M11 Branding Membership benefits expand amid dues increase
6 Complex aortic National survey of off-label treatment probes underreported outcomes data
13 Vascular heritage SVS History Work Group’s landmark project culminates in new book
www.vascularspecialistonline.com
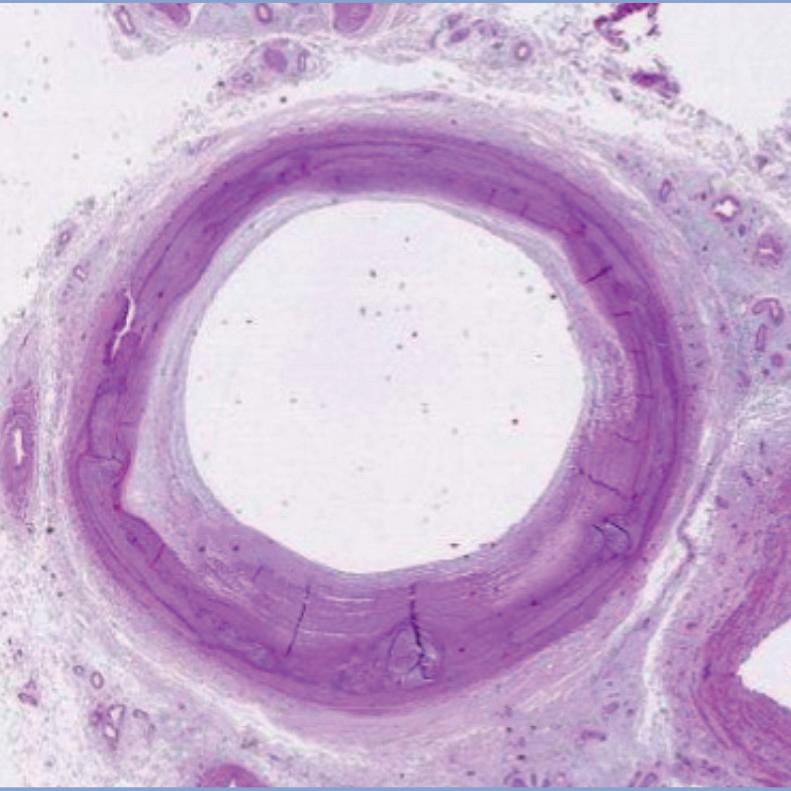
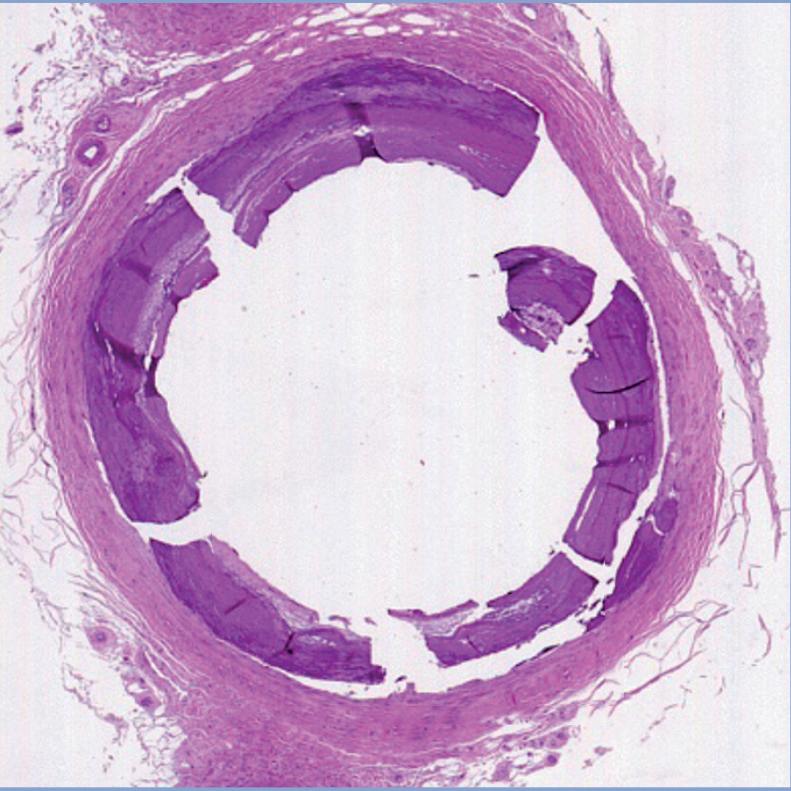
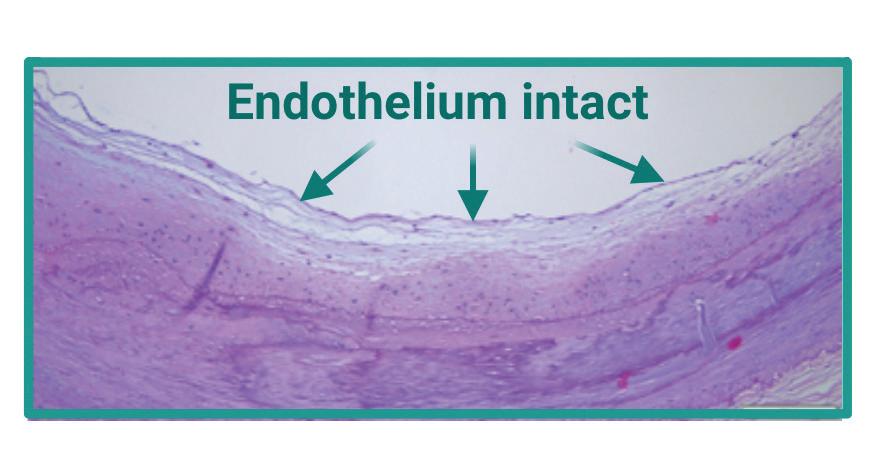
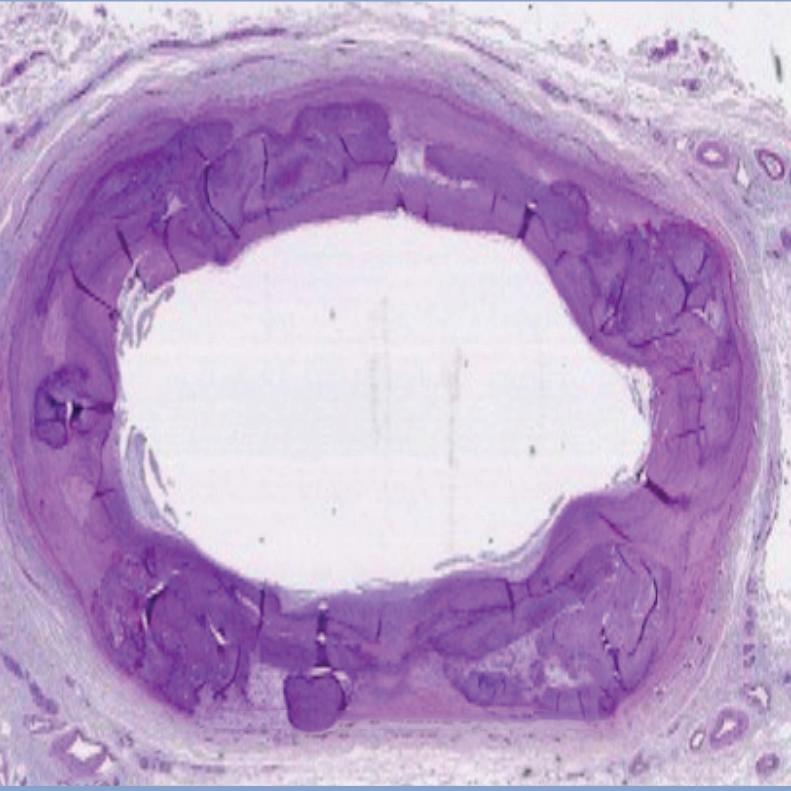
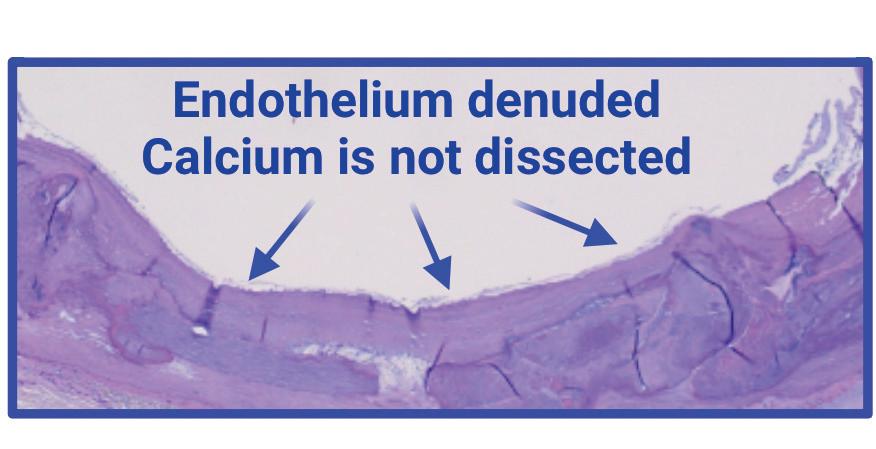
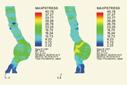
Histology of vessel wall damage after intervention: (left to right) control; plain balloon angioplasty; and orbital atherectomy plus angioplasty
ichael Conte, MD, recently used his 2024 Veith Lecture to call on young vascular surgeons on the peripheral arterial disease (PAD) frontlines to drive the space forward amid a great unmet need.
