FIGHT TO KEEP UP THE FUNDING
Community coalitions strained when federal grants run out
Addressing dental health needs PLUS When should a patient share secrets?

SPRING 2018 • VOL. 16, NO. 2 • WWW.ADDICTIONPRO.COM CREATING NEWER NORMAL HELPS FAMILIES HEAL – Page 26




















Treatment teaches new behavior. Soberlink reinforces it. Track Results Test results are stored securely in our cloud-based portal. Identity Confirmation Client’s identity is confirmed via Facial Discreet & Convenient Privately submit tests from anywhere and at Alcohol Monitoring for Continued Care Soberlink made the difference for me in my recovery. It kept me focused on my sobriety, engaged with my therapist, and gave piece of mind to my loved ones. – Soberlink Client PA-001-18-001 info@soberlink.com • 714.975.7200 • www.soberlink.com
Why Sierra Tucson?
It
NO ONE KNOWS WHAT DESPERATION FEELS LIKE UNLESS YOU’VE BEEN THERE.
Life.
I would not be alive today if it weren’t for Sierra Tucson. I believe that every person who enters those front doors by that beautiful fountain is a blessed miracle, just like me.” —Andrew S., Scottsdale, AZ.
Literally Saved My
“
are
pain that interferes with life, depression, addiction, anxiety, PTSD, or disordered eating, we are here to
you heal.
us to take the next step
your journey of change. 800-842-4487 | SierraTucson.com We work with most insurance. Where Change Begins®
It renders you hopeless. Whether you
suffering from
help
Call
on
COVER STORY
Community coalitions struggle to stay solvent
BY ALISON KNOPF
BY SYLVESTER SVIOKLA, MD
BY TOM VALENTINO
BY BRIAN DUFFY, LMHC, LADC-I
BY MICHAEL BARNES, PHD, MAC, LPC
PHD
BY MICHAEL WEINER, PHD, MCAP
BY GARY A. ENOS
GAER
EDITORIAL
Editor in Chief Julie Miller jmiller@iabhc.com
Editor Gary A. Enos genos@iabhc.com
Senior Editor Tom Valentino tvalentino@iabhc.com
Associate Editor, Reader Engagement Megan Combs mcombs@iabhc.com
SALES
All inquiries please contact
Director of the Institute for the Advancement of Behavioral Healthcare
Douglas J. Edwards (216) 373-1201 • dedwards@iabhc.com

Traffic Manager Eric Collander (216) 373-1203 • ecollander@vendomegrp.com
Please send IOs to: adtraffic@vendomegrp.com
All ad materials should be sent electronically to: https://vendome.sendmyad.com/
DESIGN
Creative Director Dave Villafañe
SUBSCRIPTIONS
Call: 1-888-244-5310, email to: VendomeHM@emailpsa.com, or visit: www.iadvancebehavioralhealthcare.com/subscribe
REUSE PERMISSIONS
Copyright Clearance Center info@copyright.com Ph: 978-750-8400
Fax: 978-646-8600
ADMINISTRATION
Chief Executive Officer Jane Butler
Chief Marketing Officer Dan Melore
Vice President, Finance Bill Newberry
Vice President, Custom Media Jennifer Turney
Director, Circulation Rachel Beneventi
Addiction Professional (ISSN: Print 1542-8435, Online 2168-460X) is published 4 times per year by Vendome Group, LLC, 237 West 35th Street, 16th Floor, New York, NY 10001-1905.
©2018 by Vendome Group. Addiction Professional is a trademark of Vendome Group, LLC. All rights reserved. No part of Addiction Professional may be reproduced, distributed, transmitted, displayed, published, or broadcast in any form or in any media without prior written permission of the publisher. To request permission to reuse this content in any form, including distribution in educational, professional, or promotional contexts or to reproduce material in new works, please contact the Copyright Clearance Center at info@copyright.com or (978) 750-8400.
EDITORIAL: Addiction Professional is the addiction treatment and prevention field’s clinical resource that examines what works for individuals with addictive disorders. Articles and opinions published in Addiction Professional do not necessarily reflect the views of Vendome Group or the Editorial Advisory Board.
SUBSCRIPTIONS: For questions about a subscription or to subscribe, please contact us by phone: 888-244-5310, online: http://www.iadvance behavioralhealthcare.com/subscribe or email: VendomeHM@emailpsa.com.
Subscription rate per year: $140 domestic, $169 outside the US. Single copies and back issues: $20 Domestic, $32 outside the US.
POSTMASTER: Send changes of address to: Addiction Professional, PO Box 11404, Newark, NJ 07101-4014.
GARY A. ENOS
CONTENTS | SPRING 2018 2 SPRING 2018 ADDICTION PROFESSIONAL WWW.ADDICTIONPRO.COM FEATURES 16 Respect, not coddling, for buprenorphine patients
20 Oral health a concern for providers to chew on
24 Secrets: How and when a patient should reveal
26 Create a newer normal to help families heal
32 Establish connection with the narcissistic patient
JD,
34 Consider a treatment strategy for life
38 Include self-awareness in counselor training
40 Center connects tech to treatment BY NEIL
DEPARTMENTS 6 Letter From the Editor Famed researcher: Disease concept is indisputable BY GARY A. ENOS 42 Process Addictions LGBT youths report eating disorders at stunning rate BY GARY A. ENOS 44 Need to Know Five facts about recovery support group options 46 Clinical Challenges Nurses fighting an opioid crisis from within BY RACHAEL ZIMLICH, RN 48 Recovery Stuart Gregory is living a productive, self-directed life while running five companies in recovery BY
BY PAUL L. HOKEMEYER,
Adolescent & Young Adult Residential Behavioral Health Services
Rosecrance offers hope through lasting recovery
At Rosecrance, we understand the impact substance use and mental health disorders have on the lives of teens, young adults, and their loved ones. Lasting recovery requires a practical approach. Our experiencedstaff provides evidence-based treatment in a healing environment.
The Rosecrance Griffin Williamson Campus is a 78-bed treatment center for teens and young adults. Located on 50 scenic acres, this beautiful facility features an on-site school, a gymnasium and fitness center, a healing garden, and a conservatory.

Program includes:
l Initial biopsychosocial assessments
l Residential and outpatient treatment
l Partial hospitalization
l Adolescent detoxification
l Gender-specific counseling
l On-site school with licensed teachers
l Integrated experiential therapies, including art, music, recreation, fitness, and horticulture
l Family education and support
l Transition planning
l Alumni Relations program
Residential Treatment
Rosecrance has residential treatment programs for:

l Teens and young adults
l Primary substance abuse (with or without mental health diagnosis)
l Primary mental health (with or without substance abuse)
l Detoxification
Our mental health program includes treatment for primary diagnosis such as:
l Mood disorder(s)
l Bi-polar disorder
l Major depression
l Anxiety disorder
l Post Traumatic Stress Disorder (PTSD)
To make a referral or for more information, call
888.928.5278
Rosecrance is a private not-for-profit organization offering behavioral health services for children, teens, adults, and families. With more than 45 locations in Northern Illinois, Wisconsin, and Iowa, Rosecrance offers comprehensive addiction and mental health services through a variety of program. Rosecrance served more than 30,000 families last year. The organization was founded in 1916.
Rosecrance Griffin Williamson Campus
RESULTS! NOT PROMISES.
Since 1987, Brown Consulting, Ltd. has assisted hundreds of mental health and addictions treatment organizations in successfully reaching their goals.
We provide a full range of consulting services.

Specialist in Regulatory Compliance. Give

Immediate Openings
Recovery Centers of America is looking for world-class business development professionals.

Join one of the fastestgrowing healthcare companies in the U.S. on the front lines of the battle against the nation’s addiction epidemic.
Competitive compensation based on experience.
Business Development Professionals responsibilities:
• Ability to establish and build relationships with potential referral sources
• Prior Business Development experience – preferably in Addiction Treatment, Behavioral Health or other Healthcare Sales (Pharma or Med. Device)
• Experience with or knowledge of Substance Use Disorder
• Self-starter – can work independently

June 25-26, 2018
Summit for Clinical Excellence
The Opioid Crisis: The Clinician’s Role and Treatment Practices
Pittsburgh
https://vendome.swoogo.com/2018-Pitt-Opioid-Summit
October 18-21, 2018
Summit for Clinical Excellence

Brain Matters: Trauma, Mindfulness and Addictions

Atlanta https://vendome.swoogo.com/2018-Atlanta-Brain-Matters
November 12-14, 2018
National Cocaine, Meth & Stimulant Summit
Ft. Lauderdale, Fla.
https://vendome.swoogo.com/stimulant-summit
4 SPRING 2018 ADDICTION PROFESSIONAL WWW.ADDICTIONPRO.COM CALENDAR
WITH ADDICTION PROFESSIONAL »
the conversations about mental health
www.addictionpro.com CONNECT
Join
CALL TODAY 833-RCA-JOBS RECOVERYCENTERSOFAMERICA.COM/CAREERS
U.S. TREATMENT CENTER SEEKS BUSINESS DEVELOPMENT
TOP
PROFESSIONALS
PENNSYLVANIA | NEW JERSEY | DELAWARE | MARYLAND | MASSACHUSETTS DANBROWNCONSULTING.COM LEARN MORE.
us a call today! 1-800-495-6786
The opioid crisis is making headlines, but another category of drugs continues to devastate communities: stimulants. Cocaine is flooding Southern states as production increases to record levels in South America. Meth remains an omnipresent scourge. And college students across the country continue to misuse prescription drugs to boost academic performance. Together these “twin epidemics” are overwhelming law enforcement and treatment providers. Yet progress is being made, as multiple stakeholders are working together to prevent stimulant use, provide access to treatment, and ensure that stimulants are part of larger societal discussions about addressing drug use.
Be
part of the discussion. Be part of the solutions.
Join us for the inaugural National Cocaine, Meth & Stimulant Summit.
•
• Psychologists
• Clinicians, counselors, social workers, interventionists

• Law enforcement: Chiefs of police, sheriffs, detectives
• Federal, state, and local officials and lawmakers
12-14, 2018 FORT LAUDERDALE, FL Register at www.stimulantsummit.com
NOVEMBER
Who Should Attend
Private Practice Therapists
• Public health and prevention officials
Famed researcher: Disease concept is indisputable
ddiction research has given rise to much new discovery in the decade since publication of the first edition of renowned academician and researcher Carlton Erickson, PhD’s “The Science of Addiction.” Now with this year’s release of the book’s second edition, Erickson says genetic and neurobiological research has led to important conclusions.
“I think the big thing, and I hope I’m not being overly biased, is that the science is in that this is a brain disease,” he says. Erickson directs the Addiction Science Research and Education Center at the University of Texas College of Pharmacy.
This is not to say that all individuals who drink or use drugs at problematic levels have a brain disease, says Erickson, who repeats this consistently in the new edition. He points out that one of the potentially huge benefits to advances in genetic research will involve being able to personalize interventions based on genetic factors, identifying potential problems early and intervening with less intensive treatments than what would be needed for someone with full-blown substance dependence.
Erickson mentions in the book’s preface an abundance of “alternative facts” or false claims that he believes are plaguing the field, with authors who proclaim addiction to be a choice causing the most concern for him.
“These are pseudo-experts, some of whom have PhDs,” says Erickson. “The people writing these books don’t see people in the treatment centers. They haven’t read about the neurobiology.”
“The Science of Addiction” seeks to educate addiction professionals at all levels on the principles and applications of neuroscience. “Through such understanding, they will be better able to empathize with their patients and apply such science to principles of treatment,” he writes.
The book lists 10 prevalent myths related to addiction that Erickson says reflect misconceptions among both professionals and the public. These statements are among those he considers most damaging: “A person cannot overdose on alcohol.” “Self-help (i.e, sheer willpower) is an appropriate way to overcome the disease of addiction.” And, “ ‘Crack babies’ are a major clinical problem.”
Erickson’s book also lists research trends that are expected to yield strong conclusions over time, in areas such as opioid overdose prevention, the relationship between age of first use of alcohol and the development of alcohol use disorders, and translational research to inform how to apply science to treatment. But Erickson reserves his greatest enthusiasm for research into genetic vulnerabilities to addiction and what such findings can ultimately produce.
“Even though this research is very, very difficult, and is moving slowly, it is like a rolling wall of water—you can’t stop it,” he says.

Editorial Advisory Board
Joseph M. Amico, MDiv, CAS, LISAC
Vice President, NALGAP, The Association for Lesbian, Gay, Bisexual, and Transgender Addiction Professionals and Their Allies
Robert Bruner, CEAP, C-SI
President, Substance Abuse Program Administrators Association
Norman G. Hoffmann, PhD
President, Evince Clinical Assessments
William Cope Moyers
Executive Director, Hazelden Center for Public Advocacy
Lorie Obernauer, PhD
President, LO Group, Recovery Coaching and Consulting
Mark W. Parrino

President, American Association for the Treatment of Opioid Dependence

Beth Sanders
Past President and Standards Chair, National Alliance for Recovery Residences
Mary R. Woods
CEO, WestBridge Community Services
LETTER FROM THE EDITOR 6 SPRING 2018 ADDICTION PROFESSIONAL WWW.ADDICTIONPRO.COM
Apply for a grant from the Institute for the Advancement of Behaviorial Healthcare Fund today! Visit: iadvancebehavioralhealthcare.com American Society of Business Publication Editors 2016 National PR IN T Award Winner Revenue of $3 million or under A | S | B | P | E Fostering B2B editoria excellence American Society of Business Publication Editors 2016 Regional PR IN T Gold Revenue of $3 million or under A | S | B | P | E Fostering B2B editoria excellence
The More You Know About Addiction Recovery, The More We Make Sense
The Program: Our exceptional success rate sets us apart from other recovery centres, because our long term program gives the brain the opportunity to heal, but that is only the beginning. Program participants also:
· Advance their education
· Receive extensive career training












































































· Develop leadership & social skills

· Build strong character
The Cost: The John Volken Academy is a registered not-for-profit society funded by private charitable foundations, friends of the Academy, supporting businesses and government. Therefore, except for a one-time intake fee, the program is free.








