Journal of Trauma and Orthopaedics


Optimal Recovery
Indicated following foot and ankle surgical cases for application in theatre or recovery or even preoperatively for trauma cases to ensure reduction of swelling. The ergonomic design ensures patient comfort, with stable elevation at heart level and without strain on the knee or hip.

OrthoFoam Adult Ramp
Indicated for all surgical cases where elevation is necessary without offloading the heel.


OrthoFoam Foot Holder
Indicated for use in surgery for foot and ankle procedures, from trauma to total ankle replacements.
OrthoFoam Knee Wedges
Simplify patient positioning for tibial or retrograde femoral nailing procedures with our range of trauma triangles.
Recover from your surgery in the comfort of your own bed with the HomeFoam version of our Ortholove® Professional Series SRE (Swelling Reduction Elevator).
Reducing postoperative swelling enhances healing and recovery and our beautifully designed HomeFoam is recommended by expert surgeons to keep your foot at the perfect height whilst relieving stresses on your knee, hip and lower back.


Journal of Trauma and Orthopaedics
In this issue...
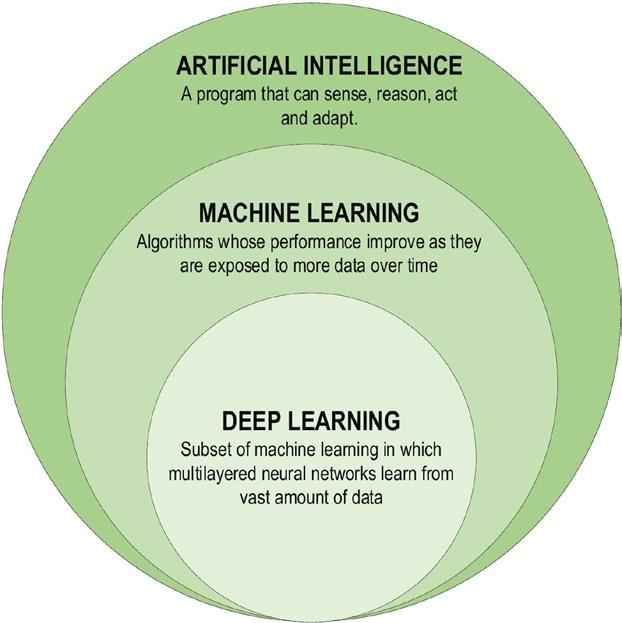
The challenge of using AI for non-traditional data modelling in predictive analytics
Justin Green, Luke Farrow, Feroz Dinah and Vipin Asopa
Advanced Clinical Practitioners in arthroplasty care

56 Subspecialty:
Incivility in orthopaedic surgery: Unmasking the hidden epidemic
Deiary Kader and Paul Banaszkiewicz


Catherine Armstrong and Rachael Daw
BOA members visit and support East Africa
Adil Ajuied, Mark Bowditch, Pranai Buddhdev and Nick Bowman 50 Medico-legal:
Professional insurance when treating elite and professional athletes
Peter Brownson, David Spencer, Andrew Wallace and Nigel Jones 54 Subspecialty:
Trauma and orthopaedic workforce –Challenges and solutions
William Allum
Advancing the surgical workforce: trauma and orthopaedics
William Allum
60 Subspecialty:
Carry on working!
Marc Patterson
63 Subspecialty:
BOTA rising to the workforce challenge
Adrian Andronic, Karen Chui, James Archer and James Allen
66 Subspecialty:
Addressing workforce issues:
The role of the SCP within the extended surgical team
Sally Stuart














JTO Editorial Team
l Deborah Eastwood (Executive Editor)
l Paul Banaszkiewicz (Editor)
l Simon Britten (Medico-legal Editor)
l Karen Chui (Trainee Editor)
l William Allum (Guest Editor)
BOA Executive
l Simon Hodkinson (President)
l Deborah Eastwood (Immediate Past President)
l Mark Bowditch (Vice President)
l Fergal Monsell (Vice President Elect)
l Hiro Tanaka (Honorary Secretary)
l Ian McNab (Honorary Treasurer)
l John Skinner (Appointed Trustee)
BOA Elected Trustees
l Simon Hodkinson (President)
l Deborah Eastwood (Immediate Past President)
l Mark Bowditch (Vice President)
l Fergal Monsell (Vice President Elect)
l Hiro Tanaka (Honorary Secretary)
l Ian McNab (Honorary Treasurer)
l Cheryl Baldwick
l Deepa Bose
l Caroline Hing
l Andrew Price
l Andrew Manktelow
l Andrea Sott
l Paul Banaszkiewicz
l Stephen Eastaugh-Waring
l Vikas Khanduja
l Dominic Meek
l Benjamin Ollivere
l Amar Rangan
BOA Staff
Executive Office
Chief Operating Officer - Justine Clarke
Personal Assistant to the Executive - Celia Jones
Policy and Programmes
Head of Policy and Public Affairs
- Gary Robjent
Head of Education and Programmes
- Alice Coburn
Programme and Committees Officer
- Eliza Heng
Educational Programmes Assistant - Maimuna May
Communications and Operations
Director of Communications and Operations
- Annette Heninger
Marketing and Communications Officer
- Pujarini Basu Nadaf
Membership and Governance Officer
- Natasha Wainwright
Publications and Web Officer
- Nick Dunwell
Finance
Director of Finance - Liz Fry
Finance Officer - Hayley Ly
Events and Specialist Societies
Head of Events - Charlie Silva
Events Coordinator - Venease Morgan
Events and Fundraising Assistant
- Emma Warwick
UKSSB Executive Assistant - Henry Dodds
Copyright
Copyright© 2024 by the BOA. Unless stated otherwise, copyright rests with the BOA. Published on behalf of the British Orthopaedic Association by: Open Box M&C
Advertising
All advertisements are subject to approval by the BOA Executive Board. If you’d like to advertise in future issues of the JTO, please contact our sales team for more information:
Email: JTOsales@ob-mc.co.uk | Telephone: +44 (0)121 200 7820 Open Box M&C, Premier House, 13 St Paul’s Square, Birmingham B3 1RB
Disclaimer
The articles and advertisements in this publication are the responsibility of the contributor or advertiser concerned. The publishers and editor and their respective employees, officers and agents accept no liability whatsoever for the consequences of any inaccurate or misleading data, opinions or statement or of any action taken as a result of any article in this publication.
BOA contact details
The British Orthopaedic Association, 38-43 Lincoln’s Inn Fields, London WC2A 3PE Telephone: 020 7405 6507
How to contact JTO
Email: jto@boa.ac.uk

From the Executive Editor
Deborah Eastwood
Congress is almost here! I can hardly believe it! Simon Hodkinson has asked us all to focus on the workforce this year with the theme of Recruit, Sustain, Retain being at the heart of all we have done. So it is totally appropriate that our Congress edition of the JTO has the workforce as our theme. As surgeons we have been working within an extended surgical team for some time and have long recognised the importance of multidisciplinary working. The names associated with various roles seem to have changed significantly over recent months and as always, change can be unsettling. The articles by Bill Allum representing the RCSE (p56) and by Adrian Andronic and Karen Chui for BOTA (p63) discuss the importance of understanding our recent workforce data. Sally Stuart (p66) discusses the extended surgical team whilst Catherine Armstrong and Rachel Daw (p40) concentrate on the role of advanced clinical practitioners. Marc Patterson (p60) reminds us that there is more to work than what we think of as the ‘routine’! He suggests we explore and expand our boundaries to reinvigorate our joy in life!
Our patients and our colleagues deserve kindness and respect and Deiary Kader and Paul Banaszkiewicz’s article (p32) is timely – we must beware of the rise of incivility and the real harm that is associated with it: they ask us to embrace the concept of radical candour or respectful confrontation and foster reciprocal respect.
It has been fun to read the SpecSoc reports and whether you are an elbow surgeon or a hip surgeon or feel that the big toe is our most important bit, the reports remind us that we are all part of one body and as such the BOA continues to work with you and for you.
If we need reminding, and I think we do from time to time, that it is the patient at the heart of all we do, then Katy Blackmore’s article (p28) asking ‘Do you see me?’ is an essential read. We must improve our ‘humanness’.
We know not all patients are the same and the elite athletes that we have been admiring recently as they throw further, run faster and jump higher are most definitely not your ‘average’ 9am appointment. The medico-legal article (p50) asks you to protect yourself whilst you accept the challenges of caring for them.
This editorial marks the end of my ‘formal’ involvement at leadership level of the BOA. I have thoroughly enjoyed the variety of tasks that I have worked on over the last few years and I must end with a big thank you to all who have helped me and worked with me at regional and national levels.
I would recommend anyone who cares about their profession to consider joining the BOA Band be it as lead guitarist, roadie or stage manager. Last year in Liverpool I asked my international speakers to incorporate a Beatles title into their talk and thus it seems fitting that I say goodbye with two corny song titles that perhaps speak for my time at BOA HQ: With a Little Help From My (Our) Friends” “We Can Work It Out!” n
Please join your colleagues for our Innovation Theatre sessions.
Essentials in Hard to Heal Fracture Management
Wednesday, 18th September, 13:30-14:00, Hall 3 Gallery
Transforming OA Care: Can Orthobiologics Interventions Postpone Surgery in Younger Patients?

Scan the QR code to register.

Mr Paul Harwood Limb Reconstruction and Trauma Surgeon, Leeds Major Trauma Centre

Mr Ansar Mahmood Consultant in Trauma and Orthopaedic Surgeon, University Hospital Birmingham

Assoc. Prof. Jane Fitzpatrick (attending virtually) Specialist Sports and Exercise Medicine Physician, Medical Director at Bioventus

Mr Graham Walsh Medical Director Health Innovation Yorkshire & Humber, Consultant Knee Surgeon
Mr
is
Stand 39 to explore our solutions that help patients resume and enjoy active lives.



Summary of Indications for Use for EXOGEN: EXOGEN Ultrasound Bone Healing System is indicated for the non-invasive treatment of osseous defects (excluding vertebra and skull) that includes:
• Treatment of delayed unions and nonunions* • Accelerating the time to heal of fresh fractures • Treatment of stress fractures
• Accelerating repair following osteotomy • Accelerating repair in bone transport procedures • Accelerating repair in distraction osteogenesis procedures
• Treatment of joint fusion
Full prescribing information can be found in product labeling Link (https://www.exogen.com/wp-content/uploads/2024/07/81087028_Sonic-2020-IFU_OUS_RevF.pdf) or by calling Bioventus Customer Care at 0800 05 16 384 (UK).
*A nonunion is considered to be established when the fracture site shows no visibly progressive signs of healing.
There are no known contraindications for the EXOGEN device. Safety and effectiveness have not been established for individuals lacking skeletal maturity, pregnant or nursing women, patients with cardiac pacemakers, on fractures due to bone cancer, or on patients with poor blood circulation or clotting problems. Some patients may be sensitive to the ultrasound gel.
Summary of Indications for Use for DUROLANE (3 mL): Symptomatic treatment of mild to moderate knee or hip osteoarthritis. In addition, DUROLANE has been approved in the EU for the symptomatic treatment associated with mild to moderate osteoarthritis pain in the ankle, shoulder, elbow, wrist, fingers, and toes. DUROLANE is also indicated for pain following joint arthroscopy in the presence of osteoarthritis within 3 months of the procedure.
Contraindications:
• DUROLANE should not be injected if the synovial joint is infected or severely inflamed.
• DUROLANE should not be injected if there is an active skin disease or infection present at or near the injection site.
• DUROLANE should not be injected intravascularly or extra articularly or in the synovial tissues or capsule.
• DUROLANE should not be injected if the patient is known to be sensitive to hyaluronic acid-based products.
• DUROLANE should not be injected in patients with pre-existing chondrocalcinosis as injection may lead to an acute attack of the condition.
Full prescribing information can be found in product labelling, or via the link: https://durolane.com/wp-content/uploads/2024/04/00057764Durolane3mlIFU90-47737-07_March_2023-Rev-G.pdf
Indications for Use for the Tenex Health TX System (with the TX1/TX2 MicroTips): The Tenex Health TX System is indicated for use in surgical procedures where fragmentation, emulsification and aspiration of soft tissue are desirable, including general surgery, orthopaedic surgery, laparoscopic surgery and plastic and reconstructive surgery. The Tenex Health TX System with the
Mr Harwood and Mr Mahmood are Bioventus paid consultants for Medical Education Programmes

Workforce challenges
Simon Hodkinson
Whilst the sun is still shinning on the South Coast it will set all too soon on my year as BOA President. It goes without saying that the last year has been a great privilege and a pleasure.
When I last wrote a piece for the JTO we were entering the summer and although there were the daily problems and seemingly ever-present, ever-growing systemic challenges, I felt that we were entering the holiday period knowing what was around the corner. Of course, 4th July changed that.
As one would hope, many of the meetings and conversations that I have had in this role, have made progress, some more than others: priorities identified and how to achieve them etc. It is now all on hold and there is as yet little idea as to how the new Government intends to move these myriad pieces of work forward.
The new Government has made it clear that the reduction of waiting lists is their priority - for the well-being of patients and of the economy - and has promised 40,000 new appointments per week by paying doctors and nurses overtime rates to take on additional shifts.
More of the same will not achieve this ambition and therefore there must be an element of working differently; more efficiently, more effectively. Post-pandemic productivity is an issue in the NHS as we all know but it is a multifaceted problem and not just down to us as surgeons.
Many of you will be aware that GIRFT requested the BOA to support a minimum number of patients in our outpatient clinics; the BOA declined to support the ‘one size fits all’ proposal. However, I made it clear the BOA would support attempts to improve productivity for the benefit of our patients as long as those attempts are not to the detriment of the quality of care our patients receive; good quality, productive services must be intelligently resourced.
In my last piece, I reported that I had been to several meetings regarding integration of primary and secondary MSK care, and I commented that around the country when these two key elements of the health service worked in collaboration it was clearly a benefit to our patients.
We are yet to hear how this project will progress, but I am pleased that we maintain a good relationship with the National Clinical Director for MSK, Lesley Kay, who will be speaking at the BOA Congress in Birmingham.
Consideration of the role of physician associates in trauma and orthopaedic surgery has been led by my colleagues, Mark Bowditch and Fergal Monsell. This work, alongside submissions by other surgical specialties is now being considered by the Royal College of Surgeons of England and we await the formal publication of a position statement from the combined UK surgical colleges.
Sadly, many of the concerns I have expressed about the T&O workforce have worsened and recent publications from the GMC have confirmed many of my fears. The BOA is looking at a range of these issues in particular those raised by the British Orthopaedic Trainee’s Association and by Training Programme Directors, including maximising training opportunities and the ‘professionalisation’ of trainers.
I raised these matters last month when I met with representatives from the Workforce, Training and Education team at NHS England, some of whom will be joining us at Congress. I came away from that meeting with the impression that they really did understand my concerns regarding recruiting people into our specialty, sustaining our trainees and young Consultants and retaining them in their later years.
Congress has a series of sessions dedicated to these issues not only in the T&O workforce but also amongst the many allied health professionals that support and augment our practise. I hope that these sessions will be stimulating, and that our discussions are robust, constructive and productive.
I sincerely hope those attending Birmingham this year will have an enjoyable and enlightening time and I look forward to meeting as many of you as I can.
Finally, it would be remiss of me in this last piece if I did not express my sincere admiration and thanks to the BOA secretariat.
This small but dedicated group of people produces a huge amount of work, and they have been of immeasurable support to me and to the Officers and Trustees of the Association in this last year. They are and will be working incredibly hard to ensure the smooth running of Congress, the vast majority of their work going completely unnoticed.
So, my grateful thanks to the team for all for the support over the past year and I would like to wish my successor, Mark Bowditch every good wish for his year as your President. n

Incoming President - Mark Bowditch
With six weeks to go, I ask myself “how did I get here!?” Soon I take over the helm from Simon Hodkinson, who I’d like to thank for using all his Navy experience to guide us through the choppy waters of the last year. Despite challenging workforce issues, he has remained calm and positive without having to yell “all hands-on deck” which I’m sure he has felt like at times!
Workforce is one of the key pillars of BOA strategy and must remain so if we are to create a sustainable T&O system. We are being asked to lead ‘recovery’, to change, do more with less, the challenges of which at times seem overwhelming.
Let’s not forget that ‘prevention is better than cure’. During the next year, I’d like to look at prevention in its broadest meaning in all our practice. Whether that is reducing injury or disease severity, complications and complaints, preventing harm to our patients, our teams or ourselves. Come up for air and reflect how to do things differently, sometimes it’s not all bad. T&O surgeons are great innovators and leaders with technology and data.
With your help, the BOA can share and influence the policy makers, setting the standards for high quality care.
Whilst hugely honoured to have the privilege of leading the BOA, my promise is that the organisation will listen to its members and be guided by our new five-year strategy. The BOA aims to be your voice, there for you, together ‘making a difference’ and transforming lives.
I’m really looking forward to meeting many of you in Birmingham, or if not, during the year ahead. n


BOA Ortho Update Course 2025 - Save the date!

The BOA Ortho Update course will take place on Saturday 1st March 2025 in Birmingham. Following on from a very successful 2024 course, we hope to carry that success over into next year’s course in Birmingham.
We are excited to announce a newly revamped and restructured BOA Ortho Update course that has something for everyone. This includes the difficult critical Case Based Discussions (CBDs) that delegates often struggle to get signed off, such as metastatic spinal cord compression and primary/secondary musculoskeletal malignancies. Improve and polish up your clinical examination skills in both a generic and diagnosisspecific manner. For the first time, we introduce the hugely popular small group teaching that involves a question-and-answer session on various orthopaedic topics, including the young adult hip, ostomies for the young arthritic knee patient and trauma scenarios.
Further information can be found at www.boa.ac.uk/OrthoUpdate


Are you receiving our emails?
BOA Committee recruitmentGet involved with the BOA!
Are you passionate about inspiring action and effecting change? Are you keen to be an active advocate and ambassador for an organisation? Are you eager to play a key role in important projects and initiatives? Committees are the engine of the BOA and Committee members are appointed for their passion, dedication, and innovation.
We have exciting opportunities for BOA members who are Home Fellows or SAS surgeons to represent, lead and effect change across the trauma and orthopaedic profession through the BOA Committees.
We are recruiting for posts in the following Committees: Orthopaedic, Trauma, and Medico-legal. Find out more at www.boa.ac.uk/get-involved.
You may apply for vacancies across multiple Committees, however, if you are successful for one, any other application(s) will automatically be removed from consideration.
Deadline for all applications: Monday 30th September
Applications are particularly encouraged from currently underrepresented groups in the BOA leadership structures including, but not limited to, women, BAME and LGBTQ+ members.
Training Orthopaedic Trainers Course (TOTs)
The underlying premise of TOTs is that if T&O trainers understand how people learn and how the T&O curriculum works, by translating that understanding into action, they should be able to improve their teaching.
Much of the work can be done at a time, place and pace convenient to participants, with attendance at live virtual meetings to supplement personal learning. The V-TOTs course will last for approximately six weeks. 2025 course dates can be found on the website at www.boa.ac.uk/TOTs
BOA Trustee Elections
Reminder that voting is open from 2nd – 30th September for the BOA Trustee election. If eligible to vote, you will have received an email with instructions from Mi Voice. (If you haven’t received it, make sure to check your junk folder). Voting members are Home Fellow, Home Member, Post CCT and SAS Year 11+. This year there are five vacancies to fill so make sure to have your say!
This year’s UKITE will run from 6th - 13th December 2024. Registration for the exam is open from 1st September. Registration is free for trainees and SAS surgeons who are BOA members provided that they register by 30th November. Late registrations are subject to a £50 fee. More information and guidance about UKITE can be found at www.boa.ac.uk/UKITE
Charity launches Major Trauma Awareness Week to
highlight long-term and complex impact of injuries on people’s lives

National charity Day One Trauma Support, in partnership with Active Care Group and PBC Biomed, is organising Major Trauma Awareness Week on 16th – 22nd September to share patient stories and encourages professionals to add their voice to the campaign.
The charity, which was founded by trauma and orthopaedic surgeon Professor Peter Giannoudis, says many major trauma patients and their families are being let down due to a lack of holistic support and signposting.
It provides non-clinical services such as emotional, practical and financial support through caseworkers within Major Trauma Centres, a network of Peer Support Volunteers, and its National Support Offer. Last year it helped more than 1,500 people and provided more than £82,000 in grants to cover immediate costs and ongoing recovery.
The charity says many more people don’t get this support, especially after discharge from hospital, leading to inadequate and disjointed rehabilitation and insufficient support for their emotional and psychological health and wellbeing.
BOA members and other health professionals are invited to join in their campaign to highlight the long term and complex impact major trauma has on people’s lives.
To find out more about the charity and how you can get involved in Major Trauma Awareness Week visit www.dayonetrauma.org/mtaw, or follow @dayonetrauma.
SAS fellowship
We are delighted to announce the second year of the SAS Education Fellowship of £3,000 for an SAS or LED member for a project of up to 12 months to support their education or career development. Deadline for applications 21st October 2024 Further information on how to apply, eligibility, and guidance can be found at www.boa.ac.uk/SAS-fellowship
Travelling fellowships
Every year, the BOA offers a number of travelling fellowships to its members to undertake a fellowship at centres of excellence in the UK or abroad to gain knowledge and experience within trauma and orthopaedic study. Applications are open 2nd September – 21st October 2024. Further information on how to apply, fellowship sponsors and guidance can be found at www. boa.ac.uk/travelling-fellowships
Mobilisation and weightbearing after orthopaedic surgery / musculoskeletal injury BOAST
The BOA have recently published a new BOA Standard (BOASt) on the mobilisation and weightbearing after orthopaedic surgery / musculoskeletal injury. This BOAST was jointly developed by the BOA and a number of stakeholders. You can read the full article here: www.boa.ac.uk/mobilisation-boast.
A full list of BOASTs can be found at www.boa.ac.uk/BOASTs
Reminder on the use of images and copyright
Just a reminder that if you are using images in a presentation, to accompany an article, in a screencast recording or any another purpose, you must ensure you have copyright or permission to use the images.
Things to consider when using images:
• Use of an image for any purpose is subject to copyright whether it is a written article or an oral presentation being recorded for re-use.
• Don’t assume that any image found online via an image search is free to re-use.
• Screenshotting or using a snip tool to ‘copy’ an image found online is a likely infringement of copyright.
• If you source an image from a website promoting copyright-free images, you are still responsible for checking the copyright status of the image.
• Check if the image is under a Creative Commons (CC) license. More information on CC license is available at: https://creativecommons.org/ share-your-work/cclicenses/
• Google Images Advanced Search is a useful tool which enables you to filter results by Usage Rights, similar to Creative Commons categories.
AI and Bots are now able to scan websites and recorded material to check for copyright infringements. Therefore, it is especially important you check any images in your work that could be potentially uploaded to the BOA website as the BOA would be liable to cover costs of any copyright infringements.
More information on use of images can be found on the BOA website at www.boa.ac.uk/ image-copyright
An update on BOA SAS activities
On taking up his post as BOA president, Simon Hodkinson spoke of the untapped potential of the SAS & LED workforce. True to his word, the BOA has been turning attention to the support and progression of the SAS/LED workforce. SAS representatives have been working to identify ways to make existing and new initiatives more accessible to our colleagues.
Last year, the SAS session at BOA Congress focused on three emerging topics: community, portfolio pathway, and the new specialist grade.
STONe

The SAS/LEDs have grown substantially in number and are a vital part of the T&O workforce. Many SAS/LED surgeons work in relative isolation from their peers and struggle for career progression.
Last year the BOA launched its SAS/LED T&O Network (STONe) as an online community where SAS/LEDs and mentors can share training opportunities. It already has over 250 members and those without BOA membership can also join (www.boa.ac.uk/SAS).
We held an online event for our members to connect with others in their region who are interested in the T&O Portfolio Pathway (TOPP). Through this, future TOPP applicants found colleagues in their deanery to share their Portfolio Pathway journey with.
Portfolio Pathway
In November 2023, the new Portfolio Pathway, replacing CESR, updated the process for entry onto the specialist register. This reduced the burden of documentation without lowering the clinical and professional standards of successful applicants. The focus, similar to that of a specialty trainee, is on achieving competencies rather than the learning course. To coin a phrase, ‘you don’t have to show you used to be a caterpillar, you just have to show that you’re a butterfly now’.
Specialist grade
For surgeons having years of expertise in one field, the specialist grade is often the most suitable route to ‘having their name at the head of the bed’.
It has particular benefits for workforce planning as it recognises experienced SAS surgeons who have demonstrated the ability to work independently and safely.
This grade is underutilised and there is a need for NHS trusts to improve availability of specialist grade posts for those already capable of working at a senior unsupervised level.