The professor and chief of vascular and endovascular surgery at the University of California San Francisco (UCSF) called on those in the vascular surgical specialty to take the lead in confronting the challenges of the global PAD burden and in furthering the science. He laid down the gauntlet. But many are already answering the call. And some have already been chosen.
One of those pressing at the leading edges of the PAD frontier is Trisha Roy, MD. The University of Toronto, Ontario, Canada-trained vascular surgeon-scientist recently received a $3.3 million funding boost from the National Institutes of Health (NIH) to push on with a cutting-edge imaging technique aimed at pinpointing who benefits from an open bypass vs. endovascular intervention, as well as more accurately tailoring device selection.
Now based at Houston Methodist DeBakey Heart & Vascular Center, Roy is deep in the throes of developing a magnetic resonance imaging (MRI)-histology technique to help distinguish plaque morphology in PAD. As she puts it, the method is “unlike anything we have right now.” Establishing how hard or soft a plaque is via computed tomography (CT), X-ray or ultrasound is not possible, Roy explains. That makes figuring out whether an individual patient would be a good or bad candidate for an endovascular intervention on the same basis falls short. “If you have something
See page 5
SVS URGES REVISIONS FOR INDEPENDENT CARDIOLOGY CERTIFICATION BOARD
By Marlén Gomez
THE SOCIETY FOR VASCULAR Surgery (SVS) has expressed conditional support for cardiology establishing an independent certification board but objects to provisions in the current American Board of Cardiovascular Medicine (ABCVM) proposal as they conflict significantly with the mission and requirements of the Vascular Surgery Board (VSB), which already issues a primary certificate issued by the American Board of Medical Specialties (ABMS).
The proposal requires critical revisions to address the underrepresentation of vascular expertise and training needed to fully care for patients with vascular disease and ensure high standards of care, the Society said.
In a detailed comment letter submitted July 10, the SVS took the lead with other vascular societies to outline concerns and suggested improvements to the ABCVM proposal, which is currently under review by the ABMS Advisory Council.
“Not surprisingly, the SVS’ perspective on the strengths and areas for improvement of the ABCVM proposal was echoed by numerous other national and regional vascular surgery societies, who joined us in providing feedback to the ABMS on this proposal. Ultimately, we are all deeply invested in assuring that the care provided to our patients with vascular disease meets the highest of quality standards in order to serve the public to the best of our ability,” said Bernadette Aulivola, MD, a member of the SVS Executive Board and the VSB of the American Board of Surgery (ABS).
The ABMS opened a 90day comment period April 24 to gather feedback on the proposed ABCVM. If approved,
See page 5
Medical Editor Malachi Sheahan III, MD
Associate Medical Editors
Bernadette Aulivola, MD | O. William Brown, MD | Elliot L. Chaikof, MD, PhD
| Carlo Dall’Olmo, MD | Alan M. Dietzek MD, RPVI, FACS | John F. Eidt, MD | Robert Fitridge, MD | Dennis R. Gable, MD | Linda Harris, MD | Krishna Jain, MD | Larry Kraiss, MD | Joann Lohr, MD
| James McKinsey, MD | Joseph Mills, MD | Erica L. Mitchell, MD, MEd, FACS
| Leila Mureebe, MD | Frank Pomposelli, MD | David Rigberg, MD | Clifford Sales, MD | Bhagwan Satiani, MD | Larry Scher, MD | Marc Schermerhorn, MD | Murray
L. Shames, MD | Niten Singh, MD | Frank J. Veith, MD | Robert Eugene Zierler, MD
Resident/Fellow Editor
Saranya Sundaram, MD
Executive Director SVS
Kenneth M. Slaw, PhD
Senior Director for Public Affairs and Advocacy
Megan Marcinko, MPS
Manager of Marketing
Kristin Spencer Communications Specialist
Marlén Gomez
Published by BIBA News, which is a subsidiary of BIBA Medical Ltd.
Publisher Stephen Greenhalgh
Content Director Urmila Kerslake
Global Sales Director
Sean Langer
Managing Editor Bryan Kay bryan@bibamedical.com
Editorial contribution Jocelyn Hudson, Will Date, Jamie Bell, Éva Malpass and George Barker
Design Terry Hawes
Advertising Nicole Schmitz
nicole@bibamedical.com
Letters to the editor vascularspecialist@vascularsociety.org
BIBA Medical, Europe
526 Fulham Road, London SW6 5NR, United Kingdom
BIBA Medical, North America
155 North Wacker Drive – Suite 4250, Chicago, IL 60606, USA
Who’s covering second? Rogue hospital human resource departments
By Arthur E. Palamara, MD
While nobody died, the procedure could have gone smoother. The patient, a corpulent man in his late 40s had been on dialysis for half of his life. Two transplanted kidneys failed, and multiple access procedures and his native arteries and veins were beyond salvage. Multiple stents were plastered within his chest, making his upper extremities impenetrable. The superior vena cava was blocked. The left iliac vein had been his lifeline for the past year and now was surrounded with pus. He came in septic. The dialysis catheter in the left groin was removed. He still needed dialysis. Somehow.
An occluded stent lay within the left external iliac vein. The veteran radiologist knew that the stent was not that old and might contain a soft “core.” Ploughing through the fat and musculature above the inguinal ligament, he skillfully aimed a needle at the center of the stent. It gave and he gently maneuvered a variety of wires into the vena cava and met with success! Several inexperienced techs worked with him as he barked orders, colorfully buttressed with a slew of profanity. The tension was high. Several times the wires came close to being pulled out but were saved at the last minute. The poor technician’s hands were uncontrollably shaking. Observing the procedure, I reassured her stating: “He doesn’t bite, just take it one step at a time.”
While the patient would not have immediately died, establishing dialysis access was critical and lifesaving. Working with an inexperienced team did little to bolster the radiologist’s confidence. Although the radiologist was one of the best in his field, he was not immune to the pressure. Extreme tension dissolves even the most placid individual’s restraint. His assistants’ inexperience increased his frustration.
Second base
Using a baseball analogy: it’s the bottom of the ninth, your team is up by one, and the opposing team is at bat. There is one out. The bases are loaded, and a ground ball is hit to the shortstop, who fields the ball cleanly and throws to second for the double play. The second baseman has failed to cover, and the ball lands in right field. Two runners score and the team has lost because of the error.
Who is covering second? That question is central to the frustration and isolation that the radiologist felt in a critical moment when he lacked confidence in his assistants. Success is exclusively up to him, and no help is on the way. What happened to those seasoned techs who had worked with him for years? Those veterans who knew what each wire, catheter and balloon did, and where they could be immediately retrieved: experienced techs could have made the job much easier and certainly less stressful. Some moved on to higher paying jobs during the pandemic when the hospital refused to meet their salary demands. Some retired, some were demoted for discourteous behavior, and some were fired.
Arthur E. Palamara
Human resource failure
Staffed as they are with non-clinical human resource (HR) employees—who know little to nothing about the positions they fill—accept candidates who correctly
check a number of boxes. Positions are staffed with employees who have agreed to work at a pre-set salary determined by financial officers who know nothing about the demands of highly complex surgical or radiologic procedures. HR personnel, abstracted as they are from real dramas of medical care, are unable to separate the wheat from the chaff. Nor do they manifest a desire to learn.
that they could not retain doctors, nurses and technicians because of outlandish salaries offered by temporary staffing companies. Yet they were happy to pay $120 per hour to a “temp” instead of giving another $10 per hour to excellent, loyal employees with recognized value to the system. As such, many of these core employees left and have not returned. Even worse, HR made no attempt to recognize key employees, nor acknowledge their fundamental contribution to the system.
by externally imposed standards of behavior that fail to portray human experience. Emotional temperance has replaced expertise; inexperienced personnel have been given responsibilities far in excess of their capabilities. This is particularly destabilizing in healthcare, and potentially dangerous for the patient. Medical error rates have increased but only the most egregious cases are reported. Moreover, lack of trained staff, while more obvious in the operating room (OR) and radiology suites, is reflected in other ways by increased length of hospital stays, longer OR turnover times, utilization of equipment, limitless diagnostic tests, and, ultimately, outrageous costs. Retention of key individuals is
Since administrators have little appreciation of what transpires when dealing with critical medical challenges, their hiring decisions are based on irrelevant factors— often social perception
paramount to achieve excellent outcomes.
blame. While adopting the DEI (diversity, equity and inclusion) philosophy is beneficial and desirable, it only works with meritocracy. Partially trained individuals eventually realize that they lack expertise and retreat from accepting responsibility, only to become resentful when confronted with a crisis. If they have the will and the stamina, they ultimately acquire the experience and enjoy the satisfaction that accompanies achievement. Unfortunately, promotions are not based on expertise, an attribute administrators fail to appreciate. Even an occasional—but rare—word of praise will suffice.
