REDUCING OR













eliminates the presence of lint and fibers in the operating room, which are identified as contributing to
*Please
A recent ResearchAndMarkets.com report predicts that the global disposable surgical devices market will reach $9.3 billion by 2028.

The goal of this course is to educate perioperative nurses in acute care with knowledge on the anesthesia selection process and the safe care of patients undergoing anesthesia.
A systematic review concluded that higher levels of noise in the OR can have a negative impact on patient outcomes and adversely affect the performance of team members.

For over 50 years, Healthmark Industries has provided innovative intelligent solutions to meet the needs of health care facilities. This year has been one of growth with Healthmark offering new products and educational services.
OR Today (Vol. 22, Issue #10) October 2022 is published monthly by MD Publishing, 1015 Tyrone Rd., Ste. 120, Tyrone, GA 30290. POSTMASTER: See address changes to OR Today at 1015 Tyrone Rd., Ste. 120, Tyrone, GA 30290. For subscription information visit www.ortoday.com. The information and opinions expressed in the articles and adver tisements herein are those of the writer and/or advertiser, and not necessarily those of the publisher. Reproduction in whole or in part without written permission is prohibited. © 2022

Summer Bryant, DNP, RN, CENP, CMSRN
The Pattern for Effective Relationships






Penne Alla Vodka

08 News & Notes
14 Q&A with BrightHospital
16 HSPA: Instrument Marking: Taping Do’s and Don’ts
18 Joint Commission: Advanced Directives in Outpatient Settings

20 AAMI: U.S. FDA Recognizes New Endoscope Guidance
22 CCI: The Perioperative Nurse Educator
24 Market Analysis: Disposable Surgery Device Market Growth Continues
25 Product Focus: Disposable Medical Supplies
30 CE Article: Perioperative Series: Anesthesia and Medication Management
52 Spotlight On:
CENP,
Bryant, DNP,
MD PUBLISHING
TODAY MAGAZINE 1015 Tyrone Rd., Ste. 120 Tyrone, GA 30290 800.906.3373 | Fax: 770.632.9090
Email: info@mdpublishing.com www.mdpublishing.com

John M. Krieg
john@mdpublishing.com
Kristin Leavoy kristin@mdpublishing.com
John Wallace
editor@mdpublishing.com
Karlee Gower
Taylor Powers Kameryn Johnson
Jayme McKelvey
Megan Cabot Emily Hise
Cindy Galindo
Kennedy Krieg
Diane Costea
Linda Hasluem
Hank Balch, President & Founder, Beyond Clean
Vangie Dennis, MSN, RN, CNOR, CMLSO, Assistant Vice President, Perioperative Services with AnMed Health System
Sharon A. McNamara, Perioperative Consultant, OR Dx + Rx Solutions for Surgical Safety

Julie Mower, Nurse Manager, Education Development, Competency and Credentialing Institute
David Taylor, President, Resolute Advisory Group, LLC
Elizabeth Vane, Health Science Teacher, Health Careers High School

Cohen Children’s Medical Center has announced the opening of the Pediatric Surgical Operating Complex, a $110 million, 24,000-square-foot, state-of-the-art home for pediatric surgery that greatly enhances the capabilities of New York state’s largest Level 1 pediatric trauma center, according to a news release.
The new Pediatric Surgical Operating Complex will specialize in cardiothoracic, neurologic and orthopedic procedures as well as general surgery, and was supported by several generous donors, including the Damaghi, Blumen feld and Feil families. The complex is the culmination of a multi-year project that began with the Blumenfeld Family Pavilion, a five-story extension at the children’s hospital built in 2013 and named in honor of the Blumenfeld fam ily’s lifetime giving to Cohen Children’s. Space was left in the master plan with new operating rooms (OR) in mind. Less than a decade later, the ORs were made possible, thanks in part to a generous gift from First Quality Enter prises, a manufacturing corporation in Great Neck, N.Y. The complex is named for the Damaghi family, who have supported Northwell for more than two decades.
“We understand that the surgical and anesthetic needs
of neonates, infants, children and adolescents are absolutely unique and quite different than those for adults,” said Charles Schleien, MD, MBA, senior vice president and chair of pediatric services at Northwell Health and the Philip Lanzkowsky Chair and Professor of Pediatrics and Anesthe siology at the Zucker School of Medicine at Hofstra/North well. “The importance of this pediatric surgical operating complex cannot be overstated. The goal was to complete this crucial project through donor support and we’re grate ful to the Damaghi family and First Quality Enterprises, and all of the members of our Cohen Children’s Advisory Board for stepping up. This is really a transformative space for patients, our community and for Northwell.”
The new complex features eight child-friendly OR suites with majestic photo walls that create an unintimidating environment. Potentially frightening surgical instruments are initially hidden, patients can enjoy their own music or videos before surgery and several play spaces populate the facility. The completion of this project will reduce wait times for pediatric and adult patients and transform care for the more than 8,000 patients who seek medical procedures at Cohen Children’s each year.






St. Bernard Hospital has selected BioVigil’s Hand Hygiene Moni toring Solution to help prevent hospital-acquired infections (HAIs) and provide peace of mind to patients, families, staff and the community. With the implementation of the BioVigil Solution, St. Bernard chose cutting edge technology and analytics to support its ongoing commitment to be among the safest hospitals serving their unique community, according to a press release.


Hand hygiene compliance is largely recognized as one of the most critical patient safety measures to avoid preventable harm. It is now more important than ever to keep both the patients and staff as safe as possible. Poor hand hygiene contributes to 1.7 mil lion HAIs annually – and 75,000 of those HAIs result in deaths.







“We wanted to share with our patients and families that we
















know patient safety is important to them. BioVigil Solution al lows us to do that through visibility, transparency and increasing compliance” said Michael Richardson, chief clinical, quality and patient safety officer. “When we decided to move to an electronic hand hygiene monitoring system, it needed to meet the needs of the organization and the employees who would be using it. The planning, contracting, installation and education process could not have gone any smoother. With onsite visits, equipment checks, and reconfiguration as needed, BioVigil could answer all our ques tions and deal with our nuances as they arose. Over a month after installation, we gathered lots of incredible data insights from their analytics to enable our leaders to monitor their department and individual employees’ overall compliance for better outcomes.”

MicroPort Navibot has received 510(K) clearance from the Food and Drug Administration (FDA) in the United States for the SkyWalker System, the company’s first robot-assisted platform for orthopedic applications. SkyWalker will initially of fer a robotically assisted total knee replacement solution that is compatible with the Evolution Medial-Pivot total knee system.

Designed based on clinical needs, MicroPort NaviBot has built a full technology research facility that has medical industry design capability, and benefits from core technological advan tages of having a self-developed, high-dexterity, and lightweight mechanical arm combined with intelligent planning and naviga tion algorithms. SkyWalker has the technical advantages of precise operation and efficient coordination, while prioritizing safety. Prior to the actual surgery, the planning system assists sur
geons in formulating personalized patient implant plans based on preoperative CT scan anatomical data as well as specific implant data. During surgery, based on actual patient alignment and anatomy, the SkyWalker system facilitates precise implant positioning to achieve the desired kinematics specific to the patient. SkyWalker then allows the surgeon to quickly proceed to resection using a high-dexterity and lightweight mechanical arm resulting in improved precision, accuracy, and efficiency.
SkyWalker is capable of providing the surgeon with informa tion that can help to achieve the desired joint line reconstruc tion while providing data to optimally balance soft tissues. MicroPort Navibot is planning to develop other orthopedic applications in the near future, in conjunction with MicroPort Orthopedics, for a more comprehensive orthopedic offering.

Arthrex and Skytron announced a partnership to offer a broad array of total room solutions designed to address the future needs and challenges of operative care facilities.

“Arthrex and Skytron share a common goal to improve surgical quality and patient care. This partnership allows us to offer the most advanced technology and operating room infrastructure in one package, a comprehensive suite of complementary products that will help surgeons treat their patients better,” said Arthrex Director of Imaging and Resection Sales Ryan Papa.
Arthrex’s Synergy brand is the fastest-growing surgical imaging solution in operating rooms worldwide. This innovative system allows health care professionals to experience the value of intercon nectivity, high-quality 4K image clarity and dynamic patientengagement applications to improve quality of care while driving
efficiency and controlling costs.

As a leader in health care efficiency, Skytron provides innovative solutions of capital equipment, architectural systems and real-time clinical business intelligence for surgical, sterile processing and inpa tient settings. This partnership will align and streamline each other’s offerings to better serve the needs of our customers and ensure a keen focus on improving surgical quality and patient care.
“This collaboration will allow Skytron and Arthrex to offer a complete package of industry-leading solutions for both the hospi tal and surgery center spaces. No one can bring a more comprehen sive package to the market,” said Skytron Vice President of Sales Operations Scott Martin. “We are truly excited about this partner ship because we know that it will enable our customers, and their patients, to be better served.”

Findings from a new study published in the American Jour nal of Infection Control (AJIC) suggest that a combination of betadine and silver colloidal gel are more effective than either material alone for inhibiting the growth of common infection-causing bacteria. The findings could help medical professionals better treat and prevent serious infections in large wounds, including burns.
“Despite substantial advancements in wound treatment and supportive care, wound infections remain a serious problem, particularly in the case of large burns,” said Jona than Kopel, Ph.D., medical student, Texas Tech University Health Sciences Center, and a study author. “Our study is the first to systematically evaluate the use of betadine alone as compared to the combination of betadine and silver col loidal gel to eliminate bacteria and the growth of biofilms.”
Large wounds such as serious burns are vulnerable to microbial invasion and the production of biofilms, micro bial colonies that can become attached to a wound surface and delay or prevent healing. While the topical antiseptic betadine is widely used in the treatment and prevention of wound infections because it has a particularly broad spec trum of antimicrobial activity, many studies have suggested it is ineffective against some bacteria. Topical antimicro bial dressings, including those containing silver, have long been used to support treatment and prevention of wound infections, and seem to provide a different microbial killing mechanism than betadine.
Kopel and colleagues measured the effectiveness of 5% betadine solution alone, silver colloidal gel (Ag-gel) alone, and the combination of 5% betadine and Ag-gel for inhibit ing the growth of five laboratory strains of bacteria: Staphy lococcus aureus (S. aureus) and Pseudomonas aeruginosa (P. aeruginosa), the predominant infective organisms in the
clinically significant microbiome of large, acute burns, as well as clinical isolates of Klebsiella pneumoniae (K. pneu moniae), Staphylococcus epidermidis (S. epidermidis), and Methicillin-resistant S. aureus (MRSA).
After incubating each of the five bacterial strains for 24 hours to grow biofilms, the researchers prepared cellu lose paper discs with each of the three test solutions and exposed the discs to the biofilms. The researchers then analyzed the concentrations of bacteria that remained in each case, using both a standard, reliable testing assay and advanced imaging. Results showed:
• The combination of 5% betadine and Ag-gel pro vided complete (100%) inhibition of all five bacterial strains tested.
• Five percent betadine alone showed little or no inhibition of P. aeruginosa, and at best approximately 90% (1 log) inhibition of the other four bacterial strains tested.
• Ag-gel alone inhibited 100% of bacterial growth (7 logs) among all bacterial strains except K. pneu moniae.
• Notably, while 5% betadine alone killed only about 90% of K. pneumoniae, betadine and Ag-gel com bined killed 100%. This reinforces the researchers’ assertion that betadine works by a different bacterial killing mechanism than Ag-gel.
“Wound infections continue to be a significant challenge for medical professionals and patients, leading to increased morbidity, mortality and health care cost every year,” said Linda Dickey, RN, MPH, CIC, FAPIC, 2022 APIC presi dent. “This study provides important new findings that could help improve infection prevention and treatment to reduce this burden.”
Encompass Group LLC recently announced all new Meta Scrubs with the M.A.M. (Meta Anti Mic) An timicrobial Finish to help fight against bacteria. The M.A.M. finish helps reduce the presence of unwanted bacteria on the surface of the fabric.
Meta Scrubs are available in men’s and women’s tops and matching pants. Two women’s tops are offered – a V-neck featuring two slanted side pockets, princess seams, and side pockets, and a ladies notch top with a mock wrap, two lower patch pockets and side slits. The men’s V-neck top features a two-layer chest pocket and side slits.
Pants in the Meta Scrubs feature the jogger style. The new men’s Axis Cargo Jogger Pant and women’s Distal Cargo Jogger Pant have a full elastic drawstring waist,
two side slanted zipper pockets, two slanted cargo pockets and dyed-to-match cuffs.
Meta Scrubs are offered in a range of sizes, from women’s XS-2X, with pants offered in Petite, and Men’s S-3X. Fabric is 77% Polyester, 20% Rayon, 3% Spandex, with Antimicrobial Finish. Colors offered include black, royal, navy and pewter.
“Encompass is excited to offer this great-looking line of men’s and women’s scrubs to the health care indus try,” said Deanna Leonard, vice president and general manager, professional health care apparel. “Meta’s unique combination of style and protection fits perfect ly with our commitment to bring products to the health care community that offer both comfort and safety.”

O R Today interviewed Hakan Ilkin, founder and CEO of BrightHospital which specializes in predictive analytics and forecasting for OR and ERs. The interview covered how such tools can address staffing issues such as utilization, nurse overwork and burnout, particularly as COVID-19 continues to create extremely demanding, high-pressure work environments.
Q: Why have hospitals continued to rely on traditional, decades-old scheduling methods?
Ilkin: Traditional scheduling methods focus on facilitating surgical pro cesses but lack analytical capabili ties and problem-solving tools to improve overall surgical through put. Hospital and OR leaders have invested in promising scheduling tools with potential, but most have increased workload and frustration among staff, and have not shown long-term improvements.
Q: How do new forecasting and predic tive scheduling tools allow OR leaders to take control of their resources?
Ilkin: The majority of tools available to OR leaders to optimize their resources are retrospective. They rely on historical practice patterns to pre
pare for the future. Next generation forecasting tools integrate historical data with predictive indicators such as surgical clinic visits to surgery conversion rates and scheduling pattern models. They can forecast surgical schedules weeks to months in advance, allowing OR leaders to make strategic allocation decisions.
Q: How can next-generation forecasting tools address current COVID-19 challenges?
Ilkin: We’ve seen significant ebbs and flows during the past couple of years as elective surgeries have been cancelled, rescheduled and cancelled again depending on the severity of the pandemic and societal reactions. Every time hospitals were subjected to these changes, OR leaders had to throw out carefully made plans and make decisions without valid information to depend on. Forecasts made by next-generation tools rely on many data streams and take into account operational changes due to COVID-19, therefore remain ing accurate during different phases of COVID-19 recovery. With these tools and changes in the surgical pipeline, such as elective surgery or clinic visit, cancellations are imme diately reflected in the forecasts and empowers OR leaders with action able information.
Q: How has the COVID-19 pandemic affected forecasting and predictive scheduling for OR leaders?
Ilkin: In the second quarter of 2020, the number of surgeries declined by more than 60%. This was widely repeated at the end of 2021 putting additional financial burden on hospi tals. Hospitals not only faced a back log of these postponed cases but also pressure to perform more surgeries per month to meet financial targets. The traditional tools available to OR leaders do not provide necessary information to meet these needs. Forecasting and predictive schedul ing methods can not only show the impact of COVID-19 to ORs in realtime, but also predict OR time that will not be used and enable OR lead ers to proactively market OR time to physicians who need it more.
Q: Can forecasting tools help to orga nize and deal with staffing shortages?
Ilkin: Yes, indeed it can. From al lowing them to adjust staff shifts to complete surgeries as early as possible, avoiding overtime and slowly closing the perennial gaps in utilization, a proactive leader can draw actionable insights from surgi cal forecasting data. Going deeper into representative daily data to analyze how the days differ from one another, and then work on more stra
tegic block scheduling to close the utilization gap, the same leader can make staffing more rational. It has long been the goal of OR managers to optimize utilization and given the pressures of Omicron and the larger nurse burnout and staffing landscape, such efforts are newly and acutely relevant now.
Q: How can forecasting data make a sig nificant measurable impact on morale and staff satisfaction?





Ilkin: One key factor of staff dissatis faction is a change to their schedules after the schedule is posted. Being asked to add shifts, asked to work overtime or take personal time be cause of un-scheduled OR time has significant impact on staff satisfaction and morale. When OR leaders have an accurate OR schedule the next
day, week, or month, they can make decisions to address OR staffing pro actively. When leadership can clearly see that the forecasted OR utilization on a specific day three weeks from today will be well below (or above) the staffed capacity, they can adjust shift needs before the staff schedule is posted. This has helped hospitals reduce overtime 10-40% and increase overall staff satisfaction.
Q: Do you have any anecdotes from OR manager customers regarding how your tools have made work less stressful for OR nurses and staff?













Ilkin: I think the most memorable discussion I had was with a pre/post op manager. It was an early day of an implementation and I did not even realize that she was receiving the information. She explained to me how
she had already started using the in formation, adjusting her staffing levels by looking at the overall forecasts and forecasts by surgeon. This interaction affirmed my core belief that health care leaders, regardless of the position, are hungry for good and actionable information. They may not be analyti cal experts, but they know what needs to be done when the information is presented to them in a clear and actionable manner. Enabling them has become a lifelong goal.
Hakan Ilkin is the founder and CEO of BrightHospital which specializes in predic tive analytics and forecasting for OR and ERs.

Figure 1. Peeling, chipped or cracked instrument marking tape can jeopardize patient safety. When detected, instruments should be removed from service until the tape and adhesive residues are removed and properly replaced.

S urgical instrument inventories come in all shapes and sizes, and today’s sterile processing (SP) professionals have the seemingly insurmountable task of knowing thousands of instruments used within their health care organizations on a day-to-day basis. Beyond that, they must sort through hundreds of tangled trays to ensure the right instruments go into the correct instrument set.
As a result, many SP departments (SPDs) use various instrument mark ing methods – mostly mechanical – to help their technicians identify surgical instrumentation to facilitate their sep aration and assembly and determine to which set or tray a given instrument belongs. This process even helps lessexperienced SP professionals carry out the set assembly process.
Health care organizations vary and so do their instrument needs; therefore, there is no one-size-fits-all solution when it comes to surgical instrument marking. The best mark ing methods for an organization will depend on the complexity of their
surgical program, the number of sets in each specialty’s inventory, the type of instrument and sterilants used, and the SP professionals’ skills.
Electrochemical, laser marking and marking tape, and dots or dipping (mechanical) options are currently available. Each method has pros and cons and needs to be carefully consid ered before a method is chosen.
Identification marking tape is one method widely used. If one’s organi zation uses this method, they must keep in mind that the Joint Com mission (TJC) is actively seeking out those instruments and scrutinizing them during their surveys. TJC will not only inspect instruments in ser vice (in sets and peel packs) but also those that sit in a bin or drawer.
Marking tape is intended to adhere to a stainless-steel surgical in strument to help with identification, organization, management, proper processing and packaging of these items. Tape comes in various colors, patterns and alphanumeric coding options that allow SP professionals to identify instruments in different ways
as they move between the SPD and operating room (OR) and other de partments. Instrument tape helps SP technicians save time by effectively organizing and identifying surgical instruments.
If instrument-marking tape methods are used within an organiza tion, the tape must be maintained. Cracked, chipped or peeling instru ment tape (See Figure 1) can harbor bioburden and harmful pathogenic bacteria. In addition, dry, flaking tape can dislodge and remain in a patient’s wound (retained foreign body), and the glues used to adhere these tapes may prevent steam from penetrating, making those instruments impossible to sterilize effectively. Ensure techni cians have a copy of the manufac turer’s instructions for use (IFU) for the product currently in use. It is also important to consider the costs involved. Maintenance is key and the costs will include the material, time it takes to apply the material, and the labor involved to maintain it. If contracting with a surgical instru ment repair service, they should be able to maintain it, usually at an additional cost. Still, SP leaders and
their teams will be responsible for rotating the instruments through this service as needed.
Not all tape is the same
Although instrument tape can be used to mark instruments, each manufacturer’s technical data should be verified and validated for use with the different sterilization methods in use in one’s organization. The tape used must be manufactured specifi cally for this purpose and withstand repeated washing and exposure to chemicals and sterilization cycles. It must also be able to adhere to the instrument during surgical proce dures and not peel or flake off.
Note: Not all marking tape can be used with all sterilization methods. The tape manufacturer’s IFU should be checked to ensure the sterilants in use at the facility can penetrate the tape during the sterilization cycle
Proper application is critical when
using marking tape. The tape should be wrapped no more than one-andone-half times around the application area of the device, and the tape should not be stretched when applied; it must lie flat, with no gaps, and it must be applied in an area that will not contact the patient or cause interference for the surgeon.
Instruments marked with tape should be carefully inspected for integrity and proper application. If the tape begins to chip or peel away from the instrument, it should be immediately removed from ser vice. All tape material and adhe sive residues should be completely removed (chemical tape removers are commercially available). Instru ments should be checked each time the instrument is processed, and the instrument must be cleaned and dried prior to re-taping. When marking tape is changed, it should be documented.
Warning: Never use a sharp object (such as a knife blade or another
instrument) to remove tape. These methods can damage the instrument’s finish and may cause employee injury.
Managing the number of instruments and surgical sets that pass through an SPD in a 24-hour period can be overwhelming. For some organizations, so many instrument trays pass through the SPD that it is not uncommon for several hundred trays to be down at the start of the new business day. Processes such as instrument marking can have a significant impact on SP processionals’ ability to process more instruments during their shift; how ever, these methods must be properly maintained and inspected each time the instruments are reprocessed.
– David Taylor III, MSN, RN, CNOR, is an executive health care consultant for Resolute Advisory Group LLC, based in San Antonio, Texas. He has served as a contributing author for HSPA since 2019.

