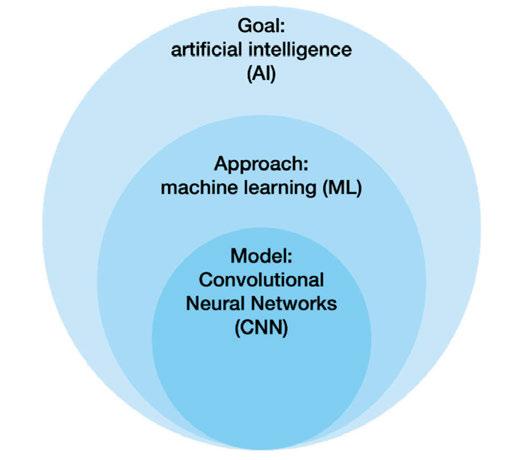
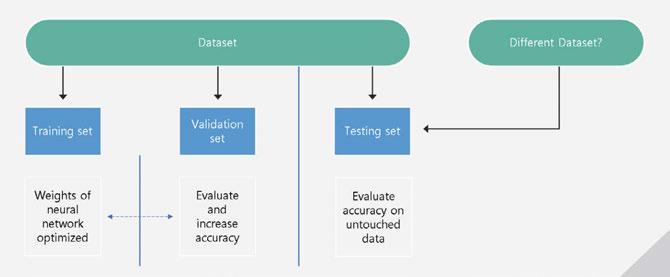
Clinical implementation of AI systems in orthodontics
Drs. Aaron Glick, John Garza, Nisha Manila, and Jennifer Chang
Shut your mouth and save your life
Dr. Michael Gunson
Improving patient compliance and predictability with hyperelastic aligners
Dr. Neil Warshawsky and Loc. X. Phan
SPARK APPROVER WEB
Use powerful Spark Approver software features in and out of the office with convenient, secure web-based access.
OPTIMIZED OPEN PLATFORM WITH DEXIS IOS INTEGRATION
Easily submit aligners with one-click captures of patient data, automatic case creation, and quick access to STL files.
GAME - CHANGING CLINICAL AND WORKFLOW UPDATES
Enjoy enhanced control and versatility with Flexible Material Choice, Integrated Hook Updates and Real-Time Approval with Passive Aligners Editing Tool.
“Ormco has a legacy of continuous, doctorinspired innovation. And it shows in this new release. As an Ormco insider, I can attest to the fact that Spark is listening to us doctors and I am thrilled with the direction that we’re going together.”
–Dr. Jeff Summers 1
Spring 2024 n Volume 15 Number 1
Editorial Advisors
Lisa Alvetro, DDS, MSD
Daniel Bills, DMD, MS
Robert E. Binder, DMD
S. Jay Bowman, DMD, MSD
Stanley Braun, DDS, MME, FACD
Gary P. Brigham, DDS, MSD
George J. Cisneros, DMD, MMSc
Jason B. Cope, DDS, PhD
Bradford N. Edgren, DDS, MS, FACD
Eric R. Gheewalla, DMD, BS
Dan Grauer, DDS, Morth, MS
Mark G. Hans, DDS, MSD
William (Bill) Harrell, Jr, DMD
John L. Hayes, DMD, MBA
Laurence Jerrold, DDS, JD, ABO
Marc S. Lemchen, DDS
Edward Y. Lin, DDS, MS
Thomas J. Marcel, DDS
Mark W. McDonough, DMD
Randall C. Moles, DDS, MS
Elliott M. Moskowitz, DDS, MSd, CDE
Rohit C.L. Sachdeva, BDS, M.dentSc
Gerald S. Samson, DDS
Margherita Santoro, DDS
Shalin R. Shah, DMD
Lou Shuman, DMD, CAGS
Scott A. Soderquist, DDS, MS
John Voudouris (Hon) DDS, DOrth, MScD
Neil M. Warshawsky, DDS, MS, PC
John White, DDS, MSD
Larry W. White, DDS, MSD, FACD
CE Quality Assurance Board
Bradford N. Edgren, DDS, MS, FACD
Fred Stewart Feld, DMD
Gregori M. Kurtzman, DDS, MAGD, FPFA, FACD, FADI, DICOI, DADIA
Justin D. Moody, DDS, DABOI, DICOI
Lisa Moler (Publisher)
Mali Schantz-Feld, MA, CDE (Managing Editor)
Lou Shuman, DMD, CAGS
Finding balance
I’ve worked for over 2 decades as an orthodontist. These have been great years. I was able to work with my father and hope that someday I will be able to work with one of my four sons in the practice. In a sense, orthodontics is my life. Treating patients has given shape to my life, connected me to my community, given me challenges, and provided interesting experiences that have changed how I see the world. I have built many friendships through my work as a lecturer and adjunct professor.
But at the same time, orthodontics is not the entirety of my life. As practitioners, we need other meaningful things in our lives to protect us from burnout. The truth is, you can’t spend all your time at work. At this point in my life, I am looking for balance. I want to spend as much time as possible with my wife and four sons without compromising my professional standards of providing quality orthodontic care and facilitating a fantastic work environment for my team.
The conventional thinking used to be that if you wanted to maximize your profitability, you needed to build a big practice, fill it with a lot of chairs, hire a large staff, and then market your practice to dentists and your community. That was what success looked like.
But I believe all of that has changed. For me, it has become more interesting to think about growing your practice without carrying big overhead costs. This can free us up to achieve the same, if not more, financial success without feeling burdened by huge operating costs and the need to work all the time. In my opinion, the best way to do that is by implementing remote monitoring into your practice.
By going All-In with DentalMonitoring, I feel free to work the way I want to. I can increase the number of patients we treat while reducing my doctor-days by streamlining our schedule. We receive clinical notifications from the AI that allow me to elevate the standard of care I can provide. The AI-driven technology allows us to eliminate some of the extraneous work for my staff, which makes them happier and more relaxed at work.
But the biggest benefit of DentalMonitoring is what it does for patients. It makes treatment easier for busy patients to finish treatment on time and trims the amount of time they need to spend in our office. This is what the future of patient choice looks like.
AI-driven remote monitoring doesn’t tell us how to treat our patients. Instead, it empowers us to transform the orthodontic experience into the best possible version for patients, staff, parents, and doctors. It’s a whole new world, and I look forward to seeing how it will change our industry for the better.
Bill Dischinger, DDS, earned his degree from the Oregon Health and Science University School of Dentistry and his certificate in orthodontics at Tufts University in Boston. An adjunct professor in the orthodontics department at the University of the Pacific in San Francisco, Dr. Dischinger is a certified Damon instructor and has taught and lectured extensively on passive self-ligation with the Damon System™ and the Spark Aligners™. He has lectured nationally and internationally on subjects including functional jaw orthopedics, Spark clear aligners, passive self-ligation, and practice management.
Dr. Dischinger has published numerous articles and written a book on a variety of subjects within the specialty of orthodontics. He is also a member of the American Association of Orthodontists, the Pacific Coast Society of Orthodontists, the American Dental Association, and orthodontic professional associations that enable him to participate in continual education and remain current on advances in orthodontic treatment. He is a key opinion leader for Ormco™, DentalMonitoring, and Propel®
Dr. Bill Dischinger
Auto-cropping,
Auto
3.5
Ultra-lightweight
Clinical implementation of AI systems in orthodontics
Drs. Aaron Glick, John Garza, Nisha Manila, and Jennifer Chang discuss the pros and cons of AI in orthodontic and general dental practice 38
Dr. Michael Gunson looks to the past and present for a view of the effects of ineffective
FINANCIAL FOCUS
5 ways to help your practice reduce credit card processing fees
Matt Rej offers tips on how to mitigate the costs of accepting credit cards 45
MILITARY MATTERS Freedom Day USA
Dr. Lou Shuman discusses how a lifetime of freedom can be repaid by giving a day for free 47
2024 — appreci-8 your potential
Numerology is the study of numbers that deal with their mystical meaning and effect on our lives. When you think of all of the numbers that surround us every day — our dates of birth, other special dates, births, anniversaries, and deaths of those near and dear to us, even your home address can have a deeper meaning. No better time to think about the power of numbers than this year. Add up the numbers in our new year, 2024, and the result is the number 8. Turn the number 8 on its side, and you get the infinity symbol — this year, you can harness the power of 8 — when opportunities to reach goals in our personal and private lives can be limitless.
Lisa Moler Founder/Publisher, MedMark Media
A little numerology research on the number 8 shows that it represents the achiever and goal-reacher. The number symbolizes good sense, a powerful presence, and strong success drive. Balance is also a hallmark of the number 8, as reflected in its symmetrical shape that promotes stability, potential, and productivity. The number 8 is ruled by the planet Saturn (as is the zodiac sign, Capricorn). Traits of this planet are perseverance and ambition, so during 2024, our “8” year, we should strive to find our places as strong leaders ready to transform our plans and words into actions.
For this Spring 2024 issue, we want to help turn your plans into prosperity with our clinical articles and marketing expertise. In our Cover Story, Dr. Mike Ragan talks about the AI-powered remote monitoring solution DentalMonitoring and how dynamic scheduling and remote monitoring are driving growth and reducing doctor days for his practice. Our CE on AI in dentistry by Dr. Aaron Glick and colleagues, points out the pros and cons of having AI-based systems in the orthodontic practice. Dr. Gunson’s CE, “Shut your mouth and save your life: the problem with interlabial gap” looks at the history of effective lip closure and how lip incompetence can affect the bite, the face, and airway. Check out the AAO Special Section to discover products and services that bring your practices to a higher level, increase your clinical success, and even protect your data from cyberattacks.
What can you do to make the most of your “8” year? Keep achieving, be strategic, and fiercely tenacious. Be a leader, but listen to your team, and let them know that the most fulfilling achievements are the ones that you reach together. Give back when you can because the karma of the number 8 is connected to the infinite balance between success and gratitude. And remember like the balanced number 8, to make time for personal life, even while you pursue professional success. 2024 is the year to turn your potential into prosperity.
With appreci-8-tion for success in 2024,
Lisa Moler Founder/Publisher MedMark Media
Published by
Publisher Lisa Moler lmoler@medmarkmedia.com
Managing Editor Mali Schantz-Feld, MA, CDE mali@medmarkmedia.com Tel: (727) 515-5118
National Account Manager Adrienne Good agood@medmarkmedia.com Tel: (623) 340-4373
Subscription Rate 1 year (4 issues) $149 https://orthopracticeus.com/subscribe/
Exclusively
Bring better workflow and comfort to your practice with the new A-dec Specialty Workstation.
Its versatile cabinet offers easy access and organization for your equipment, technology and materials, while the articulating delivery arm keeps your handpieces comfortably within reach. Customize the surfaces—and easily add on LED lights, monitor mounts, and ICVs—to perfectly suit your practice.
Efficient. Integrated. Ergonomic. It’s an ideal solution—and only from A-dec. See us in Booth #1029
a-dec.com/ortho
Going All-In with DentalMonitoring
Dr. Mike Ragan explains how dynamic scheduling helps him treat patients like family
Dr. Mike Ragan operates Ragan Orthodontics in Dallas, Texas with a simple philosophy: treat them like family.
