Expansion of portable ultrasound techniques supports life-saving differential diagnoses
Page 32
Kenneth Saltrick, President of Engineering Services in Twinsburg, Ohio, knows from his long experience that C-arm machines themselves are absolute workhorses.
For customers looking to blend the gap between expensive OEM and unreliable used assemblies, WE have your solution.
Our complete repair contains a new cable assembly, utilizing all OEM cable and components with a harvested plate and connector housing as they are proprietary items. These completely repaired products will have a significant cost savings with build quality above new OEM products and carry a warranty of 180 days, which is untouchable in the market.
CHANGING THE NARRATIVE
CHANGE
Through innovation we want to change the perspective in the imaging space.
CONTROL
We want to put the control back in the hands of the decision makers.
COST SAVINGS
We understand our customers goals and we are developing a clear pathway to measurable savings.
Dan Faulkner, CT Tech
Dan has been with Tri-Imaging for 11 years!
FEATURES
DIRECTOR’S CUT
Difficult conversations in healthcare are particularly sensitive because they directly affect patient outcomes, but they can build trust and improve performance.
COVER STORY
POCUS use continues to grow as technology provides more clinical uses for the technology.
RISING STAR
Ohio State University Lead MRI Technologist Kelly Jo Buckley is passionate about imaging.
PRODUCT FOCUS
Manufacturers share the latest and greatest in ultrasound systems.
IMAGING NEWS
Discover the latest news and trends in diagnostic imaging.
EMOTIONAL INTELLIGENCE
If employees are truly an organization’s greatest asset, then leadership must balance the needs of the organization with those of its people.
President
Vice
Kristin
Vice
Cindy
Accounting
FOCUS IN
DAVID BUCZKOWSKI, MSA, RT (R) (CT)
Corewell Health Grand Rapids Michigan Imaging Director David Buczkowski, MSA, RT (R) (CT), started his career in the 1980s. The diagnostic imaging realm has undergone many changes, through the decades.
“I started my career in 1987 as an X-ray intern. I have held many roles over the last 37 years,” Buczkowski says. His “many roles” include radiographer lead, CT lead, CT manager, pediatric operations manager, adult/peds
operations manager, senior project specialist, director of imaging/lab/respiratory therapy, and his current role of director of imaging over seven community hospitals and ambulatory imaging.
When asked about his greatest accomplishment, Buczkowski is quick to mention fatherhood along with his career achievements.
“Many doors opened for roles and promotions throughout my career. Having three young daughters during that phase of life, I completed my bachelors and
David Buczkowski is an accomplished imaging leader and a proud father of three daughters.
master’s while balancing family and work,” he explains. It is a career path that continues to reward him daily.
“I love building relationships, moving forward with projects, and trying new business models,” Buczkowski says. “Every day can be different; I am a firm believer that there is a solution for any operational situation and our great team can solve them.”
As a team leader, Buczkowski describes himself as “firm, fair and consistent.”
He adds that his goal is to be “transparent, honest and caring for the team.”
“An ex-COO I met with quarterly gave me great advice – ‘lead with influence,’” he adds. “I carry that with me today. It is best to look at any issue through many lenses and angles before making decisions. Using your strong relationships and influences can get you to making the best decision.”
Almost four decades of experience has taught Buczkowski that change happens and happens often in imaging. Looking ahead, he expects to see “continuous change, productivity increases, and new innovative technology” in imaging.
“Every imaging leader needs to embrace change rapidly and acclimate accordingly to best serve our patients,” Buczkowski adds.
He says another vital skill for imaging leaders is active listening.
“Listening is key. Respect your team and their input,” Buczkowski says. “Starting each meeting by putting the patient first can assist all with coming up with the best path forward. I am a fan of piloting things in three-month increments. So much is learned by doing experiments without doing major change management versus doing
Q&A
1. What is the last book you read? Or what book are you reading currently? I do a fair amount of travel TuesdayThursday. I enjoy audio books and “Extreme Leadership” by Jocko Willink has been my go-to.
2. Favorite movie? Any thriller or drama. “Landman” has been my favorite TV show lately.
3. What is something most of your coworkers do not know about you? Highly active with The Knights of Columbus as Grand Knight, and community outreach. Sponsor a young girl in Haiti for last 7 years so she can go to school.
4. Who is your mentor? To be honest any leader or technologist. I harvest knowledge daily and true mentorship is bidirectional and rarely carries a title.
5. What is one thing you do every morning to start your day? I look at health related magazines, surf online for hot topics, read up on politics and read the AHRA discussion
change management and then in the end seeing that it did not work.”
His advice to the next generation of leaders includes listening and honesty.
“Be open and honest in the interview process.
Going over the expectations and time commitment that will be required that first 12-18 months of learning new processes and software tools is key,” Buczkowski says. “Also, continue to remind them that they are supported by every leader, and you will never feel like you are on an island. Our imaging leadership team at Corewell Health has a system model and we all help each other regardless of geographical boundaries.”
Away from work, Buczkowski enjoys time with family. His wife, Rose, is an experienced sonographer of 35 years. He has three daughters in Erika, Megan and Lauren. And, among his greatest accomplishments is his recent new title of Grandpa. •
board online with a nice cup of coffee. Wonderful way to frame up my mind before starting work.
6. Best advice you ever received? Continue to be optimistic and kind every day. Do not sweat the small stuff. Keep that mood elevator starting with curious!
7. Who has had the biggest influence on your life? My father. From age 14 working on a farm and many jobs at an early age. Indirectly he truly created a magnificent work ethic for me to carry forward.
8. What would your superpower be? Ability to snap my fingers and go into a deep sleep, I function on little sleep. But would enjoy a solid 8 hours.
9. What are your hobbies? Mountain biking, going to a gym, great movie at the theatre and plan hiking spots when on vacations.
10. What is your perfect meal? Thai, Mexican, Steak – I am open to any new venue to experience.
RISING STAR
KELLY JO BUCKLEY, RT (R)(M)(MR) LEAD MRI TECHNOLOGIST, OHIO STATE UNIVERSITY
Ohio State University Lead MRI Technologist Kelly Jo Buckley, RT (R)(M)(MR), is currently earning a Bachelor of Biomedical Science in Diagnostic Imaging. She is an Ohio native eager to learn and make a positive impact on her community.
ICE Magazine recently found out more about her journey and her goals for the future.
Q: WHERE DID YOU GROW UP?
A: Martins Ferry, Ohio
Q: WHERE DID YOU RECEIVE YOUR IMAGING TRAINING/ EDUCATION?
A: I was accepted into a hospital-based radiology program at Ohio Valley Medical Center in Wheeling, West Virginia, that started a month after high school graduation. I took night classes at West Virginia Community College to obtain my associate degree. After passing my registry in radiology, I went on to take my registry in mammography and MRI as well.
Q: HOW DID YOU FIRST DECIDE TO START WORKING IN IMAGING?
A: I had a deep understanding and love for science. I would read for hours about anything from geology, astrology,
exploration, gardening. I was very active and loved exploring. My mom was the one who talked me into pursing radiology. I excelled in all my science classes and was intrigued by anatomy. I remember dissecting a cat and frog in biology class and my lab partner wouldn’t touch it! I loved everything about those classes and once I started in radiology I was hooked!
Q: WHAT IS THE MOST REWARDING ASPECT OF YOUR JOB?
A: One of the most rewarding aspects of working in MRI is the ability to make a meaningful difference in patients’ lives. We play a critical role in helping the physicians diagnose and treat and working with them is a gift to be able to learn from them as well. Watching how our technical expertise contributes to improved outcomes is a powerful reminder of the importance of our work.
Q: WHAT DO YOU LIKE MOST ABOUT YOUR POSITION?
A: The combination of technical expertise and patient interaction. It’s satisfying to operate advanced imaging technology while also making a patient feel comfortable and supported during their scans. I work with an amazing group of people and that makes my job even more rewarding. The ability to utilize different avenues of MRI in one day, whether it would be functional MRI, radiation oncology, OR MRI, or scanning any and all devices!
Q: WHAT INTERESTS YOU THE MOST ABOUT THE IMAGING FIELD?
A: The opportunity for learning and growth is constantly evolving with the advancements in technology. I’m always expanding my knowledge and staying at the forefront of innovation. This keeps me engaged and allows me to refine my skills. I enjoy improving processes. I’m very passionate about figuring out ways to improve work flow and productivity.
Q: WHAT HAS BEEN YOUR GREATEST ACCOMPLISHMENT IN YOUR FIELD THUS FAR?
A: Successful functional MRI program, developing a schedule template to improve patient work flow, involved in creating guidelines for conditional and non-conditional cardiac devices, involved in several committees such as the MRI optimization committee to improve turnaround times and effective utilization of order priority scoring project.
Q: WHAT GOALS DO YOU HAVE FOR YOURSELF IN THE NEXT 5 YEARS?
A: Present at a major healthcare conference. Complete my master’s in healthcare administration. •
FUN FACTS
FAVORITE HOBBY: I love the outdoors! Anything from hiking to gardening.
FAVORITE SHOW: I don’t typically watch TV, but opt to read instead.
FAVORITE FOOD: Seafood!
FAVORITE VACATION SPOT: I love traveling and seeing new things, but my family and I spend a week every year at the same beach in North Carolina.
1 THING ON YOUR BUCKET LIST: Travel outside the country
SOMETHING YOUR CO-WORKERS
DON’T KNOW ABOUT YOU: I played the trumpet in the band in elementary school.
Clock Off THE
CHRIS BEASLEY, DIRECTOR
OF RADIOLOGY
UNIVERSITY OF MISSOURI HEALTHCARE
BY MATT SKOUFALOS
Throughout his 35-year medical imaging career, Chris Beasley has experienced sweeping shifts in the job. From starting as a darkroom tech in an outpatient imaging center in the 1980s to running the radiology department at the University of Missouri Healthcare, he’s held a variety of positions at facilities across the country.
But the pace of such a career can burn out even the most stalwart of hearts. In 2019, Beasley decided he needed a break
“After many years in the business, I was really tired,” Beasley said. “I took some time off and began looking after my health. One of the ways I was doing that was walking.”
His constitutionals took Beasley through the natural beauty of the Platte River trail systems in Casper, an 11mile network of old growth trees, wildlife sanctuaries and mountain views. The scenery that surrounded him offered the freedom to let his mind wander, and when it did, Beasley found himself visualizing elements of a story that started to coalesce in his head.
“I started to get these scenes in my mind, and when I came home, I would turn those into chapters,” he said. “I think it was just a moment that I had in time where I wasn’t in the daily grind of imaging, and allowing myself to do something other than imaging.”
Beasley describes himself as a reader with a preference for audio books and an interest in science fiction and crime thrillers, especially plots that involve a heist. He counts Tom Clancy as his favorite writer.
And yet, for the clarity of the imagery in his mind and his interest in literature, Beasley was a novice writer who hadn’t ever tried his hand at fiction writing. So, he began to explore the mechanics of crafting a story from the outside in.
“You realize that sometimes getting your thoughts out is the easy part; developing and getting your thoughts across correctly is the hard part,” Beasley said. “I took a page from radiologists: I came home, and I sat down, and started telling the story through voice dictation software.”
“I would come home, describe the scenes, pull it back apart, and try to format it as a book,” he said. “I could verbally get all of my thoughts out quickly, and then turn around and become an editor.”
The support he received from his wife, Deona, who became his first editor, was invaluable in the early going, Beasley said. With her help, he had the initial draft of a novel completed in five weeks.
The tale, “Executing Justice: Concrete, Crooks, and Blood,” is a story of a group of local people who find themselves dealing with an organized crime outfit exploiting the corruption in their community. Its central character, the enigmatic Eli, is introduced as “kind of the guy who guides things from the side,” Beasley said, while the supporting characters, three ordinary citizens, find themselves drawn deeper into “a dark place.”
“The theme is that one of our basic human needs, no matter who you are, is justice,” he said. “We need things to be fair, and we need things that are not right to get set right. I think we, as consumers of entertainment, love that stuff because we see the injustices in our work and in
society, and when we see heroes that can combat that stuff, we just love that.”
Beasley said the book reflects his own moral impulses, to “do the right thing and stand up for the right things when we see something that’s unjust.”
To polish up the work, he employed freelance editors from Fiverr, and quickly learned what every novice writer discovers: how to negotiate the relationship over your work with a colleague who’s not as attached to it in the same way. When he was satisfied with the finished product, Beasley published his story directly through Amazon.com as an independent writer. The book is available at https://a. co/d/5wAqUOP
“I really enjoyed the independent aspect of it, and not having to jump through the hoops of a publisher,” he said.
