
OP 3D™ LX
next generation of cone beam technology
Vol. 35 No. 1 JANUARY/FEBRUARY 2024 $99.00 p.a.
Australasian DEN
The
Powered by
DEN TAL PRACTICE
TAL PRACTICE THE BUSINESS MAGAZINE FOR DENTISTS
dentevents presents...

SYDNEY 24-25 MAY 2024
NOVOTEL SYDNEY BRIGHTON BEACH
TWO DAYS OF LECTURES AND WORKSHOPS ON DIGITAL DENTISTRY FOR DENTISTS, SPECIALISTS, DENTAL TECHNICIANS AND DENTAL PROSTHETISTS
TWO DAYS OF LECTURES AND WORKSHOPS ON DIGITAL DENTISTRY FOR DENTISTS, SPECIALISTS, DENTAL TECHNICIANS AND DENTAL PROSTHETISTS
TWO DAYS OF LECTURES AND WORKSHOPS ON DIGITAL DENTISTRY FOR DENTISTS, SPECIALISTS, DENTAL TECHNICIANS AND DENTAL PROSTHETISTS
TWO DAYS OF LECTURES AND WORKSHOPS ON DIGITAL DENTISTRY FOR DENTISTS, SPECIALISTS, DENTAL AND DENTAL
REGISTER NOW and SAVE!
SPONSORS

INDUSTRY SUPPORTERS









Digital Dentistry & Dental Technology
The new face of digital dentistr y

Join us again or for the first time at Digital Dentistry & Dental Technology No 5 for a fun, exciting and fully immersive learning experience with the best of the best in the new age of dentistry. This year’s program will again cover Digital Smile Design
• Digital orthodontics
• Intraoral scanning
• 3D Facial Scanning
• Digital implantology
• Digital full arch restorations and full mouth rehabilitations
• Digital Dentures
• 3D Printing
• Milling
• CBCT
• Materials and applications
• Software and more with MORE Hands-on Sessions
• MORE Advanced Sessions
REGISTRATION FEES
$880 inc gst
EARLY BIRD PRICING
$550 before 24 Mar 2024
price increases $110 on the 2nd of every Month INCLUSIONS
Registration fee includes participation in TWO full days of education (12 CPD hours), all catering and Friday drinks.
Multiple lectures and workshops are being run concurrently to allow you to build your own program to suit your specific interests. Price is all inclusive.
PROGRAMME DETAILS
FRIDAY 24 MAY 2024
9.00aM - 5.00pM - education
5.00pM - 7.00pM - happy hour
SATURDAY 25 MAY 2024
9.00aM - 5.00pM - education
Check the website for details of discounted accommodation rates for the conference • Ample parking available at
12 HOURS CPD
12 HOURS CPD
Best Digital Dentistry Event TWO DAYS • 6 CONCURRENT EDUCATION STREAMS 40+ TOP
• 90+ EDUCATION SESSIONS THE BEST OF THE BEST IN DIGITAL DENTISTRY Full details of the
and presentations online www.dentaltechnology.com.au Organised by Dentevents™ a division of Main Street Publishing Pty Ltd ABN 74 065 490 655 www.dentevents.com • info@dentist.com.au • Tel: (02) 9929 1900 • Fax: (02) 9929 1999 REGISTRATION
EARLY
price
INCLUSIONS Registration
Check
•
PROGRAMME
FRIDAY
9.00
5.00
SATURDAY
9.00
2024’s
SPEAKERS
speakers
FEES $880 inc gst
BIRD PRICING $440 before 24 Jan 2024
increases $110 on the 2nd of every month
fee includes participation in TWO full days of education (12 CPD hours), all catering and Friday drinks. Multiple lectures and workshops are being run concurrently to allow you to build your own program to suit your specific interests. Price is all inclusive. VENUE DETAILS Novotel Sydney Brighton Beach - The Grand Parade, Brighton-Le-Sands NSW 2216 - Close to Sydney Domestic and International Airports
the website for details of discounted accommodation rates for the conference
Ample parking available at the hotel
DETAILS
24 MAY 2024
am - 5.00pm - education
pm - 7.00pm - happy hour
25 MAY 2024
am - 5.00pm - education
details
online www.dentaltechnology.com.au Organised
Dentevents™ a division of Main Street Publishing Pty Ltd ABN 74 065 490 655 www.dentevents.com • info@dentist.com.au • Tel: (02) 9929 1900 • Fax: (02) 9929 1999
• MORE New Products • NEW Masterclasses... and more! ONLY $440 FOR 2 DAYS OF EDUCATION (12 HOURS OF CPD) IF YOU REGISTER BEFORE Full
of the speakers and presentations
by
-
NSW 2216 - Close to Sydney Domestic and International
VENUE DETAILS Novotel Sydney Brighton Beach
The Grand Parade, Brighton-Le-Sands
Airports
the hotel











January/February 2024 Australasian Dental Practice 5 contents | REGULARS 8 briefs 10 one man’s opinion 12 mouth wide shut 16 spectrum 58 CPD centre 60 abstracts 62 the cutting edge 146 new products VOLUME 35 | NUMBER 1 JANUARY/FEBRUARY 2024 On the cover... Built on OP 3D technology, the brand new OP 3D LX imaging platform expands your 3D diagnostic capabilities with a wide range of clinical applications that support your evolving practice and enhance diagnostic confidence. Publisher & Editor: Joseph Allbeury Clinical Editor: Dr David Roessler Technology Editor: Prof. Laurence J. Walsh Infection Control Editor: Prof. Laurence J. Walsh Senior Contributing Editor: Dr Christopher CK Ho Columnists: Dr Georges Fast, Dr Jesse Green, Garry Pammer, Phillip Win, Dr David Moffet, Graham Middleton, Simon Palmer, Julie Parker, Jayne Bandy, Angus Pryor Design & Production: Jasper Communications Australasian Dental Practice™ ISSN 1445-5269 is printed in Australia and published six times per year by Main Street Publishing Pty Limited ABN 74 065 490 655 PO Box 586, Cammeray NSW 2062 Tel: (02) 9929-1900 Fax: (02) 9929-1999 Email: info@dentist.com.au © 2024 All rights reserved. The contents of this magazine are copyright and must not be reproduced without the written permission of the publisher. Permission to reprint may be obtained upon application. Correspondence and manuscripts for publication are welcome. Although all care is taken, the editor and publisher will not accept responsibility for the opinions expressed by contributors to this magazine, or for loss or damage to material submitted for publication Subscriptions: Australia and NZ: A$99.00 per year includes OralHygiene™ and eLABORATE™ magazines; Overseas Airmail: A$220.00 per year. www.dentalpractice.com.au facebook.com/dentalpracticenow twitter.com/adpmagazine instagram.com/dentevents READ ME FOR CPD management 66 Buying and selling dental practices and practice valuations! 70 Drilling down to the root cause: How to identify and solve the real problems in your dental practice 72 Practice purchase deposit FAQs 74 The best time to contact your patient marketing 76 Emails your patients will love: How to craft irresistible messages finance 80 The FIRE method for retirement




FIRST CLASS IN EFFECTIVENESS AND TASTE
• Effective – quick desensitisation and fluoride release (5 % NaF ≙ 22,600 ppm)
• Excellent handling – moisture tolerant
• Aesthetic – tooth-shaded varnish
• Universal – available in tube version, SingleDose and cartridge
• Variety of flavours – mint, caramel, melon, cherry, bubble gum, cola lime and pina colada
Contact your VOCO Dental Consultant:
VIC + TAS: Peter Kenda, Tel. 0409 390 194 | QLD: David Reyno, Tel. 0401 747 037 | NSW (North): Katrina Johnston, Tel. 0434 491 399 | NSW (South) & ACT: Buddy Ishak, Tel. 0438 065 400 | WA + SA + NT: Ronald Bangma, Tel. 0419 823 325






• B U M • • CHE Y • VOCO
® Varnish VOCO GmbH · Anton-Flettner-Straße 1-3 · 27472 Cuxhaven · Germany · Freecall 00 800 44 444 555 · www.voco.dental
Profluorid


January/February 2024 Australasian Dental Practice 7 | VOLUME 35 | NUMBER 1 JANUARY/FEBRUARY 2024 194 Smart autoclave for fast, dependable sterilisation 198 A-dec sets standard in infection control 100 Designing an efficient sterilisation room: A guide 104 Preventing needle stick injury surgery design 140 Art deco style at Spa Dental 140 84 100 READ ME FOR CPD READ ME FOR CPD clinical excellence 110 Taking on the challenge with attention to detail 120 Block selection for monolithic CAD/CAM restorations - Part 2 126 Pigeon pair: Shining 3D Wireless IOS and MetiSmile Facial Scanner 134 Biodentine™ in the treatment of Molar Incisor Hypomineralisation (MIH) in paediatric dentistry: A case report READ ME FOR CPD 126
 By Joseph Allbeury
By Joseph Allbeury
Multiple choice...
As the new year kicks off, already there are over 350 events listed on dentevents.com with more being added every day. The dental profession is once again spoiled for choice when it comes to getting educated! There are so many opportunities to upskill with everything from face-to-face bespoke hands-on workshops, to lectures to major congresses and exhibitions... so don’t miss this out!
And we’ve been busy too.
After kicking off 2024 with our 3D Printing in Dentistry event, we’re now working hard to finalise our major event for the year, Digital Dentistry & Dental Technology 2024 The 5th edition of DDDT in Sydney will again showcase the talents of our best and brightest clinicians and technicians who work with the latest digital techniques and technologies on a daily basis. The change to digital is unrelenting and this event is the place to connect with the right people and take a giant leap forward in your knowledge and understanding. DDDT24 will encompass 3D printing, intraoral scanning, 3D facial scanning, milling, CAD and CAM software, materials, smile design, digital dentures, implantology, CBCT, restorative, aligners, orthodontics and more. The multi-stream two-day event gives you complete freedom to create a programme that precisely meets your educational requirements. More at www.dentaltechnology.com.au
Leading up to that and if you’re after some tax deductibility to attach to the April school holidays - in New South Wales, ACT, South Australia and Tasmania at least - then look no further than IDEM Singapore 2024 on April 19-21. As a travel hub, there are now plenty of flights at very reasonable prices on offer to Singapore, including from Qantas and also from Singapore Airlines, the official partner airline for the event. When visiting Singapore with kids, you’re completely spoiled for choice when it comes to world class accommodation at reasonable prices, amazing dining experiences ranging from a few dollars at an outdoor market to fine dining... And then there is so much to doUniversal Studios, Sentosa Island, water parks, the Night Safari zoo, botanical gardens and more... plus Legoland and the Bintan Island resorts are only an hour away by car to Malaysia and ferry to Indonesia respectively. Plus, get excited at about the stellar educational line-up and expansive trade exhibition at www.idem-singapore.com.
Rounding off the first half of the year, we have Laurie Walsh presenting a must-attend Infection Control Update 2024 that details all of the recent changes since the adoption of the new AS:5369:2023 Reprocessing of reusable medical devices and other devices in health and nonhealth related facilities published in December 2023. Register at www.icupdate.au
Enjoy the edition...
Joseph Allbeury, Editor and Publisher
Diego Gabathuler new CEO of Geistlich

Geistlich Pharma AG has appointed Diego Gabathuler as its new CEO. As a proven leader, he brings many years of experience in the MedTech industry and will continue to drive the company’s expansion strategy in regenerative medicine. Mr Gabathuler succeeds Ralf Halbach, who departed the company in August 2023. Mr Gabathuler is a 49-year-old Swiss National who brings a broad range of experience from various management positions as well as extensive knowledge in business development and strategic marketing. Most recently, he was CEO of Ivoclar. He has expertise in the MedTech sector, excellent leadership qualities and a proven strategic acumen. His professional career also includes management positions at international digital-tech companies such as Logitech, Activision and Electronic Arts. Andreas Geistlich, Chairman of the Board of Directors, who held the CEO position on an interim basis, said “The Geistlich strategic plan includes further investment in new products, solutions and technologies in order to apply regenerative medicine in helping even more people around the world. We are convinced that Diego Gabathuler’s expertise will support us significantly in this mission.” Geistlich wishes Diego a successful start and they look forward to working with him to further advance the future of regenerative medicine. Geistlich is a global leader dedicated to advancing regenerative medicine. It has been the world market leader in the field of regenerative dentistry for many years. In addition, Geistlich is committed to providing comprehensive support to clinicians in the field of regenerative medicine through scientific research, innovative developments as well as educational programs. Geistlich is a Swiss family-owned company with a tradition since 1851. With 13 subsidiaries and 60 distributors, the company reaches around 90 markets and employs over 800 people.

8 Australasian Dental Practice January/February 2024
briefs | NEWS

 By Georges Fast
By Georges Fast
TOne man’s opinion...
“I for one cannot wait to see what additional regulatory burdens will be imposed on our profession by the release of the new standard and how many more patients will be forced into having to decide between having no dental treatment or seeking treatment offshore...”
om Peters, the author of such management classics as In Search of Excellence, A Passion for Excellence, Thriving in Chaos, etc, when speaking in Melbourne quite a number of years ago, related a story going back to World War II. It involved a USAF General who thought of mounting a radar on the side of an Air Force bomber. He got a plane out of the fleet, told the mechanics to “cut a hole here”, mount the radar through the hole and “see if it works” - it did! It was the start of “side mounted” radars on aeroplanes.
As the volume of scientific knowledge grew over the past 200 years, starting with the Industrial Revolution, one can argue that the major leaps occurred in the early years, before risk management became the dominant issue and when adverse outcomes didn’t result in monetary gains for those affected by them. A whole new industry has grown out of the combination of so-called risk assessment experts and “ambulance chasing” lawyers on the one side with publicly funded regulators on the other. This ensures that any progress occurs at a glacial pace.
Our profession is afflicted by an ever-increasing burden of regulations and requirements, often addressing potential issues that have never been shown to have caused a problem in the real clinical world and yet these regulations must be adhered to. Everyday dental practice involves treating mostly healthy individuals whose mouths already harbour considerable bacterial loads and yet we are required to apply protocols that in most cases are more onerous than those which apply in emergency rooms in public hospitals. Apparently, if our patient drinks water from a tap it is safe to do so, but if that same water is used to cool an air rotor bur, it becomes dangerous.
I for one cannot wait to see what additional regulatory burdens will be imposed on our profession by the release of the new standard and how many more patients will be forced into having to decide between having no dental treatment or seeking treatment offshore.
Having been involved with various committees over the past 40 years where I sometimes had to bite my tongue and not make public my misgivings, I am now just a “civilian” and free to do so. One of the recent committees that I served on was asked to produce material to discourage patients from seeking treatment offshore.
However, more than 50 years in practice has taught me that the standard of dental treatment is more dependent on the competency and commitment to quality of the individual dentist than it is on their country of origin. I have witnessed very high standards of restorative dentistry come from so-called third world countries and at the same time, seen diabolical treatment from countries with a high reputation for excellence in dentistry and that includes ours!
“I derive no pleasure from having made a prediction many years ago that if we kept increasing the regulatory burden on private practices without a proper cost/benefit analysis, we would price high quality dental treatment out of the reach of the general public. That’s where we are at. A valid comparison to our situation would be a driver who starts a car, places it in gear, stands on the brake and floors the accelerator.
Something
has got to give!”
I recently read that one should laser-etch - but not engrave - instruments because the scratches on the handle of a probe or Ward’s carver or mirror handle could harbour bacteria that could hide from our autoclaves. It clearly escaped the authors’ consciousness that most dentists use non-sterile gloves to carry out the bulk of dental procedures.
I derive no pleasure from having made a prediction many years ago that if we kept increasing the regulatory burden on private practices without a proper cost/benefit analysis, we would price high quality dental treatment out of the reach of the general public. That’s where we are at. A valid comparison to our situation would be a driver who starts a car, places it in gear, stands on the brake and floors the accelerator. Something has got to give!
To survive as an independent profession and to maintain some control over our working lives will require a 180-degree shift in direction from where we are being led. We don’t need a corporate structure with outside directors and articulation with other non-value-adding bodies and all the costs that this imposes on us. We can make up our own jargon and issue meaningless certificates on nicely embossed paper if people want or need to feel important. If our leaders want to gain extra corporate qualifications, then it should be their responsibility to fund this. The “frog in boiling water” analogy has never been more accurate than when used to describe our current situation.
Time to jump!
10 Australasian Dental Practice January/February 2024 spectrum | NEWS
ABSORBABLE SUTURES
MONOFAST
SYNTHETIC MONOFILAMENT SUTURES MADE FROM A COPOLYMER OF POLYGLYCOLIC ACID AND POLYCAPROLACTONE (PGCL).
NON-ABSORBABLE SUTURES
PROFIMED PTFE
SYNTHETIC MONOFILAMENT SUTURES MADE FROM POLYTETRAFLUOROETHYLENE (PTFE) POLYMER.
For more details please contact our friendly customer service on 1800 776 326 or your local Distributed by Trusted by Surgeons Worldwide
surgical sutures
 By David Moffet
By David Moffet
TIs this how they talk to everybody?...
“During my life as a dentist, there were a couple of life-changing moments where I took an incoming phone call... And if I’d never done those things, if I’d never have spoken to those people AT THOSE TIMES, my life would have certainly been worse for missing out on those opportunities...”
uesday, December 19th
Last month I phoned a dental practice to speak to the lady owner and a male voice answered the phone.
The male did not identify himself clearly, so I began by introducing myself by name and asking if the lady owner [let’s call her Dr Jones] was in the practice on this day [that I was phoning on]?
The male who answered the phone, replied to my question [with a very loud and aggressive tone]:
“What’s this about?”
Guess what?
That wasn’t the answer to the question I asked.
In fact, it was nowhere near the two most common answers I receive when I phone dental practices and ask about the owners.
Those common answers that I normally receive are: “She is, but she’s with a patient at the moment.”
Or... “I’m sorry, Dr Jones isn’t in today.”
So I replied politely, to the man with the hostile tone: “Will she be in tomorrow?”
To which the male voice replied aggressively: “She won’t be in until Sunday! What’s this about?”
I replied politely:
“That’s OK. I’ll phone back on Sunday.”
Well actually, that was a lie.
I really just wanted to end this call as quickly as possible because I had decided already that my life was too short to ever want to speak to this person ever again, nor to speak to anyone who employed someone who behaved this rudely.
Period.
But he persisted, rudely and aggressively:
“I can get her to call you back.”
I replied:
“I’m sorry. I missed your name earlier... What was your name please?”
He told me his name was Graham* [not his real name].
I replied:
“Graham, did my number come up on your phone?”
Graham replied:
“I’m out the back on a cordless. It may have come up on the reception desk set.”
I replied, curiously:
“Graham, do you have a pen and paper handy?”
Graham answered:
“No, I’m eating my lunch.”
I replied:
“That’s OK Graham. I’ll call Dr Jones back on Sunday.”
Another lie from me... I’m never phoning Dr Jones’s practice ever again!
And we ended the call there.
What was wrong with this call?
Firstly, for all dental practices, if you’re going to answer the phone while eating your lunch, or while away from your front desk, the caller doesn’t need to know this.
All the caller needs to know is that you can PROFESSIONALLY and empathetically solve their problem and give them a solution they are looking forward to.
All Graham did was tell me that the practice was understaffed to take phone calls and that the practice had no systems or protocols in place to disguise the facts that staff who were on a lunch break were being forced to answer the phone at the same time.
What Graham should have said [to any caller] is:
“Excuse me [name of caller], do you mind if I place you on hold for 15 seconds?”
And then walked to the reception desk where a computer and a notepad were handy and resumed the call.
“All the caller needs to know is that you can PROFESSIONALLY and empathetically solve their problem and give them a solution they are looking forward to... All Graham did was tell me that the practice was understaffed and had no systems or protocols in place to disguise the facts that staff who were on a lunch break were being forced to answer the phone at the same time...”
No caller to a dental practice is going to give your team member a medal when the team member tells them:
“I’m just out the back.”
There is absolutely no point in saying this. Callers don’t care.
Secondly, the role of a receptionist is to take messages and pass them along. It is not their role to decide whether the reason for the phone call is something that they think they can play judge, jury and executioner on and decide themselves whether the dentist should hear about the phone call or not.
When I was a dentist, there were a lot of times when I was treating patients that it was impossible for me to take phone calls.
All I needed to know was who called me [Name], what were their contact details [usually phone number] and when was the best time for me to return their call.
Phoning the caller back and finding out the reason for their call, well those duties were mine and mine alone. 88
12 Australasian Dental Practice January/February 2024
spectrum | NEWS
INTRODUCING THE AORALSCAN


INTRODUCING THE AORALSCAN L
AUSTRALIA’S MOST AFFORDABLE AND DOCTOR-FRIENDLY INTRAORAL SCANNER
AUSTRALIA’S MOST AFFORDABLE AND DOCTOR-FRIENDLY INTRAORAL SCANNER

Full-colour scanning, orthodontic simulator and unlimited cloud storage
$

11,990 Full-colour scanning, orthodontic simulator and unlimited cloud storage
$
11,990+GST



Price excludes a PC––we’ll assist you in finding a reliable PC or check your existing PC for compatibility
Price excludes a PC––we’ll assist you in finding a reliable PC or check your existing PC for compatibility

GO DIGITAL WITH OSSEO GROUP AND SHINING 3D
GO DIGITAL WITH OSSEO GROUP AND SHINING 3D
Osseo Group is dedicated to offering comprehensive digital dental solutions, covering every step from scanning and designing to printing or milling the final restoration. We prioritise delivering top-notch technical service and support to ensure our customers receive the best possible assistance throughout the entire process.
Osseo Group is dedicated to offering comprehensive digital dental solutions, covering every step from scanning and designing to printing or milling the final restoration. We prioritise delivering top-notch technical service and support to ensure our customers receive the best possible assistance throughout the entire process. SCAN THE QR TO LEARN
SCAN THE QR TO LEARN
IN-CLINIC DEMO
MORE AND BOOK AN
L
2024 Inter Osseo Group Systems AORALSCAN-L-MAR24
©
MORE AND BOOK AN IN-CLINIC DEMO
© 2024 Inter Osseo Group Systems AORALSCAN-L-MAR24
Not the duty of some little power hungry frustrated megalomaniac like Graham*.
Even if...
Even if your employer wants you to filter and screen his calls, as an employee, I’d hate to be responsible for making the wrong choice as to whether my boss did or did not phone somebody back who called...
When I was practising, as much as possible, I always liked to be shown [on paper] the name of someone who was calling for me, just in case it was an important call that I needed to take at that moment, if I could.
But as the owner, it was my decision.
If I needed to take the call and I could take the call, then I would.
But if I wasn’t able to take the call, I was able to instruct my employee as to when I would be able to phone that caller back... and to politely let the caller know...
There were a couple of life-changing moments...
During my life as a dentist, there were a couple of lifechanging moments where I took an incoming phone call, or I went out to speak to someone who had knocked on my dental practice door.
And if I’d never done those things, if I’d never have spoken to those people AT THOSE TIMES, my life would have certainly been worse for missing out on those conversations and the opportunities those callers had shared with me.
So let me ask you a question:
Are there team members in your practice, who through their aggressive and belligerent behaviour, could possibly be adversely determining your destiny?
P.S... As a dental practice coaching firm, we listen to recordings of incoming calls on our clients’ phones and we help their team members improve their phone skills to become the best version of themselves for their employers.
It’s surprising what we REALLY DO HEAR being said by front office employees on the phones that actually repels and deters callers from scheduling appointments for necessary dental treatment.
And the sad thing is, a lot of dental offices out there don’t record and monitor their phone calls and therefore have no idea at all as to what’s being said well and what needs to be said better...
And in reality, that’s a serious and very expensive opportunity cost going straight out the window right there... every single minute of every single day...
Just like a leaky old pipe, or a dripping tap...
And just like a leaky old pipe, or a dripping tap, bad phone skills and bad phone etiquette don’t fix themselves...
About the author
Dr David Moffet is a dentist and a #1 Amazon Bestselling author. He is the inventor of The Ultimate Patient Experience™, a simple to implement patient retention system he used to build and subsequently sell (for several million dollars) his very successful practice [of 28 years] in working class western Sydney. David recently retired from wet-fingered dentistry and now spends his time lecturing and coaching private dental clients in the USA, Canada, Great Britain, Europe and Australia and New Zealand on how to improve their practices. David can be contacted at david@theUPE.com or see TheUltimatePatientExperience.com.
Simple reasons behind our clicks on social media...
ANGUS PRYOR
In today’s digital age, social media is more than just a platform for connecting with friends; it’s a world of likes, shares and follows. But have you ever paused to wonder why we’re so inclined to hit these buttons? Read on to find out the simple yet profound reasons behind our clicks on social media.
Firstly, the act of liking a post is akin to a nod of approval. It’s a quick and effortless way to show agreement or appreciation for someone’s content. Whether it’s a friend’s holiday photo or a thought-provoking article, a like is a token of support and acknowledgement. It’s our way of saying, “Hey, I see you and I like this”.
Sharing, on the other hand, takes this a step further. When we share content, it’s because it resonates with us at a deeper level. It’s not just about acknowl-
edging the content but about endorsing it to our network. A share says, “This is worth your time”. It’s a powerful tool in spreading ideas, causes and even a bit of

humour. In essence, sharing is our way of contributing to the vast social media tapestry, weaving our tastes and beliefs into the broader conversation.
Lastly, following someone is an invitation into our digital world. It’s a sign of interest and a desire for more. Whether it’s a celebrity, a thought-leader or a brand, following them means we’re keen on their content and want a regular dose of their updates. It’s a subtle way of saying, “I’m invested in what you have to say”.
At its core, social media is about connection and expression. Every like, share and follow is a small but significant part of our digital interaction. These actions build and strengthen our virtual communities, allowing us to engage with content and creators that inspire, entertain and challenge us. So, the next time you’re scrolling through your feed and find yourself clicking these buttons, remember: you’re contributing to the dynamic and ever-evolving world of social media, one click at a time. More at
14 Australasian Dental Practice January/February 2024
dentalmarketingsolutions.com.au
spectrum | NEWS
✔ Unlimited depth of cure (self cure)
✔ Gap-free interface
✔ Only 2 steps: 15 sec prep
✔ High strength
✔ Choose: capsule or automix
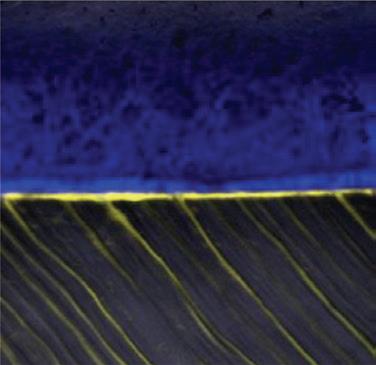

STELA GAP-FREE BONDING INTERFACE
A confocal micrograph of a gap-free Stela-dentine interface. Note the penetration depth of Stela Primer (yellow) within the dentine tubules.
Source: Dr Salvatore Sauro




STELA BULK FILL FLOWABLE SELF CURE RESTORATIVE THE FUTURE OF COMPOSITES
SCAN FOR INFORMATION ON STELA
20 µm orders phone 1300 65 88 22 | orders fax 1300 65 88 10 Call 1800 337 003 www.sdi.com.au BEFORE AFTER dentaladvisor.com RATING Stela SDI www.sdi.com.au CLINICAL EVALUATION Description Stela properties: • Self-curing composite • Unlimited depth of cure • Contains fluoride, calcium and strontium 27 CLINICAL TOTAL 468 CLINICAL 86% Key features: Self-curing composite l l Two steps l Available in syringe or capsule Photo Core Indications • Class I, II, III, & V
Photos courtesy of Prof Dr Rocio Lazo (Peru)


option.

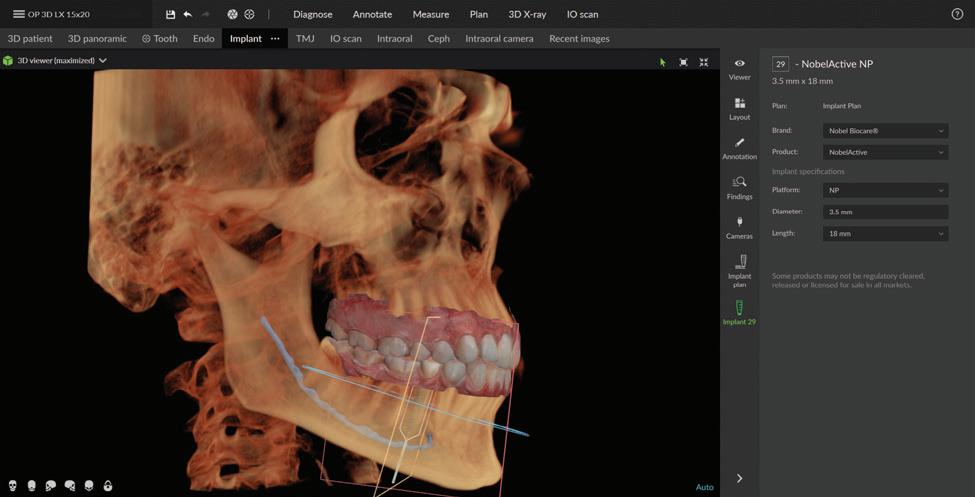
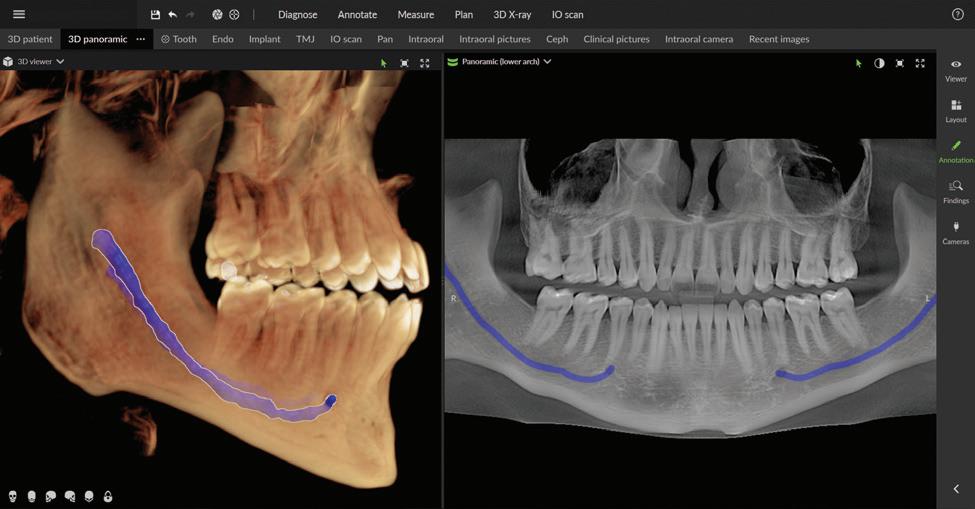
The next generation of DEXIS™ Cone Beam Technology is here
Simplify and expand your 3D diagnostics with the new ORTHOPANTOMOGRAPH™ OP 3D™ LX
Leading innovator of dental imaging technologies, DEXIS, has launched the next-generation OP 3D.
Built on OP 3D technology, the OP 3D LX imaging platform expands your 3D diagnostic capabilities with a wide range of clinical applications that support your evolving practice and enhance diagnostic confidence.
One versatile imaging platform.
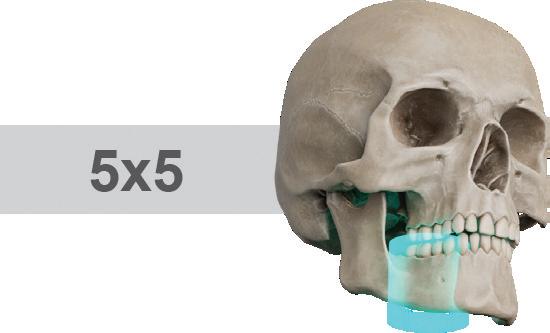
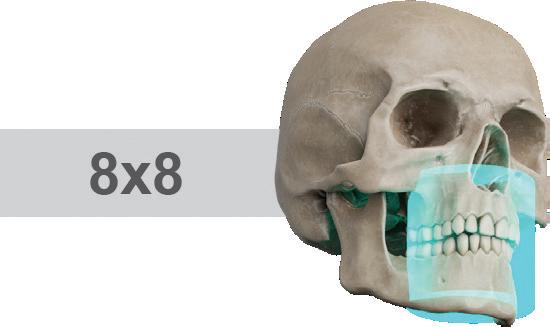
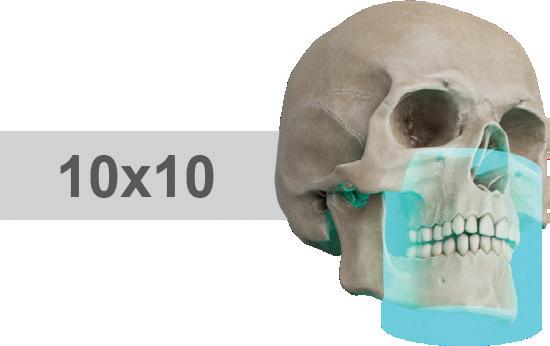
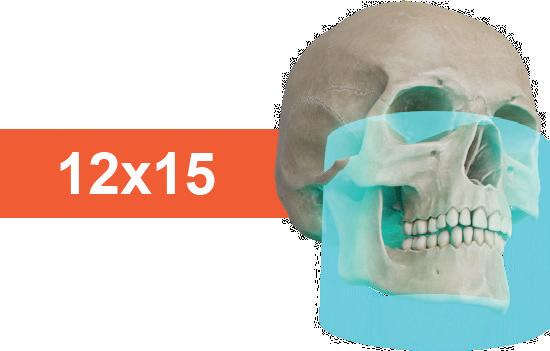
Flexible fields of view
With the largest sensor on a DEXIS OP 3D platform, this next generation system offers flexible FOV* options ranging from 5x5 up to 15x20 - the largest view option avail-
able on a DEXIS OP 3D platform to date. With 96 additional customisable FOV options and four resolutions, including endo mode and low dose mode, the OP 3D LX is the ideal solution for a wide range of dental demands.
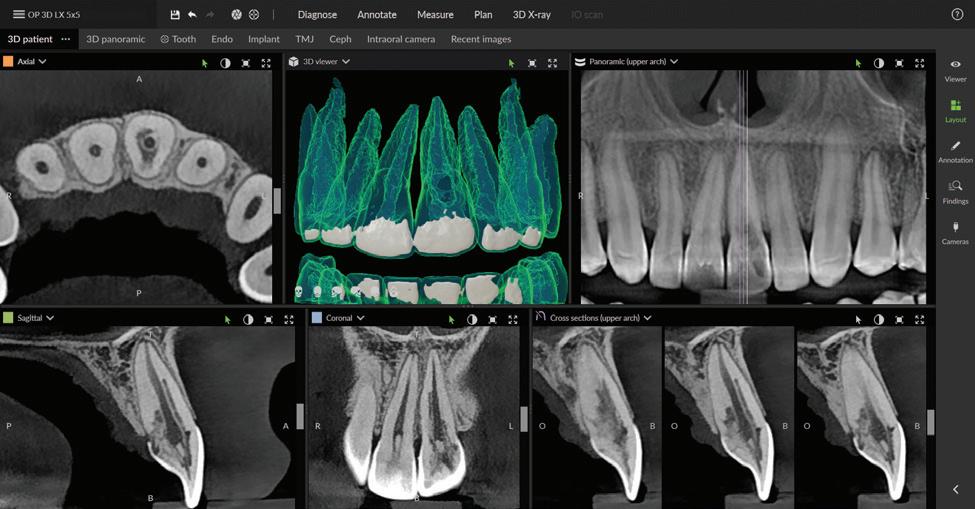
Consistent, high-quality images
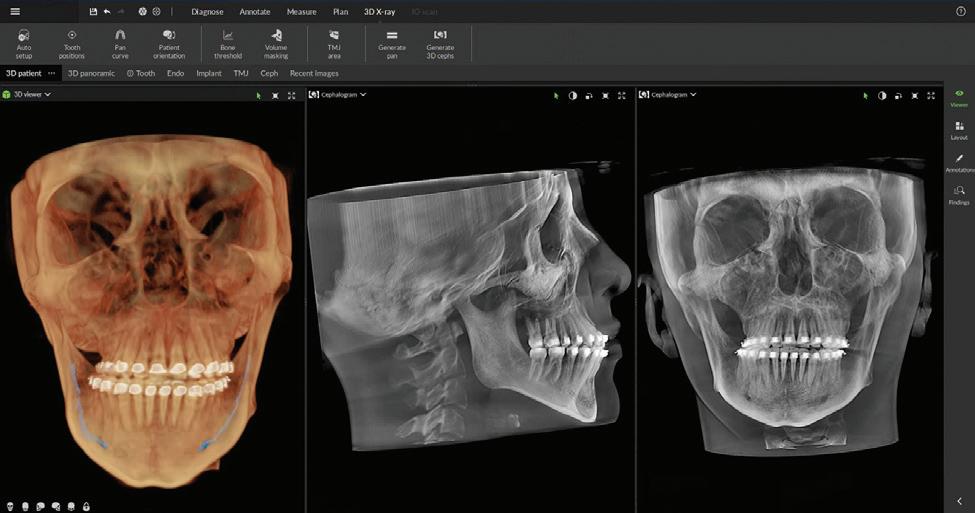
OP 3D LX offers high-resolution scans and shorter scan times while capturing the maxillofacial complex and large diagnostic areas in one non-stitched scan. In addition to panoramic, extraoral bitewing, and 3D imaging, OP 3D LX offers an optional cephalometric modality. Expand your diagnostic confidence and capabilities with the implant planning tools and noise reduction filters embedded into the system software that minimise artifacts and noise.
16 Australasian Dental Practice January/February 2024
spectrum | NEWS
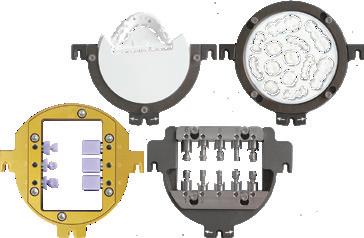
Figure 1. New DEXIS OP 3D LX.
Figure 3. Re-engineered head support.
Figure 2. Cephalometric imaging can be added as an
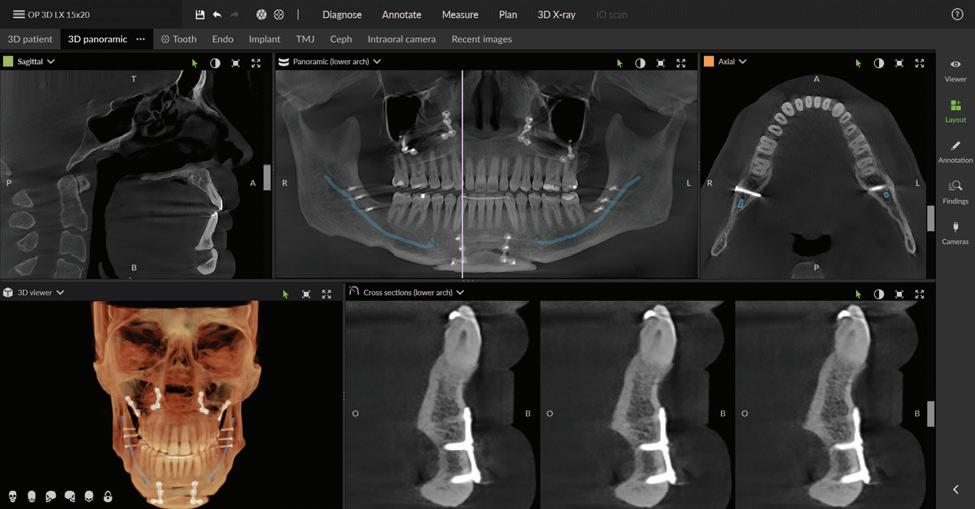

Intuitive and interactive user interface
OP 3D LX offers an intuitive user interface, allowing for anatomy visualisation, vertical adjustments and bi-directional scout modifications so that the clinical staff can capture only the structures of interest and reduce retakes.
Re-engineered head support
The new head support design provides options to scan the patient without interfering with the patient’s soft tissue profile optimised for orthodontic and surgical applications.
Cloud-based service connectivity
T
his OP 3D LX feature simplifies service and maintenance, enabling remote access to system information for simplified installation, easier maintenance and increased practice uptime.
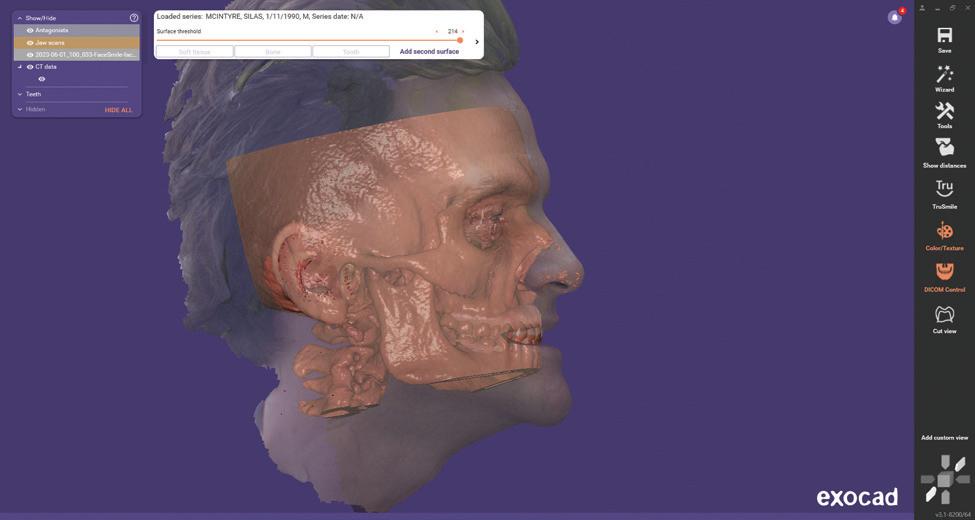
Seamless integration with new DTX Studio™ Clinic software
P acked with AI-assisted software features, DTX Studio™ Clinic complements OP 3D LX in numerous ways—for example, correcting patient positioning errors and detecting
January/February 2024 Australasian Dental Practice 17
Figure 4. Maxillofacial surgery.
Figure 6. TMJ analysis.
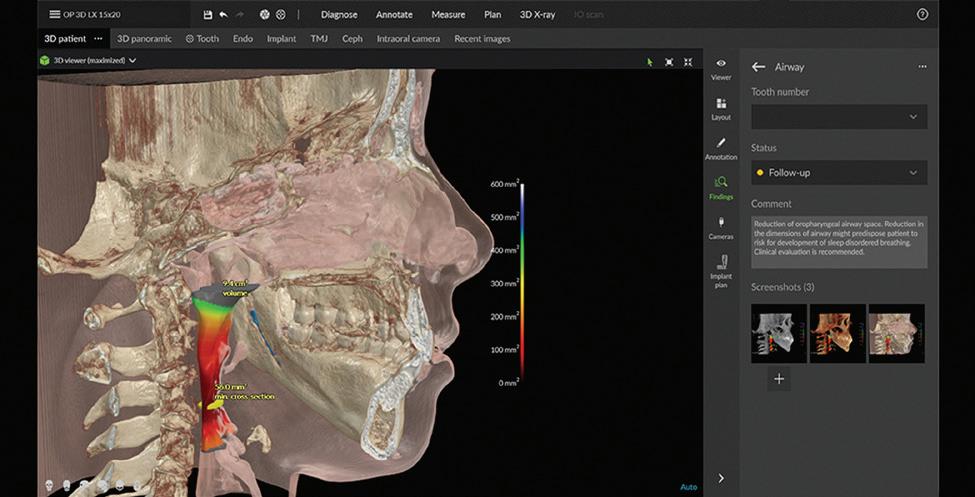
Figure 8. Airway analysis.
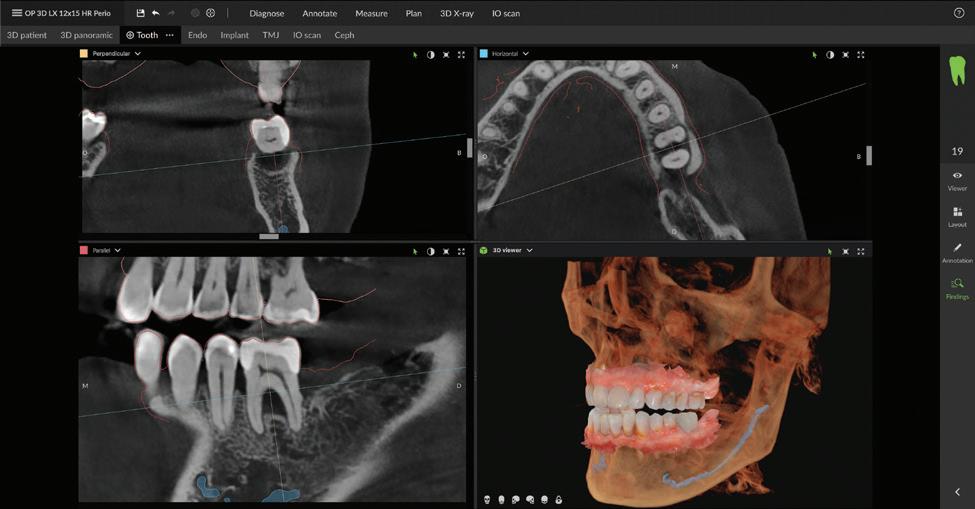
Figure 10. Periodontics.
Figure 5. Orthodontics.
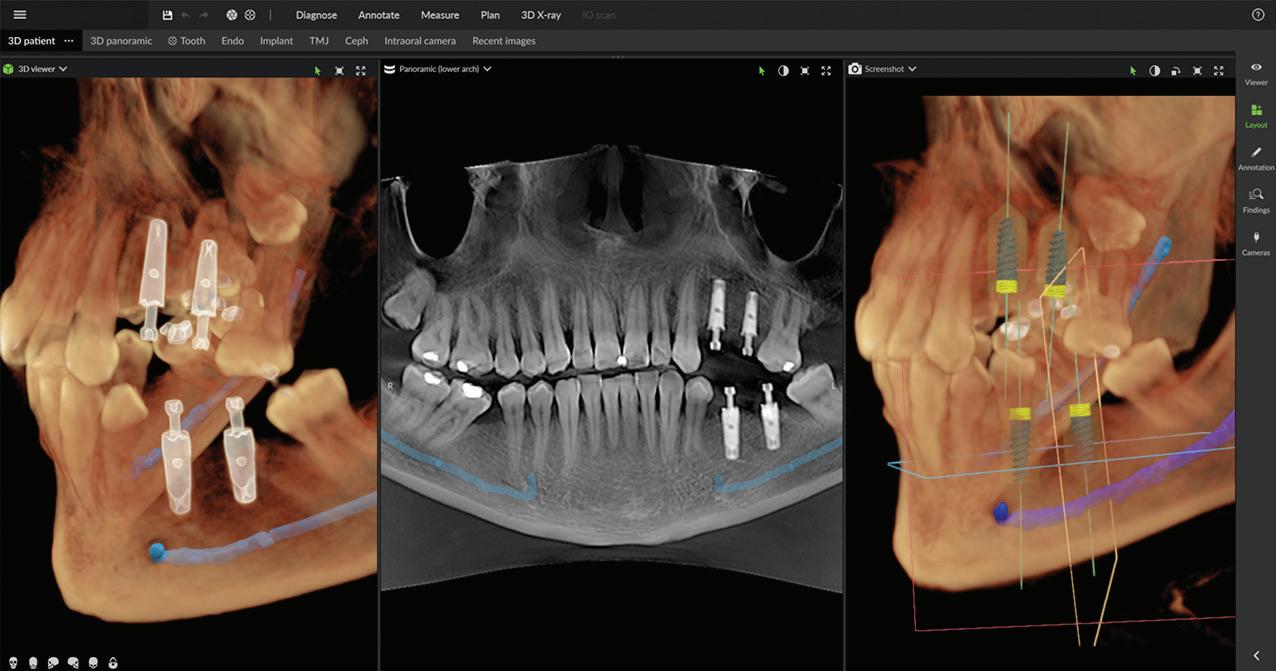
Figure 7. Implant placement.
Figure 9. Prosthodontics.
Figure 11. Endodontics.
Field of View
size (HxD)
Can be adjusted to offer up to 96 unique sizes