“When a kid walks in the door, I treat them just like I would treat my kids.” In the past year, Dr. Ragan has led his practice through the process of going All-In with DentalMonitoring, which means utilizing remote monitoring for all of his patients and shifting to dynamic scheduling. Dynamic scheduling can make both patients and other doctors nervous, as leaving each appointment with another appointment on the books has been a standard practice for a long time. But Dr. Ragan explains, “I think I can be a better practitioner and a better overall person in my practice as a leader using DentalMonitoring.”
Making changes
Dr. Ragan was an early adopter of DentalMonitoring’s remote technology, but his path to optimizing his practice schedule through monitoring wasn’t a straight line. Early on, Dr. Ragan says, “I decided to try DentalMonitoring when the first rep came in the office. I visited the headquarters in Paris and met with Philippe Salah, the CEO. He showed me the technology, and I was excited.”
But DentalMonitoring was only one of the tools he used in his practice, whereas now, it’s an essential part of his practice’s success. Previously, he says, “We tended to use it only for patients who were going to college or people who live far away from our office. I had people coming from all over the nation to see me for lingual braces, so in those cases, we used DentalMonitoring.”
Everything changed for Dr. Ragan last year when Celine Cendras-White, head of DentalMonitoring marketing, called and told him he needed to come to the 2023 DM Summit. She knew he’d been dabbling with the technology, but he still needed to see what was possible. Luckily for Dr. Ragan, he heard the commitment in her voice and booked his trip. It was at the DM Summit that “Everything changed for me.”
He’d been dealing with a certain amount of stress in his practice that he wanted to change, not just for himself, but for the patients and his team members. “I started hearing what the speakers were saying about dynamic scheduling freeing up the office. I felt like I was working my tail off, both in the office, after hours, and at home on the weekends. I was always trying to catch up. We were struggling to hire staff.”
His prior experiences with implementing new technology into his practice made him feel that he needed to wait until he thought he could handle the change. He wanted the right team around him to learn the technology. He knew it would take work to shift from how they’d been using remote monitoring for certain patients to going All-In and switching to dynamic scheduling.
Dr. Mike Ragan
But he finally realized that his thoughts about the transition were all wrong. “I thought I needed to hire and train my staff to make this happen, but I realized I was waiting for the wrong thing. I was waiting for enough staff to make the change easier on me.” Instead, by committing to the technology, he was able to decrease his reliance on his staff. The transition took effort because he was continuing to operate a busy practice while getting the protocols right and training staff and patients. In Dr. Ragan’s estimate, the All-In implementation process is a difficult month or two, but it’s not a surprise. “If you change software companies, it’s painful. When you go to 3D printing, it’s painful. When you go to 3D imaging, you don’t know what you’re looking at on the screen.”
His staff initially wasn’t thrilled about the change. They didn’t want to add anything or learn new systems. But this is where Dr. Ragan thrives as a leader. He’s not prone to big emotional outbursts. Instead, he models servant leadership, empowering his staff rather than micro-managing them. He picks the direction, gives his team the tools to succeed, and shares his vision of what success looks like. By doing that, he can convert even the most skeptical of staffers. They know, after onboarding other technology in the practice, he’s doing it to make it better.
“But if you go All-In, you are committing the time to go over the protocols. You have to spend the time to set your goals. You have to spend the time to train your staff and patients on how to scan and put in a scanning station with a mirror.”
The results speak for themselves. Dr. Ragan says, “Our summer with DentalMonitoring was different than any summer we’ve ever had, and the staff loved it. We have freedom, and we’re not as crowded.”
Now in staff meetings, if his staffers forget to fill out patient cards that only take 2 or 3 minutes, he can ask, “Do you really want to go back to 60 to 70 patients a day and work during your lunch, or be forced to stay late?”
Results
Tracking hygiene of braces patients is a game changer
In his Dallas community, Dr. Ragan and his team knew firsthand that there is a huge appetite for fewer office visits and tighter treatment timelines because kids are busy with sports and after-school activities, and families travel during the summer and holidays. DentalMonitoring has just been the latest tool to help him provide the level of care that his patients need.
Dr. Ragan has always been committed to tracking treatment time. By knowing the success metrics, he has had good reason to implement new technology in the pursuit of helping patients complete treatment sooner. Early in his career, Dr. Ragan reduced time in treatment from 2 years to 18 months through innovation. Now they’re reaching an average of 14.2 months for patients with bite correction. Dr. Ragan explains, “Our community is why we push technology. We’ve been looking for ways to decrease office visits for busy patients and busy parents for a long time. We began with indirect bonding so we had fewer brackets to reposition over time. We went to self-ligating brackets to extend the time between visits and treatment time.”
By using the AI-powered remote monitoring solution, he’s seen that his patients are falling into a bell-shaped curve. A third of his patients fall into the expected pattern, needing wire changes every 6 to 8 weeks. DentalMonitoring is actively speeding up treatment for a third of his patients, allowing him to treat based on an up-to-date knowledge of patient biology instead of treating patients based on norms from studies. For the third that is finishing slower than expected, DentalMonitoring lets his practice save office time by reducing visits. “We previously would have brought a patient like this in to learn that we weren’t ready to change wires. We would say, ‘Let’s change colors, and we’ll see you in a couple of weeks.’” DentalMonitoring provides value
in all three areas and reduces visits for all three groups, which drives profitability and reduces the workload for his team. “We can spend more time with patients during each visit, and each of those visits is purposeful. If we have to fix a broken bracket, we’ll usually do the patient visit at the same time. We used to not have the time to be able to do that before DM.”
What is your why?
Part of DentalMonitoring’s culture, inspired by Simon Sinek’s book Start With Why, is clarifying why doctors are looking to make a change to help them achieve their goals. Dr. Ragan says, “I’m not a person with a lot of hobbies. What I really love is being with my family. DentalMonitoring has freed me to visit my daughters more often. I can monitor my patients while I’m away from the office. I don’t have to worry about being stuck in a snowstorm.” By spending a little time in the DentalMonitoring dashboard, he can plan a day with his staff, and only patients who need specific intervention would need to be rescheduled.
DentalMonitoring does a lot of things to help practitioners, but there are surprise benefits. Using remote monitoring, they’ve spotted a pattern of losing brackets along one side. They’ve realized that quite often, this is because many young athletes chew on their mouthguards, as Dr. Ragan describes, “like a doggie chew toy.” When he receives notifications of these events, the first thing he does is send the patient’s mom a note and asks, “Are they chewing on their mouth guard like a doggie chew toy on the sidelines?” By communicating directly and nearly immediately with patients and parents through the DentalMonitoring app, his practice can help stop behavioral issues that will slow down treatment much sooner than was ever possible.
While he was nervous that his adult patients would be resistant to the new remote monitoring technology, he’s found that they were the quickest to embrace the streamlined orthodontic experience. Adult patients love the convenience of not needing to leave work for an aligner check.
When he thinks about the journey, he thinks that it all really began at the DM Summit, even though he was already a customer. “I wanted to be like those people on stage. I wanted to say the same thing that they did. I wanted to see the same results that they were seeing.” While he was skeptical about what his peers were saying about how remote monitoring and dynamic scheduling were driving growth and reducing doctor days, he was ambitious enough to go for it. And now, his staff is happier, his patients are happier, and he can provide committed care and clinical excellence to his patients.
Not only can he enjoy the same results as the doctors who inspired him to go All-In with DentalMonitoring, but Dr. Ragan is also up there on stages now, sharing how DentalMonitoring has helped him run his practice exactly as he wants to, where he has the freedom and lack of stress so that when anyone comes into his office, he can “treat them like family.” OP
Dr. Mike Ragan and his team in Dallas, Texas
Smarter Orthodontics
Explore how our unrivaled AI platform helps improve e ciency and increase productivity throughout the entire patient journey. October
Join DentalMonitoring for the orthodontic industry’s premiere educational experience at the beautiful Austin Fairmont Hotel! Powerhouse speakers will share proven strategies and tools for increasing clinical e ciency, improving the patient experience and optimizing your practice for growth.
Learning Objectives Mobilize your team for success with proven
strategies.
▪ Improving the quality of care:
-Take control of your clinical workflow and adjust treatments to optimize patient outcomes.
▪ Optimizing your practice growth:
-Make data-driven clinical decisions and increase revenue opportunities.
▪ Maximizing patient experience:
-Discover the science behind customer preferences and improve the quality of your interactions with patients.
▪ Di erentiating yourself:
-Use innovation to position your practice as the premium choice in your community by maximizing patient convenience.
Speakers
2-full days of education
▪ Practice optimization & growth
▪ Di erentiate, attract more patients and access new revenue opportunity
▪ Reduce workload and stress, support sta retention and optimize practice workflows
▪ Improve Patient Experience
▪ Use comprehensive data and analytics to optimize practice workflows
▪ Stay continuously connected with patients, access insights into their treatment and oral health, from observation to retention
Michelle Shimmin
Dr. Mike Ragan Dischinger
Pre-restorative orthodontic treatment for worn anterior teeth
Dr. Jane Wright illustrates the clinical and esthetic concerns that drove the treatment plan for this patient
Growing up in the orthodontic world, I have had a frontrow view of our industry and watched the evolution of bracket styles, patient requests, and product innovation. In this exciting, ever-changing field, we help people achieve a beautiful smile. It’s important and life-changing.
Through this unique perspective on the orthodontic industry, I have gained awareness of teeth straightening modalities, companies, and brands that my orthodontist father tried over the years, including what worked and what hasn’t for his patients. His curiosity and love of helping people create functional, beautiful smiles inspired me to become an orthodontist and eventually work with him in our practice.
In our two practices in Kenosha and Salem, Wisconsin, we work with children and adults with mild-to-complex malocclusions. For our adult patients seeking orthodontic treatment, I typically use esthetically pleasing clear braces or clear aligners to help resolve crowding and improve dental function. Patients with complex alignment and restorative needs often have more efficient treatment times with fixed appliances.1 In these cases, I prefer Ormco’s Symetri™ Clear brackets. Likewise, not all patients want the responsibility of remembering to wear clear aligners and sometimes prefer bonded orthodontic braces to accommodate their busy lives.
It is helpful to have an esthetic bracket to offer adult patients when doing multi-directional, pre-restorative tooth movements. Symetri Clear brackets are advanced esthetic brackets designed for refined strength, patient comfort, and easy/safe debonding and repositioning without fracturing. Its proprietary base design and patented debonding plier enable safe, easy, and non-destructive bracket removal in one piece with minimal force. It’s comprised of a combination of proprietary ceramic particles
Jane Wright, DDS, MS, is an ABO-certified orthodontist with a private practice in Kenosha, Wisconsin, and adjunct clinical faculty at Maquette University School of Dentistry in the Orthodontic Department. Dr. Wright earned her BS in Nutrition Science from the University of Minnesota, Twin Cities, and her DDS, MS, and Orthodontic Certificate from Marquette University. She is on the College of Diplomates of the American Board of Orthodontics Council.
