


Hello and welcome to the second edition of LionMed, for Summer Term 2024. Despite the hectic period of End-of-Year Exams and the ever-growing pressure of UCAT preparation (for the medics at least!), the members of Lower 6th MVD Society have once again worked hard to put together this term’s magazine. In this edition, we bring you articles on a wide range of topics – an in-depth look at the ever-present threat of Bovine TB, an overview of the feared ACL injury in footballers, and a first-hand insight into geriatric care in the UK all await you over the next 20 pages. I won’t keep you too long before you get to the articles, but as ever there are a number of thanks owed. Firstly, to Tom Cahill, who has worked tirelessly to design LionMed’s new look. Secondly, to Mr Langton, for facilitating another term of MVD meetings. Finally, to Mr Cobb, who has again enabled us to go to print. With that done, all that’s left to say is enjoy!
Sam Govier
Contributors:
Editor – Sam Govier
Designer – Tom Cahill
Writers – Tom Cahill, Kessan Konesakumar, Arya Etminan, Sam Govier, Kaspar Abraham, Kiran Broekhuizen, Ishan Patel, Anthony Aladekomo, Yangzi Tjoe
Bovine Tuberculosis are two words which strike fear into any cattle farmer. Tom Cahill reveals the devastating impact of this widespread disease…
Bovine Tuberculosis (Bovine TB or bTB for short) is a chronic respiratory disease in cattle that is having disastrous effects on the farming industry and the world beyond. Caused by the bacterium
Mycobacterium Bovis, bTB leads to a general state of illness, pneumonia, and eventual death. If an autopsy were to be performed on the corpse of a cow with late stage bTB, a number of cottage-cheese-like legions called tubercules would be found, primarily in the lungs, but often spread throughout the whole body. M.Bovis is such a successful bacterium due to its extremely well-adapted nature, something that enables its survival in their host for incredibly long periods, and something that gives them their ability to establish chronic infections with long incubation periods. However, due to being so highly adapted, its pathogenesis (the process by which an infection leads to disease) is also highly complicated. I have tried to give a simple overview but in reality, it is much more complex.
Essentially, M.Bovis causes bTB due to its ability to survive and thrive inside their host’s macrophages (a type of
phagocyte). Whilst some will be successfully engulfed and destroyed, many are able to reprogram the macrophages, allowing them to multiply rapidly. In these instances, their host’s immune system will trigger the formation of granulomas, clusters of immune cells that surround the bacteria. The aim of this is to isolate the M.Bovis so that it cannot continue to multiply. In some cases, the bacteria will be contained, and the centre of the granuloma is left to calcify, forming the cottage-cheese like legions typical of bTB. However, this is not always what happens. Normally, bacteria in granulomas would usually die due to the lack of oxygen. M.Bovis is adapted to survive through this, and instead uses the granulomas as shelters, entering a dormant state called quiescence in which it can remain alive for many months or years, only reactivating once their host’s immune system weakens. This weakened immune system could be due to anything – usually it is because of their host being infected with another disease. The newly reactivated M.Bovis can then multiply and escape, spreading to the rest of the body, causing further infection, and leading to eventual death.
Whilst primarily affecting cattle, bTB can also affect many other species, such as badgers, deer, camelids, and even humans. Inhalation of infected droplets expelled from the lungs is the usual route of TB


infection; however, the bacteria can also be ingested, particularly via contaminated milk, water, faeces, food, or spread through direct nose-to-nose contact.
The bTB situation in England has spiralled out of control, going from being a relatively unknown disease in the 1980s to one of the biggest threats to farmers today in 2024. Whilst Scotland has been declared officially bTB-free since 2009, bTB continues to spread across England at a faster and faster rate.
There are several reasons for this spread of bTB. Whilst most infections are spread from cow to cow within the same farm, we need to ask how bTB got into the farms in the first place? One of the biggest and most wellknown sources are badgers. It is estimated that in high-risk areas, 1 in 3 badgers are infected with bTB. During the night badgers will enter farms, interacting with cattle and urinating and defecating on food and water, spreading bTB as they do so. I previously mentioned that Mycobacterium Bovis has the ability to enter a dormant state within the lowoxygenated granulomas. This attribute again comes into play here. M.Bovis is able to survive in the harsh conditions of the environment for long periods of time by entering this state again, remaining a risk long after it has been deposited by badgers. There have been many initiatives to combat the impacts of badgers, such as the highly contentious badger cull and the more recent BCG badger vaccines.
However, badgers are of course not the only spreaders of bTB. Cattle movement between farms is blamed for the arrival of bTB into previously ‘clean’ areas. Thanks to the growing number of large-scale intensive beef and dairy farms since the late 1990s, the number of cattle movements have skyrocketed, bringing the number of new bTB infections up with them. bTB infected waste from these farms also spills into the wider environment as a form of industrial pollution, bringing bTB back to badgers and other wildlife. Clearly, the
spreading of bTB is a vicious circle, and farmers are being caught in the centre of it all.
To test for bTB, the government has implemented regular bTB skin tests (SICCTs), ranging from tests every 6 months in high-risk areas to tests every 4 years in low-risk areas. These tests work by injecting cattle with a small amount of bovine tuberculin - a mix of dead M.Bovis proteins. If the animal has already been infected with M.Bovis, the injection will trigger an inflammatory response, developing a lump at the injection site. An injection of avian tuberculin is also injected alongside this. If a larger lump appears in this injection site, a conclusion is made that the cow is reacting to other environmental mycobacteria that do not cause bTB. However, if the bovine tuberculin lump is larger, the cow is confirmed to have bTB and will be sent to slaughter. An advantage of this test is that it has a really high specificity (99.98%). This means there is only a 0.02% chance that any cows flagged with bTB are false positives. This means that any cow sent to slaughter will have bTB. A disadvantage however is the test’s sensitivity (50-80%). This is the measure of how many false negatives will be shown. This leads to over 1 in 5 cows being flagged as bTB free when they are really infected, making them a key contributor to the spread of disease.
