
DEXIS™ Intra-oral Scanner Solutions Simpler paths to better outcomes DEXIS™ Intraoral Vol. 34 No. 1 JANUARY/FEBRUARY 2023 $99.00 p.a. DEN TAL PRACTICE Australasian DEN TAL PRACTICE THE BUSINESS MAGAZINE FOR DENTISTS








SYDNEY 2-3 JUNE 2023
NOVOTEL SYDNEY BRIGHTON BEACH

TWO DAYS OF LECTURES AND WORKSHOPS ON DIGITAL DENTISTRY FOR DENTISTS, SPECIALISTS, DENTAL TECHNICIANS AND DENTAL PROSTHETISTS
TWO DAYS OF LECTURES AND WORKSHOPS ON DIGITAL DENTISTRY FOR DENTISTS, SPECIALISTS, DENTAL TECHNICIANS AND DENTAL PROSTHETISTS
TWO DAYS OF LECTURES AND WORKSHOPS ON DIGITAL DENTISTRY FOR DENTISTS, SPECIALISTS, DENTAL TECHNICIANS AND DENTAL PROSTHETISTS
TWO DAYS OF LECTURES AND WORKSHOPS ON DIGITAL DENTISTRY FOR DENTISTS, SPECIALISTS, DENTAL AND DENTAL
REGISTER NOW and SAVE!
SPONSORS

INDUSTRY SUPPORTERS

» Pola Light is super safe, doesn’t burn the gums, and produces the whitest natural shade over time B est of all, patients can w hiten from the comfor t of their own homes. «
 Miles Cone, DMD, MS, CDT, FACP - USA
Miles Cone, DMD, MS, CDT, FACP - USA
www.polawhite.com.au

DEXIS has relaunched its intraoral scanner range with the IS 3700 and IS 3800W building on the solid foundation of the IS 3600 with its highly accurate, continuous HD colour scanning

management
66 Business ownership disputes
70 How to generate a remarkable ROI by investing in your team
72 The dental practice generational divide: Uncovering the diamonds in the rough
74 Five steps to a high financial IQ in 2023

76 A good habit on a cancellation call marketing
78 Why your practice isn’t growing... and what to do about it finance
80 Who’s got your back?
82 Last call for temporary full expensing
facebook.com/dentalpracticenow twitter.com/adpmagazine instagram.com/dentevents



www.dentalpractice.com.au
Publisher & Editor: Joseph Allbeury Clinical Editor: Dr David Roessler Technology Editor: Prof. Laurence J. Walsh
Infection Control Editor: Prof. Laurence J. Walsh Senior Contributing Editor: Dr Christopher CK Ho
Columnists: Dr Georges Fast, Dr Jesse Green, Garry Pammer, Phillip Win, Dr David Moffet, Graham Middleton, Simon Palmer, Julie Parker, Jayne Bandy, Angus Pryor Design & Production: Jasper Communications
Australasian Dental Practice™ ISSN 1445-5269 is printed in Australia and published six times per year by Main Street Publishing Pty Limited
ABN 74 065 490 655 PO Box 586, Cammeray NSW 2062 Tel: (02) 9929-1900 Fax: (02) 9929-1999 Email: info@dentist.com.au © 2023 All rights reserved. The contents of this magazine are copyright and must not be reproduced without the written permission of the publisher. Permission to reprint may be obtained upon application. Correspondence and manuscripts for publication are welcome. Although all care is taken, the editor and publisher will not accept responsibility for the opinions expressed by contributors to this magazine, or for loss or damage to material submitted for publication
Subscriptions: Australia and NZ: A$99.00 per year includes OralHygiene™ and eLABORATE™ magazines; Overseas Airmail: A$220.00 per year.




























112 Implant restoration in the aesthetic zone using guided surgery and immediate functional loading

118 Using ceramic furnaces for chairside restorations 124 Precise and confident treatment of a complex root fracture 128 Preserving vitality after dental trauma - use of hydraulic calcium silicate cements in practice



Every two years in dentistry, a very special event takes place on the other side of the world. Over the course of five days, Cologne, Germany transforms into the global epicentre of dental ideas, technology and innovation as typically 150,000+ people descend on the city for the biennial staging of the International Dental Show, better known as IDS. For me, it’s the happiest place on earth!
By Joseph AllbeuryCompared to dental exhibitions in Australia, IDS is on an unimaginable scale with visitors struggling to take it all in even over five days - with no real possibility of engaging with every stand individually! Every manufacturer is represented with massive displays brimming with hospitality, entertainment and products galore - to visit them all in depth would take a month! Plus, there are experts on hand that can answer all of your questions on the spot regarding current products and what’s in the pipeline for the future.
Whilst many people in the dental community pencil in a visit to IDS on their “bucket list”, I’m fortunate to be going for the 12th time this year, visiting every IDS since 1999, only missing the scaled down COVID version in 2021.
If you had to describe IDS in a single word, it would be ENERGY. There is an immediate sense that there is an immense energy attached to the event that you simply never see to the same extent elsewhere. Another word would be PASSION, as there is no shortage of that on hand either.
Hundreds of millions of Euros are invested to ensure visitors have the best possible experience by exhibitors from the corners of the globe... including Australian manufacturers like SDI Limited, Myofunctional Research Co, ASIGA, BioMiniatures, Ozdent, Blender4dental, Partmaker and others.
In times past, before the internet existed and electronic communication became second nature, exhibitors at IDS would launch products that represented years of tireless toil coming up with the next big thing. Product development was literally on a two-year cycle to ensure you had something new and special to talk about in Cologne. And whilst the internet has changed much, there is still a healthy dose of NEW to be found everywhere at IDS.
IDS 2023 is particularly special because it is the 40th staging of the event and its 100 year anniversary. And it’s also the first proper staging of the event after the COVID-19 disruptions of the past few years. Like many, I will be looking forward to seeing this grand event return to normal as it truly is one of the best experiences on offer in the dental world.
And... by the time our own Digital Dentistry & Dental Technology 2023 event is staged in Sydney on June 2-3, we’re hoping to see some of the new tech from IDS filtering down under. So remember to register now for the best time you will have at an Australian dental conference in 2023.
Joseph Allbeury, Editor and PublisherSince Dr Michael Back won the Ultimate Practice Makeover in 2022, it’s fair to say life has been busy. Recently, Michael and his wife (and part time receptionist), Amy, were joined by a team of experts with the goal of taking the practice from good to great, while capturing the whole thing on camera. Expert dental coach, Dr Jesse Green, trained Michael and the team on the finer points of patient retention and boosting case acceptance. Practice Broker, Simon Palmer, advised Michael on the opportunities to grow his practice to ultimately increase its value. Host of the UPM and Practice Growth Specialist, Angus Pryor, introduced Michael and the team to a patient referral system, designed to significantly increase the referrals the practice receives. And soon, the Medifit Design + Construct crew will update the reception and waiting area to give the practice a new look befitting the significantly upskilled staff and systems that is all part of the prize. The team from New Horizons Media were there to capture the whole thing on video. The Ultimate Practice Makeover is a multi-part reality TV show tracking the journey of a dentist and team as they transform their practice with the assistance of industry experts. The show will be released later in 2023 on dentevents.tv. Stay tuned!


Dürr Dental has appointed Mr Darius Rohanian to the new role of Product Specialist for CBCT and Imaging in Australia & New Zealand. Mr Rohanian is an Oral Health Therapist who graduated from La Trobe University in 2012. Throughout his time at University, he completed a wide range of local and international placements, including clinical training in New York City. He graduated with the Australian Dental & Oral Health Therapist Association (ADOHTA) Award and La Trobe University Dental Therapy Award for excellence in both the education and treatment of children. Over the past 11 years, he has worked in leading private practices across Sydney and Melbourne. He has also spent time working as a Clinical Educator at the University of Sydney. Mr Rohanian will be responsible for Dürr’s imaging and software range, with a particular focus on the VistaVox S, the new state-ofthe-art CBCT unit that boasts unparalleled image quality. While working closely with distributors, he will also be available to clients to help with their needs. Mr Rohanian can be contacted on 0484-708-940 or darius.rohanian@duerrdental.com.

La tes t de velopm en ts in reg e n erati ve the ra pie s
Li ve su rgerie s
Hands-on wor ksho ps

Cas e sessio n

Morning with master clinici an s
Clini cal round ta ble s
Post er exhibitio n
Res ea rch net working day
Join t sessions with AAP an d SE PA
CO MMI TT EE
WilliamV Giannobile, USA
Pamela K. McClain, USA


Franck Renouard, France

Frank Schwarz, Germany
Anton Sculean, Switzerland
Istvan Urban, Hungary
Free symposium registration & invitation to research networking day






“There is plenty of anecdotal evidence of individual dentists being trained to perform a particular procedure on a patient, who is examined by somebody else, has a course of treatment ‘sold’ to them by another and this is then delegated to the various dentists working in the practice...”
Whenever I think about where our profession, the dental profession, stands today, the poem A ntigonish by Hugh Mearns keeps going around and around in my head. It begins...
“Yesterday, upon the stair, I met a man who wasn’t there He wasn’t there again today I wish, I wish he’d go away...”
My colleague, Geoff Knight, once said that trying to organise dentists was a bit like trying to herd cats. This was some 30 years ago and at the time, it perfectly described of our profession. I wonder if he still thinks that today.
In my first column in 1999, I asked whether we were taking advantage of the generally lower rate of decay and planning our patients’ treatment early enough so that they would have effective and efficient dentitions in old age. Were we getting away with poor restorative practice and avoiding confronting our patients with the need to plan for the future and maybe having to spend some money? Were we trying to save our patients money when we should be saving their teeth?

At the time most dental practices were privately owned, with the dentist having a long-term trusting relationship with their patients. It would have been unthinkable for most to recommend treatment based on the business needs of the dentist. The few dentists who were known to overservice were generally ostracised by the rest of the profession!
Two things had a monumental impact on the way dentistry has changed since then. The first was the panic that ensued after AIDS first appeared and because of the actions of one American dentist, HIV became associated with dentistry! Our professional leaders, instead of debunking this myth, proceeded to lobby for greater regulation and hence standardisation of the way dentistry needed to be practised. No regulation seemed too tough nor process too onerous in the pursuit of safety. We had so-called infection prevention experts (whose only real
qualification was appointment to infection control committees) suddenly instructing the rest of the profession how to manage their practices, ensuring that this was backed up by the registration authorities. The net result of this was that the delivery of dentistry became standardised to the extent that as long as you complied with the rules, you were largely relieved of the responsibility for what happened in your practice. You ticked off the boxes and all was O.K.
The second factor was the ability of non-dentists to own and operate dental practices. What started as a small number of practices owned and operated by member-owned mutual benefit societies escalated when some funds were de-mutualised and were sold off to insurance companies. At the same time, under the guise of increased competition and the supposed pursuit of lower dental fees, anybody could own and run a dental practice so long as the person that provided the treatment was a dentist, hygienist, therapist or prosthetist. Management of these entities was no longer the province of dental professionals, KPIs were no longer based on the quality of the dentistry or on the care taken to look after the long term needs of the patient. What matters now is hourly production figures and return on investment to the shareholders.
There is plenty of anecdotal evidence of individual dentists being trained to perform a particular procedure on a patient, who is examined by somebody else, has a course of treatment “sold” to them by another and this is then delegated to the various dentists working in the practice. Often the technical aspect of the dentistry is of a high standard which is not so difficult to do when cutting virtually virgin teeth to be veneered or crowned in the pursuit of some aesthetic nirvana promoted by various “influencers”. The fact that this then condemns the patient to a lifetime of dental treatment, replacement and maintenance is rarely if ever considered.
It was always the intention of the corporates and the health funds to turn dentistry into a product instead of a service and to wrest control of our profession from us. In this they have largely succeeded.
As I drive past the ever-increasing number of “dental studios, dental spas, smile centres”, etc, I very rarely see the name of the dentist on the hoarding outside the practice. The optimist in me keeps hoping that it is the result of some element of shame that our profession has come to this.
“Under the guise of increased competition and the supposed pursuit of lower dental fees, anybody could own and run a dental practice... Management of these entities was no longer the province of dental professionals, KPIs were no longer based on the quality of the dentistry... What matters now is hourly production figures and return on investment to the shareholders...”

With cutting-edge AI-enabled processing and up to 5 acquisition modes, the CBCT 3D Pro provides a superior level of accuracy and precision.


• 3D
• Panoramic

• Part CT
• Model and PVS impression scanning
• Cephalometric (optional arm) OR interpreted via the 3D scan
What truly sets the CBCT 3D Pro apart is its AI-enabled processing. This state-of-the-art software provides automated segmentation and reconstruction, enabling you to quickly and easily analyse 3D images with greater accuracy and efficiency than ever before.
• Doctor-friendly software interface

• Powerful features including digital endoscopy and automated airway analysis
• Global implant library
• Free and regular upgrades
Whether you’re placing implants, planning your next ortho case or simply checking for cavities, the CBCT 3D Pro’s AI capabilities make it a must-have for every dental practice.


“My experience so far is that it allows simple matching of shade, having good chameleon-like blending and furthermore, polishes very well, providing excellent aesthetics. One of the other advantages is that even if patients do decide to bleach their teeth, the shade still matches before and after...”
This issue we look into some products and equipment that I use in practice. We look at some recently released new products and elaborate on how their use can be applied in practice. Investing in the right armamentarium allows clinical practice to be simpler and more enjoyable for the wet-fingered dentist and hopefully, this column provides the reader with some of the latest “tools of the trade”

One common emergency for patients undergoing indirect restorations is the dislodgement of a provisional crown, which can happen when patients are not careful with mastication or even flossing between teeth. This can be trou blesome, especially when patients are away or not able to reattend the dental practice to have their provisional restoration recemented. Centrix have a NoMIX cement in a single-component, moisture-activated temporary cement ideal for short-term applications. It is fully compatible with acrylic, composite, PFM and ceramic materials and is eugenol free, allowing use with resin materials. And the advantage is that NoMIX requires no mixing whatsoever. I often provide these to patients to take away with them if they are going overseas or if you have any concerns with the longevity of the temporary staying in place. Simply advise the patient to apply to the inside of the provisional and affix to a moist tooth surface. NoMIX expands slightly upon setting for a tight seal and is easy to clean off prior to permanent cementation.
An exciting new facial scanning technology recently released is RAYFace from Ray dental. The technology allows a facial scan with the ease of taking a photograph with one shot (0.5s). Utilising multiple cameras, it can reconstruct a natural smile using high quality 3D data. It utilises 9 image sensors to accurately capture the depth of the subject creating realistic 3D data and as an open system, allows export to other systems. Historically, we used 2D images with photographs and exported

these to Photoshop and Powerpoint, however, this always had limitations. Being able to analyse in true 3D with the ability to export to design software such as exocad and 3Shape, allow not only the planning for optimal aesthetics but also able to assess the occlusion for prosthodontic management. It can be used in orthodontics, implantology and prosthodontics with applications within cosmetic medicine. The software has the ability to carry out smile design and the ability to show patients at their consultation appointments a trial smile in a 3D representation is revolutionary. There have been discussions on how we might be able to then digitally transfer this information to 3D print temporaries so that patients could walk away with an instant trial smile and this digital dentistry workflow will be revolutionary within dental practices.
After hearing of the innovation of Ominchroma composite resin several years ago, it seemed like a bold claim to be the world’s first universal composite that aes thetically matches every patient, from A1 to D4, with a single shade. Soon after, many dental companies released products to simplify shade matching and have much less reduced shade possibilities. Ominchroma has uniformly sized supra-nano spherical fillers (260nm spherical SiO2-ZrO2) which allow OMNICHROMA to match ALL 16 VITA classical shades. Its wide colour-matching ability eliminates the shade-taking procedure, reducing composite inventory so that clinical procedures are simplified. Having less stock - which expires - is always an advantage. My experience so far is that it allows simple matching of shade, having good chameleonlike blending and furthermore, polishes very well, providing excellent aesthetics. One of the other advantages is that even if patients do decide to bleach their teeth, the shade still matches before and after bleaching.

Dr Christopher Ho is a Specialist Prosthodontist based in Sydney, Australia. He is Head of School of the Australasian College of Dental Practitioners, Visiting Lecturer at Kings College London, Adjunct A/Prof at University of Puthisastra and Editor of the Wiley-Blackwell textbook “Practical Procedures in Aesthetic Dentistry” and “Practical Procedures in Implant Dentistry”.

Learn from orthodontic experts with our interactive Face to Face or live stream courses
Powered by
The OrthoED Mini Masters is a proven, fully accredited 2 year course that will allow you to deliver predictable, efficient, high quality and profitable orthodontic treatments for your patients.




Our 2023 Face to Face course is SOLD OUT. The live streamed course (which is available) is fully backed with full case support and mentorship to give you the confidence to take on more cases and provide predictable outcomes, every time.
• Build a solid foundation in all areas of orthodontics
• Properly diagnose and deliver treatment plans
• Save time and money on every orthodontic case
• Complete cases quickly and successfully, allowing you to take on more cases and grow your bottom line
To learn more about this program visit: https://orthotraining.com.au/orthoed-mini-masters/
Learn advanced aligner skills with this 2 day Advanced Aligner module. Learn from industry experts either through a Face to Face course or via the comfort of your home or office through a live streamed event.
• Understand when, why and how to combine fixed appliances with clear aligners
• Learn how to manage difficult tooth movements using auxiliary tools and advanced biomechanics
• Learn how to handle early treatment cases for children and teens; a rapidly growing market
• Develop a deeper understanding of the pros and cons of DIY aligner treatments to advise and educate patients accordingly
• Learn how to take on more complex, challenging cases without having to refer them to specialists
To learn more about this program visit: https://orthotraining.com.au/advanced-alignercourse/
In the OrthoED Aligner Essentials module over 3 days, you’ll learn how to provide Clear Aligner treatments confidently, profitably and successfully, even if you have no experience or have struggled with aligner cases in the past.
The OrthoED Institute teaches you the principles of aligner treatment, allowing you to take on cases with confidence. Attend a Face to Face course or learn from the comfort of your home or office through a live streamed event.

• Increase your practice profits
• Provide a better service to your patients
• Provide improved restorative treatments
• Increase your scope of practice
• Reduce referrals to specialists




• Gain a strong competitive advantage
To learn more about this program visit: https://orthotraining.com.au/aligners/
Get the ultimate certificate of acknowledgement in clear aligner treatment that will gain patient’s trust, improve your skills, and drive more patients to your practice.
Only current students and graduates of the OrthoED’s Aligner Essentials and Advanced Aligners modules are eligible for this extra qualification.
• Gain credibility and win the trust of your patients
• Prove your commitment to learning and excellence
• Demonstrate your understanding of the principles and techniques of aligner therapy through assessments and treatment planning cases
To learn more about this program visit: https://orthotraining.com.au/clear-aligner-therapy/
“Although patients do not have a dental degree, some dentists feel that they need to give each patient a full dental education before they can tell them about their impending dental treatment... when a lot of the time all the patients really want to know is how good will they look...”
I’ve been trying to remember who made the following statement:
“It takes the same effort to date a guy with money as it does to date a guy with no money, so I choose to only date guys with money.”
Or words to that effect.
I’m not sure whether it was Joan Rivers, or Joan Collins, or Joan of Arc...
In a similar vein, I do know that it was Donald Trump who said and is quoted:
“If you’re going to think, you might as well think big.”
And truth be told, small thinking and a small-minded mentality can hold you back, kill off opportunity and seriously affect what happens to you and how much success happens to you in your life.
In dentistry, it takes the same amount of time and the same amount of effort to tell a patient they need a crown on their tooth as it does to explain to them that you can patch their tooth up and see how it goes.
And it often takes less time to present a comprehensive restorative treatment plan to a dental patient than it does to present a detailed tooth-by-tooth patch up plan.
I quickly learned that most times that I tried to explain a treatment plan in detail to a patient, the patient’s eyes would start to glaze over as if I was speaking to them in double Dutch.

I found that knowing what to say and how to say it simply and effectively to patients made things far easier for those patients to receive the dentistry that was best for them.
And patients really do want what is best for them.
I consider myself to be a fairly smart person, but I don’t really know and understand how when I flick a switch at home, how the electricity flows from a pole in my street and into my house and makes a light glow so that I can see... but I’m sure glad that I know that I do need a certain number of those lights in my house so I can read comfortably and move around the rooms without tripping in the dark on the furniture.
So I’m the kind of person who doesn’t need a physics lesson from an electrician every time I go to buy a light globe...
It’s the same when I buy a car. I don’t care what processes actually take place to make the car move [be it by petrol or by electricity]. All I really want to know is how fast does the car go and how smart does it look.
And dental patients are much the same.
Although these patients do not have a dental degree, some dentists feel that they [the dentists] need to give each patient a full dental education before they can tell them about their impending dental treatment... when a lot of the time all the patients really want to know is how good will they look, or how long this treatment will last, so that they don’t need to come back and have it re-done and re-done.
The real problem is that most people are conditioned to think small and play small.
Even when we’re dealing with big numbers, we often still behave with a small-minded mentality. Like I said, it takes the same amount of work to tell a patient they need a crown as it does to explain to them they need a patch-up job. So you might as well do the work that gets the patient the result that lasts a lot longer for them, because you know that a patch-up will never be good enough.
Interestingly, I grew up in a working class neighbourhood. I didn’t have friends whose parents were rich. I didn’t know any business owners. It was all small-thinking people living there...
Fortunately for me, something changed in my thinking... I know that when I started to think bigger, big things started happening for me.
I know that since then, whenever I’ve lapsed back occasionally and played small [on the very rare occasion], it has cost me.
Playing small can cost you more money and hold you back more than you would really care to believe.
When you stop thinking small, you will stop playing small.
In reality, it makes sense to always think big anyway...
Dr David Moffet is a dentist and a #1 Amazon Bestselling author. He is the inventor of The Ultimate Patient Experience™, a simple to implement patient retention system he used to build and subsequently sell (for several million dollars) his successful dental practice [of 28 years] located in Parramatta in working class western Sydney. He can be contacted at david@theUPE.com or visit www.theUltimatePatientExperience.com.
“When I buy a car... I don’t care what processes actually take place to make the car move [be it by petrol or by electricity]. All I really want to know is how fast does the car go and how smart does it look...”


Riva Self Cure and Riva Light Cure are now 70% easier to activate. This SDI Australian innovation makes restorations faster and easier than ever before.

• Creamier, non-stick and smoother handling
• High fluoride release Superior strength
“You have tapped the retirement savings of the most vulnerable for procedures with a life expectancy of 10 to 15 years. Take a good look at yourselves, you are about to cause the demise of yet another good public health initiative!”
Australian Tax Office data released on 23 February 2023 has revealed that, in the 2022 financial year, over $171 million of retirement savings was used to pay for dental treatment. Extraordinarily, this figure doubles the FY21 figures and quadruples those for the preCOVID FY19. We’re 8 months into FY23 and I suspect the FY22 figures will be easily surpassed, if not doubled again, without immediate curtailing by the Federal Government.
Financial Services Minister Stephen Jones accused some service providers of “unconscionable behaviour”. “They are encouraging, and even pressuring, patients to tap into their super for what might be termed life-enhancing procedures like cosmetic surgery,” he said. “There are business models set up to game the system. This is deeply troubling, and I am calling this out.”
I have no doubt that legislation originally intended to allow early access to super by people experiencing severe suffering was drafted in good faith.
I advocate for this policy to remain largely intact, but I call on the unscrupulous operators to take a good look at themselves. Déjà vu: the Chronic Disease Dental Scheme (CDDS) was another great public health initiative flushed down the toilet, so to speak, by the many unscrupulous operators who gamed that system and the few who defrauded it outright.
One may pose the question, “With this track record, how can dentists ever be trusted with a Medicare-funded national scheme?”
I’d like to benchmark the Smile Solutions group against the figures just released by the Australian Tax Office.
The FY22 retirement savings of $171.3 million was accessed for dental services by 8020 individuals. That averages a staggering $21,359 per patient.
Within the Smile Solutions group, where more than 200,000 patients were seen in that financial year, a total of only 4 patients were assisted with early super access, for a total sum of $28,585 at an average of $7,146 per patient - a mere third of the national average.
This huge discrepancy in the average spend per patient may go some way towards explaining why my practice is seeing an alarmingly increasing number of new clients who have accessed their super for a mouthful of cosmetic dental veneers and crowns from other providers. As dentists, we know and understand that people experiencing extreme suffering can have that suffering alleviated with reasonable treatment plans at reasonable pricing. An average spend of $21,359 per patient is simply not reasonable.
Here is my personal message to clinicians practising in Australian dental clinics “set up to game the system”:
You may have provided wholesale cosmetic and restorative dentistry at an average ticket price of $21,000 and tapped the retirement savings of the most vulnerable in our community, for procedures with a life expectancy of 10 to 15 years. Please take a good look at yourselves, because you are about to cause the demise of yet another good public health initiative! Also spare a thought for your future selves, who in 10 to 15 years will have to face your patients needing much of your cosmetic treatment redone, having exhausted its lifespan, but who simply can’t afford to pay. Another round of early access super will no longer be government policy, because your past selves abused the system. Finally, accustom yourself to the notion of compound interest, especially when it relates to the super drain you encouraged, or pushed upon your younger patients, since $21,000 today may have a profound effect on their retirement nest egg, for a set of porcelain veneers long forgotten and a decision long regretted.
“Unconscionable behaviour” is a powerful accusation made by the Federal Minister and I call upon him to validate his allegations, audit the FY22 cases and smoke out the unscrupulous operators – before meting out collective punishment for the deplorable actions of a few.

Dr Kia Pajouhesh, a University of Melbourne graduate, established Smile Solutions in 1993. Situated in the heart of Melbourne’s CBD and incorporating the Collins Street Specialist Centre, Smile Solutions is the largest singly located dental practice in Australia engaging over 80 clinicians, including 20 board registered specialists. Together with his Core Dental chain of practices, he controls over 100 chairs across Melbourne, with a combined patient base of 350,000.

“Financial Services Minister
Stephen Jones accused some service providers of ‘unconscionable behaviour’. ‘They are encouraging, and even pressuring, patients to tap into their super for what might be termed life-enhancing procedures like cosmetic surgery...”



Less than a year after Envista purchased the highly successful intraoral scanner business of Carestream Dental, the popular CS 3600, CS 3700 and CS 3800 models have been relaunched and rebranded as the DEXIS IS 3600, IS 3700 and IS 3800W complete with an ergonomic design courtesy of Studio F. A. Porsche.

The centrepiece of the DEXIS digital dentistry universe, which includes CBCT, panoramic and intraoral x-ray units, navigated surgical solutions and software for digital dentistry, the trio of intraoral scanners offer dentists a generational choice of models to suit their clinical expectations as well as budgetary limitations.
With digital impression taking using intraoral scanners now well and truly eclipsing traditional methods in terms of accuracy, predictability, repeatability and cost-effectiveness, DEXIS is investing heavily in the newly acquired range as the uptake by clinicians grows exponentially.
The DEXIS range of intraoral scanners offer clinicians digital impressioning solutions for orthodontics, crown and bridge, implants and other applications whether for a single chair practice or a multi-chair or multi-location operation.
The three scanners represent second, third and fourth generation incarnations, with the IS 3700 and IS 3800W building on the solid foundation of the IS 3600 with its highly accurate, continuous HD colour scanning.
The entry level IS 3600 offers intuitive and accurate scanning and gives dentists the power to create vibrant, full HD 3D images to achieve outstanding clinical results. The IS 3600 scans in a continuous and uninterrupted pattern making dual arch and quadrant imaging fast and easy.
The IS 3700 incorporates patented Smart-shade matching that provides automatic selection and recording of shade information. Turbo speed scanning is proven to scan single arches in vitro in 30 seconds, faster and with better accuracy than the IS 3600 and revolutionary workflows let users navigate freely among different clinical applications, including restorative, orthodontics, implants and sleep devices.

An ergonomically optimal grip channel empowers clinicians with a balanced sense of scanner control and the optional wrist strap connects users to the device for optimal control and care of the scanner. Touchscreen capability eliminates the extra steps of operation caused by switching back and forth between the scanner and the mouse.


The flagship IS 3800W offers clinicians the freedom of wireless operation for optimal mobility and maximum flexibility. Dedicated point-to-point WiFi access ensures robust and stable transmission for a continuous and efficient scanning procedure. At 240 grams, the IS 3800W is one of the lightest and most compact intraoral scanners on the market and ergonomics are maximised following the Studio F. A. Porsche design.
With a proven scanning time of 25 seconds for a single arch, the IS 3800W’s capture speed frees up more time for
focusing on patients and the enlarged 16 mm x 14 mm field-of-view and significantly broader 21 mm depth of field captures the details you need - even in interproximal areas and subgingival margins.

The handpiece features an embedded sensor that lets you orient the digital model on screen by simply rotating the scanner, eliminating the need to use the mouse. Simply move your hand and the model follows its movement so you can stay focused on your patient.
Three styles of interchangeable autoclavable tips are provided to optimise scanning comfort.
Unlike many intraoral scanners on the market, the DEXIS IS 3700 and IS 3800W build a more detailed 2D angular distribution of colour, which includes a more accurate and complete characterisation of the tooth colour properties, leading to more accurate and reliable shadematching results.
Using an active triangulation method, the IS 3700 and IS 3800W both utilise a pattern of structured light (lines or bars) to project onto the tooth surface as illumination. The object distorts the pattern of light due to its surface shape and the IS 3700
and IS 3800W image processing and triangulation algorithms work in concert to utilise the altered light pattern to determine the shape and structure of the 3D object.
In addition to active triangulation, the IS 3700 and IS 3800W both utilise BRDF, or Bidirectional Reflectance Distribution Function, to collect shade values from 3D surfaces factoring in variations in lighting conditions.
Unlike systems that capture the RGB value from a stored mesh, the IS 3700 and IS 3800W measure the true material properties of the tooth without the influence of the scanner, resulting in more accurate colour measurement.
And thanks to triangulation, there is no strict orientation requirement - the scanner can capture the tooth shade as the scanner orientation changes. An additional benefit of triangulation and BRDF also is greater colour dimension.
practitioners with unlimited workflow capacity, smooth scanning even for edentulous situations, expanded processing options, one-click export, touchscreen and video capabilities. IS ScanFlow Premium is an additional option providing an expanded feature-set for advanced intraoral scanner users with more specific needs. IS ScanFlow is available standalone; integrated with Carestream Dental™ CS Imaging v8 and will also be integrated with Dexis DTX Studio™ Clinic.
IS ScanFlow, available to all DEXIS customers, makes intraoral scanning easy and accessible–even for those with very little experience. IS ScanFlow software allows for fast and easy acquisition of accurate, precise digital impressions.


Unlike some competitive systems that force you to select a specific workflow or application, IS ScanFlow provides
DEXIS IS Voyager and DEXIS IS Allin-One Computer provide a mobile configuration for the DEXIS IS intraoral scanning portfolio. With an exclusive and sleek design, DEXIS IS Voyager gives the user freedom to move the intraoral scanner, the connected PC and the consumables required to perform a digital impression easily from one chair to another within the practice.
Our portfolio of intraoral solutions not only makes life easier for you, it’s also great news for your patients. They will enjoy a more straightforward and comfortable scanning experience, with less chair time, and they’ll appreciate how you use the software to visualise treatments for them.

Scan the QR code for more info on DEXIS IS Solutions.


Our portfolio of intraoral solutions not only makes life easier for you, it’s also great news for your patients. They will enjoy a more straightforward and comfortable scanning experience, with less chair time, and they’ll appreciate how you use the software to visualise treatments for them.