Disclosure: Dr. Jane Wright is a paid consultant for Ormco. The opinions expressed are those of Dr. Wright. Ormco is a medical device manufacturer and does not dispense medical advice. Clinicians should use their own professional judgment in treating their patients. Teeth images have not been altered. Patient results may vary.
(polycrystalline alumina) that create a clear, esthetic appearance while meeting clinical demands. Patients like that they are resistant to staining and designed to blend well with multiple shades of enamel.2
The following is one of our adult orthodontic cases treated with Ormco’s Symetri brackets.
Case report
A 49-year-old female presented for an initial orthodontic exam with the chief complaint of bruxing and excessive wear on her teeth, especially the anterior. She was aware of the loss of tooth height and discussed restoration plans with her dentist. She had no history of previous orthodontic treatment and was wearing a maxillary flat-plane occlusal guard from her dentist. She was aware of daytime clenching and grinding but did not report any TMJ pain, clicking, or popping. Maximum opening and range of motion were within normal limits. Cephalometric
Figures 1-5: Initial dental photos
analysis showed that she had a brachycephalic skeletal pattern, but ANB and inter-incisal angles were normal. Occlusal wear in and of itself does not affect patient quality of life,3 but some patients are self-conscious about the appearance of their short, worn teeth, which is the category that this patient fits into. Her chief concern was to improve her dental esthetics.
The patient reported chronic life stress and was unaware that her teeth were not supposed to be in constant contact during the day. We discussed self-care management of the TMJs, practicing lip seal and nasal breathing while keeping the teeth separated and masseters relaxed.4 It was discussed that if she chose to pursue orthodontic treatment, she would have to discontinue her maxillary night splint until orthodontic treatment concluded, which she accepted. We discussed fabricating a new maxillary flat-plane splint after her restorative work was complete.
With the anterior tooth wear, she had lost a few millimeters from the incisal edges of her teeth, which had super-erupted to maintain contact with the lower anterior teeth. The patient had a gingival height discrepancy with teeth Nos. 6-11 due to the wear and subsequent super-eruption. She had also lost tooth structure from the incisal edges on teeth Nos. 23-26 but did not want to restore the lower anterior teeth post-orthodontic treatment. Her general dentist planned on restoring teeth Nos. 7, 8, 9, and 10 with veneers or crowns.
Treatment plan
The orthodontic treatment plan was to bond upper and lower Ormco Symetri brackets (bidimensional prescription) and intrude teeth Nos. 7-10 along with lower anterior (teeth Nos. 23-26) to establish better overbite and overjet for restorative work. Due to the loss of height of her anterior teeth, the interproximal contacts had also moved gingivally, which decreased the width of the anterior teeth (height-to-width ratios were off). In order to establish better crown ratios, the
plan was to open space mesial and distal to teeth Nos. 7-10 with open coil springs.
Though she had a rather deep bite, the Ormco Symetri bracket was low-profile and petite enough to bond the entire upper and lower braces the same day. She had no occlusal interferences with the brackets, and bite turbos were not required. The Symetri bracket’s rounded contours were comfortable to the patient, and she liked that the brackets blended with her tooth shade and met her esthetic requirements. She reported adjusting to the braces easily. The initial wires were light, 0.014 nickel-titanium archwires, and we gradually progressed into rectangular, 0.16 x 0.22 stainless steel wires for finishing. Coils were added mesial and distal to teeth Nos. 7-10 to improve the width-tolength ratios of the crowns, and teeth Nos. 7-10 were stepped up gradually to intrude them. Ideally, gingival margins of teeth Nos. 8 and 9 should be at the level of tooth No. 6 and 11, while teeth Nos. 7 and 10 should be about 1.5 mm lower5 than the centrals. As the maxillary anterior teeth were intruded, and spaces were introduced mesial and distal, the incisal angulation of the teeth also increased. This can be protective for people with a history of bruxing, in addition to leaving more inter-incisal clearance for the restoring dentist.
Despite her history of bruxing, she never broke a bracket. During treatment, power-chain, coils, and rectangular stainless-steel wires were used, and the Symetri brackets withstood all the forces and attachments applied to them by this patient. There were a few occasions where the patient’s wire was broken from her heavy occlusal forces and bruxing, but the brackets did not debond from her clenching. She worked on her “self-care” of the TMJs, decreasing her stress and increasing her awareness of tooth touching during the day.
Debonding Symetri Clear brackets
Repositioning brackets, in this case, was unnecessary, but if they had been, the Ormco Symetri bracket debonds easily without any bracket deformation or breakage. The same bracket can be re-bonded,6 which is more economical than other clear
Figure 6: Initial ceph
Figures 7-10: Images with braces, with and without coils, facial and maxillary occlusal views
bracket systems that fracture or fold while debonding and repositioning.
On the day of debonding, the patient presented with a broken wire distal to tooth No. 10 from heavy occlusal forces. Tooth No. 10 had moved lingual and was in contact with tooth No. 23, so only the lower arch was debonded. The lower anterior teeth were retained with a gold-plated stainless steel 0.020 twist wire bonded to the lingual of teeth Nos. 22-27. A new 0.16 x 0.22 TMA wire was fabricated with an additional open-coil spring distal to tooth No.10. After four weeks, tooth No. 10 was out of contact, and her upper arch was debonded.
I have found debonding Ormco Symetri bracket is similar, if not easier, than debonding stainless steel brackets. The archwires
and a-ties can stay on, and the custom Symetri Clear deboning plier quickly clicks off each bracket in one piece with no bracket breakage or folding. There is no torquing, twisting, or pulling to remove the Ormco Symetri bracket, which makes the debond very comfortable and low-stress for both patients and practitioners. Adhesive clean-up from the enamel was carried out with a green rubber wheel.
After the patient was debonded in the maxillary arch, an upper Essix retainer was fabricated and delivered the same day. She was instructed to wear it at least 12 hours/day or night to maintain the position of tooth Nos. 7-10 and their respective spacing.
Gingival health was excellent, and her dentist was ready to move forward with veneers on teeth Nos. 7, 8, 9, and 10 shortly after that. A new maxillary Essix was fabricated when she had her temporary veneers, and a final maxillary clear Essix was delivered once her restorations were complete. She was instructed to wear the upper clear retainer to bed at night, and she will also be fit for a new maxillary flat-plane splint if her clenching and grinding continue. The patient’s awareness of her bruxing improved throughout treatment, and she has reduced her daytime clenching.
This case was completed in 14 months and likely would have been completed sooner if not for her occasional broken archwires. She was delighted with the esthetics and comfort of her clear brackets and is happy with her esthetic result. The Ormco Symetri Clear bracket system helps to increase case acceptance while giving the orthodontist the control and predictability required to finish complex restorative cases efficiently.
REFERENCES
1. Murphy SJ, Lee S, Scharm JC, Kim S, Amin AA, Wu TH, Lu WE, Ni A, Ko CC, Fields HW, Deguchi T. Comparison of maxillary anterior tooth movement between Invisalign and fixed appliances. Am J Orthod Dentofacial Orthop. 2023 Jul;164(1):24-33.
2. Data on file at Ormco.
3. Kanaan M, Brabant A, Eckert GJ, Hara AT, Carvalho JC. Tooth wear and oral-healthrelated quality of life in dentate adults. J Dent. 2022 Oct;125:104269.
6. Debonded and repositioned/rebonded on the same tooth one time (1x) using Ortho Solo™ Primer and Blugloo™ Adhesive per IFU 070-2244, Rev F. Data on file with Ormco.
Figures 11 and 12: Final frontal and occlusal with spacing
Figures 13-17: Final restorative photos
How Gaidge Consult Manager came to life
A better way to manage your new patients from call to close
Mary Beth Kirkpatrick, founder of Gaidge and Gaidge 360 Consulting, has dedicated her career to understanding one fundamental principle — the less friction you introduce into a process, the greater the likelihood of achieving enhanced compliance and success. Guided by this insight, her journey began with a profound realization — the orthodontic industry was burdened by unnecessary complexities.
When consulting in practices, Mary Beth created and utilized a spreadsheet for Treatment Coordinators that allowed them to better track their new patient funnel. It included patient statuses, pending follow-up timing, new patient paperwork, insurance verification, new patient intro calls, visit outcomes, dentist information, same day starts, and more. But while this sheet helped increase patient conversions, manually inputting data and new patient info was cumbersome.
Fast forward to 2023, when Gaidge brought Mary Beth’s TC tracking spreadsheet to life as the Gaidge Consult Manager, a comprehensive tool with new patient task management, digital forms, patient follow-up, treatment, and fee presentation — all in one place.
By improving the new patient conversion process from start to finish, Gaidge Consult Manager empowers TCs and the entire admin team to be more efficient with the following essential features:
• Patient queue: View each task and completion status in a single dashboard, including appointment confirmations, intake form tracking, insurance verification, and patient details.
• Intake forms: Securely send HIPAA-compliant, newpatient intake forms via text or email. They can easily track patient activity, collect e-signatures, add branding, and choose from pre-built templates.
• Payment presentation: Present financials with an interactive payment presentation slider, with visual payment plans patients can accept from anywhere.
• Pending follow-up: Schedule reminders for pending patient follow-up, so patients never fall through the cracks.
Helping orthodontic practices thrive has always been at the core of Mary Beth’s mission. With Gaidge Consult Manager, you can see this goal come to life in your daily operations. It equips you with the tools to maintain organization, enhance efficiency, and seamlessly manage new patient and observation (obs) exams, setting a new standard for practice management and patient care.
Experience the impact of Gaidge Consult Manager firsthand. Contact us today (https://www.gaidge.com/demo) to learn how it can drive more conversions and transform your business’ operations.
Gaidge Consult Manager
Perfect Your New Patient Conversion Process
From insurance details and new patient forms to appointment confirmations, follow-up reminders, and a payment presentation tool, the new Gaidge Consult Manager has everything your team needs to close new patient and obs exams smoothly.
