The importance of suturing in dental implant surgery
Dr. Steven Vorholt
Dental sedation: an overview
Dr. Brian McGue
Expanding endodontic treatments and procedures with dental lasers


Dr. Fernando Meza
Dr. Reid Pullen helps new associate Dr. Allen Abrishami to accomplish life goals through mentorship
PROMOTING EXCELLENCE IN ENDODONTICS Summer 2023 Vol 16 No 2 endopracticeus.com Irrigation & Obturation n 4 CE Credits Available in This Issue*
Dreamin'
California


Summer 2023 n Volume 16 Number 2
Editorial Advisors
Dennis G. Brave, DDS
David C. Brown, BDS, MDS, MSD
L. Stephen Buchanan, DDS, FICD, FACD
Gary B. Carr, DDS
Arnaldo Castellucci, MD, DDS
Gordon J. Christensen, DDS, MSD, PhD
Stephen Cohen, MS, DDS, FACD, FICD
Samuel O. Dorn, DDS
Josef Dovgan, DDS, MS
Luiz R. Fava, DDS
Robert Fleisher, DMD
Marcela Fridland, DDS

Gerald N. Glickman, DDS, MS
Jeffrey W Hutter, DMD, MEd
Syngcuk Kim, DDS, PhD
Kenneth A. Koch, DMD
Gregori M. Kurtzman, DDS, MAGD, FPFA, FACD, DICOI
Joshua Moshonov, DMD
Richard Mounce, DDS
Yosef Nahmias, DDS, MS
David L. Pitts, DDS, MDSD
Louis E. Rossman, DMD
Stephen F. Schwartz, DDS, MS
Ken Serota, DDS, MMSc
E Steve Senia, DDS, MS, BS
Michael Tagger, DMD, MS
Martin Trope, BDS, DMD
Peter Velvart, DMD
Rick Walton, DMD, MS
John West, DDS, MSD
CE Quality Assurance Board
Bradford N. Edgren, DDS, MS, FACD Fred Stewart Feld, DMD

Gregori M. Kurtzman, DDS, MAGD, FPFA, FACD, FADI, DICOI, DADIA
Justin D. Moody, DDS, DABOI, DICOI
Lisa Moler (Publisher)
Mali Schantz-Feld, MA, CDE (Managing Editor)
Lou Shuman, DMD, CAGS
Collaboration is innovation
During the AAE Annual Meeting in Chicago in May, surrounded by a record-setting crowd of the brightest minds in our specialty, I was reminded of the overwhelming dedication and hard work we put in every day to save teeth and improve experiences for our patients. It is that commitment to excellence that drives us to constantly adapt and evolve in our field.
This year’s AAE made it abundantly clear that of all the changes we’ve experienced, one seems here to stay: We thrive when we work together.
In our post-pandemic world, endodontists are hungry for human interaction, flexibility, and time outside of the operatory for what matters most. The rampant burnout in the dental world is finding a foil now that we’re starting to acknowledge there is strength in numbers and great power in working alongside our peers, whether under one roof or virtually with groups that span the country or world. These realizations will echo in our industry for years to come, as they produce longevity in our careers, increase the quality of our work — and the quality of our lives. Collaboration is the ultimate key to unlocking new possibilities in endodontics. Mentorship is one of the most important forms of collaboration, and it is critical for the future of our specialty. Whether it’s generational or symptomatic of the world we live in, today’s students and new clinicians crave leadership and coaching and are actively seeking them out. They are embracing the opportunity to grow as professionals, rather than just aiming to produce more than the competition as quickly as possible, as may have once been the case.
As experienced doctors, it is our responsibility to pass on our knowledge and skills to the next generation of specialists. We owe them that care and consideration; it is a valuable opportunity to help ensure that young clinicians are well-trained, confident, and passionate about their work, and to assist them in honing their professional and personal attributes. We can provide guidance and support, helping them to navigate the challenges and opportunities that come with starting a career and mold them into better leaders.
And they can help us. The opportunity to mentor is a two-way street; those young minds can be of benefit to even the most seasoned professionals. Doctors fresh out of residency come to the table with a new library of knowledge and experience that might not have been afforded to us because the research was not yet fully developed. That knowledge can be disseminated to doctors who may have been doing things one way for a long time. That is — you can learn as much as you teach, so long as you are humble and open.
So, let’s embrace collaboration as an important form of innovation — just like a new technology or clinical breakthrough — and welcome the opportunity to work with each other and to share our experiences with a younger generation. By working together, we can continue to learn and grow throughout our careers and provide next-level oral health care to those in our communities.
© MedMark, LLC 2023. All rights reserved. The publisher’s written consent must be obtained before any part of this publication may be reproduced in any form whatsoever, including photocopies and information retrieval systems. While every care has been taken in the preparation of this magazine, the publisher cannot be held responsible for the accuracy of the information printed herein, or in any consequence arising from it. The views expressed herein are those of the author(s) and not necessarily the opinion of either Endodontic Practice US or the publisher.
ISSN number 2372-6245
Vladana Babcic Tal, DMD, serves as Chief Clinical Officer of Specialized Dental, the parent company of US Endo Partners. Dr. Babic Tal is a practicing endodontist at Cameo Dental Specialists, a five-location multi-specialty practice in Chicago and pioneer in integrated oral healthcare. She attended University of Wisconsin–Madison, then Boston University School of Medicine for a dual Master of Medical Science and International Public Health, before earning her Doctor of Dental Medicine degree at Tufts University School of Dental Medicine. She completed her post-doctorate advanced specialty training in endodontics at University of Illinois–Chicago College of Dentistry. She is a Diplomate of the American Board of Endodontics and a member of the American Association of Endodontists, American Dental Association, Chicago Dental Society, Illinois State Dental Society, and the Serbian American Medical and Dental Society. Dr. Babcic Tal serves on the Board of the Edgar D. Coolidge Endodontic Study Club and is an advisor for the Windy City Seminars-Seattle Study Club, which focuses on continuing education and interdisciplinary treatment planning for general dentists and specialists.
1 endopracticeus.com Volume 16 Number 2 INTRODUCTION
California Dreamin’
Dr. Reid Pullen helps new associate Dr. Allen Abrishami to accomplish life goals through mentorship
ENDOSPECTIVE
Review of an effective method of cleaning the root canal system


Dr. David Kelliny shares his experience with the GentleWave® System

2 Endodontic Practice US Volume 16 Number 2 TABLE OF CONTENTS PUBLISHER’S PERSPECTIVE Be the lotus Lisa Moler, Founder/CEO, MedMark Media 6 RESEARCH Role of antibiotics in the healing of periapical lesions — two case reports Drs. Amil Sharma, Stephen Cohen, Greeshma Gupta, Gregori M. Kurtzman, and Vivek Kumar Pathak discuss the applications of triple antibiotic paste (TAP) to endodontics 12 TECHNOLOGY The power of investing in technological advancements in endodontics
Anne Wiseman shares her experience of differentiating herself through innovation ........ 18
Dr.
importance
implant
22 8
STORY
CONTINUING EDUCATION The
of suturing in dental
surgery Dr. Steven Vorholt explores the many aspects of suturing for implant procedures
COVER
Cover image of Dr. Allen Abrishami courtesy of US Endo Partners.
11




“My Endo Mastery coach uncovered needed tweaks and 12 months later my net increased by 37%. With more efficient systems, I’m ready to bring on an associate and continue the upward spiral while moving towards 3 days a week.” YOU’RE INVITED TO THE NEXT LEVEL OF ENDO SUCCESS! MASTERING THE EFFORTLESS ENDODONTIC PRACTICE Friday and Saturday September 22nd/23rd, 2023 2-DAY LIVE SEMINAR DOCTORS AND TEAMS ORLANDO, FLORIDA DR, CAMERON TOWNSEND JOIN US FOR OUR NEXT EVENT. REGISTER ONLINE OR CALL: Endo Mastery (Inner Peace Seminars) Nationally Approved PACE Program Provider for FAGD/MAGD credit. Approval does not mean acceptance by any regulatory authority or AGD endorsement 5/1/2022 to 4/30/2025 Provider ID# 358761 1-800-482-7563 info@endomastery.com endomastery.com/ orlando-2023







4 Endodontic Practice US Volume 16 Number 2 TABLE OF CONTENTS PRACTICE MANAGEMENT Endodontics and billing through medical insurance Christine Taxin discusses several ways endodontists can bill through medical insurance ........................................................ 32 TECHNOLOGY Expanding endodontic treatments and procedures with dental lasers Dr. Fernando Meza sheds some light on the benefits of lasers in endodontics.................................... 34 FINANCE MATTERS A taxing situation Justin Maxwell offers suggestions for maximizing your tax strategy ..............................................................36 SMALL TALK A coach’s perspective on evolving competency Drs. Joel C. Small and Edwin McDonald show that leadership takes time and effort .................. 38 SOUND ADVICE The Endo Files: the endodontic experts podcast US Endo is amplifying the voices of specialists and industry insiders ..........................................40 Connect. Be Seen. Grow. Succeed. | www.medmarkmedia.com READ the latest industry news and business WATCH DocTalk Dental video interviews with KOLs LEARN through live and archived webinars RECEIVE news and event updates in your inbox by registering for our eNewsletter CONNECT with us on social media www.endopracticeus.com *Paid subscribers can earn 4 continuing education credits per issue by passing the 2 CE article quizzes online at https://endopracticeus.com/category/continuing-education/ 28 CONTINUING EDUCATION Dental sedation: an overview Dr. Brian McGue discusses how sedation can affect patients and dentists
Be the lotus
In an array of colors, blue, white, purple, red, or pink, lotuses are touted as symbols of peace, beauty, and longevity. I love lotus flowers. Earth.com describes them as extremely strong with the first one estimated to have sprouted millions of years ago. For all of its breathtaking beauty, the lotus flower grows out of the mud, rising above the water. As a result, it also has gained a reputation as a symbol of persistence. What does this flower have to do with anything dental, anyway? Well, like the lotus flower, on our professional and personal journeys, we may have to find the strength to grow out of somewhat messy circumstances or humble beginnings. How do we do it? Persistence, innovation, and constantly reaching for a higher standard.
One way to get out of our rut when we are stuck in the mud is by purging – getting rid of old perceptions, equipment, or materials that hold us back from growing. After freeing up some space, invite future growth by researching and adding new things that can improve life around your office and for your patients. Imaging, 3D printing, AI software, instrumentation – you name it – dental visionaries and entrepreneurs are introducing amazing inventions every day. You just have to find the ones that fit your own space and needs, and maybe even help you grow outside your comfort zone. We hope to be able to help you on your journey.
We have lots of ideas in this issue to help you expand your mind and office. In our cover story, Dr. Reid Pullen describes how his mentorship of Dr. Allen Abrishami through US Endo has given them both a valuable resource, brainstorming partner, and sounding board. In his CE, Dr. Steven Vorholt provides an overview of suturing techniques for implants and illustrates a case where all three types of sutures are used. Dr. Brian McGue discusses the benefits to the doctor and patients of using sedation in a dental practice. Dr. Anne Wiseman talks about the importance of investing in advanced technologies like CBCT, microscopes, anxiety-free injections, and GentleWave.
At MedMark, we don’t want your practices to be stuck in the mud of mediocrity. Ora Nadrich, life coach and mindfulness teacher said, “On the path of self-realization, there is no one big awakening, but many along the way of varying degrees: some small, some big; and each one of them is like the lotus flower, which grows out of muddy waters.” So my message this issue is: No matter how small or big your practice, be a lotus; keep growing, changing, and reaching for whatever it takes to make you blossom.
To your best success,
Lisa Moler Founder/Publisher MedMark Media
Published by
Publisher Lisa Moler lmoler@medmarkmedia.com
Managing Editor Mali Schantz-Feld, MA, CDE mali@medmarkmedia.com
Tel: (727) 515-5118
National Account Manager Adrienne Good agood@medmarkmedia.com
Tel: (623) 340-4373
Sales Assistant & Client Services Melissa Minnick melissa@medmarkmedia.com

Creative Director/Production Manager Amanda Culver amanda@medmarkmedia.com
Marketing & Digital Strategy Amzi Koury amzi@medmarkmedia.com
eMedia Coordinator Michelle Britzius emedia@medmarkmedia.com
Social Media Manager April Gutierrez socialmedia@medmarkmedia.com
Digital Marketing Assistant Hana Kahn support@medmarkmedia.com
Website Support Eileen Kane webmaster@medmarkmedia.com
MedMark, LLC

15720 N. Greenway-Hayden Loop #9 Scottsdale, AZ 85260
Tel: (480) 621-8955
Toll-free: (866) 579-9496 www.medmarkmedia.com
www.endopracticeus.com
Subscription Rate
1 year (4 issues) $149
https://endopracticeus.com/subscribe/
6 Endodontic Practice US Volume 16 Number 2 PUBLISHER’S PERSPECTIVE
Lisa Moler Founder/Publisher, MedMark Media


California Dreamin’
Dr. Reid Pullen helps new associate Dr. Allen Abrishami to accomplish life goals through mentorship
Dr. Allen Abrishami can’t believe his luck.
A recent graduate of the endodontics program at Nova Southeastern University in Florida, Dr. Abrishami gets to report to his dream job every day — alongside his mentor, Dr. Reid Pullen. The two practice together at Brea Endodontics in Southern California.

Dr. Abrishami wasn’t sure where he was headed after graduation, but he was exploring all his options. Most important to him was landing back home in California, as close to his tightknit family as possible. The next factor on the list? Finding a trusted mentor.

“In residency we read research papers nonstop, but so much of that research is based on lab studies. When you hear it from the messenger himself — your mentor and the endodontist who has seen the cases — you start to learn that yes, research has a lot of value in the field, but empirical evidence trumps most things,” Dr. Abrishami said. “Having someone to bounce ideas off, and learning what you don’t know is way more valuable than a thousand research papers.”
The son of two brave Jewish Persian immigrants who fled their homes during the Iranian Revolution in 1979, Dr. Abrishami was inspired to consider dentistry because of a bout of tooth pain his mother suffered when he was 15.
“I had just gotten my learner’s permit and was excited to drive anywhere I could. At that exact time, my mom was experiencing some bad dental pain … it had been 3 or 4 days, and she couldn’t sleep or eat,” he recalled. “After a few days of struggling, she finally asked me if I could drive her to the dentist.” He was excited to drive but even more excited when he learned about the powers dentists possess.
“I took her to the dentist, and it felt like what she had been experiencing for more than 3 days was gone in 3 seconds,” Dr. Abrishami said. “Obviously, I didn’t know exactly what had happened at the time, but I knew I wanted to be a dentist. I wanted to do what that guy had just done for her.” Later in school, he learned that his mother had undergone a form of endodontic treatment, so choosing a specialty was simple.
“That’s what drove my passion. I love helping patients get out of pain — helping them and bringing them relief,” he said.
Dr. Abrishami is also passionate about hard work, a character trait common in his family. “After immigrating, my parents struggled and worked hard to provide for me and my sister,” he said. “I want to be the best I can be for them and make them proud.” He completed his undergraduate education at UCLA, then graduated from the University of the Pacific School of Dentistry and a 1-year general practice residency at the University of Nevada, Las Vegas, before moving to south Florida for his endo residency. During that year, Dr. Abrishami helped organize a dinner for some of his classmates so they could connect with a doctor and
8 Endodontic Practice US Volume 16 Number 2 COVER STORY
Dr. Allen Abrishami, left, and Dr. Reid Pullen discuss a challenging case at their practice in Brea, California, just outside of Los Angeles
a support team member from US Endo Partners, a specialty dental service organization (DSO), to learn about the opportunities that existed within the group. Upon getting to know him and his goals, and hearing that he was intent on getting back home to California, the team from US Endo told him that he would be a perfect fit at Dr. Reid Pullen’s office, just outside of Los Angeles.
“I thought at first they were just selling me, but they were really listening and understood me,” Dr. Abrishami said. “They read me like a book.” A call was made, and an interview scheduled.
When he reported to his interview, Dr. Pullen apologetically messaged that he was running late because he had been surfing with his children. He showed up soon after — in a wet bathing suit and t-shirt. “Reid is an amazing endodontist, but it was clear from that moment that he also valued life outside of work and his family; that’s the kind of life I want to work toward,” Dr. Abrishami said. “The fact that he showed up in board shorts helped me know for sure that this would be a good fit.” The two also found they shared the same philosophy on patient care, a similar competitive streak, and a deeply engrained commitment to excellence.
Dr. Pullen, also a California native, opened Brea Endodontics in 2007, building the now-thriving practice from scratch. He needed another associate who could quickly go fulltime to help shoulder the growing practice load and who might eventually also choose to partner with US Endo, and he wanted the fit to be exactly right. “I wanted integrity, and I wanted someone who could start off well, but then just get better and better. And that’s exactly who Allen is,” Dr. Pullen said. “We instantly hit it off.”


