Circulation Disclosure: Total Circulation May Vary. Publisher retains the right to adjust circulation based on a number of factors including but not limited to: print and digital distribution by mail, email, and website for industry tradeshows, educational events, including nonpaid bulk copies and/or digital access provided to events, clients and educational institutions.
ISSN number 2372-6245
Transformative era of root canal therapy
The future of endodontics holds a pivotal role in the preservation of teeth and the prevention of unnecessary extractions. Root canal treatment stands as a cornerstone in dentistry, aiming to eliminate pain and effectively restore dental health.
In recent years, the landscape of dentistry has witnessed a significant surge in dental implant advancements, overshadowing the importance of preserving natural dentition. While dental implants serve a crucial role in tooth replacement, it is imperative not to overlook the significance of retaining existing teeth whenever possible.
Throughout the decades, the field of endodontics has made substantial progress in understanding and refining treatment approaches for infected teeth. From seminal works such as Miller's papers to groundbreaking studies like those of Kakehashi and colleagues1 on the role of bacteria in root canal systems, the discipline has continuously strived to enhance patient outcomes.
Innovations in instrumentation techniques (Schilder2), ranging from traditional hand files (Roane3) to modern NiTi rotary files (Walia4), have revolutionized root canal procedures. The evolution of obturation methods, including lateral condensation (Allison and colleagues5) and the Continuous Wave of Condensation (CWC) technique (Buchanan6), the use of the clinical microscope (Gartner,7 Pecora8), and micro-surgical endodontics (Kim,9 Rubinstein10) underscore the commitment to achieving optimal treatment results.
Moreover, advancements in root canal sealers, irrigation methods, and disinfection technologies have further elevated the standard of care in endodontics. The adoption of ultrasonic-activated irrigation, Er:YAG laser application (Divito,11 Jaramillo12), and multisonication (Jaramillo,13 Molina,14 Kim9) techniques has paved the way for enhanced pulp tissue debridement and disinfection, ultimately improving treatment efficacy.
As we embrace newer technologies like hydrodynamic cavitation and light-curing hydrogel root canal materials, we stand on the brink of a transformative era in endodontics. The ongoing innovations and research endeavors in the field underscore our collective commitment to advancing patient care and redefining the future of root canal therapy.
Together, let us continue to push the boundaries of knowledge, embrace emerging technologies, and uphold the principle of preserving natural dentition for the benefit of our patients and the future of root canal therapy.
References available online.
David Jaramillo, DDS, is a tenured professor at the Department of Endodontics at UTHealth School of Dentistry, having joined the faculty in 2014. Dr. Jaramillo became a full-time professor in 2004 when he accepted two positions, one at the University of Southern California (USC) and the other at Loma Linda University in California. He worked under direct supervision of Dr. Jim Simon and Bill Costerton at the Center for Biofilms at USC, and under supervision of Dr. Leif K. Bakland and Yiming Li at the Center for Dental Research and the Advanced Imaging and Microscopy Core at Loma Linda School of Medicine and at Center Facility for Advanced Microscopy and Microanalysis at UC Riverside. Dr. Jaramillo's main research focus is in the irrigation of the root canal system. He has spoken at more than 100 conferences worldwide, published over 22 peer-reviewed papers, written seven book chapters, and was recently inducted into the International College of Dentists. Dr. Jaramillo is also a very active member of the International Federation of Endodontic Associations.
David Jaramillo, DDS
Taking the endodontic procedure to the next level
A conversation with Dr. Benedict Bachstein sharing insights on his clinical experience using Odne™Fill for minimally invasive, light-cured obturation
Cover image of Dr. Benedict Bachstein courtesy of Odne.
Drs. Cassandra Wieczerza, Susan Paurazas, and Mazin Askar explore the effects of specific periapical pathologies on dental implants
Drs. Frederico Martinho and Bruno Giliolli Bisi discuss the use of guided navigation in the endodontic practice
ENDOSPECTIVE
Endodontics: no place for a snowflake
Drs. Joel Fransen, Rich Mounce, and Tom Shackleton provide seven tips for peak performance
PRODUCT
PRACTICE MANAGEMENT
The best way to eliminate financial stress
Dr. Albert (Ace) Goerig discusses how to get to profits without financial stress............................... 34
SERVICE PROFILE
Why the largest U.S. endodontic practices have quietly partnered with IDSOs
Chip Fichtner discusses how endodontists can add liquidity and a strong growth partner to their practices 36
Drs. Karen Potter, Seda Falakaloğlu, and Mustafa Gündoğar describe how multisonic technology
Dr. John Khademi discusses GentleWave®, a paradigm shift in root canal therapy ........................ 38
“I like ZenSeal because it has great radiopacity, it has great fluidity and handles well.”
-Dr. Paola López
Less Waste per Application
Efficiency
High Flowability to Fill Complex Canals
With high flowability, ZenSeal has excellent flow into accessory canals.
Excellent Sealability with Zero Shrinkage
ZenSeal adheres tightly to dentin and gutta percha with zero shrinkage.
Simplified Root Canal Procedure
Provides a simplified root canal procedure, including single cone technique.
More Uses Per Syringe
On average, ZenSeal can be used on 9 more teeth compared to EndoSequence Sealer.*
*Assuming 18 µL used per tooth
The Technique used was a single cone gutta percha point on a #2 maxillary molar. Canals were shaped by ZenFlex NiTi Files and filled with ZenFlex Gutta Percha and ZenSeal. Image provided by Dr. Paola López.
“By
changing nothing, nothing changes.”
Change is hard — some days it feels like fate is not satisfied with any stable situation that makes us comfortable and secure. Sure, no one can dispute the serenity of “business as usual” in the midst of ever-changing world issues, politics, and everyday craziness. Instead of losing sleep or stomach lining over change, let’s consider the positive aspects of being open to expanding our comfort zones, living in the moment, and having a mindset of “faith over fear.” As the title quote from Tony Robbins suggests, you have to build up some momentum in order to actually get somewhere. Let’s hear from some successful and inspirational people on how change can bring positive movement to our lives.
Lisa Moler Founder/Publisher, MedMark Media
Neurologist and psychologist Viktor E. Frankl said, “When we are no longer able to change a situation, we are challenged to change ourselves.” Some people just need a bigger push to get moving. Taking the easy route and sticking with “the familiar” is only possible until the stress of the known outweighs the fear of the unknown. So, sticking with only the activities or mindsets that are within your safety zone will eventually leave you watching others who have the ambition and confidence to move forward. You don’t want to look around in a few years and see your friends and peers busy and fulfilled with new possibilities that can change your community or your world. There is a lot of competition out there, and being a pioneer or game changer may be a challenge at first, but will head off the future frustration of a stagnating life.
Actress Sarah Parish noted, “Living with fear stops us from taking risks, and if you don’t go out on the branch, you’re never going to get the best fruit.” Overcoming fear of making the wrong decision or failing can feel daunting. But, there are a lot of ways to build your confidence, such as talking to friends, mentors, experts, attending conferences, reading MedMark publications, and listening to those who bring you inspiration. There will be learning curves and maybe even some speed bumps, but most times, innovation will lead to new and exciting ways to grow.
Our fall issue is filled with innovation and information to create productive change. In our Cover Story, Dr. Benedict Bachstein shares his experience with minimally invasive, light-cured obturation using Odne™Fill. Our CE by Drs. Frederico Martinho and Bruno Giliolli Bisi educates our readers on dynamic navigation and its role in improving outcomes and tooth survival during endodontic microsurgery. The CE by Drs. Karen Potters, Seda Falakaloğlu, and Mustafa Gündoğar explores how to achieve minimal instrumentation with multisonic technology during cleaning and disinfection. In our Clinical column, Drs. Cassandra Wieczerza, Susan Paurazas, and Mazin Askar delve into the effects of periapical pathology on dental implants and show how predictable outcomes can be achieved with proper treatment planning.
World famous performer Robin Williams said, “No matter what people tell you, words and ideas can change the world.” Don’t leave your success to chance. Change your ideas into action. Innovation will create a happier you, family, and work life. When you embrace change, the benefits will spread throughout your world!
To your best success,
Lisa Moler
Published by
Publisher Lisa Moler lmoler@medmarkmedia.com
Managing Editor
Mali Schantz-Feld, MA, CDE mali@medmarkmedia.com Tel: (727) 515-5118
National Account Manager Adrienne Good agood@medmarkmedia.com Tel: (623) 340-4373
Marketing & Digital Strategy Amzi Koury amzi@medmarkmedia.com
eMedia Coordinator
Michelle Britzius emedia@medmarkmedia.com
Social Media Manager Felicia Vaughn felicia@medmarkmedia.com
Digital Marketing & Sales Administrator Sharif Rod sharif@medmarkmedia.com
Website Support Eileen Kane webmaster@medmarkmedia.com
MedMark, LLC 15720 N. Greenway-Hayden Loop #9 Scottsdale, AZ 85260 Tel: (480) 621-8955 Toll-free: (866) 579-9496 www.medmarkmedia.com www.endopracticeus.com
Subscription Rate
1 year (4 issues) $149 https://endopracticeus.com/subscribe/
Taking the endodontic procedure to the next level
A conversation with Dr. Benedict Bachstein sharing insights on his clinical experience using Odne™Fill for minimally invasive, light-cured obturation
What motivated you to become an endodontist?
Mainly it is the level of patient contact and care, of being able to spend time with a patient and focus on one patient at a time. I also enjoy the attention to detail that the role requires and working under a microscope. There is also the satisfaction of saving teeth by providing care at the limit of what is currently possible and being on the forefront of new technologies and materials.
Benedict Bachstein, DMD, was born and raised in Germany where he completed his dental school studies with honors at the University of Munich. He then moved to Philadelphia and received his DMD from the University of Pennsylvania in 2007. Dr. Bachstein has participated in dental research and co-authored several research articles. He also has many awards including: The Award for Outstanding Clinical Performance in Fixed Prosthodontics from the Academy of Operative Dentistry, and recognition for clinical excellence by the University of Pennsylvania Department of Endodontics. Dr. Bachstein completed his specialty training in endodontics at the Albert Einstein Medical Center in Philadelphia where he also served as Chief Resident and received recognition from the American Association of Endodontists for his work. He is the past president of the Southern Dental Society of New Jersey. His professional affiliations include the American Association of Endodontists, the American Dental Association, the Academy of Osseointegration, the New Jersey Dental Association, the Southern Dental Society of New Jersey, and Alpha Omega.
Disclosure: Dr. Bachstein is an Odne™ investor.
You have a close relationship with Jefferson Einstein Philadelphia Hospital. Can you tell us more about that?
I originally moved to Philadelphia because it is the birthplace of endodontics. I chose Einstein for my specialty training and am now faculty there. Einstein has a very strong clinical program and the chairman, Dr. Frederic Barnett and I share the same values and uncompromising commitment to excellence, so it made sense for me to continue as faculty there. Dr. Barnett and Dr. Stephen Niemczyk (also faculty) have been excellent mentors to me, and I now get to pass that on by being mentor to the next generation of endodontists.
You were one of the first clinicians to use Odne™Fill in your practice. Can you tell us about your experience with it?
Odne™Fill is a material that is completely different from any of the materials I’ve used before and therefore offers us a different way to operate in the root canal system, which has the potential to be a huge advancement for our field.
If I were to try to describe it to someone who has never used it, I would say it reminded me of applying a calcium hydroxide paste, where you can literally inject the material. However, Odne™Fill is even more flowable than a paste, with a consistency just slightly thicker than water. Technique-wise, it makes me think of the progression from cold lateral obturation from years back, to the warm vertical back-filling techniques. Again, even these don’t really describe Odne™Fill as it does not require any force or compression at all; it very gently flows into the root canal morphology due to its water-like consistency.
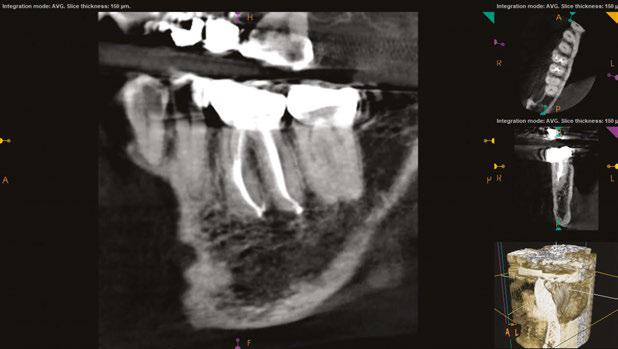
What is really exciting, beyond the tremendous benefit of the gentle back-fill technique, is that Odne™Fill seems to fill the root canal system further than what we are currently capable of. When I look at the post-op CBCT images, I see that the material seems to really cover and flow into spaces that we previously might not have been able to fill to the same extent.
Retreatment with this material is incredibly simple and easy. Of the patients for whom we have used Odne™Fill, we have not needed to retreat, but we have completed simulated cases where we intentionally retreated to test the material. Since Odne™Fill is a hydrogel, it has a pulplike consistency in its cured state, so we don’t even need to change our instruments; we can go back with the same instrument even after it has cured and easily remove the material and retreat it. This is much different than even BC sealer which is not as easy to suction back out.
I am also working with residents at Einstein for them to learn and evaluate the technique. Part of this was learning that instead of picking up a heat source, they use the Odne™Cure micro-laser curing light to cure the material,
and prior to curing, they take an X-ray to evaluate the obturation quality. We started with extracted teeth and then moved to patient cases. It was amazing to see how quickly they were able to successfully treat live cases and get great results.
What are some challenges you’ve faced with this new approach?
As with every new product, it is a new workflow to get accustomed to, not just for the endodontist, but for the assistants and the clinical team, so it took some time to adjust even though, ultimately, it simplifies the process.
We are used to materials that auto-cure, and with Odne™Fill there is a curing step that needs to be incorporated. The curing happens in two parts — first, at the apical third and then, at the pulp chamber. But once we understood the process and how to use it, it became very natural.
Figures 1A-1D: Odne™Fill light-cured in a split mold. Odne™Fill is a hydrogel, a class of biomaterials known for their excellent biocompatibility and hydrophilicity. Due to its water-like viscosity and the ultra-high hydrophilicity in its uncured state, it can flow into complex endodontic structures, such as isthmuses, deltas, and C-shaped canals. Once cured with Odne™Cure, the corresponding micro-laser curing device, it provides gap-free root canal sealing and long-term obturation. No gutta percha, no sealer needed. Prepare to ISO 20.04, then fill and cure
Pre-op and diagnosis: 74-year-old female diagnosed with necrosis with symptomatic apical periodontitis in tooth No. 19. Both mesial and distal roots follow a 2-1 configuration. 2B and 2C. Treatment: Three appointments where CaOH was applied. All canals were instrumented to ISO 30.04, with a working length of 20 mm in all 4 canals. The obturation was done with Odne™Fill and the coronal restoration with Endosquence® BC liner™ and FluoroCore 2+ for the
Figures 2A-2C: Case 1 done by Dr. John Millar, a first-year endodontics resident at the Jefferson Einstein Philadelphia Hospital (formerly Einstein Medical Center Philadelphia). 2A.
core build up
A. B.
C.