The BOA
The BOA is strongly supportive of SAS surgeons in leadership roles. Last year the governance changes approved at the AGM included allowing and indeed encouraging SAS surgeons of equivalent experience to post CCT colleagues to become trustees as well as committee members. All such surgeons can now play a key part in decision making within the association including voting for candidates in elections for all Executive positions.
The Future Leaders Programme (FLP) also encourages SAS surgeons to apply, contribute and ‘step up to the plate’ for leadership roles. These are exciting times!
SAS networking lunch
The BOA is planning to hold a networking lunch for SAS/LEDs at Congress in September. It will act as an ideal opportunity to meet and engage with the wider SAS community.
T&O SAS surgeons have an ever-increasing range of career options open to them, and the growing understanding of the role and value of SAS/LEDs in the T&O community is paving the way for this capable and enthusiastic group to strive and really ‘work at the top of their game’. n
Julie Craig and Akshdeep Bawa
OrthoLucent™ Retractors










Universal Traction Assembly
A universal traction assembly with Traction Device for standard operating room tables used to assist with fracture fixation in the acetabulum, pelvis, and femur, and designed to attach to standard operating table side rails

Stainless Steel Ratchet Frame with Arms and Blades Sets
Designed for self-retaining wound exposure, the arms and blades of the OrthLucent™ version are radiolucent and can be kept in place while using image intensification or taking an x-ray








Designed by Reza Firoozabadi, MD

Re f lections of the ABC travelling fellowship 2024
Maritz Laubscher, Groote Schuur Hospital, Cape Town, South Africa
Anand Segar, Starship Hospital, Auckland, New Zealand
Jonathan Stevenson, Royal Orthopaedic Hospital, Birmingham
Sina Babazadeh, Australian Orthopaedic Association
Xavier Griffin, Queen Mary and Barts Health, London
Tom Quick, The Cleveland Clinic, London
Ciara Stevenson, Royal Victoria Hospital, Belfast
On 2nd June 2024, seven surgeons from across the world assembled in London to represent their respective Orthopaedic Associations and embark on the ABC Travelling Fellowship. A dinner hosted by the Bone and Joint Journal, attended by previous ABC fellows Deborah Eastwood (ABC 1992), John Skinner (ABC 2004) and Fares Haddad (ABC 2004) provided entertaining stories of previous fellowships and set the expectations (of behaviour) for the coming tour. The following morning our group boarded the flight from Heathrow to Calgary full of excitement and nervous anticipation for the weeks ahead.
Calgary – Host Dr Mike Monument (ABC 2021)
Having recently completed the ABC tour himself, Dr Monument, with parenthood pending, showed kindness to our jetlag and allowed a slow start to recharge. We met Dr Richard Buckley (the first orthopaedic trauma surgeon in Calgary) who described how he became involved with AO Trauma and proceeded to co-author the peerless Hoppenfeld surgical exposures in orthopaedics.
A leadership morning at the Cumming School of Medicine provided the opportunity to meet with Dr Todd Anderson (Dean of the School of Medicine), Dr Kevin Hildebrand (Head of Department of Surgery) and Dr Jason Werle (Senior Medical Director and Chief of orthopaedic surgery. We heard how departments were organised and problems solved within government-based systems with the usual inefficiencies and constraints and about their research program.
A tour of the McCaig Institute for Bone and Joint Health left us in awe of the philanthropic donations that provide state of the art facilities for clinical and academic research.
Our academic discussions continued with the Calgary Orthopaedic Resident Research Group (CORRG) led by Dr Prism Schneider (ABC 2025) timed perfectly with the PGY5 residents receiving their fellowship exam results that afforded us the opportunity to celebrate their success. We concluded our Alberta experience with a trip to Banff to avail of the breathtaking views and incredible hospitality of Calgary Orthopaedics.
Ottowa – Host Dr Sasha Carsen (ABC 2021)
We were met at the baggage carousel with Dr Carsen’s infectious smile. What an incredible genuine and enthusiastic gentleman. He introduced us to Dr Baxter Willis, Past president of POSNA and previous Chief of Surgery at Children’s Hospital of Eastern Ontario (CHEO) who humbly talked about his fellowship with Dr Salter and the importance of mentorship living by the ethos of ‘pay it forward’. We attended trauma grand rounds chaired by Dr Steve Papp (Chief of Orthopaedics) which provided discussion of clinical cases and shared learning. A tour of the biomechanics lab taught us how collegiality within the department helped to fundraise for the Kuka robot to advance research. One of the highlights of the visit was being hosted for dinner at the Rideau Club as guests of Dr Paul Beaule with spectacular views of the Canadian Parliament.
Halifax - Canadian Orthopaedic Association meeting 12th – 15th June Dr Pierre Guy and Dr Olufemi Ayeni (Immediate past and current presidents)
We arrived at a drinks reception hosted in our honour where we had the opportunity to reconnect with our new

and longstanding Canadian friends. We each presented at the academic meeting and moderated various sessions which allowed us to debate, stimulate discussion and share learning from our own registries and research. Highlights of the meeting included dinner with the Carousel of Past Presidents – not only an opportunity to don black tie and enjoy a fine evening, but an incredible combined experience of leadership and clinical expertise.

Nashville – Dr Rick Wright, Chief of Department of Orthopaedic Surgery, Vanderbilt Orthopaedics
Running the border and heading south to the music city of Nashville where we were treated to southern hospitality of brisket and bourbon. Impressed by the facilities of the Vanderbilt campus and general scale of the unit comprising 41 operating theatres, we witnessed efficiency and resource to facilitate running two theatres simultaneously. The academic programme provided insight on how to produce big data from the MOON group (Dr John Kuhn) and MARS (Dr Rick Wright). The highlight of this stop was the listening room café - with three amazing independent female singer song writers on stage.
St Louis - American Orthopaedic Association Annual Leadership meeting, Dr Ann Van Heest (President)
Our Midwest travelling fellowship continued to St Louis. Highlights of the meeting included symposia on residency programmes, providing us with insight into how the US training system operates and how the difficulties at home about selection and training are mirrored here. The standout presentation of the meeting was by Dr Rex Marco who gave a heartfelt reflection on the use of mindfulness to survive his journey from being a prominent successful spinal surgeon to suffering a tragic accident causing tetraplegia. We learnt perspective in St Louis >>
Chicago – Hosts Dr Mike Lee (ABC 2019) and Dr Rex Haydon (ABC 2009)
The Windy City did not disappoint. We were taken on arrival for deep dish pizza and karaoke to celebrate the birthday of recently retired Professor of Orthopaedics, Dr Terry Light. The following day we saw Chicago from the river on an architecture boat tour followed by a Cubs game at Wrigley Park. Monday, we had the privilege of a private tour of the Institute for the study of Ancient Cultures Museum followed by our academic afternoon led by Dr Haydon. Our last night in Chicago was one we will never forget. Dr Haydon and his wife Nene hosted us at their family home on campus, where we celebrated the ABC legacy, sipped bourbon, ate delicious Peruvian food and watched the fireflies dance in the evening sky.
Memphis – Host Dr Derek Kelly (ABC 2019) Campbell Clinic
We made memories by staying at the Peabody hotel famous for its ducks in the fountain of the hotel foyer, taking a stroll down Beale Street and making our way to BB King’s Blues Club – home of the blues. Trauma grand rounds at Regional One followed by a tour of Le Bonheur Children’s Hospital demonstrated the devastating prevalence of paediatric ballistic trauma. Academic discussions provided insight into the rich history of the ABC association with Campbell Clinic, and we also had the opportunity to discuss how healthcare is funded in Tennessee with the CEO of Campbell Orthopaedics, Daniel Shumate. No visit to Memphis would be complete without a tour of Graceland and with our hearts full of music we made our way to Colorado.

Denver – Host Dr Evaline Burger (ABC 2000), Professor and Chair of the Department of Orthopaedics at the University of Colorado School of Medicine
We arrived for our last stop of the ABC tour in Denver as firm friends with a deep respect for each other’s practice. Offering a unique blend of outdoor adventure and world class clinical and research facilities, UC Health was fitting of our

final destination. A particular highlight was an evening at Dr Jason Stoneback’s (Consultant trauma surgeon) ranch, where he and his wife hosted traditional western education which included meeting a professional barrel racer, learning how to rope and ranch, clay pigeon shooting followed by a sunset meal from a 19th century chuck wagon. The morning of our departure we had breakfast with the Tom Gronow (CEO and President of UC Health) who gave us valuable insights into his leadership style how to promote cultural change within an organisation.
Conclusion
What is the point of the ABC travelling fellowship? Throughout the tour we were consistently overwhelmed by the generosity and enthusiasm of everyone involved in hosting the ABC fellows. Dr Stu Weinstein (ABC 1985) former president of the American Orthopaedic Association once said, “There is no greater return on investment for our profession than the ABC travelling fellowship.” Spending five weeks with like-minded individuals who share the same commitment and drive for our profession has earned us not only six treasured friends but an international network for collaborative research, a sounding board for the exchange of innovative and transformational ideas and ultimately an ABC family bonded by this incredible life changing experience. n
The Austrian Swiss German (ASG) Fellowship 2020 (postponed until 2023!)
The Austrian-Swiss-German (ASG) fellowship was set up in 1978 to facilitate an exchange programme where surgeons from the German speaking countries of Austria, Switzerland and Germany visited the UK, Canada, and the USA. A reciprocal arrangement ensued. I was privileged to be chosen by the BOA in 2019 to be part of the ASG class of 2020. COVID-19 unfortunately caused postponements until April 2023. Brian Mullis a trauma surgeon form Indiana was my co-fellow on this four-week educational trip.

Our journey began in Germany where we spent two weeks crossing the length and breadth of the country. We visited centres of excellence in Homburg/Saar, Magdeburg, Berlin, Cologne, Essen/ Mulheim, Bonn and Dusseldorf. We were hosted by former ASG fellows who hold a chair or a very high leadership position. We travelled on to Switzerland where we were hosted in Zurich before then travelling to Austria and visiting the cities of Innsbruck and Vienna. In our final leg of the journey, we finished off
being part of the South German Orthopaedic Association Conference in Baden-Baden. Here Anke Eckardt, the secretary of the ASG hosted the traditional ‘Asparagus Dinner’ for the ASG fellows at the Brenner’s Park Hotel.

“What have we learnt?” was a routine question throughout our travels. Given our seniority (nearly 10 years as a consultant), we were both set in our practices. However, we were open to learn, and learn we did. There was a clear dichotomy between trauma and orthopaedics with trauma run by general surgeons. We were witnessing a slow merger of the two. We interacted with key opinion leaders in the German Speaking countries. The hosts were all ASG fellows and we learned how their differing leadership styles grew and developed departments. The success of fostering and building teams was clearly evident. This was one of the greatest benefits of the fellowship. We have continued to be in touch with the friends we have made. I hope to contribute to the ASG and support the next generation of trainees. n
The Austrian Swiss German (ASG) Fellowship 2024
The ASG fellowship 2024 saw the 13th Class of Anglo-American ASG Fellows touring some prominent orthopaedic departments within German speaking countries, and the first group offered this opportunity since the onset of the COVID-19 pandemic caused a several year hiatus.

The fellowship group consisted of two fellows from the USA selected by the American Orthopaedic Association; Professor Deanna Mercer from the University of New Mexico in Albequerque, and Professor Nicholas Noiseux, Vice Chair of Orthopaedics and revision arthroplasty surgeon at the University Hospital of Iowa, together with myself, a locum consultant at Maidstone and Tunbridge Wells Hospitals, as the UK representative.
Over 28 days we were hosted across institutions in ten cities across Austria, Switzerland and Germany. At each institution, we had the opportunity to visit the operating theatres, interact in lively discussions with the local hosts and partake in a rigorous programme of academic symposia. On our whistlestop tour we visited Homburg (Saar), Hamburg, Berlin, Magdeburg, Cologne, Bonn, Vienna, Krems, St. Gallen and Zürich, experiencing exceptional hospitality.
The academic programme was interspersed with memorable social activities including an outing to France, a harbour boat tour, an insightful walking tour of Berlin, a Bundesliga football match, two trips to the opera, an exceptional after-dark tour of Cologne Cathedral, Vienna’s incredible Schönbrunn Palace and a trip to the mountains of Switzerland, amongst many other highlights!
The fellowship culminated in Baden-Baden at the Annual Meeting of the Association of South German Orthopaedists and Trauma Surgeons (VSOU). Following a special ASG edition session at the Conference, we attended the annual ASG Society Asparagus lunch where we were awarded our society ties and scarves.
The tour highlighted to us many of the parallels between Anglo and Germanic orthopaedic practices as well as highlighting key differences. The substantial integration between academic research and clinical practice was an intriguing element of the practice and the cost-pressures we face in the NHS were certainly less pervasive. Our varying approaches to arthroplasty rehabilitation and day-case surgery were regularly debated throughout our trip and in most cases, we are unlikely to reach consensus soon!
I would like to extend my gratitude to Nick and Deanna for their entertaining company and to all of our exceptionally generous local hosts, whom I look forward to seeing at future ASG events. I would like to thank the BOA for giving me this opportunity and most of all my wife, Dr Jean Chan and our children, for allowing me to disappear for a month on yet another travelling fellowship. n
Satish Kutty
Daniel Burchette
Conference dinner in Baden-Baden. Pictured left to right: Prof Romero, Prof N Bohler, Prof A Eckardt, Prof A Niemeier, Satish Kutty, Brian Mullis, Prof M Jäger, Prof Bernd Stöckl and Prof C Zilkens.
ASG fellows Dinner in Baden-Baden. Pictured left to right: Prof R Windhager, Prof M Jäger, Satish Kutty, Prof A Eckardt, Brian Mullis, Prof Landgraeber, Prof Romero and Prof C Zilkens.
Combined Services Orthopaedic Society (CSOS) 2024 Update
Surg Lt Cdr Tom Stevenson,
CSOS Secretary
The 2024 meeting was a truly prestigious event, where we celebrated our 50th Anniversary as a society, and was hosted in London at the National Army Museum in May 2024. Delegates were able to enjoy a two-

day Conference culminating in a formal Mess Dinner hosted at the Royal Hospital Chelsea. The theme this year provided day one as a series of presentations from trainees, showcasing their original clinical and academic research to the society, followed by a session on early consultant life. Day two was a series of keynote addresses to give reflection on ‘a life less ordinary’ as the Society enjoyed inspirational presentations on previous military campaigns over the last 50 years, as well as reflecting on current conflicts, and the future direction of travel for our military research from an impressive line-up
including: Col (Rtd) Michael Stewart CBE, Col Paul Parker, Col (Rtd) David Standley, Gp Capt Ian Sargeant OBE, Lt Col Carl Meyer, Surg Cdr Steve Mannion, Gp Capt (Rtd) Jon Kendrew, Col (Rtd) Jon Clasper CBE, Gp Capt Alexander Bennett and Col Arul Ramasamy.
We also welcomed Col Dmytro Los from the Ukrainian Armed Forces who delivered an emotive and poignant lecture about current trauma care within the Ukraine.
Maj Charles Handford was awarded the Peter Templeton Best Presentation prize, Surg Lt Cdr Louise McMenemy received the Philip Fulford Prize for Best Quickfire Presentation, and finally the Mike McErlain Travelling Fellowship was also awarded to Surg Lt Cdr Louise McMenemy.
In 2025, the Society will be hosted in Warwick for the annual meeting with the Conference being held within the Warwick Schools Foundation and a Mess Dinner at Warwick Castle. Those who are not currently receiving Society communications are invited to contact the Secretary for further information: secretary@csos.org.uk. n
British Elbow and Shoulder Society (BESS) update
Steve Drew, BESS President
BESS has just returned from another successful scientific meeting, held in Aberdeen. This year we were pleased to launch a new style programme that was very well received and we are now looking forward to developing this further when we visit Brighton in 2025. We are grateful to all who made it such a success.
We are pleased to have launched some new initiatives in the last 12 months, including a quarterly Journal Club, open to all and free of charge and our AHP Roadshow, bringing low cost AHP focused educational opportunities to members and nonmembers. The next one will be held in Leicester this November.
To raise our profile at other meetings, I will be taking a cohort of 20 Surgeons, Trainees/Fellows


and AHPs to represent BESS at SECEC this September. This cohort will form our Copeland Fellowship, our prestigious award given in honour of our founding member Steve Copeland. We are also looking forward to hosting two joint sessions at the BOA Congress this year, one with BOOS and the other with BSCOS. And later in November we will once more join forces with ORUK to run our ‘Expert to Expert’ day, Controversies in Decision Making for Shoulder and Elbow.
We continue to strengthen our support of shoulder and elbow research trials across the UK and focus on updating our management and treatment guidelines for shoulder and elbow conditions, alongside producing new ones and we are pleased to be sponsoring a place on the BOA Future Leaders Programme n












The British Orthopaedic Oncology Society (BOOS) update
Tom
The British Orthopaedic Oncology Society has had another very successful year and held its annual general meeting in Cardiff at the end of June. For the first time, we held the meeting over a full two days with day one dedicated to the treatment of metastatic disease. We held a number of interesting talks including the treatment of metastatic disease around the pelvis, hip, knee, foot and ankle as well as the upper limb with a talk about the challenges of operating around the shoulder and proximal humerus. Lead clinicians for metastatic disease were encouraged to attend across the UK and to consider how they can implement / grow / extend their provision for the treatment of MBD in their local areas. With an increasingly elderly population, this is likely to grow exponentially and it is vital that local Trusts properly support this important problem with dedicated time for a consultant-led service.


We discussed the challenge of the unknown primary and the issues around the orthopaedic surgeon often being the first to see such patients. After a very successful Conference dinner the Conference moved on to its core meeting which focused on the traditional themes of Basic Science, Arthroplasty and Operative Intervention, New Advances and Techniques and future directions in research. We awarded prizes for Best Presentation, Best Poster, Best Young Investigator and the Takeshi Takeshima prize for Basic Science which is awarded annually in memory of a young histopathologist in Oxford who sadly died of the disease in which he was an expert, Osteosarcoma, at the young age of 37. We also ran, for the first time, at conference this year, an Education Day for trainees which was well attended and aimed to give candidates a flavour of the type of questions which will be asked in the FRCS (Tr and Orth) examination.
The Society continues to be vigorous and active and welcomes new members. We will launch our Diploma in Orthopaedic Oncology accredited by the Royal College of Surgeons of England for its second diet in September 2024 and interested applicants should contact Professor Tom Cosker at Thomas.cosker@ouh.nhs.uk. We look forward to another successful conference in Dublin next year! n
World Orthopaedic Concern (WOC) update
This year has been a very exciting one for WOC-UK with a number of projects starting to feel established. Many of our members remain active around the globe and are supported in many ways - financially, logistically and scientifically. Our exceptionally dynamic BOTA sub-Committee ran another LMIC session at their annual conference and interest and feedback from this was extremely encouraging. We held our annual conference this year in June at the Aesculap BBraun Academy in Sheffield along the theme of ‘Evolving with the times’. This was well attended in person and virtually thanks to the excellent platform hosted by Medall. We had some truly thoughtprovoking talks. Our keynote was delivered by Professor Mahmood Bhutta who opened our eyes to environmental and labour harms from surgical products. Sarah Phillips spoke about how she and her team have been supporting orthopaedic surgery in Gaza over
the years and how they are responding to the increasingly difficult situation there presently. Other speakers included John Cashman from Sheffield Children’s, Howard Davies representing BOFAS, Jonathan Jones and Martin Wood representing BSSH, Guy Morris from BOOS and Sanjay Gupta and Alwyn Abraham from WOC. We also had a trainee session chaired by Professor Simon Graham and Alice Campion and an update of the FLP Programme which we actively support. Our WOC-UK commemorative medal was awarded to Lew Zirkle for his work with the SIGN nail.