Explore the New Gaidge Consult Manager
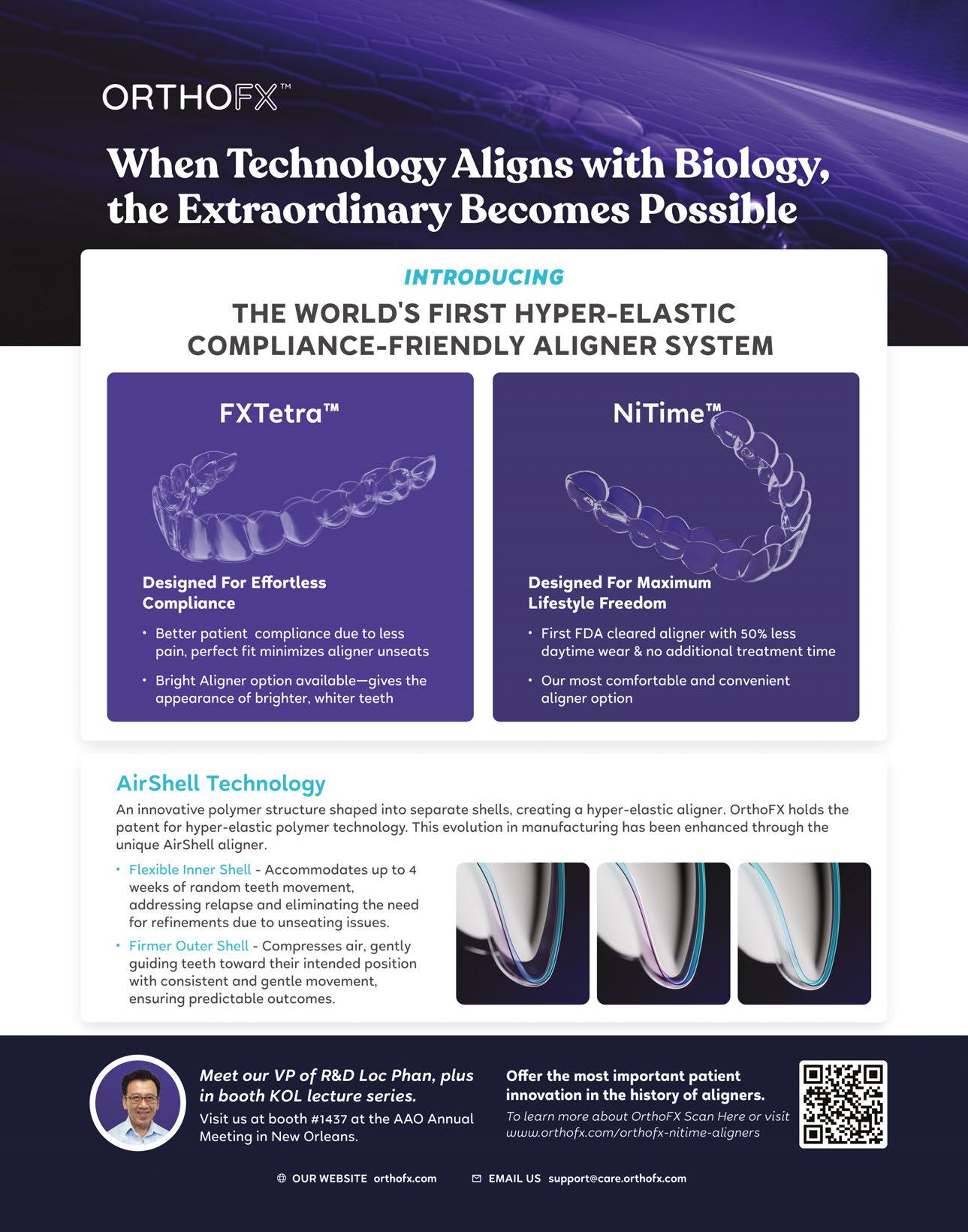
Improving patient compliance and predictability with hyper-elastic aligners
Dr. Neil Warshawsky and Loc X. Phan explore NiTime aligners and their “new generation” of aligner plastic
Abstract
Although there are numerous aligner systems, there has been a lack of industry focus on advancing the efficacy or decreasing the wear time of the clear-aligner appliance. With the introduction of new polymers from OrthoFX, a new generation of aligners is now available with “hyper-elastic” properties. Inspired by the advantages of Nitinol wires in orthodontic treatment, the NiTime Aligner is designed to be the most “compliance friendly” member of the OrthoFX polymer family. NiTime aligners provide a wide fit range and consistent forces throughout treatment, as well as the patient benefits of increased comfort and a reduced wear time.
Introduction
A new generation of aligner material
In the U.S. market today, there are more than 70 companies offering clear aligners. Where these products vary is the way each aligner brand expresses the orthodontic tooth movements. Since the beginning of aligner care, every orthodontist has been concerned about the way aligners move teeth and the potential for excessive force. In addition, the inability of aligners to complete movements without interventions such as midcourse corrections and refinements has been a pain point for doctors and patients. A related concern is the lack of patient compliance due to the typical wear time recommendation of 22 hours per day. When patients challenge the effectiveness of the appliance by inconsistent wear, the tracking of the aligner becomes extremely difficult.
To address these concerns, the ideal aligner system would have the physical properties to deliver biological efficacy while requiring significantly less wear time. OrthoFX has developed a product that meets these requirements known as NiTime Aligners. Designed with a new, patented construction, NiTime is FDA cleared for a more “compliance-friendly” wear time of a minimum 9-12 hours (contiguous wear) versus the 22 hours normally needed.
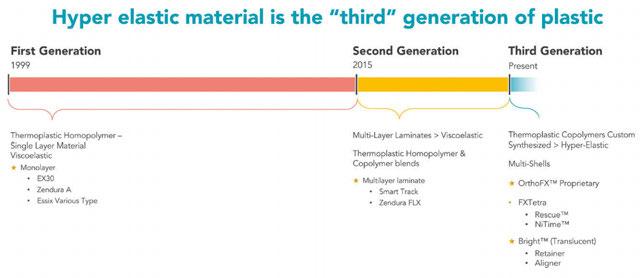
Traditionally, the industry standard aligners of today rely on viscoelastic material in their construction, which greatly limits an aligner’s effectiveness. These materials are restricted due to the principles set forth by Hooke’s Law, which states that an object’s strain (deformation) is directly proportional to its stress. OrthoFX has bypassed Hooke’s Law by developing a new aligner design and patented construction which decouple the relationship between stress and strain to deliver greater elasticity. This is attained through air shell technology that uses a torus-shaped cross section rather than the industry standard rectangular structure. OrthoFX has dubbed these material characteristics as “hyper-elastic” rather than viscoelastic to classify their family of polymer options as a new generation of aligner plastic (Figure 1).
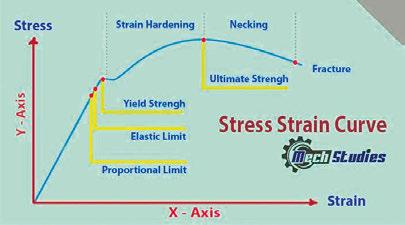
The shared goal of the orthodontic field is to utilize mechanical forces to encourage conventional tooth movement through the biological cascades of resorption and apposition. Thus, the preferred method of practitioners would be a steadily delivered, optimal force throughout the entire duration of treatment. Unfortunately, this is where many thermal plastics fail due to the characteristics of a multi-laminated material. Regardless of tertiary structure, Hooke’s Law is pervasive. The plastic properties of many industry standard aligners resemble the stress/strain curve shown in Figure 2. Note the steepness of the curve initially, as the material quickly reaches the elastic limit point. The key point of interest is the elongation at yield. Once the appliance yields, it is no longer effective as an appliance — instead, it becomes passive. This “fast to load” and “fast to die” behavior is characteristic of viscoelastic materials.
Disclosure: Dr. Warshawsky is a key opinion leader (KOL) for
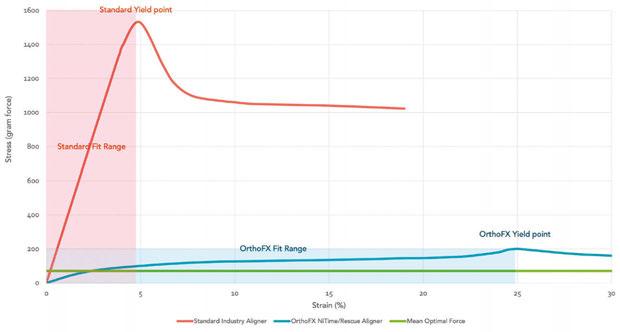
To better understand the difference in material limitations, Figure 3 illustrates actual test data of a standard industry aligner material (Zendura® FLX™) and the OrthoFX hyper-elastic aligner
Neil Warshawsky, DDS, MS, PC, operates Get It Straight Orthodontics in Chicago, Illinois.
Loc X. Phan is vice president of Research and Development for OrthoFX in Fremont, California.
OrthoFX.
Figure 1: Aligner material history timeline
material. The standard aligner material exhibits an elastic limit of approximately 5%, which is about 0.25 mm of strain/tooth movement per stage/aligner. Conversely, the OrthoFX hyper-elastic material is a half order magnitude greater in elasticity (25%), meaning it can deliver 1.25 mm of tooth movement per aligner at maximum elasticity. This allows for the OrthoFX hyper-elastic aligner to provide a wider range of fit in tandem with consistent loads during treatment.
Hyper-elasticity and fit range
The fit of the aligner is the initial, yet crucial, step to providing effective orthodontic treatment to patients. If an aligner fails to fit over the dentition, it will require mid-course corrections and refinements, which can also negatively impact patient satisfaction. To provide a broad range of fit, the hyper-elastic properties of OrthoFX aligners mimic super-elastic wire for fixed appliances (Nitinol wire). This is a critical feature for NiTime aligners, which are not worn for the standard 22 hours so can lead to the occasional dentition shift. In response, the OrthoFX NiTime Aligners offer a broad fit range to accommodate daytime shifts while continuing to move forward with the required tooth movements.
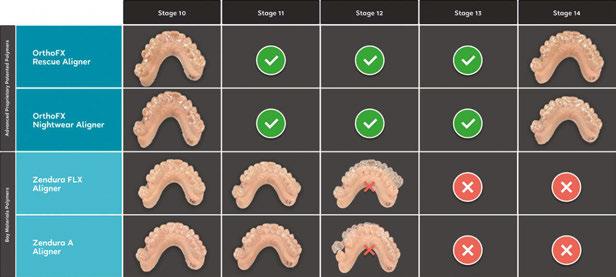
As seen in Figure 3, OrthoFX hyper-elastic aligners provide a fit range that is 5 times greater than the industry standard, while Figure 4 compares the fit ranges between an industry standard aligner (Bay Materials FLX™) and two OrthoFX aligners — NiTime and Rescue (a recovery aligner with similar elasticity to NiTime). The OrthoFX aligners have superior fit ranges by as much as +/4 aligner stages for a single aligner as compared to the industry standard aligners with just +/- 1 aligner stage.
Hyper-elasticity and optimal forces
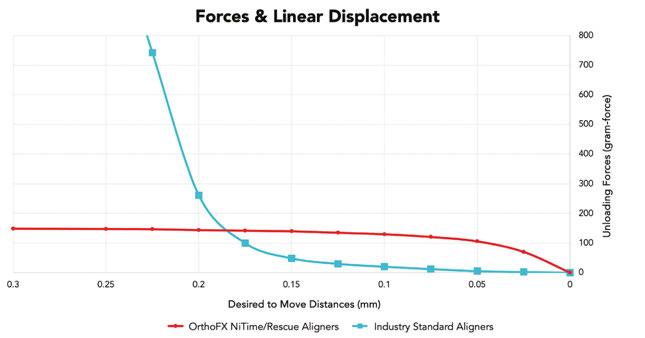
Once fit has been established, ideal forces are essential for predictable and biologically favored tooth movement. To move teeth safely and efficiently, it is important to use continuous, optimal force until the tooth reaches the desired position. Figure 5 shows the forces available for a standard industry aligner compared to an OrthoFX hyper-elastic aligner. Note the industry standard aligner’s high initial force that quickly drops below the
force required for effective tooth movement versus the constant force supplied by a hyper-elastic aligner.
