

simply.TRIOS 5 Intraoral scanning that simply makes sense
scanning
Vol. 33 No. 4 JULY/AUGUST 2022 $99.00 p.a. DEN TAL PRACTICE Australasian DEN TAL PRACTICE THE BUSINESS MAGAZINE FOR DENTISTS
Hygienic by design for minimal risk of cross-contamination. Smaller and lighter than ever for next-level ergonomics. And a ScanAssist engine with intelligent-alignment technology that makes precision
effortless, every time.
Where great dentistry meets great business


Join Christian Coachman at the DSD Residency 1
DSD Residency 1 teaches a comprehensive dental practice model that is designed to be great for dentistry and great for business. It connects the dots between clinical dentistry, team training, communication, business, management and marketing to ensure the success of your dental clinic.
“I am delighted to bring the Residency 1 course to Australia this year to present the most distilled and clear approach to Digital Smile Design: the smile business formula. Join me for an engaging three days. You won’t want to miss this!”

- Christian Coachman
Dr Luken de Arbeloa Education Content and Key Opinion Leader manager at Digital Smile Design

with Dr Fadi Yassmin Surgical And Restorative Aesthetic Dentist and owner of FY Smile
Date: 24-26 November 2022
Location: Pullman Sydney Hyde Park, College Street, Darlinghurst, Sydney
In partnership with

Reserve your seat today

On the cover... 3Shape’s brand new TRIOS 5 Wireless is a completely new, state-of-the-art intraoral scanner designed to make it easier than ever for dentists to go digital with their dentistry.

Publisher & Editor: Joseph Allbeury Clinical Editor: Dr David Roessler Technology Editor: Prof. Laurence J. Walsh Infection Control Editor: Prof. Laurence J. Walsh Senior Contributing Editor: Dr Christopher CK Ho Columnists: Dr Georges Fast, Dr Jesse Green, Garry Pammer, Phillip Win, Dr David Moffet, Graham Middleton, Simon Palmer, Julie Parker, Jayne Bandy, Angus Pryor Design & Production: Jasper Communications Australasian Dental Practice™ ISSN 1445-5269 is printed in Australia and published six times per year by Main Street Publishing Pty Limited ABN 74 065 490 655 PO Box 586, Cammeray NSW 2062 Tel: (02) 9929-1900 Fax: (02) 9929-1999 Email: info@dentist.com.au © 2022 All rights reserved. The contents of this magazine are copyright and must not be reproduced without the written permission of the publisher. Permission to reprint may be obtained upon application. Correspondence and manuscripts for publication are welcome. Although all care is taken, the editor and publisher will not accept responsibility for the opinions expressed by contributors to this magazine, or for loss or damage to material submitted for
Subscriptions: Australia and NZ: A$99.00 per year includes OralHygiene™ and




July/August 2022 Australasian Dental Practice 5 contents | REGULARS
VOLUME
| NUMBER 4 JULY/AUGUST
8 briefs 10 one man’s opinion 12 in my practice 14 mouth wide shut 16 outside in 20 spectrum 60 high tech 66 CPD centre 68 abstracts 70 the cutting edge 146 new products
33
2022
per year. www.dentalpractice.com.au facebook.com/dentalpracticenow twitter.com/adpmagazine instagram.com/dentevents management 78 Beware confusing messages from those seeking to turn dentists into their clients 82 Get your house in order 84 As a practice owner... are you driving without destination? 86 Buying back your time: A dentist’s guide to wealth creation - Part 3 88 Do your customers believe you are delivering great customer service? marketing 90 How to give your practice a marketing makeover finance 92 Budgeting for busy people READ ME FOR CPD
publication
eLABORATE™ magazines; Overseas Airmail: A$220.00

































































July/August 2022 Australasian Dental Practice 7 contents | FEATURES VOLUME 33 | NUMBER 4 JULY/AUGUST 2022 infection control 196 UVC light from 200-230 nm: A new way to improve air quality? 100 Test now to protect dental waterlines 104 Why IMS will improve your practice surgery design 140 Relocating easy as 123 Dental clinical excellence 106 Upper premolar replacement with a single implant using digital workflow 112 New SHINING 3D OrthoSimulator V2 118 Improved diagnosis confidence and patient informed consent 122 At the cross roads 128 Vital pulp therapy: A highly effective treatment 134 Guided implant placement with immediate loading: a 5-year follow-up READ ME FOR CPD READ ME FOR CPD READ ME FOR CPD 140 96 106 118
A-dec appoints new Product Manager

Back to normality...
lowly but surely, my mind is readjusting from COVID normal to the new normal, which, for all intents and purposes, ain’t too different to how life was before the recent unpleasantness.
By Joseph Allbeury
But it wasn’t as easy as simply flicking a mental switch. I have to keep reminding myself in a very deliberate way as to what I should be doing at any given point in the year based on memories of a mere few years ago. Habits had clearly changed and they need to change back!
And it seems I’m not alone.
I remember back in June, the first time I rang the bell after morning tea on the first day of Digital Dentistry & Dental Technology 2022, people looked at me quizzically. Some asked what I was ringing a bell for... while others thought for a moment and then realised that it was time for the next sessions to begin. Funny how we quickly forget.
Several months into the year and we’re flying again, domestically and internationally, dining in crowded res taurants, watching the football in stadiums packed to the gunwales and enjoying the theatre and cinema with impunity.
And of course, the Dentevents calendar is filling fast with a full range of educational opportunities through 2023.
Since the last magazine, we packed a full house for Prof. Laurie Walsh’s latest infection control update based on all the changes that occurred in July this year. And fresh from packed sessions at Digital Dentistry & Dental Technology 2022, we also ran an Intraoral Scanning for Digital Dentures course with prosthetist Sam Dias which again sold out.
Our final event for 2022 is a new Mini Smile Makeover program with specialist prosthodontist Dr Sarkis Nalbandian scheduled for November 26 in Sydney. The full day event will equip you to offer patients options for aesthetic enhance ments commensurate with their individual needs and budget. Visit www.smileacademy.com.au for details.
Next year, we have a brand new 3D Printing for Dentistry (3DPD) event over two days from February 10-11. Day 1 covers the clinical aspects of 3D printing while Day 2 looks at the technical side. You can choose to do either day or both and if you’re interested in this burgeoning area, you will find value in coming for the entire event. Keep an eye on www.3dpd.events for more info, session and speaker announcements - and note the 90 minute lunch break is designed to give you plenty of time to play with the toys.
We’ve also pencilled in our flagship Digital Dentistry & Dental Technology 2023 event for June 2-3 so please save the date for this. DDDT23 will be bigger and better than ever so keep an eye on www.dentaltechnology.com.au.

Finally, we’re still looking for readers to start contributing videos to Dentevents.TV and each month we’re offering a prize for the video thatr receives the most votes from viewers! Visit www.dentevents.tv to sign in and begin uploading. Stay safe and see you at the next big thing!
Joseph Allbeury, Editor and Publisher

AS-dec Australia has appointed of Dr Wee Teo as its new Product Manager based in Sydney. Dr Teo completed a Bachelor of Science at the University of NSW, winning the University Medal. He went on to pursue a PhD in Medicine (Oncology) at the Garvan Institute of Medical Research and the St Vincent’s Clinical School at the University of NSW. After graduating, he worked as a Clinical Trials Research Officer in oncology for the NSW Government and later as a Senior Scientist in the private sector, prior to an appointment as a Medical Device Product Manager for R-Biopharm AG, one of Germany’s leading biotechnology companies whose products include clinical diagnostics equipment. In his new role, Dr Teo will be responsible for supporting Acteon’s range of X-ray units, intraoral cameras, scanners and digital sensors. Dr Teo anticipates using his expe rience in product management and medical devices to provide technical and clinical support to external customers’ needs as well as to A-dec’s sales, marketing and technical teams - supporting new product development and launches, understanding of the dental market and strategic direction.

Impulsedents appoints new CEO
Impulsedent Dental Supplies in Queensland has appointed Thomas Kunz to the role of Chief Executive Officer. Thomas will invig orate marketing initiatives and empower the national sales efforts in Australia. With considerable experience in all facettes of sales and marketing, he will be in charge of services to clients, develop new practices of communication and enlarge the sales activities with fresh ambi tions. “Impulsedent is excited to include Thomas, who is of Swiss origin, into the team,” said Reto Herzog, Managing Director of Impulsedent. “I’m confident and looking forward to achieving new service levels with the enhanced support of Thomas.” If you have any enquiries or questions, contact Thomas Kunz on (07) 3102-3436, email thomas.kunz@impulsedent.com.au or visit the website www.impulsedent.com.au.
Organising a
dental congress, trade show
List your events on www.dentevents.com
Dentevents.com is dentistry’s continuing education cal endar and we’re looking for help in ensuring we list every dental event and education program available. Whether or not you’re the organiser of the event, you can contribute to the calendar. If you know about an event but it’s not listed at dentevents.com, then simply visit the site, select Adding Events from the menu and then select the new Express Listing option. The form takes less than a minute to complete and the event will be checked and appear on the calendar within 24 hours (or usually a lot less). The more events we can list, then more useful the calendar is in helping you and other dental professionals find the course they need.
If you’re organising any kind of post-graduate dental education, webinar, listing your event on the dentevents.com continuing calendar is now easier than ever.
No username, no password and no need to loginby simply visiting dentevents.com, clicking on Adding Events selecting Express Listing
8 Australasian Dental Practice July/August 2022
briefs | NEWS
GO EXPRESS»»
Complete all the details on the form and click SUBMIT
By Georges Fast
One man’s opinion...
“The funds had a smorgasbord of items that they could limit or exclude or group together in a manner that suited their remit to lower rebates. And we gave it to them!”
Since the release of the thirteenth edition of the ADA Schedule of Dental Services and Glossary, there has been a lot of discussion and commentary on the various online dental chat sites.
The first edition was published in 1986 as “An Australian Glossary of Dental Terms”. In 1996, this was expanded and became known as “An Australian Schedule of Dental Services and Glossary”. Prior to 1986, some (but not all) State Branches published a list of min imum recommended dental fees for various procedures and in most cases, these were the fees that the majority of dentists charged.
Each edition of “The Schedule” expanded on the number of items and resulted in the breakdown of dental treatment into many fragments. The treatment procedure and outcome remained much the same, but now the various steps to achieve that outcome acquired a life of their own.
No one involved in producing that first schedule could have ever imagined the burden that their oeuvre would impose on the profession.
From the patient’s point of view, their interest is in the fiscal cost of the total solution to their problem; from the practitioner’s perspective, what matters is the fee that needs to be charged to achieve that solution and return their desired profit.
When Dental Health Funds made their appearance, they were run by memberowned mutual benefit associations and paid a rebate based on a proportion of the fees that were charged up to a maximum annual limit. Once these funds were taken over by commercial insurance-type organisations, their primary aim became to generate a profit for their investors instead of supporting their members.
“It is my view that when the 14th Schedule is produced, it should undergo a radical culling and reflect the end result of the treatment that was carried out without delving deeply into the steps taken on the way...”
It wasn’t long before the profession was confronted by various “Business Rules” created by the funds to limit their financial exposure and what better weapon to use against us than our own expanded Schedule of Dental Services! Here the funds had a smorgasbord of items that would normally all form part of a proce dure, that they could limit or exclude or group together in a manner that suited their remit to lower rebates. And we gave it to them!
There has never been a better time to take onboard a quote from Peter Drucker: I recommend strongly a systematic abandonment policy under which every product, service, process, distribution channel or policy is put on trial for its life with the question: “Would we now go into this product, this business, into this service, knowing what we now know? If the answer is NO, don’t say ‘Lets make another study’, say ‘What do we do now?’ If you don’t have a method of systematic abandonment, you will become committed to yesterday - in violation of one of the oldest medical proverbs (possibly from Hippocrates)... “There is nothing as difficult, as expensive but also so futile as to try to keep a corpse from stinking”.
It is my view that when the 14th Schedule is produced, it should undergo a radical culling and reflect the end result of the treatment that was carried out without delving deeply into the steps taken on the way.
It might just be what is needed to stop the health funds telling us how to practise our profession.

10 Australasian Dental Practice July/August 2022
spectrum | NEWS
Online Resources for the Dental Profession... www.dentalcommunity.com.au • Update your personal details • Update your practice on dentist.com.au • Manage your subscriptions • Read 13,500 articles from past magazines • Log your CPD points • Answer CPD Questionnaires • Run your own dental events • Create online discussions • And more... www.dentevents.com • Dental education calendar • Register for all popular dental events www.dentevents.tv • Watch all the latest videos about dentistry www.dentist.com.au • Find-a-dentist in Australia www.dentist.co.nz • Find-a-dentist in New Zealand www.dentalpractice.com.au • Australasian Dental Practice™ online www.oralhygiene.com.au • Oral Hygiene™ magazine online www.elaborate.com.au • eLABORATE™ magazine online Sign up now. It’s Free.
HIGHLIGHTS
Latest developments in rege nerative therapies
Live surgeries
Hands-on workshops
Case session
Morning with master clinicians
Clinical round tables
Poster exhibition
Research networking day
Joint sessions with AAP and SEPA
SCIENTIFIC COMMITTEE
Pamela K. McClain, USA (Chair)
Istvan Urban, Hungary (Chair)
William V. Giannobile, USA
Franck Renouard, France
Frank Schwarz, Germany
Anton Sculean, Switzerland
osteology–barcelona.org be part of #OsteologyBarcelona
By Christopher Ho
In my practice...
“Unlike multilayer techniques used with conventional composites, Asteria uses only 2 layers for optimal results without compromising aesthetics.
The microstructure of the material produces a light diffusion that helps blend in with the natural tooth structure...”
This issue we look into some products and equip ment that I use in practice. We look at some recently released new products and elaborate on how their use can be applied in practice. Investing in the right armamentarium allows clinical prac tice to be simpler and more enjoyable for the wet-fingered dentist and hopefully, this column provides the reader with some of the latest “tools of the trade”
Clearfil Ceramic Primer Plus

With the increasing use of all ceramics within practice, a clinician must under stand adhesive procedures to ensure adequate bond strength for predictability and longevity. Clearfil ceramic primer plus is a single com ponent adhesive primer used to enhance bond strength between resin-based materials, as well as porcelain, composite, hybrid ceramics, metal oxide (zirconia) and lithium disilicate. It contains the adhesive phosphate containing monomer (MDP) used for adhesive bonding as well as to metal oxide. Additionally, it contains a silane cou pling agent which guarantees strong adhesion to all glass-based ceramic materials. It is a one bottle system meaning there is no mixing and has excellent shelf life compared to other silanes which need to have careful storage.
Estelite Asteria (Tokuyama)
One of my favourite composite resin materials is Asteria which is a light-cured radiopaque composite for universal use. It considerably simplifies multilayer techniques yet delivers outstanding aesthetics with excellent polishability. Unlike mul tilayer techniques used with conventional composites, Asteria uses only 2 layers for optimal results without compromising aesthetics. The microstructure of the material produces a light diffusion that helps blend in with the natural tooth structure. The chameleon like nature of the material allows a blending of the materials to natural tooth structure and it allows excellent polishability which retains its lustre over time.
Hawe X-ray film holders
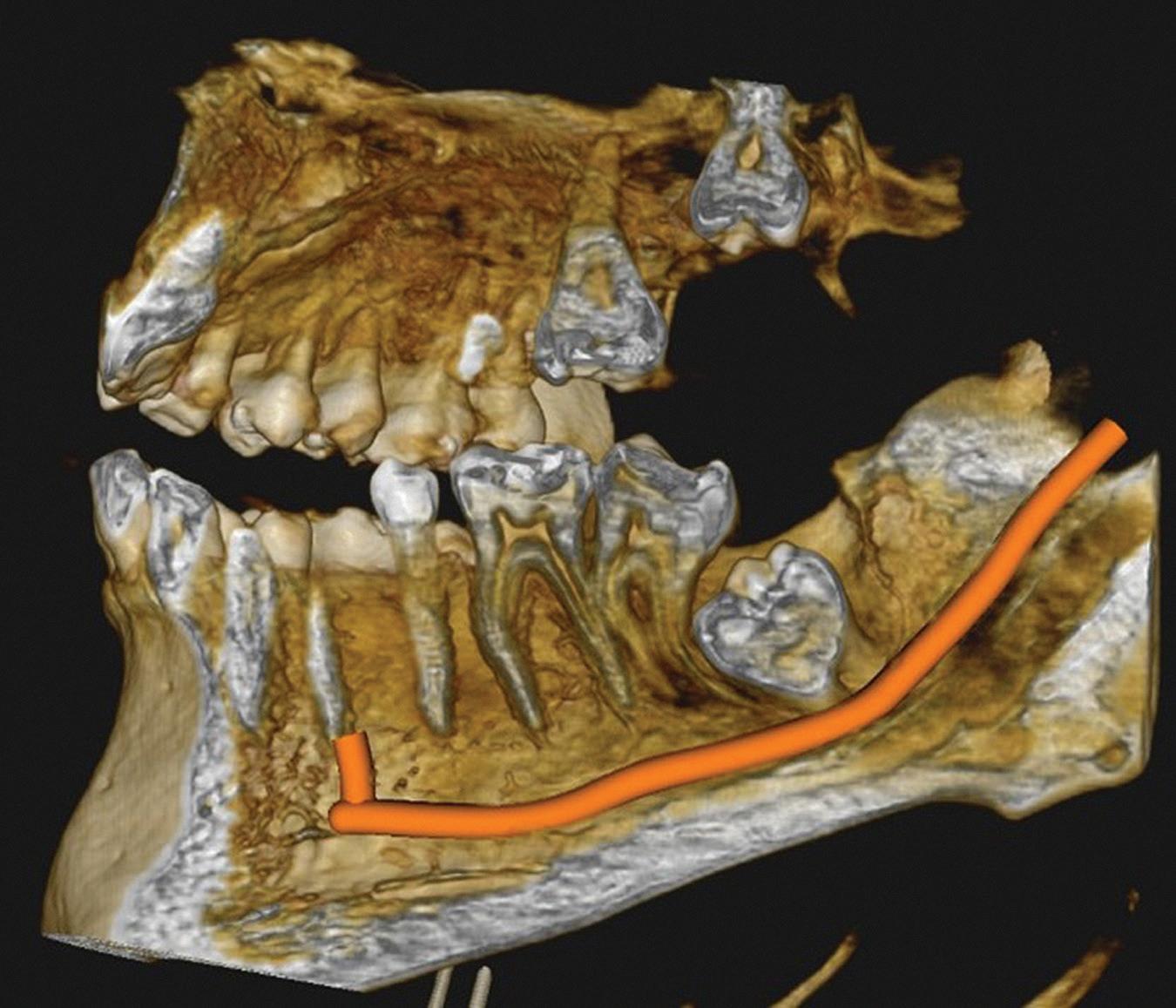
Clear radiographs are essential to accurate diagnosis and are a special test that dentists per form regularly many times throughout the day. Following the ALARA principle, we want to ensure we take a minimal number of radio graphs to ensure low radiation dosage so to repeat radiographs due to operator error should be avoided. The use of film holders allow the clinician to visualise how the radiographs should be taken to optimise the clarity of the image and ensure the diagnostic value of the image. Hawe Solutions x-ray film holders...
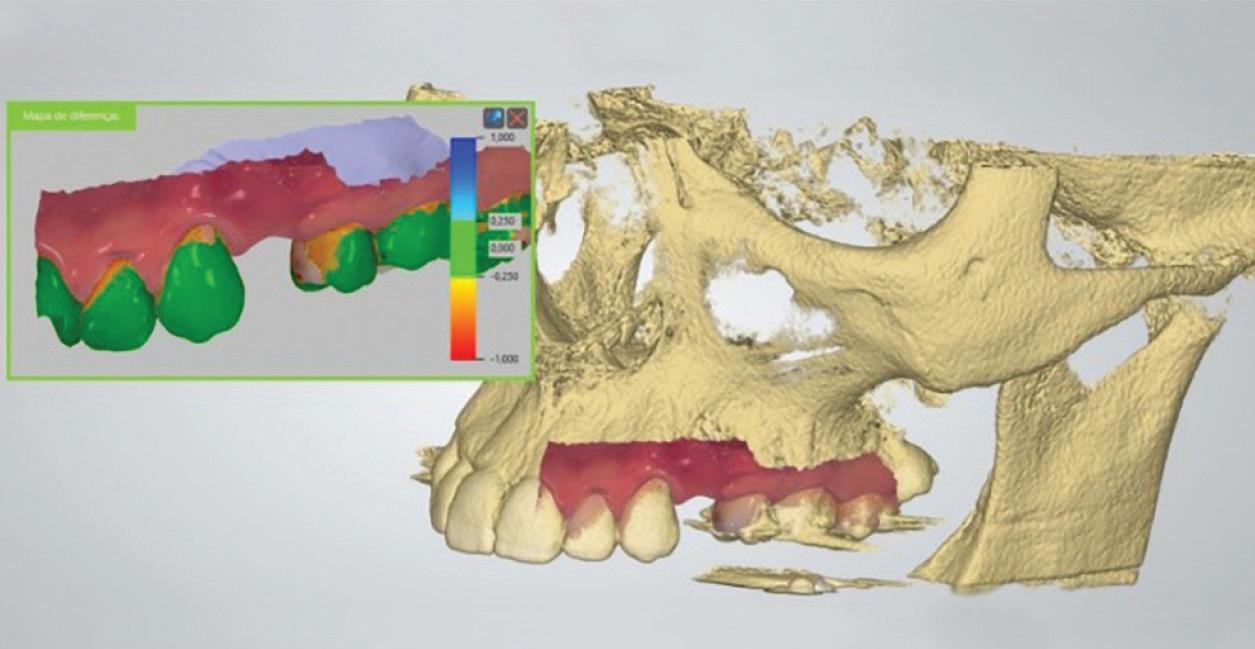
Figure 1: Radiographic Image of implants do not demonstrate bone loss due to the bisecting angle of the radiograph taken.
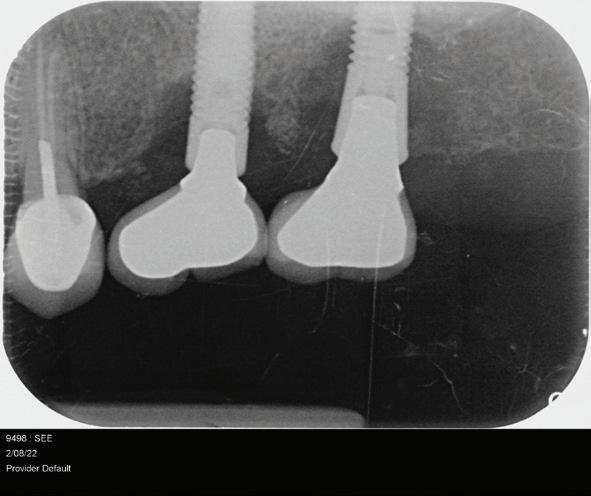
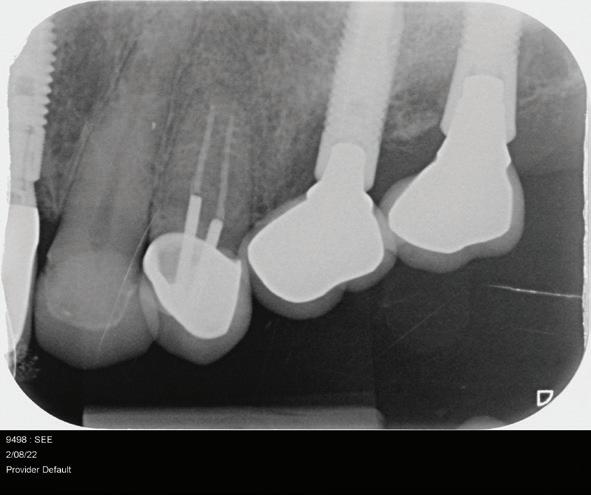
Figure 2: Radiographic image in a paralleling technique of implants dem onstrate moderate peri-implantitis with bone loss that will necessitate treatment.
• Allow exact posi tioning of the film or phosphor plate relative to the tooth - no bending and thus no distortion;
• Require no guesswork - exclusive, automatic reliance on the extraoral aiming and centring device;
• Deliver semi-reproducible images (quasi standardisation)the use of film holders allows some sense of reproducibility for assessment over time; and
• Produce optimally clear radiographs.
About the author
Dr Christopher Ho is a Specialist Prosthodontist based in Sydney, Australia. He is Head of School of the Australasian College of Dental Practitioners, Visiting Lecturer at Kings College London, Adjunct A/Prof at University of Puthisastra and Editor of the Wiley-Blackwell textbook “Practical Procedures in Aesthetic Dentistry” and “Practical Procedures in Implant Dentistry”.

12 Australasian Dental Practice July/August 2022
spectrum | NEWS

Scan for DETAILSmore New Regeneration Expert Hub covers all relevant aspects of oral tissue regeneration. VIDEO INTERVIEW EXPERT ARTICLE PODCAST INFOGRAPHIC CLINICAL CASE 1. To get inspired by clinical insights from leading experts 2. To stay up-to-date with the latest scientific studies, without reading long journal manuscripts 3. To learn about the treatment concept of your choice following a stepby-step clinical case www.regeneration-expert.com REGENERATION EXPERT HUB Expertise made accessible. Your top 3 reasons to visit the newly launched Regeneration Expert Hub!
How’s your subject matter?
By David Moffet
In June, I walked 35 kilometres in the Illawarra in a charity fundraiser walk.
It was an interesting day.
I’m a fairly brisk walker at the best of times. On a weekday at home I’ll begin my day with a 10 kil ometre walk each day just to get myself grounded and settled for the day.
When I walk at home I always listen to music for the ninety minutes or so, as opposed to lis tening to audio books or podcasts, simply because the cadence and rhythm of the music gives me a good tempo to walk to.
Now, because this fundraiser walk was a long walk, I thought I might break from tradition and listen to a book that I recently downloaded, but that did not work for me. I lasted one or two sentences before I switched back to listening to my music library.
The participants on this walk last Sunday were predominantly female for some reason. I’m not sure why that was, but I cal culated that on this walk - and there were thousands of people participating - the women outnumbered the men by between ten and twenty to one.
The interesting thing about this walk was that during the five and three quarter hours that it took me, I was only passed by two runners during that time [obviously I may have been passed by walkers while I was taking a necessary pit stop, but while I was in motion, no walker overtook me].
The reason I point this out is this: Often during the walk when I passed by walkers in conversation, I would switch off my music in case they wished, or I wished, to engage in a conversation.
Because of these “breaks of silence”, I was able to eavesdrop on a number of these walkers’ conversations, or monologs as I passed by.
Here’s what I overheard...
Predominantly, the subjects of conversation were almost always about people with problems.
Most of the conversations seemed to be discussing a third party [not present] and that third party’s problems and those problems revolved around health issues, workplace issues and relationship breakdowns.

It seemed that absolutely every conversation I was privy to eavesdropping in on was about someone with a problem and yet NEVER did I hear one person discussing a solution to those problems.
And never did I hear any person discussing someone’s good health, someone’s good job, or someone’s wonderful marriage or relationship.
Is that how the world really is?
Is that how the world really is? Or is nobody really interested in discussing happy stories? Are happy stories worth talking about?
Are happy stories worth talking about?
We know that happy stories don’t sell gossip magazines... Nobody wants to read about how wonderful the mar riage of Frederick and Mary really is, when they can always read about how Harry and William aren’t speaking to each other?
Happy stories can be your point of difference
Many years ago when I was at University, I used to work in a newsagency. There was a lady customer who used to come in regularly and was always such a “ball of energy, happiness, and enthusiasm” each and every time that she vis ited, that it prompted the owner of the newsagency to say about her once, [and I think this pre-dated the movie WHEN HARRY MET SALLY...
“Whatever she’s on, I’ll have some of that...”
This lady was always so upbeat that it became her “signature”, or her VISIBLE point of difference.
The thing is, that in this ever-increasing world of negativity out there, we each have the CHOICE to be either negative, like everybody else, or be positive and POSITIVELY DIFFERENT, to what everybody else is doing.
And when we make that choice, to behave like that lady cus tomer at the newsagency, we have the immediate ability to be able to stand out from the crowd, because everybody else is just wallowing in that world of negativity.
The choice to be different is available.
Which choice are you going to choose to take for yourself?
Will you by blend in to that world of negativity?
Or will you by choice be a positive ray of hope to the people with whom you meet?
About the author
Dr David Moffet is a dentist and a #1 Amazon Bestselling author. He is the inventor of The Ultimate Patient Experience™, a simple to implement patient retention system he used to build and sub sequently sell (for several million dollars) his successful dental practice [of 28 years] located in Parramatta in working class western Sydney. He can be contacted at david@theUPE.com or visit www.theUltimatePatientExperience.com.
14 Australasian Dental Practice July/August 2022
spectrum | NEWS
Are you living in a world of negativity?
“It seemed that absolutely every conversation I was privy to eavesdropping in on was about someone with a problem and yet NEVER did I hear one person discussing a solution to those problems...”
SUPERIOR STRENGTH & AESTHETICS
» Luna 2 has beautiful optics that mimic tooth structure and let you place fillings that disappear. It has great handling too: no stickiness on instruments and easy sculptablilty. «

Dr Susan McMahon - United States

» Handling is fantastic - much improved. It is SDI’s best handling composite yet. «


Dr Michael Chan - Australia

COMPOSITES | GLASS IONOMERS | TOOTH WHITENING | SDF RIVA STAR | CEMENTS | ADHESIVES | ETCHANTS | SEALANTS | AMALGAMS | ACCESSORIES | EQUIPMENT orders phone 1300 65 88 22 | orders fax 1300 65 88 10
337
COMPOSITES | GLASS IONOMERS | TOOTH WHITENING | SDF RIVA STAR | CEMENTS | ADHESIVES | ETCHANTS | SEALANTS | AMALGAMS | ACCESSORIES | EQUIPMENT LUNA 2 UNIVERSAL
PERFECT CREAMY & SMOOTH HANDLING HIGH FLEXURAL STRENGTH 130MPa HIGH RADIOPACITY 250% AI HIGH COMPRESSIVE STRENGTH 360MPa BPA FREE FORMULATION HIGH POLISH AND WEAR RESISTANCE
Call 1800
003 www.sdi.com.au
COMPOSITE
orders phone 1300 65 88 22 | orders fax 1300 65 88 10
Call 1800 337 003 www.sdi.com.au
Customer acquisition strategies
 By Lani Guy
By Lani Guy
Attracting new customers is always on the mind of dental practices. And it is also something which can prove very difficult to do. In this edition of Aus tralasian Dental Practice, I want to take a look at different customer acqui sition strategies that we can use within the dental industry. There is no right or wrong approach to customer acqui sition, but there are some theories and strategies that we can take straight from a business textbook and apply in our own practices. Each strategy involves different amounts of time, effort and money and each differs in the type of results they can achieve. To make the content as accessible and realistic as pos sible, I’m going to use an imaginary customer, Peter, to take us on this journey. Ready? Let’s go...
Selling to Peter
Selling to Peter’s friends
The traditional approach to sales within most industries, dentistry being no exception, is product to market. Product to market is so named because it quite literally takes the prod ucts it has and approaches the market with these products. Let’s take Peter, our market. We have many products that we could sell Peter - such as crowns, fillings, dentures, tooth whitening, braces. Some of these products are more lucrative than others when looking at gross revenue or margins. We can increase revenue using product to market by increasing sales to existing customers. We can also increase revenue by using campaigns which sell the benefits and appeal of these products to our existing customer base. This is why we see dental practices that implement key performance indicators like the number of crowns or indirect restorations per operator. However, as we operate in the health industry, we need to tread very carefully to remain ethical and avoid over-servicing when using product to market strategies.
Peter is a satisfied customer of your business. You recognise this; and also recognise that word of mouth is a powerful strategy for new customer acquisition. With this in mind, you decide to invest one hour of time to reach Peter’s networks. So what is the payoff?
• Peter has a small number of strong personal connections which are governed by high levels of personal trust. These are people who are fairly likely to heed Peter’s advice that you’re a great dentist, e.g., a sibling. These are quality leads but will be small in number;
• Peter has a larger number of middle ground contacts; people with regular personal contact with Peter but a much looser social connection where social norms rather than personal trust dominates, e.g., someone that Peter runs into every weekend at kids’ sport. These are people who might take Peter’s advice that you’re a great dentist, but only if they don’t have advice from a closer social connection. These are much better leads than a cold call but are far from a slam dunk... but also more plentiful in number; and
• Peter has a large extended virtual network that exists solely in the world of social media. These connections are very different from strong and middle ground connections because they operate on herd mentality rather than a relationship of personal trust. These leads are plentiful. But, they are separated from cold calling only by the fact that there is safety in numbers when it comes to choosing an unknown (like a new dentist).
Let’s be generous and say Peter has 20 close contacts, 50 middle ground contacts and a further 1000 contacts in his extended network. For your one hour of time, you have reached 1000 people. But because the quality of these leads differs, the conversion rate will also differ. For example, you might get 30% of his close contacts, 5% of his middle ground contacts and .01% of his extended network. Your return on investment will depend heavily on the conversion rate for each type of contact. 88
16 Australasian Dental Practice July/August 2022
spectrum | NEWS
Leads Sales Calls Follow-Up Conversion Sales OUT IN More $ Peter Leads Sales Calls Follow-Up Conversion Sales OUT 70 20 1000
“There is no right or wrong approach to customer acquisition, but there are some theories and strategies that we can take from a business textbook and apply in our own practices. Each strategy involves different amounts of time, effort and money and each differs in the type of results they can achieve...”
INTRODUCING


INTRODUCING SENSODYNE REPAIR & PROTECT DEEP REPAIR*
SENSODYNE REPAIR & PROTECT DEEP REPAIR*

INTRODUCING SENSODYNE REPAIR & PROTECT DEEP REPAIR*

Helps provide deep repair* and long-lasting protection against dentine hypersensitivity** 1-4
Helps provide deep repair* and long-lasting protection against dentine hypersensitivity** 1-4
NO.1 BRAND FOR SENSITIVE TEETH5
Builds a strong hydroxyapatite-like layer deep within the tubules of exposed dentine for deep repair* and protection** 1,3,6-9
Reparative* hydroxyapatite layer is harder than underlying dentine and resistant to dietary acid and physical brushing 2,4,7,10
Advanced Science. Deep Repair*.
Proven for effective relief and long-lasting protection against dentine hypersensitivity** 11-13
*Forms a protective layer over the sensitive parts of the teeth. Brush twice a day for lasting sensitivity protection **With twice-daily brushing. Always read label and follow the directions for use.
*Forms a protective layer over the sensitive parts of the teeth. Brush twice a day for lasting sensitivity protection **With twice-daily brushing.
*Forms a protective layer over the sensitive parts of the teeth. Brush twice a day for lasting sensitivity protection **With twice-daily brushing. Always read label and follow the directions for use.
Always read label and follow the directions for use.
References: 1. Greenspan DC. J Clin Dent 2010; 21:61–65. 2. Burwell A et al. J Clin Dent 2010; 21:66–71. 3. LaTorre G, Greenspan DC. J Clin Dent 2010; 21:72–76. 4. Earl JS et al. J Clin Dent 2011; 22:68–73.
References: 1. Greenspan DC. J Clin Dent 2010; 21:61–65. 2. Burwell A et al. J Clin Dent 2010; 21:66–71. 3. LaTorre G, Greenspan DC. J Clin Dent 2010; 21:72–76. 4. Earl JS et al. J Clin Dent 2011; 22:68–73.
5. GSK Consumer Healthcare calculation based in part on data reported by NielsenIQ and IQVIA through the IQVIA™ & NielsenIQ© RMS Sell Out] Service for the Oral Health Database, Sensitive Segment for the 52 week period ending 17/08/2021 for the Australia Grocery Pharmacy market according to the client defined product hierarchy. 6. Earl et al; J Clin Dent 2011; 22(3): 62-67(A). 7. Parkinson C et al. J Clin Dent 2011; 22(3): 74-81. 8. GSK Data on File; In vitro study number ML880; G7215/018; 2018. 9. GSK Data on File, Addendum to in vitro report ML880; 2021. 10. Wang Z et al. J Dent 2010; 38: 400-410. 11. Hall C et al; J Dent 2017; 60: 36–43. 12. GSK Data on File; Clinical Study number RH01748, 2013. 13. Hall, C et al; J Dent Res, 2017; 96 B:062 BSODR. Trade marks are owned by or licensed to the GSK group of companies. © 2022 GSK group of companies or its licensor. GlaxoSmithKline Consumer Healthcare Pty Ltd, Sydney, Australia. PM-AU-SENO-22-00121.
References: 1. Greenspan DC. J Clin Dent 2010; 21:61–65. 2. Burwell A et al. J Clin Dent 2010; 21:66–71. 3. LaTorre G, Greenspan DC. J Clin Dent 2010; 21:72–76. 4. Earl JS et al. J Clin Dent 2011; 22:68–73. 5. GSK Consumer Healthcare calculation based in part on data reported by NielsenIQ and IQVIA through the IQVIA™ & NielsenIQ© RMS Sell Out] Service for the Oral Health Database, Sensitive Segment for the 52 week period ending 17/08/2021 for the Australia Grocery Pharmacy market according to the client defined product hierarchy. 6. Earl et al; J Clin Dent 2011; 22(3): 62-67(A). 7. Parkinson C et al. J Clin Dent 2011; 22(3): 74-81. 8. GSK Data on File; In vitro study number ML880; G7215/018; 2018. 9. GSK Data on File, Addendum to in vitro report ML880; 2021. 10. Wang Z et al. J Dent 2010; 38: 400-410. 11. Hall C et al; J Dent 2017; 60: 36–43. 12. GSK Data on File; Clinical Study number RH01748, 2013. 13. Hall, C et al; J Dent Res, 2017; 96 B:062 BSODR. Trade marks are owned by or licensed to the GSK group of companies. © 2022 GSK group of companies or its licensor. GlaxoSmithKline Consumer Healthcare Pty Ltd, Sydney, Australia. PM-AU-SENO-22-00121.
5. GSK Consumer Healthcare calculation based in part on data reported by NielsenIQ and IQVIA through the IQVIA™ & NielsenIQ© RMS Sell Out] Service for the Oral Health Database, Sensitive Segment for the 52 week period ending 17/08/2021 for the Australia Grocery Pharmacy market according to the client defined product hierarchy. 6. Earl et al; J Clin Dent 2011; 22(3): 62-67(A). 7. Parkinson C et al. J Clin Dent 2011; 22(3): 74-81. 8. GSK Data on File; In vitro study number ML880; G7215/018; 2018. 9. GSK Data on File, Addendum to in vitro report ML880; 2021. 10. Wang Z et al. J Dent 2010; 38: 400-410. 11. Hall C et al; J Dent 2017; 60: 36–43. 12. GSK Data on File; Clinical Study number RH01748, 2013. 13. Hall, C et al; J Dent Res, 2017; 96 B:062 BSODR. Trade marks are owned by or licensed to the GSK group of companies. © 2022 GSK group of companies or its licensor. GlaxoSmithKline Consumer Healthcare Pty Ltd, Sydney, Australia. PM-AU-SENO-22-00121.

Helps provide deep repair* and long-lasting protection against dentine hypersensitivity** 1-4
new formula To request free Sensodyne Repair & Protect samples scan the QR code or register at gskhealthpartner.com To request free Sensodyne Repair & Protect samples scan the QR code or register at gskhealthpartner.com
It’s important to understand how advertising mediums, like social media, work within each of these network types. Failure to understand this is primarily why most social media campaigns fail to delivery their intended yields. More on this to come in the next edition of Australasian Dental Practice
Selling to market segments
The opposite approach to product to market is market to product. This is where we look at value chains and market segments. A full discussion is beyond the scope of this article, but let’s take a simplistic look. In market to product, we take our customers (aka our market) and we try to break them into meaningful groups. These meaningful groups do not, yes I repeat do not, have to have anything at all to do with den tistry. We might choose to group them on hobbies (like soccer players) or medical conditions (like diabetics). By doing so, we can use the value chain to intercept our customers upstream so that someone else does the selling for us. I just threw a lot of business terms at you, so let’s try to bring it to life by using our imaginary customer, Peter.
Peter is a diabetic. And, like all diabetics, he is managed by his GP. You know that glycaemic control and oral health is intimately related; and there would be benefit to Peter if his oral health is managed actively as part of his diabetes manage ment. You also know that Peter is managed by his GP, who also has a number of other diabetic patients (let’s say 400 patients). Now let’s take the one hour of time we previously allocated to customer acquisition. Rather than spending this hour with Peter, you choose to spend it with Peter’s GP. You now have access to the GP’s entire network of diabetic patients which are good quality leads. Moreover, through this one hour of effort, the selling will now be done upstream by their point of con tact (their GP), rather than yourself. Market to product opens up a much broader field of play for advertising and marketing than product to market; because we can engage with customers about things they are interested in rather than products they may or may not have a current interest in. Moreover, ROI (Return On Investment) tends to be high because the cost of conversion can be shifted up the value chain to other market participants - a boon any which way you look at it. Market to product is a very different way at looking at customer acqui sition and moves us away from our traditional comfort zones. However, with some practice and some good basic analysis of your market and customer base, it has the ability to yield excellent returns.
About the author
Lani Guy is a University of Queensland trained General Dentist working in private practice. In a prior life, Lani was a manage ment consultant. She has a Bachelors, Masters and Doctorate in business along with a Bachelors in psychology and has spoken globally on the topic of digital disruption and IR4.0. She has a special interest in evidence-based improvement techniques and disruptive innovation... as well as healthcare.
Most dental practices receive minor complaints all the time. Having an open, easy private complaints mechanism is quite simple and will mean that complaints to regulators will be less likely.

It could be that there is simple complaints policy available on the practice website. It could be a QR code on appoint ment cards. The pics should include where to complain, how to complain (phone, email or online, for example), who will deal with it, how long it will take, etc. A trusted person - prob ably not the dentist - should deal with it and have authority to consult with the person who is the subject of the complaint and suggest resolution.
This process which should preferably involve a conversation with the complainant by a designated person which is far pref erable to the small business system where the person dealing with the complaint may not have had training, or be inconsistent with the practice general policy. Complainants often want to be heard and the sooner it happens, the quicker they will believe that they have been heard and the practice cares about them.
Often the complaints will be about fees or clinical out comes, but a policy might mean you can resolve it locally early, so it does not fester for months before a lengthy process is commenced with a council, commission, board or ombudsman.
Contact Brad at www.bradwright.legal
18 Australasian Dental Practice July/August 2022 spectrum | NEWS
Sales
GP
Leads
Calls Follow-Up Conversion Sales OUT
Do you have a complaints policy?…
BRAD WRIGHT







Register Online Now at www.3dpd.events REGISTRATION FEES One Day $660 inc gst Two Days $990 inc gst sAVE $220 BEforE 10 DEc 2022 DATE AND TIME SYDNEY 10-11 February 2023 Starts 8.30am | Ends 5.00pm | Rego opens 8.00am See the website for venue details 3D Printing in Dentistry is presented by Dentevents, a division of Main Street Publishing Pty Ltd ABN 74 065 490 655 • www.dentevents.com • info@dentist.com.au Tel: (02) 9929 1900 • Fax: (02) 9929 1999 • 3D Printing in Dentistry™ and Dentevents™ are trademarks of Main Street Publishing P/L © 2022 Main Street Publishing Pty Ltd WHITTY KLIJNSMA ELSEY YAHYA DAY ONE - FEB 10 - CLINICAL n Selecting the right printer for your practicedo you really get what you pay for? n The 3D printed crown - is it a reality? n Workflows for designing and printing temporaries n 3D printing software apps n Designing and printing surgical guides & splints n Workflows for producing chairside aligners n Is printing the solution for digital dentures? n What is accuracy in 3D printing? DAY TWO - FEB 11 - TECHNICAL n Selecting the right printer for your laboratory n Modern 3D printing technologies for dentistrya comparison n Workflow and manufacturing optimisation n Workflows for printing digital dentures n Correct methods for cleaning and post curing printable resins n Materials update and future directions n Safety and regulatory compliance n Effective troubleshooting of printer errors Join Australia’s leading experts on dental 3D printing at this two day event exploring the applications of 3D printing in both the clinic and the laboratory. Visit the website for information and additional speakers. THIS EVENT IS DESIGNED FOR DENTISTS, SPECIALISTS, DENTAL PROSTHETISTS & DENTAL TECHNICIANS
3Shape launches all-new TRIOS 5 Wireless intraoral scanner
3Shape’s brand new TRIOS 5 Wireless is a completely new, state-of-the-art intraoral scanner designed to make it easier than ever for dentists to go digital with their dentistry.
A breakthrough in intraoral scanners, TRIOS 5 Wireless makes scanning smoother and faster with its all-new ScanAssist intelligent alignment technology that comes housed in a redesigned, compact and hygienically optimised scanner - to deliver the highest standard in imaging performance and infection control.
With over 50 improvements in ease of use and design, TRIOS 5 Wireless is 3Shape’s smallest and lightest scanner to date and is perfectly balanced to fit comfortably in any hand.
TRIOS 5 Wireless delivers an unprecedented level of scanning simplicity. An LED ring and haptic sensory feedback guide you while you scan to make digital impression taking smoother and faster than ever. And now with ScanAssist technology, which minimises misalignment and distortion in 3D models, you can scan your patients in any direction you want - just create the scan path that works best for you.
TRIOS 5 Wireless also features a closed autoclavable scanner tip protected by scratch-free sapphire glass. The scanner body has been designed for easy cleaning and disinfection.
“At 3Shape, we have strived for perfection through five gen erations of intraoral scanner evolution. Using state-of-the-art scan software and artificial intelligence to deliver sharper colours, improved accuracy and increased efficiency, we believe TRIOS 5 surpasses all expectations. With its ergonomic and well-balanced look inspired by classic Danish design, TRIOS 5 Wireless simply makes sense,” said Jakob Just-Bomholt, 3Shape CEO.
• Optimise your scans while you scan, guided by LED ring and haptic feedback and driven by the all-new, robust ScanAssist engine that minimises misalignment and distortion in 3D models to make impression-taking so simple that you can create your own scan strategy or scanning routine.
• All-day battery life with Smart Power Management that auto matically switches TRIOS 5 to sleep-mode to save energy when not in use. Up to 66 minutes of scan time per battery.
• Precision 3D models with no need for a calibration tool - that means you no longer need to calibrate your scanner every 14 days like with other intraoral scanner models.
• LED ring and haptic feedback guide you while you scan to make scanning easier. Two-button design for improved software navigation and scan analysis.
A new standard in infection control
TRIOS 5 Wireless reimagines intraoral scanner design. It is so easy to clean because it is hygienically sealed up to its battery inlet with no cracks or crevices that can accumulate soil or con taminants. A sapphire glass window encloses the autoclavable tip to create a sturdy microbial barrier between patient and scanner. TRIOS 5 Wireless also includes ultra-thin, snug and near-invis ible single-use sleeves to cover the scanner body and minimise risk for cross-contamination.
Powered by 3Shape Unite
TRIOS 5 Wireless is 3Shape’s most streamlined scanner ever. The sleek, pen-grip scanner is optimally balanced to fit com fortably in any hand. TRIOS 5 is 30% more compact and weighs just 300 grams (with battery) and is only 266 mm long. In com parison, some competitor scanners weigh up to 470 grams and are more than 330 mm in length. And you can take your TRIOS 5 any where using TRIOS Share to scan from every PC in your practice.
Like all 3Shape TRIOS scanners, TRIOS 5 Wireless includes the 3Shape Unite platform with it for free. Together, TRIOS and 3Shape Unite seamlessly to connect you to over 2000 dental companies, treatment solutions, practice management systems and labs, represented as apps on the dental world’s most open and collaborative platform. Doctors can also take advantage of 3Shape engagement apps, included free with TRIOS 5 Wireless, to help boost treatment acceptance.
Peace of mind service
At the heart of TRIOS 5 is the ScanAssist engine, which fea tures intelligent-alignment technology to make scanning even easier. Dental professionals will enjoy the built-in LED ring and haptic sensory feedback that guide you while you scan to make digital impression-taking smoother and faster. In fact, intraoral scanning with TRIOS 5 is so easy to do that you create the scan path you prefer. Highlights include:
TRIOS 5 Wireless owners can take advantage of two TRIOS service agreement options: TRIOS Care, which delivers focused onboarding, extensive training and unlimited support for practitioners, including express replacement if your scanner is damaged and TRIOS Only - a scan-ready free service agreement with no monthly costs. TRIOS 5 is 3Shape’s fifth-generation model of the world’s most recognized intraoral scanner bringing industry-leading scanning experiences, award-winning design, and unparalleled clinic-to-lab workflows – powered by 3Shape Unite.
Discover more about the 3Shape TRIOS 5 Wireless by visiting 3shape.com/trios5
20 Australasian Dental Practice July/August 2022
Smallest and lightest intraoral scanner to date
Simply effortless - introducing intelligent-alignment technology
spectrum | NEWS
simply.TRIOS
5
Intraoral scanning that simply makes sense
Hygienic by design for minimal risk of cross-contamination. Smaller and lighter than ever for next-level ergonomics. And a ScanAssist engine with intelligent-alignment technology that makes precision scanning effortless, every time.
Anyone who relies on a fixed wage, exchanging their time for money has ZERO LEVERAGE When they stop working, the income stops!
Conversely, if someone’s income is not related to their personal efforts, then they have leverage.
Having lots of employees is what we normally think of when we consider gaining business leverage. But it’s much more than that.
Leverage tips for dentists
Use technology that saves you clinical time. Lasers? Scanners? Milling machines?. Use technology that increases clinical accuracy and efficiency. Micro scope? CBCT? Use technology that improves diagnostics. Bite analysers. Electronic shade guides.
Don’t do anything that a team member can do
Clinicians should leverage the use of hygienists/therapists/employee den tists, dental assistants and team members. Any dentist who does their own hygiene work is wilfully lowering their hourly rate. This is anti-leverage.
Train your team to do more patient communications. It’s possible for a clinical coordinator to take radiographs and full mouth photos. They can have a detailed discussion about what is vis ible. They then can guide the patient to “discover” their own problems.
Scale up your practice
The bigger your patient base, the more opportunities you’ll have for leverage. It’s much easier to achieve leverage in a large practice.
You want to achieve 2 key outcomes: You want more patients choosing optimum treatment. Note: this needs to be achieved without applying any sales pressure and it needs to be rejection proof (If you know how to do that, you’re an advanced communicator);
You want more patients to refer friends and family. Ideally you’re using your communications skills to grow; not spending dollars. Free growth is 100% leveraged growth!
Metrics to measure leverage
Your re-appointment rate should be over 90%. This will explode your patient base and this allows for even more leverage.
Track the clinician/owner’s hourly rate. If you want to spend more personal clinical hours because you love it... fine. But if you reach a point where you have a practice that doesn’t require your time and the practice is profitable, then you’re lev eraged. The higher the income, the more leverage you have.
The ultimate leverage metric is Take Home Profit/Time spent on the practice.
To achieve 100% leverage is the holy grail of business success because it gives you solid reliable income and life style choices. Normally, we don’t think of dentistry as an ideal leverage busi ness model... but it really is if you put your mind to it. It clearly requires smart communications skills and systems.
More at www.sernik.com
GO DIGITAL INTRAORAL SCANNERS
have become very affordable and the quality, speed and dimensional accuracy of all scanners on the market has come to a point where there is really no excuse not to own at least one. Get yourself some software that allows you to dabble with simple designs, there is software that comes with intraoral scanners and even free software on the internet so cash outlay is not required for some and this will help you understand what is going on in digital dentistry. Don’t forget to have a look at a few online seminars on digital dentistry and check out www.dentevents.tv, it’s like You Tube for Dentistry. And it’s free.
BACKUP
YOUR DATA: There is nothing worse than
losing all your data due to a failed hard drive. To retrieve data from a crashed drive is ridiculously expensive and so inconvenient, it’s not funny. There are so many ways you can inexpensively backup data yourself so shelling out tons of cash is not needed. RAID arrays are like having an instant backup as they have 2 or more hard drives writing the same data, so if one drive fails you have the other as the backup. Cloud services are a great way to backup as well and once setup, they are automatic and really are a very inexpen sive way to backup. A Google™ Drive backup is only $16.80 a month for 2TB.
UPDATE YOUR COMPUTERS:
Computers are not expensive to own, however I’m amazed how many clients I work with still use outdated operating systems and antiquated hardware.You can easily buy computers with just the specifications for what you need without going into hock and in fact most people buy well over what they really need, thinking they’re future proofing–well you can’t as things will always change. Try not to have all your programs on one computer. For example, if you have a 3D printer, buy a dedicated computer to run it, don’t use the office computer; the same for any technology you have - get a computer for the purpose.
22 Australasian Dental Practice July/August 2022
3 things every dentist should start doing now…
TERRY WHITTY
briefs | NEWS 1 2
Achieving business leverage in dentistry… DR MICHAEL SERNIK
“To achieve 100% leverage is the holy grail of business success because it gives you solid reliable income and lifestyle choices...”
The truth about dentists & TikTok...
So what’s the big deal about TikTok?
TikTok is the fastest growing social media app in the world and has the 3rd largest social following, with over 1 billion active users every month.

The average user spends 95 MINUTES A DAY on TikTok!
How can dentists benefit from
TikTok?
If you’ve had any experience with TikTok, you may assume it’s just for young people or dancing videos! This is no longer the case. The current target audience is between 17-60.
TikTok uses an algorithm (a complex set of equations that analyse myriad data) which favours localised content. This means, despite being a global app, it has a strong focus on showing content that is trending (i.e. popular) in your country. This means it’s easier to get a higher
What Google wants...
Google wants to be the number one source of information on the internet and it’s pretty much there already. The reason Google is so popular is because when you Google something, it pretty much nails what you’re looking for in the search results. Mostly anyway.
If patients want to find a dentist, then Google is now the number one place they start. So what happens when you Google “Dentist in your suburb” ? Is your practice showing up? Because if it’s not, then you have no idea how much potential business you’re missing out on.
If you have a website, then make sure you connect with Google through the Search Consule feature which can be located at search.google.com/search-console
If you don’t have a website at all, then think seriously about getting one! And whether or not you have a website, make sure you have your details listed on sites like www.dentist.com.au which ranks highly in all Google searches.
reach of your content to the right audi ence, particularly using hashtags. For example... #teethwhitening
and simple, with a number of pre-existing templates for you to use. Use little snip pets of what you do and how you do it to capture attention. Even if you don’t see yourself posting as regularly on TikTok as other platforms, you can re-purpose the content you create in TikTok onto other platforms. With Instagram now moving to “reel first” in your newsfeed, it makes re-purposing material a no brainer.
TikTok - the verdict
How “techy” do I need to be to use TikTok?
TikTok is primarily a video sharing platform and you can capture users’ attention with informative and educa tional videos. The TikTok app has in-built features that make content creation fun
Consistency trumps perfection. Take advantage of the templates within TikTok to make short, catchy videos. Then use the same content on other plat forms such as Instagram and Facebook.
If you’re ready to take the plunge into producing more video content, jump onboard with TikTok now and ride that wave of growth. Most dentists don’t use it, so get in early before the competition arrives.
More at www.anguspryor.com
Does your website work if you type in www.name.com.au and name.com.au. If your website has been correctly set-up, both should work. If they don’t, contact your developer to fix this issue.
Does your website have a “lock” symbol next to the URL when you look at it in a browser. The lock symbol indicates the website is using a Secure Socket Layer, which means it has an active SSL certificate in place, a further form of protection. Google also apparently gives greater priority to secure websites. Check your website at https://www.digicert.com/help and if need be, talk to your developer about installing an SSL certificate on your site. It’s simple and inexpensive.

Does your website show a © date anywhere on it that is not © 2022. If so, then get this updated. You are telling Google your site is out of date!

How does your website look on your Smartphone and Tablet? Websites created recently should be “responsive”, meaning they resize and reformat according to the device you’re on. Having a responsive website makes it easier for people to connect with you and… you will rank better in Google searches. You can test your site here - https://search.google.com/test/mobile-friendly - to see if it’s considered to be mobile friendly by Google.
Does your website feature a broken Google map? A few years back, Google introduced charges in some cases for showing Google maps on your website which resulted in all maps being disabled at the time. In order to display a Google map on your website, your devel oper needs make the appropriate changes. You can still use the map at no charge, but the code needs to be updated.
July/August 2022 Australasian Dental Practice 23
ANGUS PRYOR briefs | NEWS
Top 3 mistakes dentists make with marketing…
It’s not surprising that dentists struggle with marketing - let’s face it, how much time is spent during a dental degree focusing on marketing your future prac tice? Zero! Now that you’re out, here are the top 3 mistakes we see dentists making with their marketing...
You don’t take marketing seri ously! The competition in dentistry is at an all-time high. Every day in Aus tralia, 3 new dentists start practising, one hangs up their drill and one new practice opens. Every. Single. Day. Highly suc cessful Rich Dad, Poor Dad author Robert
Kiyosaki famously said “I’m not the best author, just the best marketed author.” Dentists must adopt the same approach to succeed. Be the best clinician... but also be the best marketed clinician!
Trying to be all things to all people: Every practice has a sweet spot - a particular patient demographic who love the type of dental experience you offer. Identify that group and focus your marketing towards them. If you try to be all things to all people, you’ll fail to be anything much to anyone. Ironi cally, even potential patients outside the
ANGUS PRYOR
marketing you do to your sweet spot, will still respond positively.
Producing marketing to impress other dentists: I wish I was joking, but I’m amazed at how dental websites I see that honestly, seem like they’re written for other dentists, not patients. The text on the site talks about all manner of technical things that other dentists may find inter esting, but your prospective patients don’t understand or don’t care about. Be hyper focused on speaking to potential patients... and leave impressing your colleagues to storytelling over a drinks at conferences.
The Julie Parker Practice Success Podcast
Julie Parker
68 episodes
Listen to discover management insights and strategies for a suc cessful dental practice. Julie also interviews key people in the dental industry who have advice and services to help you and your team achieve greater success.
The Dental Head Start Podcast

Dr David Keir
178 episodes
The Dental Head Start podcast is made to help dental students become great dentists. You can’t Google the path to dental success, but you can learn from those already there. We interview dentists who have achieved what you’re striving for and get the story behind the strug gles, the successes and the advice they want you to hear. Get the head start you need in your dental career.
The Savvy Dentist Podcast

Dr
Jesse Green
375 episodes
Create a dental practice and a business life you love with Dr Jesse Green as he interviews successful dentists, entrepreneurs and athletes. Listen in as guests share their stories, ideas and business techniques that you can take back to your practice to have more patients, more profit and less stress. This is the podcast where great dentistry meets great business.
Send your favourite podcast info to joseph@dentist.com.au so we can feature it in an upcoming edition


24 Australasian Dental Practice July/August 2022
1 2 3
briefs | NEWS

GET LISTED 1 million visitors a year... 9,675 dental practices... 27,690 clinicians... And counting... Get listed today! The easiest dental marketing you will ever do! ™ www.dentist.com.au SCAN to Add or Update Your Practice
Infection control in dental practice design…
Whilst infection control has always been an impor tant consideration in dental practice design, the COVID-19 pandemic has highlighted the vital role that infection control plays in keeping dentists, staff and patients safe.
Building infection control strategies into your practice design is an effective way to minimise the risks and keep your practice operating now and in the future should troubled times again arise.
Complying with social distancing requirements in a confined space can be challenging. Creating an effective and efficient patient flow at the practice design stage helps to minimise the time patients spend in contact with each other. In larger practices and certain specialities, the prac tice can be designed to have a circular patient flow so it is one-way traffic as much as possible. In smaller practices, it’s often possible to utilise the disability com pliance rules with corridors designed for
wheelchair turns to facilitate passing areas for maintaining distancing requirements.
Material selection also plays an impor tant role in infection control. For counters and benches, solid surface materials such as Corian™ and Austaron™ are non-
Where laminates are used, post formed tops are preferred in lieu of joins which may harbour unwanted germs.
Careful consideration should be given to all touch points, including door handles, handrails and latches to select surfaces that are easy to clean and disinfect. Metal lics and solid surfaces provide a balance of aesthetics, durability and ease of care.
porous, durable and easy to keep clean and disinfected. These products also have an antimicrobial range suitable for oper ating theatres and scrubs. In addition, HEPA filtered air conditioning systems can be incorporated into high risk areas to help minimise airborne pathogens.
Visible controls help to communicate the importance of infection control to patients visiting the practice. These con trols can include dedicated hand sanitiser stations designed to minimise repeat con tact and clear screens at reception areas, putting physical protection between your staff and patients without losing the critical visual connection.
Building a solid infection control strategy into the design of your practice is an investment in the security of your healthcare career.
More at www.medifit.com.au
26 Australasian Dental Practice July/August 2022 briefs | NEWS
GEOFF RAPHAEL
“Creating an effective and efficient patient flow at the practice design stage helps to minimise the time patients spend in contact with each other...”
Say goodbye to neck and back pain!
The uniquely designed PENTAX deflection prism allows the surgeon to view the surgical site with the greatest depth of field and enhanced vision, whilst maintaining the best possible working posture.

