


“Internal government data shows nearly 2,000 patients on average kept in ‘unconventional spaces’ like hallways and break rooms in January — the highest number ever recorded.”
The Trillium, September 9, 2024


“Internal government data shows nearly 2,000 patients on average kept in ‘unconventional spaces’ like hallways and break rooms in January — the highest number ever recorded.”
The Trillium, September 9, 2024
In 2018, Doug Ford assured voters that he would get rid of hallway health care if he were elected premier. But six long years later, it’s a bigger problem than ever.
Hallway health care - patients waiting for hours or days in hospital corridors, storage areas, and other “unconventional spaces” - is a clear indication that public hospitals are being understaffed and underfunded.
Ford’s Conservative government keeps expanding private health care, saying they’re improving things. So why are more patients waiting in hallways? Why are millions of people unable to find primary care? Why can’t people get the timely home and long-term care services they need? So many questions...and zero accountability.


















By Michael Wolfson
For the first time, a new study has estimated life expectancy across neighbourhoods in Canada’s largest cities – the first in Canada to drill down below the levels of provinces and cities to census tracts, the smallest level of geography that can support estimates of life expectancy.
The results are disturbing.
Along with my colleagues, we examined 3,348 census tracts in Canada’s 15 largest cities, as well as ones with robust data in the largest U.S. cities. Variations in life expectancy across geographic areas are widely observed, and are generally associated with socio-economic factors such as income poverty rates and median household incomes. While overall life expectancy in Canada was about three years longer among the cities studied, we found differences as much as 20 years between one census tract and another, all within a single large city.
Of Canada’s 15 largest cities, Victoria had the widest range in life expectancies, while Oshawa had the smallest range. Victoria, St. Catharines, Ont., and Winnipeg had the largest associations between life expectancy and income poverty rates and median family incomes, while Vancouver and Toronto had the weakest associations.
Our results showed substantial differences in life expectancy among cities within the same province. These results are especially notable given the frequent claims that health care is provincial jurisdiction, and hence
NOVEMBER 2024 ISSUE
EDITORIAL: Oct. 15
ADVERTISING:
Display – Oct. 25 | Material – Oct. 31
Monthly Focus:
Emergency Services/Critical Care/Trauma/ Emergency: Innovations in emergency and trauma delivery systems. Emergency preparedness issues facing hospitals and how they are addressing them. Advances in critical care medicine. Technology: An update on the impact of technology, including robotics and artificial intelligence on healthcare delivery.
Emergency Care Focus
their responsibility. The implication of these findings is that something about municipalities also has important effects on life expectancy and health inequalities.
Perhaps surprisingly, we also found the range of life expectancies across census tracts in Canada’s largest cities could be just as wide as within the six largest U.S. cities, where variations ranged up to about 20 years. However, there was a major difference when it came to income poverty rates: the U.S. cities showed a much stronger link between life expectancy and poverty than in Canada’s six largest cities.
This is puzzling. On the one hand, the largest cities in both countries show similarly wide variations in life expectancy across census tracts. On the other, income poverty rates accounted for much more of these health inequalities in the U.S. cities than in Canada.
What could be driving these health inequalities in Canada, if not the usual socio-economic status measures?
While Canada has purportedly “universal” health care (despite major gaps in dentistry, drugs and longterm care) that is certainly much more universal than in the U.S., this cannot be a strong explanation. There were differences in Canadian life expectancy inequalities across cities within the same province.
Another possibility is that Canada is significantly more egalitarian than the U.S. (though less egalitarian than some other OECD countries), which is evident not only in terms of income inequality, but also in scholastic achievement.
Continued on page 6
EDITORIAL: Nov. 8
ADVERTISING: Display – Nov. 22 | Material – Nov. 26
Monthly Focus:
Medical Imaging /Year in Review/Future of Healthcare/Accreditation/Hospital Performance Indicators:
Overview of advancements and trends in healthcare in 2023 and a look ahead at trends and advancements in healthcare for 2024. An examination of how hospitals are improving the quality of services through accreditation. Overview of health system performance based on hospitals performance indicators and successful initiatives hospitals have undertaken to measure and improve performance. A look at medical imaging techniques for diagnosis, treatment and prevention of diseases.
Annual Radiology Supplement
THANKS TO OUR ADVERTISERS Hospital News is provided at no cost in hospitals. When you visit our advertisers, please mention you saw their ads in Hospital News.
610 Applewood Crescent, Suite 103 Vaughan Ontario L4K 0E3 TEL. 905.532.2600|FAX 1.888.546.6189 www.hospitalnews.com
Editor Kristie Jones editor@hospitalnews.com
Advertising Representatives
Denise Hodgson denise@hospitalnews.com
Publisher Stefan Dreesen stefan@hospitalnews.com
Accounting Inquiries accountingteam@mediaclassified.ca
Circulation Inquiries info@hospitalnews.com
Director of Print Media
Lauren Reid-Sachs
Helen Reilly, Publicist Health-Care Communications
Bobbi Greenberg, Health care communications
Sarah Quadri Magnotta, Health care communications
Dr. Cory Ross, B.A., MS.C., DC, CSM (OXON), MBA, CHE Vice President, Academic George Brown College, Toronto, ON
ASSOCIATE PARTNERS:

Hospital News is published for hospital health-care professionals, patients, visitors and students. It is available free of charge from distribution racks in hospitals in Ontario. Bulk subscriptions are available for hospitals outside Ontario.
The statements, opinions and viewpoints made or expressed by the writers do not necessarily represent the opinions and views of Hospital News, or the publishers.
Hospital News and Members of the Advisory Board assume no responsibility or liability for claims, statements, opinions or views, written or reported by its contributing writers, including product or service information that is advertised.
Changes of address, notices, subscriptions orders and undeliverable address notifications. Subscription rate in Canada for single copies is $29.40 per year. Send enquiries to: subscriptions@ hospitalnews.com
Canadian Publications mail sales product agreement number 42578518.

Researchers at Lawson Health Research Institute and Western University are using a new brain imaging technique to detect preserved consciousness in the intensive care unit (ICU) at London Health Sciences Centre (LHSC) in patients that appear to be in a coma following a severe brain injury.
In a groundbreaking discovery published in The Proceedings of the National Academy of Sciences (PNAS), researchers used functional near infrared spectroscopy (fNIRS), a portable brain imaging technique, to examine whether unresponsive patients in the ICU had preserved consciousness by recording brain activity at their bedside.
For the study, the research team led by Dr. Karnig Kazazian, Dr. Androu Abdalmalak, and Dr. Derek Debicki used fNIRS to determine if patients can feel pain, hear their surroundings, and perhaps most crucially, retain preserved conscious awareness. They first tested this technique on more than 100 healthy individuals before using fNIRS to identify a patient in the intensive care unit who, despite being unresponsive, was able to demonstrate appropriate brain responses to the instruction “imagine playing a game of tennis,” which showed that they were aware.


cordings. It also expands on recent advances made the research team using fMRI and EEG in patients with severe brain injury.
“These findings could fundamentally change the way patients are cared for,” said Dr. Kazazian, Research Associate at Lawson Health Research Institute and LHSC, and Associate Scientist and medical student at Western University’s Schulich School of Medicine & Dentistry. “Deploying a simple tool like fNIRS at the bedside has the potential to provide clinicians information about preserved brain function that standard clinical tools are not capable of doing”.
This discovery builds on more than 20 years of research from renowned Western neuroscientist Dr.Adrian Owen, who first discovered that some unresponsive patients are entirely aware based on results from brain re-
“Families of patients with severe brain injuries want to know whether their loved ones will be able to recover from their injuries,” said Dr. Debicki, a Neurologist at LHSC, Assistant Professor of Neurology at Schulich Medicine & Dentistry and Scientist at Lawson. “fNIRS is an exciting new tool that we can use at the bedside in the ICU to improve the way we answer this very important, complex question.”
Beyond making predictions about outcomes, fNIRS may provide a unique opportunity to interact with patients who are aware but unable to be physically interactive.
“The next steps are incredibly exciting, as expanding the testing to a larger group of patients will enable us
to explore the potential of using fNIRS to communicate with ICU patients, potentially unlocking groundbreaking advancements in patient care,” said
Dr. Abdalmalak, a former Research Associate in the Owen Lab at Western University’s Schulich School of Medicine & Dentistry. n H

People who initiate a premature or “before medically advised” (BMA) hospital discharge have a 10-fold increase in the risk of drug overdose in the following month, according to new research in CMAJ (Canadian Medical Association Journal).
Patients leave hospital prematurely for a range of reasons, including improperly treated pain, cravings, stress that accentuates psychiatric issues, conflicts with hospital staff, and restrictions on movement or visitors. Hospital patients who initiate a BMA discharge are up to 3 times more likely to die in the following year than people who undergo routine physician-advised discharge. “Before medically advised” discharge has also been called “patient-initiated” or “against medical advice” discharge.
Continued from page 4
“For a long time, front-line doctors and nurses have wondered if BMA discharge increases subsequent overdose risk,” says Dr. John Staples, study senior author and a clinical associate professor at the University of British Columbia in Vancouver, BC. “For patients with substance use disorder, a long hospital stay can sometimes be a period of drug abstinence, potentially reducing opioid tolerance and interrupting access to [addiction] treatments. After these patients leave hospital, persistent pain and untreated addiction might prompt heavier-than-usual drug use. All these factors can increase the risk of subsequent overdose.”
To understand the link between BMA discharge and drug overdose, researchers conducted a study that examined health data on 189 808 hospital admissions occurring between
Further, and notwithstanding the American rhetoric about being the land of opportunity, Canadians experience twice the rate of movement up (and down) the income ladder from one generation to the next than in America. And while there is increasing attention in the U.S. to “deaths of despair,” there is growing evidence that a more pervasive cause of shorter life expectancies is chronic stress.
But something other than national-level differences in inequality must be at work. The significantly stronger associations within each of the six largest U.S. cities between life expectancy and poverty rates could be ascribed to greater racial segregation across U.S. cities. While Canada also suffers from racial and other forms of discrimination, recent analyses suggest something more general: there is more socio-economic segregation across U.S. neighbourhoods, including but not exclusively by race.
In part, these broader differences in socio-economic segregation may derive from very different local government structures. In the U.S., wealthy sub-
urbs can “opt out” of supporting poorer neighbourhoods in the same city by creating their own local governments and school boards. In contrast, recent waves of municipal and school-board amalgamation in Canada’s largest cities mean local public goods such as schools are more equitably distributed, with many fewer locally elected authorities.
The findings in our study raise important questions. While Canada’s largest cities appear to have substantially reduced the link between income poverty and life expectancy compared to their American counterparts, why are the variations within them as wide as those in the U.S.? Even though health care is a provincial and territorial responsibility, why can these patterns be so different from one city to the next within the same province? Is municipal and school-board amalgamation a “hidden gem” of public-health policy?
Now that we have the data, addressing these questions could reframe the discourse on health and health care policy in Canada. n H
Michael Wolfson is a former assistant chief statistician at Statistics Canada and current member of the University of Ottawa’s Centre for Health Law, Policy and Ethics.
2015 and 2019 in British Columbia, Canada. A total of 6440 (3.4%) of these admissions ended with patients leaving hospital against medical advice. They found that patients with a BMA discharge were more likely to be younger males with psychiatric illness, substance use disorder, or a history of illicit drug use. The rate of fatal or nonfatal illicit drug overdose in the first 30 days after departure from hospital was 10 times higher after BMA discharge than after physician-advised discharge. “Before medically advised” discharge was associated with subsequent overdose even after accounting for other risk factors for overdose.
“These findings indicate that patients initiating a BMA discharge are
at high risk of overdose, that BMA discharge may be a causal contributor to subsequent overdose, and that patients initiating a BMA discharge (especially those with a history of substance use disorder) should be offered urgent clinical and social supports to reduce overdose-related harms,” write the authors.
They suggest there are opportunities to improve medical care for these patients.
“Hospitals and health systems should develop evidence-based protocols to prevent BMA discharge and should explore novel means of postdeparture outreach to reduce the risk of drug overdose after hospital discharge,” the authors advise. n H
Improved continuity of care protective for persons with lower-extremity
After a lower-extremity amputation (LEA), an improved continuity of clinical care – particularly integration within primary and specialist care – would better assist in the management of LEA and related conditions, suggests a new study.
“After a LEA, patients were more at risk for emergency-department (ED) visits and hospital readmission within a year of initial discharge if they had higher comorbidity (two or more medical conditions) and lower continuity of care,” says Dr. Sara Guilcher, lead author of the study, and senior adjunct scientist at ICES, affiliate scientist at the St. John’s Rehab Research Program at Sunnybrook Research Institute (SRI), and Associate Professor at the University of Toronto.
Recently published in PLOS One, the researchers found that overall, 62 per cent of patients with a LEA visited the ED, and 60 per cent were re-admitted to acute care within the year.
The most common reasons for acute re-admissions and ED visits related to infections (urinary tract, pulmonary and sepsis), congestive heart failure/myocardial infarctions, diabetes,
chronic obstructive pulmonary disease, and wound-related care. Persons with LEA were more at risk for ED visits if they had higher comorbidity, lower continuity of care, and living in areas of lower income.
Common risk factors for rehospitalization included having lower continuity of care, increasing comorbidity, and having a diagnosis of chronic obstructive pulmonary disease. However, sex differences were also identified, with females being at risk for re-hospitalization if they had a previous diagnosis of a mental health condition.
“LEA is a life-altering procedure, with significant negative impacts to patients, care partners, and the overall health system,” adds Dr. Sander Hitzig, senior author of the paper and program research director & senior scientist for the St. John’s Rehab Research Program at SRI. “There is a need to improve transitions from the acute setting to next point of care to ensure care is coordinated and integrated for persons with LEA who are more at risk.”
The study was funded by the Physician Services Inc. Foundation and the Ontario Association for Amputee Care. n H
Targeting vaccination programs for respiratory syncytial virus (RSV) to older adults with underlying health conditions is a cost-effective way to reduce disease, according to a new modelling study in CMAJ (Canadian Medical Association Journal).
RSV infections cause major illness, especially in infants and older adults, and rates of infection increase with age. There are now vaccines available to prevent disease caused by RSV in adults, and vaccination campaigns may reduce the incidence in older adults and associated health care costs.
To understand the potential impact of RSV vaccinations, researchers created a model to assess the cost-effectiveness of vaccine programs in different age groups with different medical risk. Most existing cost-effectiveness studies have focused on adults aged 60 and older, but in this study, researchers focused on adults aged 50 and older. They analyzed a combination of age-only, medical risk–only and ageplus medical risk–based vaccination strategies.
“Strategies focused on adults with underlying medical conditions that place them at increased risk of RSV disease are more likely to be cost-effective than general age-based strategies,” writes Dr. Ashleigh Tuite, the Centre for Immunization Programs at
the Public Health Agency of Canada and the Dalla Lana School of Public Health, University of Toronto, Toronto, Ontario, with coauthors. “We found that vaccination of older adults may be less costly and more effective
than no vaccination and that vaccinating people aged 70 years and older with chronic medical conditions is likely to be cost-effective based on commonly used cost-effectiveness thresholds.”
The research team notes that in some settings with higher risk of disease and higher health care costs, such as remote communities in Canada’s north, broader vaccination programs across age groups may be cost-effective.n H
Anew study by the Centre for Addiction and Mental Health (CAMH), entitled Mental Health Service Use Before First Diagnosis of a Psychotic Disorder and published in JAMA Psychiatry, found that nearly 75 per cent of young Ontarians with a psychotic disorder had at least one mental health service visit within the three years prior to their first diagnosis of the disorder.
The retrospective cohort study –one of the largest of its kind – suggests that youth with a psychotic disorder are nearly four times as likely to have a previous mental health-related hospital admission, twice as likely to have a mental health-related emergency department visit, and more likely to have a past diagnosis of substance use disorder compared to youth diagnosed with a mood disorder.
“Our findings suggest that these factors – prior mental health-related
hospital admissions and emergency department visits, and prior diagnosis of substance use disorder – may indicate increased risk for a psychotic disorder,” says Dr. Nicole Kozloff, Co-Director of the Slaight Family Centre for Youth in Transition at CAMH. “These results are remarkably consistent with other jurisdictions outside Canada, and should guide further research into detecting and intervening earlier in the course of psychotic illness.”
As part of the study, the researchers used information held by ICES on health service use and other linked data to examine previous mental health use in Ontarians aged 15-29 years who were later diagnosed with a psychotic disorder between April 1, 2012 and March 31, 2018. The team identified more than 10,000 individuals with a first diagnosis of psychotic disorder and matched them with individuals who were diagnosed with a mood disorder.
“Those at risk for psychosis are ‘hiding in plain sight,’” says Dr. Aristotle Voineskos, Vice President, Research at CAMH and Director of the Campbell Family Mental Health Research Institute. “These data provide a very different picture of who is at risk for psychosis, and also suggest the opportunity moving forward to examine whether effective treatment for prior conditions may change the risk for psychosis.”
The early findings from this research inspired the launch of the Toronto Adolescent & Youth (TAY) Cohort Study at CAMH. This five-year study is tracking 1,500 children and youth presenting for mental health services, examining their biology, education and cognition, social factors, and service use patterns. The goal is to increase understanding of who is at risk for psychosis and, most importantly, how to mitigate that risk via earlier intervention. n H
Recently published in JAMA, findings of the HeLiX Randomized Clinical Trial, an 8-year multicentre trial, demonstrate that among patients undergoing liver resection for a cancer-related indication, tranexamic acid did not reduce bleeding or blood transfusion but increased perioperative complications.
11 hepatopancreaticobiliary sites across Canada and the United States participated in the placebo-controlled, randomized trial including Ontario Hospitals Sunnybrook Health Sci-
ences Centre, Unity Health Toronto, University Health Network, London Health Sciences Centre, Kingston General Hospital and Hamilton Health Sciences.
Liver resection is an optimal treatment for patients with primary or metastatic liver malignancies, with 15 to 25 per cent of these patients receiving perioperative blood transfusions. Intraoperative blood loss and transfusion are major risk factors for postoperative morbidity and mortality and are strongly associated with long-term cancer recurrence and lower overall survival.
Previous studies have found that in a variety of surgical procedures, tranexamic acid – a medication used to treat or precent excessive blood loss – reduces the probability of receiving a blood transfusion. However, this evidence is largely derived from cardiac and orthopedic surgery, in which bleeding often occurs from small vessels. As a major abdominal surgery, intraoperative bleeding during liver resection often occurs from large vessels. The Hemorrhage During Liver Resection: Tranexamic Acid (HeLiX) trial was conducted as a response to the gaps in evidence sup-
porting the use of tranexamic acid in cancer surgery like liver resection. “We wanted to see if tranexamic acid had a significant impact on red blood cell transfusion in major abdominal surgeries like liver resection, as it does in other types of surgery,” explains Dr. Paul Karanicolas, scientist in the Odette Cancer Research Program at Sunnybrook and principal investigator of the study. “The results of the trial have a significant impact on the use of tranexamic acid, emphasizing a cautious approach to the adoption of tranexamic acid in certain surgical procedures.” n H
Anew study from Unity Health Toronto researchers evaluates the use of CHARTWatch, the artificial intelligence (AI) early warning system developed at St. Michael’s Hospital that monitors hospitalized patients in real-time and identifies those at high risk of unexpected death or transfer to an intensive care unit (ICU) and sends alerts so that doctors and nurses can intervene early.
The study, published in the Canadian Medical Association Journal on Sept. 16, shows a significant 26 per cent reduction in unanticipated mortality after the tool was implemented on the St. Michael’s general internal medicine (GIM) ward.
“As AI tools are increasingly being used in medicine, it is important that they are evaluated carefully to ensure that they are safe and effective,” says lead author Dr. Amol Verma, General Internist at St. Michael’s who led the development and implementation of CHARTWatch.
“Our findings suggest that AI-based early warning systems are promising for reducing unexpected deaths in hospitals.”
One of the primary sources of unplanned admission to the ICU is the unexpected deterioration of hospitalized patients, which prompted researchers at Unity Health Toronto and the University of Toronto to develop this AI tool and study its effectiveness.
“This important study evaluates the outcomes associated with the complex deployment of the entire AI solution, which is critical to understanding the real-world impacts of this promising technology,” says co-author Dr. Muhammad Mamdani, Vice President of Data Science and Advanced Analytics at Unity Health Toronto.
“We hope other institutions can learn from and improve upon Unity Health Toronto’s experiences to benefit the patients they serve. Unity Health Toronto is a collaborative leader already helping to spread our AI tools via innovative partnerships with more to come.”
The study analyzed data from 13,649 patients aged 55 to 80 years old

