by Dr. Warren Umansky, PhD
Discussions about autism are popping up everywhere: in social media, in magazines and newspapers, on tv talk shows. It is meaningful to you personally because your 2½-year-old child seems to show a lot of the characteristics that are described in these discussions. The day care director has shown some concern, as well. What do you do?
A. Wait a while longer before doing anything. She’s too young to do anything anyway.
B. Hire a tutor to come and work with her at home.
C. Talk with her pediatrician as soon as possible.
D. Read as much as you can about autism and decide if she is on the autism spectrum.
If you answered:
A. The American Academy of Pediatrics recommends that pediatricians screen for autism at 18 and 24 months, but many identify signs and symptoms at earlier ages. Don’t wait to seek professional help.
B. If your child is on the autism spectrum, there are professionals who are specially trained to help these children. Depending on the state, services often are provided at no charge or are covered by private insurance. See below to find out more.
C. Your pediatrician can make or rule out a diagnosis of autism spectrum disorder, or refer you to a specialist who can. There are many resources available to help your child and you. Until age three, most states offer early intervention services through the public health department. Specially trained early interventionists can come to your home or go to the child’s day care center to work with your child (and you). In Georgia this program is called Babies Can’t Wait, and in South Carolina the program is BabyNet. The early interventionist also can help arrange other therapies that your child needs (such as occupational, speech, or physical therapy) and assist in the transition to public schools. When your child turns three, the public schools become responsible for providing early intervention services. This, too, can take a variety of forms and include other therapy services. Contact the ChildFind office (usually part of the special education department) at your local school system. There also are many Applied Behavior Analysis (ABA) programs in most communities. These are specialists in working with children of all ages on the autism spectrum, and they can do so in a variety of settings (day care, school classroom, home, or their own classroom). Most insurance plans now cover ABA therapy.
D. Indeed, read all you can from reputable sources but leave diagnosis to the experts.
The evidence is growing that early intervention for children on the autism spectrum leads to much improved outcomes. If you have any concerns about how your young child is developing, start by talking with your pediatrician and then based on that discussion, consult other experts.
Dr. Umansky has a child behavioral health practice in Augusta.
Perhaps you’ve heard of ear candling, a practice which, depending on your point of view, either holds an honored spot in the Medical Mythology Hall of Fame, or is one of Big Medicine’s great coverups.
For the uninitiated, ear candling describes a procedure that places a cone-shaped device in the ear canal, after which a candle or smoldering wick is inserted in the cone. The heat allegedly creates a gentle vacuum which extracts ear wax and other impurities.
According to its proponents, the benefits of ear candling extend far beyond simple ear wax removal. The purported benefits include improved hearing, smell and taste; relieving sinus pressure, earaches, vertigo, and tinnitus; and far beyond, including purifying the mind, strengthening the brain, fortifying the central nervous system, releasing blocked energy, and aligning the chakras. And that’s just a partial list.
You might think that a procedure with so many benefits would be offered at many a doctor’s office, but it’s most likely to be offered in one of two settings: either a spa/salon or a Tupperware-style party (remember those?).
One its most basic level — as a way to remove ear wax — candling is already suspect.

(assuming an intact eardrum).
There have been cases where the ineffectiveness of candling was compounded by injuries, usually burns from candle wax, or, ironically enough, the wax from the candle causing ear canal obstruction. There have been numerous cases of perforated eardrums and even a few fires.

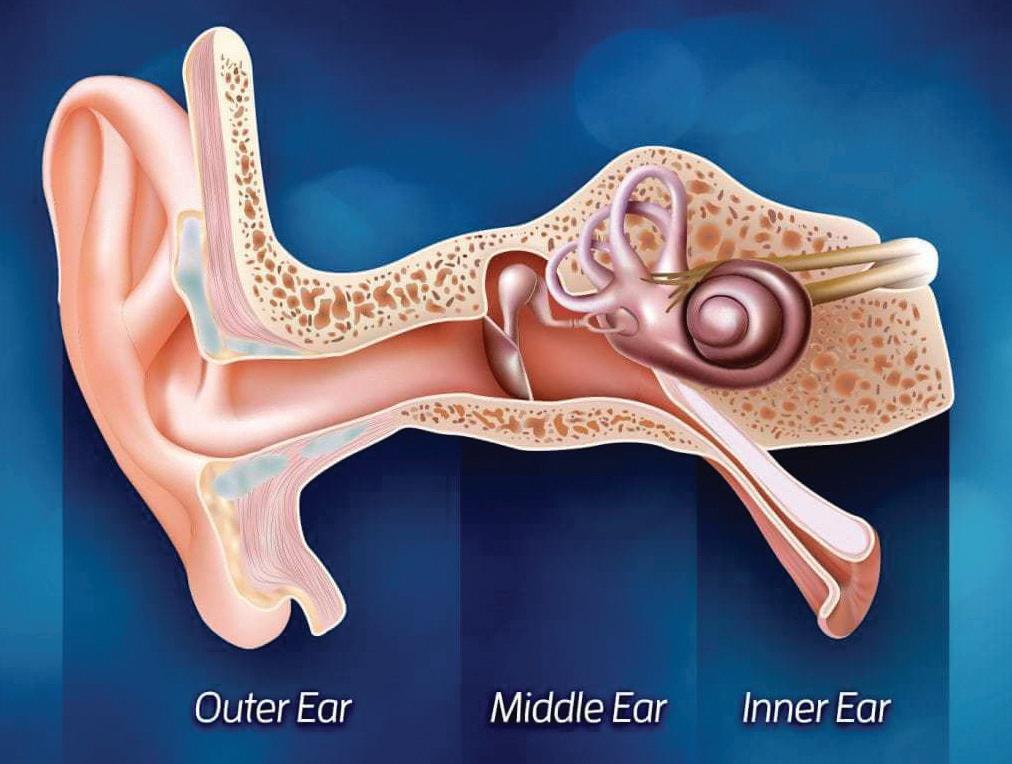
Wax is thick and somewhat sticky, and experts say the vacuum necessary to remove ear wax would rupture the eardrum. In any case, investigators who have extensively tested various candling products report no vacuum created and no ear wax removed. In any event, ear anatomy does not afford access to sinuses, the Eustachian tubes (the downward-sloped structure above “Inner Ear” in the diagram below), or the brain
The FDA has been on the warpath against ear candling since the 1990s, with limited success. A number of companies have been fined and/ or forced out of business due to false and fraudulent claims, and the agency has tried to publicize the quackery involved. In response, companies offer candles “for entertainment only.” In Canada the sale of ear candles is illegal for any reason since HealthCanada considers any alleged use other than ear wax removal (such as “for entertainment”) to be bogus, and it considers the ear wax use as bogus too.
The bottom line for at least 99% of the population is that ear wax doesn’t need professional intervention to be removed; the body takes care of the process easily and naturally, and if there is an accumulation of wax that is creating an obstruction, it should be removed by a physician or other healthcare professional using proper instruments, not a burning candle.
Let’s face it: water is boring. Where’s the sugar? The fizz of carbonation? Sure, there’s no hangover, but that’s because there’s no buzz either. Water isn’t even fattening.
Water is no fun at all. And yet we’re supposed to drink how much water every day? And supposedly the vast majority of us are chronically dehydrated. Well, no wonder.
If only water could somehow be transformed into something a little more exciting, maybe we would drink more of it.
But wait. What if we didn’t have to drink our water? What if we could eat it instead?
Guess what? We can! In fact, we not only can eat water; we should!
Not that there’s anything terribly wrong with drinking water. But it’s pretty uneventful. Compare that with popping a handful of strawberries down the hatch. Delicious! And strawberries are over 90% water. A cup of sliced strawberries contains more than 5 oz. of water plus fiber, vitamin C, and antioxidants. And did we mention they’re also delicious?
Or how about the water celebrated in our front cover artwork? Watermelon, as its name would suggest, is another delicious source of water, like strawberries measuring over 90% water content. Recent research found that watermelon, rich in antioxidants, offers benefits ranging from heart health to weight



