“Being from the north and Indigenous, we have our set of challenges. Serving our marginalized population without support is unjust. Now is the time for change to be action.
The Ford government could release billions of dollars for health care so that we can have the funding to do our job the way it’s supposed to be done.”
Ontario deserves better.
The race is on to protect infants from RSV this season
By Dr. Darine El-Chaâr
Ottawa mother Jessica Cohn still vividly remembers crumpling to the hospital floor when a team of doctors told her that her one-month-old may need to be intubated. Her healthy full-term newborn son Eitan had been diagnosed with RSV, a highly contagious virus that can be deadly for infants. While infants with some medical conditions are at higher risk, most infants diagnosed with severe RSV disease each year are healthy infants like Eitan. Eitan did recover, but for parents like Jessica, the emotional distress leaves a lasting mark.
RSV is very contagious and causes seasonal epidemics, like the flu, with cases peaking in the fall and winter months. In addition to the psychology trauma RSV inflicts on families, the disease also puts strain on our pediatric units. A significant portion of RSV-related hospitalizations are admitted to the ICU and over 60% of those admissions are for children under 6 months old.
The economic impact of these RSV-associated hospitalizations is high, with an estimated cost of $9,000 per case in Ontario.
Until this year, protections against RSV for healthy infants in Canada were limited to basic hygiene and keeping children away from people with colds. Now, Health Canada has approved two new products that offer protection against RSV.
• Nirsevimab is a monoclonal antibody which can be given to newborns and infants in their first RSV season and to high-risk children up to 24 months of age in their second RSV season, and
• RSVpreF a maternal RSV vaccine that can be given to pregnant people who are between 32-36 weeks pregnant. The vaccine protects babies 0 to 6 months through protection from their mothers.
These tools have incredible promise for reducing the impact of RSV in Ontario and across Canada, but several barriers stand in the way including low awareness, and in some provinces, cost.
In Ontario, both Nirsevimab and RSVpreF are available free of charge to eligible parents and infants. This is not the case in most provinces where parents must pay out of pocket for RSVpreF. Nirsevimab is funded through publicly funded programs, but is not available in all provinces. These restrictions limit options for parents. In most cases however, it is a lack of awareness preventing both doctors and patients from having informed discussions about the available options.
We need policymakers to act now to bridge knowledge gaps for parents and healthcare providers and to equip healthcare providers with the communication tools to support informed-shared decision making. We need clear and consistent communication about the availability of RSV protections in Ontario and how parents can access them. But most importantly, we need to reach parents now to inform them about their options. We need both a broad and tailored approach to communicating with parents, making sure that information is accessible and relevant to all pregnant people in all communities.
When Jessica Cohn was pregnant with her third child, her first since Eitan, she could only dream of a vaccine that could protect her child from this ex-
Continued on page 6
UPCOMING DEADLINES
FEBRUARY 2025 ISSUE
EDITORIAL: Jan. 8
ADVERTISING: Display – Jan. 24 | Material – Jan. 28
Monthly Focus:
Gerontology/ Public Health and Preventive Medicine/Rehabilitation/Wound Care: Geriatric medicine, aging-related health issues and senior friendly strategies. Developments in rehabilitation techniques for a variety of injuries and diseases. Effective approaches for disease prevention and health promotion. Innovation in the treatment and prevention of wounds.
+ WOUND CARE SUPPLEMENT
MARCH 2025 ISSUE
EDITORIAL: Feb. 7
ADVERTISING: Display – Feb. 20 | Material – Feb. 24
Monthly Focus:
Facilities Management and Design/Health Technology/Greening Healthcare/Infection Control: Innovative and efficient healthcare design, the greening of healthcare and facilities management. An update on the impact of technology, including robotics and artificial intelligence on healthcare delivery. Advancements in infection control in hospital settings.
+ INFECTION CONTROL SUPPLEMENT
THANKS TO OUR ADVERTISERS Hospital News is provided at no cost in hospitals. When you visit our advertisers, please mention you saw their ads in Hospital News.
Helen Reilly, Publicist Health-Care Communications
Bobbi Greenberg, Health care communications
Sarah Quadri Magnotta, Health care communications
Dr. Cory Ross, B.A., MS.C., DC, CSM (OXON), MBA, CHE Vice President, Academic George Brown College, Toronto, ON
ASSOCIATE PARTNERS:
Hospital News is published for hospital health-care professionals, patients, visitors and students. It is available free of charge from distribution racks in hospitals in Ontario. Bulk subscriptions are available for hospitals outside Ontario.
The statements, opinions and viewpoints made or expressed by the writers do not necessarily represent the opinions and views of Hospital News, or the publishers.
Hospital News and Members of the Advisory Board assume no responsibility or liability for claims, statements, opinions or views, written or reported by its contributing writers, including product or service information that is advertised.
Changes of address, notices, subscriptions orders and undeliverable address notifications. Subscription rate in Canada for single copies is $29.40 per year. Send enquiries to: subscriptions@ hospitalnews.com
Canadian Publications mail sales product agreement number 42578518.
Navigating mental health with technology
The COVID-19 pandemic triggered a sharp rise in eating disorders, particularly among youth. Demand for treatment has remained high, underscoring the urgent need for accessible, innovative solutions.
UHN’s National Eating Disorder Information Center (NEDIC) is addressing this ongoing challenge with JEM, a new 24/7 chatbot designed to connect individuals with essential resources and supports.
For 40 years, NEDIC had provided information, guidance, referrals and real-time support to Canadians affected by eating disorders and their caregivers. Before the pandemic, the service reached 3,500 individuals annually through its toll-free helpline and live chat service. That number has since grown to over 6,000 each year.
JEM is a rules-based artificial intelligence (AI) chatbot. It guides users through predefined scripts and decision trees to NEDIC’s most important and popular resources — such as explainers on the causes and types of eating disorders, and coping skills for managing emotions or balancing social media usage.
“JEM helps us connect people to resources that might help them understand what their options are and where they can go,” says Sara Marini, NEDIC’s Technical & Administrative Coordinator, and a past member of the team that answers the helpline and chat service.
This non-intrusive, easily accessible tool allows individuals to take the first step toward seeking support without feeling pressured to engage in conversation. With two-thirds of NEDIC users opting for chat and 40 per cent of traffic occurring evenings and weekends, JEM addresses a critical need to access resources outside traditional hours.
“We want people to know that JEM is not replacing human interaction,” says Suzanne Phillips, Program Manager, NEDIC. “Our helpline team is still available every day (Monday to
Thursday, 9 a.m. to 9 p.m.; Friday, 9 a.m. to 5 p.m.; Saturday and Sunday, 12 p.m. to 5 p.m. All times EST.).
“We know that not everyone wants to receive information in the same way, and that someone may not be ready to talk to a person.”
JEM is a rules-based artificial intelligence (AI) chatbot that guides users through predefined scripts and decision trees to NEDIC’s most important and popular resource. (Photo: NEDIC)
While chats on JEM are private and not monitored, ensuring individual confidentiality, users can opt to connect with a real person via NEDIC’s Live Chat during service hours or access 988, Canada’s Suicide Crisis Helpline, available 24/7 via phone or text for crisis support.
Unlike generative AI, which learns from user data and may generate unsuitable responses, JEM’s rule-based system ensures safety by providing clear and reliable responses for those seeking health-related support. If users ask questions beyond its parameters, JEM responds with: “I’m just a simple bot, so I’m still learning. Try using my buttons to start a conversation.”
“We have a responsibility to meet people where they are, which includes leveraging technology,” says Sara. “While we understand hesitations around chatbots, we know that younger demographics are more comfortable using these tools, and eating disorders often begin in adolescence or early adulthood, making early intervention crucial for better outcomes.”
JEM was initially developed by a research team led by Dr. Gemma Sharp at Monash University in Australia. NEDIC, connected with like-minded organizations in the United States, United Kingdom, Ireland and Australia that support those affected by eating disorders, heard about the work and was intrigued.
“We had the opportunity to meet with Dr. Sharp and her team and learn more about JEM,” says
JEM IS A RULES-BASED ARTIFICIAL INTELLIGENCE (AI) CHATBOT. IT GUIDES USERS THROUGH PREDEFINED SCRIPTS AND DECISION TREES TO NEDIC’S MOST IMPORTANT AND POPULAR RESOURCES — SUCH AS EXPLAINERS ON THE CAUSES AND TYPES OF EATING DISORDERS, AND COPING SKILLS FOR MANAGING EMOTIONS OR BALANCING SOCIAL MEDIA USAGE.
Suzanne. “We recognized its potential to provide individuals with accessible, immediate support, complementing the services we already offer.”
NEDIC has adapted JEM for the Canadian context, becoming the first organization to modify it for a different geographic region. Australian expressions were removed, and Isabel Legault, NEDIC’s Senior Direct Client Support Worker, re-recorded the accompanying videos that teach coping skills. New imagery was also added throughout to enhance JEM’s visual appeal.
JEM was soft-launched in September to test its effectiveness, and was later publicized in NEDIC’s newsletter in November. The service has received positive reviews.
The chatbot is part of NEDIC’s multi-year expansion strategy, supported by a $2 million gift from the Slaight Family Foundation. The funding has enabled extended live chat support hours, translation of resources into multiple languages and the creation of new materials addressing the unique eating disorder experiences of 2SLGBTQ+ individuals and those from Black, Indigenous and people of colour (BIPOC) communities. While JEM does not replace professional treatment or provide personalized guidance, it serves as a vital tool, directing individuals to appropriate help when they need it most. Its launch marks a promising development in leveraging technology to enhance access to support for those affected by eating disorders. n H
COVID-19 vaccine cuts risk of disease in half when administered during pregnancy
Alarge multistate study, conducted by the Centers for Disease Control and Prevention’s (CDC’s) VISION Network, has found that COVID-19 vaccination given during pregnancy offered 52 per cent protection, cutting risk of a COVID-19-associated emergency department or urgent care visit in half. This is especially significant because there is an increased risk of severe COVID-19 during pregnancy requiring hospitalization and potentially causing adverse pregnancy outcomes.
However, if received less than six months prior to pregnancy, vaccination effectiveness declined provid-
ing only moderate protection against COVID (28 percent). If received more than six months prior to pregnancy, vaccination provided little protection (6 percent) against COVID.
Similar to findings in previous VISION studies of those who were not pregnant, protection provided by vaccination against COVID for those who were pregnant waned over four to six months. Also, similar to COVID vaccines for individuals who are not pregnant, effectiveness was comparable to that of the flu vaccine.
The study looked at geographically and racially diverse data from electronic medical records captured
during routine healthcare delivery. There was no difference in the protection provided by COVID vaccination by age or race in the study population of 7,677 pregnant 18- to 45-year-olds.