admitted to the GIM unit (9,626 in the pre-intervention period and 4,023 using CHARTWatch) and 8,470 admitted to subspeciality units that did not use CHARTWatch.
“The CHARTWatch project started at Unity Health when we asked patients, clinicians, hospital leaders, what would you want to use artificial intelligence for? If you could predict one thing that AI would tell you, what should that be?” says Verma.
“And one of the leading priorities of everyone was to be able to predict in advance which patients might become so sick in hospital that they need ICU or might die.”
During the 19-month-long intervention period, 482 patients in the GIM became high-risk, compared with 1,656 patients who became high risk in the 43-month-long pre-intervention period. There were also fewer non-palliative deaths in the CHARTWatch group than in the pre-intervention group (1.6 per cent versus 2.1 per cent).
“If I were a patient, I would be so relieved to know that we have this

kind of system,” said co-author Dr. Yuna Lee, Division Head and General Internist at St. Michael’s.
“So when the patient gets a high risk alert, they’re going to be assessed by senior staff right away. And also they’re also going to have quite close monitoring by nursing staff, so they check on them every one to two hours.”
CHARTWatch inputs more than 100 aspects of a patient’s medical history and current health status that are routinely stored in the hospital’s electronic medical record. It analyzes the interactions between these inputs and how they change over time. With that information, it’s able to categorize each patient by their risk for deterioration and send an alert to prioritize treatment.
“The team lead receives a high risk CHARTWatch alert and then she would inform the primary nurse,” says Emme Rose Villanueva, Registered Nurse at St. Joseph’s Health Centre. “Then we would closely monitor the patient, prioritize high risk alert ver-
sus the stable ones, and do necessary interventions as needed.”
The study is one of the first rigorous studies evaluating how CHARTWatch can benefit hospital patients in Canada and shows the potential real world impact of AI on the health care sector.
“Every time I hear the alarm I tell the nurses, whoever has the patient, and then also inform the doctor,” said Alicia Feruelo, Team Leader and Registered Nurse at St. Joseph’s Health Centre. “From the first time it’s been used, I could only remember one transfer to ICU.”
Damian Jankowicz, Vice President and Chief Information & AI Officer, says he hopes AI tools like CHARTWatch will continue to have a profound impact on patients.
“Hopefully with reduced administrative burden on our providers, they will have more time to spend with our patients and really focus on the patient needs,” he says.
“I hope that AI will be able to distill the incredible amounts of information that’s coming at our clinicians into important components and really bring their clinical judgment to the forefront.” n H
By Anna Sharratt
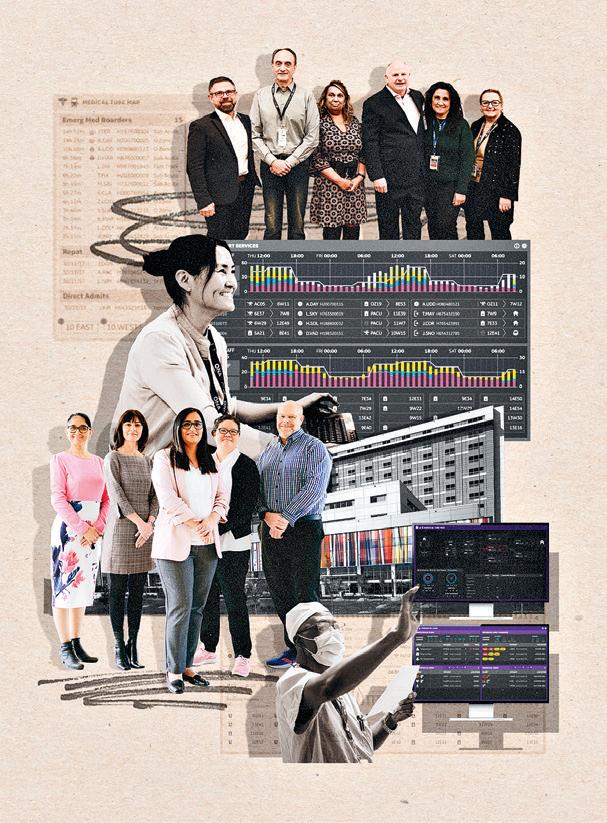
If you stand outside Humber River Health, you’ll see a steady stream of Ubers, taxis, other cars, and ambulances delivering patients to the bustling hospital’s Apotex Emergency Department (ED), which serves almost 140,000 patients every year. Yet despite having one of the busiest EDs in Ontario, Humber has a reputation for being one of the safest hospitals in Canada.
The proof is in the numbers: 66 per cent fewer cases of hospital harm than the provincial average, a 10 per cent year-over-year reduction in sepsis cases, a 40 per cent year-overyear decrease in code blues – medical emergencies that can include heart
attacks or respiratory distress – and a medication error rate of 0.009 per cent.
Humber’s commitment to safety and quality care is further exemplified by its ranking among the top five Ontario hospitals in every category of the American College of Surgeons’ 2023 National Surgical Quality Improvement Program (NSQIP). Humber is the only hospital in the province to achieve this distinction.
The secret to Humber’s safety successes? For starters, Humber’s culture of safety is the focal point for staff at every level of the organization, according to Amanpreet Ghuman, Director of Quality and Patient Safety.
Continued on page 11




With the support of donor funding, St. Michael’s Hospital has opened a state-of-the-art hybrid biplane operating room for advanced neurovascular procedures. The firstof-its-kind in Canada, Operating Room 19 (also known as ORX) features the combined functionalities of a hybrid operating room with the advanced imagining technologies of a radiological suite.
ORX gives clinicians the ability to perform multiple procedures or surgeries at the same time, while having access to real-time, high-resolution imaging from two different X-ray machines to guide their work. This combination will allow for greater efficiency and patient safety, says Dr. Vitor Mendes Pereira, neurosurgeon at St. Michael’s and Schroeder Chair in Advanced Neurovascular Interventions.
“This hybrid biplane operating room offers the possibility of doing a full range of neurovascular procedures, including minimally-invasive and endovascular. It also opens up the possibility of doing open surgeries and minimally-invasive surgery combined,” he says.
Before ORX opened, if a patient required multiple specialized interventions, they would usually be performed separately and in different parts of the hospital. This workflow requires extra time and planning to prepare and transfer patients – many who are

in critical condition. Now, with the hybrid biplane operating room, the patient doesn’t need to leave the OR, and clinicians can provide both interventions in one session, he says.
For example, for certain cancer patients, clinicians in ORX can reduce the blood flow to a patient’s tumour, allowing a surgeon to immediately remove it with less bleeding. Previously this pre-surgical procedure would have to be done separately from the actual tumor removal, requiring additional time and resources, Pereira says. ORX could also accommodate trauma patients who require multiple surgeries, eliminating the need for intra-hospital transfers, he says.
This more efficient operating room will allow for better mapping and planning of care for complex patients, says Pereira.
“ORX was designed to have many different specialties working in the room together, including surgery, trauma, cardiac, oncology and medical imaging. This will reduce the number of procedures for patients and ultimately be safer,” he says. “We have a very unique set up. There is no other facility like this in Canada.”
Director of Medical Imaging Jeff Kerk says having integrated imaging technology built directly into the operating room is a game changer.
“This innovation allows for real-time, high-resolution imaging during surgical procedures, ensuring that surgeons have the most accurate information at their fingertips. The result is greater surgical precision, shorter operative times, and ultimately, better outcomes for our patients,” Kerk says.
“The Medical Imaging team is excited to be a part of this transformative step forward in healthcare delivery, with advanced medical radiation technologists and interventional registered nurses providing essential technical, diagnostic, and clinical support.”
ORX is being set-up to support the latest telerobotic systems, which will allow the St. Michael’s team to further their research on robotic-assisted surgery, says Neurovascular Research Program Manager Nicole Cancelliere.
Cancelliere, who co-leads the RADIS Lab and was part of the team that performed the world’s first robotic neurovascular intervention in 2019, says local robotics has shown many benefits to date, including increasing surgical precision and safety, helping to reduce surgeon fatigue and decreasing staff exposure to the radiation emitted from X-ray machines.
The innovative work of RADIS Lab in ORX will allow our surgeons to one day treat patients in another hospital using telerobotics, she says.
“Remote robotic neurovascular surgery will allow faster treatment of patients in remote communities, suffering from time sensitive diseases, such as stroke, which can have a significant impact on improving patient outcomes,” Cancelliere says. n H
“Our leaders know what risks are present and how to address those proactively,” she says. “We use that data to take action.”
During orientation, trainees are put through a rigorous set of simulations that prepare them for a range of scenarios, from handling a code blue to de-escalating a violent patient situation. “This process ties in all of our safety concepts for everybody before they even start,” explains Derek Hutchinson, a Director of Professional Practice at Humber.
Overseeing operations is Humber’s Command Centre, an innovative centralized data tracking system that allows clinicians to track patients and their vitals in real time. The first of its kind in Canada, this “mission control”

uses data algorithms to identify where in the hospital an issue is occurring –whether it has to do with staffing in a particular unit, an uptick in ED admissions, or a patient who is deteriorating – so staff can take action before an issue worsens.
The Command Centre also ensures that potential delays in patient care can be addressed promptly and efficiently, rather than being reported at the end of the day. The Command Centre’s Early Warning Systems, such as the Clinical Deterioration tile, have significantly reduced critical events by proactively identifying and mitigating potential issues. Any concerns are flagged and immediately sent through to a variety of departments, which in turn work collaboratively with other divisions to address them.
Ghuman’s team tracks patient safety events, conducts reviews, and cre-
ates a report highlighting trends and opportunities for improvement. “If anything is significant, we will roll out education in collaboration with the programs,” she says.
In addition to its staff, Humber also has Patient and Family Advisors (PFAs), a dedicated volunteer group of former and current patients and family members. This team of more than 50 individuals focuses on quality improvement at the unit and corporate level, highlighting any gaps or issues for hospital staff¬ and leaders. Most importantly, they have the ear of management.
“We seek their guidance around patients’ expectations when it comes to their care and how we can better meet those expectations,” explains