Figures 3A-3C: Case 2 done by Dr. John Millar, a first-year endodontics resident at the Jefferson Einstein Philadelphia Hospital (formerly Einstein Medical Center Philadelphia). 3A. Pre-op and diagnosis: 31-year-old female diagnosed with symptomatic irreversible pulpitis with symptomatic apical periodontitis in tooth No. 30. 3B and 3C: Treatment: The mesiobuccal and mesiolingual canals were instrumented with BlueShaper® Z3 files at a working length of 23 mm. The distal root canal was instrumented with XP-Endo® Shaper and Finisher at a working length of 21 mm. The obturation was done with Odne™Fill and the coronal restoration with Endosquence® BC liner™ and FluoroCore 2+ for the core build up
I also find that the contrast of the material during application takes getting used to. It is light blue, turning transparent once cured, but we are used to the bright orange of gutta percha.
Given its water-like consistency, I have found the microscope to be very helpful for greater control in applying the material.
Would you recommend Odne™Fill to other endodontists?
In general, if there’s a new product, there are several questions that I always ask to determine if it is worth adopting. Does it improve the treatment outcome, and does it have the potential to improve the standard of care? Does it make our current treatment more efficient? Meaning, does it make the treatment easier for the patient and make it faster and easier for us to achieve the same level of care?
Odne™Fill does make treatment and re-treatment more efficient and is less technique-sensitive compared to other obturation methods. This means less chair time for patients. And simplicity is one of the most appealing aspects for me.
Any treatment that preserves tooth structure, while ensuring adequate disinfection of the root canal system, leads to improved tooth resistance, lower prevalence of fractures, and improved outcomes. The Odne™System (which includes Odne™Clean, the company’s root canal debridement technology), is a tremendous improvement to current minimally invasive root canal technology and potentially, to outcomes. The Odne™System uses 190µm tips, which are smaller than what is currently available, such that the minimal preparation needed is ISO 20.04. This is a huge advantage for minimally invasive approaches. The main reason we traditionally instrumented the root canal to size 35 is to make sure that it would accommodate the needed tools to irrigate and clean. Odne™Clean recently received FDA clearance and joined the family of new minimally invasive root canal debridement devices, and Odne™Fill provides an obturation solution for the resulting minimally instrumented canals.
Another interesting consideration is regarding the preservation of tooth structure. Up until now, we have been shaping the
canal to fit the cone — this principle will become obsolete, as Odne™Fill can flow into any kind of geometry.
One of my values is to always look to further improve the care I provide. For this, it is important for me to always stay abreast of science and education as innovation drives all progress. Odne’s science-based approach aligns with this value. The Odne team truly looked at the science first before they even considered putting this in a clinician’s hand. They took time to look at the foundations of this material — the biocompatibility, the properties, and what could be achieved with this new material. It was a very thorough pre-clinical process, unlike other companies we’ve encountered that try to make claims about something being the next greatest material when it hasn’t gone through a thorough evaluation process. The researcher line-up at AAE 2024 for Odne was impressive, and clinical studies are ongoing with renowned researchers.
In summary, I’d say that any product that has the potential of either improving the quality of care or making treatment more efficient and easier for both the patient and clinician are products that I would use in my practice, would recommend to colleagues, and importantly, would further the development of our profession. I think Odne™ products have the potential to do exactly that. EP
A.
B.
C.
Treatment considerations of endodontics and implants
Drs. Cassandra Wieczerza, Susan Paurazas,
and
Mazin Askar
explore the effects of specific periapical pathologies on dental implants
Introduction
The goal of dental implants is to restore the patient’s masticatory function as well as esthetics. To achieve this goal, it is vital to obtain proper osseointegration of the implant and maintain health of surrounding tissues. With a prevalence rate of 19.53%,1 the development of either apical peri-implantitis or retrograde peri-implantitis (RPI) is a concern with long-term success of the dental implant. RPI and apical peri-implantitis are diagnosed by radiographic or cone-beam computed tomography (CBCT) evidence of bone loss in the apical region of an implant, with or without clinical signs. The etiology of these pathologies is an inflammatory response leading to progressive loss of the bone supporting the implant.2 In cases of implant failure related to endodontic infection, two possible etiologies of peri-implantitis
Cassandra Wieczerza, DDS, earned her doctoral degree at the University of Michigan School of Dentistry in 2016. Upon graduation, Dr. Wieczerza followed her husband to Texas and then Colorado while he fulfilled his commitment with the United States Army. Following this time, Dr. Wieczerza and her family returned to Michigan where she continued her career in general dentistry for an additional 2 years. After 7 years in general practice, Dr. Wieczerza returned to school to pursue a postdoctorate degree in endodontics at the University of Detroit Mercy. She is currently a second-year resident and is eagerly looking forward to her future practice in endodontics.
Susan Paurazas DDS, MS, MHSA, is a Clinical Professor and Program Director of Graduate Endodontics at the University of Detroit Mercy School of Dentistry and a Board-certified endodontist. Dr. Paurazas is a speaker at local, regional, and national continuing education courses. Dr. Paurazas has served on multiple committees of the American Association of Endodontists, including the Research and Scientific Affairs committee and is chair of the Educational Affairs Committee. She is actively involved in the American Dental Education Association as chair of the Council of Advanced Education Programs. Dr. Paurazas maintains a private endodontic practice in New Baltimore, Michigan.
Mazin Askar, BDS, MS, teaches in the Postgraduate Endodontics Residency Program at University of Detroit Mercy School of Dentistry. He has special interest in Microsurgical Endodontics. He received his BDS degree in dentistry from the University of Baghdad, Iraq and a Certificate and Master’s Degree in endodontics from the University of Minnesota. He has received several teaching awards. His areas of interest include microbiology of the root canal system, metallurgy of the root canal file systems, cytotoxicity and genotoxicity of different root canal materials, and tissue reaction to the growth factors.
Disclosure: All authors report no conflicts of interest with the products mentioned in this article.
are the presence of periradicular lesions of an adjacent tooth and implant placement into a previously infected site.3,4,5,6 A 2016 literature review by Sarmast, et al., found that the most common etiology of RPI was the presence of periradicular periodontitis of an adjacent tooth.7 This discussion and case presentation aims to address the possible effects of adjacent and/or previous periapical pathology on dental implants.
Can endodontic lesions affect adjacent implants?
When treatment planning a dental implant, it is vital to evaluate the pulpal and periapical status of teeth adjacent to the edentulous site. Previous reports have shown cases in which periapical pathology of an adjacent tooth spreads to an otherwise healthy and osseointegrated implant.3,4,8 Whether the periradicular pathology was present at the time of implant placement or developed following placement, one thought is that adjacent pathology can contaminate the implant fixture. If contamination occurs shortly after implant placement, then proper healing and thus osseointegration cannot occur, leading to a failed implant.8 Consequently, the health status of the pulp should always be assessed on teeth adjacent to the implant site. Periapical radiographs alone are insufficient to detect periradicular periodontitis, since 30%-50% of mineral content of bone must be destroyed prior to detection with 2-dimensional imaging.9 Thus, if pulp necrosis or periapical periodontitis is found during clinical or radiographic exam, CBCT should be considered to evaluate the presence and extent of pathology. An integrative review by Costa, et al., provides evidence supporting the superiority in sensitivity and specificity of CBCT over radiographs in evaluating the presence of bone defects around implants. Measurements of detected lesions using CBCT are accurate to a degree of 1 mm when compared to the actual defect.10 Necessary root canal treatment or extraction should be completed prior to implant placement to prevent possible cross-contamination.4
Two important factors when considering adjacent periradicular pathology are the time between the resolution of infection and implant placement and the distance between the infected tooth and implant. Zhou, et al., studied the stability of 128 implants placed adjacent to endodontically treated teeth. Their evidence shows that less than 2 mm between the implant and adjacent tooth increases risk of the RPI. A correlation was also seen between increased success and extending the time between endodontic treatment and implant placement.3
While periradicular lesions of untreated or root canal treated teeth can negatively affect the adjacent implant, this does not mean failure of the implant is imminent. If the infected adjacent natural tooth develops a lesion after implant placement or was
not resolved prior to implant placement, efforts must be made to resolve any periradicular pathology as soon as it is detected. A 2019 case series by Sarmast, et al., shows that performing adequate non-surgical root canal treatment of an infected tooth adjacent to an infected implant will allow the complete healing of both.11 Thus, the interdisciplinary relationship between implant surgeons and endodontists is vital to maintain the health of natural teeth as well as dental implants.
Does placing an implant in the site of previous periapical periodontitis affect outcome?
One proposed reason for infections around the implant apex is the placement of said implant in the site of persistent apical periodontitis following endodontic treatment. To investigate this etiology, Saleh, et., al studied the incidence of retrograde peri-implantitis when implants replaced teeth with failed apicoectomy. While not statistically significant, this study showed increased incidence of RPI when implants were placed in sites of persistent apical periodontitis.5 Another study comparing success of implants placed in sites with periapical pathology and those placed in pristine sites found a 98.1% and 98.2% success rate respectfully. They concluded that the difference in survival was not affected by the presence of previous periapical pathology.6
A systematic review by Chrcanovic, et al., also concluded that implants may be immediately placed after extraction of an endodontically or periodontally infected tooth with adequate healing and osseointegration.12 When evaluating implants placed in sites with chronic periapical lesions, one randomized prospective trial showed a 92% success rate with immediate placement. In cases where a 3-month waiting period between tooth extraction and implant placement was observed, the implant success rate increased to 100%; however, this increase was not of significant difference.13
While evidence shows implants are successful when placed in previously infected sites, suggested treatment guidelines should be followed to achieve success. These include thorough debridement of the implant site prior to placement, guided bone
regeneration between the bone and implant, and prescribing systemic antibiotics.12,14
Case report
A 48-year-old female patient presented to the graduate endodontic clinic with a referral to evaluate and treat tooth No. 11 through the existing crown. The patient’s chief complaint was, “I was told a year ago I had an infection, but it hasn’t bothered me. They told me I needed a root canal to get rid of the infection.” The patient had no significant health history or any known drug allergies. Dental history for tooth No.11 included multiple restorations followed by a final core and crown in 2019. The adjacent tooth, No. 12, was replaced with an implant in 2018 and restored in 2019, 6 months following final crown of tooth No. 11. Upon examination of records, a periapical radiolucency on tooth No. 11 was visible on the day of crown fabrication and delivery (Figure 1). There was no note of this lesion in the patient’s record. An updated radiograph was taken during a periodic oral exam in September of 2023 showing clear delineation of the periapical radiolucency on tooth No.11 (Figure 2).
Upon presentation to the endodontic clinic, the patient was asymptomatic. Extraoral exam revealed no signs of acute infection and no lymphadenopathy. Intraoral exam showed no signs of acute infection and no sinus tracts. The crown on tooth No. 11 had adequate margins, contacts, and no recurrent decay was detected. Endodontic testing revealed negative responses to cold, percussion, and palpation. Probing depths of tooth No.11 and adjacent implant No. 12 were equal to or less than 3 mm, and no mobility was recorded. Radiographic examination revealed a periapical radiolucency present on the distal aspect of the root apex extending toward implant No. 12. Diffuse calcification in the coronal portion of the canal was observed, and no caries was noted (Figure 3).
As previous literature has identified the negative effect between periradicular periodontitis of natural teeth and adjacent implants, a limited field of view CBCT (Carestream Dental S 8200 3D, Atlanta, Georgia) was exposed to properly define the periapical radiolucency. Measuring from the apex of tooth No. 11 to a line perpendicular to the long axis of the implant,
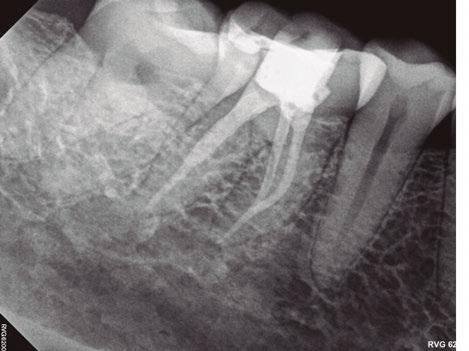
Figure 1 (left): Periapical radiograph taken at the time of tooth No. 11 crown delivery in 2018 with a periapical radiolucency extending distally toward implant No. 12. Figure 2 (right): Updated periapical radiograph taken in 2023 during a periodic oral exam showing clear delineation of a periapical radiolucency associated with tooth No. 11
Figure 3: Periapical radiographs taken during endodontic consultation in 2023. Periapical radiolucency originated from tooth No. 11 and extended toward implant No. 12. Calcification was appreciated in the coronal portion of the canal space on tooth No. 11
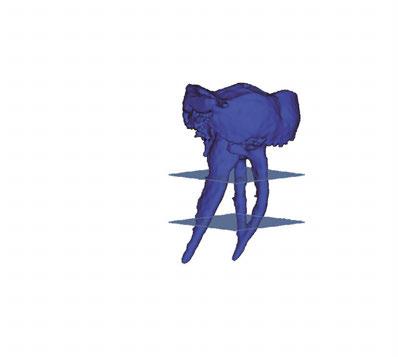
5A-5B: CBCT was taken during initial endodontic exam in 2023. 5A. Coronal CBCT
revealed a 6.1 mm x 3.0 mm hypodensity extending from the apical and distal aspect of No. 11. 5B. Sagittal
slices revealed the presence of bone between tooth No. 11 and implant No. 12
spacing of 3.4 mm between the two was noted (Figure 4). The recommended amount of space between a natural tooth and dental implant should be 1.5 mm-2 mm, proving adequate spacing in this case.15 Coronal views of the CBCT evaluation revealed a 6.1 mm x 3.0 mm hypodensity extending from the apical and distal aspect of tooth No. 11 (Figure 5A). Sagittal slices revealed the presence of healthy bone morphology between the distal border of the hypodensity on tooth No. 11 and implant No. 12, thus the hypodensity did not extend to the implant (Figure 5B). Reference was made to the Treatment Options for the Compromised Tooth: A Decision Guide published by the AAE in 2017 to determine prognosis.16 In evaluating the coronal tooth structure, tooth No. 11 had a well-fitting crown with adequate margins, no need for crown lengthening, and required only routine endodontic treatment placing it in the favorable category. The periodontal condition of tooth No. 11 was also favorable with probing depths equal to or less than 3 mm and a normal periodontium. Lastly, the apical periodontitis was expected to resolve following non-surgical root canal treatment.16 Thus, tooth No. 11 was diagnosed as pulpal necrosis with asymptomatic apical periodontitis with a favorable prognosis. Nonsurgical root canal treatment was planned, and informed consent was obtained.
