Companion Quarterly
OFFICIAL NewsLetter OF the COmpANION A NIm AL veter INA r IAN s br ANC h OF the NzvA

Volume 34, No. 2 | June 2023
Tracheal intubation in cats

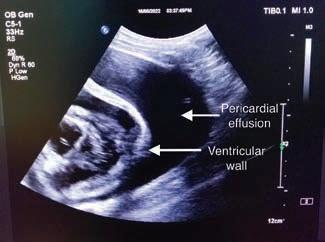
Pericardial mesothelioma in a German Shepherd
A galah with zinc toxicosis
Rat bait is not always an anticoagulant: cholecalciferol poisoning in a dog
Puppy heart murmurs: when to worry and what can be done
E XECut IVE Comm I tt EE 2023 cav@vets.org.nz

President Natalie Lloyd
Vice President
Simon Clark
Secretary
Sally Aitken
treasurer
Kevanne McGlade
Committee members
Nina Field
Toni Anns
Becky Murphy
Shanaka Sarathchandra
Head of Veterinary Services

Sally Cory
EDI to RIAL Comm I tt EE
Sarah Fowler (Editor)
Ian Millward
Juliet Matthews
Aurore Scordino
Shanaka Sarathchandra
Address for submitting copy/
correspondence
Sarah Fowler
66 Callum Brae Drive, Rototuna, Hamilton 3210
T (H) 07 845 7455 | M 027 358 4674
E sarah.fowler@gmail.com
Advertising manager
Tony Leggett
NZ Farmlife m edia Ltd
Agribusiness Centre
8 Weld St, Feilding
T 027 4746 093

E tony.leggett@nzfarmlife.co.nz
NZVA website

www.nzva.org.nz
CAV website
www.nzva.org.nz/cav
Copyright
t he whole of the content of the Companion Quarterly is copyright, t he Companion Animal Veterinarians Branch of the NZVA (CAV) and t he New Zealand Veterinary Association (NZVA) Inc.



Cover credit
Cover from Pixabay
Newsletter design and setting
Penny May
T 021-255-1140
E penfriend1163@gmail.com
Disclaimer
t he Companion Quarterly is a non peer reviewed publication. It is published by the Companion Animal Veterinarians Branch of the NZVA (CAV), a branch of the New Zealand Veterinary Association Incorporated (NZVA). t he views expressed in the articles and letters do not necessarily represent those of the editorial committee of the Companion Quarterly, the CAV executive, the NZVA, and neither CAV nor the editor endorses any products or services advertised. CAV is not the source of the information reproduced in this publication and has not independently verified the truth of the information. It does not accept legal responsibility for the truth or accuracy of the information contained herein. Neither CAV nor the editor accepts any liability whatsoever for the contents of this publication or for any consequences that may result from the use of any information contained herein or advice given herein. t he provision is intended to exclude CAV, NZVA, the editor and the staff from all liability whatsoever, including liability for negligence in the publication or reproduction of the materials set out herein.
Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 1 CON teN ts 2 Editorial 4 CAV activities and meeting highlights 6 CAV Noticeboard 8 News in brief 10 Tracheal intubation in cats Colette Jolliffe 20 A case of zinc toxicity in a galah (Eolophus roseicapilla) Lisa Stuart 30 Rat bait is not always an anticoagulant! Cholecalciferol rat bait poisoning in a dog. Neil Stuttle 34 Pericardial mesothelioma in a 6-yearold German Shepherd dog Charlotte Bellaton 40 Puppy murmurs: when to worry and what can be done Kayla Gardiner, Keaton Morgan 44 ISFM Research Roundup 48 Companion Animals NZ update 49 Healthy Pets NZ update 50 Massey news 51 Committee biographies 52 Authors' guidelines Companion Quarterly Helps you solve personal and work problems, including: Relationship problems Drug and alcohol issues Work issues Change Stress Grief 0508 664 981 24-Hour Freephone Confidential Counselling Service Vets in Stress Programme Volume 34 | No. 2 | June 2023 ISSN No. 2463-753X
20 10 44 34
Is the “Gold standard” still gold standard?
Gold-standard care is defined as a treatment or procedure widely deemed to be the best available.
After graduating from veterinary school a couple of eons ago I started my first job with the intention to provide every patient I saw with gold-standard care.
In reality, on finishing my first year, I could say that I aimed high but often found myself striking out when it came to selling that gold standard to my clients.
o ver the last few months, I have heard growing unease with that term “gold standard”. Leaders and influencers in our profession have expressed a concern that the aim to shoot high, to always be reaching for that kind of platinum care, may actually be putting our clients under unrealistic pressure. It may not always be the right thing for our patient. And maybe, the constant striving for that level of care is also putting unnecessary pressure on ourselves and our teams.
I first heard Jody Lulich refer to this concept many years ago in a presentation on lower urinary tract disease, an area where he is quite the guru. He had a lot of pearls that day, but the pearl I remember the best, was a discussion about using the “small rocks” first. Do the easy and economical things that make good medical sense first so there is room in the virtual “jar” (an analogy for our clients’ financial reserves), when you need to utilise those “big rocks”, i.e., perform the more expensive tests and treatment options.
Don’t get me wrong – I am a firm believer that we need to practice great medicine. I am not suggesting that it’s ok to take a short cut. We still need to provide a good level of care for our patients. We need to work to try to determine the underlying cause for our patient’s presenting symptoms and treat that cause with effective and safe medications or surgical procedures. t here is no doubt that most of the time we will need reliable diagnostics to help us with reaching a diagnosis. But we should also appreciate that the physical examination and a thorough history are as valuable a diagnostic tool, as many of the other tools we have at our fingertips, and they are an integral part of the “art” of being a great GP veterinarian. I have heard it discussed among feline practitioners that goldstandard care may be at odds with feline-friendly practice. How can we provide feline-friendly care, to those little animals who so dearly love to be in control, if every cat we see receives a gamut of procedures every time they come into the clinic? t he challenge of treating cats is in minimising the impact of their experience in the consultation room. If that goes poorly, we risk the cat’s caregiver not wanting to bring the cat back. So, can we think about what procedures are necessary for that cat on that day, and maybe defer some in order to minimise impact? t his may well mean that we end up with a cat that is more comfortable about coming into the clinic, allowing us to ultimately provide better holistic care for that animal.
Finally, how does the concept of gold-standard care make us feel about ourselves? How do we feel when, like my experience as a new graduate, we don’t manage to convince people to accept our gold-standard treatment suggestions? Do we feel like we should have communicated our plan in a more concise way? or perhaps we could have delivered the information in a better manner? Should we have pushed a little harder? Could we have used different words? Do we beat ourselves up with the thought that our colleague could have done better than we did in that moment, for that patient?
If we can perhaps spend some time on our history and physical examination, being careful and gentle with our patients so their experience is not a negative one. If we can be responsible with the finances of our clients, understanding the power of the human-animal bond, often meaning people will do anything for their pet, sometimes beyond their own means. And if we can ultimately be a little gentler on ourselves, understanding that the gold standard may sometimes be an unrealistic and unachievable goal, then I believe that we will have patients and customers that are more likely to return regularly.
t his allows us the opportunity to provide better care over the life of that pet, strengthens our bonds with our clients, and helps us to dial back that constant pressure we put ourselves under, just a touch.
to read more on this topic, please see:
Skipper A, Gray C, Serlin R, O'Neill D, Elwood C, Davidson J. 'Gold standard care' is an unhelpful term. Veterinary Record 189, 331, 2021, https://doi.org/10.1002/vetr.1113

 Natalie Lloyd, CAV President
Natalie Lloyd, CAV President
Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 2 eDI tOR IA l
[Photo credit: Joanna Reichert from Pixabay]

Activities of the CAV e xecutive Committee
CAV held their first committee meeting for the year in march. It was great to see the energy and enthusiasm for the planned project work which we will be starting to share with our members in due course.
t he year is flying by, and over the first quarter CAV have been busy with code of welfare reviews. We continue to contribute as a key stakeholder in the rewriting of the Code of Welfare: Dogs before it is circulated for wider consultation prior to presentation to the National Animal Welfare Advisory Committee (NAWAC) in october. t he committee has also provided valuable feedback on the draft updated Code of Welfare: Cats, also prior to NAWAC submission.
We are extremely grateful to members for their response and feedback on the proposed regulations on subgingival dental procedures and prolonged tethering in dogs following public consultation. CAV were able to provide feedback to mPI with overwhelming support for the subgingival dental procedures regulation, which will allow Allied Veterinary Professionals (AVP) to perform these procedures again with urgency. We asked that this regulation be progressed in an expedient manner for the benefit of our members and the animals they care for. We are aware that the proposed suite of regulations on prolonged tethering in dogs is more complex in nature and again are
grateful to our membership for providing feedback.
CAV are looking forward to their next committee meeting in June, especially since this will also mark the start of the NZVA Centenary conference ( tākina Events Centre, Wellington, 28–30 June 2023). l

Companion Quarterly – a call for contributions
Do you have a clinical case to share, need to tick off a task on your CPD plan or want to earn some pocket money?
CQ publishes case studies, clinical updates, reviews etc. on topics that are of interest to companion animal veterinarians. An award of $300 is paid for all published articles, with the chance to win the Best Article of the Issue and Best Article of the Year (thanks to tCI Glenbred).
Please send your contributions to the Editor at sarah.fowler@gmail.com
microsoft Word format is preferred and photographs/images are welcome, preferably 2 megapixels or higher, and sent as a separate attachment (rather than embedded within the Word document).

Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 4 WOR k ING tO pROmO te AND supp OR t COmpANION ANI m A l pRAC t ICe IN N e W Z e A l AND

The CAV Noticeboard

Hill’s Pet Nutrition and CAV present: Educating the Educators Scholarship
Applications are now open for the Hills/CAV Educating the Educators Scholarship. t his scholarship provides assistance for advanced veterinary practitioners to attend advanced-level continuing education events, in exchange for articles, reports and presentations on their area of interest. Successful applicants are usually specialists in their field, but we also support those who have developed advanced skills in an area of special interest.
t hrough this partnership, we recognise the importance of supporting our leading veterinarians’ participation in international conferences, to ensure they remain up to date and able to disseminate this knowledge to the

wider CAV membership.


t he scholarship is open to both CAV members and non-members and there are two funding rounds each year, in march and September. t he closing date for this application round is 30 September.
We gratefully acknowledge Hill’s Pet Nutrition as the principle sponsor.

For more information, check out the CPD section of the CAV website (https://www.nzva.org.nz/branches/cav/ scholarships/), or email Sally Cory at cav@vets.org.nz.

Healthy Pets NZ Project Grant 2023
Healthy Pets NZ is a charitable trust that acts as the research funding arm for CAV. Funding applications are invited in march and September for research projects that will enhance companion animal health and welfare.
See the Healthy Pets NZ website (www. healthypets.org.nz) to find out how we

WINNER
Article of the Issue

Isobel McEwen & Keaton Morgan
are supporting projects on analgesia for ovariohysterectomy, treatment of squamous cell carcinoma and FIV prevalence. Any queries on how to make an application or donate please email healthypetsnz@gmail.com.
march 2023 | Volume 34(1) | Pp 20–24
Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 6
"Pacemaker implantation for persistent atrial standstill"
Ne W s IN BRI ef
CAV Annual General meeting and committee election
t he 2023 Annual General meeting (AGm) of the Companion Animal Veterinarians Branch of the NZVA will be held in June preceding the NZVA conference.
Date: tuesday 27 June 2023
Time: 4.30pm
Location: online via Zoom, please email cav@vets.org.nz for link.
Canine leptospirosis factsheet
leptospirosis are common after heavy rain and flooding, so this is an important resource to have on hand following Cyclone Gabrielle, and in other severe rain events.
t he NZVA and CAV have created a factsheet on canine leptospirosis for veterinary teams. outbreaks of


t he fact sheet can be downloaded at https://nzva.org.nz/assets/For_vet_ professionals/Companion_Animals/ c800659aa1/Canine_Leptospirosis.pdf or found on the Companion Animal Health and Welfare section of the NZVA
WsAVA m ichael J. Day scholarship Award sponsorship
Calling all veterinary students! WSAVA is accepting applications for the 2024 WSAVA michael J. Day Scholarship. Don’t miss this opportunity to apply for financial assistance for research into an aspect of small companion animal infectious disease, clinical vaccinology or immunology.

t he recipient will spend 2–3 months carrying out their research in a host university or academic environment of their own selection. t hey will receive a grant of up to uS$15,000 to support them in carrying out their project. Full details and guidance on the application process, together with eligibility criteria are available here: https://wsava.org/news/ events-courses/applications-invited-forthe-2023-wsava-michael-j-day-scholarship/. Applications close on 3 September 2023. l

CAV would like to thank tCI Glenbred for taking over sponsorship of the awards for best article published in each issue of Companion Quarterly and best article of the year. l

Positions and Resources page of the NZVA website (https://nzva.org.nz/resource/ companion-animal/). t his page contains NZVA’s companion animal-related policies, guidelines and position statements (e.g. policies on first digit amputation in dogs and euthanasia of dogs and cats) along with fact sheets, guidelines, webinars and posters generated by CAV on a range of important topics (managing reactive dogs, brachycephalics, puppy socialisation). l
CAV 50-year Anniversary CpD awards cont.
As described in the march issue of Companion Quarterly, in commemoration of its 50 th birthday CAV awarded three lucky members a $500 CPD voucher to be redeemed at any NZVA event with a companion animal focus or stream. one of those three vouchers went to a 2004 graduate Kathleen Limpus, a companion animal veterinarian at VetCare tauranga.
Kathleen says that her favourite part of being a vet is getting to know her patients, and their families, over their lifetime, and even into the next generation. When informed of her win, she replied, “ t hank you so much for the award, I am looking forward to keeping up to date with my CPD over the year, with a subscription to the Webinar Vet.” l
Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 8
[Photo credit: Compare Fibre for Unsplash]
[Photo credit: Dominik QN for Unsplash]
[Photo credit: Stagridge Kennels]
Cl INICA l upDAte tracheal intubation in cats
COlette JOll I ffe
Introduction
tracheal intubation provides several functions. It protects the patient’s airway from obstruction due to reduced muscle tone under anaesthesia; protects against aspiration of saliva, blood or gastric contents; allows administration of oxygen, volatile agent and positive pressure ventilation; and enables suction of the airway.
Poor technique during tracheal intubation can cause laryngospasm, laryngeal oedema, haemorrhage, vagal stimulation, arrhythmias and tracheal damage, ranging from transient inflammation to tracheal rupture. use of inappropriately small internal diameter tubes can increase resistance to flow of gas and the work of breathing, leading to hypoventilation. Small diameter tubes also increase the risk of tube obstruction by mucus, blood or other debris. Inappropriately large tubes can traumatise the airway. Cuffed tubes have been associated with tracheal trauma in cats including tracheal mucosal ischaemia, stenosis and tracheal rupture. t his article will discuss equipment and techniques used for tracheal intubation in cats.
selection of tube type
t here are many different endotracheal (E t ) tubes available for use in veterinary patients. t he material, diameter and shape of the tube required may depend on the patient and the procedure.
tube material
Endotracheal tubes may be made of rubber, silicone rubber or polyvinyl chloride (PVC) (Figure 1). Red rubber tubes and silicone tubes are re-usable and this is reflected in the price. Polyvinyl chloride tubes can be clear, siliconised, or ivory. t hese tubes are inexpensive as they are designed for single use, although it is common in veterinary practice to re-use them after cleaning. t he PVC tubes soften at body temperature and are reported to conform to the shape of the trachea. Generally tracheal intubation is technically easier using the stiffer tubes such as red rubber rather than the soft ivory PVC or silicone rubber tubes. Soft tubes are often straight rather than curved, which may also make intubation more challenging. However, softer tubes are less likely to cause damage to the larynx during insertion, and cause less pressure on the tracheal wall during anaesthesia as they conform better to the shape of the trachea. With good patient positioning and some practice, these tubes are easy to use.

Cuffed tubes
Endotracheal tubes may be cuffed or plain (uncuffed). Inflation of the cuff provides a seal between the tube and the tracheal mucosa, preventing pollution of the atmosphere with anaesthetic gases, aspiration of saliva or gastric contents, and facilitating the provision of positive pressure ventilation. However, the use of cuffed tubes in cats has been associated with tracheal injury including rupture. t he mucosal perfusion pressure of the trachea is between 20 and 30 mmHg, hence if the cuff exerts a pressure greater than this, ischaemia will occur. High pressure/ low volume cuffs are more likely to cause tracheal ischaemia, necrosis and subsequent stenosis when overinflated due to the small area of trachea over which the force is exerted. Low pressure/high volume cuffs exert the force over a larger area, resulting in a lower pressure on the tracheal mucosa (Figure 2). Cuffs of tubes manufactured from different materials have different properties (Figure 3).

