Reduces bad breath material AND improves oral hygiene and other whole body effects* by stimulating ‘good’ nitrate reducing bacteria which create nitrites and nitric oxide (visit nutritionfacts.org below).
Portable, handy and reusable. With anatomically shaped toothpick.
*Tongue cleaning is much more important than we realised - new studies show why. Scan code to watch this amazing evidence based video...
Oral Health Care
patient-requested whitening brand*
On the cover... Portable, handy, reusable and with an anatomically shaped toothpick, Piksters SupaGRIP® Tongue Cleaner both reduces bad breath material and improves oral hygiene.
Integrating periodontal care in the general dental practice has many benefits accordimng to Dr Annamaria Sordillo
A NEW CONCEPT FOR TOOTHPASTES: THE USE OF MICROFIBRILLATED CELLULOSE?
Over the past 70 years, the fundamental design of toothpastes has been based on the concept that abrasives should be included... until now reveals Prof. Laurie Walsh
DYNAMIC IMPACT OF COMPOSITE BONDING ON PATIENTS’ LIVES
Cass Wyllie poses the question, Who says all teeth must bow to the porcelain throne?
ODYSSEY
Clinicians need to have a working knowledge of endotoxin in order to assess its impact on their clinic practice explains Prof. Laurie Walsh
Publisher & Editor: Joseph Allbeury
www.oralhygiene.com.au
times
Cammeray 2062
How oral bacteria can aggravate rheumatoid arthritis
Periodontal disease is one of the most prevalent dental conditions worldwide. Most often caused by the formation and accumulation of bacterial biofilm around the teeth, the inflammatory effects of periodontal bacteria can go well beyond the mouth, leading to systemic effects. Over the past few decades, clinical studies have revealed that the periodontal pathogen Aggregatibacter actinomycetemcomitans (A. actinomycetemcomitans) is closely related to the onset and worsening of rheumatoid arthritis (RA), a serious autoimmune disease that affects joints. However, what goes down at the molecular level remains largely unexplored and unclear.
In a recent study published online on 15 August 2024 in the International Journal of Oral Science, a research team from Tokyo Medical and Dental University (TMDU) in Japan sought to fill this knowledge gap through detailed mechanistic studies in an animal model.
The researchers first conducted preliminary experiments to confirm whether A. actinomycetemcomitans infection influenced arthritis in mice. To this end, they used the collagen antibody-induced arthritis mouse model, which is a well-established experimental model that mimics several aspects of RA in humans.
They found that infection with this specific bacterium led to increased limb swelling, cellular infiltration into the lining of the joints and higher levels of the inflammatory cytokine interleukin-1β (IL-1β) within the limbs.
Notably, these symptoms of worsening RA could be suppressed by administering a chemical agent called clodronate that depletes macrophages - a type of immune cell. This demonstrated that macrophages were somehow involved in aggravating RA caused by A. actinomycetemcomitans infection.
Further investigation using macrophages derived from mouse bone marrow revealed that A. actinomycetemcomitans infection increased the production of IL-1β. In turn, this triggered the activation of a multiprotein complex known as the inflammasome, which plays a key role in initiating and modulating the body’s inflammatory response to infections.
The researchers added yet one more piece to this puzzle using caspase-11-deficient mice. In these animals, inflammasome activation due to A. actinomycetemcomitans was suppressed. Most importantly, caspase-11-deficient mice exhibited less deterioration of arthritis symptoms, hinting at the important role that caspase-11 plays in this context.
“Our research findings provide new insights into the link between periodontal pathogenic bacteria and the exacerbation of arthritis through inflammasome activation, offering important information on the long-debated relationship between periodontal disease and systemic diseases,” said Professor Toshihiko Suzuki, one of the lead authors of the study.
With any luck, these efforts will contribute to the development of novel therapeutic strategies to manage RA. “The findings of this research may pave the way for advances in clinical treatments for RA induced by infection with A. actinomycetemcomitans. Our suggestion to inhibit inflammasome activation could attenuate the expansion of inflammation to joints, resulting in a recovery from arthritis symptoms,” said lead author Dr Tokuju Okano. “Moreover, the outcome of our work could contribute to the development of treatment strategies for not only arthritis but also other systemic diseases, such as Alzheimer’s disease, which is also related to periodontal pathogenic bacteria,” he added with eyes set on the future.
Tokyo Medical and Dental University. “Shedding light on how oral bacteria can aggravate rheumatoid arthritis.” ScienceDaily. ScienceDaily
The oral cavity contains numerous microorganisms, including antimicrobial-resistant bacteria. These microorganisms can be transmitted via respiratory particles from patients to healthcare providers and vice versa during dental care. To track the spread of particles, we used Staphylococcus aureus bacteria in irrigation solutions during standardized dental procedures using different scaling devices and rinsing solutions during dental biofilm removal (guided biofilm therapy), using an EMS Airflow-1 with erythritol powder, or an EMS ultrasonic scaler on a typodont model in a phantom simulation head. A Staphylococcus aureus bacteria suspension was injected into the mouth of the model to mimic saliva. Different suction devices (a conventional saliva ejector or a prototype suction device) and rinsing solutions (water or 0.1% chlorhexidine) were used. To assess contamination with S. aureus, an air-sampling device was placed near the oral cavity of the phantom head and samples of surface areas were collected. S. aureus was detected by air sampling when the airflow was used with a conventional saliva ejector. Compared to the conventional saliva ejector, suction collects splatters in a more efficient way. No indicator bacteria were found when the airflow was used with high volume suction. with airflow was used. No growth was observed during treatments with the ultrasonic piezo instrument or the prototype suction device. Notably, a rinsing solution of chlorhexidine digluconate decreased the level of bacteria compared to water. Although our findings indicate the potential for airborne bacterial transmission during routine prophylactic procedures with an airflow device, this risk can be lowered by CHX rinsing and by using high volume suction, as both appear to reduce air contamination.
Eco friendly, with superior functionality
SupaGRIP®Eco Floss Picks 100pk
100% recycled and recyclable handle and super strong fine floss with scrubbing fibres. Like Gorilla floss (800 denier), but finer for easier insertion (400 denier) and better patient compliance.
• Gives pleasant scrubbing feel preferred by some over PTFE.
• Softer, more flexible handle to get around corners.
Have you tried SupaGrips? They may surprise you with their simplicity and effectiveness. Dental colleagues sometimes ring me saying - “ I know you make Piksters, but I think your best product is actually SupaGrips. I keep one on me all the time.
Dr Erskine-Smith
20% OFF use code: sgeco20
• Super slim and flexible toothpick, almost unbreakable with normal toothpick use.
On-sell to patients (RRP $8) or refer them to piksters.com or
Review: ISDH 2024 Seoul, South Korea
By Tabitha Acret
In July this year, I was lucky enough to attend and present at ISDH in Korea.
ISDH is the International Dental Hygiene Symposium held every two years by the International Federation of Dental Hygiene. This year, the hosting country was Korea and it was held in Seoul. The symposium brought together professionals, researchers and clinicians from around the world, fostering an environment of collaboration, innovation and education.
As a delegate, I had the privilege of experiencing firsthand the diverse range of presentations, trade and networking opportunities that the event offered. Presenters from the UK, Holland, USA, Korea, Ireland, Italy, Germany, Canada, USA, Japan and Australia presented on a range of subjects, giving an insight into new research and clinical findings from around the globe.
I was able to listen to presentations on minimal interventions, transgender oral health, mental health, mentoring, academic leadership, motivating patients and latest technologies
Australia had a strong presence at the symposium with invited speakers Dr Nicole Storman, Dr Julie Satur and Cathryn Carboon and further oral presentations from Associate Professor Melanie Aley, Dr Rosin McGrath, Andrew Terry, Melinda Lawther, Ron Knevel, William Carlon-Jones and myself. We also represented well in the awards with Cathryn Carboon winning the sustainability award, Amanda Tinnery from Adelaide coming second for her company neomorph mouthguards for innovations and Melosh Naicker winning best poster presentation.
Attending the symposium in Korea also offered a rich cultural experience. We arrived a couple of days earlier and wandered the streets of Seoul, taking in temples, visiting the DMZ, eating street food and of course sampling some Korean skin care!
The cultural immersions add a unique dimension to the symposium, making it not just an academic event but also a
memorable personal experience. Korea was my fourth ISDH and one of my favourite aspects now is catching up with friends from all over the world every two years and getting to discuss our common struggles and finding out new approaches
The next ISDH will be in Milan Italy–my diary is marked and I can’t wait!
About the author
Tabitha Acret is a dedicated and passionate award-winning Dental Hygienist. She studied a BOH at Newcastle University, Graduate Certificate in Public Health and is a current Masters student. Tabitha has become one of the most sought-after Hygienists and Educators in Australia and internationally with a fast-growing and loyal customer base of patients, dental professionals and media. Tabitha was previously the National Vice-President for the DHAA and has volunteered in many roles for the Association. She also has a passion for educating with students, working as a Clinical Educator at Sydney University and Newcastle University as well as working in private clinical practice and as a Clinical Educator.
Feel the difference Soft ergonomic handles and advanced instrument coatings reduce finger force and forearm fatigue for the same effect at the instrument tip.*
GRACEY 11/12 SD
• For molars and premolars.
• For mesial surfaces.
LM211-212SDES
GRACEY 7/8 SD
• For premolars and molars.
• For buccal and lingual surfaces. LM207-208MSDES
*SCAN CODE to see how the LM Test & Feel Machine works.
Why choose sharp?
‘Sharpen-free’ micro coating
Enjoy full control and improved tactile sense while easily and e ectively removing the calculus.
Saves time & money in the long run. Long-lasting superior sharpness. Improved productivity & clinical results.