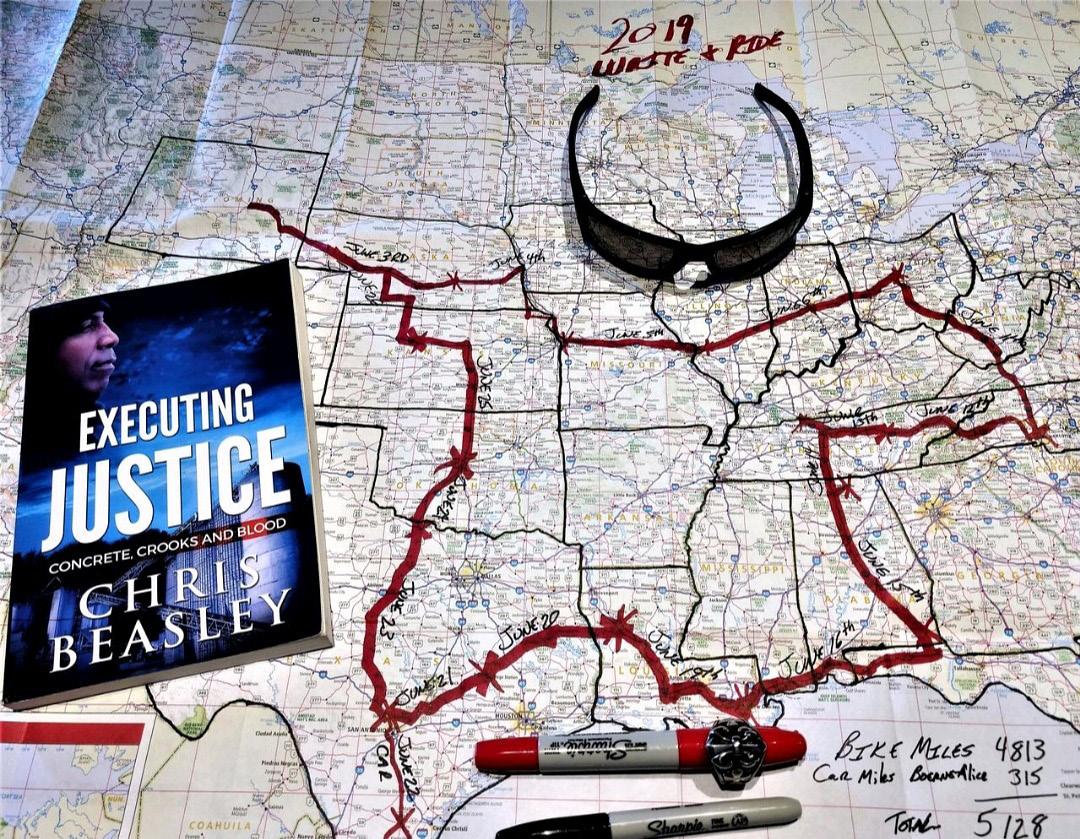
After the story was completed, Beasley promoted it with a multistate motorcycle tour that doubled as an opportunity to visit some former colleagues and coworkers from throughout his career.
“It was really a way to reconnect with folks that I had met over the previous 20 years,” Beasley said. “That was the best part. Any time I get a chance, I take my bike out when the weather’s good and I go for a ride.”
Although Beasley said he enjoyed the experience of writing, self-publishing, and promoting his work, he doesn’t believe he’ll have the capacity to revive the experience until retirement. The opportunity that presented itself to him the first time isn’t likely to come around again in his current work schedule.
“Doing what I do every day, I don’t have the emotional bank account to do it,” Beasley said. “Being in a very scientific career that is also financially driven; to escape all of that, I could escape into the story. You can take the fiction anywhere you want.”
... one of our basic human needs, no matter who you are, is justice.
He rode his Kawasaki Concours 14, a sport touring bike, from Wyoming to North Carolina, Tennessee, and down to Florida; then back through Alabama, Mississippi, Louisiana, Texas, Oklahoma, and Kansas before returning home. In all, his journey took him through 17 different states over a month and a half.
Even so, Beasley said, the opportunity to stretch his mind and heart into areas outside of his vocation were invaluable life experiences, and he would encourage anyone else to follow their curiosity in the same way.
“I think that everybody needs a moment in their life to explore a world outside of their profession, and that’s what it was for me,” Beasley said. “Everybody needs a way out of the grind to feed their soul, and for me that is through writing.” •
Chris Beasley promoted his novel and reconnected with friends during a multi-state motorcycle trek.
Imaging News
A LOOK AT WHAT’S CHANGING IN THE IMAGING INDUSTRY
FIRST U.S. INSTALLATION OF MAMMOMAT B.BRILLIANT MAMMOGRAPHY SYSTEM
GRACE Breast Imaging & Medical Spa of Iowa, with locations in Urbandale and Clive, recently became the first healthcare facility in the United States to install the new Mammomat B.brilliant. The first completely redesigned mammography platform from Siemens Healthineers in over a decade, the Mammomat B.brilliant includes new 3D image acquisition and image reconstruction technology as well as features for full-field digital mammography, or two-dimensional breast imaging; breast biopsy; and titanium contrast-enhanced mammography.
“At GRACE, our primary goal is to provide exceptional breast care to women,” said Andrea Lamphiear, MD, founder of GRACE Breast Imaging & Medical Spa. “Our decision to acquire the nation’s first Mammomat B.brilliant mammography system was driven by the cutting-edge technology of Siemens Healthineers, which offers unparalleled image quality for early breast cancer detection. We believe this will best help us expand our vision of providing individualized breast care in a wellnessbased and serene environment and making healthcare feel like self-care, while also allowing us, as radiologists, to have the best chance of finding breast cancer
at its earliest stage.”
Building on the 50-degree wide-angle image acquisition capabilities that are the hallmark of Siemens Healthineers and offering the widest angle available, the Mammomat B.brilliant introduces PlatinumTomo 3D technology that enables this wide-angle tomosynthesis acquisition in under five seconds. Wide-angle tomosynthesis technology separates overlapping layers of breast tissue to help visualize otherwise obscured lesions.
The system’s fast detector and new X-ray tube use flying focal-spot technology adapted from Siemens Healthineers computed tomography scanners to visualize microcalcifications more clearly. New UltraHD image reconstruction technology reduces metal artifacts, crisply visualizes calcifications, and offers customizable image settings. The system also provides a synthetic 2D image with no additional radiation exposure to the patient, reducing the radiologist’s need for full-field digital mammography images. Other features improve patient comfort, enhance user workflow, and improve user ergonomics compared to the system’s predecessor, the Mammomat Revelation.
MC2 X-RAY SYSTEM ACHIEVES FDA CLEARANCE
OXOS Medical has announced that its MC2 Portable X-ray System has achieved FDA 510(k) clearance and is now available for sale.
The MC2 device is portable and cordless, allowing healthcare practitioners to simplify the process of taking X-rays in traditional and nontraditional spaces. MC2 will have a profound impact on imaging by giving clinics:
In addition to static imaging capabilities, MC2’s 9” Class detector offers Dynamic Digital Radiography (DDR) – a first for a device of this size – as well as Fluoroscopy. When practitioners can quickly access accurate images, they can diagnose the patient swiftly and return them to regular activity.
Practitioners using the MC2 can take X-rays efficiently with easy training and setup, helping reduce office wait times and getting patients the care they need quicker. The device’s Viewfinder allows for quick positioning and alignment
of the X-ray beam, and its Patented Positioning System assists in alignment for image capture.
MC2’s lightweight, ergonomic design makes it easy to move the device to the point of need and will allow clinicians to maximize their limited space. In addition, MC2’s small scatter area and low radiation output can reduce the space and infrastructure needs required by larger systems.
Premium Quality
Exceptional Value
Impressive Warranty
MC2 is the latest release from OXOS, which launched the Micro C portable X-ray device in 2021. For the last three years, this portable solution has been used by clinics and athletic departments and has also brought X-ray capabilities to previously underserved areas.
“Everything we do at OXOS is about helping providers move into a new era of imaging,” said Dr. Gregory Kolovich, chief medical officer and OXOS co-founder.
“MC2 will simplify the imaging process, empowering clinicians to provide X-ray imaging using a device a fraction of the size. We can’t wait for practices to see the difference themselves.”
Replacement X-ray tubes for Radiography, R/F, Mobiles, C-Arms, And Mammography systems
• One-year-old company with 67 years of experience manufacturing and supplying X-ray tubes.
• High-quality components from IAE SpA, Europe’s premium X-ray tube manufacturer for 75 years.
Made in the USA with US and European components.
For a product list and prices contact us at:
Email: info@X-RayAmerica.com
Phone: 1.854.999.6888
Global: IAE.it
US Headquarters: X-RayAmerica.com
SUTTER HEALTH, GE HEALTHCARE ENTER PARTNERSHIP
Sutter Health and GE HealthCare have announced a seven-year strategic enterprise partnership, known as a Care Alliance, that aims to increase access to innovative imaging services and create a more seamless and coordinated experience for clinicians and patients across the Sutter Health system. The long-term collaboration will increase access to essential diagnostic care across California, providing patients with advanced technology in their own communities that can help enable quicker appointment scheduling, accelerated diagnostic imaging scan results, early diagnoses, greater convenience, and more consistent and timely care. This Care Alliance marks one of GE HealthCare’s largest ever enterprise strategic partnerships.
For Sutter, this alliance will help achieve faster access to novel equipment and technology solutions, as well as provide an innovative service delivery model with enhanced, reliable equipment availability. It is grounded in key goals, including expanded access to care, improved patient experience, more consistency regardless of care location, increased patient capacity, greater system integration and interoperability, and a timely refresh of needed equipment. It centers on several areas of collaboration, including optimized technology, an innovative service delivery model, advancing service line care at destination centers of excellence and digital integration.
The first key focus area of the Care Alliance is an accelerated technology program across the Sutter Health system that will focus on some of the most advanced AI-powered imaging technology and digital solutions available to patients, including PET/
CT, SPECT/CT, MRI, CT, X-ray, nuclear medicine and ultrasound. GE HealthCare’s interventional, mammography, diagnostic cardiology, maternal and infant care and anesthesia solutions will also be included in Sutter Health’s ambulatory care centers, helping to address the growing need for care outside of the traditional hospital setting. This comprehensive technology refresh covers the breadth of GE HealthCare’s portfolio of solutions, providing clinicians with innovative options to meet changing patient needs more efficiently and quickly.
Imaging and ultrasound solutions, enabled by digital and AI advancements, will be implemented across the entire healthcare system over several years, reducing variation and providing the innovation clinicians need to best serve patients.
The strategic partnership also supports Sutter Health’s larger access strategy, which includes opening dozens of new care sites across Northern California in the next few years. Additionally, it will further support the health system’s expansion of advanced service lines and destination centers of excellence including areas such as heart and vascular care, cancer care and neurosciences.
Sutter Health will adopt technology at a more rapid pace with an accelerated upgrade schedule, including the latest software releases to prevent obsolescence and keep technologies current over the long-term. The service delivery model will help ensure consistent operations and minimize unexpected disruptions –with patient safety, efficiency and reliability in mind.
The agreement will also include significant investment in Sutter Health’s workforce development programs.
CLARIUS ANNOUNCES ULTRASOUND SOFTWARE INNOVATIONS
Clarius Mobile Health recently announced availability of new ultrasound innovations including enterprise software to manage a fleet of Clarius ultrasound scanners, new capabilities powered by artificial intelligence (AI), and built-in CPT medical codes to assist with billing and reimbursement in the United States.
“We’re especially excited to introduce the Clarius Enterprise Software Solution tailored to meet the needs of our growing base of large healthcare institutions that are managing the use of multiple Clarius scanners,” says Clarius CEO Ohad Arazi. “This latest software release, which includes so many unique features, clearly demonstrates the limitless ability of our R&D team to deliver ground-breaking innovations across multiple clinical segments in ultrasound.”
Clarius offers a range of AI-powered specialty ultrasound scanners designed to provide high-definition imaging for multiple clinical applications. They deliver detailed imaging that is equivalent to the best traditional cart-based systems for a small fraction of the cost. Clarius 12.0 App for iOS and Android smart devices includes new capabilities for clinicians in various specialties.
Simplifying The Imaging Equipment Ownership Experience
Image One Medical is the only Engineer-Owned medical equipment service group that is fully dedicated to Florida’s amazing base of Imaging Centers, Hospitals, and Cancer Treatment Centers. We have a mission: Self perform on every aspect of our business. Specialize on specific modalities: Pet CT, CT & MRI, and Focus in a key geographic region.