Contact: Jo.Hart@dechra.com
Red rubber tubes have high pressure/ low volume cuffs due to the thickness of the cuff material which requires a high pressure for inflation. PVC tubes
Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 10
BVet med CertVA Dipl eCVA
mRCVs, Centre for small Animal studies, Animal Health trust
f igure 1. from left to right: clear pVC, red rubber and silicone rubber et tubes
a b
f igure 2. Different types of et tube cuffs. (a) low pressure/high volume cuff showing large contact area with the tracheal wall. (b) high pressure/low volume cuff showing a small contact area.

can have low pressure/high volume, intermediate, or high pressure/low volume cuffs because the cuff wall is thin and inelastic. However, when deflated, these cuffs do not conform well to the contours of the tube, which may necessitate the use of a smaller internal diameter tube (Figure 4). Also, they do not protect the airway against aspiration as effectively as high pressure/ low volume cuffs due to wrinkles in the cuff which may allow passage of fluids. Application of a water-based gel to the cuff reduces the risk of aspiration. t his phenomenon has not been investigated in cats where it is possible that the small size of the trachea and hence any wrinkles in the cuff may not be sufficient to allow liquids to pass. Silicone tube cuffs are usually medium pressure/ medium volume and the soft elastic material conforms well to the contour of the tube, enabling passage of a large diameter tube (Figure 4).



low pressure/high volume cuffs tended to be more severe due to their longer length. most of the cats had undergone dental procedures. t he most likely cause of tracheal rupture in these cases was over-inflation of the cuff, possibly in an attempt to prevent aspiration of water and debris, although use of stylets and excessive movement of the tube during the procedure were also suggested as possible causative factors. A plain tube combined with a throat pack will provide adequate protection from aspiration during dental procedures, and it is recommended to disconnect the E t tube from the anaesthetic breathing system each time the patient is repositioned during the procedure to minimise traction and twisting of the E t tube within the trachea. occlusion of the lumen of the tube may occur due to over-inflation of the cuff, either by prolapse of the cuff over the end of the tube or by compression of the tube lumen (Figure 5).
It has been well demonstrated that cuff pressure cannot be assessed by subjectively estimating the pressure or volume of the pilot balloon. Cuff pressure can be measured using a pressure manometer attached to the pilot balloon, but depending on the type of cuff, this may not reflect accurately the pressure exerted on the tracheal wall. t he most practical way to assess cuff inflation is to connect the tracheal tube to the breathing system and inflate the lungs with oxygen while listening for sounds of gas leakage around the E t tube (Figure 6). t he cuff can then be inflated slowly to the point where there is no audible leakage.
t he use of nitrous oxide as part of the carrier gas mixture can alter cuff pressure. Due to its low blood:gas solubility coefficient, nitrous oxide diffuses into the air-filled cuff and expands it further, resulting in increased pressure on the tracheal mucosa. t he magnitude of the expansion depends on the percentage of nitrous oxide delivered and the material of the cuff. Nitrous oxide diffuses more easily across red rubber than PVC tube cuffs. In human practice there are various devices designed to negate this effect. For veterinary patients, if using nitrous oxide, it may be wise to slightly deflate the cuff and reassess cuff pressure by the method described above after five to ten minutes of anaesthesia. Cuffed tubes can be used without cuff inflation if required.
plain tubes
If an uncuffed or plain tube is used, the internal diameter of the tube
t here have been reports of tracheal rupture in cats associated with the use of cuffed E t tubes, both high pressure/ low volume and low pressure/high volume cuffs. t he tears associated with

Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 12
f igure 3. from left to right: plain ivory pVC tube; high pressure/low volume cuffs on a clear pVC and a red rubber tube; medium pressure/medium volume cuffs on a silicone rubber and a siliconised pVC tube; low pressure/high volume cuff on a reinforced tube.
f igure 4. Different cuff materials. l eft: low profile cuff on a silicone rubber tube, showing the murphy eye; right: bulky, inelastic cuff on a siliconised pVC tube.
a b
f igure 5. Obstruction of the et tube by over-inflation of the cuff. (a) compression of the lumen of the tube; (b) prolapse of the cuff over the end of the tube.
f igure 6. Assessment of et tube cuff inflation. The anaesthetist inflates the cuff while listening for leakage of gases while an assistant inflates the patient’s lungs.

is likely to be larger than that of a cuffed tube for the same size trachea, resulting in decreased resistance and work of breathing, and decreased risk of obstruction of the tube by mucus. t here is also less risk of tracheal rupture, although one reported case of tracheal rupture involved a cuffed tube which was not inflated. A close fitting plain tube is required to prevent pollution of the environment with anaesthetic gases and inhalation agents, especially if positive pressure ventilation is to be imposed. Aspiration of saliva, blood or debris from dental procedures can be prevented by packing the pharynx ideally with a throat pack or with dampened swabs.
For each patient the advantages and disadvantages of use of a cuffed tube should be assessed. For example, in a cat with megoesophagus the risk of regurgitation and aspiration may outweigh the risk of tracheal rupture and a cuffed tube should be considered.
l ength of the tube
t he optimal position of the E t tube is with the distal end in the mid to distal cervical region and the proximal end level with the incisor arcade. If the tube is too long there is a risk of bronchial intubation with resulting ventilation perfusion mismatching. In the event of tracheal rupture following intubation, the prognosis for survival following surgical repair is worse if the rupture is close to the carina. If the E t tube protrudes from the mouth this results in increased apparatus dead space with potential for decreased alveolar ventilation and carbon dioxide rebreathing. t here may be increased risk of kinking and movement of the tube.
Width of the tube
t he internal diameter (ID) of the E t tube is marked on the tube and sometimes on the pilot balloon of the cuff. In general, use of the largest diameter tube that can be inserted without causing damage to the larynx or trachea (i.e. with no resistance) is advantageous. A wider tube will give less resistance to breathing and is less likely to become obstructed by mucus, lubricating gel or mucosa. For a given tracheal diameter, an appropriate plain tube is likely to have
a wider ID than a cuffed tube, because of the bulk of the cuff itself. t his is less true of silicone rubber tubes, whose cuffs are very low profile when not inflated (Figure 4). An average 4 kg cat’s trachea will usually accommodate a 4.5 mm ID plain tube.
Bevel
E t tubes are bevelled to aid visualisation of the larynx and insertion of the tube. Some bevels have a hole opposite the aperture called a murphy eye (Figure 4). t his is a safety feature to enable passage of gases should the opening of the tube become lodged against the tracheal wall.
preparation for intubation
Before the cat is anaesthetised equipment for intubation should be prepared.
tubes
t he size and conformation of the cat should be assessed visually to estimate the likely appropriate ID of the E t tube to be inserted. Gentle palpation of the trachea may also be useful. t here are no published guidelines on selection of tube size, this must be based on clinical judgement and experience. Several tubes of different internal diameters should be available. t he required length of the tube should be estimated, for example by measuring a tube against the cat. t he tube should be cut if necessary. If cuffed tubes are used, the cuffs should be inflated for a few minutes before induction of anaesthesia to check for leaks.
laryngoscope
Although intubation can be performed without a laryngoscope, a laryngoscope or other light source should always be readily available in case of difficult intubation. A laryngoscope is useful to depress the base of the tongue to provide good illumination of the larynx. An appropriate short blade should be fitted and the light tested prior to induction of anaesthesia (Figure 7). tube ties tape or bandage may be pre-tied around the E t tubes to tie the tube in place after intubation. A dry swab may be useful to hold the tongue.

l ocal anaesthetic
Due to the sensitivity of the feline larynx, the mucosa should be desensitised with local anaesthetic prior to intubation to help avoid laryngospasm. Intubeaze (Dechra Veterinary Products) is the only spray bottle licensed for this use in New Zealand.
lubrication
t he E t tube may be lubricated with a water based gel such as KY jelly or with local anaesthetic gel, although no products are licensed for this purpose.
skilled assistance
t he most important requirement is a skilled assistant who can position the patient for the intubation procedure, secure the tube and assist with cuff inflation.
Intravenous access
Ideally an intravenous catheter should be placed to enable administration of incremental doses of injectable anaesthetic agent during the intubation procedure. Alternatively a syringe and needle can be taped in position for this purpose. Intravenous injection of incremental doses helps to ensure adequate depth of anaesthesia during intubation.
technique
once anaesthetised, the patient should be placed in the preferred recumbency for tracheal intubation. t his may be
Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 14
a b
f igure 7. (a) laryngoscope with a short m iller blade; (b) testing the light.

sternal, left or right lateral or dorsal recumbency depending on the preference of the anaesthetist.
sternal and lateral recumbency
t he assistant should extend the patient’s head and neck by lifting the lips and grasping the cat behind the maxillary canine teeth with the thumb and forefinger of one hand. An alternative technique is to thread a piece of bandage behind the maxillary canines and use the bandage to extend the head (Figure 8). t he assistant or the anaesthetist then pulls the tongue forward by grasping it gently with fingers or a dry swab. If the tongue tip is within the mouth, the laryngoscope blade or a tongue depressor should be used to pull the tongue forward to avoid injury to fingers.
enable visualisation of the larynx. t his technique can be performed without assistance, but there may be increased risk of regurgitation and aspiration.

laryngoscopy
t he larynx is visualised, ideally using a laryngoscope. For a right-handed person, the tongue is held in the left hand or by the assistant. t he laryngoscope is held in the right hand and positioned with the tip at the base of the tongue. Depression of the base of the tongue causes the epiglottis to rotate rostrally, enabling visualisation of the vocal folds (Figure 9). t he laryngoscope should not be used to pull the epiglottis forwards unless it is absolutely necessary, as touching the epiglottis and other laryngeal structures should be kept to a minimum to avoid iatrogenic damage. t he laryngoscope can then be held by the left hand
leaving the right hand free for applying local anaesthetic and inserting the E t tube (Figure 10).
laryngeal desensitisation
t he larynx is usually desensitised using a lidocaine spray. It is possible to use injectable lidocaine 2% solution applied using a syringe and an intravenous catheter to spray the larynx, but this is not licensed, and care should be taken not to exceed the toxic dose. When using Intubeaze, the bottle must be held upright or the spray generated is inadequate. t his should be factored into the decision as to which recumbency to position the patient. For example, the (right handed) author’s preferred technique is to position the cat in left lateral recumbency, and operate the Intubeaze bottle with the right hand while holding the tongue and laryngoscope with the left hand.
t he lidocaine needs 30 to 90 seconds to take effect before intubation is attempted. It is imperative that the cat is adequately anaesthetised before tracheal intubation is attempted. Attempts to intubate the trachea with the cat too lightly anaesthetised may result in excessive coughing and laryngospasm, potentially necessitating a tracheostomy. maintenance of intravenous access allows titration of the depth of anaesthesia to optimise intubation conditions.


tracheal intubation
(a) the assistant holds the patient’s maxilla between thumb and forefinger. (b) the maxilla is held with tape.
Dorsal recumbency
t he patient is positioned in dorsal recumbency, and the anaesthetist uses a laryngoscope to raise the mandible and push the tongue upwards to
once the larynx is desensitised the E t tube is advanced through the rima glottidis between the vocal folds. If the arytenoid cartilages are moving with respiration, the tube should be advanced during maximal abduction. t he tube should not be forced through a closed glottis. t here should be no resistance to the passage of the tube. t he tube is then secured in place using a tie made of woven bandage or other suitable material which is usually tied behind the head or around the mandible caudal to the canines. once the tube is secure, it can be connected to the breathing system and oxygen supplied. If cuff inflation is required cuff pressure should be assessed by the method described above (Figure 6). It is recommended to secure the tube before cuff inflation to minimise movement
Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 16
a b
f igure 8. positioning the patient for intubation.
f igure 9. Viewing the larynx using a laryngoscope.
f igure 10. The anaesthetist holds the tongue and laryngoscope with the left hand, leaving the right hand free for spraying with local anaesthetic or intubation.

of the inflated cuff within the trachea. once the cuff is inflated administration of anaesthetic agent (and nitrous oxide if used) can be started.
preparation for a potentially difficult intubation
Before anaesthesia, the risk of problems during tracheal intubation should be assessed for each patient. If the risk of complications is considered to be high, e.g. in patients with upper respiratory tract noise or suspected nasopharyngeal polyp, preparations for alternative intubation techniques and emergency procedures should be made (Figure 11).
needle passed between tracheal rings. t his can be attached to a size 3.5 ID 15 mm E t tube connector and connected to an anaesthetic breathing system. Apparatus for this procedure should be prepared prior to anaesthesia in high risk cases. A transtracheal needle can also be used for retrograde wireguided orotracheal intubation. Lastly, a sterile tracheostomy kit should be available.
e xtubation
A skilled assistant must be available. Pre-oxygenation by mask or flow-by technique should be considered as this will increase haemoglobin saturation and provide more time for intubation before hypoxaemia occurs.
A laryngoscope is invaluable for aiding visualisation and access to the larynx. A blunt stylet may be useful to stiffen the E t tube. A stylet or a dog urinary catheter threaded through an E t tube can be passed through the larynx, and the tube guided over it once access to the trachea is achieved (Figure 12). Care must be taken to avoid iatrogenic damage to the larynx and trachea if a stiff stylet is used for this. Suction and throat swabs should be available if regurgitation or haemorrhage is likely. Suction can be achieved using a dog urinary catheter and a large syringe if a suction machine is not available.
If orotracheal intubation proves impossible, oxygen can be insufflated using a transtracheal 18 G hypodermic
Prior to extubation, the pharynx and larynx should be examined to detect the presence of debris, blood, gastric contents etc, particularly following dental procedures, gastroscopy, gastro-intestinal surgery, and in cases of megoesophagus. A laryngoscope may be useful for this. t he unwanted material can then be removed by swabbing or suction. Any throat packs or swabs should be removed. t he cuff must be deflated before extubation. Some anaesthetists recommend extubation early, when the ‘ear twitch’reflex returns, to minimise coughing and irritation of the larynx. o thers recommend extubation at the return of oral and pharyngeal reflexes. t iming of extubation may depend on the patient, e.g. brachycephalic patients should be extubated late to minimise the risk of upper respiratory tract obstruction. t he patient should be monitored for post-extubation upper respiratory tract obstruction until fully awake, although airway oedema may not develop for several hours. Patients considered at risk of obstruction should be closely monitored and equipment
for emergency intubation should be prepared and readily available.
Conclusions
tracheal intubation is routine in feline patients. An understanding of possible complications and their prevention is paramount in reducing morbidity. As with any clinical technique, adequate preparation is the key to a trouble-free procedure.

Acknowledgements
t hanks to michelle Higman, Elizabeth Leece and Andy Sparkes for the photographs used. t his article was sponsored by Dechra Veterinary Products.
References
Al-Shaikh B, Stacey S. Essentials of Anaesthetic Equipment (2nd edn), Churchill livingstone, e dinburgh, uk , pp 55–71, 2002
Davey A, Moyle JTB, Ward C. Ward’s Anaesthetic Equipment (3rd edn), WB saunders Company ltd, l ondon, uk , pp 120–166, 1992
Hardie EM, Spodnick GJ, Gilson SD. tracheal rupture in cats: 16 cases (1983–1998). J Am Vet Med Assoc 214, 508–512, 1999
Hartsfield SM. Airway management and ventilation. In: lumb and Jones’ Veterinary Anaesthesia (3rd edn). Thurmon JC, tranquilli WJ, Benson GJ (eds). Williams and Wilkins, Baltimore, usA, pp 515–556, 1996

Mitchell SL, McCarthy R, Rudloff E et al . tracheal rupture associated with intubation in cats: 20 cases (1996–1998). J Am Vet Med Assoc 216, 1592–1595, 2000 Wong WT, Brock KA. tracheal laceration from endotracheal intubation in a cat. Vet Rec 134, 622–624, 1994 l

Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 18
f igure 12. A dog urinary catheter has been passed into the trachea and an et tube is threaded over it to achieve tracheal intubation (the same patient as figure 11).
f igure 11. A bleeding pharyngeal mass obscures the larynx.

A case of zinc toxicity in a galah (Eolophus roseicapilla)
Case history
A 2-year-old female galah (Eolophus roseicapilla) was presented with a 2-day history of inappetence, vomiting, passing loose droppings and a ‘fluffed up’ appearance. t he bird had vomited frequently for the past 2 days but not on the day of examination.

t he bird’s normal diet was varied and consisted of vegetables, pellets, seed, vitamins and willow tree branches. It had been in the owners’ possession since it was fledged. t here were no other aviary birds on the property, and it had not received anthelmintics since it had been in their possession.
t he bird had free range of the property for part of each day so access to unspecified plants in the garden was a possibility. A recently purchased zinc-galvanised cage had some flaking of the coating on it, however the owner felt the bird was becoming unwell prior to arrival of the new cage. Approximately 3 weeks ago a bird toy in the shape of shoe had been purchased from which metal eyelets were now missing.
Clinical findings
on distance examination, the bird was sitting fluffed up in the carry cage. t here was accumulation of bright green faecal material on the feathers around the vent and crusted material in the chest feathers. Prior to closer examination the patient was placed in a darkened, warm, humid environment for 30 minutes to recover from travel and reduce stress. on close examination the bird was in ideal body condition and weighed 265 g. t he crusting in the chest feathers was consistent with vomited crop contents. t he crop was empty. No abnormalities were detected on coelomic palpation. No dyspnoea was present.
t he problems identified from the history and the clinical examination were vomiting, diarrhoea, reduced appetite and lethargy. t he history was indicative of vomiting rather than regurgitation. Differential diagnoses for vomiting include dietary indiscretion (toxins, plants, spoiled food), infections (proventricular dilatation disease (PDD), bacterial, fungal, gastric yeast), psittacosis (Chlamydia psittaci ), heavy metal intoxication (lead or zinc), or metabolic (hepatopathy, sepsis, pancreatitis) (Bowles et al. 2007). In assessing this list, dietary indiscretion
Contact: lisas@vetsouth.co.nz
was considered most likely given the free-range time outside, and heavy metal intoxication was quite possible given the damaged toy. PDD is considered to be exotic to New Zealand according to mAF Biosecurity (2009), although it is widely distributed in caged parrots in Australia. Psittacosis was lower on the differential list as this often presents with respiratory as well as gastrointestinal clinical signs.
Diagnostic findings
Based on the differential list, a plan was formulated to check serum biochemistry for metabolic disorders, haematology for evidence of infectious disease, serum concentrations of heavy metal and radiographs for signs of gastrointestinal tract dilation, obstruction and any significant changes to the coelomic organs.
t he patient was pre-oxygenated while being maintained in a warm environment. using a gas mask, light anaesthesia was induced with isoflurane (Isoflurane medsource NZ Ltd, Ashburton NZ) delivered at 2 L/minute via facemask, starting at
Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 20
CA se R ep OR t
lIsA s tuARt BVsc (dist), pGCertsc

