ALSO IN THIS ISSUE
Closing the Mentorship Distance New programme could reduce complication rates and improve outcomes for trainee surgeons.

ALSO IN THIS ISSUE
Closing the Mentorship Distance New programme could reduce complication rates and improve outcomes for trainee surgeons.
ESCRS expanding treatment opportunities in underserved areas.
Maximising Refractive Surgery Outcomes with Lenticule Extraction Pursuing the goal of sharp vision at all distances.
CXL for Infectious Keratitis Can adjunctive CXL improve outcomes in diffcult cases?
With the participation of the Hellenic Society of Intraocular Implant and Refractive Surgery


Beyond Cataract Camps
Draws Global Audience, Strengthens Ties
ESCRS Updates; Two Videos Added to ESCRS 100; Eleven Ophthalmologists Earn FEBOS-CR Credential
18 Committing to Better Patient Care
Helena Prior Filipe MD
19 Refractive EDOF with the Benefits of Monofocal
José Manuel Díez del Corral Belda MD
22 Maximising Refractive Surgery Outcomes with Lenticule Extraction
Pooja Khamar MD, PhD
23 CXL for Infectious Keratitis
Jennifer Rose-Nussbaumer MD
24 Making the Right IOL Decisions
28 Unpacking PACK-CXL Options
Boris Knyazer MD, MSc
29 Femto-CAIRS for Keratoconus
Shady T Awwad MD
30 Addressing CXL’s Limitations
Farhad Hafezi MD, PhD, FARVO; Mark Hillen PhD; and Emilio Torres-Netto MD, PhD, FWCRS
32 PRIMA Implant Study Shows Promise
Frank G Holz MD
Closing the Mentorship Distance
Kevin M Barber MD and Rengaraj Venkatesh MD 16 Bridging the Gap Between Local and Global
Ronald Yeoh MBBS, FRCOphth; Filomena Ribeiro MD, PhD, FEBO; Durval M Carvalho Jr MS, MSurg, MChir, MCh; Jacqueline Beltz BMedSci, MBBS(Hons), MSurgEd, FRANZCO; Stephen D McLeod MD; and Vance Thompson MD
Ruth Lapid-Gortzak MD, PhD
25 ESCRS Refractive Surgery Guidelines a Work in Progress
Jesper Hjortdal MD, PhD
26 Improving Graft Survival in High-Risk Eyes
Claus Cursiefen MD, PhD
27 Stabilising with PACE-CXL
Farhad Hafezi MD, PhD, FARVO
34 Could Awareness Lead to ESCRGS?
Iqbal K ‘Ike’ Ahmed MD, Elena Arrondo MD, and Henny Beckers MD, PhD
36 Gaining a Core Outcome Set
Francesco Oddone MD

Publisher Filomena Ribeiro
Executive Editor
Stuart Hales
Editor-In-Chief
Sean Henahan






Senior Content Editor Kelsey Ingram
Creative Director
Kelsy McCarthy
Graphic Designer
Jennifer Lacey
Circulation Manager
Lucy Matthews
Contributing Editors
Cheryl Guttman Krader
Howard Larkin

Roibeárd O’hÉineacháin
Contributors
Laura Gaspari Soosan Jacob
Timothy Norris
Colour and Print CitiPost


Advertising Sales
Roo Khan
MCI UK
Tel: +44 203 530 0100 | roo.khan@wearemci.com
EuroTimes® is registered with the European Union Intellectual Property Office and the US Patent and Trademark Office.

Published by the European Society of Cataract and Refractive Surgeons, Runway East Borough Market, 20 St. Thomas Street, London, SE1 9RS, UK. No part of this publication may be reproduced without the permission of the executive editor. Letters to the editor and other unsolicited contributions are assumed intended for this publication and are subject to editorial review and acceptance.
ESCRS EuroTimes is not responsible for statements made by any contributor. These contributions are presented for review and comment and not as a statement on the standard of care. Although all advertising material is expected to conform to ethical medical standards, acceptance does not imply endorsement by ESCRS EuroTimes. ISSN 1393-8983


There is a huge unmet need for advanced eye care in lowand middle-income countries. In the past, volunteer organisations would send cataract surgeons to these areas to do surgery in what were known as cataract camps. However, in recent years, this approach has been modified, with a new emphasis on not only providing cataract surgery but also teaching young ophthalmologists in these areas how to do the surgery themselves through intensive training courses led by volunteer surgeons from more prosperous parts of the world. New technology—such as surgical simulators, virtual reality, telemedicine, and online mentoring—is playing an increasing role in this effort.
In addition, there is also a new emphasis on social equity, making sure care is available to all regardless of gender, age, or social status. We want to make sure vulnerable groups get access to high quality eye care, particularly surgery. There is plenty of evidence to show that women don’t have equal access, along with children, elderly people, and the disabled.
The ESCRS, itself a charity, has dedicated resources to improving eye care in underserved areas for many years. In the past three years, we have reviewed our experiences and sharpened our focus on where we can do the most good. Working with the International Agency for the Prevention of Blindness (IAPB), our Charity Committee chose three large collaborative projects to pursue in addition to other projects already underway.
Those projects include two in Africa: one is in Mozambique with Eyes of the World, a Spanish organisation that has worked there for many years, and the second in Malawi with the Blantyre Institute for Community Outreach (BICO). A smaller project in South Sudan supports Dr Lado, a Sudanese ophthalmologist.
The focus on training is particularly important in another ESCRS project with the Community Eye Health Institute at Cape Town University in South Africa. This concentrates on training the trainers and bringing people from all Sub-Saharan Africa to Cape Town, where they have an intensive course working in dry labs using artificial eyes and surgical simulators to improve their skills and pass on some of that knowledge to others in more remote areas. The ESCRS also supports the College of Ophthalmology of Eastern Central and Southern Africa (COECSA), which dedicates a great part of its annual meeting to wet labs and training, specifically on phaco surgery.
ESCRS charity projects extend beyond Sub-Saharan Africa to include ongoing support for surgeons in Ukraine and the St John’s Eye Hospital in Jerusalem.
For more information on our ongoing projects, and how to support them, please visit https://www.escrs.org/about-escrs/charities-supported-by-the-escrs/.
Dr Tom Ogilvie-Graham, Managing Director, ESCRS
EDITORIAL BOARD

Medical Editor
Noel Alpins (Australia)
Bekir Aslan (Turkey)
Roberto Bellucci (Italy)
Hiroko Bissen-Miyajima (Japan)
John Chang (China)
Béatrice Cochener-Lamard (France)
Oliver Findl (Austria)
Nino Hirnschall (Austria)
Soosan Jacob (India)
Vikentia Katsanevaki (Greece)
Daniel Kook (Germany)
Boris Malyugin (Russia)


Marguerite McDonald (US)
Cyres Mehta (India)
Sorcha Ní Dhubhghaill (Ireland)
Rudy Nuijts (The Netherlands)
Filomena Ribeiro (Portugal)
Leigh Spielberg (The Netherlands)
Sathish Srinivasan (UK)
Robert Stegmann (South Africa)
Ulf Stenevi (Sweden)
Marie-José Tassignon (Belgium)
Manfred Tetz (Germany)
Carlo Enrico Traverso (Italy)

ESCRS’s vision is to educate and help our peers excel in our field. Together, we are driving the field of ophthalmology forward.
Physicians from as far away as Cambodia and Curaçao joined more than 16,000 fellow ophthalmology professionals and industry personnel in Barcelona in September for an event that broke new ground as well as records for attendance and exhibition space.
The 2024 ESCRS Annual Congress, the Society’s 42nd such meeting, drew ophthalmologists from every continent except Antarctica as well as 300-plus exhibitors and more than 1,300 ophthalmic nurses, technicians, and allied professionals. They were treated to a display of scientific research, handson training, lively debates, new technologies, and in-depth discussions that encompassed issues ranging from whether femto-LASIK is the standard procedure in corneal refractive surgery to implementing electronic instructions for use (eIFU) with IOLs.
The Congress continued its tradition of offering strong programming for eye surgeons at all career levels, including 80 wet labs, 111 instructional courses, 12 ‘getting it wrong’ videos, and 4 research symposia. New this year were dry labs, which used model eyes instead of animal material to simulate ocular surgery, and a surgical training lab with more than a dozen training devices from Haag-Streit, Alcon, and HelpMeSee. Attendees could register for up to three sessions in the lab, and each session was guided by a trainer using a curriculum developed by the manufacturer.
Highlights of the Congress included the following:
ESCRS Tablao. Taking centre stage at the Congress was the Tablao, a concept built on the successful launch of the ESCRS Arena at the 2023 Annual Congress in Vienna. Tablao is a colloquial term for the Spanish word tablado (‘floorboard’) and is also a place where flamenco shows are performed; tablao is also the term for the platform floor on which a flamenco dancer dances. The ESCRS Tablao hosted debates between teams of ophthalmologists on several topics:
• My first option: EDOF IOLs
• What doctors want to know from industry and what industry wants to know from doctors
• Femto-LASIK is the standard procedure in corneal refractive surgery
• How should I start refractive surgery
• A simulated curriculum should be mandatory in cataract surgery training
IOL anniversary museum. Another star attraction at the Congress was a tunnel museum celebrating the 75th anniversary of the first intraocular lens implantation, performed by Sir Harold Ridley. Complete with selected period museum pieces, the tunnel allowed visitors to walk through Ridley’s office and operating theatre and learn how the idea of implanting a lens came to him, how the IOL was designed and implanted, and how the wider profession reacted to this unprecedented innovation in the field of cataract surgery.
Leadership and business innovation. The Congress featured a day-long lineup of sessions on leadership and business innovation, including an instructional course on becoming an entrepreneur, a session on shared decision making, and a presentation about low-cost marketing tactics. A joint luncheon workshop with ESONT examined how to successfully implement innovative technology in a practice.
Global Refractive Summit. As part of ESCRS President Filomena Ribeiro’s goal to build a more inclusive Society and profession, the Congress featured a first-ever Global Refractive Summit that addressed topics ranging from refractive surgery and endothelial disease to new phakic IOL sizing parameters and prediction models. Joining ESCRS in the daylong event were representatives of several national societies, including the Brazilian Association of Cataract and Refractive Surgery (BRASCRS), the American Society of Cataract and Refractive Surgery (ASCRS), the Asia-Pacific Association of Cataract and Refractive Surgeons (APACRS), and the American Academy of Ophthalmology (AAO).
“The Barcelona Congress was not only a significant milestone with over 16,000 participants, but it also continued our commitment to inclusivity,” said President Ribeiro. “With delegates from 126 countries, we strengthened connections with ophthalmological societies worldwide, creating a collaborative environment that benefits all.”

Two more videos have been added to the ESCRS 100 library, bringing the total number of videos to nearly three dozen and furthering the Society’s efforts to be a leading source of continuous education for ophthalmologists in Europe and around the world.
The two videos—“Reading a Topography” by Daniel Chang and “Removing Viscoelastic after ICL” by Bruce Allan—are the latest instructional aides to be added to the ESCRS 100 series. The series comprises short (100-second) instructional videos related to all fields of cataract and refractive surgery.
The ESCRS 100 series launched in April 2023 and includes videos on topics such as extracapsular cataract extraction, secondary IOL implantation, and slit lamp epithelium debridement. Additional videos are being added nearly every month.
Eleven more eye surgeons have earned the right to use the FEBOS-CR credential after passing an exam at the 2024 ESCRS Annual Congress in Barcelona.
The FEBOS-CR exam is one of a handful of European ophthalmic subspecialty exams, along with glaucoma, paediatric, and strabismus. ESCRS, in collaboration with the European Board of Ophthalmology (EBO), organizes the annual exam in cataract and refractive surgery to formally recognize subspecialty training and expertise in these fields. By developing exam criteria and standards, ESCRS and the EBO harmonize and improve training across Europe and define the expected level of knowledge and skills a subspecialist should acquire to solve complex, difficult cases.
Successful candidates earn the right to use the FEBOS-CR credential to show they—
• hold a superior theoretical and practical knowledge;
• can deal with more challenging cases and a complex case mix;
• appreciate the importance of evidence-based medicine and its purpose in developing scientific knowledge and clinical practice of the subspecialty; and
• are, or have the ambition to become, trainers and leaders in the cataract and refractive surgery subspecialty.
FEBOS-CR candidates must be independent surgeons with a varied case mix who regularly deal with complex situations. They must also be willing to have their expertise and theoretical knowledge tested by a rigorous theoretical examination and interviews with some of the top opinion leaders in European and worldwide ophthalmology.
“The level should be advanced, since the final goal is getting a structured fellowship programme in different fields of ophthalmic subspecialists in Europe,” says Marie-José Tassignon MD, PhD, who led the development of the exam and chairs the FEBOS-CR exam committee. “Successful candidates have shown high skills in education and surgical skills within their subspecialty and should be able to run clinical trials. This explains why the application process is a bit more daunting for the primarily surgically oriented subspecializations like FEBOS-CR.”

ESCRS expanding treatment opportunities in underserved areas.
BY LAURA GASPARI
Last June, three people sat under a tree in a village in a remote region of Mozambique, in southeastern Africa. They spoke with community leaders about the importance of eye care and how it should be accessible to everyone. Those three people were Filomena Ribeiro, Mark Wevill, and Tom Ogilvie-Graham, visiting one of the charity projects supported by the ESCRS in Sub-Saharan Africa, following the mission of providing eye care for everyone globally. According to the World Health Organization (WHO), eye healthcare is a vital issue in Africa. Around 26.3 million people are visually impaired, and among these, 20.4 million have low vision and 5.9 million are estimated to be blind. WHO reports the continent holds 15.3% of the world’s blind population. While most vision issues affecting the African population are treatable, the average number of ophthalmologists per million people is 2.5, compared to 76 per million in Europe. As our world becomes increasingly interconnected, global ophthalmology has shifted its focus to developing sustainable systems for eye care delivery in resource-limited settings. ESCRS heard the call and concentrated efforts on projects in Africa, working shoulder to shoulder with skilful partners, carefully chosen from an extensive list according to their expertise and experience.



Currently, the ESCRS has two major projects in Africa: one in Mozambique with Eyes of the World, a Spanish organisation that has worked there for many years, and the second in Malawi with the Blantyre Institute for Community Outreach (BICO). A smaller project in South Sudan supports Dr Lado, a Sudanese ophthalmologist.
“A principle we have is we want to support organisations that already have a good record providing services because they are experts,” said cataract and refractive surgeon and surgical trainer Mark Wevill.
There is also financial support, maximising the benefit to people in need of eye care, but ESCRS wants its support to go somewhere deeper.
“We want to be able to partner in a fuller sense, offering our expertise to add value with some of these projects,” said Tom Ogilvie-Graham MD, managing director of the ESCRS.
ESCRS President Professor Filomena Ribeiro has demonstrated this aim by going to Mozambique to see how the project is going and to speak directly with locals. “It is incredibly good for ESCRS members to see our president, early in her term of office, taking time out to go all the way to Mozambique to visit one of our projects,” Dr Ogilvie-Graham remarked. “It demonstrates the level of commitment that we have in this area.”