To be eligible you must be:
· Committed to change your life
· Between the ages of 18-32
· Able to participate in the program



 His Holiness the Dalai Lama honored our founder John Volken with the Dalai Lama Humanitarian Award for effectively changing lives.
Vancouver, BC. Oct. 21, 2014
His Holiness the Dalai Lama honored our founder John Volken with the Dalai Lama Humanitarian Award for effectively changing lives.
Vancouver, BC. Oct. 21, 2014
Program Participants Adopt a Whole New Life-style MIND, BODY & SPIRIT Freedom we are not just treating addiction we are treating people... from Phone Today Toll-Free for More Informaiton 1-855-592-3001 www.volken.org Phoenix, AZ Seattle, WA Vancouver, BC Addiction
Finding order in the Steps
I read Brian Duffy’s article about chaos in recovery (Winter 2018 issue). I like that the author said it is his opinion, and I agree with him. I also have been working in the field of addiction treatment for many years. This is one of those things that is hard to put your finger on, but it explains why early recovery is so stressful. Not enough focus has been put on this part of the problem in substance use treatment, and maybe it can’t be. I’d like to share some of my thoughts on this with you.



I always take a look at what is there already in the 12 Steps. Although they are not very popular these days, the five original slogans that used to hang in all meeting rooms cover this beautifully and simply. “Think, think, think,” “Easy does it,” “Live and let live,” “First things first” and “But for the Grace of God.” I think they definitely address the chaos.
Also, the structured environment of the old therapeutic community programs also worked on the chaos, creating new skills of thinking and behaving and organizing the world physically. Today’s programs emphasizing comfort and décor don’t do that.
Being in a controlled environment that requires structure was healing, and created new skills over time. (I guess jail does that too, but with overtones that are not so helpful.)
I have been working with opiate addicts in the last couple of years. I ponder why they are so clueless about the need for recovery and so willing to revisit their preferred mental state. Maybe chaos has to do with this. Certainly, the need to restructure life in order to get the drug on time builds a completely new set of life skills that support the goal. Forget everything else; just stay on focus.
Another group beset by chaos
Brian Duffy’s article on chaos is very interesting, and I’ve shared with my colleagues. I’d like to add a third group [of those with chaos in their lives]: the people that come from both a family riddled with substance abuse and chaos and who also suffer from substance abuse themselves and have developed a truly dysfunctional lifestyle.
Doreen Schenkenberger Partners for Progress Anchorage, Alaska


LETTERS 8 SPRING 2018 ADDICTION PROFESSIONAL WWW.ADDICTIONPRO.COM
VOL. 16, NO. EMBRACE WHAT CLICKS WITH PATIENTS— Page 14 Peers’ roles in treatment remain ill-defined Professionals perpetuate patients shame PLUS PROVIDERS DIRECTLY ADDRESS RELATIONSHIP DYNAMICS EARLIER IN TREATMENT OCTOBER 18-21, 2018 Atlanta, GA | Hyatt Regency Atlanta The National BRAIN MATTERS Trauma, Mindfulness and Addictions Summit Returns to Atlanta ‘s Get Your Super Saver Pass NOW Very limited quantity What to Expect: • National Industry leader in behavioral and addiction conferences • Nationally Approved Continuing Education Provider • Cutting-Edge content. Field-Leading Experts • Stay at the iconic Hyatt Regency in downtown Atlanta Stefanie
Carnes, PhD, LMFT, CSAT-S, Clinical Sexologist, CEO, IITAP
Featuring: Earn up to 24 CE Hours
Tim Desmond, LMFT Polly Young-Eisendrath, PhD, Diplomate Jungian Analyst
Kathy King Alpine, Calif.



2018 Title Sponsor National Conference on Addiction Disorders Furthering recovery by engaging clinicians in conversations based on analytics, cutting-edge research, and trust
more about Dominion Diagnostics online at: www.dominiondiagnostics.com | @domdiag
Learn
Part of the addiction treatment and recovery community for more than two decades, Dominion Diagnostics delivers the most sophisticated, actionable clinical information to treatment professionals, and supports them with the latest technologies and best education available as they work to improve outcomes.


10 SPRING 2018 ADDICTION PROFESSIONAL WWW.ADDICTIONPRO.COM
FIGHT FUNDING TO KEEP UP THE
ederal Drug-Free Communities (DFC) funding is the lifeblood of substance use prevention in many communities, offering 120 grant awards of $125,000 each per year aimed at curbing the opioid epidemic and other drug problems locally. Each grant lasts for up to five years. Grantees are allowed to apply for a second round at any time, but they apply as a new applicant, with no special standing to get a renewal. No DFC recipient can earn more than two grant cycles. The basis for all of this is sustainability—keeping the program going in the community after the federal grant has run out.
In general, the DFC program has been a success, because it is based on the concept of the hometown’s responsibility of dealing with its drug issue. Community buy-in from the start is essential to achieving sustainability. In order to apply for a DFC grant, a local anti-drug coalition must have been in existence for six months prior to applying, and must have communitywide involvement from groups ranging from
schools to businesses to health professionals to everyday citizens. Local grantees also must match every federal dollar up to $125,000 a year.

The program has grown from $10 million at its start in 1998 to $95 million in 2016. However, there has been enough funding for only 32.7% of those who have applied since the beginning of DFC. And while many of the more than 2,000 DFC recipients have achieved sustainability, some have not. Poorer and more remote areas have tended to struggle the most.
ABOUT DFC
The Drug-Free Communities Support Program, administered through the Office of National Drug Control Policy (ONDCP) and with grantees trained by Community Anti-Drug Coalitions of America (CADCA), advances evidence-based prevention programming. Grantees are selected by ONDCP and the Substance Abuse and Mental Health Services Administration (SAMHSA). Included in the grantee training is how to implement seven strategies to change communities and achieve reductions in youth drug use. Examples of the strategies include enhancing skills, changing consequences with incentives and disincentives,
Community coalitions in rural America feel the strain when federal grants run out
BY ALISON KNOPF
WWW.ADDICTIONPRO.COM 11
and modifying or changing policies.
The model is to “change the culture across the community about drugs in general,” says Sue Thau, public policy consultant for CADCA. Thau tells Addiction Professional that some communities that once couldn’t find workers because nobody could pass a drug test are now thriving because of DFC-funded coalitions’ efforts.
Every DFC grantee must have a sustainability plan in year one. “We have a full-time technical assistance manager” who can help with developing such a plan, says Thau. Sustainability does not have to be at the full $125,000-a-year level, she notes.
It’s important to point out that the program has a rigorous outcomes management and evaluation system, says Thau. “Every grantee gets their data back, so they can show population-level outcomes,” she says.
In a random sample of DFC grantees conducted in 2013, it was found that of 182 coalitions, 82% were still in existence 10 years after the first grant.
RURAL CHALLENGES
But sustainability has been proving difficult in some rural areas. Nancy Hale, president and CEO of Operation UNITE, a Kentucky not-for-profit started in 2003 by U.S. Rep. Harold “Hal” Rogers, knows her state’s successes and its needs. Bell County in eastern Kentucky had a DFC grant that was not renewed for a second cycle.
“They were doing tremendous things. There was a lot of programming, but when the grant cycle ended, there was no way for them to sustain it,” Hale says.
Even though Bell County had only one DFC cycle, much good was accomplished, and the effects lasted long after the grant ran out, says Donnie Caldwell, who headed up the local effort for UNITE Bell County. “The lasting results were there,” says Caldwell. “I’m thankful because it did save lives.”
Without the consistent source of funding, however, the community work must be done by volunteers, and many times volunteers don’t have the time, he says. “Once we don’t have funded, paid individuals out doing it because they’re taking on other jobs and have other responsibilities, we lose the commitment,” he says.
Caldwell adds, regarding the federal support, “$125,000 a year doesn’t pay for a lot of people. But it helps for securing facilities like the gym and the movie theater and the ad promotion. We did a movie commercial—a trailer, with local kids.”
With the declines in the local coal industry, financial support from the community is minimal, says Caldwell. Over the last 10 to 15 years, local fundraising from banks is almost impossible to secure.
The First Tee program, a partner of Operation UNITE, is the coalition vehicle in Bell County. It has an annual budget
12 SPRING 2018 ADDICTION PROFESSIONAL WWW.ADDICTIONPRO.COM COVER STORY
"The value of community coalitions is you can spread the awareness of the changing patterns of drug use and try to get out ahead of it. If you don’t have that good network, you can’t get ahead of it.”
—Dale Morton, Operation UNITE
Join Us! Be part of the solution at the National Conference on Addiction Disorders, Aug. 19-22 in Anaheim, Calif. Register at: vendome.swoogo.com/ncad-2018
of $60,000, and as of February, there was only $3,000 in the bank. “Folks don’t have the checkbook available,” Caldwell says.
Couldn’t the coalition simply apply for another DFC grant? “We can,” says Caldwell. “But sadly, it takes someone basically full time to be able to put up a competent product.” The application would take someone working diligently for “weeks and months,” he says, adding, “I don’t see a volunteer being able to do this.”
Still, Caldwell has no regrets about the five years spent with the DFC. “We saved hundreds if not thousands of lives here, because we educated the young people,” he says. “I feel very good about the work we did for those five years.”
But he sounds ambivalent about going back to that work. “It wears on you—not the dealing with the kids, that was great. But there’s no down time. You’re getting a phone call when you’re putting your kids to bed, and you have to talk someone through suicide,” he said. “You can’t say, ‘Can I call you back in the morning?’ ”
Another rural community in eastern Kentucky did manage
to achieve sustainability, but misses the DFC funding. “Our DFC grant ended a few years ago,” says Glenda Shrum of the Knott Drug Abuse Council, based in Hindman in Knott County. “We have sustained our coalition and have built a good community network among partners.”
That said, the coalition did lose one full-time employee, with its other employee working only two days a week through the Kentucky Agency for Substance Abuse Policy (ASAP). “This has hindered us in many ways,” Shrum says. “We could do so much more with a little more money. We have many local partners who work alongside and support us. We partner with the local health

WWW.ADDICTIONPRO.COM 13 COVER STORY
HazeldenBettyFord.edu 866-959-0118 6362-1 (12/17) © 2017 Hazelden Betty Ford Foundation Earn your master’s degree. Study the science of addiction and mental health counseling online or on campus. Accredited by the Higher Learning Commission Financial Aid Opportunities Available 6362-1_GSAddictionProf_PrintAd_7x4.875_Fx.indd 1 12/14/17 1:36 PM
department, board of education, community action agency, law enforcement and the ministerial association.”
Successes in Knott County have included helping families seeking treatment, collecting unused medications, holding community events such as recovery rallies and town hall meetings, and helping to develop county ordinances related to substance use.
VIEW FROM UNITE
Some Kentucky communities have been able to get county government to give them several thousand dollars a year to keep coalition efforts going, says Debbie Trusty, education and treatment director for Operation UNITE, which has 32 of its own anti-drug coalitions throughout the state. “But in the poorer counties, everyone is strapped, including law enforcement,” she says. “When the funding stops, they don’t have the money to do what they did before.”
Hale says UNITE is proud of being able to bring law enforcement, treatment and education together. “Hal Rogers definitely was a pioneer in this,” she says. “We’ve been contacted by several states to look at how we started, replicating some of our programs.”
In addition to The First Tee, other programs crafted in Kentucky include the National Archery in the Schools Program and Hooked On Fishing—Not On Drugs. “You don’t have to start from scratch,” says Dale Morton, UNITE’s communications director. “The value of community coalitions is you can spread the awareness of the changing patterns of drug use and try to get out ahead of it. If you don’t have that good network, you can’t get ahead of it.”
Morton adds, “If you’re talking about sustainability, the one piece of advice I would give a DFC recipient is not to wait until the end of your funding cycle to start thinking about it. It’s not something that can be done overnight. In the early stages of having a grant, in addition to focusing on the specific mission, you need to be bringing your partners on board and looking at ways these programs can continue at the end of the grant.”
Also, it is important to make sure “you have a leader who is very passionate about the issue, because that leader will make sure that things get done,” Morton says.
Finally, Hale says coalitions are needed even when improvements have occurred.
“Just because things are going well, that doesn’t mean you don’t need a coalition anymore,” she says. Different drugs start trending. “You always have to be prepared,” she says. “Yes,
COALITIONS CAN OVERCOME CHALLENGES
Despite the challenges outlined by some of the leaders interviewed for this article, it is possible for low-income, rural communities to have sustainable Drug-Free Communities coalitions. Here are three examples:
• Jackson County, W.Va. Under the leadership of Amy Haskins, the Ripleybased Jackson County Anti-Drug Coalition has conducted initiatives that included a multifaceted media campaign on prescription drug use, a pill identification training for law enforcement officers, and advocacy efforts to promote wider use of the state’s prescription drug monitoring program.
• Carter County, Ky. Run by Shelly Steiner in Ashland, Ky., the Carter County Drug-Free Coalition has helped bring about a rise in college- and career-readiness scores from 23% in 2010 to 76.5% in 2016. Initiatives have included health professional training in polypharmacy and addiction, and a communitywide drug-free workplace initiative.
• Scioto County, Ohio. Lisa Roberts, program director of the Scioto County Coalition, credits her coalition’s success to the National Coalition Academy run by CADCA. The coalition’s initiatives have included implementing an adult and caregiver education effort on prescription drug misuse and piloting Ohio’s first community-based naloxone education and distribution program.
we want youth use to go down. But we also want our young people to never use drugs, whether it’s tobacco or marijuana or abuse of prescription drugs. Prevention is ongoing. You don’t just stop when things get better.”
14 SPRING 2018 ADDICTION PROFESSIONAL WWW.ADDICTIONPRO.COM COVER STORY
Alison Knopf is a freelance writer based in New York.

