02 Guest editorial Track your wRVUs, because nobody else does it better
10 Branding SVS launches patient-facing website as part of long-term vascular surgery branding campaign
18 Brand new column VS launches its latest comment section addition: The Outpatient 22 SVS Foundation Applications open for 2025 James S.T. Yao Resident Research Award
www.vascularspecialistonline.com
NOVEL
MEASURE SUGGESTS 20% OF ELECTIVE CAROTID REVASCULARIZATIONS FAIL TO ACHIEVE A TEXTBOOK OUTCOME
By Bryan Kay
ONE-IN-FIVE PATIENTS
failed to achieve a textbook outcome after undergoing carotid endarterectomy (CEA), transcarotid artery revascularization (TCAR) or transfemoral carotid artery stenting (TF-CAS), a Vascular Quality Initiative (VQI) analysis that tested a novel, patientcentric textbook outcome metric found.
“Having a non-textbook outcome was prognostic of an inferior five-year survival” among asymptomatic carotid stenosis patients who underwent any of the three carotid revascularization procedures, Jesse Columbo, MD, presenting author of the multi-institutional study, told the 2024 New England Society for Vascular Surgery (NESVS) annual meeting in Portland, Maine (Oct. 25–27).
“Hospital transfer, non-home living status and severe comorbidities were predictive of a non-textbook outcome.”
The findings come in the wake of the Centers for Medicare & Medicaid Services (CMS) Medicare coverage expansion for carotid stenting to standardrisk patients, with a physicianpatient shared decision-making interaction now required to form part of the preoperative assessment process.
See page 7
Service: Giving back
Pioneering American Venous Forum (AVF) and Eastern Vascular Society (EVS) efforts aimed at breaking down barriers to care and educating patients in economically challenged communities on vascular disease have yielded early gains over the first two events staged this year. The vascular surgeons behind these outreach programs—or days of service—tell Vascular Specialist of their plans for the events going forward, an idea they hope catches on among other societies.
By Bryan Kay
See page 12
Medical Editor Malachi Sheahan III, MD
Associate Medical Editors
Bernadette Aulivola, MD | O. William Brown, MD | Elliot L. Chaikof, MD, PhD
| Carlo Dall’Olmo, MD | Alan M. Dietzek MD, RPVI, FACS | John F. Eidt, MD | Robert Fitridge, MD | Dennis R. Gable, MD | Linda Harris, MD | Krishna Jain, MD | Larry Kraiss, MD | Joann Lohr, MD
| James McKinsey, MD | Joseph Mills, MD | Erica L. Mitchell, MD, MEd, FACS | Leila Mureebe, MD | Frank Pomposelli, MD | David Rigberg, MD | Clifford Sales, MD | Bhagwan Satiani, MD | Larry Scher, MD | Marc Schermerhorn, MD | Murray L. Shames, MD | Niten Singh, MD | Frank J. Veith, MD | Robert Eugene Zierler, MD
Resident/Fellow Editor
Saranya Sundaram, MD
Executive Director SVS
Kenneth M. Slaw, PhD
Senior Director for Public Affairs and Advocacy
Megan Marcinko, MPS
Manager of Marketing
Kristin Spencer
Communications Specialist
Marlén Gomez
SVS Consultant
Beth Bales
Published by BIBA News, which is a subsidiary of BIBA Medical Ltd.
Publisher Stephen Greenhalgh
Content Director Urmila Kerslake
Global Sales Director Sean Langer
Managing Editor Bryan Kay bryan@bibamedical.com
Editorial contribution Jocelyn Hudson, Will Date, Jamie Bell, Éva Malpass and George Barker
Design Terry Hawes
Advertising Nicole Schmitz nicole@bibamedical.com
Letters to the editor vascularspecialist@vascularsociety.org
BIBA Medical, Europe
526 Fulham Road, London SW6 5NR, United Kingdom
BIBA Medical, North America
155 North Wacker Drive – Suite 4250, Chicago, IL 60606, USA
Erica L. Mitchell, MD, Nicolas J. Mouawad, MD, and Issam Koleilat, MD
If you were in the audience at the 2024 Southern Association for Vascular Surgery (SAVS) annual meeting, you might have been taken aback by the presentation from UT Health San Antonio and the San Antonio VA Medical Center, presented by Luke D. Perry, DO, and co-authored by Alissa Hart, MD, Reshma D. Brahmbhatt, MD, and Lori D Pounds, MD: “Work for a dollar get reimbursed a dime: An analysis of the dire need for coders trained in vascular billing,” the paper was entitled. The authors described that only 42% of the cases for three procedure types were coded correctly, with only 67% of work relative value units (wRVUs) captured. This is a tragedy not just for individual compensation, but also division and department financial accounting, and justification for practice growth, i.e., adding surgeons, advance practice providers (APPs), equipment or otherwise. Our administrators don’t really know what we do on a daily basis, nor do they understand the intricacies of our work and operations. Regardless, the wRVU has now become the currency by which we (“they”) measure our work “effort” and productivity, even though wRVUs do not really measure “physician effort,” the work that we do to take care of patients safely, the education we provide, the research we conduct, and the administrative tasks we must complete by day’s end. Our work is also being measured by other surrogates, including the numerical metrics of number of operations, average case length, on-time starts, and average length of stays. So, while you may feel overworked by the end of the week, you may not be working hard enough according to the administrators, because the measured metrics are not above the median.
In a healthcare economy increasingly reliant upon productivitybased compensation models, knowing the minutiae can mean the difference between getting a bonus or not. Each and every wRVU adds up by the year’s end. Consider codes G2211 and the recent inpatient coding changes: a difference of 0.7 wRVUs per patient encounter could mean more than 360 wRVUs at the end of the year if you have 10 relevant encounters per week. That’s just two a day!
Tracking your “work productivity” is particularly critical if you have coders and billers separate from you and your practice, if you have others who code your procedures, and if you just want to know what your wRVUs amount to.
This small group of authors, impressed by the “Work for a dollar get reimbursed a dime” analysis, convened to develop the table provided (see page 6) as a reference for the everyday vascular surgeon. We’ve included the most common procedures that we perform on a daily basis in hopes that we can help our fellow vascular surgeons better account for their daily wRVU earnings. This list will allow you to quickly identify how many wRVUs each procedure carries, and, more importantly, the associated global period associated with a procedure. Did you know that your evaluation and management (E&M) note the day after an inpatient angiogram is a billable encounter? You do now.
The table is based on 2024 Centers for Medicare & Medicaid Services (CMS) numbers, where any and all can look up any procedure at their whim by Current Procedural Terminology (CPT) code. If you just want the wRVU value and the global period, use the first row. The remaining rows are related to reimbursement adjustments based on geographic locations. This table doesn’t even get into the nuances—for instance, adding the diagnostic angiogram
codes, if relevant, when you are also doing an intervention, the additional code for brachial plexus decompression during rib resection, modifiers, multiple procedures, etc. It also doesn’t explain the “rules” and allowances of bundled billing versus component billing. But at least it will get you started. Also captured here is the opportunity cost of your time. So, that challenging open aneurysm repair that takes eight hours is still only about 34 wRVUs. But six or seven vein cases will get you pretty close to that with none of the postoperative headache, and probably less musculoskeletal strain and emotional stress. Not that we’re advocating for patient or case selection based on this; we’re just saying that the next time you get called in to put a stitch in an iliac vein that was traumatized by a laparoscopic port, and you’re done in 30 minutes, be grateful for the quick and easy 26 wRVUs. Knowledge is power. Imagine what you could do with this information. Because, if we don’t know what and how much we do, how can we expect others to know accurately? And, as always, a plug for the Society for Vascular Surgery (SVS) coding course: take your coders, attend yourself. It’s only two days—and an invaluable experience.
While you may feel overworked by the end of the week, you may not be working hard enough according to the administrators, because the measured metrics are not above the median
SHERAZUDDIN QURESHI is a clinical assistant professor of surgery at Northwestern Medicine, RYAN MEYER is a vascular surgeon at RWJBarnabas Health, ERICA L. MITCHELL is a professor of surgery at the University of Tennessee Health Science Center, NICOLAS J. MOUAWAD is chief of vascular surgery at McLaren Bay region, and ISSAM KOLEILAT is also vascular surgeon at RWJBarnabas Health.
continued on page 6
30-day results of the ROADSTER 3 study demonstrate that TCAR, using the ENROUTE® Transcarotid Stent System in conjunction with the ENROUTE® Transcarotid Neuroprotection System, is safe and effective in patients at standard risk for adverse events from carotid endarterectomy. With indisputable clinical and patient benefits, ENROUTE® TCAR is the less invasive standard in stroke prevention.
The ROADSTER Trials: Demonstrating Consistent, Low Adverse Event Rates Across All Risk Levels
Stroke (ITT)
Stroke (PP)
S/D/MI (ITT)
S/D/MI (PP)
ABOVE AND BEYOND FOR ABOVE AND BELOW
Extend Your Capabilities with the New Peripheral IVL Workhorse
See how Dr. Siah enabled wound healing in a patient with CLTI using Shockwave E8
Pre-Amputation
Case Courtesy of Dr. Michael Siah
Peripheral IVL Important Safety Information
In the United States: Rx only.
SCAN TO LEARN MORE ABOUT THE CASE:
Indications for Use—The Shockwave Medical Intravascular Lithotripsy (IVL) System is intended for lithotripsy-enhanced balloon dilatation of lesions, including calcified lesions, in the peripheral vasculature, including the iliac, femoral, ilio-femoral, popliteal, infra-popliteal, and renal arteries. Not for use in the coronary, carotid or cerebral vasculature.
Contraindications—Do not use if unable to pass 0.014” (M5, M5+, S4, E8) or 0.018” (L6) guidewire across the lesion-Not intended for treatment of in-stent restenosis or in coronary, carotid, or cerebrovascular arteries.
Warnings—Only to be used by physicians who are familiar with interventional vascular procedures—Physicians must be trained prior to use of the device—Use the generator in accordance with recommended settings as stated in the Operator’s Manual.
Precautions—use only the recommended balloon inflation medium—Appropriate anticoagulant therapy should be administered by the physician—Decision regarding use of distal protection should be made based on physician assessment of treatment lesion morphology.
Peripheral IVL into the treatment of patients with chronic limbthreatening ischemia
Anand Prasad, MD, an 18-year veteran of vascular and endovascular medicine with a particular interest in peripheral arterial disease (PAD) in patients with chronic kidney disease (CKD), explores the deliverability of the Shockwave E8 catheter below the knee in patients with advanced disease.
Below-the-knee (BTK) intervention in patients with chronic limb threatening ischemia (CLTI) represents a challenging area in our field. The length, calcification and smaller size of tibial vessels, coupled with patient comorbidities such as diabetes and CKD, and the consequences of procedural failure, all converge in these patients. 1,2 Traditionally, plaque modification with atherectomy devices has been the primary mode to address vessel calcium. Although effective in many cases, atherectomy carries a risk of distal embolization, vessel perforation, and a variable impact on deep and superficial calcium, depending on the specific device used.
Shockwave Medical’s introduction of intravascular lithotripsy (IVL) into the endovascular field has been revolutionary for the treatment of calcium. In my own practice, the use of IVL has provided multiple benefits, including replacing atherectomy for many cases, reducing flow-limiting dissections, and improving vessel preparation prior to adjunctive therapies.
Most recently, our center has used the newest iteration of Shockwave’s IVL family of peripheral catheters extensively: the Shockwave E8 catheter. The Shockwave E8 provides a broad range of IVL sizes, which span utility above and below the knee. Key features include diameters of 2.5–6.0mm, 80mm balloon length with evenly spaced emitters, 150cm working length for distal vessel reach, 400 pulses available at 2Hz (two pulses per second). As many operators use lower-profile access, the smaller balloon sizes, 2.5–4.0mm, are compatible with 5F sheaths. In my experience, the versatility of these Shockwave E8 features can replace the use for Shockwave S4 and Shockwave M5+ catheters in many vessel sizes.
A key challenge with IVL therapy in the BTK circulation has been deliverability. To date, pre-IVL vessel preparation with gentle balloon dilation or use of atherectomy were the primary means to help advance the Shockwave devices. Shockwave E8 has been easier to deliver, despite the longer length relative to the Shockwave S4, in large part due to more extensive (45cm) hydrophilic coating, coupled with a novel tapered tip. These latter features have been particularly
helpful to me when treating chronic total occlusions (CTO), as well as distal tibial lesions. The following case highlights many of these capabilities of the Shockwave E8 in CLTI patients.