Creating effective groups
HR departments and most hospitals have yet to acknowledge the importance of creating “effective groups,” a concept that is vitally important in healthcare. From heart transplant groups to interventional radiology to nursing floors, teams are the cornerstone of excellent outcomes.
TCAR Procedures
Together, we’re advancing the future of carotid intervention.
This TCAR milestone is a testament to your passion and expertise in delivering a transformative, patient-preferred* approach to carotid intervention. You are laying the foundation for healthier, brighter tomorrows.
And we’re ENROUTE to so much more.
Scan to see how ENROUTE ® TCAR has transformed lives on the journey to 100,000. silkroadmed.com/100K
COMMENT& ANALYSIS
CORNER STITCH
The good, the bad and the bloody: Reflections on the road to residency
By Blake Murphy, MD
As my third year of residency comes to a close, that little thing called The Match feels like a distant fever dream. The memories of Electronic Residency Application Service (ERAS) application anxiety now tinted with the rose-colored glasses of a surgical resident entering her much-needed research years. Every summer, however, the residency application process starts anew. Like many colleagues, matching into residency was filled with some staggering highs and notable lows. So, for the vascular surgery residents of tomorrow, I encourage you to shoot your shot!
Find your footing and your mentors
As someone batting less than 500 on the day of United States Medical Licensing Examination (USMLE) Step 1, the weak points in my application were well defined. Even with solid clinical grades and an extensive advocacy background, the climb to surgical residency felt like tackling Mount Everest. Thankfully, honest feedback from thoughtful mentors provided invaluable guidance—focused on
centering my lived experience. My work as a primary care scribe, data analyst, and advocacy fellow in Washington, DC meaningfully informed my answer to “why medicine” and “why vascular surgery.” As a non-traditional medical student, creating a framework to highlight my unique strengths was crucial for success on the interview trail. And if we’re being honest, my Step 2 CK (clinical knowledge) score improved massively—thanks in large part to dedicated work around test anxiety.
Survive and thrive on the interview trail
The cost of applying to more than 40 programs was dulled by the thrilling prospect of color-coded Excel spreadsheets and enabling email alerts for interview invites. Before the spreadsheets, however, came honest reflection about my priorities in surgical training—mainly the importance of living in an urban environment, exposure to vascular trauma and complex aortic work, and access to dedicated research years. On the interview trail, I clearly communicated
how my priorities as a future vascular surgeon-in-training aligned with my programs of interest. After each interview, I took time to digest the experience and updated my rank list in real-time. While momentarily tedious, this practice saved hours, if not days of deliberation in the weeks leading up to rank list certification. Last but certainly not least, I militantly tackled my post-interview follow-up emails—for which my future self is grateful.
Trust the process
Trusting the process is always easier in retrospect. Even during my Halloween COVID-19 wedding in 2020—amidst the first round of interview invites—real uncertainty about my future was front of mind. Looking back, the process of organizing an application, completing interviews and honest self-reflection was just good practice for surgical training. You must trust the knowledge, confidence and purpose you have cultivated. The Match is simply about finding a training program that challenges you to be the best person and vascular surgeon you can be. It should come as no surprise—this looks different for every applicant. Nevertheless, I promise your first open abdominal aortic aneurysm repair, tibial bypass or trauma thoracic endovascular aortic repair (TEVAR) is truly just a blink away.
BLAKE MURPHY is a an integrated vascular surgery resident at the University of Washington in Seattle.
DECODING DIFFERENCES FOR PROPER BILLING AND REIMBURSEMENT PAYMENT
THE SOCIETY FOR VASCULAR Surgery (SVS) has partnered with KarenZupko and Associates (KZA), a consulting and education firm, to create vascular surgery coding resources for SVS members and their coding staff. The resources include on-demand courses for purchase and frequently asked questions (FAQs) and answers.
The on-demand courses will be released each quarter, with the third and latest course released in June. The new course, entitled “Co-Surgeon and Assistant: What’s the Difference?”, helps staff understand the importance of the differentiation between co-surgeons and assistants when it comes to the important area of coding and reimbursement.
In the past, Medicare noted that this type of coding error has resulted in improper billing, leading to a report by the Office of Inspector General recommending payor scrutiny of their use.
GUEST EDITORIAL WHO’S COVERING SECOND? ROGUE HOSPITAL HUMAN RESOURCE DEPARTMENTS
opportunity to solve problems and refine processes to enhance care. When denied the chance to fulfill their expectations, they become disillusioned and filled with moral outrage. Then they leave.
Some years ago, at the inception of robotic surgery, a small hospital in upstate New York was matched against an Ivy League competitor in Manhattan. The researchers went back five years later to look at the results and found the smaller hospital enjoyed better outcomes than their prominent competitor. The smaller hospital was able to train and retain the same team of surgeons and nurses while the larger, world-renowned hospital suffered numerous defections. The smaller hospital experienced cultural growth, and a sense of pride and shared identity. Their leadership was respected and inspired the team members to achieve superlative results.
That was, of course, before the pandemic, an event to which many hospital systems lay blame for their failures. While partially true, valuable team members who could have been retained were allowed to leave for wont of small increases in salary and lack of recognition of their contribution.
Instead, these professionals were never acknowledged as integral and criticized for their lack of loyalty. HR departments now complain that Gen Z and millennials lack commitment. But also true is that when hiring new physicians and key team members, existing doctors’ recommendations are often ignored. Since administrators have little appreciation of what transpires
continued from page 2
when dealing with critical medical challenges, their hiring decisions are based on irrelevant factors—often social perception. They, their institutions and the patients would be better served if they spent more time on the front line of medicine to gain an understanding of what is really essential.
Transactive memory
Loyalty to an institution and accomplishing highly complex tasks are accomplished by developing what is known as “transactive memory,” through which collective intelligence is achieved and shared.
Returning to the baseball analogy, the second baseman would instinctively know to cover the “bag,” as the scrub tech instinctively knows to hand over a Crafoord clamp when blood is gushing from the aorta. But creating a staff capable of achieving those goals requires an investment of time, money and patience.
Regretfully, our capitalistic, fragmented, patient-unfriendly, expensive healthcare system seems loathe to make that commitment. Patients are not ignorant; they will respond to and seek excellent care. Ultimately, a healthcare system espousing these virtues will be both medically and financially rewarded. And their employees much happier.
ARTHUR E. PALAMARA is a vascular surgeon practicing in Hollywood, Florida, for 44 years. He is active in county, state and national medical organizations.
Once completed, participants should be able to describe the difference between cosurgery and assistant surgery, list the key documentation necessities and understand the reimbursement differences of coversus assistant surgeons. The course will provide a detailed explanation of payor rules and documentation imperatives, as well as clinical scenarios.
The two previous on-demand courses covered surgical modifiers in vascular surgery and nonphysician provider (NPP)/ advanced practice provider (APP) billing and coding for vascular surgeons. The remaining courses published later this year will cover the evaluation and management of clinical scenarios for vascular surgeons, and relative value unit compensation and contracting.
The courses provide American Academy of Professional Coders with continuing education credits.
New FAQs are being added to the SVS website on a monthly basis. They are sorted by category and aimed at answering questions and helping to avoid coding errors down the road. Categories range from aneurysms to venous disease and cover every vascular bed and area in between.
Each fall, the SVS hosts an in-person Coding and Reimbursement Workshop now open for registration. To access more information on this workshop and the other coding resources, visit vascular.org/ CodingInquiries.—Kristin Spencer
FROM THE COVER: ‘CHOOSING THE RIGHT DEVICES FOR THE RIGHT PATIENTS’
that is a long, long, long occlusion but is very soft and easy to cross, you can’t tell that apart from a rock-hard dense collagen lesion with CT scans, X-ray or ultrasound right now,” she tells Vascular Specialist. “The only way we can test is by trying—and that is why we do endovascular-first for most of these patients.”
This raises a point of both challenge and excitement for Roy. Or, as Conte referred to it in his Veith Lecture at the 2024 Vascular Annual Meeting in Chicago: “opportunity.”
That endovascular-first approach was challenged by the landmark outcomes reported from the BEST-CLI trial. Key among its findings was that, for many patients with adequate saphenous vein, bypass surgery was a better option, Roy observes. High failure and immediate technical failure rates for endovascular interventions were reported. “The problem is that [bypass] is so much more invasive. So the question that we had with this NIH grant was: is it a matter of bypass being better for PAD patients full stop?”
Or, Roy considers, perhaps there is a way patients can be better selected for endovascular treatment. “We know that the most common mode of failure is the inability to cross a lesion because it’s too hard or too stiff.” Those immediate technical failure rates amount to about 15–20%. “We want to bring that down to 0% by selecting the right patients that you can treat.”
Which is really only the opening gambit in this MRI-histological quest.
“Once you get your wire across, how do you actually open the blood vessel in an effective way?” Roy continues. “We know that PAD plaques are very variable, and depending on what a plaque is made out of, it’s going to be more or less amenable to a certain device. Each of these devices are made for specific types of plaque. So, if you’re talking about something that’s a big nodular chunk of calcium, that’s going to be different from the eggshell calcium around the perimeter, which is different from soft thrombus, and so on.”
