CENSUS 2023 AND REPORT ON MATERNITY: THE RAPIDLY CHANGING DEMOGRAPHICS OF AOTEAROA P.36
STANDARDS REVIEW I TE REO MĀORI (IN TE REO MĀORI) P.40
EDITOR
Hayley McMurtrie
E: communications@nzcom.org.nz
ADVERTISING ENQUIRIES
Hayley McMurtrie
P: (03) 372 9741
MATERIAL & BOOKING
Deadlines for March 2025
Advertising Booking: 1 February 2025
Advertising Copy: 10 February 2025
Welcome to Issue 115 of Midwife Aotearoa New Zealand
It is hard to believe we are already sharing the December issue of Midwife Aotearoa.
In this issue, the College co-presidents discuss the importance of unity. As I write, tens of thousands of New Zealanders are gathered at Parliament for a hīkoi in opposition to the Treaty Principles Bill. As a Tiriti-honouring organisation, the College stands in support of a united and proactive approach to affirming and protecting tino rangatiratanga and mana motuhake for Māori, strengthening relationships for all New Zealanders. Unfortunately, the timing of this magazine has prevented us from featuring the powerful images of this historic event of the nation uniting to support the enduring principles of the Tiriti.
The cover story dispels some of the myths surrounding artificial intelligence, showing that many of us are already using AI without necessarily realising. We also celebrate the first Midwifery Standards Review conducted entirely in te reo Māori and reflect on the valuable lessons this offers.
The feature on early pregnancy ultrasound illustrates how, when midwives are empowered to respond directly to whānau needs within their communities, we move closer to achieving equitable outcomes.
I hope you are staying up to date with our regular updates in the email newsletter Pitopito Kōrero in between magazines.
If you are not receiving these updates or have any feedback, please contact us at communications@nzcom.org.nz. The newsletter aims to reduce the number of emails sent to members, while keeping you informed of all the important developments within the profession.
On behalf of the National Office, I wish all members a restful festive season and hope you find time to relax with your whānau.
Meri Kirihimete me te Hape Nū Ia Hayley Square
HAYLEY MCMURTRIE
COMMUNICATIONS MANAGER
Email: communications@nzcom.org.nz
from the co-presidents
Bea Leatham
He kokonga whare ka kitea
He kokonga ngākau e kore e kitea
The corners of the whare can be seen
The corners of the heart cannot
Kotahitanga, or unity, is a word that’s become synonymous with the late Kiingi Tuheitia and his call for Māoridom to stand proudly, as one. And in a heartfelt display of manaakitanga, it was my co-president Debbie Fisher who was the first to reach out when he passed, approaching myself and Alison, to ask what the College could – or should – do at such a time.
Manaakitanga is more than ‘hospitality’. It’s about upholding one another’s mana, and I believe Debbie’s intention that day was to do just that, for all Māori members.
Along with whanaungatanga, hononga and aroha ki te tangata, manaakitanga is one of the many precursors to kotahitanga and I firmly believe that if we can get the basics right, we’ll be steering our waka towards the same, collective vision.
The construction of any whare requires a solid foundation upon which it can be built. And if the foundation lacks integrity, the stability and longevity of the whare will be compromised. Our journey towards kotahitanga could be likened to that process. Right now, we’re still working on the foundations, and it’s likely to require a few more layers before we can all feel confident enough to build upon it. But we’re moving in the right direction.
The partnership agreement established between the College and Ngā Māia is a tohu of this and, as we undertake a co-governance
review, we are collectively impelled to revisit our values. Manaakitanga encourages and reminds us to embrace the differences and acknowledge that we all have our unique mana, strength and purpose.
I’m encouraged that as a profession and an organisation, meaningful steps towards kotahitanga have been taken. The focus is shifting; the groundwork has begun.
I’d like to thank my Tiriti partner Debbie for her aroha and support throughout this first year of co-presidency. The above whakatauāki refers to hearing and seeing actions that align to what one feels. It not only reflects the feeling of kotahitanga, but it also echoes the intentional value of working in partnership. I appreciate the partnership Debbie and I have fluidly created and I look forward to embedding manaakitanga, whanaungatanga and kotahitanga within our organisation and our profession!
Ngākau nui, ngākau whakaiti Square
Debbie Fisher
It’s hard to believe nearly 12 months have passed since Beatrice and I began our roles as co-presidents. I’ve really appreciated and enjoyed working alongside Beatrice – it seems as though we’ve worked together for years.
The past year has been incredible; learning from our tangata whenua co-president and the full Board has been an enriching experience and, together, we’re excited to be creating space for mahi to progress towards a meaningful Te Tiriti partnership approach.
As College members, you each are also part of this mahi, with your regional chairs
bringing your voices to important national discussions. Active participation in your local region is all about building kotahitanga | unity, supporting each other as midwives to continue challenging the status quo and managing the stressors of workforce shortages and significant fiscal constraints. I highly recommend taking up an opportunity to be a regional chairperson or co-president for the College – you’ll find it a rewarding experience, I’m sure.
Recently, I’ve been talking with several local wāhine | women who are keen to become midwives themselves. Why would they want to, you might ask, given our current climate? But what they’ve all shared is that they’ve held onto the dream of becoming a midwife for so long. It is inspiring listening to why they see midwifery as such a powerful and honourable role in their communities, and this inspiration is a timely reminder for us all.
Midwifery is more than contracts and working in places made of bricks and mortar. This was so evident through the recent court case, as midwifery presented itself professionally and with the highest degree of integrity.
As we come to the end of the year, I hope you can all enjoy the festive season and have some downtime to relax with your loved ones. As we look towards 2025, let’s continue to build kotahitanga and take care of each other; we’re all midwives and we need to nurture the relationships that make our jobs rewarding, easier and safer.
And remember, you each hold a position that is respected and valued in your community – whether you work in a hospital, primary facility, community setting, as an educator or as a researcher. You also never know whether you might plant a seed of possibility for someone you come into contact with, inspiring them too to become a midwife in the future. Square
MIDWIFERY MODELS OF CARE
Hot off the press, the World Health Organization (WHO) published a global position paper on Transitioning to midwifery models of care in October 2024. This paper, developed through collaboration with 100+ individuals and partners, outlines the definition and guiding principles of these models and provides the rationale for transitioning to them.
The paper lays out the considerable evidence base which demonstrates the positive impact midwifery models of care have on maternal and newborn outcomes, in all settings. It is the first of two documents. The second (yet to be published) document will be an implementation guide, intended to inform policy changes needed to enable midwives to work in a midwifery model of care within a wider integrated health system.
The document defines and describes a midwifery model of care as 'a model in which the main care providers for women and newborns, starting from pre-pregnancy and continuing all the way through the postnatal period, are educated, licensed, regulated midwives who autonomously provide and coordinate respectful high-quality care across their full scope of practice, using an approach that is aligned with the midwifery philosophy of care.'
Midwifery models of care enable women and whānau to be at the centre of care, optimising the physiological, social and cultural processes around birth. They can be contextualised for any setting and respond to the unique needs of whānau.
In midwifery models of care, midwives provide integrated care, addressing the needs of each individual woman and newborn, within functional and enabling health systems, equipped with necessary resources and streamlined consultation and referral processes. They collaborate within networks of care as part of interdisciplinary teams, characterised by equality, trust and respect. This approach guarantees that every woman and newborn receives personalised care, tailored to their health needs.
Midwifery models of care are adaptable to all levels of care and contexts, including home, community, and hospital-based settings, the public and private
from the chief executive, alison eddy
A model of care is about how services are conceptualised and organised, how roles and responsibilities are delineated and how services are delivered.
sectors and public-private partnerships, resource constrained environments, and humanitarian and crisis settings. This ensures wide accessibility, equity and relevance across different cultural contexts for women, newborns partners, families and communities.
A common assumption is that midwifery models of care relate exclusively to continuity of midwifery care, but the meaning of the term is more expansive than this. A model of care is about how services are conceptualised and organised, how roles and responsibilities are delineated and how services are delivered. Within a midwifery model of care the woman and her baby (in the context of her whānau) are at the centre of care. Midwives coordinate care, working within a philosophy that recognises the importance of cultural, social, psychological as well as physiological dimensions. Midwifery models of care can be provided in any setting, including hospitals.
“Transitioning to midwifery models of care” refers to the process of re-orientation of health systems away from the currently prevalent fragmented and risk-orientated model of care to a midwifery model of care in which women and newborns, starting from pre-pregnancy and continuing all the way through the postnatal period, receive equitable, person-centred, respectful, integrated and high quality care, provided and coordinated by midwives working within collaborative interdisciplinary teams.
Aotearoa re-orientated its system to accommodate a ‘midwifery model of care’ from the 1990s, and this model is now firmly embedded at the core of our maternity service. Aotearoa is one of the few (if not the
only) countries in the world where continuity of midwifery care is central to primary maternity care delivery and midwives working within maternity facilities are enabled to work autonomously. The WHO document is a timely reminder that the rest of the world is still trying to catch up with what we have achieved.
There are many factors in our favour in Aotearoa which enabled the relatively rapid transition to a midwifery model of care from 1990 onwards:
• a small country with a single national health system and universal access to publicly funded maternity care
• a regulation model which permits midwives to practise autonomously across their full scope of practice
• a funding model which enables midwives to self-determine how they provide continuity of care (within contractual and professional expectations)
• an undergraduate education model through which midwives develop the necessary competence to practise across the full scope from graduation
• an integrated system, with referral pathways and accessible specialist services within a functional health system
Although our unique context has no doubt been a large contributor to the success of establishing our current system, it was not always easy. It took time for the role of autonomous midwives within our system to become widely accepted, respected and normalised, by the public and the other professional groups who we work alongside. It has also taken time to establish the resources necessary to support midwives to work and function effectively in a midwifery model of care.
Although Section 94 (the Notice) enables continuity of care, it only provides fees for modules of care or services provided. The Notice expects continuity of care, yet no value is placed on it. Community midwifery practice requires a significant level of organisation and coordination at a practice level, as well as considerable administration. The structures and systems needed to support community midwifery practice are not currently recognised or resourced. The form of the Notice is outdated too; it has not kept pace with modern commissioning principles. It would require major revision to meet the true resource requirements of our model of care. For example, while midwives are a readily accessible workforce who are capable
of providing services such as HPV screening and maternal immunisation, there is no funding mechanism available to midwives who provide these services.
The evidence base for continuity of care is strong and the recent WHO publication provides a clear mandate for it to remain central within our maternity service. However, over recent years workforce shortages have led to work-around solutions being developed which have in turn normalised a reduction in access to continuity of care and choice of care provider. Are we drifting away from a midwifery model of care and moving towards a “fragmented and risk-orientated model” – the antithesis of what the midwifery model is intended to achieve?
The midwifery model is not broken nor is it unsustainable. The building blocks which have enabled our current system to be established and embedded are fundamentally unchanged. We just don’t have the right funding model, structural support, and wider system integration to sustain and support the midwifery workforce and drive equity goals. The College has advocated strongly for a new funding model for primary maternity services for many years now (including through the recent Class Action case taken on behalf of LMC midwives). Change is now finally on the horizon with the establishment of a Health New Zealand convened Technical Advisory Group. This group is being asked to ‘inform the design and development of a commissioning framework (the Framework) for maternity services’. The intention is to develop a national description of the ‘requirements and expectations’ of community maternity services and the ‘quality dimensions’ that might then be ‘regionally commissioned’
After more than three decades, the profession has a wealth of experience about what it takes to sustain continuity of care, and what is needed to strengthen it. While a degree of midwifery self-determination is essential to sustaining continuity of care, midwives must be valued and supported by the system. Implementing support for group practice models is an important part of protecting sustainable ways of working for community midwives, but they need to be able to choose who they work with to ensure successful group dynamics. Watch this space, after nearly a decade of frustration and lack of progress, something may finally be about to happen.
As always, the College will engage with this new design project in good faith and with a clear understanding of the solutions we need to strengthen and support the midwifery model of care. Square
joan donley midwifery research forum
The College’s biennial Joan Donley Midwifery Research Forum, held in New Plymouth over 24-25 October 2024, provided a wonderful opportunity for midwifery colleagues to come together to celebrate the profession and the research that informs our future.
Thanks to Elaine Gray and her organising team who were well supported by the Taranaki region, Ngā Maia rōpū, the schools of midwifery, and Tania Fleming, the College Education Advisor. Tania summed up the proceedings at the end of the final day:
“To Joan Donley – in your memory may we always do you proud! In the 1980s and 1990s Joan challenged midwives to step out from under the nursing umbrella and reclaim midwifery as an autonomous profession. I suspect that Joan would be challenging us again to reclaim our midwifery ways of knowing, being and doing! She equally would be proud of the breadth and depth of research and the exciting direction our midwifery researchers are taking our profession in”.
Once again the forum included presentations on a diverse range of topics relevant to midwifery in Aotearoa, from clinical (episiotomy does not protect women from experiencing severe perineal tears during spontaneous vaginal birth!), to education, abortion, exercise, teenage pregnancy, continuity of care, quality assurance, the autonomy paradox, innovative research methods and many more. We heard about equity, inclusivity, manaakitanga and whanaungatanga | the development of relationships being the key to quality midwifery care. These relationships, centred on trust, are essential for providing culturally safe care for whānau across Aotearoa.
Midwife researchers were encouraged to publish their work in an academic journal so it can inform midwifery practice – and the College Journal is an excellent forum for this. Thank you to all the midwives who presented their work, chaired sessions, and attended the forum.