Clinical application
Localised diagnostics
Endodontic evaluation, single implant sites, and pathoses
Single arch
Implant planning, surgical guide creation, and impacted canines
Compact dual arch
Mandibular and maxillary treatment planning of dental implants in both arches
Complete dentition
Mandible and maxilla with 3rd molar region, and lower maxillary sinusesideal for multiple implants or periodontal evaluation
Entire dentition
Mandible and maxilla, bilateral TMJ, sinus, and pharyngeal airway
Maxillofacial complex
Mandible and maxilla, bilateral TMJ, upper and lower airway, soft tissue profile, OMS, and orthodontic analysis
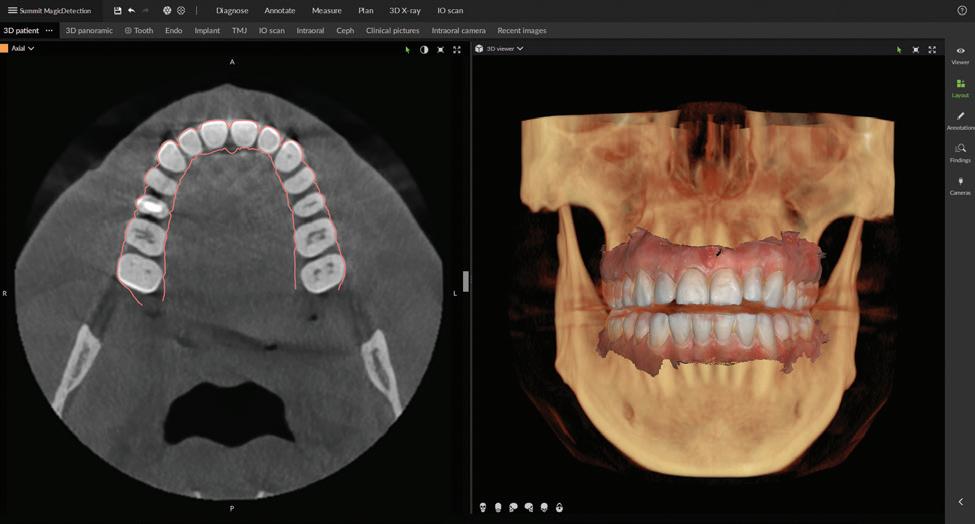
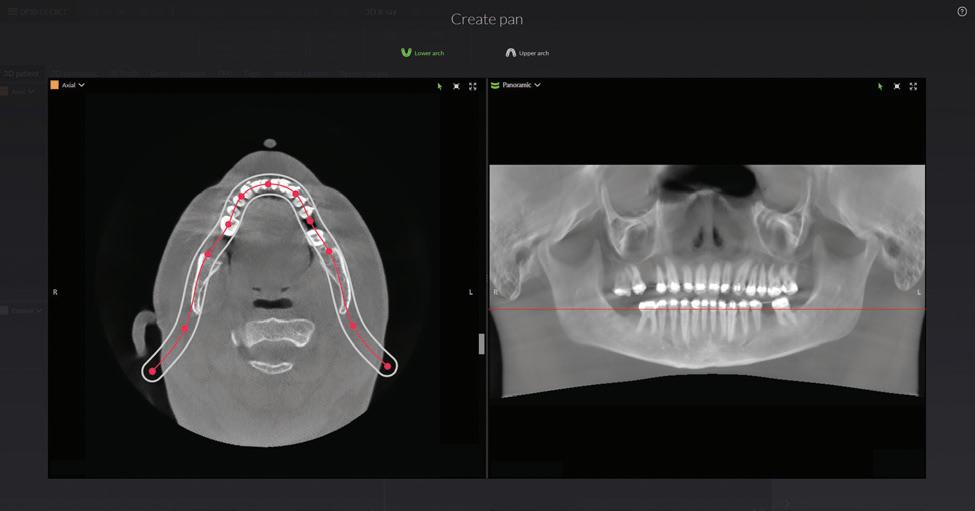
landmarks, annotating mandibular nerve canals, tracing patientspecific panoramic curves for mandible and maxilla and merging CBCT and intraoral scan data for improved implant planning. These intuitive award-winning software features support a more efficient workflow allowing you to spend less time in the software and more time with your patient.
For more information about the new DEXIS OP 3D LX, visit www.dexis.com/en-au
About DEXIS
DEXIS is a leading global brand in digital radiography for 70+ years. Today, DEXIS has brought together the most trusted brands in 3D imaging, intraoral scanning solutions and diagnostic software to provide you with a complete digital diagnostic solution. Their innovative award-winning technology enhances the way you diagnose, accelerates your workflow and delivers simpler treatment paths with better patient outcomes.
About Envista Holdings Corporation
Envista is a global family of more than 30 trusted dental brands, including DEXIS, Nobel Biocare, Ormco and Kerr united by a shared purpose: To partner with professionals to improve lives. Envista helps its customers deliver the best possible patient care through industry-leading dental consumables, solutions, technology and services. Our comprehensive portfolio, including dental implants and treatment options, orthodontics and digital imaging technologies, covers a broad range of dentists’ clinical needs for diagnosing, treating and preventing dental conditions as well as improving the aesthetics of the human smile. With a foundation comprised of the proven Envista Business System (EBS) methodology, an experienced leadership team and a strong culture grounded in continuous improvement, commitment to innovation and deep customer focus, Envista is well equipped to meet the end-to-end needs of dental professionals worldwide. Envista is one of the largest global dental products companies, with significant market positions in some of the most attractive segments of the dental products industry.
18 Australasian Dental Practice January/February 2024 spectrum | NEWS
Figure 12. Merge CBCT and intraoral scans.
Figure 13.Automatic focal trough.
Figure 14. Mandibular nerve canal annotation.
* Optional field of view.
Field of view options up to 15x20 without stitching
Enhanced user interface
Seamless integration with DTX Studio™ Clinic Imaging

Improved patient positioning
Cloud-based service connectivity
Built on the ORTHOPANTOMOGRAPH™ OP 3D™ technology, with the same consistent, high-quality images, upgradeable options, and installation footprint – the OP 3D LX is a multimodality imaging platform that expands your 3D diagnostic capabilities.

Discover the
with OP 3D LX. Get your demo today
Innovation Expanded.
possibilities
Authenticity on social media wins customers...
In the bustling world of social media, where every brand seems to be vying for attention, there’s one strategy that outshines all others - authenticity! Being genuine isn’t just a nice-to-have, it’s a must-have in today’s digital landscape. Here’s why authenticity on social media can be your golden ticket to winning customers and earning their loyalty.
Firstly, let’s talk trust. Social media users are savvy; they can spot a hard sell a mile away. But when a brand shows its true colours - whether that’s through behind-the-scenes glimpses, honest responses to feedback, or showcasing real-life uses of their products - trust begins to build. This trust is fundamental. It transforms casual browsers into loyal customers who feel a personal connection to your brand.
one that resonates with your audience. Whether it’s the journey of creating your product, the challenges you’ve overcome, or simply day-to-day operations, these stories foster a deeper, more emotional connection. People remember stories far longer than they recall a sales pitch.
ANGUS PRYOR
your brand. Engaged customers are more likely to become repeat customers and even brand ambassadors.
Moreover, authenticity sets you apart. In a sea of curated content and perfect images, raw and real content stands out. It shows you’re not just a faceless brand; you’re humans talking to humans. This relatability is priceless in forging strong customer relationships.

Then there’s the power of storytelling. Authentic content often tells a story,
Engagement is another key aspect. Authentic interactions not only draw people in but also encourage them to engage - like, comment, share and beyond. This isn’t just about numbers; it’s about creating a community around
If we’ve learnt anything about social media in 2023, it’s that nothing stays the same. While the main players in social media are reasonably consistent from one year to the next, appearing strongly in each of them is a constantly evolving field.
One area that is getting a lot of attention is the ubiquitous Reel. A Reel is a short piece of video, typically between 15 and 90 seconds, designed to capture people’s attention.

Reels can be used on Facebook, Instagram, YouTube (aka Shorts) and TikTok, so there is the potential to use the same material multiple times on different channels.
Reels/videos achieve a double whammy in terms of engaging potential patients because...
There is a growing trend of users watching more video onlineCISCO found that 80% of internet traffic in 2020 was video, compared to just 50% in 2016 while online video consumption has been on the rise with the current average viewer spending 17 hours a week watching digital videos in 2023; and
Social media platforms prioritise “Reels” over text or images i.e. if you a deliver an identical message via Reels or a different technique, the Reel will almost certainly get more views.
Here are some other benefits of Reels: Stand out from other dentists: in the past few months at live events, I’ve asked literally hundreds of dentists in Australia whether they are using video to promote their practice. Based on my
Authenticity on social media isn’t just a trend; it’s a powerful approach to creating lasting relationships with your customers. By being real, you’re not just earning likes; you’re building a community of loyal customers who believe in your brand and its story.
Remember, in the world of social media, genuine connections beat polished pitches any day.
More at dentalmarketingsolutions.com.au
survey, only around 5-10% are doing so which is a huge opportunity you can capitalise on;
Communication and virality: Reels allow you to create captivating videos that leave a lasting impression. They offer potential virality by being featured on content feeds plus dedicated Reels sections, helping you expand your audience and gain brand exposure; and Authentic Connection: With Reels, you can share behindthe-scenes, educational material and entertaining content in a friendly and conversational tone to establish a genuine connection.
In summary, utilising Reels in your social media strategy in 2023 can help you capture attention, boost your reach and create meaningful connections with your audience.
20 Australasian Dental Practice January/February 2024
briefs | NEWS
More at dentalmarketingsolutions.com.au Do I REELY have to use Reels in social media?... ANGUS PRYOR 1 • • • 2

Ph 9655 1919
• Fax 9655 1818
• admin@commodorefitouts.com.au
www.commodorefitouts.com.au
166 Arcadia Road, Arcadia NSW 2159
• Fax 9655 1818
• admin@commodorefitouts.com.au
www.commodorefitouts.com.au
Dental W orkspace C O M Dental & Medical Fitouts C O M M O D O R E Digital
OF QUALITY DENTAL AND MEDICAL WORKSPACE SPECIALISTS
A TRADITION
166 Arcadia Road, Arcadia NSW 2159 Ph 9655 1919
C O M M O D O R E Dental W orkspace C O M Dental & Medical Fitouts C O M M O D O R E Digital
AND MEDICAL WORKSPACE SPECIALISTS
cabinetmakers and detailed joiners
A TRADITION OF QUALITY DENTAL
Infection Control UPDATE 2024
4.5 hr FACE-TO-FACE LECTURE + 1.5 hr VIDEO
MELBOURNE | JUNE 14 • SYDNEY | JUNE 15
Presented by Emeritus Professor Laurence Walsh AO BDSc, PhD, DDSc, GCEd, FRACDS, FFOP (RCPA), FDTFEd
This course will discuss recent developments in infection control, with the major focus being on instrument reprocessing, following the release of the AS 5369 Standard in December 2023. The online video component (90 mins) covers New infection control terminology used in 2024; Online resources to support implementing modern infection prevention and control; The journey leading to AS 5369; and an explanation of how the standards system works in Australia, including the interactions between ISO, EN and Australian standards and the concepts that underline the standards landscape. The latter video also summarises the normative ISO and EN standards for AS 5369. As a bonus feature, there is another video on the history of infection prevention and control over the past 150 years.
TOPICS for the 4.5 hour face-to-face session include:
n The importance of precleaning at the chairside.
n What happens when instrument reprocessing is delayed.
n Key requirements for the proper use of ultrasonic cleaners and washer disinfectors.
n How to assess the outcomes of the cleaning process.
n Workflow, PPE and hand hygiene for the reprocessing area.
n Design elements of the reprocessing area and the concepts of physical and spatial segregation of work areas.
n The requirements for sterilising handpieces.
n Proper use of bespoke sterilisers running S cycles.
n Protocols for using air-removal and steam penetration tests.
n Correct use of chemical indicators.
n Tests for the integrity of packaging systems.
n Implementation of low temperature sterilisation.
n Criteria for load release from sterilisation.
n Definitions of non-conforming items.
n Environmental conditions for instrument storage.
n Record keeping requirements.
n Batch control information, including for high level disinfection.
dentevents presents...
Register Online Now at www.icupdate.au
6 HOURS CPD
A vital update on recent changes to infection control following the release of the new AS 5369 Standard in December 2023

All the changes to Infection Control for 2024
Laurie Walsh is a specialist in special needs dentistry who is based at the University of Queensland in Brisbane, where he is an emeritus professor. He has been working in clinical microbiology for over 27 years, with more than 200 publications in this field and has been teaching microbiology and infection control at postgraduate level for the more than 25 years, including for the ADA and RACDS. Laurie has contributed to the development of national standards since 1992, including standards for masks, gloves, faceshields, ultrasonic cleaners and most recently, for instrument reprocessing (the AS 5369 standard). He was also involved in the development of the CDNA BBV guidelines, the second edition of the Australian Commission on Safety and Quality in Health Care standards and the ADA IC guidelines.
REGISTRATION FEES

Dentists $660 inc gst
Earlybird 550 inc gst *
Others $330 inc gst
Earlybird $275 inc gst
* Early bird ExpirEs 15 May 2024
DATE AND TIME
Melbourne Friday, 14 June 2024
Sydney Saturday, 15 June 2024
Starts 8.30am | Ends 2.30pm
Rego opens 8am
See the website for venue details
Register Online Now at www.icupdate.au
*
Infection Contol Update 2024 is presented by Dentevents, a division of Main Street Publishing Pty Ltd ABN 74 065 490 655 • www.dentevents.com • info@dentist.com.au Tel: (02) 9929 1900 • Fax: (02) 9929 1999 • Infection Contol Update 2024™ and Dentevents™ are trademarks of Main Street Publishing P/L © 2024 Main Street Publishing Pty Ltd
FULL UPDATE!
ASIGA reveals two new printers at 3D Printing in Dentistry event in Sydney

Fnent brand in the 3D printing industry and has become a market leading manufacturer in dentistry, best known for their robust and reliable 3D printing technologies.
Not only this, but Asiga have also embraced the rapid development of 3D printing materials by providing their customers with “plug & play” profiles for most, if not all, market leading dental 3D printing materials. Their library now boasts more than 500 qualified material profiles from many of the world’s best known and respected material manufacturers. To offer such freedom in a rapidly evolving industry is testament to Asiga’s objective: to provide their customers the best possible outcome in an everevolving landscape.
At 3D Printing in Dentistry 2024 in Sydney, Asiga revealed two new 3D printers, the Max 2 and the Ultra. The Max 2 is a significantly updated version

of their hugely popular MAX with a major packaging upgrade and a remarkable new user interface. The Ultra, however, is the show stopper stealing, positioning itself as arguably the most advanced dental 3D printer ever.
Housing the latest 4K DLP imaging technology alongside the full suite of Asiga’s robust layer monitoring technologies, the Ultra delivers manufacturing certainty but with a new focus for the sector –design. It is clear that Asiga has taken note and listened to their customers to bring to market a product where the end-user is front and centre.
You cannot help being drawn to the Ultra. It all starts with their new and beautifully designed user interface which feels like something straight from a market leading tablet/phone manufacturer. Menu navigation, infographics and the responsiveness of the user interface screen all have a high quality feel and draw you in for more.
A feature that will most definitely have you hooked is their new touchless entry, an engineering marvel in itself. Asiga
surely had a lot of fun with this and with a simple hand-wave gesture, the hood opens effortlessly and is so silent that it leaves you helplessly opening and closing the hood. Once you have satisfied your desire to play with the hood, it is clear that the attention to detail and build quality of the Ultra is nothing short of exceptional.
A magnetic build platform, simple material tray clamping, internal lighting and wide range of connectivity options all help in the presentation of a cleverly refined 3D printer for both the dental laboratory and dental clinic.
Another key feature to the Ultra is a new infrared heating system which warms materials to 70°C. This opens doors to new polymer technologies where high impact and hardness are key material properties. This is an exciting time for 3D printing and dentistry in general and these new products from Asiga will certainly be turning heads.
For more information on Asiga and these new 3D printers, visit www.asiga.com.
24 Australasian Dental Practice January/February 2024 spectrum | NEWS

All-new A-dec 300 Pro delivery system
A-dec has launched its next generation A-dec 300 Pro delivery system, opening up a whole world of connectivity and simplified equipment integration, management and maintenance.
Harnessing full internet connectivity and a larger, more interactive 5” capacitive touchpad, A-dec 300 Pro delivery provides more functionality, more versatility and a more forwardthinking future-proof design. It also features the option of an all-new ergonomically advanced “Continental” delivery system.
Simply put, A-dec 300’s already popular, modular and compact design has been made even better with enhanced features. Now enabled with A-dec+, the A-dec 300 Pro offers all the powerful performance you need for the way you practice today. With more possibilities for the needs of tomorrow.
Fits today. Flexible tomorrow
A-dec 300 Pro is an easily customisable system that lets you choose the features you want for the way you practice. It’s a system that can truly grow with your practice. Adding handpieces and ancillary equipment to the A-dec 300 Pro controller is simple and straightforward. Pick up an electric handpiece or scaler and the settings and adjustments are automatically displayed – and can be programmed to display either motor speed – or bur speed, for precise control. This feature is especially useful when using speed-increasing or speed-reducing handpieces.
When using an Acteon Satelec scaler, the colour coded tip intensity is automatically displayed on the screen, giving added visual support to the operator. The new delivery system can also be configured to accommodate other popular scaler models.
A “connected” experience
Add the A-dec+ Gateway unit to access A-dec+ software, a digital foundation for integrating the latest clinical products and future technologies. A-dec’s updatable software platform helps you work more efficiently and predictably for the life of your practice giving you an holistic view of all your equipment in the one place on the A-dec app. As technology evolves and becomes more intelligent, the A-dec+ Gateway keeps you and your practice up to date – opening doors to new possibilities. It also keeps track of your maintenance requirements and logs system upgrades and allow easy diagnostics by the user or service technicians.
Accessible comfort
E verything you need is easy to position and comfortably within reach on the A-dec 300 chair and A-dec Pro delivery system. Close-in to your patient, your posture is healthy, your view is clear, and your reach is minimal. Thoughtful chair design keeps the experience comfortable for your patients, too.
What’s even more exciting is the all-new A-dec 300 Pro continental delivery system, providing unrivalled flexibility and ergonomics for the operator, enabling you to stay focused in a

healthy work position, minimising eyestrain and unnecessary breaks in concentration or twisting to reach the dynamic instruments.
Everything is there within easy reach in your peripheral view. The soft rubber flex arms gently support the handpiece, taking the strain off your wrists and hands, and then guide you back to the control head when replacing the instrument.
Evolved performance
W hy work harder when you can work smarter? The A-dec 300 Pro makes practicing simple and seamless, bringing advanced features together with legendary A-dec quality and reliability, allowing you to keep your full focus on the patient.
Lasting peace of mind
R eliable. Well designed. Future-ready. Rest assured, your A-dec equipment is ready to work reliably—patient after patient, day after day, for years to come. Despite the advanced electronics and touchscreen convenience, the time proven reliability of the A-dec delivery system has been maintained and actually improved. The capacitive touch screens have been designed for a 20+ year life and have no moving parts, unlike membrane or button style controllers.
A-dec 300 is the perfect launchpad for your A-dec Pro adventure either as a turnkey complete dental unit when ordered with a new A-dec patient chair, or as a fully upgradable delivery system.
Learn more at australia.a-dec.com
26 Australasian Dental Practice January/February 2024 spectrum | NEWS


All inclusive pricing – no additional fees for shipping or model printing.
Save up to 20% on all lab work with Cyberdent volume discounts.
Make the Switch this year.
Work at a time that suits you with our online provider portal, CyberConnect.
Start the new year with Cyberdent dental laboratory and receive your first case free!*
Start the new year with Cyberdent dental laboratory and receive your first case free!*
Start the new year with Cyberdent dental laboratory and receive your first case free!*
Start the new year with Cyberdent dental laboratory and receive your first case free!*
Your partner in digital dentistry - simply scan and send.
Start the new year with Cyberdent dental laboratory and receive your first case free!*

All inclusive pricing – no additional fees for shipping or model printing.
Start the new year with Cyberdent dental laboratory and receive your first case free!* cyberdent.com.au | 1300 789 368
All inclusive pricing – no additional fees for shipping or model printing.
All inclusive pricing – no additional fees for shipping or model printing.
All inclusive pricing – no additional fees for shipping or model printing.
Save up to 20% on all lab work with Cyberdent volume discounts.
All inclusive pricing – no additional fees for shipping or model printing.
All inclusive pricing – no additional fees for shipping or model printing.
Save up to 20% on all lab work with Cyberdent volume discounts.
Save up to 20% on all lab work with Cyberdent volume discounts.
Save up to 20% on all lab work with Cyberdent volume discounts.
Save up to 20% on all lab work with Cyberdent volume discounts.
Work at a time that suits you with our online provider portal, CyberConnect.
Save up to 20% on all lab work with Cyberdent volume discounts.
Work at a time that suits you with our online provider portal, CyberConnect.
Work at a time that suits you with our online provider portal, CyberConnect.
Work at a time that suits you with our online provider portal, CyberConnect.
Work at a time that suits you with our online provider portal, CyberConnect.
*Receive your first case free when you submit four or more cases in your first month as a new Cyberdent provider. Up to a maximum value of $300.00. Offer ends 31st March, 2024.
Your partner in digital dentistry - simply scan and send.
Work at a time that suits you with our online provider portal, CyberConnect.
Your partner in digital dentistry - simply scan and send.
Your partner in digital dentistry - simply scan and send.
Your partner in digital dentistry - simply scan and send.
Your partner in digital dentistry - simply scan and send.
cyberdent.com.au | 1300 789 368
cyberdent.com.au | 1300 789 368
Your partner in digital dentistry - simply scan and send.
cyberdent.com.au | 1300 789 368
cyberdent.com.au | 1300 789 368
*Receive your first case free when you submit four or more cases in your first month as a new Cyberdent provider. Up to a maximum value of $300.00. Offer ends 31st March, 2024.
*Receive your first case free when you submit four or more cases in your first month as a new Cyberdent provider. Up to a maximum value of $300.00. Offer ends 31st March, 2024.
Start the new year with Cyberdent dental laboratory and receive your first case free!* cyberdent.com.au | 1300 789 368
*Receive your first case free when you submit four or more cases in your first month as a new Cyberdent provider. Up to a maximum value of $300.00. Offer ends 31st March, 2024.
*Receive your first case free when you submit four or more cases in your first month as a new Cyberdent provider. Up to a maximum value of $300.00. Offer ends 31st March, 2024.
*Receive your first case free when you submit four or more cases in your first month as a new Cyberdent provider. Up to a maximum value of $300.00. Offer ends 31st March, 2024.
*Receive your first case free when you submit four or more cases in your first month as a new Cyberdent provider. Up to a maximum value of $300.00. Offer ends 31st March, 2024.
am
Make the Switch this year.
ADP Ad Make the switch this year 2024.indd 1 1/3/2024 10:01
ADP Ad Make the switch this year 2024.indd 1 1/3/2024 10:01
am Make the Switch this year.
ADP Ad Make the switch this year 2024.indd 1 1/3/2024 10:01
am Make the Switch this year.
cyberdent.com.au | 1300 789 368
ADP Ad Make the switch this year 2024.indd 1 1/3/2024 10:01
am Make the Switch this year.
ADP Ad Make the switch this year 2024.indd 1 1/3/2024 10:01 am
Make the Switch this year.
ADP Ad Make the switch this year 2024.indd 1 1/3/2024 10:01 am

Excitement builds as IDEM 2024 emerges as
the pinnacle event in dental innovation for Asia
Pacific
IDEM 2024, the International Dental Exhibition and Meeting and the leading dental exhibition and conference in the Asia Pacific, is poised to captivate and inspire dental professionals from around the region with its highly anticipated event happening in April at Marina Bay Sands, Singapore. The exhibition is set to present a well-rounded experience for all participants, with over 500 exhibitors from 33 countries showcasing their latest products and innovations together alongside a comprehensive 3-stream scientific conference featuring more than 30 speakers from around the world.
“We are delighted to collaborate again with our esteemed partners to present IDEM 2024 to the dental community. Following the resounding success of IDEM as an inperson event in 2022, we eagerly
anticipate the amalgamation of innovation and expertise that will undoubtedly mould the future landscape of dentistry,” said Mathias Kuepper, the Managing Director and Vice President Asia-Pacific of Koelnmesse Pte Ltd.
Over 30 conference sessions
Anticipated by professionals and enthusiasts alike, the 13th edition of IDEM stands as a cornerstone in the dental community where attendees can learn from an impressive line-up of renowned experts. The SDA Masterclass by the father-andson duo, Dr David S. Alleman and Dr Davey Alleman, will kick off the conference programme, offering a half-day conference session and half-day workshop on biomimetic dentistry.
Over 30 conference sessions and workshops will feature a wide range of topics
by notable speakers such as Dr Alberto Miselli covering the “Umbrella Concept” and Dr Andrea Bazzucchi sharing the latest advances in digital workflow synergy. Other conference sessions and workshops include global expert Dr Roberto Sorrentino’s “Restorative Materials and Luting Agents in Prosthodontics” and Dr Paulo Monteiro’s insights and expertise in “Anterior Indirect Restorations”.
Oral Health Therapy forum
The 5th edition of the Dental Hygienist and Therapist Forum (DHTF) will take place from 20-21 April 2024, providing a dedicated platform for hygienists and therapists to engage in meaningful discussions and knowledge-sharing, with an interesting variety of topics such as oral ulcers, paediatric patient management, digital workflows and oral care for older adults.
28 Australasian Dental Practice January/February 2024
spectrum | NEWS

Dr Lawrence Yong, President of the Singapore Dental Association, shared, “I am thrilled to welcome dental professionals from around the world to IDEM 2024. This conference is a powerful testament to Singapore’s unwavering commitment to advancing dental science and education. I am particularly enthusiastic about the conference sessions, which will delve into burning topics within our field—offering valuable insights that attendees can readily apply in their practices the next day.”
Asian Speaker Series
Attendees can also look forward to the inaugural “Asian Speaker Series”, an innovative platform designed to spotlight diverse talents from within the region. A collaborative effort between the regional and national dental associations to offer a more diverse take on the latest developments in dentistry, explore riveting industry topics such as “Treating the Paediatric Patient”, “Oral Care for the Dependent Older Adult” and delve into complex topics such as “The Systoles and Diastoles of Implant Dentistry” and “Prognosticating Periodontal Treatment Outcomes Using Artificial Intelligence”.

Expansive trade exhibition
The heart of IDEM 2024 lies within its exhibition, spanning a fully booked 17,000 square meters and hosting over 500 exhibitors who will present a diverse range of products and services, showcasing the latest industry innovations. It will host 11 pavilions (China, France, Germany, Italy, Japan, Singapore, South Korea, Spain, Switzerland, Taiwan and the USA), underscoring the wide scope of the dental industry showcased at the event.
Antonio Garcia Rebollar, Trade and Economic Counsellor, Spanish Embassy in Singapore, representing the Spain Pavilion, expressed, “We are thrilled to be part of this dynamic and highly acclaimed event. Newly supported by ICEX Spain Trade and Investment, our pavilion is a testament to the innovation and excellence within the Spanish dental industry. We look forward to engaging with the international community, sharing our expertise and contributing to the vibrant exchange of ideas that IDEM 2024 represents.”
January/February 2024 Australasian Dental Practice 29
spectrum | NEWS

This unprecedented gathering of industry leaders and innovators such as GC Asia, Straumann, 3M, imes-icore GmbH and many more, creates an immersive experience designed to inspire and inform dental professionals. Attendees can expect to engage with the latest industry offerings, witness live demonstrations and explore groundbreaking solutions that have the potential to reshape the landscape of dentistry.
3M, one of IDEM 2024’s sponsors, expressed, “IDEM provides a unique platform for industry leaders to connect, share knowledge and contribute to advancing dental science. We eagerly anticipate the exciting interactions and collaborations that will unfold. Attendees can look forward to scientific education, new products and hands-on demonstrations” – said Kae Moe Wong, Asia Area Marketing Leader.
In addition to the established players, IDEM 2024 welcomes more than 40 firsttime exhibitors this edition. These new companies bring forth a diverse array of products, ranging from orthodontics and endodontics to prosthodontics and paediatric dentistry. The inclusion of these innovative companies reflects IDEM’s commitment to staying at the forefront of emerging trends and technologies in the dental field.
imes-icore GmbH, an innovator in digital and dental CAD/CAM production systems, shares their excitement in their first participation as an exhibitor. “IDEM 2024 is the epitome of international collaboration and innovation. As a first-time exhibitor, we are thrilled to be part of this gathering, showcasing our solutions of
“The exhibition includes over 500 exhibitors from 33 countries alongside a comprehensive 3-stream scientific conference featuring more than 30 speakers from around the world...”
the best possible automated and validated workflows to a diverse audience.”
Unparalleled networking
IDEM 2024 provides an unparalleled platform for networking, fostering connections and gaining exclusive opportunities for meaningful business discussions and relationship-building. The event will be complemented with IDEM360+, an all-in-one digital platform
and app that enables participants to do business matching, find networking opportunities, schedule meetings, navigate around the event and more. Visitor badges will also be made digital from this edition and accessed via the IDEM360+ app.
Register now
Online registration is ongoing. Trade visitor registration is free and conference delegate tickets are available at a discounted price before 12 April 2024. Visit www.idem-singapore.com for more information and to register.
About IDEM Singapore
The award-winning trade fair, IDEM, is a biennially-held three-day B2B trade fair and convention for the dental industry. Styled as the Leading Dental Exhibition and Conference in the Asia Pacific Region, the conference brings in world-class speakers in general dentistry, while the exhibition is the largest dental B2B trade fair in the Asia Pacific. Riding on its continuous success since 2000, IDEM will enter its 13th edition in 2024 and maintain its position as a leading dental trade and continuing education platform in the Asia Pacific.
30 Australasian Dental Practice January/February 2024 spectrum | NEWS



SCAN TO REGISTER Organised by Supported by Connect with us IDEM Singapore IDEM Singapore idem.sg Held in 19-21 APRIL 2024 Marina Bay Sands, Singapore THE LEADING DENTAL EXHIBITION AND CONFERENCE IN ASIA PACIFIC Endorsed by USE PROMO CODE* ADP-YE3GPV TO ENJOY 10% OFF IDEM 2024 CONFERENCE TICKET Promo code will expire on 11 April 2024 and cannot be used in conjunction with other discounts. www.idem-singapore.com
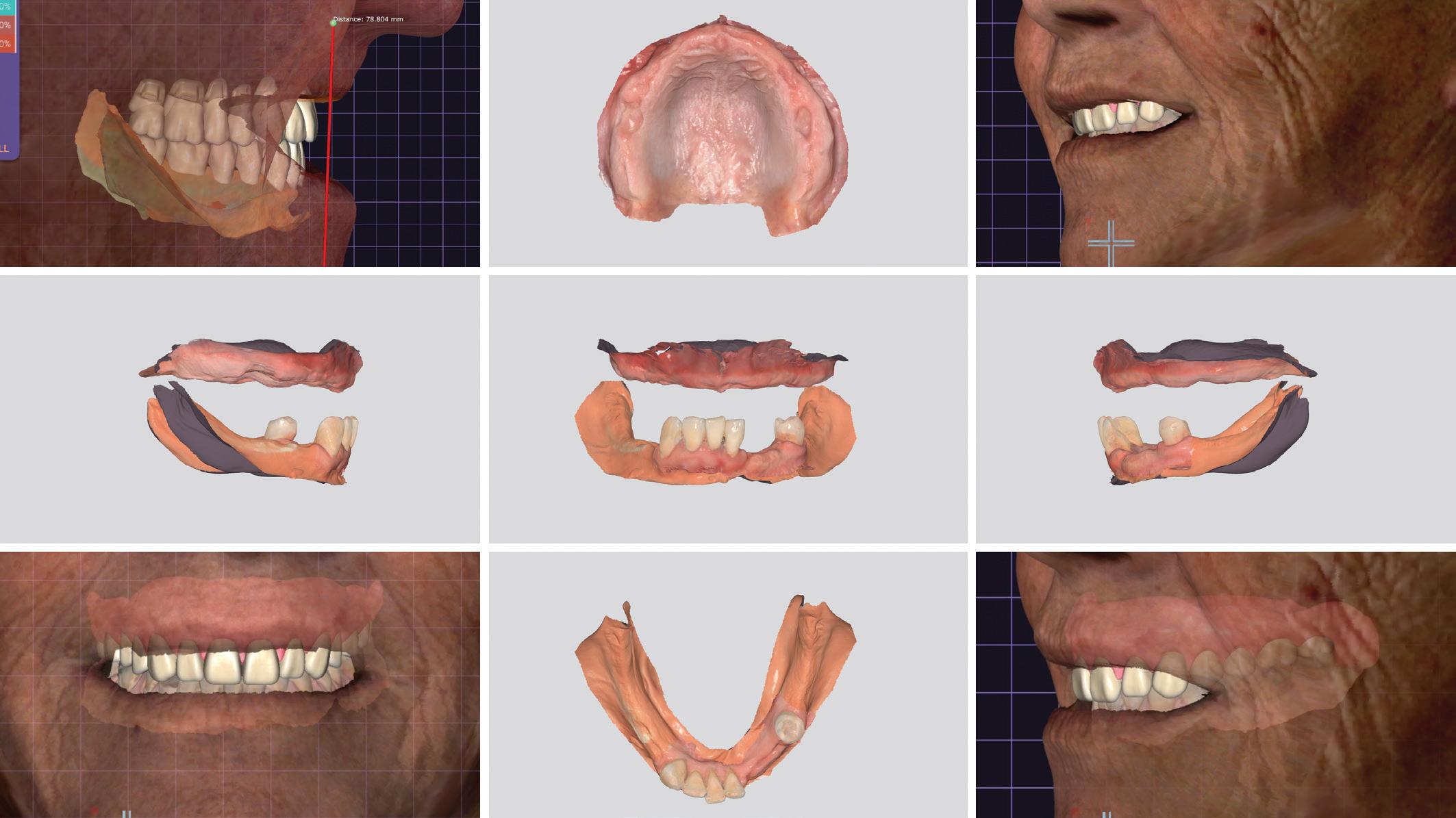
Intraoral scanning for Digital Dentures
Workflows for fabricating Full and Partial dentures digitally
NEW 2-DAY INTENSIVE MASTERCLASS
SYDNEY - JUNE 21-22 | AUCKLAND - JULY 26-27
Presented by Sam Dias, Dental Prosthetist
This event is both a lecture documenting why you should choose digital dentures today as the optimal solution for your dental practice or denture clinic together with a LIVE systematic run-through of the process for fabricating both full and partial digital dentures. You will be able to follow Sam Dias as he explains the step-by-step process he uses in his four clinics across Sydney every day.
A demonstration of accurate intraoral scanning and prosthetic design ensures that the outcome won’t be compromised while saving time and money for you and your patient.
The session will conclude with a Q&A session discussing options leading to self-design or aided design as well as the finishing and polishing process.
This course will cover the following...
DAY ONE
1. Impression vs Scanning - A discussion and slide presentation comparing intraoral scanning and traditional impressions, including a live scan of dentures will be shown. The scanning process will be shown step-by-step and the many different impression techniques currently used will be reviewed, and details of how these can be carried on to the digital world shown.
2. Clinical workflows for correctly scanning different types of denture cases.
3. Preparing scans before export to fellow colleagues and or labs to minimise errors and patient discomfort, REVIEWS!
4. Adding mesh and articulator adjustment. Combining multiple scans and adjusting the setup of the virtual articulator will be shown.
5. Wizard and model analysis tools explained.
6. Digital denture teeth selection- How to select the correct digital denture teeth library will be discussed as well as the use of the measure tool plus patient notes and extra scans. Denture teeth library options and applications will be discussed.
7. Digital denture teeth setups - Digital denture teeth setup tips and tricks for faster and more effortless setups will be detailed.
8. Denture teeth options, different materials for multiple applications, such as printed, milled and carded.
9. Denture base design - Key principles to bear in mind when designing your denture bases plus a guide to troubleshooting.
dentevents presents...
Register Online Now at www.ios.events
HOURS CPD
12
techniques plus a guide to material selection and achieving better outcomes.
3. LIVE Carded Teeth modification and milled teeth finishing and tweaking before Bonding. 4.

Register Online Now at www.ios.events REGISTRATION FEES Registration $1200 + gst Early Bird $900 + gst DATE AND TIME SYDNEY Fri-Sat, 21-22 June 2024 AUCKLAND Fri-Sat, 26-27 July 2024 Intraoral Scanning for Digital Dentures is presented by Dentevents, a division of Main Street Publishing Pty Ltd ABN 74 065 490 655 • www.dentevents.com • info@dentist.com.au Tel: (02) 9929 1900 • Fax: (02) 9929 1999 • Intraoral Scanning for Digital Dentures™ and Dentevents™ are trademarks of Main Street Publishing P/L © 2024 Main Street Publishing Pty Ltd Starts 9 am Ends 5 pm Opens at 8.30am DAY TWO
1. Continued denture design with a group discussion and clarification of denture designs. 2. 3D printing - 3D printing
LIVE
denture teeth, Milled Teeth and Printed
Step-by-step bonding
with tips and tricks.
LIVE
the gaps.
Carded
Teeth -
technique
5.
Staining technique - Techniques for staining and filling in
6. Finishing and polishing - Tips to achieve a great outcome.
7. Discussion + Q&A Session.

What are the benefits of adding orthodontics into your general practice?
Adding orthodontic services to a general dental practice can offer several benefits, enhancing the overall patient experience and contributing to practice growth. Here are some potential advantages:
1. Comprehensive patient care
Benefit: Offering orthodontic services allows for more comprehensive patient care within the same practice. Patients can receive a broader range of dental services without the need for external referrals.
2. Increased revenue streams
Benefit: Orthodontic treatments can be financially rewarding. Adding orthodontic services creates an additional revenue stream for the practice, potentially boosting overall financial performance.
3. Enhanced patient retention
Benefit: Providing orthodontic services in-house can increase patient loyalty. Patients may be more likely to stay with a practice that offers a full spectrum of dental services, including orthodontics.
4. Competitive advantage
Benefit: Offering orthodontic services can set a practice apart from competitors. It positions the practice as a one-stop-shop for dental needs, attracting patients seeking convenience and comprehensive care.
5. Improved case management:
Benefit: Managing orthodontic cases inhouse allows for better coordination of care. The dental team can seamlessly integrate orthodontic treatments with other dental procedures, providing an holistic approach to oral health.
6. Enhanced practice reputation
Benefit: A practice that incorporates orthodontic services may gain a reputation for being progressive and forward-thinking. This positive image can attract new patients and build trust within the community.

7. Optimised scheduling and efficiency
Benefit: Having orthodontic services within the practice streamlines scheduling and coordination of appointments. It improves overall practice efficiency by reducing the need for patients to visit multiple locations for different treatments. 88
34 Australasian Dental Practice January/February 2024
spectrum | NEWS


Growth Through Education ®
8. Personalised treatment plans
Benefit: Offering orthodontic services allows for the creation of personalised treatment plans tailored to each patient’s needs. This individualised approach can lead to higher patient satisfaction and better treatment outcomes.
9. Increased patient referrals
Benefit: Satisfied orthodontic patients are likely to refer friends and family to the practice, contributing to a broader patient base. Word-of-mouth referrals can be a powerful marketing tool.
10. Educational opportunities for staff
Benefit: Integrating orthodontic services provides educational opportunities for the dental team. Ongoing training and skill development contribute to professional growth and a more versatile team.
11. Adapting to market demand
Benefit: With the increasing demand for orthodontic treatments, incorporating these services allows the practice to meet patient needs and stay relevant in a competitive market.
“Proper planning, investment in training and ongoing commitment to excellence are key factors...”
12. Opportunity for practice differentiation
Benefit: Offering orthodontic services can be a unique selling point for the practice. It differentiates the practice in the market and attracts patients seeking a comprehensive dental solution.
Dr Geoff Hall says “it’s important for a dental practice to carefully evaluate the potential benefits and challenges before adding orthodontic services. Proper planning, investment in training and ongoing commitment to excellence are key factors in maximising the advantages of incorporating orthodontics into a general practice.”
The OrthoED Institute offers a range of course options for studying orthodontics. The flagship course is the 2-year Mini Masters program which is delivered as nine modules over two years and is hosted by myth-busting orthodontist, Dr Geoff Hall. The program includes pre-course reading material, theory, practicals, case examples, treatment planning sessions, troubleshooting, hands on components, full case support over 2 years as well as a plethora of post course resources.
For more info, visit www.orthoed.com.au, email info@orthoed.com.au or call (03) 9108-0475.
36 Australasian Dental Practice January/February 2024 spectrum | NEWS
“Communication and service has always been exceptional, and I have no hesitation in recommending Credabl across the board.“
Dr Andrea King, Dentist

Getting more from my finance partner, means my patients get more from me.
Professional and personal finance solutions, tailored for you and turned around fast. When you partner with Credabl, you can expect all that and more. With a team of experienced finance specialists, we understand the medical sector so you can look forward to finance solutions that help you get on with business and looking after your patients.
You always get more with Credabl.

1300 27 33 22
credabl.com.au



Practice Purchase • Commercial Property • Goodwill Loans • Overdraft Facilities • Home Loans • Car Loans • Equipment & Fitout Finance • SMSF Lending The issuer and credit provider of these products and services is Credabl Pty Ltd (ACN 615 968 100) Australian Credit Licence No. (ACL) 499547.
Specialist finance provider, Kooyong Group, becomes Avant Financial Services
Doctor, dentist and veterinarian finance specialist Kooyong Group has become Avant Financial Services, a division of Avant Mutual, having been a part of the Financial Services specialty area of Avant for several years. Avant Financial Services provides doctors, dentists and vets with the most extensive range of finance solutions under the leadership of industry veteran, Paul Freeman.
Avant Financial Services continues to provide exceptional service and the most extensive range of finance solutions, which now includes an expanded practice finance product suite of equipment loans, car loans and commercial property finance.
As CEO of Avant Financial Services, Mr Freeman brings more than three decades of financial services and medical lending experience to the business.
Mr Freeman said, “The many years that doctors, dentists and vets spend in training and the complexity of modern practice often requires a specialist funding partner.
“Our investment in technology allows doctors to secure the funding they need quickly and seamlessly...”
“Kooyong had a track record of saving doctors, dentists and vets time and money by understanding what lenders require, doctors’ unique income streams, career journeys and most importantly, credit character, which can make the process of financing a home, investment property, motor vehicle, medical equipment or practice quicker and easier.
“We will continue this service commitment under the Avant Financial Services brand, allowing time-poor specialists to secure finance solutions that are tailored to their needs.”
Avant Financial Services expands finance solutions
In addition to offering brokered practice finance solutions, Avant Financial Services now are providing doctors access to new practice finance products including business equipment, motor vehicles and commercial property loans under the Avant brand.
Mr Freeman said, “The launch of these products, coupled with Avant’s ability to broker loans with strategic lending partners, means Avant Financial Services gives doctors the most extensive range of finance options available from a single medical finance provider. Plus, Avant’s heritage and mutuality provide the Financial Services team the significant point of differentiation amongst the lending market in being the only finance provider who use doctors’ money to finance doctors’ practice growth, with profits going back to the membership.”

