRAINING APDVS launches vascular surgery curriculum e-book for medical students
By Marlén Gomez
THE ASSOCIATION OF PROGRAM DIRECTORS in Vascular Surgery (APDVS) has released a new ebook designed to enhance vascular surgery education for medical students. According to developers, the aim of The APDVS Medical Student Curriculum is to broaden the medical student’s clerkship curriculum, in line with the APDVS’s goal to provide a solid foundation in vascular surgery pathology and treatment.
“Unfortunately, the notion that assessment drives education holds true. Vascular surgery has very limited representation on the surgery shelf and Step exams and so finding the motivation to study vascular topics can be tough. For students on vascular surgery rotations, intrinsic motivation plays an equal if not larger role than extrinsic motivation. We created a resource that makes intrinsically motivated vascular surgery studying accessible, level-appropriate and interesting,” said Ezra Schwartz, MD, co-editor and lead developer of the project.
The ebook covers key domains of vascular surgery, offering both the fundamentals and opportunities for deeper dives. Originally published in January 2023, the APDVS Medical Student Curriculum project was years in the making. The idea was born from research spearheaded by Chelsea Dorsey, MD, of the University of Chicago, where she did a national needs assessment to understand the curriculum for medical students.
The results revealed that neither the American College of Surgeons (ACS) nor the Society for Vascular Surgery (SVS) provided curriculum recommendations for medical students rotating on a vascular surgery service, resulting in a gap in education geared towards medical students with minimal knowledge of vascular services.
Two studies by Dorsey et al are particularly relevant to the goals of the ebook: “Vascular surgery curriculum for medical students: A national targeted needs assessment”
VASCULAR PRACTICE
and “The value of a vascular surgery curriculum for clinical medical students: Results of a national survey of nonvascular educators.”
“[These articles] demonstrate the need to have a standardized curriculum and use the Delphi method to determine the topics that we should prioritize,” said Schwartz.
Critical contributors have supported the ebook’s development, including Sharif Ellozy, MD, director of the New York Presbyterian Hospital (Columbia and Cornell Campus); Adam Johnson, MD, of Duke Health, the Audible Bleeding Vascular Surgery Exam Prep project and the SVS Resident Student Outreach Committee (RSOC). Additionally, Schwartz credits his thesis mentor, Traci Wolbrink, MD, of Boston Children’s Hospital, founder of the modular online learning platform OPENPediatrics.
The ebook includes supplementary materials, such as slide decks, pre- and post-reading questions and teaching cases
“Unfortunately, the notion that assessment drives education holds true. Vascular surgery has very limited representation on the surgery shelf and Step exams and so finding the motivation to study vascular topics can be tough” EZRA SCHWARTZ
SVS ENCOURAGES PARTICIPATION IN COMPENSATION SURVEY
THE SOCIETY FOR VASCULAR Surgery (SVS) is encouraging members to participate in the 2024 Compensation Survey, a key initiative designed to provide vascular surgeons with tailored insights into compensation, productivity and practice data. This effort, conducted in collaboration with Phairify—a webbased data collection and visualization platform—aims to help SVS members make informed career decisions by offering exclusive access to detailed information that is specific to their specialty and practice situations.
The SVS Compensation Survey,
which launched at the 2023 Vascular Annual Meeting (VAM), has already seen significant participation from members, with 22% completing the survey by the end of 2023—exceeding the initial 20% target.
As 2024 progresses, the SVS is urging both new participants and those who took part last year to update their data to ensure the most accurate and up-to-date information is available.
The survey, designed with busy physicians in mind, takes approximately 15 minutes to complete. It is fully anonymous, allowing participants to
developed by the APDVS in addition to highlighting highly relevant outside content such as Audible Bleeding podcast episodes. One advantage of publishing an ebook is the ease of releasing updates, with the title set to continue to create and share additional slide decks, questions and podcast episodes, the developers said.
“We strive to present each chapter in the preferred modalities for every learner type. This means sharing the information in a traditional textbook style, a PowerPoint presentation, a podcast, etc. We want students to be able to learn the material on their way to the hospital if they’re biking or on public transportation,” summarized Schwartz.
“We want to cover all learning styles because everyone learns differently, and time is a limited resource in the life of a medical student. We want to make sure that people can learn vascular surgery in the way they prefer.”
There are three main points developers hope to convey to the vascular community: that the ebook is comprehensive, utilitarian and concise.