Fort Myers I Fort Lauderdale I Tampa I Orlando
FLORIDA BASED
Dealer and servicer of PET CT, CT and nuclear medicine
• Equipment service: full coverage plans
• Equipment sales: installation, relocation and project management
• Mobile coach construction, refurbishment, maintenance and management OUR EXPERTISE
• Self performing team of in-house engineers
• High level problem solving for Siemens and GE PET CT, CT and nuclear medicine
• In-house inventory of 40+ systems and parts for repair
• 24 hour service with quick uptime guarantee
SIEMENS HEALTHINEERS, ASRT EXPAND TRAINING PARTNERSHIP
GLOBALLY
Siemens Healthineers and the American Society of Radiologic Technologists (ASRT) will expand an existing partnership to bring top-quality training for radiologic technologists, or radiographers, to underserved countries around the world for the first time. Educating radiographers to operate imaging or radiation therapy equipment is crucial, as the machines enable physicians to diagnose and treat diseases including cancer and cardiovascular disease.
The multiyear partnership will make ASRT’s curriculum and educational content, which are regarded as an industry gold standard, available for foundational and advanced training in both in-person and virtual forms. Training will be vendor-neutral for as broad an impact as possible. ASRT, founded more than 100 years ago, is the largest association for medical imaging and radiation therapy professionals in the world. Siemens Healthineers, which has activities in more than 180 countries, will bring local know-how so that content can be tailored to local circumstances or requirements. This builds on an existing 30-year partnership which included Siemens Healthineers as a charter partner of the ASRT Foundation Corporate Roundtable and supporter of a clinical advancement scholarship program. One of the first activities under the extended partnership, will be to jointly develop a curriculum to train 50 radiographers from Ukraine. The training will be delivered in hybrid form – in person at the Siemens Healthineers Academy in Poland and
PRELIMINARY
online over the next two years.
“Too often in low-resource countries, medical equipment sits unused – often still in its original packaging – because no one is trained to use it,” said Hagen Weissapfel, head of education and service, Siemens Healthineers Access to Care. “We recognize that skilled people are the backbone of any healthcare system, and that building workforce capacity is key.”
Workforce shortages affect healthcare systems across the world, but scarcity in low- and middle-income countries is severe. In high-income countries there are 93 radiologists per million people, but Sub-Saharan Africa has only two per million, according to the International Atomic Energy Agency. Building capacity is crucial, and Siemens Healthineers is committed to providing six million hours of training by 2030 as part of new sustainability targets announced last November.
“ASRT’s mission is to advance and elevate the medical imaging and radiation therapy profession and to enhance the quality and safety of patient care,” said Melissa Culp, head of member engagement at ASRT. “With our colleagues at Siemens Healthineers, we are raising awareness of the profession, ensuring high standards of educational preparedness and strengthening the workforce pipeline globally.”
FINDINGS FROM POCUS STUDY REVEALED
Butterfly recently announced preliminary findings from a seminal study conducted by Rutgers Robert Wood Johnson Medical School (RWJMS) and Robert Wood Johnson University Hospital (RWJUH), an RWJBarnabas Health facility, demonstrating the impact of point-of-care ultrasound (POCUS) on patient outcomes and hospital efficiency. A late-breaking clinical trial presentation of the data was disseminated at the European Association of Cardiovascular Imaging’s EchoEuro-Imaging Conference in Berlin, Germany in December 2024.
The study focused on using cardiopulmonary POCUS for patients admitted to the hospital with shortness of breath without an identifiable cause. It was designed as a prospective, head-to-head comparison of hospital physicians who utilized Butterfly iQ+ and/or iQ3 POCUS devices versus those who did not use POCUS. Results showed a significant reduction in both hospital length of stay (LOS) and healthcare costs. Patients experienced an average LOS reduction of over four days. Lower-acuity patients saw their LOS reduced from 6.7 to 5.6 days. For higher-acuity patients,
LOS was reduced from 39 to 16.7 days. These reductions also translated into substantial financial savings, with lower-acuity patients experiencing up to 50% cost reduction.
Dr. Partho Sengupta, Henry Rutgers Professor of Cardiology and Chief of Cardiovascular Medicine at RWJMS and RWJUH, and principal investigator of the study, said, “This study is an important demonstration that point-of-care ultrasound can serve as a practical tool for stratifying patient acuity, reducing hospital resource utilization, and improving patient flow. The preliminary findings support the growing body of evidence advocating for POCUS as an essential component of modern hospital care and underscore the need for broader adoption of POCUS to improve outcomes and address healthcare inefficiencies.”
Daily use of lung ultrasound (LUS) emerged as a key factor in accelerating discharge for lower-acuity patients, demonstrating how this technology can facilitate more efficient and effective patient management.
The full study is anticipated to be published in the first half of 2025.
BANNER UNVEILS NEW IMAGING SUITE
A transformative endoscopy and interventional radiology suite recently opened at Banner Boswell Medical Center. The wing is equipped with the most advanced technology for complex biopsies, therapies and endoscopies, thanks to a $15 million investment funded in part by Sun Health, a philanthropic partner of Banner Boswell and Banner Del E. Webb Medical Center.
The Banner Boswell Medical Center Interventional Radiology and Endoscopy Suite will all now be housed in a single area, with procedure rooms that are triple the size of the current suites. It is supported by the latest software and algorithms, allowing for a reduction in radiation doses per procedure (to patients and providers), while also achieving a far superior end image. That enhanced visualization will give providers more confidence in taking on additional and more intricate cases, positively impacting patient experiences and outcomes.
“We also have the ability to create simple and fast 3D imaging in this suite,” said Gordon Weimer, director of medical imaging at Banner Boswell. “We can generate CT-like images in just 2.5 seconds with less blurriness. It’s game changing for all of us.”
The system is also pre-programmable for various image-guided procedures, which will cut the set-up times needed by Banner staff. With a single touch, this feature alone can eliminate up to six manual steps, saving more time for individualized cases. Scope processor upgrades have also enhanced the efficiency and safety in sterilizing processes. In addition, the integrated technology communicates directly with one’s medical record – allowing Banner nurses to document changes in real time.
“In so many ways, we are taking the current space forward by 17 years – this is tremendous for our patients, providers and staff,” said Erica Dorward, chief operating officer of Banner Boswell. “We are grateful to the Sun Health Foundation and the many generous donors who have made this transformative space possible.”
UNITED IMAGING EXPANDS MANUFACTURING SPACE
United Imaging has signed on for additional production and office space in greater Houston. The new space in Pearland, Texas will more than triple the total size of the company’s current manufacturing square footage that’s now at their North American headquarters on Kirby Drive. It was only just over four years ago that the company opened that current production facility. United Imaging has been steadily increasing U.S. production since then, with products in all four imaging modalities it currently sells achieving local production in Texas over the last four years. All critical spare parts are already stored in Houston and in stocking locations across the country.
“With the steadily spiking demand and manufacturing capacity also has come an increase in hiring,” said Jeffrey M. Bundy, Ph.D., CEO of United Imaging Healthcare North America. Since 2021, U.S. headcount growth has averaged 60% annually.
The proximity to Houston’s ports provides strategic opportunity the global company has been investing in for years, with increasing operations in South America and across the world. United imaging also announced recently its first product registrations in Canada. It has installations in 75+ countries worldwide since 2011, and earlier this summer announced its 30,000th unit installed globally, which was in the U.S. •
SPONSORED BY:
DIRECTOR’S CIRCLE
Ultrasound technology continues to redefine the standards of imaging with its non-invasive nature, diagnostic versatility and constant advancements. In this exclusive March 2025 Director’s Circle roundtable, industry leaders and experts delve into the critical aspects of ultrasound devices shaping modern medicine. From evaluating image quality and advanced functionality to the nuances of equipment procurement and staff training, this discussion highlights the strategies, challenges and exciting innovations that are influencing the field. Whether you’re navigating procurement decisions or considering the latest trends, this dialogue offers insights for healthcare professionals invested in ultrasound excellence.
Participants in the March 2025 Director’s Circle roundtable on ultrasound are:
• AdventHealth West Florida Division Director of Radiology Rebecca Kitta
• Banner Imaging Associate Manager-Medical Imaging Kalen Terry
• Corewell Health Senior Imaging Specialist-Ultrasound Danielle Tiefenthal
Q: WHAT ARE THE MOST CRITICAL FEATURES OR SPECIFICATIONS YOU LOOK FOR IN AN ULTRASOUND MACHINE?
Kitta: When considering ultrasound units, I tend to prioritize features and specifications that align with clinical needs, operational efficiency, and long-term investment value. The most critical considerations
I consider include imaging quality, portability and ergonomics, artificial intelligence (AI) and automation, interoperability and connectivity, specialty-specific customizations, durability and maintenance, and last but certainly not least cost efficiency
Terry: The most critical features or specifications that I am looking for in an ultrasound machine are image quality, transducer types, doppler capabilities, high-definition display, user friendliness, and advanced software options such as liver packages to include Elastography, UDFF/ UGAP, and advanced OB software for our sites in Colorado.
Tiefenthal: Ultimately, we’re looking for image quality, and by that we’re looking at resolution with increased depth/penetration. We’re looking for quality of the grayscale image when Color Doppler is on, how crisp and sensitive is the Spectral Doppler. Aside from the quality of the basic ultrasound imaging functions, I’m looking for the advanced functions like SMI/microvascular flow, how user friendly is elastography and 3D imaging? What is the wide view, convex, and dual screen imaging like? Does dual screen imaging reduce your FOV more than you’d like or does it keep your whole FOV. These things matter to every exam we perform, it’s important to have a solid understanding of what the machine can do. It’s also important to understand the probe selection, and which functions are compatible with those probes as not all technology is available on every probe.
REBECCA KITTA
Q: HOW MANY ULTRASOUND SYSTEMS ARE CURRENTLY IN USE IN YOUR DEPARTMENT, AND WHAT IS THEIR AVERAGE AGE?
Kitta: Today we have approximately 56 ultrasound systems installed. The average age is 7 years old.
Terry: We currently have 53 ultrasound units across Banner Imaging, average age 8 years.
Tiefenthal: Corewell Health West region has about 60 ultrasound machines within imaging across several locations. In 2024, we were fortunate to do a large install of 42 new machines, and 8 upgraded machines so I have a very young fleet to manage, and it has been an incredible experience. Prior to this install the average age of our machines was about 10 years old, which is a little higher than our typical life cycle replacement age.
Q: ARE THERE ANY SPECIFIC CHALLENGES YOU FACE WITH YOUR CURRENT ULTRASOUND EQUIPMENT?
Kitta: Today our challenges are centered around having different system vendors or models in most ultrasound departments. This presents workflow challenges. Additionally, with new techs entering the workforce, this presents issues with training and leveraging technology available on each system.
Terry: Currently, our biggest challenge is that we have a few different platforms, each with their own unique level of technology. While our newer units deliver high-quality images with ease, our older units are very dependent on the technologist to utilize their physics expertise and knobology skills to obtain a diagnostic image. Older units also require more frequent repairs over time.
Tiefenthal: Currently, with a very young fleet of equipment, we’re fortunate to have very few issues. We do have some units that are older that have issues with dropping presets, diminished image quality, and things that we typically see with aging technology – but we
work through it. We have a great team of in-house service engineers who partner with vendor service teams. I personally partner with applications support and we work together to optimize units the best we can.
Q: WHAT FACTORS ARE MOST IMPORTANT WHEN SELECTING A NEW ULTRASOUND SYSTEM?
Kitta: Image quality, AI, technologist and patient safety, vendor training and support, and cost are the most important considerations to me when purchasing a new ultrasound system.
Terry: When I am evaluating an ultrasound machine, I am looking for image quality, user friendliness, reliability, and cost. Ultrasound machines are becoming more intuitive, which increases efficiency, and in a fast-paced clinical setting, that is imperative. It is crucial to have a machine and technologist that can perform highquality ultrasounds to provide comprehensive diagnostic information. I also need a machine that is durable and reliable. It needs to be able to withstand frequent use and provide consistent performance over time, with minimal down time. I also must consider affordability. The cost of maintenance, transducers and software upgrades all need to be considered to ensure the long-term sustainability of the equipment. These factors together help ensure that the ultrasound machine will meet clinical needs, improve patient outcomes and maintain operational efficiency.