Procedure
The patient was anesthetized with topical benzocaine and 3.4mL Septocaine (Articaine hydrochloride 4% and epinephrine 1:100,000) (Septodont, Saint-Maur-Fosses, France) via buccal and lingual infiltration. A rubber dam was placed, and the root canal system was accessed through the crown. Working length was obtained with Root ZX II apex locator (J. Morita, Kyoto, Japan) and verified with a periapical radiograph to be 24 mm. The tooth was then mechanically instrumented with WaveOne® rotary files (Dentsply Sirona, Charlotte, North Carolina) using 10mL of 6% NaOCl throughout the procedure. A final irrigation with EDTA (3mL) and SmartLite Pro EndoActivator™ (Dentsply Sirona, Charlotte, North Carolina) for 1 minute, followed by 6% NaOCl and activator for 1 minute was completed prior to obturation. Obturation was performed with EndoSequence® BC sealer (Brasseler
6A-6D: 6A. Preoperative periapical radiograph of
proper working
radiograph of tooth No. 11 confirmed proper master cone
periapical radiograph of tooth No. 11 verified length control and appropriate obturation
Figure 4: Sagittal CBCT slice revealed 3.4 mm of space between the apex of tooth No. 11 and the mesial border of implant No. 12
Designed to be accessible to all clinicians, ACE is a workflow that lets you anatomically shape, clean and seal with fewer products, saving time and money while still delivering superior clinical outcomes.
Shaping : single adaptive instrument to maximize dentin preservation while also maximizing clinical efficiency
Disinfection : all-in-one solution that can tackle tissue dissolution, smear layer removal and disinfection in one step
Obturation: zero shrinkage, bonded obturation that provides maximum antibacterial effect and biocompatibility SCAN THE QR CODE TO LEARN HOW ADOPTING ACE CAN REDUCE YOUR INVENTORY BY UP-TO 60% or visit BrasselerUSADental.com/ACE
USA, Savannah, Georgia) and gutta percha via continuous wave condensation. EndoSequence BC liner blue (Brasseler USA, Savannah, Georgia) was placed over the gutta percha at the canal orifice, and the tooth was temporized using a cotton pellet and Fuji IX placed in the access (Figure 6). Following completion of the root canal, the patient was scheduled for a 3-month reevaluation and referred to her provider for definitive restoration. Healing was observed at the 3- and 6-month postoperative visits. Periapical radiographs were exposed at each visit revealing bony healing (Figure 7). The patient reported no pain or symptoms following nonsurgical root canal treatment. At both visits, percussion and palpation were negative. A CBCT was captured at the 6-month postoperative exam to evaluate healing. Coronal CBCT slices revealed a reduction in lesion size to 3.5 mm x 1.6 mm. Sagittal slices also showed reduction in lesion and maintained health of bone surrounding implant No. 12 (Figure 8). A 2011 article by Ng outlines eleven factors that, if present, improve periapical healing following primary non-surgical root canal treatment.17 Only two of these eleven factors, absence of a preoperative periapical lesion and size of the preoperative periapical lesion, were not met in this case report. Along with this and the 2017 AAE Treatment Options for the Compromised Tooth: A Decision Guide article, the final prognosis for healing is favorable.16
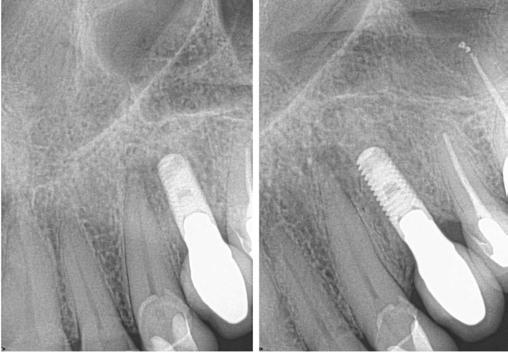
Figures 7A-7C: 7A. Immediate postoperative periapical radiograph. 7B.Periapical radiograph of tooth No. 11 at the 3-month reevaluation showing a reduction in size of the periapical radiolucency. 7C. Periapical radiograph of tooth No. 11 at the 6-month reevaluation showing a further reduction in the size of the periapical radiolucency.
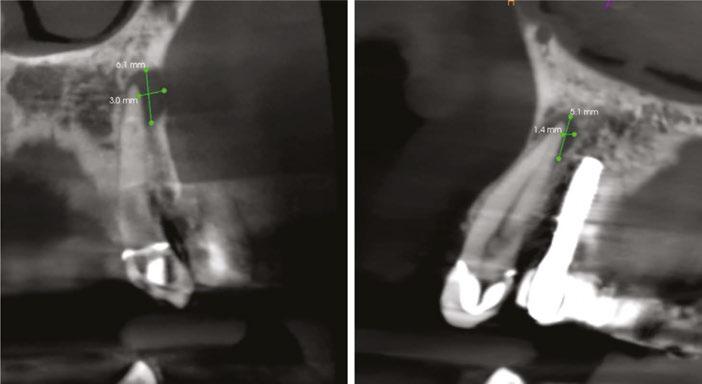
Figures 8A-8B: CBCT was taken at the 6-month postoperative visit. 8A. Coronal CBCT slices revealed a reduction in lesion size to 3.5 mm x 1.6 mm. 8B. Sagittal CBCT slices revealed a reduction in lesion size and maintained health of bone surrounding implant No. 12
Conclusion
Current evidence suggests the risk of an implant developing peri-implantitis is higher when the adjacent tooth has periapical pathology than it is when placed in an extraction site with previous infection. When planning a dental implant, pulp sensibility testing and proper radiographic and, if necessary, CBCT evaluation must be done on teeth adjacent to the implant site prior to placement. When endodontic therapy is indicated, treatment should be completed prior to implant placement. With increased time between root canal therapy and healing of an adjacent periapical lesion and implant placement, a decrease in development of peri-implantitis is expected. It is also important to maintain adequate space of at least 2 mm between the implant and adjacent tooth to help prevent retrograde peri-implantitis. Per the reviewed literature, it can be accepted that the presence of periapical pathology in the planned implant site had no statistical significance in healing when compared to implants placed in pristine sites. Interdisciplinary communication between the implant surgeon and endodontist is key in obtaining long term success of cases when periapical pathology is diagnosed in teeth adjacent to an implant or future implant site. With proper treatment planning, predictable outcomes can be achieved.
REFERENCES
1. Diaz P, Gonzalo E, Villagra LJG, Miegimolle B, Suarez MJ. What is the prevalence of peri-implantitis? A systematic review and meta-analysis. BMC Oral Health. 2022 Oct 19;22(1):449.
2. Schwarz F, Derks J, Monje A, Wang HL. Peri-implantitis. J Periodontol. 2018 Jun;89 Suppl 1:S267-S290.
3. Zhou W, Han C, Li D, Li Y, Song Y, Zhao Y. Endodontic treatment of teeth induces retrograde peri-implantitis. Clin Oral Implants Res. 2009 Dec;20(12):1326-1332.
4. Shaffer MD, Juruaz DA, Haggerty PC. The effect of periradicular endodontic pathosis on the apical region of adjacent implants. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998 Nov;86(5):578-581.
5. Saleh MHA, Khurshid H, Travan S, Sinjab K, Bushahri A, Wang HL. Incidence of retrograde peri-implantitis in sites with previous apical surgeries: A retrospective study. J Periodontol. 2021 Jan;92(1):54-61.
6. Fugazzotto P. A retrospective analysis of immediately placed implants in 418 sites exhibiting periapical pathology: results and clinical considerations. Int J Oral Maxillofac Implants. 2012 Jan-Feb;27(1):194-202.
7. Sarmast ND, Wang HH, Soldatos NK, Angelov N, Dorn S, Yukna R, Iacono VJ. A Novel Treatment Decision Tree and Literature Review of Retrograde Peri-Implantitis. J Periodontol. 2016 Dec;87(12):1458-1467.
9. Bender IB. Factors influencing the radiographic appearance of bony lesions. J Endod. 1982 Apr;8(4):161-170.
10. Costa JA, Mendes JM, Salazar F, Pacheco JJ, Rompante P, Câmara MI. Analysis of peri-implant bone defects by using cone beam computed tomography (CBCT): an integrative review. Oral Radiol. 2023 Jul;39(3):455-466.
11. Sarmast ND, Wang HH, Sajadi AS, Munne AM, Angelov N. Nonsurgical Endodontic Treatment of Necrotic Teeth Resolved Apical Lesions on Adjacent Implants with Retrograde/Apical Peri-implantitis: A Case Series with 2-year Follow-up. J Endod. 2019 May;45(5):645-650.
12. Chrcanovic BR, Martins MD, Wennerberg A. Immediate placement of implants into infected sites: a systematic review. Clin Implant Dent Relat Res. 2015 Jan;17 Suppl 1:e1-e16.
13. Lindeboom JA, Tjiook Y, Kroon FH. Immediate placement of implants in periapical infected sites: a prospective randomized study in 50 patients. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006 Jun;101(6):705-710.
14. Waasdorp JA, Evian CI, Mandracchia M. Immediate placement of implants into infected sites: a systematic review of the literature. J Periodontol. 2010 Jun;81(6):801-808.
15. Liu W, Zhu F, Samal A, Wang HL. Suggested mesiodistal distance for multiple implant placement based on the natural tooth crown dimension with digital design. Clin Implant Dent Relat Res. 2022 Dec;24(6):801-808.
16. American Association of Endodontists. Treatment Options for the Compromised Tooth: A Decision Guide. 2017. www.aae.org/treatmentoptions.
17. Ng YL, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of non-surgical root canal treatment: part 2: tooth survival. Int Endod J. 2011 Jul;44(7):610-625.
“It’s
Endodontic Artistry
Endo Direct
Endo Direct was established in 2023 with the sole mission of offering premium quality endodontic products at the best prices available. Endo Direct has quickly emerged as a trusted leader among dental professionals catering specifically to the needs of endodontic specialists.
Products and services
Endo Direct offers a comprehensive range of products essential for endodontic procedures, including:
• NiTi files
• Stainless steel files
• Bioceramic sealer
• Irrigants
• Motors and obturation devices
Our platform serves as a one-stop shop for all endodontic consumable needs, ensuring dental professionals have access to high quality products at the very best price.
At Endo Direct, customer satisfaction is paramount. We prioritize transparency, reliability, and affordability in all aspects of our operations. Our dedicated customer support team is readily available to assist dental professionals in selecting the right products, resolving issues, and ensuring a seamless purchasing experience.
Endo Direct makes the best files! Their Cyclone System is the perfect combination of cutting efficiency, flexibility, and durability. They are awesome.” — Dr. Todd Schultz, Endodontist, Endodontics Limited, Langhorne, Pennsylvania
EndoDirect.com remains dedicated to expanding its product portfolio, enhancing customer support initiatives, and fostering strategic partnerships to better serve the evolving needs of the specialty. We are committed to maintaining and growing our position as a leader in the endodontic specialty through innovation, integrity, and excellence.
For more information, visit Endo Direct’s website at www.endodirect.com, email at info@endodirect.com, or call 833-378-3588.
This information was provided by Endo Direct.
Case courtesy of Dr. Todd Schultz, Endodontist, Langhorne Pennsylvania
ProShape Cyclone System
Sealer
Dynamic navigation system: a revolutionary technology for endodontic microsurgery
Drs. Frederico Martinho and Bruno Giliolli Bisi
discuss the use of guided navigation in the endodontic practice
Over the past decade, technology has revolutionized endodontics. The ultimate goal of technology is to improve root canal treatment outcomes and tooth survivability rates.1,2 Root canal treatment failure is an ongoing issue despite technological advances; therefore, the search for new technology continues.3
Treating persistent apical periodontitis (PAP) is routine for an endodontist,4 and non-surgical root canal treatment (NSRCR) is one of the treatments for PAP.5 However, NSRCR can be affected by numerous factors.5 Endodontic microsurgery (EMS), which has been widely explored lately, is also a treatment option for PAP. The introduction of new technologies, including magnification and ultrasonics, and the development of new endodontic sealers and retro-filling materials have revolutionized EMS.1
Guided EMS has recently received a lot of attention.7 New technologies have enabled surgeons to treat more complex cases with more predictable outcomes. It allows the surgeon to deliver a more accurate and efficient minimally invasive treatment.2
Frederico Martinho, DDS, MSc, PhD, is currently a Clinical Professor in Endodontics at the University of Maryland School of Dentistry since 2017. He has lectured nationally and internationally and published over 100 scientific articles in peer-reviewed journals. He has received Journal of Endodontics publication awards and an honorable mention in 2017, 2018, and 2022. He is a member of the Scientific Advisory Board of the Journal of Endodontics and a reviewer for numerous endodontic and dental journals. Dr. Martinho has authored cutting-edge technology scientific articles in endodontic microsurgery. He is currently a member of the Research and Scientific Affairs Committee and the Special Committee for the Endodontic Educator Fellowship Awards from the American Association of Endodontists Foundation (AAEF). He is the 2022 recipient of the Educator Fellowship Award from the AAEF.
Bruno Giliolli Bisi, DDS, MSc, PhD, candidate, is currently a visiting scientist at the Division of Endodontics at the University of Maryland School of Dentistry, a PhD Candidate at the University of São Paulo (Brazil), and also a Clinical Professor in Endodontics at Metodista University of São Paulo (Brazil). Dr. Bisi is an active member of the American Association of Endodontics (AAE), the Brazilian Endodontics Society (SBENDO), and the Brazilian division of IADR (SBPqO). He has worked as an endodontist for 10 years part-time and is now developing research related to dynamic navigation.
Disclosures: Drs. Martinho and Bisi report no financial relationships to disclose.
Educational aims and objectives
This self-instructional course for dentists aims to discuss the details regarding dynamic navigation for more accurate and efficient minimally invasive endodontic treatment.
Expected outcomes
Endodontic Practice US subscribers can answer the CE questions by taking the quiz online at endopracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
• Define dynamic navigation.
• Realize some comparisons between static navigation and dynamic navigation during endodontic treatment.
• Identify some systems that employ dynamic navigation.
• Identify components of a dynamic navigation system.
• Recognize some aspects of the learning curve for guided navigation.
• Realize some of the benefits of dynamic navigation.
• Identify some possible future beneficial updates to guided navigation systems.
CREDITS
Guided EMS requires pre-surgical planning in planning software, and the surgery can be delivered under static or dynamic navigation.
Static navigation requires printing a 3D surgical guide.9 Several studies have shown that surgical guides improve EMS accuracy and efficiency when compared to freehand.3 However, surgical guide design and production have a complex workflow with numerous steps that can be time-consuming and require multiple appointments.4 Additionally, the software for surgical planning, 3D printing, and other related functions requires some surgical knowledge and training.