Being on the front line means having a winning strategy. In the past, charity projects involved surgeons going to these remote places in Africa, organising cataract camps, and performing surgeries, then returning home. While it is true that some people benefit from this approach, it is not sustainable, Dr Ogilvie-Graham pointed out.
“What we are looking to do is to provide sustained support and to build on something,” he said.
So, the focus is on training ophthalmologists and the ancillary staff—the nurses, technicians, and optometrists.
“The emphasis has shifted a lot now—it is on upskilling and training African surgeons to do more surgeries and to do them better,” Dr Wevill said. Moreover, African countries often have stricter regulations regarding permission to perform surgeries, while training does not involve any bureaucratic issues.
The focus on training is particularly important in another ESCRS project with the Community Eye Health Institute at Cape Town University in South Africa.
“It concentrates on training the trainers and bringing people from all Sub-Saharan Africa to Cape Town, where they have an intensive three-day [workshop] in dry labs using artificial eyes and even simulators to improve their skills and


pass on some of that knowledge to others in more remote areas,” Dr Ogilvie-Graham said.
The catalytic effect of this project can really be effective, Dr Wevill said, adding ESCRS members can take an active part in training their African colleagues, maximising the benefits and the impact. ESCRS also supports the College of Ophthalmology of Eastern Central and Southern Africa (COECSA), which dedicates a great part of its annual meeting to wet labs and training, specifically on phaco surgery.
Yet challenges remain numerous in Africa. First, it is important to evaluate the risks and be careful.
“We would avoid conflict zones and do a risk assessment,” Dr Ogilvie-Graham explained. “Occasionally, there are certain regions with groups that might be criminal or politically motivated. We want to avoid taking personnel from ESCRS and exposing them to that kind of risk.”
It’s precisely for this reason that ESCRS secures a trusted partner. Reaching remote locations within African countries poses a real challenge because of the difficulties of travelling by road or finding an aircraft: sometimes roads are impassable due to the weather conditions or the lack of transportation—something that already undermines patient
accessibility to hospitals and clinics in the main cities to receive proper eye treatments.
“The projects aim to make eye care accessible and set up more rural eye clinics. For some people, it is a long or expensive journey to the city,” Dr Wevill said. For example, Eyes of the World trains people in the villages to recognise eye problems and refer to experts on those who need help.
Unfortunately, there are more disadvantaged categories than accessibility, such as the elderly, disabled people, and, above all, women. Women’s health is regarded as less important than that of men, as both Dr Ogilvie-Graham and Dr Wevill mentioned.
Traditionally, men are the breadwinners who decide where to allocate the scarce family resources.
“In Africa, healthcare is paid out of pocket, without insurance or government provisions, so the man gets the most benefit,” Dr Wevill said.
“It is a cultural change, which was also the aim of that meeting under the tree: to make men understand that women’s health is also important and to make women understand they have the right to have family resources spent for their healthcare.”
For this reason, gender equality is another selection criterion for partners in these projects for ESCRS.
Finally, raising awareness of eye care is extremely important. Many people in remote areas do not know they can get their visual impairment, such as cataracts or uncorrected refractive errors, cured. In his experience, Dr Wevill noted many refer to the local herbalist for a cure or accept blindness as a natural part of life, which in most cases it is not.
ESCRS wants its charity projects to last and to expand their benefits to reach the highest number of people. Both Dr Wevill and Ogilvie-Graham stressed the Society plans to continue the Mozambique, Malawi, and South Sudan projects while strengthening the Cape Town project for more extensive training possibilities. The ESCRS also wants to expand its reach beyond anglophone countries, as indicated by the programme in Mozambique, where Portuguese is the primary language. New collaborations will come out in the future, especially with innovative technologies.
“Telemedicine can help. Surgeons from Europe can assist their colleagues in Africa. One just needs good connectivity, cameras, and bandwidth,” Dr Wevill said. “But that is something for the future.” Training is the key strategy to follow.
“We took out this new strategy and are investing a lot in it,” Dr Ogilvie-Graham said. “And despite the difficulties, this is a long-term commitment for ESCRS.”
Filomena Ribeiro MD, PhD, FEBO is head of ophthalmology at Hospital da Luz Lisboa, Portugal, and ESCRS president.
Tom Ogilvie-Graham MD is managing director of the ESCRS.
Mark Wevill MBChB, FRCS (Edinburgh), FCS (SA) is a cataract and refractive surgeon in Birmingham, UK, and a surgical trainer at the University of Cape Town Community Eye Health Institute Surgical Skills Laboratory.

Non-profit organisations look to innovative, scalable virtual reality training systems.
CHERYL GUTTMAN KRADER REPORTS
Virtual reality (VR) simulation-based training programmes for manual small-incision cataract surgery (MSICS) can help to increase the number of skilled providers in low- and middle-income countries and thereby reduce the personal, economic, and social burdens associated with what remains the leading cause of blindness in the world.
Since introducing simulation training for MSICS in 2005, Orbis International launched a new tool in 2024 that will accelerate the utilisation and benefits of simulation training by allowing increased accessibility, according to Hunter Cherwek MD, Orbis Vice President of Clinical Services and Technologies.
“We believe our new VR training solution is a perfect tool for helping us fulfil our goals to democratise and globalise the best in ophthalmic education, training, and technology,” he told EuroTimes
Created in cooperation with FundamentalVR, a for-profit company that develops VR surgical training platforms, the new tool integrates VR, haptic feedback, cloud assessment data, and off-the-shelf hardware in an affordable, durable, and portable platform—features that make it ideal for training surgeons in the countries where Orbis works.
It benefits users by being an autonomous learning system that provides automated performance monitoring, feedback, and guidance on next steps. Before being able to use the simulator, however, surgeons must first demonstrate commitment and competency through an online learning programme, Dr Cherwek said.
In addition to training on their own, surgeons can participate in connected learning via access to remote surgical mentorship provided by clinical faculty members. Users can
also supplement their learning with Cybersight, Orbis’s telemedicine and e-learning platform.
“Simulation training is a valuable step in the journey towards surgical competency, and our new virtual reality system provides a great tool and environment for building knowledge, confidence, and communication that together make a surgeon better prepared to provide optimal patient care,” Dr Cherwek said.
“Moreover, it is being used to train other key members of the surgical team based on the idea that the knowledge gained by personnel supporting the surgeon will improve communication and efficiency in the operating room.”
Dr Cherwek noted the new VR simulator was developed through scientific research and input from a community of users. An initial prototype was distributed to centres across four continents in seven countries (Bangladesh, China, Ethiopia, India, Mongolia, the United Kingdom, and the United States) for rigorous study. The applied user feedback helped create a refined version that was launched at partner hospitals in Bangladesh, China, Ethiopia, India, and Mongolia.
“We did not want to design a high-tech, overly engineered tool and present it as a solution without getting direct input from users,” Dr Cherwek said.
Orbis is also working to incorporate the VR training solution as a component of surgery simulation training in residency programmes in various countries. It recently sponsored a major workshop in Bangladesh that brought representatives from all the country’s residency programmes together to support the development of a standardised national training curriculum.
VR training through HelpMeSee Targeting eradication of blindness caused by cataract through the innovation of simulation-based training, HelpMeSee created its first VR simulator prototype in 2014 and introduced it for surgeon training the next year. By the end of 2023, about 2,500 surgeons trained on a HelpMeSee platform, with an expected 1,500 more to complete the course in 2024, said Bonnie Ann Henderson MD, President, Chief Executive Officer, and Head of Global Innovation and Technology at HelpMeSee.
“The amount and quality of ophthalmic training by doctors in low-resource regions is extremely variable, and a potential consequence of that variability is compromised patient outcomes. Simulation training levels the playing field,” she said. “By allowing surgeons to practice again and again, simulation technology can increase operator skills and confidence, which leads to better surgical outcomes. Better outcomes benefit patients who undergo the operation but are also important for eradicating cataract blindness because they increase willingness of people in the community to have cataract surgery.”
Our mission is to train surgeons using technology to improve the quality and safety of surgical outcomes.
Dr Henderson noted that HelpMeSee is the only non-profit creating and providing high-fidelity virtual reality simulators with haptic feedback.
“Our mission is to train surgeons using technology to improve the quality and safety of surgical outcomes,” she told EuroTimes. “We deliver this training at no or minimal cost in low-income regions of the world.”
The HelpMeSee programme combines an interactive ebook, facilitated discussions with a certified instructor, and guided sessions on the HelpMeSee Eye Surgery Simulator. The current simulator system integrates high-quality computer graphics with a physics model of surgical activities in MSICS and provides tactile feedback.
Results of a randomised controlled pilot trial evaluating scleral tunnel construction performance among novice surgeons showed the group trained on the HelpMeSee MSICS system made fewer errors compared to the control group of surgeons who received traditional training. The company is further investigating the effectiveness of its simulation-based training by conducting a multicentre prospective masked trial at Aravind Eye Hospital (India), Moran Eye Center (Salt Lake City, US), and Copenhagen Academy for Medical Education and Simulation (Denmark).
For more information, please visit orbis.org and helpmesee.org.
European Registry of Quality Outcomes for Cataract and Refractive Surgery
One-stop-shop Registries in Ophthalmology registries.ESCRS.org
European Cornea and Cell Transplantation Registry
European Registry for Childhood Cataract Surgery
Accountability. Benchmark. Patient Care. Research. Outcomes & Risks.

Addressing a need in underserved regions, distance surgical mentorship offers a viable strategy with multiple benefits.
CHERYL GUTTMAN KRADER REPORTS
Success in reducing the global burden of cataractrelated blindness will depend on increasing the supply of skilled cataract surgeons practising in low- and middle-income countries. Live distance surgical mentorship appears to offer a safe, effective, economical, and eco-friendly approach to meeting the latter need.
Kevin M Barber MD is president of Advanced Centers for Eyecare (ACE) Global, a non-profit organisation aiming to eradicate cataract blindness in the developing world by teaching, training, and mentoring ophthalmic surgeons. Fellows become eligible for distance mentorship only after completing wet lab and simulator training and demonstrating competency in the operating room while working under the guidance of an in-person mentor.
ACE Global has focused its efforts in Honduras, where distance mentoring happens with a high-quality 3D visualisation system to livestream the surgery and a teleconferencing platform for communication between the mentor and mentee.
“With this set-up, the mentor shares the surgical microscope view and can see the mentee’s hands and the screen on the phaco machine. The mentor can communicate verbally with the operating surgeon who wears headphones and visually with hand gestures or drawings displayed on a tablet next to the operating surgeon,” Dr Barber explained. “However, distance mentorship can also be done with a lower cost setup, substituting an action or cell phone camera and webcam for the 3D visualisation system.”
The same set-up could be implemented for remote mentoring and live streaming in surgical fields, which are done under a microscope.
Findings in a prospective, investigator-masked case series showed distance surgical mentorship improved both skill and efficiency of young surgeons.1 Mentees in the project were four Honduran ophthalmologists, of whom three had recently completed residency training and the fourth expressed a need for improving phacoemulsification surgical skills. They received live, remote expert guidance during 25 cases. Changes in performance over time were assessed by comparing outcomes data from three randomly selected cases completed early during the mentorship programme versus three randomly selected cases performed towards its end.
The analyses showed statistically significant improvements in both median Ophthalmology Surgical Competency Assessment Rubric (OSCAR) score and case duration over time. Improvements were also seen in the odds of major complications and self-rated competence, although the changes were not statistically significant.
At Aravind Eye Hospital in Pondicherry, India, distance mentoring of junior surgeons for performing manual small incision cataract surgery (MSICS) was introduced out of necessity during the COVID-19 pandemic and continues today. Illustrating Dr Barber’s comment about not needing sophisticated technology, the Aravind set-up uses the GoPro sports action camera for recording coupled with a GoPro Operations Live on Facebook (GOLF) to link the mentor and mentee.
“Although the distance mentorship is done using a closed-circuit system that is limited to doctors working at Aravind Eye Hospital, the same set-up could be implemented for remote mentoring and live streaming in surgical fields, which are done under a microscope,” Rengaraj Venkatesh MD said.

Currently, all residents and fellows at Aravind Eye Hospital receive one month of mandatory MSICS training provided by an in-person senior ophthalmologist. Thereafter, they progress to a one-month step-up training period where they independently perform one case per day for another 25 cases.
“Junior residents and fellows who have performed fewer than 200 MSICS cases are encouraged to continue operating using the distance mentoring set-up with a dedicated senior medical officer monitoring their surgeries. With this approach, when a junior resident encounters some difficulty, the medical officer can type comments to provide guidance or encourage the resident to call for help,” Dr Venkatesh explained. “Additionally, we use the recorded videos for 30-minute, end-of-day online teaching discussions focused on highlighting mistakes and improving surgical techniques.”
Anecdotally, participation in the distance mentoring opportunity has helped reduce complication rates and improve surgical outcomes for beginners. Now, a study is about to launch, designed to formally document whether this remote mentoring accelerates the surgical learning curve and reduces complication rates for junior surgeons, Dr Venkatesh said.
In the study, residents entering their step-up training are randomised to complete it with or without remote monitoring. Researchers will analyse changes in OSCAR scores for the two groups as the primary outcome.
By eliminating the need for travel, distance surgical mentorship avoids the accompanying ecologic footprint and has time and cost-saving benefits that could lead more ophthalmologists to volunteer their services. Dr Barber said there are some unique considerations for distance mentoring.
“There is a need to be more specific with verbiage and to tweak one’s teaching skills in certain ways when mentoring remotely,” he noted. “All new mentors are required to observe sessions conducted by experienced mentors and be observed by an experienced mentor during their first mentoring session.”
Drs Barber and Venkatesh spoke at ASCRS 2024 in Boston, US.
For citation notes, see page 40.
Kevin M Barber MD is in private practice at Central Florida Eye Specialists, Deland, Florida, US, and President of ACE Global. kbarber@acecaresglobal.org
Rengaraj Venkatesh MD is the Chief Medical Officer of Aravind Eye Hospital, Pondicherry, India. venkatesh@aravind.org
Learn more about ACE Global!

New training programmes seek to reach hard-to-reach areas to meet growing patient needs.
HOWARD LARKIN REPORTS
Meeting the burgeoning eye care needs of rapidly ageing populations across diverse locations will require greater collaboration among ophthalmic societies worldwide, according to a panel of society leaders discussing the topic at the ESCRS Annual Congress in Barcelona. Close cooperation with patients, governments, regulators, and industry will also be needed to foster the innovation required to manage demands that outpace growth in ophthalmologist supply.
With 60% of the world’s population and the largest land mass, Asia is a prime example of the challenges, said Ronald Yeoh, president of the International Ocular Implant Club and past president of APACRS. Across four dozen countries with hundreds of languages, geographic conditions range from lowland tropical cities to remote mountain, desert, and island villages.
“In big cities, it is no issue, but getting out to the rural areas is difficult. It can create quality issues. Education and delivery of clinical services are challenges,” Dr Yeoh said. He sees encouraging national societies and different countries to participate in education and outreach programmes as essential.
Europe faces a similar landscape, but to a lesser extent, said Professor Filomena Ribeiro MD, PhD, ESCRS president. “We have the EU, which tries to provide equality among all countries.” Still, access to services varies, and multiple governments, payment schemes, and cultures make standardisation and collaboration challenging.
Brazil faces similar issues reaching patients in remote areas such as the Amazon, said Durval M Carvalho Jr, president of BRASCRS. “We access by river, trying to give more to isolated people. It’s not easy for us, we have a lot of patients. We did one million cataract surgeries last year, but it’s not enough.”
Two years ago, Australia addressed the same problem by creating a training programme to train rural and remote