Respect, not coddling, for buprenorphine patients
A physician in recovery sees patients soar with an assist from buprenorphine
BY SYLVESTER SVIOKLA, MD
he opioid scourge continues unabated. People continue to die at a record rate in spite of ever-increasing news coverage of illicit drug use. How can this be?
While friends, family members and others not dependent upon drugs view the flood of information with appropriate alarm, active opioid users do not. They wonder about the newer, stronger street drugs, especially fentanyl, and what it must feel like to find some. Most are sure they will use it wisely. Most do not think they will die. Some do think they might, but are willing to risk it.
How do I know they think this way?
I am recovering from opioid addiction (17-plus years), and the thought does not shock me. More importantly, there is a recurrent behavior that provides empirical evidence that impaired thinking pervades the drug-using community.
The promulgation and use of the first aid medication naloxone (Narcan) by healthcare providers, law enforcement and education institutions has offered a window into opioid use and attempts to treat it. Naloxone also is being given
to many individuals with opioid addiction who leave various treatment settings for use should they relapse. Consequently, large numbers of patients who relapse are being given the drug, and most are arriving at emergency rooms alive rather than dead. Though this represents progress in initial survival, there is much more to the story.
One would think that these patients would be relieved to have cheated death and would be ready to start a serious attempt at beginning treatment. But this rarely describes the actual scenario. Although naloxone has allowed the patient’s breathing to begin again and can help restore a viable blood pressure, the patient quickly awakens in full-blown opioid withdrawal. Under these circumstances, the patient will agree to most any follow-up plan, as long as it starts tomorrow. The immediate need to relieve the worst withdrawal the patient has yet endured becomes paramount in the patient’s mind. The individual must use again, as soon as possible. He will leave, against advice if necessary, leaving loved ones and friends bewildered. Chances are, if he doesn’t die, he will be back again.
In my capacity as medical director of Phoenix House in Rhode Island, I have seen scores of patients admitted for detoxification and treatment as they continue in their addiction. Many readily admit to having suffered multiple overdoses requiring naloxone reversal within a one-year period. They are aware they are lucky to be alive, and often offer no promises that it will not happen again.
Although the public is baffled by such behavior, we providers cannot be. Respecting the power of a disease that so often brings the patient to the edge of death mandates our attention and resolve to avoid being deceived by our patients.
MEDICAL SERVICES 16 SPRING 2018 ADDICTION PROFESSIONAL WWW.ADDICTIONPRO.COM
A BOOST FROM MEDICATION
It is in the milieu of an opioid treatment center that the patient has the best chance for success. The patient should be offered medication-assisted treatment options. They include: methadone maintenance clinics; naltrexone, orally or in the form of monthly Vivitrol injections; and buprenorphine-assisted recovery. Here I will discuss the latter, as I believe it has been proven to work best for the majority of opioid-dependent patients. This medication has several qualities that make it ideal for those patients who wish to stop using now.
Buprenorphine is a partial agonist (activator) of the mu (opioid) receptors in the brain. It is at these receptor sites where nearly all the damage caused by opioid addiction starts and develops. Here is where tolerance for the opioid occurs. Tolerance is a need to take more of the drug, in use over a shorter period, in order to achieve the same result as when it was first taken. It is also at these receptors where healing can begin quickly by employing the appropriate introduction of buprenorphine into a formally scheduled treatment program.
The patient must be induced (started on the drug) when he/she is in sufficient opioid withdrawal. The state is best determined by a trained provider who uses history, physical examination and urine drug screen results. Although the sublingual medication enters the peripheral blood system as soon as it dissolves in the mouth, it will take another 45 minutes for it to cross the blood/brain barrier. The buprenorphine then will quickly attach itself to every mu receptor it can find. Those empty receptors are demanding activation by more opioid to stop the tremendous life-controlling dysphoria that has brought the patient near death and now to treatment.
The affinity (adhesiveness or stickiness) of buprenorphine for these mu sites is stronger than that of the common drugs of abuse and will immediately bond with the receptor and not allow other opioids to occupy that space. But instead of fully activating these sites, it will only

partially turn them on. This amount of site activation will immediately begin the reversal of the patient’s discomfort, but will not activate the receptors enough to reinstate the “high” initially felt by the patient. This limited amount of activation will, however, eliminate the desire to take more of the opioid of choice.
In addition, this small amount of mu activation will provide a slight energetic boost, but is not so energy-producing that the drug develops the tolerance that occurs with all other abusable opioids (including methadone). Practically speaking, this means that the newly induced buprenorphine patient will not feel better by taking more than his particular prescription dosage, but will instead begin to feel dysphoric and nauseated. This absolutely discourages and most often prevents overuse.
After the first few days of dose adjustment, the patient often begins to feel “as well as I did before I started using opioids.” These are frequent comments I hear, as the terrifying craving that had ruled these individuals’ lives actually disappears while they are on their regular dose of buprenorphine. They often
-Praise
ÑR. Nikki Myers, founder of Y12SR: The Yoga of 12-Step Recovery
MEDICAL SERVICES WWW.ADDICTIONPRO.COM 17
MAY 2018
978-1-942094-64-7 144 pages • $16.95 • 8 x 10 centralrecoverypress.com
active and personalized way for
in
to extend and
their yogic investigation
ISBN: 978-1-942094-63-0 E-book:
An
people
recovery
strengthen
of the Twelve Steps.
for Yogic Tools for Recovery“...filled with wisdom and practices to deepen recovery from any addiction.”
will share with me that they previously had felt despair over ever finding a way out of their dilemma. The patient now feels that recovery is possible. As powerful and specific as this medication is, the patient is now only beginning the journey to recovery, a journey not thought likely or even possible before.
CONTINUING TREATMENT
At the very beginning of buprenorphine-assisted recovery, sessions with qualified chemical dependency professionals are necessary to help the patient understand that cross-addiction will jeopardize recovery. The use of other mind-altering drugs poses a major impediment to recovery. Although most with an opioid addiction will say that neither alcohol, marijuana, benzodiazepines nor cocaine are their “drug of choice,” I insist upon an approach that helps the patient stop even infrequent use of substances.
Sometimes a higher level of care is necessary to help the patient stop other drug use. In cases where the patient refuses to comply, I will suggest transfer to another provider who is less strict about the use of concomitant mind-altering drugs. That threat is often sufficient to ensure compliance. If the patient has a comorbid disorder and had remained opioid-free, then I take responsibility for coordinating care with the other provider of any necessary prescription medications.
The ability to refer a patient to an intensive outpatient program (IOP) or for individual counseling is essential to being able to serve a patient well. Although I ask patients to refrain from beginning an attempt at detoxification from buprenorphine until they have had six straight months of
FIVE TIPS FOR ADDICTION PROFESSIONALS
1. Doctors who are familiar with treating addiction and who obtain an “X” number in order to prescribe buprenorphine should realize that the patient with an opioid addiction doesn’t lose all bad habits in the first month or two he/she is placed on buprenorphine. Normal doctorpatient relations and treatment plans are based on a truthful exchange between the two parties. This is not true with most who have an addiction. In order to help and not enable your patient, assume that an unbelievable story is probably just that: a lie. Always use urine drug screens as reality checks. Your patient’s dishonesty will decrease as he/she sees less need for it every day.
2. The near ubiquity of very inexpensive illicit imported fentanyl is causing it to be added to cocaine, marijuana and most other supplies of dealers. Realistic looking “Perc30s” have been found to contain no oxycodone but only illicit fentanyl. The incredibly powerful strength of this drug offers another reason to insist upon no use outside of prescribed buprenorphine.
3. Be certain that the drug screen that is employed in treatment specifically tests for fentanyl.
4. Marijuana use, with or without a medical marijuana card, has no place in the treatment of opioid addiction. All claims to the contrary are baseless.
5. Reduction in criminal penalties for the purchase of illegal buprenorphine on the street, as recommended by some treating entities, is dangerous. It is just as likely to bring the purchaser to a bad end as it is to expose him/her to its benefits. As my experience has shown, buprenorphine-assisted recovery is a process, not just a terrific medication— much as I believe it to be.
— Sylvester Sviokla, MD
MEDICAL SERVICES 18 SPRING 2018 ADDICTION PROFESSIONAL WWW.ADDICTIONPRO.COM
Although most with an opioid addiction will say that neither alcohol, marijuana, benzodiazepines nor cocaine are their “drug of choice,”
I insist upon an approach that helps the patient stop even infrequent use of substances.
drug-free urines, that does not usually present a problem. By that time, most patients are beginning to thrive. They are getting good jobs, promotions and newer cars, and are regaining family members’ trust.
They are at first in no hurry to start dropping their dose. Since I have told them prior to induction that slow reduction of buprenorphine dosage takes years, not months, my patients are in for the long haul. When they begin detox, the early phase will require at least four months to reduce daily dosage by 4 mg (i.e., from 16 mg per day to 12 mg per day). They are reassured that they may slow down the rate or even stop it at any time in the process without penalty.
I am currently waivered to treat 275 opioid-dependent patients. My proudest accomplishment is to be able to report that after a recent review of calendar years 2016 and 2017, 13 patients (all of whom had at least tried heroin) who had never owned a home before were able to purchase one for the first

time. All are between 22 and 45 years of age and have been with me for two to five years, and all but three are on a lower dose of buprenorphine than when they began.
This clearly represents more than “not using.” This represents a thriving recovery. This is most rewarding to me as a provider. Helping more patients on this road to buprenorphine-assisted recovery will do much to help reduce the stigma associated with opioid addiction.
Sylvester “Skip” Sviokla, MD, is a graduate of Harvard College and Harvard Medical School. After a successful 25-year emergency medicine practice, he lost his medical license due to opioid addiction. His struggle back to board certification is chronicled in the memoir From Harvard to Hell … and Back, published by Central Recovery Press. The author affirms that he has never received compensation from a maker of buprenorphine-containing products and does not own stock in such companies.

MEDICAL SERVICES WWW.ADDICTIONPRO.COM 19
Oral health a concern for providers to chew on
Substance use disorders wreak havoc on users’ teeth and gums, leaving them more susceptible to additional health concerns
mong the many ways in which substance use disorder wreaks havoc on a person’s well-being, oral health often is an overlooked component. Nevertheless, the effects that illicit substances and misuse of prescribed medications can have on teeth, gums and the oral cavity can also lead to other health concerns, all of which greatly hinder recovery.
For that reason, Mark Calarco, MD, the national medical director for American Addiction Centers (AAC), says his aim for AAC facilities is to be true medical homes for clients, and not only places that directly treat addictions and co-occurring disorders.
“Sometimes, we think of oral health as being secondary behind those other issues in priority, but the research is showing it’s just as critical as any other aspect,” Calarco says.
“Meth mouth”—severe tooth decay and gum disease—is a commonly known result of methamphetamine use, as illustrated by a 2015 National Institute on Drug Abuse study in which 96% of methamphetamine users in were found to have cavities1. But other substances,
BY TOM VALENTINO
from opioids to cocaine to even marijuana, have been shown to cause damage to the mouth. A 2005 study appearing in the British Dental Journal found that 95% of all illicit drug users surveyed reported experiencing dry mouth, while 75% experienced a “chewing” sensation, 56% felt pain or tenderness in their jaw muscle or jaw joint, and 52% developed a habit of grinding their teeth2
UNDERSTANDING THE EFFECTS
Dry mouth in particular opens the door to a series of other oral health problems, says Harold Katz, DDS, founder of the California Breath Clinics.
“Healthy mouths are always in balance, which means you have plenty of saliva,” Katz says. “Saliva does a lot of beneficial things. Not only does it keep your breath fresh, it prevents tooth decay and gum disease because of the enzymes in saliva, as well as minerals and oxygen.” A lack of saliva can also eventually lead to the beginning of gingivitis, bleeding gums and the loss of teeth, Katz adds.
Oral health problems stemming from substance use put patients at an increased risk for other ailments as well. The oral cavity is its own microbiome with its own set of bacteria, says Calarco. Imbalances in that microbiome heighten the potential for heart attack, cardiovascular disease and type II diabetes.
Both Katz and Calarco note that pregnant women face even more risks, including preterm labor and miscarriages. When patients have bleeding gums, the open wound sites created in the mouth allow toxins to enter the bloodstream and cross the placenta, affecting the baby, Katz says.
MEDICAL SERVICES 20 SPRING 2018 ADDICTION PROFESSIONAL WWW.ADDICTIONPRO.COM
Various substances heighten the risk for oral health ailments:
• Opioids: Heroin causes sugary food/drink cravings. Other complications include: grinding teeth, oral fungus, viral infections, loss of sensitivity (which could lead user to ignore cavities or gum disease).
• Alcohol: Increased plaque buildup, rapid tooth decay, tooth stains.

