



Higginbotham Public Sector (833) 453-1680 www.mybenefitshub.com/santafeisd
BCBSTX (866) 355-5999 www.bcbstx.com/trsactivecare
RediMD (866) 989-2873 Option 3 www.redimd.com
Code to Register: santafeisd HEALTH
GCEFCU (281) 487-9333 www.gcefcu.org
Cigna (800) 244-6224 www.cigna.com
Cigna (800) 754-3207 www.cigna.com
EMERGENCY MEDICAL TRANSPORTATION
MASA (800) 423-3226 www.masamts.com
Cigna (800) 754-3207 www.cigna.com
New York Life (888) 842-4462 www.newyorklife.com/
CHUBB (888) 499-0425
Higginbotham (866) 419-3519 https://flexservices.higginbotham.net/ Flexclaims@higginbotham.net
EMPLOYEE ASSISTANCE PROGRAM (EAP) F INANCIAL WELLNESS AND ID PROTECTION
Lincoln Financial Group (888) 628-4824 GuidanceResources.com
Cigna (800) 244-6224 www.cigna.com
Lincoln Financial Group (800) 423-2765 www.lfg.com
Cigna (800) 754-3207 www.cigna.com
MetLife (800) 438-6388 www.metlife.com
Experian (855) 797-0052 www.experian.com
• Login and complete your benefit enrollment from 8/5/24 - 8/16/24
• Enrollment assistance is available by calling Higginbotham Public Sector at (866) 914-5202, Monday - Friday 8am-6pm. Bilingual assistance is available
• Update your profile information: home address, phone numbers, email, beneficiaries
• REQUIRED: Provide correct dependent social security numbers
Employee benefits made easy through the Benefits App!
Text “BENEFITS” to (214) 831-4286 and get access to everything you need to complete your benefits enrollment:
• Benefit Resources
• Online Enrollment
• Interactive Tools
• And more!
Text “BENEFITS” to (214) 831-4286


1
2
3
www.mybenefitshub.com/santafeisd
4
CLICK LOGIN
5
Enter your Information
• Last Name
• Date of Birth
• Last Four (4) of Social Security Number
NOTE: THEbenefitsHUB uses this information to check behind the scenes to confirm your employment status.
Once confirmed, the Additional Security Verification page will list the contact options from your profile. Select either Text, Email, Call, or Ask Admin options to receive a code to complete the final verification step.
Enter the code that you receive and click Verify. You can now complete your benefits enrollment!
During your annual enrollment period, you have the opportunity to review, change or continue benefit elections each year. Changes are not permitted during the plan year (outside of annual enrollment) unless a Section 125 qualifying event occurs.
• Changes, additions or drops may be made only during the annual enrollment period without a qualifying event.
• Employees must review their personal information and verify that dependents they wish to provide coverage for are included in the dependent profile. Additionally, you must notify your employer of any discrepancy in personal and/or benefit information.
• Employees must confirm on each benefit screen (medical, dental, vision, etc.) that each dependent to be covered is selected in order to be included in the coverage for that particular benefit.
All new hire enrollment elections must be completed in the online enrollment system within the first 31 days of benefit eligible employment. Failure to complete elections during this timeframe will result in the forfeiture of coverage.
Who do I contact with Questions?
For supplemental benefit questions, you can contact your Benefit Office or you can call Higginbotham Public Sector at (866) 914-5202 for assistance.
Where can I find forms?
For benefit summaries and claim forms, go to your benefit website: www.mybenefitshub.com/santafeisd. Click the benefit plan you need information on (i.e., Dental) and you can find the forms you need under the Benefits and Forms section.
How can I find a
For benefit summaries and claim forms, go to the Santa Fe ISD benefit website: www.mybenefitshub.com/santafeisd. Click on the benefit plan you need information on (i.e., Dental) and you can find provider search links under the Quick Links section.
If the insurance carrier provides ID cards, you can expect to receive those 3-4 weeks after your effective date. For most dental and vision plans, you can log in to the carrier website and print a temporary ID card or simply give your provider the insurance company’s phone number, and they can call and verify your coverage if you do not have an ID card at that time. If you do not receive your ID card, you can call the carrier’s customer service number to request another card.
If the insurance carrier provides ID cards, but there are no changes to the plan, you typically will not receive a new ID card each year.
The amount of coverage you can elect without answering any medical questions or taking a health exam. Guaranteed coverage is only available during initial eligibility period. Actively-at-work and/or preexisting condition exclusion provisions do apply, as applicable by carrier.
Applies to any illness, injury or condition for which the participant has been under the care of a health care provider, taken prescriptions drugs or is under a health care provider’s orders to take drugs, or received medical care or services (including diagnostic and/or consultation services).
A Cafeteria plan enables you to save money by using pre-tax dollars to pay for eligible group insurance premiums sponsored and offered by your employer. Enrollment is automatic unless you decline this benefit. Elections made during annual enrollment will become effective on the plan effective date and will remain in effect during the entire plan year.
Marital Status
Change in Number of Tax Dependents
Change in Status of Employment Affecting Coverage Eligibility
Gain/Loss of Dependents’ Eligibility Status
Judgment/ Decree/Order
Eligibility for Government Programs
Changes in benefit elections can occur only if you experience a qualifying event. You must present proof of a qualifying event to your Benefit Office within 31 days of your qualifying event and meet with your Benefit Office to complete and sign the necessary paperwork in order to make a benefit election change. Benefit changes must be consistent with the qualifying event.
A change in marital status includes marriage, death of a spouse, divorce or annulment (legal separation is not recognized in all states).
A change in number of dependents includes the following: birth, adoption and placement for adoption. You can add existing dependents not previously enrolled whenever a dependent gains eligibility as a result of a valid change in status event.
Change in employment status of the employee, or a spouse or dependent of the employee, that affects the individual’s eligibility under an employer’s plan includes commencement or termination of employment.
An event that causes an employee’s dependent to satisfy or cease to satisfy coverage requirements under an employer’s plan may include change in age, student, marital, employment or tax dependent status.
If a judgment, decree, or order from a divorce, annulment or change in legal custody requires that you provide accident or health coverage for your dependent child (including a foster child who is your dependent), you may change your election to provide coverage for the dependent child. If the order requires that another individual (including your spouse and former spouse) covers the dependent child and provides coverage under that individual’s plan, you may change your election to revoke coverage only for that dependent child and only if the other individual actually provides the coverage.
Gain or loss of Medicare/Medicaid coverage may trigger a permitted election change.
Supplemental Benefits: Eligible employees must work 20 or more regularly scheduled hours each work week. Eligible employees must be actively at work on the plan effective date for new benefits to be effective, meaning you are physically capable of performing the functions of your job on the first day of work concurrent with the plan effective date. For example, if your 2024 benefits become effective on September 1, 2024, you must be actively-at-work on September 1, 2024 to be eligible for your new benefits.
Dependent Eligibility: You can cover eligible dependent children under a benefit that offers dependent
coverage, provided you participate in the same benefit, through the maximum age listed below. Dependents cannot be double covered by married spouses within the district as both employees and dependents.
You are performing your regular occupation for the employer on a full-time basis, either at one of the employer’s usual places of business or at some location to which the employer’s business requires you to travel. If you will not be actively at work beginning 9/1/2024 please notify your benefits administrator.
Please note, limits and exclusions may apply when obtaining coverage as a married couple or when obtaining coverage for dependents.
Potential Spouse Coverage Limitations: When enrolling in coverage, please keep in mind that some benefits may not allow you to cover your spouse as a dependent if your spouse is enrolled for coverage as an employee under the same employer. Review the applicable plan documents, contact Higginbotham Public Sector, or contact the insurance carrier for additional information on spouse eligibility.
FSA/HSA Limitations: Please note, in general, per IRS regulations, married couples may not enroll in both a Flexible Spending Account (FSA) and a Health Savings Account (HSA). If your spouse is covered under an FSA that reimburses for medical expenses then you and your spouse are not HSA eligible, even if you would not use your spouse’s FSA to reimburse your expenses. However, there are some exceptions to the general limitation regarding specific types of FSAs. To obtain more information on whether you can enroll in a specific type of FSA or HSA as a married couple, please reach out to the FSA and/or HSA provider prior to enrolling or reach out to your tax advisor for further guidance.
Potential Dependent Coverage Limitations: When enrolling for dependent coverage, please keep in mind that some benefits may not allow you to cover your eligible dependents if they are enrolled for coverage as an employee under the same employer. Review the applicable plan documents, contact Higginbotham Public Sector, or contact the insurance carrier for additional information on dependent eligibility.
Disclaimer: You acknowledge that you have read the limitations and exclusions that may apply to obtaining spouse and dependent coverage, including limitations and exclusions that may apply to enrollment in Flexible Spending Accounts and Health Savings Accounts as a married couple. You, the enrollee, shall hold harmless, defend, and indemnify Higginbotham Public Sector from any and all claims, actions, suits, charges, and judgments whatsoever that arise out of the enrollee’s enrollment in spouse and/or dependent coverage, including enrollment in Flexible Spending Accounts and Health Savings Accounts.
If your dependent is disabled, coverage may be able to continue past the maximum age under certain plans. If you have a disabled dependent who is reaching an ineligible age, you must provide a physician’s statement confirming your dependent’s disability. Contact your Benefit Office to request a continuation of coverage.
Description
(IRC Sec. 223)
Approved by Congress in 2003, HSAs are actual bank accounts in employee’s names that allow employees to save and pay for unreimbursed qualified medical expenses tax-free.
Employer Eligibility A qualified high deductible health plan
Contribution Source Employee and/or employer
Account Owner Individual
Underlying Insurance
Requirement High deductible health plan
Minimum Deductible
Maximum Contribution
Permissible Use Of Funds
Cash-Outs of Unused Amounts (if no medical expenses)
Year-to-year rollover of account balance?
$1,600 single (2024)
$3,200 family (2024)
$4,150 single (2024)
$8,300 family (2024) 55+ catch up +$1,000
Employees may use funds any way they wish. If used for non-qualified medical expenses, subject to current tax rate plus 20% penalty.
(IRC Sec. 125)
Allows employees to pay out-of-pocket expenses for copays, deductibles and certain services not covered by medical plan, taxfree. This also allows employees to pay for qualifying dependent care tax-free.
All employers
Employee and/or employer
Employer
None
N/A
$3,200 (2024)
Reimbursement for qualified medical expenses (as defined in Sec. 213(d) of IRC).
Permitted, but subject to current tax rate plus 20% penalty (penalty waived after age 65). Not permitted
Yes, will roll over to use for subsequent year’s health coverage.
Does the account earn interest? Yes
Portable?
$570 Rollover - At the end of the plan year, any remaining balance $570 or less will be forwarded to the next plan year. An amount remaining above $570 will be forfeited.
No
Yes, portable year-to-year and between jobs. No
Major medical insurance is a type of health care coverage that provides benefits for a broad range of medical expenses that may be incurred either on an inpatient or outpatient basis.
For full plan details, please visit your benefit website: www.mybenefitshub.com/santafeisd

