P.12 | PROFESSIONAL OF THE MONTH ANTHONY PHOENIX P.14 | DEPARTMENT OF THE
| ROUNDTABLE RTLS
Quickly
CONTENTS
P.12 SPOTLIGHT
p.12 Professional of the Month: Anthony Phoenix
p.14 Department of the Month: TRIMEDX/Sentara Clinical Engineering Department
p.16 Next Gen: Reed Stewart
p.18 Association of the Month: The California Medical Instrumentation Association (CMIA)
P.22 INDUSTRY UPDATES
p.22 News & Notes
p.29 Ribbon Cutting: IoMT Solutions
p.30 Welcome to TechNation
p.32 ECRI Update
p.34 AAMI Update
P.36 THE BENCH
p.36 Biomed 101
p.39 Tools of the Trade
p.40 Webinar Wednesday
p.43 MedWrench Shop Talk
P.44 FEATURE ARTICLES
p.44 Roundtable: RTLS
p.52 Cover Story: The Future of HTM: Increasing Innovation and Efficiency
P.56 EXPERT ADVICE
p.56 Careers Now
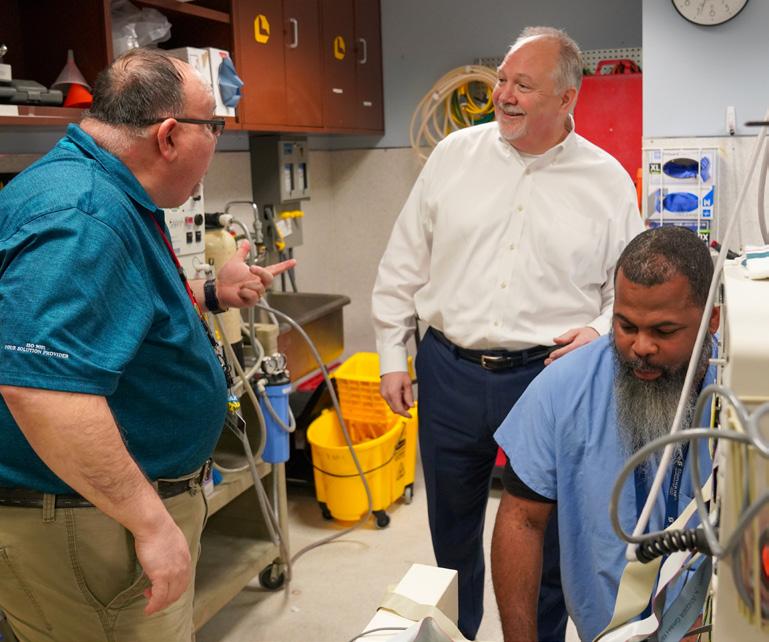
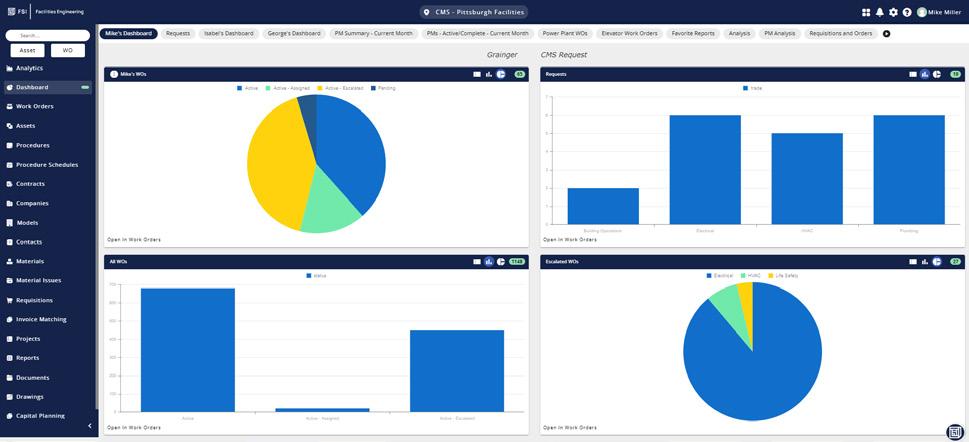
p.59 Company Showcase: FSI
p.63 Right to Repair
p.64 The Future
p.66 Cybersecurity
p.68 SPONSORED: Altamont Software
p.70 Networking Notes
p.72 Health-ISAC
PUBLISHER John M. Krieg
VICE PRESIDENT Kristin Leavoy
VICE PRESIDENT Jayme McKelvey BUSINESS DEVELOPMENT
EDITORIAL John Wallace
CONTRIBUTORS Roger Bowles
K. Richard Douglas
Jim Fedele
Joie Marhefka
Manny Roman
Steven J. Yelton
ACCOUNT Megan Cabot
EXECUTIVES Emily Hise
ART DEPARTMENT Karlee Gower
Taylor Hayes
Alicia Brown
DIGITAL SERVICES Cindy Galindo
Kennedy Krieg
Haley Harris
EVENTS Kristin Leavoy
WEBINARS Linda Hasluem
HTMJOBS.COM Kristen Register Sydney Krieg
ACCOUNTING Diane Costea
CIRCULATION Joanna Manjarrez
p.75 Biomed Brainbuster
p.82 Time Capsule
p.76 Preferred Vendors
p.78 Service Index
p.81 Alphabetical Index
EDITORIAL BOARD
Rob Bundick, Director HTM & Biomedical Engineering, ProHealth Care
Carol Davis-Smith, CCE, FACCE, AAMIF, Owner/ President of Carol Davis-Smith & Associates, LLC
Nadia ElKaissi, CHTM, Biomedical Engineer, HTM, VA Central Office (19HTM)
Bryant Hawkins Sr., Site Manager, Children’s Hospital of New Orleans
Earl Morris Jr., BMET, Director of Clinical Engineering, Harrison County Hospital
Leticia Reynolds, Clinical Engineering Operations Manager at UCHealth Parkview Medical Center
Make
the year you invest in your future with
Make 2025 the year you invest in your future with a career in Healthcare Technology Management. CBET offers 100% online programs tailored to fit your life, equipping you with the expertise to succeed in this rapidly evolving industry. Whether you're starting fresh or enhancing your current role, our programs empower you to reach new
Healthcare Technology Management. CBET offers 100% online programs tailored to fit your life, equipping you with the expertise to succeed in this rapidly evolving industry. Whether you're starting fresh or enhancing your current role, our programs empower you to reach new heights.
offers 100% online
fit your life, equipping
with the expertise to succeed in this rapidly
industry. Whether you're starting fresh or enhancing your current role, our programs empower you to reach new heights.
Lab Training
VR Lab Training
PROFESSIONAL OF THE MONTH Anthony Phoenix
BY K. RICHARD DOUGLAS
Anthony Phoenix is the director of biomedical engineering at Eskenazi Health in Indianapolis, Indiana. Phoenix had his interest in biomed piqued while pursuing a business major in college and changed his plans.
“As a college student studying business management, I was introduced to the biomedical engineering profession at a career fair held on campus. I thought that the work was interesting because I liked working with my hands and taking things apart to see how they work. I shadowed a biomed technician for the day at the local downtown hospital, then decided to switch my major,” he says.
Phoenix says that he started taking HTM courses with the idea to graduate and work as an in-house biomed technician.
“I attended school at Purdue University’s downtown Indianapolis campus, IUPUI, and graduated from the HTM program in 2002. I then went on to finish my B.S. degree in EET in 2006,” he says.
Since finishing training, Phoenix has come up the professional ladder, starting out as an entry level biomed technician (BMET I) in 2002, and promoted to BMET II and BMET III through 2006.
“I left the hospital setting in
2008 to work for Eli Lilly, a pharmaceutical company as an analytical instrument technician working on mass spectrometry, gas chromatography and HPLC (High Performance Liquid Chromatography) equipment. I returned to the hospital setting as an in-house radiology engineer in 2010. In 2021, I was promoted to the clinical engineer manager position, and most recently in 2021, was promoted to the director of biomedical engineering position,” Phoenix says.
The different roles that Phoenix has held have added to his areas of specialization.
“As an experienced biomed, I focused on OR equipment including anesthesia machines. As a radiology engineer, I
“The thing I like best about what I do for a living is that every day, I get to be a hero.”
specialized in MRI and nuclear medicine equipment, but also worked on CT, mammography and general X-ray equipment. As a manager, I was responsible for the day-to-day operations of the department as well as team performance metrics and regulatory accreditation reports. In my current role as director, I am primarily responsible for both the operational department and replacement capital equipment budgets,” he says.
DIRECTOR DECISIONS
Moving up the HTM professional ladder does come with some challenges.
“Throughout the years I have encountered many challenges. The biggest special challenge that comes to mind is the response to COVID. During that time, the biomed department was faced with the challenge of working onsite, responding to service calls, maintaining equipment PM completion as well as facilitating the extremely high demand of respiratory equipment,” Phoenix says.
He says that the department added over 700 pieces of equipment to its inventory during the COVID response and converted over 140 acuity adaptable rooms to critical care rooms by adding critical care patient monitors and central monitoring throughout the acuity adaptable space.
“Another challenge that I have encountered is related to medical equipment cybersecurity. We could see the demand for this skill set continue to grow as we continue to integrate our medical equipment with other network systems in the hospital. We created a new position, manager of clinical systems and medical equipment cyber security, on the biomed team to specifically address this challenge,” Phoenix says.
He explains that this position is responsible for potential incidents by an identifying risk score associated with medical equipment, then mitigating that risk by taking targeted actions on the medical equipment.
“As the director of the biomedical engineering department, I find myself being more involved in many projects. With the continued technology advancements, the medical equipment that the biomed team is responsible for maintaining is now integrated and connected to other systems which creates special circumstances for the HTM professional to troubleshoot. These projects associated with medical equipment integrations continue to be at the forefront of my responsibilities,” Phoenix says.
He says that capital equipment replacement planning is also a continued project that he facilitates.
“Because Eskenazi was built in 2013, and all of the medical equipment was new at that time, all of the medical equipment is aging at the same rate. Part of my responsibilities, as related to capital equipment replacement planning, is to develop a five-year capital plan to know what fleets of equipment we should replace early, what equipment we should replace on
time and what equipment we can safety push out a year or two and replace a little later,” Phoenix says.
Phoenix says that choosing biomed as a college student was the best decision he could have made. He reflects on the field as many HTM professionals view it.
“I value all of my experiences as a BMET and radiology engineer, getting to work on fascinating medical equipment. The thing I like best about what I do for a living is that every day, I get to be a hero. When I show up, there is usually a patient and/or a caregiver that is having a negative experience with their equipment. I love being able to fix the problem and making their day better. I appreciate their sincere gratitude when the problem is resolved and they can now move forward with providing their patient with the best care possible,” he says.
When not managing a biomed department, Phoenix enjoys boating, camping, riding ATVs and watching his sons’ youth sports games (football, basketball, baseball).
He has been married for 16 years and has two boys; 16 and 13 years old.
While a business major may lead to a worthwhile career, the decision to pursue HTM can present many opportunities. This biomed director has embraced his experience to evolve his career to the benefit of others.
BIOMETRICS
FAVORITE BOOK:
“Baby Steps Millionaires” by Dave Ramsey
FAVORITE MOVIE:
“Old School”
FAVORITE FOOD:
Pizza. (pepperoni, sausage, ham, bacon, mushroom, green pepper) or (ham, jalapeno, pineapple)
FAVORITE PART OF BEING A BIOMED DIRECTOR?
I enjoy leading my team to success. I appreciate my teams feedback and ideas then implement those to make positive changes. I see myself as kind of a “fire fighter” because I put out fires all day long. When someone comes to me with a problem, “a fire”, I do my best to bring them to a positive resolution that we can both be proud of. I enjoy engaging with the senior leaders of the organization and look to them for feedback on my performance. I love being part of an industry that is constantly evolving, and I appreciate the fact that every day brings new challenges.
DEPARTMENT OF THE MONTH
TRIMEDX/Sentara Clinical Engineering Department
BY K. RICHARD DOUGLAS
Virginia Beach is one of the better-known resort cities along the east coast, drawing tourists every summer from further north and from other eastern states.
Visitors will often hear the loud F/A-18 Super Hornets flying in and out of Naval Air Station Oceana. Not far from the naval air station, in the opposite direction from the tourist beaches, is Sentara Princess Anne Hospital.
The clinical engineering team at Princess Anne are known for taking on interns and junior volunteers and acting as good ambassadors for the HTM profession.
The TRIMEDX department is comprised of four techs, an imaging tech, an assistant manager and site manager.
Members include Senior Site Manager Sandy Mason, CHTM; Assistant Manager Tai Steede Sailor; Senior Technician Corinne Davis, CBET; Christina Taylor, CBET, BMET III; Chris Johnson, BMET II; Michelle Wiggs, BMET I; and Cassie Redburn, Imaging Tech I.
“Here at Sentara Princess Anne Hospital, the clinical engineering department is a six-member shop, comprised of five BMETS and one imaging technician. We utilize our shop to better the HTM field for our fellow technicians by providing a space for internship and skill bridge candidates, as well as sponsor high school volunteers, building recognition of our field with the youth,” Mason says.
“We also provide leadership training for current TRIMEDX technicians. All of this allows for us to support the system that is 12 hospitals (2,800-beds) and supporting imaging centers, senior care centers, outpatient clinics, primary care physician offices, outpatient therapy centers and homecare, all throughout Virginia and North Carolina,” she adds.
The department supports Princess Anne Hospital, a 176-bed acute care facility, and the surrounding campus that includes a plastic surgery center, advanced imaging center, pain management center, comprehensive breast center, four outpatient therapy centers, two urgent care centers and a variety of specialty clinics and physician practices.
“Service contracts are obtained by both TRIMEDX and Sentara; but all are managed by TRIMEDX. The customer will reach out to us for support. We follow up and ensure the maintenance is completed during its allotted schedule,” Mason says.
She says that the team’s CMMS tracks the PM schedule and opens work orders proactively when the PMs are due along with all other contracted services provided.
The department also coordinates with IT to harden the threat surface and network devices.
“We are actively involved in the CE/IT arena. The devices are monitored, threats assessed, and software patches applied and/or any approved remediation activity completed. We also work closely with IT for integration into the patient record and/or any device safety and/or drug library monitoring systems,” Mason says.
Data collection is done throughout the life cycle of all devices.
“Originally at incoming inspection, we collect all appropriate information to include (but not limited to) make, model, SN, MAC address, operating system, applications software revision and photos. This information is validated and if necessary updated whenever we touch the unit – annually at a minimum,” Mason adds.
INFUSION CONFUSION
The department has even achieved positive results when confronted with competing projects.
“We recently opened a new wing, which allowed us to move the stroke/med surg department closer to ICU and stepdown to create better flow for our patients. Also added was a new wound care clinic that features two hyperbaric chambers. This was occurring at the same time as our department was moved to a different part of the hospital,” Mason says.
She says that the CE team was able to validate and reallocate many devices to cover the needs of the new unit assisting with reducing unnecessary capital expenditure, standardizing like units and doing their part to allow clinical staff to ensure patient safety.
“We actively worked with the PACs department, IT and clinicians to move towards a new PACs system. We coordinated and performed all changes with minimal interruption to patient flow or uptime. By being flexible and working with the various impacted departments we were able to complete an average of 45 modalities per week for a four-week period. The system went live with no issues,” Mason says.
In addition to tackling multiple projects simultaneously, the team has put its collective minds together to problem-solve.
“One of the issues that is prevalent and frustrating to
our healthcare system is the movement of infusion devices when patients are transferred to a different level of care. This results in many smaller facilities struggling to have the appropriate number of devices to ensure appropriate patient care. We identified that one [of the] most common drivers of the devices leaving those facilities was that the patient transportation organization, that the health system partnered with, was transferring the devices with the patients. The reasons for this were not that they had devices that used different disposables but that their devices were not able to utilize that drug library approved by the system,” Mason says.
She says that by coordinating with the pharmacy and the transportation company, the CE team was able to offer a solution to where the devices could be updated by CE on a periodic basis – as new library changes are approved and pushed – so that the patient could be placed on the devices owned by the transportation staff therefore keeping the number of devices leaving the facility to a minimum.
“We have recently enacted this drug library solution and are already seeing a week over week reduction in devices leaving the facilities therefore helping to ensure safe, timely and appropriate patient care and a reduction of clinical staff time obtaining the proper device,” Mason says.
Aways from work, the team is actively involved with the Virgina Biomedical Society (including a board member) and AAMI.
As Navy jets fly overhead, patients and clinicians at Sentara Princess Anne are assured that the country is protected and the medical devices they depend on are professionally managed.
Pictured from left to right are TRIMEDX/Sentara Clinical Engineering Department members Christina Taylor, Cassie Redburn and Michelle Wiggs.
NEXT GEN POWERED BY YP AT MD Reed Stewart R
eed Stewart serves as a BMET III at Betsy Johnson Hospital-Cape Fear Valley Health System. He began his HTM career by earning an associate in applied sciencebiomedical equipment technology from Durham Technical Community College.
TechNation recently interviewed Stewart to find out more about his interest in HTM and his goals for the future.
Q: WHERE DID YOU GROW UP?
A: Dunn, North Carolina
Q: WHERE DID YOU RECEIVE YOUR HTM TRAINING/ EDUCATION?
A: Durham Technical Community College
Q: HOW DID YOU FIRST DISCOVER HTM?
A: Viewing available local college programs, and discovered the program at Durham Tech.
Q: WHY DID YOU CHOOSE TO GET INTO THIS FIELD?