• Amphetamines: Grinding teeth, jaw damage, dry mouth.
• Cocaine: Powdered form rubbed into the gums creates mouth sores and damages tooth enamel, while snorting damages upper palate tissues. Cocaine use can also lead to jaw and mouth-related muscle spasms and grinding teeth.
• Marijuana: Oral cancer, dry mouth, vomiting, tooth enamel damage.

• Meth: Dry mouth, gum disease, grinding teeth, increased cravings for sugary foods and drinks.
• Tobacco: Smoking and chewing tobacco increases risk of oral/throat cancer. Other risks: gum disease, halitosis.
Source: https://americanaddictioncenters.org/how-does-drug-abuse-affect-teeth-health/
MEDICAL SERVICES WWW.ADDICTIONPRO.COM 21 ORAL HEALTH IMPACTS BY SUBSTANCE
714.375.1110 Fax: 714.242.9700 www.damorehealthcare.com www.patmoorefoundation.com Healing with Heart™ Crisis Stabilization, Residential Mental Health, Detoxification & Dual Diagnosis Treatment. We are a treatment center that created a new recipe for compassion: Gracious Redundancysm Boundaries Positive Reinforcements
While oral health issues often surface during addiction treatment, the inverse is common as well.
Harold Katz, DDS, founder of the California Breath Clinics, tells Addiction Professional that it is often dental professionals who are the first to identify a patient’s potential substance use disorder because individuals with SUDs tend to stay away from physicians.
“It’s pretty easy for a dental professional to look and see something isn’t quite right,” Katz says. “Today, if people can sneak around and are addicted to opiates and no one can tell, sometimes the dentist can tell by the constant dry mouth, increase in tooth decay and increase in gum disease.”
issues,” he says. “When patients are going through the withdrawal process and treatment, all of the sudden, that pain will rise to the surface and be very acute. If you’ve ever had bad tooth pain, you know it can be excruciating.”
OPIOID ALTERNATIVES POST-SURGERY
During many cases of addiction treatment, it is discovered clients will require extensive dental work to address damage incurred through substance use. Such surgery could cause intense pain for the client, but given their substance use history, prescribing opioids isn’t a safe and viable option. In these situations, Calarco recommends the following alternative pain management modalities:
• Topical analgesics, such as lidocaine and clove oil
• Nonsteroidals, such as ketorolac and naproxen
• Acupuncture
• Bridge, a neuro-stimulation device that attaches to the earlobe that targets withdrawal-related pain
• Auricular therapy
“It’s that whole continuum of drugs directly and indirectly leading to a domino effect in causing a lot of disease processes,” Calarco says.
ORAL HEALTH IN TREATMENT
Self-neglect, particularly with regard to oral health, is a common theme among those with substance use disorders, making the re-establishment of good oral hygiene practices a key part of addiction treatment, Calarco says.
Katz recommends that patients brush their teeth twice per day with two minutes per brushing. He also recommends treatment centers provide non-alcoholic mouthwash and toothpaste, and to also use a toothpaste with fluoride to remineralize the tooth enamel. Lastly, Katz recommends daily flossing to remove food particles, which promotes faster healing of gums.
Calarco, meanwhile, says that when addiction treatment patients are in detox, be prepared for patients to experience increased oral pain, including pain in the jaw and headaches, if they have underlying dental health issues.
“[Opioids] can mask a lot of underlying, serious dental
• Ice, heat, ultrasound or a battery-powered transcutaneous electrical nerve stimulation unit, which uses a lowvoltage electrical current to deliver pain relief through skin patches
Calarco also notes that many of these modalities can be combined or “stacked” to provide additional comfort.
Tom Valentino is Senior Editor of Addiction Professional.
1. https://www.mouthhealthy.org/en/az-topics/m/meth-mouth
2. https://www.nature.com/arti cles/4812050flossing to remove food particles, which promotes faster healing of gums.
Join Us!
To further explore this important topic, the Institute for the Advancement of Behavioral Healthcare is launching the National Cocaine, Meth & Stimulant Summit in 2018, along with a series of e-newsletters and webinars on this issue.
To receive the e-newsletter and details on the upcoming conference, visit: iabhc.com/stimulants
MEDICAL SERVICES 22 SPRING 2018 ADDICTION PROFESSIONAL WWW.ADDICTIONPRO.COM
SUBSTANCE
USE SPOTTED BY DENTISTS
Life-changing steps forward.



steps forward

When your patients are not responding to treatment, The Retreat at Sheppard Pratt can help. Our residential program offers individualized, compassionate and comprehensive care that empowers residents to manage even the most challenging mental health disorders. The Retreat is part of the Sheppard Pratt Health System, ranked among the nation’s top psychiatric hospitals by U.S. News & World Report for the past 27 years. For more information, visit our website or contact us.
retreat.sheppardpratt.org
410.449.2831
Secrets: How and when patients should reveal
Clinicians can help patients understand when it’s safe to share
BY BRIAN DUFFY, LMHC, LADC-I
e’re as sick as our secrets.”
It’s a commonly held belief. Whether it’s Catholics in the confessional, 12Step recovery participants doing their fifth Step, or individuals participating in talk therapy, acknowledging past unhealthy behaviors and expressing a desire to improve has great therapeutic value.
There is a caveat, however: Not every secret needs to be revealed. The secrets we’re discussing here are the ones that can lead to guilt and shame if they remain bottled up.
At many recovery meetings, the chairperson (or the entire group) will say something like: “Who you see here, what you hear here, when you leave here, let it stay here.” The group usually responds: “Hear, hear.” This serves as a good reminder of the importance of anonymity, confidentiality and trust.
Unfortunately, people talk. People gossip. There is nothing to stop the flow of rumors, misinterpretations and outright lies that might emanate from recovery meetings.
So, what is the correct hierarchy of sharing? How will patients learn what to share, when to share and with whom to share?
Addiction professionals find themselves in a unique position to provide guidance on these sometimes perplexing issues.
IN A PUBLIC FORUM
A public forum could include any self-help gathering, from a church group, health club or recovery meeting to an informal gathering of like-minded individuals. Although the group may claim to be respectful of secrets, there is no
guarantee because no one in the group is legally obligated to maintain confidentiality. Ironically, many experts believe gossip serves as an important part of our evolution, useful in forming healthy peer groups.
Professionals’ advice to clients should be this: Talk in generalities in these settings. Avoid anything you wouldn’t want people to read in the local newspaper, including criminal behavior, sexual practices and family secrets. Avoid discussing details of past trauma, even though it might be tempting to do so. This could retraumatize the client or others in the group.
Finally, resist the temptation to “perform,” to tell hilarious stories that entertain the crowd but contain too much personal information. Individuals in early recovery commonly make this mistake.
WITH A TRUSTED ADVISER
Sharing with a trusted adviser involves some gray area, because every relationship is different. As Anton Chekhov said, “You must trust and believe in people, or life becomes impossible.” Ernest Hemingway said, “The best way to find out if you can trust somebody is to trust them.” A bit more cynical, Ronald Reagan said, “Trust, but verify.”
The bottom line is it’s never completely obvious whom we should trust and with what information. Our patients might need our help in navigating these waters. A group facilitator, a 12-Step sponsor or a long-term close friend might very well be trustworthy resources. But they are not contractually obligated to observe one’s confidence. They are human and often lack training in maintaining appropriate boundaries. So, the “Who do I trust?” decisions will ultimately rest with the individual.
COUNSELING 24 SPRING 2018 ADDICTION PROFESSIONAL WWW.ADDICTIONPRO.COM
1 2
WITH A LICENSED CONFIDANT
This is the category where one can realistically assume that privacy will be assured. However, even therapists violate their code of conduct, though this occurs rarely. If they do share someone’s secrets, they risk losing their license to practice. This is equally true of ministers, psychiatrists, doctors and lawyers. Other providers of professional services (teachers, yoga instructors, probation officers, spiritual advisers, massage therapists, physical therapists, etc.) also might be placing their licenses at risk by violating boundaries. Patients should discuss confidentiality issues to better understand the protection and limits provided by professionals involved in their care.
Of course, there are exceptions. Most professionals are “mandated reporters” who must advise authorities if a patient is suicidal, homicidal, reporting child abuse or elder abuse, or intending to harm someone. But beyond those exceptions, one can reasonably assume one’s information will not be shared with anyone.
Insurance reports, by the way, can be a slippery area for our patients. The information, often in progress notes provided by the therapist and available to the insurance company, is generally wrapped in non-specific language. The most intimate details usually are not specifically addressed. This is considered protected health information and held in the highest confidence. While all health records are protected under the Health Insurance Portability and Accountability Act (HIPAA), mental health records are held to an even higher standard of secrecy. This should ease patients’ anxiety about talking freely to a trained professional.
It is important for people in recovery to unload, to share secrets with another person. But a hierarchy of sharing exists, and we can help patients avoid embarrassing mistakes by stressing that there are some things that they can say in a group, but others that they should save for a sponsor or trusted friend/ adviser. And then there are things they shouldn’t even tell their sponsor. They
should save those highly personal stories for their licensed therapist, minister, doctor, psychiatrist, etc.—people who are trained “secret keepers” and whose license status hinges on their ability to do so.
COUNSELING WWW.ADDICTIONPRO.COM 25
Patients should discuss confidentiality issues to better understand the protection and limits provided by professionals involved in their care.
Ranked #1 in the country for psychiatric care. addiction a ects everyone ■ Proven treatments for positive therapeutic outcomes ■ Harvard Medical School-a liated clinicians ■ Luxurious, ultra-private locations 877.850.4550 mcleanhospital.org McLean helps people break the habit. From science teachers to CEOs, 3
Brian Duffy, LMHC, LADC-I, is a mental health counselor at SMOC Behavioral Healthcare in Framingham, Mass.
Create a newer normal to help families heal
The focus in treatment should shift from individual to family recovery
BY MICHAEL BARNES, PHD, MAC, LPC
hen working with families struggling with addiction, it is common to hear family members say, “I wish my loved one would get sober so that we can get back to normal!” This comment makes sense, as families view the period when a loved one is using as an anomaly and inconsistent with how they functioned without the active addiction. They believe that the person with the addiction is the person with the problem, and they cling to the belief that their own struggles are only transient realities that will go away when their loved one achieves sobriety. They attend family programming to better understand their loved one’s problem, to support their loved one’s recovery and to facilitate their family’s journey back to normal.
Unfortunately, many addiction professions hold this same notion. They believe the value of family participation in the treatment process lies in supporting their clients’ recovery efforts. They fail to recognize the significance of the family disease process on addiction formation and addiction resolution. While a supportive family becomes a valuable asset to the treatment process, it falls far short of treating addiction as a family disease.
If addiction is to be treated as a family disease, with genetic and
transgenerational transmission, we must accept that the illness affects every member of the family. It also affects how current and future generations either inhibit or support addiction and recovery. As one generation after another is affected by epigenetic influences, childhood trauma and dysregulation of the autonomic nervous system, normal family functioning becomes skewed by family members’ unconscious coping with the elephant in the room.
With each new generation, family members are predisposed to addiction long before their first drink or drug. Therefore, treatment providers must recognize that each family member’s experience of normal functioning is influenced as much by personal and family history as it is by their current struggles with a loved one’s addiction.
UNDERSTANDING A NORMAL FAMILY EXPERIENCE
The concept of organization is important to understanding how families perceive what is normal. From the time that we were born, our family leaders established rules, roles, boundaries and routines that created repetitive, consistent and patterned interactions. These organizing principles created stable thoughts, feelings and behaviors that allowed the family to live within a desired value system and to achieve desired goals.
Family organization is shaped through a process of positive and negative feedback. On a day-to-day basis, family leaders reinforce or extinguish thoughts, feelings and behaviors, through consistent patterns of verbal and nonverbal parental interventions. Parental interventions are influenced, positively and negatively, by relationships with authority figures within their own family of origin. Primary family relationships set the foundation for establishing the stable patterns that promote family values and goal achievement.
Rules can take the form of overt and covert communication
COUNSELING 26 SPRING 2018 ADDICTION PROFESSIONAL WWW.ADDICTIONPRO.COM
patterns, allowable limits to emotional experience and expressions, obedience to leader authority, conflict management and resolution, and rule flexibility to meet age-appropriate developmental needs and growth. Roles may include expectations for child care, financial management, chauffeur duties and enlistment of older siblings to manage younger siblings while family leaders are engaging in other role-determined behaviors. Boundaries govern the flow of information within the family system and with the outside world. They can take the form of family subsystem boundaries that shield children from parental relationship issues and prevent the triangulation and parentification of children. They often include limits to time spent with friends or with the television and computer, and also the holding of family secrets. Rituals take the form of religious or spiritual practices, participation in birthday celebrations, and time spent with extended families. Over time, stable patterns evolve into routines, which in turn become a hard-wired and mostly unconscious organizational system that feels normal to each family member.
As family members leave the nest, these same organizational negotiations take place in the formation of new families. New family leaders utilize the organizing principles from their own families of origin as templates for negotiating desired stable patterns for their newly forming family. Within this process, rules, roles and boundaries will evolve. Some will be similar to those of one family of origin and others to the other family of origin. Over time, the new family will evolve hard-wired stable patterns that create a hybrid organization that once again will become the lens for what is normal.
FAMILY STRESS, PROBLEMS AND CRISES
Family stress theory defines a problem as any stressor that requires the family to initiate an existing coping strategy and to expend existing resources to solve the issue. A crisis is defined as any problem for which a family does not have a coping strategy or appropriate resources to resolve. Until a family either identifies a new understanding of the problem or develops new resources, it is forced to expend resources consistently to solve the problem, while living with the consequences of the unresolved crisis on a daily basis.
Addiction and trauma are experienced by families as crises, in that they rarely have sufficient understanding and resources needed for individual and family healing. Over time, the addiction becomes increasingly resistant to resolution, and
family members must adapt to the loved one’s progressing symptoms. As the addiction and trauma remain unresolved, “build-up” stressors in the form of employment, financial, legal, relationship or behavioral problems become additional crises that demand attention. As families continue to put forth effort to resolve the addiction and trauma symptoms, they become exhausted by the need to address these other