The authors of this study note that their findings, derived from real-world data, indicate the protection provided by either monovalent or bivalent COVID vaccination for those who were pregnant or became pregnant was lower as compared with previous studies, likely due to changes in virus subvariant predominance in 2022-23.
Other VISION Network studies have had similar findings in non-pregnant populations.
“The VISION Network did this study to examine the effectiveness of the COVID-19 vaccine for individuals who were pregnant, because there have been a lot of questions as to whether pregnant people should be vaccinated or not,” said study co-author Brian Dixon, PhD, MPA. “Our data show that for Covid-19, vaccines are protective of pregnant persons, supporting CDC guidelines that recommend COVID vaccination.” Dr. Dixon is director and a research scientist with the Clem McDonald Center for Biomedical Informatics at Regenstrief Institute and a professor at the Indiana University Indianapolis Richard M. Fairbanks School of Public Health. n H
Federal needle exchange programs are to reduce health care costs, blood-borne infections
New research suggests that every dollar spent in Prison Needle Exchange Programs (PNEPs) in Canadian federal prisons will save $2 in infection treatment costs, making the case for further investment in these programs. The research is published in CMAJ (Canadian Medical Association Journal).
“Needle exchange programs are evidence-based strategies that prevent
Continued from page 4
transmission of blood-borne viruses, reduce injection-related infections, improve access to medical care, and facilitate entry into substance dependence programs for people who inject drugs,” writes Dr. Farah Houdroge, Disease Elimination Program, Burnet Institute, Melbourne, Australia, with coauthors.
The World Health Organization has set a target of reducing hepatitis C
The race is on
tremely common disease. We cannot afford to squander the incredible opportunity we have to save another parent the trauma of seeing their tiny child in a hospital bed, struggling to breathe. We have the tools to prevent RSV this season, but we
need act now so parents can make the right choice for them and their families.
For more details on the Federation of Medical Women and the recently published Maternal RSV White Paper, please visit fmwc.ca. n H
Dr. Darine El-Chaâr is a Maternal Fetal Medicine (MFM) physician at The University of Ottawa.
infections to fewer than two per 100 people who inject drugs per year as part of an elimination strategy for hepatitis C. In 2024, Canada unveiled its 2024–2030 Sexually Transmitted and Blood-Borne Infection Action Plan that emphasized support for harm reduction programs and expanding the PNEP.
Researchers from Canada and Australia sought to assess the return on investment for Canada’s PNEP, and the potential impact of scaling it up, as part of efforts to eliminate bloodborne infections in prisons. Using a modelling study, they found that expanding the program to 50 per cent of people in all federal prisons who inject drugs from 2025 to 2030 would prevent 15 per cent of new hepatitis C cases and eight per cent of injection-related infections compared with the status quo.
“This study adds to the growing body of evidence supporting PNEPs as effective harm reduction strategies that are also cost saving. Given that they show both health and economic benefits, PNEPs should be a priority
not just in Canada, but globally,” the authors conclude.
In a related commentary, authors argue that more comprehensive interventions to make substance use in correctional institutions safer, and specifically reduce related risks of acute death, are needed. “Prison-based programs aimed at mitigating the health harms of substance use by correctional inmate populations should be carefully evaluated as part of their implementation, as has been done in the related research with specific respect to needle exchange programs. Without systematic expansion of and increased access to such programs, prisoners in Canada will remain at unnecessarily high risk of ill health and death from the adverse consequences of substance use,” the authors conclude.
“Cost–benefit analysis of Canada’s Prison Needle Exchange Program for the prevention of hepatitis C and injection-related infections” and “The burden of drug overdose deaths among correctional populations: implications for interventions” were published December 16, 2024. n H
Working toward achieving the Quintuple Aim using holistic patient data
Anew demonstration study from the Canadian Institute for Health Information (CIHI) combined patient-reported survey data with clinical outcomes and costing data on hip and knee replacements for the first time. The report determined that there were statistically significant correlations between patient reported experience measures (PREMs) and clinical outcomes, PREMs and patient reported outcome measures (PROMs), and costs and PROMs.
By using patient reported data alongside other data sources, this demonstration report was able to measure how socio-demographic factors influence outcomes, experiences, and costs associated with hip and knee replacement surgeries. For example, data determined that patients aged 75 and older had higher rates of hospital harm and readmission to hospital; lower favourable patient experience, lower improvement in functional status, quality of life and satisfaction with surgery; and
higher inpatient hospitalization costs compared with younger age groups.
Equity is a vital component of health care delivery and is a priority for health care systems in Canada. Examining measures across patient groups helps identify inequities in outcomes and experiences and inform strategies to optimize care for all patients receiving hip and knee replacements.
Using different sources of heath data to assess the value of health care interventions aligns with the Quintu-
Lung cancer screening CTs find coronary artery disease in 83 per cent of cases
Lung cancer screening with low-dose chest computed tomography (CT) may detect more than just lung cancer. As new research in CMAJ (Canadian Medical Association Journal) shows, these CTs can identify coronary artery calcium, a strong risk factor for coronary artery disease (CAD), in patients without cardiac symptoms.
“Lung cancer screening, although primarily geared towards reducing deaths from lung cancer, also has an opportunity to help tackle the second most common cause of premature death in middle-aged adults, through the identification and risk stratification of coronary atherosclerosis,” writes Dr. Gary Small, University of Ottawa Heart Institute, Ottawa, Ontario, with coauthors.
In a study of 1486 patients screened for lung cancer between March 2017 and November 2018 as part of the Ontario Health Lung Cancer Screening Pilot for People at High Risk, coronary artery calcium was detected in 83 per cent (1232) of patients, with high levels in 30 per cent (439). More than half of patients (52%) were male, mean age was 66 years, and 68 per cent (1017) were current smokers.
As lung cancer is the leading cause of cancer deaths in Canada, screening programs across the country have introduced low-dose CT for people at risk of lung cancer. These CTs can also easily identify coronary calcification, a marker of coronary artery disease, the most common cause of cardiac death.
“If appropriate therapeutic responses are instituted, lung CT findings could affect survival from 2 leading causes of death: lung cancer and coronary artery disease,” the authors write.
The success of this pilot program will be affected by how clinicians interpret and manage findings of coronary artery calcium. However, clinicians must be aware that there could be harms such as inappropriate investigation after coincidental detection.
The authors urge more research into how to manage patients with coincidentally detected coronary artery calcium but suggest “continued attention to cardiovascular disease prevention is warranted and could be amalgamated into lung cancer screening initiatives to promote health.” n H
ple Aim – a framework that emphasizes the importance of optimizing health care systems to achieve health equity by focusing on an improved patient experience, better patient outcomes, lower costs, improved provider experience, and overall health equity.
THE FUTURE OF MEASURING THE PATIENT EXPERIENCE
Originally launched in 2014, in the spring of 2024 CIHI updated its Canadian Patient Experiences Survey on Inpatient Care (CPES-IC) to better meet evolving health system needs and better reflect current patient priorities. This standardized tool allows hospitals to receive qualitative feedback from patients in a timely, standardized, and user-friendly way.
“It is important to collect patient-reported data to leverage the potential that this type of information can provide when linked with other health care data,” said Dr. Jason Werle, Orthopaedic Surgeon, Alberta. “This will ultimately improve patient-centred care and the patient experience.”
More robust patient data combined with synergistic analysis across clinical and administrative data sources will help identify challenges patients and health care providers experience and will empower decision makers, practitioners, and patients to deliver and receive better patient-centred care. n H
Pregnancy enhances natural immunity to block severe flu
McGill University scientists have discovered that pregnancy may trigger a natural immunity to boost protection against severe flu infection.
Contrary to the common belief that pregnancy increases vulnerability to infections, researchers found that it strengthened an immune defense in mice, blocking the Influenza A virus from spreading to the lungs, where it can cause severe infection.
“Our results are surprising because of the current dogma, but it makes sense from an evolutionary perspective,” said co-lead author Dr. Maziar Divangahi, Professor in McGill’s Faculty of Medicine
and Health Sciences and Senior Scientist at the Research Institute of the McGill University Health Centre (RI-MUHC).
“A mother needs to stay healthy to protect her developing baby, so the immune system adapts to provide stronger defenses. This fascinating response in the nasal cavity is the body’s way of adding an extra layer of protection, which turns on during pregnancy.”
EXPLORING BENEFITS FOR PREGNANCY AND BEYOND
The researchers used a mouse model to observe how a certain type of im-
mune cell activates in the nasal cavity of mice during pregnancy, producing a powerful molecule that boosts the body’s antiviral defenses, especially in the nose and upper airways.
“Influenza A virus remains among the deadliest threats to humanity,” said first author Julia Chronopoulos, who carried out the research while completing her PhD at McGill.
“This natural immunity in pregnancy could change the way we think about flu protection for expectant mothers.”
The Public Health Agency of Canada recommends pregnant wom -
en and pregnant individuals get the flu vaccine, as they are at high risk of severe illness and complications like preterm birth. The new insights offer promise for more targeted vaccines for influenza, which is among the top 10 leading causes of death in Canada.
“The broader population could also benefit, as our findings suggest the immune response we observed could be replicated beyond pregnancy,” said co-lead author Dr. James Martin, Professor in McGill’s Faculty of Medicine and Health Sciences and Senior Scientist at the RI-MUHC. n H
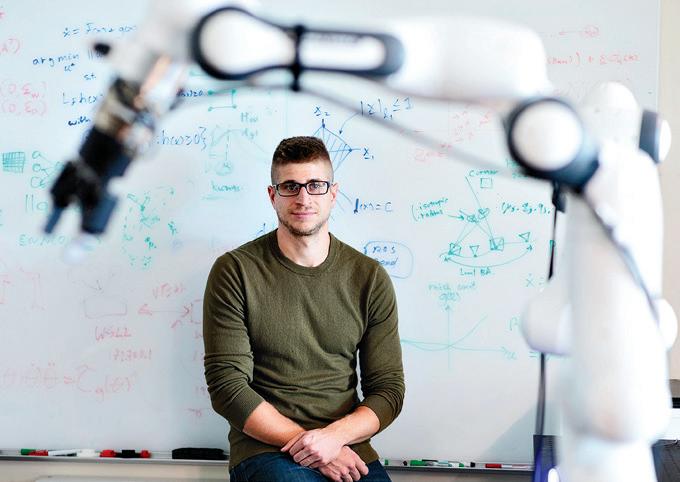
Building robot brains
How one KITE scientist is changing the way robots think. Literally.