This brings to the fore an important biographical detail
FROM THE COVER SVS URGES REVISION FOR INDEPENDENT CARDIOLOGY CERTIFICATION BOARD
continued from page 1
this new board would become a voting member of the ABMS. There is concern in the vascular community that both the public and other providers may become confused or misunderstand the expertise and extensive training of vascular surgeons who have a primary ABMS certificate in vascular. The SVS and co-signatories support the initiative for an independent cardiology board, the Society pointed out, but stressed that the current proposal falls short in several key areas.
Underrepresentation of vascular diseases
The SVS letter highlights the critical expertise and years of experience required to provide high-quality care for patients with vascular diseases such as peripheral arterial disease (PAD), cerebrovascular disease and renovascular disease. With more than 200 million people worldwide
continued from page 1
“ Once you get your wire across, how do you actually open the blood vessel in an effective way?”
TRISHA ROY
from Roy’s own trajectory—and how it interplayed with the development of the MRI technique.
She first started to work on the imaging modality as a PhD student in Canada. Back then, about a decade ago, Roy was more or less focused on the mechanical properties of plaques. Upon arriving in the U.S., the plethora of endovascular devices at the disposal of surgeons and interventionalists—unknown north of the border—helped drive exploration of
suffering from PAD alone, the SVS argues that the proposal does not adequately address the significant health burden posed by these conditions, or the amount of training or case volume to care for patients.
Lack of specific credentialing pathways
The proposed board lacks clear pathways for credentialing in vascular disease, the SVS continued, emphasizing the necessity of detailed training paradigms and requisite case numbers for vascular procedures to ensure consistent expertise among practitioners. According to Aulivola, “The ABMS requires that its boards ‘create independent, external assessments and conduct comprehensive evaluations of the knowledge, clinical competence, performance and experience, of such candidates through initial and continuing certification.’ The current proposal lacks clarity in both areas, with the suggestion that continuing certification assessments would be delegated to specialty societies rather than being directly overseen by the board itself. This is a significant concern when it comes to assuring that the care of patients with vascular disease meets established standards.”
Quality improvement and practice standards
The proposal does not adequately outline plans for quality improvement programs,
the device-vessel wall-plaque morphology interaction. In essence, without the ability to differentiate different types of plaques, “we’re not able to make informed decisions about who’s going to benefit from what device,” she says. “So that’s why the mainstay, especially for below-the-knee disease, is still balloon angioplasty. And our results are dismal—up to 70% having re-narrowing within just three months.”
Another detail of the U.S. dimension, not available back home sans evidence in support of its use: atherectomy. “I come to the States and it’s used a ton here,” Roy observes. “I can see why—you know balloon angioplasty is not going to work; maybe atherectomy can help in some patients? We don’t know who or what, we say, ‘But let’s give it a try,’ as this is kind of their last chance.”
Cue the contemporary backdrop to atherectomy: overuse, questions of harm and worsening results, and mainstream media scrutiny. “We are looking at that right at the vessel wall level,” Roy points out. “We’re taking the legs of real patients who undergo amputation because we were not able to save their legs, characterizing those plaques, then using orbital atherectomy and comparing that with plain balloon angioplasty. We are making real observations of whether it helps in terms of the vessel wall damage, or are we still doing a lot of dissections? Or does it make any difference at all?”
Into the longer distance, Roy wants to see an outcome whereby a more precision level of care for PAD patients is achieved. “What I envision is that we are using MRI for patients we think need revascularization and individualizing our care based on what the patient’s individual anatomy is,” she explains. “I think that can reduce our failure rate—so, that 20% going down to 0%, but also ultimately making us more successful because we’re choosing the right devices for the right patients.”
The knowledge gleaned from the research thus far has also helped inform new device development. “Right now, we are using coronary devices and applying them to the leg,” says Roy, adding: “They haven’t been very effective.”
the SVS said, underscoring the importance of quality registries, such as the Vascular Quality Initiative (VQI), in improving patient outcomes and maintaining high standards of care. The VQI provides the continuous feedback necessary for vascular providers to verify national benchmark levels, said SVS Secretary William Shutze, MD, an advocate of the proposal.
Potential public confusion
The SVS stressed that the interchangeable use of “cardiovascular medicine” and “cardiology” in the proposal could lead to public confusion over qualifications and areas of expertise, possibly misleading patients regarding the extent of cardiologists’ training in vascular diseases. According to Shutze, cardiology has multiple subspecialties, including but not limited to electrophysiology, heart failure and structural heart, all of which are laserfocused on their domain.
“The nomenclature of the new board elevated them as vascular-proficient providers. That is not the case,” Shutze said. “If the proposal is approved with the current name-granting, this board authority and domain over the vascular space, it will not advance vascular care but diminish it.”
Public safety risks
The proposed certification raises concerns about the impression that all cardiologists
can fully manage vascular diseases, but the SVS pointed out that most cardiologists lack comprehensive training in medical, surgical and endovascular treatment for these conditions. “With the comment period closed, we now await the ABMS decision. If approved, we will congratulate them and work with the new board to address the noted deficiencies in vascular education and training. If rejected, we will learn from the process as we consider our Board’s options. Should revisions be requested, we will collaborate with the proposed new board, too,” said Shutze.
According to Aulivola, the SVS has offered to work with ABCVM proponents to enhance their proposal, particularly in areas concerning the care of vascular disease, where significant overlap with care provided by VSB-certified vascular surgeons exists. The aim is to fulfill the ABMS’ mission of improving healthcare quality.
“The SVS is excited to partner with our colleagues in cardiology to develop improved training paradigms and quality improvement initiatives that will allow those interested in contributing to the care of vascular patients to do so with rigor and expertise,” added SVS President Matthew Eagleton, MD.
For more information and to view the full comment letter, visit vascular.org/ CVMComments.
COMPLEX AORTIC Survey of offlabel treatment of complex repair pinpoints factors behind underreported outcomes data
By Bryan Kay
THE POTENTIAL FOR COST AND TIME TO BE KEY factors in low levels of outcomes data reporting emerged during a national survey of the off-label use of approved endovascular devices for complex aortic aneurysm repair.
Grayson S. Pitcher, MD, an assistant professor of vascular surgery at the University of Rochester in Rochester, New York, and colleagues conducted targeted sampling to identify vascular surgeons with experience in off-label treatment complex repair, disseminating an electronic survey to 291 individuals that achieved a response rate of 38%.
The researchers found that from an estimated number of elective cases totaling nearly 1,800 per year, the majority—1,307—were performed at medical centers without a Food and Drug Administration (FDA) physician-sponsored investigational device exemption (PS-IDE).
“Estimates of off-label repair are underrepresented in the literature in the U.S.,” Pitcher et al report. “Physician-modified endograft [PMEG] has become the dominant modality. Underreported outcomes data appear to be limited by non-standardized PS-IDE reporting to the FDA, the lack of VQI [Vascular Quality Initiative] participation and prospective institutional data collection, and limitations imposed on publication and presentation.”
Pitcher first presented the survey findings during the 2024 Vascular Annual Meeting (VAM) in Chicago (June 19–22), and they have since been published in the Journal of Vascular Surgery. During VAM 2024, Pitcher reminded delegates of the FDA bar for the off-label use of approved devices: deep knowledge of the product, use based on sound scientific rationale, and use and effects record-keeping. “Unfortunately, the 2013 advisory statement from the SVS was contradictory,” he said, recommending against the performance, presentation and publication of off-label procedures. “This has resulted in a lack of transparency to clinical practice and outcomes data, despite an increase in off-label cases.”
Pitcher told VAM attendees the survey was aimed at not only estimating national volume but better understanding the behaviors of vascular surgeons performing off-label endovascular repairs of complex aortic aneurysms.
Covering a total of 89 institutions in 38 states—including four with Cook Medical device PS-IDEs and 11 other PS-IDEs—the survey showed that 43% of sites perform more than 15 cases per year and that PMEG (63%) was
“There is a need for access to commercially available devices and transparent outcomes”
GRAYSON S. PITCHER
the common and preferred technique, with a market share dominated by Cook, Pitcher reported. “What stands out among this group [of surgeons] is that this is a young group: the majority of respondents were less than 45 years of age, within the first 10 years of practice, and [with] the majority having the technical skills and requisite technical skills having trained at a center with a PS-IDE,” he said.
An exit survey demonstrated that only 29% of respondents always referred to PS-IDE centers “with multiple barriers for referral listed,” Pitcher continued. Only 61% participated in the VQI and 57% maintained an institutional database, he added.
“This study highlights an underrepresented population and the barriers that inhibit referrals to PS-IDE centers,” Pitcher explained. “We felt the best way to visualize this was to use the Dartmouth Atlas hospital referral regions [HRRs] where each outlined area represents a regional healthcare market where patients are referred for major cardiovascular surgery,” he said, pointing to a patchy map of the continental U.S. depicting coverage of PS-IDE centers and those with off-label use. “Even with off-label use in the U.S., only 20% of HRRs are represented.”
Pitcher acknowledged limitations, including recollection bias and the limited number of vascular surgeons surveyed. “There is a need for access to commercially available devices and transparent outcomes, with the majority of respondents in this survey interested in a national collaborative,” he concluded.