Master’s in Health Sciences in Addictions Studies
COUNSELING WWW.ADDICTIONPRO.COM 27
If addiction is to be treated as a family disease, we must accept that the illness affects every member of the family.
NOW AVAILABLE FULLY ONLINE Providing Graduate Education in Addictions Studies since 1985 Accredited through the National Addictions Studies Accreditation Commission and the Illinois Alcohol and Other Drug Abuse Professional Certification Association Be Part of the Solution 1 University Parkway, University Park, IL 60484 For more information or to apply, contact us at www.govst.edu/CHHS/ASBH or 708.534.4910 GOVERNORS STATE UNIVERSITY
Professionals A Vision for
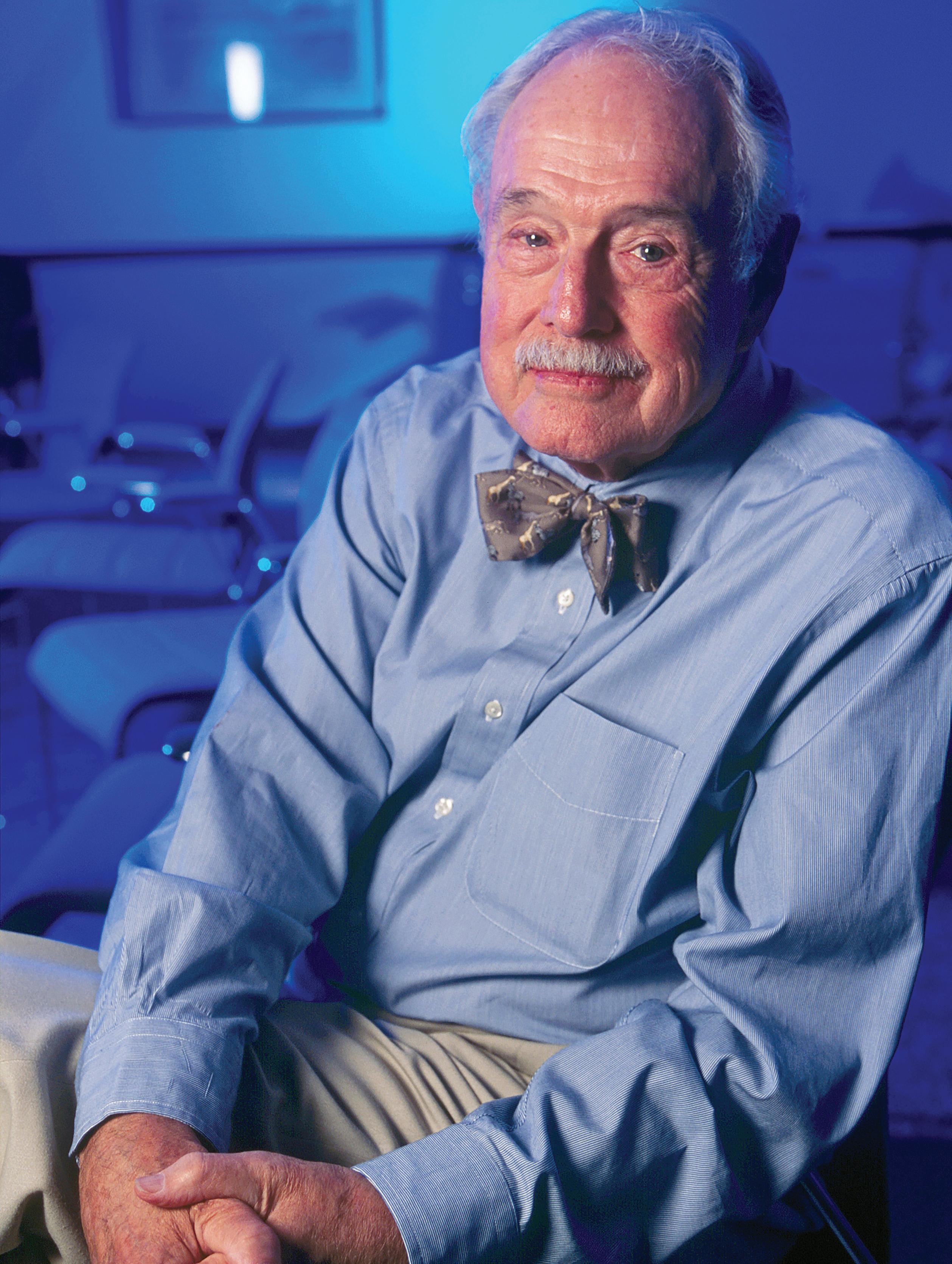 Photo by Billy Howard
Photo by Billy Howard
Our founder, Dr. Douglas Talbott, was a pioneer who spent decades advocating for those battling the disease of addiction. It was a personal issue for him, so he understood the difficult struggle to maintain his medical career and family life while desperately needing to address his addiction. At that time, there was no one pointing the way, so he took up the challenge. A graduate of Yale University and Columbia Medical School, he blazed trails, developing innovative new methods that resulted in lasting recovery for professionals like himself and anyone battling addiction. Today, Dr. Talbott’s legacy lives on in everything we do and every patient we treat.
Talbott Recovery offers:
• Treatment for co-occurring addiction and mental health issues
• Licensed Professionals program
• Adult and Young Adults program
• Pilots program
• Groups for family members
• 72-hour professional assessments
• Mirror Image program
Wherever you are in Georgia, Talbott Recovery is nearby. Our Atlanta campus is conveniently located near Hartsfield-Jackson Atlanta International Airport, making it ideally situated to serve metro Atlanta and a wide range of suburbs. In addition to Talbott Recovery, we offer convenient outpatient treatment in Dunwoody and Columbus.

While you’re in treatment at Talbott, your time with your family is very valuable to us. They have the opportunity to be part of your treatment weekly — to be part of your treatment at home and at Talbott. All of that is integrated into the experience.
in Need Talbott Recovery ... carrying out the vision of Dr. Talbott for over 30 years. TalbottRecovery.com | 866-494-7787
-Jennifer Angier, CEO of Talbott Recovery
stressors simultaneously. Within this process, family members’ perceptions of the crisis and of one another begin to change.
For many families, living with the crisis will shift their focus from fundamental values and goals to surviving the crisis. This typically results in significant organizational shifts and changes to the family’s rules, roles and boundaries. As stable patterns shift to coping with the addiction, trauma and stressor build-up, coping strategies such as hypervigilance, control, enabling and enmeshment become the norm. It is within this process that we see the establishment of a new normal in terms of family organization.
It is important to recognize that the stable patterns associated with the new normal might not represent a shift at all. Many partners and parents who experienced their own childhood trauma or grew up in families with addiction, trauma and mental health issues may have entered into the process of new family development with impaired perceptions about coping with these kinds of crises. Their pre-existing
emotional, behavioral and cognitive stable patterns make it especially difficult to resolve these crises in their own family. Hypervigilance, control, enabling and enmeshment may have been a critical part of the organizational negotiation long before the crisis occurred.
FAMILY RECOVERY: A NEWER NORMAL
The goal of family healing is the creation of new emotional and interactional stable patterns that allow family members to initiate desired change and growth. A prerequisite for this type of family healing is a perceptual shift from focusing on the addicted family member’s need to achieve recovery to accepting the need for family healing. This promotes family creation of a “newer” normal that advances resource development needed to resolve the crises that have plagued the family.
For many families, this becomes a hard pill to swallow. Families that are newer to the treatment process tend to be more open to hearing this message. They are desperate for resolution and need a more direct and hierarchical therapeutic relationship. Families that are organized around the addiction and trauma are sensitive to perceived judgment and blame. Over time, attempts by professionals to help them recognize increased control, enabling and enmeshment are experienced as blaming. These families tend to respond better to a slower collaborative therapeutic relationship, where they remain the expert on the family experience and the therapist is the “curious” expert in the therapeutic process.
Once the therapeutic relationship has been developed, education offers a critical starting point for perceptual change. The educational process should begin with a focus on the loved one’s struggles to achieve recovery, co-occurring mental health issues, trauma, and how childhood trauma, family trauma and attachment struggles have complicated recovery efforts.
Families initially can be quite defensive when discussing childhood issues. When this information is presented in an educational, evidence-based and non-blaming way, family members become curious about their loved one’s struggle and begin to understand why achieving recovery has proven so difficult. In time, they often become open to questioning how these same issues may have posed a challenge in their own lives.
Once perceptions have been challenged, family members begin to risk speaking, feeling and trying on new interactional behaviors. The experience of these organizational changes
COUNSELING 30 SPRING 2018 ADDICTION PROFESSIONAL WWW.ADDICTIONPRO.COM
The educational process should begin with a focus on the loved one’s struggles to achieve recovery, cooccurring mental health issues, trauma, and how childhood trauma, family trauma and attachment struggles have complicated recovery efforts.
promotes new rules, roles and boundaries that create a “newer” normal that can sustain recovery. At this point, families become open to a comprehensive intergenerational assessment of addiction, trauma, mental health and other struggles that may have influenced how the client and the family have attempted to deal with the active addiction and associated trauma. Within this process, it is important to assess how values, goals and stable patterns have evolved. Asking parents or partners to discuss what they looked like in their own family of origin offers a good starting point. Then, one can assess how they were negotiated prior to the addiction and how they changed during the active addiction. Ultimately it is important to discuss the values, goals and stable patterns that family members believe will be needed to sustain recovery.


THE ULTIMATE MESSAGE


As most treatment programs have become increasingly traumainformed and trauma-integrated, it is important to include

transgenerational trauma education in our family programs. We must help family members understand the reality that a loved one’s achievement of sobriety does not resolve the family’s problems. Once armed with this new information, families can be challenged to stop waiting for their loved one to get sober and to allow their own healing process to serve as a model for recovery.
The ultimate message is that families who heal together create an environment that is inhospitable to active addiction. Conversely, when families wait for their loved one to get sober, they often create an environment that is inhospitable to the recovery of all family members.
Michael Barnes, PhD, MAC, LPC, is Chief Clinical Officer for Foundry Treatment Center in Steamboat Springs, Colo. He has more than 35 years of experience in addiction and mental health counseling, and his expertise is in developing trauma-integrated addiction treatment and in working with families. He can be reached at mike.barnes@ foundrytreatmentcenter.com.