Understanding and incorporating a patient’s right to make decisions about their plan-of-care plays an integral role in overall health care outcomes. Honoring end-oflife choices in ambulatory settings is complex, since determination whether a health care organization will venerate a patient’s choice may vary based on services provided and specific patient populations served. It is also challenging for health care organizations to balance patient rights against possible ethical challenges.
Protecting patients’ rights to advanced directives is not new. Decades ago, The Patient Self Determination Act of 199O highlighted patients’ rights by amending titles XVIII (Medicare) and XIX (Med icaid) of the Social Security Act. The amendment required hospitals, skilled nursing facilities, home health agencies, hospice programs and health maintenance organizations to inform patients of their rights, under state law, to make decisions concerning their medical care.1
Almost 20 years later, in 2009, Centers for Medicare and Medicaid Services (CMS) revised Conditions for Coverage (42 CFR § 416.50) progress ing patients’ rights further by requiring ambulatory surgery centers (ASCs) to query all patients about advance direc tives and to provide information about their policies on advance directives and applicable state law. Furthermore, the document stated that ASCs must pro vide patients with official state advance directives forms, if requested.2
The Joint Commission defines an advance directive as a document or documentation allowing a person to give direction about future health care or to designate another person(s) to make health care decisions if the individual loses decision-making capacity. Advance direc tives may include:
• Living wills – generally describe an in dividual’s wishes regarding end-of-life care, should they become perma nently unconscious at the end of a terminal illness. An advance directive, while similar to a living will, is not limited to a terminal illness. It may also apply to events, such as a stroke, dementia or coma which leave the individual unable to communicate their wishes.
• Durable powers of attorney – allow the individual to name an individual as a medical decision-maker on their behalf if they lose the ability to make their own decision.
• Do-not-resuscitate (DNR) orders instruct medical staff not to enact life-saving measures, such as car diopulmonary resuscitation or an automated external defibrillator.3
Patients receiving care in an outpa tient setting may have completed one or more of these types of patient direc tive documents. Therefore, it is impor tant that staff and practitioners provid ing care are familiar with various forms of advanced directives that may impact how care is provided within their settings. Because laws and regulations vary from state to state, ASCs should work closely with their legal counsel to determine what types of directives are available. Such decisions should be considered legal and enforceable.
John C. Wallin The Joint Commission
Physicians must respect a patient’s wishes, since advance directives are legally recognized documents, however, they can refuse to comply if they consider the directives to be an objection of conscience or deem the patient’s wishes medically inappropriate. Health care organizations are required to create written policies that specify whether they will honor advance directives and provide those documents to patients, upon request.
Honoring end-of-life choices is partic ularly challenging in ambulatory surgery and procedural settings. Patients receiv ing care in these facilities are generally undergoing “elective” procedures which are often performed under moderate or deep sedation or anesthesia. Medica tions used during such procedures may induce side effects or adverse reactions that, if untreated, could potentially be life-threatening. However, such untow ard reactions are often easily treated using non-invasive advances, such as the administration of reversal agents or short term ventilatory support.
Patients whose advance directives indicate that they do not want any life-saving measures enacted under any circumstance, force health care organi zations and practitioners to determine whether they will comply with such choices. Therefore, informing patients of the health care organization’s advanced directives policies is a critical step in assisting a patient with the choice to proceed with a procedure or not. Discus sions about advanced directives need to occur when the patient is most receptive to making an informed decision about whether to proceed with a procedure.
Other settings, such as dialysis centers caring for end stage renal failure patients
or oncology infusion/radiation services, present different chal lenges. Often patients receiving care in these settings have chosen to forego any life-saving interventions should a life-threatening event occur while receiving care. Again, health care organiza tions should share written information about their policies with patients and their family members, including a description of applicable state health and safety laws, and if requested, official state advance directive forms.
In settings where a patient’s choice will be honored, staff should know the patient’s wishes and be prepared to support them, should such an event occur. Health care organizations may wish to consider organizing a support team to respond to such events. In addition to nursing, staff from social services, pastoral care, medical staff and leadership could be considered as members of such a team.
In summary, health care organizations must establish policies and procedures that address patient self-determination decisions that may impact the organization’s ability to provide care, treat ment or services in a manner consistent with patient choice.
Understanding state-specific regulatory requirements and educating staff and practitioners is key to consistent, compliant advanced directive implementation. Health care organizations can take the following steps to ensure their facility is prepared:
• Involve nursing and medical leadership and staff responsible for regulatory and accreditation compliance in the develop ment of advanced directive policy and procedures.
• Identify staff who are responsible for providing information to patients regarding their advanced directive rights.
• Communicate through identified staff the facility’s position on advance directives and explain to each patient whether theirs will be met.
• Work with legal counsel to determine both state and federal regulatory requirements.
For questions regarding Joint Commission accreditation requirements, please send standards-related questions via the online question submission process: http://web.jointcommission.org/sigsubmission/sigquestionform.aspx.

– John C. Wallin is associate director of the Standards Inter pretation Group at The Joint Commission
1 https://www.congress.gov/bill/101st-congress/housebill/4449
2 https://www.cms.gov/Regulations-and-Guidance/Guidance/ Transmittals/downloads/r56soma.pdf
3 https://www.nationwide.com/lc/resources/investing-andretirement/artictles/advance-directive-vs-living-will

Nova’s unique heating element uses a novel carbon veil technology. This technology has been proven as a heater in car seats for years.

The Carbon veil is manufactured in a similar manner to paper, so it is readily available and a consistent methodology to warm patients.





To learn more or schedule an evaluation - Scan code (encompassgroup.com/patient-warming)


Maintains Performance
The veil is so flexible it can be cut and/or spilled on and yet still maintains performance.


 INDUSTRY Imagine effective patient warming with no noise, air movement or excessive heat.
INDUSTRY Imagine effective patient warming with no noise, air movement or excessive heat.
The U.S. FDA has recognized ANSI/AAMI ST91:2021, Flexible and semirigid endoscope processing in health care facilities as a guidance document “appropriate for meeting requirements for medical devices under the Federal Food, Drug, and Cosmetic Act.” Additionally, five other new or updated AAMI standards were added to the federal regulator’s list.

ANSI/AAMI ST91:2021 was spe cifically designed to establish a state of the art for cleaning and storing medical devices such as flexible bronchoscopes and various endo scopes. After five years of research and discussion, the new document represents the consensus of clini cians, industry, and sterilization pro fessionals from around the world. The guidance accounts for new technologies and modern insights concerning medical device clean liness. The revised standard also
reflects and expands upon 2021 rec ommendations issued by the FDA in the interest of helping health care providers prevent infections caused by or related to reprocessed urologi cal endoscopes.
And that’s no coincidence. FDA representatives were involved in the development of ST91, working alongside numerous other members of AAMI’s Endoscope Reprocessing Working Group (ST-WG 84). In ad dition to accounting for regulatory concerns, the new standard comes with extensive appendices citing peer-reviewed research and data to support the requirements and rec ommendations of the document.
“We wanted to make sure that everybody’s voices were heard and that all comments were discussed and resolved properly,” said Mary Ann Drosnock, director of Clinical Affairs at Healthmark Industries and a member ST-WG 84 since its inception. “There was no question afterwards. This guidance is about patient safety and we have the data baked in to support it.”
The document’s predecessor, ST91:2015, was similarly recog nized by the FDA in August 2015, but is now superseded. According to
the FDA, it will continue to accept declarations of conformity, in sup port of premarket submissions, to ST91:2015 until July 9, 2023. After this transition period, declarations of conformity to the 2015 version will no longer be accepted.
Another newly recognized AAMI sterilization standard is ANSI/ AAMI/ISO 11737-1:2018, Ster ilization of health care products - Microbiological methods - Part 1: Determination of a population of microrganisms on products. This standard specifies requirements and provides guidance on how to measure and characterize the popu lation of viable microorganisms on or in a health care product, compo nent, raw material, or package – an essential step in ensuring a product will not cause a patient infection.
ANSI/AAMI/ISO 11737-1:2018 is a national adoption of an ISO standard. The ISO standard was also recognized by the FDA and su persedes a version which does not include 2021 amendments.
AAMI TIR101:2021, Fluid deliv ery performance testing for infusion pumps is a new addition to the list.
This document outlines methods for testing the fluid delivery of an infu sion pump in order to provide clini cally relevant data of how the pump will perform. According to the FDA, “this document is applicable to sy ringe pumps, container pumps, and volumetric infusion pumps for all indicated delivery modes including enteral, patient controlled analgesia, or epidural and prescribed infusate sources … This document does not establish criteria for the clini cal acceptability of infusion pump performance, provide guidance for test method validation, or address uncertainty of measurement.”
ANSI/AAMI CN27:2021, Gen eral requirements for Luer activated valves (LAVs) incorporated into medical devices for intravascular ap plications is also newly recognized. Although LAVs have been incor porated into medical devices for intravascular applications for sev eral decades, a lack of harmonized practices among manufacturers has made aligning terminology and comparing performance claims par
ticularly difficult. This new standard is designed to improve understand ing common terminology, minimum requirements, and test methods for LAVs among manufacturers, regula tory agencies and end users.
The recognition of ANSI/ AAMI HA60601-1-11:2015 [In cluding AMD1:2021], Medical Electrical Equipment -- Part 1-11: General requirements for basic safety and essential performance -Collateral Standard: Requirements for medical electrical equipment and medical electrical equipment and medical electrical systems used in the home healthcare environ ment (IEC 60601-1-11:2015 MOD) [Including Amendment1 (2021)] means that after December 17, 2023, the FDA will only recognize declarations of conformity that account for the general medical electric equipment safety standard with its 2021 amendments, reflect ing modern industry consensus. This modified national adoption of an IEC standard ensures the basic safety and performance of elec

tronic medical equipment in the home health care environment — an essential standard in this era of telemedicine.
Similarly, the FDA has recog nized 2021 amendments for ANSI/ AAMI ES60601-1:2005/(R)2012 & A1:2012, C1:2009/(R)2012 & A2:2010/(R)2012 (Cons. Text) [Incl. AMD2:2021], Medi cal electrical equipment - Part 1: General requirements for basic safety and essential performance (IEC 60601-1:2005, MOD) [In cluding Amendment 2 (2021)]. The main document and amendments provide requirements for the safety and essential performance for all medical electrical equipment, while the newly recognized second amendment addresses changes to terminology and references since the main document was finalized in 2005 and first amended in 2012. There are additional updates to clauses to keep current with tech nology as well as to address ques tions received since the first amend ment was published.
P erioperative nurse educators are essential to the work of perioperative nursing and are often charged with fulfilling a variety of roles in addition to staff education. Such roles may include learning facilitator, change agent, mentor, leader, champion for scientific inquiry and/or a partner for practice transitions (Harper & Maloney, 2022). Thus, it might be more appropriate to refer to perioperative nurse educators as perioperative nursing professional development (NPD) practitioners.
This title encompasses the broad nature of their work and contributions to health care organizations. But such titles are not common in perioperative nursing and would require a change in perspective on this essential role. Embracing the full potential of periop erative nurse educators recognizes the unique and crucial responsibilities of these health care professionals (Wool forde, 2019).
Perioperative nurse educators may be unaware of a variety of key resourc es available to support the periopera tive NPD practitioner and the valuable networking opportunities found with the Association for Nursing Profession al Development (ANPD). The mis
sion of ANPD is to “advance quality health care by defining and promoting nursing professional development practice.” (“About ANPD,” n.d.) Additionally, ANPD develops and publishes the “Nursing Professional Development Scope and Standards of Practice,” which outlines the scope of NPD practice as well as the standards and related competencies for NPD practitioners.
There is also opportunity for the perioperative NPD practitioner to broaden their personal profes sional development via credentials related to the NPD specialty. The base credential in Nursing Professional Development, NPD-BC, is offered via the American Nurses Credential ing Center (ANCC). The NPD-BC certification is a competency-based examination that “provides a valid and reliable assessment of the entrylevel clinical knowledge and skills of registered nurses in the nursing professional development specialty.” (“Nursing professional development,” n.d.) However, the professional devel opment opportunities for the periop erative NPD practitioner do not stop there.
For those perioperative practitio ners that function at the NPD special ist level and who are prepared at the graduate level in nursing or a related field and certified in NPD (e.g., NPD-
BC), there is the opportunity to pursue certification via the Nursing Professional Development AdvancedBoard Certified (NPDA-BC) certifica tion program. This portfolio-based certification program, administered by the Competency & Credentialing Institute (CCI), “acknowledges the professional achievement of a nursing professional development special ist who fulfills all NPD roles and responsibilities while demonstrating adherence to professional practice and performance standards.” (Nursing professional development advanced,” n.d.)
The advanced certification assesses the knowledge and skills of an NPD specialist with at least 5 years’ experi ence utilizing a peer-reviewed profes sional portfolio to validate a candi date’s demonstration of advanced levels of knowledge and skills in NPD. The NPDA-BC portfolio articulates the candidate’s competency for each of the six throughputs of the NPD Practice Model – education, role de velopment, collaborative partnerships, inquiry, onboarding/orientation and competency management. (Harper & Maloney, 2022)
There are various advantages to this innovative method of certifica tion. First, portfolios are a portable avenue by which to evaluate and validate competencies that are often

more abstract and difficult to assess via the more common knowledgebased tests. (Byrne et al., 2007) Sec ond, portfolios allow for the assess ment and evaluation of one’s actual work and/or practice. (Schnipke & Wiley, 2019).
CCI nurses believe that the ANPD resources and these innovative NPD credentials will facilitate the professional growth and strengthen the practice of perioperative nurses. But this change will require a shift in perspective from nursing education to nursing professional development. At CCI, we believe it is time to begin that pivot to an emphasis on profes sional development over the span of a career.
To learn more about the innovation of the NPDA-BC certification visit https:// www.cc-institute.org/npda-bc/learn/.

– Tabitha Kinlaw, MBA, MSN, RN, NPDBC, CNOR, ONC, is a nurse manager - education and development at the Competency and Credentialing institute.
– James X. Stobinski, Ph.D., RN, CNOR, CNAMB, CSSM(E), is the CEO of the Competency and Credentialing Institute.
About ANPD. (n.d.). Association for Nursing Professional Development. Retrieved on July 19, 2022, from https://www.anpd.org/page/about
Byrne, M., Schroeter, K., Carter, S., & Mower, J. (2009). The professional portfolio. An evidencebased assessment method. Journal of Continuing Education in Nursing, 40(12), 545-552.
Harper, M. G., & Maloney, P. (2022). Nursing professional development: Scope & standards of practice (4th ed.). ANPD.
Nursing professional development advanced –board certified. (n.d.). Competency & Creden tialing Institute. Retrieved on July 19, 2022, from https://www.cc-institute.org/npda-bc/learn/
Nursing professional development certification. (n.d.). American Nurses Credentialing Center. Retrieved on July 19, 2022, from https://www. nursingworld.org/our-certifications/nursingprofessional-development/
Schnipke, D., & Wiley, A. (2019). Selection and use of item types.
In J. Henderson (Ed.), Certification: The ICE handbook (3rd ed., pp. 289-322). Institute for Credentialing Excellence.
Woolforde, L. (2019). Nursing professional de velopment practitioner or nurse educator: What’s your response? Journal for Nurses in Profes sional Development, 35(3), 174–175.
A recent report from ResearchAndMarkets.com report predicts that the global disposable surgical devices market will grow in the coming years.
The growing prevalence of chronic dis eases, such as cardiovascular, neurologi cal, urological, and infectious disorders, is expected to drive the overall market.
Chronic diseases are a global health care concern, with over half of the adult population in the U.S. suffering from them, resulting in over 75% of the total health care expenditure. Thus, a rise in infectious and chronic diseases is expected to create a significant de mand for disposable surgical devices.
Cancer has become a significant health care burden and a leading cause of death across the globe. According to the WHO, almost 1 in 6 deaths can be attributed to this disease. Estimates from the same source indicate that over 70% of cancer-related deaths typically occur in middle- and low-income coun tries. Thus, a steady rise in the number of curative, preventive and diagnostic
cancer surgeries has been observed globally, creating a high demand for disposable surgical equipment.
The growing number of road ac cidents is expected to augment the demand for disposable surgical instru ments. According to the WHO, around 10 million people are injured or dis abled due to road accidents every year, creating a demand for surgeries. Such wounds are commonly managed using surgical sutures. Hence, the increasing number of road accidents is expected to positively impact demand for dis posable surgical sutures and staplers.
The increasing government initia tives for the usage of disposable medi cal devices to avoid hospital-associated infections are expected to boost the usage of single-use devices. The grow ing number of surgical procedures is expected to increase the need for disposable surgical devices.