A: I’ve always had a desire for technology and repairing mechanical/electrical systems. My dad also always encouraged me to get a job in the healthcare field, so biomed is a perfect combination of the two.
Q: WHAT DO YOU LIKE MOST ABOUT YOUR POSITION?
A: I enjoy the amount of value that I feel from performing this job, from the feeling of helping the users resolve their issues to explaining our little-known field to people outside of the healthcare world.
Q: WHAT INTERESTS YOU THE MOST ABOUT HTM?
A: I enjoy learning the real-world relationships between a piece of electrical equipment and its applications to the human body. Being able to see and understand the technology that bridges physical
readings to analytical data is very interesting to me.
Q: WHAT HAS BEEN YOUR GREATEST ACCOMPLISHMENT IN YOUR FIELD THUS FAR?
A: Receiving employee of the year in our clinical technology services department this year.
Q: WHAT GOALS DO YOU HAVE FOR YOURSELF IN THE NEXT 5 YEARS?
A: I would like to continue to learn how to service more equipment in house, and possibly start branching into more in-depth imaging service.
FUN FACTS
FAVORITE HOBBY: Saltwater fishing
FAVORITE SHOW OR MOVIE: “The Hateful Eight”
FAVORITE MEAL: Homemade lasagna
WHAT WOULD YOUR SUPERPOWER BE?
Being able to read nurses’ handwriting would be an incredible power
1 THING ON YOUR BUCKET LIST: Scuba diving a shipwreck
SOMETHING YOUR CO-WORKERS DON’T KNOW ABOUT YOU:
My wife and I are thinking about having a baby soon
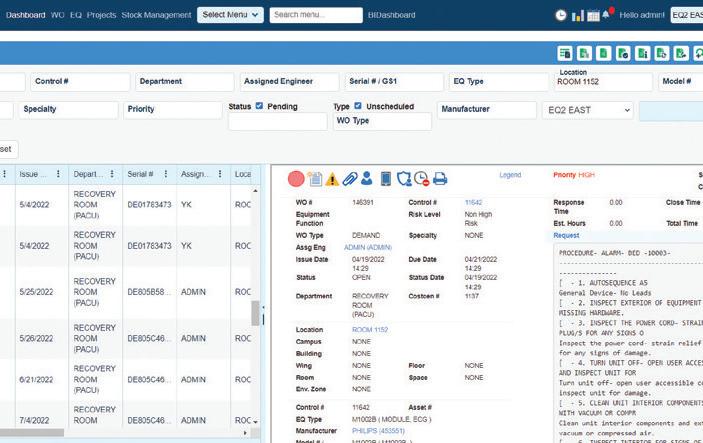
LOOKING FOR A CMMS THAT IS DESIGNED FOR HTM BY HTM EXPERTS?
EQ2 HEMS – is focused entirely on healthcare maintenance management
Management and Technicians achieve more in less time
Integrate with all of your existing systems
Compliance and AEM made easier with the right tools and reports
Our system helps you keep your devices protected
Data and information that shows leadership how your department saves the hospital money
Years
ASSOCIATION OF THE MONTH
The California Medical Instrumentation Association (CMIA)
BY K. RICHARD DOUGLAS
Few states in the continental U.S. have more natural beauty than California. The expansive state offers coastal communities, wine country, tourist destinations like Disneyland and the Golden Gate Bridge and production of twothirds of the nation’s fruit and nut crops.
The state contains approximately 400 hospitals, which equates to a lot of medical equipment and a lot of healthcare technology management professionals.
The California Medical Instrumentation Association (CMIA) is one of the country’s oldest and largest HTM organizations. The statewide organization includes eight local chapters. It was founded in 1972 and incorporated in 1992. TechNation previously highlighted CMIA in 2019; pre-pandemic.
From 1974 to 1981, the group met once annually at Cottage Hospital in Santa Barbara, California. The group became a model for subsequent biomed association formations in several states.
Current CMIA leadership includes the Chair Byron Webster and Chair Pro-Tem Jason Velick. Additional leaders include Conference Chair Jennifer Nichols, Secretary Emily Hickerson and Treasurer Karie Heiselt.
“The CMIA was established by a group of dedicated professionals in the biomedical engineering field who recognized the need for a statewide organization to support and advance the profession. While specific founding members are not detailed in our records, their collective vision has significantly contributed to the growth and success of the association,” Velick says.
He says that since the group’s inception in 1972, CMIA has grown into a thriving statewide non-profit organization dedicated to serving the needs of the biomedical community through eight local chapters. The association focuses on promoting education, facilitating information exchange, and fostering a sense of community among clinical biomedical engineering professionals in California.
The local chapters keep HTM professionals in each region apprised of what is going on.
“Each of the CMIA’s eight local chapters holds regular meetings, typically on an every-other-month basis. These meetings provide members with opportunities for professional development, networking and information exchange. While in-person attendance is encouraged to foster community engagement, some chapters offer online simulcasts to accommodate members who cannot attend physically, ensuring broader participation,” Velick says.
He says that the organization actively collaborates with local biomedical technical schools and community colleges to support educational programs and provide students with industry insights.
“These partnerships include guest lectures, workshops, and internship opportunities, bridging the gap between academic training and professional practice,” Valick says.
To bolster this commitment, the group offers scholarships to support students pursuing careers in biomedical engineering and related fields.
“These scholarships aim to alleviate financial barriers and encourage academic excellence among aspiring professionals. Details about eligibility criteria and application processes are available on the CMIA website,” Valick adds.
CONNECT WITH CMIA
As a large, multi-chapter association, it is safe to anticipate that any annual conference would be comprehensive and a large undertaking. CMIA brings together many attendees
from far and near.
“The CMIA hosts an annual conference known as ‘CMIA Connect,’ which serves as the premier educational event for healthcare technology management professionals in California. The conference features keynote speakers, educational sessions, networking opportunities and exhibits showcasing the latest advancements in medical instrumentation. For instance, the 2024 CMIA Connect was held at the Hilton Anaheim Hotel from January 18-20, 2024,” Valick says.
He says that the 2024 event featured a range of educational sessions, keynote presentations from industry leaders and an exhibit hall showcasing cutting-edge medical technologies.
“Attendees had ample opportunities for networking and professional development. Plans for the upcoming conference include expanding the educational tracks, increasing exhibitor participation and enhancing interactive sessions to provide attendees with a comprehensive learning experience,” Valick adds.
attract new members to the field.
Education and training are often the primary focuses of biomed associations. CMIA identifies this activity as only one of their objectives.
“Beyond education, the CMIA emphasizes networking opportunities, professional development and advocacy for the biomedical engineering profession. We host events that encourage collaboration among members and support initiatives that advance the field. Additionally, the CMIA is committed to community outreach, aiming to inspire the next generation of biomedical professionals,” Velick says.
With more veteran biomeds exiting the profession, it has become incumbent on biomed associations to help back-fill those positions by encouraging more interest in the field.
With more veteran biomeds exiting the profession, it has become incumbent on biomed associations to help back-fill those positions by encouraging more interest in the field.
“The CMIA addresses the impending workforce gap by engaging with educational institutions to promote careers in healthcare technology management. We participate in career fairs, offer mentorship programs, and provide resources to students and early-career professionals. Additionally, the association leverages social media and professional networks to reach a broader audience and
Many state biomed associations had to make substantial adjustments during the pandemic and some had their operations thrown off substantially. CMIA moved to a digital format to accommodate the disruption of in-person events.
“The COVID-19 pandemic necessitated a swift transition to virtual platforms for meetings, conferences and educational sessions. The CMIA adapted by hosting webinars and online workshops, ensuring that members continued to receive valuable content and opportunities for engagement. This shift also highlighted the importance of digital resources, leading to the development of a knowledge base accessible to members statewide,” Velick says.
In the state with the largest population, the statewide HTM association does not disappoint. CMIA continues to be a pioneer and thought leader among biomed associations and keeps the states’ biomeds connected.
New chapter formed 12/10/24. The 8th chapter of the CMIA is the Coachella Valley chapter. Featured is the current chair Byron Webster and the Chair Pro Tem Jason Velick along with the new officers for the Coachella Valley chapter.
CLICK. WATCH. EARN!
CLICK. WATCH. EARN!
LIVE WEBINARS
FEBRUARY 5
SPONSORED BY
TOOLS OF THE TRADE
Save the date for this live webinar. Participation is eligible for 1 CE credit from the ACI.
FEBRUARY 12
SPONSORED BY
WEBINAR WEDNESDAY
Save the date for this live webinar. Participation is eligible for 1 CE credit from the ACI.
FEBRUARY 26
SPONSORED BY
WEBINAR WEDNESDAY
Save the date for this live webinar. Participation is eligible for 1 CE credit from the ACI.
PODCAST
SPONSORED BY
“The Key to Growth in the HTM Industry and MMS sponsored Bringing together Women Leaders in HTM”
ON-DEMAND
SPONSORED BY Tools of the Trade demo
SPONSORED BY
“Going beyond “Where’s my thing?” Asset Management that increases utilization and automates PAR”
All webinars, podcast, and product demos are eligible for 1 CE credit from the ACI.
RTLS Asset Tracking
Delivers room-level intelligence without room-level hardware
AI-enabled location intelligence
SaaS model that eliminates upfront hardware expense and expeites ROI
Less than 50% hardware vs. legacy platforms
No Wi-Fi impact
NEWS & NOTES
Updates from the HTM Industry
UCONN CLINICAL ENGINEERING INTERNSHIP PROGRAM ATTENDS MD EXPO
BY CAROL DAVIS-SMITH
The UCONN campus welcomed our arrival with a beautiful fall day. We only had one day on campus because we took the opportunity to align our Fall 2024 CE Week with the MD Expo New England conference which was supported by MD Publishing, TechNation and the New England Society for Clinical Engineering (NESCE).
DAY 1 – FALL 2024 CE WEEK
Day 1 was our day on the UCONN Storrs campus, so we took the opportunity to get outside and take a new class photo!
The rest of the day was spent in workshop-like activities. We began by sharing our course registrations and rationales behind those choices in an effort to optimize our MD Expo experience. Our discussion was
very interesting because many of the interns had never attended a conference and session titles are sometimes hard to interpret. One lesson learned – don’t rely on the title, read the description. All of us had at least one “ah ha” moment as we listened to each other’s thoughts about why they chose (or didn’t choose) certain sessions. Another lesson learned – our perspectives are formed by our individual experiences, values, and interests; therefore, we can enrich our perspectives by listening.
In the afternoon, we explored the process and concept behind forecasting medical equipment replacement needs. Most of you know this is a passion of mine and a bit of a “Goldilocks” exercise – i.e., finding just the right “fit” for determining what, when, and why to replace. The interns were randomly placed in three groups that rotated through three stations – Technical criteria, Clinical
criteria, and Business/Financial criteria. Each group charted criteria they thought was important, what data was required, and how it would be evaluated. The interns were then asked to stand next to the station with which they (individually) had the most comfortable and/or confidence. Each station selected a first-year and second-year intern to present the criteria to the larger group. A fascinating discussion ensued during which we (again) all learned something new. A third lesson learned – Forecasting is about objectively identifying what needs to be replaced at what time and why; it is not determining how to spend a defined budget; that comes later in the process.
DAYS 2, 3, AND 4 – FALL 2024 CE WEEK
The rest of CE Week was spent at the MD Expo New England.
Some of the UCONN CE interns were fortunate enough to get front row seats for the session on working with Peri-Op Nurses.
The exhibit hall was a first-time opportunity for many UCONN CE interns to see so many vendors in one place. Because of our prep work on Day 1, many were able to make excellent use of the exhibit hall time to find answers to challenges at their hospitals. Some second-year CE interns also used the opportunity to explore potential career paths.
We even had Exhibit Hall Vendor BINGO winners!
The interns joined in the fun at the MD Expo Young
Professionals reception. This was an opportunity to meet new and rising leaders in the HTM/CE community in a more informal situation.
The next morning, it was a quick breakfast then back into networking and the educational sessions.
The Octoberfest Finale Party was an opportunity to regroup and compare experiences.
With that, we wrapped up our Fall 2024 CE Week. We had an intense week of learning, networking, and even a bit of fun. I would be remiss if I did not extend a huge Thank You to the MD Expo and NESCE teams who helped make this experience possible and provided all of these and more photos on their website.
I also want to thank the host hospitals and health systems, for providing the real-world experience so valuable to our interns.
Last, but certainly not least, thank you to everyone who shared my posts with your networks! That visibility is so very important. Reach out to me if you’re interested in learning more about the UCONN Clinical Engineering Internship program or if you would like to hire one of our talented students!
— Carol Davis-Smith, MS, CCE, FACCE, AAMIF, is the UCONN BME Clinical Engineering Internship Program Director.
INDUSTRY UPDATES
AGILITI LAUNCHES NEW ADAPT LINE OF THERAPEUTIC SUPPORT SURFACES
Agiliti, a nationwide manufacturer and provider of medical device solutions to the health care industry, recently announced the launch of its Adapt Line of therapeutic hospital support surfaces, clinically engineered to enhance patient comfort and help reduce the risk of pressure injuries resulting from prolonged bed rest.
“The introduction of the Adapt Line marks a significant milestone for Agiliti, establishing its position as a branded innovator of medical technology,” said Tom Leonard, CEO of Agiliti. “We are now one of the only manufacturers of therapeutic support surfaces backed by an extensible platform of medical device management, maintenance and clinical service solutions. For more than eight decades, Agiliti has been the nation’s leading provider of ready-access medical technology and service solutions. We are proud to bring more of our clinical capabilities to market with this important new product line.”
The Adapt Line includes three models: Adapt Air Pro, Adapt Air and Adapt Convertible – designed to meet the needs of patients across a wide range of acuity levels. Each model is built for optimal pressure injury prevention and treatment with proprietary immersion and alternating pressure algorithms. In connection with a recent clinical study evaluating existing pressure injuries among 84 critically ill patients, 100% of clinicians surveyed (n=33) recommended Adapt Air Pro for its ease-of-use, management of pressure distribution and microclimate.
Other key features of Adapt Line include:
• Adapt Pump: A quiet and easy-to-use pump that works across all Adapt Line models, designed to maintain surface inflation during transport and provide up to eight levels of customizable support for better patient outcomes.
• Next-Gen Microclimate Management: A specially formulated top
COGNOSOS LAUNCHES FAST LANE FEATURE
Cognosos has announced the launch of Fast Lane, a low latency feature for its hospital staff safety and duress solution, Cognosos Guardian. Fine-tuned and custom-built for the chaotic nature of hospital environments, Fast Lane introduces a high-priority communication pathway designed to expedite critical information through the network, ensuring that hospital staff receive the timeliest assistance in emergencies.
Approximately 40% of health care employees have experienced workplace violence in the last two years. With this increasing rate of verbal and physical abuse directed at health care workers, 80% of hospital staff have reported feeling safer with dedicated duress solutions.
“Hospitals are challenged with finding IT-friendly, end-to-end communication systems that are also reliable, accurate and fast,” said Jeff Stiffler, senior director of product, Cognosos. “Staff safety solutions hinge on three critical elements: a discreet way to notify
cover fabric, AirSpace mesh, and the Adapt Pump ensure non-stop, targeted airflow beneath the entire patient/surface interface.
• Proprietary CoreShield: A waterproof top cover and RF-welded seams give the Adapt Convertible foam-based model superior construction to withstand the rigors of care, resist fluid ingress and support higher levels of infection prevention.
• Capacity Expansion: The Adapt Line provides options to extend length, width and weight capacity through patented technology to transform from 35 to 48 inches wide; from 82 to 86 inches long; and, up to a max weight capacity of 1,000 lbs.
• Vertical Cell Technology: The Adapt Air Pro is designed with twenty 8-inch air cells with vertical cell technology to maximize immersion and envelopment while providing two clinically-effective pressure redistribution therapies – leading to 37% more immersion compared to similar 6-inch surfaces
“Nearly 3 million U.S. patients per year are treated for pressure injuries related to support surfaces – costing hospitals upward of $17.8 billion,” said Tim McCarty, general manager of beds and therapeutic support surfaces at Agiliti. “Support surface selection plays a critical role in injury prevention and treatment, and the features of the new Adapt Line are proven to help both prevent pressure injuries and accelerate their healing.”
Along with its manufactured lines of beds and therapeutic support surfaces, Agiliti provides rapid access, management and maintenance of life-saving medical equipment across the medical, surgical and procedural space. These solutions have been shown to help clinicians improve patient care and drive greater efficiency among health care networks.
security, accurate location tracking of the incident, and effective communication to the necessary personnel. If any one of these fails, the system fails. Cognosos Guardian already encompasses these features. The addition of Fast Lane enhances communication speed by providing a dedicated alert pathway.”
Cognosos Guardian includes a discreet, wearable staff duress button that upon activation allows hospitals to locate the employee who is wearing the badge in real-time – regardless of whether they are moving within a facility, outside in pathways, or a parking lot or garage. Cognosos is the only company that provides this coverage indoors and outdoors with minimal installation requirements.
“In critical moments, every second counts. We created Cognosos Guardian with Fast Lane so healthcare workers could focus on their work rather than worry about how long it might take for help to arrive. This innovation reinforces our commitment to improving the safety and well-being of staff and patients,” continued Stiffler.
BIOMEDICAL EQUIPMENT TECHNOLOGY ALUM RETURNS TO TEACH AT TSTC
Texas State Technical College alumnus Armando Ortiz Jr. has fond memories of when he and his father walked the stage at TSTC’s spring commencement in 2013 and received associate degrees in biomedical equipment technology from TSTC’s Harlingen campus.