“As vascular surgery continues to evolve and differentiate itself from general surgery, the surgical curricula at many medical schools can leave students poorly equipped to have meaningful discussions about complex issues in vascular surgery,” said Mark Basilious, a fourth-year medical student at Weill Cornell Medical College in New York City and co-editor of the ebook. “This resource is an effort to democratize knowledge in this niche field and make it accessible to trainees everywhere. We are deeply grateful for the enormous contributions of our student and trainee authors, and we extend our heartfelt thanks to our expert senior authors for volunteering their time to review the product as it rolls out.”
Drayson Campbell, a fourth-year medical student at the Ohio State University College of Medicine, feels the opportunity to contribute to a practical, convenient and accessible resource for medical students like himself has been incredibly fulfilling. Based on his experience, transitioning from standardized pre-clinical curricula to caring for vascular surgery patients has presented a steep learning curve.
“Numerous challenges exist in navigating the complex practice guidelines written for trainees and attending vascular surgeons, and these are amplified by the gap in medical education. The ability to contribute to a resource written for medical students in their clinical years to facilitate the next generation’s transition has been a satisfying way to give back to the community that has given me so much,” said Campbell.
To learn more about the needs assessment research, visit vascular.org/APDVS-ebook.
provide information without concerns about privacy. The survey covers a wide range of topics, including compensation, call frequency, productivity, bonuses, benefits and practice settings, among others.
Members can use this data to compare their financial situation with their peers across various demographics, such as geographic location, gender, race, age and practice type (academic vs. private practice).The platform’s focus on privacy and security ensures that all data is de-personalized and inaccessible to any external agencies.
Participation in the survey also unlocks additional benefits for SVS members. Upon completing the survey, members gain access to comprehensive benchmarking data, allowing them to review their
compensation and productivity relative to peers. The initiative was developed in response to ongoing requests from SVS members for more transparency and data-driven insights into vascular surgery compensation. The SVS Financial Compensation Task Force, responsible for overseeing the work, worked closely with Phairify from January 2023 through May 2023 to design the survey.
The survey is open to all SVS Active and Early Active members residing in the U.S. Participation is free, and the data is completely anonymous. Once a sufficient number of responses (a minimum of 10) are collected for a given data field, participants gain immediate access to the compensation benchmark data.
Visit vascular.org/Compensation.— Marlén Gomez
SVS PRESIDENT CHAMPIONS
CONTINUITY, COLLABORATION AND UNIFIED FUTURE
By Marlén Gomez
As Matthew Eagleton, MD, continues with the duties of president of the Society for Vascular Surgery (SVS), his vision for the organization extends well beyond his yearlong term. Eagleton brought a wealth of experience to the position, not only from his current role as system chief of vascular and endovascular surgery for Mass General Brigham and co-director of the Fireman Vascular Center at Massachusetts General Hospital, but also from his years of dedication to advancing vascular care and education. However, his approach to leadership emphasizes continuity, collaboration and a commitment to long-term goals that surpass the influence of any single president.
Reflecting on his journey, Eagleton traces his passion for vascular surgery back to his roots in upstate New York, where he grew up in a small farming community near Rochester. Influenced by his father, a retail
pharmacist, and his mother, a high school science teacher, Eagleton’s early exposure to medicine laid the foundation for his future career. After receiving his medical degree and completing his general surgery residency at the University of Rochester, he further specialized in vascular surgery at the University of Michigan. This journey through these institutions and his advanced training at the Cleveland Clinic, where he became a leader in the field, is one he credits in shaping his perspective on surgery and leadership.
Throughout his career, Eagleton has been guided by numerous mentors, from Seymour Schwartz, MD, who sparked his interest in surgery, to vascular surgery pioneers like James DeWeese, MD, Richard Green, MD, and Ken Ouriel, MD. These influences not only guided his professional path but also instilled in him the importance of mentorship, collaboration and long-term planning—principles that now inform his leadership at the SVS.
One of the key messages Eagleton emphasizes is that the role of SVS president cannot be viewed as an isolated position of power. Instead, it is part of a larger, ongoing effort that requires the collective wisdom and contributions of the entire SVS Executive Board, the SVS Strategic Board of Directors and the membership.
“Each president has the opportunity to champion specific issues that can provide immediate improvement in our ability to provide quality vascular care,” said Eagleton. “In addition, we have invested in a number of projects, as part of our long-term strategic plan defined by the Strategic Board of
Directors, that we must not lose focus on as they will have a tremendous impact on the future of vascular care globally.”