management, cancer protection, and diabetes regulation.
What about cantaloupe? Sure, it’s 90% chewable water, but it also offers a healthy serving of beta-carotene-delivering vitamin A, more than an entire day’s worth of the recommended daily intake in a single cup.
You say you like your water just a little on the crunchy side? Got you covered.
A tasty fresh salad is basically that — crunchy water. Consider:
• Cucumbers are about as watery as foods come, at 95% water. That’s amazing, isn’t it? Along with the water, cucumbers are rich in vitamin K, a clotting factor that benefits people who cut themselves slicing cucumbers.
• Celery is also 95% water, plus it’s loaded with antioxidants.
• Zucchini is another member of The 95% Club, plus it’s loaded with vitamin C and antioxidants.
• Tomatoes are 94% water and super-low in calories, yet high in vitamins A and C, antioxidants, potassium and, incidentally, flavor.


Clinical studies have established that wellhydrated people develop fewer chronic health conditions, like heart and lung disease, and live longer than those who don’t get enough fluids. Staying hydrated seems to slow down the aging process. So by all means, do your best to drink sufficient water every day. But don’t forget to eat plenty of water too. +


How’s that for an extremely simple question? Or is it actually extremely complex?
After all, it isn’t the skull itself that hurts, nor is it the scalp. As for the brain itself, brain surgery can be performed (and sometimes is) without general anesthesia while the patient is wide awake and alert. That’s because the brain doesn’t even have pain receptors. Yet paradoxically, the brain “feels” 100% of the pain we experience; it is the organ through which all of our pain, whether it’s a stubbed toe or our hair is on fire, is recognized, processed and experienced.
So the answer to our question is a lot more than just, “a headache is when your head hurts.”
Broadly speaking, most headaches arise from “referred pain.” The pain may be perceived as a headache, but it’s actually being referred over from another source, like a tension or stress headache caused by tightened muscles in the neck and shoulders, or from a clenched jaw.
But that still doesn’t answer our question; in fact, it implies that pain may not even be real; it’s imaginary.
Rest assured (or lose sleep) pain is real. All of it, say researchers, even though it can be flavored by our individual mix of physical and psychological ingredients. So pain isn’t something to ignore. It provides an important alert that something is wrong and needs attention.
Although the brain has no pain receptors (nociceptors), there are plenty of body parts in the immediate vicinity that do. The brain’s cellophane-like wrapping, the dura mater and pia mater, have them. Changes in temperature and blood flow — common examples might be called brain freeze or ice cream headaches — can result in headaches. Another common cause of headaches is dehydration, something experts say most of us are chronically affected by. When we’re dehydrated, even mildly, the brain shrinks enough to pull away from the skull and puts pressure on nearby nerves. Blood vessels in the brain can also narrow, another headache trigger
In summary, all pain — at least its perception — is in the brain, but no pain is actually in the brain. Are we clear?

www.AugustaRx.com The
Direct editorial and advertising inquiries to: Daniel R. Pearson, Publisher & Editor E-mail: Dan@AugustaRx.com
AUGUSTA MEDiCAL EXAMINER P.O. Box 397, Augusta, GA 30903-0397 (706) 860-5455
www.AugustaRx.com • E-mail: Dan@AugustaRX.com
www.Facebook.com/AugustaRX