Ortiz’s father recently retired from Toyota, where he performed maintenance on an assembly line. Ortiz himself worked in the biomedical equipment field for 12 years and this fall returned to TSTC as an instructor in the biomedical equipment technology program.
“I’ve been an instructor for four months,” he said. “It’s been my privilege to coach our students to be the best biomedical technicians in the country.”
Before Ortiz graduated from TSTC, he had an internship at General Electric in Houston that transitioned into a full-time job as a biomedical equipment technician with the same company in Corpus Christi. Before returning to TSTC to teach, he helped open and operate a Harlingen medical facility as its chief technology officer.
Ray Longoria is team lead for TSTC’s biomedical equipment technology program in Harlingen.
“Armando’s teaching approach emphasizes hands-on learning and real-world scenarios,” he said. “By having his students troubleshoot medical devices under realistic conditions, he equips them with technical and critical-thinking skills and problem-solving abilities, which are essential for their careers.”
Ortiz said his new role provides him with a new kind of fulfillment.
“I have a passion to make a difference with my students,” he
said. “I am transparent about the kind of events and repairs they will experience. That will prepare them for their career success.”
TSTC offers an Associate of Applied Science degree in biomedical equipment technology at its Harlingen and Waco campuses, as well as an Associate of Applied Science degree in medical imaging systems technology specialization at the Waco campus.
According to onetonline.org, the average annual salary for medical equipment repairers is $50,600 in Texas, where the number of jobs in that field was forecast to increase 18% between 2020 and 2030.
Registration continues for the spring semester at TSTC. To learn more, go to tstc.edu.
Welcome to GMED ONE, where we have been setting the gold standard in biomedical repair services since 2011. As a leader in the field, we pride ourselves on our reputation for excellence, trust, and unparalleled service.
Our mission is to provide fast, reliable repairs on a wide range of medical equipment, ensuring that healthcare professionals can continue to deliver the highest quality care to their patients.
The latest news and events from TechNation
MD EXPO ENHANCES SCHEDULE IN 2025
MD Publishing announced the spring MD Expo is set for April 15-17 in Southern California. MD Expo SoCal continues the long history of delivering excellent educational opportunities, networking events and a solutions-filled exhibit hall.
MD Expo SoCal also features:
• Welcome Reception
• Networking Lunch
• Extended Exhibit Hall Grand Opening
• Several Hands-On-Training (H.O.T.) Workshops
MD Expo strives to provide healthcare technology management professionals with a unique, intimate and rewarding conference second to none. Clinical engineers, biomedical technicians, directors and managers, procurement/asset managers and others responsible for medical technology will gather in a one-of-a-kind warm and welcoming environment to network with peers, learn the latest technologies and advances in HTM.
As always, MD Expo offers free registration for hospital
employees, students and members of the U.S. Armed Forces.
MD Expo returns to Pechanga Resort Casino in the Temecula Valley, minutes from the beautiful Temecula Wine Country and Old Town Temecula. It is one of the largest casino resorts in the United States.
MD Publishing and TechNation thanks sponsors AllParts Medical, AIMS3, Prescott’s, USOC Bio-Medical Services, EQ2, PM Biomedical and MW Imaging for their support.
Find out what everyone has been talking about; this is one event you can’t afford to miss!
WEBINAR WEDNESDAY COMPLETES SUCCESSFUL 10 YEAR CELEBRATION
Webinar Wednesday benefitted from amazing presenters, generous sponsors, new Tools of the Trade demonstrations and more in 2024 as it tallied 3,437 registrations in 2024.
The Webinar Wednesday series averaged 123 registrations per webinar. Highest registration and attendee numbers for 2024 were recorded by Fluke and Pronk.
Highest rated presenters for the year were Rigel’s Lewis Lennard and Healthmark’s Jahan Azizi.
Attendees praised Webinar Wednesday throughout the year. Attendees were asked “What does Webinar Wednesday provide the industry?”
“A lot of great information on new equipment,” said Jason Chaffin, lead BMET with St. Luke’s Vintage.
“Up-to-date information about innovations in industry,” stated Rafik Mesropyan, CBET, Loma Linda University.
“This event provides a great support system for HTM employees to stay active in the industry and the AAMI standards,” said Alec Hadley, field services manager with ReNew Biomedical.
“A chance to bring valuable information to various professionals around the globe,” said Isaiah Ledesma, biomedical engineering technology instructor at St. Philip’s College.
“Provides helpful insight into new and emerging technologies,” said Jody Butler, biomedical equipment technician with
Memorial Hospital of Sweetwater Memorial.
“Webinar Wednesday provides the industry insight to resources that we may not have known about otherwise as well as helpful information pertaining to changes in the industry,” shared Robert Wentworth, vice president of biomedical operations for VIKAND.
“Updates, useful information to be informed in this fast-paced industry,” said Rafik Mesropyan, CBET, with Kaiser Permanente.
View on-demand recordings of the 2024 webinars and register for upcoming webinars at WebinarWednesday.live.
RECORD NUMBER OF VOTES FOR TECH CHOICE AWARDS
The Tech Choice Awards continue to grow as they shine a spotlight on the important and amazing work HTM professionals complete on a daily basis.
The 2025 Tech Choice Awards (also known as the Wrenchies) had more than 6,500 votes.
MD Publishing’s Jayme McKelvey released the number of votes recorded as of December 2024 . She also said it is an honor for TechNation to celebrate HTM prtofessionals again this year.
“I love the Tech Choice Awards because they provide a unique opportunity to celebrate outstanding achievements and the incredible individuals behind them,” McKelvey said. “It’s deeply rewarding to help shine a well-deserved spotlight on men and women whose hard work and dedication often go unrecognized. These moments of recognition inspire others and create a sense of pride and appreciation within our industry. TechNation is truly honored to bring the Tech Choice Awards to the biomedical and HTM industry, and we are looking forward to celebrating the 2025 winners at MD Expo SoCal.”
Finalists were selected during a month-long nomination process.
The Tech Choice Award categories are:
• Professional of the Year – sponsored by Renovo Solutions
• Department of the Year – sponsored by USOC Medical
• Young Professional of the Year – sponsored by Prescott’s
• ISO Employee of the Year – sponsored by Elite Biomedical Solutions
• Director/Manager of the Year – sponsored by MW Imaging
• Lifetime Achievement Award – sponsored by Tri-Imaging Solutions
• Military BMET of the Year – sponsored by College of Biomedical Technology Equipment
• Humanitarian Award – sponsored by Healthmark
• Women in Leadership Award – sponsored by Avante Health Solutions
• Educator of the Year – sponsored by Maull Biomedical
• Outstanding Vendor of the Year
• Association of the Year – sponsored by MultiMedical Systems
• Industry Influencer of the Year – sponsored by Soma Tech Intl
The top nominees for each category were highlighted in the October 2024 issue of TechNation with voting allowed until January 10, 2024. Wrenchies will be awarded with the winners selected based 100% on votes from those who make up the HTM industry. Winners will be announced in the March issue of TechNation and highlighted in a special digital supplement.
NOMINATIONS OPEN FOR 40 UNDER 40: CELEBRATE THE RISING STARS OF HTM
TechNation is thrilled to announce that nominations are now open for the 2025 40 Under 40, powered by YP at MD. Now in its fourth year, this prestigious program shines a spotlight on the next generation of leaders in the healthcare technology management (HTM) industry.
Each year, TechNation honors a diverse group of accomplished young professionals who are driving innovation, excellence, and progress in HTM. Last year’s honorees exemplified the intelligence, creativity, and dedication that make this field so impactful—and now it’s time to recognize the next wave of outstanding talent!
If you know an exceptional HTM professional under 40, we encourage you to nominate them for this honor. Applications are
open now at 1technation. com/2025-40-under-40/, with a submission deadline of April 25. Don’t wait — help us highlight the best young biomeds shaping the future of HTM!
The YP at MD program, supporting the 40 Under 40, is a dynamic community of young professionals in the HTM field. Members benefit from exclusive networking opportunities at MD Expos, HTM Mixers, and through online platforms, fostering connections and sharing ideas for a bright future in HTM.
For more details about YP at MD, visit 1technation.com/yp.
Control Capital Cost and Ensure Safe, Uninterrupted Patient Care
Objectively develop a systematic, multi-year capital budget replacement plan with help from ECRIʼs expert team on your timetable that meets strategic goals, controls maintenance costs, and minimizes risk.
Uncover the hidden costs of aging technology
Mitigate chances of sudden device failure
Identify potential hazards with existing devices
Enhance Capital Equipment Planning
Learn more at home.ecri.org/predictive-replacement-planning or contact us today at 610-825-6000, x5891.
RIBBON CUTTING
IoMT Solutions
The Internet of Medical Things (IoMT) encompasses a large amount of devices used in the medical industry. These include personal devices, biomedical, telemedicine, monitoring devices, computers, printers, testing equipment, remote monitors and life saving devices. All of these devices store data.
“IoMT Solutions recycles medical devices, parts and accessories,” explains Melanie Haga. “We destroy any hard drives or data bearing component, and then the raw materials are melted down for re-use.”
“Because of our licenses and certifications, IoMT Solutions is one of the easiest and safest ways for manufacturers and health care facilities to manage device recalls. We offer secure logistics and detailed reporting to satisfy FDA requirements and our customer portal allows access to all documentation 24/7/365,” she adds. “While we can pick up devices from a warehouse or hospital, many of our customers create a customer returns solution so that their recalled, returned or upgraded products can be sent directly to us from the end user.”
Haga explained more about the business in a question-and-answer session with TechNation magazine.
Q: HOW DOES YOUR COMPANY STAND OUT IN THE MEDICAL EQUIPMENT FIELD?
A: Many recyclers are actually remarketers. They will refurbish items and resell them. This is a dangerous practice,
as it allows medical devices to be sold second hand, with no guarantee that data has been cleaned.
Because we shred any data that resides in the device, we eliminate the risk of a data breach. Additionally, removing those devices from the used marketplace allows manufacturers to retain control prices and peripherals.
Our parent company, Back Thru The Future Technology Disposal, has been in business for over 30 years and has been a leader in the secure destruction of IT equipment.
Q: WHAT IS ON THE HORIZON FOR YOUR COMPANY?
A: We would like to work with manufacturers and consultants to have our disposal services built into the initial product development. This satisfies FDA chain of custody requirements. Our disposal process also ensures an environmentally sound product, since the materials will be recycled, and it means that no patient data is recoverable.
Q: IS THERE ANYTHING ELSE YOU WOULD LIKE OUR READERS TO KNOW?
A: IoMT Solutions is a division of Back Thru The Future Computer Recycling Inc., located in New Jersey. We are certified as both a “Woman-Owned Business” and SBA qualified Small Business. We have over 30 years of providing regulatory compliant computer recycling and electronic destruction services.
F or more information, visit www.IoMTSolutions.com.
WELCOME TO THE TECHNATION COMMUNITY!
INTERLIGHT
Q: WHAT PRODUCT, SERVICE OR SOLUTIONS DOES YOUR COMPANY PROVIDE TO THE INDUSTRY?
Interlight carries thousands of specialty replacement bulbs and batteries that serve every lighting & battery application used throughout hospitals and surgery centers. Here at Interlight, we offer an extensive cross reference list for not only bulbs and batteries but patient monitoring accessories as well. Interlight has operated since TV tubes were still in regular use. Whether it’s in the office, operating room, biomed shop, OEM light sources, Interlight has the light bulb or battery you need. By maintaining one of the largest inventories in the world, along with an unsurpassed cross reference, Interlight leverages technology to create a one-stop-shop for all your lighting, parts and battery needs.
Q: TELL US WHAT DIFFERENTIATES YOUR COMPANY FROM THE COMPETITION?
What sets us apart from other medical lighting distributors is that we also operate as a source for “legacy” bulbs that are considered EOL (End of Life). Rather than having to make a capital purchase for a new light source we can provide the spare bulb that was no longer manufactured by the OEM so your equipment can still operate with no issues. We offer same day shipping whether it’s domestic or international, as well blind drop shipping for resellers and dealers.
Q: WHY DID YOU CHOOSE TECHNATION FOR ADVERTISING?
Having personally exhibited at MD Expo’s in the past, I can say without a doubt that when it comes to medical equipment there is NO better exposure than TechNation magazine. When it comes to networking the MD Expo’s were always a hit so it was a no brainer for me to start advertising with TechNation. The support you get from everyone at MD Publishing is simply the best and I can’t wait to work more with them in the future!
For more information, visit interlightus.com.
ALTAMONT
SOFTWARE
Q: WHAT PRODUCT, SERVICE OR SOLUTIONS DOES YOUR COMPANY PROVIDE TO THE INDUSTRY? CaptureWare Video
Q: TELL US WHAT DIFFERENTIATES YOUR COMPANY FROM THE COMPETITION?
Our connectivity platform. It provides an enterprise approach that simplifies EHR access to all medical imaging information and eliminates the myriad of desktop applications sprinkled throughout healthcare institutions. Our platform provides a common toolset for centrally managing, configuring, and deploying our suite of document, SR data integration, digital media, eForm, photo, and video capture applications with enterprise security and scalability.
Q: WHY DID YOU CHOOSE TECHNATION FOR ADVERTISING?
The TechNation readership is our target audience. Biomedical and Healthcare Technology Management professionals are burdened with managing video and image integration across the healthcare system. They are involved in assessing, influencing, and recommending next-generation technology.
For more information, visit altamont.com.
Jeff Van Etten, Sales Director
Chris Barnett, President
METROPOLIS INTERNATIONAL
Q: WHAT PRODUCT, SERVICE OR SOLUTIONS DOES YOUR COMPANY PROVIDE TO THE INDUSTRY?
Metropolis is the largest stocking dealer of all types of imaging equipment in the New York Metro area. We are about to celebrate our 20th year and we offer all imaging modalities, from all manufacturers.
Q: TELL US WHAT DIFFERENTIATES YOUR COMPANY FROM THE COMPETITION?
We also offer service and warranty contracts for customers local to us at a great discount compared to the OEMs. Metropolis, unlike 90 of the dealers out there, is FDA registered and is the leading wholesale dealer for various modalities. Being FDA registered, allows Metropolis the flexibility to help other dealers with equipment as well. We also get all of our inventory direct, so our prices are great and reasonable for even the most discernable customer. Lastly, our longevity and overall experience in the industry, from a C-arm, to an MR in being able to handle the most difficult projects is second to none!
Q: WHY DID YOU CHOOSE TECHNATION FOR ADVERTISING?
Leon Gugel, President
TechNation provides Metropolis with a wide and easy way to reach and connect with existing, as well as new customers and vendors from around the world.
For more information, visit metropolismedical.com.
Medical equipment everywhere, yet nowhere?
Safe, timely and effective care is jeopardized because the equipment that makes it possible is everywhere … and yet nowhere at the same time.
Real-time locating system (RTLS) technology not only allows you to see where equipment is located across your health system, it also helps distribute assets more effectively, optimize your fleet and reduce costs.
ECRI UPDATE
Top 10 Health Technology Hazards for 2025
Providing safe and effective patient care requires identifying sources of danger or difficulty with health technologies and taking steps to reduce the risk.
ECRI produces its annual Top 10 Health Technology Hazards report to help in this effort.
The full report, accessible to ECRI members at https://ly.ecri. org/2025Top10Hazards, probes the system issues that contribute to each hazard and provides detailed recommendations to prevent harms. For non-members, an Executive Brief is available for complimentary download at https://ly.ecri.org/2025hazards.
ECRI identified the following topics as warranting high-priority attention in 2025.
1. RISKS WITH AI-ENABLED HEALTH TECHNOLOGIES
Artificial intelligence offers the promise of increasing the efficiency and precision of medical diagnoses, treatments, and services; but improvements are not guaranteed. Placing too much trust in the AI model may lead to inappropriate patient care decisions.
The potential for preventable harm exists if, for example, biases are present in the data used to train the AI model, if the model is not well matched to the target patient population, or if the model’s performance is not monitored over time. Further, AI solutions can yield disappointing results if organizations have unrealistic expectations, fail to define goals, provide insufficient governance and oversight, or don’t adequately prepare their data for use by the AI application.
2. UNMET TECHNOLOGY SUPPORT NEEDS FOR HOME CARE PATIENTS
The safe and effective use of complex medical devices in the
home setting requires more than just user training for patients and family members, it requires adherence to sound technology management practices. These include assessing device usability in the context of the user’s abilities, mitigating any physical or structural limitations in the intended area of use, and supplying the appropriate accessories, as well as providing sufficient training for proper device operation and maintenance.
Inattention to such practices can lead to events and errors going undetected, readings from the device being misinterpreted, or care delays and other harm from unresolved device malfunctions.
3. VULNERABLE TECHNOLOGY VENDORS AND CYBERSECURITY THREATS
The practice of health care increasingly depends on the availability and performance of systems hosted by external (i.e., third-party) vendors. While there are many benefits to the use of scheduling and billing services, electronic health records (EHRs), and other services provided by third-party vendors, the arrangement also involves risks that must be managed.
Past instances of unauthorized access, disruption to services, or other adverse cybersecurity events that incapacitated or degraded operations at the vendor have had downstream effects for health care providers. Incidents have left providers without access to critical services, reliable data, or effective communications channels with their partnering care providers. Such eventualities put patients in harm’s way by delaying, degrading or preventing care.
4. SUBSTANDARD OR FRAUDULENT MEDICAL DEVICES AND SUPPLIES
Large-scale instances of substandard or fraudulent (e.g., counterfeit) products reaching the U.S. market have become startlingly common. Patients or staff can be harmed if medical devices or supplies (e.g., syringes,
isolation gowns) do not function as intended.