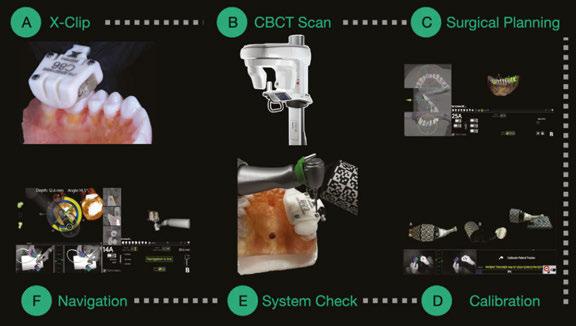
The Dynamic Navigation System (DNS) is a new technology in endodontics, and it is like a GPS for the handpiece and the drill.5 DNS has a more straightforward workflow (Figure 1) and is less time-consuming than static navigation.6 Previous studies revealed DNS’s high accuracy and efficiency for EMS.7 DNS enables the surgeon to deliver a minimally invasive EMS. Its high accuracy allows endodontists to conduct EMS in more difficult cases, such as areas with no direct visualization and close to vital anatomical structures. To date, DNS has been explored for different EMS steps, including bone window,8 osteotomy, and
root-end resection (RER).9 DNS can improve the accuracy and efficiency of EMS performed both by novice and experienced endodontists.10
Dynamic Navigation System
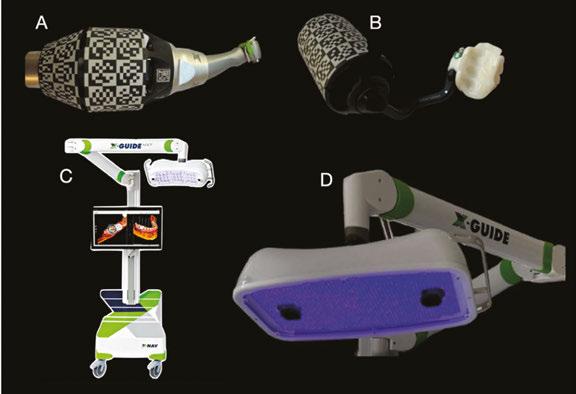
Currently, only a few companies offer DNS. These include the X-Guide® (X-Nav Technologies, Lansdale, Pennsylvania), the Navident (ClaroNav, Toronto, Canada), the ImplaNav™ (Bres Medical, Ingleburn, Australia), and the Denacam (Liestal, Switzerland). All these DNS systems share a similar navigation concept despite different manufacturers. These DNS software applications are overall very user-friendly with a straightforward workflow.
DNS has numerous components. The main components include a central console, a display for the user interface, a section in the upper part containing motion-tracking cameras, and a lighting system, which varies from manufacturer to manufacturer (Figure 2). The cameras identify the DNS trackers that are attached to the patient’s face and to the handpiece and create a precise 3D model of the surgical site and the handpiece’s relation to the site regarding the angle, spatial position, and drilling depth.5
To plan for DNS surgery, the cone beam computed tomography (CBCT) Digital Imaging and Communications in Medicine (DICOM) file is directly uploaded into the DNS software. A key advantage of the DNS is that it does not require separate software to open and visualize the CBCT scan. Once the CBCT scan DICOM file is in the DNS software, the surgeon can plan the EMS procedure. After surgical planning, the DNS software requires a calibration step, in which the software recognizes the trackers attached to the handpiece and the patient’s dentition and memorizes their geometry to ensure that the handpiece and the drill are accurately represented on the planned drilling path. It has been suggested that the pre-surgical steps should not take more than a total of 15 minutes.6 After calibration, the DNS software becomes live for navigation, guiding the user to the drill at the correct angle and position. The DNS software guides drilling in real-time, and when the desired depth is reached, the DNS software indicates to stop, and the procedure is completed.
DNS has a learning curve like other technologies. It is crucial to undergo thorough training before treating a patient although the DNS is easy to operate, which makes the DNS learning curve less steep. A relatively low number of trial attempts are sufficient to calibrate the operator on DNS prior to the surgery.11 A previous study showed that after 20 trial attempts, both novice and experienced endodontists delivered EMS more accurately and efficiently than freehand.5 Overall, the DNS has a less challenging learning curve and is easy to fit into the surgeon’s existing EMS workflow.
Dynamic Navigation System EMS studies
Early studies evaluated the accuracy and efficiency of DNS for osteotomy and RER.9,10,12,13 Accuracy is a primary concern when
performing EMS (Figure 3), especially in areas close to important anatomical structures, in which small deviations could lead to partial or irreversible damage to local structures. Surgical time
Figures 1A-1F: X-Guide workflow. 1A. X-Clip fit. 1B. CBCT scan. 1C. Surgical planning. 1D. DNS trackers calibration. 1E. System check. 1F. Live navigation screen
Figures 2A-2D: DNS trackers for the X-Guide software (X-Nav Techologies, Lansdale, Pennsylvania). 2A. Handpiece tracker assembled. 2B. Patient’s tracker attached to the X-Clip. 2C. X-guide system. 2D. Tracking camera using violet light
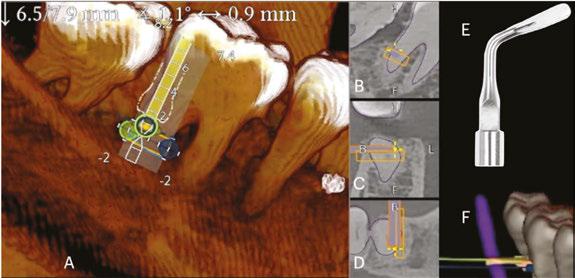
Figures 3A-3F: Root-end resection using DNS (X-Guide software). 3A. Live navigation for the linear cuts. 3B-3D. Live navigation screen representation over the axial, coronal, and sagittal CBCT scan plans. 3E. Ultrasonic tip (P1B, Helse Ultrasonics, SP, Brazil). 3F. DNS 3D- live navigation
is critical for EMS, and cutting down the EMS time is desirable. Optimizing the EMS surgical time with technology could avoid operator and patient fatigue, loss of anesthesia, and excessive bleeding, which can affect visibility and the outcome of the surgery. It is worth highlighting that the longer the surgical time, the higher the risk of technical error. Therefore, keeping the surgical time short using technology could also help to prevent mishaps.
Early studies have compared the accuracy and efficiency of DNS to the freehand method.13 Despite no fair comparison, it was still important at that time to prove that the DNS technology could enable the surgeon to conduct a more accurate and efficient EMS than the freehand existing method.
EMS involves many steps, including osteotomy, root-end resection, root-end cavity preparation, and root-end filling.14 All these steps are crucial for EMS success.15 Each EMS step can be a source of error, and cumulative errors can ultimately impact the EMS outcome and longevity of the tooth. To date, DNS has been mainly explored for osteotomy, bone-window cut, and root-end resection.8,9,10,12,13 Previous studies have demonstrated the high accuracy and efficiency of DNS for osteotomy and root-end resection.9,16 Most of these studies indicated 2D- and 3D-deviation metrics below or close to 2 mm.10,12 Moreover, these studies also showed a lesser root-end resection angle compared to freehand surgery.9
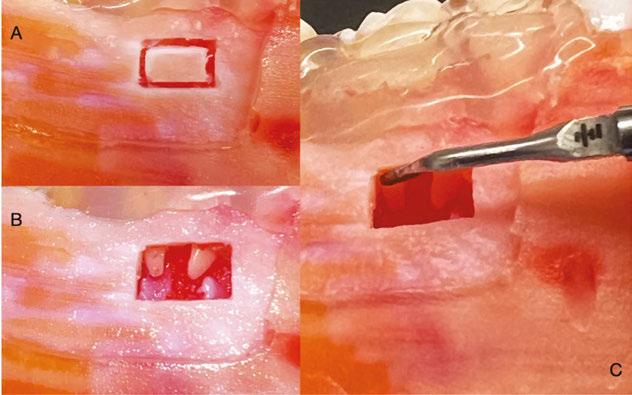
Bone window or “bony lid” surgery was introduced in 1987 for direct surgical access to the apical root of mandibular molars for root-end resection16 (Figure 4). It is an alternative surgical method to conventional osteotomy using burs or drills. The procedure involves preparing and removing a bone window, which is then reinserted into its original position after the surgery. One advantage of bone window surgery is that it preserves and maintains bone that would have been removed by conventional osteotomy with burs (Figure 4). The bone window works as an autogenous graft without substitute materials for guided tissue regeneration providing essential bone remodeling factors, including osteoinductive molecules, proper scaffolding, and osteogenic cells.18,19
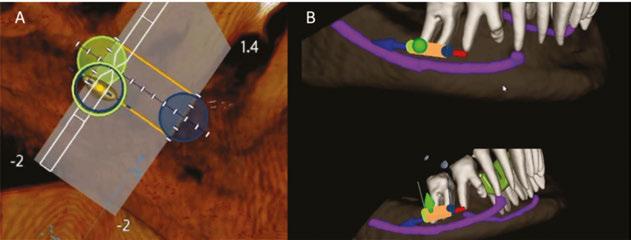
Recently, DNS was successfully applied for a bone-window surgery8 study which was the first to integrate X-Guide software into a piezoelectric device for bone window cutting in EMS (Figure 5). The authors showed that DNS improved the accuracy and efficiency of EMS piezosurgery. Piezosurgery’s many advantages include the ability to perform minimally invasive procedures, preserve neurovasular structures, control bleeding, and reduce thermal damage.23,24 The piezosurgery preserves more of the cancellous properties and more osteocytes than traditional osteotomy.22 Moreover, piezosurgery offers less edema, less trismus, reduced pain, and improved quality of life after the surgery.23
The DNS has several applications in endodontics.24,25 In addition to EMS, DNS has been mainly tested for intraosseous
DNS will be updated with new features as the technology evolves. Endodontic techniques and applications are encouraged. Recent studies integrated DNS into augmented reality (AR) headsets for mixed reality.26 AR is one of the biggest technology trends in the medical field. DNS integration into the AR headset allowed the surgeon to overlay the high-definition AR content of the live output display from the navigation system near the surgical site through the Microsoft HoloLens 2 AR headset. AR integration with DNS improved surgeons’ hand-eye coordination and also overcame 3D DNS’s disadvantage, which was the need to simultaneously pay attention to both the surgical site as well as the output of the DNS display. The HoloLens AR headset allowed the operator to remain focused on the surgical site while drilling for RER and osteotomy without having to look away at the DNS monitor.16 The DNS has attracted attention from both clinicians and researchers lately. As the DNS technology advances, more studies are needed to evaluate the clinical accuracy and efficiency
DNS for EMS.
of
EP
Figures 4A-4C: Bone window cut with DNS. 4A. Linear cuts for the bone window using Ultrasonic tip (P1B, Helse Ultrasonics, SP, Brazil). 4B. Bone window. 4C. Distal root-end resection following the bone window
Figures 5A-5B: DNS Live screen for the bone window cut. 5A. Representation of the straight-cutting alignment and guidance on bone window procedure. 5B. 3D pre-surgical planning for bone window cut
REFERENCES
1. Dioguardi M, Stellacci C, La Femina L, Spirito F, Sovereto D, Laneve E, Manfredonia MF, D’Alessandro A, Ballini A, Cantore S, Lo Muzio L, Troiano G. Comparison of Endodontic Failures between Nonsurgical Retreatment and Endodontic Surgery: Systematic Review and Meta-Analysis with Trial Sequential Analysis. Medicina (Kaunas). 2022 Jul 4;58(7):894.
2. Connert T, Zehnder MS, Amato M, Weiger R, Kühl S, Krastl G. Microguided Endodontics: a method to achieve minimally invasive access cavity preparation and root canal location in mandibular incisors using a novel computer-guided technique. Int Endod J. 2018 Feb;51(2):247-255.
3. La Rosa GRM, Peditto M, Venticinque A, Marcianò A, Bianchi A, Pedullà E. Advancements in guided surgical endodontics: A scoping review of case report and case series and research implications. Aust Endod J. 2024 Aug;50(2):397-408.
4. Buniag AG, Pratt AM, Ray JJ. Targeted Endodontic Microsurgery: A Retrospective Outcomes Assessment of 24 Cases. J Endod. 2021 May;47(5):762-769.
5. Martinho FC, Griffin IL, Corazza BJM. Current Applications of Dynamic Navigation System in Endodontics: A Scoping Review. Eur J Dent. 2023 Jul;17(3):569-586.
6. Martinho FC, Bisi BG, Gavini G, Griffin IL, Tordik PA. Comparison of the Accuracy and Efficiency of Two Dynamic Navigation System Workflow for Fiber-post Removal: Small versus Large Field-of-view Registration Workflows. J Endod. 2024 Jun 28:S0099-2399(24)00363-00367.
7. Geo TG, Saxena P, Gupta S. Static vs. dynamic navigation for endodontic microsurgery - A comparative review. J Oral Biol Craniofac Res. 2022 Jul-Aug;12(4):410-412. Epub 2022 May 17. Erratum in: J Oral Biol Craniofac Res. 2024 Jul-Aug;14(4):358-359.
8. Martinho FC, Griffin IL, Tordik PA. Piezoelectric Device and Dynamic Navigation System Integration for Bone Window-Guided Surgery. J Endod. 2023 Dec;49(12):1698-1705.
9. Dianat O, Nosrat A, Mostoufi B, Price JB, Gupta S, Martinho FC. Accuracy and efficiency of guided root-end resection using a dynamic navigation system: a human cadaver study. Int Endod J. 2021 May;54(5):793-801.
10. Martinho FC, Aldahmash SA, Cahill TY, Gupta S, Dianat O, Mostoufi B, Price JB, Griffin I, Tordik PA. Comparison of the Accuracy and Efficiency of a 3-Dimensional Dynamic Navigation System for Osteotomy and Root-end Resection Performed by Novice and Experienced Endodontists. J Endod. 2022 Oct;48(10):1327-1333.
11. Wang W, Zhuang M, Tao B, Wang F, Wu Y. Learning curve of dynamic navigation-assisted zygomatic implant surgery: An in vitro study. J Prosthet Dent. 2024 Jul;132(1):178.e1-178. e12.
12. Martinho FC, Rollor C, Westbrook K, Aldahmash SA, Fay GG, Rivera E, Parsa A, Price JB, Tordik PA. A Cadaver-based Comparison of Sleeve-guided Implant-drill and Dynamic Navigation Osteotomy and Root-end Resections. J Endod. 2023 Aug;49(8):1004-1011.
13. Aldahmash SA, Price JB, Mostoufi B, Griffin IL, Dianat O, Tordik PA, Martinho FC. Real-time 3-dimensional Dynamic Navigation System in Endodontic Microsurgery: A Cadaver Study. J Endod. 2022 Jul;48(7):922-929.
14. Floratos S, Kim S. Modern Endodontic Microsurgery Concepts: A Clinical Update. Dent Clin North Am. 2017 Jan;61(1):81-91.
16. Martinho FC, Griffin IL, Price JB, Tordik PA. Augmented Reality and 3-Dimensional Dynamic Navigation System Integration for Osteotomy and Root-end Resection. J Endod. 2023 Oct;49(10):1362-1368.
17. Khoury F, Hensher R. The bony lid approach for the apical root resection of lower molars. Int J Oral Maxillofac Surg. 1987 Apr;16(2):166-170.
18. Mittal M, Vashisth P, Arora R, Dwivedi S. Combined endodontic therapy and periapical surgery with MTA and bone graft in treating palatogingival groove. BMJ Case Rep. 2013 Apr 18;2013:bcr2013009056.
