





FALL 2017 • VOL. 37, NO. 4 • WWW.BEHAVIORAL.NET INVESTORS SEEK FOLLOW-ON DEALS: PAGE 20 Involuntary
for addiction? IT Vendor Survey PLUS
commitment
STAKEHOLDERS HOPE TO HOLD DRUG COMPANIES ACCOUNTABLE FOR THE OPIOID CRISIS







Trauma Informed EHR Performance Dashboards Revenue Cycle Management Look no futher for a complete EHR! (716) 810-9755 www.10e11.com h
COVER STORY
BY JULIE MILLER
BY DOUG TIEMAN
EDITORIAL
Editor in Chief Julie Miller
(216) 373-1204 • jmiller@iahbhc.com
Senior Editor Tom Valentino
(216) 373-1225 • tvalentino@iabhc.com
DESIGN
Creative Director Dave Villafañe
SALES
Director of the Institute for the Advancement of Behavioral Healthcare
Douglas J. Edwards (216) 373-1201 • dedwards@iabhc.com

Project Manager, Directories/Design Showcase
Erin Beirne (216) 373-1217 • ebeirne@vendomegrp.com
Traffic Manager Judi Zeng
(212) 812-8976 • jzeng@vendomegrp.com
Please send IOs to adtraffic@vendomegrp.com
All ad materials should be sent electronically to: https://vendome.sendmyad.com/
REPRINTS
Erin Beirne (216) 373-1217 • ebeirne@vendomegrp.com
CUSTOMER SERVICE/SUBSCRIPTIONS
Call: 1-888-244-5310, email to: VendomeHM@emailpsa.com, or visit: www.iadvancebehavioralhealthcare.com/subscribe
REUSE PERMISSIONS
Copyright Clearance Center info@copyright.com Ph: 978-750-8400
Fax: 978-646-8600
ADMINISTRATION
Chief Executive Officer Mark Fried
Chairman Jane Butler
Chief Marketing Officer Dan Melore
Vice President, Finance Bill Newberry
Director, Custom Media Jennifer Turney
Director, Circulation Rachel Beneventi
BY JULIE MILLER
BY ALISON KNOPF
Behavioral Healthcare Executive (ISSN 1931-7093, Online 2167-9649) is published four times per year by Vendome Group, LLC, 216 East 45th St., New York, NY 10017. ©2017 by Vendome Group.
Behavioral Healthcare Executive is a trademark of Vendome Group, LLC. All rights reserved. No part of Behavioral Healthcare Executive may be reproduced, distributed, transmitted, displayed, published, or broadcast in any form or in any media without prior written permission of the publisher. To request permission to reuse this content in any form, including distribution in educational, professional, or promotional contexts or to reproduce material in new works, please contact the Copyright Clearance Center at info@copyright.com or 978.750.8400. For custom reprints, e-prints, or logo licensing, please contact Erin Beirne at 216.373.1217 or email ebeirne@vendomegrp.com.
BY TOM VALENTINO
SUSAN ROMANO
BY JOANNE SAMMER
EDITORIAL: Behavioral Healthcare Executive is the practical resource for intelligence that executives can apply to meet current leadership, financial, clinical, technology, and compliance needs in the mental health and substance abuse fields. Behavioral Healthcare Executive is indexed in the National Library of Medicine’s MEDLINE/PubMed database. Articles and opinions published in Behavioral Healthcare Executive do not necessarily reflect the views of Vendome Group or the Editorial Advisory Board.
SUBSCRIPTIONS: For questions about a subscription or to subscribe, please contact us by phone: 888-244-5310, online: http://www.iadvance behavioralhealthcare.com/subscribe or email: VendomeHM@emailpsa. com. Subscription rate per year: $140 domestic, $169 outside the US. Single copies and back issues: $20 Domestic, $32 outside the US.
POSTMASTER: Send changes of address to: Behavioral Healthcare Executive, PO Box 11404, Newark, NJ 07101-4014
CONTENTS | FALL 2017 2 FALL 2017 BEHAVIORAL HEALTHCARE EXECUTIVE WWW.BEHAVIORAL.NET
EDITOR'S LETTER 6 The almighty Google has changed its policy on addiction treatment advertising
IN THIS ISSUE
PERSPECTIVES 8 We must become patient-centric
BY THE NUMBERS 10 What the DEA uncovered in this year’s report
MILLER NEED TO KNOW 12 The opioid commission files its final repor t
MANAGEMENT 20 Follow-on deals build out investment por tfolios
22 Prep work is critical for accreditation
BY JULIE
BY TOM VALENTINO
CLINICAL TRENDS 28 Involuntar y commitment for addiction disorder treatment remains controversial BY JILL SEDERSTROM 32 Brain injur y assessments must include mental health, other evaluations BY JULIE MILLER TECHNOLOGY 36 HIT vendors share their insight on the future
DESIGN FOCUS 42 Environments must consider patient flow
46 Quick tips for geothermal HVAC systems
BY
As more states launch legal attacks against pharmaceutical manufacturers, many wonder if the effort will drive any real change BY BRIAN ALBRIGHT
Therapy Notes
Behavioral Health



ProgressEvaluationNote


Scheduling & To-Do Lists

Optimize how you manage appointments, notes, and billing. Your To-Do list automatically keeps track of notes you need to write, pending billing actions, and much more. Sync your calendar to your smart phone to view your schedule on the go.
Electronic
Streamline your billing with seamlessly integrated electronic













claims, ERA payment posting, credit card processing, and more. Submit insurance claims with a single click. Easily generate patient statements, superbills, revenue reports, and more.


View Features and Sign Up Today at www.TherapyNotes.com My experience with TherapyNotes has been fantastic!
the system is easy to navigate,
flexible, and extremely clinically
technical and customer support has been efficient,
and
I am leaving another EHR system for TherapyNotes...gladly. I'm very happy that you've created such a quality product. Thank you! Dr. Christina Zampitella, FT, Licensed Clinical Psychologist Many more stories on TherapyNotes.com! Special Offer! Just for Addiction Professional and Behavioral Healthcare Executive Readers! Sign Up and Receive Your First 2 Months FREE! Use Promo Code: APFLMG Cloud-Based SOFTWAR E iPad Mac Windows Robust Notes & EMR
your clients’ growth with powerful form-based notes, each uniquely designed for behavioral health. Go paperless by uploading your patient files into TherapyNotes. All of your data is secure,
and backed up automatically. Automatic Reminders Automatic text, phone, and email reminders to reduce no-shows and decrease expenses Custom Client Portal TherapyPortal, your own custom client portal for appointment requests Unlimited Support Superior, unlimited phone and email support included with your TherapyNotes account ...AND MANY MORE FEATURES!
Firstly,
thorough,
intuitive. Secondly,
fast,
very personal.
Document
encrypted,
11:30AM Appt with Kyle Called in to say he may be a little late Appt with Kyle 12:00PM Appt with Susan Remember to collect paperwork Appt with Susan Create a Progress Note for your appointment on 4/16 appointment on 4/16
Billing
Claim for John with Acme 12/2 $100 90791 12/9 $75 90832 https://www.therapynotes.com Acme Insurance Company Submit Claims
insurance
Diagnosis: Presenting Problem: Treatment Goals: Electronically Sign this Note Treatment Plan DSM-5 anxiety Online Practice Management Software for
CARF-BHExecMag_thirdpagesquare_2017.pdf
EVENT CALENDAR
December 4-6, 2017
Treatment Center Investment & Valuation Retreat
Scottsdale, Arizona
The Treatment Center Investment & Valuation Retreat brings together owners and senior executives from the addiction treatment and recovery community to meet with key members of the investment and financial community for an exclusive three-day educational, business, and networking event.
https://vendome.swoogo.com/TCIV-2017

April 2-5, 2018
National Rx Drug Abuse & Heroin Summit
Atlanta
The National Rx Drug Abuse & Heroin Summit is where solutions are formulated, stakeholders convene, and change begins. Be part of the international discussion on addressing the opioid crisis by attending the 2018 Summit.
https://vendome.swoogo.com/2018-rx-summit/












April 30-May 2, 2018
Treatment Center Executive & Marketing Retreat
Hilton Head, South Carolina
The second annual Treatment Center Executive & Marketing Retreat provides CEOs, CFOs, COOs, directors, senior marketing/business development/admissions leaders, and other executives with the tools they need to effectively and ethically grow their services in a rapidly changing market.
https://vendome.swoogo.com/2018-Executive-MarketingRetreat
August 19-22, 2018
National Conference on Addiction Disorders
Program Areas:
■ Assertive Community Treatment
■ Assessment and Referral
■ Case Management/Services Coordination
■ Community Housing & Integration
■ Comprehensive Suicide Prevention
■ Court Treatment
■ Crisis Programs
■ Day Treatment & Out-of Home Treatment
■ Detoxification/Withdrawal Support


■ Diversion/Intervention & Prevention
■ Employee Assistance

■ Health Home
■ Inpatient & Outpatient Treatment

ons s










Accreditation assures the persons served, funders, and partners that an organization is committed to continually improving services, encouraging feedback, and serving the community.

■ Integrated Behavioral Health/Primary Care



























■ Intensive Family-Based Services
■ Partial Hospitalization
■ Prevention
■ Residential Treatment
■ Student Counseling
■ Supported Living
■ Therapeutic Communities
■ Opioid Treatment Programs
■ Criminal Justice
■ Juvenile Justice
■ Medically Complex
■ Autism Spectrum Disorders
To learn more about CARF and how accreditation can help your organization, please contact Michael Johnson at mjohnson@carf.org or (888) 281-6531 ext. 7101.

Anaheim, Calif.
Join addiction treatment and behavioral healthcare professionals of all types who are working together to advance recovery at the 2018 National Conference on Addiction Disorders.

https://vendome.swoogo.com/NCAD-2018
Join
The




Boca Raton, Florida
http://iadvancebehavioralhealthcare.com
4 FALL 2017 BEHAVIORAL HEALTHCARE EXECUTIVE WWW.BEHAVIORAL.NET
Join the conversations about behavioral health business operations on social media. Follow us @BehavioralHlth
Facebook LinkedIn
@Editor_JMiller
Us in Your Local Area
Behavioral Healthcare Panel Series
Behavioral Healthcare Executive Panel Series inspires dialogue with local professionals on hot topics in a lunch’n’learn format at locations across the country each year. Nashville, Tennessee Denver, Colorado New Jersey
Phoenix, Arizona Orange County, California
C M Y CM MY CY CMY K
■ Eating Disorders 1 10/30/2017 8:38:21 AM
CHECK OUR WEBSITE FOR MORE DETAILS!

Solutions Offered at NCAD:
• How to evaluate new treatment modalities and clinical tools for addiction
• How to enhance treatment modalities and clinical tools such as mindfulness, CBT, DBT, and ACT
• How to remain pro table/solvent when reimbursement realities change
• How to engage in partnerships and collaboration with the larger health community
• And much more
THE
AND PRODUCED BY
National Conference on Addiction Disorders offers solutions to the most pressing challenges faced by those working in the addiction field. AUG 19-22, 2018
WWW.NCADCON.COM —As to Disney properties/artwork: © Disney
SAVE
DATE! FOUNDED
The
Disneyland® Hotel | Anaheim, CA
The most extensive educational experience for professionals working in addiction prevention, treatment, aftercare, and management, with dedicated topics for clinicians, executives, and marketers!
Google policy remains a work in progress
Ever since the almighty Google changed its policy on how addiction services are handled in search tools, the treatment industry has wrestled with mixed feelings. The search engine giant began by eliminating paid AdWords for certain addiction treatment terms—thousands of them—because many of the terms were known to be linked to fraudulent and unethical operations.
The list of taboo words isn’t being made public for obvious reasons, but you can bet that “addiction treatment in Florida” is on that menu. No one can pay for preferential rankings related to that search term anymore.
But where does this new environment leave the ethical providers?
Most of the good guys are pleased by Google’s policy and see it as a reasonable way to reduce the ability of the bad guys to lure vulnerable folks into their clutches with $90-per-click AdWords. However, smaller treatment centers are worried that the increased reliance on organic search will still leave them at the bottom of the rankings.
For example, a search for “addiction treatment in Florida” will yield many unpaid results, but there is still an algorithm driving certain links to the top. The centers that tend to have the advantage are those that know how to make digital search work in their favor and have invested time and money—a lot of money—into ensuring that result.
Smaller organizations with frugal marketing budgets often believe that they can’t keep up. They’re challenged to find the resources to maintain multiple sites, refresh the content daily and drive authentic, positive reviews from patients, especially when there’s so much clinical work to be done.
Google has pledged to continue to consult with trustworthy industry leaders on improving the governance of search results, such as the National Association of Addiction Treatment Providers and Facing Addiction. Smaller treatment centers have some opportunity to weigh in proactively through this collaborative process.
Algorithms driving search results are never going to be perfect, but it’s encouraging that leaders are looking for better ways to connect consumers with all the best quality providers rather than just those who pour a lot of cash into their websites.
ADVISORY BOARD
David Chernof, MSW, LCSW, MBA
Consultant, Behavioral Help, LLC; Associate Clinical Director, Queen of Peace Center
Patrick Gauthier
Director, AHP Healthcare Solutions