Excessive force over an extended duration can cause root resorption and eventually tooth loss, which is a direct effect of tissue remodeling from inflammation known as “undermining resorption.” Furthermore, this process fails to deliver desired orthodontic tooth movements due to sterile necrosis of the locally required cellular activities. The main area of concern, for the delivery of optimal force and duration is the periodontal ligament.1 Excessive forces are detrimental to the PDL, causing hyalinization of the ligament and Sharpe’s fibers attaching the
Figure 2: Mech studies: typical stress strain property of plastic
Figure 3: Comparing fit range flexibility of FLX Aligners and OrthoFX hyper-elastic aligners*
Figure 4: Fit range comparison of four different aligner types*
Figure 5: Forces and displacements comparison*
root to the bone, thereby creating extreme pain for the patient.
OrthoFX hyper-elastic aligners follow neo-Hookean principles that generate the optimal force required for tooth movement over the entire duration of patient wear, to follow the “frontal resorption” biological process. Over a 7-day cycle of consistent force delivery, NiTime Aligners can achieve higher efficiency with greater patient comfort and a more convenient wear time. In fact, wear time is reduced from the recommended 22 hours per day to 9 to 12 hours contiguously each day, at minimum. This reduction in daily aligner wear does not extend the total treatment duration and can significantly improve patients’ daytime quality of life leading to happier, more satisfied patients. The more satisfied the patient, the more likely they are to consistently follow through in their care.
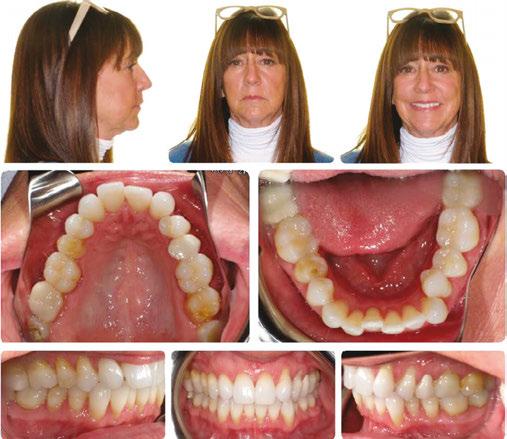
Figures 6 through 9 demonstrate a patient successfully treated with NiTime Aligners following the patient’s rejection of other systems. Figures 6 and 8 display pre- and posttreatment photos of a patient that presented with a Class II malocclusion and normal OB/OJ. This patient has teeth Nos. 7 and 10 missing congenitally. Note that the patient was treated as a child and has a canine substitution due to the missing lateral incisors. Recession was noted on tooth Nos. 2,3, 4, 5, 9, 11, 13, 14, 22, 24, 26, and 27. The patient tried labial and lingual brackets unsuccessfully, as well as a leading clear aligner to correct her malocclusion as an adult. In all three treatments, the patient could not tolerate the mechanics due to increased discomfort and was unable to complete therapy.
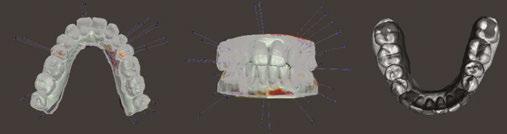
It is important to note that there was no refinement required for this case, and the patient finished in 26 weeks with 26 trays. Although the patient presented with significant recession, it did not worsen with treatment. As demonstrated in Figure 9, teeth aligned as planned by the OrthoFX treatment plan shown in Figure 7. Overlays of the actual results with the original treatment plan indicate a high level of predictive accuracy. Not only was a satisfactory result produced from the patient wearing the aligners, but the accuracy is quite high for the NiTime material despite the patient wearing it significantly less than the traditional 22 hours per day.
Conclusion
To ensure the predictable completion of aligner orthodontic treatment, flexibility in aligner dentition fit and the application of biologically desired forces are imperative. These attributes are unattainable with the industry’s outdated generation of viscoelastic material. The hyper-elastic properties of OrthoFX polymers provide a wide range of fit and optimal forces to deliver results efficiently, while providing patients a higher degree of comfort and convenience.
REFERENCE
1. Ren Y, Maltha JC, Kuijpers-Jagtman AM. Optimum force magnitude for orthodontic tooth movement: a systematic literature review. Angle Orthod. 2003 Feb;73(1):86-92.
* Internal data generated by OrthoFX R&D
Figure 6: Class II malocclusion pretreatment
Figure 9: Overlays of the actual results with the original treatment plan
Figure 8: Class II malocclusion posttreatment. Left column pretreatment. Right column posttreatment 22 stages
Figure 7: Predicted results from the OrthoFX treatment plan
Protecting your practice from hackers
We are all experiencing constant dangerous threats in our digital lives with ongoing attempts to phish for login credentials, personal details, banking information, and more. These threats come in the form of email scams, suspicious texts, payroll and wire fraud, etc. Think about how many you receive personally. Now multiply that by the number of staff you employ who could unknowingly allow hackers access to your orthodontic practice’s network and systems with one wrong click.
Keeping patient and sensitive data safe
Our robust Black Talon Academy Cybersecurity Awareness Training program significantly reduces your “click-risk” and empowers your staff to recognize well-disguised malicious attempts to breach your network. Regular training tailored to help each team member understand and identify the latest cyberthreats within their daily workflows in a practice is crucial. All team members must know the signs of phishing, the subtleties of social engineering scams, and the importance of
strong password habits. Taking time to analyze links and emails for malicious intent must become second nature for everyone.
Staff training should be your first line of defense in the cyber war
Significantly reduce your practice’s exposure to a debilitating attack by cultivating a culture of awareness. Empower your team, fortify your defenses, and proactively protect with informed awareness.
BrandHouse Dental — Your practice.
Your brand. Your products
BrandHouse Dental helps offices provide and sell their own brand of fully customized dental and bleaching products. From retainer delivery and bleaching products to branded electric toothbrushes, BrandHouse Dental has everything you need to elevate your practice’s brand.
Each of our products is FDA registered and ISO certified to ensure that you are providing your patients with the highest quality of products. Our packaging is fully customizable with full-color printing and high-quality rigid and magnetic closing boxes to showcase your custom-branded products.
BrandHouse Dental simplifies the process of the design with our fully online design-proofing software that puts you in
you with all printing proofs along with a full 3D rendering of your products for you to approve before we begin production.
Provide and sell your own brand of professionally manufac-
Redefine orthodontics with ClearCorrect ® at AAO 2024!
Ever wondered why aligners lose their initial force over time? Explore ClearCorrect’s cutting-edge technology at Booth No. 3019 as we unveil a solution to this common issue. Did you know our aligners retain 10x more initial force compared to competitors?1 Discover how this innovation transforms treatment efficiency!
Tired of additional attachments and patient discomfort? Break free from tradition with ClearCorrect’s high trimline design, 2.5x more retentive than scalloped aligners.2 Learn how this feature enhances patient comfort and simplifies treatment procedures.
Rediscover ClearCorrect! Your Path to Healthier, Confident Smiles
Explore Orthodontic Excellence with ClearCorrect at Booth #3019!
Join us at Booth #3019 in reshaping orthodontic standards!
Seeking aligners that stand the test of time? Explore how ClearCorrect’s ClearQuartz material ensures long-lasting reliability. Our proprietary aligners, engineered for 4x more tear resistance1 without staining, elevate durability standards. Visit Booth No. 3019, and discover the ClearCorrect difference at AAO 2024! Redefine orthodontic excellence with ClearCorrect.
1. Data on file; compared to 0.030” single layer polyurethane
2. Cowley DP, Mah J, O’Toole B. The effect of gingival-margin design on the retention of thermoformed aligners. J Clin Orthod. 2012 Nov;46(11):697-702; quiz 705.
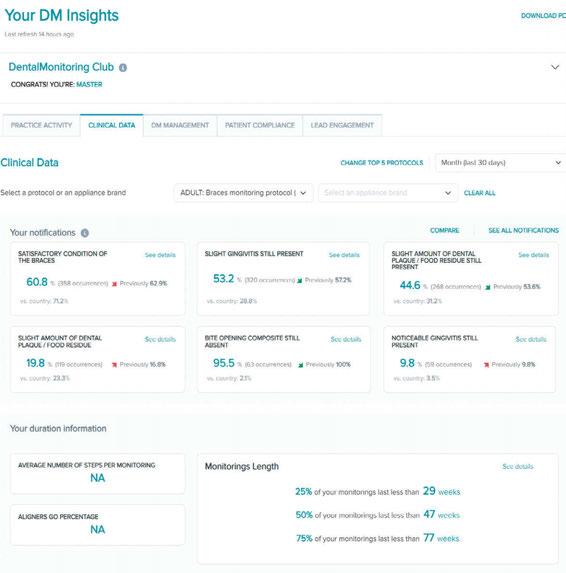
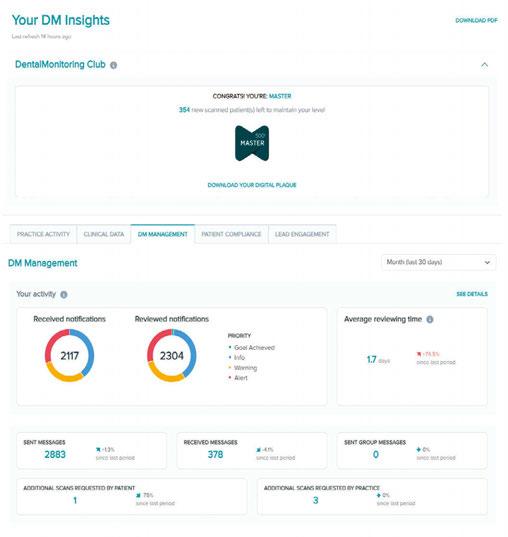
DentalMonitoring with DM Insights
Convenience for patients, clinical control for doctors
DentalMonitoring gives orthodontists the power to monitor their patient’s treatment progress remotely. Doctors are now able to have weekly updates, using scans created with the ScanBoxpro, the patient’s smartphone, and the DentalMonitoring patient app. The platform monitors 130+ intraoral observations including hygiene, gum disease, wire passivity, aligner fit, and tooth movement. Unlike other monitoring systems that add more demands on a busy clinician’s time, the intraoral observations from DentalMonitoring are automatically delivered to the practice. Notifications and reminders can be automated for all patients, which makes encouraging patient compliance more effective. The DentalMonitoring app also improves direct communication between patients and the practice staff by eliminating the problems of missed calls and voice messages. Instead, patients text the practice, and the
staff knows exactly how to respond because they have real-time observations about what is happening inside the patient’s mouth.
The simplicity of remote scanning, which works for all orthodontic treatment types, phases, and appliance brands, helps doctors and staff streamline their schedules. Regular scanning makes treatment more convenient for patients while providing even more clinical control for orthodontists.
Every piece of data from remote monitoring flows into DM Insights, an industry-first data hub that clinicians use to discover patterns and trends in their practice. Doctors utilize DM Insights real-time data analytics to identify recurring issues and take action, retrain staff, improve procedures, or compare the effectiveness of certain appliances over time.
Focus on the clinical side of care, let DentalMonitoring AI do the rest.
You’re the doctor and DentalMonitoring is the digital solution to help drive clinical excellence while optimizing treatment outcomes.