Ghuman. “And we’re always looking for more former patients and family members to join.”
Hutchinson notes that Humber’s Corporate Patient and Family Advisory Committee (PFAC) has an unusually high engagement rate and has made significant contributions to hospital policies and quality improvement initiatives.
While the general public wouldn’t be familiar with the behind-the-scenes dedication to safety, patients are well aware, with the Canadian Institute for Health Information finding that 87 per cent of patients would recommend Humber as a place to receive care.
The pride Humber’s staff¬ take in ensuring every patient is expertly cared for can be heard in the passionate way Ghuman and Hutchinson speak on the topic. “Things are working well, but we don’t plan to stop,” says Ghuman. “We’re constantly striving for improvement.” n H

According to the Canadian Cancer Society, lung cancer is the deadliest form of cancer in both males and females, accounting for one quarter of all cancer deaths in Canada. Twelve years ago, two physicians at William Osler Health System (Osler) set out to change that narrative with the launch of a lung cancer screening program to serve its growing communities. Based on the results of a recent Osler study, the program has positively impacted the lives of more than 150 patients and families.
Osler’s Lung Cancer Screening Program was the first of its kind in a community hospital in Canada. Today, it is the longest running multidisciplinary lung cancer screening program in the country outside of a research/pilot study, combining the significant expertise of Osler’s talented health care professionals in diagnostic imaging, thoracic surgery and medical oncology.
“Thanks to a $300,000 grant from the Lung Ambition Alliance, we were able to conduct a retrospective study of more than 5,000 patients who participated in our program between 2012 and 2019,” said Dr. Marc Ossip, Chief, Diagnostic Imaging, William Osler Health System and one of the screening program’s founders. “Over the eight-year period, Osler detected a high rate of cancers – primarily early stage – which is so critical given that catching cancer early often leads to a much better outcome.”
Patients entering the program had to meet specific criteria: aged 55 to 77 years, a significant history of smoking, no prior lung cancer, no prior CT scan within 12 months of having an initial Low-Dose Chest CT scan (LDCT), and former smokers must have quit the habit within the previous 15 years. The median age for participants was 63 years, with more than 60 per cent of them being male. Patients were referred through a family physician or specialist.
“What we were seeing as thoracic surgeons back in 2012 was that the majority of patients were coming to the hospital with late-stage lung can-

cer,” said Dr. Kashif Irshad, Division Head, Thoracic Surgery, William Osler Health System, who partnered with Dr. Ossip to create the program and is one of its most ardent champions. “For us, at Osler, a lung cancer screening study in the New England Journal of Medicine, at that time, crystallized that we needed to create an evidence-based lung cancer screening program to better serve our communities. I am grateful that we have a supportive hospital executive team that agreed.”
Given there was no dedicated funding available for the program, the hospital tapped into its budget to cover associated costs. The results of Osler’s eight-year study validate that the investment has made a significant positive difference in the health of people in its communities.
The study revealed that more than 680 new patients entered the program each year, with an average program growth rate of 27.6 per cent. To date, the Lung Cancer Screening Program recorded over four per cent cancer detection rate, which is higher than similar major studies. Of those patients requiring lung biopsies, more than half were malignant and another 12 per cent were suspicious for cancer. As a result of the program, the clinical stage of lung cancer detected was primarily early stage (Stage I or 2).
Thoracic surgeons typically present complicated patient cases at weekly multidisciplinary rounds to get the input of the entire team. This collaborative group includes a molecular pathologist, radiologist, radiation doctor, and medical oncologist. If lung cancer is found early and surgery is required, this often means a less-involved surgery, such as the removal of a lobe or section of a lung.
“Not only are we finding cancers early, we’re discovering that involvement in the screening program is triggering many patients to re-evaluate their smoking habits whether cancer is detected or not,” said Dr. Irshad, who notes that the program also links patients to a smoking cessation program in their own community if wanted.
Given most lung cancer screening programs are in highly specialized centres, those living in smaller communities have limited or no access to them. Osler’s experience demonstrates that multidisciplinary lung cancer screening programs are effective and can be implemented on a much broader scale in community hospitals across the country with excellent outcomes.
“Osler recognized that establishing a lung screening program was the right thing to do and took the steps to make it a reality for our community,” said Dr. Parneet Cheema,
Medical Director of Cancer Care and Head of Cancer Research, William Osler Health System. “We work seamlessly as a team across diagnostic imaging, thoracic surgery and medical oncology to screen and treat these patients. As the study showed, it saved the lives of many people whose cancer would have otherwise gone undetected.”
The program was recently approved for funding through Cancer Care Ontario (CCO) as a designated Ontario Lung Cancer Screening location. It was also profiled at the World Conference on Lung Cancer in San Diego in September 2024, and will be featured at the Radiology Society of North America’s Annual Meeting in Chicago in December 2024.
Osler’s cancer care program offers a wide range of high quality and compassionate cancer care services including prevention, screening, diagnosis and treatment. The organization is currently working diligently on plans for a comprehensive Cancer Care Centre at Brampton Civic Hospital that will bring new and expanded cancer care services – including radiation therapy –closer to home.
Family physicians and specialists who wish to refer patients to Osler’s Lung Cancer Screening Program can do so by downloading the referral form from Osler’s website. n H


The toxic drug crisis is a long-standing public health emergency, but many are unaware of the brain injury epidemic that underlies it. As researchers investigating the intersections between brain injury, mental health and substance use, we want to shed light on one of the more under-recognized consequences of drug toxicity in Canada: overdose-induced brain injury” says Dr. Mauricio A. Garcia-Barrera, Professor of Psychology at the University of Victoria.
It is known that 16 Canadians died every day between 2016 and 2023 from toxic drugs, amounting to 42,494 deaths.
Beneath these numbers lie thousands of unaccounted survivors with overdose-induced brain injuries – what we refer to as the hidden epidemic. By definition, any loss of consciousness is a hypoxic event, so any overdose with a loss of consciousness is a potential brain injury. “Howev-
er, this relationship is not common knowledge among health-care service providers, people who use substances and their family members,” says Cole J. Kennedy, Clinical Neuropsychology PhD student at the University of Victoria.
“Even in hospitalization cases, routine brain injury screening and assessment is not common practice after overdose. Our research identified the need for accurate recognition and diagnosis of brain injury as a top priority.”
Kennedy’s recently published study outlines stakeholders’ top ten priorities for research addressing the intersections of brain injury, mental health and addictions, as part of the team’s larger investigation.
The three-year BC Consensus on Brain Injury, Mental Health & Addictions research project was designed to reach a consensus on the priorities and solutions to best serve people experiencing the intersections of brain
injury, mental health and addictions in BC.
Using a community-engaged approach, the group examined these intersections with a closer look at particular sub-topics each year, including overdose and brain injury, intimate partner violence and brain injury, and housing and homelessness as is relates to brain injury.
Recommendations emerging from the three years include:
• Provision of integrated care, in which access to services and supports is facilitated by servicing co-morbidities within a single and continued process.
• Informed services by adequate screening for brain injury, mental health, and addictions as co-existing problems, that is supported by a collaborative approach to care across health professionals.
• Increased education about brain injury across health professionals, members of the legal and police system, and many other professionals
The Master of Health Administration (Community Care) program prepares graduates to effectively manage and lead organizations in the dynamic and growing Community Care sector.
and volunteers servicing survivors of brain injury.
• Increase access to services, including long-term housing, improve existing services, create personalized care, and increase research requires increased and continuous funding and resourcing from government, as well as federal policy to support longterm impact of these efforts. The project represents a unified stance from leading experts and stakeholders across BC, emphasizing the urgent need for comprehensive legislation addressing the interconnected challenges of brain injury, mental health and addiction.
The BC Consensus on Brain Injury has been instrumental in the progression of Bill C-277, the National Strategy on Brain Injury Act. Bill C-277 received a unanimous vote in the House of Commons on June 12, 2024, and will now be studied by the Standing Committee on Health before advancing to the Senate floor. n H
format allows students to work full-time while completing the program in 16 months
By Meg Stypa
Each time a person enters a hospital, they entrust their care providers to keep them safe and help them heal. With this level of responsibility, the stakes are high and even seemingly simple errors can prove catastrophic.
While health care organizations are focused on improving patient safety, preventable harm persists and continues to impact patient care. The impact is significant at a system level, with the Canadian Institute for Health Information reporting that Canada’s unintended hospital harm rate increased from 5.4 to 6.0 per 100 hospitalizations from 2021-2022 to 2022-2023
Believing that safe, compassionate care for every patient is the only standard, Mackenzie Health began a journey to zero harm in November 2019. With an emphasis on leadership commitment and support, the organization developed and implemented a fivepart strategy for cultural and process redesign that engaged stakeholders at all levels. This set the stage to improve the patient safety culture across the organization.
In 2022, after opening Cortellucci Vaughan Hospital during a pandemic and amidst a global health human resources crisis, Mackenzie Health recognized the opportunity to accelerate this journey by adopting principles of a High Reliability Organization – principles used in high-stakes industries such as aviation and nuclear power, where errors can lead to catastrophic outcomes.
“At Mackenzie Health, we are committed to actively promoting a culture of transparency, accountability and continuous improvement. This commitment has helped us establish a strong foundation of safety and high reliability across the entire organization,” says Mary-Agnes Wilson, Executive Vice President, Chief Operating Officer and Chief Nursing Executive. “We’ve seen that the HRO approach, which teaches

skills and behaviours that help prevent human error, foster collegiality and ensure patient-centred care, has positively impacted both our quality of care and the patient experience.”
The improvement to patient safety is evident in several key results. Mackenzie Health has reduced its pressure injury rates by 51 per cent, its central line associated bloodstream infections (CLABSI) by 34 per cent and patient falls with an injury have decreased by 41 percent. Since implementing HRO tools and principles, Mackenzie Health has seen a 28 per cent decrease in serious safety events, a 42 per cent decrease in patient complaints and 20 per cent fewer cases of hospital harm than the national average.
Mackenzie Health attributes these positive results to a fundamental cultural shift made possible by the organization embracing a new approach to work. As of September 2024, 83 per cent of all staff and physicians have completed HRO universal skills train-
ing. Organization-wide education also includes leader-specific HRO skills training, which focuses on instilling the principles of HRO, promoting a safety-first mindset and ensuring the timely identification and resolution of problems. Additionally, 76 per cent of leaders at Mackenzie Health have been trained on the Just Culture policy. This policy ensures that the organization continues to promote a fair and open environment that encourages learning from errors in a non-punitive way so that everyone feels safe speaking up for safety.
“One of the most telling indications of the safety-first culture we’re creating is that staff feel more comfortable coming forward with safety concerns,” explains Altaf Stationwala, Mackenzie Health’s President and CEO. “We encourage staff and physicians to openly discuss errors and near misses, as a willingness to report incidents is crucial to learning from them.”
Since 2022, Mackenzie Health has seen a 23 per cent increase in patient safety event reporting while continu-
ing to see a reduction in serious safety event rates. Near miss reporting rates have increased to more than 25 per cent and reporting of employee safety events has increased by nine per cent.
Leadership has played a critical role in reinforcing this safety-first mindset. In June of 2023, Mackenzie Health launched Daily Leadership Safety Huddles, where leaders meet to report on safety events each day. A threetiered model allows safety information to flow from frontline workers to executives and vice versa, ensuring that operational sensitivity is maintained and safety concerns are promptly addressed.
With such promising early gains, Mackenzie Health is eager to continue on the journey it has started.
“We’re proud of our accomplishments in the first few years, but our work is certainly ongoing,” says Altaf Stationwala. “As we continue making progress, we’ll continue to share our experience because the more we learn as a collective, the closer we’ll get to the goal of zero harm.” n H
Anovel longitudinal outreach program for people with opioid use disorder (OUD), set into motion in the emergency department at Vancouver General Hospital, was associated with better health outcomes. Led by Vancouver Coastal Health Research Institute researcher and emergency room physician, Dr. Andrew Kestler, the outreach program resulted in greater participant housing, retention in substance use care and initiation of opioid agonist therapy.
Published in Substance Abuse Treatment, Prevention and Policy, the study builds on previous research findings linking the rapid transition to community care programs with better treatment retention among people with OUD. Initiated by emergency department team members, many programs involve referral to mental health and addictions teams or opioid agonist therapy (OAT), which substitutes medications, such as buprenorphine/ naloxone or methadone, for opioids to reduce the harms associated with substance use disorders and support recovery.
“The emergency department presents an opportunity to act by offering in-the-moment services to patients who may have experienced opioid poisoning or are managing multi-

ple comorbidities at once, such as wounds and mental illness, as well as facing homelessness,” notes Kestler.
“The emergency department encounter can open the door to connecting people with OUD to peer navigators and other resources for longer-term follow-ups.”
Kestler and his team’s first-of-itskind, year-long intensive community outreach program for people with OUD integrated regular check-ins on top of the standard of care. Initiated in the emergency department, the program offered a mix of in-person and telephone conversations with patient-centered care options. Outreach team members facilitated well-being check-ins and offered information on community supports, such as substance use care and housing.
“We have a greater understanding now that simply referring to follow-up care from the emergency department is more of a barrier for people with OUD who want to explore community-based care options than, for example, accompanying them to a community-based care facility directly from the hospital.”
Long-term follow-ups resulted in greater housing and treatment retention
Eighty-four adults from the Vancouver area aged 18 years of age or older participated in the study. All had