FROM $3995+GST
learn more and
QR code or
To
book an in-office demo, scan the
visit osseogroup.com.au/pentax
The Ultimate Practice Makeover begins!
Earlier this year, more than 100 dental practices from all around Aus tralia applied to win the 2022 Ultimate Practice Makeover - a $100,000 makeover including a $40,000 fit out from Medifit, a compre hensive marketing makeover from Dental Marketing Solutions, high-level coaching and consulting from a hand-picked team of experts and much more.
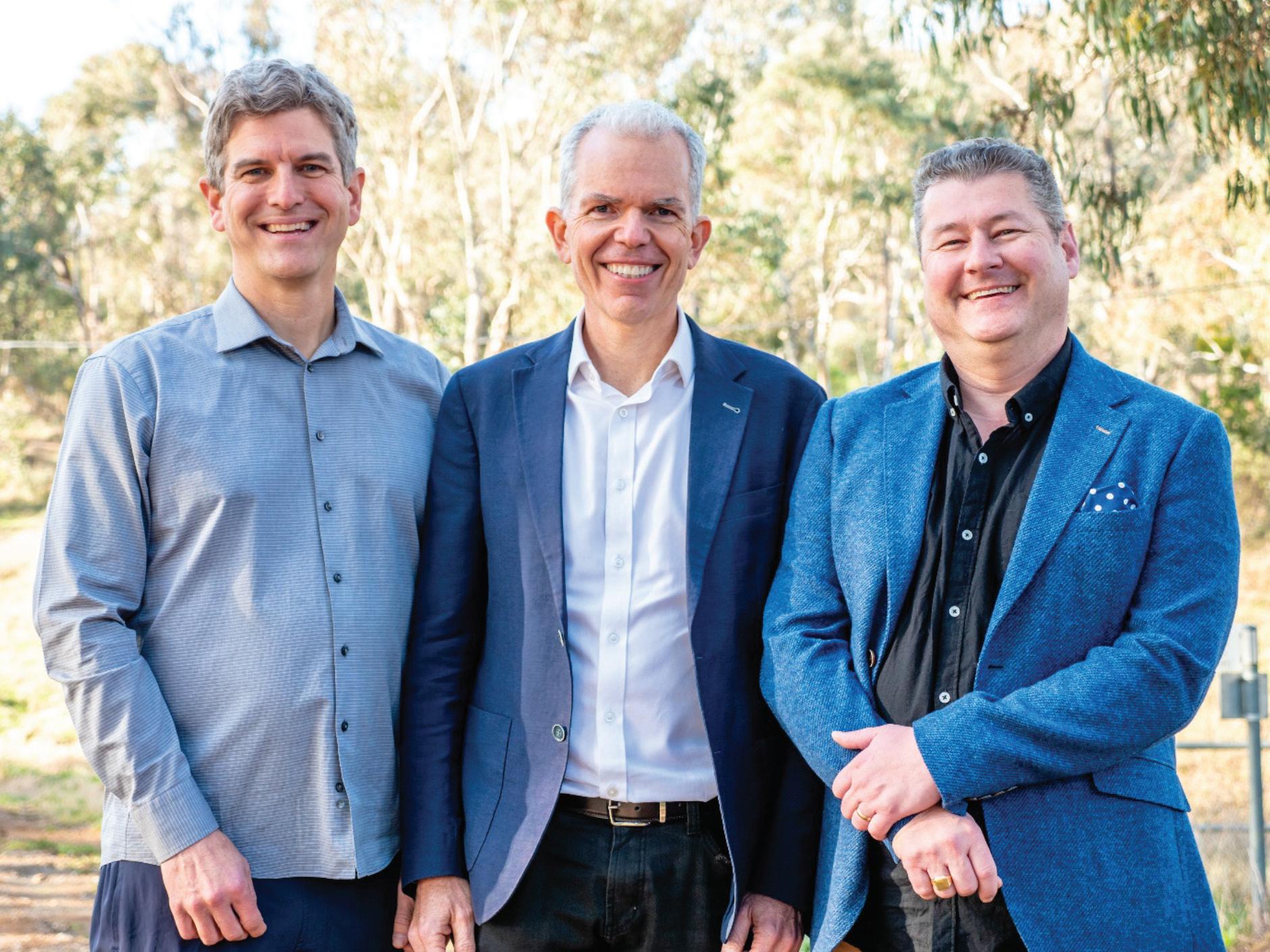
After a rigorous selection process, the lucky winner was Dr Michael Back of Authentic Dentistry in Canberra. Michael said “when I found out that I’d won, I was really, really excited. It’s an oppor tunity to lean on experts who have an area of expertise where I do not... it’s a great opportunity to tap into something that I wouldn’t otherwise do.”
Apart from Michael’s practice receiving the makeover, the whole experience will be captured in the Ultimate Practice Makeover reality TV show, allowing the dental community to share the experience.
Dental Marketing Solution’s CEO and the show’s host, Angus Pryor, shares Michael’s enthusiasm for the project.
“This is going to be an amazing expe rience. We’ve pulled together the top experts in the dental field to pretty much ‘throw the kitchen sink’ at the practice. It’s basically everything we could think of to take the practice from good to amazing in the shortest possible time.”
Medifit National Marketing & Business Development Manager, Marton Jakab, visited the practice recently to start the planning process for the fit out.
“There quite a few options for the prac tice,” Marton said. “Our goal is to give new patients a ‘wow’ experience when they walk through the door. We’ll work with Michael to come up with something that not only looks great, but has high functionality for Michael’s team.”
Every aspect of the implementa tion of the Ultimate Practice Makeover is being filmed in the style of a reality TV show to provide unique insight into the consultancy process. The Ultimate Practice Makeover will be released at www.dentevents.tv in 2023.
The Ultimate Practice Makeover includes...
n Reception and waiting area upgrade to provide patients with the best possible first impression of your practice from Australia’s leading surgery builder, Medifit Design and Construct valued at up to $40,000
n Full marketing review and strategy development by Dental Marketing Solutions valued at $5,500
n 12 month subscription to Channel D to engage your patients in the waiting area including a TV valued at $3,100
n Full business identity branding package including logo, colours, style guide and more valued at $1,000
n Brand new website and Search Engine Optimisation (SEO) package to max imise your Google rankings in organic searches valued at $12,000
n Online marketing including premium listing upgrade on www.dentist.com.au to expose your practice to 1 million potential new patients a year valued at $2,000
n New uniforms, patient welcome packs from Erkine Oral Care and more valued at $2,500
n Tablet with SpeedPix™ loaded for better case conversions valued at $1,500
n Marketing consultancy for 6 months valued at $10,000
n Training for you and your team valued at $2,000
n Telephone answering training valued at $3,500 from Call Tracking Excellence
n Treatment presentation coaching valued at $2,000 from Dr Jesse Green
n New practice management software valued at $5,000 from Centaur Software
n And more...
28 Australasian Dental Practice July/August 2022 spectrum | NEWS
Ultimate Practice Makeover 2022 winner Dr Michael Back from Authentic Dentistry in Canberra with Ultimate Practice Makeover host Angus Pryor and Marton Jakab from major sponsor Medifit Design and Construction.


TOGETSTARTED: 1300002239 CLEAREX.COM.AU Threeturnkeysystemstotransformyouraligner practiceintoarevenuegeneratingmachine. UNLOCKTHEOPPORTUNITY MASSIVEPRACTICEGROWTH $900
month,CAEmembershipcanpayforitselfby savingupto$900percaseinalignerlabfees. 4X 2.ALIGNEREDUCATIONPROGRAM Comprehensiveclinicaltrainingdesignedtoenable youtotreatmorecomplexcasespredictablyand efficiently,resultinginquadruplingnewcasestarts. $250K 3.ALIGNERBUSINESSPROGRAM Traintheentireteamtosuccessfullypresentand closemoretreatmentusingprovenprocessesand scriptingtoaddanaverageof$250,000in additionalannualprofit.
Growthareestimates. Actualresultsmayvaryfromresultsshownhere.
1.EXCLUSIVEBUYINGGROUP Ifyourpracticeisalreadystartingonecaseper
*ActualSavings,CaseSubmissions,andProfit











Digital Dentistry & Dental Technology SYDNEY 2-3 JUNE 2023 NOVOTEL SYDNEY BRIGHTON BEACH TWO DAYS OF LECTURES AND WORKSHOPS ON DIGITAL DENTISTRY FOR DENTISTS, SPECIALISTS, DENTAL TECHNICIANS AND DENTAL PROSTHETISTS dentevents presents... INDUSTRY SUPPORTERS SPONSORS











Full details of the speakers and presentations online www.dentaltechnology.com.au Organised by Dentevents™ a division of Main Street Publishing Pty Ltd ABN 74 065 490 655 www.dentevents.com • info@dentist.com.au • Tel: (02) 9929 1900 • Fax: (02) 9929 1999 REGISTRATION FEES $880 inc gst EARLY BIRD PRICING $220 before 2 Dec 2022 price increases $110 on the 2nD of every month INCLUSIONS Registration fee includes participation in TWO full days of education (12 CPD hours), all catering and Friday drinks. Multiple lectures and workshops are being run concurrently to allow you to build your own program to suit your specific interests. Price is all inclusive. VENUE DETAILS Novotel Sydney Brighton Beach - The Grand Parade, Brighton-Le-Sands NSW 2216 - Close to Sydney Domestic and International Airports Check the website for details of discounted accommodation rates for the conference • Ample parking available at the hotel PROGRAMME DETAILS FRIDAY 2 JUNE 2023 9.00am - 5.00pm - e D ucation 5.00pm - 7.00pm - happy hour SATURDAY 3 JUNE 2023 9.00am - 5.00pm - e D ucation 12 HOURS CPD Join us again or for the first time at Digital Dentistry & Dental Technology 2023 for a fun, exciting and fully immersive learning experience with the best of the best in the new age of dentistry. This year’s program will cover Digital Smile Design • Digital orthodontics • Intraoral scanning • Digital implantology • Digital full arch restorations and full mouth rehabilitations • Digital Dentures • 3D Printing • Milling • CBCT • Material and applications • Software and more with MORE Hands-on Sessions • MORE Advanced Sessions • MORE New Products • NEW Masterclasses and more! ONLY $220 FOR 2 DAYS OF EDUCATION (12 HOURS OF CPD) IF YOU REGISTER BEFORE 2 DECEMBER 2022 (SAVE 75%)
Next Smile launches national network of All-on-4® Dental Implant Clinics

Agroup of renowned local clinicians have launched a bold play to set-up a national network of dental centres specialising in the delivery of All-on-4® treatment under the Next Smile™ brand. B ased on the clinically proven Malo Protocol philosophy of the pioneer of Allon-4®, Prof. Paulo Malo, and supported by Nobel Biocare, who own the All-on-4® brand, Next Smile Australia hosted its launch event recently on the Gold Coast with its entire Australian clinic network.
Dr Larry Benge, Dr Tony Rotondo and Rob Dulieu employed former Nobel Bio care General Manager ANZ, Peter Jeffers as CEO to transition their formerly loose cooperation under the Malo Dental name to a formal network of surgical clinics, accredited regional access centres and a full training regime centred around All-on-4® .
“Next Smile Australia is basically a nationally branded dental implant busi ness, which primarily focuses on All-on-4® and the All-on-4® treatment concept,” Mr Jeffers said. “We’re the first true nationally branded All-on-4® business and the way that we work is by having All-on-4® surgical super clinics in most of our main population centres. We then have Next Smile Accred ited Partners who provide local access in more geographically diverse locations that are selected and trained to undertake parts of the All-on-4® treatment, including initial consultation, post-surgical reviews and the fitting of the final prosthetics. And then we have All-on-4® training hubs.
“For our Next Smile Accredited Part ners, we have developed a really good commercial referral model where we essentially share the journey of the patient to ensure they receive the best possible delivery of all All-on-4® treatment.
“To give that context, if you’re in Dubbo, where we have an Accredited Partner, it means a patient in that region can access part of the treatment journey for All-in-4 in Dubbo, like the initial consultation and scans and then transi tion to Sydney, to our super clinic, for the surgery. They then transition back to the Accredited Partner for final pros thetics and ongoing maintenance. This reduces the number of appointments necessary and ensures the patient has the best possible outcome and experience.”
Mr Jeffers said that in addition to providing a surgical pathway for Allon-4® patients referred from Accredited Partners, Next Smile will also undertake direct to patient marketing to increase the awareness of the treatment option.
“We have a national brand and go-tomarket strategy for patient acquisition via direct patient marketing,” he said.
32 Australasian Dental Practice July/August 2022
spectrum | NEWS
“We’re trying to tap into the market opportunity. We know that by 2050, for example, over 25% of the population will be over 65. We know that a large pro portion of these will be fully or partially edentulous. We know that by making the patient more aware of the treatment, we can help them by bringing this great All-on-4® treatment to them.
“From a commercial perspective, our surgical super clinics and Accredited Part ners can tap into this market opportunity with us because we’re providing the infra structure, we’re providing the training through Next Smile education and we’re providing marketing tools to basically drive more patients to their practice. And we share part of the revenue and ensure the patient experience is optimal.
“Treatment is delivered using the clinically researched and proven Malo protocol using the Nobel Biocare Speedy Groovy implant system invented by Prof. Malo specifcally for All-on-4 ® and the surgery is being completed by clinicians who have been fully trained and already delivered thousands of cases.
“We are focussed on using the right tools, the right branding, the right mar keting and the right product in order to essentially bring the best possible outcome to the patient. There’s a massive opportu nity out there to tap into but delivering treatment involves a complex surgical procedure and as a result, the opportunity is not available to every practice.
“We know from our market research that patients present themselves to den tists who maybe don’t know or understand how to communicate about All-on-4® as a treatment option. So they tend to either refer them out to a specialist or they simply prescribe a denture. So what we’re trying to do through our marketing is highlight through direct-to-patient communica tion is here’s what All-on-4® is and you should try and talk to your local dentist about it.
“So if we can send them to our branded partners, they’re going to have a much better conversation about this option, versus potentially getting an outcome which is not right for them.”
Mr Jeffers said that the Next Smile super clinics currently located in Melbourne, Ballarat, Brisbane, Robina, Sydney and Wollongong are full service centres while Accredited Partners focus on completing the prosthetics only.
“Again, if we use somewhere like Dubbo in regional New South Wales as an example, it’s a large area that our Local Access Partner can tap into. A patient in the Dubbo area can effectively come into our accredited partner, have their initial consultation, scan and work-up. Then, the Local Area Partner transitions the patient to our Bondi Junction super centre in Sydney for the surgery.
“Here, they also get their first provi sional set of teeth with Rob Dulieu. They receive their final set of teeth and ongoing maintenance back in Dubbo.
“So from a patient perspective, it’s very smooth, easy and accessible and the surgical treatment will be completed by a clinician with hundreds of cases under their belt using the Malo protocol.”
“We know that by 2050, over 25% of the population will be over 65. We know that a large proportion of these will be fully or partially edentulous. We know that by making the patient more aware of the treatment, we can capitalise on this and bring the All-on-4 to them...”
Mr Jeffers said another key feature of their patient centric approach is to offer a transparent price for treatment.
“We try to include the pricing in our marketing and we try to market to the sweet spot where effectively all is included in one price. We charge $27,000 for a single arch with two bridges. That includes the whole journey for the patient apart from the anaesthetic costs, which are separate. So from a patient perspective, it’s smooth and easy. They’re getting the clinically-proven and researched protocol - which is the two bridge protocol - and we’re using Speedy Groovy implants from Nobel Biocare. And at the end of it, we also offer a warranty.”
Mr Jeffers said that despite many patients having received All-on-4 ®, the treatment remains little known.
“We’re trying to offer All-on-4 ® as a treatment outcome which is as easy and accessible as possible for the patient. Because I know from my experience and
background that whilst lots of patients in Australia have received All-on-4 ® , there’s still a massive opportunity. Through our market research, we found there’s still a huge swathe of people who don’t know what All-in-4 is and they still suffer with removable dentures or partial dentures or don’t go to the dentist at all. So what we’re actually trying to do is bring it to the masses by making it really easy for people to receive treatment.
“And for the dentist, we’ve effectively made a turnkey package for All-on-4 ® It makes it really easy for them and it makes it really easy for the patient. It’s taken us a while to figure this out, but we’re now starting to see the fruits of our success, particularly over the last 12 to 18 months. We know that we are the big gest group and we know that we are the biggest in terms of cumulative volume of cases completed in Australia. So now we are opening up to expand nationally and bring on more Accredited Partners.”
Mr Jeffers said that working closely with Dr Larry Benge has been the key to making Next Smile a reality.
“Larry has been very, very successful with All-on-4® for many, many years. He was the original trailblazer in Australia, along with one or two others like Tony Rotondo. Education is a big part of Next Smile and this is where Larry excels.
“So one of Larry’s key roles, aside from providing excellent patient care, is to assist with the education and group den tist succession planning as well because he’s been doing All-on-4® the most and doing it the longest and he’s treated the most cases. So where possible, Larry will continue to build his Melbourne practice with his dentists there, but also support our other dentists around the country.
“The other thing that we’re very con scious of is giving back. So we’re setting up the Next Smile Foundation which will be our philanthropic arm. We will treat patients in need on a pro bono basis, as fun damentally, Next Smile is about helping patients improve their quality of life.
“Overall, our model is essentially to support the dentist to treat more patients by providing the expertise in a more coor dinated, formalised national way, in order to try and bring more awareness of the All-on-4® procedure to more patients.”
For more information on Next Smile, visit www.nextsmile.com.au
July/August 2022 Australasian Dental Practice 33
spectrum | NEWS
Bringing All-on-4® back to its roots
Dr Larry Benge is one of the pioneers of All-on-4® in Australia and has seen the popularity of the protocol grow sig nificantly in recent times. Now, with the launch of Next Smile™, he sees an oppor tunity to guide clinicians offering the procedure a path back to its roots.

I’ve been on the All-on-4® journey with Professor Malo since 2007 when I first went to Portugal and I’ve seen what the gold standard of All-on-4® is in terms of how it should be done. Having been on this journey, I’ve also seen first-hand the problems that can occur and I’ve also seen how very rewarding it is when the process is done in a particular way.
What’s happened now, though, is that like every other technique in dentistry, when something comes into vogue, everybody jumps onto the bandwagon. The result is that the All-on-4® procedure is not being done well by many, many people because they often take a concept and they change it to suit their own ends and that has consequences.
In general terms, what I’ve seen over the years - and I managed Asia for a long time for the Malo Clinic - are problems caused by the procedure being done incorrectly. And it’s not like when you do a filling or a crown and you have a complication, this is big in terms of the problems that can occur if the procedure doesn’t go well. So this group we’ve formed, Next Smile, has the opportunity to get clinicians together that are highly trained, that have gone and invested time in learning and are all committed to a particular gold standard of quality. We all use the same implant, we use the same procedures, we follow the same protocol - the Malo protocol, the protocol with the research behind it that has been tried and tested over many years - and combined, this results in very pre dictable outcomes for patients.
Next Smile was born based on the need to establish a group that had serious clinical credibility that could first and foremost provide a great platform for edu cating dentists on the Malo protocol. Most dentists only do one or two All-on-4® cases a year, if that, whereas the members
of this group are doing over a thousand arches a year. It’s a significant difference in surgical ability. We want to provide a pathway for all dentists interested in incorporating All-on-4® into their prac tices a way to ensure their patients receive the outcomes they are investing in.
So this is really about taking back All-on-4 ® and when patients buy All-on-4 ®, helping to ensure they’re getting what they’re paying for - a contin ually researched, tried and tested solution. Because it’s a big investment for the patient. It’s a lot of money; a lot of people
buying power in terms of implants, com ponents and all those sorts of things. So that’s really been the journey.
Peter Jeffers was running Nobel Biocare at the time we were discussing forming this group, so I head-hunted him to run it. He’s very experienced in the industry.
My relationship with Paulo Malo goes back many years and I speak to him two or three times a day, every day of the year. So we’re always working on how the pro tocol could be improved and developing strategies for teaching it, so that gives me my personal stimulation as well because
go into their superannuation to have this treatment and they deserve to receive what they’re paying for.
And, personally, by me being really at the tail end of my career, Next Smile is a chance to create a legacy that helps bring young clinicians - and so far we have some very impressive young dentiststhrough significant training programs in a great environment. So it becomes a legacy for someone to take over when I retire. So all those things together have been contributing to this project.
We also thought that if we become the leading All-on-4® body in this country, then we now have the reputation to allow us to control the results out there a little better and we would also benefit from being in a bigger group, with obvious
not only do I work on the clinical side, I also work on the business side.
So we’ve just moved into a huge super centre in Melbourne which has two oper ating theaters - it’s like a hospital - so it’s an environment that oral surgeons can use with proper theaters, proper beds, proper recovery. It’s in an environment that’s a very safe environment. No stone is unturned. The laboratory’s also there, so it’s a one stop shop. Any complicationsand we know there can be complications - it’s fixed on the spot so you don’t have to go anywhere else. So I think that’s peace of mind for people that we look after from beginning to end.
For more information on Next Smile, visit www.nextsmile.com.au
34 Australasian Dental Practice July/August 2022
| NEWS
spectrum
Australia’s no.1 Googleranked dental marketer.
PERSONAL Development
Australia’s no.1 Googleranked dental marketer. you’ll hear from Dr Mark Costes who has built nothing short of a dental empire. Yet, for a man of great achievement, Mark is a man of great humility and willingness to share what he has learnt along the way.

you’ll hear from Dr Mark Costes who has built nothing short of a dental empire. Yet, for a man of great achievement, Mark is a man of great humility and willingness to share what he has learnt along the way.
You’ll hear from Pete Williams from Deakin University in Melbourne.
He’s a serial entrepreneur, (part time academic) and best-selling author of ‘Cadence: a tale of fast business growth’,where he reveals7 key levers to growing faster.
You’ll hear from Pete Williams from Deakin University in Melbourne. He’s a serial entrepreneur, (part time academic) and best-selling author of ‘Cadence: a tale of fast business growth’,where he reveals7 key levers to growing faster.
clinical psychologist, Kasey Compton, talks about her new book ‘Fix This Next for Health care Providers’. She discusses the simple system that shows you exactly what to fix next in your quest for practice growth.
clinical psychologist, Kasey Compton, talks about her new book ‘Fix This Next for Health care Providers’. She discusses the simple system that shows you exactly what to fix next in your quest for practice growth.

SOMETHING HEY PODCAST LISTENER
HERE’S
JUST FOR YOU ! A BRAND-NEW PODCAST PRACTICE GROWTH HQ is your home for all things practice growth. YOUR MULTI AWARD WINNING HOST ANGUS PRYOR is an Amazon-best-selling author International speaker and PRACTICE GROWTH HQ DROPS EVERY WEDNESDAY With great content on MARKETING Tactics BUSINESS Strategies TEAM Building IN EPISODE 2 IN EPISODE 1 IN EPISODE 3 Practice Growth HQ is available now on all popular podcast channels visit www.PracticeGrowthHQ.com NOW TO CHECK IT OUT. HERE’S SOMETHING HEY PODCAST LISTENER
Development You’ll enjoy learning
thought-leaders, industry experts, best-selling authors, and thriving practice owners as they
their very best tips, tools, and strategies to help you
PERSONAL
from
reveal
grow your practice faster.
JUST FOR YOU ! A BRAND-NEW PODCAST PRACTICE GROWTH HQ is your home for all things practice growth. YOUR MULTI AWARD WINNING HOST ANGUS PRYOR is
author International
and IN THIS WEEKLY PODCAST PRACTICE GROWTH HQ
MARKETING Tactics BUSINESS Strategies TEAM
IN
IN
IN
an Amazon-best-selling
speaker
DROPS EVERY WEDNESDAY With great content on
Building
EPISODE 2
EPISODE 1
EPISODE 3
Helping Hand Grants return to support medical, dental and veterinary practices
Specialist medical lender Credabl is delighted to announce the return of its Helping Hand Grants for healthcare practices across Australia. The 2022/23 grants have offi cially launched - both direct applications from practices and nominations from the general public are being accepted until 31 December 2022. The recipients will be announced on 13 March 2023.
The grants are designed to support practice growth, showcasing the amazing contributions occurring in local communi ties and to help drive patient numbers and engagement.
The grants are valued at over $10,000 and will be awarded to up to five medical practices around Australia across the med ical, dental and veterinary professions.
Each grant includes a cash incen tive, practice growth and management coaching from industry partners including Health Business Network, Prime Prac tice and Vettr, a Delonghi Nespresso coffee machine, 50,000 Qantas Points* for their business and a digital guide book filled with great tips to help boost patient numbers.
This year’s judging panel are Dr Kris tina Cain (Dentist and Business Owner of SmileChix), Dr Geoff Toogood (Car diologist and Founder of Crazy Socks 4 Docs), Dr Garnett Hall (Veterinary Sur geon, Founder and CEO at VetChip and President of AVA WA), Stafford Ham ilton (CEO at Credabl), Glen Stewart (Chief Risk Officer at Credabl) and Kelly Gall (Finance Specialist at Credabl).
Stafford Hamilton, Credabl CEO and Co-founder, says the return of the Helping Hand Grants is a way to continue to shine a light on hard-working healthcare practices right across Australia.
“At Credabl, we have seen first-hand how hard the past few years have been on medical practices, emotionally and finan cially. The Helping Hand Grants enable us to support up to five businesses whilst also acknowledging the challenges many prac
tices are currently facing – from patient retention and community engagement to financial hardship,” Hamilton said.
For previous winner Family Dental Yamba in Yamba, NSW, the last two years had significantly impacted the practice’s growth plans, like many others.
“Thanks to the grant, we were able to complete our practice renovations and upgrades despite the floods and other challenges. Without Credabl’s help and support, these dreams would not have become a reality and we are forever grateful!” said dentists, Aninke Lippert and Willem Espag.
the financial attention they deserve in both their personal and professional lives. With niche finance knowledge and specialist skills, Credabl is your partner on call.
About Health Business Network
APPLY NOMINATE
Our 2020/21 Helping Hand Grant recipients also included Brentford Dental in Victoria, Cygnet Clinic in Western Australia, Modbury Veterinary Clinic in South Australia and Family Health Clinic in Queensland.
Medical, dental and veterinary busi nesses can directly apply for a Helping Hand Grant via the dedicated program page, while patients and clients can nomi nate a doctor, dentist or vet by visiting the nomination page (T&Cs apply).
About Credabl
Credabl is a team of finance special ists providing tailored solutions for medical, dental, veterinary and accounting professionals. Through simplified, cus tomised and digitised solutions, Credabl ensures that medical professionals receive
H
ealth Business Network (HBN) is the one-stop-shop for all your medical business needs. Whether you’re starting out, or an established doctorpreneur wishing to expand, HBN is Australia’s trusted leader in medical prac tice growth and strategy. From business plans and cash flow forecasting, through to marketing, manager mentoring and profitable operational planning, HBN is the one-stop-shop for all your medical business needs.


About Prime Practice
rime Practice is a global dental practice management and consultancy com pany that provides training and business solutions to the dental community across Australia, New Zealand, South East Asia, China, North America and Europe.
P
About Vettr
Vettr is a buying group with a differ ence. Vettr is different because they know that pricing is only one component of your business. They will help you take an objective look across all the aspects of your practice to come up with a plan to help you achieve your goals.
About Qantas Business Rewards
Qantas Business Rewards is the loyalty program that allows your business to earn Qantas Points on your everyday busi ness expenses. Plus, your business can save on flights, manage your travel and redeem your Qantas Points on a range of products and services to benefit your busi ness. All you need is a valid ABN to join.
36 Australasian Dental Practice July/August 2022 spectrum | NEWS
Give your dental practice a helping hand with Credabl.

Would a $10,000 helping hand be a welcome treat for your practice?

The Helping Hand Grants are back to support medical practices.
Valued over $10,000 and awarded to up to five practices around Australia, the grants are designed to help your practice grow. Each grant includes a cash incentive, practice growth and management coaching from industry partners including Prime Practice, a Delonghi Nespresso coffee machine, 50,000 Qantas Points* for your business and a digital guidebook filled with great tips to help boost patient numbers.
If you own, manage or work for a dental practice, tell us why a Helping Hand Grant would support your business.




Scan the QR code to apply now or visit credabl.com.au/helpinghand22
Applications close 31 December 2022. T&Cs apply.
Helping Hand Grants brought to you by Participating partners




T&Cs apply.
*A business must be a Qantas Business Rewards Member to earn or receive Qantas Points for business. A one-off join fee of $89.50 including GST normally applies, however this will be waived for Credabl Pty Ltd (ACN 615 968 100) customers if they join at www.qantasbusinessrewards.com/credablfree. Membership and Qantas Points are subject to Qantas Business Rewards Terms and Conditions (www. qantas.com/au/en/business-rewards/terms-and-conditions). Qantas Points for business are offered under the Credabl Terms and Conditions (www.credabl.com.au/qbr/terms-and-conditions).

IDEM excites industry professionals with its grand return this October 2022
IDEM 2022, themed “Building Resilience in Dentistry”, will be held from 7-9 October at the Sands Expo and Convention Centre, Marina Bay Sands. Organised by Koelnmesse and the Singapore Dental Association, IDEM 2022 will feature over 30 scientific conference sessions, including hands-on workshops, a full-day masterclass and exhibits com plemented with hybrid elements to ensure an holistic experience for all participants. This is the first physical IDEM after a hiatus brought about by the pandemic.
“As organisers of IDEM, we are excited to bring back the exhibition and confer ence face-to-face after four years. While continuing education has been ongoing digitally, based on feedback we have received from our partners, exhibitors and delegates, the in-person experience cannot be replaced. A physical event will ensure that participants will once again get to con nect face-to-face with speakers, exhibitors and peers to learn about the latest develop ments in dentistry,” said Mathias Kuepper, Managing Director of Koelnmesse Pte Ltd. IDEM Singapore is the leading dental exhibition and conference in the AsiaPacific region. This year, participants at IDEM 2022 can look forward to a series of programmes specially curated for the dental community.
Full-day SDA Masterclass
Conducted by Maurizio Tonetti, Chair Professor of Shanghai Jiao Tong University School of Medicine, Director of the Shanghai Preimplant Innovation Center and Executive Director of the European Research Group on Periodon tology will present on the topic Implants in Stage III and IV Periodontitis Patients: Benefits and Risks.
“We have curated a slew of exciting conference sessions for IDEM 2022,” said Dr Lawrence Yong, President, Singapore Dental Association. “The IDEM conference will provide participants the opportunity to learn about the latest in clinical research and pick up practical skills as well.”

“We are excited to have our SDA Mas terclass Speaker Maurizio Tonetti as part of the IDEM Conference and remain committed to delivering the best experi ence for all delegates by continuing to bring them high quality continuing educa tion sessions,” added Prof Patrick Tseng, Scientific Chairperson of IDEM 2022.
Trade Exhibition
with over 40 new international exhibi tors participating for the first time. In addition, long-standing pavilion partners such as Germany, Switzerland and the United States will once again be present at the IDEM Exhibition Hall, bringing the international dental industry to one central location in the Asia Pacific.
AOHTS@IDEM
The Association for Oral Health Thera pists Symposium in collaboration with IDEM brings together the AOHT Annual Congress and IDEM’s Dental Hygienist and Therapist Forum (DHTF).
IDEM360+
While the conference will take place in person, it is supplemented by IDEM360+, a digital platform that ena bles participants to do business matching, find networking opportunities with the onsite lead generation feature, book meeting slots, watch on-demand content from the scientific programme after the actual event day and more.
I
DEM 2022 includes a 14,000m2 allencompassing exhibition showcasing close to 500 exhibiting brands with exhibitors from more than 30 countries,
Online registration is ongoing. Pre-show rates will be available at a discounted price before 2 October 2022. For more info visit www.idem-singapore.com

38 Australasian Dental Practice July/August 2022 spectrum | NEWS

THE LEADING DENTAL EXHIBITION AND CONFERENCE IN ASIA PACIFIC www.idem-singapore.com NEW VENUE Organised by Endorsed by Held in Supported by Connect with us IDEM Singapore IDEM Singapore idem.sg @IDEMSingapore Singapore Dental Association 7-9 OCTOBER 2022 MARINA BAY SANDS SINGAPORE NEW DATES: ENJOY 10% DISCOUNT* ON YOUR TICKETS WITH PROMO CODE: IDEMADPMCR9B *Promo Code will expire on 2 August 2022 and cannot be used in conjunction with other discounts.
dentevents presents...
MINI SMILE MAKEOVER
A ONE DAY LECTURE IN SYDNEY ON NOVEMBER 26, 2022
Presented by Dr Sarkis Nalbandian, specialist prosthodontist
Specialist Prosthodontist Dr Sarkis Nalbandian is one of Australia’s leading cosmetic dentists. In this one day program, he offers a specialist’s perspective on the MINI SMILE MAKEOVER concept to enable you to offer patients options

for aesthetic enhancements commensurate with their individual needs and budget. Treat ment options to address discolourations, fluorosis, white spot lesions, diastemas and more will be detailed encompassing a range of solutions including composite and porce lain veneers. Equip yourself with a range of solutions to address common aesthetic issues cost-effectively and minimally invasively.
TOPICS include Diagnosis | Critical thinking in patient assessment | Case selection | Indications and contraindications for composite and porcelain veneers Smile Design | Non-invasive treatments

Register Now: www.smileacademy.com.au
Dr Sarkis Nalbandian
BDS (Hons), Grad.Dip.Clin.Dent (Oral Implants) (Syd), MClinDent (Prosth) (King’s College London), DClinDent (Prosth) (Syd), FIADFE, FPFA, FRACDS, MRACDS (Prosth)

Dr Sarkis Nalbandian is a specialist prosthodontist. His special interests include non-invasive treatments of white spot lesions, the application of composites and porcelain technology for treating complex functional and aesthetic problems, along with the application of piezosurgery in implantology, accelerated orthodontics (PAOO) and bonding to zirconia.

Dr Nalbandian is a founder and course director for the International College of Dental Practitioners (ICODP.COM) and has a specialist
private referral practice in Sydney focusing on Aesthetics, Prosthodontics, Implant surgery, TMD & Facial Pain.

Dr Nalbandian has lectured both locally and internationally on Aesthetics, Dental Implants and Complex Prosthodontics.


He is a contributor and consultant to postgrad uate master’s degree programs in Restorative Dentistry and Prosthodontics at King’s College, University of London and doctorate program at University of Sydney.
LIMITED PLACES! REGISTER TODAY Register Now: www.smileacademy.com.au
REGISTRATION FEES Dentists $660 inc gst Early Bird $440 inc gst save $220 - register by october 26 DATES AND TIMES SYDNEY CBD Saturday, 26 November 2022 Starts 9am | Ends 5pm | Rego opens 8.30am For venue location and information, please visit www.smileacademy.com.au Mini Smile Makeover is presented by Dentevents, a division of Main Street Publishing Pty Ltd ABN 74 065 490 655 • www.dentevents.com • info@dentist.com.au Tel: (02) 9929 1900 • Fax: (02) 9929 1999 • Smile Academy™ and Dentevents™ are trademarks of Main Street Publishing P/L © 2022 Main Street Publishing Pty Ltd 6 HOURS CPD
Upload your videos to Dentevents.TV now and win a smartphone gimbal
Dentevents.TV has launched a brand new feature to allow anyone working in dentistry to upload and share videos that’s easier than ever. Simply login at www.dentevents.tv and click “Upload Video” to get started.
Whether you have a webinar recording, a product hack, a clinical technique, a product review or unboxing, a diatribe on difficult patients or some wisdom or humour about dentistry, you’re invited to share your video with your peers through the site.
Plus, the author of the video that receives the most votes before November 30 will receive a DJI OM 5 Smartphone Gimbal Stabiliser (Phone not included) to help you make even better videos in the future.
“Dentevents.TV has continued to grow in popularity following its launch during the first COVID lockdown, but moving forward, we need to attract more con
tent to take it to the next level,” said Dentevents.TV publisher Joseph Allbeury. “We have a great catalogue of dental videos available free and on demand 24/7 from a variety of sources already, but now we’re looking for more content created by members of the dental community.
“Many people working in dentistry are already prolific content creators and we want to engage with these people and encourage them to use dentevents.tv as an additional way to share their videos with their peers.
“Part of this is making it far easier to load videos and part of this is incentivising videos creators to share their content.”
Up until now, the only way to post videos on Dentevents.TV was by logging in to the www.dentalcommunity.com.au website,
clicking Manage Your Videos and then uploading your video. However, now you can upload videos directly through the Dentevents.TV website.
The latest videos all appear under
“Recently Added” and a new “VOTE” button has been added to enable anyone to vote for the videos they like.
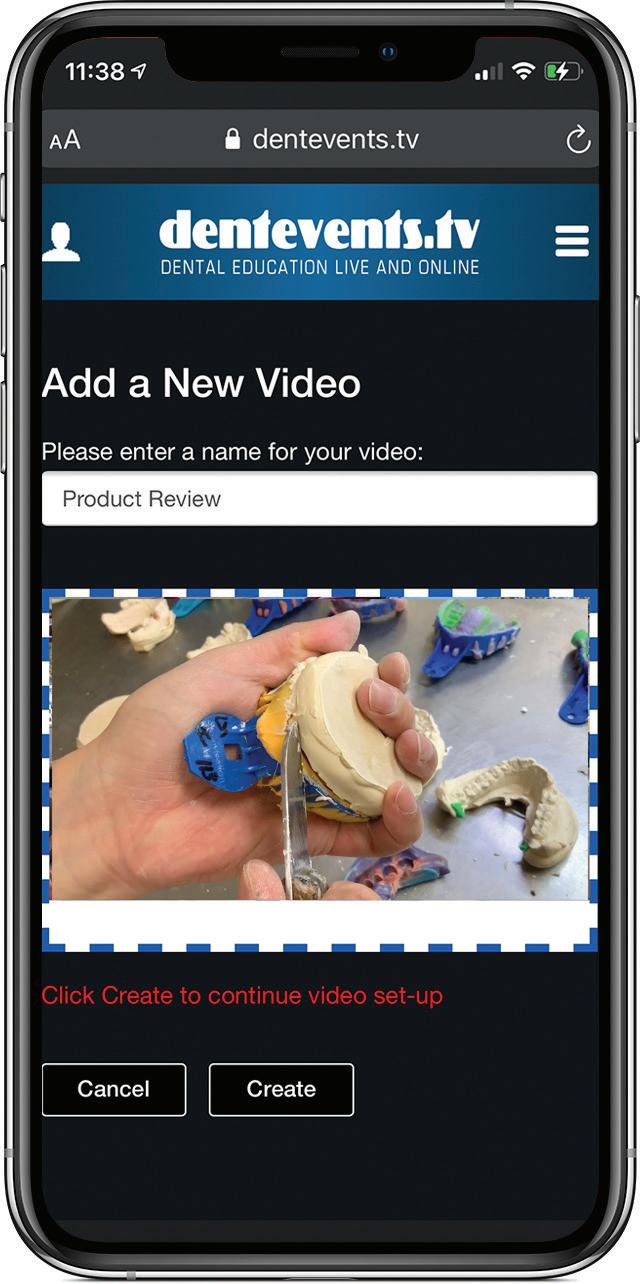
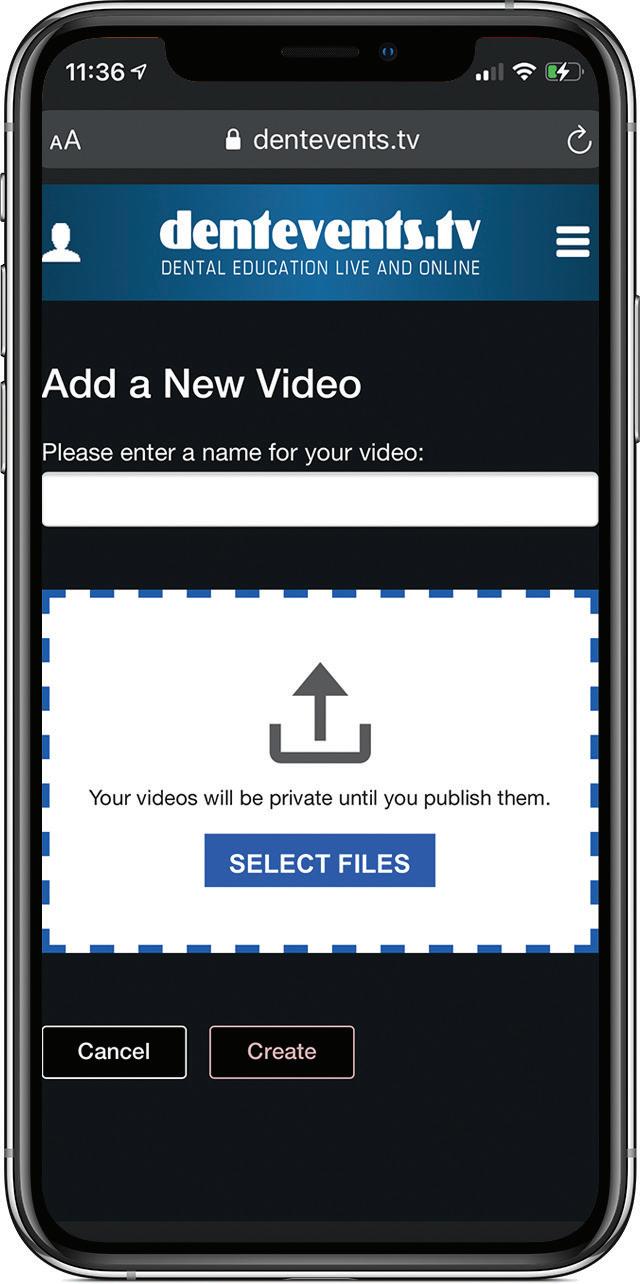
“You have to login to Dentevents.TV to watch the videos and vote,” Mr Allbeury said. “Each person can only vote once for a video, but they can also vote for multiple videos. So if you load a video onto the site, then it’s in your interests to encourage your friends to login as well and vote for it. The VOTE button acti vates after you have watched the video.”
For more info, visit Dentevents.TV. It’s free to login and watch any of the videos 24/7.
42 Australasian Dental Practice July/August 2022 spectrum | NEWS
STREAMING NOW ON-DEMAND
www.dentevents.tv
Dentevents.TV is a brand new dental video streaming service Watch a growing list of hundreds of videos related to dentistry all in one place
High-speed sintering in just 20 minutes
Amann Girrbach’s HighSpeed Zirconia Kit allows users to sinter zirconia restorations in only 20 minutes. Consisting of the HighSpeed Ceramill Therm DRS sintering furnace and the specifi cally developed Zolid DRS zirconia, the High-Speed Zirconia Kit provides the per fect basis for the ultra-fast fabrication of highly aesthetic zirconia restorations. The restorations can be sintered in just 20 min utes and offer maximum efficiency with a natural appearance due to the perfectly coordinated 16 Vita shades with inte grated shade and translucency gradient.
The focus of the development was clearly on the issue of safety, as only durable restorations are of benefit to the
laboratory, the clinician and the patient. For this reason, numerous studies were already conducted by renowned external institutes during the development phase. The result was conclusive: the fast sin tering cycle has no relevant influence on optical or mechanical properties. In addi tion, the high flexural strength of > 800 MPa and the associated classification as a Class 5 zirconia provides an additional safety cushion.
Both laboratories and dental practices benefit from this innovative high-speed sintering process enabling them to add the so-called “Same Day Crown” to their service offering. Due to the extremely shortened sintering process, single-tooth crowns and three-pontic bridges can be realized in just one day, from preparation to final insertion.
What’s more, the fabrication of other indications can also be shortened consid erably, for example, an implant restoration consisting of a zirconia abutment and a crown. Whereas previously at least two days had to be allowed for in planning this type of restoration, it can now be fabri cated easily in less than 24 hours with the High-Speed Zirconia Kit.
The High-Speed Zirconia Kit offers every user an efficient and profitable process extension for the fabrication of zirconia in everyday routines - while at the same time maintaining natural aesthetics and maximum safety.
For more information, contact Innovatio Dental Supplies on Tel (02) 8575-8675, sales@innovatiodentalsupplies.com.au or see www.innovatiodentalsupplies.com.au
44 Australasian Dental Practice July/August 2022
spectrum | NEWS





PA R AMOUNT PROCESSING VERSATILE,CLINICAL LY PROVEN , ESTHETIC ZIRCONIAFOR THE HI G HEST REQUIREMENTS zolid zirconia YEARS AMANNGIRRBACH YEARS AMANNGIRRBACH 15 10 YOU DON’T LIKE SURPRISES? THEN TAKE ZOLID. Zolid-Webinars: Program and dates at academy.amanngirrbach.com/en/webinar #NoSurpriseZirconia www.amanngirrbach.com/zolid Amann Girrbach AG Tel +43 5523 62333-105 www.amanngirrbach.com Tel 02 8575 8675 sales@innovatiodentalsupplies.com.au www.innovatiodentalsupplies.com.au
Laurence Walsh AO is a clinically active specialist in special needs den tistry who is based at the University of Queensland in Brisbane. Laurie has been teaching infection control and clinical microbiology for over 25 years at postgrad uate level and has been the chief examiner in microbiology for the RACDS for the past 20 years. He has presented invited courses and lectures on infection control across Australia and internationally. Laurie has written over 60 articles on infection control and in addition published over 320 journal papers and a further 190 technical reports and literature reviews. He serves on two committees of Standards Australia (personal protecting equip ment; and instrument reprocessing) and in recent years has been an adviser to the Communicable Diseases Network of Australia and the Australian Commission on Safety and Quality in Health Care. Laurie has been a member of the ADA Infection Control Committee since 1998. He has contributed to various protocols, guidelines and checklists and manuals used in Australia.





Register Now: www.boosterinjection.com.au REGISTRATION FEES Dentists $660 inc gst Others $330 inc gst REGISTRATION INCLUDES n On-Demand access to 26 Online Learning Videos (Over 6 hours of education). n Online Learning Companion Booklet. n Suggested Reading Material Booklet. n Access to regular Q&A Webinar(s). n Online Questionnaire to earn 6 Hours of CPD. Infection Contol Boot Camp is presented by Dentevents, a division of Main Street Publishing Pty Ltd ABN 74 065 490 655 • www.dentevents.com • info@dentist.com.au Tel: (02) 9929 1900 • Fax: (02) 9929 1999 • Infection Contol Boot Camp™ and Dentevents™ are trademarks of Main Street Publishing P/L © 2020 Main Street Publishing Pty Ltd dentevents.tv
Register Now: www.boosterinjection.com.au REGISTRATION FEES Dentists $660 inc gst Others $330 inc gst REGISTRATION INCLUDES n On-Demand access to 26 Online Learning Videos (Over 6 hours of education). n Online Learning Companion Booklet. n Suggested Reading Material Booklet. n Access to regular Q&A Webinar(s). n Online Questionnaire to earn 6 Hours of CPD. Infection Contol Boot Camp is presented by Dentevents, a division of Main Street Publishing Pty Ltd ABN 74 065 490 655 • www.dentevents.com • info@dentist.com.au Tel: (02) 9929 1900 • Fax: (02) 9929 1999 • Infection Contol Boot Camp™ and Dentevents™ are trademarks of Main Street Publishing P/L © 2020 Main Street Publishing Pty Ltd FULL UPDATE! All the changes to Infection Control Guidelines in 2020 dentevents.tv
Professor
All Zirkonzahn implant abutments include a warranty for up to 30-years

As one of the world’s largest manufacturers of implant prostethic components, Zirkon zahn use a high-quality medical titanium alloy (Ti-6Al-4V ELI according to ASTM F136 and ISO 5832-3) and meet the strictest quality criteria (ISO 13485 MDSAP; Medical Device Directive 93/42/EEC; EU Regulation 2017/745 on medical devices). All components are conceived and manufactured at Zirkonzahn production sites in South Tyrol, Italy and in addition to the legally prescribed warranty obligation - the company offers up to 30 years warranty on all Zirkonzahn implant abutments used (titanium bases, Multi Unit Abutments, Multi Unit Abutments Angled and Raw-Abutments® as well as the corresponding screws). Within the current Zirkonzahn war ranty regulation, they explicitly also include implants from other manufacturers used with Zirkonzahn implant abutments.
Zirkonzahn Implant Prosthetic Components
For more than 140 implant systems, the Zirkonzahn Portfolio consists of a great range of TGA approved products: regular titanium bases, Scanmarkers, White Scanmarkers, ScanAnalogs (laboratory analogues used as Scanmarkers), impression copings, laboratory analogues, Multi Unit Abutments, Raw-Abutments and healing caps. All implant prosthetic components are 100% integrated into the Zirkonzahn workflow via corresponding libraries. Exocad® and 3Shape® users are also able to download and implement Zirkonzahn components for free in their design software through a dedicated portal (Zirkonzahn Library Down load Center). The product line has been recently expanded with new innovations and new products (See Table 1).
Table 1. New products and innovations
n Zirkonzahn LOC-Connector, a snap attachment system for implants and bars to fix removable dental prostheses on the implant.
n Multi Unit Abutment 17°, characterised by a 17° angle and two different anti-rotation connection types to compensate for any implant inclinations.
n Titanium Base K85, with the chimney height adjustable to the individual tooth length.
n Titanium Base K80 Angled Screw Channel, with a chimney height adjustable to the tooth length and the possibility to tilt the screw access channel from 0° to 30°.
n White Metal Scanmarkers, reusable Scanmarkers to acquire the implant position and orientation during intraoral and model scans.
All components are developed and produced at the Zirkon zahn Molaris I and II production sites in South Tyrol, Italy. Here, highly accurate techniques and versatile pro CNC machinery with turning, grinding and coating systems are used to produce milling tools, implant abutments and machine parts.
To exlore the renewed range of prosthetic components from Zirkonzahn, visit www.zirkonzahn.com and check if they are compatible with your implant system!
48 Australasian Dental Practice July/August 2022
spectrum | NEWS
Figure 1. Zirkonzahn’s wide range of TGA approved implant prosthetic components available for more than 140 implant systems.





























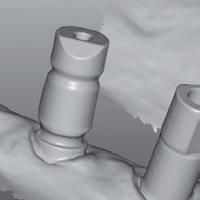

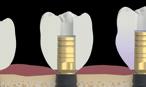
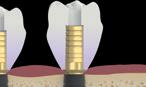




ZIRKONZAHN LIBRARY DOWNLOAD CENTER With the free Zirkonzahn Library Download Center, all components are also available for exocad ® and 3Shape users IMPLANT PROSTHETIC COMPONENTS – EVERYTHING UNDER ONE ROOF UP TO 30-YEAR WARRANTY high quality by zirkonzahn White Metal Scanmarkers – For acquiring implants position and orientation during intraoral or model scans Titanium base K85 – With adjustable chimney height Zirkonzahn Multi Unit Abutment 17° – With an angle of 17° to compensate for any implant inclinations and with two different connections Zirkonzahn LOC-Connector –Snap attachment for implants and bars used to fi x removable dental prostheses on the implants Titanium base K80 Angled Screw Channel (ASC) – With adjustable chimney height and screw access channel (0°-30°) *NEW COMPONENTS, MORE OPTIONS! NO LIMITATIONS! USE OUR TGA APPROVED COMPONENTS WITH MORE THAN 140 IMPLANT SYSTEMS Zirkonzahn Worldwide – T +39 0474 066 680 – info@zirkonzahn.com – www.zirkonzahn.com
Cameras boost case acceptance
Intraoral cameras have become something of a game changer in progressive dental practices, offering far more than a convenient diagnostic aid.
Increasingly, intraoral cameras like the Sopro 717 and high-end SoproLIFE and SoproCARE diagnostic cameras with built-in caries detection and periodontic functions, are providing added value in terms of patient communication, case acceptance and patient retention.
A-dec Product Marketing Manager, Shal Hafiz says more and more patients are becoming involved in their treatment planning and are self-diagnosing both aesthetic and functional flaws.
Intraoral cameras help to demonstrate treatment value visually by communicating information to the patient in real time through visuals rather than words. This makes the practitioner’s job much easier, overcomes miscommunication and greatly boosts case acceptance, ongoing treatment and the patient’s trust.
Mr Hafiz says there is a strong argument that cameras should be introduced into all consultations to aid diagnosis, provide a medico-legal patient record and to aid patient education, treatment planning and case acceptance.
He said the popular Sopro 717 has become the workhorse of many practices because of its ease of use, high resolution images and its compatibility with digital workflow.
“This enables live images to be captured at the swipe of a button and then easily saved to the patient record, so that patients’ oral health can be studied more closely on a large screen and monitored over time or utilised for future reference.”
Mr Hafiz said what is most interesting to hear is the amount of “self-diagnosis” patients do when they see their teeth close-up.
“Patients are opting in for both cosmetic and functional treatments to address anything from cracks and replacing old restorations to ortho and implants. This is not only a great ‘practice builder’ in terms of return-on-investment, but probably more importantly builds patient trust in their practitioner. There is simply nothing like ‘seeing it with their own eyes’ to buy into the recommended treatment plan,” Mr Hafiz said.
A-dec is making the choice of intraoral camera easy for practi tioners with a range of Acteon’s leading Sopro intraoral cameras and diagnostic aids which integrate easily into the A-dec delivery system. This allows images to be displayed on a video monitor in real time, as well as captured for further diagnosis and patient consultation. One of the most popular cameras, the Sopro 717, provides up to 115x magnification, helping locate problems that are not easily visible to the naked eye or even when using loupes.
For more in-depth analysis and to support minimally inva sive dentistry, A-dec also offers the advanced SoproLIFE (Light Induced Fluorescence Evaluation) caries detection aid with its unique diagnostic and treatment modes. In diagnostic mode, using reflected fluorescent light, SoproLIFE can detect demin eralised dentine and carious lesions which may not show up on X-rays or during a physical examination.
In treatment mode, the caries detection function helps the prac titioner pinpoint the extent of the caries during excavation of the tooth under magnification, so that only infected tissue is removed.
In this way, the use of SoproLIFE improves the accuracy of both diagnosis and treatment.
SoproCARE also uses fluorescent light to help identify biofilm and early plaque build-up without messy disclosing solutions, which makes it especially useful for hygienists and oral health therapists. It also includes a caries detection function.
Intraoral cameras also aid in early detection of other oral health problems. What might start out as an appointment for a simple clean may reveal early-onset caries, gum disease, cracks and fissures - and even suspicious oral lesions such as mouth cancers - allowing these conditions to be identified early and referred on for further investigation and treatment as needed.

Mr Hafiz said the complete Acteon range of cameras were part of the Sopro Imaging software suite which enabled images to be captured, filed and shared on an open-source database – together with images from Acteon X-ray machines, PSPIX phosphate plate scanners and Sopix or U-SENSE digital sensors.
The Sopro range of cameras and Acteon X-ray units, PSPIX phosphor plate imaging devices and Sopro digital sensors are available from A-dec in Australia.
Contact 1800-225-010 for year nearest authorised A-dec dealer or visit australia.a-dec.com or acteongroup.com for more info.
50 Australasian Dental Practice July/August 2022 spectrum | NEWS


ENHANCE YOUR VISION Scan the QR code or call 1800 225 010 to contact your local A-dec dealer JAD2200041
IT’S TIME TO
Carestream Dental’s CS 9600 wins Cellerant Best of Class Award again!
Carestream Dental’s intelligent CS 9600 CBCT imaging system has received its fourth Cellerant Best of Class Technology Award. The machine combines powerful imaging, advanced software and artificial intelligence (AI) to make it Carestream Dental’s “smartest” imaging system to date.

The five-in-one system’s intuitive fea tures make patient positioning easier for first-time-right imaging every time and AI technology automatically detects and traces the Frankfort plane. The CS 9600’s pre-set programs, quality control tools and ability to automatically detect when the wrong accessory is selected all go into making the system a winner.
“When you can avoid mistakes that lead to retakes you have more time for diagnosis and patient care,” said Stephane Varlet, global product line manager for extraoral imaging, Carestream Dental. “Years ago, I helped a doctor who was unhappy with the image quality of his system—upon closer inspection it turns out that an accessory was inserted incor rectly. That kicked off the inspiration for the CS 9600: A system that doesn’t just
capture high-quality images but make it easier and more intuitive to capture those images.”
Those easy, intuitive features are what led to the CS 9600 being selected to receive the 2022 Cellerant Best of Class Technology Award by a panel of the most prominent technology leaders in dentistry. Since the inaugural presentation in 2009, the Best of Class Technology Awards have grown to occupy a unique space in dentistry by creating awareness in the community of manufacturers that are driving the discussion as to how practices will operate now and in the future.
The CS 9600 is available in three edi tions with 10, 12 and 14 fields of view (FOV)s. In addition to 2D and 3D imaging and object scanning, practices have the option to include face scanning or a scanning cephalometric arm. Addition ally, the optional CS UpStream program helps Carestream Dental’s support team monitor historical performance and pre vent downtime and maximize system availability. Today, there are nearly 2,000 CS 9600 systems installed worldwide that have captured a combined 5 million acquisitions.
The CS 9600 is also the recipient of a 2021, 2020 and 2019 Cellerant Best of
Class Technology Award, as well as a 2019 Edison Award seal in the Medical/ Dental Diagnostics category and the Krak dent Medal of the Highest Quality from the International Fair KRAKDENT® .
For more info on the Cellerant Best of Class Awards and the 2022 Winners, go to cellerantconsulting.com/bestofclass.
For more information about the CS 9600, visit carestreamdental.com/CS9600. Learn more about Carestream Dental, and all its innovative solutions, at carestreamdental.com/en-au
Cellerant Consulting Group
F ounded and led by CEO Lou Shuman, DMD, CAGS, Cellerant provides strategic dental market insights, clinical expertise, implementation resources and support to accelerate growth for client dental companies. Cellerant ser vices include new concept incubation, clinical product evaluation, product development, continuing education pro gram development and CE sponsorship, strategic branding and marketing, online marketing, content marketing and dental media relations management.
52 Australasian Dental Practice July/August 2022
spectrum | NEWS
The CS 9600 has won more Best of Class Technology Awards than any other extraoral imaging system.
Seeing the difference makes a difference
See CBCT in a new light with CS 8200 3D NEO EDITION. It is the versatile 4-in-1 imaging system that creates new possibilities with capabilities such as an intuitive user interface, 9 fields of view and low-dose panoramic imaging. carestreamdental.com/8200 anz-enquiries@csdental.com

CS 8200 3D NEO EDITION Extended capabilities for new opportunities
1800 223 603
Periodontology a key focus at IDS as the greatest show celebrates 100 years

Two new “fixed stars” are giving periodontology a clear direction: the valid S3 guideline and the COVID-19 triggered insight into the close connection between oral health and general health. Both impulses generally bring about opportuni ties for the dental practice, especially for the periodontal team and in a wider sense also for the dental laboratory. The 40th International Dental Show (IDS) shows the possibilities and offers the opportu nity for a professional exchange like no other industry event - coming up soon in Cologne from 14 to 18 March 2023.
The S3 guideline of the European Fed eration of Periodontology (EFP) has been implemented in Germany for peridontal therapy since mid-2021. This has caused a row of positive impulses. In this way, the “periodontal explanation and therapy dis cussion” (ETD) and the “patient-specific oral hygiene instruction” (OHI) can be invoiced according to the nationwide fee schedule (BEMA). This underlines the sig nificance of consistent periodontal therapy and prophylaxis. Its main goal is to involve the patient in all four therapy stages. This is why domestic oral care, where applicable smoking cessation and optimal diabetic control already play important roles. For example, periodontitis encourages a row of diabetes-related secondary diseases and can increase the mortality rate.
This shows the close connection between oral health and general health. Furthermore, periodontitis is linked to rheumatism, heart attacks, strokes and chronical respiratory diseases. This has only become evident to a high number of patients as a result of the findings of the COVID pandemic. A broad cross-section of the public knows: Thorough periodontal therapy and prophylaxis can help prevent a severe case of COVID-19. Because COVID-19 patients with periodontitis are at higher risk of having a more severe case of the disease. Hence, the patient may pos sibly have to be admitted to intensive care or require artificial respiration.
Patients take note of such strong restric tions to the quality of life and can be won over for consistent prevention and therapy. The periodontal team encounters a strong readiness to carry out precautionary meas ures because the periodontal therapy and prophylaxis is considered to be essential due to the COVID-19 catalyst. And thanks to the far-reaching state-paid services pursuant to the new S3 guideline, the nec essary measures can normally be invoiced much more simply than before and are thus easier to calculate economically.
As is the case for domestic oral care, periimplantitis is also gaining in signifi cance in the dental practice. In contrast to periodontitis, special features have to be heeded. For example, special nonvibrational ultrasonic systems that purely work with vertical oscillations can be implemented for the removal of tartar and calculus. An airflow device may need an application to clean pockets that are much deeper than just two millimetres subgin gival. A swab soaked in CHX can be used as an antiseptic measure. A tight connec tive tissue collar can then be applied for example with the help of a very strong alkaline pH value. Subsequently the activity of the osteoclasts are reversibly inactivated using a collagenase inhibitor to prevent bone from growing and/or to balance out the bone remodelling.
The trusted aids are available for domestic oral care: Toothbrushes, tooth paste, dental floss, etc. Mouthwashes also prove to be effective in reducing the risk of a COVID infection which - according to surveys carried out at the Claude Bern hard Lyon University - already reduce the viral load in the mouth by 71% after just one single rinsing and which support the immune system in fighting an infection.
Especially in the case of periimplantitis, it is recommended to use antibacterial and anti-inflammatory toothpaste on an inter dental brush in addition to the customary cleaning routines. In this way, the active ingredients reach the boundary surfaces between the implant and the tissue while brushing one’s teeth. The background of this strategy is that unlike a natural tooth, the implant receives no special protection through the gingival crevicular fluid.
Manual tools and ultrasonics are used for the professional removal of plaque.
In the case of well-advanced periodon titis, soft tissue surgery may be necessary in line with the S3 guideline in therapy stage 3. For the subsequent tissue regener ation, autologous blood concentrates such as PRF (platelet-rich fibrin) could play a more significant role in future. They are obtained from the centrifugation of patient blood from the peripheral blood vessels.
“The differentiated approaches show how individually the therapy and prophylaxis of periodontitis and periim plantitis are contemplated and carried out,” summed up Mark Stephen Pace, Chairman of the Association of German Dental Manufacturers (VDDI). “Since the respective measures have an impact on much more than the mouth, going to the dentists is an essential element in a com prehensive prevention strategy. As the leading trade fair of the dental industry, IDS 2023 offers the ideal opportunity to inform oneself about current concepts and tools for successful and efficient dental care and to engage in an exchange with professionals.”
IDS takes place in Cologne every two years. It’s taking place for the fortieth time in 2023 and was founded 100 years ago. For info, see www.ids-cologne.de
54 Australasian Dental Practice July/August 2022 spectrum | NEWS
OrthoED’s MiniMasters is a fully accredited 2-year orthodontics course with an optional post-graduate diploma. Using comprehensive and sound principle-based training, GP’s will learn to think for themselves, treat a range of cases,
OrthoED’s MiniMasters is a fully accredited 2-year orthodontics course with an optional post-graduate diploma. Using comprehensive and sound principle-based training, GP’s will learn to think for themselves, treat a range of cases, and foresee problems before they arise.
OrthoED’s MiniMasters is a fully accredited 2-year orthodontics course with an optional post-graduate diploma. Using comprehensive and sound principle-based training, GP’s will learn to think for themselves, treat a range of cases, and foresee problems before they arise.
GP’s will also receive ongoing case support from our myth-busting orthodontist, Dr Geoffrey Hall. So at the end of the course, they will be fully equipped to complete cases more efficiently, confidently, and with predictable outcomes every time.
GP’s will also receive ongoing case support from our myth-busting orthodontist, Dr Geoffrey Hall. So at the end of the course, they will be fully equipped to complete cases more efficiently, confidently, and with predictable outcomes every time.
GP’s will also receive ongoing case support from our myth-busting orthodontist, Dr Geoffrey Hall. So at the end of the course, they will be fully equipped to complete cases more efficiently, confidently, and with predictable outcomes every time.

