Correspondence: Please send all correspondence to The Editor at PO Box 782, Kent Town, SA 5071, or email editor@hepatitissa.asn.au .
Editor: James Morrison
Regular Contributors: Cecilia Lim, Joy Sims
Some photos in this publication may have been altered to disguise identifying details of members of the public.
This resource was prepared and printed on Kaurna Country.
Disclaimer: Views expressed in this newsletter are not necessarily those of Hepatitis SA. Information contained in this newsletter is not intended to take the place of medical advice given by your doctor or specialist.
We welcome contributions from Hepatitis SA members and the general public.
SA Health has contributed funds towards this program.
ISSN 2651-9011 (Online)
Australasian Viral Hepatitis Conference
The 14th Australasian Viral Hepatitis Conference for 2024 was held in early August on the beautiful lands of the Larrakia People in Darwin. This year’s conference had a different feel to it: much as in the classic Australian movie The Castle, it was the vibe, and this was commented on by numerous people I spoke with.
There were presentations from across Australia and the region covering all aspects of viral hepatitis. On the first morning, I attended a pre-conference meeting held by the Kirby Institute on ‘Implementation Process Mapping of Hepatitis C Point-ofCare Testing’. Participants shared their experiences and the creative ways they are engaging with the community to increase testing, including the use of incentives other than cash (like linking up with the courts to have people’s fines reduced when they are engaging with their service, or providing top-ups to bus cards). There are also a lot of mobile clinics getting around Australia, ranging from fully decked-out vans to the back of someone’s Camry. One thing that definitely came out of this meeting was how creative and passionate people are
Delegates
in coming up with new ways to reach the community, and in going to where they are. The Kirby Institute will pull together all of the discussions which will then allow other services to implement new strategies.
When the conference officially commenced, we were welcomed to the beautiful lands of the Larrakia People by Yvonne Odegaard, whose clan group is Saltwater Crocodile, Dangalabba, a proud Saltwater woman and traditional owner. Following Yvonne was the Convenor’s Welcome; Associate Professor Jane Davies talked about our need to work together to build connections, foster partnerships and collaborate to reach the 2030 viral hepatitis elimination goals.
Afterwards I attended the session on implementing the national hepatitis strategies. There was talk of the money being invested in viral hepatitis through the national budget, but how it wasn’t enough. Some good news, though, is that there is mention of implementing needle and syringe programs in custodial settings, and implementing universal hepatitis B screening for all adults born before the year 2000 whose hepatitis B status is unknown. The panel was asked what they thought was the most important items in the national strategies, and the consensus was that ending stigma and increasing investment for community-based organisations to increase their amazing work so that decisions on whether, say, they could renew their $350 Survey Monkey subscription didn’t need to cause a financial crisis.
The morning of day two also had a focus on what needs to be done to reach our elimination targets, and began with Professor Ed Gane from the University of Aukland
taking part in a Saltwater Ceremony performed by Larrakia Elder Richard Fejo on the Darwin Waterfront
discussing the Māori people of New Zealand and the great success of the New Zealand program in the pursuit of elimination of hepatitis B. He talked about the new, simplified guidelines New Zealand has, and— as we are not on track to eliminate hepatitis B in any country—we need to screen whole populations. However, this will put immense burdens on health care systems as we find those undiagnosed patients. We should also consider treating everyone living with hepatitis B who is over the age of 30, as suppressing the virus will reduce liver cancer incidence.
Afterwards I attended a new format of tabletop presentations: think ‘speed dating’ where there are 6 tables, 6 presenters, 10 people per table, and every 10 minutes the presenter moves to the next table and gives their presentation again. I really enjoyed this format, and look forward to participating in them again. The first presentation was from Derbarl Yerrigan Health Service workers Jessamy, Lakhbinder, and Cameron, who discussed how their service is working to optimise the management of hepatitis B through utilising ‘Communicare’, a patient record system, to analyse data, create clinical items, and manage recalls for patients living with hepatitis B, as well as partnering with a tertiary hepatology team. Through this audit, they were looking to identify patients
with chronic hepatitis B, past hepatitis B infection, isolated anti-HBc, non-immunity to hepatitis B, and close hepatitis B contacts. A total of 777 patients who would benefit from a review were identified. The team are prioritising 51 regular patients with chronic hepatitis B, ensuring their management is optimal as per the guidelines.