The kit contains a variety of instruments for basic extraction socket or implant surgery.
We are proud to offer stoma®, a traditional manufacturer of precise dental instruments made with passion for perfection. Strict manufacturing processes and rigorous testing ensure that all Geistlich products exceed expectations and meet established regulatory requirements.
Goldman-Fox Scissors, 13cm, curved, toothed
Periosteal elevator, Prichard, straight
Periodontal probe (PCPN22, 2-4-6-8-10-12)
Hy-grip handle, dia. 8mm x2
Bone curette, Lucas, 2.5mm, toothed, DE


Periosteal elevator Buser, 17 cm
Scalpel blade holder, straight Forceps, advanced, anatomic TC, 1.3 mm, straight
Forceps, advanced, surgical 1:2 teeth, 1.3 mm, straight
Micro needle holder, Barraquer, TC, 1.2 mm, straight, 18cm
MEGA "Rhodium Front Surface" Mouth Mirror, size 4, dia. 22mm plane (12PK)
Optional:

Gingevectomy knife, Orban O 1-2, contra-angled
STO-19924.00
Images are not to scale.
P.i.c tray with 2 racks for 7 instruments, 1 rack for tweezers, 2 holding bolts and cover made in germany

Twitter has been around for a while, but the benefits of Twitter for dentists have been anything but static.
Initially, Twitter offered a very restrictive 140 characters per “Tweet” (i.e. post) before increasing the limit to 280 characters in 2017. The platform is popular for keeping up-to-date with news events.
After a steady decline in popularity in recent years, Twitter’s benefit for dentists was probably a lost cause as it lay in 13th place among the plethora of social media options available.
However, a couple of recent changes may cause a rethink.
In June 2022, Twitter released a feature called “notes”. Notes allows you to post more than the 280-character limit, meaning you can post blog-style articles which can work well for dentists. You’re also able to add in images and gifs.
with NCA ANZ Pty Ltd
Since Elon Musk bought Twitter in October 2022, there are rumours that the character limit will increase again and a new long-form of tweets will supposedly be released early in 2023. This could allow you to educate your users in a more comprehensive way. Twitter is also still growing in Australia and there are currently 5.8 million Australian Twitter users (mainly in their 20s and 30s).
So is the “new” Twitter worth exploring for dentists?
For practices with limited resources to invest in social media, Twitter is still a long way down the list of priorities. Facebook (21.5 million users) and Instagram (13.5 million users) are higher priorities.
However, the more online presence you have, the more beneficial it is to your practice. Think of social media as a giant funnel, where each post and each platform help each other in creating brand awareness for your business/practice.
Twitter sits in the middle of the funnel, where people know what they want but require a little more information.
If you’ve got the time, jump on board... otherwise keep Twitter on the back shelf for possible future use.
Bring your practice up to the latest scientific compliance for infection control. Pass ALL current and future accreditations. We do all the work and offer a Turn Key Solution.
We undertake a complete run through of your practice and...

s Custom write all practice operation manuals and procedures for infection control
s Custom write all WHS/HR policies and procedures
s Train and certify all staff members to ASNZ 4815:2006
s Certify your practice to ASNZ 4815:2006

s Provide ongoing service and support
The manuals and documents have no expiration date and encompass all the current scientific methods utilised in international infection control.
Total Infection Control (TIC) takes your practice into the 21st Century. Utilising the latest international scientific standards, these short videos provide a complete course for dental infection control, complete with CPD certificates upon completion.

n Individual login for each staff member
n Access to all areas of infection control
n Easy to understand - Next generation of training
n Comical and entertaining
n Easy to use
n Multiple choice quiz
Your staff will become competent and confident in their knowledge of infection control in dentistry, holding strong scientific knowledge, without the need of expensive classroom style training.




The various of the state governments are known to be moving on medical practitioners’ payroll tax liability. The AMA is pushing back. One wonders how long until the dental profession is within the sights of the OSR or equivalent in each state.
The ADA is now asking for an exemption similar to that sought by the AMA to the effect that the private dental practices will be exempt in some unspecified ways from payroll tax. The problem is that this presently has to be done on a state-by-state basis; national claims will only go so far.
Recent cases such as NSW Thomas and Naaz Pty Ltd v Chief Commissioner of State Revenue [2022] NSWCATAP 220 show just how difficult a conventional independent contractor arrangement can be to NOT be characterised as a relevant contract (meaning the contract’s amounts do amount to “wages”).
In other words, simply having the payments receipted by the practice, did not change the nature of the payment to have been payment for services. On appeal, the Court of Appeal (Commissioner of State Revenue v The Optical Superstore
BRAD WRIGHTand employed staff, then the obligation is clear. It is difficult to avoid Payroll Tax where a practice has a “payroll” including relevant contracts exceeding or approaching the threshold in each state. Each state has different legislation and it is best to get advice in your state.

Practice owners might consider paying an amount of the relevant percentage in their state as a contingency in the event that a payroll tax assessment should be done.
Pty Ltd as Trustee for OS Management S Trust and Ors [2019] VSCA 197), in a unanimous judgement, held that the ordinary meaning of “payment” embraced a payment of money to a person beneficially entitled to that money.
Of course, with less contentious amounts such as wages to non-clinical
The usual persons to advise as to liability are appropriate accountants or lawyers with relevant State Revenue experience.
Cautious practitioners with large PAYE payrolls and a significant amount paid to contractors or service and facility users might seek advice about these matters in coming months.
best available knowledge on the performance of your practice relative to others. Our

Synstrat has spent many years collecting data on dental practices. We provide you with
service has assisted many dentists Australia wide to create significant wealth. We
business accounting, practice valuation and financial advice services
•Do you need us to value the practice?
•What rent can it afford?
• How do you structure to meet tax planning requirements?
• What changes should you make to the practice business plan?



Safe and effective powder jet treatment with a feel-good factor
Th e Lunos prophylaxis system from Dürr Dental offers a range of products to help with all aspects of the prophylaxis session. The Lunos Prophy Powders Gentle Clean and Perio Combi, as well as the MyLunos powder jet handpiece, ensure that patients receive an air-polishing treatment that is both effective and comfortable.

The MyLunos handpiece is ideal for reprocessing manually and automatically and can be disassembled into its component pieces for placement into an ultrasonic bath and sterilisation unit. The handpiece’s precise balance allows for ergonomic, fatigue-free working, while the convenient exchangeable chamber approach gives much flexibility while saving a tonne of time. The powder container may be easily changed on the handpiece, preventing the inconvenience
of having to stop treating the patient to complete a time-consuming refilling operation. Powder containers are available in four colours: blue, orange, mint green and purple. These different colours can be used to help with the organisation and planning of prophylaxis treatments. For example, the container colours can be assigned to certain treatment rooms or specific powder variants.
Lunos Prophy Powders Gentle Clean and Perio Combi are the latest-generation of low-abrasive prophy powders made mostly of the water-soluble disaccharide trehalose. As an abrasive material, Trehalose is gentle on surfaces while still providing effective cleaning and this leads
to more comfort for patients and minimal invasiveness during treatment. Additionally, Trehalose’s excellent solubility protects suction systems and preserves their value. It is ideal to offer different flavours or a neutral option during prophylaxis treatments for patient comfort, accommodating different tastes and preferences while considering those who have allergies.
Lunos Prophy Powder Gentle Clean is available in the flavours Neutral (for patients at risk of allergies), as well as Orange and Spearmint. It is suitable for supragingival cleaning and removing extrinsic discolouration for general hygiene appointments, around orthodontic
brackets or before fissure sealants. The 30 μm particle size of Lunos Prophy Powder Perio Combi makes it perfect for recall appointments. It effectively removes biofilm subgingivally, makes it easy to clean around implants and removes slight discolouration supragingivally. This neutral-tasting powder is ideal for patients who are sensitive to flavours.
For more information on how MyLunos can improve your practice, contact Dürr Dental’s Product & Hygiene Specialist, Mina Farag, on 0437-799-323 or email mina.farag@duerrdental.com. Alternatively, you can contact your local Henry Schein Relationship Manager today.











Since its foundation, Ivoclar has become one of the world’s leading companies in the dental industry, consistently bringing customer-focused innovations to the market. 2023 marks the dental company’s 100-year anniversary. Through those many years, Ivoclar has become associated with numerous world-class products, services, training and education offerings, all of which have significantly influenced the dental industry.
To continue and honour that tradition, while simultaneously looking ahead into the next century, Ivoclar Academy will be hosting a global webinar series, “Celebrating a Century of Innovation with 100 Minutes of Education”, open to anyone who wishes to register.
Available on demand beginning April 21st, 2023, this free webinar series that includes special guests from around the world, evaluates the past, present and future of innovation in dentistry. Separated into five parts for the ultimate viewing convenience, this webinar will cover the following topics: a look back at how far the dental industry has come; current ways to improve patient satisfaction in a clinical setting through efficient aesthetics; the impact of all-ceramic materials; and how a digital denture workflow can benefit the dental laboratory, clinicians and the patient.
The webinar series will conclude with a panel discussion where a wide range of industry experts from around the world will discuss the future of our profession and the opportunities and challenges that lie ahead. Dr Saiesha Mistry will discuss aesthetic dentistry trends throughout Asia, Dr Roshan Parikh will comment on the growth of group practices, Sascha Heinze will analyse advancing technology for dental professionals from a laboratory perspective and Dr Victor Clavijo will touch on social media and patient education.
The program boasts some of the industry’s most well-known presenters, including Dr Eduardo Mahn, Dr Lyndon Cooper and Dr Andrea Ricci. Additionally, Ivoclar’s Dr Thomas Hirt and Dr George Tysowsky will be presenting.
Ivoclar has a long history of educating dental professionals. As early as the 1950s, the company’s dental laboratory specialists started offering its customers practical demonstrations on how to use its products. Since then, the advanced learning and education opportunities provided have expanded significantly.

“We are excited to host such an exciting program in 2023. It honours our beginnings as leaders in the dental education field, while also serving as a thank you to all of our dedicated customers and partners, who helped make this milestone a reality,” said Dr George Tysowsky, Head of Global Training and Education for Ivoclar.

With all educational activities now falling under the umbrella of the Ivoclar Academy, the company offers courses and resources specifically developed for clinicians, hygienists and technicians across all levels of experience. Ivoclar Academy offers content through partnerships with over 800 industry leaders and experts across the globe and at 70 Ivoclar Academy inperson training centres throughout the world. The more recently launched Ivoclar Academy digital platform is a one-stop educational resource centre. Here, customers can find out more information and register for cutting-edge in-person learning, while taking advantage of contemporary virtual education offered by dental experts from across the globe - all in one easy-to-navigate place. Furthermore, Ivoclar Academy offers both virtual and on-site tailored learning programs for key product workflows and large groups. The type of training experience can be selected and personalised. Learn from the Ivoclar Academy experts online, in-office, at partner training centers or other suitable locations.

The uniquely designed PENTAX deflection prism allows the surgeon to view the surgical site with the greatest depth of field and enhanced vision, whilst maintaining the best possible working posture.

To learn more and book an in-office demo, scan the QR code or visit osseogroup.com.au/pentax
A-dec Australia has announced a new partnership with Dürr Dental that sees the introduction of the Hygoclave steriliser into the Australian market.


The Hygoclave 40 and Hygoclave 50 range is known throughout Europe and international markets for its ease of operation and efficiency in the dental practice, thanks to its fast operating cycles and flexible drying programs.
The Hygoclave can process dental instruments in as little as 30 minutes, including drying using the “B” Flash cycle with minimal water and power use. Drying time can be extended or run as a separate program to accommodate hard to dry hollow loads.
Simple one-touch controls on the coloured 5” (125mm) touch screen can commence a sterilisation cycle or produce a batch report. A compact printer for producing barcode labels and batch reports is also available.
The intuitive layout of the icon-based user interface with its colour touchscreen display means there is no need to go deep into menus, as all the key functions you need for your day-to-day work are just a matter of clicks away.
For example, you can access the most recently performed sterilisation and test program and run it again directly from the home screen. The Hygoclave has a dedicated interface for connection to practice management and hygiene management software, as well as internal storage capacity for over 100,000 reports which are captured automatically.


An automated door locking mechanism and integrated user management system guarantees secure and easy workflows and the system offers a carefully designed universal program to ensure reliable reprocessing of even complex, hollow shapes.
Hygoclave has extremely flexible water supply options, making it easy to adapt to any practice. The system can be filled manually via the externally accessible tanks, via a suction system from a canister of treated water, or by means of a fully
automated fresh water supply via a connection to an optional Dürr Dental or other water treatment system. As an added safeguard, a water quality tester is built into the unit.

Hygoclave is manufactured from quality stainless steel and special high temperature and ionised water-resistant plastics and is available with either a 17L or 22L chamber to suit the needs and throughput of the practice.
The product is also easy to maintain and service-friendly due to its intelligent design which offers the following benefits:
• Modular, simple design allows fast access to all components;
• Helpful service functions via touch screen/graphical user interface; and
• Easy routine maintenance.
Dürr Dental has a proud 80-year record in developing hygiene and medical technology. The Hygoclave range is now available from authorised A-dec dealers across Australia.
For more information, call A-dec toll free on 1800-225-010 for your nearest dealer.
5“ high-resolution colour touch display for intuitive navigation
3-fold flexible fresh water supply with integrated quality control
All in view and documented thanks to connection to the practice network
With Hygoclave 50, Dürr Dental and A-dec offers dental practices a professional Class B solution that combines impressive performance with a well thought-out operating concept – for maximum efficiency and exceptional user friendliness designed to cope effortlessly with tough day-to-day working environments. Available with a volume of 17 or 22 litres. More information under www.duerrdental.com
High-performance sterilization- and drying system
This is an exclusive training course on the BioMiniatures Miniature Implant system, offering an opportunity to be the first to learn about this innovative system. The course includes hands-on education on the use of Miniature Implants for full and partial arch rehabilitation using a minimally invasive approach. Miniature Implants are narrow diameter implants with a unique self-drilling and self-advancing design which allows placing implants in very narrow alveolar ridges without needing complex and risky bone augmentation procedures. The course will enable you to restore dentitions in severely atrophic ridges with simplicity and confidence. This will include both surgical and prosthetic procedures.







There are many reasons to visit the International Dental Show (IDS) from 14 to 18 March 2023 in Cologne - and the first of them is very special:
#1
This opportunity is once in a lifetime: “100 Years of IDS - and I am here!”

#2
As an international showcase for dental innovations, the IDS presents all proven concepts and products, as well as current new products - in a form more comprehensive than that of any other industry.
#3
The IDS has been reliably fulfilling its claim to leadership in the dental trade fair landscape for 100 years as the largest forum of the entire dental community for expert exchange and personal conversations.

#4
Seeing and understanding make the IDS so valuable. Visitors experience all concepts and products right up close here. And this is why they can validly evaluate the extent to which a device, material, etc is suitable for their practice or their lab.
#5
At the IDS, visitors can already sense the trends of tomorrow today. The trade fair, which is celebrating its 100th anniversary in 2023, is already pointing the way to the next 100 years. One’s own practice and lab can be sensibly positioned on this trend basis.
#6
Health consciousness, which has especially increased in the past three years and the related patient wishes call for clear answers. The IDS is the right forum to enter into a dialogue about this and develop a strategy for the practice or lab.
#7
The IDS is an ideal event for team building!
#8
The IDS combines internationality with short routes. For visitors from Germany, the Benelux and other neighbouring countries, the renowned trade fair city of Cologne can be reached very quickly. And with the free travel ticket that visitors receive in addition to the admission ticket for the IDS, public transport in the extended network of the Rhine-Sieg transport system (VRS) and the Rhine-Ruhr transport system (VRR) can be used at no charge.
#9 A comprehensive update on the state-of-the-art, technical discussions, personal conversations with customers and partners, team building –all this together makes the IDS visit an experience you will not forget. Every visitor can derive decisions from it that will positively influence daily business.
the VDDI (Association of the German Dental Industry), is pleased to announce. “Patients have learned to intensively appreciate their health and are now much more aware of the importance of their oral and dental health for their general health. An ever increasing number of patients understand that investments in their dental health are at the same time investments in their own quality of life. Which is why it especially pays in this phase for dentists, dental technicians and their teams to orient themselves and set the recovery course for the future of their practice and their lab on a well-founded basis.
“The starting point is the 40th IDS 2023 from 14 to 18 March in Cologne.”
#10
Anyone who has attended the IDS in recent years will confirm that the atmosphere at this trade fair is unique. That can’t be described. You have to have experienced it!
“The world and the dental world are turning smoothly and more quickly again after the uncertainty of the past three years”, Mark Stephen Pace, Chairman of
The IDS (International Dental Show) takes place in Cologne, Germany every two years and is organised by the GFDI Gesellschaft zur Förderung der Dental-Industrie mbH, the commercial enterprise of the Association of the German Dental Industry (VDDI), and is staged by Koelnmesse GmbH. Over 150,000 visitors regularly attend.
For more information on IDS 2023March 14-18, visit www.ids-cologne.de





































Indonesia Dental Exhibition & Conference (IDEC) 2023 is back physically for the first time since the onset of the pandemic. It will return across three days from 15-17 September 2023 at the Jakarta Convention Center as an in-person event, expecting over 250 exhibitors and 20 international group pavilions with an expected 5000 local and international visitors spanning 2500 square metres of exhibition space. IDEC 2023 will also offer over 18 seminars conducted by over 20 speakers over the 3 days.

“We’re excited to bring back IDEC after the postponement in 2021. Participants will be able to connect with each other once again and meet key stakeholders of the dental industry in Indonesia to learn and discover the latest dental health developments,” said Mathias Kuepper, Managing Director of Koelnmesse Pte Ltd. “The continued collaboration between Koelnmesse, Traya and Indonesia Dental Association (PDGI) is an encouragement to bring IDEC to greater heights over future editions.”
“Indonesia’s trade fairs are roaring back to life and we are eager to bring together the local and international dental industry with IDEC,” said Andy Wismarsyah, Director of PT Traya Eksibisi Inter-
nasional. “We look forward to welcoming attendees back in person and bringing attendees an improved and refreshed IDEC 2023.”

“IDEC returns with the theme The Transformation of Dental Health Resiliency, with the vision of providing a platform for participants to pick up new skills and knowledge and continuously future-proof their skillsets,” said Dr Usman Sumantri, President of the Indonesian Dental Association.
For more information, please visit the IDEC 2023 website at www.indonesiadentalexpo.com.





A dental practice is usually one of the most valuable assets in a dentist’s life. When it comes time to sell, many will do so with little understanding of the value of what they are selling and how to present it effectively to a buyer. Others delay putting their practice on the market at an optimal time, fearful of what to do next and afraid of a loss of their identity.
This course explains:
6 HOURS CPD
• How to prepare your practice for sale to optimise the price, terms and compatibility with a purchaser
• Which exit strategy is right for your practice and why
• When is an optimal time to maximise the return for your asset
• Pitfalls owners fall into that devalue their practice in the final years of ownership
• Steps owners can take to improve the outcome in the final years of ownership
With more than 20 years’ experience in dental practice sales, Simon Palmer has extensive knowledge of and insight into the complexities and sensitivities involved in buying and selling dental practices. Simon’s business - Practice Sale Search - sells more than 100 practices per year. He is a regular writer/contributor to dental publications and journals, and is regarded as an expert on dental practice purchases and sales in Australia and New Zealand.

n Exit planning: how do you get your practice ready to sell?
n What are the pros and cons of the exit options/ strategies available to you?
n Succession Planning: What do you need to do now to prepare?
n What is the likely profile of the buyer for your practice and what will they be looking for?
n Valuing Dental Practices: What/ where is the value in your practice?

n How do you handle staff discretion, confidentiality and disclosure?
n Legal agreements
n Effective strategies for transferring patients effectively from seller to buyer

n What to do next post sale: post-sale strategies
n Tax implications and strategies when selling
n Expert finance, legal, accounting speakers
In the heart of the Italian Alps, with the fundamental values of discipline, innovation, trust and responsibility, the family-run company Zirkonzahn provides innovative solutions for the dental sector. Under the motto “Everything under one roof”, all Zirkonzahn’s milling materials, hardware equipment, software, implant prosthetic components and tools are conceived and developed in-house, in order to guarantee constant controls over the production process and therefore comply with the company’s high-quality standards. In their homeland, South Tyrol, Italy, Zirkonzahn has their headquarters, main education centres, a dental laboratory and operates five production sites, all located within a few kilometres from the head office. Purchasing raw materials only from specially selected suppliers, the company develops new visions and technologies providing dentists and dental technicians with dedicated, simplified instruments for a smooth and reliable workflow, from the implant planning procedures to the final restoration.
In order to meet the patient’s growing demand for fast and aesthetic solutions without compromising on quality, some of the latest technologies launched in the market greatly simplify the production process of dental restorations. With the new, highly accurate Detection Eye intraoral scanner, the patient’s jaw can be easily digitised in less than 60 seconds, making the impressiontaking more comfortable for the patient and ensuring real-time scan with realistic colours and preparation borders. The scanner has been designed to be lightweight, compact and ergonomic and the scanning areas do not need to be pre-treated with powder, which simplifies the acquisition process. Once the data have been captured, they can be easily and quickly loaded into the Zirkonzahn.Software for the model design. The created model can be then milled in one of the five milling units of the new M2 comfort line or 3D printed using the P4000 Printer.

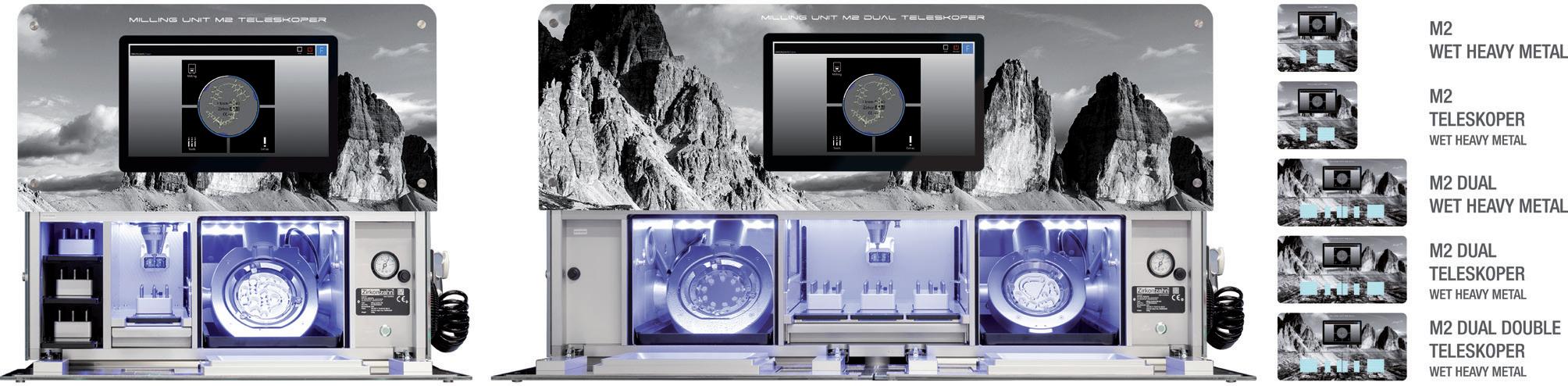
Fully automatic, flexible and vibration free, the M2 milling unit comfort line exemplifies precision and flexibility. With the M2 Wet Heavy Metal, the M2 Teleskoper, the M2 Dual Wet Heavy Metal, the M2 Dual Teleskoper and the M2 Dual Double Teleskoper, the comfort line comprises five milling machines with fully automatic 5+1 axis simultaneous milling technology.
The highlight is the extra-large Teleskoper Orbit (ø 125 mm): in combination with special interchangeable holders, it allows the processing of all common soft and hard material blanks of ø 95, 98, 106 or even 125 mm. With the Teleskoper Orbit, blanks can be removed and reinserted back into the orbit at the same position with high precision in the micron range.
In addition, the pre-set Ultraspeed programs of the Zirkonofen Turbo, perfectly adapted to each kind of Zirkonzahn zirconia, allow to sinter small zirconia structures in about 1 hour and 30 minutes only, with no variation of flexural strength, colour and fit values. This cuts processing time by 81% and reduces electrical consumption by 73%.


No limitations! With the extra-large Teleskoper Orbit, it is now possible to mill material blanks with Ø 95, 98, 106 or even 125 mm, as well as glass ceramics and Raw-Abutments® blanks. Discs can be removed and reinserted back into the orbit at the same position with high precision in micron range - this is particularly useful for the two-stage fabrication of immediate restorations in case of implant-supported prostheses (Double Milling technique).

Optimal material and colour selection: monolithic sample teeth available in the shape of upper incisor, upper incisor with minimal cutback for further characterisation, lower incisor and premolar.
Prettau® zirconia is the material of choice for functional and aesthetical solutions - from single crowns to monolithic full arches. The Prettau line includes different zirconia typologies available as discs (Ø 95 or 98 with step) as well as mini blanks. In the last years, the company’s range of zirconia typologies has recently embarked even more on the path of monolithic design with the new Dispersive® versions. In this case, ceramic layering and manual colouring are not necessary anymore, since materials are already provided with a very smooth, natural colour transition during the manufacturing process. However, for an even more patientspecific result, structures can be further characterised with colouring liquids or, alternatively, a minimal cutback can be applied for the subsequent application of a slight layer of Fresco Ceramics. Developed for both gingival and vestibular regions, these new ceramic pastes do not require staining anymore. Prettau 3 Dispersive is the latest material developed by the company and is characterised by a triple gradient of colour, translucency values and flexural strenght (Gradual-Triplex-Technology).
With the new Zirkonzahn Shade Guides, the patient’s tooth colour can be precisely determined on the basis of monolithic zirconia sample teeth.
In this way, it’s possible to determine the most suitable Prettau zirconia material in a safe and quick manner: if the shade guide and the material of the zirconia prosthesis are identical, it is ensured that the colour of the restoration corresponds 1:1 with the natural tooth colour of the patient.
The colour spectrum is inspired by the VITA® Classical shade range and is comprised of 16 dentine colours (A1-D4) and 3 bleach shades.
As one of the world’s largest manufacturers, Zirkonzahn’s implant prosthetics components are made with high-quality medical titanium alloy and meet the strictest quality criteria. The wide portfolio, which includes Scanmarkers, White Scanmarkers, ScanAnalogs (laboratory analogues used as scanmarkers), impression copings, laboratory analogues, Multi Unit Abutments, Raw-Abutments® and healing caps also comprises:
• Zirkonzahn LOC-Connector, a snap attachment system for implants and bars to fix removable dental prostheses on the implant;
• Multi Unit Abutments 17°, characterised by a 17° angle to compensate for any implant inclinations and with two different anti-rotation connection types which allow intermediate positions;
• Titanium Bases K85, with the chimney height adjustable to the individual tooth length;
• Titanium Bases K80 Angled Screw Channel, with a chimney height adjustable to the tooth length and the possibility to tilt the screw access channel from 0° to 30°; and
• White Metal Scanmarkers, reusable scanbodies to acquire the implant position and orientation during intraoral and model scans.
All components - available for more than 140 implant systems - are warrantied up to 30 years, including the implants from other manufacturers used with Zirkonzahn implant abutments.

All Zirkonzahn’s innovative products have been conceived to improve the techno-clinical team working process in a smooth and time-efficient manner.
In cooperation with various research institutes, the company constantly develops new and intelligent solutions for creating a 100% patient-oriented, natural-looking restoration.
Find out more about Zirkonzahn by visiting www.zirkonzahn.com or follow the company on social media!







EVERYTHING FOR YOUR WORKFLOW




In the heart of the Italian Alps, with the fundamental values of discipline, innovation, trust and responsibility, we produce everything on our own. Purchasing raw materials only from specially selected suppliers, we develop new visions, dental materials, tools and technologies all under one roof. We provide dentists and dental technicians with technical support as well as educational trainings, to help them stand out in terms of quality and excellence.
INTRAORAL SCANNER AND 3D PRINTER





A complete package for a smooth digital workflow
ZIRKONZAHN SHADE GUIDES









With monolithic Prettau® zirconia sample teeth for optimal material and colour selection








ZIRKONOFEN TURBO

With pre-set programs for sintering small zirconia structures in about 1 hour and 30 minutes



M2 MILLING UNIT COMFORT LINE
Machines with one or two milling chambers and the extra-large Teleskoper Orbit Ø 125 mm
IMPLANT PROSTHETICS
TGA approved components for more than 140 implant systems and with up to 30-year warranty









































PRETTAU® DISPERSIVE®







Zirconia typologies with natural colour gradient or with Gradual-Triplex-Technology

Piksters has won a Canstar Blue Award for “Most Satisfied Customers” for the “Dental Floss & Picks” category, coming in above big name multi-national players such as Oral-B, Sensodyne and Colgate.
“Piksters was the favourite pick of shoppers in Canstar Blue’s dental floss and pick ratings, winning 5-star reviews for ease of use, effectiveness, packaging convenience, taste and overall satisfaction,” read the Canstar Blue citation.

Earning a Canstar Blue Award is a tribute to Piksters’ commitment to their customers which echoes Megan Doyle’s (Canstar Blue CEO) statement - “When you see the Canstar Blue Award logo, know that you’ve got a dedicated team and brand behind you every step of the way.”
“The gap between your teeth is where most big dental problems start. We have been working on easier and better ways to clean that gap for 30 years and it’s nice to see we’re having some success,” said Dr Craig Erskine-Smith BDS, CEO of Erskine Oral Care (parent company of Piksters).
The Piksters “Dental Floss & Picks” range includes:
• Piksters Interdental Brushes
• Piksters Interpik
• Piksters Pikstix
• Piksters HydroPik Water Flosser
• Piksters Eco Charcoal Floss Picks
• Piksters SupaGRIP Floss Picks
• Piksters Gorilla Floss
Piksters is known for their leading interdental brush widely distributed throughout dental, grocery and pharmacy channels. Oral care is their specialty. Piksters’ products span across categories such as floss, toothbrushes, toothpaste and teeth whitening. The company strives to bring innovative, new and improved products to the market that represent high quality and value to dental professionals and consumers.
Learn more at the consumer website www.piksters.com and for dental professionals www.pikstersdental.com

Dental treatments are inherently associated with potentially infective aerosols, as well as splashes of blood and saliva. This study measured the extent of contamination of protective eyewear during different dental treatments and also the efficacy of the subsequent disinfection procedures for that eyewear. A range of different aerosol-producing dental treatment modalities were performed in clinic, using normal dental suction, namely supragingival cleaning, subgingival periodontal instrumentation, endodontic access and root canal treatment and cavity preparation within carious teeth. The 53 face shields worn by the students, dentists and dental assistants who performed these procedures were analysed using forensic techniques. To detect blood contamination, luminol solution was applied onto the surface of the face shields. A special forensic test paper was used to visualise saliva contamination. The face shields were decontaminated and then the same analyses were conducted. Macroscopically detectable contamination was found on 60.4% of face shields. Contamination with blood was detected on all shields after dental treatment. The area covered by blood was measured (median 330 pixels) and was equivalent to 0.3% of the total surface. The extent of blood contamination differed between treatments, with the most found after professional tooth cleaning (median 1,087 pixels). There were also significant differences in the extent of saliva contamination between the different measurements. Decontamination procedures for the face shields removed all saliva but left traces of blood (covering 0.02% of the total surface area). Decontamination procedures for face shields are effective against saliva contamination. However, after decontamination, macroscopically clean face shields may have up to 12% surface contamination with blood. Based on the results, it may be concluded that protective eyewear is essential for each dental practitioner. Decontamination of face shields after each patient is equally essential.
Bergmann N, et al. Blood and saliva contamination on protective eyewear during dental treatment. Clin Oral Investig. 2022; 26(5): 4147-4159.