‘Sharpen free’
Superior sharpness
Highest rated ergonomics
Minimum maintenance Diamond-like features
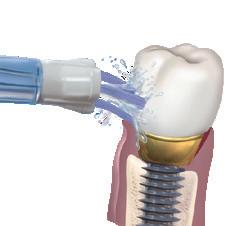
The Waterpik™ Water Flosser:
more effective than interdental brushes for removing plaque
Comparison of water flosser and interdental brush on plaque removal:
A single-use pilot study
Objective
To determine the efficacy of a Waterpik™ Water Flosser vs interdental brushes for plaque removal.
Methodology
Twenty-eight subjects completed this one-time use study. Subjects were randomly assigned to one of two groups: Waterpik™ Water Flosser (WF) plus manual tooth brushing or interdental brushes (IDB) plus manual tooth brushing. Plaque scores were obtained using the Rustogi Modification of the Navy Plaque Index (RMNPI). Subjects were instructed on the use of their interdental product. Post-cleaning scores were obtained after a supervised brushing and use of the interdental device. Scores were recorded for whole mouth, marginal, approximal, facial, and lingual regions for each subject.
Results
The Waterpik™ Water Flosser group was significantly more effective than the IDB group for removing plaque from all areas measured.
Specifically, the WF was 18% more effective for whole mouth and marginal areas, 20% for approximal areas, 11% for facial areas, and 29% for lingual areas.
Conclusion
The Waterpik™ Water Flosser and manual toothbrush removes significantly more plaque from tooth surfaces than interdental brushes and a manual toothbrush after a single use.
What more information? Book your free Professional Education session today by visiting waterpikshop.com.au/lunch
American Express® expands partnership with HICAPS
Coinciding with the roll-out of HICAPS’ new best-in-class Trinity Payment Terminals, American Express has expanded its partnership with the leading healthcare claiming solution. This enables tens of thousands of healthcare providers across Australia to accept American Express and gives American Express Card Members the ability to earn Membership Rewards® points when visiting a HICAPS provider.
The new Trinity Terminals, currently being rolled out, will see 90,000 HICAPS providers set up to accept American
Express payments including dentists, chiropractors, physiotherapists, general practices and more. The rollout is expected to be complete by the end of 2024.
The HICAPS Trinity Terminals are designed to streamline the patient payment experience with fast claim processing among 100% of private health insurers in Australia. For practices, this reduces the need to manually input claims, transactions and quoting - cutting down on administration.
Robert Tedesco, Vice President & General Manager of Global Merchant Services at American Express said: “Digitisation and automation is a priority for many businesses wanting to simplify the payments process, both for customers and themselves. This announcement bolsters our commitment to supporting healthcare providers by removing friction at the checkout, while allowing our Card Members to earn reward points for essential health services.
“71% of American Express Card Members say they are more likely to return to a business that accepts American Express. With that, we hope healthcare providers will see increased customer loyalty and repeat business with American Express automatically enabled in their payment process.”
Simon Terry, from HICAPS said: “One of the most common pain points for both practices and patients when it comes to paying a health bill is speed and flexibility. HICAPS is dedicated to delivering ease, speed and reliability and since 2014, we’ve achieved this in partnership with American Express.
“We’re proud to support more than 90,000 healthcare providers across Australia and today’s announcement will help further reduce administration and complexity for practices, while offering more choice to patients.”
For more info, visit www.hicaps.com.au
Periodontal patients: The balance between referral and in-house treatment
Integrating periodontal care in the general dental practice
By Dr Annamaria Sordillo, DDS
General dental practitioners are often the first to diagnose patients with periodontal disease and outline the appropriate course of care.1 The typical “periodontal patient journey” develops as follows:
1. Screening;
2. Periodontal assessment - including a complete periodontal chart, radiographs and photos and a risk assessment;
3. Non-surgical periodontal treatment; 4. Re-assessment (4-6 weeks later)including an updated periodontal chart to ascertain the effectiveness of the treatment; and 5. Regular supportive periodontal therapy (3-6 monthly, based on the risk level). Today most general practitioners effectively screen for periodontal disease2,3 and there is a growing trend of retaining more periodontal treatment within the practice.3 In this shifting landscape, general dentists, hygienists and oral health therapists have the opportunity to significantly contribute towards the best care of periodontal patients.
TIn-house periodontal treatment: advantages
he latest National Oral Health Plan 2015-2024 performance monitoring report shows an unfavourable increase in the prevalence of moderate and severe periodontitis in Australia, affecting almost one third of the adult population.4 With only 270 specialist periodontists in Australia, it is clear that they cannot fully service the current need.5 Additionally, the majority of the dental workforce resides in metropolitan areas, forcing people in regional and remote areas to endure either long drives or extensive waiting times to be able to see a specialist.6 Building the confidence of general practitioners could create more accessible and timely care for the millions of Australians affected. In the dental environment, the highest efficiency and satisfaction can be obtained when every team member is utilised at the best of their abilities. If general practitioners contribute to the management of periodontal patients, specialists can dedicate themselves to the more complex cases and procedures. This approach is also effectively true when OHTs and hygienists are employed and empowered in the general practice.3,7
Interestingly, a recent US-based survey revealed employing hygienists results in more patients referred to a periodontist. This is likely because hygienists and OHTs are very well-trained and focused on periodontal health, increasing the awareness and education, enhancing screening and diagnosis and benefiting both the patients and the practice.8 Finally, non-clinical factors, such as fear and financial constraints, can significantly delay pursuing a referral.9 Due to the increasing cost of living, private specialist care can become prohibitive. In such cases, providing solid treatment as a general practitioner is better than no treatment at all. Additionally, patients often choose us for a reason. An established relationship means we are familiar with the patient, their personality, their needs and anxieties. Being able to provide treatment is great not only for their continuity of care, but also for the business’ patient retention.
When
to retain and when to refer
In Australia, there are no set rules dictating when a general practitioner must refer a patient to a periodontist. Practitioners are trained to assess patients and based on their scope of practice and
clinical skills, make a decision. Interestingly, guidelines from the British Society of Periodontology10 suggest that even complex cases may be cared for in a general dental practice, based on the clinician’s experience and the patient’s risk factors and desires. Most practitioners would agree that a referral is advised for advanced disease (Stages III-IV), medically compromised or frail patients, particularly young patients and those with peri-implantitis. Local complexities such as furcation involvement and vertical bony defects also warrant consideration. Patients who are difficult to motivate toward good oral hygiene are also good candidates for specialist treatment.
Non-clinical factors are equally impor tant; is the patient willing and financially able to seek specialist care? Do they live far from the nearest periodontist and can they travel? Is the waiting period exces sively long? Are they anxious about seeing a new practitioner? Do you feel confident stepping slightly outside your comfort zone and taking on a case?
Regardless of the reason, it is your obligation to offer the patient a specialist referral for a second opinion or full man agement and this conversation should be documented in the patient’s file.
Referral to a periodontist is also strongly recommended when, despite initial non-surgical treatment, the disease progresses or relapses. Even with good overall healing and perfect compliance, stubborn residual bleeding pockets might persist, which may require advanced periodontal care or surgery.
sary examinations, records to send and any treatment to commence. By clearly communicating what you are comfortable managing, specialists will know when they can confidently refer the patient back to your care. Moreover, specialists
Periodontal patient retention = Revenue
GThe importance of education
AFinally, when in doubt, ask your periodontist. A quick phone call or email often provides the clarity needed to make the appropriate decision.
Cultivate the relationship with your specialists
General practitioners should carefully consider which specialist they will trust with their patients’ care. How do they work? What’s their philosophy and does it align with yours? How do they ensure good results? How do they communicate with you? Do not be afraid to initiate and grow communication with your periodontist. A specialist can help your clinic develop a mutually beneficial protocol and referral pathway, detailing which type of patients to refer, the neces-
n evident discrepancy still exists between clinicians’ confidence in diagnosing periodontal disease and their confidence and willingness to undertake the active treatment.2 This lack of confidence seems to mainly come from the level of training the clinician has received and their perceived experience.2,11 Therefore, the first step to is to undertake further training. The availability of periodontal-focused continuous education courses is on the rise, with periodontists themselves offering a share of their incredible knowledge to empower general practitioners and foster strong, fruitful collaborations. An excellent starting point is the EMS Swiss Dental Academy, where webinars, in-person courses and in-house training from local and international GBT® experts can help build a high standard of periodontal care in your practice.
iven the prevalence of periodontal disease, retaining periodontal treatment in-house can significantly contribute to both business revenue and the clinician’s financial reward. Even if a referral is necessary early in the patient’s journey, there are still valuable steps you can take. A thorough and complete assessment before referral is not only advised but also greatly appreciated by specialists, allowing them to better know the patient. This includes periodontal charting, radiographs, photos and sometimes even initial supragingival debridement and oral hygiene instructions, all of which are within the scope of any general practitioner. Completing the initial assessment not only enhances your clinical records, but also reassures the patient that you are actively involved in their care, rather than simply passing them on to someone else.
Based on the average revenue as per ADA Dental fees survey of 2022, the initial comprehensive assessment of a periodontal patient including an x-ray could earn the practice $400+, with an additional $120 if the initial supragingival debridement is provided.
If the active treatment is performed in house, it can generate between $571 and $992, plus around $113 for the reassessment. Finally, maintenance therapy becomes a regular and reliable source of work and income for the practice.
How Guided Biofilm Therapy® can help
C onsistent clinical results rely on established protocols. Guided Biofilm Therapy - GBT is an emerging and successful approach designed to address a wide range of patients and clinical needs, from the everyday preventative check-ups and cleans to the treatment of periodontal disease, providing several advantages.
Improved communication with the patient
GBT prioritises patient engagement and motivation before any debridement begins. Fear of failing to communicate with periodontal patients can hinder practitioners’ confidence2 and getting patients on board is one of the
biggest hurdles when the “simple clean” they thought they needed turns into a more demanding course of treatment. Using a plaque disclosing agent is a great way to initiate conversation and check and maintain motivation along the way.