ophthalmologists, noted Jacqueline Beltz, co-president and secretary/treasurer of AUSCRS. It combines taking specialty and surgical simulation training in cities with rotations in rural areas.
Creating peer-to-peer support networks for rural surgeons is an important part of the programme, Dr Beltz said. Working with payers to create viable funding models is another feature. “It takes a lot of collaboration. If it doesn’t work, we need to try something else.”
Adopting sustainable practices, such as using the ESCRS-recommended cat pack, can help ophthalmologists do more with less. However, regulations at every level can create barriers, Prof Ribeiro said.
Stephen D McLeod MD, CEO of the AAO, agreed. “There’s no question individual choices are a big part, but you run into roadblocks of what is allowed by regulatory agencies.” Long-term advocacy is required to change regulations. “It’s frustrating, but you need to keep pushing. It is an important component of a long-term solution.”
National and international societies can help by jointly creating evidence-based guidelines for reusing and recycling medical supplies and standardising requirements for electronic medical records and devices, Prof Ribeiro added. Better educating trainees to avoid complications, which are expensive and time consuming, is another key to increasing efficiency.
Making the most of new technologies, such as telemedicine, remote monitoring, and gene therapy, also helps maximise
efficiency, said Prof Vance Thompson MD, president of the ASCRS. “We all have teams supporting us who are willing to work as long as we train them well.”
At a time of decreasing reimbursement and increasing costs, effective practice management is critical, Prof Thompson added. Understanding that patients are willing to invest to receive better care is part of the solution. “We need to be better not only at keeping up our surgical and medical skills, but the business of what we do.”
While radiology and cardiology have the most approved AI applications, its use in ophthalmology is growing, Dr McLeod noted. He suggested that radiology applications are largely binary—either there is pathology or there is not—and cardiology applications are largely volumetric. Dermatology, on the other hand, is more pattern recognition and, therefore, harder for AI to assess.
“Ophthalmology is kind of in the middle,” he said. “Applications in [radiology and cardiology] are much more straightforward, but we will catch up.”
Dr Yeoh questioned that ophthalmology is behind, particularly with retinal imaging. “It depends on who you ask. Young doctors are fine with AI.” Currently it may be more useful for large-scale screening than individual case decision-making, he added. “We need to figure out how to make it more clinically relevant.” For example, AI may have a role in deciding which IOL is best for a given patient.
All comments were made during iNovation Day at the 2024 ESCRS Congress in Barcelona. Jim Mazzo of Neurotech Pharmaceuticals chaired the session.
Ronald Yeoh MBBS, FRCOphth is the medical director and founding partner of Eye & Retina Surgeons, Singapore, a faculty member at the Singapore National Eye Centre, board member of the APACRS, and president of the International Ocular Implant Club.
Filomena Ribeiro MD, PhD, FEBO is head of ophthalmology at Hospital da Luz, Lisbon, Portugal, associate editor of the Journal of Cataract and Refractive Surgery , and president of the ESCRS. filomenajribeiro@gmail.com
Durval M Carvalho Jr MS, MSurg, MChir, MCh is a cataract and glaucoma surgeon at Centro Brasileiro da Visão, Brasilia, Brazil, and president of the BRASCRS.
Jacqueline Beltz BMedSci, MBBS(Hons), MSurgEd, FRANZCO is an ophthalmologist at Eye Surgery Associates, Melbourne, Australia, and co-president/ secretary-treasurer of AUSCRS.
Stephen D McLeod MD is CEO of AAO and former head of ophthalmology at the University of California, San Francisco, US. mcleods@vision.ucsf.edu
Vance Thompson MD is founder and director of Vance Thompson Vision and professor of ophthalmology at the University of South Dakota Sanford School of Medicine, both in Sioux Falls, South Dakota, US, and president of the ASCRS. thompsov@siouxvalley.org
Organisation dedicated to fostering education opportunities offers mentoring, team developments, and online learning tools.
LAURA GASPARI REPORTS
The Ophthalmology Foundation is committed to ophthalmic education, faculty development, and improving eye care around the world, emphasised Helena Filipe MD, discussing the organisation in a symposium.
Specifically, the foundation works with eye care professionals, societies, and organisations to enhance and provide ophthalmic education, with a special commitment to remote, low-resourced settings and underserved regions.
“The main mission of the Ophthalmology Foundation is to assist ophthalmologists [in becoming] better educators and to provide training opportunities through sponsored fellowships,” Dr Filipe said.
The organisation’s focus and passion for faculty education means providing ophthalmic educators with effective educational tools, useful resources, and evidence and experience-based strategies ready to use in their teaching activities.
The six main programmes proposed are all accessible to anyone for free by creating an account on the Ophthalmology Foundation website (ophthalmologyfoundation.org/). They cover teaching skills for ophthalmic educators, courses to become leaders in education, mentorship programmes, faculty development symposia and workshops at national and regional congresses, simulation-based education to optimise learning and skills development, and finally the accreditation of residency training programmes. Moreover, the Ophthalmology Foundation YouTube channel offers educational videos with useful tips and tools for ophthalmology.
A one-to-one mentoring programme follows the classic dyadic model, where experienced ophthalmologists can enrol as mentors, find younger and less experienced ophthalmologists, and build a team relationship from which both can benefit: the mentors would be able to develop leadership and coaching skills while the mentees can progress further in their professional and personal lives.
There is also a group mentoring programme focused on teamwork to develop an organisational-based project and promote continuing professional development (CPD). The latter integrates mentoring formats such as peer mentoring, co-mentoring, and group facilitation to create inclusive and supportive environments and amplify the impact and reach of organisational projects. The Ophthalmology Foundation places significant importance on learning via simulation, which benefits physicians’ performance development and protects patient safety and best outcomes through its efficacy and satisfactory results in ophthalmic training.
“The area of CPD offers a series of focused short pieces of content on CPD fundamentals (microlearning) that can be friendly and quickly accessed following just-in-time learning needs and interests,” Dr Filipe said.

Finally, the Ophthalmology Foundation’s newest initiative centres on international standardised online examinations covering essential topics within visual sciences, optics, refraction, instruments, and clinical ophthalmology.
“We are all volunteers, passionate about medical education,” she said. “We welcome those who would like to join any of these projects or eventually propose another that could also be embraced by the Ophthalmology Foundation.”
Dr Filipe presented during the 2024 ESCRS Congress in Barcelona.
Helena Prior Filipe MD is a Consultant Ophthalmologist at the Hospital de Egas Moniz, Lisbon, Portugal. She is the Chair of the Continuing Professional Development and Simulation-Based Education subcommittees for the Ophthalmology Foundation. hpriorfilipe@gmail.com
Access the Ophthalmology Foundation’s library of videos here.
PureSee IOL studies indicate high patient satisfaction.
TIMOTHY NORRIS REPORTS
Poor night vision outcomes and reduction in contrast sensitivity are among the greatest concerns regarding the implantation of presbyopia-correcting IOLs. First highlighted by an ESCRS survey, this issue has recently been valued more by the industry and has received more consideration for the common photic phenomena associated with PCIOLs like halo, glare, and starbursts. For this reason, designs for the next generation of EDOF IOLs aim to address these vision quality issues, according to José Manuel Díez del Corral MD.
Dr del Corral discussed the results from two recent studies investigating the quality and depth of vision of Johnson & Johnson’s TECNIS PureSee IOL, a purely refractive EDOF lens with an anterior surface that is the same as any monofocal-plus IOL. The posterior surface instead includes a continuous and smooth change in the profile, without rings or separated optical zones. With these changes, it maintains a dysphotopsia profile comparable to that of a monofocal lens, enabling a consistent and extended depth of focus from distance to near.
The first study was a prospective, randomised, two-way masked trial of 60 patients bilaterally implanted with either TECNIS PureSee IOL or a monofocal-plus Eyhance IOL. This study took place in six sites in Australia and New Zealand. The second study was a post-market prospective study on 38 patients with bilateral TECNIS PureSee implants, conducted in three sites in Europe and still ongoing.
Results from the first study showed that at least 50% of eyes obtained an intermediate visual acuity within 0.2 logMAR. The PureSee IOL also had 0.7 D more range of vision at 0.2 logMAR than the monofocal counterpart and non-inferiority in the distance vision.
In the second study, uncorrected and corrected binocular visual acuity (UCDVA and BCDVA) were excellent results at all distances (-0.09 distance, 0.08 intermediate, and
50%
Results from the first study showed that at least 50% of eyes obtained an intermediate visual acuity within 0.2 logMAR.
89%
The results of the studies showed a high quality of vision at all distances, dysphotopsia, and contrast sensitivity compared to a monofocal IOL and an overall satisfaction of 89%.

0.20 logMAR near uncorrected and 0.13 distance, 0.08, and 0.17 logMAR distance-corrected VA). Monocular UCDVA was 0.01±0.09 logMAR and BCDVA was 0.08±0.07 logMAR. The lens provides over 2.5 D of continuous range of vision, binocularly at 0.2 logMAR or better, which is a very nice range of focus, he added. Most patients achieved visual acuity of 0.2 logMAR or better, not only for distance or intermediate, but also for near vision.
Regarding the quality of vision, almost every patient was happy except for a few who experienced some dysphotopsia. In addition, both studies showed similar degrees of contrast sensitivity and low light performance with the comparison monofocal lens.
The results of the studies showed a high quality of vision at all distances, dysphotopsia, and contrast sensitivity compared to a monofocal IOL and an overall satisfaction of 89%, with almost every patient recommending it to family and friends, Dr del Corral concluded.
Dr Díez del Corral presented at the 2024 ESCRS Congress in Barcelona.
José Manuel Díez del Corral Belda MD is Medical Director at the Clínica Oftalmológica Díez del Corral, Madrid, Spain, and Medical Advisor EMEA Johnson & Johnson Vision. jmddcb@yahoo.es

Sponsored by






Performing cataract surgery in a patient who has glaucoma or who is taking IOP-lowering medication is a very common clinical scenario. In the United Kingdom, we’ve adopted combined procedures at a fairly significant rate, and we now have enough data to answer the question of whether patients gain benefit from the simultaneous placement of an iStent inject® W (Glaukos Corp.) or other trabecular bypass stent versus doing cataract surgery alone. Due to these volumes, I think we can now say there is a new gold standard of glaucoma management in which we consider surgical IOP control, if medically appropriate, in eyes requiring cataract surgery.


BY LAURA CRAWLEY, BSC (HONS), MB CHB (HONS), MRCP, FRCOPHTH
A safe and proven technology for earlier intervention.

BY LAURA CRAWLEY, BSC (HONS), MB CHB (HONS), MRCP, FRCOPHTH

much more towards the range of normal and mild.


For those patients who’ve been on the traditional pathway of glaucoma diagnosis, (topical medication then
PFurthermore, treatment group’s safety profile was favorable and similar to that of the control group throughout the 2-year follow-up.
BY LAURA CRAWLEY, BSC (HONS), MB CHB (HONS), MRCP, FRCOPHTH
erforming cataract surgery in a patient who has glaucoma or who is taking IOP-lowering medication is a very common clinical scenario. In the United Kingdom, we've adopted combined procedures at a fairly significant rate, and now have enough data to answer the question of whether patients gain benefit from the simultaneous placement of an iStent inject® W (Glaukos Corp.) or other trabecular bypass stent versus doing cataract surgery alone. Due to these volumes, I think we can now say there is a new gold standard of glaucoma management in which we consider surgical IOP control, if medically appropriate, in eyes requiring cataract surgery.

erforming cataract surgery in a patient who has glaucoma or who is taking IOP-lowering medication is a very common clinical scenario. In the United Kingdom, we've adopted combined procedures at a fairly significant rate, and we now have enough data to answer the question of whether patients gain benefit from the simultaneous placement of an iStent inject® W (Glaukos Corp.) or other trabecular bypass stent versus doing cataract surgery alone. Due to these volumes, I think we can now say there is a new gold standard of glaucoma management in which we consider surgical IOP control, if medically appropriate, in eyes requiring cataract surgery.
and similar to that of the control group throughout the 2-year follow-up.
and similar to that of the control group throughout the 2-year follow-up.
In contrast, the effect of phacoemulsification alone on openangle glaucoma is likely attenuated from 2 years on. cataract surgery alone may lower IOP initially, the effect is not necessarily permanent.

For those patients who've been on the traditional pathway of glaucoma diagnosis, (topical medication then surgery), we want to maximize the chance of surgical success should they need filtration later on. Again, in the clinical trials with the longest-term follow-up of patients receiving an iStent implant, the device reduced patients’ medication burden, more so than other factors.4-7
In contrast, the effect of phacoemulsification alone on open-angle glaucoma is likely attenuated from 2 years on.2 Meaning, although cataract surgery alone may lower IOP initially, the effect is not necessarily permanent.
In contrast, the effect of phacoemulsification alone on open-angle glaucoma is likely attenuated from 2 years on.2 Meaning, although cataract surgery alone may lower IOP initially, the effect is not necessarily permanent
NO LONGER A
COMBINED CATARACT AND MIGS PROCEDURES: NO LONGER A QUESTION OF BENEFIT
COMBINED CATARACT AND MIGS PROCEDURES: LONGER A QUESTION OF BENEFIT
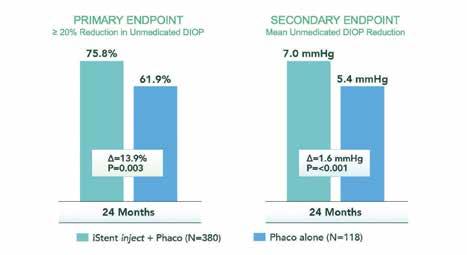
From my own experience and patients' outcomes, when I seek the safest and most effective options for lowering IOP that won’t negate other interventions the patient might need in the future, the iStent inject® W (Glaukos Corp.) fits into that category of treatment nicely. For example, pivotal study for the iStent inject®, published in 2019, was a prospective, multicenter, randomized, controlled trial of 505 total patients who were randomized 3:1 to receive either phacoemulsification and the iStent inject® (n=387), or phacoemulsification alone (n=118). Patient follow-up was performed over years, with annual washouts. The study met effectiveness endpoints: (primary) a reducof ≥ 20% in unmedicated diurnal IOP and (secondary) a mean reduction in unmedicated diurnal IOP (Figure 1).1 Furthermore, the treatment group’s safety profile was favorable
From my own experience and patients’ outcomes, when I seek the safest and most effective options for lowering IOP that won’t negate other interventions the patient might need in the future, the iStent inject® W (Glaukos Corp.) fits into that category of treatment nicely. For example, the pivotal study for the iStent inject® , published in 2019, was a prospective, multicenter, randomized, controlled trial of 505 total patients who were randomized 3:1 to receive either phacoemulsification and the iStent inject® (n=387), or phacoemulsification alone (n=118). Patient follow-up was performed over 2 years, with annual washouts. The study met its effectiveness endpoints: (primary) a reduction of ≥ 20% in unmedicated diurnal IOP and (secondary) a mean reduction in unmedicated diurnal
From my own experience and patients' outcomes, when I seek the safest and most effective options for lowering IOP that won’t negate other interventions the patient might need in the future, the iStent inject® W (Glaukos Corp.) fits into that category of treatment nicely. For example, the pivotal study for the iStent inject®, published in 2019, was a prospective, multicenter, randomized, controlled trial of 505 total patients who were randomized 3:1 to receive either phacoemulsification and the iStent inject® (n=387), or phacoemulsification alone (n=118). Patient follow-up was performed over 2 years, with annual washouts. The study met its effectiveness endpoints: (primary) a reduction of ≥ 20% in unmedicated diurnal IOP and (secondary) a mean reduction in unmedicated diurnal IOP (Figure 1).1 Furthermore, the treatment group’s safety profile was favorable
In a meta-analysis of 13 studies (778 eyes) of iStent implantation alone out to 5 years, Healey et al found that the iStent provided well-sustained reduction in IOP, as well as reduced medication usage.3 Reducing medication usage is important, not only because of the issues of toxicity and compliance, but across the UK, we've seen real challenges to the supply chain of some of the most commonly used drops. Healey et al found a 60% reduction in medication dependence, which is the average of what we see across iStent trials. In turn, removing this insult to the ocular surface would likely push scores on the Ocular Surface Disease Index
In a meta-analysis of 13 studies (778 eyes) of iStent implantation alone out to 5 years, Healey et al found that the iStent provided well-sustained reduction in IOP, as well as reduced medication usage.3 Reducing medication usage is important, not only because of the issues of toxicity and compliance, but across the UK, we’ve seen real challenges to the supply chain of some of the most commonly used drops. Healey et al found a 60% reduction in medication dependence, which is the average of what we see across iStent trials. In turn, removing this insult to the ocular surface would likely push scores on the Ocular Surface Disease Index much more towards the range of normal and mild.
chance of surgical success should they need filtration later on. in the clinical trials with the longestterm follow-up of patients receiving an iStent implant, the device reduced patients’ medication burden, more so than other factors
In a meta-analysis of 13 studies (778 eyes) of iStent implantation alone out to 5 years, Healey et al found that the iStent provided well-sustained reduction in IOP, as well as reduced medication usage.3 Reducing medication usage is important, not only because of the issues of toxicity and compliance, but across the UK, we've seen real challenges to the supply chain of some of the most commonly used drops. Healey et al found a 60% reduction in medication dependence, which is the average of what we see across iStent trials. In turn, removing this insult to the ocular surface would likely push scores on the Ocular Surface Disease Index