0.5% and increasing by 0.5% every 30 seconds until a sufficient plane of anaesthesia for radiography was reached at 1.5%. t he patient was stable with an uneventful recovery following blood collection and radiography.
Blood was collected from the right ulnar vein with pressure applied after venipuncture to reduce haematoma formation. As the total volume collected must be <0.5–1% of bodyweight including any haematoma which forms (Doneley 2018), tests had to be prioritised to give maximum information. A serum biochemistry screen ( table 1) was immediately processed inclinic using the Vetscan Avian/Reptilian Profile Plus rotor on the Vetscan VS2 machine (Abaxis Inc. union City CA, uSA) to reduce post-collection artefact (Hoppes et al. 2015). Results were compared to two reference ranges for psittacines as a reference range for Eolophus spp. could not be found. Sufficient blood was collected to allow measurement of lead concentrations in blood and zinc concentrations in serum (New Zealand Veterinary Pathology, Hamilton, NZ). A microhaematocrit sample was assessed in-clinic as having a packed cell volume of 44% (reference rang 38–48%; Adamcak et al. 2000) and a blood smear assessed in-clinic showed no significant abnormalities. t here was insufficient sample to request a full haemogram at the external laboratory.
t he following abnormalities (according to the reference ranges applied) were observed: mild increase in potassium concentration, decrease in creatine kinase activity and decrease in phosphorus concentration. Based on these results, hepatopathy was ruled out and the supportive treatment plan remained unchanged.
Lateral and ventrodorsal radiographic views (Figure 1) of the whole bird showed the presence of four radiopaque particles in the ventriculus which had a similar radio-opacity to the metal marker and the metal leg band on the patient. t here was no dilation of the gastrointestinal tract suggesting obstructive disease. t hese observations sent heavy metal toxicosis to the top of our differential list despite not yet having the results of zinc and lead testing.


table 1. s erum biochemistry results measured in-clinic for a female galah with a 2-day history of innappetence and vomiting.
c Extrapolated from reference ranges for albumin and globulin d Converted to SI units using the website http://www.endmemo.com/medical/unitconvert
Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 22
Reference ranges Analyte Units Measurement Cockatooa Psittacinesb Aspartate aminotransferase (AS t ) Iu/L 309 52–203 90–380 Bile acids (BA) µmol/L 35 23–70 Not recorded Creatine Kinase (CK) Iu/L 0 34–204 110–875 uric acid (uA) µmol/L 207 190–327 59.48–684.02 Glucose (GLu) mmol/L 14.8 12.8–17.6 6.94–19.43 Calcium (CA) mmol/L 2.12 2.2–2.7 2.0–3.38 Phosphorus (Phos) mmol/L 0.63 Not recorded 0.94–2.13 total Protein ( t P) g/L 34 35–44 30–50 Albumin (ALB) g/L 16 Not recorded 13–32 Globulin (GLoB) g/L 17 Not recorded 13–19 Albumin/globulin ratio 0.94 1.5–4.3 0.68–2.46 c Potassium (K+) mmol/L 5.1 3.2–4.9 2.2–4.6 d Sodium (Na+) mmol/L 140 152–164 134–156 a Lumeij and o verduin 1990 b Hoppes et al. 2015
a b
f igure 1. l ateral (a) and ventrodorsal (b) radiographic views of a galah with a 2-day history of innappetence and vomiting.

A crop swab and faecal sample taken a day prior to this consultation had been submitted to Gribbles Veterinary Pathology (mosgiel, NZ). Both samples were submitted for culture (but not cytology). t his revealed a heavy growth of Streptococcus spp. in the faecal sample but no growth from the crop swab. t he presence of Streptococcus spp. in the faecal sample was interpreted as normal faecal flora (Alan Fudge, pers. comm., Veterinary Information Network).
t he tests for blood lead and serum zinc concentrations were performed at New Zealand Veterinary Pathology and the results reported 2 and 6 days respectively after the samples were submitted ( table 2). t he serum zinc concentration was so high that it required retesting by the laboratory. t he delayed reporting meant chelation therapy could not be discussed with the owner while the bird was still in clinic.
Analyte Measurement (units) Comment from laboratory
Zinc 207 µmol/L Zn levels >30 are diagnostic of zinc toxicity. t his is an extremely high zinc level, compatible with zinc toxicity.
Lead <0.03 mg/L Wildbase, massey university recommends that avian blood lead concentrations should not exceed 0.1 mg/L.
treatment
While the bird was sedated for blood sampling and radiography, its maintenance fluid requirement (13 mL based on a rate of 50 mL/kg/day) was administered as lactated Ringer’s solution (LRS; Baxter Healthcare Ltd, Auckland, NZ) SC over the dorsum in three sites. A recommendation was made that the bird was hospitalised so that fluid therapy could be continued via crop and/or SC supplementation while the results of final diagnostics were obtained. However, this was declined and treatment as an outpatient was initiated with 0.5 mg/kg metoclopramide (metoclopramide HCl; Baxter Healthcare Ltd, Auckland, NZ) given orally 2–3 times daily, with oral electrolytes (oralade; macahl Animal Health Ltd, uK). While there are no pharmacokinetic studies, there are anecdotal recommendations to use metoclopramide to improve crop motility and control regurgitation (Bowles, 2007). t he plan was that if vomiting continued and or fluid intake was insufficient then the patient would be admitted to the hospital.
t he patient was re-examined and admitted to hospital the following morning as it was not drinking at home. Supportive treatment started with oral fluid therapy as protracted vomiting was not occurring. If oral fluids were insufficient then the next option would have been intermittent SC fluids, followed by IV or intraosseous access if needed. maintenance fluid requirements had been calculated at 13.25 mL/day and the bird was estimated to be 5% dehydrated after 24 hours at home with minimal fluid intake. Aiming to replace the first 50% of the dehydration loss within the first 24 hours, this gave a goal of 20 mL fluids/day plus any ongoing losses. t he estimated safe crop volume for medium parrots is 10–15 mL and large parrots is 20–30 mL (Lisa Argilla, pers. comm.; Wismer 2009). t he fluids were
administered to the galah at a rate of 5 mL every 2–3 hours which was well within the crop volume guidelines. LRS was selected for the first two doses of crop fluids. When this was tolerated with no vomiting, oralade was added in a 1:1 ratio to the LRS for the next two feeds. t here was no vomiting through day 1 of hospitalisation and by later in the day the patient was starting to eat fruit and vegetables out of the nurses’ hands. No vomiting was observed at any stage while in the hospital. During day 2 of hospitalisation, oral fluid supplementation using oralade and LRS in a 1:1 ratio for a total of 20 mL was repeated. t he patient continued to eat when hand fed and later in the day started voluntarily drinking as well. t he faeces were still bright green but the urates were white. Body weight remained stable at 265 g.
t he patient was discharged for supported feeding at home while we awaited the results of the heavy metal testing. Follow-up phone calls with the owner confirmed that the bird was drinking well with an improving appetite but was still quiet. t he faeces continued to gradually return to their normal colour and consistency.
Six days after the initial presentation, the serum zinc concentration was reported as 207 µmol/L consistent with zinc toxicity. For recommendations for treatment for zinc toxicity see Box 1. By the time the zinc results were available, the owner reported that the bird’s behaviour, eating and drinking habits had returned to normal. t hey declined another hospital admission and more intensive therapy at this stage. t he decision was made to start ½ teaspoon psyllium (metamucil, Procter & Gamble, Auckland, NZ) daily, added to 60 mL baby food, diluted peanut butter or fruit and vegetables to encourage metal items to pass through the gastrointestinal tract.
Box 1. Treatment recommendations for heavy metal toxicosis in birds (Green 2004)
1. Fluid therapy with LRS to prevent renal damage from dehydration and potential chelation toxicosis, and to offset the fluid loss due to polyuria. Fluid rates of up to 100 mL/kg/hour are recommended and the oral route can be used if gastrointestinal tract is working.
2. Warm environment of 28–30°C with a humidification source.
3. Chelation therapy – administration of an agent that binds to zinc forming non-toxic complexes which can then be excreted.
4. Catharsis (e.g. psyllium) to encourage metal items to pass through the gastrointestinal tract.
5. If seizures develop, then use of diazepam may need to be considered.
A plan was made to repeat the measurement of serum zinc concentration and radiography 2.5 weeks after the initial presentation to see if the zinc particles had been excreted, if the zinc concentration was reducing and revisit whether chelation therapy was required. At this revisit, the bird had maintained its weight and had no history of further vomiting or diarrhoea. Radiography showed only one radiopaque particle remaining in the ventriculus. t he serum zinc concentration had reduced from 207 µmol/L to 48.7 µmol/L, consistent with the reduced amount of radiopaque material in the
Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 24
table 2. measurement of concentrations of zince in serum and lead in blood of a galah presenting with innappetence and vomiting

ventriculus (assuming that this material had contributed to the zinc toxicosis). Based on this improvement, chelation therapy was not pursued. Addition of psyllium to the diet was continued for a further 2 weeks. t he patient made an uneventful recovery and no further monitoring was performed.
Discussion
Just as with other veterinary species, the first step of managing and treating a sick bird is a thorough history and clinical examination to allow differential diagnoses to be considered and the most appropriate diagnostic tests to be performed. Distance examination and minimising stress prior to and during handling are even more important in birds than other veterinary species.
With regards the differentials under consideration for this case, infectious causes (e.g. by food contamination), toxins (heavy metal, plants, other environmental contaminants), foreign body ingestion, pancreatitis, secondary causes of vomiting such as hepatic or renal disease, were all under consideration. Parasitism seemed less likely differential given the bird was not in an aviary situation and exposed to frequent faecal contamination in the environment, however given it had some outdoor access, this could not be completely discounted. Pancreatitis in birds is rarely documented antemortem but should be suspected in birds showing abdominal pain or gastrointestinal dysfunction. Similar to mammals, hyperamylasaemia can be suggestive of pancreatitis, but it is not present in all affected birds and amylase is not included on the Vetscan Avian/ Reptilian rotor.
A crop swab and faecal sample collected the day prior to the initial consultation were submitted for bacterial culture. In retrospect, rather than a culture of the crop contents, a swab would have yielded more information faster. Alan Fudge recommends swabbing the crop with a saline-moistened swab and using this to make a saline wet mount, followed with a Gram's stain. t his can be used to look for bacteria, yeasts and flagellates such as Giardia or Trichomonas in some bird species. Gram staining of fecal smears are a commonly used
tool in parrots to assess enteric health with low numbers of Gram-positive bacteria predominating in the healthy psittacine gastrointestinal tract. Evans et al. (2014) looked at the agreement of faecal Gram stains with culture results in 21 healthy parrots and found that Gram's stains and bacterial culture may need to be performed with a parallel testing strategy to limit the likelihood of misclassifying the microbial flora of psittacine patients. Performing a faecal Gram stain would have been a quicker way of identifying if there was bacterial overgrowth and if antibiotics or other diagnostic work-up was indicated while waiting for the culture results. A faecal egg count could also have been performed to see if there was any indication for anthelmintic treatment.
By the time the test results indicating zinc toxicosis was received, the patient was clinically improving. t he movement of metal particles through the gastrointestinal tract of a bird is very different to that of a mammal (Green, 2004). t he ingested particles are often trapped with the ventriculus contents and are gradually ground into smaller particles, creating a greater risk of metal poisoning for birds. Lead and zinc toxicosis can produce similar signs affecting multiple organ systems including the gastrointestinal tract, nervous system, kidneys and haematopoietic system. Zinc is not sequestered in bone or other tissue like lead, so once it is cleared from the gastrointestinal tract there is no concern about mobilisation from bone increasing circulating concentrations again months after the initial ingestion. Zinc toxicosis is more often seen in caged birds due to more potential sources of zinc being available domestically. Clinical signs can include regurgitation, diarrhoea, anorexia, lethargy, depression, ataxia, seizures, feather picking, polyuria/ polydipsia, anaemia and sudden death.
Diagnosis of zinc toxicosis may be supported by presence of hypochromic microcytic anaemia, increased alanine aminotransferase (ALt ) activity and increased blood glucose. Interestingly these anomalies were not recorded in this case – however the Vetscan Avian rotor does not measure ALt activity. Zinc is an essential dietary trace element and
some amount of zinc is expected to be present in the serum of healthy birds however it should be <30–55 µmol/L depending on the reference range used by the reporting laboratory (NZVP, Lisa Argilla, pers comms.). t he concentration recorded in this galah (207 µmol/L) could therefore be considered extremely high. When reviewing the management of this case, daily weighing of the patient was a useful tool. It also would have been ideal to have weighed any food or water left in the cage so that the actual voluntary intake could be calculated. t here was not an effective assessment of whether the bird had abdominal pain which required analgesia (e.g. butorphanol). Fluid therapy was appropriate for maintenance and to correct for fluid losses from vomiting. Birds should not be fasted due to their high metabolic rate and energy requirements (Doneley, 2001), which is why oralade was added into the oral fluids to replace electrolytes and some energy until the patient was eating.
t he galah’s serum zinc concentrations were high enough initially that starting chelation therapy would have been appropriate. However, as it was starting to improve when the diagnosis was confirmed, the owners declined this treatment and opted to retest and monitor. When the zinc concentration was re-checked, it had dropped from 207 µmol/L to 48.7 µmol/L; chelation therapy was still justifiable (but again declined). Recommendations for chelation therapy are to administer calcium EDtA at a dose of 25–50 mg/kg Im every 12 hours for 5 days then reassess serum zinc concentrations 2 days later and repeat the treatment if needed (Lisa Argilla, pers. comm.). Calcium EDtA can be compounded by a veterinary compounding pharmacy (e.g. optimus Healthcare Ltd, Penrose, Auckland NZ) to give a volume suitable for injection into the patient. While receiving chelation therapy, supportive treatment with fluids, warmth and rest are important.
Conclusion
Heavy metal intoxication should always be considered in any bird showing gastrointestinal signs. Zinc toxicity is more common than lead toxicity in pet
Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 26

birds due to more exposure to this metal within their living environment. management of avian cases is possible and rewarding in general practice: just follow the same process as for all other patients – a good history, a diagnostic plan and supportive care while the treatment plan is sorted.
Acknowledgments
t hanks to Lisa Argilla (Wildlife Hospital Dunedin) for taking the time to discuss this case and her recommendations regarding zinc toxicosis management in parrots.
Relevant Reading
Adamcak A, Hess LR and Quesenberry KE. Intestinal string foreign body in an adult umbrella Cockatoo (Cacatua alba). Journal of Avian Medicine and Surgery 14, 257–63, 2000
Bowles H, Lichtenberger M, Lennox A. emergency and critical care of pet birds. Veterinary Clinics of North America: Exotic Animal Practice 10, 345–94, 2007
Doneley RJT. Acute pancreatitis in parrots. Australian Veterinary Journal 79, 409–11, 2001
Doneley RJT. Clinical Pathology of Exotic Pets. https:// www.vin.com/apputil/content/defaultadv1. aspx?pId=22915&catId=124640&id=8896524 (accessed 16 April 2023). World small Animal Veterinary Association Congress proceedings, 2018
Evans EE, Mitchell MA, Whittington JK, Roy A, Tully TN. measuring the level of agreement between cloacal Gram's stains and bacterial cultures in Hispaniolan Amazon parrots ( Amazona ventralis). Journal of Avian Medicine and Surgery 28, 290–6, 2014
Green C. Heavy metal toxicoses in birds. Companion Animal Society Newsletter 15 (3), 24–8, 2004
Hoppes SM, Boyd JD, Brightsmith DJ. Impact of delayed analysis in avian blood biochemical values measured with the Abaxis Vets can Vs2. Journal of Avian Medicine and Surgery 29, 200-9, 2015
Lumeij JT, Overduin LM. plasma chemistry references values in psittaciformes. Avian Pathology 19, 235-44, 1990
MAF Biosecurity New Zealand. Import Risk Analysis: Psittacine Hatching Egg s draft, pp 62–5, https://www.mpi.govt.nz/ dmsdocument/6076-psittacine-hatching-eggs-draft-import-riskanalysis-august-2009, (accessed 19 April 2023). Wellington, NZ, 2009
Wismer T. Managing Toxicoses in Exotic Animals. Wild West Veterinary Conference 2009, 2009 l
t his article was written as part of the requirements for receiving the Dechra/CAV "A week with ..." scholarship

Would you like to see your pet on the cover of Companion Quarterly?

We now have a new cover photo for each issue of Companion Quarterly. This means we are always on the lookout for suitable photos. Photos selected for the cover must be landscape orientation (or able to be cropped to this), crisp and well focused, and of high resolution (at least 300 DPI). They must also be well composed and interesting.
Please send any suitable images to the Editor (sarah.fowler@gmail.com). If however you have a favourite snap of your furfamily that’s not quite up to cover standards, please send that in too: photos that are not selected for the cover may be printed on the back inside cover.
Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 28

CA se R ep OR t
Rat bait is not always an anticoagulant!
Cholecalciferol rat bait poisoning in a dog.
NeI l s tuttle, BVsc
Introduction
In New Zealand pest control baits containing cholecalciferol (vitamin D3) are commonly used for control of possums. However it is also available for use as a rodenticide as Selontra soft gel blocks. Cholecalciferol is as a pest bait used due to its properties of breaking down in contact with soil, light and heat, insolubility in water, low toxicity in birds and a low risk of secondary poisoning. once ingested cholecalciferol is absorbed completely and rapidly from the jejunum. It is metabolised by the liver and kidney and excreted mainly in the faeces. Cholecalciferol acts as a positive regulator of calcium homeostasis. Excessive amounts of cholecalciferol lead to hypercalcaemia by increasing calcium and phosphorus absorption from the intestinal tract, mobilising of calcium and phosphorus from bone and decreasing renal excretion of calcium. It generally takes 12–24 hours for hypercalcaemia and hyperphosphatemia to develop (Parton et al. 2018) with hyperphosphatemia preceding the hypercalcemia by up to 12 hours. t he effects of hypercalcaemia are caused by calcium being deposited (metastatic calcification) in the heart, blood vessels, kidneys, liver and lungs. t he most common clinical signs associated with hypercalcaemia are polydipsia, polyuria and anorexia. Weakness vomiting and constipation can also occur (Chew 2001).
t his report describes diagnosis and treatment of a dog that ingested an unknown amount of rat bait containing cholecalciferol.
Contact: neil.stuttle@vshb.co.nz
Case history
“Herbie” a 2-year-old, male, Jack Russell/ Shih tzu cross was presented to the clinic with anorexia and vomiting. t he owners reported that Herbie had ingested some rat poison blocks 2 days earlier, but were unsure the total amount Herbie had eaten. t he rat bait Herbie had ingested was Selontra Soft Bait (BASF New Zealand Ltd., Auckland, NZ) blocks containing 0.75 g/kg cholecalciferol.