Case report Introduction
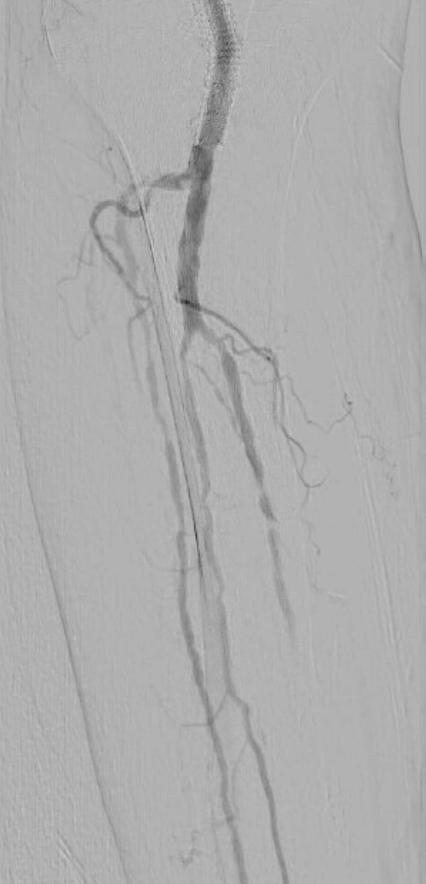
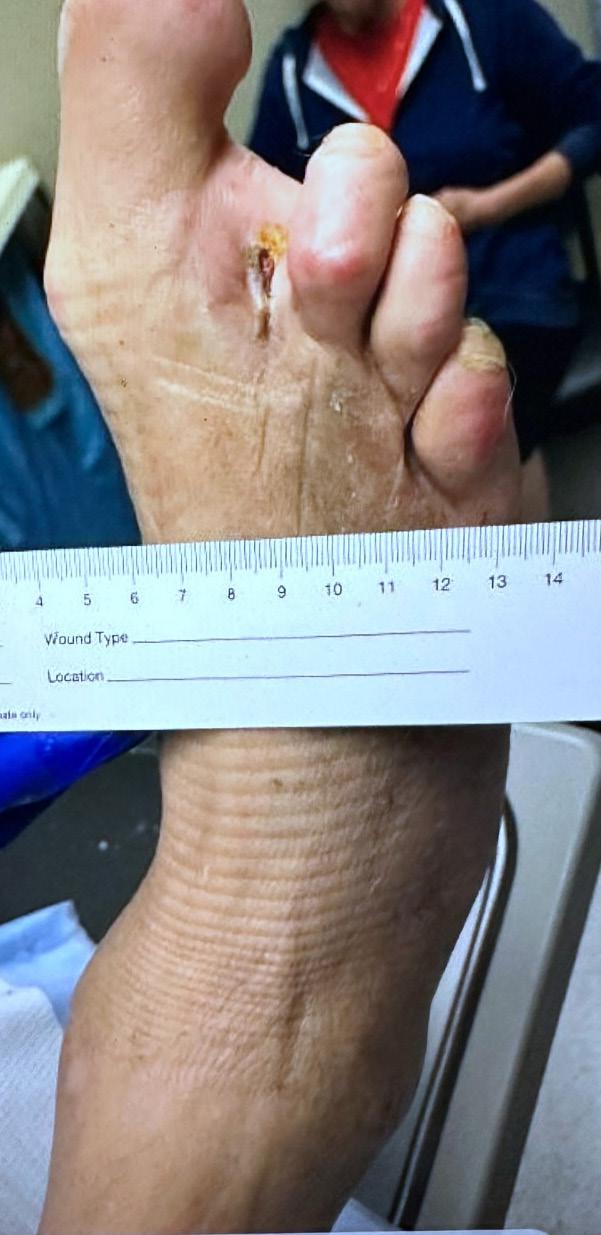
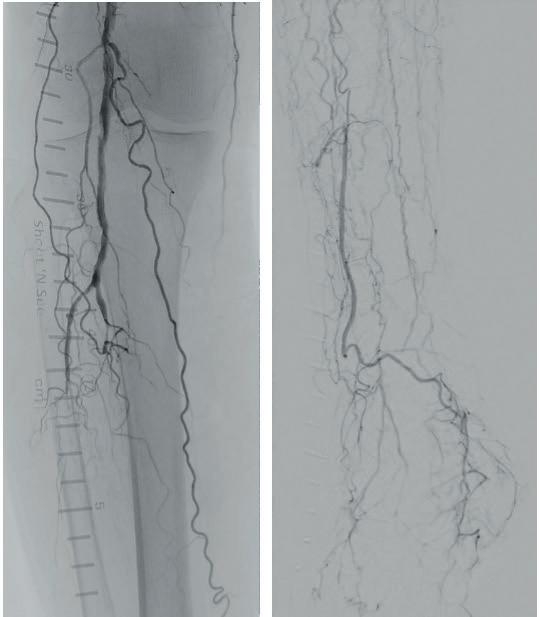
A 75-year-old female patient with diabetes and end-stage kidney disease (ESKD) presented with progressive right second toe swelling ulceration with gangrene and rest pain (Figure 1). There was extensive osteomyelitis and underlying tissue injury which required a planned amputation of the second toe. We were consulted prior to amputation for angiography, which demonstrated patent inflow vessels but severe BTK tibial disease. The baseline angiogram is shown in Figure 2. There was no inline flow to the foot, with occlusion of the anterior tibial, posterior tibial and peroneal arteries (Figure 2a). There was reconstitution of the peroneal artery, with partial filling of the posterior circulation via the posterior communicating artery. There was reconstitution of the anterior circulation with a visible small dorsalis pedis artery (Figure 2b).
Procedural overview
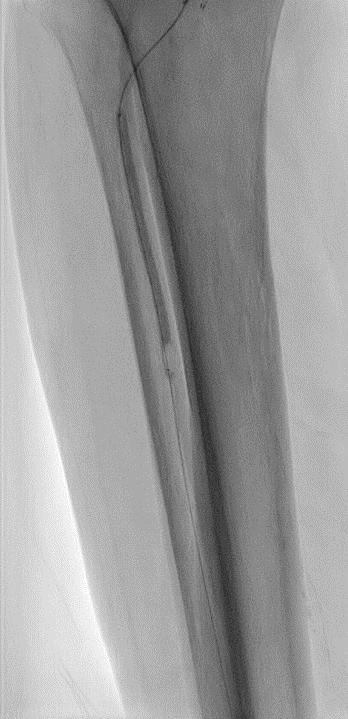
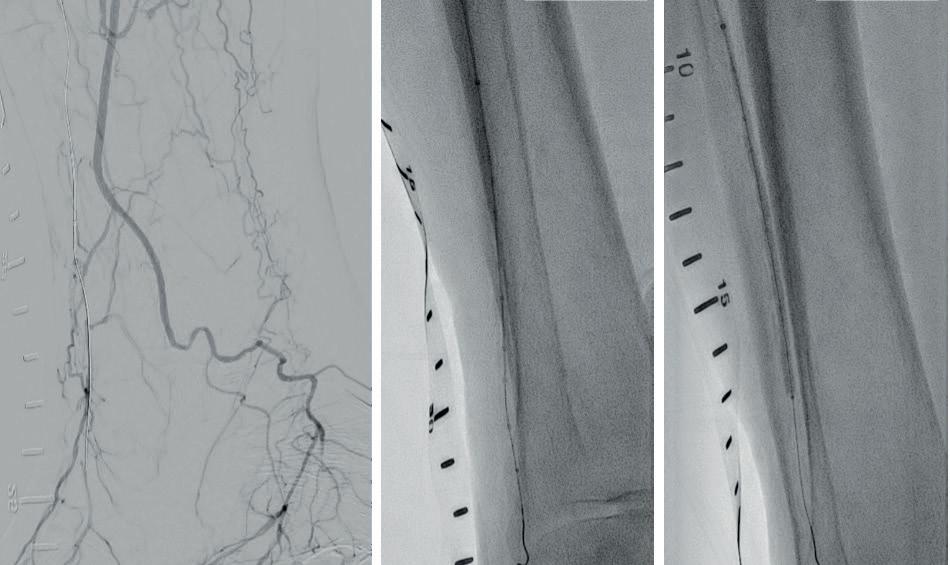
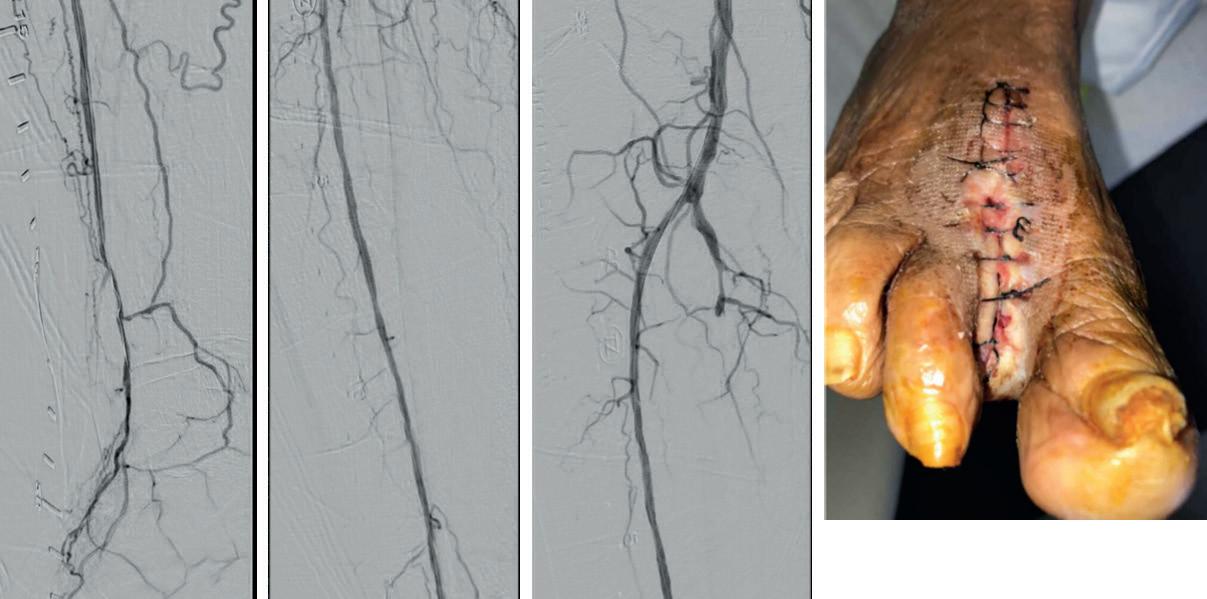
Given the angiosome of the tissue loss, we elected to pursue opening the anterior tibial CTO. Access with a 5F, 70cm sheath was used from a contralateral femoral approach. Using a 0.014” microcatheter and wire escalation, we were able to cross into the true distal lumen of the distal anterior tibial circulation using a 12-gram tipped guidewire (Figure 3a). A 2.5mm Shockwave E8 was used for multiple treatments along the entire length of the CTO segment (Figures 3b, 3c). Post IVL therapy, angiography showed brisk flow through the anterior tibial and into the distal anterior circulation of the foot (Figures 4a-c). This improvement in circulation allowed for this patient to undergo her planned second toe amputation with primary close (Figure 4d).
Conclusion
The key takeaway points for this case were the deliverability of the Shockwave E8 and the ability to treat longer segments versus
the Shockwave S4. In addition, in many cases the Shockwave E8 can serve as the primary or final therapy without the need for additional angioplasty. This catheter continues the evolution of treatment options for patients with BTK disease.
References
1. Feraresl R, et al. J Cardiovasc Surg. 2018 Oct;59(5):655-664
2. Mustapha JA, et al. Circ CV interventions. 2016;9e003468.
ANAND PRASAD is a professor of medicine and director of interventional cardiology at UT Health San Antonio and University Health in San Antonio, Texas. He is a paid consultant of Shockwave Medical. The views expressed are those of the author and not necessarily those of Shockwave Medical
SPL-73445
Peripheral Safety Information
In the United States: Rx only.
Indications for Use—The Shockwave Medical Intravascular Lithotripsy (IVL) System is intended for lithotripsy-enhanced balloon dilatation of lesions, including calcified lesions, in the peripheral vasculature, including the iliac, femoral, ilio-femoral, popliteal, infra-popliteal, and renal arteries. Not for use in the coronary, carotid or cerebral vasculature
Contraindications—Do not use if unable to pass 0.014” (M5, M5+, S4, E8) or 0.018” (L6) guidewire across the lesion-Not intended for treatment of in-stent restenosis or in coronary, carotid, or cerebrovascular arteries.
Warnings—Only to be used by physicians who are familiar with interventional vascular procedures—Physicians must be trained prior to use of the device— Use the generator in accordance with recommended settings as stated in the Operator’s Manual.
Precautions—use only the recommended balloon inflation medium—Appropriate anticoagulant therapy should be administered by the physician— Decision regarding use of distal protection should be made based on physician assessment of treatment lesion morphology. Adverse effects–Possible adverse effects consistent with standard angioplasty include–Access site complications –Allergy to contrast or blood thinner–Arterial bypass surgery—Bleeding complications—Death— Fracture of guidewire or device—Hypertension/Hypotension— Infection/sepsis—Placement of a stent—renal failure—Shock/ pulmonary edema—target vessel stenosis or occlusion— Vascular complications. Risks unique to the device and its use—Allergy to catheter material(s)— Device malfunction or failure—Excess heat at target site. Prior to use, please reference the Instructions for Use for more information on indications, contraindications, warnings, precautions and adverse events. www.shockwavemedical.com/IFU
GUEST EDITORIAL TRACK YOUR wRVUs, BECAUSE NO ONE ELSE DOES IT BETTER
continued from page 2 ACTIVITY
The following is an edited version of a table composed by the authors that contains procedures commonly performed by vascular surgeons. It is based on 2024 CMS numbers and contains CPT codes, wRVU values and the global period.
Procedures – Aortic Aneurysm
TEVAR - no coverage of left subclavian
TEVAR - coverage of left subclavian 33880 34.58 90
Percutaneous access for large sheath
Dialysis revision without thrombectomy 36832 13.50 90
Dialysis revision with thrombectomy 36833 14.50 90
Basilic vein transposition AVF 36819 13.29 90
Fistulagram 36901 3.36 0
Fistulagram with angioplasty of the outflow vein 36902 4.83 0
Fistulagram with stent of the outflow vein 36903 6.39 0
Fistulagram with PMT 36904 7.50 0
Fistulagram with PMT and angioplasty 36905 9.00 0
Fistulagram with PMT, angioplasty and stent 36906 10.42 0
Fistulagram with central vein angioplasty (add-on) 36907 3.00 zzz
Fistulagram with central vein stent (add-on) 36908 4.25 zzz
Fistulagram with embolization (add-on) 36909 4.12 zzz
Percutaneous fistula – one access site 36836 7.20 0
Percutaneous fistula – separate access sites 36837 9.30 0
Repair blood vessel with graft not vein – neck 35261 18.96 90
Repair blood vessel with graft not vein –upper extremity 35266 15.83 90
Repair blood vessel with graft not vein –intra-abdominal 35281 30.06 90
Repair blood vessel with graft not vein –lower extremity 35286 17.1 90
FROM THE COVER NOVEL MEASURE SUGGESTS 20% OF ELECTIVE CAROTID REVASCULARIZATIONS FAIL TO ACHIEVE A TEXTBOOK OUTCOME
continued from page 1
The crucially important carotid revascularization effectiveness measures of stroke, death and myocardial infarction (MI) are, of course, “irrefutably important,” Columbo told NESVS 2024, but—referencing his group’s prior work—he pointed to data showing patients prioritize additional aspects of their perioperative care, and drew further reference to another crucial factor: to obtain reimbursement, the required interaction must involve the personal preferences of beneficiaries.