Pitcher was asked about a discrepancy between a lower level of those taking part in database collection and a higher number expressing interest in being part of a registry. Pitcher noted that respondents reported that the limitation was cost and time, suggesting the potential of a VQI lite to ease data input.
DUAL IMPACT
Fracture medial arterial calcium while debulking intimal morphologies
BELOW THE KNEE
Proven success in below-the-knee arteries, where calcium tends to be more prevalent2
SAFETY
Safety at the forefront. Treat with confidence by minimizing the risk of embolization and dissection3
RISK INFORMATION
Caution: Federal (USA) law restricts the use of the system by or on the order of a physician. Refer to Directions for Use and/or User Manual provided with the product for complete Instructions, Warnings, Precautions, Possible Adverse Effects and Contraindications prior to use of the product. INDICATIONS FOR USE
The Auryon Atherectomy System and Auryon Atherectomy Catheters with aspiration are indicated for use as atherectomy devices for arterial stenoses, including in-stent restenosis (ISR), and to aspirate thrombus adjacent to stenoses in native and stented infra-inguinal arteries. The Auryon Atherectomy System and Auryon Atherectomy Catheters without aspiration are indicated for use in the
1. Rundback et al. Treatment effect of medial arterial calcification in below-knee after Auryon laser atherectomy using micro-CT and histologic evaluation, Cardiovascular Revascularization Medicine, 2023,ISSN 1553-8389, https://doi.org/10.1016/j.carrev.2023.06.027.
2. Paul D. Bishop, Lindsay E. Feiten, Kenneth Ouriel, Sean P. Nassoiy, Mircea L. Pavkov, Daniel G. Clair, Vikram S. Kashyap, Arterial Calcification Increases in Distal Arteries in Patients with Peripheral Arterial Disease, Annals of Vascular Surgery, Volume 22, Issue 6, 2008, Pages 799-805, ISSN 0890-5096, https://doi.org/10.1016/j.avsg.2008.04.008.
3. Rundback J, Chandra P, Brodmann M, et al. Novel laser-based catheter for peripheral atherectomy: 6-month results from the Eximo Medical B-LaserTM IDE study. Catheter Cardiovasc Interv. 2019;94(7):1010-1017.
CAROTID STENTING
CEA and TCAR should be ‘first-line’ interventions for weekend carotid revascularization, researchers advise
By Jocelyn Hudson
PATIENTS WHO UNDERGO CAROTID REVASCULARization at the weekend have increased odds of complications and mortality, with transfemoral carotid artery stenting (TFCAS) posing the highest risk and transcarotid artery revascularization (TCAR) the lowest, compared to carotid endarterectomy (CEA). This is one of the key findings of new observational research published online ahead of print in the Journal of Vascular Surgery (JVS).
Lead author Mokhshan Ramachandran, MD, senior author Mahmoud Malas, MD, and colleagues—all from University of California San Diego in San Diego, California, where the latter is chief of vascular and endovascular surgery— state in their research article that outcomes for weekend surgical interventions are known to be associated with higher rates of complications and mortality compared to weekday interventions.
The aim of the group’s study was to assess the “weekend effect” for the three available carotid revascularization meth-
ods—CEA, TCAR and TFCAS—noting that research on the topic is currently only available regarding CEA.
To do this, the researchers queried the Vascular Quality Initiative (VQI) for patients undergoing CEA, TCAR and TFCAS over a six-year period, from 2016–2022. They employed Chi-square and logistic regression modelling to analyze outcomes including in-hospital stroke, death, myocardial infarction (MI), and 30-day mortality by weekend versus weekday intervention.
Providing more details on their study methods, Ramachandran et al write that they used backward stepwise regression to identify significant confounding variables, and that logistic regression of outcomes was substratified by symptomatic status.
Furthermore, they used secondary multivariable analysis to compare outcomes between the three revascularization methods by weekend versus weekday interventions.
Overall, Ramachandran and colleagues analyzed 155,962 procedures in their study, comprising 103,790 CEA, 31,666 TCAR and 20,506 TFCAS. Of these, the authors specify, 1,988 CEA, 246 TCAR and 820 TFCAS received weekend interventions.
In JVS, the authors report that they observed no significant differences for TCAR, and increased odds of in-hospital stroke, death and MI for CEA and TFCAS procedures conducted at weekends.
In addition, Ramachandran et al ymptomatic TCAR patients had nearly triple the odds of 30-day mortali ty, and that odds of in-hospital mortality were nearly tripled for asymptomatic CEA and asymp tomatic TFCAS patients.
Finally, they reveal that CEA and TCAR had no significant differences for all outcomes, while TFCAS was
AAA MACHINE LEARNING-BASED MODEL COULD AID IN DETERMINING ENDOVASCULAR ANEURYSM REPAIR SUITABILITY
By Jocelyn Hudson
RESEARCHERS AT THE UNIVERSITY Medical Center Groningen in Groningen, The Netherlands, and the University of Twente in Enschede, The Netherlands, have developed a prediction model that they say could assist in the preoperative identification of patients who are unlikely to achieve sufficient endograft apposition after endovascular aneurysm repair (EVAR).
Willemina van Veldhuizen, MD, and colleagues from the University Medical Center Groningen, including members of the Virtual Stenting study group, shared their work in a paper published online ahead of print in the European Journal of Vascular and Endovascular Surgery (EJVES). By way of background, the authors first underline an association between
challenging infrarenal aortic neck characteristics, such as short apposition (less than 10mm circumferential shortest apposition length) on the first postoperative computed tomography angiography (CTA), and an increased risk of type Ia endoleak after EVAR. It was the study team’s aim to develop a model to predict postoperative shortest apposition length in patients with an abdominal aortic aneurysm (AAA) based on the preoperative shape.
associated with increased odds of stroke and death compared to CEA and TCAR.
In the conclusion of their findings, Ramachandran and colleagues summarize that weekend carotid revascularization is associated with increased odds of complications and mortality, adding that asymptomatic weekend patients perform worse in the CEA and TFCAS groups.
“Among the three revascularization methods, TFCAS is associated with the highest odds of perioperative stroke and mortality. As such, our findings suggest that TFCAS procedures should be avoided over the weekend, in favor of CEA or TCAR,” the authors write. They continue that, in patients who are poor candidates for CEA, TCAR offers the lowest morbidity and mortality for weekend procedures. Sharing the take-home message from their research, Ramachandran et al posit that CEA and TCAR procedures should be the “first-line” interventions for weekend carotid revascularization.
“Among the three revascularization methods, TFCAS is associated with the highest odds of perioperative stroke and mortality. As such, our findings suggest that TFCAS procedures should be avoided over the weekend”
without complications and 54 treated with EVAR who went on to experience a late type Ia endoleak.
In terms of methods, the authors detail that they obtained the infrarenal shortest apposition length from the first postoperative CTA, which they subsequently binarized between those under 10mm in length and those equal to or longer than 10mm.
The researchers then used the principal component scores that were statistically significant between the shortest apposition length groups as input for five classification models, and subsequently determined area under the receiver operating characteristics curve (AUC), accuracy, sensitivity and specificity for each classification model.
Willemina van Veldhuizen
Van Veldhuizen et al note that they developed a statistical shape model to obtain principal component scores, with the dataset comprising 147 patients in total: 93 treated with standard EVAR
Van Veldhuizen and colleagues report in EJVES that, of the 147 patients included in the study, 24 had an infrarenal shortest apposition length of less than 10mm and 123 had a shortest apposition length of 10mm or more.
The authors share that the gradient boosting model resulted in the highest AUC of 0.77 and that, using this model, 114 (78%) patients were correctly classified, with sensitivity (less than 10mm apposition
was correctly predicted) and specificity (equal to or longer than 10mm apposition was correctly predicted) at 0.7 and 0.79, respectively.
Van Veldhuizen et al summarize that the model they present can predict the binarised shortest apposition length of an endograft into the infrarenal aortic neck for treatment of a AAA on the first postoperative CTA scan, with an accuracy of 78%.
Given that a shortest apposition length of less than 10mm has been associated with higher risks of type Ia endoleak, the researchers posit that their model “could help vascular specialists in the preoperative phase to accurately identify patients who are unlikely to achieve sufficient apposition after EVAR.”
In the discussion of their findings, the authors acknowledge a series of limitations to their study, including the fact that the data they used came from different datasets, which may have created a selection bias, they note.
Looking down the road, van Veldhuizen and colleagues suggest that their prediction model “should be externally validated with a consecutive patient series that includes patients with an early type Ia endoleak before it can be used as a patient-specific virtual stenting tool in clinical practice.”
SOCIETIES SEEK CONSENSUS ON NIVL MANAGEMENT AMID
OF RIGOROUS DATA’
By Jocelyn Hudson
THE DIAGNOSIS AND MANAGEMENT of non-thrombotic iliac vein lesions (NIVL) is the focus of a newly published set of consensus statements from the Vascular Interventional Advances (VIVA) Foundation, the American Venous Forum (AVF), and the American Vein and Lymphatic Society (AVLS).
The report, authored by Kush Desai, MD, from Northwestern University Feinberg School of Medicine in Chicago, and colleagues, appears as an open access article in the American Heart Association (AHA) journal Circulation: Cardiovascular Interventions
Imaging considerations for diagnosis, patient selection and technical considerations for stent placement, and optimal post-procedure medical therapy and surveillance are all covered in the document.