A goal of substance use care is to shorten the time between relapses, giving people enough breathing space to establish social supports that can facilitate their recovery.
clinically confirmed OUD and were not on OAT at the time of program initiation. Sixty participants completed at least one follow-up questionnaire – provided at the one-, two-, six- and 12-month marks – with eight participants completing all four questionnaires that were part of the research team’s survey protocol.
Researchers surveyed for participant demographic information, as well as frequency of drug use, OAT status, engagement in community care, motivation to engage in treatment, health-related quality of life, housing status and the perceived helpfulness of the outreach program. Study outcomes measures were informed by completed follow-up questionnaires, along with phone and in-person conversations between participants and care team members.
On average, study participants self-reported an increase in substance use care engagement, primarily in the form of clinic visits, from 22 per cent at baseline to 65 per cent at the one-month mark, 81 per cent at two
months, 73 per cent at six months and 74 per cent at the one-year close of the study. Participants also went from no abstinence in illicit opioid use for a full week at baseline to nine to 15 per cent of participants reporting abstaining from opioid use for seven consecutive days.
Forty-two per cent of participants began OAT within their first month participating in the program. After one year in the program, 56 per cent of participants were on OAT. At the outset of the program, 32 per cent of participants had fixed housing, which increased to 48 to 59 per cent at follow-up.
Kestler plans to pursue additional follow-up research with study participants to see whether longer-term program engagement can yield greater retention in substance use care and stable housing.
“We need more information about the role of continued connections to community care supports and support networks in substance use treatment and recovery,” states Kestler. n H

The Centre for Addiction and Mental Health (CAMH) results from the 2023 Ontario Student Drug Use and Health Survey (OSDUHS), revealing a worrying decline in overall mental health among Ontario students.
Key findings show that 38 per cent of students rate their mental health as fair or poor, while a similar number (37 per cent) reported experiencing elevated stress levels. In addition, more than half (51 per cent) of students indicate a moderate-to-serious level of psychological distress, a figure that has doubled over the past decade. Onein-five (19 per cent) students report harming themselves on purpose and one-in-six (18 per cent) had serious thoughts about suicide in the past year.
The data were collected between November 2022 and June 2023 among 10,145 students in grades 7 to 12 in 235 schools in 46 school boards across Ontario. The 2023 OSDUHS reports provide one of the most comprehensive snapshots of youth mental health and drug use in the province, offering valuable insights into both current conditions and long-term trends.
“These results paint a concerning picture of youth mental health in Ontario,” said Dr. Hayley Hamilton, Co-Director of the Institute for Mental Health Policy Research, and survey lead. “Currently more than half of Ontario students report symptoms of depression and anxiety and a third of students (31 per cent) rate their ability to cope as fair or poor. This trend points to a generation under increasing stress and the need for continued and increased investments in youth mental health.”
On a more positive note, the survey revealed a significant decline in drug use among Ontario youth over the past several decades. Seventeen percent of students reported using cannabis in the past year, a number that has decreased since 2019, the year after can-
nabis was legalized for adults. Alcohol use among students has also steadily declined over the past 25 years, with only about one-third (36 per cent) reporting consumption in the past year. Similarly, the percentage of students smoking cigarettes has substantively dropped, reaching just 3.2 per cent in 2023. Additionally, about one in eight students (13 per cent) reported vaping in the past year, a figure that has declined since 2019.
Of note however is that, for the first time, the percentage of female students using certain drugs has surpassed that of males. Specifically, girls are more likely than boys to use cannabis (21 per cent vs. 15 per cent), vape (18 per cent vs. 9 per cent), and drink alcohol (39 per cent vs. 33 per cent).
“While we’ve seen significant decreases in alcohol and cannabis use among youth over the past few decades, the elevated rates of drug use among girls relative to boys is certainly concerning,” noted Dr. Leslie Buckley, Head of the Addictions Division. “We need more data to better understand what is underlying this trend, but it may speak to increased pressure specifically for girls.”
More than three-quarters (78 per cent) of students report spending three or more hours per day in front of an electronic screen in their free time. In addition, the vast majority (94 per cent) of students use social media daily. About one-quarter (23 per cent) of students spend five hours or more on social media every day.
Dr. Alexia Pollilo, Staff Scientist at the Slaight Family Centre for Youth in Transition, commented: “While there is some evidence linking increased use of electronic screens with poor mental health in kids and teens, there’s just not enough data at this point to conclude that social media causes increased distress among youth. Today’s young people are navigating a digital landscape that’s become integral to

their lives, bringing both opportunities and challenges. We need more targeted research on social media’s impact to develop evidence-based guidelines and strategies that promote a healthy digital engagement.”
The survey reveals that climate change continues to weigh heavily on students’ minds. About one-in-six (18 per cent) report being very or extremely worried about climate change, while just under half (45 per cent) say they feel depressed about the future due to this issue. These figures are consistent with those from 2021, when these questions were first introduced, underscoring the ongoing environmental anxiety faced by this generation of young people.
The OSDUHS survey asked youth about barriers to seeking mental health support. One-third (33 per cent) of students report that they felt they needed mental health support from a professional during the past year, but did not seek it. The most common reasons cited for not seeking help are thinking they could manage it
themselves, being afraid of what others would think about them, and being “too busy.”
“Let this be a call to action for parents and young people,” added Dr. Buckley. “It’s crucial that we continue to break down barriers to seeking support. If you’re struggling, please know that help is available and that asking for it is a sign of strength, not weakness.”
The Institute for Mental Health Policy Research at CAMH has conducted the Ontario Student Drug Use and Health Survey (OSDUHS) every two years since 1977. The OSDUHS is the longest-running ongoing school survey of adolescents in Canada, and one of the longest running in the world. The survey results are described in two reports – one for mental health and the other for drug use – and include data on drug use, mental health, physical health, gambling, bullying, and other risk behaviours, as well as identifying risk and protective factors among Ontario students. All data are based on self-reports derived from anonymous questionnaires. The survey was administered in classrooms by the Institute for Social Research (at York University) on CAMH’s behalf. n H
National Infection Control Week
October 14-18, 2024












Hamilton residents living in north and east-end neighbourhoods with L8L and L8H postal codes and mountain neighbourhoods with an L8V postal code develop almost double the amount of sepsis compared to those living elsewhere in the city, a study published in the Canadian Journal of Anesthesia has found.
Any type of infection can lead to sepsis, including bacterial, viral or fungal infections, and as many as one in three people with this disease will die. Common causes include pneumonia, kidney, bladder or bloodstream infections; wounds or burns that become infected; or infections at catheter sites. Sepsis can happen at home or in hospital if an inpatient develops an infection. Preventing hospital-acquired sepsis is strategic priority for HHS.
Several Hamilton communities – including neighbourhoods in these postal codes – have long been identified as facing increased challenges, such as more difficulty accessing health care, higher rates of poverty, and language barriers.
The study’s findings tell us what’s happening in these postal codes in regards to sepsis, says Fatima Sheikh, the McMaster University PhD candidate who led the study. But the data doesn’t reveal why.
“We know `the what.’ Now we need to understand `the why,’ and importantly, how we work with our communities to reduce these inequities,” says Sheikh, who is also an HHS health equity specialist.
Collecting health equity data is critical to understanding ‘the why.’
Back in 2010, the Hamilton Spectator’s Code Red coverage revealed significant disparities in health outcomes across the city, including a difference of 21 years in average age of death, in
communities just five minutes apart. A follow-up series by the Spectator 10 years later found little had changed, and in some cases the health equity gap had actually widened, in spite of significant efforts to close the gap.
“That to me was mind blowing,” says Sheikh, who first learned of the Code Red project as an undergraduate student.
At the time of Sheikh’s sepsis study, close to 18 per cent of Hamilton residents lived in the three postal code regions, with the remaining 82 per cent making up the rest of the city’s population.
“Our research found 33 sepsis cases per 100,000 residents in these three postal code areas, compared to 15 per 100,000 residents in the rest of the city,” says Sheikh. “It’s almost twice as many in the three postal code areas, yet this represents such a small sliver of our city’s population. That, to us, was staggering.”
As an HHS health equity specialist, Sheikh is part of the hospital’s equity, diversity and inclusion (EDI) team that is leading an initiative to collect health equity (CARE) data from patients, confidentially and voluntarily.
Health equity data will help HHS health-care teams to better understand the diverse needs of patients, identify and address challenges that prevent equitable access to health care, and improve culturally-sensitive care.
This initiative aims to tackle healthcare disparities and develop ways to measure and evaluate how collecting health equity data is helping. Taking steps to close the health-equity gap should also help reduce sepsis rates in systemically disadvantaged neighbourhoods.
“Understanding health equity data is essential for creating a health-care system that truly values and respects the diverse needs and experiences of all individuals,” says Rochelle Reid, senior lead and strategic advisor for EDI at HHS. “By collecting and utilizing

CARE data, we can foster a culture of inclusivity, empathy, and equity, ultimately leading to better health outcomes and an equitable approach to patient care.”
Preventing sepsis is a strategic priority for HHS, as is equity, diversity and inclusion, says Dr. Alison Fox-Robichaud, an HHS critical care physician and the scientific director of Sepsis Canada. She is also the HHS chair in sepsis research.
“This study and the work by our EDI team are important steps in ensuring we have the knowledge and resources to improve sepsis care and prevention for all city residents.”
The collection of equity data began as a pilot program at the HHS Boris Clinic and HHS Ron Joyce Children’s Health Centre in 2023, where more than 2,400 patients volunteered to provide information about their race, ethnicity and preferred language.
A working group was also formed to connect HHS team members with community members to ensure that the collection of health equity data is respectful, inclusive and equitable,
Researcher, Fatima Sheikh
and to develop guidelines and policies for the use of data at HHS.
“Data collection is certainly important,” says Sheikh. “But we recognize that there are people and stories behind these data, so we can’t just report the numbers. We’re committed to working with communities, and we’re starting to do that at HHS.”
The hospital holds a seat on the Greater Hamilton Health Network’s Health Equity Table, Kids Health Alliance Data Collection Working Group and continues to work with Ontario Health West Equity Diversity and Inclusion team to support and coordinate health equity efforts regionally. For next steps, HHS is now working to make health equity data collection standard practice across many of the hospital sites beginning with establishing a process to collect this data using e-Check-in and MyChart.
MyChart is a free, secure, online tool is available to all HHS patients and provides easy access to their hospital health record, and an opportunity to voluntarily provide personal information related to health equity. n H
By Colette Ouellet
ffective infection prevention and control (IPC) programs save lives.
COVID-19 tragically uncovered gaps in IPAC programs and practices in numerous long-term care homes in Canada. Globally, it shed additional light on the lack of effective IPC programs in many countries and regions. Over the past ten years, several major outbreaks have demonstrated that the rapid spread of infectious organisms through a community can be significantly amplified in healthcare settings, particularly where IPC infrastructure is not steadfastly in place. This was true with the Ebola virus, Middle Eastern respiratory syndrome, and H1N1, in addition to COVID-19. While efforts and investments were made during the pandemic to improve the situation, additional supports are necessary to create
sustainable, effective IPC structures and to prevent transmission of infections in all healthcare settings.
A dedicated team of IPC experts within the World Health Organization (WHO) has designed a Global Action Plan and Monitoring Framework on IPC1, supported by a resolution passed at the May 2022 World Health Assembly. With a breathtakingly ambitious timeline, the WHO team, in close collaboration with external stakeholders, augmented the plan with an implementation structure and a global monitoring framework. The plan is based on eight strategic directions organized at the national, regional, and facility levels. This trailblazing strategy builds on existing key WHO documents as well as the recommendations and standards presented in the WHO core components2 and minimum requirements
for IPC programs3. It is work that will substantially assist in moving toward the 2030 vision of ensuring everyone accessing or providing healthcare will be safe from associated infections. While low and middle-income countries will benefit most dramatically from this foundational work, the burden of healthcare-associated infection spares no country. Without effective IPC programs, supported by political commitment and financing, the incidence of antimicrobial resistance (AMR) will rise, fanned by spread in healthcare settings, and the harm experienced by patients and healthcare workers due to preventable nosocomial infection will continue to occur across the healthcare continuum.
IPAC Canada is a member of the Global Infection Prevention and Control Network (GIPCN), a collab-
orative group under the WHO IPC Global Unit, whose ultimate aim is to reduce healthcare-associated infection, including outbreaks, and address the global burden of AMR. Recently, representatives from IPAC Canada were pleased to have been invited to a pivotal meeting that brought together leaders from across the world to exchange experience and insights to inform strategic approaches for implementing the Global Action Plan. We are honoured to provide support to the global community to improve IPC efforts worldwide and are committed to supporting work done through the Public Health Agency of Canada (PHAC) to ensure that Canada has a sustainable national action plan in place with appropriate reporting structures to allow ongoing monitoring of our progress, programs, and impact. n H
Infection Prevention and Control professionals and healthcare providers interested in the prevention and control of infections in all healthcare settings
Sessions will be live streamed.
FUNdamentals of IPAC in Long Term Care
Clinical Rounds
Cultivating Compassionate Leadership for a More Just World | Presenter: Celina Caesar-Chavannes Balancing IPAC Care vs Rules
Persuasive Conversations
Decolonizing Healthcare: Culturally Sensitive Care for Indigenous
Peoples | Presenters: Dr. James Makokis and Anthony Johnson
D EADLINE DATE : January 31, 2025
Abstract submission to open September 2024. Watch for announcement.
To register, submit an abstract, or obtain program updates, visit the conference website at: ipac-canada.org/ipac-canadaannual-conference
IPAC Canada
Telephone: 1.204.897.5990
Toll Free: 1.866.999.7111
Email: info@ipac-canada.org ipac-canada.org
atients who develop a periprosthetic joint infection (PJI) after a total hip replacement have more than a five-fold increased risk of mortality within 10 years, according to new research published in the Journal of Bone and Joint Surgery.
In one of the largest studies to date of patients with PJI after total hip arthroplasty (THA), researchers from ICES, Sunnybrook Research Institute and the Department of Surgery at the University of Toronto’s Temerty Faculty of Medicine looked at the longterm (10 year) mortality risk of PJI for 175,432 adults receiving their first hip replacement in Ontario, Canada. The study was funded by ICES and Arthritis Society Canada.
About 1 in 7 Canadian adults live with osteoarthritis, a number that is expected to grow as baby boomers age and life expectancies increase. Joint replacement procedures can lessen pain and
improve quality of life for people who are dealing with this progressive disease.
“Most hip replacement surgeries are very successful, but unfortunately, about one to two percent of patients develop infections of the prosthetic joint. It is well established that such infections impact patient health over the long-term, but this research provides compelling evidence that it can even lead to death,” says lead author Dr. Raman Mundi, an assistant professor in Temerty Medicine’s Department of Surgery and a surgeon-scientist in the Division of Orthopaedic Surgery at Sunnybrook Health Sciences Centre.
The researchers found that among adults receiving their first hip replacement from 2002 to 2021, 868 patients (0.5%) required further surgery for a PJI within one year of hip replacement.
Patients with a PJI within the first year had a significantly higher 10-year mortality rate than those who didn’t develop an infection (11.4% versus 2.2%)
STERIS is a leading global provider of products and services that support patient care with an emphasis on infection prevention. WE HELP OUR CUSTOMERS CREATE A HEALTHIER AND SAFER WORLD by providing innovative healthcare, life sciences and dental products and services.
STERIS Healthcare’s complete focus is in the peri-operative environment. We partner to understand where you are today, create a plan together, and provide full solution sets to support the Operating Room (OR), GI / Endoscopy Suites and Medical Device Reprocessing Area (MRDA) environment. Our commitment is to help Customers solve their biggest challenges, leverage opportunities for growth, and advance the care of patients. We put the full power of our market leading solutions and our people to work every day in order to help Customers elevate patient care.
To learn more about how STERIS can help you, call STERIS Canada Sales ULC at 800-661-3937 or visit www.steris.com/healthcare-canada.