The novel metric—the work of Columbo, a vascular surgeon at Dartmouth Hitchcock Medical Center in Lebanon, New Hampshire, and colleagues from the University of Florida in Gainesville, and the University of Alabama Medical Center in Birmingham—includes stroke, transient ischemic attack (TIA), MI, cranial nerve injury, reperfusion syndrome, return to the operating room (OR), access site complications, death within 30 days, discharge to a facility, and a postoperative length of stay of two days or more.
“The context of a textbook outcome composite adjunct has been championed by several other surgical specialties, most notably surgical oncology,” noted Columbo. “It has been documented as capturing a patient-centric snapshot of the anticipated successful outcome of the surgery. However, to date, vascular surgery has not adopted the use of textbook outcomes in clinical practice.”
RATES OF MAE AND REINTERVENTION FOLLOWING F/BEVAR REMAIN ‘STABLE,’ AORTIC RESEARCH CONSORTIUM DATA SHOW AAA
Latest study out of consortium details trends and outcomes after F/BEVAR procedures carried out over an eight-year period under consortium of 10 physician-sponsored IDEs.
By Bryan Kay
DESPITE INCREASING REPAIR extent and complexity, rates of technical failure, adverse events and reintervention remained “stable” following fenestrated and branched endovascular aneurysm repair (F/BEVAR) for abdominal aortic aneurysms (AAAs), a newly presented analysis of U.S. Aortic Research Consortium (ARC) data show. The positive outcomes are “likely secondary to evolutions in minimally invasive techniques and devices,” the ARC investigators report.
Aiming to create such a patient-centered outcome measure to inform shared decision-making conversations surrounding carotid revascularization, the research group established a cohort of elective patients in order to evaluate the likelihood of a textbook outcome. Mining VQI data from 2016–2023 resulted in a patient group further divided into CEA (51,000), TCAR (15,000) and TF-CAS (6,000) cohorts.
Patients had a mean age of 71.6 years, approximately 40% of each cohort was female, and most were White, with those who had a recent MI, on home oxygen and with heart failure important minorities in each cohort, Columbo said. “Notably, 1% of patients who underwent CEA had a history of a prior ipsilateral carotid procedure, compared to 14% of TCAR patients and 22% of TF-CAS patients,” he revealed.
“Across the three cohorts, most patients had a textbook outcome, but a slightly higher percentage of patients who underwent TF-CAS achieved a textbook outcome.”
Stroke and MI were found to be low across the three groups, while return to the OR and access site complications were approximately 2%, while 30-day mortality was low, Columbo pointed out. “Nearly 20% of these asymptomatic patients were discharged on postoperative day two or later.”
Sensitivity analyses showed that the driver of the greater level of textbook outcomes among those treated via TF-CAS—postoperative length of stay—did not endure into
The data were presented by first-named author Eric Finnesgard, MD, a vascular surgery resident at UMass Chan Medical School in Worcester, Massachusetts, during the 2024 New England Society for Vascular Surgery (NESVS) annual meeting in Portland, Maine (Oct. 25–27). Finnesgard collected the R. Clement Darling Jr. Award—given for an outstanding original paper from a resident, fellow or medical student—for the work.
The analysis laid out a cumulative 30day major adverse event (MAE) rate of 10% and a one-year secondary intervention rate of 18%, with adjusted observed-minusexpected cumulative sum used to evaluate outcomes over time.
In the case of 30-day MAEs, which occurred in 240 patients, Finnesgard demonstrated a cumulative event rate oscillating around the baseline—reflecting “a stable process that is achieving expected outcomes over time,” he told NESVS 2024. For one-year reinterventions, of which there were 435 performed, the cumulative event rate followed a similar pattern, again reaching expected outcomes over time.
Survival at 30 days was 97.3%.
days three and four, when the there was no statistically significant difference between the three treatment modalities.
Analysis of five-year survival curve data revealed a rate of 92% among CEA patients who had textbook outcomes versus 86% for those who did not. The data were similar for TCAR and TF-CAS: 91% vs. 85% and 90% vs. 82%, respectively.
“ The context of a textbook outcome composite adjunct has been championed by several other surgical specialties, most notably surgical oncology”
JESSE COLUMBO
“You’ll note that, in each case, the results for patients who underwent elective procedures for asymptomatic carotid stenosis appear roughly similar, and patients who had a textbook outcome had superior survival across the cohorts,” Columbo said. Columbo acknowledged study limitations, including an inability to quantify the impact of the distinct components of the composite textbook outcome. “A successful textbook outcome after any carotid revascularization in current practice was surprisingly less likely than may have been anticipated, Columbo concluded.
“The correlation between textbook outcomes and fiveyear survival substantiates it as a useful quality measure for patients considering carotid revascularization.”
The novel patient-centric textbook outcome measure at hand may offer value to shared decision-making interactions between physicians and patients as they discuss carotid procedure options in the wake of the CMS coverage expansion, he added.
how total device components, dissections and the proportion of thoracoabdominal aortic aneurysms (TAAAs) increased across the study period, while technical failure rates and hospital stays remained stable. Fusion imaging, low-profile devices and completely transfemoral repair were increasingly adopted over time, he continued, and there were nonsignificant downward trends in fluoroscopy times, procedure times, radiation dosage and blood loss throughout the study.
Significant determinants of 30-day MAEs included index procedure, technical failure, TAAA, patient age, operative time and baseline renal function. For secondary interventions, significant determinants included index procedure, off-the-shelf device use, technical failure, total target vessels incorporated and prior aortic dissection.
“These data demonstrate trends toward treatment of more complex and extensive aortic disease over the study period,” Finnesgard said, acknowledging study limitations that included the retrospective nature of the analysis and an inability to account for previous operator experience.
Therapy at Yale University in New Haven, Connecticut, queried Finnesgard over the nature and outcomes of the reinterventions, as well as the study’s “incredibly low” paraplegia rates. Kuwayama said “the functional question” around reintervention is: “Are the aneurysms actually successfully excluded?” Finnesgard detailed that 85% of the interventions were performed percutaneously for endoleaks, with type IIIc and Ic the most common, but said he did not have outcome data from these reinterventions on hand, and further acknowledged that “successful aneurysm exclusion” is “a the key metric we need to strive for.” On the paraplegia question, Finnesgard pointed toward practice changes over time—such as a shift toward staged procedures—as significantly helping patients, alongside “big changes to our multimodal protocols for management of spinal cord ischemia” postoperatively.
ARC data guide debate
The analysis included 2,377 F/ BEVAR patients—derived from ARC’s 10 prospective, non-randomized, physician-sponsored investigational device exemption (IDE) studies and treated between 2015–2023— with a median follow-up of 2.3 years. Finnesgard detailed
“These multicenter data demonstrate that, despite an increase in practice complexity, cumulative event rates have actually remained relatively stable.”
Discussant David P. Kuwayama, MD, director of aortic surgery in the Division of Vascular Surgery and Endovascular
Meanwhile, the analysis’ senior author, Andres Schanzer, MD, chief of vascular surgery at UMass, made the case for superior outcomes from F/BEVAR over open repair using ARC’s vast dataset during a debate at the 2024 VEITHsymposium in New York City (Nov. 19–23): “While open and endovascular repair are valuable, I believe it is time to stop starting and ending every talk with ‘Open repair is the gold standard,’ because it really no longer is.”
Eric Finnesgard
Research suggests arm vein is the best alternative bypass conduit in patients with CLTI
By Jocelyn Hudson
A NEW ANALYSIS has found arm vein to be the most suitable alternative conduit to great saphenous vein (GSV) in chronic limb-threatening ischemia (CLTI) patients, particularly in below-knee bypass targets. Prosthetic grafts also represent an adequate option, the researchers add, while advising that the use of biological grafts in this setting should be limited.
The research—a retrospective analysis of prospectively collected data from the Vascular Quality Initiative (VQI)—were recently published in the Journal of Vascular Surgery (JVS) following its presentation at the 2024 Western Vascular Society (WVS) annual meeting (Sept. 7–10) in Colorado Springs, Colorado.
First author Mohammed Hamouda (pictured), MD, senior author Ann C. Gaffey, MD, both from UC San Diego in San Diego, California, and colleagues write in JVS that, while the optimal conduit for infrainguinal bypass is single-segment GSV, this is not aways available in patients with CLTI. Therefore, suitable alternatives conduits are warranted.
The authors pored over 9,165 infrainguinal procedures from across a 20-year study period. These included 417 arm vein grafts (4.55%), 7,520 prosthetic grafts (82.05%), and 1,228 biological grafts (13.4%).
Hamouda et al report in their results that, compared to arm vein grafts, patients receiving prosthetic grafts had higher odds of infection (adjusted odds ratio [aOR] 2.89, p=0.045) and higher hazard of one-year mortality (aOR 1.51, p=0.035). On the other hand, the investigators continue, patients receiving biological grafts had higher risk of graft occlusion (aOR 4.55, p=0.04) and infection (aOR 2.78, p=0.046), as well as higher hazard of one-year mortality (aOR 1.53, p=0.04), amputation (aOR 1.72, p=0.019) and amputation or death (aOR 1.52, p=0.005) compared to arm vein grafts. Finally, the authors note that, after stratifying by bypass configuration, arm vein grafts had the highest overall survival and amputation-free survival among the three alternative conduits.
BEST-CLI: TRIAL RESULTS ENDURE IN ANALYSIS OF PATIENTS WHO PRESENTED WITH DIABETES
DIABETES AFFECTS APPROXIMATELY
70% of patients with chronic limb-threatening ischemia (CLTI) and is associated with more severe presentation, driven mostly by higher rates of wounds and infections, according to a recently presented retrospective analysis of BEST-CLI randomized controlled trial data. Investigators further found that CLTI patients without diabetes presented with more severe ischemia, were more likely to undergo major reinterventions, and that the trial’s seminal finding endures: bypass outperformed endovascular intervention when a single-segment great saphenous vein (SSGSV) graft was used as a conduit.
The data were presented during the 2024 annual meeting of the New England Society for Vascular Surgery (NESVS) in Portland, Maine (Oct. 25–27) by Cassius Iyad Ochoa
COMPLEX PAD
Chaar, MD, associate professor at Yale School of Medicine in New Haven, Connecticut, on behalf of the BEST-CLI trial investigators.
Of note among baseline characteristics in the cohort of 1,777 patients, those with diabetes were more likely to be younger and significantly more likely to be Hispanic (17.1% vs. 4.7%), Chaar noted. Meanwhile, diabetes patients were more likely to have cardiovascular comorbidities such as hypertension, hyperlipidemia and coronary artery disease (CAD), but those without diabetes were more likely to be smokers and to have chronic obstructive pulmonary disease (COPD).
Chaar also pointed out how diabetes patients had a significantly higher rate of previous minor amputation of the index limb at 18.6% vs. 6% for non-diabetes patients.
Procedurally, patients with diabetes had
Two-year LIFE-BTK data show sustained benefits of drug-eluting resorbable scaffold for below-the-knee arteries
THE LATEST RESULTS FROM THE LIFE-BTK CLINICAL trial demonstrate the long-term effectiveness of the Food and Drug Administration (FDA)-approved Esprit BTK everolimuseluting resorbable scaffold system (Abbott) in patients with the most severe form of below-the-knee (BTK) peripheral arterial disease (PAD), with the device showing sustained benefits over balloon angioplasty and fewer repeat procedures at 24 months.
Two-year trial data were presented by Brian DeRubertis, MD, chief of the Division of Vascular & Endovascular Surgery at NewYork-Presbyterian and Weill Cornell Medicine in New York City during the 2024 Vascular Interventional Advances (VIVA) meeting in Las Vegas (Nov. 3–6).
The LIFE-BTK trial evaluated Esprit BTK in more than 260
significantly less ischemia than those without, Chaar reported. “So, their ABIs [ankle-brachial indices] were higher—and not just ankle pressure, but their toe pressure was higher as well.” But patients with diabetes had significantly higher WIfI wound and foot infection grades, and, overall, had a higher WIfI stage compared to those without, he added. Meanwhile, there was no difference in the revascularization strategies used between the two patient groups.
In terms of the trial’s primary outcome, Kaplan-Meier analysis showed significantly higher rates of major adverse limb events (MALEs) or all-cause death (53.5% vs. 46.4%), above-ankle amputation of the index limb (17.8% vs. 9.9%), and all-cause death (34.4% vs. 26.0%) in the diabetes group at three years, Chaar revealed. “Interestingly, those curves were flipped when looking at major reinterventions: patients with diabetes had significantly decreased incidence of major reintervention [18.2% vs. 24.3%].”
Under multivariate analysis, the researchers also looked to determine whether WIfI grades compounded the impact of diabetes. “The initial regression showed that diabetes was independently associated with the primary outcome, but when you repeated the model with WIfI, that trend was still there but the significance was lost,” Chaar explained. “However, WIfI was significantly associated with the primary outcome.”
The analysis mirrors the BEST-CLI trial’s overall findings, the investigators found: that is, lower rates of major reintervention, above-ankle amputation, and MALE or all-cause death in patients who underwent bypass with SSGSV compared with endovascular procedures, irrespective of diabetes status. “Patients with diabetes had worse overall outcomes after lower extremity revascularization for CLTI, probably related to more advanced disease on presentation,” Chaar concluded,—Bryan Kay
Brian DeRubertis presents LIFE-BTK data during VIVA 2024
patients worldwide with BTK PAD, comparing treatment to balloon angioplasty—the current standard of care
Results after two years showed that 90.3% of patients in the Esprit BTK arm did not require a reintervention at 24 months. The trial also showed sustained efficacy at 24 months.
Furthermore, compared to balloon angioplasty, patients treated with Esprit BTK had significantly greater freedom from chronic limb-threatening ischemia (CLTI) at 61.5% vs. 32.8% for balloon angioplasty.
Additionally, at one year, the trial’s powered secondary endpoints revealed that Esprit BTK had a higher rate of reducing vessel re-narrowing (35.2% improvement) compared to balloon angioplasty, DeRubertis reported.—Jocelyn Hudson and Bryan Kay
Cassius Iyad
Ochoa Chaar at the NESVS podium
ARTIS pheno Cutting-edge robotic imaging
For vascular interventional procedures
Meet the robotic C-arm that answers the diverse challenges of today’s vascular interventional procedures.
• Benefit from our experience with over 1,350 Hybrid OR and interventional radiology suite installations worldwide.
• Profit from a versatile system that is ready for current and future demands.