As part of the course, you’ll enjoy modules on
As part of the course, you’ll enjoy modules on
As part of the course, you’ll enjoy modules on
Diagnosis, treatment planning, risk management, and
Enrol in OrthoED’s Mini Masters 2023 program today.
Email geoff@orthoed.com.au or call 1300 073 427 secure one of the limited spots available for face to face or online learning.
Visit
www.orthotraining.com.au/testimonials and hear what other students say about

The OrthoED Mini Masters is back and better than ever!
in OrthoED’s Mini
Diagnosis, treatment planning, risk management, and the art of excellent case presentation Orthodontic brackets, wires, auxiliaries, bracket placement and indirect bonding and biomechanics Orthodontic bracket prescriptions, risk analysis, orthodontic mechanics for nonextraction and extraction cases Early orthodontic treatment, including facial growth and dental development Clear Aligner therapy Aesthetic and accelerated orthodontics, TMJ and sleep apnoea Advanced biomechanics Management of severe skeletal and dental discrepancies IDT and management of difficult orthodontic problems and malocclusions, digital smile design (DSD) Want to learn orthodontics the easy and predictable way? More hands-on training Two extra days of Aligner education A live stream option of the program, plus, All the latest orthodontic knowledge in the industry! OrthoED’s best-selling course was SOLD OUT for 2022, but enrolments for 2023 are now OPEN! We’ve made some significant improvements to our course! The OrthoED Mini Masters 2023
Do you want to stop referring patients outside your practice? Are you interested in practising orthodontics but scared about getting it wrong?
Enrol
Masters 2023 program today. Email geoff@orthoed.com.au or call 1300 073 427 secure one of the limited spots available for face to face or online learning. Visit www.orthotraining.com.au/testimonials and hear what other students say about the OrthoED program and why they all give 5 star reviews every time
now comes with:
The OrthoED Mini Masters is back and better than ever!
case presentation
wires, auxiliaries,
and
Early
dental
Clear Aligner therapy Aesthetic and accelerated orthodontics, TMJ and sleep apnoea Advanced biomechanics Management of severe skeletal and dental discrepancies IDT and management of difficult orthodontic problems and malocclusions, digital smile design (DSD) Want to learn orthodontics the easy and predictable way? More hands-on training Two extra days of Aligner education A live stream option of the program, plus, All the latest orthodontic knowledge in the industry! OrthoED’s best-selling course was SOLD OUT for 2022, but enrolments for 2023 are now OPEN! We’ve made some significant improvements to our course! The OrthoED Mini Masters 2023 now comes with: Do you want to stop referring patients outside your practice? Are you interested in practising orthodontics but scared about getting it wrong?
the art of excellent
Orthodontic brackets,
bracket placement and indirect bonding
biomechanics Orthodontic bracket prescriptions, risk analysis, orthodontic mechanics for nonextraction and extraction cases
orthodontic treatment, including facial growth and
development
The OrthoED Mini Masters is back and better than ever! Enrol
auxiliaries,
bracket prescriptions, risk
mechanics for nonextraction and extraction cases
orthodontic treatment, including facial growth and dental development Clear Aligner therapy Aesthetic and accelerated orthodontics, TMJ and sleep apnoea Advanced biomechanics Management of severe skeletal and dental discrepancies IDT and management of difficult orthodontic problems and malocclusions, digital smile design (DSD) Want to learn orthodontics the easy and predictable way? More hands-on training Two extra days of Aligner education A live stream option of the program, plus, All the latest orthodontic knowledge in the industry! OrthoED’s best-selling course was SOLD OUT for 2022, but enrolments for 2023 are now OPEN! We’ve made some significant improvements to our course! The OrthoED Mini Masters 2023 now comes with: Do you want to stop referring patients outside your practice? Are you interested in practising orthodontics but scared about getting it wrong?
in OrthoED’s Mini Masters 2023 program today. Email geoff@orthoed.com.au or call 1300 073 427 secure one of the limited spots available for face to face or online learning. Visit www.orthotraining.com.au/testimonials and hear what other students say about the OrthoED program and why they all give 5 star reviews every time Diagnosis, treatment planning, risk management, and the art of excellent case presentation Orthodontic brackets, wires,
bracket placement and indirect bonding and biomechanics Orthodontic
analysis, orthodontic
Early
and foresee problems before they arise.
How can you make a practice more efficient?
Dentistry has gone through many changes over the past two years with factors such as the pandemic and staff shortages to name a few. All dentists and practice staff understand these challenges well, yet finding ways to work with them and remain efficient as a business is the key to navigating them, both now and for the future.
The solution
Practice efficiency is not necessarily about speeding up treatment time but about streamlining all the peripheral, but necessary, elements of a dental appoint ment, leaving more time for the clinical aspects and reducing the frustrations often experienced at the front desk.
Introduce patient portal
Patient Portal allows practices to send forms direct to a patient’s mobile device, prior to an appointment, ena bling patients to complete forms at home, in advance. This benefits the practice, reducing the time needed for adminis trative tasks and avoiding duplication of effort. Better still, patients spend less time in the surgery, which is a real bonus especially if they are busy or anxious.
Offer online appointment booking
The technology required to streamline these workflows is already here, along with the expert help and advice to integrate the systems that can transform the future of your practice. EXACT, the leading prac tice management solution, helps dental practitioners like you to automate many of the tasks that would have once been des ignated to admin staff, not only elevating practice efficiency but providing your team with the time they need to:
• Focus on delivering an enhanced patient experience;
• Manage their workload more effectively and reduce work-related stress; and
• Drive success and hit those all-impor tant practice KPIs.
Here’s just a few ways how...
This, alongside tools such as automated recalls/reminders and remote form filling, means that as a practice you can ultimately rest easy knowing your dental software is taking care of the “boring stuff” while you can get back to delivering your vital services safely.
The switch
While transitioning to a new Practice Management System can feel daunting, EXACT offers support every step of the way, allowing you to turn challenges into success.

O
nline booking is now considered the norm. Integrating this small change can make a dramatic difference to the patient’s overall experience, providing a higher level of convenience and less admin work for the reception team.
Streamline form filling
Creating a digital workflow for forms smooths out the experience for patients and reduces duplications and the chance of error. Clinipad provides a streamlined way for patients to update their medical history and consents, as well as including a host of other forms. Completed forms are submitted electronically and sent direct into the patient’s file - eliminating the need for scanning and document filing.
Their hands-on approach, means they take the stress away from you; guiding you at every stage, with all the tools and support you need to run a great business, so you can focus on more of what matters - patient care.
“The transition was much easier than I thought it would be. EXACT is very log ical,” said Dr John Collins from Collins Dental House in Perth.
With its combined range of software solutions and expert advice, EXACT will work with you to unlock the full potential of your practice. To join the thousands of dental practices across Australia that manage and grow their business with EXACT software, contact sales@henryscheinone.com.au or visit www.exactdental.com.au
56 Australasian Dental Practice July/August 2022 spectrum | NEWS
EXACT provides dentists all of the tools and data they need to make their patient experience better and their practices more profitable.
Receive customised support through our customer success programme
Optimise practice workflow efficiency
Hone skills of best practice with expert guidance and resource
Empower patients to take control of their contactless journey
Discover how automation can streamline admin tasks to free up your team’s time Visit
at
us
exactdental.com.au
Inaugural ADX in Brisbane this October 27-29
Australia’s premier dental event, ADX is heading to Brisbane for the first time! The Australian Dental Industry Association (ADIA) is busy preparing three full days of ADX, to be held from 27-29 October 2022 at the Brisbane Con vention and Exhibition Centre, 10am to 6pm. ADX Brisbane will host 150 exhibitors in 400 booths across 10,000 m2 of exhibition space, featuring the latest oral health tech nology and innovation the Australian dental industry has to offer.
And that’s not all! There’s plenty of action running alongside the exhibition, with two major breakfasts, free childcare, Learning Lab sessions and an expert CPD program presented by ADAQ. The Continuing Professional Development Program helps oral health profes sionals enhance their clinical practice and improve patient outcomes. The program includes more than 50 expert speakers delivering 60 sessions over the 3 days.
To further maximise the education offering at ADX Bris bane, ADIA will also hold business-focused Learning Lab sessions throughout the exhibition, welcoming a variety of pro fessional speakers. While the CPD Program provides further clinical education, the Learning Labs prioritise skills that sup port efficiency and profitability in your business.
The Opening Breakfast at 7.45am on Thursday 27 October is the perfect way to kick off your first day at ADX Brisbane. Net work with friends and colleagues and enjoy a great meal, before entertainment and mascots lead visitors to the exhibition floor.
The Women in Dentistry Breakfast is a great way to start your weekend on the final day of ADX Brisbane. Celebrate and support the success of women in dentistry over a delicious breakfast accompanied by an inspirational speaker and quality networking on Saturday, 29 October, again at 7:45am.
ADX Brisbane also lets you take the pressure off with free on-site childcare. Professionals will ensure your child is happy, entertained and rested while you make the most of your ADX Brisbane experience and networking opportunities. Free child care at ADX Brisbane will be available for the whole show including the breakfasts.

For further details about ADX Brisbane, visit the website at www.adxbrisbane.org.au
International Update
Oral microbes are dispersed during dental treatment and reduc tion methods have been proposed. Methods to mitigate dispersion or microbial load, such as dental suction, dental dam and antimicrobial mouthrinses, have been studied, but few authors have examined the effect of dental unit waterline (DUWL) disinfectants on microbes contained within dental bioaerosols and their effect on viruses has not been studied. Products are available for peri odic DUWL disinfection, including those intended for continuous use at concentrations safe for patients This study investigated the effect of the DUWL disinfectant product ICX on viral dispersion in dental bioaerosols. It also established a dual-tracer system using live bacteriophage and fluorescein supported by optical particle measurement. Bacteriophage MS2 was used as a viral tracer and fluorescein as a fluorescent tracer. Validation experiments were conducted to exclude interference of one tracer with the other or of DUWL disinfectants on detection methods. Simulated “saliva” containing the tracers was infused into the mouth of a dental man nequin during 10 minute dental procedures with an air turbine handpiece (n = 3 replicates). Aerosols and droplets were sampled in an enclosed dental operatory using air samplers and settlement onto sterile filter papers. Bacteriophage was quantified using plaque assays and reverse transcription quantitative polymerase chain reaction (RT-qPCR). Fluorescein was quantified fluorometrically. The effect of DUWL disinfectants on total aerosol concentration was assessed in separate experiments using an optical particle counter. DUWL disinfectants reduced bacteriophage viability and interference between tracers was not observed. In simulated clinical procedures, the disinfectant ICX reduced bacteriophage detection substantially (P < 0.001; 2-way analysis of variance). MS2 RNA was detected in all experimental samples but not negative controls. Samples positive on RT-qPCR but not plaque assays may indicate that virions at distant sites are nonviable. Fluorescein tracer showed good agreement with the bacteriophage tracer. DUWL disinfectants designed for continuous presence in irrigants reduce the dispersion of viable virus in dental bioaerosols during simulated procedures. Their use may therefore be important for routine infection con trol and as a mitigation factor during infectious disease outbreaks. Future studies should explore this using a range of viruses and other microbes.
Allison JR et al. Waterline disinfectants reduce dental bioaerosols: a multitracer validation. J Dent Res. 2022. 1010(10):1198-1204.

Waterline treatment agents reduce the dispersion of viruses in dental aerosols
spectrum | NEWS 58 Australasian Dental Practice July/August 2022
• Opening Breakfast • Free childcare • Free business growth seminars • Latest technology & innovations • Women in Dentistry Breakfast • Australian Dental Association Queensland professional CPD program Brisbane Convention & Exhibition Centre Highlights include: REGISTER NOW AUSTRALIA’S PREMIER DENTAL EVENT See you at 27 - 29 October 2022 @ausdental / ADX expo @ ad x expo adxbrisbane.org.au FREEENTRY #ADXexpo #ADXBrisbane
Top 10 things to consider when buying an intraoral scanner
By Dr Ahmad Al-Hassiny
Buying an intraoral scanner is one of the most important investments in your dental career. It used to be tough to convince dentists to go digital; now it’s clear that digital is not only the future, but it’s also the here and now. By not adopting digital dentistry, you’re offering your patients substandard service.


The benefits of intraoral scanning are endless...
• It’s a huge timesaver: Instead of forcing your patient to sit still for 3-5 minutes and then sending impressions to the lab that have numerous errors you didn’t know about, you can now take digital impressions in under 45 seconds and ultimately have a higher hourly rate per day (if you know what you’re doing);
• Much more comfortable: You put a lot of effort into making your dentistry suave, impressive and ele gant, however, this is completely undermined when you take out the messy gloop that feels disgusting in the patient’s mouth to take a physical impression; and
• Exceptional accuracy: Intraoral scans are extremely accurate and reduce the need for redos if you know what you’re doing. This helps speed up your workflows, impresses your patients and eliminates needless stress in your life. Never forget - operator error is the number one reason for any issues!
60 Australasian Dental Practice July/August 2022
But, there’s one thing working against you when trying to buy an intraoral scanner for your dental clinic.
The intraoral scanning market has a lot of players and they all want your money. So, a lot of the information you find out there is incredibly biased.
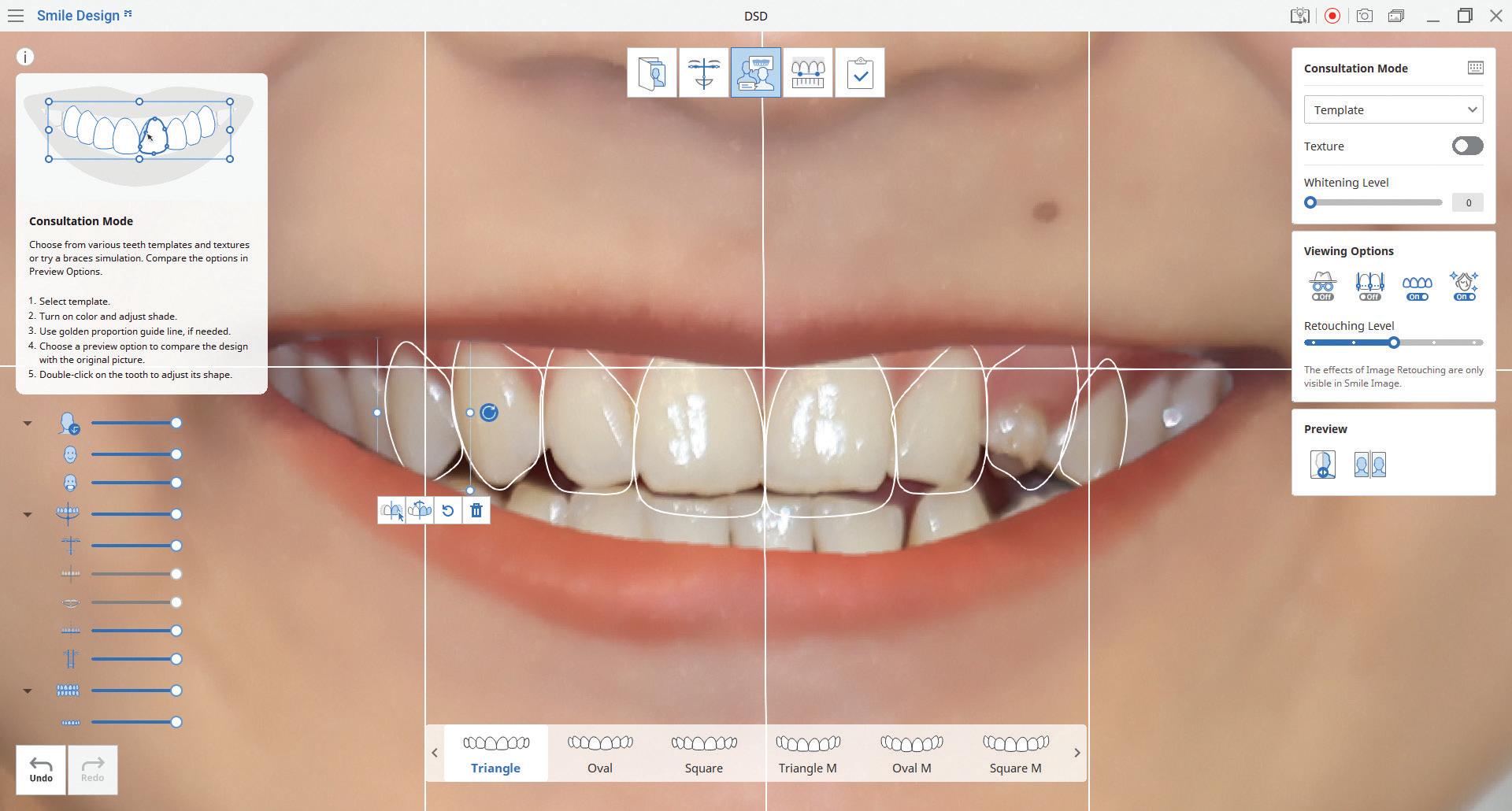
Below are some things you need to consider when purchasing an intraoral scanner, but if you’re looking for unbiased reviews on nearly every intraoral scanner available, check out our scanner reviews. They’re completely free and you can even download the full pdf so you can print it out and make comparisons (See the link at the end of the article. Disclaimer: It’s worth noting that the pricing and avail ability of intraoral scanners is dependent on your location, as such, some of our reviews might contain different infor mation than what you will see on your distributor’s website).
Support
How well you’re going to be supported AFTER buying your intraoral scanner is probably the single most important thing to consider.
Before purchasing, many companies will persuade you that they’re only a phone call away if something goes wrong. However, when the time comes to actu ally support you, you’re greeted with an automated answering machine and your emails never get a response.
Support encompasses a few different areas. Such as:
• Training;
• Support and troubleshooting;
• Continuing education and community forums;
• Do they follow up after you’ve expressed the need for help?
• If they release new features, will they tell you about them or train you?
• Are they motivated to support you or simply see you as a walking dollar sign?
The truth is, there’s a lot of similarities between various brands of scanners. What really sets each company apart is how they look after the people that have purchased from them or how good their distributor network is.
If something goes wrong, you want to know that you can get in contact with someone who knows what they’re talking about - not just passed off to some sales rep who knows less than you do.
Figure 1. Make sure training and support are available before purchasing a scanner.
Figure 2. Check what software comes with the scanner and whether it suits your needs.
For example, 3Shape has a great academy that offers a multitude of study materials, YouTube tutorials and training. Medit also have an academy and they’re renowned for their customer support. The Institute of Digital Dentistry also offers a wide range of online training on dif ferent intraoral scanners as part of our affordable Membership.
2. Cost
While support will help you separate the good from the bad, cost is prob ably going to be the one thing that dictates what scanner you’ll start researching.
The good news is that the price of scan ners has decreased dramatically over the years. There used to only be a few scan ners on the market, all retailing for around $50,000 to $60,000. Nowadays, you can get some great quality scanners for as little as $12,000. For example, Medit has some great low-cost intraoral scanners that are really high quality.
On the other hand, the Primescan is one of the most high-tech scanners available and the gold-standard for same day den tistry - however, it is priced accordingly.
You can find a great scanner to fit any budget, you just need to decide how much you can spend and what you want it for.
3. What software comes with your scanner?
Depending on what you want to do with your scanner, seeing what additional software comes with it is really important.
Some scanners come with software that is just for scanning and exporting files. That’s it. Others come with a full suite of patient engagement tools such as orthodontic simulators, smile design, etc. Lastly, some scanners are made for CAD/CAM and have full CAD software included for production in-house.
It’s important to think about what you want a scanner for and ensuring you are getting the right software. 88
July/August 2022 Australasian Dental Practice 61 high | TECH
For example, 3Shape and Medit have some great apps such as Ortho Simula tion, Smile Design and Model builders. CEREC has basically no ‘apps’ but has arguably the best chairside CAD software for crown and bridge work.
If you’re considering a scanner, it is crucial to consider what is important for you. Are patient engagement tools critical or do you just want an impressionreplacement device?
4. Image quality
Image quality is incredibly important when purchasing an intraoral scanner. If you buy one that has substandard image quality, it can make sending the scans to your lab an absolute nightmare.
Luckily, most companies are mostly open about their image quality, especially if you get in contact with a sales rep and ask about it so you can compare.
If you can’t find the image quality spec ifications you need, you can always look up photos of our scanner reviews online and see how the image quality compares amongst different brands.
5. Open source or closed
Whether or not open source mat ters to you is entirely based on what you want to do with your scanner. Thankfully, every single scanner on the market is now open sourced to some degree - meaning scans can be exported in STL format.
Open source
Closed system
I
f you plan on simply scanning and then sending to your lab, you should check with your lab to see what file format they are comfortable with to make collabora tion as easy as possible.
The most common file types for are:
• STL - monochrome;
• OBJ - colour; and
• PLY - colour.
STL is the file type most commonly exported. But many scanners these days can also export OBJ and PLY which are colour files, which might help with identifying margins of equi- or subgingival preparations.
If you’re going to buy a scanner, defi nitely look into this and ensure your lab is comfortable using OBJ or PLY files.
If you plan on sticking with one brand, like Dentsply Sirona, then arguably a “closed” system is actually not such a bad idea.
It’s similar to Apple in terms of phi losophy. All your technology will work in conjunction with each other, which means everything is simplified and comes with an easy-to-follow workflow.
Having a connected ecosystem of soft ware and hardware can make life easier for you, however, it does limit flexibility in the future.
If you’re going to be venturing into CAD/CAM, in-office milling and other aspects of digital dentistry, when you start looking into milling machines you will come across closed systems.
For example, CEREC Chairside does not enable any third party scanner to be used with its chairside software. In saying that, closed systems like CEREC can be beneficial as they work a lot more seam lessly and less piecemeal than combining multiple systems together.
6. What treatments
While we’re big advocates for moving your workflow in-house and only referring really difficult things to your lab, the truth is a vast majority of clinicians are happy to just take scans and then send them off to the lab.
This is completely fine! 88
62 Australasian Dental Practice July/August 2022
do you want to offer?
high | TECH
Figure 3. Image quality is incredibly important when choosing an intraoral scanner.
THE AORALSCAN 3 IOS
AI INSIDE EVERY SCAN
With unprecedented scan speeds allowing you to scan a quadrant in 25 seconds, a full arch in 1 minute, and an entire ortho case in 3 minutes, the AORALSCAN 3 IOS promises faster appointment times and a more comfortable patient experience.
When you’re done scanning, its hassle-free exporting of STL and full-colour PLY scans, along with the license-free operation, means you can send to as many or as few labs as you like.
Every scanner package comes pre-installed with a suite of intuitive, doctor-friendly software, including:
Scan software - Intraoral scanning
Ortho simulator - Chairside orthodontic simulation
Healthcheck - Intraoral scaner + intraoral camera

Lab cloud - Seamlessly send scans your lab
Model builder - Base and export models to a chairside printer
Unlike many other scanners on the market, there are no ongoing license fees, and updates are free and automated, ensuring you enjoy the latest features as they’re released.
When you buy the AORALSCAN 3 IOS from Osseo Group, you’ll receive the scanner, PC, trolley, and ongoing clinical and technical support for one low price.
Visit osseogroup.com.au/aoralscan or scan the QR to learn more.
Visit osseogroup.com.au/demo or scan the QR to arrange an in-office demo.
$22,000+GST
ONLY
ANZ2022-1-AORALADP
However, it’s important to be honest with yourself and look into your future.
If at some point, you’re going to want to explore how you can do more than just take scans and send them off, you need to get an intraoral scanner that’s going to allow you to do more.
Are you eventually going to start doing digital implantology? Is smile design something that you could use to improve case acceptance and patient communica tion? Will you decide that 3D printing is something that interests you?
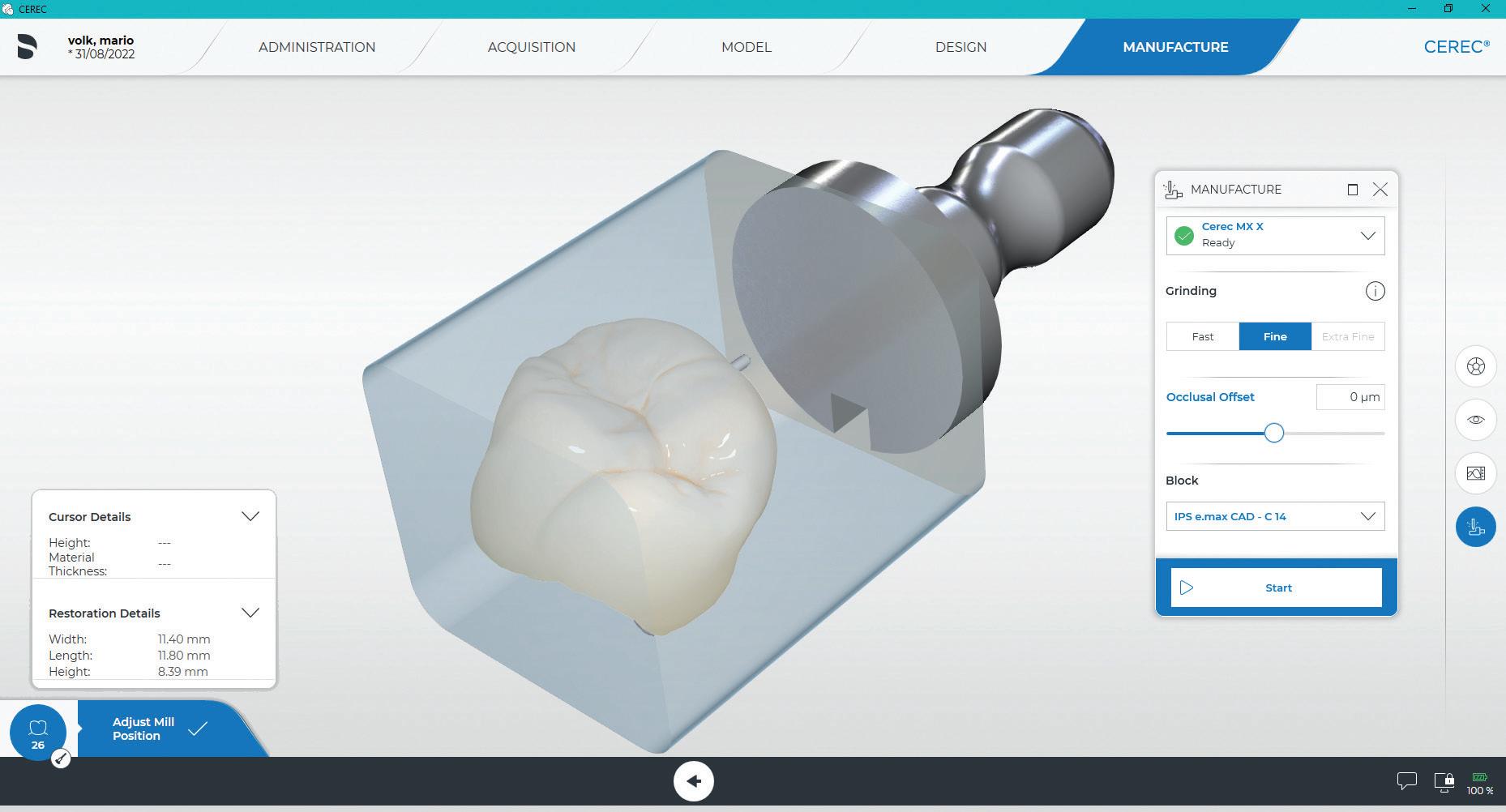
Whatever you decide to do, it’s impor tant to think about the future when you start looking for intraoral scanners that enable some form of CAD workflow. That way, you don’t back yourself into a corner and only offer one treatment.
8. Distributor reputation
As is the case when buying anything, it’s important to look at reviews from other dentists to see if the company you’re purchasing from is reputable. We are talking about the distributor now.
Google reviews, talk to fellow dentists, ask around in forums.
You want to be purchasing from a com pany that is known to be reputable and helpful. Like we said prior, support is key!
It’s also important to realise in some countries you can buy the scanner directly from the manufacturer (e.g. buying directly from 3Shape) while most of the time you will have to buy the scanner from a distributor.
10. Ease of use
Your definition of ease of use comes down to what you’ve purchased your intraoral scanner for and who’s going to be using it.
• Will you be teaching your clinical staff?
• Will you be collaborating with your lab?
• Are you a beginner in digital dentistry and need to learn the protocol?
All of these questions will dictate how important ease of use is. Some scanners are simply easier to use than others with many tutorials and sometimes an entire educa tion platform you can access freely. It is important to consider how easy the scanner will be to use for you and your staff.
And thats our top ten list!
When venturing into CAD/CAM, you will need software such as that sold by CEREC, 3Shape or exocad. Some scan ners have direct integrations to these software and some others do not.
7. Size of the scanner
The size of your intraoral scanner is defi nitely something you want to be aware of. You’re going to be holding it quite a bit, so make sure that it’s comfortable!
You will also want to compare the weight of different scanners you’re considering.
Additionally, you might find that wire less scanners are more comfortable for you, in which case you might want to con sider a wireless scanner such as TRIOS 4, TRIOS 3 wireless, CS 3800 or Medit i700. Check out our unboxing of the latest wire less intraoral scanner on the market - the Medit i700 Wireless.
Once again, check out our scanner reviews as we compare the ergonomics and size of each scanner.
Figure 4. Dentsply Sirona’s “closed” CEREC system does offer several advantages.
9. On-going fees
While subscription fees are mostly on the out for the majority of the digital dentistry industry, it’s impor tant to at least check if there will be any unexpected and/or ongoing costs when purchasing your scanner.
This can be in the form of:
• Membership fees;
• Annual fees/Subscription fees;
• “Clubs”;
• Fees for when you export files; and/or
• Ongoing equipment costs such as tips, consumables, etc.
As mentioned, subscription fees are mostly on the way out in the digital dentistry industry... but there are still companies that insist on charging you yearly fees, so keep a look out!
About the author
Dr Ahmad Al-Hassiny is a global leader in digital dentistry and intraoral scanners, carrying out lectures as a KOL for many leading brands. He is one of the few in the world who owns and has tested all main stream scanners and CAD/CAM systems in his clinic. Dr Ahmad Al-Hassiny is also the Director of The Institute of Digital Dentistry (iDD), a world-leading digital dentistry education provider. iDD offers live courses, masterclasses and an online training platform with a mission to ensure dentists globally have easy and afford able access to the best digital dentistry training possible.
Dr Al-Hassiny is in private practice in New Zealand.
Scan the QR code to view IDD intraoral scanner reviews or visit https://instituteofdigitaldentistry.com/intraoral-scanner-ios-reviews

64 Australasian Dental Practice July/August 2022 high | TECH
“Whatever you decide to do, it’s important to think about the future when you start looking for intraoral scanners that enable some form of CAD workflow. That way, you don’t back yourself into a corner...”
An


easy way to make a great impression
ivoclar.com Making People Smile Visit: bit.ly/3wrbIKR TELL ME MORE VivaScan® Compact and intuitive solution [1] for your entry into intraoral scanning Effortlessly easy integration into your practice [1] Lightweight and ergonomic design for a comfortable scanning experience [1]
[1] GlebovaT, Product Validation Report VivaScan, Test Reports, Ivoclar Vivadent, 2021.
Shining light on common misconceptions about the role of light in dental bleaching

Why
Question 1. Using an LED array in combination with a suitable whitening gel shows a gain in the effectiveness of the treatment in the order of:

a. 8-10%
b. 12-20% c. 24-28% d. 30-45% e. 50-62%
Question 2. Teeth are relatively transparent to wavelengths...
a. From visible green through to the near infrared region. b. In the far ultraviolet range. c. In the mid ultraviolet range. d. All of the above.
Question 3. Warming a bleaching gel with light facilitates the break down of hydrogen peroxide and can improve the overall bleaching effect that is gained:
a. True b. False
Question 4. Examples of whitening systems which use photodegradation are the...
a. HiSmile Vio 405 nm violet light. b. Smartbleach™ 535 nm visible green LED array. c. Deka Smartlite™ 532 nm KTP laser. d. All of the above.
Question 5. Studies show that violet light has no effect in reducing yellow stains unless an intervening oxidant is used like hydrogen peroxide...
a. True b. False
INSTRUCTIONS:
UVC light from 200-230 nm: A new way to improve air quality?
The problems of contamination of the dental working environment with particles of patient origin are well-known and similar con cerns exist for operating theatres, especially when more complex procedures such as organ trans plantation and the placement of joint prostheses are being undertaken.

The literature indicates that particular problems around contaminated material in the air occur during procedures such as ultrasonic scaling and the use of air powder polishing devices and high-speed air turbine drills. These problems are magnified when the operatory is small in size and has limited fresh air exchange through the air-conditioning system, hence allowing concentrations of particu lates in the air to increase over time in bursts, as various procedures are undertaken.
As well as aerosols generated during procedures, there are also issues with the movement of people in and out of rooms. This issue has been well docu mented in operating theatres, where the movement of personnel and the associated opening and closing of doors greatly increases aerosol concentrations.
While common sense would suggest that a simple approach using high efficiency particle air filtration may be highly effective at reducing the concentra tion of aerosols, to date the literature around this has reported mixed results, with real world studies involving aerosol sensors showing no benefit from area HEPA filters in the dental operatory.
On the other hand, recent literature supports the value of high volume evacuation (HVE) as an effective mitigation strategy that reduces aerosol concentrations, particularly when used with a wide bore tip and especially when that tip has a conical end that increases the surface area at the collecting end.2-4
Question 6. Which wavelength of light causes significant cellular and molecular injury, including damage to DNA?:
a. 200 nm b. 207 nm c. 222 nm d. 254 nm e. 289 nm
Question 7. Particular wavelengths of light that are of interest in infection control are 207 nm and 222 nm because:
a. Light in this spectral range can be generated cheaply by LEDs. b. Elemental mercury is not required in the light source. c. It can kill bacteria without causing harm to living tissue in humans. d. All of the above.
Question 8. Ultraviolet lamps emit light that... a. Is carcinogenic. b. Causes keratitis. c. Causes cataracts. d. Damages your DNA. e. All of the above.
Question 9. Light from 200 to 230 nm is...
a. Unable to penetrate through the stratum corneum of the skin. b. Unable to penetrate through the cell membrane of a human cell. c. Readily able to penetrate bacteria and viruses because of their much smaller size. d. All of the above.
Question 10. UVC light at 222 nm has been shown to kill:
a. Influenza viruses. b. Coronaviruses including SARS-CoV-2. c. Multi-drug resistant bacteria. d. All of the above.
Australasian Dental Practice™ is now offering PAID subscribers the ability to gain 2 Hours CPD credit from reading articles in this edition of the magazine and answering the questions above. To participate, log in to the Dental Community website at www.dentalcommunity.com.au (call (02) 9929-1900 if you do not have a login) and click on the CPD Questionnaires link; select the Australasian Dental Practice Jul/Aug 2022 questionnaire and then click START. A score greater than 80% is required to PASS and receive CPD.
ONLINE CPD CENTRE
70 Australasian Dental Practice July/August 2022 the cutting EDGE
By Maria Lucas and Laurence J. Walsh AO
This article explores the role of light in dental bleaching from several different perspectives, emphasising the translation from the scientific principles to the explanation given to patients. Clinicians typically learn information about bleaching techniques and the role of light both from continuing professional education courses and from training materials provided by manufacturers for their individual systems. This represents the beginning of a journey rather than its entirety. Let us begin with the dental clinician’s perspective (from Maria Lucas).
clinicians choose to use a system that also has a light An important reason why some clinicians may choose to use a light is to remain comparable and on trend with what patients are asking for and what patients feel may work best for them. Patient perception is important to consider when running a suc cessful dental practice; The introduction of initial “in office” power bleaching methods Zoom, the old “BriteSmile” and other laser or LED devices were sold to dentists/business owners on the presumption that the “light” did the work to lighten and brighten the teeth; READ ME FOR CPD
96 Australasian Dental Practice July/August 2022
By Emeritus Professor Laurence J. Walsh AO
infection
READ ME FOR CPD
CONTROL
A-dec’s dental unit waterline testing service can provide accurate results in just minutes.

Test now to protect dental waterlines
 By David Petrikas
By David Petrikas
waterline bottles, however, it was also important to monitor water quality and apply a periodic shock treatment as per guidelines.
“A-dec ICX Renew shock treatment, launched in May this year, is the perfect complement to A-dec’s self-contained water line system to ensure the highest quality water is delivered to patients.” ICX Renew is an odourless formula that clears deposits and contamination which can build up over time, without harming plastic tubing or corroding dental unit components, unlike some harsh treatments.
The latest ADA Infection Control Guidelines suggest a shock treatment if CFU (colony forming units) reach 200 CFU/mL.
Question 1. The Water Control System analyses DUWL biofilm in: a. 60 seconds b. 2 minutes c. 5 minutes d. 15 minutes
Question 2. Once mixed, the ICX Renew solution is: a. Clear b. Blue c. Pink d. Cloudy white
Question 3. ADA guidelines recommend action when the bacterial load in dental unit water reaches: a. 100 CFU/mL b. 200 CFU/mL c. 300 CFU/mL d. 400 CFU/mL
Question 4. When high bacterial counts are found, waterlines need to undergo shock treatments using: a. ICX Renew b. ICX c. Distilled water d. Chlorhexidine gluconate
Question 5. ICX and ICX Renew are non-corrosive and will not corrode or clog waterlines or harm dental tubing, diaphragms, ‘O’ rings and other soft components:
a. True b. False
At the cross roads
The medical management of gangrene during the American Civil War was to amputate a limb above the infection site to prevent ongoing bacterial proliferation into surrounding tissues (Figure 1). During a lecture in 2000, Dr Graham Mount, a pioneer in the clinical use of glass ionomer cement, described dentistry as “The only health care profes sion that still treats an infectious disease by amputation”.

In the last few years, dental technology has made significant advances to facilitate the diagnosis and replacement of tooth structure by either partial or complete amputation of teeth. Sadly, all this amazing technology remains based upon the principles of the medical management of infectious diseases over 150 years ago, especially when there are so many more conserva tive treatment options currently available.
The medical management of dental caries Dental caries is a bacterial infection of tooth structure caused by changing circumstances within the oral environment. There are defence mechanisms in the dentine pulp complex that are capable of slowing or reversing the rate of caries proliferation.
Arrested caries are an example of how, in a favourable oral environment, teeth are able to remineralise caries infected den tine (Figure 2). As the collagen matrix within the dentine has been denatured by the carious process, normal dentine is unable to form and remineralisation occurs by the deposition of min eral salts from the dentinal tubules and saliva. The dark colour of arrested caries is due to the inclusion of sulphur ions into the remineralising tissues.
Arrested caries can be compared to scar tissue, where the dermis is unable to reform, so a protective layer of scar tissue (arrested caries) is laid down to cover the wound area to prevent bacterial incursion into the tissues beneath.
The current medical manage ment of a dermal infection is to: Clean the wound; Place a medicament to enhance the natural healing process; and Isolate the infected site from a hostile environment and enable the healing process to occur. These same principles can be applied to the management of dental caries.

Clean the wound Carious dentine contains a high degree of surface bioload con sisting of bacterial plaque and other debris present within the mouth. Infected surface dentine may be so badly broken down to be breaking away from the surface of the caries. Within the carious dentinal tubules, necrotic debris and bac teria are present that can interfere with the healing process. Surface preparation consists of removing badly broken-down infected dentine and the bioload from the surface of the caries and into the infected dental tubules. Broken down infected dentine can be removed with a small excavator, gently levering it from the surface of the caries. Bioload can be efficiently removed to facilitate penetration of medicaments and GICs, from the surface of the caries and into the dentinal tubules, by the application of 37% phosphoric acid for 15 seconds, washing with water and gently air drying. Polyacrylic acid will not remove bioload from the dentinal tubules (Figure 3).
Apply a medicament to enhance healing (remineralisation)
Fluoride release from glass ionomer cement (GIC) has a limited effect in arresting caries and has been used extensively for caries management in remote communities (ART), however GIC cannot be relied upon for total caries management and requires additional pharmacological assistance to be truly effective. Ozone gas has been used as an effective caries management tool but its use is limited due to lack of an efficient delivery system.
Question 16. A traditional problem with using AgF or SDF to arrest dental caries is:
a. The affect is limited and temporary. b. The arrested caries are stained black. c. an efficient delivery system is lacking. d. All of the above.
Question 17. In the ART acronym, the A stands for: a. Aesthetic b. Asymptomatic c. Atraumatic d. Anterior
Question 18. The application of potassium iodide with AgF or SDF... a. Scavenges any remaining free silver ions to form silver iodide. b. Results in a creamy coloured white precipitate. c. May be contraindicated for patients who are pregnant or have thyroid issues. d. All of the above.
Question 19. The bond strength of Glass ionomer cement... a. Is weak chemically to enamel and dentine. b. Does not need to be high as the interface is stress free. c. Is enhanced by the prior application of SDF and AgF. d. All of the above.
Question 20. Silver fluoride compounds have long been used to arrest caries since the early...
a. 1890’s b. 1900’s c. 1950’s d. 1970’s POWERED BY THE
READ THE ARTICLES BELOW AND ANSWER THE QUESTIONS ONLINE AT WWW.DENTALCOMMUNITY.COM.AU - 2 HOURS OF CPD 100 Australasian Dental Practice July/August 2022 A -dec dealers have stepped in to help dental prac tices with a new end-to-end waterline maintenance approach and routine waterline testing service. A-dec Product Marketing Manager, Shal Hafiz, said it was important to ensure dental unit waterlines remained uncontaminated to avoid unpleasant experiences with poor water quality in clinics and the potential health risks for patients and staff. He said dental unit waterlines needed periodic maintenance to ensure they met ADA guidelines and that a systematic approach was the only way of ensuring ongoing dental unit waterline quality. “Recently, more A-dec dealers have begun offering water line testing as part of A-dec’s recommended ‘Maintain Monitor Shock’ regime, which provides peace of mind to all dental practices that their waterlines are kept within safe limits.” The rapid and accurate water testing system uses state-of-theart equipment to detect contamination at very low levels, so that the required treatment regime can be implemented to maintain or correct water quality issues. The testing is part of the “A-dec 360 Maintenance” approach which includes regular waterline maintenance, backed up by waterline quality monitoring and periodic shock treatment. Shock treatment Mr Hafiz said daily waterline maintenance was easy with a proven solution like A-dec ICX tablets for self-contained
infection CONTROL
READ ME FOR CPD
Practice July/August 2022
122 Australasian Dental
READ ME FOR CPD
By Dr Geoff Knight AM, BDSc, MSc, MBA, PhD clinical EXCELLENCE Figure 1. 170 years ago, the medical model for treating gangrene was to amputate a limb above the infection. Figure 2. Arrested caries demonstrates a tooth’s ability to remineralise caries into dental scar tissue.
retrieve your FREE
Call (02)
1900 or
To
Dental Community Login:
9929
Email info@dentist.com.au
A summary of the latest research
By Emer. Prof. Laurence Walsh AO
Real time monitoring of aerosols
Aerosol mitigation: Suction tip shapes matter


Human exposure to infectious aerosols results in the trans mission of diseases such as influenza, tuberculosis and COVID-19. Most dental procedures generate a significant number of aerosolised particles, increasing transmission risk in dental set tings. Since the generation of aerosols in dentistry is unavoidable, some clinics have started using intervention strategies such as area-filtration units and extraoral evacuation equipment, especially under the recent constraints of the COVID-19 pandemic. How ever, the effectiveness of these devices in dental operatories has not been studied. Therefore, the ability of dental personnel to effi ciently position and operate such instruments is also limited. To address these challenges, this study utilised a realtime sensor network for assessment of aerosol dynamics during dental restoration and cleaning procedures with and without intervention. The strategies tested during the procedures were (i) local area HighEfficiency Particle Air (HEPA) filters and (ii) Extra-Oral Suction Devices (EOSD). The study was conducted at the University of Washington School of Dentistry in Seattle USA using a network of 13 fixed sensors positioned within the operatory and one wearable sensor worn by the dental operator. The sensor network provided time and space-resolved particulate matter (PM) data. Three-dimensional (3D) visualisation informed aerosol per sistence in the operatory. It was found that area filters did not lower the overall aerosol concentration in dental offices in a significant way. A decrease in PM concentration by an average of 16% was observed when EOSD equipment was used during the procedures. The combination of real-time sensors and 3D visualisation can provide dental personnel and facility managers with actionable feedback to effectively assess aerosol transmission in medical set tings and develop evidence-based intervention strategies.

Makhsous S et al. Methodology for addressing infectious aerosol persis tence in real-time using sensor network. Sensors 2021; 21: 3928.
The aim of this study was to determine the impact of various aerosol mitigation interventions and to establish duration of aerosol persistence in a variety of dental clinic configurations. Aerosol measurement studies were performed in endodontic, orthodontic, periodontic, paediatric and general dentistry clinics in St. Louis, Missouri from July to October 2020. Aerosol sen sors in the form of an optical aerosol spectrometer, the inlet of which was positioned 20 cm in front of and 10 cm above the patient’s mouth without interruption of the procedures performed by the dentist. Wearable particulate matter sen sors were to measure real-time aerosol concentration from the vantage point of the den tist during routine care in a variety of clinic con figurations (e.g. open bay, single room, par titioned operatories). It compared the impact of aerosol mitigation strate gies (e.g. ventilation and high-volume evacuation (HVE) and prevalence of particulate matter) in the dental clinic environment before, during and after high-speed drilling, slow-speed drilling and ultrasonic scaling procedures. Dental suction was used in all configurations with an 8.2 mm tip with aflow rate 74 standard cubic feet per minute at 7.0 Hg (2095.44 LPM). The concentra tion of aerosol was highest when using a high-speed drill in a dental operatory space with little ventilation. The largest aer osol concentrations were generated by ultrasonic scaling and high-speed drilling of anterior teeth. Conical HVE had higher efficiency for removing aerosol plumes than the standard-tip HVE. When aerosols were detected in the environment, they were rapidly dispersed within minutes of completing the aerosolgenerating procedure. Few aerosols were detected in dental clinics, regardless of configuration, when conical HVE was used. Thus suggests that fallow time can be reduced to 5 minutes, which likely occurs during routine patient care. Dentists should consider using conical HVE rather than standard-tip evacuators to reduce aerosols generated during routine clinical practice. Conical HVE is likely more efficient in reducing emissions from high-speed drilling than standard-tip HVE because of the rela tively large surface area available for conical HVE to evacuate aerosols from the dental environment. Furthermore, when such effective aerosol mitigation strategies are employed, dentists need not leave dental chairs fallow between patients because aerosols are rapidly dispersed.
Choudhary S et al. Comparison of aerosol mitigation strategies and aerosol persistence in dental environments. Infect Control Hosp Epidemiol. 2022, 1–6. doi:10.1017/ice.2022.26
68 Australasian Dental Practice July/August 2022 abstracts | 2022
INTERNATIONALLY RENOWNED ULTRASONIC SCALERS, LASERS AND SURGICAL MOTORS
Trusted by 200,000+ dentists and specialists across Australasia and worldwide, Woodpecker dental are the safe choice for quality, doctor-friendly, and affordable small dental equipment.
Osseo Group is the new home of Woodpecker equipment and is steadily releasing their latest range of small equipment, including:
Implanter surgical motor
• Easy-to-use touchscreen
• Auto-calibration for accurate torque
• Ultra-quiet pump and motor design
• Lightweight, balanced high-torque motor
PT-A scaler and air polisher
Easy-to-use touchscreen
• Solution reservoir or in-line use
• Pure-sine scaler transducer for patient comfort


• Ultra-small handpieces
• Powder-water suppression for patient comfort
X16+ Dual-wavelength laser
• Easy-to-use touchscreen
• Dual infrared and ultraviolet wavelengths
• Rechargeable and completely wireless
• Includes all photomodulation therapy tips LX16+
BOOK A DEMO PLACE AN ORDER
dual-wavelength laser $8495
$8495
PT-A scaler + air polisher
$4995 ANZ2022-7-WoodpeckerADP.indd 1 1/7/2022 12:19 pm
Implanter surgical motor
Shining light on common misconceptions about the role of light in dental bleaching
 By Maria Lucas and Laurence J. Walsh AO
By Maria Lucas and Laurence J. Walsh AO

This article explores the role of light in dental bleaching from several different perspectives, emphasising the translation from the scientific principles to the explanation given to patients.
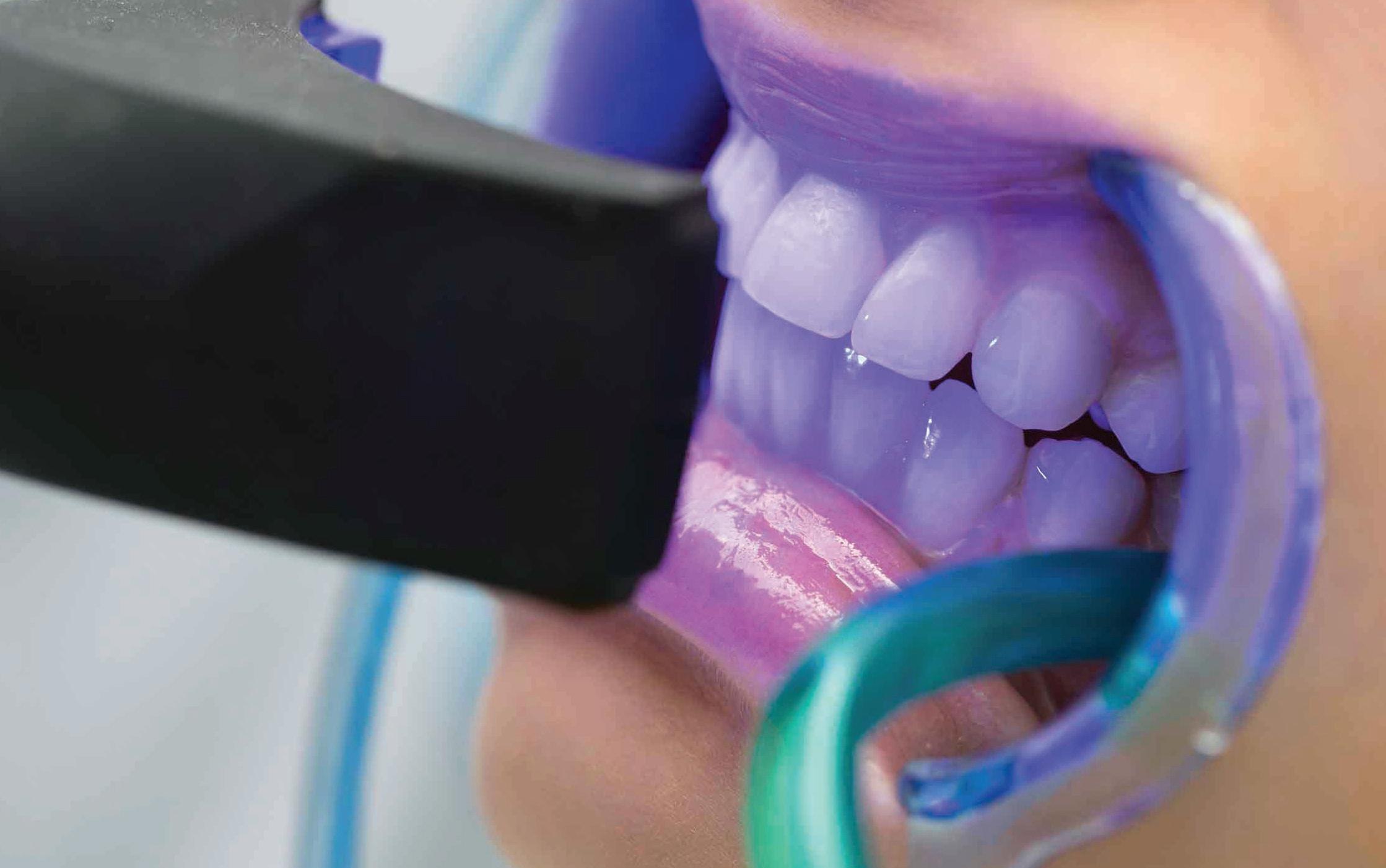
Clinicians typically learn information about bleaching techniques and the role of light both from continuing professional education courses and from training materials provided by manufacturers for their individual systems. This represents the beginning of a journey rather than its entirety.
Let us begin with the dental clinician’s perspective (from Maria Lucas).
Why clinicians choose to use a system that also has a light
• An important reason why some clinicians may choose to use a light is to remain comparable and on trend with what patients are asking for and what patients feel may work best for them. Patient perception is important to consider when running a suc cessful dental practice;
• The introduction of initial “in office” power bleaching methods - Zoom, the old “BriteSmile” and other laser or LED devices were sold to dentists/business owners on the presumption that the “light” did the work to lighten and brighten the teeth;
70 Australasian Dental Practice July/August 2022 the cutting | EDGE
READ ME FOR CPD
• Patients often affiliate “the light” with a procedure that works or is well known. The question could be asked as to whether they have become accus tomed to what they see in the cosmetic area outside dentistry and in online social media; and
• Clinicians often consider both the actual effectiveness of the treatment that is being offered, as well as what patients want and expect, in order to keep chairs booked up.
What the manufacturers told users about the role of light
• The typical information coming to clinicians from manufacturers is that the light or light source activates the initiators in bleaching gel and also helps to catalyse (speed up) the chem ical reactions of hydrogen peroxide to make the process of whitening occur faster;
• Typically, some emphasis will be placed on the fact that the light is not ultra violet (this is always emphasised) and hence not harmful and that the energy and warmth from the light heats the gel up and this speeds up chemical reactions that occurs;
• Advice can sometimes be that the pro cess of bleaching from the gel will work without a light, but that applying light speeds up the process; and
• Manufacturers sometimes say that patients perceive that using light helps the process work faster.
How clinicians explain the use of light to patients
• Clinicians often repeat to patients what has been told to them by the manufacturers of the product they are using. In my experience, clinicians adhere to the manufacturer’s instruc tions for the product they are using on patients and don’t stray from what has been advised.
• It is common to inform patients that the “light source” helps to activate and speed up the chemical reaction which occurs as a result of the hydrogen per oxide breaking down to whiten and lighten the discoloured molecules in the tooth.
How we ensure the appropriate light intensity and exposure time
• Clinicians follow manufacturer’s instructions for appropriate use of the product they are using. Both light intensity and light exposure time are also based on the manufacturer’s instructions;
• My personal experience with Zoom is based on using 4 x 15 minute light intervals with the option of changing the light intensity. The exposure time period is set, but can be varied in terms of “sessions” based on the level of comfort of the patient and how much sensitivity they are experiencing; and
• It is common knowledge Zoom bleaching will induce sensitivity but that it is transient. The manufacturer recommends using fewer intervals or to reduce the light intensity if the patient is experiencing sensitivity. Hence light intensity and exposure time are chosen based on the features of the patient, e.g. Do they suffer from gen eralised tooth sensitivity? Are they taking photosensitive medications that may render them inappropriate for the procedure? Do they have underlying medical conditions we need to be aware of?, etc.
What the science says
Photodegradation
This is the starting example because it is the form of interaction which we all see in our everyday lives. We notice that the curtains and fabrics that hang in windows positioned on the western side of our house become brittle and fade in colour over time. When our car is parked in an open-air car park for most of its life, we notice how the paint colour fades. We notice the same thing on the painted areas of our house, especially on the northern and western sides which get more direct sun exposure. When we buy certain medi cines, we notice that they are provided in brown glass bottles to prevent ambient light from degrading them.
When we attend an art gallery, we notice a sign that says that flash photography is not permitted and paintings are positioned to prevent direct exposure to sunlight (Lightinduced fading of paintings was reported in 50 BC by Vitruvius. In 1782, the first comprehensive and successful book on the effect of solar light on pigments and dyes in paintings is written by Senebier).
N
ow let us move on to explore the science of photochemistry (from Laurie Walsh).
It is sometimes amusing when one sees commentary in dental publications questioning the role of light in dental bleaching. If one was to train in photo biology or attend classes for chemical engineering (both of which I have done), one would soon discover that the major processes by which light can alter dental bleaching are standard foundation knowl edge in chemical engineering.
The second part of this article helps to explain how the various ways that light can interact with different sub strates in a way that is relevant to dental bleaching. Note that some products and systems may use several of these pro cesses in parallel. It all comes down to the selection of the wavelength of the light source and the formulation of the gel.
All of these basic phenomena share a common causal pathway, which is that of photodegradation. What is happening here is that short wavelength light is being absorbed into the substrate, where it is causing the decomposition of the molecules that absorb the light. Short wavelengths of light (such as visible violet) carry more photon energy than long wavelengths (such as visible red), which is why they are better at breaking chemical bonds in the target.1
In the case of coloured light, the absorbing molecule will be opposite the colour wheel from the incident light source. For example, visible violet and visible blue light absorb most strongly in molecules that are yellow.2,3 This is why tetracycline antibiotics are stored in a brown glass bottle. There is a consid erable literature showing the impact of different wavelengths of light on tetracy clines, which reveals the potent influence of violet and cyan light, while green and red light have little, if any, effect.
The use of violet light for photodeg radation has been the subject of many studies on the dental literature. A key take-home message from the studies is that violet light can reduce yellow stains without an intervening oxidant (such as hydrogen peroxide).4,5
July/August 2022 Australasian Dental Practice 71
the cutting | EDGE
A classic example of this process is seen in the way that visible green light interacts with the red coloured quinone complex that forms when tetracycline molecules are bound strongly into tooth structure. This explains both why intense green light from an array of LEDs or from a KTP laser is highly effective at degrading this quinone molecule and like wise, why ambient sunlight in patients who were exposed to first-generation tet racyclines during tooth development and developed marked discolouration of their teeth as a result, causes the incisal half of their anterior teeth to become lighter over time.6-8 The same lightning effect is not seen on posterior teeth and the same indi viduals. A recent 27 month study tracked the colour of tetracycline stained teeth and showed that ambient light alone was able to cause substantial beneficial colour change.9 When one uses filters to remove the green component, this beneficial effect no longer occurs.2
Examples of current systems which use photodegradation are the Vio 405 nm violet light which is part of the HiSmile™ PAP+™ in office bleaching system, and Smartbleach ™, where the light source can be a 535 nm visible green LED array (Smartbleach 3LT®) or a 532 nm KTP laser such as the Deka Smartlite™
Photothermal reactions
The chemistry of bleaching using hydrogen peroxide is oxidation and this process is enhanced when tempera tures are elevated. An everyday example of a photothermal process is the increase in temperature which occurs in a car with black exterior paint, as compared to a car with white exterior paint. The white paint is highly effective at reflecting all visible light wavelengths, whereas the opposite is true for the black exterior paint, which absorbs all visible light wavelengths. The absorbed energy causes increased molec ular vibrations, which means that the object gets hotter. The same phenomenon occurs when standing in bright sunshine wearing a black shirt, versus wearing white clothing. A photothermal process does not require a short wavelength of light and will work with longer wave lengths such as near infrared light.
Given that hydrogen peroxide bleaching gels have water as a major com ponent, it makes sense to also consider
1. Percentage absorption of light passing through 1 mm of enamel or 1 mm of Ultradent Opalescence Boost™ bleaching gel. Calculated from references 37-39.
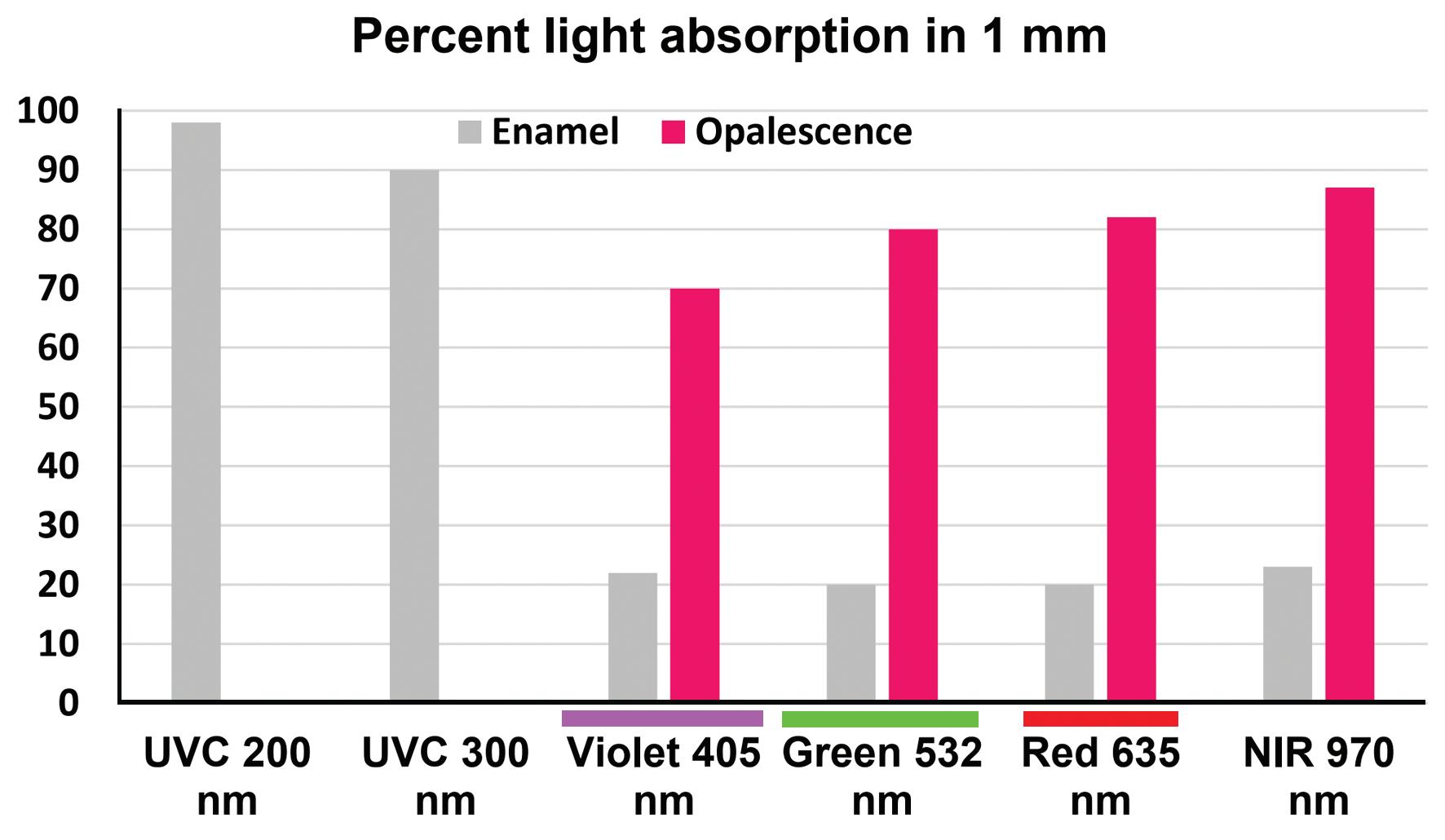
intense energy sources that can absorb strongly into water, such as lasers in the middle and far infrared regions. His torically, photothermal processes were the first way that intense light was used to accelerate bleaching reactions. The
bleaching gels, with orange or red col ours that will absorb strongly light from a conventional 470 nm dental curing light. Some gels use various forms of titanium dioxide microparticles to alter their light absorbing properties. An example of the effective absorption of light over a range of visible light wavelengths is shown in Figure 1. Note in this example, the strong absorption of light by the coloured bleaching gel at a range of wavelengths in the visible and near infrared region.
improvement can be gained using a broad wavelength light source (such as a lamp with appropriate filtration) or a narrow spectrum light source such as an LED), or a monochromatic light source (a laser).
Provided that suitable absorbing col oured molecules (chromophores) are present, an intense light source will warm a bleaching gel. This facilitates the break down of hydrogen peroxide10-12 and can improve the overall bleaching effect that is gained.14-17
From a design perspective, it is essen tial to match the light source to absorbing molecules in the gel. To the water base of the gel, various pigments can be added. This explains why some commercial bleaching products have highly coloured
The key limitation of the photothermal approach is that excessive heating of the gel or direct absorption of light that is transmitted through the gel into the enamel will heat the tooth surface and this in turn can cause thermal stress to the dental pulp leaving the patient to experience a poorly localised C fiber pain response. Note from Figure 1 that this direct absorption of light by enamel is very low for visible and near infrared light, but is very high for short wavelength ultraviolet light. Overall, it is important to avoid excessive light exposure (prolonged time at high intensity) as this will cause heat-related stress to the dental pulp18-21 and increase pain sensations during in-office bleaching.22,23
Manufacturers have learnt the hard way that light sources operating in the short wavelength ultraviolet spectrum are highly problematic in terms of direct heating of enamel and also causing prob lems such as photo-eruptive lesions and sunburn to the oral tissues and perioral facial skin. This is why current systems typically use visible light wavelengths.
72 Australasian Dental Practice July/August 2022
the cutting | EDGE
Figure
“Light causes the decomposition of the molecules that absorb the light. Short wavelengths of light carry more photon energy than long wavelengths, which is why they are better at breaking chemical bonds...”
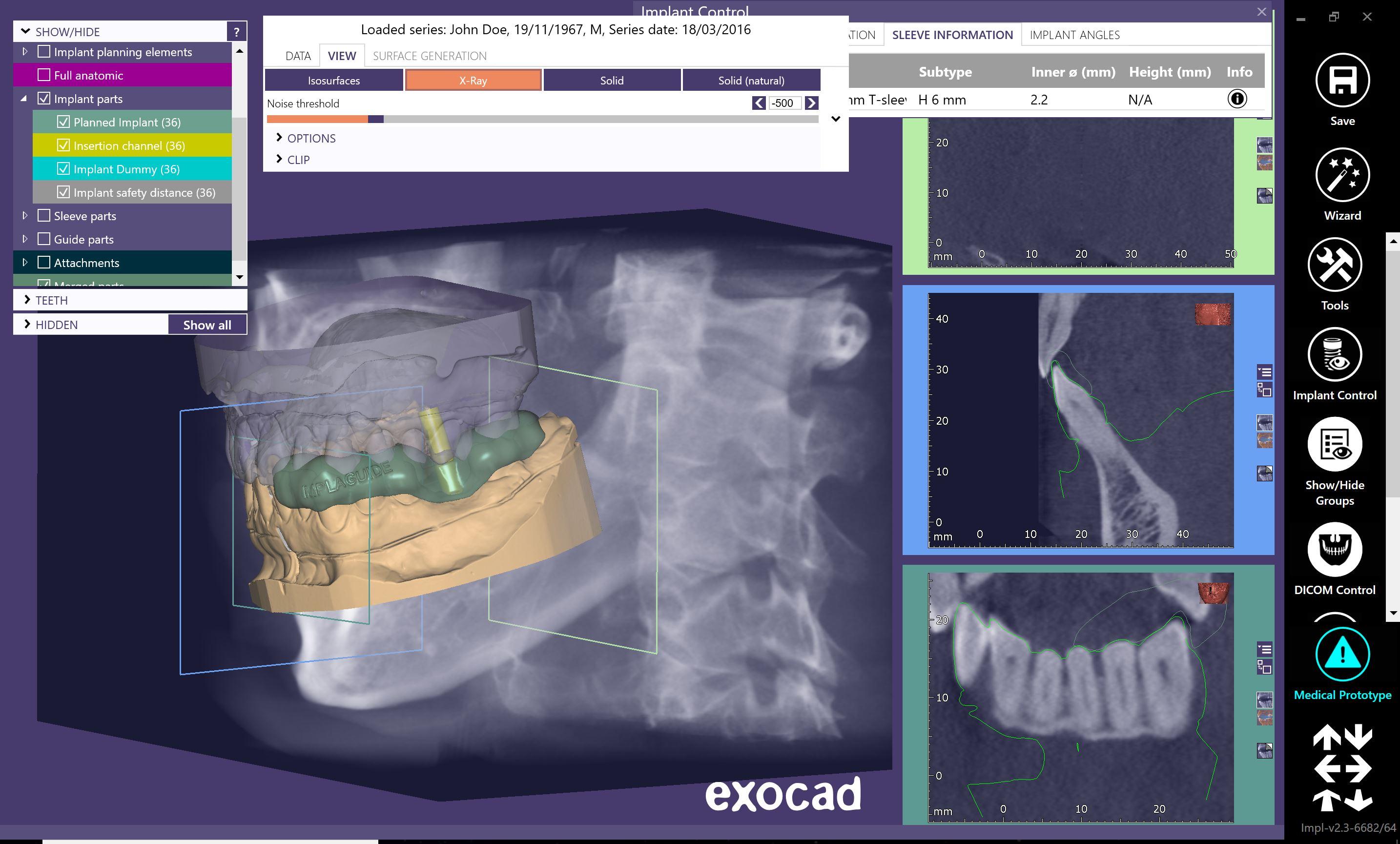