JoinCAEandgainaccesstoalloftoolsyou needtodrivemassivegrowthforyour clearalignerpractice.
Saveupto$900onalignerlabfeesand loweryouroverheadonotherdental servicesyouuseeverydaywiththe ExclusiveBuyer’sGroup .




Treatmorealignercasesmoreconfidently andefficientlywithcomprehensiveand ongoingclinicaltrainingusingthe AlignerEducationProgram .
Presentandclosemoretreatmentwith provenprocessesandscriptingdesigned toworkforalltypesoftreatmentinthe AlignerBusinessProgram .
Evenifyouarenewtoalignertherapy,CAEcanhelptransform yourpracticeintoanalignerrevenue-generatingmachine. 1300002239CLEAREX.COM.AU

222 nanometre lighting



Far-UVC lighting is an autonomous and continuous sanitation system that is safe for humans and animals – using 222-nanometer wavelength, and is also maintenance free.
Far-UVC lighting is an autonomous and continuous sanitation system that is safe for humans and animals – using 222-nanometer wavelength, and is also maintenance free.

Far-UVC lighting is an autonomous and continuous sanitation system that is safe for humans and animals – using 222-nanometer wavelength and is also maintenance free.
Together with the two primary methods for minimising exposure to airborne diseases (including COVID-19) – wearing a mask and social distancing, far-UVC has been proven to effectively sanitise the indoor air around us.
Together with the two primary methods for minimising exposure to airborne diseases (including COVID-19) – wearing a mask and social distancing, far-UVC has been proven to effectively sanitise the indoor air around us.
Together with the two primary methods for minimising exposure to airborne diseases (including COVID-19) – wearing a mask and social distancing, far-UVC has been proven to effectively sanitise the indoor air around us.

Far-UVC can be widely applied to safeguard populated spaces such as shopping centres, hospitals, schools, offices, public transport systems and gyms.
Far-UVC can be widely applied to safeguard populated spaces such as shopping centres, hospitals, schools, offices, public transport systems, gyms... and dental surgeries.
Far-UVC can be widely applied to safeguard populated spaces such as shopping centres, hospitals, schools, offices, public transport systems and gyms.
Available in Australia from Medisupply Pty Ltd
Unit 33/110 Inspiration Drive, Wangara WA 6065 www.medisupply.net.au | info@medisupply.net.au
For more information on FAR UVC AFRICA and this immediately available and highly cost-effective solution, please visit www.faruvcafrica.com or contact: 082 578 3755
For more information on FAR UVC AFRICA and this immediately available and highly cost-effective solution, please visit



FAR UVC light at 222nm destroys viruses and bacteria and is the only product that offers REAL TIME air and surface sanitation.

UVC light at 222nm is effective against viruses including SARS-CoV-2 (COVID) and Influenza together with multi-drug resistant bacteria in the air, on living human tissue and on surfaces. Unlike UVA and UVB light, UVC does not penetrate the stratum corneum of the skin nor the cell membrane of a human cell.
The placement of fixed or mobile UVC lighting units in dental treatment rooms including during invasive, implant and oral surgical proceduces can add a further line of defence to your infection control protocols.

FAR-UVC lighting is the first safe, effective, autonomous and continuous disinfection system for occupied spaces.
Visit www.medisupply.net.au for product and technical information, scientific research and studies, recent installations and more...
Ceiling mounted
Wall mounted
Mobile units
Hand sanitisers
Motion activated
 By Dr Ahmad Al-Hassiny
By Dr Ahmad Al-Hassiny
Transitioning from a traditional dental workflow to a digital workflow offers a unique set of challenges for practitioners steeped in conventional analog techniques.
Digital dentistry has transformed our dental practices here in Wellington, New Zealand and continues to revolutionise the field of dentistry. For us, it has been a 15-year undertaking to transform our five dental clinics from the comfort zone of status-quo dentistry to a fully digital workflow.
Today, each clinic is equipped with intraoral scanners, CAD/CAM equipment and all the latest materials and technologies the profession offers (Figures 1-3). In fact, we are so passionate about the possibilities of digital dentistry that we opened New Zealand’s first digital dentistry training centre where like-minded dental professionals from around the globe gather for live and online courses. Our mission at the Institute of Digital Dentistry (instituteofdigitaldentistry.com) is to ensure dental professionals gain the knowledge and confidence they need to use digital dentistry effectively and efficiently.

The knowledge and confidence we gained from our journey to achieve high-quality same-day restorations have completely changed how we practice dentistry and the perception of our patients on how dentistry is practised.



Our patients are “wowed” by our ability to provide them with single-visit restorations, which has become a significant selling point to families and friends and an enormously profitable and free marketing tool for our practice.
Patients love the concept of leaving the practice with a new, beautiful, life-like smile (Figures 4-5) or, more simply, a same-day crown.

Need some guidance in digital dentistry?
IDD membership unlocks a catalogue of helpful videos that can take you from digital dentistry novice to a knowledgeable expert. It’s affordable and you can cancel anytime.
Scan the QR code to view membership offers perfect for dentists of every skill level, or as a great way to train your team to lessen your workload. Start a free 7 day trial of IDD membership here: https://www.instituteofdigitaldentistry.com/online-membership

No more temporaries; no waiting for weeks for the final restorations; and few, if any, final adjustments after seating (Figures 6-9).
Of course, our journey, like yours, is only possible with proven technologies and research-based materials that provide the combined trifecta of strength, aesthetics and workflow efficiency. Over the years, we have placed more than 10,000 digitally-driven restorations, 90% of which were fabricated from a single allceramic material (IPS e.max®, Ivoclar).

Whether a single crown or a quadrant, we rely on materials that provide the highest quality aesthetics while maximising our time, workflow efficiency and profit, as well as the comfort and convenience of our patients.
For example, suppose we find decay mesial or distal to a crown preparation, which is quite common. In that case, we can simply prep the site, restore with an inlay or onlay milled from a complementary material (Tetric® CAD, Ivoclar) and bond both at the same appointment (Figures 10-15).

Perfecting a digital workflow that is efficient, maximises timesaving processes and increases profitability requires constant tweaking as the field of digital dentistry continues to evolve.
In Part II, I will share the workflow processes we have found the most efficient and helpful tips and techniques we have incorporated to ensure we provide optimum dental care in a single visit.


Exceptionally smart and elegant, Aoralscan 3 improves the overall clinical experience for you and your patient –allowing users to easily acquire vivid digital impressions in a fast, accurate, and more comfortable way.
The Aoralscan 3 comes with a wide range of intelligent functions which guarantee a more comfortable chairside experience and efficient clinic-to-lab collaboration.
SCANNER PACKAGES STARTING FROM $15,990+GST
BOOK AN IN-CLINIC DEMO

Scan the QR code and our nearest Account Rep will come to you!
LEARN MORE
Scan the QR code to learn more about device features and our digital solutions.
ONLINE – ANYWHERE, ANYTIME
Create an account, browse our full range, compare prices, then hit the checkout – there’s no waiting, phone calls or arduous paperwork required!
Dr Ahmad Al-Hassiny is a global leader in digital dentistry and intraoral scanners, carrying out lectures as a KOL for many companies and industry. He is one of the few in the world who owns and has tested all mainstream scanners and CAD/CAM systems in his clinic. Dr Ahmad is also the Director of The Institute of Digital Dentistry (iDD), a world-leading digital dentistry education provider. iDD offers live courses, masterclasses and an online training platform, with a mission to ensure dentists globally have easy and affordable access to the best digital dentistry training possible.







Recording patient-specifi c information with the PlaneSystem ® and the Face Hunter 3D facial scanner improves diagnostic planning, reduces chair time and increases patient satisfaction. Individual position of the maxilla, occlusal plane and 3D face scans are accurately transferred 1:1 into the Zirkonzahn software and combined without loss in information (fig. 1, 2, 3). The 3D virtual patient provides the restorative team in the clinic and lab with the ideal planning tools for high quality functional and aesthetic dental splints and rehabilitations.



 Fig. 1
Digital patient analysis with the PlaneSystem® and the Face Hunter
Fig. 2
Fig. 1
Digital patient analysis with the PlaneSystem® and the Face Hunter
Fig. 2
PQuestion 1. How many litres of air does HVE remove?
a. 100 litres per minute
b. 150 litres per minute
c. 200 litres per minute
d. 250 litres per minute
e. 300 litres per minute
Question 2. An alternative to HEPA air filtration is...
a. An open window
b. UVC light treatment
c. Reverse osmosis
d. All of the above
Question 3. Air quality can be improved by using a preprocedural antimicrobial mouthwash on every patient...
a. True
b. False
Question 4. Activated carbon filters absorb...
a. Aerosol particles

b. Volatile gases
c. Carbon dioxide
d. All of the above
Question 5. Aerosol particles settle onto surfaces in...
a. 1 to 2 hours
b. 2 to 3 hours
c. 3 to 4 hours
d. 4 to 5 hours


AQuestion 6. Total confirmed cases of COVID-19 globally exceed:
a. 550 million
b. 660 million
c. 770 million
d. 1 billion
Question 7. Australian data grossly under represent the true number of current COVID cases because...
a. Up to 40% of cases are asymptomatic.
b. Only GP doctors can order PCR tests.
c. Positive RAT test results are often not reported.
d. All of the above.
Question 8. Symptoms of LONG COVID are found in what percentage of the population:
a. 1.5-2%
b. 2-3%
c. 3-5%
d. 6-7%
Question 9. An antiviral drug used to treat COVID-19 is...
a. Penciclovir
b. Paxlovid
c. Promethazine
d. Peramivir
Question 10. An Omicron sub-variants in circulation during late 2022 is known as:
a. BA.1
b. BA.2
c. BA.3
d. XBB
e. All of the above



Question 11. What has been working silently to reduce the viability of viruses and the dispersion of pathogens from the mouth?
a. Rinses containing chlorhexidine
b. Listerine





c. Waterline disinfectants












d. Quaternary ammonium compounds
e. All of the above
Question 12. Ingredients that inactivate SARS-CoV-2 include:


a. Povidone iodine
b. Chlorhexidine
c. Essential oils
d. Hydrogen peroxide
e. All of the above
Question 13. Excipients used for the long-term stabilisation of mouth rinses that also exert potent antiviral actions include:
a. Surfactants
b. Flavours
c. Ethanol
d. All of the above
Question 14. Intact virus particles can be found in symptomatic COVID-19 infected patients in their:
a. Saliva
b. Dental plaque
c. Crevicular fluid
d. All of the above
Question 15. The mouth rinse active ingredient that worked fastest in terms of the rate of reduction in viral load is:













a. Chlorhexidine
b. Povidone iodine
c. Essential oils
d. Hydrogen peroxide
Question 16. IMS Cassettes take up too much space...
a. True
b. False
Question 17. Packing IMS Cassettes takes too long...
a. True
b. False
Question 18. IMS Cassettes make it more difficult for team members...
a. True
b. False
Question 19. IMS Cassettes take up too much space in autoclave...



a. True
b. False
Question 20. IMS Cassettes make staff turnover more difficult...

a. True
b. False

Surgical masks are contaminated during dental treatments and can itself be a source of further contamination, posing a threat to dental staff and patients. The aim of the study was to investigate mask contamination during dental treatments, when wearing a face shield and having patients perform a pre-procedural mouth rinse with chlorhexidine (CHX). This was a prospective, randomised study. A total of 306 treatments were included: 141 single-tooth restorations and 165 treatments involving the total dentition (supra- and subgingival ultrasonic scaling for periodontal debridement). The treatment was delivered by second and third year dental students over an appointment of 60-90 mins. For all types of treatment, a lingual low speed saliva ejector was used with a 3.3 mm diameter tip (suction flow rate 1.1 litre/sec), as well as high-volume evacuation (8.0 mm tip, 6.0 litre/sec) held by an assistant near the aerosol source. The students wore tieband medical surgical masks on top of FFP2/KN95 masks, with a face shield (Clever One) over the top. There were 3 intervention groups (each with n = 102). In group 1, participants rinsed for 60 sec with 0.1% CHX or with water before treatment. As a control, a non-rinsing group was included. A face shield was used above the surgical mask. After treatment, the front surface of the masks were imprinted onto agar plates which were incubated at 35°C for 48 hours. Colonies were counted. Bacteria were classified by phenotypic characteristics, biochemical assay methods and matrix-assisted laser desorption/ionisation time of flight mass spectrometry. The following results were obtained. Rinsing with water before treatment reduced CFU significantly in comparison with not rinsing group (mean 47 CFU versus 80 CFU for nonrinsing), while CHX was even better again (24 CFU), giving a further statistically significant reduction of bacterial contamination of the surgical mask. Mask contamination with bacteria was found routinely, with no significant differences between single tooth restorations or total dentition periodontal treatments.
The most common bacteria recovered were Streptococcus spp., Staphylococcus spp., Micrococcus spp., and Bacillus spp., which represent both the oral flora and the skin flora. We conclude that a pre-procedural mouth rinse is useful and it will reduce the bacterial load on the surface of the surgical mask. However, contamination of the mask’s outer surface cannot be prevented completely by rinsing, nor even by applying a face shield.
Gund MP et al. CHX and a face shield cannot prevent contamination of surgical masks. Front Med (Lausanne). 2022; 9: 896308.
Oral health care settings carry a potentially higher risk of causing cross-infection between dentists and patients and among dental staff members due to close contact and use of aerosol-generating procedures. Past studies of COVID-19 infections in dentists and dental care professionals have come from studies in the United States, UK, France and China, with the largest study (from the US) reporting a prevalence of 0.9% for confirmed or probable cases of COVID-19 infection among 2,195 dentists. The present prospective study estimated COVID-19 incidence rates among a cohort of 644 Canadian dentists over a 6-month period from July 29, 2020 through February 12, 2021. This was after a lockdown and restrictions on dental care to only emergencies during March 2020. Early in the reopening phase during May, 2020, Canadian dental regulatory authorities published detailed infection control and prevention protocols for providing oral health care. Most of the sample had their primary practices in Quebec and Ontario and were serving a metropolitan or urban community An online questionnaire, adapted from the WHO’s Unity Studies protocols for assessment of COVID-19 risk among health care workers, was used to collect data on self-reported COVID infections every 4 weeks. 226 participants were also randomly invited from this group to provide saliva samples every 4 weeks to test for asymptomatic cases of infection. No SARS-CoV-2 was detected in any of the saliva samples from 224 participants during the study period. The median age of the dentists was 47 years; most were women (56.4%) and were general dental practitioners (90.8%). Only 6 of the 644 participants reported COVID-19 infections during the study period, giving an incidence rate of 5.10 per 100,000 person days (95% CI, 1.86 to 9.91). The incidence proportion was estimated to be 1,084 per 100,000 dentists (95% CI, 438 to 2,011) which was lower than the rate in the Canadian population during the same period (1,864 per 100,000 people (95% CI, 1,859 to 1,868). During the period of the study, the use of N95 respirators or higher-specification respirators was low - because of shortages - but it increased over time, as more of this PPE became available. Uptake of vaccinations is not a possible explanation for the observed low infection rates, as the study was beyond more than 4 months of the 6 month duration follow-up at the time the COVID-19 vaccination campaigns began in Canada. At the time of data analysis, the proportion of participants who had received at least 1 dose of the COVID-19 vaccine was low (only 5%), so this cannot explain the lower infection rates seen in dentists versus the general community during the study period. Overall, the low infection rate observed among dentists should be reassuring to the dental and general community. This lower rate may have been a reflection of an array of interacting factors, including but not limited to preprocedure screening of patients and adherence to rigorous infection prevention and control protocols used during these procedures.
Madathil S et al. The incidence of COVID-19 among dentists practising in the community in Canada: A prospective cohort study over a 6-month period. J Am Dent Assoc. 2022; 153(5): 450-459.




 By Emeritus Professor Laurence J. Walsh AO
By Emeritus Professor Laurence J. Walsh AO

Prior to the COVID-19 pandemic and the recognition in early 2020 that airborne transmission of the virus was highly likely in certain situations, limited attention had been paid to the issues of aerobiology that are unique to a dental practice setting. During the pandemic, there has been an explosion of interest from manufacturers who have seen a more receptive market for devices and technologies that aim to improve air quality in dental practice. While there is clearly commercial opportunism at play here, one needs to recognise that there were devices already on the market prior to the pandemic that were very useful for addressing specific issues around air quality.
The first notable example was the introduction of medical HEPA filter systems with a snorkel or elephant trunk design over 25 years ago, as part of the rollout of air abrasion in dentistry. These devices, which still exist today and still function extremely well, were intended to remove nuisance particles of alumina from the air, recognising that the spread of such particles was highly likely to occur despite the use of high-volume evacuation. Those who have used alumina particles for air abrasion dentistry will recognise the problems of the fine layer of dust.
The second notable pre-pandemic example was the inclusion in some dental practices of devices with medical HEPA air filters that were designed to reduce environmental allergens such as pollens, because the staff of the practice or their patient pool was particularly prone to asthma or atopic disease caused by such common allergens.
The physical removal of these submicron sized particles by such systems is highly effective. As with the previous example, both types of system were designed to be of high quality, have easily replaceable filters and have a low total cost of ownership, because the filters would often have a service life of up to
The more recent tech
uring the pandemic, a plethora of air filter devices hit the market, many of which lacked the medical HEPA air filter performance characteristics of the pre-pandemic technology. Some marketed systems lacked HEPA filters and instead had activated carbon (which will absorb volatile gases but not aerosol particles). Many of these recently marketed systems have a high total cost of ownership, with a short stated filter life. Hence, the question must be asked, why has quality suddenly gone backwards in this specific field? And even more importantly, are such devices even necessary in the first place? Advertisements and social media advertising for such devices routinely lumped dental practice in the same situation as hospitals and medical centres, but is that actually correct?
Back to the basics
hen faced with any new challenge, be that in the realm of infection prevention and control, or in the realm of work health and safety, there is a basic algorithm that can be followed to guide one’s thinking. The process begins with a formal assessment of risk. This includes assessing the nature of the hazard, how frequently it is present and what existing risk control measures are in place and how well these are working. This is designed to address the question, is something more needed than what we are already doing? (Question one). There are a range of professional tools such as nomograms which can be used to calculate risk score precision to guide purchasing discussions.

If that assessment of risk results in a finding that an additional control measure is necessary to manage the hazard (in this case, infectious aerosols being present and posing a risk to staff and patients), then one moves on to explore issues of the effectiveness of the new control measure. In essence, one is asking, does this work? (Question 2). Under the situations encountered in the workplace, which are quite different between the waiting room, the dental operatory and the sterilising room, will the device work to reduce risk?
One then moves on to consider the issues of practicability and implementation. This is designed to answer the question, how do we make this work at its best? (Question 3). In the case of air filtration devices, where do we put them, how long do we leave them running, how do we know that they are working properly and how do we know that the filter needs to be replaced?
For question 1, the answer will depend on the unique situation of the dental practice. For all the scenarios considered below, it is assumed that the standard management methods described in the ADA Risk Management Principles for COVID-19 are being followed (such as preappointment triage and the routine use of a preprocedural antimicrobial mouthwash).
Consider the situation of a mobile dental van or dental caravan. There is no waiting room to consider and there may be no sterilising room because a back to base approach is being used for instrument management or disposable instruments are being used. In this case, the dental van or caravan is the operatory. It has a relatively small total air volume, with less height from the floor to the ceiling than one would find in a typical building. On the other hand, the van or caravan has operable windows, which can be opened to bring in fresh air. This is unlike the situation of a typical fixed building where the windows are not operable but remain closed.
The van or caravan will typically have a small air-conditioning system, which depending on its design, may or may not be able to bring in outside air.
Knowing if the air-conditioning only recirculates air is important since this will influence the risk assessment for aerosolrelated tasks.
If the patients being seen are only undergoing examinations, the generation of aerosol from the triple syringe being used will be relatively limited. Whether the clinician is working with an assistant who can provide high-volume evacuation during patient appointments is also an essential consideration.
This example highlights the importance of not only the physical dimensions of the working space and its ability to exchange air with the outside world, but also the nature of the procedures being undertaken.
Consider the situation of a sole clinician dental clinic with a single operatory, a small sterilising room and a small combined waiting room and reception area. For such a small footprint, if the clinic is located within a shopping centre or mall, there may be three outlets for ducted central air-conditioning, but only one return air inlet. This is typically the case because such an approach reduces construction costs for the air-conditioning components, with the assumption that the tenants would be small businesses - rather than dental clinics where aerosols are being generated. In this situation with a single point for return air, aerosols floating within the environment of the practice only have four possible fates. The first is that they will move slowly through the air current created by the air-conditioning system to eventually reach the return air inlet. Often this inlet is located in a corridor, rather than in one of the individual spaces mentioned above. The inlet can readily be determined by the fact that air movement will draw in a sheet of paper held over the inlet. Inlets are also typically covered by a simple square grill. The second fate is that the aerosol will be inhaled by staff or patients. Because of their small diameter, being less than 5 µm, these particles will settle in the air sacs in the deeper areas of the lungs, where they can cause respiratory infections. The third fate is that the aerosol particles settle out onto surfaces. This normally takes 3 to 4 hours, so is relevant for the end of the day. The fourth fate is that some aerosol particles exit via the single front door of the practice.
This example highlights the importance of understanding where the inlets for ducted air-conditioning systems are located within the dental practice. Outlets which provide the delivered conditioned air are typically located on the ceiling with a diffuser that distributes the air. This makes them easy to locate and identify. Tracking down the return air is, however, much more important when considering risks of aerosol transmission.
Consider the situation of a multi-chair dental practice that has areas that have an open plan design, with dividers or joinery between the chairs. Here the issue was that aerosol that is generated on one dental chair can pass into the environment of other dental chairs. A further consideration is that in a multi-chair dental practice, the throughput of patients will be higher because of the larger number of available chairs. The nature of the clinical work being undertaken is also important. If all of the patients are orthodontic cases having adjustments, there will be a large number of individual patients, but the time that each is within the dental chair will be short and the nature of the procedures being done are less likely to generate aerosol. On the other hand, if a patient is having a deband of their fixed appliances, this will be a long appointment and will generate a large amount of aerosol because of the powered devices that are being used. The same would be true if a dental chair was being used for ultrasonic scaling, especially if the operator did not have their own dental assistant and was only able to use low-volume evacuation.
This example highlights the importance of considering the type of aerosol generating procedures that will be done and the physical pathways through which aerosols may move. Particles which are coolant water have a much lower density than particles of human saliva, hence any spray that is dispersed into the air a long way from a dental chair is likely to be just water and contain no patient material.
To address the question, do air filtration devices work, one needs to consider that some of the studies of such devices use situations that are completely unrealistic.
For example, they are done in rooms with the air-conditioning (of whatever type) turned off, or they are tested clinically in procedures without the use of either low volume suction (saliva ejector), or even more importantly, high-volume evacuation. One needs to remember that HVE will remove 250 litres of air per minute, so when this is placed within the mouth close to the aerosol generating device, it gives a massive reduction of aerosols that leave the confines of the mouth. Any study of an air filtration device that does not also have the simultaneous use of normal high-volume evacuation is fundamentally flawed and appears to have been set up to make the air filtration system perform better than it would in real life.
An approach that is based on prevention and reduction (patient triage, pre-procedural rinses, HVE) will always be more effective than one which starts off with a large aerosol cloud and hopes to somehow capture that.
Now moving on to discuss the issues of practicability, if a risk assessment reveals that one particular area of the practice has an unacceptable level of risk, then it would be appropriate to consider improving the air handling in that area. In many dental clinics, it is far more likely that the area of greatest risk is the reception area and waiting room, not the dental operatory. This is because the waiting room of a dental practice generally gets the least attention when dental practices are being designed and it is often undersized.
As an example of contemporary and award-winning design, when we designed the reception and waiting areas of the UQ Oral Health Centre in Brisbane, these all have both internal and outside waiting areas for patients to sit, with the appropriate environmental controls for the outside areas to be pleasant at most times of the year and patients sitting in the outside areas are still also easily within the eye line of the receptionist. There is also sufficient spacing that patients can achieve social distancing in the inside and the outside areas.
Staying with the same design example, having delivery air and return air in the same room creates air circuits that prevent aerosols leaving the room (Figure 1).
Likewise there are rooms designed deliberately with negative pressure. Given that this design work was undertaken in 2009, more than a decade before the pandemic, it has stood up well under the challenges of recent times. A lesson from this particular design is the importance of considering the distribution of return air inlets. This means considering the reflected ceiling plan and designing the ceiling with the same level of attention that one would normally give to the floor plan.
If a decision is made that air quality should be improved in the reception area, there are a range of different systems which are available to improve air quality using filtration. Remember that any system which has moving air will by definition generate noise because of that air movement. Considering the decibel rating of the device and its location is therefore very important. A range of mobile and wall mounted HEPA air filter units are available which could be suitable in such situations.
If the risk assessment process reveals that there are still risks in the dental operatory, then consideration needs to be given to simple measures such as reducing the coolant flow level on air turbine drills and ultrasonic scalers. This dramatically reduces the amount of aerosol that is generated, without causing problems of overheating. Some dental handpieces now come with specific valves for closing off some of the coolant spray outlets.
The next consideration is to use a high volume suction tip that has a large diameter (8 or 10 mm) and a conical or flared tip, which alters the air movement pattern to enhance aerosol removal.
The next step would be to ensure that low volume suction is used routinely with all patients. In the case of clinicians who are working alone without dental assistant support (as may be the case with some dental hygiene appointments), then the use of fixed suction systems, including those combined with lighting, such as IsoLight™ becomes more important, as does having patients clean their teeth thoroughly before attending for supragingival scaling.
One should also consider the benefits of alternatives to HEPA air filtration such as UVC light treatment. Several systems are available that can incorporate UVC treatment within existing air-conditioning equipment.
If a snorkel or trunk design of air filtration devices is used, some practical considerations include: trip hazards from the power cables, noise, visual hindrance from the collector and steric hindrance from the system. This latter problem will be worse if the dental chair has a sidemounted element supporting the operating light, spittoon, monitors, etc, since this already influences the seated position of the dental assistant. Having an air filter device also present could make it difficult for the dental assistant to fulfil their tasks properly.
When considering the various physical facilities within which dentistry is undertaken, there is “no one size fits all”. This is why it is so important to consider the elements that alter risk and some of the simple measures discussed above they can reduce the risk of aerosols, before jumping over the steps and proceeding to try to implement a solution that may not be ideal for that particular work environment. In a way, it’s very much like prescribing antimicrobials: as much as necessary, but as little as possible.
Emeritus Professor Laurence J. Walsh AO is a specialist in special needs dentistry who is based in Brisbane, where he served for 36 years on the academic staff of the University of Queensland School of Dentistry, including 21 years as Professor of Dental Science and 10 years as the Head of School. Since retiring in December 2020, Laurie has remained active in hands-on bench research work, as well as in supervising over 15 research students at UQ who work in advanced technologies and biomaterials and in clinical microbiology. Laurie has served as Chief Examiner in Microbiology for the RACDS for 21 years and as the Editor of the ADA Infection Control Guidelines for 12 years. His published research work includes over 390 journal papers, with a citation count of over 18,300 citations in the literature. Laurie holds patents in 8 families of dental technologies. He is currently ranked in the top 0.25% of world scientists. Laurie was made an Officer of the Order of Australia in January 2018 and a life member of ADAQ in 2020 in recognition of his contributions to dentistry.