any Medical Examiner readers no doubt instantly recognize the smiling face of Dr. Ruth Westheimer, who died in July at age 96.
The very fact that she even survived childhood is something of a miracle, given that she was born to a Jewish family in Germany and grew up as the Nazis were coming to power. In fact, both of her parents were killed in Nazi concentration camps. They met their fate because, while their 10-year-old daughter was sent off to a school in Switzerland for her own safety, the parents stayed behind in Germany to care for Dr. Ruth’s elderly grandmother.
Born in 1928 as Karola Ruth Siegel, Dr. Ruth acquired her last name from husband #3 in 1961 following two brief marriages that didn’t work out, and her first name living in Palestine after World War II when it was suggested that Karola was too German. She went by Ruth K. Seigel in case her parents came looking for her. She later learned her father had been murdered by the Nazis in 1942, while the exact circumstances surrounding her mother’s death are unknown. The World Holocaust Remembrance Center database lists her mother as “disappeared/murdered.”
There are a number of fascinating chapters to Dr. Ruth’s life. There is her post-war stint in what is now the IDF, the Israeli Defense Forces, where she was trained as a sniper, in part because of her 4-foot 7-inch height (although she has said she never shot anyone). She saw action in the 1947-1949 Palestine war and was seriously wounded on her 20th birthday in a mortar attack that killed two girls right next to her.
There is her time studying at the University of Paris (the Sorbonne) beginning at age 22 with her first husband, a medical student. She earned an undergraduate degree there despite the lack of a high school education, and went on to teach psychology at the Sorbonne.
There is her time in the United States, beginning with her immigration in 1956, where with the aid of a couple of scholarships and working as a maid for 75 cents an hour (later raised to $1 an hour), she earned a degree in Sociology in 1959, followed in 1970 by a Doctor of Education (Ed.D.) degree from Columbia University. She trained as a sex therapist at Cornell Medical School before a 7-year internship under Helen Singer Kaplan, founder of the first clinic in the U.S. for sexual disorders at a medical school.
There are other chapters, but the one for which she became famous as a sex therapist happened by chance. She had given a speech to New York area broadcasters about the need for sex education programming. The community affairs manager of one radio station offered her $25 per week for a 15-minute show in the dead-air time slot of Sundays at midnight. In no time, the show averaged 250,000 listeners, was expanded to a full hour at 10 pm, and was syndicated across the U.S. Soon after, her Lifetime TV show was added, becoming the network’s #1 draw at 2 million average weekly viewers.
She was the author of 45 books on sex and sexuality, and is lauded by many for fostering education and awareness about important subjects that had been taboo, doing so forthrightly with good taste, humor, and candor. +
There are some questions that are so easy you think they must be trick questions because the answers seem so obvious.
Here are a few, just to make you feel like you are an authority on something.
1. Is it a best friend’s job to immediately clear your computer history when you die?
2. Don’t you just hate the moment during an argument when you realize you’re wrong?
3. Is there a great need for a sarcasm font?
4. Is there any good way to fold a fitted sheet?
5. Was learning cursive really necessary?
6. Wouldn’t obituaries be a lot more interesting if they told you how the person died?
7. Can you remember the last time you weren’t at least kind of tired?
8. Don’t bad decisions make good stories?
9. If ballet dancers were taller, would they still have to dance on their toes?
10. Are Ebony, Jet, and BET racist organizations?
11. Don’t you feel a little panic when you exit out of Word and it asks if you want to save any changes to your ten-page research paper that you swear you didn’t make any changes to?
(most of the time)
A series by Bad Billy Laveau
12. Does “Do not machine wash or tumble dry” mean you never wash the garment – ever?
13. Don’t you hate getting all dressed up and putting on your best confident moods and going out and not seeing anyone of importance the entire day?
14. Do you keep some people’s phone numbers in your phone just so you know not to answer when they call?
15. Don’t you agree that Kay Jewelers is wrong and that on the weekend more kisses begin with Jack Daniels than Kay?
16. Have you ever watched a movie that you saw when you were younger and suddenly realize you had no idea what the heck was going on the first time you saw it?
17. Hadn’t you rather carry 10 plastic grocery bags in each hand than take two trips to bring in your groceries?
18. Do women look sexier in tight clothes?
19. Shouldn’t red lights last longer so you can finish your text?
20. Is there any difference

between boredom and hunger?
21. When someone is boring you at a party and you didn’t hear what they said, do you nod and smile rather than say, “What did you say?”
22. Don’t you just love the sense of camaraderie when an entire line of cars teams up to prevent a jerk from cutting in at the front?
23. Is it true that you can wear underwear once, shirts three times and slacks two weeks between washings?
24. Is it true they don’t make bells as loud as they used to?
25. Doesn’t a red light mean STOP? A green light means GO? And a yellow light means GO A LITTLE FASTER?
26. Do you have to drink to have fun? Obviously, no one does, but why start a fire with flint and sticks when they’ve invented the lighter?
27. When someone says, “I’m not book smart, but I’m street smart,” don’t they really mean, “I’m not smart at all, I just imagine I’m smart”?
28. Have you ever wanted to say to a total stranger, “Excuse me, would you like me to show you how to discipline your child?”
29. Is there any good reason chocolate shouldn’t be a food group rather than a treat?
Editor’s note: This column originally appeared in the Nov. 19, 2010 issue of the Medical Examiner
The newest newsstand location where you can pick up your FREE copy of the latest Medical Examiner is at the US Post Office Summerall Station at the intersection of Pine Log and Silver Bluff Roads in Aiken.
BY J.B. COLLUM