Substandard or fraudulent devices may be more susceptible to failure or malfunction, leading to misdiagnoses or injuries. Additionally, the disruptions and recalls that these products cause can stress the supply chain, leading to product shortages; and the need for corrective actions can cost time and money, as health care organizations must review inventories for affected items.
5. FIRE RISK IN AREAS WHERE SUPPLEMENTAL OXYGEN IS IN USE
In the acute care setting, OR staff are typically well aware of fire risks during surgery. Outside the OR, however, ECRI’s investigations suggest that increased attention is needed to prevent fires in areas where supplemental oxygen is being delivered.
The three elements needed for a fire – an oxidizer, a fuel and an ignition source – can be present wherever oxygen is delivered. Ignition sources can range from the obvious (e.g., an electrosurgical unit pencil) to the unsuspected, such as a defibrillator, heated humidifier, fiberoptic light source or damaged electrical cord.
6. DANGEROUSLY LOW DEFAULT ALARM LIMITS ON ANESTHESIA UNITS
Certain anesthesia units can be configured such that the default alarm limits (those active whenever a new surgical case is started) will be set to zero or a similarly unsafe lower limit. In effect, this disables the alarm at the start of the case. ECRI has investigated numerous incidents in which inappropriate default alarm limits caused dangerous conditions to go undetected, in some cases leading to brain damage or death.
While anesthesia providers can set lower alarm limits to zero when needed during a procedure, ECRI recommends against configuring the unit such that the lower limit defaults to zero (or some other unsafe lower limit).
7. MISHANDLED TEMPORARY HOLDS ON MEDICATION ORDERS
The need to suspend (or hold) the administration of a drug based on clinical circumstances is a common occurrence during patient care. Yet errors can arise if organizations lack carefully vetted workflows for documenting hold order parameters in the EHR.
The Institute for Safe Medication Practices has found that errors associated with hold orders often can be attributed to uncertainty about what a hold order means, how the order should be communicated or what process should be followed. Failure to hold a medication when indicated, or neglecting to either restart or discontinue a held medication as circumstances require, can lead to patient harm.
8. INFECTION RISKS AND TRIPPING HAZARDS FROM POORLY MANAGED INFUSION LINES
The improper management of infusion lines and connectors creates multiple opportunities for harm. Healthcare-associated infections are one example. Infections can result if care
providers don’t clean and disinfect an infusion line connector before access, if they touch the insertion site or tubing with contaminated gloves, or if they don’t follow sterile technique when preparing the infusate.
Another circumstance that can lead to harm is if infusion lines are allowed to dwell on the floor. This creates a tripping hazard that can lead to patient or staff injuries from a fall, as well as patient harm if the infusion line becomes dislodged.
9. SKIN INJURIES FROM MEDICAL ADHESIVE PRODUCTS
Medical adhesive products are used for a variety of applications, such as dressing wounds, securing IV lines or attaching ECG electrodes. But not all adhesives are the same, and not all patients will respond similarly to an adhesive product.
Inappropriate choices or errors in use can lead to skin tears, blisters, adverse reactions like contact dermatitis, or other forms of injury. While most skin injuries resolve within a few days, they nevertheless cause unnecessary discomfort and pain. Additionally, they can leave patients susceptible to infection, which can lead to more severe consequences.
10. INCOMPLETE INVESTIGATIONS OF INFUSION SYSTEM INCIDENTS
With so many patients receiving infusion therapy, adverse events associated with the use of infusion pumps are not unusual. Organizations that lack the expertise or resources to conduct a thorough investigation of such incidents will be poorly positioned to prevent future ones.
Of concern is that investigations involving infusion systems can be particularly challenging due to the variety of potential contributing factors. Issues related to the pump hardware and software, the IV administration set and other accessories, and the actions of the user all must be examined. Additionally, staff must know what to do (and what not to do) to facilitate an investigation.
AAMI UPDATE
Illinois Clinical Engineering Association Celebrates Legacy and Innovation at Record-Breaking Conference
The Clinical Engineering Association of Illinois (CEAI) celebrated a landmark moment during its 14th annual conference, where record-breaking attendance underscored the growing importance of grassroots associations for professionals in the healthcare technology management (HTM) field. In a series of on-site interviews, CEAI founders Alan Moretti and Joe Bandra, alongside current CEAI President Kelley Harris and Vice President Greg Czajka, reflected on CEAI’s origins, growth and enduring contributions to the profession.
According to CEAI, the 2024 run of their annual conference reached its highest attendance figure yet, with more than 215 participants. AAMI Vice President of HTM Danielle McGeary expressed her gratitude for the chance to take part in the event, noting its vibrant atmosphere and the professional value it provided.
“It’s truly remarkable to see such a dedicated group of professionals come together to share knowledge and build connections,” she said.
The event was marked by an impressive array of presentations, workshops and networking opportunities. Moretti was quick to commend the new generation of CEAI leadership for the event’s success.
“This has been our most attended conference yet,” he exclaimed. “The leadership team, led by Kelley and Greg, truly blew it through the roof. It’s humbling to see
how far this organization has come.”
“CEAI has always been about bringing people together, and this event exemplifies that spirit. The turnout is proof of the community’s commitment,” Harris said.
FROM GRASSROOTS BEGINNINGS TO INSPIRING THE NEXT GENERATION
CEAI was founded in 2005 when Moretti and Bandra identified a need to unify Illinois’ HTM professionals. Inspired by an ad hoc meeting at Triton Community College, they organized the first gathering at Loyola University Chicago. While uncertain about the initial turnout, they were thrilled when over 35 attendees arrived. “That first meeting showed us the energy and need for something like CEAI,” Moretti explained.
This enthusiasm catalyzed 12 additional grassroots meetings in 2005 and 2006, culminating in the formal establishment of CEAI and the election of its first officers in 2007. Today, CEAI has grown into a thriving organization that continues to shape the HTM landscape in Illinois.
One of CEAI’s cornerstones is its investment in education and the development of future leaders. The association has awarded more than $40,000 in scholarships to date, a point of pride for founders and members alike. Several scholarship recipients, who are now working in the HTM field, attended this year’s conference.
Bandra, who personally donated $10,000 to the scholarship fund, shared his excitement. “It’s incredible to see students we’ve supported now excelling in their
careers. That’s what CEAI is all about – creating opportunities and building the future of HTM,” he said. Harris echoed this sentiment, highlighting the importance of mentorship and education. “The scholarship program isn’t just about financial support. It’s about fostering a pipeline of talent and inspiring young professionals to carry the torch forward,” he said.
ADVICE FOR EMERGING ASSOCIATIONS
The success of CEAI has inspired HTM professionals in other regions to consider forming their own associations. McGeary commended CEAI for its legacy of leadership and community-building. “You’ve created something that not only serves Illinois, but also sets an example for HTM organizations nationwide. The dedication and vision here are inspiring,” she said. Moretti and Bandra offered practical advice, emphasizing the importance of energy, planning and financial sustainability. “No money, no mission. You need sponsors, exhibitors and committed members to make something like this thrive.”
Bandra noted that building strong digital infrastructure is also key. From the start, “having a well-designed website helped CEAI connect with members and communicate effectively.” In today’s world, that’s not optional – it’s essential, he said.
Reflecting on 14 years of progress, Moretti and Bandra also acknowledged the contributions of collaborators like the late Pat Lynch and Robert Shu, who were instrumental in drafting CEAI’s bylaws and operational framework. “It truly took a village to get CEAI to where it is today.”
As CEAI continues to grow, its focus remains on education, collaboration and leadership succession. This year’s record-breaking conference is a testament to its success and the unwavering commitment of its members. With its strong foundation, CEAI is poised to drive innovation and excellence in HTM for years to come.
Preventative maintenance is a proactive approach that involves regular inspections, testing and servicing of equipment to prevent potential failures before they occur. In the field of healthcare technology management (HTM), preventative maintenance is a core responsibility in ensuring the safety of patients and healthcare providers. For example, sensors that monitor flow rates and pressure can degrade over time in an infusion pump. If not replaced, they might fail to detect anomalies, causing the pump to malfunction and potentially harm the patient. Healthcare delivery organizations (HDO) must comply with stringent regulations and standards to ensure patient safety. Regular maintenance service records are required to demonstrate that medical devices are maintained according to manufacturer guidelines.
HDO are required to measure preventative maintenance (PM) completion but how can an HDO measure the quality of its preventative maintenance? VISN 2 New York and New Jersey Healthcare Network started our journey towards high
reliability in seeking to measure PM quality. The objective for PM quality is that PMs are conducted according to manufacturer requirements or AEM requirements.
The PM quality life cycle in VISN 2 starts with HTM staff reviewing the service manual and identifying the OEM PM frequency, which is then manually input in the CMMS model table instead of just setting up the PM schedule according to this frequency. Because the data of OEM PM frequency is catalogued in CMMS by model, reports can easily identify any deviations from OEM requirement. “None” frequency is also documented to identify an accurate count for missing PMs. A PM checklist workgroup meets to create PM checklist questions based on the service manual. CMMS admin then implements checklist using checklist rules so that PM generates with PM checklist. If an external technician is completing the PM, the checklist can be skipped, and service report attached instead. Before each PM, the assigned technician reviews the service manual for revisions. Some PMs generate a quality assurance (QA) work order, with closing code of Pass or Fail. During the QA, the manager reviews the latest service manual to identify if PM frequency revisions are incorporated in the process. The manager inspects the medical device to review the service logs and PM sticker on the device. A fail closing code are utilized on the QA work order if PM documentation, procedure or
frequency does not meet OEM requirements.
There are a few CMMS limitations that currently mitigate complete PM quality tracking. Currently, there is no CMMS PM suppression capability so if there are multiple maintenance definitions, multiple PM work orders generate when frequencies align such as semi-annual and annual. This makes it difficult for the front-line staff to streamline their work to complete both PM tasks for different work orders on the same device.
To measure the effectiveness of the quality life cycle process, a few metrics may be utilized. First, QA fail percentage, which can be monitored to find areas of improvement with processes or training. QA fail percent is proportion of QA fail divided by QAs generated times 100. Some examples include vendor service report missing, missing procedure step, mismatch of vendor PM month to CMMS PM month, missing part for PM kit, etc.
The second quality metric is OEM PM conformance. OEM PM conformance provides a quantitative composite measure of whether OEM PM frequency is met for models where OEM PM frequency is noted. OEM PM conformance is the proportion of devices without missing PM or wrong PM schedules divided by number of medical equipment times 100. As the percentage of inventory impacted by OEM PM decisions increases over time, OEM PM conformance increases in reliability. Data hygiene is important to note for this metric. To accurately measure the OEM PM conformance, the assets in the inventory must have accurate naming by model.
Another metric is percentage of vendor PM wos without service reports. This is the proportion of vendor PM wos without service reports divided by the number of vendor PM wos. Since checklists are bypassed for vendor PM work, service reports are utilized to ensure PM quality.
The PM checklist is another way to ensure that a PM is conducted according to manufacturer requirements. To err is human, so checklists act as a cognitive net that helps BMETs remember essential steps, especially in complex tasks. Checklists also establish a baseline for performance, ensuring individuals do not overlook critical details. The standard documentation ensures an entry-level BMET reviewing the PM history will understand what steps were performed. In addition, checklists can be designed to fail automatically based on out-of-range value and generate a corrective maintenance (CM) work order. While checklists provide structure, they should complement professional judgement rather than replace it.
In conclusion, implementing a PM quality program is crucial for healthcare organizations to ensure patient safety, regulatory compliance and optimal equipment performance. By adopting a systematic approach to PM quality measurement, as demonstrated by VISN 2 New York and New Jersey Healthcare network, HTM departments can significantly improve their maintenance practices. This includes careful documentation of OEM requirements, creation of comprehensive PM checklists, regular quality assurance checks, and continuous monitoring of key metrics such as QA fail percentage, OEM PM conformance and vendor PM work order documentation. While challenges remain such as CMMS limitations and the need for quality data hygiene, the benefits of a well-executed PM quality program are clear.
As medical technology continues to advance, the importance of high-quality preventative maintenance will only grow, making it an essential focus for healthcare organizations striving for operational excellence and high reliability.
Arleen Thukral, M.S., CCE, CHTM, is a VISN 2 Healthcare Technology Manager with New York/New Jersey VA Health Care Network.
LIVE DEMO: FEB. 5 at 2PM ET
Registration on WebinarWednesday.live.
Eligible for 1 CE credit from the ACI.
TOOLS OF THE TRADE
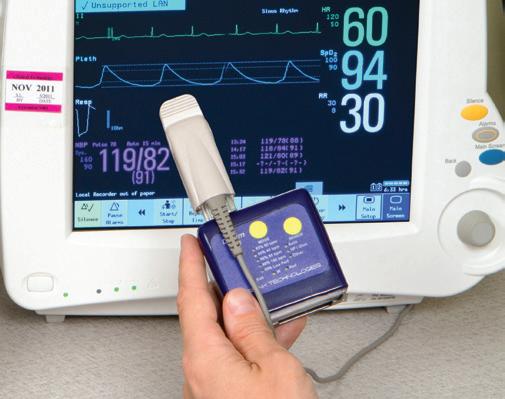
The Rigel SafeTest 60+ is a robust and reliable medical safety analyzer designed for high-volume testing of medical and laboratory equipment. It ensures compliance with NFPA 99 standards by performing essential applied parts tests, including patient current leakage and insulation measurements to guarantee electrical safety. A key enhancement in the SafeTest 60+ is the introduction of dynamic pass/fail thresholds during measurement. This feature streamlines the testing process by automatically providing clear, real-time
results and reducing the risk of errors. Built for clinical engineering teams, hospitals and service organizations, the SafeTest 60+ is both powerful and user-friendly. Its rugged design and advanced functionality make it ideal for maintaining the safety and reliability of critical equipment. With its focus on precision, efficiency and ease of use, the SafeTest 60+ is an indispensable tool for HTM professionals.
For more information, visit rigelmedical.com/gb/.
CLICK. WATCH. EARN.
Kontakt.io.com
All webinars, podcast, and product demos are eligible for 1 CE credit from the ACI.
TOOLS OF THE TRADE LIVE DEMO – PRONK MOBILIZE WIRELESS
The recent TechNation Tools of the Trade Live Demo featured the Pronk Mobilize Wireless Solution. Pronk’s Julio Castro guided attendees through the many helpful uses of Mobilize before fielding questions during an informative Q&A session. Sponsored by Pronk Technologies, the webinar is eligible for 1 credit from the ACI.
Pronk Mobilize is a multi-level solution that provides flexibility to connect test equipment to Pronk’s Mobilize App to streamline and automate medical device testing. Mobilize can be adapted to fit a biomedical engineer’s testing and documentation needs. It includes various operating modes that enable biomeds to automate testing on a single or combination of Mobilize-compatible test equipment including automated electrical safety, vital signs simulation, IV pump, defibrillator and ventilator testing – all as part of a test protocol/ procedure that the engineer defines.
Mobilize includes automated step-by-step electronic procedure features. It includes user-controllable options to adapt procedures according to the particular configuration of the medical device and test equipment at hand.
A third operating mode provides the ability for a biomed to create a library of test protocols that can be loaded instantly for executing automated testing with wireless connectivity to the test equipment.
Joshua Moffett, a biomedical equipment technician with Kansas City Orthopaedic Institute won a $100 Amazon gift card as part of the Webinar Wednesday 10th anniversary celebration. A recording of the webinar is available for on-demand viewing at WebinarWednesday. live.
Attendees were asked, “What was your single biggest takeaway from today’s product demo?”
“Connectivity of test equipment,” said James Whitaker, CE Lead Technician, CHI St. Luke’s Memorial Lufkin.
“The ability to connect older devices to Mobilize and the ease of use of the product,” said Ryan Mueller, a biomedical equipment technologist with the Richmond Road Diagnostic & Treatment Center.
“I really liked the checklist tests,” said Brian Dodds, biomed/ materials manager at Minidoka Memorial Hospital.
“Ease of generating procedures and reports,” RS Medical Engineer Mark Moore said.
“The quality, usability, and technology streamlining PM testing,” said Joseph Trujillo, a biomedical engineering manager with Hoag Hospital Newport Beach.
“GOING
BEYOND ‘WHERE’S MY THING?’ ASSET MANAGEMENT”
The recent Webinar Wednesday session “Going beyond ‘Where’s my thing?’ Asset Management that increases utilization and automates PAR” was sponsored by Kontakt.io and eligible for 1 credit from the ACI.
Presenter Tim Young asked, “Is RTLS tracking alone enough for today’s clinical engineers?” Beyond location visibility, modern health systems need an asset management solution that automates PAR-level inventory management, gives clear insights with AI analytics and increases mobile equipment utilization.
In 2025, the RTLS market will shift, driven by the growing dominance of scalable, cost-effective technologies like Bluetooth Low Energy (BLE). And the asset management solutions that will rise to the top will be simple to install, easy to use and maintained in the cloud.
Whether you’re looking to increase utilization, right-size inventory, or simply want to know what’s available beyond “Where’s my thing?” – this webinar with Kontakt.io illustrated the many benefits of an asset management solution that’s easy to use, quick to deploy and future-proof with open APIs and cost-effective technology.
Young also fielded questions from attendees. He shared his knowledge and expertise with insightful answers relevant to HTM professionals. A recording of the webinar is available for on-demand viewing at WebinarWednesday.live.
Attendees provided feedback regarding the session in a post-webinar survey. Attendees were asked “What does Webinar Wednesday provide the industry?”