Dr. Abrishami added with a laugh, “He and I joke that we’re endodontic partner soulmates.”
Because the two had established a relationship and personal rapport, the transition from school to work was easier than expected for Dr. Abrishami. “I didn’t feel nervous at all about how I was going to get along with Reid or what his expectations of me were. He’d already made me feel so comfortable,” he remembered.
The first days on the job weren’t perfect by any stretch of the imagination but it didn’t take long to find a groove. “For the first few weeks, Reid was with me more than he was supposed to be. We share a day on Wednesdays, but he would come in periodically other days to kind of check in on me,” Dr. Abrishami said. “There were definitely times where I had to be bailed out because I didn’t really know my clinical skills well enough to be able to say how much time I needed for a procedure.”
Dr. Abrishami said timing was his biggest limitation in the beginning. “In the beginning, there was a period of transition where my abilities and the expectations from the practice team were a bit misaligned, but within the first 2 or 3 days, we all felt each other out; by the second week we were hitting the ground running. Everyone understood that I was fresh out of school and that I needed a little extra time for tougher cases.”
9 endopracticeus.com Volume 16 Number 2 COVER STORY
Dr. Allen Abrishami consulting with a patient about root canal therapy (left). Dr. Reid Pullen invests time in mentoring and developing his valued teammates, from associate doctors to assistants (right)
US Endo is such a large, supportive organization, so you don’t get pushback about the specific materials that you want to use and how you want to provide care to patients. Whatever works best in my hands, I can guarantee we’re going to have it in the office.”
— Dr. Abrishami
Dr. Pullen repeatedly assured Abrishami that getting the job done correctly and in the best interest of the patient was of ultimate concern to him — not the timing.
“I told him, ‘It doesn’t matter what your speed is right now. I want you to do A+ work. If you do A+ work, you can take as long as you need,’” Dr. Pullen recounted. And that made all the difference in Dr. Abrishami’s level of confidence. “I think the most important thing for a more timid, inexperienced endodontist is to walk into a room and feel like the quality of the work is more important than how much they’re producing. It works wonders,” Dr. Abrishami said.
In addition to the encouragement and validation Dr. Pullen continues to provide Dr. Abrishami in these early days of practice, he also serves as a valuable resource, brainstorming partner, and sounding board. They frequently speak on the phone during Dr. Abrishami’s drives home after work if they haven’t been in the office together, talking through problems encountered during the day and deciphering why potential missteps occurred.
“One of the most valuable things Reid has taught me is to stop what you’re doing in the moment after making a mistake, clear your mind, and ask yourself, ‘Why did you do that?’ Not in an accusatory way, but to figure out why, exactly, the event happened,” Dr. Abrishami said. “Then, if it’s something you can control, start brainstorming right then and there to figure out how you can change it next time.”
Dr. Abrishami likened having a mentor close by to having a safety net. “Endodontics is a very nerve-racking field to come into; you know that there is a plethora of mistakes you could make,” he said. “If you can take the aspect of being by yourself out of the equation, it makes starting out a lot more comfortable and makes the quality of your work go up, too.”
Though as a talented resident he had other options, Dr. Abrishami is certain joining the team at Brea Endodontics and US Endo was the right move for him — although he was the only resident in his group to select a DSO-affiliated practice.

“I can’t even think of a scenario where I would’ve gone out on my own. The idea of setting up shop right out of residency was so intimidating,” Dr. Abrishami said. “US Endo is such a large, supportive organization, so you don’t get pushback about the specific materials that you want to use and how you want to provide care to patients. Whatever works best in my hands, I can guarantee we’re going to have it in the office.”
Dr. Abrishami said that he is thrilled to have complete clinical autonomy in the way he treats his patients and doesn’t feel pressure to complete a certain number of cases, which helps where timing is concerned.
“Reid and I tend to be pretty competitive people in general, so we’re constantly looking at our reports and trying to be the best we can be,” he said. “But at the same time, nobody’s ever knocking on our door to tell us, ‘Hey, you guys aren’t producing enough,’ or ‘You’re not doing enough,’ or ‘You need to pick up the pace.’ I couldn’t be happier being associated with US Endo.”
Dr. Abrishami said he couldn’t imagine having a better start to his career, given all the support he has at his fingertips. “Fresh out of school, you tend to hit a lot of different limitations and restrictions. You realize quickly what you can and can’t do with the arsenal of information you’ve been given during the last 10 years of education,” Dr. Abrishami said. “Practicing has been great so far, and so much of that is because I have a wonderful mentor in Reid. And, honestly, I couldn’t even ask for a better person to spend a day with. I’m so grateful to be here.”
And Dr. Pullen is grateful to have him. “US Endo found me, I think, probably the best associate in the entire nation, and I feel extremely lucky,” Dr. Pullen said. “Allen is a fantastic clinician, but also a fantastic human being with a great heart. It’s been a pleasure to go to work with him.” EP
10 Endodontic Practice US Volume 16 Number 2 COVER STORY
Dr. Allen Abrishami with a patient
Review of an effective method of cleaning the root canal system
Dr. David Kelliny shares his experience with the GentleWave® System

“Ilove my GentleWave® System.” That’s how I answer and start a conversation with anyone who asks me about the GentleWave Procedure. I have been a user and a believer for 5 years. The GentleWave Procedure is an advanced endodontic treatment that utilizes a combination of different technologies to improve the success rate of root canal treatment. This procedure is a minimally invasive technique that uses a combination of sound waves and fluid dynamics to create a powerful vortex that cleans and disinfects the root canal system.
The traditional method of root canal treatment involves the use of rotary and hand files and irrigation solutions to clean and shape the root canal system. While this method has been reasonably effective for many years, it has its limitations. One of the main challenges is the presence of complex anatomical structures within the root canal system that are difficult to access and clean thoroughly. These structures can serve as a haven for bacteria and other microorganisms, leading to treatment failure.
The GentleWave Procedure, on the other hand, overcomes these limitations and improves the outcomes of root canal treatment. The specially designed Procedure Instrument (PI) creates acoustic energy in the irrigation solution. The acoustic waves and fluid agitation used in the procedure can reach areas that are difficult to access with traditional instrumentation, facilitating the removal of bacteria and debris from the tooth. This helps to reduce the risk of reinfection and improves the overall success rate of the treatment.
One of the major benefits of the GentleWave Procedure is that it can significantly reduce the time required for root canal treatment. Because the procedure is more efficient than traditional methods, it can often be completed in a single visit, saving patient’s time, and reducing the need for multiple appointments.
Dr. David Kelliny earned his bachelor’s degree in Dental Surgery from Cairo University in 1992. He graduated with a Doctor of Dental Surgery degree from University of Southern California in 1998 and earned a Certificate in Endodontics also from USC in 2001. Dr. Kelliny is currently a part-time Clinical Assistant Professor at the Herman Ostrow School of Dentistry of USC post-graduate Endodontic program and has been teaching at USC since 2002; he is involved in teaching and lecturing residents on various aspects of Endodontics with a specific emphasis on surgical endodontics, 3D endodontics and dental implants. Dr. Kelliny is a member of the American Dental Association, California Dental Association, Western Los Angeles Dental Society, American Association of Endodontists, American Dental Society of Anesthesiology, and International Congress of Implantologists.
Disclosure: The author declares that there are no conflicts of interest in connection with this article.
Additionally, the GentleWave Procedure is less invasive than traditional methods, which can help to reduce doctor discomfort and speed up the healing process. In fact, research shows 97.7% of patients experience healing within 12-months.1
The GentleWave Procedure has several advantages over traditional root canal treatment. First, it is a minimally invasive technique that preserves more tooth structure, reducing the risk of tooth fracture and improving the long-term prognosis of the tooth. Second, it is a more efficient method of disinfection, enabling thorough cleaning of even complex anatomical structures within the root canal system. Third, it reduces the risk of treatment failure and the need for retreatment. Studies have shown that the procedure is effective at removing bacteria and debris from the root canal system, which can significantly improve the success rate of root canal treatment.
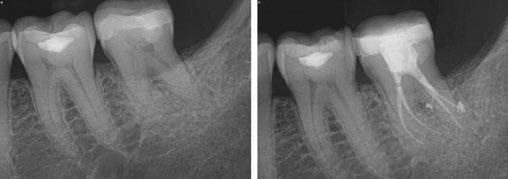
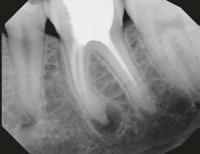
Let’s examine a case of a 58-year-old male who presented to my office in pain. He was referred as an emergency for consultation and treatment on either tooth No. 18 or 19. The patient presented with pain that had been on and off for over a month. The patient’s chief complaint was pain to cold and hot that lingered and now was spontaneous. On examination, tooth No. 19 responded to pulp testing within normal limits and was negative to percussion. Tooth No. 18 had a lingering sensitivity to cold, and a diagnosis of irreversible pulpitis and symptomatic apical periodontitis was made.
As you can see from final radiographs, the GentleWave Procedure’s ability to clean out and clear all portals of exit is on clear display here. I would not have had a similar outcome if I did not use the GentleWave Procedure.
In conclusion, the GentleWave Procedure is an advanced and highly effective method for cleaning the root canal system during endodontic treatment. The procedure offers numerous benefits, including that it reduces treatment time, is less invasive, and has a high success rate. As such, the GentleWave Procedure represents a significant advancement in the field of endodontics and offers a promising treatment option for patients. Review additional clinical studies and practice case studies at GentleWave.com/Doctor.
GentleWave® is a trademark of Sonendo, Inc.
11 endopracticeus.com Volume 16 Number 2 ENDOSPECTIVE
1. Sigurdsson A, Garland RW, Le KT, Woo SM. 12-month Healing Rates after Endodontic Therapy Using the Novel GentleWave System: A Prospective Multicenter Clinical Study. J Endod. 2016 Jul;42(7):1040-8.
EP
Figure 1: Radiograph of tooth No. 18. The image on the right illustrates how the GentleWave Procedure cleans and clears all portals of exit
Role of antibiotics in the healing of periapical lesions — two case reports
Drs. Amil Sharma, Stephen Cohen, Greeshma Gupta, Gregori M. Kurtzman, and Vivek Kumar Pathak discuss the applications of triple antibiotic paste (TAP) to endodontics
Abstract
This study investigated the latest findings and notions regarding triple antibiotic paste (TAP) and its applications in dentistry, particularly endodontics. TAP is a combination of three antibiotics — ciprofloxacin, metronidazole, and minocycline. Despite the problems and pitfalls research pertaining to this paste has unveiled, it has been vastly used in endodontic treatments. The paste’s applications vary, from vital pulp therapy to the recently introduced regeneration and revascularization protocol. Studies have shown that the paste can eliminate root canal microorganisms and prepare an appropriate matrix for further treatments. This combination is able to remove diverse groups of obligate and facultative gram-positive and gram-negative bacteria, providing an environment for healing. In regeneration protocol cases, this allows the development, disinfection, and possible sterilization of the root canal system, so that new tissue can infiltrate and grow into the radicular area. TAP has diverse uses as an antibacterial intracanal medication. Nevertheless, despite its positive effects, the paste has shown drawbacks. Further research concerning the combined paste and other intracanal medications to control microbiota is imperative.
Introduction
There is no greater association between the basic science and the practice of endodontics than that of microbiology. One of the strongest factors contributing to the controversies often encountered in the endodontic field is the lack of understanding that the disease processes of the pulp and periradicular tissues
Amil Sharma, BDS, MDS Endodontics, is a Reader in the Department of Conservative Dentistry and Endodontics at Modern Dental College and Research Centre, Indore, Madhya Pradesh, India.
Stephen Cohen, DDS, MA, FICD, FACD, is a Diplomate of the American Board of Endodontics and author of Pathways of the Pulp.
Greeshma Gupta, BDS, MDS Endodontics, is Consultant Endodontist in Gwalior, Madhya Pradesh, India.
Gregori M. Kurtzman, DDS, MAGD, FPFA, FACD, FIADFE, DICOI, DADIA, DIDIA, is in private practice in Silver Spring, Maryland.
Vivek Kumar Pathak, BDS, MDS Endodontics, is a Reader Department of Conservative Dentistry and Endodontics at Maharana Pratap College of Dentistry.
generally have a microbiological etiology. The vast majority of diseases of dental pulp and peri radicular tissues are associated with microorganisms. After the microbial invasion of these tissues, the host responds with both nonspecific inflammatory responses and with specific immunologic responses to encounter such infections. Pulp diseases are the main cause of the invasion of endodontic spaces by oral microbial flora. The survival of bacteria and fungi in this environment depends on a series of factors that involve the presence of nutrients, the environmental conditions of anaerobiosis, the pH value, competition/ cooperation with other microorganisms, and the microenvironmental characteristics. The environment determines which microorganisms survive, and some can survive under unfavorable conditions.
The very first aim of endodontic treatments is to eliminate as many bacteria as possible from the root canal system and create an environment in which no remaining microorganisms can survive.15 Ideally, this can only be obtained through the use of a combination of aseptic treatment techniques, chemomechanical preparation of the root canal, antimicrobial irrigation, and intracanal medicaments.15,16 Approximately 50% of root canal peripherals and ramifications may remain uninstrumented during preparation of the root canal.17 In this condition, the remaining necrotic tissues may act as a nutrition source for the surviving bacteria.18,19 Thorough and systemic mechanical instrumentation, irrigation, and use of inter-appointment medication can perhaps reduce this phenomenon. Medicaments can play an important role in the preparation of the root canal for further therapies;17 for example, in necrotic pulps and active exudation.20 Calcium hydroxide has long been used as an inseparable part of root canal treatment in necrotic cases, resulting in less signs and symptoms. Traditionally, calcium hydroxide has been used in open-apex teeth with necrotic pulp tissues for inducing a bridge and preparing the root canal space for forthcoming therapies. Without the use of inter-appointment intracanal medications, such successful results are far-fetched.20,21
The type of intracanal medication depends upon the precise diagnosis of the tooth condition, a thorough knowledge of the type of microorganisms involved, and finally, their mechanisms of growth and survival. The presence of bacteria within the root canal is the main factor of endodontic disease, and therefore, the use of an antimicrobial agent is essential. Many forms of intracanal medicaments, apart from antibiotics and calcium hydroxide, have been used in an attempt to accomplish the
12 Endodontic Practice US Volume 16 Number 2 RESEARCH
above aim.22 These mainly include chlorhexidine and ethylenediaminetetraacetic acid.23
Currently, the common antibiotic-containing commercial pastes are Ledermix® (Lederle Pharmaceuticals, Wolfratshause, Germany) and Septomixine Forte (Septodont, Saint-Maur, France).24,25 Both preparations have corticosteroids as antiinflammatory agents. However, neither of these pastes can be considered suitable for use against endodontic microbiota owing to their inappropriate spectrum of activity.17,23 Several studies have investigated different root canal antibiotic agents.26
Recently, another combination of antibiotics, called triple antibiotic paste (TAP) was introduced especially for the regeneration and revascularization protocol and the treatment of open apex teeth with necrotic pulp. This material has also shown other applications in endodontics.25 Initially, TAP was largely developed by Hoshino and colleagues,24 who investigated the effectiveness of the paste on the removal of microorganisms from the root canals.27 Researchers have also used TAP in vitro to disinfect Escherichia coli-infected dentin.27 Later, particular attention was given to the antibiotic paste and its effect against microorganisms present in carious dentin and infected pulp. The outcome showed excellent results in the eradication of the bacteria from the radicular system.28
TAP is a combination of ciprofloxacin, metronidazole, and minocycline.29 Metronidazole, as a nitroimidazole compound, is particularly toxic to anaerobes and is considered an antimicrobial agent against protozoa and anaerobic bacteria. Minocycline is bacteriostatic and shows activity against gram-positive and gram-negative bacteria. It also causes an increase in the amount of interleukin-10, which is an inflammatory cytokine. Moreover, ciprofloxacin — as a synthetic fluoroquinolone — possesses fast bactericidal action and exhibits high antimicrobial activity against gram-negative bacteria, and with limited activity against gram-positive ones. Many anaerobic bacteria are resistant to ciprofloxacin. Hence, it is often used with metronidazole in treating mixed infections to compensate for its limited scope.30 Therefore, TAP can affect gram-negative, gram-positive, and anaerobic bacteria, and this combination can be effective against odontogenic microorganisms.31
If the TAP is to be used, ciprofloxacin, metronidazole, and minocycline should be mixed equally (1:1:1)2,25,32 to a final concentration of 0.1–1.0 mg/mL.33,34
Applications of TAP in endodontics
The applications of TAP in endodontics can be considered as follows:
1. In the regeneration and revascularization protocol of the pulp
2. As an intracanal medicament for the treatment of:
A. Periapical lesions
B External inflammatory root resorption
C. Root fracture
D. Primary teeth
3. As an intracanal agent to control flare-ups
4. As a medicated sealer (to prevent possible re-infection)
5. As an addition to gutta-percha points in root canal obturation (known as medicated gutta-percha points)
6. As an intracanal medicament loaded on a scaffold
Materials and methods
Case 1
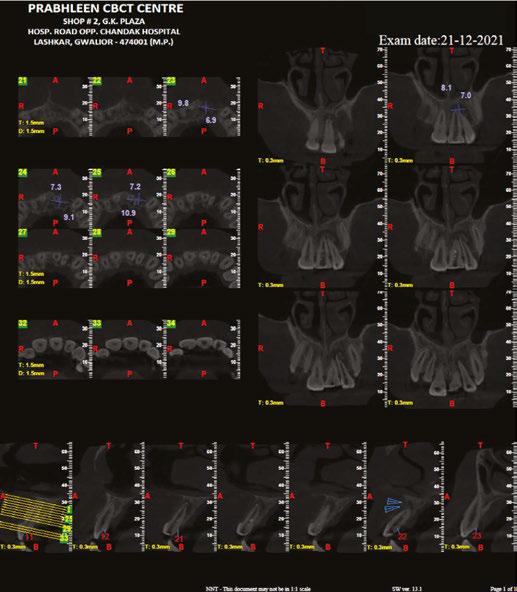
A 19-year-old female patient reported to the Department of Conservative Dentistry and Endodontics, IDEAS Dental College, Gwalior, India, with a chief complaint of pain in the upper front teeth. She gave a history of mild intermittent pain in the region of the upper front teeth. Her further history revealed that the patient had a blow to her front teeth when she was 10 years old. No treatment was performed after that.
On intraoral examination, it was seen that the patient had mild discomfort on vertical percussion with respect to her upper maxillary left central and lateral incisors. The patient also complained of discomfort while palpating the mucobuccal fold corresponding to these incisors. An intraoral periapical radiograph showed the presence of large periapical radiolucency with irregular outline corresponding to upper maxillary left central and lateral incisors. Pulp sensibility tests (thermal and electric pulp tests) were then performed to determine the teeth responsible. As per the tests, it was concluded that only the maxillary central left and lateral incisors were the culprit.
The patient was reluctant for any sort of surgical procedure as she described an intense fear of any surgical intervention. Therefore, a non-surgical approach was chosen to treat this case of asymptomatic apical periodontitis associated with necrotic pulp. Access opening was carried out under proper aseptic conditions for both the upper central incisors. The working length was determined, and canals were shaped with K-files (Dentsply-Maillefer, Ballaigues, Switzerland) to an apical preparation of ISO size No. 80. During the preparation, the canals were irrigated with 2.5% NaOCl (Novo Dental Products Pvt. Ltd., Mumbai, India),
13 endopracticeus.com Volume 16 Number 2 RESEARCH
Figure 1: Preoperative image
17% ethylenediaminetetraacetic acid (B.N. Laboratories, Mangalore, India), and 0.2% chlorhexidine (Vishal DentocarePvt. Ltd., Ahmedabad, India) with in between saline flush to remove the necrotic debris from the pulp space. The access cavity was sealed with zinc-oxide-eugenol temporary restoration (Dental Products of India, Mumbai, India). The next day, the patient returned with severe pain with respect to both teeth. On examination, it was seen that both the maxillary central left and lateral incisors were severely tender to percussion. It was concluded that it was a case of mid-treatment flare-up. The canals were opened again. Pus discharge was allowed to drain. Canals were dried, followed by closed dressing. The patient was put on systemic antibiotics (Amoxicillin; Amox 500 mg 3 times daily 5 days) and analgesics (Ibuprofen; Brufen 400 mg twice daily for 3 days).
On the recall visit after 4 days, it was seen that the patient still had mild tenderness and that the canals were still weeping on the removal of the temporary restoration. The canals were once again irrigated with chlorhexidine, and an intracanal medicament, TAP, was placed. The TAP was prepared as described by Takushige, et al.,9 using commercially available tablets of ciprofloxacin (Cifran 500 mg, Ranbaxy Laboratories Ltd., India), metronidazole (Metrogyl 400 mg, J.B. Chemicals and Pharmaceuticals Ltd., India) and minocycline (Minoz 50 mg, Ranbaxy Laboratories Ltd., India). Following the removal of the enteric coating of the tablets, the contents were pulverized using a mortar and pestle and mixed with propylene glycol to obtain a paste form. The paste was packed into the canal using a hand plugger, and the access was sealed with zinc-oxide-eugenol temporary restoration (Dental Products of India, Mumbai, India). The patient was then recalled after 2 weeks, and the canals were then free of any exudate. The TAP was again placed as an intracanal medicament. On her next visit after 2 weeks, a slight greenish tinge was noticed in the upper central incisors, which was not very significant.
Since both the teeth were asymptomatic, antibiotic paste was removed, and the canals were obturated with gutta percha (Dentsply-Maillefer, Ballaigues, Switzerland)