The next project that was of interest was ASHM’s ‘Beyond the C’ program and the work was presented by Adi and Grace from ASHM. This program is recruiting GP practices and funding them to perform clinical audits on their patient software system to identify individuals who may benefit from hepatitis C testing and treatment. Since the program launched in December 2022, 183 practices have submitted an expression of interest, and 60 have formally commenced the project. From these practices, approximately 990 people that require testing and or treatment have been identified.
The final presentation of interest was Lana Richardson from Hepatitis Queensland, who presented ‘Strength in Partnership’. Lana discussed how as a non-indigenous organisation, Hepatitis Queensland is very aware of the importance of cultural safety and community involvement and have implemented a number of strategies to ensure the success of their Hep Check program. Those include the inclusion of their Aboriginal and Torres Strait Islander Liaison Officer, following cultural protocols, creating meaningful connections and having continuous engagement utilising multiple modes of interaction.
The afternoon session I attended was discussing the UNSW’s project trialling a universal precautions approach to stigma reduction in health care. There were a few presentations in this session looking at how this project might work if Australia had a health system that would assume that all people who enter a health service might be fearful of being treated negatively or excluded in some way, thus creating an approach where, just as healthcare workers
assume all blood and bodily fluids are potentially infectious, the same could be true for people who have experienced stigma. It wouldn’t mean ‘everyone would be treated the same’, more that staff would be trained to understand the plethora of issues that can create a stigmatising environment. This seems to be a really intriguing way to tackle such a huge issue. It doesn’t just relate to STIs and BBVs, but anything: obesity, gender, race, religion, etc. It is certainly a huge task ahead of the project team, but one that needs to happen.
The last day started with a hugely thoughtprovoking talk by Dr David Carter from the University of NSW, who is leading the Health+Law Research Partnership, which aims to improve access to justice and high quality of life for those living with hepatitis B or HIV in Australia by removing legal barriers to testing and treatment. He was able to connect everyday goings-on to the laws that surround us on a daily basis; laws which we probably don’t even think about, but that, for people living with hepatitis B or HIV, are regularly confronting, and often with negative impacts. The Health+Law team have conducted interviews with people living with hepatitis B to ascertain the legal issues they have had in the past, and what would better support them into the future.
Following David’s presentation, Dr Jacqui Richmond and Dr Amanda Wade presented on GP perspectives on hepatitis B models of care in a low-prevalence area in regional Victoria. They have conducted semi-structured interviews with key hepatitis B healthcare providers in the Barwon South West region, and found that hepatitis B was perceived to be a rare, complex condition by the GPs, which affected their confidence to independently manage patients. Of the 20 interviewees, six were trained hepatitis B s100 prescribers, but none of them had prescribed treatment and were not confident to do so without consulting a specialist. They reported that GPs in lowprevalence areas or those with low caseloads need support, and one of those supports included collaboration with a specialist nurse
to build their confidence and access to case management and clinic audit support.
Dr Jacqui Richmond also presented at the final tabletop session and discussed how there was a huge underrepresentation of nurses and the work that nurses do. One of the reasons for this was that the majority of the work that nurses completed—the followup phone calls, the home visits, the talking with families—is not recorded, so their work was underreported and thus undervalued. Jacqui stated that this needs to be done better so data collection occurs and the highly valuable work that nurses are doing is captured, and there is evidence to support expanding the workforce. Jacqui also stated that nurses have done a lot to get to where we are today with our elimination efforts, but this is still not being recognised.
All in all, it was such a wonderful conference, and I am fortunate to have been able to go. The next Viral Hepatitis Conference is to be held in August 2025 on Narrm Country in Melbourne, we hope to see you all there.
Dr Jacqui Richmond presenting at the closing ceremony
Shopping Centre Fibroscans: Popular as Hot Cakes
A liver health scan would not be on your “toget” list when you visit your local stores, so shoppers at the Arndale Shopping Centre in Kilkenny, north-west of Adelaide, were pleasantly surprised by the opportunity for a free check, and eagerly took up the offer.
