Managing Nonadvanced Systemic Mastocytosis: An Expert Roundtable Session
Educational Objectives
• Describe the pathophysiology of nonadvanced systemic mastocytosis (SM), including the effects of driver mutations on mast cell (MC) activation and the rationale for new targeted therapies
• Assess symptoms and analyze laboratory and genetic testing results to differentially diagnose nonadvanced SM and classify subtype
• Discuss recent clinical trial evidence and regulatory status for new and emerging targeted treatment options, including selective tyrosine kinase inhibitors and their role in treating SM
• Formulate individualized treatment plans reflecting clinical evidence for treatment efficacy and safety, patient-reported outcomes, and shared decision making
WHAT IS THE ROOT CAUSE OF SM?
SM Is a Rare Clonal MC Disorder
• Systemic mastocytosis (SM) is characterized by the abnormal expansion and accumulation of MCs in 1 or more organ systems1
• SM affects approximately 1 in 10,000 people1
Nonadvanced SM (~88%-95%)2-4 Advanced SM (~5%-12%)2-4
•Bone marrow mastocytosis (BMM) [WHO only]
•Indolent SM (ISM; 88% of cases)3
•Smoldering SM (SSM)
• No apparent gender or ethnic bias5
•SM with associated hematologic neoplasm (SM-AHN [WHO], SM-AMN [ICC])
•Aggressive SM (ASM)
•Mast cell leukemia (MCL)
• Life expectancy is equivalent in patients with ISM vs control population6,7
ICC, International Consensus Classification of Myeloid Neoplasms and Acute Leukemias; MC, mast cell, WHO, World Health Organi zation.
1. Brockow K. Immunol Allergy Clin North Am. 2014;34(2):283-295 2. Cohen SS, et al. Br J Haematol. 2014;166(4):521-528; 3. Ungerstedt J, et al. Cancers (Basel). 2022;14(16):3942; 4. Mesa RA, et al. Cancer. 2022;128(20):3700-3708; 5. American Society of Clinical Oncology (ASCO). 2023. https://www.cancer.net/cancer-types/mastocytosis/statistics; 6. Lim K , et al. Blood. 2009;113(23): 5727-5736; 7. Cohen SS, et al. Br J Haematol. 2014;166(4):521-528.
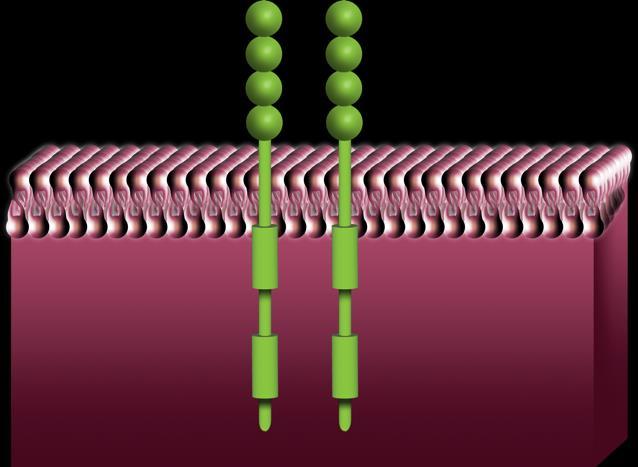
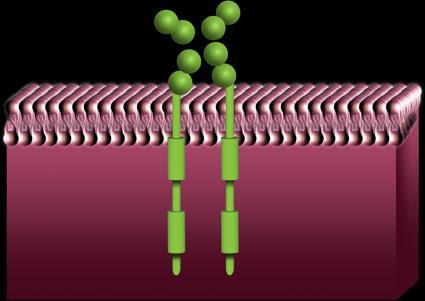
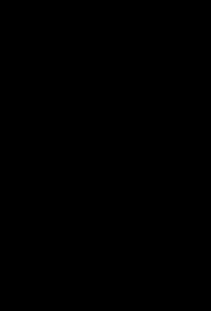
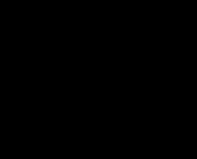
KIT D816V Mutation in SM
Wild Type KIT
KIT D816V causes constitutive activation of the KIT receptor and downstream signaling
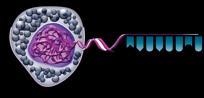
SCF binds KIT and activates signaling pathways that control MC differentiation, maturation, migration, proliferation, survival, and cytokine production.