 By Graham Middleton
By Graham Middleton
Owners of shared dental practices invariably practice in associateship rather than partnership for the obvious reason that some are more talented, have better hands, have developed particular skills and generate more personal referrals than other dentists in the same practice. By contrast, vets practice in partnership as several vets routinely consult, diagnose, operate on and attend to aftercare of individual patients. Small and medium businesses use a variety of structures.
Regardless of structures, disputes between owners keep breaking out. Often jealousy is the cause. Sometimes, an accountant who does not understand the internal workings of the type of practice or business, despite doing the tax returns, fuels disharmony by suggesting to a client that they are being treated unfairly. Often it is a marketing consultant without a significant client base in the personal service professions who claims to be able to show a dentist, accountant or veterinarian how
to grow their practice but does not recognize that practices are personal relationship businesses and that overwhelmingly most new patients/clients are referred by existing patients or clients. Successful accountants use lead in services aimed at specific segments of the market; successful dentists receive most new patients by personal referral of existing patients as do vet practices.
Many accountants fail to look behind the surface of the annual financial returns to recognise which dental, vet practice or business owner is the main drawcard, or whether a busy dentist is attracting surplus referrals to a practice whilst others are not producing significant personal referrals. The cause invariably rests with their communication with patients. Many accountants endorse business strategies without understanding client businesses or recommend inappropriate strategies to clients. I have seen structures created by accountants which created feather beds for the least productive associates while reducing the incentive of a practice’s main drawcards. This was definite proof that the accountants had not graduated from bean counting class to business strategic thinking.
“I have seen structures created by accountants which created feather beds for the least productive associates while reducing the incentive of a practice’s main drawcards...”
33 years of close involvement with the financial outcomes of an Australiawide dental and veterinary client base, as well as other businesses including practice performance benchmarking, advice on practice purchases, continuing operation, practice sales and dispute resolution, taught me that most fees paid by dentists and veterinarians to marketing and business consultants was money poured down the drain. It is essential that a person you consult has substantial experience in advising dentists. To varying degrees, this observation also applies to a spectrum of other small businesses. Lawyers were poor at resolving disputes between associates, often inflaming them, prolonging settlement and adding vastly to costs.
Afew dentists have advanced their skill base substantially beyond their peer group. They are difficult to replace in the short term, with some generating a multiple of the annual fees of an average dentist. Some are able to successfully mentor a younger dentist buying an associateship who has worked in their practice and been prepared to develop their dentistto-patient communication and practice management skills, as well as their kit of clinical skills.
These practice-owners should not be confused with owners of “restrictedto practices”, who are basically dental specialists albeit without the formal qualification who in return for patient referrals by general dentists restrict their practice to particular procedures. They undertake not to compete as general dentists and may have negligible transferable saleable goodwill.
The key to buying an associateship is the ability of the existing principal to assist the new associate to fill their book thereby transferring goodwill. Having done so for a period, it becomes the responsibility of the new associate to generate their continuing fees by creating a high proportion of follow-on appointments and developing their own referral base. Communication and empathy with patients are as important as clinical skills; often more
so. One determinate of goodwill value is the ability to handover clients. The more advanced the treatments offered in a practice, the longer will be the mentoring process but the eventual income reward can be far greater. These skills are not taught at dental school.
Dentistry is a highly personal activity. Overwhelmingly, almost all general dentists gain most new patients by personal referral as a result of successfully bonding with their established patients through both personal communication and clinical skills. A practice internet website is important for referred patients to confirm how to make appointments and their location and availability of parking but is rarely a source of many unreferred patients. Letter box leaflets and regular local newspaper advertisements have usually proved to be a waste of money.
The three-way bond between vets, pet owners and pets has long proved to be a powerful force. When a long-term veterinary practice owner retires, having sold their practice to a corporate owner and completed a contractual earn out period, it is common for nearby privately-owned practices to receive an influx of patients from the corporate practice as the threeway bond between vet, pet and owner has been broken. The more advanced the treatments offered by a dental practice, the greater is the need for mentoring potential associates—but the greater also is their associate’s reward if they successfully grow their advanced dental client list and commensurate skills. The difficulties of some dental corporates suggest that they suffer similar problems to veterinary corporates.
Successful accounting practices, like dentists, are relationship businesses. I recall an accountant who, about 15 years ago, was one of several partners in a prominent practice. I prefer to call him “Bob” (as in Bob the practice builder). Bob built a client list of successful business owners over many years. He spent much personal work time visiting his business clients, attending their board meetings, understanding their problems and assisting them to adopt solutions. Bob learned continuously by observing problems to avoid or successful strategies from his constant
cycle of business contacts and brought authoritative advice to meetings. His advice was succinct and based in experience. He added value to client business decision processes, cautioning against risky strategies and suggested improvements to proposed or existing strategies.
Clients valued Bob’s input regarding him as their de-facto board member. His time in the accounting office was small, sometimes only a few hours per week, as he spent most of his time attending client businesses. On a daily basis, he communicated instructions back to his staff of tasks to be performed for clients or issues to be flagged via telephone or email including recommendations arising from meetings with clients to be confirmed quickly by email.
Both directly and indirectly, he built the majority of the practice fee base, particularly with the larger business clients. The referrals sourced by other partners were fewer and their client’s businesses were much smaller than those of Bob’s premium client list. Bob expected them to create opportunities on their own initiative, but their impact on practice profitability was minor.
The other partners underestimated Bob’s impact and exaggerated their own. They became jealous of his influence over premium clients and confused their qualifications as accountants as giving them equal status with Bob. Clients knew differently. It was also obvious to the staff. Significant business referrals invariably came to Bob who identified their needs and solutions. He was selective as to those he kept as personal clients due to his time constraints and those he introduced to other partners to have periodic financials completed. Premium clients were wedded to Bob because of the quality of his business advice. Bob’s personal staff took pride in helping his clients as efficiently as possible.
Partners enjoyed enhanced income due to Bob’s effort in building the practice. He was the practice rainmaker. It was not Bob’s qualification which grew the practice—it was his ever-increasing store of business experience enabling him to assist clients to make relevant business decisions and caution them away from strategies found wanting elsewhere.
The accounting function did not excite clients, most of whom had a good understanding of their own figures. Nationwide there are a huge number of accountants but only a tiny proportion are effective at providing timely and valuable business advice.
One of the partners, Julius, had a desire to become the practice managing partner but knew that Bob would never accept this change. He persuaded other partners to let him put a retirement proposal to Bob. Julius and the other partners made the cardinal error of not consulting Bob as to the content. Julius met with Bob one-on-one and handed a completed buyout proposal to Bob with the words, The conditions in this proposal are not negotiable
Bob took a brief glance at the document which contained unacceptable conditions that he would never have advised to a client. The content of the proposal and its delivery by Julius as a “fait accompli” were offensive. As the conditions were not negotiable, he put it away and did not reply. He was at the zenith of his influence with clients and continued to generate valuable referrals for several more years but his trust in the other partners—particularly with Julius—was diminished.
Eventually, tensions created a partnership dispute resulting in Bob’s buy out and retirement. Soon, some of the most capable staff began seeking employment elsewhere. The remaining partners were not practice builders. Within a couple of years, many staff had left. Clients found partners lacking in the depth of Bob’s business experience and sought accountancy and business advice elsewhere.
There was a steady loss of clients and quality referrals dried up. The practice that Bob had built steadily diminished. Within a few years, it had an ageing and reducing client list serviced by ageing partners. New employees were informed by existing staff and did not remain long. They moved on to growing practices elsewhere. The remaining partners were unable to replicate Bob’s rainmaking and placed their individual wants above the overall practice good.
Partners sought solutions to the decline in the practice and for a time they blamed their former partner. They realised too
late how much the practice’s reputation and their income had been due to Bob. Their jealousies, enhanced by Julius’s ambition to be managing partner, had led them into strategic error. The practice became top heavy with ageing partners and a shrinking client list. As older clients moved on or sold their businesses and retired, the practice decline quickly became irreversible. Within about six or seven years, it had receded from having a substantial business presence to being one of many suburban accounting practices offering no advantage over competitors.
I recall interviewing an accountant applying for a job. I posed the question, “Why do you want to move from your current practice?” He replied by saying, “It has not had a new client in a long time and a couple of its most valuable clients
rates complemented by growing their kit of dental skills and being recognised as team players in the practice.
Where a practice contains a significant specialty element, the growth of the assistant dentist’s fee base, dental skills and the ability of the owner to support the new associate are key elements of a contractual transaction, but the long-term rewards in such a practice can be substantially greater than in a more traditional practice. Maintaining a strong relationship between the vendor associate(s) and the buying associate is vital, with a clear understanding of practice management standards and protocols established in advance of ownership change. New associates who try to introduce radical changes after purchase are quickly reminded that the deal remains what was agreed prior to signing the buy-sell contract.
Jealousy and conflict between associates limit long term opportunity and in extreme circumstances, can become catastrophic. See “When associateships break down into legal conflict” , Australasian Dental Practice Volume 25, Number 1, Jan/Feb 2014 and also “Conflict Resolution: Associateship disputes, partner disputes, marriage property settlement disputes”, Australasian Dental Practice Volume 25, Number 2, Mar/Apr 2014.
died recently. As the practice diminishes in size, the interesting accounting assignments are reserved for partners and there is no career growth for me!”.
Successful practice owners generate follow-on appointments and new client referrals by creating trust in their patients. They fill their own surgeries and create additional appointments for assistant dentists. They monitor assistant dentists to measure the proportion of follow up appointments and personal referrals created. They also expect assistant dentists to take on some work which they choose not to do personally. Assistant dentists signal their readiness to purchase associateships via a growing clinical fee base, including improving patient referral and retention
The best single owner practices are long established 2- or 3-surgery nonpreferred provider practices located in established middle-class suburbs of major cities and in significant regional cities. They must have suitable premises available to purchase or for long term lease. Their annual fees as well as their fees generated in recent months—evidenced by recent bookings and patient invoicing— are consistently good. Purchasers can enjoy a reliable income immediately from the day of purchase. The best two associated owner practices have no more than four surgeries, including one each for the associates. In virtually all privately owned dental practices, the lion’s share of profit is generated in the owner’s surgeries.
“A dentist boldly starting a new practice near long-established practices has zero patients on day one and no referral base. An established practice nearby has a large existing patient list, which are also its referral base...”
Those brave enough to start new practices must navigate a long period of producing insufficient income to cover expenses. It’s rare to find a location, other than in remote areas, which can produce a steady income immediately after opening. These are not attractive to most professionals’ lifestyles and do not offer attractive education opportunities for their families.
A dentist boldly starting a new practice near long-established practices has zero patients on day one and no referral base. An established practice nearby has a large existing patient list, which are also its referral base. It will continue to be busy while the new entrant struggles to generate sufficient fees to cover its costs including finance, rent, materials and wages of minimum staff.
Recently developed suburbs usually are designed so as to force dentists into expensive rental premises located in shopping centres. The younger population in these suburbs tend to have young families, substantial mortgages and below average family income. They are unlikely to afford quality dentistry in the early years of family formation.
The other extreme are exclusive suburbs with too many competing dental practices, many of which are located in small premises with very expensive rent. About 20 years ago, I was consulted in quick succession by young dentists seeking advice on a practice advertised for sale in Melbourne’s most exclusive suburb. The gross fees were good for a single dentist, but the rent was several times the average percentage of fees paid by dentists, there was no space for a second surgery and difficulty in parking nearby. The financials indicated that after paying rent, the owner struggled to produce net income matching the percentage of employed dentists. I advised successive dentists to buy elsewhere.
I recall being consulted about purchasing solo owner practices which had developed upmarket practices located in capital city CBDs. When young dentists asked me

to advise whether they should purchase one, my reply was to ask them whether they could persuade clients to accept the expensive treatment plans which produced over three times the annual fee income of an average dentist? And whether they had a matching skillset? Invariably, they agreed that they would be unable to replicate the advanced premium treatment plans of the current owner and were advised to search for a practice in which they could confidently replace the vendor.
Along-term client, a skilled veterinary surgeon, had owned a vet practice in the wealthy Melbourne suburb of Toorak. He found that despite having the external
The information contained in this article is unsolicited general information only, without regard to the reader’s individual financial objectives, financial situation or needs. The information contained in this article is general in nature and you should consider whether the information is appropriate to your needs and where appropriate, seek professional advice from an accountant or financial adviser. It is not specific advice for any particular individual and is not intended to be relied upon by any person. Before making any decision about the information provided, you should consider the appropriateness of the information in this article, having regard to your objectives, financial situation and needs and consult your professional adviser. Any indicative information and assumptions used here are summarised, are not a product illustration or quote and also may change without notice to you, particularly if based on past performance. This notice must not be removed from this article.
trappings of wealth in the form of expensive houses, valuable motor vehicles and children attending exclusive private schools, many residents were cash flow poor, having large mortgages and huge lifestyle costs. They were unwilling to pay for essential surgery if their pet dog suffered an accident, if indeed they had a pet. Later, he bought a small practice in the established working-class suburb of Clayton and became very successful. The Clayton residents, typically two income families, long-established owners of modest homes, had small mortgages drove modest vehicles and their children attended public schools. And they had good cash flow! They willingly paid for necessary surgery on their pets. The Clayton working class had much better cash flow than many of the wealthier citizens of Toorak!
Graham Middleton disposed of his interest in Synstrat group on 30 June 2020 and won’t be starting another business; he spent the later 33 years of his working life advising health professionals on business and financial matters. Dentists were the most numerous of his clients. He is the author of the recently published Financial Success for Dentists. Dentists may obtain a copy by making a donation of minimum $60 to the Delany Foundation a registered charity which assists schools in Ghana, Kenya and Papua New Guinea then email Graham at graham. george.middleton@gmail.com. A copy will be sent to you. All proceeds go to the Delany Foundation for its good work. Graham has paid for the printing and mail costs personally.
“Recently developed suburbs usually are designed so as to force dentists into expensive rental premises located in shopping centres. The younger population in these suburbs tend to have young families, substantial mortgages and below. average family income...”
 By Julie Parker
By Julie Parker
WWhen it comes to business, there are costs and then there are costs.
Many “costs” are just that: a “cost” to the business without any direct financial return. Examples would be repairing items that are broken through simple carelessness, utilities, rent and equipment maintenance.
These are all necessary for the operation of your dental practice, but they do not directly generate any money.
Then, there are other “costs” that can give the business good returns on investment. Marketing would fall into this category, so too would the costs of introducing a new service to offer to patients.
Another cost to the business that can generate a remarkable return is an investment in your team.
I often have dental practice owners and managers contact me with concerns around the low or declining performance of their teams. When I ask what investment has been made in the team, the answer is usually “not much”.
When it comes to team training, of course there are “costs”. The costs include the fee paid to the training consultant or organisation, the wages of

the team members while they participate in the training and the loss of income if the practice has been required to close off the appointment books for time taken for the training. Additional non-cost concerns can be whether the team members will be engaged and enthusiastic about the training and whether the necessary changes in systems and behaviours will be implemented so the practice can achieve more desirable outcomes.
Given the above obstacles, I appreciate the resistance some (perhaps most?) practice owners and managers experience when faced with investing into team development. However, without such adequate investment, team performance will rapidly deteriorate and the repercussions will end up costing your practice dearly.
A key principle for the operation of your practice is to deeply appreciate that “everything counts”. It is similar to your health: everything does, indeed, count. The issue with your teams is that the failure to invest does not immediately result in bad results and so it is tempting to put off the investment.
• High staff turnover, leading to high expenditure in time, energy and money to recruit and train new people.
• Team dysfunction leading to poor patient experiences and stress for the managers and owners.
• Increased team absenteeism as stress in the workplace increases, requiring the need to employ temp staff.
• The patient experience at your practice suffers and patients leave for a better service. Your practice will then need to spend more on marketing and promotion.
• Low performance at reception leads to poor new caller conversion, low rebooking rates, bad patient complaint management, inefficiency in scheduling and inadequate patient follow-up.
All these factors mean lost opportunities to be productive and failure to reach financial targets. On the flip side, when you do invest in your team - and providing training is not the only way - you build a team of efficient, productive, caring and happy team members. And, instead of costing you money, they are making your practice strong and healthy, just like you become when you invest in your own behaviours around your health!
Improve the physical environment. If it has been a while since any improvements have been made, give the practice a facelift. A fresh coat of paint, new waiting room seating, better lockers for the staff... your team will be happier and have more pride if their physical environment is modern and professional.
Bring on additional staff. Never more so than now have team members been “under the pump” with their duties. With so many team members having to take sick days during the pandemic, it has become usual to have heavy workloads. Bringing on a steri nurse or floater can help you remain staffed despite sick days and provide wonderful support to the whole team. Bookkeepers, social media virtual assistants and hiring cleaners can make sure that existing team members are not overwhelmed with their daunting list of responsibilities.
Celebrations. Rewarding the team for their continued efforts with regular celebrations can do wonders for morale and team performance.
Time off or extra holidays. If your team or individual team members deserve a reward for particularly strong performances, why not give them bonus paid time off? Imagine how appreciated you would feel if you were given a four-day weekend for being awesome?
Personal development. Paying for your team to attend self-development seminars can have a substantial impact on their personal, emotional and spiritual awareness, leading to greater happiness, willingness to accept and embrace responsibility and to contribute to your practice.
Provide regular perks. Bringing in a mobile masseuse for your team members every month or a mobile car-detailer to spruce up their cars every quarter will foster a strong culture of caring and appreciation.
Give of yourself. Be interested in your team members. Provide support. Show them that you genuinely care about them. Show your appreciation.
Investing in your team is a win-win for all aspects of your practice, with remarkable benefits.
• Greater job satisfaction;
• Increased staff loyalty;
• Greater team harmony;
• Decreased management and team stress;
• More easily attract recruits with team recommendations; and
• Exposure to more ways to improve and broaden skills.
• More friendly, energetic atmosphere;
• Improved patient experiences;
• Positive patient reviews; and
• Stronger commitment.
• Increased new caller conversion;
• Improved treatment acceptance rate;
• Higher new patient referrals;
• Increased patient retention;
• Improved follow-up with recall and incomplete treatment patients;
• Improved systems; and
• Fewer mistakes.
• Increased revenue;
• Reduced wastage;
• Improved management of challenges, problems and obstacles;
• Better ability to identify and take advantage of opportunities; and
• Reduction of barriers to your success.
When considering the costs of operating your business, I encourage you to look at the “costs” of investing in your team as an investment in the future of your dental practice with a remarkable ROI. The benefits listed above clearly show that such investment is definitely money well spent!
In my next article, I will calculate the horrific costs to your practice of replacing a team member whom you don’t want to lose!
Julie Parker Practice Success provides dental teams with coaching and training so they can work together and achieve successful outcomes for their dental practice. For more information, please contact Julie on 0407-657-729 or julie@julieparkerpracticesuccess.com.au
 By Simon Palmer
By Simon Palmer
At first glance, many would assume that young and older dentists would have a shared perspective when it comes to what it takes to run a practice - after all, they have chosen the same profession and job description. However, in reality, there is often a generational divide that exists in their perspectives.
The practice of dentistry has changed enormously in the past 25-35 years. From the technology and compliance needed, to the equipment and materials, to the clinical range offered and the marketing that is allowed to bring in patients, there is actually very little about the modern practice of dentistry that has remained untouched or would have been the same when senior dentists (55+) started practice.
It is only natural that some of these senior dental practice owners are perhaps more conservative when it comes to adopting change and, as such, many of the practices for sale by senior dentists have a more traditional approach to practice operations.
While some short-sighted buyers will look at a traditionally-run practice and be turned off by the amount of change and reinvestment that would be required in order to update it, savvier buyers will recognise the massive opportunity that exists in these practices. For example:

Many older dentists (those that are 55+ years old) started dentistry and built solid practices in a very different competitive landscape in the Australian dental industry.
• There were less dentists per head of population; and
• Advertising was almost illegal. You could have a brass plaque outside your practice and an announcement in the paper when you started the practice, with lettering of a limited font size, but that was about it.
They built solid businesses and loyal patient bases on the back of hard work and good service. Many of these business owners have been able to maintain their practices in the face of strong competition, even though many still have a more traditional and conservative approach to their practice’s marketing. While they may have a website (though not all do), many:
• Still spend money on traditional advertising avenues like Yellow Pages and mailed-out appointment reminders;
• Haven’t embraced Google AdWords, online reviews or a social media presence; and
• Have poor signage (even though they have the physical location for great exposure).
Apractice that is achieving a revenue of $1M without advertising has more potential than a practice with the same revenue that is advertising. If a practice is popular and grossing good revenue without modern advertising, imagine what would be possible if this was updated. Imagine what could be built on the foundation that is there.
Thirty-plus years ago, it was rare to find a general dental practice offering treatments like orthodontics and dental implants. Many built and maintained successful practices on purely general clinical work and referred out all orthodontics, endodontics, implant surgery and prosthodontics to specialist practitioners.
Nowadays, a large and growing percentage of general dentists under the age of 40 have undertaken further clinical education and training and feel competent to be able to offer extended treatment options, like orthodontics (including Invisalign) and/or dental implants.
Apractice that is achieving a revenue of $1M without offering extended treatment options, like ortho and implants, has more potential than a practice with the same revenue that is offering these treatment options.
If you’re a young dentist who can provide extended clinical options and you’re looking to purchase a practice, you would do well to recognise that there is sometimes a large amount of dental work that is being referred out in a practice with a conservative clinician range, which you could introduce in house.
In order to get a sense of this, ask the practice for an Item Performance Report from their dental software (this report breaks the revenue down into item codes).
Younger dentists are so used to having access to OPGs, digital X-rays, etc, they cannot imagine practising without them. The truth is, that this equipment
has only been around for a relatively short period of time. It used to only be financially viable in larger clinics and many senior dentists are still running their practices without them.
While many younger dentists who are looking at buying a clinic that doesn’t have an OPG or 3D CBCT unit or modern, up-to-date equipment may moan about the extra investment needed, the savvier buyer will dig deeper and realise that, while this is true, adding an OPG introduces efficiencies and a far greater diagnostic capability to a practice and could easily pay for itself in a short period of time in a practice with a large patient base. A practice with a large patient base, without easy access to an OPG, could be sitting on a significant amount of undiagnosed treatment.
Often, looking at more traditionallyrun practices can be similar to finding a diamond in the rough. At first glance, they may look like they need some work. However, if you invest the time to do some polishing, there is massive underlying value that just hasn’t been fully realised yet.
Simon Palmer is the Managing Director of Practice Sale Search, Australia’s largest dental practice brokerage. If you’d like more info on practice sales or want to have a confidential discussion about your practice’s circumstances, email Simon at info@practicesalesearch.com.au or call 1300-282-042.

 By Dr Jesse Green
By Dr Jesse Green
If there’s one skill that I wish every dental practice owner could snap their fingers and magically acquire, it would be financial literacy and intelligence. That’s not to discredit the existing financial understanding that gets you to the point of practice ownership.
In fact, I don’t think there’s a single dental practice owner out there who opened the doors to their business without some degree of financial intelligence.
But there’s no denying it’s often a major sticking point.
We spend years in dental school learning how to hone our clinical skills and become brilliant and talented dentists – only to walk out the door into a practice and know little about the business side.
It’s not a system that sets us up to run successful dental practices. It’s a great shame, because we all have powerful reasons that compelled us to open a practice in the first place.
We want to build beloved local institutions that serve our communities; We want to create a business on our terms, that functions to our unique values and visions; And of course, we want to build generational wealth that looks after us and our families for years to come.
None of which is possible without profits. And profits only come with (you guessed it) financial intelligence.
By taking the time to develop your financial intelligence, you will begin to know your business intimately – inside and out. You’ll be able to understand what’s happening on any given day and make great decisions based on real-time data. This ultimately gives you more control, because you can adapt and pivot quickly in response to certain factors that arise on a daily basis. When you know your numbers, you know your business is on a path of stability and continued growth.
So, if you need to up your financial literacy this year, here are five ways to do so.
I’m sure you’ve heard this generic, yet well-intentioned piece of advice a million times before. But it really is that important, so I’ll say it again.
All dental practice owners who successfully scale their businesses start by setting a goal.
This goal will be based on your fiveyear, three-year and 12-month targets. The categories of these goals typically revolve around revenue, ideal lifestyle numbers and time based at work.
For example, I’ve had clients set the goal of reducing clinical days. Great, right? They ended up eliminating clinical days entirely!
Isn’t that incredible?! But with a generic goal like “make more money”, they would never have gotten there. Your goals need to be specific to your practice, your priorities and you as a person.
This plan acts like the roadmap from where you are now to where you want to be. On that journey, it’s important to understand what milestones you need to meet so you know when you’re on course or if you’ve become lost.
Again, a major issue is that these roadmaps tend to be too generic to help you make any real progress. You need concrete numbers, timelines and milestones so you know when you’re on or off track – and how to course correct and when.
3. Determine what to measure and
For each practice there will be a set of key drivers that dictate performance.
I refer to these as “critical drivers”. These are the levers that you can pull to reliably generate results.
You can identify these by asking “when I’ve had a good month financially, what did I do differently?” And on the flipside, “when I’ve had a bad month financially, what did I do differently?”
These metrics can then be measured daily, weekly, monthly, quarterly and annually so that you always know if you’re on-track.
Building these into the rhythms of your practice will ensure they stay top of mind and keep you laser-focused on your goals.
We need to be super clear about the language we use when setting these goals and creating plans, because they inadvertently shape our behaviour and can dictate real outcomes.
Do you want to bring in more revenue? Because there are only ever three ways you can do that, which are:
• See more patients;
• Increase the average amount each patient spends; or
• Increase the frequency of transactions.
But bringing in more revenue can often be expensive and doesn’t guarantee you’ll be left with a profit margin you’re happy with.
If you want to increase your profits, don’t create goals around revenue. You’ll only end up swamped in costs and frustrated at the outcomes.
Cashflow is oxygen for a businesswhen businesses run out of cash, they go broke. There’s a distinct difference between profit and cashflow, in that a business won’t necessarily go broke when they run out of profit, but will when they run out of cash. Our job as business owners is to maximise that cashflow.
Cashflow is created by turning assets into cash - your physical assets, database assets, patient base, team and intellectual property assets.
When it comes to maximising cashflow, there are six ways we can go about it:
• Maximise your revenue (as above);
• Decrease the cost of goods sold;
• Decrease operating expenses;
• Get in any money owed quickly;
wages bill, for instance. Rent or mortgage, inventory, repairs, marketing, taxes. These are holes we expect.
But I see way too many dental practices leaking money where they don’t need to.
Small inefficiencies, under-utilised assets and clumsy workflows are where most practices make or break their profitability. And that’s great news for you because that means the smaller the hole, the easier it is to fix.
You just have to know how to spot these leaks and plug them.
After 20+ years working as a dentist and owning my own multi-7-figure practices, as well as working with hundreds of dental practice owners across Australia, I’ve spent a lot of time looking at leaky practices.
I’ve seen what does and doesn’t work, developed reliable solutions and been able to replicate these awesome results up and hundreds of times over.
So, I figured I’d put pen to paper and outline the most common profit leaks I see – as well as how to fix them.
I compiled them in a FREE guide, aptly called Plug Your Leaky Practice. It contains 19 of the most common profit leaks and how to solve them.
• Push out your payables as far as possible; and
• Reduce your inventory or work-inprogress costs.
Once you’ve got that free cash flow, then you can choose whether you pay yourself a dividend, reduce debt, or indeed rinse and repeat the cycle and build more assets and go from there.
Now, these are all crucial steps to building your financial IQ so that you can enjoy a profitable practice.
But a lot of dental practices come unstuck when they develop “leaks”.
What do I mean by that?
Think of your dental practice as a bucket. Revenue comes in and hopefully fills the bucket up.
But hold on - you have a lot of expenses to consider.
Each expense is like a hole in the bucket that your hard-earned money slowly trickles out of.
Now, some expenses are important and cannot (and should not) be avoided. Your
The focus is on simple, quick and effective solutions that you can easily implement into your practice. So, once you spot the leaks, you can get plugging right away!
It’s a completely FREE guide and super simple to download - you’ll have it in your inbox in 20 seconds easily. Just follow the QR code and it’s all yours. Here’s to a financially free 2023!

Dr Jesse Green is a leading business coach for dentists, author of Retention and a sought-after speaker. Jesse shares his knowledge, skills and experience as a practice owner through the Savvy Dentist Academy, a digital hub of training, events, courses and resources for practice owners who want to earn more and work less. Get your personalised plan to grow and scale your practice by booking a Practice Growth Call. To book, call the Savvy Dentist team on 1300-668-384 or visit https://savvydentist.com/growthcall
“I see way too many dental practices leaking money where they don’t need to. Small inefficiencies, underutilised assets and clumsy workflows are where most practices make or break their profitability...”
Iam just calling to cancel my appointment, says your patient.
“That’s okay. Thank you for letting us know,” say your team. No cancellation is okay, but there are times when patients do need to cancel their appointments. There are many patients who make and confirm an appointment only to fall sick and then cancel their appointment. But are you in the habit of not finding out the reason for their cancellation, accepting the cancellation and making it very easy for your patients to do so?
I know it can seem a little awkward and sensitive when asking patients why they need to cancel their appointment for treatment and care and still want to be understanding and empathetic.
So what is the best way to handle these cancellation calls and really help patients stay on track where possible?
A cancellation spells delayed treatment and care for your patient as well as a change in your appointment book, which means less production for the day and maybe an appointment that is never filled.
My advice is to ask every patient who calls to cancel their appointment, the reason for their cancellation.
Here is the BEST way to do it:
“Is everything okay?” “Your appointment for Tuesday with Dr Incredible is very important.”
“Is there a reason why you need to cancel your treatment?”
Keep in mind that every appointment your patient has confirmed is the time that has been reserved for their dental treatment and care. It is not JUST an appointment time!
Ensure you discuss the treatment and care during your conversation with the patient and not just the appointment time.
During the cancellation call, you want to stay focused on the urgency and importance of your patient’s treatment and care.
Look at the dentist’s clinical notes and refer to them as you speak with your patient. It is a much easier and effective conversation with your patient when you can refer to a higher authority, i.e. the dentist.
Avoid asking the patient if they would like to make another appointment. This question can get a NO response.
You want to make sure the Cancellation Call ALWAYS has a next step for your patient.
The BEST next step is an appointment to continue treatment and care.
Maintain good habits during the Cancellation Call and give your patients the opportunity to KEEP their appointment by finding out the reason for the cancellation. Then try to offer a suitable solution so they can keep their appointment and not delay their treatment and care.
Call Tracking Excellence is not a product IT’S A RESULT!
With Call Tracking Excellence your team will learn the SAME exact processes Jayne used to:

1. Dramatically improve new patient call-in conversions to booked appointments.
2. Retain existing patient appointments and...
3. Prevent ongoing losses from appointment cancellations.
Visit the website to find out how to get started. It’s that easy!
www.calltrackingexcellence.com

Once you know the cancellation reason, you can try to offer a solution so your patient can keep their appointment.
If there is no solution to offer, then reschedule the appointment immediately.
“Let’s confirm another appointment for you right now.”
Jayne began her career as an educator. After spending several years teaching, she made the jump to practice management, serving as a Practice Manager for a renowned dentist in Sydney for more than 25 years, giving her first-hand experience at what works when it comes to building and maintaining patient relationships, how to convert leads over the phone and most importantly - what it takes to reach your practice goals. As the CEO and Founder of Dental Phone Excellence, Jayne helps practices convert more calls into appointments, reduce cancellations and nurture effective patient communication that will result in increased profitability. Her past experience as an educator combined with her passion for practice management gives her a unique set of skills that allows your team to fully understand and take advantage of the tools she presents.
For more information on what to say and ask your patients, call 1300-378-044 or email jayne@thedpe.com



If your practice isn’t growing, there is good news and bad news. The good news is that the cause of the lack of growth is relatively simple to diagnose. The bad news is that your practice isn’t growing!

In this article, we will unpack why your practice isn’t growing... and what to do about it.
The most likely reason your practice isn’t growing is due to your new patient numbers.
For most dental practices, growth in the business is closely tied to the number of new patients coming into the practice each month.
In years gone by, achieving solid levels of new patients wasn’t too difficult. This simply reflected
the fact that in relative terms, there were a moderate number of dentists for lots of potential patients.
In recent times, however, the ratios between practising dentists and the Australian population have been getting steadily worse.
For example, in the last five years, the Australian population grew by around 7%. Over the same length of time, the number of practising dentists grew by 17% - almost 2 1/2 times faster.
What this means is the competition for new patients is increasing and practices need to get better at attracting new patients to continue a reasonable growth trajectory.
While word of mouth is a helpful tool in increasing new patient numbers, this is no longer enough - due to the much higher levels of choice of dentists and increasingly sophisticated marketing options.