I orea te tuatara ka patu ki waho A problem is solved by continuing to find solutions Square
“To Joan Donley – in your memory may we always do you proud! In the 1980s and 1990s Joan challenged midwives to step out from under the nursing umbrella and reclaim midwifery as an autonomous profession. I suspect that Joan would be challenging us again to reclaim our midwifery ways of knowing, being and doing!”
eLearning
The College is currently offering two eLearning courses with more planned for launch in the New Year. The courses available are practicalities of mentoring in Aotearoa and Te Tiriti o Waitangi and we are receiving great feedback about both courses. Te Tiriti o Waitangi is subsidised for members and can be applied to the Midwifery Council’s mandatory cultural safety education requirements for the 2024–2027 cycle.
Practicalities is a pre-requisite for midwives considering becoming a mentor in any of the College's mentoring programmes. It has a great deal of useful information for any midwife supporting another professionally. This workshop is fully funded for College members. The courses are available through the College website education tab. Square
college guidance review process
The College team have implemented a new process for reviewing and updating College guidance documents, including Consensus Statements, Practice Guides and Keteparaha.
We have reviewed all existing and proposed guidance documents and developed a programme of work based on order of priority. Our team have six guidance updates currently in progress, and will continue working through the list as these progress. We are also developing a tool that members will be able to use to request the review of existing guidance or development of new documents. Members will also see new formatting and branding elements for the College reflected in draft guidance documents as they are developed. Square
abortion reversal statement now on web
The College’s board has approved the publication of a statement on the practice known as “abortion reversal”. This term refers to a non-evidencebased procedure whereby a pregnant woman/person who has taken mifepristone medication to induce an abortion then attempts to reverse this process by taking progesterone in an unlicensed way.
The claims of success made about abortion reversal are not reputable. Concerning reports about the arrival of the practice in Aotearoa have
prompted the Ministry of Health | Manatū Hauora, RANZCOG and RNZGP to release statements which provide clarity for clinicians that this procedure is not supported and should not be offered in Aotearoa.
The College supports this stance, and has published a statement for midwives on its Practice Updates webpage: https://www.midwife.org. nz/midwives/professional-practice/practice-updates/ Square
college governance review
As stated in the September edition of the magazine, the College board has recently commissioned a report on the organisation’s governance structure.
The report, completed by Kathie Irwin and Jo Cribb within a te Tiriti partnership model was informed by a series of wānanga around the motu with Māori midwives and their supporters (as identified by the current tangata whenua board members) and interviews with current or previous tangata tiriti board members and ex-presidents, and key leaders from the MMPO and MERAS.
The board considered the report at its November meeting which was held at Te Māhurehure marae. Although the experience of tangata whenua and tangata tiriti members of the College and its governance model differs, there was clear agreement between all who participated in the interviews and wananga that change is needed. The report's recommendations include moving to a smaller, skill-based, Tiriti-based governance board, with a mixture of elected regional representatives and appointed members to ensure that the board composition includes the necessary mixture of skills and perspectives. The report also recommended that the College seek to adapt its regional structures to make them more flexible and responsive to members needs. The board has agreed to release a discussion paper which includes context, background and the recommendations for members' to consider. Members will have the opportunity to consider and discuss the recommendations over the coming months. Square
terms of reference for the governance review (summary). with reference to the college’s commitment to Te Tiriti, and its wider constitutional objectives:
How does the College ensure that its governance arrangements: are fit for purpose, meet the expectations of ‘good governance’ and include the necessary skill sets, experience and diversity for effective present and future governance needs, ensure the values of the organisation are reflected in its arrangements and decision-making processes enable it to confront the challenges, manage risk in a rapidly changing environment and maximise the opportunities for the midwifery profession in Aotearoa New Zealand?
What is the optimal structure across the country within national and regional structures to: enable members' voices to come together nationally to inform the organisation and the profession, and the College’s strategy and operations, to ensure transparency in decision making and policy? What structures are needed within the College to ensure all voices are honoured?
What is the most effective means of incorporating consumer/ whānau perspective in the College’s structures?
November board meeting at te Māhurehure marae, Tāmaki Makaurau.
bulletin
primary maternity service notice fee increase
Health NZ | Te Whatu Ora has announced an increase to fees within the Primary Maternity Services Notice. The overall amount of the increase is 2.51%; however, this uplift will be applied into selected fees within the Notice rather than across the board. The increases take effect from 1 July 2024 and once changes have been implemented, a back payment will be applied where applicable.
The increases will be applied to the Additional Care Supplements (ACS) and the Rural Practice and Travel Supplements (RPaTS). College staff have consulted with a work group from the College board (including Ngā Maia representatives) and provided advice to Health NZ on where the uplifts are needed the most. Given that a planned uplift to the ACS fees in 2023 was not applied, there was general agreement that this is a priority area for increased investment.
The ACS was designed to address areas of midwifery practice that have traditionally been under-funded within the Notice, and in particular acknowledges the extra time involved in in supporting the equitable provision of midwifery care.
The total claimable amounts within the ACS modules are capped and one of the areas the uplift will be applied to is the raising of these claiming caps. The College advocated strongly to have all caps removed, however, this was not possible with the level of increase allocated this year.
Due to the timelines required for the IT work, additional tasks related to the ACS criteria will be conducted in two stages.
Stage 1 (implementation by the end of 2024)
The ACS maximum amounts have increased for claims related to pregnancy, labour and birth, as well as postnatal care.
immunisations are more important than ever.
A new webinar, Immunisations in Pregnancy, www.immune.org.nz/education/ webinars, provides support for health professionals having important conversations with hapū māmā and whānau around the importance of antenatal and on-time immunisations.
The webinar covers clinical information, how to build immunisation confidence with hapū māmā and whānau and address any concerns, as well as where to find useful resources. Square
principles for quality and safe prescribing document
The College also advocated strongly for a significant increase to be applied to the acute after-hours call-out category, and to make it claimable for each call-out. Although the 2.51% increase does not allow for a substantial increase to this fee, Health NZ has agreed that the acute call out fee will be classified as ‘high’ which attracts a $90 fee and will be claimable per call-out, capped as per above. The College will continue to advocate for further increases to this funding as we recognise that this does not fully compensate midwives for this important aspect of LMC practice. Square
immunisations
in pregnancynew webinar recording
With the rise in cases of pertussis across many regions in New Zealand, antenatal
A number of principles for safe prescribing have been developed by the seven responsible authorities (RAs) who regulate prescribers to promote safe prescribing and ensure best prescribing practice. This document presents a set of principles to assist health practitioners who prescribe (prescribers) to undertake and maintain quality prescribing practice when prescribing therapeutic products.
This collaborative approach and development of joint principles has been greatly influenced by overseas competence frameworks and the Medical Council of New Zealand’s statement on good prescribing practice. The document is available on the guidance for practice page of the College website: www.midwife.org.nz/ wp-content/uploads/2024/09/Principles-forquality-and-safe-prescribing_17Sep2024_JointRelease.pdf Square
BRIGID BEEHAN
MIDWIFERY ADVISOR
redesigning midwifery standards review: shaping the future of MSR
A quality assurance programme for midwives plays a crucial role in maintaining, sustaining and improving the quality, safety and effectiveness of midwifery care. It provides a framework for accountability, continuous improvement and person-centred, whānaufocused care within the profession.
In 2023, the College established a coleadership model for the Midwifery Standards Review (MSR) programme. Soon after, the College began examining how MSR, a component of the quality assurance activities and programmes offered by the College, could best meet the diverse needs of midwives across Aotearoa.
In April 2024, the College commissioned a comprehensive literature review to support the evaluation of the current MSR process. The aim of the review was to address various questions relating to competency maintenance and professional development, both in midwifery internationally and within other regulated health professions in Aotearoa. The review also included searches of te ao Māori frameworks relevant to professional development and considered literature related to existing components of the MSR programme.
The areas covered in the review were:
• Continuing competence and professional development requirements in Aotearoa’s health professions
• Continuing competence and professional development requirements in international midwifery
• Published te ao Māori approaches to professional development
• Evidence that supports the inclusion of the current elements of the MSR within competency maintenance, professional development and quality assurance processes
The review presented a wide range of literature in the context of midwifery in Aotearoa. While the material accessed highlighted the need for more robust evidence on the effectiveness of competency maintenance methods, the key elements of the MSR were supported by the available evidence, particularly in relation to improving professional practice.
Many of the elements within the current MSR process are reflected in competency and professional development programmes across other health professions in Aotearoa and midwifery programmes internationally.
The literature review highlighted that additional components, seen in other programmes, may be worth considering for inclusion within a future or revised programme for the Aotearoa midwifery context.
Following the literature review, the College drew upon data from the Midwifery Council’s 2023 recertification survey and insights from the College’s cultural review report. These resources have informed discussions and planning for the discovery stage of the redesign of the MSR process.
As part of the discovery stage a questionnaire was circulated to members within the College’s e-newsletter to gather input from stakeholders on the programme's future direction. Over the past four months,
College midwifery advisor co-leads for quality assurance have facilitated 16 in-person and virtual focus groups with a range of stakeholders. Their contributions have been invaluable.
The focus groups centred on critical questions, such as:
• What aspects of a midwife’s quality assurance programme would positively contribute to ongoing culturally safe care for whānau?
• What is essential in the midwife’s quality assurance programme to ensure it is a culturally safe experience for the midwife?
• If you were tasked with building a new quality assurance programme for midwives, what would it look like?
The next step is to analyse the data and compile a report from the discovery phase. The report will include recommendations for what a future MSR quality assurance process might encompass. Based on these findings, and in consultation with the Council, we anticipate the steps following this will involve establishing an advisory group and beginning the potential re-design phase in early 2025. We are working closely with the Council to ensure they are well-informed and that the voices of the profession are heard. Both the literature review and the report from the questionnaire and focus groups will be presented to the Council at their December meeting.
Look out for the academic publication of the literature review, which we hope to publish in the College Journal next year. Square
VIOLET CLAPHAM MIDWIFERY ADVISOR
second midwife support
In 2018 the College successfully negotiated with the Ministry of Health to implement a new funding module into Section 88 of the Primary Maternity Services Notice (now referred to as Section 94). This new module (DB15) provides payment for the back up support services midwives often provide to each other at births to ensure safety and sustainability in practice. The successful implementation of the Second Midwife Support module was a hard-won victory that came after many years of College advocacy and negotiation on behalf of LMC midwives.
The feedback the College has had since the inception of the second midwife fee is that it has made a significant difference to LMC midwives in practice, with many of them referring to it as a ‘game-changer’ in allowing them to access support and relief when needed. There has at times, however, been confusion about when it is appropriate to invoke use of the second midwife support service, and when it is not. This article offers practice guidance by way of clarification about claiming the second midwife fee.
The second midwife fee is available to provide relief or support for the LMC midwife (or her LMC back-up) when providing midwifery care during labour and birth in any setting (home, birthing unit or hospital) for the following circumstances:
• When the midwife is tired (fatigued) due to a woman’s labour being long or due to previous midwifery work
• If the midwife becomes unwell during attendance at a labour and birth
• If a midwife has an unanticipated personal crisis during attendance at a labour and birth
• As a second midwife at a home birth
• If the midwife requires support from a midwifery colleague to provide safe care
The second midwife fee is claimed separately from the LMC midwife labour and birth fee by the second midwife herself when:
• The second midwife has provided midwifery care for a minimum of 90 minutes (requires in-person attendance and must be documented)
• The second midwife has an authorisation to claim from the Primary Maternity Services Notice (can be the back-up LMC midwife but attending as a second midwife)
Examples of when it is not appropriate to claim the second midwife fee include:
• When the woman does not have an LMC midwife and care is being provided by employed midwives
• To relieve an LMC, so she can leave and carry out other planned midwifery work (such as an antenatal clinic)
• Routine use of second midwife support at every birth an LMC attends in a birthing
unit or hospital setting (as opposed to for homebirths where a second midwife would routinely attend)
• When it is more appropriate for clinical responsibility to be transferred to obstetric and core midwifery staff (for example, situations of high clinical risk like extreme preterm birth or fulminating pre-eclampsia)
The College continues to see the significant benefit and value of the second midwife fee being available to midwives to support sustainability and safety of practice. This guidance is offered in response to the many contacts the College receives for advice on appropriate use of second midwife support. Midwives are encouraged to read the wording of the Second Midwife module in the Primary Maternity Services Notice (2021) and can direct further questions to the MMPO team (if claiming through the MMPO). College advisors are also available if further clarification is needed. Square
Credit: Rebecca Claridge Photography.
VIOLET CLAPHAM MIDWIFERY ADVISOR
online certification of stillbirth by midwives
key messages
• When a person dies in Aotearoa, a medical certificate of cause of death must be completed by a health practitioner.
• There is a specific form for recording fetal and neonatal deaths: The Medical Certificate of Causes of Fetal and Neonatal Death (HP4721).
• Since 2018 medical practitioners and nurse practitioners have been able to submit medical certificates of cause of death online.
• The online service has recently been expanded to include stillbirth and neonatal death certificates.
• Midwives are now able to complete online certificates for stillborn babies.
• The online certification system is managed by the Death Documents service (a collaboration between the Department of Internal Affairs and Health New Zealand).
The form which needs to be completed for stillbirths or neonatal deaths is the Medical Certificate of Causes of Fetal and Neonatal Death (HP4721). A medical practitioner or nurse practitioner can complete the certificate for a liveborn baby who dies within 28 days of birth. In the case of a stillbirth, if no medical practitioner was present at the birth of a stillborn baby, a midwife who was present at the birth may complete the HP4721 certificate instead.