Go ahead and sign up for the Houston rodeo –
are covered with


Learn the Terms.
• Premium: The monthly amount you pay for health care coverage.
• Deductible: The annual amount for medical expenses you’re responsible to pay before your plan begins to pay.
• Copay: The set amount you pay for a covered service at the time you receive it. The amount can vary based on the service.
• Coinsurance: The portion you’re required to pay for services after you meet your deductible. It’s often a specified percentage of the costs; e.g., you pay 20% while the health care plan pays 80%.
• Out-of-Pocket Maximum: The maximum amount you pay each year for medical costs. After reaching the out-of-pocket maximum, the plan pays 100% of allowable charges for covered services.
A Health Savings Account (HSA) is a personal savings account where the money can only be used for eligible medical expenses. Unlike a flexible spending account (FSA), the money rolls over year to year however only those funds that have been deposited in your account can be used. Contributions to a Health Savings Account can only be used if you are also enrolled in a High Deductible Health Care Plan (HDHP).
For full plan details, please visit your benefit website: www.mybenefitshub.com/santafeisd
A Health Savings Account (HSA) is more than a way to help you and your family cover health care costs – it is also a tax-exempt tool to supplement your retirement savings and cover health expenses during retirement. An HSA can provide the funds to help pay current health care expenses as well as future health care costs.
A type of personal savings account, an HSA is always yours even if you change health plans or jobs. The money in your HSA (including interest and investment earnings) grows tax-free and spends tax-free if used to pay for qualified medical expenses. There is no “use it or lose it” rule — you do not lose your money if you do not spend it in the calendar year — and there are no vesting requirements or forfeiture provisions. The account automatically rolls over year after year.
You are eligible to open and contribute to an HSA if you are:
• Enrolled in an HSA-eligible HDHP
• Not covered by another plan that is not a qualified HDHP, such as your spouse’s health plan
• Not enrolled in a Health Care Flexible Spending Account, nor should your spouse be contributing towards a Health Care Flexible Spending Account
• Not eligible to be claimed as a dependent on someone else’s tax return
• Not enrolled in Medicare or TRICARE
• Not receiving Veterans Administration benefits
You can use the money in your HSA to pay for qualified medical expenses now or in the future. You can also use HSA funds to pay health care expenses for your dependents, even if they are not covered under your HDHP.
Your HSA contributions may not exceed the annual maximum amount established by the Internal Revenue Service. The annual contribution maximum for 2024 is based on the coverage option you elect:
• Individual – $4,150
• Family (filing jointly) – $8,300

You decide whether to use the money in your account to pay for qualified expenses or let it grow for future use. If you are 55 or older, you may make a yearly catch-up contribution of up to $1,000 to your HSA. If you turn 55 at any time during the plan year, you are eligible to make the catch-up contribution for the entire plan year.
To get started with your new HSA, you will enroll with Santa Fe ISD. Afterwards, Gulf Coast Educators FCU will service your HSA, and mail your new benefit cards to the address listed in THEbenefitsHUB. You will have the option to make pre-tax deductions straight from your paycheck, or transfer funds as you are able.
• Always ask your health care provider to file claims with your medical provider so network discounts can be applied. You can pay the provider with your HSA debit card based on the balance due after discount.
• You, not your employer, are responsible for maintaining ALL records and receipts for HSA reimbursements in the event of an IRS audit.
Participant Account Web Access: www.gcefcu.org
Participants may call Gulf Coast Educators FCU and talk to a representative during regular business hours, Monday - Friday, 7 am to 7 pm CST, and on Saturday from 9 am to 12 pm CST. Participants may also log into their GCEFCU online banking account at any time to view their balance, account history, and make transfers to their HSA.
This is an affordable supplemental plan that pays you should you be inpatient hospital confined. This plan complements your health insurance by helping you pay for costs left unpaid by your health insurance.
For full plan details, please visit your benefit website: www.mybenefitshub.com/santafeisd
Prepared for: Santa Fe Independent School District