Some of the key takeaways from this year’s EGS plenary session were new goals for designing future clinical trials in glaucoma. It was agreed that outcomes should target at least a 20% reduction in medications for patients, if not complete elimination. Because it was the first MIGS device brought to market, the iStent inject® is the only drainage device that has pivotal trial data showing significant durable improvements in visionrelated quality-of-life measurements. 8 The device also has subjective patient data on metrics like general vision, ocular pain, and driving. But what’s most exciting, although relatively new, are functional measures.
Some of the key takeaways from this year’s EGS plenary session were new goals for designing future clinical trials in glaucoma. It was agreed that outcomes should target at least a 20% reduction in medications for patients, if not complete elimination. Because it was the first MIGS device brought to market, the iStent inject® is the only drainage device that has pivotal trial data showing significant durable improvements in vision-related quality-of-life measurements.8 The device also has subjective patient data on metrics like general vision, ocular pain, and driving. But what's most exciting, although relatively new, are functional measures.
A meta-analysis conducted by Gillmann et al produced evidence that the iStent slows the rate of functional vision loss (Figure 2).9 That's interesting; we've not really seen this outcome until very recently, and


much and traditional ical mize they clinical patients reduced than QUALITY-OF-LIFE year’s designing It at patients, brought only data ments surements. patient ocular exciting, tional et slows (Figure seen
A meta-analysis conducted by Gillmann et al produced evidence that the iStent slows the rate of functional vision loss (Figure 2).9 That’s interesting; we’ve not really seen this outcome until very recently, and it warrants further research and debate. Still, it helps us give patients more information about what might happen if their IOP control is suboptimal, and how we can influence it.
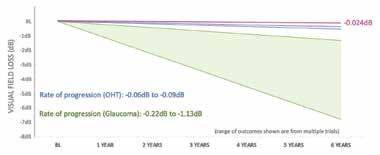
Figure 2. Researchers compared the observed visual field mean deviation progression following implantation of iStent technologies (pink line) with the rates of progression reported in the literature for ocular hypertension (blue lines) and glaucoma (green lines). (Data adapted from Gillmann K, et al. BMJ Open Ophthalmology . 2024. 9)
Figure 2. Researchers compared the observed visual field mean deviation progression following implantation of iStent technologies (pink line) with the rates of progression reported in the literature for ocular hypertension (blue lines) and glaucoma (green lines). (Data adapted from Gillmann K, et al. BMJ Open Ophthalmology. 2024.9)
Figure 2. Researchers compared the observed visual field mean deviation progression following implantation of iStent technologies (pink line) with the rates of progression reported in the literature for ocular hypertension (blue lines) and glaucoma (green lines). (Data adapted from Gillmann K, et al. BMJ Open Ophthalmology
Sponsored by
Sponsored by
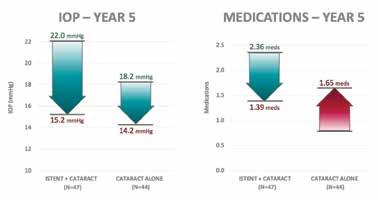
My colleagues and I at Imperial College reviewed our 5-year results in an observational, retrospective, singlecenter, longitudinal cohort study of 47 patients who received the first-generation iStent at the time of cataract surgery. Our control group was 44 patients who had undergone cataract surgery alone. We found that IOP was reduced in both groups immediately after surgery, but the cataract-alone patients needed increasing medications over 5 years of follow-up to maintain their target IOPs (Figure 3). Those who received the firstgeneration iStent had a lower medication burden at 5 years (Figure 3).
Perhaps more exciting were the data from our visual field analysis: those who had the iStent experienced a stabilization of their visual field—we didn’t see further significant loss or further reduction in the mean deviation. In contrast, the visual fields of those who underwent cataract surgery alone deteriorated (Figure 4). These data reflect previous reports that even patients who receive regular follow-up care can lose their visual field function over time. And again, even though our patients tell us that they take the drops every day, we know from a multitude of evidence that they don’t. So, removing that patient-dependent factor should translate into longer-term visual field stabilization. In our study, 26% of patients were medication-free at 5 years.
Figure 4. An observational, longitudinal, 5-year outcome for the change in visual field mean deviation before and after cataract surgery combined with the first-generation iStent (n=47) versus cataract surgery alone (n=44). The two groups were matched for age, visual field mean deviation, and glaucoma diagnosis. (Glaucoma Unit, Imperial College Healthcare, NHS Trust, unpublished data.)
Figure 4. An observational, longitudinal, 5-year outcome for the change in visual field mean deviation before and after cataract surgery combined with the first-generation iStent (n=47) versus cataract surgery alone (n=44). The two groups were matched for age, visual field mean deviation, and glaucoma diagnosis. (Glaucoma Unit, Imperial College Healthcare, NHS Trust, unpublished data.)
evidence that they don’t. So, removing that patient-dependent factor should translate into longer-term visual field stabilization. In our study, 26% of patients were medication-free at 5 years.
deviation, and glaucoma diagnosis. (Glaucoma Unit, Imperial College Healthcare, NHS Trust, unpublished data.)
Figure 3. An observational, longitudinal, 5-year outcome for the change in visual field mean deviation before and after cataract surgery combined with the first-generation iStent (n=47) versus cataract surgery alone (n=44). The two groups were matched for age, visual field mean deviation, and glaucoma
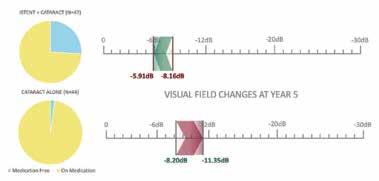
Figure 4. An observational, longitudinal, 5-year outcome for the change in visual field mean deviation before and after cataract surgery combined with the first-generation iStent (n=47) versus cataract surgery alone (n=44). The two groups were matched for age, visual field mean deviation, and glaucoma diagnosis. (Glaucoma Unit, Imperial College Healthcare, NHS Trust, unpublished data.)
Figure 4. An observational, longitudinal, 5-year outcome for the change in visual field mean deviation before and after cataract surgery combined with the first-generation iStent (n=47) versus cataract surgery alone (n=44). The two groups were matched for age, visual field mean deviation, and glaucoma diagnosis. (Glaucoma Unit, Imperial College Healthcare, NHS Trust, unpublished data.)
References
evidence that they don’t. So, removing that patient-dependent factor should translate into longer-term visual field stabilization. In our study, 26% of patients were medication-free at 5 years.
In summary, I think the safety and efficacy of the iStent inject® W has been proven in both randomized control trials and in the real-world setting. I believe this device offers not only significant benefits for our patients, but for us surgeons, as well as for the healthcare system at large and the financial model within which we have to operate. The iStent inject® W procedure is incredibly elegant and safe, and I think it should be among our first considerations for cataract surgery patients with high IOP, controlled or not. It feels like a missed opportunity if we don't offer a secondary procedure that does not have an impact on the cataract surgical procedure but can potentially change the patient’s quality of life and/or their treatment outcome n
In summary, I think the safety and efficacy of the iStent inject® W has been proven in both randomized control trials and in the real-world setting. I believe this device offers not only significant benefits for our patients, but for us surgeons, as well as for the healthcare system at large and the financial model within which we have to operate. The iStent inject® W procedure is incredibly elegant and safe, and I think it should be among our first considerations for cataract surgery patients with high IOP, controlled or not. It feels like a missed opportunity if we don’t offer a secondary procedure that does not have an impact on the cataract surgical procedure but can potentially change the patient’s quality of life and/or their treatment outcome.
1. Samuelson TW, Sarkisian Jr SR, Lubeck DM, et al. Prospective, randomized, controlled pivotal trial of an ab interno implanted trabecular microbypass in primary open-angle glaucoma and cataract: two-year results. Ophthalmology 2019;126(6):811-821.
In summary, I think the safety and efficacy of the iStent inject® W has been proven in both randomized control trials and in the real-world setting. I believe this device offers not only significant benefits for our patients, but for us surgeons, as well as for the healthcare system at large and the financial model within which we have to operate. The iStent inject® W procedure is incredibly elegant and safe, and I think it should be among our first considerations for cataract surgery patients with high IOP, controlled or not. It feels like a missed opportunity if we don't offer a secondary procedure that does not have an impact on the cataract surgical procedure but can potentially change the patient’s quality of life and/or their treatment outcome n
2. Armstrong JJ, Wasiuta T, Kiatos E, et al. The effects of phacoemulsification on intraocular pressure and topical medication use in patients with glaucoma: a systematic review and meta-analysis of 3-year data. J Glaucoma. 2017;26:511–522.
LAURA CRAWLEY, BSC (HONS), MB CHB (HONS), MRCP, FRCOPHTH
1. Samuelson TW, Sarkisian Jr SR, Lubeck DM, et al. Prospective, randomized, controlled pivotal trial of an ab interno implanted trabecular microbypass in primary open-angle glaucoma and cataract: two-year results. Ophthalmology 2019;126(6):811-821.
3. Healey PR, Clement CI, Kerr NM, et al. Standalone iStent trabecular micro-bypass glaucoma surgery: a systematic review and meta-analysis. J Glaucoma. 2021;30(7):606-620.
2. Armstrong JJ, Wasiuta T, Kiatos E, et al. The effects of phacoemulsification on intraocular pressure and topical medication use in patients with glaucoma: a systematic review and meta-analysis of 3-year data. J Glaucoma. 2017;26:511–522.
4. Hengerer FH, Auffarth GU, Conrad-Hengerer I. 7-year efficacy and safety of istent inject trabecular micro-bypass in combined and standalone usage. Adv Ther. 2024;41(4):1481-1495.
In summary, I think the safety and efficacy of the iStent inject® W has been proven in both randomized control trials and in the real-world setting. I believe this device offers not only significant benefits for our patients, but for us surgeons, as well as for the healthcare system at large and the financial model within which we have to operate. The iStent inject® W procedure is incredibly elegant and safe, and I think it should be among our first considerations for cataract surgery patients with high IOP, controlled or not. It feels like a missed opportunity if we don't offer a secondary procedure that does not have an impact on the cataract surgical procedure but can potentially change the patient’s quality of life and/or their treatment implanta
time of cataract surgery. Our control group was 44 patients who had undergone cataract surgery alone. We found that IOP was reduced in both groups immediately after surgery, but the cataract-alone patients needed increasing medications over 5 years of follow-up to maintain their target IOPs (Figure 3). Those who received the first-generation iStent had a lower medication burden at 5 years (Figure 3).
evidence that they don’t. So, removing that patient-dependent factor should translate into longer-term visual field stabilization. In our study, 26% of patients were medication-free at 5 years.
needed increasing medications over 5 years of follow-up to maintain their target IOPs (Figure 3). Those who received the first-generation iStent had a lower medication burden at 5 years (Figure 3). Perhaps more exciting were the data from our visual field analysis: those who had the iStent experienced a stabilization of their visual field—we didn't see further significant loss or further reduction in the mean deviation. In contrast, the visual fields of those who underwent cataract surgery alone deteriorated (Figure 4). These data reflect previous reports that even patients who receive regular follow-up care can lose their visual field function over time. And again, even though our patients tell us that they take the drops every day, we know from a multitude of
Perhaps more exciting were the data from our visual field analysis: those who had the iStent experienced a stabilization of their visual field—we didn't see further significant loss or further reduction in the mean deviation. In contrast, the visual fields of those who underwent cataract surgery alone deteriorated (Figure 4). These data reflect previous reports that even patients who receive regular follow-up care can lose their visual field function over time. And again, even though our patients tell us that they take the drops every day, we know from a multitude of
Sponsored by SEPTEMBER/OCTOBER 2024 | SUPPLEMENT TO CATARACT
Imperial College Healthcare NHS Trust, London
3. Healey PR, Clement CI, Kerr NM, et al. Standalone iStent trabecular micro-bypass glaucoma surgery: a systematic review and meta-analysis. J Glaucoma. 2021;30(7):606-620.
5. Salimi A, Watt H, Harasymowycz P. Long-term outcomes of two first-generation trabecular micro-bypass stents (iStent) with phacoemulsification in primary open-angle glaucoma: eight-year results. Eye Vis (Lond). 2021;8(1):43.
6. Neuhann TH, Neuhann RT, Hornbeak DM. Ten-year effectiveness and safety of trabecular micro-bypass stent implantation with cataract surgery in patients with glaucoma or ocular hypertension. Ophthalmol Ther. Published online ahead of print June 21, 2024.
Private practice at Clinica London and The London Clinic drlauracrawley@gmail.com
4. Hengerer FH, Auffarth GU, Conrad-Hengerer I. 7-year efficacy and safety of istent inject trabecular micro-bypass in combined and standalone usage. Adv Ther. 2024;41(4):1481-1495.
5. Salimi A, Watt H, Harasymowycz P. Long-term outcomes of two first-generation trabecular micro-bypass stents (iStent) with phacoemulsification in primary open-angle glaucoma: eight-year results. Eye Vis (Lond). 2021;8(1):43.
7. Ferguson TJ, et al. Trabecular micro-bypass stent implantation with cataract surgery in open-angle glaucoma: 9 year results. Presented at: the ASCRS Symposium on Cataract, IOL and Refractive Surgery; May 5-8, 2023; San Diego, CA.
Financial disclosures: Speaker (Glaukos Corporation)
6. Neuhann TH, Neuhann RT, Hornbeak DM. Ten-year effectiveness and safety of trabecular micro-bypass stent implantation with cataract surgery in patients with glaucoma or ocular hypertension. Ophthalmol Ther. Published online ahead of print June 21, 2024.
8. Samuelson TW, Singh IP, Williamson BK, et al. Quality of life in primary open-angle glaucoma and cataract: an analysis of VFQ-25 and OSDI from the iStent inject® pivotal trial. Am J Ophthalmol. 2021;229:220-229.
9. Gillman K, Hornbeak DM. Rates of visual field change and functional progression in glaucoma following trabecular microbypass implantation of iStent technologies: a meta-analysis. BMJ Open Ophthalmol. 2024;9(1):e001575. Published online ahead of print Feb 15, 2024.
1. Samuelson TW, Sarkisian Jr SR, Lubeck DM, et al. Prospective, randomized, controlled pivotal trial of an ab interno implanted trabecular microbypass in primary open-angle glaucoma and cataract: two-year results. Ophthalmology. 2019;126(6):811-821. 2.. Armstrong JJ, Wasiuta T, Kiatos E, et al.The effects of phacoemulsification on intraocular pressure and topical medication use in patients with glaucoma: a systematic review and meta-analysis of 3-year data. J Glaucoma. 2017;26:511–522. 3..Healey PR, Clement CI, Kerr NM, et al. Standalone iStent trabecular micro-bypass glaucoma surgery: a systematic review and meta-analysis. J Glaucoma. 2021;30(7):606-620. 4. Hengerer FH, Auffarth GU, Conrad-Hengerer I. 7-year efficacy and safety of istent inject trabecular micro-bypass in combined and standalone usage. Adv Ther. 2024;41(4):1481-1495. 5.Salimi A, Watt H, Harasymowycz P. Long-term outcomes of two first-generation trabecular micro-bypass stents (iStent) with phacoemulsification in primary open-angle glaucoma: eight-year results. Eye Vis (Lond). 2021;8(1):43. 6. Neuhann TH, Neuhann RT, Hornbeak DM. Ten-year effectiveness and safety of trabecular micro-bypass stent implantation with cataract surgery in patients with glaucoma or ocular hypertension. Ophthalmol Ther. Published online ahead of print June 21, 2024. 7. Ferguson TJ, et al.Trabecular micro-bypass stent implantation with cataract surgery in open-angle glaucoma: 9 year results. Presented at: the ASCRS Symposium on Cataract, IOL and Refractive Surgery; May 5-8, 2023; San Diego, CA. 8. Samuelson TW, Singh IP, Williamson BK, et al. Quality of life in primary open-angle glaucoma and cataract: an analysis of VFQ-25 and OSDI from the iStent inject® pivotal trial. Am J Ophthalmol. 2021;229:220-229. 9. Gillman K, Hornbeak DM. Rates of visual field change and functional progression in glaucoma following trabecular microbypass implantation of iStent technologies: a meta-analysis. BMJ Open Ophthalmol. 2024;9(1):e001575. Published online ahead of print Feb 15, 2024. iStent inject® W IMPORTANT SAFETY INFORMATION
7. Ferguson TJ, et al. Trabecular micro-bypass stent implantation with cataract surgery in open-angle glaucoma: 9 year results. Presented at: the ASCRS Symposium on Cataract, IOL and Refractive Surgery; May 5-8, 2023; San Diego, CA.
8. Samuelson TW, Singh IP, Williamson BK, et al. Quality of life in primary open-angle glaucoma and cataract: an analysis of VFQ-25 and OSDI from the iStent inject® pivotal trial. Am J Ophthalmol. 2021;229:220-229.
9. Gillman K, Hornbeak DM. Rates of visual field change and functional progression in glaucoma following trabecular microbypass implantation of iStent technologies: a meta-analysis. BMJ Open Ophthalmol. 2024;9(1):e001575. Published online ahead of print Feb 15, 2024.
LAURA CRAWLEY, BSC (HONS), MB CHB (HONS), MRCP, FRCOPHTH
n Imperial College Healthcare NHS Trust, London
n Private practice at Clinica London and The London Clinic
LAURA CRAWLEY, BSC (HONS), MB CHB (HONS), MRCP, FRCOPHTH
n drlauracrawley@gmail.com
n Imperial College Healthcare NHS Trust, London
n Financial disclosures: Speaker (Glaukos Corporation)
n Private practice at Clinica London and The London Clinic
n drlauracrawley@gmail.com
n Financial disclosures: Speaker (Glaukos Corporation)
INDICATION FOR USE: The iStent inject® W, is intended to reduce intraocular pressure safely and effectively in patients diagnosed with primary open-angle glaucoma, pseudo-exfoliative glaucoma or pigmentary glaucoma. The iStent inject® W, can deliver two (2) stents on a single pass, through a single incision. The implant is designed to stent open a passage through the trabecular meshwork to allow for an increase in the facility of outflow and a subsequent reduction in intraocular pressure. The device is safe and effective when implanted in combination with cataract surgery in those subjects who require intraocular pressure reduction and/or would benefit from glaucoma medication reduction. The device may also be implanted in patients who continue to have elevated intraocular pressure despite prior treatment with glaucoma medications and conventional glaucoma surgery. CONTRAINDICATIONS: The iStent inject® W System is contraindicated under the following circumstances or conditions: • In eyes with primary angle closure glaucoma, or secondary angle-closure glaucoma, including neovascular glaucoma, because the device would not be expected to work in such situations. • In patients with retrobulbar tumor, thyroid eye disease, Sturge-Weber Syndrome or any other type of condition that may cause elevated episcleral venous pressure. WARNINGS/PRECAUTIONS: • For prescription use only. • This device has not been studied in patients with uveitic glaucoma. • Do not use the device if the Tyvek® lid has been opened or the packaging appears damaged. In such cases, the sterility of the device may be compromised. • Due to the sharpness of certain injector components (i.e. the insertion sleeve and trocar), care should be exercised to grasp the injector body. Dispose of device in a sharps container. • iStent inject® W is MR-Conditional; see MRI Information below. • Physician training is required prior to use of the iStent inject® W System. • Do not re-use the stent(s) or injector, as this may result in infection and/or intraocular inflammation, as well as occurrence of potential postoperative adverse events as shown below under “Potential Complications.” • There are no known compatibility issues with the iStent inject® W and other intraoperative devices. (e.g., viscoelastics) or glaucoma medications. • Unused product & packaging may be disposed of in accordance with facility procedures. Implanted medical devices and contaminated products must be disposed of as medical waste. • The surgeon should monitor the patient postoperatively for proper maintenance of intraocular pressure. If intraocular pressure is not adequately maintained after surgery, the surgeon should consider an appropriate treatment regimen to reduce intraocular pressure. • Patients should be informed that placement of the stents, without concomitant cataract surgery in phakic patients, can enhance the formation or progression of cataract. ADVERSE EVENTS: Please refer to Directions For Use for additional adverse event information. CAUTION: Please reference the Directions For Use labelling for a complete list of contraindications, warnings and adverse events. © 2024 Glaukos Corporation. Glaukos, iStent®, iStent inject
Understanding how the features of one proprietary platform translate into optimal clinical results.
CHERYL GUTTMAN KRADER REPORTS
Refractive surgeons interested in adding lenticule extraction as an option for correcting myopia/myopic astigmatism can now choose among procedures from multiple femtosecond laser manufacturers. According to Pooja Khamar MD, PhD, however, smooth incision lenticule keratomileusis (SILK) performed with the ELITA platform offers many unique features that she believes provide an edge for delivering fast and flawless vision outcomes.
“Refractive surgery today is not just about achieving a clear cornea and 20/20 uncorrected vision,” she explained. “Patients are demanding sharp vision for all distances to support their dynamic lifestyles, and they want the ‘wow’ factor of having super vision on day one after surgery.”
Outlining the factors that set the ELITA femtosecond laser and SILK apart from competitors, Dr Khamar highlighted the laser’s operating parameters and the unique biconvex shape of the SILK lenticule. Laser energy and spot separation are two factors that affect postoperative day-one outcomes, and ELITA offers the combination of a low pulse energy (40–45 J) and short spot-to-spot distance (~1 micron) to optimise results.
“Lower energy equals better quality of vision, and because the ELITA spots are almost connected, there are no tissue bridges. Therefore, the lenticule can be extracted with a no-dissection technique that leaves a very smooth interface behind,” she said.