The requirements for certification of stillbirths are set out in the Burial and Cremation Act 1964, Section 46A. The certificate records information about the mother, pregnancy and birth, in addition to
information about the birthweight, gestation and cause of death of the baby.
Moving to an online service means faster updating of National Health Index (NHI) records with dates of death, reducing the risk of deceased persons being invited to attend health appointments. Documents submitted online are immediately available for funeral directors to view (for deaths they are providing services for). This means they can commence the burial and cremation arrangements sooner, and it is easier for them to notify the death to the Department of Internal Affairs for registration.
The Death Documents team are now working on assisting midwives and health practitioners working in hospital maternity and neonatal units to register and use Death Documents, and to update the Health NZ Death Documents Viewer to receive the new forms. LMC midwives are also able to register to access the online system.
To find out more about this online service, go to https://www.tewhatuora.govt.nz/ health-services-and-programmes/burial-andcremation-act-1964/death-documents-project
As a registered user of Death Documents online, midwives will be able to:
• complete a certificate of cause of death for a stillborn baby (HP4721), once you have the NHI number of the deceased baby to enter on the form
• amend a certificate you have created online
• search and view documents completed by other practitioners
• print a certificate you (or another practitioner) have created
• revoke a HP4721 certificate you have submitted, e.g. if you accidentally entered the wrong NHI number on the form
The system will pre-populate the forms with your credentials. Users will be alerted if a document already exists for the NHI you are certifying. Midwives will need to be a ‘verified RealMe’ user to access the online system.
To register to become a user of the online Death Documents tool, go to https:// deathdocs.services.govt.nz. Midwives can also access a range of helpful tips by clicking on the Help using death documents button on the Death Documents home page. Further assistance is available to navigate the site through the Give us your feedback button on the home page. By entering your name and contact details, someone from the Death Documents support team will follow up.
Guidance on how to complete a paper or online Medical Certificate of Causes of Fetal and Neonatal Death (HP4721) can be found on the Health NZ | Te Whatu Ora website (www. tewhatuora.govt.nz). Square
definition of stillbirth in the Births, Deaths, Marriages, and Relationships Registration Act 2021
Stillbirth means the issue of a stillborn child from its birth mother. Stillborn child means a dead foetus that:
(a) weighed 400 g or more when it issued from its birth mother; or
(b) issued from its birth mother after the 20th week of pregnancy.
VIOLET CLAPHAM MIDWIFERY ADVISOR
notifiable diseases
WHAT IS A NOTIFIABLE DISEASE?
Some diseases pose a risk of harm to the public because of their contagiousness, severity or frequency. Such diseases can be classified as ‘notifiable diseases’ which means that health practitioners, or staff working in laboratories, have a statutory obligation to notify public health officials about the case. The notification process enables follow-up treatment, as well as public health measures to be undertaken to minimise the spread of the disease and risk of harm to the public. This article sets out information about notification processes that midwives need to be aware of and the current notifiable diseases which have relevance to midwifery practice.
MIDWIFERY RESPONSIBILITIES
Although it is important for midwives to be aware of which diseases are notifiable, and it is possible that a midwife is the health practitioner who has ordered the
Due to the contagiousness and severity of the diseases which are notifiable, it is highly likely that midwives will be referring women to other health practitioners or services for treatment and care.
laboratory test which confirms the presence of a notifiable disease, midwives may or may not be directly involved in the notification process. Due to the contagiousness and severity of the diseases which are notifiable, it is highly likely that midwives will be referring women to other health practitioners or services (such as sexual health services or obstetric specialists) for treatment and care. In these circumstances, midwives should check with the service or practitioner to whom they are referring, that they are taking responsibility for the notification process. If not, the midwife will be required to complete the notification. This should include an explanation to the woman of the statutory requirement for notification, the information that the midwife is required to share and the likely outcome, e.g. possible follow-up treatment for the woman and her close contacts.
For full information, including the notifiable diseases list, notification forms, and disease information sheets, please go to www.cph.co.nz/health-professionals/ notifiable-diseases The following table sets out the currently notifiable infectious diseases. When an update is issued the College will notify members.
NOTIFYING DISEASES
Health practitioners must ‘forthwith’ notify when, in attending their client/patient, they have reasonable suspicion that the patient has a notifiable disease. The diseases that must be notified are listed in Schedule 1 (infectious diseases) and Schedule 2 (non-infectious diseases) of the Health Act 1956. Notifiable diseases that midwives may encounter in
practice include measles, mumps, rubella, hepatitis B and C, syphilis, Covid-19, HIV, AIDS, gonorrhoea and invasive group A streptococcal infection.
WHO TO NOTIFY
Health practitioners must notify the medical officer of health of their local public health unit. If the disease is listed in Section A of Part 1 of Schedule 1 (mostly foodborne illnesses such as acute gastroenteritis), health practitioners must also notify the local authority (Council). When a disease is diagnosed by a laboratory, those in charge of the laboratory must notify the requesting health practitioner as well as the medical officer of health.
THE NOTIFICATION PROCESS
Health practitioners must notify the local medical officer of health by electronic means (e.g. email) unless this is impractical, in which case they must notify by post or hand delivery.
These requirements should not discourage health practitioners from notifying urgent cases by telephone in the first instance, but notification should be promptly followed by the completed prescribed form contained in Schedule 2 of the Health (Infectious and Notifiable Diseases) Regulations 2016 (the HIND Regulations).The health practitioner will (for living patients) use either:
• Form 1: the general disease form (i.e. for diseases listed on Sections A or B of Part 1 of Schedule 1 of the Health Act) or,
• Form 2: when the disease is listed on Section C of Part 1 of Schedule 1 of the Act.
DISEASES NOTIFIABLE BY HEALTH PRACTITIONERS AND LABORATORIES TO THE MEDICAL OFFICER OF HEALTH
SECTION A - DISEASES NOTIFIABLE TO A MEDICAL OFFICER OF HEALTH AND LOCAL AUTHORITY
Acute gastroenteritis*
Campylobacteriosis
Cholera
Cryptosporidiosis
Giardiasis
Hepatitis A
Legionellosis
Listeriosis
Meningoencephalitis – primay amoebic
Salmonellosis
Shigellosis
Typhoid and paratyphoid fever
Yersiniosis
SECTION C - INFECTIOUS DISEASES NOTIFIABLE TO MEDICAL OFFICER OF HEALTH WITHOUT IDENTIFYING INFORMATION OF PATIENT OR DECEASED PERSON
Acquired Immunodeficiency Syndrome (AIDS)
Gonorrhoeal Infection
Human Immunodeficiency Virus (HIV) infection
Syphilis
SECTION B - INFECTIOUS DISEASES NOTIFIABLE TO MEDICAL OFFICER OF HEALTH
Anthrax
Brucellosis
Creutzfeldt Jakob disease (CJD) and other spongiform encephalopathies
Diphtheria
Hepatitis B
Hepatitis (viral) not otherwise specified
Hydatid disease
Invasive pneumococcal disease
Leptospirosis
Measles
Monkeypox
Neisseria meningitidis invasive disease
Novel coronavirus capable of causing severe respiratory illness
Plague
Q fever
Rheumatic fever
Rubella
Tetanus
Verotoxin-producing or Shiga toxin-producing Escherichia coli
Non-seasonal influenza (capable of being transmitted between human beings)
Pertussis
Poliomyelitis
Rabies and other lyssaviruses
Rickettsial diseases
Severe Acute Respiratory Syndrome (SARS)
Tuberculosis (all forms)
Viral haemorrhagic fevers
*Not every case of acute gastroenteritis is necessarily notifiable, only those where there is a suspected common source or from a person in a high risk category (for example, a food handler, an early childhood service worker) or single cases of chemical, bacterial, or toxic food poisoning such as botulism, toxic shellfish poisoning (any type) and disease caused by verotoxin or Shiga toxin-producing Escherichia coli.
When the patient has died of a notifiable infectious disease, the health practitioner must notify the medical officer of health ‘forthwith’ using the post-mortem form prescribed in the HIND Regulations.
SEXUALLY TRANSMITTED INFECTIONS
Sexually transmitted infections included within Schedule 1 of the Health Act which are notifiable include HIV, AIDS, gonorrhoea and syphilis. These diseases are notifiable on a non-identifying basis (the name of the infected person is not recorded) and listed on Section C of Part 1 of Schedule 1 of the Health Act.
Other infectious diseases, listed in Part 2 of Schedule 1 of the Health Act are not notifiable, but medical officers of health and others may exercise statutory powers in managing them. Some of them are sexually transmitted, e.g. chlamydia, herpes, venereal granuloma and venereal warts.
TUBERCULOSIS
Notification and management of tuberculosis is now included in the Health Act with other
notifiable, infectious diseases. Tuberculosis is in the general category of infectious diseases that are notifiable on an identifying basis and listed in Section B of Part 1 of Schedule 1 of the Health Act.
NEW REQUIREMENTS FOR INVASIVE GROUP A STREPTOCOCCAL INFECTION
From 1 October, 2024, invasive group
A streptococcal infection (iGAS) has been added to Aotearoa New Zealand’s schedule of notifiable diseases. This places new legal requirements on health practitioners and laboratories for the management and reporting of both suspected and confirmed iGAS cases.
iGAS CASE DEFINITION
iGAS is defined as detection of group A Streptococcus bacteria (GAS, Streptococcus pyogenes, Strep A) via culture or nucleic acidi testing (e.g. polymerase chain reaction, PCR) in a specimen from a normally sterile site of the body—an anatomical location where bacteria are not normally present in a healthy person.
NOTIFICATION AND REPORTING OF iGAS
The case definition for an iGAS infection includes:
• a confirmed case – defined by meeting laboratory definitive criteria
• a probable case – defined by meeting both clinical criteria and laboratory suggestive criteria.
Clinicians are responsible for notifying their local medical officer of health of both confirmed and probable cases of iGAS that meet the case definition.
CONFIRMED CASE NOTIFICATION
Most iGAS cases are expected to be notified via a direct laboratory notification based on a set of specimen sterility guidelines as outlined by the case definition:
• group A Streptococcus detected in specimens from sterile sites (e.g. blood cultures) will be notified via direct laboratory notification (DLN) as confirmed cases of iGAS.
• group A Streptococcus in specimens from non-sterile sites (e.g. skin, throat and genital swabs) will NOT be notified.
PROBABLE CASE NOTIFICATION
The probable case definition is intended to identify people with iGAS whose laboratory evidence does not meet the confirmed case definition, but who are likely to have close contacts who could benefit from chemoprophylaxis. Hospital clinicians are required to notify probable cases when they meet the following clinical criteria, and when there is suggestive laboratory evidence that group A Streptococcus is the likely causative organism:
• peripartum infections up to 28 days post birth, or
• neonatal sepsis
Peripartum infections are defined here as clinically suspected bacterial infections of the genital tract or its surrounding tissues, occurring at any time between the onset of rupture of membranes or labour, and the 28th day postpartum (e.g. chorioamnionitis, endometritis, maternal/puerperal sepsis).
Peripartum infections include intrapartum and postpartum infections. This definition of peripartum infection has been adapted for use in this context from the WHO definition of ‘maternal peripartum infection’.
Laboratory suggestive evidence constitutes detection of group A Streptococcus from a non-sterile site (e.g. a woman presenting with postpartum endometritis with group A Streptococcus detected on a vaginal swab would constitute a probable case of iGAS).
IGAS CONTACTS AND CLOSE CONTACTS
Health information should be provided by the local public health service to close contacts of all iGAS cases. An information sheet has been developed for close contacts, which is being made available in the new Communicable Disease Manual chapter on iGAS.
NEW CHEMOPROPHYLAXIS
GUIDANCE FOR CLOSE CONTACTS OF iGAS CASES
For cases of iGAS in a mother-neonate pair, it is recommended that the close contact within the pair (i.e. the mother of the
neonate is infected, or vice versa) receives antibiotic chemoprophylaxis to reduce their risk of developing iGAS. The public health service will facilitate the provision of chemoprophylaxis to these close contacts.
Chemoprophylaxis is NOT routinely recommended for other close contacts of iGAS cases although the public health service may occasionally request clinician support to help quickly provide chemoprophylaxis to close contacts when needed.
Obstetrics and gynaecology departments should be prepared to notify probable cases of iGAS in adults (i.e. cases of peripartum infection where group A Streptococcus is detected on a non-sterile site specimen).
For example, a woman who is diagnosed with chorioamnionitis, endometritis or maternal/puerperal sepsis within 28 days of giving birth and has group A Streptococcus detected on a vaginal swab will fall under this category. Group A Streptococcus detected on a vaginal swab is not notifiable via direct laboratory notification (as it was taken from a non-sterile site) and so the case must be clinically notified by the practitioner who requested the testing. Square
CAROLINE CONROY MERAS CO-LEADER (MIDWIFERY)
skill mix and staff mix in our maternity services… keeping our new graduate midwives safe
As maternity services welcome an increasing cohort of new graduate midwives to fill midwifery vacancies, how do we keep our new graduates safe as they develop the confidence to work in our busy, understaffed maternity service?.
The care capacity demand management (CCDM) programme is achieving good outcomes for maternity services in highlighting the increasing acuity and the midwifery staffing needed to provide the required care. For the last few years the challenge has then been for maternity services to recruit into the additional midwifery staffing positions identified as an outcome of annual FTE calculations.