• Advance your case mix in your hybrid operating room or interventional suite.
siemens-healthineers.us
‘This is just the beginning’:
SVS launches patient-facing website in opening salvo of long-term branding campaign
By Marlén Gomez
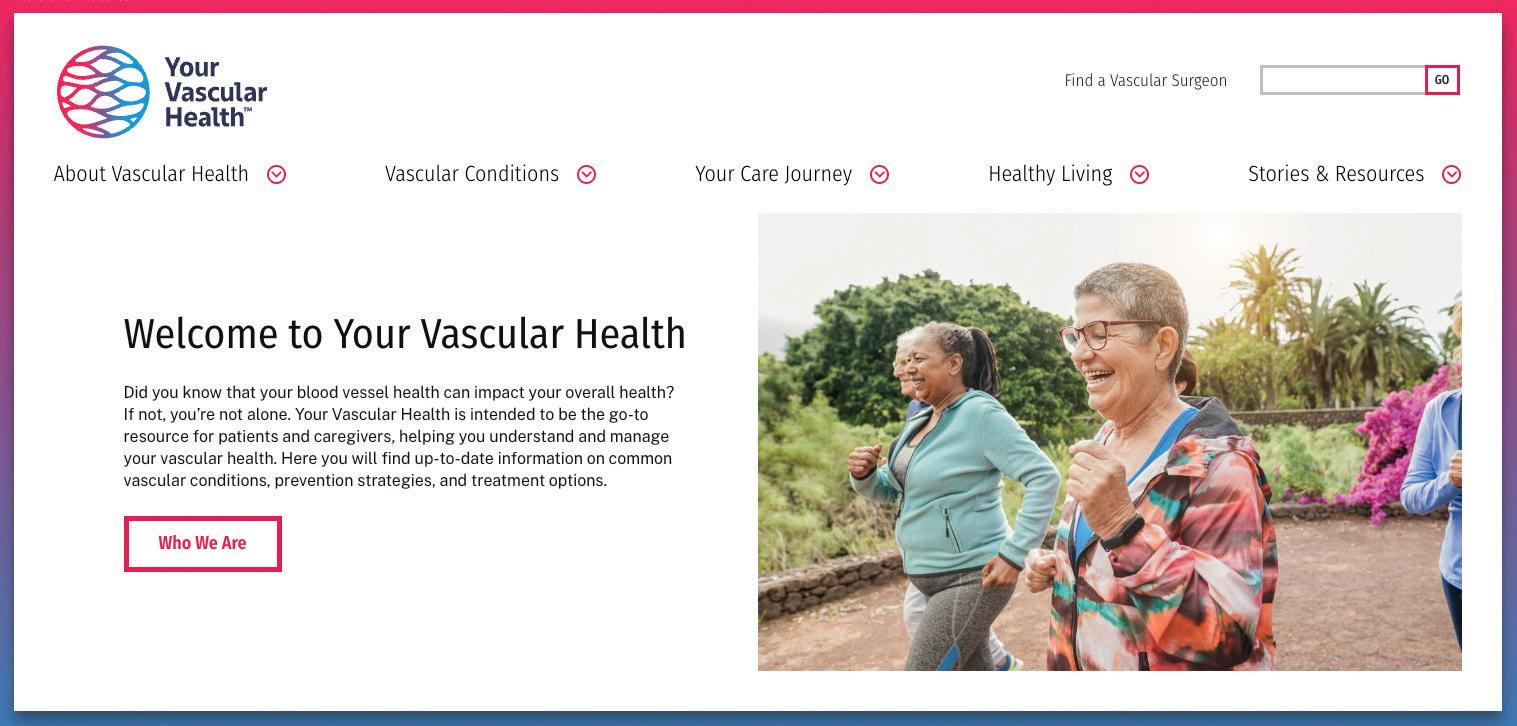
The Society for Vascular Surgery (SVS) has launched a new patient-facing website aimed at bridging the information gap between members of the public and their vascular care providers. Your Vascular Health allows patients to navigate the complexities of vascular health with accurate, easy-to-understand resources.
A cornerstone of the broader SVS branding initiative, it is central to efforts aimed at enhancing public awareness of vascular disease and highlighting the critical role vascular surgeons play in managing these conditions.
More than just a digital brochure, the site serves as a comprehensive tool to empower patients and caregivers to make informed decisions about their vascular health. It provides credible, in-depth information on conditions like peripheral arterial disease (PAD), aneurysms, deep vein thrombosis (DVT), and carotid artery disease, among others.
Guided by the latest clinical research and expert recommendations, the platform aims to be the go-to resource, offering support at every stage—whether patients are learning about vascular health for the first time, undergoing testing or managing a condition, according to William Shutze, MD, SVS secretary and a key spokesperson for the campaign.
The branding initiative’s origins predate the pandemic, when the organization rolled out initial toolkits aimed at educating patients and referral sources like primary care doctors.
According to Shutze, the effort intensified in 2023 following an extensive communications retreat designed to refine the SVS’s messaging strategy. “We spent much time honing our understanding of the different target audiences. We then developed messaging that would resonate best with each group, whether patients, referral physicians, healthcare executives, or medical students. That was our blueprint, and we’ve built upon that foundation to arrive at the point we’re at today.”
This blueprint helped build the foundation for the website, the most patient-centric aspect of the campaign. It offers visitors information on various vascular conditions through patient education flyers, treatment options and ways to connect with qualified vascular care providers.
Shutze emphasized the importance of offering actionable insights, stating, “We designed this site to give patients real, tangible information about how they can improve their lifestyle for better vascular health. It’s not just about listing symptoms or treatments. We want to empower patients with the knowledge that they can take control of their condition, whether through lifestyle changes or knowing when and how to seek medical intervention.”
Lifestyle resources include blog articles that focus on how patients can make daily lifestyle changes—such as diet, exercise and smoking cessation—significantly impacting vascular health. A physician directory functions as a searchable database of board-certified vascular surgeons,
underscoring the long-term scope of the effort—much like the continuous branding strategies employed by major corporations. “We’re not treating this as a one-and-done situation,” he said. “For the campaign to be truly effective, we’ll need sustained effort over the coming years. Think about how companies like Coca-Cola never stop branding—they evolve and refresh their message but keep at it. We’re taking the same approach with vascular health.”
Shutze believes that for the initiative to reach its full potential, all SVS members must participate. “Our national efforts are critical, but just as important are the local efforts made by individual surgeons and care providers,” he said. “We’re giving our members the tools to brand themselves and their practices to participate actively in this larger movement.
“This is just the beginning. We’re on a journey to ensure that patients everywhere know how to take charge of their vascular health and that they understand the critical role vascular surgeons play in that journey.”
complete with biographies and areas of expertise, and helps patients find the right specialist for them. Real-life accounts from patients undergoing vascular treatments are featured, offering inspiration and reassurance for those embarking on their healthcare journeys.
“We designed this site to give patients real, tangible information about how they can improve their lifestyle for better vascular health”
WILLIAM SHUTZE
Features aimed at maximizing accessibility for the user include condition-specific information, from which patients can learn about common and complex vascular conditions, their symptoms, risk factors and the latest treatment options.
The introduction of Your Vascular Health coincided with the launch of another significant aspect of the SVS’ branding efforts: on Oct. 23, the Society unveiled the findings of a comprehensive consumer survey that sheds light on public perceptions and misconceptions about vascular disease. The survey revealed that 82% of respondents are unfamiliar with the medical specialty that has the most comprehensive training for treating vascular diseases—vascular surgery. The results will help shape ongoing SVS efforts to raise awareness, both on a national scale and within local communities, via a threeyear public awareness campaign called “Highway to Health—Fast Track Your Vascular Health,” Shutze explained.
Shutze was at the forefront of this media effort, participating in interviews across TV, radio and other platforms.
“We’re hitting the ground running with a six-hour media blitz,” he explained as he prepared to hit the airwaves. “We’ll be discussing the survey results and promoting the new website, ensuring that the public knows about the vast resources available to them.”
While Your Vascular Health marks a milestone in the SVS’s branding campaign, it is only the beginning. Shutze said,
The new patient-facing website, Your Vascular Health, marks a major move aimed at bridging the information gap between vascular surgeons and member of the public
THE SVS NEEDS YOUR EXCELLENCE IN COMMUNITY PRACTICE AWARD NOMINATIONS!
THE SVS IS SEEKING NOMINATIONS FOR ITS annual Excellence in Community Practice Award. Formerly known as the Excellence in Community Service Award, the honor is bestowed on a member who has exhibited outstanding leadership within his or her community as a practicing vascular surgeon.
Nominations will be reviewed by the SVS Section on Ambulatory Vascular Care (SAVC)—the SVS Community Practice is now folded into this new entity— which will the determine the award recipient.
Past recipient Manish Mehta, MD, a vascular surgeon and director of Vascular Health Partners in Albany, New York, says others should consider applying due to the award’s role in highlighting “the important work that so many community practice vascular surgeons are doing.”
The 2025 nomination period is open, with a deadline to apply for the award of Sunday, Dec. 15.—Marlén Gomez
POWER AND PRECISION:
RISK INFORMATION
Caution: Federal (USA) law restricts the use of the system by or on the order of a physician. Refer to Directions for Use and/or User Manual provided with the product for complete Instructions, Warnings, Precautions, Possible Adverse Effects and Contraindications prior to use of the product. INDICATIONS FOR USE
FROM THE COVER SERVICE: GIVING BACK
continued from page 1
Former SVS president named ACS president-elect
THE AMERICAN College of Surgeons (ACS) elected Anton N. Sidawy, MD, as its president-elect during the ACS annual business meeting on Oct. 22. He served as president of the Society for Vascular Surgery (SVS) in 2010.
Sidawy is currently the Lewis B. Saltz chair and professor of surgery at The George Washington University School of Medicine and Health Sciences in Washington, D.C.
Sidawy’s career spans several decades and includes 180 peerreviewed articles, 60 book chapters, and numerous national and international presentations.
He served as editor-in-chief of the Journal of Vascular Surgery (JVS), launching two additional titles: the Journal of Vascular Surgery-Venous and Lymphatic Disorders (JVS-VL) in 2013 and the Journal of Vascular Surgery-Cases, Innovations and Techniques (JVS-CIT) in 2015.
In addition to his editorial work, Sidawy has authored three influential textbooks, including Basic Science of Vascular Disease (1997), Diabetic Foot: Lower Extremity Arterial Disease and Limb Salvage (2006), and the 9th and 10th editions of Rutherford’s Vascular Surgery and Endovascular Therapy, released in 2018 and 2022, respectively.
Sidawy has been an ACS fellow since 1987 and has played a key role in shaping the future of surgery. He has served on both the ACS Board of Governors (2001–2007) and the Board of Regents (2015–2024), including a term as chair of the Board of Regents from 2021–2022. Notably, he led a joint effort by the ACS and SVS to establish the Vascular Verification Program (Vascular-VP) aimed at broadening quality in care.
In his upcoming term as president of the ACS, Sidawy envisions focusing on the wellbeing of fellows, the quality of surgical care, and improving the practice environment for surgeons. He remains deeply committed to the ACS’s mission to “heal all with skill and trust,” a vision he plans to continue championing in his new role.
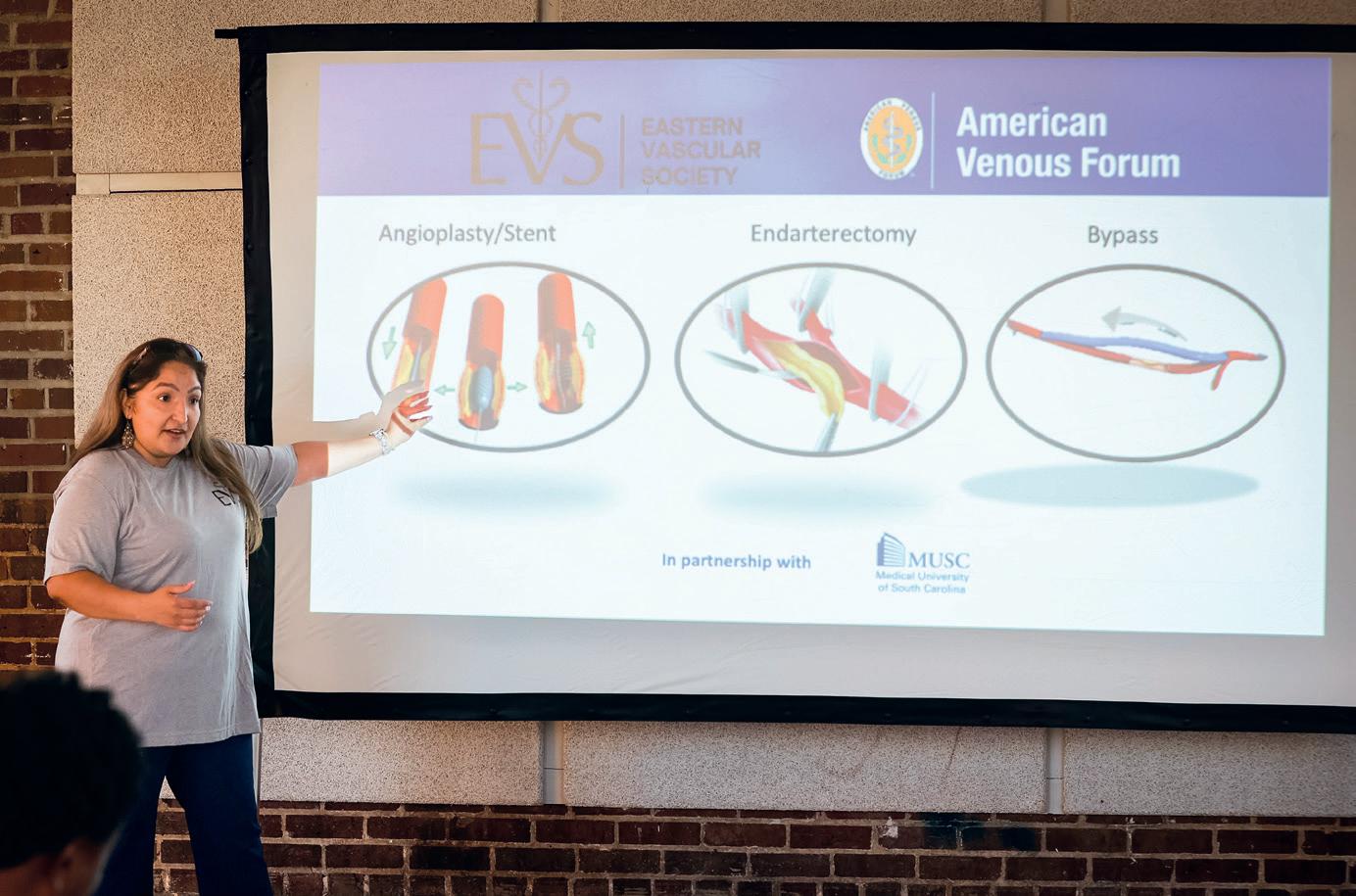
“I’m determined to make these work, I’m not giving up. There is something to this.” Kathleen Ozsvath, MD, is observing the scene at a local community center close to the heart of Charleston, South Carolina, where the EVS and AVF are staging a day of service as part of the former’s annual meeting program currently taking place in town.