Implant Surgical Guides Precise - Easy - Affordable • Any Implant System • Setup Included • Fast Turnaround • Fully Guided • Pilot Drill Guides • Edentulous Cases • Scan Appliances • Free Planning Software Talk to us today and we will help you plan and construct a guide for your next case FIRST CASE HALF PRICE * www.implaguide.com.au TGA NOTES : We have always worked within the guidelines of the TGA and now with the new regulations we continue to do so. If you have any concerns please don’t hesitate to contact us for more information. Another Quality Product From 1300 878 336 Implant Surgical Guides Precise - Easy - Affordable • Any Implant System • Setup Included • Fast Turnaround • Fully Guided • Pilot Drill Guides • Edentulous Cases • Scan Appliances • Free Planning Software Talk to us today and we will help you plan and construct a guide for your next case FIRST CASE HALF PRICE * www.implaguide.com.au TGA NOTES : We have always worked within the guidelines of the TGA and now with the new regulations we continue to do so. If you have any concerns please don’t hesitate to contact us for more information. Another Quality Product From 1300 878 336 Implant Surgical Guides Precise - Easy - Affordable • Any Implant System • Setup Included • Fast Turnaround • Fully Guided • Pilot Drill Guides • Edentulous Cases • Scan Appliances • Free Planning Software Talk to us today and we will help you plan and construct a guide for your next case FIRST CASE HALF PRICE * www.implaguide.com.au TGA NOTES : We have always worked within the guidelines of the TGA and now with the new regulations we continue to do so. If you have any concerns please don’t hesitate to contact us for more information. Another Quality Product From 1300 878 336 Implant Precise - - Aff Any Implant Setup Fast Turnaround Fully Guided Pilot Edentulous Scan Free to we you construct a for CASE HALF * www.implaguide.com.au TGA have within of s you have to contact for more information. Product From 1300 Implant Surgical Guides Precise - Easy - Affordable • Any Implant System • Setup Included • Fast Turnaround • Fully Guided • Pilot Drill Guides • Edentulous Cases • Scan Appliances • Free Planning Software Talk to us today and we will help you plan and construct a guide for your next case FIRST CASE HALF PRICE * www.implaguide.com.au TGA NOTES : We have always worked within the guidelines of the TGA and now with the new regulations we continue to do so. If you have any concerns please don’t hesitate to contact us for more information. Another Quality Product From 1300 878 336 Implant Surgical Guides Precise - Easy - Affordable • Any Implant System • Setup Included • Fast Turnaround • Fully Guided • Pilot Drill Guides • Edentulous Cases • Scan Appliances • Free Planning Software Talk to us today and we will help you plan and construct a guide for your next case FIRST CASE HALF PRICE * www.implaguide.com.au TGA NOTES : We have always worked within the guidelines of the TGA and now with the new regulations we continue to do so. If you have any concerns please don’t hesitate to contact us for more information. Another Quality Product From 1300 878 336 Implant Surgical Guides Precise - Easy - Affordable • Any Implant System • Setup Included • Fast Turnaround • Fully Guided • Pilot Drill Guides • Edentulous Cases • Scan Appliances • Free Planning Software Talk to us today and we will help you plan and construct a guide for your next case FIRST CASE HALF PRICE * www.implaguide.com.au TGA NOTES : We have always worked within the guidelines of the TGA and now with the new regulations we continue to do so. If you have any concerns please don’t hesitate to contact us for more information. Another Quality Product From 1300 878 336 Implant Surgical Guides Precise - Easy - Affordable • Any Implant System • Setup Included • Fast Turnaround • Fully Guided • Pilot Drill Guides • Edentulous Cases • Scan Appliances • Free Planning Software Talk to us today and we will help you plan and construct a guide for your next case FIRST CASE HALF PRICE * www.implaguide.com.au TGA NOTES : We have always worked within the guidelines of the TGA and now with the new regulations we continue to do so. If you have any concerns please don’t hesitate to contact us for more information. Another Quality Product From 1300 878 336 Implant Surgical Guides Precise - Easy - Affordable • Any Implant System • Setup Included • Fast Turnaround • Fully Guided • Pilot Drill Guides • Edentulous Cases • Scan Appliances • Free Planning Software Talk to us today and we will help you plan and construct a guide for your next case FIRST CASE HALF PRICE * www.implaguide.com.au TGA NOTES : We have always worked within the guidelines of the TGA and now with the new regulations we continue to do so. If you have any concerns please don’t hesitate to contact us for more information. Another Quality Product From 1300 878 336 Implant Surgical Guides Precise - Easy - Affordable • Any Implant System • Setup Included • Fast Turnaround • Fully Guided • Pilot Drill Guides • Edentulous Cases • Scan Appliances • Free Planning Software Talk to us today and we will help you plan and construct a guide for your next case FIRST CASE HALF PRICE * www.implaguide.com.au TGA NOTES : We have always worked within the guidelines of the TGA and now with the new regulations we continue to do so. If you have any concerns please don’t hesitate to contact us for more information. Another Quality Product From 1300 878 336
A typical bleaching product that can undergo photothermal activation will also work without exposure to the light and the user instructions will indicate that applying light will enhance the effect of the agent, but is not a critical requirement.
Examples of photothermal activa tion include SDI Pola Office Plus™ and Ultradent Opalescence Boost™. The ben efits of photothermal enhancement vary between products depending on which light-absorbing agents have been included in the gel. This explains why variations in the role and importance of light have been reported in the literature.24-28
Photocatalytic processes
Because this technology is not deployed in bleaching systems sold in Aus tralia, some readers will be unfamiliar with the broad concept involved. As the name suggests, a light-sensitive catalyst is used. When exposed to the relevant wavelengths of light, reactive oxygen species are generated, which then are the active components for bleaching. Tita nium dioxide is a widely used material in photocatalytic processes in industry, as it has a wide absorption pattern in the visible spectrum and in the adjacent near infrared and ultraviolet regions. In fact, the absorption spectrum can be altered by the introduction of various changes in the titanium dioxide, such as doping with nitrogen atoms.
Using a broad spectrum photocatalyst, the choice of light source becomes less important, although as already discussed, using a shorter wavelength will bring more energy from absorption as each photon carries greater energy. An example of a bleaching gel which uses a titanium dioxide photocatalyst is GC Tion™.
Photochemical processes
Colour vision and photosynthesis are perhaps the best-known examples in everyday life of photochemical processes. In such reactions, the light wavelength triggers a specific chemical reaction and is a critical requirement for it to occur.
The concept of using photochemical processes for degrading coloured mol ecules is a standard approach within chemical engineering for the treatment of highly coloured wastewater. A particular chemical process developed for such an
application is the photo-Fenton reaction, where iron ions and short wavelength (blue, violet or ultraviolet) light combine together to give much greater breakdown of highly coloured molecules.
The photo-Fenton reaction forms the fundamental basis for what happens when an LED array is used in combination with a suitable gel in current versions of Zoom! dental bleaching systems. A range of clin ical and laboratory studies have assessed the added value of the photo-Fenton reaction above the fundamental Fenton reaction driven by the same gel, which is not light dependent. Across all the lit erature, the improvement gained in the effectiveness is in the order of 24-28%.29
“Provided that suitable light-absorbing coloured molecules (chromophores) are present, an intense light source will warm a bleaching gel. On the other hand, in a photodynamic process, where light pushes the reaction, a specific photosensitiser is used, in combination with a light source that is absorbed very strongly in that photosensitiser...”
sensitiser molecules, which basically absorb the energy and then couple that into adjacent molecular diatomic oxygen, creating reactive oxygen species. As this energy transfer occurs, the photosensitiser molecule relaxes back to its ground state. Depending on the pH, there are several pathways by which it may do this, including pathways which generate light (such as luminescence and phosphorescence).6-8
An everyday example of a photo dynamic process is the activation of curcumin (turmeric) by blue and violet light that is present in ordinary sunlight. It has been known since antiquity that tur meric applied to skin wounds had a potent disinfecting action, which was greatly enhanced when the turmeric preparation on the wound was also exposed to vis ible light. The chemistry of this involves a classic photodynamic activation process, with the short wavelength light causing the molecular excitation of the turmeric, with the resulting release of reactive oxygen species.30 The feeder molecule for the reactive oxygen species is normal atmospheric oxygen dissolved in the water used in the turmeric paste.
In dental bleaching products, to enhance the supply of molecular oxygen, a feeder reaction may be used for local generation of oxygen, such as the catalytic break down of hydrogen peroxide into oxygen and water.
An example of a commercial in office bleaching gel that is based on photody namic processes is Smartbleach™ 6-8,31,32 The photosensitiser is rhodamine B, which has a maroon to magenta colour and the corresponding light sources are in the visible green region, such as a laser (argon ion 514.5 nm or KTP 532 nm) or LEDs (535 nm).
Photodynamic processes
As the Greek derivation of the term “dynamos” would suggest, in these processes the light plays a critical role in empowering (pushing) the reaction. A specific photosensitiser is used, in combi nation with a light source that is absorbed very strongly in that photosensitiser. Careful attention is paid to the pH of the environment, since this influences what happens after the light is absorbed. At the molecular level, the photosensitiser mol ecules become electronically excited and then undergo a decay process. The process is not inherently damaging to the photo
Concurrent irradiation
ome light sources designed for bleaching may contain more than one light source. The rationale behind this is that the secondary light source is not designed to contribute to the bleaching process, but rather to attenuate pulpal responses of the patient from hydrogen peroxide and its derivatives during the treatment. To achieve this, the secondary light source needs to have a wavelength that can cause photobiomodulation (PBM) effects by absorbing in cytochrome oxi dase enzymes within mitochondria.33-35
S
74 Australasian Dental Practice July/August 2022
the cutting | EDGE
Dental Advisor rates
• Dental Advisor rates
• Fast acting, delivering whiter teeth in as little as 5 days
• Fast acting, delivering whiter teeth in as little as 5 days
• Formulated to safely remove long term stains
• Formulated to safely remove long term stains
• Fast acting, delivering whiter teeth in as little as 5 days
• Fully rechargeable for future tooth whitening treatments
• Fully rechargeable for future tooth whitening treatments
• Formulated to safely remove long term stains
• Remineralisation to strengthen the teeth
• Remineralisation to strengthen the teeth
• Fully rechargeable for future tooth whitening treatments


• Extra hydration to minimise sensitivity
• Extra hydration to minimise sensitivity
• Remineralisation to strengthen the teeth
• No custom tray required
• No custom tray required
• Extra hydration to minimise sensitivity
• Available in 6% and 9.5% hydrogen peroxide
• Available in 6% and 9.5% hydrogen peroxide
• No custom tray required
• Available in 6% and 9.5% hydrogen peroxide
The results were great in a short amount of whitening time. Also, it was very easy to use.
The results were great in a short amount of whitening time. Also, it was very easy to use.
Dental Advisor evaluator comment
Dental Advisor evaluator comment
The results were great in a short amount of whitening time. Also, it was very easy to use.‹‹ Dental
Pola Light ++++ or 87% clinical rating.
• Dental Advisor rates Pola Light ++++ or 87% clinical rating.
Pola Light ++++ or
1238 uses with ease of
1238 uses with ease of use and lack of tooth sensitivity.
• 88% of Dental Advisor evaluators rated it either equal or better than their existing take home LED whitening.
80% would recommend Pola Light to a colleague.
Call 1800 337 003 www.sdi.com.au
1300 65 88 10 Call 1800 337 003 www.sdi.com.au
A NEW
TAKE HOME TOOTH WHITENING SYSTEM WITH LED LIGHT TECHNOLOGY
ADVANCED
NOW YOUR PATIENTS CAN ENJOY A BRIGHTER, MORE CONFIDENT SMILE IN 5 DAYS.
EASY TO USE E T
47 CLINICAL EVALUATORS TOTAL USES
CLINICAL RATING
LIGHT 2021
1238
87% POLA
NOW ALSO AVAILABLE IN 9.5% orders
orders
›› A NEW
HOME TOOTH WHITENING SYSTEM WITH LED
TECHNOLOGY
phone 1300 65 88 22 |
fax
ADVANCED TAKE
LIGHT
NOW YOUR PATIENTS CAN ENJOY A BRIGHTER, MORE CONFIDENT SMILE IN 5 DAYS.
EASY TO USE E T
47 CLINICAL EVALUATORS TOTAL USES
CLINICAL RATING
POLA LIGHT 2021
1238
87%
NOW ALSO AVAILABLE IN 9.5% orders phone 1300 65 88 22 | orders fax 1300 65
10
88
›› A NEW ADVANCED TAKE HOME TOOTH WHITENING SYSTEM WITH LED LIGHT TECHNOLOGY NOW YOUR PATIENTS CAN ENJOY A BRIGHTER, MORE CONFIDENT SMILE IN 5 DAYS.
EASY TO USE FROM JUST 20 MINUTES A DAY WHITER TEETH IN FIVE DAYS PROFESSIONALLY USED AND RECOMMENDED 10 MINUTES WHITENING PER DAY EASY TO USE WHITER TEETH IN TEN DAYS PROFESSIONALLY USED AND RECOMMENDED
47 CLINICAL EVALUATORS TOTAL USES 1238 CLINICAL RATING
POLA LIGHT 2021
87%
Advisor evaluator comment OFFICIAL 2021 TEETH WHITENING PARTNER NOW ALSO AVAILABLE IN 9.5% orders phone 1300 65 88 22 | orders fax 1300 65 88 10
››
Call 1800 337 003 www.sdi.com.au
Suitable wavelengths occur from the visible red region (from 630 nm) through to the near infrared region (to around 1100 nm). These wavelengths alter the behav iour of neurons and reversibly impair neural transmission without causing damage.36 A secondary light source can be an LED or a diode laser.
Why should there be controversy about the role of light in bleaching?
A s explained above, the fundamental photochemistry behind light in bleaching processes is well known. The observation of chemical effects of light is as old as humanity itself and photochem ical processes are the subjects of multiple
“There
cases
poorly conducted laboratory studies of photothermal bleaching which lack relevant controls... A well-designed study should explore the effect of the gel used alone, light used alone and the combination of the gel with the appropriate light, at a sufficient intensity for the appropriate time...”
recent standard chemistry texts. 40,41 From a pure chemistry perspective, the electronic excitations that are required to trigger photochemical, photodynamic and photophysical events (including photo degradation) require energies roughly in the interval 100-1000 kJ/mol (1 to 10 eV) as this is sufficient to break bonds or cause other major molecular rearrangements. Hence, the corresponding wavelengths go from the ultraviolet region right through the visible spectrum (400-700 nm) and extend as far as 1200 nm in the near infrared region.40 This aligns with wave lengths used with contemporary dental bleaching systems.
Despite the wealth of material on the topic of photochemistry in the dental liter ature as well as in the industrial literature
Table 1. Key clinical take home messages
n Become informed of what mechanisms bleaching systems are using light to achieve.
n Follow manufacturer advice regarding limits for light intensity and exposure time. Use separate additional timers if these are not built into the system.
n Use the supplied positioning devices to locate the light source at the proper working distance.
n Check that products are used well within their expiry date.
n Protect the patient’s eyes from intense light using the recommended protective eyewear, retractors, etc as supplied by the manufacturers.
and in the patent literature and the occur rence of everyday examples such as those mentioned above, there are those who deny any value to using light to enhance bleaching. Perhaps their core knowledge of photochemistry is limited.
In some cases, they have drawn upon the results of poorly conducted labora tory studies of photothermal bleaching which lack relevant controls and so they are unable to properly distinguish between the effect of light versus no light. A welldesigned study should explore the effect of the gel used alone, light used alone and the combination of the gel with the appropriate light, at a sufficient intensity for the appropriate time. As well, some authors have only looked at studies using photothermal processes (where improve ments will be small if the gel lacks the appropriate absorbing molecules) and have ignored literature on the other mechanisms discussed above. A narra tive review or a systematic review is only as good as the selection process that is used for the included papers. Excluding papers on processes other than photo thermal systems is a common error in such reviews on the question of light and dental bleaching.
The comment can also be made that some manufacturers of various light systems could have better informed clini cians regarding the mechanisms at play and in particular provided information about how their system is designed to maximise the interaction between light and the relevant target. Armed with that information, clinicians could have greater confidence that there is a worthwhile ben efit in using the light source provided by the manufacturer.
Get the photochemistry right!
f one uses an incorrect light source that is not absorbed in the target, then one cannot expect to see any beneficial actions. On the other hand, if one uses a powerful light source for an extended period that is fixed in position over the teeth, it is self-evident that some heating of the teeth could occur, both through absorption in the gel, as well as by absorp tion within the tooth structure itself. This is where consideration around how well the light is absorbed within the structure of the tooth is very important.
I
As can be seen in Figure 1, teeth are relatively transparent to wavelengths from the visible green through to the near infrared region. However, teeth absorb strongly in the far and middle ultraviolet range, due to absorption into apatite min eral.37,38 Not surprisingly, when an intense UVC or UVB lamp is applied to teeth for a prolonged period, the enamel becomes hot and there is thermal stress at the level of the pulp. This was the cause of problems with the first generation of Zoom! and one of the reasons why there was subsequently a change in the light source used with this
76 Australasian Dental Practice July/August 2022
the cutting | EDGE
are some
of
All methods of light activation of bleaching products need to use pathways that are effective for improving the final result from the procedure...”
particular bleaching system. Other reasons included photo-eruptive lesions within the mouth and around the oral tissues and UVB-induced erythema (sunburn) caused by ultraviolet B and C light exposure.
In summary, all methods of light acti vation of bleaching products need to use pathways that are both effective for improving the final result, while at the same time considering the complexity and cost of the light source and the relevant safety implications for staff and patients. Key points for safety and effectiveness are listed in Table 1.
About the authors
Maria Lucas is an oral health therapist in full time private practice. She completed her OHT training at the University of Adelaide in 2007 and later undertook the Adult Restorative Course at the University of Sydney. Maria has a special interest in tooth whitening and is a co-director of the Institute of Aesthetic Teeth Whitening, a training company devoted to education in tooth whitening. She has a keen interest in business development and in supporting not for profit entities that provide health care for disadvantaged communities in the Asia Pacific region.
Emeritus Professor Laurence J. Walsh AO is a specialist in special needs dentistry who is based in Brisbane, where he served for 36 years on the academic staff of the University of Queensland School of Den tistry, including 21 years as Professor of Dental Science and 10 years as the Head of School. Since retiring in December 2020, Laurie has remained active in hands-on bench research work, as well as in supervising over 15 research students at UQ who work in advanced technolo gies and biomaterials and in clinical microbiology. Laurie has served as Chief Examiner in Microbiology for the RACDS for 21 years and as the Editor of the ADA Infection Control Guidelines for 12 years. His published research work includes over 330 journal papers, with a citation count of over 15,400 citations in the lit erature. Laurie holds patents in 7 families of dental technologies. He is currently ranked in the top 0.25% of world scientists. Laurie was made an Officer of the Order of Australia in January 2018 and a life member of ADAQ in 2020 in recognition of his contributions to dentistry.
References
1. Coluzzi DJ, Convissar RA, Roshkind DM, Walsh LJ. Laser Fundamentals. In: Convissar RA (ed) Principles of Laser Dentistry, 3rd edition, 2022. St Louis: Elsevier Mosby.
2. Bennett ZY, Walsh LJ. Factors affecting the rate of oxidation and resultant discolouration of tetracyclines contained in endodontic medicaments and irrigants. International Endodontic Journal. 2015; 48(4):373-379.
3. Athanassiadis B, Abbott PV, Walsh LJ. A critical analysis of research methods and experimental models to study tooth discolouration from endodontic materials. International Endodontic Journal, 2022; 55 (Suppl.2): 370–383.
4. Zanin F. Recent advances in dental bleaching with laser and LEDs. Photomedicine and Laser Surgery 2016;34:135-136.
5. Kury M, et al. Effect of violet LED light on in office bleaching protocols: a randomized con trolled clinical trial. Journal of Applied Oral Science 2020;28:e20190720
6. Walsh LJ, Liu JY, Verheyen P. Tooth discolouration and its treatment using KTP laser-assisted tooth whit ening. Journal of Oral Laser Applications 2004;4(1):7-20
7. Verheyen P, Walsh LJ. Bleaching using the laser.
In: Moritz A, Beer F, Verheyen P, Wernisch J, Schoop U, Blum R, Walsh LJ. Oral Laser Application. Berlin: Quintessence, 2006
8. DeMoor RJG, Verheyen J, Diachuk A, Verheyen P, Meire MA, De Coster PJ, Keulemans F, De Bruyne M, Walsh LJ. Insight into the chemistry of laser-activated bleaching. The Scientific World Journal. 2015: 650492.
9. Athanassiadis B, Abbott PV, Walsh LJ. Develop ment and reversal of discolouration in roots filled with Ledermix or Doxymix pastes stored in the dark for three months then daylight for twenty four months. European Endodontic Journal 2022, in press.
10. Baxendale J, Wilson J. The photolysis of hydrogen peroxide at high light intensities. Transactions of the Faraday Society 1957;52:344-356.
11. Garcia Einschlag F, et al. Effect of temperature on hydrogen peroxide photolysis in aqueous solution. Journal of Photochemistry and Photobiology, Part A Chemistry. 1997;110:235-242
12. Haywood VB. In-office bleaching: lights applica tions, and outcomes. Current Practice 2009;16:3-6.
13. Ontiveros JC. In-office vital bleaching with adjunct light. Dental Clinics of North America 2011;55: 241-253.
14. Tavares M, et al. Light augments tooth whitening with peroxide. Journal of the American Dental Associa tion 2003;134:167-175.
15. Luk K, et al. Effect of light energy on peroxide tooth bleaching. Journal of the American Dental Association 2004;135:194-201.
16. Sulieman M, et al. Comparison of three in office bleaching systems based on 35% hydrogen peroxide with different light activators. American Journal of Den tistry 2005;18:194-197.
17. Ziemba SL, et al. Clinical evaluation of a novel dental whitening lamp and light-catalyzed peroxide gel. Journal of Clinical Dentistry 2005;16:123-127.
18. Zach L, Cohen G. Pulp response to externally applied heat. Oral Surgery Oral Medicine Oral Pathology 1965;19:515-530.
19. Seale NS, et al. Pulpal reaction to bleaching of teeth in dogs. Journal of Dental Research 1981;60:948-953.
20. Baik JW, et al. Effect of light enhanced bleaching on in vitro surface and intrapulpal temperature rise. Journal of Esthetic and Restorative Dentistry 2001;13:370-378.
21. Eldeniz AU, et al. Pulpal temperature rise during lightactivated bleaching. Journal of Biomedical Materials Research,Part B: Applied Biomaterials 2005; 72:254-259.
22. Kossatz S, et al. Effect of light activation on tooth sensitivity after in-office bleaching. Operative Dentistry 2011;36:251-257.
23. He L-B, et al. The effects of light on bleaching and tooth sensitivity during in-office vital bleaching: A sys tematic review and meta-analysis. Journal of Dentistry 2012;40:644-653.
24. Marson FC, et al. Clinical evaluation of in office dental bleaching treatments with and without the use of light-activation sources. Operative Dentistry 2008;33:15-22.
25. Calatayud JO, et al. Clinical efficacy of a bleaching system based on hydrogen peroxide with or without light activation. European Journal of Esthetic Dentistry 2010;5:216-224.
26. Buchalla W, Attin T. External bleaching therapy with activation by heat, light or laser – a systematic review. Dental Materials 2007;23:586-596.
27. Alomari Q, El Daraa E. A randomised clinical trial of in-office dental bleaching with or without light activation. Journal of Contemporary Dental Practice 2010;11:E017-024.
28. Gurgan S, et al. Different light-activated in-office bleaching systems: a clinical evaluation. Lasers in Med ical Science 2010;25:817-822.
29. Bennett ZY, Walsh LJ. Effect of photo-Fenton bleaching on tetracycline stained dentin in vitro. Journal of Contemporary Dental Practice. 2015;16(2):126-129.
30. Walsh LJ. Back to the roots: applications of curcumin (turmeric) in dentistry. Auxiliary. 2015; 25 (3): 26-28.
31. Kuzekanani M, Walsh LJ. Quantitative analysis of KTP laser photodynamic bleaching of tetracycline-dis coloured teeth. Photomedicine and Laser Surgery 2009; 27(3):1-5.
32. Bennett ZY, Walsh LJ. Efficacy of LED versus KTP laser activation of photodynamic bleaching of tetracycline-stained dentine. Lasers in Medical Science 2015;30(7):1823-8. doi: 10.1007/s10103-014-1675-4.
33. Walsh LJ. Laser analgesia with pulsed infrared lasers: theory and practice. Journal of Oral Laser Appli cations 2008;8(1):1-10.
34. Liang R, George R, Walsh LJ. Pulpal response fol lowing photo-biomodulation with a 904-nm diode laser: a double-blind clinical study. Lasers in Medical Science 2016;31(9):1811-1817.
35. Walsh LJ. Clinical applications of low level laser therapy: current use and future potential. Australasian Dental Practice 2015 May-June 26 (3): 82-84.
36. Chan A, Punnia-Moorthy A, Armati P. Low-power pulsed Nd:YAG laser irradiation for pre-emptive anaes thesia: A morphological and histological study. Laser Therapy 2014;23(4):255-62.
37. Spitzer D, Ten Bosch JJ. The absorption and scat tering of light in bovine and human dental enamel. Calcified Tissue Research 1975;17;129-137.
38. Li R et al. Optical properties of enamel and trans lucent composites by diffuse reflectance measurements. Journal of Dentistry 2012; 40S: e40-e47.
39. Anagnostaki E et al. A Spectrophotometric study on light attenuation properties of dental bleaching gels: potential relevance to irradiation parameters. Dentistry Journal 2020;8:137.
40. Albini A. Photochemistry: Past, Present and Future. Springer: New York, 2016.
41. Persico M, Granucci G. Photochemistry: A Modern Theoretical Perspective. Springer: New York, 2018.
July/August 2022 Australasian Dental Practice 77
the cutting | EDGE
Beware confusing messages from those seeking to turn dentists into their clients
By Graham Middleton
“Wealthier investors can feel somewhat of an ego surge when they are offered to be classified as professional investors, but rarely does this convey an actual advantage...”
Igained my first dental clients soon after joining a firm known as APMA, which soon after rebadged itself as SAI following an ownership separation. I left SAI in 1994 to form Synstrat Group in partnership with Bill Dewez, a chartered accountant. By prior agreement, we transferred our existing clients from SAI to Synstrat Group. I retired from Synstrat on 30 June 2020, having spent over 33 years advising dentists on a range of business strategy and financial decisions. Prior to 1987, I had spent 2 years working for Shell, 20 years in the reg ular army, most of it as an officer and two years as Director, Human Resources of the Attorney Generals Department of Victoria - all valuable experiences.
It is critical to know the extent of your adviser’s knowledge of dental practice financial outcomes
Long ago, I came to the realisation that to be a trusted advisor to dentists or veterinarians, I needed to learn a lot about their business models and identify what made some very successful while
others, some of them probably equally talented, did not gain the long-term financial security enjoyed by their colleagues. This led me toward deeper analysis of their practice financials, leading to establishment of benchmarking databases. Benchmarking, in turn, disclosed weaknesses in practices; often the prac tice owner was either unaware of these weaknesses or, in many cases, sensed that something was wrong but could not identify it. In turn, this helped greatly with practice valuations. You cannot be an effec tive financial adviser to dentists without detailed knowledge of their performance as practice owner operators, the financial structure of their practice and the split of debt between practice related assets and non-business debt including home loans.
Valuations which came as a shock
Sometimes a valuation exposed raw nerves when a dental practice owner had an inflated idea of the performance and value of their practice and a low valuation touched upon a raw nerve. At other times, the recipient took it as a signal to address the short comings in order to raise the value of their practice.

78 Australasian Dental Practice July/August 2022 practice | MANAGEMENT
Sometimes, on receiving a valuation required for dispute resolution, a lawyer was surprised at the value. I recall an instance of the lawyer representing the wife of a veterinary practice owner being shocked at my value of the hus band’s practice which was attached to a Melbourne suburban home in built on premises which were sub-standard. When the lawyer protested that the husband had already offered more in settlement negotiations, my advice was “this prac tice is a dump and has many deficiencies; my strong advice to your client through you is to accept the settlement offer and move on”.
Many of the investment schemes tar geting dentists ignore the huge amount of evidence indicating that for many dentists, their four best investments are:
1. Their long-term home. This is usually a step up from their first home;
2. Their dental practice from which they draw the vast bulk of their income;
3. Their practice premises with the excep tion of some country dentists paying very low rent. Premises ownership also permits long term control of the fitout infrastructure including plumbing, wiring and dental cabinetry, most of which is unsalvageable if a practice is moved but which is extremely costly to replace; and
4. Their family superannuation fund once combined dentist and spouse combined superannuation assets are likely to pass $500,000 in the coming financial year.
There are very solid reasons why this strategic quad of investments is para mount in the vast majority of successful dentist’s net wealth.
Beware of those who tell you dif ferently because almost certainly they are window dressing some scheme which should be avoided like a dose of COVID.
selves as “forensic accountants” in order to feast upon partnership disputes and marital breakdowns presented themselves as able to value a myriad of business types but lacked expert knowledge of any. Over many years, I was sometimes asked to value dental or veterinary practices for legal support purposes and the opposing party’s lawyers had engaged a forensic accountant who demonstrably had no knowledge of the relevant benchmarks and who simply manipulated figures to present a heavily distorted value which was either extremely high or extremely low dependent on the interest of their client toward an over value or under value outcome. Sometimes I was able to persuade both party’s lawyers that pro ceeding to court with a flawed valuation was not advisable, apart from the mag nitude of the additional costs involved. On other occasions when unable to deter court action, I was able to arm my client’s barrister with a list of questions to put to the opposing expert (forensic accountant) to demonstrate to the court the individu al’s lack of expertise concerning dental or veterinary practice appraisal and valu ation experience. Questions such as how many dental practices do you currently provide accounting or advisory services to? Or how many dental practices have you valued? Or what is the most widely accepted dental remuneration formula and like questions quickly exposed a lack of industry specific knowledge.
Lawyers who profit by prolonging disputes
My advice to couples in dispute was to remove as many items from the dispute as possible by selling directly owned shares and investment properties other than practice premises and having up to date superannuation fund financials. Ensure that practice financials are as up to date as possible. If the dispute starts late in a financial year, wait until post 30 June and have the practice accountant complete annual financials as quickly as possible, then expedite valuation. Ideally both par ties should agree a common valuer and it is essential that the valuer concerned have substantial experience of valuing dental practices.
Financial schemes: The vital test
There has been no lack of schemes pushed at dentists and other profes sionals over many years. The first vital test is to ask, “is there a financial market where I can sell this investment?” - for example, while there is a visible acces sible housing market and a share market, investments in timber plantations, olive groves, chocolate factories, viticulture vineyards, etc, lacked the essential ingre dients of a vibrant secondary market on which investments could be readily sold at realistic market value.
Practice valuation exposed many den tists’ accountants as being inadequate in their advice. Some accountants set themselves up as valuers without bench marking data and few if any dental clients trusting that they could bluff their way through until they had gained sufficient expertise. Some who advertised them
Unfortunately, some family law spe cialist lawyers go to considerable lengths to prolong disputes to generate income. Family law specialists come in quads, being each party’s solicitor and each party’s barrister; when a valuation from a forensic accountant is considered by that party’s solicitor who refers it to a barrister who refers it back with questions to the solicitor to ask of the other party’s solicitor who refers to that party’s valuer and barrister, a circle of legal fee genera tion ensues and if 30 June passes, then one of the solicitors calls for new valuations and the legal fee merry-go-round con tinues. I observed over many years that the eagerness of lawyers to prolong disputes was directly proportional to their view of the likely value of the assets in dispute.
The commercial property collapse of the early 1990s exposed unlisted property trusts’ weaknesses. Investors who had bought into what they thought to be sound strategies were suddenly left locked into syndicates and unlisted property trusts with many of these syndicates having significant but internal gearing which had leveraged off the high inflation of the 1980s but which was utterly destructive in the early 1990s. Government and Reserve Bank actions forced interest rates up and inflation down. This destroyed the internal leverage of these unlisted property syndi cates and unit trusts.
Beware offers to include dentists with substantial income or assets into the clas sification of professional investors. While less scrupulous advisors will pretend that this is giving them access to certain investments not generally available, the reality is that many investments packaged in minimum lots of $500,000 have poor characteristics. Naturally, wealthier inves tors can feel somewhat of an ego surge when they are offered to be classified by
July/August 2022 Australasian Dental Practice 79
Exposing lack of dental specific knowledge of “forensic accountants”
practice | MANAGEMENT
capital assets or income as professional investors, but rarely does this convey an actual advantage.
The reality is that most of the above types of investments, including those packaged for “professional investors”, lack the intrinsic qualities of the dental quad, i.e. home, practice, practice prem ises and super fund. With respect to super funds, it is best to be a little patient and wait until the combined superannuation assets of the members (generally husband and wife) are likely to reach $500,000 in the year in which a self-managed super fund is established. Beware of advisors who then advise your SMSF to invest in managed investments therein. Internal costs of most managed investments are the precise reason why investors set up SMSFs and buy shares, bank hybrids, exchange traded funds and listed real estate investment trusts direct. Exchangetraded funds generally have far lower management expense ratios than do managed funds.




General Advice Warning
The information contained in this article is unsolicited general information only, without regard to the reader’s individual financial objectives, financial situation or needs. The information contained on this article is general in nature and you should consider whether the informa tion is appropriate to your needs, and where appropriate, seek professional advice from an accountant or financial adviser. It is not specific advice for any particular individual and is not intended to be relied upon by any person. Before making any decision about the informa tion provided, you should consider the appropriateness of the information in this article, having regard to your objec tives, financial situation and needs and consult your professional adviser. Any indicative information and assumptions used here are summarised, are not a product illustration or quote and also may change without notice to you, particularly if based on past performance. This notice must not be removed from this article.

About the Author
Graham Middleton disposed of his interest in Synstrat group on 30 June 2020 and won’t be starting another business. He spent the later 33 years of his working life advising health professionals on busi ness and financial matters. Dentists were the most numerous of his clients. He is the author of the recently published Finan cial Success for Dentists. Dentists may obtain a copy by making a donation of a minimum of $60 to the Delany Foundation, a registered charity which assists schools in Ghana, Kenya and Papua New Guinea, then email Graham at graham.george.middleton@gmail.com. A copy will be sent to you. All proceeds go to the Delany Foundation for its good work. Graham has paid for the printing and mail costs personally.

80 Australasian Dental Practice July/August 2022 practice | MANAGEMENT
8 great websites for dental professionals www.dentalcommunity.com.au professional portal www.dentalpractice.com.au magazine www.oralhygiene.com.au magazine www.elaborate.com.au magazine www.dentevents.com events calendar www.dentevents.tv dental video streaming www.dentist.com.au find a dentist - australia www.dentist.co.nz find a dentist - new zealand






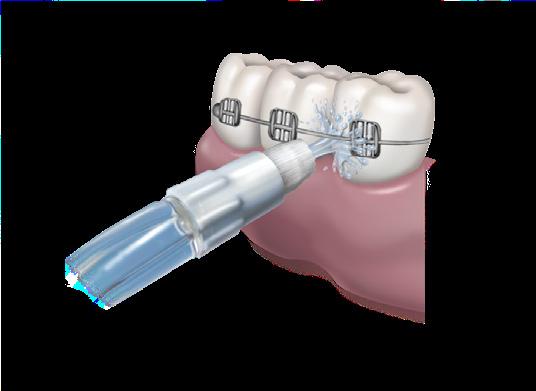



Visit www.waterpik.com.au for more information or email professionalau@waterpik.com Lunch on us!* Book your free lunch and learn NOW and find out how Waterpik can benefit your practice and patients. Take advantage of our Professional Trial Offer with up to 60% off 1 BOOK The Easy and Most Effective Way to Floss!™ *Dependent upon location of practice. Sessions via face to face or Zoom. 1. Terms & Conditions apply. Please visit Waterpik.com.au/shop for more information. 2. Independent clinical studies. Go to Waterpik.com.au for details. Clinically Proven Results Untreated Treated Removes up to 99.9% of plaque from treated areas2 Up to 50% more effective for improving gum health vs floss2 Up to 2X as effective for improving gum health around implants vs string floss2 Up to 3X as effective for removing plaque around braces vs strong floss2 waterpik.com.au/shop professionalau@waterpik.com
Get your house in order
By Julie Parker
What do you think of when I say, “get your house in order”?
It may mean getting your financial affairs in order. Or it may mean finding some solutions to some ongoing problems you might have.
Another meaning to “get your house in order” is to improve or correct the way you do things. And this is a meaning that I find powerful.
Many people are faced with the ques tion at some point in life: “how can I be happier?” They know they don’t feel as happy, satisfied... passionate as they would like to be. But, when asked by ther apists and friends “specifically, what do you want?” they are at a loss. What they truly desire seems so long ignored that they can’t even see it anymore.
For those people, might I suggest that it is time to “get your house in order”?
I have developed a process that can be helpful in creating a happier life. It’s called “getting your house in order” and it goes like this. It can be used for home or for your practice or elsewhere.

Allocate about an hour of your time and find a quiet space. Equip yourself with a pad and pen.
You are going on a tour of your “house”.
At the top of each page, write the name of each room in your house. There will be “front porch”, “living room”, “kitchen”, “master bedroom”, “kid’s bedroom”, etc.
Using a whole page for each room of your house, draw a table with four rows and four columns (Figure 1).
Starting on your first page, consider the following questions when contemplating the space you hold in that particular room of your house. Enter your answers under the column “Current Reality”.
• What is your mood when you are in this room?
• What are you doing when in this room?
• What are you thinking when in this room?
• What are you feeling when in this room? To give you an example, someone who is unhappy with aspects of their life may have answers similar to the following:
Living room
• What is your mood when you are in this room? Tired.
• What are you doing when in this room? Watching television.
• What are you thinking when in this room? Nothing much. Maybe that I should be using my time better.
• What are you feeling when in this room? A little disappointed.
Kitchen
• What is your mood when you are in this room? Frustrated as making meals is a constant chore.
• What are you doing when in this room? Cooking meals, eating.
• What are you thinking when in this room? What to eat/prepare/shop for.
• What are you feeling when in this room? Impatient and a little resentful.
Backyard
• What is your mood when you are in this room? Okay... neither a positive or a negative mood.
• What are you doing when in this room? Taking garbage out, weeding.
• What are you thinking when in this room? I wish I had more time to spend out here and make it nicer and better maintained.
• What are you feeling when in this room? Guilty for neglecting this space.
Once you’ve moved through each room and area of your house and made com ments about the space you hold in each of them, consider what a happy, successful and optimistic space you could hold instead. Close your eyes and imagine a happier reality for yourself and what envi ronment you need to create to foster those feelings of happiness. Enter these com ments on the second column titled “Happy Reality”. For example, this could be:
Living room
• What is your mood when you are in this room? Excited to spend time doing anything I choose.
• What are you doing when in this room? Reading, having friends over, watching programs on television that are educational, enlightening or inspiring.
• What are you thinking when in this room? All sorts of things. Books, con versations with friends and insightful television push me to think differ ently and broaden my perspective and awareness. Life is interesting!
• What are you feeling when in this room? Elated.
Kitchen
• What is your mood when you are in this room? Happy - I love delicious food!
• What are you doing when in this room? Trying different ways of cooking, having family meals.
• What are you thinking when in this room? How can I make meals more delicious? How can I make new, adven turous meals?
• What are you feeling when in this room? Enjoying family time and finding out how others’ days went.
82 Australasian Dental Practice July/August 2022
practice | MANAGEMENT
Living room
CURRENT REALITY HAPPY REALITY SHIFT (NEW ACTIONS)
MOOD DOING THINKING FEELING
Backyard
• What is your mood when you are in this room? Calm, happy, soulful.
• What are you doing when in this room? Breathing in fresh air. Admiring the plants, flowers and weather.
• What are you thinking when in this room? Thinking about each area of the backyard of the memories of building and maintaining the space and garden.
• What are you feeling when in this room? Gratitude to have this beautiful space to come and replenish my spirit.
The third column is where you identify specifically what actions you can take to shift from Current Reality to Happy Reality. Continuing with our example, this could be:
Living room
1. Set my current favourite book beside the chair I will read in.
2. Scroll through and select a couple of documentaries that I want to watch this week on streaming.
3. Invite my sibling over for morning tea with the intention of connecting.
Kitchen
1. Establish the routine of eating at the table with my family for dinner.
2. On Sunday, just for enjoyment, select a cake to bake to eat as a treat throughout the week.
3. Eat slowly and savour the flavours and enjoyment of eating.
Backyard
1. Start a herb garden.
2. Set aside 20-minutes every day to sit in the backyard and enjoy the aromas, the sound of the birds and look at the garden.
3. Get rid of any trash and garbage that is staring at me to manage.
Using this “getting your house in order” process is helpful because it helps you identify the small, routine actions that you can take that will quickly achieve happier results.
You won’t have to wait for weeks or months to start seeing progress. Progress is achieved instantly.
You might also find that identifying larger, long-term goals easier once you get your house in order. As you start
achieving happiness in several aspects of your life, your mindset will start to shift to one that is more powerful and open to seeing that which you were blinded to in the past.
This process can be used for your work place as well. Consider the space you currently hold when you enter your dental practice, your surgery to see patients, your staff meetings and the connections you make with your co-workers.
A happy life is up to us.
We quickly discover that no one else arrives to do this for us.
So, if you feel as though you could be living a happier life but don’t know where to start, then maybe it is time to get your house in order.
About the author
Julie Parker Practice Success provides dental teams with coaching and training so they can work together and achieve successful outcomes for their dental practice. For more information, please contact Julie on 0407-657-729 or julie@julieparkerpracticesuccess.com.au
July/August 2022 Australasian Dental Practice 83
| MANAGEMENT
practice
Tired Watching television Nothing much. Maybe I should be using my time better
A little disappointed
As a practice owner... are you driving without destination?
 By Simon Palmer
By Simon Palmer
When dentists decide to get into ownership, they spend many hours ana lysing possible practices to buy or sites to start up in. They fill spreadsheets with costings and projections, competition analysis, ideas and business plans before they act.

When they are in practice, they spend countless hours agonising over how they are going to make their practice work for them. They develop systems and procedures, stress about which supplies, lab
and advertising they will commit to, go to clinical and business courses... all to make sure they are at the top of their game, so that they can offer a quality, efficient service of integrity to their clients.
With the methodical nature in which dentists get into ownership and run their practices, it is quite paradoxical that they spend nearly no time thinking about how they would like it all to end - and let’s face it - it will end. Someday, somehow, the prac tice that you currently own will one day no longer be yours and this end of practice ownership can either come on your terms or on someone else’s.
84 Australasian Dental Practice July/August 2022
practice | MANAGEMENT
Far too many dentists ignore this inevi tability. They turn up to work, day after day and year after year, as if each day and year will be like the one that preceded it... working with little vision about what it is building towards and what it will all look like when it’s time to bow out.
“With the methodical nature in which dentists get into ownership and run their practices, it is quite paradoxical that they spend nearly no time thinking about how they would like it all to end - and let’s face itit will end...”
The way most dentists own a practice is akin to driving a car without a destination, without ever checking how much petrol is in the tank. Sure, the car may be nice and comfortable, they may be enjoying the journey, but when the tank starts to run dry (and it will in one way or another), the destination that they end up at may be undesirable and they may be left with few choices when they get there.
In 1989, Stephen Covey published his famous book, “The 7 habits of highly effective people”. It is consistently rated by business institutions in the top business self-help books in the world. While not all of the habits outlined in his book are relevant to exit planning, one certainly is. Habit number 2 in the book is to “Begin with the end in mind”. The takeaway point of this chapter is that if we take the time to be goal focused in our approach to our
lives and businesses, we are much more likely to get outcomes that are right for us. What this means for you as a dental business owner is asking and having answers for the following questions for yourselves:
1. What financial figure do you need to reach, in order to retire comfortably?
2. Is there an approximate date or age that you are hoping to work until? Or retire before?
3. Are there any bucket-list trips, hob bies/interests (outside of dentistry) or relationships (kids, grandkids) that you would like to dedicate more time to while you are healthy and young enough to enjoy them?
4. Do you know what your practice is approximately worth and how that value is increasing or decreasing over time?
5. Do you know what your practice’s likely buyer profile looks like? (Is it likely to be a corporate, an aggregator, an experienced owner-operator or a new grad?)
6. Do you know what that buyer profile is likely to be looking for (Pro tip: a cor porate is looking for something very different to an owner-operator)?
If you know answers to these questions, you can work backwards and take steps to ensure that, when you reach your exit date, your practice is optimally placed to attract the best possible buyer, to offer the best possible price and terms to facilitate the exit that is best for you.
This doesn’t mean working harder. There are many, many variables that, if positioned correctly, can make a differ ence when you get to the finish line. For example: ensuring that you have a long lease on the premises; the zoning permit on your premises is correct for use; reducing key-man dependence; having
written agreements with employees, con tractors and partners; making sure that financials are clear and not mixed up with other business interests; not taking excessive holidays in your final years; timing reinvestment to ensure that it is reflected in revenue and profit before you sell; etc, etc. A far more comprehen sive list can be found at our exit seminar (www.exitacademy.com.au).
A dentist’s practice is usually one of their most valuable assets. If dental practice owners applied the same methodical pro cess to exiting ownership that they applied to entering and operating their practice, its sale would be able to make a massive difference in their (and their family’s) lives post sale.
“If dental practice owners applied the same methodical process to exiting ownership that they applied to entering and operating their practice, its sale would be able to make a massive difference in their (and their family’s) lives post sale...”
About the author
Simon Palmer is the Managing Director of Practice Sale Search, Australia’s largest dental practice brokerage. If you’d like more info on practice sales or want to have a confidential discussion about your practice’s circumstances, email Simon at info@practicesalesearch.com.au or call 1300-282-042.
July/August 2022 Australasian Dental Practice 85
practice | MANAGEMENT
AUCKLAND SYDNEY MELBOURNE 17 September 22 October 29 October AUCKLAND SYDNEY MELBOURNE 17 September 22 October 29 October AUCKLAND SYDNEY MELBOURNE 17 September 22 October 29 October
Buying back your time:
A dentist’s guide to
By Dr Jesse Green
hen we think of currency, we tend to imme diately think of money, finances, capital and our business. But really, there are three major currencies we hope to generate as practice owners; time, money and purpose.
Money can be found in many dif ferent places and show up in different ways. Time, on the other hand, is the only resource that isn’t renewable. It cannot be replenished as once it’s gone, it’s gone. It’s also one of our most valuable assets and a great equaliser and it’s something most dental practice owners are often complaining about not having enough of...
A lot of dentists are type A perfectionists who are in the habit of giving away a lot of their time. They have a team to manage and patients to treat and find themselves caught in the middle overworked and with little time for themselves or to focus on the key areas of their business.
Needless to say, that’s not what you got into practice ownership for.
You don’t want to grow to resent your practice and the people around you for gobbling up your time - you want your time to be intentional, given willingly and used effectively. You also need to be the leader of a pack that does its job well while you do what you love to do - dentistry.
In short, you want to take control of your business so you can also have a life.
With that in mind, I wanted to share with you some reflections on how to get back more of your time - or at least spend it where you should to get the most out of your efforts and keep the stress of running a practice under control.
wealth
creationPart 3
WAs a dental practice owner, you often find yourself wearing different hats and switching between roles very quickly. From dentist to receptionist to accountant to marketer, it tends to fall on your shoul ders. However, just because we can do everything, doesn’t mean we should.
When you overburden yourself with work that your team members should be taking care of, your routine becomes overwhelming and you have no time to run the actual business and also treat your patients. The appointments keep piling up while you tend to emergencies and postponements disturb your schedule. Eventually, you will need to work longer hours and will ultimately put yourself under a lot of stress.
So, what’s the most effective and efficient way out? Delegate.
Remember when you recruited team members and were looking forward to off loading tasks from your plate? Now’s the time to actually delegate tasks and respon sibilities to the team you have built with a lot of time, effort and expense.
Instead of doing it all on your own, trust your team and let them share the load. By leading your team and saving yourself precious time, it allows them to do the heavy-lifting for your business and you can then focus on your core expertise and skills.
Be an effective leader, delegate responsibilities and tasks and buy back time
When your employees are disen gaged and unmotivated, or when you take ownership of your dental prac tice more than you should, you’ll always find yourself answering questions, filling
up your entire day with small tasks, leaving you overworked, unproductive and stressed.
You’ll sit down at the end of the day and wonder why you haven’t got any time left for your goals and priorities, much less to spend time with yourself and working “on” your business...
You might have your processes, tools and even your workplace culture to blame for all this, but it all boils down to a lack of effective leadership. As a leader, you need to make your team feel like you are one of them. Inspire your team not only to perform well in their jobs but also to find purpose within the roles they’re performing.
When everyone realises their responsi bility, you’ll save more time and energy for what you love to do and what needs your attention the most. Besides, you’re going to be a much better practice owner, dentist, leader, parent, partner and friend when you can give each person your atten tion and have the energy to recuperate between responsibilities.
Now, the question is how exactly are you going to do that? Here are a few things you need to do to see that happen.
Partner with your team
W

hen you partner with your team, they’ll have an undeniable urge to work harder. It’s human nature - many people thrive when they feel they are trusted and needed to make success happen.
Leaders will also benefit by showing their team that they are one of the pack and are actually willing to trust and work alongside them. It makes employees feel comfortable and they in turn step up to give their best to their leader and their team.
86 Australasian Dental Practice July/August 2022 practice | MANAGEMENT
Delegate tasks
By delegating tasks to your staff, you’ll be giving them more respon sibility which many employees thrive on. Remember, however, that delegation starts with getting over our own ego.
When our business is our brainchild, it can be hard to let go of the feeling that we know best.
We have this idea that we know our own business so intimately, that no one else can match our skill sets.
Subconsciously, we might not be making the space for our employees to succeed.
When they stumble and trip and make mistakes, it gives us the excuse to take back the reins. And then, we’re back where we started, wearing all the hats and with no time.
Delegating tasks lets you focus on things that can make your practice more profitable. Have your team members deliver on what you have hired them for and keep your focus on dentistry - some thing that you’re meant to do.
You’ll save your own precious time and you can make the most of it by directly helping your patients and growing your business.
Train your employees
Play to your employees’ strengths and skills
A gain, you have to choose the right person for the job. You might instinc tively know who the right person is, or you might need to consult other team members and ask around. Don’t be afraid to ask your team “Who would like to take the role? Who wants to level up on their responsibilities? Do you have the capacity to take this on right now?”
And while failure is just part of the game, you do want to ensure you aren’t actually setting people up to fail. Give them what they are capable of and play to their strengths and skills so that you don’t have to intervene or bother all the time so that things may not get messed up.
After all, your ultimate goal is to buy your time back.
Define the desired outcome
need to innovate and build the financing option into case presentations to operate more efficiently.
Being patient and sharing your experi ence with your team members gives them the confidence to start all over again and get you the outcome you had previously defined for the given task or deliver on new milestones.
Deliver constructive feedback so your staff learn and take more on
G
ive feedback to your team where needed and help them improve. Your constructive feedback will not only help your staff learn, but they’ll be ever-ready to take more on.
As a result, you’ll free up more of your time to focus on other important things.
A
s a leader and the owner of your dental practice, you know how cer tain tasks need to be done and what should be the desired outcome. So, when you delegate tasks, communicate to your employees what needs to be done, by when and WHY. Take the extra ten min utes to explain the strategy and context around the task, explain what it will look like when done right and how this benefits the practice in the big picture.
Owning and running a practice is no small task - you have many responsibili ties on your mind as well as your patient load, team’s welfare, financial responsi bilities, strategic decision making... and this is all on top of your own personal issues like family, health, home, etc.
S
uccessful delegation of tasks is only possible when you have trained your employees for their roles. You may have hired the best people for the job, but it may take a little on-the-job training for them to perform to their potential, so it’s important to realise that mistakes are learning opportunities.
You have employed these people, so trust them to grow your business with you.
Giving our employees the space to fail empowers them to be 100% accountable for their own work - which ultimately frees up time for you. Now you have a piece of the business you no longer have to worry about.
When you’re delegating, there are a few things to consider such as attitude, existing skill set, workload and whether they’re up to the task. When every aspect is taken care of, it will lead to suc cessful delegation and you can expect the desired results.
Try not to helicopter and hover over the person taking on the task, but do have someone on hand should that person need to clarify or ask questions - whether it’s yourself or someone else.
It will give them the confidence and the inspiration to give their best and achieve the desired outcome.
Be patient and be prepared to give guidance
Even when you have the right person on the job and have given them the neces sary training to perform delegated tasks, errors are inevitable. As a leader, you need to stay patient when that happens and should provide guidance on where things went wrong and how they should go about it in the future.
For instance, if your employee failed to achieve their target for accounts receiv able where your practice does not use outside patient financing much, you may
When we get burnt out, we feel less fulfilled with our choices and end up working twice as hard for less satisfac tion and financial reward. Obviously, this isn’t ideal and something needs to be done about it. The more burnt out, over whelmed and fatigued you are - the less effective you work.
Practice ownership is a marathon, not a sprint. You need to pace yourself with a sustainable schedule, look after your mind and body and make the process enjoyable. And that’s only possible when you del egate tasks and lead effectively.
About the author
Dr Jesse Green is the founder of the Practice Max mastermind, the host of The Savvy Dentist Podcast - Australia’s #1 Dental podcast and the author of the Amazon Bestseller “Retention! How to Plug the #1 Profit Leak in Your Dental Practice”. Delegating and being an effec tive leader are not the skills taught at a dental school. To become the very best leader for your team and get more time and more freedom in your business, join us at the Practice Max Mastermind by visiting https://savvydentist.com/practice-max
July/August 2022 Australasian Dental Practice 87
practice | MANAGEMENT
Do your customers believe you are delivering great customer service?
 By Jayne Bandy
By Jayne Bandy
I’m sure you already know how important it is to all businesses to deliver consistent GREAT CUSTOMER SERVICE.
But what if, the Great Cus tomer Service you are delivering is not so great in the eyes of your customers?
Are you getting your cus tomer service wrong?
You might be trying to be everything to everyone, only to be diluting the impact of your customer service delivery.
So, how do you know if you are hitting the mark with your customers, when it comes to the delivery of customer service?

Do you sit there hoping you don’t get bad reviews and phone call complaints, or do you make sure you are on top of it and consistently ask your customers for feed back to guide you?
I’m the sort of person that gives both positive and negative feedback when I personally receive good and bad customer service.
I usually do what most people do when they receive bad customer service. Yes, I have a rant about how disappointed I am and tell a few people before I speak to the people who have delivered the bad customer service.
This is the dangerous time for busi nesses. The time between when the customer is either extremely or mod erately disappointment and angry and finally contact you.
After all there is an exchange for the services you provide, and people can feel ripped off if they have not been happy with your customer service.
One of the biggest issues people have when they received bad customer service is being ignored or made to feel unimportant.
A story from my friend
A person I know very well, finally received an email from a company that had failed to reply in an acceptable time frame. The email was quite generic and impersonal and started by letting her know they prided themselves on delivering great customer service to their valued cli ents. My friend was not receiving great customer service and was not feeling like a valued client. Why would you tell your customer you deliver great customer ser vice when you did not?
The best and only way to ever give great customer service is to consistently
show it in your actions. Anyone can tell you how great they are.
You need to SHOW IT!
Ok, let’s go back to consistently asking customers for their feedback.
Now when you ask your customers for feedback you will get good feedback, but you do open yourself up to receive bad feedback if your customer service has been bad. So be prepared.
I always see negative customer service feedback as a GIFT.
Your customer has given you the gift of awareness and the gift of opportunity to make positive changes.
You benefit and the customer benefits after you make the changes needed to improve your customer service.
There is nothing worse than not knowing your customer service is BAD!
88 Australasian Dental Practice July/August 2022 practice | MANAGEMENT
Eventually someone comes forward to tell you about your bad customer service but it’s often too late for all the customers you have lost because you had no idea your customer service was awful.
If you are concerned that you are not delivering customer service to your patients the way you should be, then start by asking your customers for their feed back and remember feedback is only as good as what you do with it. Again, you may not like what you hear but take the feedback seriously and make changes.
Your customer service may be failing on the very first phone call, you may not be making your patients feel loved when they arrive at your front door, you might not be listening to your patients and matching what they want as well as what they need.
One of the worst stories I heard was a Dental Practice who thought they were doing everything right until they discov ered they had lost patients because of how a team member was speaking to them on the phone.