Midwifery has experienced significant midwifery workforce shortages but these shortages are starting to be addressed by an increasing cohort of new graduate midwives being recruited into our maternity services. However, these midwives need support from experienced midwives to develop their confidence in decision making and clinical skills. If the appropriate support is not able to be provided to new graduate midwives or early career midwives, this impacts on the retention of these midwives and can result in them leaving the profession far too early in their career.
THE ROLE OF MIDWIFE CLINICAL COACHES
The creation of the midwife clinical coach role was an outcome of the Midwifery Accord work 2019-2021. The midwife clinical coach’s role is to support new graduate midwives, return to practice midwives, and new to service midwives, working alongside them as they grow their confidence in the workplace. Some districts have invested in these roles to ensure there is a midwife clinical coach on each shift 24/7, but other districts will need to increase the role’s FTE as the number of new graduate midwives increases, if they want to provide appropriate levels of support.
The success of the midwife clinical coach role has allowed the designated senior midwife on the shift to focus on providing clinical leadership and managing the shift.
The role has also supported the retention of experienced midwives in the workplace, by providing a career opportunity that is still clinically focused.
USING THE CCDM TOOLS
Trendcare data has been good in highlighting the care required and the acuity on maternity wards but is currently not able to show if the rostered staff on any shift provide the right staff mix. The next version of Trendcare should improve this.
Staff mix and skill mix is highlighted in the variance response indicator score (VIS) tool (the VIS tool was described in Midwife Aotearoa, September 2023, pp 12-13).
The midwife clinical coach hours should be shown in the allocate staff screen as ‘clinical support’ where they are part of the ward budget. In situations where they are providing clinical care as part of a VRM response their hours should be should as ‘clinical in department’ .
The VIS score reflects the ‘moment in time’ on any shift, providing a visual indicator to the hospital as to whether staffing is appropriate for the acuity in the ward or
unit at that time. The coordinating midwife should be completing a VIS scoring at the beginning of each shift and as changes in workload or available staff occur during the shift. It is important that the skill mix and staff mix indicators are used correctly, as outlined below.
SKILL MIX
• Indicate where staff do not have the required skill set for that maternity area or where there is no senior midwife on duty in a secondary or tertiary ward. Re-VIS if a midwife has left the ward (e.g. gone to theatre, escort, ED) and this has impacted on available skill mix.
STAFF MIX
It is important that roster gaps are not normalised. Indicate when:
• The staffing on the shift does not reflect the approved CCDM roster. This may differ from the actual number of staff rostered. In most maternity units the registered staff mix should be 100% midwifery.
• The HCA or clerical staff are absent and midwives are doing these tasks
• There are casual staff absent and midwives are doing their tasks
• There are casual or locum midwives working who are unfamiliar with the ward area
• You have a midwife ‘on-call’ due to roster shortages and this is not part of the CCDM roster model for your ward
• Re-VIS if a midwife has left the ward, as this has changed the staff mix
DEEMED PROFESSIONALLY UNSAFE
• Indicate if, as the coordinating midwife, you believe the clinical situation is unsafe. This might be a situation where the number of midwives on the shift is less than the agreed minimum staffing, there is no experienced or senior midwife to coordinate, or the workload exceeds the available staff. Re-VIS as situations arise and, if possible, complete a datix or safety-first form to highlight the situation and actions taken.
There may be times when a coordinating midwife may find themselves as the only experienced midwife on a shift and the other staff members are new graduate and early career midwives. In situations of high acuity or where the needs of the women or babies
are complex, and the coordinating midwife recognises that it would be unreasonable to ask the new graduate midwives to provide the care needed without additional support, this should be indicated in the VIS score.
When there is high acuity care needs and staff or skill mix challenges the coordinating midwife should ensure this is indicated in the VIS score. There may be a need to indicate ‘deem the situation professionally unsafe’. This is likely to place the ward into amber or red VIS scoring enabling the coordinating midwife to activate the maternity escalation plan and request additional support and assistance. Incident reports (datix or safety first) should be completed in situations where assistance is not able to be provided.
Using the CCDM tools correctly will assist in supporting our new graduate midwives and early career midwives, as well as ensuring we are not normalising unsafe staffing within our maternity services. Square
For MERAS Membership merasmembership.co.nz www.meras.co.nz
Miranda Hall, Midwife Clinical Coach and MERAS workplace representative, with new graduate midwife Maddi Barton.
WAYNE ROBERTSON
EXECUTIVE DIRECTOR, MMPO
empowering midwives and enhancing maternity care across aotearoa
In recent months, against the backdrop of shifting government priorities and tightening health sector budgets, the MMPO has been proactive in expanding resources to support LMC community midwives across Aotearoa. Through initiatives that blend digital innovation, practical tools and unwavering advocacy, the MMPO has provided vital backing to midwives as they navigate an evolving healthcare landscape.
Key initiatives this year have reinforced the MMPO’s commitment to ensuring midwives can deliver the best possible care to māmā, pēpi and whānau, while also experiencing professional and financial well-being.
SUPPORTIVE CONTRIBUTIONS TO
LMC MIDWIFE CLASS ACTION
A significant accomplishment for LMC midwifery this year was the successful completion in September of the College-led legal Class Action case, with the judge’s final decision pending. The MMPO played an active role by providing essential data insights and leveraging its extensive knowledge of LMC midwifery to help demonstrate the impact of midwifery work and business claims under Section
94 (formerly Section 88). This support added strength to the Class Action for fair remuneration and underscored MMPO’s dedication to advocating for midwives’ rights and financial security.
FLEXIBLE WORKFORCE SOLUTIONS FOR SUSTAINABLE CARE
In recent periods defined by resource constraints and healthcare transformation, the MMPO’s strengthening of the “flexible workforce (locum)” model has been critical in supporting both LMC community midwives and facility-based midwives. By moving beyond the traditional “locum” approach, the MMPO has introduced adaptable workforce options that enable and sustain midwives to provide uninterrupted, quality
care in both community settings and facility environments. This flexibility approach helps ensure continued access to maternity care for all māmā, pēpi and whānau by providing an integrated support system that strengthens the sustainability of the midwifery workforce and enables midwives to thrive in their essential roles.
STRENGTHENING DIGITAL CAPABILITIES WITH TIAKI AND BADGERNET
The MMPO’s digital initiatives continue to lighten the administrative load for midwives, providing tools that streamline workflows and improve financial management. The Tiaki platform, now fully enhanced to support Section 94 claims, offers midwives
an efficient system to manage business operations, while further developments are planned to enhance data insights that can inform future advocacy.
PRACTICAL FINANCIAL TOOLS AND INSURANCE
Recognising the importance of financial stability for selfemployed midwives, the MMPO continues to offer group midwifery equipment insurance and support to access Xero accounting software. These resources help midwives manage their finances, from cash flow to tax compliance, enabling them to streamline their operations, which reduces stress and frees them to focus on delivering high-quality care.
HOW WE SEE OUR ROLE IN SUPPORTING MIDWIVES
The MMPO staff receive immense satisfaction in seeing the positive impact of these initiatives and being able to help midwives navigate financial, digital and workforce challenges. As one team member put it, “What satisfies me most about my work is knowing that LMC midwives can get on with caring for their women, assured that MMPO is there to advocate for them, keep their data safe and ensure timely payments”. Another team member noted the empowerment that digital tools like Xero bring to midwives, observing that these tools enable midwives to “become more proficient with their day-to-day operations… saving them valuable time and money”.
Others reflected on the overarching mission that guides their work: “Our purpose is to support midwives in any way we can, every day”, and “It’s rewarding to advocate for the value of LMC community midwives and show them that they are valued”. This shared sense of purpose has allowed MMPO to foster a supportive environment that resonates deeply within the midwifery community.
REFLECTION
Amidst a year of uncertainty and sector-wide challenges, the MMPO welcomes the collaborative role it plays in advocating for and empowering midwives across New Zealand. From making valued contributions to the Class Action to developing flexible workforce models and more relevant digital tools, MMPO has shown resilience, adaptability and dedication to the needs of the midwifery community. Through our steadfast support, the MMPO is ensuring a sustainable future, where midwives, māmā, pēpi and whānau alike will benefit from a robust and responsive maternity care system. Square
MMPO provides self employed community midwives with a supportive practice management system. www.mmpo.org.nz / mmpo@mmpo.org.nz / 03 377 2485
Hono Ngā Hononga Ora CULTIVATING POSITIVE CONNECTIONS
2025 NZLCA ONLINE CONFERENCE
8th February to Sunday, 2nd March 2025
See a wide range of outstanding presentations
• Cultivating Positive Connections Using a Mahi Ngātahi Care Model
• Lactation Aids Over Time and the Ethical Considerations for Their Use
• Helping Families Who Combine Breast & Formula
• Endocrinology: Understanding Hormone Mechanisms for Optimal Milk Supply
• A Breastfeeding Paradox: Evolving Science, Competing Values, and Conflicting Interests
• Biodynamic Craniosacral Therapy and Breastfeeding
• A Systematic Review and Meta-Analysis of Relaxation Practices for Lactating Mothers
• Expressing Dynamics: Recommendations When Exclusive Expressing is Needed
• And much more!
TAMARA KARU NGA MAIA GENERAL MANAGER
treaty principles bill, māori erasure, and the battles for our health
I wish I could focus this piece on celebrating the positive strides in Māori health, like congratulating the new Māori Midwifery Council members, acknowledging the success of Te Ara o Hine and Tapu Ora's programmes with the largest cohort of Māori and Pacific new midwives graduating in 2025, expressing our sincere gratitude to the inspiring speakers that generously shared knowledge in Otaki at Hui-a-Tau 2024, or recognising the brave and powerful testimony of whānau who this week received a long-awaited apology from parliament for the atrocities inflicted on them by the state while in care.
However, the current attacks on our rights and on our health demand attention. Right now, Māori are imploring the hearts and minds of Aotearoa to recognise the rights of Māori by demonstrating their right to protest the Treaty of Waitangi Principles Bill. Backed by ACT's David Seymour, this bill promises a homogenised "One People" of New Zealand. The motivation for this bill is rooted in colonial sanitation,
erasure and inequality, excusing this government from its duties to those most in need. This dangerous waste of resource and the early axes expose their agenda. Public sector reforms and the refusal to adopt the UN Declaration on the Rights of Indigenous Peoples (UNDRIP) show that, despite Māori efforts, the rules still serve their authors.
In healthcare, the powerful are causing harm. Pae Ora could have transformed our system but, instead, we see disestablishment. Midwives and the whānau we serve have much to lose. The senseless removal of investment and leadership destabilises care. It's underhanded, dishonest and threatens the very services our communities depend on.
Māori midwifery services, already underfunded, face even more uncertainty. The potential loss of investment in successful innovations is devastating. These programmes have proven to improve outcomes for wāhine and pēpi. Without them, we risk widening health inequities.
The constitutional rights articulated in Te Tiriti are inalienable, not gifts from those in power able to be removed at a whim. Yet here we are in a fight to protect our rights, our health and our future.
So I am looking for a silver lining and it could be this. My generation needed to witness and absorb a threat of this kind, to honour and know the work of the agents of change before our time, those who laid the foundations for Māori and the midwifery we know and love today, and to galvanise our commitment and resolve as Te Iwi Māori and as midwives. In the hopeful words of Ani Mikaere, "this government will soon be an unpleasant memory, Te Tiriti will always be here, because we (Māori) will always be here. We still have a lot of work to do. This government changes nothing."
Dr Tina Ngata reminds us that the empire will fall at the will of the people, and that power is in knowing this history of colonial harm and acknowledging the privilege that we have to do something about it. This peaceful demonstration is the collective resistance against the “Act” of historical erasure. Square
TISH TAIHIA CLINICAL MIDWIFE MANAGER, NGĀ HAU MĀNGERE
changing the south auckland narrative
According to Midwifery Council of New Zealand workforce data, the majority of practising midwives reported their base as the Auckland area. The metropolis that is the Tamaki Makaurau/Auckland region is further divided into three districts of Counties Manukau, Auckland and Waitematā.
In February this year, Stats NZ reported that for the first time in 20 years the country had seen a decline in the national birthrate.
However, Counties Manukau saw an increase of births for the 2023 year, numbering over 7500. Approximately a third of those pēpi identified as being Pacific. With the significance of those numbers, it has become sadly evident that the midwifery workforce has declined in Counties Manukau, specifically those who were self-employed.
This has huge implications for this community which, according to the Perinatal and Maternal Mortality Review Committee reports over the years, carries the ’ongoing burden of higher rates of adverse outcomes for Māori, Pasifika and Indian whānau’.
Pasifika Midwives Aotearoa (PMWA) was established to address the dire numbers of Pacific midwife practitioners who could not satisfy the numbers required to be reflective of its thriving community in the provision of best care. In spite of our best efforts, it is obvious that one solution is to continue to support the profession’s understanding and acceptance of the Te Tiriti principles of matauranga Māori. These guides underpin care for all, Pacific and non-Pacific.
‘HARD TO WORK IN A COMMUNITY THAT YOU DON’T UNDERSTAND’
LMC Dinah Otukolo (Tongan/European) who has been a midwife for 7 years, expresses her deep belief in finding the best way to be of service to the community is to see if she is the right person to give whānau support for their maternity journey.
Although confident in secondary settings, primary care is what she has chosen to specialise in, to ‘protect’ space that gives positive experiences and satisfaction for whānau.
From her ‘Meet & Greet’ appointment to the discharge with personal touches (beautifully stickered Well Child Record book), Dinah believes this is the opportunistic time to pass on health messaging that will endure past the pregnancy and birth.