Hospital Care coverage provides a benefit according to the schedule below when a Covered Person incurs a Hospital stay or undergoes a broad range of medical treatments or care resulting from a Covered Injury or Covered Illness
Who Can Elect Coverage:
Eligibility for You, Your Spouse and Your Children will be considered by Your employer.
You: All active, Full-time Employees of the Employer who are regularly working in the United States a minimum of 20 hours per week and regularly residing in the United States and who are United States citizens or permanent resident aliens or non-United States citizens legally working and living in the United States (Inpats) and their Spouse, Domestic Partner, or Civil Union Partner and Dependent Children who are United States citizens or permanent resident aliens or Spouse, Domestic Partner, or Civil Union Partner or Dependent Child Inpats and who are legally residing in the United States.
You will be eligible for coverage on the first of the month after date of hire or Active Service. Your Spouse/Domestic Partner: Up to age 100, as long as you apply for and are approved for coverage yourself. Your Child(ren): Birth to age 26; 26+ if disabled, as long as you apply for and are approved for coverage yourself.
Available Coverage:
The benefit amounts shown in this summary will be paid regardless of the actual expenses incurred and are paid on a per day basis unless otherwise specified. Benefits are only payable when all policy terms and conditions are met. Please read all the information in this summary to understand the terms, conditions, state variations, exclusions and limitations applicable to these benefits. See your Certificate of Insurance for more information.
Benefit Waiting Period:* None, unless otherwise stated. No benefits will be paid for a loss which occurs during the Benefit Waiting Period.
NOTE: This insurance is NOT a substitute for comprehensive or major medical insurance coverage.
Hospital Admission
No Elimination Period. Limited to 1 day, 1 benefit(s) every 365 days.
Hospital Chronic Condition Admission
No Elimination Period. Limited to 1 day, 1 benefit(s) every 90 days.
Hospital Stay
No Elimination Period. Limited to 30 days, 1 benefit(s) every 90 days.
Hospital Intensive Care Unit (ICU) Stay
No Elimination Period. Limited to 30 days, 1 benefit(s) every 90 days.
Hospital Observation Stay
24 Elimination Period. Limited to 72 hours.
Newborn Nursery Care Admission
Limited to 1 day, 1 benefit per newborn child. This benefit is payable to the employee even if child coverage is not elected.
per 24-hour period $500 per 24-hour period
Abuse Facility Care
No Elimination Period. Limited to 30 days, 30 day lifetime maximum.
Mental Illness and Nervous Disorder Facility Care
No Elimination Period. Limited to 30 days, 30 day lifetime maximum.
Wellness Treatment, Health Screening Test and Preventative Care Benefit*
Also includes COVID-19 Immunization, Tests, and Screenings. Virtual Care accepted.
Costs are subject to change. Actual per pay period premiums may differ slightly due to rounding.
Benefit Amounts Payable: Benefits for all Covered Persons are payable at 100% of the Benefit Amounts shown, unless otherwise stated. Late applicants, if allowed under this plan, may be required to provide medical evidence of insurability.
Benefit-Specific Conditions, Exclusions & Limitations (Hospital Care):
Hospital Admission: Must be admitted as an Inpatient due to a Covered Injury or Covered Illness. Excludes: treatment in an emergency room, provided on an outpatient basis, or for re-admission for the same Covered Injury or Covered Illness (including chronic conditions).
Hospital Chronic Condition Admission: Must be admitted as an Inpatient due to a covered chronic condition and treatment for a covered chronic condition must be provided by a specialist in that field of medicine. Excludes: treatment in an emergency room, provided on an outpatient basis, or for re-admission for the same Covered Injury or Covered Illness (including chronic conditions).
Hospital Stay: Must be admitted as an Inpatient and confined to the Hospital, due to a Covered Injury or Covered Illness, at the direction and under the care of a physician. If also eligible for the ICU Stay Benefit, only 1 benefit will be paid for the same Covered Injury or Covered Illness, whichever is greater. Hospital stays within 90 days for the same or a related Covered Injury or Covered Illness is considered one Hospital Stay.
Intensive Care Unit (ICU) Stay: Must be admitted as an Inpatient and confined in an ICU of a Hospital, due to a Covered Injury or Covered Illness, at the direction and under the care of a physician. If also eligible for the Hospital Stay Benefit, only 1 benefit will be paid for the same Covered Injury or Covered Illness, whichever is greater. ICU stays within 90 days for the same or a related Covered Injury or Covered Illness is considered one ICU stay.
Hospital Observation Stay: Must be receiving treatment for a Covered Injury or Covered Illness in a Hospital, including an observation room, or ambulatory surgical center, for more than 24 hours on a non-inpatient basis and a charge must be incurred. This benefit is not payable if a benefit is payable under the Hospital Stay Benefit or Hospital Intensive Care Unit Stay Benefit.
Newborn Nursery Care Admission: Must be admitted as an Inpatient and confined in a Hospital immediately following birth at the direction and under the care of a physician.
Benefit-Specific Conditions, Exclusions & Limitations (Additional Care Benefits):
• Excludes routine health examinations or immunizations or for visits
by a Physician or other licensed health care professional while confined to a Hospital.
• Some benefits require services to be performed, prescribed or recommended by a Physician
• Substance Abuse Facility Care: Must be confined in such facility due to a Covered Injury or Covered Illness at the direction and under the care of a physician or licensed health care professional. Care must begin within 30 days of a 1 day(s) Hospital or ICU Stay. Benefits are not payable during same period as a Hospital, ICU stay or other Facility Stay. Facility stays or care provided within 90 days for the same or a related Covered Injury or Covered Illness is considered one stay or one period of care. Benefits for care beginning during the Benefit Waiting Period will payable after such period. For a Substance Abuse Facility, the facility must charge room and board for treatment services. The exclusions that apply to this benefit are in the Common Exclusions Section, except: (5) Voluntary ingestion of any narcotic, drug, poison, gas or fumes, unless prescribed or taken under the direction of a Physician and taken in accordance with the prescribed dosage; (6) Operating any type of vehicle while under the influence of alcohol or any drug, narcotic or other intoxicant including any prescribed drug for which the Covered Person has been provided a written warning against operating a vehicle while taking it. “Under the influence of alcohol”, for purposes of this exclusion, means intoxicated, as defined by the law of the state in which the Covered Injury or Covered Illness occurred.
• Mental Illness and Nervous Disorder Facility Care: Must be confined in such facility due to a Covered Injury or Covered Illness at the direction and under the care of a physician or licensed health care professional. Care must begin within 30 days of a 1 day(s) Hospital or ICU Stay. Benefits are not payable during same period as a Hospital, ICU stay or other Facility Stay. Facility stays or care provided within 90 days for the same or a related Covered Injury or Covered Illness is considered one stay or one period of care. Benefits for care beginning during the Benefit Waiting Period will payable after such period. The exclusions that apply to this benefit are in the Common Exclusions Section, except: (1) Intentionally selfinflicted Injury, suicide or any attempt thereat while sane or insane.
Dental insurance is a coverage that helps defray the costs of dental care. It insures against the expense of routine care, dental treatment and disease.
For full plan details, please visit your benefit website: www.mybenefitshub.com/santafeisd
Our dental plan helps you maintain good oral health through affordable options for preventive care, including regular checkups and other dental work. Premium contributions are deducted from your paycheck on a pretax basis. Coverage is provided through Cigna
You may select the dental provider of your choice, but your level of coverage may vary based on the provider you see for services. You could pay more if you use an out-of-network provider.
DHMO Plan
• You choose your primary-care dentist when you enroll. To find a participating dentist, visit http://ldc.lfg.com and select Find a Dentist. (You can also print your dental ID card from this site once your coverage begins.)
• This dental plan offers a detailed list of covered procedures, each with a dollar copayment (see the Summary of Benefits on Benefits Portal for details). You pay for services provided during your visit.
• Emergency care away from home is covered up to a set dollar limit.
• You can change your primary-care dentist at any time by calling the customer service number listed on your dental ID card.
• Covers most preventive and diagnostic care services at no charge
• Also covers a wide variety of specialty services - lowering your out-of-pocket costs with no deductibles or maximums
Vision insurance provides coverage for routine eye examinations and can help with covering some of the costs for eyeglass frames, lenses or contact lenses.
For full plan details, please visit your benefit website: www.mybenefitshub.com/santafeisd
Cigna Health and Life Insurance Company
Cigna Vision serviced by EyeMed
Santa Fe Independent School District
C1 PPO Comprehensive Plan
Welcome to Cigna Vision
Lined
Lens Enhancements / Options: Oversize lenses Rose #1 and #2 Solid Tints Polycarbonate Lenses Progressives Plastic Dye Tints
Photochromic – Glass or Plastic
Scratch Coating
Ultraviolet (UV) Coating
Anti-Reflective (AR) Coating
Hi-Index Lenses
All
Contact Lenses Retail Allowance: Frequency*: one pair or single purchase per 12 month
Frame Retail Allowance Frequency*: one per 12 month
* Your Frequency Period begins on January 1 (Calendar year basis)
Definitions:
Copay: the amount you pay towards your exam and/or materials, lenses and/or frames
Coinsurance: the percentage of charges Cigna will pay. Customer is financially responsible for the balance.
Allowance: the maximum amount Cigna will pay. Customer is financially responsible for any amount over the allowance.
In-Network Coverage Includes**:
• One vision and eye health evaluation including but not limited to eye health examination, dilation, refraction, and prescription for glasses;
• Retinal Screening for non-medically necessary retinal imaging, which takes digital pictures of the inside of the eye. Does not replace dilation.
• Contact Lens Professional Services including the fitting, evaluation and two follow-up visits, covered under the contact lens materials allowance, unless otherwise stated above