The free Fibroscan clinic by viral hepatitis nurse, Jeff Stewart, was part of an awareness raising activity carried out with Relationships Australia PEACE Multicultural Services and Hepatitis SA for the 2024 World Hepatitis Day campaign.
Speaking to Seven Network News, Hepatitis SA Education Coordinator, Jenny Grant, explained that the liver scan would take only about 15 minutes and people would get their results on the spot so they can see “the shape of their liver and where it’s at”. Results are recorded in a written report which
participants can take to their GP for followup action if needed.
The Hepatitis SA team offered printed information about hepatitis in different languages, and had conversations with community members as they waited their turn. PEACE workers were able to advise people on where they might get further support and counselling in languages other than English, should the need arise.
Relationships Australia PEACE Multicultural Services Program Manager, Memoona Rafique, said bringing services such as liver health scans into the community “is extremely important as there is a lot of stigma around hepatitis, getting tested or treated”.
In South Australia, over 16,000 people live with hepatitis B or hepatitis C. About 30% of
Educators Jen (L) and Yingbin (R) with viral hepatitis nurse Jeff (Centre)
people in the state with hepatitis B, and 20% of those with hepatitis C, are undiagnosed. Hepatitis B and hepatitis C are the leading causes of liver cancer, the fastest growing cause of cancer-related deaths in Australia. In all, 49 people received liver scans that day. Eight people who missed out got on the waiting list and Hepatitis SA took a call from someone who had seen the news on TV, asking if a similar event could be held down south. PEACE and Hepatitis SA workers spoke to a more than 100 people, in addition to the 49 who were fibro-scanned.
Fibroscan: What is it?
Until about 10 years ago, liver fibrosis had to be determined by a biopsy. This was an invasive procedure which required preparation and the surgery. FibroScan is the commercial name for a relatively recent ultrasound based technology known as transient elastography or TE. In 2013, it was approved by the American FDA for use in assessing liver fibrosis and has gradually replaced liver biopsies as the standard monitoring tool for diagnosing and assessing liver damage.
The scan is performed at the bedside in a clinic or similar setting, with the FibroScan machine and a probe similar to those used for ultra-sound scans in pregnancies. There is no pain and no need for sedation. Results can be read immediately off the screen. The time taken to complete a scan may vary depending on each individual, the size of the liver and the tissues surrounding the organ. You can get a fibroscan from your closest liver health clinic or some private radiology services. If you think your liver might be at risk, contact your nearest viral hepatitis nurse—see the contact details on the inside back cover of this magazine.
ABOVE: From the Seven News story
LEFT: Viral hepatitis nurse Jeff demonstrates the Fibroscan on on Relationships Australia worker Andy INSET: Arndale Shopping Centre, Kilkenny
Into the Community for World Hepatitis Day
South Australia has done well initially in eliminating hepatitis. More than half of people in the state with hepatitis C have been cured, but now momentum has slowed. With the hepatitis B elimination targets, we still lag behind the national averages in treatment and care uptake, as well as diagnosis.
One of the strategies for accelerating progress to reach our 2030 targets is to go into communities, to raise awareness, and take services directly to them. The successful liver scan clinic at a local shopping centre in Arndale (see previous pages) was just one of a number of outreach activities popping up during the 2024 World Hepatitis Day campaign.
Barbecue, Chat and Test
Community Access and Services SA (CAaSSA) is a grass-roots organisation in Adelaide’s west which offers services including aged care, disability support, drug and alcohol services, gambling, mental health and wellbeing support, and adult education. Originally set up by Vietnamese immigrants to meet the needs of their community, CAaSSA has grown and now works with a range of other immigrant communities, including those from regions of higher hepatitis prevalence such as the Middle East, Africa and Southeast Asia.
During 2024’s World Hepatitis Day (WHD) campaign, CAaSSA workers saw the opportunity to start conversations by hosting a friendly barbecue, an information table and, with support from Hepatitis SA, bring hepatitis C point-of-care testing to their communities.
Hepatitis SA’s Hepatitis C Treatment, Support and Information Coordinator, Lisa Carter, said 17 people were tested at the
event on the day, many of whom would not have considered doing so had the risk factors for blood-borne virus not been explained to them.
Provided under the Australian National Point of Care Testing Project, the testing clinic offered hepatitis C antibody tests and, in appropriate situations, hepatitis C RNA, HIV and hepatitis B tests as well.