Nancy Hale
Program Director, Operation UNITE
Andrew Kessler
Founder and Principal, Slingshot Solutions
Jean Krisle
Founder and CEO, 10,000 Beds
Edward R. Jones, PhD
Senior VP for Strategic Planning, Institute for Health and Productivity Management
Ron Manderscheid, PhD
Executive Director, National Association of County Behavioral Health and Developmental Disability Directors
Steven Millette Director, Gloo Inc.
Linda Rosenberg
President/CEO, the National Council on Behavioral Health
Raymond Tamasi
President, Gosnold on Cape Cod
Doug Tieman
President/CEO, Caron Treatment Centers
Mary Woods CEO, WestBridge
Julie Miller, Editor-in-Chief

LETTER FROM THE EDITOR 6 FALL 2017 BEHAVIORAL HEALTHCARE EXECUTIVE WWW.BEHAVIORAL.NET
APPLY NOW! New micro-grants are available from the Institute for the Advancement of Behavioral Healthcare at iadvancebehavioralhealthcare.com. American Society of Business Publication Editors 2017 Regional PR IN T Award Winner Revenue of $3 million or under A | S | B | P | E Fostering B2 B editorial excellence
CREATE A POSITIVE OUTLOOK
Exterior windows for behavioral health facilities must guarantee safety and security for patients and staff. The strength of windows should be proven per rigorous ASTM testing. Equally important, they should foster serenity and contribute to an environment’s healing properties. Hope’s steel windows provide maximum safety and security with minimal framing to offer an enduring elegance and homelike comfort.
» Long life cycle and low maintenance
» Energy ef cient and contributes toward LEED certi cation








































» Wider views and bountiful natural light


» Human impact resistant

» Optional Health & Life Safety features such as integrated blinds, concealed mechanics, and controlled operation


















THE WORLD’S FINEST WINDOWS AND DOORS SINCE 1912 HOPE’S WINDOWS, INC. . (716) 665-5124 . SALES@HOPESWINDOWS.COM
Why values and ethics are good for business
BY DOUG
t is a privilege to be a trusted and integral part of a person’s recovery from addiction. Most of us in the field take this responsibility seriously, and we are fully invested in the recovery of patients and their families. So, I am deeply troubled when I see facilities cutting corners and bending the rules to increase revenue or profit. These actions are not only short-sighted from a business standpoint, but also highly unethical and potentially dangerous to those who have entrusted us to help them recover.
Frankly, the treatment field lacks a consistent set of regulations, recognized best practices or outcomes—which leaves room for unethical practices such as patient brokering or overbilling. Caron and other leaders are working with National Association of Addiction Treatment Providers to establish appropriate standards.
Money-making gimmicks are not treatment, nor are they sustainable in the long run. Businesses that depend on loopholes or lax enforcement to keep themselves solvent are ultimately doomed to fail, no matter how much “good work” they feel they provide to the community.
Of course, every organization, whether for-profit or notfor-profit, must be in good shape financially to produce its product or offer its service effectively. But there must always be an appropriate balance between the mission of the work and an expected financial performance. The mission must always come first.
Taking an ethical approach and putting best practices and standards in place may not always appear financially beneficial to addiction treatment organizations in the short-term, but
the effort will pay off by sustaining the business for the long run. The emphasis must be on empowering individuals and their families to recover from addiction and begin the life-long journey of recovery. However, one of the benefits of being a not-for-profit, is that we don’t answer to investors. Therefore, we can engage in treatment, research, prevention and charity care.
If we want the addiction treatment industry to be recognized as a legitimate healthcare sector, then we need to act like one. That means becoming patient-centric rather than customerservice-centric. Patient-centric treatment focuses on always doing what is right for a person’s long-term health, even if it causes dissatisfaction or affects profit margins.
A business that emphasizes ethics and values will ultimately be stronger. People want to participate in an organization that is making a difference. It starts with attracting and retaining the right people as staff members, but it spreads to volunteers, donors, investors and referring physicians, and extends to patients and their families.
Treatment can be profitable, of course, but quality of care comes first.

PERSPECTIVES 8 FALL 2017 BEHAVIORAL HEALTHCARE EXECUTIVE WWW.BEHAVIORAL.NET
Doug Tieman is president and CEO of Caron Treatment Centers.
Join Us! The second annual Treatment Center Executive & Marketing Retreat provides CEOs, marketing/business development, and other executives the tools they need to effectively and ethically grow their services in a rapidly changing market. Join us April 30 - May 2, 2018, in Hilton Head, South Carolina. vendome.swoogo.com/2018-Executive-Marketing-Retreat
We must become patient-centric and focus on long-term health
TIEMAN

I N T R O D U C I N G
THE NUMBERS
DEA reports new drug threats
The opioid crisis continues to outpace all other concerns
BY JULIE MILLER
New national data indicates troubling trends around methamphetamine, cocaine, new psychoactive substances and marijuana, according to the 2017 National Drug Threat Assessment from the Drug Enforcement Administration.
13 % 95.5 %
Percentage of total prescriptions written in the United States that are for controlled substances
12 %
Increase in the percentage of workplace urine drug tests that come back postive for cocaine as recorded between 2015 and 2016
The reported purity level of methamphetamine sampled by DEA in the first half of 2016
80.9 % 40 KG
Percentage of DEA’s field divisions reporting that heroin availability was high in the first half of 2016 (17 out of 21 divisions)
The amount of fentanyl found in March 2016 in a pickup truck in Bartow County, Georgia—the largest recorded amount ever seized
10 FALL 2017 BEHAVIORAL HEALTHCARE EXECUTIVE WWW.BEHAVIORAL.NET
The Black Sheep of Healthcare: Behavioral and Mental Health

Many people do not hesitate to visit a doctor when they suspect they have strep throat, a broken arm, or any other common yet inhibiting illness. Why is it then that there are still many people who refuse to seek treatment for addiction or other mental illnesses? There is still a stigma and perception of vulnerability and weakness when it comes to admitting that one needs this type of healthcare, but part of the reason might be that even those in the healthcare industry see behavioral and mental health as the black sheep of care.
What is causing this “black sheep” image?
Corruption
Dishonest marketing tactics provide insight into dishonest care tactics. “Black hat” marketing, patient brokering, and even hijacking a facility’s name and number to trick potential patients are tactics only tolerated in behavioral and mental health when compared to other types of healthcare.
Limited Resources
Poor or Unenforced Regulations
Yes, there are several strict guidelines and rules that behavioral healthcare professionals need to follow. However, many mental health professionals say that most regulations are only enforced by California and New York. Couple this with insurance denying coverage, and you have billing and admission chaos.
DREAMSCAPE AD
Overcoming a Bad Reputation
The main government resource for mental and behavioral healthcare is the Substance Abuse and Mental Health Services Administration (SAMHSA), and even that is under scrutiny. Luckily, it seems like progress is being made in DC with regards to improving SAMHSA.
A quick trigger for institutionalization and the misguided use of lobotomies and electroshock therapy have given society a frightening (and now fortunately outdated) view of mental healthcare. While we are past these types of careless practices, the mental connection is still there.
These and more perceived slights against behavioral healthcare are being overcome each and every day, but it is up to all mental health professionals to take a good look at what their facilities and colleagues are doing to enforce positive change. There is quality care to be had for those that need it; all we need to do is showcase it in the right way.
For more information on how to provide a better service to those in need, visit: behavioral.net/BH-Black-Sheep
IT’S TIME TO GET THE KIND OF SEO RESULTS YOU NEED.
As a Google Partner and Google AllStar, Dreamscape Marketing is dedicated to helping addiction treatment centers increase their admissions through our industry expertise and leading-edge digital marketing strategies. LET US TAKE YOUR ADDICTION TREATMENT CENTER TO THE NEXT LEVEL OF SUCCESS.
more at https://www.dreamscapemarketing.com/

SPONSORED CONTENT
Learn
NEED TO KNOW
Executives mixed on opioid commission report
The President’s Commission on Combating Drug Addiction released its long-awaited report on November 1 with recommendations on how the nation should fight the opioid crisis. The commission’s report contained 56 strategies that included expanding drug courts to all federal court jurisdictions, making continuous training a requirement for prescribers to be licensed, and mandating prescribers to check prescription drug monitoring databases to ensure patients are not “doctor shopping.”
The commission’s recommendations received mixed reviews from executives in the field. The fowllowing comments are excerpts of statements published by industry leaders following the release of the report:
Mark Dunn, director of public policy, NAATP: “Not only is enforcement [of the Mental Health Parity and Addiction Equity Act] on the list, the commission recommends that monetary penalties be assessed on insurers who fail to comply. A uniform tool to monitor compliance and transparency regarding reasons for denials would also be a very positive development. Better screening by healthcare professionals for substance use disorder would be a substantial step forward in addressing this health crisis as would easier access to appropriate care. Elimination of the IMD 16-bed exclusion for Medicaid patients, which the president has already taken steps to implement, is another positive outcome.”
Chuck Ingoglia, senior vice president, public policy and practice improvement, National Council for Behavioral Health: “While the report recommends some positive steps forward, it starves the country for the real resources it needs to save American lives. In addition to no increased federal spending, the report doesn’t recommend expanding the Excellence in Mental Health and Addiction Act, which would allow more Americans to access comprehensive, coordinated treatment services. Block granting addiction treatment resources may ease some regulations but does nothing toward combatting the opioid epidemic. After all, if there is no treatment available for Americans, how are we going to cure the epidemic?”
Andrew Kessler, principal, Slingshot Solutions: “I was very pleased with the commission’s recommendations on workforce and Medicaid reimbursement. We are in need of a highly trained workforce, and one that can stay on the job at a respectable wage. As Congress and others demand ‘greater access to treatment,’ few have stopped to realize that we are not where we need to be in terms of credentialed, qualified professionals. We need to be in this for the long haul, and if we want the best and the brightest, we must pay for the best and the brightest.”
Gary Mendell, founder and CEO, Shatterproof: “I hope they continue to build off President Trump’s declaration last week, and the commission’s report today, by fully implementing all of their proposed recommendations. They should especially prioritize implementing improved provider education, adoption of the CDC guideline, medication-assisted treatment access and expanded naloxone use. However, today’s recommendations fail to address comprehensive addiction treatment. The country needs a national standard of care for addiction treatment programs.”
B. Douglas Hoey, CEO, National Community Pharmacists Association: “The commission proposed that the relevant federal agencies and pharmacy associations work collaboratively to train pharmacists on best practices for evaluating the legitimacy of opioid prescriptions, as opposed to penalizing pharmacists for denying inappropriate prescriptions. It’s important to assure that remedies implemented through legislation or regulation allow patients with legitimate pain management needs to access appropriate medication. That means that compliance requirements should not overreach so that needful patients are made to suffer.”
recovery 12 FALL 2017 BEHAVIORAL HEALTHCARE EXECUTIVE WWW.BEHAVIORAL.NET
Parity regulations and training requirements lauded, however, lack of additional funding disappoints
BY TOM VALENTINO
A draft of the commission’s full list of 56 recommendations can be viewed here: https://tinyurl.com/OpioidReportNov17



CALL 833-RCA-JOBS www.RecoveryCentersofAmerica.com/Careers JOIN OUR TEAM TODAY! NOW HIRING! As the fastest growing addiction treatment provider in the country our mission is to save 1 million lives one neighborhood at a time. We’re looking for dynamic healthcare professionals who share our passion. Contact us today and together we can make a difference. It’s coming to work everyday knowing you’re making an impact on someone’s life. “ ” Immediate openings for full time & part time DANVERS, MA EARLEVILLE, MD MAYS LANDING, NJ WESTMINSTER, MA Join us in the fight against the opiod epidemic
STAKEHOLDERS HOPE TO HOLD DRUG COMPANIES ACCOUNTABLE FOR THE OPIOID CRISIS
 BY BRIAN ALBRIGHT
BY BRIAN ALBRIGHT
Dozens of lawsuits filed by counties, cities and states against opioid manufacturers aim to hold the big drug companies accountable for the opioid crisis one way or another. The suits, citing fraud and consumer protection laws, have been filed by large cities like Chicago and smaller towns like Bridgeport, Conn.; by states led by Republican and Democratic governors; and from nearly every region of the country.

“Almost all of [the lawsuits] are claiming that the marketing of the products was fraudulent and misrepresented to the general public and to the physician constituency,” says Chip Babcock, an attorney with the Austin, Texas-based law firm Jackson Walker L.L.P.