COUNSELING WWW.ADDICTIONPRO.COM 31
www.RetreatAddictionCenters.com | 855.859.8810 Palm Springs, FL | Ephrata, PA | New Haven, CT Premier
Retreat Premier Addiction Treatment Centers is a network of inpatient and outpatient facilities offering a full continuum of care for individuals struggling with addiction. Our services range from medically monitored detox to outpatient rehabilitation provided by a credentialed and compassionate staff. We work with most major insurance companies, offer 24/7 admissions and complimentary transportation.
Addiction Treatment Centers®
Establish connection with the narcissistic patient
Too many programs engage in clinical pandering with the high-worth population
BY PAUL L. HOKEMEYER, JD, PHD
ou’re an idiot, Hokemeyer. Actually, let me clarify that. You’re a [expletive] idiot.”
I was sitting across the room from a senior executive of a pharmaceutical conglomerate, who felt compelled to put me in my place. (The identifying details of the case vignettes in this article have been changed to protect the integrity of the patients and treatment professionals.) If the truth were told, I probably deserved it. We had met only once before and had not yet established a therapeutic alliance. My clinical intervention that invoked his reaction was ambitious, formulated not to pander to but to gauge the level of his narcissistic presentation.
The patient had come into treatment after being backed into a corner by his wife. After 30 years of marriage, she had had enough of his drinking and philandering and had hired one of New York’s most prominent divorce lawyers to execute her departure. The only reason the patient agreed to see me was to avoid an expensive and embarrassing divorce.
As he said, “She’s asking for half of my net worth. I can’t believe how greedy she’s being … especially after all I’ve done for her. She said she’d hold off pursuing this if we met.” Although from a financial standpoint he would remain extraordinarily wealthy after the proposed settlement, his pride and ego would be crushed in what he would consider a tactical defeat.
Going into our engagement, I suspected he would rate high on the narcissistic scale. Men and women like him frequently do. They have attained extraordinary success in the financial and professional realms of their lives, but have failed miserably in those that require intimacy. They think they have gotten where they are by manifesting the dominant cultural message “nice guys finish last,” and they view emotional vulnerability as a liability to be avoided at all costs.
The intervention that garnered his hostile reaction was my attempt to see if he had any capacity to empathize with his wife. I had asked, “Well, have you ever thought maybe she’s been impacted by the mistresses you’ve kept over the years?”
On a very deep level I knew he had, but that he had submerged those thoughts and their accompanying feelings deep below his consciousness.
His emotionally charged response to my question was clinically rich. It enabled me to gauge his psychic composition, but it also required me to retreat and make tactical reparations. If I got into a power struggle with him, I would lose. He’d be out the door and racing back down the cobbled path of his self- and relational destruction. Instead of responding through my bruised ego, I needed to assuage his. I said, “I’m sorry if I’ve offended you. I’m just trying to get a sense of where your wife is in all of this.”
My short-term goal was to obtain data I would subsequently use in a long-term treatment strategy that is highly effective in working with narcissistic executives. Central to the strategy is recognizing that deeply embedded narcissism such as his would never be completely removed but could be softened. To do this, I would have to keep him engaged in the following three-step treatment process:
1. Establish a therapeutic alliance that meets him in his narcissistic personality presentation;
2. Craft clinical interventions that allow him to intellectually appreciate the value of intimacy; and
3. Provide concrete tools that enable him to tolerate the extraordinary discomfort he will feel from a new way of relating to himself, other human beings and the world around him.
SOME PROGRAMS’ SHORTCOMINGS
Unfortunately, too few treatment professionals and programs
COUNSELING 32 SPRING 2018 ADDICTION PROFESSIONAL WWW.ADDICTIONPRO.COM
have the resources to accomplish this labor- and time-intensive task. This is particularly true in the recent deluge of “executive treatment programs” that are more concerned with filling beds than providing culturally competent and clinically relevant care to patients. Instead of working in the patient’s narcissistic personality presentation, these programs either engage in clinical pandering or lose the patient through culturally insensitive interventions.
Clinical pandering is essentially babysitting, using the patient as narcissistic supply (where individuals use objects and people to enhance their self-image) or feeding a patient’s narcissistic ego to garner a financial reward in the form of elevated fees or generous donations. Culturally insensitive interventions are subtler, manifesting in hostile countertransference reactions (conscious and unconscious) to the patient. These result in the patient emotionally shutting down or physically leaving treatment.
Recently, I learned of a case in which one of the field’s most talented family therapists referred an ultra-high net worth patient to an executive treatment facility that mishandled her cultural presentation. Shortly after arriving into treatment, the high-profile woman was challenged by the clinical team for being “too vain.” The patient, a former model, would only appear in the psychotherapeutic community “perfectly coiffed and attired.” Instead of seeing the patient’s physical presentation as an essential part of her being and connecting to her in it, the staff used it to demean her and drive her away. While she remained physically present in treatment for 28 days, as demanded by her husband, she did so in a superficial and compliant way.
A more culturally and clinically effective strategy would have been to allow the patient to be herself in treatment until she got her “sea legs.” During this time, her clinician could establish a therapeutic alliance that met her “in her vanity” rather than attempting a culturally insensitive extraction of it. While the attachment was occurring, the therapist would artfully inquire into the patient’s psychic composition and interject subtle questions that would provide bits of personal and relational insights.
In this regard, interventions that are a hybrid of questions and statements are highly effective. As it relates to the treatment of this particular patient, statements such as, “You’re a beautiful woman. Does that ever get exhausting?” would have provided her with ego gratification as well as an opportunity for connection through insight. Simultaneous with this individual
work, the patient would be connecting with her psychosocial community—men and women whom she viewed as her peers, outside of the structured psychotherapeutic dyad—to test and share her clinician’s interventions.
Handled in a culturally sensitive way, the patient would have become open to maximizing the rich opportunities she was afforded in treatment. Instead, she felt judged and yet again misunderstood. After 28 days of external compliance, she jumped into her private jet and flew back to self-soothe in the isolation of her Park Avenue penthouse, convinced that treatment doesn’t work for people like her.
ETHICAL OBLIGATION
Treatment professionals and facilities that market to executives and ultra-high net worth individuals have an ethical responsibility to provide clinical services that address these patients’ unique and challenging compositions. Rather than profit centers, these patients are human beings who exist in a culturally distinct intrapersonal, interpersonal and sociocultural space.
Executive treatment is not purely a function of amenities. Yes, a culturally relevant holding environment is part of the equation, but the real value comes from the maturity, intelligence and artfulness of the treatment team working interpersonally with a vulnerable population.
Paul Hokemeyer, JD, PhD, is a family and addictions therapist who works as a clinician and patient advocate to elite individuals and families around the world. His research and experience is the subject of a book to be published by Hazelden Publishing in the summer of 2018. In addition to maintaining a private clinical and consulting practice, Hokemeyer is senior clinical fellow at Caron Treatment Centers. He can be contacted at drpaulnyc@yahoo.com.

COUNSELING WWW.ADDICTIONPRO.COM 33
Clinical pandering is essentially babysitting, using the patient as narcissistic supply or feeding a patient’s narcissistic ego to garner a financial reward in the form of elevated fees or generous donations.
Consider a treatment strategy for life
Lifespan recovery managment would more closely reflect the nature of addiction
BY MICHAEL WEINER, PHD, MCAP
rominent addiction research leaders
John F. Kelly, PhD, and William White in 2011 published an article titled “Recovery Management: What If We Really Believed that Addiction Was a Chronic Disorder?”1 The answer to that question might be that we would be providing care for our patients over the course of a lifetime.
The hope would be for long periods of stability that would require only monitoring. However, symptoms of a chronic disease tend to recur. At those times, interventions could be rapid and the recommended level of care would depend upon the severity of the symptoms and the level of risk. I’m referring here to symptoms of and risk for a substance use disorder as stated in the 2013 ASAM (American Society of Addiction Medicine) Criteria and in the DSM-5.
What we have been doing is treating a series of episodic occurrences as though one episode was totally unrelated to the other. I frequently hear people in the process of recovery say something like, “I’ve been to treatment three times.” That perception is understandable. If a person has been admitted on multiple occasions to residential treatment for a substance use disorder, each treatment was likely to
look the same (another first Step, another story, etc.). There’s an assumption that a person needs to start from scratch.
But every time this happens, shame accumulates.
“Lifespan recovery management,” on the other hand, treats a chronic substance use disorder over the course of time. The intensity of care always matches the severity of symptoms and the level of risk. The critical factor is that even when symptoms are inactive, the disorder is monitored. The lowest level of care would take the form of an annual recovery checkup.2
This sounds a lot like treatment for any other chronic disorder, doesn’t it? No shame attached.
LEVEL-OF-CARE CONSIDERATIONS
Initially, residential care is likely to make sense. As a culture, we tend not to recognize the severity of substance use disorders until the symptoms become severe. If the disorder is caught early, a lower level of care, such as intensive outpatient, might be recommended. Again, symptoms and risk would dictate the determination.
The length of stay in any level of care needs to depend upon how quickly or slowly symptoms can be treated. Withdrawal from one drug might take longer than withdrawal from another. Age, history and body weight also are factors.
Let’s forget notions about a 28-day program. As David MeeLee, MD, says, we do treatment, we don’t do time. Lifespan recovery management means that we don’t make time frame recommendations. We make recommendations based upon symptoms and risk.
A person can be discharged from the residential level of care when the objectives for that level have been met. This likely will mean that the patient can now function at a lower level
RECOVERY SUPPORT 34 SPRING 2018 ADDICTION PROFESSIONAL WWW.ADDICTIONPRO.COM
of care with a minimal risk of recurrence.
What happens upon transfer to a lower level of care is critically important. The term “aftercare” is a relic. It has to go. It should have gone 20 years ago. What happens next is not an “afterthought.” Research continues to show that people who are committed to and follow at least a five-year plan are highly likely to remain abstinent.3
It is logical that an intensive level of outpatient care would follow the completion of residential objectives. This is the same as for a person leaving a hospital after being treated for diabetes. Initially after hospital discharge, outpatient care is delivered frequently.
The patient with diabetes will be monitored for a lifetime. People with substance use disorders need the same. Under lifespan recovery management, a person with a substance use disorder would always have an addiction specialist (an MD board-certified in addiction medicine) on his/her medical team.
Getting through the medical and emotional upheavals of life is not always easy. Staying motivated to follow a program of recovery does not remain consistent. There are marriages and divorces, joys and sorrows. There are geographical changes, career changes, and probably much more. One might ask, “How does anyone remain abstinent through all of that?” The answer is that not many do. Recurrences happen.
However, recurrences do not have to be shameful, nor do they have to be a disaster. They can be short-lived. People perceiving themselves to be in treatment over the course of a lifetime will have an addiction specialist to reach out to, in a manner similar to the person with diabetes reaching out to an endocrinologist. People with other chronic diseases always have had a safety net, a place to land. People with substance use disorders need one too.
NEW PARADIGM REQUIRES NEW LANGUAGE
Early in 2017, the Office of National Drug Control Policy (ONDCP), then directed by Michael Botticelli, made recommendations regarding the language we use on a daily basis in the field of substance use disorder treatment and recovery. The recommendations reflect a movement away from language that has been judgmental and toward one that is consistent with healthcare.
You can see from this article that I have adopted the recommendation, as part of person-first language, that the term “relapse” be replaced with “recurrence.” This gets us away from the baggage that comes with references to relapse. As William
White explains, the general public linked relapse to low moral character rather than sickness.
It follows, then, that the term “relapse prevention” be replaced with “recovery management.”
Also, “I’ve been to treatment five times” would be eliminated in the framework of recovery management. “I’ve been to treatment five times” means “I’ve failed five times.” Treatment is managed. It is not a series of acute episodes. Similarly, “this is my first time in treatment” would lose its meaning.
And isn’t “ambivalence” a more accurate description of a new patient’s state of mind than “denial”? Ambivalence gives the therapist something to work with.
It is not possible to eliminate shame from addiction treatment and recovery, and to move toward lifespan recovery management, without changing the language. Change is not always easy, and it takes practice. Let’s begin.
Michael Weiner, Ph.D., MCAP, has held faculty positions at the University of North Carolina and at the Rochester Institute of Technology. He has been a director and researcher for Behavioral Health of the Palm Beaches/ Seaside since 1999. He is currently in private practice at Veritas Palm Beach.

References
1. Kelly JF, White WL. What If We Really Believed that Addiction Was a Chronic Disorder? In Kelly JF and White WL (eds.). Addiction Recovery Management: Theory, Research & Practice. New York City: Springer; 2011.
2. White WL. Recovery Checkups. Retrieved from http://www.williamwhitepapers.com/ blog/2014/03/recovery-checkups.html
3. Skipper GE, DuPont RL. The advantages of long-term monitoring. Retrieved from http://www.addictionpro.com/article/ advantages-long-term-monitoring
RECOVERY SUPPORT WWW.ADDICTIONPRO.COM 35
Events
The Institute is a trusted educational resource that helps address daily challenges. Our conferences convene thought leaders that share clinical best practices, discuss how to effectively and efficiently operate a behavioral healthcare organization, and strategize solutions for addressing the opioid epidemic. Join us at an upcoming event to network with peers and take home valuable tools. Learn more about us and how we can help you at www. iadvancebehavioralhealthcare.com.
National Events
APRIL 22-25, 2019 | ATLANTA, GA
Be part of the discussion at the largest national gathering of stakeholders working together to address the opioid crisis. Prevention, treatment, law enforcement, public health, and many others exchange best practices and hear from state and federal officials at the annual Rx Summit. www.nationalrxdrugabusesummit.org

AUGUST 19-22, 2018 | DISNEYLAND, CA
Addiction professionals annually convene at NCAD to share what’s working: Clinicians hear from thought leaders on delivering treatment, while executives of behavioral healthcare organizations learn how to run more effective, more efficient, and ethically minded businesses. www.ncadcon.com
NOVEMBER 12-14, 2018 | FORT LAUDERDALE, FL
The opioid crisis is making headlines, but another category of drugs continues to devastate communities: stimulants. Join other stakeholders to explore how to address and treat stimulant use.
www.stimulantsummit.com
DECEMBER 10-12, 2018 | SCOTTSDALE, AZ
Senior executives of treatment centers, and those investing in these enterprises, discuss growth strategies and market dynamics at this exclusive, three-day educational and networking event.
www.treatmentcenterretreat.com
APRIL 30-MAY 2, 2018 | HILTON HEAD, SC
TCEM provides CEOs, CFOs, COOs, directors, senior marketing/business development/ admissions leaders, and other executives with the tools they need to effectively and ethically grow their services in a rapidly changing market. www.executiveandmarketingretreat.com
Interested in attending an event? Contact Ellen Kelley at ekelley@iabhc.com or 216-373-1223.
Photography: Pete Winkel GPA
President Obama addressed Institute attendees in 2016.
Matt Bevin, Governor of Kentucky, addressed Institute attendees in 2017.
and CE
CE Hours CE Hours
CME
Hours
National-Regional Events
CE Hours
The Summits for Clinical Excellence bring together thought leaders on cutting-edge topics in multi-day national and regional conferences. Summits on mindfulness, trauma, process addiction, and shame appeal particularly to private practice behavioral healthcare professionals. Other Summits address the national opioid crisis from a regional perspective and engage a diverse group of stakeholders. Many Summits offer treatment ethics continuing education credits.
• PITTSBURGH, PA June 25-26, 2018
The Opioid Crisis: The Clinician’s Role and Treatment Practices
www.pittsburghopioidsummit.com
• ATLANTA, GA October 18-21, 2018
Brain Matters: Shame, Trauma, and Process Addictions www.atlantasummitconference.com
• NEW ENGLAND November 8-9, 2018
The Opioid Crisis: Strategies for Treatment and Recovery www.newenglandopioidsummit.com