On imaging, Desai et al advise: “In a patient considered for NIVL treatment, an invasive
diagnosis with the complementary use of venography and IVUS [intravascular ultrasound] is recommended.” In addition to this, the authors stress the importance of “dynamic” IVUS evaluation of NIVL, which they explain includes breath hold and maneuvers that increase intra-abdominal pressure.
The writing group further advise that intervention below the thresholds of >50% area reduction or >61% diameter stenosis on IVUS at the NIVL is not recommended, and that use of venography thresholds alone for diagnosis and treatment of NIVL is “less well established.”
Finally in this section, Desai and colleagues state that axial imaging with computed tomography (CT) or magnetic resonance imaging (MRI) “can help confirm the presence of anatomy that may be associated with a clinically significant NIVL.” They stress, however, the importance of clinical evaluation and venography and/or IVUS being central to the final diagnosis and intention to treat.
On the topic of patient selection for NIVL stent placement, the authors recommend that stenting “may be appropriate” in certain circumstances, for example in the presence of either asymmetrical edema significantly affecting quality of life (QoL), progressive Clinical-Etiology-Anatomy-Pathophysiology (CEAP) class 4–6 venous disease, or venous claudication with minimal superficial venous disease.
The authors warn, however, that stent placement for NIVL is “inappropriate” in patients with minimal-to-no symptoms and in
asymptomatic patients to prevent possible future venous thromboembolism (VTE) events.
In their final recommendation of this section, Desai et al write that stenting “may have a role” in some cases with QoL-impacting chronic pelvic pain of venous origin in the presence of parauterine veins with or without pelvic venous reflux.
The report also includes four consensus recommendations on technical considerations for stent placement, including firstly that the choice of stent size and length in NIVL “should depend on IVUS for diameter/length measurements with compulsory fluoroscopy for length measurements.”
This section of the report also addresses stent migration, which Desai and colleagues highlight can have “devastating consequences.” As a result, the authors stress that measures to mitigate the possibility of stent migration and complications are “mandatory.”
Desai and colleagues continue that sizing based on the normal reference vessel is “generally recommended” and that stents for
NIVL should be extended into the straight portion of the external iliac vein to limit complications including stent migration.
The authors advise against routine use of anticoagulation or antiplatelet therapy for untreated NIVL, opening their recommendations for optimal medical therapy and surveillance for NIVL patients. They go on to highlight that, in treated patients with NIVL with no evidence of previous VTE, there is “no consensus that anticoagulation or antiplatelet therapy is necessary.”
Furthermore, they recommend that an assessment of thrombotic risk in patients with NIVL should be made and, should anticoagulation or antiplatelet therapy be indicated, the agent, dose and duration “should be tailored accordingly.” The final recommendation the authors make in this section is to encourage routine early and long-term clinical surveillance following stent placement.
Finally, the document outlines future direction in research and education on the topic of NIVL diagnosis and management. “Evidence-based appropriateness of treatment and longitudinal management of patients with NIVL should be supported by long-term prospective trials,” Desai et al write.
“Evidence-based appropriateness of treatment and longitudinal management of patients with NIVL should be supported by long-term prospective trials” KUSH DESAI ET AL
Open repair of dissected infrarenal aortic aneurysm
Dittmar Böckler, Heidelberg, Germany
EDITED CASE
BEVAR with an inner-branch design
Mark Farber, Chapel Hill, United States
EDITED CASE
TEVAR after debranching by axillary-axillary bypass
Kazuo Shimamura, Osaka, Japan
PRESENTATION
Best practice: Risk strati cation of TAAA patients
Tara Mastracci, London, United Kingdom
SVS Foundation’s Step at
VAM
challenge raises more than $30,000
THE RECENT SVS VASCULAR ANNUAL Meeting (VAM 2024) was more than a gathering of medical professionals to discuss advancements in vascular health. It featured the Step at VAM challenge, an inspiring event highlighting the importance of physical activity that raised over $30,000 for the SVS Foundation.
Participants collectively walked over 575,000 steps in less than three days, promoting vascular health awareness through their efforts. The event saw enthusiastic participation, with one standout participant: Greg Westin, MD, from the Indiana University School of Medicine, was named VAM’s top walker after covering 24 miles.
Westin expressed gratitude to the challenge organizers and appreciated the convenience of VAM’s walking location, which had a gym available. His room was on the 31st floor, giving him “plenty of stairs to climb!”
PAD, a chronic disease where plaque builds up in the arteries of the legs, affects more than 10 million people in the U.S. and walking aids in its prevention and treatment.
“Walking is a fundamental human activity that keeps us healthy,” said SVS Foundation Chair Joseph Mills, MD. “It’s great to see this campaign succeed in not only raising PAD awareness but also funds for the SVS Foundation.”
Registration for the 2024 Challenge opened on Aug. 1, and walkers can sign up as individuals or form teams. Everyone who registers will receive a commemorative Step Challenge T-shirt.
This year’s sponsors for the event include presenting sponsor Advanced Oxygen Therapy, Inc. (AOTI), superior sponsor W. L. Gore & Associates (Gore), as well as Abbott and the Society for Vascular Nursing (SVN).
TWith the success of the Step Challenge at VAM 2024 and the enthusiasm building ahead of the September event, the SVS Foundation continues to lead the charge in promoting positive vascular health. Organizers want everyone who can to join the movement, walk for a cause and contribute to a healthier vascular future.
) body of titles—subscription free for Active, Trainee, Graduated Candidates and Associate members. Additional member updates are available via the electronic newspaper, which inform members about the latest news and , the Society’s online community, provides an exclusive platform for members to engage in discussions, share insights and collaborate with peers worldwide. Members enjoy reduced pricing for key events such as the Vascular Annual Meeting (VAM), the Vascular Research Initiatives Conference (VRIC), the Complex Peripheral Vascular Intervention (CPVI) Skills Course and
The sixth edition of the Vascular Education and Self-Assessment Program (VESAP6) offers a structured approach to continuous learning and gives members access to the latest educational materials to stay current with evolving
The SVS offers mentorship programs, leadership opportunities on councils and committees and scholarships that support members at all stages of their careers, from emerging professionals to seasoned experts. Research grants are available for vascular surgeons, ensuring innovative work
CONGRESS SAVE THE DATE: SVS’ INAUGURAL LEADERSHIP AND ADVOCACY CONFERENCE
With its rich history and political significance, Washington, D.C., provides the perfect setting for the SVS’ collective mission to advance vascular health advocacy. From exploring effective leadership qualities to discussing strategies for effective lobbying, every session will be meticulously designed to inspire and empower.
The challenge at VAM 2024 was just the beginning. As part of Peripheral Artery Disease (PAD) Awareness Month in September, the SVS Foundation is gearing up for the third annual Vascular Health Step Challenge. This initiative encourages participants to walk 60 miles throughout September, symbolizing the 60,000 miles of blood vessels in the human body.
To register, visit vascular.org/ STEP2024.
The SVS professional government affairs staff advocates on behalf of members to influence federal legislative and regulatory processes that directly impact their practices and patients. This advocacy ensures that member voices are heard in decisions affecting their lives, livelihoods and patients, providing essential support and representation. An advocacy conference will take place in 2025, allowing
he Society for Vascular Surgery’s (SVS) Advocacy team is thrilled to announce the inaugural Leadership and Advocacy Conference, set to take place Sept. 14–16, 2025, in Washington, D.C. The event is designed to bring together passionate vascular surgeons nationwide to engage in meaningful dialogue, share insights and collaborate on an advocacy agenda designed to protect and promote the future of vascular surgery.
Mark your calendars to participate in this transformative experience that will enhance your leadership skills and amplify your voice in vascular advocacy. Over the course of three days, attendees will have the unique opportunity to participate in a series of dynamic workshops, keynote presentations, and panel discussions. Additionally, attendees can visit Capitol Hill and directly engage with lawmakers and their staff. The conference promises to equip both seasoned advocates and those new to advocacy with the tools and knowledge necessary to serve as a champion for the field of vascular surgery and its patients.
“Surgeon involvement in managing change and solving the challenges of our health care system has never been more important. I am incredibly excited that the SVS is working to position vascular surgeons at the forefront, building knowledge and skills within our ranks, leveraging the expertise we have, and bringing it all to Congress’s doorstep,” said SVS Advocacy & Policy Council Chair Megan Tracci, MD, JD.
Save the date and prepare to participate in an experience that will impact professional journeys and the broader healthcare landscape.
Matthew Eagleton
status
By Kristin Spencer
THE SOCIETY FOR VASCULAR SURGERY (SVS) Executive Board (EB) unanimously approved the transition of the Young Surgeons Section (YSS) from a pilot section to a full section during their annual retreat held July 26–27. The decision is a reflection of the section’s many accomplishments and commitment to its mission.
The SVS implemented membership sections to give different subsets of the organization an opportunity to provide added member value and voice in Society initiatives. In 2022, the EB approved the section to begin its pilot phase to represent members within their first 0–10 years of practice, a demographic of membership that has been growing rapidly over the years. The formal mission of the YSS is to foster and accelerate the learning and career development of SVS members within their first decade in clinical practice.