Tiefenthal: It’s important to look at all aspects of the purchase. Of course, imaging quality is at the top of the list, that’s why we’re all here, but vendor applications support, and service support should be part of the discussion as well. How local is apps support? Are they responsive when there are questions? The machine goes down or is having issues, how long until parts can arrive? Do they have loaner probes if you’re in a pinch? These are all things that matter to your organization’s operations outside of being able to provide excellent image quality. I recommend working with vendors to set up equipment
KALEN TERRY
COREWELL HEALTH
DANIELLE TIEFENTHAL
demos, get hands on, scan patients and/or volunteers, push buttons and really be sure the equipment meets the needs of the department. Not only does this allow you to manipulate the presets and test image quality across many types of patients, but it also allows you to meet and work with the applications and sometimes service teams. You really get to work with the whole team and get an idea of the support that comes with purchasing.
Q:
HOW DO YOU ENSURE THAT RADIOLOGISTS AND SONOGRAPHERS ARE ADEQUATELY TRAINED ON NEW ULTRASOUND SYSTEMS?
Kitta: We work closely with our vendors to assure that each unit is installed appropriately. We then have the vendor’s ultrasound specialist on-site for training. We have lead technologists who help to assure each person attends training and coordinates additional training as needed.
Terry: To ensure our staff is adequately trained on new systems, we have vendor-supported onsite training with clinical applications specialists. We block our schedules to allow enough time for the technologists to learn the new machine, while working with the vendor to fine tune settings, and to adjust and refine technique. The apps specialist stays on site with the technologists as they scan patients to address any questions the tech may have or to make real-time adjustments if needed. We have had great apps specialists over the years that are very hands on, thorough and helpful! Once our technologist(s) are proficient in using the new machine, we offer peer-topeer training to additional technologists. Our vendors have been great about checking in with us regarding how the system is performing and the image quality. They prioritize our feedback and will return to adjust settings when needed. Our radiologists are involved in our onsite demos prior to purchasing machines. I work with our CMO, Dr. Khan, to communicate any information or changes that need to be sent to our radiologist groups.
Tiefenthal: The partnership you build with your vendor can be incredibly beneficial in this area. If you’re purchasing new equipment, I would recommend outlining a detailed installation plan – provide your vendor with a list of key functions, exams, etc. to help the apps team know how to best support your team’s needs. Schedule adequate time with applications and give the department leaders enough time to prepare their patient and staff schedule. Of course, that doesn’t cover the sonographers who enter the organization after initial installation, so we find it helpful to keep a library of tip sheets available to help guide our teams on functions of the machine. We also have an onboarding plan that allows for time to become familiar with the machines. In the event we have radiologist in need of equipment training, we
either partner with our vendor or have them work with an experienced sonographer to get familiar with the machine. Physicians also have access to the tip sheets if they find them helpful.
Q: WHAT TRENDS OR DEVELOPMENTS IN ULTRASOUND TECHNOLOGY ARE MOST EXCITING OR RELEVANT TO YOUR DEPARTMENT?
Kitta: For me, the most exciting trends in ultrasound today are furthering the development of AI including deep learning imaging, high-resolution imaging that utilize microbubble contrast enhancement, and multi-modality integration for enhanced diagnostics specifically in the interventional radiology and oncology spaces. These advancements are pushing ultrasound beyond traditional diagnostic roles and into therapeutics and other areas, making it more accessible, versatile and impactful.
Terry: Being that we have so many systems across a large geographical area, I am very intrigued by fleet management software. When a change is needed to be implemented, I currently travel to the sites myself to adjust protocols or settings, or must schedule with an application specialist, which can take weeks. I recently learned about GE’s software Verisound, which would allow me to make configurations remotely in minutes. I think this would allow us to be more efficient as a department, but also provide our patients consistent ultrasounds with standardized protocols, regardless of which Banner Imaging they receive their care from.
Tiefenthal: We’re currently working to implement the use of Liver Fat Quantification technology (ATI/UGAP) into our exams where appropriate. Ultrasound is constantly evolving; we work hard to stay informed as to what technology is available or possibly coming to market and then assess if it is something that would benefit our exam quality. Not all technology will serve the department in the same way so it’s important to evaluate the benefit of each function as they often come at a cost. Purchasing a new technology that won’t be used, doesn’t offer significant quality improvement, or isn’t billable may have negative impacts on future replacement purchases.
Q: WHAT ELSE SHOULD ICE MAGAZINE READERS KNOW ABOUT ULTRASOUND DEVICES?
Kitta: Ultrasound is being used more broadly each year. Assuring that ultrasound systems meet quality standards, and the staff is trained appropriately on the technology the system has is extremely important.
Terry: While ultrasound technology is improving and becoming more intuitive and user friendly, ultrasound is still a very tech-dependent modality. Modern ultrasound systems determine the quality and clarity of the images,
but the technologist must utilize their expertise to obtain the best possible image to assist the radiologist in providing a diagnostic report.
Tiefenthal: Ultrasound devices continue to evolve, and they are not one size fits all. It is important to do your homework, demo, ask questions, and make sure the units you’re looking at truly meet the needs of the department. With POCUS becoming more popular, we’re seeing great advancement in handheld and portable devices which is exciting. It can be easy to lose track of ultrasound because a new unit doesn’t require facility changes like a new CT or MRI, but the advancement in ultrasound technology continues to be fast-paced and updating ultrasound equipment will continue to be a need in many service lines. Ultrasound can evaluate more and more areas of the body that it didn’t in the past because of the new technology, making ultrasound competitive in ways it historically wasn’t. For organizations to be able to offer improved and specialized services, they need to be able to replace aging technology more often. This may present barriers but, ultimately, it’s great to continuously see the demand for the modality as a whole continue to grow. •
PRODUCTS
Market Report
Ultrasound Market Clearly on the Rise
The global ultrasound devices market size was estimated at $9.79 billion in 2023 and is anticipated to expand at a compound annual growth rate (CAGR) of 4.24% from 2024 to 2030, according to Grand View Research.
The market growth is poised to be driven by the rising usage of ultrasound equipment for diagnostic imaging and treatment, along with the increasing prevalence of chronic and lifestyle disorders. Other factors influencing market growth include increased demand for minimally invasive surgeries and frequent developments in ultrasound imaging technology. Ultrasound is a leading diagnostic tool in medical imaging, compared to other diagnostic imaging systems, since it is less expensive and faster. Moreover, as it does not utilize ionizing radiation or magnetic fields, it is safer than other imaging technologies.
Diagnostic and therapeutic uses for ultrasonic medical devices are extensive. Specific therapeutic applications of ultrasound, from oncology to cardiology, have grown in popularity. The development of wireless transducers, appbased ultrasound technology, fusion with CT/MR, laparoscopic ultrasound, and the expansion of ultrasound device applications in 3D imaging and shear wave elastography are expected to support market growth.
Fortune Business Insights also reports market growth.
The global ultrasound equipment market size was $9.32 billion in 2023 and is projected to grow from $9.99 billion in 2024 to $17.55 billion by 2032, exhibiting a CAGR of 7.3% during the forecast period (2024-2032), according to Fortune Business Insights. Moreover, the U.S. ultrasound equipment
market size is projected to grow significantly, reaching an estimated value of $4.35 billion by 2032, driven by increasing demand for compact ultrasound devices with potential benefits.
Ultrasound is considered to be one of the safest, noninvasive diagnostic procedures to examine internal organs.
Recent advancements in this technology and introduction of innovative equipment, along with the developing healthcare facilities in emerging countries, have influenced market players to develop easily operable devices. Additionally, the growing prevalence of chronic diseases and expansion of applications of these systems are some of the major factors anticipated to propel the global ultrasound equipment market growth during the forecast period.
Some of the leading market players are developing advanced devices and systems integrated with artificial intelligence (AI). The AI algorithms are aimed to improve quality of the image and interpretation. It can be used to analyze ultrasound images in real-time in turn offering valuable insights and assistance in accurate diagnosis to healthcare professionals. Furthermore, the integration of AI in ultrasound equipment leads to enhanced accuracy and efficiency of ultrasound examinations, resulting in better patient outcomes. This step is being propounded to overcome certain limitations associated with the conventional devices such as the long duration of time required to conduct the examination, poor image qualities in certain cases, high dependency on technicians to acquire and interpret images, and so on. Thus, the introduction of advanced systems with artificial imaging by key players is expected to boost the growth of the market during the forecast period. •
Product Focus
ULTRASOUND
*Disclaimer: Products are listed in no particular order.
1
FUJIFILM ARIETTA 750 DEEPINSIGHT ULTRASOUND SYSTEM
The ARIETTA 750 DeepInsight (DI) ultrasound system is designed to provide superior image quality, excellent noise reduction, stable penetration and high spatial resolution. Fujifilm’s DeepInsight uses cognitive technology to distinguish between echo signals and electrical noise, as well as transmission and reception technology, to obtain high-quality images even in deep and challenging regions of interest, supporting more efficient ultrasound exams. The system offers an array of advanced imaging techniques combined with a variety of efficiency tools based on automated image analysis and protocol-based operation. For example, the system’s eFocusing focal-free scanning provides homogenous image quality and improves sensitivity for both near and far field screening. In addition, tissue structure clarity is further enhanced through Carving Imaging, based on Fujifilm’s advanced image processing technology. Together, these technologies ensure high image quality and consistency for both routine and complex examinations, ultimately contributing to faster diagnoses. The ARIETTA 750 DeepInsight ultrasound system monitor arm and console are ergonomically designed to offer a wide range of movement for enhanced operator comfort. Examinations are further streamlined through the Protocol Assistant, which can pre-register procedures and parameters.
EXO IRIS
Exo Inc. is a health information and devices company modernizing medical imaging. Its mission is to empower healthcare professionals with real-time, high-performance handheld ultrasound technology that improves patient outcomes. Key features of Exo products include:
• Powered by patented silicon technology and real-time AI for highperformance imaging.
• Compact and cost-effective compared to traditional cart-based systems.
• Simple user interface and AI capabilities delivered by our patented SweepAI artificial intelligence technology, making ultrasound imaging easy for even novice users.
• Delivers deep tissue imaging and detailed visuals of fine structures, making it ideal for scanning major organs and guiding IVs or needlebased procedures.
• Exo Works Workflow Software: Seamlessly integrates with Exo Iris (or any other ultrasound system) for fast, efficient documentation and exam review.
• Enables healthcare professionals to access and manage scans from anywhere in seconds.
By combining advanced imaging, artificial intelligence, user-friendly design, and efficient workflow solutions, Exo is transforming the way medical imaging is performed, ensuring better decisions and improved care.
SIEMENS HEALTHINEERS ACUSON SEQUOIA 3.5
The latest release of Acuson Sequoia, a Siemens Healthineers ultrasound system, leverages artificial intelligence (AI)-powered features to enhance clinical performance. Acuson Sequoia features AI Abdomen, an industry-first technology that reduces sonographer hand motion by up to 89% compared with manual exams, and up to 44% compared with protocol exams. AI Abdomen improves workflow with an algorithm that automatically recognizes and labels 17 anatomical views and calculates 12 key measurements. The algorithm enhances diagnostic accuracy, reduces variability, and helps standardize exams across users with real-time organ-identification and freeze-measurement of organs. The new HLX transducer uses proprietary 2D Shear Wave technology to better identify and display stiff lesions in the breast. The HLX transducer provides the company’s highest-frequency penetration and resolution, giving clinicians the necessary diagnostic information to reduce false negatives. The transducer addresses the musculoskeletal clinician’s need to visualize large in-motion tissues and small, superficial structures. The lightweight HLX transducer, designed with an ergonomical grip and narrow shape, allows for tight access, and reduces strain during scans. Acuson Sequoia also includes notable liver quantification tools, Ultrasound Derived Fat Fraction (UDFF) and Auto Point Shear Wave Elastography (Auto pSWE), which provide quantification of liver tissue stiffness and hepatic steatosis in a single acquisition.
GE HEALTHCARE LOGIQ E10 SERIES
The LOGIQ E10 Series is designed to keep imaging departments at the forefront of clinical imaging and operational excellence. It provides a new standard in imaging so clinicians can scan, diagnose, and treat a wide range of patients across a broad spectrum of conditions with a high level of confidence. With robust, standard features and scalable options professionals can configure the optimal system to meet radiology, cardiac, OB/GYN, vascular, breast, and musculoskeletal imaging needs. Pair the Vscan Air CL wireless dual probe with a LOGIQ console to scan and then display, optimize, save, and review images with the power of LOGIQ processing. Plus, it’s AI-based tools help in diagnostic confidence and workflow efficiency.