• One pair of standard prescription plastic or glass lenses, all ranges of prescriptions (powers and prisms) including Oversize, Rose #1 or #2 Solid Tint and Polycarbonate lenses. | 20% savings on all additional lens enhancements/ option you choose for your lenses, not shown on the Schedule of Vision Coverage above.
• One pair of Elective conventional contact lenses or a single purchase of a supply of disposable contact lenses – in lieu of lenses and frame benefit, (may not receive contact lenses and frames in same benefit year).
• Coverage for Therapeutic contact lenses will be provided when visual acuity cannot be corrected to 20/70 in the better eye with eyeglasses and the fitting of the contact lenses would obtain this level of visual acuity; and in certain cases of anisometropia, keratoconus, or aphakis; as determined and documented by your Vision eye care professional. Contact lenses fitted for other therapeutic purposes or the narrowing of visual fields due to high minus or plus correction will be covered in accordance with the Elective contact lens coverage shown on the Schedule of Vision Coverage.
• One frame for prescription lenses – frame of choice covered up to retail plan allowance, plus a 20% savings on amount that exceeds frame allowance;
** Coverage may vary at participating discount retail and membership club optical locations, please contact Customer Service for specific coverage information.
*** Provider participation is 100% voluntary; please check with your Eye Care Professional for any offered discounts.
• Orthoptic or vision training and any associated supplemental testing
• Medical or surgical treatment of the eyes
• Any eye examination, or any corrective eyewear, required by an employer as a condition of employment
• Any injury or illness when paid or payable by Workers’ Compensation or similar law, or which is work-related
• Charges in excess of the usual and customary charge for the Service or Materials
• Charges incurred after the policy ends or the insured’s coverage under the policy ends, except as stated in the policy
• Experimental or non-conventional treatment or device
• Magnification or low vision aids not shown as covered in the Schedule of Vision Coverage
• Any non-prescription (minimum Rx required) eyeglasses, includes frame, lenses, or contact lenses
• Spectacle lens treatments, “add-ons”, or lens coatings not shown as covered in the Schedule of Vision Coverage
• Prescription sunglasses lens “add-ons”, or lens coatings not shown as covered in the Schedule of Vision Coverage
• Two pair of glasses, in lieu of bifocals or trifocals
• Safety glasses or lenses required for employment not shown as covered in the Schedule of Vision Coverage
• VDT (video display terminal)/computer eyeglass benefit
• Claims submitted and received in excess of twelve (12) months from the original Date of Service
• Up to 40% off additional complete pairs of glasses (frame and lenses)
• 20% off any item not covered by the plan, including nonprescription sunglasses, but excluding professional services
Interested in Laser Vision Correction service such as LASIK? Visit your MyCigna.com and search for Healthy Rewards® for details.
Disability insurance protects one of your most valuable assets, your paycheck. This insurance will replace a portion of your income in the event that you become physically unable to work due to sickness or injury for an extended period of time.
For full plan details, please visit your benefit website: www.mybenefitshub.com/santafeisd
If you had an unexpected illness or injury and were unable to work, how long would you be able to pay your bills and take care of your family? Disability insurance pays a portion of your salary if you’re unable to work due to a covered disability.
By purchasing coverage through your employer, you also benefit from cost-effective group rates and convenient payroll deduction.
Eligibility:
If you are an active employee working at least 20 hours per week, you will be eligible immediately.
Initial Enrollment: If you are eligible on or before the policy’s effective date, you may enroll for coverage during the Initial Enrollment without submitting any evidence of good health.
New Hires: If you were hired after the policy’s effective date, you may elect coverage once eligible without submitting any evidence of good health.
Annual Enrollment: During annual enrollment, you may enroll for the first time or make coverage changes, if already participating, without submitting any evidence of good health.
*The Pre-Existing Condition Limitation, as outlined in the Benefit Reductions, Conditions, Limitations and Exclusions section, will apply.
Please refer to the “Maximum
Schedules below for more details
Maximum Benefit Period Schedule
Premium Plan
The later of your SSNRA* or the Maximum Benefit Period listed below.
Age When Disability Begins
Age 62 or under
Age 63
Age 64
Age 65
Age 66
Age 67
Age 68
Age 69 or older
Select Plan
Maximum Benefit Period
The later of your SSNRA* or the date the 42nd Monthly Benefit is payable.
The later of your SSNRA* or the date the 36th Monthly Benefit is payable.
The later of your SSNRA* or the date the 30th Monthly Benefit is payable.
The date the 24th Monthly Benefit is payable.
The date the 21st Monthly Benefit is payable.
The date the 18th Monthly Benefit is payable.
The date the 15th Monthly Benefit is payable.
The date the 12th Monthly Benefit is payable.
For Disabilities Resulting From an Accident
The date the 36th Monthly Benefit is payable.
Age When Disability Begins
Age 62 or under
Age 63
Age 64
Age 65
Age 66
Age 67
Age 68
Age 69 or older
Maximum Benefit Period
The later of your SSNRA* or the date the 42nd Monthly Benefit is payable.
The later of your SSNRA* or the date the 36th Monthly Benefit is payable.
The later of your SSNRA* or the date the 30th Monthly Benefit is payable.
The date the 24th Monthly Benefit is payable.
The date the 21st Monthly Benefit is payable.
The date the 18th Monthly Benefit is payable.
The date the 15th Monthly Benefit is payable.
The date the 12th Monthly Benefit is payable.
*SSNRA means the Social Security Normal Retirement Age in effect under the Social Security Act on the Policy Effective Date.
Pre-existing Condition Limitation:
We will not pay benefits for any period of Disability caused or contributed to by, or resulting from, a Pre-existing Condition. A “Preexisting Condition” means any Injury or Sickness for which you received medical treatment, care or services including diagnostic measures, took prescribed drugs or medicines within 12 months before your effective date of insurance.
The Pre-existing Condition Limitation will apply to any added benefits or increases in benefits. This limitation will not apply to a period of Disability that begins after you are covered for at least 12 months after your effective date of insurance, or the effective date of any added or increased benefits.
We will waive the Pre-Existing Condition Limitation for the first 4 weeks of Disability even if you have a Pre-Existing Condition. The Disability Benefits as shown in the Schedule of Benefits will continue beyond 4 weeks only if the Pre-Existing Condition Limitation does not apply.
You may elect to increase or decrease coverage during Annual Enrollment. If you are insured for the maximum benefit amount allowed based on your Covered Earnings and you receive an increase in Covered Earnings, the Pre-Existing Condition Limitation will not apply to the increased amount if you elect, during the following Annual Enrollment, to increase your benefit to the new maximum amount.
If you are insured under the disability plan you may enroll in a plan option with a shorter Benefit Waiting Period during a subsequent annual enrollment. If you become Disabled and are subject to the Pre-Existing Condition Limitation for any period of Disability caused or contributed by, or resulting from, a Pre-Existing Condition, benefits may be paid on a limited basis as outlined in the PreExisting Condition Waiver provision. Once benefits have been exhausted under the Pre-Existing Condition Waiver provision they may recommence if the Benefit Waiting Period of the previously elected option and all other provisions of the plan are satisfied.
If you are insured under the disability plan you may enroll in a plan option with a shorter Benefit Waiting Period during a subsequent annual enrollment. If you become Disabled and are subject to the Pre-Existing Condition Limitation for any period of Disability caused or contributed by, or resulting from, a Pre-Existing Condition, benefits may be paid if the Benefit Waiting Period of the previously elected option and all other provisions of the plan are satisfied.
What is disability insurance? Disability insurance protects one of your most valuable assets, your paycheck. This insurance will replace a portion of your income in the event that you become physically unable to work due to sickness or injury for an extended period of time. This type of disability plan is called an educator disability plan and includes both long and short term coverage into one convenient plan.
Pre-Existing Condition Limitations - Please note that all plans will include pre-existing condition limitations that could impact you if you are a first-time enrollee in your employer’s disability plan. This includes during your initial new hire enrollment. Please review your plan details to find more information about preexisting condition limitations.
How do I choose which plan to enroll in during my open enrollment?
1. First choose your elimination period. The elimination period, sometimes referred to as the waiting period, is how long you are disabled and unable to work before your benefit will begin. This will be displayed as 2 numbers such as 0/7, 14/14, 30/30, 60/60, 90/90, etc.
The first number indicates the number of days you must be disabled due to Injury and the second number indicates the number of days you must be disabled due to Sickness
When choosing your elimination period, ask yourself, “How long can I go without a paycheck?” Based on the answer to this question, choose your elimination period accordingly.
Important Note - some plans will waive the elimination period if you choose 30/30 or less and you are confined as an inpatient to the hospital for a specific time period. Please review your plan details to see if this feature is available to you.
2. Next choose your benefit amount. This is the maximum amount of money you would receive from the carrier on a monthly basis once your disability claim is approved by the carrier.
When choosing your monthly benefit, ask yourself, “How much money do I need to be able to pay my monthly expenses?” Based on the answer to this question, choose your monthly benefit accordingly.
Choose your desired elimination period.
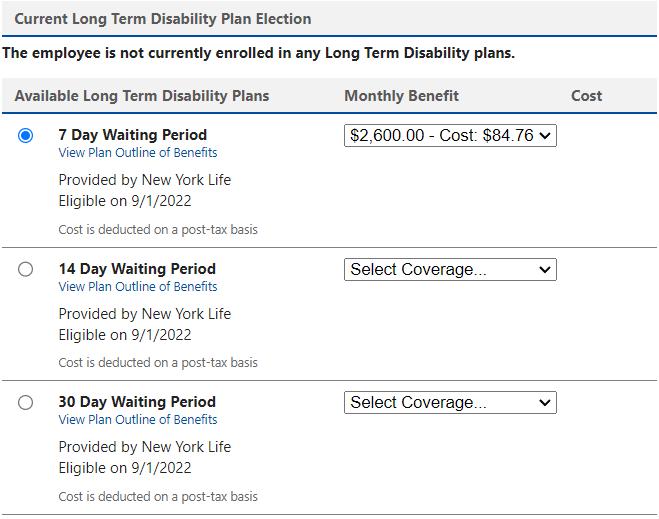
Choose your Benefit Amount from the drop down box.
Group term life is the most inexpensive way to purchase life insurance. You have the freedom to select an amount of life insurance coverage you need to help protect the well-being of your family.
Accidental Death & Dismemberment is life insurance coverage that pays a death benefit to the beneficiary, should death occur due to a covered accident. Dismemberment benefits are paid to you, according to the benefit level you select, if accidentally dismembered.
For full plan details, please visit your benefit website: www.mybenefitshub.com/santafeisd