I’ve often found myself at the crossroads of life’s various challenges and opportunities where I could make good choices and work hard to follow through, or I could make bad choices. Usually though, I make the good choice, but the follow through is where I fail. At this stage of life, one gains a wealth of experiences. Especially someone like me who has taken the wrong path or tried to take to good path and then slipped on a banana peel and slid down the mountainside and into the quicksand. I have shared many embarrassing moments before, but I feel like I have held back too much and I must confess even more embarrassing and perhaps even felonious things, to clear my conscience and to let my failures help you not to make the same mistakes. The moment seems the right to really open up and share with you all...
Hey folks,
JB Collum Jr here. Sorry to barge in, but my dad was about to get way too deep into “TMI” territory. So let’s lighten things up a bit, shall we? This is the third time I’ve been forced to hijack one of his articles, and this time it’s to discuss a different aspect of handling your aging parents.
Hey folks, Jr here. Sorry to barge in, but my dad was about to get way too deep into “TMI territory. So, let’s lighten things up a bit, shall we? This is my third time hijacking one of his articles, and this time it’s to discuss a different aspect of handling your aging parents. When we see our parents showing signs of slowing down, we want to rush in and take over. No longer viewing them as capable as they once were. While the occasional help with newer technology is appreciated, sometimes you need to step back. Yes, it is obvious my father is getting older both mentally and physically, but he still has a surprising amount of vigor and understanding.
When we see our parents showing signs of slowing down, we want to rush in and take over, no longer viewing them as capable as they once were. While the occasional help with newer technology is appreciated, sometimes you need to step back. Yes, it is obvious my father is getting older both mentally and physically, but he still has a surprising amount of vigor and understanding.
Recently, he decided to buy a shed and recruited me into helping finish it over the summer. To help us out he put an air conditioner inside to reduce some of the heat. Despite that, the current lack of any insulation means we’re still in a hot box that drenches us in sweat. My father tries to keep the sweat away with a tied handkerchief around his forehead, it works for about a minute before it drips past his meager defenses. Despite the heat, his larger frame, and age, he just keeps going! I am wiped out after two hours, three on my best days, and he still has the stamina to keep going while cracking a joke about my work ethic. “Millennials” he curses under his breath as he sighs and shakes his head derisively.
Recently, he decided to buy a shed and recruited me to help finish it over the summer. To help us out he put an air conditioner inside the shed. Despite that, the current lack of any insulation means we’re still in a hot box that drenches us in sweat. My father tries to keep the sweat away with a tied handkerchief around his forehead. That works for about a minute. Despite the heat, his larger frame, and age, he just keeps going! I am wiped out after two hours, three on my best days, and he still has the stamina to keep going while cracking a joke about my work ethic. “Millennials,” he curses under his breath as he sighs and shakes his head derisively.
When his health challenges do crop up, I have learned to pause and listen carefully before jumping into caregiver mode. In a recent scare, my dad complained of chest pains. It so happened to be the night before we were to work on the shed. Combining past issues he had, and perhaps a selfish desire to not have to work in the world’s worst sauna, I pushed for him to rest in the morning. Turns out he was right about it being simply indigestion from what he had eaten. This proved to be a humbling reminder that not every symptom is a sign of serious trouble.
In summary, don’t be so quick to treat your parents as if they are incapable. The transition for children from receiving care to providing care is gradual. While this transition is different for everyone, it should involve mutual respect and understanding. To sum it up: support your aging parents without undermining their autonomy. They will surprise you, or in the case of my dad, taunt you, with what they are still readily capable of. Speaking of which, I need to go. My dad just challenged me to a rematch of who can last longer in the shed without melting and I need to find a hiding spot in the air-conditioned house!
-JBC Jr out. Back to Dad’s story now.
When his health challenges do crop up, I have learned to take pause and listen carefully to him before jumping into caregiver mode. In a recent scare, my dad complained of chest pain. It so happened to be the night before we were to work on the shed. Combining past issues he hpped on a banana peel and slid down the mountainside and into the quicksand. I have shared many embarrassing moments before, but I feel like I have held back too much and I must confess even more embarrassing and perhaps even felonious things, to clear my conscience and to let my failures help you pped on a banana peel and slid down the mountainside and into the quicksand. I have shared many embarrassing moments before, but I feel like I have held back too much and I must confess even more embarrassing and perhaps even felonious things, to clear my conscience and to let my failures help you pped on a banana peel and slid g moments before, but I feel like I have held back too much and I must confess even more embarrassing and perhaps even felonious things, to clear my coom what he had eaten. This proved to be a humbling reminder that not every symptom is a sign of serious trouble. In summary, don’t be so quick to treat your parents as if they are incapable. The transition for children from receiving care to providing is gradual. While this transition is different for everyone, it should involve mutual respect and understanding. To sum it up: support your aging parents without undermining their autonomy. They will surprise you, or in my case taunt you, with what they are still readily capable of. Speaking of which, I need to go. My dad just challenged me to a rematch of who can last longer in the shed without melting and I need to find a hiding spot in the air-conditioned house!
Despite the jail time and injuries, the experience was one of the most profound lessons I have ever learned. I have laid bare my soul and confessed all to you, my dear readers. I only hope that my sacrifice will somehow help you in your lives. I’m so glad I got that off my chest.
J.B. Collum is a local novelist, humorist and columnist who wants to be Mark Twain when he grows up. Reach him at johnbcollum@gmail.com



Nearly all of us — even doctors and nurses — are sometimes patients. Perhaps you were recently injured playing your favorite sport, or years ago you somehow got hurt without even leaving your favorite recliner. Maybe you have a personal COVID-19 story or one involving your family. Maybe you were diagnosed with a dreaded disease, were mugged in a dark and lonely parking lot, or you stubbed your toe in the safety of your own bedroom. On the other hand, perhaps you needed medical attention 5,000 miles from home.
Whatever your medical experience, we’d like to hear your story for our Everyone Has a Story feature. It can be frightening or funny, ordinary or extraordinary, just a few paragraphs long or quite a lengthy tale, bylined or anonymous. We’ll publish your medical adventures as often as we receive them. Hopefully that will be often.
Send your submissions for Everyone Has a Story to the Augusta Medical Examiner via e-mail: info@AugustaRx.com or to PO Box 397, Augusta, GA 30903-0397. (The Medical Examiner reserves the right to accept, reject, or edit any submission at its sole discretion.)

...wherein we share amusing medical tales we have overheard, or that have been shared with us.
“We once had a patient brought in to the ER who had been shot in the butt from the side.
1 bullet, 4 holes.
It was perfectly, and I mean perfectly aligned to go through both butt cheeks at exactly the same angle and spot.
You’d need a level to recreate it.”
READERS: What have you heard? Please share! EMAIL: Dan@AugustaRx.com or MAIL: PO Box 397, Augusta




by Kim Beavers, MS, RDN, CDCES Registered Dietitian Nutritionist, Chef Coach, Author
Kim on Facebook:
This unique twist on pasta salad makes a delicious side dish or entree sure to become a family favorite.
Ingredients
• 4 slices bacon
• 3 medium cloves garlic, sliced (sliced garlic is much milder than chopped or minced)
• 4 medium-large ripe tomatoes (about 1½ pounds); you can also use cherry or grape tomatoes
• 1 tablespoon extra-virgin olive oil
• 1 teaspoon sea salt
• Freshly ground white or black pepper (white pepper has a wonderful taste, different from black)
• 1 cup mixed fresh herbs, (lots of basil), or 2 teaspoons dried herbs
• 1 pound pasta, preferably thin whole grain spaghetti
• 1 bunch of assorted lettuce, washed and dried
• Freshly grated Parmigianino Reggiano
Directions
Bring 4 quarts of salted water to a boil in a large pot for cooking the pasta.
Cook bacon over medium heat until crispy. Remove and drain on paper towels. When cool, break into pieces.
Pour off all but 1 tablespoons bacon fat. Add garlic and olive oil to the pan and sauté over low heat until

soft.
Cut tomatoes into 1/2-inch cubes. Shake over a colander to remove seeds and some of the juice. Add to the hot pan and sauté for 2-3 minutes, until just warmed. Add salt and pepper; remove from heat.
Wash and dry the herbs. Tear the leaves into pieces. Stir the herbs into the tomato mixture. Taste for salt and pepper and adjust seasonings if necessary.
While preparing the sauce, cook and drain the pasta. Toss the hot pasta with the tomato sauce, bacon and lettuce. Mix well. Transfer

portions to pasta bowls and serve immediately with the Parmesan.
Yield: 8 Servings
Nutrition Breakdown: Calories 300, Fat 10g (3.5g saturated, 2g monounsaturated), Cholesterol 15mg, Sodium 420mg, Carbohydrate 40g, Fiber 9g, Protein 14g, 182mg Potassium.
Percent Daily Value: 35%
Vitamin A, 35% Vitamin C, 20% Iron, 10% Calcium Carbohydrate Choices: 2 ½ Carbohydrates
Diabetes Exchange Values: 1 Vegetable, 2 Starches, 1 Medium Fat Protein, 1 Fat