14 Endodontic Practice US Volume 16 Number 2 RESEARCH
Figures 2-4: 2. Working-length radiograph CBCT of the involved tooth. 3. Master cone radiograph. 4. Postoperative radiograph
Figures 5 and 6: 1- year follow-up CBCT image
and AH Plus® sealer (Dentsply, De Trey, Konstanz, Germany) using the lateral compaction technique. An interim glass ionomer restoration was then placed. The patient was asked to get the core build up and full coverage crowns from the place where she was going to continue her further studies. As she could not find time, she came back to the institution for the completion of the treatment during her vacation. On examination, the teeth were asymptomatic, and post-obturation radiograph taken after 18 months showed an increase in periradicular bone density suggestive of progressive healing.
Case report 2
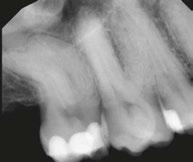
A 19-year-old male reported to the Department of Conservative Dentistry and Endodontics at the Institute of Dental Education and Advance Studies (IDEAS), Gwalior, Madhya Pradesh, India, with a complaint of pain in her upper left front region with medical history status of trauma 5 years prior. Two months earlier, he noticed the formation of the sinus tract in relation to her central incisor with purulent discharge. An intraoral examination revealed that the RCT was already attempted, which did not relieve patient’s issues. An extraction was advised, but the patient was not willing to undergo an extraction. There was presence of a sinus tract and inflamed gingiva in relation to the tooth. The electronic pulp test was negative. An intraoral periapical radiograph showed periapical radiolucency so a CBCT was recommended. At the same appointment, the root canal treatment was initiated on her central and lateral incisor. An access cavity opening was done, and hemorrhagic, purulent exudate was found. The working length was estimated using electronic apex locator (RAYPEX® 6 VDW Inc.; Munich, Germany). Biomechanical preparation was done with K-file 10–40 using a step-back technique. During the instrumentation, the canal was irrigated copiously with 3% sodium hypochlorite solution using a 27-gauge endodontic needle after each instrument. Drainage was performed until the discharge through the canal ceased. The canals were irrigated, and the smear layer was removed with 17% EDTA followed by 3% sodium hypochlorite. The canals were dried, and a triple antibiotic paste consisting of ciprofloxacin, metronidazole, and minocycline (100 mg of each drug in 0.5 ml total volume) was placed with the help of a lentulo spiral. The dressing was changed after every month for 3 months until the teeth showed no symptoms. On intraoral examination, the teeth showed complete resolution of sinus as soft tissues were found healthy, and the canals were


15 endopracticeus.com Volume 16 Number 2 RESEARCH
Figure 7: Preoperative radiograph
Figure 9: 1-year follow-up CBCT
Figure 10: 1-year follow-up CBCT
Figure 8: CBCT of involved tooth
dry. Final irrigation was done with 2% chlorhexidine, and canals were obturated with gutta percha using a lateral compaction technique. The restoration was accomplished with composite.
Discussion
A “Comparison between the Antimicrobial Effects of Triple Antibiotic Paste and Calcium Hydroxide Against Enterococcus Faecalis” suggested that the triple antibiotic paste with either 2% chlorhexidine or normal saline would be the preferred medicament against E. faecalis and, among its three components, minocycline has the greatest antibacterial effect.1
Comparative analysis of tooth discoloration induced by conventional and modified triple antibiotic pastes used in regenerative endodontics was carried out, and it was inferred that modified TAP with clindamycin did not induce clinically visible discoloration up to 3 weeks after placement. In this, minocycline or doxycycline were replaced by clindamycin. However, further in-vivo research is needed.2
Regarding the discoloration caused by TAP, which is composed of ciprofloxacin, metronidazole, and minocycline, Kim, et al.,14 showed that minocycline was the main cause of tooth discoloration due to TAP. Thus, it has been suggested to use other antibiotics such as cefaclor,23,24 fosfomycin,24 amoxicillin,13,20,24 or Augmentin12 instead of minocycline or DAP (ciprofloxacin and metronidazole)25 instead of the classic TAP.21 In another study, Kahler, et al.,13 indicated that despite replacement of minocycline with amoxicillin, 10 out of 16 teeth that underwent regenerative treatment showed coronal discoloration. Also, replacement of minocycline with cefaclor and doxycycline in another study did not prevent visible coronal discoloration of teeth following application of these drugs for three weeks.25 Thus, strategies to prevent coronal discoloration following the use of antibiotic compounds must be studied in further detail. However, TAP is one of the most commonly used intracanal medicaments for disinfection in regenerative endodontic procedures and is one of the suggested medications in the American Association of Endodontists guidelines. Considering the risk of coronal discoloration following the use of TAP, future studies are required to assess the antibacterial effects of lower concentrations of TAP on the biofilm. Lower concentrations of TAP have easier clinical application and better penetration into the root canal system, although they can be washed from the root canal system and need a scaffold. Also, production of nano-TAP can be an interesting topic for future research. It should be noted that considering the critical role of stem cells in endodontic regenerative treatments and the coronal discoloration potential of TAP, future studies are required to find a medicament with the least side effects for this treatment protocol.
TAP was used as the medicament of choice for the non-surgical endodontic therapy in the present case as previous studies have shown its effectiveness in the elimination of the microorganism from the root canal system.6,9,11 Hoshino, et al.,11 in their in-vitro study on the antibacterial efficacy of metronidazole, ciprofloxacin, and minocycline alone and in combination against the bacteria of infected dentin, infected pulps and periapical lesions showed that they are incapable of complete elimination of bacteria, when used alone. However, in combination, these drugs were able to consistently sterilize all samples.
Hence the concept of lesion sterilization and tissue-repair therapy; i.e., the combination of the above-mentioned drugs can be employed in infected teeth with large periapical lesions where diverse microflora can be encountered. In accordance with the previous study, the present case reports also demonstrated favorable healing of the large periapical lesion with non-surgical endodontic therapy using TAP.7,12
Calcium hydroxide, which is the commonly used intracanal medicament, has shown limited effectiveness in disinfecting the root canal system because of the dentinal protein buffering and its inability to eliminate certain microorganism especially within biofilms.5 Long-term calcium hydroxide placement has shown to result in higher incidence of root fracture either due to the disruption of the link between the hydroxyapatite crystals and the collagenous network in dentin or because of the reduced organic support due to denaturation and hydrolysis.13 Hence, the use of TAP can overcome these disadvantages of calcium hydroxide. TAP is also biocompatible as evident from its use in regenerative endodontics.14
Petrino, et al., (2010), while applying revascularization protocol using a triple antibiotic paste and a coronal seal of mineral trioxide aggregate on six immature teeth with apical periodontitis discovered that all six teeth showed resolution of periapical radiolucencies, and three showed root development.
Several studies have shown the effect of TAP in controlling endodontic flare-ups34 in diabetic patients between treatment appointments. Interestingly, TAP has shown to be more effective than calcium hydroxide in these patients.35 The combination of the three existing antibiotics seems to be able to defeat bacterial resistance and subsequently result in increased antimicrobial action.36 The anti-inflammatory ability of minocycline can synergistically assist in treating the disease.
Conclusion
If endodontics is to succeed, root canal microbiota should be properly reduced. Endodontic treatments rely mainly upon the elimination and possible eradication of the involved microbiota and their various virulent features from the root canal system. Biomechanical instrumentation, though an essential step, does not always provide such an environment in the root canal system. Non-instrumentation methods such as tooth repair and strategies towards maintaining a situation for regeneration and revascularization of the pulp should be considered, in which local use of drugs, particularly antibiotics, has shown their significance. Among the combination of antibiotics, TAP, owing to its effectiveness on different microorganisms and its diverse applications and triumphs, is of particular interest in endodontics. However, development of resistant bacterial strains and tooth discoloration are some of its pitfalls. Nonetheless, TAP seems to be a successful combination of drugs in root canal disinfection, possible coronal canal sterilization, and pulp regeneration and revascularization protocol. All currently available antimicrobial materials for radicular irrigation and medication have their own benefits and limitations; the search for creating the ideal irrigant and inter-appointment medicament continues.
EP
16 Endodontic Practice US Volume 16 Number 2 RESEARCH
References available online or upon request.