As stated, any cow flagged with bTB is immediately sent to slaughter. Whilst farmers do get compensation for any animal taken away, this does not cover anything else, such as the loss of future milk or calves produced. A single cow being flagged with bTB puts a farmer’s entire livelihood at stake. Immediately, their farm will be locked down, with no cows being allowed to enter or leave. Milk restrictions are brought in – the sale of raw milk is immediately halted, and any other milk must be pasteurised. Subsequent tests will occur every 60 days for a minimum of 120 days, or until all cows are deemed bTB free. Only once official bTB-free status has been returned are lockdowns and restrictions lifted. This is an incredibly stressful period for any farmer, and I personally have been told of events whilst on work experience where farms over 150 cows strong have had their whole herd wiped out and taken to slaughter. Over 38,000 positive cattle were
slaughtered in 2021 alone, and over the next 10 years, bTB is estimated to cost the taxpayer £1 billion. Clearly, something has to be done.
Over the past 50 years continual steps have been taken to prevent the spread of bTB, however evidently, something is not working. This is a huge frustration for vets, farmers, and government officials alike
“A vet’s instinct is to control disease, either by curing it or preventing it. At the moment it is very frustrating that we’re not able to do either of those things with TB.” – Bridget – vet,
As I have already mentioned, the government mandated badger culls have been a very contentious issue over the last 10 years. Questions have been put as to whether it is effective or not, with the Badger Trust stating that since the cull began in 2013, there has been no reduction of bTB levels in England, even though 72% of the UK’s badgers are estimated to be killed by 2025. Over 230,000 badgers have been killed since the cull began in 2013, costing an average of £6785 per badger. Is this really the right way to go about eradicating bTB?
Badger vaccines using the same BCG vaccine as used in humans have been introduced, only costing £293 pounds per badger. This is proving effective, but as it can only prevent further spread of bTB, and not cure already infected badgers, it has its limitations The current vaccine is also required annually and is only available as an injectable vaccine. However, with the development of an oral vaccine, rollout could soon be made a lot easier and more effective.
A BCG vaccine for cattle is also in development. Currently, it is entering phase 3 of trials, and if all goes smoothly its nationwide rollout could begin in a few years’ time. The biggest hurdle to developing this vaccine was creating a new skin test alongside it. As the vaccines work by triggering an immune response to a small number of bacteria, the BCG vaccine
would sensitise cattle to the current skin tests used. It is estimated that around 80% of BCG vaccinated cattle would flag as positive for being infected with bTB. Now however, a new skin test has been developed (DIVA format of the same test). This DIVA test is based on the immune response of 3 antigens found in bTB infected animals but not in BCG vaccinated animals. Now that this test has been developed, the full focus can be put on the testing and development of the BCG vaccine, which soon could play in key part in the elimination of bTB in England.
Finally, some less medical-based approaches have been made which have proved successful. This includes increased biosecurity around farms, brought in through badger proofing gates, fences and water tanks. As well as this, cattle movement controls have been increased, such as the introduction of pre and post movement testing, requiring cattle moving out of an annually or more frequently tested herd to require a negative skin test passed a maximum of 60 days before moving.
A combination of all these methods is required in some capacity to eradicate bTB in England and Wales. Personally, I believe that the scale of the
and enhanced farmers’ biosecurity measures – bTB levels reduced significantly because of this. The likely future Labour government has stated that they will take a similar stance, vowing to end the badger cull whilst making England bTB free by 2038. In my eyes this is a step in the right direction.
“I actually want to beat [bTB]. And we can do that with vaccines and biosecurity measures.” – Daniel Zeichner, Shadow Farming Minister
Even though a bTB-free future for England may seem lightyears away, the tide is changing. With a potential BCG vaccine being rolled out as soon as 2025, and a potential change in governmental approach, bTB may eventually be a thing of the past. It will take time, care, and continued research, but one day, farmers will no longer have to fear the kiss of death that a bTB diagnosis often has.


Many people will suffer from insomnia at some point in their lives, but what actually causes this damaging disorder? Kessan
Roughly 30% adults worldwide suffer from insomnia with around 10% of all adults meeting the criteria for insomnia disorder But what is Insomnia? Insomnia is sometimes described as disturbed sleep with long sleep latency (time taken to go from fully awake to sleeping); waking up frequently and going long periods of time without sleep. This is why some believe insomnia is not just a disorder, but rather a symptom or a sign. Despite this, in this article we will define insomnia a disorder. The National Cancer Institute defines a disorder as - ‘an abnormal condition that affects the body's function but may or may not have specific signs and symptoms. A disorder may indicate that a specific disease is present, but there is usually not enough evidence to make a diagnosis’.
It is believed that insomnia is a disorder of hyperarousal experienced throughout the whole day. Hyperarousal is an unusually increased responsiveness to stimuli, with this potentially being shown via a state of hypervigilance throughout the day. One model of the evolution of insomnia proposes that that the hyperarousal can be explained by both physiological and cognitive models of insomnia. The cognitive model proposes that ruminations
about stresses in life disrupt the sleep, causing episodes of insomnia. Once the individual experiences the negative consequences associated with insomnia their ruminations and worries shift from the stress to the sleep itself. Supporting this are studies which suggested that hyperarousal is due to physiologic or neurophysiologic factors.
The neuroendocrine system is the system that is responsible for the control of homeostasis and other processes in the body via hormones and transmitters. Many studies measured urinary free cortisol excretion (a hormone produced by your two adrenal glands, which sit on top of each kidney). They measure the plasma of healthy patients and patients with insomnia, and the evidence suggested that insomniacs had a higher level of urinary free cortisol in both their urine and blood plasma (there was a positive correlation between time awake and level of urinary free cortisol) suggesting that is associated with pathology of chronic insomnia.
Physiological arousal is measured via: the whole body metabolic rate, neuroendocrine measures, functional neuroimaging and any vary in heart rate. A study completed recently compared healthy sleepers to those with insomnia, and it showed insomniacs showed significantly metabolic rate and the variability of the heart was decreased in all stages of sleep (there are 5 stages of sleep: wake,
N1, N2, N3 and REM. Each stage leading to progressively deeper sleep.)
