This is the third most common type of cancer in the world and according to The American Cancer Society, 52,900 patients in the US will die from it this year. Most of the time, there are no symptoms. See what you can do to prevent this deadly disease. P. 14
Rochester Doc: 'My Path In and Out of Addiction'
Dr. Mark Winsberg, the former medical director of Rochester Regional Health chemical dependency department, talks about his addiction and how he was able to overcome it. P.10
Gambling: The Silent Addiction Impacting All Ages P.9
Still Taking a Low-Dose
Aspirin Every Day?
Many Americans don't see anything wrong with taking daily low-dose aspirin, even though experts have concluded its risks outweigh its benefits, a new survey has found.
Nearly half (48%) of people incorrectly think that the benefits of taking low-dose aspirin daily to reduce the risk of heart attack or stroke outweigh the risks, according to the survey from the Annenberg Public
Policy Center of the University of Pennsylvania.
“Habits backed by conventional wisdom and the past advice of health care providers are hard to break,”
Kathleen Hall Jamieson, the center's director, said in a news release.
“Knowing whether taking a low-dose aspirin daily is advisable or not for you is vital health information.”
For years, healthy seniors were advised to take low-dose aspirin to
reduce heart attack and stroke risk.
The rationale was that aspirin acts as a blood thinner, reducing the risk that a blood clot could cause a heart attack or stroke by clogging an artery.
But in 2019, the leading heart groups — the American College of Cardiology and the American Heart Association — reversed that recommendation in a set of new guidelines. The groups concluded that daily
aspirin for healthy seniors 70 and older wasn't worth the risk of gastrointestinal bleeding.
"If you're over 70, taking aspirin to prevent a first heart attack or stroke could do more harm than good," the AHA now says on its website.
Aspirin still is recommended for people with diagnosed heart disease who don't have an increased risk of bleeding. This updated guidance has failed to break through decades of advice supporting daily low-dose aspirin, the poll found.
Nearly 1 in 5 U.S. adults who have no personal or family history of heart problems report routinely taking low-dose aspirin. According to survey results:
• 10% say they take it “basically every day.”
• 6% take it “a few times a month.”
• 2% take it “a few times a week.”
Younger adults were more likely than older folks to correctly report that the risks of aspirin outweigh the benefits, the survey showed.
About 29% of 18- to 29-year-olds with no personal or family history of heart disease correctly said the risks of daily aspirin outweigh benefits, compared with 11% of those 40 to 59 and 7% of those 60 and older, researchers found.
That's likely because the younger folks haven't been exposed as much to the outdated guidance supporting aspirin use, researchers said.
The survey involved 1,771 people polled Nov. 14 to 24, 2024, and has a margin of error of plus or minus 3.3 percentage points.
Everybody deserves to live a healthy life. At Excellus BlueCross BlueShield, we understand that people are facing rising costs in healthcare. And that’s why we’re here to make sure no one faces them alone. We are advocates for our members and communities; working to ensure care is as effective and efficient as possible.
To learn more visit ExcellusBCBS.com or scan the QR code.
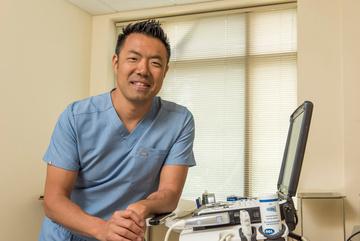
Meet Your Doctor
By Chris Motola
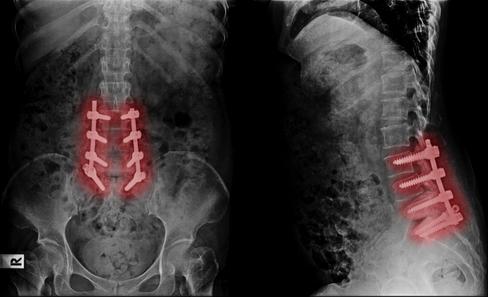
Matthew C. Talbott,
M.D.
Top doctor at Finger Lakes Health talks about why his hospitals have some of the shortest ER wait times in the state and why he thinks AI will help free up time for physicians to spend more time with patients
Q: You've been chief medical officer of UR Medicine Finger Lakes Health for a year now. What was that first year like?
A: I love challenges. I'm an ER physician by training and came out to Finger Lakes Health in 2008. And during that first decade or so, I worked clinically and got involved in leadership. I took over the ED [emergency department] leadership in 2016. So my mentors here, the previous medical director Jason Feinberg and our CEO Dr. Acevedo really knew the importance of having a succession plan. So my year prior to becoming CMO [chief medical officer] I was an associate CMO. A lot of the quality initiatives that we've done in the emergency department
So my leadership here has evolved through the emergency department as director and now more in a system-wide role. So that's really given me great energy to improve and continue the successes that we've had and different disease processes like stroke and chest pain and things like that.
Q: Geneva General Hospital and Soldiers and Sailors Memorial Hospital have two of the shortest ER wait times in the state. How did you pull that off?
A: That's something that we're very proud of. We've had the shortest door-to-doc times for the last 10 years or so and CMS data at both hospitals has also shown that. It's really a culture of not accepting patients staying in the waiting room do is called “pull to full,” so we pull physical space in the emergency -
throughout it's very satisfying.
Q: How about the rest of the process? Have you improved treatment times as well?
A: It's not just the door-to-doc times that we've had a lot of success on, but also if you look at recent national and regional data, we have some of the best treat-to-release times too. So that's the time between when you're seen and when you're discharged. The efficiencies we've been able to adopt through the lab, through radiology are really interdisciplinary. Patients have so many choices now. When I started in 2008, there were no urgent cares in the area. Now we have one in Seneca Falls, in Geneva. So people are going to pick where they know they're going to have quality, but also where it's a more efficient use of their time.
Q: What advantages does coming from an emergency medicine background have when you reach a system-wide administrative role?
'We've had the shortest [ER] door-to-doc times for the last 10 years or so and CMS data at both hospitals has also shown that. It's really a culture of not accepting patients staying in the waiting room for long periods of time.
Q: Why did that contractor model become so popular?
120,000 patients a year with Strong Memorial Hospital.
a physician in triage to at least get the care of those
only have one physician staffing our emergency
that we're not going to leave a patient in the waiting room. the staff. I've seen the satisfaction. When you promote
A: I think one of them is that we are a specialty that really has to be able to effectively communicate with all types of sub-specialty services, whether it's working with the hospitalist team to transfer someone from the ED to the inpatient side or consulting with surgical teams. When you're working with different specialties there can be disagreements, so being that person at the bedside of the patient you're really able to drive what the patient needs. Those communication skills have really served me as I've transitioned to an administrative role here as well as in our collaboration with UR Medicine. We have a lot of those synergies where I think working across different service lines across the medical spectrum helps in a lot of ways.
Q: What are some of the challenges you see coming down the pipeline?
A: Every day we have more and more regulation. The human resources required to keep up with those regulations is significant. We want to deliver the highest quality care that we can, but physicians are often constrained with the electronic medical record and the time that it takes to complete and get through those documentation requirements. I think AI is going to play a big role in the next five to 10 years and take some of that burden off the physicians and allow them to be back at the bedside more. Also, as we've come out of COVID a significant amount of our nursing staff is contracted through outside agencies. So there's more turnover there than there used to be. So a lot of our initiatives have been focused on getting nurses to come back in-house. It helps to improve quality and standardize and streamline processes. So I think things to watch in the next decade will be how much AI can lessen the burden on providers on the documentation end, and how can we incentivize nurses to come back to the bedside as employees.
A: There's no single answer. As I'm sure you're aware with COVID, a lot of things became remote. People, because they were staying at home, weren't getting as ill, having as much trauma. Volumes went down at the ER. But you also had places that had very sick patients with COVID that affected the mental health of medical community. A lot of nurses retired or took remote jobs doing non-patient-facing activities. To be honest I think a lot of the agency nurses did enjoy that flexibility of having more control over their own work environment and lives. I think COVID did accelerate some of those trends.
Q: How do you get them back?
A: I think we have to be a welcoming work environment and make sure the nurses have what they need to do their job. We have a nursing leadership team that supports all of those things. We had much lower nursing turnover rates in the last 18 months. We've also had some success bringing back nurses who had left for other hospitals or contractors. We're trying to make sure they have a say in their own environment and a clinical ladders program that encourages growth. And I think we'll have more success as we grow those initiatives.
Lifelines
Name: Matthew C. Talbott, M.D.
Position: Vice president, medical affairs & chief medical officer at UR Medicine Finger Lakes Health
Hometown: Springfield, Ohio
Affiliations: UR Medicine Finger Lakes Health (Geneva General Hospital, Soldiers and Sailors Memorial Hospital
Organizations: American College of Emergency Physicians; American Board of Emergency Medicine
Young adults keep dying at higher-than-expected rates, falling prey to drug overdose and poor health, a new study says.
The death rate among adults 25 to 44 was 70% higher in 2023 than it would have been had pre-2011 trends continued, researchers reported in a new study published Jan. 31 in JAMA Network Open.
“Although mortality rates decreased after the core pandemic years, excess mortality remained higher than expected based on prepandemic levels,” the research team led by Elizabeth Wrigley-Field, an associate professor of sociology at the University of Minnesota, concluded.
This trend started prior to the COVID-19 pandemic, with early deaths among adults 25 to 44 nearly 35% higher than expected in 2019.
Then during the pandemic, excess deaths among young adults nearly tripled compared with 2019, researchers found.
By 2023, the pandemic-era death surge among young adults had subsided somewhat, but early deaths remained 70% higher than expected.
“These results suggest the possibility of a worsening mortality crisis unless these trends are reversed,” researchers concluded.
Drug overdoses accounted for nearly 32% of deaths among young
adults in 2023, researchers found. About 14% died in accidents, nearly 9% due to alcohol use and 8% in homicides.
“The largest portion of 2023 excess mortality was driven by drug poisoning, but many other external and natural causes exceeded what prior trends would have projected,” researchers wrote.
Even diseases usually thought of as affecting older people, like heart disease and diabetes, are contributing to early deaths among young adults, said physician Sanjey Gupta, senior vice president and director of emergency medicine for Northwell Health in Hempstead on Long Island.
“Unfortunately, we have a much higher percentage of our youth who suffer from some of the diseases that we used to attribute to old age," Gupta, who was not involved in the study, said in a Northwell Health news release.
"So hypertension and diabetes and obesity — we're encountering children with these illnesses. And as they are aging, they're getting the ad ditive effect of having these diseases for long term,” he added.
The two distinct phases of increasing early deaths, before and after 2020, might indicate that the pandemic continues to stalk the health of young adults, researchers said.
SERVING MONROE AND ONTARIO COUNTIES
A monthly newspaper published by Local News, Inc. Distribution: 33,500 copies throughout more than 1,500 high-traffic locations.