Significant investment in technology
Across Avant’s practice finance products, the business equipment loan is designed for the purchase of practice equipment and motor vehicles and provides funding for up to $250,000 without financials, under a fast-track approval process.
Mr Freeman said, “Avant Financial Services is not weighed down by legacy systems, which has allowed us to rapidly adopt new technologies that significantly streamline our processes, while always keeping the client experience front of mind.
“Doctors, dentists and vets are busy seeing patients and don’t have time for paperwork. Our investment in technology allows doctors to secure the funding they need quickly and seamlessly.
“Avant Financial Services are commited to meeting the finance needs of doctors. We have a new name, but our dedication to delivering outstanding service to doctors remains at the heart of what we do, and we are excited about the opportunities that lie ahead with Avant,” concluded Mr Freeman.
38 Australasian Dental Practice January/February 2024
spectrum | NEWS

The best & brightest PENTAX AND LUMADENT DEFLECTION PRISM LOUPES BOOK A DEMO Scan the QRs or call 1300 029 383 to book an in-clinic demo © 2024 Inter Osseo Group Systems PENTXLUMA-MAR24 ERGOPRISM FROM $3195+GST Normally $3395 - 4995 PRISMVUE NF2 FROM $3495+GST Normally $3995
Rise

In today’s competitive landscape, dentists in Australia and New Zealand are navigating through increasingly challenging times. With growing competition and tighter economic circumstances, the need to stretch every marketing dollar further has never been more crucial.
That’s where The Ultimate DIY Dental Marketing Pack comes in – your comprehensive solution to not just survive, but thrive in these testing times.
Meticulously crafted for dental practice owners and managers in Australia and New Zealand, this pack isn’t just another marketing toolkit; it’s a strategic partner in your journey towards attracting new patients and securing your practice’s future.
Why choose this?
n Unprecedented Comprehensive Pack: Everything you need in one easy-to-use DIY package.
n Significant Savings: $8,080 value for just $997! Act quickly and save 88%!
n Prepared by experts: Heavily curated content based on more than 10,000 hours of 1 on 1 consulting with dentists in Australia and New Zealand by Angus Pryor and his team.
What’s Inside?
Perpetual DIY Marketing Pack
n 12-Month Marketing Calendar: plan and execute your marketing efforts with precision. Includes monthly marketing themes, promotional activities, list of key international days, and more. $500 value.
n 24 x Social Media Posts: engage and grow your audience all year. Includes caption library of over 100 customisable social media captions, professional image library, 24 professionally designed Canva templates to level up your practice’s social media image. $2400 value.
n 24 x Professionally-Written Patient Emails: Keep your patients informed, interested and thinking about you! Send just one of these emails to your patients and you could reap thousands in additional business. $2400 value.
n 12-Month Dentist.com.au Upgrade: Enjoy thousands of additional views of your practice listing. Elevate your online presence and appear strongly in surrounding suburbs. $795 value.
n Automated Reminder System: Dental life gets busy, so this system helps you always know where you’re up to, allowing you to stay on track effortlessly. $360 value.
One-off bonuses
n Google Business Profile Checklist: Appearing strongly in Google is Marketing 101 for dentists and an essential part of your online presence is your Google Business Profile (formerly Google My Business). This checklist gives you the clear steps for success. $200 value.
n 12-Point Website Self-Audit: Your website is a virtual calling card for your entire business. What does it say about you? This 5-minute check will give you everything you need to independently assess whether you practice comes across as a hero or a zero. $500 value.
n Competitor Assessment: Looking for answers about the competition in your local area? This 5-minute assessment will help you gauge your competition and suggest next steps. $995 value.
n The Dental Practice Profit System book: No.1 Amazon bestselling book from Australia’s no.1 Google-ranked dental marketer, Angus Pryor. $30 value. Take advantage of this Limited Time Offer! This incredible offer is only available for a limited time. Seize the opportunity to elevate your dental practice!
Sign up at https://diy-marketing.com.au
40 Australasian Dental Practice January/February 2024
spectrum | NEWS
above the challenges – Elevate your dental practice! The ultimate DIY dental marketing pack – Save 88%!
every dentist in australia every dentist in new zealand and every dental practice...
n Australia and New Zealand have over 25,000 dental practitioners
n dentist.com.au and dentist.co.nz lists every practitioner free of charge
n For 20 years, the Australian public has relied on www.dentist.com.au to find and connect with you. Now we have introduced the service to New Zealand
n Over 1 million searches are made every year
n Visit dentist.com.au or dentist.co.nz to check your details are correct
n Visit www.dentalcommunity.com.au and login to update your details any time without cost
info@dentist.com.au
™ www.dentist.com.au Call (02) 9929 1900 or
email



THE ULTIMATE DIY DENTAL MARKETING PACK – SAVE 88%!
Rise Above the Challenges – Elevate Your Dental Practice!
In today’s competitive landscape, dentists in Australia and New Zealand are navigating through increasingly challenging times. With growing competition and tighter economic circumstances, the need to stretch every marketing dollar further has never been more crucial.
That’s where The Ultimate DIY Dental Marketing Pack comes in – your comprehensive solution to not just survive, but thrive in these testing times.
Meticulously crafted for dental practice owners and managers in Australia and New Zealand, this pack isn’t just another marketing toolkit; it’s a strategic partner in your journey towards attracting new patients and securing your practice’s future.
WHY CHOOSE THIS?
Unprecedented Comprehensive Pack: Everything you need in one easy-to-use DIY package.
Significant Savings: A $8,080 value for just $997! Act quickly and save over 90%!
Prepared by experts: Heavily curated content based on more than 10,000 hours of 1 on 1 consulting with dentists in Australia and New Zealand by Angus Pryor and his team

READY
NEED MORE INFO? Use this QR code or visit DIY-marketing.com.au for more details and discover how you can revolutionise your dental practice today!
TO ELEVATE YOUR PRACTICE?
WHAT’S INSIDE? PERPETUAL DIY MARKETING PACK
12-Month Marketing Calendar: plan and execute your marketing efforts with precision. Includes monthly marketing themes, promotional activities, list of key international days, and more. $500 value
24 Social Media Posts: engage and grow your audience all year. Includes caption library of over 100 customisable social media captions, professional image library, 24 professionally designed Canva templates to level up your practice's social media image. $2400 value
24 Professionally-Written Patient Emails: Keep your patients informed, interested, and thinking about you! Send just one of these emails to your patients and you could reap thousands in additional business. $2400 value
12-Month Dentist.com.au Upgrade: Enjoy thousands of additional views of your practice listing. Elevate your online presence and appear strongly in surrounding suburbs. $795 value
Automated Reminder System: Dental life gets busy, so this system helps you always know where you’re up to, allowing you to stay on track effortlessly. $360 value
ONE-OFF BONUSES
Google Business Profile Checklist: Appearing strongly in Google is Marketing 101 for dentists, and an essential part of your online presence is your Google Business Profile (formerly Google My Business). This checklist gives you the clear steps for success. $200 value
12-Point Website Self-Audit: Your website is a virtual calling card for your entire business. What does it say about you? This 5-minute check will give you everything you need to independently assess whether you practice comes across as a hero or a zero. $500 value
Competitor Assessment: Looking for answers about the competition in your local area? This 5-minute assessment will help you gauge your competition and suggest next steps. $995 value
The Dental Practice Profit System book: no.1 Amazon bestselling book from Australia’s no.1 Google-ranked dental marketer, Angus Pryor. $30 value
LIMITED TIME OFFER!
$8,080VALUE JUST $997!
This incredible offer is only available for a limited time. Seize the opportunity to elevate your dental practice!
Dr Claire Wilson, VIC “Definitely Angus has a great organisation. You will get value for money.”
“My experience with Angus and the team has been really excellent. They’ve helped my business grow.”
Dr Brian Chen, NSW
“Honestly, it’s the best money I’ve ever spent. Because it’s all about return on investment. And this is the best return on investment I’ve ever done.”
Dr Geoff Hall, VIC
Zirkonzahn opens new facility in Sydney
After openings in Toronto and New York City, the Italian company lands in the southern hemisphere with Zirkonzahn Australia
The countdown has started! In the north of Sydney, Zirkonzahn will soon open a brand-new facility: Zirkonzahn Australia - the company’s 14th location worldwide, following the latest openings in Toronto and New York City. Only a few minutes from the city centre, the facility will host educational training on Zirkonzahn products and devices for all dentists and dental technicians who wish to know more about the company’s workflow and work philosophy.
The training courses offered on-site are part of the Zirkonzahn School - the wide, well-structured, and targeted educational programme developed by the Italian company with the aim of teaching the use of its equipment and materials with no knowledge gaps.
But that’s not all - Zirkonzahn Australia will also feature a logistics department
for supplying materials without delivery delays. Moreover, the on-the-ground CAD/CAM expert, Rian Barnard, will support clients and potential customers in the creation of their workflow with Zirkonzahn products, explaining and showing the different components as well as answering all technical questions. With the new opening, Zirkonzahn customers and potential clients from Australia can now see first-hand all the company’s innovations and solutions without flying to the headquarters in Italy (which is, however, always worth a visit: Zirkonzahn’s doors are always open to dentists and dental technicians wishing to discover where all products are manufactured and enjoy the typical South Tyrolean culture that has shaped Zirkonzahn since the beginning).
What started as a one-person business is now a workplace for more than 300 employees all over the world, in various
facilities and training centres. In South Tyrol, Italy, Zirkonzahn has its headquarters, main education centres, a dental laboratory and five production sites. The company also owns 26 facilities and education centres in ten different countries.
Dental technology 100% made in Italy
In the heart of the Italian Alps, with the core values of discipline, innovation, trust and responsibility, the family-run company Zirkonzahn has been providing solutions and approaches for the dental sector since its foundation in 2003. The know-how and skills developed during the years are inherited from father to son, both Master Dental Technicians, ensuring continuity to clients and building with customers lasting relationships based on mutual trust. 88
44 Australasian Dental Practice January/February 2024
spectrum | NEWS













high quality by zirkonzahn
high quality by zirkonzahn

*NEW COMPONENTS, MORE OPTIONS! NO
*NEW COMPONENTS, MORE OPTIONS! NO LIMITATIONS!



IMPLANT PROSTHETIC COMPONENTS – EVERYTHING UNDER ONE ROOF UP TO 30-YEAR WARRANTY
IMPLANT PROSTHETIC COMPONENTS – EVERYTHING UNDER ONE ROOF UP TO 30-YEAR WARRANTY
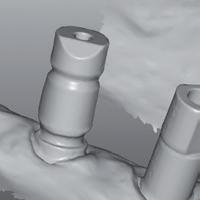

White Metal Scanmarkers
White Metal Scanmarkers

For acquiring implants position and orientation during intraoral or model scans
For acquiring implants position and orientation during intraoral or model scans











Titanium base K80 Angled Screw Channel (ASC)

Titanium base K80 Angled Screw Channel (ASC)
With adjustable chimney height and screw access channel (0° – 30°); also available in different gingival heights
With adjustable chimney height and screw access channel (0° – 30°); also available in different gingival heights
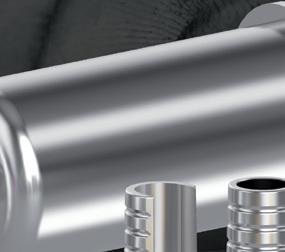


Zirkonzahn LOC-Connector
Zirkonzahn LOC-Connector
Snap attachment for implants and bars used to fi x removable dental prostheses on the implants
Snap attachment for implants and bars used to fi x removable dental prostheses on the implants





Zirkonzahn Multi Unit Abutment 17° and Zirkonzahn Multi Unit Abutment 30°
Zirkonzahn Multi Unit Abutment 17° and Zirkonzahn Multi Unit Abutment 30°

With an angle of 17° or 30° to compensate for any implant inclinations and with two different anti-rotation connections which allow intermediate positions
With an angle of 17° or 30° to compensate for any implant inclinations and with two different anti-rotation connections which allow intermediate positions





Titanium base K85
Titanium base K85
Available in different gingival heights and with a chimney height adjustable to tooth length
Available in different gingival heights and with a chimney height adjustable to tooth length
ZIRKONZAHN LIBRARY DOWNLOAD CENTER
ZIRKONZAHN
LIBRARY
DOWNLOAD CENTER
With the free Zirkonzahn Library Download Center, all components are also available for exocad ® and 3Shape users
With the free Zirkonzahn Library Download Center, all components are also available for exocad ® and 3Shape users
Zirkonzahn
info.australia@zirkonzahn.com
LIMITATIONS! USE OUR TGA APPROVED COMPONENTS FOR MORE THAN 140 IMPLANT SYSTEMS
Australia –
Zirkonzahn Worldwide – T +39 0474 066 680 – info@zirkonzahn.com – www.zirkonzahn.com
USE
MORE
Australia – info.australia@zirkonzahn.com
Worldwide – T +39 0474 066 680 – info@zirkonzahn.com – www.zirkonzahn.com
OUR TGA APPROVED COMPONENTS FOR
THAN 140 IMPLANT SYSTEMS Zirkonzahn
Zirkonzahn
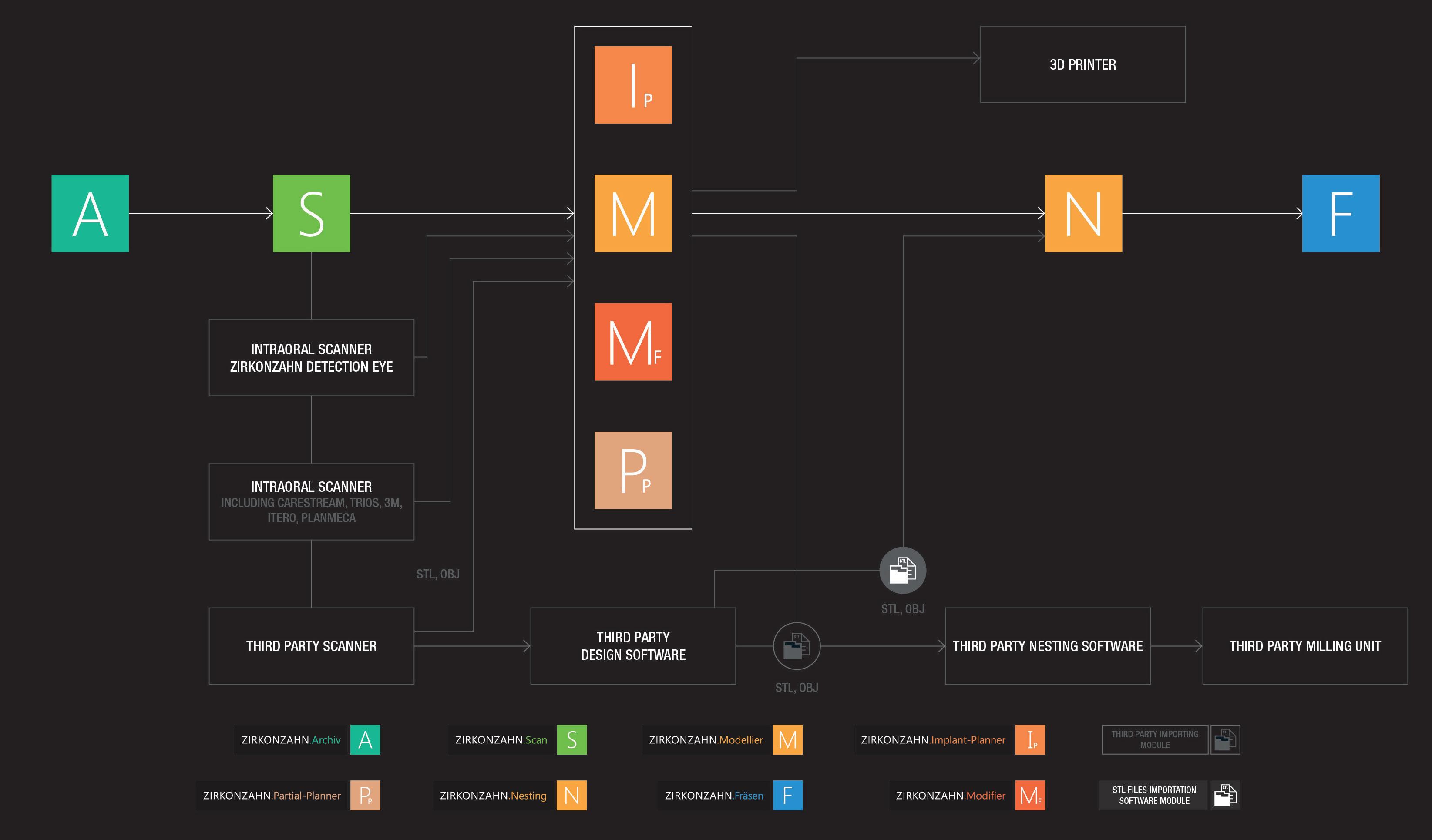
From patient diagnostics to the final restoration, Zirkonzahn’s main goal is to optimise the collaboration and communication between dentists and dental technicians, providing clinics and laboratories with dedicated instruments forming an optimum match in the complete workflow. Under the motto “Everything under one roof”, all milling units, dental materials, hardware, software, tools and implant prosthetic components are conceived and developed in-house to guarantee constant control over the production process and therefore comply with the highest quality standards. Only in this way, all products can be perfectly coordinated with each other. From Zirkonzahn, clients don’t just buy “a product”. They buy a whole work philosophy that includes the conception of a seamless and well-coordinated dental workflow - with the possibility of switching from digital to analogue and vice versa - a complete package of services and reliable support. With the company’s multilingual helpdesk, customers can benefit from comprehensive technical support with extremely short response times
provided by a dedicated team, ready to quickly solve all customer’s needs at any workflow stage.
Zirkonzahn is open
Always developing innovative technologies and searching for smart, unconventional solutions, all hardware components and software modules generate open data formats (e.g. STL, OBJ) which are therefore compatible with all open CAD systems, milling units or 3D printers. Of course, also open data (scans or design files) from other manufacturers can be processed with Zirkonzahn’s wide range of products. In this way, customers can benefit from a complete system which can be personalised und upgraded according to different combination possibilities to meet all one’s requirements. Moreover, the CAD/CAM system design can be customised on request in all colours and different styles, expressing every attitude.
With our products, we offer a complete solution to produce high-quality dental restorations.
Always at your side to face the future
In dentistry as in the broader world, whoever is up-to-date with the latest news in their field demonstrates competence, professionalism and versatility. Any dentist would be excited to work with a dental technician who, along with the excellent restorations delivered, can offer an incomparable advisory service on the latest effective working techniques to meet all of a patients’ demands. From new working methods to new materials, through the most advanced CAD/ CAM technologies, any new Zirkonzahn invention aims at bringing clinic-lab communication to new levels and finding an ever-increasing balance between function, aesthetics and technical simplification. As in all battles, the duel against the lazy and dull routine can only be won with passion and perception. Looking forward to this new year together, Zirkonzahn will always be at its customers side to walk together. With trust and mutual support, we will be each other’s source of change!
46 Australasian Dental Practice January/February 2024
spectrum | NEWS



100 % FROM THE DOLOMITES – EVERYTHING FOR YOUR WORKFLOW we


In the heart of the Italian Alps, with the fundamental values of discipline, innovation, trust and responsibility, we produce everything on our own. Purchasing raw materials only from specially selected suppliers, we develop new visions, dental materials, tools and technologies all under one roof. We provide dentists and dental technicians with technical support as well as educational trainings, to help them stand out in terms of quality and excellence. 100 % FROM THE DOLOMITES – EVERYTHING FOR

In the heart of the Italian Alps, with the fundamental values of discipline, innovation, trust and responsibility, we produce everything on our own. Purchasing raw materials only from specially selected suppliers, we develop new visions, dental materials, tools and technologies all under one roof. We provide dentists and dental technicians with technical support as well as educational trainings, to help them stand out in terms of quality and excellence.



























SHADE GUIDES INTRAORAL SCANNER AND 3D PRINTER SINTERING FURNACES



MILLING UNITS Ø 95 Ø 98 Ø 106 Ø 125


















M2 Comfort Line with extra-large Teleskoper Orbit (Ø 125 mm)












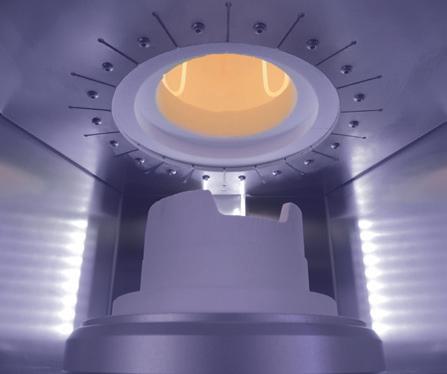


Zirkonofen Turbo
IMPLANT PROSTHETIC COMPONENTS ZIRCONIA PRETTAU® LINE





Prettau® 3 Dispersive®
MEET US AT ADX SYDNEY (20 – 23 MARCH 2024, BOOTH 1143) AND JOIN OUR LECTURE TO DISCOVER ALL OUR PRODUCTS!

are zirkonzahn
ZIRCONIA PRETTAU® LINE
MORE INFORMATION MEET
JOIN
ALL OUR
Zirkonzahn
–
Zirkonzahn Worldwide – T +39 0474 066 680 – info@zirkonzahn.com – www.zirkonzahn.com SHADE GUIDES INTRAORAL SCANNER AND 3D PRINTER SINTERING FURNACES Zirkonofen Turbo MILLING UNITS Ø 95 Ø 98 Ø 106 Ø 125 M2 Comfort Line with extra-large Teleskoper Orbit (Ø 125 mm)
YOUR WORKFLOW we
IMPLANT PROSTHETIC COMPONENTS
Prettau® 3 Dispersive®
US AT ADX SYDNEY (20 – 23 MARCH 2024, BOOTH 1143) AND
OUR LECTURE TO DISCOVER
PRODUCTS!
Australia
info.australia@zirkonzahn.com
are zirkonzahn
MORE INFORMATION
Zirkonzahn Australia – info.australia@zirkonzahn.com Zirkonzahn Worldwide – T +39 0474 066 680 – info@zirkonzahn.com – www.zirkonzahn.com

Exiting Your Dental Practice and Maximising Your Outcome
How to get the right result when selling one of your greatest assets
*organised in conjunction with the australian dental association in new south wales and victoria
A dental practice is usually one of the most valuable assets in a dentist’s life. When it comes time to sell, many will do so with little understanding of the value of what they are selling and how to present it effectively to a buyer. Others delay putting their practice on the market at an optimal time, fearful of what to do next and afraid of a loss of their identity.
This course explains:
• How to prepare your practice for sale to optimise the price, terms and compatibility with a purchaser
• Which exit strategy is right for your practice and why
• When is an optimal time to maximise the return for your asset
• Pitfalls owners fall into that devalue their practice in the final years of ownership
• Steps owners can take to improve the outcome in the final years of ownership 6
dentevents presents...
Register Now: www.exitacademy.com.au
HOURS CPD
SYDNEY* : MAR 9 | AUCKLAND : APR 5 | MELBOURNE* : MAY 11 ADELAIDE : JUN 1 | BRISBANE : JUN 22 | MORE DATES ONLINE


Presented by Simon Palmer
With more than 20 years’ experience in dental practice sales, Simon Palmer has extensive knowledge of and insight into the complexities and sensitivities involved in buying and selling dental practices. Simon’s business - Practice Sale Search - sells more than 100 practices per year. He is a regular writer/contributor to dental publications and journals, and is regarded as an expert on dental practice purchases and sales in Australia and New Zealand.
TOPICS INCLUDE
n Exit planning: how do you get your practice ready to sell?
n What are the pros and cons of the exit options/ strategies available to you?
n Succession Planning: What do you need to do now to prepare?
n What is the likely profile of the buyer for your practice and what will they be looking for?
n Valuing Dental Practices: What/ where is the value in your practice?
n How do you handle staff discretion, confidentiality and disclosure?
n Legal agreements
n Effective strategies for transferring patients effectively from seller to buyer
n What to do next post sale: post-sale strategies
n Tax implications and strategies when selling
n Expert finance, legal, accounting speakers

Register Now: www.exitacademy.com.au
Dentevents is a division of Main Street Publishing Pty Ltd ABN 74 065 490 655 • www.dentevents.com • info@dentist.com.au • Tel: (02) 9929 1900 • Fax: (02) 9929 1999
VITAL INFORMATION for anyone within 5 years of EXITING

Quality is everything: Catching up with Prof. Anton Sculean
By Joseph Allbeury
Professor Anton Sculean is chairman of the Department of Periodontology and currently the Head of Research at the School of Dental Medicine, University of Berne, Switzerland. His research interests focus on periodontal wound healing, regenerative and plastic-aesthetic periodontal surgery, use of antibiotics, antiseptics and novel approaches such as lasers and photodynamic therapy in the treatment of periodontal and periimplant infections. While presenting at Osteology Barcelona, we caught up with Dr Sculean to hear about the specialised instruments he has designed together with STOMA.
Thank you very much for your time. I was fascinated to hear that you’ve designed a range of instruments with STOMA that support the clinical procedures you’ve pioneered. Can you please tell us more about these.
Of course. So I’m doing a lot of soft tissue surgery around teeth and also around implants.
In doing so, I’m trying to preserve as much soft tissue as possible. For this, of course, you need instruments that are tiny and sharp.
At the same time, I need a way to lift the papillae and prepare the flap, the so-called tunnel flap, because usually, I don’t have any vertical releasing incisions in order to get access to the defect.
Therefore we need instruments that are designed in a specific way. With the different shapes of tunneling instruments, for example, which look like small periosteal elevators, but in a very tiny design, straight or bent, or even a novel type of instrument that is designed to lift a papilla.
With these instruments, I can manage the soft tissues in a way that is less traumatic for the tissues, and of course, it increases the chances of successful regeneration.
50 Australasian Dental Practice January/February 2024
spectrum | NEWS
JA AS
The clinical techniques you’ve developed obviously came before the instruments, so you used other instruments at first?
Of course, in the beginning, we didn’t have “tunneling” instruments or mini tunneling instruments. So I used larger periosteal elevators or even a modified Orban knife.
I realised quite early on that these instruments traumatise the tissues because of their size. It is very difficult to work in the depth of the defect, to reach the depth of the residual with larger instruments. For two decades now, I have had an excellent

collaboration with STOMA and together, we have developed new designs. And we’re still in the process of improving everything and we learn every day - but the idea is always the same. We try to traumatise the tissue as little as possible and be gentle with the tissues, because the defect will then heal by itself. In this way at least, the chances are much higher for this to occur.
Why did you choose to partner with STOMA?
It’s difficult to remember that far back because we’ve known each other for 20 or 25 years. I think we originally met at a dental meeting and just started discussing how we could cooperate. We started the collaboration by running some courses together and I would also try out some of their instruments on my patients and provide feedback. We realised that certain instruments needed modifications. Now we have new tweezers, for example, and tissue pliers and needle holders in specific designs that allow for more gentle handling of the tissues and more precise suturing techniques.
And you’ve developed three kits with STOMA?
Yes. So the “basic surgery set” contains the curettes, the periodontal probes, elevators, retractors and periotomes. We have the “micro surgery kit” with a micro periosteal elevator specifically designed to maintain the papilla and also to harvest connected tissue, for example, from the palate. And we have the “plastic esthetic surgery kit” that contains the tunneling instruments in various shapes.
Are these kits specifically for periodontists or are they being used by general dentists?
They are mainly used by specialists - periodontists and oral surgeons - but also by GPs who are trained in certain procedures. It’s a range of instruments that are used in all kinds of indications where we need gentle handling of soft tissues.
With so many instruments on the market, what factors should clinicians and surgeons think about when they’re choosing instruments?
That’s a very good question. In periodontology, generally, if you want to be gentler with the soft tissues, try to avoid using very large instruments. It’s obvious that if you’re working with tiny areas of tissue, you do not use a large instrument because the chance that you will destroy the tissue is higher. So, coming from this way of thinking, we try to decrease the sizes of the instruments to make them more tissue-friendly and at the same time, with specific angulation for specific areas of the dentition. If you work, for example, in the maxillary area in the anterior front or in the lateral area or maybe on lingual defects, the access is different. And we have even developed some specific instruments for the so-called lingual tunneling that is quite demanding from a technical point of view.
So how do STOMA instruments excel?

One word – quality. I have STOMA instruments from over 15 years ago that I still use today. So from that point of view, it’s excellent because it’s like a Mercedes. You buy it one time and in most cases, you have it for decades. I think that that’s maybe the most important value and characteristic of STOMA - high quality. STOMA instruments are a little bit more expensive than some other instruments, but it’s a very good investment because if you take care of the instrument, you can have it for decades. Some other instruments you have to throw away after a few months. So, that’s very important.
And how does the process of developing new instruments with STOMA work?
January/February 2024 Australasian Dental Practice 51
JA JA JA JA JA JA JA AS AS AS AS AS AS spectrum | NEWS

Another good question. If we take the example of the tunneling instruments, in the beginning, we only had large instruments. I realised that it would be useful to have smaller sizes for use in the interior area of the mandible. The tissue is very thin. So, if you have a very large instrument, you have a higher chance of tearing the tissue majorly and distally. So I said, “Okay, let’s try to develop a narrower one”. Through this process, I realised that a small change can make a big difference.
We also modified the needle holder. In the old design, you don’t get the thread when you make the knot. This was very annoying because sometimes, you make the knot and it didn’t have this oblique groove. So, the suture stays stuck in the needle holder. Then you had to repeat the procedure. It was very annoying. Now, with this oblique groove, this never happens. With this groove, in fact, the suture is sliding over the instrument. So, this is excellent.
So these are the kind of small improvements we make.
So, do they hand make a prototype and give it to you to test?
Usually, yes. We discuss it and then I have an idea about a novel instrument. Martin Mazzeo from STOMA is very good at designing or bending different kind of metals. Then he shows it to me and I try it. I say, “Oh, this is nice, but you could do it better here or there”. So, he’s improving it and then I try it again and then at a certain moment I tell him, okay, that’s perfect.
Thank you very much for your time and insight.
Thank you very much.
“If you want to be gentler with the soft tissues, try to avoid using very large instruments. It’s obvious that if you’re working with tiny areas of tissue, you do not use a large instrument because the chance that you will destroy the tissue is higher...”

52 Australasian Dental Practice January/February 2024 spectrum | NEWS
AS AS AS JA JA
Hi, I’m Layla! Let me introduce you to Geistlich myGuide®.

This new learning journey covers all areas of regenerative dentistry and is structured in three patient types.
Geistlich myGuide® is a new learning journey to boost your skills in regenerative dentistry. A variety of e-learning modules, clinical videos and cases, assessments and Geistlich vLab® online hands-on courses have been created for you to learn how to treat your implant, perio and peri-implantitis patients. More details on: www.geistlich-myguide.com
Meet the patient types



implant patient
Amari
The
The perio patient
Josy
peri-implantitis patient
details
Lee The
More
on learning portal
Five-in-CS 9600 3D system is now a five-time Cellerant Best of Class
Technology Award Winner
This advanced dental imaging machine is now the winningest extraoral system of all

Continual innovation and market-leading technology has earned Carestream Dental’s CS 9600 CBCT system its fifth-straight Cellerant Best of Class Technology Award. The system combines advanced hardware with powerful software to make sure doctors are always practising on the cutting edge.
Available in three editions with 10, 12 and 14 fields of view (FOVs), the CS 9600 is sized to meet doctors’ needs so they can focus on the smallest detail of root morphology or zoom out to see the full picture, including the TMJ and sinuses. But the system doesn’t just capture high-quality images, it employs automation, guided assistance and artificial intelligence to capture the right image the first time.
Patient positioning is easier and more intuitive so users can avoid mistakes that lead to retakes and instead focus on diagnosis and patient care. Plus, in addition to 2D and 3D imaging and object scanning, practices have the option to include face scanning or a scanning cephalometric arm, turning this five-time winner into an intuitive five-in-one system.
It’s not just imaging that makes the system a winner; upgradeable software modules mean that the CS 9600 is always evolving to meet doctors’ needs as their practices grow. No matter the type of treatment a practitioner offers today, when it’s time to scale up, the CS 9600 can expand to handle prosthetic-driven implant planning, upper airway analysis and more.
Third-party intraoral scanners can even be integrated into the CS 9600’s workflow so doctors can handle the most advanced treatment and care. The latest feature of CS Imaging version 8—the imaging hub that centralises and displays all a user’s Carestream Dental imaging data—lets users combine scans from intraoral scanners with images captured by their CS 9600 so they can do even more for their patients.
Cellerant Best of Class Awards
The CS 9600 was selected to receive a 2023 Cellerant Best of Class Technology Award by a panel of prominent dental technology leaders. The Best of Class Technology Awards create awareness in the dental community of manufacturers that are leading the way in how practices will operate today and in the future. In addition to five Best of Class Technology Awards, the CS 9600 won a 2019 Edison Award seal in the Medical/Dental Diagnostics category and the Krakdent Medal of the Highest Quality from the International Fair KRAKDENT®.
For more info on the Cellerant Best of Class Awards and the 2023 winners, go to cellerantconsulting.com/about-best-of-class
For info about the CS 9600, visit carestreamdental.com/CS9600 or contact Carestream Dental on (02) 9919-4500 or email anz-enquiries@csdental.com
54 Australasian Dental Practice January/February 2024
spectrum | NEWS
CS 9600 Cone Beam CT

Smarter and Better Than Ever.
The smart way for your team to capture the high-quality images you need to achieve faster diagnoses and treatment plans. The CS 9600 features multiple advances including video-aided positioning guides and an intuitive SmartPad to enable you and your staff to achieve highquality, precise images on the first try, every time. And intuitive software and innovative metal artifacts reduction tools help you reach a more confident diagnosis.

For more information, please visit: carestreamdental.com/CS9600


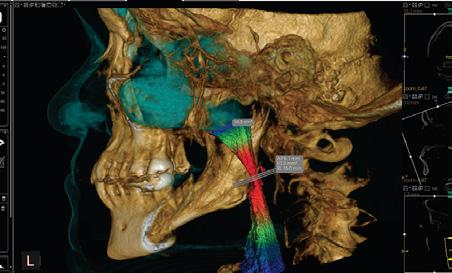
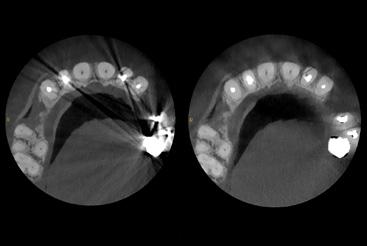
© 2023 Carestream Dental LLC. 1197258034
Digital Dentistry & Dental Technology
May 24-25, 2024

Digital Dentistry & Dental Technology is back for a 5th edition in 2024 in Sydney on May 24-25. The two-day, multi-stream event is proving as popular as ever with its unique format, allowing delegates to create their own event within an event.

“We’re looking forward to celebrating 5 editions of Digital Dentistry & Dental Technology with the biggest and best event yet,” said Dentevents’ Joseph Allbeury, the organiser and publisher of this magazine. “We’re already working with sponsors and supporters to bring in top international speakers to present alongside the stellar local talent from Australia and New Zealand we always feature. Back in 2019, we had over a dozen internationals alongside speakers from Australia and New Zealand and now that COVID is behind us, we’re hoping to bring back the international flavour.”
Digital Dentistry and Dental Technology 2023 presented delegates with a choice of over 90 education sessions including 18 workshops - 94 hours of content - in 8 concurrent streams presented by 46 speakers over two days at the Novotel Sydney Brighton Beach.
Topics covered included 3D printing, intraoral scanning, 3D facial scanning, milling, CAD and CAM software, materials, smile design, digital dentures, implantology, CBCT, restorative, aligners, orthodontics and more.
“If you’ve never attended before, have been multiple times or attended every event, we would encourage you to take advantage of the 75% off early bird discount available and register for only $220 until November 24.”
For more info or to register for Digital Dentistry & Dental Technology 2024, visit www.dentaltechnology.com.au
International Update
Infection alters views of future vaccination
COVID-19 vaccinations significantly reduce disease severity, hospitalisations and deaths, but in 2023, uptake of vaccines including booster doses was relatively low. Perceptions about the benefit and safety of COVID-19 vaccines are important determinants of vaccine uptake. This remains particularly important given that research evidence regarding the protection against COVID-19 offered via different types of immunity (e.g. infection-induced/ vaccine-induced/hybrid) is ever-changing. However, public perceptions of this changing body of evidence and the extent to which they may influence vaccination perceptions and intentions have not been studied in detail. In this study, whether people in the USA think COVID-19 vaccination is less beneficial or safe for someone who has already had COVID-19 was we examined, compared to someone who has not. Whether COVID-19 vaccine benefits and safety perceptions and intentions (for primary and booster doses) vary was also examined. An online survey of 1,733 US adults was undertaken (mean age 41 years, 66.4% were non-Hispanic White and 66.0% were female). Half (53.1%) had received ≥1 dose of a COVID-19 vaccine and 27.6% reported prior COVID-19 infection. Overall, respondents believed COVID-19 vaccines are less beneficial and less safe for someone who had already had COVID-19. Those who experienced COVID-19 after being vaccinated believed that the vaccines are less beneficial and less safe than those who had not. Over 40% of the respondents felt that a COVID-19 vaccine did not even offer a moderate benefit for someone else with prior history of COVID-19 infection and 30% felt that a COVID-19 vaccine was unsafe. Benefit and safety perceptions of COVID-19 vaccination varied according to COVID-19 infection history. Vaccinated respondents who had personally experienced COVID-19 postvaccination perceived COVID-19 vaccines as less beneficial and less safe for someone else compared to vaccinated respondents who had not personally experienced COVID-19 post-vaccination. Intentions to receive primary and booster doses among those eligible did not differ based on the respondents’ prior COVID-19 infection history, possibly due to stronger or more immediate influences of other demographic or cognitive factors. There are several important public health implications. Evidence indicates that COVID-19 vaccination is highly beneficial, including for individuals who have previously experienced COVID-19. To address low uptake, these findings highlight the need to more effectively communicate changes in the clinical understanding of COVID-19 immunity, as the public appears to underestimate the benefits and safety of COVID-19 vaccination for those who have had a COVID-19 infection. These findings also stress the importance of tailoring communications to peoples’ COVID-19 history and vaccination status. Moving forward, communicators should also be mindful not to convey overoptimistic information about vaccine efficacy when promoting vaccines for COVID-19 and other diseases.
Thorpe A, et al. Impact of prior COVID-19 infection on perceptions about the benefit and safety of COVID-19 vaccines. American Journal of Infection Control 2024;52(1):125-128.
spectrum | NEWS 56 Australasian Dental Practice January/February 2024



Instrument reprocessing solutions
Instrument reprocessing solutions
Instrument reprocessing solutions
has revolutionised sterilisation by offering a compact, dedicated line that provides unparalleled performance! Decontamination Washing Drying Disinfection Sterilisation
Mocom has revolutionised sterilisation by offering a compact, fully dedicated line that provides unparalleled performance!
Mocom has revolutionised sterilisation by offering a compact, fully dedicated line that provides unparalleled performance!
Disinfection
Washing Drying
Sterilisation




Decontamination Washing Drying Disinfection
M: 0427 816 459 • F: (02)46328456 • sales@mocomaustralia.co m.au • www.mocomaustralia.com.au
459 • F: (02)46328456 sales@mocomaustralia.co m.au • www.mocomaustralia.com.au


Question 1. A change from disposable gowns to reusable gowns has been estimated to reduce...
a. Energy consumption by 64%
b. Greenhouse gas emissions by 66%
c. Solid waste generation by 84%
d. All of the above
Question 2. Low-temperature vaporised hydrogen peroxide (VHP) sterilisation is better for the environment because...
a. The chamber only needs to be heated to around 40°C.
b. Packaging used for instruments processed using VHP can be recycled.
c. Water used in the process does not need to be distilled.
d. All of the above.
Question 3. The big contributor to environmental impact of disposable over reusable instruments occurs...
a. From transport and disposal costs.
b. Due to greenhouse gas emissions in the manufacturing process.
c. From electricity consumption during the manufacturing process.
d. Due to the raw materials consumed.
e. All of the above.
Question 4. A single disposable gown has an estimated carbon footprint of carbon dioxide gas equivalents of almost...
a. 100 grams
b. 500 grams
c. 1 kg
d. 2 kg
Question 5. The everything disposable mindset that dominated during the height of the pandemic is sustainable going into the future...
a. True
b. False
Question 6. Every dental clinic is now required to have a washer disinfector...
a. True
b. False
Question 7. Ultrasonic cleaners are being phased out for dental practice....
a. True
b. False
Question 8. A Class 2 or PCD must be included in every steam steriliser cycle...
a. True
b. False
Question 9. There are no major changes between AS 5369 and AS/NZS 4815...
a. True
b. False
Question 10. Using a particular device in the steriliser to test its performance protects the practice from all possible prosecutions relating to infection control...
a. True
b. False
62 Australasian Dental Practice January/February 2024 the cutting EDGE Changing to more sustainable dental practice in the post-pandemic era By Emeritus Professor Laurence J. Walsh AO A cross the years of the COVID-19 pandemic, many dental clinics have found that their use of disposable items has increased dramatically. This article challenges that mindset, prompting a rethink of decisions on two key elements that can lower the environmental impacts of dental practice: disposable gowns and d isposable instruments. Reusable gowns Prior to the pandemic, reusable linen gowns were the norm in many dental schools and in private and public dental clinics for many years. Hence, it is relevant to ask the question as to why clinics cannot return to this as a normal practice for non-surgical dental procedures. Modern reusable gowns are typically made of cotton, polyester or blends of cotton and polyester. READ ME FOR CPD 84 Australasian Dental Practice January/February 2024 Infection control challenges for 2024 By Emeritus Professor Laurence J. Walsh AO As we begin a new year, it’s useful to flag a number of the issues that will emerge during the coming 12 months, to prompt thought, reflection and discussion. Washer-disinfectors Automated mechanical cleaning of reusable medical devices (RMDs) is a mainstay of modern instrument reprocessing practices, with ultrasonic cleaners and washer disinfectors (WD) being the two most commonly used technologies in dental practice reprocessing areas. Both of these approaches are included and discussed in the new December 2023 Australian standard on reprocessing of RMDs that will be discussed below. The Australian standard that applies to ultrasonic cleaners used in healthcare facilities (AS 2773) was updated in late 2019. This reinforces the point that ultrasonic cleaners will continue to be used in reprocessing (Figure 1). A key consideration when considering which of these two methods to use with a particular device is the manufacturer’s instructions for reprocessing. Under the Essential Principles requirements when devices are approved by the Therapeutics Goods Administration (TGA), RMDs that are designed by the manufacturer for reuse on multiple patients must have comprehensive documentation on reprocessing. READ ME FOR CPD infection CONTROL
ONLINE CPD
INSTRUCTIONS: Australasian Dental Practice™ is now offering PAID subscribers the ability to gain 2 Hours CPD credit from reading articles in this edition of the magazine and answering the questions above. To participate, log in to the Dental Community website at www.dentalcommunity.com.au (call (02) 9929-1900 if you do not have a login) and click on the CPD Questionnaires link; select the Australasian Dental Practice Jan/Feb 2024 questionnaire and then click START. A score greater than 80% is required to PASS and receive CPD.


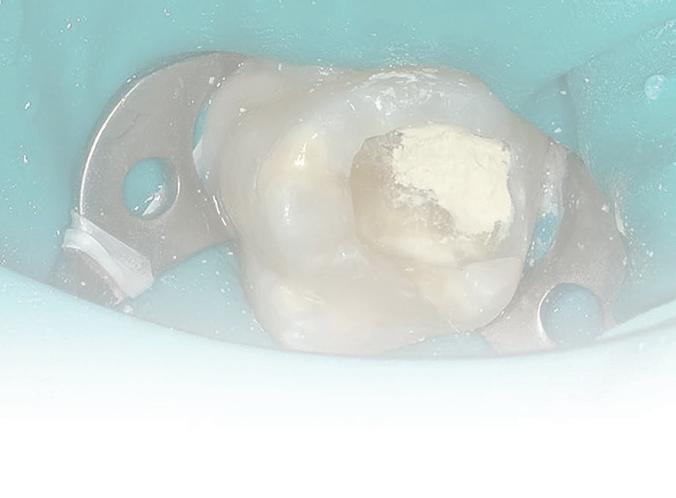

Question 11. How effective is post-exposure prophylaxis in preventing HIV from needle stick injuries?
a. 20%
b. 40%
c. 60%
d. 80%
Question 12. The new version of the Ultra Safety Plus is called the...
a. Ultra Safety Plus Snap
b. Ultra Safety Plus Twist
c. Ultra Safety Plus Pro
d. Ultra Safety Plus Lock
Question 13. The risk of transmission following a skin puncture injury is dependent on:
a. The level of virus in their blood.
b. The amount of blood involved.
c. The type of needle or syringe in question.
d. The time that has elapsed since the needle was used.
e. All of the above.
Question 14. The risks of acquiring HIV from a contaminated needle are:
a. 0.23%
b. 0.56%
c. 1.8%
d. 6-30%
Question 15. Following the implementation of Ultra Safety Plus, a study found that the number of avoidable needle stick injuries reduced to an average of:
a. 14.8 per 1 million hours worked.
b. 8.3 per 1 million hours worked.
c. 11.8 per 1 million hours worked.
d. 7.3 per 1 million hours worked.
e. 0 per 1 million hours worked.
To retrieve your FREE Dental Community Login: Call
Question 16. How many children worldwide have Molar Incisor Hypomineralisation (MIH):
a. 5%
b. 15%
c. 25%
d. 35%
Question 17. The etiology of MIH has been linked to...
a. Acute and chronic childhood illness
b. Dioxins
c. Antibiotics
d. Ear-nose-throat infections
e. All of the above
Question 18. The porous enamel structure associated with MIH...
a. Leads to rapid wear and post-eruptive enamel breakdown.
b. Can lead to dentine hypersensitivity.
c. Makes bonding less reliable.
d. Can lead to chronic pulp inflammation.
e. All of the above.
Question 19. Long-term restorative treatment for hypomineralised teeth requires up to ten times more treatment and retreatment than teeth without MIH...
a. True
b. False
Question 20. Biodentine has been shown to have better results as an Indirect Pulp Capping material because...
a. It has a high pH of 12.
b. It releases calcium and silicon ions.
c. It creates a superior seal.
d. The crystallisation of the calcium silicate hydrate gel reduces porosity, increases hardness with time and increases compressive strength.
e. All of the above.
READ THE ARTICLES BELOW AND ANSWER THE QUESTIONS ONLINE AT WWW.DENTALCOMMUNITY.COM.AU - 2 HOURS OF CPD 104 Australasian Dental Practice January/February 2024 S harps injuries in dental practice remain a concern today even though dentistry adopted preventive practices in the 1980s. An Australian study found 27.7% of dentists had experienced at least one sharps injury in the previous 12 months and 16.1% of these involved a contaminated instrument that had been previously used on a patient. Furthermore, the most common devices to cause sharps injury in the previous 12 months were needles (14.4%). Hollow-bore needle injuries are of particular concern, since they are likely to contain residual blood and are associated with an increased risk for blood-borne virus transmission. Of the 57 documented cases of occupational HIV transmission to healthcare personnel reported to CDC from June 1995 to December 2002, 50 (88%) involved percutaneous exposure. Of these, 45 (90%) were caused by hollow-bore needles and half of these needles were used in a vein or an artery.2 The risk Blood-borne viruses that could potentially be transmitted by a sharps injury include hepatitis B and C, as well as HIV. The risk of transmission following a skin puncture injury is dependent on: Whether the person who previously used the object had an infection; The level of virus in their blood; The amount of blood involved; The type of needle or syringe in question; The time that has elapsed since it was used; and The nature of the injury. So in dentistry, the most likely source of a blood-borne virus transmission is the local anaesthetic needle, being hollow and injected into a vascular rich area. It is estimated that up to 14% of inferior dental nerve blocks result in an intravascular injection and with an infiltration may too puncture a blood vessel.
FADI, FPFA infection CONTROL READ ME FOR CPD 134 Australasian Dental Practice January/February 2024 Biodentine™
By Dr Lance Kisby M olar Incisor Hypomineralisation (MIH) has become one of the most pressing issues in paediatric dentistry. MIH is a qualitative defect of unknown etiology in enamel development, presenting as demarcated opacities of variable extent and severity (Figure 1, Tooth 11). In 2003, the European Academy of Paediatric Dentistry defined MIH as a systemic condition and qualitative enamel defect of systemic origin that affects at least one first permanent molar (Figure 2-3), which can also be associated with permanent incisors. However, recent studies have shown it can affect second permanent molars, permanent canines, bicuspids and second primary molars.1,2,3,4,5 Hypomineralised second primary molars (HSPMs) can be considered a predictor for MIH in permanent teeth. Prevalence and distribution MIH is considered a worldwide clinical problem with a global prevalence of 14.2%, ranging from 0.5% to 40.2%. Worldwide, 25% of children have MIH.2 Lopes has shown that MIH has, in general, a prevalence of 13.5%; 36.3% of MIH teeth are moderately to severely affected; and MIH is present in 3.6% of second primary molars. Distribution of MIH was seen more in males at age nine years old, with molars affected more than incisors. The mandible was affected more than the maxilla and the right side was affected more than the left side.8 clinical EXCELLENCE READ ME FOR CPD
Preventing needle stick injury By Dr Greg Mahoney, BDSc, PhD, MSc (Dent), GradDipClinDent,
in the treatment of Molar Incisor Hypomineralisation (MIH) in paediatric dentistry: A case report
BY THE
POWERED
9929
Email info@dentist.com.au
(02)
1900 or
A summary of the latest research
By Emer. Prof. Laurence Walsh AO
Surgical respirators in clinical settings

One of the main infection prevention and control measures introduced during the COVID-19 pandemic was the focused application of respiratory protection to ensure health worker safety and the effective use of personal protective equipment. However, user acceptance of these strategies is paramount in sustainable compliance. During the periods of very high transmission of SARS-CoV-2, most health workers in NSW wore P2/N95 respirators. The effectiveness of any respirator is dependent on achieving and maintaining an adequate seal for the duration of its use. If respirators do not meet acceptable standards for comfort and compliance with donning, the ability to maintain an appropriate seal may be reduced, potentially leading to respirator leak and patient and health worker infection. This study explored various aspects of respirator use in NSW. The aim of the study was to understand the relationship between respirator comfort and user experience. A cross-sectional study was conducted in NSW (Nov-Dec 2022) using an anonymous self-administered online questionnaire. Of 2,514 respondents, 65% reported to have used a respirator every working day, with only a few using a respirator once weekly or less (9%). Almost all respondents had completed at least one fit test (96%) prior to the survey. Some 59% experienced discomfort from wearing a respirator. The most reported adverse effect was difficulty communicating (64%), followed by skin irritation or acne (62%) and headache (56%). Despite somewhat less favourable ratings on comfort and communication, NSW health care workers were in favour of respiratory protection. However, a focus on tolerance of respirators and strategies to address adverse effects from prolonged respirator use must be considered when implementing policies and procedures. The NSW Health respiratory protection program provides strategies such as frequent breaks, increased hydration, avoidance of makeup while wearing a respirator and skin protection with regular moisturising to reduce pressure injuries. Moreover, resources must be allocated to improve the design, breathability and sustainability of a respirator along with education and training on how to use respiratory protection safely and effectively.
Jain S, et al. Evaluation of health worker acceptance and tolerance of respirators in clinical practice—An Australian perspective. American Journal of Infection Control 2024;52(1):46-53.