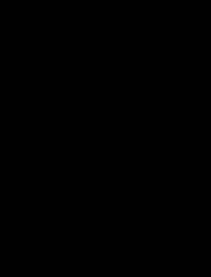
MC Mediators
Environmental stimuli
Preformed mediators (found in granules):
•Histamine
•Tryptase
•Heparin
FcεR1, high-affinity IgE receptor 1; GPCR, G protein-coupled receptor; IL, interleukin.
Giannetti MP. Ann Allergy Asthma Immunol. 2021;127(4):412-419.
Lipid mediators (synthesized from arachidonic acid):
•Leukotrienes
•Prostaglandins
Chemokines/Cytokines:
•IL-4
•IL-6
•TNF
Known Triggers for MC Activation Events1
Triggers Examples
Venoms
Food
IgE-mediated
Medications
Allergens
MRGPRX2 Medications
Acute infection
Pain
Environment
Stressors
Fatigue
Physical triggers
Surgery
Procedures
Vaccinations
Bee, wasp2,a, mixed vespids, fire ants
Alcohol consumption
Ask Dr. Fahrenholz for example
Pollen, pet dander, dust mites
Opioids, NSAIDs, some antibiotics (eg, vancomycin), contrast dyes
Viral, bacterial, or fungal
Emotional, physical
Heat, cold, sudden changes in temperature, sun/sunlight
aHymenoptera venom was recently identified as the most common trigger in ISM; bPerioperative management should be considered.
1. Adapted from NCCN. 2024. https://www.nccn.org/professionals/physician_gls/pdf/mastocytosis.pdf; 2. Niedoszytko M, et al. Allergy. 2024 Sep;79(9):2470-2481 3. Farmer I, Radha DH. Curr Hematol Malig Rep. 2024 Aug
27 [Epub ahead of print].
WHAT ARE THE COMMON SIGNS AND SYMPTOMS OF NONADVANCED SM?
Patients with SM experience an average of 14 SM-related symptoms in their lifetime.
Suboptimal Identification and Delayed Diagnoses Increase Overall Patient Burden
• Delayed diagnosis due to the rarity of SM and the broad spectrum of signs and symptoms that are shared by other, more common disorders1,2 –Puts patients at risk of life-threatening anaphylaxis, organ dysfunction, and severe osteoporosis
• Prior to diagnosis, patients had seen an average of 6 HCPs3
The median time from symptom onset to diagnosis of SM is 6 years.3
HCP, health care provider. 1. Ungerstedt J, et al. Cancers (Basel). 2022;14(16)3942; 2. Mikkelsen CS, et al. Dermatol Reports. 2014;6(1):5199; 3. Mesa RA, et al. Cancer. 2022;128(20):3691-3699.
WHAT ARE THE DIAGNOSTIC CRITERIA FOR NONADVANCED SM?
Jon, Initial Serum Testing
• CBC/Differential
• CMP
• Basal serum tryptase (BST)
• High sensitivity KIT D816V mutation analysis (eg, ddPCR, ASO-qPCR)
Benefits of High-Sensitivity KIT D816V Assays (ddPCR, ASO-qPCR)
• Most reliable for KIT D816V analysis, especially with a low VAF1-3
–0.01-0.03% sensitivity vs 3-5% sensitivity of NGS
• ddPCR detected KIT D816V mutations in 95% of PB samples vs 28% by NGS vs 80% by local detection –Consider testing BM samples if the PB is negative in a patient with a high suspicion of disease4 –Recommended by NCCN and ICC Guidelines to avoid false negatives4,5 • 80% of patients positive for KIT D816V in PROSPECTOR had BST <20 ng/mL6
1. Greiner G, et al. Clin Chem. 2018;64(3):547-555; 2. George T, et al. Blood. 2020;136(suppl 1):7-8; 3. Boggs NA, et al. Blood Adv. 2023;7(13):3150-3154; 4. NCCN. 2024. https://www.nccn.org/professionals/physician_gls/pdf/mastocytosis.pdf; 5. Arber DA, et al. Blood. 2022;140(11):1200-1228; 6. Hartmann K, et al. Presented at: EAACI; May 31-June 3, 2024; Valencia, Spain. Abstract 403.
Jon, Testing Results
• BST, 26.2 ng/mL • CBC/Diff, normal • CMP, normal • PB: KIT D816V positive; VAF: 0.08% • Biopsy of skin lesions – increased number of dermal CD117+/tryptase+ MCs • No organomegaly
Colonoscopy results:
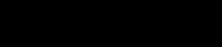
The REMA Score
aFor tryptase values ranging from 15-25 ng/mL, proceed with BM evaluation when REMA score ≥1. MIS, mastocytosis in skin. Alvarez-Twose I, et al. Int Arch Allergy Immunol. 2012;157:275–280; Zanotti R, et al. Mediterr J Hematol Infect Dis. 2021;13(1):e2021068.