“Our findings underscore the need for arthroplasty surgeons and infectious disease experts to work together on prevention efforts and follow best practice guidelines for patient care,” says senior author Dr. Bheeshma Ravi, an adjunct scientist with ICES, surgeon-scientist with the Division of Orthopaedic Surgery at Sunnybrook Health Sciences Centre and assistant professor of surgery at Temerty Medicine.
The authors provide several reasons for why they believe the association between PJI and mortality is likely causal and not correlational. First is that the association was quite strong, with the authors controlling for variables such as age, sex, income and health status. Second is that there is precedent that major orthopaedic events (for example, hip fractures) can directly increase risk of mortality. And finally, this study builds on existing evidence that used smaller cohorts of patients and shorter follow-up times.
“Ultimately, we need to develop effective strategies to prevent and cure these infections to reduce the longterm risk to patients,” adds Ravi.
“Joint replacement surgery is the mainstay of definitive management for millions of patients living with end-stage osteoarthritis. Although the risk of infection is quite low for the individual patient, given that tens of thousands of hip replacements are performed annually in Canada, and 70% are directly due to arthritis, it is crucial from a public health perspective to find strategies that reduce infection risk even further. Funding this research has allowed us to quantify this risk and provides necessary data to inform
future prevention strategies,” says Dr. Siân Bevan, Chief Science Officer at Arthritis Society Canada.
The article, “Association Between Periprosthetic Joint Infection and Mortality Following Primary Total Hip Arthroplasty,” was published in the Journal of Bone and Joint Surgery.
Sunnybrook Research Institute (SRI) is the research arm of Sunnybrook Health Sciences Centre, an internationally recognized academic health sciences centre fully affiliated with the University of Toronto. With well-established programs in basic and applied sciences which span across three scientific platforms and ten clinical programs, SRI is developing innovations in care for the more than 1.1 million patient visits the hospital provides annually. Recognized as a Centre of Excellence in focused ultrasound, SRI has one of the most comprehensive and successful focused ultrasound research programs in the world, with technical, scientific and clinical experts accelerating progress in the field. Learn more at Sunnybrook.ca/research.
ICES is an independent, not-forprofit research and analytics institute that uses population-based health information to produce knowledge on a broad range of healthcare issues. ICES leads cutting-edge studies and analyses evaluating healthcare policy, delivery, and population outcomes. Our knowledge is highly regarded in Canada and abroad and is widely used by government, hospitals, planners, and practitioners to make decisions about healthcare delivery and to develop policy. For the latest ICES news, follow us on X, formerly Twitter: @ICESOntario n H
V-PRO™ maX 2 Sterilizer is the first and only sterilizer cleared and validated for select 3D materials. Now you can process a broader range of items, including 3D printed anatomical models and patient specific surgical guides.*
Facing the Future Together.


recent CAMH youth-led qualitative study of attitudes and beliefs among transitional-aged youth (aged 16-29) with mental health concerns has found that lived experience of mental illness impacts their decision-making about whether to get a COVID-19 vaccine. The article, entitled Understanding attitudes and beliefs regarding COVID-19 vaccines among transitional-aged youth with mental health concerns: a youth-led qualitative study, has been published in the journal BMJ Open. In order to ensure the findings resonated with the study’s target population, the study took a youth-led approach. The researchers conducted interviews with 46 young people with mental health concerns as well as six family members between September 2021 and August 2022, a period when COVID-19 vaccines were widely
available and 73 per cent of the population had received at least one shot. The research team included Youth Engagement Specialists from CAMH’s Margaret and Wallace McCain Centre for Child, Youth and Family Mental Health, plus an advisory committee of eight lived experience Youth Advisors.
The CAMH team involved in the study also created a variety of public education resources intended to reduce vaccine hesitancy among young people with mental illness, including a resources aimed both for youth and clinicians.
The study found that the main reason for vaccine hesitancy in this population was lack of trust in the vaccine itself, in healthcare providers, and in government. The study also found lived experience of mental illness played a role in whether transitional-aged youth decided to get a COVID-19 vaccine.
trusted loved ones, and specialized vaccine clinics with low-stimulation setups and personalized approaches can help address these issues.
• Encourage Open Conversations: Encourage open, non-judgmental conversations about vaccines by normalizing hesitancy and feelings of doubt. Health care providers should reduce stigma and provide clear, evidence-based, and accessible information to foster informed decision-making.
Previous research has shown that people with mental illness, including youth, have a 65 per cent higher risk of contracting COVID-19, and that people between 18 and 34 are seven times more likely to be vaccine-hesitant than people over 65.











• Address Trust Concerns: Better understand and address youth’s trust concerns regarding vaccines, healthcare providers, the healthcare system, and government policy makers to improve vaccine acceptance. Participants who were vaccine hesitant often cited decreased trust in institutions and relied increasingly on information from their social networks, increasing the risk of mis/ disinformation exposure.
• Acknowledge Historical Harms: Acknowledge and rectify historical and ongoing harms perpetrated by healthcare systems and governments against racialized communities to boost vaccine confidence and uptake. Participants expressed concerns over the lack of acknowledgement of previous harms when encouraging and enforcing vaccination, emphasizing the need for governments and healthcare organizations to demonstrate trustworthiness.
• Impact of Mental Health: Understand the impact of acute mental health concerns, such as psychosis, on vaccine decisions, and develop strategies to reduce susceptibility to mis/disinformation and needle phobia. Providing plain language vaccine information, support from
“These statistics suggest that youth with mental health concerns may have even higher rates of vaccine hesitancy,” says Senior Author Alexxa Abi-Jaoudé, Communications Coordinator, CAMH Education. “The insights into attitudes towards vaccines gleaned from this study are highly relevant to not just ongoing vaccination efforts for new COVID-19 strains, but for other transmissible diseases and future pandemics as well. Our youthled work here illustrates the need for youth-specific public health and clinical resources to encourage vaccination in this population, and that the lived experience of youth must be embedded in the development of those resources.”
The study also found that different kinds of mental illness can have positive or negative effects on vaccine hesitancy. While previous research has shown young people with anxiety may be more likely to engage in risk-reducing behaviours like getting a vaccine, some participants in the study with lived experience of acute psychosis said they had negative views of vaccination that improved after the episode of psychosis had passed.
“When I was in that state of mind, I was like, ‘This is going to be bad for my body, they are putting toxins in me,” said one study participant. “After I was put on medication and came back to
being aware of what reality is, I was like ‘This is stupid, I should just get vaccinated. It’s not really an infringement on people’s rights or anything. It’s about public safety.”
Aloha Narajos is a Youth Engagement Specialist who was part of the Youth Engagement Initiative engaged in the co-creation of the study and the public education resources related to the study. She remarked:
“When speaking with youth about vaccine hesitancy what came across clearly is that scare tactics don’t work. In addition, the use of scientific jargon can be harmful to youth’s understanding of vaccines and making informed decisions. Rather than using language where it seems as if folks don’t have a choice or confusing them with technical language, instead provide all the right and applicable information so youth can make a well informed decision on their own accord.

“The young people also talked about how social media had influenced their decisions and their knowledge of vaccines. I think because in most cases,
social media is a huge part in a young person’s life; it’s one of the big ways they’re able to connect with others in their lives, and to get information.

This could be leveraged as an important tool to combat vaccine hesitancy if delivered in a clear, simple way from an organization they trust.” n H

- 20,











By Molly Giroux
Four years after the COVID-19 pandemic devastated long-term care homes, those hit hardest in Ontario are rebuilding with an enhanced focus on infection prevention and control thanks to new Infection and Prevention Control (IPAC) Hubs.
Isobel and Arthur Meighen Manor, owned and operated by the Salvation Army is a 168-bed long-term care home in midtown Toronto. It was one of the hardest hit homes in 2020 when the first wave of the pandemic took the lives of 48 residents, and made more than half its staff ill.
“Our goal is to provide the best quality of care to our residents,” says Monica Klein-Nouri, registered nurse and Executive Director of Meighen Manor, “but at the onset of the pandemic we were completely unprepared.”
At the time, infection control was not embedded into long-term care facilities in Ontario. “The roles fell on nurses, which in reality is only a sliver of their responsibilities and knowledge,” says Klein-Nouri.
Plagued by limited resources and staff shortages, the pandemic exposed critical gaps in the health-care system, leading to a re-evaluation of how we care for our most vulnerable populations and the start of a new relationship between hospitals and long-term care homes in the province.
In April 2020, Sunnybrook Health Sciences Centre offered support to Meighan Manor by leveraging its connections through the North Toronto Ontario Health Team and mobilizing a team of infection prevention and control experts to help manage the COVID-19 outbreaks that had taken hold of the long-term care home. The relationship was formalized and expanded in the fall when Ontario Health introduced Infection Prevention and Control (IPAC) Hubs. Local
networks of infection prevention and control expertise were established across the health system to enhance infection control practices in community-based congregate living settings, such as long-term care homes.
Sunnybrook was paired with 18 congregate care homes in north Toronto, including Meighan Manor. Known as the North Toronto IPAC Hub, homes were provided with continuous seven-day per week access to hospital infection prevention and control support, including testing, vaccine delivery and clinical support as needed.
The Hub also assessed each homes’ infrastructure, such as heating, ventilation and air conditioning systems, trained staff on IPAC protocols, and created better connections to hospital resources when needed.
“The Hub has become the new normal of how Sunnybrook integrates with its local community partners,” says Dr. Jerome Leis, Medical Director of Infection, Prevention and Control at Sunnybrook and co-lead of the North Toronto IPAC Hub. “We have moved from the initial crisis to a longitudinal partnership where our focus is on prevention.”
Through the implementation of the Hub, homes saw measurable improvements to disease surveillance, detection, management, and interventions that can improve resident outcomes.
The North Toronto IPAC Hub remains committed to supporting congregate care homes by continually enhancing infection prevention and control capabilities well beyond COVID-19.
Each home now benefits from bi-weekly visits by a certified IPAC professional who works with the team to address the home’s unique and evolving needs on issues such as infection surveillance, antibiotic-resistant organisms, environmental cleaning protocols, facility renovations, and co-developing protocols for a range of infection-related threats.

Homes are now also provincially mandated to designate an IPAC lead of their own. These leads are working with the Hub to skill-up and become certified practitioners themselves. Webinars and weekly meetings offer training and critical information to help their homes stay on top of emerging threats.
Annual conferences, held in collaboration with Michael Garron Hospital, also equip them with the latest recommendations and implementation challenges that they can share with their peers. “These conferences are helping us navigate new issues that can impact our residents and are equipping us with the skills we need to keep them safe,” says Klein-Nouri.
As IPAC Hubs were being implemented throughout Ontario, a new Fixing Long-Term Care Act mandated that long-term care homes use an ethical framework for policy decisions affecting residents and stakeholders.
“No such framework existed within the IPAC community,” says Heather Candon, Director, Infection Prevention and Control at Sunnybrook and co-lead of the North Toronto IPAC Hub. “We needed a structured ap-
proach to decision-making, so we adapted one.”
Developed by the North Toronto IPAC Hub and leading ethicists at Sunnybrook, the Ethical Infection Prevention and Control (EIPAC) Framework provides a step-by-step process to help teams make decisions about infection control measures such as visitation, isolation, masking and understand their impact on residents and their families.
The first-of-its-kind framework has since been adapted to other health-care sectors and is recognized by Infection Prevention and Control Canada and internationally by the Association for Professionals in Infection Control and Epidemiology as a tool that addresses a broader need within the profession.
By leveraging the strong relationships established through the Hub, homes are better prepared to address infection prevention and control issues beyond COVID-19. “There is still so much work to do within the sector when we consider other emerging threats to the safety of residents,” says Dr. Leis, “and capacity-building is a long-term quality improvement journey.”
Hospitals and community partners working as a team to support the health and well-being of our most vulnerable populations is here to stay. n H




Patients and staff are seeing a lot more blue at hospitals in the Fraser Health region.
First introduced to Fraser Health in 2023 for high-infection and outbreak areas, Highlight is now being used for everyday cleaning and disinfecting. Initially, blue coloring was added to bleach wipes. Now, the same hue is compatible with hydrogen




KEEPING GERMS AT BAY IS AN ONGOING CHALLENGE IN HEALTH CARE. AS MICROBES THAT CAUSE INFECTIONS BECOME MORE RESISTANT TO THE DRUGS DESIGNED TO TREAT THEM, EFFECTIVE CLEANING AND DISINFECTING PLAYS A CRITICAL ROLE IN PATIENT CARE.
peroxide (HP) wipes, which are commonly used in health care settings.
To date, Surrey Memorial Hospital, Langley Memorial Hospital, Abbotsford Regional Hospital, Royal Columbian Hospital and Fraser Canyon Hospital have all implemented the hydrogen peroxide version of Highlight. Eagle Ridge Hospital and Ridge Meadows Hospital will join the blue wave this month, with other acute sites and all owned-and-operated long-term care sites onboard by the end of 2024.
With Highlight, each wipe is colored with a blue dye as it is fed through a device attached to the top of a cannister. When housekeeping staff wipe down surfaces, the blue fades to clear as the surface is fully cleaned and disinfected. If color remains, additional cleaning is required.
“Along with implementing Highlight HP region-wide, we are also collecting data to verify the effectiveness and the infection control benefits,” says Jody Miller Elliot, Director of
Housekeeping Strategies and Initiatives, Fraser Health. “Testing results so far indicate a significant reduction in surface contamination, with a 30 per cent reduction in colonizing clusters (bacteria) with Highlight compared to cleaning with microfibre cloths.”
Highlight works in conjunction with other forms of disinfection including: UVGI robots, UVGI pods and Adenosine Triphosphate (ATP) testing. Combined, they reduce the risk of infections such as Clostridioides difficile (C. difficile), carbapenemase-producing organisms (CPO), Candida auris (C. auris) and methicillin-resistant Staphylococcus aureus (MRSA).
“Our housekeeping staff have really embraced this cleaning protocol,” says Jody. “Housekeeping is often the entry point into health care, and many of our staff move into other roles in Fraser Health with a solid foundation on what it takes to help prevent hospital acquired infections. I’m really proud of that.” n H

EFFECTIVE AGAINST
(norovirus/rotavirus), butnot all non-enveloped viruses.

