Eagleton is acutely aware of the challenges that come with leader ship transitions and the potential for disruption in long-term initiatives. He stresses the importance of continuity within SVS leadership, ensuring that the Society’s core objectives— improving patient care and serving its membership—remain steadfast despite changes in administration. This commitment to continuity is reflected in the way the SVS Executive Board (EB) operates, providing critical guidance to the president on key decisions, helping to maintain focus on the Society’s mission and ensuring that the SVS remains aligned with the needs of its diverse membership.
president alone who makes decisions about what we’re doing,” Eagleton explains. “The EB functions critically, providing guidance on how we should react, what we should invest in and what to avoid. It’s important that we have diverse voices within the Executive Board so that we can understand the many different facets and interests of the SVS.”
“Anytime there is a major issue, it’s not the
“We have long-standing projects that go on for years, and we have to have a leadership structure that listens to and recognizes the needs of our constituents”
MATTHEW EAGLETON
This emphasis on diversity and collaboration within the leadership team is essential to Eagleton’s vision of a more unified Society. He recognizes that the SVS represents a wide range of vascular surgeons, from those in private practice to those in academic settings, and that the Society must find ways to bring these different groups together. As Joseph Mills, MD, highlighted in his 2024 SVS presidential address, unity is key to determining the future of the specialty, and it is a message he intends to continue to champion throughout his presidency. In addition to fostering unity, Eagleton is focused on ensuring that the SVS plays a larger role in the global political dynamics of vascular care. He sees the SVS as a crucial voice in advocating for the specialty. A major part of this effort will involve an education campaign to help the world better understand what vascular surgeons offer.
As Eagleton embarks on his year as SVS president, his vision is clear: leadership is not about short-term gains or individual achievements but about guiding the Society toward a future where vascular surgery is better understood, more unified and more
Matthew Eagleton
impactful. Through collaboration, continuity, and a commitment to the long-term goals of the SVS, Eagleton hopes to leave a lasting legacy that benefits both the Society and the patients it serves.
“Our vision is longer than my 12-month term. We need to focus on this goal, and it’s up to all of us in leadership to ensure that SVS stays on track to achieve it,” said Eagleton.
SVS president convenes 2024 EB retreat
The SVS EB gathered at its headquarters in Rosemont, Illinois, this summer, tackling over 40 strategic, policy and governance issues as it set the course for the year ahead. “The annual EB retreat is a critical meeting,” said SVS President Matthew Eagleton, MD. “The SVS strategic plan and program portfolio are expansive, and this retreat allows the EB to establish focused priorities for the next 11 months, define desired outcomes and ensure that governance structures and resources are aligned to achieve those priorities.”
The retreat’s discussions centered on the long-term health, vitality and trajectory of vascular surgery as a specialty. Key focus areas included the SVS branding campaign, the Society’s response to the proposed new American Board of Medical Specialties (ABMS) American Board of Cardiovascular Medicine (ABCVM) and the ongoing work of the Vascular Certification Board (VCB) Task Force. “The next six to 12 months could bring significant changes for vascular surgery, and we need to be prepared for multiple scenarios,” said Eagleton.
The EB outlined specific measures of success for its branding initiatives and developed key messaging for each target audience in preparation for a major launch in September-October. With the ABMS expected to decide on the proposed ABCVM as early as October, the EB also prepared responses for various potential outcomes. The VCB Task Force met in person the day before the retreat and also considered the potential impacts of a new ABCVM. “The outcome of the ABMS decision will almost certainly influence discussions and decisions about the optimal structure of the Vascular Surgery Board (VSB),” said Michael Dalsing, MD, task force chair.
The VCB Task Force will deliver its final report in November, with presentation to the SVS Strategic Board scheduled for Janu-
The SVS is set to stage an advovacy conference in the capital
ary. Additional priority initiatives and decisions discussed during the retreat included:
● SVS Advocacy Leadership Conference: Preparations are underway for the inaugural conference and Hill visit in Washington, D.C., in September 2025
● SVS education needs assessment: The board agreed to design the following needs assessment, focusing on early- and mid-career vascular surgeons, to guide the launch of a comprehensive support approach for these groups
● SVS Gala transition: The board approved transitioning the SVS Gala at the Vascular Annual Meeting (VAM) to a milestone event celebrating SVS anniversary years, with more informal events in between
● PMEGs best practices paper: At the Food and Drug Administration’s request, the
SVS was approved to develop a “best practices” paper on physician-modified endografts (PMEGs)
● Young Surgeon Section: The board approved the Young Surgeon Section as a full-standing section of SVS
● Section mergers: The board approved merging the Section on Outpatient and Office Vascular Care (SOOVC) with the Community Practice Section to form the new Section on Ambulatory Vascular Care (SAVC)
● Senior Members Provisional Section: A new provisional section for senior members was approved
● APP Section: The Advanced Practice Providers (APP) Steering Committee was approved to design and launch a new APP Section within the SVS, merging with the Physician Assistant Section
● Inter-society relations: The board approved SVS’ support of vascular society milestone events, provided that inter-society relations are in good standing
● SVS EB at-large members: Plans for the nomination and selection of five at-large members of the SVS EB were approved
● DEI Committee priorities: The top priorities of the Diversity, Equity and Inclusion (DEI) Committee for the coming year were accepted
● SVS HQ space assessment: The board agreed to assess future headquarters space needs
“The health and vitality of our specialty and members will be front and center during my year as president,” said Eagleton.