• ≥2 is considered to be associated with high probability of SM • Can be used to predict MC clonality and SM in patients suffering systemic MC activation symptoms without MIS
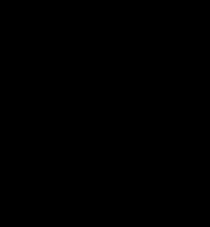
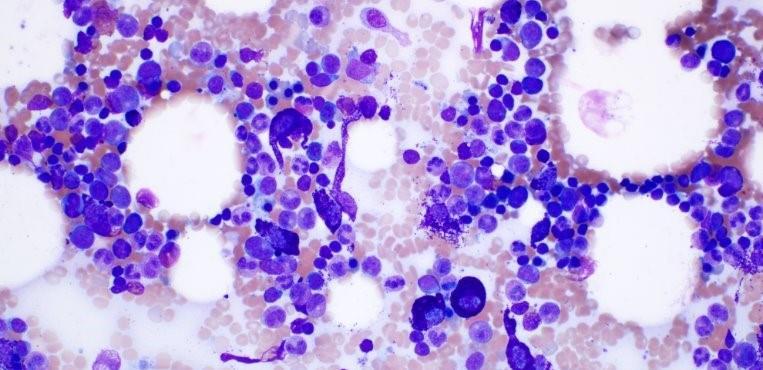
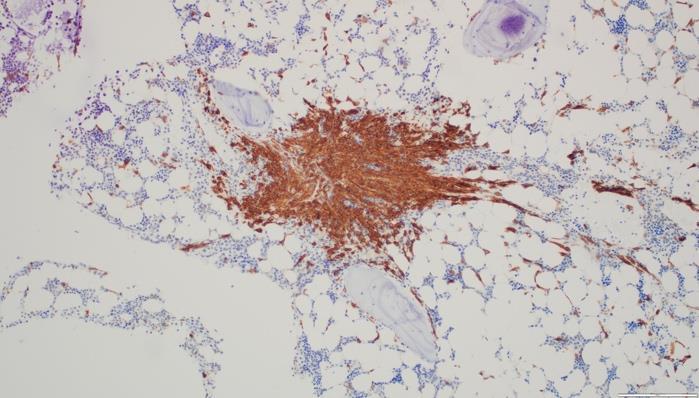
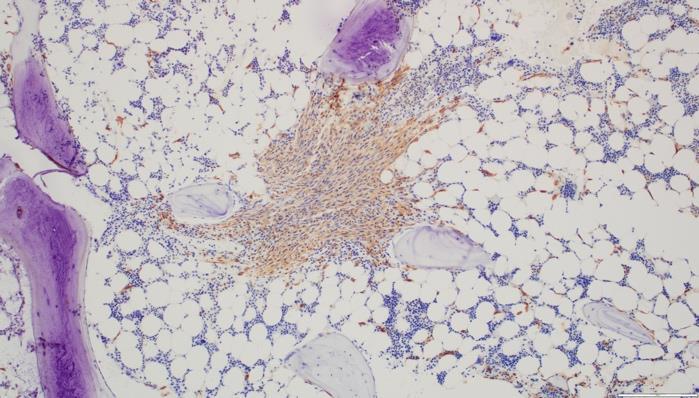
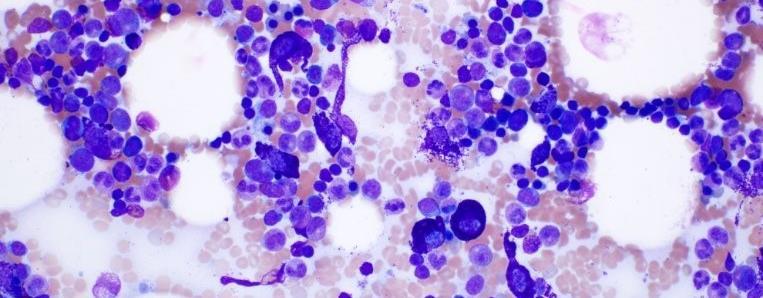
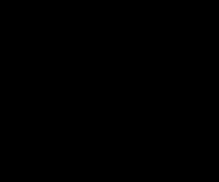
BM Aspirate and Biopsy in an Adult With Suspected SM
Cytogenetics
• HαT
• FISH for AHN-related abnormalities
• Myeloid gene panel (NGS)
• FIP1L1-PDGFRA if D816V negativea
Flow cytometry
CD2
CD25
CD30
CD34
CD117
Immunohistochemistry
Tryptase
CD25
CD30
CD117
BM, bone marrow, FIP1L1-PDGFRA, FIP1L1 factor interacting with Papola and CPSF1; FISH, fluorescence in situ hybridization; HαT, hereditary alpha tryptasemia.