By Glynis Ratcliffe
t’s morning, and an older woman who is recovering from a stroke sits at the kitchen table. Her adult son, who has temporarily moved into the family home to help, makes coffee for his mother before heading to work, placing the mug on the table as he leaves. The woman can’t wait for that first sip, but there’s a problem: her stroke has caused some weakness on
one side of her body, which makes it difficult for her to lift and hold things, like her morning brew.
Imagine if, attached to the table, was a robotic arm that “sees” the coffee-filled mug through its cameras. Using neural networks and artificial intelligence (AI) to process the visual information, it recognizes the coffee. Then, another algorithm, trained using reinforcement learning, autonomously
controls the robotic arm to pick up the mug and pass it without spilling.
While this scenario isn’t yet possible, Dr. Brokoslaw Laschowski hopes it will be soon. Why? The Research Scientist and Principal Investigator at the KITE Research Institute at University Health Network (UHN) is working to create intelligent robots to help people with physical disabilities. The novelty of his robotics research stems
from his expertise in computational neuroscience.
“I research brain-inspired algorithms and brain-machine interfaces,” he explains. “With regards to the first, I develop machine learning algorithms to mathematically model human perception, cognition, and motor control. These ‘artificial brains’ can then allow robots to think and control themselves.”
While AI has existed for half a century, and deep learning (a technology designed to recreate how the human brain processes information and is considered the foundation of modern AI) was developed in the 1980s, integrating AI into the physical world is a problem that computer scientists are still trying to solve.
“Even the most sophisticated robots developed to date, such as the Boston Dynamics backflip robot, aren’t fully autonomous,” he adds. “It’s one of the grand challenges we face as a field –bringing artificial intelligence into the real world.”
UNDERSTANDING THE BRAIN
From his undergrad and master’s degrees in neuroscience and kinesiology to a second master’s and PhD in engineering, Dr. Laschowski has always been captivated by how the brain works. For instance, during his second master’s degree in mechanical and mechatronics engineering at the University of Waterloo, he developed mathematical models based on optimal control theory to model how the brain optimizes and controls human movement.
“I love research. The exploration and creation of new theories and technology – it’s addictive. I’m completely obsessed,” he says. “I didn’t just want to study neuroscience at the cellular level; I’m interested in mathematically modelling how the neural computations in the brain see, think, and control movement – an area known as computational neuroscience.”
Dr. Laschowski began to wonder how he might apply his mathematical and machine-learning models of the brain to robotics. After seeing someone walking with an early version of a robotic prosthetic leg, he immediately knew his next area of focus: giving intelligence to robots that physically assist humans.
“I thought to myself, ‘I understand a little bit about how the human brain controls a biological leg. What if we created an artificial brain to control a robotic leg?’” he explains. “That’s how it all started.”
TRAINING ROBOTS TO SEE
Dr. Laschowski, who is a Core Faculty Member of the Robotics Institute at the University of Toronto (U of T) and Director of the Neural Robotics Lab, has received considerable media attention for his robotics research, such as being featured in a keynote talk by the President and CEO of NVIDIA. However, he emphasizes that he specializes in developing the “brains” that power robotic systems rather than the physical robots themselves.
A key component of that process is giving robots the ability to see, which involves far more than cameras. If you think about how humans see, the eyes are only the first step of the process –the sensors that take in visual information. The visual cortex and other parts of the brain are then responsible for processing and understanding that information.
Although cameras are the first step in giving robots “vision,” they still require an artificial brain to process the visual information. Over the years, Dr. Laschowski and his lab have developed neural networks that mimic how neurons in the human brain work in order to process visual information from cameras like the ones mounted on their custom-built smart glasses. These neural networks then become the foundation with which robots learn to perform movements in the real world, such as walking down the street or picking up a coffee cup.
In addition to modelling how the human brain processes visual information, Dr. Laschowski is also developing models to reverse engineer how the brain controls movement. These brain-inspired controllers can be programmed into robots to behave similarly to humans.
TRAINING ROBOTS TO THINK
Dr. Laschowski likens the training of his learning algorithms to his new role as a father, providing his young daughter with a safe environment in which she can learn to walk and feed herself. “When we train our reinforcement learning algorithms, there’s a
certain amount of exploration. The artificial brain, like the human brain, learns by interacting with the environment and experiencing failures and rewards,” he says.
In humans, the neural networks in the motor cortex and other parts of the brain are responsible for motor control, such as when you pick up a coffee cup. “One of the goals of my research is to mathematically model these neural computations, which, in addition to advancing our scientific understanding of the brain, can also be used to direct robots to move like humans,” he explains.
Researchers at the Neural Robotics Lab use computer simulations to teach their reinforcement learning algorithms to mimic human movements in an effort to reverse engineer human motor control. Within the simulation, their algorithms learn these brain-inspired control policies. Once the researchers recreate human-like movements on the computer, they transfer their brain-inspired controllers from the simulation to physical robots.
However, Dr. Laschowski stresses his research is mainly mathematical and computer-based, noting that people often assume he’s the one building physical robots. “I don’t even have a screwdriver in my lab,” he says, laughing.
The vision and brain technology his lab is developing can be applied to many different machines, such as prosthetics, robotic arms, humanoids, and exoskeletons. For instance, imagine a boy with a spinal cord injury
who uses a robotic exoskeleton for walking assistance. He could wear the lab’s smart glasses, which then connect wirelessly to the robot.
“As he’s looking around while wearing our glasses, this system, which is the boy and the robotic exoskeleton together, acts like an autonomous car, where now the robot could control itself because the neural networks on our smart glasses have the ability to see,” Dr. Laschowski explains.
The same boy could instead choose to use the lab’s brain-machine interface to control the robot with his thoughts, such that the lab is also developing algorithms to decode movement intent from brain recordings. Alternatively, a hybrid of the two technologies – where sometimes the artificial brain has autonomous control, but the boy could take over manual control when he wants by using the brain-machine interface – could be the best option.
“The long-term vision for my research is to study, along this spectrum of autonomy, what level of control individual people prefer, which remains one of the major unsolved research questions in the field,” he says. Ultimately, Dr. Laschowski is working diligently to give robots intelligence by developing artificial brains and interfacing with the human brain. He hopes these intelligent robots will soon be used to assist people with physical disabilities in the real world, just like that older woman who, despite her stroke, wants to enjoy her morning coffee. n H
Glynis Ratcliffe is a freelance writer.
KITE Affiliate Scientist Dr. Brokoslaw Laschowski is building artificial brains that power robotic prosthetics.
Health care hackathon rapidly spreads and scales Stop the Pop
By Shauna Mazenes
indy Kim and Jessica Cheng knew there was a problem, and it was their job to fix it.
The two advanced practice nurse educators were told too many patients on their units at UHN’s Toronto General Hospital (TGH) were getting post-operative pneumonia – a respiratory infection following a surgical procedure that can lead to more serious complications.
“It really increased our sense of urgency. We knew we had to do something fast,” says Mindy.
“We needed to get to the root cause and find a solution our teams could use,” adds Jessica.
Led by Tiffany Tram and Mikha Alegria, quality improvement specialists in UHN’s Sprott Department of Surgery, the pair implemented a project with their teams that significantly reduced those rates on their units – 72 per cent on General Surgery over two years, and 100 per cent on Surgical Oncology over four months. The initiative is called Stop the POP.
Now, they’ve shown other surgical teams how they can do the same at UHN’s first health care hackathon.
A health care hackathon is an event that brings multidisciplinary teams together to collaborate and solve a problem in a short period of time to improve patient care. Led by the Sprott Centre for Quality & Safety, this hackathon focused on how to successfully increase the uptake and sustainability of Stop the POP on all surgical inpatient units across UHN.
“We’ve been working hard on this event for a year,” says Alexandra Boasie, Senior Manager of Transformation & Quality, who spearheaded the hackathon, which was held on Nov. 15.
“We’re excited to launch an initiative that ensures the safest care for all surgical patients being looked after at Sprott, while equipping teams with practical quality improvement skills for future change.”
Stop the POP is an evidence-backed pneumonia prevention bundle consisting of five patient interventions: using incentive spirometers, maintaining oral hygiene, practicing deep breathing and safe coughing, staying elevated while in bed, and getting up and moving more frequently.
Building on TGH General Surgery’s successful piloting of Stop the POP over the past two years, the goal of the hackathon was to rapidly spread and scale these proven strategies by showing other teams how they did it, and how to do the same – but in ways specific to their team and unit.
“The hackathon is a novel approach to quality improvement that we’re adopting here in the Sprott Department of Surgery,” says Dr. Thomas Forbes, Surgeon-in-Chief at UHN. “Patient care and patient experience is our primary focus at UHN and quality improvement is a constant priority.
“This is a new and innovative opportunity to improve patient outcomes, speed-up recovery time, prevent further complications and reduce the burden on the health care system.”
The Sprott Centre for Quality & Safety developed a roadmap for each of the seven surgical teams attending the hackathon to articulate the problem, then adapt and adjust solutions according to local challenges and patient needs respective to their clinical spaces.
While Gifty Mahama, currently a nurse manager at UHN’s Toronto Western Hospital, successfully carried out Stop the POP on General Surgery in 2017, the project didn’t last for various reasons, such as lack of resources, documentation issues and competing priorities on the unit.
Tiffany, Mikha, Jessica and Mindy worked closely with their teams to tackle these barriers and maintain engagement by creating contests for staff to compete in, distributing checklists for patients to keep them involved and consistent, using graphics and
videos to communicate Stop the POP for those with language barriers, and putting the materials together in a central package that nurses could hand to patients at once, saving time.
Jessica says finding innovative ways to keep staff and patients engaged is at the core of this work.
“We truly believe that’s the key to supporting the successful implementation of Stop the POP on nuanced units,” she said at the event.
Mindy says sharing the results with her team was another key component in keeping staff engaged.
“It builds a sense of confidence when our nurses, the ones who are on the floor delivering these interventions, see the work they’re doing is making a difference,” Mindy told hackathon participants.
By the end of the hackathon, each team developed their own ideas and action plans to implement Stop the POP on their units, such as educating patients and families about the importance of oral health, documenting data in one central flow sheet to save time and measure results, getting patients up for breakfast every morning, and leveraging the support of personal support workers.
Dr. Keyvan Karkouti, Anesthesiologist-in-Chief at UHN, says spreading awareness about quality improvement techniques is invaluable in this space, but more important is the teamwork.
“Effort and collaboration are necessary to make change,” he says. “These are tough issues that require multiple processes, stakeholders and collaboration.
“Without that teamwork, we’re not going to have an impact. That is the greatest value in all of this.”
UHN Patient Partner David Johnston, a retired industry-leading quality improvement expert, attended the hackathon. He says it was interesting to see the same frameworks he used in the private sector being applied to improve patient care.