In Florida, former Representative Gwen Graham has made a potential lawsuit against pharma companies part of her platform as she runs for governor. In other states, people affected by addiction have begun suing drug manufacturers as well as individual physicians. Thirty-six states have also filed an anti-trust lawsuit against the makers of Suboxone (buprenorphine naloxone).
In Ohio, the suit filed by Attorney General Mike DeWine is considered one of the strongest and exemplifies the types of charges made by other claimants. Ohio alleges that drug company efforts to overstate the benefits of prescription opioids while downplaying addiction risks directly led to the current addiction and overdose crisis. The suit claims that the drug companies have triggered a public nuisance under the Ohio Product Liability Act and that marketing practices violated the Ohio Consumer Sales Practices Act, the state’s Medicaid fraud statute and the Corrupt Practices Act.
“The United States is the largest consumer of painkillers by far,” says Matthew Chase, executive director of the National Association of Counties (NACo). “There were aggressive attempts to push out these pharmaceuticals.”
In September, a West Virginia attorney filed to have 66 similar cases consolidated. In addition, 41 state attorneys general have teamed up to investigate drug company marketing and sales practices, issuing subpoenas to Endo, Johnson & Johnson, Allergan, Teva, AmerisourceBergen, Cardinal Health, McKesson and Purdue Pharma. These could be the first steps toward a universal settlement, similar to the $206 billion agreement reach by 46 states and “Big Tobacco” in 1998.
The claimants in most of the prescription-opioid cases want to see an end to what they characterize as aggressive and misleading opioid marketing as well as help in shouldering the enormous cost to states, counties and cities now dealing with rising levels of addiction and overdose deaths. According to a study by the Centers for Disease Control and Prevention’s (CDC’s) National Center for Injury Prevention and Control, the economic burden of overdose, abuse and dependence in the United States topped $78.5 billion in 2013. Even if the Big Tobacco settlement serves as a precedent, communities will continue to wonder if the legal action will make any impact on the opioid crisis.
DECADES OF AGGRESSIVE MARKETING
“This is an epidemic that began in 1996, and the CDC has been very clear about why,” says Andrew Kolodny, MD, co-director of the Opioid Policy Research at the Heller School for Social Policy and Management, and executive director of Physicians for Responsible Opioid Prescribing. “As the medical community began to prescribe opioids more aggressively, the rates of addiction and overdose deaths went up.”
Just as the lawsuits assert, Kolodny says that drug company marketing practices drove a rapid increase in prescriptions.
“The messaging—and most of it came from the drug companies—was that patients were suffering needlessly, the risk of addiction had been overblown, opioids were safe and effective for long-term use, and we should be using them for many more people with pain,” he says.
 Chip Babcock
Andrew Kolodny
Matthew Chase
Chip Babcock
Andrew Kolodny
Matthew Chase
Pharmaceutical manufacturers funded professional societies, specialists within their own speaker’s bureaus and even programs for the Joint Commission in order to push the message that more patients needed lengthier prescriptions for opioids in order to handle pain that had previously been treated using alternative methods.
ANOTHER BIG TOBACCO?
Babcock says that while the scope of the lawsuits and the speed at which they are proliferating are similar to the landmark case against Big Tobacco, there are some details that make the Big Pharma cases unique.
“Tobacco never enjoyed a government endorsement, and in fact, the government actively warned that tobacco was harmful to human health,” Babcock says. “In contrast, the FDA has approved opioid drugs as safe, and highly trained medical professionals have prescribed the drugs for their patients. Because there is a federal regulatory scheme in place, the pharmaceutical companies are claiming that federal law pre-empts the state laws. These consumer protection statutes would have to give way to federal interests in regulating the sale, marketing and supply of drugs.”
In addition to the FDA’s authority providing some defense to pharma companies, there are also other stakeholders in the healthcare system that are culpable. State pharmaceutical boards, distributors, hospitals, large pharmacy chains like CVS and Walgreens, and individual physicians have also played a role, and in some cases have already been held liable and fined by the federal government.
FEW CHANGES
This is not the first time manufacturers have faced off against states over opioids. A decade ago, Purdue was sued over its aggressive marketing of OxyContin, but very little changed after the company settled.
“The settlements weren’t significant enough,” Chase says. “It didn’t change the behavior. In fact, these issues accelerated after that round of litigation.”
In that case, the lawsuits focused on Purdue’s branding of OxyContin as a less-addictive alternative because of its extended release formulation.
“But that was the least of what Purdue did,” Kolodny says. “What caused the epidemic was the campaign to change the culture of opioid prescribing. The settlement didn’t focus on
PLAINTIFFS PILE ON
Below is a list of some of the states that have filed lawsuits against drug manufacturers, distributors and other entities related to the opioid crisis. In addition, a coalition of 41 attorneys general have also issued joint subpoenas. While this list does not include the counties or municipalities that have filed separately, it does reflect the scope of the legal challenges currently underway.
STATES FILING LAWSUITS
• Arizona
• Illinois
• Kentucky*
• Louisiana
• Mississippi
• Missouri
• New Hampshire
• New Jersey
• New Mexico
• Ohio
• Oklahoma
• South Carolina
• Washington
• West Virginia*
• The Cherokee Nation
*Have reached a settlement
what they had really done, so they were able to keep doing it.” Purdue and three executives paid more than $630 million in federal fines, and the executives were convicted of criminal charges. It is estimated that Purdue’s OxyContin business has generated more than $31 billion in revenue.
There are already other settlements in the works, but most of these lawsuits have only been filed within the past few months.
While a settlement might help counties cover the cost of services related to treating a staggering number of individu-
COVER STORY 16 FALL 2017 BEHAVIORAL HEALTHCARE EXECUTIVE WWW.BEHAVIORAL.NET
DOMINION DIAGNOSTICS

Furthering recovery by engaging clinicians in conversations based on analytics, cutting-edge research, and trust
Part of the addiction treatment and recovery community for more than two decades, Dominion Diagnostics delivers the most sophisticated, actionable clinical information to treatment professionals, and supports them with the latest technologies and best education available as they work to improve outcomes.


Learn more about Dominion Diagnostics online at: www.dominiondiagnostics.com | @domdiag
2017 Title Sponsor National Conference on Addiction Disorders
als with opioid addiction—including those who have turned to illegal substances such as heroin—advocates hope to see comprehensive changes as a result of the lawsuits.
“From a county official perspective, these lawsuits are less about money and more about behavioral change,” says Chase. “We’re seeing through our jails, through child protective services and through foster care, dramatic increases in our caseloads. And ultimately we’re seeing huge increases in the workload of our coroners. Our number-one priority is behavioral change around the way these drugs are prescribed.”
Kolodny says the best result might be an end to what he calls the false marketing of opioids as safe and effective for long-term use. For example, Pfizer settled in two instances by agreeing to stop funding advocacy groups that promote the use of opioids.
Chase says counties want to see a change in federal policy that alters incentives for physicians, accelerates education for providers and reaches out to consumers so that they are better aware of the risks of the medication.
“We can reduce demand and change incentives,” Chase says. “That’s really the key, in addition to penalties. If pharmaceutical companies are still making tremendous profits off of this, they are going to keep flooding the market.”
FUNDING TREATMENT
If there are substantial settlement funds available, the experts have a number of ideas for the best use of that money. Treatment is at the top of the list.
“We have a significant backlog and a lack of professional treatment options, particularly in rural areas,” Chase says. “There’s an enormous demand for treatment. As law enforcement officials say, there’s no way we’re going to arrest our way out of this crisis. These pain pills are so addictive that it takes professional abuse counseling to get folks off of them.”
The approach to the crisis should also be smarter.
Eric Sun, MD, PhD, of the Department of anesthesiology, perioperative and pain medicine at the Stanford University School of Medicine, has conducted a number of studies on the distribution of chronic opioid users. According to a recent study his team conducted, three-quarters of all opioid prescriptions are prescribed to 10% of patients, and 59% of all prescriptions go to just 5% of patients. Broad approaches that make it harder for all patients to obtain painkillers penalize some while not effectively addressing the minority

of chronic users.
“Opioids are not effective for long-term treatment of pain with the exception of cancer,” Sun says. “What can we do to address [patients] where they are and reduce what they are taking? That’s a clinical issue, not a legislative one. We can identify those patients and reduce their opioid use.”
Prescriber practices also need to be improved, Kolodny says.
“We are still massively overprescribing,” he says. “Doctors have had this drilled into them for more than a decade that they need to prescribe these drugs more frequently.”
Kolodny also says that there should be funding for programs directed at correcting the misinformation that led to overprescribing in the first place. He advocates for easier access to treatment with buprenorphine, with a payment system that supports that access.
“This case cuts across almost every layer of delivery of medical services,” Babcock says. “It continues to escalate in its expense for states and municipalities in order to take care of people who have now become addicted. It is one of the biggest medical crises outside of tobacco we’ve ever faced.”
And the answers can’t come too soon for most communities.
The Pharmaceutical Research and Manufacturers of America declined to comment on any of the legal actions noted in this article.
Join Us!
The National Rx Drug Abuse & Heroin Summit is where solutions are formulated, stakeholders convene and change begins. Be part of the international discussion on addressing the opioid crisis by attending the 2018 Summit, April 2-5, 2018, in Atlanta.
https://vendome.swoogo.com/2018-rx-summit
COVER STORY 18 FALL 2017 BEHAVIORAL HEALTHCARE EXECUTIVE WWW.BEHAVIORAL.NET
Brian Albright is a freelance writer based in Ohio.
Eric Sun