Further questioning revealed Herbie was also drinking and urinating significantly more than normal.
Clinical examination
on clinical examination Herbie was quiet and responsive. t he oral mucous membranes were pink with a capillary refill time of < 2 seconds. mild drooling was present. Skin turgor was within normal limits. on chest auscultation lungs sounds were clear and the heart rate was 120 beats per minute, with a regular rhythm and no murmur. t he abdomen was soft and comfortable on palpation. Herbie’s rectal temperature was 38.6°C and he weighed 8.7 kg.
Diagnostic findings
A jugular blood sample was taken and a comprehensive diagnostic serum biochemistry profile (see table 1) was run on a Vetscan VS2 Chemistry Analyser (Zoetis New Zealand, Auckland, NZ) to determine the severity of metabolic effects. It was decided not to obtain a complete blood count or urinalysis as
easurements in red and blue text are greater or less than the reference range respectively
Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 30
[Photo courtesy of Herbie's owners and the author]
Concentration in serum at time after ingestion a Analyte (units) Reference range 2 days 4 days 5 days 11 days 42 days total calcium (mmol/L) 2.15–2.95 3.83 >4 3.73 3.01 2.73 Albumin (g/L) 25–44 40 39 31 44 42 Globulin (g/L) 23–52 23 33 45 25 24 t P (g/L) 54–82 62 72 76 68 62 Glucose (mmol/L) 3.3–6.1 6.5 6.5 6.9 6.3 5.7 Amylase (u/L) 200–1,200 358 401 376 485 595 ALt (u/L) 10–118 64 49 100 134 39 ALP (u/L) 20–150 29 70 111 459 33 Phosphate (mmol/L) 0.94–2.13 2.42 1.92 0.82 1.25 1.89 Creatinine (µmol/L) 27–124 75 147 90 82 83 urea (mmol/L) 2.5–8.9 12.9 11.8 13.3 7.9 7.6 Na+ (mmol/L) 138–160 150 155 148 153 152 K+ (mmol/L) 3.7–5.8 3.3 4.0 3.0 4.5 4.1 a m
table 1. s erum biochemistry results for a 2-year-old terrier cross dog that ingested rat bait containing cholecalciferol.
the results were unlikely to change the treatment approach.
Based on the clinical exam and serum biochemistry data Herbie’s problem list was as follows:
l Anorexia
l Vomiting/nausea
l Polyuria/polydipsia
l Hypercalcaemia
l Hyperphosphataemia
l Increased BuN
l Hypokalaemia
t he biochemical changes were all supportive of a diagnosis of vitamin D toxicity. If a urine sample had been obtained this would be expected to show hyposthenuria, proteinuria and glucosuria ( t illey et al. 2004).
treatment and outcome
to correct dehydration, Herbie was started on IV fluids (compound sodium lactate; Baxter Healthcare Ltd, Auckland, NZ) with 20 mmol/L potassium chloride to manage the existing hypokalaemia. IV fluids were administered at a rate of 100 mL/kg/day (Chew 2001). maropitant (Cerenia; Zoetis) was administered slow IV at 1 mg/kg once daily to treat nausea/ vomiting. Herbie was also started on furosemide (Baxter Healthcare Ltd.) 2.5 mg/kg IV once daily to decrease serum calcium concentration through diuresis.
o ver the following 48 hours Herbie was stable but remained quiet, anorexic, polydipsic and polyuric. A repeat blood sample was taken to assess serum analytes ( table 1, 2 days). Concentrations of total calcium and creatinine in serum had increased while the concentration of urea level decreased but was still elevated above the normal range. Concentrations of phosphate and potassium in serum were now in the normal range.
In order to further reduce serum calcium concentrations, it was decided to start Herbie on dexamethasone (Dexa 0.2 injection; PHENIX NZ) IV 0.15 mg/kg twice daily along with an infusion of 1.3 mg/kg pamidronate disodium (Pamisol; Pfizer NZ Ltd., Auckland, NZ) in 150 mL 0.9% saline given as an IV infusion over 2 hours. Following the infusion Herbie
was maintained on IV fluids (0.9% saline) at 100mL/kg/day.
A day later Herbie was eating and appeared brighter. A repeat blood sample was taken for serum biochemistry analysis ( table 1, 4 days) which revealed a reduction in serum calcium concentration, though Herbie was still hypercalcaemic. t he concentration of creatinine was now within normal limits but the BuN was mildly increased. Hypokalaemia was present along with hypophosphataemia.
Herbie was switched onto 2.5 mg/kg furosemide and 1.5 mg/kg prednisone both given orally twice daily. oral potassium supplementation (1000 mg) was also started (Kaminox, Vetplus), given twice daily. Herbie’s diet was changed to a kibble with a low calcium concentration (Hill’s K/D; 0.57% calcium Dm).
o ver the next 24 hours Herbie continued to eat well and was much brighter. t he IV fluids were discontinued and Herbie was discharged home on oral furosemide, prednisone and oral potassium at the doses described above.
Herbie was seen again 1 week later. t he owners reported he was bright and eating well. He was still drinking and urinating substantially more than usual. t he clinical exam was unremarkable.
Herbie had lost 100 g in body weight. A blood sample was taken for serum biochemistry ( table 1, 11 days). t he total calcium concentration was still marginally elevated. t he serum concentration of phosphate, urea and potassium were now within the normal reference ranges.
Herbie was weaned off the prednisone, kaminox and furosemide over the following 2 weeks and continued on Hill’s K/D diet. Herbie was seen 1 month later. t he owners reported his rate of drinking and urinating had returned to normal. He was bright, alert and responsive. Herbie had gained 1 kg in weight. A blood sample was taken to assess serum biochemistry ( table 1, 41 days). t he total calcium concentration was now within the reference range. Herbie was re-introduced onto a standard commercial diet. No further follow-up examinations were scheduled.
Discussion
t his report describes diagnosis and treatment of a dog that ingested an unknown amount of a rat bait containing cholecalciferol. toxicity of cholecalciferol has been reported with a dose as low as 3 mg/kg but is more likely with doses >10 mg/kg (Parton et al. 2018). It was uncertain the exact amount Herbie had ingested but given his clinical signs it was presumed to be at least 10 mg/kg. In Herbie’s case his owners were aware of the ingestion of cholecalciferol and so the reason for the subsequent hypercalcaemia was apparent. t his however is not always the case and the cause of hypercalcaemia is often not initially known. Hypercalcaemia can be transient and inconsequential (common), persistent and inconsequential or persistent and pathological (Chew 2001). Inconsequential hypercalcaemia can be caused by haemoconcentration, post-feeding, lipaemia and EDtA/citrate contamination. Puppies and kittens
< 12 weeks old have significantly higher normal concentrations of calcium in serum than adult dogs/cats (mackay 2022). t he most common pathological causes of hypercalcaemia in dogs are neoplasia (e.g. lymphoma, anal gland adenocarcinoma) and vitamin D toxicity. In cats the most common causes are renal failure and idiopathic (mackay 2022).
Calcium exists in three fractions in plasma: 35% is in the ionised (biologically active) form, 10% is chelated and 55% bound to albumin (mackay 2022). most in -house biochemistry analysers measure the concentration of total serum calcium. In clinically normal animals serum ionised calcium is typically proportional to the level of serum total calcium. Ideally serum concentration of ionized calcium is measured when there is a disease state resulting in hypercalcemia. t he concentration of ionised calcium is reduced in patients with renal failure and hypoalbuminaemia, and increased in patients with moderate to severe metabolic acidosis (Chew 2001). Serum samples for measurement of ionised calcium need to be stored anaerobically before analysis as concentrations are affected by exposure to oxygen and changes in pH. If pH decreases calcium is displaced from binding sites and the
Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 31
ionised serum levels increase. If pH increases more calcium is bound and the ionised serum levels decrease. If stored anaerobically at 4°C samples are stable for up to 72 hours (Chew 2001). In this case ionised calcium concentration was not measured due to logistics of storage and transport to an external laboratory. treatment of hypercalcaemia is best targeted towards the underlying cause, e.g. removal of parathyroid adenoma or chemotherapy for lymphoma. In Herbie’s case, the cause was vitamin D toxicosis so the management was supportive and aimed to reduce the degree of hypercalcaemia until the concentration of absorbed cholecalciferol reduced to below clinically significant levels.
If Herbie was presented within 4–6 hours of ingestion then emesis would have been induced and activated charcoal administered orally every 8 hours for 48 hours (Romine 2022). t his is due to vitamin D being fat soluble and the likelihood of enterohepatic recirculation. Herbie was presented 48 after ingestion so decontamination in this case was not possible. In Herbie’s case supportive therapy was undertaken to reduce serum concentration of calcium to less toxic levels.
Parental fluids were administered to correct dehydration. Haemoconcentration contributes to increased serum ionised calcium concentration. t he ideal parental fluid type is 0.9% saline at 100–125 mL/kg/day (Chew 2001). In Herbie’s case lactated Ringers solution (LRS) was initially chosen due to concurrent hypokalaemia. After 48 hours the fluids were changed to 0.9% saline based on increasing calcium concentration and normal potassium concentration in serum. on reflection, 0.9% saline could have been used initially with increased potassium supplementation to reduce calcium concentrations. one litre of LRS contains 2.7 mEq of calcium which would be adding to the already high concentration of calcium in the blood.
o nce the patient is hydrated, 2–4 mg/ kg IV furosemide, given SC or orally every 12 to 8 hours is used to decrease serum calcium concentration through diuresis.
After 48 hours, despite this treatment, the concentration of calcium in Herbie’s serum had increased (from 3.83 to >4.00 mmol/L) so he was started on glucocorticoids and pamidronate. Corticosteroids exert their effect by reducing bone resorption, decreasing intestinal calcium absorption and increasing renal calcium excretion (Chew 2001). However they should be withheld if a definite diagnosis has not been established. t he administration of glucocorticoids in this case resulted in the steroid-induced elevation of the ALP isoenzyme and AS t in the day 5 and 11 blood results. Initial serum biochemistry results showed no evidence of liver disease and after treatment activities returned to within normal limits by day 42. Pamidronate is a diphosphonate that works by inhibiting osteoclastic bone resorption (mackay 2022). Pamidronate was sourced from a local pharmacy by external prescription and is relatively inexpensive (~ $40). Biphosphates are the standard of care in human oncology for treating hypercalcaemia of malignancy and prevention of pathological fractures associated with metastatic bone disease.
Herbie’s serum calcium concentration began to drop 24 hours after treatment with pamidronate and dexamethasone. Herbie also clinically improved in his demeanour and appetite. once he began eating, Herbie’s calcium concentrations were further managed with a restricted calcium diet. Low calcium diets are only helpful in substantially lowering serum calcium concentrations where hypercalcaemia is caused by the action of excess vitamin D metabolites (Chew 2001). Hill’s Canine K/D was chosen as it contains 0.57% calcium on a dry matter (Dm) basis. Standard dog food generally contains 1.0–1.7% calcium Dm
o ther possible treatment options in this case included calcitonin treatment to treat hypercalcaemia and haemodialysis and lipid infusion therapy to help clear the toxin. Calcitonin acts to reduce osteoclast activity and inhibits the formation of new osteoclasts. Calcitonin can be used as an alternative to bisphosphonate (e.g. pamidronate) treatment or following bisphosphonate treatment if there has not been a
sufficient response ( t illey et al. 2004). t he dose of calcitonin is 4u/kg SC once or twice daily (Nelson et al. 1998). many patients have a limited response and may become refractory to treatment so it needs to be combined with other treatments as discussed above ( t illey et al. 2004). Give the good response to the pamidronate infusion in this case, calcitonin treatment was not considered.
Haemodialysis is the process of exchanging water, solutes and toxins across a semi permeable membrane. toxins that are not tightly protein bound and are small enough to fit through the artificial membrane pores can effectively and quickly be removed. However, as it is generally a specialist procedure, haemodialysis is unavailable to most patients.
Intravenous lipid emulsion (ILE) therapy is another potential treatment of cases of vitamin D toxicosis given the lipophilic nature of cholecalciferol. Lipid emulsions are sterile mini-emulsions of oil and water. t he oil component consists of neutral long chain triglycerides or a mixture of medium and long chain triglycerides. ILE was first used in the early 2000s to treat local anaesthetic toxicities in humans. t here are growing case reports that ILE is useful in treating veterinary patients with lipid soluble toxins (Epstein et al. 2013). t he mechanism of action is still being investigated and is currently thought to be due to a “shuttle” effect. t his is where the liposomes scavenge toxins from lipid-rich tissues and carry them to other organs where metabolism and elimination can occur. Case reports have shown benefits in cats with permethrin toxicity (Di Pietro et al. 2022) and in dogs with avermectin/milbemycin toxicities (Epstein et al. 2013). t here are no reports to the author’s knowledge treating cholecalciferol toxicity with ILE.
t his case also highlights the need for client education in early presentation following a toxin ingestion. Presentation to the clinic immediately after ingestion in this case for induction of emesis and activated charcoal would have likely to have been sufficient in preventing the toxic dose being absorbed.
on reflection on the management of this case, fluid therapy with 0.9% saline
Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 32
supplemented with potassium would have been started instead of LRS to minimise administration of exogenous calcium. In hindsight corticosteroid treatment could have been started earlier in the clinical management of the case, and indeed was considered at the time of initial treatment. It was decided to hold off administering this treatment until the response to IV fluids and furosemide could be assessed. If in this case, a large toxic dose of cholecalciferol was known to be ingested, then treatment corticosteroids and pamidronate would have been started earlier.
Herbie made a complete clinical recovery and continues to do well at the time of writing.
References
Chew D. Hypercalcaemia in dogs: approach to diagnosis and treatment. https://www. vin.com/doc/?id=3843801 (accessed 7 may 2023). Proceedings World Small Animal Veterinary Association Congress, 2001