“I tell people all the time that I’m just glad to be here. Four years ago, I didn’t think I would be,” says David, who survived Stage 3 prostate cancer at UHN.
“It’s opportunities like this – not only sharing, listening and learning from each other, but using measurable data and guided strategies –that can really make a difference in a patient’s life, if not save one altogether.” n H
Seven surgical teams came together at UHN’s first health care hackathon with the shared goal of improving patient safety and quality of care.
Shauna Mazene works in communications at University Health Network.
Photo: UHN
A North American first: Southlake Health celebrates 1,000th sutureless heart valve surgery
Only six healthcare organizations worldwide have reached this milestone in cardiac care
Southlake Health has successfully implanted 1,001 sutureless heart valves, becoming the first hospital in North America to meet this major milestone using the Perceval valve. The Perceval valve is the only fully sutureless heart valve currently used in aortic valve replacement surgery around the world. The surgery was completed by Kevin Teoh, MD, a leading cardiac surgeon who also implanted the first Perceval valve in North America.
“Southlake Health continues to build on a century of leading edge care, bringing innovative cardiac procedures and technologies, like Perceval surgical sutureless heart valves, closer to home,” said Derek McNally, Executive Vice President, Clinical Services and Chief Operating Officer, Southlake Health. “We’re incredibly proud of the world-class team at the Regional Cardiac Centre. They are at the forefront of ground-breaking research and ensure patients can access the latest advancements – because they deserve nothing less.”
Only six healthcare organizations worldwide have implanted 1,000 sutureless heart valves. Southlake is the only hospital in North America to reach this milestone, a testament to the dedication to providing leading edge cardiac care through its Regional Cardiac Care Program. All other organizations to reach this milestone are in Europe.
The 1,000th implant was completed by Dr. Teoh, a renowned cardiovascular surgeon and Master Proctor of the Perceval sutureless heart valve training program. Dr. Teoh’s significant experience with this technology began in 2011 when he participated in the first-ever Perceval implant in North America at Sunnybrook. His leadership and expertise have been instrumental in establishing Southlake as a global leader in sutureless valve technology.
The same day as the 1,000th procedure, Stacy O’Blenes, MD, the
Division Head of Cardiac Surgery at Southlake Health, also implanted the 1,001st Perceval sutureless heart valve.
“This incredible achievement reflects not only Southlake’s commitment to leading edge cardiac care, but also the dedication of our exceptional healthcare team,” said Dr. Teoh. “Less invasive technology like the Perceval valve supports faster recovery times and improved outcomes for patients.
We are honored to have played a key role in bringing this technology to more than a thousand patients as part of their cardiac care journey.”
“As the Regional Cardiac Centre, Southlake cares for cardiac patients from as far north as Muskoka to as far south as North York,” said Elizabeth Lalingo, Director, Department of Cardiac Health, Southlake Health.
“Our commitment to patients and excellence, drives us to innovate, so that every patient who walks through our doors can be confident that they’re receiving comprehensive, leading edge care.”
The Regional Cardiac Care Program at Southlake was an early
adopter of the Perceval valve, an innovative heart valve made from bovine pericardium that is used in aortic valve replacement surgery. The valve’s sutureless and collapsible design enables minimally invasive access and simplifies surgical implantation to support faster recovery times and reduce the risk of post-operative complications when compared to traditional valve replacement surgeries. Southlake has become a recognized leader in the field, offering patients access to this innovative procedure, closer to home.
“Congratulations to Dr. Teoh, Dr. O’Blenes and the team at Southlake Health for gaining their place in the Perceval 1000 Club and for being the first to reach it in North America,” said Christian Mazzi, Chief Executive Officer, CORCYM. “This achievement is a testament to their trust in our Perceval valve as an innovative solution for their patients suffering from aortic stenosis.”
As a Level 7 Regional Cardiac Program, Southlake’s contributions to advancing cardiac care extends far beyond the operating room. The
highly-skilled team of medical staff and staff provide almost every type of cardiac care, with the exception of heart transplants and Extracorporeal Membrane Oxygenation (ECMO), to patients who no longer need to travel far distances to Toronto. As leaders in their fields, the team actively participate in ground-breaking research and are often the first to perform leading edge procedures in Ontario, Canada and even the world. Southlake continues to collaborate with international experts to enhance cardiac care and improve patient outcomes globally. n H
Bursary supports bereavement midwifery research
Hamilton Health Sciences (HHS) midwife Spencer Sawyer could be the first hospitalist midwife in the country to specialize in bereavement support for patients during and after a pregnancy loss. Hospitalist midwives work in hospitals, providing direct care to patients during their pregnancy, labour and delivery, and postpartum.
“To my knowledge there are no other dedicated bereavement midwife roles across Canada,” says Sawyer, who cares for patients at HHS McMaster University Medical Centre (MUMC). Located in the same building as HHS McMaster Children’s Hospital (MCH), MUMC is the regional referral centre for high-risk pregnancies and deliveries, handling among the most complex cases in the province.
“Many high-risk pregnancies benefit from the leading-edge, innovative work by our maternal-fetal medicine team, including our incredible physicians, nurses, and nurse practitioners who often prevent high-risk pregnancies from resulting in loss,” says Sawyer. “But sadly, in some cases, a pregnancy loss is unpreventable.”
The hospitalist midwifery team saw an opportunity for a bereavement specialist in addition to services already available to patients experiencing pregnancy loss. Sawyer felt passionate about taking on that role, and worked with departments including maternal fetal medicine, prenatal diagnostics, labour and delivery, and post-partum care to develop this specialized portfolio of work.
He’s also exploring best practices through research, by pursuing a master’s of midwifery degree part-time at McMaster University. His master’s project, focusing on the specialized role of a bereavement midwife, could pave the way for this position to be introduced at other Canadian hospitals.
“My goal is to grow and improve what we’re doing already for the benefit of other midwives interested in this specialty,” says Sawyer, who joined HHS in 2022. His position is funded through the province’s expanded midwifery care model.
BURSARY SUPPORTS MASTER’S PROJECT ON BEREAVEMENT MIDWIFERY
While hospitals overseas, mostly in the United Kingdom and Australia, employ bereavement midwives, the role has yet to find a significant foothold in North America.
A scoping review published in the Canadian Journal of Midwifery Research and Practice in 2023 helped outline the role midwives could play in providing this care, says Sawyer. The review, by the school of nursing at Thompson Rivers University in British Columbia, highlighted the unique role of bereavement midwives in improving bereavement care in pregnancy loss.
Sawyer hopes to eventually have his master’s project made publicly available to further share the benefits of this specialty. He’s grateful to the HHS Volunteer Association (HHSVA) for awarding him a bursary to do his master’s.
“The HHSVA bursary made it much easier for me to pursue my master’s degree while at the same time developing this role both academically and professionally,” says Sawyer.
The HHSVA is a non-profit organization that supports patient care at HHS through the operation of cafes, cafeterias, gift shops and hospital parking. All profits generated are donated to enhance patient care. This includes providing educational opportunities for staff so they can deliver the very best patient care.
“We take great pride in our partnership with HHS in helping to support the delivery of excellence in patient care,” says Tracy Rivers, the HHSVA’s executive director.
“It’s a driving force for our team, and our customers can feel proud knowing that their purchases help raise funds for equipment donations and staff education support, such as health professionals’ bursaries to support some incredible work and studies like Sawyer is pursuing.”
COMPASSIONATE CARE
When patients receive news that they are losing, have lost, or may be presented with difficult decisions about their pregnancy, Sawyer consults them about their options, provides support, and connects them to other members of the HHS health-care team including genetic counsellors, neonatal specialists, social workers, nurses, psycho-spiritual care providers and the quality of life and advanced care team.
“These teams provide vital patient support and are the foundation that makes my role possible,” says Sawyer, who’s also available to patients in the postpartum period for clinical care, and as a resource and support person.
UNIQUE CONCERNS
As a clinician, Sawyer can provide answers to many questions patients may have related to their unique set of circumstances.
For example, patients and family members are often unsure how to engage with their baby after delivery. “Research suggests that for many families seeing, holding, and making memories with their baby can help them engage with and process their loss, and I can provide them with that evidence-based information, while exploring whether the evidenced-based approach resonates for each individual family,” says Sawyer.
They also often wonder what their baby will look like, and Sawyer can apply the clinical information about a loss to sensitively help families anticipate what it might be like to meet and see their babies. Other niche in-
formation includes letting patients know about medications to suppress lactation and explaining parameters for post-partum bleeding so they can assess their own wellbeing more accurately. He’s also available, on call, to answer questions, provide emotional support, and connect them to other HHS health-care professionals.
INSPIRING ROLE MODELS
Sawyer was inspired by family members to pursue a career in health care. He spent most of his childhood living with his mother, who ran a single parent household while putting herself through nursing school. “I would help her study, which peaked my own interest in health care,” says Sawyer, adding that his grandmother was also a nurse, in the neonatal unit.
After joining HHS in 2022, Sawyer found himself assisting with some of the more challenging pregnancies, offering emotional and social support, and helping some families navigate loss.
“Growing up with such strong role models, I really strove to be a helper, and my work as a bereavement midwife fills my cup in a way I never anticipated.”
Sawyer adds that he’s grateful to his colleagues, mentors and managers for supporting his work and contributing to his growth and development as a midwife. “As my work here at MUMC continues, I’m committed to expanding pathways for a greater diversity of midwives to have the opportunities to work in highly impactful, innovative ways.” n H
From roots to research in advancing burn care and treatment
adi Khalaf was a toddler living in Iraq with his family when U.S. forces invaded in 2003. In search of safety, his family relocated to Syria when Khalaf was five years old, followed by a move to Canada when he was eight, where they settled in Burlington.
“I was very young, but those experiences shaped me into who I am,” says Khalaf, now a 23-year-old McMaster University student pursuing a master’s degree in biochemistry and biomedical sciences, with a focus on research aimed at helping burn patients. He’s investigating burns in older adults for his thesis, with an internationally recognized team of experts at the Hamilton Health Sciences (HHS) Centre for Burn Research. The team’s research focuses on developing treatments and
therapies to improve outcomes in people with severe burn injuries.
Khalaf grew up listening to his family recount their experiences with explosions, traumatic injuries and limited access to health care, which inspired him to study burns and explore new and improved ways to treat them. Before starting his master’s degree, Khalaf worked for three summers at Dr. Marc Jeschke’s burns lab in Toronto and then Hamilton at the burn research centre where Jeschke’s lab is now based. Jeschke is a globally recognized burn surgeon and researcher, vice president of research for HHS and medical director of the regional burn program at HHS Hamilton General Hospital (HGH). He’s also Khalaf’s primary mentor.