Participants also received information about hepatitis B and together with their families, were referred to their own GPs for testing. Arabic and Vietnamese interpreters were present to facilitate the process, and viral hepatitis nurses were on hand via telephone, if required, to arrange for liver scans in the work-up for treatment, and to quickly and easily arrange prescriptions for direct-acting antiviral treatment.
Hepatitis SA Needle and Syringe Program Peer Projects Coordinator Carol Holly was on hand at the event to provide harm minimisation information.
Art, Craft and Education
Aboriginal Community Connect (ACC) is a one-stop service provided by Uniting Communities. It supports First Nations people who want to change their use of alcohol and other drugs, and to stay connected to their culture and community. ACC has shared houses in north-west Adelaide, Mount Gambier, Murray Bridge and Renmark.
Hepatitis SA has been working with ACC in Prospect to share hepatitis-related information and education through art and craft projects. For 2024 World Hepatitis Day, the participants put together some special artwork to showcase what they’ve learnt in that journey.
In all, some 15 people participated in the project over three weeks. ACC’s Social and Emotional Wellbeing Worker, Nat Loadsman, said learning about hepatitis testing and treatment was important for the community. “Raising awareness encourages action. About 70% of our clients have been tested,” he said. “We’ve spoken about having another project later, maybe creating a montage of the artwork, and sharing a healthy lunch.”
Hepatitis SA Education Coordinator Jen Grant said it was a wonderful project to work on. “Sharing knowledge and producing some beautiful artwork with health messages—it was a privilege to work with ACC and their community. Hepatitis SA looks forward to working with ACC into the future.”
Square Dance, Tai Ji and More
Chinese Welfare Services (CWS) in the city has been in Adelaide for over 30 years. It is one of two peak Chinese community service organisations in Adelaide. CWS provides a range of aged care-related services and runs classes and activities that include fitness, dance, and Cantonese opera. It also runs a weekend Chinese language school in the city.
For WHD 2024, CWS created an informative display ad, distributed through their newsletter and social media, encouraging members to find out more about viral hepatitis.
Community members were encouraged to participate in the week’s square dance and
taiji activities, where hepatitis B education was incorporated into the schedule.
Hepatitis SA educator Jesse Chen, fluent in both Cantonese and Mandarin, was able to engage with participants, explaining the basics of hepatitis B, how it could be prevented and how they could get tested, including how to approach their GPs to request testing should they think they might be at risk.
CWS Executive Officer, Kam Chiu said both events were “highly successful”, attracting 75 participants. “The Square Dance Group and Fitness Tai Chi Group activities were wellreceived, encouraging physical fitness and healthy living, contributing to the overall goal of raising awareness about viral hepatitis,” he said.
“The brief educational sessions on Hepatitis B raised significant awareness among the participants. The distribution of sample letters and flyers helped participants understand what a referral letter looks like and its general content.”
Artwork by community members at Aboriginal Community Connect - Prospect
CWS Executive Officer, Kam, with participants at the end of a session
Goods Administration, meaning it can now be used widely in Australia.
This test is a single-use, rapid, flowthrough test of the kind many people will be familiar with in the form of home COVID tests. Instead of a nose or mouth mucous swab, however, the INSTI test uses a small amount of blood taken via a fingerprick. When mixed with the supplied reagents in the correct way, the test is able to detect hepatitis C antibodies. It can also detect these antibodies in human venous whole blood, blood serum, and EDTA plasma (blood plasma combined with ethylenediaminetetraacetic acid, which acts as an anticoagulant, allowing the plasma to stay liquid).
The test results are available as quickly as 60 seconds.
The plan is for these kits to be made available across Australia in hepatitis C point-of-care testing sites. A quality assurance panel is being developed to make sure the tests are used reliably and consistently.
Hepatitis SA’s Lisa Carter explained why it’s such an improvement. “In AOD, NSP, Correctional, Homelessness and Mental Health Service settings particularly, we find that people feel that even the 20-minute
60-Second Hep C Test Approved
antibody tests take too long. So, a oneminute INSTI test will really be the gold standard, helping us to scale up testing in these settings, which we need to do if we want to reach our global elimination targets here in Australia.”