The ResearchAndMarkets.com dis posable surgical devices market report states that electrosurgical devices are expected to witness the fastest growth over the forecast period due to the growing usage of disposable electro
surgical devices in outpatient settings, such as ambulatory surgical centers.
By application, general surgery held the largest share in 2020 owing to the growing demand for general surgeries to avoid the transmission of infec tion, which is increasing the need for disposable surgical devices.
The plastic and reconstruc tion surgery application segment is expected to grow at the fastest rate over the forecast period. The growing number of plastic surgeries in vari ous countries, such as the U.S., Brazil and Mexico, is expected to propel the need for disposable surgical devices for the same. North America held the largest share in 2020 on account of the high prevalence of chronic diseases in countries, like the U.S., and the growing adoption of disposable surgical devices in the region, accord ing to the report.
Asia Pacific is expected to reg ister the fastest growth rate during the forecast period due in part to the increasing number of road accidents in the region and the presence of a large patient pool seeking surgery.
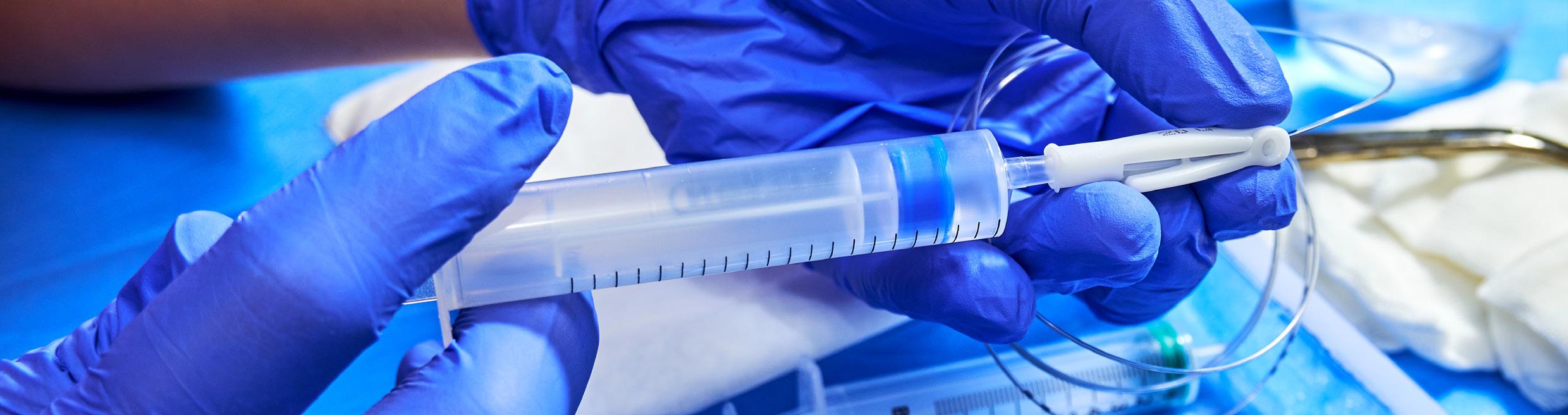
The lightweight, self-retaining single use retractor features unique cam locks that al low single-handed adjustment on the frame. The multiple frames and hooks allow the Galaxy II LUX Connect to be used in a vari ety of procedures including ENT, colorectal, orthopaedic, gynaecological and other open surgeries. LUX Connect can be used with the Galaxy II retractor, or on its own. Plug in, bend it, straighten it and shape it. Dispose of it when you are done. No heavy head gear, just light, where it needs to be.

Medgluv Perioperative Professional Resistant Gloves feature textured fingertips that enables grip, wet or dry. They have a tear-resistant beaded cuff that eases donning and offer color-coded sizing to identify different sizes. The gloves offer excellent sensitivity for touch perception and dependable protection. They meet and exceed NIOSH recommendations for Fentanyl. They also meet both ASTM D6978-05 and USP 800 Personal Protection Equipment requirement for use of select chemotherapy gloves.

Encompass Group LLC offers a wide variety of single-use apparel for patients, pediatrics, and staff, along with single-use bedding, patient care, personal protective equipment (PPE) and bed side accessories. Every item is developed with high-quality performing materials and fabrics. Disposable patient apparel features generously sized garments, which help reduce the incidence of cross-contamination, and are available in blue and green nonwoven materials. Encompass Group LLC also offers disposable washcloths, cleaners and bedding in multiple fabrics, colors and styles. All pediatric apparel, safety footwear and bedding items meet the required standards and specifica tions and are available in a variety of sizes, colors and prints, in SBPP or SMS fabrics.

To learn more, visit encompassgroup.net.
Easily contain fluids and streamline OR cleanup procedures with Flagship Surgical’s EcoDri-Safe Absorbent Rolls. These economical, disposable floor pads are ideal for use wherever fluids build up, including in the OR, around scrub sinks and on lab station floors. The super absorbent, dis posable floor pads eliminate expensive laundry costs and reduce OR turnover times. EcoDri-Safe Rolls help prevent slips and falls, and minimize the transmission of harmful contaminants to health care providers. OR clean-up times are significantly reduced and, with efficient disposal, these pads help prevent cross-contamination. The super ab sorbent pad material is manufactured with up to 33% recycled materials. An impermeable, non-slip poly backing (optional) promotes safety by lock ing liquid within the absorbent material, and helps keep the pad firmly in place. EcoDri-Safe Rolls are available in 100-foot rolls, both with and without the impermeable, non-slip poly backing, and are perforated every 20 inches for easy tear-off.
To learn more, visit flagshipsurgical.com.


For health care systems looking to de crease the amount of plastic in single-use products in the OR, the NewGen Surgi cal Needle Counter (NGSNC) outer box is made with 100% plant-based bagasse, a post-agricultural by-product from sugar cane upcycled to create fiber pulp; giving the needle counter a 95% plastic reduc tion by weight and reduces Scope 3 CO₂e by over 50%. The NGSNC, used by major hospital systems, eliminated over 20 tons of plastics with this one product. Designed to perform clinically like its plastic counterpart, the NGSNC provides secure closure with audible feedback, adhesive tabs and a full-surface magnet that provides space for larger needles and blades.

Jac-Cell USA Wound Drains are manufactured from high-grade biocompatible silicone material for enhanced patient comfort and tensile strength. They are ideal for postop erative wound drainage using high and low vacuum systems.

To learn more, visit jaccell.com.




CIVCO’s TEE Probe Transport Trays are designed to streamline probe turnover, helping to make the transportation of expensive, delicate TEE ultrasound probes as safe and efficient as possible. The revers ible push tab-locked lid makes clean/dirty indication easy, and the disposable molded fiber tray and paper lid are made from recyclable materials, eliminat ing time and resources needed to clean a reusable tray. The tray’s special OEM-approved design helps reduce the risk of cross-contamination by separating the high-level disinfected transducer shaft from the low-level disinfected cable and connector. The TEE Transport Tray meets probe manufacturer transducer coiling requirements, helping facilities stay compliant with national transport standards.
To learn more, visit civco.com
Ambu’s new aScope 5 Broncho HD System marries the benefits of reusable endoscopes with every advantage of singleuse endoscopes. Building on more than a decade of single-use expertise, Ambu offers bronchoscopy like you’ve never seen it before. The fifth-generation scope provides exceptional imaging, excellent maneuverability, and smart, functional design. With a new, sterile scope every time, there’s no worry about cross-contamination, or finding and cleaning equipment. Invented for the fast-paced work of thoracic surgeons, the scope is portable, intuitive and lightweight. Ambu’s fullyintegrated solution simplifies workflow while improving patient and clinician safety.
Swann Morton is the recognized global leader in surgical blade manufacturing, making more than 300 million blades a year. The high-quality British blades are manufactured to ISO 13485 standards with an open edge grinding technology resulting in a difference you can feel. One side of the blade is micro-serrated providing enhanced tactile feel for improved control while cutting. All of the blades go through 200 percent visual inspection, meaning there are no defects in the finished product. Swann Morton surgical blades perform consistently each use and are available in a range of sizes suitable for operations across all surgi cal disciplines, from Cincinnati Surgical or a preferred distributor.