“It’s a partnership of specialists and we are all specialty strong.” - Partner Doctor (2022) 305 - 206 - 7388 | Specialty1partners.com YOUR SPECIALTY IS OUR SPECIALTY. The Only Doctor-Founded, Doctor-Led Specialty Partnership Organization.
The power of investing in technological advancements in endodontics

Dr. Anne Wiseman shares her experience of differentiating herself through innovation
Some patients experience feelings of anxiety or dread when visiting a dentist or endodontist, underscoring the importance of creating a patient experience that is exceptionally comfortable and soothing. When I designed my office, I worked with an interior designer to make it feel more like a spa retreat than a dental office. I heavily invested in creating a welcoming space for patients, incorporating features such as a massage chair in the waiting room, a fireplace, live flowers, noise-canceling headphones for a ceiling mounted TV, weighted blankets, a therapy dog, and soothing ice packs for after appointments.
That said, creating the ideal patient experience isn’t just about ambiance. For me, it’s also about investing in advanced technologies that streamline my practice and enhance patient care.
Investing in the right technology
It’s exciting to invest in the latest gadgetry, especially if it can significantly improve practice workflows, cut down on procedure times, reduce repeat visits, and more. In turn, this improves the overall experience for patients.
The key to identifying the right technology is to prioritize what capability you would most like to gain or enhance. Do your due diligence to ensure that there is solid foundation of scientific evidence that proves effectiveness before investing. In my practice, I’ve implemented a variety of technologies including:
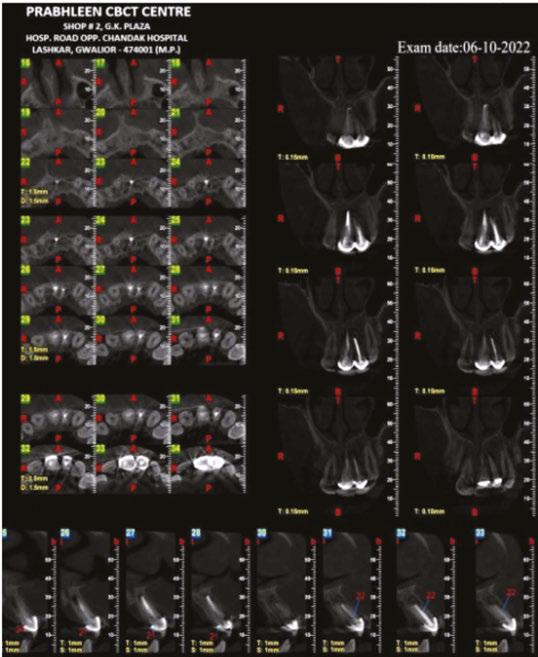
Radiograph of a 30-year-old male who presented with pulp necrosis and symptomatic apical periodontitis. The canals were very long and dilacerated. Dr. Wiseman performed minimal instrumentation in this case due to the dilacerated and calcified canals. The GentleWave procedure was completed. Radiographs viewed are the preoperative 2D and 3D images and the postoperative image. The final radiograph reveals sealer flowing into the isthmus between MB1 and MB2


• J. Morita F40 CBCT for high-resolution, three-dimensional imaging
• Global A Series™ microscopes, magnification for enhanced precision
Anne Wiseman, DDS, MSD, completed a Bachelor of Science at the University of Nebraska at Kearney. She joined the US Navy in 2002 and in 2005, earned her Doctor of Dental Surgery degree at the University of Nebraska Medical Center in Lincoln, Nebraska. She was then stationed in San Diego, California. After completing a 1-year advanced education in general dentistry, she was stationed at Camp Pendleton, California. She found great reward in the field of endodontics as it alleviated patient’s pain at a crucial point in their life — prior to their deployment. After an honorable 3-year tour in the Navy, she made the decision to further her education in the specialty of endodontics. Dr. Wiseman completed a 26-month post-graduate residency earning a Master of Science in Endodontics from the University of Washington. She then completed a 1-year surgical implant fellowship at Loma Linda University. She is Board-certified and practices in Sioux Falls, South Dakota.
Disclosure: Dr. Wiseman is a KOL for Sonendo®
• The DEXIS™ NOMAD™ system, a portable x-ray system
• The DentalVibe®, for anxiety-free dental injections
• The GentleWave® System from Sonendo®, an advanced technology for root canal treatment
The importance of understanding the technology
Working in dentistry can be both challenging and humbling. Almost every endodontist has worked through a time when they believed they could do something easily, but it turned out to be much more complicated than they originally anticipated. Dental technology earns its stripes in instances like this. Endodontists and their technology partners help inspire and develop instruments to successfully navigate the myriad complexities of saving teeth.
And while innovative technology can certainly make things simpler, it’s important to keep in mind that there is still a lot of activity that happens behind the scenes. With this, endodontists and their teams must dedicate time and resources to understanding how to properly use the technology that they’ve invested in and how to best integrate it into their practice workflows.
18 Endodontic Practice US Volume 16 Number 2 TECHNOLOGY
Dr. Wiseman performing the GentleWave procedure on a patient while he watches TV mounted on the ceiling


Summer2023 Vol16 No2 endopracticeus.com Irrigation&Obturation n 4 CE CreditsAvailable inThis Issue* California Dreamin' Dr.ReidPullenhelpsnewassociate Dr.AllenAbrishamitoaccomplishgoalsthroughmentorship Theimportanceofsuturing indentalimplantsurgery Dr.StevenVorholt Dental sedation: an overview Dr.BrianMcGue Expandingendodontic treatments and procedureswith dental lasers Dr.FernandoMeza ENDODONTICS Communicating periodontalissuesacross dentalimplantplatforms Drs.StuartSegelnickand MeaA.Weinberg Dentalinfections,part2 —prophylaxis:helpavoid antimicrobial resistanceWiyannaK.Bruck,PharmD, andJessicaPrice Practicespotlight Dr.JasonPutnam:owninghisfuture Winter2022 Vol15 No4 endopracticeus.com Implant&EndoConnection n 4 CE CreditsAvailable inThis Issue* JudyMcIntyre, DMD,MS 1 year print $149 1 year digital only $79 Connect. Be Seen. Grow. Succeed. | www.medmarkmedia.com Address the Endodontic Complexities You Face Everyday with... 3 EASY WAYS TO SUBSCRIBE VISIT www.endopracticeus.com EMAIL subscriptions@medmarkmedia.com CALL 1.866.579.9496 SUBSCRIBERS BENEFIT FROM: 16 continuing education credits per year Clinical articles enhanced by high-quality photography Analysis of the latest groundbreaking developments in dentistry Technology reviews of the latest products Practice management advice on how to make endodontics more profitable Real-life profiles of successful endodontic practices Endodontic Practice US 4 Issues • • • • • • • • • • • • 16 CEUs
In a similar vein, endodontists should always be prepared to explain a new technology to their patients. While many patients aren’t eager to know all of the details, there are circumstances under which a patient may ask how a technological process works and its benefits. I build rapport with each patient to discern how granular an explanation they need for peace of mind. Sharing details with curious patients can help answer questions and curb worries or anxieties. Some patients even want to watch the procedure! The video camera on the Global A Series microscope can beam the procedure to the ceiling-mounted TV, so they can witness their tooth being saved in real time.
Overall patient sentiment
My patients have an overwhelmingly positive response to the technology I’ve incorporated into my office.
Integrating CBCT into my practice has greatly increased diagnosis accuracy and case treatment planning strategy; resulting in heightened effectiveness and faster healing times. Patients love viewing CBCT images of their teeth! It opens up a whole new world of understanding about their dental health.
The NOMAD system enables more mobility and efficiency, as I am no longer confined to the limited movement of a wall-mount unit. Patients are impressed with digital technology and the speed at which the radiographic images of their teeth can be visualized and shared among providers. We always share these high-resolution images with their dentist in a detailed treatment report.
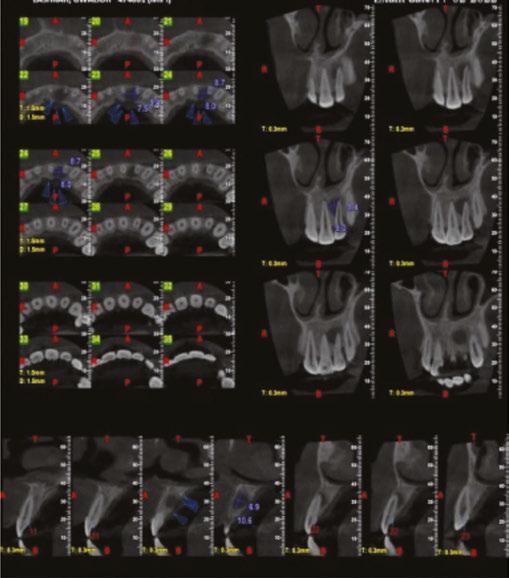
Radiographs of a 61-year-old female who presented with pulp necrosis and asymptomatic apical periodontitis. Dr. Wiseman performed minimal instrumentation in this case due to the dilacerated and calcified canals. The mesial canal has a 45 degree curvature in the apical 1/3 of the root. The GentleWave procedure was completed. Radiographs viewed are the preoperative 2D and 3D images and the postoperative image




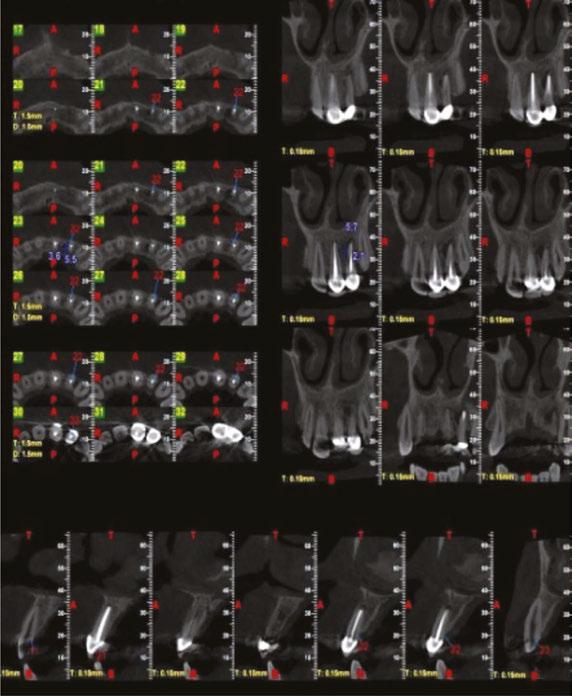
Radiographs of an 80-year-old male who presented with pulp necrosis and asymptomatic apical periodontitis. Dr. Wiseman performed minimal instrumentation in this case due to the dilacerated and calcified canals. The mesial canal has a 45 degree curvature in the apical 1/3 of the root. The GentleWave procedure was completed. Radiographs viewed are the preoperative 2D and 3D images and the postoperative image

I have integrated a customized anesthesia technique to minimize discomfort during the dreaded numbing portion of the appointment. I often have patients ask me what I am doing while numbing them, as it is so comfortable they may not even know that the numbing process is taking place. The DentalVibe technique provides a nice distraction so patients don’t have to feel the injection discomfort associated with anesthesia.
Radiographs of a 15-year-old male who presented with previous treatment and asymptomatic apical periodontitis. When Dr. Wiseman removed all the gutta percha, the mesial canals were blocked. The GentleWave procedure was completed. The final radiograph reveals sealer that was able to flow into the apical 1/3 of the mesial roots. Radiographs viewed are the preoperative 2D and 3D images and the postoperative image



Root canals are perhaps one of the most dreaded procedures among patients, even causing some to delay necessary treatment. To help combat this, I utilize the GentleWave System, a technology that enables a minimally invasive procedure. My patients have been pleasantly surprised by the fast recovery time – some have even found it hard to believe that they’ve had root canal therapy at all. Many patients even fall asleep during treatment, which is a testament to my team and these technologies working seamlessly together.
Our Google reviews validate the comfort our patients experience from the technologies we’ve utilized. Our schedule reflects the successful case outcomes utilizing this array of innovation that our referring doctors have come to expect.
What next?
Make sure to ask the important questions before committing to a technology, and evaluate whether it’s the best move for your business at that moment in time. As a practice owner, don’t be
impulsive. Be sure to inquire about costs of disposables and any extended maintenance and warranty plans. Keep in mind that investing in new technology might not be right for every practice at every stage of growth. As your business continues to expand, using advanced, effective technological instruments is an impactful way to enhance what matters most – patient care –and differentiate your office from others.
As innovative technologies continue to emerge, it’s essential that endodontists work diligently to vet what is fad and what is the future. I believe there can be a misleading narrative that with the use of technology, all procedures, like root canals, are easy now. In reality, all of the technologies I use work in concert with each other and my team. They do not negate the fundamentals of dentistry; case selection, clinical acumen and academic rigor will always win the day. For providers, keeping your sword sharp with continuing education is ultimately the best investment you can make.
If you’re interested in learning more about how I maintain an inviting office, the benefits of our technologies and more, you can visit my website at https://www.wisemanendo.com/.
20 Endodontic Practice US Volume 16 Number 2 TECHNOLOGY
EP
Do what you do best and we’ll handle the rest. We aren’t your typical DSO. When you partner with HighFive Healthcare, you join an exclusive network of top endodontists dedicated to exceptional patient care. Our doctor-owned practices and seasoned team of experts nurture a fun and collaborative culture like no other. While we optimize and scale the business side of endodontics, clinical autonomy is left in your skilled hands. Together, we’ll help you take ownership of something bigger than a single practice and support you as you create your own tomorrow.
Learn more at high5health.com