Critical illness insurance can be used towards medical or other expenses. It provides a lump sum benefit payable directly to the insured upon diagnosis of a covered condition or event, like a heart attack or stroke. The money can also be used for non-medical costs related to the illness, including transportation, child care, etc.
For full plan details, please visit your benefit website: www.mybenefitshub.com/santafeisd
Prepared for: Santa Fe Independent School District

Critical Illness insurance provides a cash benefit when a Covered Person is diagnosed with a covered critical illness or event after coverage is in effect.
Available Coverage:
The benefit amounts shown will be paid regardless of the actual expenses incurred. The benefit descriptions are a summary only. There are terms, conditions, state variations, exclusions and limitations applicable to these benefits. Please read all of the information in this Summary and your Certificate of Insurance for more information. All Covered Critical Illness Conditions must be due to disease or sickness.
The benefit amount shown will be paid regardless of the actual expenses incurred and is paid on a per day basis. Also includes COVID-19 Immunization, Tests, and Screenings. Virtual Care accepted. $50 1 per year
If you are a new hire you are not required to provide proof of good health if you enroll during your employer’s eligibility waiting period and you choose an amount of coverage up to and including the Guaranteed Issue Amount. If you apply for an amount of coverage greater than the Guaranteed Issue Amount, coverage in excess of the Guaranteed Issue Amount will not be issued until the insurance company approves acceptable proof of good health. Guaranteed Issue coverage may be available at other specified periods of time. Your employer will notify you when these periods of time are available. Your Spouse must be age 18 or older to apply if evidence of insurability is required.
Covered Person: An eligible person who is enrolled for coverage under the Policy.
Covered Loss: A loss that is specified in the Policy in the Schedule of Benefits section and suffered by the Covered Person within the applicable time period described in the Policy.
When your coverage begins: Coverage begins on the later of the program’s effective date, the date you become eligible, the first of the month following the date your completed enrollment form is received, or if evidence of insurability is required, the first of the month after we have approved you (or your dependent) for coverage in writing, unless otherwise agreed upon by Cigna. Your coverage will not begin unless you are actively at work on the effective date. Coverage for all other Covered Persons will not begin on the effective date if the covered person is confined to a hospital, facility or at home, disabled or receiving disability benefits or unable to perform activities of daily living.
When your coverage ends: Coverage ends on the earliest of the date you and your dependents are no longer eligible, the date the group policy is no longer in force, or the date for the last period for which required premiums are paid. For your dependent, coverage also ends when your coverage ends, when their premiums are not paid or when they are no longer eligible. (Under certain circumstances, your coverage may be continued. Be sure to read the provisions in your Certificate about when coverage may continue.)
30 Day Right to Examine Certificate: If a Covered Person is not satisfied with the Certificate of Insurance for any reason, it may be returned to us within 30 days of receipt. We will return any premium that has been paid, and the Certificate will be void as if it had never been issued.
Cancer insurance offers you and your family supplemental insurance protection in the event you or a covered family member is diagnosed with cancer. It pays a benefit directly to you to help with expenses associated with cancer treatment.
For full plan details, please visit your benefit website: www.mybenefitshub.com/santafeisd