Di Pietro S, Falcone A, Arfuso F, Pennisi M, Piccione G, Giudice E. treatment of permethrin toxicosis in cats by intravenous lipid emulsion. Toxics 10, 165, 2022
Epstein SE, Hollingsworth SR. Ivermectin induced blindness treated with intravenous lipid therapy in a dog, Journal of Veterinary Emergency and Critical Care 23, 58–62, 2013 Mackay Bruce. Calcium disorders - highs and lows in small animal patients. Online Veterinary Conference 2022, Vet e ducation, James Cook university, Ql D, 2022
Nelson RW, Couto CG. (e ds) Small Animal Internal Medicine, 2nd e dtn, pp 826–9, mosby Inc., st l ouis. mO, usA, 1998
Parton K, Bruere AN, Chambers JP. (e ds) Veterinary Clinical Toxicology, 3rd e dtn. pp 131–4, massey university press, palmerston North, NZ. 2018
Romine J. Calcium and vitamin D disorders. Proceedings New Zealand Veterinary Association Conference, Companion Animal Branch, pp 15–6, 2022
Tilley LP, Smith FWK. (e ds) The 5-Minute Veterinary Consult, Canine and Feline, 3rd e dtn. pp 1356 –7. lippincott Williams & Wilkins, philadelphia, pA, usA, 2004 l
Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 33
s tu DeN t CA se R ep OR t pericardial mesothelioma in a 6-year-old German shepherd dog
CHAR l O tte Bell AtON, BVscV
Abstract
Canine mesothelioma is a rare form of neoplasia in dogs which is challenging to diagnose and treat and is usually associated with a poor prognosis. mesothelioma of the thoracic cavity can involve the pleural space and/ or the pericardial sac and this diffuse cavity involvement often requires an invasive method of biopsy to confirm the diagnosis. t his case report describes the presentation, diagnosis, treatment and outcome of mesothelioma of the pericardial/pleural spaces in a 6-year-old German Shepherd dog that presented for lethargy, inappetence and a distended abdomen. Initial pericardiocentesis suggested septic pericardial disease. However the subsequent development of marked pleural effusion prompted surgical intervention, allowing relief from cardiac tamponade via a sub-total pericardiectomy and confirmation of the diagnosis by histopathology. ultimately the treatment was unrewarding, with rapid return of pleural fluid prompting euthanasia.
Introduction
Canine pericardial mesothelioma is a rare, spontaneous, neoplastic disease of dogs that can arise from either the peritoneum, pericardium or pleura and less commonly from the tunica vaginalis (Nabeta et al. 2019; moberg et al. 2021; Lajoinie et al. 2022). Indeed, it represents only 0.2% of all canine neoplasms but nevertheless is a serious disease that
Contact: bellatoncharlotte@gmail.com
is rapidly fatal due to progression of the pericardial effusion into cardiac tamponade (macDonald et al. 2009; Nabeta et al. 2019; Scheuermann et al 2020). t he cavitary effusion associated with mesothelioma is thought to be due to the blockage of lymphatic drainage as a result of diffuse thickening of the tissue (moberg et al. 2021). Less commonly, mesothelioma can spread into regional lymph nodes and other regional organs (macDonald et al 2009; moberg et al. 2021). t he cause of mesothelioma development in dogs is not well understood but Glickman et al (1983) suggest a possible association with asbestos exposure and related compounds found in powdered flea products and pesticides.
mesothelioma is challenging to diagnose without tissue for histological assessment. Indeed, cytology of the pericardial effusion has poor sensitivity to differentiate mesothelioma from reactive mesothelium (mesothelial hyperplasia) or carcinoma (milne et al 2021). ultrasonography of the thoracic and pericardial cavities usually does not offer greater differentiation of diseases causes, due to the diffuse, granular distribution of the cancer. Even magnetic resonance imaging (mRI) is unlikely to be useful as although it can highlight pericardial thickening, it is not able to differentiate the origin of this thickening (Gallach and mai 2013). Hence, confirmation of mesothelioma requires biopsy and histology of the affected tissue with special stains and immunohistochemistry (milne et al. 2021). Due to its typical location, obtaining biopsy samples can be a challenging and invasive procedure to perform.
t he aim of this case report is to describe the clinical presentation and clinical findings, histopathological results,
treatment and outcome of a case of pericardial mesothelioma in a dog that presented to the massey university Veterinary teaching Hospital (muV t H). t he diagnostic challenge in such cases and current available treatment options for canine mesothelioma will also be discussed.
Case history and initial clinical findings
A 6-year-old, female, spayed German Shepherd dog presented initially to its primary veterinarian for lethargy, inappetence and a distended abdomen. Clinical examination revealed increased respiratory effort and ultrasonography ( t FAS t/AFAS t scan protocols) showed significant pericardial effusion with severe cardiac tamponade. Abdominal radiographs ruled out gastric dilation and volvulus. Pericardiocentesis was performed and 640 mL of serosanguinous fluid with a PCV of 18% was obtained. Cytology revealed a haemorrhagic and inflammatory effusion composed predominantly of neutrophils (85–95%) with occasional extracellular rod-like bacteria. Reactive mesothelial proliferation was also noted at this time. Given the inflammatory nature of the effusion and the few bacteria observed, the diagnosis considered most likely at this time was septic pericarditis and the dog was prescribed a 4-week course of 15 mg/kg amoxycillin/clavulanic acid twice daily. microbial culture came back negative but a septic aetiology was still considered, and the course of antibiotics was pursued in case this was a false negative result.
one month later the dog represented in respiratory distress and thoracic ultrasonography confirmed recurrence of pericardial fluid (Figure 1).
Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 34
Pericardiocentesis was repeated and 500 mL of haemorrhagic fluid was drained. A sample of this was again submitted for cytological interpretation yielding a similar cellular composition. t he differential diagnosis list under consideration at this time was septic pericarditis, idiopathic haemorrhagic pericardial effusion and haemangiosarcoma. As the effusion still contained inflammatory cells, the dog was prescribed a further antibiotic course of 5 mg/kg clindamycin twice daily.
twelve days later the dog represented with a weak pulse and pale mucous membranes and a further 706 mL of fluid was drained from its pericardial sac.
t horacic radiography and abdominal and cardiac ultrasound were repeated. Imaging did not reveal any noticeable tumour at the heart base, on the right atrium or within the pericardium. At this stage the dog was presumed to have idiopathic pericardial disease and 1 mg/kg prednisone at 1 mg/kg SID was dispensed. A recheck ultrasound examination performed 3 weeks later did not show any considerable fluid build-up.


However 1 week later, a large volume of serosanguinous fluid was drained from the pericardial sac but the respiratory effort did not improve. Subsequent thoracic radiography (Figure 2) and showed an unstructured interstitial pattern, lobar signs, cardiac border effacement, increased soft tissue opacity in the sternal region and reduced lung fields consistent with pleural effusion. A further 2.5 L of fluid was drained from the pleural cavity. Referral to the mu V t H was offered in order to discuss potential surgical intervention to relieve the tamponade.
Clinical findings upon referral
on arrival at the muV t H 10 weeks after the initial problem was identified by the referring veterinarian, the dog presented with muffled heart sounds and tachypnoea. t he heart rate was 88 beats per minute with a strong and synchronous pulse.
t he case was reviewed and the chief differential was considered to be neoplasia of a diffuse nature. Idiopathic pericarditis was considered less likely due to the extent
of pleural fluid that seemed to be overwhelming pleural drainage and given the lack of response to two courses of antimicrobials an infectious course was considered unlikely. Exploration and biopsy of the thoracic cavity and pericardial sac were considered necessary for a diagnosis. t horacoscopy for pericardial window and biopsy and an open thoracotomy which would allow a sub-total pericardiectomy were discussed. t he latter offered a higher probability of thorough thoracic inspection but with higher morbidity. t he owner elected open surgery.
surgical and histopathological findings
under general anaesthesia with mechanical ventilation, a median sternotomy was performed. Extensive miliary nodules were found covering the mediastinum and outer pericardium. o ther patches of nodular disease were present on the thoracic wall’s pleural surface on the left side. An impression smear of the nodular disease was prepared intra-operatively and sent to the IDEXX laboratory (Palmerston North) for a S tAt read. mesothelial cells with atypia and neutrophilic infiltration were diagnosed but no definitive diagnosis of neoplasia was possible based on the cytology. Biopsies of the pericardium were then taken and fixed in 10% buffered formalin for histopathological analysis. A sub-total pericardiectomy was performed preserving the phrenic nerve pathways and the sternotomy was closed routinely.
t he histology revealed diffusely thickened pericardium and mediastinum with a moderate amount of pleomorphic cuboidal to polygonal cells consistent with neoplasia (Figure 3). Features of malignancy such as mild anisokaryosis, small nucleoli and stippled chromatin were also observed. t he mitotic index was low and there was a prominent amount of neutrophils alongside haemosiderophages. t hose observations are highly suggestive of mesothelioma but metastatic carcinoma could not be fully ruled out.
Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 35
f igure 1. Cardiac ultrasound of a 6-year-old German shepherd dog representing for respiratory distress showing a significant amount of pericardial effusion.
f igure 2. Right lateral recumbency thoracic radiograph of a 6 yearold female German shepherd dog presenting for respiratory distress. The radiograph shows an unstructured interstitial pattern, lobar signs, cardiac border effacement and increased soft tissue opacity in the sternal region (pleural effusion).
Following surgery, the dog recovered well and was initially maintained on a constant rate infusion of ketamine (0.003 mg/ kg/minute) and fentanyl (0.003 mg/kg/hour) for pain control and chest drain care was performed every 4 hours. t he dog no longer required opioids for analgesia 24 hours after surgery and was bright and ambulatory. t he drain production decreased from 0.6 mL/kg/hour 24 hours following the surgery, to 0.19 mL/kg/hour 48 hours after surgery and to 0.36 mL/ kg/hour 60 hours after surgery. Despite mildly increased respiratory effort and tachypnoea the drain was not producing much fluid and so was pulled out 3 days after surgery. t he dog was discharged 2 days later with 12 mg/kg paracetamol to be given twice daily for post-operative pain management. Chemotherapy options were discussed but not instituted due to limited efficacy and high cost.
t he pleural effusion recurred 1 month following the surgery and therefore the option of placing a PleuralPort (https:// norfolkvetproducts.com/products/pleuralport/) to provide palliative drainage was offered. However, the owner elected to not pursue any further treatment and the dog was euthanised
1 month after the surgery due to a deteriorating state and nonresolving respiratory distress.
Discussion
t his case report highlights some of the challenges in establishing a diagnosis of canine mesothelioma. At presentation, the clinical signs are non-specific, as they are related to cavitary effusion which may have multiple aetiologies. moreover, the cytological features of reactive mesothelial cells, mimic the features of neoplastic mesothelial cells (macDonald et al. 2009; Gallach et al. 2013; milne et al. 2021; moberg et al. 2021; Lajoinie et al. 2022), making differentiation of the two using cytology very difficult. In the initial management of this case, septic pericarditis was placed at the top of the differential list due to the inflammatory nature of the fluid cytology despite negative culture. t he cytology report mentioned a prominent neutrophilic population in the effusion but no degenerate neutrophils were noted. occasional rod bacteria were also seen but none were intracellular. t hese findings are suggestive, but not strongly indicative, of a septic effusion. As mentioned in the study by milne and others (2021), cytology has only 56% sensitivity for the diagnosis of mesothelioma and it is not unusual to see non-degenerate inflammatory cells on cytology of a mesothelioma (Stevens et al. 2014; moberg et al. 2021). Septic pericarditis in dogs is not a common diagnosis and is usually associated with a penetrating wound, local extension of infection or a migrating foreign body (Johnson et al. 2004; Botha et al. 2017). Pleural effusion secondary to neoplastic disease is actually more common. Indeed, Scheuermann and others (2020) report that 60–70% of pericardial effusion cases in dogs occur secondary to a neoplastic aetiology with haemangiosarcoma, mesothelioma and chemodectoma being the most common causes. t he same study further categorises mesothelioma as being responsible for 20% of cases of neoplastic pericardial effusion while the study of macDonald and others (2009) reports an incidence rate of 14% for pericardial mesothelioma when pericardial effusion is present.


When the effusion culture was negative, it was interpreted as a false negative result and the course of antibiotics continued. However, the occasional bacteria seen on the initial cytology may have been due to contamination of the sample either at the time of the collection or while preparing the microscope slide, or were erroneously identified as bacteria.
Imaging can offer useful information in terms of ruling out other causes of pericardial effusion, such as a migrating foreign body, heart base tumour or cardiac haemangiosarcoma and it can also reveal a diffusely thickened pericardium (macDonald et al. 2009; Gallach and mai 2013). But due to mesothelioma’s growth pattern of diffuse thickening of the tissue and miliary nodules, imaging is not a definitive diagnostic tool for mesothelioma. C t and mRI are the imaging modalities of choice in most studies as they allows soft tissue structures and discrete masses to be visualised. Nevertheless, ultrasonography, in the hands of an experienced radiologist, has been reported to also be an acceptable method for ruling out heart base tumours or cardiac haemangiosarcoma as a cause of pericardial effusion (macDonald et al. 2009; Nabeta
Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 36
a b
f igure 3. photomicrographs of a section of the outer pericardium of a dog with pericaridial mesothelioma. A) l ow power image showing neoplastic infiltrative mesothelial cells forming papillar structures. B) High power image showing neoplastic infiltrative mesothelial cells with neutrophilic inflammation and low numbers of lymphocytes and plasma cells.
et al. 2019). macDonald et al. (2009) state that the sensitivity and specificity of ultrasound to detect cardiac masses is 82% and 100% respectively. t he sensitivity can increases up to 88% with repeated echocardiographic exams. In this case, cardiac ultrasonography did not reveal any discrete mass in the right atrium nor at the heart base. Advanced imaging via C t or mRI were offered to the client in order to investigate the other possible causes of pericardial effusion, but due to the cost of either procedures and the limited information they were expected to provide, the owner did not elect to pursue C t or mRI.
t he development of new diagnostic tools as means to get a definitive diagnosis without an invasive method of sampling has been investigated. milne et al. (2021) investigated the accuracy of diagnosing mesothelioma using cell block immunohistochemistry, as this requires a less invasive sample collection method. However, these authors concluded that whilst a diverse panel of stains is helpful to distinguish reactive mesothelial cells from neoplastic cells, the definitive diagnosis remains nonetheless difficult. Hence, as other literature suggests, the definitive diagnosis of mesothelioma currently relies on the conjunction of clinical signs, cytology, imaging, histology and immunochemistry of biopsies (Lajoinie et al. 2022).
In this present case, the amalgamation of clinical signs of recurrent, non-septic pericardial effusion, the developing pleural effusion and the lack of distinguishable mass on ultrasound made mesothelioma the most probable diagnosis. However, surgical biopsies were needed for a definitive diagnosis. In order to obtain a tissue diagnosis, thoracoscopic or open surgical biopsy were required. Biopsies of the mediastinum and pericardium were taken during open thoracic surgery via sternotomy and subsequent histology supported the diagnosis of canine pericardial mesothelioma.
In terms of management of this case, the current recommendations for treatment of recurrent pericardial effusion were discussed with the owner prior to surgery. t here is a lack of
gold-standard treatments for recurrent pericardial effusion in dogs, despite several technique being described. t he first option was making a thoracoscopic pericardial window to allow the fluid to drain into the pleural space and be reabsorbed via lymphatic drainage. t he second option was to perform a subtotal pericardiectomy, which involves resecting the parietal pericardium ventral to the phrenic nerve, thus removing most of the causative tissue and relieving permanently the cardiac tamponade. t his latter surgery is either performed via sternotomy or thoracoscopy. t he choice of the surgical approach is determined by the requirement for haemostasis during the surgery with sternotomy offering a greater capacity for limiting haemorrhage.
Studies by Scheuermann and others (2020) and Case and others (2013) demonstrate that sub-total pericardiectomy, specifically for managing pericardial mesothelioma, increases the median survival time (mS t ) significantly compared to intermittent pericardiocentesis or to the pericardial window technique. Indeed, dogs receiving a sub-total pericardiectomy had a mS t of 10.3 months compared to 8.6 months for those that received a pericardial window. In this case, the presence of marked pleural fluid accumulation warranted investigation beyond the limits of thoracoscopy in our hands. t he surgical approach was via sternotomy as this allowed better visualisation of the pericardium and pleural space, allowed quantification of the extent of the disease, as well as better control of haemorrhage and preservation of the phrenic nerve while removing the parietal pericardium.
Adjunctive chemotherapy has shown only marginal benefit by increasing the mS t from 195 days to 234 days after resection of the pericardium (moberg et al. 2021). more favourable response was reported by Lajoinie and others (2022) who reported that chemotherapy increased the mS t to 366 days compared to 74 days for dogs who did not receive chemotherapy. t he chemotherapeutic agents used in this study were cisplatin with carboplatin given intracavitary and carboplatin with doxorubicin given IV.
However, this study did not differentiate which chemotherapeutic agent was associated with the better outcome and 41% of dogs received several different drugs in their protocol. Additionally, chemotherapy is associated with adverse reactions in 28% of cases (moberg et al 2021) and decreases the quality of life temporarily. t herefore, although this was discussed, the owner declined to pursue chemotherapy due to the guarded prognosis and the likely decline in quality of life it would have caused.
t he pleural effusion recurred within 1 month after surgery, and the owner was offered the palliative option of placing a PleuralPort to facilitate the drainage of the pleural cavity. A PleuralPort was advised over pleuraperitoneal shunt or pleurovenous shunt as these are associated with metastatic spread of the disease in the peritoneum and thrombosis formation, respectively (Brooks and Hardie 2011).
PleuralPorts are reported to be welltolerated in dogs, and can be an effective way to drain the thorax at home without the repeated need for veterinary intervention, hence reducing the cost and the risk of potential iatrogenic trauma caused by repeated thoracocentesis (Brooks and Hardie 2011; moberg et al. 2021). moreover, Brooks and Hardie (2011) stipulate that the placement of the port is minimally invasive and that they are well-tolerated as they are made of inert material, thus can remain in the thorax for an extended period (months) as well as providing an adequate alternative for palliative care. However, the same study also reported port blockage and pneumothorax as the most common complications associated complications with PleuralPort devices. Additionally, in this specific case, given the amount of fluid being produced by the pleura and the small bore of the Huber needles available, regular and prolonged manual drainage would have been required. Consequently, considering the cost, the requirement of another surgery, the anaesthetic risk, the care needed to keep the port clean and patent and the diagnosis and prognosis of the condition, the owner declined the installation of the PleuralPort.
Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 37
Conclusion
As causes of pericardial effusion in dogs haemangiosarcoma and mesothelioma are more common than septic pericarditis. However, despite a predisposition of German Shepherds to haemangiosarcoma, this condition was ruled out relatively early in the diagnostic course due to the absence of a discrete mass in the right atrium on cardiac ultrasound and thoracic radiography. Septic pericarditis was also ruled out via negative culture and the lack of response to antibiotic therapy. As the disease progressed, idiopathic pericardial effusion was thought to be the most probable diagnosis. However after the condition progressed to pleural effusion, the suspicion of malignant mesothelioma became more likely and surgery was advised to provide a definitive diagnosis and manage the condition procedure. Sternotomy and sub-total pericardiectomy were performed as this is described as the most successful surgery to manage pericardial mesothelioma in the literature, and the dog recovered well. Histopathology of biopsies confirmed a diagnosis of malignant mesothelioma. Chemotherapy was offered but not strongly advised, as despite the reported increase in mS t, it is only palliative and may lower the quality of life for a transient period at least. Eventually, significant pleural effusion recurred. Placement of a PleuralPort was proposed but declined by the owner due to cost and the poor prognosis regardless. t he dog was euthanised 1 month after surgery due to recurrent and worsening signs of respiratory distress.
t his case report demonstrates the diagnostic challenge posed by mesothelioma as well as the associated poor prognosis and the lack of efficient treatment available in veterinary medicine.
Acknowledgements
t hank you to the staff of the surgical and anaesthesia departments of the muV t H. Susan Piripi performed the cytology and histopathology and Andrew Worth was the attending clinician and surgeon.
References
Botha WJ, Mukorera V, Kirberger RM. s eptic pericarditis and pneumopericardium in a dog with an oesophageal foreign body. Journal of the South African Veterinary Association 88, a1496, 2017, https://doi.org/10.4102/ jsava.v88i0.1496
Brooks AC, Hardie RJ. use of the pleural port device for management of pleural effusion in six dogs and four cats. Veterinary Surgery 40, 935–41 2011, https://doi.org/10.1111/j.1532950x.2011.00901.x
Casamián-Sorrosal D, Fournier D, Shippam J, Woodward B, Tennant K. s eptic pericardial effusion associated with pulmonary and pericardial botryomycosis in a dog. Journal of Small Animal Practice 49, 655–9, 2008.,https://doi.org/10.1111/j.17485827.2008.00605.x
Case JB, Maxwell M, Aman A, Monnet EL. Outcome evaluation of a thoracoscopic pericardial window procedure or subtotal pericardectomy via thoracotomy for the treatment of pericardial effusion in dogs. Journal of the American Veterinary Medical Association 242, 493–8, 2013, https://doi. org/10.2460/javma.242.4.493
Gallach RG, Mai W. Cardiac m RI findings in a dog with a diffuse pericardial mesothelioma and pericardial effusion. Journal of the American Animal Hospital Association 49, 398–402, 2013. https://doi.org/10.5326/jaaha-ms-5925
Glickman LT, Domanski LM, Maguire TG, Dubielzig RR, Churg A. mesothelioma in pet dogs associated with exposure of their owners to asbestos. Environmental Research 32, 305–13, 1983
Johnson JM, Martin MW, Stidworthy MF. s eptic fibrinous pericarditis in a cocker spaniel. Journal of Small Animal Practice 44, 117–20, 2004, https://doi. org/10.1111/j.1748-5827.2003.tb00131.x
Lajoinie M, Chavalle T, Floch F, Sayag D, Lanore D, Ponce F, Chamel G. Outcome of dogs treated with chemotherapy for mesothelioma: A retrospective clinical study on 40 cases and a literature review. Veterinary and Comparative Oncology 20, 825–35, 2022, https://doi.org/10.1111/vco.12843
MacDonald KA, Cagney O, Magne ML. e chocardiographic and clinicopathologic characterization of pericardial effusion in dogs: 107 cases (1985–2006). Journal of the American Veterinary Medical Association 235, 1456–61, 2009, https:// doi.org/10.2460/javma.235.12.1456
Milne EM, Piviani M, Hodgkiss- Geere HM, Piccinelli C, Cheeseman M, Cazzini P, Ressel L, Marcos RJ, Marrinhas CS, Santos MS, et al . Comparison of effusion cell block and biopsy immunohistochemistry in mesothelial hyperplasia, mesothelioma, and carcinoma in dogs.Veterinary Clinical Pathology 50, 555–67, 2021, https://doi. org/10.1111/vcp.13002
Moberg HL, Gramer I, Schofield I, Blackwood L, Killick D, Priestnall SL, Guillén A. Clinical presentation, treatment and outcome of canine malignant mesothelioma: A retrospective study of 34 cases. Veterinary and Comparative Oncology 20, 304–12, 2022, https://doi.org/10.1111/vco.12777
Nabeta R, Nakagawa Y, Chiba S, Xiantao H, Usui T, Suzuki K, Furuya T, Fukushima R, Uchide T. pericardial mesothelioma in a dog: The feasibility of ultrasonography in monitoring tumor progression. Frontiers in Veterinary Science 6, Article 121, 2019. https://doi.org/10.3389/fvets.2019.00121
Rivera PA, Borgarelli M. Cardiovascular images: constrictive pericarditis and tricavitary effusion in a dog with pericardial mesothelioma. Journal of Veterinary Cardiology 32, 55–9, 2020. https://doi.org/10.1016/j.jvc.2020.09.005 Scheuermann LM, Gordon-Evans WJ, Nault AJ. systematic review of the treatment options for pericardial effusions in dogs. Veterinary Surgery 50, 20–8, 2020, https://doi.org/10.1111/ vsu.13475
Stevens BJ, Montgomery SA, Phillips KL, Wester MW, Jennings SH. pathology in practice. Journal of the American Veterinary Medical Association 245, 57–9, 2014, https://doi.org/10.2460/ javma.245.1.57 l
Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 38