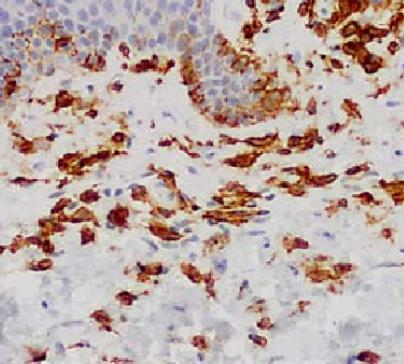
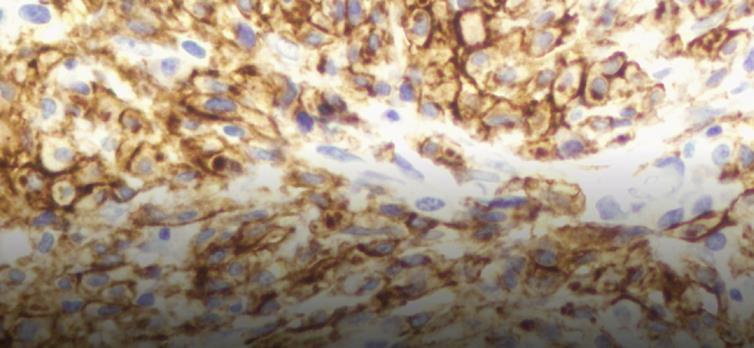
• MCs, slightly increased (3%),75% spindleshaped, 25% mature round/oval forms
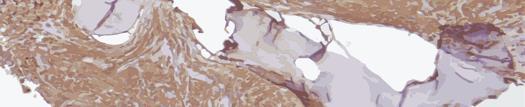
Biopsy
• Few dense aggregates with >15 MC
• MC in aggregates, CD25+, CD117+, Tryptase+, CD30- abnormal spindle-shaped morphology
• Burden of MC,10%
CD117+ Tryptase+
Images courtesy of Anton Rets, MD, PhD.
Serum tryptase level >20 ng/mL (in the case of known HαT, tryptase levels should be adjusted) KIT D816V (or any other mutation causing ligand-independent activation of KIT)
>25% of MC are immature or atypical (type I or II) in BM smears or spindle-shaped in MC infiltrates detected in sections of BM or ECO
Detected on MC in BM, blood, or other ECO
ECO, extracutaneous organ; WHO, World Health Organization. Khoury JD, et al. Leukemia. 2022;36(7):1703-1719; NCCN. 2024. https://www.nccn.org/professionals/physician_gls/pdf/mastocytosis.pdf. Images courtesy of Tracy George, MD and Anton Rets, MD, PhD.
Pitfalls in SM Diagnostic Criteria
• BST variability1
–HαT affects BST levels, so adjustments should be done
–Tryptase is not reliable when AHN is present
–Tryptase <20 mg/mL does not rule out SM
• Negative KIT D816V in PB does not rule out SM (often negative even by high-sensitivity methods in low MC burden)2
• Be aware of overlapping findings between monoclonal mast cell activation syndrome (MMAS) and SM3
1. Boggs NA, et al. Blood Advances. 2023;7(13):3150-3154; 2. Arock M, et al. Leukemia. 2015;29(6)1223-1232; 3. Jackson CW, et al. Int J Mol Sci. 2021;22(20):11270.
• Large osteolytic lesions or pathological fractures
• Malabsorption with weight loss
aB- and C-findings possible.
ANC, absolute neutrophil count.