RECRUITING | SCHEDULING OPTIMIZATION | SCALABILITY | BRANDING & MARKETING | PAYROLL | IT SERVICES | AND MORE
Most endodontists have to master multitasking. Ours just have to master root canals.
The importance of suturing in dental implant surgery
Dr. Steven Vorholt explores the many aspects of suturing for implant procedures
Editor’s note: In recognition of our editorial focus on implants, we offer an article that provides an overview of suturing techniques during implant procedures.
Suturing and incision design are the bookends to a successful implant surgery. With either of the bookends done poorly, the entire surgery is at risk. While surgical suturing may seem like a topic for beginners only, it is important to revisit and have a firm grasp so you can build on these basics for the benefit of your patients. The three suturing techniques discussed in depth in this continuing education article form the basis for all dental implant suturing. You must be a master of these techniques before you can adequately grow into the master implantologist.
There are several suturing techniques that can be used in dental procedures, each with its own advantages and disadvantages. In this article, we will discuss the benefits of the top three dental suturing techniques: simple interrupted sutures, interlocking continuous sutures, and horizontal mattress sutures and also discuss the types of dental sutures commonly used.
Suturing is the process of closing the wound after dental implant surgery. The sutures help to hold the gingiva in an ideal place, promote healing, and prevent infection. The proper technique and choice of suture material can significantly impact the success of the implant. Proper suturing is essential after dental implant surgery for the following reasons:
1. Promotes healing: Proper suturing helps to keep the implant in place and allow the surrounding tissues to heal properly.
2. Reduces the risk of infection: Suturing helps to close the wound and prevent bacteria from entering the surgical site, reducing the risk of infection. Proper suturing techniques and the use of sterile materials can help to minimize the risk of postoperative infection.
3. Minimizes discomfort and bleeding: Good suturing techniques can help to minimize postoperative discomfort and bleeding, which are common after dental implant surgery. Proper suturing can also reduce the need for pain medication and promote a faster recovery.
Choosing the right suture material
Choosing the right suture material is essential for the success of the implant. The ideal suture material should be strong,
Steven Vorholt, DDS, FAAID, DABOI, practices exclusively as a traveling dental implant surgeon in Phoenix and Tucson, Arizona. He has completed his Fellow in the AAID and earned his Diplomate in the ABOI. For more information on his lecturing and clinical practice, visit www.stevenvorholtdds. com. Dr. Vorholt also authored a guest chapter in a new book by Drs. Bart Silverman and Richard Miron called Modern Implant Dentistry, published summer 2023 by Quintessence Publishing. http://www.quintpub.com/
Educational aims and objectives
This self-instructional course for dentists aims to provide an overview of the benefits of the top three dental suturing techniques the types of dental sutures commonly used for implant procedures.
Expected outcomes
Endodontic Practice US subscribers can answer the CE questions by taking the quiz online at endopracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
• Identify why proper suturing is essential after dental implant surgery.
• Realize some characteristics of ideal suture material for certain types of procedures.
• Identify the armamentarium of instruments needed for suturing.
• Realize some techniques for suturing.
• Observe a patient case that uses the top three techniques.
2 CE CREDITS
flexible, and biocompatible. There are several types of suture materials available, including:
1. Non-absorbable sutures: Non-absorbable sutures are made of materials that do not break down in the body and must be removed after the wound has healed. Examples of non-absorbable sutures include silk, nylon, and polypropylene.
2. Absorbable sutures: Absorbable sutures are made of materials that break down in the body over time and do not require removal. Examples of absorbable sutures include gut and polyglycolic acid.
3. Monofilament: Monofilament sutures have smooth microstructure and therefore prohibit or vastly lessen bacterial migration along the length of the suture.
4. Braided: Braided sutures are more apt to allow migration of bacteria and oral fluids and have a higher likelihood of infections. However, braided sutures are easier to throw secure knots and maintain knot stability.
The choice of suture material will depend on the location of the implant, the type of surgery performed, and the patient’s individual needs. It is essential to choose a suture material that is biocompatible and suitable for the specific procedure.1
Armamentarium
The armamentarium for suturing varies based on the surgeon’s preference and the type of suturing being attempted.
22 Endodontic Practice US Volume 16 Number 2 CONTINUING EDUCATION
Generally, it involves a needle holder, tissue forceps, and scissors. Each of these tools has several variations available to the implant surgeon.2
Needle Holders
Needle holders are instruments for gripping, driving, and grabbing suture needles. Not to be confused with hemostats which are generally more aggressively toothed instruments meant for hemostasis control, needle holders are often cross-hatched to allow gentle but firm control of the suture needle itself (Figure 1). The needle should be held ½-⅔ the way back towards the swage (the connection point on the suture and needle) on the body of the needle. Care should be taken to avoid grabbing the needle on the swage to avoid breaking the thread free, and care should be taken to avoid grabbing the needle by the point to avoid breaking, bending, or dulling the needle.
Insertion of the suture needle into the tissue should be perpendicular to the tissue for maximum cutting efficiency. Approaching the tissue at an acute angle can lead to shallow bites, torn tissue, and poor adaptation of the incision line. Needles should not be pushed through tissue but turned through with the wrist movement to allow for maximum cutting efficiency. When the needle exits the tissue, it should not be grabbed by just the tip of the needle; this may blunt or bend the needle tip leading to poor future bites and trauma to the tissue.3
Traditional needle holders have finger-ring handles and are available in differing lengths and tooth patterns. The needle holder is held in balance with the thumb and ring finger in the finger-rings and the middle and index finger stabilizing and guiding the passage of the needle through tissue.
Locking needle drivers come in two main varieties, the Mathieu (and variations) and the Castroviejo (Figure 2). Both needle drivers allow the surgeon to gently engage the auto-locking and unlocking portion of the instrument for better handling. The Mathieu-style needle holder is held in a palm grasp and is generally meant for use with thicker tissue and suture materials, while the Castroviejo is a more delicate instrument more widely used with finer suture materials 5-0 and thinner. The Castroviejo is held in a pen-grasp.
Tissue Forceps (Figure 3)





When engaging tissue margins for accurate suturing, the more mobile tissue should be engaged first, and the more secure tissue should be engaged second. A popular idiom to remember this is to “bring the ship to shore.” Bites should be equidistant depths from the incision line on either side of the incision to ensure equal pressure along the incision line. Tissue forceps can help stabilize mobile tissue for the initial bite and also help in retraction of more secure tissue.
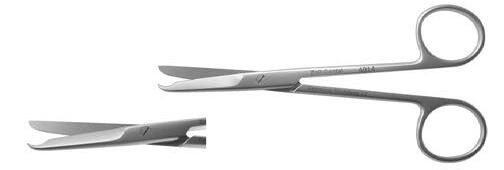
Scissors
Any type of dental scissors can be used for suture removal and trimming, though several variations are available to help overcome common issues — longer scissors, angled cutting blades, hooked tips to facilitate embedding suture removal, etc. (Figure 4). Scissors should be maintained with adequate sharpness to avoid splitting or fraying sutures or accidentally pulling delicate sutures.



23 endopracticeus.com Volume 16 Number 2 CONTINUING EDUCATION
Figure 1: Needle holders have cross-hatch patterns for grabbing needles, differing from hemostats which have aggressive teeth for clamping vessels, but are routinely incorrectly utilized for needle driving. The tool on the left is the hemostat
Figure 2: Locking needle drivers Castroviejo and Mathieu styles allow for more precise control with smaller diameter suture materials
Figure 4: Suture scissors have different angles for easy access to hard-toreach areas of the mouth. Hooked variations help to cut sutures at follow-up appointments by facilitating gently getting underneath the suture at the healed site. All intruments shown are from Zoll Dental
Figure 3: Tissue forceps have many varieties for different levels of access, tissue control, delicacy of the tissue being held, and features like suture slots
The length the suture “ears” should be cut is determined by the location, suture material, and surgical technique employed. Sutures with high shape memory should be cut longer to avoid irritation to the adjacent oral tissues and avoid early unraveling of the knots. Suture materials with low shape memory and braided materials can generally be cut shorter and maintain knot stability and low irritation. Approximately 3 mm to 5mm of ear length is acceptable and works well in most clinical situations.
Top three suture techniques
Simple Interrupted Sutures
Simple interrupted sutures are the most commonly used suturing technique in dental procedures (Figure 5). This technique involves placing individual sutures at regular intervals along the wound edge and tying each stitch separately. Simple interrupted sutures are easy to place and provide excellent wound closure.
Benefits of simple interrupted sutures
1. Precise wound closure: Simple interrupted sutures provide precise wound closure, ensuring that the edges of the incision are well approximated.
2. Reduced tension: These sutures help to distribute the tension evenly along the incision, reducing the risk of wound dehiscence and promoting faster healing.
3. Versatility: Simple interrupted sutures can be used in a variety of dental procedures, including extractions, flap surgeries, and implant placements.
Technique
1. Begin in the middle of the wound with the first stitch (bisecting incision technique) to ensure the wound margins are adapted correctly along the length of the incision.4
2. Take a 2 mm to 4 mm bite from the wound margin starting with the more mobile tissue (typically the buccal), and take another bite directly across the wound margin to the same depth as the first bite. This ensures equal tension on either side of the wound.


3. Begin the suture throw with a surgeon’s knot (2 forward, 1 backward) to cinch the knot and stabilize the suture. Add additional throws as necessary depending on the suture material chosen.5
4. Cut the ears of the suture 5 mm minimum to avoid early untying of the suture material. Stiffer suture material should have the ears trimmed longer to avoid causing the patient pain postoperatively.
5. Continue throwing simple interrupted sutures 3 mm to 5mm apart until the length of the incision is closed.

Interlocking continuous sutures
Interlocking continuous sutures are a variation of the continuous suturing technique (Figure 6). This technique involves placing a continuous suture along the wound edge and interlocking the stitches at regular intervals. Interlocking continuous sutures provide excellent wound closure and reduce the risk of suture failure.
Benefits of interlocking continuous sutures
1. Reduced risk of suture failure: Interlocking continuous sutures distribute tension more evenly along the incision, reducing the risk of suture failure and promoting faster healing.
2. Efficient placement: This technique is faster to place than simple interrupted sutures, reducing the time required for the suturing process.
3. Reduced trauma: Interlocking continuous sutures reduce trauma to the tissue by minimizing the number of times the needle passes through the tissue.
24 Endodontic Practice US Volume 16 Number 2 CONTINUING EDUCATION
Figures 5A and 5B: Simple interrupted sutures are the simplest and effective in quickly approximating tissue
Figures 6A and 6B: Examples of interlocking continuous sutures, convenient for longer span surgical sites for more efficient closure in time and suture material
Technique
1. Beginning at the most posterior segment of the incision, throw a simple interrupted suture and leave the knot placed buccal to the incision line.
2. Trim the tail only; do not cut the length with the suture needle.
3. Take an equal bite 3 mm to 5 mm more anterior to your initial bite.
4. Prior to cinching the loop, twist the loop 1 to 2 times (depending on suture material — sutures with less friction, i.e., PTFE, can be twisted more than braided sutures, i.e., PGA) and pass the needle through the loop.
5. Carefully cinch the new segment of suture material and align the interlocking knot buccal to the incision line.
6. Complete throws and interlocking loops along the length of the incision until reaching the end. Leave the loop long enough to tie to, and cut all 3 suture ears to appropriate length for suture security and patient comfort.
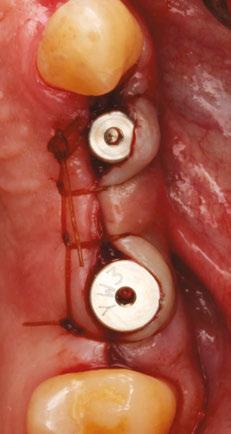
Horizontal mattress sutures
Horizontal mattress sutures are a technique used to close wounds under tension, such as those in the oral cavity. This technique involves placing stitches parallel to the incision, with each stitch passing through the tissue on either side of the incision (Figure 7). The mattress is typically the first suture throw to help close a wound, finished with either of the two previously dis-
cussed techniques. Its ability to reduce tension vectors across the incision line is key to its success in postoperative implant surgery.
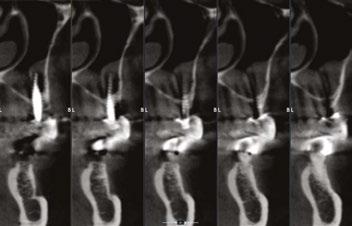
Benefits of horizontal mattress sutures
1. Effective at closing wounds under tension.
2. Minimal tension on the wound edge.
3. Reduces the risk of wound dehiscence.
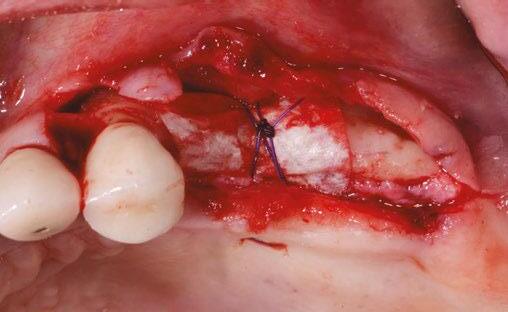

4. Helps to maintain downward pressure on a membrane and bone graft.
Technique
1. Begin with a bite 7 mm to 10 mm apical to the incision line (typically at the mucogingival junction) on the distal buccal of the incision.
2. With your next bite, exit the lingual tissue at similar depth to the initial buccal bite.
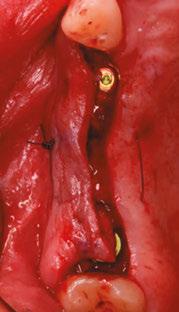
3. Re-bite the lingual tissue 5 mm to 10 mm mesial at the same depth.
4. Exit the buccal tissue perpendicular to the third bite — the four bites now forming a square with two threads crossing the crest/membrane.
5. Tie with a surgeon’s knot and any additional throws as needed depending on the suture material.
Building on the basics
Let’s review a recent case that showcases the rationale and techniques of the top three. It is common to utilize several suturing techniques in surgical closure, especially in larger grafting cases. In the following case, a lateral sinus lift was performed, and all three techniques were used to their full effect. Simple interrupted sutures are used to close small incisions and place tissue margins accurately back in place; horizontal mattress sutures are used to hold membranes in place and relieve tension over the incision line, and running interlocking continuous sutures are used to close longer incisions with watertight closure for maximum healing potential via primary closure.
A patient presented with a failing bridge on the upper left that is supported by three mini implants. The implants directly perforate the sinus and only ~2mm of residual bone height remains on the crest (Figure 8). The mini implants were removed, and a

25 endopracticeus.com Volume 16 Number 2 CONTINUING EDUCATION
Figures 7A and 7B: Horizontal mattress sutures are useful for helping to secure membranes in grafting situations and relieving tension in longer span incisions
Figures 8A and 8B: The pre-op condition of the patient with mini implants engaging minimal bone and perforating the sinus. The patient’s implant supported bridge was loose and causing discomfort
Figure 9: A periosteal biting mattress engages only the periosteum in the buccal vestibule and exit and re-enters on the lingual tissue, helping to secure the membrane tightly over the window and crest
Figure 10: Simple interrupted, papilla sling, and horizontal mattresses can be seen to achieve primary closure without any sutures over the main body of the incision. Passive closure requires that closure is obtainable without tension directly over the incision line, as seen here

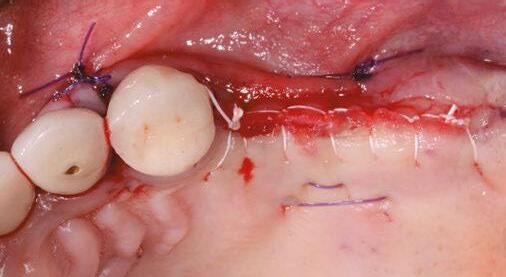
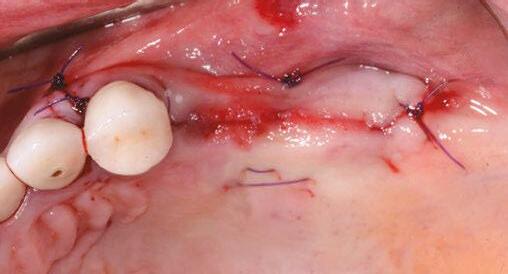
lateral window sinus lift was performed. Over the window and crest, a pericardium membrane was positioned to close all perforations into the sinus. Pericaridum membranes are resorbable membranes made from either human or porcine pericardium. The tissue that surrounds the heart is known to be extremely resistant to tearing (a leading reason for pericarditis being potentially fatal), and facilitates great handling properties as a dental material. It can be easily tacked or sutured, and maintains its shape memory for ease of placement over a defect. A periosteal-biting mattress suture is thrown first to help pin the membrane down on the buccal plate and crest (Figure 9). Next, simple interrupted sutures are used to put the vertical incision in the posterior back in position and the vertical incision in the anterior. Third, a papilla sling is used mesial to tooth No. 11 to tightly reposition the gingiva around the canine. A papilla sling suture functions by using a tooth as a pivot point to “sling” around and help reapproximate tissue. Only the buccal papilla are engaged, and the suture is passed underneath proximal contacts (if necessary) to facilitate wrapping around the lingual of the tooth. This suture is very useful for coronally advancing flaps or maintaining the coronal position of papillas after flap release. Fourth, a horizontal mattress suture is placed at the depth of the mucogingival junction to help approximate the flap margins, relieve tension at the incision line, and evert the tissue (Figure 10). Lastly, a PTFE running double-interlocking continuous suture is used to complete the final closure of the surgical site (Figure 11).
Two weeks post-op photos show great tissue response and health thanks in large part to meticulous suturing of the case (Figure 12).
Conclusion
Proper suturing technique is essential for successful dental procedures. By understanding the benefits and techniques of the top three dental suturing techniques, dentists can choose the appropriate technique for each procedure and promote faster healing, reduce the risk of infection, and minimize discomfort and bleeding for the patient.
REFERENCES
1. Moy RL, Waldman B, Hein DW. A review of sutures and suturing techniques. J Derma-
tol Surg Oncol. 1992 Sep;18(9):785-795. doi: 10.1111/j.1524-4725.1992.tb03036.x. PMID: 1512311.
2. Yag-Howard C. Sutures, needles, and tissue adhesives: a review for dermatologic surgery. Dermatol Surg. 2014 Sep;40 Suppl 9:S3-S15. doi: 10.1097/01.DSS. 0000452738.23278.2d. PMID: 25158874.
3. Moy RL, Lee A, Zalka A. Commonly used suturing techniques in skin surgery. Am Fam Physician. 1991 Nov;44(5):1625-34. PMID: 1950960.
4. Davis B, Smith KD. Oral Surgery Suturing. [Updated 2023 Jan 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www. ncbi.nlm.nih.gov/books/NBK572089/.
5. Romeo A, Rocha CL, Fernandes LF, Asencio FA, Zomer MT, Fujimoto C, Ussia A, Wattiez A, Koninckx PR, Kondo W. What is the Best Surgeon’s Knot? Evaluation of the Security of the Different Laparoscopic Knot Combinations. J Minim Invasive Gynecol. 2018 Jul-Aug;25(5):902-911. doi: 10.1016/j.jmig.2018.01.032. Epub 2018 Feb 5. PMID: 29421249.