‘FOUND MY NICHE WITH SUPPORTIVE PRACTICE PARTNERS AND SUSTAINABLE TIME OFF’
Having undertaken her midwifery degree straight from secondary school, Hillary Khan (Samoan/Bangladeshi) went straight into LMC practice as a new graduate also 7 years ago.
When asked what would attract and retain midwives to work within Counties Manukau, she states that there is no one singular thing because ‘money alone would not fix it’.
Hillary has found great satisfaction in working with a primary focus, with the right practice partners who are flexible in providing secondary care should their clients change acuity, and with covering in times of personal priorities.
There is infinite potential to look at new models of service delivery for a population that has rising acuity and co-morbidities, but to also fulfil the needs of whānau searching for ways to improve their health and wellbeing.
*PMWA would like to acknowledge the passing of Samoan midwife, Therese Stowers in August this year after a 19-year career at Wellington Hospital before doing LMC practice – fa’afetai mo lau tautua (thank you for your service). Square
Positive Birth Stories – Whānau at Ngā Hau Māngere birthing centres first year celebration in 2020.
AMELLIA KAPA
REGISTERED MIDWIFE
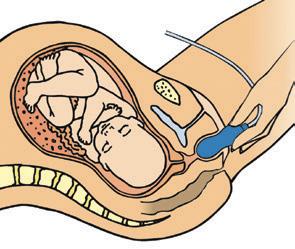
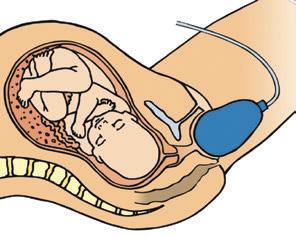
BASIC EARLY PREGNANCY ULTRASOUND FOR MIDWIVES: A ROAD LESS TRAVELLED
Shelley Tweedie’s unyielding commitment to whānau in Te Tai Tokerau has seen her navigate a path taken by only a handful of Aotearoa-based midwives thus far, officially gaining accreditation to perform basic early pregnancy ultrasound in July this year. She shares her motivations with Amellia Kapa and offers insights for midwives interested in pursuing the training.
Shelley Tweedie may not whakapapa to Te Tai Tokerau but her actions are reflective of someone deeply invested in her community. Choosing to complete her elective placement in Northland in 2015 as a final year midwifery student, Shelley made the trip up from her then-home of Christchurch to experience the winterless north, having no inkling she would relocate to the region four years later, with whānau in tow.
“I didn’t do that placement with the intention of practising up north but my experiences as a student in Te Tai Tokerau were all positive. My tāne and I were at a point where we were ready for a change, so we moved up for the fishing, warmer weather, beaches and the beautiful community. Being in a place with such a high Māori population is also a natural setting for me that feels like home, so we relocated with our three children in 2019.”
A far cry from Christchurch, Te Tai Tokerau faces its own unique challenges both geographically and
socio-economically, but Shelley (Ngāti Maniapoto) wasn’t deterred, diving straight into mahi. “Initially, I worked at Kaitaia Hospital to get a feel for the system. Then in 2020, I went out as an LMC in the Far North, working on-call up until the beginning of this year.”
“At the end of last year, I became the clinical midwife manager at Kaitaia Hospital,” she continues, “which is quite a different role because it’s not so much hands-on midwifery but it’s still really rewarding. To be effective in this role, you need someone who not only knows the community but can also advocate for whānau and promote an environment where we work collectively to sustain one another and maintain a positive culture. We’re so isolated up here; we’re so far away from obstetric help or paediatric input, so it’s vital we all work together. When we do that well, it naturally flows on positively to whānau.”
The motivation to branch off into pregnancy ultrasound was rooted in a desire to improve outcomes
for whānau facing a potentially heartwrenching decision. “It came out of wanting to provide an early medical abortion service in Kaitaia because, in the past, it’s only been available in Whangārei. For years, it’s been a massive undertaking for people to access a termination in this region, and the barriers they’ve faced have often been insurmountable.”
The inequity has left many whānau powerless, despite knowing the decision they would have made if the financial barriers and geographical distance were removed, as Shelley explains. “For someone who’s pregnant but wanting a termination, travelling two or three hours to Whangārei may not be achievable. Some would carry on with an unwanted pregnancy as a result, while others would still access an abortion, but at a high cost financially and personally. Having to arrange childcare and transport, as well as sitting on the local ultrasound waiting list, resulted in unnecessary delays, often dragging out timeframes for whānau receiving early abortion care.”
Offering early abortion closer to home was the obvious solution but it required timely access to ultrasound, which had historically been a challenge in Kaitaia. “For many years, the ultrasound service in Kaitaia had been stretched and unable to meet the needs of the community. Many had experienced long wait times of up to four weeks for a pregnancy ultrasound. If someone needed a dating scan, it hadn’t been possible to squeeze someone in urgently and build the clinical picture needed for that whānau to make their decision.
In 2023, following the abortion law reforms, Te Tatau o te Whare Kahu | Midwifery Council published a statement showing its support of registered midwives carrying out basic early pregnancy ultrasound, provided they have completed an endorsed education programme and remain engaged in ongoing credentialling.
We do have a local scanning service within our hospital but it was often booked out weeks in advance, with limited time slots. It was vital to explore early pregnancy ultrasound accreditation to provide a complete and less fragmented early abortion service.”
In 2023, following the abortion law reforms, Te Tatau o te Whare Kahu | Midwifery Council published a statement showing its support of registered midwives carrying out basic early pregnancy ultrasound, provided they have completed an endorsed education programme and remain engaged in ongoing credentialling.
The shift meant Shelley could get to work right away. Her first step was to register as a member of the Australasian Society for Ultrasound in Medicine (ASUM), who provide accreditation and administer the online theory course.
“After becoming an ASUM member, the next step was enrolling in the Certificate in Allied Health Professional UltrasoundBasic Early Pregnancy Ultrasound course, which included a unit on ultrasound physics. Upon completion of the online education and assessments, the next requirement was to attend a practical ultrasound course by one of ASUM’s approved training providers, the Australian Institute of Ultrasound.”
Currently, there aren’t any approved training providers in New Zealand, so Shelley approached the institute to find out what the options were. “They were really accommodating and had designed a bespoke course for Aotearoa-based midwives, specific to the work we’d be carrying out,” she recalls. “Alongside another midwife from Kaitaia, I went to the Gold Coast to attend that workshop with a sonographer and was able to gain ultrasound experience with arranged volunteers.”
Having completed both the theory and practical courses, the last step was gaining accreditation, which Shelley explains practitioners have a two-year window to achieve. “To become accredited, you need to have a primary clinical supervisor here in Aotearoa, who’s willing to do three assessments with you. You also need to carry out 25 ultrasounds, keeping a log of each, and have those reviewed by your supervisor and compared to a formal ultrasound. Once all of that is complete, the paperwork is sent back to ASUM and you receive your accreditation.”
Upon accreditation, Shelley explains that a midwife is then able to perform early pregnancy ultrasound to confirm intrauterine pregnancy and gain measurements to estimate gestational age. “We’re not diagnosing abnormalities,” she clarifies. “If the ultrasound doesn’t align with the clinical picture, or we’re unable to gain reliable findings, we refer people for formal ultrasound.”
Shelley explains that, due in part to how new this pathway is for midwives, the most challenging aspect of the whole process was finding a supervisor in New Zealand who was willing to support her. “For any midwives interested in pursuing this path, you need to know how vital that supervisor is. It’s a huge part of the accreditation process. We definitely need more supervisors who will support midwives to step into this work but, in some cases, you may have to arrange for remote supervision and revision of cases, which is the arrangement I had. I met with my supervisor regularly online and had access to ongoing support and mentoring throughout.”
Being able to provide basic early pregnancy ultrasound in her community now means whānau have more options available to them if they are facing an unplanned or unwanted pregnancy. “We offer a medical abortion service for women up to 10 weeks’ gestation,” Shelley explains, adding that a scan isn’t always necessary. “If a woman is sure of her LMP and is less than 10 weeks pregnant, we don’t need to do a scan before they access abortion. But if she’s unsure of her LMP, has experienced any spotting or bleeding, or has a history of ectopic pregnancies, a scan is indicated. The great thing is, we can now go and get our bedside scanner and I can perform the scan right then and there – on the day we discover they need one – rather than referring and waiting for an ultrasound to be available, causing an unnecessary delay which may place them outside of the timeframe for early medical abortion. Time is of the essence for some of these women, and now we have a solution.”
The early abortion service has been running for seven months now and Shelley acknowledges it’s a whānau-centred process, from start to finish. “Women are always offered counselling, although it’s no longer compulsory for them to attend since the legislation changed. As long as they’re less than 10 weeks pregnant and they want to proceed, we give them the medication and they can take it home with them, provided
they live within an hour’s drive of the hospital and have reliable transport. We provide phone support the day they take the treatment at home, and then offer a follow-up appointment a week after their termination to check in and ensure their hCG levels are coming down.”
Shelley is quick to point out that while the service is undoubtedly meeting the needs of her community, there’s still room for improvement. “It’s not a full service, in the sense that early surgical terminations are not yet an available option for those who would choose that over a medical termination. So it’s not a truly equitable choice, in comparison to places where all of the options are available and accessible. If it was really equitable, people would have both options because some people might prefer a surgical procedure, but the challenge of travelling to Whangārei for it becomes a factor in their decision-making process.”
For now though, Shelley is confident the introduction of this service has been meaningful for those who’ve accessed it. “Collectively, our local health providers work
hard to bring a great service to our region but often face challenges of being underresourced. Many of our GPs, for example, are at capacity and working hard to meet the needs of our community. Being able to offer this service closer to home makes all the difference for whānau.”
Shelley hasn’t sought formal feedback on the service yet but the response from whānau thus far has been heartening.
“Women have expressed high levels of gratitude and thanks – one person came back a few weeks later to drop off some chocolates, so it’s an interesting place to be as a midwife. It’s a reminder that people don’t always come to us with wanted pregnancies. We might have young people coming in to access this service, women at the other end of their journey who’ve had eight children, or women who are in the process of leaving unsafe relationships. It’s a privilege to be able to provide support when people are seeking abortion care; to enable them to empower themselves throughout their decision-making process, as hard as that choice may be. And providing
what the college is doing...
The College has been working with Hauora Taiwhenua | Rural Health Network and the University of Otago to develop a New Zealand based early pregnancy ultrasound education programme for midwives, meaning that the education would be more accessible and affordable, and negate the need for midwives to travel to Australia to access the practical component of the training.
At this stage, Otago University is hoping to pilot a programme in the first quarter of next year. Through the Hauora Taiwhenua | Rural Maternity and Maternity chapter, we have sought expressions of interest for midwives to undertake the education and are exploring possible funding opportunities to enable midwives to access the New Zealand based training at no cost.
kind, compassionate care without judgment is an honour.” Square
Early pregnancy ultrasounds in the community give whānau more options for unplanned pregnancies.
ZAHRA SHAHTAHMASEBI JOURNALIST
THE AI AGE IS COMING: WHAT DOES THIS MEAN FOR THE HEALTH SECTOR?
When you hear the words ‘artificial intelligence’, it can be hard not to immediately think of science-fiction movies, sentient robots or talking computers. The arrival of ChatGPT in 2022 exacerbated this, sparking conversations fuelled with anxiety over jobs lost to machines and a society run by computers.
The reality is, most of us already use artificial intelligence (AI) on a regular basis, says Dr Reza Shahamiri, senior lecturer in software engineering at the University of Auckland | Waipapa Taumata Rau. He says a good example is predictive text that suggests the next character or words to type, based on the context of the other words around it, and every time you ask Siri, Google or Alexa to answer a question or play a song on Spotify, you’re also engaging with AI.
We have been using the technology for years now, Reza says. “But it is recent innovations, like ChatGPT, that has thrown AI more into the public spotlight. So now there’s increased awareness about AI but at the same time a lack of awareness about what it actually is.”
MACHINES
THAT LEARN
Reza describes AI as an umbrella term that refers to a range of technologies where we teach computers to perform certain tasks based on inputs we provide to it.
One of the expressions of AI is ‘machine learning model’ (MLM). Email filtering, autocorrect, Apple’s Face ID and Netflix’s recommended watch list are all examples of machine learning, as is the ability for email programmes to recognise common aspects of junk email so it can send them immediately to the spam folder.
Large language models (LLMs) also exist under the AI umbrella. An example is text-to-speech software where the algorithm in the computer has been taught, using a vast amount of written data, to understand the statistical relationships between words and then translate that to be read aloud in a human-sounding voice.
WHERE IT ALL STARTED
Development of AI tools began at pace in the 1950s and 1960s thanks to the work of computer scientists. However, the limitations of computing at the time prevented further progress, leading to what was called an ‘AI-winter’, says Arindam Basu, associate professor at the University of Canterbury | Te Whare Wānanga o Waitaha School of Health.
The resurgence of AI in the last 10 years is due to the advances in computing power, Arindam explains, allowing the technology to become more sophisticated. This has led to generative AI, or Gen AI, as the latest breakthrough, where MLMs have gone from being able to predict, to being able to create and generate new content based on the data inputs it has processed.
“It can replicate human creativity to some extent,” says Arindam. “If you provide a machine with a set of statements and meanings, and then ask for a picture of a
cat with a green background, it understands the meanings of the words and can combine them to create something new.”
This ability has been the cause for major concern and anxiety around plagiarism, privacy and data ownership, particularly among writers and artists whose work now exists in the datasets that AI content generators like ChatGPT and Cici AI are pulling from, often against their wishes and without their consent. While these concerns are valid, Reza reminds us that AI can only act based on the inputs it receives, so it is down to the humans training it to be diligent in sourcing their data ethically, as well as removing biases where possible.