Foot traffic has been brisk. Local residents are flowing in to hear short presentations on peripheral vascular health, and how both peripheral arterial disease (PAD) and venous insufficiency develop. Key, the talks are being delivered by nurse practitioners in simple, engaging language. Christina Guarin, NP, from the Department of Surgery at the University of Texas Medical Branch (UTMB) in League City, Texas, is in the middle of one, telling assembled members of the public about the signs and symptoms of PAD and how they can spot potential claudication. Across the room, a vascular surgeon and another nurse practitioner are performing ankle-brachial index (ABI) screenings. The remit is simple: reach local communities where they are and build awareness of vascular disease. Ozsvath—one of the chief architects of the event alongside Misaki Kiguchi, MD, the vascular surgery residency program director at MedStar Washington Hospital Center in Washington, D.C.—is energized. “We plan to do this again at the next AVF in February in Atlanta. I think it’s extremely important for societies to give back in this way,” she tells Vascular Specialist. “We teach our trainees, we teach our young surgeons, we teach one another at these academic meetings, but I think it’s also important that we help and reach out to our patients.”
This is the second such community outreach day those involved have organized this year. The first took place during the AVF’s annual gathering, VENOUS 2024, in Tampa, Florida, in March. The group learned much from that initial foray, Ozsvath observes. The first go round, they involved advanced practice providers (APPs) like nurse practitioners, as well as local doctors to ensure familiar points of contact, in addition to industry partners. Learning from that experience, Ozsvath, Kiguchi and company made sure to enlist industry help at an earlier juncture in a bid to increase foot traffic. It worked. “In Tampa, we had people who went out into the street, walked up to people and knocked on doors,” says Ozsvath, looking back a few weeks after the event. “We did the same thing in Charleston, but had a lot more out there. We also asked several local industry reps to put this out there in advance. The local doctors we included also made sure to advertise it to their patients. We were more aggressive—and pointed—in the appropriate directions.”
The initial idea grew out of a societal equity project to perform a day of service with providers, giving them venous disease education so they could try to treat patients in need, explains Kiguchi. The theory goes that, if primary care providers are not up-to-date on what is available for deep vein thrombosis (DVT), superficial venous disease or pulmonary embolism (PE), then what hope is there for
“I think it’s extremely important for societies to give back in this way. We teach our trainees, we teach our young surgeons, we teach one another at these academic meetings, but I think it’s also important that we help and reach out to our patients”
KATHLEEN OZSVATH
disadvantaged patients. “It then evolved into trying to treat people in underserved communities, where we would do a small day of service at the meetings themselves, bringing everyone together,” she says. “It doesn’t necessarily benefit each of us in terms of practice development because we’re coming from out of town, but what we’re trying to do is allow people in the area to understand what venous disease is and to tell them the resources there are in the community to get evaluated.”
INDUSTRY INVOLVEMENT PROVED fruitful. Jobst provided a tranche of compression stockings to be handed out to those who attended, for instance. Some volunteered their time on the night, fanning out into the surrounding community to help draw residents to attend. Scott Dooney, an area vice president with Advanced Oxygen Therapy, Inc., was one. “I think I walked probably two miles in the community,” he recalls. “I talked to anybody. I went solo, and we all wore scrubs. I had interactions with a guy cleaning his car, I went to the playground and talked to a gathering. I handed out the leaflet for the event and explained what we were trying to accomplish. Simply: ‘If you have diabetes in your family, anybody who has had issues with any type of ulcer on their foot—we’re doing a free screening down here at the community center building, we’re going to have some education and there is something to eat. You can also get screened. Bring your significant other and any family members.’”
Other volunteers, including a group led by local vascular surgeon A. Sharee Wright, MD, a clinical associate professor of surgery at Medical University of South Carolina (MUSC), helped corral a family reunion who had gathered in a local restaurant to the event. Current AVF president Ruth Bush, MD, associate dean for educational affairs at the John Sealy School of Medicine at UTMB, was also
part of the team on the ground coaxing in passersby, dressed in scrubs like many of her colleagues as a means of gentle greeting.
The sartorial code was deliberate.
“We didn’t want to appear intimidating,” explains Ozsvath. The language used followed suit. Ultimately, the idea was to blend into the community. To not appear formal. “I personally pride myself very much on speaking to people the way I want to be spoken to and try to explain things in a manner people are going to understand,” continues Ozsvath. “When I speak to patients in an office, I speak to them eye-to-eye so I’m not looking down on them. Those are the things that make people feel better and more comfortable.”
Martin Sylvain, a longtime industry leader in the vascular space and consultant, helped co-ordinate industry involvement. He also took part on the day. “The idea was to make it neighborhood-based so people could access the event with ease, walking a block or two to get there, and to provide food and refreshments. If they were to take place at a medical center where people had to take a bus, for example, people might be less likely to attend,” Sylvain says. “It was a great example of industry partnering with vascular surgery to create awareness for vascular disease at the local level.”
Kiguchi looks at the device company par-
ticipation through a slightly different lens. Ordinarily, their participation at meetings is through traditional sponsorship opportunities like booths, and breakfast and lunch symposia, she notes. “But there is a push to be more involved in community outreach because that is where the patients are. Think about the fact that you’re educating people who are already at the meeting, at these booths, at these lunch meetings, and you’re kind of educating the people who are already educated. So, there is a movement to educate people who really need the education.”
Kiguchi also highlights the importance of community involvement. “One of the main things we realized from Tampa is that the people in these communities we work in don’t plan. So, right before the events begin, we need people out there corralling people in. And we did that. We went around a couple of hours before, into places like Section 8 housing, and invited people along.”
Come VENOUS 2025 in Atlanta (Feb. 16–19)—scene of the next day of service event—Ozsvath and Kiguchi want to piggyback on local community health events. “Reaching out to communities in the church, communities in volunteer programs—not reinventing the wheel but going to these events—is going to increase foot traffic,” Kiguchi says. Eventually, the organizers hope the idea is adopted by other regional
and national meetings, hopefully coalescing around a fixed day or weekend on the calendar for vascular surgery outreach, she adds. From the administrative angle, AVF CEO John Forbes, another of the volunteers present at the EVS day of service, observes the
“More so now, the first person people are going to see for venous or arterial disease is the nurse practitioner”
MISAKI KIGUCHI
scene and marvels at the big step made from version one in Tampa to 2.0 in Charleston. “The longer-term vision is to scale this even bigger, and provide knowledge to the public that is widespread.”
Venous disease education is a particular focus of the outreach. As Ozsvath tells it, “venous disease is underdiagnosed, undertreated, and it is hard enough to teach providers about venous disease, because it is not something we necessarily learn in medical school.” Hence, the need to go directly to the patients, “especially those who may have less access to care,” she adds, and why the host fa-
cilities of the events are in underserved areas.
It’s not just venous disease, Kiguchi says: these events also offer an opportunity to focus in on PAD and highlight how the disease process can manifest. Again, the role of nurses in disseminating the information—just as Guarin did alongside Debbie Williams, RN, clinical lead at Vascular Associates in Albany, New York, in Charleston—comes to the fore. “More so now, the first person people are going to see for venous or arterial disease is the nurse practitioner,” Kiguchi reflects. “We really wanted them to be at the forefront. That is something we learned from the AVF in Tampa. There, I did the presentations along with Ruth [Bush] and Kathleen [Ozsvath], but these APPs are fully capable of evaluating these patients on their own. They are more readily available. Us surgeons get called into the operating room, and we have limited time. It makes the most sense that these providers are able to be the ones who evaluate these patients first. So we thought, if these are the folks that these patients are going to see first anyway, then why shouldn’t they be the ones giving the presentations.”
RUNNING IN TANDEM WITH THE effort to give back amid a vascular disease knowledge vacuum is the ever-present issue of vascular surgery’s identity problem. “If you ask the average person, ‘What is a vascular surgeon?’, they don’t know,” says Ozsvath. “Even a lot of physicians will ask, ‘What do you do again? So you must work on the heart.’ These are the things that we, as a group of professionals, have not done a good job of: get out there to explain to people what it is we do.”
Equally as important, Ozsvath argues, is working across specialty boundaries in a similar way to how the outreach effort operates. “This is also about the other specialties we overlap with: interventional radiology, cardiology, cardiothoracic surgery; there are a lot of people in these specialties who do similar work,” she explains. “For patients, that can get confusing. They might think: ‘Do I go to a radiologist to get my veins done, or do I go to a cardiologist? He’s doing my heart; do I go to them for my veins also?’ What really matters is not so much what your specialty is, but whether or not you have the experience and the knowledge to treat a specific disease entity.”
In this climate, collaboration is key, Ozsvath adds, speaking to Vascular Specialist from the vantage point of a cardiac cath lab. “I did eight cases here today. I love working here. They treat me with open arms, and I work really well with the cardiologists. We share patients. I think that goes a lot further with relationships—and also better with our patients. It’s the same thing with the day of service programs. I tell patients all the time: this is a team sport. We’re in this together. It’s your body. You need to be educated so you can make the best decision for you and I’m here to help.”
Left: the day of service draws to a close with the departure of the last group of visitors. Top right: Christina Guarin conducts a lecture. Middle (l to r): Kathleen Ozsvath, Ruth Bush and Misaki Kiguchi. Bottom (clockwise from left): Compression stockings, on display and boxed up; and residents take in a talk
Tackling difficult acute limb ischemia cases with an endovascular-first approach using Lightning Bolt 7 computer assisted vacuum thrombectomy
Adam Reichard, MD, discusses the use of Lightning Bolt 7® computerassisted vacuum thrombectomy (CAVT TM) as a first-line option across a wide spectrum of challenging lower extremity acute limb ischemia (ALI) cases, including patients with Rutherford classification IIb ALI.
Two cases stick out for Reichard where he used Lightning Bolt 7 (Penumbra) computer-assisted vacuum thrombectomy (CAVT) as his firstline therapy for patients who require urgent management for lower extremity ALI.
Both patients were diagnosed with Rutherford IIb lower extremity acute limb ischemia. And both saw clinical improvement following use of the Lightning Bolt 7 device, notes the vascular surgeon in the TriHealth hospital system based in Cincinnati, Ohio.
For Reichard, the specter of Rutherford IIb cases is a key point of contention.
The level of threat to the limb is so great, open surgery would be the traditional approach. Yet, as Reichard has observed in recent years, the landscape has shifted. In these patients, an endovascular-first approach is increasingly the go-to option. For evidence, he points to the STRIDE study, which looked at 30-day outcomes after firstline use of the Indigo and Lightning portfolios in cases of ALI, including Rutherford I, IIa and IIb patients.
“If you’re talking to vascular surgeons who treat this disease pathology, they would agree that it is routine to start with an endovascular approach in someone who has Rutherford I or IIa ischemia, but, when you get into IIb territory, and you know it’s a more threatened limb, then people might be a little more reluctant,” Reichard explains. “However, the STRIDE study did a great job showing that, even in patients with Rutherford IIb ALI, at 30 days you’re going to salvage more limbs and mortality is going to be lower if you start with percutaneous thrombectomy, including computer-assisted vacuum thrombectomy technology, as opposed to open surgery.”
Thirty-day outcomes from STRIDE—a prospective, single-arm observational study carried out at 16 international sites among 119 patients with lower extremity ALI— showed rates of 98.2% for limb salvage, 89.4% for patency, 3.4% for mortality and 4.2% for periprocedural major bleeding.1 This compares to rates of 83.1% (limb salvage),2 78.6% (patency),3 13.2% (mortality),4 and 21% (major bleeding)5 in the setting of
open surgery, as recorded in the literature.
During his fellowship years, Reichard watched as endo-first took hold. “When I first started in practice, it wasn’t too long after the Lightning Bolt 7 catheter had been released,” he says. “I got the opportunity to use it in training, as some of my mentors had embraced endovascular-first for lower extremity ALI, and I saw how effective it was. When I went out into practice, I told myself that was going to be my practice pattern when it was appropriate.”
You do your on-table angiogram at the end of the case to see what your outflow looks like. More often than not, you’re going to end up doing adjunctive endovascular procedures trying to touch that up.”
Reichard argues that, in this case, taking an endovascular-first approach from an open exposure provided visibility on the outflow vessels, ultimately proving to be “more effective and efficient.”
The gravity and complexity of an ALI diagnosis weigh heavily. In-hospital and 30day mortality rates are up to 9% and 15%, respectively, Reichard points out. Amputation rates can reach 15% at discharge and 25% at 30 days, he continues.
“Something that is most important to consider is that if a patient comes in with ALI, mortality at five years is almost 50%, so obviously there is a lot of morbidity and mortality associated with this issue.”
Reichard recalls of those first two patients he treated, both Rutherford IIb: “They had pain, sensory dysfunction and motor dysfunction, and traditionally we would have taken them to the operating room for a cutdown and open embolectomy or thrombectomy.”