$100
Employee or spouse: $5,000
Child(ren): $7,500
Diagnosis of cancer
Hospital confinement
Hospital confinement ICU
Radiation therapy, chemotherapy, immunotherapy
Alternative care
Medical imaging
Skin cancer initial diagnosis
Attending physician
Hospital confinement sub-acute ICU
Waiting period: 0 days
Benefit reduction: none
$300 per day – days 1 through 30
Additional days: $600
Maximum days per confinement: 31
$600 per day – days 1 through 30
Additional days: $600
Maximum days per confinement: 31
Maximum per covered person per calendar year 12-month period: $10,000
$75 per visit
Maximum visits per calendar year: 4
$500 per imaging study
Maximum studies per calendar year: 2
$100 per diagnosis
Lifetime maximum: 1
$50 per visit
Maximum visits per confinement: 2
Maximum visits per calendar year: 4
$300 per day – days 1 through 30
Additional days: $300
Maximum days per confinement: 31
Childcare: $100 per day per child
Maximum days per calendar year: 30
Family care
Adult day care or home healthcare:
$100 per day
Maximum days per calendar year: 30
$100 paid upon receipt of first covered claim for cancer; only one payment per covered person per certificate per calendar year
Employee or spouse: $10,000
Child(ren): $15,000
Waiting period: 0 days
Benefit reduction: none
$300 per day – days 1 through 30
Additional days: $600
Maximum days per confinement: 31
$600 per day – days 1 through 30
Additional days: $600
Maximum days per confinement: 31
Maximum per covered person per calendar year 12-month period: $20,000
$75 per visit
Maximum visits per calendar year: 4
$500 per imaging study
Maximum studies per calendar year: 2
$100 per diagnosis
Lifetime maximum: 1
$50 per visit
Maximum visits per confinement: 2
Maximum visits per calendar year: 4
$300 per day – days 1 through 30
Additional days: $300
Maximum days per confinement: 31
Childcare: $100 per day per child
Maximum days per calendar year: 30
Adult day care or home healthcare: $100 per day
Maximum days per calendar year: 30
Prescription drug in-patient
Private full-time nursing services
U.S. government or charity hospital
Renewability
Portability
Per confinement: $150
Maximum confinements per calendar year: 6
$150 per day
Maximum days per confinement: 5
Days 1 through 30: $300
Additional days: $600
Maximum days per confinement: 15
Per confinement: $150
Maximum confinements per calendar year: 6
$150 per day
Maximum days per confinement: 5
Days 1 through 30: $300
Additional days: $600
Maximum days per confinement: 15
Conditionally Renewable Coverage is automatically renewed as long as the insured is an eligible employee, premiums are paid as due, and the policy is in force.
Portability Employees can keep their coverage if they change jobs or retire while the policy is in-force.
Continuity of coverage Included
Pre-existing conditions limitation
A condition for which a covered person received medical advice or treatment within the 12 months preceding the certificate effective date.
Waiver of premium Included
If the certificate replaced another cancer indemnity certificate or individual policy, your coverage under the certificate shall not limit or exclude coverage for a pre-existing condition or waiting period that would have been covered under the policy being replaced.
Continuity of coverage
Benefits payable for a pre-existing condition or during the waiting period will be the lesser of the benefits that would have been payable under the terms of the prior coverage if it had remained in force; or the benefits payable under the certificate.
Time periods applicable to pre-existing conditions and waiting periods will be waived to the extent that similar limitations or exclusions were satisfied under the coverage being replaced.
Continuity of coverage is only extended to the benefits provided under the certificate. The certificate may not include all the benefits provided under the prior coverage.
Cancer means carcinoma in situ, leukemia, or a malignant tumor characterized by uncontrolled cell growth and invasion or spread of malignant cells to distant tissue. Cancer is also defined as cancer which meets the diagnosis criteria of malignancy established by the American Board of Pathology after a study of the histocytologic architecture or pattern of the suspect tumor, tissue, or specimen.
Carcinoma in situ means a malignant tumor which is typically classified as Stage 0 cancer, where the tumor cells still lie within the tissue of the site of origin without having invaded neighboring tissue.
The following are not considered cancer: Pre-malignant conditions or conditions with malignant potential; non-invasive basal cell carcinoma of the skin; non-invasive squamous cell carcinoma of the skin; or melanoma diagnosed as Clark’s Level I or II or Breslow less than .75mm.
Plan descriptions Refer to the Certificate of Coverage for details specific to each plan.
No benefits will be paid for a date of diagnosis or treatment of cancer prior to the coverage effective date, except where continuity of coverage applies. No benefits will be paid for services rendered by a member of the immediate family of a covered person.
We will not pay benefits for other conditions or diseases, except losses due directly from cancer or skin cancer.
We will not pay benefits for cancer or skin cancer if the diagnosis or treatment of cancer is received outside of the territorial limits of the United States and its possessions. Benefits will be payable if the covered person returns to the territorial limits of the United States and its possessions, and a physician confirms the diagnosis or receives treatment.
Do you have kids playing sports, are you a weekend warrior, or maybe accident-prone? Accident plans are designed to help pay for medical costs associated with accidents and benefits are paid directly to you.
For full plan details, please visit your benefit website: www.mybenefitshub.com/santafeisd

Prepared for: Santa Fe Independent School District
Available Coverage:
This Accidental Injury plan provides 24 hour coverage. The benefit amounts shown in this summary will be paid regardless of the actual expenses incurred and are paid on a per day basis unless otherwise specified. Benefits are only payable when all policy terms and conditions are met. Please read all the information in this summary to understand terms, conditions, state variations, exclusions and limitations applicable to these benefits. See your Certificate of Insurance for more information.
Accidental Death and Dismemberment Benefit
Examples of benefits include (but are not limited to) payment for death from Automobile accident; total and permanent loss of speech or hearing in both ears. Actual benefit amount paid depends on the type of Covered Loss. The Spouse and Child benefit is 50% and 25% respective of the benefit shown.
Wellness Treatment, Health Screening Test & Preventive Care Benefit*
Wellness Treatment, Health Screening Test and Preventive Care Benefit:* Benefit paid for all covered persons is 100% of the benefit shown. Also includes COVID-19 Immunization, Tests, and Screenings. Virtual Care accepted.
Sports Accident Benefit
Organized and Personal Sports Activity
Limited to 10 per year
Portability Feature: You, your spouse, and child(ren) can continue 100% of your coverage at the time your coverage ends. You must be under the age of 100 in order to continue your coverage. Rates may change and all coverage ends at age 100. Applies to United States Citizens and Permanent Resident Aliens residing in the United States. Only available to United States Citizens, Permanent Resident Aliens and non-United States Citizens working in the United States lawfully (Inpats) while residing in the United States. Employee’s Monthly
Costs are subject to change. Actual per pay period premiums may differ slightly due to rounding.
Coverage Type: Benefits are paid when a Covered Injury results, directly and independently of all other causes, from a Covered Accident.
Covered Accident: A sudden, unforeseeable, external event that results, directly and independently of all other causes, in a Covered Injury or Covered Loss and occurs while the Covered Person is insured under this Policy; is not contributed to by disease, sickness, mental or bodily infirmity; and is not otherwise excluded under the terms of this Policy.
Covered Injury: Any bodily harm that results directly and independently of all other causes from a Covered Accident.
Covered Person: An eligible person who is enrolled for coverage under this Policy.
Covered Loss: A loss that is the result, directly and independently of other causes, from a Covered Accident suffered by the Covered Person within the applicable time period described in the Policy.
Hospital: An institution that is licensed as a hospital pursuant to applicable law; primarily and continuously engaged in providing medical care and treatment to sick and injured persons; managed under the supervision of a staff of medical doctors; provides 24-hour nursing services by or under the supervision of a graduate registered Nurse (R.N.); and has medical, diagnostic and treatment facilities with major surgical facilities on its premises, or available to it on a prearranged basis, and charges for its services. The term Hospital does not include a clinic, facility, or unit of a Hospital for: rehabilitation, convalescent, custodial, educational, or nursing care; the aged, treatment of drug or alcohol addiction.
When your coverage begins: Coverage begins on the later of the program's effective date, the date you become eligible, or the first of the month following the date your completed enrollment form is received unless otherwise agreed upon by Cigna. Your coverage will not begin unless you are actively at work on the effective date. Coverage for all Covered Persons will not begin on the effective date if hospital, facility or home confined, disabled or receiving disability benefits or unable to perform activities of daily living. When your coverage ends: Coverage ends on the earliest of the date you and your dependents are no longer eligible, the date the group policy is no
longer in force, or the date for the last period for which required premiums are paid. For your dependent, coverage also ends when your coverage ends, when their premiums are not paid or when they are no longer eligible. (Under certain circumstances, your coverage may be continued. Be sure to read the provisions in your Certificate.)
30 Day Right To Examine Certificate: If a Covered Person is not satisfied with the Certificate for any reason, it may be returned to us within 30 days after receipt. We will return any premium that has been paid and the Certificate will be void as if it had never been issued.
This document provides only the highlights. All claims for a covered loss must meet specific Benefit Conditions and Limitations and are otherwise subject to all other terms set forth in the group policy.
Common Exclusions:* In addition to any benefit specific exclusions, no payments will be made for losses which directly or indirectly, is caused by or results from: • intentionally self-inflicted injury, including suicide or any attempted suicide; • committing an assault or felony; • bungee jumping; parachuting; skydiving; parasailing; hang-gliding; • declared or undeclared war or act of war; • aircraft or air travel, except as a commercial passenger or Aircraft used by the Air Mobility Command (unless owned, leased or controlled by Subscriber); • sickness, disease, bodily or mental infirmity, bacterial or viral infection or medical or surgical treatment, except bacterial infection from an accidental external cut or wound or accidental ingestion of contaminated food; • activities of active military duty, except Reserve or National Guard active duty training lasting 31 days or less; • operating any vehicle under the influence of alcohol or any drug, narcotic or other intoxicant; • voluntary use of drugs, unless taken as prescribed and under direction of a physician; • services or treatment rendered by a physician, nurse or any other person who is: employed by the subscriber, living with or immediate family of the Covered Person, or providing alternative medical treatments. Actual policy terms may vary depending on your plan design and location
Comprehensive coverage and care for emergency transport.
Our Emergent Plus membership plan includes:
Emergency Ground Ambulance Coverage1
Your out-of-pocket expenses for your emergency ground transportation to a medical facility are covered with MASA.
Your out-of-pocket expenses for your emergency air transportation to a medical facility are covered with MASA.
When specialized care is required but not available at the initial emergency facility, your out-of-pocket expenses for the ground or air ambulance transfer to the nearest appropriate medical facility are covered with MASA.
Should you need continued care and your care provider has approved moving you to a hospital nearer to your home, MASA coordinates and covers the expense for ambulance transportation to the approved medical facility.