“Minimal collagen disturbance and minimal distortion of Bowman’s membrane with SILK give patients a ‘wow’ effect with good quantity and quality of vision as measured by the Ocular Scatter Index.”
A biconvex lenticule shape is another distinguishing feature. Dr Khamar showed biomechanical simulations illustrating that because the biconvex lenticule has a smaller change in curvature from centre to periphery compared to plano-convex lenticules, which are cut in other lenticule extraction procedures, SILK causes minimal change in asphericity and spherical aberration. Consequently, patients have good depth perception with better night vision and preserved depth of focus post-SILK.
“A lot of patients who have had laser refractive surgery (especially the low myopes) tell me they are happy with the outcome, but they complain about experiencing a lag when changing focus from far to near,” Dr Khamar said. “Our research shows that depth of focus in post-SILK eyes is as good as in unoperated emmetropic eyes.”
Because it preserves depth of focus and spherical aberration, SILK can also be a good option for pre-presbyopic patients who tend to be happy with their outcomes after laser refractive surgery, except for poor near vision quality, she added.
“Looking at patients aged 38 to 50 years, we found that the depth of focus and visual performance at near was similar in the SILK-operated eyes and untreated emmetropes,” Dr Khamar said.
Listing other advantages, she said the biconvex lenticule minimises impact on peripheral cornea nerves, allowing for faster neuroregeneration and better maintenance of tear film optics. Cornea remodelling after SILK is also more regular than traditional laser refractive procedures.
“Therefore, the chance of pseudoregression or erratic epithelial remodelling is reduced,” Dr Khamar said.
Finally, when astigmatic correction is needed, the risk of residual astigmatism is reduced because ELITA features manual cyclorotation adjustment.
Dr Khamar spoke on this topic during the ESCRS Refractive Surgery IME Forum, “Maximizing visual quality through enhanced precision and safety,” at the 2024 ESCRS Congress in Barcelona.
Pooja Khamar MD, PhD is a consultant in the department of cataract and refractive surgery, Narayana Nethralaya, Bengaluru, Karnataka, India. dr.poojakhamar@gmail.com
Used as an adjuvant, the procedure holds promise for addressing an unmet need.
CHERYL GUTTMAN KRADER REPORTS
Cases of progressive infectious keratitis (IK) requiring therapeutic transplant are a reminder of the need for better treatments than just topical antibiotics, and emerging experience suggests that adjunctive corneal cross-linking (CXL) may be a solution, according to Jennifer Rose-Nussbaumer MD.
Describing research with her involvement, Dr RoseNussbaumer said results from an initial pilot study conducted in collaboration with researchers at Aravind Eye Care System in India were positive enough to justify further study of riboflavin CXL as an adjuvant procedure to treat eyes with bacterial keratitis.1 Due to its limited size, the study could not detect statistically significant differences between groups. Encouragingly, however, eyes treated with Dresden protocol CXL plus topical antibiotics had a higher negative culture rate after 24 hours and lower rates of perforation and therapeutic transplant compared to controls managed with antibiotics alone.
Subsequently, NIH funding was obtained to conduct the SCUT II (Steroids and Cross-linking for Ulcer Treatment II) trial, a collaboration between Dr Rose-Nussbaumer and colleagues at the University of California San Francisco; University of Miami, Florida; and Aravind Eye Care System. Started in 2022, SCUT II enrolled 280 patients with bacterial ulcers and randomised them to topical moxifloxacin with sham CXL and placebo, moxifloxacin plus difluprednate and sham CXL, or moxifloxacin, steroid, and riboflavin CXL following the Dresden protocol.
“Results are expected soon,” Dr Rose-Nussbaumer said. “It was interesting that approximately 10% of the participants screened for inclusion in this study were not able to participate because they were already blind in their fellow eye. That finding speaks to the importance of identifying interventions able to improve infectious keratitis outcomes as they may lead to bilateral blindness in high-risk populations.”
Ongoing research is also investigating whether high fluence protocols of riboflavin-based CXL may offer greater efficacy in treating bacterial keratitis. In addition, interest has turned to rose bengal photodynamic antimicrobial therapy (RB-PDAT) for bacterial, fungal, and Acanthamoeba keratitis. While results of a randomised study yielded disappointing results using Dresden protocol CXL as an adjunct to topical antifungal therapy in eyes with fungal keratitis, in vitro studies show greater efficacy of RB-PDAT versus riboflavin-PDT for inhibiting filamentous fungi growth as well as common bacterial keratitis pathogens.2–4
Results of a pilot study conducted at the University of Miami showed therapeutic keratoplasty was avoided in 13 (72%) of 18 eyes treated with RB-PDAT for IK unresponsive to medical therapy.5
“These eyes were deemed in need of a transplant because of severe, progressive disease,” Dr Rose-Nussbaumer said. “Impressively, one of the successes occurred in a patient with both keratitis and scleritis caused by multidrug-resistant Pseudomonas. Improving the outcome in that situation is quite a big ask.”
Now, RB-PDAT for Acanthamoeba or fungal keratitis is being studied in the NIH-funded REAGIR (Rose Bengal Electromagnetic Activation with Green light for Infection Reduction) study randomises patients to medical therapy alone plus sham RB-PDAT or medical therapy plus RB-PDAT.
“Enrolment of 330 patients has been completed at the Federal University of São Paulo in Brazil and Aravind Eye Hospitals, and we are looking forward to sharing results from this study in the near future, too,” she said.
Dr Rose-Nussbaumer spoke on this topic at the 2024 ESCRS Congress in Barcelona.
For citation notes, see page 40.
Jennifer Rose-Nussbaumer MD is Associate Professor of Ophthalmology, Stanford Byers Eye Institute, Palo Alto, California, US. rosej@stanford.edu

Use of presbyopia-correcting lenses in post-corneal refractive surgery patients requires attention to multiple considerations.
CHERYL GUTTMAN KRADER REPORTS
Implantation of a multifocal intraocular lens (MFIOL) or an extended depth of focus (EDOF) IOL in cataract surgery patients having a history of a corneal refractive procedure is a controversial topic given the lack of rigorous evidence to inform the decision. Some published data show that good results are possible, but cataract surgeons should think about a number of issues when deciding if and how to proceed with using a presbyopia-correcting lens in this patient population, said Ruth Lapid-Gortzak MD, PhD.
“There are no randomised clinical trials showing which lens is better after what kind of corneal refractive procedure, and cohort studies show that results of IOL calculation accuracy in eyes with previous corneal refractive surgery lag behind those achieved in untreated eyes,” Dr Lapid-Gortzak observed.
“However, a meta-analysis and systematic review of available retrospective studies evaluating presbyopia-correcting IOLs implanted in post-corneal refractive laser surgery eyes found that the predictability outcomes were not so bad.”1
In the absence of evidence-based guidelines, cataract surgeons must rely on expert opinion, and Dr Lapid-Gortzak provided her perspective.
Noting two strategies for approaching these cases, Dr Lapid-Gortzak said she favours performing cataract surgery within the limitations of what current practice allows and performing a touch-up when necessary. The alternative involves a staged approach in which corneal sphericity is restored before performing cataract surgery.
“Although the approach I take is not academic, it is practical, has wider applicability, and does not subject all patients to a possibly unnecessary extra procedure that certainly adds cost and risk.”
Regarding IOL selection, optical design is one of the main considerations, and data indicate diffractive IOLs offer better image quality than those with refractive or asymmetric optic technology.2 Asphericity is also important as available evi-
dence indicates visual quality is better when eyes with a history of laser vision correction surgery for myopia are implanted with a negative spherical aberration (SA) IOL; eyes with hyperopic correction likely will do better with an SA-neutral IOL.
Dr Lapid-Gortzak also outlined several ocular-related factors to consider when evaluating patient candidacy for a presbyopia-correcting IOL. Attention should be paid to tear film regularity and cornea surface, as it should for any patient wanting a presbyopia-correcting lens. With that in mind, Dr Lapid-Gortzak advised against implanting an MFIOL or EDOF IOL in eyes with a history of conductive keratoplasty or radial keratotomy, given their irregular topography. She also suggested proceeding with caution in high myopes (axial length >26 mm) and eyes ablated for >5 D myopia or >2 D hypermetropia.
Furthermore, surgeons should look for signs predicting a high likelihood of patient dissatisfaction.
“Judge how well patients understand what they are told in the informed consent, beware of men in the 40- to 50-yearold age range who have good uncorrected distance vision for far because they think everything is seen at arm’s length, and beware of patients in the midst of a stressful life event,” said Dr Lapid-Gortzak.
“Most importantly, remember that saying ‘no’ to a patient wanting a presbyopia-correcting IOL is also sound advice.”
Dr Lapid-Gortzak spoke on this topic during Cornea Day at the 2024 ESCRS Congress in Barcelona.
For citation notes, see page 40.
Ruth Lapid-Gortzak MD, PhD is a Medical Specialist in Ophthalmology at Amsterdam University Medical Centers, Amsterdam, Netherlands. r.lapid@amsterdamumc.nl

Challenges involve keeping up to date on current treatments.
LAURA GASPARI REPORTS
The ESCRS work to achieve a consensus on guidelines on corneal refractive surgery is ongoing, but there are still many challenges to face, according to Jesper Hjortdal MD, PhD.
The last 30 years have marked a real revolution in refractive surgery, full of many breakthrough inventions. Surgeons now have a lot of procedures available when it comes to refractive surgery. So, many questions come to mind. “Which procedure should we perform? Which variation should we select to obtain the best and safest outcome in each individual patient?” Professor Hjortdal asked.
In this regard, common guidelines are the best strategy to answer all these questions, but a thorough evaluation must be put in place considering different aspects such as patient selection, contraindications, efficacy, safety, predictability, and stability.
He explained that guidelines are designed following the PICO (Patient, Investigative condition, Comparison condition, Outcome) process, used in evidence-based practice to frame a clinical or healthcare-related question. Also, evidence is commonly classified according to an ‘evidence pyramid,’ where systematic reviews and meta-analyses are on top; single publications, randomised clinical trials, and cohort studies are in the middle; and finally, expert opinions and background information are below. All the evidence must be evaluated using the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) approach.
“You create the quality of evidence into high, moderate, low, and very low,” he said. “High means that there is a lot of confidence that the true effect lies to what it has been estimated, while low means there is little confidence.”
Under these premises, the ESCRS decided to develop guidelines for cataract and refractive surgery in 2020 on the
initiative of Professor Rudy Nuijts. After the pandemic period, Jos Kleijnen led the Kleijnen Systemic Reviews (KSR) team in the official start of their work in 2022, finding and grading all the papers on the subject. The refractive surgery group is led by Professors Béatrice Cochener-Lamard and Thomas Kohnen, with PhD students Victoria Kauer and Joujke Wanten.
As Jesper Hjortdal recalled, the group focused on many PICO questions to address the issue, grading the existing literature.
“Many publications had quite low or very low confidence in what they reported. So, the challenge in writing evidence-based guidelines in refractive surgery is that there are many techniques and variations, and very few are addressed by randomised controlled trials,” he reported.
“Mainly, these treatments take place in private settings, or the companies support them with selected patients. Also, it is difficult to find studies on long-term stability as we tend to lose patients to follow-up after some years.”
However, while the cataract guidelines are published, the work is ongoing for the refractive ones, and the guidelines will most likely be available before the next ESCRS meeting in Copenhagen.
“Our group is confident that such guidelines will improve safety and outcomes for future patients,” Prof Hjortdal concluded. “It will be a contribution, especially for those countries that do not have their own national recommendations.”
Prof Hjortdal spoke at the 2024 ESCRS Congress in Barcelona.
Jesper Hjortdal MD, PhD is Professor of Ophthalmology at the Aarhus University Hospital, Denmark. jesper.hjortdal@clin.au.dk

Ongoing clinical trial explores a novel application for corneal cross-linking.
CHERYL GUTTMAN KRADER REPORTS
Preclinical studies and early clinical data show that corneal cross-linking (CXL) can induce regression of corneal blood and lymphatic vessels, improve visual acuity in eyes with corneal neovascularisation, and may improve graft survival after subsequent penetrating keratoplasty (PK), said Claus Cursiefen MD, PhD.1,2
Based on that promising evidence, a randomised, multicentre, prospective controlled exploratory investigator-initiated trial is now underway in Germany to further test whether preconditioning pathologically vascularised eyes with CXL before high-risk corneal transplantation is a means for promoting graft survival.3
“If successful, CXL will be the first approach to promote graft survival in high-risk transplants worldwide,” Dr Cursiefen said. “However, further research will be needed to identify optimal protocols and refine the indications.”
Dr Cursiefen and colleagues at the University of Cologne have conducted much of the previous research investigating this novel application of CXL. He conceived the study and led the proposal for obtaining funding as well as the protocol development. The study is supported by a grant from the German Federal Ministry for Education and Research. As of September 2024, patients had been enrolled at six of seven participating centres.
Eligible participants are randomised to intervention with CXL or no pre-treatment (control arm) before transplantation. CXL can be repeated once if the initial treatment does not cause sufficient vessel regression. In addition, fine needle diathermy can be done on the day of transplantation to treat any remaining corneal blood vessels.
Graft survival at 24 months is the primary endpoint of the study. The effect of CXL on corneal vessel regression, recurrence of corneal neovascularisation after CXL and after transplantation, visual acuity, safety, and vision-related quality of life are among the secondary endpoints.
Treatment rationale
Interest in developing interventions to treat neovascularisation before corneal transplant derives from data indicating that about 75% of PKs worldwide are performed in highrisk recipients with pathologically prevascularised eyes and knowing the risk of post-PK graft rejection increases as the degree of vessel growth increases. Additionally, animal models have shown lymphatic vessels in the cornea, despite being clinically invisible, have an even greater negative impact on graft survival after high-risk corneal transplantation compared with blood vessels.