“INSTI tests are also less expensive than the current GeneXpert technology used for quick hep C RNA tests, and are both extremely accurate when used correctly, as well as simple enough to be used by staff when they’re visiting peers at various health and community services,” she said.
These rapid antibody tests makes larger scale screening quicker and easier, so only people testing positive for HCV antibodies
Image by tohamina on Freepik
Image supplied by Insti
need to then take the one-hour RNA test to confirm if they currently have the virus. The chemicals used in the new INSTI tests are also shelf-stable and compared with other tests, these new tests themselves are also less fragile in terms of handling in the field.
“It will work better in prisons as we’d be able to target RNA testing with use of the INSTI more quickly than the current 20-minute test allows, and it is just more realistically achievable to test people in custody during induction than doing traditional needle-andsyringe testing or 20-minute rapid antibody tests,” Lisa explained.
“In the future [these tests] may be deemed suitable for self- testing campaigns (increasing confidentiality, particularly in rural and remote locations, where people are often related or are known to those working in healthcare or Needle and Syringe Program (NSP) sites, or to GPs, hospitals and pharmacies.”
Anything that helps us all in achieving our goal of Hep C elimination in Australia is vital. The availability, speed and relatively inexpensive nature of the INSTI HCV Antibody test kits will be a valuable weapon in that fight.
How Emergency Departments Fail the Mentally Ill
The prevalence rates of mental illness in people living with viral hepatitis are significantly higher than those rates in the general population.Some research suggests that the prevalence of HCV infection in patients with severe mental illness may be as high as nine times that of the general population. This means that someone living with hepatitis B or hepatitis C is much more likely to present at an emergency department with an acute mental illness.
Unfortunately, a serious disconnect between hospital emergency departments and the National Disability Insurance Scheme (NDIS) is failing people with mental health conditions, as new research from the University of South Australia shows that they frequently receive inadequate care within emergency departments, potentially putting thousands of vulnerable people at risk.
Funded by MIND Australia, the study, published in the International Journal of
Mental Health Nursing, found that people with psychosocial disabilities (disabilities caused as a result of poor mental health) not only experience distress when dealing with the NDIS, but also face further serious problems when they present to emergency departments requiring emergency care.
Speaking with NDIS participants, the nationwide study found that when participants disclosed that they had NDIS support, clinicians wrongly assumed that the NDIS provides medical and mental health crisis care, which it does not–this is entirely the job of hospital emergency departments.
It’s a concerning finding, particularly following the discrimination, non-inclusivity and lack of equality experienced by people with a disability, identified in the NDIS review and the disability royal commission.
In Australia, 1.1 million people have a psychosocial disability which causes
limitations or restrictions in their everyday activities. Additionally, 58% of these people also have an anxiety or emotional condition, 42% have problems with memory or periods of confusion, 41% have behavioural conditions, and 40% have a mental illness (such as schizophrenia). 86% also have at least one other disabling condition (63% physical disability; 38% intellectual disability; and 33% sensory disability).
UniSA researcher and PhD candidate
Heather McIntyre said that the disconnect between the NDIS and emergency departments is failing people with psychosocial disabilities.
“Time and time again we hear about people experiencing distress when they contact the NDIS – they fight to be heard, fight for support, and are often dismissed, so the last thing they need is to go through this again when they require emergency care,” she explained. “This is particularly concerning for people with a mental health
FROM PARTICIPANTS IN THE STUDY
“I find a lot of time you have to fight…It’s a battle…a bit of a fulltime job…I keep on top of all the legislation, the wording, the changes…No-one has their facts straight, no-one knows what they’re talking about. There’s not clear information unless you’re researching 24/7 yourself.”
“But the system wasn’t designed for psychosocial disabilities and you can see it…it’s like saying to someone, if you need a critical surgery, do you want to keep your right hand or your leg? Which one?”
“And they don’t see that they’re causing emotional distress… [they say] that there’s this fancy Candyland [NDIS], you can go through and everything will be fixed.”
condition, especially those with fluctuating psychosocial disabilities who may struggle with communication.
“Because many emergency department staff aren’t aware of the limitations of NDIS supports, they wrongly assume that the NDIS provides a higher level of care than it does. This leaves many people with a psychosocial disability being discharged [from] emergency without appropriate treatment and returned to the situation that caused them to present in the first place.