This is where the need for constant awareness, and education around AI’s use in our day-to-day lives, is paramount.
“Like any other tool, we can use it to help people or we can use it to harm people but it’s not the technology that is in question, it is the person who uses the technology,” says Reza. “We can pick up a hammer, build a house with it... or really hurt each other. We don’t blame the hammer.”
AI IN HEALTHCARE
Both Reza and Arindam believe that the area where AI tools stand to make the most impact is in health.
Already image processing tools have been trained to look at a medical image and examine it pixel by pixel for any anomalies. Last year, a Swedish study investigated the clinical safety of using AI to read mammograms (Lang et al., 2023).
AI technology offers the possibility of improving the quality of healthcare in Aotearoa, while making the system more efficient. The technology has the potential to improve accuracy in diagnoses, allow for fairer allocation of resources and remove barriers to accessing healthcare.
The 80,000 female participants were split into two groups; one group had their mammograms read by an AI system first, then by a radiologist. The second group followed standard procedure with the scan being read by two different radiologists. Results found that the AI group had similar rates of breast cancer detection as the standard group, leading the researchers to determine that not only was AI-assisted reading safe, but it also reduced the screenreading workload for radiologists.
In surgery, robotic arms controlled by a medical professional can be used to conduct precise surgeries with minimal invasiveness, says Reza. These types of surgeries have been shown to result in better patient outcomes, with faster recovery times and reduced complications, he adds.
Reza is currently working on various projects using AI technology, including programmes that help people with speech impairments communicate better with others; that can identify autism in children earlier; and that can predict dementia in individuals by analysing speech patterns and flaws in memory. “Assume Siri in your phone can listen to your parents’ conversations and if it realises there are signs of developing dementia, then it could raise the alarm. Because, as of yet, there is no cure for dementia, so the best tool we have is to diagnose it as early as possible and then manage its development.”
Arindam says AI and MLMs can be used to create a digital twin of a patient to which different treatment options can be delivered and analysed. “It allows you to work through ‘what ifs’. The digital replica of a pancreas from a diabetic patient, for example, could allow you to virtually administer insulin to monitor changes in blood sugar without risk to the patient.”
VISION FOR THE FUTURE
Where AI can really shine is by offloading the pressures on the health system, particularly when it comes to workforce, says Reza. Dame Juliet Gerrard, former Chief Science Advisor to the Prime Minister | Kaitohutohu Mātanga Pūtaiao Matua ki te Pirimia, agrees. In their report, Capturing the benefits of AI in healthcare for Aotearoa New Zealand, Dame Juliet and her co-authors (2023) write of their vision for AI and primary healthcare in Aotearoa. The report tells of the immense pressures on health professionals and services in Aotearoa, especially post COVID-19.
While far from a panacea, AI offers opportunities to strengthen the health system, the authors say. Their vision describes the year 2035 and a GP, Jade, working at a practice in the Auckland suburb of Newmarket. The rollout of AI support across the healthcare system has changed the game for Jade, allowing her to stay on top of her workload while working at the top of her scope. She can collect information on patients prior to their arrival using a preliminary consultation conducted through a personalised AI module on their phones; an AI assistant can scribe appointments, take notes and provide a range of treatment options; and patient data can be collected for use by the practice using smartwatches. Data collected is tightly held for medical purposes only, but can be fed into a whānau or iwisharing system where members and their GPs can be alerted to general risk factors without any specifics. Specialist monitoring and virtual simulations can also be set up to help patients better manage conditions from home; sophisticated mammograms can compare past and present images to screen for abnormalities; and a chatbot tool can translate medical information into any language.
Overall, the Gerrard report says that AI technology offers the possibility of improving the quality of healthcare in Aotearoa, while making the system more efficient. The technology has the potential to improve accuracy in diagnoses, allow for fairer allocation of resources and remove barriers to accessing healthcare.
A more easily achievable potential of the technology is the automation of administrative tasks – typing up patient notes, putting together routine communications or scheduling appointments, which often are anecdotally listed as some of the most time-consuming tasks for health professionals. Heidi is an example of an AI scribe created specifically for use in medical consultations. It can record appointments, take notes and create instant referral letters.
INTEGRATING AI INTO MIDWIFERY EDUCATION AND PRACTICE
An Australasian Institute of Digital Health article (Bichel-Findlay & Scanlon, 2024) lists current AI technologies being used by nurses and midwives, which include virtual reality, voice assistive technology and image recognition. The benefits of these tools come from the ability of AI to quickly
search large volumes of data for patterns, trends and anomalies to identify patients at risk or to provide specific interventions, as well as taking over mundane tasks like administration and note-taking.
In a recent scoping review, Kranz and Abele (2024) list the potential benefits of integrating AI into midwifery education and practice. They say such tools in midwifery could improve quality of care, safety, optimise decision-making and simplify administrative tasks, while increasing precision and productivity.
Their review also acknowledges the importance of adapting and evaluating the midwifery curricula to prepare students for a future where AI plays a significant role in their practice. The authors add that programmes like ChatGPT could enhance midwifery education by supporting students in research and writing skills, with personalised learning materials, and by simulating clinical scenarios.
However, both the above articles admit that integrating clinical practice and AI doesn’t come without risks.
ETHICAL CHALLENGES
Ethical sourcing of the training datasets becomes even more important when dealing with people’s health and personal information. Ensuring this is obtained with consent and respect, and with the data representative of the population you’re dealing with, is paramount.
No training set is perfect, and the jury is still out on who should be held accountable if the AI does make a mistake. As Reza identifies, the tool’s accuracy is only as good as the training data provided to it.
The Chief Science Advisor report (2023) identifies that there are many challenges to contend with before AI reaches the authors’ 2035 vision. AI has the potential to spark scepticism and fear, write the authors, and research suggests that Aotearoa as a nation is less positive about it compared to globally. Consent, data sovereignty, governance, equity and the risk of a digital divide need to be considered, with the report recommending that the use of AI in healthcare must:
• Implement Te Tiriti o Waitangi and recognise tikanga Māori
• Be safe and effective
• Be for equity
• Be effectively controlled
• Be evaluated and trusted
At the time of writing, Te Whatu Ora | Health NZ (2024) has issued a statement saying that, although it is investigating the use of AI in clinical coding of hospital admissions, it did not endorse its employees to use any of the available generative tools in patient care as they had not been validated for safety and effectiveness. Health NZ has established the National Artificial Intelligence (AI) and Algorithm Expert Advisory Group to continue to provide advice and guidance in this space.
Meanwhile, approximately 400 GPs across Aotearoa are already testing the use of GenAI tools in taking patient consultation notes, but not in offering advice or making decisions (McBeth, 2024). The Royal New Zealand College of General Practitioners (RNZCGP, 2017) acknowledges the impact AI will have, enabling GPs to improve diagnostics, predict outcomes and provide more personalised healthcare for patients. RNZCGP writes of algorithms capable of detecting cancerous skin lesions; imaging tools capable of providing at-home diagnoses; and various projects, including IBM’s Watson for Oncology, to provide evidence-based, patient-centred treatment plans for people with cancer.
Similarly, Arindam talks about tailored treatments, where the AI tool takes into account all aspects of an individual to design a specific treatment plan for them. “What excites me about AI is that we are probably the last generation of humans who experienced the old style of care – one size fits all.”
He says there is the need for AI ideas and possibilities to be well communicated across society because all of us will interact with AI, either as the consumer or the operator. He cautions against a sole reliance on AI tools, however, stressing the importance of always using them with due diligence and careful supervision. And while this technology has the opportunity to support health equity, countries with constrained resources won’t have the capital to invest in it unless the data and knowledge is shared freely across the globe, says Arindam.
RETAINING THE HUMAN TOUCH
When asked to describe AI in one word, Reza pauses to think before answering: “Revolutionary”. However, he adds that for health, this vision is always for AI tools that health professionals can use and will never replace the practitioner themselves.
“AI does not make a decision by itself, AI does not do the diagnosis, [it] does not care for us,” he says. “In healthcare, AI is a tool that a [health professional] utilises to work better but, at the end of the day, it’s their decision to come up with a diagnosis, to come up with assessments.”
And whether AI is reading x-rays or is a virtual medical assistant, there is no doubt the AI age is coming and society –including healthcare providers – needs to keep pace with the developments or risk being left behind. Square
References available on request
VIOLET CLAPHAM MIDWIFERY ADVISOR
artificial intelligence in midwifery
Practising midwives may already be engaging with AI technologies without being aware of it, such as using predictive text, auto-fill functions on forms or voice to text technology.
Artificial Intelligence is developing at a rapid rate and some of the potential future applications for midwifery include enabling clinicians to:
• Process and analyse large amounts of clinical information or data
• Record, summarise and transcribe clinical consultations
• Interpret CTG tracings
• Make early identification and diagnosis of diseases (such as breast cancer)
• Analyse complex data to provide personalised insights and recommendations for care
• Analyse data and provide personalised insights into a woman’s cycle length, ovulation and fertility
• Use sophisticated practice management, accounting and referral tools that are intuitive and highly automated
• Make real-time predictions about the need for induction or caesarean birth
A WORD OF CAUTION
Whilst the rapidly evolving potential of AI is exciting, the College urges midwives to be cautious in the way they incorporate it into their professional practice. For example, midwives remain fully accountable for documentation they have initiated in a woman’s clinical record, even it if is generated by a programme underpinned by AI editing or transcription software. Any such records need to be checked and edited to ensure accuracy and completeness. Midwives must also ensure they uphold the legal requirements of the Code
of Health and Disability Services Consumers' Rights and the Privacy Act. AI is not without its challenges, limitations and potential risks in relation to privacy and security.
In addition, women may be hesitant to share personal health data with AI systems and may be concerned about personal privacy, or about their data being used behind the scenes to develop AI algorithms, particularly if they are not confident that their data will be kept secure. Midwives should take care to gain fully informed consent before entering a woman’s data into electronic systems.
AI systems are only as good as the data they receive, and if the data are biased, the AI system and outputs may also be biased. There is still a lot of work to be done to ensure that AI algorithms are developed and tested using population-representative data sets that capture the full range of women’s health needs and experiences and are validated by human experts.
Whilst the rapidly evolving potential of AI is exciting, the College urges midwives to be cautious in the way they incorporate it into their professional practice.
A further concern is the potential replacement of human clinicians with autonomous AI systems. In addition to the potential for this to place women and babies at risk of unsatisfactory outcomes, the reality is that AI-based technologies lack consideration for human emotions and have a limited ability to sympathise and consider the emotional well-being of humans. Considering the role midwives have in providing humanistic pregnancy and labour support, scepticism about the ability of AI to connect with humans and replace midwifery decision making is understandable.
AUGMENTING HUMAN CARE
The great potential of AI lies in its ability to help shape a more reliable healthcare system that consistently delivers safe and quality care. However, midwives need to be actively engaged in the testing, implementation, use and evaluation of AI. They also need to contribute to the data sets that support the technical infrastructure, the research to determine efficacy and effects on clinical decision making, and the bioethical implications of AI.
Rest assured that, ultimately, because delivering midwifery care is relational by nature and requires “uniquely human skills like empathy, persuasion and big picture integration” (Davenport & Kalakota, 2019, p. 98), most experts agree that AI will not replace clinicians but, rather, it will change how practitioners spend their time and it will augment their care provision for the benefit of women and babies. Square
References available on request
A large tranche of data from the 2023 census (released in October, 2024) demonstrated the diversifying demographics of our population, as also seen in the latest birthing population data from the Report on Maternity (Health NZ | Te Whatu Ora 2024, reporting data for 2022). The New Zealand Disability Survey was also undertaken in 2023 but data reporting is not yet available – this will hopefully provide some insight for midwives and maternity services in future once it is published. This article explores the recently published information about who we are as a nation and who we serve as midwives, with some considerations for midwifery practice.
Please note: The language used in this report aligns with that of the publication being cited.
POPULATION GROWTH
The Aotearoa population grew by almost 300,000 between the 2018 and 2023 censuses, a 6.3% increase. The regions with the highest growth were Tasman (10.3% increase); Canterbury (8.9%); Waikato (8.9%); and Northland (8.3%, possibly because of outward drift due to the cost of living in Auckland). There was also moderately high growth in Bay of Plenty, Gisborne and Taranaki. Three-quarters of the population lives in the North Island.
With population growth comes increasing economic activity but also pressure on housing and infrastructure. Housing ownership increased slightly between 2018 and 2023, and there was an improvement in healthy housing (in all areas except Gisborne, partly due to Cyclone Gabrielle). However, for those renting, the median weekly rent paid by households increased by almost a third and
Midwives will be familiar with the realities for many whānau who experience significant challenges in meeting their basic needs, which means some are unable to afford essential healthcare during pregnancy.
there was also a sharp increase in the number of people living in mobile homes, improvised shelters or sleeping rough. Midwives will be familiar with the realities for many whānau who experience significant challenges in meeting their basic needs, which means some are unable to afford essential healthcare during pregnancy, including prescriptions, ultrasound scans and travel to appointments.
FERTILITY RATES AND PARITY
While the population growth in 2023 included a 3% increase in the number of women aged 15-49, there was a 3% decrease in the number of births that year. As a result, 2023 had a record-low fertility rate of 1.56 births per woman, which is well below the ‘replacement rate’ (2.1 births per woman), as it has been since 2013 (Stats NZ, 2024).