“Excellent real-time updates,” said Mark Moore, an engineer with RS Medical.
“Good information relating to the Biomed World,” Tenet Healthcare Biomed Manager Frank Nichols said.
“Great insight and keeps me up to date on the latest in the industry,” said Thomas Shoots, biomedical engineering supervisor with Northern Arizona Healthcare.
“Remote continuing education opportunity,” Brian Simson, proprietor, Ventura Biomedical Services.
Webinar Wednesday would like to thank the sponsor – Kontakt.io. Kontakt.io optimizes processes and resources by revealing how patients and equipment move through the care delivery process. Using AI, IoT, and RTLS, Kontakt.io helps health systems uncover waste, streamline capacity, improve workflows, and make staff and patients feel safer, seen and valued. For more information, visit kontakt.io.
TRAINING
Unlock your engineering team’s full potential with our in-depth, hands-on training courses at our state-of-the-art Center of Technical Excellence facility in
Our Courses
Arcadis -Avantic/Orbic/Varic
GE Innova x100
Basic Principles of MRI Imaging
GE Excite Product Family
GE Innova IGS/Discovery
Siemens Axiom Artis
Siemens Artis Zee Cath Lab
Basic Principles of CT
GE CT 5X-7X, Brightspeed and Optima/Rev-EVO
Siemens Emotion 6/16 - Perspective CT
Siemens Sensation 10/16/40/64
Siemens Definition AS
Siemens Go Series CT
GE Precision
Siemens Multix Fusion
Siemens Ysio
Siemens Luminos Agile Max
Basic Ultrasound/PM
GE Logiq 9/Vivid 7 UL
GE Logiq E9/Vivid E9 UL
GE Logiq-Voluson Midrange Training (P7/P9/S8/E8/F6/F8
MedWrench is an online resource for medical equipment professionals (biomeds, HTMs, imaging professionals, etc...) to engage with their peers about medical equipment repairs, source parts and locate a service company. The following are examples of how the MedWrench community members help each other in the website’s forums.
HOLOGIC - SELENIA DIMENSIONS
Q: Error 38:15. Which is a patient movement detection, anyone have an idea as to what could cause this when there is no patient? What could cause this with no patient present? Please refer to last two entries in this discussion for clarification of PMC.
A: Check PMC fan
A: If we are talking about the two fans located behind the detector it is not them causing the error. Strangely enough I can not create the error by moving or any other means, any other suggestions will be greatly appreciated.
A: PMC is power module control. It’s at the bottom of the gantry. Remove 2 screws top of gantry and that top cover off. Then lift those 2 front covers and slide bottom cover you should see the PMC at the bottom.
A: Wow! Was I way off base, thank you for setting me straight I had found the stuff regarding patient movement by searching the error code on Google, talking about leading one down the wrong path!
A: Just wanted to let everyone know it was the fan inside the PMC chassis, causing the 38:15 error, replaced the fan and system is working correctly. Thank you for your help.
SAMSUNG - WS80A ELITE
Q: I recently bought a used Samsung WS80A, and I am getting an error message that says “Failed to connect a trackball and a keyboard”, but the trackpad and keyboard are working fine. Could someone please help me with this? Do I need an admin password to restore settings? A software update?
A: This implies the system encountered an issue during the connection process for these peripherals and suggests a simple troubleshooting step: restarting the system. Restarting often resolves hardware connection issues caused by temporary glitches or incomplete initializations.
A: This recommends a straightforward troubleshooting step: restarting the system. It also shows that the system experienced a problem during the connection procedure for certain devices. Hardware connection problems brought on by brief hiccups or insufficient initializations are frequently fixed by restarting.Complete rows or columns to score points block blast
A: Most likely a faulty keyboard.
For more FREE forum information, visit medwrench.com/forums.
ROUNDTABLE RTLS
Real-time locating systems continue to be a hot topic in healthcare. A RTLS system can help locate medical devices, track patients, assist with handwashing goals and more. TechNation contacted several companies within the RTLS sphere to find out more about the latest offerings and features.
Participants in this Roundtable article on RTLS are:
• Kapil Asher, senior director of enterprise IoT solutions, global head of healthcare and education practices, Kontakt.io
• Ron Borden, head of operations, Vizzia Technologies
• Jeff Stiffler, director of healthcare product marketing, Cognosos
• Mike Zimmer, manager, solutions engineering, FSI
Q: HOW CAN RTLS IMPROVE PREVENTIVE MAINTENANCE SCHEDULES?
ASHER: RTLS significantly enhances preventive maintenance (PM) schedules by introducing efficiency, precision and
predictive capabilities. Key benefits include:
• Streamlined Device Locating: RTLS enables biomedical engineers to instantly locate devices needing preventive maintenance by leveraging real-time location data. Engineers can apply filters for devices closest to upcoming PM deadlines (or those currently unutilized), preventing unnecessary interruptions to in-use devices and optimizes time spent locating assets
• Optimized Equipment Fleet Size: RTLS helps hospitals optimize their equipment fleet size by identifying underutilized equipment and redistributing or decommissioning them. This reduces the number of devices, resulting in fewer PMs, cost and time savings while maintaining the same level of service quality.
• Utilization-Based Maintenance: RTLS systems analyze asset utilization data throughout a maintenance cycle. For instance, if a device is used only 10% of the time, it may require less intensive maintenance compared to one used 75-80%. Such insights facilitate the adoption of Alternative Equipment Maintenance (AEM) strategies instead of routine PMs, reducing resource strain without compromising functionality.
• Predictive Maintenance Models: Integrating AI and RTLS data allows for predictive maintenance based on usage patterns. This approach proactively addresses potential issues before they arise, reducing equipment downtime and enhancing overall reliability. Predictive maintenance also
minimizes unnecessary maintenance cycles by employing “just-in-time” interventions, aligning with actual device needs rather than fixed schedules
BORDEN: Vizzia continues its emphasis on innovation by collaborating with clinicians and technology leaders to further enhance its InVIEW software platform. The company has recently released several new integrations that power today’s smart hospital, to include computerized maintenance management system (CMMS) applications. APIs with AIMS and Nuvolo improve preventive maintenance (PM) workflows and location syncing. The real-time locating of valuable medical devices for critical firmware updates or product recalls greatly assists biomedical engineers with asset management across multiple healthcare facilities.
KRAIMER: Biomedical technicians spend more than 200 hours per year searching for equipment in need of maintenance. Equipment they know they should have is nowhere to be found, jeopardizing the integrity of PM routines. With RTLS, filterable dashboards help staff drill down to specific equipment on specific floors or wings to identify the locations of equipment in need of maintenance. This increased visibility to the entire fleet offers a more organized and structured approach to locating equipment. When RTLS is interfaced with the hospital’s CMMS, technicians can also receive visual cues or alerts for assets that are past their PM date, helping proactively manage equipment.
STIFFLER: RTLS systems offer significant potential to streamline maintenance and reduce associated burdens. While seemingly straightforward, accurately locating and accounting for 100% of inventory often presents the most significant challenge. Beyond simple location tracking, RTLS platforms provide valuable data on asset utilization and historical location patterns. This rich data empowers organizations to make more informed maintenance decisions, optimizing schedules and resource allocation.
ZIMMER: Having a last-known location associated to a piece of mobile medical equipment assists BMETs in finding the equipment. Less time looking, more time ensuring the device is in top notch condition and available for patient use. These time savings have a cumulative effect, of course, increasing operational efficiency across the team and inventory utilization.
Q: WHAT PROTOCOLS OR STANDARDS SHOULD BMETS FOLLOW WHEN INTEGRATING RTLS WITH HOSPITAL EQUIPMENT?
ASHER:
Regulatory and Safety Standards
• HIPAA Compliance: While RTLS for asset tracking and PM management does not usually require patient data, it is necessary to ensure any data collected by RTLS is handled per HIPAA regulations to protect data security.
• SOC2 Type 2: This compliance demonstrates that the system
has undergone rigorous third-party audits to safeguard sensitive patient and facility data.
Open Standard Network and Communication Protocols
• Bluetooth Low Energy (BLE): Adopt BLE for cost-effective, low-power communication between RTLS tags and gateways. BLE is open standard and provides flexibility to BMETs to choose tracking devices from multiple vendors rather than a single monopolistic vendor limiting choices in form factors and other environmental specifications (size, weight, adherence methods etc.)
• Wi-Fi Standards: Ensure data backhaul from readers utilizes ubiquitous infrastructure like Wi-Fi rather than a proprietary parallel network that can prove to be expensive and cumbersome to install and maintain.
Data Integration Protocols
• RESTful APIs: Leverage REST APIs to integrate RTLS data with asset management or maintenance systems, enabling real-time updates on equipment location and status.
• CMMS Integration: Ensure compatibility with computerized maintenance management systems (CMMS) using standard integration methods (e.g., API or file import/export).
• HL7 and FHIR: Use HL7 or FHIR standards for integration with hospital information systems, including electronic health records (EHRs).
BORDEN: It’s important to establish user standards, naming and data protocols. Oftentimes, different hospital units or teams have colloquial or abbreviated names for assets that may or may not align to the biomed or IT team’s nomenclature. This tends to cause confusion and difficulty locating the correct asset or medical device throughout the hospital system – defeating the purpose of tracking them overall. We recommend getting on the same page with the name of each asset tracked so every hospital team can look at the dashboard and understand where or what is missing, what is in-service, and where the nearest needed medical device or asset is located. This reduces the time spent searching and maximizes that asset’s utilization.
KRAIMER: Asset tag configuration is a critical implementation step but should really be considered early in the search for an asset tracking solution. A customersuccess minded RTLS partner can help health systems understand their options. Some key considerations we often experience in the field:
• Attach tags to equipment using a trial-and-error method. Start with a small batch to identify the most effective attachment location and method for each equipment category. The type of tracking technology used is also a consideration for placement. With some technologies, tags need to be fully exposed to be detectable. Other technologies, such as Bluetooth Low Energy (BLE), can be covered, however the tag cannot be surrounded by metal. Otherwise, signal strength can be affected. Once you have a controlled and regulated
approach, then you can scale it to the entire fleet.
• Understand cleaning protocols to ensure tags stay operational for their expected lifespan. Knowing your tag’s ingress protection (IP) rating and acceptable cleaners that won’t degrade its plastic can help inform both where on a device the tag should be attached and long-term workflow for care and cleaning.
• Designate appropriate staff to proactively replace asset tag batteries. Low battery reports emailed on a standard cadence are helpful to stay on top of this critical task. We also recommend that battery replacement for RTLS tags be done during the PM process, to lessen the number of ad hoc battery changes that must be done.
ZIMMER: This may best be answered by someone in the RTLS arena; however, BMETs should ensure that the network infrastructure in use at their facility is compatible with whichever solution they are moving forward with. Additionally, the solution may not always need to be an active RTLS tag, oftentimes low-cost passive technologies may be leveraged to support workflows.
Q: CAN YOU DESCRIBE A SCENARIO WHERE RTLS IMPROVED EQUIPMENT UTILIZATION OR OPERATIONAL EFFICIENCY?
ASHER: Kontakt.io partnered with a national health system to deploy the industry’s largest RTLS project across 180 facilities and 30 physical locations, impacting 500,000 assets and 41,000 licensed beds. Using Kontakt.io’s asset management solution, the health system is seeing a 10X annual ROI of $40 million, a 75% reduction in rentals, and a 14.5% reduction in nurses’ time searching for devices.
BORDEN: GE Healthcare estimates that the utilization of medical equipment averages only 42%. RTLS has increased utilization rates to approximately 75%. Piedmont Healthcare is the largest provider in Georgia with 25 hospitals caring for more than 4 million patients. Piedmont’s use of RTLS has increased device utilization by 20% and increased worker productivity by 90%.
KRAIMER: One of our long-standing customers increased their pump utilization by 133% while decreasing pump inventory by 33%, thanks to RTLS. Originally, the hospital set out to replace an aging fleet of IV pumps, planning to purchase even more than the number in the current fleet. But after conducting a manual study, they learned their existing inventory had only a 30% utilization rate, which is actually very common. Despite these numbers, staff voiced concerns about having too few pumps. These contradictions were clear drivers in their decision to implement RTLS, which gained them evidence-based data to help inform and right-size their fleet. Knowing that RTLS would help nurses find pumps when they needed them, they decreased their pump acquisition from 900 units to 600, saving them more than $1 million in expenses.
STIFFLER: A customer success story demonstrated a remarkable 92% reduction in annual equipment loss after implementing our platform. This significant improvement not only alleviated clinician frustration stemming from equipment unavailability and time-consuming searches but also translated to substantial cost savings. The 92% decrease in equipment loss represents a significant financial recovery that can be redirected towards other critical priorities within the healthcare system.
ZIMMER: Two use cases spring to mind. Many of our customers will integrate their RTLS solution to FSI’s CMMS. This integration will refresh the last-known location of medical devices on the asset record, as well as update the asset’s location on a floorplan (viewable within FSI’s solution). This leads to the aforementioned increase in operational efficiency when performing maintenance on the devices.
Secondly, I know that many health systems will leverage either active or passive tracking technologies to support their equipment distribution processes and teams. Oftentimes there are designated clean and dirty
Jeff Stiffler Cognosos
Mike Zimmer FSI
Ron Borden Vizzia Technologies
Kapil Asher Kontakt.io
Jeanne Kraimer Midmark RTLS
rooms – these spaces can be monitored by RTLS solutions so that when a certain threshold of dirty equipment in the designated dirty room is reached a request is sent to Central Supply to pick them up, sanitize them, partner with BMETs if they need to be PMed and make available for use. This kind of solution naturally assists in balancing the utilization of the devices within a particular fleet.
Q: WHAT ARE PRIMARY CONCERNS OR CHALLENGES WITH RTLS IMPLEMENTATION?
ASHER: Implementing RTLS in a hospital to track assets and equipment presents several technical, operational and organizational challenges. These include:
• Infrastructure limitations: Hospitals have complex layouts with thick walls, metal equipment and electronic devices that can interfere with the wireless signals (for example, RFID, Wi-Fi, or Bluetooth) used by RTLS.
• Integration with existing systems: Hospitals often rely on multiple legacy systems for asset management, patient care and operations. Integrating RTLS with these systems can be technically challenging and time-consuming.
• Staff training and adoption: Hospital staff need adequate training to use RTLS effectively. Without proper education, the system may be underutilized or misused.
BORDEN: It starts with selecting the appropriate technology platform that will support both current and future use cases for each healthcare facility. Once the RTLS solution has been selected, it’s critical to have an onsite support partner that can properly and fully implement all the components (i.e., hardware installation of sensors and tags, and software integrations). Followed by the training of clinical and technical staff on how to leverage the data analytics dashboards and reporting tools.
KRAIMER: One challenge we sometimes see in health systems is they fail to plan for RTLS coverage in areas where they really need it, resulting in assets “disappearing” from tracking dashboards. Detailed planning and strategy meetings with your RTLS partner will help account for all areas in need of coverage, especially maintenance areas. Another consideration is having a process for tagging rental equipment to help prevent loss. Resources and budgets are already thin, so it is critical that rented devices stay within defined boundaries of the hospital to avoid excess spending. Be sure to set up alerts for when certain rental equipment gets close to an exit or unauthorized areas.
STIFFLER: Real-time location systems (RTLS) face several key challenges during implementation. The most obvious is ensuring the infrastructure installation provides sufficient facility coverage while minimizing disruption to patient care.
With that said, considerable planning goes in before the first sensor is installed to ensure the teams have addressed platform interoperability, cybersecurity and connectivity. Once the platform is up and running, one of the more underappreciated challenges is addressing change, especially if the platform is helping introduce a new process or PAR management. Lastly, the system must deliver on the outcomes it was established to address.
ZIMMER: Healthcare organizations need to understand the value a RTLS solution provides at a deep level and make sure to have the means to measure that value realization. The concern or feedback I hear from many customers is that the implementations are costly and difficult to justify to senior leadership within their organization. This understanding of the return on investment helps mitigate that pushback.
Q: DO YOU HAVE SUGGESTIONS FOR IMPROVING RTLS OR THEIR INTEGRATION INTO BIOMEDICAL WORKFLOWS?
ASHER: To improve RTLS integration into biomedical workflows:
• Open standard technology: The biggest advantage of BLE is its open-source protocol. This is the only technology that allows interoperability between tags and the location service infrastructure. BLE lets users choose tags from multiple vendors and does not lock them within a monopolistic ecosystem. This creates a price and technological competition that benefits the customers. Moreover, modern network infrastructure, such as lighting, tablets, TVs, etc., all have BLE capabilities, allowing the creation of a dense location service infrastructure that is unmatched by any previous generation asset tracking technologies. BLE is also inherently a low power-consuming protocol that enjoys a longer battery life compared to all other active technologies, making maintenance of the system easier. Combined with cloud software, BLE truly can meet most HTM requirements from a data-sharing point of view.
• Ease of Deployment and Maintenance: Deploy quickly with minimal disruption, integrate into existing network infrastructure and automate monitoring and maintenance.
• Scalability: Leverage the same solution platform for additional use cases, such as staff safety, patient flow optimization and hand hygiene compliance. Build on a cloud-managed, enterprise-grade architecture to expand usage to thousands of beds across multiple facilities without hidden fees.
BORDEN: Smart hospitals are integrating RTLS into more of their existing workflows. The Vizzia InVIEW software
platform integrates seamlessly with several applications to streamline workflows and enhance safety. Key InVIEW integrations include Epic, Microsoft Entra ID, Get Well 360, Lynx Systems and Workday HR.