Dr.Alison Fox-Robichaud’s passion for research dates back to her teenage years, when she spent the summer between high school and university working at a McMaster University research lab.
“From the time I graduated high school, and every summer in university, I worked in a lab,” says Fox-Robichaud, who has gone on to build an illustrious career as a Hamilton Health Sciences (HHS) critical care physician, national sepsis expert and researcher at the Thrombosis & Atherosclerosis Research Institute (TaARI) of HHS and McMaster. She is also the HHS chair in sepsis research.
“Dr. Fox-Robichaud has been instrumental, locally and nationally, in raising awareness of sepsis including its long-term impacts,” says Dr. Marc Jeschke, vice president of research and chief scientific officer for HHS.
“As well as caring for our sickest patients, her leading-edge research focuses on saving lives and improving the quality of life for sepsis patients and survivors, and she is accomplishing this through various unique and highly-impactful approaches.”
Fox-Robichaud is sharing more about her roles in health care including sepsis research for World Sepsis Day on Sept. 13.
Fox-Robichaud also mentors the next generation of doctors as a professor of medicine at McMaster University and as director of medical education at HHS. As a young adult, her own mentor was her mother -- Dr. Jo-Ann Fox-Threlkeld, a professor emeritus at McMaster. Fox-Threlkeld worked in a research lab and was one of the first nurses in Canada to earn a PhD in physiology. “My mother was a nurse scientist, and my role model,” says Fox-Robichaud.
Fox-Robichaud cares for critically-ill patients, including people with sepsis, in HHS Hamilton General Hospital’s intensive care unit (ICU), while also researching sepsis. This disease is

“DR. FOX-ROBICHAUD HAS BEEN INSTRUMENTAL, LOCALLY AND NATIONALLY, IN RAISING AWARENESS OF SEPSIS INCLUDING ITS LONG-TERM IMPACTS”
caused by an out-of-control response to an infection, and is the deadliest health condition in the world, killing more people globally than cancer.
Back in her student days, her internal medicine residency experience in Calgary set her course to become a bench-to-bedside sepsis researcher. “I found the ICU in my second year of residency and I have not looked back,” says Fox-Robichaud, adding that this was also the time in her life when she developed a keen interest in sepsis research and caring for patients with this disease.
“When doing my residency I came to realize that that the one disease I felt passionate about was sepsis.”
While completing her residency, she spent all her electives and any spare time working in a lab. “I was bound and determined to be a bench clinician scientist.” Bench clinician scientists are physicians or other health-care professionals who care for patients and also conduct wet lab research, which involves handling liquids, biological matter and chemicals.
After completing her residency, Fox-Robichaud returned to McMaster, where she was hired as a bench scientist focused on critical care. She worked for close to seven years in that position before taking on the role of
Dr. Alison Fox-Robichaud is an HHS critical care physician and scientific director of Sepsis Canada. She has been instrumental, locally and nationally, in raising awareness of sepsis. Her leading-edge research focuses on saving lives and improving the quality of life for sepsis patients and survivors, and she is accomplishing this through various unique and highlyimpactful approaches.
local principal investigator on her first clinical trial involving sepsis patients. Many research projects followed over the years including being site lead for large Canadian Institutes of Health Research (CIHR) studies and leading some industry-funded studies. She is currently the lead for an HHS drug repurposing study looking at treating patients with sepsis in the ICU. She is also the local principal investigator for another three clinical trials currently underway, and one about to start.
Over the past few years, Fox-Robichaud also became involved in health services research, related to reducing sepsis rates. Preventing hospital-acquired sepsis is strategic priority for HHS.
Health services research focuses on improving the efficiency and effectiveness of health professionals and the health-care system through changes
to practice and policy. It can include studying social factors, financing systems, organizational structures and processes, health technologies, and personal behaviours affecting access to health care, the quality and cost of health care, and, ultimately, people’s health and well-being. This branch of research led to her becoming scientific director for Sepsis Canada.
In 2017, the World Health Organization identified sepsis as a global health priority, urging countries to take steps to reduce the burden of sepsis through improved prevention, diagnosis and management.
In response, the CIHR funded Sepsis Canada – a national research network aimed at further understanding the causes of sepsis; improving prevention, detection, and management; and supporting recovery and rehabilitation.
“Some of the research I’m most passionate about is finding tools to more quickly recognize sepsis,” says Fox-Robichaud. “Whether it’s in hospital or in the community, we need better tools to recognize sepsis. Early warning system scores are one of those tools.”
One of her early health services projects was the development of the Hamilton Early Warning Score (HEWS) at HHS. HEWS is used by hospital care teams to recognize the early signs of diseases in order to intervene and management them early.
Fox-Robichaud is also interested in research aimed at supporting sepsis survivors. Post-sepsis syndrome affects up to half of sepsis survivors, with long-term side effects that can include difficulty sleeping, severe muscle and joint pain, decreased cognitive function, kidney failure and respiratory problems.
By Shaelyn Winters
People with substance use disorders are up to three times more likely to have a mental health issue in their lifetime, compared to those without a substance use disorder. Navigating concurrent disorders – a term used to refer to co-occurring addiction and mental health issues – can be overwhelming, but a clinic at St. Michael’s Hospital is working to help.
The Pathways Clinic provides outpatient psychiatric care aimed at identifying and treating mental health disorders in the context of substance use disorders. The clinic was established in September 2023 after psychiatrists at St. Michael’s noticed a steady increase in the number of psychiatric referrals for patients with concurrent disorders.
“Our clinicians used to receive one-off assessments for patients with concurrent disorders but the number of referrals and the rate at which patients were presenting with comorbidities became more consistent in recent years,” says Samantha Boumeester, Clinical Leader Manager of Addictions and Withdrawal Management Services at St. Michael’s. “It got to a point where we realized that having easy, dedicated access to psychiatric care for these patients was urgently needed.”
The clinic is led by a multidisciplinary team comprised of a registered nurse, case manager, peer support specialist and two psychiatrists. It offers time-limited individual and group supports for up to one year, with the goal of mental health and addiction stability and referral to a community clinic or provider, such as a family physician, who can provide ongoing care on a long-term basis.
Upon receipt of a referral, a nurse reaches out to the patient to determine if they are still interested in receiving treatment. The patient is then booked for a consultation with one of the clinic’s two psychiatrists and other recommended team members, who
can clarify lingering questions about the referral.
“Our clinic provides access to psychiatrists but also an allied health team, which includes a peer support specialist who has lived experience with both addictions and mental illness,” says Dr. Anita Kang, one of the psychiatrists in the Pathways Clinic. “Our case manager helps us navigate addictions resources in the city, which can be challenging for patients to find on their own.”
In the clinic’s early days, referrals were limited to St. Michael’s clinicians. Today, the clinic accepts referrals both inside and outside of Unity Health Toronto, provided that the patient lives within the St. Michael’s catchment area and has a health care provider who will resume care following the program’s one year duration. People experiencing homelessness are also welcome at the clinic.
“We’ve learned a lot from previous clinics with regards to the referral process,” says Kang. “It’s important to keep it low barrier, to help people attend. I think we’re doing a good job branching out, not just in the hospital, but in the community as well.”
The frequency of follow-up appointments is dependent on the patient’s psychiatric illness and the type of treatment required. While the program offers supports for up to one year, it’s flexible for patients who require further assistance, says Boumeester.
“The goal is stabilization of patients’ mental health concerns and their substance use disorder,” she says. “That could be done with a stable medication regimen, therapy, connecting them to a family doctor if they don’t already have one, or setting them up with any other kinds of services that they might need.”
Support from the Rapid Access to Addiction Medicine Clinic (RAAM)
“There isn’t a lot of research into survivorship, so we don’t understand this patient population well,” says Fox-Robichaud. “I’m very interested in studies looking into how we can help our sepsis survivors at HHS.” n H Shaelyn Winters works in communications at Unity Health.
Recognizing how the stigmatization of mental health and substance use disorders may prevent patients from receiving care, the Pathways Clinic works collaboratively with other addictions services at Unity Health.
It’s this coordination between services that distinguishes Pathways from other similar clinics in the Greater Toronto Area, says Dr. Karen Shin, Chief of the Department of Psychiatry at St. Michael’s.
“We’re fortunate at St. Michael’s to have a complement of services, including inpatient addiction medicine consultations, a rapid access addiction medicine (RAAM) clinic and an emergency department that frequently supports patients with acute substance use intoxication and withdrawal,” she says. ”These teams work closely together to move suitable patients into Pathways for further care.”
RAAM is an urgent care dropin service for people with substance use disorder. Many of the Pathways team members also support the RAAM in the hopes of building trust with RAAM patients who may later attend Pathways for ongoing personalized services.
“It can be a challenge to provide care for patients with severe substance use disorders and mental illness, because those patients are often the ones that have the hardest time coming to the clinic,” says Kang. “Our allied health teams in RAAM and Pathways are so knowledgeable and reliable, and they’re really good at forming deep relationships with their patients.”
Consultations for new patients occur every Tuesday and Thursday. While the average wait time for an appointment with a psychiatrist can take many months, the Pathways clinic triages patients urgently – the current wait time is about one month.
Though the clinic hasn’t yet established a formal channel to receive patient feedback, this hasn’t discouraged patients from expressing gratitude for the clinical team.
“I think a lot of patients like having additional supports from our multidisciplinary team – at least that’s what I hear from my patients,” says Kang. “We’d love to expand the clinic across the city one day, but we’re taking baby steps for now.” n H
Many cancer patients are living longer, thanks to new and better treatments and cures made possible through research.
But what about life after cancer treatment? There’s an emerging area of research aimed at helping cancer survivors enjoy the very best quality of life in the months and years after completing treatments like chemotherapy, radiation therapy and surgery.
Researchers leading these quality-of-life studies include Hamilton Health Sciences (HHS) psychologist Dr. Karen Zhang, who cares for cancer patients at HHS Juravinski Hospital and Cancer Centre (JHCC). Zhang is also a researcher with the Escarpment Cancer Research Institute, a joint institute of HHS and McMaster University. As a psychologist, Zhang is especially interested in research that understands and addresses the psychosocial aspects of cancer care.
“I see a lot of room for research and innovation that explores how to help people live better with cancer, as well as after cancer treatments have ended,” says Zhang. “I’m especially passionate about studies aimed at developing programs to help people manage better.”
Projects that Zhang is currently working on include the breast cancer research study, I-CAN Manage Cancer Pain. Zhang is the co-principal investigator along with Dr. Greg Tippin, a psychologist with the HHS Michael G.DeGroote Pain Clinic, the largest academic university-affiliated pain clinic in Canada.
This pilot feasibility study brings together HHS health-care professionals from the JHCC and the pain clinic to explore pain management for breast cancer survivors in the months and years after finishing treatment. Health-care professionals involved in the study include psychologists, oncologists, a pain specialist, nurse, physiotherapist and occupational therapist.

“We want to help people better manage their pain, so they can live their best lives,” says Zhang.
The study, which has the potential to be expanded in the future, focuses on patients diagnosed with Stage 1 to 3 breast cancer who continue to experience pain in the months and years after treatment.
Common reasons for chronic pain include neuropathy – a side effect from chemotherapy that causes tingling or numbness in the feet or hands and can spread to legs and arms. In severe cases, it can affect people’s ability to do everyday activities including returning to work, says Zhang.
People can also experience prolonged post-surgical pain from their mastectomy or incisions. And some medications can also cause pain symptoms.
An HHS Foundation grant of just over $48,000 made it possible to hire a research coordinator to help organize the study and recruit participants.
“The importance of supporting research cannot be understated,” says Anissa Hiborn, the HHS Foundation’s CEO.
“Health journeys don’t end once a person leaves a hospital or treatment plan, and Dr. Zhang’s research work in pain management can help so many women in their quality of life after breast cancer. Donor dollars are making a tangible difference in improving our region’s health care and I’m proud of the community’s generosity.”
The research team will recruit approximately 30 study participants through the JHCC, Wellwood support centre and the BRIGHT Run fundraiser for breast cancer research.
These study volunteers are divided into three cohorts, each taking part in six-week virtual interprofessional pain management program developed by the study team and modeled a validated chronic pain intervention. The goal of the program is to help survivors better manage their pain symptoms so that they can cope better with the aftermath of their cancer journey.
“Rather than reinventing the wheel, we were able to adapt an already validated intervention program for our study participants,” says Zhang.
Sessions are led by HHS psychologists, nurses, occupational therapists and physiotherapists, and offer strategies for self-managing pain that includ-
ed exercise, breathing techniques, and relaxation and mindfulness exercises.
“Some strategies are more psychological in nature, while others focus on exercise or information,” says Zhang. “Our study really concentrates on leveraging our expertise to help people cope through self-management.”
The program hasn’t been fully evaluated yet, as the study is still in the process of data collection. However, verbal feedback from participants has been positive so far. “We’re currently running focus groups with participants to get their feedback,” says Zhang, adding that she appreciates opportunities to collaborate with so many experts at HHS, including her pain clinic colleagues.
Next steps could include a randomized control trial to help determine the effectiveness as standard program for breast cancer survivors.
“There’s a lot we don’t know yet about supporting patients during and after cancer treatment,” says Zhang.
“With my research, I’m trying to identify gaps where our standard clinical services may not be meeting psychosocial needs of patients. That’s where I see a lot of room for research and innovation to help people live better with cancer, and after cancer.” n H
The BC Health Coalition launches Platform for Public Health Care and 6 Priority Solutions As the provincial election begins, the BC Health Coalition is launching a platform that puts public health care and the people who rely on it first. The public health care advocacy organization is using the platform to raise the bar on what commitments the provincial parties make.
“Recent polling shows that improving our public health care system is one of the most important issues that people in British Columbia care about. But beyond the political slogans, we need to know if parties will actually commit to real solutions that will heal and strengthen our public healthcare system,” says Ayendri Riddell, Director of Policy and Campaigns at the BC Health Coalition.

