Educational Objectives
• Describe key pathophysiologic processes and persistence in severe asthma development, including the roles of TSLP and implications for treatment
• Discuss the clinical profiles and recent trial results with newer biologic therapies for severe asthma
• Construct biologic-based treatment regimens for patients with severe asthma to maximize asthma control, prevent exacerbations, and incorporate shared clinical decision making
TSLP, thymic stromal lymphopoietin.
BIOLOGIC THERAPIES FOR SEVERE ASTHMA

Real-world Use and Disparities
E. Gonzalez, MD
FDA-Approved Biologics for SA
Agent Target Indication(s)
Omalizumab IgE
Reslizumab IL-5
Mepolizumab IL-5
• Moderate-to-severe, persistent asthma inadequately controlled with ICS; (+) skin test or in vitro reactivity to aeroallergen; age ≥6 years
• Symptomatic CSU despite H1 AH; age ≥12 years
• Nasal polyps with inadequate response to INCS; age ≥18 years
• Severe asthma, eosinophilic phenotype; age ≥18 years
• Severe asthma, eosinophilic phenotype; age ≥6 years
• CRSwNP; age ≥18 years
• EGPA; age ≥18 years
• HES that lasts for ≥6 months without identifiable nonhematologic secondary cause; age ≥12 years
Benralizumab IL-5R
• Severe asthma, eosinophilic phenotype; age ≥12 years
• Moderate-to-severe asthma, eosinophilic phenotype OR OCS-dependent; age ≥6 years
Dupilumab IL-4Rα
Tezepelumab TSLP
• Inadequately controlled CRSwNP; age ≥18 years
• Moderate-to-severe atopic dermatitis inadequately controlled with topical therapy OR contraindication to topical therapy; age ≥6 years
• Severe asthma; age ≥12 years
AH, oral H1-antihistamine; CRSwNP, chronic rhinosinusitis with nasal polyps; CSU, chronic spontaneous urticaria; EGPA, eosinophilic granulomatosis with polyangiitis; FDA, US Food and Drug Administration; HES, hypereosinophilic syndrome; ICS, inhaled corticosteroids; IgE, immunoglobulin E; IL, interleukin; INCS, intranasal corticosteroids; OCS, oral corticosteroids; R, receptor; SA, severe asthma. Drugs @ FDA. https://www.accessdata.fda.gov/scripts/cder/daf/.
6
Biologic therapies have revolutionized the treatment of severe asthma by reducing asthma exacerbations as demonstrated in randomized placebo-controlled trials.
The State of Biologic Use in Severe Asthma
1M patients have severe asthma in the US1
40% (400K) have been seen by a specialist
65% (260K) are prescribed a biologic
35% (140K) are not on a biologic despite uncontrolled SA or chronic OCS use3
60% (600K) are assumed to be managed by primary care
Almost all of asthma biologics prescribed in the US are prescribed by specialists, and those specialists are more accessible to certain groups of people than others.4
1. American Lung Association. Severe Asthma. Available at https://www.lung.org/lung-health-diseases/lung-disease-lookup/asthma/learn-about-asthma/types/severeasthma#:~:text=Of%20the%20more%20than%2025,by%20the%20frequency%20of%20symptoms. Accessed January 23, 2023;
3
2
2. Most JF, et al. J Allergy Clin Immunol Pract. 2021;9(10):3662-3671; 3. Panettieri RA, et al. Ann Allergy Asthma Immunol. 2022;129(4):467−474; 4. Mayo Clinic. Advancing the Science. Available at https://advancingthescience.mayo.edu/2022/01/06/big-data-helps-in-understanding-asthma-biologic-use-outcomes/. Accessed January 23, 2023.
Disparities in Biologic Use in the US
Patients with the highest rate of receiving biologic therapy
White, adult females
Annual income of >$75,000

1:
Managed by specialist
Patients with highest rate of asthma mortality and ED visits due to asthma
Black, adult females Black, Hispanic, and Indigenous individuals in the US face the highest burden of asthma compared with White Americans.
Although biologic therapies represent a new dawn in medical care, the benefits are not accessible to all patients.3 There is a clear gap between the number of people receiving biologics and those who would benefit from these therapies.4