Editor & Publisher: Wagner Dotto • Writers: Deborah J. Sergeant, Chris Motola, George Chapman, Gwenn Voelcker, Anne Palumbo, Jim Miller, Mike Costanza Eva Briggs (MD), Mark Winsberg (MD), Jennifer Faringer, Brian Burger, Joe Murabito
Advertising: Anne Westcott (585-421-8109) • Linda Covington (585-750-7051)
No material may be reproduced in whole or in part from this publication without the express written permission of the publisher. The information in this publication is intended to complement—not to take the place of—the recommendations of your health provider. Consult your physician before making major changes in your lifestyle or health care regimen.
an fusion, screws, egenerative
moments. Stop d pain mean fusion, screws, e l d
your last stop
e
Healthcare in a Minute
By George W. Chapman
Infant Mortality Among Black People: Astounding
It’s been said here several times that the U.S. gets the worst bang for the buck when it comes to the cost of care versus results.
With the cost per capita of more than $14,000 a year, we rank around 40th in overall mortality. And nothing says how poorly we perform more than Black infant mortality. Per 100,000 births, it is three
Deferred Resignation Offer to VA Nurses
If any group has earned the right to receive healthcare, it is our veterans. Yet the White House is offering VA nurses, the govern ment's largest group of employees, deferred resignations. This is being done before any valid analysis and done when half of our VA hospitals are operating under severe staffing shortages. The nurse union is encouraging their members not to take the bait. When care eventually deteriorates further due to nurse shortages and the VA is finally allowed to hire more nurses, where do the powers that be think they will come from? The VA cares for more than 9 million veterans.
times higher than the mortality rates for Whites (14), Hispanics (12) and Asians (11). The infant mortality rate for Black infants is astounding 50 per 100,000.
The mortality report leaked out just after the official "temporary pause" on external federal health agency communications. (Pausing all federal health communication is a to-
down certain web pages by the new administration. The agencies are: CDC, OPM, FDA and HHS. The lawsuit is brought by the Public Citizens Litigation Group. One can only hope that science, not politics, determines what information is available to us all let alone our providers and researchers. Will any of these agencies even exist in the future? Scary. A judge has since ordered the pages reinstated.
Fentanyl Deaths
Physicians Suing the Government
Doctors for America is suing several federal agencies over the removal of several web pages from websites covering a broad range of health-related (scientific and validated) data used daily by providers and researchers. In fairness, the agencies being sued were mandated to take
The leading cause of death among 18-45-year-olds remains fentanyl overdoses. In 2023, more than 107,000 of us died from an OD with 70% being from the opioid fentanyl. While measures are being taken to slow down, if not stop altogether fentanyl smuggling into the U.S., a new drug developed by the school of pharmacy at the University of the Pacific can save lives. naloxone is the chemical in Narcan which is used to counter overdoses. Narcan lasts up to two hours when delivered as a nose spray. Researchers at U of P found that the HD-5 molecule when added to naloxone allows Narcan to be delivered via
tally different problem. In the future, will we ever know what’s wrong?) Studies have shown that more Black docs lead to better outcomes. Unfortunately, the number of Blacks attending medical school has dropped off sharply the past several years. Attempts to curtail health insurance for at-risk populations will only exacerbate the mortality problem.
injection versus nose spray. Consequently, the medication lasts in the body for a week preventing overdoses for longer and more often.
Impact of Tariffs
No matter what the final outcome of the tariff war with Cana da, it will inevitably increase the cost of medical equipment we import from our friendly neighbors to the north. Medical equipment has typically been exempted from tariffs per the free trade agreement that existed between the US, Mexico and Canada. Guess who signed it? Anyway, unless the medical equipment exemption continues, we can expect higher costs for MRIs, ventilators, wheelchairs, pace-makers, insulin pumps and orthopedic implants. In 2022, Canada imported $5 billion of medical equipment from the US or 38% of their total medical imports. We imported $3 billion from Canada. Clearly, the trade imbalance favored the U.S. Any tariff on Canadian medical equipment will negatively impact both cost and access to both countries.
Reducing Drug Costs
The U.S. could make substantial inroads toward reducing the exorbitant cost of care in the US by hundreds of billions if Congress would simply take the handcuffs off CMS negotiators and let them negotiate the price of all drugs with Big Pharma on behalf of all 335 million citizens. But our purchasing power has been stilted/controlled by the powerful drug lobby which has reluctantly agreed (gun to head) to striking deals per the Inflation Reduction Act (IRA) on 10 drugs for 2026 for our 60 million Medicare recipients. (We actually had to pass a law to allow Medicare the ability to get our consumers the best bang for our bucks.) Instead of taking the 10-drug limit as a win, Big Pharma continues to lobby for the repeal of the Inflation Reduction Act. Will our newly created Department of Government Efficiency dare take on the drug lobby and recommend negotiating all drug costs and not just a few at a time? We'll see. In the meantime, with the initial 10 prices to take effect in 2026, CMS has indicated the second round of 15 drugs to be negotiated per the IRA. These 15 new prices take effect in 2027. Among them are: Ozempic, Rybelsus, Wegovy and Trelegy. Instead of thwarting physician, hospital and nursing facility reimbursement, CMS should be laser focused on going after the fat in drug prices.
Uninsured Will Increase
To reduce costs, the White House is proposing to cut $2.5 billion from Medicaid by disen rolling 25 million people that qualified for coverage during the pandemic via expanded eligibility. Currently, Medicaid covers more than 70 million people. If the Affordable Care Act is repealed, even more than the 25 million on Medicaid will lose affordable insurance they purchased via the health exchanges. In 2023, our uninsured rate was at an all time low of 8%. If Medicaid is cut and the ACA repealed, the uninsured rate could jump up to 15% or four million per year through 2034. This significant loss of insurance will create more uncompensated care for already struggling clinics, emergency rooms, hospitals and health systems. Making matters worse, patients without insurance tend to postpone or delay care so when they finally seek care they are much sicker. To make up for these losses, providers will be forced to negotiate higher rates with commercial carriers thereby forcing commercial insurance rates up. Is it time we gave serious consideration to a national health plan? We can't stop a boat from sinking if we only plug some of the holes. We need a new boat.
George W. Chapman is a retired healthcare business consultant who worked exclusively with physicians, hospitals and healthcare organizations. He used to operate GW Chapman Consulting based in Syracuse.
By Eva Briggs, MD
Vaccines For All
As I am writing this article, the availability of many vaccines might be in jeopardy in this country.
In fact, at the current moment the vaccine information sheets (VIS) have disappeared — then reappeared — from the Centers for Disease Control’s (CDC) website.
VIS provide written information about each vaccine and by law must be provided to every patient or their parent-guardian, whenever a vaccine is given.
I’m old enough to have seen some diseases that are now far less common because of vaccination. I want to share some of my personal experiences to help foster an understanding of why vaccines are important.
First, chickenpox which is also called varicella.
Part of my family practice training in residency included a rotation in the neonatal intensive care unit (NICU). If a mother has had chickenpox, she will pass antibodies to her infant that protect the baby during the newborn period. That’s why the varicella vaccine is not given immediately after birth as those maternal antibodies would block the vaccine and prevent it from doing its job. This vaccine was licensed in the U.S. in 1995, so it was not available during my residency training in 1984-1987. One patient that I cared for was born to a mother who contracted chickenpox at the time her baby was born. The baby ended up covered from head to toe in the tiny blisters characteristic of the disease. She survived after a long hospitalization in the NICU. I don’t know whether she suffered scarring or other long-term aftereffects.
One of my fellow residents contracted chickenpox during his training. He didn’t wind up hospitalized, but he too was covered in blisters and missed about two weeks of work. When I was a teenager, I used to babysit. One of the kids I babysat for developed a serious bacterial infection of his chickenpox lesions and required hospitalization.
Then there is measles. This virus is one of the most contagious diseases. A measles patient can breathe virus particles into the air which can linger for hours after the patient leaves the room. My husband’s best childhood friend developed subacute sclerosing panencephalitis as a teen-
ager. This disease is due to reactivation of dormant measles virus from an earlier typical case of measles. The measles virus slowly destroys the brain. Essentially his friend Doug developed dementia as a teenager. Over several years it robbed his cognitive abilities, his speech, his motor functions, even the ability to swallow, until Doug died as a young adult.
It was incredibly stressful for his family, and his mother who was probably only in her 40s died shortly after of sudden cardiac arrest.
Another one of my husband’s friends, his college freshman roommate, contacted measles as an adult. In adults, measles can attack the testicles (or ovaries in women). This made him so sick and miserable that he wound up hospitalized, missing weeks of school and ultimately dropping out of college.
As an interesting historical note, at that time Crouse Hospital in Syracuse still had a leftover sign on the building from the Hospital of the Good Shepherd which they had previously taken over. I remember seeing this sign when we walked over to visit our friend in the hospital.
I also remember Hemophilus influenza type B (H. flu).
Before there was a vaccine, every parent whose small child used daycare (and plenty of others) feared this bacterial scourge capable of causing meningitis which could kill or disable a child. One of my oldest child’s daycare classmates contracted H. flu at age 2 and was rendered permanently hearing impaired.
As a resident, it seems like every week I cared for at least one child seriously ill due to H. flu. The improved vaccine for this illness was licensed in 1987.
Whatever your political leanings, I feel strongly that it is important to preserve the availability of affordable vaccines for all.
Eva Briggs is a retired medical doctor who practiced in Central New York for several decades. She lives in Marcellus.
By Gwenn Voelckers
Practical tips, advice and hope for those who live alone
This Much I Know: 25 Things I've Learned About Living Alone
Editor’s Note: The column below was published years ago and has been updated by the author in celebration of the 20th anniversary of her solo trip to Paris and the launch of her “Live Alone and Thrive” column. We think the column’s uplifting insights remain as timely and relevant as ever. Enjoy!
This year marks the 20th anniversary of my solo trip to Paris to celebrate turning 50. It also marks the anniversary of a decision I made that changed my life.
It was in the "City of Light" that I decided to create a workshop series designed to help women live on their own with more confidence and joy.
Since launching the workshop in 2005, I have learned and experienced so much. I have also been inspired by the courageous, resourceful women and men I've met along the way who are now living alone with pride and gusto.
They reinforce what I practice every day and what I shared in my Live Alone and Thrive workshop (now on hiatus since COVID -19) — namely, that the relationship with ourselves is the most enduring of all and that it is worth nurturing.
Most of these women and men have overcome some very real and often painful obstacles, but they now embrace their independence and are busy leading interesting, full lives.
They are making it on their own. They have challenged, as have I, the age-old belief that marriage, as it has been traditionally defined, is the only state in which we can be truly happy,
fulfilled, secure and complete.
Whether divorced, widowed or a confirmed bachelor or bachelorette, they are not spending their time bemoaning their fate. They have conquered uncertainty and adversity and are the stronger for it.
They have taken their lives into their own hands and have come to appreciate the choices and opportunities that living alone has to offer.