Effective and comfortable debridement
Let’s be honest, long and repetitive sessions of scaling and root planing (SRP) are uncomfortable for both the patient and the clinician and the postoperative sensitivity can deter many patients. Unlike old-style SRP which primarily focuses on calculus removal and “smoothening” of the root surface, GBT shifts the attention to biofilm, the living cause of periodontal disease and aims to be minimally invasive on any surface. The first step of GBT involves complete biofilm removal through Airflowing, a gentle stream of air, water and erythritol powder.
The Airflow MAX® handpiece is ideal for supra-gingival areas and sulci up to 4mm of depth, while the Perioflow® handpiece is used in pockets up to 10mm of depth. Once all biofilm is removed, the long and thin Piezon PS® ultrasonic tip gently removes all the calculus and debrides the root surface. GBT demonstrated excellent treatment outcomes, particularly in reducing deep pockets (PPD≥5.5mm)12 and positively shifting in the pocket microbiome.13
However, the main advantage of GBT is the increased patient comfort. The reduced use of ultrasonic and manual instruments provides a better overall patient experience, which is fundamental for maintaining their willingness to continue treatment and causes less fatigue to the clinician.14
Easy maintenance
Maintenance therapy for periodontal patients is a life-long commitment. However, repeated SRP may lead to removal of root cementum and dentinal hypersensitivity, potentially reducing longterm patient compliance.15 GBT excels in maintenance care. As all the stubborn calculus was eliminated during active treatment, biofilm is once again the main target and Airflow MAX and Perioflow are the instruments of choice. This gentler approach ensures long-term success.16
Time saved
GBT typically requires less treatment time than conventional SRP, both during the initial treatment14 and the maintenance phase.15 The increased time-efficiency contributes to the overall financial advantage of adopting GBT in the practice.
Overall, while referral to specialists remains essential in certain cases, inhouse treatment can be a valuable option. By leveraging in-house treatment capabilities and cultivating strong relationships with specialists, dental practices can deliver comprehensive periodontal care while maximising business success and patient outcomes.
About the author
Dr Annamaria Sordillo grew up in Italy, were she obtained her combined Bachelor and Masters degree in Dentistry with Honours. She moved to Sydney in 2017 to be with her Australian husband and she now lives and works in general practice in the Hunter region of New South Wales. For the last 7 years, she has been collaborating with a research group in Periodontology led by Prof Magda Mensi at the University of Brescia, Italy and she has co-written several international research papers. Dr Sordillo has an interest in periodontology, preventative and restorative dentistry and is a Swiss Dental Academy Trainer and Educator.
References
1. Brown LM, Bowman P, O’Rourke VJ, Mercado F, Marshall R, Parsons S. Periodontal Referral Patterns in Australia: 2000 Versus 2015. J Periodontol. 2017 Sep;88(9):869-875. doi: 10.1902/jop.2017.160774. Epub 2017 May 18. PMID: 28517973
2. Darby IB, Angkasa F, Duong C, Ho D, Legudi S, Pham K, Welsh A. Factors influencing the diagnosis and treatment of periodontal disease by dental practitioners in Victoria. Aust Dent J. 2005 Mar;50(1):37-41. doi: 10.1111/j.1834-7819.2005. tb00083.x. PMID: 15881304
3. Kraatz J, Hoang H, Ivanovski S, Ware RS, Crocombe LA. Periodontal diagnosis, treatment, and referral patterns of general dental practitioners. J Investig Clin Dent. 2019 Aug;10(3):e12411. doi: 10.1111/ jicd.12411. Epub 2019 Apr 21. PMID: 31006957
4. National Oral Health Plan 2015–2024: performance monitoring report - https://www.aihw.gov.au/reports/ dental-oral-health/national-oral-health-plan-2015-2024/ contents/our-oral-health-a-national-perspective/periodontitis-prevalence#
5. Dental Board of Australia – Registrant Data, Reporting period: 01 January 2024 to 31 March 2024. https://www.dentalboard.gov.au/about-theboard/statistics.aspx
6. Dentists, specialists and allied practitioners in Australia: Dental Labour Force Collection, 2006 - https://www.aihw.gov.au/getmedia/0b50f218a1a4-4dd3-8a4b-d09d2645feef/11915.pdf?v=20230 605171922&inline=true
7. Hopcraft M, McNally C, Ng C, Pek L, Pham TA, Phoon WL, Poursoltan P, Yu W. Attitudes of the Victorian oral health workforce to the employment and scope of practice of dental hygienists. Aust Dent J. 2008 Mar;53(1):67-73. doi: 10.1111/j.18347819.2007.00012.x. PMID: 18304244.
8. Zemanovich MR, Bogacki RE, Abbott DM, Maynard JG Jr, Lanning SK. Demographic variables affecting patient referrals from general practice dentists to periodontists. J Periodontol. 2006 Mar;77(3):341-9. doi: 10.1902/jop.2006.050125. PMID: 16512747.
9. Dockter KM, Williams KB, Bray KS, Cobb CM. Relationship between prereferral periodontal care and periodontal status at time of referral. J Peri-
11. Sum J, O’Rourke VJ. Factors affecting periodontal disease referral and the adherence to guidelines among general dentists. Aust Dent J. 2018 Dec;63(4):394-401. doi: 10.1111/adj.12641. Epub 2018 Jul 25. PMID: 29947419
12. Divnic-Resnik T, Pradhan H, Spahr A. The efficacy of the adjunct use of subgingival air-polishing therapy with erythritol powder compared to conventional debridement alone during initial nonsurgical periodontal therapy. J Clin Periodontol. 2022 Jun;49(6):547-555. doi: 10.1111/jcpe.13623. Epub 2022 Apr 22. PMID: 35373340; PMCID: PMC9321595
13. Mensi M, Caselli E, D’Accolti M, Soffritti I, Farina R, Scotti E, Guarnelli ME, Fabbri C, Garzetti G, Marchetti S, Sordillo A, Trombelli L. Efficacy of the additional use of subgingival air-polishing with erythritol powder in the treatment of periodontitis patients: a randomized controlled clinical trial. Part II: effect on sub-gingival microbiome. Clin Oral Investig. 2023 Jun;27(6):2547-2563. doi: 10.1007/ s00784-022-04811-4. Epub 2022 Dec 20. PMID: 36538094; PMCID: PMC10264538.
14. Vouros I, Antonoglou GN, Anoixiadou S, Kalfas S. A novel biofilm removal approach (Guided Biofilm Therapy) utilizing erythritol airpolishing and ultrasonic piezo instrumentation: A randomized controlled trial. Int J Dent Hyg. 2022 May;20(2):381-390. doi: 10.1111/idh.12533. Epub 2021 Jul 19. PMID: 34218516
15. Zappa U, Smith B, Simona C, Graf H, Case D, Kim W. Root substance removal by scaling and root planing. J Periodontol. 1991;62(12):750–4.
16. Tan SL, Grewal GK, Mohamed Nazari NS, Mohd-Dom TN, Baharuddin NA. Efficacy of air polishing in comparison with hand instruments and/or power-driven instruments in supportive periodontal therapy and implant maintenance: a systematic review and meta-analysis. BMC Oral Health. 2022 Mar 23;22(1):85. doi: 10.1186/s12903-022-02120-6. PMID: 35321688; PMCID: PMC8944123
Question 1. Building the confidence of general practitioners in periodontal care is vital because...
a. Almost 33% of adults need treatment.
b. There are too few specialist periodontists.
c. Specialist care is limited in regional and remote areas.
d. All of the above.
Question 2. A non-clinical factor to consider before referring to a specialist periodontist is...
a. Is the patient willing and financially able to seek specialist care.
b. Does the patient live far from the nearest perio and can they travel.
c. Is the waiting period excessively long.
d. Is the patient anxious about seeing a new practitioner.
e. All of the above.
Question 3. Using Guided Biofilm Therapy, biofilm in a 10mm deep pocket would be removed using...
a. Scaling and root planing.
b. The Piezon PS ultrasonic tip.
c. The Perioflow handpiece.
d. The Airflow MAX handpiece.
Question 4. Using Guided Biofilm Therapy, biofilm in a 4mm deep pocket would be removed using...
a. Scaling and root planing.
b. The Piezon PS ultrasonic tip.
c. The Perioflow handpiece.
d. The Airflow MAX handpiece.
Question 5. The main advantage of GBT is...
a. It’s easier to smooth the root surface.
b. Increased patient comfort.
c. Efficient calculus removal.
d. All of the above.
INSTRUCTIONS:
Question 6. The extent of abrasion cause by toothbrushing is influenced by the...
a. Amount of abrasive particles in the toothpaste.
b. Force applied during brushing.
c. Hardness of the toothbrush bristles.
d. Length of brushing at any particular site.
e. All of the above.
Question 7. High-level evidence indicates that using toothpaste...
a. Doubles the amount of plaque removed.
b. Completely removes all plaque.
c. Does very little to the extent of plaque removal.
d. Removes plaque only after brushing for more than 2 minutes.
b. Attending regular check up and clean appointments.
c. Maintaining at-home whitening.
d. Avoiding using your teeth as bottle openers.
e. All of the above.
Question 16. Endotoxin (ET) is also known as...
a. Polynucleotide
b. Phospholipid
c. Lipopolysaccharide
d. Glycosaminoglycan
e. Liposome
Question 17. One of the largest concerns with ET is when it...
a. Is present in drinking water.
b. Gains access to systemic circulation.
c. Is present on dental instruments.
d. Is present in the gastrointestinal tract.
Question 18. The TGA Medical Device Standards Order (Endotoxin Requirements for Medical Devices) sets the exposure limit for endotoxins at...
a. 1 ng per device
b. 2 ng per device
c. 3 ng per device
d. 4 ng per device
Question 19. Endotoxins that dry onto instrument surfaces do not remain biologically active after normal steam sterilisation...
a. True
b. False
Question 20. Endotoxin is a fundamental component of the cell wall of...
a. Gram-negative bacteria
b. Gram-positive bacteria
c. Mycobacteria
d. Corynebacteria.
dentevents presents...