To grow your new patient numbers, you need to get intentional about your marketing. 20 years ago, that might have meant an ad in the Yellow Pages. Fast forward to today and intentional marketing requires a range of marketing activities working together in unison.
QUESTION: Have you updated your marketing activities in the last 1-2 years? Have you reviewed the results of your marketing activities? If not, this may be one of the reasons you’re not growing.
Attracting new patients is not enough.
I’ve seen practices bringing in enquiries from 100 new patients a month and yet barely grow. How is this possible?
The answer is “conversion”.
There are two ways in which conversion happens inside a dental practice. The first is the conversion of enquiries to appointments. The second is the conversion of treatment plans into treatment actually going ahead. We will deal with these separately.
It’s simply not enough to drive lots of people to your website and/or have your phone ringing off the hook every day with enquiries from potential patients. What we also need is the ability to convert high numbers of these enquiries into appointments (and for the patients to turn up for those appointments).
The first step to boosting this enquiry to patient conversion is to track patient behaviour once potential patients visit your website and/or speak to your team on the telephone.
If you have online booking on your website (which I recommend), it is simple to track the ratio of visitors to your website compared with the number of online bookings made. You should expect the conversion rate to be somewhere between 1% to 10% - the higher, the better.
Similarly, you should track the rate of conversion (enquiries into appointments) by your team answering the telephone. Some practices achieve a 90% conversion rate on the telephone; for others, it can be as low as 50%. Start with tracking, then train your team to increase the results.
The second type of “conversion” is where you make an ethical treatment recommendation for a patient and they go ahead with the treatment... or they don’t.
Again, the key here is to track the success of each conversion, by healthcare professional. Based on my experience, the conversion rate between two different dentists at the same practice (even in adjoining surgeries) can be quite stark.
If the conversion rate is low, then communication skills training is essential for boosting treatment conversion.
It is typical for a practice to literally have hundreds of thousands of dollars of treatment that has been proposed to patients but never taken up! A sobering thought.
QUESTION: Do you know what percentage of visitors to your website make an appointment? What percentage of callers to your practice make an appointment (and show up)? If these numbers are low, this may be why your practice is not growing.
Ihope you’re feeling well right now, because after I drop this bomb, you may be feeling a little sick in the stomach. Consider this:
How big would your practice be if you had never, ever lost a patient?
I asked this question at a training course and heard practices advise, two times larger, three times larger and even up to 10 times larger than they are now. Wow!
Some level of attrition (lack of retention) is inevitable, but much is avoidable. To my way of thinking, there are really only two “legitimate” reasons for a patient to move on.
If a patient moves far away from your practice, typically, you are going to lose them as a result.
For example, I recently moved from New South Wales to Victoria and as a result, I changed dentists. I don’t care how amazing the experience was with my first dentist in New South Wales, I’m still changing to a new dentist - for me, it would be a 10-hour drive!
The second reason for a lack of retention is an unfortunate part of life. If your patient dies, well, clearly they’re not going to be a patient any more, are they.
But, apart from that, the remaining 90-99% of your patients could continue to see you if you provide an amazing experience and/or a sufficiently compelling enough reason for them to do so.
For some people, they are not retained because they’ve had a negative experience with your practice and don’t want to come back. For some people, you haven’t given them a sufficiently compelling reason to come back. Some people may have fallen on hard times financially and struggle to pay the fees.
But in my view, a lack of retention for most practices comes down to an average level of service and/or an ineffective recall process.
To improve your retention:
1. Measure your current retention rateanyone who hasn’t visited you for 18 months is usually considered not to have been retained;
2. Provide an excellent service so that patients want to come back - do you ever ask your patients how you’re doing?
3. At the time of each appointment, give your patient a compelling (medical) reason to return.
QUESTION: Do you know what your retention rate is? Have you asked your patients about their experience with you? Do you give them a compelling reason to return? If you’re answering no to some or all of these questions, this may be why your practice is failing to grow.
If your practice is not growing, it’s either because you’re failing to attract, convert and/or retain your patients. Answering the questions above will give you an indication of which of these reasons is most likely to be the largest cause of your lack of growth.
Angus Pryor is the winner of the 2022 Australian Business Awards for Marketing Excellence and Australia’s number one Google-ranked dental marketer. He is a #1 Amazon bestselling author, marketer and international speaker. Visit www. DentalMarketingSolutions.com.au for more information.
If you’re looking for practical help (in Sydney, Melbourne or Brisbane), join me and Dr Jesse Green for an evening’s workshop titled “Attract, Convert, Retain”. See www.attractconvertretain.com.au for all the details.
etting older is a fact of life and while most of us hope to live to a ripe old age with all our faculties, it is not something we can take for granted. There is an increasing awareness around what we can do to help our health and longevity. Diet and exercise are common and there is an industry built around that goal. We’re also becoming more aware of the links between oral health and heart disease, amongst others - something that is easy to ignore but just as important. And there is always that proverbial bus that might run us over! We live in a world where “it will never happen to us” - until it does.
Rather than be fatalistic about it though, there are steps you can put in place to allow you to protect you and your loved ones in the event of a crisis. Just as you shouldn’t ignore a visit to the dentist, you shouldn’t ignore appointing someone in
Gyour life to be your spokesperson should you lose capacity (temporarily or permanently) for whatever reason.
Many of you may have appointed a power of attorney (PoA) already, but is it enduring?
By establishing a Power of Attorney (PoA), you are legally appointing a person or an organisation to make decisions, sign documents and act on your behalf in respect to your financial matters. As you’re outsourcing the responsibility for some of your most important financial decisions, you should have unwavering confidence and trust in whom you establish as your PoA. You will want to make sure your PoA has your best interests ahead of their own.
One of the limitations of a Power of Attorney is that it generally ceases when the person suffers a loss of mental capacity. This is where an Enduring Power of Attorney (EPOA) is appropriate, as it does not cease on mental incapacity. However, much like an insurance policy, it is nearly impossible to establish after the fact.

Most of the time when an EPOA is required, it’s to assist a family member in their later years. Older parents or family members may have started to lose mental capacity and require assistance with daily living. When it comes to financial responsibility, most of the time an EPOA is required to help assist with managing bank accounts, investments, Medicare and Aged Care. The EPOA therefore has the legal right to handle what can be a significant amount of wealth on your behalf, which is termed a “fiduciary duty”. An EPOA has a fiduciary duty to act honestly, reasonably and in the best interests of their client.
This responsibility should not be taken lightly as there are steep consequences for breaching fiduciary duty. Quite often breaches occur but are not even considered by the EPOA. For example, an adult child acting as an EPOA for a parent may feel it’s OK to have the parent cover the renovation costs to their home, in order for the parent to move in. Whereas it might be better for the parent to receive the appropriate care from an Aged Care facility.

Another potential breach in fiduciary duty occurs when an EPOA might incur a large expense that they are unable to manage themselves. They may see their parent’s assets as a solution to their problem and justify the “borrowing” as receiving their inheritance slightly early. This situation is referred to as inheritance impatience and is a form of elder abuse.
One of the ways to prevent abuse by an EPOA is to have joint EPOAs. It may be worth having an EPOA that is a family member and one that is a trusted friend or lawyer who has no financial interest. They must both agree on an action and hopefully this will lead to decisions made in your best interest.

APower of Attorney can act on your behalf while you still have the capacity to understand and make decisions but is ineffective should you lose capacity to understand the decisions being made.

An Enduring Power of Attorney can act on your behalf beyond your capacity to make or understand decisions and/or have the ability to communicate and act upon your wishes. It is in your best interests to have communicated your thoughts and desired outcomes well in advance.
At Profile we help with these decisions on a regular basis. Should you want any guidance or simply a chat about your estate planning, we’re happy to help.
This communication is issued by Profile Financial Services Pty Ltd (ABN 32 090 146 802), holder of Australian Financial Services Licence and Australian Credit Licence No. 226238. It contains information and general advice only and does not take into account any investor’s individual objectives, financial situation or needs. It should not be relied on by any individual. Before making any decision about the information provided, investors should consider its appropriateness
having regards to their personal objectives, situation and needs, and consult their adviser. Any indicative information and assumptions used here are summarised, are not a product illustration or quote, and may change without notice to you, particularly if based on past performance.

Scott Ungaro is a Senior Financial Adviser at Profile Financial Services Pty Ltd (AFSL 226238) a privately owned and self-licensed fee-based financial planning firm that specialises in working with dental professionals he is also is an accredited Aged Care Professional. Profile focus on implementing strategic advice and have a solid understanding and working knowledge of dentist’s structures and investment issues. Scott is also an accredited Aged Care Professional. Scott can be contacted on (02) 9683-6422, scott.ungaro@profileservices.com.au or see www.profileservices.com.au
Whether you’ve just started working, own your own practice or are considering retirement, Profile Financial Services can help you plan and secure your financial future. Just like good dentistry, in investing, prevention is better than cure! A sound financial plan can help anticipate and avoid risks before they damage your portfolio.
How safe are your investments?

To find out, contact Profile now to book an obligation-free initial meeting: (02) 9683 6422 Or visit our website www.profileservices.com.au

Regardless of market conditions, reviewing your current business plans and strategies should always be top of mind and you should ask yourself what your approach to investing into new equipment should be. If upgrading or purchasing new technology and equipment fits within your plans, then considering the investment and ensuring you have access to capital for the purchase are crucial.
Temporary full expensing was extended by the ATO to 30 June 2023 - and then it stops. While many have called for the measure to become permanent to help curb inflation, it did not receive any further mention in the October 2022-23 Budget. Subject to any further announcements, from 1 July 2023, all accelerated depreciation measures will have ended. Instant asset write-off will revert to a $1,000 asset cost cap and is limited to taxpayers with aggregated turnover less than $10 million.
It’s the last chance for eligible practice owners to take advantage of the setting while it’s around. After all, making significant business purchases can be much more beneficial beyond its primary purpose - i.e. cash flow, savings for other expenses or upgrades, increased patient satisfaction and also a boost to staff morale.
Another major consideration ahead of the 30 June 2023 cut-off is the supply of stock. Ongoing delays from overseas manufacturers, plus a spike in sales and stock shortages, could mean that leaving purchases to the last minute may see deliveries and installation fall outside of EOFY. So avoid cutting it too close and missing out by getting in early and beating the crowds.
When it comes to financing the goods, it’s been widely assumed that you must pay cash in order to get the write-off. However, you can actually borrow funds
to acquire the eligible assets. Facilities such as a chattel mortgage, or equipment loan, may meet the criteria. You can also buy from multiple sources or buy multiple eligible items under one invoice.
Here are a few general rules for the measure to confirm with your accountant.
• For assets you start to hold, and first use (or have installed ready for use) for a taxable purpose from 6 October
• Assets that fall into this scheme include medical equipment and devices, dental chairs, IT equipment including servers, computer and phone hardware, along with scanners, copiers etc. Plus, practice furniture, cabinetry, white goods and so on; and

• All work vehicles to the extent that they are used for business purposes. The team at Credabl is always here to support your plans with bespoke funding solutions. You can chat live on their website 24/7 at http://www.credabl.com.au or call one of their specialist lenders on 1300-273-322.
2020 to 30 June 2023, the instant asset write-off threshold does not apply. You can immediately deduct the business portion of the asset under temporary full expensing;
• Goods can be new or second-hand;
• Goods are first held from 6 October 2020 and first used or installed by 30 June 2023;
• You can make numerous claims across many tax invoices or with multiple items on the one invoice;
• It’s not a one-time-only offer, just so long as each purchase meets the criteria;
• If financed, the goods must be under a specific loan type, as not all facilities are appropriate;
This article is a guide only and does not constitute any recommendation on behalf of Credabl Pty Ltd (ACN 615 968 100) or any of its related bodies corporate (Credabl). The information in this article is general in nature and we have not considered your personal objectives or financial circumstances or needs when preparing it. Before acting on this information you should consider if it is suitable for your personal circumstances. Credabl is not offering financial, tax or legal advice. You should obtain independent financial, tax and legal advice as appropriate.




Professional and personal finance solutions, tailored for you and turned around fast. When you partner with Credabl, you can expect all that and more. With a team of experienced finance specialists, we understand the medical sector so you can look forward to finance solutions that help you get on with business and looking after your patients.

You always get more with Credabl.
1300 27 33 22
credabl.com.au
me.
“Communication and service has always been exceptional, and I have no hesitation in recommending Credabl across the board.
“
Dr Andrea King, Dentist
As we enter the 4th year of the pandemic, it’s fitting to reflect on the successes of 2022 and to ponder the challenges of 2023, knowing that there is a larger “toolbox” of interventions and a growing evidence base to support recommendations that are aimed at reducing risks of acquiring infection in the workplace.

The big picture
As of January 2023, total confirmed cases of COVID worldwide exceed 660 million and the number of deaths surpassed 6.6 million. A simplistic assessment of the ratio of deaths to cases gives approximately 1% as an overall mean fatality rate, but that grossly underestimates the dramatic impact of COVID in certain subpopulations (such
as the elderly and the medically frail). In data published by the Australian government’s Department of Health, in a typical week across the summer of 2022-2023, there were around 230 deaths, bringing the tally for Australia to over 16,500 by the end of 2022.
A plot of the cumulative number of deaths in Australia shows sudden increases in the gradient when a wave occurs, as in July 2022 and again in December 2022. Driving these waves in 2022 was the enormous infectivity of the Omicron variants and sub-variants (such as BA.4 and BA.5), which have been the dominant circulating strains in Australia during 2022 (Figure 1A). These are far more infectious than the previous Alpha and Delta strains that circulated during 2020 and 2021. Omicron transmission by the aerosol route explains transmission through aerosol-generating behaviours, pathways and contamination of air when people are present in very dense or crowded environments.
The total prevalence of COVID infection in Australia has now surpassed the 50% mark. In other words, more people have had Covid in Australia than people who have not. Beyond this glaring statistic, current published Australian data grossly under represent the true number of current cases, since (1) up to 40% of cases are asymptomatic; (2) only GP doctors can now order PCR tests; and (3) people using RAT tests often will not go online to report their RAT test results. Long gone are the days of people lining up in large numbers to get PCR tests. Hence, the true numbers of people who are infected at any one time is now becoming rather “fuzzy”.
One place where data are more complete is for residential aged care facilities. These have shown waves of infections in both staff and in patients in July 2022 and December 2022. Those align with peaks of infection in waves that occurred in the community. An ongoing concern is that workers may bring the infection into their aged care workplace, giving it to residents. As well, between the various waves, there has been persistence of cases in aged care, even when there were few or no cases in the community (Figure 2B). One implication of this is that nursing homes could be a reservoir for outbreaks in the general community.

Unlike the previous 2 years, COVID in 2022 was different because rates of people being admitted to intensive care units and placed on ventilators were both very low, despite spikes in the rate of hospitalisations when waves of infection occurred (Figure 1B, Figure 2A). Even during the July 2022 and December 2022 waves, COVID was not a major reason for ICU admission or going onto a ventilator. This is a very different situation from what was occurring in 2020 and 2021, where COVID cases overwhelmed hospital ICU facilities and created shortages in available ventilators.
There are likely several reasons why this occurred.
1. Some level of herd immunity is now emerging, since large proportions of the population have had at least one bout of infection;
2. Extremely high vaccination rates, particularly for third and fourth vaccine doses; and
3. The availability of several highly effective antiviral drugs in early 2022 and an important change in Australian government policy in early July 2022, which made these drugs widely available to those in the community by prescription from a general medical practitioner. Since all three of these factors lower the severity of disease, there is also a growing time period between the onset of infection and death. The pattern in 2020 and 2021 was that when people had severe infections, they would take between 7 and 10 days to succumb. This time period is now stretching out. This is not only because of better antiviral therapy, but also because of a greatly enhanced evidence base on how to better manage more severe COVID cases once they are admitted to hospital.
Uptake of 4 doses of a vaccine has been strong in Australians who are 60 years of age and above (Figure 3A), as one would expect, because these individuals are well aware that their age is a risk factor for severe infection. Unvaccinated individuals tend to be younger. Vaccination rates for people who have had all 4 doses are lower in the Northern Territory and in Western Australia than in other parts of the country. This low uptake is even more problematic because of the very dispersed population in both of those jurisdictions.
An interesting development of recent times is the bivalent COVID vaccine from Moderna for use in people who are 18 years of age or older.
This targets the original strain and also the Omicron strains and like other vaccines, provides protection from severe disease. There are also clinical trials underway in Australia of vaccines that cover not only COVID, but also influenza and respiratory syncytial virus (RSV) with the concept being to have a “universal annual booster” to cover several respiratory viral infections in the one injection. Bundling all the components into one injection may reduce vaccine fatigue and hesitancy.
The Australian government’s decision to expand the use of antiviral medicines (Molnupravir, Paxlovid, etc) in the community by prescription in early July 2022 has likely been a major factor in “sparing the ventilators” throughout 2022. Despite large numbers of cases in the community and hence considerable numbers of hospitalisations, a lower proportion of cases ended up in ICU on a ventilator than in past years. This point has not been widely discussed in the mass media, despite it being one of the success stories of 2022.

The eligibility criteria that are used for prescriptions for oral antiviral agents are:
1. Being over 70 years of age, regardless of whether there are symptoms or additional risk factors. A positive PCR test result is sufficient justification;
2. Being 50 years of age or older, with two additional risk factors (e.g. moderate or severe asthma, disability, medical frailty, heart failure, etc); or
3. Those of Aboriginal or Torres Strait Islander background aged over 30 with one additional risk factor.
This approach is a good way to target these expensive but highly effective medicines to those who are most likely to experience the most severe disease. PBS usage data from July to December 2022 show a massive uptake of prescriptions on the PBS as those two waves occurred (Figure 3B).
Patients using these medicines were mostly adults aged 70+ and 50+ as one would expect. This targeted program using antiviral drugs is certainly being taken up well and has been effective at keeping down demand for ICU beds and for ventilators.
There are concerns relating to the 2023 lunar New Year in late January and what that might lead to in a world that is “living with COVID”. This applies all around the world due to people travelling at pre-pandemic levels.
Omicron has been generating sub-variants with BA.4, BA.5 and XBB being in circulation during late 2022. These accounted for most of the cases during the second half of 2022. With some Omicron sub-variants (such as BA.2), transmissibility is greatly increased. Given the known history of COVID and of coronaviruses in general, it is highly likely that further variants and sub-variants will emerge. How transmissible they will be and whether these will become “variants of concern” or just “variants of interest” remains to be seen.
COVID-19 is vastly different from other respiratory viral infection pandemics in the past, where people who were infected either recovered or died and there were no long-term after-effects. With COVID, while most people will get a mild to moderate illness and recover without long-term side effects, others will experience severe disease and ongoing health problems, caused by the virus being present in multiple organs outside the respiratory tract. The reason for long term disease is persisting virus and as a result, ongoing inflammation. COVID is more than just an “ordinary” respiratory viral infection and SARS-CoV-2 is different from circulating endemic coronaviruses because it is neurotrophic. Persisting inflammation in the brain explains why people with long COVID notice issues with attention, sleep, memory, smell and taste.
There is an emerging public health problem of long COVID in those who experience more severe infections. In many parts of the world, more than half the population has had at least one bout of infection and while only 3-5% of people will get long COVID, that can mean 1.52.5% of the entire population will have it. Long COVID can cause over 100 different symptoms and clinical presentations.
An important point is that the single biggest risk factor for getting long COVID is having a severe case and being hospitalised and ventilated. With fewer people with severe infection dying, more are at risk of going on to get long COVID. Early use of antiviral medicines limits disease severity so it should reduce the chance of long COVID developing.
All current strategies for infection prevention and control are based on attacking one of the links in the chain of transmission. The ADA recommendations for risk management during the COVID pandemic were updated in October 2021 and are based on the hierarchy of risk controls, moving from actions that are extremely effective down to those that are less effective and/or less predictable.
In the operatory, aerosol generating procedures can be altered (reduced coolant water with scalers or air turbines) and various measures can be applied to reduce risks from aerosols. Turning down water flow rates costs nothing and can be done quickly. Many clinicians perform restorative procedures with excessively high water flow rates. They probably do this because of what they learnt at dental school in the sim lab as students. Perhaps they do not know that dental school simulation labs tend to use unusually high water flow rates for handpieces because dental students burn plastic teeth and natural teeth because of poor technique and blunt burs!
In the waiting room, the challenge is from aerosol generating behaviours (breathing, speaking, etc). Studies of air filters from waiting rooms during waves of infection have recovered viral particles from these waiting room air filters - but not from the same type of filters used in the operatory. This reflects how well the multiple (layered) containment measures used in the operatory work. Said another way, it
Figure 3. Panel A shows the age distribution of vaccine uptake, by the number of vaccine doses. The blue arrow shows that the older cohorts are more likely to have had 4 vaccine doses. Panel B shows PBS data for March 2022 to December 2022 for COVID-19 antiviral medicines prescribed for use in the community. The arrows show the 2 major waves of infection - July (orange) and December (red). Note how each wave has triggered intense usage of these medicines.

could be more likely that people will get a COVID infection from being in a waiting room than the operatory. Hence, we need to keep people who are actively infected (and who thus have high viral loads in their secretions) out of the practice by triage before the appointment.
There is now good data from multiple studies showing that the protection afforded by layered measures is extremely high. Going forward into the future, we can have confidence that these measures are able to keep us safe at work while also reducing risks to our patients.
Emeritus Professor Laurence J. Walsh AO is a specialist in special needs dentistry who is based in Brisbane, where he served for 36 years on the academic staff of the University of Queensland School of Dentistry, including 21 years as Professor of Dental Science and 10 years as the Head of School. Since retiring in December 2020, Laurie has remained active in hands-on bench research work, as well as in supervising over 15 research students at UQ who work in advanced technologies and biomaterials and in clinical microbiology. Laurie has served as Chief Examiner in Microbiology for the RACDS for 21 years and as the Editor of the ADA Infection Control Guidelines for 12 years. His published research work includes over 390 journal papers, with a citation count of over 18,300 citations in the literature. Laurie holds patents in 8 families of dental technologies. He is currently ranked in the top 0.25% of world scientists. Laurie was made an Officer of the Order of Australia in January 2018 and a life member of ADAQ in 2020 in recognition of his contributions to dentistry.
BDSc, PhD, DDSc, GCEd, FRACDS, FFOP (RCPA), FFDT (RCS Edin)
Learn from Australia’s leading authority on infection prevention and control in dentistry about recent changes in infection control including from the Dental Board of Australia (July 2022), the ADA (4th edition guidelines August 2021 and the ADA Risk management principles for dentistry during the COVID-19 pandemic (October 2021)), the new guidelines from NHMRC (May 2019), Hand Hygiene Australia (Sept 2019) and the CDNA (Dec 2018) as well as recent changes in Australian Standards and TGA regulations that are relevant to infection control. The course provides a summary of how those changes interlink with one another and also covers practical implementation of the new requirements and what it means for everyday dental practice. Hear about the why and the how and keep up-to-date with the changes that are happening.
This one day course will cover changes in regulations and guidelines from 2018 to 2022 including:
n Risk-based precautions.
n Hand hygiene and hand care practices.
n Addressing common errors in personal protective equipment.
n Biofilm reduction strategies.
n Efficiency-based measures to improve workflow in instrument reprocessing and patient changeover.
n Correct operation of mechanical cleaners and steam sterilisers.
n Wrapping and batch control identification.
n Requirements for record keeping for instrument reprocessing.
n Correct use of chemical and biological indicators.
8 HOURS CPD
Laurie Walsh is a specialist in special needs dentistry who is based at the University of Queensland in Brisbane, where he is an emeritus professor. Laurie has been teaching and researching in the areas of infection control and clinical microbiology for over 25 years and was chief examiner in microbiology for the RACDS for 21 years. His recent research work includes multiple elements of infection control, such as mapping splatter and aerosols, COVID vaccines and novel antiviral and antibacterial agents. Laurie has been a member of the ADA Infection Control Committee since 1998 and has served as its chair for a total of 8 years, across 2 terms. He has contributed to various protocols, guidelines and checklists for infection control used in Australia and represented dentistry on 4 committees of Standards Australia and on panels of the Communicable Diseases Network of Australia and of the Australian Commission on Safety and Quality in Health Care.




































 By Emeritus Professor Laurence J. Walsh AO
By Emeritus Professor Laurence J. Walsh AO

In Australia during the COVID-19 pandemic, there has been a consistent recommendation to have dental patients use mouth rinses at the start of the dental visit as one of the layers of risk reduction, in combination with other measures such as high-volume evacuation. This article summarises the key findings published in the last 18 months of work in this field, developing further the literature around how preprocedural mouth rinses can be used effectively as a risk reduction measure in dental practices. My previous articles on this topic reviewed laboratory microbiological studies of viral inactivation by mouth rinses and their components (such as excipients). Now, during the pandemic, several research groups have undertaken clinical studies using commercial products and hence one can now move beyond laboratory studies to discuss how various mouth rinses have performed in the setting of the pandemic, where issues such as acceptability and feasibility may be quite different from studies undertaken at times outside a pandemic.
ACochrane review that appeared in August 2022 1 used standard, extensive Cochrane search methods, and included literature published up to February 2022, focusing only on randomised controlled trials. The Cochrane review was designed to assess the effects of preprocedural mouth rinses used in dental clinics to minimise incidence of infection in dental healthcare providers and reduce or neutralise contamination in aerosols. A total of 17 studies were included in this Cochrane review and all of the participants in the included studies were adults (830 participants aged 18 to 70 years).
None of the 17 studies actually measured the incidence of COVID-19 infection in dental staff. Instead, they measured the extent of reduction in the level of bacterial contamination, at distances of less than 2 metres from the patient’s mouth (larger droplets) and more than 2 metres (aerosols). There are some obvious limitations to following such an approach and the studies were measuring bacteria rather than viruses.
In that regard, it is unclear what size of reduction in bacterial levels represents a clinically useful reduction in levels of virus.
Compared with no rinsing or rinsing with water, reductions were found for chlorhexidine, essential oils (Listerine™) and quaternary ammonium compounds such as benzalkonium chloride. The evidence from head-to-head comparisons was limited and inconsistent.




Several important limitations were noted. The studies did not provide any information on costs, change in microorganisms in the patient’s mouth or
adverse events such as temporary discolouration, altered taste, allergic reactions or hypersensitivity. The studies did not assess acceptability of the intervention to patients or feasibility of implementation for dentists.
Not surprisingly, the authors of the Cochrane review pointed out that further studies are needed that measure the effect of rinses on infectious disease risk among dental healthcare providers and on the infectivity of contaminated aerosols.
Similar conclusions were reached in an October 2021 systematic review,2 which included 13 studies. That review also focused on whether using mouth rinse could influence the risk of infection or the rate of progression of infection. The commonly used antimicrobial mouth rinses were found to exert significant virucidal activity against SARS-CoV-2 in saliva. They concluded that the


effective mouth rinses were povidone iodine, chlorhexidine and essential oils, but again noted how the available studies did not assess actual COVID-19 infection outcomes. Overall, these and other systematic reviews undertaken over the past 2 years have reinforced recommendations regarding the use of mouth rinses, albeit with the caveats already mentioned.
One must remember that the formulations used in different clinical studies around the world are not directly comparable, because even the same product type may have different excipients when manufactured by another company. These excipients, such as ethanol, surfactants and flavours, can in themselves exert potent antiviral actions, which can amplify the effect of the named active ingredients. This is also why there is not always a direct correlation between testing a single pure active ingredient in the laboratory and testing a commercial preparation with the same active ingredient in the laboratory, or in clinical practice.

Anarrative review published in July 2022 3 included a useful summary of 13 laboratory studies which tested, in the laboratory, the antiviral efficacy of povidone iodine, chlorhexidine, essential oils, hydrogen peroxide and benzalkonium chloride. All these active ingredients inactivated different clinical strains of SARS-CoV-2 after 15 or 30 seconds of contact. The authors of this review concluded that, based on these laboratory studies, rinses with these active ingredients could reduce the viral load in the oral cavity and, thereby, the likelihood of transmission of SARS-CoV-2 during dental procedures.

This same narrative review also included nine controlled clinical trials, which showed reductions in SARS-CoV-2 viral load in patients who were infected, with somewhat lower efficacy for hydrogen peroxide and a slightly lower duration of effect, which may be due to its inactivation by salivary enzymes. They commented on the high acceptability of mouth rinses with concentrations of hydrogen peroxide below 1.5%, but cautioned that going below 1% appeared to considerably reduce the therapeutic action on the virus.
The authors also noted that 1% povidone iodine seemed to work faster than other mouth rinse types in terms of the rate of reduction in viral load. A 1% concentration of povidone iodine is below the levels that are considered irritant or toxic to the oral mucosa.
The review also pointed out the useful features of quaternary ammonium compounds such as cetyl pyridinium chloride, which in most studies gave results comparable to those of chlorhexidine. They also included in their review studies which showed reductions in viral load after rinsing with Listerine.
Perhaps the most useful contribution of the narrative review, however, is its discussion of the various pathways and mechanisms that may be operating when mouth rinses are used. These include the mass dilution effect, which will be discussed later. While it is clear that the active ingredients and some of the excipients in mouth rinses can disrupt viral envelopes or act on viral proteins, it is important to discount the notion that the active mouth rinse components work by cytotoxic effects on virally infected cells. All oral antiseptics exhibit antiviral activity when used at levels that are not cytotoxic to human cells.
One of the most interesting studies published in early 2022 tested the presence of SARS-CoV-2 genetic material on HEPA filters from portable air cleaners that had been used in a dental facility in Spain for three months during one of the Covid-19 pandemic peaks.4
Based on the measured levels of carbon dioxide (around 900 ppm), the ventilation in the clinic where the study was done was rated as poor.
The researchers compared the filters in the waiting room where patients had not yet undergone mouth rinsing, with those in the treatment rooms where patients had undertaken mouth rinsing. The particular mouth rinse used in that study was 1% hydrogen peroxide used for 60 seconds.
Importantly, viral load was only found in filters that had come from the waiting room - but not in those from the treatment rooms.
As the study was conducted during a major pandemic peak (in this case, the third wave in Spain), it provides a useful real-world assessment of the efficacy of mouth rinses.
predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. when it comes to the perfect fit, Hu-Friedy is just right.
DENTISTS LOVE OUR STAINLESS STEEL PEDO CROWNS:
predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. it comes to the perfect fit, Hu-Friedy is just right.
DENTISTS LOVE OUR STAINLESS STEEL PEDO CROWNS:

Septanest : the first choice of dentists with over 150 million injections per year, provides you high quality you can trust

reserved.


One of the limitations in the available literature is that the molecular methods which are used to detect and quantify viral load will not be able to distinguish between viable versus non-infective viral particles. Studies do not culture samples to confirm the presence of viable infectious virus. This might seem like an unfair criticism, since laboratories that can do this are very few in number around the world and require special laboratory conditions such as biosafety level 4 precautions.
There are always continual developments in formulations, with several new types of materials entering the mouth rinse category that may be of interest, including molecular iodine, beta-cyclodextrin + Citrox® (flavonoids), hypochlorous acid, octenidine, d-limonene and iota-carrageenan.5,6 Preliminary laboratory studies of antiviral actions of all of these have been undertaken over the past 18 months, but those results remain to be confirmed in other laboratories and documented in randomised controlled clinical trials.
In patients with symptomatic infection, their very high viral loads and the rate of release of virus from infected cells in the oral tissues limits how much suppression can be achieved using mouth rinses. After all, the use of a preprocedural mouth rinse is not a panacea. Results from studies conducted in a general dental practice setting may well be different from those conducted in the COVID-19 ward of a local hospital, where patients will have been admitted because of serious illness. Those patients will have a very high viral load. Proper triage of dental patients will prevent those with serious acute COVID-19 illness from presenting to dental practice.
Indeed, there is good evidence from studies published in late 20227 that in patients with symptomatic COVID-19 infection, intact virus particles will be found not only in the saliva, but also in dental plaque and in crevicular fluid. This is because the oral cavity can be a niche for viral infection, with replication of the virus occurring in oral tissues, including the salivary glands. This is why such
studies have demonstrated the presence of oral epithelial cells that contain virus and have microscopic features of active viral infection, including vacuoles filled with particles ready to be released.
Finally, when considering the strategy of using mouth rinses, one should remember that part of their action is bulk dilution of the saliva and other oral fluids by the volume of the mouth rinse used and then by the water rinse which then follows it. Given that the typical volume of saliva at rest in the mouth is in the order of 1.5 mL, this dilution effect can be greater than 50-fold. There is also further dilution of the saliva that occurs during a dental appointment because of the irrigants that flow through the dental unit waterlines, into the triple syringe and into various dental handpieces. In a paper which appeared in September 2022, the important finding was reported that commonly used dental unit waterlines disinfectants reduce the viability of viruses.8 This was demonstrated using the virus Bacteriophage MS2 as the target. This phage infects Escherichia coli and has structural similarity to several human viral pathogens (e.g., rhinoviruses, adenoviruses, coronaviruses). The water line treatment products that were tested comprised A-dec ICX™ (silver nitrate and hydrogen peroxide) and Alpro Apron™ which contains chloramine-T and polyhexanide biguanide. Both agents reduced the viability of this phage and when present in waterlines, reduced dispersion of viable virus into the simulated dental clinical setting.
The authors of that study commented that water line disinfectants have been
working silently to reduce the viability of viruses and the dispersion of pathogens from the mouth within aerosols and droplets. One could consider them having an action somewhat like a mouth rinse, but one that is present at all times. One could also conclude that such waterline disinfectants work in partnership with mouth rinses as a mitigation factor during infectious disease outbreaks/pandemics.
Looking to the future, there is likely to be ongoing interest in the antiviral actions of mouth rinses. One can expect greater recognition of the ways that residues of mouth rinse ingredients that are substantive and can be released over time (such as chlorhexidine) may work in partnerships with waterline disinfectants to keep levels of virus in the saliva low.
1. Nagraj SK et al. Preprocedural mouth rinses for preventing transmission of infectious diseases through aerosols in dental healthcare providers. Cochrane Database Syst Rev 2022; 8(8): CD013826.
2. Verma SK et al. Effectiveness of mouthwash against viruses: 2020 perspective. A systematic review. Minerva Dent Oral Sci. 2021;70(5):206-213.
3. Bernal CGG et al. Oral antiseptics against SARSCoV-2: a literature review. Int. J. Environ. Res. Public Health 2022; 19: 8768.
4. Burgos-Ramos E at al. Is hydrogen peroxide an effective mouthwash for reducing the viral load of SARS-CoV-2 in dental clinics? Saudi Dent J. 2022; 34(3): 237-242.
5. Garcia-Sanchez A et al. Virucidal activity of different mouthwashes against the salivary load of SARS-CoV-2: a narrative review. Healthcare 2022; 10: 469.
6. Garcia-Sanchez A et al. Efficacy of pre-procedural mouthwashes against SARS-CoV-2: a systematic review of randomized controlled trials. J. Clin. Med. 2022; 11: 1692.
7. Belhaouari DB et al. Microscopic observations of SARS-CoV-2 like particles in different oral samples. Eur J Oral Sci. 2022; 130: e12903.
8. Allison JR et al. Waterline disinfectants reduce dental bioaerosols: a multitracer validation. J Dent Res. 2022; 101(10): 1198–1204.
Emeritus Professor Laurence J. Walsh AO is a specialist in special needs dentistry who is based in Brisbane, where he served for 36 years on the academic staff of the University of Queensland School of Dentistry, including 21 years as Professor of Dental Science and 10 years as the Head of School. Since retiring in December 2020, Laurie has remained active in hands-on bench research work, as well as in supervising over 15 research students at UQ who work in advanced technologies and biomaterials and in clinical microbiology. Laurie has served as Chief Examiner in Microbiology for the RACDS for 21 years and as the Editor of the ADA Infection Control Guidelines for 12 years. His published research work includes over 390 journal papers, with a citation count of over 18,300 citations in the literature. Laurie holds patents in 8 families of dental technologies. He is currently ranked in the top 0.25% of world scientists. Laurie was made an Officer of the Order of Australia in January 2018 and a life member of ADAQ in 2020 in recognition of his contributions to dentistry.