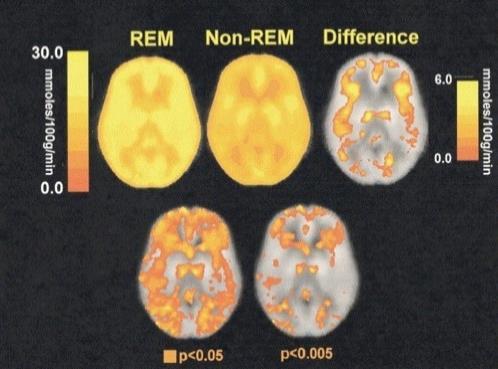
Positron emission tomography (PET) have also been used to try find the cause of insomnia. This method produces detailed 3D images of the inside of the body, in this scenario it was used to measure cerebral glucose metabolism, which is believed to be an indirect measure of the brain’s metabolism. When comparing the PET of a healthy patient to a patient with insomnia, the patient with insomnia showed greater cerebral glucose metabolism during the wake and REM (non-rapid eye movement) sleep stages. The Insomniac patients also presented with a decrease in the relative metabolism from wake to non-REM sleep, suggesting potentially some neural networks may be the cause of their inability to fall asleep, which also explains the hyperarousal and other related symptoms (such as those relating to emotion-regulation and cognitive system).
Although all these studies are very promising and suggest reasons for why some individuals present with insomnia, we still don’t have a definitive reason for what cause it, let alone if it is a disorder or just a symptom. It is a hard disorder to diagnose but hopefully new research being carried out currently will help us get an answer.
SPM maps of metabolic rate during REM and non-REM sleep
It is now common knowledge that smoking presents a serious threat to our health, but why exactly is this? Arya Etminan explains the evidence…
The practice of smoking all around the world has been believed to exist since as early as 3000 BC. Tobacco was first introduced to England in the 16th century and at the time it was purported to have many medicinal properties – a belief which the majority shared until the 1960s.
Gradually since then, more and more evidence has been found against smoking, and more recently against vaping – believed to be a better alternative to help with quitting smoking. When it comes to vaping, due to how new they still are, we are unaware of the effects they may have in the long term. However, Hookah/Shisha – which is a vaporising instrument like vaping – can be used to predict possible side effects of vaping. There are some differences, however, such as the fact that vapes do not contain tobacco while Shisha does. This can pose many dangers (which are in fact worse than cigarettes) such as carbon monoxide poisoning links to high risks of cancer (especially lung, bladder, and oral cancers) and heart disease.
Cigarettes themselves are also known to be extremely harmful with side effects such as many lung diseases due to the tar and risks of cancer due to the presence of carcinogens.
Going into more depth, smokers are at greater risk of cardiovascular disease, as smoking can damage blood vessels making them thicken or grow narrower – increasing your blood pressure.
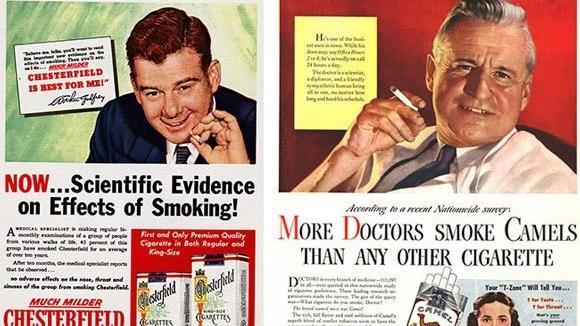
Until the 1960s companies paid doctors to claim that their cigarettes were “healthier” than the competition. However, the truth soon came out…
Smoking is also linked to respiratory disease as the tar and other chemicals in cigarette smoke cause alveoli in the lungs and airways to become damaged. This makes the body susceptible to diseases such as COPD, emphysema, and chronic bronchitis.
The increased risk of all types of cancers is also linked to smoking as carcinogens and other poisons in tobacco smoke can increase the mutation rate of DNA
Other than these three main dangers that smoking can pose. Smoking can also affect the behavior of one’s offspring (are more likely to become smokers themselves) and even reduce fertility in both males and females.
More recent research from an article in early February 2024 claims that smoking also has long term effects on the immune system. This finding was made at the Institut Pasteur. The experiment consisted of using 1000 healthy individuals with ages ranging from 20-70. With an analysis of the data, it revealed that the response of a human’s body to pathogens (called an inflammatory response) was heightened in smokers. The studies showed that smoking disrupts adaptive immune mechanisms, and the impacts can persist for up to 10-15 years. These long-term effects were linked to the potential of modifying expression of the genes which are involved in immune cells.
Given all these horrifying effects that smoking can cause, to deter the population from smoking, UK government law now requires cigarette manufacturers to feature at least one of the text warnings on the packaging.

26 years ago, the medical world was rocked by claims that the MMR vaccine –routinely administered to millions of schoolchildren – was linked to an increased incidence of autism and gastrointestinal issues among the UK’s child population. In this article, Sam Govier explores the ensuing scandal and its lasting impacts…
In the early 1990s, the British government was deeply concerned about the rise in measles cases in the general population. In the 1980s, there had been at least 50,000 cases in all but 2 years, and at least 80,000 cases in 6 of the 10 years. Action had to be taken, and in November 1994 a mass-vaccination program began. 92% of 7.1 million English schoolchildren received the MR vaccination and from 1996 the MMR vaccination, in an effort to eradicate the disease. The plan was successful, with cases decreasing to just 3,962 in 1997.
MMR stands for measles, mumps and rubella – the three diseases against which the vaccine offers protection. It is offered to all children in the UK at two developmental milestones. The first dose is administered at one year, followed by a pre-school booster at three years and four months. It is a live vaccine, meaning it contains live, but weakened,
versions of the three viruses. When injected, these stimulate the body’s immune system to produce memory cells. The memory cells remain in the blood after the immune response has ended and allow a much quicker secondary immune response to occur should the patient be re-infected in the future. This dramatically reduces the severity of any symptoms, and in most cases prevents the patient from actually becoming infected. Although the three vaccinations are offered separately in some countries, the NHS only offers the combined version and since it was introduced globally, over 500 million doses have been administered.
In 1996, Andrew Wakefield began investigating what he believed was a link between autism, bowel disease and the MMR vaccine. Although respected in the medical community - Wakefield was an honorary consultant in experimental gastroenterology and a senior lecturer at the Royal Free Hospital School of Medicine (now a part of UCL) – he was otherwise unknown. That all changed, however, on 28th February 1998 when his paper (titled “Lleallymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in children”) was published in The Lancet, a well-known and respected British medical journal.
Speaking from the Royal Free Hospital at a press conference timed to coincide with the paper’s publication, Wakefield claimed a link existed between the MMR vaccine and a new disease he
named ‘autistic enterocolitis’. He stated that as a result of his investigations, he ‘couldn’t support the continued use of the three vaccines [measles, mumps and rubella] given in combination’ and he called for the MMR vaccination program to be halted and replaced by single vaccines. His claims immediately hit the headlines.