ED, emergency department. 1. Inselman JW, et al. J Allergy Clin Immunol Pract. 2020;8(2):549-554.e1; 2. Asthma and Allergy Foundation of America. Asthma Disparities in America. Available at https://aafa.org/asthma-allergy-research/our-research/asthma-disparities-burden-onminorities/#:~:text=The%20burden%20of%20asthma%20in,asthma%20rates%2C%20deaths%20and%20hospitalizations. Accessed January 1, 2023; 3. Burchard EG, Borrell LN. N Engl J Med. 2021; 385(24):2297-2298; 4. Mayo Clinic. Advancing the Science. Available at https://advancingthescience.mayo.edu/2022/01/06/big-data-helps-in-understanding-asthmabiologic-use-outcomes/. Accessed January 23, 2023.

2
:
Factors Contributing to Disparities in Biologic Use
Race and Ethnicity1

Biological Behavioral Sociocultural Environmental
Built Environmental and Health System
• Severe and poorly controlled asthma disproportionately affects the Black population2
– Asthma mortality is 4x as high among Puerto Ricans and Black Americans as among White Americans
Genetics
Nutrition Smoking
Microbiome
Diet
Education
Socioeconomic Status
Health Insurance
Health Literacy
Therapy Adherence
Psychosocial Stressors
Housing
Neighborhood
Quality of Indoor Air
Outdoor Air/Pollution
Access to Health Care
Access to Quality Foods
• Black and Hispanic populations represent only 5% and <1% of clinical trial participants, respectfully2

1. Perez MF, Coutinho MT. Yale J Biol Med. 2021;94(3):497-507; 2. Burchard EG, Borrell LN. N Engl J Med. 2021; 385(24):2297-2298.
Health disparities, including access to biologics, are multifactorial.
The lack of racial and ethnic diversity limits the generalizability of trial results.2
NEWER THERAPEUTIC TARGETS FOR SEVERE ASTHMA
M. Kraft, MD
Newer Therapeutic Targets for Asthma
Current
and Emerging Therapies
Target Mechanism Agent Stage of Development
• Tezepelumab, anti-TSLP
• FDA Approved
Alarmins
TSLP IL-33 IL-25
• Epithelial tissue damage → release of alarmins (epithelial cell-derived cytokines) → drive inflammatory responses by activating dendritic cells and mast cells
• Itepekimab, anti-IL-33
• Phase 2 – Completed; Development Terminated in Asthma
• Ecleralimab, inhaled anti-TSLP
• Phase 2a – Development Terminated in Asthma
Mast cells
• IgE cross-linking → Mast cell degranulation → mediators including histamine, tryptase, chymase, carboxypeptidase Th1
• Masitinib, TKI
• Phase 3 – Completed
• Imatinib, TKI
• Phase 2 – Completed
TKI, tyrosine kinase inhibitor.
Hinks TSC, et al. Eur Respir J. 2021;57(1):2000528; Weschler ME. Respir Care. 2018;63(6):699-707; Sze E, et al. Allergy. 2020;75(2):311-325; Clinicaltrials.gov. https://clinicaltrials.gov/ct2/home. Accessed February 6, 2023.
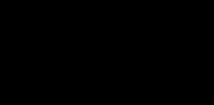
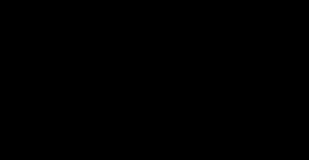
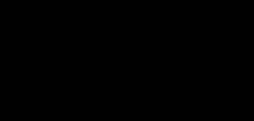
Pivotal Phase 3 Navigator Trial1
Annualized Rate of Exacerbations
• SAFETY
– Serious AE
• Tezepelumab, 9.8%