SOCIETY BRIEFS
Compiled by Marlén Gomez and Kristin Spencer
SVS set to disseminate educational needs assessment survey to members
THE SVS HAS CALLED ON MEMBERS to detail their educational and professional development needs in order that it can seek to better support vascular surgery careers.
The Society will be sending out an educational needs assessment surgery to members and other vascular surgery constituents from September into early October. This survey is aimed at helping the SVS to map out future education priorities.
“This is one of the three key surveys that the SVS Executive Board weighs in on and approves the SVS to send out,” said SVS Education Council Chair Kellie Brown, MD.
The first assessment survey was sent out in 2021 and received 767 responses. The usable sample was 585, the number SVS hopes to exceed this time around. The 2021 assessment produced data that showed the need for more coding and reimbursement resources.
The SVS is encouraging all vascular surgery specialists to participate in the needs assessment in order to map out educational needs for the next three years. Those who complete the assessment will be entered into a draw to win one of 10 Amazon gift cards (ranging from $100–$200 in value). Email education@vascularsociety.org
SVS EMPOWERS SURGEONS WITH PATIENT-REPORTED OUTCOMES TOOLKITS
THE SVS QUALITY IMPROVEMENT COMMITTEE
has developed toolkits aimed at enhancing patient care and outcomes by integrating patient-reported outcomes (PROs) into clinical practice. These resources are set to transform how healthcare professionals interact with and understand their patient experiences and health statuses.
“Patient-reported outcomes are invaluable in understanding the full scope of our patients’ well-being and the effectiveness of our interventions,” said Ashley Vavra, MD, chair of the SVS Quality Improvement Committee. “These toolkits provide vascular surgeons with the necessary resources to incorporate patient perspectives directly into their care plans, ensuring a more holistic approach.”
PROs are essential metrics that allow healthcare providers to assess medical interventions’ effectiveness by capturing patients’ firsthand accounts of their health and experiences. This approach offers a direct, unbiased insight into patient perspectives, free from the influence of clinicians or other intermediaries.Two primary categories of stand out: satisfaction scores and healthrelated quality of life (HRQOL). The toolkits include resources on survey administration, data collection and an inventory of existing PROs.
For more information on the toolkits, visit vascular.org/Quality.
STEPPING UP FOR VASCULAR HEALTH: CHALLENGE COMMENCES
THE 2024 SVS FOUNDATION’S Vascular Health Step Challenge kicked off Sept. 1 with over 400 registrants committed to walking 60 miles throughout September in honor of Peripheral Arterial Disease (PAD) Awareness Month. With over 60,000 miles of blood vessels in the human body, walking is a common prescription that vascular surgeons give their patients to decrease their risk of PAD or to manage their symptoms.
SVS members and people from across the world have signed up to support the third annual iteration of the challenge. Registrants have come from places as far flung as India, Mexico, Vietnam and Brazil as part of the global commitment to vascular health.
The mission of the SVS Foundation is to optimize the vascular health and well-being of patients and the public through support of research on circulatory disease. Recently, the foundation announced that funds raised from the challenge will support a new Vascular Care for the Underserved (VC4U) grant for SVS and Society for Vascular Nursing (SVN) members.
It isn’t too late for walkers who still want to sign up: registration will remain open through the end of September. Donations toward individual walkers, teams and the general campaign will be accepted throughout September as well. Visit vascular.org/ Step2024 for more details.