Make sure this is NEVER YOU!
About the author
Jayne began her career as an educator. After spending several years teaching, she made the jump to practice manage ment, serving as a Practice Manager for a renowned dentist in Sydney for more than 25 years, giving her first-hand experience at what works when it comes to building and maintaining patient relationships, how to convert leads over the phone and most importantly - what it takes to reach your practice goals. As the CEO and Founder of Dental Phone Excellence, Jayne helps practices convert more calls into appoint ments, reduce cancellations and nurture effective patient communication that will result in increased profitability. Her past experience as an educator combined with her passion for practice management gives her a unique set of skills that allows your team to fully understand and take advantage of the tools she presents.
For more information on what to say and ask your patients, call 1300-378-044 or email jayne@thedpe.com
July/August 2022 Australasian Dental Practice 89
practice | MANAGEMENT ACCOUNTING & FINANCIAL SERVICES FOR DENTISTS DON’T RISK SECOND BEST Synstrat has spent many years collecting data on dental practices. We provide you with the best available knowledge on the performance of your practice relative to others. Our proven service has assisted many dentists Australia wide to create significant wealth. We are able to provide you with business accounting, practice valuation and financial advice services tailored to the dental profession. Buying A Practice? •Do you need us to value the practice? •What rent can it afford? • How do you structure to meet tax planning requirements? • What changes should you make to the practice business plan? The Synstrat Group www.synstrat.com.au ALSO AVAILABLE: 50 Rules for Success as a Dentist Buying and Selling Specialist Dental Practices Speak to Paul Steel or David Collins on (03) 9843 7777 or email dental@synstrat.com.au NOW AVAILABLE: Synstrat Dental Stories TO RECEIVE THE BOOK You can either e-mail dental@synstat.com.au with your request for the book together with your postal address or go to www.synstrat.com.au, navigate to the Synstrat Publications area and fill in the form. You will then be forwarded the book.
Dental
I listened
you
for YOU! Your
the
The
Phone Excellence Online Master Class dentalphoneexcellencemasterclass.com
to
and finally my Master Class is here ONLINE just
team do not need a day off work to attend this Master Class. YOUR TEAM can complete
Dental Phone Excellence Master Class right there in your practice at their own pace. The BEST part of my Master Class is that you have it FOREVER! dentalphoneexcellencemasterclass.com
How to give your practice a marketing makeover
 By Angus Pryor, MBA (Marketing)
By Angus Pryor, MBA (Marketing)
If your service is good but your new patient numbers are not, you probably need a marketing makeover. In this article, we look at the exact steps to make this happen at your practice.
Step 1. Find your ideal patient
E very single dental practice in Australia has a sweet spot for the types of patients that they serve best. Trying to be all things to all people is a recipe for disaster and must be avoided.

The first step in your marketing makeover is to look at your data and identify the common charac teristics of the patients that have historically been the best value for your business. To do this, run a
report of the top 30 spenders at your practice in the last year. Almost every practice management soft ware can do this. If need be, ask your provider how to generate this.
The reason we go after the top 30 spenders is this group is a combination of patients:
• With a need for more dental services than just an annual check-up and clean; and
• Who have trusted you to pay for those more expensive services.
This is the group we want more of - they trust you and they’re willing to spend. If you were to target patients without regard to their historic spending habits, you might end up attracting patients who don’t care about their oral health and won’t follow your treatment recommendations. That makes for unhappy dentistry.
90 Australasian Dental Practice July/August 2022 marketing | INSIGHTS
Once you’ve identified the top 30 spenders, look at their demographic data such as their age, gender, suburb, occu pation, educational background, family composition and so on.
There will be a spectrum but if you kind of squeeze them all together, you will come up with the series of averages i.e. among the top 30 patients, the average age is 45, the most common gender is female, their occupation is a teacher, etc. This aggregate person is what is known in marketing as your “avatar”.
Step 2. Personify your ideal patient
Now that you know the profile of your ideal patient (your avatar), we want your marketing to speak directly to that person. This next step in the process is kind of fun. Firstly, give your avatar a name, e.g. Mary.
Next, get together with your team and try to “look through the eyes of Mary” at your practice. This means asking ques tions like “what would Mary tell her friends about this practice?”, “what does Mary love about this practice?“, “what fears have we helped Mary to overcome?”. These kinds of insights are essential for attracting more “Marys” to your practice.
Step 3. Get the messaging right
It’s a surprise to some people, but the actual words that you use to describe what you do and the unique offer that you make to your potential patient, is really the most important part of your marketing.
Attractive images and broad exposure of your message form part of the picture, but the precise words you use are very, very important.
In my experience, this messaging is the one area most practices get wrong. Their messaging is frankly more often written for other dentists (“we have abc technical skills and xyz equipment”, etc) rather than speaking directly to your all-important avatar in a way they understand.
To avoid dentist-focused messaging, aggregate all of the feedback from the ses sion at Step 2 above and then hand this text over to a professional copywriter.
You could do this writing yourself, but this step is so important that it’s better to get a professional involved. Once you have received perhaps a page of text from the
copywriter that vividly describes what you do for your avatar and you’re happy with it, it’s time to start spreading that message.
Step 4. Marketing funnel
5. A strong presence in social mediagiven declining visibility for business social media pages (unless you pay for ads), this step is about reassuring people who come to check what you’re like;
N
ow that you know who your ideal client is and you have a message that speaks directly to them, it’s time to set up a marketing “funnel” that drives your potential patients to your practice.
This funnel comprises three parts: a. Your unique message distributed in var ious marketing “channels” where your avatar is likely to hang out’ b. These messages drives potential patients to your website; and c. The website asks visitors to make an appointment.
An important part of part a of this pro cess is to think about where your avatar actually hangs out. Channels to attract a 60-year-old are very different to those that attract a 20-year-old. Fortunately, you can play the odds and start in order of the most popular channels and work your way down to the least popular channels - more on that below.
Note: In a competitive, “noisy” mar ketplace, relying on just one form of external marketing is fraught with danger and more likely to be completely unsuc cessful. Prospective patients need to see your message multiple times before they decide to become a patient.
Put it this way, would you go and see a movie after hearing about it just once? Probably not. By the time you actually attend, you’ve seen or heard about it mul tiple times via multiple “touch points” (social media, TV ads, bus shelters, etc). It’s the same for marketing your practice.
In our experience, the following is the hierarchy of channels to market your ser vices to - ordered from most likely to be successful to least likely to be successful:
1. A strong “organic” presence in Google - this means appearing on the map and showing up in the unpaid listings;
2. Google ads - this system is completely separate to point 1 above but provides a good addition;
3. An internal referral system - good patients refer good patients, make it easy for them to do so;
4. Boosting your Google reviews - poten tial patients look for your Google reviews to reassure them that visiting your practice is the right choice;
6. Local marketing - this can include sponsoring sports teams, community groups, schools, ads at cinemas, etc;
7. Letterbox drops - can work, often doesn’t; and
8. Radio, TV, newspaper - problematic because most people won’t travel far to the dentist - can work in regional areas.
Step 5: Capture more data
Once your marketing makeover is in place, the final step is to capture information on what’s working and what’s not. On your new patient form, make sure that you ask your new patient to identify ALL the places that they came across you, not just one.
Otherwise, they’re likely just to indi cate the last place that they became aware of you rather than all of them. As noted above, successful marketing in 2022 is not about one marketing message in one place, but rather the aggregate of many touch points.
From time to time, aggregate the feed back from your new patient forms and adjust your marketing channels from there. If you find no one ever mentions a particular marketing channel that you use, then it may be time to kill it and move onto something else.
Conclusion
n an increasingly competitive envi ronment like dentistry, having sound marketing activities really is a must. Implementing the steps above for a mar keting makeover maximises your chances of attracting a steady flow of new patients to your practice.
I
About the author
Winner of the ADIA 2020 Marketing Award and Australia’s number one Google-ranked dental marketer, Angus Pryor is a #1 Amazon bestselling author, marketer and international speaker. Want a makeover but need some help with the process? Visit www.AngusPryor.com and book a free call.
July/August 2022 Australasian Dental Practice 91
marketing | INSIGHTS
Budgeting for busy people

 By Lena Ridley
By Lena Ridley
We are hearing (and feeling) the reality of cost-of-living increases and rising interest rates this year. The need to have and understand your personal budget (and practice budget if you have one) is more important than ever in this current environment. The truth is, budgeting is not an easy task and it’s one that most of us partially avoid. We hope that somehow, we will continue to manage living comfortably within our means and accu mulating wealth through some mystical process whereby intention is translated into results without any intervening hard work! Unfortunately, this rarely happens.
It’s a basic fact of human nature that we are inclined to avoid tasks that are painful and repeat those that bring us happiness. The relevance to budgeting? Compare spending an evening at home drawing up a budget plan to relaxing watching TV or going out with friends. Compare home renovations, a nice new car, travel, eating out and so on with boring old investing or paying off the mortgage. It’s more fun and much easier to spend now and hope the future will take care of itself.
For professionals and small business people such as dentists, the process can be even harder. Taking time to plan per sonal financial success often takes a back seat as we instead focus on business and career success. We figure, if we invest lots of time and energy in making the business more successful, that is bound to pay off for me personally in the long run - isn’t it? The sad truth is it often does not. Part nerships fall over, bankruptcies, illness and divorces dissipate business and career achievements and people are left with little personally to show for a lifetime of hard work.
The good news is it is within the con trol of almost all of us to live an enjoyable lifestyle now while still making sensible provision for the future. We have seen clients who never earned or drew more than about $40,000 a year, but neverthe less managed to accumulate seven figure sums by retirement. We have also seen (new) clients with personal incomes north of $400,000 per year who are in debt and have very little accumulated yet for their future.
There is strength in helping people understand the old-fashioned unsexy vir tues of thrift, forward planning and hard work. It is not quite as bad as blood, sweat and tears that I have to offer. But there is
a war on, in a way, or at least a battlethe battle for personal financial freedom in times of rising costs.
So how do you win the battle?
While budgeting can be tough, there are ways to make the process easier. Thank fully, there are plenty of apps out there to help you. You can track every receipt using some apps or take a broader view with others. Bank apps can help you cat egorise every transaction in your bank account; other companies can be used to manage your money and budget for you; and some are run in conjunction with your financial adviser taking a more holistic approach. The core tenants of each remain the same...
92 Australasian Dental Practice July/August 2022
finance | INVESTMENT
1. Set up a
personal balance sheet
Your personal balance sheet will vary according to your stage of life. It should include assets and any associated liabilities/debts attached to those assets. TIP: It is a good first goal to ensure your assets are greater than your debts!
Younger dentists will often have more debt on their personal balance sheet that will typically comprise their home, their share of a practice and most likely a motor vehicle. Mid-career dentists should start to see a fall in their level of debt, or at least a change in the type of debt from non-deductible (such as a home) to deductible (such as for investment). Those aiming to retire within the next 5 years or so should see a healthy net asset position that comprises superannuation, personal investments (property and shares) and the value of their practice. There should be little if any debt by this stage - or at least a strategy to pay it off at a point in time such as at time of retirement.
2. Plan your income for the year
The next step is to project how much income you are going to earn for the year. Dentists are often in a position where they can significantly influence or even directly control their personal income or drawings from the business. If you have been in business or have been employed for some years, there is a known pattern of
3. Decide your Net Asset Improvement (NAI) goal



This goal states by how much you want your net worth to improve over the year. Your NAI goal can cover asset accumulation (i.e., contributing to superannuation), debt reduction, or a com bination of both (It should not include any projected asset price improvement, as this is beyond your direct control).
What is a realistic goal for NAI? If you do not know where to start, there are a couple of approaches that can help:
income. This is typically a function of the number of days (and hours each day) you choose to work as well as the type of work that you undertake. Now is a very good time to review, assess and project your income for calendar year 2023. Most den tists will revisit this at the end of financial year, but I encourage you to set a realistic goal for the next calendar year now.
• One rule of thumb is to decide a set proportion of your income to commit to using for NAI. If you have no figure in mind, I generally suggest starting with a figure of around 20% of your incomeit may be more if your expenses are low and less if you are at a high expenses stage (such as paying private school fees, significant mortgage repayments, etc). I would generally suggest a minimum of 10% of income be considered, how ever. If this is problematic, then a major re-think of spending may be required!
July/August 2022 Australasian Dental Practice 93
finance | INVESTMENT Whether you’ve just started working, own your own practice or are considering retirement, Profile Financial Services can help you plan and secure your financial future. Just like good dentistry, in investing, prevention is better than cure! A sound financial plan can help anticipate and avoid risks before they damage your portfolio. How safe are your investments? To find out, contact Profile now to book an obligation-free initial meeting: (02) 9683 6422 Or visit our website www.profileservices.com.au even fOr yOur SAFety FirSt FinAn ci Al A FFA irS Wealth managers for the dental industry FOr OVer 30 yeArS BUilDinG WeAltH SecUrity AFSl 226 238 Profile_SafetyAd_v3.indd 1 18/03/11 2:04 PM
“TIP: It is a good first goal to ensure your assets are greater than your debts!”
• An alternative approach is to calculate the amount you will need to commit each year to ensure you are on track to deliver the income you require once you stop work. The calculations can be complex and small changes to the assumptions you use can have a very big impact on whether you are likely to achieve your overall goals. Financial advice is gen erally very helpful here. Your adviser can also help ensure you are making the very best possible use of the funds you can afford to commit to NAI - working out, for example, whether you would be better off reducing debt compared with making concessional contributions to superannuation and so on.
So have you created a budget yet?
If you have followed the process, you will have the following three inputs:
1. A personal balance sheet;
2. The income that you are going to earn over the next 12 months; and
3. An NAI goal.
The difference between the last two numbers represents the amount you can afford to commit to expenses this yearyour “expenses budget”. For many people, the process can stop here. You simply direct the amount you have decided on to your chosen NAI goal (debt reduc tion or asset increase) and anything that is left in the bank account after that rep resents your expenses budget and can be spent as required.
Other people may wish to go one more step and understand at least at a high level, the makeup of their expenses each year.
Discretionary expenses are simply what’s left over after you’ve subtracted fixed expenses from your expenses budget. This can be allocated to holidays, eating out, movies, gifts, donations, etc.
This analysis is very handy to do - it can identify whether your NAI goal is realistic or show areas where additional savings could be made. It is very common for clients to find, after going through
It is very common for clients to find, after going through this exercise, that a high proportion of their income could be devoted to NAI based on estimated expenses - and yet, for several years, no savings have been achieved! In some cases, we see debt has been steadily increasing even though income has been high and theoretically there should have been plenty available to invest. Never underestimate the power of discretionary expenses to eat away at your financial plans!
At Profile Financial Services, we have a range of tools to assist our clients to for mulate their budgets, as well as providing guidance on estimating expenditure for given stages of life and lifestyles, based on our extensive experience with many clients in the dental industry. We are also able to illustrate what level of asset accu mulation is required to support a lifestyle once the income from a dental practice stops. I strongly encourage you to for mulate your planned expenditure sooner rather than later, as the biggest enemy is time - and that is one factor that neither you nor I can control.
Remember - it’s not what you earn, it’s what you keep that matters!
Adapted from an original article from 2011 authored by Phillip Win.
General advice warning
Your fixed expenses usually include minimum loan repayments, elec tricity, water, gas, council rates, telephone (fixed and mobile), internet, health insur ance, life insurance, car insurance and car registration. This may sound a bit daunting, but all you need is a copy of your last two bills for electricity, water, gas, council rates, telephone and a quick snapshot of the direct debits for insur ances and you have your fixed expenses expenditure figure. You may also have additional expenses you consider nonnegotiable (such as private school fees).
this exercise, that a high proportion of their income could be devoted to NAI based on estimated expenses - and yet, for several years, no savings have been achieved! In some cases, we see debt has been steadily increasing even though income has been high and theoretically there should have been plenty available to invest. Never underestimate the power of discretionary expenses to eat away at your financial plans!
I hope I have convinced you of the importance of budgeting and illustrated some practical ways that this daunting task can be made a little easier.
This communication is issued by Profile Financial Services Pty Ltd. (ABN 32 090 146 802), holder of Australian Financial Services Licence and Australian Credit Licence No. 226238. It contains infor mation and general advice only and does not take into account any investor’s indi vidual objectives, financial situation or needs. It should not be relied on by any individual. Before making any decision about the information provided, inves tors should consider its appropriateness having regards to their personal objec tives, situation and needs, and consult their adviser. Any indicative informa tion and assumptions used here are summarised, are not a product illustra tion or quote, and may change without notice to you, particularly if based on past performance.
About the author
Lena Ridley is the CEO at Profile Financial Services Pty Ltd (AFSL 226238), a pri vately owned and self-licensed fee-based financial planning firm that specialises in working with dental professionals. Profile focus on implementing strategic advice and have a solid understanding and working knowledge of dentists’ structures and investment issues. Pro file can be contacted on (02) 9683-6422, email admin@profileservices.com.au or see www.profileservices.com.au
94 Australasian Dental Practice July/August 2022
4. Understand your fixed vs discretionary expenses and how you will keep a track of them
finance | INVESTMENT

3 FOR OPTIMAL TEMPORARIES Safe and quick processing • Intraoral time: just 45 seconds • 1:1 mixing ratio ensures homogeneous blend Outstanding aesthetics • Natural appearance • Available in 8 shades Long-lasting • High compressive strength • Excellent fracture resistance VOCO GmbH · Anton-Flettner-Straße 1-3 · 27472 Cuxhaven · Germany · Freecall 00 800 44 444 555 · www.voco.dental Structur 3 1.Processing! 3. Durability! 2. Aesthetics! Gloss without polishing! Order now! The proven crown and bridge materialVOCOfrom For more information please contact VOCO Australia P/L: David Reyno · Tel. 0401 747 037
UVC light from 200-230 nm: A new way to improve air quality?
By Emeritus Professor Laurence J. Walsh AO
The problems of contamination of the dental working environment with particles of patient origin are well-known and similar con cerns exist for operating theatres, especially when more complex procedures such as organ trans plantation and the placement of joint prostheses are being undertaken.
The literature indicates that particular problems around contaminated material in the air occur during procedures such as ultrasonic scaling and the use of air powder polishing devices and high-speed air turbine drills.1-3 These problems are magnified when the operatory is small in size and has limited fresh air exchange through the air-conditioning system, hence allowing concentrations of particu lates in the air to increase over time in bursts, as various procedures are undertaken.
As well as aerosols generated during procedures, there are also issues with the movement of people in and out of rooms. This issue has been well docu mented in operating theatres, where the movement of personnel and the associated opening and closing of doors greatly increases aerosol concentrations.
While common sense would suggest that a simple approach using high efficiency particle air filtration may be highly effective at reducing the concentra tion of aerosols, to date the literature around this has reported mixed results, with real world studies involving aerosol sensors showing no benefit from area HEPA filters in the dental operatory.4
On the other hand, recent literature supports the value of high volume evacuation (HVE) as an effective mitigation strategy that reduces aerosol concentrations, particularly when used with a wide bore tip and especially when that tip has a conical end that increases the surface area at the collecting end.2-4
96 Australasian Dental Practice July/August 2022
infection | CONTROL READ ME FOR CPD
While the use of germicidal ultraviolet lamps is well known historically, their use has not been popular because of the inherent problems of 254 nm ultraviolet light, which causes significant cellular and molecular injury, including damage to DNA. As a result, such light sources can only be used when no people are in the area that is being treated. Light at this wavelength is absorbed strongly into DNA, causing strand breakages and hence having mutagenic effects.5
Friendly photons
Moving to a shorter wavelength of light is a useful strategy because it then falls outside the absorption spectrum of DNA, but instead into the absorption spectrum of proteins. The extremely strong absorption of light from the 190-230 nm range into human tissues is well-known6,7 and it is responsible for the extreme safety of laser vision correction surgery, where laser light with a wavelength around 200 nm is used to selectively ablate cells on the surface of the eye, without any risk of penetration into deeper structures (and thus no risk of damage to the retina).
There is now considerable interest in using ultraviolet C (UVC) light for area disinfection, as a replacement for the older and more dangerous 254 nm ultraviolet lamps which emit light that is both carcinogenic and also readily able to cause keratitis and the generation of cataracts.
Particular wavelengths of interest are 207 nm and 222 nm.8 Light in this spectral range can be generated by LEDs or by filtration from a more broad-spectrum light source such as a krypton-bromine or krypton-chlorine excimer lamp (excilamp), which is relatively inexpensive and does not contain elemental mercury, which is a common ingredient in lamps that generate longer ultraviolet light wavelengths.
Effects on pathogens
Wavelengths of light from 200 to 230 nm have been shown to kill bacteria without causing harm to living tissue in animals or humans.8-16 The light is unable to penetrate through the stratum corneum of the skin (which has a thickness of between 5 and 20 µm). Likewise, the light is unable to penetrate through the cell membrane of a human cell, since the light intensity is reduced by half a distance of approximately 0.3 microns, which means that it is unable to penetrate through the membrane of a human cell (typically 10 to 25 µm in diameter). On the other hand, it is readily able to penetrate bacteria and viruses because of their much smaller size.
The ability of ultraviolet light to kill viruses and resistant bac teria is similar for 254 nm light and for the wavelengths from 200 to 230 nm. From a practical standpoint, having a light which is not dangerous to humans changes the way that one could deploy such a light source in a work environment. There has been particular interest in using such light sources in operating theatres16 to reduce the incidence of surgical site infections, including the concept of continuous irradiation of the germicidal wavelengths of light during the surgical procedures. The underlying rationale is that the majority of surgical site infections result from bacteria that fall directly onto the surgical wound from the air. If there was contin uous exposure of germicidal UVC light during surgical procedures, this should inactivate pathogens that fall onto the wound area.
In oral surgical procedures undertaken in office-based prac tice settings, the physical set up is, of course, different from the operating theatre of a major hospital, but nevertheless the concept of using a continuously running invisible light source may merit further exploration. A powerful feature supporting its use is that it would not be necessary to shield the eyes or the skin from the light source when it is in operation.
Application to the COVID-19 pandemic
Recent studies have shown that UVC light at 222 nm is highly effective against a range of viruses including human influ enza viruses17 and endemic strains of coronaviruses as well as SARS-CoV-2,18 as well as against bacteria including those with multi-drug resistance. Adding to this, recent clinical trials con ducted on either healthy volunteers or patients with pressure ulcers have shown no indications of skin inflammation or DNA damage, but a large reduction in the number of bacteria recovered from swabbing the surface of the skin.20
Suggested applications for 200-230 nm light currently include health care facilities, operating theatres and occupied public spaces where large numbers of people may be found and where airborne transmission of coronaviruses can be expected to occur.15,18 Sugges tions have also been made to include airports, schools, restaurants and public transportation vehicles as an inexpensive and safe way of reducing the spread of airborne mediated viruses. Based on cur rent regulatory limits, which for this range is an energy density of 23 mJ per square centimetre over 8 hours,19 achieving 90% inacti vation of viruses would require approximately 8 minutes, 99% in 16 minutes and 99.9% inactivation in 25 minutes. Such exposure times are practical for these types of environments and would also align with the timing of typical dental appointments, if such light sources were to be deployed in a waiting room or in a dental operatory.
This is a rapidly evolving topic and it will be interesting to follow the pathway by which UVC light sources operating in the range of 200 to 230 nm gain approval from the Therapeutic Goods Administration for claims that are made regarding their disinfecting actions.
July/August 2022 Australasian Dental Practice 97 infection | CONTROL
About the author
Emeritus Professor Laurence J. Walsh AO is a specialist in special needs den tistry who is based in Brisbane, where he served for 36 years on the academic staff of the University of Queensland School of Dentistry, including 21 years as Pro fessor of Dental Science and 10 years as the Head of School. Since retiring in December 2020, Laurie has remained active in hands-on bench research work, as well as in supervising over 15 research students at UQ who work in advanced technologies and biomaterials and in clinical microbiology. Laurie has served as Chief Examiner in Microbiology for the RACDS for 21 years and as the Editor of the ADA Infection Control Guidelines for 12 years. His published research work includes over 330 journal papers, with a citation count of over 15,400 citations in the literature. Laurie holds patents in 7 families of dental technolo gies. He is currently ranked in the top 0.25% of world scientists. Laurie was made an Officer of the Order of Aus tralia in January 2018 and a life member of ADAQ in 2020 in recognition of his contributions to dentistry.
References
1. Han P et al. Splatters and aerosols contamination in dental aerosol generating procedures. Appl Sci. 2021; 11(4):1914.
2. Pulich A et al. Simulated and clinical aerosol spread in common periodontal aerosol generating proce dures. Clin Oral Invest 2022 https://doi.org/10.1007/ s00784-022-04532-8 1 June 2022
3. Makhsous S et al. Methodology for addressing infectious aerosol persistence in real-time using sensor network. Sensors 2021; 21: 3928.
4. Choudhary S et al. Comparison of aerosol miti gation strategies and aerosol persistence in dental environments. Infect Control Hosp Epidemiol. 2022, 1–6. doi:10.1017/ice.2022.26
5. Pfeifer GP, Besaratinia A. UV wavelengthdependent DNA damage and human non-melanoma and melanoma skin cancer. Photochem Photobiol Sci. 2012; 11(1): 90-97.
6. Goldfarb AR, Saidel LJ. Ultraviolet absorp tion spectra of proteins. Science 1951; 114(2954): 156–157.
7. Kreusch S. et al. UV measurements in microplates suitable for high-throughput protein determination. Anal Biochem. 2003;313(2): 208–215.
8. Welch D. et al. Far-UVC light: A new tool to control the spread of airborne-mediated microbial dis eases. Sci Rep. 2018; 8(1):2752.
9. Buonanno M. et al. 207-nm UV light - a promising tool for safe low-cost reduction of surgical site infec tions. I: in vitro studies. Plos One 2013; 8(10): e76968.
10. Buonanno M. et al. 207-nm UV light-a prom ising tool for safe low-cost reduction of surgical site infections. II: In-vivo safety studies. PLoS One 2016; 11(6): e0138418.
11. Buonanno M. et al. Germicidal efficacy and mam malian skin safety of 222-nm UV light. Radiat Res. 2017; 187(4): 483-491.
12. Ponnaiya B. et al. Far-UVC light prevents MRSA infection of superficial wounds in vivo. Plos One 2018; 13(2): e0192053.
13. Narita, K et al. Disinfection and healing effects of 222-nm UVC light on methicillin-resistant Staph ylococcus aureus infection in mouse wounds. J Photochem Photobiol. B 2018; 178(Suppl C): 10-18.
14. Narita K. et al. Chronic irradiation with 222-nm UVC light induces neither DNA damage nor epi dermal lesions in mouse skin, even at high doses. PLoS One 2018; 13(7):e0201259.
15. Welch D et al. Far-UVC light: A new tool to control the spread of airborne-mediated microbial dis eases. Sci Rep. 2018; 8(1): 2752.
16. Fukui T et al. Safety of 222 nm UVC irradiation to the surgical site in a rabbit model. Photochem Photo biol. 14 March 2022, DOI: 10.1111/php.13620
17. McDevitt JJ et al. Aerosol susceptibility of influ enza virus to UV-C light. Appl Environ Microbiol. 2012; 78(6):1666–1669.
18. Buonanno M et al. Far-UVC light (222 nm) efficiently and safely inactivates airborne human coro naviruses. Sci Rep 2020;10:10285.
19. ICNRP. The International Commission on NonIonizing Radiation Protection, Guidelines on limits of exposure to ultraviolet radiation of wavelengths between 180 nm and 400 nm (incoherent optical radia tion). Health Phys 2004; 87(2), 171-186.
20. Fukui T et al. Exploratory clinical trial on the safety and bactericidal effect of 222-nm ultraviolet C irradiation in healthy humans. PLoS ONE 2020;15(8): e0235948.
98 Australasian Dental Practice July/August 2022
infection | CONTROL
ENHANCED HAND CARE FOR DENTAL PROFESSIONALS

Introducing
SafeTouch®
Advanced Pure Accelerator Free Medical Examination Gloves
A glove that’s clean and gentle on the skin Often chemical accelerators like Thiurams, Thiazoles and Carbamates are added in the glove manufacturing process to enhance its strength and elasticity. These chemical accelerators in the gloves are known to be common contributor in causing Allergic Contact Dermatitis (ACP), type IV hypersensitivity. The Medicom SafeTouch® Advanced Pure accelerator free gloves emphasise the fundamental needs for safety and allergy care.

Scan the QR code to request your promotional sample pack today!


Proud Leader In Infection Control Since 1988
Contact us at email: cs@medicom-australia.com | Phone: 1300 818 168 or visit au.medicom.com
140222-DN-AD-043-MAU V1
A-dec’s dental unit waterline testing service can provide accurate results in just minutes.
Test now to protect dental waterlines
By David Petrikas
A-dec dealers have stepped in to help dental prac tices with a new end-to-end waterline maintenance approach and routine waterline testing service.
A-dec Product Marketing Manager, Shal Hafiz, said it was important to ensure dental unit waterlines remained uncontaminated to avoid unpleasant experiences with poor water quality in clinics and the potential health risks for patients and staff.
He said dental unit waterlines needed periodic maintenance to ensure they met ADA guidelines and that a systematic approach was the only way of ensuring ongoing dental unit waterline quality.
“Recently, more A-dec dealers have begun offering water line testing as part of A-dec’s recommended ‘Maintain / Monitor / Shock’ regime, which provides peace of mind to all dental practices that their waterlines are kept within safe limits.”
The rapid and accurate water testing system uses state-of-theart equipment to detect contamination at very low levels, so that the required treatment regime can be implemented to maintain or correct water quality issues.

The testing is part of the “A-dec 360 Maintenance” approach which includes regular waterline maintenance, backed up by waterline quality monitoring and periodic shock treatment.
Shock treatment
Mr Hafiz said daily waterline maintenance was easy with a proven solution like A-dec ICX tablets for self-contained waterline bottles, however, it was also important to monitor water quality and apply a periodic shock treatment as per guidelines.
“A-dec ICX Renew shock treatment, launched in May this year, is the perfect complement to A-dec’s self-contained water line system to ensure the highest quality water is delivered to patients.”
ICX Renew is an odourless formula that clears deposits and contamination which can build up over time, without harming plastic tubing or corroding dental unit components, unlike some harsh treatments.
The latest ADA Infection Control Guidelines suggest a shock treatment if CFU (colony forming units) reach 200 CFU/mL.
100 Australasian Dental Practice July/August 2022
infection | CONTROL
READ ME FOR CPD
Unwanted guests in your waterlines?
When you SHOCK, let ICX RENEW.
Unwanted visitors like bacteria love to colonise in your dental unit waterlines. A daily waterline maintenance protocol with A-dec ICX® waterline treatment tablets, along with periodic ICX Renew™ shock treatments, will help reduce these nasty microorganisms.


For complete trademark information, visit a-dec.com/legal/trademarks.
To find out more, visit australia.a-dec.com
© 2021
A-dec Inc. All rights reserved.
“Shock treatments are required peri odically to clean dental unit waterlines and more often if dental units have been left unused for any period, such as over a holiday break,” Mr Hafiz said.
“It is good practice to test microbial levels in water lines regularly - at least every six months, as this is a good pro tocol to ensure dental unit waterline quality is not forgotten,” Mr Hafiz said.
“Monitoring requirements will depend on your area’s water quality and the clin ic’s individual requirements. Initially, test water once a month. If the results pass your specified action level (i.e. 200 CFU/ mL), then reduce the testing protocol to at least every six months.”
Mr Hafiz said the A-dec 360 Main tenance system took the uncertainty out of dental unit waterline mainte nance, ensuring water quality, staff and patient safety was maintained, and that equipment was protected.
“Some testing systems are tedious and inaccurate and take up to 72 hours to produce a result, which could mean you are using contaminated water on patients while awaiting your test results. A-dec’s water testing system produces an accurate result in just minutes, without the need for cumbersome and potentially inaccurate manual counts. If your test triggers an action level, simply treat your dental units with ICX Renew liquid shock treatment.”
ICX Renew has a visual indicator which turns the dental unit waterline water blue, indicating the shock treatment is at work in the waterline. After the prescribed sitting time, the lines are flushed until they are clear and are then ready to be refilled with clean water and an ICX tablet matching the size of the self-contained water bottle for ongoing daily maintenance.
Mr Hafiz said both ICX and ICX Renew are non-corrosive and will not corrode or clog waterlines or harm dental tubing, diaphragms, ‘O’ rings and other soft components.
He said the digital waterline testing ser vice should be implemented as part of a regular service call. “The digital waterline test, A-dec ICX tablets and ICX Renew shock treatment are all available from your local A-dec dealer for complete endto-end care of your dental unit waterlines.”
Contact A-dec on 1800 225 010 or visit: australia.a-dec.com to find your nearest authorised A-dec dealer to arrange a dental unit waterline test today.
ICX Renew Shock Treatment

Fast-acting ICX Renew liquid shock treatment removes odour and foul-tasting bacteria in dental unit waterlines. Just mix the two solutions together into an empty water bottle, run through the lines and soak overnight. After completing the shock treatment, flush the lines with water and resume your regular use.
n Penetrates and removes the buildup of odour and foul-tasting bacteria
n Blue colour lets you know the solution is hard at work in the waterlines
n Non-corrosive and gentle on equipment
n Will not corrode or clog waterlines
n Odourless formula
ICX Waterline Treatment Tablets
The effervescing ICX formula does the work for you, preventing the accumulation of odour and foul-tasting bacteria. Simply add one tablet to an empty selfcontained water bottle before each filling. ICX continues working in the system with each treatment, protecting the waterlines from further contamination and reducing the need for frequent shock treatments

n Maintains dental unit waterline effluent ≤ 10 CFU/mL
n Eliminates odour and foul-tasting bacteria
n Reduces buildup of deposits
n Continuously present in water as a preventive, proactive solution
n Remains active in water up to two weeks during periods of equipment non-use
n Eliminates the need to purge waterlines at night
n Compatible for use with restorative bonding materials
n Gentle on your dental equipment
102 Australasian Dental Practice July/August 2022 infection | CONTROL






munglobal.com.au
A brand by
Why IMS will improve your practice
Funning a dental practice takes a lot of work. Although all practices are different and face unique challenges, one common issue is optimal instru ment management. For many practices, switching to an Instrument Management System (IMS®) provides innumerable ben efits; however, practices may be reluctant to switch. Practices may have to recon figure their sterilisation area, purchase new instruments or retrain employees, but the return is worth the investment! Whether it’s reduced sharps injuries, enhanced organisation, cost reductions, increased patient counts or another benefit, practices that adopt IMS see measurable results.
Over the years, Hu-Friedy has profiled practices that implement IMS to explore the variety of ways that it positively impacts practices. Here are examples:
Reducing sharps injuries
Large organisations like Pacific Dental Services (PDS) are always looking for measurable, data-driven ways to improve safety and ensure regulatory compliance across their network of dental practices. To better understand the impact of IMS, PDS identified two practices with an opportunity to reduce sharps injuries to trial the cassette-based system. After implementing IMS in those practices, PDS compared the results after a year with equivalent control practices.
The findings were unmistakable. Not only were sharps injuries reduced to zero for the two practices during the trial period, but both practices experienced improved efficiency, as instruments were repro cessed eight minutes faster on average, freeing up time to spend with patients.
Following this successful experiment, PDS expanded it to more locations to verify the findings, which generated iden tical results. With such positive outcomes, Hu-Friedy worked with PDS to imple ment IMS in over 100 practices.
“Now that we’ve implemented these cassettes in approximately 100 locations, the feedback continues to be the same,” said one PDS compliance manager. “Staff really love the cassettes. They love the efficiencies of the cassettes.”
Keeping up with expansion
s Floss & Co. began to get busier, staff struggled at first to manage an increase in patients. There were simply not enough scalers to keep up and all instruments were either in use or in repro cessing. At first, Dr Izzy Naem looked to solve the problem by purchasing more instruments, but the real issue wasn’t the number of instruments. It was about improving process efficiencies and finding better ways to keep instruments better organised.
So, when Dr Naem instead decided to switch to the IMS system, the practice was able to save 15 minutes per patient per chair, relieving some of the stress that the staff were experiencing.
“We don’t have to think about the instruments,” Dr Naem said. “Where they’re at, where to put them, where to store them. It’s all in the cassette. It was safer and it was easier.”
With improved efficiency and organi zation, the practice was able to continue expanding and saw a 40 percent increase in new patients. By switching to IMS, Dr Naem was able to increase revenues and provide a better experience for his staff and growing patient base.
Improving efficiency
Simplifying complexity
or Dr Steven Koos of ORA Oral Surgery & Implant Studio, proper organisation is key to practice success. Since ORA specialises in various oral surgery procedures, it’s important to have setups ready for each unique procedure and organising the correct instruments can be complicated and time-consuming.
F
Adopting IMS simplified instrument prep with the introduction of versatile and customisable cassettes that keep instru ments organised and in one place for each procedure, from chairside to cleaning to storage. “My surgical team has really embraced the Hu-Friedy IMS Cassette System because it’s enabled them to com bine the cleaning and sterilisation and organisation and storage of a vast array of instruments into one integrated package and it works well,” Dr Koos said.
Additionally, implementing cassettes has made it easier to hire and train new team members and open new locations without affecting the quality of care pro vided to patients.
Where can you improve?
C
W
hen Dr Edward Lin and his team at Orthodontic Specialists expanded from three doctors to four, the number of instruments used in their facility rose accordingly. Additionally, Dr Lin was concerned about protecting his invest ment in premium instruments. After trying other solutions with unsatisfac tory results, the team began using IMS, enabling them to see 60 to 120 patients a day efficiently.
Cassettes were fundamental to enabling Dr Lin’s practice to successfully expand: “To work without the Hu-Friedy IMS System would be pure chaos,” Dr Lin said. “I couldn’t tolerate it because instru ments are going to get lost. Instruments will get damaged. It would be physically impossible to be able to see the number of patients that we see in a clinical day without the IMS System.”
hairside efficiency is the key to a productive practice. Maximizing this efficiency is possible when the exact pro cedural set ups needed for each patient are always at your fingertips. Hu-Friedy’s dental Instrument Management System standardises and combines the cleaning, sterilisation, storage and organisation of instruments in one integrated cassette system, creating real results that can save your practice up to 5-10 minutes per pro cedure. There are numerous advantages to adopting IMS and while each practice profiled here chose to make the switch for different reasons, the results are uni versal: better efficiency, improved safety, enhanced patient experience and an increased bottom line.
If your practice does not already use an instrument management system, you can request more information from a Hu-Friedy representative on how a cas sette-based system can directly benefit your practice.
104 Australasian Dental Practice July/August 2022
A
infection | CONTROL
INFINITY
SERIES™ CASSETTES
INFINITY SERIES™ CASSETTES
INFINITY SERIES™ CASSETTES
INFINITY SERIES™ CASSETTES
The most sophisticated solution for instrument management
The most sophisticated solution for instrument management
The most sophisticated solution for instrument management
The most sophisticated solution for instrument
That’s right, you deserve it. You deserve the peace of mind and confidence of knowing that you are employing the most contemporary method of processing instruments. As dentistry’s innovator of the cassette-based instrument management system, Hu-Friedy is proud to bring you the modern design and functionality of the Infinity Series Cassettes which include:
That’s right, you deserve it. You deserve the peace of mind and confidence of knowing that you are employing the most contemporary method of processing instruments. As dentistry’s innovator of the cassette-based instrument management system, Hu-Friedy is proud to bring you the modern design and functionality of the Infinity Series Cassettes which include:
Ensure predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. You’ll quickly discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. Because when it comes to the perfect fit, Hu-Friedy is just right.
That’s right, you deserve it. You deserve the peace that you are employing the most contemporary
Ensure predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. You’ll quickly discover why dentists favor our impeccable fit.
• An open hole pattern that promotes water flow throughout the cassette
That’s right, you deserve it. You deserve the peace of mind and confidence of knowing that you are employing the most contemporary method of processing instruments. As dentistry’s innovator of the cassette-based instrument management system, Hu-Friedy is proud to bring you the modern design and functionality of the Infinity Series Cassettes which include:
Ensure predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. You’ll quickly discover why dentists favor our
• An open hole pattern that promotes water flow throughout the cassette
WHY DENTISTS LOVE OUR STAINLESS STEEL PEDO CROWNS:
file. Available upon request.
• An open hole pattern that promotes water flow throughout the cassette
designs. Data on file. Available upon request.
• Color-coded silicone rail system that significantly reduces instrument contact and allows for more water flow while protecting the instruments during reprocessing
©2020 Hu-Friedy Mfg. Co., LLC. All rights reserved. HFL-482AUS/1220
• Ideal height and mesio-distal width

• Color-coded silicone rail system that significantly reduces instrument contact and allows for more water flow while protecting the instruments during reprocessing
• Color-coded silicone rail system that significantly reduces instrument contact and allows for more water flow while protecting the instruments during reprocessing
©2020 Hu-Friedy Mfg. Co., LLC. All rights reserved. HFL-482AUS/1220
• Pre-trimmed and pre-crimped for simple placement
• Easy-to-use, ergonomic latch that allows for one-handed opening
All
• Accurate occlusal anatomy that matches the natural tooth
• Easy-to-use, ergonomic latch that allows for one-handed opening Performing at your best means having confidence in what you do. Experience Infinity Series™ Cassettes, and improve the efficiency of your practice, while helping protect your patients, your staff and your instrument investment.

©2020 Hu-Friedy Mfg. Co., LLC. All rights reserved. HFL-482AUS/1220
To learn more about how IMS can enhance your practice visit Hu-Friedy.com/Infinity
VISIT US ONLINE AT HU-FRIEDY.COM/PerfectFit
Hu-Friedy Mfg. Co., LLC, 1666 E. Touhy Ave., Des Plaines, IL 60018 | Hu-Friedy.com
• Easy-to-use, ergonomic latch that allows for one-handed opening Performing at your best means having confidence in what you do. Experience Infinity Series™ Cassettes, and improve the efficiency of your practice, while helping protect your patients, your staff and your instrument investment. VISIT US ONLINE AT HU-FRIEDY.COM/PerfectFit
©2016 Hu-Fried y Mfg. Co., LLC. All rights reserved.
Performing at your best means having confidence in what you do. Experience Infinity Series™ Cassettes, and improve the efficiency of your practice, while helping protect your patients, your staff and your instrument investment. VISIT US ONLINE AT HU-FRIEDY.COM/PerfectFit
All company and product names are trademarks of Hu-Friedy Mfg. Co., LLC, its affiliates or related companies, unless otherwise noted.
©2016 Hu-Fried y Mfg. Co., LLC. All rights reserved.
©2017 Hu-Friedy Mfg. Co., LLC. All rights reserved.
©2016 Hu-Fried y Mfg. Co., LLC. All rights reserved.
©2021 Hu-Friedy Mfg. Co., LLC. All rights reserved.
INSTRUMENT MANAGEMENT
IS EVERYTHING Find
Orders 1300 65
22 www.henryschein.com.au
FIT
the right one with Hu-Friedy
88
Orders 0800 808 855 www.henryschein.co.nz
of
Hu-Friedy is now a proud member
company and product names are trademarks of Hu-Friedy Mfg. Co., LLC, its affiliates or related companies, unless otherwise noted. 1) Compared to other leading scaler designs. Data on file. Available upon request.
working ends, ensuring you have sharp, long lasting blades to efficiently remove calculus while applying less pinch force when holding the handle.
How to Scale in Perfect Harmony at Hu-Friedy.com/Harmony
is now a proud member of
Learn
Hu-Friedy
All company and product names are trademarks of Hu-Friedy Mfg. Co., LLC, its affiliates or related companies, unless otherwise noted. 1) Compared to other leading scaler
less pinch force when holding the handle.
PER-Harmony-PrintAd-HFG-Introduces-HFL-482AUS-A4-2012.indd 1 12/11/20 11:53 YOU DESERVE INFINITE CONFIDENCE.
Learn How to Scale in Perfect Harmony at Hu-Friedy.com/Harmony
INSTRUMENT MANAGEMENT
impeccable fit. Perfect for your patients. Easy for you. Because when it comes to the perfect fit, Hu-Friedy is just right. WHY DENTISTS LOVE OUR STAINLESS STEEL PEDO CROWNS:
Ideal height and mesio-distal width
Pre-trimmed and pre-crimped for simple placement
Accurate occlusal anatomy that matches the natural tooth FIT IS EVERYTHING Find the right one with Hu-Friedy Orders 1300 65 88 22 www.henryschein.com.au Orders 0800 808 855 www.henryschein.co.nz To learn more about how IMS can enhance your practice visit Hu-Friedy.com/Infinity ©2017 Hu-Friedy Mfg. Co., LLC. All rights reserved. Hu-Friedy is now a proud member of All company and product names are trademarks of Hu-Friedy Mfg. Co., LLC, 1) Compared to other leading scaler designs. Data on file. Available upon request. ©2020 Hu-Friedy Mfg. Co., LLC. All rights reserved. HFL-482AUS/1220 working ends, ensuring you blades to efficiently remove less pinch force when holding Learn How to Scale in Perfect Hu-Friedy.com/Harmony PER-Harmony-PrintAd-HFG-Introduces-HFL-482AUS-A4-2012.indd 1 Hu-Friedy is now a proud member of All company and product names are trademarks of Hu-Friedy Mfg. Co., LLC, 1) Compared to other leading scaler designs. Data on file. Available upon request. ©2020 Hu-Friedy Mfg. Co., LLC. All rights reserved. HFL-482AUS/1220 less pinch force when holding Learn How to Scale in Perfect Hu-Friedy.com/Harmony PER-Harmony-PrintAd-HFG-Introduces-HFL-482AUS-A4-2012.indd 1 INSTRUMENT MANAGEMENT INFINITY SERIES™ CASSETTES The most sophisticated solution for instrument management That’s right, you deserve it. You deserve the peace of mind and confidence that you are employing the most contemporary method of processing instruments. innovator of the cassette-based instrument management system, Hu-Friedy you the modern design and functionality of the Infinity Series Cassettes An open hole pattern that promotes water flow throughout the cassette • Color-coded silicone rail system that significantly reduces instrument for more water flow while protecting the instruments during reprocessing • Easy-to-use, ergonomic latch that allows for one-handed opening Performing at your best means having confidence in what you do. Experience the efficiency of your practice, while helping protect your patients, your VISIT US ONLINE AT HU-FRIEDY.COM/PerfectFit ©2016 Hu-Fried y Mfg. Co., LLC. All rights reserved. Ensure predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. You’ll quickly discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. Because when it comes to the perfect fit, Hu-Friedy is just right. WHY DENTISTS LOVE OUR STAINLESS STEEL PEDO CROWNS: • Ideal height and mesio-distal width • Pre-trimmed and pre-crimped for simple placement • Accurate occlusal anatomy that matches the natural tooth FIT IS EVERYTHING Find the right one with Hu-Friedy Orders Orders 0800 808 855 www.henryschein.co.nz To learn more about how IMS can enhance your practice visit Hu-Friedy.com/Infinity ©2017 Hu-Friedy Mfg. Co., LLC. All rights reserved. Hu-Friedy is now a proud member of All company and product names are trademarks of Hu-Friedy Mfg. Co., LLC, its affiliates or related companies, unless otherwise noted. 1) Compared to other leading scaler designs. Data on file. Available upon request. ©2020 Hu-Friedy Mfg. Co., LLC. All rights reserved. HFL-482AUS/1220 working ends, ensuring you have sharp, long lasting blades to efficiently remove calculus while applying less pinch force when holding the handle. Learn How to Scale in Perfect Harmony at Hu-Friedy.com/Harmony Hu-Friedy is now a proud member of All company and product names are trademarks of Hu-Friedy Mfg. Co., LLC, its affiliates or related companies, unless otherwise noted. 1) Compared to other leading scaler designs. Data on
•
•
•
less pinch force when holding the handle.
PER-Harmony-PrintAd-HFG-Introduces-HFL-482AUS-A4-2012.indd 1 12/11/20 11:53 AM YOU
Learn How to Scale in Perfect Harmony at Hu-Friedy.com/Harmony
DESERVE INFINITE CONFIDENCE. INSTRUMENT MANAGEMENT
Perfect for your patients. Easy for you.
WHY DENTISTS LOVE OUR STAINLESS STEEL PEDO CROWNS:
Because when it comes to the perfect fit, Hu-Friedy is just right.
• Ideal height and mesio-distal width
for
• Pre-trimmed and pre-crimped
simple placement
FIT IS EVERYTHING Find the right one with Hu-Friedy Orders 1300 65 88 22 www.henryschein.com.au Orders 0800 808 855 www.henryschein.co.nz To learn more about how IMS can enhance your practice visit Hu-Friedy.com/Infinity ©2017 Hu-Friedy Mfg. Co., LLC. All rights reserved. Hu-Friedy is now a proud member of All company and product names are trademarks 1) Compared to other leading scaler designs. Data ©2020 Hu-Friedy Mfg. Co., LLC. All rights reserved. working ends, ensuring blades to efficiently less pinch force when Learn How to Scale Hu-Friedy.com/Harmony Hu-Friedy is now a proud member of All company and product names are trademarks 1) Compared to other leading scaler designs. Data ©2020 Hu-Friedy Mfg. Co., LLC. All rights reserved. less pinch force when Learn How to Scale Hu-Friedy.com/Harmony PER-Harmony-PrintAd-HFG-Introduces-HFL-482AUS-A4-2012.indd 1 YOU DESERVE INSTRUMENT
• Accurate occlusal anatomy that matches the natural tooth
MANAGEMENT
innovator
cassette-based
VISIT US ONLINE AT HU-FRIEDY.COM/PerfectFit ©2016 Hu-Fried y Mfg. Co., LLC. All rights reserved. Ensure predictable
your
patients with
You’ll
dentists
WHY
OUR STAINLESS
Ideal
width
placement • Accurate
FIT IS EVERYTHING Find the right one with Hu-Friedy Orders 0800 808 855 www.henryschein.co.nz To learn more about how IMS can enhance your practice visit Hu-Friedy.com/Infinity ©2017 Hu-Friedy Mfg. Co., LLC. All rights reserved.
method
of the
instrument management you the modern design and functionality of the Infinity • An open hole pattern that promotes water flow throughout • Color-coded silicone rail system that significantly for more water flow while protecting the instruments • Easy-to-use, ergonomic latch that allows for one-handed Performing at your best means having confidence in the efficiency of your practice, while helping protect
outcomes for
littlest
Hu-Friedy Stainless
quickly discover why
favor our impeccable fit. Perfect for your Because when it comes to the perfect fit, Hu-Friedy is just right.
DENTISTS LOVE
STEEL PEDO CROWNS: •
height and mesio-distal
• Pre-trimmed and pre-crimped for simple
occlusal anatomy that matches the natural tooth
case report
Upper premolar replacement with a single implant using digital workflow
By Dr Nelson Silva, Professor in the Department of Restorative Dentistry at UFMG

For aesthetic and functional reha bilitation of upper Premolar #24, Dr Silva used the TRIOS® intraoral scanner and 3Shape’s Implant Studio® software for the implant planning and designing of the surgical guide, as well as 3Shape Dental System™ for the making of the final prosthesis.

The digital implant workflow
Initially, the patient information was entered into the system and the digital impressions from TRIOS and the CT scans were loaded. The tooth of interest was selected for the reverse prosthesis planning and subsequent implant plan ning. A surgical guide has been designed and manufactured to provide precision and predictability in the surgery. Finally, the implant abutment was selected and the crown was made with the 3Shape Dental System software.
106 Australasian Dental Practice July/August 2022
clinical | EXCELLENCE
1.
Figure 2.
The 35-year-old female patient pre sented for aesthetic and functional rehabilitation of one upper premolar (#24). Her general health history showed no contraindications for rehabilitation using implants. The possibility of a graft to improve the vestibular structure of the given region was discussed, but the patient wasn’t interested in the procedure.

The patient’s information was entered in the system and the digital impressions from TRIOS and the CT scans were loaded in the Implant Studio session window (Figure 2). The tooth of interest was selected for the reverse prosthesis plan ning and subsequent implant planning.
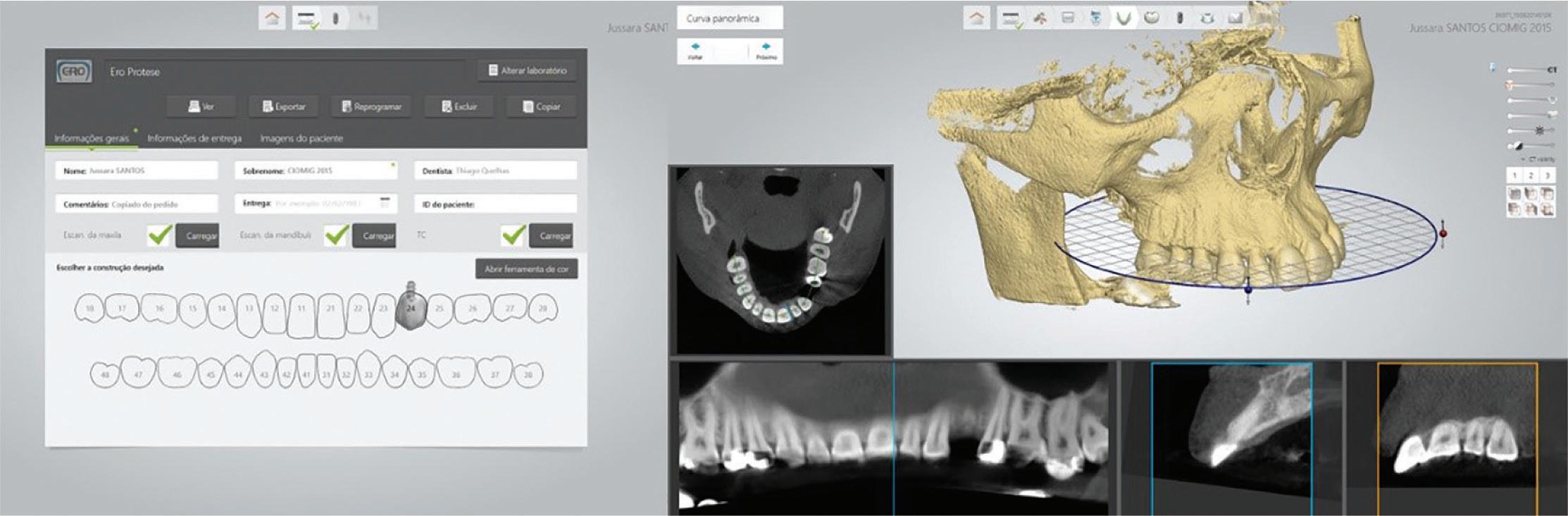
Note that the CT file uploaded to Implant Studio allows for an overall assessment of the case, as well as specific sections of it, demonstrated in the following.
Then, the CT and the intraoral scan were aligned (Figure 3). To check the alignment, the system offers a colour scale, which makes it possible to quantify the accu racy of this alignment. The first step for the implant planning is the virtual wax-up of the related tooth, which will guide the planning of the implant position and subsequent design of the surgical guide.
Figure 3.
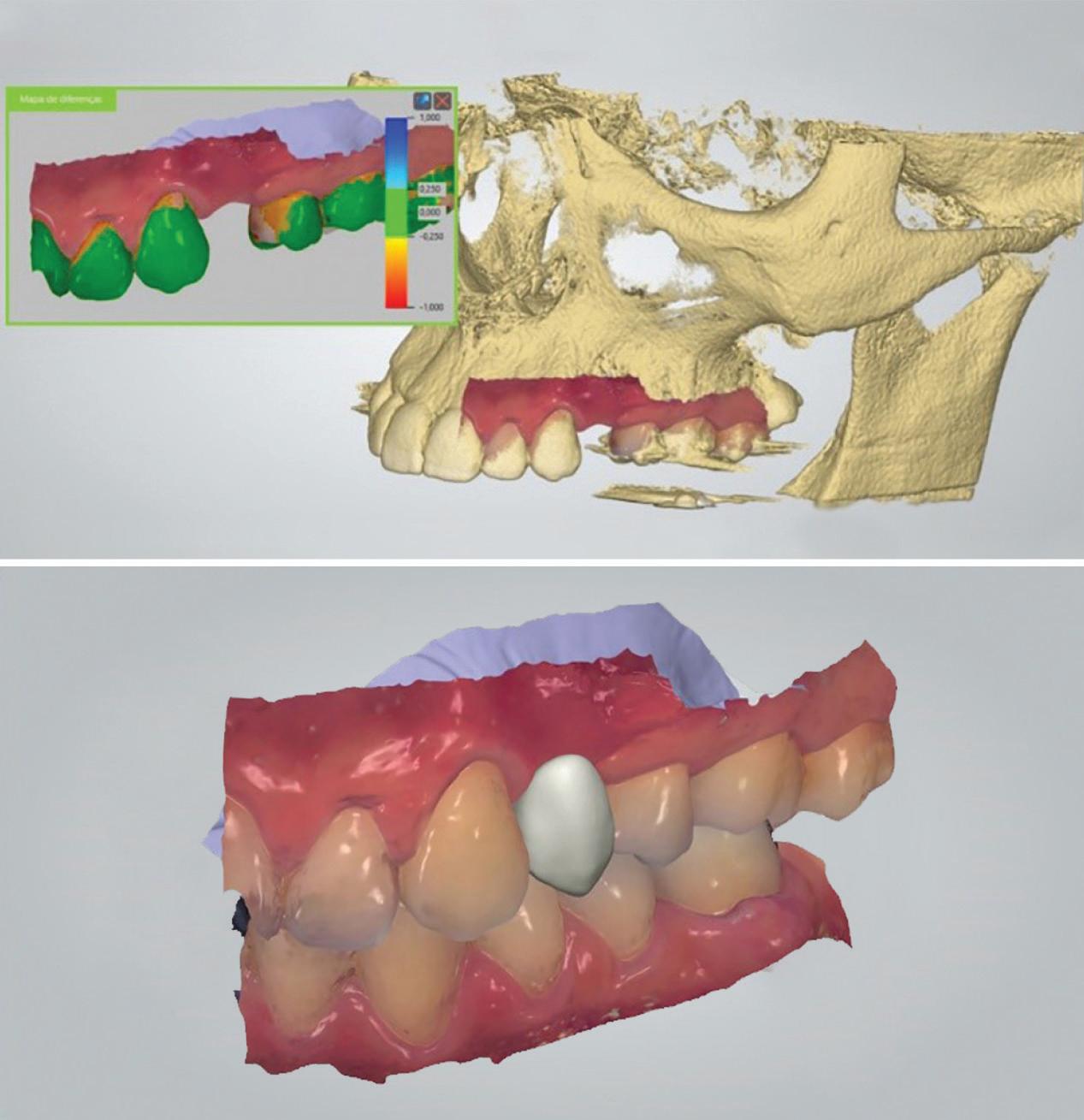
July/August 2022 Australasian Dental Practice 107
clinical | EXCELLENCE
Figure
Intraoral scan for aesthetic and functional rehabilitation of upper Premolar tooth 24.
With the virtual wax-up set, the posi tioning of the implant in 3D is planned. Implant Studio has accurate and opti mised positioning and visualisation tools (Figure 4).

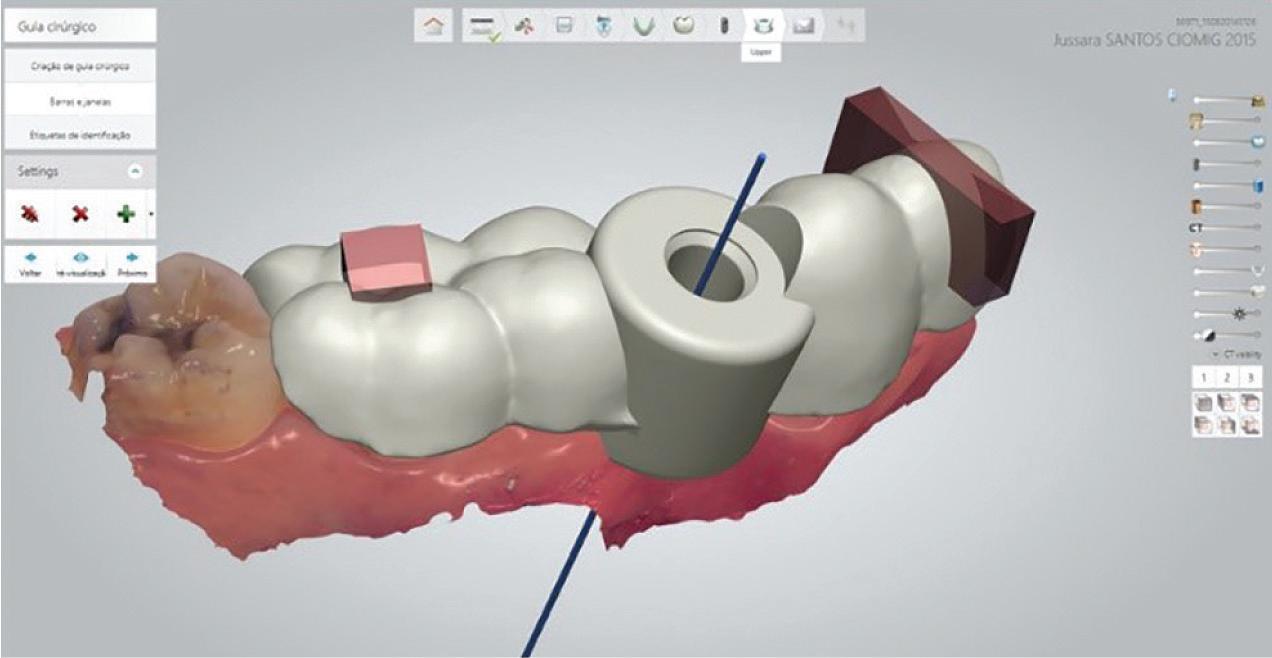
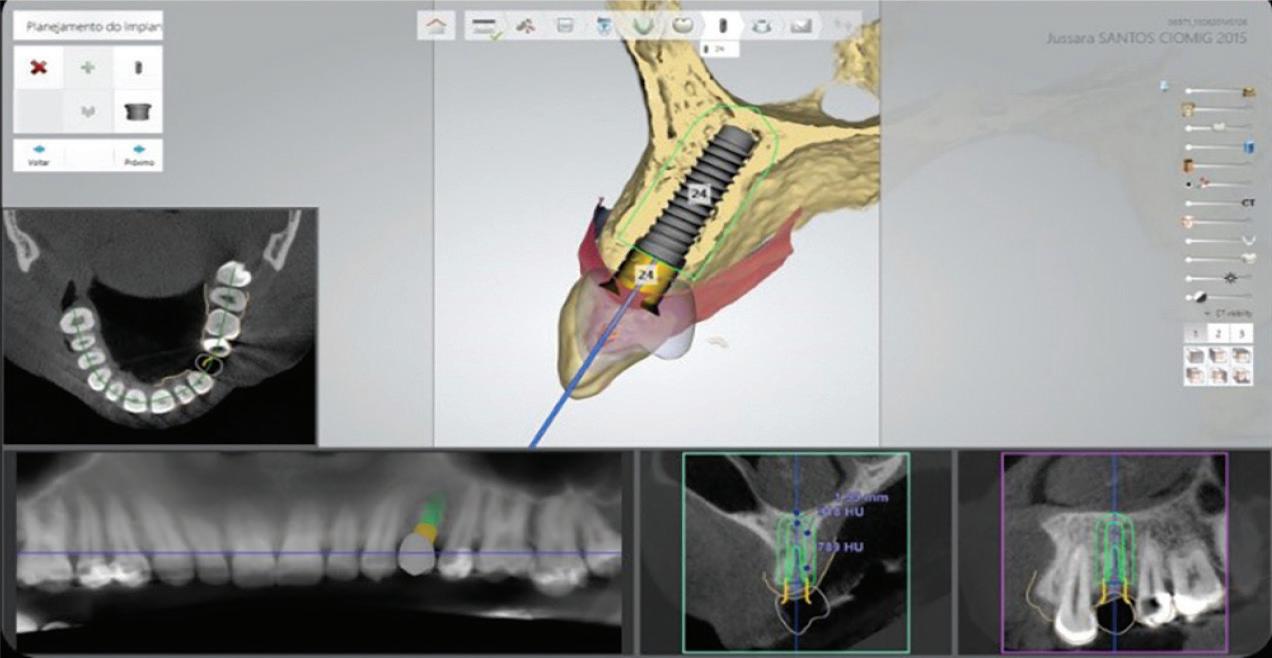
After the implant placement, the sur gical guide is designed and customised for each case (Figure 5). Subsequently, the digital file of the guide is sent (in STL format) to be prototyped or milled in an optimal and precise way.
Figure 4.
Figure 5.
By looking at Figure 6, you can see the milled surgical guide in “A” and the prototype in “B”. Observe that in this example, the guide that was milled and offers a greater translucency, but the decision to use one or the other depends on the working philosophy adopted. In addition, it is possible to show that

regardless of the method of manufacturing the guide, it has an accurate and stable fit for the surgery. In image “C”, it is possible to see the implant with the healing abutment placed and in the image “D”, you can see the emergence profile set for aesthetic optimisation.