Carol, a Facebook friend from Augusta, asks:
“My friends swear by the Carnivore Diet. What is it, and is it healthy? ”
Thanks for this interesting question, Carol. The Carnivore Diet is a fad diet and an extreme one at that, with significant nutritional issues. The diet is a very high protein diet that stresses zero carbs and advises you eat only foods of animal origin. It is an “ultra” keto diet. Even most keto diets typically allow some carbs (usually 10% of calories), which the Carnivore Diet does not. Foods typically allowed on the Carnivore Diet are meats, chicken, eggs, dairy and fish. Completely eliminated from this diet is any food from the plant kingdom. That means that the Carnivore Diet is a diet with no fruit, veggies, nuts, beans, tofu, seeds of any type, or whole grains or other type of grains.
Do you really need to ask me about the” healthfulness” of such an eating plan? Probably not. It doesn’t take a nutrition scientist to realize that this is a very out-of-balanced way of eating that emphasizes the wrong foods. At the same time, this diet tells you to eliminate foods that we know are important sources of nutrients.
Why would people go on the carnivore diet? Besides everything else, it is an expensive way of eating. This diet is touted, without concrete evidence, to help you lose weight, improve your mood, improve your immunity, and help you control your blood glucose concentration. A “typical” Carnivore Diet meal plan might be this: for breakfast, bacon and eggs; for lunch, ground beef cooked in tallow (tallow is animal fat often used in candle-making); and for dinner, venison steak with bone marrow. Yum, yum…not!
The Carnivore Diet is not based on evidence and peer-reviewed data. It is, rather, based on social media gossip and the feelings and emotions of trainers, Facebook, Tik-Tok and Instagram fitness influencers, life coaches, etc. You can go to TikTok and see people eating plates filled with steak and nothing else, bars of butter and dozens of eggs.
Dental College of Georgia and is past Vice Chair of the

Social media postings like those are what we call “anecdotal evidence.” You do not want to use anecdotal evidence to evaluate nutrition recommendations. Major pitfalls of this way of eating are 1) this regimen is an extreme keto diet. It eliminates whole food groups: fruits, veggies, grains and beans. Because of this, it is inadequate in fiber, vitamins and minerals. It may lead to Vitamin C and folic acid deficiencies. Secondly, this diet will raise your LDL cholesterol (the so-called “bad” cholesterol), will raise your blood pressure and increase your risks of heart attacks, strokes, peripheral vascular disease, diabetes and certain types of cancer. Carol, if you are searching for an evidenced-based and data-supported pattern of eating, there is no doubt that The Mediterranean or The DASH eating plans fit the bill. The Carnivore Diet does not.
What’s the “No-Nonsense Nutrition” advice for today? If you are the type of person who likes to go against the grain, ignores science, and instead uses testimonials on social media as a basis for your decision making, then the Carnivore Diet is the diet for you. On the other hand, if you want evidence, data, science and peer-review, then stick to The Mediterranean or DASH way of eating. It will lower your risk of cardiovascular disease, strokes, and specific types of cancer. And by the way, it’s great for the planet, too.
County Board of Health. You can find out more about Dr. Karp and the download site for the public domain eBook, Nutrition for Smarties, at www.wbkarp.com Dr. Karp obtains no funding for writing his columns, articles, or books, and has no financial or other interests in any food, book, nutrition product or company. His interest is only in providing freely available, evidenced-based, scientific nutrition knowledge and education. The information is for educational use only; it is not meant to be used to diagnose, manage or treat any patient or client. Although Dr. Karp is a Professor Emeritus at Augusta University, the views and opinions expressed here are his and his alone and do not reflect the views and opinions of Augusta University or anyone else.









This is a very disturbing story. It involves one of the toughest humans I have ever met and involves some pretty gory imagery. You have been warned.
I received a 20-minute-out warning that a trauma code had been called for a young woman. Her car had slid off a gravel road. She had been ejected from her car right into a tree. (Why? Because she wasn’t wearing her seatbelt!)
The EMTs wheeled her into the trauma bay seated cross legged, leaning forward in the middle of a backboard with no c-collar on. Her face below the nose was a bloody ruin. She was covered in blood. She was leaning forward slightly. In her hand was a small Yankauer portable suction tip. With it she was calmly suctioning away blood that was pooling around her fully visible vocal cords.
The EMTs, who were used to horrific injuries, were visibly disturbed. They gave their report as we lifted the backboard up. She sat in the center of it like a sad, bloody Buddha. We held her steady on the board and lifted the girl and the board up and over onto a hospital gurney. She remained motionless through it all, just suctioning away the blood. Calmly focused on saving her own life.
The EMTs told her story to the trauma team. She had been driving down a gravel road and lost control. Her car rolled and she was thrown out the window into a tree. A branch had caught her full in the mouth. It had torn her jaw away and broken it. Her tongue, with no support, was lying on her neck allowing me to see the top of her trachea with her vocal cords visible. To this day the memory is upsetting.
They had found her wide awake under the tree, on all fours, bleeding briskly from her face. Apologetically the EMT explained, “She just flat refused to lie on the backboard. We tried and she fought us. We were sucking the blood out of her—well, her mouth, and she just grabbed the sucker right out of my hand and took over. She rode here just like this.”
The trauma surgeon looked at the girl and back at me: “Can’t do anything until that airway is controlled.”
I walked around to her front. Her eyes were a brilliant blue and laser focused on the trauma team. I introduced myself and asked if she knew that she was in the ER. Barely perceptible head bob. She was absolutely “with it.” I turned a wall suction canister on high and approached to assess her airway. She flung her hand out beseechingly for the