IMS™ Cassettes may be physically bigger than pouches, but that doesn’t necessarily mean that they take up more space. IMS

Cassettes help facilities better organise their reprocessing flow, freeing over two linear metres of counter space. They are also easily stacked, sterilised and stored in a more organised fashion than pouches. One cassette can do the job of multiple pouches during a single procedure - saving you extra space. Plus, they are made of durable, lightweight stainless steel.

Myth 2: Packing IMS Cassettes takes too long
IMS Cassettes eliminate time-consuming steps to streamline reprocessing, which can save facilities an hour or more each day. IMS
Cassettes systematically organise instruments according to procedure type, allowing for more focus on patients and less time spent looking for missing instruments. Instruments don’t need to be scrubbed by hand and they don’t need to be sorted and pouched. That time saved adds up quickly. On average, practices that use IMS Cassettes see a time savings of 5 to 10 minutes per procedure.1 Over the course of a day, that saves an hour or more.
With IMS Cassettes, team members are left with less sorting, less guess work, less forgotten instruments and less chance of mislabeling or mispacking instruments. Dental assistants and hygienists can feel confident walking into every operatory knowing they have the correct instruments and leaving more time to spend with the patient.


Myth 4: IMS Cassettes take up too much space in autoclave

Keeping procedures in a cassette helps to prevent overloading of the steriliser. Without the use of cassettes, pouches are frequently overstuffed. This leads to overloading the steriliser and the risk of not achieving full sterilisation. HuFriedyGroup IMS Cassettes have a patented design that permits optimal penetration of steam to instruments during sterilisation. Revolutionary hole pattern design provides more access to instruments during cleaning and sterilisation.


Myth 5: IMS Cassettes make staff turnover more difficult.

IMS Cassettes help facilities create a system for managing their procedural setups. Each setup includes all of the instruments that are needed to help with onboarding and standardising care throughout a single facility and even across multiple locations. Training new hires or temporary staff on patient prep, reprocessing and operatory breakdown is simpler with IMS Cassettes.
Myth 6: IMS Cassettes are not worth the investment
IMS Cassettes can make an immediate impact on a facility’s bottom line, with the time saved allowing them to see new patients and bring in tens of thousands of dollars in new revenue. IMS Cassettes also protect instruments and reduce costs of purchasing new instruments. Dental instruments are kept together throughout the cleaning process, reducing the potential for instrument breakage or loss. It’s no wonder IMS Cassettes have a 95% satisfaction rating.2
The most sophisticated solution for instrument management
The most sophisticated solution for instrument management
The
The most sophisticated solution for instrument management
Ensure predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. You’ll quickly discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. Because when it comes to the perfect fit, Hu-Friedy is just right.
Ensure predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. You’ll quickly discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. Because when it comes to the perfect fit, Hu-Friedy is just right.
That’s right, you deserve it. You deserve the peace of mind and confidence of knowing that you are employing the most contemporary method of processing instruments. As dentistry’s innovator of the cassette-based instrument management system, Hu-Friedy is proud to bring you the modern design and functionality of the Infinity Series Cassettes which include:
That’s right, you deserve it. You deserve the peace of mind and confidence of knowing that you are employing the most contemporary method of processing instruments. As dentistry’s innovator of the cassette-based instrument management system, Hu-Friedy is proud to bring you the modern design and functionality of the Infinity Series Cassettes which include:
The
That’s right, you deserve it. You deserve the peace of mind and confidence of knowing that you are employing the most contemporary method of processing instruments. As dentistry’s innovator of the cassette-based instrument management system, Hu-Friedy is proud to bring you the modern design and functionality of the Infinity Series Cassettes which include:
That’s right, you deserve it. You deserve the peace of mind and confidence that you are employing the most contemporary method of processing instruments. innovator of the cassette-based instrument management system, Hu-Friedy
• An open hole pattern that promotes water flow throughout the cassette
• An open hole pattern that promotes water flow throughout the cassette
Ensure predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. You’ll quickly discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. Because when it comes to the perfect fit, Hu-Friedy is just right.
• An open hole pattern that promotes water flow throughout the cassette

Ensure predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. You’ll quickly discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. Because when it comes to the perfect fit, Hu-Friedy is just right.
WHY DENTISTS LOVE OUR STAINLESS STEEL PEDO CROWNS:
• Color-coded silicone rail system that significantly reduces instrument contact and allows for more water flow while protecting the instruments during reprocessing
WHY DENTISTS LOVE OUR STAINLESS STEEL PEDO CROWNS:
• Color-coded silicone rail system that significantly reduces instrument contact and allows for more water flow while protecting the instruments during reprocessing
• Ideal height and mesio-distal width
• Easy-to-use, ergonomic latch that allows for one-handed opening
WHY DENTISTS LOVE OUR STAINLESS STEEL PEDO CROWNS:
• Color-coded silicone rail system that significantly reduces instrument contact and allows for more water flow while protecting the instruments during reprocessing
WHY DENTISTS LOVE OUR STAINLESS STEEL PEDO CROWNS:
• Ideal height and mesio-distal width
•
• Ideal height and mesio-distal width
• Easy-to-use, ergonomic latch that allows for one-handed opening
• Pre-trimmed and pre-crimped for simple placement
• Ideal height and mesio-distal width
• Accurate occlusal anatomy that matches the natural tooth
• Pre-trimmed and pre-crimped for simple placement
Performing at your best means having confidence in what you do. Experience Infinity Series™ Cassettes, and improve the efficiency of your practice, while helping protect your patients, your staff and your instrument investment.
• Pre-trimmed and pre-crimped for simple placement
• Accurate occlusal anatomy that matches the natural tooth
• Accurate occlusal anatomy that matches the natural tooth
• Pre-trimmed and pre-crimped for simple placement
Performing at your best means having confidence in what you do. Experience Infinity Series™ Cassettes, and improve the efficiency of your practice, while helping protect your patients, your staff and your instrument investment.
• Easy-to-use, ergonomic latch that allows for one-handed opening Performing at your best means having confidence in what you do. Experience Infinity Series™ Cassettes, and improve the efficiency of your practice, while helping protect your patients, your staff and your instrument investment.

©2016 Hu-Fried y Mfg. Co., LLC. All rights reserved.
©2016 Hu-Fried y Mfg. Co., LLC. All rights reserved.
©2016 Hu-Fried y Mfg. Co., LLC. All rights reserved.
• Accurate occlusal anatomy that matches the natural tooth
 By Joseph Allbeury
By Joseph Allbeury
The uptake of automated instrument cleaning using thermal washer disinfector units continues to increase as dental practices update their infection control workflows and equipment. The trend is as much driven by the need to comply with a Standards-driven push to move away from manual instrument cleaning as it is to increase efficiency and make better use of valuable human resources.
We spoke to Jim Owen from MOCOM Australia about this growing trend in infection control solutions and why installing a washer disinfector is a good idea.
QThank you for your time, Jim. So why are washer disinfector units becoming the new normal in dental sterilisation rooms?
AI think the big driver for installing washer disinfectors in 2023 will continue to be as a way of future proofing your practice. The new draft standard AS 5369:2021, which will replace AS/ NZS4187 and AS/NZS4815, reiterates the need to move away from manual instrument cleaning so we’re only going to see more and more interest in automated systems.
There are also myriad benefits to using a washer disinfector over manual cleaning. It’s a validated process so you know its
cleaning effectively. It allows for better use of staff time. There is significantly less risk of sharps injuries due to reduced handling.
Many practices are on an efficiency drive so for a staff member to be able to load the washer disinfector and then move on to other duties while the instruments are automatically cleaned has a multitude of benefits.
QIs a washer disinfector an alternative to an ultrasonic bath?
AIt’s a better alternative. A lot of practices do use ultrasonic baths to assist in instrument cleaning but the fact remains that you still need to manually
handle the instruments. You still need to rinse the instruments afterwards and you still need to dry the instruments before sterilisation. And you need to drain the chemicals out of the bath. If you’re short on space, we have a bench top washer disinfector (Mocom H10 Tethys) that completely automates that process and for larger clinics, the under-bench models offer even greater productivity. You load the dirty instruments and the unit does the rest.
AThe short answer is yes you can. In our under-bench units, there’s an accessory for this. The handpieces fit into a silicon holder that allows water and chemicals to be “pushed” through the handpiece mechanism to remove any bioburden. It’s one size fits all handpieces.
Our bench top unit, the Tethys H10, is also now able to process handpieces using an accessory. Up until recently, you couldn’t process handpieces in the H10 because it uses ultrasonics during the washing phase. And as we know, you can’t put rotary instruments in an ultrasonic bath. With the new firmware update, however, it enables the ultrasonic function to be turned off and with the addition of the handpiece accessory, you can now process up to six handpieces at a time.
In both cases, once removed, the handpieces should be lubricated prior to sterilisation.
It is of course important for practices to clean their handpieces internally as well as lubricating them and we often see this first step overlooked.
AInstrument cassettes are actually perfect for use in our washer disinfectors and mitigate the risks of sharps injury even further. Instruments can remain in the cassettes during cleaning and drying in the washer disinfector and once completed, wrapped or bagged for sterilisation. If practices are utilising instrument cassettes, like Hu-Friedy’s IMS, MOCOM has two accessory racks that allow up to 12 of the very large cassettes to be processed at a time in our full size under-bench washer disinfector.
Using cassettes have also been shown to save time and increase efficiency. Instruments are loaded into the cassette chairside after use and closed up for transport to the sterilization area. The entire cassette is placed in the washer disinfector unopened. The instruments inside are cleaned and dis-
is it opened. So the instruments inside are never misplaced, dropped or damaged and risks of a sharps injury is negligible.
So whereas using a washer disinfector alone increases your efficiency considerably, when used in conjunction with a cassette system, the gains are even greater.

Do the instrument cassettes fit in the sterilisers?
infected and dried at the end of the cycle. The still unopened cassette is then bagged or wrapped and placed into an autoclave for steam sterilization. The instruments in the cassette are then ready for patient use. Only when the cassette is chairside again
We have multiple chamber racks available for the sterilisers as well. As cassette systems have become larger and more popular, having sterilisers that can accommodate these is obviously important. And sometimes you find with different brands of sterilisers that the standard chamber rack doesn’t accommodate cassettes very well. At MOCOM we have a couple of options that basically utilise the width of the round chamber better so you can get those bigger cassettes in. We also have what we call a modular tray rack where the shelves can be adjusted to the different heights of the cassettes. And we also have three chamber sizes available with the 28 litre model being fairly unique for bench top dental sterilisers. Its larger diameter obviously allows you to fit more in but also accommodates larger instrument cassettes with ease.

QHow long does the washer disinfector take to process a load?
AA full cycle with our largest D60 under-bench model utilising threephase power - which includes pre-rinse, wash, thermal disinfecting and dryingtakes around 90 minutes. There are also shorter cycles. The D60 has 16 cycles to select from and some of the shorter cycles don’t include the pre-rinse. We tend to recommend using the full cycle because the Standard says that if you’re using a washer disinfector, you should be using a cycle with a pre-rinse.
QWhen you say a validated process, what does that mean?
AIt means that you’re getting the same cleaning result every time because a technician has validated that the process is successful. It means the unit has been tested to ensure it is cleaning thoroughly, time after time.
Soil tests and process challenge devices should also be used at regular intervals per guidelines.
QHow are the chemicals dispensed?
APart of the validated process is the automated dispensing of chemicals to ensure the correct amounts are used. There is a chemical cleaner and an acid neutralizer. There are two 5-litre bottles that sit side-by-side next to the machine, normally inside a cupboard.
QDo washer disinfectors record cycle data?
AThe units do record cycle data - disinfection level and how long it’s disinfected for and at what temperature. The unit can send cycle data to a computer and then this can be read with the software provided. There’s also an option for an external printer to print cycle data. Like sterilisers, you’re meant to record this information with thermal disinfectors as well.
QMOCOM are based in Perthwhat’s the support network like?
AService and support is critical when selling sterilisers and washer
disinfectors so we have a large national service network in place. We have multiple service technicians in each state so there is a choice of service providers. Technicians attend regular training sessions at our HQ and technical office in Perth to ensure they
are up-to-date with product updates. Spare parts are also available for overnight shipping nationwide, so any downtime is minimised.
QAny final words of advice?
AThere’s been a lot of talk about the use of washers disinfectors becoming mandatory. It’s already recommended in the Standard that you should always be using a washer disinfector where possible, unless the instruments cannot withstand the rigors of the cleaning process.
So installing a washer disinfector the next time you update your sterilisation area is future proofing your practice against any changes that may occur. It will also deliver a range of other benefits to your practice that will pay for itself time and again.
Thank you for your time.
MOCOM sterilisers and washer disinfectors are available from Henry Schein.

A typical MOCOM customer experience...
“This is my 2nd MOCOM Autoclave and I would not hesitate to recommend the MOCOM autoclave to all my colleagues due to the reliability of the machine and most importantly, the after sales service that I receive from your company.
“It is the best service I have received in 43 years in dental practice!

“My dental nurse / receptionist of 36 years and I have only good words to say about your company, the service we receive is second to none. In today’s world, reputation is very underrated; to Jeanette and myself it is the most important part of our work. Henry Schein said to me to select the MOCOM autoclave due to its reliability, quality and after sales service, they were correct. We were then introduced to Utech as they commissioned the first MOCOM autoclave we bought; they also said that MOCOM was the best autoclave they dealt with. They also are a very well run, reliable company. We wouldn’t use anybody else. It is these connections that make our dental practice pretty well stress free in terms of the autoclave everyday .
“Thanks again for sorting the door jamming problem out so professionally. My late father always said to buy quality, as you remember this in years to come, long after you have forgotten about the price. This is my MOCOM experience.”
Dr David Rosenthall, Eastwood, Sydney





CYCLE TYPES: B and S
WATER SUPPLY: One way.
Auto water fill & manual top fill water function
Anthos Australia Tel: 1300-881-617 www.anthos.com.au info@anthos.com.au
RRP (inc GST): $POA
MIN. CYCLE TIME:
(Wrapped, Solid, Drying, 134oC) 22 minutes
MAIN CYCLE TIMES (inc. DRYING):
Universal 134 42 min 134oC
Universal 121 58 min 121oC
Unwrapped Hollow 22 min 134oC
Wrapped Solid 33 min 134oC
INTERNAL: 250 mm Ø x 350 mm (17 L)
EXTERNAL: W: 480 x H: 500 x D: 600 mm
WARRANTY: 3 Years or 3000 cycles
SERVICE: All States and NZ
Loan units available.
PRINTER: On-screen cycle release; Opt’l cycle & barcode printer.
DATA LOGGER: USB pen drive or Automatic download of cycle data to software
CYCLE TYPES: B and S
WATER SUPPLY: One way.
Auto water fill & manual top fill water function
MIN. CYCLE TIME:
(Unwrapped, Hollow, Drying, 134oC) 25 minutes
MAIN CYCLE TIMES (inc. DRYING):
Universal 134 46 min 134oC
Universal 121 63 min 121oC
Unwrapped Hollow 25 min 134oC
Wrapped Solid 39 min 134oC
WARRANTY: 3 Years or 3000 cycles
SERVICE: All States and NZ
Loan units available.
PRINTER: On-screen cycle release; Opt’l cycle & barcode printer.
Anthos Australia Tel: 1300-881-617 www.anthos.com.au info@anthos.com.au
RRP (inc GST): $POA
INTERNAL: 250 mm Ø x 450 mm (22 L)
EXTERNAL: W: 480 x H: 500 x D: 600 mm
CYCLE TYPES: B and S
WATER SUPPLY: One way. Auto water fill & manual top fill water function
MIN. CYCLE TIME: (Unwrapped, Hollow, Drying, 134oC) 28 minutes
MAIN CYCLE TIMES (inc. DRYING):
Universal 134 56 min 134oC Universal 121 69 min 121oC
Unwrapped Hollow 28 min 134oC
Wrapped Solid 45 min 134oC
DATA LOGGER: USB pen drive or Automatic download of cycle data to software
WARRANTY: 3 Years or 3000 cycles
SERVICE: All States and NZ
Loan units available.
PRINTER: On-screen cycle release; Opt’l cycle & barcode printer.
Anthos Australia Tel: 1300-881-617 www.anthos.com.au info@anthos.com.au
RRP (inc GST): $POA
INTERNAL: 280 mm Ø x 450 mm (28 L)
EXTERNAL: W: 480 x H: 500 x D: 600 mm
DATA LOGGER: USB pen drive or Automatic download of cycle data to software
CYCLE TYPES: B and S
WATER SUPPLY: One way. Auto water fill & manual top fill water function
MIN. CYCLE TIME: (Wrapped, Solid, Drying, 134oC) 22 minutes
MAIN CYCLE TIMES (inc. DRYING):
Anthos Australia Tel: 1300-881-617 www.anthos.com.au info@anthos.com.au
RRP (inc GST): $POA
INTERNAL: 250 mm Ø x 350 mm (17 L)
EXTERNAL: W: 480 x H: 500 x D: 600 mm
WARRANTY: 3 Years or 3000 cycles
SERVICE: All States and NZ
Loan units available.
PRINTER: On-screen cycle release; Opt’l cycle & barcode printer.
DATA LOGGER: USB pen drive or Automatic download of cycle data to software
CYCLE TYPES: B and S
WATER SUPPLY: One way.
Auto water fill & manual top fill water function
MIN. CYCLE TIME: (Wrapped, Solid, Drying, 134oC) 25 minutes
MAIN CYCLE TIMES (inc. DRYING):
Universal 134 44 min 134oC
Universal 121 61 min 121oC
Unwrapped Hollow 25 min 134oC
Wrapped Solid 37 min 134oC
WARRANTY: 3 Years or 3000 cycles
SERVICE: All States and NZ
Loan units available.
PRINTER: On-screen cycle release; Opt’l cycle & barcode printer.






Anthos Australia Tel: 1300-881-617 www.anthos.com.au info@anthos.com.au


RRP (inc GST): $POA
INTERNAL: 250 mm Ø x 450 mm (22 L)
EXTERNAL: W: 480 x H: 500 x D: 600 mm
DATA LOGGER: USB pen drive or Automatic download of cycle data to software
CYCLE TYPES: B and S
WATER SUPPLY: One way. Auto water fill & manual top fill water function
MIN. CYCLE TIME:
(Unwrapped, Hollow, Drying, 134oC) 28 minutes
MAIN CYCLE TIMES (inc. DRYING):
Universal 134 54 min 134oC
Universal 121 67 min 121oC
Unwrapped Hollow 28 min 134oC
Wrapped Solid 43 min 134oC
WARRANTY: 3 Years or 3000 cycles
SERVICE: All States and NZ
Loan units available.
PRINTER: On-screen cycle release; Opt’l cycle & barcode printer.
Anthos Australia Tel: 1300-881-617 www.anthos.com.au info@anthos.com.au
RRP (inc GST): $POA
INTERNAL: 280 mm Ø x 450 mm (28 L)
EXTERNAL: W: 480 x H: 500 x D: 600 mm
DATA LOGGER: USB pen drive or Automatic download of cycle data to software
CYCLE TYPES: B and S
WATER SUPPLY: Closed loop. Built in Deminuses tap water and recycles. 5L per 50 cycles.
MIN. CYCLE TIME:
(Wrapped, Solid, Drying, 134oC) 22 minutes
MAIN CYCLE TIMES (inc. DRYING):
Universal 134 40 min 134oC
Universal 121 56 min 121oC
Unwrapped Hollow 22 min 134oC
Wrapped Solid 31 min 134oC
WARRANTY: 3 Years or 3000 cycles
SERVICE: All States and NZ
Loan units available.
PRINTER: On-screen cycle release; Opt’l cycle & barcode printer.
Anthos Australia Tel: 1300-881-617 www.anthos.com.au info@anthos.com.au
RRP (inc GST): $POA
INTERNAL: 250 mm Ø x 350 mm (17 L)
EXTERNAL: W: 480 x H: 500 x D: 600 mm
DATA LOGGER: USB pen drive or Automatic download of cycle data to software
CYCLE TYPES: B and S
WATER SUPPLY: Closed loop. Built in Deminuses tap water and recycles.
5L per 50 cycles.
MIN. CYCLE TIME: (Wrapped, Solid, Drying, 134oC) 25 minutes
MAIN CYCLE TIMES (inc. DRYING):
Universal 134 44 min 134oC
Universal 121 61 min 121oC
Unwrapped Hollow 25 min 134oC
Wrapped Solid 37 min 134oC
WARRANTY: 3 Years or 3000 cycles
SERVICE: All States and NZ
Loan units available.
PRINTER: On-screen cycle release; Opt’l cycle & barcode printer.
Anthos Australia Tel: 1300-881-617 www.anthos.com.au info@anthos.com.au
RRP (inc GST): $POA
INTERNAL: 250 mm Ø x 450 mm (22 L)
EXTERNAL: W: 480 x H: 500 x D: 600 mm
DATA LOGGER: USB pen drive or Automatic download of cycle data to software
CYCLE TYPES: B and S
WATER SUPPLY: Closed loop. Built in Deminuses tap water and recycles.
5L per 50 cycles.
MIN. CYCLE TIME: (Unwrapped, Hollow, Drying, 134oC) 28 minutes
MAIN CYCLE TIMES (inc. DRYING):
Anthos Australia Tel: 1300-881-617 www.anthos.com.au info@anthos.com.au
RRP (inc GST): $POA
INTERNAL: 280 mm Ø x 450 mm (28 L)
EXTERNAL: W: 480 x H: 500 x D: 600 mm
WARRANTY: 3 Years or 3000 cycles
SERVICE: All States and NZ
Loan units available.
PRINTER: On-screen cycle release; Opt’l cycle & barcode printer.





DATA LOGGER: USB pen drive or Automatic download of cycle data to software
More detailed information on all models listed in the marketplace is available online... www.dentalcommunity.com.au/products/autoclaves---sterilisers

Detailed specifications to allow you to easily compare products
Articles, Videos and other information
Full list of distributors for each products so you can shop around
Constantly updated with new products, models and information
CYCLE TYPES: S
WATER SUPPLY: One Way
MIN. CYCLE TIME: (Wrapped, Hollow, Drying, 134oC) 18 minutes
MAIN CYCLE TIMES (inc. DRYING):
Handpiece - clean, sterilise & lubricate 18 min 134oC
Ultrasonic handpieces and 22 min 134oC tips - Clean disinfect & sterilise

WARRANTY: 1 Parts / 1 Labour
SERVICE: All States. Loan units available whilst in warranty
PRINTER: Data Log printer included
Dentsply Sirona
AU: 1300-552-929 NZ: 0800-336-877 clientservices@dentsplysirona.com
INTERNAL: 1.8L
EXTERNAL: W: 350 x H: 380 x D: 370 mm

CYCLE TYPES: B and S
WATER SUPPLY: One Way
MIN. CYCLE TIME:
(Wrapped, Hollow, Drying, 134oC) 30 minutes
MAIN CYCLE TIMES (inc. DRYING):
Universal 45-50 min 134oC
Quick B 40 min 134oC
Quick S 20 min 134oC
Gentle 60 min 121oC
Dentsply Sirona
AU: 1300-552-929 NZ: 0800-336-877 clientservices@dentsplysirona.com
INTERNAL: 250 mm Ø x 350 mm (17 L)
EXTERNAL: W: 425 x H: 485 x D: 630 mm
WARRANTY: 2 Parts / 2 Labour
SERVICE: All States. Loan units available whilst in warranty
PRINTER: Data log printer included
DATA LOGGER: External data logger and flash card optional
CYCLE TYPES: B and S
WATER SUPPLY: One Way
MIN. CYCLE TIME: (Wrapped, Hollow, Drying, 134oC) 12 minutes
MAIN CYCLE TIMES (inc. DRYING):
Universal 33 min 134oC
Quick B 20 min 134oC
Quick S 12 min 134oC
Gentle 48 min 121oC
Dentsply Sirona
AU: 1300-552-929 NZ: 0800-336-877 clientservices@dentsplysirona.com
INTERNAL: 250 mm Ø x 450 mm (23 L)
EXTERNAL: W: 470 x H: 565 x D: 690 mm
WARRANTY: 2 Parts / 2 Labour
SERVICE: All States. Loan units available whilst in warranty
PRINTER: Optional barcode
Label-Printer

DATA LOGGER: Integrated compact flash card ETHERNET
CYCLE
MAIN CYCLE TIMES (EXCL. DRYING):
Rubber/Plastic 18.40min+ 121oC
Henry Schein Halas AU Tel: 1300-658-822
Henry Schein Shalfoon NZ Tel: 0800-808-855
INTERNAL: W: 180 x H: 35 D: 280 mm
EXTERNAL: W: 415 x H: 150 x D: 483 mm
WARRANTY: 1 Year Parts / Labour
SERVICE: All States and NZ
PRINTER: Optional - attach via RS232 serial printer port + LAN
DATA LOGGER: Integrated data logger with USB port
CYCLE TYPES: S
WATER SUPPLY: One way
RRP (inc GST): $POA
MIN. CYCLE TIME: (Solid Unwrapped 134oC) 9 minutes
MAIN CYCLE TIMES (EXCL. DRYING):
Solid/Unwrapped 8.45min+ 134oC
Hollow/Unwrapped 10.50min+ 134oC
Hollow/Wrapped 15.30min+ 134oC
Rubber/Plastic 20.20min+ 121oC
Henry Schein Halas AU Tel: 1300-658-822





Henry
INTERNAL: W: 180 x H: 75 D: 380 mm
EXTERNAL: W: 577 x H: 190 x D: 483 mm
WARRANTY: 1 Year Parts / Labour
SERVICE: All States and NZ
PRINTER: Optional - attach via RS232 serial printer port + LAN

DATA LOGGER: Integrated data logger with USB port


CYCLE TYPES: B and S
WATER SUPPLY: One Way
RRP (inc GST): $POA
MIN. CYCLE TIME: (Wrapped, Hollow, Drying, 134oC) 30 minutes
MAIN CYCLE TIMES (inc. DRYING):
45 min 134oC Quick B 35 min 134oC Quick S 18 min 134oC Gentle 20 min 121oC
NSK Oceania Pty Ltd
AU Tel: 1300-443-321 NZ Tel: 0800-443-321 www.nskoceania.com.au





A-dec Australia dealers Tel: (02) 8332-4000 or 1800-225-010
CYCLE TYPES: B and S
WATER SUPPLY: Mains connected water treatment system
RRP (inc GST): $POA
INTERNAL: 240 mm Ø x 384 mm (17 L)
EXTERNAL: W: 445 x H: 428 x D: 532 mm
MIN. CYCLE TIME: (Flash, Drying, 134oC) 32 minutes
MAIN CYCLE TIMES (inc. DRYING):
54 min 121oC
B 30 min 134oC
INTERNAL: 250 mm Ø x 370 mm (17 L)
EXTERNAL: W: 493 x H: 484 x D: 654 mm
WARRANTY: 1 Parts / 1 Labour
SERVICE: All States
PRINTER: Barcode label printer
DATA LOGGER: External data logger and USB card or via Wi-Fi dongle
WARRANTY: 3 Years* or 2000 cycles
(* If registered on website)
SERVICE: Authorised Dealers and Service Partners in ALL States.
PRINTER: Optional Hygoprint Easy external printer
DATA LOGGER: Yes


CYCLE TYPES: B and S WATER SUPPLY: Mains connected water treatment system
RRP (inc GST): $POA
CYCLE TIME: (Flash, Drying, 134oC)
minutes MAIN CYCLE TIMES (inc. DRYING):
WARRANTY: 3 Years* or 2000 cycles
(* If registered on website)
SERVICE: Authorised Dealers and Service Partners in ALL States.
PRINTER: Optional Hygoprint Easy external printer
DATA LOGGER: Yes
INTERNAL: 250 mm Ø x 450 mm (22 L)
Tel: (02) 8332-4000 or 1800-225-010
EXTERNAL: W: 493 x H: 484 x D: 654 mm
CYCLE TYPES:
WARRANTY: 3 Years* or 2000 cycles (* If registered on website)
SERVICE: Authorised Dealers and Service Partners in ALL States.
PRINTER: Optional Hygoprint Easy external printer
DATA LOGGER: Yes. VistaSoft Monitor ready
A-dec Australia dealers Tel: (02) 8332-4000 or 1800-225-010
INTERNAL: 250 mm Ø x 370 mm (17 L) EXTERNAL: W: 493 x H: 484 x D: 654 mm
CYCLE
WARRANTY: 3 Years* or 2000 cycles
(* If registered on website)
SERVICE: Authorised Dealers and Service Partners in ALL States.
PRINTER: Optional Hygoprint Easy external printer
DATA
Yes. VistaSoft Monitor ready
CYCLE
MIN. CYCLE TIME: (Wrapped, Solid, Drying, 134oC) 18 minutes
MAIN CYCLE TIMES (inc. DRYING):
WARRANTY: 2 Parts / 2 Labour Conditions Apply
SERVICE: All States
Loan units available.
PRINTER: Optional ink ribbon printer or Label Printer


DATA LOGGER: Opt. compact flash card drive or via ethernet
CYCLE
Device Technologies
Tel: 1800-672-675 • www.device.com.au customers@device.com.au
WARRANTY: 2 Parts / 2 Labour Conditions Apply
SERVICE: All States
Loan units available.
PRINTER: Optional ink ribbon printer
DATA LOGGER: Opt. compact flash card drive or via ethernet



WARRANTY: 2 Parts / 2 Labour Conditions Apply
SERVICE: All States
Loan units available.
PRINTER: Optional ink ribbon printer
DATA LOGGER: Opt. compact flash card drive or via ethernet
WARRANTY: 2 Parts / 2 Labour Conditions Apply
SERVICE: All States
Loan units available.
PRINTER: Optional ink ribbon printer
Technologies
Tel: 1800-672-675 • www.device.com.au customers@device.com.au
DATA LOGGER: Opt. compact flash card drive or via ethernet