©2017 Accumedic Computer Systems, Inc.
Talk About AccuMed™ EHR
Automation Modernize and automate your referral process with AccuMed™ EHR Direct Messaging. Harness our cutting-edge technology to enable secure, electronic sharing of continuity of care documentation directly with the client’s treatment team. Take it to the next level and implement secure scheduling so clients can receive their referral and confirmed follow-up appointment, all during the initial visit. Come learn more about AccuMed™ EHR and how IT can work for YOU at www.accumedic.com Learn more about our intelligent EHR (800) 765-9300 | info@accumedic.com | www.accumedic.com
Let’s
& Electronic Referral
of care
“Provide immediate and secure electronic
referrals to promote
continuity
and peace of mind”
Follow-on deals build out portfolios
Investors aim to build a continuum and leverage the platform
Ongoing deal activity in the behavioral health sector indicates its sustained, strong position for investment. In fact, private equity interest is accelerating with an upward trend among add-on deals—the secondary transactions that build the portfolio after the initial platform deal.
“One major driver of growth in healthcare-based investment is the deal after the deal,” says Robert Aprill, analyst with Provident Healthcare Partners, an investment banking firm.
In 2016, there were a record 49 follow-on deals in the behavioral health space, according to data from the Braff Group, a mergers and acquisitions advisory firm. In the past, value was attributed largely to size, but that’s changing.
“Today, as at-risk population health and global payment models continue to gain traction, we are likely to see follow-on deals reflect the needs of payers, accountable care organizations and other contractors as they seek to coordinate care over tighter geographic footprints and across multiple behavioral health subsegments,” says Dexter Braff, president of the Braff Group.
LOWER TRANSACTION VALUE
The multiples in follow-on deals are significantly lower than the original platform investment. According to Tom Schramski, president and managing partner of Vertess, a mergers and acquisitions advisory firm, secondary transactions might involve targets with $5 million to $10 million in annual revenue with adjusted EBITDA of $1 million to $2 million. With add-on deals, it’s not just about scale or revenue.
“What investors are looking for more and more is to build out the continuum of care,” Schramski says.
Although the secondary acquisitions tend to be smaller in scale and sophistication, the acquiring organizations can benefit from the multiple arbitrage, Aprill says.
BY JULIE MILLER
For example, a $100 million business formed from a platform deal might go on to acquire a $10 million business, but the acquired asset is instantly worth more because it gains the added scale and other strategic advantages already established in the portfolio. Advantages might include the platform’s existing payer contracts or its technology backbone, for example.
“You might be able to generate higher profits from that business just from leveraging the size and scale of the larger platform,” Aprill says. “It’s no longer a smaller group. It’s now worth more.”
SELLING POINTS
There are a number of assets that investors might look for in follow-on deals. Quality and clinical alignment remain first and foremost, of course, but beyond that, investors are primarily seeking transactions that will fill the gaps in their portfolios. It’s particularly true in the addiction treatment space.
“For example, there are a lot of providers that don’t have medication assisted treatment,” says Schramski. “But they’re looking for that now because it gives them a strong advantage, especially if they’re in-network because they’ll get more referrals if they have a more complete opportunity for people to get treatment.”
He says detox is another attractive target right now because many organizations don’t offer the service and because it represents the front end of the treatment model where many patients first connect with care services. The initial contact is valuable because of the potential to serve that patient long-term through the full continuum.
Behavioral health secondary deals can also add competencies with new service lines, such as treatment of co-occurring disorders, says Chris Rogers, managing director at Ziegler, a specialty investment bank. Creating an ecosystem within be-
20 FALL 2017 BEHAVIORAL HEALTHCARE EXECUTIVE WWW.BEHAVIORAL.NET MANAGEMENT
havioral health will position an organization to move toward the new accountable-care models of reimbursement.
“To improve patient care, you’re seeing a more holistic approach,” Rogers says. “It’s an offensive move in terms of inpatient care but a defensive move to prove to payers that outcomes are trackable and are improving under the care model the company’s implementing, which will impact how reimbursement discussions go with payers.”
Integration with the health system at large will be the most significant challenge for the future. An organization that is able to integrate behavioral health with primary care would have a strong competitive advantage to leverage with payers, Schramski says.
INVESTMENT FOR GROWTH
Most investment groups are looking to grow and diversify by entering new geographic areas and reaching additional patient populations.
“Generally those investments are well thought out in terms of geographic expansion and what areas in the region make sense,” Aprill says. “And maybe it’s more conducive and financially beneficial to the partnership to acquire a practice instead of building a de novo location.”
For example, he says, a provider that delivers at-home autism services might want to grow by establishing brick-and-mortar treatment centers. Rather than building from the ground up, acquiring a network of centers might make more sense financially.
When considering today’s reimbursement landscape, followon deals might bring along an opportunity to leverage the organization’s payer mix as well.
In residential addiction treatment, self-pay has been the dominant structure, but increasingly, more organizations are making the leap to in-network commercial insurance contracts because they see the model as a necessity in the new era of healthcare delivery. An add-on deal could be a viable opportunity to gain or expand in-network capabilities, and experts say that in-network status has become more desirable in the past five years among financial buyers looking for acquisition targets.
However, once a platform has secured in-network status, an add-on that is only self-pay could be brought into the model more easily, says Michael Fassett, analyst with Provident Partners.
“You utilize the payer contracts from the platform’s perspective and apply those to the add-on acquisition for immediate synergy,” Fassett says. “And in behavioral health, by integrating
with the platform group, you can be more efficient.”
He says the time required to collect payment from patients or from payer contracts can be reduced as an organization builds scale.
PATIENT SUBPOPULATIONS
A follow-on deal could bring along with it a new patient subpopulation. For example, the adolescent addiction treatment market is highly fragmented with few platform-sized organizations, Schramski says. And the therapeutic approach to treating that subpopulation needs to be distinctly different and individualized.
“If you have a decent adolescent program with good clinical fidelity, you’re going to be attractive,” he says.
Other emerging subpopulations might include older adults with alcohol use disorders—a market for which there is increasing and unrecognized demand. Many seniors are enrolled in Medicare Advantage plans, which are delivered by commercial managed care organizations and include more services than traditional Medicare.
Finally, experts note that behavioral healthcare executives themselves can be assets in platform deals as well as followon deals. A strong leadership team is invaluable to investors because they will rely on the leaders’ industry experience to evaluate potential acquisition targets, identify like-minded clinical philosophies and to contribute to the enterprise growth strategy moving forward.
“Talent gets you through times that money can’t,” says Schramski. “Financial buyers put a premium on that.”
Julie Miller is Editor in Chief of Behavioral Healthcare Executive.
Join Us!
The third annual Treatment Center Investment & Valuation Retreat brings together owners and senior executives from the addiction treatment and recovery community to meet with key members of the investment and financial community for an exclusive three-day educational, business and networking event, December 4--6, 2017, in Scottsdale, Arizona.
https://vendome.swoogo.com/TCIV-2017
MANAGEMENT WWW.BEHAVIORAL.NET 21
Follow best practices in accreditation
Preparation for site visits and surveys will serve you well
The four accrediting bodies in behavioral healthcare have different standards and measure different things. However, there are some similarities when it comes to the site visit or survey portion of the process.
CHOOSE THE BEST TIMING
Decide when you want to be accredited, and then make sure you use the time well, says Carl Noyes, CEO of Retrospect Consulting Group and lead behavioral healthcare surveyor for the Accreditation Commission for Health Care (ACHC), who has been doing behavioral health surveys for 35 years. If you need to be accredited by a certain date, for example, you are going to need to plan ahead. It takes months before the site visit takes place, so don’t procrastinate.
“Agencies that don’t leave enough time to prepare often find themselves rushed,” says Noyes. After the site visit, it takes months before the accreditation actually takes place.
2STUDY UP ON THE APPLICATION
Some organizations actually start to write new policies and procedures before they even know what the accreditation measures call for, says Noyes. The self-study, which all the accrediting bodies require, is essential. Use the self-study time, which is typically six to nine months, to assess your practices and align them with the standards, says the COA’s Kerry Deas, quality improvement manager for the Council on Accreditation (COA). “If you put all of that time in up front, then you usually don’t have much to do after the site visit,” Deas says.
BY ALISON KNOPF
PICK YOUR DOCUMENT GATEKEEPER
Someone on staff must be in charge of the final approval of all documents that are presented in the site study. This needs to be one person, not a committee, who reviews the materials for compliance with the accreditor but also with state and federal rules. 4
MAINTAIN A SINGLE MANUAL
Some organizations have one policy manual for accreditation and a separate one for state and federal policies. Your policies and procedures should be compiled in one manual, says Noyes. Don’t waste your money on templated manuals, either.
“I’ve seen providers spend an inordinate amount of money on a template accreditation policy manual and pull it off the shelf on the day surveyors come,” says Noyes. “It’s very obvious, and any experienced surveyor will ask if there is one set or two sets of manuals. It doesn’t show the agency in the best light, and frankly, it’s a liability. You can see a staffer doing what they think is the appropriate thing, and then something goes wrong, and it comes out that there are two policy manuals.” 5
TAKE THE HIGH ROAD
It’s not unusual to identify conflicts between state rules and accreditation rules, but experts recommend that treatment centers always aim to comply with the strictest standards to ensure full compliance. For example, ACHC requires a supportive employment specialist be including on an ACT (Assertive Community Treatment) team, but some states don’t have this require-
22 FALL 2017 BEHAVIORAL HEALTHCARE EXECUTIVE WWW.BEHAVIORAL.NET MANAGEMENT
3
1
ment. ACT teams work with individuals with serious mental illness. One of the ways to help them stay in recovery is to help them find employment, for example, says Noyes.
APPOINT A SURVEYOR LIAISON
Your liaison can be someone on staff or an outside consultant, but it should be someone who is well versed on the standards of the accrediting organization. That person should have sufficient rank in the organization to be able to motivate employees to get things done.
TAKE NOTES
7
Peter Vance, LPCC, CPHQ, field director for survey management and development in accreditation and certification operations for the Joint Commission, recommends that organizations assign a scribe to follow the surveyor, taking notes. This gives the program the opportunity to have an internal person who is keeping track and monitoring everything that’s being said and done.
“There are lots of things discussed through the survey process that may not show up on the report, but are good as consultative material,” Vance says.
He recommends that the scribe use an old-fashioned paper and pencil method for notes. “We don’t encouraging recording, because we’ll be interacting with clients,” he says.
CONDUCT A MOCK SURVEY
8
You can prepare a trial run by bringing an expert on site who might see details your leadership has overlooked. The best time to do this is six months before the real survey. “This will allow time for the provider to make any necessary changes,” Noyes says.
9
REMEMBER THAT COMPLIANCE TIME VARIES
CARF requires six months of compliance for all applicants. The Joint Commission requires that applicants have certain benchmarks met on the day of the survey. ACHC assigns a “readiness date,” at which time the organization must be in compliance. For example, let’s say you applied to become ACHC accredited in January, and you aim for June 1 to be full compliance. Any admission, staff hire or process must be in compliance from that date going forward.
PRESENT YOUR MATERIAL STRATEGICALLY
Surveyors will expect your materials to be presented in an organized fashion rather than as a heap of binders with an excess of information.
“It comes off as desperation, as if you don’t know what you really want,” says Noyes. “A much better practice is to take your comprehensive manual, create another column, and crosswalk it to standards.”
The documents should be bound and indexed. Also, appoint a knowledgeable staff person who can find and explain documents as needed. Deas of COA notes that reviewers will ask for additional documents during the site visit, beyond what is included in the self-assessment. Documents can be electronic or in paper format, says Deas says, but the main point is that you must clearly label how your documents correspond to standards.
DON’T CHERRY-PICK
Surveyors are aware of the motivation to present your organization in the best light, but cherry picking patient records for review will not be successful.
“Often organizations try to find a ‘best record’ to review,” says the Joint Commission’s Vance. “That’s not necessary. We want to see samples of all the records.”
He says the purpose of accreditation isn’t to score well as much as it is an opportunity to find areas where you can improve.
Noyes says he might ask for records created by recent hires and several created by longtime staff. He will also ask for a list of all clients admitted in the last three months and choose several of those at random.
“We recognize that some staff are better at writing treatment plans than others,” he says. “Some are better at working with clients than others, but everyone should meet a list of minimal standards.”
CARF surveyors additionally talk to the client served, according to Brian J. Boon, PhD, president and CEO of CARF.
“We ask them to tell us about their experience and what orientation was like,” he says. “We may talk to family members. We talk to referral sources. The file is just one data point.”
WWW.BEHAVIORAL.NET 23 10
11
6
It all started with one One Agency that knew there had to be a better way
One Agency that knew technology could be a resource, an ally, a simplifier.
One Agency Partnering with One visionary young company.
Both committed to increasing the Quality of Care and Life for all in Behavioral Health
Seventeen years later, One Partner Agency in One State is now over 300 and One, in 30 one states.
Credible thanks each and every one of our Partner Agencies for their service and commitment.
C Credible drives each and every one of our Partner Agencies to further leverage technology
Credible encourages our Partners to join together to push the bounds of collaboration and cooperation to new levels.
Credible is proud to Partner with so many quality Agencies from coast to coast
The Power of One, delivering Benefits to Many.
There is room for more.
In June of 2000, Credible Behavioral Health started for one reason:
U Use technology to improve the quality of care 17 years and 350+ Agencies later,
Credible is the first Enterprise SaaS company delivering fast, secure, clinical, billing, mobile, reporting, and data mining functionality. And Credible delivers software efficiently while implementing in as little as 4.5 months.
Credible delivers real, tangible benefits to our Partner Agencies:
l A proven, reliable, secure and easy to use web-based solution
l Monthly innovation, real state-specific service, live phone help

l An independent, financially strong, lasting company; founder owned and founder run
l Mission-based and built to stay that way
301.652.9500 | partnership@credibleinc.com | credibleinc.com
The Power of One. The Benefits to Many. Now It ’s Your Turn!
AIM FOR CONTINUOUS IMPROVEMENT
The purpose of accreditation is to improve your service, not just to get a gold star or to facilitate third-party reimbursement. Look at the site visit and the entire survey process as a way to make your services better for patients.

For example, CARF’s reviewers are all peers, which means that they work in behavioral health organizations that serve the similar populations.
“That’s why the orientation of accreditation from our perspective is quality improvement,” says Boon. “Yes, you have to have your package prepared. But you also have to be open for conversation and for improvement.”
DON’T SKIMP ON DATA METRICS

How do you use your data? It should be to improve services, results and outcomes. Most organizations struggle with this because data analysis is labor
intensive, says Boon. He recognizes that in treating chronic mental illness and substance use disorders, good outcomes may not necessarily equate to full recovery. Reduced hospitalizations, clients’ maintaining engagement in social support systems and adhering to medication regimens can be considered in the outcomes measures.
BE HONEST
When the reviewers come to your site, tell them the truth, even if it doesn’t seem to paint your organization in the best light because the surveyors want to drive accreditation success.
“If a procedure isn’t quite meeting the standard, or if you don’t have an element at all, it helps to be honest with your reviewers,” says the COA’s David Haynik, LMSW, director of quality improvement. “If you hide the fact that evidence is lacking, you’re closing off communication with that group of reviewers.”
Accreditors’ goal is different than that of regulatory or compliance entities, such as state or federal agencies, Vance says. Accreditors aim to partner and work with an organization to identify a risk, which requires trust.
NO WINING AND DINING
In general, organizations can have snacks, water, coffee or food for a working lunch, but there are boundaries. Don’t offer surveyors dinner out or offer them “welcome baskets.” COA would actually prefer that organizations not pay for lunch, especially if it could be perceived as valuable and as “trying to persuade,” says Haynik.
And Vance of the Joint Commission says not to be disappointed if the reviewers opt not to join you for a working lunch. “The surveyor may politely decline because they want to do a working lunch on their own,” he says. Alison Knopf is a freelance writer based in New York.
MANAGEMENT 26 FALL 2017 BEHAVIORAL HEALTHCARE EXECUTIVE WWW.BEHAVIORAL.NET 12
13
14
15
THE COMPLAINT PROCESS
All four accrediting organizations have a complaint process for patients/clients/consumers and staff (because staff need to be able to report complaints as well). Most offer a toll-free number that is posted prominently in the facility.