19. Lee SM, Yu YH, Wang Y, Kim E, Kim S. The Application of “Bone Window” Technique in Endodontic Microsurgery. J Endod. 2020 Jun;46(6):872-880.
20. Hennet P. Piezoelectric Bone Surgery: A Review of the Literature and Potential Applications in Veterinary Oromaxillofacial Surgery. Front Vet Sci. 2015 May 5;2:8.
21. Bharathi J, Mittal S, Tewari S, Tewari S, Duhan J, Sangwan P, Kumar V. Effect of the Piezoelectric Device on Intraoperative Hemorrhage Control and Quality of Life after Endodontic Microsurgery: A Randomized Clinical Study. J Endod. 2021 Jul;47(7):1052-1060.
22. Mouraret S, Houschyar KS, Hunter DJ, Smith AA, Jew OS, Girod S, Helms JA. Cell viability after osteotomy and bone harvesting: comparison of piezoelectric surgery and conventional bur. Int J Oral Maxillofac Surg. 2014 Aug;43(8):966-971.
23. Al-Moraissi EA, Elmansi YA, Al-Sharaee YA, Alrmali AE, Alkhutari AS. Does the piezoelectric surgical technique produce fewer postoperative sequelae after lower third molar surgery than conventional rotary instruments? A systematic review and meta analysis. Int J Oral Maxillofac Surg. 2016 Mar;45(3):383-391.
24. Mekhdieva E, Del Fabbro M, Alovisi M, Scotti N, Comba A, Berutti E, Pasqualini D. Dynamic Navigation System vs. Free-Hand Approach in Microsurgical and Non-Surgical Endodontics: A Systematic Review and Meta-Analysis of Experimental Studies. J Clin Med. 2023 Sep 8;12(18):5845.
25. Vasudevan A, Santosh SS, Selvakumar RJ, Sampath DT, Natanasabapathy V. Dynamic Navigation in Guided Endodontics - A Systematic Review. Eur Endod J. 2022 Jun;7(2):81-91.
26. Martinho FC, Qadir SJ, Griffin IL, Melo MAS, Fay GG. Augmented Reality Head-Mounted Device and Dynamic Navigation System for Postremoval in Maxillary Molars. J Endod. 2024 Jun;50(6):844-851.
Continuing Education Quiz
Dynamic navigation system: a revolutionary technology for endodontic microsurgery
MARTINHO/BISI
1. For endodontic microsurgery, to date, dynamic navigation systems have been explored for _________.
a. bone window
b. osteotomy
c. root-end resection (RER)
d. all of the above
2. DNS software applications that are currently available _______.
a. are overall very user-friendly with a straightforward workflow
b. require a long and grueling onboarding process
c. need specialty technicians to use properly
d. have complicated interfaces
3. (With the DNS) The cameras identify the DNS trackers that are attached to the patient’s face and to the handpiece and create a precise 3D model of the surgical site and the handpiece’s relation to the site regarding the ________.
a. angle
b. spatial position
c. drilling depth
d. all of the above
4. To plan for DNS surgery, the _______ is/are directly uploaded into the DNS software.
a. digital photographs
b. treatment notes
c. cone beam computed tomography (CBCT) Digital Imaging and Communications in Medicine (DICOM) file
d. 2D X-rays
5. A key advantage of the DNS is that it does not require separate software to open and visualize the CBCT scan.
a. True
b. False
6. A previous study showed that after ________ trial attempts, both novice and experienced endodontists delivered EMS more accurately and efficiently than freehand.
a. 5
b. 10
c. 20
d. 30
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://endopracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://endopracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 070
Date Published: September 13, 2024
Expiration Date: September 13, 2027
2 CE CREDITS
7. Optimizing the EMS surgical time with technology could avoid _______, which can affect visibility and the outcome of the surgery.
a. operator and patient fatigue
b. loss of anesthesia
c. excessive bleeding
d. all of the above
8. _________ is/are an alternative surgical method to conventional osteotomy using burs or drills.
a. Root end dissection
b. Bone window or “bony lid” surgery
c. osteotomies
d. none of the above
9. Piezosurgery’s many advantages include the ability to perform minimally invasive procedures, preserve neurovascular structures, control bleeding, reduce thermal damage, and improve healing.
a. True
b. False
10. Recent studies integrated DNS into ________ .
a. a joystick format
b. augmented reality (AR) headsets for mixed reality
c. a video game format
d. a format that has no learning curve
To provide feedback on CE, please email us at education@medmarkmedia.com
Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
Endodontic management of periapical lesions using the GentleWave procedure with minimal instrumentation
Drs. Karen Potter, Seda Falakaloğlu, and Mustafa Gündoğar describe how multisonic technology can clean and disinfect teeth
Endodontic treatment aims to restore and preserve the health of apical tissues so that patients can achieve a functional and asymptomatic tooth structure. Removal of infected tissue and bacteria appears to increase the success rate of endodontic treatment.1,2 Due to the inadequacies of mechanical debridement alone and complex anatomy, many different irrigation and activation techniques have been used. Adequate irrigation is the key to successful endodontic treatment because it is the only way to reach areas untouched by instrumentation.3-5
The GentleWave® system (GWS) (Sonendo® Inc, California) uses multisonic technology to deliver irrigation solutions from the tip of a procedure instrument into the pulp chamber and canal system. These solutions are degassed to prevent energy loss.6 GWS consists of a console and three different handpieces
Karen Potter, DDS, has provided endodontic care in San Clemente, California for almost 15 years. She graduated from the University of Southern California Magna Cum Laude with degrees in Spanish and Natural Sciences. She then went to dental school at the UCLA School of Dentistry, and after that she attended her Endodontic residency program at the University of Iowa. Her research project in residency regarding the placement of dental implants by endodontists has been published in the JOE and cited frequently.
Seda Falakaloğlu, DDS, graduated from Ege University, Faculty of Dentistry in Turkey, receiving her dental degree in 2011. She worked as a research assistant in the Department of Endodontics at Dicle University Faculty of Dentistry and became qualified to become an endodontist in 2017 and has worked as an associate professor in the Department of Endodontics, Faculty of Dentistry at Istanbul Health and Technology University, Istanbul, Turkey, since 2023.
Mustafa Gündoğar, DDS, graduated from Marmara University, Faculty of Dentistry in Turkey with his dental degree in 2005. He attended the Endodontics Program of Graduate Study offered by Institute of Health Sciences at Marmara University and graduated with a PhD degree in Endodontics in 2011. He is currently working in the Department of Endodontics, Faculty of Dentistry at Medipol University, Istanbul, Turkey as an associate professor. Dr Gündoğar has been working at the Regenerative and Restorative Medicine Research Center (REMER) since 2020. Dr. Gündoğar is a social media influencer with more than 55K followers on Instagram. He is the founder of ENDOTALKS Library, the first patented endodontic education platform on social media.
Disclosure: Dr. Potter is a Key Opinion Leader for Sonendo®
Educational aims and objectives
This self-instructional course for dentists aims to review management of endodontic cases with periapical lesions using minimal instrumentation.
Expected outcomes
Endodontic Practice US subscribers can answer the CE questions by taking the quiz online at endopracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can: Review the keys to successful endodontic treatment.
• Define how the GentleWave System uses multisonic acoustic energy to transmit the irrigation solution to the root canal system.
• Observe two case reports to show management of periapical lesions.
2 CE CREDITS
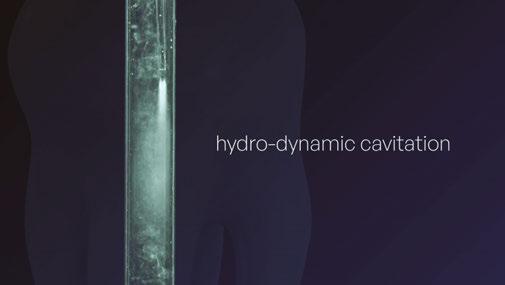
(Anterior/Premolar, Molar, and Cleanflow PI). Integrated flow diverters in these handpieces convert the degassed solution flow into a spatter, which interacts with the stationary liquid. This movement in the negative pressure environment allows the continuous formation and bursting of microbubbles within the root canal system to create hydrodynamic cavitation. As a result of this mechanical movement, multisonic acoustic energy is generated that transmits the irrigation solution to the root canal system.7-9
This article deals with managing two endodontic cases with periapical lesions using GWS and minimal instrumentation. The aim is to discuss the clinical outcome of GWS and offer clinicians treatment guidance.
Case reports
Case 1
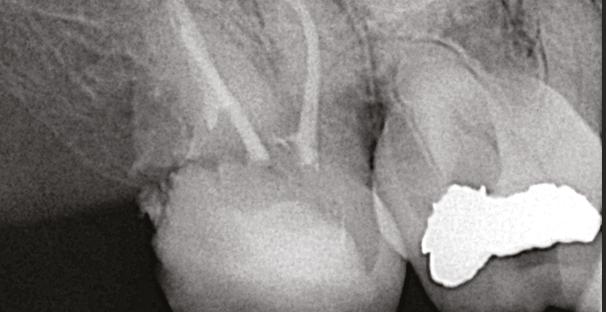
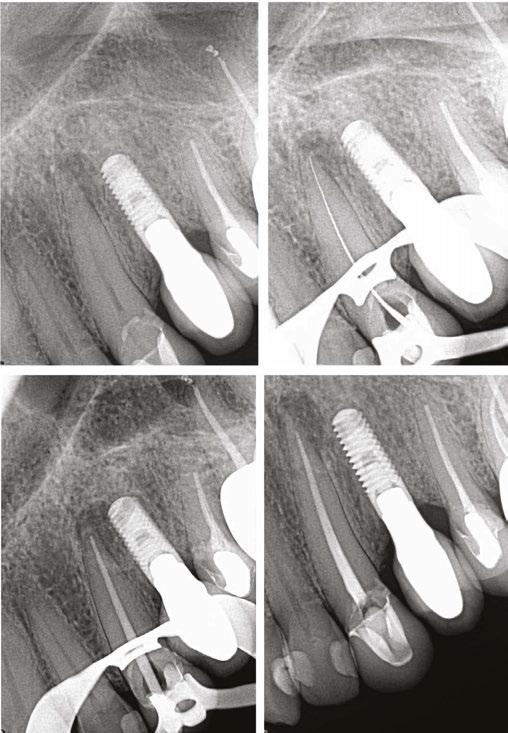
A 43-year-old female patient with a noncontributory medical history was referred with a chief complaint of a bad toothache that was very painful to touch. The patient reported a history of trauma and had been told that tooth No. 8 had been dead for years. There was a history of internal bleaching 4 years prior with some success, but the shade had regressed. Clinical examination of the right first maxillary central revealed fluctuant swelling of
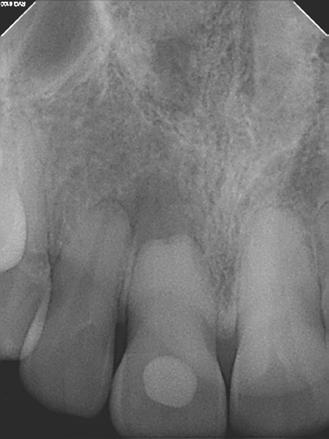
the labial gingiva. Radiographic examination revealed a lingual composite restoration and a blunted root tip with calcific metamorphosis. Also, a periapical lesion was associated with the root canal (Figure 1A). The patient’s history of symptoms and the clinical examination indicated a pulpal diagnosis of pulp necrosis and an acute apical abscess. After a review of options with the patient, root canal treatment with internal bleaching was recommended to retain the tooth, and the patient consented to care.
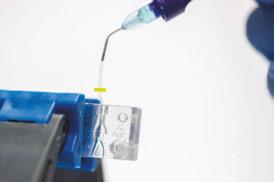
A standard anesthesia protocol (lidocaine with 1:100.000 epinephrine and articaine with 1:200.000 epinephrine through buccal and palatal infiltration) was followed, and the tooth was isolated with a rubber dam. A dental operating microscope was utilized for creating a minimally invasive, straight-line endodontic access opening. After patency and working length were established, mechanical instrumentation was prepared with No. 20 variable taper SlimShaper® file (Avalon Biomed, Houston, Texas). Following minimal preparation, debridement and disinfection were completed utilizing the GWS, where sodium hypochlorite (NaOCI) + distilled water + ethylenediaminetetraacetic acid (EDTA) + distilled water were delivered using Multisonic UItracleaning technology (Figure 1B). After the cleaning process, the root canal was dried using sterile paper points. A single cone technique employing gutta percha and bioceramic sealer (EndoSequence® BC Sealer HiFlow; Brasseler USA, Savannah, Georgia) was utilized during obturation. A coronal seal was placed, and the access cavity was sealed with temporary filling material. The patient was advised to return to the referring general dentist for internal bleaching.
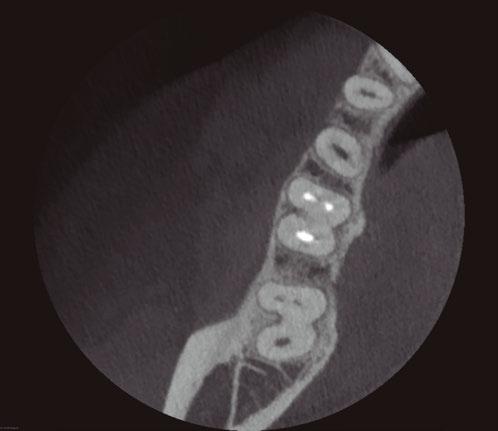
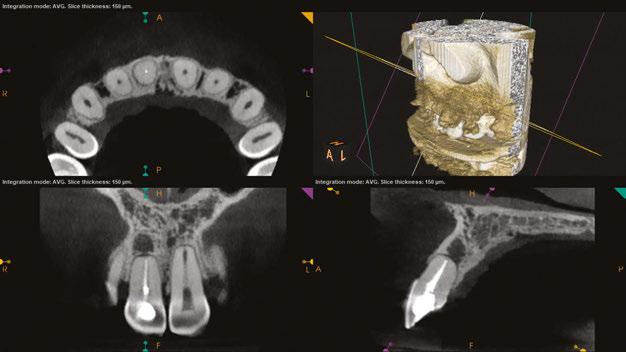
tissue lesions, or root resorption radiographically. After 2 years of GWS, cone beam computed tomography (CBCT) images show intact lamina dura and growth of trabecular bone in Figure 1D.