At the AGM, I took over chairmanship from Alberto Gregori, whose outstanding achievements in WOC I need to acknowledge. Alwyn Abraham was voted in as Chairman-elect and the post of treasurer is now out for expressions of interest. We have an active committee-at-large who are instrumental in helping us steer our global efforts. Our next event is at the BOA Congress in September and we already have a great list of speakers lined up. n
Cosker, BOOS President
Ashtin Doorgakant, WOC Chairman



Honorary Fellowships
The BOA is pleased to announce the recipients of the 2024 Honorary Fellowship, which will be presented at BOA 2024 Congress.

Andrew Carr
Professor Andrew Carr ChM DSc FRCS
FMedSci is a surgeon and clinical scientist, whose work over 40 years has influenced the evaluation of surgical procedures including the increased involvement of patients in assessing clinical outcomes. The Oxford Scores are used globally to direct health policy. He has pioneered the use of large-scale randomised trials of surgery including the controversial use of placebo surgical controls. He holds the Nuffield Professorship of orthopaedics at Oxford University, is a fellow of Worcester College, Oxford and was head of the Nuffield Department of Orthopaedics, Rheumatology and Musculoskeletal Sciences for 21 years during which time it grew to over 450 research staff and PhD students.
Professor Carr was born in Bradford and studied medicine at Bristol University before training in Sheffield, Oxford and Melbourne. He founded and directed the Botnar Institute of Musculoskeletal Sciences and was Director of the NIHR Biomedical Research Unit. He was Divisional Director of the Nuffield Orthopaedic Centre during its merger to form Oxford University Hospitals NHS Foundation Trust and was instrumental in the move of the Kennedy Institute to Oxford. He is a Nuffield Medical Trustee, a Trustee and Council member of the Royal College of Surgeons of England, Deputy Chair of the Board of Trustees of Bristol University and one of the 25 most cited surgical researchers globally with over 40 publications in the Lancet, BMJ, Science Translational Medicine, Cell and Nature Biotechnology. He has received numerous national and international awards, is an NIHR senior investigator and a fellow of the Academy of Medical Sciences. n

Lisa Hadfield-Law
Having spent 20 years in clinical practice and 20 years in surgical education, Lisa Hadfield-Law has been immersed in both cultures and has, therefore, been in a unique position to provide educational and leadership support. She has managed an orthopaedic/trauma service at a teaching hospital and has insight into the circumstances and challenges facing surgical teams.
A surgical educator since 1992, Lisa has trained over 15,000 surgeons in all surgical specialties from 68 different countries across Europe and the rest of the world. She has 20 years of trauma nursing experience both in the UK and abroad and was Head of Nursing at St Bartholomew’s Hospital, London. She served as BOA Education Advisor from 2012 to 2024.
Lisa continues as a Surgical Educator in the UK and abroad and is currently Education Advisor to AOUK&I. Her current focus is leadership for surgeons and dentists and she leads the Future Leaders Programme both for the BOA and for the Royal College of Surgeons of Edinburgh (RCSEd). She is also a Convenor for the RCSEd Foundations in Surgical & Dental Leadership programmes. Lisa is Honorary Fellow of the Faculty of Surgical Trainers for RCSEd and serves on the Faculty of the Surgical Trainers Advisory Board. n

Brigitte Scammell Presidential Merit Award
Professor Scammell retired in 2022, having dedicated 40 years of service to the NHS, with 26 years as a consultant orthopaedic surgeon at Nottingham University Hospitals NHS Trust, and as a clinical academic at the University of Nottingham. She trained in Birmingham, Southampton, Basingstoke and Lord Major Treloar Hospital, Alton, and completed her training with a fellowship in lower limb arthroplasty and trauma in Toronto. As a clinical academic she received a Lord Dearing award for teaching and learning excellence; served as the Admissions sub-Dean for Medicine, interviewing future medical students at home, in Malaysia and Thailand; became the first female Professor of Orthopaedics in the UK; and the first female Dean and Head of School of Medicine, University of Nottingham. She feels very fortunate as academic life brought opportunities to teach in China and present team research across the world. She has supervised more than 35 DM/PhD students, being especially proud when students received prizes for their work. Academically she has most enjoyed the reward that comes from teaching and mentoring students, and staff, to overcome challenges and achieve their dreams.
Professor Scammell has also served as the Secretary and President of the British Orthopaedic Research Society, and on national committees including the British Foot and Ankle Society, the British Orthopaedic Association, and the Surgical Advisory Committee. She was honoured to receive the BORS President’s medal and the Tony Mitchell medal from the Nottingham Medico-Chirurgical Society in 2022, and last year she was thrilled to receive an Award of Fellowship ad hominem of the Royal College of Surgeons Edinburgh. She is grateful to be able to lead an active ‘retirement’. She has two part-time roles, as a trustee/board member for the charity Framework Housing Association providing a full range of services to homeless people, and as Director of the Trent Simulation and Clinical Skills Centre at Nottingham University Hospitals NHS Trust. She continues to supervise PhD students and mentor medical students. This still allows time to pursue her hobbies, and to spend time with friends and family. n
The BOA is pleased to announce the recipient of the 2024 Presidential Merit Award, which will be presented at BOA 2024 Congress.

Sarah Stapley
Sarah has been a Consultant in Trauma and Orthopaedics since 2004, based in Portsmouth Hospitals University Trust and has had a diverse training pathway including fellowships in Wrightington and Toronto. She served with the Royal Navy for 33 years, frequently leading health care delivery in isolated and extreme locations with limited resources. Sarah understands how education, and the effect a good mentor has on an individual, and this has continually driven her to encourage trainees of all levels to seek their potential. She has undertaken roles as Surgical Tutor, Training Programme Director at both core and higher specialty level, and as Defence Professor of Trauma and Orthopaedics. Sarah has undertaken several unusual leadership roles, as a Deployed Medical Director (Camp Bastian Hospital) in Afghanistan, Consultant Advisor in Trauma and Orthopaedics to the Royal Navy and as the UK Representative on the NATO COMEDS futures advisory panel. She has also sat on the National Selection Design panel for ST3 interviews and still interviews regularly for both levels of trainee.
Sarah has been a member of the BOA since she was a trainee. She has sat on the BOA Education Committee, as a Council member and now as the Council member for BADS. She is the co-opted BADS Council member from the BOA. n
BOA Annual Congress 2024
17th – 19th September, ICC Birmingham www.boa.ac.uk/Congress
Programme update
The theme for this year’s flagship event will be ‘Recruit, Sustain, Retain: The T&O Work Force’, taking place from 17th – 19th September at the ICC, Birmingham.

This year’s Howard Steel Lecture will be delivered by John McFall, former British Paralympic sprinter, and European Space Agency (ESA) astronaut reserve. In 2022 John was selected to take part in ESA’s feasibility study ‘Fly!’ to improve our understanding of, and overcome, the barriers space flight presents for astronauts with a physical disability.

The BOA’s Presidential Guest Lecture from Dr Ann Van Heest, President American Orthopaedic Association (AOA). Dr Van Heest presently serves in several national leadership positions, Vice Chair of Education in the Department of Orthopaedic Surgery at the University of Minnesota, a Director at the ABOS, and a member of the ACGME orthopaedic RRC. She is also the past president of Ruth Jackson Orthopedic Society, and on the BOD for Perry Initiative.

The Robert Jones Lecture will be delivered by Professor Deborah Eastwood. She is an Associate Professor of Paediatric Orthopaedic Surgery, UCL. She works at Great Ormond St Hospital and the Royal National Orthopaedic Hospital. Professor Eastwood also works in the generality of paediatric orthopaedic surgery but has a particular interest in children with overgrowth syndromes, metabolic bone diseases and those with neurological problems. She is also the surgeon for the GOSH Ponseti service.
Our Hunterian Lecturers will be:

• Hannah James – An ST8 on the Warwick Rotation and current NIHR Academic Clinical Lecturer at Warwick Clinical Trials Unit. She completed an award-winning PhD investigating patient benefit from cadaveric simulation for postgraduate T&O trainees.



A paediatric Consultant at the Royal Hospital for Children. He has a longstanding interest in education, is Director of the Avon Centre for Musculoskeletal Education and Projector at the Grand Academy.
• Matthew Costa –Professor of Orthopaedic Trauma Surgery at the University of Oxford and Honorary Consultant Trauma Surgeon at the John Radcliffe Hospital, Oxford. His research interest is in clinical and cost effectiveness of musculoskeletal trauma interventions.

• Imran Ahmed – An orthopaedic registrar on the Warwick Orthopaedic Rotation and previous NIHR doctoral research fellow at the Warwick Clinical Trials Unit.
Other sessions from the BOA include:
• BOA Diversity and Inclusion Session
• BOA Congress Theme Plenary - Recruit, Sustain, Retain
• BOA Ortho Committee Session - ReadySteady Go - Elective Hubs for High Risk Patients - Performance and Impact
• BOA Big Debate/Question Time - Physician Associates in T&O: Ensuring a Safe and Collaborative Future
• BOA SAS Session - Retaining and developing SAS/LED Orthopaedic surgeons
• BOA Medico-legal Committee SessionAsk the Expert - The ‘Difficult’ Joint Report
• Industry Thought Leader Session
• BOA Radiation and Exposure in Theatre Session
We will also once again be working closely with the specialist societies to deliver a mix of revalidation and hot topic sessions. The full details of the programme can be found on the Congress website at www.boa.ac.uk/ programme
Registration
General Registration is open for both BOA members and Non-members, and will close at 23:59 on Monday 2nd September! Full details can be found at www.boa.ac.uk/registration
Accommodation
Book your exclusive accommodation rates online, through BCD M&E with HotelMap, the BOA Annual Congress 2024’s official hotel booking partners. Find out more at www.boa.ac.uk/accommodation
BOA App
Make sure to download the BOA App to access the BOA Annual Congress programme, and other event information to make the most of your experience before, during and after the Congress. Available to download from the Apple App Store and GooglePlay.
Exhibition and sponsorship opportunities
Thank you to all our Industry Sponsors at this year’s exhibition. We are delighted to welcome over 80+ exhibitors, including our Diamond and Platinum sponsors - Heraeus Medical GmbH, IBSA UK, Smith & Nephew, along with our Gold sponsors Getinge, Medacta, Orthofix, Summit Medical, IGEA Medical & All Aces Medical Couriers.
A full listing of our exhibitors can be found at www.boa.ac.uk/exhibitor-list
• Fergal Monsell –

The power of one platform



To experience RI.HIP on CORI◊ Surgical System visit us at the BOA stand 18 or click here to learn more. read read more here



Conference Listing 2024/25:
BORS (British Orthopaedic Research Society) www.borsoc.org.uk
09-10 September 2024, Sheffield
BOA (British Orthopaedic Association) www.boa.ac.uk
17-20 September, Birmingham
BOSTAA (British Orthopaedic Sports Trauma and Arthroscopy Association) www.bostaa.ac.uk
7 November 2024, Twickenham
BSSH (British Society for Surgery of the Hand) www.bssh.ac.uk
14-15 November 2024, Belfast
BTS (British Trauma Society) www.britishtrauma.com
20-21 November 2024, Bristol
BSS (British Scoliosis Society) https://britscoliosis.org.uk
21-22 November 2024, Birmingham
BOTA (British Orthopaedic Trainee Association) www.bota.org.uk
26-29 November 2024, Manchester







We specialise in casing and packaging solutions for orthopaedic implants, medical equipment and have supplied many of the world’s leading medical organisations.
We specialise in casing and packaging solutions for orthopaedic implants, medical equipment and have supplied many of the world’s leading medical organisations.
Our flight cases are made in our 70,000 sq ft factory in the UK using the highest quality materials to ensure that your vital
Our flight cases are made in our 70,000 sq ft factory in the UK using the highest quality materials to ensure that your vital equipment is fully protected in transit.

BOFAS (British Orthopaedic Foot & Ankle Society) www.bofas.org.uk
29-31 January 2025, Brighton
BHS (British Hip Society) www.britishhipsociety.com 5-6 March 2025, Harrogate
BRITSPINE
www.BritSpine.com 12-14 March 2025, Manchester
BSCOS (British Society for Children’s Orthopaedic Surgery) www.bscos.org.uk
13-14 March 2025, Brighton
BLRS (British Limb Reconstruction Society) www.blrs.org.uk
27-28 March 2025, Newcastle
BSSH (British Society for Surgery of the Hand) www.bssh.ac.uk
23-25 April 2025, Majorca
BASK (British Association for Surgery of the Knee) www.bask.ac.uk
29-30 April 2025, Harrogate
equipment is fully protected in transit. We design and manufacture cases to your exact specification. A range of pull-out drawers, shelves, lift-out trays, doors and shutters can be integrated into the case. With an in-house design team and advanced computer aided design and CNC routing facilities, we can produce custom foam interiors to
house implant samples, instruments and any other equipment.
Trifibre Ltd 17 Boston Rpad
Gorse Hill Industrial Estate Leicester LE4 1AW
We design and manufacture cases to your exact specification. A range of pull-out drawers, shelves, lift-out trays, doors and shutters can be integrated into the case. With an in-house design team and advanced computer aided design and CNC routing facilities, we can produce custom foam interiors to house implant samples, instruments and any other equipment.
Telephone: 0116 232 3166
Email us: info@trifibre.co.uk Web: www.trifibre.co.uk
Trifibre Ltd 17 Boston Rpad
Gorse Hill Industrial Estate Leicester LE4 1AW
Telephone: 0116 232 3166
Email us: info@trifibre.co.uk
Web: www.trifibre.co.uk




Download the App


The Journal of Trauma and Orthopaedics (JTO) is the official publication of the British Orthopaedic Association (BOA). It is the only publication that reaches T&O surgeons throughout the UK and every BOA member worldwide. The journal is also now available to everyone around the world via the JTO App. Read the latest issue and past issues on the go, with an advanced search function to enable easy access to all content. Available at the Apple App Store and Google Play – search for JTO @ BOA


Abstract and Innovation Theatre
New for this year, the 2024 selected abstracts will be presented in the Abstract and Innovation Theatre in the Exhibition Hall. With over 800 abstracts submitted, there will be presentations from healthcare professionals from across the UK and overseas on a wide range of orthopaedic topics.
Also, join us in the Abstract and Innovation Theatre and discover the latest innovative products and solutions to the market. We have a great line-up planned, with sessions from Bioventus and others. Register and join us! Limited spaces are available and seats are on a first come first serve basis. Visit our website for further details www.boa.ac.uk/abstract-innovation-theatre n


BIOS at 25: The Silver Jubilee

Sunil Garg is a Consultant Orthopaedic Surgeon at the James Paget University Hospital, Great Yarmouth. He is the BIOS President 2023-25.

Nanda is a Consultant Orthopaedic Surgeon at University Hospitals of North Tees and Hartlepool and Honorary Professor at Teesside University. He is the Treasurer for BIOS (2024-2026) and is a member of BOA Education and Careers Committee.
Sunil Garg and Rajesh Nanda
Jawaharlal Nehru’s Independence speech at the stroke of midnight 77 years ago ushered in the birth of two great nations. Nehru spoke of the tryst with destiny made by colonised people, redeemed as they won freedom from the British Empire. At the end of the twentieth century, Britons voted the NHS as one of their greatest ever achievements. This monumental institution has ensured that the United Kingdom and South Asia have remained linked.
Particularly in its early years, doctors from the Indian Subcontinent formed the backbone of the NHS and as the NHS celebrates its 76th birthday, the specialism of trauma and orthopaedics continues to be enriched by the Indian contribution. With this background, the formation of an association of orthopaedic surgeons of Indian origin in the UK was a logical step.
Birth of a Society
In the early summer of 1999, exciting things were happening around the UK including a Cricket World Cup. As the South African and the Indian teams were locked in a group match at Hove, a handful of enthusiastic British orthopaedic surgeons of Indian origin, led by Bisal Muddu assembled in nearby Eastbourne to sow the seeds of the Indian Orthopaedic Society UK (IOS-UK). Bisal became the founder-president and his colleague Babu
Peravali, the founder secretary, invited likeminded colleagues from across the UK for the inaugural meeting, hosted by Ravi Koka.
The society has grown steadily and now celebrates its silver jubilee with over 600 life members, representing all surgical grades. The Society celebrates its core Indian connection but is equally proud to be essentially a body of British surgeons who happen to be of Indian origin. With this in mind, a unanimous decision was taken by the Society at its AGM in Liverpool 2015 to change its name from ‘Indian Orthopaedic Society of United Kingdom’ to ‘British Indian Orthopaedic Society (BIOS)’ and adopted the motto ‘Excellence through Education’
BIOS has made giant strides on many fronts fulfilling its stated goals but remains primarily an educational and cultural body, promoting and nurturing orthopaedic ties between the UK and India. This is an organisation that aims to be inclusive, not exclusive.
The Society as a BOA affiliated society continues its close association with both the BOA and the IOA with a presidential exchange at BIOS, BOA and IOA meetings. The bridge underpinned by BIOS linking Indian and British orthopaedics is built on strong foundations, nurturing the science and art of orthopaedics across the two continents.
Rajesh
(From Left to Right) – Joseph Dias (Past President BOA), Bisal Muddu (Founder President BIOS), Sunil Garg (President BIOS), Amit Sinha (Past President BIOS), Murti Gollapudi (Past President BIOS), Mark Bowditch (Vice President BOA), Gautam Chakrabarty (Past President BIOS), Rajesh Nanda (Chair, Organising Committee BIOS 2024), Amit Tolat (Immediate Past President BIOS), Anand Arya (Past President BIOS) and Ram Chaddha (President IOA).

Indian Summer
The ‘Indian Summer’ concept was the brainchild of Bisal Muddu and the inaugural event took place as a part of the 2004 Annual BOA Congress in Manchester. A delectable combination of invited lectures from eminent Indian Orthopods, a spicy Indian Dinner and even spicier Bollywood themed entertainment enthralled the delegates. The second event was held in 2009 garnering equally enthusiastic reviews for both the quality of the science and the artistry of the Indian themed entertainment. It is now a triennial event and firmly established in the BOA Congress calendar.
A reciprocal event in India mirroring the UK Indian Summer became a reality at the Chennai IOACON in 2013, under the name, ‘British Autumn’ where senior British orthopods gave a series of lectures to an appreciative audience.
BIOS educational activities
BIOS draws on the vast expertise of its members in areas of mentoring, education, training and leadership and via its membership organises many educational sessions throughout each year. Increasingly, this content has been delivered online. Over the last few years BIOS has organised regular virtual sessions covering the breadth of orthopaedics both for trainees as well as established surgeons. BIOS has organised and presented not only the annual BOABIOS session at Congress but also a similar annual IOA-BIOS session. It has also had the opportunity of its members presenting invited guest lectures at various regional state meetings in India.
BIOS funds a place on the BOA Future Leaders Programme and this year started a CESR support and mentorship programme for our SAS colleagues.
Indo British travelling fellowships
This flagship educational programme from BIOS has arranged a number of opportunities for young Indian orthopaedic surgeons to visit UK in an observer capacity for 2-3 week fellowships with the aim of providing exposure to British T&O concepts. Fellows end the fellowship by attending the annual conference of BIOS or the BOA.
BIOS also sponsors trainees from BOTA and its wider members to visit centres of excellence in India for a similar period and attend the IOA Congress attended by approximately 5,000 orthopaedic surgeons from India and abroad. Over the years, several orthopaedic trainees and Consultants from the UK have visited state of the art arthroplasty, sports and trauma centres in India and exchanged ideas.
The 25th Annual British Indian Orthopaedic Society Conference
Our Silver Jubilee meeting was held in Newcastle 5th – 6th July 2024, organised
by Professor Rajesh Nanda and his team. The theme of the conference was ‘Utilising the Wisdom of Experience’. The conference showcased the achievements and contributions of the Indian orthopaedic surgeon with speakers including past and present members of the BOA presidential line: Professor Joe Dias, Ananda Nanu, Mark Bowditch and Professor Amar Rangan as well as Vikas Khanduja President-elect of SICOT and researcher Professor Hemant Pandit. Dr Ram Chaddha, President of the IOA gave an insightful talk, ‘My Ten Mistakes – Journey of a Spine Surgeon’. There were also lectures by Professor Mike Reed on AI in Orthopaedics and Professor Paul Banaszkiewicz on Resilience in Orthopaedics: Dealing with Setbacks. The invited guest lecture was delivered by retired general surgeon, author and equality advocate, David Sellu, who spoke on Experience of a GMC Investigation.
In a special session, the contributions of the society’s past presidents were highlighted and acknowledged with thanks for their outstanding leadership and service.
For the first time, in collaboration with BOMSA, BIOS organised a parallel session for medical students, incorporating lectures and workshops on plastering and suturing skills, application of an Ex-Fix and basic AO principles.
There were also several free paper sessions (abstracts published in BJJ), posters and an exciting JAM session (Just a minute) that was well received by all. Visiting fellows from India presented their reports and their learnings from the NHS. CESR and medico-legal revalidation were other popular sessions.
BIOS continues to develop its educational activities both within the UK and in India. It will continue to be the bridge between our two organisations, BOA and IOA, helping to forge better relations and improve the exchange of ideas that is beneficial to our patients. We take this opportunity to invite JTO readers to attend the BOA-BIOS session at Congress on Wednesday 18th September. n

BIOS at Indian Orthopaedic Conference 2023 at Lucknow, India supporting the Women in Orthopaedics session.
BIOS Council members.
Do you see me? A patient perspective
Katy Blackmore

Katy Blackmore – After some dark days during which Katy experienced a short course of talking therapy, she became curious enough to rethink her career path. Katy became a personcentred counsellor and she has worked in several settings including HM Prison Service, a UK Adoption charity, the homicide division of Victim Support UK, primary schools and pupil referral units.
She currently specialises in working with trauma and supporting parent/ child relationships both privately and within a school and early years setting. Alongside this, Katy is developing a social enterprise project www.embracingempathy.co.uk aiming to support cultures of empathy within our healthcare systems.
As I write to you, the medical professionals, I wonder, what is the most important message to hear from my own patient story. Shall I speak about my presentation as a toddler, the subsequent diagnostic and reparative journey and the vast array of procedures I have undergone? Or perhaps you should hear about my experience of chronic pain and the many ways I have sought to manage this on a day-to-day basis? And would it not be productive to enlighten you about my experience of being at the sharp end of a power imbalance inevitably manifested from professionals assuming the expert position? But… no, I want to talk about Shame
Aged 18 months my parents realised that I was not walking the way my brother had, I was referred to the local orthopaedic surgeon and
diagnosed with bilateral CDH which set me on a course of corrective surgery that had mixed results. My left hip surgery was successful, but my right hip refused to respond. At age seven, my parents were told that there was little chance that I would walk again. However, a timely referral to GOSH gave me new hope. A successful Colonna procedure enabled me to walk for a short time. Puberty brought uneven leg growth, requiring two lengthening surgeries over four years. But by age 18, I could again walk unaided, and I enjoyed nearly three years at university before I was struck by a car just ahead of my finals. This led to more surgery at RNOH, including a titanium nail in my tibia that I still have today.