Diabeticfootproblemssignificantly impairthe quality of lifeofdiabetic patients. Each year in theUnitedStates, thesecomplications lead tomore than 750,000 new diabeticfootulcers and 70,000 lower extremity amputations. This extraordinarythreedaysymposium will promotebetterunderstandingof the unmet management needs ofDiabeticLower Extremity (DLE) complications and thenewtherapeuticapproachesthat arecurrentlyunder development. dlesymposium.com This CME meeting will focus on the management of diabetic lower extremity and other chronic wounds. The meeting will include top experts from all over the world and will facilitate
Peter Gloviczki steps up for PAD
CLINICAL&DEVICENEWS
Compiled by Jocelyn Hudson and Bryan Kay
SCOREPAD seeks to address ‘alarmingly high’ mortality in CLTI patients with underlying coronary disease
A NEW RESEARCH LETTER UNDERSCORES THE need to improve long-term survival following lower extremity revascularization for chronic limb-threatening ischemia (CLTI), setting out a randomized controlled trial to examine the impact of coronary artery ischemia testing in these patients.
The letter, authored by Dainis Krievins, MD, of Pauls Stradins Clinical University Hospital in Riga, Latvia, Andrejs Erglis, MD, of University of Latvia in Riga, and HeartFlow’s senior advisor for medical affairs, Christopher K. Zarins, MD, was recently published online ahead of print in the European Journal of Vascular and Endovascular Surgery (EJVES).
Krievins and colleagues first detail that patients undergoing lower extremity revascularization for CLTI or claudication have “poor” long-term survival due to coexisting coronary artery disease (CAD), which they note is “often asymptomatic, undiagnosed and undertreated.”
Diving into the available data on the topic, Krievins et
Inari Medical updates
ClotTriever XL IFU amid FDA recall notice
THE FOOD AND DRUG ADMINISTRATION (FDA) has issued a Class I recall—the most serious type—for Inari Medical‘s ClotTriever XL, 30mm device due to reports of patient injury, and death from device entrapment and pulmonary emboli (PE).
The device remains on the market with updated instructions for use (IFU), with all devices and lot numbers with labeled dates prior to Aug. 1 affected. The FDA recall was categorized as a “correction,” addressing a problem with a medical device in the place where it is used or sold rather than removing it from the market.
There have been four reported injuries and six reports of death, the FDA noted. The serious adverse events occurred in patients who had the ClotTriever catheter inserted through the jugular vein; thrombus that is fibrotic, organized and/or adherent; clot formed by tumor cells; and extremely large clot that can’t be removed in pieces.
On July 19, 2024, Inari sent all affected customers an Urgent Medical Device Labeling Correction letter covering IFU updates, recommending that they view the letter and updates, then share it with any relevant personnel and/or device users; share this information with any organization where the ClotTriever XL catheter may have been transferred; and complete the
al highlight an “alarmingly high” mortality rate in these patients that is evident throughout the literature. They state, for example, that the recent BASIL-2 and BEST-CLI randomized controlled trials reported a five-year mortality rate for patients with CLTI that exceeded 50% and was three times higher than the risk of amputation. They also note a 10–12% annual mortality rate following lower extremity revascularization in studies including both patients with CLTI and those with claudication—namely SWEDEPAD, SAFE-PAD and VQI Vision.
The authors point out that the mortality rate in these patients is not only high, but has remained unchanged over the past 40 years, contrasting a “marked decline” in the mortality rate among patients with symptomatic CAD in association with coronary revascularization as a mainstay of treatment. Current annual mortality for patients with CAD is only 1–2%, the researchers point out, as per the ISCHEMIA, FAME 2 and SCOT-HEART trials.
Krievins and colleagues state that guidelines recommend no cardiac testing of patients without cardiac symptoms prior to vascular surgery procedures, despite patients with PAD with combined CAD having “invariably worse outcomes.”
Against this backdrop, Krievins et al detail that they have embarked on a multicenter, randomized clinical trial to determine whether non-invasive diagnosis of silent coronary ischemia together with ischemia-targeted coronary revascularization can improve the outcome of patients following lower extremity revascularization.
The SCOREPAD (Selective coronary revascularization in peripheral artery disease patients after lower extremity
Customer Acknowledgement Reply Form as soon as possible.
The FDA recommended that, based on its review of the reported adverse events, users consider the device to be contraindicated for the removal of fibrous, firmly adherent or calcified material, and be aware that the use of a clot capture device—for example an embolic protection device—”has not yet been demonstrated to be effective in the venous vasculature.”