This is reflected in the birthing data, with a gradual increase in the proportion of women and people giving birth to their first baby compared with a subsequent baby, and a slight decrease in the
FIGURE 1.
proportion of people having a third or more birth, particularly since 2013 (Figure 1). Maternal age has also shifted significantly. In 2013, half of the birthing population was aged 30 or more. By 2022, 58% of birthing people were aged 30 or more after year-on-year age increases.
MIGRATION
With a low birth rate, most of the population growth in Aotearoa is due to net migration, which is contributing to the rapid diversification of our society. In 2023, 28.8% of the population was born overseas. Unfortunately, migration status data are not included in health and maternity reports but the proportion of the birthing population with a migrant or refugee background is very likely to be higher than in the general population. Researchers of migrant health are currently looking into this.
The 2023 census indicated that tāngata whenua who live in Aotearoa are the second-largest ethnic group and are now nearing the one million mark, with 904,100 Māori recorded in 2023 – an annual population increase of 1.5%.
ETHNICITY
The 2023 census indicated that tāngata whenua who live in Aotearoa are the second-largest ethnic group and are now nearing the one million mark, with 904,100 Māori recorded in 2023 – an annual population increase of 1.5%. The largest ethnic group is still NZ European/Pākehā; however, the proportion has decreased over the last three censuses.
The Indian New Zealand population has surpassed Chinese New Zealanders to become the third largest ethnic group. The other fast-growing ethnic populations were Māori, Asian, Pacific peoples, and Middle Eastern/Latin American/African (MELAA).
Similar patterns are seen in the birthing population, although the Report on Maternity combines European and Other ethnic groups, which reduces the visibility of some communities (Figures 2 and 3).
With migration and diverse ethnic groups come the sounds of more than 160 languages ringing out in Aotearoa. Te reo Māori speakers numbered 213,849 in the 2023 census, a 15% increase since 2018. After English, the ten most widely spoken languages are (in order) te reo Māori, Samoan, Northern Chinese, Hindi, Tagalog, Sinitic (Chinese) languages, Yue, French, Punjabi and Afrikaans.
SEX, GENDER AND LGBTIQ+
Census 2023 included the first collection of data on Aotearoa New Zealand’s sex, gender and LGBTIQ+ ‘concepts’. Four data fields were included: 1) sex at birth; 2) gender (the transgender status variable was derived from the answers to these two questions); 3) sexual
FIGURE 2. PERCENTAGE OF THE BIRTHING POPULATION BY PRIORITISED ETHNIC GROUP
3. PERCENTAGE OF THE BIRTHING POPULATION BY PRIORITISED ETHNICITY (ASIAN ETHNIC GROUPS)
identity; and 4) variations of sex characteristics. A Rainbow/LGBTIQ+ indicator was derived from these four data fields.
Data are reported for the population aged 15 years and over, among whom 4.1% reported a sexual identity other than heterosexual (including ~1/3 gay or lesbian, ~1/2 bisexual, and ~1/8 sexual identity not elsewhere classified); 0.7% were transgender (including ~1/5 transgender males, ~1/5 transgender females and ~3/5 another gender); and 0.4% were intersex.
Stats NZ (2024) explained in a news release that “0.4 percent of the census usually resident population had a gender other than male or female. The category includes all genders that are not male or female. This group is sometimes referred to as ‘non-binary’… People who had another gender were on average younger than the general population, with a median age of 24.8 years compared with 38.1 years. Over half (59.8%) of the adult population who had another gender were aged 15-29 years.”
Data on gender and sexuality are poorly collected in the maternity dataset and not yet reported; however, the age structure of the gender diverse population suggests that the majority are within a reproductive age bracket.
MIDWIFERY PRACTICE FOR A DIVERSIFYING POPULATION
Cultural Safety and Kawa Whakaruruhau remind us that culture includes many aspects, including indigeneity, ethnicity, age or generation, sex, gender, sexual orientation, religious or spiritual belief, disability and socioeconomic status. With a rapidly diversifying population, Cultural Safety continues to provide an essential
framework for midwifery practice. The College’s draft Cultural Safety consensus statement recently underwent member consultation and publication is anticipated in 2025. It is also timely that the Midwifery Council has added Cultural Safety and Turanga Kaupapa to the midwifery recertification programme, so midwives will have access to more education opportunities.
Education in care for culturally and linguistically diverse (CALD) communities is also important, enabling midwives to deepen their understanding of cultural values, cross-cultural communication and working with interpreters. We are excited to announce that the College’s eLearning course on midwifery care for former refugee whānau will be launched early in 2025. Online courses about working with interpreters, cultural competence and working with migrants and refugees are also fully funded for midwives –register at www.ecald.com.
Working with professional interpreters is essential when the midwife does not speak the language of the woman receiving care, to ensure communication both ways is understood and to enable informed decision making. Telephone and video interpreting services are fully funded for LMC midwives via Connecting Now (contact the College or MMPO for access details), and employed midwives can request access through their districts or employers.
Guidance on culturally safe care for gender diverse whānau is available in Warming the Whare for Trans People in Perinatal Care (Parker et al., 2023).
He waka eke noa – we’re all in this together. Square
References available on request
FIGURE
TE PAEA BRADSHAW MĀORI MIDWIFERY ADVISOR
midwifery standards review i te reo māori (in te reo māori)
Titiro Whakamuri, Kōkiri whakamua - look back and reflect so you can move forward.
The Midwifery Standards Review (MSR) is a unique process developed by the College to reflect the partnership model of midwifery practice. It provides midwives with a mechanism and opportunity to formally reflect on their midwifery practice with the assistance of specially educated reviewers. But what if a midwife wanted to complete her MSR solely in te reo Māori?
The College is pleased to share the recent success of a MSR pilot i te reo Māori (in the Māori language).
Earlier this year, the College received a tono (request) by a midwife to complete her MSR using tō tatou reo Rangatira. We were thrilled to support a review team who were both willing and able to facilitate this. Afterwards, I had the privilege of discussing what this experience meant for all involved.
Their feedback was unanimous: “It was beautiful doing it in a Māori way”. The whole review was led by the midwife, and the
The midwife began with a karakia she had prepared, and shared her whakapapa in the review.
reviewers said, “it felt like a whole new way”. Speaking in te reo enabled the reviewers and midwife to discuss the review material in its entirety, rather than as separate components, “the midwife let Tūranga Kaupapa guide the review”. The midwife began with a karakia she had prepared, and shared her whakapapa in the review. Surprisingly “we were all from Te Tai Tokerau. He tohu nā ngā atua, nā ngā tīpuna, nā rātou tēnei huarahi i hora” (it was a sign, like a pre-destined pathway from the heavens that our ancestors had guided us to). Similarly, another comment was, “the tīpuna put us all in the right place at the right time”.
The reviewers said they were “buzzing” and detailed how they felt that there was “no assimilation, when you put a Māori framework into play to do a MSR, it really showcased te ao Māori, and our innate way of practising; we were all able to be ourselves, and she talked about Kōhanga, Wānanga, Kura Kaupapa (Māori education streams). These things are important to all of us, and it’s relevant to the mahi we are doing”. Furthermore, the midwife came away from her MSR feeling “celebrated and excited”.
"Feedback was mostly shared through kōrero, whakarongo and titiro, it doesn’t usually get the space or the mana if the only feedback being considered is the feedback submitted in the portal. It needs to continue to happen this way, it felt groundbreaking, it was history in the making”.
Reflecting was so easy and natural, “as reviewers we felt uplifted too, obviously the
midwife felt safe, it’s our reo (language), our framework (Tūranga Kaupapa), our lens, our practice, the mana was hers and it was celebrated, she got to talk about all the amazing things she was doing and that doesn’t always fit the prescribed material as it is currently. Because the midwife is working and practising in an area she is connected to, she is innovative and invested in what she is doing. When we got to the PDP, she knew
what she wanted to do, and she had the answers, which is how it should be.
For anyone thinking about undertaking a MSR in Te Reo Māori, the participants in this review were clear about the following points:
• Let the midwife being reviewed lead
• Indigenising MSR is important and validating to Tūranga Kaupapa
• Request a Māori reviewer team, not just ‘a’ Māori reviewer
• Celebrate and uphold the mana of whānau, the taonga of Tūranga Kaupapa and the mana of midwifery
• It is important that the reviewers connect with each other first, so the MSR space is an ahuru mōwai (safe, nurturing haven)
Influencing change in the MSR space through this pilot was a clear example of the potential benefits to the profession if we continue to honour Te Tiriti, and foster cultural safety within our College processes. If you change the reo, you change the framework, you give mana to another way of being and you whakamana a different lens. This is an important consideration when trying to grow and sustain a Māori midwifery workforce which can then influence better health outcomes for whānau Māori.
E rere ana ngā mihi huhua ki a koe e hoa, nāhau tēnei mānuka I takoto mai, ki a kōrua anō hoki, ōku hoa tēnei mānuka I hiki. Mei kore ake koutou katoa tēnei kaupapa I rangatira ai. Square
Comfort and safety for babies newborn-2 years
More restful, safer sleep and helps prevent flat head
• More restful, safer sleep limb and hip movement
Goes over any type of swaddling, sleeping bag or sleepwear, for a snug and more restful sleep
• Ensures swaddling, sleepwear, Sleepingbag use is safer and cosier
Natural, flexible body, limb and hip movement
safely lasts two babies aged 0-2 yrs
• Excellent for babies requiring varied sleep positions or cot elevation est 1992 Helps keep young babies comfortably o the tummy; older babies turn freely within the wrap Use code ‘NZCOM’ for 20% OFF
The World’s Safes t Baby Wrap w w.safet sleep.com
TRUSTED • SAFE • UNIQUE
EPI-NO is clinically proven to of an intact per ineum, reduce episiotomy, and is safe to use
EPI-NO is a dual pur pose CE approved medical device designed muscles from ear ly in pregnancy, and again postpar tum The per ineal stretching exercises commence concur rently after Week 36.
EPI-NO Childbir th Tr aining has been accepted in Austr alia & New Zealand for over 15 year s as an effective prepar ation for women choosing a natur al vaginal bir th
EPI-NO Patient Brochures can be requested for New Zealand via info@starnbergmed.co.nz
Over 65,000 EPI-NO births in Austr alia and New Zealand. Available in over 20 countr ies wor ldwide www.starnbergmed.co.nz
Available online with shipment from Auckland and at selected phar macies.
‘The human body performs to maximum trained and prepared. Childbir th is no exception ’ Dr Wilhelm Hor kel, Star nberg (EPI-NO nventor)
Germany
CAROL BARTLE POLICY ANALYST
THE MARKETING OF COMMERCIAL MILK FORMULA IN AOTEAROA
NEW ZEALAND - VARIED AND LESS THAN IDEAL INFORMATION
There is a surfeit of misleading marketing about commercial milk formula (CMF) aimed at parents who may be unclear about the differences between breastfeeding and formula, confused about the differences between formula brands, and hoping to find the ‘best’ product for their babies. This may lead to purchases of the most expensive product to get what parents think is the ‘best’ available on the market, and also lead to using CMF for longer than necessary.
Marketing of any kind can influence purchasing decisions. Winstanley and Cressey (2008) reported that parents taking part in a survey about the preparation of powdered infant formula in NZ were ‘information hungry’ and that the information on products was seen as ‘available, authoritative and trusted’. In March 2020, the Ministry for Primary Industries (MPI) released a report from a 2019 survey of caregivers’ beliefs about the risk of improper infant formula preparation and their understanding of infant formula preparation risks. Participants were caregivers in Australia (n = 600) and in NZ (n = 733). Caregivers were reported to have high confidence in their formula preparation techniques, with 84% stating they were either very or extremely confident. There was a low level of awareness of the potential risks of formula “if not prepared according to the instructions on the label,” with only 33% of caregivers indicating their awareness of a risk of bacterial infection. Reported practices in preparing and storing formula feeds were reported as “varied, and less than ideal”, despite the responses to a further question
about instructions on the label, where 87% of respondents viewed the importance of exactly following the preparation and storage instructions on a tin of formula as “very important” or “extremely important”.
The information on CMF products is in itself “varied and less than ideal”. For example, powdered CMF is not a sterile product, but this fact is not declared on the majority of product labels. There is a range of different preparation instructions which are not consistent with the World Health Organization optimal recommendations. Any bacteria that may be present in the powder will not be controlled if parents follow the preparation instructions, which are often for boiled and then fully cooled water. Powdered infant formula preparation needs to control potential pathogen growth to minimise illness risk. Optimal reconstitution requires freshly boiled water left to cool for no more than 30 minutes, so the water remains at a temperature of at least 70°C to inactivate any bacteria already present in the product (Baby Friendly Initiative UK, NHS, 2022).
Campbell and Soboleva (2015) undertook a Ministry of Health funded review of the reconstitution of powdered infant formula and the advice from this review is used on the Health NZ | Te Whatu Ora website (2024). The modelling described in this review recognises that using boiled water (>70oC) showed the greatest exposure reduction of any potential bacteria present in powdered infant formula. Unfortunately, reported negative reactions from consumers to this advice were reported, and this was seen as reason for NZ to abandon the optimal recommendations, while suggesting that improved information to eliminate widespread misunderstanding was required.
Potential bacteria present in CMF can be a source/cause of Cronobacter Sakazakii infection, which in infants is associated with severe neurologic disability and death. The Campbell and Soboleva review (2015) suggests that the global incidence of infection is rare but, in reality, it may be the reporting of these infections which is rare as most countries, including most US states, do not require mandatory reporting, so the true incidence is unknown (Strysko et al., 2020).