CYCLE TYPES: B and S
WATER SUPPLY: One Way RRP (inc GST): $POA
MIN. CYCLE TIME: (Wrapped, Solid, Drying, 134oC) 20 minutes
MAIN CYCLE TIMES (inc. DRYING):
Universal B 13-43 min 134oC
Quick S 12-33 min 134oC
Prion B 28-58 min 134oC
WARRANTY: 2 Parts / 2 Labour Conditions Apply
SERVICE: All States Loan units available.
PRINTER: Bar Code Label-Printer
DATA LOGGER: Standard USB drive or via ethernet Device Technologies
Tel: 1800-672-675 • www.device.com.au customers@device.com.au

Gentle 25-62 min 121oC
INTERNAL: 380 mm Ø x 450 mm (53 L)
EXTERNAL: W: 636 x H: 590 x D: 715 mm

WARRANTY:
PRINTER:
DATA
via ethernet
CYCLE
WARRANTY: 2 Parts / 2 Labour Conditions Apply
SERVICE: All States
Loan units available.
PRINTER: Optional ink ribbon printer or Label Printer
DATA LOGGER: Opt. compact flash card drive or via ethernet
WARRANTY: 2 Parts / 2 Labour
Conditions Apply
SERVICE: All States
Loan units available.
PRINTER: Optional ink ribbon printer or Label Printer
Device Technologies
Tel: 1800-672-675 • www.device.com.au customers@device.com.au
mm Ø x 450 mm (22 L)

EXTERNAL: W: 460 x H: 500 x D: 680 mm
DATA LOGGER: Opt. compact flash card drive or via ethernet

CYCLE TYPES:
and S WATER SUPPLY: One Way RRP (inc GST): $POA
CYCLE TIME:
Solid, Drying, 134oC) 30 minutes
MAIN CYCLE TIMES (inc. DRYING):
43-55 min 134oC Quick B 30 min 134oC Quick S 23 min 134oC




Prion 56-62 min 134oC
Gentle 56 min 121oC
Device Technologies
Tel: 1800-672-675 • www.device.com.au customers@device.com.au
INTERNAL: 440 mm Ø x 720 mm (105 L)
EXTERNAL: W: 650 x H: 1600 x D: 910 mm
WARRANTY: 2 Parts / 2 Labour
Conditions Apply
SERVICE: All States
Loan units available.
PRINTER: Optional ink ribbon printer or Label Printer


DATA LOGGER: Opt. compact flash card drive or via ethernet

CYCLE TYPES: B and S
WATER SUPPLY: One Way
RRP (inc GST): $POA
MIN. CYCLE TIME:
(Wrapped, Solid, Drying, 134oC) 31 minutes
MAIN CYCLE TIMES (inc. DRYING):
Universal 41-60 min 134oC
Quick B 31 min 134oC
Quick S 23 min 134oC
Prion 56-65 min 134oC
Gentle 56 min 121oC
Device Technologies
Tel: 1800-672-675 • www.device.com.au customers@device.com.au
INTERNAL: 440 mm Ø x 740 mm (110 L)
EXTERNAL: W: 650 x H: 1600 x D: 1010 mm
WARRANTY: 2 Parts / 2 Labour Conditions Apply
SERVICE: All States
Loan units available.
PRINTER: Optional ink ribbon printer or Label Printer
DATA LOGGER: Opt. compact flash card drive or via ethernet
CYCLE TYPES: B and S
WATER SUPPLY: One Way
RRP (inc GST): $POA
MIN. CYCLE TIME:
(Wrapped, Solid, Drying, 134oC) 38 minutes
MAIN CYCLE TIMES (inc. DRYING):
Universal 57-78 min 134oC
Quick B 38 min 134oC
Quick S 29 min 134oC
Prion 65-73 min 134oC
Gentle 65 min 121oC
Device Technologies
Tel: 1800-672-675 • www.device.com.au customers@device.com.au
INTERNAL: 440 mm Ø x 1340 mm (200 L)
EXTERNAL: W: 650 x H: 1600 x D: 1530 mm
WARRANTY: 2 Parts / 2 Labour Conditions Apply
SERVICE: All States
Loan units available.
PRINTER: Optional ink ribbon printer or Label Printer

DATA LOGGER: Opt. compact flash card drive or via ethernet
CYCLE TYPES: S
WATER SUPPLY: One Way or Recycled
RRP (inc GST): $POA
MIN. CYCLE TIME: (Wrapped, Solid, Drying, 134oC) 25 minutes
MAIN CYCLE TIMES (inc. DRYING):
Universal 40-53 min 134oC
Quick 25-33 min 134oC
Prion 54-67 min 134oC
Gentle 56-71 min 121oC
Device Technologies
Tel: 1800-672-675 • www.device.com.au customers@device.com.au




INTERNAL: 250 mm Ø x 450 mm (22 L)
EXTERNAL: W: 425 x H: 485 x D: 660 mm
WARRANTY: 2 Parts / 2 Labour Conditions Apply
SERVICE: All States
Loan units available.
PRINTER: Optional ink ribbon printer
DATA LOGGER: Opt. compact flash card drive or via ethernet

CYCLE TYPES: S
WATER SUPPLY: One Way or Recycled
RRP (inc GST): $POA
MIN. CYCLE TIME: (Wrapped, Solid, Drying, 134oC)
Technologies Tel: 1800-672-675 • www.device.com.au customers@device.com.au
INTERNAL: 250 mm Ø x 450 mm (22 L) EXTERNAL: W: 425 x H: 485 x D: 660 mm

WARRANTY: 2 Parts / 2 Labour Conditions Apply SERVICE: All States
Loan units available.
PRINTER: Optional ink ribbon printer
DATA LOGGER: Opt. compact flash card drive or via ethernet

CYCLE TYPES: S
WATER SUPPLY: One Way or Recycled
MIN. CYCLE TIME: (Wrapped, Solid, Drying, 134oC) 24 minutes
MAIN CYCLE TIMES (inc. DRYING):
Universal 39-53 min 134oC
Quick 23-31 min 134oC
Prion 54-68 min 134oC
WARRANTY: 2 Parts / 2 Labour
Conditions Apply
SERVICE: All States
Loan units available.
PRINTER: Optional ink ribbon printer
RRP (inc GST): $POA
Gentle 54-70 min 121oC
INTERNAL: 250 mm Ø x 350 mm (18 L)
DATA LOGGER: Opt. compact flash card drive or via ethernet Device Technologies Tel: 1800-672-675 • www.device.com.au customers@device.com.au
EXTERNAL: W: 425 x H: 485 x D: 570 mm
CYCLE
WARRANTY: 2 Years or 2000 cycles
SERVICE: Authorised Dealer Technicians in ALL States.
PRINTER: Optional LisaSafe; can be used to print barcodes
DATA LOGGER: ioDent & USB drive, wireless & LAN connectivity

CYCLE TYPES:
B and S
WATER SUPPLY: Integrated tank with option of demineralisation system
MIN. CYCLE TIME:
(Wrapped, Hollow, Drying, 134oC) 28 minutes
MAIN CYCLE TIMES (inc. DRYING):
B Universal 134 28-63 min 134oC
B Prion 134 42-77 min 134oC
B Universal 121 42-82 min 121oC
S Fast 21-25 min 134oC
W&H Australasia Pty Limited
Tel: 1300-613-988
RRP (inc GST): $16,990.00
INTERNAL: 230 mm Ø x 420 mm (28 L)
EXTERNAL: W: 492 x H: 455 x D: 614 mm
WARRANTY: 2 Years or 2000 cycles
SERVICE: Authorised Dealer
Technicians in ALL States.
PRINTER: Optional LisaSafe; can be used to print barcodes
DATA LOGGER: ioDent & USB drive, wireless & LAN connectivity
CYCLE
28-55 min 134oC
B Prion 134 40-68 min 134oC
B Universal 121 42-76 min 121oC
S Fast 21-25 min 134oC
W&H Australasia Pty Limited
Tel: 1300-613-988
WARRANTY: 2 Years or 2000 cycles
SERVICE: Authorised Dealer Technicians in ALL States.
PRINTER: Optional LisaSafe; can be used to print barcodes
DATA LOGGER: ioDent & USB drive, wireless & LAN connectivity
INTERNAL: 195 mm Ø x 400 mm (22 L)
EXTERNAL: W: 465 x H: 452 x D: 646 mm
CYCLE TYPES: B
WATER SUPPLY: Integrated tank with option of demineralisation system
MIN. CYCLE TIME: (Wrapped, Hollow, Drying, 134oC) 33 minutes
MAIN CYCLE TIMES (inc. DRYING):
B Universal 134 33-64 min 134oC
B Prion 134 48-79 min 134oC
B Universal 121 79 min 121oC
W&H Australasia Pty Limited
Tel: 1300-613-988
RRP (inc GST): $12,990.00
INTERNAL: 195 mm Ø x 440 mm (22 L)
EXTERNAL: W: 465 x H: 452 x D: 646 mm
WARRANTY: 2 Years or 2000 cycles
SERVICE: Authorised Dealer Technicians in ALL States.
PRINTER: Optional LisaSafe; can be used to print barcodes
DATA LOGGER: ioDent & USB drive, wireless & LAN connectivity
CYCLE TYPES: S
WATER SUPPLY: Integrated tank with option of demineralisation system
MIN. CYCLE TIME:
(Wrapped, Hollow, Drying, 134oC) 39 minutes
MAIN CYCLE TIMES (inc. DRYING):
S Universal 134 39-45 min 134oC
S Prion 134 53-60 min 134oC
S Gentle 121 62-66 min 121oC
S Unwrapped 134 21-27 min 134oC
W&H Australasia Pty Limited
Tel: 1300-613-988
RRP (inc GST): $10,990.00




INTERNAL: 195 mm Ø x 440 mm (22 L)
EXTERNAL: W: 465 x H: 452 x D: 646 mm
WARRANTY: 2 Years or 2000 cycles
SERVICE: Authorised Dealer
Technicians in ALL States.
PRINTER: Optional LisaSafe; can be used to print barcodes




DATA LOGGER: ioDent & USB drive, wireless & LAN connectivity

CYCLE TYPES: B and S
WATER SUPPLY: One way.
Auto water fill & manual top fill water function
MIN. CYCLE TIME:
(Wrapped, Solid, Drying, 134oC) 22 minutes
MAIN CYCLE TIMES (inc. DRYING):
Universal 134 42 min 134oC
Universal 121 58 min 121oC
Unwrapped Hollow 22 min 134oC
Wrapped Solid 33 min 134oC
WARRANTY: 3 Years or 3000 cycles
SERVICE: All States and NZ
Loan units available.
PRINTER: On-screen cycle release; Opt’l cycle & barcode printer.
Henry Schein AU Tel: 1300-658-822
Henry Schein NZ Tel: 0800-808-855
RRP (inc GST): $POA
INTERNAL: 250 mm Ø x 350 mm (17 L)
EXTERNAL: W: 480 x H: 500 x D: 600 mm
DATA LOGGER: USB pen drive or Automatic download of cycle data to software
CYCLE TYPES: B and S
WATER SUPPLY: One way.
Auto water fill & manual top fill water function
MIN. CYCLE TIME:
(Unwrapped, Hollow, Drying, 134oC) 25 minutes
MAIN CYCLE TIMES (inc. DRYING):
Universal 134 46 min 134oC
Universal 121 63 min 121oC
Unwrapped Hollow 25 min 134oC
Wrapped Solid 39 min 134oC
WARRANTY: 3 Years or 3000 cycles
SERVICE: All States and NZ
Loan units available.
PRINTER: On-screen cycle release; Opt’l cycle & barcode printer.
Henry Schein AU Tel: 1300-658-822
Henry Schein NZ Tel: 0800-808-855
RRP (inc GST): $POA
INTERNAL: 250 mm Ø x 450 mm (22 L)
EXTERNAL: W: 480 x H: 500 x D: 600 mm
DATA LOGGER: USB pen drive or Automatic download of cycle data to software
CYCLE TYPES: B and S
WATER SUPPLY: One way. Auto water fill & manual top fill water function
MIN. CYCLE TIME: (Unwrapped, Hollow, Drying, 134oC) 28 minutes
MAIN CYCLE TIMES (inc. DRYING): Universal 134 56 min 134oC Universal 121 69 min 121oC
Unwrapped Hollow 28 min 134oC
Wrapped Solid 45 min 134oC
WARRANTY: 3 Years or 3000 cycles
SERVICE: All States and NZ
Loan units available.
PRINTER: On-screen cycle release; Opt’l cycle & barcode printer.
Henry Schein AU Tel: 1300-658-822
Henry Schein NZ Tel: 0800-808-855
RRP (inc GST): $POA
INTERNAL: 280 mm Ø x 450 mm (28 L)
EXTERNAL: W: 480 x H: 500 x D: 600 mm
DATA LOGGER: USB pen drive or Automatic download of cycle data to software
CYCLE TYPES: B and S
WATER SUPPLY: One way. Built in Demin Filter allows tap water usage.
MIN. CYCLE TIME:
(Wrapped, Solid, Drying, 134oC) 22 minutes
MAIN CYCLE TIMES (inc. DRYING):
134 40 min 134oC
WARRANTY: 3 Years or 3000 cycles
SERVICE: All States and NZ
Loan units available.
PRINTER: On-screen cycle release; Opt’l cycle & barcode printer.
Henry Schein AU Tel: 1300-658-822
Henry Schein NZ Tel: 0800-808-855
RRP (inc GST): $POA
INTERNAL: 250 mm Ø x 350 mm (17 L)
EXTERNAL: W: 480 x H: 500 x D: 600 mm
DATA LOGGER: USB pen drive or Automatic download of cycle data to software
CYCLE TYPES: B and S
WATER SUPPLY: One way. Built in Demin Filter allows tap water usage.
MIN. CYCLE TIME: (Wrapped, Solid, Drying, 134oC) 25 minutes
MAIN CYCLE TIMES (inc. DRYING):
Universal 134 44 min 134oC
Universal 121 61 min 121oC
Unwrapped Hollow 25 min 134oC
Wrapped Solid 37 min 134oC
WARRANTY: 3 Years or 3000 cycles
SERVICE: All States and NZ
Loan units available.
PRINTER: On-screen cycle release; Opt’l cycle & barcode printer.







Henry Schein AU Tel: 1300-658-822
Henry Schein NZ Tel: 0800-808-855
RRP (inc GST): $POA
INTERNAL: 250 mm Ø x 450 mm (22 L)
EXTERNAL: W: 480 x H: 500 x D: 600 mm
DATA LOGGER: USB pen drive or Automatic download of cycle data to software
CYCLE TYPES: B and S
WATER SUPPLY: One way. Built in Demin Filter allows tap water usage.
MIN. CYCLE TIME:
(Unwrapped, Hollow, Drying, 134oC) 28 minutes
MAIN CYCLE TIMES (inc. DRYING):
Universal 134 54 min 134oC
Universal 121 67 min 121oC
Unwrapped Hollow 28 min 134oC
Wrapped Solid 43 min 134oC
WARRANTY: 3 Years or 3000 cycles
SERVICE: All States and NZ
Loan units available.
PRINTER: On-screen cycle release; Opt’l cycle & barcode printer.
Henry Schein AU Tel: 1300-658-822
Henry Schein NZ Tel: 0800-808-855
RRP (inc GST): $POA
INTERNAL: 280 mm Ø x 450 mm (28 L)
EXTERNAL: W: 480 x H: 500 x D: 600 mm
DATA LOGGER: USB pen drive or Automatic download of cycle data to software
CYCLE TYPES: B and S
WATER SUPPLY: Closed loop. Built in Deminuses tap water and recycles.
5L per 50 cycles.
MIN. CYCLE TIME:
(Wrapped, Solid, Drying, 134oC) 22 minutes
MAIN CYCLE TIMES (inc. DRYING): Universal 134 40 min 134oC Universal 121 56 min 121oC
Unwrapped Hollow 22 min 134oC
Wrapped Solid 31 min 134oC
WARRANTY: 3 Years or 3000 cycles
SERVICE: All States and NZ
Loan units available.
PRINTER: On-screen cycle release; Opt’l cycle & barcode printer.
Henry Schein AU Tel: 1300-658-822
Henry Schein NZ Tel: 0800-808-855
RRP (inc GST): $POA
INTERNAL: 250 mm Ø x 350 mm (17 L)
EXTERNAL:
DATA LOGGER: USB pen drive or Automatic download of cycle data to software
CYCLE TYPES: B and S
WATER SUPPLY: Closed loop. Built in Deminuses tap water and recycles.
5L per 50 cycles.
MIN. CYCLE TIME: (Wrapped, Solid, Drying, 134oC) 25 minutes
MAIN CYCLE TIMES (inc. DRYING):
Universal 134 44 min 134oC Universal 121 61 min 121oC
Unwrapped Hollow 25 min 134oC
Wrapped Solid 37 min 134oC
WARRANTY: 3 Years or 3000 cycles
SERVICE: All States and NZ
Loan units available.
PRINTER: On-screen cycle release; Opt’l cycle & barcode printer.
Henry Schein AU Tel: 1300-658-822
Henry Schein NZ Tel: 0800-808-855
RRP (inc GST): $POA
INTERNAL: 250 mm Ø x 450 mm (22 L)
EXTERNAL: W: 480 x H: 500 x D: 600 mm
DATA LOGGER: USB pen drive or Automatic download of cycle data to software
CYCLE TYPES: B and S
WATER SUPPLY: Closed loop. Built in Deminuses tap water and recycles.
MIN. CYCLE TIME: (Unwrapped, Hollow, Drying, 134oC) 28 minutes
MAIN CYCLE TIMES (inc. DRYING):
WARRANTY: 3 Years or 3000 cycles
SERVICE: All States and NZ
Loan units available.
PRINTER: On-screen cycle release; Opt’l cycle & barcode printer.





5L per 50 cycles.
0800-808-855
RRP (inc GST): $POA
INTERNAL: 280 mm Ø x 450 mm (28 L)
DATA LOGGER: USB pen drive or Automatic download of cycle data to software Henry Schein AU Tel: 1300-658-822
EXTERNAL: W: 480 x H: 500 x D: 600 mm

A72-year-old male patient presented with an extraction 3 months prior following a failed root canal treatment on a supported bridge on 13-22. He requested fixed prosthodontics for the missing teeth. The patient is a medical doctor and more concerned with functional rather than aesthetic success.
The patient’s general periodontal condition is fair with medical history of cardiovascular disease (Warfarin, 5 mg per day). Clinical and radiographic evaluation was performed on the initial visit.
The patient was presented with the following treatment options for the replacement of the anterior maxilla. The first option was a 3-unit fixed prosthetic using teeth #14, #22 and #23 as abutments. Second, an implant restoration for the replacement of the edentulous space at teeth #13, #11, #21 and #22 was determined to be the more conservative option. Option number 2, the replacement of the edentulous space at teeth #13, #11, #21 and #22 with implants, was accepted.
An extensive extraoral followed by an intraoral examination was performed (Figures 1 and 2). The occlusion on the right and left side showed an unclassified molar relationship due to the missing tooth (Figures 3 and 4). The SAC classification for implant dentistry was used.
An implant site-specific evaluation was then carried out, including an evaluation of the inner occlusal space, in addition to both a hard- and a soft-tissue assessment, showing good ridge dimensions and keratinized tissue volume.
Keratinized tissue width was 8 mm. The CT scan revealed the buccolingual cortical width was 7 mm, mesio-distal width was 32 mm. The CT scan revealed the buccolingual cortical width at 7 mm. From the panoramic radiograph, the crest to the floor of the nose was 16mm (Figure 3). An intraoral periapical radiograph was also taken (Figures 4-6).
Solutions featured
3Shape TRIOS intraoral scanner

3Shape Dental System


3Shape Implant Studio




The patient was scanned using an intraoral scanner (TRIOS, 3Shape). CBCT scans (GiANO, Newtom) and digital impressions were merged using 3Shape Implant Studio® software.



Implant placements (CAMLOG, Henry Schein) were planned using software (Implant Studio) to identify direction and positioning and to create the CAD/CAM guide surgical template.




A CBCT was taken before and after implant placement. During surgery, the drilled template was used as a drill guide. The implant-supported bridge for #13 to #11 and #21 were designed using 3Shape software (Dental System™).
One hour before surgery, the patient was given 2g of Amoxillin (400 mg) and Ibuprofen (1 g) (or paracetamol).
Intraoral scanning that simply makes sense
Hygienic by design for minimal risk of cross-contamination. Smaller and lighter than ever for next-level ergonomics. And a ScanAssist engine with intelligent-alignment technology that makes precision scanning effortless, every time.

Preparation of the implant bed started with a bone drill sequence. It was planned to place the definitive prefabricated abutment and provisional restoration immediately after surgery.


After implant placement, postoperative CBCTs were recorded and compared with the preoperative scan using the McNemar test.
During the restorative phase, an impression was taken at implant level. This scan set assists in determining the dimensions for assuming the axial alignment and gingival height. An appropriate space was obtained and a good emergence profile of the cement-retained restoration was selected for the case. All information gathered before the actual surgery, together with the guided surgical template, ensured an accurate, functional and aesthetic final restoration.
Acomprehensive pre-operative workup is essential for planning the number and type of implants, as well as in identifying the optimum location for implant placement.


Prosthesis design and manufacture based on three-dimensional imaging data facilitates the preparation of a guide for the surgical intervention.
Using a prosthetically-driven workflow (3Shape Implant Studio) by first placing virtual crowns helped to ensure proper depths and angulations. Implants were then positioned to accommodate the maximum amount of bone, while establishing optimal support to achieve an aesthetic outcome for the proposed restoration.

The result was less post-operative morbidity, due to the surgery being minimally invasive. A guided surgery technique and immediate functional loading helped to create a more predictable procedure.
The digital workflow increases patient satisfaction because the procedure provides an immediate aesthetic and functional restoration.
• More efficient communication between the dentist, dental technician and patient;

• Diagnostic and restorative software tools allow for the precise, predictable placement of dental implants;

• Detailed visualisation of the prosthetic outcome prior to the actual treatment due to intraoral scanning, digital treatment planning, guided surgery and CAD/CAM software;


• Guided surgery technique and immediate functional loading create a predictable procedure; and
• Patient satisfaction increased due to immediate provisionalisation and an aesthetic and functional restorative outcome.
Patients must meet the right criteria for being treated with a digital workflow. The restorative team needs a thorough understanding of the techniques and limitations in the digital workflow to ensure a high success rate in the aesthetic zone.
Master of Science Program in Implant Dentistry (International Program), Rodolphe Saidnattar (Dental technician/ Digital advancement technology, Accord Corporation Limited).
Dr Suriyan graduated with a Doctor of Dental Surgery in 1997 from Chulalongkorn University in Bangkok, Thailand. She completed a post-graduate qualification in oral and maxillofacial surgery at Chiang Mai University and an International oral and maxillofacial surgery qualification at the Prince of Songkla University. Dr Suriyan has a Master of Public Health from Sukhothaithammatirat University, an MSc Implant dentistry from Mahidol University and a PhD from Chulalongkorn University. She completed the IMC Master Implant Dentistry Program at Muenster University, Germany and is a Fellow of the International Congress of Oral Implantologists. Dr Suriyan practices at the Prachatipat Hospital in Prathumtani Province, Thailand, Lectures in the MSc Implant Dentistry program at Thammasat University and acts as a Research Consultant.

 By Dr Andreas Kurbad
By Dr Andreas Kurbad
Ceramic furnaces are a necessary part of the process chain for dental ceramics. They have been part of the dental repertoire for centuries. At the latest since the introduction of zirconia for dental applications, sintering furnaces have come into use alongside conventional ceramic furnaces. Sintering requires significantly higher temperatures than firing. Sintering furnaces are therefore designed differently than ceramic furnaces and they are usually installed in a separate room in the dental practice.
The chairside workflow involves the fabrication of indirect restorations directly in the practice. This has become possible with the advent of CAD/CAM technologies. Modern ceramic materials in particular can be easily processed by machining and are therefore especially suitable for this workflow. By nature, ceramic restorations are ready to be placed in the oral cavity straight after the milling process without the need for post-processing. However, a ceramic furnace is required for those restorations that are to be additionally customised (by glazing, staining, layering) after the milling process or for restorations that are made of materials that generally require post-processing.
The latter are ceramic materials that cannot be processed directly in one of the commonly used milling machines because their final strength is too high. Therefore, these materials are supplied in a form that can be easily machined and they only achieve their final properties in a downstream firing process (sintering, infiltration or crystallisation).
The chairside process requires in-office furnaces to meet particular requirements. Since space is often limited and there is no designated laboratory area, chairside furnaces should have a small footprint. The aim is therefore to come up with a combination furnace that can do both sintering and firing in one device–one furnace for all applications. In addition to the footprint, the noise and heat emission of the furnace also needs to be considered, as these furnaces are usually not installed in a separate room. Processing time presents another decisive factor. Many chairside applications involve single-visit restorations with all the clinical and technical steps being performed in one appointment. This means that the processing times should be as short as possible, as the patient’s willingness to wait is limited. Against such a background, it is necessary to reduce the time required to achieve the parameters that give the material its final properties. Another option is to combine several working steps into one to save time (e.g. crystallisation, staining and glazing in a single step). Still another option is to use a furnace that is embedded in a system. Data relevant to the firing process is collected in the course of the CAD/CAM process and then transmitted to the embedded furnace, which is connected to the overall system. In this way, the processing times can be additionally optimised.
The Programat CS furnace from Ivoclar was the first genuine ceramic furnace for chairside applications. It made sense to introduce the furnace when the IPS e.max CAD lithium disilicate ceramic was launched. Conventional furnaces of the time were not equipped to process the parameters involved in a two-stage firing process. The Programat CS offers a small footprint and can be accommodated even
in relatively small dental practices. The furnace is connected to a vacuum pump and is therefore also suitable for use in conjunction with the layering technique. It comes with a clearly defined range of factory-set firing programs that cover all essential options. Custom programs can be entered additionally. The Programat CS furnace proved to be very popular, especially because of its compact dimension and relatively low price.
The Programat CS2 and CS3 are further developments of the original CS furnace. They are somewhat larger and, like their predecessor, are equipped with a vacuum pump.
Major changes relate to the number of programs and the level of user friendliness (touchscreen, program structure). Although almost identical to the CS2, the CS3 offers a few additional features, such as the Digital Shade Assistant (DSA) to analyse and determine the tooth shade.
With the introduction of the CEREC SpeedFire furnace, several innovations became available. The furnace was the first to be able to sinter zirconia restorations in a time short enough to be useful for chairside restorations thanks to its induction heating technology. Induction heating had never been used in a ceramic furnace before.


Furthermore, the furnace features a considerably smaller firing chamber than conventional ceramic furnaces to enable it to achieve the required temperature quickly. However, the small firing chamber is a decisive shortcoming of this furnace. Even medium-sized bridges are too large to fit into its firing chamber and yet this kind of restorations are of particular interest when using zirconia.
In addition, the induction heating system does not allow the installation of programs for long sintering processes and yet long sintering is essential for improving the aesthetic results. SpeedFire is a system-based furnace and can only be used in conjunction with the complete CEREC system. The advantage of this is that the data relevant to the restoration is sent to the furnace and can be used to optimise the firing parameters. There is no doubt that this kind of coupling helps improve the reliability of the system.
Operating errors can be minimised. The disadvantage is that only those restorations can be fired that have been routed through the system. This can lead to problems if, for example, the order gets lost due to connection errors or if changes are made at a later stage. Finally, the CEREC SpeedFire does not allow firing under vacuum.

The CS4 furnace was introduced by Ivoclar to offer fast sintering processes with a furnace of the Programat CS range. Compared to its predecessor, the CS4 is relatively large.

On the plus side, the furnace features an optimally dimensioned firing chamber. The furnace uses heating technology that is based on conventional heating elements and does therefore not match the extremely short processing times of the CEREC SpeedFire. The CS4 cannot be used for vacuum firing processes either. For this reason, the process for crystallising lithium disilicate has been optimised to such an extent that it can be carried out without vacuum. In addition, the furnace can be used for staining and glazing both glass and oxide ceramics and is therefore a truly universal device. The furnace does not offer the long sintering times of typically up to 10 hours used in slow sintering processes. However, sintering times of over 4 hours can be set up as a custom program in the free programming section.

Sintering times of this length are likely to improve the aesthetic properties of many zirconia materials. The shortest processing times are 27 minutes for zirconia (IPS e.max ZirCAD) and 17 minutes for lithium disilicate (IPS e.max CAD).



Ivoclar has recently introduced a newly developed furnace: the CS6. While the CS6 has a similar footprint to the CS4, its height is smaller. It is a stand-alone unit (Figure 1). Although the furnace has a network connection, it does not need to be linked up to operate. The firing programs can be executed straight away.
When you look at the furnace, you will immediately notice that the operating mechanism has changed. With Ivoclar furnaces, the head containing the heating elements is usually lowered over the objects to be fired. This is different with the new furnace: here the restorations are lowered into the firing chamber, similar to an elevator system (Figure 2).
The dimensions of the firing chamber are kept small to ensure that the processing temperature is reached swiftly. Having a diameter of 55 mm and a height of 40 mm, the firing chamber of the CS6 is nonetheless noticeably larger than that of the CEREC SpeedFire (38 mm diameter, 20 mm height). These dimensions should offer enough space for accommodating indirect restorations made at chairside. The 55/19 block size can be taken as a maximum benchmark size because current milling machines cannot process blanks that are any larger than that (Figure 3). In spite of this, the pre-installed programs only allow the processing of three-unit restorations as the largest size, according to the instructions for use from Ivoclar.
The CS6 furnace uses a new pre-drying mechanism: Similar to a chimney, warm air is guided from the firing chamber past the objects, enabling them to dry quickly and effectively. Pre-drying is involved in the programs for crystallisation, glazing and wet sintering. In the cooling phase, the firing chamber can be completely closed to speed up the cooling process. The cooling process can be additionally accelerated by repositioning the object from the firing tray to the object tray provided for this purpose.
A special pair of tweezers is supplied with the furnace to grab the restorations, which are still very hot at this point. These tweezers have ceramic tips to prevent the objects from cooling down at the contact points (Figure 4). If some areas of the restoration cool down too quickly, cracks or tears may develop.
Combined with special heating elements, the compact dimension of the heating chamber enables speedy processing times. This configuration ensures that the firing temperatures are accurately maintained at all times and calibrations can be performed directly by the operator. The induction heating technology of the SpeedFire furnace does not allow this. The type of heating elements used in the
furnace is an open system device. This means that the furnace can be customised to include individual firing programs in addition to the pre-installed programs. As a result, the furnace covers almost the entire range of materials available for the in-office workflow...”
CS6, however, are not suitable for longtime sintering. To make up for this, the furnace features a special technology that enables the zirconia restorations to reach an ideal level of translucency. In other words, the CS6 is the first sintering furnace that allows zirconia to be sintered under vacuum. All factory-set sintering programs use vacuum for the sintering process. Vacuum causes the pores of the material to close as the air between the particles is extracted. Once a certain temperature is reached, fresh air is pumped into the firing chamber. Zirconia starts to acquire its shade only after oxygen has been supplied. By using vacuum and purging with fresh air, the sintering process is accelerated and the translucency of the restoration improved.