WHO criteria for associated hematologic neoplasm met (eg, dysplasia, monocytosis, eosinophilia)
Figure adapted from Mannelli F. Ann Hematol. 2021;100(2):337-344; Khoury JD, et al. Leukeumia. 2022;36(7):1703-1719; Zanotti R, et al. Leukemia. 2022;36(2):516-524.
venom immunotherapy. 1. NCCN. 2024. https://www.nccn.org/professionals/physician_gls/pdf/mastocytosis.pdf; 2. Pardanani A. Am J Hematol. 2023;98:1097-1116; 3. Mesa RA, et al. Cancer. 2022;128(20):3691-3699. More than one half of patients take ≥3 prescription medications and ≥3 OTC medications.3
Ann, 58-year-old female
• Diagnosed with ISM 9 years ago
• Hepatomegaly (18cm) but no splenomegaly
• QoL severely impacted by:
– History of osteoporotic fractures
– Frequent nausea, vomiting, abdominal pain after eating and exposure to smells
• There can be overlap in inhibition (eg, avapritinib inhibits mutant KIT and PDGFRA2)
• Currently, targeted therapies are available only through specialty pharmacies3
• There is a risk of bleeding and thromboembolism associated with TKIs4
– Risk varies depending on the therapy
• A subset of patients with ISM (with other non-KIT mutations) show faster progression and would benefit more from earlier treatment with targeted therapy5
Preliminary reports suggest TKIs are effective in reducing or preventing anaphylaxis.
aNot indicated for nonadvanced disease and utility limited by gastrointestinal toxicity; Avapritinib is the only TKI currently FDA approved to treat ISM.
1. Akin C. Immunol Allergy Clin N Am. 2023;43:743–750; 2. Trullas-Jimeno A, et al. ESMO Open. 2021;6(3):100159; 3. Blueprint Medicines. https://www.ayvakithcp.com/AYVAKIT_Product_Pricing_Sheet_HCP.pdf; 4. Deb S, et al. Cancer Med. 2020;9(1):313-323; 5. Muñoz-González JI, et al. Blood. 2019;134(5):456-468.
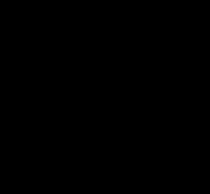
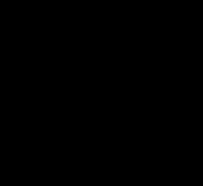
Avapritinib Met Primary Endpoint in Patients With ISM
Phase 2 PIONEER Trial
Avapritinib Targets the KIT
Receptor on the MC1,2 Avapritinib Significantly Improves TSS Score3
Avapritinib Met Key Secondary Endpoints in Patients With ISM
Phase 2 PIONEER Trial1
Avapritinib Significantly Improved Clinical Markers and Symptoms
Avapritinib Improved on a 30% Reduction in Symptoms vs Placebo
Avapritinib Treatment for ISM
• 25 mg orally QD on an empty stomach
– (ASM: 200mg orally QD)
– Not recommended for patients with platelet counts <50 x 109/L
• Avoid coadministration with strong and moderate CYP3A inhibitors and inducers
• AEs: peripheral and periorbital edema, dizziness, flushing, photosensitivity
• To date, increased bleeding has not been reported in patients with ISM who are taking avapritinib
– Ensure patient does not have a history of intracranial hemorrhage before prescribing
• Monitoring: lab monitoring (CMP, CBC/Diff) and visit at 3 and 6 months after starting medication, then every 6 months
adverse event. Adapted from Drugs@FDA. https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/212608s013lbl.pdf.
Elenestinib
Phase 2/3 HARBOR Trial Part 1 (ISM)
• Does not penetrate CNS
• Selectively inhibits KIT D816V while preferentially sparing WT KIT
• Primary endpoints: Safety, PK, PD
– Well-tolerated at all dose levels for median 35 weeks
– No treatment-related SAEs or AEs that led to drug discontinuation
• All AEs grade 3 or less
• Part 2 (anticipated 2024)
Secondary Endpoints
Significant Dose-Dependent Improvements After 12 Weeks of Elenestinib PD, pharmacodynamics;
aN= 39 adult patients with ISM per WHO criteria with moderate to severe symptoms (ISM-SAF TSS ≥28), who were randomly assigned to BSC + Elenestib 25mg
Bezuclastinib1,a
Summit Phase 2 (ISM and SSM) Part 1a and 1b Results
• Minimal CNS penetration1
• High selectivity: does not inhibit PDGFRA, PDGFRB, FLT3, CSFR12
• Part 1a: Primary endpoints: Safety, PK, MC Biomarkers, Symptom Improvement at 12 weeks1
– No treatment-related SAEs; majority of TEAEs at 100-200mg QD were low grade and reversible; no dose reductions
– No bleeding
• Part 2: 24-week treatment (open)
• Still enrolling Significant Improvements After 12 Weeks of Treatment
Part 1b: Mean % Change from Baseline3,4
aN=54 adult patients with ISM or SSM per 2016 WHO criteria with moderate to severe symptoms (on ≥2 anti-mediator therapies), who were randomly assigned 1:1:1 to BSC +placebo or BSC + bezuclastinib: Part 1a, N=20, 100mg QD, 200mg QD; Part 1b, N=34, 100mg QD (n=11), 150mg QD (n=11), placebo (n=12)for 12 weeks, followed by open-label extension (N=18); bP=0.046. N/A, not available.