Infection Control BOOT CAMP
29 VIDEOS - 8+ HOURS OF EDUCATION
Presented by Emeritus Professor Laurence Walsh AO BDSc, PhD, DDSc, GCEd, FRACDS, FFOP (RCPA), FFDT (RCS Edin)
8
Learn from Australia’s leading authority on infection prevention and control in dentistry about recent changes in infection control including from the Dental Board of Australia (July 2022), the ADA (4th edition guidelines August 2021 and the ADA Risk management principles for dentistry during the COVID-19 pandemic (October 2021)), the new guidelines from NHMRC (May 2019), Hand Hygiene Australia (Sept 2019) and the CDNA (Dec 2018) as well as recent changes in Australian Standards and TGA regulations that are relevant to infection control. The course provides a summary of how those changes interlink with one another and also covers practical implementation of the new requirements and what it means for everyday dental practice. Hear about the why and the how and keep up-to-date with the changes that are happening.
COURSE TOPICS
This one day course will cover changes in regulations and guidelines from 2018 to 2022 including:
n Risk-based precautions.
n Hand hygiene and hand care practices.
n Addressing common errors in personal protective equipment.
n Biofilm reduction strategies.
n Efficiency-based measures to improve workflow in instrument reprocessing and patient changeover.
n Correct operation of mechanical cleaners and steam sterilisers.
n Wrapping and batch control identification.
n Requirements for record keeping for instrument reprocessing.
n Correct use of chemical and biological indicators.
Laurie Walsh is a specialist in special needs dentistry who is based at the University of Queensland in Brisbane, where he is an emeritus professor. Laurie has been teaching and researching in the areas of infection control and clinical microbiology for over 25 years and was chief examiner in microbiology for the RACDS for 21 years. His recent research work includes multiple elements of infection control, such as mapping splatter and aerosols, COVID vaccines and novel antiviral and antibacterial agents. Laurie has been a member of the ADA Infection Control Committee since 1998 and has served as its chair for a total of 8 years, across 2 terms. He has contributed to various protocols, guidelines and checklists for infection control used in Australia and represented dentistry on 4 committees of Standards Australia and on panels of the Communicable Diseases Network of Australia and of the Australian Commission on Safety and Quality in Health Care.
REGISTRATION INCLUDES
n On-Demand access to 29 Online Learning Videos (Over 8 hours of education).
n Watch and re-watch at your leisure 24/7
n Digital Online Learning Companion.
n Digital Suggested Reading Material.
n Online Questionnaire to earn 8 Hours of CPD.
Oral Hygiene Abstracts 2024
By Emer. Prof. Laurence Walsh AO
Isopropyl alcohol wipes are effective for disinfecting smartphones in the workplace
Smartphones in healthcare settings pose infection risks due to harbouring pathogenic bacteria. The microbiota found on smartphones resembles that observed on the hands of healthcare workers and between 9% and 25% of smartphones are contaminated with pathogenic bacteria. The inanimate surfaces of the phone serve as reservoirs for pathogenic micro-organisms. This is an issue because smartphones have become a fundamental tool in our daily lives and clinical practice and their touch screens require repeated finger contact. This study assessed the effectiveness duration of two sanitization methods, 70% isopropyl alcohol wipes and ultraviolet-C (UVC) boxes, assessing the reduction in total bacterial load 3 hours post-sanitization. A randomised trial with two intervention arms (IPA wipes and UVC boxes) was designed. As participants, 71 healthcare workers from a university hospital were recruited, stratified by ward and block randomised within each ward to control confounders (62% nurses, equally from Neonatal Intensive Care, Geriatrics, and Intensive Care departments; physicians 21% and medical residents 17%). Initial bacterial load reduction was significant with both disinfection techniques and no different between the 2 options. However, when assessed again 3 hours after sanitizing, levels of bacteria had begun to return, approaching baseline levels in the UVC group. Bacterial levels were lower after using the IPA wipes, indicating some residual efficacy. This study highlights the necessity for guidelines on smartphone sanitisation methods in healthcare and reinforces the need for educational initiatives for both healthcare workers and patients who use smartphones, tablets and other devices. The use of 70% isopropyl alcohol-impregnated was more intuitive and practical than using UVC boxes, making it easier to sanitise the phone surface repeatedly throughout the work shift. Further work is needed to determine optimal sanitisation intervals.
Lontano A, et al. Pilot randomized experimental study evaluating isopropyl alcohol and ultraviolet-C radiation in the disinfection of healthcare workers’ smartphones. Journal of Hospital Infection 2024; 148: 105-111.
Quats in 2-in-1 wipes are not the cause of degradation of plastics
Surface cleaning and disinfection is a key part of breaking the chain of transmission and reducing the risk of healthcare associated infections (HAIs). However, if cleaning and disinfectant formulations are incompatible with surface materials, frequent application can cause premature failure of plastics due to Envi ronmental Stress Cracking (ESC). Material compatibility should be considered when selecting cleaning and disinfecting products. Wipe formulations are comprised of active (biocides) and inactive (co-formulants) chemicals. A single formulation may contain multiple potential ESC agents at varying concentrations, influencing the overall ESC risk. Moreover, interactions amongst these ingredients can further alter the ESC potential. Hence, predicting ESC solely based on individual ingredient tests is challenging. This study evaluated the tendency of 2-in-1 wet wipes to cause ESC in commonly found healthcare plastics. These disinfectant and detergent products (2-in-1) contain a range of ingredients which make up their formulation. A total of 8 ready-to-use 2-in-1 wet wipes were evaluated for their ability to cause ESC in 13 plastic surfaces. Polymers were exposed to fluid extracted from wipes at a fixed strain of 0.5% for 7 days and assessed for cracking, crazing and tensile strength. The severity of ESC caused by wipes varied. Products with higher pH (>8.0) were responsible for 74% of failures, with 22 of the 39 tested plastics visibly cracking. All wipes tested contained quaternary ammo nium compounds (QACs), such as benzalkonium chloride, and didecyldimethylammonium chloride, as active ingredients. These were combined with co-formulants such as solvents, preservatives, biocide potentiators, stabilisers and pH buffering agents. Each of these other ingredients have the potential to act as ESC agents, with differing severity based upon their molecular structure, concentration and conditions such as pH, humidity and temperature. Factors such as pH levels, co-formulants and the specific type and grade of plastic are crucial deter minants of material compatibility. The results indicate that the QACs were not the primary cause of ESC, rather the small/medium amines or alcohols that were included in the products, as these gave a greater propensity for plastic cracking. Overall, each disinfectant wipe formulation exhibited a unique spectrum of microbial efficacy and had a unique potential to cause surface damage to plastics. This damage may result in device failures that could compromise patient and staff safety.
Jennings J, et al. Chemical resistance testing of plastics – Material compatibility of detergent and disinfectant products. Journal of Hospital Infection 2024 DOI: 10.1016/j.jhin.2024.04.023.
When you SHOCK, let ICX RENEW.
Unwanted visitors like bacteria love to colonise in your dental unit waterlines. A daily waterline maintenance protocol with A-dec ICX® waterline treatment tablets, along with periodic ICX Renew™ shock treatments, will help reduce these nasty microorganisms.
A new concept for toothpastes: The use of micro-fibrillated cellulose
By Emeritus Professor Laurence J. Walsh AO
Over the past 70 years, the fundamental design of toothpastes has been based on the concept that abrasives should be included, to remove external stains from the surfaces of teeth and improve the disruption of dental plaque biofilm.1-3 Over the past 20 years, different toothpastes have been developed that specifically target patients with cervical dentine hypersensitivity. As well as including agents with desensitising actions, these toothpastes have much lower abrasivity
In the past 5 years, an opposite trend has also occurred with some recent toothpastes including higher levels of abrasive particles, including charcoal, in an attempt to increase the removal of extrinsic stains. This poses a risk for abrasive wear of teeth.4-7 The fundamental challenge here is that when a toothpaste has greater abrasivity, the impacts of this will be seen much more on exposed dentine and root surfaces than on the enamel. This has been a major challenge in toothpaste design since the 1940s.8-10 The extent of abrasion which occurs will be influenced by factors such as the force applied during brushing, the hardness of the toothbrush bristles that are used and the length of brushing at any particular site.
Figure 1. A. Scanning electron microscope view of the micro-fibrillated cellulose fiber network that was incorporated into toothpaste. B. V-shaped brushing machine used to test toothpaste performance. C. Samples with external stains from a tea and coffee mixture prior to brushing. D. The same samples after brushing, showing reduction in external stains. E. Sample preparation for standardised laboratory assessments of toothpaste performance. Image A is courtesy of NovaFlux Inc, Princteton, New Jersey, USA. Images B-E are courtesy of Therametric Technologies Inc., Noblesville, Indiana, USA. This lab did the PCR tests described in reference 28.
With the advent of nanotechnologies, there is an opportunity to break the long-held paradigm of toothpaste design and to reimagine the design of toothpastes, so that they can achieve enhanced cleaning of dental plaque biofilm, as well as better removal of extrinsic stains, but without necessarily posing a great risk for abrasion.
The challenge of lubricants and dilution
To understand how this could be achieved, one has to enter the world of engineering tribology, which is the field of science that focuses on the wear of objects. One of the key concepts in tribology is that the presence of lubricants lowers the effectiveness of abrasive particles.
In the case of conventional toothbrushing, viscosity modifiers (such as glycerin) and surfactants can alter the way that individual abrasive particles in the toothpaste come into contact with the tooth surface that is being cleaned.