A nesthesia administration has become increasingly safer, but is not without risk. Patient- and family-centered care and the desire to save costs has led to a shift in perioperative care needs from “stabilize and admit” to “stabilize and discharge.” Each patient undergoing anesthesia requires competent, professional nursing staff to assist in timely and safe medication administration, maintenance, and recovery. Knowledge of anesthetic techniques, agents, and adjuvants is vital to this competence.
The goal of this course is to educate perioperative nurses in acute care with knowledge on the anesthesia selection process and the safe care of patients undergoing anesthesia.
All surgical procedures pose a risk. There fore, patients should be in the best pos sible health before surgery. This optimal state of health includes both physical and psychological wellness. The physical state of the patient is assessed at a pre-anesthe sia assessment and includes their health history, a thorough physical examina tion, and diagnostic testing done prior to surgery. The patient is given instructions on pre-operative fasting requirements, smoking cessation, if applicable, and taking or holding their normal daily medications (Sweitzer, 2021). The patient can also be referred to a specialist for surgical clear
ance at this time. These baseline findings help the team to formulate a plan of care. Depending on the patient’s age, comor bidities, and the procedure, testing may include (Rothrock, 2014; Sweitzer, 2021):
• A blood type, screen, and crossmatch
• A pregnancy test
• A complete blood count
• A basal metabolic panel
• A coagulation panel
• An electrocardiogram
• Urinalysis, used to detect urinary tract infections, metabolic disorders, or kidney disorders
• Cardiovascular biomarkers, such as a C-reactive protein (CRP) and betanatriuretic peptide
An increased CRP level has been linked to an elevated risk for development of post-operative delirium (Dillon et al., 2017).
The pre-operative assessment may also determine the patient’s psychologi cal status. Patients commonly experience fear and anxiety surrounding the surgical experience. Evidence shows a connection between pre-operative anxiety and pro longed recovery times, increased hospital length of stay, increased pain levels, and delayed wound healing (Ali et al., 2013; Geers et al., 2018; Turksal et al., 2017). It is important to try to address questions and allay fears prior to the procedure to prevent these outcomes.
The anesthesia provider will perform their own assessment of the patient and classify the patient into one of six groups to determine the physical status of the pa tient. The assignment of a physical status is based on the patient’s physiological condi tion and is not related to the proposed
Relias LLC guarantees this educa tional program free from bias. The planners and authors have declared no relevant conflicts of interest that relate to this educational activity. See Page 43 to learn how to earn CE credit for this module.
After taking this course, you should be able to:
• Define the different types and stages of anesthesia.
• Describe anesthetic agents and adjuvants commonly used for the perioperative patient.
• Identify perioperative prepara tion, complications, and nursing interventions.
surgical procedure. The American Society of Anesthesiologists (ASA) Physical Status (PS) Classification System is as follows (ASA, 2019a):
• An ASA1 or PS1 patient is a normal healthy patient. For example, a pa tient with no smoking history and no or minimal alcohol use.
•
An ASA2 or PS2 patient has a mild systemic disease. Examples include a pregnant patient, a current smoker, a social alcohol drinker, or a patient with well-controlled type 2 diabetes, hypertension, or asthma.
• An ASA3 or PS3 patient has more than one severe systemic disease. Examples include a patient with poorly-controlled type 2 diabetes,
hypertension, chronic obstructive pulmonary disease (COPD), or a body mass index (BMI) greater than 40; a patient with an implanted pacemaker; a patient with coronary artery disease or a history of stent placement; a patient with end-stage renal disease on dialysis; and a patient with a history of a stroke.
• An ASA4 or PS4 patient has a severe systemic disease that is a constant threat to life. Examples include a pa tient who had a heart attack or stroke within the previous three months, a patient with ongoing cardiac ischemia or heart failure, and a patient with end-stage renal disease who is not on dialysis.
•
An ASA5 or PS5 patient is not expected to live without surgery. Examples include a patient with a ruptured abdominal aortic aneurysm, a massive trauma, a large intracranial bleed, an ischemic bowel, or multior gan dysfunction.
• An ASA6 or PS6 is a patient who has been declared brain-dead and is on life support, whose organs are being removed for donor purposes.
Another screening tool, the STOPBang questionnaire, is used to assess the patient’s risk for obstructive sleep apnea (OSA) (Chung, et al., 2016). A Mal lampati score, evaluating the ability to visualize the airway relative to the tongue, and evaluating the patient’s dentition for airway risks related to loose teeth, is used to supplement this information (Sweitzer, 2021). These assessment data, as well as the patient’s history and physical exami nation, allow the anesthesia team to make a plan regarding the type of anesthesia to be used, the need for advanced equipment or monitoring (for example, arterial line monitoring or a video laryngoscope for intubation), as well as any pre- or intraop erative medications that may be needed.
In the pre-operative area on the day of surgery, the nurse will assess the patient, obtain vital signs, review the patient’s
chart and labs, and assist in obtaining informed consent for the surgery and anesthesia administration. Consent forms ensure that the patient is aware of the pro cedure to be performed, the alternatives to surgery, the risks and benefits of surgery, and legally documents the patient’s understanding and permission to proceed (Shah et al., 2020). The anesthesiologist and surgeon are responsible for ensuring the patient’s level of understanding and that consent is obtained (Rothrock, 2014).
During the pre-operative process, teaching is reinforced, questions are answered, and any patient allergies, implants, and issues with previous surgical procedures are documented, if not already completed.
Once all team members and the room are ready, the patient is brought into the operating room (OR). Because the room is kept cold, a warm blanket or forced air warming device is usually placed over the patient, and the patient is secured on the operating table by a safety belt. Vital sign and cardiac monitoring equipment are attached. A calm, quiet environment is essential for an effective anesthetic induc tion. With sedation, safe and adequate amnesia, anesthesia, analgesia, and immo bility are the anesthesia provider’s overall goals. The administration of anesthesia has three phases: Induction, maintenance, and emergence (Siddigui & Kim, 2021):
1. Induction begins when the anesthetic is administered and ends when the incision is made. Anxiety-relieving medications, such as midazolam (Versed®), block memory of the procedure, while a sedative-hypnotic, such as propofol (Diprivan®), induces un consciousness. Older adult patients with multiple comorbid conditions or those with baseline myocardial impairments may alternatively receive etomidate (Amidate®) (King, 2020). For general anesthe sia, an endotracheal tube (ETT) or a laryngeal mask airway (LMA) will be inserted and connected to a
mechanical ventilator to maintain the patient’s airway. Verification of correct artificial airway placement is done by continuous waveform capnography, also known as endtidal carbon dioxide (EtCO2) monitoring and monitoring of vital signs and breath sounds (Palmer, 2013). Neuromuscular blocking agents or muscle relaxants, such as succinylcholine (Anectine®) or rocuronium (Zemuron®), are used to facilitate exposure of the surgi cal site and help with intubation (Rothrock, 2014).
2. The maintenance phase begins with the surgical incision and ends near the completion of the procedure. Gases such as isoflurane (Forane®), sevo flurane (Ultane®), and desflurane (Suprane®) are used for maintenance in conjunction with a sedative such as propofol or dexmedetomidine (Precedex®) (Palmer, 2013; Ro throck, 2014). During this phase, the anesthesia provider maintains the level of anesthesia and monitors vital functions. The anesthesia provider may not require assistance from the nurse; however, the team should remain alert to any unanticipated need for medication or supplies that are unavailable in the anesthesia cart. Usually, no emergent needs arise. At this time, the perioperative nurse may update the patient’s record and generally does other intraoperative tasks to assist the surgical team.
3. The emergence phase begins at the end of anesthesia as the patient is awakening and ends when the patient is successfully transferred to the post-anesthesia care unit (Rothrock, 2014). Reversal medications may be used if the sedation and neuromus cular blockade have not adequately worn off. If the medication is wearing off, the patient may be allowed to wake up unassisted; however, contin uous observation for residual sedation or blockade should be maintained. Patients with a risk for aspiration are
at high risk during emergence, so suctioning should be readily available (Berkow, 2020). Older adults and children are more likely to experi ence emergence delirium, a state of dissociation, and hypo- or hyperactiv ity upon wake-up (Griner & Kremer, 2019). Ensuring patient safety, reorienting the patient, and maintain ing hemodynamic stability are the primary goals for this event.
Rapid sequence induction is per formed for patients who are at high risk for pulmonary aspiration (Caro, 2019). Patients will receive pre-oxygenation, followed by simultaneous or rapid one-by-one dosages of a benzodiaz epine, such as midazolam, a paralytic, such as succinylcholine, and a sedative, such as propofol, immediately prior to intubation. The nurse is responsible for maintaining vigilance for complica tions, such as aspiration during rapid sequence induction. The anesthesia provider may need assistance during intubation to maintain an open airway, suction secretions, or access additional supplies. Suction must be available to help remove any secretions that may obstruct the provider’s vision during intubation. The nurse may also serve as an additional set of eyes and ears for unanticipated events.
The bispectral index (BIS) monitor can help the anesthesia provider monitor the optimal anesthesia level during general anesthesia and, to a lesser extent, the actual analgesia level (Rothrock, 2014). The system uses five electrodes placed on the patient’s forehead to measure sedation via electroencephalography recordings, on a scale of 0 to 100 (Lopez, 2016):
• 0 corresponds to no brain activity
• 90 to 100 corresponds to alertness
• 40 to 60 is an appropriate score during general anesthesia or deep sedation
Peripheral nerve stimulation, or “trainof-four,” is used to monitor the depth of neuromuscular blockade on the ulnar, me dian, or facial nerves (Adeyinka & Layer, 2020). Electrical impulses are delivered
to the nerves, and the number of twitches corresponds to a percentage of block ade. The normal goal is two out of four twitches or approximately 85% paralysis while under anesthesia. It is important to note that a return of four twitches is generally used in conjunction with clinical evaluation of muscle strength using a head-lift for 5 seconds, grip strength, and respiratory evaluation (Brull & Kopman, 2017; Renew, 2020).
Surgery is performed by a variety of anes thetic methods. Three concepts are vital to understanding these techniques and their effects on perioperative patients. Analge sia is defined as the lack of normal pain sensation (Venes et al., 2013). Amnesia, an essential element of general anesthesia and a desired element of regional and sedation techniques, is the absence of awareness of stimuli and events (Drain, 2013a).
Anesthesia is a partial or complete loss of sensation with or without the loss of con sciousness (Venes et al., 2013). The Asso ciation of periOperative Registered Nurses recommends that patients receiving ALL forms of anesthesia should have physiolog ical and psychological monitoring during and after the procedure (AORN, 2020).
Emergency resuscitative equipment, such as suction and oxygen supplies, medica tions, artificial airways, and a defibrillator, should be readily available.
Moderate sedation, also known as con scious sedation, is a medication-induced minimization of consciousness, during which the patient is still able to respond to verbal commands without touch or with only light touch (ASA, 2018a/b). No intervention should be needed for the patient to maintain spontaneous ven tilations. Patients are generally given an anxiolytic only, for example, midazolam (Versed®), or an anxiolytic and an opioid, usually fentanyl (Sublimaze®). An anes thesia provider does not need to perform moderate sedation; it can be performed by the procedural physician or a nurse with critical care training and a physician order, depending on the scope of practice
for the applicable State’s Board of Nursing (AAMSN, 2020; ASA, 2018a/b).
Local anesthesia is the injection of a nerve-blocking medication such as lido caine (Lidoderm®) into tissue to create a numbing effect to prevent pain during a procedure. It can be done while the patient is awake and undergoing minor procedures, such as small biopsies, wound stitching, and skin tag removals; or it can be done in combination with other types of anesthesia to improve pain manage ment at the direct surgical location. Locals are divided into two classes: amino amides and amino esters. Amino amides are more commonly used as they are more stable and produce fewer allergic reactions. Ex amples of amino amides include lidocaine, bupivacaine (Marcaine®), and ropiva caine (Naropin®). Examples of amino esters include procaine (Novocain®) and tetracaine (Pontocaine®). Dosing needs to be monitored carefully, as excess doses can cause central nervous system and cardiovascular toxicity (Cherobin & Tavares, 2020). Pain management for some procedures can also be achieved by combining IV sedation and local anesthe sia injected at the incision site; this is called local standby with sedation.
Monitored anesthesia care (MAC), a deeper level of sedation than moderate sedation, involves opioids and benzodi azepines given in combination with IV anesthetic agents. The anesthesia provider ensures an anxiolytic and analgesic state, while the surgeon generally provides local anesthesia at the surgical site. During MAC anesthesia, the patient maintains their own airway with spontaneous respirations, usually with only minimal or no assistance from the anesthesia provider; for example, the patient may only require a chin lift, nasopharyngeal or oropharyn geal airways (NPA/OPA), or supplemental oxygen. The main way to differentiate this method from general anesthesia is that NO artificial airway is inserted. This level of sedation must be performed and main tained by a qualified anesthesia provider, in case of a rapid need to switch to general anesthesia (Das & Ghosh, 2015).
General anesthesia is a combination of medications that produces unconscious ness, amnesia, analgesia, skeletal muscle relaxation, and sensory blockade (Drain, 2013a). It can be administered via inhala tion, IV, or both routes. General anesthesia without the use of inhalation agents is known as total intravenous anesthesia (TIVA). The patient undergoes insertion of an artificial airway, normally a laryn geal mask airway or endotracheal tube, to maintain a patent airway during the procedure. The two types of blades com monly used for intubation are the straight Miller blade and the curved Macintosh blade (Greenberg & Morrison, 2017). A portable video-assisted laryngoscope, such as a Glidescope™ or McGrath™, may be used for instances in which the patient has a known difficult or reactive airway. The LMA does not proceed past the glottis into the trachea, so it is less invasive, decreasing the risk of laryngospasm or bronchospasm; however, the risk of aspira tion is greater with this device (Bosson & Gordon, 2018). Procedures for patients who are at increased risk for aspiration, such as those with gastroesophageal reflux disease (GERD), morbid obesity, or an unknown NPO time, and procedures involving abdominal insufflation must be done with intubation.
Regional anesthesia involves injecting local anesthesia into a nerve or cluster of nerves to interrupt nerve impulses to the sensory, motor, and sympathetic nervous system at a specific surgical site (Moos, 2013). It is normally used in conjunction with monitored anesthesia care. Re gional anesthesia is generally used as a safe alternative to general anesthesia with the added benefit of prolonged pain manage ment for extremity or lower abdomen procedures. For lower extremity proce dures, a popliteal block or femoral nerve block is often used; for upper extremity procedures, an interscalene or brachial plexus block may be used. Nerve blocks are also becoming more common for large abdomen and chest wall surgeries, via the use of fascial plane blocks, such as the qua dratus lumborum (QL) and transversus
abdominis plane (TAP) blocks.
The volume and type of medica tion used and the site of instillation affect the intensity and duration of blockade (Moos, 2013). The anesthesia provider administers regional anesthesia by injecting a local anesthetic along a nerve pathway into clusters of nerves supplying an area that needs numbing (Rothrock, 2014). The advantage of this anesthesia is that it suppresses the pain impulse without causing a generalized depression of the entire nervous system. However, nerve blockade carries a risk of pneumothorax, pleural or vascular puncture, Horner syndrome, and dia phragmatic hemiparesis (Elsharkawy et al., 2019; Mavarez, 2020). The patient should be assessed for breathing dif ficulty, signs of local anesthetic toxicity, nerve damage following resolution, residual weakness following resolution, and site-specific complications. Contra indications to receiving a block include:
• Local anesthetic allergy
• Infection or open skin at the site where a block will be performed
• Venous thromboembolism
• Chronic neurological disorders
• Recent or current thrombolytic therapy
The nurse helps the anesthesia provid er with positioning the patient to facilitate the procedure. When regional anesthesia is used on one extremity, the anesthesia provider uses a double tourniquet and inserts an IV catheter in the operative extremity, while avoiding the surgical site. The extremity is raised and exsanguinated. The proximal tourniquet cuff is inflated, and local anesthetic is injected into the IV catheter. If the patient feels discomfort, the distal cuff is inflated, and the proximal cuff is deflated. This maneuver ensures that the anesthetic remains in place in the distal extremity, and NOT in sys temic circulation, until the tourniquet is deflated. The anesthesia provider and the perioperative nurse monitor the tourni quet inflation time and report the number of minutes the tourniquet has been in place; a maximum “tourniquet time” is 1
to 2 hours to prevent neuromuscular and vascular compromise (Kumar et al., 2016).
During a spinal block, a type of re gional anesthesia, the anesthesia provider injects anesthesia into the subarachnoid space, the cerebrospinal fluid surround ing the spinal cord, one time with a needle, usually between the L3 and L4 vertebrae for lower extremity procedures. The anesthesia works quickly to numb the entire lower body. The nurse or the nursing assistant may help reassure the patient while providing support for positioning during administration. The patient is observed for hypotension after successful anesthesia is achieved.
In epidural anesthesia, medication is injected into the space outside of the dura, and often, an epidural catheter is left in place to allow for titration of medica tion via an infusion pump; alternately, bolus injections can be performed by a qualified provider. The spinal level of the epidural varies based on the procedure. The epidural catheter may be secured in place for hours or days, and medications are regulated to control pain.
For caudal anesthesia, the epidural space is approached through the caudal canal in the sacrum. It requires a greater amount of anesthetic to fill the epidural space. Caudal anesthesia is often used for pediatric surgery, surgical procedures per formed on the perineum, and in the lower extremities (Rothrock, 2014).
The care of patients with regional and spinal anesthesia should include an assess ment of the sensory and motor function at the block site and its surrounding area. Hypotension and shivering are common due to vasodilation caused by the sym pathetic blockade that leads to decreased venous return and cardiac output. For spinal blocks, the return of motor func tion should be documented based on the patient’s ability to progressively move the toes, feet, and thighs, and the ability to lift the extremities. Return of sensory function is demonstrated by the ability to distin guish sensations of cold or touch. Docu mentation should include notation of the spinal dermatome level at which sensation
has returned; for example, “the patient has a weak toe wiggle and sensation to cold at the dermatome level T12/L1.”
Pre-operatively, patients are generally given a benzodiazepine to induce mild sedation and amnesia as well as calm the patient. The most common medication is midazolam (Versed®), as it is shorter-act ing, water soluble, and causes less venous irritation than alternate options, such as diazepam (Valium®) or lorazepam (Ativan®). If diazepam is used, administer it by slow IV push in a large-bore IV due to the risk for thrombophlebitis. Adverse effects of benzodiazepines include drowsi ness and slow wakening, somnolence, dis orientation, post-operative delirium, and respiratory depression, especially if used in combination with opioids and other seda tives (Bounds & Nelson, 2020).
Flumazenil (Romazicon®) is a ben zodiazepine antagonist, used to reverse severe adverse effects, such as respiratory depression. Nurses should be alert for the possibility of re-sedation occurring as the flumazenil wears off (Bounds & Nelson, 2020). Benzodiazepines are con traindicated in patients with untreated glaucoma due to a risk for the increase in intraocular pressure with administra tion and should be used with extreme caution in older adults due to the risk for accumulation of metabolites (Bounds & Nelson, 2020; Lingamchetty et al., 2020). Evidence suggests a correlation between pre-operative benzodiazepine use and increased post-operative opioid use. This finding, in addition to safety concerns related to use, may necessitate changes in practice recommendations in the near future (Rishel et al., 2020).
Sodium thiopental (Pentothal®) and methohexital (Brevital®) are histori cally known sedative agents that are no longer commonly used due to the risks for hypotension, bronchospasm, and pro longed effects with repeat dosing, which
can cause delayed awakening, somnolence, and respiratory depression post-operative ly. Methohexital is sometimes used for induction of patients undergoing electro convulsive therapy (ECT) (King, 2020). It is important to note that barbiturates do not provide analgesia, and alternative medications must be given for pain con trol (Nagelhout, 2014a). Extravasation of thiopental can cause severe tissue necrosis (Skibiski & Abdijadid, 2020).
Propofol (Diprivan®) is a lipid-soluble medication that is approximately twice as potent as sodium thiopental and com monly used for induction and mainte nance of general anesthesia (King, 2020). Propofol produces dose-dependent de pression of the central nervous system, but it has a rapid onset of 30 to 45 seconds, with a short half-life of 40 minutes, result ing in a quick return to baseline. Other central nervous system depressants, such as opioids, increase the hypnotic effect of propofol. The nurse should be aware that propofol administration causes a burning sensation in the veins. It is important to have appropriate IV access with a largebore IV needle; patients may benefit from having lidocaine injected into the IV first to prevent burning. Other adverse effects include muscle spasms and vasodilation that can lead to hypotension; this may be more prominent if the patient is older or has a history of left ventricular dysfunc tion. Fluid resuscitation and administra tion of one or multiple vasopressors may be required to maintain the patient’s blood pressure while receiving propofol (Nagelhout, 2014a). Of the available induction agents, propofol is the safest for use in pregnancy; however, it can cross the placenta and depress the fetal central ner vous system, so post-operative monitoring of the fetal heart rate should be initiated (Folino et al., 2020).
Etomidate (Amidate®) is often used as an alternative to propofol during induction of anesthesia for patients with cardiac disease, for emergent surgeries,
or on hypotensive patients with ongoing volume resuscitation (Nagelhout, 2014a). It has less of an effect on blood pressure, heart rate, myocardial contractility, and cardiac output than the other sedatives (King, 2020). Adverse effects include involuntary muscle contractions, tremors, nausea, and vomiting. Etomidate does not have any analgesic qualities, so concurrent opioid administration is necessary. One important note about this medication is that it can cause myoclonic jerking upon administration; usually, this goes unnoticed due to simultaneous paralytic and opioid administration (Rozycki et al., 2016). This medication should be used with caution in patients with adrenal insufficiency, due to suppression of cortisol. If used in this patient population, the patient should also receive a glucocorticoid, such as dexa methasone (Decadron®).
Dexmedetomidine (Precedex®) is used to provide anxiolysis, sedation, and analgesia with minimal respiratory depression (Das & Ghosh, 2015). Due to its opioid-sparing analgesic effects, this medication has quickly gained popularity in the proce dural anesthesia field. However, it is not routinely used due to a variable half-life with repeat or prolonged dosing, and a lack of ability to measure the sedation level, resulting in difficulty timing the infusion for emergence (Khorsand, 2020; Reel & Maani, 2020). It is often given as an adjunct with other medications and can prolong the duration of analgesia when given with peripheral nerve blocks (Reel & Maani, 2020). Nurses monitoring patients who have received dexmedeto midine should be alert for hypotension, bradycardia, and hypothermia.
Clonidine (Catapres®) is another alpha-2 agonist that is more commonly used to treat hypertension, but it has also been used for adjunctive pain man agement, particularly in patients with chronic pain, such as patients undergo ing extensive spinal surgery (Carr & Ferguson, 2019).
Ketamine (Ketalar®) is a nonbarbiturate, anesthetic medication. This medication is commonly used in the OR as patients maintain their normal pharyngeal and laryngeal reflexes, resulting in less risk for airway obstruction (Rosenbaum et al., 2020). Ketamine also produces both analgesia and sedation, making it an excel lent option for patients with chronic pain or expected severe pain post-operatively. It is contraindicated in patients with hypertension and increased intracranial pressure (ICP), due to increased cerebral blood flow and contractility resulting in an increased cardiac output, heart rate, and blood pressure (Caro, 2019). Adverse effects include a risk for hallucinations, dissociation, and emergence delirium. This risk can be minimized by avoiding early verbal or tactile stimulation, decreasing the dose, and administering ketamine in conjunction with a benzodiazepine, such as midazolam (Rosenbaum et al., 2020).
Sevoflurane (Ultane®), a volatile an esthetic, is the most commonly used agent for both inhalation induction and maintenance for both adults and children, as it is potent while being less pungent and bronchodilating (Hays, 2020). Inhala tion induction is indicated for patients with poor or unobtainable IV access or a fear of needles, such as pediatric patients. Inhaled induction takes minutes of deep inhalation, as opposed to seconds with IV induction. Despite being an expensive medication, it is still frequently used as it allows for rapid changes in anesthetic depth with quick recovery.
Nitrous oxide, the only non-volatile gas, may or may not be given as an adju vant to accelerate the onset of induction and provide analgesia and anxiolysis. It is also commonly used as a maintenance agent to affordably deepen sedation and reduce the need for high doses of alternate agents. Nitrous oxide should NOT be given to patients with gaseous distension of any compartment, due to
the risk for adverse reactions related to further expansion. For example, patients with bowel distention, a pneumothorax, or intraocular gas who receive nitrous ox ide could experience vomiting, a tension pneumothorax, or ocular vision loss. It also should be avoided for patients with vitamin B12 deficiency due to inactiva tion of B12 with use and the risk for subsequent neurotoxicity.
Desflurane (Suprane®) and Isoflurane (Forane®) are less likely to be used for in duction due to airway irritability and pun gency, but may be used as maintenance gases (Hays, 2020). Both of these agents are associated with increased cough ing during emergence and are generally avoided in patients with any pre-existing airway disease, such as asthma or COPD (Clar et al., 2020). Desflurane is most appropriately used for maintenance dur ing short procedures, while isoflurane is chosen for longer procedures due to lower cost and high potency. Another agent, halothane (Fluothane®), is no longer used in the U.S. due to the availability of safer substances and the risk for halothaneinduced hepatitis (Hays, 2020).
The minimum alveolar concentra tion is the lowest amount of an anes thetic that eradicates movement or a response to pain in 50% of patients (Hays, 2020). This value is used to as sign potency to inhaled agents and is an important concept for dosing decisions. A low minimum alveolar concentra tion indicates a potent anesthetic; a high minimum alveolar concentration indicates a less potent anesthetic. The minimum alveolar concentration will be higher for movement than for awareness or memory, allowing for relative safety in prevention of awareness while under anesthesia. However, certain patient conditions can influence the minimum alveolar concentration:
• Age, hypothermia, central nervous system depression, and antihyper tensive medications decrease the minimum alveolar concentration.
• Hyperthermia and chronic alcohol
use increase the minimum alveolar concentration.
This is also important in regard to the additive effects of other inhaled medica tions, such as sevoflurane and nitrous oxide. Anesthesia providers may moni tor the continuous end-tidal anesthetic concentration relative to the minimum alveolar concentration level or use BIS monitoring to guide anesthetic decisions (Hays, 2020).
The most common side effect of inhaled anesthesia is post-operative nausea and vomiting (PONV); antiemetics should be administered prophylactically unless otherwise contraindicated. All agents also carry the risk for delirium and laryngospasm. Isoflurane and sevoflurane are highly fat-soluble and thus result in longer emergence times (Hays, 2020). A more serious complication is malignant hyperthermia, most commonly caused by a combination of a volatile anesthetic, such as isoflurane or sevoflurane, and the muscle relaxant succinylcholine (Miller et al., 2020a). Inhalation agents, namely des flurane and isoflurane, are very irritating to the airway, potentially causing coughing, laryngospasm, or bronchospasm (Miller et al., 2020a). Management of adverse effects is by symptomatic treatment, as there are no reversal agents for these medications. Clearance of these medications is achieved by optimizing ventilation and supporting oxygenation, by encouraging coughing and deep-breathing once awake.
Neuromuscular blocking agents are prin cipally used to relax and paralyze skeletal muscles to assist with ease of endotra cheal intubation and muscle retraction within the surgical field, and decreas ing anesthetic needs (Khorsand, 2020). These medications do not have analgesic, amnesic, or anesthetic properties, and are classified according to their action on the neuromuscular junction: Depolarizing or nondepolarizing. Dosing is based on body
weight. Succinylcholine (Anectine®) is the only depolarizing neuromuscular blocking agent currently available in the U.S., and there is no reversal agent for this medication (Nagelhout, 2014b). Succi nylcholine should not be used in patients receiving digitalis (Digoxin®) or in those with chronic renal insufficiency due to a risk for arrhythmias and hyperkalemia (MacLeod-Glover, 2016). Of note, this medication can, in rare instances, trigger malignant hyperthermia. This will be discussed later in this course.
Nondepolarizing neuromuscular blocking agents include intermediateacting rocuronium (Zemuron®), ve curonium (Norcuron®), cisatracurium (Nimbex®), atracurium (Tracrium®), long-acting pancuronium (Pavulon®), and a newer medication, gantacurium. The selection of which medication to use is based on the drug availability, duration of the procedure, the patient’s comorbid conditions, and monitoring needs during surgery (Khorsand, 2020). Adverse effects may include (Nagelhout, 2014b):
• Anaphylaxis
• Cardiac dysrhythmias
• Post-blockade myalgia
• Sustained blockade
• Prolonged weakness
Certain medications, including local anesthetics, antibiotics, antidysrhythmics, and diuretics, can potentiate the ef fects of neuromuscular blocking agents, contributing to a prolonged recovery (Nagelhout, 2014b). The nurse should regularly assess the respiratory rate, quality of respirations, oxygen saturation, and end-tidal carbon dioxide levels, and report adverse findings to the anesthesia provider. The most serious post-operative complication is inadequate reversal; the patient will present with uncoordinated, short, jerky respirations with poor gas exchange. This has been described as a “floppy fish” gasping for air.
Reversal agents for nondepolarizing neuromuscular blocking agents include neostigmine (Prostigmin®), edropho nium (Enlon®), and pyridostigmine (Regonol®). A newer medication, sugam
madex (Bridion®), is gaining popularity. Patients who receive sugammadex should be instructed to use a non-hormonal contraceptive for 1 week following ad ministration of this drug, as it can decrease progesterone levels, thus negating the effects of traditional hormonal contracep tives (Stanford Medicine, 2020). It is rec ommended that an anticholinergic, such as atropine or glycopyrrolate (Robinul®), is given with the reversal agent to prevent adverse effects such as bradycardia, bron choconstriction, and hypotension (Drain, 2013b; Nagelhout, 2014b).
Local anesthetics disrupt the permeabil ity of nerve cells to sodium, resulting in an interruption of normal sensory, mo tor, and sympathetic pathways (Garmon & Huecker, 2020). They are divided into amides and esters. Amides are the more stable anesthetics (for example, lidocaine [Xylocaine®], mepivacaine [Polocaine®], prilocaine [Citanest®], bupivacaine [Marcaine®], ropivacaine [Naropin®]). Lidocaine, mepivacaine, bupivacaine, and ropivacaine are com monly used for injections at surgical sites or for regional anesthesia that are “nerve blocks.” Esters are more likely to produce allergic or hypersensitivity reactions, and include medications such as tetracaine (Pontocaine®), benzocaine (Anbesol®, Orajel®, Hurricaine®), procaine (Novocain®), and chloropro caine (Nesacaine®). Another difference between these groups of anesthetics are the areas where they are hydrolyzed: amides in the liver and esters in the plasma by cholinesterase. This is impor tant to note in the event that the patient has pre-existing liver disease or pseudo cholinesterase deficiency, as metabolism of these medications may be slowed, increasing the risk of toxicity (National Institute of Diabetes and Digestive and Kidney Diseases, 2017).
Benzocaine spray or a similar topical anesthetic spray is often used to numb the mouth and throat for oral procedures or upper esophagogastroduodenosco
pies (EGDs) (Aegis Anesthesia, 2020). Tetracaine, lidocaine, bupivacaine, and ropivacaine are the most common local anesthetics used for spinal anesthesia.