1. Bose P, et al. Blood. 2023;142(Suppl 1): 77; 2. Akin C. Immunol Allergy Clin N Am. 2023;43:743–750; 3. Modena B, et al.. Poster 694. Presented at: American Academy of Allergy, Asthma & Immunology Annual Meeting; February 23-26, 2024; Washington, DC. Poster 694; 4. Triggiani M, et al. EMJ Allergy Immunol. 2024;9[1]:26-36.
THE ROLE OF MULTIDISCIPLINARY MANAGEMENT
What are the patients’ needs?
Multidisciplinary Management of Nonadvanced SM
As compared to pre-diagnosis, patients with SM had increased:
• Numbers of hospital admissions
• Emergency room visits
• Urgent care visits
• Specialty provider visits
–Greatest increases noted in hematology/oncology, allergy/immunology, dermatology, and gastroenterology
Tse KY, et al. J Allergy Clin Immunol. 2024;3(4):100316.
• What type of monitoring and education does Jon need?
Routine Monitoring
• Patients with stable SSMa should be monitored every 6 months and those with stable ISMa every 12 months, for changes in:
– Serum tryptase level
– CBC/Diff
– CMP
– Weight
– Physical examination, including skin/lesions
• Regression of MPCM lesions does not correlate with changes in underlying ISM
– QoL/Symptom burden: ability to participate in daily activities, ability to eat, respiratory symptoms under control, sleep
• Use MSAF or MQLQ
• DEXA scan every 1 to 3 years for patients with osteopenia/osteoporosis
If laboratory results or symptoms change, therapeutic adjustment should be considered.
aPatients with unstable SSM or ISM should be seen more frequently until stabilized. Adapted from Brockow K, et al. Arch Dermatol. 2002;138(6):785-790; NCCN. 2024. https://www.nccn.org/professionals/physician_gls/pdf/mastocytosis.pdf.
Anaphylaxis Management Is Critical to Successful Management1
• Educate patients on trigger avoidance
• All SM patients should be trained in supine positioning
• All SM patients should be advised to carry 1 or 2 epinephrine auto-injectors to manage anaphylaxis
• Consider adding omalizumaba to treatment plan2
aOmalizumab is not FDA-approved for SM or recurrent anaphylaxis.
• NSAIDs (unless the patient is already taking a drug from this class)
• Rocuronium
• Mivacurium
• Procaine
• Tetracaine
• Calcium channel blockers
• Centrally acting alpha 2 adrenergic stimulants
• Aldosterone antagonists
• Fentanyl (may require adjunctive treatment with ondansetron)
• Tramadol
• Pancuronium
• Vecuronium
• Bupivacaine
• Lidocaine
• Levobupivacaine
• Ketamine
• Midazolam
• Propofol
• Sevoflurane
• Mepivacaine
• Prilocaine
• Ropivacaine
Patient Resources and Action Plans
NCCN Guidelines for Patients®
Systemic Mastocytosis, 2022
TMS provides multifaceted support to patients, families, and medical professionals through education, advocacy, and collaboration.
GARD helps patients find information, services, experts, financial aid, and support groups.
NORD is a patient advocacy organization committed to the identification, treatment, and cure of rare disorders through programs of education, advocacy, research, and patient services.
ECNM is a group dedicated to improving diseaserecognition, diagnosis, and therapy in patients with mastocytosis in Europe.
Conclusions
• The pathophysiology of nonadvanced SM is complex and clinical presentation varies
• High sensitivity assays are the most reliable for KIT D816V analysis, especially with a low VAF
• Traditional management of nonadvanced SM is largely preventive and symptom directed
• Multidisciplinary management is essential
• Avapritinib is FDA-approved to specifically treat the symptoms and underlying etiology of ISM
– Other selective TKIs are under investigation and may soon provide additional therapeutic options
• Patient education (triggers, anaphylaxis, and ER action plans) are necessary to help minimize the significant burdens of SM