In addition, during brushing, the physical brushing action and the stimulation caused by the flavours in the toothpaste cause a profound stimulation of saliva production. The stimulated saliva then dilutes the toothpaste and the salivary mucins also act as lubricating agents. These lubricating effects reduce the opportunity for abrasive particles to be trapped between the end of the bristles and the tooth surface while the bristle end is moving during a brushing stroke. These issues have all been described in the tribology literature,11-14 however they are rarely mentioned in dental publications.
Against this background, when one considers the literature on the effectiveness of toothbrushing, it is perhaps now less surprising that routinely used toothbrushing methods and conventional toothpastes typically leave dental plaque biofilm remaining in many areas of the mouth after brushing. In fact, several clinical studies15-18 and the most high-level evidence of the effectiveness of brushing, from systematic reviews,19 indicates that the addition of toothpaste to a brushing routine adds very little to the extent of plaque removal.
Entangled fibre networks for enhanced cleaning
One way to better remove dental plaque is to employ special particles with a mesh-like structure that can create a large amount of shear stress as they move across a surface, creating a type of nano scrubbing action. For toothbrushing, these particles can be propelled by the action of the toothbrush bristles, as well as by the fluid movements that occur in the mouth. This means the special particles can reach places that may not be accessed by the ends of toothbrush bristles.20,21
Mesh-like particles can be made from wood pulp, which can be treated to create microscopic fibrils of varying dimensions. Because of entanglement, the clusters of microscopic fibrils do not separate into their constituent fibrils during brushing. An example of this type of technology is NanoClean™, a form of micro-fibrillated cellulose (MFC) (Figure 1A). This material is insoluble in water and is classified as a “generally recognised as safe” (GRAS) ingredient by the US FDA.
The special mesh-like particles themselves can have powerful cleaning actions, depending on the speed at which they move across a particular surface. This can occur because of the fibers making direct contact with stacks of bacteria within the dental plaque biofilm and the stacks becoming entangled with the fibers, causing the stacks to be detached from the surface. This entanglement concept is also the basis of technologies used to remove body fluids and biofilms from the narrow channels of medical devices such as endoscopes.22,23
One can take this concept even further and trap within the meshwork of MFC particular abrasive particles that are designed for optimal cleaning and removal of external stain, such as high polishing silica. The silica particles are then dragged over the tooth surface as the MFC clusters move across the tooth surface.20,21
Removal of extrinsic stains
In conventional toothpastes, various insoluble abrasive particles from the toothpaste may be pushed along the tooth surface by the toothbrush bristles and some particles may theoretically even be sandwiched between the bristle end and the tooth surface, causing them to be pushed into the surface. The likelihood of such interactions occurring is reduced because of the dilution and lubrication events described above.
The standardised test for removal of extrinsic stains is the pellicle cleaning ratio (PCR) test. This compares the removal of a mixture of external stains from the enamel surface (Figure 1 B-D). The stain mixture applied to the teeth includes tea and coffee. The PCR results are highly predictive for clinical performance for extrinsic stain removal.24-27
When a very small amount of silica is loaded into MFC, impressive removal of extrinsic stains from tooth services can be achieved. This was shown in a recent laboratory study which used a novel fluoride toothpaste (Protegera™) containing 7% by weight high cleaning silica entangled into MFC. The PCR results were comparable (not significantly different) to several commercial toothpastes marketed specifically for whitening actions caused by removal of extrinsic stains (Figure 2).28
The cleaning efficiency index (CEI) calculations factor in both stain removal properties and dentine abrasion. The MFC toothpaste was found to be superior to six well-known commercial toothpastes that are marketed for their effects on appearance (Figure 3). When dentine abrasion was tested using standard methods,7,29-31 the MFC toothpaste had far lower dentine abrasivity than toothpastes that are marketed with whitening claims (Figure 4).28
Clinical performance for dental plaque removal
Arecent clinical study compared dental plaque removal using the novel MFC fluoride toothpaste to a commonly used fluoride toothpaste (Crest Cavity Protection™), assessing supervised use as well as unsupervised at-home use over a period of one week, in 82 adults with moderate plaque deposits (a mean plaque score greater than or equal to 2.0 at baseline).32
Figure 2. Pellicle cleaning ratio results for 6 toothpastes. Protegera (black bar) is the brand containing microfibrillated cellulose. There is no significant difference between the PCR values for the first 4 toothpastes. Based on data from reference 28.
Figure 3. Cleaning efficiency index results for the same 6 toothpastes shown in Figure 2. The highest CEI value is found for Protegera. Based on data from reference 28.
Figure 4. Data for dentine abrasion. Note the low value for Protegera (black bar), the brand containing microfibrillated cellulose. Based on data from reference 28.
Figure 5. Percent whole mouth plaque reduction was greater for Protegera (black bars) than for Crest Cavity Protection (blue bars) by 3 to 4 fold, at each of the points of comparison in a one week randomised clinical trial. Based on data from reference 32.
Overall, when compared to the conventional toothpastes, the MFC toothpaste was at least three times and up to four times more effective in whole-mouth plaque reductions (Figure 5), 5 times more effective on approximal surfaces (Figure 6) and 7 times more effective on lingual surfaces.32 This benefit was gained without the subjects changing their toothbrush or their toothbrushing method. The latter two findings are important, since approximal and lingual surfaces are typically the most difficult to clean. The explanation for these effects is that the MFC fibre networks with their entrapped silica abrasive particles are moving within the slurry of toothpaste diluted with saliva. The particles are cleaning those tooth services without needing direct contact between the bristles of the tooth brush and that tooth surface. The safety assessment conducted as part of the clinical trial showed no adverse soft tissue or hard tissue effects from the
Figure 6. The percent plaque reduction on approximal surfaces in a 7 day clinical trial was greater for Protegera (black bars) than for Crest Cavity Protection (blue bars) by 3 to 5 fold, at each of the measurement sites. Based on data from reference 32.
MFC toothpaste.28 Overall, the novel toothpaste had a similar mouth feel to a conventional toothpaste.
Advantages of a cleaner tooth surface
With greater removal of dental plaque biofilm and external stains, one would expect to see that the fluoride component of the MFC toothpaste would be highly efficacious. Standardised laboratory tests have revealed that there is greater efficacy than for a toothpaste with the same fluoride ingredient and concentration, giving a statistically greater reduction in enamel solubility for an acid challenge.28 It was effective at delivering fluoride for remineralisation of enamel lesions, causing fluoride uptake into those lesions and increased surface microhardness.
Conclusions
Incorporating MFC technology into a toothpaste can enhance multiple aspects of its performance, whilst at the same time reducing its abrasivity. This technology approach is disruptive because it challenges the long-held view that powerful stain removal requires large amounts of abrasives. Without changing the design of a toothbrush or the method of its use, worthwhile gains in performance can be achieved by this change to the toothpaste. As well, this technology approach opens the prospect of “liquid cleaning” applications where a toothbrush is not used and where the normal fluid motions of saliva can propel the MFC clusters around the mouth.
“This technology approach is disruptive because it challenges the long-held view that powerful stain removal requires large amounts of abrasives. Without changing the design of a toothbrush or the method of its use, worthwhile gains can be achieved by this change to the toothpaste...”
About the author
Emeritus Professor Laurence J. Walsh AO is a specialist in special needs dentistry who is based in Brisbane, where he served for 36 years on the academic staff of the University of Queensland School of Dentistry, including 21 years as Professor of Dental Science and 10 years as the Head of School. Since retiring in December 2020, Laurie has remained active in hands-on bench research work, as well as in supervising over 15 research students at UQ who work in advanced technologies and biomaterials and in clinical microbiology. Laurie has served as Chief Examiner in Microbiology for the RACDS for 21 years and as the Editor of the ADA Infection Control Guidelines for 12 years. His published research work includes over 400 journal papers, with a citation count of over 20,000 citations in the literature. Laurie holds patents in 8 families of dental technologies. He is currently ranked in the top 0.25% of world scientists. Laurie was made an Officer of the Order of Australia in January 2018 and a life member of ADAQ in 2020 in recognition of his contributions to dentistry.
References
1. Forward GC. Role of toothpastes in the cleaning of teeth. Int. Dent. J. 1991; 41: 164-170.
2. Ashley P. Toothbrushing: Why, when and how? Dent. Update 2001; 28: 36-40.
3. Lippert F. An introduction to toothpaste - its purpose, history and ingredients, Monogr. Oral Sci. 2013; 23: 1-14.
4. Hunter ML, Addy M, Pickles MJ, Joiner A. The role of toothpastes and toothbrushes in the aetiology of tooth wear. Int. Dent. J. 2002; 52 (Suppl. S5): 399-405.
5. Lewis R, Dwyer-Joyce RS. Wear of human teeth: A tribological perspective. Proc. Inst. Mech. Engin. Part J. J. Engin. Tribol. 2005; 219: 1-18.
6. Addy M, Hunter ML. Can tooth brushing damage your health? Effects on oral and dental tissues. Int. Dent. J. 2003; 53 (Suppl. S3): 177-186.
7. Schemehorn BR, Moore MH, Putt MS. Abrasion, polishing, and stain removal characteristics of various commercial dentifrices in vitro. J. Clin. Dent. 2011; 22: 11-18.
8. Manly RS. The abrasion of cementum and dentin by modern dentifrices, J. Dent. Res. 1941; 20: 583-595.
9. Epstein S, Tainter ML. Abrasion of teeth by commercial dentifrices, J. Am. Dent. Assn. 1943; 30: 1036-1045.
10. Kitchin PC, Robinson HB. How abrasive need a dentifrice be? J. Dent. Res. 1948; 27: 501-506.
11. Lewis R, Dwyer-Joyce RS, Pickles MJ. Interaction between toothbrushes and toothpaste abrasive particles in simulated tooth cleaning. Wear 2004; 257: 368-376.
12. Lewis R, Dwyer-Joyce RS. Interactions between toothbrush and toothpaste particles during simulated abrasive cleaning. Proc. Inst. Mech. Eng. Part J. J. Eng. Tribol. 2006; 220: 755-765.