Wakefield’s study, on which his article was based, focused on 12 patients aged between 3 and 10 years old – 11 boys and 1 girl. All had presented to paediatric gastroenterologists (doctors who deal with stomach issues in children) suffering from a seemingly simultaneous onset of developmental symptoms commonly associated with autism, and diarrhoea and abdominal pain. Wakefield believed this was a result of inoculation with the MMR vaccine – the study claimed 8 of the children had been vaccinated within 2 weeks of the onset of symptoms.
Immediately after the study’s publication, public interest skyrocketed. Parents across the country panicked as television channels broadcast the press conference to the nation. This was not helped by the intense – and unbalanced – coverage the study received across all forms of media. This coverage tended to focus on the headline of the study, that the MMR vaccine caused autism, rather than the evidence which underpinned it. Furthermore, stories tended to be written by journalists, rather than healthcare professionals or other knowledgeable correspondents. This led to the public being fed the information the study’s author wanted them to hear, rather than examining the intricacies of the study, which would later come under extreme scrutiny.
The ultimate consequence of the study – and to an arguably greater extent, the media coverage which surrounded it – was a dramatic drop in vaccine uptake among the UK population. In 2001, 24% of parents believed that the MMR vaccine presented a greater danger to their children than contracting measles, mumps or rubella. This caused vaccine coverage (the percentage of the population who have received the vaccine and are protected against infection) to fall to below 80% in 2-year-olds – it had sat at 92% throughout the early 1990s.
Proving immediately controversial, the study has since been subject of numerous investigations…
The results of these investigations have repeatedly shocked the nation. They have found a wide variety of issues with how the initial study was conducted and published. Crucially, it has been discovered that Wakefield himself had a number of undeclared conflicts of interest.
Firstly, in 1996, 2 years before the study was published, Wakefield had been recruited as an expert witness by Richard Barr, a lawyer planning a class action lawsuit claiming vaccines had damaged children. Research into the MMR study began only after Wakefield had been hired, and the study served to provide evidence for the case. This, along with the £55,000 gained from the Legal Aid Board for MMR research, was not disclosed to The Lancet before publication.
Secondly, in 2004 journalist Brian Deer, who had led the initial investigation into the study, claimed that the study had been performed in an unethical manner. Claims were made that children involved had had invasive procedures performed on them without the correct ethical approval. The Lancet was quick to deny the allegations, pointing out that the study stated, “Investigations were approved by the Ethical Practices Committee of the Royal Free Hospital NHS Trust, and parents gave informed consent”. In 2012, however, the High Court ruled in Walker-Smith v General Medical Council that the study had in fact been carried out without ethical approval, “either because the investigations were carried out before approval was given or because the children’s condition did not meet the selection criteria or because they were carried out in breach of the conditions of approval.”. It emerged that some of the children had been exposed to unnecessary tests such as colonoscopies, lumbar punctures and barium meal scans, which were found to be against their clinical interests.
In 2011, the British Medical Journal (BMJ) reported that Wakefield had planned to capitalise on the publicity of his study by launching a new company named Carmel Healthcare Ltd, of which he would own 37%. This company was to produce diagnostic tests for the ‘Autistic Enterocolitis’ identified by the study – a condition which did not actually exist. This company forecasted profits of up to £28,000,000 in their 3rd year and was also owned by the father of one of the children featured in the study.
In 2007, the General Medical Council (GMC) began a case against Wakefield, accusing him of professional
misconduct in the study. Allegations included that he “was being paid to conduct the study by solicitors representing parents who believed their children had been harmed by MMR”; that he “ordered investigations ‘without requisite paediatric qualifications’… contrary to the children’s clinical interests”, that he “conducted the study on a basis not approved by the hospital’s ethics committee” and that he “showed callous disregard for any distress or pain the children might suffer”.
Although Wakefield refuted all the allegations, the GMC ruled that all the accusations were proven – the judgment stated that he had “failed in his duties as a responsible consultant” and acted “dishonestly and irresponsibly” in performing the study. The GMC imposed the most severe punishment possible – striking Wakefield off the medical register, barring him from practicing medicine in the UK.
In 2010, immediately following the GMC report, the Lancet retracted the study – 12 years after it was first published. Richard Horton, the Lancet’s editor, stated that “It was utterly clear, without any ambiguity at all, that the statements in the paper were utterly false… I feel I was deceived”.
As mentioned above, the impact on the MMR vaccine campaign was immediate, with coverage dropping by 12% 3 years after the study was published. Although coverage improved once the validity of the study was brought into question, this left an entire age band with insufficient coverage. In 2008, cases of measles in the UK hit 5000 for the first time since 1996, remaining at this level until 2010, when they dropped again to 2235.
The real effect, however, was not limited to the MMR vaccine. Although the safety of vaccines had been debated before, the study was the first time that it had been questioned in an official study. This sparked widespread fear among the British population, which extended to various other vaccines offered to children, leading to increased levels of vaccine refusal.
The study gave apparent weight to the growing anti-vax movement, which grew massively in strength once the results were published. Seemingly backed by scientific data, ‘anti-vaxxers’ began to campaign with increased vigour as the public demanded answers. This has led to newly-introduced vaccines being treated with increased distrust, most recently with the COVID-19 vaccination programmes. Each time a new vaccine is avoided by these groups, the nationwide coverage drops, placing the whole population at increased risk –most illnesses require an incredibly high immunity rate to be eliminated (for example, it is estimated that 95% immunity is required to eliminate measles).
It is clear that the 1998 Lancet Scandal severely damaged trust in the healthcare system and turned many against vaccination programs. It also led to widespread distrust for the monitoring and drug approval agencies, such as NICE (the National Institute for Health and Care Excellence) and MHRA (the Medicines and Healthcare products Regulatory Agency), as well as the manufacturers of vaccines –whom many felt had knowingly produced dangerous products. Although vaccination coverage has since rebounded, we continue to see the effects throughout society and covering various vaccines. It certainly seems that public opinion may never return to how it was before the study.
As for its future effects? We may just have to wait and see.