After some dark days post-finals, I realised that I had been harbouring childhood medical trauma and began my own therapeutic journey to understand and heal these wounds from childhood that were impacting on my adult life. I discovered latent ‘Toxic Shame’ at the root of my life story, informing every decision, instilling every feeling that I faced in the moment. I had never experienced my body as my own, having been repeatedly exposed to strangers in the most undignified ways. I watched my family in pain as they were exposed to my pain: all of this made me feel wrong inside. To feel right, I was as ‘good’ as I could be, cried as little as possible, was courageous and brave in the face of each new procedure, and did my best to take care of others around me to feel validated. My cup always had to be half-full in a world that felt empty and unsafe. All my efforts failed to take away the ‘wrongness’ within. The trouble with compliance and painted on smiles is, of course, that my shame was banished into the
depths of my soul only to leak out in other ways… perfectionism, a reliance on alcohol, an inability to hold boundaries or say no to people, feeling I had no voice and crippling anxiety, I could go on…
So, what is Shame? The Oxford English dictionary definition is ‘a painful feeling of humiliation or distress caused by the consciousness of wrong or foolish behaviour’. We need to acknowledge this feeling to set our moral compass, stick within the boundaries of what is right and behave appropriately towards self and others. Now whilst I wasn’t ‘wrong’ to have been born with a disability, constant intimate exposure to painful, dehumanising procedures, knowing that loved ones were suffering at my expense led to an internalised sense of shame and feeling that my whole being was in fact wrong. This is when healthy shame becomes toxic. John Bradshaw stated that “shame as a healthy human emotion can be transformed into shame as a state of being… [which] is to believe that one’s being is flawed, that one is defective as a human being. [Shame] becomes toxic and dehumanising”1
Throughout my childhood, I suffered trauma from countless physical procedures alongside the additional complex layer of trauma associated with my compromised feelings of worth. Long-term such high psychological distress levels in individuals with trauma exposure are associated with elevated inflammatory markers. Various studies over recent decades have explored the link between childhood trauma and inflammation, which can lead to chronic diseases, for example cardiovascular issues and psychiatric conditions such as depression. Research findings from a study on childhood trauma and adult inflammation concluded that there was “strong evidence that childhood traumatic events significantly impact on the inflammatory immune system, with trajectories reaching into adulthood, thus offering a potential molecular pathway by which early trauma confers vulnerability to developing psychiatric and physical disorders later in life”2. Perhaps, no wonder that tonsilitis and other illnesses were ever-present throughout my childhood. This is important for all healthcare professionals to hold in mind when interacting with patients in an ever-stretched healthcare system.
Whilst much of this impact was unavoidable, there have also been many distressing interactions with healthcare staff which, whilst unintended could have been avoided. Professionals entering the room who did not acknowledge me, nurses standing over me, dressing my wounds whilst talking to
each other about my body parts, receptionists who worked only to script, and consultants who talked over me and worked hard to avoid eye contact when addressing me. Every time I was faced with a substandard interaction my complex trauma was compounded, my selfworth was further diminished, and I was silenced again.
Only when I was 20 years old did I meet a consultant who treated me with a level of compassion and empathy that helped me feel truly seen as a person and not a set of medical records. They would look directly into my eyes, wait patiently to hear my thoughts, and had a natural capacity to empathise with my experiences. Alongside this, an ever-supportive network of family and friends, pockets of gold standard healthcare provision and my determination to recover from my trauma has helped me find my voice and place myself in a position of strength that can be used to help both myself and others.

It has led me to a personal project that focuses research on how to create a culture of empathy within our healthcare systems to support both professionals and service users in their positions, bolstering staff within highly pressurised environments and reducing the impact of internalised shame in their patients. Brene Brown sees empathy as “the natural antidote to shame [ ] If we can share our story with someone who responds with empathy and understanding, shame cannot survive.”
Empathy is defined as “the action of understanding, being aware of, being sensitive to, and vicariously experiencing the feelings, thoughts, and experience of another”
Developing empathy is crucial for establishing relationships and behaving compassionately towards others.
“Only when I was 20 years old did I meet a consultant who treated me with a level of compassion and empathy that helped me feel truly seen as a person and not a set of medical records. They would look directly into my eyes, wait patiently to hear my thoughts, and had a natural capacity to empathise with my experiences.”
Experiencing empathy with a medical professional whom I knew was held in high esteem helped me to consider myself, for the first time, through a more compassionate lens. I reached out to a couple of therapists in my twenties, but it was only in my early thirties as a young mother and a practicing counsellor myself that I really began my own discovery of self and journey towards the self-compassion necessary to heal from my toxic shame. Gentle encouragement from my clinical supervisor led me into the therapy room not as the ‘good’ therapist or the ‘good’ wife and mother, but as me. I started to feel for myself, to acknowledge my losses and appreciate my struggle to endure painful situations. I found I was able to access many needs within me that had laid dormant, and for the first time in my life I could find ways to meet these needs with intention and care. I realised I had been denying so much of my pain that it was impossible for me to know when I needed to take care of myself in even the most basic of ways like sitting down to rest a while or remembering to eat. So powerful is the neuroscience of our >>
emotions that it was about a year or more after my therapist had suggested a daily ritual of putting lotion on my body, that I realised I had routinely covered only the top half of my body, neglecting my legs! My poor legs, I had denied them for decades, and yet they had survived so much, done so much for me, only for me to disown and disconnect from them completely. Today I can acknowledge and be proud of my body and its battle scars, my body tells my story, and my voice, now unsilenced, protects and advocates for me and others who I care about.
NHS England states that “Compassion is how care is given through relationships based on empathy, respect and dignity. It can also be described as intelligent kindness and is central to how people perceive their care.” For me this concept underpins quality of care within all systems, in fact it should be at the heart of all human interactions. However, turning concept into widespread practice is not easy, and twelve years on there is still an ongoing need to improve consistency in the quality of interactions between healthcare professionals and service users. Systems are shaped by people who have feelings, and who need to know how to care for themselves and each other. We all have a lived experience, a narrative that forms and shapes our intentions and actions, much of which we do on autopilot.
It is easy to become comfortable with our environments and routines, humans thrive on routine, but this does not always produce best practice.
Years ago, I attended A&E with a severe facial cellulitis. After a misdiagnosis by the duty consultant, a junior doctor listened to my opinion then strategically waited for a staff changeover, which lead to a second opinion garnering swift appropriate treatment. This caring individual looked me in the eyes with concern and listened to me. They were committed to hearing me and challenged their own system of practice to do so, which made all the difference to the outcome. Perhaps this highlights a need to challenge internal hierarchies that at times foster a culture of fear in communications up the chain.
I understand the bigger picture of an extremely pressurised service with more demand than supply and staff who are also feeling underappreciated and ‘unseen’. I will not be another voice complaining about a provision that heals and that has enabled me to walk without aid. I wish to give back to a system of people who service humanity at its most vulnerable; to help that system heal. Compassion and empathy must start within; you and the work that you do within the healthcare profession is invaluable, and
I’ve Got This
‘Dear Little me, I’ve got this. You rest now, you’ve earned it. You’ve done so well, you have survived the poking and prodding, Enduring the subtle cruelty of a system that cannot see. You are still here, Amazing You!’
‘Dear Little me, I see you are still frozen in your fear, No voice to tell of the horrors in the There and Then nor the Here and Now. Silent compliance is your saviour. And yet it holds you back, sweet one.’
‘Dear Little me, Life has taught us the value of fight… Don’t you see? You are not frozen in fear anymore, unable to run or push back. Together we have a voice now.’
‘Dear Little me, I will take the reins today. I love you little one, And I’ve got this.’
By Katy Blackmore
to take good care of others you must take good care of yourselves first. Years of personal therapy has taught me that this is no small task, and at times I do forget to practice what I preach. Nonetheless, I am committed to starting each new day holding on to the promise I have made to me to view myself and others through a compassionate lens.
It is this that I would like you to take home today; with each new day consider what you need, to be the best version of yourself, for both you and those around you. When you go into work tomorrow, take the time to ask at least one of your colleagues how they are, and really listen to their answer. When you see your first patient instead of looking through the lens of the procedure you are planning, look into their eyes and imagine being in their shoes; what would you hope for from your doctor if it was you? Lead with your humanity. There will never be enough hours in the day to complete all our ‘to-do’ lists, there will always be deadlines and hierarchy and system pressures. But we cannot escape our humanness and at our core this must be honoured, not only for ourselves but for all those around us. In a world that teaches us daily to disconnect, we must fight back with commitment to a human connection, to feeling for ourselves and for others so that we allow our needs to be met within our imperfect systems. In your interactions, you have the power to limit your patient’s trauma, and to create a better quality of everyday life for yourselves and others around you. I see you; I see the heavy weight of responsibility carried when others look to you to fix them, the stress and burnout of a system under pressure, and the never-ending, often thankless, list of tasks to be done. And I see the individuals you serve; I see their fear at the unknown and feel their pain as they navigate the trauma of illness and suffering. Our humanity connects us; we are all one and in order not only to exist but to thrive we must remember this.
“When humanness is lost the radical difference between the bodies in the pit and people walking on the street is lost.”
Edward Bond, Playwright
‘Love and work are the cornerstones of our humanness.’
Sigmund Freud n
References
1. Bradshaw, John. (2015). Healing the Shame that Binds You. Health Communications, Inc., Deerfield Beach, FL 33442.
2. Baumeister D, Akhtar R, Ciufolini S, et al. Childhood trauma and adulthood inflammation: a meta-analysis of peripheral C-reactive protein, interleukin-6 and tumour necrosis factor-α. Mol Psychiatry 2016;21(5):642-9.
NEW THOMAS SPLINT & ACCESSORIES








Incivility in orthopaedic surgery: Unmasking the hidden epidemic
Deiary Kader and Paul Banaszkiewicz

Deiary Kader is a consultant specialising in knee arthroplasty and sports injury surgery at the South West London Elective Orthopaedic Centre (SWLEOC), where he serves as the Director of Research. Professor Kader is committed to the clinical integration of AI in orthopaedics. He is the founder of NGMV Medical Volunteers & Life Academy, was a war reconstruction surgeon for the ICRC in Lebanon, and is currently serving as a surgeon for Swisscross in Iraq.

Paul Banaszkiewicz is a Consultant trauma and orthopaedic surgeon working at the Queen Elizabeth Hospital Gateshead. He is a fellow of the Higher Education Academy, fellow of the Academy of Medical Educators and has a Master’s degree in Medical Education from Newcastle University. He is a Visiting Professor at Northumbria University, a BOA Council Trustee, JTO Editor and the current BOA Education and Careers Chair.
In the fast-paced, high-pressure environment of healthcare, particularly within orthopaedic surgery, incivility is an under-acknowledged yet pervasive issue that can significantly corrode the pillars of healthcare.
Unprofessional and disruptive behaviour in the surgical environment can take many forms. Surgeons and managers may display such conduct towards one another, their juniors, and other staff members, creating a toxic work atmosphere. These behaviours can range from overt acts of rudeness and intimidation to subtler forms of disrespect and undermining, manifesting in dismissive exchanges, non-constructive criticism, passing blame for mistakes, withholding information, and passive-aggressive behaviours. Such actions not only create a hostile work environment but also fuel stress, stifle collaboration, and disrupt the fabric of cohesive team dynamics. Moreover, they adversely affect staff retention, productivity, and morale.
Reports of unprofessional behaviour vary among staff, with black and minority ethnic employees experiencing this more often. In addition, evidence indicates women are more commonly targeted than men1,2
But why does this happen, and what are the consequences of such behaviours? This article explores the impacts, causes and remedies for incivility, specifically addressing orthopaedic surgeons and the broader healthcare community.
The impact of incivility
The cost of incivility extends beyond hurt feelings, it has tangible consequences:
• Reduced team efficiency: Incivility disrupts the workflow and can lead to poor patient outcomes. Indeed, a single rude remark was found
to reduce the effectiveness of doctors and nurses by over 50% during a simulated critical scenario3.
• Medical errors go unchallenged: Stress and distraction from uncivil behaviour can lead to mistakes. In a 2003 survey conducted by the Institute for Safe Medication Practices (ISMP) on workplace intimidation, 40% of those surveyed acknowledged that they refrained from querying orders they were uncertain about, preferring to presume they were accurate, rather than confront a prescriber whom they viewed as intimidating4
• Diminished morale and turnover: Continuous exposure to a toxic work environment leads to higher staff turnover rates.
• Patient satisfaction: An uncivil environment can spill over into patient care, affecting their experience and trust in the healthcare system.
• Higher complication rate: A detailed US study involving 200 surgeons and 13,653 patients found that patients treated by surgeons with higher reports of unprofessional behaviour faced a notably higher risk of surgical and medical complications5. Consider the consequences when a surgeon encounters unprofessional behaviour from a colleague just before surgery. Such distractions elevate the likelihood of surgical mistakes and complications, compromising patient safety.

Figure 1: Incivility. The red bird is being mocked and made fun of by the three other birds.
Furthermore, they can heighten the risk of injury to the surgical team and severely damage team cohesion and the overall work environment.
• Cost to the NHS: A cautious estimate suggests that the cost of unprofessional behaviour to the UK’s NHS amounted to approximately £2.28 billion per year when considering factors such as sickness absence, employee turnover, reduced productivity, compensation and litigation costs6

Why, then, do surgeons, renowned for their precision and skill, fall prey to uncivil behaviour?
With a demanding unwritten code of conduct that emphasises relentless commitment and emotional stoicism, it is no surprise that the pressures of the job can manifest in uncivil behaviour.
Professionals in healthcare, particularly surgeons, operate within an unspoken ethos that prioritises patient care above all. This ethos includes:
• Dedication to long hours: Coming in early, staying late, and working nights and weekends is commonplace.
• High volume of procedures: The expectation to perform a large number of procedures often with complex demands.
• Multitasking under tight deadlines: Meeting simultaneous deadlines for different tasks and patients.
• Emotional restraint: Keeping personal issues and emotions from affecting professional responsibilities.
Such relentless standards, while aiming to uphold the highest quality of patient care, can inadvertently foster an environment where stress is high and the bandwidth for civility is low. For many, the job becomes not just a profession but an identity, and with identity so closely tied to performance, the stakes of every interaction are raised.
The psychology behind surgeon incivility
Several psychological and systemic factors contribute to this conundrum:
• Stress and burnout: The constant high-pressure environment can lead to emotional exhaustion, reducing an individual’s ability to engage positively with colleagues.
• Dehumanisation: With a focus on technical excellence, surgeons may start viewing patients — and by extension, colleagues — as tasks rather than humans, leading to depersonalisation.
• Lack of resources: Staff shortages and resource constraints increase the pressure on individuals, which can result in frustration and a higher propensity for incivility.
• Fear of error: The knowledge that a single mistake can have dire consequences may create a defensive workplace atmosphere.
• Competitive culture: The drive to be the best can sometimes overshadow the collaborative nature of healthcare, leading to aggression and disrespect.
• Challenges in expressing emotions - rethinking British stoicism: The British cultural norm of the ‘stiff upper lip’ may contribute to suppressing emotions and inhibiting open communication. Recognising that emotions are not weaknesses but natural responses that can guide more mindful interactions is crucial for fostering transparency. Emotions act as a complementary immune system, not only safeguarding our mental wellbeing but also assisting in interpreting and comprehending our environment. They facilitate our processing of and responses to social and emotional signals, leading to clearer communication and a deeper level of understanding. When we fail to express these emotions, it can result in a build-up of stress and anxiety, compromising our physical health and straining interpersonal relationships. Expressing emotions, therefore, is crucial for maintaining both our psychological balance and the quality of our connections with others.
How rudeness reduces mental bandwidth
The concept of cognitive bandwidth, demonstrated by Miller’s Law, offers insight into the profound impact incivility can have. Cognitive bandwidth, akin to a mental window, represents an individual’s capacity to concurrently process multiple thoughts or tasks. This bandwidth
essentially sets the pace at which we can consciously absorb and respond to information. Miller’s Law, suggesting that the average person can hold about seven items (plus or minus two) in their working memory, highlights the finite nature of our cognitive resources.
Incivility disrupts this cognitive balance, encroaching on our mental bandwidth. When faced with negative interactions, a significant portion of our cognitive capacity is diverted towards managing these stressors, leaving less available for critical thinking and decisionmaking. This is particularly pertinent in high-stakes environments like hospitals, where staff members’ varying capacities to withstand negativity can markedly influence their mental well-being and job performance. The repercussions of diminished cognitive bandwidth in such settings are significant, with hospital staff who are preoccupied with uncivil interactions more prone to errors, memory lapses, and a lack of innovative problem solving.
Addressing the root causes
To tackle incivility, it is essential to understand and address its root causes:
• Mentorship and advocacy: The link between surgical skills and stress levels is undeniable. Evolving surgeons often face higher stress, impacting their performance. A targeted solution is a well-structured mentorship programme that offers direct access to experienced surgeons’ insights and reassurance. However, the effectiveness of such a programme largely depends on the developing surgeon’s emotional intelligence, including their willingness to seek support and accept guidance. With the right mind-set, a mentorship programme can significantly alleviate stress and enhance the skills and confidence of the doctor, leading to a more proficient and composed surgical team. Additionally, within this mentorship framework, the advocacy role of experienced surgeons becomes crucial as it ensures that developing surgeons receive personalised support, guidance, and opportunities essential for their professional growth and success.
• Leadership development: Healthcare workers often perceive courteous surgeons as leaders, regarding them as competent individuals. This perception highlights the importance of cultivating leadership skills among surgeons, emphasising emotional intelligence and strategies to navigate the pressures of the profession with grace and civility. >>
Figure 2: Incivility in the surgical setting.
Features
• Promoting reciprocity: Simple acts of kindness and civility can set off a chain reaction: as team members receive support from their peers, they are motivated to extend it to others. The impact of reciprocity on workplace dynamics cannot be overstated, resulting in a more harmonious work environment.
• Adequate staffing and resources: Ensuring that the healthcare system is adequately staffed and resourced can reduce the pressure that contributes to uncivil behaviour.
• Encouraging open dialogue: Creating safe channels for feedback and discussion can help alleviate misunderstandings and tension.