The burn research centre is within the Thrombosis and Atherosclerosis
FEBRUARY 2025
FEBRUARY FOCUS: Wound Care/ Gerontology/Public Health and Preventative Medicine/Rehabilitation: Geriatric medicine, aging-related health issues and senior friendly strategies. Developments in rehabilitation techniques for a variety of injuries and diseases. Effective approaches for disease prevention and health promotion. Innovation and treatment and prevention of wounds. WOUND CARE SUPPLEMENT
Advertising Booking Deadline January 24th
Material Deadline January 28th For more info email advertising@hospitalnews.com
Research Institute (TaARI), located in the David Braley Research Institute building. The Braley building is next door to HGH, where the Regional Burn Program is located, so researchers are right beside the patient population they’re working to help.
The HGH regional burn program is one of only two burn units in the province caring for adults with severe burns. The other is in Toronto.
THE POWER OF MENTORSHIP
“Research has found that many older adults, including younger seniors in their 60s and in good physical shape, don’t survive burns,” says Jeschke. “We are one of few research centres in the world studying the impact of burns on older adults on cellular and molecular as well as genetic levels.”
This means that Khalaf is on the front line of cutting-edge research that could advance care for burn patients worldwide. This unique learning experience has inspired him to follow in Jeschke’s footsteps, with a career goal of becoming both a medi-
MARCH 2025
MARCH FOCUS: Facilities Management and Design/Health Technology/Greening Healthcare/Infection Control:
Innovative and efficient healthcare design, the greening of healthcare and facilities management. An update on the impact of technology, including robotics and artificial intelligence on healthcare delivery. Advancements in infection control in hospital settings.
INFECTION CONTROL SUPPLEMENT
Advertising Booking Deadline February 20th
Material Deadline February 24th For more info email advertising@hospitalnews.com
cal doctor and a researcher exploring innovative new burn treatments.
BURNS AND OLDER ADULTS
Age-related factors that make older adults more susceptible to burn injuries include thinning skin, decreased sensation and deterioration of judgement and coordination. Yet it’s not completely understood why older adults haven’t benefited from the ongoing improvements in burn care, says Jeschke. It’s vital research, considering Canada’s aging demographic.
Over the next 20 years, Canada’s senior population is expected to grow by 68 per cent, according to the Canadian Institute for Health Information.
“It’s not just a vulnerable population; it’s also an expanding one,” adds Khalaf. “We need to start figuring out ways to mitigate these poor outcomes. Part of my project involves figuring out why older adults don’t recover well from burns, and exploring treatments and drugs that could help them respond to that trauma.” n H
EDITIONS
APRIL FOCUS: Healthcare Transformation/ eHealth and EHR/Mobile Health:
ANNUAL E-HEALTH SUPPLEMENT Programs and initiatives that are transforming care and contributing to an effective, accountable and sustainable system including virtual care. Innovations in electronic/digital healthcare, including mHealth and the Electronic Health Record (EHR).
Advertising Booking Deadline March 21st, 2024
Material Deadline March 25th, 2024 For more info email advertising@hospitalnews.com
Safe Medication Practices for Restless Legs Syndrome
By Samir Kanji, Laura Brady, and Certina Ho
Having a good night’s sleep is essential for our well-being. Restless legs syndrome (RLS), a neurological disorder, can disrupt sleep patterns and may significantly impact quality of life. It is known to be the fourth leading cause of insomnia, with up to 85% of individuals with RLS finding it difficult to fall or stay asleep. By understanding the condition and adopting safe medication practices, patients can better manage symptoms and their sleep quality.
WHAT IS RESTLESS LEGS SYNDROME (RLS)?
RLS is characterized by an uncomfortable urge to move the legs, particularly when resting or sitting
still. Symptoms typically worsen in the evening or at night but tend to improve with movement, such as walking or stretching. While RLS can occur at any age, it is most commonly diagnosed between the ages of 40 and 60, with symptoms often beginning earlier if RLS is associated with a family history. Risk factors may include pregnancy, anemia (low iron levels), Parkinson’s disease, and end-stage kidney disease. RLS is associated with a higher risk of depression and anxiety, and treating these conditions in RLS patients requires caution, as certain antidepressants may worsen RLS symptoms.
DRUG-INDUCED RLS
As previously mentioned, there are medical conditions like anemia
and Parkinson’s disease that are known risk factors for RLS. However, more attention should be given to drug-induced RLS, as there is emerging evidence supporting that there might be an association between certain drug classes and RLS, such as antidepressants, antipsychotics, and antiepileptics.
Although the exact causes of drug-induced RLS are unclear, some theories suggest that decreased iron levels in the substantia nigra, a region of the brain associated with RLS, may play a role. Emerging theories also indicate that neurotransmitters like dopamine and serotonin may be involved. Medications that increase serotonin levels have also been shown to raise the risk or severity of RLS. Furthermore, an imbalance between dopamine and thyroid hormone levels has been suggested as another contributing factor to RLS. These theories help explain why antidepressants, antipsychotics, and antiepileptics may trigger or worsen RLS, as they all impact the pathways in the brain that are related to dopamine, serotonin, or thyroid hormones.
For medication management of RLS, dopamine receptor agonists (e.g., pramipexole, ropinirole, rotigotine) could be considered to reduced RLS symptoms and improve sleep quality. Gabapentin or pregabalin are typically recommended for initial treatment to help patients with severe sleep disturbance or insomnia associated with RLS. If iron deficiency is causing RLS, then iron supplements may help. If RLS is associated with medication use (i.e., drug-induced), and is affecting the patient’s quality of life, then consulting the prescriber or primary care provider about switching medications may be necessary.
SAFE MEDICATION PRACTICES FOR RLS
MANAGEMENT OF RLS
Management of RLS may involve non-medication approaches and medication-use measures that are customized to the patient’s needs and symptoms. Non-medication interventions may include:
• Reducing caffeine, nicotine, and alcohol intake
• Practicing good sleep habits and getting adequate rest
• Exercising regularly
• Massaging, stretching, or using heating or vibrating pads on affected areas
The International Restless Legs Syndrome Study Group (IRLSSG) developed an evidence-based best practice guide for long-term medication management of RLS, available at https://pubmed.ncbi.nlm.nih. gov/23859128/. In general, medications for RLS are effective for durations ranging from one to five years. When starting a medication for RLS, beginning with a low dose can help minimize side effects. It is important for patients to follow the prescribed dose and avoid adjusting doses on their own. Open communication and regular check-ins with the healthcare team can help manage potential side effects and make optimal lifestyle adjustments. The “5 Questions to Ask About Your Medications” (https://www.ismp-canada.org/medrec/5questions.htm) resource can facilitate meaningful discussions between the patient and healthcare providers to optimize medication therapy management. n H
Samir Kanji and Laura Brady are PharmD Students at the Leslie Dan Faculty of Pharmacy, University of Toronto; and Certina Ho is an Assistant Professor at the Department of Psychiatry and Leslie Dan Faculty of Pharmacy, University of Toronto.
Creating space for leadership development and mentorship conversations
By Dr. Andy Smith
In today’s fast-paced world, where meetings are often back-to-back and priorities seem endless, it can be difficult to carve out time for meaningful leadership development and mentorship conversations. Yet, it is these very moments of connection and reflection that often drive the most profound personal and professional growth. As the CEO of Sunnybrook Health Sciences Centre, I’ve found that one of the most powerful ways to foster these conversations is through a dedicated, deliberate practice of walking. While walking has worked for me, my key message is not about the method but about making time and space for authentic conversations that help develop future leaders.
Mentorship and leadership growth require more than occasional advice or feedback. They thrive when given focused, intentional attention. This is why I’ve intentionally made space for leadership conversations by dedicating time to walk with colleagues, emerging leaders, and community partners.
It started several years ago when I first started in my role as vice president when a vice president at a peer hospital and I began walking together. Both of us were recovering from joint surgeries, so we took to the ravines that connect our two hospital catchments. Over time, these walks evolved into something more. They became a time to step away from our offices and truly connect with one another, discussing everything from organizational culture to leadership challenges. By taking the conversation outside the traditional setting of a meeting room, we were able to engage more creatively and reflect more deeply. As I moved into the CEO role at Sunnybrook, that peer became
the CEO of Orillia Soldiers Memorial Hospital, and I continue to value these walking conversations as a vital part of my leadership practice.
Walking provides a unique opportunity to slow down and think. There’s something about moving through nature, whether it’s a forest, a park, or a city street, that opens up the mind. Research supports the idea that physical movement, especially walking, enhances mental clarity, sparks creativity, and fosters deeper reflection. When you walk with someone, you’re not sitting across from them at a desk. Instead, you’re side by side, engaging in a dynamic flow of conversation, where ideas can emerge more organically. The rhythm of the walk allows you to focus on the conversation without the usual distractions of emails, phones, or meeting agendas.
The power of these walks isn’t just about the physical movement, but the mindset it encourages. Whether it’s a challenging leadership decision, a tough conversation with a team member, or a moment of self-reflection, walking provides a space to think through solutions in a more relaxed, open way. I’ve walked with emerging leaders who needed guidance on how to approach quality improvement projects or navigate the complexities of organizational change. And more often than not, they walk away with clearer heads and new ideas. I often receive notes of thanks afterwards, with many participants sharing how the conversation helped them think more clearly or feel more confident about their next steps.
A central question I always ask during these walks is simple yet powerful: How can I help you today? It’s a question that puts the focus on the other person, allowing them to identify what they need in order to move forward. Whether it’s overcoming a specific challenge or brainstorming
solutions to a larger problem, this question encourages reflection and clarity. It’s a way of empowering others to take ownership of their development, while also providing the support they need to succeed.
Another important aspect of these mentorship conversations is the reminder that leadership and problem-solving in healthcare are not about us as individuals. It’s easy to become fixated on our own role or success, but the heart of leadership is about the people we serve—the patients, our teams, and the communities we support. By helping others refocus on what matters most—the people and teams they lead—many of the challenges they face can be reframed, leading to clearer and more compassionate solutions.
The beauty of mentorship is that it’s not a one-size-fits-all approach.
Each person has different needs, preferences, and learning styles. What’s important is that we make time for it, whether it’s through a walk in nature, a structured meeting, or an informal chat during a commute. These conversations, however they happen, are the cornerstone of effective leadership development.
I encourage you to create dedicated time for leadership conversations and mentorship, whether it’s through walking, talking, or another approach that works for you. Ask the questions that matter, focus on the people you serve, and take the time to listen. These moments of connection will not only help you grow as a leader, but will also help others around you develop the skills, confidence, and perspective they need to lead effectively in the future. And for some of us, walking will also serve as great rehabilitation post-surgery. n H
Dr. Andy Smith, President & CEO, Sunnybrook Health Sciences Centre
Dr. Andy Smith is President & CEO, Sunnybrook Health Sciences Centre.