Case 2
A postoperative radiograph is presented in Figure 1C. At the 2-year recall, the patient was asymptomatic. Upon clinical and radiographic examination, there was no painful response to percussion or palpation, no presence of mobility, fractures, soft
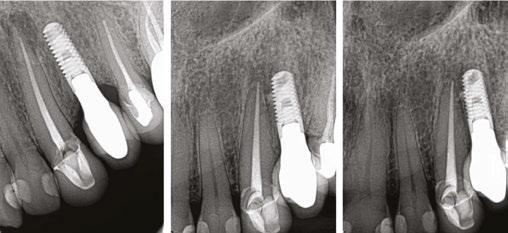
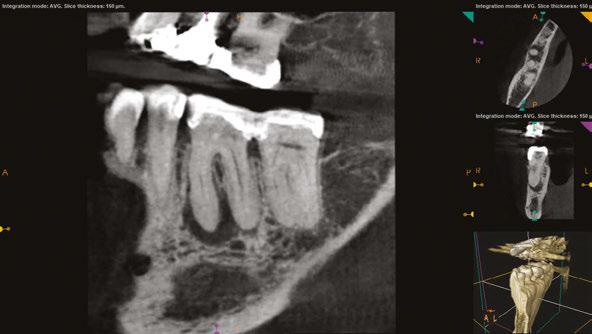
A 75-year-old female patient with a noncontributory medical history was referred with a chief complaint of dull pain in the lower right quadrant for 1 month, worsened by pressing on the gum. The patient reported a history of crown preparations of teeth Nos. 30 and 31, 1 week prior. Gingival swelling for several days had partially subsided since starting antibiotic therapy. Clinical examination of the right first maxillary molar (No. 30) revealed negative sensitivity to percussion and a mild pain response to palpation. There was a vestibular swelling over the mesial root of tooth No. 30. Vitality testing elicited a negative response. Radiographic examination revealed a large periapical lesion on the mesial root of tooth No. 30 (Figure 2A). The patient’s history of symptoms and the clinical examination indicated a diagnosis of
Figure 1A (left): Preoperative image of Case 1. Figure 1B (middle): Image of GentleWave. Figure 1C (right): Post-GentleWave procedure radiograph of Case 1
Figure 1D: 2-years post-GentleWave procedure recall with healing periapical lesion of Case 1
pulp necrosis and an acute apical abscess. After a review of options with the patient, endodontic therapy was recommended to retain the tooth.
After standard local anesthesia and isolation protocols, the temporary crown was removed, and the tooth was accessed under the dental operating microscope. Upon entry to the pulp chamber, necrotic tissue and purulence was noted from the mesial canals. After patency and working length were established, mechanical instrumentation was prepared with at No. 20 variable taper SlimShaper file. Following minimal preparation, debridement and disinfection were completed utilizing the GWS, where sodium hypochlorite (NaOCI) + distilled water + ethylenediaminetetraacetic acid (EDTA) + distilled water were delivered using Multisonic UItracleaning technology. After the cleaning process, root canals were dried using sterile paper points. A single cone technique employing gutta percha and bioceramic sealer were utilized during obturation (Figure 2B). A coronal seal was placed, and the temporary crown was re-cemented with TempBond™ (Kerr).
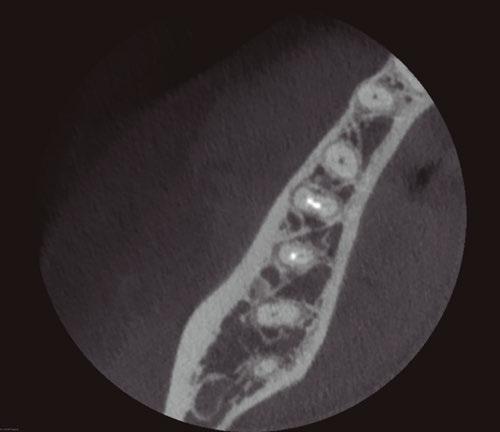
Upon completion of endodontic therapy with the GWS, at the 6-month recall, the tooth was asymptomatic (Figure 2C). The CBCT was taken, and images showed complete healing of the apical bone (Figure 2D).
Figure 2B: Post-GentleWave procedure obturated root canal system of Case 2 Figure 2C: 6-month recall postoperative radiograph of Case 2
Figure 2D: CBCT images with no evidence of periapical lesion of Case 2
Figure 2A: Preoperative images of Case 2
Discussion
The primary goal of endodontic treatment of pulpal infected teeth and periapical lesions is to eliminate the infection and prevent microorganisms from infecting or re-infecting the root and surrounding tissues.10 In this article, we evaluated the efficacy of GWS on the healing of periapical lesions. The patients with periapical lesions in their teeth healed after endodontic therapy with the GentleWave Procedure which allows better irrigation and canal anatomy contact with the irrigants then standard irrigation techniques.
The concept of minimally invasive preparation to save root dentin by instrumenting smaller file sizes in root canals has been discussed for years. Preserving the dentin structure in its natural form is one of the main factors improving the prognosis after endodontic treatment.11 Notwithstanding, the GWS is a minimally invasive alternative treatment for root canal therapy. GWS reduces the need to shape the roots using extensive instrumentation, thus preserving dentin for minimal invasive endodontic technique. In the literature, in-vitro GWS studies have shown that a statistically significant clean root canal system was observed even when molars were shaped with No. 15/.04.7-9 This remarkable effect results from the combined washing effect, multisonic energy, and the dissolving action of NaOCl and EDTA irrigating solutions. Cavitation releases energy from imploding, microscopic vacuum, and gas bubbles, allowing the freed force to dissolve and break down pulpal tissue.12 In our cases, the root canals were prepared with a No. 20 variable taper SlimShaper file. This preparation size adheres to GWS’s minimally invasive root canal preparation philosophy, which achieved successful results.
Sigurdsson, et al., reported that treatment of sizable periapical lesions with the GWS resulted in a success rate of 97.7% at 12-month re-evaluation.13 Essentially, unsuccessful root canal treatments are often the result of microorganisms remaining in the canals after treatment. The lack of success is probably due to the limitations of traditional chemomechanical instrumentation and the difficulties in accessing the morphological complexities in the root canals.10 The success of GWS in removing microorganisms from anatomical complexities was able to facilitate both the healing of the periapical lesion and the regrowth of the alveolar bone.14,15 Healing depends on the disinfection process’s effectiveness and the host’s response to the debris or biofilm remaining in the root canals, so lesion healing is a dynamic process.16 GWS has been shown to remove the smear layer and biofilm effectively.17,18 In addition, Haapasalo, et al., reported that GWS greatly improved the effectiveness of tissue dissolution compared to other irrigation methods.8 The rapid organic tissue ability and effective removal process could contribute to the healed periapical lesions in our cases. Noticeably, one of the cases presented healed after 6 months. This rapid healing has been consistent with a prospective clinical study using GWS.19 In these case reports, both teeth were cleaned and disinfected during the GWS with no evidence of reinfection, clinical signs, or symptoms present at the 6 month and 2 year recalls. These case reports demonstrate the ability of the GWS to clean and disinfect teeth with apical periodontitis and minimally instrumented canals.
Conclusion
The cases presented in this paper highlight the use of multisonic energy technology as the GentleWave System, in managing teeth with periapical lesions. Although more extensive clinical studies need to be utilized, these clinical cases show that the GentleWave System improves the success of endodontic treatment results with minimal instrumentation.
REFERENCES
1. Vera J, Siqueira JF Jr, Ricucci D, Loghin S, Fernández N, Flores B, Cruz AG. One- versus two-visit endodontic treatment of teeth with apical periodontitis: a histobacteriologic study. J Endod. 2012 Aug;38(8):1040-1052.
2. Sjögren U, Figdor D, Persson S, Sundqvist G. Influence of infection at the time of root filling on the outcome of endodontic treatment of teeth with apical periodontitis. Int Endod J. 1997 Sep;30(5):297-306.
3. Burleson A, Nusstein J, Reader A, Beck M. The in vivo evaluation of hand/rotary/ultrasound instrumentation in necrotic, human mandibular molars. J Endod. 2007 Jul;33(7): 782-787.
4. Susin L, Liu Y, Yoon JC, Parente JM, Loushine RJ, Ricucci D, Bryan T, Weller RN, Pashley DH, Tay FR. Canal and isthmus debridement efficacies of two irrigant agitation techniques in a closed system. Int Endod J. 2010 Dec;43(12):1077-1090.
5. Gu LS, Kim JR, Ling J, Choi KK, Pashley DH, Tay FR. Review of contemporary irrigant agitation techniques and devices. J Endod. 2009 Jun;35(6):791-804.
7. Molina B, Glickman G, Vandrangi P, Khakpour M. Evaluation of Root Canal Debridement of Human Molars Using the GentleWave System. J Endod. 2015 Oct;41(10): 1701-1705.
8. Haapasalo M, Wang Z, Shen Y, Curtis A, Patel P, Khakpour M. Tissue dissolution by a novel multisonic ultracleaning system and sodium hypochlorite. J Endod. 2014 Aug;40(8):1178-1181.
9. Charara K, Friedman S, Sherman A, Kishen A, Malkhassian G, Khakpour M, Basrani B. Assessment of Apical Extrusion during Root Canal Irrigation with the Novel GentleWave System in a Simulated Apical Environment. J Endod. 2016 Jan;42(1):135-139.
11. Murdoch-Kinch CA, McLean ME. Minimally invasive dentistry. J Am Dent Assoc. 2003 Jan;134(1):87-95.
12. Chen B, Szabo D, Shen Y, Zhang D, Li X, Ma J, Haapasalo M. Removal of calcifications from distal canals of mandibular molars by a non-instrumentational cleaning system: A micro-CT study. Aust Endod J. 2020 Apr;46(1):11-16.
13. Sigurdsson A, Garland RW, Le KT, Rassoulian SA. Healing of Periapical Lesions after Endodontic Treatment with the GentleWave Procedure: A Prospective Multicenter Clinical Study. J Endod. 2018 Mar;44(3):510-517.
14. Patel S, Wilson R, Dawood A, Foschi F, Mannocci F. The detection of periapical pathosis using digital periapical radiography and cone beam computed tomography - part 2: a 1-year post-treatment follow-up. Int Endod J. 2012 Aug;45(8):711-723.
15. Vandrangi P. Evaluating Penetration Depth of Treatment Fluids into Dentinal Tubules Using the GentleWave System. Dentistry. 2016;6(3).
16. Zhang MM, Liang YH, Gao XJ, Jiang L, van der Sluis L, Wu MK. Management of Apical Periodontitis: Healing of Post-treatment Periapical Lesions Present 1 Year after Endodontic Treatment. J Endod. 2015 Jul;41(7):1020-1025.
17. Choi HW, Park SY, Kang MK, Shon WJ. Comparative Analysis of Biofilm Removal Efficacy by Multisonic Ultracleaning System and Passive Ultrasonic Activation. Materials (Basel). 2019 Oct 25;12(21):3492.
18. Zhang D, Shen Y, de la Fuente-Núñez C, Haapasalo M. In vitro evaluation by quantitative real-time PCR and culturing of the effectiveness of disinfection of multispecies biofilms in root canals by two irrigation systems. Clin Oral Investig. 2019 Feb;23(2):913-920.
19. Sigurdsson A, Le KT, Woo SM, Rassoulian SA, McLachlan K, Abbassi F, Garland RW. Six-month healing success rates after endodontic treatment using the novel GentleWave™ System: The pure prospective multi-center clinical study. J Clin Exp Dent. 2016 Jul 1;8(3):e290-298.
Continuing Education Quiz
Endodontic management of periapical lesions using the GentleWave procedure with minimal instrumentation POTTERS, ET AL.
1. Adequate irrigation is the key to successful endodontic treatment because it is the only way to _______.
a. boost energy loss
b. reach areas untouched by instrumentation
c. interact with stationary fluid
d. none of the above
2. The primary goal of endodontic treatment of pulpal infected teeth and periapical lesions is to eliminate the infection and prevent microorganisms from infecting or re-infecting the root and surrounding tissues.
a. True
b. False
3. ___________ is one of the main factors improving the prognosis after endodontic treatment.
a. Internal bleaching
b. Preserving the dentin structure in its natural form
c. Avoiding antibiotic treatment
d. Identifying the type of infection
4. GWS _____________, thus preserving dentin for a minimally invasive endodontic technique.
a. reduces the need for radiographs
b. increases the need to shape the roots
c. reduces the need to shape the roots using extensive instrumentation
d. breaks down gas bubbles
5. In the literature, in-vitro GWS studies have shown that a statistically significant clean root canal system was observed even when molars were shaped with _______.
a. No. 15/.04
b. No. 15/.15
c. No. 20/.20
d. No. 30/.30
6. This remarkable effect results from the combined washing effect, multisonic energy, and the dissolving action of ______ irrigating solutions.
a tetracycline
b. NaOCl and EDTA
c. MTAD
d. chlorhexidine
7. Sigurdsson, et al., reported that treatment of sizable periapical lesions
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://endopracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://endopracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 070
Date Published: September 13, 2024
Expiration Date: September 13, 2027
2 CE CREDITS
with the GWS resulted in a success rate of ________ at 12-month re-evaluation.
a. 67.2%
b. 74.3%
c. 82.6%
d. 97.7%
8. The lack of success (of root canal treatment) is probably due to the limitations of traditional chemomechanical instrumentation and the difficulties in accessing the morphological complexities in the root canals.
a. True
b. False
9. Healing depends on the disinfection process’s effectiveness and the host’s response to the ________ remaining in the root canals, so lesion healing is a dynamic process.
a. debris
b. biofilm
c. irrigating solution
d. both a and b
10. In addition, ________, reported that GWS greatly improved the effectiveness of tissue dissolution compared to other irrigation methods.
a. Chen, et al.
b. Vandrangi, et al.
c. Haapasalo, et al.
d. Sigurdsson, et al.
To provide feedback on CE, please email us at education@medmarkmedia.com
Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
Endodontics: no place for a snowflake
Drs. Joel Fransen, Rich Mounce, and Tom Shackleton provide seven tips for peak performance
Practicing endodontics at a high level requires a sustained focus. Distraction can result in iatrogenic mishaps that may negatively impact the final result. There are a plethora of external factors vying for our attention while treating patients. As a result, it is vital to prioritize one’s attention on the task at hand, so as to perform clinical endodontic treatment to the best of our abilities.
This article will provide clinicians with insight to optimize performance, especially in challenging circumstances. The examples used are endodontic, but the advocated principles are applicable to general dentistry.
1. Mental toughness
Managing patient anxiety and expectations are often more difficult than the clinical procedure. Patients can be abrasive, uncooperative, and uncommunicative before, during, and after root canal treatment. Continual exposure to stressed people can lead to professional burnout if one does not recognize the challenge and take steps to do better than just cope.
What is mental toughness? How does one develop it?
Being a 21st century dentist is no place for a snowflake. Mental toughness is the armor we need to deliver consistent results in inconsistent situations — in other words, getting the best possible results even in adverse environments. Staying positively focused is crucial to be the stable deliverer of great treatment on technically tough teeth on stressed or misbehaving patients.
Joel Fransen, DMD, is a certified endodontist based in Richmond, British Columbia. He attained his endodontic qualifications in the great Lone Star State of Texas. He is the first ever registered endodontic specialist in the Yukon Territory. He also travels to Northern British Columbia to provide endodontic care. Outside of the office, Dr. Fransen enjoys speed skiing, cycling to raise funds for oral cancer research, and he tries to convince his family to enjoy supporting Liverpool FC and F1 as much as he does. He can be contacted at: joelendo@gmail.com.