Air treatment systems: State of the evidence
The COVID-19 pandemic increased the focus on preventing contamination with airborne pathogens (e.g. viruses, bacteria and fungi) by reducing their concentration. Filtration, UV or ionisation technologies could contribute to air purification of the indoor environment and inactivation of micro-organisms. The aim of this study was to identify relevant literature and review the scientific evidence presented on the efficacy of filter and germicidal technologies in air purification devices used to capture and inactivate micro-organisms and airborne viruses in practice. A scoping review was performed; after applying exclusion criteria, 75 studies were included. Data support the inactivation efficiencies of ultraviolet germicidal irradiation (UVGI) and ionisation applications in laboratory studies. Based on the results of these laboratory studies, it may be concluded that filtration, UVGI and ionisation technologies have an effect on various micro-organisms under different environmental conditions and these can inactivate micro-organisms and viruses. However, these studies are not representative of a practical situation. For example, no continuous aerosol emitting source in a room is used to investigate inactivation of microbiological contaminants. Studies that do work with aerosolised micro-organisms often study the decrease in a room which explains filtration, however, not inactivation of these pollutants. Overall, the laboratory studies do not adequately represent the practical situation in which the purifier systems are used. As well, the number of studies performed in practical situations is limited. Hence, based on the literature, no unambiguous conclusions can be drawn regarding the effectiveness of air purification technologies in clinical practice. Demonstrating the effectiveness of these air purifiers in practice will prove to be very challenging. As well, studies into the effect of by-products on human health of UVGI systems and ionisation systems are needed.
Kompatscher K, et al. Scoping review on the efficacy of filter and germicidal technologies for capture and inactivation of micro-organisms and viruses. Journal of Hospital Infection 2023;12:39-48.
60 Australasian Dental Practice January/February 2024 abstracts | 2024
















SOLUTIONS FOR 3D DENTURES ARE HERE fabdent.com.au Get onboard the 3D denture revolution, yes you can Scan, Design and Print or Mill today Contact us today ! 1300 878 336 exocad or 3Shape CAD ! Intraoral or Lab Scanners ! Asiga and Shining 3D New Printers ! ULTRA MAX 2 ACCUFAB CEL AoralScan Wireless DSEX - PRO G DWX-53DC

Changing to more sustainable dental practice in the post-pandemic era
By Emeritus Professor Laurence J. Walsh AO

Across the years of the COVID-19 pandemic, many dental clinics have found that their use of disposable items has increased dramatically. This article challenges that mindset, prompting a rethink of decisions on two key elements that can lower the environmental impacts of dental practice: disposable gowns and d isposable instruments.
PReusable gowns
rior to the pandemic, reusable linen gowns were the norm in many dental schools and in private and public dental clinics for many years. Hence, it is relevant to ask the question as to why clinics cannot return to this as a normal practice for non-surgical dental procedures.
Modern reusable gowns are typically made of cotton, polyester or blends of cotton and polyester.
62 Australasian Dental Practice January/February 2024 the cutting | EDGE
READ ME FOR CPD
It is important to know the composition of the gown because this influences how it is machine dried. Gowns with more cotton can tolerate a higher temperature in the dryer and will take longer to dry than those with more polyester and vice versa.
Even without including any pre-soaking in sodium hypochlorite, the processes that are used for machine washing and machine drying exert antimicrobial actions, but do not lower the splash resistance of the gown to any measurable extent. Modern reusable fabrics typically have superior resistance to fluid splashes when compared to disposable gowns, albeit at the cost of greater weight and also less breathability. Of interest, a majority of clinicians (over 80%) have reported feeling comfortable and safe when wearing reusable gowns.1,2
From a life cycle analysis (LCA) point of view, a reusable gown incurs costs for acquisition, laundering and eventual replacement. One can expect gowns to be laundered and reused 75 times before being replaced.3
There are also impacts from water use for washing and the release of water containing detergents into the waste stream and on the use of mains electrical power for operating the washer and dryer. The latter can be offset if electricity is generated by photovoltaic cells, hydro, wind or other zero-emission methods.
Disposable gowns represent a significant component of the waste generated by dental and other healthcare facilities over the past 5 years. Environmental impacts occur from the manufacture of the gowns, their transport to the point of use and disposal. Little has been done to attempt to recycle the polypropylene of disposable gowns, because of the risks that would pose to those working in recycling due to potentially infectious material being present on the gown caused by splashes of patient fluids.4
Overall, across different items of PPE used in dentistry, greenhouse gas emissions are greater for disposable gowns than for disposable gloves or surgical masks. A change from disposable gowns to reusable gowns has been estimated to reduce energy consumption by 64%, greenhouse gas emissions by 66% and solid waste generation by 84%.5 If fabrics in reusable gowns are designed for even longer use than the nominal 75 use cycles, the benefits of the change to them would be
even larger.5,6 This is why further research into the degradation of the fabrics used in gowns and their splash resistant properties, with repeated laundering, is needed. The polypropylene used in disposable gowns is derived from fossil fuels and this polymer generates during its production around 3 kg of carbon dioxide equivalent
manufacturer (typically in Asia) to Australia. It has been estimated that a single disposable gown has a carbon footprint of almost 1 kg of carbon dioxide gas equivalents. That is based on the assumption that the gown when disposed goes to landfill rather than for incineration. Incineration increases greenhouse gas emissions.8-10
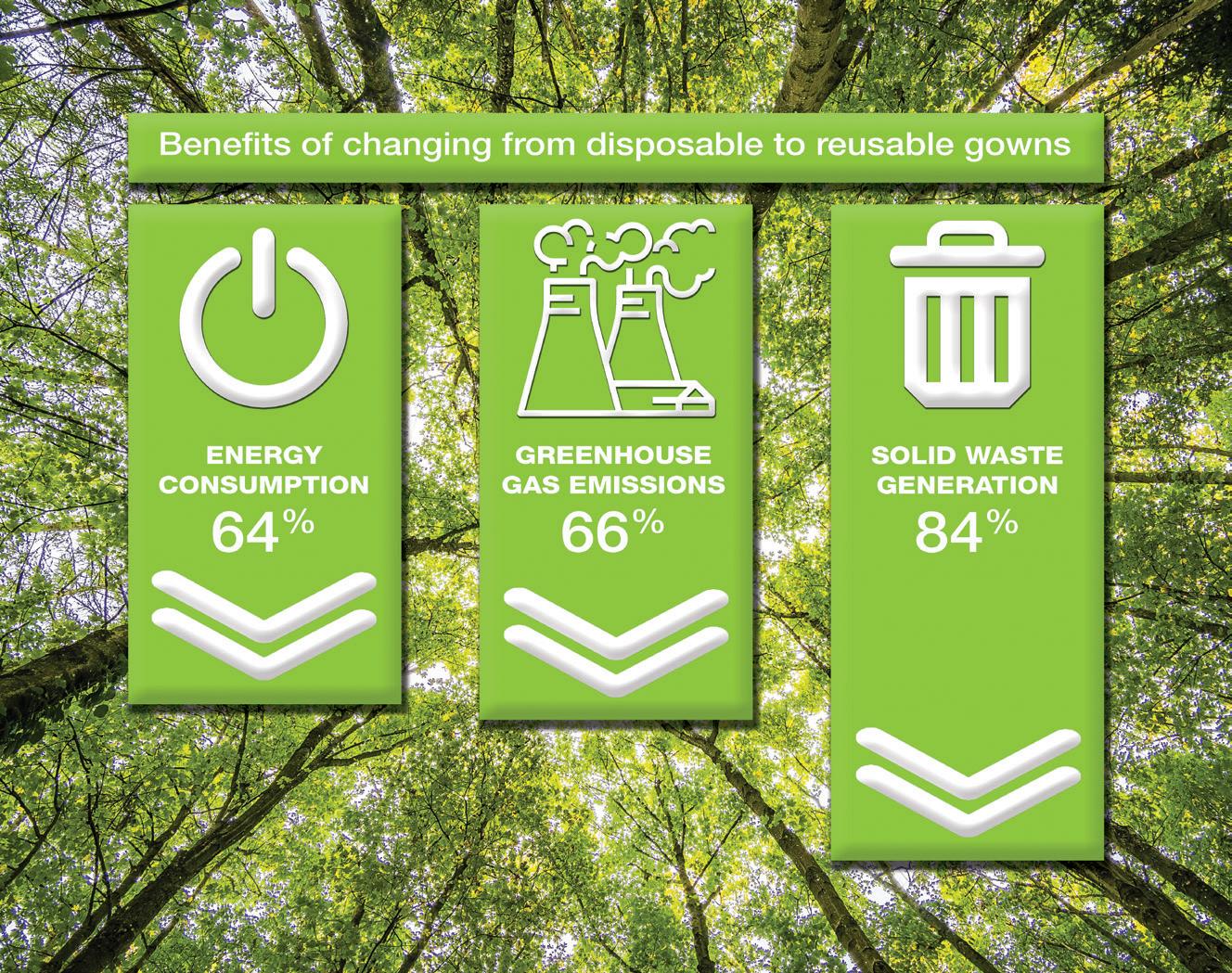
Disposable instruments
“Disposable gowns represent a significant component of the waste generated by dental and other healthcare facilities over the past 5 years. Environmental impacts occur from the manufacture of the gowns, their transport to the point of use and disposal...”
Another trend which emerged during the COVID-19 pandemic was for more dental clinics to use kits of disposable dental instruments, ranging from simple kits containing a dental mirror and some probes, through to single use sterile extraction forceps, to single use implant surgical kits. From a purely manufacturing point of view, when considering the processes involved in casting, finishing and polishing metal alloys, the differences between disposable and reusable dental instruments are quite small, in terms of greenhouse gas emissions. Similar raw materials and amounts of electricity will be used.
per kilogram of polypropylene manufactured.7 Most polypropylene production is undertaken in China, with the raw material then being exported to manufacturers who produce the disposable gowns. Thus, there is shipping of the polypropylene raw material and then subsequently shipping of the disposable gowns from the gown
The big contributors to environmental impact with disposable instruments occur because of transport and disposal costs, whether that is into landfill or by incineration. On the other hand, a normal reusable instrument, when properly cared for, should give a long period of clinical use, after which it is discarded and replaced.
January/February 2024 Australasian Dental Practice 63
the cutting | EDGE
the cutting | EDGE
Most estimates place the use life of regular non-surgical and surgical instruments at around 10 years.11
As with reusable gowns, there are reprocessing costs associated with reusable instruments. Costs for staff time figure large in such calculations, however the use of mechanical cleaning systems and better instrument management approaches (such as instrument cassettes) can considerably reduce these staff time costs by improving the efficiency of reprocessing by as much as 5 times.
One must factor in the electrical energy used for steam sterilisers, heat sealers, washer disinfectors and other equipment, as well as the electrical energy required for air-conditioning the reprocessing area and for providing relevant heating and lighting. There are additional con-
“Using alternative methods of sterilisation may further reduce the direct costs and environmental impacts of reprocessing reusable dental instruments...”
siderations for water usage, including the cost of specially treated deionised water for steam sterilisers and for the usage of various chemicals as part of the cleaning process. To date, there have not been detailed calculations of all these individual environmental impacts for reprocessing reusable instruments in dentistry. Having said that, calculations of this type have been undertaken for medical instruments and these show very large costs savings when instruments are reused, compared to the single use alternative.12
Using alternative methods of sterilisation may further reduce the direct costs and environmental impacts of reprocessing reusable instruments in the dental setting. As an example of this, one can compare lowtemperature vaporised hydrogen peroxide (VHP) sterilisation to steam sterilisation. VHP does not require water to be free of ions and hence there are no costs for distillation, deionisation or reverse osmosis. Total electrical energy consumption is very low for several reasons. The first of these is that the chamber does not need to be heated to 134°C, but rather only to around 40°C, which is necessary to keep the hydrogen
peroxide in the vapour form, to stop it condensing. Secondly, the only direct heating that is required is for the small nozzle where the hydrogen peroxide is converted from the liquid phase to the vapour phase. This nozzle tip is heated to just 55°C. On the other hand, with a steam steriliser, a sizeable volume of water must be heated to convert the water into steam and both the chamber and the load items within the chamber must also be heated to reach the 145°C operating temperature of the holding cycle.
A second consideration is that the packages used for VHP are made of a material (DuPont Tyvek™) that can be recycled. Unlike used disposable surgical gowns, used sterilisation packages made of Tyvek are not contaminated and so these do not pose a risk to those involved in recycling processes. At the present time, such
recycling is only available in North America, but it is possible that it will extend to Australia in the future.
Conclusions
Staff working in practices make decisions about where and when to use disposable gowns and disposable instruments. When making those decisions, they should consider both the direct costs to the practice (the financial expense for purchase and shipping), as well as the environmental impact those decisions have. The “everything disposable” mindset that dominated many dental clinics during the height of the pandemic is not a situation that is sustainable going into the future. Now is the time to think “back to the future”.
About the author
Emeritus Professor Laurence J. Walsh AO is a specialist in special needs dentistry who is based in Brisbane, where he served for 36 years on the academic staff of the University of Queensland School of Dentistry, including 21 years as Professor of Dental Science and 10 years as the Head of School. Since retiring in December 2020, Laurie has remained active in hands-on bench research work, as well as in supervising over 15 research students at UQ who work in advanced technologies and biomaterials and in clinical microbiology. Laurie has served as Chief Examiner in Microbiology for the RACDS for 21 years and as the Editor of the ADA Infection Control Guidelines for 12 years. His published research work includes over 400 journal papers, with a citation count of over 20,000 citations in the literature. Laurie holds patents in 8 families of dental technologies. He is currently ranked in the top 0.25% of world scientists. Laurie was made an Officer of the Order of Australia in January 2018 and a life member of ADAQ in 2020 in recognition of his contributions to dentistry.
References
1. McQuerry M, et al. Disposable versus reusable medical gowns: a performance comparison. Am J Infect Control 2021;49:563-70. doi: 10.1016/j.ajic.2020.10.013.
2. Belkin NL. Reusable personal protective equipment refutes savings claims of disposable counterparts. Hosp Mater Manage 1992;17(10):14-7.
3. Rizan C, et al. Environmental impact of personal protective equipment distributed for use by health and social care services in England in the first six months of the COVID-19 pandemic. J R Soc Med 2021;114:250-63.
4. Singh N, et al. Environmentally sustainable management of used personal protective equipment. Environ Sci Technol 2020;54:8500-8502.
5. Varangu L, et al. Reusable personal protective equipment in Canadian healthcare: Safe, secure, and sustainable. Healthc Manage Forum 2023;36(4):207-16.
6. Vozzola E, et al. An environmental analysis of reusable and disposable surgical gowns. AORN J. 2020;111:315-25.
7. Kutralam-Muniasamy G, et al. A critical synthesis of current peer-reviewed literature on the environmental and human health impacts of COVID-19 PPE Litter: new findings and next steps. J Hazard Mater 2022;422:126945.
8. De-la-Torre GE, Aragaw TA. What we need to know about PPE associated with the COVID-19 pandemic in the marine environment. Marine Pollut Bull 2021;163:111879.
9. Kumar H, et al. COVID-19 creating another problem? Sustainable solution for PPE disposal through LCA approach. Environ Dev Sustain 2020;23:9418-32.
10. Zhao W, et al. Comparative life cycle assessments of incineration and non-incineration treatments for medical waste. Int J Life Cycle Assess 2009;14:114-121.
11. Spry CN. Care and handling of basic surgical instruments. AORN J 2007;86(Suppl 1):S77-81.
12. Donahue LM, et al. A comparative carbon footprint analysis of disposable and reusable vaginal specula. Am J Obstet Gynecol 2020;223:225.e1-7. https://doi.org/10.1016/j.ajog.2020.02.007.
64 Australasian Dental Practice January/February 2024


• Computer Designed
• Perfect Fit
• Patented Material
• Laser Cut
• Smooth edges
• 3D Printed Model
• Perfect Fit
• Upper &/or Lower
• All scans accepted


The Solution For Your Retention Issues fabdent.com.au
Quality Retainers for all your patient needs. Contact us today ! 1300 878 336 The Original CAD Retainer ! All retainers supplied with a 3D printed model. Ask about discounts on multiples.
Buying and selling dental practices and practice valuations!
Things dentists need to know: Part 1
By Graham Middleton
“If a seller and buyer each seek advice from uninformed accountants, it is usual that the seller’s greatly overestimates value and the buyer’s greatly underestimates value. Neither is helpful...”
Ibegan advising dentist and veterinarians in 1987 and began valuing practices about three years later. This became a core competency I used as a founding partner of Synstrat Group in 1994 and by the time I departed Synstrat, in 2020, I had valued hundreds of practices located in every state plus the Northern Territory and ACT and advised a multitude of dentists, many of whom became lifelong friends.
Dentists with business problems
Many of the “valuation” enquiries I received were in fact requests for help with dental business problems in which case the dentist’s hidden agendas were identified and dealt with but valuation not proceeded with. 33 years of examining dental financials, including benchmarking dental practice efficiency, doing tax planning for dentists, helping dentists negotiate practice buy and sell agreements or sensitive dental associateships, gave me a rewarding insight into the Australian dental profession. I was fortunate to enjoy dental client relationships Australia-wide and to observe the differences in practice of financially very successful dentists and some who have struggled.
Practice brokers lack objectivity
Ichose not to become a practice broker as that would have destroyed objectivity in the services offered to dentists. Like real estate agents, brokers have greater motivation to achieve listings and sales rather than getting the best price for their clients. Practice owners frequently voice criticism that their broker was more concerned with talking down their sale price/conditions than representing them in negotiations. Like real estate, it is effectively the buyer who pays the agent’s commission. Agents will talk down a seller to gain a quick commission.
Dealing with brokers
Practice brokers ask potential buyers to sign confidentiality agreements before inspecting a practice. If it looks promising at first inspection then advise your definite interest but that you need to make some personal checks by appointment with the owner. That is when you ask to check the patient records billings and level of recent appointments. If that checks out, your accountant then asks for the financial records, including supporting tax returns. Be aware that brokers like to hand over “sanitised” financials which have had some
66 Australasian Dental Practice January/February 2024 practice | MANAGEMENT
purported-to-be private expenses removed. Your accountant must stand firm and insist on the actual financials and supporting tax returns plus any supporting documents. Remember that should you find a significant flaw in practice and financial records, you can pull out.
Knowing your own practice.
Often sales processes reveal that dentists have not understood their strengths and weaknesses and expose themselves to shocks during the selling process. Most accountants simply churn out tax returns for a variety of small businesses and individuals with no idea regarding how a dental practice compares with key benchmarks. These accountants are inadequate in representing their dental clients if a sale process reveals weakness whereas their client had assumed that they would have been advised by their accountant of issues that they should have addressed long before listing for sale.
Practice managers negative impact on profit and sale price.
Unfortunately, most practice managers —other than courtesy titles given to experienced receptionists—are profit destroyers rather than profit enhancers.
“Innocent” asked for a practice valuation and was shocked at the low figure. He sought deeper analysis and I pointed out that his non-clinical staff cost as a percentage of practice fees was extraordinarily high. With superannuation and work cover insurance, the “manager” was costing his practice $110,000 per year—and this was quite a few years back. The remainder of the non-clinical staff together cost as much as the average of all dental practices. The manager was not saving on other staff and her cost effectively reduced the capital value of his practice by around $400,000. He took a deep look at what the manager actually did and found out that with the assistance of a visiting bookkeeper and a bit of tightening of dental patient appointments and chairside assistants’ hours, he could dispense with the manager, reducing non-clinical staff overhead by $110,000. The practice manager’s position had long been redundant. A couple of years later he was able to sell his significantly more profitable practice for its true value.
Preparing to buy a dental practice.
The first thing to understand is that the vast majority of accountants and financial advisers know “diddly squat” about the differences between good and mediocre dental practices.
If they do have one or two dental clients, their interaction is invariably limited to completing annual tax and financial returns, but they are clueless as to how their clients’ practices compare with wellperformed practices or what to advise a buyer to look for beyond averaging the last three years’ profits.
Accountants’ advice seriously lacking
While many accountants have signage proclaiming that they give “business advice”, most do tax returns and confine advice to tax issues.
There is no point in comparing a dental client with a plumbing contractor or an Australia Post and lottery agent. Wisdom does not appear to improve with size of accounting practices. I have seen accountants from top-end-of-town accounting groups badly let down dentists with misinformed advice.
If approached for advice by a prospective practice buyer, a majority of accountants are inclined to suggest that it is overpriced without an idea as to what a realistic price range for similar practices is.
If a seller and buyer each seek advice from uninformed accountants, it is usual that the seller’s accountant greatly overestimates value and the buyer’s accountant greatly underestimates value. Neither helps their clients.
The accountant who wrecked “Tom’s” career
Tom was an employed dentist of about seven years’ experience. His boss offered to sell him the practice and work for him part time on a declining basis. The asking price was realistic, perhaps slightly above market, but not enough to warrant Tom walking away.
Tom consulted an accountant who unbeknown to Tom had few if any dental clients. The accountant proclaimed the practice far too expensive but offered
no comparative data. Armed with the accountant’s assessment Tom confronted his boss, who had approached him in good faith, suggesting that the price being asked was very unfair. Relations broke down. Tom left and spent more years as an employee in other practices, regretting what had occurred and was financially much worse off over a long career as a result.
The accountant suffered no loss for pretending that he had knowledge of dental practices and wrongly proclaiming that the practice was far too expensive.
What Tom should have done
Tom should have taken care to maintain good relations with his boss hoping that he could become the buyer to whom his boss wanted to hand over the practice.
Once his boss broached the subject of sale, Tom would have had meaningful personal discussions with his boss, dwelling on how long he wanted to continue working and for how many days.
He would have discussed protocols for a gradual handover of his surplus patients and shedding some to Tom and another assistant filling up the vacated days.
He would have gently asked whether his boss could be a little flexible on price, perhaps pointing out that in a direct sale, he was forgoing the cost of a broker.
At all times, he would have been polite, continuing to be deferential to his boss, who would come to realise that selling to Tom was his best chance of sale to a dentist to whom he was happy to leave his long-term patients in the care of and work for in the post-sale phase down of his dental career.
Three years financials:
Recent performance is much more important
The fees produced in the most recent month are a lot more relevant than the fees three years ago, particularly if most of the current financial year has elapsed. Buyers should seek proof of recent fees by demanding proof in the form of statements of the account into which fees are banked to determine whether income is being maintained. Bank lenders will demand three years financials, but the present state of the practice is far more important to the buyer.
January/February 2024 Australasian Dental Practice 67
MANAGEMENT
practice |
Hidden messages in practice records
Personal inspection of practice invoicing and treatment numbers is essential to understand the opportunity in what is being sold. A practice conducted by a pair of aging dentists who have limited their treatments to simple drill and fill procedures may have a wealth of patients who will welcome more advanced restorative treatments if given the option. Such a practice may be a great buy.
Conversely, a practice where a ruthless owner has shamelessly oversold highpriced procedures may have mined the practice dry as well as having left ethical clouds hanging over it. Only personally digging into treatment records and billings will inform a buyer as to how worthwhile a practice purchase is. Almost without exception, accountants—even some who profess expertise in advising dentists—are found wanting when advising purchasers.
Sell before fees deteriorate
It is important to maintain fees if intending to sell and this suggests that selling before the owner’s energy level deteriorates is important. Once a practice’s fees are in decline, it may mean that its patients have stopped referring their friends. I observed over many years that practice owners could reduce successfully to 4.5 clinical days per week then to 4 clinical days, but if they moved to 3 clinical days, there was usually a huge fall in practice profitability. Other critical staff, receptionists and employed dentists eased up, realising that their boss had lost the impetus to push the practice’s performance. Overall fees and profits plummeted. The lesson is to sell before reducing personal output below 4 days per week. No other individual will maintain the practice standards of a busy owner who cares.
Buy the practice not the company
Some dentists began their practices within a company structure, having zero goodwill in the beginning. If buying an established practice, it is vital to buy it from the company, not within the company, as it brings with it a potentially
huge future capital gains tax trap since its cost base to the company is zero and a company precludes the benefit of halving the goodwill value for tax purposes. I have known practice brokers to go to considerable lengths to persuade buyers to take the company who only end up having to sell the practice from the company many years later and finding that its cost base within the company created a huge taxable cost on sale of the practice after finding that no buyer would buy the company, only the practice from the company.
When buying a practice
1. Don’t buy it in a company; and
2. Buy in your own name or jointly with your spouse and in due course consider forming a company, not to own the goodwill, but to operate it under license so that the goodwill remains personal property and also enables you to take advantage of capital gains tax concessions when sold in the distant future. A company can be licensed to manage and conduct the practice part way through the first year of ownership, say after eight months. Timing is important because of tax issues.
3. There are advantages in operating via a company under a license agreement rather than a trust.
Preparing to sell your practice
• Appearance and presentation are important to buyers. Buyers need to be able to imagine themselves working in your practice. They must also view a practice as seen by patients on their first visit. Worn carpet and poorly presented waiting rooms are a turn-off. Pleasing surgeries with natural light and attractive ceiling pictures in patient’s vision when lying back in a dental chair are positives. Potential buyers who are put off probably will not come back.
• Know how your practice compares. Knowing your DEBDIT percentage relative to other practices and fixing weaknesses in the couple of years before sale is necessary to getting an acceptable sale price. Refer to my book Financial Success for Dentists for more detail.
The practice owner who destroyed his best buyer
Titus was miserable with a dollar. He was reluctant to spend on new carpet or repainting and the appearance of his practice had deteriorated somewhat. He had a loyal patient list, albeit their referrals had dropped off. It was a two-chair practice and Titus had a long-term employee dentist, John, who was prepared to buy the practice at a fair price. John planned to immediately replace the carpet and update the décor. Potentially it was a good deal for both and John thought he had a deal. Titus discovered a dental corporate who would pay a higher price for the practice but there was a catch; they would only do so if John signed a long-term contract with them. Titus was considered to be too old to fit their plan. Titus demanded that John pay the higher price or sign the corporates contract so he could sell. John was angry at Titus using him as a bargaining chip to get a higher price from the corporate and told Titus in blunt terms what he could do with that proposal. The dental grapevine picked up the message that John had fallen out with Titus and a dentist nearing retirement approached him to buy their practice. John bought the other practice and Titus no longer had a buyer for his practice as the corporate was no longer interested. Titus’s stinginess, lack of empathy with John and strategic misjudgement destroyed his sale.
Why buying, an established practice usually works better than doing a practice start-up
Starting a practice in an established suburb faces huge hurdles as existing practices in the area have large patient lists which are their referral base. The new start-up has zero referral base and may face years of struggle before it achieves a large enough fee base to reward the dentist after paying unavoidable expenses. Meanwhile a regular stream of newly referred patients attend established practices nearby.
The start-up near a new suburb is confronted with first homeowners with young families and poor cash flow who often cannot afford more than very basic treatment. New planned suburbs often force dentists into expensive shopping centre rentals making it near impossible to gain a significant return on investment.
68 Australasian Dental Practice January/February 2024 practice |
MANAGEMENT
The difficulties faced by start-ups is an underlying reason why established practices often have substantial goodwill value.
Over the years I occasionally got approached by a dentist desperately seeking advice on how to on-sell a recently started practice which was unable to cover its expenses and faced liquidation. I was unable to advise a solution. I came to realise that while successful practices are obvious, there are an unknown number of start-up failures because they disappear quietly with former premises usually filled quickly by some other type of business.
Don’t fall for marketing consultants’ blarney: Existing patients and their referrals are a practice’s lifeblood
Over many years, I spoke to many dental groups and conducted many informal audience surveys. They revealed that overwhelmingly, the biggest source of new patients are existing patient referrals of friends, family members and co-workers. They got little return on practice advertising cost including from internet sources.
While every modern practice has a website, it is mainly visited by persons who have already been referred and go to the site to find contact details for appointments and to check location.
Periodically, when benchmarking a new client’s practice, I found a significant marketing cost but inevitably it was not reflected in the practice performance. On questioning the dentists concerned, they indicated that the overwhelming majority of new patients were patient referrals despite heavy advertising.
Dentists who attempt start-ups competing against long-established practices thinking that some marketing consultant’s internet strategy will bring quick success are destined to learn an expensive lesson.
Breakaway strategies lacking patient connectivity.
Bondie and Chrissie worked in a longestablished practice owned by Harry. He had promised them first right of refusal when he decided to sell indicating that he would likely work for them on a reduced time basis for a couple of years. Harry had indicated that his decision to sell was imminent.
Harry owned the premises which had ample patient parking. There was a big patient list, the practice name being well established.
Bondie and Chrissie were persuaded by a friend’s friend—Smooth, a marketing consultant—to start up their own practice locally. As they had treated many local patients, they expected to avoid paying for Harry’s practice.
Smooth indicated he had strategies to ensure their success. They secretively rented premises in a building adjacent to a nearby shopping centre.
When fit-out and equipping was completed, they gave Harry their notice. Their strategy was a lot more expensive than they had bargained for as they realised the cost of fit-out and the myriad of things that they had taken for granted in Harry’s practice.
Smooth’s internet magic produced very little and they found that only a trickle of patients that they had previously treated were making appointments.
Harry was peeved but had been able to find other dentists. Since most patients only seek treatment periodically and had the contact number for Harry’s practice in their phones, most continued to make appointments at Harry’s practice. They were familiar with its location and knew that it had reliable parking.
Harry’s receptionist efficiently booked them into one of the new dentists’ and most remained bonded to Harry’s practice. Its name, telephone number, web page and parking created inertia favouring Harry’s practice. He received only a trickle of requests for dental records from Bondie and Chrissie indicating that they were struggling. Smooth had failed them badly.
In due course they observed another dentist buying Harry’s practice with Harry continuing to work a couple of days per week. Through a staff contact, they learned that Harry’s now former practice remained as busy as ever.
Advice to dentists on business matters
These days, I provide occasional advice to dentists who make donations to the charity I support, the Delany Foundation.
There is more to follow in the next issue of Australasian Dental Practice.
PFurther valuable advice
lease read my book Financial success for dentists. See my website at grahamgeorgemiddleton.com for further details and valuable information. Payment for the book is via donation to the Delany Foundation a registered charity. All costs of printing and mailing are met by me personally.
General Advice Warning
The information contained in this article is unsolicited general information only, without regard to the reader’s individual financial objectives, financial situation or needs. The information contained in this article is general in nature and you should consider whether the information is appropriate to your needs and where appropriate, seek professional advice from an accountant or financial adviser. It is not specific advice for any particular individual and is not intended to be relied upon by any person. Before making any decision about the information provided, you should consider the appropriateness of the information in this article, having regard to your objectives, financial situation and needs and consult your professional adviser. Any indicative information and assumptions used here are summarised, are not a product illustration or quote and also may change without notice to you, particularly if based on past performance. This notice must not be removed from this article.
About the Author
Graham Middleton disposed of his interest in Synstrat group on 30 June 2020 and won’t be starting another business; he spent the later 33 years of his working life advising health professionals on business and financial matters. Dentists were the most numerous of his clients. He is the author of the recently published Financial Success for Dentists.
Dentists may obtain a copy by making a donation of minimum $60 to the Delany Foundation a registered charity which assists schools in Ghana, Kenya and Papua New Guinea then email Graham at graham. george.middleton@ gmail.com. A copy will be sent to you. All proceeds go to the Delany Foundation for its good work. Graham has paid for the printing and mail costs personally.
January/February 2024 Australasian Dental Practice 69
practice | MANAGEMENT

Drilling down to the root cause: How to identify and solve the real problems in your dental practice
By Julie Parker
As a dental practice management consultant, I often come across practice owners who are constantly battling symptoms rather than addressing the root cause of their problems.
If you’ve ever found yourself trying to fix issues such as a gappy schedule or high staff turnover, it’s essential to pause and reflect: could these problems merely be symptoms of a more profound issue?
Think about how you operate as a clinician. When a patient comes to you with an abscess, you do not limit your thoughts to simply treating the infection. Instead, you consider what caused the infection in the first place. Is there decay present? A periodontal issue? As a skilled practitioner, you know that providing antibiotics is not enough. You know you have to find the CAUSE of the infection and treat that. Otherwise, the infection will return.
A similar approach is useful when addressing the problems that occur in the operation of your dental practice.
And there are always problems!
For example, let’s look at the common problem of a gappy appointment book. Many practice owners will say to me that they need to solve this “problem” by getting more patients booked in. However, without identifying the root cause of the growing downtime in the appointment book, we’re addressing the symptom only and not the cause.
Root Cause Tool
SYMPTOM (Problem)
Enter the challenge your practice is currently experiencing CAUSE
List 3 aspects of your dental practice that influence, or cause, the SYMPTOM
SOLUTION/S
For each CAUSE, provide 1-3 actions that you could take that will help resolve the root problem CAUSE #1 ACTIONS
A gappy appointment book can have several causes, such as:
n Decreasing treatment plan conversion rate;
n Fall in the quality of your customer service;
n Inadequate management of the recall strategy;
n Lack of follow-up with patients who have incomplete treatment, or;
n Increase in patient cancellations.
70 Australasian Dental Practice January/February 2024
practice | MANAGEMENT
CAUSE
CAUSE
FOR CAUSE
FOR CAUSE #1 CAUSE #2 ACTIONS FOR
#2
#3 ACTIONS
#3
Managing the problem simply by getting more new patients in the book might address the short-term problem of the gappy schedule (like antibiotics for the abscess), however, the practice will still suffer long term as those new patients don’t return because the root cause of patients failing to return has not been resolved.
To help dental practices tackle the inevitable problems with their day-to-day operations, I have developed a helpful resource called the Root Cause Tool (See figure opposite).
This tool takes you through the following steps...
1. Identify the symptom.
2. List three issues that may be causing the symptom.
3. Consider strategies (or treatments) that can help fix the true causes of the symptoms identified.
When faced with a symptom, consider three causes that would likely be influencing the outcome.
For example, if your appointment book is looking sparse, you might consider your treatment plan conversion rate; recall strategy; and management of incomplete treatment. Then, for each of these causes, identify what actions you could take to get a different outcome.
So, if a cause is a reducing treatment plan acceptance rate, actions you could take could be:
n Conduct a team training session where you brainstorm and role-play ideas on how to improve;
n Find an online course that could deliver new insights that your team have not yet considered (such as a Julie Parker Practice Success/Dental Business Mastery mini-course like Achieving Patient Engagement); and/or
n Analyse your practice reports and have the provider who achieves the highest conversion rate mentor the rest of the team.
Just like any business, dental practices encounter ups and downs in performance. Uncovering the underlying factors that are causing your dental practice to
underperform at this moment is essential for identifying and implementing the most sustainable and effective strategies for long-term success.
If you would like to access the Root Cause Tool , head over to our website dentalbusinessmastery.com.au and go to the Free Resources page. Download the fillable form and use over and over again to help you manage your dental practice towards greater success.
About the author
Julie Parker is a Dental Practice Management Consultant and Team Educator. At the age of 33, Julie became the first non-dentist to own a dental practice in Australia. Julie is Co-Founder of Julie Parker Practice Success and CoFounder of Dental Business Mastery. Visit julieparkerpracticesuccess.com.au and dentalbusinessmastery.com.au to find how Julie can help your dental practice be more successful. You will find information about consulting programs, online courses, podcasts, free downloads and more.
ACCOUNTING & FINANCIAL SERVICES FOR DENTISTS DON’T RISK SECOND BEST
Synstrat has spent many years collecting data on dental practices. We provide you with the best available knowledge on the performance of your practice relative to others. Our proven service has assisted many dentists Australia wide to create significant wealth. We are able to provide you with business accounting, practice valuation and financial advice services tailored to the dental profession.
Buying A Practice?
•Do you need us to value the practice?
•What rent can it afford?
• How do you structure to meet tax planning requirements?
• What changes should you make to the practice business plan?
January/February 2024 Australasian Dental Practice 71
practice | MANAGEMENT
The Synstrat Group www.synstrat.com.au ALSO AVAILABLE: 50 Rules for Success as a Dentist Buying and Selling Specialist Dental Practices Speak to Paul Steel or David Collins on (03) 9843 7777 or email dental@synstrat.com.au NOW AVAILABLE: Synstrat Dental Stories TO RECEIVE THE BOOK You can either e-mail dental@synstat.com.au with your request for the book together with your postal address or go to www.synstrat.com.au, navigate to the Synstrat Publications area and fill in the form. You will then be forwarded the book.

Practice purchase deposit FAQs
By Simon Palmer, Wilson Twist and Harry Nicolaides

There are many misconceptions about the role that a deposit plays in a practice sale/purchase transaction. Is it negotiable? Is it refundable? Who holds the deposit? When and how is it released?
To provide some clarity in this regard, we thought we would answer some practice sale deposit FAQs.
Q1
WWhat is the usual amount of a deposit in a business sale?
hile the standard deposit amount is 10% of the purchase price, it can be negotiated to be a higher or lower amount, depending on the commercial terms agreed to by the parties.
Q2
At what stage in the purchase/sale does the purchaser need to pay a deposit?
U sually, a deposit is paid by the purchaser to the deposit holder upon execution (signing) of the formal, binding contract of sale, or by a specified date shortly after the contract is signed.
Q3
Who holds the deposit? Can the deposit holder use the money?
Depending on the scale of the transaction, the deposit is usually held by the vendor’s agent or the vendor’s lawyer. In either case, the deposit is usually held in a trust account (a special kind of bank account maintained by agents and lawyers). The deposit is held until one of the parties to the transaction becomes entitled to it under the contract of sale. The deposit holder is not permitted to access or use the deposit funds (and would be in for some serious consequences if they did!).
Q4
At what stage in the purchase/sale of the business does the deposit become non-refundable?
O
nce the deposit is paid, it is dealt with under the formal contract of sale. Often, if a contract is subject to purchaser conditions (such as finance, due diligence, premises lease approval, etc), the contract might specify that if the condition does not eventuate, then the deposit is returned in full
72 Australasian Dental Practice January/February 2024
practice | MANAGEMENT
to the purchaser. If a contract is signed unconditional or becomes unconditional, then generally speaking, the deposit is “non-refundable”.
At what stage in the purchase/ sale of the business does the deposit get released?
This depends on what is written in the contract.
Generally, the deposit is released:
• Back to the purchaser if the contract is not unconditional and one of the conditions precedents are not met (e.g., unsatisfactory due diligence of the contract subject material, failure to obtain suitable finance, the premises lease not being assigned, etc.);
• To the vendor at the settlement/completion of the transaction; or
• To the vendor if the purchaser defaults on completion or an intermediary pre-condition (failure to satisfy due diligence as incoming tenant, etc).
Some purchasers offer to pay a deposit with their offer (i.e., before a formal contract is signed). What are some of the implications of this?
Offering to pay a deposit prior to contract is sometimes used by prospective purchasers as an incentive for their offer to be accepted. However, such an arrangement without a formal contract in place comes with significant risk for all parties involved - including the deposit holder.
Without a contract of sale signed by both parties, it is very difficult to know if all parties are on the same page about how the deposit is to be held and distributed. As such, a deposit should only be paid once the formal, binding obligations of the parties are agreed and signed.
The purchaser has asked for a reduced deposit... does this mean that they are not serious about the transaction?
Not necessarily. A purchaser will often be relying on finance to purchase a business. This finance is only released by the lending institution at settlement.
A deposit is payable on exchange of signed contracts BEFORE the finance becomes available.
This means that the purchaser often needs to pay the deposit before finance is available out of their savings. On a large deal, with a significant purchase price, a serious purchaser may simply not have enough of their own funds saved to pay the usual deposit percentage amount.
If the purchaser defaults on an unconditional signed - but not completed – deal... What are the damages a vendor can seek from a purchaser? What role does the deposit pay in these damages?
The damages that are payable if a buyer defaults ultimately depends upon what the contract says.
Assuming the purchaser has withdrawn from the contract (without a proper basis), damages seek to compensate the vendor to the extent that the vendor has been financially disadvantaged by the purchaser not completing the sale.
Losses which are commonly suffered and which may be recoverable, include:
• Any loss of value (e.g. if the vendor sells the practice to another purchaser for a lower amount);
• Any operating losses or capital expenditure which are reasonably incurred by the vendor seeking to minimise any loss in value;
9 March 5 April 11 May 1 June 22 June
• A readvertising fee; and
• Other fees and charges associated with the intended sale, such as bank fees (this can include legal fees).
The deposit plays an important role in these damages:
• Some contracts provide that the deposit may be retained by the vendor, in full, if the purchaser causes the contract to not complete;
• The deposit becomes the first and most accessible part of the damages paid to the vendor, HOWEVER, the purchaser may be liable for damages that far exceed the deposit amount; and
• The vendor may have to take legal action against the purchaser in order to recover the rest of the damages they are entitled to.
The deposit is, in any circumstances, important security for the vendor for any losses they might suffer.
About the authors
Simon Palmer is the Managing Director of Practice Sale Search, Australia’s largest dental practice brokerage. If you’d like more information on practice sales or want to have a confidential discussion about your practice’s circumstances, email Simon Palmer at info@practicesalesearch.com.au or call 1300-282-042.
Wilson Twist is a senior associate in the K&L Gates Brisbane real estate group. He has experience across a range of commercial real estate matters.
Harry Nicolaidis is a partner at K&L Gates Brisbane. For legal advice about your practice sale/purchase, Harry Nicolaidis can be contacted at harry.nicolaidis@klgates.com.
January/February 2024 Australasian Dental Practice 73
SYDNEY AUCKLAND MELBOURNE ADELAIDE BRISBANE
practice | MANAGEMENT Q5 Q6 Q7 Q8
The best time to contact your patient
By Jayne Bandy
When is the best time to contact a patient?
Anytime is the best time of course!
Within reason.
The crack of dawn or midnight will not go down well.
In the past, we’ve been a little hesitant contacting patients in case it’s not the best time for them.
We call patients, sometimes in the hope they will pick up that phone, but alas this is easier said than done nowadays!
A text message has become a great way to shoot off a message to patients who can then read it immediately or when they have a moment to check their phone.
But there are certain times when you really need to speak with your patient over the phone.
One of these times is when you need to get patients back for their incomplete treatment where no appointment has been scheduled.
This is the time when you may need to have a serious conversation with your patient regarding urgency and importance and the consequence of delaying treatment. This is near impossible to do in a text message. During these calls, your patient may have questions and even objections that can easily be handled on a phone call.
The biggest problem faced by practices is when you try to call your patient, even at a time that you believe is best, you most often get a voicemail and must leave a message.
The next problem is most dental practices do not know how to leave a great phone message and have lost sight of the purpose of the message they leave.
What is the purpose of the phone message you leave?
Yes, it’s for the patient to you call back immediately.
So, what kind of phone message will achieve this?
The phone message you leave needs to let your patient know who you are and where you’re calling from and what the call is in regard to.
My advice, always, is to avoid telling the patient too much.
You want your message to be a little cryptic and mysterious.
Remember, you want your patient to call back to find out more.