“Destroying the vessels pretransplant with fine needle cautery has been shown to improve graft survival rates, but this procedure is somewhat invasive, may need to be repeated, and can lead to vessel rebound,” Dr Cursiefen said.
“CXL is a noninvasive technique that can destroy cellular structures in the upper layers of the cornea—and it is also widely available.”
An initial preclinical study performed in a murine model of experimentally induced corneal neovascularisation showed CXL with riboflavin induced corneal blood and lymphatic vessel regression and significantly improved subsequent graft survival.1 The procedure also showed promise in a retrospective review that included five patients.2
“Temporary pretransplant lymphangio-regression using corneal cross-linking of the recipient may become an easily available tool to promote high-risk graft survival worldwide,” Dr Cursiefen concluded.4
Dr Cursiefen spoke on this topic during Cornea Day at the 2024 ESCRS Congress in Barcelona.
For citation notes, see page 40.
Claus Cursiefen MD, PhD is Professor of Ophthalmology and Vice-Rector for Research and Innovation, University of Cologne, Cologne, Germany. claus.cursiefen@uk-koeln.de
Performed with advanced technologies, PACE-CXL procedure stops ectatic progression and improves vision.
CHERYL GUTTMAN KRADER REPORTS
Phototherapeutic keratectomy (PTK)-Assisted Customised Epi-on corneal cross-linking (PACE-CXL) in eyes with progressive keratoconus or other keratectasia halts further corneal steepening and rehabilitates vision because it both stabilises and regularises the cornea. Importantly, the effect on corneal shape is achieved without removing any stromal tissue, said Farhad Hafezi MD, PhD.
Developed at the ELZA Institute by Dr Hafezi and colleagues, the customised CXL procedure selectively “pushes down the cone.” Although it involves excimer laser use to selectively remove epithelium over the area of greatest steepening via an epithelial map-driven PTK, the CXL portion of the procedure is responsible for the treatment benefit, Dr Hafezi said.
“Some colleagues have said PACE-CXL is nothing new because they can stabilise the cornea and improve vision with the Athens or Cretan protocol combining topography-guided PRK with CXL,” he said. “That is true, but in these procedures, the remodelling effect comes from removing 50 microns of stroma with the excimer laser. In PACE-CXL, the stroma is not touched, and the entire effect comes from cross-linking. The excimer laser is just a very precise tool for creating the epithelial map-driven PTK.”
Epithelial map-driven PTK is done using a software addon of the MS-39 (Schwind eye-tech solutions), a combined Placido ring/anterior segment OCT-based corneal topographer tomographer (CSO Italia), and the AMARIS (Schwind eye-tech solutions) excimer laser. CXL is performed with the C-eye device (EMAGine Switzerland) and is an epi-off/epi-on approach in which there is increased riboflavin saturation and oxygen availability over the site of localised epithelial removal. After irradiating the entire cornea, the epi-off area is treated again with another round of fluence. Together, the gradient differences in riboflavin, oxygen, and energy result in greater flattening at the cone relative to other areas of the cornea and much greater flattening compared to earlier generation CXL procedures, Dr Hafezi said.


The procedure results in immediate flattening and regularisation of the cornea, as cone depression leads to a coupling effect in which the surrounding tissue steepens. Remodelling occurs with epithelial regrowth, leading to some loss of the flattening effect. Topographic stability is usually achieved by month six.
“The thickness map does not change after PACE-CXL because the stroma is not removed, and the demarcation line follows the pattern of the gradient in the CXL effect,” Dr Hafezi said.
Thus far, surgeons at the ELZA Institute have performed PACE-CXL in more than 300 eyes, of which more than 150 have been followed for up to one year.
“Once the remodelling is complete, there have been cases where regularisation of up to 20 D has been observed with CDVA improvement of up to six lines,” Dr Hafezi said.
Because PACE-CXL does not remove stroma, Dr Hafezi said he is comfortable performing the procedure in younger patients with whom he would not perform an Athens or Cretan protocol. PACE-CXL is also being done to regularise the cornea and enhance biometry measurements before cataract surgery in older patients with stable keratoconus. Considering the need for longer follow-up to understand the longterm flattening effect of PACE-CXL, however, the procedure is only being performed in myopic eyes with a Kmax of at least 50 D.
Dr Hafezi spoke at the 2024 ESCRS Congress in Barcelona.
Farhad Hafezi MD, PhD, FARVO is the Chief Medical Officer of the ELZA Institute in Zurich, Switzerland, and Professor of Ophthalmology at Geneva University (Switzerland), NYU Langone (US), the USC Roski Eye Institute (US), and Wenzhou Medical University (China). fhafezi@elza-institute.com
Safety and effectiveness make it a top option for early IK intervention.
CHERYL GUTTMAN KRADER REPORTS
Clinicians should not hesitate to consider using photoactivated chromophore for infectious keratitis-corneal cross-linking (PACK-CXL) as an adjunctive treatment for eyes with infectious keratitis (IK) because it is safe and has the potential to benefit patients regardless of the infection’s aetiology or severity, said Boris Knyazer MD.
“Identifying the causative pathogen at presentation in eyes with IK can be challenging. Standard of care involves obtaining material to send to the microbiology lab and starting broad-spectrum antimicrobial therapy while waiting for the culture report. In these cases, however, PACK-CXL is another option we can include in our armamentarium, and I believe it should be used as early as possible,” said Dr Knyazer.
“It is true that PACK-CXL is probably most effective for treating bacterial keratitis, less so for fungal infections, and maybe even less for treating mixed infections and Acanthamoeba keratitis. However, it is possible to get positive and useful results no matter what the causative organism(s). Do not be concerned about using an accelerated protocol with high-fluence irradiation, because existing evidence shows this more efficient technique is also safe and effective.”
Its use as an IK treatment with the standard Dresden protocol was first reported in the literature in 2008.1 In 2019, a systematic review and meta-analysis of 46 studies with 435 patients summarised outcomes for PACK-CXL performed with a 5.4 J/cm2 total fluence.2 The authors concluded that compared to standard antimicrobial treatment alone, adjuvant PACK-CXL had benefits regarding shortening the mean time to complete corneal healing and accelerating corneal infiltrate resolution. The addition of PACK-CXL had no significant effect on epithelial defect size, visual acuity, or risk of adverse events.
“However, these conclusions were only for IK caused by bacteria and fungi, as there was insufficient evidence on use of PACK-CXL for treating Acanthamoeba and mixed IK,” Dr Knyazer said.
A first report of high-fluence PACK-CXL was published in 2020.3 It described findings from an in vitro study that suggested the higher fluence could increase eradication of various bacteria.
Prompted by that report, Dr Knyazer and colleagues conducted a pilot clinical trial evaluating the safety and efficacy of adjuvant accelerated high-fluence PACK-CXL using a total fluence of 10.0 J/cm2 applied as 30 mW/cm2 for approximately 5.5 minutes. They treated 20 patients with moderately severe bacterial, fungal, or mixed-origin IK. Three patients were treated twice (Figure 1).
The results supported the procedure’s safety—no complications were observed and endothelial cell density counts were essentially unchanged. Mean time to re-epithelialisation was 8.2 days, and no eyes required keratoplasty.





1. Slit lamp and OCT images. (A) Initial presentation: infiltrated cornea with haze, oedema and hypopyon; (B) Incomplete resolution of ulcer on day 5 post the first high-fluence PACK-CXL; (C) Slit lamp image at 8 days after the second high-fluence PACK-CXL procedure; (D) OCT taken prior to the PACK-CXL procedure showing distinct corneal oedema and deep stromal infiltrate; (E) OCT taken at 8 days after the second PACK-CXL procedure with distinct reduction of stromal infiltrate, improvement of corneal thickness, and a deep demarcation line at 260 µm.
Dr Knyazer highlighted the fact that the procedure is performed at the slit lamp with C-Eye device (EMAGine AG, Zug, Switzerland) without the need for additional staff.
“It doesn’t matter how old the patients are. We treated patients aged as young as 16 years and as old as 96, and they were all able to sit for this relatively short procedure without any problems,” he said.
“Our series also included one patient with a history of schizophrenia and an individual with muscular dystrophy treated while sitting in a wheelchair. Imagine having to transfer that patient onto a surgical bed.”
PACK-CXL continues to evolve as ongoing studies are investigate novel chromophores and light sources for irradiation.
Dr Knyazer spoke on this topic during Cornea Day at the 2024 ESCRS Congress in Barcelona.
For citation notes, see page 40.
Boris Knyazer MD, MSc is Associate Professor of Ophthalmology Ben-Gurion University of the Negev, and Head of Cornea and Cornea Transplantation Unit, Department of Ophthalmology, Soroka University Medical Center, Be’er Sheva, Israel. knyazer@bgu.ac.il
Utility of the allogenic segments continuing to broaden with ongoing innovations.
CHERYL GUTTMAN KRADER REPORTS
Corneal allogenic intrastromal ring segments (CAIRS), developed by Dr Soosan Jacob in 2015, became a valuable option for treating keratoconus that offered several advantages compared with the use of synthetic intracorneal ring segments (ICRS). Subsequently, using a femtosecond laser to craft customised corneal segments (femto-CAIRS) brought more versatility to this safe and effective procedure, and the applications are continuing to expand, said Shady T Awwad MD.
“Compared to ICRS, CAIRS technically does not cause melts because the segments are allogenic, and because they have the same index of refraction as the cornea, they can be used where PMMA segments do not dare to go. Specifically, CAIRS can be placed higher up and in a tighter optical zone, allowing their use in thin corneas and more advanced cones,” said Dr Awwad.
“On top of those benefits, the idea of using a femtosecond laser for customising the thickness, size, and shape of the segments and creating asymmetric segments was very appealing. I think this femto-CAIRS technique is really where the CAIRS procedure shines.”
Dr Awwad and colleagues teamed up with Fabian Müller PhD of Ziemer Ophthalmic Systems to develop dedicated CAIRS software for the LDV Z8 femtosecond laser. The segments are cut with the donor cornea mounted on an artificial anterior chamber with guidance by optical coherence tomography (OCT). A published article reported a positive experience with femto-CAIRS using asymmetric segments, describing outcomes of four eyes of two patients with irregular keratoconus.1
The team has also reported the benefit of using CAIRS as a secondary intervention in eyes with keratoconus that developed anterior stromal necrosis overlying synthetic ICRS.2 Compared with eyes managed with ICRS removal alone, eyes that underwent CAIRS insertion into the same tunnels following ICRS explantation had better visual and topographic results.
Additionally, Dr Awwad suggested the future of CAIRS will include a combination approach where the segments are inserted first to ‘debulk’ a large cone, followed one to three months later by customised transepithelial PRK and corneal cross-linking.

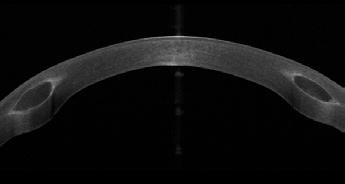
“It is a huge task to obtain good results using an excimer laser to treat a steep cone. Our group and others have shown that in cases where Kmax is over 50.0 D, the repeatability of topography measurements is poor and around 2.5 D, while when Kmax is 50.0 D and lower, it is around 1.0 D. In addition, the excimer laser procedure involves significant stromal ablation,” he explained.
“Flattening the cone first with the additive technology minimises tissue consumption with the laser procedure and improves its repeatability.”
Dr Awwad also reviewed research his group has done to understand the underlying mechanism for CAIRS efficacy.3 Using segmental tomography to follow changes in epithelial and stromal thickness and elevation after CAIRS, the team showed the corneal flattening and regularisation benefits were mediated by epithelial thickening central to the segments combined with anterior stromal flattening. Delineation of the time course for these changes also helps to explain the postoperative clinical course that sometimes shows a peak improvement in vision after one week due to a paradoxical thinning of the epithelium over the flattened cone, followed by a very mild regression due to a compensatory epithelial thickening over the cone, but still showing a clear improvement compared to preoperatively.
Dr Awwad spoke during Cornea Day at the 2024 ESCRS Congress in Barcelona.
For citation notes, see page 40.
Shady T Awwad MD is Professor of Clinical Ophthalmology and Head of Cornea and Refractive Surgery, American University of Beirut Medical Center, Beirut, Lebanon. sa11@aub.edu.lb