4
CLARIUS MOBILE HEALTH
ULTRA-SPECIALIZED ULTRASOUND
One handheld scanner cannot deliver for all clinical applications. That’s why Clarius is making accurate, easy-to-use, and affordable ultrasound available to medical professionals in every specialty. From facial mapping at 1 cm to diagnosing aortic aneurysms at 40 cm, Clarius helps get clear imaging at the bedside for accurate diagnoses and safe procedures. Ultraportable and wireless, you can easily carry scanners from patient to patient, whether they’re in the next room or in another building. Clarius offers clinically validated artificial intelligence solutions to save time, enhance learning, and improve decisionmaking. AI-powered Clarius handheld wireless ultrasound scanners connect to iOS and Android devices, delivering highresolution ultrasound images traditionally only available with bulkier, high-end systems at a fraction of the cost. Clarius scanners are available in over 90 countries worldwide. Learn more at www.clarius.com.
• The fastest growing HTM talent network in the country.
MAGAZINE NEWS MAGAZINE NEWS
• 350+ open opportunities throughout the United States.
» A variety of posting options ranging from single-job postings to 12-month unlimited memberships.
“My HR department advertised on various government sites and our web site but we did not get a single applicant in over 120 days. Fairbanks Alaska is hard to recruit for but I took out an ad on HTM Jobs and got two good applicants in less than 30 days I am hiring them both. Thanks HTM Jobs.”
Featured Employers: Agiliti, Renovo Solutions, TRIMEDX, Erbe USA Inc., Dartmouth-Hitchcock, Sutter Health, and more!
- D. Anderson, Tanana Chiefs Conference
Decision-Making at the Point of Care
Expansion of portable ultrasound techniques supports life-saving differential diagnoses
BY MATT SKOUFALOS
Since its emergence subsequent to the Gulf War of 1990, point-of-care ultrasound (POCUS) has been leveraged in broader and broader use cases in various healthcare settings. Portable ultrasound technology, which sprang from a U.S. Department of Defense (DOD) Defense Advanced Research Projects Agency (DARPA) challenge grant for the development of a diagnostic technology that could reach soldiers in the battlefield during combat, led to the creation of the first widely produced portable ultrasound device, the Sonosite 180.
Coupled with the emergence of the FAST exam (Focused Assessment with Sonography for Trauma), which was developed by trauma surgeon Gail Rozycki, the first, cart-based, portable ultrasound systems began to find practical use in civilian healthcare environments.
Rob Ferre, MD, the POCUS program director for Indiana University School of Medicine and the system-wide POCUS director for the Indiana University Health System in Indianapolis, Indiana, marks that inflection point as the change that began taking diagnostic ultrasound technology from the imaging suite into the emergency department.
“Back then the machines were huge, and they never moved,” Ferre said, “but that new, highly portable form factor really started moving ultrasound into the emergency department.”
In 2001, the American College of Emergency Physicians released its first guidelines for the use of ultrasound imaging in the emergency department. Thereafter, when other specialties from pulmonary critical care to hospital medicine to anesthesia began leveraging the technology, the term POCUS was coined. In 2023, the Accreditation Council for Graduate Medical Education (ACGME) named POCUS a requirement of residency training in family medicine, and now more than half of all medical schools have some approved POCUS curriculum, Ferre said.
“It’s become a bigger deal,” he said.
Ferre traces the ubiquity of POCUS to the development of ever-smaller ultrasound devices, specifically, the Butterfly iQ, which lowered the cost for a handheld portable ultrasound scanner to a few thousand dollars. That was a game-changer for educators.
“Just like when Sonosite 180 came along in the ’90s, Butterfly took the ability to do mass training to the next level,” he said. “Now that POCUS was affordable, how do we develop more experts in the field, and how do we find space in the curriculum for instruction?”
By distributing POCUS systems at white-coat ceremonies, as has become popular to do at medical schools across the country, physicians-in-training now have the opportunity to pick up the technology as they learn anatomy, which offers a practical tie-in for both modes of learning.
“They’re learning to use a modality that’s in clinical practice and for physical exams,” Ferre said. “Now, because we are in a new paradigm where we’re trying to get students to use an imaging modality that’s used in clinical practice, we’re getting them to use this, and we’re making it cheap and available throughout medicine.”
Adding ultrasound technology at the point of education has led to the emergence of a grassroots group of students who are looking to then learn how to incorporate the technology into clinical practice, Ferre said. He believes that the addition of POCUS into such curricula has even become a signifier to medical students that they’re at an institution that embraces innovation.
Beyond that, Ferre spoke about the work that POCUS manufacturers have done to “remove the proximity to education” for training new users of the technology. By adding in access to diagnostic assistance tools and artificial intelligence (AI)-powered image recognition algorithms, device-makers are “helping the new user, and giving the user who feels uncomfortable an added boost” to embracing POCUS.
“I call it ‘just-in-time learning,’” Ferre said.
“As I’m using the device, can I quickly refer to some educational materials? If I want to refresh my memory, how can I do it?” he added. “It helps overcome some of the reluctance to adopt the technology.”
Those same utilities also make POCUS a technology ideally suited for use by “downstream healthcare workers” who might not have the same levels of medical training as a physician or modality specialist, but who can quickly pick up specific use cases for which POCUS is particularly suited, Ferre said.
“We know that vascular access is difficult,” he said. “If I can give a nurse or phlebotomist a technology that can help them perform the procedure more easily, then why shouldn’t I? Lung ultrasound is another one of those very good, easy-to-learn applications that has a good use case. It’s just pattern recognition, and you add some AI tools, and it’s helpful.”
Ferre sees far greater adoption of POCUS by practitioners in traditional medical specialties – like cardiology, obstetrics and gynecology, and vascular surgery – and for specific use cases. In circumstances where the physician doesn’t need a comprehensive
imaging study, and needs answers to “very specific, focused questions” at the point of care, POCUS has the ability to deliver that information very quickly.
“Some of the low-hanging fruit that applies to most specialties is lung ultrasound,” Ferre said. “Lung ultrasound was never a thing developed by radiologists because chest X-rays were so ubiquitous, and ultrasound is not good at looking at air-filled structures like the lung. That changed with research and data, initially from trauma surgeons. Lung ultrasound was further developed by intensivists and emergency physicians. As a result, we now know that the surface of the lung is easily imaged by ultrasound, and a lot of the pathology exists at the surface of the lung. It’s much better than chest X-ray for heart failure or pneumonia, and it’s really easy to learn it.”
“In obstetrics, if you’re doing an anatomic survey to find any problems with the baby, you’re never going to do that with a handheld,” Ferre said. “But if you show up for delivery, everyone’s going to say, ‘Is the baby’s head down? It turns out your physical exam is not as good as just looking [with an ultrasound device]. Even though breech presentations are only three percent of deliveries, it’s significant.”
Ferre believes growth in the adoption of POCUS will
continue to be organic and based on use cases. Rather than an orders-based deployment of the technology, he believes physicians are better served by developing encounter-based workflows to document and capture POCUS images that can be sent to the patient’s chart.
“As an ER physician, if I want a CT scan of the head, I order it,” he said. “That order communicates to the tech that a CT needs to be done; it’s triggered because somebody went to the electronic health record and ordered it. Clinicians who use ultrasounds at the bedside don’t order themselves to do anything, so that doesn’t work. We’ve got to build an entirely new system, and that is complicated. There’s millions of dollars in healthcare organizations to support order-based workflows, and almost none spent for encounter-based workflows. We need to change that paradigm and support clinicians who are at the forefront of innovation and improving patient care.”
Training the next generation of POCUS experts doesn’t only happen in medical school. Dr. Davoren Chick, chief learning officer for American College of Physicians (ACP), said there’s a significant opportunity to drive adoption of the technology among internal medicine physicians in a continuing education setting.
Chick, who has used and taught POCUS in a hospital setting, said that ACP delivers hands-on skills development courses, peer mentoring, and extended review and feedback for those physicians “who didn’t learn POCUS during their initial training years but would like to refine and improve and expand their skill set.”
The ACP approach comprises online interactive, multimedia, and hands-on training seminars, as well as a six-month virtual mentorship program, which takes the form of virtualized, interactive, livestreamed sessions that offer POCUS learners “continual feedback on their directly observed scanning and resulting images; what worked well and what didn’t,” she said.
“People can join up as individuals or pairs to engage in months-long scanning guidance and feedback that allows a POCUS expert to develop their manual skills,” Chick said. “Then, they work on refinement of a POCUS imaging portfolio, and we provide a certificate at the completion of a capstone project.”
“There’s a lot that needs to be trained and refined,” Chick said.
but its specific use cases within their area of expertise.
“That’s the whole point of appropriate level of training and making sure that within each discipline, each discipline is defining appropriate uses,” Chick said. “A lot of people are doing this because they’re good doctors who want to learn and expand their skill set, and this is something that reinvigorates their practice. We’re also doing a lot of retraining of hospital physicians and others looking for support in their differential diagnoses.”
Point-of-care ultrasound is rewriting the books of medicine, expediting diagnosis and transforming patient care at the bedside.
“There’s the cognitive skills that need to be trained (What am I looking at?), and then there’s the manual stuff (How do I get that image?), the clinical decision-making (When do I do this? Which probe?) and finally, patientcentered scanning.”
Just as with every aspect of a physician’s scope of practice, Chick spoke about the importance of good judgment governing the use of POCUS. The technology itself is a tool that’s only as good as its users and their decision-making skills with it, she said; to effectuate that, they must be properly trained not only on the modality,
Organizationally, “POCUS is a team effort,” Chick said, particularly for reimbursement and external reporting. She emphasized the need for collaboration among informatics and device management teams for underlying supportive mechanisms including image filing and retention, compliance issues, risk management, and credentialing. For those individual physicians who work with POCUS as a component of diagnostic and clinical decision-making, she emphasized the importance of recognizing “the limits of your skill set with that instrument.”
“Internal medicine physicians have great respect for radiology and radiologists, and have no interest in trying to become one,” Chick said.
“There’s no sense of competition here. Physicians using POCUS to support their day-to-day work are doing it in a way that’s not a replacement for necessary radiology and guidance- and guideline-based radiology techniques.”
“This is not a competition; this is a way in which physicians in the field are supporting their own work to manage complexity of decision-making,” she said.
Radiologist Victor V. Rao, global clinical content manager and POCUS educator at the Inteleos Pointof-Care Ultrasound Certification Academy, said that
Rob Ferre, MD Nilam Soni
Victor V. Rao Dr. Davoren Chick
POCUS continues to demonstrate its value to physicians in individual moments that deliver life-saving clinical information at the point of care, and which provide a vital clinical tool for highly accurate, enhanced physical examinations.
In one instance, while he was training a primary care physician in rural South Carolina, Rao recalled a female patient who presented with mild lower abdominal pain. A quick POCUS examination revealed that the patient was not only pregnant – of which she had been unaware – but was also about to undergo a spontaneous abortion. The patient disclosed that she’d previously had three pregnancy losses in the second trimester, and had never delivered a child. This condition had been not diagnosed earlier in this patient due to lack of availability of ultrasound.
“She had a condition called incompetent cervix,” Rao said. “We quickly called an obstetrical service; they rushed her in and performed a cerclage procedure, and the pregnancy was saved. The patient later delivered a normal, healthy fetus at term.”
Another physician wasn’t as lucky, he said, when a young female patient, who presented with redness and swelling in the legs, was treated for cellulitis with broad spectrum antibiotics. She unfortunately died of a massive pulmonary embolism that was related to an undiagnosed deep vein thrombosis (DVT). Had the physician been able to diagnose the DVT with an ultrasound study, and immediately begin anticoagulation treatment, he might have saved her life, Rao said.
He described similar cases in which POCUS was used to help successfully treat patients who were being treated for congestive heart failure exacerbation but had been suffering from chronic obstructive pulmonary disease (COPD) exacerbation. Both these conditions may present similarly, but require different treatments, and ultrasound is able to differentiate between the two in a couple of minutes.
“The thing about POCUS is you end up saving lives,” Rao said. “There are many stories out there, but the big impact is when you save a life or when you help deliver proper treatment to the patients using POCUS.”
Anecdotes such as these illustrate how “POCUS is rewriting the books of medicine,” said Nilam Soni, an academic hospitalist at the University of Texas School of Medicine in San Antonio. Soni, who also leads point-ofcare ultrasound training for the Department of Veterans Affairs nationally, said that the technology fundamentally changes “the whole approach to the way we assess patients” by expediting differential diagnosis at the bedside.