The FDA noted in the recall that U.S. customers with questions about the recall should contact their local Inari sales representative, Inari Customer Care at 877-923-4747, or its quality department at QA@inarimedical.com
First-in-human study of SonoThrombectomy system completed
SonoVascular device
SONOVASCULAR HAS announced the successful initiation of its first-in-human (FIH) study of the company’s SonoThrombectomy system, an ultrasound-facilitated, thrombolytic-enhanced platform that utilizes multiple mechanisms of action to treat patients with venous thromboembolism (VTE). The catheter-based system combines microbubble-mediated cavitation with low-dose thrombolytic delivery to treat clots with no blood loss.
revascularization) trial, will enroll up to 600 patients with CLTI or severe claudication and no known CAD after successful open or endovascular lower extremity revascularization, Krievins and colleagues share in EJVES . The patients will be randomized to either coronary computed tomography angiography (CTA) plus computed tomography-derived fractional flow reserve (FFRCT; HeartFlow) with ischemiatargeted coronary revascularization in addition to best medical therapy (BMT) or BMT alone with no elective coronary revascularization, which they note is the current guideline-directed standard of care.
The primary endpoint of the trial is a composite of cardiac death, myocardial infarction (MI) and urgent (unplanned) coronary revascularization during two-year follow-up, the authors detail. Extended follow-up will continue out to five years.
“Patient enrollment began in February 2024 and more than 80 patients have been randomized so far,” Krievins et al report in EJVES, who go on to say that the trial is seeking to include up to 10 additional sites in Europe and the U.S.
“Patient enrollment began in February 2024 and more than 80 patients have been randomized so far”
DAINIS KRIEVINS ET AL
GORE® TAG® Conformable Thoracic Stent Graft with ACTIVE CONTROL System
INDICATIONS FOR USE IN THE U.S.: The GORE® TAG® Conformable Thoracic Stent Graft is intended for endovascular repair of all lesions of the descending thoracic aorta, including: isolated lesions in patients who have appropriate anatomy, including: adequate iliac/femoral access; aortic inner diameter in the range of 16-42 mm; ≥ 20 mm non-aneurysmal aorta proximal and distal to the lesion. Type B dissections in patients who have appropriate anatomy, including: adequate iliac/femoral access; ≥ 20 mm landing zone proximal to the primary entry tear; proximal extent of the landing zone must not be dissected, diameter at proximal extent of proximal landing zone in the range of 16-42 mm.
CONTRAINDICATIONS: Patients with known sensitivities or allergies to the device materials; patients who have a condition that threatens to infect the graft. Refer to Instructions for Use at eifu.goremedical.com for a complete description of all applicable indications, warnings, precautions and contraindications for the markets where this product is available.
Products listed may not be available in all markets.
GORE, Together, improving life, ACTIVE CONTROL, TAG and designs are trademarks of W. L. Gore & Associates. 2023 W. L. Gore & Associates, Inc. 231209692-EN OCTOBER 2023
Dainis Krievins
GORE® TAG® Conformable Thoracic Stent Graft with ACTIVE CONTROL System
Help your patients live their lives with a TEVAR device backed by 5-year clinical data. Choose the GORE® TAG® Conformable Thoracic Stent Graft with ACTIVE CONTROL System for clinical outcomes that address long-term patient needs.
W. L. Gore & Associates, Inc. Flagstaff, Arizona 86004 goremedical.com
* No reported compressions, fractures or type III endoleaks.
1. W. L. Gore & Associates. Evaluation of the GORE Conformable TAG® Thoracic Endoprosthesis for Treatment of Acute Complicated Type B Aortic Dissection. NLM Identifier: NCT00908388. Published May 25, 2009. Updated October 27, 2017. Accessed June 7, 2022. https://clinicaltrials.gov/ct2/show/NCT00908388
2. W. L. Gore & Associates. Evaluation of the GORE Conformable TAG® for Treatment of Traumatic Transection. NLM Identifier: NCT00917852. Published June 10, 2009. Updated August 25, 2017. Accessed June 7, 2022. https://clinicaltrials.gov/ct2/show/NCT00917852
3. W. L. Gore & Associates. An Evaluation of the GORE Conformable TAG® Thoracic Endoprosthesis for the Primary Treatment of Aneurysm of the Descending Thoracic Aortic. NLM Identifier: NCT00874250. Published April 2, 2009. Updated August 25, 2017. Accessed June 7, 2022. https://clinicaltrials.gov/ct2/show/NCT00874250
Please see accompanying prescribing information in this journal.
Products listed may not be available in all markets.
GORE, Together, improving life, ACTIVE CONTROL, TAG and designs are trademarks of W. L. Gore & Associates.