A long-acting formulation of liposomal bupivacaine, called Exparel®, is com monly injected by surgeons within the surgical site to assist in pain management for up to 72 hours following a procedure.
The decision on which medication to use and the amount is based on the type and length of the procedure (Rothrock, 2014). The primary adverse effects to watch for are contact dermatitis, allergic reactions, and local anesthetic toxicity.
Opioids produce analgesia, euphoria, and sedation. Examples include morphine (MS Contin®) (the gold standard to which all others are compared), fentanyl (Subli maze®), remifentanil (Ultiva®), sufentanil (Sufenta®), alfentanil (Alfenta®), and hydromorphone (Dilaudid®). Remifent anil is commonly used as a continuous infu sion during procedures requiring total IV anesthesia. Opioid administration can cause vasodilation and bradycardia, so the nurse should be aware of adverse effects, such as hypotension or syncope (Chen & Ashburn, 2015). Other adverse effects may include (Khorsand, 2020):
• Somnolence
• Urinary retention
• Constipation
• Nausea and vomiting
• Respiratory depression
• Pruritus
• Opioid-induced hyperalgesia
• Acute tolerance
Meperidine (Demerol®) is generally not used for perioperative pain manage ment due to its metabolite, normeperi dine, which causes central nervous system excitability (Drain, 2013c). The reversal agent for opioids is naloxone (Narcan®), which can reverse adverse effects such as respiratory depression. Opioid-sparing technique and enhanced recovery after surgery (ERAS) protocols recommend using the smallest amount of opioid neces sary for the shortest period of time to
ensure analgesia while preventing adverse outcomes (Khorsand, 2020).
Nurses administering opioids should consider if the patient is opioid tolerant, which may occur if the patient takes opioids regularly at baseline, or opioid naïve, as dosages may need adjustment to achieve the desired effect. Fentanyl is commonly used in the perioperative setting because of its rapid onset of 1 to 5 minutes and short duration of action. For medications such as morphine and hydromorphone, nurses should con sider that onset and duration times are extended, and the patient is at risk for delayed respiratory depression. Onset and duration times should be evaluated prior to nursing administration of any opioid to prevent adversely administering excess doses. Opioids in the perioperative area are generally given in small increments to achieve the desired effect, and titrated for safe patient outcomes.
Although not anesthetic agents, premedi cation prior to surgery to prevent pain, minimize opioid use, and optimize patient recovery is now standard procedure. The medications used vary based on the type of surgery, surgeon preference, and contra indications to use. Excluding regional and spinal techniques, oral and IV non-opioid medications to pre-emptively manage pain may include (Mariano, 2021):
• Acetaminophen (Tylenol®, Ofirmev®)
• Non-steroidal anti-inflammatory drugs (NSAIDs)
• Ketorolac (Toradol®)
• Celecoxib (Celebrex®)
• Meloxicam (Anjeso®)
• Gabapentin (Neurontin®)
Antiemetics may be given pre-, intra-, or post-operatively depending on the patient’s risk for PONV, the risk of PONV disrupting the surgical site, and the patient’s preference (Feinleib et al., 2021). Facility policy and perioperative algorithms may dictate the number of antiemetics to be used for prophylaxis and rescue therapy post-operatively. Ensuring
the patient is adequately hydrated using goal-directed fluid therapy is another means of prevention. Medications for nausea prevention may include:
• Ondansetron (Zofran®)
• Promethazine (Phenergan®)
• Dexamethasone (Decadron®)
• Diphenhydramine (Benadryl®)
• Metoclopramide (Reglan®)
• Transdermal scopolamine (Transderm Scop®)
Many other classes of medications may be used on a case-by-case basis to maintain hemodynamic stability during and after procedures. This includes medi cations such as:
• Anticholinergics, such as atropine or glycopyrrolate (Robinul®)
• Anti-hypertensives, such as vasodila tors, beta-blockers, or angiotensinconverting enzyme (ACE) inhibitors
• Antacids, such as famotidine (Pep cid®)
• Bronchodilators, such as albuterol (Proventil®)
• Diuretics, such as furosemide (Lasix®)
• Insulin
• Vasoconstrictors, such as phenyleph rine (Neo-synephrine®) or ephedrine (Akovaz®, Corphedra®)
Hypotension is a decrease in systolic blood pressure greater than 20% to 30% of baseline, or a blood pressure less than 90/60 mmHg (National Heart, Lung, and Blood Institute, 2021). It is the most frequent perioperative complication, and may be related to bleeding, dehydration from NPO status, fluid loss or lack of fluid replacement, perioperative medications, or parasympathetic nerve stimulation. Prior ity nursing interventions include:
• Providing oxygen and assessing the patient’s mental status and level of consciousness.
• Assessing perfusion via vital signs, skin color, and capillary refill: A mean arterial pressure (MAP) greater than 65 mmHg indicates adequate organ perfusion.
• Ensuring adequate urine output.
• Administering fluid boluses per orders; usually in amounts of 250 to 500 mL.
• Limiting or reducing sedation or pain medications that are contributing to hypotension.
• Placing the patient in Trendelenburg position, if not contraindicated.
• Administering corrective medications per orders.
Vasopressors and inotropes are often used for the correction of hypotension intra- and post-operatively. Vasopres sors raise blood pressure by increasing systemic vascular resistance, contractility, and heart rate, with a resultant increase in cardiac output (London, 2020). Examples include ephedrine (Akovaz®, Corphe dra®), phenylephrine (Neosynephrine®), vasopressin (Vasostrict®), norepinephrine (Levophed®), and epinephrine. Phen ylephrine and ephedrine are the most common perioperative choices. Ephedrine has both alpha and beta effects, so it cor rects hypotension with the added benefit of bronchodilation. All these medications should be used with caution in patients with pre-existing cardiac dysfunction.
Hypertension is an increase in systolic blood pressure greater than 20% to 30% of baseline, or a blood pressure greater than 140/90 mmHg. Causes are extensive and may include (London, 2020):
• Pre-existing hypertension and missed medications
• Pain leading to catecholamine release and vasoconstriction
• A full bladder
• Hypoxemia
• Fluid overload
• Hypothermia and shivering Anti-hypertensives can be used for short-term management, but the underly ing cause needs to be treated; for example, emptying the bladder, medicating for pain, or rewarming the patient. Primary antihypertensives include (London, 2020):
• Sodium nitroprusside (Nitropress®), which decreases the blood pressure
by peripheral vasodilation to decrease the afterload.
• Hydralazine (Apresoline®), which causes peripheral vasodilation by relaxation of smooth muscles.
• Calcium channel blockers, such as nifedipine (Adalat®) or nicardipine (Cardene®), which relax coronary smooth muscle and dilate periph eral arteries.
• Beta-blockers, such as labetalol (Normodyne®), metoprolol (Lopres sor®), and esmolol (Brevibloc®), which act by a mixture of alpha- and beta-blocking effects.
Hydralazine is a common choice for hypertensive patients with bradycardia (London, 2020). Labetalol is a com mon choice for hypertensive patients with tachycardia. Beta-blockers should be avoided in hypovolemic patients, those at high risk for bronchospasm, and those with bradycardia (Miller et al., 2020b). Esmolol is commonly used intraoperatively, as it has a rapid onset and short duration of action.
Total spinal anesthesia, or a “high spi nal block,” is a rare occurrence, and can be caused by excessive spread of local anesthetic by unintentional injection of epidural medication into the subarachnoid or subdural space, inadvertent transfer of medication via a dural tear, or overdose (Ituk & Wong, 2020). Clinical signs may appear directly following administration, or later with a change in the patient’s posi tion, usually from supine to sitting upright. Signs include:
• Loss of consciousness
• Upper extremity sensory and motor changes
• Nausea and vomiting
• Anxiety
• Hypotension
• Bradycardia to asystole
• Respiratory distress or apnea
Treatment focuses on hemodynamic stability until elimination of the medica tion. The patient may require intubation and the use of advanced cardiovascular
life support (ACLS) protocols for man agement; expect fluid and vasopressor administration.
Also known as plasma cholinesterase deficiency, pseudocholinesterase defi ciency occurs when there is an insufficient amount of enzyme needed to hydrolyze succinylcholine and ester local anesthetics (GARD, 2016). This results in a prolonged duration of neuromuscular blockade, which can last for hours after the pro cedure is complete. The patient may be alert and aware, but unable to move. Signs include irreversible “floppy” muscles, ap nea, hyperkalemia, and hypoalbuminemia. Patients with baseline liver or renal failure, malnutrition, severe anemia, and recent pregnancy are at highest risk. As there is no reversal for succinylcholine, treatment involves prolonged mechanical ventilation until the medication wears off. Support the patient and family during this time, as it can be a very frightening experience.
Local anesthetic systemic toxicity (LAST) is caused by systemic absorption of a local anesthetic, either by accidental intravascular injection or the administration of excess medication, and is a medical emergency (Behm et al., 2018). Amino esters are more likely to cause LAST, and early recognition is key to preventing rapid deterioration of the patient’s condition. Early signs include:
• Circumoral numbness: Numbness most commonly occurs around the lips, mouth, and fingertips
• A metallic taste in the mouth
• Dizziness
• Blurred vision
• Ringing in the ears, also known as tinnitus
• Decreased hearing
Late signs include:
• Restlessness
• Tremors and twitching
• Seizures
• Decreased cardiac function, lead ing to bradycardia, hypotension, and dysrhythmias
Treatment of LAST includes rapid initiation of IV 20% lipid emulsion, also known as intralipids, bolused at 1.5 mL/ kg, followed by a continuous infusion at 0.25 mL/kg/minute to a maximum of 10 mL/kg (Behm et al., 2018). Cardiovascu lar and respiratory support with oxygen and ventilation may be needed, based on the severity of symptoms; amiodarone (Nexterone®) is first-line treatment for ar rythmias. Lidocaine and calcium channel blockers should NOT be used for cardiac support as they may worsen existing hypotension (Warren & Pak, 2021). Once stable, the patient should remain under continuous hemodynamic monitoring in the event of reoccurrence.
Normothermia is a core temperature of 36°C to 38°C or 96.8°F to 100.4°F. Anesthesia blunts innate thermoregulation in the hypothalamus, and causes periph eral vasodilation, which reduces core body heat (Hooper, 2021). The surgical patient also experiences heat loss via:
• Radiation heat waves.
• Evaporation through sweating, exhal ing, and insensible fluid loss.
• Conduction to objects, such as a cold OR table, and the use of cold blankets.
• Convection to surrounding air.
The combination of these factors often leads to perioperative hypothermia, a body temperature less than 36°C or 96.8°F. Planned hypothermia is indicated for certain cardiovascular and neurological procedures to decrease oxygen require ments or lower intracranial pressure (ICP). Unplanned hypothermia is a complication of anesthesia, occurring in up to 70% of patients (Hooper, 2021). Patients at age ex tremes and those with spinal anesthesia are at higher risk for unplanned hypothermia.
Treatment of hypothermia can be both passive and active (Hooper, 2021). Passive warming is indicated for patients with body temperatures nearing hypothermia, shivering, or who complain of being cold. Passive interventions include increasing
the room temperature, applying warm blankets, and covering exposed skin. Ac tive warming is indicated for hypothermic patients. Active interventions include the use of a forced-air warming device, such as a Bair Hugger™, warming of IV fluid or blood products, and the placement of a targeted temperature management sys tem, such as the Arctic Sun®. Literature supports the use of prewarming measures to prevent post-operative hypothermia (Riley & Andrzejowski, 2018).
Patients with hypothermia should receive serial temperature checks every 15 minutes until normothermia is achieved, and assessments should ensure that peripheral vasoconstriction is not interfer ing with surgical site perfusion (Hooper, 2021). Shivering with hypothermia increases the use of oxygen stores, and the patient should be continually assessed for signs of hypoxia until symptoms subside. Meperidine (Demerol®) is a narcotic analgesic that may be used in small doses of 12.5 to 25 mg IV to decrease postoperative shivering in the adult patient; pediatric dosing is 0.25 to 0.5 mg/kg IV. Meperidine is contraindicated in patients with pre-existing seizure disorders and those taking monoamine oxidase inhibi tors (MAOIs) (RxList, 2021).
Febrile, or hyperthermic, patients have body temperatures greater than 38°C or 100.4°F. Fevers are not uncommon in the immediate post-operative period, from operative days 0 to 3. Low-grade fevers are often caused by inflammation, disrup tion of normal homeostatic mechanisms by anesthetic medications, and exposure to foreign material during surgery (Weed et al., 2020). High fevers greater than 38.3°C or 101°F should receive treatment with acetaminophen (Tylenol®), and a full work-up to determine the underlying cause, and most importantly, to rule out malignant hyperthermia or allergic reac tion to medication or transfusion products. Causes could include urinary tract infec tion, aspiration, medication-induced fever, or surgical site infection, although these causes are unlikely to present with fever until more than 5 days post-operatively
(Weed et al., 2020)
Malignant hyperthermia is a rare, inherited condition, in which exposure to certain volatile inhalation anesthetics and the commonly used paralyzing agent succinyl choline (Anectine®) results in a hyper metabolic response (MHAUS, 2020). This response causes an uncontrolled increase in body temperature, metabolism, and muscular breakdown. Malignant hyper thermia can be fatal, even when rapid treatment is initiated. Signs and symptoms include:
• An unexpected sudden increase in carbon dioxide (CO2) production
• Muscle rigidity
• Tachycardia, arrhythmias, and hemo dynamic instability
• Cyanosis, skin mottling, and a falling oxygen saturation
• Extreme hyperthermia with body temperatures in excess of 43.3°C or 110°F
• Metabolic or respiratory acidosis
• Hypoxia
• Hyperkalemia
• Elevated serial creatine kinase
• Myoglobinemia and myoglobinuria
Management of malignant hyperther mia should be rapid and coordinated, with guidelines in place for each facility. A cart containing equipment and medications for emergent intervention should be readily available. If malignant hyperthermia is sus pected, actions include (MHAUS, 2020):
• Stopping the surgery as soon as pos sible.
• Hyperventilating the patient with 100% oxygen to flush out inhaled volatile anesthetics.
• Rapidly cooling the patient using IV infusions of cold isotonic saline and bags of ice.
• Administering dantrolene sodium (Dantrium®) 2.5 mg/kg as an IV bolus to decrease muscle contraction.
• Addressing metabolic imbalances and dysrhythmias.
Dantrolene sodium is a skeletal muscle relaxant that blocks calcium release from
the sarcoplasmic reticulum, the action responsible for muscle contraction. It re quires reconstitution with 60 mL of sterile water and a large volume of medication, so the team will need many hands to assist in preparation. A newer formula tion of dantrolene, called Ryanodex®, requires reconstitution with only 5 mL of sterile water but is more expensive with a shorter shelf-life, and thus is less likely to be on hand during a malignant hyperther mia crisis. During recovery, avoid giving the patient calcium channel blockers as this can worsen hyperkalemia and hypo tension when administered together with dantrolene sodium. Ongoing manage ment includes repeated blood gases and biochemistry tests, further infusions of dantrolene as needed, and hemodynamic and renal monitoring and support.
Respiratory depression, or hypoventilation, is a slow respiratory rate or ineffective breathing pattern that causes retention of CO2, also known as hypercarbia or hypercapnia (Schick, 2021). Hypoxia is an oxyhemoglobin saturation level less than 90%. Primary perioperative causes include:
• Residual anesthetic agents and seda tives.
• Inadequate reversal or excess volume of opioids.
• Poor excursion or respiratory effort related to incisional pain.
• Weakness due to pre-existing neu romuscular diseases or prolonged neuromuscular blockade.
Presentation includes a decreased respiratory rate, shallow respirations, and increased EtCO2 on continuous wave form capnography.
Assess the patient’s breath sounds, chest excursion, and respiratory effort on arrival, and at frequent intervals (Schick, 2021). Equipment for rapid oxygen administration and suctioning of secretions should remain at the bedside at all times.
Assess the patient’s level of sedation using a verified scale, such as the Richmond Agitation-Sedation Scale (RASS) or the
Pasero Opioid-Induced Sedation Scale (POSS), according to facility policy. The perioperative nurse should seek to rectify the causal factor, in addition to providing supplemental oxygen, encouraging cough ing and deep breathing exercises, incentive spirometry, repositioning the patient, and verbal or tactile stimulation for sedated patients. Every patient receiving anesthesia is at risk for respiratory compromise.
OSA is caused by pharynx obstruction, usually as a result of edematous or swollen soft tissue of the throat or neck, a large tongue, or a foreign body (Chung et al., 2016; Schick, 2021). Patients at risk for sleep apnea and those with pre-existing OSA may need a sleep study before surgi cal clearance, depending on the procedure. Patients with OSA should be instructed to bring their continuous positive airway pressure (CPAP) device to the hospital on the day of surgery for use during anesthet ic recovery. A series of questions regarding Snoring, Tiredness, Observed apnea, blood Pressure, BMI, Age, Neck circumference, and Gender, called the STOP-Bang analy sis, is commonly used to screen patients for their risk of OSA prior to surgery. The total score ranges from 0 (low) to 8 (high) risk of OSA.
Nursing interventions for patients exhibiting OSA include:
• Stimulating the patient with voice or touch.
• Elevating the head of the bed greater than 30°.
• Applying supplemental oxygen, as needed, or a bi-level positive airway pressure (BiPAP) or CPAP machine.
• Repositioning the head to optimize the airway.
• Lifting the chin and thrusting the jaw forward to relieve the obstruction.
• Placing a rolled towel underneath the shoulders.
• Inserting an adjunctive airway, such as an NPA or OPA.
• Maintaining respirations with positive-pressure ventilation with
a bag-valve mask, if the respiratory rate falls below 10 to 12 breaths per minute.
• Notifying the anesthesiologist if there is no return of spontaneous respira tions.
• Administering naloxone (Narcan®) per order, or assisting the provider with reintubation if there is no re sponse to treatments.
Be sure to review the chart and pa tient’s medical history to confirm there are no contraindications to these interventions to protect the patient’s safety (OdomForren, 2015). For example, a patient with a medical history of epistaxis, cranial surgery, facial fractures, or a low platelet count should not have an NPA inserted. A patient with chronic cervical neck pain or cervical surgery may not be able to tolerate or achieve hyper-extension of the neck or lifting of the chin. Stimulation of the patient’s gag reflex with an OPA may cause vomiting in a semi-arousable or awake patient, increasing the risk for aspiration. An OPA should be used only in an unconscious patient.
Atelectasis is a common intra- and post-operative complication that results in basilar alveolar collapse (Marley, 2021). It is caused by intraoperative positioning, diaphragmatic dysfunction related to compression of lung tissue, neuromuscular blockade, and mechani cal ventilation, and sedative effects on normal breathing patterns post-opera tively. The patient with atelectasis is at risk for the development of hypoxemia and pneumonia. Auscultation may re veal diminished breath sounds or crack les, and supplemental oxygen should be used as needed. Primarily, the patient should be encouraged to initiate incen tive spirometry and effective cough ing and deep breathing exercises to re-expand the basilar alveoli. Patients in pain should receive cautious pain medi cation and be provided with a pillow for splinting incisions, while practicing
lung expansion exercises.
Aspiration is regurgitation of stom ach contents or inhalation of foreign material, such as food, blood, or teeth (Schick, 2021). Pre-surgical fasting guidelines generally state no solid foods for 8 hours prior to surgery, with the allowance of clear liquids until 2 hours prior to the surgery start time. These times may be extended depending on the surgical procedure and if the patient is known to have delayed gastric emptying or severe GERD. Signs of aspiration include unexplained tachycardia and tachy pnea, frequent coughing, crackles on auscultation, sudden bronchospasm, hypoxemia, interstitial edema, or acute respiratory distress syndrome. Medications are commonly given preand intraoperatively to reduce the risk of nausea, vomiting, and aspiration; these include:
• Proton pump inhibitors, such as pantoprazole (Protonix®)
• Antacids, such as sodium bicarbonate (Alka-Seltzer®)
• Antiemetics, such as ondansetron or promethazine
• Anticholinergics, such as scopolamine or glycopyrrolate
• Antihistamines, such as diphenhydr amine
Nursing interventions include (Schick, 2021):
• Frequent respiratory monitoring to assess for rhonchi or crackles.
• Administering the above medica tions or initiating non-pharmacologic techniques to reduce nausea, such as aromatherapy with peppermint, placement of an alcohol swab by the nose, or acupressure.
• Suctioning of secretions or emesis. Keeping the head of the bed elevated and, if not contraindicated, rolling the patient to one side to allow for better drainage of secretions.
Laryngospasm is the involuntary closure of the vocal cords caused by secretions, blood drainage, or irritation of laryngeal reflexes during emergence from anesthesia (Marley, 2021). The patient most commonly presents with:
• High-pitched wheezing or inspiratory stridor, indicative of a partial laryngo spasm
• Absence of air exchange, indicative of complete laryngospasm
• Paradoxical chest and abdominal movement
• Hypoxia and bradycardia
• Tracheal deviation
Laryngospasm is an airway emer gency, and the attending anesthesiologist should be notified immediately. If the patient experiences laryngospasm, stay with the patient and remove the offend ing source, when possible, via suctioning the airway, asking the patient to cough, or turning the patient to one side to promote drainage (Cooper, 2020). If the patient is experiencing a complete laryn gospasm, do NOT ask them to cough, as coughing against a closed airway can result in pulmonary edema. Ap ply positive-pressure ventilation with a bag-valve mask at 100% oxygen to break the spasm. If these actions do not break the spasm, a low-dose of propofol can be given to deepen anesthesia, followed by 0.25 to 0.5 mg/kg of IV succinylcholine to relax the airway. Enlist help in gather ing supplies in the event that emergent reintubation is needed. Following resolu tion, the patient remains at risk for the development of pulmonary edema and should remain under close monitoring.
Bronchospasm is constriction or closure of the bronchial smooth muscle caused by airway irritation (Marley, 2021). It is more common in patients with pre-existing re active airway diseases, such as asthma and COPD, but patients with recent upper respiratory infections and tobacco smokers are also at risk. Signs include:
• Cough
• Expiratory wheezing
• Dyspnea, tachypnea, and prolonged expirations
• Accessory muscle use and an in creased work of breathing Nursing interventions include (Marley, 2021):
• Notifying the anesthesiologist.
• Removing the irritant, if possible, by oropharyngeal suctioning.
• Administering oxygen.
• Administering inhaled bronchodila tors or beta2-agonists, such as alb uterol (Ventolin®) or anticholinergic bronchodilators, such as ipratropium bromide (Atrovent®), or a combi nation agent, such as ipratropium bromide and salbutamol (DuoNeb®) per order.
• Administering an IV loading dose of 5 mg/kg, followed by an infusion at 0.5 mg/kg/hour of the bronchodilator aminophylline hydrate.
• Gathering supplies for emergent reintubation, if necessary.
Emergence delirium is characterized by a state of excitement upon emergence from general anesthesia. Risk factors include age extremes, pre-existing mental health conditions, pre-operative anxiety, and the use of the anesthetic gases sevoflu rane, desflurane, isoflurane, or halothane intraoperatively (Mamaril, 2021). The surgical team can assist in preventing the occurrence of emergence delirium by providing emotional support and fre quent updates pre-operatively, choosing rapid-acting IV sedatives over those with a prolonged duration of action, and allowing for a slow emergence from anesthesia (Zafirova, 2019). Physiological etiologies, such as pain, hypoxemia, hypercarbia, and hypovolemia, should be considered and assessed; always suspect and treat the patient for hypoxia FIRST.
The presentation of emergence delir ium can differ between patients, but may include severe restlessness, combativeness,
crying, screaming, moaning, kicking, flail ing, non-purposeful movements, disorien tation, incoherence, a glassy eyed appear ance, or unresponsiveness. Delirium is generally time-limited, lasting from 10 to 30 minutes; episodes not resolving within 1 hour can be classified as post-operative delirium, and warrant further work-up to prevent neurocognitive decline (Windle & Mamaril, 2021). During the acute phase, protect the patient from injuring them selves and others, protect surgical sites, and ensure the patient does not inadvertently remove any lines or drains. Initiate treat ment for any expected causes, such as pro viding pain medication for pain, oxygen for hypoxia, and a warming blanket for hypothermia. Reuniting the patient with the caregiver or support person can assist in reorienting the patient. Generally, medi cations are not given unless the patient is violent. The American Geriatrics Society discourages the use of benzodiazepines to treat emergence delirium in the older adult patient (Zhang et al., 2018).
Delayed awakening is a prolonged emergence from anesthesia and continued sedation with unresponsiveness in the re covery room (Pai, 2020). It may be a com mon phenomenon in some patients, and the surgical history should be reviewed for any reports of slow awakening prior to this incident (Schick, 2021). Older adult patients metabolize medications at a slower rate, and potentiation of multiple sedative agents may contribute to delayed awakening. Assess the patient for any hemodynamic instability or hypothermia that could explain the delay.
The anesthesia provider should be notified if the patient remains unarousable beyond 30 to 60 minutes following the last administered anesthetic or sedating adjuvant agent (Pai, 2020). Stimulate the patient frequently and remain with the patient to support the airway. Ensure there are no clinical indicators of carbon dioxide retention, with support from arte rial blood gas analysis. The patient should
also be assessed for prolonged neuromuscular blockade, via the use of a peripheral nerve stimulator. Additionally, obtain point-ofcare testing for hyper- or hypoglycemia, and perform a thorough neurological examination to rule out causes such as stroke. Administer reversal agents, as indicated, to assist in returning the patient to baseline status.
The patient who reports knowledge of the events while under anesthesia should receive immediate referral to the attending anesthesia provider (AANA, 2021). Document the patient’s report and provide emotional support to the patient, who may have experienced great fear during the event. Generally, the patient remembers activities that happened just prior to or just after the surgery or dream awareness. In rare cases, intraopera tive awareness has been reported; 1% to 1.5% of cases occur in high-risk surgical patients, such as those undergoing major trauma and cardiac procedures (Rothrock, 2014). In any instance, the an esthesia team should be notified so the event can be documented and avoided in any further surgeries.
Now that you have finished viewing the course content, you should have learned the following:
• The different types and stages of anesthesia
• Anesthetic agents and adjuvants for the perioperative patient
An 84-year-old man arrives to the pre-operative holding area prior to a planned ureteroscopy with stent placement procedure for treatment of a kidney stone. The patient’s past medical history includes poorly controlled hypertension, type 2 diabetes, hyper lipidemia, severe GERD, and OSA.
1. Based on this patient’s history, what American Society of Anesthesiologists (ASA) Classification would be assigned to this patient?
A. ASA 1
B. ASA 2
C. ASA 3
D. ASA 4
2. The anesthesia team decides to use general anesthesia based on the patient’s medical history and risk for aspiration. The patient has lactated ringers, running into a 20 gauge IV in the left antecubital, and undergoes rapid sequence intubation with midazolam, succinylcholine, and propofol. Directly prior to sedation, the patient complains of burning pain in the left arm. What is the MOST likely cause?
A. Midazolam
The content for this course was created by Nicole Strickland, BA, BSN, RN, CPAN.
Nicole Strickland, BA, BSN, RN, CPAN has cared for medical-surgical, stepdown, and ICU-level neurology and postanesthesia care patients. She holds a BA in English from Temple University and worked as a medical editor for the National Board of Medical Examiners before returning to school to obtain a BSN from Duke University. She has devoted much of her nurs ing career to training nurses and nursing students as a Certified PeriAnesthesia Nurse (CPAN). She now continues her passion for nursing research and education as an acute care SME writer for Relias.
American Association of Moderate Sedation Nurses: https://aamsn.org/ American Association of Nurse Anesthetists: https://www.aana.com/ American Society of PeriAnesthesia Nurses: https://www.aspan.org/ Malignant Hyperthermia Association of the United States: https://www.mhaus.org/
For the full list of references, visit ortoday.com
B. Excess fluid administration with LR
C. Propofol
D. Succinylcholine
3. The procedure is completed within 30 minutes without incident, and the patient is brought to the recovery room. On waking up, the patient is oriented to self only, and tries to climb out of bed. What BEST describes this behavior?
A. Emergence delirium
B. Over-sedation
C. Local anesthetic toxicity
D. Pseudocholinesterase deficiency
A 64-year-old female is scheduled for a breast biopsy and lumpectomy. The patient is admitted to the preoperative holding area with vital signs as follows:
• A. Blood pressure 142/94 mmHg
• B. Temperature 36.8°C (98.4°F)
• C. Heart rate 100 beats per minute
• D. Respiratory rate 24 breaths per minute
• E. Oxygen saturation by pulse oximeter is 98% on 2 L of oxygen via nasal cannula
The patient has a history of well-controlled hyperten sion, sleep apnea, and post-operative nausea and vomit
ing (PONV). During the pre-operative evaluation, the anesthesiologist has assigned the patient a physical status of ASA2 on the classification system from the American Society of Anesthesiologists.
1. Which of the following is REQUIRED in the initial preoperative nursing assessment for this patient?
A. An arterial blood gas analysis
B. Vital signs
C. A chest X-ray
D. An electroencephalogram
2. An IV is started, the consent forms are signed, the nurse completes the pre-operative teaching and checklist, and the anesthesiologist administers dexamethasone (Decadron®) for nausea prevention. During induction in the OR, the nurse stands by the anesthesiologist to help during intubation. Which of the following is a nursing responsibility during intubation of the patient?
A. Applying cricoid pressure to prevent aspiration
B. Administering inhaled gases
C. Suctioning the airway
D. Pushing propofol into the IV line
3. The procedure is performed without incident, and the patient is taken to the recovery room. Prior to receiving a report from the anesthesia provider, the patient awakens and states that their mouth tastes like metal and their ears are ringing. What should the nurse immediately suspect?
A. Malignant hyperthermia
B. Local anesthetic systemic toxicity
C. Pseudocholinesterase deficiency
D. Overdose of opioid
Earlysignsincludecircumoralnumbness,ametallictasteinthe mouth,dizziness,blurredvision,andtinnitus,orringingintheears.
whileaventilatorissetup.Thealternateoptionsareanesthesia providertasks,unlessthenursehasadditionalcriticalcaretraining andcertification.3.B,Localanesthetictoxicityiscausedbysys temicabsorptionofalocalanestheticandisamedicalemergency.
torytests,andinformedconsentdocumentsarerequiredpriorto surgery.2.C,Thenursemustbeavailabletoassisttheanesthesia providerduringthecriticaltimeofinduction.Thiscouldinclude handingsuppliestotheanesthesiaprovider,suctioningtheairway toallowforbettervisualizationduringintubation,orproviding respiratorysupport,suchasprovidingbag-valvemaskventilations
1. Read the Continuing Education article.
2. Go online to ce.nurse.com to take the test for $12. If you are an Unlimited CE subscriber, you can take this test at no additional charge. You can sign up for an Unlimited CE membership at https://www.nurse.com/ sign-up for $49.95 per year.
Courses must be completed by 6/30/2024
3. If the course you have chosen to take includes a clinical vignette, you will be asked to review the vignette and answer 3 or 4 questions. You must answer all questions correctly to proceed. If you answer a question incorrectly, we will provide a clue to the correct answer.
4. Once you successfully complete the short test associated with the clinical vignette (if there is one), proceed to the course posttest. To earn contact hours, you must achieve a score of 75%. You may retake the test as many times as necessary to pass the test.
5. All users must complete the evaluation process to complete course. You will be able to view a certificate on screen and print or save it for your records.
In support of improving patient care, OnCourse Learning (a Relias LLC company) is jointly accredited by the Accreditation Council for Continuing Medical Education (ACCME), the Accreditation Council for Pharmacy Education (ACPE), and the American Nurses Credentialing Center (ANCC), to provide continuing education for the healthcare team.
CASESTUDY21.B,Vitalsigns,labora
Itisimportanttohaveappropriateaccesswithalarge-boreIV; patientsmaybenefitfromhavinglidocaineinjectedintotheIVfirst topreventburning.3.A,Emergencedeliriumischaracterizedbya stateofexcitementuponemergencefromgeneralanesthesia.The patient’sage,administrationofmidazolam,andtheshortlengthof procedurewithrapidemergenceallplacethispatientatincreased riskofemergencedelirium.
C,Propofoladministrationcausesaburningsensationinthevein.
ASA3,duetomorethanonemoderatetoseverecomorbidity.2.
CASESTUDY11.Answer:C,Thispatientwouldbeclassifiedas
OnCourse Learning is also an approved provider by the Florida Board of Nursing, the District of Columbia Board of Nursing, and the South Carolina Board of Nursing (provider #50-1489). OnCourse Learning’s continuing education courses are accepted by the Georgia Board of Nursing. Relias LLC is approved by the California Board of Registered Nursing, provider #CEP13791.
Nurse.com
You can take this test online or select from the list of courses available. Prices subject to change.
Questions or for a complete listing of our courses
Phone: 877-843-8374 Email: nursesupport@relias.com
F or over 50 years, Healthmark Industries has provided innovative intelligent solutions to meet the needs of health care facilities. 2022 has been a year of growth, offering new products and providing new educational services.