“The CS6
The furnace head can be moved into a “service position” for cleaning. The firing chamber can be accessed by swivelling the furnace head sideways. The chamber can be cleaned with a vacuum cleaner equipped with a HEPA filter, if necessary.
At this point, it is also possible to remove pieces that have fallen off the tray because they have not been placed properly (Figures 5 and 6).
The CS6 furnace is an open system device. This means that the furnace can be customised to include individual firing programs in addition to the pre-installed programs for processing the materials from Ivoclar. As a result, the furnace covers almost the entire range of materials available for the in-office workflow. Setting up customised programs is a breeze thanks to the logical structure of the menu and the large touchscreen display (Figure 7).
The furnace features a pre-installed program for processing the leucitereinforced IPS Empress CAD blocks, as they are materials from the Ivoclar range. Other conventional glass-ceramic blocks, such as the VITA MK II (VITA Zahnfabrik) and GC Initial LRF (GC) can also be processed in the furnace after the relevant firing parameters have been entered.
IPS e.max CAD is the classic material for this type of furnace and the CS6 is optimally geared to processing it. The furnace offers a speed crystallisation (16 minutes) and a super speed crystallisation (11 minutes) program in addition to the conventional crystallisation program. While the latter requires essentially the same amount of time as the other furnaces from Ivoclar, the former two programs provide substantial time savings for in-office applications and they are only available on this furnace. A newly designed IPS Speed Tray is supplied for the crystallization process. IPS Object Fix auxiliary firing paste and firing pins are used for the crystallisation process, like before with the other furnaces (Figures 8 and 9). As is already known, a special firing protocol is used for the MO and Impulse blocks. If staining and glazing are not carried out
directly in the course of the crystallisation process, a program option allows these processes to be performed separately.
Restorations that have been milled from comparable blocks of a different lithium disilicate material can also be crystallised in the furnace, if required. For this purpose, a custom program containing the relevant parameters has to be set up on the furnace, which is really easy to do.
Given its innovative vacuum technology, the CS6 ceramic furnace appears to be especially advantageous when it comes to sintering zirconia restorations. Different sintering programs are available for the two kinds of zirconia
Needless to say, the furnace is also suitable for sintering materials from other manufacturers, such as Chairside Zirconia (3M), VITA YZ (VITA Zahnfabrik) or Katana (Kuraray Noritake).
Staining and glazing programs are additionally available for all the materials. Restorations made of zirconia are directly placed on the firing table, as is customary for Ivoclar (Figure 10).
Ivoclar was the first manufacturer of ceramic furnaces who realised early on that it makes sense to support the chairside workflow with a purpose-designed furnace and that this can lead to a significant increase in the range of treatment options available in the dental practice.
This is why it is particularly encouraging that the new CS6 furnace offers intelligent solutions that provide fresh impetus to creating indirect dental restorations at chairside with the help of high-end technology. At least some of these restorations can be provided as single-visit treatment options. The compact design and the extremely short processing times are instrumental in achieving this. Innovative solutions such as the vacuum sintering process have led to a leap in quality. As the clinical cases show, attractive and aesthetically pleasing results can be achieved in addition to having the advantage of saving time.
blocks (LT / MT Multi) available from Ivoclar. An optional pre-drying phase can be added to the program. The LT variant can be processed in 22 minutes - a processing time that is definitely suitable for in-office applications. MT Multi requires about an hour (55 minutes in the Speed mode) for processing and therefore presents more of a challenge when used in-office. The resulting restorations, however, show really good and even excellent aesthetic properties. The vacuum firing process offsets the loss of translucency resulting from the short processing times. As mentioned above, the furnace does not support long sintering processes. However, the operator can set up individual programs that last longer than the pre-installed ones.
Dr Andreas Kurbad has been running his own dental practice specializing in cosmetic dentistry and implantology since 1990. He has been a CEREC user since 1994. Moreover, Dr Kurbad has given lectures and courses on the subject of all-ceramic restorations and CAD/CAM procedures since 1996. He is a member of the editorial boards of the International Journal of Computerized Dentistry, Quintessenz Zahntechnik and Digital Dental News. Dr Kurbad is the author of publications on various subjects including epidemiology, periodontology, restorative dentistry, CAD/CAM techniques and metal-free restorations. In addition, he is the co-author of the textbook “CAD/ CAM und Vollkeramik – Ästhetische Restaurationen in der Praxis”.
“The vacuum firing process offsets the loss of translucency resulting from the short processing times.
As mentioned, the furnace does not support long sintering processes. However, the operator can set up individual programs that last longer than the pre-installed ones...”
A complex premolar root fracture case using the new CS 8200 3D Neo Edition CBCT system from Carestream Dental
By Dr Giuliano Fragola, DDS, MS, MSc, PhD
A45-year-old female patient presented with pain in the teeth of the first quadrant and the sensation of slight mobility when she chewed. Her overall condition was good – she was a non-smoker, with good oral hygiene. The dental history revealed that she had undergone endodontic treatment about 15 years previously and she had a full contour crown in place, which was causing no issues.


In trying to identify the source of the pain, extensive visual inspection and percussions were carried out, but these alone were not enough to diagnose the problem.


A 3D x-ray was therefore indicated to assess potential subgingival or bone complications. The new CS 8200 3D Neo Edition from Carestream Dental was used to take the image, with the MAR tool (Metal Artefact Removal) delivering precise and very clear images for diagnosis and treatment planning.
It can be very difficult to see a root fracture of this nature due to reflections from existing crowns, which are typically paced over endodontically-treated teeth, but this technology overcomes this problem.
Having used digital imagin g technologies from Carestream Dental since the late 1990s, I completely trust the quality of the equipment available.
The images demonstrated bone loss around the sites of the 14 and 16 (Figures 1a and 1b), which explained the mobility and positive percussion.
Using different 3D views, a complex root fracture was diagnosed in the first premolar (14) (Figure 2), along with complete bone loss between the roots of the first maxillary molar (16) and a small sinus floor bone perforation (Figure 3). This provides a very useful tool for the clinician, facilitating communication with the patient and encouraging their engagement with treatment from the very beginning.
With CS 8200 3D Neo Edition image, it was easy for the patient to visualise the problem and understand the proposed treatment so she felt confident to accept it and proceed straightaway.
There was only one viable treatment option available in this case – the 14 and 16 both had a hopeless prognosis and so would require extraction and restoration.
The procedure was explained to the patient in full, including benefits, limitations and potential risks to ensure informed consent to proceed.
Both teeth were extracted as atraumatically as possible and then left to heal for approximately six months, when dental implants would be placed.
The patient refused a removable denture, preferring restoration with an implant-retained prosthesis instead. Given the complexity of this case, a new CBCT scan was indicated post hard and soft tissue healing to assess bone volume remaining for implant placement planning.
The patient was very satisfied with the treatment outcome, appreciating the quick and precise diagnosis and treatment delivery based on the information obtained. She commented “I’m absolutely impressed by the images shown by the dentist with the fracture lines. I completely understand that extraction is the only option.”
At this stage, we are waiting for the soft and hard tissue to fully heal before deciding how to proceed.
A new CBCT scan may be indicated post healing to analyse the bone volume and density and to support the planning procedure for implant placement and restoration. This scan would be used to help determine whether bone grafting will be required and if it can be delivered simultaneously with implant placement.


Even with the second CBCT scan, the patient would still be exposed to less radiation in the long-term compared to the alternative – multiple periapical x-rays at different angles. The CBCT low dose mode is ideal for reducing exposure without compromising image quality.
From a professional perspective, good results were achieved in this case. The new CBCT scanner was instrumental in ensuring accuracy and confidence at every stage in the treatment, from diagnosis to treatment planning and delivery. It was also beneficial in supporting and improving communication with the patient, enhancing their understanding of the procedure and ensuring quick but confident informed consent.
The CS 8200 3D Neo Edition helps to obtain precise, highquality images with the lowest possible dose of radiation. Being able to select the FOV with a simple and quick view shot and to manage the scattering with digital formatting are further benefits.
Dr Giuliano Fragola is a renowned dental surgeon, ITI Fellow and international speaker. He utilises his skills and experience by working as an ITI online Academy reviewer, a KOL for various dental organisations and in his own private practice in Madrid, Spain.

From a statistical viewpoint, one in three adults experience dental trauma during the course of their life, very often during their childhood. Appropriate primary dental care is a priority to ensure the teeth concerned can be preserved for the long term. Pulpotomy plays a key role in such care. Removing a part of the dental pulp can preserve the remaining vital pulp tissue and avoid root canal treatment.
The clinical case study below demonstrates the use of pulpotomy with an hydraulic calcium silicate cement.
A dental trauma poses a challenge in everyday practice due to the heterogeneity of cases and treatment options. From a statistical viewpoint, 33% of adults experience dental trauma during the course of their life;1 and there is pulp involvement for 6.4-18.3%.2 Deciduous teeth are affected by dental trauma more often (22.7%) than permanent teeth (15.2%).3 Various therapies are indicated, depending on the extent of the trauma. This article aims to discuss primary care for crown fractures with pulp involvement.
In the first step, comprehensive anamnestic and clinical diagnostics are essential for adequate emergency care after a dental trauma.

Correct diagnosis and assessment of the pulp condition are the cornerstones of long-term success in therapy with regard to measures aimed to preserve vitality. The therapy decision is based on the relationship between the duration of unsterile pulp exposure and the extent of pulp inflammation.4 The latter is characterised by histological damage to the odontoblast layer, vasodilation and granulocyte infiltration into the exposed tissue. The longer the exposure lasts, the more pronounced the inflammatory reactions will be; if left untreated, complete pulp necrosis can occur.4
Treatment options include direct capping, partial and full pulpotomy or root canal treatment. In case of direct pulp capping, a capping material is applied directly to the pulp wound while, in the case of pulpotomy, part of the pulp tissue is removed before the capping is applied (partial pulpotomy: about 1-3 mm; full pulpotomy: coronal pulp is removed). In contrast, the entire pulp tissue is removed during root canal treatment.

The success rate after direct capping over the pulp exposed to the oral cavity is around 80%;5,6 direct capping is inferior to partial pulpotomy with the same indication (94-96% success rate).7,8 The reason for this is that potentially infected tissue is retained during capping and may cause the inflammatory process to progress. In contrast, a partial pulpotomy eliminates this tissue before the pulp stump is capped and is indicated for after up to 48 hours of unsterile exposure.4 A full pulpotomy can be recommended for a period of 48-96 hours, depending on the clinical status of the pulp.4 Root canal treatment

should be performed in the case of longer pulp exposure.9
Both calcium hydroxide preparations (Ca(OH)2) and hydraulic calcium silicate cement can be used to dress the pulp wound after a pulpotomy. The use of calcium hydroxide has a long history in dentistry; the material was specified in relation to dental trauma and resorption back in 1930.10 Although calcium hydroxide offers good biocompatibility and induces the formation of a hard tissue barrier,11 the material’s mechanical stability is inadequate and it is also not permanently impervious to bacteria due to an irregularly shaped hard tissue barrier.12 Hydraulic calcium silicate cements offer an alternative and are superior to conventional calcium hydroxide compounds due to their biocompatibility, stability and impermeability to bacteria.12
In the following case study, a 31-year-old male patient came to the Interdisciplinary Walk-In Centre at the Charité Center for Oral Health Sciences CC 3 in Berlin in April 2020, around 28 hours after a dental accident. The patient had suffered a syncope incident of unknown origin and received initial medical treatment in a hospital. He was unable
to remember the cause of the accident. On reflection, it was suspected that he had fallen on a stair edge. Once the medical history was obtained, comprehensive intra- and extraoral radiographic diagnosis was performed. External skull injuries were ruled out; there were no pathological findings at the trigeminal pressure points and the patient had no problems with temporal and spatial orientation. There were no definite or possible signs of fracture to the maxilla or mandible. The sensitivity tests on teeth 13-23 were positive; Tooth 11 was sensitive to percussion. Moreover, Tooth 11 presented a crown fracture with pulp involvement and a mobility grade of I (Figures 1a-b). A root fracture was considered unlikely due to the radiographic and clinical presentation.
The preoperative radiograph showed a defect in the coronal hard tissue which extended into the pulp chamber (Figure 2). Due to an exposure time of less than 48 hours and the specific dental findings, partial pulpotomy was discussed as a treatment option with the patient. From a clinical viewpoint, a fibrin coating appeared on the exposed pulp and light red bleeding was induced after initial probing (Figure 3).
Dr Sascha Herbst has been a senior consultant in the Department of Oral Diagnostics, Digital Dentistry and Health Services Research, under the direction of Prof. Falk Schwendicke, at Charité - Universitätsmedizin Berlin in Germany since 2020. Since 2016, Dr Herbst has been working exclusively in endodontics. As a certified member of the Deutsche Gesellschaft für Endodontologie und zahnärztliche Traumatologie (German society of endodontics and dental traumatology), he is a renowned guest author and lecturer in his field of expertise.
Using a dental dam to ensure completely dry conditions, infected tissue was gradually removed with a sharp, sterile diamond while irrigating with 1% sodium hypochlorite (NaOCl). Once 3 mm of pulp tissue was removed, haemostasis could be obtained with a sterile foam pellet and 1% NaOCl (Figure 3) within 3 minutes (Figure 4). The pulp stump was then covered with Biodentine™ calcium silicate cement (Septodont). After a curing time of



12 minutes, the cavity was cleaned using a sandblaster (Microetcher CD, Danville Materials). A temporary adhesive restoration was applied using an etch-and-rinse technique with OptiBond FL (Kerr), CeramX Duo A1 and Ceram X Flow A2 (Dentsply Sirona) since the patient was unable to tolerate prolonged procedures due to his physical state (Figure 7). A radiographic examination was then performed to check the pulpotomy (Figure 8).

The tooth was subsequently permanently restored in another place using a customised wax-up and a direct composite core.

After six months, teeth 13-23 presented themselves as vital and insensitive to percussion. No anomalies were detected on radiographic images (Figure 9). After 18 months, Teeth 13-23 also responded in the same way to cold and presented no pathological findings clinically and radiographically (Figures 10-11).


predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. it comes to the perfect fit, Hu-Friedy is just right.
IS
the right one with Hu-Friedy
LOVE OUR STAINLESS STEEL PEDO CROWNS:
predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. comes to the perfect fit, Hu-Friedy is just right.
LOVE OUR STAINLESS STEEL PEDO CROWNS:
Septanest : the first choice of dentists with over 150 million injections per year, provides you high quality you can trust
In this case study, the treatment decision to use pulpotomy was straightforward since all criteria had been met for predictable treatment: the duration of pulp exposure was less than 48 hours, there was a positive reaction to cold and haemostasis was achieved within a few minutes. Conventional root canal treatment offers an alternative to pulpotomy but is significantly more invasive. Based on the clinical findings, the decision was made in favour of a minimally invasive attempt to preserve vitality. This offers advantages such as a shorter duration of treatment, preservation of the pulp proprioception and avoidance of further loss of hard tooth tissue due to root canal preparation.

The reason for choosing Biodentine among the wide range of calcium silicate cements was largely due to the tooth region affected since very high aesthetic standards are applied to the anterior teeth. Studies show that, compared to cements with zirconia, the risk of tooth discolouration is significantly increased when hydraulic calcium silicate cements are used with bismuth oxide as a radiographic contrast agent and if there is contact with blood or sodium hypochlorite.13,14 As a result, a tricalcium silicate cement was used with zirconia as a contrast agent, in this case,
Biodentine. However, the disadvantage is the comparatively reduced x-ray opacity, making the distinction between cement and physiological tooth structures somewhat more difficult in the x-ray image (Figures 8-10).15

Pulpotomy after dental trauma is a reliable, minimally invasive treatment for preserving pulp vitality. Hydraulic calcium silicate cements deserve particular interest as a first choice material since they excel due to their excellent biocompatibility, mechanical stability and associated high success rate.
1. L. Levin, P.F. Day, L. Hicks, A. O’Connell, A.F. Fouad, C. Bourguignon, P.V. Abbott, International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: General introduction, Dent Traumatol 36(4) (2020) 309-313.
2. I. Gomes, Partial Pulpotomy with Mineral Trioxide Aggregate in Permanent Incisors with Complicated Crown Fracture: 5-Year Follow-Up, Case Rep Dent 2020 (2020) 8855331.
3. S. Petti, U. Glendor, L. Andersson, World traumatic dental injury prevalence and incidence, a metaanalysis-One billion living people have had traumatic dental injuries, Dent Traumatol 34(2) (2018) 71-86.
4. M. Cvek, P.E. Cleaton-Jones, J.C. Austin, J.O. Andreasen, Pulp reactions to exposure after experimental crown fractures or grinding in adult monkeys, J Endod 8(9) (1982) 391-7.
5. A.B. Fuks, S. Bielak, A. Chosak, Clinical and radiographic assessment of direct pulp capping and pulpotomy in young permanent teeth, Pediatr Dent 4(3) (1982) 240-4.
6. J.J. Ravn, Follow-up study of permanent incisors with complicated crown fractures after acute trauma, Scand J Dent Res 90(5) (1982) 363-72.
7. M. Cvek, A clinical report on partial pulpotomy and capping with calcium hydroxide in permanent incisors with complicated crown fracture, J Endod 4(8) (1978) 232-7.
8. L. Haikal, B. Ferraz Dos Santos, D.D. Vu, M. Braniste, B. Dabbagh, Biodentine™ Pulpotomies on Permanent Traumatized Teeth with Complicated Crown Fractures, J Endod 46(9) (2020) 1204-1209.

9. M. Hargreaves, Berman L.H., Cohen´s Pathways of the Pulp, (2016) 763-788.
10. L.I. Grossman, Pioneers in endodontics, J Endod 13(8) (1987) 409-15.
11. U. Schroder, L.E. Granath, Early reaction of intact human teeth to calcium hydroxide following experimental pulpotomy and its significance to the development of hard tissue barrier, Odontol Revy 22(4) (1971) 379-95.
12. A.M. Zaen El-Din, H.H. Hamama, M.A. Abo El-Elaa, M.E. Grawish, S.H. Mahmoud, P. Neelakantan, The effect of four materials on direct pulp capping: An animal study, Aust Endod J 46(2) (2020) 249-256.
13. M.A. Marciano, M.A. Duarte, J. Camilleri, Dental discoloration caused by bismuth oxide in MTA in the presence of sodium hypochlorite, Clin Oral Investig 19(9) (2015) 2201-9.
14. A. Adl, S. Javanmardi, A. Abbaszadegan, Assessment of tooth discoloration induced by biodentine™ and white mineral trioxide aggregate in the presence of blood, J Conserv Dent 22(2) (2019) 164-168.
15. M. Kaur, H. Singh, J.S. Dhillon, M. Batra, M. Saini, MTA versus Biodentine™: Review of Literature with a Comparative Analysis, J Clin Diagn Res 11(8) (2017) ZG01-ZG05.
edifit Design & Construct recently completed the design and interior fitout of the Centre for Oral Medicine and Facial Pain for Drs Alissa Jacobs, Jacinta Vu and Hosam Ehd in the Perth suburb of Como in Western Australia.

Drawn to dentistry with a common desire to help people and use their skills in a practical and hands-on way, the trio found shared interests in Oral Medicine due to its problem-solving nature
Mand the ability to make a real impact on people’s lives.
The trio had never planned to own their own practice but after working individually in several practices, they found themselves with the need and desire to create a place to practice oral medicine together in their own style and environment. The Centre for Oral Medicine and Facial Pain was subsequently born.
The objective for the new practice was to create a warm, welcoming environment where patients, practitioners and the entire team feel valued and where everyone leaves feeling better than when
they entered. With the Centre for Oral Medicine and Facial Pain, these objectives have been met.
They came across Medifit from recommendations from colleagues in the industry. After interviewing numerous companies, it became evident that Medifit’s systems delivered superior results and the choice was easy. Medifit demonstrated very early on that they were a safe pair of hands to help Hosam, Jacinta and Alissa execute their vision. This was their first time starting a practice so teaming up with an experienced and established company was a priority for them.


Medifit’s Sam Koranis was able to leverage Medifit’s 21 years in the industry and draw upon his experience as a CPA to help with advice and assist with lease negotiations, ensuring the trio positioned their new practice for success.
With just over 200m2 to work with, the practice contains four chairs, with space for a future fifth consult as the practice grows.
The Medifit team worked closely with the dentists to understand their vision for the practice and created a design that not only met their functional needs but also reflected the warm, wel-



coming environment they wanted to create and remained within their nominated budget.
The use of natural light, neutral colours and comfortable seating helped to create a calming atmosphere.
The team also paid close attention to the flow of the practice, ensuring that patients could move easily through the space and that staff could work efficiently. Careful consideration was given to the locations and layout of each consult room to maximise the day-to-day productivity.



The thing that the dentists were most excited about for their new practice is the ability to create the pace, the culture and the environment that they wanted. Positive feedback from staff and patients has reaffirmed their decision, with regular comments on how wonderful the space is and how the feel of the practice is amazing.

Dr Hosam Ehd added “The experience with Medifit can be best summed up as both enjoyable and easy. From the initial proposal, all the way to handover, the team was very transparent and easy to communicate with. The quality of work has been exceptional and we found the whole process to be smooth with minimal stress.”
Medifit has successfully helped to create a dental practice which is warm, welcoming and comfortable for both patients and staff and gives Hosam, Jacinta and Alissa the opportunity to take the next steps in their respective careers.
Sam Koranis has the final word. “I would like to thank Hosam, Jacinta and Alissa for the opportunity to help create the Centre for Oral Medicine and Facial Pain. Assisting such fantastic individuals to achieve their dreams of establishing a successful practice is a privilege that myself and the entire Medifit team are very grateful for. I wish them every success for the future”.
The Practice
The Practice Centre for Oral Medicine
Principal Dr Alissa Jacobs, Dr Jacinta Vu and Dr Hosam Ehd
Type of Practice Oral Medicine and Facial Pain
Location Como, Perth, Western Australia

Size 203 square metres
No of chairs 4 + 1
The Team
Design Medifit Design & Construct
Construction Medifit Design & Construct

Equipment
Dental Units Belmont Eurus and Belmont Clesta E3
Autoclaves Mocom Classic 22 L
Suction Cattani Turbo Smart A
Software Gentu
Since 2002, Dentists and Dental Specialists all around Australia have trusted Medifit to create state of the art practices with individual interior designs that boost productivity and enhance levels of care.





Whether it’s your first practice or your latest, we’ll help you create a dental practice that reflects your personal style and complements the way you work - and we do it with a friendly, no fuss approach using proven best practices.
Contact Medifit today for a no obligation consultation and experience our award winning service.
• SITE ASSESSMENTS
• LEASE NEGOTIATION
• FEASIBILITY STUDIES
• COUNCIL SUBMISSIONS
• ARCHITECTURAL DESIGN
• INTERIOR DESIGN
• BUILDING CONSTRUCTION
• PRACTICE FIT-OUTS
• RENOVATIONS / REFRESHES
• BRANDING & MARKETING
Young Hurstville dentist, Dr Lena Qiu, has successfully established a stylish and functional practice in a quiet corner of the thriving southern Sydney suburb.
A local, Dr Qiu’s foray into dentistry started with her graduating with a Bachelor of Oral Health at the University of Sydney and working for some years as an oral health therapist. She then continued her studies, completing a Doctor of Dental Medicine at the University of Western Australia to become a dentist.
After spending several years working, combined with dental studies, the lure of home never left, leading to her wanting to practice dentistry close to where she grew up.
“I have been in the dental industry for 16 years. I grew up and went to primary school across the road at Hurstville Public School and I attended St George Girls High School, which is also in the area.
“I wanted to build a space where I could treat the locals for years to come, just like family, in a boutique style setting. Every detail has been chosen to give a sense of warmth and a feeling of home. ‘Meili’ means ‘beautiful’ and is the name of my daughter.
“I wanted to create a beautiful and calm space for families to come and improve their oral health. I want everyone to feel comfortable, calm and not feel that the space is too clinical and not just rush them through treatment like a medical centre. It is a place to come and choose your favourite show/song to watch with/ without headphones and even sit and have a cup of tea while waiting.”
By David PetrikasThis decision to name the practice Meili Dental Care also enabled a clever logo design to be produced, resembling a molar rendered in striking gold above gloss black lettering.

Dr Qiu went in search of help to create the new practice. After approaching four dental surgery design companies, she enlisted the help of Craig Exley of Commodore Medical & Dental Fitouts to come up with a plan and a design to accommodate two surgeries and convey the modern, quality feeling she was after.
“Craig has had some very good reviews and he was very easy to work with. I emailed his designer with several different styles I liked and pictures I found on Google and they got back to me with some ideas and also helped pick out different finishes, right down to the style of the cabinet handles.
“I wanted a more high-end look, not like lots of dental clinics which have the typical ‘healthcare’ look in blue (or some in bright green). There are a lot of dental clinics around and I wanted to stand out and not have the look of a health fund or corporate practice,” she said.

The resulting setup is something of a Tardis, with two fully equipped surgeries each with a premium A-dec 400 dental unit and Acteon X-ray unit, chair mounted monitor (and separate desktop computer monitor) and ceiling mounted entertainment screen.
Most importantly, Dr Qiu wanted to incorporate ample storage space which is achieved by a combination of floor to ceiling cupboards and both overhead and below bench cabinets in the surgeries.


There’s even a separate OPG room, plus a small staff amenity area and kitchen, complete with meals nook, refrigerator and sink and locker storage, plus a discrete rear exit.


A bonus was the ability to remotely locate the compressor in the underground carpark which both frees up space inside the compact surgery and eliminates noise inside.
In fact, the only challenge was not an engineering one but negotiating approvals from the body corporate and local council which thankfully Craig Exley from Commodore Medical & Dental Fitouts was able to assist with.

Every dental practice is unique. That’s why A-dec offers a full line of dental chairs, with a wide variety of options and price points, all designed for comfort, performance, and reliability.



From the entry-level A-dec 200, the stylish A-dec 300, to the classic A-dec 400 and the premium A-dec 500, there’s an A-dec chair to fit your practice, your personal style, and your budget.
To see our award-winning family of A-dec dental chairs – scan the QR code and find the one that’s right for you.
Design-wise, although the choice of marble and natural timber has become very popular, the unique combination of purple soft furnishings with the woodgrain and marble finishes manages to give the practice an individual look.
The timber wall cladding extending above the upholstered built-in waiting room benches in particular imbues a warm feel, while a completely mirrored wall makes the area feel lighter and much more spacious.
The Practice
The Practice Meili Dental Care
The Principal Dr Lena Qiu
Practice Type General
Location Hurstville, Sydney, New South Wales
Size 60 square metres
No of chairs 2
The Team
Colour & Design Commodore Medical & Dental Fitouts

Construction Commodore Medical & Dental Fitouts
Project Manager Craig Exley
Installer Dental Installations, Miranda

Equipment
Dental Units A-dec 400 x 2

Sterilisation W&H Lisa Automatic steriliser
Imaging Acteon DC X-ray units
Acteon PSPIX phosphor plate scanner SoproCARE intraoral camera with caries detector
Orthophos XG OPG
Compressor Cattani AC200
Suction Cattani Turbo SMART B
Software D4W Cloud
The logo and illuminated signage on the marble finish reception desk and the bold gold logo and gloss black lettering on the waiting room wall reinforce the “high end” quality feel, despite the compact size of the practice.
The use of marble finishes on the reception desk and white walls throughout the rest of the practice also reflects natural lighting well inside the space, despite the absence of windows down the side of the building.
After evaluating options to equip the practice, Dr Qiu worked closely with Tanya McRae and Darren Welsh from local A-dec dealer Dental Installations located at the nearby suburb of Miranda.
“I found Tanya and Darren were honest and helpful and took the time to walk me through the available options, build a relationship and support me through the purchase process,” Dr Qiu said.
Reliability and good after-sales support was a key consideration, together with an ambidextrous delivery system. This made the choice of A-dec 400 with traditional delivery system a no-brainer as she employs three other dentists.
“I looked at other chairs but when I went to the A-dec showroom the A-dec 400 turned out to be the ‘happy medium’ for me and is so much more cushioned than older style chairs and is just so comfortable,” Dr Qiu said.


























Information contained in this section is provided by the manufacturers or distributors. Australasian Dental Practice does not assume responsibility for the accuracy of the data.

With the Hygoclave 50, Dürr Dental offers dental practices a professional Class B steriliser that combines impressive performance with a well thought-out operating concept – for maximum efficiency and exceptional user friendliness designed to cope effortlessly with tough day-to-day working environments. With the intuitive operation of its graphical interface, the high-resolution
125mm touch screen delivers comfortable standalone operation of all functions. Colour-coded icons on the home screen make for incredibly easy navigation and offer fast access to key functions and the integrated user management system. There, the most recently executed sterilisation and test cycles can be conveniently started via quick access or program starts can be freely programmed Stainless steel and plastic are used across the board in the sterilisation process to prevent the the risk of highly corrosive demineralised water dissolving ions from the materials.
Available: A-dec Dealers
Tel: 1800-225-010
www.duerrdental.com/en/AU
The Smile Lite MDP2 Mobile Dental Photography by Prof. Louis Hardan - the ultimate evolution in mobile dental photography – is here. It’s equipped with three groups of next generation “SunLike“ LEDs and each group can be lit up individually. A dimmer function gives you the possibility to set four different illumination levels. The increased light power is perfect
for posterior shots and the new integrated ergonomic handle provides stable support. The back of the Smile Lite MDP2 is equipped with a universal adapter that is adjustable and fits any smartphone with a width between 55-85mm.

Available: Alphabond Dental Tel: (02) 9417-6660
info@alphabond.com.au
www. alphabond.com.au


Just in time for changes to teeth whitening products able to be dispensed by dentists, the Pola Light patient kit with Pola Day 9.5% hydrogen peroxide gel now has premium packaging crafted to elevate the appeal of Pola Light above less effective pharmacy and online solutions on the market. This gives clinicians the confidence and support to convince customers of the benefits of professional tooth whitening.
Pola Light is easy and comfortable to use at home, with treatment options from just 20 minutes a day. The gels are fast acting and are formulated to safely remove long term stains in as little as 5 days. The high viscosity, neutral pH tooth whitening gel ensures the greatest patient comfort in a take home kit.

Available: SDI Limited www.sdi.com.au
With cutting-edge AI-enabled processing and up to 5 acquisition modes - 3D; Panoramic; Part CT; Model and PVS impression scanning; and Cephalometric (with optional arm) - the CBCT 3D Pro provides a superior level of accuracy and precision. What truly sets the CBCT 3D Pro apart is its AI-enabled processing. This state-of-the-art software provides automated segmentation and reconstruction, enabling you to quickly and easily analyse 3D images with greater accuracy and efficiency than ever before.
Available: Osseo Group
1300-029-383
osseogroup.com.au
TGA NOTES : We have always worked within the guidelines of the TGA and now with the new regulation we continue to do so. If you have any concerns please don’t hesitate to contact us for more information.
TGA NOTES : We have always worked within the guidelines of the TGA and now with the new regulation we continue to do so. If you have any concerns please don’t hesitate to contact us for more information.
TGA NOTES : We have always worked within the guidelines of the TGA and now with the new regulation we continue to do so. If you have any concerns please don’t hesitate to contact us for more information.
TGA NOTES : We have always worked within the guidelines of the TGA and now with the new regulation we continue to do so. If you have any concerns please don’t hesitate to contact us for more information.


Another Quality Product From
Another Quality Product From
Another Quality Product From
Another Quality Product From



For





and recent relapse cases. Pay for the exact amount of treatment you need—no more, no less.
For mild cases, up to 24 sets of aligners, including one revision and one set of retainers.
48
For severe cases, as many aligners as you need for five full years, including replacements, revisions, and retainers. OsseoGroup Scan the QR code or visit clearcorrect.osseogroup.com.au to become a ClearCorrect provider.