• Creating a culture of support: Fostering an environment where asking for help is normalised can decrease the perceived need for stoicism.
• Mindfulness and reflection: Taking the time to reflect on one’s behaviour and its impact can lead to greater self-awareness and civility.
• Resilience and emotional intelligence training: Equipping surgeons with tools to manage stress and engage empathetically can mitigate the rise of uncivil actions.
• Civility Quotient (CQ) Awards: Create an award programme that recognises individuals or teams with the highest ‘Civility Quotient’ based on feedback from peers, supervisors, and patients. Positive reinforcement of civil behaviour can shift the culture.
Radical candour: A pathway to change
It is imperative to clarify that advocating for civility doesn’t equate to diminishing professional rigour or fostering a laissezfaire environment. Rather, the essence lies in balancing stringent work standards with a culture of respect and motivation. This equilibrium is appropriately captured in the radical candour framework, which promotes a balanced blend of genuine empathy and straightforward feedback, advocating for leaders to deeply care while maintaining openness with their team. It is structured around two pivotal elements: demonstrating real concern for individuals beyond their professional capacities, and delivering candid, unambiguous feedback, even when it involves
challenging discussions. This underscores the importance of combining sincere care with directness, avoiding counterproductive attitudes such as obnoxious aggression (critique devoid of empathy), ruinous empathy (excessive empathy that avoids crucial feedback, potentially harming individual or team performance due to unclear guidance and unaddressed errors), and manipulative insincerity (ineffective and disingenuous feedback). By adhering to this model, leaders are encouraged to foster a supportive yet honest environment, ensuring that feedback is delivered with both kindness and clarity7
Leaders, by genuinely caring for their team members, not only as professionals but as individuals, promote a foundation of trust and loyalty. Concurrently, direct and respectful challenges serve as impetuses for improvement and growth, ensuring that complacency finds no foothold. This method, centred on compassionate leadership coupled with clear expectations, not only mitigates workplace incivility but also enhances the overall team vitality, nurturing a workspace where respect, transparency, and highperformance merge, thereby optimising the collective output.
This article aims to draw the attention of regulatory authorities and healthcare governing bodies to the critical issue of unprofessional conduct and disruptive behaviours exhibited by a minority of doctors. It highlights the importance of addressing unprofessional behaviours promptly and effectively to avert dysfunction in workplaces and mitigate risks to patient safety. By tackling these issues head-on, we can ensure that healthcare institutions
remain places of healing and trust, where the focus is on patient care and the well-being of both staff and patients is prioritised.
Conclusion
While the culture of healthcare, particularly in orthopaedic surgery, has historically valued stoicism and relentless dedication, it’s time to acknowledge that these values can coexist with, and indeed be enhanced by, a commitment to civility. The costs of incivility are too great to ignore, from the wellbeing of healthcare professionals to the safety of patients. By understanding the underlying causes of incivility, embracing radical candour (respectful confrontation), and fostering an environment of support and reciprocity, orthopaedic surgeons can lead the way in creating a more respectful, effective, and caring healthcare system. n
References
1. NHS Staff Survey (NSS). NHS Staff Survey 2022 National results briefing. 2023 [cited 2024 Mar 10]; Available at: www. nhsstaffsurveys.com/results/national-results
2. Keller S, Yule S, Zagarese V, Parker SH. Predictors and triggers of incivility within healthcare teams: a systematic review of the literature. BMJ Open. 2020;10(6):e035471.
3. Riskin A, Erez A, Foulk TA, et al. The Impact of Rudeness on Medical Team Performance: A Randomized Trial. Pediatrics. 2015;136(3):487-95.
4. Institute for Safe Medication Practices (ISMP). Intimidation: Practitioners Speak Up About This Unresolved Problem (Part I). ISMP Medication Safety Alert! Acute Care 2004;9(5):1-3.
5. Cooper WO, Spain DA, Guillamondegui O, et al. Association of Coworker Reports About Unprofessional Behavior by Surgeons With Surgical Complications in Their Patients. JAMA Surg. 2019;154(9):828-34.
6. Kline R, Lewis D. The price of fear: Estimating the financial cost of bullying and harassment to the NHS in England. Public Money & Management 2018:39(3);166-74.
7. Scott K. Radical Candor: How to Get What You Want by Saying What You Mean. Pan Macmillan; 2017.
Figure 3: Radical candour - Combining sincere care with directness to uphold stringent work standards.

Solving the most pressing healthcare challenges
Johnson & Johnson MedTech are developing next generation MedTech solutions to tackle the most pervasive and complex health challenges for people around the world.
Join us at this year’s British Orthopaedics Association annual congress as we showcase how Johnson & Johnson MedTech are solving the most pressing health challenges, through our offering across orthopaedics, surgery, and services & solutions.
Stand 33 will be our central congress hub, where delegates can experience live demonstrations and expert sessions across surgical specialties including Robotics, Joint Reconstruction, Trauma and Extremities, Sports, Services & Solutions, and Wound closure.
Scan the QR code to see our full schedule.



Justin Green has recently completed his Clinical Research Fellowship with NAHR, BHS and ORUK, exploring the application of digital technologies in determining longitudinal outcomes in hip preservation surgery. He is currently reading for a PhD in Artificial Intelligence at Newcastle University with an interest in ethics and responsible application of AI in healthcare. Justin acts a Clinical Safety Officer and member of the AI Clinical Safety Board at Northumbria Healthcare NHS Foundation Trust and contributes to the NortHFutures Digital Skills collaborative.

Luke Farrow is a Scottish Research Excellence Development Scheme (SCREDS) Clinical Lecturer based in Aberdeen. He is currently in the final stages of a Clinical Academic Fellowship exploring how to make improvements in the clinical care pathway for those awaiting hip and knee replacement through the use of AI. He leads the Aberdeen AI Healthcare Collaborative (AAHC) and is the current BOA Associate Sub-Speciality Lead for Elective Orthopaedics. Luke has particular research interests in the use of routinely collected healthcare information and clinical applications of AI in T&O.
The challenge of using AI for non-traditional data modelling in predictive analytics
Justin Green, Luke Farrow, Feroz Dinah and Vipin Asopa
Much has been written about the use of predictive analytics in orthopaedics in terms of predicting outcomes of surgery, optimising operational efficiency, etc1. Predictive analytics has classically been applied to ‘traditional’ datasets such as tabular continuous or discrete data in order to identify trends and relationships. However, artificial intelligence (AI) can also handle ‘non-traditional’ data such as unfiltered social media text and images through natural language processing (NLP) and computer vision (CV), to reach a predictive output. However, explaining how AI reaches such predictions can be problematic, especially with complex setups like convoluted neural networks (CNNs) and graphical neural networks (GNNs). Such ‘black box’ analytics are opaque and pose challenges in relation to data quality and output, privacy, trusting the output and ethical considerations2
This article will start with a description of using predictive analytics with non-traditional (NT) data. It will then discuss the model complexity vs. explainability to optimise accuracy and user confidence. Lastly, the importance of reporting guidelines regarding predictive analytics in healthcare will be discussed.
Predictive analytics and non-traditional data
NT data refer to data that cannot be easily handled by traditional statistical tools or methods because the data does not fit neatly into the fields, or it may be too unstructured or varied to fit into a traditional database. The data may also be too large: examples include the billions of search engine uses undertaken
on a daily basis, resulting in huge amounts of information. Such data volumes may be measured in Petabytes to Exabytes (1,000 to 1 million TB) and is typically termed ‘Big data’.
Machine learning (ML) allows big data to be processed in a stream, i.e. analysed and acted upon in near real-time, rather than being collected and stored for later batch processing because of the above challenges. Other examples of challenging data include newer forms of personal data produced by various connected digital platforms such as social media posts, or devices like smartphones, fitness trackers, computer tablets, smart home devices, medical devices, etc., resulting in large amounts of unstructured text, numerical and image data. Because this type of data is not systematically structured or stored, its analysis has only become possible thanks to advances in AI and redictive analytics. Previous analysis of large amounts of data, such as that found in the Facebook and Instagram ecosystems relied on traditional statistical methods and simple algorithms, requiring human intervention. These were far less efficient than modern AI-based techniques such as CNNs and more recently, GNNs, as discussed below.
Graph data is another form of NT data. It is a non-linear data structure representing relationships between entities (Figure 1). The most common applications include social networks (connections between friends or followers) and recommendation systems (personalised suggestions while the customer is still browsing). Graph data can also be used to describe group dynamics in a team sport, to find the shortest route in a navigation programme, and to identify spread of information or even diseases among social networks.


Feroz Dinah is a Consultant Hip and Knee Surgeon based in the Epsom and St Helier Hospitals NHS Trust. He also works closely with the research department in the South West London Elective Orthopaedic Centre. He has a keen interest in the application of robotic surgery and AI in trauma and orthopaedics.

Vipin Asopa is a Specialist Hip and Knee Surgeon at South West London Elective Orthopaedic Centre, Epsom. His research interests include the use of artificial intelligence to improve patient outcomes following surgery.
The presence of different interconnected data sources, found in various domains, from social networks, recommendation systems, science and cybersecurity, has fuelled the rapid evolution of GNNs3. These networks can model and understand complex relationships and make sense of the interlinked data to help solve real-world problems better than traditional ML models (e.g. CNNs).
Deep learning (DL), a subset of ML, is a powerful method that can be used to analyse the unstructured NT data described above (see Figure 2). It is based on artificial neural networks using multiple layers that simulate the human brain3. NLP and CV are applications of DL that help with data analysis. Examples of NLP include language translation and speech recognition, while medical applications include the analysis of clinical, patient communication and research summarisation, if necessary, after conversion from image or sound data to textual data1. Similarly, CV examples include object

detection (autonomous surveillance), image classification (medical radiology, dermatology and pathology) and face recognition, with orthopaedic applications including implant positioning and gait analysis1
Although DL algorithms perform best after being developed/trained on large datasets, they require significant computational resources including specialised hardware4 Furthermore, DL needs vast amounts of labelled training data, and the performance of a trained algorithm depends heavily on how the training data represents the data being analysed. If the dataset is small or noisy, the model can overfit to the training data and will not be applicable to unseen data. This can cause models to learn and propagate biases present in the training data, leading to unfair or discriminatory outcomes. This can raise ethical questions, particularly around privacy, consent, and fairness. DL models are often criticised for their lack of transparency and interpretability and explainability, making it difficult to understand how decisions are made5. This is addressed below.
Making AI models less opaque: Explainable AI (XAI)
The term ‘black box’, originally coined during World War II to describe aircraft components housing sensitive data, was first applied to AI in 1961, to denote analysis or interpretation through unknown means. More recently, the term has evolved to signify the opaque nature of ML models6. ML and DL models, construct non-linear relationships in data. This enables more complexity and in turn results higher accuracy than traditional statistical models. The complexity of the relationships however generates a lack of clarity in the modelling structure. When the arrays are interrogated as to which factors in training data leads to the particular conclusions it can become too complex to interpret. This opacity has earned them the name ‘Black Boxes’, highlighting the difficulty in understanding and interpreting their inner workings. Lack of transparency raises trust and accountability concerns with users, especially in critical applications such as healthcare.
To address this, Explainable Artificial Intelligence (XAI) proposes a shift from the black box model to a fully transparent AI by devising methods and tools to mitigate the opacity in models, without degrading their accuracy and performance. This, it is hoped, would make the judgments of complex models understandable and expected, by revealing the internal mechanisms in a comprehensible manner7
XAI can be represented in various ways, from mathematical equations to visual representations such as scatter plots. >>
Figure 1: Diagrammatic representation of graph data. Graphs lack a predefined structure for data storage (left side), and there is no inherent knowledge of node-to-neighbour relationships, as illustrated on the right side. Left side is amenable to CNNs, right side requires GNNs.
Figure 2: Deep learning as a subset of machine learning (from AlZubaidi et al. Review of deep learning: concepts, CNN architectures, challenges, applications, future directions. J Big Data. 2021;8,:53).
Features
An example of XAI in medical imaging is employing saliency mapping, a process where areas of an image a model considers important in generating a prediction, are highlighted providing a visual indication of the regions of interest which are determining the outcomes. The use of saliency mapping as a tool, has shown promising results in implant identification and models predicting the risk of implant failure or loosening8 improving the interpretation features. Similarly, LIME (Local Interpretable Modelagnostic Explanations) approximates complex models with simpler, interpretable models locally around a prediction, offering insights into individual decisions. SHAP (SHapley Additive exPlanations) values, based on cooperative game theory, provide a unified measure of feature importance in predictive analytics, making it possible to understand the contribution of each feature in the data to the model’s output.
Generative AI, seen in LLMs, has been used to create new content such as text, images, and sound, also faces significant challenges regarding explainability. In the context of orthopaedics, generative AI has been used to simulate and visualise surgical outcomes in arthroplasty. For example, a group led by Bardia Khosravi from the Mayo Clinic9 applied Generative Adversarial Networks (GANS) to create high-fidelity synthetic pelvis radiographs which were used for DL-based image analysis. The synthetic images were indistinguishable from real images and showed equivalent performance when assessed by DL models. However, the use of synthetically generated images to train other algorithms raises questions of whether this is a suitable way to train algorithms and, in turn, the validity of the decision making that arises from these. This makes the results difficult to interpret. The challenge lies in understanding how these models generate specific outputs from the given inputs, particularly when the training data may contain inherent broad variation in structure and biases. A systemic review reported that the diagnostic accuracy of LLMs was significantly worse than clinicians10. To ensure that patient safety in an autonomous clinical decision-making scenario is maintained, transparency and assurances in LLMs is vital, and assurances in performance should be validated to a level that is at least as good as, if not better, than clinicians.
The lack of overall transparency with how AI algorithms work is a barrier to humans trusting and accepting these tools. It highlights the need for a robust approach to the development, training, testing and reporting of AI algorithms in healthcare.
Reporting guidelines for predictive analytics in orthopaedics
One of the other key advancements helping drive improvements around the potential clinical integration of AI based predictive analytics is the formation of associated development and reporting guidelines.
The Clinical Practice Integration of AI (CPIAI) framework11 is one proposed application using the IDEAL principles12 of surgical innovation to AI applications in T&O. It identifies the steps required from the beginning of an AI based research proposal through to eventual clinical deployment and includes six stages:
• Stage 0 – Concept outline
• Stage 1 – Algorithm development
• Stage 2a – External validation
• Stage 2b – Prospective assessment
• Stage 3 – Clinical impact assessment (Randomised Controlled Trial)
• Stage 4 – Implementation and model surveillance
The majority of current work in T&O using AI based predictive analytics falls into stage 1, with very few progressing beyond this to build the evidence base for necessary regulatory approvals and eventual clinical practice integration13. The application of NLP for prediction of selection for hip and knee arthroplasty surgery has previously demonstrated the importance of external validation in the accurate assessment of predictive capability, given a significant drop in model performance when tested on new external data sources14
Another key aspect to the development of AI based predictive analytics is the use of reporting checklists. These serve not only as guidance to researchers who are developing AI algorithms, but also provide for a robust system of assessment of quality and diligence. Several reporting checklists have been developed specifically for AI applications for various research methodology, including predictive analytics15-18
The main checklist in this regard is the Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis AI (TRIPOD+AI) statement15, which was published by Collins et al. following a modified Delphi process. This checklist establishes 27 criteria across the domains of study title, abstract, introduction, methods, results and discussion.
One of the key changes to the original TRIPOD guidance is an emphasis on the importance of fairness in the evaluation of AI. Points considered include evaluation of model performance based on key subgroups (for example different sociodemographic profiles which will vary dependent on the target application), as well as reporting standards that include patient and public involvement, and open science principles. The development of the associated Prediction model Risk Of Bias ASsessment Tool (PROBAST+AI) is still underway and will further help delineate assessment of the quality and risk of bias in prediction models16
Other checklists such as the Developmental and Exploratory Clinical Investigations of DEcision support systems driven by Artificial Intelligence (DECIDE-AI)17 and Consolidated Standards of Reporting Trials-Artificial Intelligence (CONSORT-AI)18 statements are also important in relation to further improving and reporting predictive analytics, particularly as a research proposal moves towards clinical practice integration (CPI-AI stages 2b and 3). The DECIDE-AI checklist particularly focuses on early-stage clinical evaluation of AI systems, including predictive analytics and includes 17 specific reporting items with a particular focus on proof of clinical utility, safety, and human factors, in preparation for large-scale trials. The final consideration is the CONSORT-AI statement that covers the conduct of Randomised Controlled Trials related to AI interventions and adds a further 14 new checklist items to the original CONSORT statement.
These reporting standards, when added to the CPI-AI framework, can provide a clear pathway for safe and evidence-based development and deployment of predictive AI in T&O.
Conclusion
This article has highlighted the challenges around analysing the huge amount of NT data produced by personal and other electronic devices which could help with patient care. Newer methods of AI, capable of dealing with such huge amounts of varied data have been described. Safeguards about using and reporting the use of AI models in healthcare have been explained. The importance of these cannot be underestimated to help improve the quality of research and assist the future integration of predictive AI into clinical practice. n
References
References can be found online at www.boa.ac.uk/publications/JTO


Advanced Clinical Practitioners in arthroplasty care
Catherine Armstrong and Rachael Daw

Catherine Armstrong qualified as a Physiotherapist from the University of Ulster and worked as a Physiotherapist before going on complete a PhD at Manchester University. Catherine has worked in physiotherapy and advanced clinical practice for over 30 years, specialising in arthroplasty care. She was the president of the Arthroplasty Care Practitioners Association (ACPA) from 2020-2022. She currently works as a Consultant Therapist in arthroplasty and lower limb MSK at Liverpool University Hospital Foundation Trust.

Rachael Daw trained as a Physiotherapist at the University of Liverpool and worked for the NHS for nearly 20 years, specialising in care and surveillance for upper limb arthroplasty. Rachael completed a Master’s degree in Advanced Practice in Healthcare in 2016 and went on to be a lecturer in Advanced Clinical Practice at the University of Liverpool, before joining the RCP in 2022 where she is now a Senior Educationalist.
Over the last decade, demand for joint arthroplasty surgery in the UK has increased significantly. In many centres, Advanced Clinical Practitioner (ACP) roles, typically fulfilled by specialist nurses or physiotherapists, have been developed to alleviate service pressures and enhance outcomes for the growing number of patients undergoing arthroplasty surgery. ACPs in arthroplasty care are involved across the entire patient journey, requiring expertise across the four pillars of advanced clinical practice.
The National Joint Registry for England, Wales and Northern Ireland (NJR) has recorded significant increases of hip, knee and shoulder replacements over the last decade1, trends which are also reflected in the Scottish Arthroplasty Project2 Increasing numbers, coupled with pressures on services, have meant that new models for providing care for these patients are
essential to improve equitable access to services and reduce waiting times.
Arthroplasty clinics where ACPs substitute for surgeons for routine post-operative care, were originally pioneered in the UK in the 1980s and have since been replicated worldwide with the aim of reducing pressure on surgeon-led services. Evidence suggests that these ACP clinics are safe and effective, and patient satisfaction is equal to that for surgeon-led clinics3-6. Most ACP led clinics have primarily targeted patient cohorts undergoing lower-limb arthroplasties, however more recently specialist ACP-led services for shoulder and elbow arthroplasty have developed to meet emerging demands.
ACP-led arthroplasty care is largely fulfilled by advanced practice physiotherapists and advanced nurse practitioners3,4, as illustrated by the membership of the Arthroplasty Care Practitioners Association (ACPA)7, see Figure 1.

Figure 1: Arthroplasty Care Practitioners Association (ACPA) Membership by parent profession.




To our knowledge, there are no studies that have investigated the relative advantages of either of the parent professions, and the decision of who to employ in these roles would appear to be dependent on the local service requirements. Regardless of parent profession, the role domains of the ACP in arthroplasty care including clinical practice, leadership, research, and education and professional development4 define a skill-set clearly commensurate with the four pillars of Advanced Clinical Practice set out in the Multi professional Framework (MPF) for Advanced Clinical Practice8.
Clinical
practice
Pre-operative care
Post-operative inpatient length of stay has decreased significantly in recent years due to the evolution of rapid recovery protocols. These protocols place a greater burden on service requirement for pre-operative care to ensure that timely and safe discharge will be possible. In many UK centres, ACPs are often responsible for pre-operative assessment of patients to evaluate their fitness for surgery, provide necessary education regarding procedures and post-op protocols, make referrals for post-operative care packages and rehabilitation, and support discharge arrangements. In some centres (with appropriate training) ACPs may also consent patients for surgery.
Peri-operative care
In 2012, the Peri-operative Care Collaboration defined roles for non-medically qualified professionals including Surgical Care Practitioners (SCP)9. SCPs are registered healthcare professionals who have extended their scope of practice to work as members of the surgical team. Under the supervision and direction of a consultant surgeon (but not independently) they can perform surgical intervention in addition to pre-operative and post-operative care10. Currently the extended role of the SCP continues to develop and may be fulfilled by ACPs.
As with all ACP roles, SCPs must ensure that they remain within the limits of their
competence, skill, and experience11,12 and within their scope of practice where this has been defined. ACPs must therefore have the requisite experience and education to demonstrate satisfactorily their competency in the appropriate areas of surgical practice.
Post-operative care
ACPs contribute to all stages of postoperative care from early review to long-term surveillance. The role of the ACP includes patient assessment, physical examination and ordering routine imaging as well as any additional investigations such as blood tests or ultrasound scans. ACPs can also facilitate effective communication between the surgical team and other healthcare providers and, where they have evaluated the need, referral to other services.
infection and aseptic prosthetic loosening. ACPs can effectively identify when patients need orthopaedic consultant review, and therefore have the potential to initiate early investigation and treatment of complications3,5. Effective management of patients with identified complications relies on clear and efficient pathways between the ACP and consultant services.
Research
As well as the opportunity to review clinical progress, clinical encounters offer an opportunity to evaluate outcomes and collect data14. ACPs in arthroplasty care are often responsible for essential data collection, contributing to clinical trials and working with industry and joint registries to inform evaluation and development of prostheses and procedures. Data collection might include a variety of objective clinical measurements and patient reported outcome measures (PROMS) which the arthroplasty ACP must be competent in implementing and evaluating. The ACP may also inform patients about potential research projects, consent patients for participation and collect data for research outcomes. To support this the ACP must have knowledge and competency with research procedures, ethics and governance, requiring training such as the NIHR’s Good Clinical Practice15
Education
To independently fulfil the service and care requirements of patients undergoing arthroplasty surgery ACPs require advanced clinical skills and expertise in relevant musculoskeletal assessment, along with evaluation of investigations. Specialist training in image interpretation is often a requirement for individuals undertaking such roles. Currently in the UK there is no specified or standardised educational route to competency in the specialised skills required for ACP in arthroplasty care, however, ACPA have developed a competency framework, that may provide guidance on training for the role, and also run bespoke image interpretation courses to facilitate practitioner learning7

One of the key purposes of long-term review clinics in arthroplasty care is to identify complications, particularly in asymptomatic patients and instigate risk management as necessary13. It is therefore vital that the ACP working autonomously in this scenario understands the scope of normal presentations and the presentation of possible complications, which may or may not be symptomatic, including
The Multi–Professional Framework for ACP8 promotes an advanced skill set encompassing four pillars of advanced practice which should be at Masters Level or equivalent. Self-awareness and reflection are essential for the individual to recognise their own learning needs to satisfy the specific requirements of their role. Supervision from experienced colleagues and support for continued professional development are also critical for developing the novice to meet the ACP requirements and for sustained development throughout their career. Voluntary membership of special interest groups can also provide networking and development opportunities, educational and support (see Table 1).
Experienced arthroplasty ACPs are experts in the field with breadth and depth of clinical and professional knowledge related to their area of practice. Due to their unique position, working almost exclusively with a specific patient cohort, these ACPs rapidly gain extensive ‘patient mileage’ and are at the forefront of clinical and policy developments, making them well placed to offer education and advice to patients, junior colleagues, and the extended MDT. >>
Figure 2: The Four Pillars of Advanced Clinical Practice, HEE 2017 8 .
Arthroplasty Care Practitioners Association (ACPA) https://acpa-uk.net/ Association of Surgical Care Practitioners (ASCP) https://www.aoscp.co.uk
British Orthopaedic Association
British Hip Society
https://www.boa.ac.uk/
https://britishhipsociety.com/
British Association for Surgery of the Knee https://baskonline.com/ British Elbow and Shoulder Society https://bess.ac.uk/
The Centre for Advancing Practice
https://advanced-practice.hee.uk/

Leadership and management
The ACP with responsibility for arthroplasty clinics must ensure that the services offered are in keeping with local and national guidelines and that patients can make contact with appropriately skilled professionals in the right place, at the right time.
It is acknowledged that leadership is not just about service management, but should also encompass clinical and professional leadership, as well as leadership in health policy and health systems16. In the arthroplasty community there are several examples of ACP-led regional and national developments and contributions to national policy demonstrating the potential impact of this influential group of professionals.
Future developments and challenges
There is ongoing debate in orthopaedic communities regarding the long-term follow-up of patients following arthroplasty surgery, in terms of the frequency, duration, location and personnel involved in reviewing patients, and recent guidelines from the National Institute for Clinical Excellence (NICE)17 were inconclusive in providing firm recommendations. Despite these challenges, it is understood that follow-up is essential and ACPs can have an important role in providing efficient best quality services for patients. For many years there has been a move towards providing a virtual clinic model for routine arthroplasty follow-up care14. This enables patients who have uncomplicated arthroplasty to have a remote appointment, and X-ray, without attending for a face-toface consultation. ACPs are ideally placed to provide this virtual link and to provide a triaging portal for patients to get in touch if they have concerns.
Conclusion
Advanced practice roles in arthroplasty care have been long established and are frequently fulfilled by nurses or physiotherapists. The ACP in arthroplasty care will require a skill set that encompasses expertise across all four pillars of the HEE framework8 and in many cases will develop beyond the level of expert to influence patient care. The ACP is integral to patient experience throughout all stages of their journey and will continue to be vital to the delivery of efficient and cost-effective services as they evolve in the future. n
References
References can be found online at www.boa.ac.uk/publications/JTO
Figure 4: Jenna Bardsley, Advanced Physiotherapy Practitioner, performing objective strength test with dynamometry on a shoulder patient in arthroplasty clinic.
Table 1: Special interest groups and societies to support the ACP in Arthroplasty Care.