“We will investigate immediately anything that could cause imminent danger,” says Carl Noyes, surveyor for the Accreditation Commission for Health Care (ACHC).
Complaints can also be an unplanned part of a survey. A month before the CARF survey, a notice is posted with the date of the visit so patients can talk to surveyors directly.
Joint Commission standards require that programs have complaint procedures posted, but there is a separate process for complaints presented directly to surveyors, says Peter Vance, LPCC, CPHQ, field director for the Joint Commission. “If it’s beyond the actual survey, we have another program that would follow up with that. We interact with them during the site visit as well,” he says
In general, accrediting organizations urge patients to talk to the organization to resolve their complaints, but sometimes patients are fearful, says Brian J. Boon, PhD, president and CEO of CARF. CARF might also suggest they go to the local advocacy or protection agency in the state to resolve the problem. The bottom line is that the organization’s accreditation at risk. “One of the commitments of being CARF accredited is that you are focused on the persons served,” says Boon.
The president/CEO of COA handles all consumer complaints personally. Consumers can call or report on the website. Having an internal grievance process is part of being a good human services organization. “Many times when we receive those complaints, we start by going back to the organization to make sure that they have their own internal process,” says Kerry Deas, quality improvement manager for COA.
Unfortunately, consumers of behavioral health services might be viewed as difficult populations, more likely to make unfounded complaints. “I can’t think of an example where any complaints were the result of a deteriorating mental health condition,” says COA’s David Haynik, LMSW. “I have a clinical background, and we have a lot of social workers here.” All complaints should be taken seriously, he says.
POWER of FURNITURE Designed for Behavioral Health.

S afety is a primar y concern for all BHC organizations. Furniture designed and built for the unique needs of behavioral healthc are is an impor tant component of risk management to ensure the safet y of patients, visitors and staff.
Furniture and components can be used as weapons or to inflic t self-harm. Therefore, the right furniture designed specifically for behavioral healthcare and psychiatric environments is crucial to successful therapies and treatments.
Eliminating furniture and fixtures that can be broken in to shards, and used as weapons, preventing contraband and eliminating ligature points are tall orders but necessar y for the best patient results.
Some considerations for Secure Furniture are:
1. Anti- Contraband Bedroom: allows patients or residents to have private time while allowing staff easy inspec tion for contraband items. The anti- contraband design replaces drawers and doors with finished, open spaces Open shelving also prevents small, break able par ts like drawer boxes, drawer fronts and hardware.

2. Metal Furniture: (aka steel furniture) gives your facility a sleek, modern look without sacrificing on toughness. High- qualit y metal furniture is resistant to chemic al treatments and easily cleanable.
Metal furniture is also great for the prevention of bed bugs and other pests

3. Molded Furniture: is design for increased

strength Molded plastic lounge chairs, beds, desks and tables are available with bolt- down or weight- down options It c an handle high levels of use and abuse, but also has fewer crevices so it can be trusted to help reduce bed bug concerns. It can also be easily cleaned.
Residential st yle furniture is t ypically the first choice bec ause feeling like “ home” provides therapeutic suppor t through offering patients a comfor table environment where they will be more willing to par ticipate in healing. Sterile, institutionlike furnishings c an be a distrac tion to patients and can prevent healing. For tunately, there are solutions that deliver both safety and residential styling.
The Right Furniture plays a vital role for Behavioral HealthCare Facilities. The right furniture can help your facility look like a place where people can heal.
Contac t Furniture Concepts today to talk to a furniture exper t about investing in the right furniture for your patients.
800 969 4100 info@furnitureconcepts.com
WWW.BEHAVIORAL.NET 27 ® FURNITURE CONCEPTS Home of TOUGH STUFF!
w w
l l
w.furnitureconcepts.com
T H E B.H._Advertorial_Fall_ 2017 furniture Concepts.qxp_Layout 1 10/30/17 8:42 AM Page 1
Would commitmentinvoluntary save lives?
Interest in civil commitment for addiction grows, but hurdles could impede implementation
BY JILL SEDERSTROM
As the opioid crisis continues to grow, the possibility of involuntary commitment for overdose patients is gaining more attention from advocates who see it as a necessary tool in the battle to save lives. However, many experts also acknowledge that there are significant legal and practical issues that still need to be addressed before the controversial strategy could be fully effective.
Involuntary commitment for patients with mental health concerns is a wellestablished practice in many states across the country, but using similar laws to force people with addiction disorders—who are outside the criminal court system—into substance use treatment is a much newer concept.
Many, like Charlotte Wethington, see the such a move as a powerful option to help patients who have either overdosed, so they might get the help they need to survive. Wethington, who lost her son Casey to an overdose in 2002, helped create Casey’s Law in Kentucky in 2004. The law gives parents, friends or relatives a pathway to intervene and get a patient into involuntary treatment for substance use disorders for a period of up to 360 days.
“The bottom line is you have to be
alive to recover,” she says. “So, if recovery is our ultimate goal, then we need to use all the tools that we have in our toolbox to make that happen...or at least to facilitate that happening.”
An increasing number of state officials, parents and law enforcement officers have expressed interest in creating similar laws in other states.
“It’s certainly an area of great interest,” says Sherry L. Green, chief executive officer of the National Alliance for Model State Drug Law. “We’ve received a number of requests, including from some governors and drug policy directors, to look into the possibility of drafting language for an effective civil involuntary commitment law.”
According to Green, more than half of all states that have some process written into existing laws that would allow for civil commitment; however, in some states, healthcare professionals, parents and loved ones are not aware such laws exist.
Green says this lack of knowledge is a sign that many of the laws are not being used consistently.
“A lot of states started with involuntary commitment under mental health, and that’s fairly well fleshed out at the state levels. Those mental health commitment laws tend to be used extensively, and then when they were broadened to include substance use disorders, that’s less consistent and less used,” she says.
GETTING HELP TO THOSE IN NEED
Residents in the state of Florida have access to the Hal S. Marchman Alcohol and Other Drug Services Act of 1993 (Marchman Act). Under this law, someone with direct knowledge of another person’s substance misuse is able to petition the court
CLINICAL TRENDS 28 FALL 2017 BEHAVIORAL HEALTHCARE EXECUTIVE WWW.BEHAVIORAL.NET
to intervene in a two-step process.
Mark Astor, JD, founder of Drug and Alcohol Attorneys in Boca Raton, Fla., says the first step is petitioning the court to have the individual involuntarily assessed for treatment. This can be done on an ex-parte basis, meaning the subject of the filing doesn’t have to be aware of the proceedings. If the assessment is granted, the sheriff’s department collects the individual and brings him or her in for assessment on a five-day hold at a treatment facility of the petitioner’s choosing.
After that, a second petition is filed to secure involuntary treatment for the individual for a period of up to 90 days, although Astor says the treatment can be extended twice if necessary. There is also a hearing, he says, adding that the individual is entitled to contest the filing and have their own counsel.
Astor sees the law as a benefit in Florida, particularly because of the large number of people who come from out-of-state for treatment, often leaving family and friends many miles away.
“The Marchman Act at least enables the family to run to the courthouse and say, ‘Judge, my kid walked out of treatment,’ and can initiate something,” he says. “I think it’s a safety net for families.”
But while Astor notes the law’s advantages, he says it is not utilized nearly enough in Florida. There continues to be a lack of knowledge among treatment centers, parents and even emergency medical personnel about the law and its potential to initiate people into what could be life-saving treatment.
LEGAL AND PRACTICAL CHALLENGES
The involuntary commitment laws face logistical hurdles as well. Jessica Hulsey Nickel, president and chief executive officer of the Addiction Policy Forum, says communities that institute such laws need to ensure they have enough providers to serve patient needs.
“How well this works really does depend on having treatment capacity available,” she says.
Many state officials, Green says, are already struggling to find enough beds for those patients who actively want help for their addiction and are ready for treatment.
“They feel like they can’t really prioritize reserving treatment beds for people who don’t really want to be there in the first place,” she says.
There’s not only a need to increase the number of treatment centers overall, but many of those facilities would also need to be secured to ensure the safety and treatment efficacy of
involuntary commitment patients.
“If you are committing someone to an unsecured facility, and because it’s involuntary and you don’t have any means of actually keeping them there, they can just walk out,” Green says.
Massachusetts, which allows for civil commitment under what’s known as section 35, solved this problem by creating several locked commitment facilities.
Massachusetts Gov. Charlie Baker, who also sits on the White House opioid commission, wanted to go a step further by requiring patients who were taken to the emergency room after overdosing to be involuntarily held for up to 72 hours. However, the policy was met with controversy and ultimately failed.
Raymond V. Tamasi, president and founder of Gosnold on Cape Cod—The Innovation Center, says even with the existing section 35 guidance, such commitments aren’t simple.
“It’s only available during certain times when the court is in session, so it really is a little bit awkward and cumbersome,” Tamasi says.
Green says one of the legal challenges with involuntary commitment laws is determining what level of deterioration or addiction a person has to demonstrate to warrant being involuntarily sent to treatment.
“If you look at the common reasons under involuntary commitment laws and why you can successfully commit someone involuntarily, you find it’s because they are a danger to themselves or others, or they lack the ability to basically care for themselves,” she says.
However, what that means for people with a substance use disorder and what specific evidence is necessary to prove that criteria has not been fully fleshed out yet in the courts.
“At what point in the deterioration of addiction are we going to say, ‘This person fits this criteria,’” Green says.
For that reason, much of the focus has been on individuals who have survived overdoses.
THE ROLE FOR TREATMENT CENTERS
Within states that do have involuntary commitment laws in place, experts say, many treatment centers and medical centers don’t fully understand these laws or highlight their potential use with the loved ones of prospective clients. Therefore, they avoid leveraging the policies.
Attorneys who specialize in the addiction field can assist treatment centers as they explore the concept. Astor says he is willing to work with treatment centers as a free resource and
WWW.BEHAVIORAL.NET 29
to offer consultations to help clients understand what information they need to secure an involuntary commitment in the state of Florida.
Controversy remains among medical professionals, addiction specialists and state officials about whether the benefits of involuntary commitment outweigh the harms of impeding on civil liberty.

“I believe personally that this is a tool that some families in the community definitely need when someone is in crisis and is in harm’s way,” Hulsey Nickel says.
Others, such Tamasi, question whether treatment centers can adopt other proactive strategies to help patients get into treatment that don’t have the controversy of involuntary commitment. Gosnold has begun partnering with hospitals and local law enforcement to place addiction professionals at the sites where individuals with substance use disorders might interact with community service personnel. For example, staff members might do ride-alongs with police or speak to patients
in emergency rooms.
The strategies, he says, have been effective, with an estimated seven out of 10 potential patients approached agreeing to begin treatment.
“Obviously you need a little bit of everything,” Tamasi says. “And we need to step outside of the box and do as many things as we possibly can. I’ve always been struck by the fact that treatment centers pretty much wait. The whole system of addiction treatment is built around someone getting to the point where they’re so desperate, they absolutely have to place that call. And that’s just not the way.”
CLINICAL TRENDS 30 FALL 2017 BEHAVIORAL HEALTHCARE EXECUTIVE WWW.BEHAVIORAL.NET
is a freelance writer based in
REPLACE YOUR BEAT UP BOOTH USING OUR $500 CREDIT AS PART OF OUR FALL PROMOTION | CALL US AT (877) 958-9180 OR VISIT WWW.DREAMSCAPEMARKETING.COM FOR MORE INFORMATION DISCOUNTED TRADESHOW BOOTH & DIGITAL DISPLAYS FOR 2018
Jill Sederstrom
Kansas.
At Work in Behavioral Health Centers
“There’s
team.”
According to a recent survey by Coleman Parkes on behalf of the Workforce Institute at Kronos, only 10% of respondents rated employee engagement as “very strong,” and only 21% said the same about employee productivity. While some turn their attention to human resources, 71% of HR managers state incompatible workforce systems as their biggest challenge.
Workforce management has become an exercise in corralling paperwork, struggling with compliance, and untangling red tape. While all these aspects are of extreme importance to behavioral healthcare centers, they become cumbersome and begin to affect the quality of patient care as well as the happiness and engagement of employees.
“We’re more tangled up in compliance and legislation in our industry, and I think that makes a difference.”