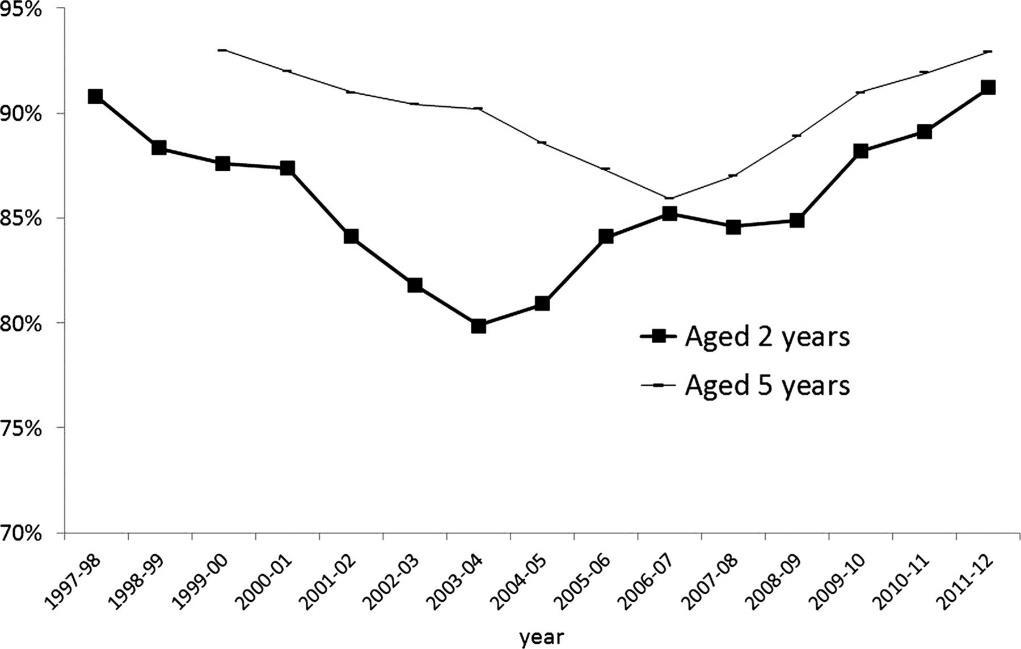
MMR vaccination coverage by year for 2 and 5 year olds in the UK year-by-year.
Since its creation in the 1990s, the TPLO has become the backbone of orthopaedic practice in small animal and referral surgeries. Tom Cahill delves into the intricacies of this life-changing surgery…
Whilst on work experience at a small animal vets, I was luckly enough to observe a tibial plateau levelling osteotomy (TPLO) on a boxer called Luna. This was the first complex surgery I ever saw, and I was so intrigued by the theory behind it that I decided to research the surgery further. Below, I have tried to give a short insight into TPLOs, why they are used, and how they are done.
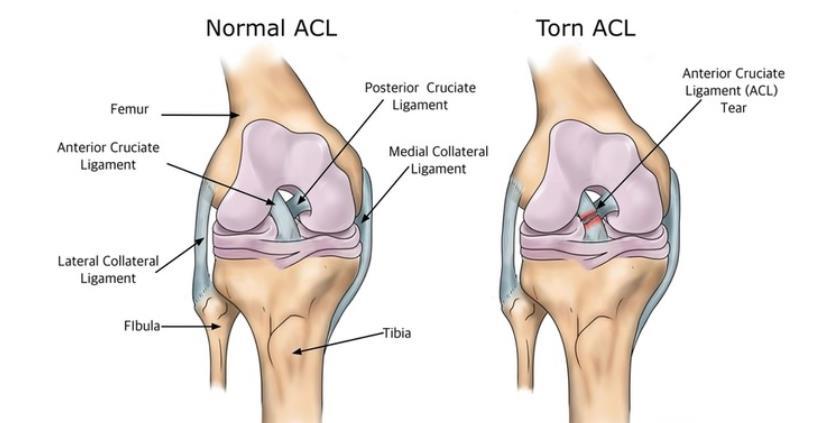
The TPLO was devised in the 1990s by Dr Barclay Slocum and is used to stabilise the knee joint following the rupture of the cranial cruciate ligament (CrCL) in dogs (the equivalent of humans tearing their ACL – see pages 15-16). This knee joint consists of 2 ligaments that cross over each other, joining the femur (thigh bone) and tibia (shin bone) together so that the knee can function as a hinged joint. The cranial cruciate ligament is the front facing ligament that attaches the femur to the tibia and can be ruptured for a number of reasons:
The knee joint is only supposed to move forwards and backwards. Therefore, if a sudden twist occurs in this joint, its ligaments can become damaged. This is most commonly seen when dogs are running and suddenly change direction, putting the majority of their weight through this one joint. The cranial cruciate ligament is usually most badly effected, and it can either tear completely, or be damaged enough that the joint becomes unstable, both leading to lameness.
Damage to the cranial cruicate ligamment can also be caused by degenerative disease, where it is stretched and weakened, but not damaged enough to be flagged as an issue to vets by owners. This results in dogs continuing to walk and exercise, damaging the liagment even further, and eventually leading to it tearing completely.
With a torn CrCL, the femur will slide backward relative to the tibia, causing pain for the dog, and damaging the
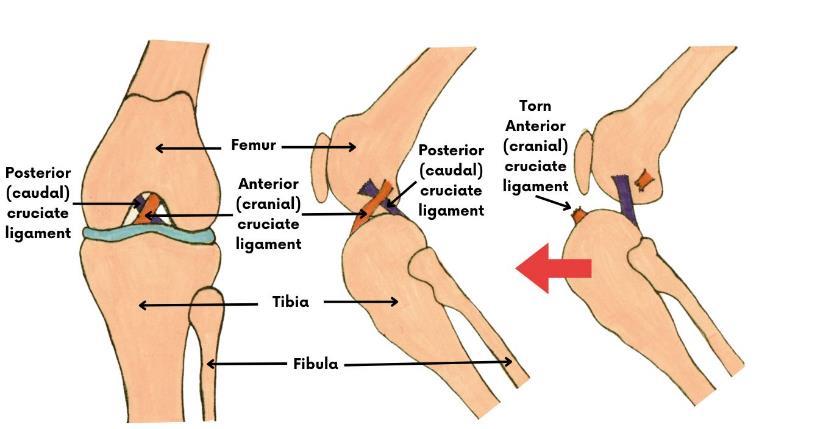








A diagram showing the arrangement of the knee joint before and after the tearing of the cranial cruciate ligament.
surrounding cartialage and bones, eventually leading to osteoarthrits. Therefore, surgery is almost always required to rectify this. A TPLO is one of the most common surgeries used, but works in a fascinating way. Rather than repairing or replacing the CrCL, it removes the need for it entirely.