BOA members visit and support East Africa
Adil Ajuied, Mark Bowditch, Pranai Buddhdev and Nick Bowman

Adil Ajuied is a Consultant knee surgeon at Guy’s & St Thomas’ London. While on fellowship in South Africa, Adil had the opportunity to deliver charitable medical care alongside his fellowship. It was this time that inspired him to seek out new opportunities to support developing word orthopaedics in Tanzania.

During their visitation, the team spent most of their time at the Muhimbili Orthopaedic Institute (MOI) in Dar es Salaam, Tanzania, in addition to visiting the Mnazi Mmoja Referral (MMR) hospital in Zanzibar and an orphanage for blind children during their stay.
MOI is the national reference centre for orthopaedics for both Tanzania and East Africa performing 30-40 major cases per day receiving consultant-fellows for advanced training internationally from much of East Africa, including South Sudan, Kenya, Uganda, Zambia, Malawi, and Rwanda. The institute is a Sign Nail training centre, as well as representing the only Multi Trauma Centre in the country. MOI also delivers elective services, in addition to being a tertiary centre for subspecialties such as paediatrics, arthroplasty, sarcoma, neurosurgery and sports medicine.
What was the goal of the project?
The aim of the group was to deliver specialist clinical care, not usually available, via a local tertiary hospital through direct surgical care, education and training, as well as making a substantial donation of implants and equipment. Simultaneously, and most critically, the group aimed to leave a legacy of enhanced care and ongoing clinical and educational engagement.
The group were aware that within the space of orthopaedics and trauma, there is significant need throughout East Africa, and while much of this need is trauma, the area less frequently focused upon is elective orthopaedics. Furthermore, it is well established that the regions demand far out strips the resources available.
In an attempt to match the clinical strength of the group to the local needs, and therefore

Mark Bowditch is a Consultant Orthopaedic Surgeon East Suffolk North Essex NHS FT Trust and is the BOA Vice President.
Top left to right - Elizabeth Turp, Andrew Pearse, Adil Ajuied, Stephen Dugmore, Martin Goddard, Pranai Buddhdev, Nick Bowman. Bottom left to right- Michael Risebury, Giles Heilpern, Jo Dartnell.

Pranai Buddhdev is a Consultant paediatric orthopaedic surgeon at Mid & South Essex NHS Trust and a member of the BSCOS Education Committee. Pranai is on the Executive board of the Hip Hope Network, an international organisation promoting paediatric hip health worldwide and has a keen interest in promoting global paediatric orthopaedics and improving health infrastructure in Tanzania.

Nick Bowman is a Consultant knee surgeon and works in Tunbridge Wells in Kent. He has a passion for delivering medical care and teaching in developing counties and has worked in Ghana, Malawi and most recently Tanzania.

maximise clinical impact MOI was identified as the ideal host institution. While being the national tertiary reference centre, clinical demand out striped the available resources and equipment. Furthermore, it was very clear early on during their engagement and interaction, that there were outstanding and highly talented local consultants surgeons with the potential to be up skilled.
In preparation for the group visitation, two members of the group conducted a pre-visitation site assessment in 2022. It was during this visit that the team first had the opportunity to assess the clinical needs of the local population, the key resources requiring donation, and critically began the process of building the friendships and relationships with local clinicians and hospital management that would allow for the surgical visitation in late 2023.

We in the UK, and wider western medicine, are accustomed to exhaustive educational and training opportunities through conferences, instructional, dry bone and cadaveric courses. These resources are not available through East Africa, and the cost of travelling abroad to access this education training is prohibitively expensive.
Who went?
The group was comprised of eight BOA-Home Fellow Consultant orthopaedic surgeons and two members of senior Smith & Nephew staff who made an invaluable contribution by way of project management and technical support.
Martin Goddard Wimbledon
Giles Heilpern Kingston
Andrew Pearse Worcester
Michael Risebury Basingstoke
Stephen Dugmore UK
The consultant surgeons (St Roch Society) were drawn from across the UK, six of whom primarily specialised in knee surgery, and, two paediatric orthopaedic surgeons. The group have been established approximately 10 years earlier, focusing primarily on education >>
Donations arrive at the Muhimbili Orthopaedic Institute.
Donations inventoried and packed at storage depot in north London.
Table 1: Members of the St Roch Society.
Surgeons
Adil Ajuied London
Pranai Buddhdev Broomfield
Nick Bowman Tunbridge Wells
Jo Dartnell Tunbridge Wells
Smith & Nephew Project Team
Elizabeth Turp UK

and training. It was during one of these educational meetings that a member of the group, Nick Bowman, presented on his personal experience of having worked in Malawi. It was this presentation and subsequent discussions that planted the seed for the Tanzania visitation.
The surgical team identified very early on that given the nature of the clinical care and education they hoped to deliver, project management and technical support was going to prove essential. The group turned to their primary industry partner, Smith & Nephew, and saw Elizabeth Turp, and Stephen Dugmore join the team. It was noted by the surgical team that the contributions of Elizabeth and Stephen were invaluable both in the pre-departure planning and equipment donation phase, as well as on the ground during the visitation.
What did they do?
Once the team had completed their assessment of the equipment and implant needs, donations were sought in the UK, collected and inventoried before being shipped to Dar Es Salaam. Donations were gratefully received from industry, hospitals, and charitable sources (Table 2).
Smith & Nephew
Hospital Innovations
OSSUR Orthopediatrics
Fortius Clinic
Guy’s & St Thomas’ hospital NHS trust
Broomfield hospital NHS trust
Royal Tunbridge Wells NHS trust
Vista Orthocycle

These donations included, but were certainly not limited to; three fully equipped arthroscopy stacks, shaver systems, fluid pumps, surgical instrument sets, trauma and sports implants, simple and advanced negative pressure dressings, knee braces, ankle boots, TLSOs, clutches and personal protective equipment. The volume of goods required an entire shipping container for dispatch, and were valued at approximately £1.5-2 million. The shipment received all the requisite UK and Tanzanian regulatory clearances and exemptions prior to dispatch.
Prior to departing for Tanzania, the group arranged multiple remote Zoom calls with the local clinical team at MOI, which allowed the teams to review cases and discuss clinical workload as well as planning daily schedules of activities etc. This also gave the respective teams an opportunity to establish and build relationships.
Upon arriving at MOI and following a short orientation and induction, the UK team quickly established a daily routine and programme. These would begin at 7am with a Trauma meeting, followed by a daily orthopaedic grand round seminar where two to three lectures

were delivered and lively Q&A Sessions were enjoyed by all.
The teams would then divide into pairs and proceeded to theatres, ward rounds, or clinic. The teams would deliver two to three operating lists per day, completing approximately six to nine procedures per day. Every day ended with a round-table debrief of both the successes, as well as any challenges faced and strategies were put in place to enhance the next day’s activities.
The highlight of the trip?
The group report that they found the entire trip spectacularly rewarding and fulfilling and that it is so difficult to pick out any one particular highlight. However, one day does standout for the group members, which interestingly occurred away from the hospital.
Over their first weekend, they had the opportunity to go and visit and support a >>

Michael Risebury on the visit to orphanage.
Giles Heilpern examines a patient in clinic.
Martin Goddard leading a grand round meeting.
Andrew Pearse and Nick Bowman, reconstructing a multi-ligament knee injury.



local orphanage for blind children and those with disabilities, (The Sathya Sai School and Orphanage). During this visit, the group members made a charitable donation and distributed toys kindly donated by one of their benefactors. Since returning to the UK the team have maintained links with the orphanage, and continue to support their amazing work.
What where some of the takeaways?
Andrew said, “Tanzania is very under-resourced in terms of healthcare. It’s a desperately poor country and they have no funds for medical equipment and implants. In all my years as a surgeon, I’ve never

had to use domestic equipment in an operating theatre setting, however this is routine at MOI. MOI is a specialist orthopaedic hospital and treats people from across the entire country and neighbouring countries. They are amazing people and it was rewarding and humbling to be able to make a contribution.”
Giles commented, “The gratitude of the patients they treated and the doctors they trained and collaborated with was overwhelming. They have so little and yet achieve so much. Everything is reused including such simple things as scalpel blades. We take for granted the abundance of resource that we have here. I sincerely hope that as well as treating some patients our education and training contribution will lead to the better treatment of many more. And note to self – ‘I will endeavour to never again complain about lack of equipment’. We do not appreciate how fortunate we are! Many thanks to all those that supported this trip.”
Martin said, “The challenges the group encountered were immense but the resilience and determination of the local clinicians inspired him every step of the way. The gratitude and relief on the faces of our patients, young and old, were immeasurable. It was a humbling experience to witness the transformative power of healthcare, as we saw hope being restored and lives being changed for those less fortunate.”
What are plans for the future?
Since their return to the UK, the group has held almost monthly virtual MDT meetings with their Tanzania colleagues, and continue to be in regular dialogue. The group has also been able to secure donations to fly in three of the consultants from MOI, for a

UK visitation, during which they will attend multiple cadaveric mini-lab courses, and will have the opportunity to visit multiple UK orthopaedic centres where members of the St Roch Society work. This will be a unique educational and training opportunity for these Tanzanian colleagues and will be their first trip to Europe.
Members of the group will be returning for a further visit in July 2024, and the group will also be contributing faculty to the second East African Arthroscopy Course in July 2024. n

Donated Pico dressing applied to tibial wound, in patient with osteomyelitis.
Muhimbili Orthopaedic Institute’s originally had only one arthroscopy stack, which utilised a PC monitor as a screen.
One of three new stacks donated to Muhimbili Orthopaedic Institute.
By the end of the visitation, the local theatre staff had nicknamed the stacks!
Arthrosamid® — The first and only synovial scaffold2,3administered via a single injectable for long-lasting pain relief.4,5


Proven1 Pain relief treatment1

Statistically significant reduction in pain maintained at 3 years.4,5 Learn more about our reproducible results here by scanning the code.


References: 1. Arthrosamid®, Instructions For Use. Release Date March 2022. 10082-003; 2. Christensen, L., et al. (2016). Histological Appearance of the Synovial Membrane after Treatment of Knee Osteoarthritis with Polyacrylamide Gel Injections: A Case Report. Journal of Arthritis. Vol 5: 217; 3. Christensen, L., et al. (2016). Synovial incorporation of polyacrylamide hydrogel after injection into normal and osteoarthritic animal joints. Osteoarthritis and Cartilage. Vol 24(11):19992002. DOI:10.1016/j.joca.2016.07.007; 3. Data on file; 4. Bliddal, H., et al. (2023) A Prospective Study of Polyacrylamide Hydrogel Injection for Knee Osteoarthritis: Results From 3 Years After Treatment. Osteoarthritis and Cartilage. Vol 31(5): 682-683; 5. Bliddal, H., et al. (2024) 3 year follow-up from a randomized controlled trial of intra-articular polyacrylamide hydrogel injection in subjects with knee osteoarthritis. Poster LB-31, OARSI 2024 World Congress on Osteoarthritis.





Peter Brownson is a Consultant Orthopaedic surgeon based in Liverpool. He specialises in shoulder and elbow surgery and he is a past President of BESS. Over the last 25 years, he has treated elite athletes from a wide range of sports and he was the upper limb surgeon for Liverpool Football Club from 2000 to 2017. He serves as an Expert Witness for McCollum Consultants.

David Spencer is a partner in Clyde & Co LLP. With over 20 years of experience in litigation, specialising in a wide range of catastrophic and fatal injury claims, David also heads our sports practice group. He is responsible for coordinating our sports law offerings across insurance, claims and risk, and regulatory. David is also the appointed panel solicitor for liability claims involving the UK Governing Bodies of two and four-wheeled motorsport. He is a member of the Forum of Insurance Lawyers (FOIL) Sports Law Sector Focus Team.
Professional insurance when treating elite and professional athletes
Peter Brownson, David Spencer, Andrew Wallace and Nigel Jones
The terms ‘elite’ and ‘professional’ are commonly used to refer to individuals with the potential to earn money from sport, media or endorsements.
The treatment of such elite and professional sports people is recognised as an area of particular risk when it comes to clinical negligence claims. There are several reasons for this.
Firstly, athletes may have a higher earning capacity when compared to the average patient. Secondly, the impact of a minor injury may be disproportionately significant. Thirdly, third parties such as professional clubs or sponsors may have a stake in the sportsperson’s wellbeing.
With regard to professional indemnity insurance for doctors involved in the treatment of professional athletes, the first point of reference may be the GMC professional guidance of indemnity which states: “The GMC requirement is to hold ‘adequate and appropriate insurance or indemnity arrangements in place covering the full scope of your medical practice... for liabilities that arise from your practice as a doctor whenever a claim is brought’.”
In terms of what constitutes adequate and appropriate to the GMC, they state that “the law says appropriate cover is cover against liabilities that may be incurred in practising as a doctor having regard to the nature and extent of the risks of practising as such.”
Whilst this GMC wording is a good start it does not necessarily help us to the extent necessary when considering the level of cover required when treating an elite athlete. Perhaps more pertinent guidance can be found within the Faculty of Sport and Exercise Medicine’s professional code Section1.71: “You must ensure that you have adequate indemnity protection against damages, claimants’ costs and defence costs relating to a claim brought by a patient’s employer, club, agent, sponsor or event organiser in relation to alleged negligent treatment of a patient.”
This statement highlights two important points: firstly, it is essential for doctors treating elite and professional athletes to recognise that not only may claims from professional or elite athletes be of a higher value than those from the average lay person, and secondly that there is every possibility that the doctor will not only receive a claim from the patient but also from the club whose asset has been damaged, players agent, sponsors etc. This is referred to as third party cover. In other

Andrew Wallace has worked exclusively in shoulder surgery for over 25 years and has been at the forefront of the development of arthroscopic techniques for the management of shoulder instability, cuff tears and arthritis with a particular interest in elite athletes. Following training in Australia, Scotland and Canada and academic posts at Imperial College and in the NHS, he was a founding member of the Fortius Clinic in London. He has extensive experience in dealing with athletes from international and premiership rugby and football, as well as cricket, martial arts, equestrian and other disciplines within sport.

Dr Nigel Jones is a Consultant in Sport and Exercise Medicine and works at Spire Liverpool Hospital and Rehab 4 Performance. He is the current Chief Medical Officer for British Cycling and Prior to this he was Doctor to the England Men’s Senior Rugby Union Team. He has also worked at Liverpool Football Club, the English Institute of Sport, and the British Boxing Board of Control. Nigel is a former Chair of Education for the Faculty of Sport and Exercise Medicine (FSEM), and the British Association of Sport and Exercise Medicine (BASEM). Nigel has many years’ experience as an Expert Witness in Sport and Musculoskeletal Medicine.

words, medical malpractice insurance as opposed to professional indemnity insurance is additionally required to respond to a claim from a third party such as a football club.
Historically, such third-party cover has not been provided by providers of medical indemnity. To quote from the Medical Protection Society website, “our advice to specialists/consultants treating sports people for injuries incurred during the course of their employment is to ensure that they conduct themselves in such a way that the duty of care is limited to the patient and not to the patient’s employer. In order to minimise the liability, we strongly advise members who treat elite or professional athletes that they should:
• Not enter into a written or oral contract with a third party (i.e. someone who is not their patient) to treat the professional or elite sportsperson for reward.
• Only accept referrals from other independent healthcare professionals, and not from clubs directly or from healthcare professionals working for them.
• Address any professional fee notes to the patient and not a third party. If fees are to be settled by a third party, the patient should be asked to forward them on. Alternatively, written confirmation may be obtained from the patient that all fee notes should be sent to the club, employer or their medical insurers.
It is important to note that what constitutes a written or oral contract with a third party is not defined but factors that might be considered relevant would include hospitality, free match tickets etc. This issue was
highlighted in the case of West Bromwich Albion Football Club v El-Safty [2005] EWHC 2866 (QB). The claim related to negligent advice and subsequent unsuccessful knee surgery performed by the defendant Consultant Surgeon on a West Bromwich Albion (WBA) player. WBA claimed ’millions of pounds’ in damages from the Defendant for the losses which it alleged it had suffered in consequence of his negligence; the loss of value of the contract, the cost of replacing him and lost wages. The action was brought both in contract and in tort. The Defendant denied there was a contract with WBA and denied he owed any duty to WBA in tort. The existence of any duty in contract or tort was tried as a preliminary issue. The Court at first instance found that there was no contract between WBA and the Defendant as WBA’s physiotherapist had referred the player to the Defendant as a health professional, as opposed to instructing the Defendant for reward. The claim for a liability in tort also failed. WBA unsuccessfully appealed to the Court of Appeal (see [2006] EWCA Civ 1299).
As an aside, the player concerned issued his own separate claim for damages of c. £7 million against the same defendant (Appleton v El Safty [2007] EWHC 631 (QB)). The negligent advice was admitted and the Court awarded damages of £1.5 million on consideration of expert quantum evidence.
The area of third-party cover came under further scrutiny and entered the public domain in 2019 when Sunderland Football Club attempted to sue their club team doctor for £13 million. In response, the doctor pursued a counter-claim for an indemnity / contribution against the club’s former physiotherapist >>
© Nigel Jones

and doctor. The claim related to an alleged failure by the club doctor to raise concerns about a player’s chronic knee issue at a signing on medical. Although subsequently the claim and counter claims were abandoned, it highlighted the potential issues facing doctors treating professional athletes.
Whilst the vast majority of orthopaedic surgeons will not be employees of a particular elite sport organisation e.g. a football club, some ‘Club Doctors’ will be. It is imperative that these doctors establish what vicarious liability cover is provided by their employer, and what is not. Those on a service level agreement will have no vicarious liability cover.
Arranging appropriate cover may be relatively straightforward, however, what of adequacy?
As the previous summary identifies, multi-million-pound claims for damages from ‘average’ athletes (Mr Appleton was described in his litigation as a footballer with a ‘low profile’) are not uncommon.
Damages for the injury itself (general damages for pain, suffering and loss of amenity) may be the least expensive part of the claim, however the claim can (and will) be developed to include loss of income, loss of potential income, loss of bonus (personal and club), loss of sponsorship, loss of benefit of sell on clauses, lost opportunity in management and even punditry.
In addition, claims inflation is an ongoing concern in the insurance industry, where all
claims are more expensive, year on year. The concern might not necessarily be when the next Mr Appleton makes a claim, but when the claimant was going to be the next Ronaldo, McIlroy, or Hamilton.
And damages are only one element; “ … You must ensure that you have adequate indemnity protection against damages, claimants’ costs and defence costs.”
In complex claims, as professional athlete claims can often be, the claimant’s litigation costs might reasonably exceed £1 million, and the costs of defending a claim to trial is unlikely to be too far behind.
So, how much indemnity is enough?
Dedicated medical insurance schemes have been developed that provide additional levels of protection in terms of level of medical indemnity (up to £20 million rather than the more usual £10 million) and third-party liability. Probably the most well-known of these is provided by SEMPRIS but other schemes do exist.
However, when taking out professional indemnity through such schemes, it is important to note that the increased level of protection comes at a price. Firstly, the costs of such indemnity are increased. Secondly, professionals undertaking the treatment of professional athletes may subsequently find that they are effectively locked-in to the same insurance provider, even if they
cease treating professional athletes, as new insurance providers may be unwilling to provide retrospective cover for athletes treated previously or at the very least will require details of all professional athletes treated previously together with a log of previous claims.
In summary, it is essential that surgeons check with their insurance providers that they have both appropriate and adequate cover before commencing treatment.
The treatment of elite athletes is extremely challenging for many reasons:
• The increased risk and size of potential negligence claims
• Exposure to third party claims
• Increased reputational risk for the surgeon
• Increased complexity of diagnosis and surgical treatment
• Increased urgency of diagnosis and treatment
Consequently, ideally, what are often highly complex or controversial decisions should be made in collaboration with colleagues, with the consent of both the player and the club/agent.
Finally, it is important to state that the increased risks and costs of indemnity cover should be reflected in the fees levied on the player/club for their treatment. n
© Nigel Jones