26 Endodontic Practice US Volume 16 Number 2 CONTINUING EDUCATION
EP
Figure 11: Final closure finished with interlocking continuous PTFE sutures for watertight secure closure
Figures 12A and 12B: Two week post-op reveals minimal erythema and maintained tissue closure
Continuing Education Quiz
The importance of suturing in dental implant surgery
VORHOLT
1. Sutures help to _________.
a. hold the gingiva in an ideal place
b. promote healing
c. prevent infection
d. all of the above
2. The ideal suture material should be ________.
a. strong
b. flexible
c. biocompatible
d. all of the above
3. Monofilament sutures have and therefore prohibit or vastly lessen bacterial migration along the length of the suture.
a. smooth microstructure
b. rough microstructure
c. multiple filaments
d. braided structure
4. (Regarding insertion of the suture needle into the tissue) Approaching the tissue at ______ can lead to shallow bites, torn tissue, and poor adaptation of the incision line.
a. an acute angle
b. an obtuse angle
c. a right angle
d. reflex angle
5. The Castroviejo-style needle holder is held in a palm grasp and is generally meant for use with thicker tissue and suture materials, while the Mathieu is a more delicate instrument more widely used with finer suture materials 5-0 and thinner.
a. True
b. False
6. Sutures with _______ should be cut longer to avoid irritation to the adjacent oral tissues and avoid early unraveling of the knots.
a. a braided shape
b. low shape memory
c. high shape memory
d. a rougher texture
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://endopracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://endopracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 690
Date Published: June 16, 2023
Expiration Date: June 16, 2026
2 CE CREDITS
7. ________ help to distribute the tension evenly along the incision, reducing the risk of wound dehiscence and promoting faster healing.
a. Simple interrupted sutures
b. Interlocking continuous sutures
c. Horizontal mattress sutures
d. Purse-string sutures
8. With simple interrupted sutures, cut the ears of the suture 5 mm minimum to avoid early untying of the suture material.
a. True
b. False
9. __________ reduce trauma to the tissue by minimizing the number of times the needle passes through the tissue.
a. Simple interrupted sutures
b. Interlocking continuous sutures
c. Horizontal mattress sutures
d. Buried sutures
10. _________ help to maintain downward pressure on a membrane and bone graft.
a. Simple interrupted sutures
b. Interlocking continuous sutures
c. Horizontal mattress sutures
d. Subcutaneous sutures
To provide feedback on CE, please email us at education@medmarkmedia.com
Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
27 endopracticeus.com Volume 16 Number 2 CONTINUING EDUCATION
Dental sedation: an overview
Dr. Brian McGue discusses how sedation can affect patients and dentists

Sedation of dental patients is not a new concept. Dentists in the United States have been sedating patients for more than 150 years. In the mid-19th century, Horace Wells and William T.G. Morton were dentists who demonstrated that the perioperative use of sedation for dental procedures was beneficial.1 Wells attempted to demonstrate the use of inhaled nitrous oxide as a sedative for a dental extraction at the Massachusetts General Hospital in 1845. Though the sedation Wells performed was not deemed a success, Morton was very successful a year later, again at the Massachusetts General Hospital, while sedating a patient with ether.
At the beginning of the 20th century, sedation of patients for medical procedures became more widespread, and the medical specialty of anesthesiology was created. Technical advances coupled with scientific research and discoveries in pharmacology advanced sedation to become a safer and more predictable procedure. The overwhelming use of sedation, however, was in the field of medicine. Outside the widespread use of intravenous sedation by oral surgeons, dentists generally did not use sedation techniques beyond the use of nitrous oxide for very lightly inhaled anxiety control.
Dentists began to do more sedation in the 1990s when oral conscious sedation began to become popular.2 The use of an orally administered sedative pre- or peri-operatively became widespread for dentists to alleviate anxiety during dental procedures. The nature of current dental practice appears to be evolving to a more surgical focus with the accelerated use of implants. With this evolution, the use of sedation has become prevalent as dentists strive to make their patients more comfortable during these surgical procedures.
The increased use of sedation by dentists can be attributed to many factors. Some of these factors are obvious and some are not. This article will try to address some of these reasons.
Educational aims and objectives
This self-instructional course for dentists aims to discuss the benefits of using sedation in the dental practice.
Expected outcomes
Endodontic Practice US subscribers can answer the CE questions by taking the quiz online at endopracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
• Realize some history of dental sedation.
• Identify reasons how dental sedation can increase patient comfort.
• Define anterograde amnesia from sedation and how this expands certain patients’ treatment options.
• Realize some reasons to decrease use of local anesthetic.
• Realize how using sedation can combat “compassion fatigue” in the dental office.
Why do we sedate patients?
Patient anxiety and comfort
Patient anxiety and comfort are the most obvious reasons for sedation. The American Dental Association estimates that 100 million Americans do not seek dental care.3 Severe debilitating fear of the dentist has been estimated to prevent 60 million people from entering a dental office. Sedation is a method for lowering this barrier and permits patients to receive dental treatment. If a dentist is attempting to build a patient base, this group of patients can be an aid in that endeavor.
Brian McGue, DDS, is a fulltime practicing general dentist with a private practice in Chesterton, Indiana. His practice has a comprehensive focus offering a variety of restorative and surgical treatments with an emphasis on full-mouth rehabilitation while using sedation for patient comfort. Dr. McGue and his wife, Susan, lecture on the topic of sedation and run hands-on workshops for dentists interested in incorporating oral and IV sedation into their practices at The Pathway in Tempe, Arizona (www.thepathway.com) and the 3-D Dentists facility in Raleigh, North Carolina, and Nashville, Tennessee (www.3ddentists.com). Together they have authored three textbook manuals on sedation. Dr. McGue is a fellow of the Academy of General Dentistry and a member of the American Dental Society of Anesthesiology, the International Anesthesia Research Society, and an educational member of the American Society of Anesthesiologists. Dr. McGue and Susan McGue can be reached at stayintheboxsedation@gmail.com.
Patients also have fear of specific dental procedures. The fear of some of these procedures can be understood. Third molar removals, implant procedures, multiple extractions, endodontic procedures, etc., can involve complex procedures, loud sounds, unpleasant sensations, and disconcerting instrumentation that can elevate a patient’s negative perceptions. However, the fear of some other procedures may not be as well understood by dental practitioners. From personal experience in my practice, two patients that we perform dental prophylaxis on every 6 months request sedation. Though many dental team members perceive receiving dental prophylaxis as a non-stressful, pleasant experience, there is a segment of the population that feels a sense of foreboding when they consider their routine dental prophylaxis.
Additionally, it may not be simply fear of a dental procedure that keeps a patient from seeking care — it may be the fear of sitting still for an extended length of time. Sitting in a dental chair with one’s mouth open for an extended time may be a source of stress for some people. Sedation helps with this because many of
28 Endodontic Practice US Volume 16 Number 2 CONTINUING EDUCATION
2 CE CREDITS
the sedation medications used in the dental office can cause the sensation of time compression. A 2-hour procedure can feel like a 15-minute procedure for a sedated patient.
Primum non nocere (First do no harm)
As health care providers, we have an ethical responsibility to not harm a patient. Iatrogenic injuries can occur in the dental office — most dental practitioners have inadvertently caused a minor injury to a patient. Nicking a tongue with a bur, retracting a patient’s cheek too aggressively, or having a tissue flap tear while reflecting are all examples of minor injuries that can occur but most likely do not have any long-term effects. Some injuries though are not obvious or even physical.
Mental trauma can occur from dental treatment. As mentioned before, dental procedures, even procedures that appear non-threatening, can create a lot of anxiety for patients. Most dentists can relate to having to manage an extremely fearful patient who had a previous negative dental experience. As dentists, it behooves us not to be the practitioner who created the negative experience that so traumatized a patient that he/she avoided dental care for years.
Anterograde amnesia
The primary class of medications used in sedation dentistry is benzodiazepines. Benzodiazepines are known to cause anterograde amnesia. Anterograde amnesia is the loss of memory of during the time the patient is under the influence of a certain medication. Patients simply don’t remember the procedure for which they were sedated. Many patients are happy with not having memory of the procedure. This type of patient arrives for the appointment, goes to “sleep,” and “wakes” up after the procedure is concluded. Almost all sedations done in dental offices are conscious sedations where the patient is awake and responsive so the patients are not asleep even though many think they were.
Anterograde amnesia can be a practice builder. If a patient has a painful tooth, and the dentist is able to sedate them, do an endodontic procedure, and a CAD/CAM crown during the sedation, the patient can emerge from the sedation with an asymptomatic white tooth. These patients will tell other potential patients about their positive experience and help build your practice.
Decreased use of local anesthetic
When we train dentists to perform sedations, we encourage the use of online services that check the patient’s own medications against the administered sedation medications for interactions and also the local anesthetics we are intending to use on the patients. Many of the attendees at our courses are surprised by the lack of interactions with sedation medications but are more astonished by the significantly higher number of interactions between the patient’s medications and the local anesthetics.
Many local anesthetics are vasoconstrictors and can cause an increase in heart rate and blood pressure. Physiologically, these changes can be detrimental to the patient and can precipitate a medical crisis. As dentists, one of our goals in treating patients is to try to reduce inherent risks for the patient. Sedation is one method of lowering how much local anesthetic we are required to use to properly anesthetize a patient for a procedure.
An article written by J.B. Murray in the Journal of Psychology in 19714 looked at decades of psychological research and was able to definitively conclude from his research that apprehensive patients have a lowered threshold of pain. In other words, a nervous patient will feel pain quicker and at lower stimulus levels then a non-anxious patient. As dentists, we already inherently know this. In the dental chair, it is the nervous patient that is harder to numb.
Prior to Murray’s article, there had already been connections made between the perception of pain and apprehension. In his 1960 book, Pyschophysiologic Approach in Medical Practice, William Schottstraedt5 theorized that pain and apprehension have a circular relationship. Pain causes apprehension, apprehension heightens one’s perception of pain, which then causes more apprehension.
If we can break the chain of apprehension through sedation, then we can lower the patient’s perception of pain, and thus, use less local anesthetic.
Higher quality of dentistry
Can the patient’s behavior negatively impact the quality of dentistry a dentist is trying to provide? As dentists, we all will answer “yes” to this question. We have all had the apprehensive patient who will not listen to our instructions, sit still during the procedure, and/or be overly dramatic when they perceive they’ve felt something.
By removing a patient’s negative behavior from the equation, the dental team can focus on the technical aspects of the procedure. One can equate this to placing an isolation device to get better visualization on the area we are treating. Another analogy

29 endopracticeus.com Volume 16 Number 2 CONTINUING EDUCATION
Figure 1: Sedation can be part of any dental practice
is using a surgical guide to place an implant. The guide is just another tool we can pull off of our shelf in order to increase the level of the quality of dentistry we are providing. Similarly, sedation simply can be another tool to remove factors that may interfere with the quality of treatment.
Sedation enables the dental practitioner to perform and learn higher levels of dentistry

The profession of dentistry is unique and amazing. One of the reasons for this is the ability to continually expand and refine one’s clinical skills throughout a career. Very few professions are geared in this way. Continuing education courses offer a way to expand technical skills that can be honed with continued use of those new skills in practice.
Sedation is a tool that can be used in order to relax the patient, take their behavior out of the equation, and let the dental team focus on learning and refining these new skills. It has been said that “repetition is the moniker of learning.” Sedation is one way to have those early repetitions be in a lower stress environment for both the practitioner and the patient. This allows the dental team to focus on what they are learning in the early stages of their development.
Learning these higher levels of dental treatment is a win-win for both dentist and patient. For dentists, it can combat job burnout, promote long-term job satisfaction, and allow dentists to treat patients in a more comprehensive way. For patients, having the dentist able to perform higher levels of dentistry is advantageous because they can have most of their dental work done in one office and have more dentistry done in one appointment which helps them avoid multiple days off of work.
Compassion fatigue
Compassion fatigue is a clinical term that is applied to health care workers, educators, first responders, members of the clergy, and funeral home workers.6 For health care workers, there is a clear definition of compassion fatigue:
“The ‘cost of caring’ for others in emotional or physical pain. Defined as occupational burnout in conjunction with vicarious traumatic stress, which is caused by indirect exposure to stress. Finding emotional energy to calm and reassure apprehensive patients and maintain a confident demeanor while your patient is exhibiting fear or panic can be draining. The potential for negative energy transfer is substantial. Health care workers are generally very sympathetic and empathetic toward others. That is why they are in health care.”7
As dentists, we have all probably experience compassion fatigue at some point. I like to make the analogy that we all start the day with a large vat of compassion. Throughout the day, we ladle out compassion to whomever needs it. Eventually, toward the end of a long day at the dental office, the vat is dry. We leave the office and arrive home to our spouses, children, and/or pets, and many of them also want some love or compassion. Unfortunately, at this time of the day, the vat may be empty. Unchecked compassion fatigue can create burn-out, exhaustion, and mental illness.
Conclusion
Sedation can dramatically lower the amount of compassion a dental team has to ladle out because sedated patients are much less anxious.
Dentists have been sedating patients in their offices for a long time. In fact, in the early history of sedation and anesthesia, dentists were at the forefront of its development. In today’s modern dental practice, sedation has become widely used. For many dentists, it is a way to build a practice, expand their skills, and decrease their own stress level. The science of sedation will continue to evolve and most likely help to expand the options in the dental office.
REFERENCES
1. American Society of Dental Anesthesiologists. History. https://www.asda.org/ about-us-2/. Accessed April 17, 2023.
2. Donaldson M, Gizzarelli G, Chanpong B. Oral sedation: a primer on anxiolysis for the adult patient. Anesth Prog. 2007 Fall;54(3):118-28; quiz 129.
3. Beaton L, Freeman R, Humphris G. Why are people afraid of the dentist? Observations and explanations. Med Princ Pract. 2014;23(4):295-301.
4. Murray JB. Psychology of the pain experience. J Psychol. 1971 Jul;78(2d Half):193-206.
5. Schottstaedt, W. W. Psychophysiologic approach in medical practice. Chicago: The Year Book Publishers; 1960.
6. Cocker F, Joss N. Compassion Fatigue among Healthcare, Emergency and Community Service Workers: A Systematic Review. Int J Environ Res Public Health. 2016 Jun 22;13(6):618.
7. McGue, BC, Susan M. Oral Conscious Sedation. Stay in the Box Sedation [Course Manual]. 2021;(1), 4-5.
30 Endodontic Practice US Volume 16 Number 2 CONTINUING EDUCATION
EP
Figures 2A and 2B: 2A. Continuing education courses offer a way to expand technical skills. 2B. Dr. McGue and his wife, Sue, recently published a new Oral Conscious Sedation manual
Continuing Education Quiz
Dental sedation: an overview McGUE
1. In the mid-19th century, _____________ were dentists who demonstrated that the perioperative use of sedation for dental procedures was beneficial.
a. Horace Wells and William T.G. Morton
b. Ben Johnson and James Gutmann
c. Anton van Leeuwenhoek and Phillip Pfaff
d. Edwin Maynard and Edwin Truman
2. Severe debilitating fear of the dentist has been estimated to prevent ________ people from entering a dental office.
a. 500,000
b. 5 million
c. 60 million
d. 125 million
3. Third molar removals, implant procedures, multiple extractions, endodontic procedures, etc., can involve ________ and disconcerting instrumentation that can elevate a patient’s negative perceptions.
a. complex procedures
b. loud sounds
c. unpleasant sensations
d. all of the above
4. Dental procedures, even procedures that appear non-threatening, can create a lot of anxiety for patients.
a. True
b. False
5. ________ are known to cause anterograde amnesia.
a. Cepahlosporins
b. Benzodiazepines
c. Prilocaine
d. Pilocarpine
6. ________ is the loss of memory of during the time the patient is under the influence of a certain medication.
a. Transient Global Amnesia
b. Dissociative Amnesia
c. Anterograde Amnesia
d. Retrograde Amnesia
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://endopracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://endopracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 340
Date Published: June 16, 2023
Expiration Date: June 16, 2026
2 CE CREDITS
7. Many local anesthetics are vasoconstrictors and can cause an increase in heart rate and blood pressure.
a. True
b. False
8. A study by J.B. Murray in the Journal of Psychology noted that a nervous patient will feel pain ________ then a non-anxious patient.
a. quicker and at lower stimulus levels
b. more slowly and at lower stimulus levels
c. quicker and at higher stimulus levels
d. more slowly and higher stimulus levels
9. _________ is defined as occupational burnout in conjunction with vicarious traumatic stress, which is caused by indirect exposure to stress.
a. Traumatic Burnout Disorder
b. Dental Professional Stress Disorder
c. Compassion Fatigue
d. Emotional Energy Deficit Disorder
10. Sedation is a tool that can be used to __________.
a. relax the patient
b. take the patient’s behavior out of the equation
c. let the dental team focus learning and refining new skills
d. all of the above
To provide feedback on CE, please email us at education@medmarkmedia.com
Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
31 endopracticeus.com Volume 16 Number 2 CONTINUING EDUCATION
Endodontics and billing through medical insurance