• PHOENIX, AZ February 20-22, 2019
The Opioid Crisis: The Clinician’s Role and Treatment Practices www.arizonaopioidsummit.com
• CHICAGO, IL March 6-7, 2019
The Opioid Crisis: Strategies for Treatment and Recovery
www.chicagoopioidsummit.com
• CHICAGO, IL March 6-9, 2019
Local Events
The National Conference on Alcohol and Addiction Disorders convenes panel discussions across the country in a lunch & learn format. Clinicians hear about treatment practices, while those on the business side of the field share strategies for managing and marketing behavioral healthcare organizations.
www.iabhc.com/local
Upcoming events:
Virtual Events
Hear from experts on clinical, managerial, and other topics in our frequent, free-to-attend Webinars.
www.iabhc.com/webinars
attending an event? Contact Ellen Kelley at ekelley@iabhc.com or 216-373-1223.
The National Conference on Trauma, Addictions, and Mindfulness: Where Freud Meets Buddha www.chicagosummitconference.com Interested
in
Baltimore Chicago Columbus, OH Denver Detroit King of Prussia, PA Long Island Memphis Nashville New Orleans Phoenix Pittsburgh Providence Salt Lake City San Diego Washington, DC
CE Hours
CE
Hours
Include self-awareness in counselor training
An academic program embeds self-care topics into its curriculum
BY GARY A. ENOS
ddiction counselors today see patients with increasingly complex problems in healthcare systems of similarly growing complexity. Often, they are required to see more patients with fewer resources. If their academic training does not address the real threat of burnout and potential turnover out of the profession, one can expect a worsening of a problem that currently plagues all of healthcare.
“From day one of orientation, we’re talking self-care,” Stephen Delisi, MD, assistant dean at the Hazelden Graduate School of Addiction Studies, tells Addiction Professional
“When we hear back from our students, they’ll say, ‘We didn’t necessarily fully appreciate at first how important self-care was, but we kept hearing about self-care. By the end of the program, we were fully aware,’ ” Delisi says.
The topic of self-care hits home for Delisi, a longtime addiction psychiatrist who maintains a clinical practice in addition to his administrative duties. His medical training certainly did not focus much on physician self-care, and one byproduct of that is seen in presentday doctor surveys in which half of respondents report feelings of burnout.
Students at the Hazelden graduate school see self-care topics embedded throughout the academic curriculum, from introductory courses in the first semester to professional development training in the final semester. Delisi says the school’s ties with a working treatment organization, the Hazelden Betty Ford Foundation, have improved its overall awareness of why these topics need to be incorporated into clinicians’ academic training.
Another goal here involves the effort to grow clinicians into future leaders within their organizations. “We’re trying to increase the leadership aptitude of the next generation of counselors,” Delisi says. “If [we can develop] a healthier culture, that will help with burnout and turnover.”
IMPORTANCE OF MASTER’S TRAINING
In discussing trends in higher education for clinicians, Delisi emphasizes first the continued establishment of the master’s degree as the degree of choice, both for individuals who are newly entering the field and those advancing their training and credentials.
Again, the changes occurring in the treatment environment offer a model for what needs to be happening at the academic level. Delisi points to how Hazelden Betty Ford’s clinical model has dramatically transformed, to the surprise of many nationally at first.
“Why do we now have patients on Vivitrol, and Suboxone, and specialized opioid support groups?” he says. “Higher education has to be keeping up with that. How does the curriculum equip the next generation for those integrated treatment approaches?”
In today’s behavioral health treatment organizations, it is
BUSINESS OPERATIONS 38 SPRING 2018 ADDICTION PROFESSIONAL WWW.ADDICTIONPRO.COM
the master’s-level clinicians who are securing the unit manager and program director jobs, Delisi says. The master’s degree also offers the only pathway to the licensed professional clinical counselor (LPCC) credential. Having more LPCCs on staff in an organization can allow treatment facilities to hire fewer psychologists and to be able to use them more in a consulting capacity, he says.
An ever-present question in recent years has been whether the master’s degree will move from highly desirable to mandatory for any clinical practice in addictions. Delisi identifies some components of the field where this might be true. For example, front-line staff in treatment organizations that address co-occurring substance use and mental health disorders in a truly integrated fashion will need to be master’strained professionals, he says.
Also, as the field collaborates with larger health systems, the master’s-trained professional will serve as the entry point for integration with primary care, he says. “If you’re going to have addiction professionals in medical homes, they’re going to need a master’s,” Delisi says.
EVOLUTION OF CURRICULUM
Delisi outlines several areas in which the Hazelden school has sought to broaden its curriculum for today’s clinicians:
• It has expanded its advanced course in differential diagnosis as part of an effort to broaden its offerings that address co-occurring disorders.
• Its examination of evidence-based practices now goes well beyond the traditions of 28-day treatment to address areas that include contingency management, 12-Step facilitation, cognitive-behavioral therapy, dialectical behavior therapy and motivational interviewing.
• Other components that have expanded at the graduate school include multicultural diversity, the effects of trauma and adverse childhood experiences, and neurobiology.
Applications of technology also are growing in importance. Today’s clinicians no longer have to be familiar with an electronic health record only—they also must be prepared to conduct therapy groups online and offer access to treatment for individuals in remote communities. Hazelden students have the opportunity while in the program to interact with
clinicians who are employing telehealth strategies in their practices, Delisi says. Today’s clinicians in training, whether new to the field or expanding their professional expertise, are becoming savvy observers of the directions in which professional practice is moving. Delisi says this is playing out not only in their interest in applications of technology, but also in outpatient levels of care that are growing in importance in today’s cost-conscious and more integrated environment.
Delisi sees the continued attention around the opioid crisis as a major factor for many individuals pursuing a career as an addiction professional. “The national discussion occurring because of the opioid epidemic is shedding light on the larger issue of addiction in general,” he says.
But the training should not reflect an effort to “solve” discrete crises, he says, because the waning of one drug phenomenon inevitably will give way to the rise of another, he says. “The goal should be one of addressing addiction as a disease,” Delisi says.
BUSINESS OPERATIONS WWW.ADDICTIONPRO.COM 39
Gary A. Enos is Editor of Addiction Professional.
In today’s behavioral health treatment organizations, it is the master’s-level clinicians who are securing the unit manager and program director jobs.
Center connects tech to treatment
A facility’s clients engage in an online environment from the point of admission
BY NEIL GAER
ashburn House is an addiction recovery center located in Worcester, Mass., serving individuals with substance use disorders. We opened a medically monitored withdrawal management (detoxification) program and a clinically managed inpatient program last year, recently expanding to 52 beds. We also operate outpatient levels of care and a 42-bed sober living community. Our care is structured around four overarching goals: evidence-based treatment; well-structured, repeatable processes; engaged clients; and seamless transitions as clients step down and reintegrate.
We believed that if we could incorporate technology into day-to-day treatment and connect clients to it, we could achieve these goals. We would have one treatment approach that we could evolve as we learned and grew. We would have engaged clients, as most are millennials and members of the digital generation. And, with the right technology, we should even be able to smoothly hand off to the next phase of treatment.
TECHNOLOGY INTRODUCED AT ADMISSION
Upon admission to our inpatient program, clients are set up with a laptop, allowing them access only to the online environment that we have built. We start with the Texas Christian University Client Evaluation of Self and Treatment surveys, conducting them online. The surveys that we use assess motivation, engagement, psychological and social functioning, and trauma. We follow TCU’s protocol for when to assess the client. We conduct three of the surveys multiple times, the last time being post-discharge. Our implementation of the surveys automatically calculates the client’s score, comparing the results with the TCU benchmarks and ultimately against facility-
specific data. We are not shy about showing the results to the clients. This helps them see—and believe in—the progress they are making.
Washburn House structures treatment by assigning worksheets tailored to the objective of a client’s individualized plan. Clients fill these out (again online), our counselors review and discuss them with the clients, and clients can iterate if need be. Clients can even self-assign worksheets.
Our case managers also plan transitions using the same technique of assigning a series of worksheets. Discharge planning begins immediately, but the client and the case manager develop the plan together over the course of the treatment stay.
Importantly, the clients take these worksheets (both the transition plans and all the therapeutic assignments) with them when they move on from Washburn House and reintegrate into their communities. The goal is not to discharge our clients with a paper portfolio, as it can easily be lost or discarded. Instead, the portfolio lives in their phones and, for those few without a phone, it is accessible via a browser. Being able to reference it later gives clients another way to see how much progress they have made, and it offers reminders if needed.
One dimension of our treatment involves helping clients be more reflective and become less reactive to their triggers. To help teach this, we use daily check-ins that offer an inspirational quote and then ask a quick “How do you feel today?” We begin the daily check-ins during the client’s inpatient stay, with the care team receiving alerts when there are problems. We continue them post-discharge, thus providing a little more continuity across each level of step-down. We can monitor ongoing progress, and we are maintaining a lifeline back to us should the client need it.
40 SPRING 2018 ADDICTION PROFESSIONAL WWW.ADDICTIONPRO.COM BUSINESS OPERATIONS
IMPLEMENTATION CHALLENGE
Interestingly, our biggest challenges have not been in integrating the technology into the treatment itself. Clients have really taken to completing the surveys and assignments online. We were initially concerned whether clients would engage with the daily check-ins, but then one client pointed out, “What’s the first thing you do in the morning? Check your phone for messages.” As long as we kept it light, they were all in.
For us, the first challenge was figuring out how to manage the logistics of intake and onboarding (i.e. provisioning laptops for new clients, making the initial set of assignments, etc.). Part of this stemmed from being a new treatment center, but another part was that we have added steps to the process. Our platform for all of this allowed us to structure that into a repeatable workflow once we determined the best way to do it.
The other big challenge involved integrating with other followup programs at organizations outside of the Washburn House continuum. We are still working with many of these organizations on how our clients might continue with the TCU surveys and daily check-ins. If clients stay within the Washburn House
continuum, we can continue to incorporate use of technology in both our outpatient programs and our sober living community.
A goal for us is to make a client’s portfolio available to the downstream care teams, since we know greater continuity of care improves outcomes. As we grow and develop stronger ties with other programs, we expect to institute this. The platform’s sharing data across organizations and managing workflow across transitions were key reasons we implemented the system.
Going forward, we expect to leverage technology more, seeing it become integral throughout the cycle of care. Telepresence/video chat for remote counseling, social networking-type technologies for support groups, etc.—these capabilities are certain to boost outcomes further. For, as one of our clients put it: “I like it; it’s like you’re not alone.”
Neil Gaer is the CEO at Washburn House, a private substance abuse treatment center in Worcester, Mass. He has more than 25 years of experience at various social and human services organizations. Prior to joining Washburn House in January 2017, Gaer was president of SEG Consulting.

Timberline Knolls is a residential treatment center located on 43 beautiful acres just outside Chicago, offering a nurturing environment of recovery for women ages 12 and older struggling to overcome eating disorders, substance abuse, mood disorders, trauma and co-occurring disorders.

While there’s life, there’s hope.
Rooted in the principles of recovery and emphasizing spiritual growth, Timberline Knolls combines clinical services, education and expressive therapies to enhance the continuum of life-changing care. Striving to provide the most effective and highest quality individually tailored treatment, Timberline Knolls gives its residents hope again.
BUSINESS OPERATIONS WWW.ADDICTIONPRO.COM 41
40 Timberline Drive | Lemont, Illinois 60439 | 1.877.257.9611 www.timberlineknolls.com | info@timberlineknolls.com
LGBT youths report eating disorders at stunning rate
Data shows more than half of the surveyed population between age 13 and 24 has been diagnosed with an eating disorder
BY GARY A. ENOS
ecause health concerns in the LGBT population generally are considered to be an under-researched topic, the release of any comprehensive data in this area rarely escapes notice in the professional community. In the case of results of a newly released survey on eating disorders among LGBT young people, however, these fresh numbers are both noteworthy and utterly staggering.
Cosponsored by the National Eating Disorders Association and unveiled as part of the annual awareness week activities that it spearheads in February, the survey of more than 1,000 young people ages 13 to 24 found that more than half (54%) had received an eating disorder diagnosis at some point in their young life. Moreover, of those individuals who had not received this diagnosis, 54% said they suspected they had an undiagnosed eating disorder.
Such numbers did not appear to surprise Philip McCabe, a health educator at the Rutgers University School of Public Health and president of NALGAP, The Association of Lesbian, Gay, Bisexual, Transgender Addiction Professionals and Their Allies. However, McCabe tells Addiction Professional , “As a trainer on LGBT issues, I find many clinicians are surprised when I share information
on eating disorders with gay and bisexual youth.”
McCabe adds, “This raises several areas of concern—first, not all addiction professionals have received training on eating disorders. Unless the client self-discloses, it is not always included during the assessment.”
WHAT THE NUMBERS SHOW
The online survey also was conducted by Reasons Eating Disorder Center and The Trevor Project, the latter being an organization seeking to end suicide in the LGBT population. It took place from early January to early February of this year and included individuals identifying as a sexual orientation other than heterosexual and/or a gender identity other than cisgender, which is defined as identifying with one's gender of birth. A detailed questionnaire explored disordered eating diagnoses and behaviors, as well as any history of suicidal ideation or behavior.
The survey found that transgender youth face a disproportionate risk of having an eating disorder, with 71% of transgender respondents who identify as straight having been diagnosed with an eating disorder. However, cisgender LGBTQ females (the Q stands for both queer and questioning in the survey) reported the highest prevalence of eating disorder diagnoses of any gender identity in the survey, at 54%. By comparison, the prevalence of eating disorders among cisgender males was 31%, and the prevalence of eating disorders among transgender females was 12%. A total of 39% of transgender males reported an eating disorder diagnosis.
The researchers reported that across all subpopulations in the survey, the most common habits of disordered eating were fasting, skipping meals and eating minimal amounts. Bulimia was the most common eating disorder diagnosis that cisgender and transgender females had received.
The survey also illustrated a close link between the presence
PROCESS ADDICTIONS 42 SPRING 2018 ADDICTION PROFESSIONAL WWW.ADDICTIONPRO.COM
of an eating disorder and suicidality. Responses indicated that 58% of LGBTQ youths who had been diagnosed with an eating disorder have considered suicide. Suicidal thoughts were more common among young people who had been diagnosed with bulimia, the researchers reported.
An introduction to the survey document from Amit Paley, CEO of The Trevor Project, states that the findings “are alarming and highlight the need for further research to improve the lives of LGBTQ young people in this country.”
CORRELATIONS GO UNRECOGNIZED
“There is a correlation between body dysphoria, poor body image, combined with how individuals who experienced trauma and minority stress, that is not always understood,” says McCabe in reaction to these findings on eating disorders in the young LGBTQ population. He adds, “This survey helps to shed light on the greater health risks of LGBTQ youth and young adults.”
Paley adds in the survey document, “The unique stressors
that LGBTQ-identified people experience, such as coming out and harassment in schools or the workplace, can impact levels of anxiety, depression, low self-esteem, and unhealthy coping mechanisms such as substance abuse. All of these can be contributing factors in the development of an eating disorder and are common co-occurring conditions.”