13. Lewis R, Barber SC, Dwyer-Joyce RS. Particle motion and stain removal during simulated abrasive tooth cleaning. Wear 2007; 263: 188-197.
14. Bongaerts JHH, Rossetti D, Stokes JR. The lubricating properties of human whole saliva. Tribol. Lett. 2007; 27: 277-287.
15. Parizotto SP, Rodrigues CRMD, Singer JDM, Sef HC. Effectiveness of low cost toothbrushes with or without dentifrice, in the removal of plaque in deciduous teeth. Pesqui Odont. Bras. 1993; 17: 17-23.
16. Paraskevas S, Timmerman MF, van der Velden U, van der Weijden GA. The additional effect of dentifrices on the instant efficacy of toothbrushing. J. Periodontol. 2006; 77: 1522-1527.
17. Paraskevas S, Rosema NA, Versteeg P, Timmerman MF, van der Velden U, van der Weijden GA. The additional effect of a dentifrice on the instant efficacy of toothbrushing: A crossover study. J. Periodontol. 2007; 78: 1011-1016.
18. Zanatta FB, Antoniazzi RP, Pinto TM, Rösing CK. Supragingival plaque removal with and without dentifrice: A randomized controlled clinical trial. Braz. Dent. J. 2012; 23: 235-240.
19. Valkenburg C, Slot DE, Bakker EWP, Van der Weijden FA. Does dentifrice use help to remove plaque? A systematic review. J. Clin. Periodontol. 2016; 43: 1050-1058.
20. Labib ME, Perazzo A. Oral cavity cleaning composition method and apparatus. U.S. Patent 20210121386, 29 April 2021.
21. Labib ME, Perazzo A, Winston AE, Tabani Y, Manganaro JL, Franz LL, Sohn SY, Kuchar C. Oral cavity cleaning composition, method and apparatus U.S. Patent 202100330557, 28 October 2021.
22. Labib ME, Duhkin SS, Tabani Y, Lai CY, Manganaro JL, Materna P, Roberston JC. Compositions for Cleaning and Decontamination. U.S. Patent 10,266,793, 23 April 2019.
23. Labib ME, Duhkin SS, Tabani Y, Lai CY, Manganaro JL, Materna P, Roberston JC, Sohn SY. Cleaning Composition with Superabsorbent Polymer. U.S. Patent 11,345,878, 31 May 2022.
24. Stookey GK, Muhler JC. Laboratory studies concerning the enamel and dentin abrasion properties of common dentifrice polishing agents. J Dent Res. 1968 Jul-Aug;47(4):524-32. doi: 10.1177/00220345680470040301.
25. Stookey GK, Burkhard TA, Schemehorn BR. In vitro removal of stain with dentifrices. J. Dent. Res. 1982; 61: 1236-1239.
26. Pontefract H, Courtney M, Smith S, Newcombe RG, Addy M. Development of methods to enhance extrinsic tooth discoloration for comparison of toothpastes. 1. Studies in vitro, J. Clin. Periodontol. 2004; 31: 1-6.
27. Pontefract H, Courtney M, Smith S, Newcombe RG, Addy M. Development of methods to enhance extrinsic tooth discoloration for comparison of toothpastes. 2. Two-product clinical study, J. Clin. Periodontol. 2004; 31: 7-11.
28. Labib M, Perazzo A, Manganaro JL, Tabani Y, Durham CJ, Schemehorn BR, McClure HC, Walsh LJ. Stain removal, abrasion and anticaries properties of a novel low abrasion dentifrice containing micro-fibrillated cellulose: in vitro assessments. J. Dent. 2024; 2024. Doi: 10.1016/j.jdent.2024.105038
29. Grabenstetter RJ, Broge RW, Jackson FL, Radike AW. The measurement of the abrasion of human teeth by dentifrice abrasives: a test utilizing radioactive teeth. J. Dent. Res. 1958; 37: 1060-1068.
30. Bull WH, Callender RM, Pugh BR, Wood GD. The abrasion and cleaning properties of dentifrices. Brit. Dent. J. 1968; 125: 331-337.
31. Joiner A, Pickles MJ, Matheson JT, Weader E, Noblet L, Huntington E. Whitening toothpastes: effects on tooth stain and enamel, Int. Dent. J. 2002; 52 (Suppl 5): 424-430.
32. Labib ME, Perazzo A, Manganaro J, Tabani Y, Milleman KR, Milleman JL, Walsh LJ. Clinical assessment of plaque removal using a novel dentifrice containing cellulose microfibrils. Dent. J. 2024; 12: 7.
High-performance sterilization- and drying system
5“ high-resolution colour touch display for intuitive navigation
3-fold flexible fresh water supply with integrated quality control
All in view and documented thanks to connection to the practice network
With Hygoclave 50, Dürr Dental and A-dec offers dental practices a professional Class B solution that combines impressive performance with a well thought-out operating concept – for maximum efficiency and exceptional user friendliness designed to cope effortlessly with tough day-to-day working environments. Available with a volume of 17 or 22 litres. More information under www.duerrdental.com
The dynamic impact of composite bonding on patients’ lives
By Cass Wyllie, BOHT (Newcastle)
Who says all teeth must bow to the porcelain throne?
Throughout my career, I’ve been a witness to the beauty of natural teeth being subjected to a lifetime of work through invasive smile transformations involving porcelain veneers and crowns. Often, patients have concerns about just one or two teeth, yet end up with a full porcelain grin from molar to molar. The common excuse is, “You won’t be able to achieve a perfect colour match if we only address the one or two teeth of concern”.
While porcelain definitely has its time and place, in more cases than not, you can achieve the same results without the detrimental effects that porcelain can have on your teeth. As an Oral Health Therapist, it is ingrained in us to preserve rather than restore. This constantly had me thinking about what I could offer that was minimally invasive, required no enamel reduction and was affordable so everyone could have the option to enhance their smiles. That’s when I discovered the world of composite bonding.
Composite bonding is a dental procedure where toothcoloured composite resin is applied to the teeth to repair damage and improve appearance. This method has had a dynamic impact on my patients’ lives. I’ve treated patients who otherwise might have been unable to afford porcelain, patients who didn’t want to subject their teeth to a lifetime commitment to porcelain, patients who had been told they needed orthodontic alignment to close gaps and patients with small chips or uneven edges. All of these patients shared one common outcome: Improved confidence that was always under the surface, just needing a helping hand to truly shine through.
I’ve been fortunate enough to treat patients for all these reasons through composite bonding in a way that requires no enamel reduction, is pain-free, quick, cost-effective and provides aesthetic results in one minimally invasive, toothfriendly package.
Transform your smile: Real-life success stories of composite bonding
In the following cases, composite is minimally applied, covering only the essential tooth surface to achieve the patient’s desired results. The photos demonstrate the seamless transition and colour match between the tooth and composite.
TCase study one: Chipped incisal edges
Background
he patient had undergone Invisalign treatment. After treatment, their chief concern was the chipped and uneven edges of teeth 11, 21 and 23.
Procedure
EMS biofilm discloser and complete prophylaxis using EMS Airflow, etch, Scotchbond, Mylar strip, 3M Filtek A1 body and flowable. Final polish with coarse, fine Softflex disc, and high polishing wheels.
The truth about maintenance
You might wonder if adding something to the tooth requires lifelong maintenance. The answer is yes and no. Maintenance does not differ from what most patients already do without composite bonding. This includes adequate at-home biofilm removal, attending regular check and clean appointments, maintaining at-home whitening and avoiding using your teeth as tools. All of this will keep the composite looking fresh up until
Case study two: Adding length to laterals and closing diastema
Background
The chief concern was that the patient felt their centrals appeared more pronounced and they wanted to close the gap and add length to the laterals.
Procedure
EMS biofilm discloser and complete prophylaxis using EMS Airflow, etch, Scotchbond, BioClear Matrices system, 3M Filtek A1 body and flowable composite.
Case study three: Wanting the orthodontic-free alternative
Background
The patient wanted to close the gaps between her teeth but did not want to go through orthodontics.
Procedure
ZOOM in-chair whitening, composite bonding procedure seven days after whitening to allow the reactive molecules within the tooth to dissipate. EMS biofilm discloser and complete prophylaxis using EMS Airflow, etch, Scotchbond, BioClear Matrices system, 3M Filtek A1 body and white flowable composite.
and likely beyond the expected shelf life. When it comes time for renewal, it’s easily removed with a tungsten carbide bur and can be redone or left as is.
So, the next time a patient walks through your door, please consider composite bonding as a potential front-runner in the treatment options.
To see more before and afters, you can follow me on my socials @thecompositecollective
The relevance of endotoxin in instrument reprocessing - An odyssey
By Emeritus Professor Laurence J. Walsh AO
Clinicians need to have a working knowledge of endotoxin in order to assess its impact on their clinic practice and ensure that the methods used for reprocessing instruments ensure positive clinical outcomes. Endotoxin (ET) is also known as lipopolysaccharide (LPS) and is composed of lipid A, the core polysaccharide and the O-antigen polysaccharide. This article provides an overview of the key issues to inform how risks from endotoxin are assessed.
The famous ancient epic Greek poem the Odyssey is a suitable model for the discussion since it captures the sense of journey and wandering. A relevant example of this wandering is endotoxin (ET) being displaced off the surface of surgical instruments and then causing local inflammation and in a worst-case scenario, adverse systemic effects such as fever.
Where ET comes from
ET is a fundamental component of the cell wall of Gram-negative bacteria.1 Because of the widespread presence of such bacteria in water, soil and other environments, there are well-developed mechanisms for tolerating ET in drinking water and on foods.2 The human body contains considerable amounts of ET within the gastrointestinal
tract because of the large load of both viable and non-viable Gram-negative bacteria found in the gut. This high local concentration of ET explains why the allowed limits for final rinsing of medical endoscopes in an automated endoscope reprocessor (AER) in ISO 15883 Part 4 and in AS 5369:2023 are set at 3 ng/mL (30 endotoxin units (EU)/mL). By way of context, this level is approximately 3-fold higher than the normal range found in reticulated water.