Did you know?
51.3 million emergency responses occur each year
MASA protects families against uncovered costs for emergency transportation and provides connections with care services.
Source: NEMSIS, National EMS Data Report, 2023
MASA is coverage and care you can count on to protect you from the unexpected. With us, there is no “out-of-network” ambulance. Just send us the bill when it arrives and we’ll work to ensure charges are covered. Plus, we’ll be there for you beyond your initial ride, with expert coordination services on call to manage complex transport needs during or after your emergency — such as transferring you and your loved ones home safely.
Protect yourself, your family, and your family’s financial future with MASA.
A Flexible Spending Account allows you to pay for eligible healthcare expenses with a pre-loaded debit card. You choose the amount to set aside from your paycheck every plan year, based on your employer’s annual plan limit. This money is use it or lose it within the plan year.
For full plan details, please visit your benefit website: www.mybenefitshub.com/sampleisd
www.mybenefitshub.com/santafeisd


The Health Care FSA covers qualified medical, dental and vision expenses for you or your eligible dependents. You may contribute up to $3,200 annually to a Health Care FSA and you are entitled to the full election from day one of your plan year. Eligible expenses include:
• Dental and vision expenses
• Medical deductibles and coinsurance
• Prescription copays
• Hearing aids and batteries
You may not contribute to a Health Care FSA if you contribute to a Health Savings Account (HSA)
The Higginbotham Benefits Debit Card gives you immediate access to funds in your Health Care FSA when you make a purchase without needing to file a claim for reimbursement. If you use the debit card to pay anything other than a copay amount, you will need to submit an itemized receipt or an Explanation of Benefits (EOB).
The Dependent Care FSA helps pay for expenses associated with caring for elder or child dependents so you or your spouse can work or attend school full time. You can use the account to pay for day care or baby sitter expenses for your children under age 13 and qualifying older dependents, such as dependent parents. Reimbursement from your Depend ent Care FSA is limited to the total amount deposited in your account at that time. To be eligible, you must be a single parent or you and your spouse must be employed outside the home, disabled or a full-time student.
• Overnight camps are not eligible for reimbursement (only day camps can be considered).
• If your child turns 13 midyear, you may only request reimbursement for the part of the year when the child is under age 13.
• You may request reimbursement for care of a spouse or dependent of any age who spends at least eight hours a day in your home and is mentally or physically incapable of self-care.
• The dependent care provider cannot be your child under age 19 or anyone claimed as a dependent on your income taxes.
• The maximum per plan year you can contribute to a Health Care FSA is $3,200. The maximum per plan year you can contribute to a Dependent Care FSA is $5,000 when filing jointly or head of household and $2,500 when married filing separately.
• You cannot change your election during the year unless you experience a Qualifying Life Event.
• In most cases, you can continue to file claims incurred during the plan year for another 90 days after the plan year ends.
• Your Health Care FSA debit card can be used for health care expenses only. It cannot be used to pay for dependent care expenses.
• Review your employer's Summary Plan Document for full details. FSA rules vary by employer.
Health care reform legislation requires that certain over-the-counter (OTC) items require a prescription to qualify as an eligible Health Care FSA expense. You will only need to obtain a one-time prescription for the current plan year. You can continue to purchase your regular prescription medications with your FSA debit card. However, the FSA debit card may not be used as payment for an OTC item, even when accompanied by a prescription.
Higginbotham Portal
The Higginbotham Portal provides information and resources to help you manage your FSAs.
• Access plan documents, letters and notices, forms, account balances, contributions and other plan information
• Update your personal information
• Utilize Section 125 tax calculators
• Look up qualified expenses
• Submit claims
• Request a new or replacement Benefits Debit Card
Register on the Higginbotham Portal
Visit https://flexservices.higginbotham.net and click Register. Follow the instructions and scroll down to enter your information.
• Enter your Employee ID, which is your Social Security number with no dashes or spaces.
• Follow the prompts to navigate the site.
• If you have any questions or concerns, contact Higginbotham:
∗ Phone – 866-419-3519
∗ Questions – flexsupport@higginbotham.net
∗ Fax – 866-419-3516
∗ Claims- flexclaims@higginbotham.net
Legal plans provide benefits that cover the most common legal needs you may encounter - like creating a standard will, living will, healthcare power of attorney or buying a home.
For full plan details, please visit your benefit website: www.mybenefitshub.com/santafeisd