Call Tracking Excellence is not a product IT’S A RESULT!
With Call Tracking Excellence your team will learn the SAME exact processes Jayne used to:
1. Dramatically improve new patient call-in conversions to booked appointments.
2. Retain existing patient appointments and...
3. Prevent ongoing losses from appointment cancellations. Visit the website to find out how to get started. It’s that easy! www.calltrackingexcellence.com
“Hi John, it’s Jayne from Active Dental. I’m calling in regard to your appointment. Can you please call me back on ________ as soon as you can this afternoon.”
Can you see I have let the patient know who I am, where I’m from and why I was calling.
Now think about it. This patient has no appointment. The patient hears the phone message and is trying to work out which appointment.
The patient is now more driven to call you back to find out more. Now you have control of the conversation with the patient. They have called you back.

You now have an opportunity on the phone to schedule an appointment for the patient that they do not have booked in yet.
So, back to the best time to call a patient.
Anytime is the best time because this is what usually happens - you end up leaving a short message for the patient to call you back at a time that suits them.
Giving a time frame when you need the patient to call you back is important as is avoiding giving too much information in the message. You want your patient to call you back to find out more.
Now you can have a great conversation with your patient, schedule and confirm their appointment and go tell your dentist how great you are at following up your patients!
To find out how I can teach your team to know what to say and ask your patients, to help them make more kept appointments and prevent cancellations, call me on 1300-378-044 or email jayne@thedpe.com
About the author
Jayne began her career as an educator. After spending several years teaching, she made the jump to practice management, serving as a Practice Manager for a renowned dentist in Sydney for more than 25 years, giving her first-hand experience at what works when it comes to building and maintaining patient relationships, how to convert leads over the phone and most importantly - what it takes to reach your practice goals. As the CEO and Founder of Dental Phone Excellence, Jayne helps practices convert more calls into appointments, reduce cancellations and nurture effective patient communication that will result in increased profitability. Her past experience as an educator combined with her passion for practice management gives her a unique set of skills that allows your team to fully understand and take advantage of the tools she presents.
74 Australasian Dental Practice January/February 2024 practice | MANAGEMENT
Organising a dental event, lecture, congress, trade show or webinar?


GO EXPRESS»»»»»
If you’re organising any kind of post-graduate dental education, event or webinar, listing your event on the dentevents.com continuing education calendar is now easier than ever.
No username, no password and no need to login - add your event by simply visiting dentevents.com, clicking on Adding Events and then selecting Express Listing.
Complete all the details on the form and click SUBMIT
An email containing a link to edit or update the event will be sent to you that also allows you to track the approval status.
After the event is checked, it will be posted to dentevents.com.
Advanced functionality
For event organisers who already use Dentevents to manage their events through www.dentalcommunity.com.au and use the registration, payment and ticketing tools, this system should continue to be used as normal.
Tools for event organisers
Dentevents.com offers event organisers a full suite of marketing, ticketing, payment, registration and event management tools cost-effectively and on-demand.
Full information is available at the newly updated Dentevents.com website.
Visit www.dentevents.com Published by Main Street Publishing Pty Ltd • PO Box 586 Cammeray NSW 2062 • Call (02) 9929 1900

Emails your patients will love: How to craft irresistible messages
By Angus Pryor, MBA (Marketing)

In today’s fast-paced digital landscape, emails are an essential part of our daily lives and indeed, some (though not all) dentists regularly use email to communicate with their patients.
Yet, with inboxes getting more crowded by the day, the challenge is to make emails not just reach your patients but also resonate with them on a deeper level, cutting through the noise. In this article, we unpack how to create emails your patients will love.
Personal touch in emails
Connecting beyond names
I n 2024, personalisation is key and much more than just using the recipient’s name. It’s about creating a connection that feels genuine and personal. This can be achieved by segmenting your email list and creating content that caters to specific patient interests and needs. When an email feels tailor-made for the reader, it instantly becomes more engaging and noteworthy.
76 Australasian Dental Practice January/February 2024
Strategies for effective segmentation
Segmentation means not treating everyone the same. Most practice management software systems have the capacity to “tag” patients based on whatever category you like, for example “Kids”, “Cosmetic” and so on.
Once you have your patients tagged, you can easily email all patients with (or without) that tag on a particular topic. For example, you could send a back-to-school email to all patients that have a “kids” tag.
If you’re worried this somehow feels like big brother, be aware it’s much better for the clients to get emails about things that interest them rather than content that’s completely irrelevant.
By dividing your audience into different groups based on their unique characteristics and preferences, you can craft messages that should be much better received than a one-size-fits-all approach.
Subject lines that captivate
First impressions matter
Your subject line is critical for your email and probably the number one mistake dentists make in communicating with their patients.
It’s crucial to make the subject line as engaging and relevant as possible - but there is an art to it.
Aim to spark curiosity while staying true to the content of your email. Misleading subject lines can damage trust and reduce the effectiveness of your future communications.
Crafting effective subject lines
The best subject lines are concise, clear and enticing. You should keep them to a maximum of about 12 words but fewer is usually better – we went for 10 words in this article. The key is to build curiosity and value.
As we’ve done, “how to” emails can work well, but there are a myriad of other headlines you can go for. Using numbers in headlines is helpful too – e.g. 5 ways to save money at the dentist.
Headlines often include an element of intrigue or urgency but should always be aligned with the actual content of the
email - otherwise they can be spammed as “clickbait”. Regularly testing different subject lines and analysing open rates (i.e. how many people open it) can provide valuable insights into what works best with your audience.
Designing visually appealing emails
The power of visuals
Since humans are highly visual beings, the aesthetic appeal of your email plays a crucial role in capturing and maintaining the reader’s interest. A clean, attractive design with relevant images or graphics can significantly enhance the readability and appeal of your email.
“Once you have your patients tagged, you can easily email all patients with that tag on a particular topic. For example, you could send a back-to-school email to all patients that have a “kids” tag.
If you’re worried this somehow feels like big brother, be aware it’s much better for the clients to get emails about things that interest them rather than content that’s completely irrelevant...”
OOptimising email layouts
rganising your email content into easy-to-read sections with clear headings and bullet points not only makes your emails more scannable but also guides the reader through your message. Striking the right balance between text and visuals helps make your emails inviting and not overwhelming.
Brevity and relevance
Conciseness is key
In our time-strapped world, brevity in emails is highly valued. Get to your point quickly and ensure every part of your email adds real value to the reader. Unnecessary fluff can lead to disengagement and a lost opportunity to connect.
Ensuring content relevance
Each element of your email should serve a clear purpose, whether it’s to inform, persuade or entertain. Avoid diluting your main message with irrelevant content, as this can detract from the overall impact of your email.
For most emails, keeping it to a page is desirable. Few people, other than skilled copywriters, can keep people’s attention for more than a few paragraphs, particularly when most people are only moderately interested in the dentist.
Clear and compelling calls-to-action
Guiding your readers
AIf you looked back over time at my articles in Australasian Dental Practice, you’d discover that there is almost always a face in the image. Even from babies, our eyes are attracted to faces.
You may be excited to email an announcement about your new piece of equipment, for example, but it’s faces (rather than bits of equipment) that our eyes are drawn to. Show the result of the equipment (smiling faces) rather than the equipment itself in your cover image.
well-crafted call-to-action (CTA) is essential in guiding the reader on what to do next. Whether it’s visiting a website, calling the practice or reading a blog post, your CTA should be clear, prominent and enticing.
If you’re struggling to think of a CTA, you may need to rethink why you’re sending the email in the first place.
One of the most appealing words to the human brain is “new”. If you have something new to talk about, then the CTA can be relatively straightforward: Come meet that person, book an appointment, read more, etc.
January/February 2024 Australasian Dental Practice 77
marketing | INSIGHTS
marketing | INSIGHTS
Effectiveness of your CTAs
Astrong CTA can significantly boost the conversion rate of your email. If you have a very strong CTA, then put it through the email more than once. For example, add “call us today” after paragraph 2, in the middle of the page and at the end of the page.
Enhancing engagement through storytelling
The art of narrative in emails
Incorporating storytelling into your email marketing can dramatically increase engagement. A good story not only captivates readers, but also makes your message more memorable.
You can share stories about your brand, services or patient experiences to create a deeper emotional connection with your audience.
Ideally, your story has a point that you want to leave with the reader. A good question to ask is “If there was only one thing I want the reader to take away from this email, what is it?”.
Creating resonating stories
Stories should be relatable and authentic, reflecting real-life experiences, challenges, or successes. When readers see themselves reflected in your narratives, it fosters a stronger bond with your practice. In 2024, more than ever, people are looking for a human connection.
Once you start using stories in your email (and realise you need to generate more in the future), you may be surprised to find them popping up everywhere.
Optimising for mobile devices
The need for mobile-friendly
design
With the increasing use of smartphones for email, ensuring your emails are mobile-friendly is crucial. This means optimising layouts, images, and text for readability on smaller screens, increasing the likelihood of your email being read and acted upon.
Testing for mobile optimisation
S end a test email and view it on multiple devices – desktop, tablet, and mobile phone – to make sure whichever way the reader accesses it, the email will be easy to consume.
Based on that feedback, you might need to be simplifying designs, increasing font sizes, and/or ensuring that CTAs are easily clickable on a touchscreen.
CTAs, and pay attention to feedback and preferences from your audience. This ongoing process of adaptation ensures that your email marketing remains effective and relevant over time.
Summary
Email marketing is not dead, as some people claim. It has the benefit of a broad distribution to your patients at a very low cost. However, as noted in this

Regular analysis and adaptation
Harnessing data for improvement
Now that you’re in the habit of sending emails, regularly analysing the performance of your email campaigns is vital for continuous improvement. Metrics like open rates, click-through rates, and conversion rates can offer insights into the effectiveness of your strategies.
It’s fair to say that open rates for email are going down over time (comparing one year with the next), but you can buck the trend by producing better quality content.
Adapting based on insights
Use data to refine your approach. Experiment with different elements like subject lines, content, layout, and
article, it does require some planning to get and maintain a good result.
By implementing these strategies, your emails will not only capture attention in crowded inboxes but also forge deeper connections with your patients.
About the author
Multi-award-winning Practice Growth Specialist, Angus Pryor, is an author, marketer and international speaker. He is the #1 Google-ranked dental marketer in Australia. In 2023, Angus’ team at Dental Marketing Solutions received the ADIA’s marketing award. More details are at www.DentalMarketingSolutions.com.au. For a smarter, cheaper solution to finding great team members doing particular tasks, there is a solution. To find out how to unlock the gold in your practice from incomplete treatment plans, reactivations and more (and to access free sources), visit www.DentalStars.com.au.
78 Australasian Dental Practice January/February 2024
















Subscribe Today! Earn 2 CPD Hours every edition Only $99 per year or $165 for 2 years Click Subscribe at... www.dentalpractice.com.au Paid subscribers can access all past editions of Australasian Dental Practice and complete any of the CPD questionnaires by logging in at www.dentalcommunity.com.au

The FIRE method for retirement
By Scott Ungaro
As financial advisers, we get asked all sorts of questions from buying a house to investing for the future. We also get asked about the latest financial literature, celebrities or philosophies. One of the more common questions I am asked is in regards to the FIRE method for retirement.
The FIRE method, which stands for “Financial Independence, Retire Early”, is a personal finance and lifestyle movement that aims to achieve financial independence and retire at a relatively young age, often well before the traditional retirement age of 60-65.
The goal of FIRE is to have enough savings and investments to support one’s desired lifestyle without the need for traditional employment.
Here’s how the FIRE method works:
1. Financial Independence
Achieving financial independence means having enough savings, investments and passive income streams to cover your living expenses without relying on a traditional job. In other words, you have enough money to sustain your desired lifestyle indefinitely.
2. Retire Early
The “Retire Early” part of FIRE means leaving your traditional full-time job or career at a younger age than is typical. While some FIRE enthusiasts aim to retire in their 40s or 50s, the specific age varies from person to person based on their financial goals and circumstances.
Key principles of the FIRE method:
1. Frugality
F IRE advocates typically embrace a frugal lifestyle to save as much money as possible. This includes minimising unnecessary expenses, budgeting carefully and avoiding lifestyle inflation.
2. Saving and investing
F IRE followers prioritise saving a significant portion of their income, often aiming to save 50%+. They invest their savings in various assets, such as stocks, bonds, real estate and index funds, to generate passive income and wealth over time.
3. Minimalism
M any FIRE adherents adopt minimalist lifestyles, focusing on owning fewer possessions and simplifying their lives to reduce expenses and clutter.
4. Side hustles
S ome FIRE enthusiasts pursue side businesses or part-time work to supplement their income during the early retirement phase.
5. Emergency fund
B uilding and maintaining an emergency fund is crucial to cover unexpected expenses and ensure that early retirement plans aren’t derailed by unforeseen financial setbacks.
6. Continuous learning
F IRE followers often emphasise ongoing learning, both in personal finance and other areas, to adapt to changing circumstances and stay financially savvy.
80 Australasian Dental Practice January/February 2024
|
finance
INVESTMENT
7. Safe withdrawal rate
A central concept in FIRE planning is the “safe withdrawal rate”. This is the rate at which retirees can withdraw money from their investments without depleting their portfolio too quickly. The commonly cited safe withdrawal rate is 4% annually, adjusted for inflation, but this can vary based on individual circumstances.
It’s important to note that achieving FIRE requires discipline, dedication and a clear financial plan. It may not be suitable for everyone, as it involves significant lifestyle changes and financial sacrifices in the short term to achieve long-term financial independence. Additionally, individual circumstances and financial goals vary, so what works for one person may not work for another. Consulting with a financial adviser and carefully evaluating your own situation is advisable if you’re interested in pursuing the FIRE method for retirement.
General advice warning
This communication is issued by Profile Financial Services Pty Ltd. (ABN 32 090 146 802), holder of Australian Financial Services Licence and Australian Credit Licence No. 226238. It contains information and general advice only and does not take into account any investor’s individual objectives, financial situation or needs. It should not be relied on by any individual. Before making any decision about the information provided, investors should consider its appropriateness having regards to their personal objectives, situation and needs, and consult their adviser. Any indicative information and assumptions used here are summarised, are not a product illustration or quote, and may change without notice to you, particularly if based on past performance.
Whether you’ve just started working, own your own practice or are considering retirement, Profile Financial Services can help you plan and secure your financial future. Just like good dentistry, in investing, prevention is better than cure! A sound financial plan can help anticipate and avoid risks before they damage your portfolio.
How safe are your investments?

To find out, contact Profile now to book an obligation-free initial meeting: (02) 9683 6422 Or visit our website www.profileservices.com.au
About the author
Scott Ungaro is a Senior Financial Adviser at Profile Financial Services Pty Ltd (AFSL 226238), a privately owned and self-licensed fee-based financial planning firm that specialises in working with dental professionals. Kurt’s passion for planning is to help people make their own, wellinformed financial choices by breaking down complex information and situations and identifying the important issues that need to be addressed. He has a particular interest in helping people plan for and transition to their retirement. Kurt holds a Bachelor of Agricultural Economics (Majoring in Corporate Finance, Economics and Agricultural Economics) and an Advanced Diploma of Financial Planning. He is a member of both the Financial Advice Association of Australia (FAAA) and the Self-Managed Super Association. Scott can be contacted on (02) 9683-6422, scott.ungaro@profileservices.com.au or visit www.profileservices.com.au).


January/February 2024 Australasian Dental Practice 81
finance | INVESTMENT
even fOr yOur SAFety
FinAn ci Al A FFA irS Wealth managers for the dental industry FOr OVer 30 yeArS BUilDinG WeAltH SecUrity AFSl 226 238 Profile_SafetyAd_v3.indd 1 18/03/11 2:04 PM
FirSt
Infection Control BOOT CAMP
ON DEMAND ONLINE LEARNING PROGRAMME
29 VIDEOS - 8+ HOURS OF EDUCATION
Presented by Emeritus Professor Laurence Walsh AO BDSc, PhD, DDSc, GCEd, FRACDS, FFOP (RCPA), FFDT (RCS Edin)
Learn from Australia’s leading authority on infection prevention and control in dentistry about recent changes in infection control including from the Dental Board of Australia (July 2022), the ADA (4th edition guidelines August 2021 and the ADA Risk management principles for dentistry during the COVID-19 pandemic (October 2021)), the new guidelines from NHMRC (May 2019), Hand Hygiene Australia (Sept 2019) and the CDNA (Dec 2018) as well as recent changes in Australian Standards and TGA regulations that are relevant to infection control. The course provides a summary of how those changes interlink with one another and also covers practical implementation of the new requirements and what it means for everyday dental practice. Hear about the why and the how and keep up-to-date with the changes that are happening.
COURSE TOPICS
This one day course will cover changes in regulations and guidelines from 2018 to 2022 including:
n Risk-based precautions.
n Hand hygiene and hand care practices.
n Addressing common errors in personal protective equipment.
n Biofilm reduction strategies.
n Efficiency-based measures to improve workflow in instrument reprocessing and patient changeover.
n Correct operation of mechanical cleaners and steam sterilisers.
n Wrapping and batch control identification.
n Requirements for record keeping for instrument reprocessing.
n Correct use of chemical and biological indicators.
dentevents presents...
8 HOURS CPD Register Now: www.boosterinjection.com.au






Laurie Walsh is a specialist in special needs dentistry who is based at the University of Queensland in Brisbane, where he is an emeritus professor. Laurie has been teaching and researching in the areas of infection control and clinical microbiology for over 25 years and was chief examiner in microbiology for the RACDS for 21 years. His recent research work includes multiple elements of infection control, such as mapping splatter and aerosols, COVID vaccines and novel antiviral and antibacterial agents. Laurie has been a member of the ADA Infection Control Committee since 1998 and has served as its chair for a total of 8 years, across 2 terms. He has contributed to various protocols, guidelines and checklists for infection control used in Australia and represented dentistry on 4 committees of Standards Australia and on panels of the Communicable Diseases Network of Australia and of the Australian Commission on Safety and Quality in Health Care.
REGISTRATION FEES
Dentists $660 inc gst
Others $330 inc gst
REGISTRATION INCLUDES
n On-Demand access to 29 Online Learning Videos (Over 8 hours of education).
n Watch and re-watch at your leisure 24/7
n Digital Online Learning Companion.
n Digital Suggested Reading Material.
n Online Questionnaire to earn 8 Hours of CPD.
Register Now: www.boosterinjection.com.au
Infection Contol Boot Camp is presented by Dentevents, a division of Main Street Publishing Pty Ltd ABN 74 065 490 655 • www.dentevents.com • info@dentist.com.au Tel: (02) 9929 1900 • Fax: (02) 9929 1999 • Infection Contol Boot Camp™ and Dentevents™ are trademarks of Main Street Publishing P/L © 2023 Main Street Publishing Pty Ltd FULL UPDATE! All the changes to Infection Control Updated in 2022 dentevents.tv
Infection control challenges for 2024
By Emeritus Professor Laurence J. Walsh AO
AAs we begin a new year, it’s useful to flag a number of the issues that will emerge during the coming 12 months, to prompt thought, reflection and discussion.
Washer-disinfectors
utomated mechanical cleaning of reusable medical devices (RMDs) is a mainstay of modern instrument reprocessing practices, with ultrasonic cleaners and washer disinfectors (WD) being the two most commonly used technologies in dental practice reprocessing areas. Both of these approaches are included and discussed in the new
December 2023 Australian standard on reprocessing of RMDs that will be discussed below. The Australian standard that applies to ultrasonic cleaners used in healthcare facilities (AS 2773) was updated in late 2019. This reinforces the point that ultrasonic cleaners will continue to be used in reprocessing (Figure 1).
A key consideration when considering which of these two methods to use with a particular device is the manufacturer’s instructions for reprocessing. Under the Essential Principles requirements when devices are approved by the Therapeutics Goods Administration (TGA), RMDs that are designed by the manufacturer for reuse on multiple patients must have comprehensive documentation on reprocessing.
84 Australasian Dental Practice January/February 2024
READ ME FOR CPD infection | CONTROL
This will indicate whether the device can be cleaned in an ultrasonic cleaner, or whether a washer disinfector is needed. As an example of this, several modern air turbine high speed handpieces have been designed to be compatible with cleaning in a washer disinfector, as they are able to tolerate the highly alkaline detergents that are used, without undergoing corrosion. A separate device will be needed for lubrication of these handpieces once they have been cleaned. Washer disinfectors will be fitted with couplings onto which the handpieces will be attached. These couplings will ensure that the range of liquids that are dosed into the chamber are delivered to the internal aspects of the handpieces.
“One of the key changes in the document is the scope... This provides a uniform thinking approach across different settings, which will simplify assessment by public health regulators in the future...”
International standards that relate to WD are found within the ISO 15883 series. Some of these have been updated in recent years, particularly those relating to the use of performance assessment using soil tests. An example is part 5 of the series from 2021 which focuses on performance requirements and test method criteria for demonstrating cleaning efficacy. This type of testing can occur in 2 different contexts: type testing, under simulated use conditions, with defined test soils, soiling methods and RMDs that are representative; and performance qualification (PQ) testing under everyday clinical conditions with loads that are soiled from clinical use. In type testing, various synthetic soils can be applied onto dental RMDs, while in PQ, a range of different soil test devices are available commercially. Test strips can be placed in parts of the chamber that are more difficult for the spray jets to reach, so that the effectiveness of cleaning can be assessed. While there is a minimum requirement in the ISO 15883 series for daily assessment of performance, it is best practice to use soil tests in every WD cycle. The test strips should be visibly free of any soil at the completion of the cycle.

Motors and scalers
In addition to the point made above regarding the compatibility of certain models of handpieces with a WD cycle, another key consideration is what happens to the electric motor that is driving the handpieces. Many clinics now use red band handpieces on electric motors, rather than air turbine handpieces, since the former provide higher and more consistent torque and generate less noise during operation. A number of companies now make electric motors that are designed for steam sterilisation and the instructions for these dictate that steam sterilisation is to be undertaken between individual patient use. This means that the clinic needs to have a sufficient inventory of electric motors as well as handpieces.
Similar comments apply to modern piezoelectric ultrasonic scalers. Many common brands of these scalers have barrels that are designed for steam sterilisation. This is stated in the user instructions and is also, like dental handpieces, indicated by a symbol that is printed on the side. Clinics need to ensure that they have a sufficient inventory of barrels as well as scaler tips to
meet their usage requirements. Adding to this, most brands of ultrasonic scaler provide specific advice around the types of materials that are suitable for wiping over the barrel before it is packaged for sterilisation. Products give specific advice around the correct method of packaging the tip (often located within the mandrel), barrel and O-rings to ensure proper steam sterilisation.
Navigating the selection and use of chemical indicators
The ISO (the International Organization for Standardization) is a worldwide federation of national standards bodies, of which Standards Australia is a member. ISO standards are used extensively as normative references for Australian Standards, and in many cases, full-text adoption of ISO standards is undertaken in Australia and in other countries to achieve uniformity. When new ISO standards that relate to infection control are published, a key consideration is whether their target audience is manufacturers of products, or end users. This point of the intended readership is often made in the ISO standard in its introduction section.
January/February 2024 Australasian Dental Practice 85
| CONTROL
infection
Figure 1. A benchtop ultrasonic cleaner used for mechanical cleaning of dental instruments. Note the glass partition that separates the reprocessing area from the adjacent dental operatory.
infection | CONTROL

Table 1. Common myths and falsehoods
Every dental clinic is now required to have a washer disinfector.
Ultrasonic cleaners have been outlawed for dental practice.
A Class 2 or PCD must be included in every steam steriliser cycle.
There are no major changes between AS 5369 and AS/NZS 4815.
Using a particular device in the steriliser to test its performance protects the practice from all possible prosecutions relating to infection control.
Like Australian standards, when a new ISO standard is published, that cancels and replaces earlier editions. Typically, the introduction to the new standard will state the documents that have been superseded, to remove any doubt around this point. In the case of ISO 11140 Part 6, Sterilisation of healthcare products - chemical indicators - Type 2 indicators and process challenge devices for use in performance testing of small steam sterilisers, which was published in November 2022, the previous standard which is superseded is EN 867 Part 5. This is an essential point since any marketing of chemical indicators for small steam sterilisers that continues to refer to EN 867 Part 5 is outdated and irrelevant. The fact that a manufacturer would still indicate EN 867 Part 5 on their marketing materials reveals that they are unaware of the new ISO standard, and
raises the question that their products may not conform to the requirements of the new 2022 standard. It is also important to clarify that the scope of ISO 11140 Part 6, as indicated by its name, relates only to small steam sterilisers. This classification includes those with chamber volumes of less than 60 litres (This definition comes from EN 13060). Large sterilisers use tests that are described under EN 285. Another key point regarding ISO 11140 Part 6 is that its application is for steam sterilisers running B cycles (i.e. pre-vacuum types).
ISO 11140 Part 6 introduces some changes in terminology in its Annexe D and these changes should also be reflected in information provided to market air removal and steam penetration tests. The new terminology includes “reference porous load” and “reference hollow device”.
The latter term replaces the previous terminology of “hollow load type A”. The standard also points out that when a test for air removal and steam penetration uses tubing that is made out of plastic polymer rather than metal, the polymer system will have a restricted number of uses and must not be used beyond that point as its performance and reliability will be affected.
Implementing the new reprocessing standard
On 15 December 2023, Australian Standard AS:5369:2023 Reprocessing of reusable medical devices and other devices in health and non-health related facilities was published. This document has a history that dates back to the two families of ancestor standards of instrument reprocessing, the hospital based series (AS 2014:1994 which became AS/ NZS 4187:2003 and then AS 4187:2014) and the office-based practice series (AS/ NZS 4815:2001 which became AS/NZS 4815:2006). The new AS 5369 supersedes the previous 4187 and 485 series, and unified both, being built on the platform of the 4187 series with modern ISO layout, definitions and nomenclature. The new standard was the result of over 3 years of work, involving 2 public consultation rounds and the committee addressing over 700 public comments on 2 versions.
One of the key changes in the document is the scope, which has extended beyond health care facilities, to include the effective and safe reprocessing, storage, handling and transportation of reusable medical devices and other devices used in skin penetration and skin aesthetic procedures and other treatments. This provides a uniform thinking approach across different settings, which will simplify assessment by public health regulators in the future.
The new standard has a strong emphasis on local facility level risk assessments to inform procedures, since the standard is not written as a step-by-step procedural document. Examples of topics for these local risk assessments include ergonomic considerations in the reprocessing area, physical and operational segregation of work areas within instrument reprocessing
86 Australasian Dental Practice January/February 2024



The Solution For Perfect Splints Everytime fabdent.com.au • Any Design • HD PMMA Milled • Flexion Milled • POM Resin Milled • 3D Print Option • Perfect Fit • Upper or Lower • All scans accepted You can’t beat a professionally made DigiSplint for quality, value and longevity everytime ! The Original CAD Digital Splint ! Contact Us Today ! 1300 878 3367

Following appropriate advice
F(Figure 2), air movement and air exchange in the reprocessing area, water used for instrument cleaning and water used for the final rinsing of instruments. The information on water quality requirements is based on the second amendment of AS/ NZS 4187:2014, which was specifically around that topic.
A number of topics have transferred directly from the 2014 4187 standard to the 2023 5369 standard. These include following the Spaulding classification, how the performance of steam steriliser cycles is assessed and the correct sequence for start of day tests for a pre-vacuum steriliser (a door seal air leak test followed by a daily Bowie-Dick test, with the later use of a process challenge device being completely optional). Each practice will need to undertake a gap analysis between their current processes and what is described in the new 5369 standard and then progress through implementation.
inally, the Dental Board of Australia expects all registered dental practitioners to follow current advice and high-level evidence. Clinicians should be alert to any advertising materials or courses that continue to cite ISO or Australian standards that have been superseded, since these are clearly outdated and inaccurate. People also need to be cautious about incorrect advertising claims. Some of the most common myths that the author has debunked on multiple occasions are in Table 1. People need to be particularly careful about statements that are made by anonymous people on social media including Facebook and LinkedIn. Some people making such posts are not qualified or informed on the topics that they are posting on and the information can be misleading. Sadly, we live in the age of misinformation and disinformation and this is why the onus on finding the best quality information sits with each registrant.
About the author
Emeritus Professor Laurence J. Walsh AO is a specialist in special needs dentistry who is based in Brisbane, where he served for 36 years on the academic staff of the University of Queensland School of Dentistry, including 21 years as Professor of Dental Science and 10 years as the Head of School. Since retiring in December 2020, Laurie has remained active in hands-on bench research work, as well as in supervising over 15 research students at UQ who work in advanced technologies and biomaterials and in clinical microbiology. Laurie has served as Chief Examiner in Microbiology for the RACDS for 21 years and as the Editor of the ADA Infection Control Guidelines for 12 years. His published research work includes over 400 journal papers, with a citation count of over 20,000 citations in the literature. Laurie holds patents in 8 families of dental technologies. He is currently ranked in the top 0.25% of world scientists. Laurie was made an Officer of the Order of Australia in January 2018 and a life member of ADAQ in 2020 in recognition of his contributions to dentistry.
88 Australasian Dental Practice January/February 2024
infection | CONTROL
Figure 2. Another view of the same glass partition that establishes physical segregation between the dental operatory and the instrument cleaning section of the adjoining reprocessing area.
Scan with your camera to learn more
Australia: 1800 643 603
New Zealand: 0800 167 626
orders.anz@kerrdental.com

Gutta Percha Points
Use your ZenFlex confidently and precisely. ZenFlex Gutta Percha Points match canals shaped by ZenFlex NiTi Files. Choose the corresponding size, taper and length to meet the needs of each root canal procedure.
Points designed to match canals shaped by ZenFlex NiTi Shaping Files
Zero natural rubber latex
Flexible matches to a wide range of canal depths
Reliable fill and seal with a seamless glide path

NEW! ZenFlex™ Gutta Percha Points Designed to Work Seamlessly with ZenFlex NiTi Shaping Files
©2023 Kerr Australia Pty Ltd, Level 4, 7 Eden Park Drive, Macquarie Park NSW 2113, Australia

MOCOM streamlines sterilisation at Tomaree Dentistry in coastal NSW
Tomaree Dentistry in the picturesque Port Stephens region of New South Wales, two and a half hours north of Sydney, is streamlining its infection control practices by utilising innovative solutions from MOCOM that are perfect for small clinics and large. We asked them about their practice and choices...
Q Good morning, please tell us about your practice?
A Of course. Tomaree Dentistry is a long standing practice in Nelson Bay, having provided general dentistry to the local community for 30 years. We focus mainly on the mature, older patient with much of our work involving restorations, crown and bridge work, dentures, implant restorations and oral hygiene. We have 4 treatment rooms currently used by our two dentists and supported by 7 staff.
Q Describe the infection control workflow - Steri to chair side and back
A Treatment rooms are stocked with instruments that have been processed in the sterilising room each session and as required throughout the day. Before each patient, the chair side is set up with necessary items for the dentist and DA. At the end of treatment, the procedure tray is taken to the sterilising room for processing.
Q What is your sterilisation area like and what equipment do you use?
A We have a left to right circular flow in our sterilisation room. Treatment trays land in the processing bay ready for reprocessing. Trays are sorted with handpieces going through the MOCOM Thalya Plus handpiece maintenance unit and instruments go into the MOCOM Tethys H10 benchtop washer disinfector. Once both cycles are finished, the handpieces and instruments are moved to the packaging area. We use self-seal bags and once packaged, they go through the autoclave. We have MOCOM autoclaves with printers. Once that cycle is finished, the bags are inspected and a printed label attached.
90 Australasian Dental Practice January/February 2024
infection | CONTROL
Instrument reprocessing solutions
Instrument reprocessing solutions
Instrument reprocessing solutions
has revolutionised sterilisation by offering a compact, dedicated line that provides unparalleled performance! Decontamination Washing Drying Disinfection Sterilisation
Mocom has revolutionised sterilisation by offering a compact, fully dedicated line that provides unparalleled performance!
Mocom has revolutionised sterilisation by offering a compact, fully dedicated line that provides unparalleled performance!
Disinfection
Washing Drying
Sterilisation
Decontamination Washing Drying Disinfection
M: 0427 816 459 • F: (02)46328456 • sales@mocomaustralia.co m.au • www.mocomaustralia.com.au
459 • F: (02)46328456 sales@mocomaustralia.co m.au • www.mocomaustralia.com.au
Q Are there dedicated staff working in infection control?
A
We have one dedicated staff member in our sterilising room. All assistants and front desk staff are at times required to assist there as well. All staff and dentists participate in infection control training.

Q Regarding the MOCOM Thalya Plus handpiece unit, what was the catalyst for purchasing this?
A
Our principal dentist, John Cropley, saw the Thalya handpiece unit at a trade show. He was wanting equipment that not only oiled the handpieces but cleaned internally as well - with the aim to improve the systems in our sterilising protocols. We previously oiled our handpieces in an oiler and staff used a can of spray to clean handpieces internally before processing further. The Thayla Plus provides both procedures during its cycle - we have found it to be a more efficient process and the handpieces are lasting longer than we had experienced prior to installing the Thalya.
Q And why did you choose MOCOM Sterilisers?
A
We have two MOCOM autoclaves. These have a reputation for reliability and our previous experience with this brand meant we have stayed with MOCOM. Although we are a small
MOCOM Thalya PLUS
M OCOM Thalya PLUS handpiece maintenance unit treats up to 4 instruments simultaneously including turbines, micromotor handpieces and scalers. The complete Thalya PLUS cycle consists of 6 stages:
n Duct purge
n Internal cleaning
n Internal and external disinfection
n Lubrication
n Excess oil purge
n Drying
The 4 instruments are treated simultaneously and the entire cycle lasts about 12 minutes.
MOCOM Tethys H10 PLUS
M OCOM Tethys H10 PLUS is a compact benchtop, thermal washer disinfector that offers four phases that are all performed in a single, rapid, automatic process:
n Decontamination
n In-depth ultrasound washing
n Effective thermal disinfection
n Forced-draught drying
One cycle eliminates risks for the operator and efficiently completes the four phases that precede instrument packaging and sterilisation in a fast 35 minute cycle.
practice, we are busy and having two machines allows us to keep our treatment rooms well-equipped and allows for efficient and productive days. We find the autoclaves work well and notifications within the system allow us to keep on top of maintenance of the equipment.
Q
Does the practice use instrument tracking and if so, how does the MOCOM equipment work in with this.
A The autoclaves have printers attached. At the end of each cycle, staff check each bag for tears or punctures and then attach a label to each one. Sterilising room forms are then completed so as to keep a record of all loads that are processed and a barcode label is attached here as well. These labels, with barcodes, allow for tracking of instruments from the load and cycle through to the patient they are used on. In the treatment rooms, the barcodes are scanned into the patient’s chart at the time of treatment. Autoclave details are saved and records kept of all cycles.
Q Can you sum up the benefits of using MOCOM equipment in the operation of the practice?
A Our practice uses MOCOM equipment for oiling, cleaning, disinfecting, sterilising and tracking. We have found the equipment has helped us fine tune our infection control procedures within our sterilising room, allowing our staff to work efficiently and feel reassured that standards are being met.
92 Australasian Dental Practice January/February 2024
infection | CONTROL






T o t a l H a n d p i e c e M a i n t e n a n c e . Clean. Disinfect. Lubricate. Purge. Dry. In 12 minutes. Replace Manual with Mechanical. Clean. Disinfect. Lubricate. Purge. Dry. In 12 minutes. Replace Manual with Mechanical. Clean. Disinfect. Lubricate. Purge. Dry. In 12 minutes. Replace Manual with Clean. Disinfect. Lubricate. Purge. Dry. In 12 minutes. Replace Manual with Mechanical. M: 0427 816 459 | P: (08) 9244 4628 E: sales@mocomaustralia.com.au | W: www.mocomaustralia.com.au
Smart autoclave for fast, dependable sterilisation
By David Petrikas
A-dec is providing Australian dental practices with access to one of Europe’s best sterilisation solutions, Dürr’s Hygoclave range.
The Hygoclave was launched in Australia at ADX Melbourne in 2023 after successful prior “road testing” in local dental practices where it proved a far superior experience to existing brands in terms of ease of use, effectiveness, speed and reliability.


Although the Hygoclave is a relatively new introduction to the Australian market, Dürr has a proud history in infection control solutions, extending some six decades back to 1965.
This has culminated in the more recent development of a superior autoclave, incorporating advanced technology and simplicity of operation with fast and secure B class cycles meeting users’ needs.
power use - illustrating both its efficiency and environmental credentials.
The Hygoclave represents the next generation of sterilisers, marked by a clear and intuitive touchscreen, one-touch operation capability, flexible water connection options and inbuilt water quality testing. The Hygoclave has proven quick, quiet and a delight to use, winning instant fans among those who have experienced it.
A-dec Australia has thrown its full support behind the Dürr Hygoclave range, with the appointment of Dr Wee Teo, who is highly experienced in clinical devices, as Dürr product manager to provide technical and clinical support for the Dürr Hygoclave range to A-dec customers.
Smart cycles
Dr Teo said the Hygoclave can process dental instruments in as little as 30 minutes, including drying using the 134oC B Flash cycle with minimal water and
“The 134oC B Standard sterilisation program ensures reliable reprocessing of instruments. And being a ‘smart’ machine, drying time is automatically extended according to load size - while additional vacuum cycles can be pre-selected on the Hygoclave 50 using the 134oC B Standard Plus program to accommodate hard to dry complex, hollow loads,” he said.
“The result is properly processed, dry loads every time.”
Dr Teo said feedback from dental practices is that the Hygoclave is a joy to use with next to no training thanks to the intuitive layout of its colour touchscreen display and easy to understand icon-based buttons. Key day-to-day functions are just a simple button-press away.
“It has a simple, easier-to-understand and smarter user interface,” Dr Teo said.
“For example, one press on the coloured 5” [125mm] touch screen can select the
94 Australasian Dental Practice January/February 2024
infection | CONTROL
Dr Wee Teo



With Hygoclave 50, Dürr Dental and A-dec offers dental practices a professional Class B solution that combines impressive performance with a well thought-out operating concept – for maximum efficiency and exceptional user friendliness designed to cope effortlessly with tough day-to-day working environments. Available with a volume of 17 or 22 litres.
More information under www.duerrdental.com
your local A-dec dealer 1800 225 010
your local A-dec dealer 1800 225 010
Hygiene is in our DNA. The Hygoclave 50. 3-fold flexible fresh water supply with integrated quality control All in view and documented thanks to connection to the practice network 5“ high-resolution colour touch display for intuitive navigation High-performance sterilization- and drying system Integrated dust protection filter Contact
Contact

most recently used sterilisation cycle to be used again; produce a batch report; or initiate a test program directly from the home screen without having to go deep into menus to set parameters.”
Traceability
An automated powered door with locking mechanism and integrated user management system guarantees secure and easy workflows, supporting full traceability back to an individual operator and cycle.
The Hygoclave has a dedicated interface for practice management and hygiene software, as well as internal storage capacity for a massive 100,000 cycles, which are automatically captured in accordance with ADA Infection Control Guidelines. It can also produce barcode labels and batch reports on an optional attached Dürr printer to assist with labelling and storage of sterilised items.
The premium Hygoclave 50 is also “future proof” with an interface for remote monitoring and operation via Dürr’s VistaSoft Monitor mobile app and computer software.
VistaSoft Monitor enables remote cycle history backup and downloading of reports to a user’s PC, together with remote service diagnostics ability. The latter is expected to be a popular feature among Australian users by enabling ser-

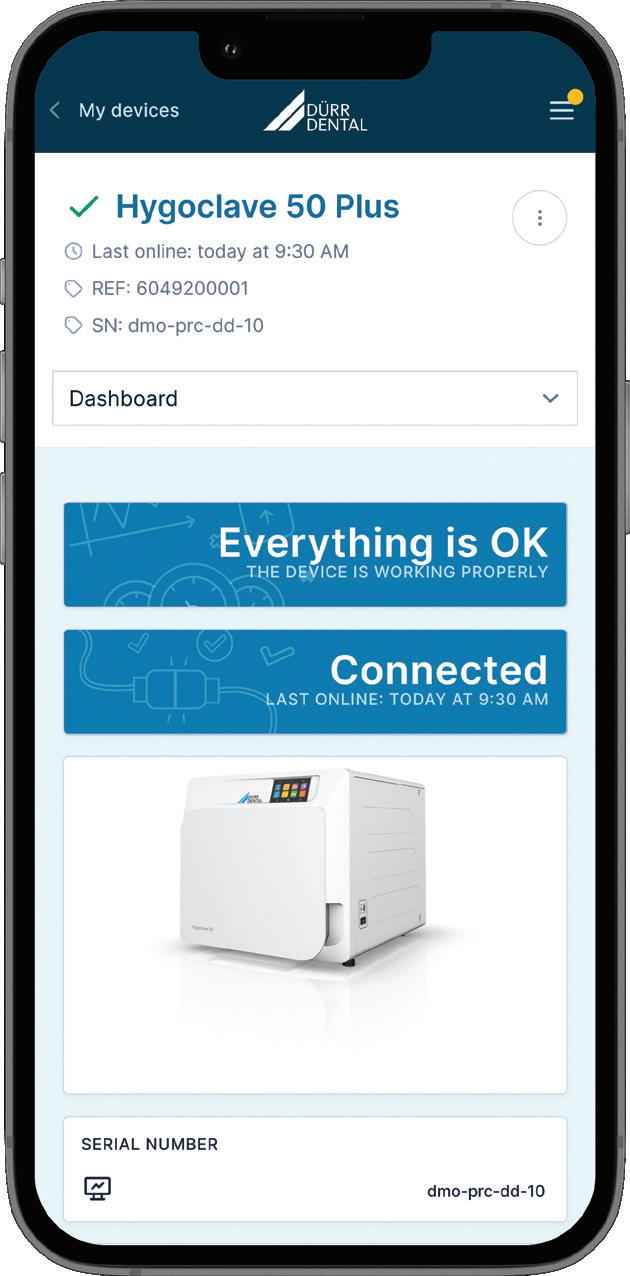
vice items to be identified and ordered ahead of time by equipment technicians to help speed up servicing.
These convenient features are available to users using the free VistaSoft Monitor program exclusive to the Hygoclave 50.
Flexible water supply options
Another unique feature of Hygoclave 50 is its extremely flexible water supply options, making it easy to install in any practice, as well as its built-in automatic water quality test function with alerts should water quality fall below acceptable levels.
The Hygoclave 50 can be filled manually via the internal tanks accessed by top-mounted “butterfly” door covers; alternatively, via a suction system from a canister of treated water; or by being connected to a fully automated Dürr water treatment system.
Hygoclave is manufactured from quality stainless steel and special high temperature and ionised water-resistant plastics for sustained trouble-free operation. It is available with either a 17L or 22L chamber matching the size and throughput of the practice.
The product is also easy to maintain and very service-friendly due to its intelligent and modular design, making internal access easy which has already won a big thumbs up from dental equipment technicians in Australia.
To find out more about Hygoclave, contact A-dec on 1800-225-010 or your nearest authorised A-dec dealer.
96 Australasian Dental Practice January/February 2024
infection | CONTROL











NEW Over half of dental professionals experience neck and back pain. Preserve your career Reduce neck discomfort Improve your posture HDL Ergo™ 5.0x Deflect discomfort with Schedule your free in‑office demo, scan the code or call 1800 643 603
A-dec sets standard in infection control
By David Petrikas
When it comes to infection control in the dental surgery, A-dec has you covered.
As one of the world’s most respected manufacturers of dental equipment, A-dec has also developed a comprehensive asepsis program known as A-dec 360™.
A-dec 360 is a complete end-to-end system to make sure your dental units are fully maintained and do not pose a risk of infection to your staff or patients. In keeping with ADA Guidelines, A-dec recommends a three-step: “Maintain, Monitor & Shock” approach to keeping water lines clean.
Monitoring requirements will depend on your water quality and the clinic’s individual requirements. Initially, test water once a month. If the results pass your specified action level (i.e., 200 CFU/mL using the ADA guidelines), then reduce the testing protocol to at least every six months.
A-dec 360 includes the tools to maintain dental unit water lines on a daily basis using A-dec’s convenient ICX tablets. Each time you refill the water reservoir, you simply drop an ICX tablet into the reservoir to ensure the water is effectively treated against microbial contamination.

Periodically, as part of your clinic’s infection control protocol and to comply with ADA guidelines for water quality, dental unit water lines may require a shock treatment with A-dec’s ICX Renew. This is especially the case if the dental units have sat idle for an extended period.
Once treated with ICX Renew and flushed clear, the self-contained dental unit water system is ready for routine treatment with ICX tablets at each refill
“From beginning to end, the thoughtful design of A-dec delivery systems ensures the highest level of infection control...”
to maintain water quality. A-dec’s authorised dealers offer a digital water testing service to diagnose dental unit waterline quality on the spot.
A-dec builds asepsis right into its chair design, starting with their fully self-contained dental unit water system, using A-dec’s proprietary microbial-resistant AlphaSan tubing and a control block design that prevents water stagnating. Each time a handpiece is picked up, the control block is automatically flushed with fresh water.
The new “Vaporiser” feature - exclusive to the A-dec Pro delivery systems - purges the turbine with a blast of highspeed air, preventing aerosols and water being drawn back into the turbine head, helping eliminate potential contamination. It also avoids the last drop from dripping onto the patient when the handpiece is removed from the oral cavity.
A-dec’s NLZ electric motor, suitable for contra angle and speed-increasing and speed-decreasing handpieces is also favoured by many for its quiet, powerful operation and reduced production of aerosols compared to high-speed turbines.
At the end of the day, an “auto flush” function on the new A-dec Pro delivery systems purges all tubing to ensure only fresh water is in the dental unit water lines.
Externally, A-dec’s smooth surfaces make for easy positioning of barriers and rapid cleaning between patients. This is especially the case with the streamlined control head and upholstery of the latest A-dec 300 and 500 Continental delivery systems.
From beginning to end, the thoughtful design of A-dec delivery systems ensures the highest level of infection control for you, your team and importantly, your patients.
Learn more at australia.a-dec.com
98 Australasian Dental Practice January/February 2024
infection | CONTROL

When you SHOCK, let ICX RENEW
Unwanted visitors like bacteria love to colonise in your dental unit waterlines. A daily waterline maintenance protocol with A-dec ICX® waterline treatment tablets, along with periodic ICX Renew™ shock treatments, will help reduce these nasty microorganisms. To find out more, visit australia.a-dec.com

For complete trademark information, visit a-dec.com/legal/trademarks.
.
© 2021 A-dec Inc. All rights reserved.
Unwanted guests in your waterlines?