This raises the interesting issue of dental instruments that are being used for non-surgical procedures in the oral cavity, an environment where there are, like the gut, large numbers of Gram-negative bacteria and the ubiquitous presence of ET. This means that the level of ET on instruments is insignificant from an exposure perspective compared to ET already present in the mouth.
Endotoxins in the oral cavity
ET derived from oral bacteria is far more potent than its counterpart found on bacteria from the gut, even within the same genus of bacteria (e.g. Fusobacteria). One of my studies in the late 1980s documented this unusually high potency of ET from oral bacteria versus gut bacteria, in terms of the ability to stimulate the production of inflammatory cytokines such as interleukin-1.3
ET from oral bacteria plays a significant role in maintaining the chronicity of gingivitis insights where mature plaque biofilms are present. ET stimulates local immune cells and drives the expression of markers such as Class II major histocompatibility complex antigens and adhesion molecules, which increase the functionality of immune cells and stimulate their trafficking through the gingival tissues, respectively.4-7 ET is a major driver of local inflammatory responses to periodontal bacteria, especially when they have been killed, since this releases large amounts of ET into the local environment.8 Most individuals produce antibodies to the ET released by periodontal pathogens.9
Systemic effects of endotoxin
One of the largest concerns with ET is when it gains access to the systemic circulation. This can occur in certain med-
infection | CONTROL
ical procedures, as shown by case reports of ET on medical devices causing issues. Each of these medical contexts has significant differences from dental procedures:
• Joint (hip/knee) replacement surgeryvery large instruments and devices are used, which can carry large amounts on their surface. Prolonged procedure;
• Interventional cardiology proceduresdevices are located within the circulation;
• Renal dialysis - there is prolonged contact (over hours) with the circulation; and
• Cataract surgery - the extremely small volume of the anterior chamber of the eye and compromised local defences make inflammation very problematic.
animal models of inflammation.11,12 This is why, around the world, pharmaceutical manufacturers are required to produce medicines, sterile saline and sterile distilled water that have very low levels of ET (below 0.25 EU/mL) (Table 1).
Impact of ET on instrument surfaces
The classic paper on how much endotoxin dose is needed for specific adverse effects is a 2002 review by Anderson et al.13 It defines the “No Observed Effect Level” (NOEL), which is the threshold level below which ET
Table 1. Key reference standards for endotoxin
WHO Decontamination and reprocessing of medical devices for health-care facilities 2016.
Washer-disinfectors: ISO 15883-1:2018 for WDs - Water for the preparation of sterilization and disinfection products - Part 1: Quality of water. An ET limit of 0.25 EU/ mL in ISO 15883, for medical devices that are intended to come into contact with the bloodstream or other normally sterile areas of the body. Also found in the UK Health Technical Memorandum 01-01: Management and decontamination of surgical instruments (medical devices) used in acute care Part D: Washer-disinfectors.
Automated endoscope reprocessors: 30 EU/mL in in AS 5359:2023. Also in UK HTM 01-06 Part B.
Intravenous fluids (including medicines): 0.25 EU/mL. TGA Medical Device Standards Order (Endotoxin Requirements for Medical Devices) 2018. Also in the US, UK and other pharmacopeias for pharmaceutical requirements, and in the European Union Guidelines to Good Manufacturing Practice (EU Guidelines to GMP) 2021.
Final rinse water: 10 EU/mL in USA AAMI TIR 34:2014; Replaced in 2023 by ANSI/ AAMI ST108:2023 - Water for the Processing of Medical Devices. ANSI/AAMI ST108 is designed for all healthcare facilities in the United States, including hospitals, clinics, ambulatory surgery centers, endoscopy centers, and offsite reprocessing facilities.
Most stringent final rinsing water: 0.25 EU/mL (25 pg/mL) in AS 5359:2023.
Exposure to ET can also occur when patients receive intravenous medicines or intravenous biological agents and when they undergo treatments that are extra-corporeal, where blood is taken from the body and then returned to it (e.g. extracorporeal photochemotherapy and harvesting haematopoietic stem cells for transplantation.10 Likewise, it is a major issue with recombinant cytokines and biological agents. Many of these are prepared using coliform bacteria such as E. coli and so considerable effort must be put into removing ET contaminants. I had to deal with similar issues when I was isolating and purifying cytokine antagonists and using these for intravenous therapy in
elicits no adverse health effects, such as fever. The NOEL concept has been used widely in ET research and informs national requirements, such as the 2018 TGA Medical Device Standards Order (Endotoxin Requirements for Medical Devices).14 This sets the exposure limit at 2 ng per device, or for fluids, at 0.25 EU/mL. An amount of 2 ng per person in contact with the bloodstream will cause fever. This limit of 2 ng per device is also the limit used in the USA by the Center for Devices and Radiological Health (CDRH) for products that directly or indirectly contact the cardiovascular system and lymphatic system (Table 1).15
infection | CONTROL
The US Centers for Disease Control and Prevention (CDC) Guideline for Disinfection and Sterilization in Healthcare Facilities 2008, which was last updated in 2019, makes the point that “Users of ultrasonic cleaners should be aware that the cleaning fluid could result in endotoxin contamination of surgical instruments, which could cause severe inflammatory reactions”.
In Appendix A.7.2.3.1 of AS 5369:2023, a risk-based approach has been taken in terms of the maximum endotoxin levels for final rinse water that are given in Table 7.2 for surgical instruments that are used in sterile body cavities. This was designed to cover the highest possible medical settings where the risks of ET contamination are wellknown, namely orthopaedic surgery, interventional cardiology, renal dialysis, ophthalmic surgery and so on. These same informative appendix also discuss how for untreated reticulated tap water the facility should undertake risk assessment on the issue of water quality. That same risk assessment should also guide decisions around the frequency of monitoring of ET levels in water.
A key point in this informative appendix is that the standard discusses how a particular clinic should conduct a risk assessment to determine whether tap water as supplied is of suitable quality, based on the findings of the local risk assessment. When undertaking that risk assessment, each clinic must consider that the context of the threshold level given in Table 7.2 refers to instruments that are used in sterile body cavities and is based on high-risk medical settings. The mouth is not a sterile body cavity and the standard does not give any advice regarding rinse water for nonsurgical instruments that would be used in dental practice. It is also important to note that surgical instruments used in dentistry are not dosing endotoxin continuously into a patient’s circulation over prolonged periods of time.
Practical considerations
F or items that have been through the ultrasonic cleaner, thorough rinsing with tap water is required to remove traces of the ultrasonic cleaning fluid, prior to a brief final rinse. For surgical instruments, the purpose of that brief final rinse is to ensure that the traces of water
that remain on the item are relatively free of contaminants, such as ET and viable bacteria. Hence, as those instruments then dry off before being packaged, as the water evaporates very little, ET dries onto the instrument surfaces. Any ET which remains on the surface will remain biologically active after normal steam sterilisation, because of the heat resistant nature of ET.
For the length of final rinsing (which will be in seconds), the first place to go is
Some clinics that do large amounts of implant placement, sinus lifts, third molar removal and other invasive surgical procedures where bone is accessed and mucoperiosteal flaps are raised have tackled the issue of ET in rinse water by performing the final rinse using water from a reverse osmosis (RO) system. As an example, a typical small RO system is the Melag MELAdem 47. This produces around 3-5 litres of treated water (permeate) per hour. This rate varies because
Table 2. Endotoxin exposure limits
In fluids (e.g. medicines, saline) given intravenously...
• 2 ng (20 EU) per adult intravenously (20 EU)
• 25 pg/mL (0.25 EU/mL) for infusions
• 0.5 ng (5 EU) per kg of body weight per hour or 10 ng (100 EU) per m2 of body surface area per hour
Ingested from water or food...
• Greater than 500-4500 mg/kg body weight
Implantable medical devices...
• 2 ng (20 EU) per device
On instruments...
• 2 ng (20 EU) per device
Intraperitoneal administration...
• Lethal dose (LD50) is 27 mg/kg body weight
Inhaled...
• 500 ng per exposure (e.g. during a shower)
• 1 ng/m3 of air for gradual onset of fever
• 9 ng/m3 of air for rapid onset asthmatic effects
Based on refs 13, 16 and 17
always the manufacturer’s instructions. It will vary depending on the complexity, size and shape of the item and whether or not items are in cassettes, etc.
The volume of rinse water that remains on dental instruments is very small due to the small size of the instruments. Careful measurements reveal that 50-150 microlitres is the applicable range. At typical tap water ET levels, on a single instrument, this would not give the threshold amount to meet the NOEL threshold (2 ng per instrument) (Table 2). This is why local risk assessments need to consider factors that modulate the risk, such as the number of instruments used in sterile sites and the duration of surgical procedures.
of 1) the local mains water pressure - which must be 2-6 bars; 2) the water temperature – (less output when the climate is very cold); and 3) the life of the mixed-bed resin cartridge and other cartridges. It has a maximum storage of 10.5 litres of treated water (permeate) in a pressurised tank. The RO process runs until the pressure tank is full and then it shuts off. This system has a production efficiency of 20-25%, so for each 1 litre of permeate produced, around 4 litres of waste water will be sent down the drain. The RO system pressure tank then connects to steam sterilisers and to an outlet tap via 6 mm hoses. In this case, the water outlet pressure is 4 bar, which is more than sufficient for the short final rinse.