• Improve access and quality of seniors care
• Protect funding for public healthcare from being used as profits
• Create sustainable working conditions for all health care workers
just proposing band-aids, or worse –poison pills that will undermine public health care,” says Riddell.

The BC Health Coalition is raising the bar by launching a platform for public health care and calling on all political parties to commit to six priority solutions: Guarantee access to on-going Prima-
Provide coverage for medicines that
Rapidly reduce surgical wait-times
“We all know there are many challenges facing our public healthcare system, but what we need to know from all of the parties during this election is what will be their prescriptions that will heal and expand health care. We will be examining the party commitments to see if they will actually help to heal the public system or if they are
The BC Health Coalition is a B.C.wide non-partisan, non-profit coalition of community members, health care workers, researchers, NGO and community service providers. We base our policy positions on peer-reviewed research and on our mission to strengthen and defend the public health care system.
Please visit our website, https:// www.bchealthcoalition.ca/ to learn more about our work. n H
By Hyun Uk Lee and Certina Ho
Over the past few months, John, a 58-year-old with advanced gastric (or stomach) cancer, has been undergoing intravenous (IV) chemotherapy, requiring regular hospital visits for infusions. Recently, his doctor introduced the option of oral (i.e., taken by mouth) chemotherapy in tablet form, allowing John to take his medications at home. Chemotherapy involves the use of drugs to target and kill cancer cells. Chemotherapy can be delivered in different routes of administration, depending on the type of drugs involved, the treatment objectives, and what and where the cancer is. Most chemotherapy drugs are given IV or intravenously (i.e., directly into the bloodstream via a vein using a needle or a small plastic tube – a catheter). Oral chemotherapy involves taking chemotherapy drugs by mouth, usually in the form of tablets or capsules, which are absorbed through the digestive system before entering the bloodstream. While both forms of chemotherapy may serve the same purpose, sometimes the route of administration may affect the patient experience in significant ways. Imagine being able to receive treatment without regular visits or commute to the hospital, without needles or tubes, and without hours spent in a chair or bed connected to an IV, etc., oral chemotherapy is an option of taking cancer treatment at home. Understanding these two options could be the key to not just a more convenient but a more empowered approach to managing health and wellness.
Instead of frequent visits to the hospital for IV infusions, patients can take their chemotherapy medication(s) at home. This is particularly valuable for individuals who may have logistical barriers to frequent hospital visits. Oral chemotherapy reduces the time/
costs spent on commuting, waiting for appointments, and/or undergoing IV infusions, which may significantly improve a patient’s quality of life.
However, it is important for patients to follow their prescribed regimen carefully. Missing doses or taking the medication incorrectly may impact effectiveness of oral chemotherapy. Readers can learn more about “Taking Oral Chemotherapy at Home” on the Cancer Care Society website.
Several studies have investigated the efficacy of oral chemotherapy in comparison to IV treatments. For example, in the case of John’s advanced gastric (or stomach) cancer, a 2018 study was conducted in 126 Chinese patients. It was found that the oral chemotherapy option could be just as effective, if not more so, than the IV option and have similar safety profile in certain cases.
However, in 2019, a U.S. study reported that when patients experienced challenges in adherence to their oral chemotherapy at home, they experienced higher number of cancer-related symptoms and lower quality of life, suggesting that oral chemotherapy may not be as effective if patients are not able to adhere to the medication regimen accordingly.
Both oral and IV chemotherapy come with side effects, and these can vary depending on the drug(s) and the patient’s individual response. Common side effects of oral chemotherapy include nausea, vomiting, and diarrhea, while IV chemotherapy may lead to neutropenia, which may increase the risk of infection. [Our July 2024 edition covered “common side effects of chemotherapy and safe medication use considerations”)

One of the advantages of oral chemotherapy is the reduced risk of infection, as patients do not require a tube or catheter for drug administration, which are common sources of complications in the IV treatment option. However, oral chemotherapy also comes with the expectations of patients adhering strictly to their medication regimen/schedules at home, which can sometimes be more challenging than attending scheduled IV sessions at the hospital. In addition, it is also important to store and handle oral chemotherapy drugs at home safely.
Cost is another factor that patients need to consider when deciding between oral and IV chemotherapy. While oral chemotherapy reduces the number of hospital visits and associated costs, the medications could be more expensive. Patients should consult their healthcare providers and/or their third-party insurance (if applicable) to understand the financial implications of their treatment options.
Oral chemotherapy represents a significant advancement in cancer treatment, providing patients with a convenient alternative to traditional IV methods. In John’s scenario, oral chemotherapy has demonstrated comparable efficacy to IV chemotherapy, offering a valuable option for his advanced gastric cancer treatment. However, patients must carefully weigh the benefits of convenience and reduced hospital visits against the importance of adhering strictly to their medication regimen, managing potential side effects, storage, and safe handling of their medications at home.
As with any cancer treatment, it is essential to discuss all options and your concerns with your healthcare providers to determine the best possible medication therapy management. Oral chemotherapy may not be suitable for everyone, but for many, it offers a new level of freedom and flexibility in their cancer care journey. n H
Young adults who had undiagnosed and unmanaged high blood pressure as children face a higher risk of suffering a life-threatening heart attack or stroke as early as their late twenties or early thirties. These are people in the prime of their lives, when they’re building careers, getting married, starting families or buying their first homes, and their children are also at higher risk of developing this medical condition.
High blood pressure, also called hypertension, is present in six to eight per cent of children and is becoming increasingly common. Yet studies show it’s largely underdiagnosed.
Hamilton Health Sciences (HHS) pediatric kidney specialist Dr. Rahul Chanchlani is concerned for the future of these young people, and he’s leading a study aimed at developing an online screening tool, or calculator, that family doctors, pediatricians and even parents can use to predict risk and intervene early, so dangerous health complications due to hypertension can be prevented.
And because the study is international in scope, this innovative screening tool will have the potential to be used worldwide, preventing life-threatening illnesses and saving health-care systems millions of dollars.
Chanchlani led a study that was published in the Journal of the American Medical Association (JAMA) Network Open in January. Results showed that less than 25 per cent of children have their blood pressure checked during visits to their family doctor.
Hypertension Canada guidelines recommend annual blood pressure checks for all children between the ages of three to 17, with more frequent checks for those considered at risk. Yet routine screening rarely happens at the primary care level in Canada, partly because the need had never been clearly identified.
There’s a lack of awareness, even in medical circles, about the dangers of hypertension in children, says
Chanchlani. “I’m not blaming primary care providers. Family doctors are overburdened. Regular blood pressure checks for children aren’t part of their routine practice, and they may not have blood pressure machines for kids, with the smaller sized cuffs or they may lack the nursing support to check blood pressure.”
Chanchlani runs the Pediatric Hypertension Clinic at HHS McMaster Children’s Hospital (MCH), where his patients include kids with high blood pressure for reasons including heart defects, kidney disease, genetic conditions or lifestyle issues like being overweight.
He also leads groundbreaking, award-winning research addressing the under-diagnoses of pediatric hypertension in Canada.
A study led by Chanchlani, published in JAMA Pediatrics in May, found that Canadian children diagnosed with hypertension have twice the risk of having a major heart attack, stroke or even dying as early as their late 20s or early 30s.
Chanchlani’s research included analyzing the health records of thousands of Ontario children as far back as 1996 using data from The Institute for Clinical Evaluative Sciences of Ontario (ICES), an independent, non-profit research organization. The study tracked outcomes of more than 25,000 children diagnosed with high blood pressure, comparing them to a control group of about 120,000 children who didn’t have hypertension.
“We followed these children from 1996 to 2022, and found that those with high blood pressure were at twice the risk of having major cardiovascular events such as heart failure, heart attack or stroke within 20 years of their diagnosis.”
Chanchlani’s research aims to reduce the future adverse outcomes of hypertension by showing the huge benefits of early detection and intervention.
When young children have high blood pressure, it’s often related to health conditions like heart defects or kidney disease, or some other medical
Dr. Rahul Chanchlani is leading a study aimed at developing an online screening tool, or calculator to detect high blood pressure in youth.

conditions. But with older kids heading into their teen years, it tends to be triggered by lifestyle issues like being sedentary, overweight, obese, and/or eating too much salt. These older kids would especially benefit from a screening tool and early detection, because in their case high blood pressure can be prevented or managed when caught early.
Going back 25 or 30 years, studies show that two to three per cent of Canadian children were diagnosed with high blood pressure. Today, it’s significantly higher at six to eight per cent. And that’s likely low, because children aren’t routinely checked. In addition, one-third of Canadian children are considered overweight or obese, making them more at risk.
Improving screening at the primary-care level is the key to identifying kids with high blood pressure early, in order to prevent serious health complications down the road.
Chanchlani’s ALERT-BP study, made possible through funding from the HHS Foundation and Kidney Foundation of Canada, aims to develop a risk prediction tool, or calculator, for detecting high blood pressure in kids as young as five using data from
birth cohort studies in Canada, the United States and the United Kingdom, and testing the prediction tool model in those countries.
Two of the Canadian cohorts are in based in Hamilton, led by HHS physicians. The South Asian Birth Cohort (START) was led by Dr. Sonia Anand, an HHS vascular medicine specialist and senior researcher at the Population Health Research Institute, a joint institute of HHS and McMaster University. The other is the FAMILY Atherosclerosis Monitoring in Early Life study led by Dr. Katherine Morrison, a researcher and the medical director of the Pediatric Weight Management and Pediatric Lipid Clinics at MCH.
Next steps before launching the study include receiving ethics board approval, working on data sharing agreements, recruiting a masters student with expertise in statistics and partnering with the HHS CREATE (Centre for Data Science and Digital Health) team to explore incorporating machine learning and AI when developing this risk prediction tool.
Staffed with experts in software engineering, AI and data sciences, CREATE works with hospital clinicians including physicians to develop new ideas and create digital solutions that fundamentally reimagine how health care is delivered. n H
The Ontario government is investing in two programs in York Region that will expand diagnostic services in long-term care homes and help reduce hospital and emergency room visits.
The new Community Paramedicine for Long-Term Care Plus (CPLTC+) program builds off the existing Community Paramedicine for Long-Term Care program and allows community
paramedics to deliver diagnostic services like bloodwork, ultrasound and urinalysis for long-term care residents. The government is also providing funding to long-term care homes to receive equipment and training for diagnostic services within existing longterm care homes.
“We are investing in diagnostic care so seniors can receive the right care in the right place,” said Natalia Kusendova-Bashta, Minister of Long-Term
Care. “This funding will help longterm care residents access care in their own homes and help reduce avoidable hospital visits and 911 calls.”
The CPLTC+ program in York Region will be administered in nine homes by York Region Paramedic Services.
The government is also investing $6 million provincewide to continue the Equipment and Training Fund in 2024-25. Launched last October as
part of the Your Health Plan, the fund helps long-term care homes train staff and buy diagnostic equipment so they can provide better care for residents. Investments are targeted to help buy equipment that can detect and prevent conditions that most often lead to preventable hospital visits, such as urinary tract infections, falls, pneumonia and congestive heart failure. Last year, the Equipment and Training Fund supported more than
In a historic moment for seniors care in Canada, Providence Living at The Views, the nation’s first public long-term care home based on the concepts of a dementia village, welcomed its inaugural residents this summer. The state-of-the-art care home village in Comox, British Columbia, represents a significant step forward in providing compassionate, person-centred care for seniors with and without dementia.
Natividad “Naty” Parinas, mother of Eddie Parinas, a contestant from the ninth season of The Amazing Race Canada, was the first resident to make the journey from the previous existing long-term care home, The Views at St. Joseph’s, to the new care home village. Accompanied by her son and daughter-in-law, Allie Sellers, who was also a contestant on the show, Parinas was greeted with a poignant ribbon-cutting ceremony at the main entrance of Providence Living at The Views. Mark Blandford, President & CEO of Providence Living, and Kathy MacNeil, CEO of Island Health, personally portered Parinas to her new home.
The move-in day was a heartwarming display of community support and

meticulous planning, as nearly 90 volunteers and staff members came together to ensure a smooth transition for the 156 residents. Remarkably, the entire move was completed in less than six hours, with Parinas leading the way as the first resident to settle into the new care home village.
A partnership between Providence Living, the province and Island Health with funding also from St. Paul’s Foundation and Comox Valley Healthcare Foundation, Providence Living at The Views marks a departure from the traditional institutional model of long-term care, focusing in-
stead on creating a warm, home-like environment that prioritizes autonomy, social engagement, and first-class medical care.
“Today, we celebrate a new era in seniors’ care in Canada,” said Mark Blandford. “Providence Living at The Views embodies our commitment to redefining long-term care by putting the well-being and dignity of our residents at the heart of everything we do. We are proud to offer a public care home village that is accessible to all, regardless of financial means.”
The successful move-in day was a testament to the dedication and collaboration of the staff, volunteers, and community partners. From the careful coordination of transportation to the attention to detail in ensuring residents’ comfort and safety, every aspect of the move was meticulously planned and executed.
As Canada’s aging population continues to grow, the need for innovative, person-centred long-term care solutions has become increasingly pressing. Providence Living at The Views serves as a model for the future of seniors’ care, demonstrating that exceptional care can be provided in a public setting, making it accessible to all who need it.n H
700 projects at close to 220 homes across Ontario. In York Region, the investments included:
• Simcoe Manor Home for the Aged in Beeton purchased a bladder scanner and urinalysis analyzer to support the diagnosis and treatment of urinary tract infections, and cameras to support virtual health
• Mackenize Health Long-Term Care Facility in Richmond Hill purchased a doppler and electrocardiogram machine, and associated staff training to use this equipment, to support the diagnosis and treatment of congestive heart failure
• Mon Sheong Richmond Hill LongTerm Care Centre purchased a bladder scanner, urinalysis analyzer and oximeter to support the diagnosis and treatment of urinary tract infections and congestive heart failure.
• The Ontario government is investing $9 million this year across the province in the Equipment and Training Fund and the CPLTC+ program.
• Along with York Region, CPLTC+ is being rolled out by paramedic services in Cochrane District, Hastings-Quinte, Middlesex-London, Ottawa and the Region of Durham.
• As par t of its plan to fix long-term care and address sector waitlists, the government is building 58,000 new and upgraded long-term care beds across the province.
• Ontario is offering incentives of up to $25,400 to students and recent graduates of personal support worker education programs to launch careers in long-term care homes and in the home and community care sector.
• The Ontario government is investing up to $4.9 billion to create thousands of new positions for personal support workers and nurses in long-term care.