This much I know:
1. Living alone doesn’t mean being alone. A single text or phone call can bridge the gap and foster connections.
2. Rediscovering your true self and identifying those things that bring meaning and joy into your life can turn living alone into an adventure of the spirit.
3. Loneliness is not a state of being reserved for single people. Were you ever lonely while you were married?
4. Accepting party invitations is worth doing, even if you suspect the party will be mostly couples. Remind yourself that guests often separate into groups of women and men, so singles blend right in.
5. Figuring out how to hire a contractor, buy a car or even replace the flapper valve in your toilet — all by yourself — can be very gratifying!
6. Sitting in solitude allows you to listen to your inner voice, process loss and begin a journey of self-awareness and compassion. Enlightenment can follow.
7. Pursuing a volunteer activity, part-time job, academic degree or
deeper role in your congregation can be invigorating and fun.
8. The stereotyped image of single women and men as desperate and miserable is exaggerated and just plain untrue. Not a believer? Check out this article about an older adult living by herself and thriving: A Centenarian Thrives Living Alone, Active and Engaged. Simply Google the title and be inspired!
9. Traveling solo can awaken your sense of adventure and passions you never knew existed. Whether it’s Paris or Poughkeepsie, traveling by yourself creates space for these discoveries.
10. Doing a random act of kindness is a great antidote when you’re feeling lonely and sorry for yourself.
11. Friends matter. Reach out. Nurture your friendships. Honor your commitments.
12. Turning your home into a personal retreat that reflects your own tastes, without compromise, can be liberating. Energizing. Even healing.
13. Letting go of the idea that you need to be married to have any chance of being happy and fulfilled is essential. This idea will only keep you mired in self-pity. “Build thy home in thy heart and be forever sheltered.” Anonymous
14. Treating yourself well builds self-esteem. Prepare healthy meals. Get enough sleep. Exercise. You’re worth it. Tell yourself so by taking good care of yourself.
15. Managing your own schedule becomes easier on your own. You can prioritize your time however you want, leading to greater productivity and personal growth.
16. Getting out of your comfort zone is worth the discomfort. Try something new — tap dancing, a cooking class, book club, drumming circle — or whatever piques your interest. It’s a great way to have fun and meet new people.
17. Isolating on holiday, birthdays, Sundays, etc. is for the birds. Solitary confinement is punishment for criminals, not single people. Make plans.
18. Comb your hair. Lose the sweats. Put a smile on your face. It’s
important to create your own positive feedback. Looking your best can bring people, compliments and joyful energy your way.
19. There’s no shame in asking for help. It’s not a sign of weakness. On the contrary, asking for help shows courage and resourcefulness.
20. Self-confidence and humor can lead to rewarding relationships; neediness and desperation can thwart them.
21. Doing anything alone means you enjoy life and your own good company; it’s a reflection of your independence.
22. Expanding your definition of love beyond romantic love will stand you in good stead. Embrace passionate friendships — those relationships in which you can be yourself and feel completely comfortable.
23. Hanging out with negative people is a real downer. Put yourself with uplifting people who make you feel good about yourself and about life.
24. Living alone and loving it takes practice. Know that there is always someone you can call or something you can do to improve your situation.
25. Building your home in your heart can deliver peace as well as power. Harness that potential and your contentment will know no bounds.
Don’t I know it!
Gwenn Voelckers is the author of “Alone and Content: Inspiring, empowering essays to help divorced and widowed women feel whole and complete on their own.” She welcomes your thoughts on this column as well as topic suggestion for future essays at gvoelckers@rochester. rr.com.
Gambling: The Silent Addiction Impacting All Ages
By Jennifer Faringer
Problem Gambling Awareness Month in March is a time to ensure our communities understand the risks and impact of this concerning behavior on youth, young adults, older adults and families.
Consider these statistics:
• Approximately 85% of adults in the United States have gambled at least once in their lives and 60% have in the past year. About a third may not gamble at all and many gamble infrequently.
• Approximately 1% or two million adults meet the criteria for a problem gambling disorder, while another 2% to 3% or four to six million would be considered problem gamblers.
• Ten percent of gamblers account for 65% to 80% of all wagers.
Wider access and availability play a significant role in the likelihood of developing an addiction.
For example, in 2022 when mobile sports betting was legalized,
an individual could gamble at any time without leaving home by simply using their mobile device. New York now ranks third in the total amount of dollars wagered in the U.S. with $1.55 billion collected in taxes.
This comes with a price. Consider the cost:
• Crime (robbery, embezzlement, fraud)
• Business (loss of productivity, unemployment-related employer costs)
• Bankruptcy
• Illness (stress, anxiety, depression)
• Treatment
• Family (divorce, child abuse and neglect, domestic violence)
• Social connection (loss of social capital —employer, family, friends)
While teens and young adults are impacted by problem gambling, so are older adults, a segment of the population that is often overlooked.
The environmental factors for older adults differ from those experienced by youth and young adults. Older adults may be retired, have more time on their hands and may be seeking social interaction. Like so many addictions, gambling starts as a social connector and all too often ends in social isolation with the gambler betting alone.
Seniors may believe gambling is a way to foster a sense of independence. Their gambling activity may be a form of emotional escape. Senior centers and churches sponsor regular trips to casinos, normalizing and celebrating it as an activity without warning the seniors of the potential risks.
Know the warning signs
• Do you experience mood swings based on winnings and losses?
• Do you neglect other responsibilities to concentrate on gambling activities?
• Do you experience impatience with loved ones because they are interrupting your gambling activities?
• Are you willing to eat less or go without food so that you can gamble?
• Do you gamble with money needed for necessary expenses such as household supplies, groceries, medication, electricity and rent or mortgage?
• Are you spending your retirement funds or thinking about cashing in a life insurance policy for gambling money?
• Do you fantasize about big winnings and believe you will win back all your losses?
If you answered “yes” to any of these warning signs know that help is available.
For more information on problem gambling, visit NCADD-RA’s website at www.ncadd-ra.org/ services/finger-lakes-addiction-resource-center/ to find resources, including the Problem Gambling Services Directory and a flyer with the active Gambler’s Anonymous (GA) Meetings in Monroe County.
Jennifer Faringer is the director of the National Council on Alcoholism and Drug Dependence – Rochester Area (NCADD-RA).
“From my room to the food to the excellent doctors and techs…they took what could
have been an unpleasant experience and made it great.”
That’s just one of the comments we’ve received from a patient who has had postsurgical rehab at St. Ann’s. We’re proud to offer first-class care that gets you healthy and home as soon as possible.
Life’s Unexpected Turns: My Path In and Out of Addiction
By Mark Winsberg, M.D
Iam the youngest of four kids born to my parents in the span of six years. My father, Cornell-educated with a master’s degree in soil science, was just finding his way into farming in South Florida when I entered the scene.
My mother, also a Cornell student in home economics, had to cut her college career one semester short of graduating when my oldest sister was born.
I still find it hard to fathom how my parents held it together while Dad went from college student to fertilizer salesman, to dairy farmhand, to partner with another farmer and eventually to buying our 300acre farm, while Mom almost single-handedly raised us four kids.
I was a good student, a good athlete and good at holding my own in almost any social situation. But maybe because I was the youngest child, I came to the erroneous conclusion that I wasn’t and
would never be smart enough, strong enough or good enough to truly fit into my family or anywhere else for that matter. Ignoring mountains of evidence to the contrary, I spent much of my life trying to prove that assumption true.
Maybe that’s why my past is made up of such a crazy array of social and work situations.
Like the dog in the kids’ story “Are You My Mother?” it seemed I could never find my place in the world.
I was a farm boy, drove tractors, baled hay, raised cattle and dug ditches.
My playmates were the Black and Puerto Rican farmworker kids on the farm and in town, the lawyers’ and doctors’ kids in the advanced classes at school. I worked on a dairy farm, did house construction,
spent two years as a welder-pipefitter, lived in a kibbutz in Israel picking bananas and learning Hebrew.
I went to three different elementary schools, two junior high schools, two high schools, four undergrad colleges, two medical schools (graduated from Stanford Medical School), completed a residency in family medicine and ended up working in and becoming the medical director of a small emergency room outside of Rochester for 17 years.
I did well in every one of those environments, but the loop playing in my head always said, “You’re stupid, you’re weak and you don’t belong here.”
Alcohol and drugs first entered my life when I was about 16.
The self-demeaning brain loop was becoming intolerable when I met Bob, the first-chair drummer in the marching band (I was second chair). Bob invited me to a “church party,” which turned out to consist of meeting in the church parking lot, going to 7-Eleven for dollar bottles of Strawberry Hill, then heading to the beach to get drunk. That kicked off a six-month period of getting stoned at Bob’s house every day before school, getting stoned at rock concerts on the weekend and finally feeling like I fit in.
However, by the end of that time, the loop was back, louder than ever. I didn’t feel like I fit in anymore and realized I was being used because I was the one who always had money and a car.
Addicts and alcoholics often try to stop this disease on our own — drinking beer instead of liquor, using weed instead of cocaine, only using on weekends, etc. Another common tactic is the “geographic cure.” At the end of my teenage drug phase, I opted for that one. I suddenly decided to attend a small private hippie high school in the wilds of British Columbia, Canada. I told my parents I
was going and since I had the money saved up from farm work and other jobs, I went. And it worked — at least for the alcohol and drugs.
It wasn’t until much later that I figured out I was really trying to flee the self-demeaning brain loop.
Drugs and alcohol didn’t play a significant part in my life again until my early 40s. If you looked at my life from the outside at that time, you’d wonder why anyone in that situation would start using drugs.
I was the medical director of the ER, well respected by my colleagues and patients. My wife, also a doctor and I had two wonderful daughters, had paid off our medical school loans and owned our home outright.
But what you wouldn’t see was that toxic brain loop that never quit playing. That loop, combined with the stress of working in the ER day after day, left me subconsciously searching for a pressure relief valve. That valve appeared in the form of a drug called Ultram (a combination of Tramadol and Tylenol), which hit the market in the late ’90s as a new non addictive pain reliever. The drug company’s reps would deliver grocery bags full of samples to the ER, encouraging us to hand them out to patients. I don’t remember exactly when I tried it for some ache or pain, but I do remember thinking it didn’t do much for pain. However, it did make my 12-hour ER shifts easier. It was quieting “the loop,” giving me a weird distance from the intensity of patients and a sense of calm amidst the ER storm. Later, researchers discovered tramadol has opiate-like and antidepressant-like effects, is highly addicting and is now classified as a narcotic.
Thus, I was inadvertently taking a narcotic and thinking I had everything under control.
Within a few months, I was taking three or four tablets at a time throughout the day, drinking tons of caffeine (standard ER fare) and adding a muscle relaxant to keep me from feeling too wired. When I got home, I drank wine and took Benadryl to sleep. This cycle continued for almost four years. My wife repeatedly asked if I was using drugs, but I always lied and would often turn the tables, acting hurt or angry that she would even ask.