“It’s an inequitable and unsafe approach that is putting thousands of people at risk.”
The study demonstrates that there is an urgent need to strengthen service integration between the NDIS and emergency departments. “Communication between the two services is not occurring seamlessly, which affects continuity of care. This needs to change,” Heather McIntyre noted.
“We must start at the pointy end: emergency department clinicians need more training and education to better understand how the NDIS works and how to best support people with a disability. They need to learn how to support people with neurodiversity and hearing impairments, how to build trust and how to really listen, as well as to provide low sensory environments. But equally, stronger connections and pathways must be established between NDIS providers and emergency departments so that everyone is on the same page.
“With budget cuts to the NDIS of $14 billion over the next four years, peoples’ disability supports will further be reduced, resulting in more emergency department presentations when supports are insufficient. In emergency departments we need to step up care, not ration care, if we are to support people with disabilities who already feel abandoned by the health system.”
Life After Hep C: Meal Plans for Health and Convenience!
I was cured of hepatitis C back in the year 2000 on my second attempt, using a combination of Interferon and Ribavirin. This was long before the much better and more well-tolerated direct-acting antivirals were available.
When I still had hep C, liver biopsies showed level-2 fibrosis but soon after my cure (perhaps a year or two), a pair of FibroScans showed that the fibrosis had reversed back to zero, which was fantastic news! But I must admit that although I thought that I was looking after my health, my diet was not fantastically healthy.
A routine annual blood test taken over a year ago showed elevated cholesterol levels that prompted my GP to start me on a statin drug to lower the cholesterol. After about six months on the statin I found myself experiencing muscle aches and a general body weakness and fatigue.
I told my GP that I didn’t want to take them anymore, and that I would try to lower my cholesterol through diet. My blood tests had also shown that my glucose levels were starting to climb. I realised that I needed to be a bit stricter with my diet.
The GP referred me to a dietician. After I explained that I wasn’t all that fond of cooking nutritious meals with fresh food as I would always end up throwing a lot of food away, the dietician explained that there are healthy options for people that don’t like to cook: home-delivered meal plans.
I decided to give it a try. In my case I used Lite ‘N Easy, and after more than a year I am still enjoying their meals and my blood tests have all returned to normal levels. I think that they are fairly priced. I only order for five days of the week, but that is completely optional, and I get free delivery on a Friday.
The breakfast and lunch meals are packaged in a plastic bag for the day and usually include a piece of fruit (an orange, an apple or a mandarin or a punnet of grapes, or perhaps an energy bar or sometimes a sweet cake or pikelets).
Fruit is something that I wouldn’t often buy in the past so this is a great option for me. Breakfast and lunches come in a choice of three for each day and are probably a healthier option than the frozen dinners as the sodium level in the frozen meals range
from around 220mg to 280mg per 100g, which is lower than supermarket options but might be a bit high for some. The frozen dinners have a lot more options with 66 to choose from, and I have enjoyed most of them.
There’s no doubt that my diet is a lot healthier than it was in the past and my blood tests are proving this. I wouldn’t hesitate in recommending meal plans to anyone in a similar situation to mine.
I always leave the empty foam esky (including the plastic bags) out for the delivery driver on Fridays to take away when they drop off the next set of meals, so apart from remembering to order the meals each week, the whole process is very easy.
two people, for each supplier. Note that most also offer introductory deals that can dramatically reduce the cost of the first or first few orders.
READ MORE:
There are other suppliers that provide a similar experience, so if you are interested, it would pay to research and see which option suits you best. I just happened to find one that suited me on the first try.
Directly comparing different meal plans is difficult because no two offer exactly the same number of meals, range of ingredients, and number of meals per day, in a way that lets you easily see which is the best value for money. However, at the time of writing, the following is a rough guide to the cost, with delivery, of one week’s dinners for
EveryPlate: $70.99
Family Cook: $102.30
: $114.99
Youfoodz: $141.89
CHOICE has also reviewed and rated these and other meal plans recently, and you can see their conclusions at bit.ly/foodkits.
Fred Robertson Hepatitis SA Peer Mentor
For other ideas, check out Hepatitis SA’s ‘Eating Low Sodium’ series, or have a look at our publications on healthy eating for your liver.