• MetLaw covers—you, your spouse and dependents.
• Telephone and office consultations for an unlimited number of personal legal matters with an attorney of your choice
• E-Services—Attorney locator, law firm e-panel, law guide, free, downloadable legal documents, financial planning, insurance and work/life resources
Estate Planning Documents
• Simple and Complex Wills
• Trusts (Revocable and Irrevocable)
• Powers of Attorney
• (Healthcare, Financial, Childcare)
• Healthcare Proxies
• Living Wills
• Codicils
Document Review
• Any Personal Legal Documents
Family Law
• Prenuptial Agreement
• Protection from Domestic Violence
• Adoption and Legalization
• Guardianship or Conservatorship
• Name Change
Immigration Assistance
• Advice and Consultation
• Review of Immigration Documents
• Preparation of Affidavits and Powers of Attorney
Elder Law Matters
• Consultations and Document Review for issues related to your parents including Medicare, Medicaid, Prescription Plans, Nursing Home Agreements, leases, notes, deeds, wills and powers of attorney as these affect the participant
Real Estate Matters
For More Information:
Visit our website info.legalplans.com and enter access code: GetLaw or call our Client Service Center at 1-800-821-6400
Monday - Friday from 8 a.m. - 7 p.m. (Eastern Time).
• Sale, Purchase or Refinancing of Your Primary, Second or Vacation Home
• Eviction and Tenant Problems (Primary Residence)
• Home Equity Loans for Your Primary, Second or Vacation Home
• Zoning Applications
• Boundary or Title Disputes
• Property Tax Assessment
• Security Deposit Assistance (For Tenant)
Document Preparation
• Affidavits
• Deeds
• Demand Letters
• Mortgages
• Promissory Notes
Traffic Offenses*
• Defense of Traffic Tickets (excludes DUI)
• Driving Privilege Restoration (Includes License Suspension due to DUI)
Personal Property Protection
• Consultations and Document Review for Personal Property Issues
• Assistance for disputes over goods and services
Financial Matters
• Negotiations with Creditors
• Debt Collection Defense
• Identity Theft Defense
• Personal Bankruptcy
• Tax Audit Representation (Municipal, State or Federal)
• Foreclosure Defense
• Tax Collection Defense
Juvenile Matters
• Juvenile Court Defense, including Criminal Matters
• Parental Responsibility Matters
Defense of Civil Lawsuits
• Administrative Hearings
• Civil Litigation Defense
• Incompetency Defense
• School Hearings
• Pet Liabilities
Consumer Protection
• Disputes over Consumer Goods and Services
• Small Claims Assistance
Family Matters™**
• Available for an additional fee
• Separate plan for parents of participants for Estate Planning Documents
• Easy Enrollment - online or by phone
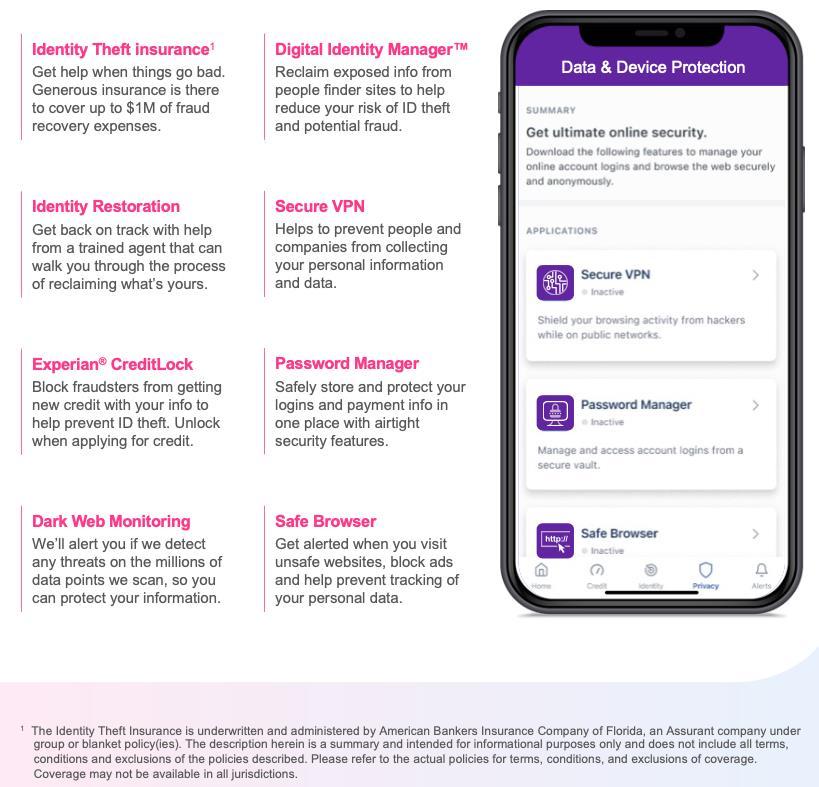
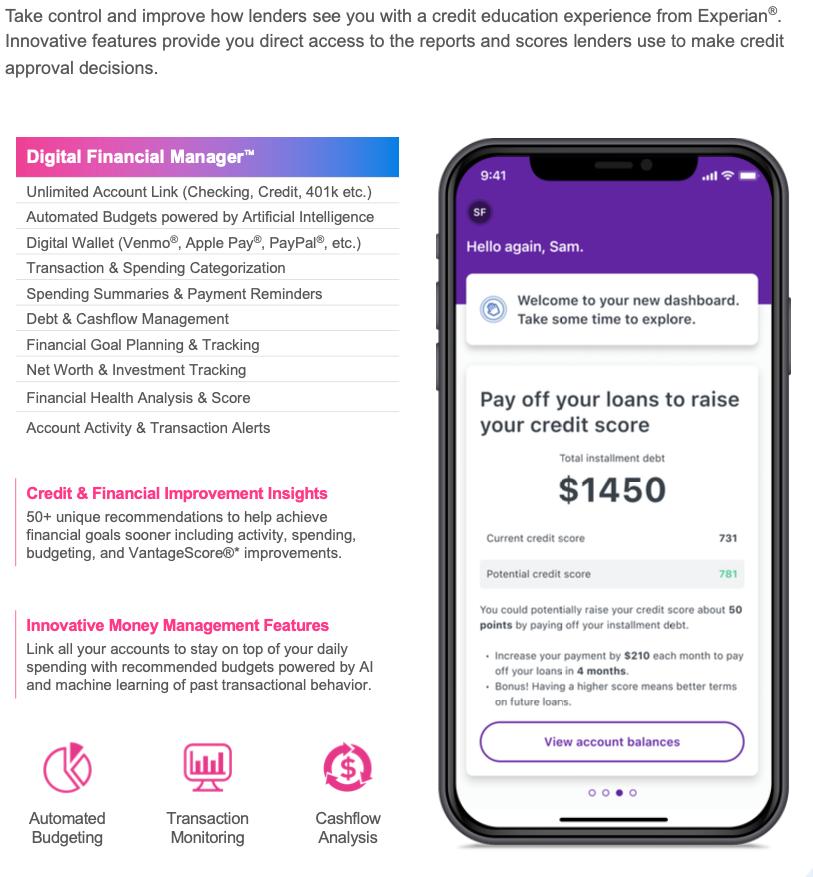
As identity theft and fraud continue to increase, an evolving suite of products helps you monitor any potential threats to your identity and alerts you if there are any areas of concern. You will also have access to a full financial wellness platform and proactive digital privacy tools that can help you keep passwords and other personal information private and secure while surfing the web.
For full plan details, please visit your benefit website:www.mybenefitshub.com/santafeisd



Experian

Enrollment Guide General Disclaimer: This summary of benefits for employees is meant only as a brief description of some of the programs for which employees may be eligible. This summary does not include specific plan details. You must refer to the specific plan documentation for specific plan details such as coverage expenses, limitations, exclusions, and other plan terms, which can be found at the Santa Fe ISD Benefits Website. This summary does not replace or amend the underlying plan documentation. In the event of a discrepancy between this summary and the plan documentation the plan documentation governs. All plans and benefits described in this summary may be discontinued, increased, decreased, or altered at any time with or without notice.
Rate Sheet General Disclaimer: The rate information provided in this guide is subject to change at any time by your employer and/or the plan provider. The rate information included herein, does not guarantee coverage or change or otherwise interpret the terms of the specific plan documentation, available at the Santa Fe ISD Benefits Website, which may include additional exclusions and limitations and may require an application for coverage to determine eligibility for the health benefit plan. To the extent the information provided in this summary is inconsistent with the specific plan documentation, the provisions of the specific plan documentation will govern in all cases.