p uppy murmurs: when to worry and what can be done
Blood flow through the heart should be smooth and laminar. turbulent blood occurs with faster rates of flow and describes a chaotic and disorganised flow pathway with formation of eddy currents. When turbulent blood flow is present in the heart, it can be auscultated as a murmur, and this may or may not be associated with underlying heart disease (Spalla 2019). Determining the clinical importance of a murmur can often be the most challenging step in a diagnostic investigation as incidentally detected heart murmurs found during puppy general wellness exams may or may not require further examination (Côté et al. 2015). t he prevalence of congenital cardiac anomalies is low. However misdiagnosing or missing a pathological murmur could prove detrimental for the individual puppy as these may be associated with increased morbidity and mortality and some conditions can be treated and cured if detected early (Côté et al. 2015). t his is why distinguishing between a pathological murmur (from a cardiovascular lesion) and a non-pathological murmur (associated with a structurally normal heart) is important (Côté et al. 2015).
Characteristics of the murmur can help you differentiate between a pathological and non-pathological murmur, including the timing in the cardiac cycle (systolic, diastolic or continuous), point of maximal intensity (left or right sided, apical or basilar), and murmur grade (outlined below). In addition to auscultatory features, the patient’s signalment and physical exam findings can aid in differential diagnoses and formulating an initial case management plan (Côté et al. 2015).
Although there are many ways to grade cardiac murmurs, the most common methods are summarised below using a 6-point scale (Rishniw 2018):
l Grade I: A soft murmur that is nearly imperceptible, focal and is not immediately apparent. Both heart sounds (lubdub) are louder than the murmur.
l Grade II: A soft murmur that is focal, can be detected immediately and both heart sounds are louder than the murmur.
l Grade III: A moderate intensity murmur with heart sounds that are easily heard and are equal to the murmur intensity. typically regional but does not radiate into the lung fields.
l Grade IV: A loud murmur that is louder than normal heart sounds and radiates widely into the lung fields. t his means
Contact:
you can still hear the murmur while listening to the lungs. No palpable thrill (the ability to feel the murmur with your hands) on the chest wall.
l Grade V: A very loud murmur with a palpable precordial thrill.
l Grade VI: A very loud murmur that is audible with the stethoscope lifted 1-inch off the chest wall.
Soft cardiac murmurs (grade I–II) are commonly detected in clinically healthy puppies at their first puppy wellness examination (Pugliese et al. 2021). t hese murmurs are most likely to be non-pathological, but a pathological murmur cannot be ruled out (Sewall 2016) (Côté et al. 2015). t herefore, all murmurs identified should be noted on a patient’s medical record to accurately monitor and assess progression or changes over time (van Staveran and Szatmari 2020).
Non-pathological murmurs can also be described as innocent or functional. t hey can be heard in 15–31% of puppies <6 months old and are due to the higher cardiac output relative to cardiac size in young animals (Côté et al. 2015). Furthermore, puppies with innocent cardiac murmurs often have mild, nonpathological anaemia which lowers blood viscosity, leading to turbulent blood flow (Pugliese et al. 2021). t he following characteristics can be used to identify these murmurs: a

CARDIO CORN eR
kayla.gardiner@vsnz.co.nz
Dr. kAyl A GARDIN eR , BVsc, VsA rotating intern and Dr. k e AtON mORGAN, BVsc(hons), DACVI m (cardiology)
40 Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023
[Photo credit: Chris Arthur-Collins for Unsplash.com]
systolic, soft (grade I or II) murmur on the left side which typically disappears by 6 months of age and which is not associated with clinical signs (Côté et al 2015; Pugliese et al. 2021). Although non-pathological murmurs are common in puppies, they can also occur in adult dogs. t hese murmurs are not caused by structural heart disease but can be seen in athletic dogs, certain breeds (such as Boxers) and are associated with systemic conditions that alter blood viscosity or increase cardiac output, such as anaemia, fever, pregnancy or hyperthyroidism (Côté et al. 2015; Pugliese et al. 2021).
Pathological murmurs in puppies result from congenital heart conditions where there is a structural cardiac abnormality. t hese murmurs can be identified during puppy appointments by specific characteristics of the murmur (covered below), presence of an arrhythmia, or clinical symptoms (Pugliese et al. 2021). Possible clinical signs associated with pathological murmurs include exercise intolerance, increased respiratory rate and effort, cyanosis, ascites, or syncopal events. t hus, attention should be given to related physical exam findings, particularly mucous membrane colour, femoral pulse quality, heart rate and rhythm, and respiratory rate (Côté et al 2015).
so, when should you worry about a heart murmur?
t here are several features of a heart murmur that can give you a clue that it might be pathological. In general, loud murmurs graded III/VI or higher are likely associated with a cardiovascular lesion as these are caused by rapid, turbulent blood flow through an obstructive lesion, leaky valve, or shunt. Any murmur that is heard throughout the entire cardiac cycle (continuous or “machinery-murmur”) or only during diastole is pathological regardless of the grade. t his is also true for a murmur that is loudest on the right-side, as these are typically due to a ventricular septal defect (“hole in the heart”) or tricuspid valve dysplasia. Auscultatory features that should prompt further investigation include ≥ grade III murmurs, continuous or diastolic murmurs, murmurs loudest at right hemithorax, other abnormal heart sounds such as a gallop or arrhythmia, pulse deficits, or if the murmur is accompanied by physical findings of cardiovascular disease (Côté et al. 2015).
Additionally, congenital heart murmurs do not disappear with maturity and some such as those caused by subaortic stenosis, get louder. t herefore, puppies with a murmur during initial vaccination appointments should be re-auscultated at 6 months of age (12 months for giant breeds) (Côté et al. 2015). If a murmur is still present then further diagnostics are warranted, especially if the murmur is noted to increase in grade over time.
you have identified a murmur in a puppy that is concerning for a pathological heart murmur: what are the next steps?
t horacic radiographs can provide information on the presence of cardiac remodelling further indicating a pathological murmur. However, echocardiography (cardiac ultrasound) is the test of choice to identify the cause of the murmur and diagnose the underlying congenital heart disease that is present.
Congenital heart disease can be largely split into diseases that cause obstructions in the heart, diseases that cause a leaky valve and diseases that cause a shunt from one circulation to the other, or a mixture of all three. t he most common congenital cardiac disease in dogs is left-to-right shunting patent ductus arteriosus (PDA) and valvular pulmonic stenosis, both of which are treatable conditions with minimally invasive procedures. Early detection of congenital heart disease allows treatment to be pursued early to prevent clinical signs or improve quality and quantity of life (Rovroy and Szatmari 2021).
patent ductus arteriosus
Patent ductus arteriosus is one of the most common congenital cardiac diseases in dogs, accounting for approximately 21% of congenital heart defects (oliveria et al. 2011).
t he ductus arteriosus is a normal fetal structure that develops to shunt blood away from the pulmonary artery and the deflated lungs, into the aorta. In puppies, the ductus arteriosus functionally closes within a few days after birth as the lungs inflate and requires blood flow. PDA is a failure of the ductus to close allowing blood to
flow from the high-pressure aorta to the lower pressure pulmonary artery. t his significantly increases blood flow through the pulmonary circulation leading to volume overload. If left uncorrected a PDA will cause progressive heart enlargement and left-sided congestive heart failure (Saunders et al 2013). Patients with this congenital cardiovascular disorder do not have a normal life expectancy unless the PDA is occluded. Without occlusion, the prognosis is poor with a reported median survival of only 2 years but with occlusion the life expectancy increases by an additional 10 years (i.e., median survival time of 12 years); effectively a normal lifespan (Saunders et al. 2013).
A puppy with a PDA presenting to its first vaccination appointment will likely be asymptomatic, though some present with mild exercise intolerance, stunted growth, or signs of heart failure. A left basilar continuous murmur can be auscultated in these pups (Broaddus and t illson 2010). A continuous heart murmur is distinct and is often described as a “machinery murmur”, importantly there is no break in the cardiac cycle hence the underlying murmur sound is always present. most PDA cases will have a loud murmur and palpable thrill present, but anytime a continuous murmur is heard it should be investigated (Broaddus and t illson 2010) (Israel et al. 2003) (Pugliese et al. 2021). to hear a recording of a continuous murmur please see the university of Washington Department of medicine website: https://depts.washington.edu/ physdx/heart/demo.html
Echocardiography is necessary to confirm the diagnosis, evaluate for other concurrent cardiac conditions, and assess whether the patient is a suitable candidate for closure of the PDA.
occlusion of the PDA either by surgical ligation or minimally invasive techniques is often curative (Bureau et al. 2005) and so should be considered in these cases. minimally invasive techniques for PDA occlusion include transcatheter placement under fluoroscopic guidance of a thrombogenic device into the ductus via a peripheral vessel to promote closure (sometimes the surgical incision is so small a suture is not needed) (Singh et al. 2012). Success of implantation is high with low intraoperative mortality and low post-operative morbidity
41 Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023
(Saunders et al. 2013). minimally invasive techniques allow faster patient recovery times and avoid potential adverse complications associated with a thoracotomy to surgically ligate the PDA. With the development of a veterinary specific device, the Amplatz canine ductal occluder, this procedure is generally regarded as the treatment of choice in most cases, with a high success rate of 97% (Saunders et al. 2013; Sewall 2016).
p ulmonic stenosis
Along with PDA, pulmonary stenosis is also one of the most common congenital heart diseases in dogs with predisposition in brachycephalic breeds (oliveria et al. 2011). Pulmonic stenosis results from the abnormal development of the pulmonary valve leaflets which thicken and adhere to one-another, creating a physical obstruction to blood flow leaving the right heart. t he disease is classified according to valve morphology and anatomical location of the narrowing into sub valvular stenosis (obstruction in the right ventricular outflow tract), valvular stenosis (pulmonic valve), and supravalvular stenosis (main pulmonary artery), with valvular pulmonary stenosis being by far, the most frequent (macDonald 2006). Compensatory concentric hypertrophy of the right ventricle occurs to normalise the increased wall stress. Severe right ventricular hypertrophy can result in myocardial hypoxia, right-sided congestive heart failure, ventricular arrhythmias, and sudden death (Locatelli et al. 2013).
t he auscultatory findings of a patient with pulmonary stenosis include a left, basilar, systolic murmur. t he intensity of the murmur may vary according to the degree of obstruction, with a louder murmur indicating a more severe disease (Caivano et al. 2018). Possible clinical signs include exercise intolerance, syncope, and right-sided congestive heart failure which could include ascites/ abdominal distention or respiratory effort from pleural effusion (macDonald 2006).
t he definitive diagnosis of pulmonic stenosis is made by echocardiography with visualisation of abnormal and stenotic pulmonary valve leaflets. t he severity of pulmonic stenosis is assessed by measuring the velocity of
blood flow through the stenosis and converting this velocity to a pressure gradient. t he faster the velocity – the higher the pressure gradient. Pulmonic stenosis can then be categorised as mild (pressure gradient, < 50 mmHg), moderate (pressure gradient, 50–80 mmHg), or severe (pressure gradient, > 80 mm Hg) (Francis et al. 2011). t he risk of developing clinical signs and/or secondary right ventricular remodelling is highly dependent on the degree of valvular stenosis and pressure gradient across the stenosis (Locatelli et al. 2013).
prognosis without any intervention
mild pulmonic stenosis is generally associated with a favourable long-term prognosis for a normal lifespan without the need for intervention. Dogs with moderate pulmonic stenosis have a variable outcome but will generally have a cardiac-related death as an older-middle aged dog (Locatelli et al 2013). No clear guidelines have been established regarding the best treatment option for patients affected by moderate pulmonic stenosis and treatment plans are tailored for each patient based on echocardiographic variables and presence/absence of clinical signs (Locatelli et al. 2013; Rovroy and Szatmari 2021). Dogs classified with severe pulmonic stenosis carry a guarded prognosis for long-term survival because of the increased risk of syncope, rightsided congestive heart failure or sudden death (Francis et al. 2011). Retrospective studies show high mortality rates in dogs with severe pulmonic stenosis: 53% mortality within their first year of life and 20% annual mortality after that (Locatelli et al. 2013).
prognosis with intervention
Balloon valvuloplasty is the surgical technique of choice for most moderate and all severe pulmonary stenosis cases (Locatelli et al. 2013). t his is a noninvasive procedure via catheterisation of a peripheral vein. With the aid of a guidewire positioned across the pulmonic valve, a balloon dilation catheter is advanced across the valve and is manually and temporarily inflated to tear open the stenotic valve. Success of this procedure is normally defined as a decrease in trans-pulmonic pressure gradient by 50% from pre-procedural measurements and/or reduction in the pressure gradient to < 50 mmHg (Francis et al. 2011; Locatelli et al. 2013).
t he outcome of balloon valvuloplasty has been shown to significantly improve clinical signs in symptomatic dogs and improve survival and overall outcome when compared with dogs not treated by balloon valvuloplasty (Johnson et al 2004; Locatelli et al. 2013).
Other interventional procedures
Interventional cardiology through minimally invasive catheterization has expanded significantly in veterinary medicine (Scansen 2017). In addition to the treatment of patent ductus arteriosus occlusion and pulmonic balloon valvuloplasty for pulmonic stenosis, other interventions that an interventional cardiology service offers include coil, particle, or device occlusion of anomalous vessels/shunts for conditions such as atrial septal defects, intrahepatic shunts, arteriovenous fistulas or other intra or extra-cardiac shunts in addition to balloon angioplasty or stent implantation for a variety of vascular obstructions (Scansen 2017). transvenous artificial pacemaker implantation for bradyarrhythmias is also possible, rounding off the surgical options for various cardiovascular conditions.
References
Broaddus KD, Tillson MD. patent ductus arteriosus in dogs. Compendium: Continuing Education for Veterinarians 32, e3, 2010 Bureau S, Monnet E, Orton CE. evaluation of survival rate and prognostic indicators for surgical treatment of left-to-right patent ductus arteriosus in dogs: 52 cases (1995–2003)
Journal of the American Veterinary Medical Association 227, 1794–9, 2005
Caivano D, Dickson D, Martin M, Rishniw M. murmur intensity in adult dogs with pulmonic and subaortic stenosis reflects disease severity. Journal of Small Animal Practice 59, 161–6, 2018
Côté E, Edwards NJ, Ettinger SJ, Fuentes VL, MacDonald KA, Scansen BA, Sisson DD, Abbott JA. management of incidentally detected heart murmurs in dogs and cats. Journal of Veterinary Cardiology 17, 245–61, 2015
Francis AJ, Johnson MJ, Culshaw GC, Corcoran BM, Martin MW, French AT. Outcome in 55 dogs with pulmonic stenosis that did not undergo balloon valvuloplasty or surgery. Journal of Small Animal Practice 52, 282–8, 2011
Johnson MS, Martin M, Edwards D, French A, Henley W. p ulmonic stenosis in dogs: balloon dilation improves clinical outcome.
Journal of Veterinary Internal Medicine 18, 656–62, 2004
42 Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023
Locatelli C, Spalla I, Domenech O, Sala E, Brambilla PG, Bussadori C. p ulmonic stenosis in dogs: survival and risk factors in a retrospective cohort of patients. Journal of Small Animal Practice 54, 445–52, 2013
MacDonald KA. Congenital heart diseases of puppies and kittens. Veterinary Clinics North America: Small Animal Practice 36, 503–31, 2006
Oliveira P, Domenech O, Silva J, Vannini S, Bussadori R, Bussadori C. Retrospective review of congenital heart disease in 976 dogs. Journal of Veterinary Internal Medicine 25, 477–83, 2011
Pugliese M, Biondi V, La Maestra R, Passantino A. Identification and clinical significance of heart murmurs in puppies involved in puppy trade. Veterinary Science 8, 139, 2021
Rishniw M. murmur grading in humans and animals: past and present. Journal of Veterinary Cardiology 20, 223–33, 2018
Rovroy LB, Szatmari V. Age of puppies at referral to veterinary cardiology specialists for murmur investigation. Acta Veterinaria Scandinavica 63, 37, 2021
Saunders AB, Gordon SG, Boggess MM, Miller MW. l ong-term outcome in dogs with patent ductus arteriosus: 520 cases (1994–2009). Journal of Veterinary Internal Medicine 28, 401–10, 2014
Scansen BA. Interventional Cardiology: What's New? Veterinary Clinics North America Small Animal Practice 47, 1021–40, 2017
Sewall D. Heart murmurs in puppies and kittens. Companion Animal. 2016.
Singh MK, Kittleson MD, Kass PH, Griffiths LG. Occlusion devices and approaches in canine patent ductus arteriosus: comparison of outcomes. Journal of Veterinary Internal Medicine 26, 85–92, 2012
Spalla I. Heart murmurs in young dogs and cats: differentials, tips and additional testing. Veterinary Ireland Journal 9, 7, 2019