Fortunately for me, the drugs I was using, combined with chronic sleep deprivation from constantly switching day and night shifts, resulted in me having a seizure in front of my wife, my daughters and my parents at a restaurant in Montreal in 2003. That night, frightened by what had just happened, I finally admitted to myself that I was in trouble, that my life was out of control. The next morning, I told my wife the truth.
Physician Mark Winsberg: "Alcohol and drugs first entered my life when I was about 16. "
What followed was truly miraculous. She didn’t leave me and take the kids. She helped me get in contact with and begin treatment through The Committee for Physician Health (CPH), an organization that helps doctors with substance use problems. I was mandated to go to AA meetings, which I initially resisted, then realized was a gift that’s turned into a lifetime “habit.” I told the CEO of the hospital, the medical staff director, and my ER colleagues what I was dealing with, and every one of them responded with encouragement and support. I felt like I’d been released from prison; my life was no longer controlled by drugs.
The rest is history. I left emergency medicine five years into my recovery. A friend told me he was leaving a part-time job at the JL Norris Clinic (inpatient rehab), which I took. There, I met Dr. Charlie Morgan, the rehab medical director, who became my teacher and mentor. That led to me getting board-certified in addiction medicine. And now I’m semi-retired with my own solo, part-time addiction medicine practice after 15
years as the clinical director and then medical director of Rochester Regional Health’s chemical dependency programs.
More importantly, I’ve regained the trust and love of my family. My two daughters, now grown, have loved me through every step of my recovery. My wife has never deviated from my side, treating me with love, care, and compassion that I’ll never be able to fully repay. I’ve learned to accept help from others.
And that brain loop?
It still plays occasionally, but not continuously. And I no longer believe its toxic message, nor do I have to try to silence it with drugs or alcohol.
Physician Mark Winsberg is the former medical director of Rochester Regional Health chemical dependency department. He now operates Medical Services, PLLC in Rochester. Contact him at drmark@ winsbergmd.com or via text message at 585-565-5220. For more information, visit www.winsbergmd.com.
10 Tips If You Think You Have A Substance Use Disorder
By Mark Winsberg, M.D.
1. Acknowledge the Problem
The first step in recovery is admitting that there is a problem. Denial can be a significant barrier, and recognizing the impact of substance use on health, relationships and daily life is crucial.
2. Seek Professional Help
Addiction medicine specialists, therapists, and counselors can provide evidence-based treatments, including medication-assisted therapy (MAT) and behavioral therapies like cognitive-behavioral therapy (CBT) or motivational interviewing (MI).
3. Develop a Strong Support System
Surrounding oneself with supportive friends, family or support groups like Alcoholics Anonymous (AA) or Narcotics Anonymous (NA) can provide encouragement, accountability and emotional support.
4. Identify and Avoid Triggers
Recognizing situations, places or people that contribute to substance use can help in developing strategies to avoid or manage them. Creating a structured and substance-free environment is essential.
5. Adopt Healthy Coping Mechanisms
Replacing substance use with positive activities such as exercise, meditation, yoga or creative outlets (e.g., music, art, writing) can reduce stress and cravings.
24/7 Open Access Clinic No appointment needed On-site evaluations and referrals Call 585-627-1777
Outpatient Treatment: One-on-One Counseling Engaging Groups Medication-Assisted Treatment Call 585-467-2230
Get Help Today. 72 Hinchey Road Rochester, NY, 14624 www.delphirise.org
6. Establish a Routine and Set Goals
Having a daily routine with scheduled activities helps reduce idle time and provides structure. Setting realistic, short-term goals can provide a sense of accomplishment and motivation.
7. Address Underlying Mental Health Issues
Many people struggling with addiction also have co-occurring mental health conditions like depression, anxiety or PTSD. Seeking treatment for these conditions through therapy or medication can improve overall well-being.
8. Consider MedicationAssisted Treatment (MAT)
For some substance use disorders (e.g., opioid or alcohol addiction), medications like methadone, buprenorphine or naltrexone can help reduce cravings and withdrawal symptoms under medical supervision.
9. Educate Yourself About Addiction
Understanding addiction as a chronic disease rather than a moral failing can help reduce guilt and self-stigma, making it easier to seek treatment and stay committed to recovery.
10. Practice Self-Compassion and Patience
Recovery is a journey with ups and downs. Being kind to oneself, acknowledging progress and learning from relapses instead of seeing them as failures can improve long-term success.
Break Free From the Grip of Addiction
Addiction Looking at Trauma During Recovery
Getting to the root of substance
By Deborah Jeanne Sergeant
Substance abuse is still very much prevalent in the U.S. In 2022, 48.7 million Americans ages 12 and older experienced a substance use disorder (including drug and alcohol abuse) in the previous year, according to www.addictiongroup.org.
The organization further states that only “9.1% of those with co-occurring mental health issues and substance use disorders receive treatment for both conditions.”
Mental health issues are not the only reason that people abuse substances.
Some people begin abusing drugs like fentanyl because of physical addiction to prescribed opioid painkillers such as after an injury or surgery.
Others experience untreated mental health problems stemming from trauma and end up using substances as a harmful coping mechanism.
“Trauma plays a significant role, but it is not the only cause,” said Jennifer Faringer, director of DePaul’s National Council on Alcoholism & Drug Dependence Rochester Area and a credentialed prevention professional. “Trauma is a significant cause with many. Recognizing trauma and dealing with it can be a part of the whole counseling regimen and how trauma played a role in their mental health. We talk about trauma-informed care where you consider the impact of trauma and deal with the trauma.”
abuse
The organization focuses on prevention and operates an addiction counselor training program for candidates who want to become credentialed alcohol substance abuse counselors.
Identifying and treating trauma early can help prevent substance abuse later. Faringer said that it’s about understanding the risk. She added that it’s also important to educate the public about the myths and misconceptions about the danger of substance use and its potential impact.
“We’ve run a lot of ads in In Good Health on various drugs, alcohol and problem gambling to push back against misinformation out there,” Faringer said. “It’s risky, especially for young people. The earlier someone starts, the more likely they are to have a long-term problem with addiction. We try to interrupt it before it becomes a problem.”
Substance use does not have to include illegal drugs bought on a street corner. Some people believe that vaping or using marijuana recreationally is safe because it’s legal. Some self-medicate their anxiety or depression with over the counter or prescription medication that’s not their own or indicated for their condition.
“It may work for a little while, but they’re messing with their own neurological system,” Faringer said. “They rely on the drug to do things for them and they can’t decrease anx-
Ketamine Use Is on the Rise in U.S.
Miety without that drug. It might feel like the drug is lessening anxiety but down the road; it does more harm than good. Addiction is biological, psychological, social and physical. It affects all parts of one’s life.”
For some people, lasting, effective recovery includes cutting off the negative social influences that pull them back into addiction such as places where they obtained substances, people who encouraged and supplied them and situations that triggered substance use.
Faringer said that learning to “do things with others that are sober” often helps, along with “the ability to have fun without drinking, drugs or gambling. Learning how to socialize in a sober environment is huge. If someone comes out of treatment and goes back to the same old same old and is surrounded by a negative environment, it’s a system but not positively supportive. It’s easy to
relapse if those around them are still using.”
CORE Center and Recovery
Fitness represent two local organizations that provide help to people in recovery by providing alternatives to using substances.
“The biggest thing is to relearn or learn how to have fun without being drugged or drunk, Faringer said. “Learning how to be social in a sober environment is huge for people.”
“You want to support the family as they’re going through a journey almost as difficult. We work with families and kids. We work with families whose loved one is struggling with addiction. We try to teach them about addiction and how that has affected their family system with the goal of breaking that cycle. The family needs health and healing and help for themselves.”
any more Americans are turning to ketamine for kicks, a new study reports.
Recreational use of the anesthetic drug among U.S. adults increased 40% between 2021 and 2022, researchers say.
That follows a nearly 82% increase in ketamine use from 2015 to 2019, results show.
The more recent increase occurred mainly among young adults 26 to 34, as well as in people with a college degree, researchers found.
“These findings are consistent with other research indicating increased use among nightclub attendees in New York City along with increasing law enforcement seizures of illicit ketamine in the U.S.,” wrote the research team led by Kevin Yang,
a third-year resident physician in psychiatry at the University of California-San Diego School of Medicine.
Ketamine — also known as “Special K” or "Super K” — is typically used an anesthetic for people and animals as.
In 2019, the U.S. Food and Drug Administration (FDA) approved the use of a nasal spray ketamine derivative called esketamine (Spravato) to treat depression in adults, according to the National Institute on Drug Abuse (NIDA).
Ketamine can cause changes in how people perceive reality, the NIDA says. Users might feel like they are floating outside their bodies or dissolving into their environment.
“At higher doses, a person may experience extreme detachment from
their body and reality, which is called being in a k-hole,” the NIDA's website on ketamine says.
A ketamine overdose can cause potentially life-threatening slow and shallow breathing, particularly when combined with other drugs. Longterm use is linked to memory problems, depression and anxiety.
For the new study, researchers analyzed data gathered between 2015 and 2022 by an annual federal survey on drug use and health.
They found that the surge in ketamine use during the 2010's was largely associated with people suffering depression. Adults with depression were 80% more likely to have used ketamine between 2015 and 2019, possibly self-medicating their mood disorder.
But the increase between 2021 and 2022 occurred only in people without depression, results show.
“These findings suggest a potential shift in the relationship between ketamine use and depression, such that recreational use became less associated with depression over time,” researchers wrote in study published recently in the Journal of Affective Disorders.
People with college degrees were more than twice as likely to have used ketamine during the latest surge, compared to those with a high school education or less, results show.
And young adults 26 to 34 were 66% more likely to have used ketamine than 18- to 25-year-olds, researchers found.
Jennifer Faringer is the director of DePaul’s National Council on Alcoholism & Drug Dependence Rochester Area.
By Anne Palumbo
SmartBites The skinny on healthy eating
Boosting Immunity But One of Clementine’s Many Benefits
As winter drags on, many of us slump into a winter funk. Me? I’ve taken whining to an indecent level this year. And, honestly, it may have lasted indefinitely had I not spotted a bag of cheery clementines at the grocery store last week.
Clementines!
If there’s one fruit that brightens my mood, it’s the seedless clementine.
Clementines (like tangerines and satsumas) are a special variety of mandarin oranges. While both navel oranges and mandarins are healthy citrus fruits, they have some key differences that set them apart. Navel oranges are larger, more acidic and harder to peel, while mandarins are smaller, sweeter and a breeze to peel.
This potent little fruit delivers over a quarter of our needs for vitamin C, a powerhouse vitamin that contributes to wound healing, helps keep skin healthy and glowing, and boosts the immune system.