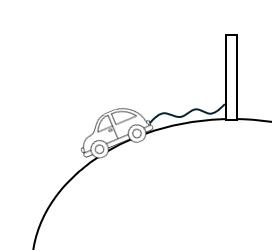
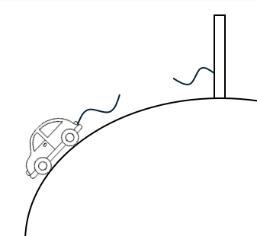
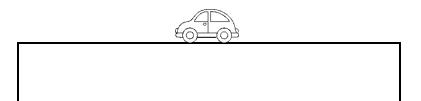
Imagine a car tied to a post on a hill. In this instance, the car represents the femur, and the hill represents the tibia. The car is connected to the top of the hill by a rope – the cranial cruciate ligament. If this rope holds, the car will stay where it is. However, if we add excess weight to the car and the rope snaps, the car will roll down the hill - the equivalent of the femur sliding down the tibia. Rather than replacing the rope, where it could snap again, we could instead level the hill. If the car was on flat ground, we wouldn’t need a rope in the first place. We could add as much weight to the car as we like, but it would stay exactly where it was. This is what a TPLO does. It literally means, ‘a bone cut which levels the tibial plateau’, and prevents the femur from being able to slide backwards, therefore stabilising the joint.
A TPLO consists of making a moon shaped cut in the tibia, and then rotating the upper segment until the
A diagram representing the car on the hill analogy.
angle between the tibia and femur is approximately level. This can range between 2-14 degrees, with 5 degrees being the angle most vets aim for. A metal plate will then be screwed onto the 2 sections of tibia, holding them in place, and allowing them to heal into their new shape.
One of the biggest benefits of a TPLO is its quick recovery time. Dogs can walk on the operated leg from 24 hours after the surgery, and if strict advice regarding exercise is followed, they can return to full physical activity after only 6 months. Apart from post-operative infections, other complications are uncommon, mostly due to the procedure almost always being performed by specialist surgeons who carry out this complex procedure 100s of times a year. A disadvantage is that because of this, TPLOs are a lot more expensive than a more routine surgery like a bitch spay that can be done by your everyday vet. The rupture of the cranial cruciate ligament is not an uncommon issue, especially in certain breeds such as Boxers and Labradors, meaning dogs and owners of varying socio-economic backrounds will be effected. This means that for many owners, a TPLO may not be a feasible option, and other less effecive routes will have to be explored. As well as this, due to the complex nature of TPLOs, dogs are likely to be under general anaethetic for longer periods of time than most surgeries, increasing the risk of anaesthetic related complications during the surgery.
Nonetheless, the TPLO is highly effective, and has delivered countless lifechanging results to dogs and their owners. Since its genesis in the late 90s, the TPLO has became commonplace in veterinary practices all over the world, and will continue to be used for the forseeable future. It was fascinating to be able to see this procedure in action, and is something that one day I hope I will be able to carry out as a future vet.

Before and after X-rays of a TPLO.
There are many different types of investigative scans that are used in different situations within medicine. These scans allow physicians to visualize the internal structures and systems of the body with high accuracy. Kaspar Abraham examines their vital importance…
X-ray Imaging - X-ray imaging uses electromagnetic radiation to penetrate tissues and create images of bones, organs, and foreign objects. It is widely used for detecting fractures, assessing joint injuries, and diagnosing pulmonary conditions like pneumonia. X-rays remain indispensable in clinical settings.
Computed Tomography (CT) Scan - CT scans, also known as CAT scans, revolutionized diagnostic radiology with their ability to produce cross-sectional images of the body. By combining X-rays and computer processing, CT scans offer detailed views of internal structures in 3D. They are instrumental in diagnosing conditions such as tumors, vascular diseases, and traumatic injuries, providing valuable information for treatment planning.
Magnetic Resonance Imaging (MRI) - MRI uses magnetic fields and radio waves to produce detailed images of soft tissues, organs, and the central nervous system. MRI scans give a better contrast resolution compared to other scans, MRI is very important in diagnosing neurological disorders, musculoskeletal injuries, and cardiac conditions. It is particularly useful for visualizing the brain, spinal cord, and joints with exquisite detail.
Ultrasound Imaging - Utilizing high-frequency sound waves, ultrasound imaging is a non-invasive technique ideal for visualizing internal organs and fetal development. Widely used in obstetrics and gynaecology,
ultrasound scans enable monitoring of pregnancies and diagnosing conditions such as gallstones, kidney stones, and abdominal masses. Its portability and real-time imaging make it an essential tool in various medical specialties.
Positron Emission Tomography (PET) Scan - PET scans involve the injection of a radioactive tracer, which emits positrons that interact with surrounding tissues. By detecting these interactions, PET scans provide insights into metabolic activity, making them very useful for oncology, neurology, and cardiology. PET-CT imaging combines PET with CT imaging, offering comprehensive information about both structure and function.
Single-Photon Emission Computed Tomography (SPECT) Scan - SPECT scans utilize radioactive tracers to visualize internal structures. However, SPECT makes use of gamma rays emitted by the tracer, developing 3D images of organs and tissues. Commonly used in cardiology for assessing myocardial perfusion and in neurology for diagnosing conditions like epilepsy and dementia, SPECT scans play a very important role in functional imaging.
Fluoroscopy - Fluoroscopy involves real-time X-ray imaging, allowing for dynamic visualization of internal structures during various procedures. From guiding catheter placements to assessing swallowing function, fluoroscopy aids in diagnosing and treating a wide range of conditions. Its ability to capture motion makes it indispensable in interventional radiology and orthopaedic procedures.
Overall, medical scans cover many different imaging techniques with each having unique advantages in diagnosing and managing diseases. These scans enable healthcare professionals to have highly accurate insights into the human body, enabling patients to receive prompt, correct diagnoses and ensuring they receive effective treatment.

Whether human or not, the trauma experienced during birth and the demands of childcare afterwards take a huge toll on a mother’s body. Many owners, especially first-time breeders, can underestimate the care and attention required for a recovering mother, for both her sake and that of the pups or kittens.