“Traditionally, the clinician says, ‘I need to get an imaging test to evaluate X, Y, Z,’” Soni said. “The test is then performed by a sonographer who doesn’t know the patient’s history. Then the images are entered into some kind of image repository, and a radiologist reads it. The report goes back to a clinician, who has to make sense of the report and ultimately integrate the findings into the patient’s care.”
“The traditional imaging route has multiple steps, and multiple delays, and a clear disconnect in the people involved in the patient’s care,” Soni said. “When we’re using POCUS, we’re using the same technology in a clinical manner at the bedside – reducing procedural complications, helping with procedural decision-making, reducing unnecessary diagnostic testing, and delivering a better experience for the patient and provider all around.” •
Ultrasound equipment failure can be catastrophic.
Learn to service your own with our Solutionist Series videos.
When your ultrasound equipment is down, so is your business. Don’t miss our Solutionist Series videos on Ultrasound Equipment Support where you’ll learn how to service your equipment, keep your business up and running and lower your total cost of ownership.
In this 10-episode virtual training course on the Philips Epiq ultrasound platform, Larry Nguyen, Summit Imaging’s Founder and CIO, identifies common failures and provides solutions for:
• Power subsystem — power module and power regulator board
• External interfaces — control panel, touch panel, trackball, monitor and external IO
• Transducer types and applications — Doppler, linear, curved, endo-cavity and more.
• Transducer parts — a breakdown of standard and TEE
• Transducer parts and operational failures — from lens failure to cut or creased cords to CW noise and error codes
Larry Nguyen addresses lots more in our 10-episode Solutionist Series, so be sure to tune in.
“ICE Webinars always provide great timely information in a well planned format.”
- Nancy Godby, Director of Radiology, Cabell Huntington HospitalMarshall Health Network
“I attend ICE Webinars to learn more about other imaging styles and get CE credits.”
- Amanda Brunson, Manager of CT and MR Imaging Services , MUSC Health Orangeburg
“I participate in these webinars to enrich my professional knowledge and to be able to share the news in the field with my students. “
- Calin Corciova, Associate Professor, Medical Bioengineering Faculty
“I attend ICE webinars because of the variety of topics and presenters.”
- John Beall, Regional Director, United Imaging Healthcare
“I attend ICE Webinars to learn more information related to radiology and imaging technology.”
- Krista Andrews, Imaging Manager, BSHW
TEAM AND HEALTHCARE AI
PACS/IT/AI
BY MARK WATTS
This may be the right time to apply AI in your healthcare organization. You could be faced with care coordination challenges unlike any other. A new payment structure calls for a new AI-driven workflow.
TRANSFORMING EPISODE ACCOUNTABILITY
MODEL (TEAM): A NEW ERA IN MEDICARE CARE
TEAM is a groundbreaking initiative by the Centers for Medicare & Medicaid Services (CMS) aimed at enhancing the quality of care for Medicare beneficiaries undergoing specific surgical procedures. This model addresses the fragmented care that patients often experience, which can lead to complications, avoidable hospitalizations and increased healthcare costs. In this article, we will explore the key points of the TEAM model, its goals, approach, and the impact it aims to have on the healthcare system. Additionally, we will discuss how AI can enable healthcare organizations to excel under this new program.
INTRODUCTION TO THE TEAM MODEL
TEAM is an episode-based, alternative payment model that will be mandatory for selected acute care hospitals. The model is set to
launch on January 1, 2026, and will run for five years, ending on December 31, 2030. The primary objective of TEAM is to improve the coordination and quality of care for Medicare beneficiaries undergoing specific surgical procedures while also reducing healthcare costs.
The TEAM model has several key goals:
• Improve Quality of Care: By holding hospitals accountable for the quality of care provided during and after surgical procedures, the TEAM model aims to enhance patient outcomes and reduce complications.
• Reduce Healthcare Costs: By promoting better care coordination and reducing avoidable hospitalizations, the TEAM model seeks to lower overall Medicare spending.
• Promote Equitable Health Outcomes: The model aims to ensure that all Medicare beneficiaries receive high-quality care, regardless of their geographic location or socioeconomic status.
MODEL APPROACH
The TEAM model will be implemented in selected geographic regions across the United States, with hospitals required to participate based on their location in Core-Based Statistical
Areas (CBSAs). The model will include several key components:
• Episode-Based Payment: Hospitals will be responsible for the cost and quality of care from the time of surgery through the first 30 days after the patient leaves the hospital. This includes coordination and communication between providers across all care settings.
• Target Price: CMS will provide participants with a target price that represents most Medicare spending during an episode of care. This includes the surgery, hospital inpatient stay or outpatient procedure, and items and services following hospital discharge.
• Graduated Risk Tracks: TEAM will have different participation tracks with varying levels of risk and reward. This allows hospitals to ease into full-risk participation and accommodates different levels of risk tolerance.
INCLUDED SURGICAL PROCEDURES
The TEAM model will focus on several high-expenditure, highvolume surgical procedures, including:
• Lower Extremity Joint Replacement
• Surgical Hip Femur Fracture Treatment
• Spinal Fusion
• Coronary Artery Bypass Graft
• Major Bowel Procedure
CARE COORDINATION AND ACCOUNTABILITY
One of the critical aspects of TEAM is the emphasis on care coordination and accountability. Hospitals participating in the model will be required to:
• Coordinate Care: Ensure seamless transitions between providers and care settings, including inpatient hospital services, outpatient therapy services, skilled nursing facilities, and home health services.
• Refer to Primary Care: Connect patients to primary care services to support continued recovery and positive long-term health outcomes.
• Monitor Quality and Cost: Track and report on the quality and cost of care provided during the episode, with the potential to earn payments from CMS if spending is below the target price.
IMPACT ON HEALTHCARE PROVIDERS
TEAM is expected to have a significant impact on healthcare providers, particularly acute care hospitals. By holding hospitals accountable for the quality and cost of care, the model encourages providers to:
• Improve Care Coordination: Enhance communication and collaboration between different providers and care settings to ensure patients receive comprehensive, high-quality care.
• Focus on Patient Outcomes: Prioritize patient outcomes and recovery, reducing the likelihood of complications and avoidable hospitalizations.
• Optimize Resource Utilization: Use resources more efficiently, reducing unnecessary spending and improving the overall value of care provided.
CHALLENGES AND CONSIDERATIONS
While TEAM has the potential to drive significant improvements in the healthcare system, there are several challenges and considerations that need to be addressed, including:
• Implementation and Compliance: Ensuring that hospitals comply with the model’s requirements and effectively implement care coordination strategies can be challenging.
• Data and Reporting: Accurate data collection and reporting are essential for monitoring the quality and cost of care. Hospitals will need robust systems in place to track and report on these metrics.
• Risk Management: Managing the financial risk associated with episode-based payments requires careful planning and risk mitigation strategies.
APPLYING AI TO MEET TEAM STANDARDS
Applying AI to meet the standards for TEAM can significantly enhance care coordination, improve patient outcomes, and reduce healthcare costs. Here’s how AI can be integrated into TEAM:
• Predictive Analytics for Risk Stratification: AI can analyze patient data to predict which patients are at higher risk of complications or readmissions. By identifying these high-risk patients early, healthcare providers can implement targeted interventions to prevent adverse outcomes and reduce costs.
• Natural Language Processing (NLP) for Documentation and Communication: NLP can be used to analyze clinical notes, discharge summaries, and other unstructured data to extract relevant information. This can improve the accuracy of documentation, enhance communication between providers, and ensure that all necessary information is available for care coordination.
• Machine Learning for Personalized Care Plans: Machine learning algorithms can analyze patient data to develop personalized care plans. These plans can be tailored to the specific needs of each patient, ensuring that they receive the most appropriate care and reducing the likelihood of complications.
• AI-Driven Decision Support Systems: AI-driven decision support systems can provide real-time recommendations to healthcare providers based on the latest clinical guidelines and patient data. This can help providers make more informed
decisions, improve the quality of care, and ensure compliance with TEAM standards.
• Remote Monitoring and Telehealth: AI-powered remote monitoring tools can track patients’ vital signs and other health metrics in real-time. This allows healthcare providers to monitor patients’ progress and intervene early if any issues arise. Telehealth platforms can also use AI to triage patients and provide virtual consultations, improving access to care and reducing the need for in-person visits.
• Automated Care Coordination: AI can automate many aspects of care coordination, such as scheduling follow-up appointments, sending reminders to patients, and ensuring that all providers involved in a patient’s care are informed of any changes. This can improve the efficiency of care coordination and reduce the risk of errors.
• Quality and Cost Monitoring: AI can continuously monitor the quality and cost of care provided during an episode. By analyzing data in real-time, AI can identify any deviations from the expected care pathway and alert providers to potential issues. This can help ensure that care is delivered efficiently and within the target price set by CMS.
• Patient Engagement and Education: AI-powered chatbots and virtual assistants can engage with patients, answer their questions, and provide education about their condition and treatment plan. This can improve patient adherence to care plans and enhance their overall experience.
• Fraud Detection and Prevention: AI can analyze billing data to
detect patterns indicative of fraud or abuse. By identifying and addressing these issues early, healthcare providers can ensure compliance with CMS regulations and avoid financial penalties.
• Data Integration and Interoperability: AI can facilitate the integration of data from various sources, such as electronic health records (EHRs), wearable devices, and patient-reported outcomes. This ensures that all relevant information is available for care coordination and decision-making.
By leveraging these AI applications, healthcare providers can meet the standards set by TEAM, improve patient outcomes, and reduce healthcare costs. The integration of AI into the TEAM model represents a significant opportunity to transform the way care is delivered and ensure that Medicare beneficiaries receive high-quality, coordinated care.
The Transforming Episode Accountability Model (TEAM) represents a significant step forward in improving the quality and coordination of care for Medicare beneficiaries undergoing certain surgical procedures. By holding hospitals accountable for the cost and quality of care, the model aims to enhance patient outcomes, reduce healthcare costs, and promote equitable health outcomes. As the model is implemented and evaluated over the next five years, it will be essential to address the challenges and considerations to ensure its success and sustainability. •
— Mark Watts is an experienced imaging professional who founded an AI company called Zenlike.ai.
Being asked to write an educational article is quite an honor but not without stress. As I contemplated what to write, I used two thought processes to determine a subject. One was, does the issue occur routinely throughout my daily job? Secondly, what were the difficulties in solving the problem? This allowed me to narrow the subject matter to relevant issues encountered by biomedical engineers and field service engineers working on a variety of equipment. Although I researched this article from the view of an ultrasound engineer, I believe the problems encountered go beyond just ultrasound. So, what am I writing about? The topic is difficulties encountered with networking and troubleshooting an ultrasound system.
There are many difficulties you can encounter when dealing with network issues. The first is that each OEM uses their own proprietary interface to set up and manage network settings. Many of them are very complex and require a strong background in networking. Speaking of a strong background in networking … many of us don’t have a solid knowledge of networking principles. Although the intent of this article is not to teach you networking principles, it will certainly benefit those tasked with troubleshooting network problems. Another issue regarding networking is that some OEMs limit access to network settings by requiring passwords. To overcome this, it’s best to be proactive when purchasing the ultrasound system. As the people tasked to maintain the equipment, make sure you are actively providing critical information needed to support the systems. During
negotiations, your purchasing department has a tremendous amount of leverage. Another piece of this is that each model may have a different network user interface. An example of this is GE ultrasound equipment. They produce three unique series, the Logiq, Vivid and Voluson series systems. Although all three are GE systems, they each have their own unique network interfaces. Once we understand how to navigate the OEM interfaces for each ultrasound model, we will still need tools to help troubleshoot network problems. Let’s focus next on tools available to us for network troubleshooting.