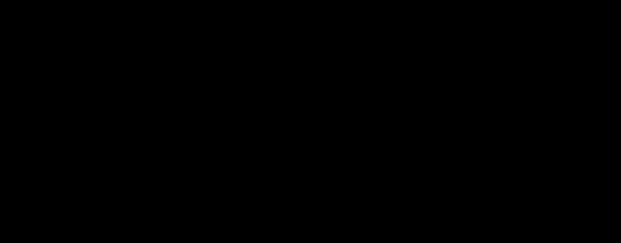
• Placebo, 13.7%
• Reductions from baseline in blood eosinophil counts and FeNO levels were also observed
recently gained approval for self-administration.2,3
aP<0.001 vs placebo. AE, adverse event; FeNO, fractional exhaled nitric oxide; Q4W, every 4 weeks; RR, relative reduction; SQ, subcutaneous. N=1061 patients aged 12-80 years with severe uncontrolled asthma requiring medium- or high-dose ICS (daily dose of ≥500 μg of fluticasone propionate or equivalent) plus ≥1 controller medication with/without OCS were randomized 1:1 to tezepelumab 210 mg SQ (n=529) or placebo (n=532) Q4W for 52 weeks. The primary endpoint was reduction in annualized exacerbation rates.
1. Menzies-Gow A, et al. N Engl J Med. 2021;384(19):1800-1809; 2. Pharmacy Times. https://www.pharmacytimes.com/view/fda-approves-pre-filled-pen-for-self-administration-oftezepelumab-ekko-to-treat-asthma. Accessed February 6, 2023; 3. European Pharmaceutical Review (EPR). https://www.europeanpharmaceuticalreview.com/news/178513/pre-filledasthma-auto-injector-pen-approved-for-self-administration-in-eu/. Accessed January 23, 2023.
Tezepelumab – Anti-TSLP
Rate 2.1 2.66 2.24 1.7 0.93a 0.79 0.89 1.04 0.0 0.5 1.0 1.5 2.0 2.5 3.0 Overall Population ≥300 cells/μL ≥150 cells/μL <150 cells/μL Placebo Tezepelumab 210 mg 56 RR % 61 RR % 70 RR % 39 RR % Tezepelumab
Other Tezepelumab Studies
Study Details Results
DESTINATION1
• Long-term extension study of tezepelumab in adults and adolescents with severe uncontrolled asthma who completed the NAVIGATOR or SOURCE studies (Phase 3)
• Sustained reductions in AAER over 104 weeks vs placebo of 58% (NAVIGATOR) and 39% (SOURCE); reduced biomarker levels vs placebo; overall long-term safety and efficacy consistent with the previous studies.
PASSAGE2
WAYFINDER3
• Real-world effectiveness and safety study of tezepelumab in a broad population of adults and adolescents with severe asthma, including underrepresented patients in clinical trials (Phase 4)
• Study to Evaluate Efficacy and Safety of Tezepelumab in Reducing Oral Corticosteroid Use in Adult Patients With Severe Asthma
(Phase 3)
• Ongoing
• Ongoing
1. Menzies-Gow A, et al. DESTINATION: tezepelumab long-term safety and efficacy versus placebo in patients with severe, uncontrolled asthma. European Respiratory Society (ERS) International Congress 2022, Oral Presentation OA9002, https://s3.eu-central-1.amazonaws.com/m-anage.com.storage.ers/abstract_2022/95944.html.pdf; 2. Lugogo N, et al. CHEST; 2022;162(suppl 4):A37-A40; 3. Clinicaltrials.gov. Study to Evaluate Efficacy and Safety of Tezepelumab in Reducing Oral Corticosteroid Use in Adult Patients With Severe Asthma (WAYFINDER). Available at https://clinicaltrials.gov/ct2/show/NCT05274815. Accessed January 23, 2023.
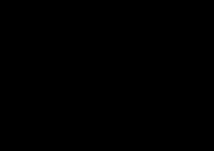
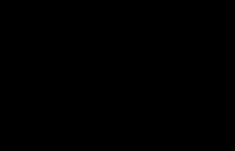
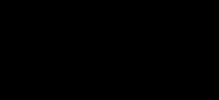
Itepekimab – Anti-IL-33
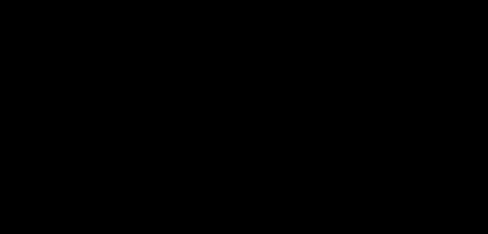





Phase 2 Study
Loss of Asthma Control Change in Eosinophil Count

While development of itepekimab has been discontinued in asthma, several studies investigating its efficacy/safety in COPD are ongoing.