Designed for the extensive reconstruction of the hip and knee joint and based on over 20 years of clinical experience of the 1st generation USTAR system. The USTAR II™ system is part of the United Orthopedic family of products designed for difficult primary and revision interventions.
Lorem ipsum
Trauma and orthopaedic workforce – Challenges and solutions
William Allum

William Allum is a Consultant Surgeon at the Royal Marsden NHS Foundation Trust. He is a Council Member of the Royal College of Surgeons of England, Elected Trustee, RCS England Workforce and Training Lead, and Chair of the Intercollegiate Extended Surgical Team Board.
Planning the surgical workforce is one of the most difficult challenges to ensure the provision of a high-quality service, meeting not only the demands of patient care but also ensuring the conditions of work and maintaining the necessary levels of recruitment and retention. This edition’s subspecialty section describes the current state of the trauma and orthopaedic (T&O) workforce from the perspectives of a consultant, trainees and a member of the Extended Surgical Team (EST).
It is very easy in such presentations to describe the negative aspects but all authors have successfully identified solutions to the challenges which face everyone. There are a number of themes which are common in all four articles and reflect the constraints which are resource related. However, there are some very positive suggestions which show from their experience how job satisfaction can be achieved despite the constraints.
By way of background, the Royal Colleges of Surgeons 2023 census provides details on demographics, working activity and working conditions. T&O faces challenges with regard to recruitment as the numbers of trainees joining training do not meet the numbers of surgeons retiring. T&O consultant surgeons are very busy and many are working frequently, or always, beyond contract. Unfortunately many surgeons are struggling with burnout challenges reflecting both the workload and conditions of service. Many trainees are struggling to gain the necessary technical competence and experience which has an inevitable impact on the confidence of the newly appointed consultant.
These themes are supported by the comparative surveys which BOTA did in 2019 and in 2022 before and after the pandemic. Adrian Andronic and Karen Chui have very clearly identified the key challenges for trainees. These are increasing training
opportunities, the appointment of a lead employer, opportunities for flexible working, opportunities for working out of programme and ensuring wellbeing. They have provided solutions such as experience of elective surgery in the independent sector, expanding access to simulation, flexible working and the potential benefit to encourage a higher proportion of women to join T&O as well as opportunities to work overseas to consolidate clinical experience.
Marc Patterson has provided a very insightful view based upon his own career. His extensive experience of a very busy clinical practice has underpinned his work and indeed has continued into his later years after ‘retirement’. He does however stress the importance of pursuing opportunities for activities such as examining and both internal and external management roles to compliment a busy clinical practice. He rightly points out that this flexibility maintains job satisfaction. He also provides very sensible advice on coming to terms with retirement and appropriate planning which combines working to suit the individual interlinking with outside interests.
The theme of this year’s annual meeting is the T&O workforce in general which includes the EST. Sally Stuart has described the background to the development and training of Surgical Care Practitioners and their very important role in supporting the service as well as providing their experience to facilitate training opportunities. This in the context of the current debate on the role of Physician Associates which she has clearly explained focussing on the different contributions of the members of the EST according to their scope of practice.
These perspectives have provided a very valuable insight into their different experiences and I think the authors have given helpful advice to aid job satisfaction for all across the T&O workforce. n




HELP SHAPE THE FUTURE OF ORTHOPAEDICS WITH US


About us
The National Orthopaedic Alliance (NOA) is a membership organisation that leads on collaboration in orthopaedics.
We are multi-disciplinary and bring together orthopaedic providers from across the UK.
Our aim is to support the delivery of consistent, high quality care for patients nationwide.





Discover NOA’s range of member benefits and help shape the future of orthopaedics with us.

info.noa@nhs.net
@NOAorthopaedics
Scan QR code to find out more nationalorthopaedicalliance.co.uk
Become an NOA member organisation
linkedin.com/company/noaorthopaedics
• We support member organisations to network, learn, share and shape the future of orthopaedics.
• We connect member organisations and foster collaboration across multiple disciplines in orthopaedics.
• We have a network of partners across the orthopaedic and MSK community.
• We have member organisations across the UK.


NOA Annual Members’ Conference 2025

• Work for an NOA member organisation and not yet registered for your FREE place to attend our next Annual Members’ Conference?
• Registration is now open for the event taking place in Birmingham on 15 May 2025.


• Don’t miss this opportunity to learn, network, and collaborate with colleagues across the orthopaedic community.
NOA ANNUAL MEMBERS’ CONFERENCE




Advancing the surgical workforce: trauma and orthopaedics
William Allum

William Allum is a Consultant Surgeon at the Royal Marsden NHS Foundation Trust. He is a Council Member of the Royal College of Surgeons of England, Elected Trustee, RCS England Workforce and Training Lead, and Chair of the Intercollegiate Extended Surgical Team Board.
In 2010, the Royal College of Surgeons of England undertook a census of all consultants working in England, Wales and Northern Ireland1. In the report, it was stated “current financial and organisational pressures within the NHS mean that the need for workforce planning is greater than ever. The NHS needs to be prepared for steep changes in the configuration of services and staffing requirements.” This statement is equally applicable now as back in 2011.
There have been a number of key events and factors which impact on the way in which we look at workforce planning. The continual adverse effect of winter pressures, coupled with the severe effect of the pandemic, both on the work force and clinical practice, and the challenges within the development of the NHS Long Term Workforce Plan,2 have all made it clear that in surgery we need to understand how the work force is working, the composition of the workforce, and the effect of conditions of work on the whole surgical team. It was within this context that the Royal College of Surgeons of England Workforce and Training Committee elected to undertake a census of the whole of the surgical workforce across the United Kingdom3
Methods
The aims of the census were to survey all members of the surgical workforce to inform workforce planning and to identify the key challenges facing the whole surgical team. It was designed to cover the whole of the UK and all specialties and all grades, including consultants, SAS surgeons, trainees, locally employed surgeons and the extended surgical team. It was undertaken by the business intelligence unit of the Royal College of Surgeons of England with the support of Royal College of Surgeons of Edinburgh and Royal
College of Physicians and Surgeons of Glasgow and the Surgical Specialty Associations. It was designed as an online survey with three domains. These were demographics of the whole surgical workforce, job plans and activity and working conditions linking to well-being and job satisfaction. The survey was questionnaire based with binary answers, drop down boxes and free text. The data has been analysed using Power BI (Microsoft) software which enables detailed interrogation of a large number of data items as well qualitative evaluation of free text comments. It has therefore been possible to identify specialty specific details which are herein described for trauma and orthopaedics (T&O).
Results
The census was completed in two months in 2023. There were 6,348 responses from the different members of the surgical team. This is estimated to represent approximately 25% of the current surgical workforce. Overall 54% of responses were from consultants, 25% from surgeons in training, 10% from SAS surgeons, 5% from locally employed surgeons, and 6% from members of the extended surgical team. In T&O there were 1,566 responses of which 59% were consultants, 23% surgical trainees, 8% SAS surgeons, 4% locally employed surgeons and 5% extended surgical team.
Demographics
The distribution by gender in T&O for consultants was 82% male and 18% female. For trainees this distribution was 67% male and 32% female. The distribution by age group is shown in Figure 1.
This distribution by age is similar to other specialties. Retirement planning is a key component of workforce planning and 31%
of consultants planned to retire in the next four years. This is considered to be earlier than initially planned by 37% of respondents. The data does suggest that there appears to be a net loss in staffing levels with more leaving the specialty than entering training.
Job planning and activity
The distribution of consultants by subspecialty is shown in Figure 2. The majority (19%) have a subspecialty interest in hip surgery including revision arthroplasty with the next highest preference being in knee surgery (16%).
The T&O workforce mainly works full time with 14% working less than full time. Just over 40% of consultants are contracted to more than 11 PAs with 56% working 1 to 1.5 SPAs. SAS surgeons are working similarly with 38% working 11 or more PAs and 68% 1 to 1.5 SPAs. Consultant job plans include two to four outpatient clinics weekly for 69%, with 35% undertaking two scheduled weekly operating sessions and 37% three scheduled operating sessions. SAS surgeons undertake similar proportions of clinics but in addition to the similar numbers of consultants undertaking two and three scheduled operating sessions, 20% are undertaking four scheduled operating sessions. These rates are higher than other specialties. The rise in revision arthroplasty has increased dual-consultant operating, largely reflecting experienced surgeons mentoring less experienced colleagues.
T&O is an acute specialty with 68% of consultants having an on call commitment (34% 1 in 5 – 1 in 8 and 38% 1 in 9 to 1 in 12). For SAS surgeons 78% have an on call commitment with 45% being resident when on call (36% 1 in 5 – 1 in 8 and 52% 1 in 9 – 1 in 12). When on call 64% are free from elective work reflecting trauma weeks which tend to occur every 6-8 weeks. The rate at which respondents always or frequently work beyond their contracted hours was 61%.
Working conditions and wellbeing
The census asked all respondents to select their top five challenges from a list of 10. The results for all for T&O are shown in Figure 3.
More than 50% of respondents cited pay and pensions, burnout and stress, access to theatre and working conditions as their main challenges. It is important to appreciate that the census was undertaken at the beginning of the industrial action by junior doctors and also as changes to pension arrangements had been announced by government. The rates of concerns amongst T&O of limited


access to theatre are equivalent to all other specialties. This reflects availability of surgeons, anaesthetists and theatre staff as well as infrastructure with the availability of operating theatres. The rate of burnout and stress is also very similar to all other specialties and this reflects the heavy workload with increasing waiting lists not the least because of the pandemic. Comments about burnout and stress are reflected in the earlier plans for retirement the high proportion of surgeons working beyond their contract and the net effect on family life with 39% not taking their full annual leave entitlement in the previous year.
Trainees and training
There were responses from 361 T&O trainees of whom 287 were higher surgical trainees and 74 in core training. Although a small sample, 62% cited access to theatre as one of their main challenges with the adverse effect on training opportunities. These limitations on training resulted in 64% citing burn out and stress as their highest challenge.
In the data for all surgical trainees 32% replied that they had considered leaving training in the previous year with the highest proportion (46%) being among core trainees. The main reasons for considering leaving training were burn out, working conditions, cost and length of training. In the specific question on the commonest responses for not recommending their specialty were lack of work-life balance, pay, lack of training opportunities and workload and working hours. There was overall frustration in the emphasis on service provision with less focus on training. Inefficiencies in the system particularly in turn-around times in theatre and short notice cancellation of training operating lists were highlighted. Therefore, trainees did not feel they were able to gain confidence in the breadth of procedures within the competence curriculum. The costs of training were also emphasised because essential courses were not covered by the study leave budget and reimbursement of upfront costs was an inefficient process. Overall trainees commented that training should be better managed with dedicated time for training and adequate on-call rota management to ensure fairness of service commitments. >>
Figure 1: Distribution of Consultations and Trainees in T&O by age.

Figure 2: Distribution of respondents by T&O Subspecialty.
Recommendations
The census has clearly shown a workforce that is struggling to provide a high quality service for patients as well as high quality training for future consultants. The recommendations from the census have been designed to provide solutions for the reported issues and have been presented as three aims. These are firstly to increase productivity to reduce waiting lists, secondly to ensure a sustainable surgical workforce and thirdly to change the way surgeons work. Waiting times are very much a systems challenge to address the problems of theatre access. Inefficiencies in the system including efficient scheduling, staffing numbers and ensuring successful implementation of the surgical hubs programme are short and medium term priorities. The Long Term
Workforce Plan has highlighted increasing numbers of consultants. Workforce capacity can also be increased by enabling consultants to work more efficiently by removing unnecessary duties which impact productivity. The census has highlighted that administration is a particular drain on consultant time which could equally be done by other members of the team. In addition to theatre work, effective transformation of outpatient work is required to ensure efficient elective recovery. This includes community clinics, one-stop services, teleconsultations and patient led review rather than traditional follow-up.
It is clear from the census that morale is low, reflecting the adverse effect of working conditions on well-being. For consultants and trained staff there needs to be better

understanding of current ways of working to improve working conditions. Variability in job planning should be readily available not only to support good clinical practice but also enable development in areas such as education training and management. For trainees there needs to be spread of best practice to ensure training opportunities are optimal. In addition, the facilities and overall support for trainees in the workplace need to be enhanced so that the surgical team is more effective. Specific initiatives such as job planning for trainees and more effective and user-friendly rota planning by trainees should be encouraged.
There is no doubt that there are challenges in ensuring surgery remains an attractive career option. The emphasis on service needs to be paralleled by an emphasis on training using every available opportunity. Trainers need to have time in their job plans to undertake dedicated training. The working lives of both trainers and trainees need to be improved as this will impact upon training experience and quality but also on job satisfaction. From the demographic details in T&O it is clear that the gender balance is shifting and there needs to be greater appreciation of less than full time working. It is also clear that there is a potential problem with more leaving than joining and measures should be clear about supporting retention of workforce as well as addressing support for those at the end of their careers who are both willing and able to continue working, supporting younger colleagues as well as the clinical service.
Conclusion
The census was designed to address a variety of topics in order to understand the composition of the workforce, the way it is working and the qualitative effect of working conditions. It has highlighted that there are common issues in T&O which are also present in other specialties. It has also identified specific challenges for T&O which need to be taken into consideration in future workforce planning to ensure maintenance of high quality patient care. n
References
1. Surgical Workforce 2010 – profile and trends. Available at: www.rcseng.ac.uk/standardsand-research/surgical-workforce-census/ workforce-reports-and-statistics
2. NHSE Long Term Workforce Plan. Available at: www.england.nhs.uk/publication/nhslong-term-workforce-plan.
3. Advancing the surgical workforce: 2023 UK Surgical Workforce Census Report. Available at: www.rcseng.ac.uk/standards-andresearch/surgical-workforce-census
Figure 3: Ranking of Top 10 Challenges.


25th November
•
•
•
•
•
•
•
•
•
•
•








Carry on working!
Marc Patterson

Marc Patterson was a consultant orthopaedic surgeon at University Hospitals Sussex NHS Foundation Trust for over thirty years working in Haywards Heath and Brighton, a level I Trauma Centre. Marc is an examiner for the Royal College of Surgeons of England (Past Chairman of the Court of Examiners) and is Chief Examiner and Secretary General of SICOT.
The work of a Consultant Orthopaedic Surgeon is a complex and satisfying role. But working for the NHS is similar to working for any huge organisation, i.e. very stressful and frustrating so within the structure of the consultant role, you have to find a way to make it work for you. You have to carve out your niche. The hamster wheel turns rapidly and, if you don’t crystallise your plan early in your career, middle age and retirement beckons quickly.
Retirement can be handled in three ways. You can retire early and sail into the sunset (literally) and never set foot in a fracture clinic ever again, you can work until you drop, or you can find a middle way which transforms your life as a satisfied surgeon to that of a satisfied retiree.
Early consultant years
After training in London and Singapore, I was appointed as a consultant in orthopaedics and trauma to the Princess Royal Hospital, a busy district general hospital in mid-Sussex in 1989. It was an active and efficient unit both for elective orthopaedics and trauma. On-call was never dull because of fast country roads and a challenging three lane main road from the end of the M23 to Brighton which encouraged daredevil overtaking, providing sufficient long bone fractures to keep up trainee’s operative numbers. Frank Horan was my senior colleague and the mentor that every new consultant needs. He was very active in politics, training and medical school circles (particularly with St Mary’s, hence the link

Helping to prepare a clinical skills station in MRCS.
with London trainees). He advised me to only undertake straightforward operations in my first year, avoid operating on staff members and to review my practice regularly and weed out procedures which plainly did not work well in my hands (this was long before regular appraisal and revalidation).
His main advice, and it is advice I have passed onto trainees ad nauseam, was to find a medical activity outside my normal day to day orthopaedic experience – examining, medical politics, sports medicine or joining international organisations etc. in an attempt to stay fresh, learn new skills and appreciate how other specialties worked, frequently leading to the realisation that everybody else was experiencing the same problems in the NHS, quite possibly worse than your own.
Becoming an examiner
you with a new perspective on education and assessment, the opportunity to meet and learn from surgeons all over the world and you might just leave a lasting contribution to the profession of surgery.
“Every exam I am involved in teaches me new skills, practices and knowledge and remains an important part of my continuing medical education. It is also a pleasure to have worked with hundreds of fellow examiners from around the world from different specialities and countries who remain lifelong friends and colleagues.”
With his encouragement and having established myself as a consultant, I became an examiner for the Royal College of Surgeons of England in the early noughties. The old FRCS was replaced by the MRCS and I became more involved in the development of the new exam, particularly communication skills, and subsequently became Chairman of the English Court. Through my connection with the MRCS, I was taken under the wing of Tony Hall and eventually took over from him as the SICOT (Societe Internationale de Chirurgie Orthopedique et de Traumatologie) Chief Examiner supervising the SICOT Diploma examination (MCQ & Viva) which was developed by him based on the FRCS.
Every exam I am involved in teaches me new skills, practices and knowledge and remains an important part of my continuing medical education. It is also a pleasure to have worked with hundreds of fellow examiners from around the world from different specialities and countries who remain lifelong friends and colleagues. Examining is also great fun!
I would therefore encourage all young established consultants to consider becoming an examiner. This challenges you, provides
In 2005 (16 years into my consultant career), Mid Sussex joined with the Royal Sussex County Hospital in Brighton creating a large teaching hospital with the new Brighton Medical School. I covered major trauma in Brighton for ten years before transferring to a weekend rota covering regular consultant-led emergency fractured neck of femur lists.
I originally had an eleven session contract (subsequently dropping one session to comply with private practice rules). This then converted to a PA contract with additional sessions to cover for management (clinical lead, MAC Chairman and BMA Consultants and Specialists Committee) and College Duties (Educational Supervisor, GP VTS work and AAC Consultant Appointments). I decided to remain on the weekend rota for a longer period than some of my colleagues because the nature of the weekend work ‘soaked up’ a number of PA sessions leaving me to continue undertaking my college work and private practice.
I continued contributing to my NHS pension under the 1995 agreement. I stopped contributing at the age of sixty as I was advised that further contributions would not be reflected in my final pension pot.
Working towards retirement
I retired at the age of 65 in 2018. I did not consider retiring and returning on a fixed term contract because (a) I didn’t want to be tied down to regular sessions and (b) the Trust didn’t want me to work on those terms! I wanted to continue working in orthopaedics for the NHS in some capacity but not full time. I therefore returned on the NHS bank after a one-month break having taken my pension. This gave me the freedom to plan my activities under my own terms and without the straightjacket of a fixed term contract. Under this scheme, I undertook NHS activity in terms of trauma ward rounds, virtual fracture clinics, fractured neck of femur lists, an element of elective hip and knee work and teaching and examining of medical students. I worked when I wanted, doing some regular work but mainly filling in gaps in the rota for leave or illness. I was available at short notice to cover gaps but if I was busy, on holiday or had other commitments, I just said no! Because I was still employed by the NHS, I was eligible for annual NHS appraisals. I continued in private practice during this period, stopping operating in 2022 but continuing outpatient and medico-legal work until this year. I continue to examine in the UK and abroad, sit on Consultant Advisory Appointments Committees and have been elected as Secretary General of SICOT so will have continuing orthopaedic input without challenging clinical work. >>

The Court of Examiners provides all the examiners for MRCS.