Patients scan using their smartphone with the DM app that has AI guided ScanAssist and the ScanBoxpro
DentalMonitoring AI crops, labels, and triages the scan.
DentalMonitoring AI automatically detects and analyses 130+ intraoral conditions.
Intraoral observation are triggered by the AI. Automated messages based on your protocols.
The doctor uses these observations to schedule appointments based on patient biology and treatment progress.
SPECIAL SECTION
Dolphin: A leader in Cloud computing
Dolphin has consistently anticipated evolving orthodontic practice trends for more than 35 years, and we’re proud to have been the first to offer Cloud computing more than 20 years ago:
• 2003: AnywhereDolphin, allowing record-sharing over the internet.
• Along the way we’ve introduced Dolphin Mobile, Dolphin MyOrthodontist, New Patient Online Forms & Scheduling, and Concierge.
What is Cloud Computing anyway?
Cloud computing is the practice of using a network of remote servers hosted on the Internet to store, manage, and process data, rather than a local server. Your software is automatically updated, and your data is regularly backed up.
Dolphin Cloud Sessions and Cloud Subscription
Dolphin Cloud Sessions is a hosted solution allowing you to enjoy full-featured Dolphin Imaging and Management software in the cloud. Cloud Subscription is a SaaS model that essentially lets you “subscribe” to the software rather than “buy” it.
Dolphin Blue
Dolphin Blue is a collection of Dolphin software modules in a web-based application. These modules include:
• Dolphin Blue Practice: an orthodontic practice management system
• Dolphin Blue Imaging: a patient imaging system for capturing, storing, and presenting patient images.
• Dolphin Aquarium: a library of patient education videos Both solutions seamlessly support practices with multiple locations. Visit www.dolphinimaging.com for more info.
THINKINGABOUT MOVINGTOTHECLOUD?
• DolphinCloudSubscriptionis a hosted solution. Your data is housedinanSSAE16TypeIIcertifiedfacilitythatadherestothe highestsecurityindustrystandards.
Custom digital workflow your patients expect, and your practice deserves
The KLOwen advantage in orthodontic practice
Conventional orthodontics requires a reactive approach to treating cases. The orthodontist must continuously diagnose and manually adjust the appliance and wait until the next visit to see if the teeth are tracking correctly. The outcome is longer treatment times, more appointments, and increased stress in the practice.
The full custom difference
KLOwen is at the forefront of transforming orthodontic practices with our full custom digital solution proven to deliver up to 41% reduced treatment time and up to 45% reduced appointments.* Our full custom digital approach empowers orthodontists and their teams with unparalleled control over
KLOwen at AAO Booth No. 1819.
their time, treatment outcomes, and the patient experience.
Each patient’s orthodontic needs are unique. Leveraging advanced digital technology and a full custom portfolio, we work closely with the orthodontist to design customized treatment plans for each patient that include a tailored bracket prescription for each tooth, ensuring maximum control and a perfect fit for all three orders.
Reduced treatment time, reduced appointments, reduced stress — we provide the tools and support needed to elevate the conventional fixed appliance treatment experience for your practice and your patients. Learn more and connect with us at www.klowenortho.com.
* https://klowenortho.com/white-paper
Carriere Motion Pro: the new standard in bite correction
We’ve taken fast, predictable, and discreet bite correction from revolutionary to essential!
The Carriere® Motion Pro™ bite corrector1 is the newest addition to the Motion portfolio and is fitted to teeth to treat the anteroposterior dimension of a patient’s occlusion, allowing clinicians to achieve a Class I platform within an average of 3 to 6 months2 of treatment and before placing brackets or aligners.
With the unique ability to treat both Class II and Class III patients with one device, Carriere Motion Pro bite corrector features a custom-designed drop-in hook to enhance treatment versatility. The wider reinforced cuspid pad hook ensures a consistent distribution of elastic forces, while the hook’s deep undercut simplifies elastic engagements and effectively secures the Carriere Motion Force™
designed to work seamlessly with Motion appliances to provide optimal results. The latest addition to the portfolio, the Carriere Motion Force 3™ Elastics, will be available soon.
The Carriere Motion Pro bite corrector also features a built-in scribe line, flat faces, straight edges, and a recessed dimple, helping to provide intuitive and accurate placement. This efficient design provides fast and predictable treatment, and the condyle-shaped joint is designed to facilitate more natural and controlled movement. With more than a million confident smiles treated using Motion, the path to a new standard is here.
1. Motion Pro bite corrector patent pending. Not avail
LightForce Orthodontics: Braces, but optimized
LightForce Orthodontics is revolutionizing orthodontic care with cutting-edge, custom bracket technology, offering personalized digital treatment plans that are precisely tailored to each patient’s unique needs. Experience the new standard of care with Lighforce’s 3D-printed, fully custom brackets, combined with indirect bonding, and digital planning. Come see us at AAO at Booth 1313.
LightForce Brackets
LightForce custom braces include a fully personalized base to fit the individual tooth morphology for complete freedom of motion for faster finishes and fewer appointments.* The 3D-printed translucent ceramic brackets are designed to meet your patients’ esthetic preferences, giving them the confidence
to smile. Our LightTrays are patient-specific indirect bonding (IDB) trays, 3D printed from a proprietary material to streamline the bonding workflow.
Digital Treatment Planning
The digital workflow you know, combined with LightPlan cloud-based software, allows you to create and approve treatment plans quickly and easily. LightPlan enables precise treatment planning with the end goal in mind, resulting in fewer appointments throughout treatment.* Features include 3D tooth and segment controls, including archwire deflection, superimposition, Bolton analysis, tooth movement table, and much more.
*Based on data published by the
Powerful Spark ApproverTM software and best-in-class Damon Ultima™ Brackets provide a trouble-free solution for your daily workflow.
Ormco has combined its premiere orthodontic technologies to provide orthodontists with even greater flexibility and more treatment options. Practices can now streamline daily workflow and achieve customized bracket positioning by leveraging Damon Ultima brackets and Spark Approver Software.
Ormco’s newest innovation features one case submission portal for both Ormco Digital Bonding cases and Spark Clear Aligner cases, one easy-to-use software platform for Ormco
Digital Bonding cases and Spark Clear Aligner cases, and the best-in-class Damon Ultima Brackets, the first true full-expression orthodontic system designed for faster and more precise finishing. These brackets are completely re-engineered to virtually eliminate play for precise control of rotation, angulation and torque.1 Plus, ODB features Ormco’s custom Jigs technology designed so that the “cap” wraps around the tooth buccally and lingually.*
Experience Ormco’s latest technology! Request a demo of Ormco Digital Bonding at go-orm.co/odb-orthopractice.
Shut your mouth and save your life: the problem with interlabial gap 1
Dr. Michael Gunson looks to the past and present for a view of the effects of ineffective lip closure issues
Biology, medicine, environmental studies, behavioral sciences, and more have improved with the application of principles from Systems Thinking. The face is obviously a complex system. The first step in Systems Thinking is to define the boundaries of the system and to explain its purpose.
“All systems seek to achieve a purpose. Whether humanmade or natural, all systems strive to do something. Systems Thinking…demands determination and consideration of the purpose – it is PURPOSE ORIENTED.”2
According to Systems Thinking then, a clinician can only be successful in treating the face if they can answer the question: “What is the purpose of the face?”
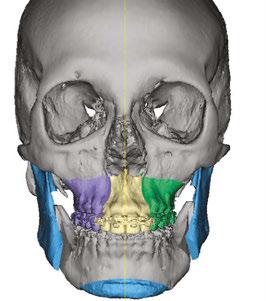
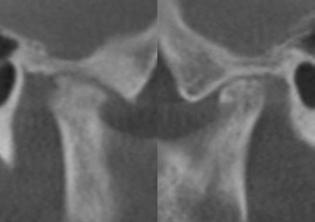
The purposes of the face, in hierarchal order, are 1) breathing, 2) eating, and 3) communicating. The brain prioritizes these purposes by causing all parts of the facial system to work together towards the three goals. When growth is inappropriate, the brain compensates to accomplish the purposes of the face often at the expense of the parts (fascia, muscles, teeth, joints, spine, etc.) These compensations may cause dysfunction, deformation, and destruction (Figures 1-4). Knowing the purposes of the face allows us to define the healthiest place for each individual part of the face. It is that position that minimizes energy expenditure as that part engages and relates with other parts in helping the face to breathe, eat, and communicate.
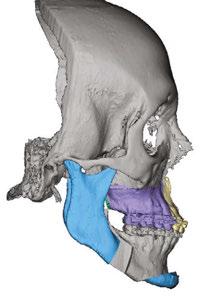
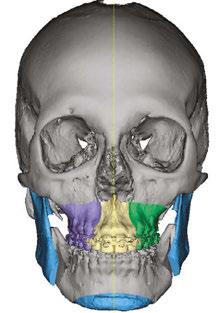
Figure 1 (left): A photo of a 69-year-old woman with a 2 mm anterior open bite and an excessive interlabial gap of 9 mm. Figure 2 (right): The sagittal slices of the above patient’s mandibular condyles reveal discontinuity of the cortical outline at the fossa and condyle (erosions). The altered condyles are flat along their path of function when she pushes her lower jaw forward to get the lips to touch in speaking, chewing, and breathing through her nose. Image captured using Dolphin® software (www.dolphinimaging.com)
Educational aims and objectives
This self-instructional course for dentists aims to provide historical background and current clinical information on the importance of lip closure to health and esthetics.
Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions by taking the quiz online at orthopracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
• Realize some history regarding the relationships of lip closure to various functions such as breathing, eating, and communicating.
• Realize how mouth breathing can have negative consequences on areas such as the bite, the face, and the airway.
• Identify some health conditions that may be associated with open mouth posture.
• Observe treatment of a patient who had a long history of pain and dysfunction due to lip incompetence issues.
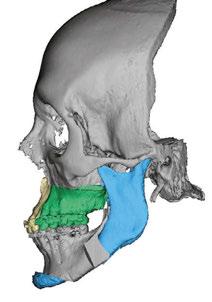
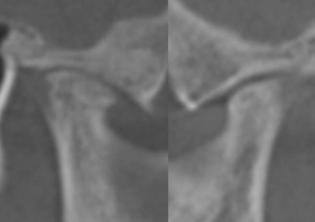
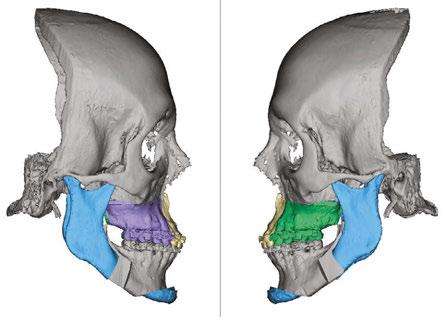
Figure 3 (left): This same 69-year-old has undergone orthognathic surgery (bilateral sagittal split osteotomies and genioplasty) to close her open bite and shorten her anterior face height. This allows her lips to touch at rest and reduces energy usage to breathe, eat, and communicate. Figure 4 (right): The energy reduction at the mandibular condyles allows them to heal as evidenced by the recortication of the bone with the disappearance of the bony erosions. Image captured using Dolphin software (www.dolphinimaging.com)
One of the most important part relationships in function is lip closure. The lips must close to achieve the following: 1) facilitate nasal breathing when awake and asleep, 2) coordinate chewing and swallowing, and 3) provide for clear and correct communication with speech and facial expression. As stated above, the parts of the face must work with the least amount of energy use;
Michael Gunson, DDS, MD, operates an oral and maxillofacial surgery private practice, limited to orthognathic surgery, in Santa Barbara, California.
in this case, the lips must close passively at rest and in function. When the lips are far from each other, the brain still insists that the lips close to breathe, eat, and communicate, but the work to close in this scenario becomes detrimental.3 Repetitive energetic movements in turn damages the parts of the facial system.