aOR=0.52 vs placebo; bOR=0.42 vs placebo; cOR=0.33 vs placebo; LABA, long-acting -agonist; OR, odds ratio; Q2W, every 2 weeks. N=296 adult patients with moderate-to-severe asthma receiving inhaled glucocorticoids plus LABAs received (1:1:1:1) itepekimab 300 mg SQ (n=73), itepekimab plus dupilumab, both 300 mg SQ (n=74), dupilumab 300 mg SQ (n=74), or placebo (n=74) Q2W for 12 weeks. LABA was discontinued at week 4 and inhaled glucocorticoids were tapered over weeks 6 through 9.
Wechsler ME, et al. N Engl J Med. 2021;385(18):1656-1668.
β ICS Taper -250 -200 -150 -100 -50 0 50 100 150 200 250 300 350 400 0 2 4 6 8 10 12 Dupilumab Itepekimab Placebo Itepekimab+dupilumab Δ From Baseline in Eosinophil Count, cells/ μ L Weeks Since Randomization LABA Withdrawal Cumulative Incidence, % 0 10 20 30 40 50 0 2 4 6 8 10 12 LABA Withdrawal ICS Taper
b a c
Weeks Since Randomization
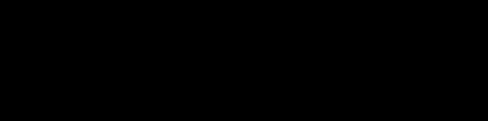
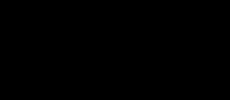
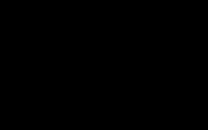
Phase 3 Study in OCS-dependent SA

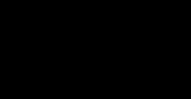
Primary analysis; no minimum baseline blood eos
Masitinib reduced severe asthma exacerbations and demonstrated a positive benefit/risk ratio in patients with severe asthma uncontrolled by OCS, irrespective of baseline eosinophil count.
P=0.01; bP=0.025. eos, eosinophils. N=355 adult patients (primary population) with severe persistent asthma uncontrolled by OCS (≥7.5 mg/day) and high-dose ICS/LABA were randomized 2:1 to oral masitinib (6 mg/kg/day) or placebo for 36 weeks. The primary endpoint was reduction of annualized asthma exacerbation rate for adjusted for overall exposure. Davidescu L, et al. J Asthma Allergy. 2022;15:737-747.
Masitinib – TKI
Exacerbation Rate Annualized
Asthma Exacerbation Rate
Annualized Severe Asthma
Moderate/Severe
a
0.48 0.34 0.0 0.1 0.2 0.3 0.4 0.5 0.6 Placebo (n=115) Masitinib (n=240) 35 RR % Subgroup analysis; blood eos ≥150 cells/µL Annualized Exacerbation Rate 0.71 0.48 0.0 0.2 0.4 0.6 0.8 Placebo (n=87) Masitinib (n=181) 38 RR %
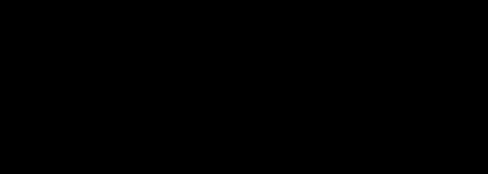
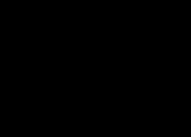
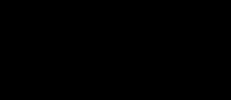
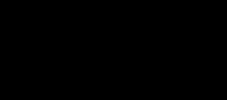
Phase 2 Proof-of-Principle Study
Airway Hyperresponsiveness
Total Tryptase Levels in Serum
Imatinib increased the methacholine PC20 by a mean of 1.20 doubling doses from baseline to month 3 and by 1.73 doubling doses from baseline to month 6. Evidence of mast cell activity was also reduced per decreased tryptase levels.
QD, once daily. N=62 adult patients with severe refractory asthma uncontrolled by beclomethasone (>960 µg/day) or equivalent were randomized 1:1 to imatinib (200 mg QD for 2 weeks then 400 mg QD thereafter) or placebo for 24 weeks. The primary endpoint was change in airway hyperresponsiveness, assessed as methacholine reactivity (PC20), from baseline to 3 and 6 months. Cahill KN, et al. N Engl J Med. 2017;376(20):1911-1920.
Imatinib – TKI
0 1 2 3 4 5 6 Baseline Month 6 Placebo Imatinib Change in Methacholine Reactivity PC 20 (doubling doses) Tryptase Level (ng/mL) -1 0 1 2 3 Baseline Month 3 Month 6 Placebo Imatinib P=0.03 P=0.94 P=0.08 P=0.08 P=0.02
BIOLOGIC THERAPY IMPLEMENTATION
Biomarkers and Predictors of Response
E. Gonzalez, MD
Blood eosinophils