Richard Mounce, DMD, is an endodontist based in Eagle River, Alaska. He is widely published in trade magazines and has lectured globally. He can be contacted at: RichardMounce@ MounceEndo.com.
Tom Shackleton, MS, DDS, is a general dentist with a practice limited to endodontics and oral medicine/orofacial pain in Calgary, AB. He is a Diplomate of the American Board of Orofacial Pain. He can be contacted at: tom@tsoralhealth.com
Mental toughness is a measure of individual resilience and confidence that often predicts success in trying circumstances where others might fail. It is a set of attributes that allow a person to become a better clinician and able to cope with difficult situations and technically challenging procedures and emerge without losing confidence. A successful outcome includes being confident enough to stop a procedure and refer in a timely manner. For instance, if a catastrophic tooth or root fracture is discovered during treatment, be brave enough to explain the unfavorable development with the patient. Face the adverse situation directly and do not cower behind staff or the extraction forceps.
If we are all honest, performing technical tasks to the best of your abilities consumes all of your conscious attention and cognitive abilities. Did Michelangelo chat with Pope Julius while lying on scaffolding and painting the Sistine Chapel? Do not believe the hype; you cannot pump out great work in automatic mode. Preoperative discussion, case preparation, and consent are all undervalued for the dividends they pay when we are in the trenches cutting teeth and finding canals.
Each of us enjoys the routine procedures we perform in “automatic mode,” allowing us to chat and joke with the patient and staff. Often a patient can mistakenly expect the same level of interaction from you during a more complex procedure. It is important to inform a patient of the uniqueness of challenging procedures and the resultant change in your behavior and demeanor. Perhaps an assistant can take over the mantle of communicating directly with the patient at these moments. Based on the risk assessment, you, your team, and the patient
The Case:
CLINICAL CASE
C LI NIC AL C AS E
by Dr. Rico Short
The patient came with discomfort on tooth #19. It had a large furcation defect and a crown that’s ill fitting, that was a “J” shaped lesion. The dx was a necrotic pulp with chronic apical periodontitis. A LFOV 3D CBCT was taken and you can see the lesion breakdown in the furcation and the lesion wraps around the distal root.
Is this a crack?
Is this a vertical fracture?
dx necrotic with periodontitis. LFOV and you see the lesion furcation around the Is this a crack? fracture?
Should this be extracted due to a periodontal defect?
Should to defect?
Post-Op
My “5” STEP Endodontic Protocol On This Case:
My “5” STEP Endodontic Protocol On This Case:
1. There was no probing or mobility and the endodontic treatment was performed in one visit.
There was no or and the endodontic treatment was performed in one visit
2. There were four canals with separate portals of exits.
2. There were four canals with separate por tals of exits.
3. I used ZenSeal™ bioceramic sealer and single cone gutta percha was used in this case.
4. The patient returned in 8 months with remarkable healing at the apex of both roots and even in the inter-radicular area where it is difficult to regenerate bone in this area.
I used ZenSeal™ bioceramic sealer and single cone gutta percha was used in this case The patient returned in 8 months with remarkable healing at the apex of both roots
About
Dr. Rico Short
About Dr. Rico Short
studied College, 1992-1995 to 3 He valedictorian GPA. of from attained a Doctor to practice
Columbus Georgia for 2 years. Dr. Short’s compassion lead him to treat underserved children who had less dental wanted their the desire him to area canal therapy.
Dr. Short was awarded a presidential scholarship and studied at Morris Brown College, from 1992-1995 to achieve a Bachelor of Science degree in 3 years. He graduated valedictorian with a 3.98 GPA. Dr. Short attended the Medical College of Georgia School of Dentistry from 1995-1999 and attained a Doctor of Dental Medicine Degree in which he graduated with honors. He went back home to practice general dentistry in Columbus Georgia for 2 years. Dr. Short’s compassion lead him to treat underserved children who had less access to dental care and help those who wanted to save their teeth. It birthed the desire for him to become excellent in one particular area in dentistry: root canal therapy.
Dr. Short has membership in several honorary dental societies. Some of them include: American Association of Endodontists, American Board of Endodontics, American Dental Association, National Dental Association, The Hinman Dental Society, Southern Endodontic Study Club, and many more local and national dental membership societies. In addition, Dr. Short has received numerous awards and recognition for his contribution to dentistry and society such as Lifetime Alumni of the Medical College of Georgia School of Dentistry; Leading Dentist In Continuing Education; The Top 40 Dentist Under 40 in America; The Character, Commitment, and Dedication Award from Morris Brown College, and many others.
Dr. Short is also a well noted motivational speaker and author. His new book “Getting to the Root of Your Problem” has opened doors for him to speak to youth groups all over the United States. His main focus is to encourage the youth to set goals and give them realistic advise on how to achieve them. Since Dr. Short was one of the first in his family to attend college moreover than to become a doctor, he encourages the youth that they can do the same if they remain focus and work hard.
several honorary dental societies. Some of them include: American Association of Endodontists, Hinman numerous for of of Dentistry; Leading Dentist In Continuing Education; The Top 40 Dentist Under 40 in America; The Character, Commitment, and Dedication Award from Morris Brown College, and many others. author. to Root Your for him to speak to youth groups all over the United States. His main focus is to encourage the youth to set goals and give them doctor, focused and work hard.
should be aware of the new ground rules for “bigger” (more complex) appointments. For instance, one may say, “Ms. Jones, your next appointment is more technically challenging than previous procedures we have performed for you. It will require my full attention, and as such, you will notice that I may be less talkative with you and my staff today.” Set the expectation properly, and you’ll notice the difference.
2. Risk assessment
Optimal sleep, nutrition, exercise, continuous learning, and review of upcoming cases are but a few of the many ways we can prepare ourselves mentally and physically to give our best.
Evaluate the mental, dental, and medical particulars of the patient and how they relate to the challenge of successfully addressing the complexities of the proposed treatment. Anticipate potential problems and plan ahead based on a rational risk assessment. In essence, this customizes treatment for the situation at hand.
Pilots know the weather in advance. We should know what “weather” we are flying into with a patient/procedure. An accurate risk assessment is the ultimate preparation task.
3. Effective communication
Effective communication is key to patient management. The technically great dentist who is socially inept will have a difficult career. Actively listening to patients’ concerns and acting upon these concerns is predictive of a good result. Frank and honest communication is central to building trust and ensuring the decision a patient makes is truly an informed one. A routine procedure for an ill-informed anxious patient is just as cognitively taxing as a technically challenging procedure for a less anxious one.
Listening carefully to patients is central to successful patient-dentist interactions. Most patient complaints and ultimately malpractice claims stem from patients who feel unheard. How do you know a patient’s expectations are unrealistic if you do not effectively communicate with them? Listening, recognizing, and addressing concerns is effective communication. That does not mean you must bend to unreasonable demands. It does mean potential issues are addressed preoperatively. For all concerned, sometimes the best treatment is no treatment.
4. Decisiveness in challenges
When faced with challenges, be decisive, calm, and act. Patients rely on us to make decisions in their best interest. We accept flight delays because of mechanical issues or severe weather systems. Pilots don’t fly faster into a storm because a delay is unacceptable. Nor should dentists fall prey to the same pressure to rush treatments. No clinician can stay on time 100% of the time and deliver top notch results reliably. For example, if the patient states they are feeling something, do not continue until the issue is resolved. Addressing such concerns can delay treatment — it is to be expected.
5. Mental preparedness
We owe it to our patients and ourselves to come to work focused primarily on our patients and not allow personal baggage to steal our concentration and prevent us from performing
at the highest level of which we are capable. Optimal sleep, nutrition, exercise, continuous learning, and review of upcoming cases are but a few of the many ways we can prepare ourselves mentally and physically to give our best.
6. Finding flow
The concept of “flow” was popularized by Psychologist Mihaly Csikszentmihalyi and can be defined as a “highly focused mental state conducive to productivity” (wiki). As clinicians, we have all experienced a moment when the procedure is flowing seamlessly, the patient is comfortable, and we are working at the apex of our skills toward an excellent result. This is flow in a dental context and represents a cruising altitude where we are on emotional and clinical auto pilot. The previous five steps can, in large measure, take the clinician predictably to an optimal state of flow.
The above stated, therein lies a challenge, especially in endodontics, as the situation can change instantly — a file fractures, a previously dry canal fills instantly with hemorrhage, the patient who was previously numb suddenly feels something, etc. Should this occur, and flow is broken, flow can be reestablished by the clinician:
• Identifying problems as they develop
• Reviewing possible means of effectively addressing the new developments
• Implementing these solution if appropriate
• Recognizing some problems warrant a cessation of the planned treatment and even a possible referral
• Asking the question, having done your utmost from technical perspective, “Has the issue at hand been effectively communicated with the patient?”
7. Self-kindness and learning from mistakes
The stoic Roman philosopher, Lucius Annaeus Seneca, said it best: “We are more often frightened than hurt; and we suffer more from imagination than from reality.”
Every problem in life and the operatory is a learning opportunity, and the valuable question is, what would I do differently if I had to do this again? What can I learn from this problem? Reflect on challenges, seek continuous improvement, and maintain a positive mindset to grow as a clinician. Every endodontist makes mistakes, but great ones learn from them. Not doing so leads to a negative feedback loop that steals our confidence and erodes our skills. Doing so is priceless.
In conclusion, mental toughness is a cornerstone of successful clinical dentistry. By embracing resilience, effective communication, and continuous learning, endodontists and dental professionals can navigate challenges with confidence and deliver exceptional patient care. We welcome your feedback.
Bio-C Sealer ION+
Bio-C Sealer ION+ is an innovative premixed bioceramic sealer, patented new material, used for root canal filling and internal resorption treatment. It is based on a new class of calcium silicate, which has a unique crystalline structure and chemical composition, different from traditional calcium silicate materials.
To obtain this new bioceramic, a mixture of silicon, magnesium, and calcium oxides is used, replacing aluminum oxide with magnesium oxide in its composition. Previous studies have shown the effectiveness of materials releasing magnesium ions in treating bone defects, promoting osteogenic differentiation and significant mineral deposition. Magnesium ions stimulate an increase in alkaline phosphatase in osteoblasts and enhance intercellular junctions, indicating a positive correlation with cellular activity.
Bio-C Sealer ION+ functions by releasing these ions in a chemically balanced environment created by an alkaline pH. Upon contact with body fluids, it forms a silica-rich gel layer on its surface, facilitating enzymatic changes that influence cellular differentiation and promote tissue formation. It aids in the repair and regeneration of tissue-bone and dentin-pulp complexes.
In clinical practice, Bio-C Sealer ION+ offers a practical, easy, and efficient procedure. It is conveniently packaged in premixed syringes with disposable intracanal tips. To preserve its physical properties, each syringe contains a small quantity of 0.5 g and is accompanied by a metallized pouch containing silica gel that protects the product from moisture.
5 reasons to choose Bio-C® Sealer ION+:
1. Resin-free and eugenol-free material: Bio-C® Sealer ION+ does not contain resin, making it easy to clean the pulp chamber only with water. It is also biocompatible, causing no postoperative pain. And being eugenol-free, it does not negatively interact with other root canal procedures such as post cementation.
2. Excellent flowability: With a flow of approximately 24 mm and micronized particles smaller than 2 µm, Bio-C® Sealer ION+ has excellent viscosity. It efficiently penetrates different branches of the complex root canal system and easily reaches the dentinal tubules, promoting a hermetic and three-dimensional filling.
3. Compatible with cold or warm technique: Bio-C® Sealer ION+ remains stable at the maximum temperature reached by equipment during root canal filling techniques that involve heating gutta percha (up to 392ºF). Unlike other sealers that degrade at temperatures close to 291.2ºF, it maintains its integrity.
4. Low solubility: With a solubility of less than 3%, Bio-C® Sealer ION+ prevents bacterial reinfection by ensuring a homogenous filling without gaps after setting. This increases the chances of successful treatment.
5. No tooth staining: Bio-C® Sealer ION+ contains zirconium oxide as a radiopaquer, allowing for excellent radiographic evaluation (≥ 7.0 mm Al) by the dentist, and unlike other products on the market that contain bismuth oxide, it does not cause tooth staining. This information was provided by Angelus.
Clinical case kindly provided by Professor João Barbizam, 12 months postoperative
Bio-C Sealer ION+ 2g box + syringe with translucent intracanal tip
The best way to eliminate financial stress
Dr.
Albert
(Ace) Goerig discusses how to get to profits without financial stress
Many doctors continue to experience financial stress that they never anticipated when they chose a “high paying” career like dentistry. Financial stress can take the joy out of life and lead to sleepless nights. Even if you are good at managing stress, there’s always an undercurrent of worry that takes energy and discipline. Here are the four most common types of financial stress:
• Cashflow distress is when every dollar you earn is earmarked for an expense or cost that must absolutely be paid. With little or nothing left over, you barely have your head above water, and you’re in constant fear of sinking.
• Debt hangover is the emotional price of monthly payments on long-term debt. This includes student loan debt, practice acquisition debt, mortgages, and auto loans. Credit cards and consumer debt with outrageous interest rates add to the burden.
Focus on the true problem
• Lifestyle limits is when your obligations are being met, but you are not living the lifestyle you want. You must budget and limit your spending much more than you expect or want, and it leads to general dissatisfaction of where you are in your life.
• Savings squeeze is when spending today is prioritized over saving for major future goals. The obvious example is not saving for the retirement you want. As years go by without making progress, stress can skyrocket (usually around the age of 40).
The first instinct of most people experiencing financial stress is to try to economize on spending. However, unless you are wildly irresponsible with your spending, there are relatively few opportunities to reduce spending in a meaningful way. Scrambling to save a few percent on dental supplies, skipping a daily coffee bar order, or avoiding team raises isn’t going to pay off your mortgage, buy the boat you want, or fund your retirement.
Albert Goerig, DDS, MS, is a Diplomate of the American Board of Endodontics and a sought-after speaker who has lectured extensively on the field of endodontics and practice success throughout the United States, Canada, and abroad. He is the author of more than 100 published articles and contributing author to numerous endodontic textbooks. Dr. Goerig has a private endodontic practice in Olympia, Washington, in the top 1% nationwide for practice profitability. He has almost 40 years of experience as an endodontic educator and practice coach to over 1,000 endodontists. www.endomastery.com | 1-800-482-7563 | info@endomastery.com
Truthfully, financial stress is almost always an income problem and not an expense problem. In the 25+ years that I’ve been coaching endodontists, I’ve never met a doctor who had unachievable financial expectations based on what is possible in endodontics. I have, however, met many doctors whose practices are underperforming financially.
The math of practice performance is quite straightforward. A recent analysis we performed across 32 Endo Mastery client practices in 21 different states showed practices collected approximately $1,500 on average for every completed case (RCT, ReTx, Apico) over the course of a year. To be clear, that’s not the average fee for treatment. It’s the total collections of the practice divided by total cases completed. Total collections would include smaller procedures, as well as exams, radiographs, and imaging for consult patients who do not proceed to treatment.