Code Orange: How SickKids plans for the unimaginable with simulation
By Danielle Orr
In a Code Orange – disaster activation, SickKids staff must mobilize and collaborate seamlessly on very short notice. Staff engage in a hospital-wide simulation as an essential way to plan and manage their response to multiple or mass casualty events.
Picture this: It’s 8 p.m. and less than zero degrees outside on a snowy December evening in Toronto. In the city’s largest stadium, a 50,000-person pop concert reverberates into the blizzard. Its echoes can almost be heard across town, straight through a bustling University Avenue to where some of its concertgoers, many of them youth, will end up by the end of the night – The Hospital for Sick Children (SickKids).
It’s respiratory virus season and the hospital is at 90 per cent capacity, with Emergency Department (ED) wait times at about eight to nine hours long. Patients and their families sit in the waiting area after hours as staff diligently admit and care for them.
Suddenly, alarms go off overhead. An announcer begins calling a Code Orange – known to staff as an external disaster or a mass casualty event.
Pagers begin to come to life across the ED, their shrill sound a call for all-hands-on-deck. Apparently, the pyrotechnics at a nearby concert malfunctioned and the resulting fire, equipment collapse, and crowd surge caused life-threatening injuries to several young people. Toronto Paramedic Services has called to say they are on the way with patients, but it’s unclear just how many will need life-saving care.
“Six minutes until EMS arrives!” someone calls out to the flurry of nurses and physicians now organizing in the trauma room.
Care teams are built within the first few minutes. A nurse and a physician are stationed in the ambulance bay. They have no idea what to expect but prepare for the worst.
What happens next in a disaster is elusive to most. But it’s the exact scenario that over 160 staff at SickKids
aimed to solidify and practice in a hospital-wide simulation this past fall.
WHEN DISASTER STRIKES
When a disaster happens in Toronto, impacted children and youth are sent to SickKids, the only designated paediatric lead trauma hospital in the Greater Toronto Area. A Code Orange is activated when a hospital expects a rapid influx of patients with severe injuries and pressure to its systems as a result. Calling the code allows departments across the hospital to prepare enough resources, space, and staff to meet the scale of the emergency.
“Multi-victim traumas and disasters are very low frequency, but very high-consequence events with significant risks to patient and staff safety,” says Dr. Natasha Collia, trauma education and simulation lead and organizer of the hospital-wide exercise.
The hospital currently engages in two Code Orange exercises – also called mega trauma simulations (MT3) – per year, and it takes months to organize an hour of practice.
The code can be called in response to a variety of incidents, like multiple vehicle or bus collisions, acts of public violence, large fires, major weather
events, or infrastructure collapses, to name a few.
Andrea Boysen, who has worked at SickKids for 31 years – 25 of those years as a frontline nurse and more recently as quality lead for the ED – has seen first-hand how crucial such simulations can be.
“I remember 9/11, I was working, and we thought they might transfer patients to us from the States. Several years later, we held our breath when an Air France plane skidded on the runway at Pearson Airport. More recently, there was the Danforth shooting,” says Boysen.
A CARE TEAM ASSESSES THEIR SIMULATED PATIENT IN THE TRAUMA ROOM
Those incidents didn’t result in a Code Orange activation for SickKids. But Boysen remembers two real activations during her time here.
“We were prepared for those real Code Oranges, and thankfully, the incidents didn’t seriously impact hospital operations. So it feels like a lot of close calls. But each is a reminder that it’s not a matter of if it happens. We need to prepare for when it happens,” she says.
The hospital has traditionally run small-scale multidisciplinary trauma simulations once per month. In 2019, co-medical director of the Trauma Program Dr. Suzanne Beno, along with Drs. Natasha Collia, Jonathan Pirie and others, evolved these simulation exercises into large-scale, hospital-wide mass casualty trauma and burn simulations. The aim was to push the system’s limits even further and combine the Code Orange preparation that was already happening within the organization.
“We see that external disasters are happening increasingly across the globe, and Toronto is not immune to that. We want patients and families to know we’re practicing constantly to work out the kinks, be precise and ready to provide the best possible care,” says Beno.
As the hospital maintains normal operations during the exercise, it was their priority to plan it in a way that would not impact patient care. Staff already engaged in pre-arranged education days were chosen for the simulation, and any others who wanted to participate were provided ample coverage in their units. Patients and families in the waiting room and other affected areas were also notified in advance.
Staff congregate in the trauma room of the Emergency Department and form care teams as they wait for “patients” to arrive.
THE “PATIENTS” START TO ARRIVE
Once the Code Orange is called for the exercise, the first button in the trauma room of the ED goes off and everyone rushes to where they need to be. The simulation begins.
The ED is impacted first, but the waves of a Code Orange spread far beyond it. In fact, this is the largest simulation the team has organized to date, with the priority to simulate how every department in the hospital becomes a key player in the real-life scenario.
A hospital Command Centre is activated, which includes a roundtable of key SickKids leaders who mobilize quickly to plan hospital operations and troubleshoot during any major colour code. It’s composed of representatives from several teams – from Protection Services, who liaise with external organizations like police, to Child Health Services, who monitor and address resource gaps across the hospital.
“We coordinate the hospital-wide response, including mass internal redeployment of staff, opening alternate care spaces and reallocating resources to keep patients and staff safe,” says Yvonne Howard, who is the Improvement Specialist – Emergency Preparedness and led the planning of the Command Centre component of the simulation.
The Command Centre also supports the Social Work team to open a Family Information Support Centre (FISC) which helps locate and reunite families with patients in this type of crisis situation. For the simulation, live actors pose as parents looking for their children.
On other levels of the hospital, beds and operating rooms need to be vacated, and quickly.
The Diagnostic and Interventional Radiology, Surgery and Critical Care teams begin anticipating patient transfers while ED teams downstairs assess the interventions or procedures their patients need.
Because the Operating Room and Critical Care may be impacted for days or weeks after a mass casualty event, the exercise is crucial for practicing patient transfers, cancelling surgeries, and ‘fanning out’ to obtain more staff. From there, they can create highly
A full care team determines their patient requires surgery and transports them carefully to surgery on the second floor.
specialized care teams, including those ready to deploy to the ED at a moment’s notice.
Outside of these areas, the blood bank prepares to service a higher volume of patients, and surgical subspecialties like Neurosurgery, Orthopaedic Surgery, and Burns and Plastic Surgery are standing by, ready to spring into action at any time.
Back in the ED, patients continue arriving in the ambulance bay and are assessed, triaged, and assigned to a team that includes a trauma team leader (TTL), two nurses, and an anesthesiologist. A medical lead (paediatric emergency physician) and a surgical lead (general surgeon) will provide oversight and leadership to these care teams.
Four simulated patients are already being cared for in the trauma room. Their teams crowd around them as other patients arrive with severe injuries.
“There is a sensory overload. You feel a sense of urgency, you feel nervous but alert. It’s loud, there are a lot of sounds, movements and distractions because of the sheer volume of people and the high clinical severity of the patients,” says Dr. Joshua Ramjist, medical co-director of the Trauma program.
A care team member stabilizes a patient in the trauma room.
In the front of the room, one patient, in this case a life-like manikin, is lying on a bed as her team quickly tends to her injuries and communicates with one another.
“I’ve got pressure on the wound.”
“Do we have blood from the blood bank yet?”
“I’m anticipating an intubation.”
The team works quickly to inspect the child. A facilitator for the exercise shares that the patient was hit by a metal bar from an overhead light from the concert stage. It had penetrated her lower abdomen.
“She’s screaming in pain,” the facilitator shares.
“Can we let the MD lead know that we need a surgeon in the room?” A member of the care team shouts.
They decide to give their patient pain medication and continue.
Meanwhile, a team across the room begins transporting their patient, who was trampled during the crowd surge at the concert, for a CT scan on the second floor. Each person wears a focused resolve, a stark contrast to the organized chaos around them.
“We make a big deal about eliciting a lot of overwhelming feelings in the sim. We want you to feel like your plastic manikin is the most important thing in the world. Because if you’ve felt those feelings before, when it happens in real life, you’ll have been there,” says Ramjist.
Once on the second floor, the team uses a practiced, swift movement to place their patient onto the CT scanner platform from the stretcher. The Diagnostic Imaging specialists take over.
In succession, they all look down at their phones as they receive word that the simulation has ended.
THE SIMULATION EVOLVES
Afterwards, all participants converge in the hospital’s Daniels Hollywood Theatre for a debrief.
The debrief is a key component to the simulation, because it informs any processes identified throughout the sim that need to be improved upon.
“All of our processes are constantly evolving, being tested, reviewed and revised through simulation,” says Leah McFeeters, a charge nurse in the ED overseeing emergency preparedness and one of the nursing leads for the exercise.
“It’s the reason we decided to implement a physician and secondary triage process to help with difficult decision making. Our blood bank process has also evolved, so we can get blood to patients even quicker than before,” says McFeeters.
Interprofessional Education Specialist and nurse Seona Dunbar addresses a crowd of participants and facilitators at the Code Orange simulation debrief, located in SickKids’ Daniels Hollywood Theatre.
Seona Dunbar, interprofessional education specialist and nurse, stands at the front of the room and facilitates conversations about what worked, and what didn’t. She is also one of the nursing leads for the exercise. Given her decades as a nurse at SickKids, Dunbar calls on Boysen, asking for her thoughts about the evolution of the simulation over time.
She takes a pause to respond.
“I’ve seen real disasters and simulated ones over the years. Each year I watch as we put so much care into fine-tuning and improving with each iteration, and that’s what will save lives. That’s why we do this, and we should be very proud,” she responds. n H
Danielle Orr works in communications at The Hospital for Sick Children.
Dr. Joshua Ramjist reviews notes made by staff regarding areas for discussion during the Code Orange simulation debrief session.
Advancing patient care through clinical education at Humber River Health
Afoundational aspect of delivering innovative, safe and equitable care lies in empowering hospital staff with the education and preparation needed to navigate the complexities of the healthcare system. Clinical education not only safeguards patient outcomes but also fortifies an organization’s ability to adapt and innovate. Humber River Health (Humber) exemplifies this culture with a variety of innovative programs designed to prepare the next generation of healthcare professionals, all while continuously developing its current staff. These initiatives reflect a commitment to fostering clinical excellence and addressing health human resource needs through immersive, hands-on learning.