FeNO IgE
≥150 cells/µL
≥20 ppb specific IgE, + skin prick
Biomarkers for T2-low inflammation have yet to be established.
Global Initiative for Asthma (GINA). Global Strategy for Asthma Management and Prevention. 2022. https://ginasthma.org.

Biomarkers for T2-High Inflammation
What Can Biomarkers Tell Us?
Biomarkers for Severe Asthma
Diagnostic biomarkers
– Screening (lung fxn) & identifying endotypes (IgE, blood eos, FeNO)
Prognostic biomarkers
– Assessing severity (lung fxn)
Predictive biomarkers
– Biologic initiation (blood eos, FeNO)
fxn, function. Wan XC, Woodruff PG. Immunol Allergy Clin North Am. 2016;36(3):547-557.
In severe asthma, biomarkers are particularly useful in identifying endotypes and in predicting response to therapy.
Predictive Biomarkers of Response
1. Medrek SK, et al. Curr Allergy Asthma Rep. 2017;17(10):69;
2. Casale TB, et al. J Allergy Clin Immunol Pract. 2019;7(1):156-164;
Biologic Agent Sputum Eosinophils Blood Eosinophils FeNO IgE Benralizumab1 ● ● Dupilumab1 ● ● Mepolizumab1 ● ● ● Omalizumab1,2 ● Tezepelumab3 ● ●
3. GINA. Global Strategy for Asthma Management and Prevention. 2022. https://ginasthma.org.
Clinical Utility of AHR A Potential Biomarker?
Tezepelumab: Phase 2 CASCADE Trial1,a Benralizumab: Open-Label Study2,b
• Improvement in AHR was significant by 8 weeks, with a mean 2.1 DD (P<0.01) change in PD10 at week 12
CI, confidence interval; DD, doubling difference; FEV1, forced expiratory volume in 1 second; LSM, least-squares mean; PD10, provoking dose of mannitol required to decrease FEV1 by 10%; PD15, provoking dose of mannitol required to induce ≥15% reduction in FEV1 from baseline 0 mannitol dose, or otherwise ≥10% reduction in FEV1 between successive nonzero mannitol doses; RDR, response dose ratio; Q4W, every 4 weeks. aN=116 patients aged 18-75 years with uncontrolled moderate-to-severe asthma treated with tezepelumab 210 mg SQ or placebo Q4W for 28 weeks (extended to up to 52 weeks if COVID-19-related disruption delayed end-of-treatment assessment). bN=21 adult patients with mannitol-responsive uncontrolled severe eosinophilic asthma treated with benralizumab 30 mg Q4W for 3 doses followed by 16-week washout.
. 2022;10(6):1497-1505.