KRAIMER: The CMMS is a foundational asset tracking interface for your RTLS, since that’s where biomedical teams primarily work. Technicians can assign RTLS tags directly in the CMMS, avoiding double-entry of data into the locating system. In turn, the RTLS provides real-time location information, which is reflected in the CMMS’ “RTLS location” field. This allows biomedical techs to locate assets much quicker, saving them steps in their daily workflow. We’ve heard of health systems investing in software development to build this interface on their own, because they didn’t realize their RTLS and CMMS vendors could work together. At Midmark RTLS, we interface to a long list of CMMS vendors and continue to add new interoperability partners.
STIFFLER: RTLS platforms can significantly enhance biomedical workflows through automated par leveling. By continuously tracking the location and availability of medical equipment, the system can optimize PAR levels based on utilization. This eliminates manual counts and ensures optimal inventory levels on each unit, minimizing stockouts and reducing the risk of delays in patient care. Furthermore, automated PAR leveling frees up valuable staff time for more critical activities.
ZIMMER: Healthcare organizations that are evaluating RTLS solutions could benefit from additional due diligence on what their options are. The technologies are always evolving and there may be more options available than they first suspect. Furthermore, RTLS providers should prioritize their tool’s interoperability with other solutions that their customers already have in place. For example, ensuring that their API’s and technical resources are apt to build connections to a CMMS, EMR or security solution.
Q: WHAT ELSE SHOULD TECHNATION READERS KNOW ABOUT RTLS PRODUCTS?
ASHER: Kontakt.io offers an all-inclusive, AI-enabled RTLS platform that covers medical devices, clinical space, staff workflow and patient flow to better orchestrate the entire end-to-end care delivery operation. The platform uses RTLS to contextualize the movements of patients, staff, and equipment, leveraging RTLS with existing systems like EMRs. Using AI, it transforms data into action that reimagines how hospitals manage resource allocation, capacity and care delivery operations and coordination.
BORDEN: The continued development of advanced RTLS solutions and sophisticated use cases is significantly increasing the value-prop for healthcare providers to reduce costs and improve care. The top two use cases beyond asset management include staff safety alerts and hand hygiene compliance. In 2024, a groundbreaking new $2 billion pediatric hospital deployed RTLS to streamline workflows and enhance care delivery.
KRAIMER: RTLS should be a hospital-wide initiative, not a one-off use case. We often see biomedical and nursing teams addressing their RTLS needs separately, out of separate budgets. Biomed chooses one RTLS to manage assets, but the health system later finds that the level of accuracy doesn’t quite fit the clinical needs to automate nurse call, manage patient flow or improve caregiver safety. This lack of planning is a waste of resources and can be costly. As a solution, hybrid technology all within one RTLS system is quickly emerging as a locating trend that not only provides innovative solutions but also meets the goals of multiple stakeholders. At Midmark RTLS, we use infrared (IR) to deliver the room-certain precision where it’s needed most (typically patient care areas), while offering BLE for near-room accuracy elsewhere to create a cost-effective, facility-wide RTLS deployment.
STIFFLER: The RTLS market is undergoing rapid transformation, driven by advancements in technology and evolving business models. Traditional RTLS systems relied on IR and ultrasound technologies and operated on-premises, requiring substantial upfront capital investment. These legacy systems are facing competition from newer technologies like Bluetooth Low Energy (BLE) and AI, which are increasingly delivered as cloud-based services (SaaS). This shift towards SaaS models significantly reduces upfront costs. Furthermore, newer technologies simplify installation by minimizing the need for extensive wiring. Many solutions now utilize plug-andplay devices or leverage AI algorithms to achieve comparable results with up to 50% less hardware deployment. Lastly, some platforms that utilize AI can provide coverage outdoors, a feat that’s long escaped most RTLS platforms.
Ultrasound equipment failure can be catastrophic.
Learn to service your own with our Solutionist Series videos.
When your ultrasound equipment is down, so is your business. Don’t miss our Solutionist Series videos on Ultrasound Equipment Support where you’ll learn how to service your equipment, keep your business up and running and lower your total cost of ownership.
In this 10-episode virtual training course on the Philips Epiq ultrasound platform, Larry Nguyen, Summit Imaging’s Founder and CIO, identifies common failures and provides solutions for:
• Power subsystem — power module and power regulator board
• External interfaces — control panel, touch panel, trackball, monitor and external IO
• Transducer types and applications — Doppler, linear, curved, endo-cavity and more.
• Transducer parts — a breakdown of standard and TEE
• Transducer parts and operational failures — from lens failure to cut or creased cords to CW noise and error codes
Larry Nguyen addresses lots more in our 10-episode Solutionist Series, so be sure to tune in.
The Ultimate Guide to HTM Jobs
Featured Employers: Agiliti, Renovo Solutions, TRIMEDX, Erbe USA Incorporated, Middlesex Health, SP Associates, and more!
htmjobs@mdpublishing.com for posting inquiries htmjobs.com to register today
A niche job board for the HTM and imaging communities
350+ open job opportunities throughout the United States Single-job postings to 12-month unlimited memberships
3300+ biomedical and imaging candidates
THE FUTURE OF HTM: Increasing Innovation and Efficiency
By K. Richard Douglas
The concept of “efficiency” comes with many meanings. It can mean doing more with less, maximizing output with minimum input, streamlining a process, making the best use of fuel or electricity, allocating resources or wasting less.
The evolution of the common light bulb in recent years is an example of efforts to achieve greater efficiency – using less power to illuminate a bulb for a longer time period.
The federal government seems very inefficient while the local fast-food restaurant is buzzing along and getting food out. Efficiency is often missing when it is not a priority. Charities are measured by how efficiently they utilize donated funds. The best charities have found ways to reduce administrative costs and efficiently use the largest percentage of donations toward their purpose.
Efficiency must be a part of business operations for a business to prosper and succeed. The same is true for hospitals and healthcare systems. Healthcare systems operate on a budget that is often determined by Medicare and Medicaid reimbursements. Hospitals rely primarily on billing insurance companies for the services they have rendered to patients.
Many of these operating revenues are derived from surgeries, diagnostic imaging, doctor services and, to a lesser extent, gift shop or food sales.
While all departments in a hospital look for ways to achieve greater efficiencies, HTM departments in hospitals worldwide have found ways to cut costs. HTM departments can also achieve greater levels of efficiency with a few tweaks.
I could assist by alleviating some of their workload. I wanted to demonstrate that others can support our technicians as well,” Collins says.
Would application of the ideas in the presentation apply to biomed departments that don’t have a dedicated operations supervisor?
“If a department lacks an operations supervisor, receptionist, or phone operator, anyone managing the front desk could assist during times of low activity,” Collins says.
KNOCKING OFF THE PMS WITH INSPECTORS
Another area for creating efficiency is to have a paraprofessional person handling many of the more routine duties that can monopolize a biomed’s time.
Collins explains that his department includes four “inspectors,” who are not biomeds, but mechanically literate individuals who are able to do PMs on high-volume, low-acuity equipment.
The inspectors have electronics training. Also, the inspector position is often a stepping-stone into a biomed position within ChristianaCare.
“Our inspectors conduct preventive maintenance (PM) on our high-volume, low-impact devices, such as scales. Clinical Engineering has assigned each off-site location a specific month to complete all necessary PMs. Additionally, we have designated asset types to be serviced in each month on a recurring basis,” Collins says. He says that individuals are selected for these roles based on their attitude and willingness to learn.
While all departments in a hospital look for ways to achieve greater efficiencies, HTM departments in hospitals worldwide have found ways to cut costs.
At the 2024 MD Expo in New England, G. Blake Collins, MBA, CBET, CHTM, FABC, director of clinical engineering for ChristianaCare Health Systems, and Theresa Street, operations supervisor with ChristianaCare Health Systems, presented the continuing education session “Increase Efficiency in Support of Clinical Engineering.” Check out the MD Expo presentation at https://tinyurl.com/47w9pxvd/
The CE department at ChristianaCare is ISO 9001 certified and has branded itself as “your solution provider.” The department will attempt to assist clinical colleagues in any way they can. At the very least, the team will connect the caregiver with the appropriate source.
What motivated Collins and Street to present on this topic?
“After learning about the various departments and their respective technologies, as well as observing the daily responsibilities of ChristianaCare technicians, I realized that
“This serves as an opportunity for them to gain experience in the biomedical equipment technician (BMET) field. We provide opportunities for learning, but it is also essential for them to take advantage of these opportunities and demonstrate the knowledge they acquire. Ultimately, our goal is to have them become BMETs and advance through the various levels of the profession,” Collins adds.
The inspectors handle 400 to 700 PMs every month. Offsite PMs are scheduled so that everything can be accomplished in one visit. The efficiencies achieved in the department allow other biomeds in CE the time to train inspectors.
THE RIGHT PERSON FOR THE JOB
The department leadership utilizes a spreadsheet that pinpoints the biomeds and the modalities that they have expertise with so they can quickly determine the primary person for a particular call. Knowing the strengths and skill sets of every biomed allows for efficiency in this area.
“During the annual reviews, each technician completes a checklist of their qualifications, while our supervisors
validate their skills, training and any new modalities they have acquired. Additionally, a spreadsheet has been created to assist me in assigning work orders based on the modalities of each technician,” Collins says.
STAFF-CENTERED SCHEDULING
Another efficiency is gained by not having a set schedule, originating from management, that determines staffing and availability.
Instead, the schedule is determined by the staff themselves based around availability and a life/work balance. Some biomeds are early risers, according to Collins, while others have family commitments that determine different hours.
“The four groups – inspectors, biomed, imaging and sterilizers – are informed a month in advance about the preventive maintenance schedules. This allows them to plan accordingly for the completion of these tasks. Family commitments will always take priority, and with approval, technicians have the flexibility to come in after regular office hours. ChristianaCare Clinical Engineering maintains a minimum staffing requirement at each campus,” Collins says.
at ChristianaCare has two members who are able to handle rounding and retrieve broken equipment.
Removing this chore from technicians increases efficiency and allows techs more time to turn a wrench. Collins says that this allows repairs to happen more quickly.
“Every Tuesday, we generate a report detailing open work orders that are not assigned to technicians. Our part-time front assistant uses this report to help locate devices while she is delivering them back to the floors. We encourage all our technicians to stay vigilant in order to help find devices and bring them down when possible. Additionally, we utilize a real-time location system (RTLS) to aid in locating devices,” he says.
In time savings, and allowing techs to focus on maintaining equipment, the efficiencies gained by the ChristianaCare CE department has improved quality of life, allowed for quick repair turnarounds and measurable savings.
He also says that this approach to scheduling allows him to keep his shop open later. At the same time, Collins says that it provides more quality of life and family life for the CE staff. In short, greater levels of efficiency are found through flexible scheduling that accommodates technicians.
ROUNDING AND RETRIEVING HELP
Another method to free up the tech’s time is for a member of the operation team to find equipment, retrieve it and bring it to the shop. Don’t require techs to do this function; it requires time away from their bench. The CE department
The department also gains more efficiency through an assistant or an operations supervisor’s involvement with the return merchandise authorization (RMA) process.
“Over time, you can create a list that the admin can use to help the technicians with generating RMAs. This process won’t happen overnight, but by gradually building this list, it will become a valuable tool to assist with the RMAs. Additionally, establish an open communication system with the technicians to facilitate follow-ups and track the equipment more effectively,” Collins says.
TRACKING PARTS
Accounting for parts and avoiding ordering duplicate parts that cannot be quickly located provides another efficiency.
In the ChristianaCare CE department, parts bins are kept along one wall. Another grouping of parts bins contain more commonly retrieved parts. The department even utilizes old file cabinets to store parts. Because the
department is ISO 9001 certified, there is a requirement of core areas of expertise.
Collins says they have developed a hybrid system using both their CMMS and a kanban system. A card that represents each part contains the number of parts that should be stocked in each bin, the number that should be par and the reorder point.
When the tech sees that the stock is low, they pick up the inventory card and drop it into a bucket. The operation’s supervisor then reorders those parts. When parts come into the department, the card is pulled, barcodes are scanned and the parts are placed in the bin
Collins says that one of the requirements of ISO 9001 is that they must segment into new parts, known-good, known-used, known-bad and unknown. He says that following this discipline prevents parts from being hoarded and unaccounted for within the department.
It proves to be efficient because parts can always be quickly located and available. There is no need to order a part that is actually on-hand but not locatable. Everything is tracked.
“Having a well-stocked parts room with high-demand items saves time during repairs. Our caregivers no longer face long delays due to shipping times for parts. As a result, the turnover rate for repaired devices increases because we have the necessary parts readily available. Our vendor provides an application that helps us determine appropriate par levels based on parts usage and purchase frequency, ensuring we don’t have underutilized parts in our inventory,” Collins says.
The department endeavors to keep three months of parts available. The parts vendor that the department uses provides reports that detail if there were bad parts or parts that had to be returned or if a tech ordered the wrong part. This data helps the department stay in compliance with ISO 9001 requirements.
If a new part also requires a core return, Street created a
bright-green sticker that goes on the part and reminds the tech to send back the broken part.
A COMMONSENSE MARKETPLACE
Many of the innovations utilized in the department provide benefits to the techs. There is more of a focus on their core responsibilities. This frees up time for more problem-solving.
The department also created a “marketplace” which allowed the team to “advertise” extra equipment that might be needed in a department. In 2022, when the department first launched the marketplace, there was a savings to the healthcare system of $192,000 from 346 requests that resulted in relocating equipment where it could continue to be utilized.
“ChristianaCare has several warehouses that store devices, furniture and accessories for the hospital. However, these warehouses were becoming overcrowded. The marketplace has facilitated communication with our caregivers regarding the items available for request. Our vendor developed an application that allows users to view what is available. The app includes pictures and descriptions of each item. Additionally, our vendor has established a delivery system to ensure these items are accessible to all of our campuses and offsite locations,” Collins says.
Marketplace relocations through October 2024 accounted for $1.6 million in savings. The marketplace, which first included only medical equipment, now includes furniture, office supplies, lamps and even artwork.
In time savings, and allowing techs to focus on maintaining equipment, the efficiencies gained by the ChristianaCare CE department has improved quality of life, allowed for quick repair turnarounds and measurable savings.
Check out the MD Expo presentation at tinyurl.com/47w9pxvd/
CAREERS NOW
How to Shine When You’re Boss-Less
BY VICKI SALEMI
Toxic bosses seem to get a lot of attention, but absentee bosses often fly under the radar. How can you advocate for yourself when your boss is missing and therefore, doesn’t have your back?
Whether you have a boss who is always MIA or don’t have a boss altogether and report to a leader at least one or more rungs higher on the company’s hierarchy, it could be challenging to be recognized for your performance if it feels like nobody’s watching. Plus, you may not get adequate support and resources to develop new skills to navigate new paths.
Some managers are being downsized and they’re not being replaced. Layoffs have surged to more than 30% lately that impacts middle managers, as per 2023 data by Live Data Technologies for Bloomberg.
You’ll need to be proactive. Seek out an internal mentor and build alliances with other departments, if you can. Especially if you previously worked for a micromanaging boss, not having boss interactions can feel liberating, at first. Be cognizant, however, of what you need to succeed: someone to go to bat for you if you have an unresolved issue, a fierce advocate during salary review meetings, and someone who sees and values your contributions to the organization.
Self-advocacy is important. Craig Guarraci, founder of Tech PM Career Path and career coach, said, “Since managers will have limited time managing many direct reports, employees will need to self-advocate more often for interesting assignments and promotions to ensure that their manager is aware of their career aspirations. Self-advocating includes being proactive as employee review season approaches.”
From an organizational perspective, Jason Walker, Psy.D., Ph.D., program director and associate professor of industrial-
organizational and applied psychology at Adler University, said, “An organization’s role, then, is to build a culture of ‘lighthouse leaders’ at all levels. Guides who provide feedback, direction and opportunity, even in flat structures. We want leaders focused on the vision and managers on the mission – removing the ‘get it done’ supervisory level will create an impact on employee satisfaction, well-being and also productivity.”
Even if you’re proactive with internal higher-ups and an organization provides guidance, there is a difference between leaders and bosses.
Roger A. Gerard, former vice president of HR in a health care system, a seasoned leadership consultant and the author of “Lead With Purpose: Reignite Passion and Engagement for Professionals in Crisis,” said, “Leaders will never be obsolete, though bosses might be. There is a difference. Bosses tend to be poor listeners and act like their opinions are law. They often use ‘blame and shame’ tactics and think it is their job to motivate their employees.”
“Real leaders, on the other hand, listen carefully to those doing the daily work, understanding that their perspectives are key to solving problems and meeting the demands of the work itself. They understand that motivation is an internal driver that people bring to their work and any use of blame/ shame undermines that motivation.”
Looking at the big picture, Gerard said these great leaders involve people in change decisions and foster co-authorship to ensure an authentic “buy-in” to organizational change.
“Engagement surveys tell us that workers who have a great relationship with their leaders are more productive, and more engaged in the work. Not so much with bosses,” said Gerard.
Vicki Salemi is a career expert for Monster, an author, a speaker and consultant, TV commentator and former corporate recruiter. Send your questions to hello@vickisalemi.com.
Broken Transducers?
Replace for Less with AIV.