The government is fixing long-term care to ensure Ontario’s seniors get the quality of care and quality of life they
need and deserve. The plan is built on four pillars: staffing and care; quality and enforcement; building modern, safe and comfortable homes; and connecting seniors with faster, more convenient access to the services they need. n H



TMS (or rTMS) is a non-invasive treatment option for treatment-resistant depression. It delivers short magnetic pulses directed at the brain to stimulate nerve cells. Patients can return to their regular activities immediately following treatment, which lasts about three to eight minutes. Ontario Shores operates two of these machines – one at the main campus in Whitby and another at the Mackenzie Richmond Hill Hospital clinic.
The magnetic coil is placed close to the left side of the head (near the left dorsolateral prefrontal cortex). Abnormalities in networks originating from this region have been identified as the pathological basis of depression.
Over three minutes, short, theta bursts emit from the coil, stimulating the area. This process is repeated daily for about six weeks, and the results are promising for many who live with debilitating depression.
Reactions vary from patient to patient. Most find it similar to the little zaps you might feel from a TENS machine, which physiotherapists use to feed a low, electrical pulse through electrodes attached to your body.
You might expect a more elaborate setup for a treatment room where a state-of-the-art machine sends stimulation into your brain in a precise way to target the microscopic nerve cells involved in mood control and depression. However, all you will find in this small room is a seat resembling a barber’s chair and an electronic box about the size of a large bread box. But don’t let the lack of racks of equipment fool you. This room has changed many lives.
Karen, a patient, entered the Brain Stimulation Clinic at Ontario Shores

on a sunny afternoon in August for a follow-up session. She was cracking jokes with Janice, the TMS technician, in no way demonstrating any traits consistent with someone with debilitating depression. She quickly got comfortable, obviously having done this dozens of times already.
“Given my condition at the time,” Karen explained, “my success rate was not all that promising, but thank goodness those worries turned out to be wrong. TMS has been a lifesaver for me.”
In fact, Karen would use the term “lifesaver” several times during this session.
Diagnosed with post-traumatic stress disorder and depression, Karen says she was a completely different person.
“I was on six anti-depressants at one time. I wasn’t the person my husband knew. I wasn’t the person I knew myself to be.”
All this time, she had been settling back into the chair while Janice was marking pre-determined points on Karen’s forehead that would provide
an exact location for the magnetic coils to be placed. She placed her glasses on the counter and laid back with seemingly no concerns at all.
Then, just like that, the session had begun. Karen continued talking away with Janice as though they were sharing a bus ride. The only indications that something was happening were three quick, high-pitched beeps from the control unit and 10 quick buzzing sounds of the theta bursts. This process would repeat several more times. Then, three minutes and eight seconds later, it was over. In the meantime, Karen had not stopped the conversation and did not acknowledge that she had just undergone an entire session.
She sits at a table in the corner of a coffee shop with a pad full of notes. On the dog-eared pages, almost a year’s worth of questions asked and answers given. This is a 70-year-old woman who describes the last 15 years of her life as “hell.” In fact, she envisions herself as “a Phoenix, rising from ashes.”
“I’ve been a Phoenix many times over the last 15 years. I’ve lost so much,” she explains. “I have fought to find meaning, hope and a measure of peace.”
Her name is Barbara Allentoff. A survivor of two bouts of cancer. But it was the death of her 20-year-old son, Matthew, in 2010 that sent her spiralling downward into a deep depression.
“Until all this happened, I was a balabusta (a Yiddish expression describing a woman who runs her kitchen and everyone comes to for advice), but I quickly lost all interest and purpose in my life.”
Barbara managed to rebound somewhat, but then came the pandemic. This time, her downfall was more severe.
She left the choir she loved so much, and her love for volunteering disap-
peared. Her days were spent weeping, and with each tear, hope faded. With the loss of her entire family, she could no longer claim to be a balabusta. Then she heard about the TMS clinic offered by Ontario Shores. It had done wonders for a friend of hers. From there, things happened pretty fast. In November of 2023, her doctor submitted a referral for her. In the first week of January 2024, she met with Dr. Amer Burhan, then Ontario Shores’ Physician-in-Chief and the leader of the TMS program. Shortly after that, she sat in a comfortable chair in the Ontario Shores TMS clinic at Mackenzie Health in Richmond Hill and received treatment five days per week for six weeks. Each treatment lasted less than 10 minutes. It was non-invasive; she only felt a slight thumping from the magnetic coil. Within four days of treatment, she felt a glimmer of hope. Three weeks later, she realized her “rise out of the ashes” had truly begun.

Back at the coffee shop, Barbara is a woman reborn.
“A year ago,” she says, “you would have been sitting here with a very dif-
*This story was shared with the permission of all parties involved.

NOVEMBER FOCUS: Emergency Services/ Critical Care/Trauma/Emergency/Health Technology:
Innovations in emergency and trauma delivery systems. Emergency preparedness issues facing hospitals and how they are addressing them.
Advances in critical care medicine.
Health Technology: An update on the impact of technology, including robotics and artificial intelligence on healthcare delivery.
FOCUS EMERGENCY CARE
Advertising Booking Deadline October 25th
Material Deadline October 29th
For more info email advertising@hospitalnews.com
ferent Barbara. I was so very sad. I was tired, not just physically. My soul was tired! Now, I see gratitude every day in life. I am journaling. If I had to write a book about my life, the title would be ‘Rising from the Ashes: How to Get the Dust Off Your Shoulders. ‘
Barbara is back with her beloved choir and volunteering again. She has regained her purpose, peace, and place as a balabusta with her extended family.
“This treatment has given Barbara her life back.”
Dr. Burhan has made it his life’s work to understand and help stimulate some of the 100 million neurons in the average human brain, each 50 times smaller than the diameter of a human hair.
Further, he must try to adjust the activity of some of the 100 trillion syn-
aptic connections, where neurons connect and communicate. Compare that number with our Milky Way Galaxy’s measly 100 billion stars.
Dr. Burhan leads one of Ontario Shores’ two TMS clinics. He was one of the first clinicians Barbara encountered as she prepared for treatment.
“She was already on two medications,” Dr. Burhan recalls, “neither of which was doing much for her severe depression.”
Dr. Burhan knows that TMS cannot be a stand-alone solution.
“By combining TMS with psychotherapy, they are complimentary to each other. We can target the brain’s cognitive networks more effectively.”
He had to decide if TMS therapy was the right option for Barbara. While it boasts a 50 percent success rate, patients must be carefully selected.
Barbara is one of the success stories.
“[In Barbara’s case] This treatment has given her life back to her.”n H


DECEMBER FOCUS: Medical Imaging /Year in Review/Future of Healthcare/Accreditation/ Hospital Performance Indicators: Overview of advancements and trends in healthcare in 2024 and a look ahead healthcare for 2025. An examination of how hospitals are improving the quality of services through accreditation. Overview of health system performance based on hospitals performance indicators and successful initiatives hospitals have undertaken to measure and improve performance. A look at medical imaging techniques for diagnosis, treatment and prevention of diseases. + SPECIAL FOCUS: ANNUAL RADIOLOGY SUPPLEMENT
Advertising Booking Deadline November 22nd
Material Deadline November 26th For more info email advertising@hospitalnews.com


JANUARY FOCUS: Healthcare Human Resources / Continuing Medical Education (CME)/ Staffing:
Continuing Medical Education (CME) for healthcare professionals. The use of simulation in training. Human resource programs implemented to manage stress in the workplace and attract and retain healthcare staff. Health and safety issues for healthcare professionals. Quality work environment initiatives and outcomes.
ANNUAL PROFESSIONAL DEVELOPMENT SUPPLEMENT
Advertising Booking Deadline Decemeber 13th, 2024
Material Deadline December 17th, 2024
For more info email advertising@hospitalnews.com
Toprovide the right care at the right time, we need the right number of staff and medical staff to meet patient demand. Fraser Health has partnered with Deloitte Canada to develop and launch scheduling tools that leverage artificial intelligence (AI) and machine-learning solutions to accurately forecast the waves in demand we see in the health system.
Thanks to a $1.5 million Scale AI award, Fraser Health and the Deloitte project team are developing three artificial intelligence models. Two will leverage patient analytics from various electronic medical records to forecast volume demands coming to the emergency and medicine departments and assist leadership in pre-determining broader staffing requirements. A third will take the forecasted patient data
and matches it with business rules, such as patient-physician ratios, to create a baseline schedule with advanced analytic capabilities to generate multiple scheduling scenarios.
A new tool to forecast trends in patients requiring emergency care is expected to launch in the coming months at Burnaby Hospital and Eagle Ridge Hospital. By better understanding when patients arrive at emergency departments, physician scheduling can be adjusted accordingly.
While current scheduling methods continue to be used, the tool will help physicians predict patient volumes and trends when preparing their manual

schedules. It will also help leaders to run different scheduling scenarios and digitally test out what the patient flow could look like.
The tool was piloted in July and the response was positive.

“Eventually, we will see the tool becoming more sophisticated and able to integrate factors such as respiratory and influenza season, outbreaks, air quality levels, and other local and regional events like concerts and festivals to more accurately predict how many patients will need care on any given day and match that demand with physician coverage,” says Sheazin Premji, executive director, Centre for Advanced Analytics, Data Science, and Innovation, Fraser Health.
with 91 per cent accuracy for the next day and 81 per cent accuracy up to seven days in advance.
“This innovative project is an example of how clinicians can use AI in a practical way to benefit themselves and their patients,” says Dr. Neil Barclay, emergency physician, Burnaby Hospital. “Being part of this project from the ground up will help us better meet our patients’ needs and provide us with a more sustainable health care system in the long run.”







Hospitalists in Burnaby are helping to inform an AI-driven surge prediction model to enable proactive decision-making about calling in additional staff based on forecasted physician workload.
The tool helps predict the number of patients requiring hospitalist care over a seven-day period. It then proactively adjusts staffing levels in the event of a surge. During validation testing, the model predicted surges
The Fraser Health/Deloitte collaboration ‘AI-Driven Physician Scheduling Solution and Workflow Optimization’ is one of nine Canadian health projects to receive $21 million in funding to pioneer the deployment of AI solutions. The initiative promotes collaboration between hospitals and AI product and solutions providers to innovate further and accelerate the deployment of AI in Canadian health care.
“Enhancing the patient experience and improving access to care is at the heart of digital transformation in Fraser Health,” says Jennifer MacGregor, vice president of Digital Patient and Provider Experience. “We are excited to be co-developing these AI tools. These partnerships are essential to drive innovation in our health system to solve some of our most challenging problems.” n H
By Alexa Battler
They’re energetic, they’re versatile, and they’re how healthcare organizations and hospital-linked research labs are quickly filling jobs that require highly specialized skills. They’re undergraduate students in U of T Scarborough’s Arts and Science Co-op program, and they have a decades-long track record of hitting the ground running in healthcare-related work placements.
Dr. Jeffrey Meyer, a senior scientist with the Brain Health Imaging Centre at the Centre for Addiction and Mental Health (CAMH), has been hiring U of T Scarborough Arts and Science Co-op students for more than 10 years and has no plans to stop. By hiring these students, his team gets support with a range of research tasks, from participant recruitment to data management. This way, they’re simultaneously propelling the next generation of healthcare workers and researchers by giving them a particularly valuable experience.
“Co-op students bring new perspectives and enthusiasm to the team and learn unique skills such as data analysis and participant interaction,” Meyer says. “They also help our team meet project demands while benefiting from practical experience, helping prepare them for future careers in research.”
These students, who Meyer says, “lend their keen energy to the lab environment,” arrive with skills both generally needed for the workforce and specific to the needs of medical and research projects, combining training from Canada’s top academics with eight months of career preparation courses. Whether it’s modern data management strategies from computer science, mathematics and statistics programs or research methodologies from the campus’ many health sciences programs, such as neuroscience, mental health studies, biotechnology, and immunology and disease, these students’ education also gives them the background needed to

“CO-OP STUDENTS BRING NEW PERSPECTIVES AND ENTHUSIASM TO THE TEAM AND LEARN UNIQUE SKILLS SUCH AS DATA ANALYSIS AND PARTICIPANT INTERACTION,”
pick up new skills and adapt to the latest technologies.
Meyer recently saw that adaptability in action when he hired a U of T Scarborough Arts and Science Coop student for a 2023 study on long COVID, published in JAMA Psychiatry. Meyer’s team used advanced brain scanning imaging agents that were developed at the Brain Health Imaging Centre at CAMH and found persistent brain inflammation in patients who experienced depression several months after getting COVID-19. The student was at first assigned to help with participant recruitment and neuroimaging data collection but ended up with a larger impact on the study.
“Initially, we expected the student to take on more administrative duties, but they quickly developed data anal-
ysis skills,” says Julie Green, research manager at the Brain Health Imaging Centre. “Their work was used in a manuscript for publication, which was recognized with an authorship.”
That’s far from the only example of a co-op student using their discipline-specific knowledge to go above and beyond researchers’ expectations. Students are frequently playing a diverse range of roles in projects — those with computer science backgrounds have done full stack web and software development for employers, and students who’ve taken courses in mathematics and statistics have contributed advanced qualitative and quantitative data analysis. Other students have worked in project management roles, with tasks such as report generation and building dashboards. Those from
life sciences, health sciences and psychological sciences programs have brought their training in U of T Scarborough’s several cutting-edge labs to clinical and pre-clinical research projects, including in dry and wet lab work and participant recruitment.
In addition, four co-op students who completed their co-op terms in the Brain Health Imaging Centre were recently listed as co-authors in the first-ever study to find a natural supplement that reduces “baby blues” and post-partum depression symptoms six months after birth. These students had their names appear in The Lancet’s science journal eClinicalMedicine, after supporting research analysts in several of the project’s stages. They helped with recruiting the study’s 100+ participants, interviewing them using psychological assessment tools, storing data using clinical research software preparing material needed for the study, and attending study visits with research personnel, among other duties.
Green says this kind of “unique hands-on research experience” is how researchers can create “a mutually beneficial environment, where the student learns essential skills while also contributing to the success of ongoing research in mental health and brain imaging.”
Behind U of T Scarborough’s Arts and Science Co-op program, which is celebrating its 50th anniversary this year, is an entire department of staff dedicated to getting undergraduate students into these roles. They advise employers by connecting them with funding organizations to support their hiring. Employers can submit job descriptions (or upload them on the university’s Co-op portal), interview and choose students to be hired for four-, eight- or 12-month work terms. They can also hire co-op students from any of U of T’s three campuses, all with support from U of T Scarborough staff. To learn more about co-op at U of T, reach out to the team at uoft.me/uoftcoop n H

OEM Reprocessed
LigaSureTM blunt tip, with seal plate removed