To alleviate these issues and free providers to take care of patients, behavioral health centers are implementing workforce management automation and other solutions. Two major benefits of workforce management automation are improved employee engagement and better business performance. For example, automated payroll processes can eliminate human error, minimize internal inflation, and ensure accurate paychecks, the last of which helps keep employees happy and less concerned with the week-to-week minutiae.
KRONOS, INC. AD
EMPLOYEE
ENGAGEMENT FOR HEALTHCARE:
Increase productivity, improve patient care, and retain a collaborative, high-quality workforce
INDUSTRY INSIGHT
This information provided by Kronos can highlight analytics that may improve workforce management, employee engagement, and patient happiness by streamlining processes that currently bog down behavioral healthcare centers.
For more information on how to:
• Improve workforce productivity
• Deliver high-quality, cost-effective care
• Minimize compliance risk

• Drive workforce engagement
Visit behavioral.net/workforce-management
To find out how advanced, clinically-focused workforce solutions can help your healthcare organization manage costs, improve productivity, manage compliance, and engage employees, visit www.kronos.com/healthcare
- Sponsored Content -
INDUSTRY INSIGHT
“There’s a requirement to do more administrative work. You might have less support or a smaller
a lack of connection at an everyday level. I think [HR] should really be focusing on the health and well-being of the workforce.”
Assess comorbidities in brain injury cases
Addiction and suicide risk must be examined
In 2013, there were 282,000 hospitalizations related to traumatic brain injury (TBI) and 56,000 deaths, according to the Centers for Disease Control and Prevention (CDC). What’s unique about the injury is that the symptoms can often be misdiagnosed as behavioral health issues, while at the same time, TBI patients are at risk for comorbid depression and addiction disorders.
Clinicians might equate sports participation or military enlistment with TBI, but other populations can experience risk. For example, while 8.5% of the population overall reports TBI, the prevalence among those incarcerated has been reported as high as 87%, according to CDC.
“About 1.7 million people in the United States have traumatic brain injury, and about 80% of those are thought to be mild,” says Nicholas DePrima, PsyD, a psychologist and neuropsychologist at Palm Beach Neuroscience Institute and St. Mary's Medical Center. “But keep in mind that information is often collected in emergency rooms, so it might be an underestimation because some people might present with symptoms later on.”
Life expectancy for those with TBI is about nine years lower than the overall life expectancy.
When considering risks, the behavioral health of a TBI patient must be evaluated both as a symptom of the injury and as a pre-existing condition. Some estimates indicate as many as half of the individuals with brain injury have some history of substance use disorder, and about 30% of brain injuries occur while under the influence of alcohol or substances, DePrima says. In addition, clinical teams must evaluate patients for attention deficit, learning disabilities, depression, stress and suicide.
“Being under the influence can affect your balance, and falls can certainly lead to brain injury,” DePrima says. “Motor vehicle accidents can lead to brain injury, and being under the
BY JULIE MILLER
influence increases that risk. And when someone is under the influence, they might engage in violent behaviors.”
Among those presenting in the hospital for brain injury, about three-fourths have alcohol in their systems at the time, according to SAMHSA. Additionally, substance misuse is associated with recurrent TBI.
According to DePrima, most brain injuries are temporary, with recovery times of weeks or months. However, the prevailing idea of a long rest after a concussion has been updated by experts, who now indicate that a briefer rest time of one to two days is often sufficient for most cases, followed by a gradual return to normal activity without exacerbating the head injury.
“Traditionally, you rest, rest, rest,” DePrima says. “But if you rest too much, you’re lying around inactive, which can increase depression, anxiety and sleep symptoms.”
The increased symptoms can be confused with symptoms from the initial head injury, he says. And comorbid conditions can make assessment even more challenging, so it’s imperative for clinicians to monitor recovery as well as providing the diagnosis.
Those with pre-existing substance misuse history are at risk to re-engage in substance use after a head injury to cope with pain, disability or emotional difficulties. It makes sense because the frontal lobe of the brain could be affected by the injury and impair judgment, resulting in risky or impulsive behavior. DePrima says lack of support or psychosocial factors could drive additional risk for brain injury patients with behavioral health disorders.
CLINICAL TRENDS 32 FALL 2017 BEHAVIORAL HEALTHCARE EXECUTIVE WWW.BEHAVIORAL.NET
Julie Miller is Editor in Chief of Behavioral Healthcare Executive.


WHERE ARE YOU HEADED? WHY? WE’RE READY TO HELP. VERTESS PROVIDES: M + A advisory services to healthcare and human service organizations Strategic consultation for healthcare leaders looking to build remarkable value Market insights that could make the difference between surviving and thriving VERTESS is a healthcare merger + acquisition and consultation firm with a strong track record in addictions treatment and behavioral healthcare. Our team members have extensive clinical experience with demonstrated results in helping executives build value in their companies, including nonprofit organizations. Our credentialed Managing Directors have each launched, built, and successfully exited their own companies, giving us a unique perspective in diverse areas of healthcare, including addictions treatment services. LET’S GET STARTED VERTESS.COM Canoeing at Vinland’s main campus in Loretto, Minnesota Vinland Center provides drug and alcohol treatment for adults with cognitive disabilities. We make all possible accommodations for cognitive deficits and individual learning styles. Located in Loretto, Minnesota — just 20 miles west of Minneapolis. 866.956.7612 • VinlandCenter.org
The Institute is a trusted educational resource that helps address daily challenges. Our conferences convene thought leaders that share clinical best practices, discuss how to effectively and ef ciently operate a behavioral healthcare organization, and strategize solutions for addressing the opioid epidemic. Join us at an upcoming event to network with peers and take home valuable tools. Learn more about us and how we can help you at www. iadvancebehavioralhealthcare.com.
National Events

APRIL 2-5, 2018 | ATLANTA, GA
Be part of the discussion at the largest national gathering of stakeholders working together to address the opioid crisis. Prevention, treatment, law enforcement, public health, and many others exchange best practices and hear from state and federal of cials at the annual Rx Summit.
www.nationalrxdrugabusesummit.org
AUGUST 19-22, 2018 | DISNEYLAND, CA
CE Credits
Addiction professionals annually convene at NCAD to share what’s working: Clinicians hear from thought leaders on delivering treatment, while executives of behavioral healthcare organizations learn how to run more effective, more ef cient, and ethically minded businesses.
www.ncadcon.com

DECEMBER 4-6, 2017 | SCOTTSDALE, AZ
Senior executives of treatment centers, and those investing in these enterprises, discuss growth strategies and market dynamics at this exclusive, three-day educational and networking event.
www.treatmentcenterretreat.com
APRIL 30-MAY 2, 2018 | HILTON HEAD, SC
TCEM provides CEOs, CFOs, COOs, directors, senior marketing/business development/ admissions leaders, and other executives with the tools they need to effectively and ethically grow their services in a rapidly changing market.
www.executiveandmarketingretreat.com
Interested in attending an event? Contact Ellen Kelley at ekelley@iabhc.com or 216-373-1223.
Photography: Pete Winkel GPA
President Obama addressed Institute attendees in 2016.
Matt Bevin, Governor of Kentucky addressed Institute attendees in 2017.
CME and CE Credits
Events
National-Regional Events
CE Credits
The Summits for Clinical Excellence bring together thought leaders on cutting-edge topics in multi-day national and regional conferences. Summits on mindfulness, trauma, process addiction, and shame appeal particularly to private practice behavioral healthcare professionals. Other Summits address the national opioid crisis from a regional perspective and engage a diverse group of stakeholders. Many Summits offer treatment ethics continuing education credits.
• NEW ENGLAND November 2-3, 2017
The Opioid Crisis: Strategies for Treatment and Recovery www.iabhc.com/newengland2017

• PHOENIX, AZ February 14-16, 2018
The Opioid Crisis: The Clinician’s Role and Treatment Practices - Featuring the 2nd Annual Arizona Opioid Summit
www.arizonaopioidsummit.com
• ORANGE COUNTY, CA March 1-2, 2018
East Meets West: Multiple Perspectives on Trauma and Addictions
www.iabhc.com/orangecounty2018
• CHICAGO, IL March 7-8, 2018
The Opioid Crisis: Strategies for Treatment and Recovery www.chicagoopioidsummit.com
• CHICAGO, IL March 7-10, 2018
The National Conference on Trauma, Addictions, and Mindfulness: Where Freud Meets Buddha www.iabhc.com/chicago2018
• PITTSBURGH, PA June 25-26, 2018
The Opioid Crisis: The Clinician’s Role and Treatment Practices www.pittsburghopioidsummit.com
• ATLANTA, GA October 17-20, 2018
Brain Matters: Shame, Trauma, and Process Addictions
www.iabhc.com/atlanta2018
Local Events
CE Credits
Virtual Events
WEBINARS
The National Conference on Addiction Disorders convenes panel discussions across the country in a lunch’n’learn format. Clinicians hear about treatment practices, while those on the business side of the field share strategies for managing and marketing behavioral healthcare organizations. www.iabhc.com/local
Upcoming events:
Hear from experts on clinical, managerial, and other topics in our frequent, free-to-attend Webinars. www.iabhc.com/webinars
CE Credits
Contact Ellen Kelley at ekelley@iabhc.com or 216-373-1223.
Interested in attending an event?
Baltimore
Boston Charlotte Chicago Dallas Denver Detroit King
Long Island Memphis Minneapolis Nashville New Orleans Orange County Phoenix Pittsburgh Providence
Lake City
Diego
Francisco
DC
Boca Raton
of Prussia
Salt
San
San
Washington,
2017 IT
S YEVRU
BY TOM VALENTINO
2017 IT VENDOR SURVEY
n increasing number of information technology vendors are partnering with residential care providers, and based on their responses in Behavioral Healthcare Executive ’s Information Technology Vendor Survey, it’s a trend that is projected to continue heading into 2018. Representatives from 69 IT firms participated in the seventh annual survey, with 95.6% indicating their organization currently works with outpatient providers. Meanwhile, 21.2% said residential care is the area they are most likely to expand, an increase of nearly 9% compared to last year, the largest jump of any of the available choices.
Two other notable takeaways from this year’s survey:
• Fine-tuning existing offerings has overtaken breaking new ground for IT vendors. This year, upgrading existing products and services was identified by 39.7% of respondents as their top priority for 2018, overtaking research and development of new products and services, which was the most popular response last year.
• Slightly more vendors (26.9% in 2017, compared to 23% in 2016) believe providers are prepared for the transition to a value-based payment model, but the majority (52.2%) still say providers are not ready.
The BHE Information Technology Vendor Survey includes snapshots of each participating organization. A full database of survey responses, which includes information about participating vendors, as well as their products, services and plans moving forward, can be downloaded for free at: behavioral.net
TECHNOLOGY 36 FALL 2017 BEHAVIORAL HEALTHCARE EXECUTIVE WWW.BEHAVIORAL.NET
VENDOR
Markets respondents directly serve
Biggest priority for 2018
WWW.BEHAVIORAL.NET 37 100% 80% 60% 40% 20% 0%
RESIDENTIAL PROVIDERS 86.8% PAYER/ MANAGED CARE 50.0% GOVERNMENT AGENCY 55.9% INPATIENT PROVIDERS 79.4%
Training and/or education for current staff Expanding staff Research and development of new products/services Upgrading existing products/services Creating connectivity with information exchanges Mergers and acquisitions of other technology firms 36.8% 4.4% 1.5% 10.3% 7.4% 39.7% Are providers prepared for the value-based payment model? 26.9% 52.2% 20.9% Not sure No Yes Download the full database of survey responses at: behavioral.net OUTPATIENT PROVIDERS 95.6%
We do not plan to expand in any of the above areas in 2018
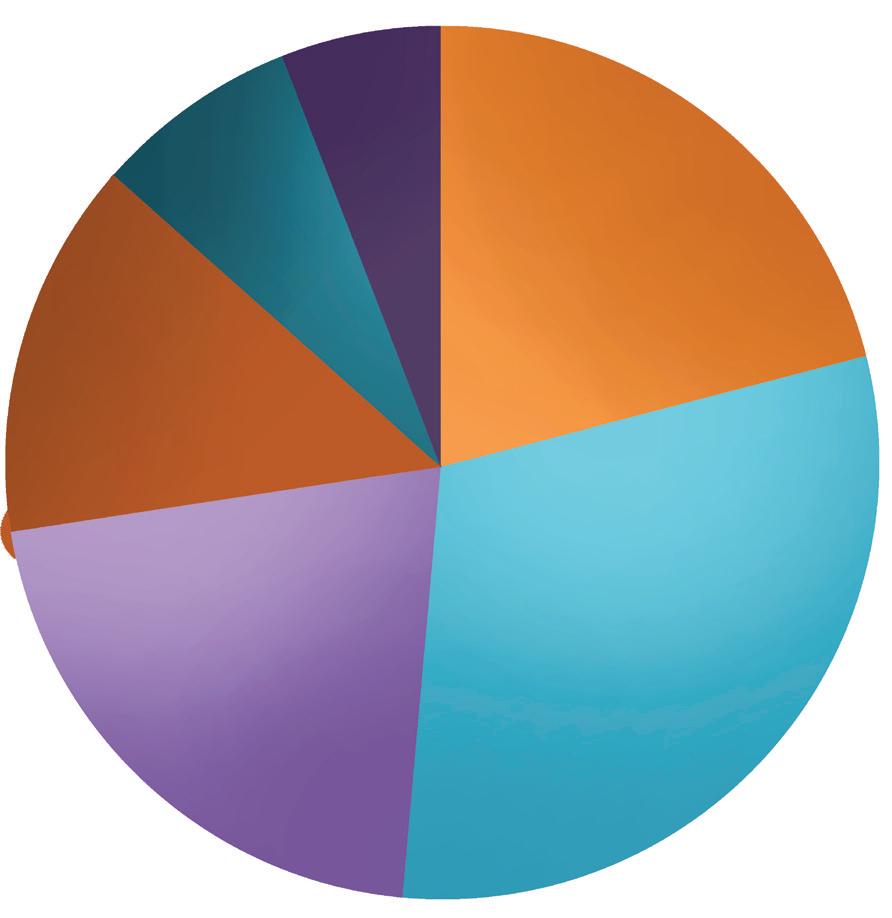