Humber holds status as a Registered Nurses’ Association of Ontario (RNAO) Best Practice Spotlight Organization (BPSO), a recognition of its unwavering commitment to evidence-based care and clinical excellence. This status signifies Humber’s dedication to implementing and sustaining RNAO’s Best Practice Guidelines (BPGs), which enhance patient outcomes, ensure consistent quality of care, and foster a culture of continuous improvement across the organization.
CORPORATE NURSING ORIENTATION THROUGH SIMULATION
Humber’s Corporate Nursing Orientation Program bridges the gap between theoretical knowledge and real-world clinical practice. Utilizing high-fidelity simulation, newly hired and existing nurses engage in hands-on scenarios that replicate diverse patient care situations – including physical assessments, wound management, clinical deterioration, and emergency interventions. This initiative fosters interprofessional collaboration, critical thinking, and evidence-based practices.
“This program is about creating a safe space where nurses can learn, practice, and refine their skills,” explains Gurmit Maghera, Manager of Simulation Lab, BPSO, Wound and Skin at Humber. “Our simulation lab is equipped to replicate real-life challenges, providing a risk-free environment for clinical problem-solving and decision-making.”
Feedback from participants highlights improved confidence, readiness for independent practice, and enhanced job satisfaction. The success of this program underscores the transformative potential of immersive learning in preparing nursing professionals to excel in today’s complex healthcare environment.
INTERPROFESSIONAL PRECEPTOR AND MENTORSHIP PROGRAMS
Humber’s Interprofessional Preceptor and Mentorship Programs represent an essential feature of its clinical education strategy. By pairing experienced clinicians with learners from various disciplines, these programs encourage cross-functional learning and professional development.
Structured workshops, practice scenarios, and reflective discussions equip participants with essential skills. This interprofessional approach creates a collaborative environment where mentors and mentees thrive. Participants often report an increase in confidence, enhanced clinical skills, and a better grasp of their roles within an interprofessional team. Meanwhile, mentors find renewed passion for their work and the satisfaction of nurturing the next generation of healthcare professionals. This progressive approach not only bolsters professional growth but also enhances patient care delivery.
INTERPROFESSIONAL BEST PRACTICE CHAMPION PROGRAM
Humber’s Interprofessional Best Practice Champion Program is a pioneering initiative dedicated to sustaining ten evidence-based BPGs and reinforcing its designation as an RNAO BPSO.
Through engaging workshops, meaningful mentorship, and collaborative projects, participants gain the essential knowledge and skills to implement, evaluate, and sustain BPGs in their practice areas. These guidelines address critical domains such as patient safety, wound care, falls prevention, pain management, and person-centered care, ensuring that the highest standards of care are consistently met. Best Practice Champions
engage in realistic, hands-on simulations that replicate clinical challenges, enabling them to implement and evaluate BPGs in a safe environment.
By fostering a culture of shared accountability, the program ensures sustainable improvements in healthcare delivery.
RESOURCE NURSES’ WORKSHOP PROGRAM
Resource nurses are pivotal in ensuring seamless patient care and operational efficiency. Humber’s Resource Nurses’ Workshop Program equips these leaders with the tools to manage complex care environments effectively.
The workshops focus on enhancing their leadership, decision-making, and problem-solving capabilities, particularly in high-pressure and complex situations. Participants engage in interactive learning experiences, including simulated-based training and collaborative discussions, which strengthen their ability to guide their teams with knowledge, resilience, and compassion.
The program also emphasizes effective communication and conflict resolution strategies for fostering a cohesive and high-performing team. Feedback from participants highlights increased confidence, improved team collaboration, and a deeper understanding of their critical role in maintaining operational excellence. This initiative strengthens Humber’s leadership framework and ensures exceptional patient-centered care, even in the most challenging circumstances.
PRECISIONOS® VIRTUAL REALITY PLATFORM
Humber recently integrated PrecisionOS®, a cutting-edge virtual reality (VR) platform, into its orthopaedic surgical training program. This technology offers an immersive, risk-free environment where surgical teams, including nurses, can refine their technical and collaborative skills. Orthopaedic surgeries demand precision and teamwork, and PrecisionOS® bridges the gap between knowledge and application. Nurses, guided by surgeons, engage in realistic simulations utilizing a VR headset to improve communication and technical competencies, ultimately enhancing patient outcomes.
LOOKING AHEAD
Humber’s comprehensive clinical education initiatives are more than just training programs—they are transformative experiences that shape the future of healthcare. From simulation-based nursing orientation to virtual reality surgical training, these programs exemplify innovation, collaboration, and a relentless commitment to excellence.
“By investing in its people, Humber River Health ensures that its workforce is prepared to meet the demands of modern healthcare,” says Gurmit “Through its visionary approach to clinical education, the organization not only safeguards patient outcomes but also inspires a brighter, more resilient future for the healthcare system.” n H
A collage of photos of Humber River Health’s Clinical Practice Leaders (CPLs), Interprofessional Preceptor and Mentorship Programs, Interprofessional Best Practice Champion Program, and PrecisionOS
Trauma Career Bootcamp allows students to explore health-care careers
Did you know that severe bleeding is the number one cause of death from traumatic injury? On Day One of Trauma Career Bootcamp, students dove into learning about safety, injury prevention and different responses to critical incidents and situations. They learned when and how to administer naloxone and were shown other treatments to reverse drug overdoses when the person is brought to the Emergency Department, along with learning how to “stop the bleed.”
There was no time as high school students entering grades 11 and 12 explored a variety of health-care careers through job shadowing and learned practical skills through hands-on activities at London Health Sciences Centre (LHSC).
The students engaged as a group when they learned through demon-
strations and practical applications on how to:
• stop bleeding from a traumatic incident,
• intubate in the Critical Care Trauma Centre (CCTC) in a simulation,
• suture and splint in the Emergency Department (ED),
• respond to a traumatic incident with Middlesex London Paramedic Services (MLPS),
• put in an IV and measure blood pressure,
• respond to a paediatric patient’s worsening condition in a simulation.
When they weren’t learning as a group, they were learning one-onone, or in very small groups, in their placements.
“Before the bootcamp started, the students shared which areas of the hospital they were most curious in learning about from a list and were
Looking to continue your education, but finding difficulty working your educational goals around professional and life commitments? Mohawk College offers a number of Health and Nursing courses through Continuing Education, with flexible delivery options to accommodate your busy schedule. Led by instructors that are subject matter experts, our courses offer the skills and knowledge you need to gain a competitive edge in your profession. Take a single course or work towards a credential; the choice is yours!
We offer a variety of post-graduate Nursing certificates, enabling you to further your skills as an RN or RPN. We work with our community partners to ensure our curriculum is relevant and meets evolving industry needs. As an example, our recent postgraduate certificate for RNs in Public Health Nursing was the first such graduate certificate in Canada, addressing a critical need for formalized training in this important area.
Interested in working in other Health related professions? We offer programs enabling you to work towards becoming an Operating Room Attendant, a Medical Device Reprocessing Technician, a Medical Laboratory Assistant, or a Perinatal Support Worker… to name but a few.
We welcome you to explore what we have to offer: mohawkcollege.ca/ce/health
given placements accordingly,” says Rai DiLoreto, Injury Prevention Specialist, Critical Care and Trauma at LHSC. “We wanted the students to be exposed to areas that were outside of their interest too, so they get to see different areas that keep a hospital running while honoring and fostering their specific areas of interest.”
The placements took place with a different roles in a variety of areas of practice at LHSC, such as:
• Physiotherapy
• Occupational Therapy
• Radiology
• Pharmacy
• Labs
• Medical Device Reprocessing (MDR)
• CCTC
• ED
• Food Services
• Switchboard
There were also new teams that joined the bootcamp this year, including:
• Trauma Observation Unit
• Minor Procedure Room (Children’s Hospital)
• The Paediatric Critical Care Unit (PCCU) and the Paediatric Critical Care Outreach Team (PCCOT) (Children’s Hospital)
• Child Life Music Therapy (Children’s Hospital)
• Paediatric ED (Children’s Hospital)
The students also had the opportunity to learn over their lunch break with special Lunch & Learn presentations from different LHSC groups: the Impact! team, Volunteer Services, the Paediatric Transport Team and an activity from a Speech-Language Pathologist that demonstrated how they support patients with swallowing and their different food/liquid needs.
The Trauma Career Bootcamp is hosted by LHSC’s Trauma Program each summer for one week. The application process for 2025 will begin in the spring. Please visit the Trauma Career Bootcamp webpage for more information. n H
Early intervention training for health professionals transforms care for children with cerebral palsy
Andrea Clelland leans forward, intently watching a baby move in a video clip. Subtle shifts in posture, reflexes, and facial expressions tell a story she’s trained to interpret. As a pediatric physiotherapist, Andrea is deeply committed to helping infants and families thrive through the early identification of infants with a high probability of cerebral palsy.
The moment was captured during a recent training session for the Hammersmith Infant Neurological Examination held by Sunnybrook’s Neonatal Follow-Up Clinic team, who are on the frontline of training teams to detect cerebral palsy and initiate interventions.
Cerebral palsy refers to a group of conditions affecting movement, coordination and posture due to a non-progressive impact on the developing brain.
While it primarily affects motor abilities, it may also involve challenges with sensation, communication, perception and cognition. Early identification and intervention play a critical role in helping children build on their strengths and achieve their full potential.
Sunnybrook’s team works closely with a multidisciplinary group of experts in cerebral palsy and neonatal neurodevelopmental outcomes, including members from Holland Bloorview, McMaster Children’s Hospital and Boston Children’s Hospital, to train clinicians to use the Hammersmith Infant Neurological Examination.
Aligned with international guidelines emphasizing early identification, the approach involves advocating for timely discussions and interventions, avoiding delays associated with waiting until 12 to 24 months. Prioritizing pa-
Certificates designed for a rapidly-changing healthcare landscape.
Anna Tersigni, Director of Quality & Risk, Chief Privacy Officer at the Canadian Mental Health Association (CMHA) in Waterloo-Wellington is a passionate and lifelong learner, having taken four OsgoodePD Certificate programs. Given her vast professional experience, she has also participated as faculty on a few programs.
If you truly want to be an informed quality/risk/health information management/privacy professional, the OsgoodePD curriculum will not only help you in your role in any healthcare organization – it will lead to much better outcomes for the vulnerable people we support...
Read more on how OsgoodePD’s certificate programs have advanced Anna Tersigni’s career and kept her inspired: osgoodepd.ca/blog-hn
Training in action: Andrea Clelland, physiotherapist from Royal Victoria Regional Health Centre (left) and Lisa Smuskowitz, physiotherapist from Sunnybrook (right).
rental voices, one of the primary goals is to offer guidance on communicating high cerebral palsy probability, emphasizing empathetic and transparent communication to support families.