bigger and harder sucking implement. An upgrade. I traded her weak portable suction for my own. In the brief instant of transfer she coughed, painting the team and me in a grotesque parody of Jackson Pollock.
I had my nurse draw up some etomidate to put her to sleep and vecuronium to relax her muscles. Her blood pressure was just 90 systolic and her heart rate was 140. Young people can keep going a long time, but when they reach their limit, they can quickly arrest, so I knew we didn’t have much time to fool around.
“Are you getting tired?” I asked. Tiny nod. Yes. “Do you understand that we need to put you off to sleep so we can help you?” Tiny nod. “Great. I’m going to slip you off to sleep and help you breathe so that we can fix your face. Do you understand?” Another tiny nod. A tear leaked down her face.
I took her IV line and looked her in the eyes. “It’s going to be all right. I’m not going to move you. I am going to send you off to sleep now.” She nodded.
I pushed the etomidate and her eyes rolled up. The intubation was ridiculously simple as her glottis was visible. I placed an anode tube and we laid her down as her limbs went slack. I gave the paralytic and began to ventilate. The team pounced.
The damage was beyond what our plastics guy felt comfortable with. She was otherwise in good shape. She was clearly going to need a team of orthomaxillofacial surgeons and plastic surgeons to repair her face. We put in a set of lines and sedated her and sent her by helicopter to the university medical center an hour away.
Later, a nurse who knew the family showed me a “before” picture of her. She was a gorgeous girl. Many weeks later the university medical center sent us an “after” picture. Seven surgeries later and she looked almost as good as she had before the accident. The only thing that was different was a thin pair of scars down either cheek. Her teeth had been replaced in a reconstructed jaw. It was a beautiful repair.
I have seen a lot of patients who have been through serious injuries. This girl impressed me because she remained focused and calm and did what she had to do to save her own life. She fought the EMTs when they tried to put her in a position that would have left her drowning in her own blood. She never indicated any pain. I don’t have any idea what became of her, but with strength and poise like that, I’m sure she recovered quite well. +
Editor’s note: the stories that appear in this series will all be anonymous, are from various sources, and may or may not be stories from the Augusta area. If you have a story to contribute confidentially, see the box on page 3 for Medical Examiner mail and email addresses.

More Americans have died on US roads since 2006 than in World Wars I & II combined
More than once in recent months, this space has mentioned the epidemic of red light runners. There was a time when you might see an occasional car squeak through after the yellow turned orange. It wasn’t exactly rare, but it wasn’t a plague upon the roadways, either.
These days you could say it’s not only common, but seeing a handful of cars run reds, even three or four or more, is the new normal.
It’s dangerous, it’s reckless, it’s rude and self-centered, it’s illegal.
We get all that.
But we’re about to shift the blame elsewhere, at least partly.
traffic spotters have observed these scenarios countless times at multiple area intersections.
These lights need to be repaired. The job of traffic engineers is to facilitate the smooth, orderly, and safe flow of traffic. That’s their job assignment.
Anyone who does a fair amount of driving around the CSR Area (a.k.a. the Central SRA) has encountered what can only be described as screwy traffic signals. Screwy is not an everyday word, but it seems to fit better than some of its synonyms, like offbeat, freakish, quirky, bizarre, and unconventional.
Whatever the best word is, this is how these traffic signals behave: they’re screwy. Let’s use the traffic signals in front of Costco as our example, although screwy lights have been observed all over town. Cars are sitting in line on Riverwatch waiting to go straight (downtown) or turn left into Costco. Or cars may be stopped on Alexander, waiting for a green to either cross Riverwatch or turn left.
Whatever the direction or the lane, eventually the red light turns green. And it stays green for maybe 5 seconds! Yes, 5 seconds! Put it like this: as soon as the light changed green all the waiting cars started to roll immediately, and Car #3 ran the yellow and was not completely into the intersection before the light turned red. The third car! That’s how short some of these greens are. And there are often more than just three cars. When there are, Cars 3, 4, 5, and sometimes 6 all run the light too.
But here’s what’s really screwy: a lot of these super-short greens are followed by super-short reds.
In other words, picture someone who’s heading downtown on Riverwatch and is just the 4th car in line when he gets a green. Even so, by the time he gets up to the light it’s already yellow. Being a law-abiding motorist he stops (and the driver behind him lays on his horn as a result) as Alexander traffic crosses in front of him. But before he has even uttered his second swear word, his light goes back to green again.
Say what?
Roving Crash Course investigators and
So let’s spend a moment considering how they are failing, and the impact (literally) these screwy lights have on the smooth, orderly, and safe flow of traffic. Following is a 2-part real-world list of outcomes. In a perfect world, neither would exist (but then, 5-second reds and greens wouldn’t either)
• Outcome #1: Motorists see their fresh green and step on the gas. Because any reasonable person has the rational expectation that their green will most likely last 15, 20, 30 seconds or longer — or in many cases as long as there is a line of oncoming cars to keep the traffic sensor activated — they don’t even notice that they just ran a red light. Nor does the driver in front of them. Or the driver in front of that car, either. Not to mention the driver(s) following.
• Outcome #2: Motorists see their fresh green and step on the gas. They also clearly see the green turn yellow seconds later. But because they’ve been sitting at a red light for two solid minutes (or so they believe, right or wrong), they feel like they are entitled to this green. They waited for it; they invested in it; they earned it, and by jimbo they’re taking it, even if it isn’t a green any more. Let the traffic gods sort it out later.
A variation on the theme above occurs when the first driver in line at a red light is playing with their phone when the light goes green. By the time they notice (or a driver behind them blasts their horn) the green has already gone yellow. Car #1 floors it through the red, followed by all the drivers who saw the whole thing happen and believe “this was my green light.”
Can you begin to see the role a traffic engineer sitting in an office miles away has on the number of cars running red lights? They are definitely part in this problem, and they can’t plead ignorance: look around you the next time you’re stopped at an intersection and count the number of cameras recording the ebb and flow of traffic. They have to know what’s going on; it’s their job.
We’re not saying it’s okay to run red lights just because the lights are screwy; it isn’t. But it isn’t okay to have malfunctioning traffic lights that go unrepaired either.