Bill Allum in the ‘Advancing the Surgical Workforce: 2023 UK Surgical Workforce Census Report’ details the problems facing the more experienced consultant1. 64% of 55-64 year old consultants plan to retire in the next four years because of unmanageable workloads, lack of time to teach and mentor, conflicts between clinical and management priorities, working beyond contracted hours, inability to take all annual leave and burnout and stress. NHS England in its 2023 paper on ‘Retaining doctors in late stage career advice’2 added health and wellbeing issues, work-life balance, caring responsibilities, pension concerns, concerns regarding performance, poor team culture and not feeling valued. Many of these concerns can of course be applied to professions other than medicine. The positive aspects of continuing to work include flexible working, adjusted clinical responsibilities, feeling supported and respected, job satisfaction, continued learning, new roles and the reduction of the impact of pension taxation.
I received one unexpected tax bill from the Inland Revenue because of the annual allowance fiasco but stopping pension contributions absolved me from further expense. From 1st April 2023, members
of the 1995 section who retire and return to the NHS can join the 2015 Scheme and build more savings. The lifetime allowance for tax-free pension saving was abolished and the annual allowance was increased meaning that for most NHS staff, pension tax charges will no longer apply. From 1st October 2023, members of the 1995 section can apply to take between 20% and 100% of their pension and carry on working, keeping pay and pension. To do this, members must reduce pensionable pay by 10%.
Phased retirement
Physical decline is often said to start at about 45 to 50 years of age but knowledge and experience are maintained far longer3 However, surgeons are terrible at selfassessment of their abilities. Rovit4 suggested three reasons why surgeons resist retiring – loss of self-esteem, fear of death and resistance to change. Surgeons’ daily work is full of excitement and responsibility. The transition from busy surgeon to retiree should therefore be gradual and allow for a personal shift in self-worth. Less on call and less complex operating is imperative but continuing orthopaedic work in a less intense atmosphere is just as rewarding and eases the transition to
full retirement. It also releases opportunities for new highly trained young surgeons. Some orthopaedic surgeons find more peace of mind by giving up their private practice first and continuing in the NHS in a different role as a senior consultant, for example mentorship.
Early planning for retirement is better both for finances and expansion of personal hobbies. Enough money, outside interests and knowing in one’s heart that self-worth is not dependent on being a doctor are all needed for successful retirement.
I don’t say that the pathway through my consultant career is right for all but it has worked for me!
1. Every new consultant needs a mentor and every old consultant should be a mentor!
2. Foster alternative interests in medicine outside your day-to-day NHS work role.
3. Medical examining can be very interesting, rewarding, exciting, educational and fun.
4. Plan for retirement early in terms of finance and outside interests.
5. A gradual reduction in clinical orthopaedic work (be that NHS or private) but retaining an interest in other orthopaedic activity makes the transition easier.
6. Continuing to work for the NHS after the age of 65 (in a different role) can be just as rewarding. n
References
1. Advancing the Surgical Workforce: 2023 UK Surgical Workforce Census Report. The Royal College of Surgeons of England 2024. Available at: www.rcseng.ac.uk/standardsand-research/surgical-workforce-census.
2. Retaining doctors in late stage career guidance. NHS England: Date last update 24 July 2023. Available at: www.england.nhs. uk/publication/retaining-doctors-in-latestage-career-guidance
3. Buckley R. The retirement conundrum: planning the end game and retiring gracefully. Bone Jt 360. 2019;8(4)1-3.
4. Rovit R. To everything there is a season and a time to every purpose: retirement and the neurosurgeon. J Neurosurg 2004;100;1123-9.
Executive Committee of SICOT.
BOTA rising to the workforce challenge
Adrian Andronic, Karen Chui, James Archer and James Allen

Adrian Andronic is an ST8 on the Yorkshire and Humber rotation and is the current BOTA Vice President. Adrian sits on multiple committees, including JCST, ISCP, and BOA Orthopaedic Committee. He has also served on the BOA Education and Careers Committee, RCSEng Learning Committee, and the HEE Training in the Independent Sector Committee. Adrian is passionate about medical education and is actively engaged in supporting trainees to achieve the highest standards of both training and clinical care, especially in light of recent challenges to training.
NHS England reports over 20 million people in the UK, almost one third of the population, have an MSK condition such as arthritis. By 2030, over 15.3 million people in the UK will be over 65 years of age, resulting in an ever-increasing demand on MSK services1
In the UK, there is a predicted net loss of staffing levels in Trauma and Orthopaedic surgery, with more leaving the speciality than those entering training. Currently, 32% of consultants plan to retire over the next four years2
BOA President, Simon Hodkinson, raised the alarms when he said, “We do not have enough qualified surgeons. On a per capita basis, we are at or near the bottom of the league in T&O workforce in the developed world”.
For the last 37 years, the British Orthopaedic Trainees Association (BOTA) has persistently and fervently fought for high standards of care for patients, for the safeguarding of training, and for the improvement and retainment of the T&O trainee workforce.
The BOTA vision is perfectly captured by the rallying call, ’No training today, no surgeons tomorrow’, beautifully coined in the trainer’s toolkit article by Miss Emily Baird, former BOTA President3
In 2022, BOTA completed its latest census data collection for T&O speciality trainees across the UK. This followed the successful 2019 study, providing a valuable comparison between pre-COVID and post-
COVID orthopaedic training in the UK. The two surveys combined gathered extensive information on training and workplace culture experiences from more than 1,350 trainees.
The 2022 census found that a startling 42% of respondents said they have considered leaving T&O training. From the census, we identified five key domains that would improve the management of the trainee workforce: Increasing training opportunities, lead employment, flexible working, out of programme working and workforce wellbeing.
Training opportunities
From the BOTA census 2022, the majority of trainees reported that their current operative exposure is insufficient to meet the training requirements of the August 2021 T&O Curriculum. To quantify this concern, the latest e-logbook data presented by the T&O SAC at the recent BOTA Regional Representative Forum Day in May 2024 in Manchester, highlighted that T&O trainees are performing 19% less elective operations compared to pre-COVID. Reasons for the low elective numbers are multifactorial and include rota gaps, theatre delays, bed pressure, increased case complexity, service provision pressures, all leading to reduced training opportunities.
“From the census, we identified five key domains that would improve the management of the trainee workforce: Increasing training opportunities, lead employment, flexible working, out of programme working and workforce wellbeing.”
Rota gaps and the impact on surgical training are worrisome and demonstrate the increasing strains of the system that we are training in. The BOTA Census 2022 found that 56% of registrar rotas have at least one gap, compared to 51% in 2019, >>
Subspecialty

Karen Chui is a Trauma and Orthopaedic Specialty Registrar in London. As BOTA President, Karen represents Orthopaedic trainees at national meetings, advocating to improve training and education opportunities for trainees. They are passionate about creating cultural change in Orthopaedics, building a compassionate profession for the modern surgeon to deliver excellent care to our patients.


and 27% reported two or more gaps in the rota, compared to 22% in 2019. As a result, 73% of respondents said they had to cover a gap at least once in the last month, compared to 67% in 2019.
Utilising the independent sector (IS) for training, in particular in NHS cases outsourced to IS, has seen improving numbers and holds promise as part of a multi-pronged approach to increase training opportunities. The BOTA Census found that 20% of trainees trained in the IS in 2022, compared to only 3% in 2019. Most trainees reported positive experiences training in the IS on NHS cases. To further incentivise training in the IS, BOTA has advocated for a training tariff and dedicated training lists in Surgical Hubs at the HEE Joint Meeting on Training in the Independent Sector advocating for trainees and NHSE Surgical Solutions meeting.
50% of trainees do not have access to simulation training based on the BOTA Census data. As previously discussed in the JTO, the BOA is in the process of becoming the first orthopaedic body to officially release a White Paper on the topic of simulation training4. Despite simulation being a valuable supplement to training and enhancing patient safety, 88% of trainees have not had robotic training and limited simulation training.
BOTA has worked closely with the BOA around the topic of the Physician Associate role in T&O surgery. We are reassured by the BOA’s position on prioritising patient safety and the training of surgeons, and will not support any situations where the use of non-medical qualified personnel adversely impacts on the experience and training of junior doctors.
Lead employment
Lead employment offers multiple benefits to trainees, including reduced paperwork when rotating through placements, fewer pay and tax code errors, standardised employment services, and access to optional salary sacrifice schemes such as the green cycle to work scheme. In 2022, 40% of trainees reported having a lead employer, which has improved from 35% previously. BOTA advocates that all nations and employers work towards having rotating trainees under one lead employer. This is reinforced by BOA President, Simon Hodkinson, who raised this issue in the past and identified it as a ’long needed change’.
The 2022 census once again indicates that the majority of trainees favour transitioning to a lead employer. Implementing an ‘NHS Passport’ would facilitate seamless transitions between trusts and allow trainees more time to be engaged in training and clinical work5
Flexible working
One of the most significant shifts between the 2019 census data and the 2022 results is the rise in trainees opting for flexible working arrangements and enrolling in Less Than Full Time (LTFT) training. LTFT training provides trainees with the opportunity to work fewer clinical days per week, accompanied by a proportional extension of their overall training period.
This has traditionally been utilised for caring roles, those with underlying health conditions and those with sporting commitments6. However, due to changes in the Gold Guide7 in 2021 and 2022, access to LTFT training is now open to a much wider range of reasons.

James Archer is BOTA Academic Representative and Census lead.
James Allen is BOTA Webmaster and Census lead.

The census results shows an increase from 4% of trainees thinking about LTFT training in 2019, to 10% in 2022, with an associated increase in the actual numbers in LTFT training from 3% to 7%. LTFT training can allow trainees to accommodate care-giving responsibilities during their training, which will hopefully attract a more diverse workforce into T&O training. This may contribute to the improvement of women in T&O, who may consider pregnancy during their training8. As we see more trainees entering LTFT training and flexible work patterns, the NHS must take this into account for workforce planning in the UK, as the traditional model of trainees entering and completing training on a specific timeline changes.
Out of programme
Out of programme (OOP) time is predominantly utilised for research, parental leave, and fellowships, a trend that has remained consistent from 2019 to 2022. However, OOP time could also be used for work in low- and middle-income countries (LMIC). The census found that 50% of trainees said they would be interested in working in LMIC, but the actual numbers of trainees working in LMIC are very low despite T&O surgeons being urgently required in LMIC. BOTA has opened its National BOTA Congress to LMIC medical students and doctors for free in the last three years.
Of those who did undertake this work, more than 80% say it did not contribute formally
to their training. This is a significant barrier for trainees as those who are interested in global surgery would like it to be paid and count towards their training. BOTA and the World Orthopaedic Concern (WOC) have released guidance on overseas placements in low resource settings9 Other publications have highlighted positive experiences by trainees in these endeavours and should be considered as training in the future10-13 .
Workforce wellbeing
The financial burden of training has been exacerbated by the ‘cost of living crisis’. The census found that trainees are struggling financially: 96% of respondents report feeling worse off financially compared to last year, 55% stating that the rising costs of living has affected their training, and 71% stating that they need to partake in additional locum shifts to mitigate these costs. This comes in conjunction to the findings of the ASiT Non-Financial Cost of Training report, with BOTA contributions, which identified the “immense non-financial burden of surgical training. It affects doctors at all stages of their career and in all specialities, irrespective of their gender or ethnicity”14
Whilst our census did not involve questions regarding the junior doctors’ industrial action, this is inextricably linked with trainees’ wellbeing. The cost of training was cited as the second most important priority for BOTA to improve upon, with training conditions being the first.
Conclusion
The BOTA census highlighted key areas for improvement with regards to the trainee workforce. The trainee workforce must be prioritised to safeguard the future consultant workforce, as ‘No Training Today, No Surgeons Tomorrow’.
The BOTA census findings were discussed at the 2024 BOTA Regional Representative Day and helped define the BOTA top five priorities for training in 2024:
1. Improving access to training opportunities
2. Reducing the cost of training
3. Improving working conditions (both with regards to rotas and the working environment)
4. Professionalising training for trainers
5. Making improvements to core training n
References
References can be found online at www.boa.ac.uk/publications/JTO
Addressing workforce issues: The role of the SCP within the extended surgical team
Sally Stuart

Sally Stuart qualified as a nurse in 1993 and instantly developed a keen interest in surgical practice and after 10 years of experiencing a wide range of surgical specialties as a scrub practitioner, was appointed as an Surgical Care Practitioner in general surgery.
After moving into academia 2019, Sally now leads the MSc in Surgical Care Practice at Edge Hill University. She is the current chair of the Association of Surgical Care Practice and is on multiple national working groups to promote the advancement of the SCP role within the extended surgical team.
In the United Kingdom, the extended surgical team (EST) includes a variety of healthcare professionals who collaborate to provide safe and effective surgical care. Those members include medically and non-medically trained and educated professionals. This article explores the impact of the non-medically trained workforce, specifically the role of the Surgical Care Practitioner (SCP) on patient care, how SCPs complement and collaborate within the EST, how they are trained and educated and how SCPs are integral to achieving the goals of the NHS Long Term Workforce Plan.
It is important to recognise that non-medically trained practitioners supporting the extended surgical team is not a new concept. Nursing support was required to assist surgeons during times of conflict, and it was in the 19th century, during Florence Nightingale’s nursing career, that the first surgical nurse assistant role was conceived, the registered nurse’s role included preparing wounds for surgery and assisting during operations1
If we proceed to the early 1990s two important policy-influencing documents emerged. There was overwhelming evidence that the junior doctors hours of work of should be reduced2 and it had been known for some time that long hours not only impacted on the physical and mental health of doctors in training but also that there was potential to harm patients. Reports supported the contention that stress associated with sleep deprivation was an important factor in unnecessary patient morbidity and mortality3. There was mention at this stage of how important non-medical practitioners would become to support surgical services. However, at this time nurses were limited to basic nursing duties and not permitted to undertake skills outside of their scope of practice due to the rules set by the
Department of Health and Social Security (DHSS) in the 1970s. In 1992, the UK Central Council, who preceded the Nursing and Midwifery Council, introduced a new scope of professional practice guidance for nurses4 which was profoundly influenced by practices in the USA5. The result of this major change was a plethora of nursing roles and the emergence of the new concept of advanced nursing practice. Within surgery, nursing roles emerged to assist surgeons. These roles were developed locally and with ‘in house’ training and education programmes6,7. However, without national standards for training and education there is the potential for confusion and variable standards. The primary objective of these roles is not to replace doctors but to produce practitioners, who use their experience, knowledge and skills to complement and collaborate with the existing surgical team8
Governance of Medical Associate Professionals
SCPs currently sit within the Medical Associates Professions (MAPs) group, alongside Physicians Associates (PA) and Anaesthetic Associates (AA). The MAPs group was established by Health Education England (HEE) in 2014 to include these professional groups under a single umbrella along with Advanced Critical Care Practitioners. HEE had intended to develop and shape postregistration education, training and careers and to support a move towards statutory regulation by the General Medical Council9 The PA and AA roles were specifically designed to find a solution to workforce shortages outlined in the NHS People Plan and have been amplified in the NHS Long Term Workforce Plan. The majority of PAs and AAs are recruited from a Biological Sciences background with limited clinical experience. The roles are currently unregulated.

In contrast, recruits to SCP training mainly come from either a nursing background with Nursing and Midwifery Council registration or an operating department practitioner background with Health and Care Professions Council registration. Entry criteria include a minimum of 18 months of post-registration experience.
The current controversy of MAPs roles in clinical practice reflects concerns surrounding patient safety and reducing training opportunities of junior doctors10. MAPs in surgery cannot and must not be used to replace surgeons. They must always work within a clearly defined scope of practice and under the supervision of appropriately qualified and experienced senior surgeons. Despite the controversies, there is evidence from both the USA11 and the UK12.13 that clearly demonstrates the positive impact MAPs skills and expertise have in improving medical care.
It has also become clear that there is a difference in governance between PA/AAs and SCPs. There is an evolving view that SCPs should no longer sit within the MAPs group due to differences in post-graduate training
“The defined role of SCPs is to assist in surgical procedures and manage pre-operative and post-operative care and play a crucial role in the extended surgical team. They help maintain continuity of care by performing tasks that can be delegated to non-medically qualified staff.”
and education, scope of practice and SCPs are already registered with a regulatory body. The Intercollegiate Extended Surgical Team Board is having preliminary discussions with NHSE Workforce, Training and Education to determine how this could develop.
The defined role of SCPs is to assist in surgical procedures and manage pre-operative and post-operative care and play a crucial role in the extended surgical team. They help maintain continuity of care by performing tasks that can be delegated to nonmedically qualified staff14 This ensures that patients receive consistent and high-quality care throughout their surgical journey. SCPs work under the supervision of consultant surgeons and assist before, during, and after surgical procedures. They are trained to perform some surgical interventions which helps streamline the surgical process. An underpinning principle of all that they do is to facilitate the training and education of surgical trainees by taking on responsibilities to allow surgical trainees to access more training opportunities. >>
Professional role of SCPs

Training and education of SCPs
The first SCP curriculum focussed on skills acquisition based on workplace learning rather than breadth and depth of knowledge and understanding. Entry requirements were non-specific and links to higher education institutes were proposed but not compulsory15 In 2014, the second edition of the curriculum was published by the Royal College of Surgeons of England following a robust and extensive review conducted by a multiprofessional working group. Changes were driven by the workforce needs of healthcare providers, where SCPs were managing the clinical care of patients and assisting with technical and operative interventions. The 2014 curriculum provided clear and systematic RCS accreditation processes for Higher Education Institutes (HEI) wishing to provide programmes, clarity of the scope of practice of SCP and assured a national standard for core and specialty knowledge and skills acquisition16
In 2022, RCS England and RCS Edinburgh published a revised SCP curriculum to set the clinical, technical and professional standards expected of a professional practitioner working in this defined role of surgical care17 addressing the needs of a rapidly evolving UK healthcare system. The overall aim of the programme is to produce competent and capable SCPs
based on the four pillars of advanced clinical practice: clinical practice, leadership and management, education and research18. The curriculum adopts a spiral approach, with each year of study progressively building on the knowledge, skills, attitudes and behaviours developed in previous years. Designed to be completed over three years, the programme is completed in two phases, with phase 1 that spans years 1 and 2 of the programme being focused on the development of generic clinical, technical and professional knowledge and skills. Phase 2 is the final year of the programme and focuses on the development of surgical specialty specific clinical, technical and professional knowledge and skills17
The curriculum is designed to ensure that all Trainee SCPs (TSCP) become self-directed and self-aware learners through a diverse range of learning and teaching opportunities both in and out of programmes. Each TSCP will focus on their personal and professional development, based on an initial learning/ training analysis, to ensure that they have opportunity to achieve their optimum potential throughout the programme, evidenced in their e-portfolios.
To commence SCP training candidates are required to be a registered practitioner, be appointed as a trainee SCP, with at least
18 months experience in surgical care and will meet the academic requirements of the RCS accredited HEI. They must identify appropriate educational and clinical supervisors who will provide and facilitate teaching, learning and assessment in practice17. In addition, other experienced medical and non-medical practitioners facilitate a multidisciplinary approach to work-place based learning.
Conclusion
The extended surgical team is a key component of the NHS Long Term Workforce Plan (LTWP), which aims to ensure a regulated, sustainable and effective healthcare workforce by expanding the number of new and extended roles to increase the breadth of skills of the multidisciplinary team to better meet the needs of patients19. This workforce expansion includes a plan to fill gaps in the current workforce and meet the needs of a growing and aging population. Overall, the extended surgical team is integral to achieving the goals of the NHS Long Term Workforce Plan, ensuring high quality, sustainable healthcare for the future. n
References
References can be found online at www.boa.ac.uk/publications/JTO
Hip Arthroplasty – A Case For Cementing
As a result of an ageing population and modern lifestyles the number of hip arthroplasties has risen sharply in developed countries with hip fracture and osteoarthritis being the most common reasons. Underlying causes such as age and frailty or a variety of comorbidities can increase the risk for fractures, infection, or general postoperative complications1-4
With a longer life expectancy and the expectancy of an active life after retirement, patients’ expectations of improvement after hip replacement surgery are increasing. To this end, a stable, reliable, and durable function of the prosthesis is not only needed in the younger but also in the elderly patient population. In addition to reducing risk factors for implant survival surgeons can improve outcomes by choosing the appropriate implant and surgical technique for a given patient.5-7
Improved Outcomes With Antibioticloaded Bone Cement
According to a recent review arthroplasty registry data did not show improved outcomes with cementless total hip implants compared to cemented fixation8. In contrast, cementless fixation shows increased implant failure and revision rates in elderly patients aged 70 years or older8. When comparing bone cements used for primary hip fixation in the UK, 66% of all cemented hip replacements in the UK are performed using PALACOS® R+G9. National Joint Registry (NJR) data shows statistically significant outcomes with PALACOS® R +G with a cumulative revision rate (2009–2024) that is 25% lower compared with all other cements brands in NJR (Figure)10
In economic terms, this means that PALACOS® R+G has a cost-saving potential of at least 21.5 € million (£16.2 million) in the UK11
Cementless Arthroplasty and Periprosthetic Fractures
Several studies and registry data show that uncemented stems increase the risk of periprosthetic fracture compared to those who have cemented stems.12-14 Therefore, a number of orthopaedic and trauma societies, such as the British National Institute for Health and Care Excellence (NICE), the American Academy of Orthopaedic Surgeons (AAOS), or the Spanish Society of Orthopedic Surgery and Traumatology (SECOT), have thus proposed that cemented fixation of hip hemiprostheses should be used in certain circumstances.15-17 Furthermore, the hybrid approach with only the femoral stem being cemented is observed to increase lately, particular for the treatment of proximal femur fractures in elderly patients with poor bone quality.18


References
References can be accessed online at: www.herae.us/boaadvertorial-sept24

The Future of Cementing
Modern Cementing Technique is an established procedure in cemented hip arthroplasty for achieving optimal cementing results.19 Closed mixing systems support surgeons and operating theatre staff with helpful tools for conveniently mixing and applying bone cement during arthroplasty procedures. Innovations such as the closed mixing system “pro” from Heraeus Medical GmbH, drive the development of medical devices to evolve to the next generation of modern cementing technique.19
We thank the patients and staff of all the hospitals in England, Wales, Northern Ireland, the Isle of Man and the States of Guernsey who have contributed data to the National Joint Registry. We are grateful to the Healthcare Quality Improvement Partnership (HQIP), the NJR Steering Committee and staff at the NJR Centre for facilitating this work. The views expressed represent those of Heraeus Medical GmbH and do not necessarily reflect those of the National Joint Registry Steering Committee or the Health Quality Improvement Partnership (HQIP) who do not vouch for how the information is presented. n
Fig. Use of PALACOS R+G ® in primary hips is associated with lower cumulative revision rates in the UK 10
I faced a GMC investigation following criticism of a handover
I’d performed a hip replacement on a 73-year-old patient with multiple co-morbidities. Due to illness, my handover to the weekend team was rushed. Tragically, after developing sepsis, the patient died.
Then I got the call. The coroner had named me an Interested Person for the inquest.
Medical Protection were there for me throughout. The inquest concluded with a Report to Prevent Future Deaths, and I faced a formal GMC investigation. My medicolegal consultant and solicitor advised me on the appropriate post-event analysis and CPD, and thankfully the GMC recognised my reflective practice and closed the matter with no further action.
The experience taught me the vital importance of the handover. I also learned the value of my Medical Protection membership. The team got me through, and saved me a lot of sleepless nights.