Although vitamin C won’t cure your cold, says research, it may shorten it. What’s more, vitamin C helps your body absorb “non-heme iron,” which is iron from plant-based foods like lentils and spinach.
If you’re worried about inflammation — a condition that can raise your risk of cancer, heart disease and other diseases — reach for a clementine. Particularly rich in antioxidants that help defend your body against an undesirable imbalance of free rad-
icals, clementines may help reduce inflammation and prevent cellular damage.
Hearts love clementines, too. From the antioxidants that protect the heart from damage to the fiber that helps lower “bad” cholesterol to the potassium that can help regulate blood pressure, these li’l “Cuties” might be better nicknamed li’l “Superstars.”
Lastly, this tangy citrus charmer helps support a healthy weight or weight loss, thanks to many factors: its decent dose of fiber that promotes a full feeling, its high-water content, and its low calorie count (only 35 per clementine). Plus, they’re ideal for kids because they’re peelable, seedless and sweet!
Anne Palumbo is a lifestyle columnist, food guru, and seasoned cook, who has perfected the art of preparing nutritious, calorie-conscious dishes. She is hungry for your questions and comments about SmartBites, so be in touch with Anne at avpalumbo@aol.com.
Helpful Tips
Look for fruits that are brightly colored, feel firm when gently squeezed, and smell strongly of citrus. Clementines will keep at room temperature for up to a week or in the fridge for up to two weeks. Wash clementines before eating to remove any residues. Like grapefruit, clementines may interfere with certain drugs: be sure to discuss concerns with your doctor.
ASIAN SALAD WITH CHICKEN AND CLEMENTINES
Salad:
6-7 cups torn romaine
2 cups shredded chicken
1 large cucumber, peeled and chopped
½ cup shredded carrot
1 green onion, thinly sliced 2-3 clementines
¼ cup cilantro, minced
½ cup chopped nuts of choice
Dressing:
¼ cup olive oil
¼ cup rice vinegar
2 tablespoons sesame oil
1½ teaspoons soy sauce
2 teaspoons honey
1-2 cloves garlic, minced ¼ teaspoon each: salt and coarse black pepper
1. In a large bowl, combine first 7 ingredients. Shake together all dressing ingredients. Just before serving, drizzle with ¼ cup dressing; toss to combine. Top individual servings with nuts; add more dressing if needed. Dressing will keep in fridge for up to 2 weeks.
Note: Save time with a rotisserie chicken.
Serves 4-6 Adapted from tasteofhome.com
Pay Attention to the Signs
By Deborah Jeanne Sergeant
Colorectal cancer is the third most common type of cancer in the world, according to the International Agency for Research on Cancer with more than 1.9 million cases diagnosed in 2022.
It’s also the second most common cause of cancer death, amounting to more than 900,000 deaths annually worldwide.
The American Cancer Society predicts that 52,900 patients in the US will die from this colorectal cancer this year.
Knowing the risk factors, early signs and prevention tools can help lower these numbers. According to the Centers for Disease Control and Prevention, risk factors include:
• Inflammatory bowel disease such as Crohn’s disease or ulcerative colitis
• A personal or family history of colorectal cancer or colorectal polyps
• A genetic syndrome such as familial adenomatous polyposis (FAP) or hereditary non-polyposis colorectal cancer (Lynch syndrome)
• Lack of regular physical activity
• A diet low in fruit and vegetables
• A low-fiber and high-fat diet, or a diet high in processed meats
• Overweight and obesity
• Alcohol consumption and tobacco use.
Although symptoms of colorectal cancer are important to note, “the most important thing to know is most of the time, there are no symptoms,” said Hannah Farley, manager of the Cancer Services Program of the Finger Lakes Region, affiliated with URMC. “It’s a pretty quiet disease. Someone could have colon cancer or precancerous polyps and have no signs.”
When colorectal cancer presents symptomatically, patients may experience blood in their stool.
“It won’t be just one time but over the course of a few weeks and months,” Farley said. “It might not be every bowel movement, but they’ll look at their stool and see a little blood present. That is a very common symptom.”
Sometimes hemorrhoids — inflamed veins in the anus and lower rectum — may bleed during a bowel movement. However, hemorrhoids typically resolve with at-home care within a week. If blood during a bowel movement continues, Farley encourages people to set up a doctor’s appointment to have it checked out.
Another possible sign of colorectal cancer is a change in bowel habits.
“They maybe have pretty reliable time when they go ‘number two,’ but they have stringy, tarry stool and can’t empty their bowels,” Farley said. “It’s especially concerning if there’s also blood in the stool.
“If you have a family history of colon cancer or personal history of polyps which can be a precursor for colon cancer, make an appointment with your primary care provider to talk about what’s going on and maybe get a referral to a gastroenterologist. You have to have a referral to see them.”
Slow growing
According to the American Cancer Society, it takes about 10 to 15 years for abnormal cells to develop into cancerous polyps. Screening can help detect polyps so healthcare provider can remove them before they become malignant.
The old standard was to begin screening at age 50. However, an uptick in earlier age diagnoses has caused that to shift to age 45. For people with a first-degree relative who experienced colorectal cancer, that age may be even younger.
Colonoscopy is considered the gold standard test, as providers can remove suspicious polyps during the procedure. Most providers would urge patients with any risk factors
to screen with colonoscopy. Patients dislike the preparation process, which includes clearing the bowels with medication or enemas. The procedure involves inserting a lighted tube in the anus, rectum and colon after air has been pumped inside. It’s generally recommended every 10 years.
Virtual colonoscopy (CT colonoscopy) scans the colon and rectum through a small tube inserted just a small distance into the anus, but the patient must still prep the bowel and have air pumped into the rectum and colon. Any suspicious polyps will require a second appointment for removal. This procedure is recommended every five years.
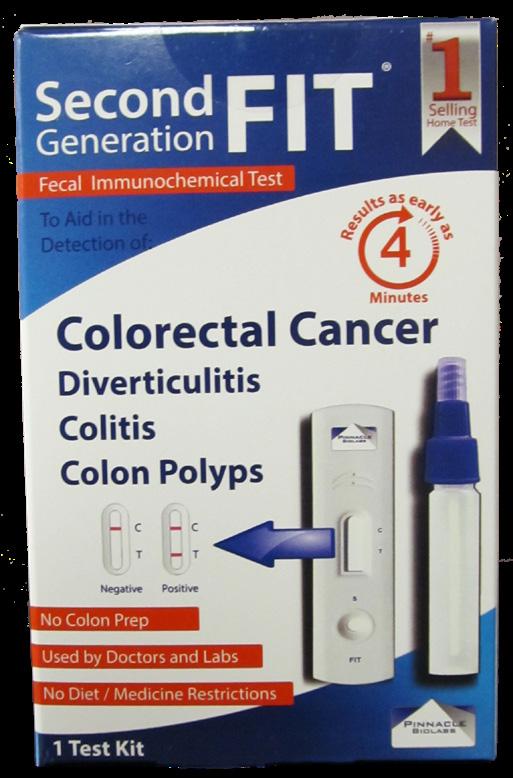
Non invasive tests include stool sampling, the fecal immunochemical test (FIT) to find small amounts of blood in the stool, a sign of polyps. It’s recommended annually.
The guaiac-based fecal occult blood test (gFOBT) can also find hidden blood in the stool. Patients can take the sample at home. Beforehand, patients must avoid certain foods and medications for a few days before the test. The gFOBT is an annual test.
Recommended for every three years, at-home stool DNA testing looks for DNA or gene changes in cells that migrate from polyps into stool. It can also detect blood in the stool. The FDA-approved DNA test is Cologuard.
Colorectal Cancer Support
Where to find help locally and virtually
By Deborah Jeanne Sergeant
The American Cancer Society predicts that 154,270 people in the US will receive a colorectal cancer diagnosis this year. As the fourth most common type of cancer in America and the second most fatal, colorectal cancer diagnosis is scary.
“I have not personally been through cancer but have been a caregiver,” said Hannah Farley, manager of the Cancer Services Program of the Finger Lakes Region, affiliated with URMC. “It’s hard. It’s emotionally draining. It’s hard to stay connected with your loved ones.”
Even people who genuinely
care about the patient can find it difficult to connect in a meaningful way.
“There’s a side to it where you feel like they don’t know what it’s like, especially if it’s a terminal diagnosis,” Farley said. “How do you have relationships? How can you take care of yourself when you have things going on in your body that can’t be stopped?”
Farley said a good support system is crucial to help patients.
The area features groups that often meet in person where a friendly smile and hug can go a long way toward restoring a sense
of normalcy in a life turned upside down. Leaders and participants in local groups often provide the most relevant, accessible resources to help patients and their families.
• Local, in-person groups include:
Cancer Support Community at Gilda’s Club, Rochester (https:// cscrochester.org)
Gastrointestinal Cancer Support Group at Wilmot Cancer Center (Contact Patrice Rogers, LMSW, at 585-275-5908 or Patrice_Rogers@ urmc.rochester.edu)
This Is Living with Cancer, New York City (https://www.thisislivingwithcancer.com/cancer-type/ colorectal)
Colorectal Cancer Alliance, Washington, DC (https://colorectalcancer.org)
• Hotlines: Cancer Helpline and Live Chat by the American Cancer Society (800-227-2345)
Counseling by CancerCare (800813-4673)
Hannah Farley is the manager of the Cancer Services Program of the Finger Lakes Region, affiliated with URMC.
Can Aspirin Reduce Colon Cancer Risk?
Daily low-dose aspirin can help prevent cancers from returning in about a third of colon cancer patients, a new study says.
Taking 160 milligrams of aspirin a day cuts the risk of cancer recurrence in half among colon cancer patients with a mutation in their PI3K genes, researchers reported at the 2025 American Society of Clinical Oncology Gastrointestinal Cancers Symposium in San Francisco.
These PI3K mutations are found in about 30% of all colon cancers, researchers said in background notes. They can make cancers more aggressive and harder to treat.
The results of this study could immediately change treatment for those colon cancer patients, researchers said.
“Aspirin has been shown to effectively reduce recurrence rates and improve disease-free survival in more than one-third of these patients,” lead researcher physician Anna Martling, a professor of surgery at the Karolinska Institute in Sweden, said in a news release.
For the study, researchers recruited more than 600 patients in Sweden, Denmark, Finland and Norway who had moderate to advanced colon cancer or rectal cancer.
The patients were randomly assigned to take either daily aspirin or a placebo for three years.
Patients taking daily aspirin had a 51% lower risk of cancer recurrence if they had a mutation in their PIK3CA mutation, compared to placebo, researchers found. Recurrence was 7.7% for people taking aspirin versus 14.1% for those on placebo.
Likewise, patients with other PI3K mutations had a 58% lower risk of cancer recurrence if they took aspirin — 7.7% for those patients versus 16.8% for those given placebo tablets.
Overall, patients who took aspirin were 55% less likely to have their cancer recur than those on placebo, researchers said.