“While the number of ‘young’ vascular surgeons is increasing, there is expected to be a surgical shortage of about 30,000 by 2030. The YSS aims to bring forth relevant education and resources to those millennials and Gen Z-ers who are entering the surgeon workforce. We hope that by offering more relevant resources to this group, we don’t see as many people leaving the specialty or the surgical field,” said Edward Gifford, MD, chair of the YSS.
Gifford recently assumed the section chair position after the 2024 Vascular Annual Meeting (VAM). Prior to VAM,
Joseph V. Lombardi, MD, MBA, FACS
Professor and Chief, Division of Vascular & Endovascular Surgery
Cooper Medical School of Rowan University
Director, Cooper Aortic Center, Camden, NJ
Joseph J. Ricotta, MD, MS, FACS
National Medical Director, Vascular Surgery and Endovascular Therapy, Tenet Healthcare Corporation
Professor of Surgery, Charles E. Schmidt College of Medicine
Program Director, Vascular Surgery Fellowship Florida Atlantic University, Boca Raton, FL PROGRAM COMMITTEE
Ali Azizzadeh, MD, Cedars-Sinai Medical Center, Los Angeles, CA
James H. Black, III, MD The Johns Hopkins University School of Medicine, Baltimore, MD
G. Chad Hughes, MD Duke University Medical Center, Durham, NC
James F. McKinsey, MD Jacobson Aortic Center Mount Sinai Medical System, New York, NY
Darren B. Schneider, MD The Hospital of the University of Pennsylvania, Philadelphia, PA
Chelsea Dorsey, MD, served as the section’s inaugural chair, and Gifford served as the vice chair. The two have led a steering committee of 12 young surgeons who have spearheaded initiatives and engaged the section’s membership at large.
The SVS leadership has championed the importance of expanding diversity of perspective and engagement. There is now a YSS representative on the SVS Nominating Committee. This change has given voice to the YSS demographic when it comes to choosing leadership for future SVS positions. Another change that was influenced by the YSS leadership was to give Early Active members of the SVS the opportunity to vote in SVS elections and serve on SVS committees. Both proposed changes were brought to the SVS membership to vote and passed in 2022 and 2023, respectively. The chair of the YSS now sits on the SVS Appointments and Nominations Committee, as well as the Strategic Board of Directors.
important, in my mind, to the overall health and growth of the SVS.”
Since its inception, the YSS has implemented two workgroups of section members to in order to thrash out different initiatives based on the results of a needs assessment. The career development and research workgroups are composed of 10 YSS members each and have worked to implement two monthly YSS-sponsored journal clubs with the Journal of Vascular Surgery (JVS), help expand the SVS mentor match program to include all SVS members and more. Additionally, members of the YSS currently serve on other committees and workgroups throughout the SVS, including the Communications and Branding Committee, Leadership Development Committee, Education Council and Compensation Study workgroup.
“Seeing these changes to the structure of long-standing SVS Committees and the voting membership has motivated me during my years as section chair to keep advocating for this demographic,” said Dorsey. “Being able to make a difference and provide a voice for this growing group of members of our organization is vitally
“We hope that by offering more relevant resources to this group, we don’t see as many people leaving the specialty or the surgical field”
EDWARD GIFFORD
While at VAM, Dorsey announced that a visiting professorship for YSS members will be added as an opportunity for application in 2025, and a scholarship program is being designed to help members travel to different conferences. The SVS is expected to emerge with more information on these initiatives in the coming months.
Gifford is excited to see membership growth throughout the section. He also plans to work with SVS leaders to get YSS members on more committees.
“Young vascular surgeons are the future of our specialty and our society. We are so excited about the approval of the section and are committed to providing resources for advocacy, collaboration, mentorship and career development for our peers,” he said. “We want all the young vascular surgeons around the country and the world to know that there is a dedicated group within the SVS to be inclusive of your needs.”
To join the YSS, members within their first 10 years of practice can email communications@vascularsociety.org
Edward Gifford
Hilton Aruba
SVS HISTORY WORK GROUP’S LANDMARK PROJECT CULMINATES IN NEW BOOK
By Marlén Gomez
THE 2024 VASCULAR ANNUAL Meeting (VAM) saw the culmination of a decade-long project by the Society for Vascular Surgery’s (SVS) History Project Work Group. The release of the book, Legends Leaders Pioneers: Surgeons Who Built Vascular Surgery, marks a significant milestone in documenting the history and evolution of vascular surgery.
Authored by the late James S.T. Yao, MD, and Walter J. McCarthy, MD, the title brings together the recollections of over 90 prominent vascular surgeons who were instrumental in shaping the field. Through in-depth video interviews conducted by the SVS History Project Work Group committee, readers are given a unique opportunity to meet these pioneers face-to-face. Each biography in the book is accompanied by a QR code, enabling instant access to the full video interview, providing an immersive historical experience.
The project, initiated by Yao in 2011 and chaired by McCarthy since 2018, captures first-hand accounts of technical advances, new devices, prosthetic materials and
the fascinating careers of these surgeons. McCarthy highlighted the project’s significance, stating, “This book is a testament to the incredible journey of vascular surgery. It preserves the voices and experiences of those who have paved the way for future generations. Their stories of innovation, perseverance and dedication are invaluable to both the vascular surgery community and the practicing vascular surgeons as inspiration to those in training or in those contemplating this career.”
Other initiators included Norman M. Rich, MD, Roger Gregory, MD, and Calvin Ernest, MD. Committee members of the project included Kenneth Cherry, MD, William Baker, MD, Mark Eskandari, MD, Melina Kibbe, MD, Peter Lawrence, MD, Richard Lynn, MD, and William Pearce, MD.
One notable feature of this book involves vascular luminaries Michael DeBakey, MD, Denton Cooley, MD, and Juan Parodi, MD. The work reflects on their mentors, including the likes of Alfred Blalock, MD, and Marie René Leriche, MD, who advanced the understanding of intermittent claudication
and lumbar sympathectomy. This book is available through Amazon. The SVS owns the copyright, and royalties from book sales support the organization.
In addition to celebrating this project, the SVS has launched a new history project—the Vascular Surgery History Archive. This initiative was featured in the VAM 2024 video titled “LEGENDS LEADERS
PIONEERS: Surgeons Who Built Vascular Surgery.” The archive aims to continue documenting the field’s evolution, and preserving the stories of current and future vascular surgery leaders.
The new archive promises to be a rich
“It preserves the voices and experiences of those who have paved the way for future generations”
WALTER J. MCCARTHY
resource for surgeons, historians and the public, ensuring that the legacy of vascular surgery’s pioneers is accessible for generations to come.
“It’s an honor to carry on the work of Dr. Yao, Dr. McCarthy, and all the others who did such an outstanding job in the Vascular Surgery History Group. Our goal with the Vascular Surgery History Archive Task Force is to create and curate a digital nexus for the history of the SVS and the specialty of vascular surgery, a central hub on the internet where information in all media is available for anyone interested in these topics. We encourage all members of the society who possess historic artifacts, information or an interest in this project to contact us,” said Craig Miller, MD, cochair of the SVS History Digital Archives Task Force.
To learn more about the project, visit vascular.org/History.
Vascular Specialist: The two-decade-long evolution of the official SVS newspaper
2004/5
Pilot issue: Twenty years ago, the late K. Wayne Johnston, MD, founding editor of the newspaper and soon to become SVS president, introduces members to the title’s pilot issue
2011
A field in motion: Born amid the endovascular revoluation, the paper continues its quest to inform SVS members with timely news of a rapidly evolving specialty. By now, George Andros, MD, has taken over as editor
2019
Tackling the issues: Under the editorship of Malachi Sheahan III, MD, the newspaper cements itself as the go-to vascular news source, developing a knack for special, issues-based editions
2015
Mischief maker: Now helmed by Russell H. Samson, MD, the paper has developed a reputation for hard-hitting columns from its reigning medical editor, in addition to its news coverage
2020
Weathering COVID: With a new publishing partner in place, the publication continues its editorial growth as a platform for news, commentary and special issues in vascular surgery
2024
Modern look: By now, the title has a rebranded look and feel, continuing a focus on covering the vascular surgery biosphere and issues close to the heart of the SVS, including its branding campaign
SOCIETY BRIEFS
Compiled by Marlén Gomez and Kristin Spencer
‘Night
at the Museum’
THE SVS FOUNDATION HOSTED ITS annual gala on June 21 at Chicago’s famous Museum of Science and Industry. This was the first of the Foundation galas to take place offsite from the Vascular Annual Meeting (VAM).
“Operation Golden Key” was an attendee favorite event of the evening. SVS Executive Director Kenneth Slaw, PhD, posed as James Bond, working the Gala floor with members of his security detail (aka other SVS staff members) and visiting attendees who had purchased keys to try and unlock his briefcase. The winner of the game unlocked $500 worth of champagne.
The evening included a touching tribute to the late James S.T. Yao, MD, a former SVS president and giant in vascular surgery who supported the SVS Foundation throughout his career. Yao’s family established the SVS Foundation’s James S.T. Yao Resident Research Award in 2024 and attended the Gala.
The night saw nearly $100,000 raised through donations, ticket sales, and both live and silent auctions.