• bit.ly/hepsalowsodium
• bit.ly/eatwell_liver
• bit.ly/hepsalowsalt
Note: neither the author nor Hepatitis SA have received any sponsorship or any other sort of inducements for this article. Please research your options to decide what is best for you.
If you’ve been diagnosed with hepatitis you’ll probably be having health care appointments and tests on a fairly regular basis. This can sometimes be overwhelming - but being prepared for what to expect and how to ask the most useful questions can lessen the stress.
The following free resources help to demystify test results, provide valuable hints in how to get the best out of appointments, how to find information about medications, and how to make sure you’re being treated respectfully by health professionals.
If you would like assistance in accessing these, or any other, resources, contact us at admin@hepsa.asn.au.
In Our Library Ready for your appointments?
Managing the stress of medical appointments
London British Liver Trust 2024. 5p.
Some tips to help prepare you for any medical appointments including: deciding what you want from the appointment, stress busting techniques while waiting; how to manage medical interactions - and how to follow up afterwards. Contains links to further information.
bit.ly/appointmentstress
Question
builder
HealthDirect & Aust Commission on Safety & Quality in Healthcare, Canberra, 2017. Interactive website and 3p. printout.
Be ready for any medical appointment by creating a
list of general questions to ask your doctor or specialist. A range of questions can be chosen to cover any queries about symptoms, tests, costs, treatment options, risks, benefits etc. and the list can be printed to take to your appointment. bit.ly/question_builder’
Worried about getting a blood test? 5 tips to make them easier (and still accurate)
The Conversation, Melbourne/ Sydney, 2023. 4p article. This article discusses the processes involved in taking blood and what happens after it’s collected. It gives advice about the best way to prepare for a variety of blood tests, tips for improving the experience, and what may happen after the test. bit.ly/five_easytips
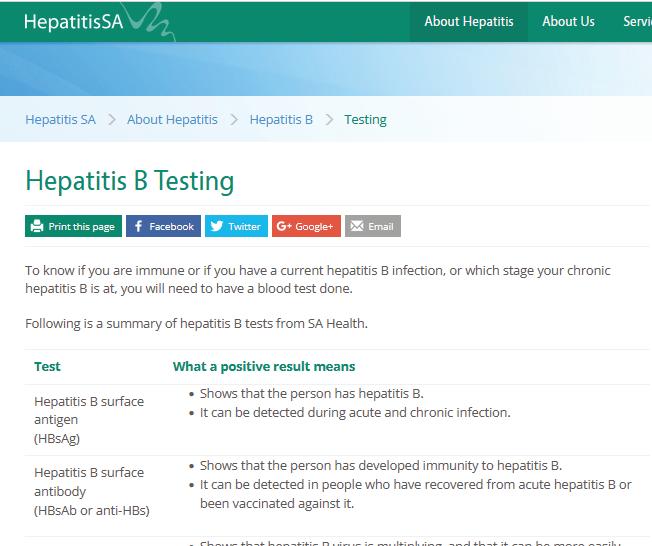
Hepatitis B testing
Hepatitis SA & SA Health, Adelaide. 1p.
A hepatitis B test (to see if you have hep B or to check for immunity) can involve terminology that is complex and can be difficult to understand, including HBsAg positive, hep B surface antibody, hepatitis B surface antigen and anti-HBs reactive. This chart explains in plain English what the tests measure and what the results indicate.
bit.ly/hepb_testresults
Charts showing this information in Chinese and Korean (produced by Hepatitis NSW) are available from bit.ly/hepb_ testing: scroll down to ‘What does your hepatitis B test result mean’.
A single page with specific questions about liver tests and what they might show, with space for notes, designed to be taken with you to GP appointments.
bit.ly/helpful_qs
What you need to know about telehealth for hep (B or C)
Hepatitis NSW, Sydney Hepatitis NSW 2022 (updated. 3p.
If you would prefer to have an appointment over the phone or via a screen (smartphone, laptop, computer or tablet) you could ask if telehealth appointments are available. This factsheet explains eligibility, benefits, how to access, additional services and follow up appointment information.
Hep C: bit.ly/telehealthc
Hep B: bit.ly/telehealthb
Take the confusion out of medications
Medsearch, Melbourne, 2024. Online search engine.