Designing an efficient sterilisation room: A guide
Adedicated sterilisation room is the backbone of any modern dental practice, serving as the cornerstone of infection control protocols and ensuring the delivery of safe, high-quality care to patients. This specialised facility plays a vital role in the sterilisation and preparation of dental instruments and materials, safeguarding against the transmission of infectious pathogens and assisting you in maintaining optimal hygiene standards.
In a dental practice, where procedures ranging from routine cleanings to complex surgeries are performed, the need for meticulous sterilisation and instrument processing cannot be overstated. A dedicated sterilisation room provides the infrastructure and resources necessary to effectively clean, disinfect and sterilise instruments, thereby mitigating the risk of cross-contamination and infection transmission between patients and staff. Central to achieving this goal is the design and layout of the sterilisation room within a dental practice.
Infection control protocols
At Medifit Design & Construct, we prioritise the implementation of robust infection control protocols in every aspect of the design process and this is evident in our steri designs. Careful use of commercial-grade finishes, laminates and non-porous solid surfaces are fundamental to our infection control approach. These materials not only facilitate ease of cleaning and maintenance but also act as a barrier against cross-contamination. The choice of surface materials can significantly impact hygiene standards, not only on the working surfaces, but also adjacent surfaces including splashbacks. Medifit are advocates for the superiority of acrylic or glass splashbacks over traditional tiles, as they offer better cleanability and hygiene standards, ensuring optimal sterilisation outcomes.
100 Australasian Dental Practice January/February 2024
infection | CONTROL

EIngress/egress options
fficient flow from dirty to clean areas is essential for infection control and operational efficiency. Our design emphasises a systematic ingress/egress pathway, beginning with a designated dirty side equipped with a stainless steel bin chute and provisions for a handpiece oiler and air point. A strategically placed sink facilitates the rinsing of contaminants, followed by stations for ultrasonic cleaning and optional washer/disinfector integration.
Central to the design are steam sterilisers (autoclaves), typically positioned centrally for accessibility. Instruments exit the autoclave into a clean area for cooling. The room includes a small hand hygiene station.

January/February 2024 Australasian Dental Practice 101
infection | CONTROL



Location in practice
Determining the optimal location for the sterilisation room is crucial for workflow efficiency and patient safety. Placing the sterilisation room centrally to dental surgeries facilitates seamless access while minimising patient exposure to the dirty side. By locating the sterilisation room away from patient areas, we mitigate potential backlogs and streamline the sterilisation process, with the goal of enhancing overall practice efficiency.
Design-informed criteria
In addition to the layout and location of the steri room within the practice, we also advocate for the integration of exhaust fans to dissipate excess moisture and maintain optimal room
conditions. Furthermore, future-proofing the design with the addition of data points enables seamless integration of advanced technologies and facilitates documentation of autoclave usage for compliance purposes.
The design of a successful sterilisation room in a dental practice requires meticulous attention to detail and adherence to best practices in infection control. By prioritising commercial-grade materials, optimising ingress/egress pathways, strategically locating the room within the practice and incorporating relevant design-informed criteria, we can minimise the potential for cross infection and ensure the creation of a safe, efficient and compliant sterilisation environment.
For more information on Medifit’s design services and expertise in dental practice construction, visit www.medifit.com.au.
102 Australasian Dental Practice January/February 2024 infection | CONTROL

Practices that work with you
Since 2002, Dentists and Dental Specialists all around Australia have trusted Medifit to create state of the art practices with individual interior designs that boost productivity and enhance levels of care.
Whether it’s your first practice or your latest, we’ll help you create a dental practice that reflects your personal style and complements the way you work - and we do it with a friendly, no fuss approach using proven best practices. Contact Medifit today for a no obligation consultation and experience our award winning service.
• SITE ASSESSMENTS
• LEASE NEGOTIATION
• FEASIBILITY STUDIES
• COUNCIL SUBMISSIONS
• ARCHITECTURAL DESIGN
• INTERIOR DESIGN
• BUILDING CONSTRUCTION
• PRACTICE FIT-OUTS
• RENOVATIONS / REFRESHES
• BRANDING & MARKETING




1300 728 133 www.medifit.com.au MULTI AWARD WINNING HEALTHCARE DESIGN & CONSTRUCTION Master Builders Excellence in Construction Awards: 2022 Best Building Fitout under $1.5m • 2021 Best Healthcare Building • 2021 Best Historical Restoration or Renovation under $1.5m Interior Fitout Association (IFA) Awards: 2020/22 Best Interior Fitout Health & Beauty • 2020/22 Best Interior Fitout Medical • 2018/19 Best Professional Suite Design • 2017/18 Best Medical Fitout • 2017/18 Best Use of Sponsors Product • 2017/18 Best Design - Professional Suites SYDNEY | MELBOURNE | PERTH | ADELAIDE | BRISBANE | CANBERRA | REGIONAL AUSTRALIA


Preventing needle stick injury
By Dr Greg Mahoney, BDSc, PhD, MSc (Dent), GradDipClinDent, FADI, FPFA
Sharps injuries in dental practice remain a concern today even though dentistry adopted preventive practices in the 1980s. An Australian study found 27.7% of dentists had experienced at least one sharps injury in the previous 12 months and 16.1% of these involved a contaminated instrument that had been previously used on a patient. Furthermore, the most common devices to cause sharps injury in the previous 12 months were needles (14.4%).1
Hollow-bore needle injuries are of particular concern, since they are likely to contain residual blood and are associated
with an increased risk for blood-borne virus transmission. Of the 57 documented cases of occupational HIV transmission to healthcare personnel reported to CDC from June 1995 to December 2002, 50 (88%) involved percutaneous exposure. Of these, 45 (90%) were caused by hollow-bore needles and half of these needles were used in a vein or an artery.2
The risk
Blood-borne viruses that could potentially be transmitted by a sharps injury include hepatitis B and C, as well as HIV. The risk of transmission following a skin puncture injury is dependent on:
• Whether the person who previously used the object had an infection;
• The level of virus in their blood;
• The amount of blood involved;
• The type of needle or syringe in question;
• The time that has elapsed since it was used; and
• The nature of the injury.
So in dentistry, the most likely source of a blood-borne virus transmission is the local anaesthetic needle, being hollow and injected into a vascular rich area. It is estimated that up to 14% of inferior dental nerve blocks result in an intravascular injection and with an infiltration may too puncture a blood vessel.3
104 Australasian Dental Practice January/February 2024
infection | CONTROL READ ME FOR CPD
A LONG-PROVEN EFFICACY
infection | CONTROL
safe & easy
Protects you and your staff from needle stick injuries
Complies with latest regulations
Intuitive device
A study demonstrated that when introduced in a dental school, Ultra Safety Plus was a the key success factor for avoiding needle stick injuries.



Passive or active aspiration:
barrel:
Available with either Sliding protective sheath:
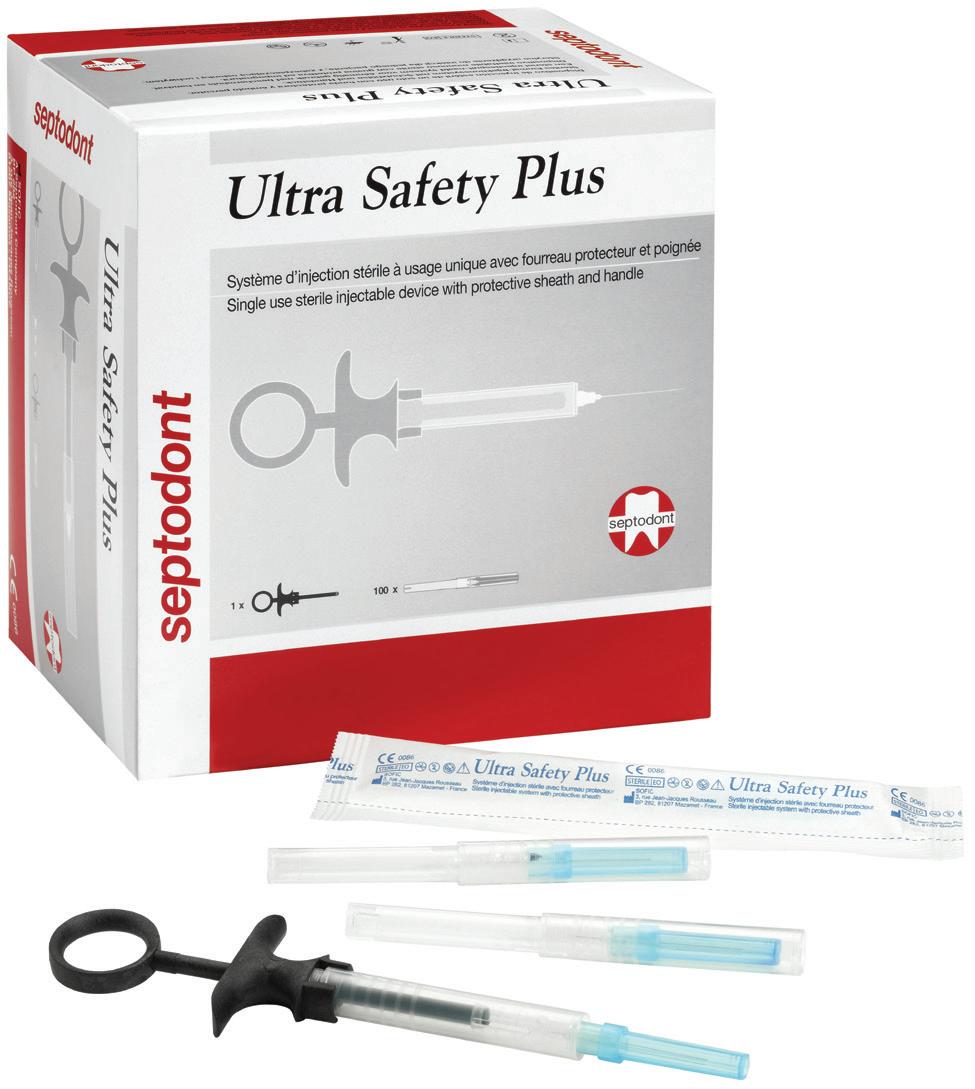
The risks of acquiring other bloodborne viruses from a contaminated needle are considerably higher than the 0.23% for HIV with 6-30% for hepatitis B and 1.8% for hepatitis C.4 Acquired hepatitis B and C cases have been reported in Australia.5,6 Following known exposure to blood borne virus, post-exposure prophylaxis (PEP) should be considered. PEP is known to be over 80% effective in preventing HIV from needle stick injuries and while oral health care workers are vaccinated against hepatitis B, there is no vaccination for Hepatitis C. Post exposure prophylaxis protocols are an essential part of everyday practice although are an expensive and time consuming process with a considerable emotional toll.7 It makes eminent sense for all dental operatories to adopt effective needle stick injury prevention protocols and safety equipment. The criteria for local anaesthetic delivery should be:
FREQUENCY OF NEEDLE STICK INJURIES

ULTRA SAFETY PLUS INTRODUCTION
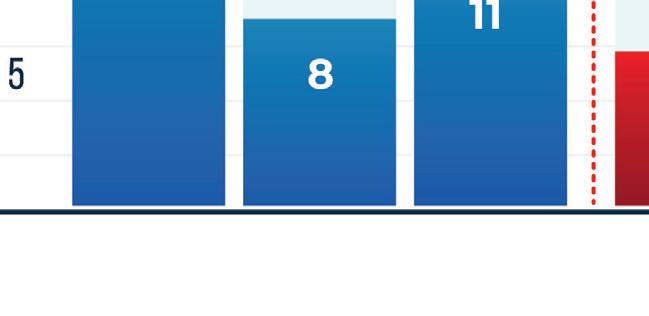
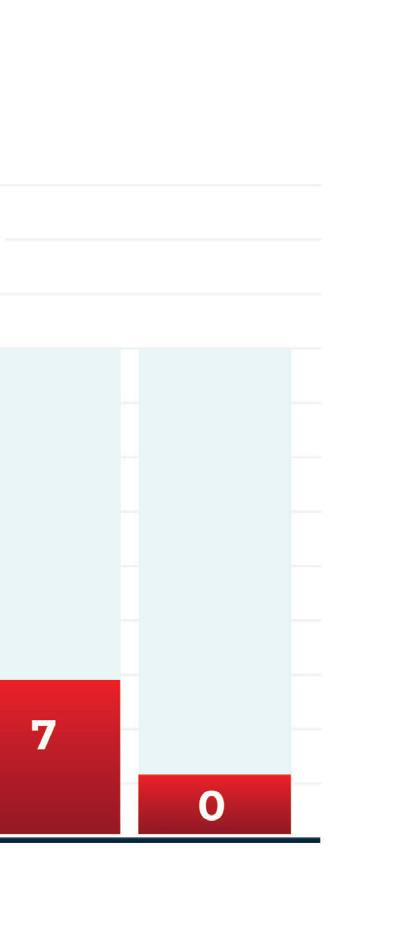
With Ultra Safety Plus, needle stick injuries decreased from an average of 11.8 to 0 injuries per 1,000,000 hours worked(1)

• Compatible with the existing local anaesthetic cartridge;
• Able to be used for all techniques for local anaesthesia;
• Single use or autoclavable;
• Proven to be effective in reducing or eliminating needle stick injury; and
• Cost effective.
Prevention
Areview of the availability of safety systems, including needleless systems, found that one system met the above criteria - the Ultra Safety Plus from Septodont. The Ultra Safety Plus™ and now the new Ultra Safety Plus Twist (also from Septodont) system – which does not require the re-sheathing or removal of a needle from its syringe – has been in my private practice for over 10 years and in that time there has been no cases of local anaesthetic needle stick injury.
Evaluating the system against the desirable criteria
Compatibility: The system uses the existing 2.2ml cartridges.
Technique: The system comes with preloaded a 27 or 30 gauge needle in short and extra short and looks, feels and acts like the traditional dental injection.
Autoclavable: It comes in single use and if desired, an autoclavable plunger.
Effectiveness at reducing needle stick injury: Zakrzewska found that the number of avoidable needle stick injuries reduced from an average 11.8 per 1,000,000 hours worked to zero in UK dental schools (Figure 3). Consequently it has been adopted by most dental school across the UK.8-10 Cost effectiveness. The University of Queensland found the cost of safety syringes was comparable to non-disposable syringes, however the reduction in the cost of managing sharps injuries was substantial.11

January/February 2024 Australasian Dental Practice 105
(1) J.M Zakrzewska et al. Introducing safety syringes into a UK dental school – a controlled study. Brit Dent J 2001 190; 88-92.
YEAR 1 YEAR 2 YEAR 3 YEAR 4 YEAR 5
protection from needle stick injuries
security
for the patient
Transparent
aspiration is clearly visible
24/09/2020
ULTRA SAFETY PLUS TWIST
Figure 3. Zakrzewska found that the number of avoidable needle stick injuries reduced from an average 11.8 per 1,000,000 hours worked to zero in UK dental schools. Consequently it has been adopted by most dental school across the UK.8-10
Figure 1. The new Ultra Safety Plus Twist from Septodont.
Figure 2. The Ultra Safety Plus from Septodont.
infection | CONTROL



The system works by sliding down a captive rigid sheath over the needle when loading up a new cartridge, exposing the needle and cap. After injection, the sheath is moved up to the first click so that the needle can be uncovered for a second injection if required. At the end of the injection, the sheath is slid up till the second click which is a one way lock to permanently lock the sheath in place over the needle, preventing sharps injuries during changeover between patients.
Adopting sharp safe methods is essential in all dental practices. The Ultra Safety Plus and Ultra Safety Plus Twist provides the dental team with the necessary tool to provide safe practice. If sharp safe habits are not expected of each team member, the risk of a sharp injury increases.
References
1. Leggat PA, Smith DR. Prevalence of percutaneous exposure incidents amongst dentists in Queensland. Aust Dent J. 2006;51(2):158-61.
2. CDC. Workbook for Designing, Implementing and Evaluating a Sharps Injury Prevention Program 14 Dec 2019]. Available from: https://www.cdc.gov/ sharpssafety/part1TEXTONLY.htm.
3. Taghavi Zenouz A, Ebrahimi H, Mahdipour M, Pourshahidi S, Amini P, Vatankhah M. The Incidence of Intravascular Needle Entrance during Inferior Alveolar Nerve Block Injection. J Dent Res Dent Clin Dent Prospects. 2008;2(1):38-41.
4. CDC. Exposure to Blood :s What healthcare personnel need to know. National Center for Infectious Diseases Divison of Healthcare Quality Promotion and Division of Viral Hepatiti. 2003.
5. Haber PS, Young MM, Dorrington L, Jones A, Kaldor J, De Kanzow S, et al. Transmission of hepatitis C virus by needle-stick injury in community settings. J Gastroenterol Hepatol. 2007;22(11):1882-5.
“The system works by sliding down a captive rigid sheath over the needle when loading up a new cartridge, exposing the needle and cap. After injection, the sheath is moved up to the first click so that the needle can be uncovered for a second injection if required. At the end of the injection, the sheath is slid up till the second click which is a one way lock to permanently lock the sheath in place over the needle, preventing sharps injuries during changeover between patients...”
6. Res S, Bowden FJ. Acute hepatitis B infection following a community-acquired needlestick injury. J Infect. 2011;62(6):487-9.
7. McAllister J. Literature review for the national guidelines for post-exposure prophylaxis after nonoccupational and occupational exposure to HIV (revised). National PEP Guidelines Expert Reference Group 2016;Australasian Society for HIV, Viral Hepatitis and Sexual Health Medicine.
8. Zakrzewska JM GIaJJ. Introducing safety syringes into a UK dental school – a controlled study. BrDent J 2001(190):188-92.
9. Zakrzewska JM BE. Use of dental safety syringes in British and Irishdental schools. . Br Dent J. 2003(195):207-9.
10. Oliver G, David DA, Bell C, Robb N. An Investigation into Dental Local Anaesthesia Teaching in United Kingdom Dental Schools. SAAD Dig. 2016;32:7-13.
11. Walsh L. Sharps injuries during patient changeover: Are you getting the point. Australasian Dental Practice January/February 2018:64-6.
106 Australasian Dental Practice January/February 2024
Please www.septodont.com BROCHURE 3 volets SEPTODONT v16 GAMME XL OK 23/09.indd 1-3
A secure lock Find the relevant details in the instructions manual 1. Introduce the pins of the handle in the notches of the barrel 2. Twist the finger grip to lock it
A INTUITIVE NEW PATENDED DESIGN Only 2 easy steps are needed for a secure assembly A secure lock Find the relevant details in the instructions manual 1. Introduce the pins of the handle in the notches of the barrel 2. Twist the finger grip to lock it ULTRA SAFETY PLUS TWIST ULTRA SAFETY PLUS TWIST 1 box of 50 sterile needles 1 sterilisable handle 1 box of 100 sterile needles + 1 STERILISABLE handle 1 box of 50 sterile SINGLE-USE handles x short - 10 mm 30 g short - 25 mm 30 g short - 25 mm 27 g long - 35 mm 27 g long - 35 mm 25 g Please visit our website for more information: www.septodont.com length gauge color code BROCHURE 3 volets SEPTODONT v16 GAMME XL OK 23/09.indd 1-3

Septanest : the first choice of dentists with over 150 million injections per year, provides you high quality you can trust


ONLINE AT Co., LLC. All rights reserved. predictable
discover
it
DENTISTS LOVE OUR
IS
the
808 855 ww ONLINE AT Mfg. Co., LLC. All rights
predictable
discover
when it
DENTISTS LOVE OUR
IS
808 855 ww
outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns.
why dentists favor our impeccable fit. Perfect for your patients. Easy for you.
comes to the perfect fit, Hu-Friedy is just right.
STAINLESS STEEL PEDO CROWNS:
EVERYTHING
right one with Hu-Friedy
reserved.
outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns.
why dentists favor our impeccable fit. Perfect for your patients. Easy for you.
comes to the perfect fit, Hu-Friedy is just right.
STAINLESS STEEL PEDO CROWNS:
EVERYTHING the right one with Hu-Friedy
Call 0508 486 252 www.ivoclar.com



> Protects you and your staff from needle stick injuries
> Complies with latest regulations
> Intuitive device
> Available with either sterile single use or sterilisable handle


Passive or active aspiration: security for the patient
Transparent barrel: aspiration is clearly visible
Sliding protective sheath: protection from needle stick injuries


Two different positions:
first Holding Position (reversible)
final Locking Position (irreversible)


Ensure predictable You’ll quickly discover Because when
Ensure predictable You’ll quickly discover Because when WHY DENTISTS
Ensure predictable You’ll quickly discover Because when

VISIT US ONLINE
Hu-Fried y Mfg.
©2016
FIT IS Find the ders 0800 808 VISIT US ONLINE
Hu-Fried y Mfg.
Ensure predictable You’ll quickly discover Because when WHY DENTISTS
©2016
ders 0800 808 VISIT US ONLINE ©2016 Hu-Fried y Mfg.
WHY DENTISTS
FIT IS Find the ders 0800 808 VISIT US ONLINE
Hu-Fried y Mfg.
WHY DENTISTS
©2016
FIT IS Find the ders 0800 808
safe & easy
ULTRA SAFETY PLUS TWIST
A LONG-PROVEN EFFICACY
A study demonstrated that when introduced in a dental school, Ultra Safety Plus was a the key success factor for avoiding needle stick injuries.
Septanest : the first choice of dentists with over 150 million injections per year, provides you high quality you can trust
With Ultra Safety Plus, needle stick injuries decreased from an average of 11.8 to 0 injuries per 1,000,000 hours worked(1)
ONLINE AT Co., LLC. All rights reserved. predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. it comes to the perfect fit, Hu-Friedy is just right. DENTISTS LOVE OUR STAINLESS STEEL PEDO CROWNS: IS EVERYTHING the right one with Hu-Friedy 808 855 ww ONLINE AT Mfg. Co., LLC. All rights reserved. predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. when it comes to the perfect fit, Hu-Friedy is just right. DENTISTS LOVE OUR STAINLESS STEEL PEDO CROWNS: 808 855 ww ONLINE AT Co., LLC. All rights reserved. predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. it comes to the perfect fit, Hu-Friedy is just right. DENTISTS LOVE OUR STAINLESS STEEL PEDO
IS
the
Hu-Friedy 808 855 ww ONLINE AT Mfg. Co., LLC. All rights reserved. predictable outcomes for
littlest
discover
when it comes to the
DENTISTS LOVE OUR
IS
808 855 ww
CROWNS:
EVERYTHING
right one with
your
patients with Hu-Friedy Stainless Steel Pedo Crowns.
why dentists favor our impeccable fit. Perfect for your patients. Easy for you.
perfect fit, Hu-Friedy is just right.
STAINLESS STEEL PEDO CROWNS:
EVERYTHING the right one with Hu-Friedy
(1) J.M Zakrzewska et al. Introducing safety syringes into a UK dental school – a controlled study. Brit Dent J 2001 ; 190; 88-92.
Call 0508 486 252 www.ivoclar.com
FREQUENCY OF NEEDLE STICK INJURIES YEAR 1 YEAR 2 YEAR 3 YEAR 4 YEAR 5 ULTRA SAFETY PLUS INTRODUCTION
Taking on the challenge with attention to detail
Rehabilitation of an anterior crown using state-of-the-art zirconia
By Dr Knut Hufschmidt

A19-year-old patient presented at our practice requesting review of, and consultation on, an unattractive singletooth restoration of tooth 21 (Figure 1).
The patient’s dentition was not affected by caries and the panoramaic radiograph that was taken showed four impacted wisdom teeth (Figure 4) that were surgically removed at a later date.
During the initial consultation, the young patient explained that she had suffered a fall during which an incisor had been fractured.
Her dentist at the time had carried out root canal therapy and restored the tooth prosthetically with a lithium disilicate crown.
The treatment outcome had been highly aesthetic to begin with, however, this changed following incorporation and the patient noticed that the anterior crown was becoming increasingly discoloured (Figures 2 and 3).
This may have been due to subsequent discolouration of the devitalised tooth.
The extremely high translucency of the glass phase of a lithium disilicate restoration can cause the dark colour of a remaining tooth to become visible, resulting in an unattractive grey effect.
As part of a detailed consultation and briefing, we explained to the patient the difficulties and challenges of a single-tooth crown in the aesthetic zone when the smile line is high and the gingiva is exposed.
In addition, we also discussed in detail the difficulty due to the fact that a preparation carried out by a previous practitioner cannot be evaluated before removing the crown. Some details cannot be corrected and the predictability of an optimum aesthetic result is reduced. The aim of a new restoration is to improve the aesthetic situation, however, only an approximation of a perfect copy of tooth 11 would be possible as the discoloured root would always be a hindrance.
Despite the risks and uncertainties presented, the young patient wanted a new restoration of the tooth so that the best possible aesthetics could be achieved. At the same time, her natural tooth colour and individual tooth setup were not to be changed.
110 Australasian Dental Practice January/February 2024
clinical | EXCELLENCE



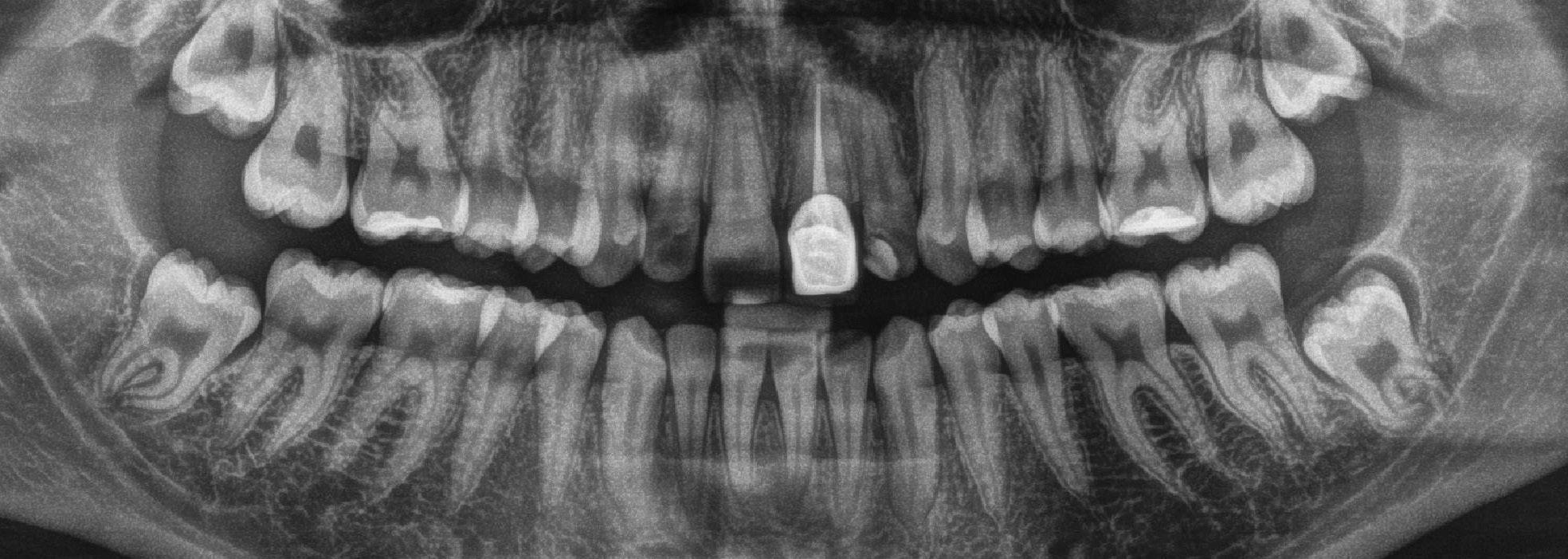
Clinical approach
Following fabrication of a study model, a vacuum-formed matrix for the temporary restoration was fabricated for the upper jaw on the model. Under local anaesthetic, the single-tooth restoration was gently removed along with the bonding material. In the labial area and in three planes, it was possible to anatomically reduce and optimise the preparation that was uncovered. When placing the circular preparation margin, the “biological width” had not been taken into consideration and the crown margin was significantly subgingival.
The gingiva was carefully pushed back with the aid of a retraction thread and the circular preparation clearly defined with a pronounced chamfer.
In the case of the long-term temporary that was fabricated in the practice, all aesthetic and functional parameters were taken into consideration and the “outer shell” of the final crown was determined.
The temporary was then bonded using eugenol-free temporary cement (Figure 5-10).
January/February 2024 Australasian Dental Practice 111
Figure 1.
Figure 2.
Figure 3.
Figure 4.
clinical | EXCELLENCE






Material selection
By contouring the margin of the temporary crown as precisely as possible and through detailed instruction and motivation of the patient regarding oral hygiene at home, it was possible to eliminate irritation and achieve firm and healthy gingiva (Figure 11).
Before taking the final impression, the temporary crown was examined using callipers in order to be able to review material-specific substance removal and correct it where appropriate.
At the same time, silicone keys were used to visualise the anatomical reduction of tooth 21 and evaluate the labial reduction in three planes.
The target shade of the restoration and the shade of the remaining tooth were defined before taking the impression for the dental laboratory and documented with photos.
Once the preparation margin had been exposed using retraction thread and PTFE tape, a conventional impression was taken using an individual tray and polyether material (Figure 12-21).
The material for the final crown was selected in consultation with the dental technician. This took place following fabrication of the working models and evaluation of the space available, the shade of the remaining tooth and the defined target shade.
Due to the discoloured and devitalised tooth and in order to avoid a “grey mask”, a material with less translucency than lithium disilicate was to be used. A state-of-the-art zirconia material with highly aesthetic properties was to be selected.
IPS e.max ZirCAD Prime (Ivoclar) was the material of choice when the decision was taken on the appropriate material.
112 Australasian Dental Practice January/February 2024
Figure 5.
Figure 7.
Figure 9.
Figure 6.
Figure 8.
Figure 10.
|
clinical
EXCELLENCE


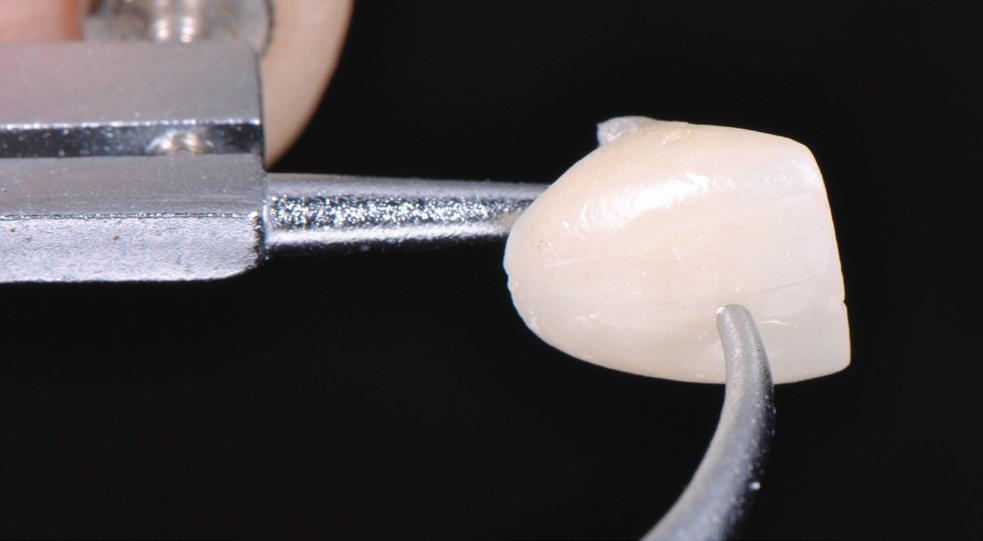


Analogue impressions and digital fabrication with hand-crafted aesthetics
This material combines two zirconia components: highstrength 3Y-TZP zirconia (1200 MPa flexural strength) in the dentine area and a more translucent 5Y-TZP zirconia (650 MPa flexural strength) in the incisal area.
The smooth progression of shade and translucency in the material discs is a further guarantee of highly aesthetic prosthetic restorations.
In terms of shade accuracy, lightness and clinical appearance, single-tooth and bridge restorations fabricated using IPS e.max ZirCAD Prime easily stand up to comparison with lithium disilicate restorations.
The finalised plaster models were scanned and the crown mould of the natural tooth (11) mirrored virtually on the remaining tooth (21). As a result of using this digital option, the fabrication of a wax-up was no longer required (Figures 22-25) and (Figures 26-28).
Following the digital design of the anterior crown, the construction was milled fully anatomically from the zirconia disc (Figures 29-30).
Generally, details were finished and the labial surface reduced minimally for micro-veneering in the pre-sintered, chalky and soft state.
January/February 2024 Australasian Dental Practice 113
Figure 12.
Figure 14.
Figure 13.
Figure 15.
Figure 11.
clinical | EXCELLENCE




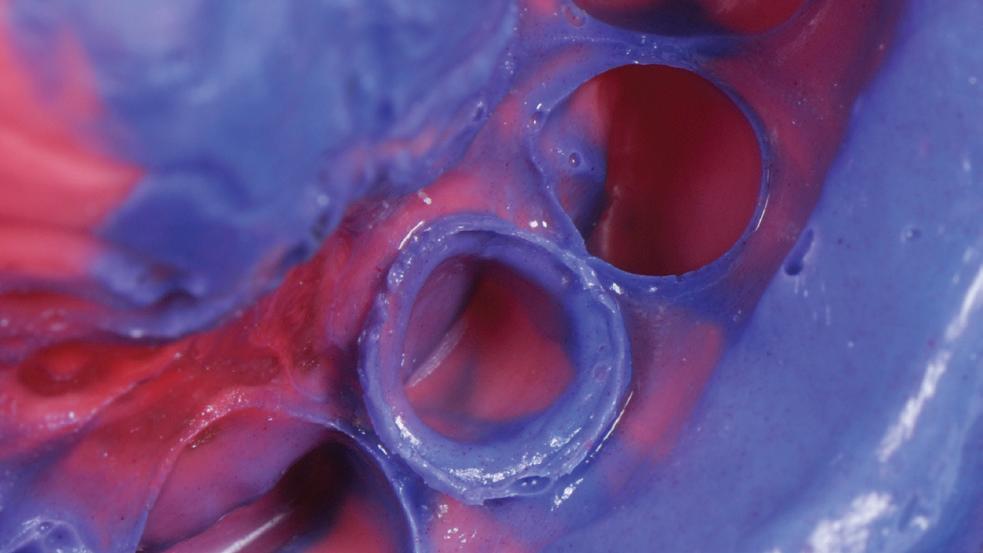

Adhesive bonding using Speedcem Plus
Once processed and modified in this way, the framework was sintered at 1530 degrees. This caused its volume to shrink by approximately 25%, resulting in the actual size high-strength zirconia framework.
To achieve a treatment outcome that was as natural as possible, a minimum labial cut-back was added followed by individual layering using IPS e.max Ceram (Ivoclar) veneering ceramic (micro-veneering) (Figures 31-34).
So that the discoloured remaining tooth was no longer visible under the new zirconia crown, a zirconia opaquer liquid was applied to the inside of the pre-sintered framework.
Thanks to material penetration, this liquid does not create additional bulk and gives the zirconia framework an opaque, nontransparent appearance from the inside at the required locations (BriegelDental) (Figures 35-36).
The inside of the restoration was delivered pre-treated by the dental laboratory.
The temporary was removed and the remaining tooth cleaned using a fluoride-free polishing paste (Proxyt) and a polishing brush (Figure 37).
During try-in of the completed restoration, different parameters were evaluated such as the fit, proximal and occlusal contact areas, functional movements and the surface texture and reflection of light. A try-in paste allowed final verification of the shade effect of the single-tooth crown (Figure 38).
To clean the surface of the remaining tooth and to increase its size, it was blasted using aluminium oxide powder (Figure 39) and the preparation margins exposed using retraction thread and twisted PTFE tape (Figures 40-42). This approach prevents subgingival penetration of the bonding material.
114 Australasian Dental Practice January/February 2024
Figure 16.
Figure 18.
Figure 20.
Figure 17.
Figure 19.
Figure 21.
|
clinical
EXCELLENCE
After try-in, the inside of the restoration was thoroughly rinsed with water and coated for 20 seconds with Ivoclean (Ivoclar) –a universal cleaning paste – in order to clean the bonding surface following contamination with saliva (Figure 43).
After cleaning, the bonding surface of the restoration was dried and the self-adhesive composite cement Speedcem Plus (Ivoclar) applied. After the restoration was placed in situ, light-curing was carried out in selected areas to bond the crown to the labial surface (Figure 44). This allowed the excess cement to be removed while still malleable without the risk of slippage and after the liquid strip gel was applied, enabled optional light curing to be carried out from all sides (Figure 45).
At the end of the bonding protocol, the retraction thread was removed (Figure 46), the bonding joint precisely inspected and any residual composite cement removed from it (Figure 47).
For quicker regeneration of the slightly traumatised gingiva, a CHX varnish (Cervitec Plus, Ivoclar) was applied using a microbrush (Figure 48).
Summary
During treatments with fixed restorations in the aesthetically demanding upper anterior area, dentists and dental technicians are faced with the complicated challenge of deciding which material should be used to achieve a treatment outcome that is as natural as possible.
In the case of all-ceramic restorations, a distinction is made between two groups of materials: glass ceramics and zirconia ceramics. Prior to the introduction of highly aesthetic zirconia ceramics for the various applications, a clear distinction had to be made between their respective application areas.


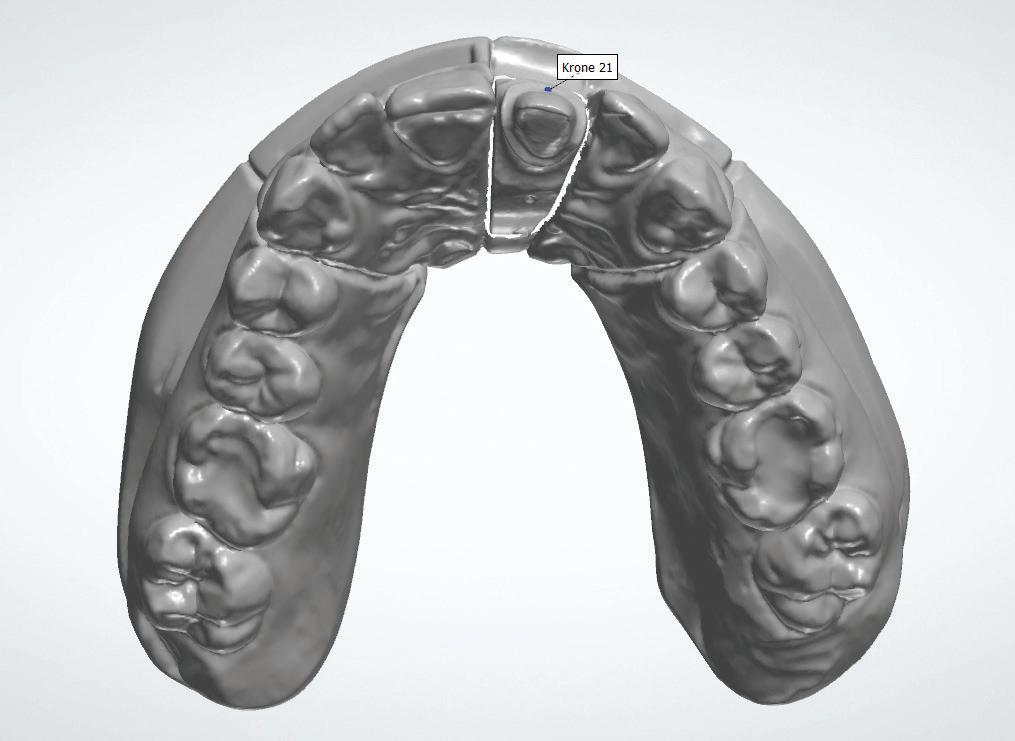
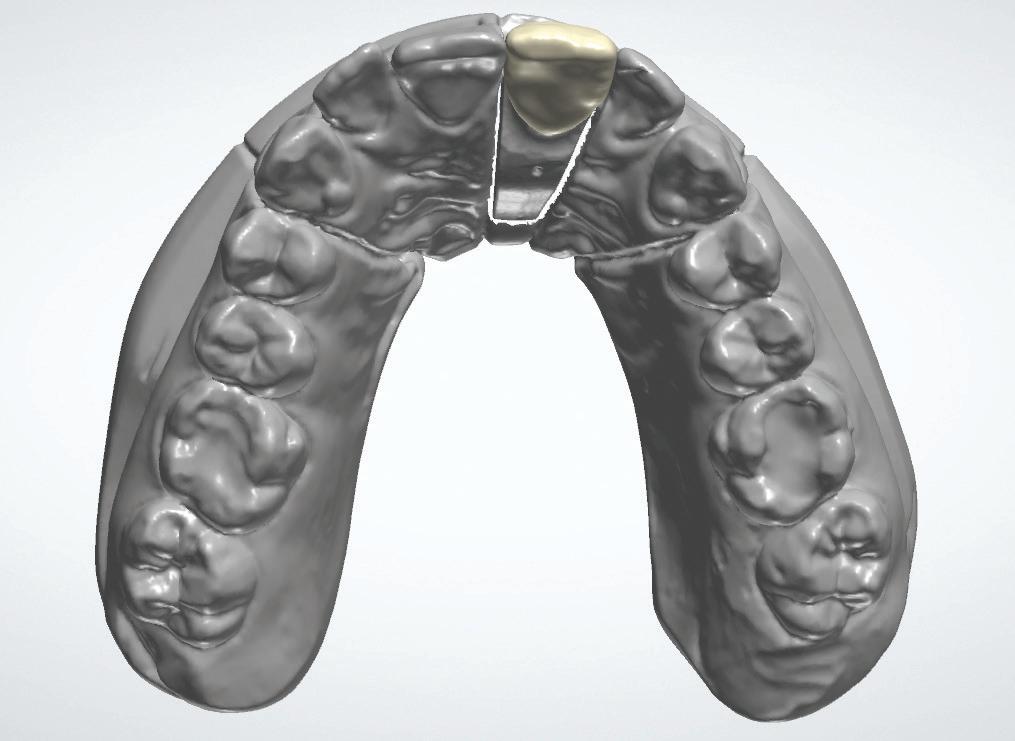


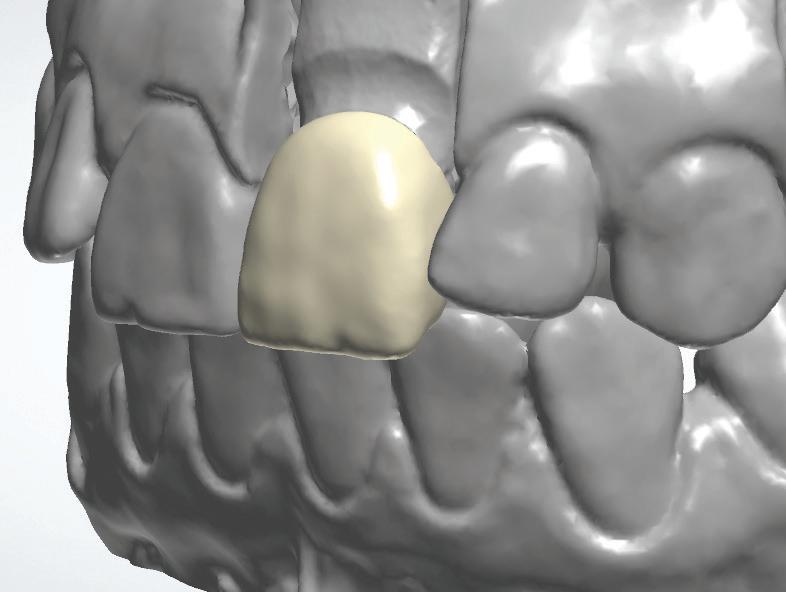
January/February 2024 Australasian Dental Practice 115
Figure 24.
Figure 26.
Figure 27.
Figure 28.
Figure 22.
Figure 23.
Figure 25.
clinical | EXCELLENCE
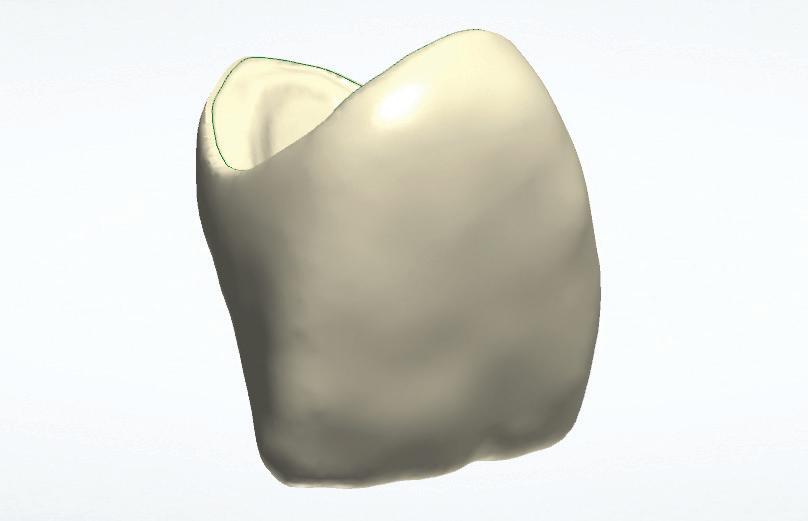



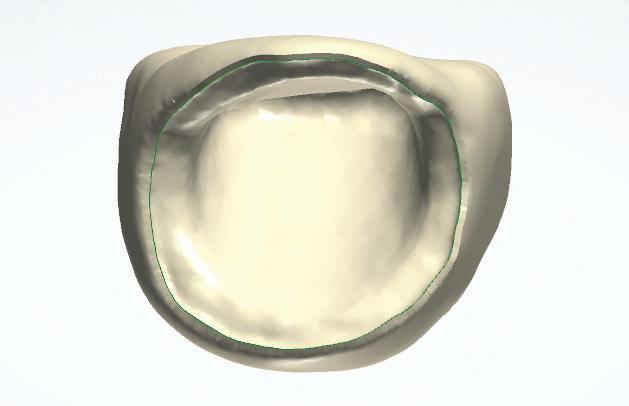



116 Australasian Dental Practice January/February 2024
Figure 29.
Figure 31.
Figure 33.
Figure 35.
Figure 30.
Figure 32.
Figure 34.
Figure 36.
clinical | EXCELLENCE






About the author
Thanks to the high strength and the outstanding aesthetics offered by the innovative IPS e.max ZirCAD Prime zirconia ceramic, this material can be used universally for all areas of application – from single-tooth crowns through to 14-unit bridges – and with all processing techniques (staining, cut-back, veneering and infiltration techniques).
The continued further development of all-ceramic restoration materials increases the predictability of the required aesthetic treatment outcome. This gives you confidence and reduces stress both in the dental laboratory and the dental practice, meeting the prerequisites for happy and satisfied patients (Figure 49).
Making people smile ;-)!!
Dr Knut Hufschmidt studied dentistry at the University of Freiburg, Germany and obtained his dental licence in 1992. After earning his doctorate two years later, he worked as an assistant dentist at a private dental practice in Kenzingen, Germany, for two years. Between 1995 and 1998, he trained as an oral surgeon at the University of Münster and the Clinic of WelsGrieskirchen, Germany. Subsequently, he opened his own dental practice, which specialises in aesthetic dentistry, implantology and full-mouth rehabilitation. Since 2003, he has been frequently invited to hold lectures on the topic of implantology. Additionally, Dr Hufschmidt has held various lectures about composite resin and all-ceramic restorations in the past three years.
January/February 2024 Australasian Dental Practice 117
Figure 37.
Figure 39.
Figure 41.
Figure 38.
Figure 40.
Figure 42.
clinical | EXCELLENCE








118 Australasian Dental Practice January/February 2024
Figure 43. Figure 45.
Figure 47.
Figure 44. Figure 46.
Figure 48.
Figure 49. Lifelike restoration – DTM Martin Loitlesberger, Gmunden, Austria
clinical | EXCELLENCE


IT’S TIME TO ENHANCE YOUR VISION Scan the QR code or call 1800 225 010 to contact your local A-dec dealer JAD2200041
Block selection for monolithic CAD/CAM restorations - Part 2
By Matt Race

Ioften get asked if we can mix and match block selection and achieve outstanding aesthetics in the same arch. To answer this simply, yes, as long as we follow the “Value Rule”. When we’re faced with certain difficulties in the mouth, our most important focal point should always be the value. If we are faced with a very dark prep alongside more aesthetic preps; or restorations that will be vastly different in thickness; or cut through interproximal preps to close diastemas or correct rotations, then we need to focus on maintaining a uniform value across the arch. The underlying dentine can cruelly influence the final shade of a restoration with respect to adjacent restorations. As too can restorations that have differences in thicknesses, where the thicker material will be lower in value than the thinner material. Closing a diastema with restorative material allows light to
refract thought the interproximal area and gives a very different aesthetic result in those interproximal areas. Generally, these areas decrease in value and look dull in retrospect to the rest of a veneer that is brightened by a lighter underlying dentine.
Case report
Kristen presented with two front teeth she was unhappy with (Figures 1-3) The 11 had been composite filled many years ago and was now very dark and the 21 was heavily discoloured. Upon assessment, it was also discovered that the zenith heights of the soft tissue across the front four teeth could also be improved upon. Surgical crown lengthening of the 11 and 22 would also improve the aesthetic outcome tenfold (Figure 4).
The shade photos were taken of the adjacent lateral incisors prior to preparation (Figures 5-6).
120 Australasian Dental Practice January/February 2024
clinical | EXCELLENCE






January/February 2024 Australasian Dental Practice 121 clinical | EXCELLENCE
Figures 1-2. Inital situation: The patient was unhappy with her discoloured centrals.
Figures 5-6. The shade photos are taken of the adjacent lateral incisors prior to preparation.
Figures 3. Inital situation - retracted view.
Figure 4. It was decided that surgical crown lengthening of the 11 and 22 would improve the aesthetic outcome tenfold.
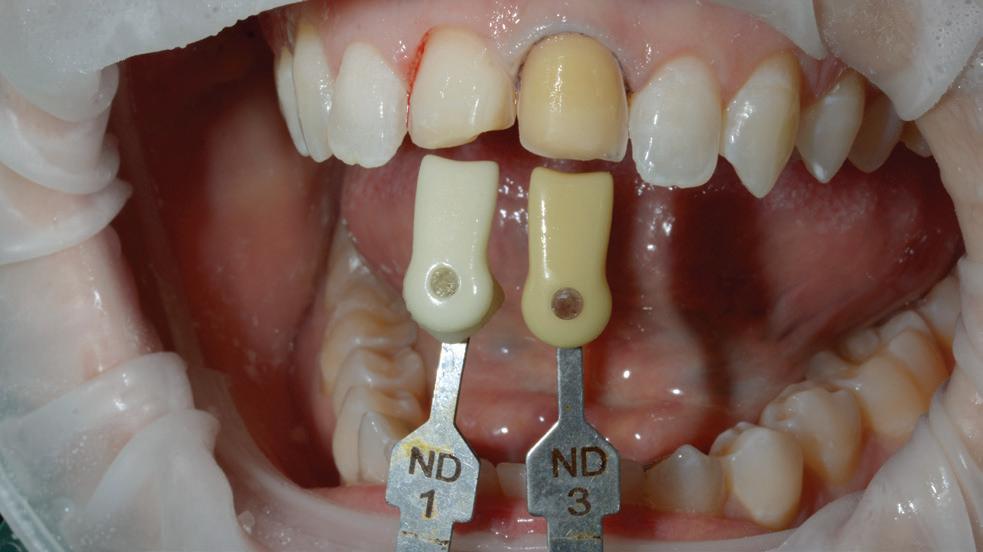


Surgical crown lengthening was performed to ensure gingival aesthetics and the teeth are prepared for restorations.
Shade photos of the preps were taken for relevant block selection (Figure 7).
The impression was taken and sent to the lab for assessment and design (Figures 8-10) After the preparation, the



discoloured 21 was more labially placed than the more aesthetic 11 preparation, increasing the difficulty of the case.
We then needed to mask the heavily discoloured preparation with a thin restoration and match it to a thicker adjacent veneer sitting over the top of a more suitable
dentine shade.
Not only would both veneers be different in thickness, but they would also have different amounts of incisal reduction, adding to the difficulty of obtaining uniform results. After assessment of the underlying dentine shades and the amount of reduction labially of both teeth, it was decided to split the shade.
122 Australasian Dental Practice January/February 2024
|
clinical
EXCELLENCE
underlying
Figure 7. Prep shades were taken for relevant block selection.
Figure 8. Digital impression.
Figures 9-10. Digital impression and restoration design.
Figures 11-12. Crystalised and glazed veneers in situ.