Van Israel N, French AT, DukesMcEwan J, Welsh EM. patent Ductus Arteriosus in the older Dog. Journal of Veterinary Cardiology 5, 13–21, 2003
Van Staveren MDB, Szatmari V. Detecting and recording cardiac murmurs in clinically healthy puppies in first opinion veterinary practice at the first health check. Acta Veterinaria Scandinavica 62, 37, 2020 l
Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 43
Isfm Research Roundup
Isfm publishes a monthly summary of the latest feline research which they have generously shared with CQ. In the April 2023 issue of Research Round-up includes a large study of common disorders affecting cats in the uk followed by the non-medical but important topic of caregiver burden (the strain of caring for sick pets or people).

f inally, there are two urinary papers, which answer some questions about upper urinary tract urolithiasis, and urethral obstruction and the effects of COVID-19 pandemic lockdowns. We hope you enjoy reading these interesting summaries.
Title: Commonly diagnosed disorders in domestic cats in the UK and their associations with sex and age
Authors: o’Neill DG, Gunn-moore D, Sorrell S, mcAuslan H, Church DB, Pegram C, Brodbelt DC.
Journal: Journal of Feline Medicine and Surgery 25, doi:10.1177/1098612X231155016, 2023.
Background: understanding the prevalence of disorders that occur in cats and the associated potential risk factors enables more targeted veterinary interventions and the opportunity to increase caregiver awareness, which, in turn, improves feline welfare.
Aims of the study: t his study aimed to look at the prevalence of disorders in cats in the uK and their associations with sex and age.
Methods: t he study used a random sample of primary care veterinary records from cats seen in 2019 using the VetCompass epidemiological research programme. All disorders were reported on and associations with age and sex were assessed.

Results: t he population demographics skewed slightly towards a younger (median age 5.76 years for females compared with 5.59 years for males) female (50.1%) population
of cats. most (88%) were non-pedigree cats and 66% of all cats had at least one disorder reported. male and older cats had a higher proportion of disorders reported, the most common being periodontal disease (15.2%), obesity (11.6%), dental disease (8.2%), overgrown nails (8.2%), flea infestation (5.1%) and heart murmurs (4.4%). Females had a statistically higher prevalence than males of poor quality of life (QoL), postoperative wound complication, overgrooming, flea bite hypersensitivity, overgrown nail(s) and hyperthyroidism. males had a higher prevalence than females for: periodontal disease, road traffic injury (RtA), heart murmur, lameness, obesity, abscess, wound and cat bite injury. Younger cats (<8 years) had a higher prevalence than older cats for four disorders: cat bite injury, flea infestation, RtA and postoperative wound complication. older cats (¦ 8 years) had a higher prevalence of lameness, abscess, cystitis, overgrooming, dental disease, constipation, being thin/underweight, osteoarthritis, haircoat disorder, anorexia, otitis externa, vomiting, cardiac dysrhythmia, weight loss, chronic kidney disease, disorder not diagnosed, periodontal disease, poor QoL, heart murmur, flea bite hypersensitivity, obesity, overgrown nail(s) and hyperthyroidism.
Limitations of the study: t his study is uK-based and findings cannot be extrapolated to other countries due to living conditions being different (risk of RtA, cat bite injury or flea infestation, for instance, are reduced in indoor cats). In addition, this is just a sample of the data, so it might not fully represent the uK and may be biased towards cats whose owners seek out and engage in veterinary care. Neuter status was not assessed as recording systems made the data unreliable.
Relevance to clinical practice: While this study is building off previous work from this group (o’Neill et al. 2014) and not necessarily showing anything ‘new’ for vets who work in general practice, this is a larger more robust data set and provides useful data to reinforce the message of the importance of annual wellness examinations in cats to monitor their weight, perform a dental assessment and check their nails, as well as carrying out other targeted diagnostics such as biochemistry.
Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 44
References
O’Neill DG, Church DB, McGreevy PD, Thomson PC, Brodbelt DC. prevalence of disorders recorded in cats attending primary-care veterinary practices in england. Veterinary Journal 202, 286–91, 2014
You can access the full article here: https://journals.sagepub. com/doi/full/10.1177/1098612X2311550
Relevance to clinical practice: Caring for sick cats has an impact on their owners. t he strains of administering medications, adjustments to lifestyle, diet and feeding and other caring tasks must be considered in chronic disease management, and as vets we need to recognise and empathise with these challenges.

References
MB Spitznagel, ASG Updegraff, MP Twohig, MD Carlson & CM Fulkerson. Reducing occupational distress in veterinary medicine personnel with acceptance and commitment training: a pilot study. New Zealand Veterinary Journal 70, 319–25, 2022
You can access the full article here: https://journals.sagepub. com/doi/full/10.1177/1098612X221145835
Title: Caregiver burden in cat owners: a cross-sectional observational study
Authors: Spitznagel mB, Gober mW and Patrick K.
Journal: Journal of Feline Medicine and Surgery 25, doi:10.1177/1098612X221145835, 2023.
Background: Caregiver burden is the strain of caring for a sick relative or pet and has been shown mainly in dogs. Some data that is available for cats suggests the burden is lower in this species, but a large group of cats and their owners have not been studied. Caregiver burden is important to understand as it can affect the human-animal bond and decisions around euthanasia.
[Note: NZVJ has published an article by this author looking at the efficacy of a programme for veterinary personnel to reduce stress, burnout and transfer of caregiver burden – see Spitznagel et al. 2022]
Aims of the study: t his study aimed to examine caregiver burden in a large group of cat owners and compare the results with dog owners in order to examine the hypothesis that owners of sick cats would exhibit lower caregiver burden than owners of sick dogs.
Methods: An online survey was used to collect data and measure caregiver burden using previously validated tools. For sick animals, the diagnosis provided by the owner was reviewed by a veterinarian to categorise the information.
Results: t he study included 1085 pet owners, including 333 owners of sick cats, 492 owners of healthy cats and 260 owners of sick dogs. unsurprisingly, owners of sick cats showed a higher burden than owners of healthy cats, but also owners of sick dogs had a higher burden than owners of sick cats.
Limitations of the study: As with all surveys, this study may have selected for motivated pet owners and it did not include owner demographics, which can affect burden.
Title: Risk factors for upper urinary tract uroliths and ureteral obstruction in cats under referral veterinary care in the United Kingdom
Authors: Geddes RF, Davison LJ, Elliott J, Syme Hm, o'Neill DG.
Journal: Journal of Veterinary Internal Medicine 37, 567–77, 2023.
Background: upper urinary tract uroliths (uutu) affecting the kidney and ureter can cause acute kidney injury and the frequency of uutu has increased significantly over the past 20 years. most utuu are calcium oxalate (Cao x), and although all uutu originate in the kidney, not all nephroliths will migrate into the ureter; risk factors for migration are unknown. Studies suggest that nephroliths may behave in a benign fashion in older cats, but in younger patients the risk of ureteral obstruction and acute kidney injury may be higher. However this has not been well studied.
Aims of the study: t his study aimed to identify risk factors associated with a diagnosis of uutu, and to examine the risks for ureteral obstruction in cats with uutu

Methods: t his was a cross-sectional study examining case records from the Royal Veterinary College referral hospital from 2009–2019. Cases were included if diagnosed with at least one urolith in the kidney or ureter on imaging. Data on various factors potentially associated with uutu, and urolith analysis results if available, were extracted.
Results: t he overall prevalence of uutu during the 10-year study period was 4.6% (521 cats). Risk factors included older
Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 45
[Image courtesy of Clinique Vétérinaire Foch]
age (>4 years), female sex, and being a Ragdoll, tonkinese, Persian, British Shorthair or Burmese (compared with nonpurebred). Cats with ureteral obstruction were significantly younger than non-obstructive cases and had a significantly greater proportion of ionised hypercalcaemia. Younger age (<12 years), being female and having bilateral uutu were risk factors for obstructive uutu t he younger the cat, the higher the risk of obstructive uutu (cats 0–3.9 years had 4.3 times the odds for obstructive uutu compared with cats >12 years) and cats with obstructive uutu were more likely to be eating exclusively dry food. Around half (51.8%) of cats with utuu were diagnosed with chronic kidney disease (CKD).
Limitations of the study: t his was a retrospective study, variable investigations were performed, there was limited utuu analysis (for instance, it was assumed that a urolith was Cao x, unless there was evidence otherwise) and dietary data were incomplete.
Relevance to clinical practice: Younger cats with nephrolithiasis should be monitored for the development of ureteral obstruction, as should those with hypercalcaemia, cats fed exclusively dry food, and cats with bilateral nephroliths.
Female cats, and Burmese, tonkinese, British Shorthair, Ragdoll and Persian cats are at higher risk of uutu, and affected cats are likely to have concurrent CKD.
You can access the full article here: https://onlinelibrary.wiley. com/doi/epdf/10.1111/jvim.16659
Cats with FIC may be more susceptible to stress and anxiety due to an imbalance in their sympathetic and hypothalamicpituitary-adrenal system and increased norepinephrine receptors in the bladder. t he CoVID-19 pandemic caused changes in routines, including cat caregivers being confined at home, which could have a positive or negative effect on cats.

Aims of the study: t his study aimed to identify whether the CoVID-19 pandemic and stay-at-home orders impacted the prevalence of uo patients presenting to emergency rooms.
Methods: t he number of cats with uo presenting to two hospitals [in the uSA] over 20 weeks was calculated for the initial period of stay-at-home orders in 2020. t his was compared with the same period in 2018 and 2019 to account for confounding factors such as season. Prevalence was calculated after also recording the total number of cats presenting with any illness during these periods and excluding cats with cystic calculi.
Results: t here was a significant increase in patients presenting with uo in 2020 at one institution, and both institutions combined when compared with 2018 and 2019 (from 4.0% of cases in 2019 to 5.9% in 2020). At the second institution the number of cats with uo also increased but did not reach significance.
Limitations of the study: It is possible that owners at home noticed uo and presented their cats more often and at an earlier stage. Diagnostic work-up varied between cats with uo and environmental/routine changes due to CoVID-19 restrictions likely varied between homes. o ther factors known to increase FIC risk were not assessed.
Relevance to clinical practice: If we needed any more evidence that stress can be associated with lower urinary tract disease in cats, this paper provides it. t he findings emphasise the importance of asking caregivers about changes to the cat’s environment and routine when investigating cases of uo
You can access the full article here: https://journals.sagepub. com/doi/full/10.1177/1098612X221149377 l
Title: Association between the COVID-19 global pandemic and the prevalence of cats presenting with urethral obstruction at two university veterinary emergency rooms
Authors: Finstad JB, Rozanski EA and Cooper ES.
Journal: Journal of Feline Medicine and Surgery 25, doi:10.1177/1098612X221149377, 2023
Background: urethral obstruction (uo) is a very common presentation to primary care hospitals. It is commonly idiopathic and associated with feline idiopathic cystitis (FIC).
Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 46

Companion Animals NZ update

sARAH OlsON, welfare officer CANZ
update from the NZ Companion Animal Register
In April, we celebrated the 2nd birthday of the new and improved NZCAR! t hanks to all the vet teams advocating for microchipping and registration.
We are committed to making the NZCAR more useful and easier to use. If you have feedback or features that you would like to see developed – reach out to us at info@animalregister.co.nz.
We constantly hear from veterinary teams how important it is that there is only one lost and found microchip database for animals in New Zealand, so it is our privilege to manage this service for you.
LostPet
We are currently redeveloping www. lostpet.co.nz and migrating the service to the NZCAR website. Losing a pet is a very stressful and emotive time. We want to make sure the process online is as streamlined as possible for guardians. t hese two complimentary services will be better managed and supported by the existing NZCAR team – meaning a more cohesive experience for guardians. t he LostPet.co.nz service is endorsed by mPI and SPCA for reporting lost and found companion animals. t his includes both cats and dogs but also horses, rabbits and other companion species.
NZVA Conference
We’re looking forward to seeing you all at the NZVA Conference Wellington in June! t his will be a great opportunity to meet and to discuss some the exciting projects we have:
l Equi trace and equine focused microchipping with NZCAR registration
l Shelter Register Aotearoa
Contact: saraho@companionanimals.nz
l LostPet redevelopment
l Accreditation – new Puppy Preschool standard
update from Companion Animals NZ
Shelter Register Aotearoa
Animal rescues and shelters in NZ are overrun with unwanted animals. Shelter personnel are stretched to the limit, with many being forced to close their doors. t he industry is unregulated and there is no concrete evidence available to quantify the size of the animal welfare ‘problem’ or understand trends in the industry.
Companion Animals NZ has established “Shelter Register Aotearoa”, an initiative to capture data on some basic metrics around animal numbers and movements within shelter/rescue organisations in NZ. t his information can then be used to help create positive outcomes for the animals and people involved in the industry.
We currently have 30 shelters that work with cats and dogs, participating the in programme. t he 9-months’ worth of data captured so far shows some interesting results. o f note, although perhaps unsurprisingly, the same trend is seen for outgoing, adopted and desexed cats. t his verifies the main reason cats leave the shelter is to be adopted, and all adopted cats are desexed before leaving. Although this is status quo for most shelters, it is encouraging to see the evidence.