Over the past few years, Healthmark has strengthened their commitment to offering new product lines that provide solutions to their customers in order for them to verify the integ rity of their equipment. The Insula tion Tester, Leak Tester Tester, Shaver Leak Tester and Cable Continuity Tester are easy-to-use devices for verifying the functionality of equip ment for safety.

The McGan Insulation Tester detects and locates defects such as pinholes, cracks and bar spots in the jacket or coating of laparoscopic and bi-polar electrosurgical instruments. It is designed specifically for electri cally testing electrosurgical instru ments. The Insulation Tester is a handheld, portable unit that tests the

insulation integrity of electrosurgi cal equipment for flaws in protective coatings applied over conductive in strument surfaces in order to prevent inadvertent tissue burns, which may occur during electrosurgical instru ment procedures.

by automated and handheld endo scope leakage testers, the Leak Tester Tester assists health care workers in reprocessing areas to make sure their endoscope leak tester is working properly by testing the functionality of the pump and the connector for leaks prior to use. The Leak Tester Tester assists in reducing the potential for cross-contamination, damage and costly repairs that result from using an endoscope with leaks.
Leak Tester Tester checks the functionality of automated and handheld endoscope leakage testers. Testing your facilities’ endoscope leak tester prior to use is a necessary step to ensure leak testing demon strates accurate results, which is why Healthmark created the Leak Tester Tester. Designed to check the accuracy of air pressure provided
The Cable Continuity Tester is de signed to test the quality of monopolar and bipolar cords, the Cable Continu ity Tester is user-friendly, durable and encased in plastic. Simply position the “ON” switch to bipolar or monopolar for the desired test. The Bipolar-OFFMonopolar switch should illuminate on the desired side. Next, insert the cable and test by lightly pulling at the connections. When complete, position the rocker to the “OFF” position. If the green light remains illuminated while Steriking Self Seal Pouches for Long Medical Devices
Leak Tester Tester Cable Continuity Testerpulling at the connections, then the cable passes testing. If the light flick ers or doesn’t illuminate, this indicates the cable failed testing. The Continuity Tester requires one 9V battery that can be replaced by sliding out of the bat tery door. Each Cable Continuity Tester comes with a 9V battery and a case.
The Shaver Leak Tester is designed for pressure testing ar throscopic shavers to help identify leaks caused by failing seals that degrade over time from repeated use and processing. The Shaver Leak Tester assists health care workers in reprocessing areas to make sure their shaver is working properly by using both a hand pump to apply pres sure and a testing stop made from polypropylene to create a temporar ily closed system within the fluid pathway of the shaver to pressure test for leaks. Utilizing positive pressure allows the user to confirm if the internal seals are fully intact or if the shaver needs to be sent out for repair. The Shaver Leak Tester helps in reducing the potential for cross-contamination, damage and costly repairs that result from using a shaver with leaks. Simply, select the appropriate brand specific test ing stop and insert the stop into the distal end of the shaver’s handpiece until it is fully seated. Then, connect the open end of the silicone tub ing attached to the pressure gauge, to the stainless-steel discharge port located at the proximal end of the handpiece. Next, use the bulb of the hand pump to apply pressure and

observe that the pressure gauge is displaying and maintaining a positive value. Confirmation of positive static pressure on the pressure gauge indi cates no leaks in the fluid pathway and is considered a passing result. The brand-specific Shaver Leak Tester stops are not interchangeable and offered for the following shavers: the Midas Rex shaver, the Stryker Formula shaver, the Stryker Small Joint shaver, the Dyonics shaver, the Conmed Linvatec shaver, and the Arthrex shaver.
Healthmark also announced the addition of the Steriking Pouches for Long Medical Devices to its Steriking Sterilization product line. Manufactured with heat-sealed up per corners that prevent dust from collecting at the opening seal to re duce the risk of contamination when opened, the Steriking Pouches for Long Medical Devices are designed as packing material for sterilization of long devices by steam.
The single-use Steriking Pouches for Long Medical Devices are con structed of heavy weight 100 gsm paper that is heat-sealed together with a multi-ply PET/PP-plastic laminate. Equipped with strong and durable multi-line parallel seams that promote a clean peel, the see-through heat and self-sealable pouches allow double pouching and have thumb notches at each end, which make the filling and opening of a pack easier.
Another new product announced by Healthmark this year is the Robotic Instrument Guards. They are de signed to protect robotic instrument tips during sterilization, transport and storage. Featuring an area to ap ply a steam dot, the Robotic Instru ment Guards are offered in the fol lowing sizes: 15mm and 30mm. The