Cures composites, luting cements, adhesives, and sealants in just 1 Second
Features:
Features:
Each click is a 1-second cure up to 2.5mm 8mm curing depth capacity
Each click is a 1-second cure up to 2.5mm 8mm curing depth capacity
Cures composites, luting cements, adhesives, and sealants
Cures composites, luting cements, adhesives, and sealants
Reduces shrinkage and debonding
Reduces shrinkage and debonding
Reduces potential for “soft bottoms”
Reduces potential for “soft bottoms”
Consistent dispersion for a deep cure
Consistent dispersion for a deep cure
Bulk fills in 3 Seconds
Bulk fills in 3 Seconds
Cures composites, luting cements, adhesives, and sealants in just 1 Second Multi-Wave Laser Training Learn
more
about and purchase Monet $4500.00 ex GST
Multi-Wave Laser
more about and purchase Monet
Training Learn
$4500.00 ex GST


Following the “Value Rule”, we elected to stick with a low translucent (LT) block to ensure sufficient masking of the underlying 21 preparation and increase the chance of uniform results across different incisal thicknesses. The 11 was milled in LTBL4 to pick up the underlying shade and match the adjacent 12 and the 21 was milled in LTBL2 to help mask the underlying discoloured core and match the adjacent 22. The underlying discolouration coupled with the thinness of the designed veneer was intended to bring these two restorations back into a shade


relationship with minimum staining. The veneers were then crystalised, glazed and returned for placement (Figures 11-12).
Figures 13-16 show the before and after of the case, highlighting the importance of the “Value Rule”.
As long as we maintain prime focus on the value, we can make necessary adjustments to the hue and chroma to get the desired outcome and deliver aesthetically pleasing veneers first time, every time.
The author wishes to thank Dr Michael Ghobrial from Sure Dental in Brisbane.
About the author
Matt Race is a Director of Race Dental, Australia’s largest Dental Laboratory, an LVI Master Technician and 3M ESPE Trainer and Demonstrator. He shares his wealth of experience as a specialist Crown, Bridge and Implant Technician, extensively training and developing this skill set in the industry. Matt is an advocate for the benefits of streamlined digital workflows and has a passion for Cosmetic Smile Design.
124 Australasian Dental Practice January/February 2024
clinical | EXCELLENCE
Figures 13-14. Before and after.
Figures 15-16. Before and after.



Pigeon pair: Shining 3D Wireless
IOS and MetiSmile Facial Scanner
By Terence Whitty


“The rise of the virtual patient will be a great asset to clinicians and technical staff because for the first time an accurate 3D representation of the patient can be manipulated on a monitor...”
The now widespread adoption of intraoral scanners has without doubt changed the landscape of dentistry forever. But it’s fair to say, it was a long time coming. While it all started with CEREC in the early 1980s when the novel system to take 3D images using an intraoral device was first introduced, it took almost two decades before iTero became another option in 2001. More slowly followed. TRIOS came in 2010.
The technology for intraoral scanning has now reached a point where all modern scanners are very good and where even spending a small amount of money will usually yield a quality and precise instrument, so the excuse of “I’m waiting for the technology to mature” or “they are too expensive” or “I’m waiting for the price to come down” are no longer valid.
Nowadays, it’s unlikely you’ll find anything that you cannot do with an intraoral scanner that you would normally do with traditional impression taking techniques. Models, crown and bridge, implant work and surgical guides, dentures of all types and splints and sleep devices just to name a few. Of course, one may have to change the technique slightly to adapt to the
technology, for example, scanning implant scan flags instead of using impression copings, but you’ll still be able to attain an excellent result using a quality intraoral scanner. This is due to the massive hardware and software developments that have been attained over the past five years or so.
Aoralscan 3 Wireless
One scanner of note is the new Aoralscan 3 Wireless intraoral scanner from Shining 3D. A quick Google search shows this company active in metrology in many areas such as aerospace, automotive, tooling, product customisation and healthcare and life sciences including dentistry. In fact, one of their industrial scanners - the Einscan Pro - is known as one of the best on the market!
The Aoralscan 3 Wireless is a new generation of intraoral scanner as it uses the latest WiFi technology which is IEEE 802.11ax, commonly known as Wifi 6. This technology, in a nutshell, is faster, more stable and more reliable than current WiFi technologies available.
126 Australasian Dental Practice January/February 2024
clinical | EXCELLENCE
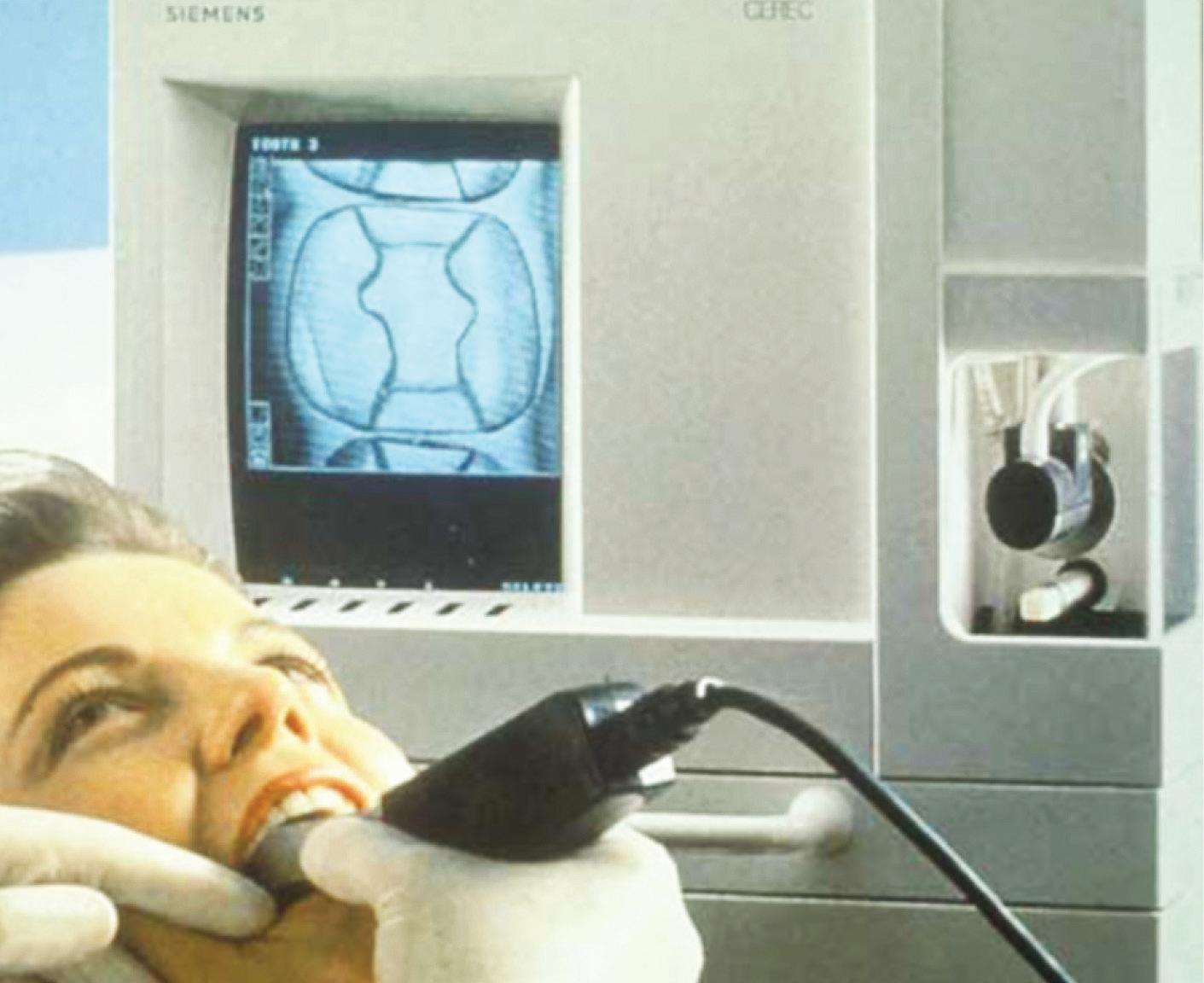
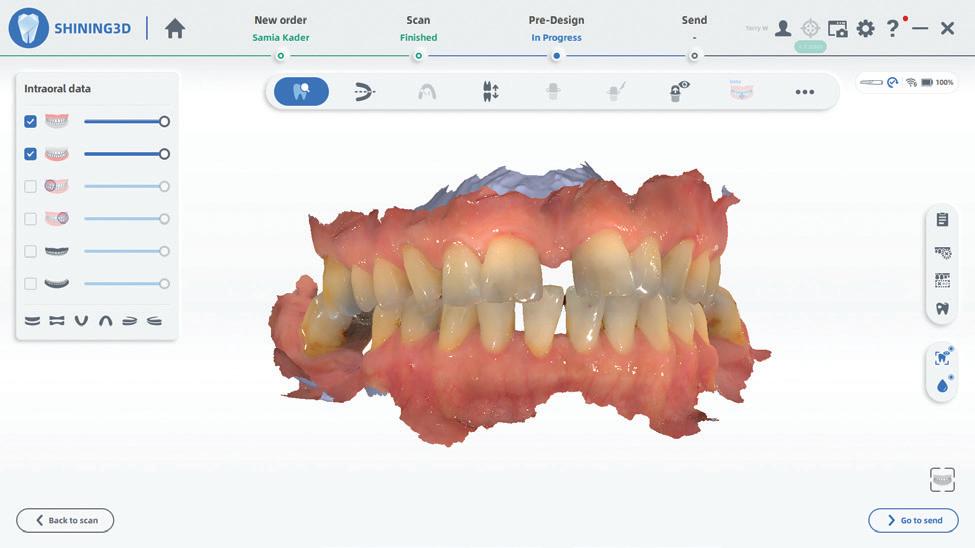
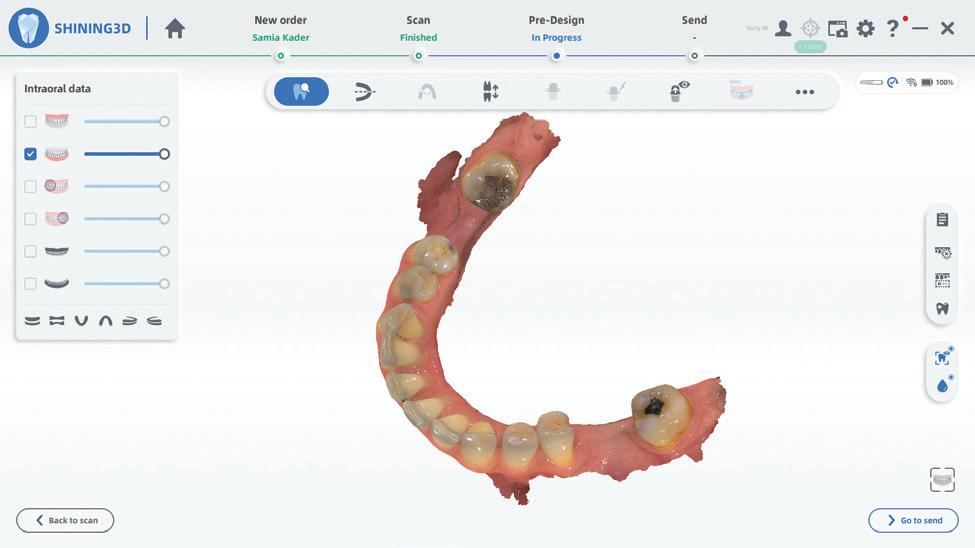
The scanner uses its own closed WiFi 6 system so it has nothing to do with your Practice WiFi. This means you will get a stable reliable signal from the base station to the scanner... always. And it works amazingly well, remaining stable over a distance far more than you will ever need, in fact at least 5 meters in the same room on my testing.
The scanner itself is light at 330 grams including the tip and a battery. It’s ergonomic and easily sits in even the smallest of hands. It has no fuss “Apple-inspired” one button operation that allows you to interact with the software and access all the functions you need. One great feature is the ability to use the scanner


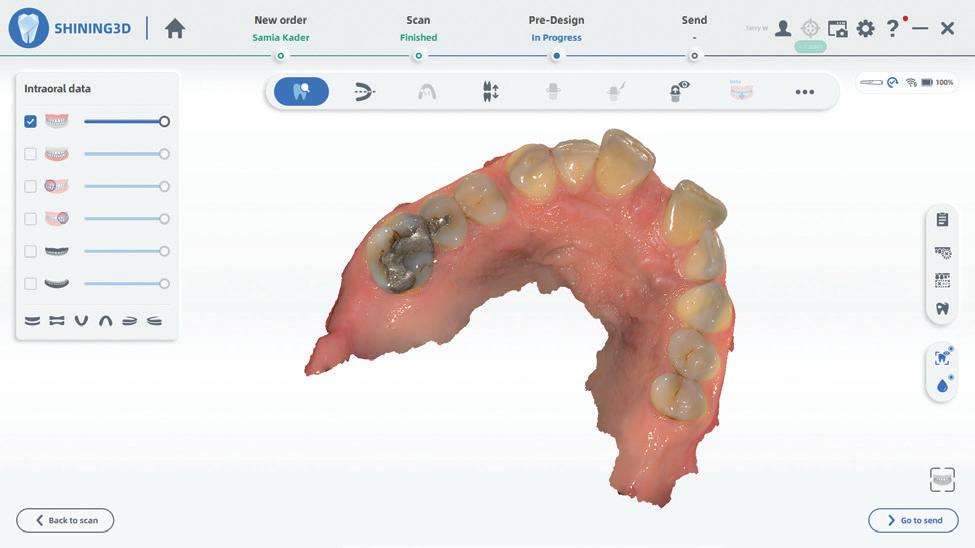

for motion function gestures where the image on the screen is controlled by movement of the scanner. This alleviates the need for a mouse or a touch screen.
The batteries last up to 2 hours each and you receive 3 batteries and a charging station in the box. Now the bonus; the scanner conveniently converts to a wired scanner by plugging in the supplied cable so you will never be without a scanner! The tips of the scanner are replaceable after 100 autoclaving cycles and come in two sizes, the small one being for children or those hard to reach places in adults. They can be swapped out instantly even during a scan.
January/February 2024 Australasian Dental Practice 127 clinical | EXCELLENCE
Figure 1. The original CEREC scanner and screen.
Figure 4. Scanning quality is excellent.
Figure 6. Full arch scan.
Figure 5. Detail including scanning of amalgam.
Figure 7. Menu for added functions.
Figure 3. Batteries and charger.
Figure 2. Shining 3D AoralScan 3 Wireless.
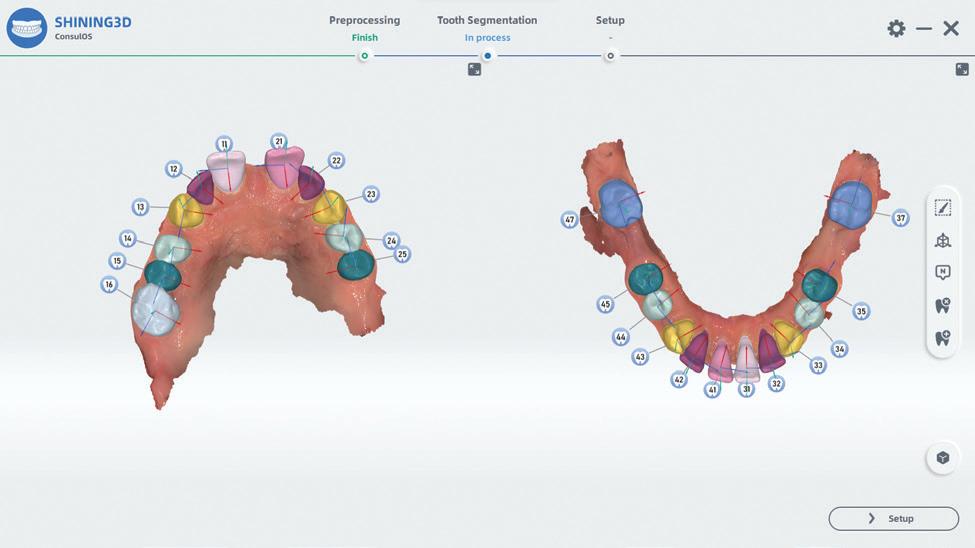
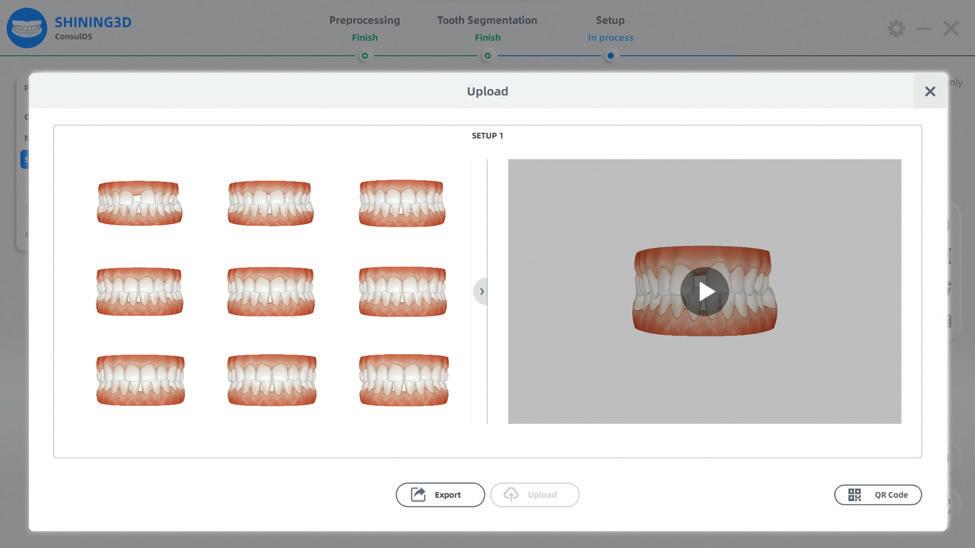

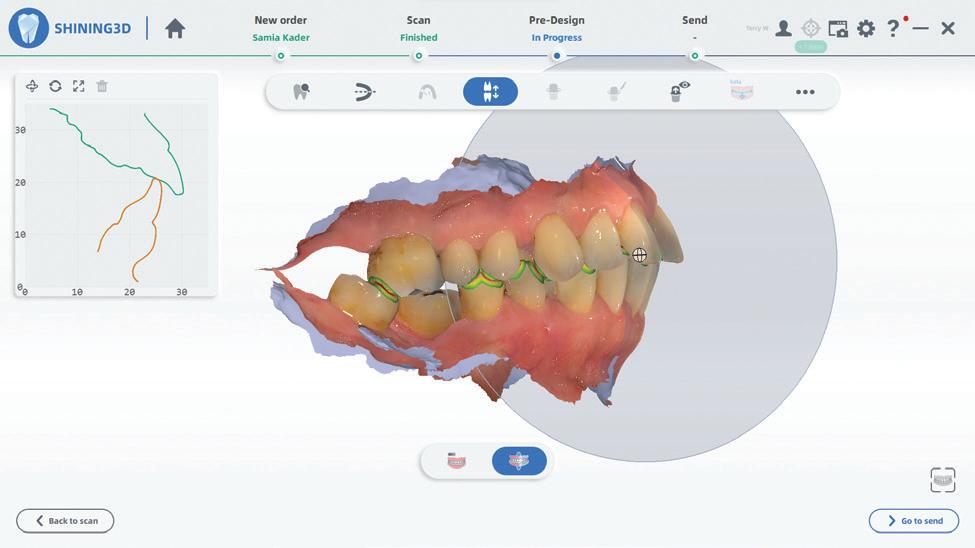
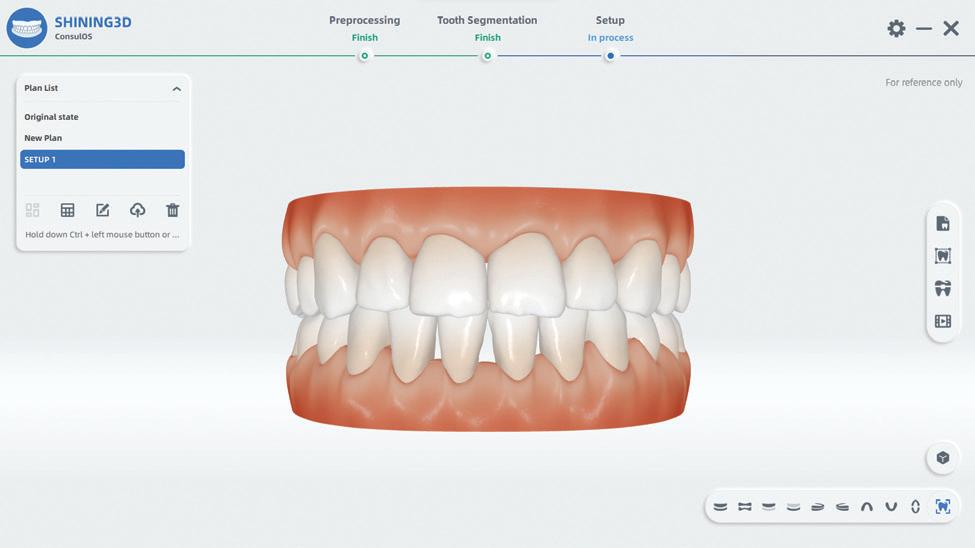
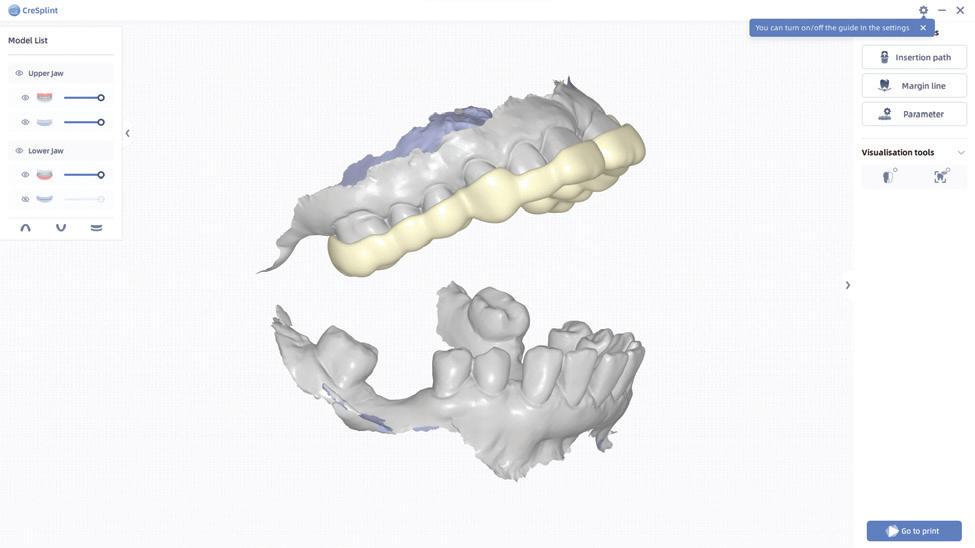
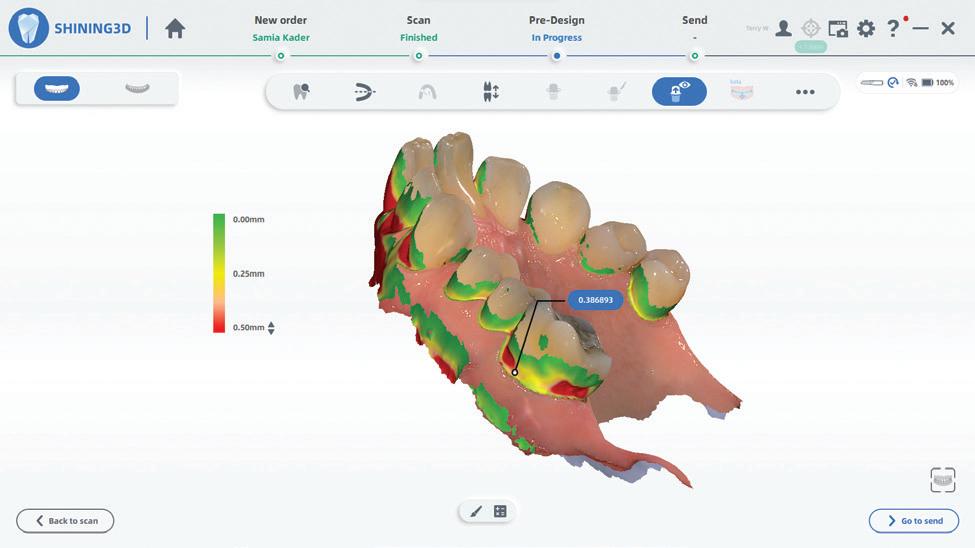
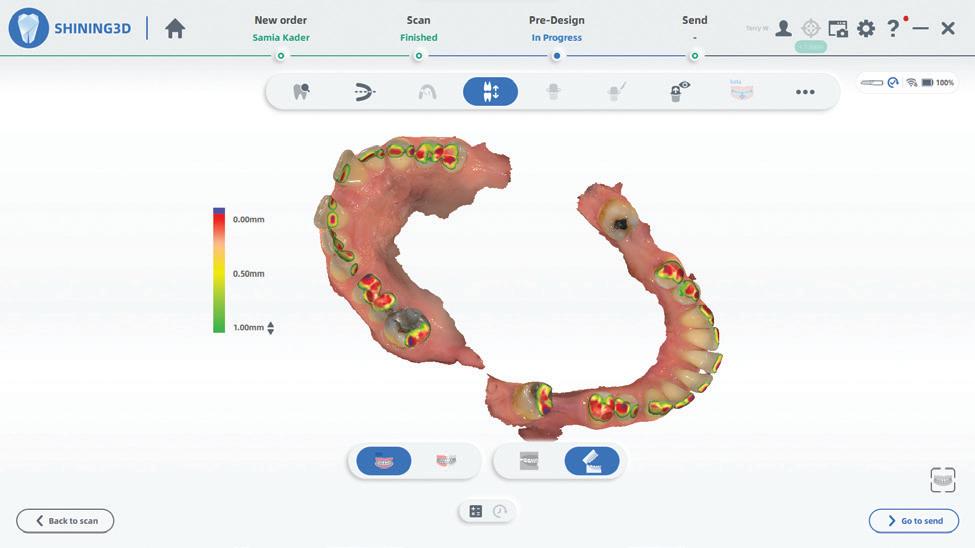
Feature-rich software
The new software that comes with the Aoralscan 3 Wireless is incredibly refined and intuitive and packed with features typically seen on scanners costing 3 times as much. It’s just very easy to use with a wizard-type interface at your fingertips, making the whole process a breeze. As a bonus, the scanning software can directly integrate with the exocad suite of CAD software, making it a very powerful system indeed.
For scanning, just setup the type of job you would like to do and the software will automatically prompt you and tell you exactly what action is needed to be executed. For example, if you wish to scan a case for two anterior implant sites, the software will tell you when to scan the tissue, when to scan the implant scan abutments (scan flags) and then when to scan the opposing teeth and of course the bite registration.
128 Australasian Dental Practice January/February 2024
Figure 8. Ortho Simulator with auto segmentation.
Figure 10. Summary and animation movie.
Figure 12. Model designer ready to print.
Figures 14-15. Occlusal mapping and cut view.
Figure 9. Auto idealisation.
Figure 11. CreSplint designs splints.
Figure 13. Undercut visualiser with measurement.

Scanning dentate or partially dentate arches is actually rudimentary and yields great results, however, there is now a special edentulous scanning algorithm that is excellent. As we all know, scanning edentulous arches is more than challenging for any scanner but this scanner does very well when you activate edentulous mode.
Bite registration
One of the most rapid actions of the software is the taking of the bite registration where a small scan is taken of the registration area and alignments are performed automatically. It’s particularly impressive as you are in control of how many areas you want to capture. Remember, you could take a registration in CR or CO or in a specific bite such as a construction bite for a splint or a sleep device. Just use your normal bite technique with wax or bite registration material and scan away, making sure there is not too much buccal overhang and you will nail it.
Oral health reporting
The software offers more features such as undercut detection, valuable when trying to get preps parallel; margin line detection; occlusion maps; and a new, interesting feature called ConsulReport, which will give you a summary of the Oral Health of the patient. After scanning, the software will generate a report which includes information such existing dental caries, missing teeth, dental calculus, pigment, missing teeth, etc. The idea here is to give patients a visual report to help relay a better understanding of their oral health, a novel idea indeed.
Ortho simulator
ConsulOS is an included orthodontic simulation module, allowing a virtual setup and a visual treatment plan for the patient. This is primarily aimed at clear aligner cases but can be adapted to traditional fixed appliances as well. Of course, we all know orthodontic simulation is a big deal these days so no
scanner is really complete without it! The software will move the teeth automatically for you and instantly give you different scenarios, for example, extraction vs non-extraction and you can even tweak the position teeth if you wish. The software will then generate a QR code that you can have the patient scan and it will download the simulation to their smart phone - what a great communication tool!
Metron Track is a module that allows you to track the patient’s differences between subsequent scans. This can be useful when tracking orthodontic treatment or evaluating wear, for example. There is a splint designer called Cresplint; a Temporary designer, CreTemp; an Indirect Bonding module, CreIBT; and a model design module so you can output directly to any of the Shining 3D 3D printers if you wish.
Dynamic bite
As an added bonus, a new Dynamic Bite function is included. The new Aoralscan 3 Wireless intraoral scanner has added the function to be able to precisely capture and record the patient’s individual jaw movements and then transfer these movements to CAD software, for example, exocad. They call this the Dynamic Bite. This really has to be seen to be appreciated. It’s already very good, but there are improvements in the pipeline to make this a really in valuable tool.
All-in-all, this a serious contender for any practice and would definitely go up against some scanners in a higher price range. It’s dripping with good value.
MetiSmile facial scanner
The new MetiSmile facial scanner, also from Shining 3D, is a revolutionary extraoral scanner that takes a 3 dimensional scan of the entire face, all in about 10 seconds. This is a very compact unit weighing in at only 800 grams, a size of only 215 x 50 x 75 mm and it can be mounted on the supplied stand or used handheld. It’s portable and easy to move between surgeries, whether it be next door or a branch practice.
January/February 2024 Australasian Dental Practice 129
clinical | EXCELLENCE
Figure 16. MetiSmile on stand.


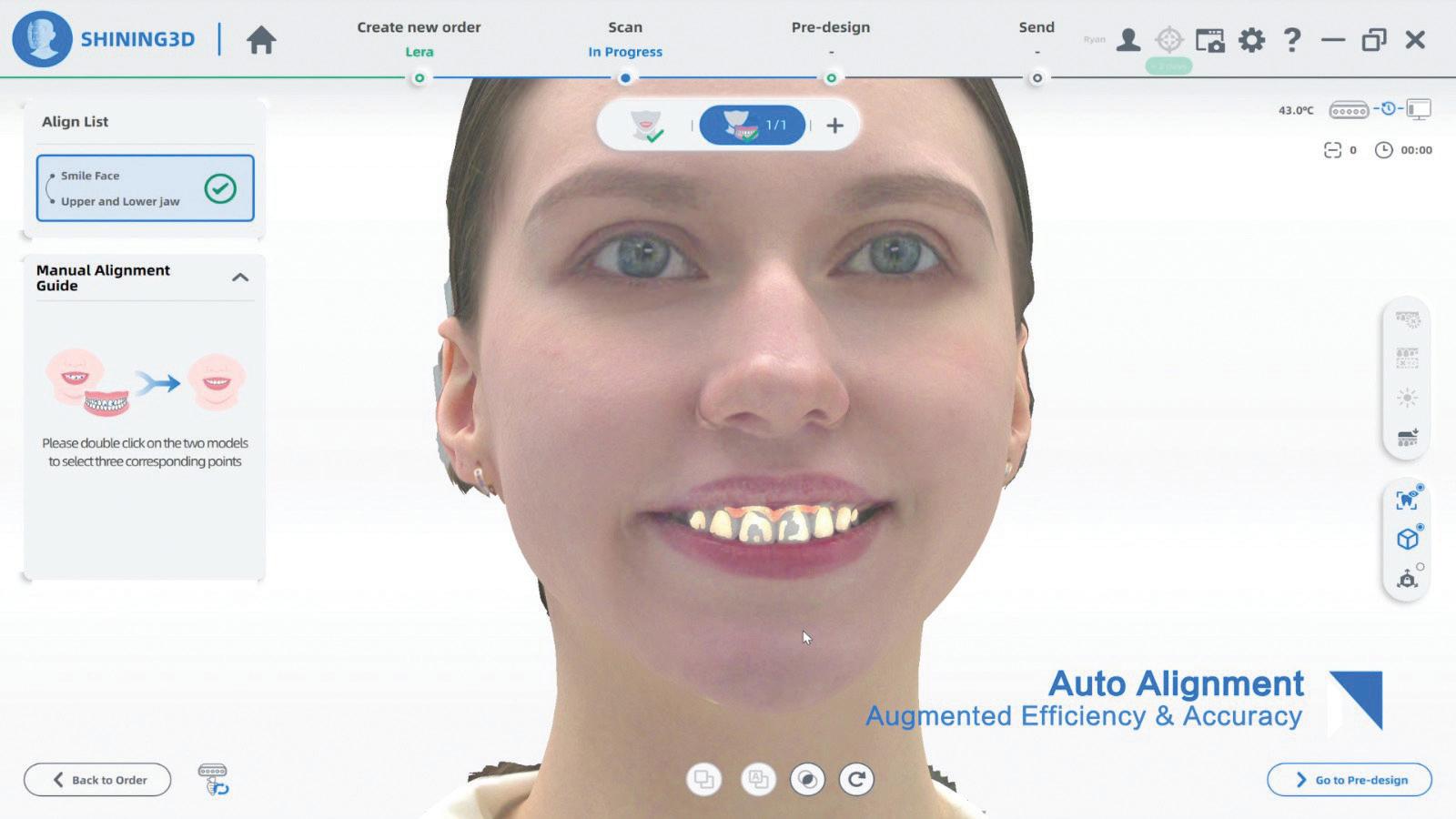

The technology of the MetiSmile uses an Infrared Vertical Cavity Surface Emitting Laser (VCSEL), not unlike that used on the iPhone for facial recognition and an array of cameras including 1.3 megapixel and 5.0 megapixel cameras to capture the data and the texture information of the patient’s face to an accuracy of 50 microns; quite accurate and impressive for a tiny unit.
With this high fidelity texture scanning, the MetiSmile can accurately record and display facial colour, so it appears realistic to the patient. Suffice to say, the technology of the hardware is modern and reliable and will give outstanding results every-time.
The software behind MetiSmile is where all the real magic happens. It’s intuitive and incredibly easy-to-use. The patient’s face is positioned in front of the camera and aligned using the connected computer’s screen. Once ready, a small countdown begins
“The technology of the MetiSmile uses an Infrared Vertical Cavity Surface Emitting Laser (VCSEL), not unlike that used on the iPhone for facial recognition...”
and image capturing will start. The patient will then be instructed to turn their head to the left and then to the right. This is all done in about 10 seconds and after a small amount of processing time, the 3D image appears on the screen. It’s really impressive to actually see the face on a screen in colour and 3D rendered. The detail is quite astounding and the colour very realistic.
130 Australasian Dental Practice January/February 2024 clinical | EXCELLENCE
Figure 19. Face scan.
Figure 17. Or handheld.
Figure 20. Merge intraoral scan.
Figure 18. Easy-to-use, the patient can sit in front of the device.
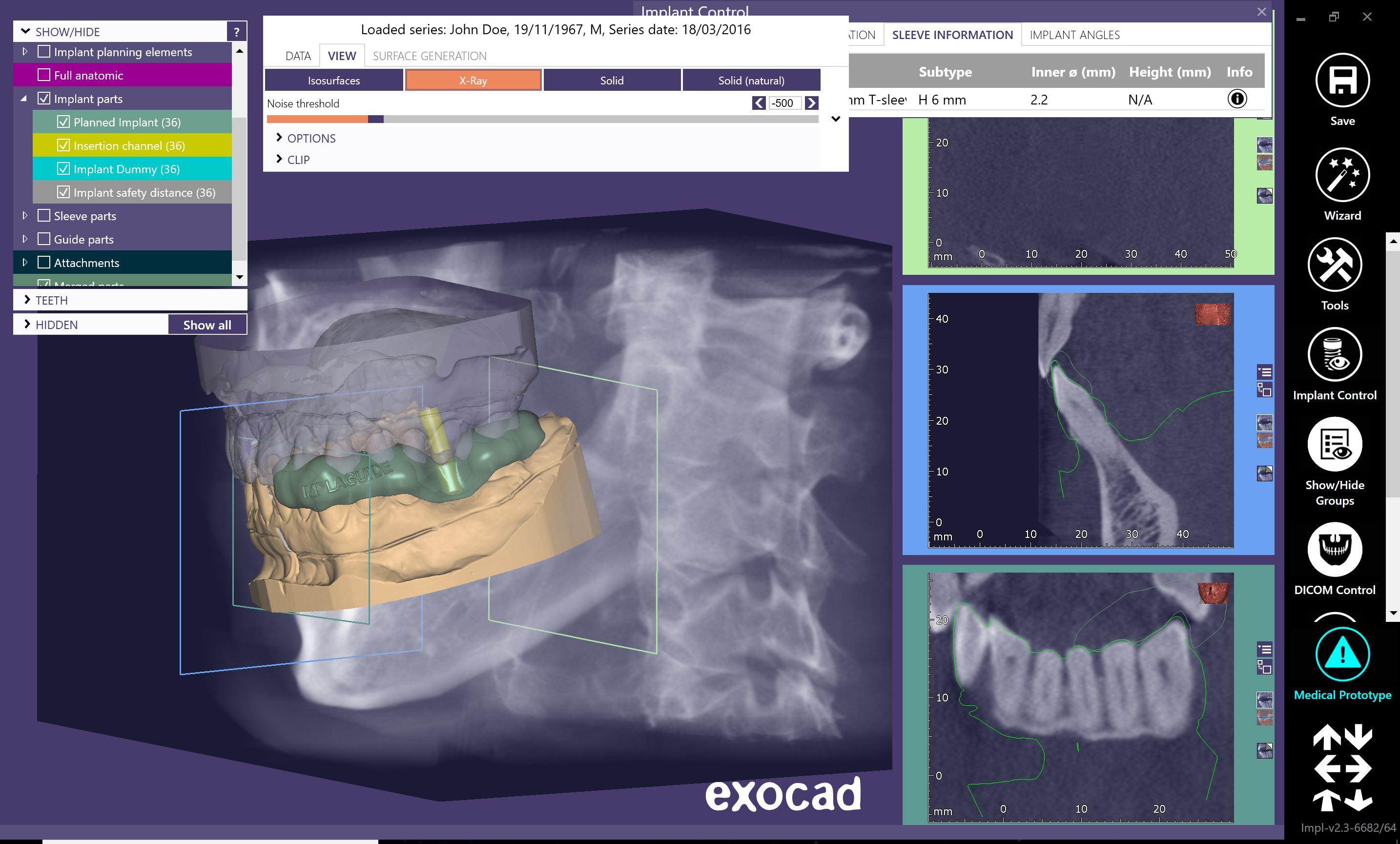