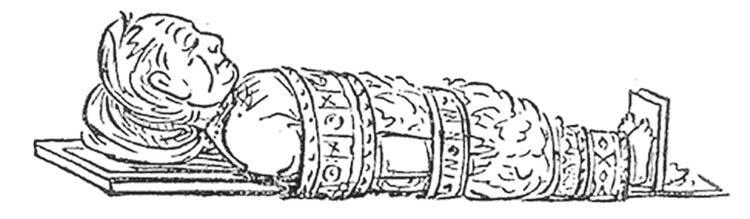
In the 1870s, a painter/explorer George Catlin observed how integral lip closure is to the entire body. Catlin traveled extensively across North and South America, visiting and painting the Native American people. After several years of close interaction, he observed that the indigenous American population was healthier than their European counterparts. Their superior health, he concluded, could be traced to the simple act of keeping their mouths closed. He published a book with art sketches called
Shut Your Mouth and Save Your Life.4 In his book, Catlin showed that mouth breathing had negative consequences in three areas: the bite, the face, and the airway.
The Bite
Catlin made the connection between lip closure and the healthy eruption of teeth into occlusion:
An Indian child is not allowed to sleep with its mouth open, from the very first sleep of its existence; the consequence of which is, that while the teeth are forming and making their first appearance, they meet (and constantly feel) each other; and taking their relative natural positions, form that healthful and pleasing regularity which has secured to the American Indians, as a Race, perhaps the most manly and beautiful mouths in the World.5 (Figures 5-6)
Burstone agrees, writing that there is a “role of lip posture as an etiologic factor in the formation of a malocclusion” and that orthodontic treatment “may not be stable if the interlabial gap is large.”6 This is shown well by Op Heij in his work regarding anterior implant placement adjacent to natural teeth. He noted an “increased vertical movement of the natural dentition” adjacent to dental implants especially in the long-faced patient.7
Malocclusion is associated with mouth breathing.8-11 In a large meta-analysis, downward-backward growth of the maxillofacial complex with narrow maxillas and dental crossbites were noted in mouth-breathing children.12,13 It is possible that repetitive application of force via lip closure causes lingual inclination of the anterior dentition. Yomo Ohno showed an association of lip forces, lingual inclination of the anterior teeth, and arch misalignment.14
The Face
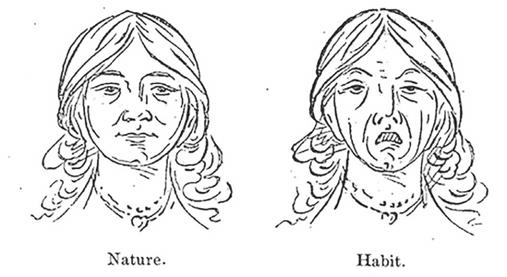
Catlin describes a pretty girl who had passive lip closure: I recollect, and never shall forget while I live, that in my boyhood I fell in love with a charming little girl, merely because her pretty mouth was always shut; her words, which were few, and always (I thought) so fitly spoken, seemed to issue from the centre of her cherry lips, whilst the corner of her mouth seemed (to me) to be honeyed together.15
Catlin’s obvious esthetic appreciation of the girl’s lip function is telling. In contrast, Catlin presents the pitiful portrait of a woman with lip incompetence:
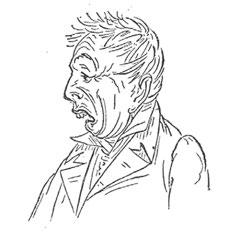
I knew a young lady many years ago, amiable and intelligent, and agreeable in everything excepting the unfortunate derangement and shapes of her teeth; the front ones of which, in the upper jaw, protruding half an inch or more forward of the lower ones, and quite incapable of being covered by the lip, for which there was a constant effort; the result of which was a most pitiable expression of the mouth and consequently of the whole face, with continual embarrassment and unhappiness of the young Lady, and sympathy of her friends.16 (Figure 7)
Dr. Ricketts concurs stating that lip incompetence “frequently results in a very unpleasant appearance of the lips and the illusion of a weak
Figure 5 (left): Catlin sketch of a European man who is mouth-breathing with excessive interlabial gap. Figure 6 (right): Catlin sketch of a mouth breather with a significant malocclusion
Figure 7: Catlin sketch of a young woman with a healthy vertical dimension, lips closed, compared to a young woman with a long anterior face height and lips apart. Notice the distress on her face and changes in esthetic appearance with deep nasolabial folds and a narrow nose
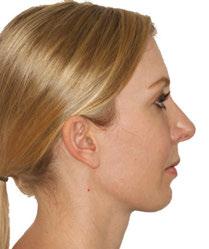
Figure 8 (left): A facial photo of a patient in repose. She has a storied history of interlabial gap secondary to anterior open bite and a long anterior skeletal face height. Figure 9 (center): A facial photo of the same patient with lips together. The esthetic changes caused by excessive efforts to get her lips to touch in function include: upper lip rhytids, deep nasolabial folds, orbicularis oris and mentalis hypertrophy, and a narrow nose. Figure 10 (right): Close-up of the same patient shows thin lips and vertical wrinkles caused by pursing her lips together in function
11: Profile facial photos of a patient with a long anterior face height with lip incompetence (left). She underwent orthognathic surgery to shorten her anterior face height, which now allows her lips to touch passively at rest (right). The esthetic outcome of lips touching in repose is thicker, more relaxed lips and a better profile
chin, and it actually is a source of embarrassment to many patients.”17 Changes in facial development start early in mouth breathers with long faces and narrow noses.18
If the lips are separated in the anteroposterior or vertical dimension, then there is muscle strain to close in function. Increasing VDO increases lower face height and lip strain with resultant facial esthetic decline.19 Ghorbanyjavadpour also showed that smaller interlabial gaps are considered more attractive. Interlabial gap causes premature aging with increasing wrinkles, deepening folds, and longer, flatter lips.21-23 (Figures 8-10)
This strain has negative facial consequences even in children. Inada wrote that interlabial gap “may induce a negative vicious cycle in the growth of the maxillofacial area, with detrimental effects on the rest of the body.”24
Treatments focused on decreasing interlabial gap reduce muscle strain and improve facial esthetics.25-27 (Figure 11)
Lip incompetence is not only associated with unhealthy facial development but it also affects the neck with related spinal curvatures such as kyphosis, lordosis, as well as pelvic tilt28,29 (Figure 12). A study showed that correction of mouth breathing and posture rehabilitation may correct early abnormalities.30
The Airway
Catlin:
…the nostrils, with their delicate and fibrous linings for purifying and warming the air in its passage, have been mysteriously constructed, and measure the air and equalize its draughts during the hours of repose.31
There is no perfect sleep of man or brute with the mouth open; it is unnatural, and a strain upon the lungs which expression of the countenance and the nervous excitement plainly show.32 (Figures 13-14)
As a society, we recognize the pathology of mouth breathing as seen in the use of the term “mouth-breather” as a pejorative reference to someone’s intelligence or health.33 The following is a quote from a medical journal in 1892:
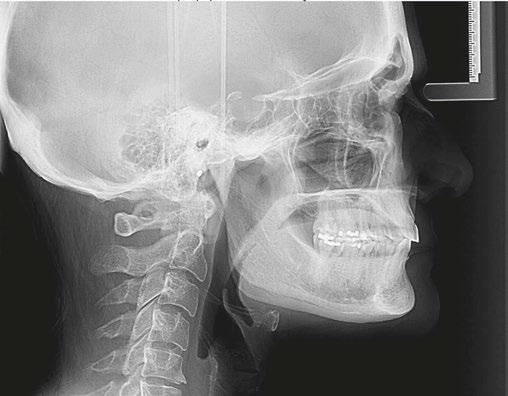
12: A lateral cephalometric radiograph of a patient with excessive interlabial gap (radiograph was taken with lips postured closed). The excessive vertical has resulted in a long history of forward head posture as she pushes to close her lips. She has developed arthritis of the spine and spondylisthesis (AP vertebral instability) secondary to her consistent forward head posture. Image captured using Dolphin software (www.dolphinimaging.com)
not allowed to sleep with his mouth open
From the condition of a “mouth-breather,” it is but a short step to one of two results more often both: deafness, and that peculiarly stupid, sleepy, inane, foolish expression of countenance so characteristic of the “mouth-breather.”34
Science has published much about the airway pathology of those with lip incompetence. Nasal congestion has been observed in mouth breathers since the late1800s.35 Allergic rhinitis and asthma seem also to be associated with open mouth
Figure
Figure
Figure 13: Catlin sketch of a native American on a papoose board who is
Figure 14: Catlin sketch of a European man in a fitful mouth-breathing sleep position
posture.36 More recently, sleep disordered breathing and obstructive sleep apnea are more prevalent in children with interlabial gap, mentalis strain, and/or mouth breathing.37,38
Clinical example
Figure 16 (left): The facial photo of the patient shows her making excessive efforts to get her lips to touch, elongating the upper lip and turning the vermillion inwards. The mentalis muscle is extremely active elevating the lower lip. She also has a forward head posture.
Figure 17 (right): The lateral cephalometric radiograph, taken in repose, shows the extent of the interlabial gap, anterior open bite, and small airway. Note the silicone chin implant which was an attempt to ineffectively correct her severe skeletal discrepancy. Image captured using Dolphin software (www.dolphinimaging.com)
A 39-year-old female with a significant open bite presents to the oral and maxillofacial surgeon’s office on referral from the orthodontist for orthognathic surgery. She has a long history of pain and dysfunction. (Figures 15-17)
Her list of complaints include the following:
• Anterior open bite
• Difficulty with lip closure — food falls out of mouth
• Muscles of mastication pain
• TMJ capsular pain
• Limited diet — soft food
• Masseter muscle spasms with tooth chatter
• Lisp
• Morning fatigue with mental cloudiness
• Exercise intolerance
• Extreme pain lower anterior teeth
• Joint noises
• Jaw posturing for comfort
She states:
“I have spent my whole life never feeling relaxed in my face because my mouth has never touched, my mouth was always open, and all the muscles would be pulling, and I could never feel relaxed.”39
Prior treatments have included
• Orthodontics — post treatment opening of anterior bite
• Dental splints x 2 — no improvement with first, worsening symptoms with second
• Physical therapy twice a week — improvement
• Anti-inflammatories — mild improvement
• Acupuncture — no effect
She was offered but refused:
• Open TMJ surgery
• Hydrocortisone TMJ injections
• Additional orthodontic treatment
• Anxiety and depression medications
• Full-mouth prosthodontic reconstruction
• Facial TENS and TMJ prolotherapy
Figure 18: The photo shows an 11 mm interlabial gap measured from stomion superior to stomion inferior. In planning for orthognathic surgery, the anterior face height must be shortened 11 mm to get the lips to touch passively prior to the teeth touching on closure
Her exam revealed:
• Interlabial gap of 14 mm
• Anterior open bite of 4 mm
• Maxillary and mandibular retrusion
• Anterior maxillary excess
• Long chin length
• Erupted third molars in occlusion
If we are to believe that her symptoms are related to her compensations, her efforts to breathe, eat, and communicate, then our goals ought to be to facilitate those actions. Her lips need to come closer together, and the teeth need to function more appropriately.