Christine Taxin discusses several ways endodontists can bill through medical insurance

Endodontics has evolved over the past decade, and its applications continue to improve the quality of dental treatment. Endodontics involves either preserving part, or all the dental pulp in health, or removing all the pulp in irreversible disease. Not only does endodontics involve treatment when a dental pulp is present, but also includes preserving teeth which have failed to respond to non-surgical endodontic treatment, or for teeth that have developed new lesions, e.g., for when retreatment or periradicular surgery is required. With the advent of new developments in the field of endodontics, there are new and exciting ways to bill for medical including for:
• Acute alveolar abscess
• Root pulp damage
• Dental implant removal
There are reasons for adding medical billing with diagnostic codes; in fact, your updated ADA coding books have the diagnostic codes in them currently.
The changes in Medicare Advantage plans being supported by every insurance company may include dental treatments; however, if your patient only has medical, or you are told by dental plan to bill medical, what can you
do?
The insurance industry is changing its dental coverage to support the patient with additional hygiene visits and with the
Christine Taxin is the founder and president of Links2Success, a practice management consulting company to the dental and medical fields. Prior to starting her own consulting company, Taxin served as an administrator of a critical care department at Mt. Sinai Hospital in New York City and managed an extensive multi-specialty dental practice in New York. With over 25 years’ experience as a practice management professional, she now provides private practice consulting services, delivers continuing education seminars for dental and medical professionals and serves as an adjunct professor at the New York University (NYU) Dental School and Resident Programs for Maimonides Hospital.
Taxin is passionate about helping dental practices reach their highest potential and increase their profitability. In her consulting work, she focuses on helping practices strengthen their communication skills, their ability to work as a team and their capacity to set goals. As a provider of continuing dental education, Taxin has been a guest speaker for Henry Schein®, Kodak Dental, Sirona, and Goetze Dental. She has presented programs to the American Association of Dental Office Managers, the PennWell Dental Group, and the New York Academy of General Dentistry. The AGD has approved her company Links2Success as a national provider of PACE continuing education credits.
medical involving more of the need to rid the patient of infections and or help them to build back function.
CBCT scans are covered by all medical plans, so whether you are charging your patient or not for this imaging, make sure you document the imaging, obtain a signed form indicating that they understand you are not billing, and allow them to bill if you are not. Remember patients who are covered by Medicare should sign a form letting them know you are not billing for this procedure.
You must be open to collaboration from the medical providers to achieve the goal of patient health. For pregnant women, that is one of the reasons for adding the letter from an ob-gyn. It is important to recognize that an infection in a pregnant woman can spread through her system and directly affect the unborn child. Offices that treat patients with conditions such as diabetes, heart conditions, lupus, arthritis, or women who are pregnant can have medical insurance cover the treatment since the infection can spread through the body. In medically compromised patients, an added bacterial load can cause key issues.
There are several treatments that are covered under medical insurance. Notice none of the covered services are the traditional root canal therapy.
Trephination is not a common procedure, but it can be useful. Here are situations when trephination might be considered:
Acute Alveolar Abscess: Surgical trephination to reduce swelling and drain pus is considered when periapical drainage is not effective or possible.
Root Pulp Damage: Trephination can offer access to the root canal system if dentin has begun to fill the canal due to trauma or decay. If the dentin has filled the canal completely, however, trephination might not be feasible.
32 Endodontic Practice US Volume 16 Number 2 PRACTICE MANAGEMENT
CDT Code

D7270 Tooth reimplantation and/or stabilization of accidentally evulsed or displaced tooth includes splinting and/or stabilization
CPT Code
21440 Closed treatment of mandibular or maxillary alveolar ridge fracture (separate procedure)
21445 Open treatment of mandibular or maxillary alveolar ridge fracture (separate procedure)
41899 Unlisted procedure, dentoalveolar structures
S02.5XXA Fracture of tooth (traumatic), initial encounter for closed fracture
D7272 Tooth transplantation (includes reimplantation from one site to another and splinting and/or stabilization)
41870 Periodontal mucosal grafting
41899 Unlisted procedure, dentoalveolar structures

K04.7 Periapical abscess without sinus
K04.8 Radicular cyst
Dental Implant Removal: If a dental implant is fully inte grated but beginning to fail, they can be quite difficult to remove. Trephination is an option if a fully integrated dental implant is beginning to fail.



• 42310 Drainage of abscess; submaxillary or sublingual, intraoral
• 42320 Drainage of abscess; submaxillary, external
In 42310, an intraoral drainage of a submaxillary or sublin gual gland is performed. In 42320, an external (extraoral) drain age of a submaxillary gland abscess can be performed. The complications within the endodontic world have the ICD10-Codes to help you bill for your patients.

• M27.51 Perforation of root canal space due to endodontic treatment
• K03.81 Cracked tooth
• K04.1 Necrosis of pulp



• K04.2 Pulp degeneration

• K04.6 Periapical abscess with sinus
• K04.8 Radicular cyst
• K08.81 Primary occlusal trauma
• K08.82 Secondary occlusal trauma
• K08.89 Other specified disorders of teeth and support ing structures
• S02.5XXA Fracture of tooth (traumatic), init for clos fx
• S02.5XXB Fracture of tooth (traumatic), init encntr for open fracture
• S02.5XXS Fracture of tooth (traumatic), sequela
Table 1: CPT Codes for Endodontic Cases CDT Code — Cross Coding When a Dental Code has a Medical Code
Expanding endodontic treatments and procedures with dental lasers

Dr. Fernando Meza sheds some light on the benefits of lasers in endodontics
Today’s patients want and even expect the highest quality of clinical care. Some patients even come prepared with their own research, whether from online or through word of mouth, that dental lasers surpass this caliber of care. Dental lasers have become an increasingly popular tool for dentists; however, education and advantages regarding endodontic applications still remain ambiguous for many in the field.
The application of laser technology in dentistry has transformed treatments and procedures, revolutionizing the way endodontists approach our most common conditions such as root canal therapy and spanning to applications including periodontal procedures such as crown lengthening. With up to 15% of people in the U.S. avoiding dental care because of misconceptions and fears, according to the American Association of Endodontists, it is pivotal for dentists to discover how dental lasers play an integral role in providing new opportunities for more efficient, precise, and comfortable treatments.1
Root canals


When it comes to root canals — removing the damaged or infected pulp inside a tooth and replacing it with a filling material, the treatment is typically performed using traditional instruments, but dental lasers are increasingly becoming more popular. Root canals are typically necessary when a tooth becomes infected or inflamed due to decay, trauma, or other factors. Traditionally, root canals have been performed using burs, files, and other mechanical instrument to remove the pulp. However, this method can be time-consuming, uncomfortable for the patient, and may not always be effective at removing all the damaged tissue. Dental lasers provide a more
Fernando Meza, DMD, is a 2002 graduate of the University of Connecticut School of Dental Medicine. Prior to dental school, he attended Vanderbilt University where he completed a B.A in Psychology. Dr. Meza then received his Certificate in Endodontics from Temple School of Dentistry in 2004. He practices at Arlington Alexandria Endodontics in Virginia.
Disclosure: During residency, Dr. Meza conducted research on the BIOLASE Waterlase All-Tissue Laser to explore the disinfecting capabilities of the laser on bacterially infected root canal systems. His research led to a publication on the Waterlase in the Journal of the American Dental Association (JADA), in July of 2007. Dr. Meza has lectured for BIOLASE in hands-on courses and provided in-office training to many endodontists in the United States and Canada. He is currently on the Fellowship track offered by the World Clinical Laser Institute (WCLI).
precise and minimally invasive alternative to traditional root canal techniques.
The main laser used at my practice is the Waterlase iPlus® All-Tissue Laser by BIOLASE® 2 It is used for both the cleaning and shaping of root canals, as well as for laser-assisted root canal disinfection following final instrumentation of the canals. By first opening the surface of the tooth to access the root canal, the dental laser uses a combination of air/water spray and laser energy to remove the diseased tissue and enhance cleaning and shaping of the canals in between the use of files, just before placing the root filling.
34 Endodontic Practice US Volume 16 Number 2 TECHNOLOGY
Figure 2: 6-month PA image showing healing of the periapical tissues
Figure 1: Retreatment case No. 31 with initial PA image
The advanced laser technology works by emitting a focused beam of light that can be adjusted to target specific tissues, offering the advantage of better performance at a deep tissue depth in soft tissue due to their precision and minimally invasive nature. In root canal procedures, the laser is used to remove the damaged pulp while minimizing collateral damage to the surrounding tissue.3 This allows for more precise removal of the damaged tissue and reduces the incidence of postoperative pain, swelling, or requiring two visits to complete treatment. The laser disrupts bacteria, biofilms, and debris resulting in faster and more effective treatments. At the same time, the enhanced disinfection achieved from activating irrigating solutions within the canal system gives the provider together with the dental assistant superior ability to clean the root canal system. While success and survival of root canal treatments can range between 85% to 95%, disinfection is key, and the enhanced precision from dental lasers reduces the chance a patient will need to undergo a retreatment, apical surgery, or extraction.
Dental lasers enhance treatment by honing in on the infected area with efficiency and power that conventional tools lack, and in some cases decreasing the reliance on burs and files. The decreased post-op pain and discomfort is a testament to proper laser use during root canal treatment which ultimately benefits both the dental provider, support staff, and patient.
By harnessing dental laser technology, dentists and their staff are now able to target bacteria and infected tooth dentin with greater accuracy, helping to preserve more of the healthy tooth structure while decreasing treatment time, and allowing care teams to see more patients.
Crown lengthening
Typically performed when a tooth is broken, decayed below the gum line, or when there is not enough tooth structure above the gum line to support a restoration such as a crown or bridge, crown lengthening commonly involves removing gum tissue to expose more of the tooth surface. Traditionally, crown lengthening has been performed using a scalpel, handpieces, and other mechanical instruments to remove the gum tissue and contour the underlying bone. However, this method can be uncomfortable for the patient and often requires stitches to close the incisions.

In laser-assisted crown lengthenings, the laser is used to precisely target the tissue, allowing for a more controlled removal of the gum tissue. This reduces the risk of bleeding, discomfort, and other complications. Additionally, laser-assisted crown lengthenings are less invasive, leading to reduced postoperative discomfort and a faster recovery time for the patient.
The laser can be adjusted to target specific areas of the gum tissue, allowing for a more controlled and accurate tissue removal. This can be particularly beneficial when performing
crown lengthening on multiple teeth or in areas where there is a high degree of complexity.

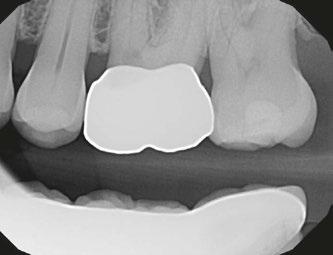
Conclusion
The industry is quickly evolving when it comes to technology. It would have been ludicrous to think in the early 2000s that just about every endodontist in the U.S. would have a CT scanner, but that is the reality now — with some having gone through a series of different ones. Dental lasers are a powerful tool, and assisting in root canals and crown lengthenings is just the beginning. As this innovative technology continues to evolve, the number of other hard and soft tissue treatments will only continue to expand further. As dental practices look to adopt innovative technology to improve care, patient satisfaction, and grow their practice, dental lasers are the next technology for endodontists to take an interest in.
REFERENCES
1. American Association of Endodontics. Endodontic Facts. From Press kit. https://newsroom.aae.org/press-kit/. Accessed May 2, 2023.
2. Biolase. Waterlase iPlus®. https://www.biolase.com/products/dental-lasers-all-tissue/ waterlase-iplus/. Accessed May 2, 2023.
35 endopracticeus.com Volume 16 Number 2 TECHNOLOGY
EP
3. Sarbadhikary P, George BP, Abrahamse H. Paradigm shift in future biophotonics for imaging and therapy: Miniature living lasers to cellular scale optoelectronics. Theranostics. 2022 Oct 17;12(17):7335-7350.
Figure 4: Preoperative image No. 14
Figure 5: Postoperative image No. 14
Figure 3: Internal resorption in the mesial root orifice of a maxillary molar
A taxing situation
Justin Maxwell offers suggestions for maximizing your tax strategy