SERIES BY PROFESSOR FARHAD HAFEZI MD, PHD; MARK HILLEN PHD; AND EMILIO TORRES-NETTO MD, PHD.
One of Dresden protocol CXL’s biggest challenges is also its simplest: it’s a slow procedure. In the 30 minutes it takes to irradiate the eye with UV energy, a surgeon could have performed two or even three routine cataract procedures. As it turns out, the slow pace of UV irradiation was—both literally and metaphorically—a strength of Dresden protocol CXL.
Photochemistry scholars will know the Bunsen–Roscoe law of reciprocity dictates that for a photochemical reaction where all reagents are in excess, the amount of reaction that occurs is dictated by the amount of light energy (fluence) introduced into the reaction. If the 5.4 J/cm² UV fluence could be delivered more quickly (i.e., with higher UV intensities), then the reaction could be completed faster. The advent of UV light-emitting diodes (LEDs) made high-intensity UV light sources inexpensive and ubiquitous, which should mean 30 minutes at 3 mW/cm² UV irradiation could be replaced with 5 minutes at 18 mW/cm². In reality, accelerating the UV fluence delivery was associated with a reduced biomechanical strengthening effect; many surgeons adopted a reasonable compromise of 10 minutes at 9 mW/cm², but this meant some efficacy was left on the table.2
The culprit was soon identified: oxygen.2,3 Oxygen is an essential, rate-limiting component of the UV-riboflavin photochemical reaction that must diffuse into the stroma from the atmosphere. As soon as UV energy is delivered, oxygen becomes rapidly depleted, and it diffuses only slowly from the atmosphere into the cornea.12,13 Accelerating fluence delivery results in diminishing returns. The emission limitation of the mercury vapour UV lamps the original Dresden team had available to them was almost fortunate—the low intensity essentially ensured the highest strengthening efficacy possible. Nevertheless, an understanding developed that the most reasonable trade-off between speed and efficacy the 9 mW/cm² / 10-minute protocol offers was a balance between procedure time and cross-linking efficacy.
However, this left efficacy on the table. Young children often have the most severe and aggressive forms of keratoconus and, despite being amongst the least able to tolerate 30 minutes of UV irradiation, are exactly the group of patients where no efficacy should be left behind. The maximum strengthening effect is most desirable here, leaving the unmet need clear: an accelerated protocol that delivers Dresden-protocol strengthening. After the importance of oxygen in the stroma was understood, ophthalmology developed accelerated CXL protocols that delivered the UV energy using pulsed light (allowing oxygen to diffuse during the periods of no UV irradiation) or the use of special goggles connected to an external 100% oxygen cylinder to accumulate oxygen over the cornea during irradiation to shrink and close the efficacy gap.
However, the Seiler (et al.) discovery in 2019 that the previously estimated corneal endothelial cell threshold for damage by UV light was too conservative14 opened another option: the delivery of UV fluences higher than 5.4 J/ cm². When high-fluence, accelerated CXL protocols were evaluated, examiners found that 9 minutes, 15 seconds of 18 mW/cm² (10 J/cm² fluence) irradiation could produce Dresden protocol-like strengthening—without requiring any of the apparatus and cost associated with supplemental oxygen apparatus.4
As the overriding issue with patients with ‘thin corneas’ (stromal thicknesses <400 µm) was the risk of UV-induced damage to the corneal endothelium, most techniques developed to address this involved artificially thickening the stroma to >400 µm. These include the use of:
• hypoosmolar riboflavin to swell the cornea prior to UV irradiation,5
• a riboflavin-soaked contact lens (contact lens-assisted CXL [CA-CXL]),6,7 and
• partial epithelium debridement, which leaves an ‘epitheli-
al island’ over the thinnest parts of the cone, thickening this region.8
However, each of these approaches has problems. Although cross-linking with iso-osmolar riboflavin results in good biomechanical strengthening effects, the amount of swelling can be unpredictable.1 As the contact lens hinders oxygen diffusion into the stroma, CA-CXL results in a reduction in a stiffening effect of approximately one-third.11 The epithelial island approach causes issues at the border between the epithelial cells and the epithelium-denuded region, refracting UV light differently at the border and causing an uneven demarcation line.9
These approaches involved modifying the cornea to fit the technique. More recently, the converse approach has been taken: modifying the technique to fit the cornea. The first proposed was the ‘M Nomogram,’ which exploits the fact different crosslinking technologies result in different demarcation line depths; the protocol delivering the deepest cross-linking effect that still retains the 70 µm safety margin is then performed. However, this does require the surgeon to have access to all the drugs and devices required to perform these protocols.10
The ELZA-sub400 protocol, developed by Professor Farhad Hafezi and colleagues, is particularly noteworthy. It individualises UV fluence based on post-epithelial removal pachymetry, ensuring effective cross-linking while preserving a safety margin for the endothelium,22 and builds on previous work that developed an algorithmic model of the UV-riboflavin-oxygen-stroma interactions.12 This protocol has been successfully applied to corneas as thin as 214 µm, expanding the eligibility of CXL to more patients, and has the advantage of simplicity. Once the surgeon knows the pre-irradiation thinnest point pachymetry measurement, they simply look at a table to determine the appropriate 3 mW/cm²-intensity UV irradiation duration to safely cross-link the cornea and leave the 70 µm safety margin. Every cross-linking device can deliver 3 mW/cm²-intensity UV irradiation, and an updated ELZA-sub400 protocol that utilises an accelerated 3 mW/cm² UV intensity will soon be released.
The first part of this series appeared in the November issue of EuroTimes
For citation notes, see page 40.

Mark
Emilio Torres-Netto MD, PhD, FWCRS is a cornea, cataract, and refractive surgeon at the ELZA Institute.

Device appears safe and effective for restoring lost central vision in patients with fovea-involving geographic atrophy.
CHERYL GUTTMAN REPORTS
Preliminary results from 12 months of follow-up in the pivotal PRIMAvera study show the PRIMA subretinal implant system can restore meaningful visual acuity (VA) in patients with advanced fovea-involving geographic atrophy (GA) and be used for reading tasks in daily life.
“Geographic atrophy due to age-related macular degeneration is a devastating disease that is never self-limiting and finally encroaches upon the fovea, destroying central vision,” said Frank G Holz MD. “Current approaches for intervention mainly aim to slow disease progression measured by a change in GA lesion growth over time. In contrast, the PRIMA system may improve functional outcomes by restoring central vision in eyes where photoreceptors are already lost and there is no longer viable foveal tissue.”
The PRIMA system, developed by the Science Corporation, consists of a camera mounted on augmented reality glasses, a small external processor, and a subretinal microchip measuring 2x2 mm wide and 30 microns thick. Images captured by the camera from the environment are processed and projected onto the microchip using infrared light. The microchip converts the infrared light signals into an electrical current that
stimulates retinal neurons. The responses of the latter cells pass through the retinal neural network to ganglion cells to exploit residual retinal signal processing.
Briefly, the surgery involves vitrectomy and the creation of a subretinal bleb by BSS injection. Then, a temporal retinotomy is created through which the microchip is delivered into the subretinal space at the macula.
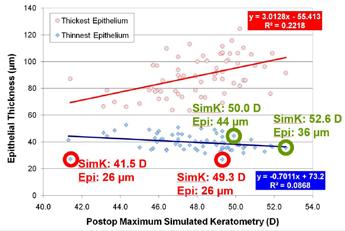
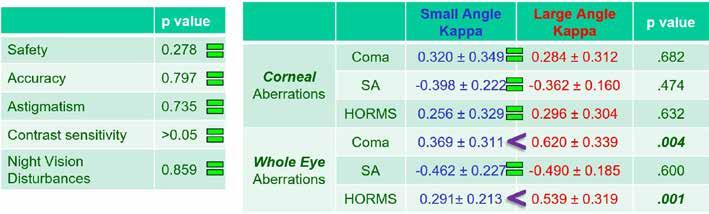
Dr Holz noted the PRIMA study was undertaken after two smaller feasibility studies conducted in France and the United States achieved positive results. He reported that in one feasibility study with data for 3 patients followed to 48 months, VA improved from baseline by a mean of 32 ETDRS letters. 1
“Importantly, there were no safety issues in adverse effects on retinal tissue above the microchip based on OCT scans,” Dr Holz said.
The system’s processor allows patients to adjust the magnifying effect of the entire system.
PRIMAvera enrolled 38 patients at 17 sites across 5 European countries. Eligible patients were aged 60 years and older and had fovea-involving GA with VA 20/320 or worse. Mean age of the participants was 79 years, and females and males were almost evenly represented. Mean atrophy size was 24.7 mm2
Preliminary results of VA testing with PRIMA at 12 months showed that compared to baseline, patients had a mean VA gain of 23 letters with the system on.
“The patient showing the greatest improvement benefited with a gain of 59 letters,” Dr Holz said. “Overall, 81% of patients achieved a gain of at least 10 letters.”
When asked about using the PRIMA system in their daily lives, 80% of patients reported using it to read letters, numbers, or words, and 31% reported it enabled them to read text from books in dimly lit environments.
“The system’s processor allows patients to adjust the magnifying effect of the entire system,” Dr Holz observed.
The safety review showed side effects were all procedure-related and mostly resolved over time. As an important safety finding, there was no evidence the average natural peripheral vision was adversely affected by the procedure or microchip.
“It seems integration of the natural peripheral vision and artificial vision is possible for patients who have the PRIMA system,” Dr Holz concluded.
Dr Holz reported at the 2024 Euretina Congress in Barcelona.
For citation notes, see page 41.
Frank G Holz MD is Professor and Chair of the Department of Ophthalmology, University of Bonn, Germany. frank.holz@ukbonn.de
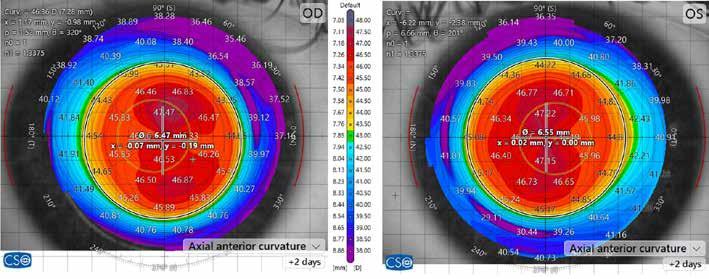
Cataract surgeons learning intervention techniques could expand early glaucoma treatment.
HOWARD LARKIN REPORTS
Today, it’s the ESCRS. Tomorrow a ‘G’ could well be add ed, Iqbal K ‘Ike’ Ahmed MD said in the iNovation Day programme at the 2024 ESCRS Congress in Barcelona.
“Just as we have seen the merger of cataract and refractive surgery over the past decade, we are seeing the synergy of cataract and glaucoma coming along quite well,” Professor Ahmed said.
Growing need and better understanding of the importance of early treatment are driving a transformation to what Prof Ahmed calls interventional glaucoma. Worldwide, the total glaucoma disease population is projected to grow from 178 million in 2024 to 198 million in 2029, or about 2.1% annually over the next 5 years, according to a Market Scope analysis. Investment in glaucoma technologies, including minimally invasive devices and sustained-release drug delivery systems, also has recovered since the pandemic, Prof Ahmed added. “This is a space that is still ripe for innovation.”


However, the percentage of cataract surgeons performing mini mally invasive glaucoma surgery (MIGS) has actually declined, from 30% in 2018 to 26% in 2023, though the ESCRS annual Clinical Trends Survey reports it has stabilised in recent years. And, on average, respondents in 2023 said only about 14% of cataract glaucoma patients qualify for MIGS.
This may be because respondents are primarily cornea and cataract surgeons unfamiliar with angle surgery, which predominates in glaucoma, said Elena Arrondo MD. Lack of awareness that a patient being treated with two or even one glaucoma drug should be considered (and even new glaucoma patients with an indication for cataract surgery) may also be an issue, said Henny Beckers MD, PhD. Better evidence of MIGS clinical efficacy and clear guidelines could help increase uptake. Reimbursement to expand patient access is also needed, according to several session panel members.




Nonetheless, Prof Ahmed said change is underway. “Our current model is very much a progression, watchful waiting, and rudimentary approach that is medication heavy, while interventions and technologies are often left until later.” Surgery, including trabeculectomy and tube shunts, is often considered for refractory glaucoma only. Even selective laser trabeculoplasty (SLT) is often withheld until maximum tolerable medical treatment has failed.
“We know there are significant problems with this paradigm, and we are hammering away to find better options,” Prof Ahmed said. Several innovations could make earlier, more aggressive treatments easier and more reliable to adopt.



Harnessing the immense data already generated in glaucoma practice using AI will drive transformative changes.
“We’ve already seen the incorporation of big data and AI in screening strategies,” he said. “As we continue to improve our diagnostic precision, this will allow us to stratify and provide a more personalised medical approach.”
Connecting diagnostic tools inside and outside the clinic will improve diagnosis and facilitate treatment customisation, Prof Ahmed added. This data will increasingly come from home and intraocular IOP sensors and virtual reality diagnostics and be analysed by AI-assisted algorithms.
Early, effective glaucoma treatment is essential before it leads to irreversible trabecular meshwork dysfunction that
reduces the effectiveness of all trabecular outflow treatment types, Prof Ahmed noted. “Glaucoma is only young once, so the question is how can we address this at the right stage?”
Already, glaucoma treatment is becoming more interventional. While medication remains dominant, first-line SLT, non-incisional MIGS, standalone and combination MIGS are all increasing. Canal surgery device and microstent volumes grew while trabeculec tomy and tube shunts remained relatively stable over

Sustained-release drug delivery is also emerging as an early treatment option, which Prof Ahmed said


“With MIGS, we’re not sure how well a patient will respond,” he added. “Drugs work really well; it’s just they don’t get in the eye enough.” More evidence of safety and long-term efficacy will help
All address the unmet patient need to provide sustained, 24/7 IOP control to prevent disease progres sion and improve quality of life by reducing reliance on eye drops. “I project this will continue over the next
Education is the key to expanding early intervention,
“There is huge room for improvement,” she said. “We should be creating awareness among patients and their doctors about how to treat according to these

Given the complexity of MIGS choices, Prof Beckers said doctors also need specific instruction on how to per form and best choose among these choices. She cited the ESCRS MIGS Masterclass as a good example of how this can be accomplished.
“We, as glaucoma surgeons, can help.”

Iqbal K ‘Ike’ Ahmed MD is professor at the University of Utah, US, assistant professor at the University of Toronto, head of ophthalmology at Trillium Health Partners, and chief innovation officer at Prism Eye Institute, all of Toronto, Canada. ike.ahmed@utoronto.ca; ikeahmed@mac.com
Elena Arrondo MD is a glaucoma specialist at IMO Institute of Ocular Microsurgery, Barcelona, Spain. international@imo.es
Henny Beckers MD, PhD is professor of ophthalmology and head of the glaucoma clinic at Maastricht University Medical Center, Netherlands. henny.beckers@mumc.nl
Committee representatives of ESCRS organise and present sessions at meetings organised by our national and sister societies. These sessions are typically delivered by a group of speakers on a current topic selected by ESCRS in person or virtually.
These sessions provide useful education as well as collaboration between societies promoting and sharing benefits across both memberships.
escrs.org/education/academies/
New guide allows easier comparison between glaucoma surgery techniques.
ROIBEÁRD O’HÉINEACHÁIN
The European Glaucoma Society (EGS) has published a core outcome set (COS) for trials in glaucoma treatment to harmonise the assessment of study results, improve the collation of results from separate studies, and compare different treatments.
“The reporting of the core outcome set in all future trials will ultimately ensure the same bar will be used in assessing old and new surgical procedures for glaucoma,” said Francesco Oddone MD.
The COS for innovation in glaucoma surgery is part of the EGS Guide on Surgical Innovations in Glaucoma. Implementing a COS should result in an agreed and standardised set of glaucoma outcomes that should be measured and reported as a minimum in all clinical trials.
Dr Oddone noted that 10 to 15 years ago trabeculectomy and non-penetrating techniques, such as deep sclerectomy and canaloplasty, dominated glaucoma surgery. Since then, the number of treatment options has expanded to include a range of new devices. Many have new mechanisms of action, including enhancement of trabecular drainage via Schlemm’s canal, subchoroidal drainage, and cyclodestruction.
He pointed out that, in contrast to pharmaceuticals, for which valid evidence of safety and efficacy is required before licensing, there is no mandatory minimum level of evidence required before surgical procedures can be used widely in patients. Instead, they frequently gain acceptance following a series of observational and cohort studies.
However, the scientific assessment of new surgical interventions is complicated by a specific set of problems, including precisely defining the procedures as they evolve and a lack of standardised outcome measures. Additional factors requiring consideration include the variations in surgeons’ skill with the procedure and the treatment preferences of patients and clinicians, Dr Oddone said.

Differences in the outcomes measured with new treatments make it difficult to meaningfully assess their safety and efficacy compared with the standard of care, he noted. In studies of trabeculectomy, the main outcome measures are intraocular pressure (IOP) reduction, complications, and re-intervention rate. The outcome variables reported in studies with the new techniques include variations in the amount of reduction achieved, the number of medications, and the proportion free of medication. There is also a corresponding ‘jungle’ of criteria for success.
This will lead all the stakeholders to have answers to the most important questions for clinical decision-making.
“The accurate assessment of the safety and efficacy of new treatments requires the use of the same outcome criteria: those relevant and important to the key stakeholders, the patients, the healthcare providers, and anyone making decisions about healthcare,” Dr Oddone said.
To develop the COS for glaucoma surgery, the EGS identified reported outcomes and descriptor measures of glaucoma trials evaluating surgical innovations from published clinical studies and systematic reviews. From this, they developed a grading system for the relevance of the reported outcomes and descriptors by electronic surveys of glaucoma experts. They concluded the process with an in-person consensus meeting of glaucoma experts.
“Clinicians can use it as a guide to critically appraise the already published literature, and policymakers will be able to make decisions based on high-grade, consistent evidence,” he said. “Finally, this will lead all the stakeholders to have answers to the most important questions for clinical decision-making, including IOP-lowering efficacy, additional postoperative interventions, visual function, structural evaluations with OCT, quality of life and patient-reported outcome measures, and safety.”
Dr Oddone presented his paper at the 16th European Glaucoma Society Congress in Dublin.
Gain extra intermediate vision without compromising the quality of far distance
Precizon Go is the newest addition to Ophtec’s premium line of cataract intraocular lenses (IOLs). This innovative lens represents a significant advancement in enhanced intermediate vision, and closes the gap between traditional monofocal and presbyopic cataract lenses.
The new Precizon Go is a purely refractive lens, precisely engineered with an ingenious technology to provide patients with enhanced intermediate vision while maintaining superior distance vision and visual quality. Its unique optics is characterized by a diopter profile with combined spherical aberrations, which extend the depth of focus without compromising vision quality.