In the first weeks post-birth (and a day or two before), mothers produce colostrum. This is a specialised type of breast milk filled with high levels of antibodies and other immunoglobulins that provide immune support to a newborn’s feeble immune system, greatly reducing mortality rates from 40% to 14%. The colostrum also acts as a laxative, allowing newborns to pass meconium, removing excess bilirubin and preventing jaundice. This is also the case in humans but infantile jaundice in humans is far less harmful than in puppies or kittens in which it can severely shorten life expectancy. This is all to labour the seemingly obvious point that a dam’s health can acutely affect her newborns soon after birth –while we can fill many of the roles a dam does, there are many we simply cannot yet fulfil.
Conditions like mastitis can have a very obvious effect on these functions. Mastitis is an infection of the mammary glands often caused (as is the case of most infections) by stagnant fluid. This explains why the illness can be more prevalent in dams with smaller litters. Infection also often occurs in the uterus due to retained foetal membranes and in this case can be far more destructive, causing discharge, severe discomfort, depression, and failure to lactate. The infection can be treated with antibiotics but with retained foetal membranes dams are often injected with oxytocin to help stimulate it passing, or in worse cases surgery is required.
Lactating is also a draining activity on a dam. Though not as common as the other conditions mentioned,
eclampsia (calcium deficiency) can still occur from breastfeeding. The discomfort caused can present as panting, excessive salivation, and whining; in severe cases muscle spasms can also be observed. Dams with this condition must have their pups hand weened after treatment otherwise the condition will return.
The cases above can all result from relatively normal births but the potential issues are multiplied during a caesarean section. The normal dangers of being under anaesthetic for a small animal apply with the additional risk of the anaesthetic crossing the placenta, in which case the foetus is at severe risk.
This can be mediated with choice of anaesthetic, but the risk is always present. The trauma caused by the incision can also be problematic potentially causing infection and risks associated with blood loss.
Childbirth can be traumatic for both owner and pet but with careful treatment and being well informed on the part of the owner can mitigate these to provide the best care for our animals.
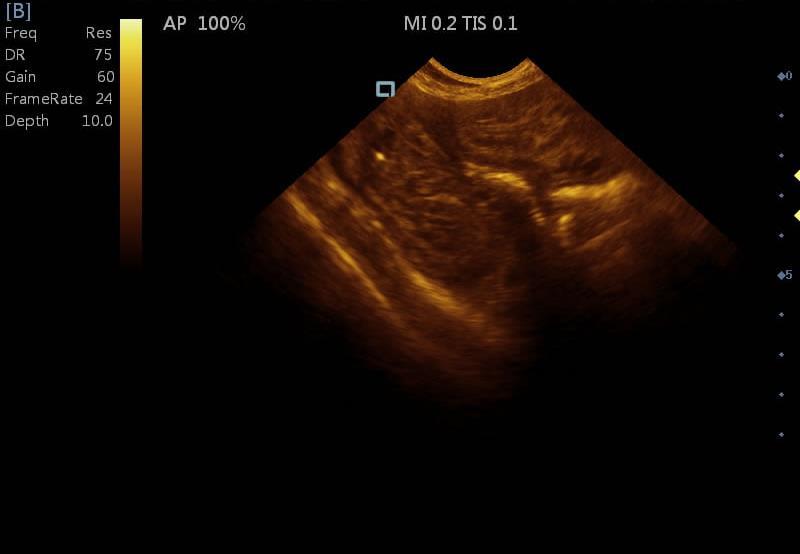
An ultrasound showing a retained foetal membrane in a dog

Anterior Cruciate Ligament (ACL) injuries are prevalent among athletes, especially those involved in sports requiring pivoting and jumping such as football, basketball and tennis. These sports involve a lot of high-impact movements and sudden changes in direction, which can put significant stress on the ACL and increase the risk of injury. In this article, Ishan Patel explores a sportsperson’s worst nightmare…
The ACL is one of the cruciate ligaments in the knee joint. It provides stability by connecting the femur (thighbone) to the tibia (shinbone) and restrains excessive forward movement and rotation of the tibia, playing a vital role in maintaining knee joint integrity during physical activities.
Changing direction abruptly while running or pivoting, especially if the athlete’s foot is firmly planted on the ground, can strain or even tear the ACL. This can also occur
due to awkward landings after a jump, particularly with poor landing technique or on an uneven surface.
Direct blows to the knee, such as tackles in football, can also cause significant stress on the ACL, leading to tears and injuries. Tyrone Mings (a football player for Aston Villa FC) sustained an ACL tear on his right knee in the opening game of the 2023-24 Premier League season. To put into perspective the severity of the injury, Mings has not been playing for nearly 10 months. In a recent image that he posted, showing his road to recovery, it can clearly be seen that there is significant muscle loss in his right leg compared to his left. There are some reasons as to why this would have occurred.
If surgery is required, there can be a period of reduced activity and immobilisation. Individuals often rely more heavily on the uninjured leg for daily activities. This increased use of the uninjured leg can lead to muscle hypertrophy (increase in muscle size) in that leg. At the same time, the injured leg experiences muscle atrophy – causing one leg to appear much skinnier than the other.
During the rehabilitation process, the focus is on restoring range of motion, strength, and stability to the injured leg. However, it takes time for the muscles to rebuild and regain their previous size and strength.
If an ACL injury is suspected, a healthcare professional will perform a thorough physical examination and may recommend imaging tests, such as MRI scans, to confirm the diagnosis.
Treatment options for an ACL depend on the severity of the case. For mild tears conservative management may be advised, which would consist of rest, ice compression, and elevation (often referred to as RICE).
On the other hand, complete tears would require surgical procedures to reconstruct the ACL. During ACL reconstruction surgery, a graft, either from the patient's own tissue or a donor, is used to replace the damaged ligament. Following surgery, a comprehensive rehabilitation program is crucial to restore strength, range of motion, and neuromuscular control in the knee joint, allowing the individual to return to normal activities and sports safely.
In conclusion, ACL injuries pose significant challenges for athletes and healthcare professionals alike, requiring prompt diagnosis and tailored treatment plans to ensure optimal recovery. By prioritising preventive measures, such as proper conditioning, technique training, and the use of protective gear, athletes can reduce their risk of ACL injuries and safeguard their long-term health.