wide, smooth design of the Robotic Instrument Guards allow individuals to easily slide robotic instruments in and out of instrument pouches. The Robotic Instrument Guards are low linting and have excellent wet and dry mechanical properties to with stand the steam sterilization cycle.
Cleaning verification continues to be a critical issue in health care across the country. News headlines often report about complications from surgeries caused by instruments and equipment that have not been properly cleaned. It has affected the health care field over the years.
Healthmark’s ProFormance monitoring tools help ensure surgi cal instruments and other equipment are reprocessed correctly. AAMI 1 and AORN 2 recommend at least weekly testing (preferably daily) of the cleaning process. These products are designed to help facilities comply with standards and ensure they are reprocessing equipment and cleaning surgical instruments effectively.
Researchers have discovered that devices that haven’t been repro cessed correctly can emerge from the
Shaver Leak Tester Robotic Instrument Guardscleaning process with bits of bone, blood and tissue from the previous procedure. These contaminants can be reservoirs for some potentially lethal bacteria. Proper cleaning and sterilization are essential for ensuring that medical and surgical devices do not transmit infectious pathogens to patients.
According to the Centers for Disease Control and Prevention (CDC), multiple studies in many countries have documented lack of compliance with established guide lines for cleaning, disinfection and sterilization. 3 Failure to comply with scientifically based guidelines has led to numerous outbreaks.
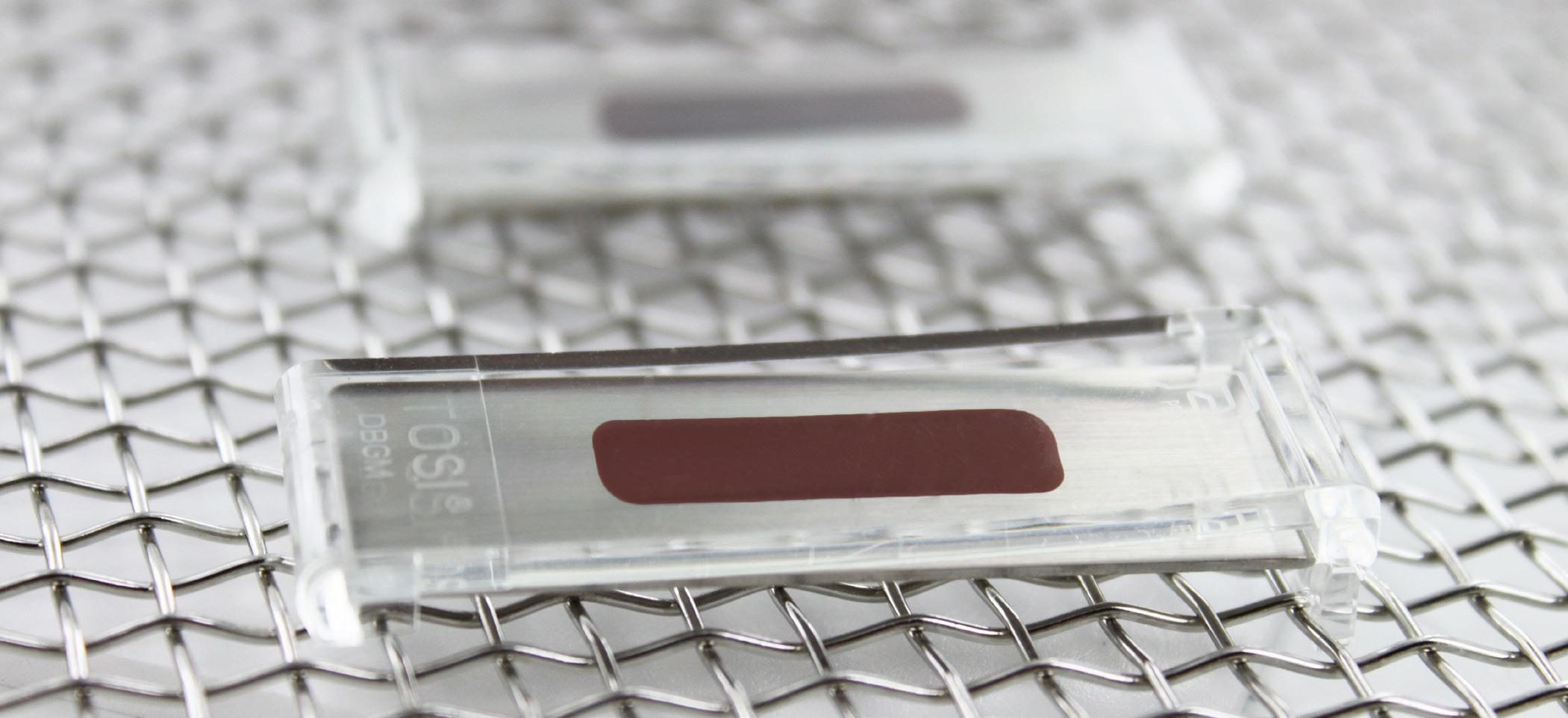
Healthmark continuously strives to create educational op portunities for health care professionals to earn CEUs. Health care professionals can register directly on the website at http:// hmark.com/education.php.
In addition to the webinars of fered, Healthmark provides a unique free service at Crazy4Clean.com. It’s a website that consists of educational games designed to teach health care professionals about proper repro cessing of instruments/equipment while earning free CEUs. At the end of each game, players receive a free CEU by completing a quiz based on what they’ve learned.
StyleYourPPE.com is a site cre ated by Healthmark where health care professionals can purchase PPE and other attire for individual use. Face masks, Cool Aids and other PPE attire are available as well as socks that are creatively designed to add a little fun to a serious dress code.
If you are looking for industry news, helpful hints and other information, Healthmark produces a weekly news letter that is distributed to thousands of readers. Each Healthmarket Digest features a story written by a member of the Healthmark team as well as a weekly coupon. You can sign up for the Healthmarket Digest weekly newsletter at Healthmarketdigest.com
For more information about Healthmark Industries, visit www.hmark.com or call 800-521-6224
1 AAMI (ST79 Comprehensive Guide to Steam Sterilization and Sterility Assur ance in Health Care Facilities)
2 AORN Recommended Practices for Cleaning and Care of Surgical Instru ments and Powered Equipment
3 https://www.cdc.gov/infectioncon trol/pdf/guidelines/environmentalguidelines-P.pdf
 TOSI
McGan Insulation
TOSI
McGan Insulation
October is Breast Cancer Awareness Month & Healthmark is all about Pink






























Choose from a variety of pink PPE apparel and accessories to show your support all month long
























hmark.com














Giving Back: Healthmark will be donating a portion of pink sales to Gilda’s Club, a cancer support community.
Sterile Processing Week is October 9-15th: Show appreciation for your sta with a “Heart of the Hospital” Fine Sign, PPE Decals or design your own Custom Headwear! 800.521.6224 healthmark@hmark.com

W hen you think of noisy environments, you probably think about a rock concert, sports stadium or airport runway. But what about the operating room?
Excessive noise can be a big problem in the operating room (OR) that leads to a number of negative consequences. Given all the different pieces of medical equipment in the OR, and the number of perioperative team members present, this noise can serve as a distraction to team members, which increases the risk of errors and jeopardizes patient safety.
“Excessive operating room noise can disrupt communication and distract clinicians during critical patient care activities,” says Emily Jones, MSN, RN, CNOR, NPD-BC, perioperative practice specialist with the Association of periOp erative Registered Nurses (AORN).
“The distractions associated with excessive noise in the operating room may interrupt patient care during critical activities,” adds Jones. “Distractions and noise contribute to the complexity of the care environment in the OR.”
Jones points to a systematic review of the perception and attitude toward noise and music in the OR published in 2021. The review concluded that higher levels of noise in the OR can have a negative impact on patient outcomes and adversely affect the performance of team members.
“This review found that excessive noise is often perceived as a source of stress in the OR,” she says.
David Taylor, MSN, RN, CNOR, the president of Resolute Advisory Group LLC, says he has been exposed to loud
noise throughout the decades he has spent working in the OR.
“My doctors have always listened to music in the OR, most of the time at high volume,” says Taylor. “This made it difficult to communicate with team members or count instruments, sharps and sponges. And anesthesia always had concerns that they could not hear their patient monitors and manage their patients.”
Taylor says that decades of exposure to excessive OR noise have left him with marked hearing loss. “None of the studies I have read have found excessive OR noise to be beneficial in any way,” he says.
Barbara L. DiTullio, DNP, RN, MA, CNOR, NEA-BC, senior clinical opera tions liaison, perioperative services at Beth Israel Deaconess Medical Center in Boston, Massachusetts, completed a study in 2019 focused on distractions that occur in the OR during wound closure and their role in suture needle injuries. In addition to other observable data, she measured OR noise in decibels to understand baseline data.
“I used the NIOSH threshold for noise in hospitals (maintaining a thera peutic environment) of 45 decibels and the WHO threshold of 35 decibels,” says DiTullio. “My baseline for procedures in the study exceeded both.”
The average decibel level DiTullio recorded during wound closure was 62, while the average peak decibel level was 104. In comparison, the average decibel level at a rock concert is between 90 and 120.
“One of the categories of distrac tion I observed was environmental noise, and this category had the highest number of occurrences observed in all cases,” says DiTullio.
Environmental noise included staff moving in and out of the OR, consolida tion and movement of people, equip ment and instrumentation, and music.
Technological interruptions were also observed, adds DiTullio, including pagers, telephones, overhead announce ments and the like.
The Joint Commission cites another study with similar results to DiTullio’s study that measured noise levels in OR trauma procedures. The average noise level here was 85 decibels, or almost double the NIOSH recommendation, and reached as high as 130 decibels.
Orthopedic and neurosurgery tend to have higher sustained noise levels with intermittent peak levels exceeding 100 decibels more than 40 percent of the time.
“Some the highest levels of OR noise come from powered surgical instruments such as high-speed drills, burs or saws used for bone dissection,” says Jones.
Meanwhile, studies focused on an esthesia have found that the noisiest pe riods during surgery are associated with induction and emergence of anesthesia. A lab study simulating OR background noise found a 17 percent reduction in the accuracy with which anesthesia residents detected changes in saturation on a pulse oximeter.
“What became clear in my study is that OR noise is distracting,” says DiTul lio. “This is true whether it’s essential communication related to the procedure, non-essential communication to help pass the time, or people entering the OR to ask a question or check on case progress.”
“Every incident may not result in a corresponding decibel increase, but each one draws attention away from the task at hand,” says DiTullio. “Even a momen tary interruption can cause harm.”
Madhavi Dave, MBA, CPPS, patient safety specialist with the Office of Quality and Patient Safety, Division of Healthcare Improvement, The Joint Commission, says he has encountered times when excessive noise impacted communication while working in the OR.
“Loud music or having many observers in the room (such as medical students and residents) are common sources of noise,” says Dave. “When this occurred, especially during critical phases of the surgery, the circulator typically addressed the situation by either letting the surgeon know that the music needed to be lowered or turned off or asking the observers to leave.”
The Joint Commission separates com mon sources of noise in the OR into two categories. The first category in cludes technological and environmental sources such as:
• Phones and paging systems (per sonal and overhead)
• Computers
• Wireless communication systems
• Music devices
• Medical equipment/devices
• Monitors and clinical alarms
• Metal equipment and instruments
• Environmental conditions (such as ventilation)
The second category includes behav ioral sources such as:
• Case-related conversations
• Non-case related conversations
• Patient care activities
• Staff entering and leaving the OR suite
“The most commonly cited sources of OR noise are non-case rel evant conversations, telephone calls, pagers and music,” says Erin Lawler, MS, CPPS, human factors engineer with the Office of Quality and Patient Safety, Division of Healthcare Improvement, The Joint Commission.
Clinical alarms are important, of course, but excessive alarms in the OR can be distracting and counterproductive.
“It’s important that alarms are kept to the minimum necessary to alert nurses to important changes in patient condition,” says Halley Ruppel, a core faculty member at the Center for Pediatric Clinical Effectiveness (CPCE) in Philadelphia. “Unfortunately, clinical alarms tend to be excessive and fre quently not urgent or actionable.”
Ruppel and her team at the Chil dren’s Hospital of Philadelphia Research Institute were recently awarded a $40,000 grant from the AAMI Foundation to explore ways to reduce alarm burdens.
“I’m interested in how we can build sustainable processes for evaluating and improving alarms and alarm management in acute care settings,” says Ruppel.
One way to do this is by giving clinical stakeholders access to up-to-date data analytics on types and frequencies of alarms occurring in their units.
“This could increase awareness and foster engagement in alarm manage ment efforts,” says Ruppel.
Ruppel and her team expect to iden tify functional specifications for alarm data analytics that can be used to develop an intervention model to test in future work. She hopes the project will optimize how technology functions in clinical care.
“Our ultimate goal is to develop a sustainable process for evaluating the dynamic clinical alarm system that nurses use while caring for patients,” says Ruppel. “Having this process in place will strengthen collaborations between healthcare technology management professionals and clinicians.”
In 2018, Glendyle Levinskas, BSN, RN, CNOR, a staff perioperative nurse at Vanderbilt University Medical Center Health System in Nashville, Tennessee, launched a project to try to deal with excessive OR noise after experiencing an event. “I was circulating one day when the increased noise level in the OR became a safety concern,” she says.
Levinskas elaborates: “The OR was crowded with multiple ongoing conver sations and music when an unexpected difficult intubation caused the anesthesia provider to call out in a loud voice, ‘Quiet in the room!’ Due to the noise distraction, she was unable to concentrate on performing a critical task for patient safety.”
Along with her colleague, research nurse special ist Elizabeth Card, APRN, FNP-BC, CPAN, CCRP, FAS
PAN, Levinskas wanted to develop evidence-based noise reduction strategies that engaged all team members in shaping sustainable solutions. They formed a task force that made a unified decision on noise reducing interventions to mitigate the increased noise levels in the OR, focusing especially on critical times of surgery.

“The measures begin with staff educa tion, noise awareness and outlined noise reducing behaviors and practices,” says Levinskas. “Specific noise reduction actions include being quiet during critical times by using the safety alert phrase, ‘Sound check.’ This should bring immediate quiet to the OR, including turning off or adjust ing music volumes, when a critical task is being performed.”
Levinskas and Card make an impor tant distinction between necessary and distracting noises. For example, an anesthesia machine, alarm or pulse oximeter beep, or move ment of carts is a necessary OR noise. Loud music, con versations about non-pro cedure related topics and unnecessary clanging of instruments are examples of distracting noises.
As part of their project, Levinskas and Card sur veyed surgical team mem bers to ask how OR noise was affecting them. Nearly half (47%) said that current noise lev els distracted them and caused stress.
Thus began a three-year process to create a culture shift to reduce distract ing OR noise. They formed a multidisci plinary OR noise reduction team with 30 members that shaped ongoing education to raise awareness about OR noise risks to health and patient safety.
“Our ultimate goal is to empower everyone in the OR with education and a mechanism to call out when noise levels impair communication and concentra tion,” says Levinskas. “It has been reward ing to see staff beginning to put the alert phrase into practice.”
The “AORN Guideline for Team Com munication” includes recommendations to help decrease noise levels and promote effective communication in the OR to create a safer environment.
“A no-interruption zone should be es tablished during critical phases of surgery
where nonessential conversation and dis tractions are stopped,” says Jones. “Critical phases may include anesthesia induction and emergence, the surgical time-out, medication management, surgical counts, critical dissections or anastomoses and specimen handling.”
ommendations to enhance team com munication and the culture of safety in the operating room for the entire perioperative team. It may be purchased at https://www.aorn.org/guidelines/ about-aorn-guidelines.
Lawler suggests that health care organizations adopt a systems approach and facilitate conditions that minimize distractions and noise that can impede concentration and communication in the OR. She lists the following recommendations from The Joint Commission:
• Create a no-interruption zone (or a “sterile cockpit”) during criti cal phases of a procedure during which non-essential conversation and activities are prohibited.
• Measure noise levels in the OR to provide evidence for noise-reduction strategies.
• Provide empirical data reflecting the efficacy of such strategies to the OR team, along with real-time information so they know when noise levels are exceeding recommended levels.
• Educate perioperative team members about the sources of OR noise, its impact on patient and staff safety, and noise reduction strategies.
“To minimize excessive noise during these critical phases, perioperative team members can refrain from non-essential conversations, lower the music volume and silence mobile devices,” Jones adds. “Any team member should feel supported in calling for a ‘safety pause’ if a distraction or interruption occurs that could affect patient safety.”
The “AORN Position Statement on Managing Distractions and Noise During Perioperative Care” contains more detailed strategies for decreasing excessive OR noise. A free PDF may be downloaded at https://www.aorn.org/-/media/aorn/ guidelines/position-statements/posstatsafety-distractions-and-noise.pdf.

Meanwhile, the “AORN Guideline for Team Communication” includes rec
• Consider equipment alternatives that produce less noise whenever possible.
• Perform simulation and training to model noise reduction strategies.
“We have long since normalized all of the noise and distractions that are experienced in the OR,” says DiTuillio. “Unfortunately, few people realize how much this impacts our daily work or how big a threat it poses to patient safety.”
Levinskas believes that team en gagement is the biggest key to reducing OR noise.
“Noise production is caused by everyone, so noise reduction calls for everyone to be involved in addressing the problem,” she says.
W
hen Summer Bryant, DNP, RN, CENP, CMSRN, was a high-school student growing up outside of Topeka, Kansas, she recalled exploring “basically every health care career there was except nursing.” The daughter of a recreational therapist and a microbiologist, her first exposure to the world of health care came when she took a job in the dietary department at a local nursing home. Although she enjoyed caring for the people there, the work nurses at the facility did seemed to consist of serving up medication, which “didn’t look exciting” to her as a young woman.
By the time Bryant enrolled at the University of Kansas, she finally began to explore nursing and discovered the career that she would make her own for the next 20 years. In 2000, she earned her bachelor’s degree of science in nursing (BSN) from the University of Kansas.
 Senior Managing Consultant, Berkeley Research Group, Healthcare Performance Improvement
SPOTLIGHT Summer Bryant
Senior Managing Consultant, Berkeley Research Group, Healthcare Performance Improvement
SPOTLIGHT Summer Bryant
She returned for a master’s degree (MS) in nursing organizational leadership in 2008, and her doctorate of nursing prac tice (DNP) in 2018.
All along the way, Bryant continued to work at the University of Kansas Health System. Her first assignments included caring for orthopedic, uro logic and otolaryngologic patients in the medical-surgical unit.
“They were there with you for just a little bit; then you got to help them go on to a rehab facility and get on their path to getting better,” she said.
Bryant continued to grow her exper tise as the facility expanded its service line but remained mostly within the med/surg area. Her reasons for staying included her interest in the patients and the variety of technologies that accompa nied the practice.

When she was offered the role of nurse manager in the trauma and general surgery unit, Bryant began par ticipating more with her local chapter of the Academy of Medical-Surgical Nurses (AMSN). After joining some committees, and eventually the AMSN board of directors, she was elected AMSN president, a role she is currently in her second year of fulfilling.
And in 2019, Bryant took on a dif ferent challenge — that of leaving the university medical center to become a senior managing consultant with the healthcare performance improve ment division of the Berkeley Research Group. Bryant said it’s been a great opportunity to leverage her doctorate in organizational nursing in addition to her years of experience in the field.
“I went from the manager role to speaking regularly with hospital execu tives about where they were, where they could go and how could they get there,” she said. “I got to immediately use my new skill set, and be able to capitalize on the knowledge I’ve had through my whole career.”
“I really enjoy what I do at this point,” Bryant said. “I feel like I get to have a bigger impact on health care because I
get to travel across the country. I don’t look narrowly anymore. My eye’s on the big picture, as compared to when I first began working as a nurse.”
Bryant also is conscious of the impact that her work in consultancy could have on the nursing profession at large, par ticularly through the lens of her AMSN leadership roles. When she’s visiting a new hospital, she considers the opportu nities she has to influence the direction of her profession on the whole.
“I think AMSN is a really great organization that I don’t think a lot of people know about,” Bryant said. “When I’m out and about, I try to connect some of those dots. One of our goals is to help people see the bigger picture. We have new competencies for medical/surgical nursing, and we hope to use those to help build programs: individual nurses can use them to see where they’re at, and health systems and institutions can use them to perform an evaluation process.”
“In nursing leadership, we’re only as strong as our weakest link,” she said. “When nursing leaders can get those nurses who are caring at the bedside involved in the decision-making process, that’s better for everybody. The nurse has a voice in how that care is provided, the CNO has buy-in from staff to implement
those changes and improve outcomes, and it helps decrease nursing turnover.”
Bryant believes that some nurses “just want to get involved” because of the nature of their personalities. As a bedside nurse, she would involve herself in a committee or work group because she wanted to be a problem-solver. She also acknowledges that not every hospital has embraced the same culture of eliciting feedback and participation from its stake holders “so they know what they need and what the gaps are before everything gets started.”
“I think you have individual initia tives and cultures that build up, so it happens more automatically,” Bryant said. “Now I speak to [different people within an organization], and get to have those conversations. The organiza tional hierarchy is gone. As consultants, we can bring our experiences from all across the country; we have access to data and colleagues, and we can pro vide successful ideas for change. We’re the outside objective observer; that 30,000-foot view looking down that can give them that perspective.”
Bryant said she also values the va riety of practice areas in which nurses can engage with their coworkers and the field at large. Although she never foresaw herself as a traveling consul tant, Bryant believes her best opportu nities have come when she took a leap of faith into something new. There’s a lesson in there for anyone looking for an opportunity to grow, she said.
“When someone says, ‘I think you should try this,’ say yes to that,” Bry ant said. “It doesn’t hurt to give it a try. And don’t be afraid to speak up; I think I wish I would have been that squeaky wheel a little bit more. The story you tell will be influential when you get to the right person.”
When she’s not traveling on as signment, Bryant spends time with her family and pets. She is a sports enthusiast, especially when it comes to Major League Soccer and college basketball.
Summer Bryant“I don’t look narrowly anymore. My eye’s on the big picture, as compared to when I first began working as a nurse.”
The motivation to lose weight, burn fat or get strong usually comes with the idea that one must really turn up the intensity of their workouts. Most gravitate to sprint intervals, box jumps and plyometrics exercises. Well, before you challenge your body with these higher intensity movements, you should really learn to absorb and control the brakes first.
For example, you wouldn’t drive a car or get on a bike without understanding how the brakes work. You wouldn’t be taught how to go down a mountain on skies before being instructed on how to slow down. The same should go before jump ing into high-intensity exercises. Prepping the body appropriately for high-intensity exercises is important because it helps stabilize and strengthen the ankle, knee and hip joints. This will decrease the chances of injury and increase the chances of improving performance. So, why not work on it?
Here are two great exercises that work on overall absorption, core and joint strength.