Findings presented at medical meetings should be considered preliminary until published in a peer-reviewed journal. The conference took place Jan. 23-25.
ADVANCED FOOT CARE
Andrea's Foot care.indd 1
5
Congenital heart disease encompasses a range of structural heart abnormalities present at birth. These defects can affect the heart's walls, valves and blood vessels, leading to improper blood flow and circulation.
CHD is one of the most common congenital conditions, impacting individuals across all demographics and often requiring lifelong management.
Advances in medical technology and surgical techniques have significantly improved survival rates and quality of life for those affected, but challenges remain in diagnosis, treatment and support.
Understanding CHD is crucial for raising awareness, improving outcomes and fostering empathy for those living with this condition.
“Learning and talking about this topic is crucial for several reasons. Enhancing maternal-fetal care is paramount,” said physician Scott C. Feitell, director of heart failure and director of cardiac intensive care unit at Rochester Regional Health. “Women can seek appropriate counseling pre-conception and ensure adequate prenatal care can lower risks of maternal-fetal harm throughout pregnancy. Many children born with congenital heart disease get lost to follow up as they outgrow their pediatricians. It is not uncommon for patients to be referred to me in the community who had heart surgery as a child, but then get lost to follow up when they leave for college.”
Feitell discusses five components to the disease.
Things You Should Know About Congenital Heart Disease
By Ernst Lamothe Jr
1.How common is it?
Congenital heart disease is one of the most prevalent birth defects, affecting approximately 1 in 100 to 1 in 200 live births globally. This means that around 40,000 babies are born with CHD each year in the United States alone.
“It is more common than we realize,” said Feitell. “Most importantly, because we have improved management, diagnosis and treatment of congenital heart disease in babies, there are now more adults living with congenital heart disease than children in the U.S.”
Physicians work with pediatric cardiologists to collaborate with options throughout their adulthood so they can monitor the situation and watch out for any additional signs.
2.What are the symp- toms?
Symptoms of CHD can vary widely depending on the specific type and severity of the defect. Common symptoms may include rapid or difficulty breathing, a bluish tint to the skin, lips or fingernails, fatigue or weakness, poor feeding or growth in infants and swelling in the legs, abdomen or eyes. Some individuals may be asymptomatic, particularly in cases of mild defects.
“Symptoms can really vary depending on the type of defect. In babies and children congenital defects can lead to low oxygen levels, it can be a cause of heart failure and may even require a heart transplant,” said Feitell. “In the modern era, most of these cases are identified in utero or immediately after birth and managed at that time.”
3.What are the causes and treatment op- tions?
The exact causes of congenital heart disease are often unknown, but several factors may contribute, including genetic predispositions and environmental influences. Some CHD cases are associated with specific genetic syndromes, while others may be linked to maternal health factors such as diabetes, certain medications or infections during pregnancy.
“The majority of congenital defects develop in utero. Many are linked to genetic diseases or abnormalities that can be inherited from parents,” said Feitell. “Sometimes certain medications or exposures such as infections during pregnancy from mom can cause a congenital defect in the baby. Certain genetic defects like Down syndrome and Turner syndrome also carry a high risk of congenital heart disease. A mother’s diabetes has also been linked to higher incidence of congenital heart disease in their infant.”
4.Family history
There can be a family history component to congenital heart disease. Having a family member with CHD may increase the risk of CHD in other family members. Genetic counseling is often recommend-
ed for families with a history of heart defects, as certain genetic conditions can be inherited.
“Definitely [there is] a family component,” he added. “Many common inherited disorders include atrial septal defects, ventricular septal defects, tetralogy of fallot, bicuspid aortic valves and many others. Women of childbearing age that have a family history of CHD, may be diabetic or have other risk factors should seek proactive counseling and assessment to minimize risks to themselves and their baby.”
5.Myths
“The single biggest misconception of CHD is that it only affects kids. Many individuals think once surgery is done as a kid then that is the end of it and nothing more needs to be done once a kid turns 18,” Feitell said. “The other misconception is that women of child-bearing age can’t take some preventive measures or seek counseling to help decision making if they are at risk of having a child with CHD. Our group runs a cardio-obstetrics program in conjunction with our high-risk pregnancy team at RRH, and women are often shocked when they are told to come to our office.”
•
•
•
Physician Scott C. Feitell is the director of heart failure and director of cardiac intensive care unit for Rochester Regional Health.
Dental Care
Periodontal (Gum) Disease 101
Periodontal (gum) disease is a broad term for conditions involving inflammation and infection of the tissues (gum and bone) that surround and support the teeth.
Gingivitis is a type of gum disease that involves inflammation of the gums. It is largely preventable and treatable with a combination of routine oral hygiene and professional cleanings.
Periodontitis, which also involves bone loss around teeth, is an irreversible condition that can be slowed down and managed with professional treatment.
adults:
• About 4 in 10 U.S. adults 30 years or older had a mild, moderate, or severe level of periodontitis in 2009–2014.
• About 1 in 2 men and 1 in 3 women 30 years or older had some level of periodontitis.
Periodontitis is more common as people age. About 60% of adults 65 years or older had periodontitis in 2009–2014.
Types
• Gingivitis
The mildest form of gum disease is gingivitis, an inflammatory condition where the gums become red, swollen and may easily bleed. Gingivitis is a reversible condition. But if left untreated, it can lead to a gum disease called periodontitis.
• Periodontitis
Periodontitis is a chronic inflammatory condition that leads to mild, moderate, or severe destruction of the supporting tissues around teeth. A main feature of periodontitis is bone loss around the affected teeth. Untreated periodontitis can also make other chronic conditions, such as diabetes, worse.
Periodontitis cannot be reversed, but it can be slowed down and managed with professional treatment. Periodontitis and cavities (tooth decay) are the two leading causes of tooth loss.
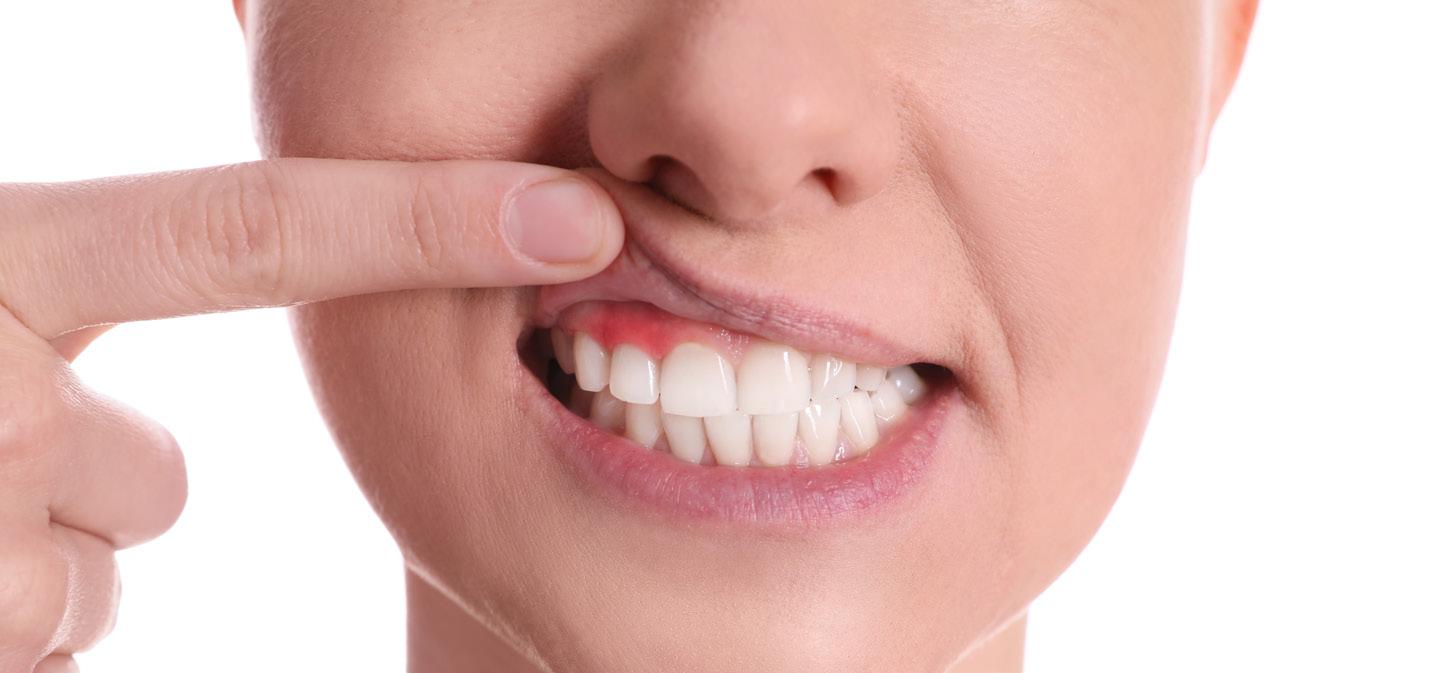
Signs and symptoms
Gum disease can often become serious before a person notices that they have symptoms. A yearly dental checkup can help to detect and prevent this condition.
Signs and symptoms of gum disease may include:
HEALTH
• Red, swollen, or tender gums.
• Bleeding gums.
• Any change in the way your teeth fit together when biting.
• Any change in how well your partial denture fits.
Causes
It is normal for some bacteria to live in a healthy mouth. Bacteria in the mouth constantly produce and dwell within a sticky, removable film on tooth surfaces called plaque. If plaque is left to build up on a tooth, it can lead to inflammation around the tooth and result in gingivitis. Plaque can be removed regularly with toothbrushing and flossing. If it is not removed, it will usually harden into tartar (also called calculus). Tartar buildup cannot be removed with toothbrushing. Professional treatment is needed to remove it.
Bacteria in buildup can spread below the gumline and lead to the formation of a periodontal "pocket." This pocket is an abnormal deepening of the space between tooth surfaces and gum tissues. Bacteria can release toxins in the pocket that make inflammation worse.
As this process continues, it contributes to the destruction of gum tissues and bone loss around the teeth, which is a main feature of periodontitis.
9.75” WIDE X 6.69” HIGH
Periodontitis is a very common type of gum disease among U.S.
Two of the most common types of gum disease are gingivitis and periodontitis.
• Gums that have moved away or downward from your teeth.
• Loose or sensitive teeth.
• Painful chewing.
Source: Centers for Disease Control and Prevention (CDC)
At Hematology-Oncology Associates of CNY, you are never just a diagnosis or a number. We see you...the whole person, with passions, hopes, dreams, histories, and loved ones who share in your journey. From diagnosis, to treatment, to survivorship – our personalized care focuses on truly understanding and planning for your unique needs. We provide genuinely compassionate support, collaborating with you, your family, and caregivers every step of the way.
Learn more about HOA today. We’ll see you and care for you – body, mind and spirit.
If You Suffer from Anxiety, You Are Not Alone, Trust Me!