The Solution For Perfect Implant Position implaguide.com.au All implant surgical guides • Edentulous Cases • Scan Appliances • Free Planning Software Talk to us today and we will help you plan and construct a guide for your next case Free Case Evaluation Send us a CBCT and a PVS Impression or Intra Oral Scan Contact us today ! 1300 878 336
clinical | EXCELLENCE
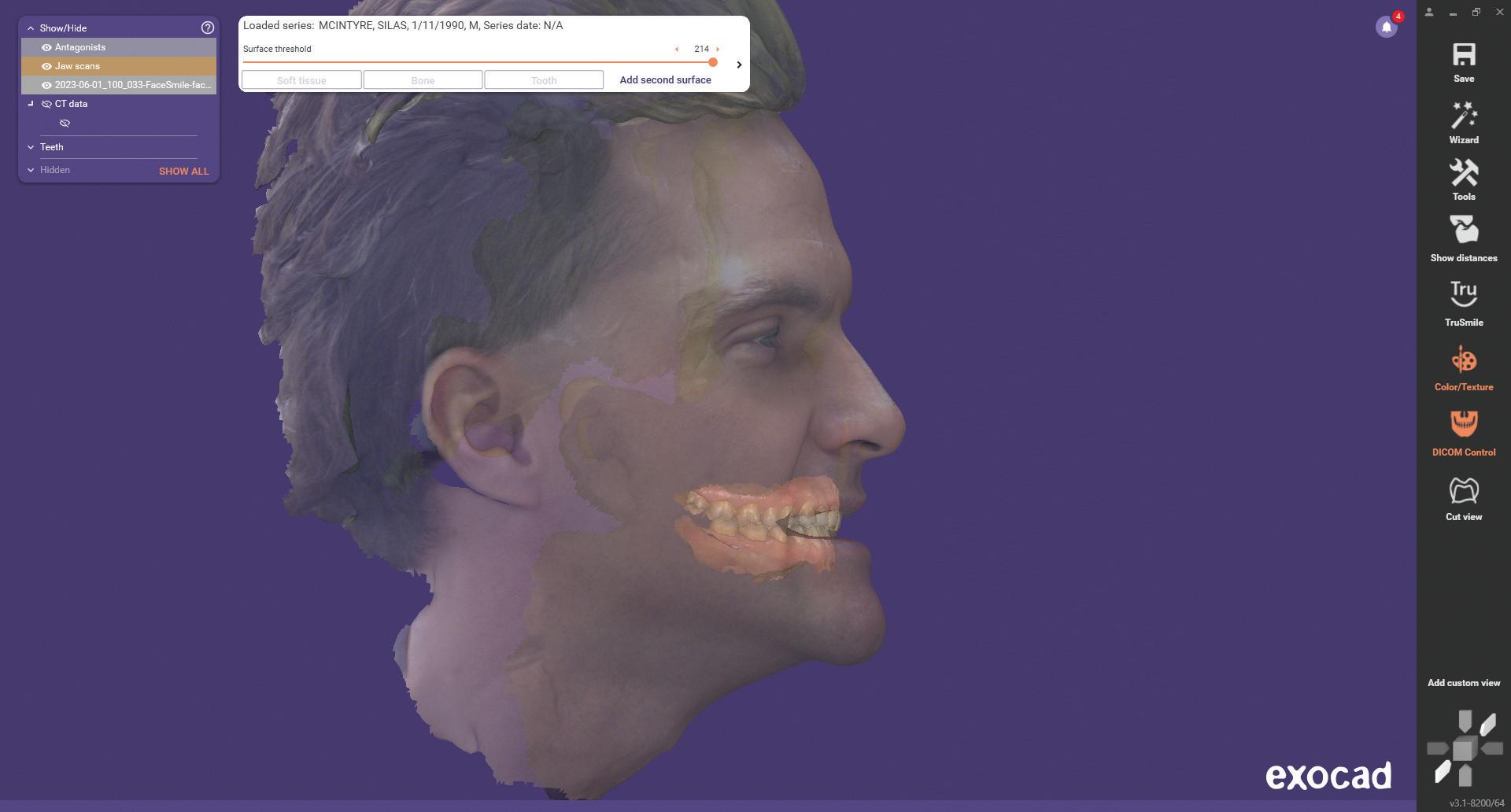
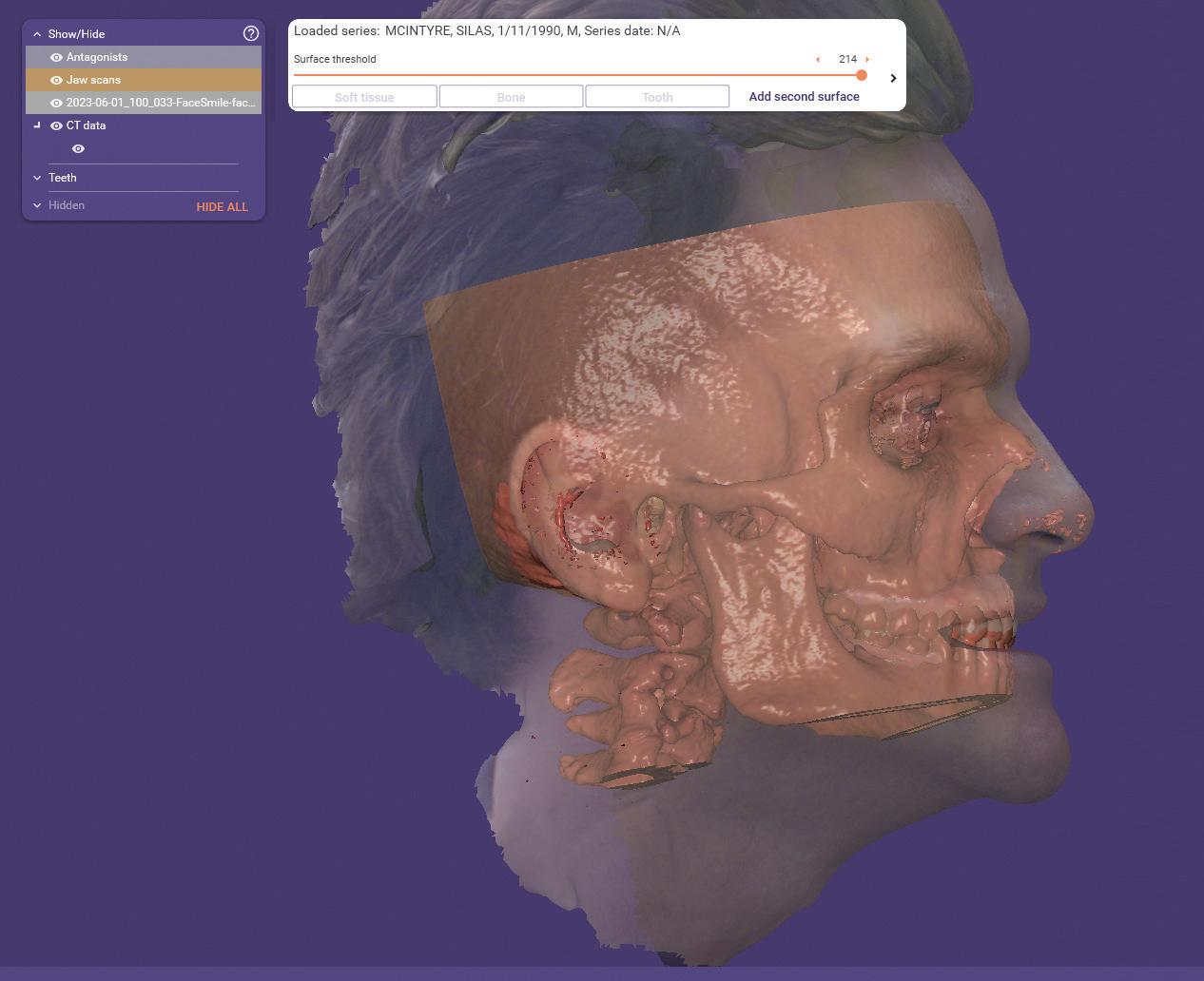
Merging scans
Now comes the really interesting part. If you take an intraoral scan (from any brand of scanner mind you), the software provided will automatically merge the facial scan of the patient and the intraoral scan. Imagine being able to see the teeth in relation to the face for treatment planning, diagnosis and communication.
The supplied software comes with an array of nifty but useful features such as a suite of facial feature measurement and comparison tools, an Ortho Simulator as well as Mandibular Trajectory Tracking.
With the right external software, MetiSmile data has the potential to digitise and replace conventional extraoral records,
“The rise of the virtual patient will be a great asset to clinicians and technicians as for the first time an accurate 3D representation of the patient can be manipulated virtually prior to treatment commencing...”
analog facebow, occlusal analysis and diagnostic wax-ups. You can also merge a CBCT scan with an intraoral scan as mentioned and see it all as an amazing 3D virtual patient. All this matched and merged data is invaluable and can easily be manipulated with a program like exocad.
The rise of the virtual patient will be a great asset to clinicians and technicians as for the first time an accurate 3D representation of the patient can be manipulated virtually prior to treatment commencing. Any restorations and appliances being designed can be viewed for size, position, colour and function in relation to the whole face. This will be revolutionary and in a short time will become the expected norm for everyone.
About the author
Terence Whitty is a well-known dental technology key opinion leader and lectures nationally and internationally on a variety of dental technology and material science subjects. He is the founder and owner of Fabdent, a busy dental laboratory in Sydney specialising in high tech manufacturing. Using the latest advances in intra- and extra-oral scanning, CAD/CAM, milling, grinding and 3D printing, most specialties are covered including ortho, fixed and removable prosthetics, computerised implant planning and guidance, TMD, sleep appliances and paediatrics.
132 Australasian Dental Practice January/February 2024
Figure 21. exocad, face scan and intraoral scan merge.
Figure 22. exocad, face scan and intraoral scan merge plus DICOM from CBCT.










• Wireless 6 Technology
• 3 Batteries
• Corded Option Included
• Amazing Software
• Ortho Simulator
• Dental Health Report
• Inbuilt Camera Mode
• Scan anything!
• Affordable Quality
Solution For Perfect Scans Every Time fabdent.com.au
The
new
is all
! Contact us today ! 1300 878 336
The
Aoralscan 3 Wireless
about unbeatable features, performance and value
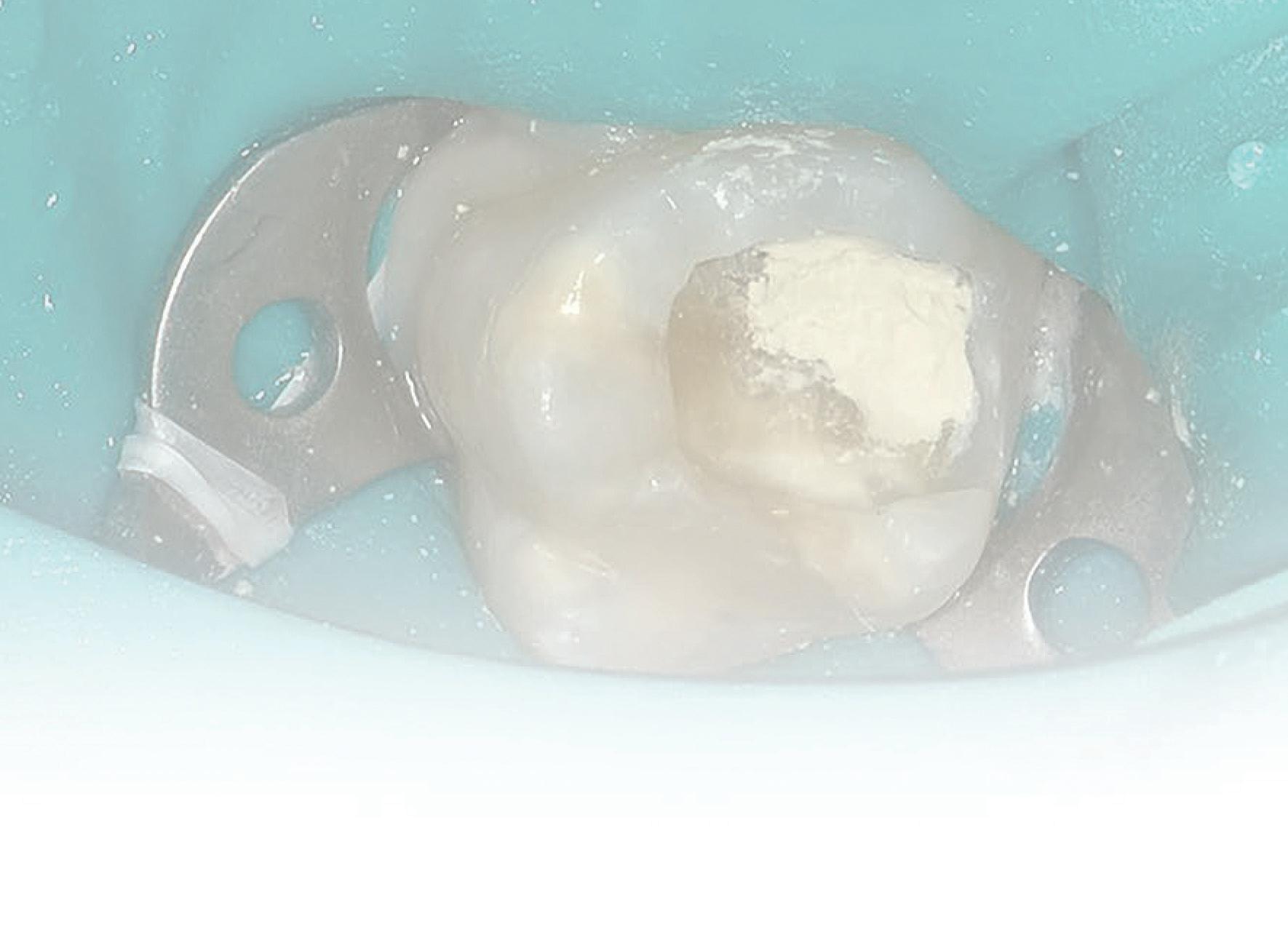
Biodentine™ in the treatment of Molar Incisor Hypomineralisation (MIH) in paediatric dentistry: A case report
By Dr Lance Kisby
Molar Incisor Hypomineralisation (MIH) has become one of the most pressing issues in paediatric dentistry.
MIH is a qualitative defect of unknown etiology in enamel development, presenting as demarcated opacities of variable extent and severity (Figure 1, Tooth 11).1 In 2003, the European Academy of Paediatric Dentistry defined MIH as a systemic condition and qualitative enamel defect of systemic origin that affects at least one first permanent molar (Figure 2-3), which can also be associated with permanent incisors.1 However, recent studies have shown it can affect second permanent molars, permanent canines, bicuspids and second primary molars.1,2,3,4,5
Hypomineralised second primary molars (HSPMs) can be considered a predictor for MIH in permanent teeth.4
Prevalence and distribution
M IH is considered a worldwide clinical problem with a global prevalence of 14.2%, ranging from 0.5% to 40.2%.6 Worldwide, 25% of children have MIH.2 Lopes has shown that MIH has, in general, a prevalence of 13.5%; 36.3% of MIH teeth are moderately to severely affected; and MIH is present in 3.6% of second primary molars.7
Distribution of MIH was seen more in males at age nine years old, with molars affected more than incisors. The mandible was affected more than the maxilla and the right side was affected more than the left side.8
134 Australasian Dental Practice January/February 2024
clinical | EXCELLENCE READ ME FOR CPD
Etiology
Though the etiology of MIH is still not fully understood, a combination of several factors which create MIH enamel formation seem to occur at the maturation stage of enamel formation. The mineralisation of the first permanent molars usually starts just before or at birth and is fully completed at four to five years of age.9
Acute and chronic childhood illness, certain adverse birth events and conditions during the neonatal period were weakly associated with MIH, while dioxins showed a moderate level of association.10 Additionally, there may be a link between the use of antibiotics, as well as ear-nose-throat infections.11
Clinical presentation
MIH can present as a lesion with clear borders which can be white, yellow or brown. An interesting feature of MIH is the asymmetry of the defects. One molar or incisor can be severely affected while the contralateral tooth may be clinically sound.8
“Though the etiology of MIH is still not fully understood, a combination of several factors which create MIH enamel formation seem to occur at the maturation stage of enamel formation...”
The enamel in MIH teeth is different than normal enamel. The hypomineralised enamel has less distinct prism edges and crystals, with larger interprismatic spaces. Thus, MIH enamel is more porous than normal, sound enamel.12
This porous enamel is easily damaged and may be subject to rapid wear and post-eruptive enamel breakdown (PEB), particularly in stress-bearing areas due to the forces of mastication. Caries risk is also elevated in porous enamel, particularly in the posterior teeth, where rapid extensive caries can be so severe as to require extraction. Exposed dentine can accelerate the development of carious lesions.1 Dentine hypersensitivity, poor aesthetics, anxiety and tooth loss can also occur.1,13,14,15
Children with MIH often complain of intense dental thermal sensitivity, especially to cold, due to chronic pulp inflammation under the hypomineralised area.16 Consequently, these patients are at greater risk of caries from poor oral hygiene due to avoiding toothbrushing, which is associated with tooth sensitivity.
Treatment challenges in MIH
Restorative treatment for MIH teeth is challenging for both the patient and the dentist. The subclinical inflammation of pulpal cells and the altered porous enamel structure make bonding less reliable, leading to defective restorations, frequent loss of restorations and frequent retreatments.



Treatment is further complicated by thermal sensitivity and the difficulty of achieving adequate local anaesthesia in MIH-affected teeth. Procedures can be more uncomfortable and painful for children as a result, leading to an increased prevalence of behavioural management problems, lack of cooperation and dental anxiety and fear.13
Successful management of MIH
Arisk assessment and early diagnosis are the key factors for an effective, successful and conservative MIH treatment.17 The choice of appropriate treatment depends on the extent of MIH. Long-term restorative treatment for hypomineralised teeth requires up to ten times more treatment and retreatment than teeth without MIH.18 Treatment can range from prophylactic strategies to highly complex restorative procedures.15
The best approach to treating MIH patients should be an individualised treatment plan according to the needs of the patient, using minimally invasive dentistry (MID) techniques.19 MID is defined as a philosophy of minimal intervention for the placement and replacement of restorations. The objective is tissue preservation, achieved by performing treatment with as little loss of tissue and damage to adjacent tissue as possible.20
This article will demonstrate how Biodentine™ (Septodont) can be used as a minimally invasive technique for immediate and long-term pain relief to achieve a successful MIH restoration with the least amount of stress and anxiety for the patient.
January/February 2024 Australasian Dental Practice 135
clinical | EXCELLENCE
Figure 1. MIH presents as demarcated opacities of variable extent and severity.
Figures 2-3. MIH is a systemic condition and qualitative enamel defect of systemic origin.
Case report
This is a case of an eight-year-old male who presented with his parent for an emergency visit complaining of pain to cold stimuli, such as water and ice cream, for over four months. The parent related that the patient had already seen four dentists who were unable to achieve adequate local anaesthesia. Pain was not experienced in any other teeth.
Figure 4 shows tooth #16 with not only a large, well-demarcated loss of enamel on the occlusal surface, but also brown spots on other areas of the occlusal and other surfaces. The tooth was sensitive to air blast. A diagnosis of MIH was made based on the history of pain to cold stimuli; no other thermal issues; severe enamel and dentine breakdown on the occlusal (posteruptive breakdown); and multiple surfaces with brown-yellow areas.
“MIH
is a qualitative defect in enamel. It creates treatment challenges including pain to cold stimuli and problems achieving adequate local anaesthesia, which contribute to subsequent behavioural issues and anxiety...”
The plan was to provide relief and comfort and to restore the function of tooth #16. This was first achieved with local anaesthesia for the rubber dam clamp. A rubber dam was placed, before removing a thin layer of slightly soft dentine and any poor enamel to reach clean, bondable enamel and dentine (Figure 5).
Because this is a newly erupted permanent tooth and the lesion is close to the mesial-buccal pulp horn, the largest of the pulp horns, it was decided to do an Indirect Pulp Capping (IPC) with Biodentine, a tricalcium silicate cement. Biodentine has been shown to have better results as an IPC than other materials.21 This is due to its high pH of 12 and the release of calcium and silicon ions, which stimulates mineralisation and creates a “mineral infiltration zone” along the dentine-cement interface, thus creating a superior sealing property compared to other materials. Biodentine




shows superior microhardness due to the continued crystallisation of calcium silicate hydrate gel, which reduces porosity, increases hardness with time and increases compressive strength.22,23,24
Biodentine was mixed, placed and condensed in the area of the mesial-buccal pulp horn (Figure 6). After Biodentine had set, excess material was removed. The area was then treated with a selective etch technique of 38% phosphoric acid on enamel only and rinsed with water for 10 seconds. A G-Premio Bond (GC) self-etch adhesive was then placed on the dentine for five seconds, air-dried and light-cured. Solare Sculpt (GC) shade A2 was placed in 1-2 mm incremental layers and light-cured at each layer. Once completed, the composite was shaped, contoured and smoothed. Anatomy was placed and G-Coat (GC), an unfilled resin, was placed over the composite and light-cured (Figure 7).
The patient returned two weeks later for a follow-up, during which the parent related that the patient had instantaneous relief after the treatment and has not had any thermal sensitivity to tooth #16 since. The parent added that he can now drink cold water and eat ice cream.
Conclusion
MIH is a qualitative defect in enamel. It creates treatment challenges including pain to cold stimuli and problems achieving adequate local anaesthesia, which contribute to subsequent behavioural issues and anxiety. In this case, Biodentine used as an indirect pulp capping represented a conservative treatment adhering to Minimally Invasive Dentistry guidelines, chosen for many positive properties that included thermal insulation and ease of restoring with a composite.
136 Australasian Dental Practice January/February 2024
clinical | EXCELLENCE
Figure 4. Initial situation.
Figure 6. Biodentine placed at mesial-buccal pulp horn.
Figure 5. Clinical situation after soft dentine removed.
Figure 7. Clinical situation after composite placed.

Irreversible Pulpitis
Irreversible Pulpitis



Biodentine™ saves pulps EVEN with signs and symptoms of irreversible pulpitis*
width Pre-trimmed and pre-crimped for simple placement occlusal anatomy that matches the natural tooth
LOVE OUR STAINLESS STEEL PEDO CROWNS: and mesio-distal width Pre-trimmed and pre-crimped for simple placement occlusal anatomy that matches the natural tooth IS EVERYTHING the right one with Hu-Friedy
Biodentine™ saves pulps EVEN with signs and symptoms of irreversible pulpitis*
outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. comes to the perfect fit, Hu-Friedy is just right.
saves pulps EVEN with signs and symptoms

saves pulps EVEN with signs and symptoms
Biodentine™ saves pulps EVEN with signs and symptoms of irreversible pulpitis*
Biodentine™ brings one-of-a-kind benefits for the treatment of up to 85%** of irreversible pulpitis cases:
Biodentine™ brings one-of-a-kind benefits for the treatment of up to 85%** of irreversible pulpitis cases:
For vital pulp therapy, bulk- lling the cavity with Biodentine™ makes your procedure better, easier and faster:
Bone Grafting
Biodentine™ brings one-of-a-kind benefits for the treatment of up to 85%** of irreversible pulpitis cases:
• Vital Pulp Therapy allowing complete dentin bridge formation
brings one-of-a-kind benefits for the treatment of
• Vital Pulp Therapy allowing complete dentin bridge formation
brings one-of-a-kind benefits for the treatment of up to 85%** of irreversible pulpitis cases:
Pulp healing promotion: proven biocompatibility and bioactivity
• Minimally Invasive treatment preserving the tooth structure
Reduced risk of failure: strong sealing properties
• Vital Pulp Therapy allowing complete dentin bridge formation
As the first all-in-one biocompatible and bioactive dentin substitute, Biodentine™ fully replaces dentin wherever it’s damaged.
• Minimally Invasive treatment preserving the tooth structure
• Immediate Pain relief for your patients’ comfort
• Immediate Pain relief for your patients’ comfort
• Minimally Invasive treatment preserving the tooth structure
Vital Pulp Therapy allowing complete dentin bridge formation
Only one material to fill the cavity from the pulp to the top
• Bio-Bulk filling procedure for an easier protocole
• Immediate Pain relief for your patients’ comfort

Similar mechanical behavior as natural dentin: ideal for bulk filling
• Bio-Bulk filling procedure for an easier protocole
Immediate Pain relief for your patients’ comfort
The final enamel restoration will be placed within 6 months.
New Biphasic Formulations allowing you to manage the pace of your bone grafting procedures: (80% ß-TCP / 20% Hydroxyapatite) 40/60 (40% ß-TCP / 60% Hydroxyapatite)
Minimally Invasive treatment preserving the tooth structure
Bio-Bulk filling procedure for an easier protocole
Innovative by nature
Innovative by nature
Innovative by nature
• Bio-Bulk filling procedure for an easier protocole Innovative by nature Irreversible Pulpitis
Innovative by nature
Innovative by nature

Please visit our website for more information
www.septodont.com
www.septodont.com
www.septodont.com
Improving on Biodentine the composite onto Biodentine full restoration in a single session
Bio-Bulk filling procedure for an easier protocole
Biodentine™ helps the remineralization of dentin, preserves the pulp vitality and promotes pulp healing. It replaces dentin with similar biological and mechanical properties.







To enjoy the clinical benefits of the first and only dentin in a capsule, ask your dental distributor for Biodentine™.



visit our website for more information
Please
Biomatlante SA Please visit our website for more information
Learn more with the Biodentine brochure ONLINE AT
LLC. All rights
predictable
HU-FRIEDY.COM/PerfectFit
reserved.
Orders 1300 65 88 22 www.henryschein.com.au 855 www.henryschein.co.nz ONLINE AT
Co., LLC. All
predictable
IS
Orders 1300 65 88 22 www.henryschein.com.au 808 855 www.henryschein.co.nz Exclusively available in Australia from Exclusively available in New Zealand from
*
our
for more
HU-FRIEDY.COM/PerfectFit
rights reserved.
outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. it comes to the perfect fit, Hu-Friedy is just right. LOVE OUR STAINLESS STEEL PEDO CROWNS: height and mesio-distal
EVERYTHING the right one with Hu-Friedy
www.ivoclarvivadent.co.nz Call 0508 486 252 Reverse the Irreversible!
Biodentine™ Please visit
website
information www.septodont.com
NEW Reverse the
Biodentine™
Irreversible!*
Please visit our website for more information www.septodont.com
*If haemostasis cannot be achieved after full pulpotomy, a pulpectomy and a RCT should be carried out, provided the tooth is restorable (ESE Position Paper,Duncan et al. 2017) ** Taha et al., 2018 NEW
* Biodentine™
visit our website for more information www.septodont.com
Reverse the Irreversible!
Please
*If haemostasis cannot be achieved after full pulpotomy, a pulpectomy and a RCT should be carried out, provided the tooth is restorable (ESE Position Paper,Duncan et al. 2017) NEW
About the author
Dr Lance Kisby is a graduate of Tufts University School of Dental Medicine, Boston, Massachusetts. He completed his Residency in Pediatric Dentistry at Floating Hospital at New England Medical Center, Boston. He was Chief of Pediatric Dentistry and Assistant Director of Dentistry at R.I. Hospital, Providence, RI. He spent 17 years in private practice in Massachusetts. He was Chief of Pediatric Dentistry at St. Mary’s Hospital in Waterbury, Connecticut. He is Board Certified in Pediatric Dentistry since 1983. He has multiple publications. He is a Fellow of the American
Academy of Pediatric Dentistry and a Master of the Academy of General Dentistry. He created two Pediatric Dental Residencies, one in Danville, Pennsylvania and the second in Wilmington, Delaware and was Program Director of both. He is currently the staff Pediatric Dentist at the Lac du Flambeau Band of Lake Superior Chippewa Indians in Lac du Flambeau, Wisconsin with the IHS. Dr Kisby has over 47 years of clinical and teaching experience bringing new and exciting techniques and insights to those dentists and staff who treat children.
References
1. Weerheijm, KL. et al. Judgement criteria for molar incisor hypomineralization (MIH) in epidemiological studies: A summary of the European meeting on MIH held in Athens, 2003. Eur. J. Paedtr. Dent. 4, 110-113.
2. de Farias AL, Rojas-Gualdrón DF, Girotto Bussaneli D, Santos-Pinto L, Mejía JD, Restrepo M. Does molar-incisor hypomineralization (MIH) affect only permanent first molars and incisors? New observations on permanent second molars. Int J Paediatr Dent. 2022 Jan;32(1):1-10. doi: 10.1111/ipd.12780. Epub 2021 Mar 17. PMID: 33629389.
3. Dietrich G., Sperling S. & Hetzer G. Molar incisor hypomineralisation in a group of children and adolescents living in Dresden (Germany). Eur J Paediatr Dent. 4, 133–137 (2003).
4. Elfrink M. E. et al. Deciduous molar hypomineralization and molar incisor hypomineralization. J Dent Res. 91, 551–555 (2012).
5. Schmalfuss A., Stenhagen K. R., Tveit A. B., Crossner C. G. & Espelid I. Canines are Affected in 16-Year-Olds with Molar-Incisor Hypomineralisation (MIH): An Epidemiological Study Based on the Tromso Study: “Fit Futures”. Eur J Paediatr Dent. 17, 107–113 (2016).
6. Balmer RC, Laskey D, Mahoney E, Toumba KJ. Prevalence of enamel defects and MIH in non-fluoridated and fluoridated communities. Eur J Paediatr Dent. 2005 Dec;6(4):209-12. PMID: 16426121.
7. Lopes, L.B., Machado, V., Mascarenhas, P. et al. The prevalence of molarincisor hypomineralization: a systematic review and meta-analysis. Sci Rep 11, 22405 (2021). https://doi.org/10.1038/s41598-021-01541-7.
8. Padavala S, Sukumaran G. Molar Incisor Hypomineralization and Its Prevalence. Contemp Clin Dent. 2018 Sep;9(Suppl 2):S246-S250. doi: 10.4103/ccd. ccd_161_18. PMID: 30294152; PMCID: PMC6169288.
9. Caruso S, Bernardi S, Pasini M, Giuca MR, Docimo R, Continenza MA, Gatto R. The process of mineralisation in the development of human tooth. Eur J Paediatr Dent 2016; 17(4): 322–326.
10. Crombie F, Manton D, Kilpatrick N. Aetiology of molar-incisor hypomineralization: A critical review. International Journal of Paediatric Dentistry 2009; 19(2): 73–83.
11. Giuca MR, Cappè M, Carli E, Lardani L, Pasini M. Investigation of Clinical Characteristics and Etiological Factors in Children with Molar Incisor Hypomineralization. Int J Dentistry, 2018.
12. Fagrell TG, Dietz W, Jälevik B, Norén JG. Chemical, mechanical and morphological properties of hypomineralized enamel of permanent first molars. Acta Odontologica Scandinavica 2010; 68(4): 215–222.
13. Jälevik B, Klingberg GA. Dental treatment, dental fear and behaviour management problems in children with severe enamel hypomineralization of their permanent first molars. International Journal of Paediatric Dentistry 2002; 12(1), 24–32.
14. Jälevik B, Norén JG. Enamel hypomineralization of permanent first molars: a morphological study and survey of possible aetiological factors. International Journal of Paediatric Dentistry 2000; 10(4): 278–289.
15. Neves AB, Americano GCA, Soares DV, Soviero VM. Breakdown of demarcated opacities related to molar-incisor hypomineralization: a longitudinal study. Clinical Oral Investigations 2019; 23(2): 611–615.
16. Mendonça FL, Regnault FGDC, Di Leone CCL, Grizzo IC, Bisaia A, Fragelli C, Oliveira TM, Magalhães AC, Rios D. Sensitivity Treatments for Teeth with Molar Incisor Hypomineralization: Protocol for a Randomized Controlled Trial. JMIR Res Protoc. 2022 Jan 6;11(1):e27843. doi: 10.2196/27843. PMID: 34989687; PMCID: PMC8778566.
17. William V, Messer LB, Burrow MF. Molar incisor hypomineralization: Review and recommendations for clinical management. Pediatric Dentistry 2006; 28(3): 224–232.
18. Kotsanos N, Kaklamanos EG, Arapostathis K. Treatment management of first permanent molars in children with Molar-Incisor Hypomineralisation. Eur J Paediatr Dent 2005; 6(4): 179–184
19. Guica MR, Lardini L, Pasini M, et al. State-of-the-art on MIH. Part. 1 Definition and aepidemiology. Eur. J Paediatr Dentl. 2020. 21(1):80-82.
20. D Ericson, E Kidd, D Mc Comb, I Mjor, MJ Noack. Minimally invasive dentistry-Concepts and Techniques in Cariology. Oral Health Prev Dent. 2003;1:59–72.
21. Selvendran KE, Ahamed AS, Krishnamurthy M, Kumar VN, Raju VG. Comparison of three different materials used for indirect pulp capping in permanent molars: An in vivo study. J Conserv Dent. 2022 Jan-Feb;25(1):68-71. doi: 10.4103/jcd.jcd_551_21. Epub 2022 May 2. PMID: 35722078; PMCID: PMC9200191.
22. Caron G, Azerad J, Faure MO, Machtou P, Yves B. Use of a new retrograde filling material (Biodentine™) for endodontic surgery: two case reports. Int J Oral Sci. 2014;6(4):250–53.
23. Grech L, Mallia B, Camilleri J. Investigation of the physical properties of tricalcium silicate cement-based root-end filling materials. Dent Mater. 2013;29(2):20–28.
24. Septodont Biodentine™ Active Biosilicate Technology™ Scientific file 2010.
138 Australasian Dental Practice January/February 2024 clinical | EXCELLENCE
outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns.
why dentists favor our impeccable fit. Perfect for your patients. Easy for you.
comes to the perfect fit, Hu-Friedy is just right.
right one with Hu-Friedy
right one with Hu-Friedy
OUR STAINLESS STEEL PEDO CROWNS:
outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. comes to the perfect fit, Hu-Friedy is just right.
OUR STAINLESS STEEL PEDO CROWNS:
Septanest : the first choice of dentists with over 150 million injections per year, provides you high quality you can trust
ONLINE
LLC.
predictable
IS
the
855 ww ONLINE
Co.,
predictable
808 855 ww IS
the
855 ww ONLINE
Co.,
IS
AT
All rights reserved.
LOVE
EVERYTHING
AT
LLC. All rights reserved.
discover
it
LOVE
EVERYTHING
AT
LLC. All rights reserved.
EVERYTHING the right one with Hu-Friedy
www.ivoclar.com
Call 0508 486 252

Art deco style at Spa Dental
If ever there was a dental practice where the surrounds matched the high-end treatments on offer, Spa Dental in the fashion district of Sydney is it. In a world where cosmetic dentistry, such as whitening, porcelain veneers, implants and Invisalign strive for the perfect look, the aesthetics throughout Spa Dental certainly set the stage for high expectations.
And in the case of Spa Dental, one of Australia’s pioneering and leading Invisalign clinics operated by Dr Sean Parsonage and Dr Lawrence Neville, the practice delivers.
Spa Dental has taken its design queue from Sydney’s glorious art deco era. The practice is located on the fourth floor of an iconic historic sandstone high-rise at 64 Castlereagh Street (once Sydney’s second-tallest building) whose signature tenant is international fashion icon, Bulgari.
From the moment you enter the decorative historic ground floor entrance, to the surgery’s “olde worldly” entrance with its black steel framed glass doors with fluted pattern glass inserts, the opulent ambience surrounds you.
Gazing past the granite-clad reception desk, the eye is drawn to a massive, dried
By David Petrikas
flower arrangement framed by a spectacular striated dark granite alcove - one of many arches used throughout the space.
More curved, natural granite is featured at each end of the transecting main hallway - one end being devoted to a patient refresh area in another alcove, complete with granite vanity and oval mirror.
Midway down the entrance hallway is a deco style waiting room with a scalloped curved salmon-pink velvet wrap-around lounge with a sheer-curtained background and distinctive patterned carpet.
Opposite is another lounge beneath a sign with the slogan: “Your Smile Our Style”.
140 Australasian Dental Practice January/February 2024 surgery | DESIGN

Adjacent to the hallway, with an entrance next to reception and through to the main hallway, is a private consult room. Here, another soft upholstered soft neutral beige lounge and matching chair feature with the same carpet in a “Neapolitan ice-cream” type pattern in caramels and brown on a light beige background.
Both the waiting room and the private consultation room feature brass deco inspired round tables on conical bases. The feeling is unmistakeably “luxe” and comforting.
The long main hallway is punctuated by a series of black arches, creating a type of “optical” effect, accentuating the perspective of depth and the ordered architectural design of the space.
The style doesn’t stop at the “public” areas of the practice. Wide arched niches crown the built-in cabinetry with its light metallic bronze doors and brown-veined smooth stone-finish benchtops and splashbacks in the main surgeries.
The dental equipment continues the luxe feel, with top-ofthe-line A-dec 500 dental chairs in black stitched upholstery providing a comfortable experience for patients.
Despite a spectacular end result, Dr Parsonage said it was quite hard to come up with a workable layout to fit the space. “We tried other designers, but they couldn’t make the layout work for us and deliver the feel that we wanted and also meet the budget.”

January/February 2024 Australasian Dental Practice 141



142 Australasian Dental Practice January/February 2024

In the end, they found a boutique design company called MXN Design Studio in Surry Hills which had an impressive portfolio of work, including commercial interiors and a previous Sydney dental fit-out.
Dr Parsonage said the design brief was centred around a “Luxe 5-star hotel feel” which has certainly been achieved.
“We wanted a grand entrance and are fortunate we have quite high ceilings which helps give a sense of space. We really wanted a bit of a statement when you came in, although there were some practical compromises because of the shape of the building.”
One of those was locating the steri room further away from the surgeries so that it now occupies a private space off one end of the hallway adjacent the staff room.
Dr Parsonage said they wanted the waiting room to be big enough to feel comfortable to give the right impact and also be located close to the front desk. Similarly, the consultation room is both private, yet easily accessible from reception, while the surgeries, private offices, steri room and staff amenities all run off the main hallway at the rear.
Design effects used to impart the desired ambience included the colour scheme, extensive use of curves, natural granite feature walls and niches, steel-framed glazed doors with fluted glass inserts and deco-inspired furnishing.
The build was done by Sheeth Builders of Marrickville, project managed by the principal, Yossef Sheeth.
When it came to equipping the surgeries, Dr Parsonage said he chose A-dec from a reliability point of view and ongoing cost of ownership as he’s used just about every other brand before.

January/February 2024 Australasian Dental Practice 143


“I’ve found other brands too expensive in terms of ongoing maintenance and if something needs to be replaced, it can be super expensive. I’m expecting A-dec to be much cheaper to maintain in the long term,” he said.
Service backup was another factor. “A-dec is a relatively simple chair from an engineering standpoint and you can do some of your own repairs and there are multiple authorised A-dec companies in Sydney that can maintain the chairs.”
Dr Parsonage first became interested in the A-dec chairs at trade shows, including IDS in Cologne, Germany and ADX in Australia and also from speaking to A-dec reps.
He then followed up with A-dec dealer, Presidental, who supplied three top-of-the line A-dec 500 chairs and one A-dec 400, plus a number of A-dec dentist and assistant’s stools. They also relocated an older patient chair from their previous practice and provided equipment training on the new A-dec equipment.
Given the need for long procedures such as sinus lifts, major bone grafts, implants and All-on-4™ procedures, Dr Parsonage said a patient chair which provided support for both the dentist and patient was an important consideration.
“I think the A-dec chairs are very ergonomic because of the thin backrest which lets you get underneath the patient
Summary
The Practice
The Practice Spa Dental
The Principals Dr Sean Parsonage and Dr Lawrence Neville
Practice Type General
Location Sydney, New South Wales
Size
200 square metres
No of chairs 5
The Team
Design MXN Design, Surry Hills, Sydney
Designers Madeleine Karrys and Marie Daaboul
Installer Presidental, Sydney
Equipment
Dental Units A-dec 500 & A-dec 400 traditional with A-dec 500 LED ceiling mounted lights
Sterilisation
Imaging
Compressor
Melag Melatherm 10 washer disinfector
Dentsply Sirona DAC Premium
Dentsply Sirona Axeos CBCT
Sirona Heliodent Plus X-ray
Dürr Vista Scan
Cattani AC300 x 2
Suction Cattani Turbo Smart Software
Dental4windows and Sidexis
because it’s not too thick,” he said. “It’s very comfortable for the patients as well because of the soft upholstery and the headrest is very easy to adjust to get it in the right position for you and the patient.”
A number of patients have commented on the comfort of the chairs, although of course most are more fixated on the procedure and the results.
The practice has a dedicated marketing team and routinely takes “before and after” photos which are featured in a “Dental Spa Smile Makeovers” hardbound book which is kept in the waiting room to showcase their quality work.
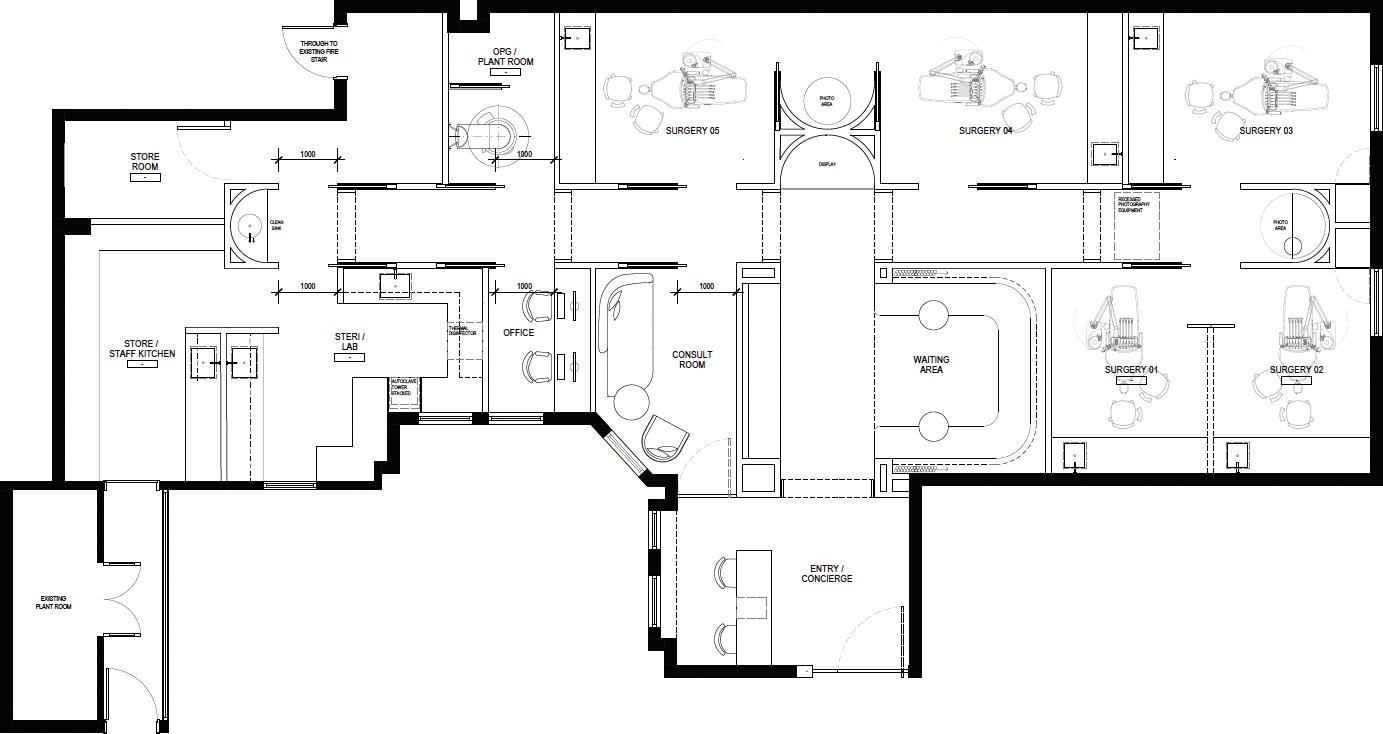


144 Australasian Dental Practice January/February 2024
A-dec 500 Pro: Experience a new level of connection.
Everything you’ve come to appreciate about the A-dec 500 dental chair, is now available with a new delivery. Enabled with A-dec+ and an updatable software platform, the A-dec 500 Pro delivery system supports your dental team with a new level of connection.
new | PRODUCTS
Information contained in this section is provided by the manufacturers or distributors. Australasian Dental Practice does not assume responsibility for the accuracy of the data.
New MOCOM THALYA handpiece care VITA MFT denture tooth

MOCOM’s new Thalya and Thaylya+ are the dentist’s latest ally for effective maintenance of rotary instruments. Simple and user-friendly, these units allow perfect lubrication and purge maintenance of turbines and handpieces. To start using the machine, just connect to the compressed air feed and the power supply. Lubrication
and purge of 4 instruments is completed in less than a minute - Duct purge; Lubrication; and oil purge in 55 seconds.
Available:
Mocom Australia
Mob: 0427-816-459
Tel: (08) 9244-4628
sales@mocomaustralia.com.au
www.mocomaustralia.com.au
New A-dec 500 Pro delivery system

The new generation A-dec Pro delivery systems - built to fit on the proven latest generation A-dec 500 and A-dec 300 patient chairs - are now being rolled out through A-dec dealers across the country. A-dec Pro heralds the new area of “Connectivity” in delivery systems, bringing tablet-style touchscreen technology and intelligent control on an allnew software-based platform.
This brings the latest technology right into the dental surgery, supporting both the operator and the entire dental team in caring for patients, now and in the future.

VITA MFT is now available in 16 VITA classical A1-D4 shades and 16 3D-MASTER shades, including 3 bleach shades. VITA MFT (Multi Functional Teeth) stand out due to their outstanding efficiency. The groundbreaking VITA Easy Centric principle simplifies the set-up process. Thanks to the predefined contact points, the teeth find the ideal position almost automati-
cally, saving time and hassle, while also increasing precision. Morphology, incisal design and the shade match with the VITA shade guides also ensure aesthetically pleasing results.
Available:
Henry Schein
Tel: 1300-658-811
lab@henryschein.com.au
www.henryschein.com.au
Cure up to 2.5 mm in 1 second!

Available:
A-dec Australia
Tel: 1800-225-010
australia.a-dec.com
The handheld Monet Laser is the first of its kind curing light. The collimated beam and consistent power of the Monet Laser create superior bond strength and a faster, deeper, more reliable cure. Cure up to 2.5 mm in 1-second! Each click of the Monet is a 1-second cure up to 2.5mm with an 8mm curing depth capacity. It cures composites, luting cements, adhesives and sealants and has been tested on over 50 brands of dental materials. Monet reduces shrinkage and debonding, reduces the potential for “soft bottoms” and features a consistent dispersion for a deep cure - Bulk fills in just 3 seconds! The compact laser includes optics for a parallel beam within the form-factor and an unrestricted rotatable head mechanism. Monet is covered by a two year warranty.
Available:
Biomedent
Tel: 1300-792-624
info@biomedent.com.au
www. biomedent.com.au
146 Australasian Dental Practice January/February 2024
Finally, your best solution for Invisible Aligners is here
Still wondering about Invisible Aligners ? Your solution is here with new TRULINE X-tra !
Free case evaluation

Free online course
Free viewing software
Realistic treatment setups - No Cartoonodontics
Precision CAD designed and CNC manufactured
Free Click retainers
48 hour turnaround on request
Trusted experience, Australia’s first Aligner brand
Satisfaction guaranteed
100% value



Mention this ad for 50% off your first case




1300 878 336 www.trulinedental.com.au
SPECIAL OFFER New Aoralscan 3L Full featured open Intra Oral Scanner $9,995 + GST FULL PRICE !