The top prize of note from the silent auction was the 2025 VAM VIP Package which was won by Mel Sharafuddin, MD. The University of Florida/Brigham and Women’s Hospital Vascular Surgery Fishing Trip Weekend was won by Peter Henke, MD.
SVS CALLS FOR NOMINATIONS
The SVS has called on its members to nominate individuals to fill five at-large positions on the Executive Board (EB) as required following a bylaw referendum passed by the membership in late 2023. This change creates flexibility and greater diversity of perspective in selecting members on the EB to address changing needs and priorities.
The Nominating Committee opened the call this month, with a closing date of September 30. The new atlarge members will be named in November and assume their roles in January 2025, coinciding with the Strategic Board of Directors (SBOD) retreat.
The initial terms for these positions are staggered to ensure continuity: one member will serve a four-year term, two will serve three years, and a further two will serve two years.
Subsequent members will serve three-year terms to prevent all five members from rolling off in the same year.
Eligibility criteria for the at-large members include being an SVS member in good standing for at least five years and demonstrating consistent service or contribution to the SVS, SVS Foundation or SVS Patient Safety Organization (PSO) through involvement in committees, subcommittees, section committees, task forces, writers’ groups or editorial groups.
Staff will contact all nominees to confirm their interest and require them to complete a short application. For any questions, email governance@vascularsociety.org
THE SVS EXECUTIVE BOARD (EB) CONVENED ON JULY 25 under the leadership of SVS President Matthew Eagleton, MD, to accelerate the implementation of key priorities identified earlier this year.
The current board includes Keith Calligaro, MD, as presidentelect, Linda Harris, MD, as vice president, William Shutze, MD, as secretary, Tom Forbes, MD, as treasurer, and Joseph Mills, MD, as immediate past president.
The EB’s July meeting followed the Strategic Board’s January review, where the Society’s Strategic Plan and priorities for the coming year were developed. The July session focused on advancing these initiatives to further the Society’s mission in the field of vascular surgery.
SUBMIT SESSION PROPOSALS FOR VAM 2025
While the 2024 Vascular Annual Meeting (VAM) only wrapped up in June and attendees are still in awe of its education offerings, it is time to start planning for the VAM 2025 program. VAM 2025 will take place in New Orleans, Louisiana, June 4-7, which is two to three weeks earlier than VAM is normally held. The call for educational session proposals opened on July 24 and will close at 3 p.m. Central Time on Wednesday, Aug. 28.
For more information regarding session proposals, visit vascular. org/VAM25Proposals
CLINICAL&DEVICENEWS
Compiled by Jocelyn Hudson, Bryan Kay and Jamie Bell
Centerline Biomedical receives FDA 510(k) clearance for new IOPS Viewpoint catheter
One-year STRIDE study data show ‘meaningful’ limb salvage, mortality and QoL outcomes
ONE-YEAR OUTCOMES FROM the STRIDE study of the Indigo aspiration thrombectomy system (Penumbra) for lowerextremity acute limb ischemia (ALI) showed target limb salvage and mortality rates of 88.5% and 12%, respectively.
Silk Road is credited with pioneering the TCAR procedure and building the Enroute transcarotid neuroprotection system (Enroute NPS) that supports the procedure with its patented flow reversal technology.
Thomas Maldonado
The data were revealed by Thomas Maldonado, MD, professor of surgery at New York University Langone Medical Center in New York City and national principal investigator of STRIDE, during VAM 2024.
The results stand up “very favorably” to historical controls for open surgery from the academic literature showing a target limb salvage rate of 65.4–82% and a mortality rate of 4.9%–42%.
“We see meaningful information both for very good target limb salvage, very low mortality, and the quality of life is significantly improved at one year,” said Maldonado.
Silk Road celebrates milestone of 100,000 TCAR procedures
SILK ROAD MEDICAL HAS ANNOUNCED the milestone of more than 100,000 transcarotid artery revascularization (TCAR) procedures having been performed to date.
CENTERLINE BIOMEDICAL recently announced that its Intra-Operative Positioning System (IOPS) Viewpoint catheter has received Food and Drug Administration (FDA) 510(k) clearance. The Viewpoint catheter is the most recent addition to the company’s patented IOPS portfolio. A press release details that Viewpoint—a low-profile 6-French catheter available in multiple tip shapes and lengths—is designed for precision access to provide three-dimensional (3D) navigation feedback to clinicians.
When Viewpoint catheters are used in combination with the proprietary algorithms of the IOPS software, Centerline Biomedical explains, clinicians can clearly visualize endovascular tools in real-time and reduce their dependency on fluoroscopy systems. The result, according to the company, is state-of-theart image-guided, real-time navigation designed to revolutionize the way endovascular procedures are performed. This is achieved while reducing exposure to harmful radiation emitted from the X-ray fluoroscopy systems that are typically used to see vessels during these procedures.
The press release continues that, at its core, the IOPS platform is designed to enhance visualization, minimize procedure times, and reduce total radiation exposure for the benefit of both patients and healthcare providers.
PRESERVE II TRIAL SHOWS ROBUST FIVE-YEAR OUTCOMES
FIVE-YEAR OUTCOMES FROM the PRESERVE II pivotal trial of Cook Medical’s Zenith branch iliac graft (ZBIS) demonstrate “sustained safety and effectiveness” when combined with the iCast (Getinge) covered stent for the treatment of aortoiliac aneurysms and preservation of hypogastric artery perfusion, new data show.
W. Anthony Lee, MD, chief of vascular surgery at Boca Raton Regional Hospital in Boca Raton, Florida, delivered the results during VAM 2024. Five-year outcomes were completed among 75% of the 40-patient cohort across 18 U.S. medical centers. Lee reported no aneurysm-related mortality, rupture, type III endoleaks, migrations or device integrity issues. Five-year freedom from all-cause mortality was 88.9%; hypogastric artery primary and secondary patency were 91% and 94%, respectively; and external iliac artery primary patency was at 95%, he told VAM 2024.
Nine patients underwent 15 secondary interventions, six ipsilateral to the ZBIS, Lee said. Freedom from type I and II endoleaks was 97.3% at five years, while aneurysm shrinkage was about 25%, he added.
“Completing the 100,000th TCAR procedure is the culmination of more than 15 years’ worth of work by members of the Silk Road Medical team and the healthcare providers we work with,” said Chas McKhann, chief executive officer of Silk Road.
Thrombolex and Aidoc announce strategic partnership to advance breakthrough PE treatment
THROMBOLEX AND AIDOC HAVE announced a strategic partnership aimed at revolutionizing the treatment of acute pulmonary embolism (PE), a press release reports.
This strategic collaboration, the release details, will leverage Aidoc’s artificial intelligence (AI) technology to accelerate patient identification and enrollment for Thrombolex’s single-session RAPID-PE study—a prospective, single-arm, multicenter, postmarket clinical registry evaluating the efficacy and safety of the Bashir endovascular catheters in the treatment of acute intermediate-risk PE.
GORE® VIABAHN® VBX
Balloon Expandable Endoprosthesis
Consult Instructions for Use eifu.goremedical.com
INDICATIONS FOR USE IN THE U.S.: The GORE® VIABAHN® VBX
Balloon Expandable Endoprosthesis is indicated for the treatment of de novo or restenotic lesions found in iliac arteries with reference vessel diameters ranging from 5 mm – 13 mm and lesion lengths up to 110 mm, including lesions at the aortic bifurcation. CONTRAINDICATIONS: Do not use the GORE® VIABAHN® VBX Balloon Expandable Endoprosthesis in patients with known hypersensitivity to heparin, including those patients who have had a previous incident of Heparin-Induced Thrombocytopenia (HIT) type II. Refer to Instructions for Use at eifu.goremedical.com for a complete description of all applicable indications, warnings, precautions and contraindications for the markets where this product is available.
5-YEAR PATENCY IN COMPLEX, REAL-WORLD SFA LESIONS.
The VIABAHN® Device demonstrated durable clinical outcomes in challenging superficial femoral artery (SFA) disease.
Gore Japan Post-Market Clinical Study1
* As used by Gore, Heparin Bioactive Surface refers to Gore’s proprietary CBAS® Heparin Surface.
Complex patient population2
▪ 24 cm average lesion length
▪ 70% chronic total occlusions
▪ 27% critical limb-threatening ischemia
▪ 48% TASC II D lesions
1. Iida O. 5-year outcomes of the Gore® Viabahn® Endoprosthesis for the treatment of complex femoropopliteal lesions in a Japanese population. Presented at the 21st Annual Vascular InterVentional Advances (VIVA); October 30, 2023–November 2, 2023; Las Vegas, NV.
2. Iida O, Ohki T, Soga Y, et al. Twelve-month outcomes from the Japanese post-market surveillance study of the Viabahn Endoprosthesis as treatment for symptomatic peripheral arterial disease in the superficial femoral arteries. Journal of Endovascular Therapy 2022;29(6):855-865.
W. L. Gore & Associates, Inc. Flagstaff, Arizona 86004 goremedical.com
Please see accompanying prescribing information in this journal.
Products listed may not be available in all markets.
GORE, Together, improving life, VIABAHN and designs are trademarks of W. L. Gore & Associates.