We rely on some basic tools that are available at little to no cost. They are invaluable when it comes to troubleshooting network problems. The first is a network switch which has activity and connectivity lights on it. These lights indicate network speed, network connectivity and network activity. This is a quick and easy way to determine if a network port is viable. Another simple tool for troubleshooting is carrying a crossover and network cable. Crossover cables are needed when connecting directly from your laptop computer to the ultrasound system computer. If used with a managed switch, a crossover cable is not needed. Please keep in mind that some lower cost switches are not managed. Carrying these extra cables can also help eliminate a damaged cable as the culprit for loss of connectivity. I also carry a short network cable and breakaway connector that I can add to the customer system to prevent damage to the system or cable. This proves invaluable on systems that are taken portable routinely. An indispensable tool is a laptop computer. These are routinely carried by field service engineers and are available to biomedical engineers. There are many uses for a laptop computer, such as pinging a network outlet to confirm an active network, testing
the customers network cable and making sure the ultrasound system can send data to the destination device. Laptops also give us access to command-line utilities. These command-line utilities include tools such as ipconfig, ping and netstat. Commands such as these allow us to determine if the network is reachable, provide detailed information about the computer’s network settings and monitor the different connections on a network. These are just a few examples of command line utilities, but you can get a comprehensive list by searching on the web. Keep in mind, when using command-line tools you may need administrative privileges. Which brings me to the last category … applications software. You can download a large selection of applications to aid in your ability to gather a variety of useful information. Many of them are freeware. An example of this is Hiren’s. We can use Hiren’s utilities to obtain the MAC address on ultrasound systems or see the file structure on a hard drive. Another application available is a DICOM emulator. There are a variety of emulators available that provide different options. In your search, make sure to choose one that meets your needs. There are some very capable emulators available, but you may have to pay to use them. For our purpose, we chose K-PACS, which is a free download and does everything we need. The intent of a DICOM emulator is to create a duplicate PACS destination device on your laptop with the same network information and see if the ultrasound system can send images
to the laptop. If the image transfer is successful, it indicates that something beyond the system is not working. If not, then it is time to start looking at settings, software corruption or hardware failure. Another category of this is DVTK, an application that specifically verifies worklist networks. When using applications to interface with your ultrasound systems make sure that you are aware of the age of your equipment. Attempting to use Hiren’s for Windows XP on a new generation system running Windows 10 is an example of an application that will not work.
In short, these are just a few of the issues that you will run into while maintaining your ultrasound systems. The list is far from all-inclusive, but it gives some guidance on where and how to complete an initial setup of your network and troubleshoot your system when its network fails. Please don’t hesitate to contact us regarding any of your ultrasound needs. •
– Jim Rickner is the director of service and training at Advanced Ultrasound Systems.
– Christopher Wright is a field services engineer at Advanced Ultrasound Systems.
WHY TOUGH CONVERSATIONS MATTER
BY NICOLE DHANRAJ DIRECTOR’S CUT
Imagine this: A team member is consistently late for their shift, delaying patient imaging schedules. Or perhaps there’s a pattern of repeat scans due to positioning errors, impacting patient care and department efficiency. As a radiology leader, addressing these issues isn’t optional – it’s necessary.
Difficult conversations in healthcare are particularly sensitive because they directly affect patient outcomes.
But these discussions, when approached thoughtfully, can build trust, improve performance and enhance the overall function of your team.
Here’s how to prepare, approach and follow through effectively.
STEP 1: PREPARE WITH PURPOSE
• Gather Your Facts
Effective preparation is key. Document specific examples to ensure the discussion focuses on facts, not opinions:
Example: “On March 10, you arrived 20 minutes late, which delayed the first patient’s CT scan and impacted the department’s entire morning schedule.”
Review QA logs, incident reports or patient feedback tied to the issue.
Check relevant policies, such as department punctuality or scan quality standards.
Being well-prepared ensures the
conversation is constructive and data-driven.
• Consider the Context
Think about the technologist’s role and individual circumstances.
Are they new and still learning department workflows?
Are they juggling personal challenges or a high workload?
Could their communication style or cultural background influence how they receive feedback?
Understanding the broader context helps you approach the conversation with empathy.
• Choose the Right Time and Place
A rushed or public conversation can escalate tension. Instead, find a neutral, private space. A conference room away from the imaging suites or a quiet meeting room near the radiology department. Arrange seating to promote collaboration. Sitting side-by-side at a small table is less intimidating than sitting across a large desk. Choose a time when the department isn’t busy, such as after peak patient hours or during a designated meeting time.
STEP 2: APPROACH WITH EMPATHY AND CLARITY
• Open the Conversation Constructively
Phrases like “We need to talk” can create anxiety. Instead, say: “I’d like to share some observations and get your perspective.” For
example, “I’ve noticed some trends with image positioning errors over the past month, and I’d like to hear your thoughts on what might be contributing to this.”
This phrasing emphasizes collaboration and signals that you value their input.
• Frame Challenges as Opportunities
Blame shuts down conversations. Instead, frame issues neutrally and factually. For example: “Here’s what I’m seeing: our repeat imaging rate for chest X-rays increased by 15% last month, with most repeats linked to incorrect patient positioning. Let’s discuss any challenges you’re facing and how we can address them together.”
This approach focuses on problem-solving and improvement rather than assigning blame.
• Focus on Behaviors, Not Character
Avoid statements like “You always make mistakes during busy shifts” or “You never communicate effectively.” Instead, zero in on specific behaviors such as “I’ve noticed recenty during evening shifts, scan delays are more frequent due to incomplete patient prep. Can we talk about what’s happening and how to prevent this going forward?”
This keeps the focus on observable actions and avoids making the technologist feel personally attacked.
STEP 3: EMBRACE SILENCE AND ENCOURAGE SOLUTIONS
• Pause for Reflection
Silence can feel awkward, but it’s essential for processing complex issues. After raising a concern, pause with: “Let’s take a moment to think this through.” You can also say, “Given the challenges with patient flow during peak hours, let’s take a minute to consider how we can streamline the process together.”
This approach invites thoughtful responses and reduces knee-jerk defensiveness.
• Invite Collaboration on Solutions
Rather than dictating changes, ask for their input: “What options do you see for moving forward?” Consider this example, “Given the increase in repeat scans, what steps do you think we could take to improve image quality and reduce repeats?”
This empowers the technologist to contribute solutions, fostering a sense of ownership and accountability.
STEP 4: FOLLOW THROUGH WITH CLARITY
End with Clear Next Steps. Avoid vague endings like, “Let’s touch base soon.” Instead, agree on a plan: “Let’s agree on next steps and set a time to check in.” You can say, “Let’s work on reviewing patient prep procedures during your next two shifts. I’ll follow up with you next Wednesday to see how it’s going and discuss any adjustments we might need.”
This ensures both parties leave the conversation with clear expectations and accountability.
Handling Resistance and Emotional Reactions
If they push back, acknowledge their perspective while redirecting the focus using such words like, “I understand this feels frustrating, and I want to support you. Let’s focus on what steps we can take to move forward.”
If emotions run high, pause the conversation if needed. You can say, “I can see this is upsetting. Let’s take a moment and regroup before we continue.”
These strategies keep the conversation productive, even in challenging moments.
Tough Conversations Build Stronger Teams
In radiology, every conversation impacts more than just the team – it impacts patient care.
Addressing tough topics with clarity, empathy and purpose resolves issues and strengthens your team’s trust and performance.
Start by making small changes in your approach. Practice opening conversations with collaborative language, like shifting from “We need to talk” to “I’d like to share some observations and get your perspective.”
Once you’re comfortable, layer in other strategies to refine your communication skills.
Each tough conversation is a step toward stronger relationships, better outcomes and a more cohesive department. Approach them with confidence – your team and your patients will benefit. •
— Nicole Dhanraj, Ph.D., SHRM-SCP, PMP, GPHR, CPSS, CRA, R.T(R)(CT)(MR), is an experienced imaging director.
BALANCING RESULTS AND RELATIONSHIPS
BY DANIEL BOBINSKI EMOTIONAL INTELLIGENCE
In the corporate world, organizations don’t crumble overnight. Devastating workplace issues often occur because of subtle, unnoticed fissures that, over time, lead to catastrophic breakdowns. Consider a company we’ll call TechNova (name changed to protect the guilty). It’s a mid-sized tech firm known for innovative solutions and a once-thriving workplace culture. The rise and fall of its research and development team illustrate what happens when leaders mismanage employees.
TechNova’s research and development department had 30 skilled professionals, and the team worked like a well-oiled machine for years. That is, until Mirriam took over as the department’s director.
Mirriam gained a quick reputation as a numbers person because her motto was “manage by metrics.” The problem? Not only did Mirriam focus solely on performance numbers, but she did so at the expense of employee well-being.
The effects weren’t noticeable at first. Over a span of four months, several seasoned team members departed, but these moves were easily explainable. Jenna, who was with the company for five years, transferred to a project management role in a different department. A man named Luis relocated to live closer to his aging parents. Another employee left for college so she could advance her career. Each exit was seen as a move for personal growth or life choices, not dissatisfaction.
However, Mirriam viewed these departures as opportunities to cut costs amidst a tightening budget. When team leads requested replacements of those who had left,
Mirriam’s response was, “We need to tighten our belts; let’s make do with what we have.”
THE DOMINO EFFECT
The reduced workforce still needed to deal with the same number of projects, which led to extended work hours and increased stress levels. Later, when the department missed a few deadlines, Mirriam began postponing vacations or cancelling them outright. This was met with much push-back, but Mirriam’s response was simply, “Our clients’ needs don’t pause for vacations.”
That went over like a lead balloon. Thinking her department could be more efficient, Mirriam hired a consulting company to assess departmental efficiency and optimize operations. Tragically, the company compiled incomplete and erroneous data, made incorrect conclusions, and then told Mirriam her team was overstaffed. Employees expressed much concern about the way the data was being interpreted, but Mirriam decided not to hire replacements when people left.
For many who were already tired of the mandatory overtime and having their vacations cancelled or postponed, this decision was the final straw. Resignations started pouring in, including those of longstanding, highly esteemed employees. In less than 12 months, a department that was once celebrated for its cohesion and excellence was now in disarray.
The reason? Leadership prioritized numbers over people.
A BROADER PERSPECTIVE
This scenario is not unique to TechNova. Similar things happened at Boeing during its push to produce the 737 MAX. Reports
The cracks in the dam are preventable; it’s leadership’s job to seal them up before the floodwaters break through.
revealed how intense pressure to meet production targets led to worker fatigue and morale issues. Employees voiced concerns about safety, but these were overshadowed by a “profits-first” mentality. The result? A loss of trust, internal disarray and a public scandal that shook the company’s foundation.
Even outside the corporate world, the consequences of poor leadership are evident. Consider the U.S. Postal Service during peak holiday seasons. Having several family members who’ve worked for the post office, I’ve heard firsthand how they get overwhelmed by being understaffed with unrealistic demands. Despite temporary hires, when leadership fails to plan adequately for high-volume periods, it leads to burnout, mistakes, delivery delays and dissatisfied customers.
THE PSYCHOLOGICAL IMPACT
Researchers have long studied the impact of leadership styles on workplace morale. According to a study published in the Journal of Organizational Behavior, leadership styles that emphasize tasks and goals at the expense of employee wellbeing can significantly erode trust and engagement. Under such conditions, employees begin to feel like cogs in a machine rather than valued contributors.
Another study, by Gallup, highlights that the number one reason employees leave their jobs is poor management. In other words, when leaders fail to recognize the human side of their workforce, they foster disengagement. This leads to decreased productivity and higher turnover rates. It’s like I said earlier: devastating workplace issues often occur because of subtle, unnoticed fissures that, over time, lead to catastrophic breakdowns.
RESTORING BALANCE
If employees are truly an organization’s greatest asset, then leadership must balance the needs of the organization with those of its people. One company that exemplifies this is Microsoft under the leadership of CEO Satya Nadella. After Nadella took the helm in 2014, Microsoft experienced a cultural transformation that emphasized both empathy and growth. These changes significantly revived the company’s internal culture as well as their bottom line.
The company now sees consistently higher scores in employee satisfaction surveys, which employees attribute to increased opportunities for development and a focus on work-life balance. Leadership also places an emphasis on more transparent communication throughout the company.
The result can be seen in Microsoft’s growth. Their annual revenue grew from $86.8 billion in 2014 to $245.1 billion in 2024.
WAYS TO BALANCE RESULTS AND RELATIONSHIPS
What can leaders do to prevent the kind of organizational decay seen at TechNova?
1. Value your team. Recognize that employees are the heart of the organization, and their well-being directly impacts performance.
2. Maintain open communication. Encourage feedback and be receptive to concerns. Dismissing genuine issues can lead to larger problems.
3. Balance metrics with humanity. While performance metrics are essential, they shouldn’t overshadow the importance of supportive work environments.
4. Adopt a proactive approach. Anticipate challenges and plan accordingly. Also, communicate openly. Teams need to know what’s going on to maintain esprit de corps and be resilient.
Bottom line, organizations like TechNova and Boeing serve as cautionary tales, highlighting the perils of neglecting the human element in an organization. Conversely, companies like Microsoft demonstrate that prioritizing employees doesn’t just boost morale – it drives long-term success.
By focusing on people as much as performance, leaders can ensure sustained success and a motivated workforce. The cracks in the dam are preventable; it’s leadership’s job to seal them up before the floodwaters break through. •
— Daniel Bobinski, who has a doctorate in theology, is a bestselling author and a popular speaker at conferences and retreats. For more than 30 years he’s been working with teams and individuals (1:1 coaching) to help them achieve excellence. He was also teaching Emotional Intelligence since before it was a thing. Reach him by email at DanielBobinski@protonmail.com or 208-649-6400.