Transducers are compatible with most popular GE/Corometrics & HP/Philips models
Functionally equivalent to OEM
Nearly identical in appearance
FDA 510k listed devices
JOIN US: htma-oh.org/join-us
SPONSOR US: htma-oh.org/sponsorship-request
WEBSITE: htma-oh.org
EMAIL: info@htma-oh.org
HELPING HEALTH CARE FACILITIES DO LESS WITH LESS
FSI CEO Discusses the Evolution of a Market-Leading Healthcare CMMS
BY ZACHARY SEELY, CEO AT FSI
No matter the person or one’s stage of life, at some point every American spends time in a hospital. Whether for preventive or corrective reasons, patients receiving care might take for granted that the heating, ventilating and air conditioning unit is working, the patient monitoring equipment operates seamlessly and the building is prepared for a disaster to ensure patient care is not interrupted.
Patients do not have to think about these things because thousands of facilities and biomedical maintenance professionals do their jobs every day. Dennis Ford, MHA, CHFM, CHC, FASHE, director of corporate facilities management support at North Carolina’s Atrium Health and the American Society for Health Care Engineering (ASHE) 2025 president-elect, succinctly relays this concept. “When we are successful in facilities operations, often nobody notices, as expectations of 100% uptime of building infrastructure systems is met,” Ford says.
While Ford and many others in the maintenance field do their job to avoid headlines about unsafe environments or regulatory noncompliance, these unsung heroes also rely on trusted technology partners to complete their work every day and to maintain a safe environment for patients. And as they navigate challenges created by labor shortages and generational transitions, aging equipment and natural disasters, FSI, is helping these health care maintenance teams adopt the philosophy of “less with less.”
INSPIRED BY HEALTH CARE MAINTENANCE PROFESSIONALS
Founded in 2002 by Joe Serwinski, FSI initially launched as a data collection company, going on-site at hospitals to provide an accurate inventory of their physical assets. The process entails
walking every square foot of a building, finding every asset and placing barcode labels on each one, recording essential information (manufacturer, make, model, location), and then double checking this work. Although it is a time-intensive task, maintaining an accurate asset inventory ensures that hospitals have a clear understanding of what exists in their environment.
The data collection business grew, and in 2006, Serwinski was approached by a customer with an interesting question: “Why collect all this information, organize it how the customer wants and then give it to another company?” This customer went on to ask, “Why not make your own software? We would use it.”
Seeing the opportunity, Serwinski moved quickly to develop a computerized maintenance management system (CMMS), which, at its most basic definition, is software for maintenance professionals to track work orders and assets, ensuring that both preventive maintenance and corrective maintenance is completed.
By 2020, FSI was serving more than 800 hospitals. But Serwinski recognized that they could do more, and in order to do so FSI needed more resources.
LESS WITH LESS: PREPARING FOR TECHNOLOGICAL AND GENERATIONAL CHANGE
As evidenced by FSI’s origin story, it has always been a “by health care, for health care” operation – gaining inspiration from those it
COMPANY SHOWCASE
serves and incorporating the insights of those using its products into the software’s DNA. That focus continues today with the company’s vision to empower health care service professionals to maintain the safest environments and most efficient operations.
This commitment to health care helped develop the concept of “less with less.” In practice, doing less with less is all about enabling health system partners to do two things. “Doing less” means prioritizing work that will lead to the greatest benefit and eliminating work that has little to no impact or value. “With less” refers to making the most with the resources available to drive the best long-term outcomes efficiently and effectively. Thus, the two-pronged approach: “less with less.”
This principle is at the heart of the FSI mission: “Our strength lies in our innate customer understanding and our commitment to enabling them to do less with less. We work in partnership with each customer, guiding them throughout each collection, implementation and process improvement, saving them time, helping to simplify and reduce waste.”
This simple concept is not without its challenges. Starting with the second “less,” there’s no doubt that health care systems have had to become creative to combat the reality of constrained resources. In facilities maintenance and health care technology management specifically, this includes the critical and complex challenges of generation transition and change in the workforce. It is estimated that the average facilities and healthcare technology management technician is 55 years old, meaning these industries are searching for a new skilled talent pool as hardworking technicians retire, exacerbating the need to find solutions that can be done “with less” without compromising the quality of work.
The challenge of “doing less,” lies in the need for solutions to streamline and prioritize operational efficiency. As the facilities maintenance industry looks to adopt technology to automate workflows and reduce idle time, not all options look alike or offer the same level of tailor-made solutions built for the day-to-day realities of health care facilities and health care technology management requirements.
THE SECRET INGREDIENT: TURNING DATA INTO ACTION
To rollout a successful “less with less” strategy, organizations must have data that provides insights to ensure they are focusing on the right type of work. While a CMMS stores the information customers need to make these data-driven decisions, a CMMS is
oftentimes only as good as the data that resides within it.
Knowing exactly what assets a hospital has and where they are located is the most important first step in maintaining a facility. Many hospitals that FSI works with, however, have lost track of this critical data, requiring cleanup efforts in order to get them on the “less with less” track.
To remedy this, FSI continues to offer in-house data collection services. By moving forward with a data collection, customers ensure that they know exactly what assets are in their system and where they are located. Furthermore, a data collection also provides a moment-in-time to standardize different fields, such as asset category, location data and nomenclature. This is especially important, as the ability to measure performance across an asset class relies on having standard naming conventions.
Once this data is in place, it’s essential for hospitals to find opportunities to take the “less with less” framework a step further by gathering insights from facilities data to make impactful decisions that will reduce wasted efforts, boost the actions that make the greatest impact and learn how to maximize the resources at hand.
FSI empowers customers to glean key insights by offering tools to visualize data in a meaningful way. Both customizable dashboards and business intelligence functionality allow customers to pre-calculate specific key performance indicator metrics, such as customer satisfaction and inspection, testing and maintenance performance, or to benchmark against health care regulatory standards from groups like ASHE. These components in FSI’s suite of solutions assist customers in arriving at insights, support decision-making and automate compliance reporting activities.
PUTTING ‘LESS WITH LESS’ INTO PRACTICE
Taking the philosophy of “less with less” and making it a daily ritual requires the right tools to prioritize beneficial tasks and eliminate less impactful work while maximizing resources and streamlining operations.
As part of the “less with less” framework, in 2024 alone FSI has developed a new mobile application that reduces work order close time by more than 33%, reinvigorated dashboarding for easier management and data visualization, built new workflow automations to eliminate manual processes, deployed a new resource center and in-application training/guides, and released integrations with other facilities management products including PartsSource, Cynerio, Fluke OneQA, ServiceNow and CRx to eliminate multiple points of data entry.
The design of these products has been inspired by FSI’s
customers and play a critical role in ensuring hospitals can save time and ensure their valuable team members are working on only the most impactful tasks. In brief, these products allow customers to do “less with less,” eliminating the work they don’t need to do with less resources.
While many CMMSs provide the necessary functionality to achieve compliance, asset management and operational efficiencies, FSI’s goal is to build a product that not only checks several fundamental boxes but also streamlines the unique workflows of a health care maintenance team – whether it’s integrating with other purpose-built tools a customer already relies on or adding new health care workflow-specific automation features that reduce clicks and increase the user-friendliness of FSI solutions.
LOOKING AHEAD: BUILDING A ROADMAP AGAINST AN EVOLVING LANDSCAPE
With the generational transition and subsequent labor
shortages, “less with less” is a strategy that more and more health care organizations will continue to adopt.
At FSI, this philosophy was developed based on firsthand experiences of health care maintenance professionals. This legacy continues as FSI leverages direct feedback to fine-tune products and empowers customers to do “less with less.”
Healthcare facilities maintenance and healthcare technology management teams should consider how they can adopt a “less with less” framework. Does the team have the tools to identify ways it could be doing less? Are the current solutions that are being used to maximize workforce and resources accomplishing the intended goal to do less?
As the healthcare maintenance industry encounters new challenges, FSI is committed to walk in lockstep with healthcare facilities teams, listening, testing and building, making “less with less” an achievable and intrinsic component to hospital operations. The highest compliment FSI’s hospital facilities customers give is that the company is more than a software vendor; FSI is a partner.
Zachary Seely is the CEO of FSI, a leader in CMMS focused on the healthcare industry. Seely holds a BA from Bates College and an MBA from the Wharton School at the University of Pennsylvania.
Contrast Injector Training
RIGHT TO REPAIR
Terumo to Stop Certifying Non-OEM Technicians
BY NATHAN PROCTOR
Terumo, manufacturer of advanced perfusion system 1 Heart Lung Machine, is informing customers that it will no longer offer training and certification for repair of that equipment. When those certifications expire, customers will be forced to contract with Terumo for the servicing of that equipment.
It’s just another example of why Right to Repair reforms are so important. Many hospitals and clinics purchase equipment that they believe they will be able to maintain, but without protections, the manufacturers can change the terms, and effectively monopolize the repair of equipment after it was purchased. Now, without competition, Terumo can charge more for their services – putting a cash-strapped hospital in a bind.
OREGON’S RIGHT TO REPAIR LAW TOOK EFFECT JANUARY 1
Oregonians are the latest Americans with a right to access parts, tools and information needed to fix their consumer devices. On January 1, a new law went into effect, requiring manufacturers of consumer electronics and appliances sold or used in Oregon to give owners of the products any parts, tools or information used by the manufacturer to conduct
repairs. The law joins laws on the books in California, New York and Minnesota covering consumer devices.
NEW MILITARY RIGHT TO REPAIR LEGISLATION INTRODUCED
Sen. Elizabeth Warren (MA) and Rep. Marie GluesenkampPerez (WA) have introduced new legislation regarding Right to Repair for the military. Similar to an earlier push to amend the National Defense Authorization Act (NDAA) to support repair, the new legislation would require contractors to include granting the military full access to parts, tools and information needed to repair a product, when they sell equipment to the Armed Forces.
The earlier amendment earned bipartisan support in committee, though did not make the final draft of NDAA.
CHECK ME OUT ON A RECENT EPISODE OF THE BEARDED BIOMED
I spoke with Chase Torres on his Bearded Biomed podcast about this push for Right to Repair for the military, and highlighted stories I’ve heard from former military biomeds about why these reforms are necessary.
Nathan Proctor is senior director of the U.S. PIRG Campaign for the Right to Repair.
THE FUTURE Students Explore Medical Imaging Opportunities
BY STEVEN J. YELTON, P.E., AAMIF
As I write this column, the Radiology Society of North America (RSNA) Conference and Annual Meeting is underway in Chicago. Throughout my career, students and perspective students have often taken an interest in pursuing a career in repair of imaging equipment.
Many years ago, I had the opportunity to attend the RSNA meeting. I wanted to further explore opportunities for my students and learn more for myself. I found this area of study to be very exciting. I was always interested in computers and new computer technology. As I toured the RSNA exhibits, I couldn’t believe the technology that I got to see. It seemed that the latest and greatest computer technology as well as imaging technology was on display. With the HTM and computer technology fields “living” so closely together, it’s understandable why HTM students would be interested in investigating these opportunities.
As I saw messages about this year’s RSNA meeting, I felt like this would be a good time to revisit imaging education and training in my column. At Cincinnati State Technical and Community College, the Biomedical Equipment Technology Program is a two-year Associate of Science (A.S.) program. As a college program, imaging education has always been a challenge. We were never able to have a significant amount of imaging equipment at the college because of cost, so partnerships with local hospitals and companies is what enables us to have a significant imaging training aspect of our HTM program.
The Cincinnati State A.S. program does not provide enough time to devote to the imaging area to achieve complete training. We try to provide a high-quality introduction to the imaging area both in classroom instruction and as part of our cooperative (co-op) education program.
We have many health care related programs in our Health Technologies Division. We try to establish working relationships between the Engineering Technologies and Health Technologies divisions at the college to provide shared services. One of the areas is scheduled maintenance and repair of medical systems including any imaging systems at the college. We are currently in the process of resurrecting this program. Over the years, participation in this program has lessened for no reason.
This collaboration not only provides real world laboratory exercises for the HTM students, but also provides timely support of equipment and will contribute to the safe and effective use of medical systems.
After participating in these programs, our hope is that graduates pursuing careers in imaging repair will continue their education in a four-year program or as part of an imaging training program. A partial list of the programs that our graduates have pursued over the years for training or employment are: RSTI (Radiological Service Training Institute), GE HealthCare, Phillips Healthcare and Hologic. You will find that many of these companies are participating at RSNA.
I am not promoting any college or training program. One of these non-college program alternatives in radiology service training that my graduates have pursued over the years is RSTI. These graduates tend to pursue RSTI training in conjunction with full-time employment. The RSTI
program is a respected program within the industry and is in Ohio near Cleveland. This makes the proximity to Cincinnati State within a drivable distance. Our graduates also pursue bachelor’s degrees from many universities in engineering and engineering technologies on a full- or part-time basis, though usually not in the imaging area primarily because of a lack of availability.
Another topic that I would like to remind everyone of is the area of certification. We have found that the Certified Radiology Equipment Specialist (CRS) is important and highly sought after by employers and graduates. The AAMI website: https://www.aami.org/home/about-aci/aci-home/cres states the following: “Healthcare technology management professionals that desire a CRES certification are expected to have experience in a wide-range of medical imaging modalities, electromechanical devices, computers, networks and software used in the delivery of healthcare.”
The AAMI website also lists the following as the requirements for CRES certification:
• Associate degree or higher in biomedical equipment technology program; OR
• Completion of a U.S. military biomedical equipment technology program; OR
• Associate degree or higher in electronics technology and one-year full-time BMET work experience, OR
• Two years of full-time BMET work experience.
*CRES Applicants for full certification: At least 40 percent of work experience over the last two years or 25 percent over the last five years must be in the designated specialty area.
I have only listed some of the certification information here and would recommend that you visit the link listed additional information for all CRES certification requirements.
As always, I hope this information helps you!
Steven J. Yelton, P.E., AAMIF; is a senior HTM engineer for a large health network in Cincinnati, Ohio and is a professor emeritus at Cincinnati State Technical and Community College where he teaches biomedical instrumentation (HTM) courses.
CYBERSECURITY FROM SMART HOMES TO
SMART HOSPITALS
A Quest for the Perfect IoMT Solution
BY NADIA ELKAISSI, CHTM
In the age of smart everything, the Internet of things (IoT) has become the backbone of countless industries. But when it comes to healthcare, IoT evolves into something more specialized: the Internet of Medical Things (IoMT). This branch of IoT focuses exclusively on medical devices and systems that connect and communicate to improve patient care. While this innovation is transforming healthcare, it also brings new cybersecurity challenges that cannot be ignored. Let’s discuss what sets IoMT apart from IoT, what you should look for in an ideal IoMT solution, and how it can help combat cybersecurity threats in healthcare.
Although both IoT and IoMT solutions are often mentioned in the same breath, it is important to recognize their differences. IoT in healthcare includes generic
connected devices like environmental sensors, smart HVAC systems or logistics trackers used in hospital operations and infrastructure. On the other hand, IoMT dives deeper – it’s all about medical devices that directly impact patient care, like infusion pumps, wearable monitors and even implantable devices like pacemakers. The stakes are higher here; a compromised IoT thermostat might leave a room too hot, but a hacked insulin pump is life-threatening.
So, what is the recipe for the ideal IoMT solution? When you are evaluating a robust IoMT solution, it isn’t just about the connectivity. It’s about building a secure, reliable and resilient system that addresses healthcare’s unique needs. Let’s dive into a few areas that you should be focusing on during the IoMT evaluation process.
1. CENTRALIZED CONTROL AND DEVICE VISIBILITY
Imagine a single dashboard where HTM and IT staff can
see every connected device – from infusion pumps to wearable monitors – in real-time. It should include detailed information such as device types, firmware versions, locations, usage history and maintenance schedules. Built with interoperability in mind, it seamlessly integrates with EHR systems, cybersecurity tools, compliance trackers and vulnerability monitors. Equipped with advanced search and reporting features, the database ensures healthcare systems can quickly identify and address issues, enhancing patient safety and operational efficiency. The ability to manage all devices in one database is not just a nice-tohave; it’s a critical for ensuring every device is functioning securely and optimally.
2. PLUG-AND-PLAY INTEGRATION
The perfect platform recognizes that hospitals and healthcare managers do not have the luxury of endless setup times. It must seamlessly integrate with medical devices without requiring drivers or additional software. This “plug-and-play” capability enhances system efficiency, streamlines operations and minimizes risk association with manual configuration or third-party software. In addition, it must also be able to integrate with other systems such as firewalls, ticketing systems, etc.
3. REAL-TIME THREAT DETECTION
Healthcare doesn’t stop, and neither do hackers. A great IoMT platform continuously monitors for anomalies, flagging suspicious behaviors like unexpected data transfers or unauthorized access attempts.
4. COMPLIANCE REPORTING
Healthcare regulations can be daunting. The perfect platform simplifies compliance by automating reporting and providing security logs, making audits less stressful. The bottom line is that the perfect IoMT management solution doesn’t just manage devices, it ensures devices stay secured. By combining real-time monitoring, threat detection and compliance reporting, it becomes the ultimate guardian of healthcare’s digital frontier. In a world where lives depend on technology, IoMT solutions ensure every beep, ping, and pulse stays protected, because in healthcare, cybersecurity is as vital as the care itself.
Nadia ElKaissi, CHTM, is a biomedical engineer in healthcare technology management with the VA Central Office (19HTM).
IT’S TIME TO DITCH THE VIDEO CAPTURE BOX & INTEGRATE ALL CLINICAL VIDEOS INTO YOUR EHR
Clinical Video is Stranded on Inaccessible Islands of Information
Clinical video is generated in many departments across a health system, including GI, surgery, urology, OB-GYN and ENT. The number and variety of scopes used during minimally invasive procedures has grown rapidly. Video recorded during these procedures is valuable for post-procedure follow-up and patient consultation, as well as teaching and research.