Based on this data and assuming 180 workdays per year, adding the equivalent of one more completed case per day on average will generate $270,000 more in annual collections. Adding two cases per day boosts collections by $540,000. Since most expenses don’t increase, almost all increased collections flow to the bottom line as improved profit. That’s a $5 million bonus over a 10-year period. Financial stress? Gone forever.
Most underperforming practices are only completing 3 to 4 cases per day, and 30% or more of the doctor’s time is being diverted into non-productive tasks that the team could perform. It’s no wonder that the doctor has financial stress. Improved clinical team efficiency, scheduling, and marketing are all effective strategies to investigate without delay. Why wait any longer? The payoff — the rest of your life without financial stress and every goal achieved — is worth the effort.
Why the largest U.S. endodontic practices have quietly partnered with IDSOs
Chip Fichtner discusses how endodontists can add liquidity and a strong growth partner to their practices
Over the last 5 years, hundreds of endodontic practices have quietly partnered with Invisible Dental Support Organizations (IDSOs). An IDSO becomes a doctor’s silent partner by buying 51% to 80% of a practice for cash up front at today’s low tax rates. Doctors remain as owners, with their brand, team, and full autonomy for years or decades. Practice performance can be enhanced with captive referral sources, and the upside in a doctor’s retained ownership can be far greater than competing alone.
IDSO partner practices benefit from the resources of a larger silent partner to reduce the administrative burdens of banking, payroll, accounting, benefits administration, compliance, credentialing, tax, and legal. Doctors can also access 30% lower costs on supplies. And practices benefit from their IDSO partner’s professional, full-time recruiting and marketing teams.
IDSO partnerships in the last 24 months, over $150 million have been for doctors in their 30s.
While there are now almost 1,000 IDSOs and DSOs in the U.S., in the last 5 years, multiple IDSOs have been formed specifically partnering with endodontic practices. They are competing with the multi-specialty and Dental Surgical Trifecta IDSOs (endo, perio, and OMS only) for great endodontic practices nationally. In an LPS process, growing practices are achieving new record values, often with six or more eager, qualified bidders from which doctors can choose the right partner.
Tens of thousands of dental practices have quietly partnered with IDSOs over the last 35 years in all 50 U.S. states. Some may have only a few practice partners and others over 700. An IDSO’s size gives them leverage in multiple areas including the cost of team benefits.
IDSOs are eager for growing endodontic practices with at least $1.5 million in collections, and the younger the doctor, the more valuable the practice. In LPS’ $1.0 billion of completed
The IDSOs act as a doctor’s silent partner. Their goal is to support a practice, not to micromanage or homogenize it to meet some corporate standard. Doctors retain full autonomy, not just clinically, but also in how they hire, pay, manage, and lead their teams. The owner doctor makes decisions, not the IDSO.
Ultimately, the IDSO can also provide doctors with a known exit strategy at retirement, years or decades in the future. Thousands of doctors have achieved dramatic increases in the value of their retained ownership over time. Some have exceeded 300%, 500%, and 1,000% or more when they selected the right IDSO partner.
Doctors today should understand the potential value of their practice in an IDSO partnership. Values achieved by LPS for larger endodontic practices in the last 6 months have exceeded 2X collections and 10x EBITDA.
Doctors who own their real estate also have two great options. They either gain an AAA credit tenant for decades, or, due to their new IDSO tenant, the value of the real estate increases in a sale to a Real Estate Investment Trust (REIT), now or in the future.
Chip Fichtner is co-founder of Large Practice Sales which completed over $1.0 billion of IDSO partnerships in 2022 and 2023. Over the past 40 years, he has built, bought, and sold public and private companies in a variety of industries, and has been featured in numerous media outlets. His tolerant wife of 34 years allows him to live on his airplane visiting clients every week. EP
To learn more about IDSOs and receive a confidential, no cost, no obligation practice valuation, doctors can contact Large Practice Sales by calling 844-405-0521, emailing endo@largepracticesales.com, or by visiting www.LargePracticeSales.com. This information was provided by Large Practice Sales.
Invisible Dental Support Organizations (IDSO) become your silent partner by purchasing 51% to 80% of your practice for cash at today’s low tax rates
Silent Partners Buy Part of Your Practice - IDSOs purchase 51% to 80% of practices for cash now at low tax rates. Doctors retain ownership and have significant upside in the equity value. Some LPS endodontic clients have achieved 3x to 7x equity returns over time.
Long-Term Wealth Building Partnership - Doctors continue to lead their practice with their brand, team and strategy for years or decades. Practices benefit from the resources of a larger, silent partner, but are not micromanaged or homogenized.
Six or More Choices in Partnership - LPS clients often have 6 to 10+ qualified bidders. LPS is the largest advisor in the U.S. which enables our clients to achieve record values that the little advisors cannot match.
√ Monetize 51%-80% of your practice value
√ Millions in cash now at low tax rates
√ Continue leading your practice
√ FULL AUTONOMY for years or decades
√ Gain the resources of a larger partner
√Grow faster, better and more profitably
√ Increase the value of your retained ownership
√ Choose the best offer from multiple bidders
√ No-cost, no-obligation practice valuation from the largest advisor to all specialties in the U.S.
877-437-3353
Your Value in Today’s Consolidation Frenzy - You should understand the value of your practice in an LPS-advised process. Doctors who deal directly with IDSOs often leave millions on the table and do not get to consider ALL of their options.
Large Practice Sales (LPS) is the largest transaction advisor to GP and specialty practices in the U.S. and has completed over $1 Billion of Invisible Dental Support Organization (IDSO) partnerships in the last 24 months.
“I am ecstatic! You guys got me DOUBLE the best offer I could get on my own! Have any doctor call me and I’ll tell them you can’t go wrong with LPS. Use my name. I am referring all my friends.”
-T.J., MD, DMD
Large Practice Sales Brings Multiple Bidders for the Highest Value in IDSO Partnerships
View the LPS Library of Webinars LargePracticeSales.com/webinars
•IDSO: What’s Changed in 2024?
•Wealth Building Strategy for Doctors of All Ages
•Specialist Options Not Available to GPs
Who moved my cheese?
Dr. John Khademi discusses GentleWave®,
Twenty-five years ago, Spencer Johnson wrote a best-selling business allegory describing the ways people react to change. In his parable, “Who Moved My Cheese?” four characters wake up one day in the maze they had studied and known to find that the cheese they had relied upon wasn’t there anymore. Johnson uses these four characters embodied by two mice (Sniff and Scurry) and two “Littlepeople” (Hem and Haw) to represent different approaches to change.
As you might guess by their names, Sniff symbolizes the ability to anticipate change. He’s constantly alert, using his keen sense of smell to detect shifts in the environment. Sniff represents those who stay vigilant and can foresee upcom ing changes, allowing them to prepare and adapt proactively. Scurry embodies quick action and adaptability. Once change occurs, Scurry wastes no time in responding. He represents those who, upon recognizing change, immediately spring into action without overanalyzing the situation. Hem personifies resistance and denial. When faced with change, Hem stubbornly refuses to accept the new reality. He complains, blames others, and clings to old ways, representing those who fear change and become paralyzed by it. Haw initially shares Hem’s reluctance but eventually embraces change. He represents the journey many people go through: initial shock and denial, followed by fear and uncertainty, and finally, acceptance and adaptation. Haw learns to laugh at his fears and move forward, symbolizing personal growth and the ability to learn from change.
a paradigm shift in root canal therapy
editorial from 2021.1 While technology has been a part of these shifts, the real changes are more fundamental, aptly described by Kuhn:
The transition from a paradigm in crisis to a new one from which a new tradition of normal science can emerge is far from a cumulative process, one achieved by an articulation or extension of the old paradigm. Rather it is a reconstruction of the field from new fundamentals, a reconstruction that changes some of the field’s most elementary theoretical generalizations as well as many of its paradigm methods and applications.2
Nearly 20 years ago, a small group of engineers embarked on a completely fresh approach to our specialty and moved our cheese. Looking back, we see that our cheese has been moved several times since the inception of our specialty as discussed in our
John Khademi, DDS, received his dental degree from the University of California San Francisco and his certificate in endodontics and MS on digital imaging from the University of Iowa. He is in full-time private practice in Durango, Colorado and was Associate Clinical Professor in the Department of Maxillofacial Imaging at USC and is Adjunct Assistant Professor at SLU. As a Radiological Society of North America (RSNA) member for over 25 years, his background in medical radiology allows him a perspective shared by very few dental professionals. He is the lead author for Quintessence’s Advanced CBCT for Endodontics: Technical Considerations, Perception, and DecisionMaking.
GentleWave® represents more than just a new technology; it’s a paradigm shift in how we approach root canal therapy. Its promise of enhanced cleaning through multisonic ultracleaning, coupled with a minimally invasive approach, challenges our long-held beliefs about what’s necessary for successful treatment. For many, this change may feel unsettling. We might find ourselves, like Hem, resistant to changing, let alone abandoning our familiar tools and techniques. By definition, advancement and progress require change. The AAE’s core purpose in their mission statement is “To advance the art and science of endodontics and to promote the highest standards of patient care.” A specialty that does not advance and progress is stagnant. Embracing progress doesn’t mean abandoning everything we’ve learned. Instead, it’s about adapting our expertise to a new modality, much like Haw eventually learned to navigate the maze in search of new cheese. It’s about recognizing that our skills in diagnosis, case selection, and understanding of root canal anatomy are more crucial than ever in leveraging this technology effectively.
Sniff and Scurry have already discovered the new cheese. As we stand at this juncture, we must ask ourselves, and our specialty this question: Will we be like Hem, clinging to the past, or like Haw, venturing forth to explore new possibilities? The choice is ours. In the world of endodontics, as in business and life, those who anticipate change, adapt quickly, and embrace new technologies are often the ones who find the freshest, most satisfying cheese.
REFERENCES
1. Khademi J. Paradigms in endodontics: CIE, MIE/RDE, NIE. Endodontic Practice US. 2021;14(2):1.
2. Kuhn TS. The Structure of Scientific Revolutions. 3rd ed. Chicago, IL: The University of Chicago Press; 1996.
The GentleWave® G4 System
Patient Care, Personalized.
The latest innovation for the GentleWave® G4 System, ProControl™ gives you the ability to adjust the percentage of concentration for NaOCl throughout the procedure, allowing for customizable root canal treatment within proven protocols for every patient, plus:
〉 Debride and disinfect undetected anatomical spaces1,2
〉 99.9% removal of biofilm3
〉 96.6% of patients report only mild or no pain within 48 hours 4
〉 97.7% healing rate at 12 months5
YOUR PATIENT. YOUR PROTOCOL.
Learn more about ProControl and how your colleagues are customizing treatment to meet the needs of each patient. GentleWave.com/ProControl
1 Wang Z et al. J Endod. 2018; 44(5):842-848
2 Molina et al. J Endod. 2015; 41(10):701-5
3 Choi HW et al. Materials (Basel). 2019;12(21):3492
4 Data on file
5 Sigurdsson A, Garland RW, Le KT, Rassoulian SA. Healing of Periapical Lesions after Endodontic Treatment with the GentleWave Procedure: A Prospective Multicenter Clinical Study. J Endod. 2018 Mar;44(3):510-517. doi: 10.1016/j.joen.2017.12.004. Epub 2018 Jan 12. PMID: 29336878
As today’s endodontists look to the future of their practices and careers, more and more are exploring practice partnerships and weighing the notion of an ideal culture and community against a lucrative financial opportunity. At Specialized Dental Partners, we know the two go hand in hand.
Specialized Dental Partners, formerly US Endo Partners, was the first Specialty DSO (SDSO) to champion endodontists. Today, we are also welcoming periodontists and oral surgeons to our community, allowing us to expand our impact and revolutionize oral health care. We are on an exciting mission to drive meaningful opportunity and growth for our team members while pursuing excellence in all we do. Together, we are delivering world-class patient experiences and brighter tomorrows for all.
“Our goal is to unwaveringly support our clinicians and their teams so that they can provide better access to care to the communities they serve,” said Specialized Dental Partners Chief Executive Officer Scotte Hudsmith.
Practice Managers engaged in expert-led sessions, gaining leadership skills, and making valuable connections during Leadership Summit 2024
“Our continued growth will accelerate by aligning endodontics, periodontics, and oral surgery so that patients have a convenient and cost-effective way to access specialty dental care when they need it.”
Strong, sustainable growth model
The Specialized Dental Partners model is attractive on multiple levels. First, we believe that the success we generate from our aligned pursuit of excellence should be rewarded. Our Partners have a stake in the company’s proven financial success. As a Partner and shareholder, you invest in your Partners, and they invest in you. Moreover, as a practicing endodontist, your work continues to produce for you at the same time as your investment.
The additional allure of Specialized Dental Partners for endodontists in all career stages is multifaceted, and throughout it all, you stay uniquely you. With Specialized Dental, you retain your clinical autonomy, practice culture, valued team members, and brand identity. Dedicated to you, your team, and your work-life balance, our team of experts supports and lifts your practice in key areas from marketing and human resources to revenue cycle management and compliance. In short, we do what we do best, so you and your team can do what you do best.
Power of community
Partners and their practice teams feel the empowering connection and support of belonging to a special community invested in each other’s success. Our annual Vision Summit brings us all together to focus on
personal and professional growth, as well as building strong friendships, and our innovative track of comprehensive development programs drives fulfillment among our clinicians. In October of 2023, nearly 300 specialists assembled in Chicago for the Summit to take advantage of connecting with peers from across the country and chart a course for the future. This past April, we expanded our commitment to supporting practices by hosting over 150 Practice Managers in Dallas at our Leadership Summit.
“Partnering with Specialized Dental is so much more than a great business opportunity. Our culture is about growth in every aspect of our lives — from improving our communication skills to leadership training, to advanced clinical training courses and beyond,” said Dr. Jeremy M. Young, Director of Partner Engagement. “What we are building is unique; I’m truly thrilled to get to be a part of it.”
Energize your future today
When it’s time to talk, talk to the first and only SDSO with proven financial results and a supportive, growthminded culture — talk to Specialized Dental Partners. We’re always in active discussions with top-tier endodontists, and we have openings for associates and recent graduates who are looking to start their careers at a flourishing practice. Learn more about Specialized Dental Partners by visiting specializeddental.com. This information was provided by Specialized Dental Partners.
Above: Dr. Kirk Coury, partner since 2018, helps chart the future of the company at the 2023 Vision Summit
Partnership supports growth, collaboration, and mutual success
The right partner for your file
X-Smart® Pro+
Endo Motor with Integrated Apex Locator
With up to 7.5 N·cm and 3,000 rpm, the X-Smart Pro+ endo motor has been specifically designed to drive Dentsply Sirona’s endodontic file systems in both continuous rotation and reciprocating modes.
Our integrated apex locator will provide the confidence for length determination while shaping. The X-Smart Pro+ features a mini contra-angle with integrated 10-lumen LED, an autoclavable handpiece sheath, a touchscreen interface that provides easy access to settings for the files you choose, and upgradeable firmware to accommodate tomorrow’s treatments.