108 Australasian Dental Practice July/August 2022
clinical | EXCELLENCE
A C B D

















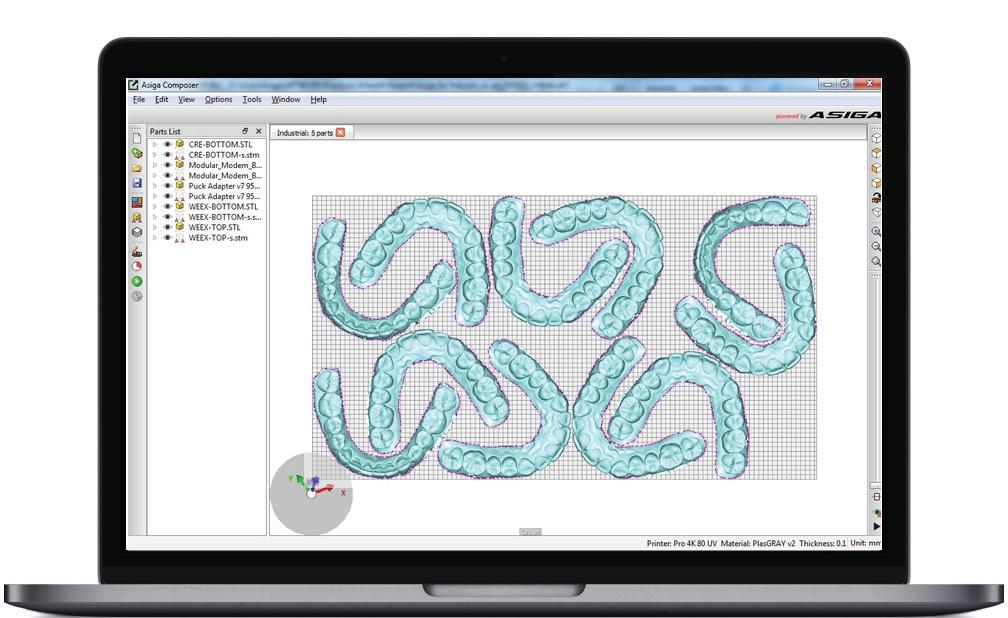










To register the implant position and for crown manufacturing, a scanbody was attached to the implant and its scanning was performed with the TRIOS (Figure 7). After scanning, the 3D images were imported into the Dental System for the purpose of designing the crown.
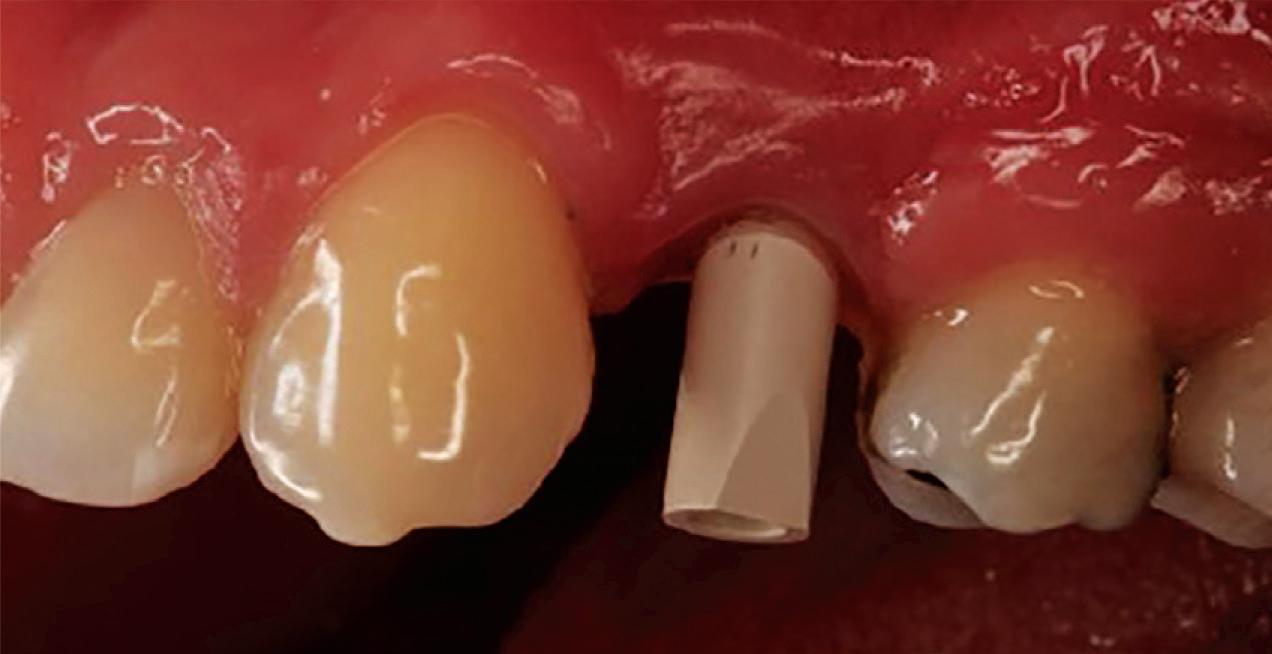
Crown placement and digital adjust ment of proximal and occlusal contacts were made in order to mill the crown with CAD/CAM technology. In this par ticular case, it was decided to copy the anatomical shape of the second premolar to re-establish better aesthetics and func tionality for the patient (Figure 8).

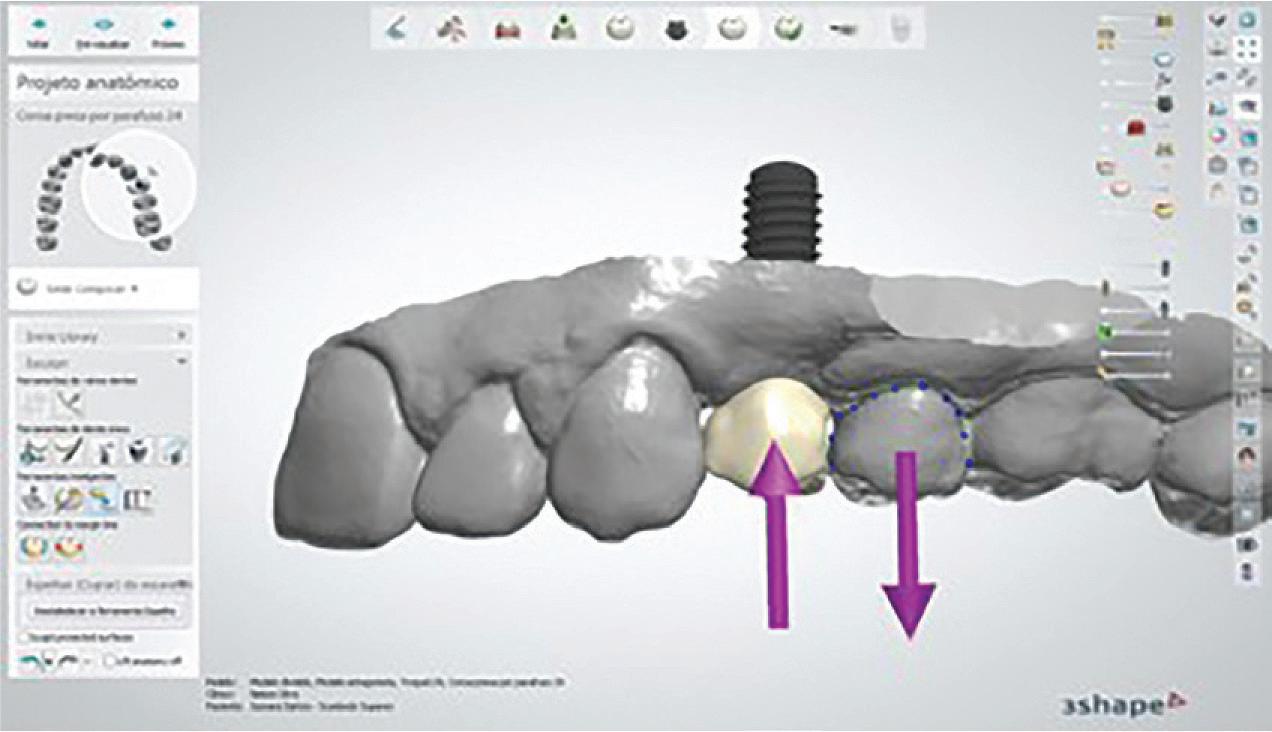
Implant and crown attached with pre cise fit was achieved, restoring aesthetics and function for the patient. Observe the similarity of the shape obtained when compared to the second premolar, showing the software’s great capacity for mimicking the anatomical details (Figure 9).
About Dr. Nelson Dr Nelson Silva is Professor in the Department of Restorative Dentistry at the Federal University of Minas Gerais (UFMG), Brazil. He holds MSc, PhD and postdoctoral degrees from the University of São Paulo / New York University. Dr. Silva served as Assistant and Associate Professor of Prosthodontics / Biomate rials at the University of New York for 11 years and published several book chapters and high impact manuscripts. His clinical and research skills involve translational research, biomaterials, disruptive technology in dentistry, labora tory and clinical aspects for the success of cosmetic restorations, partial and total removable prostheses and implants using CAD/CAM.
110 Australasian Dental Practice July/August 2022
clinical | EXCELLENCE Solutions featured 3Shape TRIOS 3Shape Dental System 3Shape Implant Studio
7.
8. Figure 9.
Figure
Figure
Superior integration. A superior partnership.
Superior integration. A superior partnership.
acceptance—made possible by a powerful partnership: 3Shape, the Straumann Group—and you.
Your ClearCorrect experience—made better with TRIOS.
Your ClearCorrect experience—made better with TRIOS.
Your ClearCorrect experience—made better with TRIOS.
Pair your TRIOS scanner with your ClearCorrect account. Select any of your recent TRIOS scans and upload them to your patient’s case page straight from the ClearCorrect doctor portal.*
Pair your TRIOS scanner with your ClearCorrect account. Select any of your recent TRIOS scans and upload them to your patient’s case page straight from the ClearCorrect doctor portal.*
Pair your TRIOS scanner with your ClearCorrect account. Select any of your recent TRIOS scans and upload them to your patient’s case page straight from the ClearCorrect doctor portal.*

3Shape TRIOS Treatment Simulator
3Shape TRIOS Treatment Simulator
3Shape
TRIOS Treatment Simulator
This feature (now with ClearCorrect branding!) simulates the results of ClearCorrect treatment compared to the patient’s current dentition, and allows you to move individual teeth in real time, or even simulate whitening treatment. TRIOS Treatment Simulator can boost case acceptance by up to 40%**—once you try it, you won’t look back.
This feature (now with ClearCorrect branding!) simulates the results of ClearCorrect treatment compared to the patient’s current dentition, and allows you to move individual teeth in real time, or even simulate whitening treatment. TRIOS Treatment Simulator can boost case acceptance by up to 40%**—once you try it, you won’t look back.
3Shape TRIOS Treatment Simulator
This feature (now with ClearCorrect branding!) simulates the results of ClearCorrect treatment compared to the patient’s current dentition, and allows you to move individual teeth in real time, or even simulate whitening treatment. TRIOS Treatment Simulator can boost case acceptance by up to 40%**—once you try it, you won’t look back.
This feature (now with ClearCorrect branding!) simulates the results of ClearCorrect treatment compared to the patient’s current dentition, and allows you to move individual teeth in real time, or even simulate whitening treatment. TRIOS Treatment Simulator can boost case acceptance by up to 40%**—once you try it, you won’t look back.


Contact your Straumann Group Specialist today to learn more or visit clearcorrect.com.au
Straumann Pty Ltd/Straumann New Zealand Limited 93 Cook Street. Port Melbourne VIC 3207, Australia
Straumann Pty Ltd/Straumann New Zealand Limited 93 Cook Street. Port Melbourne VIC 3207, Australia
AU Toll Free 1800 660 330 | NZ Toll Free 0800 408 370
Straumann Pty Ltd/Straumann
AU Toll Free 1800 660 330 | NZ Toll Free 0800 408 370 Email customerservice.au@straumann.com www.straumann.com.au
Email customerservice.au@straumann.com www.straumann.com.au www.straumann.co.nz
©Institut Straumann AG, 2021. All rights reserved. Straumann® and/or other trademarks and logos from Straumann® mentioned herein are the trademarks or registered trademarks of Straumann Holding AG and/or its affiliates.
Holding AG and/or its affiliates.
https://youtu.be/-cDebkYLH6A
* Please allow 2–3 days for new scans to populate on Doctor Portal ** Dr. Pedro Goncalves | https://youtu.be/-cDebkYLH6A
ORTHODONTICS
to
more
480.520/en/A/00
Port
| NZ Toll Free
370
2021. All rights
the
Contact your Straumann Group Specialist today
learn
or visit clearcorrect.com.au
Straumann Pty Ltd/Straumann New Zealand Limited 93 Cook Street.
Melbourne VIC 3207, Australia AU Toll Free 1800 660 330
0800 408
Email customerservice.au@straumann.com www.straumann.com.au www.straumann.co.nz ©Institut Straumann AG,
reserved. Straumann® and/or other trademarks and logos from Straumann® mentioned herein are
trademarks or registered trademarks of Straumann
+
Seamless integration, a simplified workflow, and higher case acceptance—made possible by a powerful partnership: 3Shape, the Straumann Group—and you.
* Please allow 2–3 days for new scans to populate on Doctor Portal ** Dr. Pedro Goncalves | https://youtu.be/-cDebkYLH6A
ORTHODONTICS
480.520/en/A/00
+
New Zealand Limited 93 Cook Street. Port Melbourne VIC 3207, Australia AU Toll Free 1800 660 330 | NZ Toll Free 0800 408 370 Email customerservice.au@straumann.com www.straumann.com.au www.straumann.co.nz ©Institut Straumann AG, 2021. All rights reserved. Straumann® and/or other trademarks and logos from Straumann®
Seamless integration, a simplified workflow, and higher case acceptance—made possible by a powerful partnership: 3Shape, the Straumann Group—and you.
* Please allow 2–3 days for new scans to populate on Doctor Portal ** Dr. Pedro Goncalves |
ORTHODONTICS
480.520/en/A/00
Contact your Straumann Group Specialist today to learn more or visit clearcorrect.com.au
©Institut
AG, 2021. All rights reserved. Straumann® and/or other trademarks and logos from Straumann
mentioned herein are the trademarks or registered trademarks of
and/or
+ Seamless integration, a simplified workflow, and higher case acceptance—made possible by a powerful partnership: 3Shape, the Straumann Group—and you.
www.straumann.co.nz
Straumann
®
Straumann Holding AG
its affiliates.
Your ClearCorrect experience—made better with TRIOS.
* Please allow 2–3 days for new scans to populate on Doctor Portal ** Dr.
Goncalves
Pedro
| https://youtu.be/-cDebkYLH6A
today to learn
480.520/en/A/00
integration. A superior partnership.
Pair your TRIOS scanner with your ClearCorrect account. Select any of your recent TRIOS scans and upload them to your patient’s case page straight from the ClearCorrect doctor portal.* ORTHODONTICS Contact your Straumann Group Specialist
more or visit clearcorrect.com.au
Superior
New SHINING 3D OrthoSimulator V2
By Terry Whitty
Many dentists struggle to successfully communicate the benefits and expected outcomes of aesthetic dental treatments to patients and case acceptance rates reflect this. Whereas some dentists are naturally adept at con necting with patients, the rest need to develop ways to overcome this obstacle that will eventually limit the success of their practice. Every time a patient is diag nosed and presented with a treatment plan that is not enacted, an opportunity is lost, time is wasted and potentially the patient’s oral health is compromised.
Using visual aids and personalized sim ulations to communicate is a key tool for helping patients to both accept treatment and also to have a realistic expectation of how the outcome of treatment will appear.
For many years, dentists have used various methods such as wax-ups and in mouth mock-ups to demonstrate how the patient could look with a new smile.
With the advent of smile design soft ware, this has become a very powerful tool indeed.
In orthodontics, a diagnostic wax-up, where the teeth were cut from a plaster model and reset in wax, often referred to as Kesling Setup, was a very popular method in the past as a diagnostic aid to “sell” the case to the patient. However, these setups were extremely time con suming and very expensive to produce to a high standard and often, if the case was not accepted, left people out-of-pocket.
During the digitisation of dentistry and especially with the introduction of com puter-assisted clear aligner manufacture, companies also started to create ortho dontic simulation software programs.
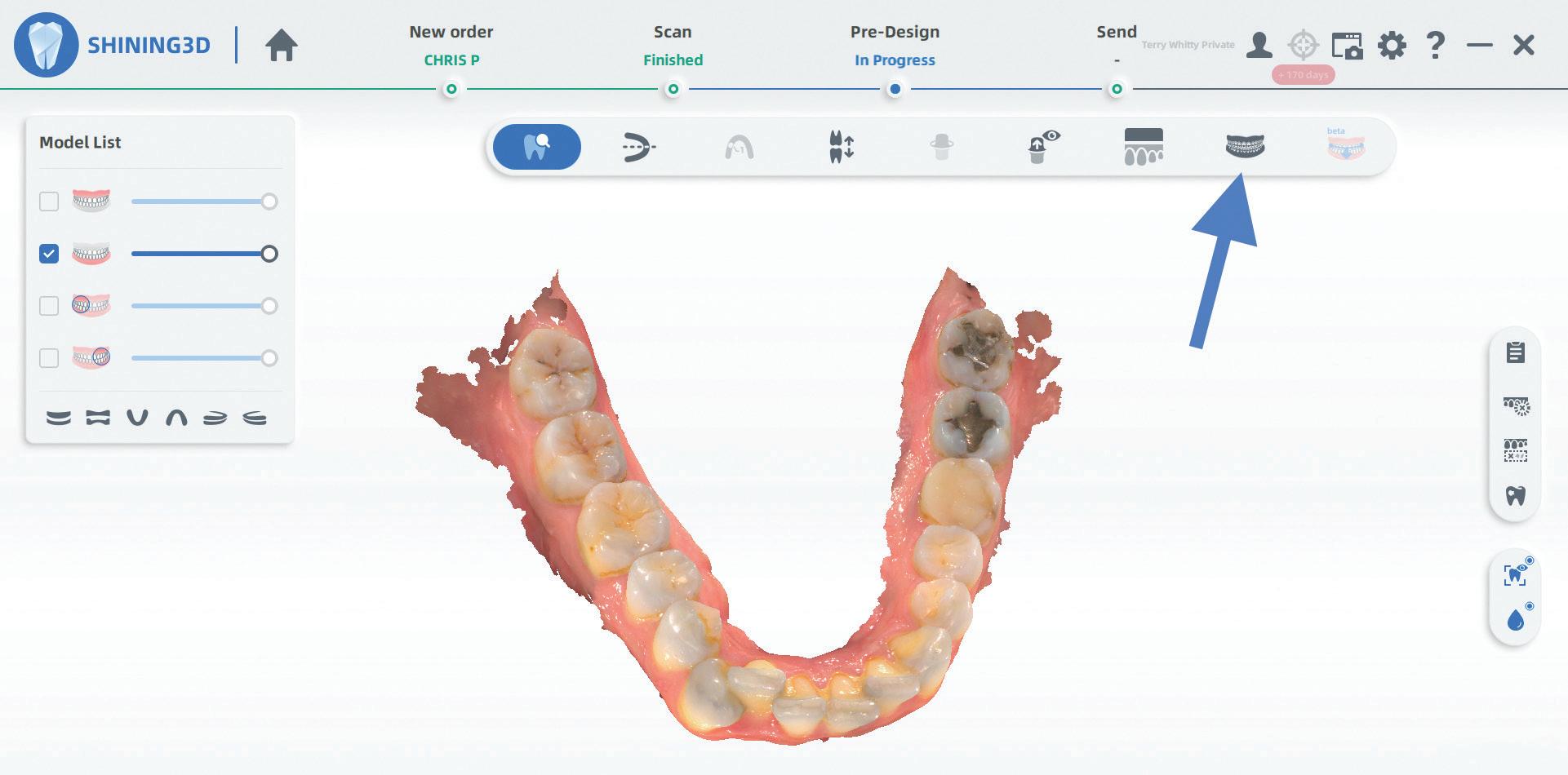
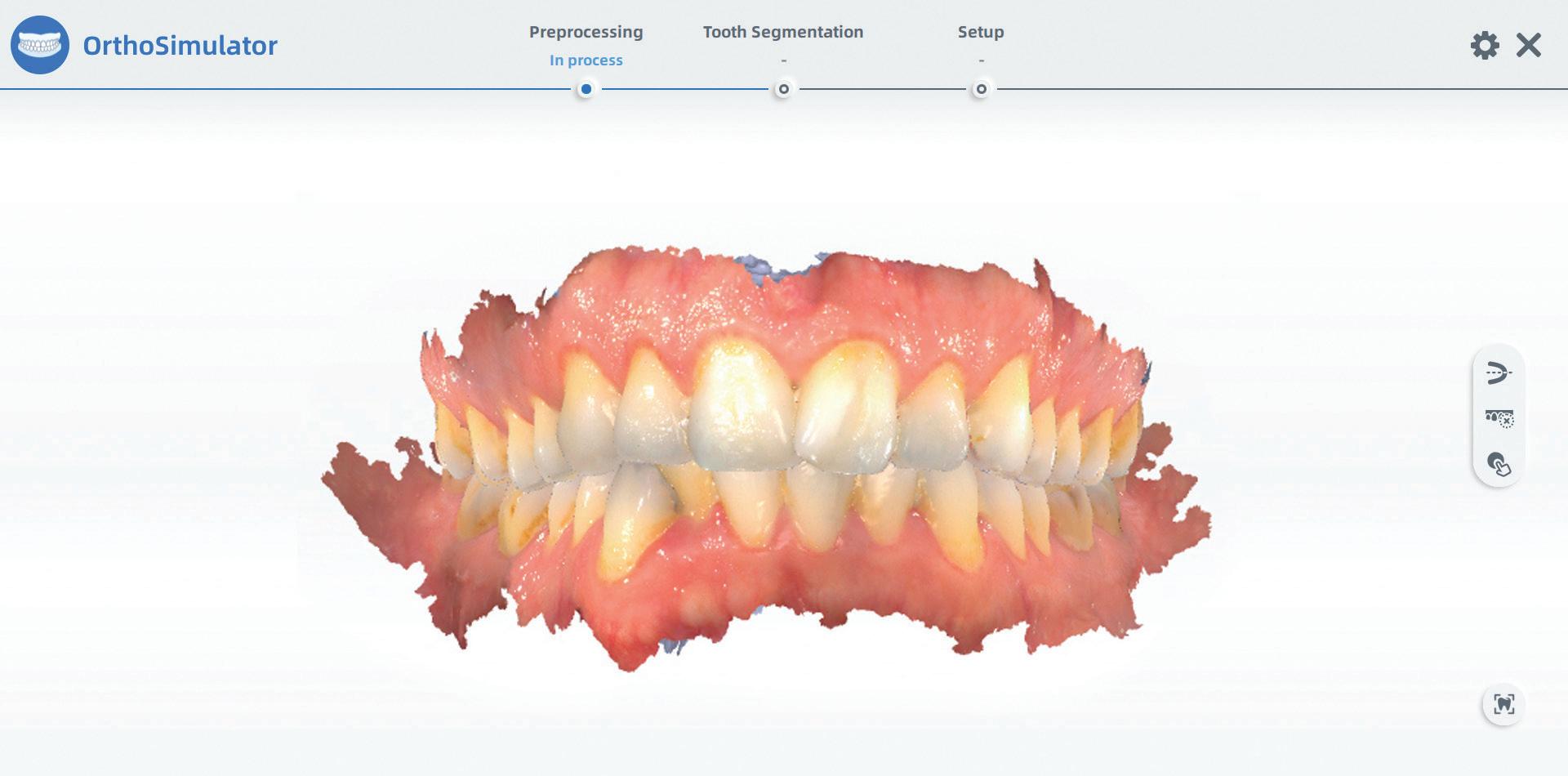
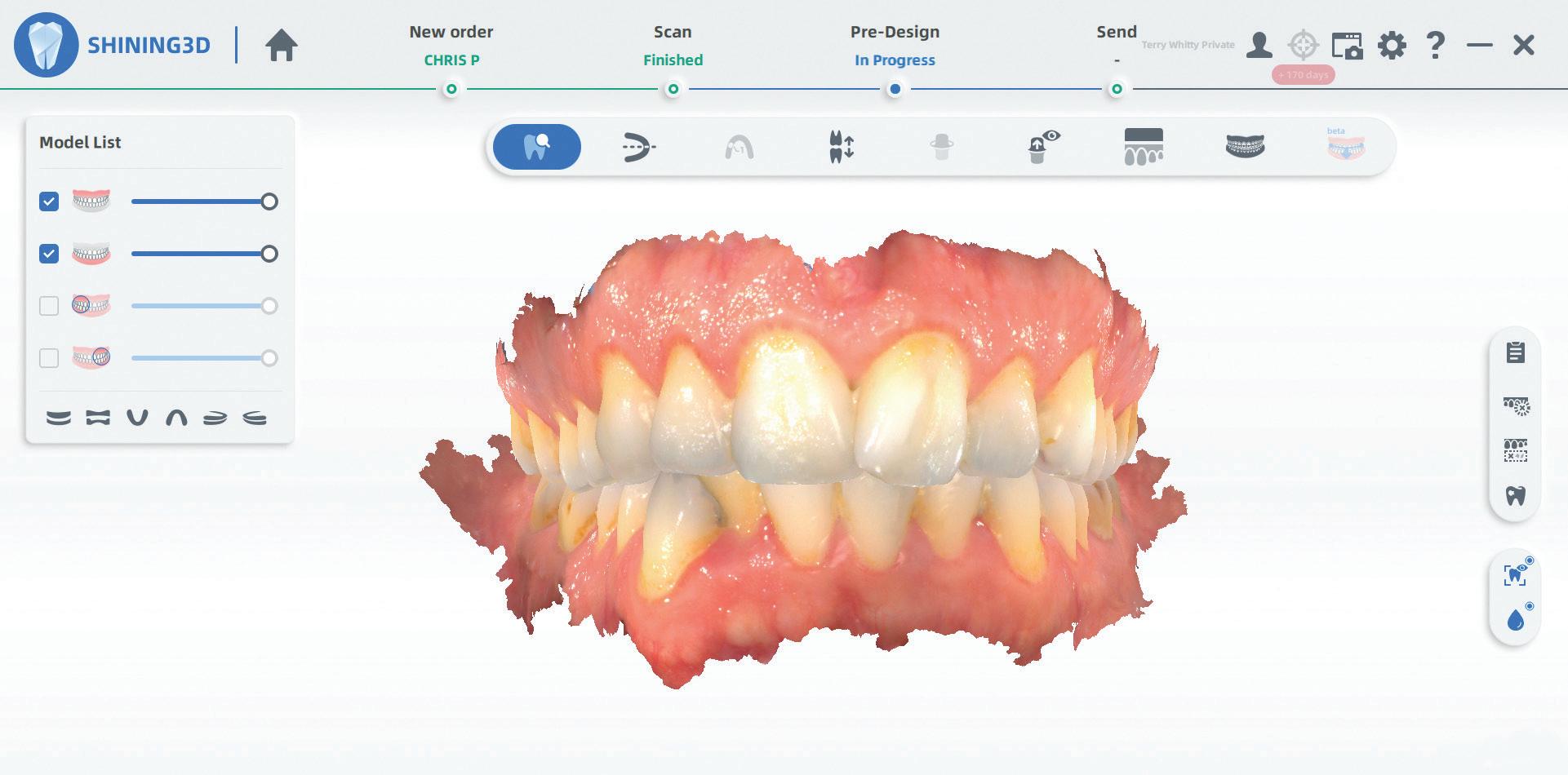
Figure 1.
Figure 2. This icon starts the OrthoSimulator.
Figure 3. OrthoSimulator start screen.
112 Australasian Dental Practice July/August 2022
Upper and lower scans from AORALSCAN 3 intra oral scanner.
clinical | EXCELLENCE
Figure 4. Adjusting scan orientation if needed.
Shining 3D AORALSCAN 3 intraoral scanner.

Figure 5. Scan smoothing of defects.
Figure 6. Edit scan mode - you can easily trim off unwanted areas of the scan.
Figure 7. Automatic tooth segmentation.
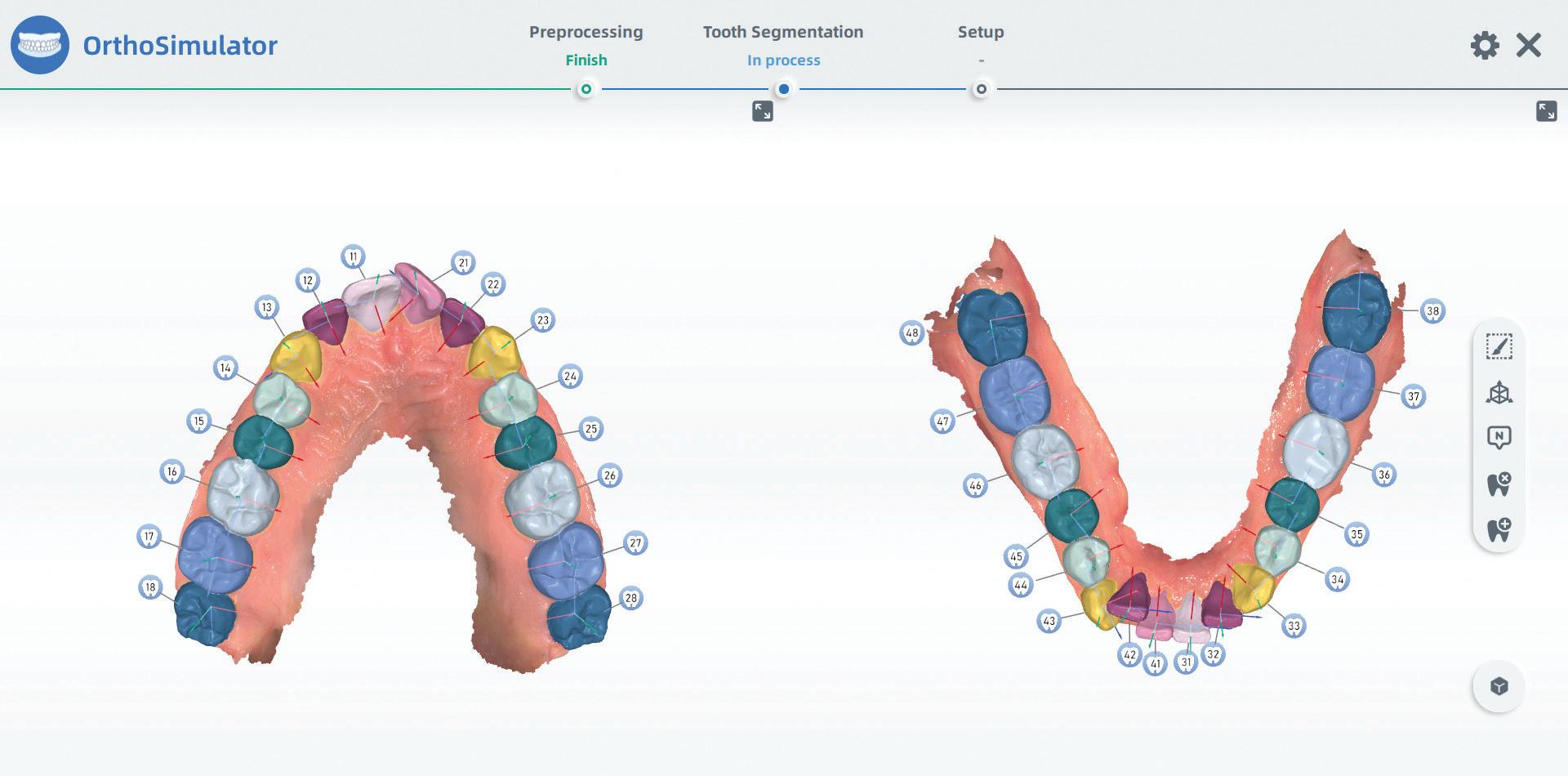
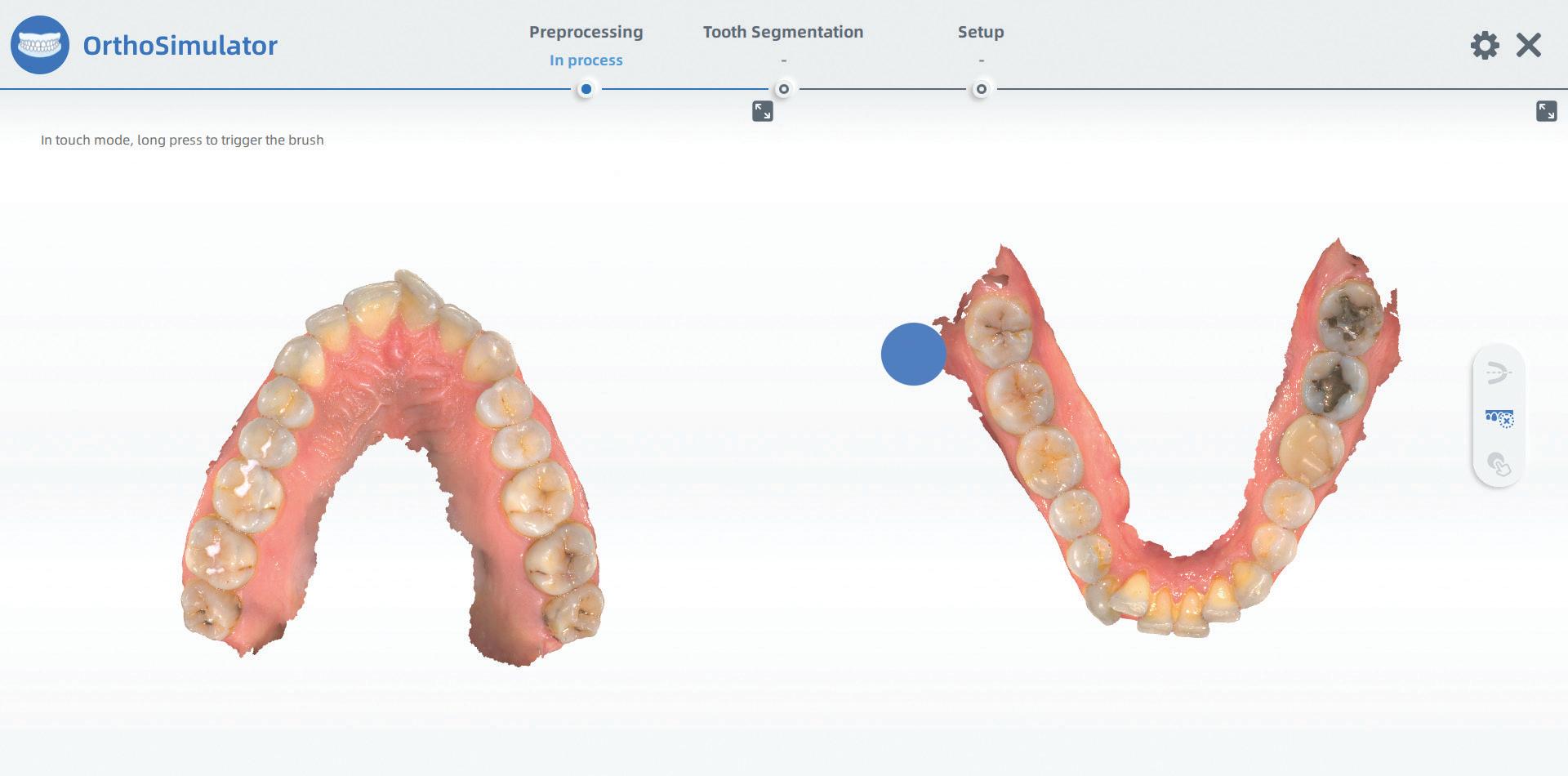
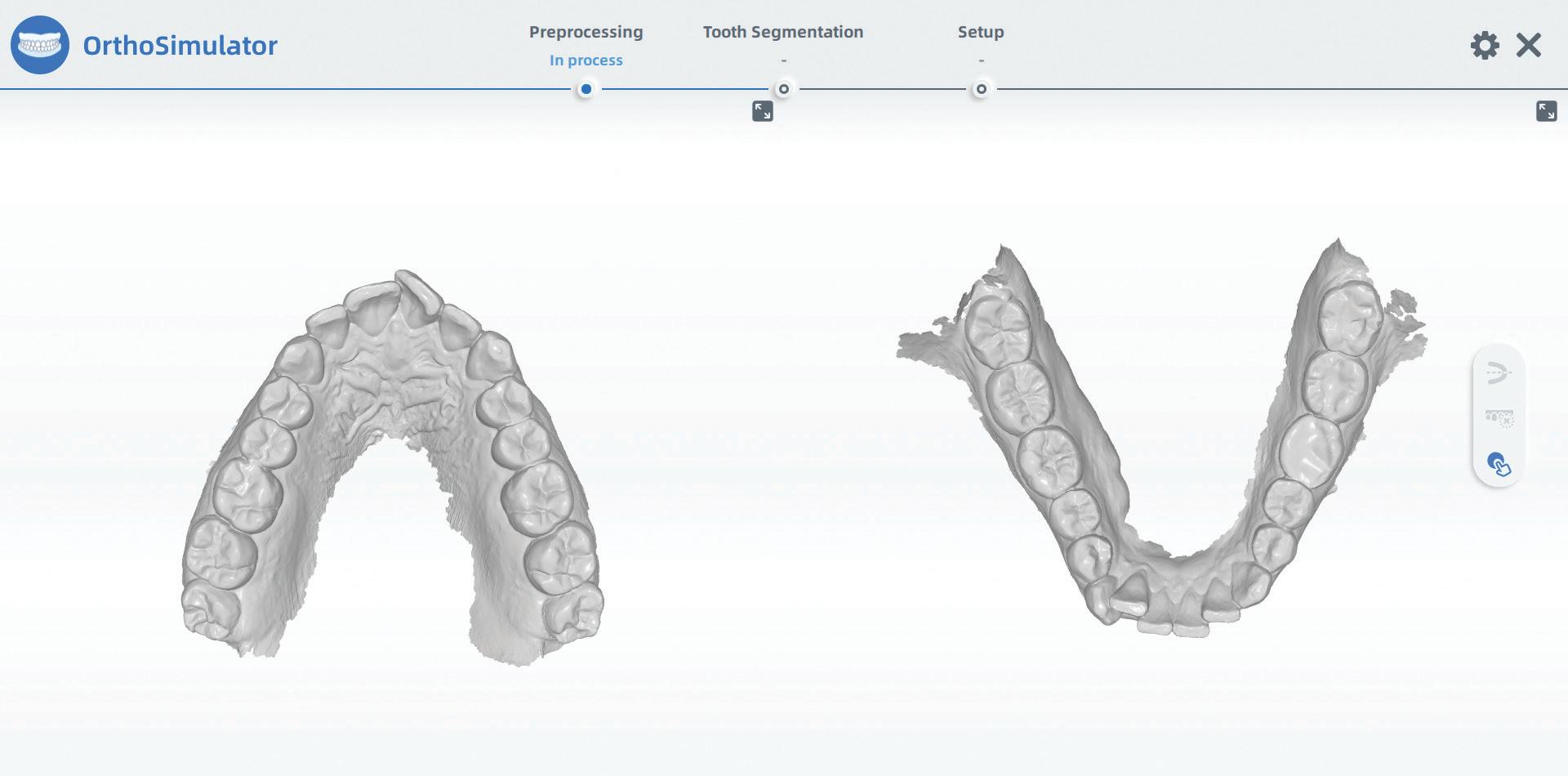
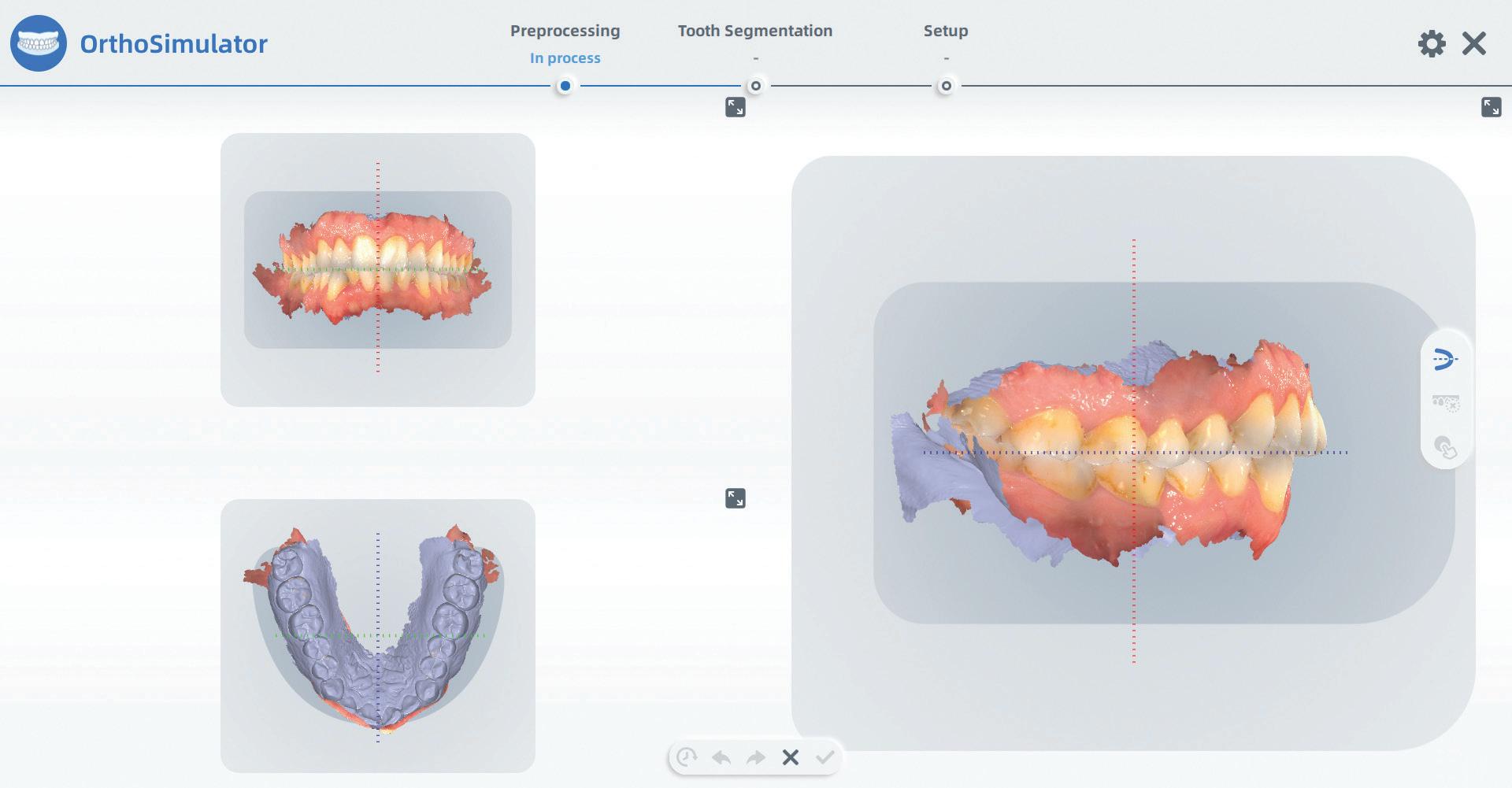
July/August 2022 Australasian Dental Practice 113
clinical EXCELLENCE
This often involved sending impres sions or scans to the software provider who would then create a virtual setup that would give the practitioner and the patient a clear idea of what the outcome may be like.
With the ever-increasing number of quality intraoral scanners coming to market, however, the incorporation of accessory software within the core pro gram is a must and from a manufacturer’s point of view, it is now becoming a bit of a feature war. Things like shade taking, caries detection, margin line detection, oral health check and model preparation for printing to name a few are all pretty much the mainstream today.
The addition of orthodontic simula tion built into the scanner software was thought of as a novelty at first, however it is now reaching a point where it seems every second patient is interested in having a look at what they may look like after orthodontics.

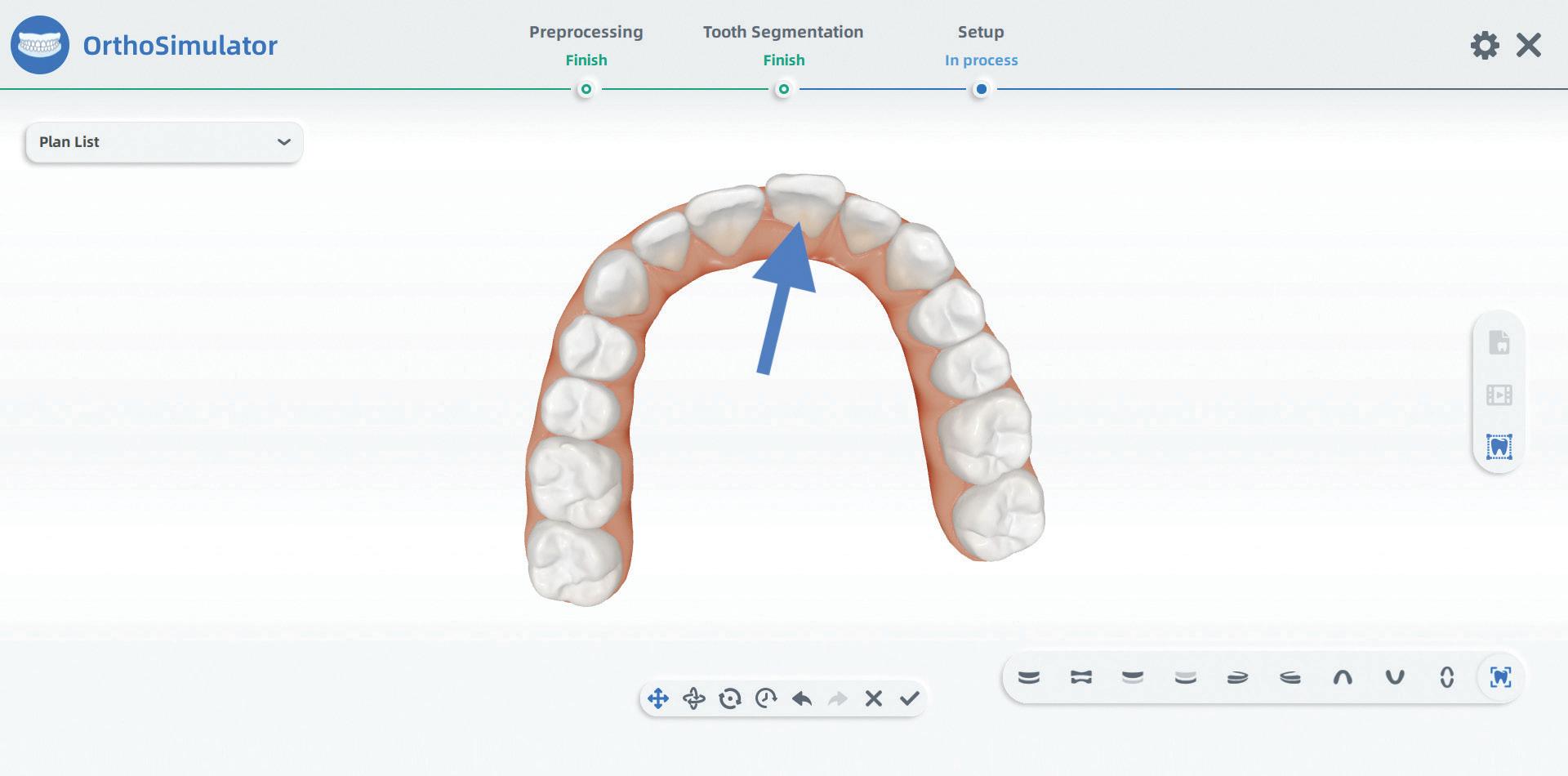
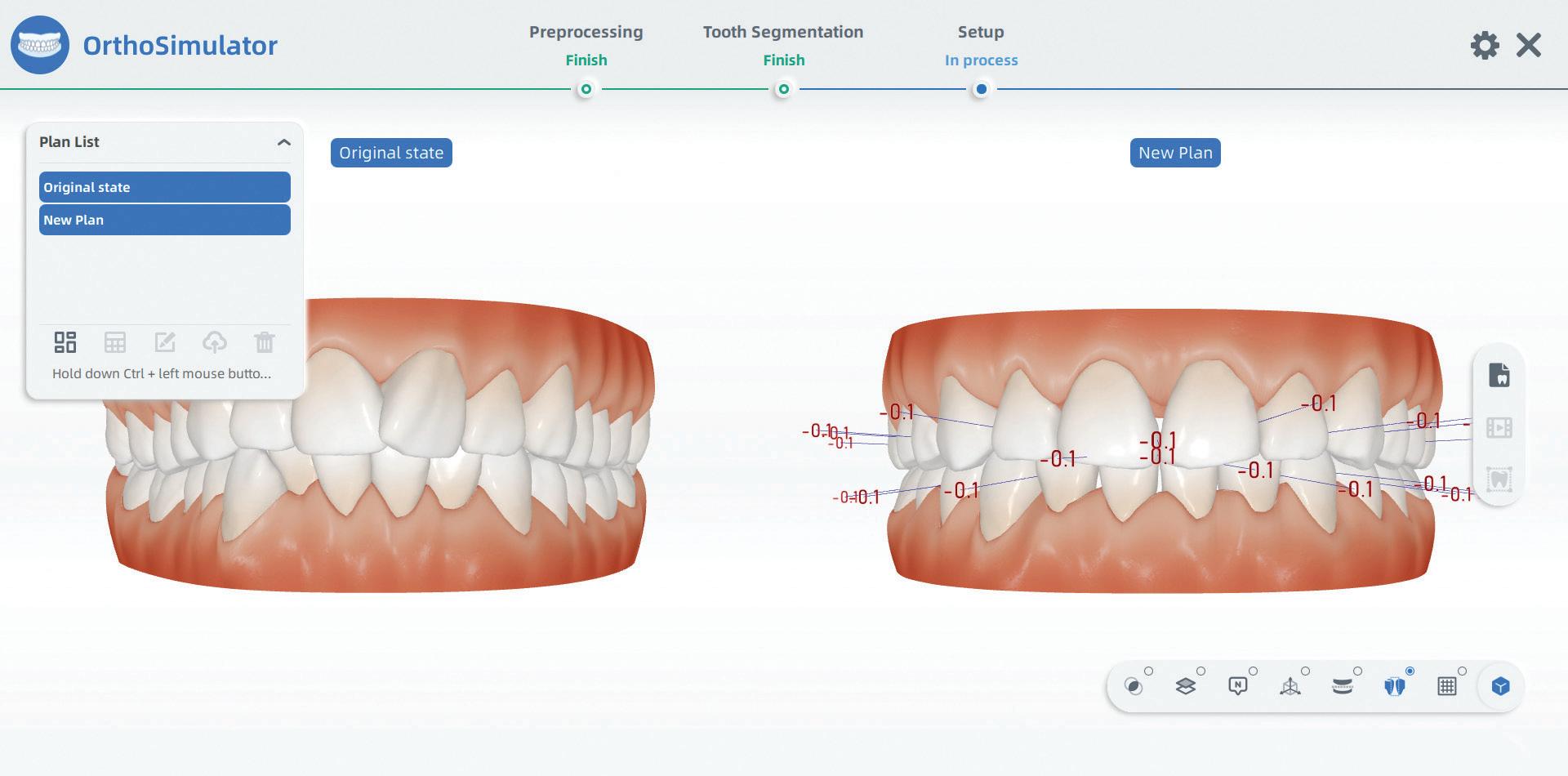
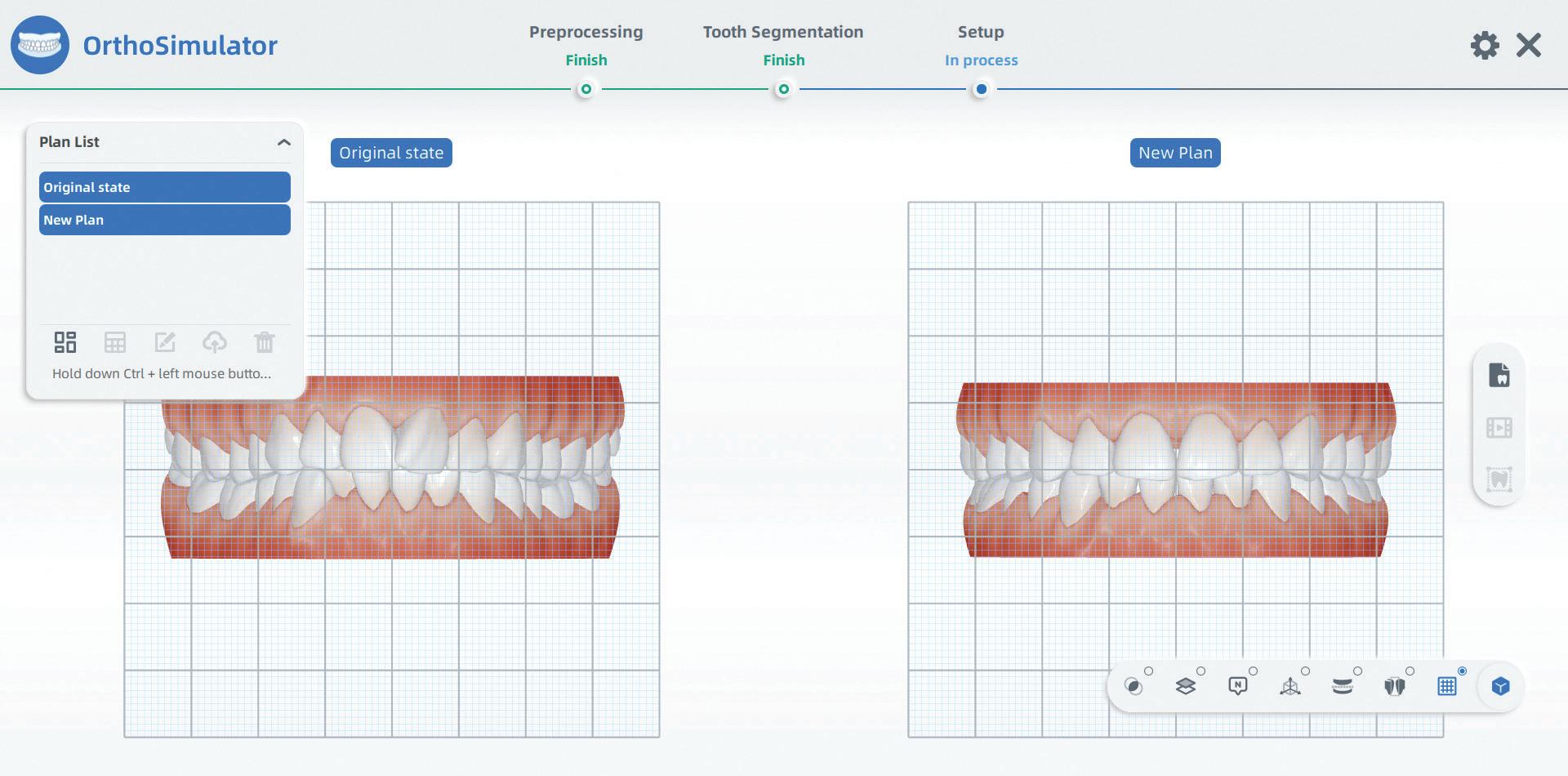
Some of these programs are very sophisticated indeed and the release of SHINING 3D’s Version 2 of the Ortho Simulator is no slouch. After scanning the patient’s upper and lower teeth and entering OrthoSimulator, the teeth are automatically segmented and a simulation
Scan the QR code below to watch the AORALSCAN 3 introductory video.
Figure 8. Automatic setup, on the left Pre Tx and on the right virtual simulation.
Figure 9. Grid visualisation.
Figure 10. Interproximal contact visualisation.
Figure 11. Easily move individual teeth in 3 dimensions with a mouse.
114 Australasian Dental Practice July/August 2022
Figure
Figure
to an idealised archform and tooth posi tion is achieved with a few clicks in no time at all while the patient is in the chair. The dentist can freely move any tooth in any direction if fine tuning is required and an animation morph from pre- to posttreatment is instantly made.
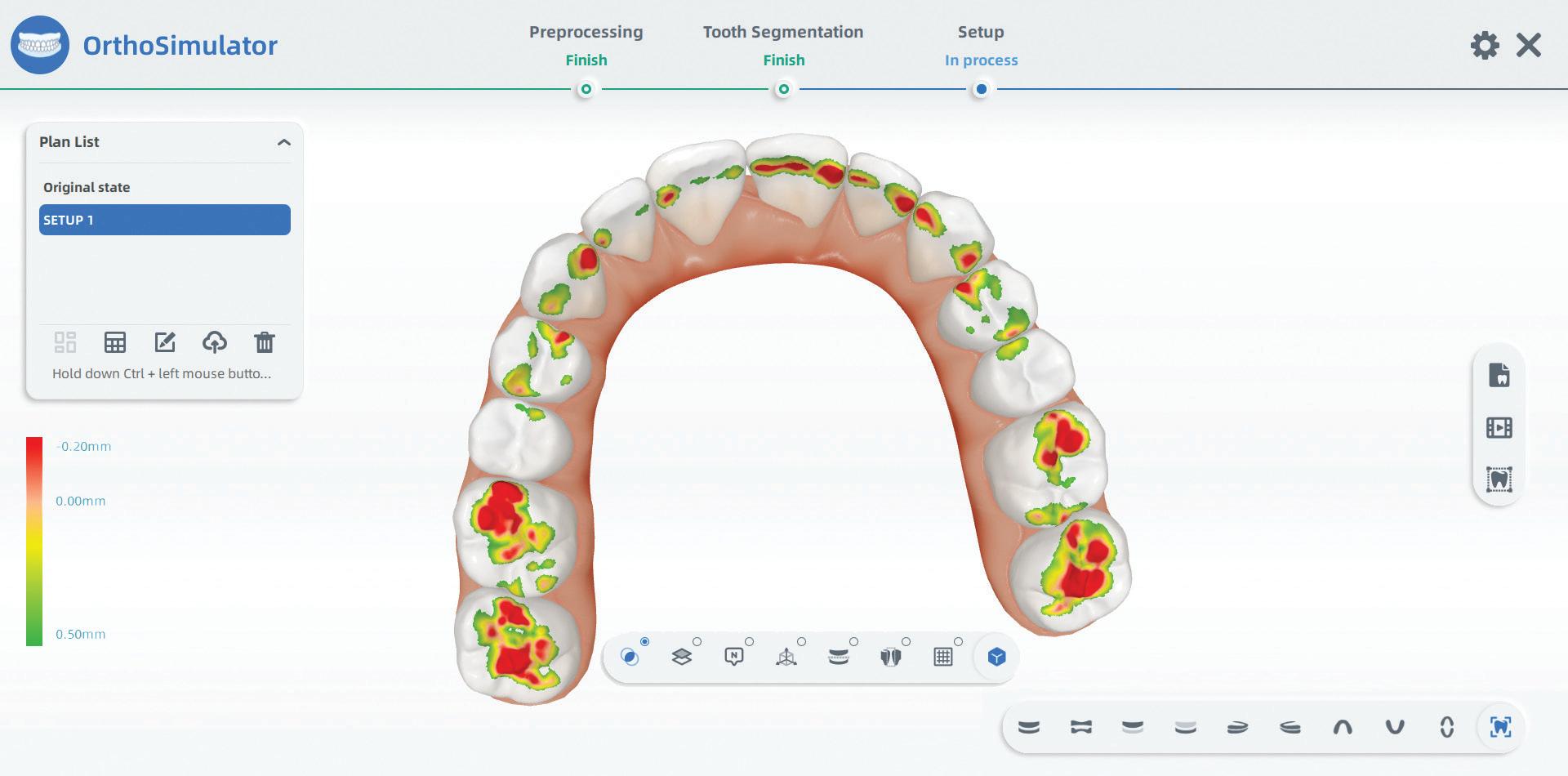
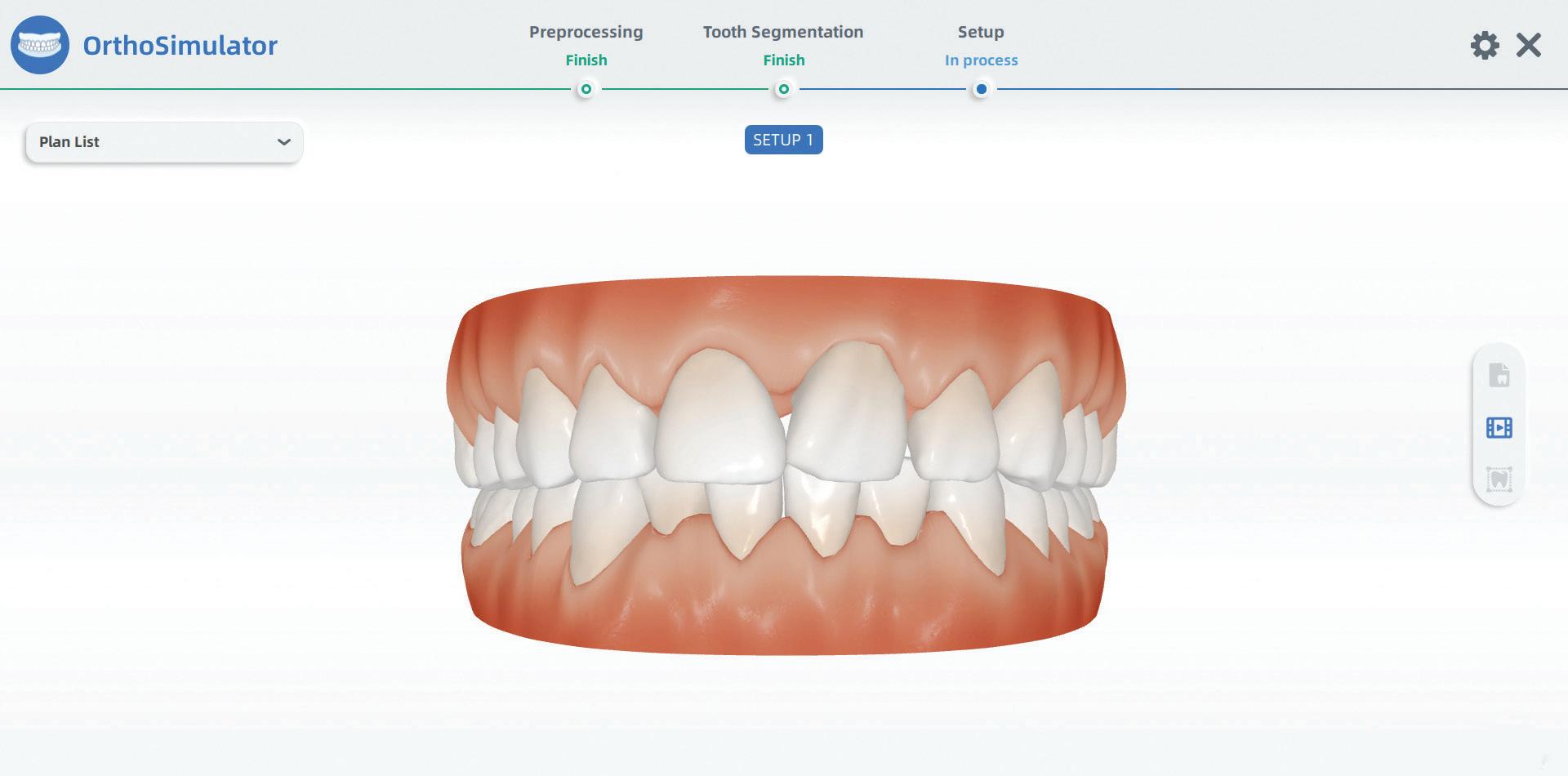
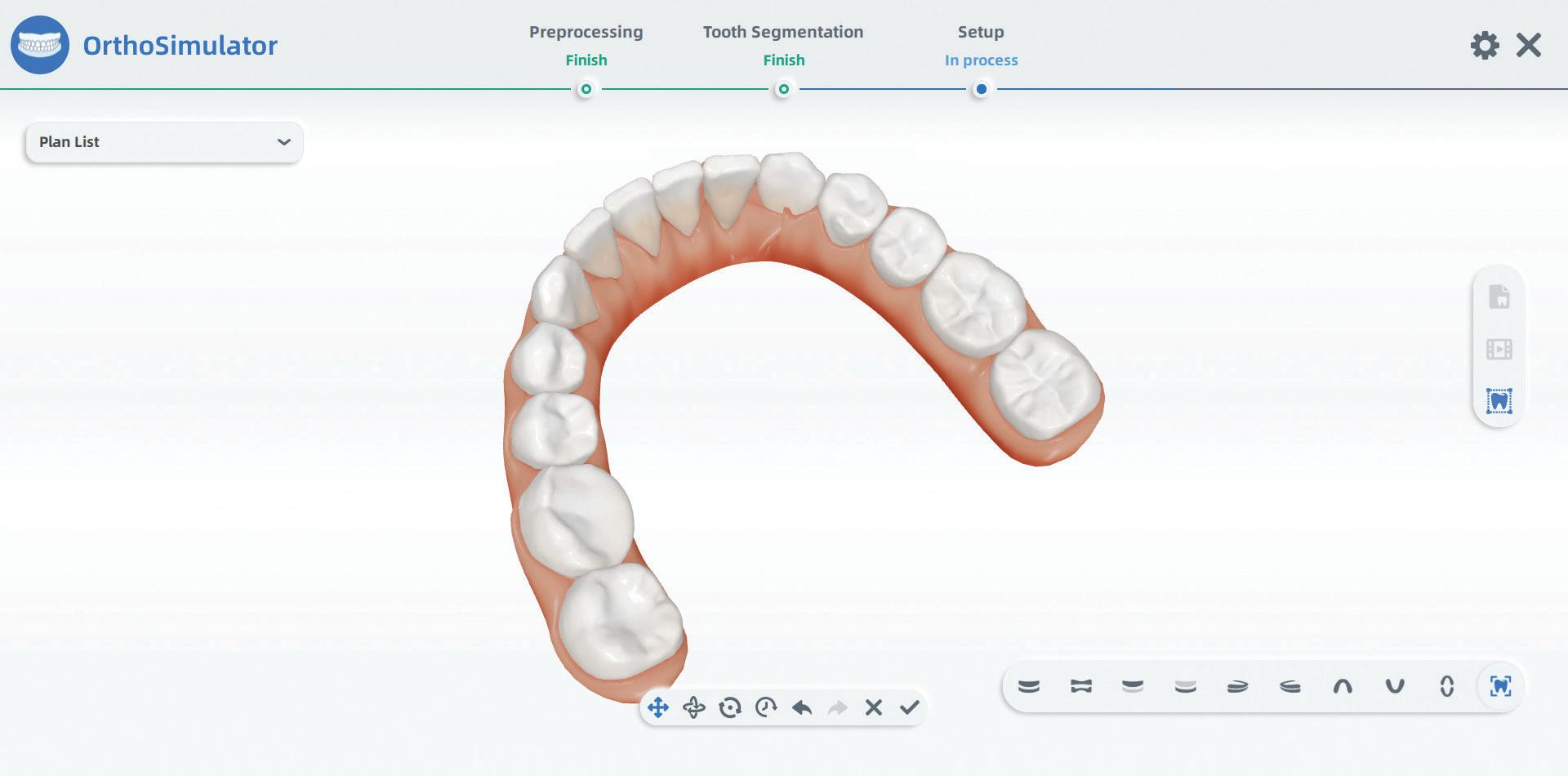
Incidentally, if extraction were a treatment option, this can now be done virtually thanks to a new feature version 2 supports... and it works very well. You can make a simulation with extraction and one without and compare the two as you can make multiple simulations for the same patient.
Once the treatment simulation is done, the patient can scan a QR code from the screen on any smartphone and the ani mation simulation with a complete set of picture views is downloaded to their phone from the cloud.
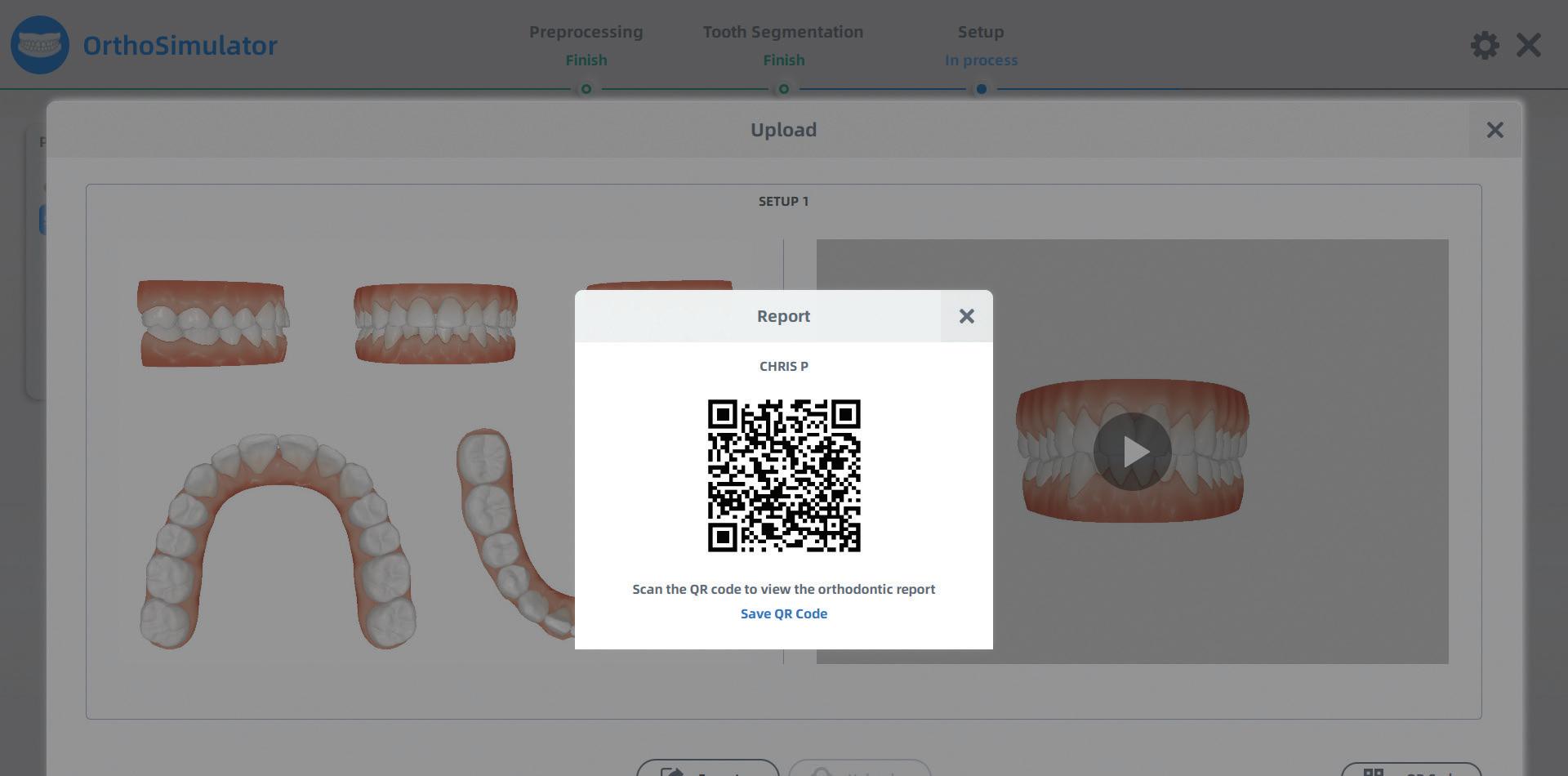
They can look at it at their leisure at any time and no doubt share with family and friends, a very powerful tool to increase case acceptance indeed.
It is important to point out to the patient that it’s only a simulation and even though the success rate is very high, achieving an exact match to the simula tion may not be possible for a multitude of reasons.
Scan the QR code below to see this case on your smartphone.