1. Diver S, et al.
Interpolated or Extrapolated PD 15 of Mannitol, mg
Lancet Respir Med. 2021;9(11):1299-1312; 2. Chan R, et al. J Allergy Clin Immunol
241.6 401.5 263.2 295.5 0 100 200 300 400 500 600 700 Baseline (n=28) End of Treatment (n=29) Baseline (n=31) End of Treatment (n=26) Difference in LSM 138.8 (95% CI 14.2 to 263.3); P=0.03 Tezepelumab Placebo
AHR is one of the hallmark features of asthma and plays a key role in its pathophysiology.
Doubling Diff -4 -3 -2 -1 0 1 2 3 4 Week 2 Week 4 Week 8 Week 12 Week 24 RDR PD 10 1st Dose 2nd Dose 3rd Dose
Clinical Utility of AHR A Potential Biomarker?
• Omalizumab, EXTRA Study1,2
– Moderate-to-severe asthma
– Lung function provocation phenotypes
• FAO+, low BDR
• FAO+, high BDR
– Results
• FAO−, low BDR
• FAO−, high BDR
• Omalizumab improved FEV1 in FAO−, high BDR group
• Omalizumab did not improve FEV1 in low BDR group, irrespective of FAO
• High BDR identified risks for exacerbation
Other AHR Studies Underway:
• The effect of dupilumab on airway twitchiness in severe asthma3
–
ISRCTN70810039
–
Currently recruiting
–
Estimated completion date, Nov 2024
BDR, bronchodilator responsiveness; FAO, fixed airflow obstruction.
1.
WW,
al. J Allergy Clin Immunol Pract. 2022;10(1):229-230;
in
Busse
et
2. Hanania N, et al. Ann Intern Med. 2011;154(9):573-582; 3. ISRCTN registry. The effect of dupilumab on airway twitchiness
severe asthma. Available at https://www.isrctn.com/ISRCTN70810039. Accessed January 23, 2023.
Assessment of BDR may be a useful guide to the presence of AHR by serving as an informative biomarker for exacerbation risks as well as a potential marker for T2-targeting agents.
BIOLOGIC THERAPY IMPLEMENTATION Evolving Algorithms and Treatment Monitoring
M. Kraft, MD
Comparative RCTs of Biologics?
Study of Magnitude and Prediction of Response to Omalizumab and Mepolizumab in Adult Severe Asthma.
(PREDICTUMAB)
– Patients with severe asthma who are eligible for both anti-IgE (omalizumab) and anti-IL-5 (mepolizumab) therapies, will be randomized to decide the first treatment to start. Patients will then be prolonged or switched to the other according to clinical response.
–
Currently recruiting
– Estimated completion date, Dec 2024
PREDICTUMAB is the first head-to-head RCT to directly compare the efficacy of 2 biologics in severe asthma.
•
RCT, randomized controlled trial. Clinicaltrials.gov. Study of Magnitude and Prediction of
to Omalizumab and Mepolizumab in Adult Severe Asthma. (PREDICTUMAB). Available at https://clinicaltrials.gov/ct2/show/NCT03476109. Accessed January 23, 2023.
Response
Biologic Selection and Switching Proposed Treatment Algorithm – UpToDate 2023
For patients with poorly controlled severe asthma, historical and laboratory workup for possible biologic add-on therapy includes the following studies:
1. Sensitivity to inhaled perennial allergens by history, skin-prick testing, or blood IgE testing
2. Peripheral blood eosinophil count
3. FeNO
4. Total IgE level
5. Focused assessment for T2 comorbid diseases
Even if previously performed, repeat measures at the time of evaluation for biologics can be helpful. Historical or current measures off OCS are strongly preferred.
Is there a severe comorbid T2 inflammatory process with limited biologic options? YES NO
Give appropriate therapy for comorbid T2 disease:
• Atopic dermatitis – dupilumab
• EGPA – mepolizumab
• Nasal polyposis – 1st line, dupilumab; 2nd line, omalizumab in childhood-onset asthma and mepolizumab in adult-onset asthma
Blood eosinophil count (cells/µL)
UpToDate. Selection of biologic agents for treatment of severe asthma in adolescents and adults. [Unpublished manuscript]. 2023.
Biologic Selection and Switching Proposed Treatment Algorithm (Continued)
UpToDate. Selection of biologic agents for treatment of severe asthma in adolescents and adults. [Unpublished manuscript]. 2023. <150 150 to 300 300 to 1500 >1500 Blood eosinophil count (cells/µL) FeNO ≥25 ppb OR sensitivity to environmental allergens? Tezepelumab Preferred Preferred Alternative Currently none available Omalizumab Alternative Tezepelumab Dupilumab Preferred Alternative Tezepelumab or omalizumab Childhood-onset asthma? YES NO NO YES
Biologic Selection and Switching Proposed Treatment Algorithm (Continued)
• Evaluate efficacy of initial biologic therapy after 4 to 6 months
• If lack of efficacy, change to alternative biologic in a different class if patient meets qualification criteria
• Trial of maintenance OCS is reasonable if no other biologic option is available
UpToDate. Selection of biologic agents for treatment of severe asthma in adolescents and adults. [Unpublished manuscript]. 2023.
Blood eosinophil count (cells/µL) Preferred Dupilumab Preferred Anti-IL-5/5R, benralizumab 300 to 1500 FeNO ≥25 ppb OR sensitivity to environmental allergens? Childhood-onset asthma? >1500 Workup for hypereosinophilic syndromes; other specific cause determined? Preferred Dupilumab Preferred Anti-IL-5/5R,
Alternative 1: Dupilumab Treatment of specific cause NO YES NO YES YES NO Alternative Tezepelumab or omalizumab Alternative
benralizumab
1: Anti-IL-5/5R, benralizumab 2: Tezepelumab or omalizumab 2: Tezepelumab or omalizumab