A further key point is that surgical cutting instruments which are reused will pose the greatest risk. Bone cutting burs can be identified as posing a particularly high risk of transferring material. Using single use burs eliminates the possibility of such transfer events occurring, whilst at the same time ensuring optimal cutting performance and minimal thermal injury to the bone. A similar logic can be applied to situations such as pulpotomy, where there are methods that involve
“Surgical cutting instruments which are reused will pose the greatest risk. Bone cutting burs can be identified as posing a particularly high risk of transferring material. Using single use burs eliminates the possibility of such transfer events occurring, whilst at the same time ensuring optimal cutting performance and minimal thermal injury to the bone. A similar logic can be applied to situations such as pulpotomy, where there are methods that involve single use burs and single use laser tips...”
single use burs and single use laser tips. Alternatively, multi-use implant burs and other higher risk items could have their final rinse undertaken with purchased sterile water.
Measuring levels of ET in water
The Limulus Amebocyte Lysate (LAL) assay is the most widely used technology for measuring ET in water. The assay involves an enzyme cascade that is triggered in response to endotoxin. Different versions of the LAL assay exist, including the traditional gel clot form as well as assays where the readout is based
infection | CONTROL
on turbidity or colour change. There are also alternative methods or variants of the LAL testing technology that use recombinant proteins in bio assays, as well as technologies for electrochemical measurement. There are also miniaturised versions of the test technology which suit on-site measurement using handheld devices, with a read-out time of around 15 minutes. The most widely used device of this type is the Endosafe® nexgen-PTS™ , which is a hand-held spectrophotometer
were typically 10 to 12.5 ng/mL (100 to 125 EU/mL). In Australian studies conducted by Dr Joanne O’Toole from the Monash University School of Public Health and Preventive Medicine and the Cooperative Research Centre for Water Quality and Treatment, similar levels were reported, up to 12 ng/mL (120 EU/mL).
Based on these results, a typical level of 10 ng/mL could be expected in most parts of Australia.
with specialised single use cartridges into which the sample is introduced for on-site measurement. AS 5369:2023 discusses commercial laboratory testing of water samples and mentions that such laboratories would be accredited, e.g. by the National Association of Testing Authorities (NATA) and/or to meet international standards for testing laboratories, namely AS ISO/IEC 17025.
Natural variations
Reported levels of ET in municipal tap water vary by season and by location. For the USA east coast, tap water ET levels in the Anderson et al. review, 13
A cold water tap has a typical flow rate of 100 mL/second, which means that approximately 1000 ng per second of ET would be delivered. A single visible water drop is 5 microliters (1/200th of a milliliter). At an ET concentration of 10 ng/mL, one visible water drop of 5 microliters will contain 0.05 ng of ET (50 pg). Since the endotoxin threshold per item is 2 ng (2000 pg), a total of 40 visible water drops containing 10 ng/ mL (100 EU/mL) would be needed to dry onto the surface of one item to leave 2 ng behind. As already mentioned, that will not be readily achievable with dental instruments because of their small size and small surface area.
infection | CONTROL
This explains why, to date, there are no reports in the literature of dental instruments being responsible for systemic ET exposures causing fevers and other adverse systemic outcomes.
Levels of ET in municipal water supply can vary due to water system factors (e.g. water trunk line repairs and other maintenance work carried out on water supply infrastructure), seasons and climatic variations (which changes the use of desalination and water recycling) and major adverse weather events (cyclones and floods). One can now consider that when the ET level rises, the number of drops of water needed to transfer 2 ng of ET onto a given instrument reduces. For example, at 50 ng/mL (500 EU/mL), only 8 drops will suffice, while at 100 ng/mL (1000 EU/mL), only 4 drops will suffice. This highlights how the potential risk of ET on surgical instruments can increase dramatically when the quality of the municipal water is compromised and when many instruments are used to enter sterile sites. In settings such as immediately after a cyclone or flood, when a “boil water” alert is issued by the local government, this will mean higher than expected levels of coliforms (such as E. coli) and other Gramnegative bacteria and also ET, since it is derived from Gram-negative bacteria. In this situation, when a dental clinic re-opens during a “boil water alert”, using small volumes of sterile water (not sterile saline, which contains ions) for final rinsing would be prudent. Likewise, mobile dental services should consider stocking supplies of sterile water during times of the year when floods can be expected to occur.
The LAL assay has an intrinsic method variability of factor 2. Sample properties (e.g. protein concentration, pH, etc.) may cause inhibition or enhancement of the LAL assay, which impacts the limit of quantification (LOQ) achievable for that specific sample. Given this and the need to identify suitable ET action limits, in the pharmaceutical industry, this action limit has been set as 6 times the threshold. For example, at a threshold of 0.25 EU/ mL, the action limit would be 1.5 EU/mL. If a water test shows levels at or above that, the clinic would consider issues such as whether there was proper sample collection and storage and if the analysis checked for interfering and enhancing substances in the sample (including those released from the sample containers).
Conclusions
Following this risk-based approach is fundamental to managing the risk that is posed for the surfaces of instruments that have been contaminated with ET coming into contact with bone or soft tissue during surgical procedures. Each clinic needs to conduct their own risk assessment regarding the suitability of water for final rinsing. This needs to
consider the types of procedures that the clinic is undertaking. Where a clinic has introduced a water treatment system to improve the quality of final rinse water, it is essential that staff are aware of the maintenance requirements for that system, since there will inevitably be requirements for servicing and replacement of particular components such as cartridges depending on the extent of use and the quality of the feedwater that is entering the system.
2. Ziegler-Heitbrock HW. Molecular mechanism in tolerance to lipopolysaccharide. J Inflamm. 1995;45(1):13-26.
3. Walsh LJ, Stritzel F, Yamazaki K, Bird PS, Gemmell E, Seymour GJ. Interleukin-1 and interleukin-1 inhibitor production by human adherent cells stimulated with periodontopathic bacteria. Arch Oral Biol. 1989;34(9):679-83.
4. Walsh LJ, Seymour GJ, Bird PS, Powell RN. Modulation of HLA-DR antigens in the gingival epithelium in vitro by heat-killed Fusobacterium nucleatum and E. coli lipopolysaccharide. J Oral Pathol. 1985;14(10):833-43.
5. Walsh LJ, Seymour GJ, Powell RN. Differential expression of Class II (DR & DQ) antigens by human gingival Langerhans’ cells and keratinocytes in vitro. J Oral Pathol. 1987;16(1):27-30.
6. Walsh LJ, Seymour GJ, Powell RN. The regulation of Langerhans cell T6, DR and DQ antigen expression: an hypothesis. J Oral Pathol. 1988;17(1):43-6.
7. Gemmell E, Walsh LJ, Savage NW, Seymour GJ. Adhesion molecule expression in chronic inflammatory periodontal disease tissue. J Period Res. 1993;29:46-53.
8. Gemmell E, Bird PS, Bowman J, Xu LJ, Polak B, Walsh LJ, Seymour GJ. Immunohistological study of lesions induced by Porphyromonas gingivalis in a murine model. Oral Microbiol Immunol. 1997; 12:288-297.
9. Pietrzak ER, Polak B, Walsh LJ, Savage NW, Seymour GJ. Characterization of serum antibodies to Porphyromonas gingivalis in individuals with and without periodontitis. Oral Microbiol Immunol. 1998;13:65-75.
10. Vowels BR, Cassin M, Boufal MH, Walsh LJ, Rook AH. Extracorporeal photophoresis induces the production of tumor necrosis factor-alpha: implications for the treatment of cutaneous T cell lymphoma and systemic sclerosis. J Invest Derm. 1992;98:686-692.
11. Walsh LJ, Lander PE, Seymour GJ, Powell RN. Isolation and purification of ILS, an Interleukin-1 inhibitor produced by human gingival epithelial cells. Clin Exp Immunol. 1987;68:366-374.
12. Walsh LJ, Au TW, Seymour GJ. Inhibition of the induction of contact hypersensitivity by an epithelial cell-derived Interleukin-1 inhibitor. Aust J Dermatol. 1989;30;48-52.
13. Anderson WB, Slawson RM, Mayfield CI. A review of drinking-water-associated endotoxin, including potential routes of human exposure. Canad J Microbiol. 2002; 48(7):567-587.
14. Medical Device Standards Order (Endotoxin Requirements for Medical Devices) 2018. URL https://www.legislation.gov.au/F2018L01280/ latest/text
15. US FDA Guidance for Industry: Pyrogen and Endotoxins Testing: Questions and Answers. URL https://www.fda.gov/regulatory-information/ search-fda-guidance-documents/guidance-industrypyrogen-and-endotoxins-testing-questionsand-answers
16. Elin RJ, Wolff SM, McAdam KPWJ, Chedid L, Audibert F, Bernard C, Oberling F. Properties of reference Eschericia coli endotoxin and its phthalylated derivative in humans. J lnfect Dis. 1981;144(4): 329-336.
17. Suffredini AF, Fromm RE, Parker MM, Brenner M, Kovacs JA, Wesley RA, Parrillo JE. The cardiovascular response of normal humans to the administration of endotoxin. New Engl J Med. 1989;321(5):280-287.
About the author
Emeritus Professor Laurence J. Walsh AO is a specialist in special needs dentistry who is based in Brisbane, where he served for 36 years on the academic staff of the University of Queensland School of Dentistry, including 21 years as Professor of Dental Science and 10 years as the Head of School. Since retiring in December 2020, Laurie has remained active in hands-on bench research work, as well as in supervising over 15 research students at UQ who work in advanced technologies and biomaterials and in clinical microbiology. Laurie has served as Chief Examiner in Microbiology for the RACDS for 21 years and as the Editor of the ADA Infection Control Guidelines for 12 years. His published research work includes over 400 journal papers, with a citation count of over 20,000 citations in the literature. Laurie holds patents in 8 families of dental technologies. He is currently ranked in the top 0.25% of world scientists. Laurie was made an Officer of the Order of Australia in January 2018 and a life member of ADAQ in 2020 in recognition of his contributions to dentistry.
Images courtesy of Prof Dr Marco Aurélio Chaves da Silva (BRAZIL)