TECHNOLOGY 38 FALL 2017 BEHAVIORAL HEALTHCARE EXECUTIVE WWW.BEHAVIORAL.NET psychesystems.com / 800.345.1514 / Laboratory software specifically designed for Pain Management and Drugs of Abuse Testing • Supports screening and metabolite confirmation • Manages automatic consistency checking with prescribed medications and/or known substances • Integrates with various EIA and LCMS based instruments Now Available! Service areas respondents are most likely to expand in 2018 30.3% 21.2% 13.6% 7.6% 6.1% 21.2% Inpatient care providers Outpatient care providers
care providers
Residential
Payer/managed care Government agency
the full database of survey responses
2017 IT VENDOR S YEVRU
Download
at: behavioral.net
The
Accumedic accumedic.com
Product: AccuMed
AdvantEdge Healthcare Solutions ahsrcm.com
Product: ARPlus
Alleva allevasoft.com
Product: Alleva
Angel Systems, Inc. angelsystemsinc.com
Product: AVENUES
Athena Software athenasoftware.net
Product: Penelope case management software

BestNotes
bestnotes.com
Product: EMR, CRM, Outcome tracking
Both Worlds Software, Inc bothworldssoftware.com
Product: Compliance Manager DUI Software
call2test LLC call2test.com
Product: Automated randomized drug and alcohol test scheduling and client notification
Cantata Health cantatahealth.com
Product: Optimum
CarePaths Inc carepaths.com
Product: eRecord
Cash Box Solutions
recoveryoutcomes.com
Product: ARMS (Advanced Recovery Management System)
Cerner Corporation
cerner.com
Product: Cerner Integrated - Community Behavioral Health
Civerex Systems Inc
civerex.com
Product: Civer-Psych
Clarity Health
clarityhealth.ca
Product: Clarity Healthcare Solutions
Clinivate, LLC
clinivate.com
Product: Clinitrak
Is
With Treatment
The landscape to promote your treatment facility is changing quickly. If you don’t have a diversified call generation plan, you may be at a disadvantage to those who’ve spent years implementing a diverse lead generation program. There is a solution.
TreatmentCalls.com has inventory every day and can route consistent, live calls to your facility within hours. Do you need 10, 25, 50 or more calls a day? You can trust our fully-compliant and high-quality programming to deliver consistent, live calls from individuals needing your care.
TECHNOLOGY WWW.BEHAVIORAL.NET 39
Google restricting your ability to advertise your facility? It is time to invest
a proven inbound call strategy.
in
by connecting People with Treatment Let Us Help YOU Reach Those in Need • You set your daily caps • You tell us how many calls you want to receive • Calls can be transferred 24/7
You pick the days of the week you can receive calls
You pick the times of day you can receive calls CALL US now at 866-670-6601 to speak with a professional account executive and begin receiving calls within hours.
Changing Lives
•
•
2017 IT VENDOR S YEVRU
following IT vendors participated in the survey
Community Data Roundtable communitydataroundtable.org
Product: Behavioral Health Outcomes Tool and Analytics
Compulink Business Systems Inc www.compulinkadvantage.com
Product: Psych Advantage
Core Solutions, Inc. coresolutionsinc.com
Product: Cx360
Credible Behavioral Health Software credibleinc.com
Product: Electronic Health Record (EHR)
DSS, Inc. dssinc.com
Product: Mental Health Suite
EchoCore EchoCore.com
Product: Echo Core +
EHR YOUR WAY ehrYOURway.com
Product: Inpatient/outpatient, autism, case management, 17 MD specialties
EnSoftek, Inc. ensoftek.com| drcloudehr.com
Product: DrCloudEHR™
ePreventions epreventions.com
Product: Behavioral Health
EscambiaSoft escambiasoft.com
Product: Addiction-EMR
Foothold Technology footholdtechnology.com
Product: AWARDS
Formdocs LLC paperclaims.com
Product: CMS-1500 Claim Forms Software
gloo gloo.us
Product: Growth Engagement Platform and data insights and marketing
Harris Public Health Solutions cocentrix.com
Product: Coordinated Care Platform
Hayver Digital Health Corporation Hayver.com
Product: Behavior monitoring for patients with chronic diseases
HCS hcsinteractant.com
Product: Interactant
HInext treatehr.com
Product: TREAT
HIPAAtrek hipaatrek.com
Product: HIPAAtrek
IMA Systems LLC imasys.com
Product: imaServe
InfoMC, Inc. infomc.com
Product: Incedo Healthcare Management System
JAG Products, LLC ClinicTracker.com
Product: ClinicTracker
Kings View Kingsview.org
Product: Telepsychiatry
Kipu Health
KipuEMR.com
Product: KipuEMR
Known Factors knownfactors.com
Product: Business Intelligence for care providers
Lightning Step Technologies LightningStep.com
Product: Lightning Step EMR
MDofficeManager MDofficeManager.com
Product: GeeseMed
MEDHOST medhost.com
Product: Enterprise Financials and Clinicals
Mediware mediware.com
Product: AlphaFlex
Medsphere Systems medsphere.com
Product: Open Vista for Mental Health
MICA Information Systems micamedical.com
Product: Intelligent Medical Software (IMS) EHR and Practice Management System
Netsmart ntst.com
Product: CareFabric
Panacea HCS panaceahcs.com
Product: CCM
Procentive procentive.com
Product: Procentive
ProComp Software procompsoftware.com
Product: CATT (Behavioral Health EHR)
PSYCHeANALYTICS, Inc. psycheanalytics.com
Product: PSYCHeDECISION
PsyTech Solutions, Inc. psytechsolutions.net
Product: Epitomax
Qualifacts Systems, Inc. qualifacts.com
Product: CareLogic
ReliaTrax ReliaTrax.com
Product: Reliatrax EMR/ Practice Management
Remarkable Health remarkablehealth.com
Product: CT|One
40 FALL 2017 BEHAVIORAL HEALTHCARE EXECUTIVE WWW.BEHAVIORAL.NET
TECHNOLOGY
2017 IT VENDOR S YEVRU
Sigmund Software
SigmundSoftware.com
Product: AURA
SMART Management, Inc. smartmgmt.com
Product: Smart System
Streamline Healthcare Solutions streamlinehealthcare.com
Product: SmartCare
swyMed swymedical.swyme.com
Product: DOT Telemedicine Backpack
Synergistic Creations (KnKt'd Health) myknktd.com
Product: KnKt'd Health
Synergistic Office Solutions sosoft.com
Product: SOS Office Manager
TenEleven Group 10e11.com
Product: electronic Clinical Record (eCR)
The Echo Group echoman.com
Product: EchoVantage
thera-LINK thera-link.com
Product: HIPAA compliant video to allow for online sessions
TheraManager+DocuTrac DocuTracInc.com
Product: TheraManager and QuicDoc Enterprise
Therapy Partner TherapyPartner.com

Product: Practice Management Software for Mental Health Professionals

Valant Valant.com
Product: Valant Platform
Vista Research Group, Inc. vista-research-group.com
Product: Patient monitoring and outcomes research
Welligent, Inc. welligent.com
Product: Welligent
Zoobook Systems LLC zoobooksystems.com
Product: Zoobook EHR
Tom Valentino is Senior Editor of Behavioral Healthcare Executive.
TECHNOLOGY Joint Commission accreditation is widely recognized and respected as a mark of distinction by referral sources, families, state agencies, business partners/investors and payers. Validate the quality and safety of the services you provide and establish your credibility as a premier program by achieving Joint Commission accreditation. Make an informed choice. Schedule an introductory call at (630) 792-5771. Visit us at www.jointcommission.org/BHCS ® Raise the Bar Elevate your quality and safety with Joint Commission accreditation.
2017 IT VENDOR S YEVRU
Healing environments advance addiction treatment
Secure spaces must consider patient flow
As healthcare institutions grapple with the opioid crisis, one increasingly important focus of their efforts to improve addiction treatment is applying innovative design concepts to both new and renovated treatment facilities.
One recent project in New York exemplifies these new approaches required for planning and designing rehabilitation and treatment facilities. Designed by Environments for Health (E4H) Architecture and completed in 2014, a new substance abuse treatment program outpatient clinic building includes:
• A methadone-dispensing clinic, maintenance program and therapy;
• An ambulatory primary-care clinic;
• A program for former users, as well as continuing-care therapy and treatment programs for neighborhood clients; and
• Staff and administrative offices.
Adjacent to a street with an elevated train line, the building has been designed to fit comfortably within the low-rise commercial streetscape. It is made of durable contemporary materials, including polished and rough masonry block, corrugated and smooth steel panels, glass curtain wall, and aluminum storefront components. Concrete Masonry Unit (CMU) rough-face finished block material was specifically chosen along the front façade at street level to aid in preventing graffiti. Its west-facing location open to the extra wide avenue and elevated train across the way, provides greater visibility to the outside and natural light to the interior spaces.
EXTERIOR
The front entry has a covered roof canopy that welcomes patients and protects them from inclement weather. A glazed finish at the stair tower on the north end provides color and highlights the
BY SUSAN ROMANO
building from the street view. On upper portions of the street façade, corrugated metal panels alternate with triple-glazed strip windows whose sound insulation mitigates elevated train noise. A secure and lighted east facing façade and alarmed monitoring system control access to the building from the rear yard. The rear façade is unit masonry with punched windows to allow natural light into the offices and consult areas.
LAYOUT
The program space is open-concept and designed to be welcoming and inclusive, with smooth traffic flow to service areas. Most of the ground level space consists of the treatment clinic and primary-care clinic. With direct access to a supervised main entry lobby, the clinic comprises a waiting room, dispensing area with bays, and security station. Windows where patients collect medication are designed to be secure yet approachable. Instead of bars or grills, unbreakable polycarbonate with clear glazing is used, with a four-by-six-inch pass-through slot. Staff wear pendants embedded with panic buttons for added security.
Also on the ground floor, for the added convenience of addiction-treatment patients, is a primary-care clinic. It is located in a separate but interconnected suite with its own waiting room. Primary care spaces include exam rooms, group therapy and counseling rooms, and staff offices.
The second floor is comprised of more consultation rooms, conference rooms and group therapy spaces. Because patients often come with multiple family members, the clinic provides a children’s play area and additional family-member waiting facilities. The third floor is comprised of administrative offices and additional consult rooms. Both upper floors have a satellite security desk station and are monitored by cameras. Guards make regular rounds through the corridors to ensure staff and visitor safety.
DESIGN FOCUS 42 FALL 2017 BEHAVIORAL HEALTHCARE EXECUTIVE WWW.BEHAVIORAL.NET
INTERIOR FINISHES
The interior of the building is finished with modest, practical and durable materials, such as vinyl composition tile flooring and vinyl base in most spaces and ceramic tile floors and base in bathrooms. Administrative offices have carpeting for both warmth and sound management. Elevator lobbies and reception areas use porcelain tile for more durable flooring as well as protective wall finishes. The clinic uses a bright, cheery color palette for accents, with different colors on each floor. These pops of paint color are used as a tool for wayfinding and allow for easy and economical updates.



NATURAL LIGHT
Natural light has been shown to aid healing, so all upstairs consult rooms are located along the exterior and have windows. Vision panels along the building’s perimeter rooms bring natural light into the center’s corridors and make spaces less gloomy and institutional. Aluminum and glass storefronts allow natural daylight to penetrate the space, including waiting rooms. All offices have clear glass sidelights next to their doors to invite ambient natural light from both the front and back of the building. This creates a sense of openness between offices and corridors allowing the natural light to brighten the area as
DESIGN FOCUS WWW.BEHAVIORAL.NET 43
PHOTO CREDIT: ENVIRONMENTS FOR HEALTH
well as staff morale. The sidelights also assist with security by allowing for visibility into each office as guards regularly walk and observe the floors.