Monitoring
Asthma Assessing Response to Biologic Agents1 1. Couillard Castonguay S, Pavord ID. Encyclopedia of Respiratory Medicine. 2021; 2nd ed (2): 411-434; 2. Runnstrom M, et al. J Inflamm Res. 2022;15:241-249.
Biomarkers in
Symptomatic Response (“I feel so much better…”) YES YES NO NO Biological Response (change in blood eos or FeNO) YES NO YES NO
“Studies exploring expected responses to biologic therapy are based largely on post-hoc analyses of registration trials or small real-world studies.”2

Metrics considered in clinical trials: Comprehensive assessment may also include: QoL, quality of life. Pepper AN, et al. J Allergy Clin Immunol Pract. 2021;9(3):1081-1088. Symptom improvement and reduction in rescue medication use Assess biologic response (4-6 month trial; up to 12-month trial for partial responders) Lung function improvement Reduction in daily OCS use QoL improvement Decrease in health care utilization Exacerbation reduction 1. Exacerbations 2. FEV1 3. Patient-reported outcomes
Assessment of Therapeutic Efficacy
Switching, Stopping, or Continuing Biologic Therapy Results From the CLEAR Study
Of 1859 patients who initiated biologic therapy, 40% switched or stopped biologic therapy
Compared with those who continued biologic therapy,
• Matched patients who switched or stopped therapy
– Were less likely to have a reduction in long-term OCS dose (aβ: -2.61)
– Had more emergency health care resource utilization (aIRR: hospitalization, 1.85; emergency room visits, 1.85)
• Matched patients who switched therapy
– Had a greater risk of exacerbation (aIRR: switched, 1.80; stopped, 1.50)
– Were more likely to have uncontrolled asthma (aOR: switched, 3.64; stopped, 2.61)
a , adjusted -coefficients; aIRR, adjusted incident rate ratio; aOR, adjusted odds ratio. N=1859 adults with severe asthma who initiated biologic therapy and had data for ≥12 months before and ≥6 months after therapy initiation were grouped by whether they continued (used first biologic for ≥6 months; n=1116), switched (discontinued first biologic <6 months after initiation and received a different biologic; n=474), or stopped (discontinued first biologic <6 months after initiation and did not receive another biologic; n=269) therapy. Ali N, et al. CHEST. 2022;162(suppl 4):A23-A27.
β β
This study highlights the importance of proper initial biologic selection. Biologics targeting multiple inflammatory pathways may address limitations of phenotyping, thus reducing switching or discontinuation.
PrecISE Study
Precision Medicine in Severe Asthma
Sponsored by the National Heart, Lung, and Blood Institute (NHLBI)
– Goal: to rapidly evaluate novel interventions in biomarker-defined subgroups of severe asthma─while seeking to refine biomarker subgroups─and to identify early markers of response to therapy1
– https://preciseasthma.org/preciseweb
Site locations
•
1. Israel E, et al. J Allergy Clin Immunol. 2021;147(5):1594-1601; 2. Runnstrom M, et al. J Inflamm Res. 2022;15:241-249.
2
The decision to initiate and maintain biologic therapy is contingent upon the recognition of the clinical relevance of biomarkers and phenotypes.
Conclusions
• 6 biologic therapies are available for the treatment of severe asthma
• Despite how these biologic agents have revolutionized the treatment of asthma, unmet needs and health disparities persist
• Treatment algorithms and validated biomarkers are available to aid in biologic treatment selection, monitoring, and switching
•
Precision management will continue to evolve as studies investigate:
–
Newer treatment targets
–
Biomarker thresholds and refined treatment eligibility
–
Outcomes in broader, underserved patient populations