The new Precizon Go IOL has demonstrated excellent performance both in bench and clinical studies.*
• Modulation Transfer Function (MTF): bench study results show similar MTF curves for both Precizon Go and Precizon Monofocal, confirming the high manufacturing standards of the new design (Figure 1)
• Simulated Defocus Curve: the simulated defocus curve obtained during bench studies demonstrate a clear advantage of Precizon Go within the defocus range of -0.50 D to -2 D (Figure 2)
“The aspherical profile of the Precizon Go IOL is a stroke of genius. It provides excellent far and intermediate vision without causing dysphotopsia and corrects the corneal positive spherical aberration according to the pupil size.”

Professor Youngsub Eom, MD, PhD, from the Korean University College of Medicine and Ansan Hospital, performed one of the first surgeries in the clinical marketing study. He remarked, “The aspherical profile of the Precizon Go IOL is a stroke of genius. It provides excellent far and intermediate vision without causing dysphotopsia and corrects the corneal positive spherical aberration according to the pupil size”.
• Visual and satisfaction outcomes: clinical outcomes highlight excellent performance at both far and intermediate distances (CDVA 0,00 ± 0,06 LogMAR, DCIVA80 0,14 ± 0,09 LogMAR & DCIVA66 0,2 ± 0,07 LogMAR), as well as high rates of patient satisfaction with 100% and 94% of patients reporting to be very satisfied or satisfied with far and intermediate vision respectively.
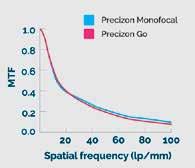
Figure 1. MTF levels of the studied IOLs at the best focus for a 4.5-mm aperture.
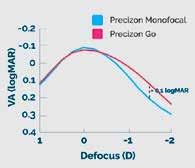
Figure 2. Defocus and LogMAR VA simulations as a function of spectacle defocus.
* The scientific data is the result of research studies conducted to evaluate the performance of the Precizon Go IOL, and/or the outcomes in patients receiving surgical implantation of the IOL. The results are summarized in a compendium and can be downloaded at www.ophtec.com/product-overview/precizon-go
Zeiss Medical Technology demonstrated its new non-ultrasound lens extraction device MICOR® 700 at the 2024 American Academy of Ophthalmology (AAO) conference. The MICOR 700 is designed for performing the Zeiss NULEX procedure and is the first handheld device for lens removal that does not require a console or a foot pedal. It also has a novel blunt tip with rounded edges designed to minimise the risk of tissue damage. In addition, ZEISS MICOR 700 features a disposable ‘plug-and-play’ system, which enables a quick set-up and breakdown in the operating room. zeiss.com
Market Scope has published its ‘2024 European Five Ophthalmic Market Report,’ which includes five-year forecasts of disease prevalence, technologies used in treatments, and market performance of ophthalmic companies in Europe’s five largest ophthalmic markets—France, Germany, Italy, Spain, and the United Kingdom. The report estimates the number of ophthalmic procedures performed will total more than 17 million in 2024 and increase to 19 million by 2029. The report also predicts cataract surgeries and intravitreal injections (IVT) will remain the most common procedures, but glaucoma laser surgery will grow at the highest rate. market-scope.com
Bausch + Lomb has announced that the US Food and Drug Administration has approved the enVista® Envy™ full range of vision IOL. Available in both toric and non-toric versions, the IOL features ActivSync optic, designed to prioritise distance vision in mesopic conditions and near vision under photopic conditions, with a favourable dysphotopsia profile and enhanced contrast vision. bausch.com
Heidelberg Engineering received FDA clearance for its Spectralis® Flex Module to capture posterior segment imaging of patients in a supine position. The Flex Module includes a moveable stand for mounting the Spectralis. Like the tabletop Spectralis, the Flex Module includes high-resolution OCT, OCT angiography, fluorescein angiography, and other imaging-only modalities. heidelbergengineering.com
Christoph Schoess, founder and long-serving managing director of Heidelberg Engineering, was awarded the esteemed Theodor Leber Medal at the German Ophthalmological Society (DOG) annual congress in Berlin. The award is presented to individuals who have made exceptional contributions to scientific ophthalmology or the DOG. heidelbergengineering.com
LENSAR has announced that more than one million robotic femtosecond laser-assisted cataract procedures have been performed using its technology. lensar.com
Aurion Biotech has announced the commercial launch of Vyznova® (neltependocel) in Japan for treating corneal bullous keratopathy. Developed by Professor Shigeru Kinoshita, the treatment consists of allogeneic human corneal endothelial cells and the ROCK-inhibitor Y-27632 and is administered by intravitreal injection. Neltependocel has received both regulatory and reimbursement approval in Japan and is currently undergoing phase 1/2 clinical trials in the US. aurionbiotech.com

Many commonly prescribed medications appear to increase the risk of keratoconus, according to the findings of a populationbased pharmacovigilance study. The study’s authors analysed data from the FDA Adverse Event Reporting System (FAERS). Their analysis showed the pharmacologic agents associated with disproportionately high reports of keratoconus included sex hormones such as progesterone and oestradiol; olopatadine, isotretinoin, methylphenidate, spironolactone; antipsychotics, such as aripiprazole and risperidone; and biologics, such as dupilumab.
R S Huang et al. “Keratoconus Cases Associated with Medication Use: A Population-Based Pharmacovigilance Study,” 18 Oct 2024. doi: 10.1097/j.jcrs.0000000000001573a.
Postoperative complication rates after IOL implantation in eyes with inadequate capsular bag support vary depending on the fixation method used, a review and meta-analysis suggest. Study authors identified 15 studies comparing two or more fixation methods and involving 1,247 eyes with inadequate capsular support. Their analysis showed when they grouped eyes according to the fixation method, the overall complication rate was non-significantly lower in the iris fixation group than in the anterior chamber (AC) and scleral fixation groups. Transient corneal oedema was significantly more common in the AC placement group (29.9%) than in the scleral (11.9%) or iris fixation group (4.1%). Vitreous haemorrhages were significantly more common in the scleral fixation group (8.5%) than in AC placement (5.4%) and iris fixation (1.4%) groups. IOL decentration/dislocation also occurred more frequently in the scleral fixation (8.9%) group than the AC (1.1%) or iris fixation (4.0%) groups.
P Kanclerz, et al. “Postoperative complication rates in intraocular lens placement and fixation methods for inadequate capsular bag support: a review and meta-analysis,” 17 Oct 2024. doi: 10.1097/j.jcrs.0000000000001572.
After the initial recovery period, keratorefractive lenticule extraction (KLEx) demonstrates comparable efficacy, safety, and accuracy outcomes compared to LASIK and PRK. The retrospective study involved 4,466 eyes of patients who underwent KLEx, PRK, or LASIK from 2019 to 2022. At six postoperative months, there was no statistically significant difference between the procedures in the percentage of eyes reaching an uncorrected distance visual acuity (UDVA) of 20/20 or better. However, at one and three postoperative months, a significantly greater number of eyes in the KLEx group achieved the same or one line better in distance visual acuity than the PRK group. At six months postoperatively, the efficacy indexes of KLEx, PRK, and LASIK were 1.09, 1.10, and 0.97, respectively. The safety indexes for the three procedures were 0.96, 1.01, and 0.81, respectively.
C Evangelista et al, “Comparing Visual Outcomes of KLEx, PRK, and LASIK Procedures in the Military,” 9 Oct 2024. doi: 10.1097/j. jcrs.0000000000001565.

JOIN the leading community and trusted source for SCIENCE, EDUCATION & PROFESSIONAL DEVELOPMENT in the fields of cataract and refractive surgery.
Closing the Mentorship Distance
Page 14
1. Barber KM, O’Connor S, Ponce J, et al. “Distance surgical mentorship in cataract phacoemulsification using a 3D visualization system,” Intl J Surgical Education (IJSED). Published online 14 May 2022.
CXL for Infectious Keratitis
Page 23
1. Prajna NV, Radhakrishnan N, Lalitha P, et al. “Cross-linking assisted infection reduction (CLAIR): a randomized clinical trial evaluating the effect of adjuvant cross-linking on bacterial keratitis,” Cornea, 2021; 40(7): 837–841.
2. Prajna NV, Radhakrishnan N, Lalitha P, et al. “Cross-linking-assisted infection reduction: a randomized clinical trial evaluating the effect of adjuvant cross-linking on outcomes in fungal keratitis,” Ophthalmology, 2020; 127(2): 159–166.
3. Arboleda A, Miller D, Cabot F, et al. “Assessment of rose bengal versus riboflavin photodynamic therapy for inhibition of fungal keratitis isolates,” Am J Ophthalmol, 2014; 158(1): 64–70.e2.
4. Roa-Tort K, Saavedra Y, Villanueva-Martínez A, et al. “In vitro antimicrobial photodynamic therapy for Pseudomonas aeruginosa (P. aeruginosa) and methicillin-resistant Staphylococcus aureus (MRSA) inhibition using a green light source,” Pharmaceutics, 2024; 16(4): 518.
5. Naranjo A, Arboleda A, Martinez JD, et al. “Rose bengal photodynamic antimicrobial therapy for patients with progressive infectious keratitis: a pilot clinical study,” Am J Ophthalmol, 2019; 208: 387–396.
Page 24
1. Sun Y, Hong Y, Rong X, Ji Y. “Presbyopia-Correcting Intraocular Lenses Implantation in Eyes After Corneal Refractive Laser Surgery: A Meta-Analysis and Systematic Review,” Front Med (Lausanne), 11 Apr 2022; 9: 834805.
2. Alio JL, D’Oria F, Toto F, et al. “Retinal image quality with multifocal, EDoF, and accommodative intraocular lenses as studied by pyramidal aberrometry,” Eye Vis (Lond), 6 Oct 2021; 8(1): 37.
Page
1. Hou Y, Le VNH, Tóth G, et al. “UV light crosslinking regresses mature corneal blood and lymphatic vessels and promotes subsequent high-risk corneal transplant survival,” Am J Transplant, 2018; 18(12): 2873–2884.
2. Schaub F, Hou Y, Zhang W, Bock F, Hos D, Cursiefen C. “Corneal crosslinking to regress pathologic corneal neovascularization before high-risk keratoplasty,” Cornea, 2021; 40(2): 147–155.
3. Wiedemann J, Hos D, Limburg E, et al. “UV light-mediated corneal crosslinking as (lymph)angioregressive pretreatment to promote graft survival after subsequent high-risk corneal transplantation (CrossCornealVision): protocol for a multicenter, randomized controlled trial,” Trials, 2024; 25(1): 169.
4. Cursiefen C, Hos D. “Cutting edge: novel treatment options
targeting corneal neovascularization to improve high-risk corneal graft survival,” Cornea, 2021; 40(12): 1512–1518.
Unpacking PACK-CXL Options
Page 28
1. Iseli HP, Thiel MA, Hafezi F, Kampmeier J, Seiler T. “Ultraviolet A/riboflavin corneal cross-linking for infectious keratitis associated with corneal melts,” Cornea, 2008; 27(5): 590–594.
2. Ting DSJ, Henein C, Said DG, Dua HS. “Photoactivated chromophore for infectious keratitis—Corneal cross-linking (PACK-CXL): A systematic review and meta-analysis,” Ocul Surf, 2019; 17(4): 624–634.
3. Kling S, Hufschmid FS, Torres-Netto EA, et al. “High fluence increases the antibacterial efficacy of PACK Cross-Linking,” Cornea, 2020; 39(8): 1020–1026.
4. Olshaker H, Achiron A, Chorny A, et al. “Accelerated high fluence photoactivated chromophore for infectious keratitis-corneal cross-linking (PACK-CXL) at the slit lamp: a pilot study,” Front Pharmacol, 2023; 14: 1229095.
Femto-CAIRS for Keratoconus
Page 29
1. Bteich Y, Assaf JF, Gendy JE, et al. “Asymmetric all-femtosecond laser-cut corneal allogenic intrastromal ring segments,” J Refract Surg, 2023; 39(12): 856–862.
2. Kozhaya K, Mehanna CJ, Jacob S, et al. “Management of anterior stromal necrosis after polymethylmethacrylate ICRS: explantation versus exchange with corneal allogenic intrastromal ring segments,” J Refract Surg, 2022; 38(4): 256–263.
3. Bteich Y, Assaf JF, Mrad AA, et al. “Corneal allogenic ring intrastromal ring segments (CAIRS) for corneal ectasia: a comprehensive segmental tomography evaluation,” J Refract Surg, 2023; 39(11): 767–776.
Addressing CXL’s Limitations
Page 30
1. Hafezi F. “Limitation of collagen cross-linking with hypoosmolar riboflavin solution: failure in an extremely thin cornea,” Cornea, Aug 2011; 30(8): 917–919. doi: 10.1097/ ICO.0b013e31820143d110
2. Hafezi F. “The Biomechanical Effect of Corneal Collagen Cross-Linking (CXL) with Riboflavin and UV-A is Oxygen Dependent,” Transl Vis Sci Technol, Nov 2013; 2(7): 6. doi: 10.1167/tvst.2.7.6
3. Kling S, Richoz O, Hammer A, et al. “Increased Biomechanical Efficacy of Corneal Cross-linking in Thin Corneas Due to Higher Oxygen Availability,” J Refract Surg, Dec 2015; 31(12): 840–846. doi: 10.3928/1081597X-20151111-08
4. Abrishamchi R, Abdshahzadeh H, Hillen M, et al. “High-Fluence Accelerated Epithelium-Off Corneal Cross-Linking Protocol Provides Dresden Protocol-Like Corneal Strengthening,” Transl Vis Sci Technol, 29 Apr 2021; 10(5): 10. doi: 10.1167/tvst.10.5.10
5. Hafezi F, Mrochen M, Iseli HP, Seiler T. “Collagen crosslinking with ultraviolet-A and hypoosmolar riboflavin solution
in thin corneas,” J Cataract Refract Surg, Apr 2009; 35(4): 621–624. doi: 10.1016/j.jcrs.2008.10.060
6. Jacob S, Kumar DA, Agarwal A, Basu S, Sinha P, Agarwal A. “Contact lens-assisted collagen cross-linking (CACXL): A new technique for cross-linking thin corneas,” J Refract Surg, Jun 2014; 30(6): 366–372. doi: 10.3928/1081597X-20140523-01
7. Wollensak G, Sporl E, Herbst H. “Biomechanical efficacy of contact lens-assisted collagen cross-linking in porcine eyes,” Acta Ophthalmol, Feb 2019; 97(1): e84-e90. doi: 10.1111/aos.13828
8. Mazzotta C, Ramovecchi V. “Customized epithelial debridement for thin ectatic corneas undergoing corneal cross-linking: epithelial island cross-linking technique,” Clin Ophthalmol, 2014; 8: 1337–1343. doi: 10.2147/OPTH.S66372
9. Omar HA, El-Agha MH, Hassaballah MA, Khalil NM. “Safety and Efficacy of Epithelial Island Crosslinking in Keratoconus with Thinnest Pachymetry less than 400micro,” Middle East Afr J Ophthalmol, Jan–Mar 2021; 28(1): 11–17. doi: 10.4103/meajo.MEAJO_186_20
10. Mazzotta C, Romani A, Burroni A. “Pachymetry-based Accelerated Crosslinking: The ‘M Nomogram’ for Standardized Treatment of All-thickness Progressive Ectatic Corneas,” International Journal of Keratoconus and Ectatic Corneal Diseases, 2018; 7(2): 137–144. doi: 10.5005/jp-journals-10025-1171
11. Hafezi F, Kling S, Gilardoni F, et al. “Individualized Corneal Cross-linking with Riboflavin and UV-A in Ultrathin Corneas: The Sub400 Protocol,” Am J Ophthalmol, Apr 2021; 224: 133–142. doi: 10.1016/j. ajo.2020.12.011
12. Kling S, Hafezi F. “An Algorithm to Predict the Biomechanical Stiffening Effect in Corneal Cross-linking,” J Refract Surg, 1 Feb 2017; 33(2): 128–136. doi: 10.3928/1081597X-20161206-01
PRIMA Implant Study Shows Promise
Page 32
1. Muqit MMK, Le Mer Y, Olmos de Koo L, et al. “Prosthetic visual acuity with the PRIMA subretinal microchip in patients with atrophic age-related macular degeneration at 4 years follow-up,” Ophthalmol Sci, 2024; 4(5): 100510.
29th ESCRS Winter Meeting Athens, Greece
April 25–28
ASCRS
Los Angeles, US
September 12–16
43rd Congress of the ESCRS
Copenhagen, Denmark
28 Feb

25 Apr


12 Sept