Strysko et al. (2020) reviewed reported cases to the US Center for Disease Control and Prevention and in the available literature between 1961-2018 and found 183 cases. Case counts were significantly higher in the final quarter of the study period, with a higher proportion of term infants and nonhospitalised infants among the US cases. Contamination of powdered infant formula was identified in 30% (21/71) of the investigations. In Aotearoa NZ notification is mandatory for suspected cases but only disease in infants less than one year old is reportable (Health NZ I Te Whatu Ora, 2024a).
Another proposed reason for not using the optimal preparation guidelines is the potential destruction of some ingredients in formula such as prebiotics and probiotics. This is a distraction from the key issue of preparation safety, as prebiotics and probiotics are unnecessary ingredients and there is no robust independent evidence to
The information on CMF products is in itself “varied and less than ideal”. For example, powdered CMF is not a sterile product, but this fact is not declared on the majority of product labels. There is a range of different preparation instructions which are not consistent with the World Health Organization optimal recommendations.
recommend these additives (Indrio et al., 2022; Lemoine et al., 2023; Skorka et al., 2018).
Given that 1) the reconstitution information on different products is inconsistent, 2) the labels do not state that the powder is not sterile, and 3) the majority of parents are likely unaware of this or of the risk of bacterial contamination, the current NZ situation regarding formula standards and Health NZ | Te Whatu Ora advice needs further review.
CLAIMS AND COSTS - HEALTH AND ECONOMIC
There is a range of marketing messages tailored to appeal to parents. However, robust, independent scientific evidence for the efficacy of added novel functional ingredients is absent or limited (Ackerberg, 2012; Cheung et al., 2023; Schulzke et al., 2011; Simmer et al., 2011; Starling, 2010; Vy, 2002; Yau, 2003). Cheung et al. (2023) examined 757 infant formula products, each with a median of two claims, and found that “… multiple ingredients were claimed to achieve similar health
Parents buying CMF products that make health and nutrition claims are being exposed to a form of puffery, which means that marketing messages ‘puff up’ the product being described... it is recognised and accepted by industry and regulators and has been described as legitimate and harmless exaggeration.
or nutrition effects, multiple claims were made for the same ingredient type, most products did not provide scientific references to support claims, and referenced claims were not supported by robust clinical trial evidence” (p. 1) The most common claim types on products examined were “helps/ supports development of brain and/or eyes and/or nervous system”, “strengthens/ supports a healthy immune system”, “helps/ supports growth and development”, “easy to digest” and “dietary management of allergy, including cow’s milk allergy”. In 2010 a mother posted on Mumsnet about what she termed “New Parent Infant Formula Selection Paralysis” (Farber, 2010):
“The few times I had to buy formula for my son, I was paralyzed by the wall of options in the grocery store. Each brand made a different claim about what their formula would do for my son's health, and the more claims there were, the more expensive the can. Even my son's paediatrician couldn't recommend a choice.”
Although that post was made fourteen years ago, there are many more brands and products making health and nutrition claims on the market now; social media and digital marketing compounds this misinformation and “formula selection paralysis” is likely to be exacerbated.
The aim of commercial marketing is to eliminate choice or to establish a strong bias towards only one choice, rather than to increase the choices for consumers (Heinig, 2006). Frick notes that companies use substantial resources to differentiate themselves from each other for the purpose of competition. This results in a market not operating efficiently to provide goods at minimum cost, with the benefits to infants of this broad range of products being unclear (Frick, 2009).
Parents buying CMF products that make health and nutrition claims are being exposed to a form of puffery, which means that marketing messages ‘puff up’ the product
being described. Puffery on consumer products is recognised and accepted as appropriate by industry and regulators and has been described as the legitimate and harmless exaggeration of advertising claims to overcome natural consumer skepticism, and also to make a product look better than those of competing brands. It is claimed that ‘reasonable consumers’ are expected to not take these claims seriously (Wilking, 2016).
This message is framed as if consumers expect advertisers to claim that their products are the best, but they will not believe these claims to be true; but this is an assumption (Adams & Maine, 1998). In the case of CMF, it certainly cannot be considered a harmless practice when marketing is aimed at parents of vulnerable newborn and young babies (Bartick & Walker, 2023). The International Code is clear about why the marketing of breast-milk substitutes (CMF) requires special treatment:
“… in view of the vulnerability of infants in the early months of life and the risks involved in inappropriate feeding practices, including the unnecessary and improper use of breastmilk substitutes, the marketing of breastmilk substitutes requires special treatment, which makes usual marketing practices unsuitable for these products”. (World Health Organization, 1981, p. 7).
The International Code of Marketing of Breast-Milk Substitutes is a set of recommendations from the collective membership of an international body in the field of health, the World Health Assembly. It does not ban the sale or use of breast-milk substitutes or any particular company’s products but, instead, it is directed at unethical marketing practices and false and misleading advertising. The Code is also clear that there are legitimate reasons for using formula/breast-milk substitutes and recommends that parents have access to accurate, safe and unbiased information.
The Code always needs to be considered alongside the subsequent, relevant World Health Assembly (WHA) Resolutions as they keep the Code, which was written in 1981, up to date. It is important that midwives and other health workers understand the Code and that they are sources of unbiased commercial-free information for parents on all aspects of infant feeding. As prime industry marketing strategies involve forming health alliances, it is essential that health workers have a clear understanding of the issues of conflict of interest, endorsement by
association and the importance of exclusive breastfeeding.
MARKETING IN AOTEAROA NEW ZEALAND: A LACK OF CONSUMER PROTECTION
Because parents and caregivers using CMF need protection from predatory marketing, the recent decision by our government to opt out of the proposed joint Australia/NZ infant formula marketing standards is alarming (TVNZ, 2024). The industry self-regulatory code of practice for marketing infant formula which operates in NZ fails to adequately protect consumers from ‘specialty’ formula marketing. Parents are buying expensive products, choosing products that make unsubstantiated claims, and also buying unnecessary products such as follow-on formula and toddler milks (Bartle et al., 2024). CMF is only necessary for the first year of life for non-breastfed infants, and follow-on formula and toddler milks are unnecessary products (Health Promotion Agency, 2022; World Health Organization, 2013). All commercial formula products have to meet nutrition and quality standards, which means there is no reason for families to spend more money on more expensive products. Interestingly, the increasing cost of CMF in the UK is being debated and, as yet, is an unresolved crisis in terms of affordability (Baby Feeding Law Group, 2023; Parmenter, 2023; UNICEF UK Baby Friendly Initiative, 2023).
Member states of World Trade Organization (WTO) with large dairyproducing industries, such as NZ, frequently use WTO processes to undermine breastfeeding and drive formula consumption by challenging protective regulations which are being adopted by other member states (Baker et al., 2021). A recent article in NZ Doctor discussed the implications of NZ withdrawing from the proposed joint Australia/NZ infant formula marketing standards (Johnston, 2024). Johnston describes how a neonatologist expressed concerns that “parents may continue to be unnecessarily persuaded to buy infant formula containing prebiotics and other ingredients without proper evidence now that the Government has pulled out of a transTasman rules review”. Toldi and Muelbert (2024) describe the government decision to opt out of the joint infant formula standard as a “step in the wrong direction for child health policy” and refer to the low rates of exclusive breastfeeding to six months in NZ
(1 in 10 babies) as to why added controls on statements made on product labels are important.
The proposed Australia/NZ infant formula standards represented a means of addressing some current legislative shortfalls and could have supported families using CMF to make informed decisions about the products they purchase. Voluntary industry agreements, rather than full implementation of the International Code into regulation and legislation, continue to be of concern in terms of the lack of protection of exclusive breastfeeding and the consequent public health implications. The influence of inappropriate CMF marketing negatively impacts immediate and long-term health outcomes for mothers and children (Becker et al., 2022). The absence and/or erosion of legal and regulatory standards means that actions to prevent misleading marketing are “underpowered and underused” (Rollins et al., 2023). Government-supported industry codes of practice distract from what is really necessary – the full International Code and resolutions. Industry codes also create a damaging illusion of effectiveness that postpones meaningful and effective action. This failure to protect breastfeeding and safe infant and young child feeding rests on the shoulders of government and action on this issue is a government responsibility. Square
key points for parents using commercial milk formula
Parents who decide to use formula for whatever reason should receive the best, most up-to-date, evidence-based information about how to choose, prepare and store formula safely.
A Stage One from birth formula can be used up until the age of one year and follow-on and toddler milks are unnecessary.
Optimal reconstitution of powdered infant formula requires boiled water left to cool for no longer than 30 minutes, so the water temperature remains at least 70˚C.
Health and nutrition claims on products are not evidence based.
All NZ products are required to meet nutrition and quality standards.
taku wāhi mahi my midwifery place
Clinical Midwife Manager of Hutt Maternity, Verity O’Connor, is personally invested in her team and the community they serve. The reverse is also true, evidenced by the fresh baking delivered to Hutt Maternity midwives several times a week. Verity shares her own story and what keeps her team ticking along.
Like many others, Verity’s desire to become a midwife was sparked by her own uplifting experience. “I had fantastic midwifery care,” she begins. “At 23 years old, I was a relatively young mum when I had my first baby, and it was the first time I really felt empowered to make the calls about what I was doing with my body and my baby. I admired my midwife because she believed in me so much. The experience changed my life, and I just knew it was what I wanted to do.”
Gaining her midwifery registration in 2005, Verity spent the next 10 years moving between providing LMC care and working in staff midwife roles at Wellington Regional Hospital. In 2016, she found herself circling back around – not only to the region where she grew up, but also the very hospital where her life began. “I was born in Hutt Hospital, grew up in the Hutt and my family’s been here for generations. When I got this job, it felt like coming home. It felt like something I not only needed to do, but wanted to do, and was ready to do.”
Now eight years into her role at Hutt Maternity, Verity describes what it is that binds the team together. “We’re connected and unified through our common goal: to provide the best care we can to our community. That sounds like lip service, but it’s not. We live in a community where there’s high
social deprivation and potential for poorer outcomes, so we’re genuinely passionate about providing e quitable care.”
A smooth interface and positive work culture also mean staff want to stay. “It’s such a fluid workforce of people going between LMC and core, so there’s no ‘them and us’ and we’re all working cohesively towards that common goal. It’s about creating the right culture in a workplace; without that, it doesn’t matter whether you have the flashiest facilities or you’re fully staffed, because none of it will make any difference.”
It’s such a fluid workforce of people going between LMC and core, so there’s no ‘them and us’ and we’re all working cohesively towards that common goal. It’s about creating the right culture in a workplace.
The flow-on effect has clearly been felt by whānau walking through Hutt Maternity’s doors, as Verity describes a special community group who regularly show their gratitude. “The ‘Oxytocin Squad’ is a group of māmā, maternity consumers and supporters, who bring in kai for us several times a week. We get pizzas on Fridays, and they’ve even organised a Givealittle page to raise funds to help new LMC midwives buy their equipment. Our external review in 2018 identified that staff needed more support and this was our community’s response. They’ve blown us away; they’re wonderful. When you’re having a tough shift and you walk in to see fresh baking on the table, knowing we’re all appreciated keeps the morale high.” Square
Above: Verity O'Connor (middle) with new graduate midwife Annie Chen (left), and third year student midwife Chloe Grey (right).
The College has a range of midwiferyrelated books, leaflets, merchandise and other resources available through our website: www.midwife.org.nz/shop
ADVERTISING POLICY AND DISCLAIMER: The New Zealand College of Midwives maintains a schedule of guidelines to exclude advertisements for products or services that are not aligned with its principles and ethics. Every effort is made to ensure that advertising in the magazine falls within those guidelines. Where advertising is accepted, this does not imply endorsement by the College of the product or service being promoted
Midwife Aotearoa New Zealand is published quarterly for the New Zealand College of Midwives. The articles and reports printed in this newsletter are the views of the authors and not necessarily those of the New Zealand College of Midwives, its publishers or printers. This publication is provided on the basis that New Zealand College of Midwives is not responsible for the results of any actions taken on the basis of information in these articles and reports, nor for any error or omission from these articles and reports and that the College is not hereby engaged in rendering advice or services. New Zealand College of Midwives expressly disclaims all and any liability and responsibility to any person in respect of anything and of the consequences of anything done, or omitted to be done, by any such a person in reliance, whether wholly or partially upon the whole or any part of the contents of this publication. The College acknowledges and respects diversity of identities through the language used in this publication. Te reo Māori is prioritised, in commitment to tāngata whenua and te Tiriti o Waitangi. To maintain narrative flow, the editorial style may use a variety of terms. Direct citation of others’ work maintains the original authors’ language, and contributing writers’ language preferences are respected. All advertising content is subject to the Advertising Standards Authority Codes of Practice and is the responsibility of the advertiser.
Contents Copyright 2024 by New Zealand College of Midwives. All rights reserved. No article or advertisement may be reproduced without written permission. ISSN: 2703–4546.
Find solutions for the biggest challenges faced by midwives today with POSTGRADUATE STUDY
Our postgraduate midwifery courses are designed to support midwives to lead positive change in rapidly moving practice environments – including promoting equity, optimising physiology, navigating childbearing in floods and disasters, and preparing for uncertain futures.
Courses can be taken individually or as part of a wider programme of study at postgraduate certificate, postgraduate diploma or master’s level.
Courses are delivered online, so you can fit your studies in around your midwifery practice.
Physiological Childbirth in Changing Times (March - June)
Resisting Racism in Reproduction (July - November)
Enhancing Preparedness: Childbearing in Disaster Conditions (July - November)
For more information, contact: anna.fielder@aut.ac.nz