There are several technical reasons why the integration of scope video into the Electronic Health Record (EHR) and enterprise Picture Archiving and Communications System (PACS) has lagged:
1. Clinical video is typically captured in a non-DICOM (nonstandard) format.
2. Clinical video scope manufacturers only recently began including native DICOM capabilities.
3. Many legacy PACS solutions cannot store and display video, forcing them to be stored locally in the medical scope, on removable media or in proprietary scope vendor archives.
There are also organizational barriers. Often, the biomedical team that services and supports clinical scopes is independent of the IT team that manages the enterprise imaging systems. Biomed may lack the experience and knowledge of the video capabilities of the enterprise PACS/VNA. This can lead to departmental purchases of isolated scope vendor solutions or perpetuating clunky “capture box” solutions instead of adopting a standards-based enterprise approach. These technical and organizational challenges are compounded by the fact that healthcare organizations typically have numerous scopes from various vendors spread across many clinical departments – which creates significant operational challenges when attempting to improve access to this valuable clinical information.
Some medical scope manufacturers provide hardware
upgrades that enable video to be exported in a standardized format. Still, they are more likely to offer a dedicated miniPACS to store the video and enable sharing with other clinical IT systems. These approaches do not align with enterprise imaging goals and strategies because they:
1. Increase costs
2. Perpetuate scope vendor-specific solutions that typically do not connect with competing vendors’ equipment using accepted standards
3. Require EHR integration to each mini-PACS solution
4. Force clinicians to learn different user interfaces to view videos from each department
The most common approach to video capture is implementing a hardware-only video capture box. Unfortunately, these capture boxes are typically expensive, and one is required for each medical scope. In addition, they cannot be centrally managed, requiring maintenance from already stretched biomed teams. Lastly, these non-IT-supported boxes are often security concerns during IT audits because of dated operating systems, custom patch administration and the potential for Protected Health Information (PHI) being stored on them. These shortcomings are significant barriers to adopting standards-based clinical video capture. They have led to their adoption only in high-volume or high-value clinical departments such as surgery and gastroenterology.
The good news is that many hospitals and health systems are on their way toward implementing enterprise imaging strategies that leverage standards to centrally store, manage and provide universal access to still images for all clinicians. It is time for clinical video to be included in these strategies so it can be accessed via the EHR and other enterprise clinical IT systems.
Challenges and Limitations with the Status Quo
The current approach of capturing clinical video in a proprietary format and locally storing it on removable media has created numerous challenges that affect the hospital’s clinical and IT operations. Let’s review some of them.
Operational Impact
• If the video is in a proprietary format, it can only be viewed on the scope that initially acquired it.
• Typically, there is no backup of the video. If the removable media is misplaced or the hard drive in the scope becomes corrupt, the clinical information may be lost.
• Removable media on the shelf inevitably becomes inaccessible as scopes are upgraded and older storage media formats become obsolete.
• Manually retrieving video files is a time-consuming process.
IT & Security Impact
• Auditable tracking of who accesses removable media is impossible. Removable media can be lost or misplaced.
• Security measures, such as the need to log into a video scope, are often not in place.
• Enterprise access controls and security measures do not exist.
• Hardware-only clinical video capture solutions cannot be centrally accessed and managed.
Clinical Impact
• Clinical comparisons are only possible if a follow-up exam is performed in the same room or on the same vendor’s equipment as a prior exam.
• Staff cannot easily retrieve and compare a current video study to a prior one for diagnostic purposes.
• There is restricted access to the video for teaching and research purposes.
• Typically, only a few high-volume, high-profit clinical departments digitize their video because of the high cost of hardware-only video capture and conversion solutions.
• Limited access to the clinical report and associated key images is also common.
Financial Impact
• The cost of removable media, the space to store it and the cost of expanding storage on an existing scope can add up.
• Hardware-only video capture solutions are expensive; one video capture box must be purchased for every medical scope.
• Purchasing a dedicated scope mini-PACS for every department is costly.
Why Connect Clinical Video to the Imaging Enterprise?
Integrating clinical video into your IT infrastructure creates an opportunity to leverage existing enterprise imaging investments. If an enterprise PACS or VNA has been implemented, enabling video to be accessible via the EHR can:
• Improve and simplify access to all caregivers inside and outside the organization.
• Increase the availability of video for teaching and research.
• Facilitate compliance with Release of Information (ROI) guidelines.
These opportunities become more attainable when adopting a modern enterprise approach to clinical video connectivity. Replacing clunky video capture black boxes with enterprise software tools provides a more cost-effective, IT friendly approach. The software should provide a common set of tools for centralizing the management of all connected video capture devices. In addition, it should be offered via an enterprise licensing model that simplifies broad implementation across all clinical departments – in a cost-effective manner that doesn’t put demands on the clinical IT department.
Summary
Replacing unmanaged video capture boxes with centrally managed enterprise software makes it easy and affordable to capture all clinical video in the DICOM standard format. Centrally managed enterprise software that makes video available to the EHR offers numerous operational, security, clinical and financial benefits. Eliminating expensive islands of clinical information is a valuable and logical extension of any enterprise imaging strategy.
For more information, visit altamont.com.
Chris Barnett, President
NETWORKING NOTES CAN Networks – A Modern Bus Network
BY GARRETT SEELEY
Imagine my surprise when I first discovered that there are several different networks in use in a modern MRI scanner. In fact, when studying at my most recent OEM school, I found several different types of networks used in the same device. It was a regular throwback to my college days. Academically, there were three principal networks topologies: a star, a ring, and a bus.
Surprisingly, each is still used in modern imaging, just not as they were originally used.
The first network is the most common and, therefore, the one I will mention the least; that is the star network. It is the common ethernet that most are very familiar with.
The second most common design for networks that I find is a bus design. There was a time when bus networks were quite popular in computer networking, however the speed and scalability of a star network eclipsed the use of bus networks for computers. Regardless, it is always amazing how older network concepts get updated and adapt to newer systems. They are reborn and rebuilt with a new purpose. One such network is a Controller Area Network (CAN). I thought that bus technology would not be used in modern electronics, however it is becoming popular for small scale sensor networks in manufacturing, automotive and, yes, medical devices. The appeal of the CAN bus is an ease of wiring combined with less hardware. It excels where speed and bandwidth are not a concern.
For example, in automobiles, a CAN bus connects over four dozen different sensors to the processors on a modern vehicle. Consider that an MRI is also completely microprocessor operated and essentially has dozens of sensors itself. All these sensors must communicate in an electrically noisy, possibly wet, physically difficult environment where temperatures can reach extremes of hot and cold. The wiring needs to be rugged and fault
tolerant, but the messages exchanged are often short lines of text. The network requires fault tolerance more than speed and this is where CAN really stands out. CAN uses a two-wire, twisted pair as a communication backbone where all the devices, called nodes, connect to the main cabling, called the bus.
Each node connects in parallel wiring to the bus. All nodes can communicate to each other on the same bus in a broadcast format where all nodes hear the same communication. To transmit, a node waits for the line to clear, and then higher assigned priority node communicate or pass in order of priority. The communication then moves to the next in priority node. This may seem inefficient, but it ensures the most critical information is transmitted first.
In CAN, both wires, simply called CAN-High and CAN-Low, are used to send the communication bits by setting voltages in a mid-range as a default, for example 2VDC. To represent a change in the bit, both wires change, CAN-High goes high, and CAN-Low goes low. This represents a zero bit. To represent a 1 bit, both lines return to the base of 2VDC. In this way, only the difference or the similarity of the voltages per clock pulse is measured as a bit by all nodes. It is this difference or not that represents the 1’s and 0’s. That is important because it gives a natural fault tolerance. If there is a spike or electrical noise, the noise is experienced on both cables in the twisted pair. This minimizes differences caused by noise, therefore
canceling the interference. Differences or no differences is basically how CAN works. The protocol includes some redundancy checks, a standard frequency, and a fixed frame bit length and then CAN becomes a small scale, noise tolerant ISO communicational standard.
A load resistor on each end of the bus ensures there are no reflected signals at the wire ends and that is all the network requires to work: nodes in parallel and end terminators. That’s it. Because this communication only needs 2 wires, CAN is generally used on a thicker conductor, offering more physical durability, hence the popularity in automotive and industrial applications. Additionally, CAN design may be changed, using a transceiver, to an optical cable. This allows for the straightforward design to have a great distance between nodes. I was quite surprised to learn about CAN as a communication technique for the sensors in an MRI. This is because the sensors do not require a lot of bandwidth, CAN represents an ideal small-scale bus for communicating to multiple sensors in a imaging device. As I started to keep an eye out for it, I noticed CAN used in other high-end scanners as well, not just in MRI applications. It seems to be common in larger medical equipment as a low priority sensor network.
This is not necessarily what a trainee can expect to find in all high-end imaging scanners, but it is common enough that elements of it will be used in multiple devices. CAN is a niche network design, preferable in small sensor networks for strings of simple devices doing small tasks. However, that statement describes a lot of designs of HTM devices. As technology grows and costs lower, we are going to find more and more sensors operating as standalone processing units reporting over a network and less as a thermocouple passing a voltage to a logic circuit. As that happens, bus networks like CAN will become more and more common.
Garrett Seeley, MS, CBET, is a biomedical equipment support specialist-imaging with VISN 17: VA North Texas Health Care System at the Dallas Veter ans Affairs Medical Center.
HEALTH-ISAC Medical Device Risk Impact Analysis for Healthcare Providers
BY PHIL ENGLERT
In the health care industry, ensuring the safety and efficacy of medical devices is paramount. Too often, cybersecurity focuses on vulnerabilities and, while important, vulnerability analysis is too narrow. Vulnerabilities are evaluated using the Common Vulnerability Scoring System (CVSS), which attempts to determine how dangerous a vulnerability is. This is useful information but considers the vulnerability risk within the component it resides in rather than the product. This limited view fails to consider the risks the vulnerability poses to a specific environment. Contextual factors such as asset importance, how the asset is used, or the controls in place, either within the product or within the network must also be considered when evaluating risk. Given these limitations, conducting a Medical Device Risk Impact Analysis (MDRIA) is a critical process that helps health care providers identify, assess and mitigate risks associated with medical devices. This essay outlines the essential components of an MDRIA.
The first step in an MDRIA is hazard identification. This involves recognizing potential hazards associated with the medical device, including those related to its design, materials and intended use. For example, a magnetic resonance imaging (MRI) scanner might pose mechanical hazards from the powerful magnets, which can attract ferromagnetic objects, potentially causing harm to patients or staff, thermal hazards from the radiofrequency
coils, especially if there is improper contact with the patient’s skin, and biological hazards from adverse reactions to the contrast agents used in some MRI procedures, which can cause allergic reactions or nephrogenic systemic fibrosis in patients with kidney issues. Identifying these hazards early is crucial for developing effective risk management strategies.
Once hazards are identified, the next step is risk assessment. This involves evaluating the likelihood and severity of harm from each identified hazard. Both qualitative and quantitative analyses are used in this process. For instance, the number and severity of CVEs provide a clear picture of the potential risks and the impact of these vulnerabilities. The number of CVEs associated with medical devices can be substantial, indicating that many medical devices and related software have known vulnerabilities that attackers could exploit. The high number of CVEs highlights the widespread security issues in the health care sector. The severity of CVEs is typically assessed using the Common Vulnerability Scoring System (CVSS), which rates vulnerabilities on a scale from 0 to 10. Higher scores indicate more severe vulnerabilities. In the context of medical devices, many CVEs fall into the high or critical severity categories. These severe vulnerabilities pose significant risks, including potential patient harm or data breaches. This step helps prioritize risks based on their potential impact on patient safety.
After assessing the risks, developing and implementing risk control measures is essential. These strategies aim to
mitigate identified risks and can include design modifications, manufacturing process changes, and clear use instructions. For example, manufacturers might improve insulation materials or add protective covers to address the risk of electrical shock from a medical device. Additionally, providing comprehensive user manuals and training can help health care providers use the device safely and effectively.
Risk evaluation involves assessing the effectiveness of the implemented risk control measures. This step ensures that the strategies effectively reduce risks to acceptable levels. For example, to mitigate the risks associated with CVEs, health care providers should implement robust cybersecurity measures, including regular patching and updates, network segmentation, access controls, and continuous monitoring to detect and respond to potential security threats in real time. This evaluation process is critical for validating the effectiveness of risk control measures and ensuring ongoing patient safety.
Even after implementing risk control measures, some risks may remain. Residual risk evaluation determines if these remaining risks are acceptable. This involves comparing the residual risks to predefined criteria for risk acceptability. For instance, if a medical device still poses a minimal risk of infection despite enhanced sterilization processes, the residual risk must be evaluated to determine if it is within acceptable limits. This step ensures that all risks, including residual ones, are thoroughly assessed and managed.
A comprehensive risk management plan outlines the entire risk management process. This plan should include roles and responsibilities, criteria for risk acceptability, and methods for identifying and evaluating risks. For example, a risk management plan for a new infusion pump might detail the healthcare technology management team’s responsibilities, the criteria for acceptable risk levels, and the procedures for ongoing risk assessment. A well-defined plan ensures that all stakeholders understand their roles and the risk management processes.
Maintaining thorough documentation of all risk management activities is crucial for ensuring traceability and accountability. This includes creating a Risk Management File (RMF) that provides evidence of how risks have been identified, assessed, controlled and monitored throughout the device’s life cycle. For example, the RMF for a medical imaging device might include records of hazard analyses, risk assessments, control measures and post-market surveillance data. Comprehensive documentation supports regulatory compliance and facilitates continuous improvement. Post-market surveillance involves continuously monitoring the device’s performance in real-world use to identify any new risks or issues arising after the device is
placed in the environment. This includes monitoring the devices within a health care provider’s network and external sources such as Health-ISAC and the manufacturer. This step is critical for detecting unforeseen problems and ensuring ongoing patient safety. For example, if a new surgical robot has a higher-thanexpected failure rate in clinical settings, post-market surveillance data can help identify the root cause and inform necessary corrective actions. Continuous monitoring and feedback loops are essential for maintaining the safety and efficacy of medical devices over time.
Conducting a comprehensive Medical Device Risk Impact Analysis is essential for health care providers to ensure patient safety and regulatory compliance. By including key elements such as hazard identification, risk assessment, risk control measures, risk evaluation, residual risk evaluation, a risk management plan, documentation and traceability, and post-market surveillance, health care providers can effectively manage risks associated with medical devices. This robust risk management process enhances patient safety and supports the development and deployment of innovative medical technologies in the health care industry.
Phil Englert is the vice president of medical device security for Health-ISAC Inc.
•
•
•
The words can appear horizontally, vertically, diagonally, and may be spelled forwards or backwards.
1. Sentara Clinical Engineering
2. Anthony Phoenix
3. Eskenazi Health Indianapolis
4. Association of the Month CMIA
5. Breaking Free from Routine
6. Roundtable on RTLS
7. Biomed Brainbuster
8. MedWrench
9. Tools of the Trade
10. Watch TechNation TV
11. Editor John Wallace
12. HTM Professional
13. Healthcare Technology
14. We Love Biomeds
15. Celebrating Fifteen Years
BIOMED BRAINBUSTER
ACROSS
1 Handled inside a business and not contracted out, 2 words
5 Very large in scale
8 US government accountability watchdog, abbr.
10 Improperly functioning
11 Surgical equipment ____ (used in operating rooms)
12 Hospital unit
13 Device, structure or part that protects against radiation or electromagnetic interference
15 ____ apnea: often requires a CPAP to address it
18 Arrange systematically
21 Immediately in medical language
22 Chemical symbol for sodium
23 Light metal used in many medical devices, symbol
25 High quality supplier of medical devices and parts, 2 words
29 Ancient Greek physician
31 Face coverings
34 Connectors that allow devices to connect to other devices and systems
35 CSI coroner’s statement, abbr.
36 Medical device for injecting or extracting fluids
DOWN
1 They deliver fluids to a patient’s body in a controlled manner, 2 words
2 They protect medical equipment from damage and stabilize its function
3 Up to this point in time
4 Abbreviation meaning “for example”
5 Emotional states
6 Having qualifications or documentation showing one’s suitability for something
7 Short for operations
9 Type of bandage
14 Measure of print or screen resolution, abbr.
16 Scan that uses a radioactive tracer, abbr.
17 It controls the ability to see, hear, speak and think
19 Computer memory
20 Prefix meaning new
24 Close off an artery or vessel
26 Doctor, for short
27 Computer design abbreviation
28 The king, in French
30 US intelligence agency focused on cybersecurity, abbr.
32 Elder, abbr.
33 Source of solar power
34 Shade of color
PREFERRED VENDORS
Need a powerful way to elevate your brand and connect with your target audience?
Becoming a Preferred Vendor attracts attention to your products or services, ensuring that your ad reaches potential customers who are genuinely interested. Plus, you are able to enhance your brand credibility and position your company as an industry leader through additional highlight in our monthly e-newsletter and preferred vendor playlist on TechNation.TV.
Anesthesia A.M. Bickford
Pronk Technologies, Inc. pronktech.com • 800-609-9802
Renovo Solutions renovo1.com • 844-4RENOVO
Tenacore LLC tenacore.com • 800-297-2241
CM
Diagnostic
SERVICE INDEX
BC
Inc
BCGroupStore.com • 314-638-3800
J2S Medical
www.j2smedical.com
844-342-5527
J2S Medical www.j2smedical.com • 844-342-5527
Pronk Technologies, Inc. pronktech.com
Ozark
Mammography
RSTI
rsti-training.com
MRI
AllParts Medical allpartsmedical.com • 866-507-4793