Senators, CPAs, and tax attorneys have long stated that most American small business owners pay more tax than is legally required. In fact, as a successful orthodontist, you have probably felt that you pay too much to the government in taxes. An independent study proved them right — they found that per $250,000 of income the average American business owner will pay about $11,000 more per year than is legally required in taxes.
Over 20 years, that’s an additional $220,000 paid to the government on top of what you are already paying them, and 100% of it is unnecessary. Fortunately, this problem is fixable, and there is a way to legally and ethically pay less tax that doesn’t require you to become a tax attorney or spend hours and hours doing something outside of your genius. In this article, we will explore one simple fix that can drastically improve or eliminate any and all unnecessary tax payments.
Whenever new orthodontists begin their business journey, one consistently offered piece of advice is: “find a good CPA.” While this advice is something every orthodontist should follow, it lacks a critical component that leads to the overpayments mentioned above. Instead, the recommendation should be to find a good tax TEAM. This is the simple fix that every orthodontist can implement today. Find a tax team versus a tax person.
The tax code is a behemoth. When you include all supporting documents, it contains over 80,000 pages. Expecting one person or one company to be an expert in all the nuances and available options is a mistake that will result in paying more taxes than is legally required.
Who then should be on this accounting team, and what roles should each team member fill?
Tax filer
The tax filer is responsible for complying with the ever-changing tax rules and regulations. These team members will compile all of your data, help you report what was made to the IRS, and tell you how much you owe in taxes. They will help you understand what is the best entity to be set up under for your given situation. They may also assist in bookkeeping, audits, providing accurate numbers as to what is going on in your business, and being a valuable resource for tax advice.
36 Endodontic Practice US Volume 16 Number 2 FINANCE MATTERS
Justin Maxwell is a wealth and tax strategist at Big Life Financial. He received a Master of Science degree from the University of Utah. He and his business partner join forces with dental and medical professional accounting teams across the country to help professionals implement effective business strategies. He can be reached at justinm@biglifefinancial.com.
Table 1
Cost segregation
Paying your kids
Tax-advantaged investing
Augusta Rule
Tax-advantaged insurance
Special entity structuring
Maximize your charitable giving
Tax credits and incentives
An owner of commercial or single family rental real estate can accelerate the depreciation taken. Most of the time, an engineer is a required member of the team.
Depending on the age of the child, entity type, and a few other factors, a business owner can potentially pay children who work in the business tax-free.
The US government incentivizes individuals to invest in specific industries/markets. The incentive they use is giving tax deductions, which at times can be quite large. A registered investment advisor who specializes in these areas must be a member of the team.
Leveraging a rule that allows an individual to rent out their personal residence up to 14 days a year tax-free and turning it into a business expense.
There are ways to save income tax and payroll tax by using a variety of insurance offerings, including health, commercial and life insurance. These are extremely niche and require a specialist to set up.
There are ways to strategically create and pair entities together (corporations and trusts) to build tax favorable environments.
Donating provides tax deductions, but there are ways to increase the tax deduction by donating to specific things or utilizing certain strategies. For example, you can create an arbitrage where you donate $1 but save $2 in taxes.
The tax code contains a variety of tax credits and incentives that may or may not be applicable, but unless a specialized tax credit professional looks at it, you can’t say for sure. These include things like the R&D, ERC, WOTC, SALT, and more.
Tax-advantaged accounts
Tax-deferred accounts
Pay the tax now, but the growth of the account is tax free. These are vehicles like the Roth IRA, cash value life insurance, etc.
Delay the tax today, but pay taxes on what you put in and the growth that occurs when you use it down the road. These are vehicles like 401K, traditional IRAs, etc.
Most people go to the “tax filer” to get their taxes done. While this team member is a vital component of the team, they should not be the only member of the team. The tax filer is what we call a tax historian, meaning they can take what has happened and tell you how it will be taxed, but unless this person is paired with a proactive tax planner, there will always be unnecessary tax payments.
Tax strategists
The tax strategists are the most often missed member of the team. These team members will be a combination of specialists, tax attorneys, and third-party administrators. However, to ensure your time is maximized, it will need to be spearheaded by one quarterbacking person or group. This quarterbacking person will bring all the needed players to the table. The tax strategist’s job is to provide quality, proactive strategy that accesses more of the tax code and focuses on lowering the tax bill. The tax filer and strategist work hand-in-hand. No decision moves forward without the consent of the other. When both parties work together, you get a tremendously powerful approach that results in using more of the tax code and paying less tax.
The tax strategist will help you as the business owner navigate through and implement the tax strategies that are most
applicable to your situation. These include but are not limited to strategies found in Table 1.
If you were going through this table and thinking:
“My tax person tells me they do tax planning, but I’ve never had anyone talk to me about all these options, or why is that I have only had a conversation about one or two items on the list?”
Then it’s time for you to upgrade your team. When people hear that, they automatically assume I should dump my old accountant. But if you go and only hire a tax filer again, you will be in a very similar situation just with a new person. The simple fix is NOT hiring a new accountant; the simple fix is creating a tax team of both a tax filer and a tax strategist. This combination results in you having the best chance of reducing your tax bill to its legal minimum.
One of the biggest problems is that most people don’t even realize that an accounting team is something they are entitled to and that these tax savings options actually exist. Yet, throughout this article, we discovered that most business owners pay more taxes than is legally required, that there is a difference between a tax filer and a tax strategist, and that there are many more legal ways to pay less tax. Most importantly, we realized that the solution is not nearly as complicated as we think it should be. The simple fix is to create a tax team filled with both tax filers and tax strategists. When action is taken on this solution, you will find your tax bill goes down. EP
37 endopracticeus.com Volume 16 Number 2 FINANCE MATTERS
A coach’s perspective on evolving competency
Drs. Joel C. Small and Edwin McDonald show that leadership takes time and effort


COMPETENT
When we observe someone performing at mastery level, they often appear to perform effortlessly, yet their performances belie the effort necessary to achieve mastery. Michael Jordan, for example, was not born as the greatest basketball player of all time. In fact, he was cut from his junior high basketball team due to a lack of skill. The same can be said for great leaders. They were not born as great leaders, but each has endured a journey to competency.
Not long ago, our studies led us to the work of Noel Burch, who in the 1970s developed a theory known as the Hierarchy of Competence. Burch theorized that the journey to mastery of any skill can best be traced through four distinct developmental phases. His theory greatly resonated with us because our personal experience of working with clinical healthcare professionals as executive leadership coaches aligned with his theory.
Unconscious incompetence
Unconscious Competence
Finding our “Voice”
• Mastery
• Habitual/intuitive
• Internal “team” narrative
• Develops peak performance
• Optimal practice culture
• Team-oriented narrative
Conscious Competence
• Transformational movement
Growth mindset
• Internal altruistic narrative
• Part of a team
• Culture developmet begins “Ugly Duckling” stage
• Aware of developing problems
• Internal narcissistic narrative
UNCONSCIOUS CONSCIOUS
Unconscious Incompetence
• Inexperienced
• Unaware Systems management
• Hierarchical
• Fixed mindset
• Reactive
• Separate from the team
Most of us began our careers with the main focus on retiring debt and making a decent living. The best we could do at this point in our career was to create and manage business systems, and with the help of mentors and consultants, to establish systems that enabled us to monitor the vital signs of a clinical dental practice. Our inexperience left us unaware that systems management in the absence of leadership could only take us so far.
Our relationship with our staff was likely hierarchical. We were their boss and felt that the best way to relate to staff was through an arms-length approach. We seldom considered or valued feedback from the staff.
We mistakenly believed that our staff had fixed capabilities with little room for growth. We believed that there would be
Drs. Joel C. Small and Edwin (Mac) McDonald have a total of over 75 years of dental practice experience. Both doctors are trained and certified Executive Leadership Coaches. They have joined forces to create Line of Sight Coaching, a business dedicated to helping their fellow dentists discover a better and more enjoyable way to create and lead a highly productive clinical dental practice. Through their work, clients experience a better work/life balance, find more joy in their work, and develop a strong practice culture and brand that positively impact their bottom line. To receive their free ebook, 7 Surprising Steps to Grow Your Practice Through Leadership, go to www.lineofsightcoaching.com.
Conscious Incompetence
• Problems with no solutions
• Implements stringent regulations
• Stressed/frustrated
Increased reactivity
• Looking for help
INCOMPETENT
a limited return on investment for staff development. As time passed, and our practices grew, we became increasingly frustrated by what we perceived to be their inability to develop to meet the increasing demands of a growing practice.
With the increased stress that often accompanies practice growth, we find ourselves reverting to habitual reactive tendencies that are counterproductive to staff development and leadership effectiveness. These destructive reactive tendencies are founded in beliefs and assumptions that we have carried with us from earlier experiences and exist at a subconscious level. Furthermore, until they are brought to a conscious level, we find ourselves incapable of corrective actions.
Conscious incompetence
The transition to conscious incompetence is driven by awareness that problems exist. For many of us, the cause of the problems is not apparent, and therefore creates additional stress and frustration as we feel incapable of finding practical solutions.
We often mistakenly identify external forces such as the economy or increased competition as the cause of our problems. It is not uncommon to blame our staff for our internal practice-related problems. Our internal narrative at this point is often narcissistic and counterproductive as we tell ourselves that “Once I fix them I can be successful.”
We attempted to resolve these problems by creating and implementing stringent and harsh corrective policies intended
38 Endodontic Practice US Volume 16 Number 2 SMALL TALK
to resolve staff issues through a command-and-control approach. These actions were the antithesis of effective leadership and often resulted in staff rebellion and/or turnover, which only further amplified the doctor’s stress and frustration.
As the levels of stress and frustration continue to rise, the doctor reverts more often to his or her reactive tendencies which have become their “go to” form of communicating and leading while under stress. This only serves to increase the growing frustration and sense of helplessness to unbearable levels.
It is usually at this point that doctors seek help in the form of coaching. Doctors often seek our help in resolving external causes for their existing problems; never realizing that they are the source of their frustration, and they have always possessed the solutions to resolving their problems. Our job as coaches is to facilitate a process through which doctors become more introspective and self-aware — a process that ultimately brings them to the conclusion that they, and they alone, are the arbiters of their future success.
We help facilitate this awareness process by administering a 360 degree leadership assessment that allows doctors to see their leadership effectiveness through the eyes of those they lead. Many of our clients have described this process as life changing. When doctors are ready to begin their leadership development journey, the magic begins.
Conscious competence
The movement from conscious incompetence to conscious competence is more of a transformational shift than a simple transition. As a doctor enters this phase, they are now aware of their need to change in order to find resolution for their existing practice problems. Their internal narrative has now shifted to become more inclusive and altruistic as they tell themselves that “Once I fix me, WE can be successful.”
Along with this transformational shift, the doctor begins to understand that even though they are the practice owner and leader, they are also part of the practice team. Much of our coaching is designed to help our clients discover the best way to walk the fine line between being both a boss and being a team member — two unique environments that, at times, may seem to be at odds with one another.
One of the most significant transformations on the part of the doctor in the conscious competence phase is the shift from a fixed to a growth mindset as they come to the believe that their staff can and must grow by scaling their capabilities to meet the demands and complexity of a growing clinical practice.
Another life-altering epiphany occurs when the doctor realizes that they have become the barrier to their staff’s growth and development. This is a pivotal inflection point in the doctor’s leadership development as they learn new ways of engaging with their team.
This is what I describe as the “ugly duckling” phase of leadership development. It is an awkward phase as one attempts to change personally while concurrently attempting to change a practice culture that presently may be less than optimal.
Much of the process involves trial and error-type experimentation as the doctor attempts to find the right leadership approach that honors both his/her authenticity and unique leadership style. Because these efforts are trial-and-error attempts, there is often frustration when the doctor realizes that their leadership development is following a non-linear path and taking longer than expected. This is where the coach offers valuable support by reminding the doctor why they are on this journey, and why they want to move forward rather than return to the previous status quo.
Unconscious competence
This is the phase where leadership becomes habitual. Just like Michael Jordan, masterful leaders respond instinctively when the game is on the line, and yet they understand that they excel because of the efforts of a supportive team. They create a practice culture that is psychologically safe, supportive, and allows each team member to be the very best version of themselves on a daily basis.
People no longer follow them because they fear them, but rather because they believe in them and trust them. They motivate their team to excel through their compelling vision and mutually shared values that serve as guidelines and perpetual reference points on how to work and exist together. The doctor’s internal narrative is now team-oriented as they tell themselves that “We, as a team, must continue to grow to ensure our future success.”
Destructive reactive tendencies have been replaced with more appropriate generative responses and supportive actions and responses. Many refer to this state of mastery as being “in the zone” or “finding one’s leadership voice.” For those leaders that are fortunate and dedicated enough to find their voice, leading appears to be second nature — almost effortless. These are the special ones who appear to have it all together. There is no second guessing or hesitation in their decisions. Leading for them becomes an intuitive experience. These are the ones we admire the most and seek as our mentors.
39 endopracticeus.com Volume 16 Number 2 SMALL TALK EP
With the increased stress that often accompanies practice growth, we find ourselves reverting to habitual reactive tendencies that are counterproductive to staff development and leadership effectiveness. These destructive reactive tendencies are founded in beliefs and assumptions that we have carried with us from earlier experiences and exist at a subconscious level. Furthermore, until they are brought to a conscious level, we find ourselves incapable of corrective actions.”
The Endo Files: the endodontic experts podcast
US Endo amplifying the voices of specialists and industry insiders
The Endo Files Podcast is a show for endodontists looking to gain insights, education, and inspiration from their peers. Each episode features a rich conversation between industry experts, highlighting personal perspectives on the specialty including clinical best practices, hot topics, work-life balance, innovative technologies, and so much more!


From harnessing mental toughness to thriving in the demanding field of endodontics, to the importance of giving back and investing your time to shape the future of the specialty and the next generation of leaders, Season One covered myriad topics appealing to specialists in every stage of career. Season Two will dig even deeper!
Season two: new co-hosts and deeper dives
New for Season Two, The Endo Files will be hosted by a rotating line-up of experts, each bringing a different perspective to the table! You’ll hear dynamic conversations led by Dr. Diwakar Kinra, Dr. Brett Gilbert, Dr. Ryan Facer, and Dr. Allen Abrishami, who will shine a light on issues pertaining specifically to residents and new associates, along with longtime industry insider and seasoned podcast host, Kim Livesay Brownell.
ICYMI: highlights from season one
• Endo Never Sleeps: Setting Boundaries and Thriving Through Grind – Dr. David Landwehr, Capital Endodontics
• Why Mental Toughness is the Endodontist’s Superpower – Dr. Reid Pullen, Brea Endodontics
• Why Chasing Excellence is More Sustainable than Chasing Perfection – Dr. Brett Gilbert, King Endodontics
• The Symbiotic Relationship Between Radiology and Endodontics, and Going Back to School – Dr. Bruno Azevedo aka “The Cone Beam Guy”
• Resident Lessons, Side Hustles, and the Importance of WorkLife Balance – Dr. Diwakar Kinra, Contemporary Endodontics
• Paying it Forward: Investing in the Specialty to Shape the Future – Dr. Scott Doyle, Metropolitan Endodontics
• Advice for Current Residents and New Endodontic Associates – Dr. Allen Abrishami, Brea Endodontics
• In Conversation with The Pulpinator – Dr. Daniel Tran, Belle Meade Endodontics
• The Case for Faster Procedures: Leaning Down to Maximize Efficiency – Dr. Tim Adams, Summit Endodontics
• Why the Patient is King, the Role of the AAE & Why Disco Diva Gloria Gaynor Was Right – Dr. Rob Roda, Roda, Bennett & Kogan
• What’s Next in Endo: A Unique Perspective on the Future of the Specialty – Dr. Steve Frost, Red Mountain Endodontics
• And more!
If you’re looking to differentiate yourself and your practice, to stay up to date on the latest happenings in the field, and to connect with other specialists on a personal level, The Endo Files is an excellent resource to add to your toolkit.
The podcast is brought to you by US Endo Partners and is available for free on all major podcast platforms, including Apple Podcasts, Spotify, and Google Podcasts. Subscribe today so you never miss an episode! EP
40 Endodontic Practice US Volume 16 Number 2 SOUND ADVICE
Hosts Dr. Diwakar Kinra and Kim Livesay Brownell discuss issues facing today’s residents on an episode of The Endo Files, recorded live at the AAE Annual Meeting
innovation through innovation through
Collaboration Collaboration
As endodontists, our passion for excellence drives us to adapt and evolve; to embrace new research and technology. But what if we put as much effort into working together as we do into perfecting our techniques? If collaboration became THE innovation that unlocks new possibilities in endo?

US Endo doctors thrive when they share ideas, insights, and best practices. We learn from one another, challenge each other, and push ourselves to be better. We win – and so do our patients.


“By working together, we can provide more comprehensive oral health care to our patients and achieve better outcomes and experiences than we can on our own.”
Scan to catch the full conversation with Dr. Babcic on The Endo Files Podcast
Dr. Vladana Babcic Tal, Cameo Dental Specialists | Partner and believer since 2022
usendopartners.com
See more every way you slice it.
The Portray System uses nanotube technology to capture multiple images from several angles over 12 degrees of movement. Its software compiles the images into a 3D volume and dissects the volume into .5 or .1mm slices you can scroll through to diagnose problems that are otherwise obscured.
portrayxray.com

See how Portray 3D Tomosynthesis lets you know more.