‘I have a happy life, a beautiful family, a thriving company, really living my best life at 37, but sometimes I feel like I just can’t breathe.’
By Shaina Zazzaro
Mental health is something that is not talked about enough and it is a very important topic for me to touch on.
I am no doctor, but I am someone who suffers from severe anxiety — and I think that is important to share with you.
If you suffer from anxiety, you are not alone, trust me. I feel like everyone must have some sort of anxiety, some worse than others.
It could be as simple as worrying about your job or something so extreme that you feel it but you don’t exactly know why you have it.
The thing about anxiety is, sometimes when people ask me “what’s wrong?” I simply cannot give them an answer.
I have a happy life, a beautiful family, a thriving company, really living my best life at 37, but sometimes I feel like I just can’t breathe.
If I can write this article — first of all, so you don’t feel alone — then I already did my job. I got your back. There are some ways that I cope with my anxiety, and I’m going to share a couple of tips with you.
For the longest time I have tried to cope without medications, going naturally. In order to do this, I make sure to eat healthy food which makes me feel better physically, and exercise often.
I would really recommend walking. Sometimes when I feel extra stressed, I’ll hop on the treadmill and go for a walk, I instantly feel a bit more at ease. I will say if you get to the point where natural coping is not enough, trust in your PCP to let them know how you are feeling and they are there to help you. That is one person that is going to be on your side and you can trust talking to, so confide in them.
What about dealing with anxiety when I can’t move around? When I’m in the car, when I’m at my desk, what then? Sometimes I’ll call a close friend, my mom or husband to vent, but sometimes I will just take deep breaths and remember to breathe. Sometimes I’ll turn on my favorite band and listen to a song I can jam to. Find something that you enjoy that works for you, but make sure it can calm you down and relax you.
I am also really big on taking time for myself — there is nothing selfish about self-care, and it is important. Take yourself to the spa, go to happy feet and get an hour-long foot rub, find a nice restaurant you can relax and have a solo quiet meal at, do something you enjoy for yourself, and don’t ever feel guilty about that.
My family heavily relies on me to be strong and in good health so I can take care of them. If I am not in good health, my children will suffer. Remember that the next time you feel guilty for taking some time to yourself.
And, last, but
not least ,if you are suffering seasonal depression, trust me — you are not alone. Splurge and take a weekend getaway in the sun, get some warmth, get some sunlight, do something fun for yourself (and your family if you are feeling wild), but there is nothing wrong with a little trip to the sun to get out of the Rochester cold (do you feel like this winter is colder than normal? I sure do)!
I hope that reading this made you feel better, and if you are struggling with anxiety, trust me you are not alone.
Follow me on Instagram @ ShainaZazzaro for some motivational videos. I’m here for you and you may not know me, but you can count me in as your new friend.
Love yourself, be happy and be healthy. Peace Out, Rochester!
Ps. I wanted to share this with you since I think it’s wonderful: There is a great new group called Roc Girl Walks that you can find and take monthly walks with, and even meet friends. Follow them on Instagram @rocgirlwalks
Shaina Zazzaro is a devoted wife and mother of two, blending her roles with a passion for health and wellness. She is the owner and chief executive officer of local meal delivery service, Effortlessly Healthy. For more information, visit www. ehmeals.com.
By Jim Miller
Service Dogs Can Help Seniors with Disabilities
Dear Savvy Senior,
What can you tell me about service dogs for seniors with disabilities? My 67-year-old father has chronic arthritis and Parkinson’s disease, and I’m wondering if an assistance dog could help make his life a little easier.
Dog Loving Leah
Dear Leah,
For people with disabilities and even medical conditions, service dogs can be fantastic help, not to mention they provide great companionship and an invaluable sense of security. But be aware that service dogs can be very expensive to purchase and the waiting list to get one can be long.
Here’s what you should know.
While most people are familiar with guide dogs that help people who are blind or visually impaired, there are also a variety of assistance dogs trained to help people with physical disabilities, hearing loss and various medical conditions.
Unlike most pets, assistance dogs are highly trained canine specialists — often golden retrievers and Labrador retrievers, and German shepherds — that know approximately 40 to 50 commands, are amazingly well-behaved and calm, and are permitted to go anywhere the public is allowed.
Here’s a breakdown of the different types of assistance dogs and what they can help with.
• Service dogs: These dogs are specially trained to help people with physical disabilities due to multiple sclerosis, spinal cord injuries, Parkinson’s disease, chronic arthritis and many other disabling conditions. They help by performing tasks their owner cannot do or has trouble doing, like carrying or retrieving items, picking up dropped items, opening and closing doors, turning light switches on and off, helping with balance, assisting with household chores, barking to indicate that help is needed and more.
Service dogs can also be trained to help people with medical conditions like epilepsy or other seizure disorders, autism, diabetes, PTSD and other psychiatric disabilities.
• Guide dogs: For the blind and visually impaired, guide dogs help their owner get around safely by avoiding obstacles, stopping at curbs and steps, navigate shopping centers and buildings, find doors, seats, pedestrian crossing buttons and more.
• Hearing dogs: For those who are deaf or hearing impaired, hearing dogs can alert their owner to specific sounds such as ringing phones, doorbells, alarm clocks, microwave
or oven timers, smoke alarms, approaching sirens, crying babies or when someone calls out their name.
Finding a Dog
If your dad is interested in getting a service dog, contact some credible assistance dog training programs. To find them, use the Assistance Dogs International website (AssistanceDogsInternational.org) which provides a listing of around 80 accredited members and 25 candidate programs in North America.
After you locate a few, you’ll need to either visit their website or call them to find out the types of training dogs they offer, the areas they serve, how long their waiting list is and what they charge. Most dog training programs charge anywhere from $10,000 to $40,000 or more for a fully trained service dog, however, most programs can assist with fundraising or grant applications for those in need. None of that cost is covered by health insurance or Medicare.
To get an assistance dog, your dad will need to show proof of his disability, which his physician can provide, and he’ll have to complete an application and go through an interview process. He will also need to go and stay at the training facility for a week or two so he can get familiar with his dog and get training on how to handle it.
It’s also important to understand that assistance dogs are not for everybody. They require time, money and care that your dad or some other friend or family member must be able and willing to provide.
Send your senior questions to: Savvy Senior, P.O. Box 5443, Norman, OK 73070, or visit SavvySenior. org. Jim Miller is a contributor to the NBC Today show and author of “The Savvy Senior” book.
The Social Security Office
From the Social Security District Office
Social Security and Scam Awareness
Social Security imposter scams continue to be widespread across the United States. Scammers use tactics to deceive you into providing sensitive information or money. If you receive a suspicious letter, text, email, or call, do not respond.
We will NEVER:
• Text or email images of an employee’s official government identification.
• Suspend your Social Security number.
• Threaten you with arrest or other legal action unless you immediately pay a fine or fee.
• Require payment by retail gift card, wire transfer, internet currency, or cash by mail.
• Promise a benefit increase or other assistance in exchange for payment.
• Mail or email “official” letters or reports containing your personal information.
• We only send text messages in limited situations, including:
• When you have subscribed to receive updates and notifications by text.
• As part of our enhanced security when accessing your personal my Social Security account.
If you owe money to us, we will mail you a letter with payment options and appeal rights. Social Security employees do contact the public by telephone for business
purposes. Ordinarily, the agency calls people who have recently applied for a Social Security benefit, are already receiving payments and require an update to their record or have requested a phone call from the agency. If there is a problem with a person's Social Security number or record, Social Security will typically mail a letter.
We encourage you to report suspected Social Security imposter scams — and other Social Security fraud — to the OIG’s website at oig. ssa.gov/report. You can find more information about scams at www.ssa. gov/scam.
Please share this information with your friends, family, and colleagues to help spread awareness about Social Security imposter scams.
Q & A
Q.: I recently retired and am approaching the age when I can start receiving Medicare. What is the monthly premium for Medicare Part B?
A.: In 2025, the standard Medicare Part B premium for medical insurance is $185.00 per month. Some people with higher incomes must pay higher monthly premiums for their Medicare coverage. You can get details at www.medicare.gov or by calling 1-800-MEDICARE.
Ask St. Ann’s
How to Plan for the Future When Choosing a Retirement Community
By Brian Burger
Our lives are filled with big decisions. For seniors, there’s one decision that’s nearly universal: should I consider moving to a senior living community?
Everyone approaches this decision differently — some rely on discussions with family and friends, while others prefer quiet reflection.
No matter how you go about it, though, it can be overwhelming trying to figure out where to start.
Knowing what to look for and what questions to ask can provide confidence and clarity when making this important decision. Beginning your search early gives you the freedom to make choices on your own terms and timeline.
Taking that first step into exploring senior communities can feel intimidating. If you just want to gather information, I absolutely encourage you to do so. Seeing communities in person helps take away a lot of the mystery, and it gives you the chance to ask all the questions you need.
What should you look for when touring a senior living community?
One of the most important factors to consider is location. Are you close to family, friends, shopping and medical services? While you can determine a location's convenience by looking at a map, experiencing it in person will help you get a feel for the environment — whether it’s a bustling city, a quiet rural area or something in between. What is the layout like? Does the atmosphere feel right to you?
Senior communities come in various shapes and sizes. At St. Ann’s Community at Cherry Ridge, our 41-acre campus provides a spacious, natural setting that allows for more activity and independence. On the other hand, communities like St. Ann’s Community at Chapel Oaks are designed so residents can enjoy dining and activities without having to step outside. With indoor connections to the club-style community center, you can get to your morning yoga class without even needing a winter coat!
When we planned our Cherry Ridge Campus, we put a lot of thought into the setting. It’s truly a unique community for the area— with woods, ponds, and beautiful outdoor spaces to enjoy, in addition to the amenities you’d expect from a senior living community.
Beyond location and layout, it’s important to consider the extra services a community offers. Does it provide transportation, on-site medical care, shopping trips, enter-
tainment, and activities? What safety features are in place? Independent living communities can offer a wide range of services, and every community is different, so doing early research is essential.
A good question to ask is: What can this community do to help me stay comfortable and happy without sacrificing my independence? For example, our transportation services allow residents to continue driving if they choose, but on a snowy Rochester day, they can opt for a warm, comfortable ride from our team of drivers instead of venturing out on their own.
Most importantly, I encourage you to think about your future needs when choosing a community. Life can take unexpected turns, and those changes can feel overwhelming if you aren’t prepared. That’s why I always recommend finding a community that offers a full continuum of care.
A full continuum of care means that, in addition to independent living, a community provides higher levels of support, such as assisted living and skilled nursing care. If your needs change, you won’t have to leave the community you’ve grown to love. Plus, as an established resident, you’ll have priority access to other levels of care.
Choosing a community like St. Ann’s with a full continuum of care allows you to maintain control over your future. You’re not just selecting a home for today; you’re making a plan that ensures you have support when you need it.