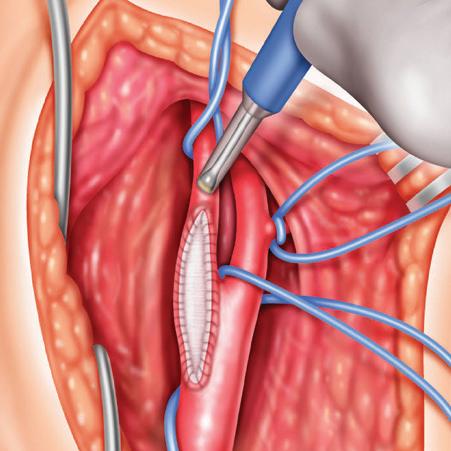
In the first case, a female patient with a prior aortobifemoral graft, Reichard explains, a Lightning Bolt 7 catheter was used in her leg from the common femoral artery down to her foot. “At the end of that case, she had palpable pulses and, a few hours after that, when I went to check on her, she said that her leg and foot felt much better, and it looked much better clinically too,” he says. “That is someone who traditionally probably would have ended up—at least— with a groin incision and a femoral dissection, but probably with a below-the-knee popliteal artery cutdown and dissection.”
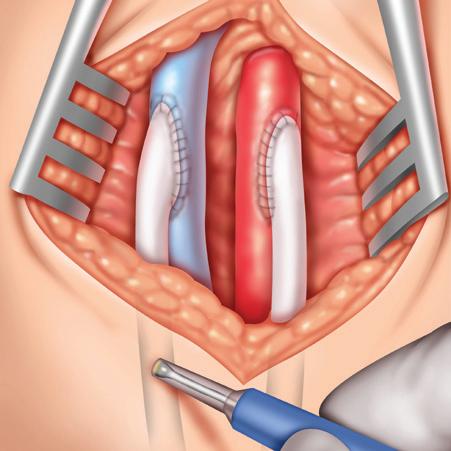
The second patient, a male in his 80s with a prior endovascular aneurysm repair (EVAR), underwent a femoral dissection and cutdown to directly access his superficial femoral artery. A Lightning Bolt 7 catheter was similarly used to thrombectomize his leg.
In this case, Reichard acknowledges a possible paradox. “People could argue that if you’re already open, and you already have the femoral vessels exposed, why not just pass a Fogarty balloon embolectomy catheter. However, my issue with that is that you’re sending a balloon catheter blindly down the leg and looking for back bleeding.
The safety and effectiveness of endovascular devices mean the shift to endo-first practice patterns like the one adopted by him and his colleagues at TriHealth are increasing, Reichard says. “We know that about 86% of patients with ALI that go for an open embolectomy or thrombectomy end up needing additional endovascular work while you are in the operating room.”
“
The STRIDE study did a great job showing that, even in patients with Rutherford IIb ALI, at 30 days you’re going to salvage more limbs and mortality is going to be lower if you start with percutaneous thrombectomy, including computerassisted vacuum thrombectomy technology”
ADAM REICHARD
The rapid development of CAVT has led to greater clinical gains as new iterations of the technology have rolled out, Reichard observes. “When the Lightning devices came out, that really mitigated blood loss during procedures. At that point, I think people were a lot less reluctant to use those devices first-line.”
As a vascular surgeon with the skills to pivot to open surgery should the need arise, Reichard says the endo-first approach infrequently leads to the need for bailout
procedures. “These devices are so effective at clearing thrombus, even in the tibial vessels, that it has really minimized the need for open surgery for tibial thrombectomies. Also, if a Rutherford IIb lower extremity ALI patient comes in and you are able to de-bulk the majority of that thrombus endovascularly, when we’re still endo, more often than not, we have the option of adjunctive catheter-directed thrombolysis, which we don’t often need to do. Once we’re open, that is taken off the table.”
Lightning Bolt 7 occupies an intriguing position in the shift toward endo-first, Reichard adds.
“The fact that the device uses a dual clot detection algorithm—pressure and flow based—is important in these cases, allowing for quicker clot detection and patent flow. What we want in these cases is effective thrombus removal, but we also want to try to mitigate blood loss. This catheter, its algorithm, effectiveness and safety are what makes it more effective in managing these patients.”
References
1. Maldonado TS, Powell A, Wendorff H, et al. Safety and efficacy of mechanical aspiration thrombectomy for patients with acute lower extremity ischemia. J Vasc Surg. 2024;79(3):584–592.e5. doi:10.1016/j. jvs.2023.10.062
2. Veenstra EB, van der Laan MJ. Zeebregts CJ, et al. A systematic review and metaanalysis of endovascular and surgical revascularization techniques in acute limb ischemia. J Vasc Surg. 2020 Feb;71(2):654–668.e3. doi:10.1016/j.jvs.2019.05.031
3. Grip O. Wanhainen A, Michaëlsson K, Lindhagen L, Björc M. Open or endovascular revascularization in the treatment of acute lower limb ischemia. Br J Surg. 2018 Nov;105(12):1598–1606. doi:10.1002/bjs.10954
4. Taha AG, Byrne RM, Avgerinos ED, et al Comparative effectiveness of endovascular versus surgical revascularization for acute lower extremity ischemia. J Vasc Surg 2015 Jan;61(1):147–157. doi:10.1016/j. jvs.2014.06.109
5. Kolte D, Kennedy KF, Shishehbor MH, et al. Endovascular versus surgical revascularization for acute limb ischemia: a propensity-score matched analysis. Circ Cardiovasc Interv. 2020;13(1):e008150
This interview was sponsored by Penumbra, Inc. Adam Reichard is a consultant for Penumbra.
Procedural and operative techniques and considerations are illustrative examples from physician experience. Physicians’ treatment and technique decisions will vary based on their medical judgment. The clinical results presented herein are for informational purposes only, and may not be predictive for all patients. Individual results may vary depending on patient-specific attributes and other factors.
Caution: Federal (USA) law restrictions these devices to sale by or on the order of a physician. Prior to use, please refer to the Instructions for Use for complete product indications, contraindications, warnings, precautions, potential adverse events, and detailed instructions for use. For the complete Penumbra IFU Summary Statements, please visit www.peninc.info/risk. Please contact your local Penumbra representative for more information.
Adam Reichard
COMMENT& ANALYSIS
HOW TO MAKE THE MOST OF YOUR RESEARCH YEAR(S)—PERSONAL GROWTH EDITION CORNER STITCH
By Saranya Sundaram, MD
I’m sure research residents everywhere have heard their fair share of unsolicited advice on this topic. But among all the voices advising me on “how to be productive” or “how to make the most impact on the vascular world,” I was lucky enough to have one mentor who asked me, “Who do I want to be at the end of this year?” That concept, which I felt myself coming back to over and over again throughout my year out, inspired me to come up with a list of ways a research year can really help you become the person you have strived to be but maybe just didn’t quite have the time to develop. This is by no means a complete list.
Spend time with family, friends, and significant others
This seems like a given, but don’t take it for granted. The generally unfiltered access to your family, friends, and significant others is something you may never get to experience again in your medical career. For me, it meant spending every birthday and holiday with my parents and sibling, maintaining
friendships that were on the verge of being forgotten, and getting to know the most incredible person in my life right now. Take every opportunity you can to prioritize your time with people (and pets!) you won’t see regularly when you return to the hospital.
Find something that is just yours
I know, it sounds cheesy, but when we make our lives about other people, we forget what makes us who we are. For one of my friends, she felt most herself when she started writing and performing music. For another friend, it was joining a tennis club and playing tournaments on the weekend. For me, it was getting back into sewing and redesigning clothing. I could spend hours not speaking to anyone and consumed just in sewing a new outfit together or fixing ones that needed altering. Now, when I find myself in a rut or just in need of some personal time, I pick something from my
What happens next? The
importance of the lame
duck session for vascular surgeons GGR
By Andrew Kenney
POST ELECTION AND WITH THE END OF THE year on the horizon, a crucial but often overlooked period in the legislative calendar begins: the lame duck congressional session. This period, which occurs between the November elections and the start of the new Congress in January, allows outgoing lawmakers a final opportunity to pass critical legislation. For vascular surgeons, the upcoming lame duck session is particularly significant, as they face a looming 2.8% Medicare reimbursement cut scheduled for Jan. 1, 2025.
Depending on the results of an election, the lame duck session is often a time when Congress acts to “clear the deck” and potentially negotiate agreements on high-priority issues previously marred by the politics of an election year. This creates a unique window for legislative compromise and action, particularly in healthcare. For vascular surgeons, this period is crucial to advocate for changes that directly impact their ability to provide care.
Starting in January 2025, physicians, including vascular
“alterations rack” and lose myself in it. It’s important to have something that grounds and reminds you of yourself when you feel lost or burnt out.
Slow down and process
You now have so much more time to process how you choose to interact with the world and the people in it. I found myself taking extra time to think through decisions, what I wanted out of my relationships with others, and whether the ways in which I responded to problems aligned with how I wanted to present myself. As someone who didn’t take much time off before they started training, I found this year offered me room to “develop myself,” especially how I deal with tough situations—this made returning to clinicals much smoother as it was easier to align myself with my personal goals and values.
Make that major event/travel
Whether it’s a wedding, family planning, or visiting your family in another country, take advantage of the time (and significantly less stressful responsibilities) to follow through with it. For me, it was planning a trip to see my grandparents in India, as I had often been stressed by the uncertainty of when I would see them
surgeons, are set to face a 2.8% cut in Medicare reimbursement under the Medicare Physician Fee Schedule (MPFS). For practices already operating under tight financial conditions, these cuts could have severe consequences. Reduced reimbursement threatens the financial sustainability of practices, limits the resources available for patient care, and places a strain on vascular surgeons who rely on Medicare payments to continue offering high-quality services.
The timing of these cuts, coupled with rising inflation and increasing costs, makes it difficult for physicians to maintain the same level of care without a corresponding increase in payments. Unfortunately, the current payment system does not adequately adjust for inflation, leaving healthcare providers to bear the brunt of escalating expenses.
Recognizing the urgency, the Society for Vascular Surgery (SVS), alongside the House of Medicine and several congressional leaders, is actively advocating to prevent these cuts and pushing for possible solutions.
given their late stage in life. It seems like the straightforward move, but I would absolutely recommend pulling the trigger if you have the means to follow through.
Learn something about the world outside of medicine
Though this may not be high on everyone’s list, it certainly increases your appreciation of life outside of the hospital. For me, I enjoyed attending a few birdwatching events that focused on the wildlife in Charleston. Through some of these Saturday kayaking events, I was able to learn about the dragon boat racing culture that was a huge part of many local lives. I also made it a point to take cooking and local wine classes around my community. It gave me an appreciation of what drives others every day. Again, this is by no means a complete list. But I welcome others to continue to share these aspects of their personal development as I believe prioritizing personal growth (though a sadly underrated practice) ultimately shapes us to contribute to this field in the best ways we can.
SARANYA SUNDARAM is a vascular surgery resident at Medical University of South Carolina in Charleston.
advocacy, communicating directly with their legislators and highlighting the real-world impact of reimbursement cuts.
The lame duck session provides a critical, but short, window to address the 2.8% Medicare reimbursement cut. For vascular surgeons, this period is key to avoiding immediate financial strain and ensuring they can continue providing high quality care.
However, the fight doesn’t end here. While preventing these cuts is the immediate priority, advocacy efforts must also focus on securing a permanent solution that aligns Medicare payment updates with inflation, ensuring longterm stability for physicians and patients alike.
The timing of these cuts, coupled with rising inflation and increasing costs, makes it difficult for physicians to maintain the same level of care without a corresponding increase in payments
The lame duck session represents the last opportunity of the congressional session to secure a temporary fix or, ideally, advance discussions on a permanent solution.
Engaging with SVS advocacy efforts plays a central role in this fight. It is essential for vascular surgeons to stay active in
As the 118th Congress wraps up, vascular surgeons must also prepare to pivot toward building new relationships with the incoming 119th Congress. Establishing these connections early will be essential for advancing broader reforms in healthcare policy. By engaging with new and returning legislators, the vascular surgery community can ensure that their priorities remain front and center in future legislative efforts.
ANDREW KENNEY is a member of the SVS advocacy staff, representing the Society in Washington, D.C.
The Doppler Designed for the Modern OR
It’s the next generation of our Trans-Q-taneous Intraoperative (TQI) Doppler System, combining the reliability and cost effectiveness of the original TQI Doppler with new, user-friendly features.
RELIABLE
VTI’s single-use surgical Doppler probes provide a higher degree of performance reliability since probe failure due to reprocessing is eliminated. You’ll reach for your Doppler with confidence!
COST EFFECTIVE
Single-use surgical Doppler probes eliminate reprocessing costs as well as the hidden expenses associated with the malfunctioning of reusable probes such as lost OR time.
EASIER TO USE
Increased Portability
In addition to its smaller size, the TQI 2.0 Doppler now features an IV pole mount and a handle for easy transport.
Greater Control
The modern design of the TQI 2.0 Doppler allows for a foot pedal for increased control from the surgical field.
Improved Sound
The TQI 2.0 Doppler System is optimized for clear audio signals for both intraoperative and transcutaneous use.
COMMENT& ANALYSIS
CONTINUED FROM PAGE 16
THE OUTPATIENT
IN FOCUS: OUTPATIENT VASCULAR PRACTICE
This month, Vascular Specialist launches its newest column, The Outpatient, which seeks to cover issues near and dear to the hearts of vascular surgeons practicing in outpatient settings such as office-based labs (OBLs) and ambulatory surgery centers (ASCs). Here, in the inaugural edition, Robert Molnar, MD, and Anil Hingorani, MD two key figures behind the creation of the newly launched Society for Vascular Surgery (SVS) Section on Ambulatory Vascular Care (SAVC)— detail the column’s aims objectives.
Welcome to the first article in a series intended to help you and your practice achieve enhanced success in delivering high quality outpatient vascular care. This is also an introduction to SAVC, formed by combining the SVS Community Practice Section (CPS) and the Section on Outpatient and Office Vascular Care (SOOVC). SAVC will leverage the collective knowledge, resources and expertise of vascular surgeons providing outpatient care to foster innovation, education, research and high quality care. Unifying the CPS and SOOVC will strengthen those vascular surgeons performing outpatient procedures in their ability to network, mentor upcoming vascular surgeons, and advocate for their practice, their patients and their communities—and, very significantly, for themselves.