July/August 2022 Australasian Dental Practice 115
12. Lower teeth adjusted.
13. Animation is available and can be moved in 3 dimensions while playing.
Figure 14. Occlusal “Heat Map” shows intersections.
Figure 15. Uploading to cloud. Use the QR code to see this case on your smartphone.
clinical EXCELLENCE
clinical EXCELLENCE
The OrthoSimulator V2 from Shining 3D is a great improvement over V1 and is now even more user friendly and for all intents and purposes, fully automated. It aids in demonstrating orthodontic treat ment plans and communicates this well to the patient and for those who crave instant gratification, it delivers this abundantly. An amazing diagnostic, edu cation and selling tool and the best news is it’s a free update for all owners of the AORALSCAN 3 Intra Oral Scanner from Shining 3D.
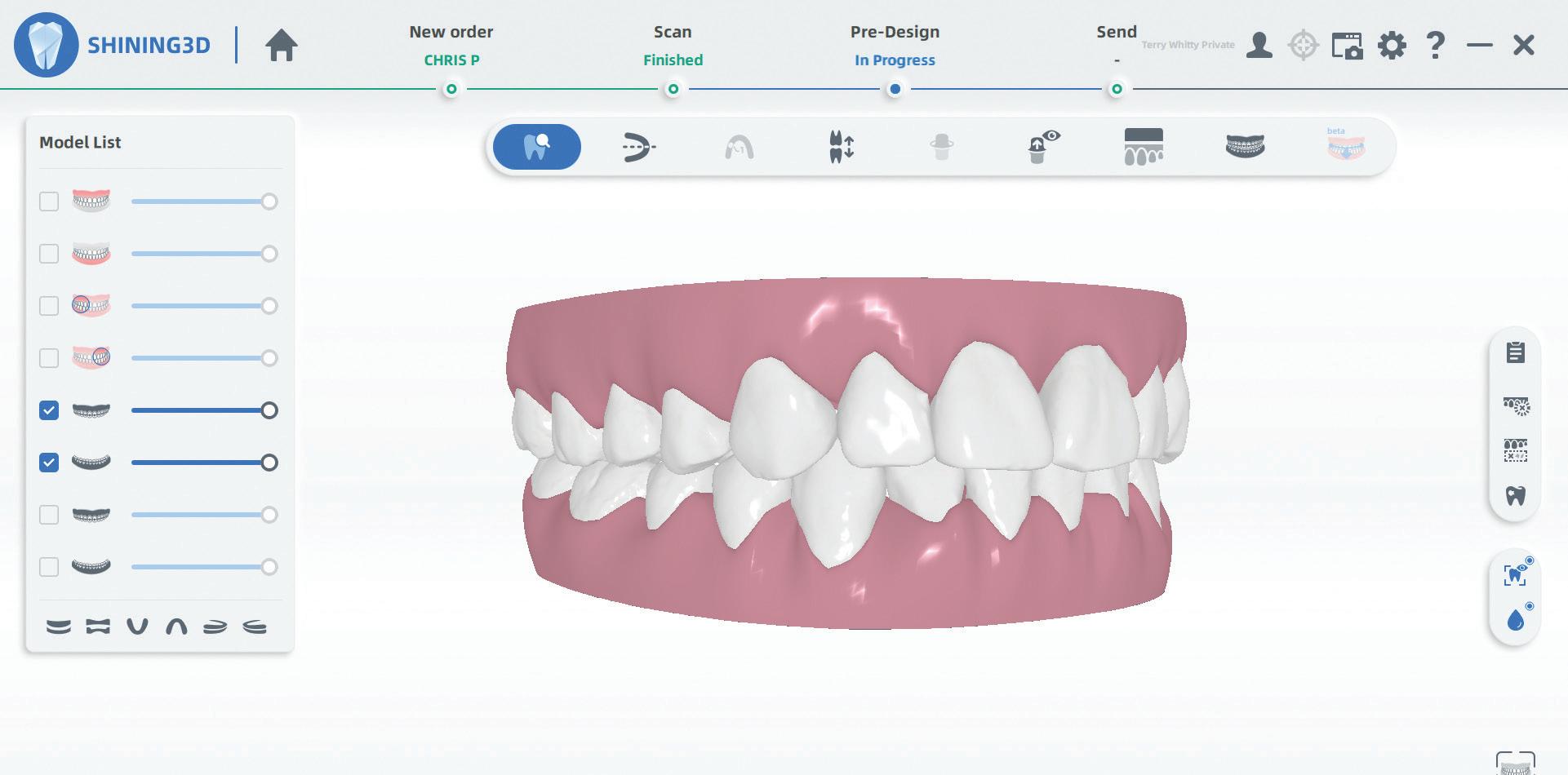
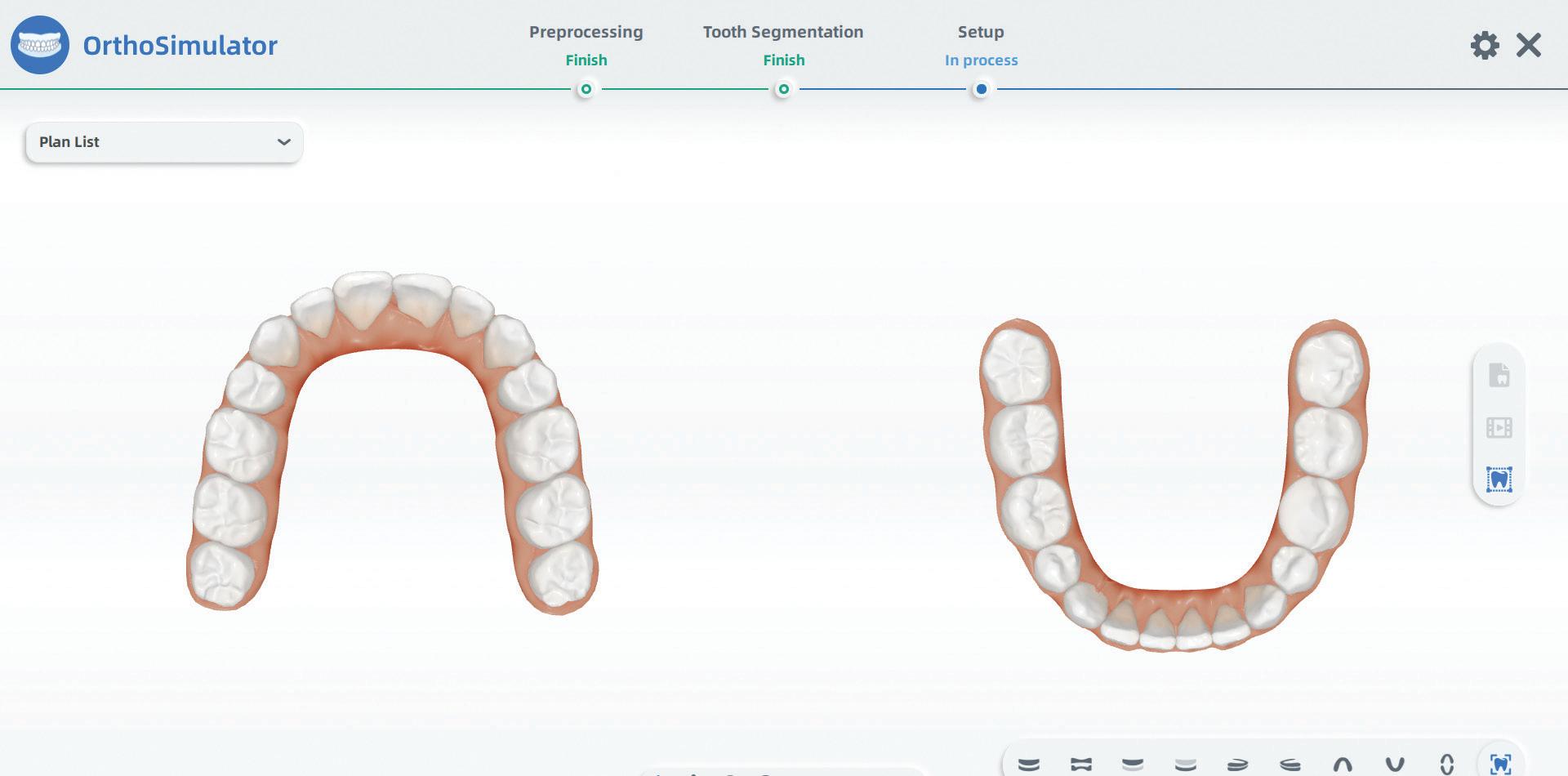
About the author
Terence Whitty is a well-known dental technology key opinion leader and lec tures nationally and internationally on a variety of dental technology and material science subjects. He is the founder and owner of Fabdent, a busy dental labora tory in Sydney specialising in high tech manufacturing. Using the latest advances in intra- and extra-oral scanning, CAD/ CAM, milling, grinding and 3D printing, most specialties are covered including ortho, fixed and removable pros thetics, computerised implant planning and guidance, TMD, sleep appliances and paediatrics.
Scan the QR code to see this case on your smartphone.

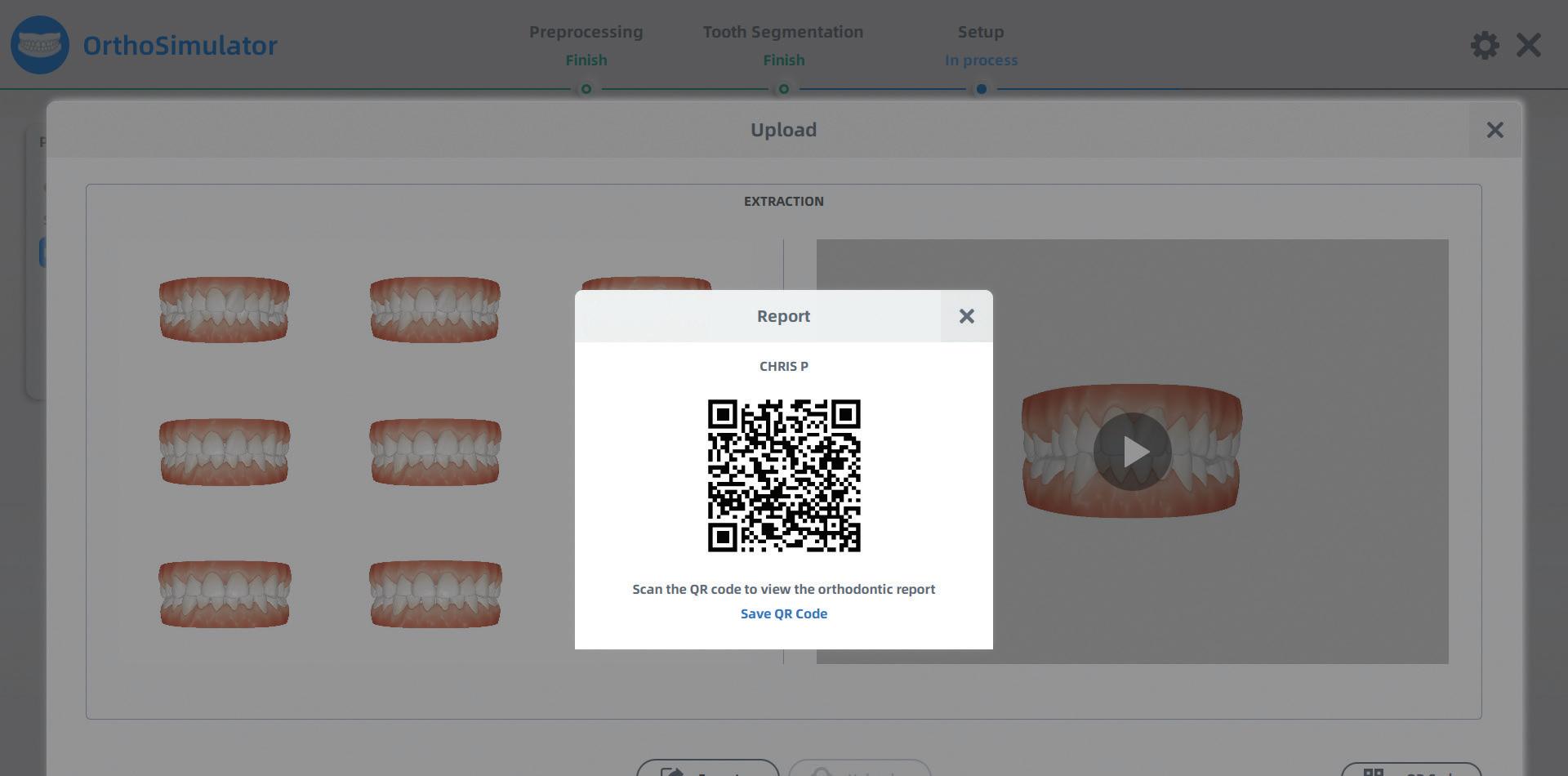
Figure 16. Instantly make a new treatment plan. Here 4 premolars were extracted.
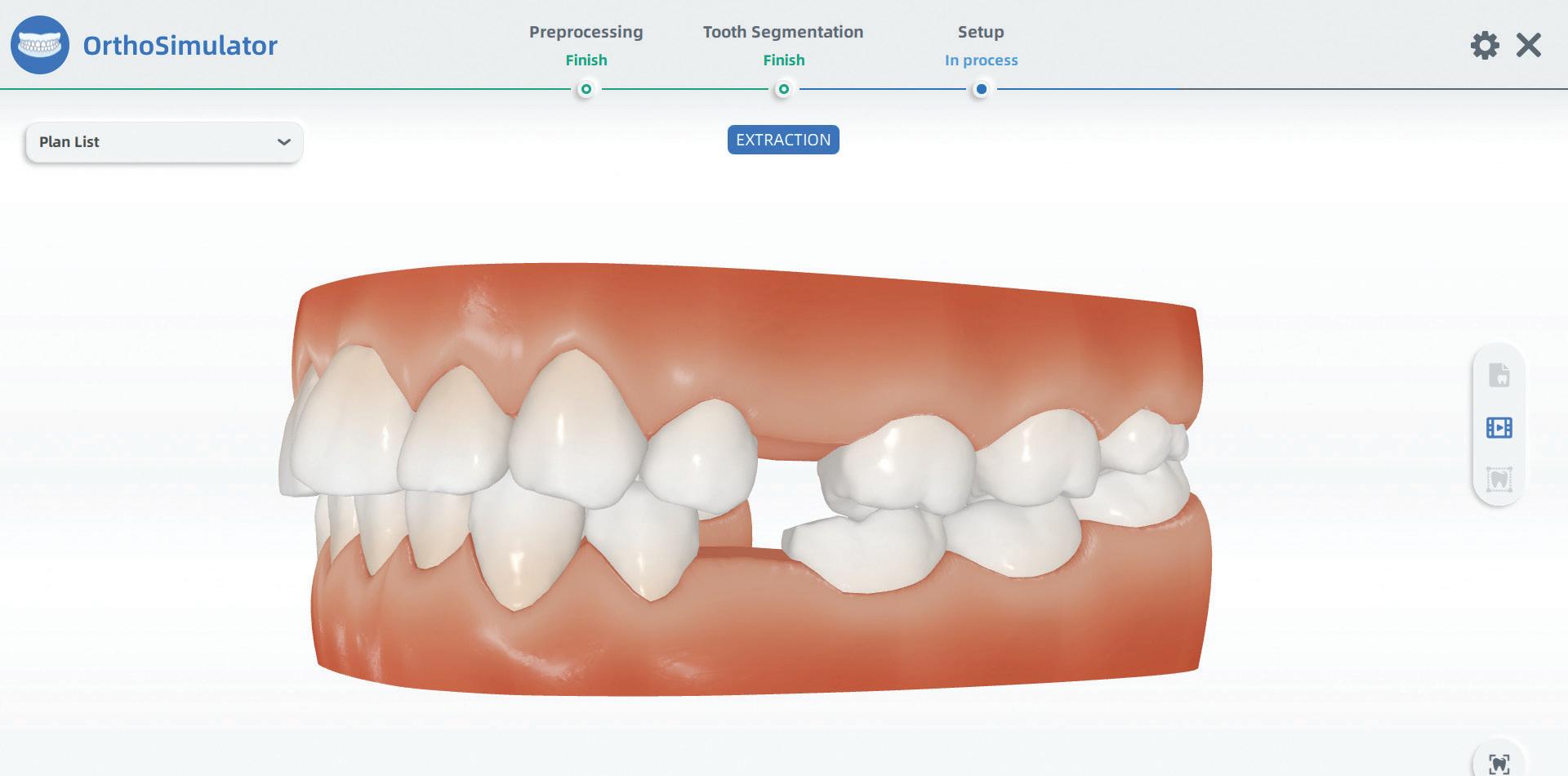
Figure 17. Extraction treatment plan simulation.
Figure 18. Extraction option uploading to cloud.
Figure 19. After exiting, the simulation models of all treatment plans are available.
116 Australasian Dental Practice July/August 2022



July/August 2022 Australasian Dental Practice 117 1300 878 336 Contact us today and we will show you how to integrate Affordable Digital Dentistry into your practice. Compatible with every major 3D printer, Mill and Software • Portable • 3 Year warranty available
Improved diagnosis confidence and patient informed consent
A case where the new CS 8200 3D Neo Edition from Carestream Dental was utilised to help diagnose and treat impacted wisdom teeth alongside numerous other oral issues in a patient
 By Dr Hubertus Schindler
By Dr Hubertus Schindler
A30-year-old male patient presented com plaining of recurrent pain in his 48. An initial evaluation showed that he had extremely impacted wisdom teeth, espe cially in the lower jaw (38 and 48) (Figure 1) with signs of coronal osteolysis which was causing him clinically observable pain. Additionally, his oral hygiene was poor and had resulted in gingivitis and calculus build-up. He had caries in multiple sites (15, 16 and 26) and there were signs of abrasion which suggested that the patient was suffering from bruxism.

A panoramic exam was done to get an overview of the general clinical situation of the patients’ mouth.
To identify the extent of the problem, the CS 8200 3D Neo Edition from Carestream Dental was used to obtain volumes for a precise diagnosis. The main benefit of this was the exceptional quality of the X-rays and how these could be used as a powerful communication tool.
As the images captured so much detail, they helped the patient to understand his medical condition and why the proposed treat ment options were necessary. This improved the quality of his informed consent. The system is very easy to use, intuitive and
118 Australasian Dental Practice July/August 2022
Figure 1. Panoramic clearly showing the impactions of teeth 38 and 48 and their close relationship with the mandibular nerve canals.
clinical | EXCELLENCE
also helped to streamline the diagnostic workflow due to its fast image acquisition and simple patient positioning.
Diagnosis and treatment
Multiple treatments were recommended based on the find ings from the diagnostic images and clinical assessment. These included:
1. Parotherapy to help treat the gingivitis and prevent bone loss from progressing any further. This would involve a process of giving the patient a series of thorough tests and questionnaires
regarding his oral hygiene habits to assess the extent of the problem, as well as taking images to accurately assess bone structure. Following this, root surface planing is often required and any teeth that cannot be sustained may be removed. The removal of subgingival calculus and any build-up along the gumline would be performed using special paro instruments and root surfaces would be cleaned and smoothed out. This would usually take 2-4 sessions.
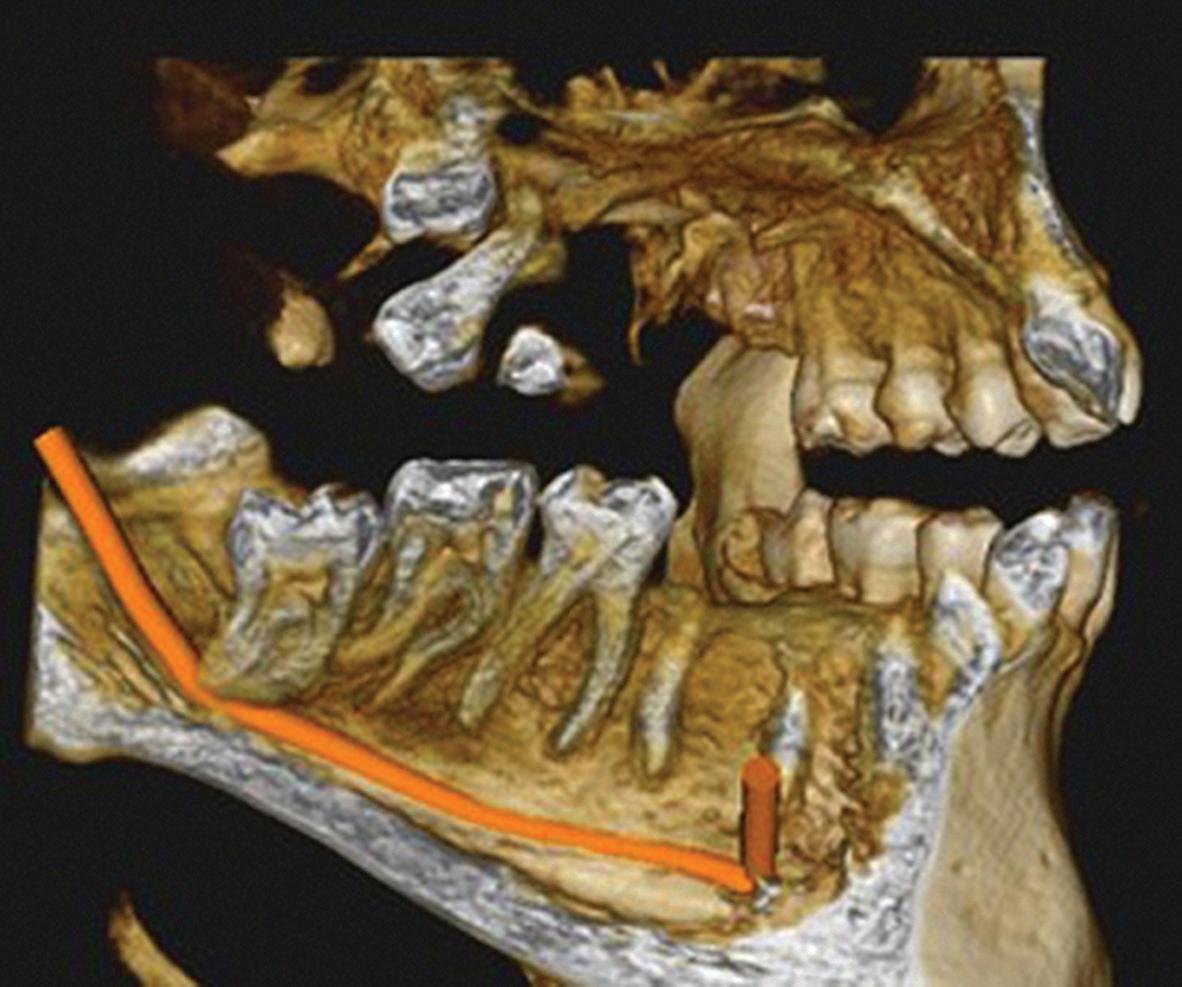
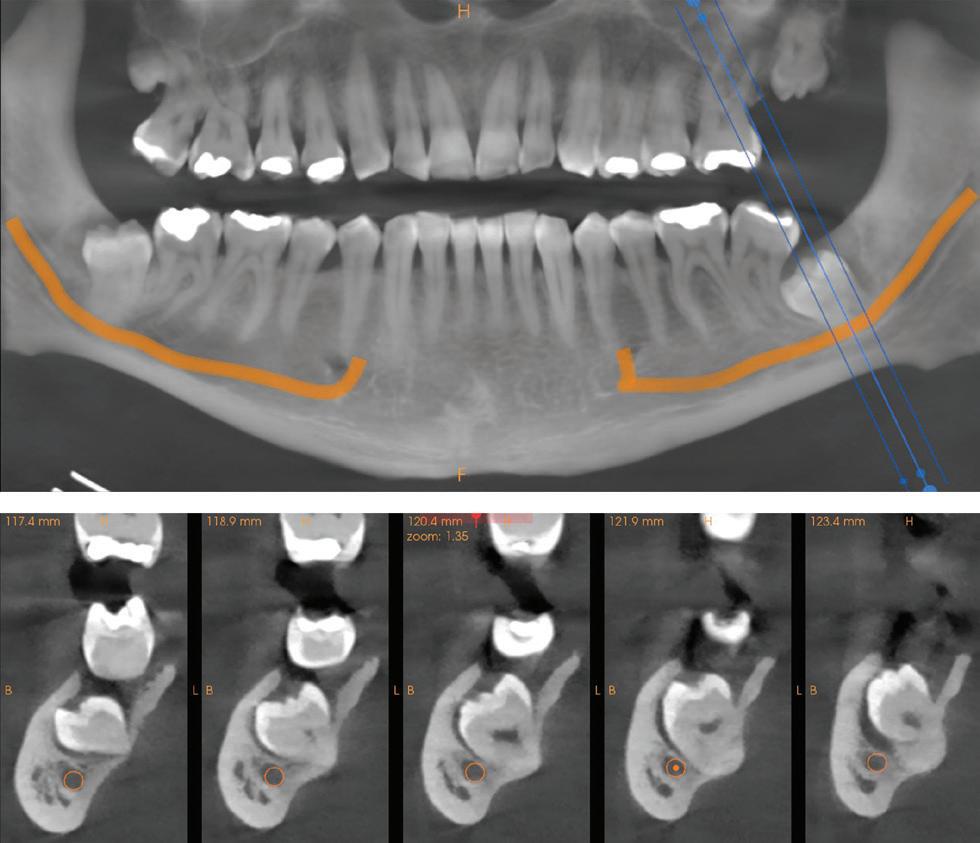
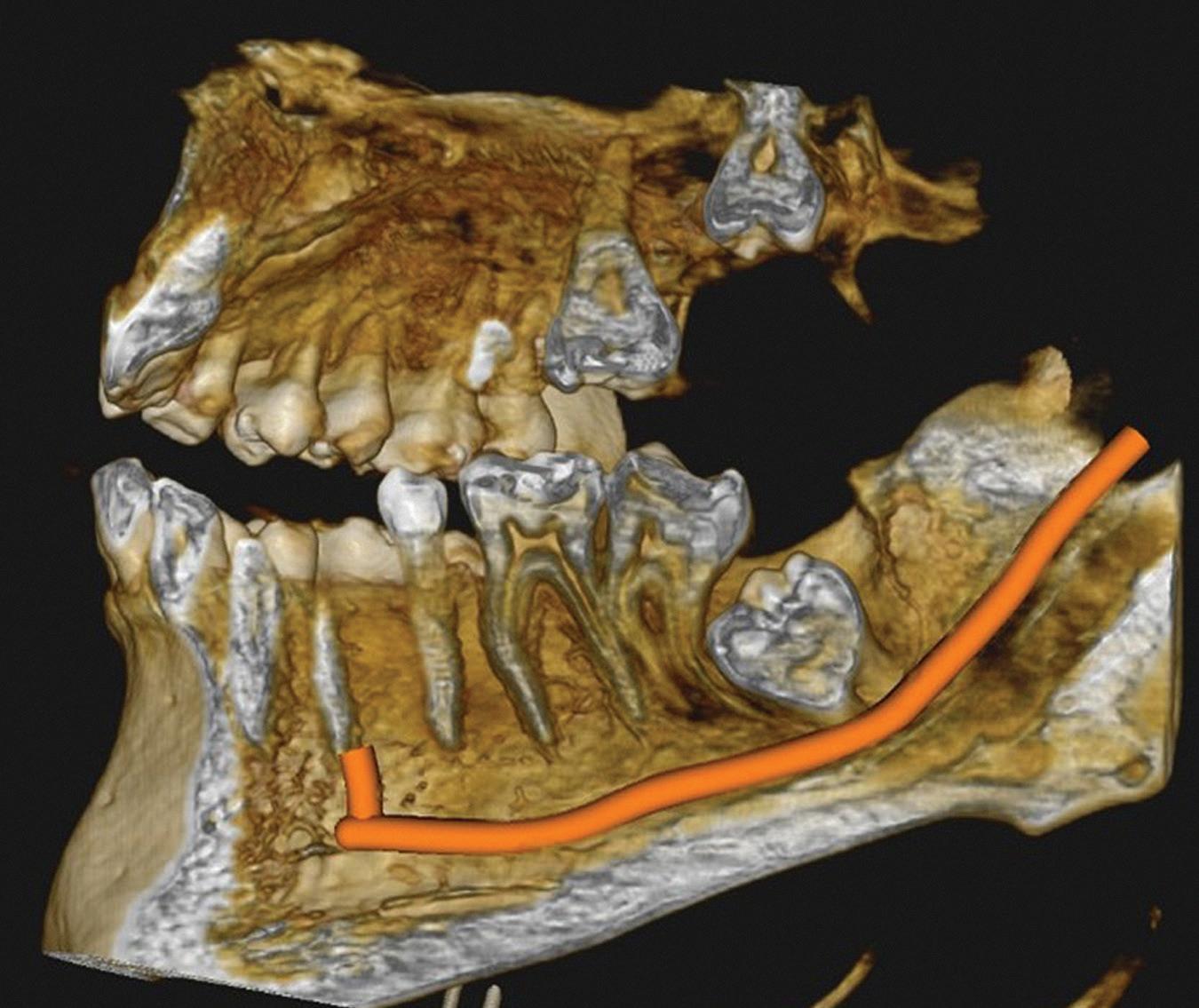
2. Restoration of the carious teeth - the teeth at sites 15, 16 and 26 needed fillings to prevent any further decay and existing caries would need to be removed.
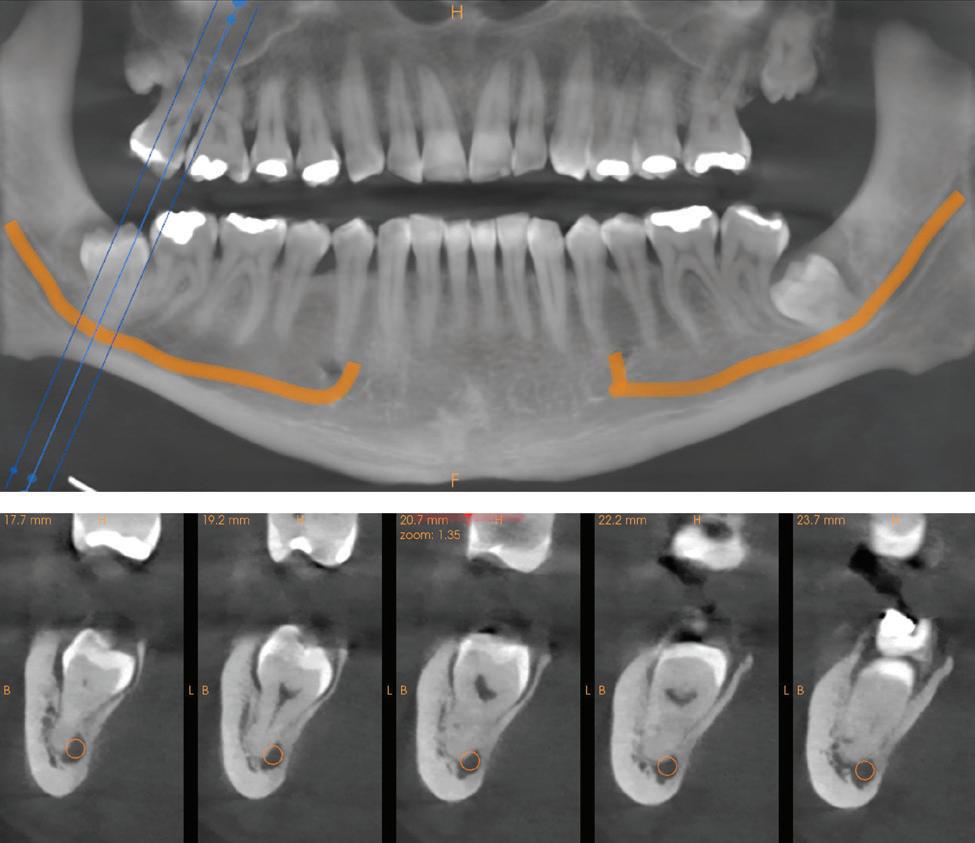
July/August 2022 Australasian Dental Practice 119
Figure 2. Reconstructed panoramic and cross sections of tooth 48, showing the contact of the root with the mandibular nerve canal.
Figure 4-5. 3D scenes showing the complex relationship of teeth 38 (left) and 48 (right) with their respective mandibular nerve canals.
Figure 3. Reconstructed panoramic and cross sections of tooth 38, showing the proximity of the tooth with the mandibular nerve canal.
clinical | EXCELLENCE
“As the images captured so much detail, they helped the patient to understand his medical condition and why the proposed treatment options were necessary. This improved the quality of his informed consent...”
3. Wisdom tooth extraction to remove the profoundly impacted wisdom teeth. The patient was warned of any potential damage to the alveolar nerve that extraction could result in.
4. A brux splint to help treat the bruxism. This measure would be to prevent further abrasion and damage to the dentition and would require extra appointments in the future for the fitting of the splint.
The patient was informed of the benefits and possible compli cations associated with each treatment option. Using the images taken by the Carestream Dental CS 8200 3D Neo Edition made this part of the process really simple, especially as the images captured had all the detail necessary to aid any conversation surrounding each treatment option and give the patient a better understanding of how every possibility would impact his denti tion moving forward. While the primary goal was the removal of the impacted wisdom teeth, I recommended that the additional treatments (parotherapy, fillings, brux splint) be completed as soon as possible - however, these would require further consent at additional consultations.
Result
Overall, the patient was very satisfied with the clarity of the medical briefing and was able to give a much better quality of informed consent due to the use of the CS 8200 3D Neo Edi tion. The system offers speed, precision and intuitive use and as my first CBCT system, it was remarkably easy to learn how to use. As mentioned before, the excellent quality of the X-rays and the fact that the patient could view them on screen made a big dif ference to this case - I had a lot more confidence as I had all the information I needed and gaining treatment acceptance was very straightforward as the patient was properly informed and had a much more detailed understanding of his particular needs.
I also liked the fact that there was no need to make an extra appointment with the patient to make a precise diagnosis and explain everything in detail as I had the images and the possibility to easily explain the treatment options with the CS Imaging 8
“Ultimately, Carestream Dental’s CS 8200 3D Neo Edition is a fantastic system that has completely transformed my workflows and optimised the way I provide treatment in practice. Not only is it easy to use and capable of capturing dynamic, high-quality images, but it also boasts a number of innovative features that have revolutionised the diagnostic process, which has made me a more confident clinician...”
software immediately at my fingertips. I would usually refer out for CBCT images and this slows the treatment process down. With the CS 8200 3D Neo Edition, it’s all instant and there when I need it.

Ultimately, Carestream Dental’s CS 8200 3D Neo Edition is a fantastic system that has completely transformed my workflows and optimised the way I provide treatment in practice. Not only is it easy to use and capable of capturing dynamic, high-quality images, but it also boasts a number of innovative features that have revolutionised the diagnostic process, which has made me a more confident clinician.
About the Author
Dr Schindler first qualified as a dental technician in 1998. He then studied human medicine and then later dentistry at the University Hospital in Vienna, during which time he also worked as a demonstrator/lecturer in the anatomical depart ment at the Medical University of Vienna. Following graduation, Dr Schindler has since worked in the University Dental Clinic in Vienna, opened his own private practice in Wiener Neudorf and undertaken advanced training in orthodontics, implantology and oral surgery.
120 Australasian Dental Practice July/August 2022
clinical | EXCELLENCE


ivoclar.com | ivde.com.au | 1300 486 252 CS 8200 3D NEO EDITION Extended capabilities for new opportunities See CBCT in a new light with CS 8200 3D NEO EDITION. It is the versatile 4-in-1 imaging system that creates new possibilities with capabilities such as an intuitive user interface, 9 fields of view and low-dose panoramic imaging. Making People Smile Seeing the difference makes the difference Tell me more https://bit.ly/38U5U39 FREE Computer, Delivery, Installation and Compliance Testing with every order!* * Offer includes travel costs up to $100. Travel costs over this are to be paid by the practice owner. Compliance Testing requirements differ in each State, based on Australian Radiation Safety Standards. Depending on your local state, the offer may include: Shielding assessment for premises, Compliance testing for premises and Compliance testing for equipment. For full details please check with one of our Equipment Specialists by contacting us. Offer valid until 31 August 2022 and may change without notice. Images indicative only. Offers not in conjunction with any other offers/discounts and not applicable to government, corporate or overseas accounts. E & OE.
CPD
At the cross roads
By Dr Geoff Knight AM, BDSc, MSc, MBA, PhD
The medical management of gangrene during the American Civil War was to amputate a limb above the infection site to prevent ongoing bacterial proliferation into surrounding tissues (Figure 1).

During a lecture in 2000, Dr Graham Mount, a pioneer in the clinical use of glass ionomer cement, described dentistry as “The only health care profes sion that still treats an infectious disease by amputation”.
In the last few years, dental technology has made significant advances to facilitate the diagnosis and replacement of tooth structure by either partial or complete amputation of teeth.
Sadly, all this amazing technology remains based upon the principles of the medical management of infectious diseases over 150 years ago, especially when there are so many more conserva tive treatment options currently available.
The medical management of dental caries
Dental caries is a bacterial infection of tooth structure caused by changing circumstances within the oral environment. There are defence mechanisms in the dentine pulp complex that are capable of slowing or reversing the rate of caries proliferation.
Arrested caries are an example of how, in a favourable oral environment, teeth are able to remineralise caries infected den tine (Figure 2). As the collagen matrix within the dentine has been denatured by the carious process, normal dentine is unable to form and remineralisation occurs by the deposition of min eral salts from the dentinal tubules and saliva. The dark colour of arrested caries is due to the inclusion of sulphur ions into the remineralising tissues.
Arrested caries can be compared to scar tissue, where the dermis is unable to reform, so a protective layer of scar tissue (arrested caries) is laid down to cover the wound area to prevent bacterial incursion into the tissues beneath.
The current medical manage ment of a dermal infection is to:
• Clean the wound;
• Place a medicament to enhance the natural healing process; and
• Isolate the infected site from a hostile environment and enable the healing process to occur.
These same principles can be applied to the management of dental caries.
Clean the wound
Carious dentine contains a high degree of surface bioload con sisting of bacterial plaque and other debris present within the mouth. Infected surface dentine may be so badly broken down to be breaking away from the surface of the caries.
Within the carious dentinal tubules, necrotic debris and bac teria are present that can interfere with the healing process.
Surface preparation consists of removing badly broken-down infected dentine and the bioload from the surface of the caries and into the infected dental tubules.
Broken down infected dentine can be removed with a small excavator, gently levering it from the surface of the caries.

Bioload can be efficiently removed to facilitate penetration of medicaments and GICs, from the surface of the caries and into the dentinal tubules, by the application of 37% phosphoric acid for 15 seconds, washing with water and gently air drying. Polyacrylic acid will not remove bioload from the dentinal tubules (Figure 3).
Apply a medicament to enhance healing (remineralisation)
Fluoride release from glass ionomer cement (GIC) has a limited effect in arresting caries and has been used extensively for caries management in remote communities (ART), however GIC cannot be relied upon for total caries management and requires additional pharmacological assistance to be truly effective.
Ozone gas has been used as an effective caries management tool but its use is limited due to lack of an efficient delivery system.
122 Australasian Dental Practice July/August 2022
clinical | EXCELLENCE
Figure 1. 170 years ago, the medical model for treating gangrene was to amputate a limb above the infection.
Figure 2. Arrested caries demonstrates a tooth’s ability to remineralise caries into dental scar tissue.
READ ME FOR
Fluoride varnish application has been shown to have limited clinical benefit.
Silver fluoride compounds are highly bactericidal and have long been used to arrest caries - silver nitrate since the early 1900’s and silver diamine fluoride was identified from early Japanese literature for arresting caries in the early 70’s. Figure 4 shows the bactericidal effects of AgI deposits on a carious dentine surface.
Aqueous silver fluoride (AgF) and silver diamine fluoride (SDF) both effectively arrest dental caries, however the side effect of staining the arrested caries black has generally limited their use for the management of caries in deciduous teeth and root caries.
Staining by AgF and SDF can largely be prevented by the immediate application of potassium iodide (KI) that scavenges any remaining free silver ions to form silver iodide, a creamy col oured white precipitate. Figure 5 shows the difference in staining of a GIC restoration when one cavity was treated with SDF and the other with SDF/KI.

The application of potassium iodide during pregnancy or patients with thyroid issues should be done in consultation with an appropriate medical practitioner.
Composite resin is a popular material for the replacement of lost tooth structure and is an excellent restorative material for cavities caused by a lost restoration without residual caries or tooth loss caused by trauma.
Composite resin relies upon the bond of resin based dental adhesives that adhere poorly to caries affected and infected den tine. In order to repair a carious lesion with composite resin, all remaining caries must be removed prior to bonding onto sound dentine and this requires the removal of a lot of remineralisable tissue. As such, composite resin is unsuitable as a restorative material to restore carious teeth.

Glass ionomer cement has a weak chemical bond to sound and carious enamel and dentine. As the interface between a tooth and glass ionomer cement is stress free, high bond strengths are not required. Furthermore, prior application of SDF and AgF enhances the bond strength of GICs to enamel and dentine (Figure 6).
High strength GICs are indicated for single surface resto rations where there are no unsupported cusps present. These include occlusal surfaces, proximal surfaces using tunnel or slot preparations and lesions at the gingival margins.
July/August 2022 Australasian Dental Practice 123
Isolate the infection from the environment to improve healing (remineralisation)
Figure 3. Etching removes debris from non-vital dentinal tubules compared to conditioning with poly acrylic acid, enabling better penetration of medicaments and restoratives into the tubules.
Figure 4. Shows the bactericidal effect of AgI deposited on the surface of carious dentine after SDF/KI treatment.
clinical | EXCELLENCE
Figure 5. Demonstrates the effectiveness of SDF/KI in preventing staining compared to SDF alone.
Figure 8. Following a 15 second etch, the caries have been treated with SDF and KI. Notice the white precipitate of AgI on the caries surface.

• Figures 7 shows a cavity prepared for a silver fluoride treated restoration, leaving significant caries in situ.

• Figure 8 shows the cavity following a 15 second etch and SDF/ KI placement. Note the white precipitate of AgI on the surface of the carious dentine.
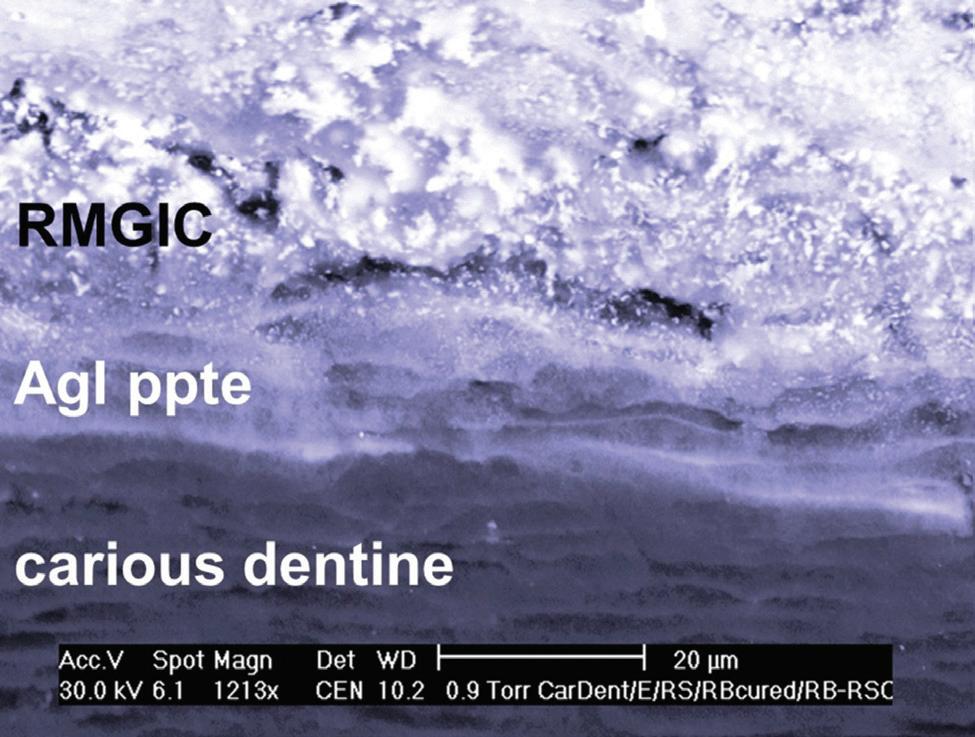
• Figure 9 shows the completed restoration.
Multi surface restorations require the extra strength of a composite resin overlay of a GIC base, or a conservatively prepared indirect restoration.

In summary, single surface restorations to remineralise caries are placed as follows:
• Remove excessive bioload with a small excavator;
• Etch for 15 seconds, wash and dry the preparation;
• Apply one or two drops of SDF or AgF onto the caries, avoiding gingival tissues;
• Immediately apply KI until the white precipitate becomes clear;
• Wash away reactant and air dry; and
• Place a GIC restoration.
The placement of multiple surface restorations follows the same steps, except a resin modified GIC is used as either a base
Figure 9. A wear resistant GIC restoration provides a simple and predictable solution for the management of single surface caries.
or lining, prior to placing a composite resin or indirect restoration overlay.
Figure 10 shows the remineralisation ability of SDF/KI on an asymptomatic carious lesion 14 months after placement and Figure 11 shows how the use of SDF/KI prevented SDF staining of the restoration over that time.
I
Opportunities
n many ways, the dental profession is at a cross roads.
The delivery of high tech treatment offers patients choices that would otherwise be unavailable to them. Unfortunately, such procedures are often highly invasive, time based treatments that do not provide permanent solutions to patient needs and have cost constraints that limit their availability. Furthermore, the enthu siasm amongst the dental profession to adopt these technologies can lead to over diagnosis and prescription of their use.
Within this mix of the treatment options available to dentists, there are clinical situations to treat carious teeth that would be better managed by using a more conservative medical-based model of care.
124 Australasian Dental Practice July/August 2022
Figure 6. The application of SDF/KI to carious dentine increases the bond strength between caries and resin modified GIC.
Figure 7. An occlusal cavity preparation with supported cusps for the restoration of caries prior to SDF/KI and a GIC overlay.
clinical | EXCELLENCE
IS EVERYTHING the right one with Hu-Friedy
predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. when it comes to the perfect fit, Hu-Friedy is just right.
IS EVERYTHING the right one with Hu-Friedy
DENTISTS LOVE OUR STAINLESS STEEL PEDO CROWNS:
predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. it comes to the perfect fit, Hu-Friedy is just right.
DENTISTS LOVE OUR STAINLESS STEEL PEDO CROWNS:

Septanest : the first choice of dentists with over 150 million injections per year, provides you high quality you can trust

ONLINE AT Co., LLC. All rights reserved.
808 855 ww
Mfg. Co., LLC.
ONLINE AT
All rights reserved.
808 855 ww
Call 0508 486 252 www.ivoclar.com
Medical caries management is based upon the treatment proto cols of Atraumatic Restorative Treatment (ART) that have been successfully used to treat caries in both established and emerging economies for a number of years. The enhancement of ART by the application of silver-based medicaments create the interesting acronym; Silver Modified ART or SMART.
SMART is a treatment model of care that:
• Enables high quality and predictable restorations over a wide range of platforms in established and emerging economies;
• Provides a virtually pain free and relaxed environment for both patients and dentists that encourages the super-efficient delivery of care;
• Dramatically reduces the need for general anaesthetics for asymptomatic and apprehensive children; and
• Lays the ground for future minimally invasive management of dental caries.


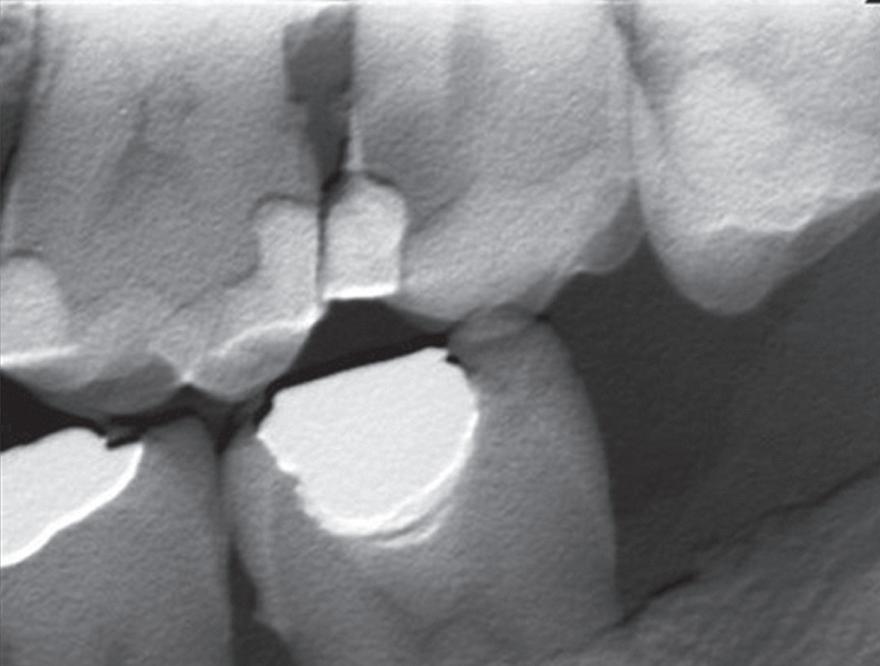
By leaving caries in situ, SMART enables the predictable, efficient and stress free delivery of restorative care with benefits to both patients and clinicians and can be readily accessible on a global scale. In reality, the coexistence of SMART and high tech dentistry offers patients the very best of care across a wide range of treatment modalities and lays the foundations for the successful evolution of the profession.

About the author
Geoff Knight AM is a general dentist from Melbourne. He is an internationally recognised speaker with a focus on preservation dentistry and has published a book on this topic - Silver Fluoride and Glass Ionomer Cement: A SMART Operative Guide for Working with Teeth. This book presents the evidence-based research for applying the cur rent medical model to restorative dentistry. The extent of caries and location on a tooth are identified and an appropriate restorative procedure described in depth for each clin ical situation, supported with over 200 colour photographs and diagrams over more than 150 pages of text. At the end of each described technique, there is a concise step by step sum mary of each procedure. This book is suitable for all restorative dentists who are seeking a less stressful and more rewarding way to practise dentistry. Available from Amazon Australia. eBook $17 - Paperback $43.45.
Disclosure: The author had a past financial interest in SDF/KI.
126 Australasian Dental Practice July/August 2022 clinical | EXCELLENCE
Figure 10. Large asymptomatic caries on multiple surface cavities shows the healing (remineralising) ability of a SMART GIC composite resin sandwich restoration.
Figure 11. A large multi surface SMART restoration treated with SDF/KI eliminates staining at the cavo margins.
