For all beginners, I highly recommend doing the Global Extension Absorb
drill first. This exercise will begin with a full global extension of the body. We do this because we don’t want to worry about leaving the ground, the focus is on how we would land if we were off the ground. So, by coming up on your toes it allows you to have enough distance off the ground to create proper force on the way down. Come up onto your toes and reach as high as possible with your arms while taking in a deep breath. Once fully extended, throw your arms down forcefully as you bring your body from a tall position to about a 90-degree squat. In the video, you should be able to hear my heels hit the floor. You’ll also notice I come to a complete stop with my arms by my side. This exercise isn’t meant to be repeated back-to-back. You want to focus on one rep at a time as you focus on the brakes. So, generate enough force into the ground to stop your body using your ankles, knees, hips and core properly to absorb that said force. The purpose of staying isolated in that position is to ensure stability.
For example, you might slam down, but be in a consistent forward lean, which would mean on the way down you didn’t drive your heels into the floor. If you are unable to stay completely still during the landing, try to slow the force down until your able to control your
body completely at the bottom position. I recommend doing 2 or 3 sets of 6 to 8 reps before getting into your high-inten sity movements.
The second exercise is a little more advanced. It is the Global Extension Split Absorb. Athletes, heavy runners, cyclists and anyone really looking to improve their athletic performance should give this exercise a try. Because of the split position, you’ll be landing with more force on the front foot/leg which will put more stress on that same ankle, knee, hip and core but slightly differently than the previous exercise. The same concepts will apply as before. You want to get fully ex tended, drive all that force into the floor and absorb with proper control. I would recommend doing about 2 or 3 sets of 5 to 6 reps per side. Now that your brakes are fully prepped, enjoy the higher inten sity movements with an added sense of strength and control. Enjoy your move ments and stay active.
– Miguel J. Ortiz is a personal trainer in Atlanta, Georgia. He is a Master Trainer for Pain-Free Performance and a Certified Nutritional Consultant with more than a decade of profes sional experience. He can be found on Instagram at @migueljortiz. You can find videos of the exercises men tioned in this column on his YouTube channel at tinyurl.com/ORTfitness.

















 By Daniel Bobinski
By Daniel Bobinski
A wonderful pattern exists in the best-selling book, “Seven Habits of Highly Effective People” by Stephen Covey. In the first three habits, what Covey calls the habits of independence, we learn that all things are created twice. First, they are created mentally, then they are created physically. In these habits of independence, Covey lays out the two-step creation process in Habits Two and Three; Begin With the End in Mind (Habit 2), and Put First Things First (Habit 3). Habit Two is the mental step of planning, and Habit Three is the physical step of acting in the order of our priorities.
This pattern duplicates in the second three habits, what Covey calls habits of inter-dependence. The habits of inter-dependence give us tools for building productive and effective rela tionships. Habit Four, Think Win-Win, is the mental step, and Habit Five is the physical process one takes to put Habit Four into practice. Habit Five is called, “Seek First to Understand; Then be Understood.”
The order is important.
1. Seek first to understand
2. Then be understood
Seeking first to understand gives
us answers for how the other person defines a win. This is the “consider ation” part of Think Win-Win, which I’ve addressed previously in this space. Remember, to be successful at this, you must truly want to understand how the other person defines a win. If people think you’re just going through the mo tions and don’t really care about their needs and desires, they won’t believe you’re genuine and the effectiveness of your relationship will suffer.
Why is the order important? Be cause as the adage goes, people don’t care how much you know until they know how much you care. People want to be heard. As Covey puts it, being heard is the psychological equivalence of air. If people don’t get air, they will fight to get it. Similarly, if people don’t feel heard, they will fight to be understood. Therefore, in accordance with Habit Five, we should seek first to understand.
At this point I should state that we can express an understanding of someone’s perspective even if we don’t agree with said perspective. Someone may tell us he believes dogs are better than cats. We can seek to understand why the person believes this without mocking or criticizing his conclusion. I’m using a simple example, but my point is that I believe that we, as a soci ety, have been steadily losing our ability to acknowledge differing points of view
without mocking or being derogatory.
The second step in Habit Five is to be understood. This is acting out the courage part of Think Win-Win. It’s standing up for what you need or desire. Brashness or rudeness have no place here. After seeking to understand the other person’s point of view, we simply express what we want.
As I mentioned, this requires a bit of courage, which comes easier to some than others. Fear of criticism, fear of failure and fear of rejection may get in our way and keep us from standing up for ourselves. We’ll address that in a future column, but for now, know that the order of how we discuss things makes a huge impact when it comes to creating effective relationships.
Daniel Bobinski, who has a doctorate in theology, is a bestselling author and a popular speaker at conferences and re treats. For more than 30 years he’s been working with teams and individuals (1:1 coaching) to help them achieve excellence. He was also teaching Emotional Intelligence since before it was a thing. Reach him by email at DanielBobinski@protonmail.com or 208-375-7606.

The nation’s blood and plasma supply dropped to historic lows during the COVID-19 pandemic. While some areas of the country have seen improvement, other areas are still struggling to meet the demand. Blood and plasma are needed on an ongoing basis to treat a variety of life-threatening conditions, which is why the U.S. Department of Health and Human Services (HHS), has launched a new campaign, Giving = Living.
The campaign aims to increase awareness of the importance of donating blood and plasma and to encourage Americans to create new, regular donation habits. Every two seconds, someone in the United States needs blood for surgeries, can cer treatments, childbirth, anemia, serious injuries and blood disorders. For many people, receiving a blood transfusion is lifesaving. Similarly, patients with rare diseases rely on medi cal treatments every day that are only available when people roll up their sleeves and give source plasma.
“A consistent supply of blood and plasma is critical to the health of our nation,” said HHS Assistant Secretary for Health Admiral Rachel L. Levine, MD. “There is no replace ment for human blood and plasma. We simply need more people to give and to give regularly. We also need donors from diverse ethnic and racial backgrounds.”
Diversity in the blood supply is important because cer tain blood types are unique to specific groups. Blood from a donor of a similar ethnic background is less likely to be rejected by a patient and often results in fewer complications after a transfusion. In addition, some people have rare blood types and need transfusions of compatible blood. Having a large, diverse pool of blood donors ensures that all patients
will have access to the blood they need, when they need it. Despite this, America’s Blood Centers estimates, that less than 20 percent of all blood donations currently come from communities of color.

The campaign, funded through the Coronavirus Aid, Re lief, and Economic Security (CARES) Act, features personal stories of people who benefit from donations:
• Heather of Dallas-Ft. Worth, Texas is an individual living with sickle cell disease who has had multiple blood trans fusions and has had to wait, sometimes days, for lifesaving blood to become available. She depends on many people who give blood.
• Earl of Scranton, Pa. was badly wounded by a roadside bomb in Afghanistan, which led to massive blood loss and a need to have his leg amputated. He survived because of several blood transfusions.
• Alice of Houston, Texas requires a plasma-based therapy to treat a rare disease called common variable immunode ficiency. This therapy helps to replace the antibodies her body should be making and is essential to her survival.
• Crystal of Birmingham, Ala. is a wife and mom of two boys who was diagnosed with two neuromuscular auto immune conditions that resulted in her going from being totally independent to suddenly being unable to feed, bathe, or dress herself. While there is no cure for her con dition, plasma-based treatments and a healthier lifestyle are helping her regain her mobility.
Organizations from across the blood and plasma industries were instrumental in creating this campaign.
Visit hhs.gov/givingequalsliving to learn more about the importance of donation and make an appointment at a donation location near you.
A few issues ago, I explained why your number one mission in the grocery store needs to be reading ingredient labels. Front of the box labels and misleading packaging is about marketing and profits, but the ingredient list is where the rubber meets the road. Most of us purchase mayonnaise so it is my favorite way to explain why label reading (and the knowledge needed to back it up) is so important.
It may seem a bit strange, but mayonnaise is really a convenience food. You may not have made homemade mayo, but it is not hard. I have made it with just egg yolk, salt, vinegar and oil. Even though I can make it from scratch, I generally buy my mayo for the added convenience. Rest assured; you can grab mayo at the supermarket. Eating better does not mean you have to make it all from scratch, but you need information to make wise choices. Use the chart and tips below to become a savvy shopper of mayo (and more.)
As you work your way from the BAD to the BEST mayonnaise, here are the key takeaways from these ingredient lists.
• Length: The BAD mayo (a popular major brand) has 15 ingredients listed. The “natural flavors” listed contain many more. The BEST one has only 6 ingredients. It is widely available as well.
• Whole ingredients: Ingredients should be recognizable food – just like the stuff you have in your kitchen. When is the last time you restocked your Calcium Disodium
EDTA? The BETTER and BEST mayonnaises have real food ingre dients.
• Fillers: See water in the BAD and BETTER choices? Mayo does not usually contain water. That’s filler and makes it cheaper to produce. Water is the top ingredient in the BAD choice meaning it is mostly water. Salt, honey and water are the three top ingredients in the BET TER mayo. You are buying sweet and salty water.
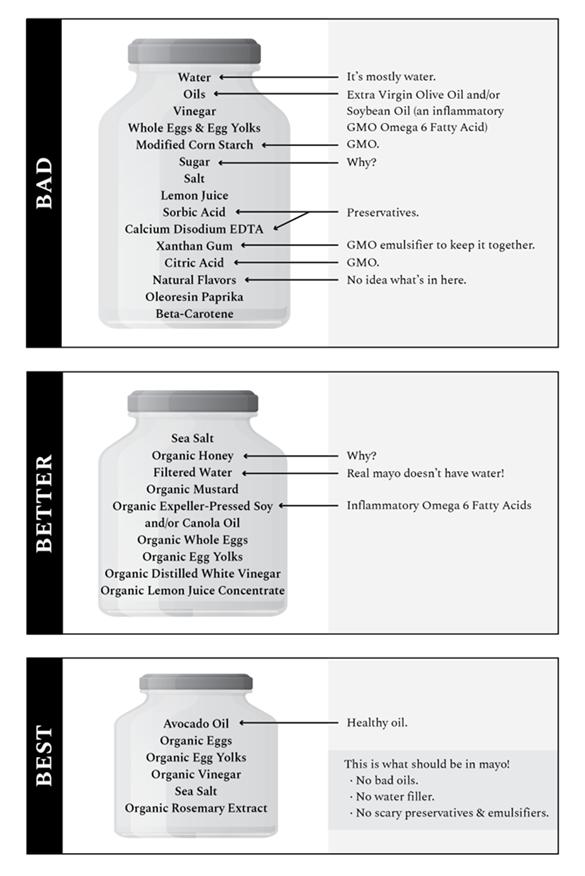
• Oils: This is a big one. Inflam matory Omega 6 oils are a huge contributor to the epic inflam mation pandemic in the United States. We need Omega 6 fats, but in a healthy balance with Omega 3 fats. Our Standard American Diet is way too rich in Omega 6 seed oils like soy, canola and corn. These oils drive inflamma tion. Inflammation is a root cause of most disease – from asthma, to arthritis, and even cancer and depression. We can help tam per down the inflammation by consuming fewer Omega 6 fats. Avoiding inflammatory seed oils is a major way to make that change. Choosing healthier fats is a pow erful tool we have to make better food choices. The BEST mayo is made with avocado oil which is a great choice.
• GMO: I avoid GMO ingredi ents when I can. GMO crops like corn, canola and soy are genetical ly engineered to withstand being
sprayed with glyphosate to kill weeds. What is the effect of glyphosate on humans?
A 2019 meta-analysis concludes that glyphosate increases the risk of non-Hodgkin lymphoma by 41 percent. 1

In 2019, researchers at Purdue University helped dis cover that the most aggressive form of breast cancer can be caused by glyphosate. 2
The World Health Organization declared glyphosate a probable human carcinogen in 2015. California fol lowed suit.
I hope I have empowered you to make impactful choices for your and your loved one’s health. The BEST mayo is also the one with the best flavor in my opinion. Real whole foods taste great.
1 Zhang, Luoping, et al. “Exposure to Glyphosate-Based Herbicides and Risk for Non-Hodgkin Lymphoma: A MetaAnalysis and Supporting Evidence.” Mutation Research/ Reviews in Mutation Research, vol. 781, no. July-September
2019, Feb. 2019, pp. 186–206, www.sciencedirect.com/ science/article/pii/S1383574218300887, 10.1016/j. mrrev.2019.02.001.
2 Purdue News Service. “Can Herbicides Cause Breast Cancer? Purdue and INSERM Scientists Discover a Piece to the Puzzle.” Purdue.edu, 2019, www.purdue.edu/newsroom/ releases/2019/Q3/can-herbicides-cause-breast-cancer-purdueand-inserm-scientists-discover-a-piece-to-the-puzzle..html. Accessed 7 Dec. 2019.
Kirsten Serrano is a nutrition con sultant, chef, farmer, food literacy educator and the best-selling author of “Eat to Your Advantage.” You can find out more about her work at SmallWonderFood.com.


• 1 tablespoon Country Crock Plant Butter with Olive Oil
• 1/2 cup chopped white or yellow onion
• 1/2 teaspoon finely chopped garlic
• 1/2 cup tomato paste
• 1 pinch red pepper flakes
• 1/4 cup (2 fluid ounces) vodka
• 16 fluid ounces Country Crock Plant Cream
• 1/4 cup (2 fluid ounces) water
• 3 cups dry penne pasta, cooked and drained
• 1/4 cup grated vegan Parmesan cheese
• 1/2 teaspoon kosher salt
• 1/4 cup loosely packed fresh basil leaves
By family featuresGathering together to enjoy a meal at the family table or a sweet treat at the end of a long day is what time with loved ones is all about. Turning to beloved classics can bring everyone running to the kitchen to share the flavors of those familiar favorites.
Savor the timeless taste of pasta with this Penne Alla Vodka, a classic dish high on flavor and low on hassle so you can have a meal ready in just 30 minutes. Plus, it offers an alternative to tra ditional recipes by using Country Crock Plant
Cream, a new dairy-free substitute for heavy whipping cream perfect for using in a variety of your favorite dishes.
Made with delicious plant-powered ingre dients, it provides the taste of heavy whipping cream without the heaviness. As a 100% vegan, dairy-free and soy-free solution, it’s a 1-for-1 swap for heavy whipping cream in cooking and baking recipes, making it ideal to have on hand year-round.
Visit CountryCrock.com for more ways to elevate weeknight meals and desserts.

Prep time: 10 minutes
Total time: 30 minutes
Servings: 5
1. In pan over moderate heat, melt plant butter. Add onions and garlic. Cover and cook until onions are translucent, about 5 minutes.
2. Add tomato paste and red pepper flakes. Cook until tomato paste starts to lightly brown.
3. Add vodka and stir well, scraping bits of browned tomato paste from bottom of pan. Cook over high heat until liquid is reduced by about half to concentrate flavors.
4. Add plant cream and water; stir to incorporate tomato paste evenly. Bring to simmer.
5. Toss in cooked pasta. Add vegan Parmesan, salt and fresh basil.
AIV Inc. 4
ALCO Sales & Service Co. 15
C Change Surgical 11
Cygnus Medical 64
C Change Surgical 11
CARTS/CABINETS
ALCO Sales & Service Co. 15
Cygnus Medical 64 Healthmark Industries Company, Inc. 47
TouchPoint Medical 9
CS/SPD
MD Technologies Inc. 55
Ruhof Corporation 2
DISINFECTION
Cygnus Medical 64 Ruhof Corporation 2-3
ALCO Sales & Service Co. 15
Cygnus Medical 64 Healthmark Industries Company, Inc. 47 MD Technologies Inc. 55
Ruhof Corporation 2-3
FALL PREVENTION
ALCO Sales & Service Co. 15 Encompass Group 19 FLUID MANAGEMENT
MD Technologies Inc. 55
GENERAL AIV Inc. 4
HOSPITAL BEDS/PARTS
ALCO Sales & Service Co. 15
Encompass Group 19 Healthmark Industries Company, Inc. 47
I.C. Medical, INC. 63
Innovative Medical Products 5
MD Technologies Inc. 55 Ruhof Corporation 2-3
TouchPoint Medical 9
ALCO Sales & Service Co. 15
Cygnus Medical 64 Encompass Group 19 Healthmark Industries Company, Inc. 47 MD Technologies Inc. 55 Ruhof Corporation 2-3
INSTRUMENT STORAGE/TRANSPORT
Cygnus Medical 64 Ruhof Corporation 2-3
ONLINE RESOURCE
OR Today Webinar Series 63
OR TABLES/BOOMS/ACCESSORIES
Innovative Medical Products 5 OTHER
AIV Inc. 4
AIV Inc. 4
Encompass Group 19
Cygnus Medical 64 Innovative Medical Products 5
Cygnus Medical 64 REPROCESSING STATIONS MD Technologies Inc. 55 Ruhof Corporation 2-3
Healthmark Industries Company, Inc. 47
SINKS
Ruhof Corporation 2-3
SMOKE EVACUATION
I.C. Medical, INC. 63 STERILIZATION
Cygnus Medical 64 Healthmark Industries Company, Inc. 47 MD Technologies Inc. 55
SURGICAL
MD Technologies Inc. 55
C Change Surgical 11 Cygnus Medical 64 Healthmark Industries Company, Inc. 47
AIV Inc. 4
TEMPERATURE MANAGEMENT
C Change Surgical 11 Encompass Group 19
WASTE MANAGEMENT
MD Technologies Inc. 55
The I.C. Medical SAFEGUARD BLUE ® Hydrophobic ULPA Filter delivers >99.9999% e iciency on all particle sizes down to 0.03 micron, including all SARS-CoV-2 particles which range from 0.06-0.14 micron.
SAFEGUARD BLUE ® Hydrophobic ULPA with Built-In Fluid Trap simultaneously ensures that evacuated surgical plumes,


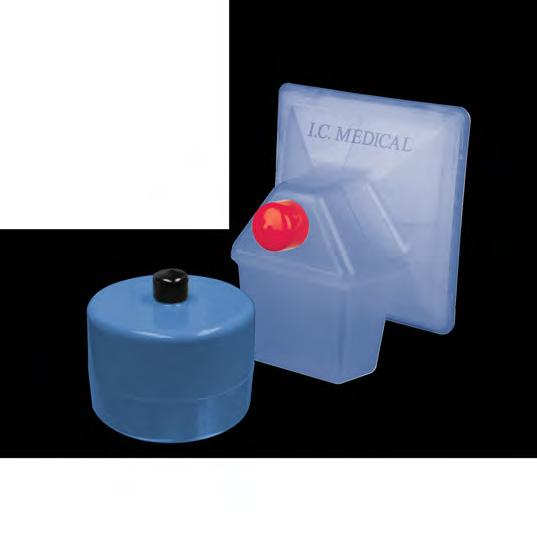

icient,