Search for the most up-to-date medicines information including reasons for use, what to know when taking, interactions with other medicines, how to use, what to do/not to do, possible
side effects, and general consumer medicine information printouts.
medsinfo.com.au
Codes of conduct
Australian Health Practitioner Regulation Agency (Ahpra), Sydney, 2022.
If you’re ever concerned about your interactions with any health practitioners: there are codes of conduct that will explain your rights to be treated fairly and with respect. Information about the codes for registered health practitioners (including dental, physiotherapy, pharmacy etc) can be found at bit.ly/ healthpractitioner_codes and information about the code for doctors is at bit.ly/doctor_code.
For a comprehensive list of resources accessible via our catalogue go to bit.ly/ prepost_testing for more pre/post test information, and bit.ly/hepsa_self_care for more information about self care and self management.
Hepatitis SA provides free information and education on viral hepatitis, and support to people living with viral hepatitis.
Postal Address:
Kaurna Country PO Box 782
Kent Town 5071
(08) 8362 8443 1800 437 222
www.hepsa.asn.au
Community News: hepsa.asn.au/ communitynews
Library: hepsa.asn.au/library
@HepatitisSA
@hep_sa
Resources: issuu.com/hepccsa
Email: admin@hepatitissa.asn.au
hepatitis A, B and C information, confidential and non-judgemental
referrals and printed
We can help. Talk to us. Call or web chat 9am–5pm, Mon–Fri
Information Support
HEPATITIS SA BOARD
Chair
Arieta Papadelos
Vice Chair
Bill Gaston
Secretary
Sharon Eves
Treasurer
Michael Larkin
Ordinary Members
Lindy Brinkworth
Bernie McGinnes
Janice Scott
Lucy Ralton
Joshua Riessen
Kerry Paterson (CEO)
Hepatitis SA has a wide range of hepatitis B and hepatitis C publications which are distributed free of charge to anyone in South Australia.
To browse our collection and place your orders, go to hepsa.asn.au/orders or scan the QR code below:
Viral Hepatitis Community Nurses
Viral Hepatitis Nurses are nurse consultants who work with patients in the community, general practice or hospital setting. They provide a link between public hospital specialist services and general practice, and give specialised support to general practitioners (GPs) to assist in the management of patients with hepatitis B or hepatitis C. With advanced knowledge and skills in testing, management, and treatment of viral hepatitis, they assist with the management of patients on antiviral medications and work in shared care arrangements with GPs who are experienced in prescribing medications for hepatitis C or accredited to prescribe section 100 medications for hepatitis B. They can be contacted directly by patients or their GPs:
CENTRAL ADELAIDE LOCAL HEALTH NETWORK
Queen Elizabeth Hospital
Phone: 0423 782 415, 0466 851 759 or 0401 717 953
Royal Adelaide Hospital
Phone: 0401 125 361 or (08) 7074 2194
Specialist Treatment Clinics
NORTHERN ADELAIDE LOCAL HEALTH NETWORK
Phone: 0401 717 971 or 0413 285 476
SOUTHERN ADELAIDE LOCAL HEALTH NETWORK
Phone: 0466 777 876 or 0466 777 873
Office: (08) 8204 6324
Subsidised treatment for hepatitis B and C are provided by specialists at the major hospitals. You will need a referral from your GP. However, you can call the hospitals and speak to the nurses to get information about treatment and what you need for your referral.
• Flinders Medical Centre Gastroenterology & Hepatology Unit: call 8204 6324
• Queen Elizabeth Hospital: call 8222 6000 and ask to speak a viral hepatitis nurse
• Royal Adelaide Hospital Viral Hepatitis Unit: call Anton on 0401 125 361
• Lyell McEwin Hospital: call Bin on 0401 717 971
Visit hepsa.asn.au - no need to log in, lots of info & pdates
Follo the HepSAY blog - hepsa.asn.a /blog
Order print resources - hepsa.asn.a /orders/ Follo s on T i er @hep_sa or Facebook @Hepa sSA
Full range of syringes and needles. Water and filters also available in limited quantities for free.
ONLINE
Viral Hepatitis & Blood SafetyEducation
Feel safer around blood, and better able to assist patients living with viral hepatitis.