It is clear that the majority of invasive vascular procedures has shifted to the outpatient arena. There are more than 1,300 OBLs and nearly 5,000 ASCs in the U.S. Nearly 80% of peripheral vascular intervention (PVI) cases are appropriately provided—and nearly 60% of these cases are currently being performed—in these sites of service. As compared to the hospital outpatient setting, OBLs and ASCs provide significant value to
the payer system, as the reimbursement rates are much less than the Hospital Outpatient Prospective Payment System (HOPPS). In addition, patient satisfaction outside of the hospital setting is extremely high. Regardless of the site of service, all vascular surgeons—whether private practice, community practice, academic affiliated/employed—are being significantly harmed by the inadequate reimbursements for providing these needed services. As we have recognized the significant cuts to our reimbursements and the inefficiencies we are forced to accept in the hospital outpatient space, we need to advocate for ourselves, our patients and our communities. As the leaders in the delivery of expert, quality and high value vascular care, we need to leverage our collective strength in advocating for our patients and our communities.
The headwinds have been—and will continue to be—significant for the foreseeable future. However, the pendulum will begin to swing in our favor once the ill-intended consequences of payor and regulator decisions lead to limited access to care, increased costs due to hospital inefficiencies, and
patient dissatisfaction. To combat these headwinds, we need to engage with each other, continue to advocate on our behalf, and share common problems and lessons learned with each other.
By bringing the CPS and SOOVC under SAVC, we will continue to promote the community practice surgeon and outpatient vascular care in the OBL and ASC settings. Specifically, we will continue to hold educational sessions at the Vascular Annual Meeting (VAM), webinars, and offer guidance in print within Vascular Specialist. We are striving to enhance all of these offerings, but we need your engagement to move the needle.
One of the projects that we continue to work on is the OBL Handbook, which is meant to help our community to open and maintain their practices by establishing and excelling in providing quality, cost-effective and needed vascular care. We certainly recognize the fluctuating reimbursements in the outpatient site of service and want to capitalize on opportunities to appropriately enhance your revenue streams by networking with those who have led the way in developing effective and highly productive practice developments.
In addition, we continue to recognize leaders in community practice with the SVS Excellence in Community Practice Award, the SAVC Presentation Award and the SAVC Research Seed Grant awards. We continue to promote the goals of the members of our section with representation from the SVS
CPVI course: Learning the latest intricate skills and techniques to treat complex PAD
VASCULAR SPECIALIST ATTENDED THE SVS Complex Peripheral Vascular Interventions (CPVI) Skills Course and spoke with participants about the hands-on learning experience designed for vascular surgeons and specialists at all stages of their careers. Over two days (Sept. 28–29), participants learned the latest techniques and innovations for treating peripheral arterial disease (PAD) through small-group simulations, using cadavers and benchtop models. Here, a small group of attendees share their experiences.
“I want to learn a bit more about distal revascularization, and I wanted to see if this course would be worthwhile for our trainees to attend in the future,” said Daragh Moneley, MD, a training program director from the Royal College
of Surgeons in Dublin, Ireland. “The hands-on stations have been excellent, particularly the industry being present and being able to demonstrate their products on actual models. It really shows the intricacies of how to use them or where you might be able to apply them. We’ll definitely encourage our trainees to attend, there’s no doubt about that”
Coding Committee, the SVS/American College of Surgeons (ACS) Vascular Verification Program (Vascular-VP) and the Postgraduate Education Committee. These are just some of the projects that we have and continue to work on to help vascular surgeons across the spectrum of our various vascular surgery practice types. We are currently engaged in ways to enhance practice revenue, given the significant cuts we have experienced for the care we provide. By engaging each and every vascular surgeon, we can promote the advocacy we deserve and share successful practice development tools and opportunities. We aim to appropriately enhance the reimbursements that each of you so significantly deserve to protect your practice and to continue to secure the finances needed to enable your continued success. We hope to enable you to compete on a level playing field through the newly launched vascular branding campaign and provide you with the marketing opportunities and SVS outreach that has been established to boost your recognition.
Therefore, if you are not currently a member, please join your colleagues in SAVC at soovc@vascularsociety.org to leverage our strength in protecting all of our futures. We need engagement, ideas and a forum to share opportunities in order to strengthen your practice.
ANIL HINGORANI is chair of SAVC, having previously held the role of chair of the SOOVC Steering Committee. ROBERT MOLNAR chaired the CPS Steering Committee.
to learn extra skills to help me take care of those patients,” she said. “I’m excited to see if I can institute deep vein arterialization, and so, coming to a course that teaches me the newer techniques and innovations that are out there to take care of my patients just makes sense.”
Alicia Stafford, MD, a vascular surgeon with Evansville Surgical Associates in Evansville, Indiana, used the course as an opportunity to add new skills to her armamentarium. “I deal with a lot of PAD and advanced diseases in the leg in my region and I felt like this course would be a good place
Amani Politano, MD, a vascular surgeon at Oregon Health and Science University used the course to brush up. “It’s been a while since I graduated from my training program and I thought that this would be a good time to get some new skills and things that I didn’t do when I trained,” he shared, “and also to get a little bit of insight into what’s maybe more cutting edge in the peripheral percutaneous world than what I remember years ago. This has definitely given me a lot more opportunity to practice some tools that I’ve heard about but maybe not done very frequently and then added some tools to my toolbox.”—Marlén Gomez
Robert Molnar and Anil Hingorani
L to r: Daragh Moneley, Alicia Stafford and Amani Politano
VASC.AI: Canadian vascular surgery researchers develop vascular-specific bot aimed at aiding education and clinical practice
By Bryan Kay
THE ADVENT OF LARGE LANGUAGE MODELS
such as ChatGPT (Open AI) has left little of the world untouched—and a quintet of University of Toronto vascular surgery researchers are bidding to harness this mode of artificial intelligence (AI) and refine it into a working model that is functionally vascular specific, capable of being used in clinical practice, research and education.
And according to research from the group recently published in the Journal of Vascular Surgery-Vascular Insights (JVSVI), they are making significant strides just 18 months on from the inception of their work.
Tiam Feridooni, MD, a vascular surgery resident at the institution in Toronto, Canada, and colleagues started to develop the model, named VASC.AI, around the same time as ChatGPT-3 was being launched, initially impressed by the mainstream application’s ability to intelligently answer questions but less so by its logical reasoning. Feridooni and colleagues tested the model on questions from the 5th edition of the Vascular Education and Self-Assessment Program (VE-
SAP5), comparing it to the evolving ChatGPT technology in three iterations: ChatGPT-3.5, -4 and -40. Across 244 textbased multiple-choice questions from six VESAP5 modules, VASC.AI significantly outperformed all three by answering 93.8% of questions correctly at the same time as ChatGPT got progressively better through version -40.
As Feridooni describes, VASC.AI is based on ChatGPT’s interface but is combined with retrieval-augmented generation (RAG), an advanced architecture that integrates specialized vascular surgery data into the model, potentially decreasing the generation of incorrect information and enhancing their educational usefulness. That input of vascular data was no small feat. Feridooni and co needed significant resources. That meant copious man hours, as well as funding. Luckily, they enlisted the help of a keen and engaged coder. Monetary help came via the research grant funding of senior author David Szalay, MD.
VASC.AI’s success is rooted in the database, made up of more than 250,000 abstracts, clinical practice guidelines and clinical trials. “The way it works in layman’s terms is we’ve basically told the model you have to draw your answer from this database of information,” explains Feridooni. “By creating this database, it has access to all of the up-to-date in-
“How do we weigh the abstracts versus the clinical trials versus the clinical guidelines? How do we make sure it is drawing from the right guidelines”
TIAM FERIDOONI
formation that a vascular surgeon would need to have access to.” The team also put about six or seven months of labor into making sure the model weighs the database’s constituent content appropriately. “That was a process in itself,” Feridooni recalls. “How do we weigh the abstracts versus the clinical trials versus the clinical guidelines? How do we make sure it is drawing from the right guidelines—for instance, if you asked about renal artery stenting, that it would pick out from the guidelines for peripheral vascular disease.”
Going forward, the research team aims to develop a similar interface for patients. “We want to help patients both pre- and postoperatively,” Feridooni explains. “If someone comes in and they learn they have an aneurysm and need surgery, by the time they have had time to digest the news, they are probably halfway home and probably have questions, and you might not see them again until the day of surgery. This will give patients the chance to ask and get accurate responses.” In the postoperative period, Feridooni says such a model could be deployed to aid triage. For example, if a patient has questions about the look and feel of their wounds, the bot could potentially distinguish between the need to visit the clinic or the emergency department.
Ultimately, the researchers want a standalone, vascular-specific large language model. “Hopefully we can gather enough information to train our own vascular-specific model so that is both faster and cheaper, and more accessible to the vascular world,” Feridooni continues, emphasizing that its fundamentals are applicable to other specialties. He sees utility across education, research and clinical practice, describing the model as “democratizing knowledge,” and even has potential as an “unbiased” arbiter in multidisciplinary discussions over how to treat patients with complex disease, he says. “AI is coming, so why not be the leaders in this rather than let it lead us.”
Tiam Feridooni
INNOVATION IN VASCULAR SURGERY: BALANCING PROGRESS WITH PATIENT SAFETY
By Jocelyn Hudson
A DEBATE AT THIS YEAR’S EUROPEAN Society for Vascular Surgery (ESVS) annual meeting (Sept. 24–27) in Kraków, Poland, centered on innovation in vascular surgery, with experts considering whether it will “change everything.” While Matt Thompson, MBBS, chief executive officer of Endologix, underscored the inherently innovative nature of vascular surgery and the inevitability of technological advancement—he urged specialists to “safely adopt new technologies or become irrelevant”—vascular surgeon Jon Boyle, MBChB, a consultant vascular and endovascular surgeon at Cambridge University Hospitals NHS Foundation Trust in Cambridge, England, championed a more cautious, patient safety-focused approach, highlighting past instances of innovation having caused harm.
In the ongoing endovascular era, Thompson put forward, several innovations—including bioresorbable stents and non-invasive devices—have refined, or are set to refine, longstanding techniques and technologies. Indeed, the presenter said, there is “still room” for endovascular innovation, despite the largely unchanging nature of its fundamental building blocks. However, these innovations will not “change everything” in vascular surgery. Instead, he argued that the next paradigm shift in the field will be defined by technological change that is happening in the wider world.
Thompson argued that the pace of technological advancement in society has already led to “enormous” changes in how people live their lives. What do technological advancements in the wider world mean for vascular surgery?
“There’s going to be some technological advance that completely changes our practice,” Thompson posited, listing wearable technology, personalized and regenerative medicine, and artificial intelligence (AI) and machine learning as just three technologies that have practice-changing potential. Thompson had a clear message here: adopt—safely—or be left behind.
‘We’ve got to be careful how we innovate’
Putting forward a counter argument, Boyle stressed the importance of striking a balance between innovation and patient safety. In several instances of innovation, Boyle
argued, “we’ve actually got it wrong—we’ve innovated, and patients have come to harm.”
He referenced data from the landmark EVAR-1 trial, noting that patients who were randomized to endovascular aneurysm repair (EVAR) “had far greater numbers of interventions out to 14 years” than the patients who received open repair. Acknowledging the age of the EVAR-1 data as a weakness of his argument, Boyle moved on to newer EVAR evidence, speaking on results from the VQI VISION study regarding the AFX graft (Endologix). The 2022 data, which illuminate reintervention and rupture rates with an early iteration of the device in the U.S., were published by Goodney et al in the British Medical Journal “When we fix an aneurysm, we’re trying to do it to prevent rupture, but the early AFX graft had a near 40% reintervention rate at eight years and a 10% rupture rate at 10 years,” Boyle informed the ESVS audience. In light of these data, Boyle remarked: “We’re fixing aneurysms, but we’re not really fixing them.” The presenter also shared similar findings with regard to fenestrated repair. He commented bluntly that “fenestration means twice the likelihood of being dead at three years,” according to data from Vallabhaneni et al ’s UK-COMPASS study, published in 2024 in the European Journal of Vascular and Endovascular Surgery (EJVES).
Boyle presented data on peripheral arterial disease (PAD), citing a growing body of evidence showing that early intervention for claudication leads to worse outcomes. Referencing an Australian study from Golledge et al, published in 2018 in the British Journal of Surgery, the presenter shared that patients with intermittent claudication who were treated early with endovascular intervention had a five-year amputation rate of 6.2% compared to 0.7% for those who received best medical therapy and exercise. “Early intervention for intermittent claudication with new devices led to a significantly higher amputation rate in this patient cohort,” he summarized.
The story is similar with carotid stenting, Boyle said. “We’ve pretty much stopped doing carotid stenting in the UK,” he said. “The reason for that,” he explained, “is that for symptomatic disease, your relative risk of stroke and death following carotid stenting is 1.7 compared to carotid endarterectomy.” Boyle returned to Endologix, this time focusing on Nellix. “We got our fingers burnt with this device,” the presenter acknowledged. “We all felt at the start this was a device that may change practice,” Boyle remembered. In the end, however, the presenter stressed that “a lot of patients came to harm as a result of being treated with this device.” Concluding, Boyle reiterated his central argument that “we’ve got to get the balance right—we need to innovate, but we need to do it in an environment where we can ensure our patients are safe.”
Matt Thompson
SOCIETY BRIEFS
Compiled by Marlén Gomez and Beth Bales
VAM 2025 abstract submission period opens
VASCULAR SURGEON-SCIENTISTS MAY submit their research for presentation at the 2025 Vascular Annual Meeting (VAM) in June through Wednesday, Jan. 8, 2025. The submission period opened Nov. 6. VAM research—both clinical and translational—is considered for presentation in several different forums that appeal to all attendees, from plenary presentations, rapidfire talks, international and video sessions, poster competitions and more.
In 2024, there was a nearly record-breaking 794 abstracts submitted, with 407 finding space on the meeting’s program.
VAM 2025 will be June 4–7, 2025, returning to New Orleans for the first time in several decades. Educational sessions will run across all four days and there will be ample opportunity for all to participate.
“Our best vascular surgical science is at the heart of the Vascular Annual Meeting,” particularly, the plenary and rapid-fire presentations, said Jason T. Lee, MD, the new chair of the SVS Program Committee, which selects the abstracts in a blinded process.
“VAM 2025 is where we will showcase the latest findings that influence care of patients with vascular disease, provide broad education to vascular surgeons and highlight the future of our specialty.”