The UK’s ageing population present new healthcare demands for the NHS and private providers to manage. Anthony Aladekomo analyses geriatric care in Britain…
Care homes are a large part of the UK, as around 450,000 people live in care homes in the UK, so they help many people care for the elderly while their health deteriorates until they sadly die. This article will cover my experience volunteering in care homes as general information about them.
Loneliness in elderly care homes is a very common issue which has been a problem for years in this country –though the individuals are surrounded by others, many feel isolated. Despite being in this communal setting, many elderly residents experience a sense of disconnection due to factors such as limited social interaction, sometimes even neglect and loss of autonomy. I experienced this in the care home – one of the elderly people I was talking to said he felt lonely as he was unable to leave the care home and unable to live by himself. He felt this was not fair as he was not allowed to make decisions for his own body. In addition, moving into a care home can be quite challenging, as it often involves leaving behind familiar surroundings and cherished relationships as people tend to visit the elderly less in care homes. Moreover, the nature of many care facilities can increase feelings of loneliness, as residents may long for the comforts of home and meaningful connections with others.
elderly in care homes is a poignant reality that demands attention and compassion. Physically, aging brings with it a range of challenges, from diminished mobility to chronic health conditions that require constant management. For many elderly residents, even the simplest tasks, such as eating and getting dressed, can become difficult feats. Moreover, mental decline, including conditions like dementia and Alzheimer's disease, adds more complexity to their care. Memory loss and confusion can profoundly impact an individual's quality of life, making it difficult for them to communicate, connect with others, and engage in meaningful activities. As caregivers strive to provide the necessary support and assistance, they must navigate the delicate balance between preserving the autonomy of the elderly and ensuring their safety and well-being. In addressing the physical and mental decline of the elderly in care homes, it is essential to prioritize empathy, understanding, and specialized care tailored to the unique needs of each resident.
From my experience volunteering in a care home there are many characteristics needed of a care home, in my opinion the most important one is patience, as I found that it is necessary when helping the elderly in many instances. A situation I can remember vividly is having to talk to an elderly man who kept repeating the same points. It felt slightly annoying constantly repeating the same conversation however it was all worth it as he seemed to enjoy our conversations. Another problem is how unfiltered the elderly can be as you hear some hurtful things while volunteering, such as an elderly woman say she wanted to electrocute
one of the workers there. However, in situations such as these it is important to keep a level head.
In conclusion, the care and well-being of the elderly in care homes are considerations that demand our collective attention and dedication. As society continues to age, it is imperative that we aim to provide compassionate, dignified, and person-centred care for the elderly. By prioritizing effective communication and promoting a culture of respect and empathy, we can create environments where our elders feel valued, supported, and cherished. Ultimately, the quality of care provided to our seniors in care homes reflects our commitment to honouring their contributions, preserving their dignity, and ensuring their golden years are characterized by comfort.
Volunteering in a care home can be a great way to help elderly people.

Yangzi Tjoe investigates the devastating disease…
Amyloidosis is a rare disease where amyloid proteins build up in organs, preventing proper function; most commonly the heart, kidneys, liver, and spleen. Unfortunately, amyloidosis cannot be cured, but it can be treated.
Symptoms
Common symptoms across most types of amyloidosis include tiredness, loss of weight, shortness of breath and swollen feet and legs. These symptoms are common to a large number of other diseases, which makes amyloidosis difficult to diagnose without proper equipment.
Amyloid proteins are the common “problem” with amyloidosis. There are over 20 different types of amyloid proteins, but they have common features which make them difficult for the body to deal with. Amyloid proteins form beta-pleated sheets, in which hydrogen bonds form between adjacent amino acids. This structure makes these proteins resistant to proteolysis – meaning enzymes cannot hydrolyse and break them down. This leads to a build-up of amyloid proteins around the body, causing amyloidosis.
Causes of amyloidosis vary widely from problems with one’s bone marrow to inflammatory conditions and age. The disease can also be inherited. These causes are independent
of each other – each cause is associated with a different type of amyloidosis.
AL amyloidosis – also known as primary amyloidosis as it is the most common form – is caused when a person’s bone marrow stops working properly and produces abnormal light chain proteins. These light chains normally help the body fight disease, but in AL amyloidosis instead replicate uncontrollably and spread throughout the body, usually building up in the heart and kidneys. This type of amyloidosis is also associated with myeloma, a type of cancer, due to the effect of both on the production of antibodyproducing cells (light chains).
Treatment, similar to that of myeloma, involves chemotherapy in order to kill malignant lymphocytes (which produce the abnormal light chains), or a drug called Bortezomib, which also inhibits the malignant lymphocytes.
These types of amyloidosis both affect the protein TTR, made in the liver. This protein normally transports the hormone thyroxine and retinol (Vitamin A) around the body. If a person has either disease, the TTR protein misfolds and forms betapleated sheets, causing a build-up of amyloid proteins in the liver, which also spreads to the heart. The causes of this type of amyloidosis are either an inherited gene (hereditary) or age (wild-type), as a mutation would have changed the DNA that codes for the TTR protein. Although there are more cases of AL amyloidosis than Wild-type, it is thought that
Wild-type ATTR is the more common type of amyloidosis.
Usually, diagnosis starts locally in a GP, where ECGs (electrocardiograms), echocardiograms, an MRI, blood tests, and urine tests may be ordered. These can look for abnormalities in the body due to the build-up of amyloid proteins, or test for the proteins themselves. If it is believed that a patient does have amyloidosis, they will be referred to the National Amyloidosis Centre at the Royal Free Hospital, which specialises in the treatment of the disease. At the centre, they can track the progress of the disease via a SAP scan, which are only available at this hospital within the UK. The SAP scan uses radioactive material (iodine-123) to detect amyloid proteins in the body, although we do not actually know how why the amyloid proteins absorb the radioactivity. However, this allows doctors to track how serious the patient’s condition is, especially when combined with ECGs and echocardiogram.
On a conceptual level, there are 3 main ways to treat amyloidosis. These are: breaking down amyloid proteins after they are made; stopping the production of amyloid proteins by killing the cells that produce them, and finally changing the genes that produce the proteins.
Although the second and third options for treatment are not really a possibility now, new innovations like CRISPR mean amyloidosis could soon be treated very easily. However, until then, doctors can only break down the proteins after they are made, unable to solve the underlying issue.

A heart with amyloidosis.