Hospitals that incorporate these design considerations underscore their commitment to serving local communities in need by finding the funding to preserve and upgrade older buildings, as well as constructing new state-of-the-art healing facilities from the ground up. Throughout the design process, the guiding principle was putting patients first – no matter their illness or treatment – and supporting their journey to recovery. Likewise, there was a clear objective to make sure clinic staff also benefitted from the design, to best support the important work they are doing in the community.
powering:

DESIGN FOCUS 44 FALL 2017 BEHAVIORAL HEALTHCARE EXECUTIVE WWW.BEHAVIORAL.NET
Susan Romano, AIA is an associate partner at E4H Environments for Health Architecture.

Find out at www.SASGroupLabs.com Or call 844.522.6468 WHAT WOULD OWNING A LAB MEAN FOR YOUR TREATMENT CENTER? There comes a time in the life cycle of an Addiction Treatment Center when it must consider all options for handling lab work. ADVERTISER INDEX Pages Pages Accumedic. 19 BestNotes 38 Brown Consulting Group .................................................... 4 CARF International. ............................................................ 4 Council on Accreditation CVR 2 Credible Behavioral Health Software 24, 25, CVR 4 Dominion Diagnostics 17 Dreamscape ............................................................... 11, 30 Furniture Concepts ........................................................... 27 Hope’s Windows and Doors 7 Kronos, Inc. 31 Panacea Healthcare Services 9 Psyche Systems ............................................................... 38 Recovery Brands LLC 44 Recovery Centers of America 13 SAS Group ....................................................................... 45 Sigmund Software. ........................................................... 26 TenEleven Group 1 The Joint Commission. 41 Therapy Notes 3 This End Up ...................................................................... 47 TreatmentCalls.com.......................................................... 39 Vertess Advisors, LLC + Vertess Consulting, LLC 33 Vinland National Center. 33 Whitehall Manufacturing CVR 3
Geothermal systems use less energy
Cumberland Heights took the leap
BY JOANNE SAMMER
hen Nashville-based Cumberland Heights had to address an aging infrastructure for heating, ventilation and air conditioning (HVAC) on its 11-building campus, it chose a geothermal system. The organization’s experience offers insight into how behavioral healthcare organizations can evaluate and manage the installation of such a system, which arguably has a much greater impact on patient and staff comfort than many realize.
Cumberland Heights opted for geothermal HVAC largely because of its energy efficiency and effectiveness. The system is designed to pay for itself within seven to 10 years through lower energy costs. Based on trends the facility has experienced since the system went online in May 2017, the system will achieve that projection, according to Butch Glover, the organization’s chief operations officer.
Geothermal systems heat and cool interior spaces by taking advantage of the consistent temperatures underground that range between 50 and 60 degrees Fahrenheit year round, which allows these systems to heat and cool using less energy with more efficiency than conventional heating systems. The systems take advantage of the fact that underground temperatures tend to be warmer in the winter and cooler in the summer than the air above ground. Air and water within the system are easier to heat or cool as they circulate underground then are forced out to heat and cool buildings.
Cumberland Heights, like many treatment centers residing in older buildings, wanted to replace its old HVAC systems due to the cost of maintaining them. In addition to creating a more energy efficient system, Glover says that the geothermal system has improved the air quality and humidity levels throughout the buildings. Since the system began running in May, “you can feel the difference in the air quality, and that gives patients a more comfortable environment,” says Glover.
The installation of a geothermal HVAC system is a complicated process that can impact many areas of patient care and operations.
1. Prepare staff and patients for the disruption. Geothermal systems reside underground and take time to install and test. Therefore, behavioral healthcare organizations must be prepared for a lot of digging on site as the installation team puts in the required wells, which can be numerous. For example, Cumberland Heights’ system has 93 wells.
“We didn’t realize how much disruption the work would cause to the campus until it started,” says Russ Taylor, director of support services. “It’s important to remember that there is a lot of mud, noise and machinery that will disrupt normal walking routes and how people get around the campus.”
2. Work with the contractor on scheduling. While there is no way to avoid some disruption, Glover and Taylor took steps to get everything back to normal as soon as the work was completed at each site. This involved everything from cleaning up to replacing the landscaping that had been removed. They recommend working closely with the contractor to discuss the schedule of work coming up so that staff has ample notice in case they needed to prepare patients for any disruption and move group sessions and meetings to less noisy and more accessible locations.
In addition, behavioral healthcare organizations must prepare the contractors for working in a behavioral healthcare environment that operates 24/7.
“The contractors had to keep us in business and realize that we can’t shut anything down,” says Glover. In many cases, that meant that the contractor had to be open to weekend and nighttime work as needed.
3. Ensure the contractor understands confidentiality. Contractors and subcontractors also had to know how to interact with staff and patients and to understand the need for confidentiality. For example, workers on the project had to be clearly and easily identified. Likewise, workers had to understand how patients might behave if they interacted and how the workers should handle those interactions if they occurred.
DESIGN FOCUS 46 FALL 2017 BEHAVIORAL HEALTHCARE EXECUTIVE WWW.BEHAVIORAL.NET
Joanne Sammer is a freelance writer based in New Jersey.
FYI
AWARDS
The National Institutes of Health (NIH) has awarded researchers at Albert Einstein College of Medicine and Montefiore Health System a five-year, $3.8 million grant for a long-term study to test whether medical marijuana reduces opioid use among adults with chronic pain, including those with HIV.
POLICY PROGRAMS
AmeriHealth Caritas, a Philadelphia-based Medicaid managed care organization, has donated $50,000 to the Pennsylvania District Attorneys Institute. The funds will be used to reimburse counties for the purchase of naloxone units.
The Joint Commission has awarded Laguna Treatment Hospital in Orange County, Calif., its Gold Seal of Approval.
The Massachusetts eHealth Institute at MassTech has awarded nearly $200,000 to four qualified electronic health record vendors to build efficient pathways for Massachusetts behavioral health providers to electronically submit reportable data to the Commonwealth’s Children’s Behavioral Health Initiative.
The International Association of Fire Fighters Center of Excellence, an addiction center that treats fire fighters battling post-traumatic stress disorder and substance use disorder, has earned the Joint Commission’s Gold Seal of Approval for behavioral healthcare accreditation.
Newport Academy, a series of adolescent treatment centers specializing in mental health, trauma, eating disorders and substance misuse, has received Gold Seal of Approval accreditation from the Joint Commission for behavioral healthcare.
Bright Futures Treatment Center, a drug and alcohol rehab center based in Boynton Beach, Fla., announced it has earned The Joint Commission's Gold Seal of Approval accreditation for behavioral healthcare and for opioid addiction treatment.

PEOPLE


AWARDS
POLICY PROGRAMS
The Association of Problem Gambling Service Administrators has announced its board officers and directors for fiscal year 2018: President Terri Sue Canale-Dalman, Chief, Office of Problem Gambling, California Dept. of Public Health; Vice President Jennifer Berg, Coordinator, Problem Gambling Services, New York State Office of Alcoholism and Substance Abuse Services; Treasurer Eric Preuss, Office of Gambling Treatment and Prevention, Iowa Dept. of Public Health, Division of Behavioral Health; Secretary Helen Ghebre, Program and Policy Consultant, Minnesota Department of Human Services Alcohol and Drug Abuse Division.
Mihaela Zdrali, PsyD, AFBPS, APA, has joined Centerstone as vice president of outpatient services for its operations in Florida.
Melissa Smith, LCSW, has joined Malibu Beach Recovery Centers as clinical director.
WWW.BEHAVIORAL.NET 47 thisendupcontract.com (800) 979-4579
PEOPLE
Beacon Health Options announced that Daniel McCoy has joined the behavioral health management organization as executive vice president and chief operating officer.
Trumpet Behavioral Health announced it has appointed Ned Carlson as chief executive officer.
Post Acute Recovery announced that John Rodolico, PhD, has joined the organization as chief clinical officer.
Diana Ramsay has joined The Tolan Group, a member of the Sanford Rose Associates Network of Offices, to lead the organization’s Behavioral Health, Human Services, Family Services and Substance Abuse Practice.
Andrea Kulberg, PhD, has been named clinical director of the adolescent mental health and eating disorder programs at La Ventana Treatment Programs in Santa Barbara, Calif.
New Directions has announced the following executive appointments: Timothy Hoffman as chief information officer, Robin Jackson as chief financial and administrative officer, and Noreen Vergara as general counsel and chief human resources executive.
The National Council for Behavioral Health has named Mohini Venkatesh as vice president of business and strategy.
Sid Goodman has been named executive director at Florida House Experience.
Danielle Gray has been named executive director of Ohio Recovery Housing.
AWARDS
PEOPLE POLICY
Beacon Health Options announced Michael S. Ramseier has been named executive vice president and market president, West Region.
PROGRAMS
New Season, a nationwide network of accredited opiate addiction recovery centers, has opened three new clinics in Mississippi: Meridian Treatment Center in Meridian, Biloxi Treatment Center in Biloxi, and Desoto County Treatment Center in Walls.
The Tennessee Highway Patrol and 15 other law enforcement agencies across the state have received 2,400 doses of naloxone nasal spray through a $250,000 grant from the BlueCross BlueShield of Tennessee Health Foundation.
Recovery Centers of America has agreed to terms on an insurance contract with Blue Cross Blue Shield of Massachusetts (BCBS) to provide treatment for BCBS policyholders at its Westminster, Mass., facility.
CleanSlate Centers, an outpatient opioid and alcohol addiction treatment provider, is relocating its headquarters from Northampton, Mass., to Nashville, Tenn., as part of a national expansion.
Summit Behavioral Health in Doylestown, Pa., has opened a multi-level eating disor-
der treatment program for women who are 18 years old and older.
Behavioral Health Group has opened a new addiction treatment center in Springfield, Mo., its second in the greater Springfield area and eighth opioid treatment center overall in Missouri.
Recovery United Pittsburgh has added an intensive outpatient program to its treatment services.
Providence St. Joseph Health and Well Being Trust jointly announced the first round of $10 million in grants and contracts to mental health and wellness initiatives to address mental health, addiction and homelessness in California.
Archstone Recovery Center of the Palm Beaches has earned accreditation and certification by the Joint Commission.
Cliffside Malibu Treatment Center has established a family program, which will integrate family members into the recovery process for those in addiction treatment.
Lucida Treatment Center, a mental health and addiction treatment center in Florida, has launched a men's primary mental health program, joining existing program offerings that address addiction and co-occurring disorders.
Gray Wolf Ranch has launched a continuum of addiction treatment services for young men, ages 15-25, on the Olympic Peninsula in
Port Townsend, Wash.
The Baltimore Station, a residential treatment program supporting veterans and others transitioning from homelessness and addiction to self-sufficiency, has been accredited by CARF International for a period of three years for both its residential program and its intensive outpatient program.
The Jason Foundation, a youth suicide prevention and awareness organization, has added Strategic Behavioral Health as a Community Affiliate that will establish affiliate offices at 10 hospitals that provide behavioral health services.
RESEARCH
Avista Pharma Solutions announced the Minneapolis Medical Research Foundation, a nonprofit subsidiary of the Hennepin Healthcare System in Minneapolis, has contracted the company to manufacture an opioid-derived small molecule, a key component of a conjugate vaccine in development to treat opioid addiction.
48 FALL 2017 BEHAVIORAL HEALTHCARE EXECUTIVE WWW.BEHAVIORAL.NET



BestCare® SOLUTIONS PATIENT-FOCUSED ADDICTION TREATMENT CENTER & BEHAVIORIAL CARE PRODUCTS 1. Showers 2. Soap Dishes 3. Grab Bars 4. Sinks 5. Shelves 6. Mirrors 7. Paper Towel Dispensers
Toilets
Adjustable Weight Hooks
Spindle-less Toilet Paper Holders
Linear Drains
Floor Drains LIGATURE-RESISTANT PLUMBING FIXTURES & ACCESSORIES NEW CONSTRUCTION/ RENOVATION / BUDGET FRIENDLY Available in a variety of colors. Some products are retro-fittable. www.whitehallmfg.com Tel: (800) 782-7706 or (626) 968-6681 Email: info@whitehallmfg.com ADA BARIATRIC UNIVERSAL DESIGN BIM/REVIT Available Ligature-resistant fixtures protect patients, staff, and reduce liability. 6 4 5 1 2 3 7 9 8 10 12 3 9 11
8.
9.
10.
11.
12.


Hundreds of Partners. One at a Time. Now it’s your Turn. The Power of One. The Benefits to Many. Now It ’s Your Turn. 301.652.9500 | partnership@credibleinc.com | credibleinc.com