The SVS Postgraduate Education Committee (PGEC), chaired by Claudie Sheahan, MD, is slated to offer sessions on topics including dialysis challenges, Enhanced Recovery after Surgery (ERAS), complex dissection care, vascular trauma and spinal cord ischemia.
To learn more about the abstract submission process, visit vascular.org/VAM. Guidelines are at vascular.org/VAM25Program.
Microlearning: The nonclinical realties of vascular surgery
IN RESIDENCY AND FELLOWSHIPS, vascular surgeons learn the techniques and skills to help them diagnose, manage and treat vascular disease.
But there are still important proficiencies to absorb. That is why the SVS has launched a series of seven free microlearning videos on “Adulting in Vascular Surgery.”
They are part of the SVS’ “microlearning videos,” shorts that answer a specific question and highlight important points on certain topics relevant to vascular surgery. It will cover topics such as medical billing, how to educate, social media and malpractice law.
Log in to access the videos at vasculearn. vascular.org.
CONSIDER VRIC A PATH TO BECOMING A SURGEON-SCIENTIST
WHEN FRANK DAVIS, MD, attended the SVS Vascular Research Initiatives Conference (VRIC) for the first time in 2014, he found not only meaningful discussions on research but also a pathway to the life he wanted. And he encourages those interested in research to attend.
The then-medical school student had taken a year off to do research and study basic science in the lab of Alan Daugherty, MD, at the University of Kentucky. Daugherty encouraged Davis to attend VRIC, telling him it wasn’t just basic research and basic biology.
Frank Davis, MD
Davis said Gilbert R. Upchurch Jr., MD, an invited speaker that year, “talked about his pathway to being a surgeonscientist and the top 10 things he learned along the way.” “It was eye-opening,” said Davis. “I saw my interest in vascular surgery and being a surgeon-scientist playing out in front of me.” His mentor Peter Henke, MD, also gave a talk on the road Davis wanted to follow. “I heard two prominent talks that showed me, ‘This can be done.’ It was a good opportunity for me to see people who are the surgeon
phenotype of who I wanted to be.” Abstracts for VRIC 2025 are now being accepted through 6 p.m. Central Standard Time on Nov. 20. The conference itself— which focuses on basic and translational vascular science in an atmosphere that fosters thoughtful discussion on research—will be held all day on April 22, 2025, at the Marriott Baltimore Waterfront in Baltimore, Maryland. VRIC will be held in conjunction with the American Heart Association’s Vascular Discovery 2025 Scientific Sessions: From Genes to Medicine, in the same location, from April 22–25, 2025. Davis, a past attendee and presenter who now has his own named lab at the University of Michigan, encourages all those interested in basic science and translational research to attend. “It’s fertile soil for junior researchers to launch their careers,” he said. It lays a “supportive groundwork and provides robust surgeon-scientist mentorship opportunities.”
Visit vascular.org/VRIC25 for more information.
Carotid Care Quality Champion program
THE SVS VASCULAR QUALITY INITIATIVE (SVS VQI) RECENTLY launched the Carotid Care Quality Champion recognition program to acknowledge select facilities nationwide for their commitment to patient safety and clinical excellence through active participation in SVS VQI’s carotid artery stenting and carotid endarterectomy registries.
This inaugural group of Carotid Care Quality Champions uses SVS VQI’s resources to monitor and enhance vascular care quality, meeting both societal and government guidelines.
Among these guidelines is the Centers for Medicare & Medicaid Services (CMS) National Coverage Decision 20.7, which requires facilities offering carotid artery stenting to establish a quality monitoring program and adhere to institutional and physician standards. By participating in the SVS VQI carotid artery stent registry, facilities can ensure compliance with CMS requirements while improving patient care.
For more information, visit VQI.org.
To maintain benefits, pay SVS dues by Dec. 31
MEMBERS HAVE UNTIL DEC. 31 TO PAY THEIR 2025 SVS MEMBERSHIP dues. Members received digital statements in October, and those with unpaid dues received paper statements at the beginning of November.
“Beyond an extensive array of valuable benefits, within the vascular community the SVS also confers the mark of professional achievement and provides a strong, dynamic and collegial network, ready to support—in a family-like style—and help each member to address various challenges of our profession,” said Ageliki Vouyouka, MD, chair of the SVS Membership Committee. “Our benefits aren’t solely for practicing vascular surgeons but for those at every stage of their career, from medical students and trainees to senior surgeons and to many other professionals who take care of vascular patients.”
Pay dues at vascular.org/invoices or email membership@vascularsociety.org
Applications open for 2025 James S.T. Yao Resident Research Award
THE SVS FOUNDATION IS accepting applications for the 2025 James S.T. Yao Resident Research Award, which supports emerging medical professionals researching vascular disease biology and innovative translational therapies. The application deadline is Jan. 8, 2025.
The recipient will present their research at the 2025 Vascular Annual Meeting (VAM), which takes place in New Orleans (June 4–7), and will receive a $5,000 prize along with a one-year subscription to the Journal of Vascular Surgery (JVS).
In 2023, the award was renamed to honor the late James S.T. Yao, MD, PhD, a pioneer in vascular surgery and his contributions to the field. The change was made possible through donations from Yao’s family. He passed away in December 2022.
“The Yao Award not only supports young researchers but also highlights the importance of foundational and translational research in vascular disease,” said Kathryn L. Howe, MD, chair of the SVS Basic and Translational Research Committee.
“It’s a tremendous opportunity for residents to have their work recognized on a national stage.”
Kevin D. Mangum, MD, PhD, a vascular surgery resident at the University of Michigan, received the 2024 award. Applicants must be general or vascular surgery residents or fellows enrolled in a U.S. or Canadian training program.
Visit vascular.org/YaoRRA.
National Nurse Practitioner Week
NATIONAL NURSE PRACTITIONER Week (Nov. 10–16) honored the dedication the essential role they play in vascular care. Show your appreciation by giving the gift of membership to the Society for Vascular Nursing (SVN).
Learn more at svnnet.org.
CLINICAL&DEVICENEWS
Compiled by Jocelyn Hudson, Will Date and Bryan Kay
DETOUR2:
Three-year data demonstrate
‘durable legacy’ of percutaneous bypass system for PAD
THREE-YEAR RESULTS FROM THE DETOUR2 study—a prospective, single-arm, international, multicenter clinical evaluation of the novel Detour system (Endologix) for fully percutaneous femoropopliteal bypass procedures—show the “durable efficacy” of the percutaneous transmural arterial bypass (PTAB) system.
Additionally, low rates of complications and deep vein thrombosis (DVT) demonstrate the favorable safety profile of this novel technique, according to data revealed at Vascular Interventional Advances (VIVA) 2024 in Las Vegas (Nov. 3–5).
Among the 202 patients enrolled and treated with the Detour system, 96% had chronic total occlusions, presenting investigator Sean Lyden, MD, chair of vascular surgery at the Cleveland Clinic in Cleveland, Ohio, told VIVA 2024 during a late-breaking clinical trial session.
Mean lesion length was 327 ± 61 mm. Primary patency through three years was 58.2%. The rates of freedom from clinically-driven target lesion revascularization (CD-TLR), major index limb amputation and all-cause mortality were 66.8%, 1.5% and 8.9%, respectively. Occurrence of deep vein thrombosis and pulmonary embolism were unchanged from two years at 4.1% and 0%.
First patient enrolled in study of integrated laser atherectomy and IVL catheter
ROYAL PHILIPS HAS ANNOUNCED enrollment of the first patient in the US THOR IDE clinical trial, which will study an innovative combined laser atherectomy and intravascular lithotripsy (IVL) catheter. Procedures that previously required the use of two different devices can now be performed in a single procedure using a single device, Philips said in a press release.
“PTAB provides a standardized technique with durable outcomes when open surgical revascularization is not viable or traditional endovascular therapy has failed,” Lyden concluded.
Endologix notes that the Detour system offers a unique approach to treating complex peripheral arterial disease (PAD), enabling physicians to percutaneously bypass lesions in the superficial femoral artery, by using stents routed through the femoral vein to restore blood flow to the leg.
The Detour system is comprised of the Endocross device and Torus stent grafts.
“These extended results from the DETOUR2 study help continue to demonstrate using the Detour system is comparable to surgical bypass but without requiring general anesthesia, which can come with additional complications and longer length of stay,” said Lyden in an Endologix press release.
“These extended results from the DETOUR2 study help continue to demonstrate using the Detour system is comparable to surgical bypass but without requiring general anesthesia”
SEAN LYDEN
Pennsylvania in Philadelphia, co-principal investigator of the THOR trial at the Penn Advanced Limb Preservation Hospital.
“Integrating atherectomy and IVL into a single device has the potential to revolutionize the treatment of patients with complex femoropopliteal lesions associated with moderate to severe calcifications.”
Endothermal ablation significantly outperforms surgery for varicose veins in long-term randomized trial
The Cardiovascular Institute of the South in Louisiana recently completed the first case using the new catheter. The care team there successfully treated a 78-year-old male with peripheral vascular disease using the device.
The goal of this pivotal study is to evaluate the safety and efficacy of using this unique laser, integrating atherectomy and IVL in a single device to treat complex, calcified lesions in a single procedure for patients with peripheral artery disease (PAD).
The prospective, single-arm, multicenter study will enroll up to 155 patients at up to 30 sites in the U.S. under an investigational device exemption (IDE) from the Food and Drug Administration (FDA).
“This innovative approach to vessel preparation could improve patient outcomes while minimizing the need for multiple therapies and interventions,” said Elizabeth Genovese, MD, an assistant professor of vascular surgery at the University of
TEN-YEAR DATA FROM THE RANDOMIZED HELP trial show that, while both endothermal ablation and conventional surgery are effective treatments for great saphenous varicose veins at 10 years, the former was associated with superior clinical and qualityof-life (QoL) outcomes. These findings have been published in the British Journal of Surgery (BJS).
First author Abduraheem H. Mohamed, senior author Daniel Carradice, MBChB, both from Hull University Teaching Hospitals and Hull York Medical School in Hull, England, and colleagues reported that they obtained data for 206 of a total of 280 patients (73.6%) at 10 years, revealing that both the ablation and surgery groups retained significant QoL improvement compared with pretreatment levels, as assessed by the Aberdeen Varicose Vein Questionnaire (AVVQ), Short Form 36 (SF-36) and EQ-5D, with a p value of less than 0.001.
ONE-YEAR DATA FROM VENOVALVE US PIVOTAL TRIAL EMERGES
ONE-YEAR DATA ON ALL PATIENTS from the VenoValve (enVVeno Medical) U.S. pivotal trial were delivered during the 2024 VEITHsymposium (Nov. 19–23) in New York City, supporting an application filed seeking premarket approval (PMA) from the Food and Drug Administration (FDA) to market and sell the bioprosthetic venous valve replacement used in the treatment of chronic venous insufficiency (CVI).
Some 55 out of 65 patients (85%) in the pivotal study who reached the one-year milestone achieved a clinically meaningful benefit of a three-point or more improvement in the revised Venous Clinical Severity Score (rVCSS). The average rVCSS improvement among the rVCSS responder cohort was 7.93 points.
The FDA had indicated that a three-point or more improvement in rVCSS would be evidence of the VenoValve’s clinically meaningful benefit, enVVeno stated. This was shown across all CEAP classes of patients (C4[b], C4[c], C5, C6) enrolled in the study.
GORE® TAG® Conformable Thoracic Stent Graft with ACTIVE CONTROL System
INDICATIONS FOR USE IN THE U.S.: The GORE® TAG® Conformable Thoracic Stent Graft is intended for endovascular repair of all lesions of the descending thoracic aorta, including: isolated lesions in patients who have appropriate anatomy, including: adequate iliac/femoral access; aortic inner diameter in the range of 16-42 mm; ≥ 20 mm non-aneurysmal aorta proximal and distal to the lesion. Type B dissections in patients who have appropriate anatomy, including: adequate iliac/femoral access; ≥ 20 mm landing zone proximal to the primary entry tear; proximal extent of the landing zone must not be dissected, diameter at proximal extent of proximal landing zone in the range of 16-42 mm.
CONTRAINDICATIONS: Patients with known sensitivities or allergies to the device materials; patients who have a condition that threatens to infect the graft. Refer to Instructions for Use at eifu.goremedical.com for a complete description of all applicable indications, warnings, precautions and contraindications for the markets where this product is available.
Products listed may not be available in all markets.
GORE, Together, improving life, ACTIVE CONTROL, TAG and designs are trademarks of W. L. Gore & Associates. 2023 W. L. Gore & Associates, Inc. 231209692-EN OCTOBER 2023
Sean Lyden
VenoVale implant
Elizabeth Genovese
GORE® TAG® Conformable Thoracic Stent Graft with ACTIVE CONTROL System
Help your patients live their lives with a TEVAR device backed by 5-year clinical data. Choose the GORE® TAG® Conformable Thoracic Stent Graft with ACTIVE CONTROL System for clinical outcomes that address long-term patient needs.
W. L. Gore & Associates, Inc. Flagstaff, Arizona 86004 goremedical.com
* No reported compressions, fractures or type III endoleaks.
1. W. L. Gore & Associates. Evaluation of the GORE Conformable TAG® Thoracic Endoprosthesis for Treatment of Acute Complicated Type B Aortic Dissection. NLM Identifier: NCT00908388. Published May 25, 2009. Updated October 27, 2017. Accessed June 7, 2022. https://clinicaltrials.gov/ct2/show/NCT00908388
2. W. L. Gore & Associates. Evaluation of the GORE Conformable TAG® for Treatment of Traumatic Transection. NLM Identifier: NCT00917852. Published June 10, 2009. Updated August 25, 2017. Accessed June 7, 2022. https://clinicaltrials.gov/ct2/show/NCT00917852
3. W. L. Gore & Associates. An Evaluation of the GORE Conformable TAG® Thoracic Endoprosthesis for the Primary Treatment of Aneurysm of the Descending Thoracic Aortic. NLM Identifier: NCT00874250. Published April 2, 2009. Updated August 25, 2017. Accessed June 7, 2022. https://clinicaltrials.gov/ct2/show/NCT00874250
Please see accompanying prescribing information in this journal.
Products listed may not be available in all markets.
GORE, Together, improving life, ACTIVE CONTROL, TAG and designs are trademarks of W. L. Gore & Associates.