Subscribe Today! Earn 2 CPD Hours every edition Only $99 per year or $165 for 2 years Click Subscribe at... www.dentalpractice.com.au Paid subscribers can access all past editions of Australasian Dental Practice and complete any of the CPD questionnaires by logging in at www.dentalcommunity.com.au
Vital pulp therapy: A highly effective treatment
By Jenner Argueta, DDS, MSc and Ana Lucía Orellana, DDS


Ahigh percentage of the population decides to visit the dentist when their teeth are con siderably affected by caries. In many cases, the patients opt for early extraction of teeth due to the costs of root canal therapy and the posterior restoration process.1,2 The importance of keeping the pulp-dentine complex vital, the search for alternatives to root canal therapy and the clinical application of minimally inva sive dentistry have led to the increased popularity of conservative approaches to pulp damage. The high success rate reported for vital pulp therapy (VPT) procedures nowadays has been a key factor in bringing a higher frequency of application of this type of therapy.3,4 The good prognosis of these procedures has been partly achieved thanks to current treatment protocols, an under standing of the biological processes involved and the materials available for use in cases of reversible pulp disease.
A good diagnosis is the most important and complex factor when taking decisions and establishing a course of treatment. Determining the exact degree of pulp inflammation is not an easy task, given the limitations of current diagnostic tests, subjective factors inherent to the patient and the correct interpretation of the clinical information by the operator.5-7 It is well-known that, for a VPT procedure to work, the pulp inflammation should be in a reversible stage (reversible pulpitis). It is important to bear in mind that current pulp sensitivity tests are not 100% reliable.6,8
Direct pulp capping clinical technique
In this clinical case, we describe the recommended technique for performing direct pulp capping in cases of frank pulp expo sure with a diagnosis of reversible pulpitis. This clinical case was selected because it is the one that occurs most frequently.
The patient attended reporting short-term pain in tooth 36 (Figure 1). Through radiography, a clinical assessment and an analysis of the patient’s clinical history, an extensive carious lesion was diagnosed (Figure 2) as the cause of the pain, due to a process of reversible pulpitis.
Complete sealing was achieved using rubber dam, a stainlesssteel clamp and a light-curing flowable dam located around the clamp to prevent bacterial contamination of the area to be treated. The caries were removed circumferentially from the coronal towards the cervical margin to limit the movement of bacteria to
“The material was placed in bulk increments as a dentinal replacement. As the material sets in 12 minutes, it was possible just to wait the indicated time and the restoration could be done in the same session...”
the pulp tissue space.9 An exploration of the cavity preparation floor showed a pulp exposure (Figures 3 and 4). It is always advis able to explore the cavity preparation floor with an endo explorer, because smaller carious-exposed pulps may be overlooked.
In cases where there is haemorrhaging in the exposed pulp region, it is necessary to apply sustained pressure for 40-60 sec onds with a cotton swab dampened with sterile saline solution,10 followed by the disinfection of the cavity with 0.5% sodium hypochlorite. After this, Biodentine (Septodont) bioactive mate rial was placed to directly cap the pulp (Figures 5 and 6). The material was placed in bulk increments as a dentinal replace ment. As the material sets in 12 minutes, it was possible just to wait the indicated time and the restoration could be done in the same session.11
128 Australasian Dental Practice July/August 2022 clinical | EXCELLENCE

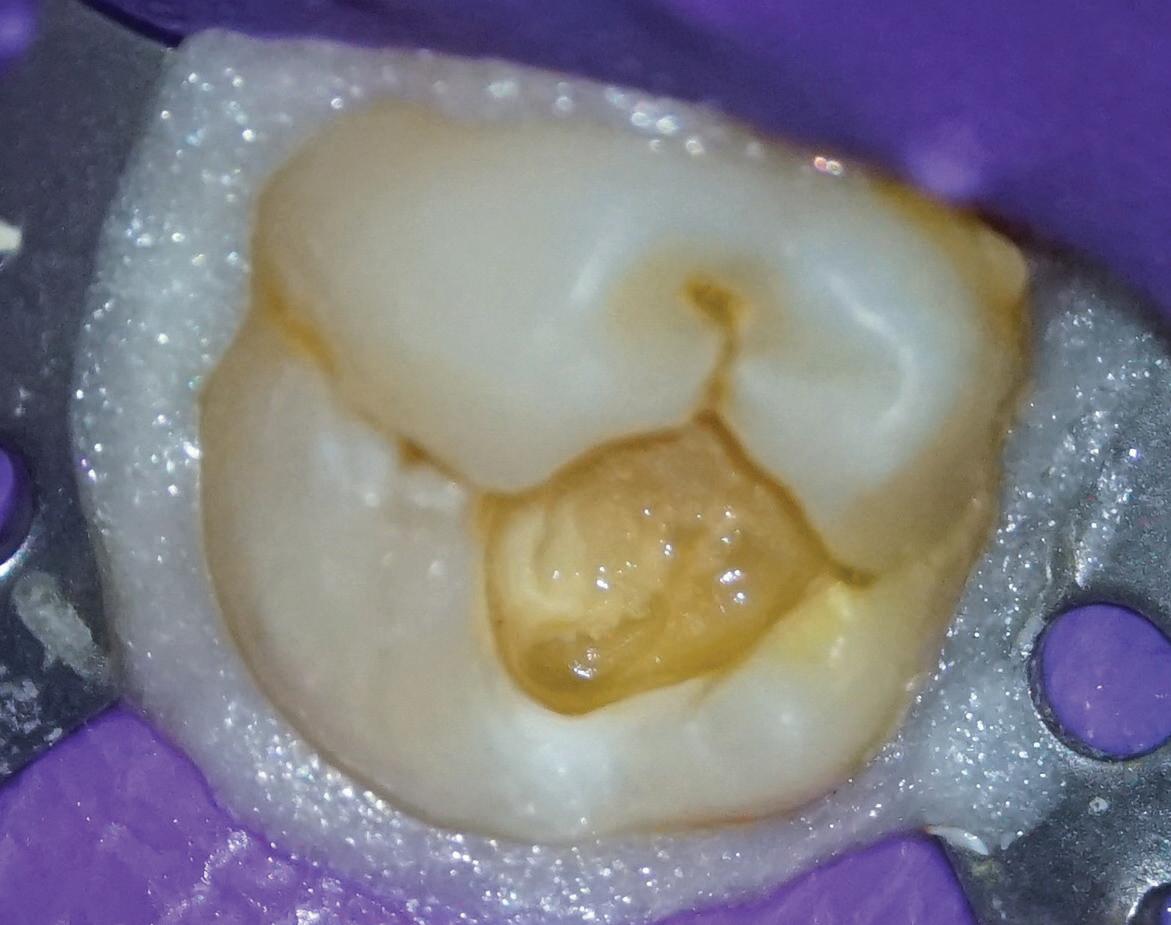
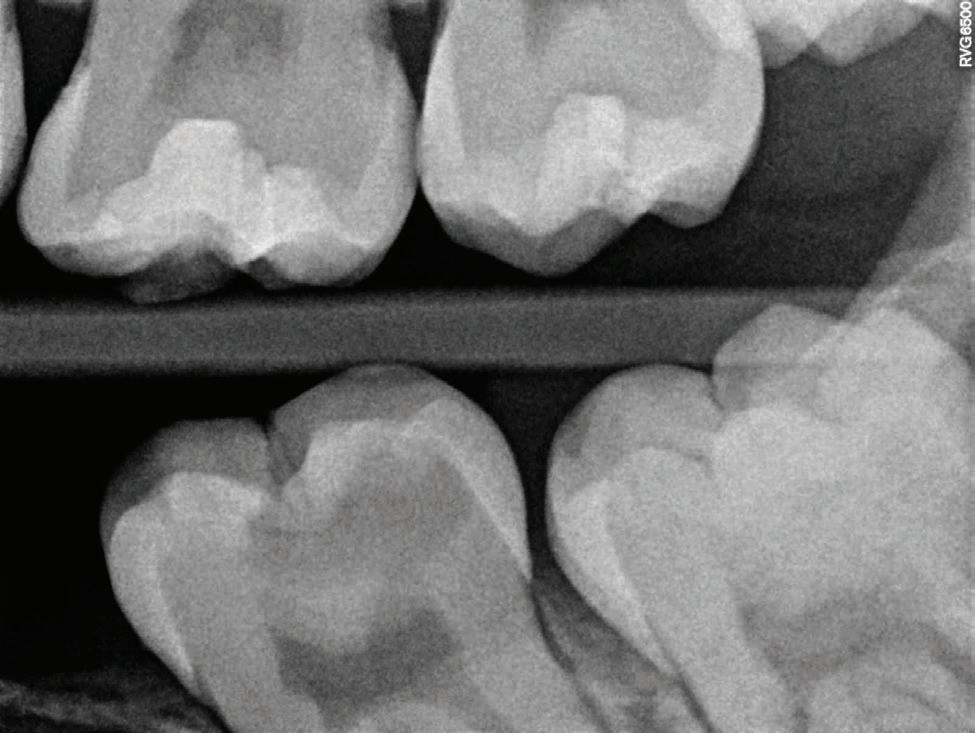



July/August 2022 Australasian Dental Practice 129 clinical | EXCELLENCE
Figure 1. Tooth 36 with deep caries. Total isolation prior to the removal of the caries.
Figures 3-4. Pulp exposure at the level of the cavity preparation floor, with minimum haemorrhaging that was easy to control.
Figure 2. Bite radiograph shows evidence of a carious lesion on tooth 36. Undermineralised tissue is found close to the mesial pulp horn.
Figures 5-6. Placing Biodentine in bulk increments using an endodontic compactor.
The definitive restoration was done afterwards, using composite resin with the oblique layer technique (Figure 7) with the aim of minimising the contraction of the material.12
The quality of the definitive restoration and its close adaptation to the dentine structure to prevent leaks are key factors in the long-term success of the procedure.
Correct marginal adaptation and the continuity of the restoration with the dental tissue can be seen in the final radiograph of the procedure (Figure 8).

An assessment was made seven days after treatment to ensure that the patient was completely asymptomatic and responded to sensitivity tests in a normal manner. A normal tissue response was obtained in all the tests.
One of the main characteristics of Biodentine is that it is easy to manipulate, it can be used as a dentine substitute due to its high compression strength and it offers good adhe sion to the tooth structure. Its characteristics mean that it is easy to place it in the region to be treated and can be used as a base for the definitive adhesive coronal restoration. Figure 9 shows the vital pulp therapy procedure.

In radiographic form, on follow-up after two years, it is possible to observe mesial pulp horn retraction. One of the most appreciated advantages of Biodentine is that it does not pigment the tooth structure, making it an ideal material for performing pulp capping in the anterior sector.
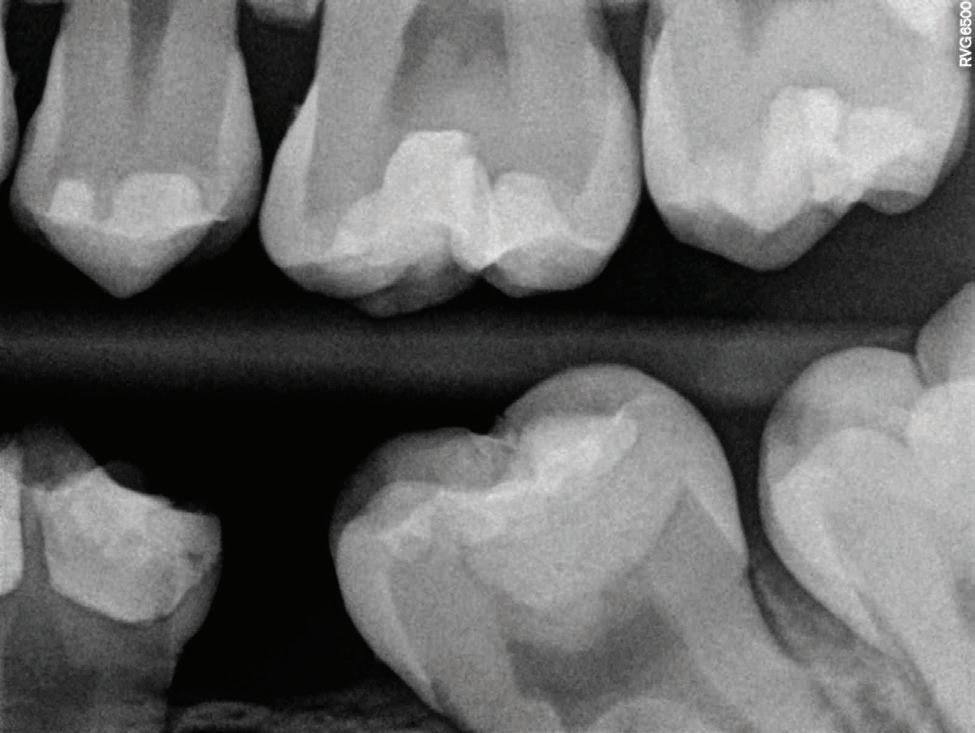
Materials used in Vital Pulp Therapy
Among the materials described to carry out pulp therapy procedures, calcium hydroxide-based cements and bioceramics10 have been mentioned. The latter are biocompatible materials that are divided into three basic groups: 1. Highresistance bioinert cements; 2. Bioactive cements that create chemical bonds with mineralised tissue; and 3. Biodegradable materials that actively participate in meta bolic processes of the organism.13 There are many materials that can be used for vital pulp therapy procedures, the bestknown being MTA and latest-generation calcium silicate-based cements such as EndoSecuence BC RRM, Biodentine and CeraPutty, among others. All the materials mentioned above belong to the bioactive cements group.
Biodentine is a dentine substitute that helps to promote dentinogenesis and shows next biological properties: alka line pH, biocompatibility, anti-bacterial capacity, release of calcium and hydroxyl ions, good margin sealing properties and insoluble when coming into contact with oral fluids. Its radiopacity is also similar to that of dentine, the setting time is approxi mately 12 minutes and it does not cause pigmentation in the dental structure.14-18 This last property makes it one of the materials of choice when it is necessary to perform treatments that involve the coronal and cervical zone, especially in anterior teeth.
130 Australasian Dental Practice July/August 2022 clinical | EXCELLENCE
Figure 7. Definitive adhesive restoration in tooth 36.
Figure 9. Vital pulp therapy at tooth 36. At the 2-year follow-up, the retraction of the mesial pulp horn can be seen.
Figure 8. Final radiograph of the vital pulp therapy procedure. The different layers of materials used and the correct marginal adaptation can be seen.
Prognosis
Obtaining the right diagnosis is essential for the success of VPT. An ideal case is one diganosed with reversible pulpitis without a history of spontaneous dental pain or long duration.6 It is generally accepted that a history of spontaneous pain or nocturnal pain are associated with the existence of a process of irreversible pulp inflammation.19,20 In such cases, the success of direct pulp capping could be questioned,21 although some studies indicate that VPT can even be successful in this kind of situation.1,22-24
As for long-term success in VPT procedures, it is extremely important to give the tooth a definitive restoration that guaran tees suitable margin sealing, because this factor, together with the absence of bacterial contamination during the procedure, are among the most important aspects to be taken into account to avoid later pulp inflammation.25,26 The reported success rate for vital pulp therapy using bioactive cements and follow-up of up to 10 years is higher than 85%,3,27 quite a high percentage for a dental procedure over that length of time.
1. Asgary S, Eghbal MJ, Fazlyab M, Baghban AA, Ghoddusi J. Five-year results of vital pulp therapy in permanent molars with irreversible pulpitis: a noninferiority multicenter randomized clinical trial. Clin Oral Investig. 2015;19(2):335-41.
2. Asgary S, Eghbal MJ. Treatment outcomes of pul potomy in permanent molars with irreversible pulpitis using biomaterials: a multi-center randomized con trolled trial. Acta Odontol Scand. 2013;71(1):130-6.
3. Mente J, Hufnagel S, Leo M, Michel A, Gehrig H, Panagidis D, et al. Treatment outcome of mineral trioxide aggregate or calcium hydroxide direct pulp cap ping: long-term results. J Endod. 2014;40(11):1746-51.
4. Holan G, Eidelman E, Fuks AB. Long-term evalu ation of pulpotomy in primary molars using mineral trioxide aggregate or formocresol. Pediatric Dentistry. 2005;27(2):129-36.
5. Fuks AB, Nuni E. Pulp therapy for the young per manent dentition. Pediatric Dentistry: Elsevier; 2019. p. 482-96.
6. Camp J. Diagnosis dilemmas in vital pulp therapy: treatment of the toothache is changing, Especially in young, immature teeth. Journal of Endodontics. 2008;34(7S):S6.
7. Taha NA, Albashaireh ZS, Alfied RG. Endodontic decision making for asymptomatic root-filled teeth with apical periodontitis - A radiographic survey. Aust Endod J. 2018.
8. Taha N, Khazali M. Partial Pulpotomy in Mature Permanent Teeth with Clinical Signs Indicative of Irreversible Pulpitis: A Randomized Clinical Trial. Journal of endodontics. 2017;43(9).
9. Schwendicke F, Dörfer CE, Paris S. Incomplete Caries Removal:A Systematic Review and Meta-anal ysis. Journal of Dental Research. 2013;92(4):306-14.
10. Hilton TJ. Keys to clinical success with pulp cap ping: a review of the literature. Operative dentistry. 2009;34(5):615-25.
Conclusions
From a completely optimistic standpoint, the ultimate aim of any dentist when carrying out a restorative and/or endodontic procedure should be to maintain pulp vitality and functionality of the tooth with an absence of symptoms.28
Based on the results reported in a number of clinical research studies,1-5,17,18,25,29-31 we can conclude that VPT on teeth with reversible pulpitis is a highly effective treatment option to maintain pulp vitality.
About the authors
Dr Jenner Argueta holds a dentistry and endodontics master’s degree in endodontics from San Carlos de Guatemala University, where he achieved multiple awards as an outstanding student. He Is the former president of the Guatemalan Endodontics Academy (2016–2020) and is a certified researcher at the Guatemalan National Council for Science and Technology. International Speaker, Faculty endodontics professor at Mariano Galvez de Guatemala University. His clinical practice is focused on microendodontics and micro-restorative dentistry.
Dr Ana Lucía Orellana is in private practice at Argueta-Orellana microscopic dental offices in Guatemala.
References
11. Magne P, Spreafico R. Deep Margin Elevation: A Paradigm Shift. the American Journal of Stetic Den tistry. 2012(2).
12. Chandrasekhar V, Rudrapati L, Badami V, Tum mala M. Incremental techniques in direct composite restoration. Journal of Conservative Dentistry. 2017;20(6):386-91.
13. Koch K, Brave D. Endosequence: melding endo dontics with restorative dentistry, part 3. Dentistry today. 2009;28(3).
14. Bekhtiar H, Hossein M, Aminishakib P, Abedi F. Human Pulp Responses to Partial Pulpotomy Treat ment with TheraCal as Compared with Biodentine and ProRoot MTA: A Clinical Trial. Journal of Endodon tics. 2017; Article In Press.
15. Malkondu O, Karapinar Kazandag M, Kazazoglu E. A review on biodentine, a contemporary dentine replacement and repair material. Biomed Res Int. 2014;2014:160951.
16. Miller AA, Takimoto K, Wealleans J, Diogenes A. Effect of 3 Bioceramic Materials on Stem Cells of the Apical Papilla Proliferation and Differentiation Using a Dentin Disk Model. J Endod. 2018.
17. Nowicka A, Lipski M, Parafiniuk M. response of human dental pulp capped with biodentine and mineral trioxide aggregate. Journal of Endodontics. 2013;39(6).
18. Villat C, Grosgogeat B, Seux D, Farge P. Conserv ative approach of a symptomatic carious immature permanent tooth using a tricalcium silicate cement (Biodentine): a case report. Restor Dent Endod. 2013;38(4):258-62.
19. Endodontics aAo. Endodontic Diagnosis. Collages for Excellence. 2013(Fall 2013).
20. Mejare IA, Axelsson S, Davidson T, Frisk F, Hakeberg M, Kvist T, et al. Diagnosis of the condition of the dental pulp: a systematic review. International endodontic journal. 2012;45(7):597-613.
21. Barrieshi-Nusair KM, Qudeimat MA. A prospec tive clinical study of mineral trioxide aggregate for partial pulpotomy in cariously exposed permanent teeth. J Endod. 2006;32(8):731-5.
22. Matsuo T, Nakanishi T, Shimizu H, Ebisu S. A clinical study of direct pulp capping applied to car ious-exposed pulps. J Endod. 1996;22(10):551-6.
23. Mejare I, Cvek M. Partial pulpotomy in young per manent teeth with deep carious lesions. Endodontics & dental traumatology. 1993;9(6):238-42.
24. Caliskan MK. Pulpotomy of carious vital teeth with periapical involvement. International endodontic journal. 1995;28(3):172-6.
25. Edwards J, Swift J, Trope M, Ritter V. Vital pulp therapy for the mature tooth – can it work? Endodontic Topics. 2003(5).
26. Rechenberg D-K, Zehnder M. Molecular diagnostics in endodontics. Endodontic Topics. 2014;30(1):51-65.
27. Daniele L. Mineral Trioxide Aggregate (MTA) direct pulp capping: 10 years clinical results. Giornale Italiano di Endodonzia. 2017;31(1):48-57.
28. Zanini M, Meyer E, Simon S. Pulp Inflammation Diagnosis from Clinical to Inflammatory Mediators: A Systematic Review. J Endod. 2017.
29. Asgary S, Eghbal MJ, Ghoddusi J, Yazdani S. One-year results of vital pulp therapy in permanent molars with irreversible pulpitis: an ongoing multi center, randomized, non-inferiority clinical trial. Clin Oral Investig. 2013;17(2):431-9.
30. Aguilar P, Linsuwuanont P. Vital pulp therapy in vital permanent teeth with cariously exposed pulp: A systematic review. Journal of Endodontics. 2012;37(5).
31. Maroto M, Barberia E, Planells P, Garcia Godoy F. Dentin bridge formation after mineral trioxide aggre gate (MTA) pulpotomies in primary teeth. American journal of dentistry. 2005;18(3):151-4.
132 Australasian Dental Practice July/August 2022
clinical | EXCELLENCE
“Vital Pulp Therapy on teeth with reversible pulpitis is a highly effective treatment option to maintain pulp vitality...”
IS EVERYTHING the right one with Hu-Friedy
predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. it comes to the perfect fit, Hu-Friedy is just right.
IS EVERYTHING the right one with Hu-Friedy
LOVE OUR STAINLESS STEEL PEDO CROWNS:
predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. comes to the perfect fit, Hu-Friedy is just right.
LOVE OUR STAINLESS STEEL PEDO CROWNS:
ONLINE AT Co., LLC. All rights reserved.
ONLINE AT Co., LLC. All rights reserved.
ONLINE AT LLC. All rights reserved.
IS EVERYTHING the right one with Hu-Friedy 855 ww
Septanest : the first choice of dentists with over 150 million injections per year, provides you high quality you can trust Call 0508 486 252 www.ivoclar.com
808 855 ww
855 ww
case report
Guided implant placement with immediate loading: a 5-year follow-up
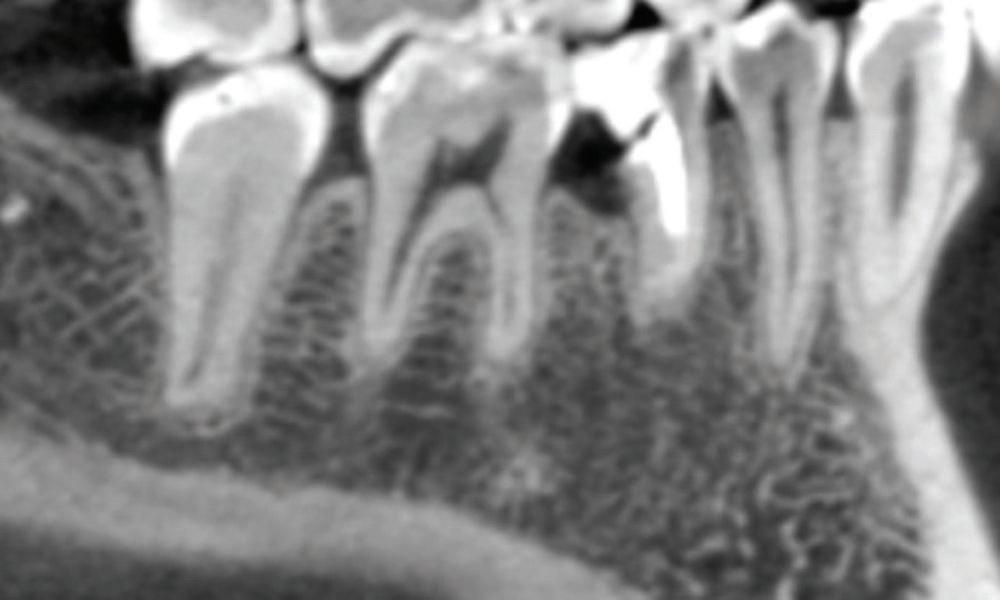 By Hani Tohme, DDS, MSc, PhD
By Hani Tohme, DDS, MSc, PhD

Figure 1.
Figure 2.
The continuous development of computer tech nology in dentistry ensures new opportunities in the field of fixed prosthodontics. Nowadays, we can easily manage implant positioning in relation to the required prosthetic outcome by utilising a precise surgical guide and a fully digital workflow.
This is very favourable, especially when imme diate implant placement and loading are involved. However, a thorough risk assessment before the treatment is also essential.
The following case report describes a successful treatment of a hopeless lower premolar with a 5-year follow-up in a young patient. The treatment included a fully digital workflow and the use of a Straumann® Bone Level Tapered implant with immediate loading and placement.

Figure 3.

134 Australasian Dental Practice July/August 2022
clinical | EXCELLENCE
Figure 4.
Figure 5.
Figure 6.
Initial situation
A25-year-old female non-smoker with no remarkable medical issues presented at our office for a consultation regarding food impaction in the right lower jaw. Her chief complaint was food getting stuck between her teeth, giving her bad breath despite her efforts to maintain good oral hygiene. She also stated that the tooth concerned had changed colour over time and that she was very dissatisfied with its aesthetic appearance.
The intraoral examination revealed tooth #45 with a failing distal occlusal provisional restoration and a greyish colour compared to the adjacent teeth. Furthermore, the gingival tissues around the tooth were inflamed and presented BoP+ in all locations.
Given these clinical characteristics, a vitality test was car ried out. The cold test was negative, but the percussion test was positive (Figures 1-2).
The radiographic examination showed a crown fracture of tooth 45 extending to the root (Figure 3).
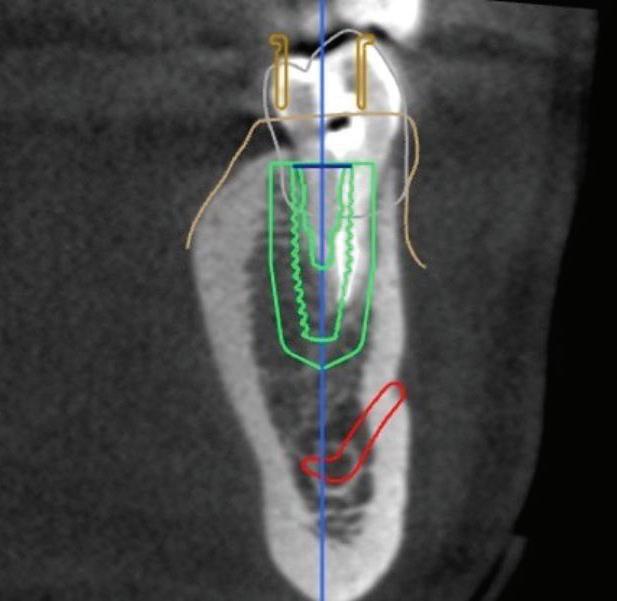
Treatment planning
After a thorough discussion of the treatment options with the patient, she opted for an immediate implant placement and provisional restoration. The corresponding treatment workflow was as follows:
• Digital planning to establish a prosthetically-driven implant position (Figures 4-5).
• Temporary crown preparation before the surgery and design of the Variobase® abutment (Figure 6).
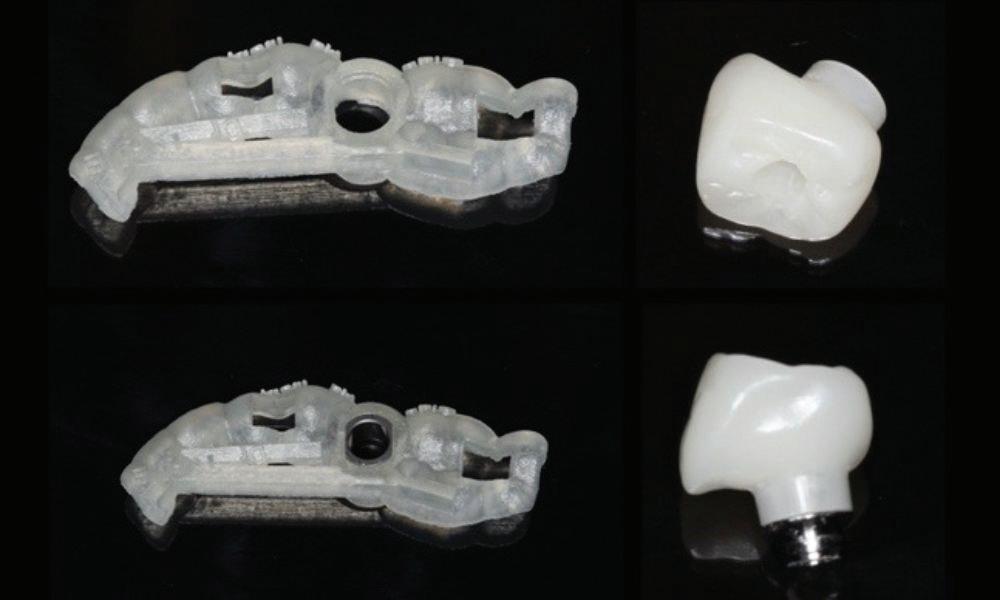
• Design of surgical guide to be completely tooth-supported to prevent rocking.
• Atraumatic tooth extraction and guided implant placement of Straumann Bone Level Tapered implant.
• Implant loading prior to achieving primary stability (35N inser tion torque, 75 ISQ).
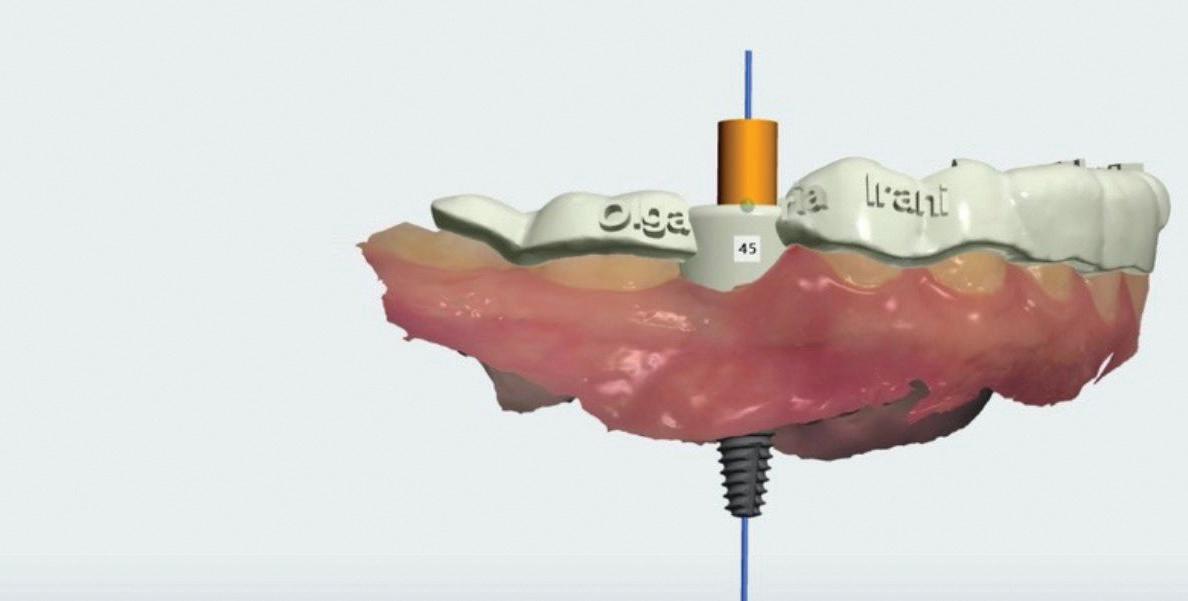
• Screw in temporary crown extraorally bonded to the Variobase.
• After healing, use the same gingival/abutment height Variobase for the digitally fabricated zirconia crown.
July/August 2022 Australasian Dental Practice 135
clinical | EXCELLENCE
Figure 7.
Figure 8.
Figure 10.
Surgical procedure
Local anesthesia with lidocaine 2% with epinephrine 1:100k was administered and an atraumatic extraction of tooth #45 was per formed. The tooth-supported surgical guide was stabilised after tooth extrac tion (Figure 7). The implant bed was prepared following the manufacturer’s instructions for guided surgery and the Straumann Bone Level Tapered Implant was placed with an optimal insertion torque (Figures 8-11).
Figure 9. Figure 11.
Prosthetic procedure
An immediate temporary crown was placed and a periapical radiograph of the implant with the Variobase was taken immediately after the surgery (Figures 12-13).
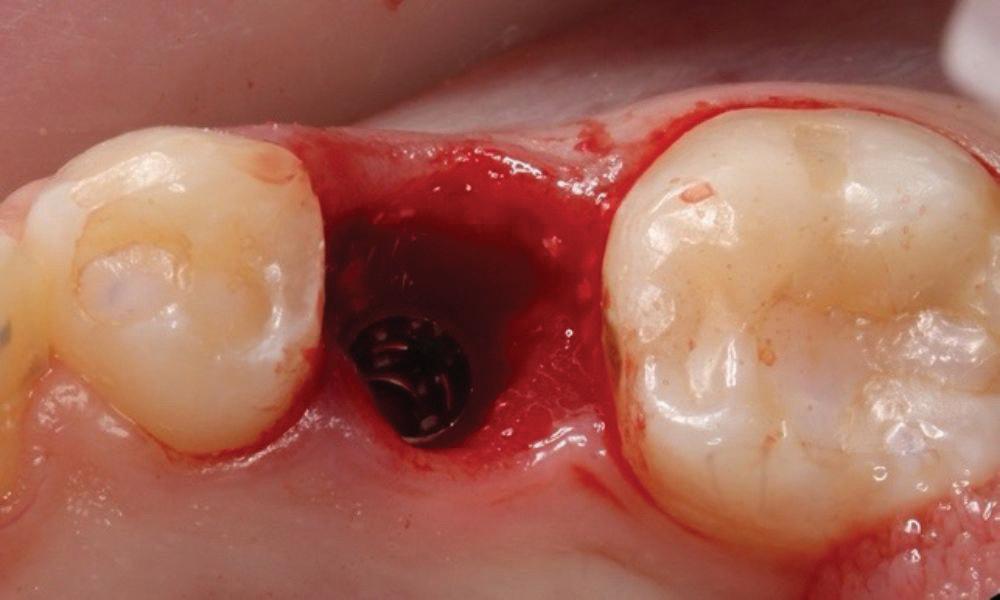


After three months of healing, the mucosal dimensions and contours were found to be preserved (Figure 14).
Following the Straumann Scanbody placement, digital impressions were taken. The intraoral scan registering the emergence profile, intraoral scanbody and antagonist was sent to the lab (Figure 15). Based on this information, the final restoration was digitally designed and fabricated (Figure 16).
At the next visit, the final crown was screwed in place and a periapical X-ray was taken as control (Figures 17-18).
After the fit of the abutment and the restoration were evaluated, the screw insertion hole was closed with Teflon and composite (Figures 19-20).
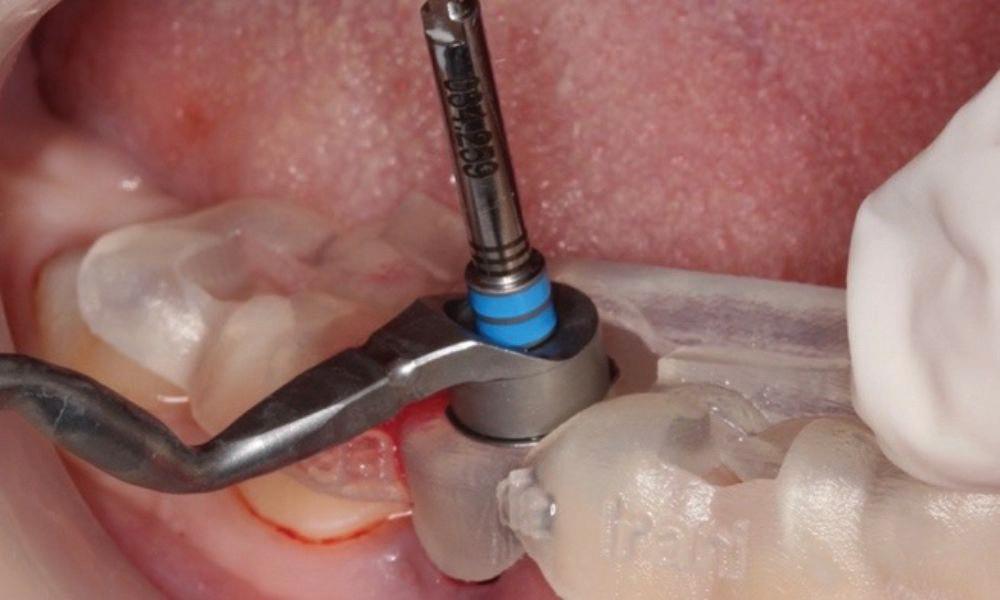
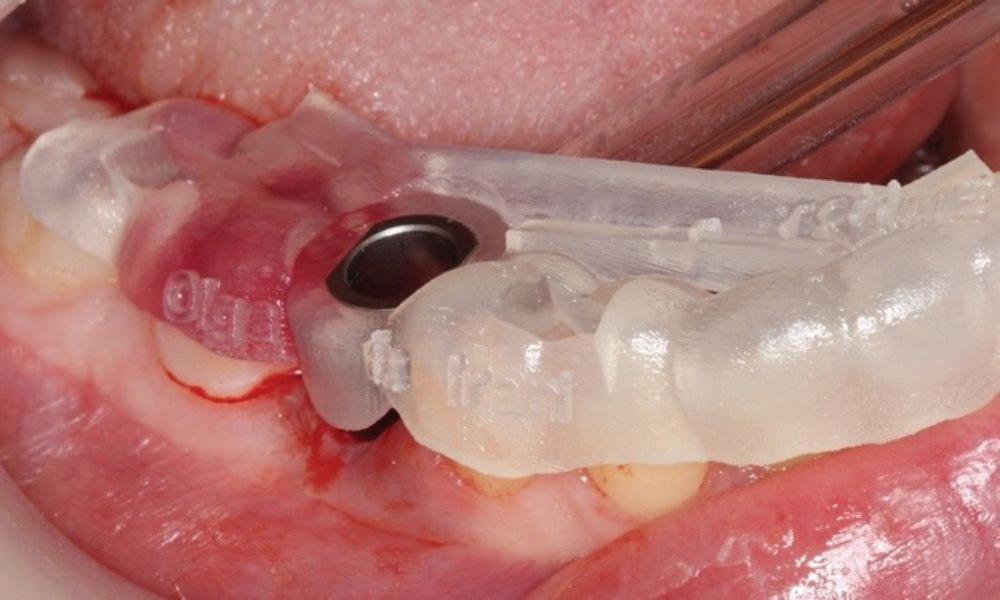
136 Australasian Dental Practice July/August 2022
clinical | EXCELLENCE
Figure 17. Figure 18. Figure 20. Figure 19.


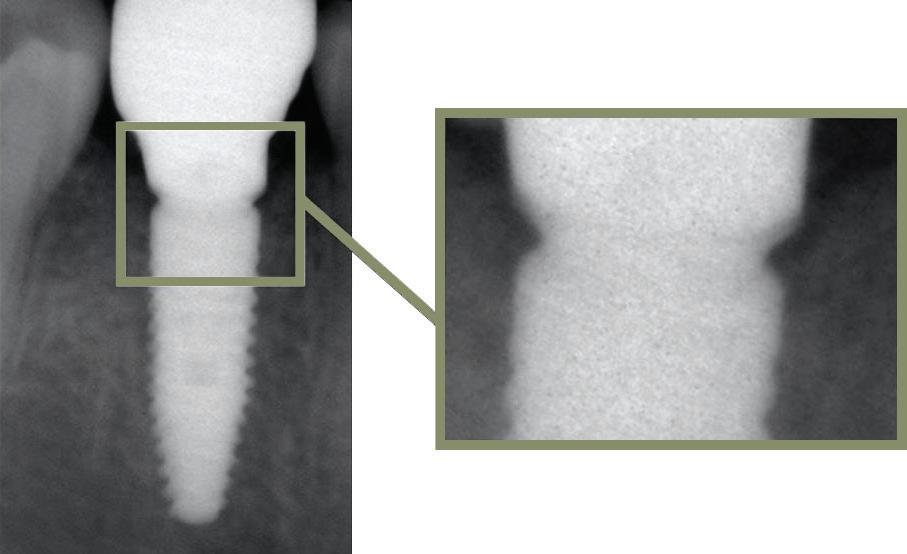

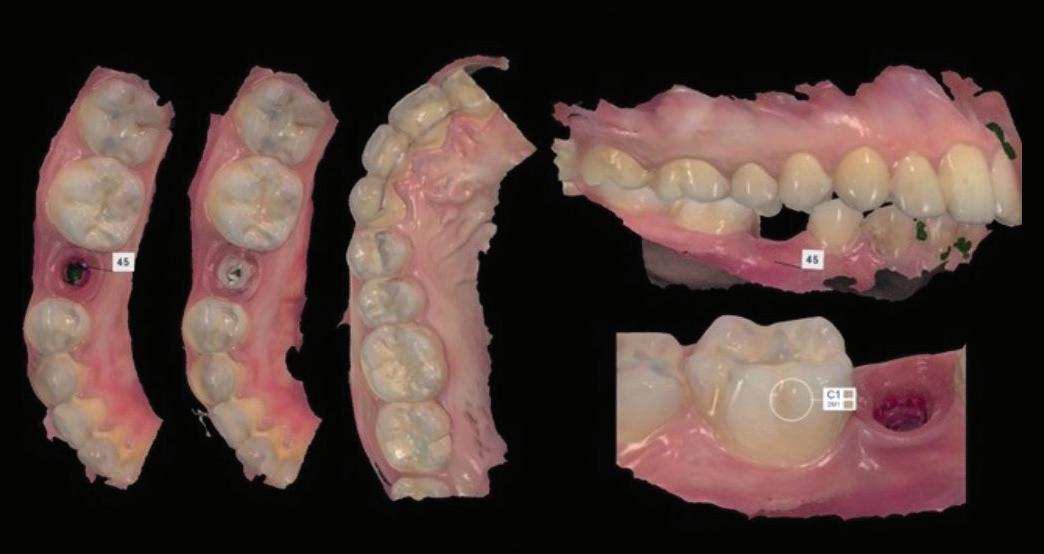

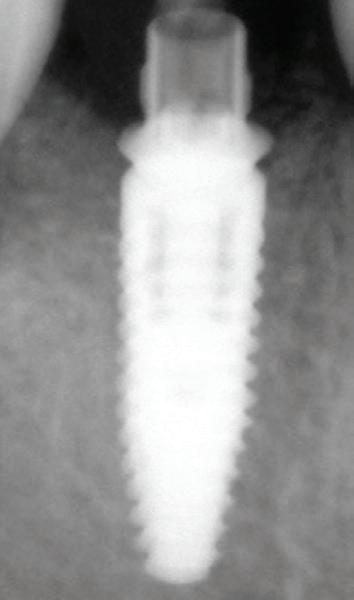


July/August 2022 Australasian Dental Practice 137 clinical | EXCELLENCE
Figure 12. Figure 14. Figure 13. Figure 16. Figure 15.
Figure 21.
Figure 22.
Figure 23. Figure 25.
Figure 24.
The patient received detailed oral hygiene instructions and participated in a yearly maintenance program with evaluation of the clinical and radiographic findings.
After 4 years, the clinical and radiographic images showed stable peri-implant hard and soft tissues (Figures 21-22).
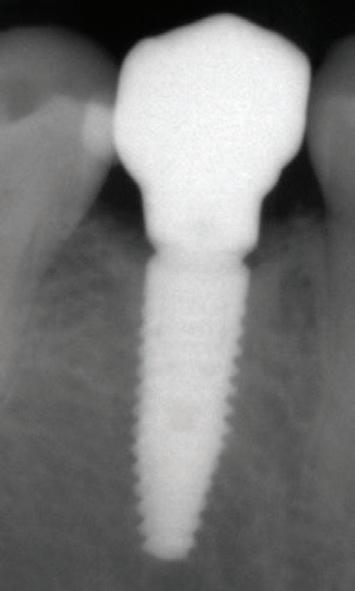
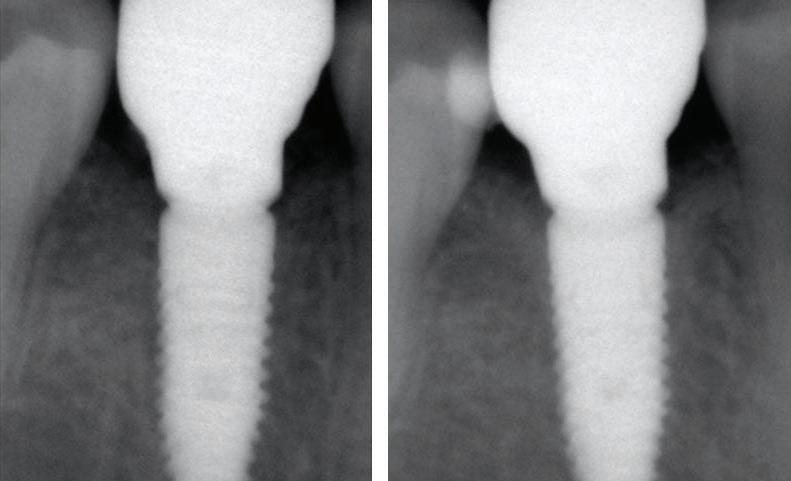
The patient returned for her 5-year follow-up and hard and soft tissues were stable according to the clinical and radiographic assessments (Figures 23-25).
Treatment outcomes
The outcome for the peri-implant hard and soft tissues was outstanding, thanks to the correct diagnosis and treatment plan, but also to the use of optimal materials and the participation of the patient in a customised maintenance program.



About the author
Dr Hani Tohme graduated in dental surgery and specialised in prostho dontics at Saint Joseph University of Beirut. He is the Founder and Head of the Digital Unit at Saint Joseph University of Beirut, Director of Prosthodontic Postgraduate Studies at Saint Joseph University of Beirut, Elected Head of Removable Prosthodontics at Saint Joseph Uni versity of Beirut and an ITI fellow and international speaker.
138 Australasian Dental Practice July/August 2022 clinical | EXCELLENCE




© Institut Straumann AG, 2022. All rights reserved. Straumann® and/or other trademarks and logos from Straumann® mentioned herein are the trademarks or registered trademarks of Straumann Holding AG and/or its affiliates.
Data Acquisition Planning Surgery Impression Design Production Post Processing Final Restoration GUIDED SURGERY Discover how Straumann® Guided Surgery delivers predictable outcomes visit www.straumann.com.au/guided More than integrated workflows. Immediate digital tooth replacement. Straumann® Guided Surgery Straumann Pty Ltd/Straumann New Zealand Limited 93 Cook Street, Port Melbourne VIC 3207, Australia AU Toll Free 1800 660 330 NZ Toll Free 0800 408 370 Email customerservice.au@straumann.com www.straumann.com.au | www.straumann.co.nz © Institut Straumann AG, 2022. All rights reserved. Straumann® and/or other trademarks and logos from Straumann® mentioned herein are the trademarks or registered trademarks of Straumann Holding AG and/or its affiliates.
05/22 Data Acquisition Planning Surgery Impression Design Production Post Processing Final Restoration GUIDED SURGERY Discover how Straumann® Guided Surgery delivers predictable outcomes visit www.straumann.com.au/guided More than integrated workflows. Immediate digital tooth replacement. Straumann® Guided Surgery Straumann Pty Ltd/Straumann New Zealand Limited 93 Cook Street, Port Melbourne VIC 3207, Australia AU Toll Free 1800 660 330 NZ Toll Free 0800 408 370 Email customerservice.au@straumann.com
| www.straumann.co.nz ©
Straumann AG, 2022. All rights reserved. Straumann® and/or other trademarks and logos from Straumann® mentioned herein are the trademarks or registered trademarks of Straumann Holding AG and/or its affiliates.
Data Acquisition Planning Surgery Impression Design Production Post Processing Final Restoration GUIDED SURGERY Discover how Straumann® Guided Surgery delivers predictable outcomes visit www.straumann.com.au/guided More than integrated workflows. Immediate digital tooth replacement. Straumann® Guided Surgery
Pty Ltd/Straumann New Zealand Limited
Cook
Port Melbourne VIC 3207, Australia
Toll Free 1800 660 330 NZ Toll Free 0800 408 370
STRA184 05/22
STRA184
www.straumann.com.au
Institut
STRA184 05/22
Straumann
93
Street,
AU
Email customerservice.au@straumann.com www.straumann.com.au | www.straumann.co.nz
Relocating easy as 123 Dental
Dr Jack Brazel has recently relocated his practice in West Leederville, part of Perth’s affluent western corridor. He didn’t move too far, taking space in the building next door.
123 Dental now occupies a tenancy in a busy neighbourhood shopping centre - a Coles complex with 2 levels of commer cial tenancies. Setting up a dental practice in a busy retail space can provide con siderable challenges during construction, but the benefits in terms of exposure and pedestrian traffic are significant.
From a young age, Jack knew that he wanted a career where he was able to help people improve their lives. After a brief stint of medical work experi ence, he discovered dentistry with its blend of technical engineering and art istry combined with the ability to have a positive and lasting impact on patients. It was a perfect match and Jack has never looked back.
Graduating in Leeds in the UK in 2011, Jack emigrated to Australia. In 2017, he purchased a three-chair practice and in the space of three years, grew the practice to the point where he needed another chair.
“I bought my current 3 chair practice 5 years ago. 2 years ago Medifit added a 4th chair for us but with my lease run ning out, I knew we needed more space so I engaged them again to build a 6 chair practice that would give us the space we need to continue to expand and provide an amazing environment for our patients and staff,” he said.
After a fruitless search for a suitable freehold property in the tightly held area, on Medifit’s Sam Koranis’ recommenda tion, Jack shifted his focus to potentially leasing the space required. When a ten ancy became available in the shopping

140 Australasian Dental Practice July/August 2022
surgery | DESIGN
centre next door, Jack took the oppor tunity and began discussion with the landlord. Taking counsel from Sam while negotiating the lease resulted in Jack securing an additional 45 square metres of space, a very generous rent free period and a contribution towards the fitout from the landlord. In addition, the project was completed in time to take advantage of the existing instant tax write offs. This financial acumen is a hallmark of Medifit projects and reflects Sam’s knowledge as a CPA and Medifit’s experience in the space.
Jack’s brief was to create a light and spacious modern practice with a luxury feel that would provide him and his staff with a beautiful working environment for at least the next decade.


July/August 2022 Australasian Dental Practice 141
Medifit’s design team responded with a stunning, timeless design solution that delivers today and into the future. Entering the practice, patients first see the recep tion counter with its bold black lines, contrasting with white fluted panels in an elegant, practical solution to welcome patients. The waiting area is cleverly deline ated by a custom joinery unit that doubles as a tv stand and a display for the practice logo along with an array of plants, books and interesting objects.



The feeling is confidently modern and assured. Crisp white walls are fur ther defined by a dark grey/brown skirting and arched mirrors that give the space a distinct, almost futuristic look. The design evokes professionalism with a hint of playfulness.
123 Dental is a six-chair practice with all chairs located around a cen tral sterilisation area for convenient access. The practice covers 259 square metres and includes the chairs and steri plus a practice manager’s office, OPG, clean prep and lab areas, a photo room, patient refresh, plant room, IT store and a generous staff room. Finishes throughout are uniformly excellent.
142 Australasian Dental Practice July/August 2022 surgery | DESIGN



July/August 2022 Australasian Dental Practice 143 surgery | DESIGN
In Jack’s own words... “We are so excited to show all of our loyal patients our new home in the coming months as well as having a practice that staff are proud to say they work at and patients are proud to say they attend.

“Medifit’s communication was amazing throughout but get ting the build finished ahead of schedule in the current climate of materials and labour shortage was really surprising!
“From the first phone call to the date of handover. Medifit made the whole experience of building a dental practice a breeze. Running a practice takes enough of your time, so knowing I could rely on them to get the job done without my involve ment for the small things helped enormously. I couldn’t be happier with the job they have done. The value adds and advice was greatly appreciated. It’s rare in today’s world to get so much free advice.”
Sam Koranis added “We are delighted with what we’ve been able to achieve for Jack. He trusted Medifit to deliver on his vision for 123 Dental and despite some challenging construction conditions imposed by the shopping centre, I’m proud that our team delivered such a great result. Jack listened and was able to benefit from Medifit’s experience while negotiating his lease and this has put himself in a great position for future practice success. We thank him for the opportunity and wish him every success.”

Summary
The Practice
The Practice 123 Dental
Principal Dr Jack Brazel
Type of Practice General
Location West Leederville, Perth, Western Australia Size 259 square metres
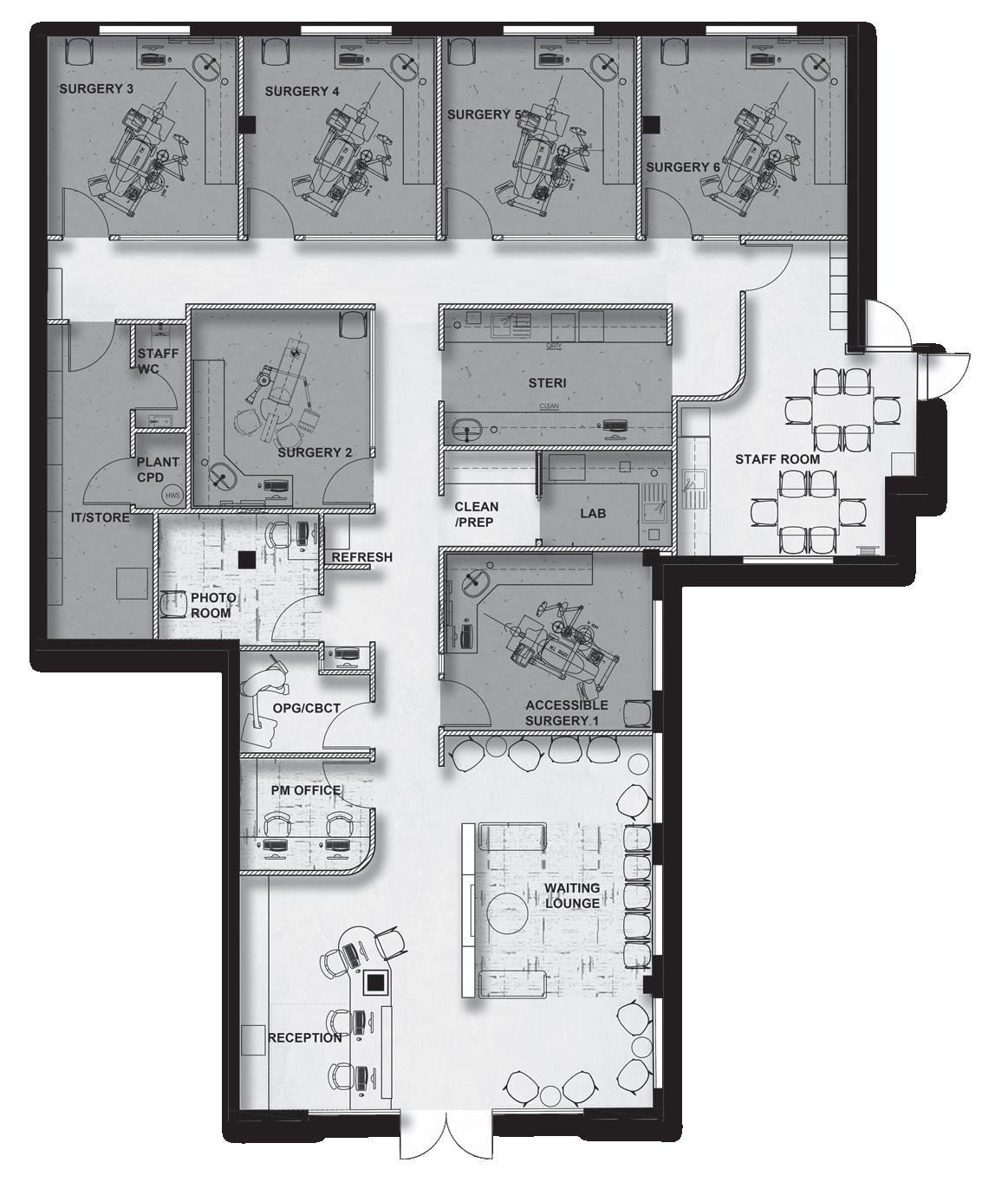
No of chairs 6
The Team Design Medifit Design & Construct Construction Medifit Design & Construct Equipment
Dental Units Kavo 1058 Life Autoclaves Mocom Futura 22 and Melag 41B+
X-Ray Planmeca ProX and Planmeca ProOne Compressor Cattani AC400 Tandem Suction Cattani Turbo Smart A Software Dental4windows
144 Australasian Dental Practice July/August 2022





1300 728 133 www.medifit.com.au MULTI AWARD WINNING HEALTHCARE DESIGN & CONSTRUCTION 2021 Master Builders Excellence in Construction Awards - Best Healthcare Building & Best Historical or Heritage Restoration or Renovation under $1.5m 2017/18 ASOFIA Best Medical Fitout • 2017/18 ASOFIA Best Use of Sponsors Product • 2017/18 & 2018/19 ASOFIA Best Design - Professional Suites Since 2002, Dentists and Dental Specialists all around Australia have trusted Medifit to create state of the art practices with individual interior designs that boost productivity and enhance levels of care. Whether it’s your
practice
your
we’ll
you
dental practice that reflects your personal style and
you
using proven best practices. Contact
for
obligation consultation
our award winning service. • SITE ASSESSMENTS • LEASE NEGOTIATION • FEASIBILITY STUDIES • COUNCIL SUBMISSIONS • ARCHITECTURAL DESIGN • INTERIOR DESIGN • BUILDING CONSTRUCTION • PRACTICE FIT-OUTS • RENOVATIONS / REFRESHES • BRANDING & MARKETING Practices that work with you
first
or
latest,
help
create a
complements the way
work - and we do it with a friendly, no fuss approach
Medifit today
a no
and experience
Information contained in this section is provided by the manufacturers or distributors. Australasian Dental Practice does not assume responsibility for the accuracy of the data.
SDI launches Pola For Aligners
SDI launches new Luna Flow composite

New Pola For Aligners from SDI utilises Pola Night 10% carbamide peroxide gel that has been carefully selected as the ideal whitening agent to suit any aligner system. The neutral pH gel ensures the greatest patient comfort in a whitening kit and the high-water content gel contains potassium nitrate
and fluoride to reduce sen sitivity and increase patient compliance. The pleasantly flavoured spearmint gel is both fresh and long lasting.
Available: SDI Limited Tel: 1800-337-003 www.sdi.com.au
Colgate Optic White Light Up
Colgate has launched a DentistExclusive Optic White Light Up Pen and matching LED device in a take-home whit ening kit that will make your teeth “up to 7 shades whiter in 5 days” if used as directed. The precision applicator pen supplied in the kit contains a patented 6% hydrogen per oxide (HP) whitening serum that is applied to the tooth surface. The unique chemistry

of the serum, when paired with the powerful indigo LED device, delivers enriched whit ening and optimum results. The kit includes the LED teeth whitening device and charging case, a USB-A charging cord and the whitening pen
Available: Henry Schein Tel: 1300-658-822 www.henryschein.com.au
SDI has launched new Luna Flow, an extra strong light-cured flowable composite. With a blend of fillers in different ultrafine sizes to optimize handling, mechanical and optical properties, Luna Flow offers high radiopacity, control over application, easy shade matching, excellent strength and wear resistance. Luna Flow is a reliable and easy universal option for liners, bases, provisionals, restoration and provisionals repairs, Class V and conservative Classes I to IV. Luna Flow was designed in two viscosities to suit all clinical needs. The regular viscosity offers superior handling and maximum control during application. This beau tiful composite flows on demand, holds its shape and does not string. The low viscosity (Luna Flow LV) offers more flow, making it perfect for liners and bases. Luna Flow is available in 12 shades, including one incisal, two opaques and two extra bleach shades. Luna Flow is an Australian innovation.
Available: SDI Limited Tel: 1800-337-003 www.sdi.com.au
Vivastyle Paint On Plus tooth whitening
Vivastyle® Paint On Plus is a unique varnish system for whitening teeth without having to use a tray. The prepara tion contains 6% hydrogen peroxide and the provitamin D-panthenol for the gentle lightening of teeth. The precise application of the varnish with a brush allows individual or crowded teeth to be effectively whitened. The varnish does not dissolve in saliva and it takes effect within 10 minutes. Customised trays and expen sive, bulky accessories are unnecessary. Vivastyle Paint On Plus satisfies the desire for natural-looking white teeth by offering effective, professional teeth whitening for in-office and at-home use. To apply, thoroughly clean your teeth, dry with a paper towel, apply Vivastyle Paint On Plus with the brush supplied, wait 30 seconds for it to dry and 10
minutes for it to take effect and then remove the varnish film with a toothbrush. Use once daily for 2 weeks with results visible after 7 days.
Available: Ivoclar Tel: 1300-486-252 www.ivoclar.com

146 Australasian Dental Practice July/August 2022
new | PRODUCTS
TGA NOTES : We have always worked within the guidelines of the TGA and now with the new regulation we continue to do so. If you have any concerns please don’t hesitate to contact us for more information.
TGA NOTES : We have always worked within the guidelines of the TGA and now with the new regulation we continue to do so. If you have any concerns please don’t hesitate to contact us for more information.
TGA NOTES : We have always worked within the guidelines of the TGA and now with the new regulation we continue to do so. If you have any concerns please don’t hesitate to contact us for more information.
TGA NOTES : We have always worked within the guidelines of the TGA and now with the new regulation we continue to do so. If you have any concerns please don’t hesitate to contact us for more information.

Another Quality Product From
Another Quality Product From trulinedental.com.au
Another Quality Product From trulinedental.com.au

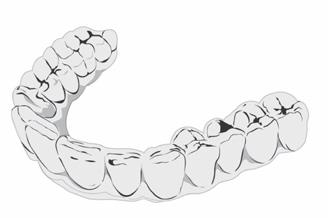

Another Quality Product From
more a
Impressions for Free Case Evaluation
trulinedental.com.au
v Clear Aligners are now more affordable than ever and made right here !
Send Any Intra Oral Scan or PVS Impressions for Free Case Evaluation 1300 878 336 trulinedental.com.au
FREE Online Course
FLEX MINI ONE
A la carte Bite sized Fun-sized




For revisions and recent relapse cases. Pay for the exact amount of treatment you need—no more, no less.
For very mild cases, up to 12 sets of aligners, including one revision.
For mild cases, up to 24 sets of aligners, including one revision and one set of retainers.
TWO
Double the fun
For moderate cases, up to 48 sets of aligners, including two revisions and two sets of retainers.
THREE UNLIMITED
The triple play
For moderate to severe cases, up to 72 sets of aligners, including three revisions and three sets of retainers.
All you can eat

For severe cases, as many aligners as you need for five full years, including replacements, revisions, and retainers.
An assortment of treatment options
Tailored to your taste

OsseoGroup
Scan the QR code or visit clearcorrect.osseogroup.com.au to become a ClearCorrect provider.