McCabe says that in discussing findings such as these, he often calls attention to a 2014 American Academy of Pediatrics study showing that gay and bisexual teen males use illicit steroids at a rate almost six times higher than straight teens.
McCabe suggests that clinicians who work with LGBTQ patients don't always grasp the full range of behavioral health issues that can be related to the experience of minority stress in this population. “Knowing how to address the concerns with LGBTQ affirmative and comprehensive evidence-based interventions requires specific training,” he says.
Gary A. Enos is Editor of Addiction Professional.
Substance Use Recovery and Wellness Program
Life changing treatment for addiction and chronic pain. Program features include:
• Detoxification
• Outpatient treatment
• Spiritual care
• Family care
• Chronic pain
We LIVE to Hope
• Recovering Alumni Association and sober living
• Relapse prevention
• Recreation therapy
Assisting our patients in meeting personal goals and guiding them on the road to recovery is why we LIVE to Hope
To request more information or to make a referral for the LLUBMC Substance Use Recovery and Wellness Program, please call 909-558-9277 or visit us on the web at llubmc.org
PROCESS ADDICTIONS WWW.ADDICTIONPRO.COM 43
MANY STRENGTHS. ONE MISSION.
NEED TO KNOW
Five facts about recovery support group options
Commitment to a group —not the group’s content— appears to make the difference
1
Leaders of organizations offering a secular alternative to 12-Step support groups felt jubilation over study results published in March in the Journal of Substance Abuse Treatment
The study found that active engagement in a mutualhelp group offers equivalent benefits no matter which type of group an individual joins.
2
Lead researcher Sarah E. Zemore, PhD, senior scientist at the Alcohol Research Group, explains that while effect sizes for Alcoholics Anonymous (AA) and its derivatives have always been large, “The number of people who stick with AA after formal treatment is quite small.” For some, the religious nature of the 12 Steps leads to a search for other options.
5
3
Zemore’s Peer Alternatives in Addiction study compared alcohol and drug use outcomes for participants in 12-Step groups and three secular alternatives: SMART Recovery, Women for Sobriety and LifeRing Secular Recovery. After adjustment for possible confounding factors, they found that substance use outcomes at baseline, six months and 12 months were about the same in all groups.
4
The “secret sauce” to members’ success in these groups was active involvement, which can take a form as simple as facilitating a meeting or helping to set up the room.
Preliminary analysis of the data showed that SMART Recovery members had a lower likelihood of abstinence from alcohol at 12 months. But the adjusted analyses uncovered a simple explanation for this: Fewer SMART Recovery members had identified abstinence as their primary goal.
44 SPRING 2018 ADDICTION PROFESSIONAL WWW.ADDICTIONPRO.COM
FOR PREVENTION, SUBSTANCE USE TREATMENT, AND RECOVERY PROFESSION ALS


Nurses fighting an opioid crisis from within
BY RACHAEL ZIMLICH, RN
hile nurses join other healthcare providers in battling the opioid epidemic on the front lines by caring for patients with overdoses or chronic substance use, they also are fighting a more private struggle.
With easy access to potent drugs and the autonomy to practice with minimal supervision, coupled with the realities of a highly demanding and stressful job, nurses might be tempted to abuse or divert the medications they steward for their patients. What’s worse is that with so much to lose, nurses might not get help until the problem hurts their patients or themselves.
In these cases, state boards of nursing are tasked with regulating licenses and addressing problems such as substance use when they occur. Nursing boards typically take a non-punitive stance in cases of problematic substance use, offering nurses an opportunity to get treatment for their disorder and retain their license. However, criminal charges can be filed by hospitals, employers or patients for neglect, theft or other issues associated with substance use or diversion among nurses.
EXTENT OF PROBLEM
The American Nurses Association estimates that as many as 15% of registered nurses may be fighting a substance use problem or are in recovery. While substance use problems aren’t necessarily more prevalent among nurses than in the general population, the issue takes on a different form among nurses because of how accessible controlled substances are to the profession.
A 2015 report published in Substance Abuse revealed that out of 300 nurses participating in a health assistance program, almost half admitted in an anonymous poll to drug or alcohol use at work, with 40% acknowledging that the use affected their professional competency.
In addition, about 60% of respondents said their problem could have been detected earlier, and that they didn’t seek help out of embarrassment and fear over losing their nursing license.
Finding ways to improve early detection and intervention is the goal of the Missouri State Board of Nursing. Mariea Snell, assistant professor and faculty coordinator of nursing at Maryville University and vice president of the state nursing board, is working to move beyond the traditionally reactive way of handling substance use problems among nurses.
Missouri has been collecting data on how and when substance use-related infractions among nurses occur, Snell says, and is working to provide analysis that will help identify trends and potential prevention and treatment interventions.
“There’s the thought that we’re seeing this more only because we’re able to detect it more,” says Snell. “This kind of problem is a combination of things. We have more opioids on the market and more access to them. And we have the technology now that detects them more frequently. I don’t believe necessarily that this is a new phenomenon. It’s just sort of a perfect storm of access and ability to detect.”
A nurse’s problems with substance use or diversion are already in full swing by the time they reach the attention of the state board, Snell says. While states have been collecting data on numerical trends, little has been done on what factors might contribute to substance abuse and diversion among nurses, and what preventive measures might be taken. Snell hopes that as Missouri’s data analysis progresses, the state board will be able to identify risk factors, as well as steps the state could take in cases of problematic use or diversion.
“We’re beginning to see those trends,” Snell says. “We see trends in settings where there’s less overall supervision but increased access.” For example, home healthcare has comparatively high rates of substance use and diversion for these reasons. “It seems to be a little too tempting for people who might have had some tendencies to begin with,” Snell says.
46 SPRING 2018 ADDICTION PROFESSIONAL WWW.ADDICTIONPRO.COM CLINICAL CHALLENGES
With easy access to potent drugs, autonomy and high-stress work, nurses face temptation to abuse or divert medications
TRENDS BY SHIFT AND UNIT
Electronic medical records and automated dispensing systems were supposed to help prevent abuse and diversion, but opportunities still exist. Snell says Missouri’s board is looking into what types of units and which shifts might be most conducive to problems, and the initial results are surprising.
“Looking at shift work, we were surprised to see no significant difference between day and night shifts,” Snell says. “We see more errors in medication administration at night, but it’s not diversion-related.”
As for the types of nursing units that are most prone to problems, Snell says the trend seems to point to the more acute units. Operating room nurses and certified registered nurse anesthetists have high rates of problematic use and diversion, and Snell says “it all comes down to access.”
Although the final analysis has not been completed, Snell shared initial data revealing that just over one-third of drug abuse issues among registered nurses occur in the hospital setting. Among hospital units, it appears that emergency departments, operating rooms, intensive care units and psychiatric units are fairly even on prevalence, she says. Problems appear most prevalent during 12-hour day shifts, she adds.
Travel nursing also poses concerns. “They’re very difficult to monitor,” Snell says of these professionals. “It’s hard because by the time [facilities] have noticed there’s a
problem, they’ve already moved on to a new assignment.”
SEEKING TO PROTECT PATIENTS
Snell hopes the investigative work being done in Missouri will benefit patients. She recalls a case in which a nurse injected a dying patient with a mixture of water and mouthwash after diverting the patient’s pain medication, and the patient died in agony. Stories such as this motivate Snell to find ways to help both nurses and patients.
“From the state board perspective, we don’t want to go around revoking licenses, but we’re there to protect the public,” she says. “We definitely feel it’s of high importance to figure out where these problem areas are.”
Snell says she is working to identify prevalence of abuse among nurses who had a prior history of drug problems, but the data aren’t available yet. In many cases, nurses with recent or significant substance use histories work under restricted licenses, but the state might have to offer more.
Missouri is now offering a self-reporting program that will allow nurses to report and address a problem in order to get help without losing their license, Snell says. “I see it as the best next step to combat this from a professional standpoint,” she says.
ADVERTISER INDEX
CLINICAL CHALLENGES WWW.ADDICTIONPRO.COM 47
Rachael Zimlich, RN, is a freelance writer based in Ohio.
Pages Pages Alkermes CVR 4 Ashley Addiction Treatment CVR 3 Brown Consulting Group 4 California Southern University .......................................... 19 Central Recovery Press 17 D'Amore Healthcare 21 Dominion Diagnostics ........................................................ 9 Foundations Recovery Network 28, 29 Governors State University 27 Hazelden Graduate School of Addiction Studies 13 IC&RC ............................................................................... 45 John Volken Academy and Lift the Children 7 Loma Linda University Behavioral Medicine Center 43 McLean Hospital 25 Recovery Centers of America............................................. 4 Retreat Premier Addiction Treatment Centers 31 Rosecrance 3 Sierra Tucson ...................................................................... 1 Soberlink CVR 2 The Retreat at Sheppard Pratt 23 Timberline Knolls 41 University Park Behavioral Health .................................... 15
Time in treatment worked in his favor
Stuart Gregory is living a productive, self-directed life while running five companies in recovery
BY GARY A. ENOS
tuart Gregory now divides his time among five companies that he runs, with his primary role at technology consultant Capstone Technology Solutions in Statesboro, Ga. His productive, self-directed life seems almost unimaginable given that a decade ago he was living in his car and initially saw substance use treatment as merely a slight improvement over what had become his default home.
Looking back, Gregory credits his treatment program’s “sheer defiance of my will” with helping him reach where he stands today. The other key ingredient, he emphasizes, was time. It took quite a while for Gregory to regress from a first joint at age 12 to the depths of despair, and likewise it would take time to find hope. He now applies that lesson to the intensive outpatient and sober living program for men that he founded, called Big Step Recovery and located in a recovery hotbed west of Savannah.
“If you can subjugate your ego to be a part of something and care about other people long enough, you can love yourself enough to stay sober,” says Gregory, who turns 35 in April.
CONTRADICTION IN YOUTH
When Gregory was first exposed to marijuana (a friend had stolen a cigarette from his sister), something that happened and something that didn’t both became important.
“That sense of ease and comfort that comes from the first hit happened,” he recalls. “And everything that [youth prevention program] D.A.R.E. had told me didn’t happen. I didn’t go out and steal someone’s TV.” The experience, and the mistrust of authority figures that it generated, would fuel his curiosity. For years, he would test the limits of his mind and body.
He says he began to experience consequences from escalating substance use around age 18, when he decided to escape an uncomfortable situation by joining the Army. “It is not a great place for a young alcoholic and drug adidict to be,”
Gregory says.
In the worst of times, he was using crack, opioids and alcohol, and was homeless. “I wasn’t suicidal in the classic sense, but death would have been a gift,” he recalls.
An acquaintance whom Gregory had known before the man had found recovery told him there was another way to live. Even though he didn’t believe him at first, a treatment facility seemed a better alternative to living in a car. He would end up spending around three years among various levels of care.
Gregory says his treatment experience has shaped the program structure at Big Step Recovery, as well as his other work (his technology company employs several people in recovery who are looking to get back into the tech arena). “One thing I’ve added, which I didn’t have a lot of myself, is lots of clinical sessions,” he says. “Our guys are getting nine to 16 hours a week of therapy. They are inundated in individual and group.”
LESSON LEARNED
Reflecting on the details of his journey, Gregory believes that the simplistic prevention messages of the field’s past need to be discarded once and for all. “If I could have sat around and ‘just said no,’ I would have, at least once,” he says. “Our taboo attitude about drugs is part of the problem.”
Comprehensive education, and plenty of patience in working with the young person, are crucial, he says. The long path has ultimately paid off for him. “I get to do what I want for the rest of my life, and what I want doesn’t hurt anybody,” he says.
Gary A. Enos is Editor of Addiction Professional.

RECOVERY 48 SPRING 2018 ADDICTION PROFESSIONAL WWW.ADDICTIONPRO.COM
Fi nd f reedom f rom pa i n.













PAIN RECOVERY PROGRAM
Ashley is a leader in pain recovery. Our comprehensive program helps reduce pain and treats co-occurring substance use disorder through evidence-based methods.
Ashley’s Pain Recovery Program offers:

• Individualized care







• Innovative treatment
• Integrated approach
Everything for recovery because recovery is everything.
800.799.HOPE (4673) AshleyTreatment.org
HELP SUPPORT YOUR PATIENTS WITH VIVITROL ALKERMES and VIVITROL are registered trademarks of Alkermes, Inc. ©2016 Alkermes, Inc. All rights reserved. VIV-002646 Printed in the U.S.A. vivitrol.com Discover VIVITROL at VIVITROL.com