Support Workforce Development with PartsSource’s 2025 Imaging Rewards Program
In the fast-evolving world of healthcare technology, staying ahead of the curve isn’t just a goal –it’s a necessity. The ability to maintain and service critical imaging equipment directly impacts patient outcomes and operational efficiency. With tight budgets and a constant demand to prioritize operational expenses, workforce development often takes a backseat. Investing in training is crucial for maintaining high-performing imaging systems and PartsSource is helping to bridge this gap.
PartsSource is excited to introduce the 2025 Imaging Rewards Program, a groundbreaking initiative designed to empower healthcare facilities by investing in their technical teams. By earning training credits through your purchases, PartsSource allows HTM leaders to fund workforce development without taking on additional financial burdens. This unique program enables teams to build their imaging training budget while meeting their ongoing procurement needs for imaging parts and glassware.
SUPPORTING WORKFORCE DEVELOPMENT
PartsSource recognizes that proper maintenance and
repair of mission-critical imaging equipment directly impacts a healthcare provider’s diagnostic imaging services operation, patient care, and bottom line. Keeping your technical staff trained and certified is essential for minimizing downtime, reducing costs, and maintaining regulatory compliance.
That’s why PartsSource is committed to the ongoing development of the healthcare technology management (HTM) workforce through comprehensive training solutions and strategic partnerships. In collaboration with the Radiological Service Training Institute (RSTI), PartsSource is ensuring imaging professionals have access to cutting-edge training and resources. RSTI offers industry-leading training courses that cover a wide range of imaging modalities, including X-ray, CT, MRI, and more. With hands-on training and expert-led instruction, your team will gain the confidence and skills necessary to keep your imaging equipment running at optimal performance levels.
WHAT IS THE 2025 IMAGING REWARDS PROGRAM?
The 2025 Imaging Rewards Program is a year-long opportunity for imaging service professionals to earn
valuable training tuition credits with RSTI – a leader in imaging equipment training. Through this program, every purchasing milestone achieved unlocks $2,000 in RSTI tuition credits, helping your facility stay equipped with the technical expertise required to maintain highperforming imaging systems. This program is designed to reward facilities for their continued investment in imaging replacement parts and glassware, ensuring that healthcare teams remain proficient in the latest service techniques and technologies.
HOW IT WORKS
Participating in the 2025 Imaging Rewards Program is simple and straightforward:
• Make Eligible Purchases: Purchase imaging replacement parts and glassware from PartsSource. Eligible items include components across all condition codes, modalities, and OEMs.
• Earn Tuition Credits: For every purchasing milestone reached, you’ll receive a $2,000 tuition credit toward RSTI training courses.
• Redeem Tuition Credits: Apply your tuition credits to RSTI courses to equip your technical team with essential skills.
PROGRAM DETAILS
• Eligibility Period: January 1, 2025, through December 31, 2025, at 11:59:59 PM PST.
• Delivery Deadline: Orders must be delivered by January 31, 2026.
• Eligible Purchases: All imaging replacement parts and glassware purchases, including all condition codes (new, used, tested, refurbished), modalities, and OEMs.
• Earn Tuition Credits: Receive $2,000 in RSTI tuition credits for every purchasing milestone achieved.*
(*Terms and conditions apply. Visit our website for full program details.)
TAKE THE FIRST STEP TOWARDS TECHNICAL EXCELLENCE
PartSource’s 2025 Imaging Rewards Program is your chance to invest in the future. By earning RSTI tuition credits through PartsSource purchases, you can empower your team to maintain and service critical imaging equipment with unparalleled knowledge and ability. Don’t miss this opportunity to invest in your team’s technical expertise and drive sustainable growth for your facility.
For more information, including terms and conditions, visit our website at partssource.com or contact your PartsSource representative today.
With the mission of ensuring healthcare is always on, PartsSource empowers providers and service organizations to maximize the clinical availability of mission-critical equipment and achieve sustainable savings and efficiencies. PartsSource connects more than 5,000 hospitals and 15,000 clinical sites with over 10,000 suppliers, enabling access to parts, services, and training through the leading technology platform for managing mission-critical healthcare equipment. Our technologydriven marketplace simplifies the supply chain for equipment service and connects thousands of providers with over 4 million mission-critical supplies and services. The PartsSource managed service (PartsSource PRO®) enables leading hospitals across the country to solve a shared set of challenges and maximize asset uptime, reduce costs, and increase procurement efficiency related to equipment maintenance. •
NEURODIVERSITY CAN TRANSFORM RADIOLOGY
BY NICOLE DHANRAJ
Our leadership within imaging plays a crucial role in building innovative, inclusive and high-performing teams.
One often overlooked area of talent acquisition is neurodiversity in radiology –hiring individuals with diverse neurological profiles, including autism, ADHD, dyslexia and other conditions.
Embracing neurodiversity goes beyond inclusivity – it’s about unlocking unique talents that drive innovation and enhance team dynamics.
WHY NEURODIVERSITY MATTERS IN RADIOLOGY
Neurodiversity in healthcare is gaining attention due to its potential to improve team performance and innovation.
Radiology demands precision, technical
proficiency and adaptability – traits often associated with neurodiverse individuals. For example, a 2019 Nature Communications study found that individuals on the autism spectrum excel in identifying anomalies in visual data, making them highly effective in detecting subtle irregularities in imaging equipment performance and quality assurance tasks (Pellicano et al., 2019).
Similarly, research from the Journal of Attention Disorders reveals that individuals with ADHD often thrive in dynamic, fastpaced environments due to their creative problem-solving skills (Kasper et al., 2017). Dyslexic professionals, according to the British Dyslexia Association, frequently exhibit advanced three-dimensional visualization abilities, crucial for tasks related to our profession (British Dyslexia Association).
DEI
By recognizing and harnessing these strengths, radiology departments can increase innovation, enhance patient care and create a more inclusive workplace.
Here’s how different neurodiverse strengths align with radiological tasks specific to imaging technologists:
• Autism: Exceptional attention to detail and pattern recognition. Imaging technologists with autism may excel in performing quality control checks, ensuring imaging protocols are consistently followed and troubleshooting equipment malfunctions
• ADHD: High energy, creativity and ability to adapt in fastpaced environments. ADHD strengths can be invaluable when managing multiple imaging procedures in busy settings, ensuring timely patient flow while adhering to safety protocols.
• Dyslexia: Strong spatial reasoning. Dyslexic imaging technologists often excel in operating advanced imaging equipment, such MRI and CT.
Creating an environment that values these abilities can lead to improved team performance, more innovative solutions and better patient outcomes.
Embracing neurodiversity within imaging is not just a
step toward inclusivity but a strategic advantage that drives innovation and enhances team dynamics.
By recognizing and leveraging the unique strengths of individuals with diverse neurological profiles, radiology departments can foster a workplace that excels in precision, adaptability and creativity. •
— Nicole Dhanraj, Ph.D., SHRM-SCP, PMP, GPHR, CPSS, CRA, R.T(R)(CT)(MR), is an experienced imaging director.
References
British Dyslexia Association. (n.d.). Dyslexia and spatial reasoning. Retrieved from https://www.bdadyslexia.org.uk/
Kasper, L. J., Alderson, R. M., & Hudec, K. L. (2017) Creativity and attention-deficit/hyperactivity disorder (ADHD): A review of conceptual and methodological issues. Journal of Attention Disorders, 21(4), 263-275. https:// journals.sagepub.com/doi/pdf/10.1177/1087054717727352
Pellicano, E., Smith, A. D., Cristino, F., & Hood, B. M. (2019). Visual processing strengths in autism spectrum disorder. Nature Communications, 10, 35494. https://www.nature. com/articles/srep35494
MEDICINE FOR THE SOUL ANXIETY CAN BE TREATED WITH CRANIAL ELECTRICAL STIMULATION THERAPY
Aclinical evidence assessment by ECRI, a global patient safety organization, found that cranial electrical stimulation relieves anxiety symptoms. The treatment was found to be more effective at relieving symptoms than fake stimulation – with or without medication –for some patients.
Cranial electrical stimulation (CES) is a noninvasive neuromodulation technique intended to treat some psychiatric disorders, including anxiety disorders, by delivering diffuse electrical stimulation through electrodes placed on the patient’s scalp or earlobes. This type of electrical stimulation is thought to normalize electrical
activity in parts of the brain that contribute to excessive fear and anxiety.
Evidence suggests some effects of CES persist for at least one month after treatment stops, and in some cases, may continue for up to six months. It is unclear if patients continue to respond to the treatment over longer periods of time.
CES is not to be confused with electroconvulsive therapy, a different, more invasive treatment that is considered a last resort therapy for treatment-resistant depression and other psychiatric pathologies.
Treatment for anxiety disorders usually involves medication, psychotherapy, or both. However, these
treatments do not work for all patients. Psychotherapy may be expensive, and it may be difficult to find a suitable psychotherapist. Some patients experience negative side effects from medication or do not want to take daily medication. Two cost studies suggested that cranial electrical stimulation may provide a cheaper alternative for patients seeking treatment.
“Cranial electrical stimulation is not widely used to treat anxiety,” said Marcus Schabacker, MD, Ph.D., president and CEO at ECRI. “Most patients bear the full cost of treatment since it’s not covered by Medicare, Medicaid or most private payer insurance companies. Usually, patients who have had this treatment have done it in a research setting, or they’ve exhausted all other options for treatment with no success. Because this treatment can be given by a nurse in a clinic, or by the patient at home, it could be more convenient than psychotherapy, and it’s scalable. It can be given with little-to-no psychiatry time.”
ECRI assessed peer-reviewed clinical literature published through mid-April of 2024 that addressed the treatment’s safety and effectiveness for anxiety, including five studies of more than 630 patients.
“This therapy has been studied since the ’60s, but until now there hasn’t been sufficient evidence showing that it’s a successful treatment option,” added Schabacker. “But
new research in the last several years sheds light on this treatment option as a way to relieve anxiety symptoms – not necessarily to replace the traditional treatment pathways of psychotherapy and medication. It’s exciting to see we now have a body of work that presents evidence of its effectiveness.”
Anxiety disorders are among the most common psychiatric illnesses. Anxiety disorders include generalized anxiety disorder, panic disorder, phobias, social anxiety disorder, separation anxiety disorder and selective mutism (i.e., the inability to speak in certain situations).
ECRI also assessed cranial electrical stimulation’s safety and effectiveness for treating depression and insomnia. However, the published evidence is insufficient to determine whether it improves symptoms for patients with depression or insomnia.
The ECRI team that generated this clinical evidence assessment helps healthcare providers, third-party payers and industry leaders make objective, evidence-based decisions on new, emerging, and existing healthcare products and interventions. These doctoral-level researchers identify, synthesize, and rate the strength and quality of the available evidence to help to drive positive outcomes, improve care quality, and lower costs. •
ICE Break
“Tomorrow
1 Concerned with identifying the cause of an illness or disease
7 Computing device
9 Traveler’s lodging
11 Theme of RSNA’s Chicago conference
13 Prefix meaning new
14 Male reproductive gland often evaluated medically with an MRI or ultrasound
16 Soft, radiant light
18 Type of drip, abbr.
20 Digital address for devices
22 The M in S.M.A.R.T. goals
25 Profit after expenses
27 _____ an exam
28 In the past
29 Computed tomography head, abbr.
33 Easily moved to different locations (desirable quality in radiology equipment)
36 Immediately, in medical lingo
38 Small container for liquids
39 Academic web domain ending
40 Wear away gradually
41 Strong and healthy
1 Lacking brightness
2 Currently fashionable
3 Device used to secure sutures in surgery
4 Decade before Y2K
5 Tube used to support blood vessels
6 Toward the interior
8 Syringe amts., abbr.
30 They inspire others to achieve more and achieve success
10 Works with other team members to achieve a common goal
Clamp shape
Standard used as a basis for moral actions 15 Be of use or benefit 17 Seven-day period
19 Ratio of 1-4 in spondyolisthesis
21 Type of scan used to evaluate the function of organs and tissues
23 Outstanding
24 Patient’s chart datum
26 graphy; type of radiography that measures body surface temperatures
31 Basic electromagnetic motion which is a basic in radiography
32 Heat measurement unit, abbr.
34 Prefix meaning two
35 “Shine a Little Love” rock grp., abbr.
37 Home security company
Radon Medical radonmedicalimaging.com • 866-723-6698