How you can help!
We need more shelters from across NZ on board to help create an accurate and robust picture of what’s going in the shelter industry. Companion animal veterinarians work with shelters and rescues every day. t hey play a vital role in helping to control the overpopulation of unwanted animals and overseeing their health and wellbeing. to help us in our pursuit to understand, monitor and resolve these animal welfare issues, we urge companion animal veterinarians to encourage their clients working with cats and dogs in the shelter industry to join Shelter Register Aotearoa
For more information, please email welfare@companionanimals.nz l
Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 48
[Photo credit: Thomas Park for Unsplash.com]
Healthy pets NZ update
CAt H WAtsON, Chair, Healthy pets NZ
It’s full steam ahead for 2023 at Healthy Pets New Zealand as we come out of the Covid19-induced coma of the last few years. We’re really excited about the increasing numbers of donors showing their support; along with more and more research grant applications each funding round. t he more we raise, the more we can support local, relevant research benefiting companion animal veterinarians in practice. Help us to help them.
Grants
two new grants were approved in march:
1. Professor Carolyn Gates: Strengthening veterinary student communication skills through postadoption preventive care consults (Discretionary grant)
Companion animals need to be provided with appropriate nutrition, health care, and social interactions to prevent medical and behavioural problems that can negatively impact their wellbeing. Veterinarians are in a unique position to counsel owners about preventive care. However, many new pet owners do not seek veterinary advice to develop a good preventive care plan and even when they do, veterinarians are not always skilled at being able to communicate with clients in a manner that encourages them to follow recommendations. In this project, we will develop a novel programme for training veterinary students in motivational interviewing (mI), which is an evidence-based communication style that uses empathy, partnership, and understanding of the clients’ perspective to empower them to make positive behavioural changes.
2. Professor Andrew Worth: Biomechanical equivalency of 3D printed titanium bone plates (Research in Practice grant)
Internal fixation using titanium bone plates is a standard method of providing stability to allow a fracture to heal. Commercially available titanium plates are press manufactured from
Contact: http://healthypets.org.nz/
a billet first reduced from a titanium ore. In medical application both pure titanium and titanium alloys are used. Laser sintering is a form of rapid prototype manufacturing (also called 3D printing) in which a laser melts titanium alloy powder to form a structure from a computer generated data file using a topographic working surface. t his computer-aided design allows a plate to be custom made for any application. In order to design a plate of sufficient strength for a patient specific application a comparison to available equivalents is desired. t he actual loading on any given device in situ is only an approximation based on biomechanical modelling. Surgical guidelines are available which relate the animals mass to the available plate sizes. t hese guidelines only relate to the testing of plates manufactured using billet and press production, not rapid prototyping. t herefore before 3D printed plates can be recommended for use in patients it is vital to ascertain the equivalence of these implants to standard plate recommendations based on patient mass. t his data is not available for laser sintered plates as manufactured in NZ and elsewhere.
Research updates
We’ve added some historical background to our website on the origins of HPNZ. t his came about as part of our contribution to the NZVA Centenary celebrations, which we’re thrilled to be a part of –congratulations NZVA!
It’s been fascinating to look back through the archives at the research funded from the start, and to be able to hear from those involved in the establishment of the trust. t hanks have to go to the efforts of Boyd Jones, Richard Squires, Ross Blanks, Stuart Burroughs, Chris Hutchings, Pieter Verhoek and the many other who have helped to ensure we have access to local funding for research that will directly benefit Kiwi vets and companion animals.
We hope to highlight some of the original research funded over the coming year, but for now we’d like to congratulate Dr Anne Haase and her team from Victoria university of Wellington for completing their project on the fostering of cats for health. t his was the very first project funded under the Human-Animal Bond
grant, with the support of Royal Canin. t he research helps fill in some of the big gaps in our knowledge about what motivates fosterers; how they care for the cats, and how they influence the health and wellbeing of both the cats and themselves. t here are some good recommendations from their report, so if you’re interested to know more, you can find the full report on our website.
partners news
HPNZ is very excited to welcome back PD Insurance as our Principal Partner. PD Insurance have been amazing partners through 2022, helping to raise the profile of HPNZ through events, interview opportunities, insurance bonuses, social media, as well as helping to share our research through their new vlogs. t heir support has meant we have been able to fund some big projects in the past year, so we look forward to bringing you lots more research in the coming years thanks to their ongoing support.
upcoming events
Healthy Pets New Zealand plans to be busy for the rest of the year, so we’d love to have at chat at one of the upcoming events. t hanks to the wonderful support from the team at PD Insurance, we’ll once again be at the NZVA Conference ( tākina Events Centre, Wellington, 28–30 June 2023), so come and talk to us and check out the research summaries at stands 214 and 215. t here will be more artwork on offer to, so come and put your bids in.

We’re also thrilled to have the support of the 4Paws marathon team and would like to encourage anyone with a dog in the vicinity of Christchurch on Sunday 1 october 2023 to sign up with your dog for one of the many events on offer. Sign up at https://4pawsmarathon.co.nz/enter/ and show your support to Healthy Pets NZ when you enter.
Dogs Day out will be back again in october too, but this time bigger and better in tauranga. Look out for more details soon on our website, or get in touch if you’d like to help out. l
Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 49
massey News

staff changes
t he inimitable Nick Cave is leaving massey after around 18 years of teaching (plus time as a resident). Nick graduated in 1991 as part of the class that spawned many academics (Wendi Roe, Janet PatersonKane, Susan tomlin, Stefan Smith and myself) and private specialists (Andrea Ritmeester, Jenny Donald, Angus Fechney, Alexander macLachlan, Richard mcKee). I look back and reflect that maybe we all took those paths in part due to the influence of the generation of teachers we were inspired by (Hilary Burbidge, Steve Fox, Colin Wilks, Stan Fenwick, Prof. Jolly amongst others). In that same way I think there will be many massey BVSc graduates that can reflect that Nick Cave challenged and inspired them along the pathway they have led. He has been a huge part of the fabric of the BSVc.
After graduation Nick left massey for private mixed practice which was followed by a stint in small animal practice working alongside the late Frazer Allan and todd Halsey in Hamilton. He joined the medicine team as a resident under ex-HoI Grant Guilford during a very productive period of gastroenterologybased clinical research. He then headed to the university of California, Davis and completed a second residency and PhD in small animal nutrition before being invited to come back home to join the medicine department in 2005. He later established a research programme in small animal nutrition and created residency positions which have led to two further specialists in this field. He has been a huge part of the academic life of the BVSc degree at massey and supervised masters and doctoral students. many former students with be able to attest to how Nick enlivened their learning with his passion for teaching. He is always at his best with an audience, captivating and witty, and a favourite on the CPD circuit as well as with undergraduates. Nick, leaving as an Associate Professor, has an international reputation in his discipline and declined many offers over the years to join the more financially lucrative private sector, preferring to devote himself to teaching the next generation of veterinarians. Now he is moving on from his massey career; to
new challenges that may yet inspire him to even greater things and we hope he will remain an active part of the veterinary community in New Zealand.
t here will be an official farewell for Nick Cave and his last day is at the end of may. I am sure there will be many massey graduates out there that will want to acknowledge his contribution to their education when next they meet. Go well Nick.
Andrew Worth
Additional staff changes:
l Hiroki Sano, recently returned from Hong Kong to the anaesthesia department is set to return to Hong Kong to a private specialist hospital. Hiroki has been a prolific researcher alongside his heavy clinical load and has contributed much to the V t H.
l Sandeep Sharma is also leaving anaesthesia for a position at the university of Sydney. t he anaesthesia department will be making use of the part-time services of Paula Larenza (a melbourne-based specialist anaesthesiologist) and locum cover whilst we recruit into the open position.
l Frank Gold and Rhea Jagdhane, both former interns and recently staffing the internal medicine service under Nick’s tutelage, are both moving on, seeking residency opportunities elsewhere. Frank and Rhea have provided an excellent service to our referral clients, rapidly acquiring expertise in their chosen discipline and we wish them ongoing success.
l Andre Grafas, also a previous intern then ECC clinician, is leaving us for an oE and we thank him greatly for his contribution to the V t H. Best of luck, Andre.
New specialist in the surgery team
It is with great pleasure that we can announce that Sacha Devereux, former resident and now faculty member, passed her European Boards examination at the first attempt and is now a specialist small animal surgeon. Her chief supervisor Kat Crosse and co-supervisors Lee and Andrew are justly proud of her achievement. t hat gives the V t H four specialist surgeons when Kat returns from maternity leave. our final year resident Sasha Polak is now running her own service with supervisor backup and hopes to credential later this year in anticipation of fellowship examination next year. t he surgical caseload is good with a few weeks waitlist for some non-urgent cases. urgent and semi-urgent cases are able to be handled according to need.
small animal referral services
As a result of our current inability to recruit specialists in internal medicine, the muV t H cannot currently offer a specialist small animal medicine referral service. We appreciate the need to still have a pathway for clients’ animals to access advanced diagnostics, emergency medicine and anaesthesia. We are recruiting veterinarians with a special interest in internal medicine to back up the referral specialist SA Surgical and ECC teams and hope to be able to handle outside medicine referrals on a more limited basis than previously.
price rises for clinical services
t here have had to be substantial price rises in the fees for veterinary services provided by the muV t H. t his mainly reflects the evolving financial structure of the university and the requirement for the Veterinary School to return more income for all operations to cover the increasing cost of delivering the programme. t he V t H, like most university clinics in the world, is not a profit generator as it might be in the private sector, due to its training role and less efficient case through-put. At the same time, we are being asked to reduce the losses and recover more costs hence the price rises. Please do not rely on historical fees and quotes when advising clients on future referrals. l

Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023 50
Executive Committee Members of the NZVA Companion Animal Veterinarians Branch
President
Natalie, Companion Animal Veterinary Advisor, Zoetis NZ, Wellington


I have been a companion animal practitioner for over 20 years with a strong interest in feline medicine, preventative health care and veterinary wellbeing. I joined the team at Zoetis in 2018 after selling my practice in Wellington. I enjoy the opportunities my role provides, meeting companion animal veterinarians across New Zealand, talking to them about the issues they face on a day to day basis, and learning where CAV can focus our member support in the most valuable way.
Additional roles: Member of WSAVA Congress Steering Committee
Vice-president
Simon Clark, Veterinarian at Pet Doctors, Hamilton

I grew up in suburban Auckland with a love of science. At high school I got a job cleaning the cattery at my local vet clinic and I’ve been in the industry ever since. I quickly found the application of science to immediate family situations fascinating. I continue to love the application of the most up-to-date science to help families. I am the CAV representative on, and Chair of, the NZVA member Advisory Group (mAG).
Additional roles: Trustee Healthy Pets NZ, CAV rep on MAG, MAG Chair and member NZVA board
Treasurer
Kevanne McGlade: community veterinarian, Massey University

I work as a companion animal veterinarian in the Community Practice small animal clinic at massey university’s täwharau ora – School of Veterinary Science in Palmerston North. Each year our final year students spend a number of weeks in the clinic. my role is to support and guide them as they take on the role of a veterinarian, conducting first opinion consultations and performing procedures to equip them for practice after graduating.
Shanaka Sarathchandra, Clinical Lead Veterinarian, Pet Doctors Hamilton

I am a 2004 massey graduate working in companion animal practice in Hamilton. I have a special interest in imaging and medicine. I am looking forward to being more involved in the veterinary community.

Toni Anns, National Sales and Key Account Manager for Companion Animals, Zoetis NZ, Auckland
I have been a member of the CAV executive committee since 2016. I currently work for Zoetis as the National Sales and Key Account manager for Companion Animals. In this role I am very privileged to be able to meet and talk with many veterinary professionals. I listen to the trials and tribulations, the challenges, the joy and the angst of veterinary life and I want to help in whichever way I can. ultimately, I would love to see elevation in the reputation of this industry and improved collaboration both nationwide and internationally. my ultimate goal is to help improve the personal satisfaction at the end of each veterinary professional’s day.
Additional roles: CAV rep on Healthy Pets NZ Trust
Becky Murphy, owner of TCI Glenbred, Feilding

I am a 2010 graduate from massey university. my practice, tCI GlenBred is devoted to canine inherited disease screening and theriogenology. I have been a member of the CAV Committee since 2018. I enjoy working with dog breeders and veterinarians to promote and improve genetic health, particularly in pedigree dogs. outside of work, my husband and I have two children, one dog, two cats, two bunnies and a very naughty pony, which keeps us very busy!
Additional roles: Member of WSAVA Hereditary Disease Committee
Secretary
Sally Aitken, Lead Companion Animal Veterinarian, VetEnt Turangi Community veterinary work is my passion; caring for animals through their life-stages. I grew up in Greymouth, worked 26 years in taupo in mixed and CA practice and am now based in turangi providing companion animal community veterinary care with VetEnt. Continuing education, ANZCVS, avian medicine, dermatology and internal medicine are my other vet passions, along with mountain-biking, tramping and raising two fantastic teenagers with my husband here in taupo.
Additional roles: CAV rep on Healthy Pets NZ Trust
Nina Field, Veterinarian, Evolution Vets and Animal Rehabilitation, Ashburton



I've been a vet for a long, long time. Eight years ago I got my certification for canine rehabilitation so have been working as a 'physio' alongside first opinion clinical practice since then. I've been on the CAV committee for 4 years now and really enjoy working and making plans with such a motivated, stimulating team.
Additional roles: CAV representative on NZ Companion Animal Trust
Ex officio members
Sally Cory, NZVA Head of Veterinary Services (Companion Animal) originally from the uK, I gained my veterinary degree from Edinburgh university. I embarked on a working holiday to NZ in 1999 and have been involved in companion animal practice since then, with recent years spent both working in and managing a Wellington based after-hours clinic. t he role of Head of Veterinary Services (Companion Animals) is an exciting new direction for me, and I am looking forward to working alongside CAV to help navigate and support our profession through a period of exciting change and progression.
Additional roles: NZVA rep on Healthy Pets NZ Trust
Sarah Fowler, Editor – Companion Quarterly (and NZVJ), Hamilton I have been the editor of Companion Quarterly (previously CAS Newsletter) since 2013. I am a 2010 massey graduate (after a starter career as a plant scientist) and worked in clinical CA practice before starting in 2016 as an assistant editor at the NZVJ. I am now editor-in-chief of NZVJ and I am stoked to have found a niche in veterinary publishing that allows me to use my previous scientific training and my veterinary qualifications.
Producing
Quarterly as a high quality source of CPD for CA
great deal of satisfaction.
Companion
vets in NZ gives me a
51 Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023
Instructions for Authors submitting articles to the Companion Quarterly
sARAH fOW leR (editor), for the Companion Quarterly editorial Committee
the Companion Quarterly is published quarterly in the first week of march, June, September and December of each year. the printing costs are covered by the advertisements. there is therefore a limit of about 55–60 pages to the size of each issue. there is a balance between political issues, articles for continuing education and other news.
Authors are expected to submit their articles and conference in a final form suitable for publication. If practitioners wish assistance with writing, please contact the editor. Also look at previous issues to see the layout.
Articles
t he article should have a title. Following the title the names of the authors, their degrees, titles, contact details should be present. Submit articles preferably by email, or disk if this is not possible.
Submit articles in adequate time for reading and alterations before publication.
Contributions must be original. Articles or extracts from articles may be completely copied only if there is permission from the original authors and source of publication. It is the responsibility of the author(s) rather than the editorial committee to obtain this permission.
t he author(s) should disclose if they have published the same article or a very similar article elsewhere.
Articles that are clearly editorials/advertising will be labelled as such at the discretion of the editorial committee. these include articles/editorials that are repeated from other publications such as VetScript and that contain obvious product placement comments.
proof reading
the authors should proof read their article looking for mistakes, spelling errors, omitted details. While the editorial committee reads through the articles, the articles should be presented error-free.
Articles and conference reports from recipients of grants and scholarships
It is the responsibility of recipients of any grants and scholarships to supply any conference reports and articles written as part of the requirements in the final form suitable for publication.
References
A list of references should be supplied if appropriate. Follow the guidelines for the New Zealand Veterinary Journal for method of reporting of references.
t he number of references should be kept to a reasonable number relative to the length of article. Keep numbers of references to a minimum when discussing a single point, i.e. do not be repetitive with numerous references when a few will do. t he editorial committee will omit references if the list is judged to be excessively long.
f igures
Good quality illustrations that clearly illustrate the necessary points should be submitted with the article.
Submit any photos or graphics in their original forms (i.e. JPG, PDF, tIF files) as they lose their clarity when extracting them from Word or Publisher documents.
If positions of figures are not obvious from the text, send a hard copy or some other form of instruction as to where they should be placed.
Figures should be clearly numbered labelled as to top and bottom where necessary. Features on the figures should be clearly labelled by the author(s).
t he figure captions should be concise and accurate, and supplied with the text on a separate page at the end of the article.
Diagrams/figures can be copied from textbooks only if there is permission from the original author and the source is clearly acknowledged. It is the responsibility of the author(s) to obtain this permission before submitting the article to the Quarterly editorial committee.
timing of article submission and publication
Articles will be published as soon as possible after submission. the newsletter goes out in the first week of march, June, September and December. Articles therefore need to be submitted at least one month before (i.e. by the end of January, April, July and october) but preferably earlier to allow one month for the collation, printing, binding and posting of the Quarterly.
Depending on when the articles are received, the size of that particular issue and the need for refereeing, at the editor’s discretion articles may be held over for a later issue.
Refereeing
Articles may be sent to appropriate people in that field of expertise for refereeing/proof
reading if the editorial committee deems this is necessary. this is to ensure accuracy within the text to protect readers, the authors CAV and the clients and the patients of veterinary practitioners.
sciQuest and the NZVA website
Selected scientific articles will be placed on the SciQuest website for access by NZVA. there will be a delay of a year to ensure that practitioners still see a benefit in becoming CAV members. the entire newsletter is now being placed on the CAV website but the most recent issues (i.e. those within a year of publication) are available only to CAV members.
Article of the issue and student article
Prizes are sponsored for the best case report and general article in each quarterly issue. t he best overall article in each category for the year is then decided in may and the overall prize awarded at the Annual dinner in June. t he members of the editorial committee will judge the articles on their clarity, conciseness, and usefulness to practitioners.
Articles that are submitted to the Quarterly as part of an obligation due to the author(s) receiving Educating the Educator or Study/ Research Grants from CAV are not eligible for the article of the issue prizes. Articles submitted by the editor and the members of the editorial committee are also not eligible for the prizes. there is a separate undergraduate student article competition.
planning a case report?
some hints as to how do so!
When writing an article take time to look at how articles in other journals are arranged. While articles for the Quarterly are not as detailed as the NZVJ the information needs to be arranged in a logical manner to make it easy for the reader to follow. therefore follow some logical headings as detailed below. Not all of these headings will need to be used in all articles and some may be combined depending on the type of case and amount and type of information available.
• Introduction
• History
• Clinical signs materials and methods
• Results (of investigations e.g. laboratory results, radiography).
• Discussion
• Conclusion
Acknowledgments
• References. l
52 Companion Quarterly: Official Newsletter of the Companion Animal Veterinarians Branch of the NZVA | Volume 34 No 2 | June 2023
LESS 00-
proGlan supports the natural mechanical emptying of anal glands
0 Natural pumpkin fibre for stool bulking
l8l Probiotic microbiome support proven to assist stool consistency 1
f8l Vitamins and natural ingredients supporting the immune response
For more information about proGlan or proHibex, call us on 0800 337 622 or visit our website at www.glapharma.co.nz
proHibex aids in the management of minor cases of diarrhoea
� BacillLts velezensis (subtilis) improves faecal firmness and dry matter content1


� Contains montmorillonite day for stool binding and bulking
� B.velezensis supports GI integrity2
proGlan'"
pr;Hibex· RE HHH.