For seniors, having a solid plan in place is one of the most empowering steps they can take. In the Rochester area, there are many senior living options available. Staying ahead of the game and narrowing down your choices early gives you the advantage of making these important decisions on your own terms. It all starts with a simple phone call. Whether you’re planning a move next week, five years from now, or just gathering information, I’m here to help. Assisting people with these decisions is not just my job—it’s my pleasure.
Brian Burger is a marketing representative for St. Ann’s Community at Cherry Ridge in Webster. Contact him at bburger@mystanns.com or 585-697-6702, or visit www.stannscommunity.com.
New
York state’s
Death by a Thousand Cuts: Nursing Homes in Crisis
‘Over my 30 years in the industry, I’ve seen challenges come and go, but this moment is unprecedented in its severity.’
By Joe Murabito
The care of our elderly is in crisis.
As the managing partner of Elemental Management Group, overseeing several nursing homes in New York state, I’ve witnessed firsthand the financial turmoil caused by the state’s unsustainable policies.
Over my 30 years in the industry, I’ve seen challenges come and go, but this moment is unprecedented in its severity.
I’m left questioning whether elected officials lack a fundamental understanding of the nursing home industry or if they simply do not care.
Regardless, there is an opportunity to educate them — as well as the public — on why this issue matters so deeply.
New York state’s nursing homes are being squeezed by two crushing forces: retroactive demands for COVID-era funding — money already spent on mandated staffing and care — and Medicaid reimbursement rates that fall far short of covering the cost of care. Together, these pressures are creating a perfect storm that threatens the future of elderly care in our state.
The Crisis at a Glance
Consider the following:
• Morningstar Residential Care Center (Oswego): This facility is being asked to repay more than $127,000 in COVID-era funding, despite operating with a Medicaid reimbursement rate less than $200 per day. Rising operational costs make this an impossible financial burden.
• Waterville Residential Care Center (Waterville): A fourth-generation, family-owned facility now facing a demand to repay $97,495 — funds used to meet state mandates for safe staffing and quality care. With Medicaid rates also less than
$200 per day, the financial strain is overwhelming.
• Elcor Health Services (Horseheads): Managed by Elemental Management, Elcor has been notified it must repay more than $323,000. Like many facilities across New York, Elcor is grappling with severe financial instability fueled by unsustainable Medicaid rates and retroactive funding demands.
These stories are not isolated. They represent the experiences of nursing homes statewide. Hundreds of nursing homes run by operators that I consider colleagues and friends are facing similar challenges. This is a systemic problem that requires immediate attention.
Why This Matters
When nursing homes struggle, the ripple effects impact everyone:
1. Displaced Seniors: When facilities close, elderly residents are uprooted, causing emotional and physical distress. Families are left scrambling to find alternative care, often far from home.
2. Strained Hospitals: Nursing homes play a critical role in transitioning patients out of hospitals. Without them, hospitals face discharge gridlocks, exacerbating an already strained healthcare system. We have proudly partnered with and support our local hospitals, including Oswego Health, to ensure continuity of care and better outcomes for our communities.
3. Diminished Dignity for Seniors: The state’s actions send a clear message that elderly care is no longer a priority, undermining the dignity and respect our seniors deserve.
A Call to Action
New York’s nursing homes cannot survive without immediate relief. Policymakers must:
• Re-evaluate Repayment Demands: Retroactive claw backs of COVID-era funding are punitive and fail to consider the reality that these funds were spent to meet state-mandated requirements.
• Increase Medicaid Reimbursement Rates: The first step to solving the rate problem is to create better wage parity and reduce the gross disparity that exists today. Level the field by establishing base rate minimums for direct and indirect
nursing homes are being squeezed by two crushing forces: retroactive demands for COVID-era funding — money already spent on mandated staffing and care — and Medicaid reimbursement rates that fall far short of covering the cost of care.
rate components. This will prevent further closures. From there, begin the process to develop a methodology that captures reasonable costs including capital improvements and that can effectively respond to market changes.
Prioritize Elderly Care: A comprehensive strategy is needed to address the growing crisis in long-term care.
The Bigger Picture
This issue is bigger than just numbers on a balance sheet. It’s about the dignity and care of our seniors, the stability of our communities and the future of healthcare in New York state. Facilities like Morningstar, Waterville and Elcor have served their communities for generations. Without intervention, their future — and the care of thousands of elderly residents — hangs in the balance.
To put it in perspective, a Medicaid reimbursement rate of less than $200 a day is unsustainable.
According to Nestment, the national average rate for a one-night stay in a hotel room is $206. Let’s remember, this is an overnight in a hotel and does not include food or entertainment. Nobody is responsible for exceptional care, nutritious meals and a meaningful quality of life for elderly residents. Yet, this is the reality faced by facilities across New York state.
I’ve spent my career advocating for quality care and the sustainability of our industry. But now, I’m calling on the state to do its part. Let’s work together to ensure that New York’s seniors receive the care they deserve and that the facilities entrusted with their care have the resources they need to succeed.
JOE MURABITO is the managing partner at Elemental Management Group, which owns or operates several senior facilities in Upstate New York, including Morningstar Residential Care Center and The Gardens by Morningstar in Oswego.
Health News
Excellus BCBS named by Forbes as America’s best midsize
employer
Excellus BlueCross BlueShield was ranked No. 8 on the Forbes list of America’s Best Midsize Employers 2025. The health plan ranked No. 1 among midsize employers in New York state and among the insurance industry nationwide. This is the third consecutive year that Excellus BCBS has been named to the list.
This award is presented in collaboration with Statista Inc., a global statistics portal and industry ranking provider.
America’s Best Employers 2025
are selected using an independent survey from a vast sample of more than 217,000 U.S. employees working for companies from all industry sectors employing at least 1,000 people within the U.S. More than 6.5 million employer evaluations were considered.
The final ranking is based on two types of evaluations:
• Personal: Given by employees themselves.
• Public: Given by friends and family members of employees or members of the public who work in the same industry.
Personal evaluations are given a higher weighting.
The results are divided into two lists: one for the top large companies with more than 5,000 U.S. employees, and another for the top midsize companies with 1,000 to 5,000.
Based on the results of the study, Excellus BCBS has been recognized on the Forbes list of America’s Best Midsize Employers 2025.
See Forbes’ full list of America’s
Best Employers on Forbes.com.
DePaul welcomes Chris Beato as VP of communications
Chris Beato has recently joined
DePaul as the vice president of communications and development. He brings over 30 years of diverse experience from Wegmans Food Markets where he served in various roles spanning human resources, marketing and food safety-quality assurance.
He has a proven track record of mentoring marketing professionals and leading multi-channel marketing
campaigns
In addition to his professional achievements, Beato has a deep passion for nonprofit work as reflected by his extensive volunteer service as a board member for AIDS Rochester, The Empire State Pride Agenda and Willow Domestic Violence Center.
During his nine years on the Willow Domestic Violence Center board of directors, he played an integral role in rebranding the agency, leading the search for its president-CEO, and contributing to successful capital campaigns that funded new housing for survivors of domestic violence.
DePaul, a progressive, private nonprofit organization founded in 1958, is committed to providing quality services including assisted living services for seniors; residential and support services to persons with mental illness in recovery, some of whom have a history of homelessness; addiction prevention and support services, vocational programs, and affordable housing.
Jewish Home’s Lilac Grove to Bring 90 New Rental Apartments for Adults Over 62
The Jewish Home campus is growing, with the construction of Lilac Grove, a 90-unit apartment complex, and the addition of 35 apartments to The Summit Independent Living, both for people over 62.
Lilac Grove will be located at Meridian Centre Boulevard and Winton Road in Brighton. Site preparation for the new build began at the beginning of January and is slated to open in fall 2026.
The new, moderately priced rental community will feature a mix of one-bedroom and two-bedroom apartments, with larger one-bedroom options with a den, ranging from 600 square feet to 860 square feet.
The four-story structure, which is adjacent to a large pond with fountains, will be surrounded by grassy lawns, trees, walking paths and a large outdoor patio with shaded dining areas and outdoor fire pits. Other amenities include a 40-vehicle carport, a versatile community room, an onsite exercise facility, a nearby on-campus deli, and access to salon services.
Lilac Grove residents also will have onsite activities programs and options for enrolling in the array of healthcare and home care services from the Jewish Home, such as licensed home care, physician services, outpatient rehabilitation, companion
care, skilled nursing and more.
The Summit is expanding
Growth at Jewish Home also includes an expansion of The Summit Independent Living, with 70 luxury apartments added in two phases.
The first phase of the project includes a new four-story residence with 35 luxury apartments slated for completion in early 2027, with groundbreaking anticipated this summer.
The one-bedroom and two-bedroom apartments are between 1,099 square feet and 1,499 square feet, with each offering a balcony or patio. There will be a covered garage for the new
residents. Amenities such as dining, activities, fitness, transportation and housekeeping are included in one monthly fee. The second phase of the expansion includes the addition of 35 new units planned for a future date.
The expansion will add new and enhanced facilities at The Summit, including a movie theater; a new community center; a new fitness and wellness center; a pickleball court; a mini market; and four dining venues — a modern bistro, a formal grill, kosher and non-kosher dining, and a daytime café and evening bar. All the common areas on the first floor of the existing Summit building will be renovated as part of this project.
“Both the new Lilac Grove and The Summit Independent Living expansion are in response to the growing population of older adults in Monroe County and the housing that is needed for our aging population,” said Michael S. King, Jewish Home president and CEO.
Chris Beato
The Summit Independent Living will add 70 luxury apartments in two phases.
Exterior rendering of Lilac Grove, , a 90-unit apartment complex The Jewish Home is building in Brighton.
ELEMENTAL MANAGEMENT GROUP
ELEMENTAL MANAGEMENT GROUP
Hybrid Nurse Aide Training Program ELEMENTAL MANAGEMENT GROUP
Hybrid Nurse Aide Training Program ELEMENTAL MANAGEMENT GROUP
Unlock the power of excellence
Equip your facility with our unstoppable HYBRID CNA program, empower your team to deliver top-notch care with the strength of a champion.
Unlock the power of excellence
Equip your facility with our unstoppable HYBRID CNA program, empower your team to deliver top-notch care with the strength of a champion.
Are you looking for an innovative way to attract CNA students? We have your answer
Are you looking for an innovative way to attract CNA students? We have your answer
Are you looking to minimize and most importantly eliminate agency use? We have your solution
Are you looking to minimize and most importantly eliminate agency use? We have your solution
Are you looking to improve morale by increasing your direct care PPD? Reach out to us to hear more
Are you looking to improve morale by increasing your direct care PPD? Reach out to us to hear more
Are you looking to captivate and motivate the newer generation by offering unique and rewarding training opportunities? Look no further contact us today
Are you looking to captivate and motivate the newer generation by offering unique and rewarding training opportunities? Look no further contact us today