Will he ever get one right?
Probably not. Questions. And answers. On page 13.
— posted by Alan Dow, MD on Aug. 24, 2024 (edited for space)
“I want you to be proud of me,” my intern replied when I asked what he wanted to get out of the rest of his year. We were wrapping up the first two weeks of July—his first two weeks of being a doctor—and having our end-ofrotation feedback session. His comment made me rethink my performance as an attending. As I have matured from a young, determined doctor to an older, occasionally paternal attending, I had not realized the importance of pride and why being proud is important.
The beginning of July is a time to be proud. Academic medical centers are filled with excitement as new interns start and other residents ascend to the next level. This was my twenty-fifth stint doctoring at the beginning of July, and I am increasingly proud of my students and residents. Not everyone who has the dream is able to become a physician. We do not celebrate this achievement enough. For some learners, we have specific reasons to be proud. Consider one of my students. She is a black woman. As we introduced ourselves to patients on rounds, several patients—specifically older black women—lit up when she introduced herself. While to me she is just another student on my team, to them she represents something more.
These women were born in the 1940s and 1950s. They lived under segregation. They experienced “separate and equal” and know it was separate but not equal. They experienced the pain of integration when explicit segregation was replaced by tacit discrimination. They saw the election of a Black president and the subsequent backlash. Now, they see a young black woman who may represent a dream they may not have been allowed to dream, much less achieve. They are proud of her.
But the story of this student’s achievement is only a part of the intersecting narratives in a hospital. We also cared for a patient whose tattoos endorsed white supremacy. Perhaps he is not the same person now as he was when he got those tattoos, but that did not matter to us. He received the best care we could offer, whatever his tattoos might represent. We seek to hold ourselves to a standard for equity that may be higher than our broader society.
Our hospitals may be society’s biggest crossroads, and that can demand a lot of us. Patients, their families, and health care workers from all different backgrounds interact with each other. We are interdependent, and diseases rarely discriminate. Even if people come to our doors with hate in their hearts, we care for them. I take pride in that.
We must be careful with pride, though. Pride can be either authentic or hubristic. Authentic pride is what I feel when I see the faces of my black patients light up when they see a learner of color. Authentic pride is when I see my learners leave our two weeks together closer to their aspiration of being a good doctor.
Hubristic pride is not based on current achievement but rather on opinions or past achievements. For example, we have built a better health care system in the United States. Yet we know it has problems: too many babies die, we lose patients to addiction, and bureaucracy hampers care. To take pride in the U.S. health care system would be hubris, ignoring the fact that authentic pride requires us to keep getting better.
As I enter my twenty-fifth year as a physician, I have a lot to be proud of. I have helped many patients and trained countless learners to be better doctors. While I take pride in these accomplishments, I need to remember the real goal is to continue to get better. I want to keep getting better as a doctor and a teacher as we work toward better care for everyone. I hope I will make my team proud.
Alan Dow is an internal medicine physician +







What are you reading?
This story about a town where a train derailed.

1. _____ Gordon 6. Around prefix (med.) 10. Within prefix (med.)
Slow (in music) 15. Ready for business 16. Incline 17. ____ Flu
18. Infant mort. cause
19. It can be posted or jumped
20. _______-Lambuth chapel
22. Post-mortem
24. ____ up, as with bread
25. Brag; boast
26. Of black & white ancestry (dated; offensive)
30. Little ball stand
31. Cage material?
34. One and all
36. Just an ordinary Joe
38. Sci-fi classic by 54-A
39. Cinemas owner
42. Kelly on TV
43. Greek epic poem
45. Short joke
47. Metal container
48. Doctrine suffix
51. Single-celled adjective
52. Rectangular pier
53. Fur scarf
54. Author of 38-A
57. Continuing
62. Parched
63. By mouth
65. Stomach woe
66. Stead
67. Flightless bird
68. Fragrant resin
69. Took a tumble
70. Management person (in short)
71. Radioactive gas, element no. 86
So then what? Yikes. What happened?
by Dan Pearson
Tons of laxatives on the train were released, contaminating the town’s water supply. Residents were forced to evacuate.


1. Common type of stone
2. Son of Jacob and Leah
3. Indigo dye
4. Thrust with a knife
5. Integrity
6. Defer; delay
7. Upon or above prefix (med.)
8. Edit or censor, as a legal document
9. Cover with Nationwide
10. Type of grease?
11. Low tide
12. Raised platform
13. Solely
21. Rotating member
23. Lower digits
26. Corpsman
27. The throat’s “little grape” (Latin)
28. Russian Premier 1917-1924
29. Extent of space
31. Nose prefix
32. Louvre Pyramid architect
33. Get on
35. Self-esteem
37. Child’s bed
40. Steroids starter
41. Yellow citrus fruit
44. Take dinner
46. Word often following little and big
49. TIA as it’s more commonly known
50. Reeves movie
52. Arabic word meaning slave or servant
54. One of two equal parts
55. Great lake
56. Monetary unit of Cambodia
58. Earthen pot
59. Like much tea
60. Captain of Twenty Thousand Leagues Under the Sea
61. Smile
64. Reverence; admiration
Simply unscramble the letters, then begin exploring our ads When you find the correctly spelled word HIDDEN in one of our ads — enter at AugustaRx.com
We’ll announce the winner in our next issue!
X A M I N E R S U D O K U
DIRECTIONS: Every line, vertical and horizontal, and all nine 9-square boxes must each contain the numbers 1 though 9. Solution on page 14.
DIRECTIONS: Recreate a timeless nugget of wisdom by using the letters in each vertical column to fill the boxes above them. Once any letter is used, cross it out in the lower half of the puzzle. Letters may be used only once. Black squares indicate spaces between words, and words may extend onto a second line.
Solution on page 14.
Use the letters provided at bottom to create words to solve the puzzle above. All the listed letters following #1 are the first letters of the various words; the letters following #2 are the second letters of each word, and so on. Try solving words with letter clues or numbers with minimal choices listed. A sample is shown. Solution on page 14.