“Early interventions are transformative for children, especially those who have spent time in neonatal intensive care units,” says Dr. Rudaina Banihani, Director of Sunnybrook’s Neonatal Follow-Up Clinic. “At Sunnybrook, we use the examination in tandem with neuroimaging and other tools like the General Movements Assessment to identify children very early at a high probability of developing cerebral palsy. This enables us to truly support children, ensuring the best motor and cognitive outcomes.”
Dr. Banihani explains that the Hammersmith Infant Neurological Examination evaluates cranial nerve function, posture, movement, muscle tone, and reflexes, with each category scored and results tracked over time to monitor progress.
The impact is evident with Kayleigh, a ‘micro-preemie’ born at 23 weeks and six days, who was identified as being at high probability of cerebral palsy by three months corrected age. Corrected age refers to a baby’s actual age in weeks (number of weeks since the date of birth), with the number of weeks the baby was born preterm subtracted. Her care team at Sunnybrook connected her family with local therapy services, and she now sees a physiotherapist and occupational therapist.
Kayleigh’s mother, Kirstin Anderson, says she’s grateful for the early identification and intervention.
“Having a preemie is overwhelming – you’re absorbing so much complex information,” she says. “Kayleigh is an amazing kid who loves finger painting and attending daycare. We’re letting
her guide her own way in life with the right supports in place.”
The Hammersmith Infant Neurological Examination is now being implemented across Canada in many Neonatal Follow-Up Clinics and care centres. Over 900 healthcare professionals have been trained, demonstrating strong engagement and a commitment to broadening awareness.
“The exam is straightforward and quick to administer,” explains Andrea, who works at the Neonatal Follow-Up Clinic at Royal Victoria Regional Health Centre in Barrie, Ontario. “It’s incredible how much it empowers families to know early on about the high probability of cerebral palsy and to have the opportunity to begin interventions that make a real difference.”
Sunnybrook’s Neonatal Follow-Up Clinic has established partnerships with Royal Victoria Hospital and other follow-up clinics across the province, improving accessibility for families within their own communities.
“This approach is accessible, efficient, and highly sensitive for identifying infants at high probability of cerebral palsy,” says Dr. Banihani. “The impact is profound: empowered families, timely interventions, and a focus on strengths and resilience. Tracking scores over time helps therapists assess the effectiveness of their interventions and adjust care plans to meet children’s evolving needs.”
A unique feature is Sunnybrook’s ongoing collaboration between Level III Neonatal Follow-Up Clinics and Level II clinics, fostering the development of expertise across care settings and strengthening shared care models. To learn more about the training sessions, please contact Sunnybrook’s Neonatal Follow-Up Clinic. n H
Photo court
esy of Doug Nicholson, Sunnybrook
Osgoode
Certificates
Learn from leaders with real-world experience in Health Law
Open to all learners, an Osgoode Certificate is a micro-credential that gives you the opportunity to learn from industry leaders with expertise and experience.
• E xpand your practical legal knowledge and skills in a targeted area
• Designed by and for working professionals
• Flexible learning options to fit your schedule
• Build your network with an influential, professional network
To preview program content, visit: osgoodepd.ca/health-hn
Upcoming health law certificates:
Certificate in Privacy Law and Information Management in Health Care
Starts January 14, 2025
Ensure health information is safeguarded. Designed for privacy officers and other professionals tasked with collecting, storing or managing health records.
Certificate in Elder Law
Starts February 5, 2025
This 5‑day intensive program is specifically designed by legal, health and elder care experts to provide you with the opportunity to tap into a deep reservoir of practical, relevant information.
Certificate in Health Law
Starts March 18, 2025
Over five comprehensive, practical one day modules, learn what you need to know about contemporary issues in health law from a diverse faculty.
Simulation training prepares the Ottawa Hospital staff for real emergencies
By Gillian Brandon-Hart
he goal here is to be better 10 minutes from now than we were 10 minutes ago,” said Dr. Glenn Posner, director of The Ottawa Hospital’s (TOH) Simulation Patient Safety Program. “If this same scenario happens in the next bed 10 minutes from now, we are going to be a well-oiled machine.”
Since 2014, TOH has been improving safety, fostering education, and sharing knowledge through their Simulation Patient Safety Program (SPSP). To learn what sets it apart, we spoke to the program’s director, Dr. Posner; lead medical facilitator, Dr. Doran Drew; and simulation educator and nursing lead instructor, Jennifer Dale-Tam.
The SPSP focuses on simulation training that takes place in the hospital or other clinical setting. It’s a part of the organization’s Corporate Strategy, which is one of the elements that make TOH’s program so unique.
Promoting interprofessional collaboration, the training resembles real-life crisis scenarios by involving real teams responding to simulated patients, while fulfilling requirements from Accreditation Canada. Simulation training also reinforces the importance of practicing and highlights what can be optimized in the healthcare system.
Dale-Tam emphasized the importance of simulation training: “It is the pinnacle of the application of knowledge and skills previously learned by the health professions.” It is a space to learn and take risks without any harm to real patients and prepares health professionals by practicing, communicating and working together as a team ensuring safe, quality patient care.
PROMOTE INTERPROFESSIONAL COLLABORATION
At HIROC, having the opportunity to hear voices from across the
healthcare system is at the cornerstone of our commitment to share valuable knowledge, all with the goal of scaling lessons learned. This is why we want to highlight interprofessional collaboration, which is key to simulation training and clinical practice, and the role of nurses, who are crucial to the healthcare system and driving safety.
“Historically, much of our training is done in silos and research is showing this does not provide the best outcomes for the patient. All health professions have a unique body of knowledge, and many a particular philosophy when it comes to patient care, but we need to understand each other and how to collaborate to achieve optimal patient outcomes,”
Dale-Tam said.
ADDRESS LATENT SAFETY THREATS
The SPSP also enables the discovery of latent safety threats (LST) that could impact quality patient care. LSTs that may not have been found otherwise can then be fixed proactively. For example, in TOH’s first simulation training session in 2014 of a cardiac arrest, they discovered the crash cart defibrillator had the incorrect pads on which would have delayed patient care in a real situation.
Similarly, simulation training offers a way to test protocols and procedures before implementing them clinically to ensure safety, and it supports TOH’s goal of creating a patient safety culture.
“One of the things we’ve been seeing when we’ve been doing our in-situ simulations is the feedback is resoundingly positive,” said Drew. “The spirit of this is actual teams practicing together just to see what things work and what things don’t, identify system issues that are going to be barriers to patient care, and provide our teams with education while they’re at work.”
DEBRIEFING MATTERS
Another key aspect of the program is debriefing. In real situations, there is little time to stop and reflect between patients, so debriefing in training offers a safer, low-stakes environment where participants feel comfortable talking about the case. Debriefing is also a main component of coaching in various high-performance fields, such as athletics and aviation – it’s all about improving learning. Medical education literature shows high-performance healthcare teams can benefit from it too.
“It’s so important to reflect on what you did well and what could’ve gone better, and we don’t do it enough in real cases because the hospital is a runaway train. You jump on for your shift and jump off at the end of your shift, but it’s always going. When you finish a case, there’s another case waiting,” Posner said.
STAY CURIOUS AND SEEK TRAINING
“My advice to someone who is building up a program at a different hospital would be encouraging them to stay curious and explore the things they’re seeing because often it’s going to relate back to their underlying mission,” Drew said. “One of the nice
things about the in-situ programs is you’re on the ground level working with people who are directly providing care, so you often are in a nice situation where you can do some root cause analysis.”
Dale-Tam recommended formal or informal training programs for simulation-based education. “There are many in Canada from organizations like Simulation Canada, the Royal College of Physicians and Surgeons of Canada, or the Canadian Association of Schools of Nursing. Looking for a mentor in the area helps too.”
She also highlighted how developing your simulation facilitation skills is critical for simulation education. “There is research coming out that learners who have participated in simulation scenarios that are facilitated by untrained faculty may develop PTSD-like symptoms even though that is not the intent of the facilitator. Participating in simulation can be scary; some may see it as a test or threat to their professional identity. A trained facilitator will put strategies in place to create that safe space for learners to take risks and see the associated outcomes before taking it into clinical practice.”
Learn more about TOH’s Simulation Program at uossc.ca. n H
Innovative medical simulation program
inspires the next generation of health-care professionals
The Canadian Surgical Technologies and Advanced Robotics (CSTAR) team at London Health Sciences Centre (LHSC) has launched an innovative curriculum in partnership with the Canadian Medical Hall of Fame Museum School to redefine health-care education for youth. Led by Scott Sumpter, Simulation Tech Consultant, and Karen Siroen, CSTAR Surgical Suite Associate, this initiative offers students from grade seven and up a fresh perspective on the many career opportunities in the health-care sector, expanding their understanding beyond traditional roles like doctors and nurses and giving them handson experience with some of the latest medical technologies.
“This unique program educates students through engaging interactive activities that capture the imag-
inations of young learners,” said Nicole Girotti, Director of Academic Operations at LHSC. “We take complex medical concepts and transform them into accessible, engaging, and enjoyable learning experiences.”
During these sessions, students explore the history of medical simulation to understand its evolution and significance in modern healthcare training. Studying the historical context helps them appreciate the advancements that have led to today’s sophisticated technologies and envision future developments in the field.
al-world applications of their learning and the impact they can have in future careers.
ly appreciative and enthusiastic about the hands-on learning experiences and interactive simulations.”
The education sessions also include guest lecturers from CSTAR’s own research division who offer a glimpse into the future of health-care technology. Students have the opportunity to hear firsthand accounts of the cutting-edge innovations and medical practices being implemented at LHSC, helping them see the re-
A standout feature of the program is the opportunity for students to receive hands-on experience with high-fidelity medical simulators. Typically used for training health-care professionals, these advanced tools enable students to dive into the inner workings of advanced medical technologies as they explore the electronics and software that drive realistic medical scenarios. This approach gives students a chance to explore fields like biomedical engineering, software development, robotics, and medical device design to broaden their understanding of the critical role of engineers and technologists in advancing health care.
“The feedback we have heard from students has been overwhelmingly positive,” said Girotti. “They are real-
Many students noted that the program helped deepen their understanding of health-care careers beyond traditional roles and sparked their curiosity and interest in diverse fields within the sector.
Looking to the future, CSTAR plans to expand this initiative and increase student recruitment efforts with the hopes of inspiring the next generation of health-care professionals. By developing a program that combines interactive learning, hands-on experiences, expert insights, and historical exploration, CSTAR is making significant strides in the future of healthcare education. Through its dynamic and engaging approach, CSTAR’s medical simulation program is a steppingstone for young minds towards a future in health-care innovation. n H