oses are dead, violets are dead, I’m a terrible gardener.
A barber, a bald man, and an eccentric professor are taking a journey together. When camping overnight, they took turns keeping watch. When it was the barber’s turn, he amused himself by shaving the head of the professor while he slept. When the professor woke up, he felt his head and said, “You idiot! You woke up the bald man instead of me!”
A husband and wife are on the 4th green when suddenly she collapses from a heart attack! “Help me dear,” she groans to her husband. The husband calls 911 on his cell phone, talks for a few minutes, then picks up his putter and lines up his putt.
His wife raises her head off the green and asks, “I’m dying over here and you’re putting?”
“Don’t worry dear,” says the husband calmly, “they found a doctor on the second hole and he’s coming to help you.”
“Well, how long will it take for him to get here?” she asks feebly.
“No time at all,” says her husband. “Every-
body’s already agreed to let him play through.”
A guy parks his car with his accordion in the back seat and walks off, not realizing that he forgot to lock the doors. About an hour later he remembered his lapse and rushed back to his car, only to find two accordions in the back seat
Moe: My earliest childhood memory is my mom taking me to the eye doctor when I was ten years old.
Joe: Ten? That’s your earliest memory?
Moe: Everything before that is a blur.
Moe: How many politicians does it take to change a light bulb?
Joe: Change? Huh?
Moe: Why did the pirate walk the plank?
Joe: I give. Why?
Moe: Because he didn’t have a dog.
Moe: Do you know how long fish should be cooked?
Joe: The same as short fish I would imagine.
Moe: Hey, you know what squirrels teach their kids about traffic safety?
Joe: Tell me.
Moe: Be sure to run both ways before you cross the street.
Moe: Mind if I use your Wi-Fi password?
Joe: Sure. It’s taped under the modem.
Later...
Moe: Am I spelling this right? t-a-p-e-d-u-nd-e-r-t-h-e-m-o-d-e-m?
Staring at my phone all day has certainly had no Effect on ME!
By popular demand we’re making at-cost subscriptions available for the convenience of our readers. If you live beyond the Aiken-Augusta area, or miss issues between doctor’s appointments — don’t you hate it when that happens? — we’ll command your mail carrier to bring every issue to your house!
NAME
Choose six months for $24 or one year for $42 . Mail this completed form with payment to
Dear Advice Doctor,


My boss has an odd habit that affects my ability to perform my job. He’ll ask me to do something, maybe a task that might take awhile, and then he’ll stand there and watch me do it - or at least start doing it. I can’t function with somebody looking over my shoulder like that. He’s cramping my style big time. Any suggestions?
— Under the microscope
Dear Under,
That can indeed be an unpleasant and uncomfortable feeling. I’ve been there myself, and no doubt many people reading this can also relate.
I remember one time I had cramps so bad while I was running that I fell to the ground. It took a several minutes to get back to normal, but I walked the rest of the way that day.
The whole subject of spasms and cramps is actually a fascinating one that is under a lot of study, and even medical debate into the causes and treatments. With all of our medical advancements, there is still so much we don’t know.
And the two — spasms and cramps — are completely different. Technically speaking, a cramp involves some kind of electrical activity, whereas a muscle spasm can be caused chemically, like as the result of dehydration or an electrolyte imbalance.
But those descriptions are too broad to accurately describe the conditions completely. For example, menstrual cramps are the result of natural uterine contractions as the uterus works to expel its lining. Sometimes the triggers for the contractions (prostaglandins) are present in higher than normal levels, which can lead to menstrual cramps. Endometriosis, uterine fibroids, and other conditions can also cause or contribute to menstrual cramps.
Among the most annoying scenarios are leg muscle cramps that occur at night, just when you want to finally rest after a long day.
The good news is that the vast majority of cramps resolve quickly with stretching, massage and rest, and in most cases they are not medically significant. The exceptions occur when cramps are frequent and severe and have a serious impact on daily living and quality of life — and as in your case, the ability to do your job.
In such situations, consult your doctor for assistance.
Thanks for writing, and I hope I answered your question.
Do you have a question for The Advice Doctor about health, life, love, personal relationships, career, raising children, or any other important topic? Send it to News@AugustaRx.com. Replies will be provided only in the Examiner.

The Mystery Word in our last issue was:
...cleverly hidden in a doctor photo in the p. 16 ad for AIYAN DIABETES CENTER
If that’s your name, congratulations! Send us your mailing address using the email address in the box on page 3. The new Mystery Word is on page 12. Start looking!
...wherein we hide (with fiendish cleverness) a simple word. All you have to do is unscramble the word (found on page 12), then find it concealed within one of our ads. Click in to the contest link at www.AugustaRx.com and enter. If we pick you in our random drawing of correct entries, you’ll score our goodie package!
SEVEN SIMPLE RULES: 1. Unscramble and find the designated word hidden within one of the ads in this issue. 2. Visit the Reader Contests page at www.AugustaRx.com. 3. Tell us what you found and where you found it. 4. If you’re right and you’re the one we pick at random, you win. (Winners within the past six months are ineligible.) 5. Prizes awarded to winners may vary from issue to issue. Limited sizes are available for shirt prize. 6. A photo ID may be required to claim some prizes. 7. Other entrants may win a lesser prize at the sole discretion of the publisher. 8. Deadline to enter is shown on page 12.



Dr. Eric Sherrell, DACM, LAC
Acupuncture Clinic 4141 Columbia Road 706-888-0707 www.AcuClinicGA.com

Chiropractic Health Center

William M. Rice 108 SRP Drive, Suite A 706-860-4001





















OH, THE THINGS PATIENTS SAY WHILE DRIFTING INTO SLEEP UNDER ANESTHESIA I am an anesthesiologist, and when people meet me they will commonly relate a “this is what happened to me in the operating room” story. But this is not a story about what a patient said, but rather what someone said to a patient.
Several years ago, I was at a get together with friends when a couple I knew introduced me to their son who was visiting them from out of town.
Their son was an attorney who had recently graduated from law school and passed the bar exam. He wasn’t a trial attorney, he explained, but rather a corporate attorney who worked in-house to provide legal services for a company to keep them out of court.
When he found out that I was an anesthesiologist, he launched into his “this happened to me” story.
He was going to have knee surgery and had been wheeled into the OR and placed on the operating table. As the anesthesiologist was attaching the EKG stickers and the BP cuff to him, the patient jokingly said, “I think I should tell you that in law school I got an “A” in the class on how to sue doctors.”
He told me the anesthesiologist didn’t immediately react, but continued his preparations for the procedure. When everything was ready, an oxygen mask was placed over the lawyer’s face, and he started to feel the medicine (likely propofol) flowing into his veins via IV.
It was precisely at that moment that the anesthesiologist leaned down and whispered into his ear “I think I should tell you that in med school, I got a “D” in the class on how to wake up lawyers.” Then the lights went out.
This attorney laughed out loud as he related this story and didn’t seem bothered by it at all.
+