Figure 15: An intraoral photo of the patient described in the clinical example. She has a large anterior open bite and is only touching on her 3rd molars
The first step to close her lips was to remove the 3rd molars which allowed over 3 mm of anterior closure. Immediately following extractions, she reports increased exercise tolerance and elimination of her lisp. She comments: “Two weeks post-op, I ran 4 miles straight without stopping once. I no longer felt 9 months pregnant. I now wake up every morning refreshed. I wake up now without an alarm clock and feel wonderful.”
Because she still had 11 mm of interlabial gap, she required orthognathic surgery (Figure 18). The surgery was planned with the intent of closing her lip incompetence. The maxilla was impacted 4 mm, the open bite was closed by 4 mm, the chin was shortened by 2 mm, and the whole complex was counterclockwise rotated. Virtual surgical planning allows us to track the amount of vertical reduction in the anterior to assure correction of lip incompetence (Figures 19-20). After surgery, she reported complete cessation of muscle spasticity, headaches, and jaw posturing. She said: “Right out of surgery, the first time I felt my lips touch was one of the most emotional experiences because I never felt something so nurturing before…I’ve never had that feeling before in my life, and to get it for the first time was remarkable and to feel at peace.”40 (Figures 21-22)
Conclusions
Figures 19 and 20: The desired three dimensional virtual surgical movements are seen in this and the following figures. The anterior vertical reduction is accomplished by 1) impacting the anterior maxilla, 2) closing the open bite with counterclockwise rotation of the mandible, and 3) shortening the chin with genioplasty. Images captured using Dolphin software (www.dolphinimaging.com)
Figure 21 (left): The frontal dental photo shows correction of the open bite. Figure 22 (right): The profile photo after orthognathic surgery shows improved lip function with significantly decreased lip strain at lip closure and an improved profile with better lip curl and chin projection. The mentalis muscle thickness will continue to atrophy with continued disuse
After reviewing the literature about the deleterious effects of lip incompetence on the facial health of patients, it ought to be in the forefront of every clinician’s treatment plan to assist patients in getting their lips together. Dentists can reduce vertical dimension through oc clusal equilibration. Orthodontists can close anterior open bites by managing transverse discrepancies and with posterior intrusion mechanics. Thin lips can be enlarged carefully by cosmetic surgeons with fat or dermal fillers. And orthognathic surgery can effectively treat excessive anterior vertical heights by impacting the anterior maxilla, closing open bites, and reducing chin lengths. The relief that patients feel when correcting lip incompetence is dramatic as we are literally “shutting our patients mouths to save their lives.”
REFERENCES
1. Burge S. System Purpose. 2015. https://www.burgehugheswalsh.co.uk/Uploaded/1/ Documents/System-Purpose.pdf (Accessed March 8, 2024).
2. Schlossberg, L, Harris, S. An electromyographic investigation of the functioning perioral and suprahyoid musculature in normal occlusion and Class II, Division 1 dysplasia cases. Am J Orthod. February 1956; 42(2):153.
4. Ibid, 46.
3. Catlin G. Shut Your Mouth and Save Your Life. Pantianos Classics. Reprint adapted from revised edition 1890.
5. Burstone CJ. Lip posture and its significance in treatment planning. Am J Orthod. 1967 Apr;53(4):262-284.
6. Op Heij DG, Opdebeeck H, van Steenberghe D, Quirynen M. Age as compromising factor for implant insertion. Periodontol 2000. 2003;33:172-184.
7. Mattar SE, Anselmo-Lima WT, Valera FC, Matsumoto MA. Skeletal and occlusal characteristics in mouth-breathing pre-school children. J Clin Pediatr Dent. 2004 Summer;28(4):315-318.
8. Granja GL, Leal TR, Lima LCM, Silva SED, Neves ÉTB, Ferreira FM, Granville-Garcia AF. Predictors associated with malocclusion in children with and without sleep disorders: a cross-sectional study. Braz Oral Res. 2023 Oct 27;37:e106.
9. Ma Y, Xie L, Wu W. The effects of adenoid hypertrophy and oral breathing on maxillofacial development: a review of the literature. J Clin Pediatr Dent. 2024 Jan;48(1):1-6.
10. Otsugu M, Sasaki Y, Mikasa Y, Kadono M, Sasaki H, Kato T, Nakano K. Incompetent lip seal and nail biting as risk factors for malocclusion in Japanese preschool children aged 3-6 years. BMC Pediatr. 2023 Oct 26;23(1):532.
11. Zhao Z, Zheng L, Huang X, Li C, Liu J, Hu Y. Effects of mouth breathing on facial skeletal development in children: a systematic review and meta-analysis. BMC Oral Health. 2021 Mar 10;21(1):108
12. Souki BQ, Pimenta GB, Souki MQ, Franco LP, Becker HM, Pinto JA. Prevalence of malocclusion among mouth breathing children: do expectations meet reality? Int J Pediatr Otorhinolaryngol. 2009 May;73(5):767-773.
13. Ohno Y, Fujita Y, Ohno K, Maki K. Relationship between oral function and mandibular anterior crowding in early mixed dentition. Clin Exp Dent Res. 2020 Oct;6(5):529-536.
14. Catlin, 75.
15. Ibid. 79.
16. Ricketts RM. Esthetics, environment, and the law of lip relation. Am J Orthod. 1968 Apr;54(4):272-289.
17. Al Ali A, Richmond S, Popat H, Playle R, Pickles T, Zhurov AI, Marshall D, Rosin PL, Henderson J, Bonuck K. The influence of snoring, mouth breathing and apnoea on facial morphology in late childhood: a three-dimensional study. BMJ Open. 2015 Sep 8;5(9):e009027.
18. Sun J, Lin YC, Lee JD, Lee SJ. Effect of increasing occlusal vertical dimension on lower facial form and perceived facial esthetics: A digital evaluation. J Prosthet Dent. 2021 Oct;126(4):546-552.
19. Ghorbanyjavadpour F, Rakhshan V. Factors associated with the beauty of soft-tissue profile. Am J Orthod Dentofacial Orthop. 2019 Jun;155(6):832-843.
20. Oliveira AC, Dos Anjos CA, Silva EH, Menezes Pde L. Aspectos indicativos de envelhecimento facial precoce em respiradores orais adultos [Indicative factors of early facial aging in mouth breathing adults]. Pro Fono. 2007 Jul-Sep;19(3):305-312.
21. Demir R, Baysal A. Three-dimensional evaluation of smile characteristics in subjects with increased vertical facial dimensions. Am J Orthod Dentofacial Orthop. 2020 Jun;157(6):773-782
22. Qadeer TA, Jawaid M, Fahim MF, Habib M, Khan EB. Effect of lip thickness and competency on soft-tissue changes. Am J Orthod Dentofacial Orthop. 2022 Oct;162(4): 483-490.
23. Inada E, Saitoh I, Kaihara Y, Murakami D, Nogami Y, Kubota N, Shirazawa Y, Ishitani N, Oku T, Yamasaki Y. Incompetent lip seal affects the form of facial soft tissue in preschool children. Cranio. 2021 Sep;39(5):405-411.
24. Yogosawa F. Predicting soft tissue profile changes concurrent with orthodontic treatment. Angle Orthod. 1990 Fall;60(3):199-206.
25. Yu YH, Kim YJ, Lee DY, Lim YK. The predictability of dentoskeletal factors for soft-tissue chin strain during lip closure. Korean J Orthod. 2013 Dec;43(6):279-287.
26. Zide BM, McCarthy J. The mentalis muscle: an essential component of chin and lower lip position. Plast Reconstr Surg. 1989 Mar;83(3):413-420.
27. Milanesi JM, Borin G, Corrêa EC, da Silva AM, Bortoluzzi DC, Souza JA. Impact of the mouth breathing occurred during childhood in the adult age: biophotogrammetric postural analysis. Int J Pediatr Otorhinolaryngol. 2011 Aug;75(8):999-1004.
28. Yi LC, Jardim JR, Inoue DP, Pignatari SS. The relationship between excursion of the diaphragm and curvatures of the spinal column in mouth breathing children. J Pediatr (Rio J). 2008 Mar-Apr;84(2):171-177.
29. Corrêa EC, Bérzin F. Efficacy of physical therapy on cervical muscle activity and on body posture in school-age mouth breathing children. Int J Pediatr Otorhinolaryngol. 2007 Oct;71(10):1527-1535.
30. Catlin, 30.
31. Ibid. 27.
32. Oxford English Dictionary. Mouth-Breather. https://www.oed.com/search/dictionary/?scope=Entries&q=mouth+breather. (Accessed March 8, 2024).
33. Fanning, AM. Deafness and the care of the ears. The Popular Science Monthly, December 1892:212.
34. Cassells JP. “Shut Your Mouth and Save Your Life:” Being Remarks on Mouth-Breathing, and Some of Its Consequences, Especially to the Apparatus of Hearing: A Contribution to the Ætiology of Ear-Disease. Edinb Med J. 1877 Feb;22(8):728-741.
35. Georgalas C, Terreehorst I, Fokkens W. Current management of allergic rhinitis in children. Pediatr Allergy Immunol. 2010 Feb;21(1 Pt 2):e119-126.
36. Oh JS, Zaghi S, Peterson C, Law CS, Silva D, Yoon AJ. Determinants of Sleep-Disordered Breathing During the Mixed Dentition: Development of a Functional Airway Evaluation Screening Tool (FAIREST-6). Pediatr Dent. 2021 Jul 15;43(4):262-272.
37. Fitzpatrick MF, McLean H, Urton AM, Tan A, O’Donnell D, Driver HS. Effect of nasal or oral breathing route on upper airway resistance during sleep. Eur Respir J. 2003 Nov;22(5):827-832.
38. Patient. Interview conducted by Dr Alan Marcus May 22, 2018.
39. Ibid.
• 16 CE credits available per year
• 1 subscription, 2 formats – print and digital
• 4 high-quality, clinically focused issues per year
Shut your mouth and save your life: the problem with interlabial gap GUNSON
1. The lips must close to _________.
a. facilitate nasal breathing when awake and asleep
b. coordinate chewing and swallowing
c. provide for clear and correct communication with speech and facial expression
d. all of the above
2. After several years of close interaction, George Catlin observed that the indigenous American population was healthier than their European counterparts. Their superior health, he concluded, could be traced to _________.
a. their discovery of dental tools
b. their traditional vegan diet
c. the simple act of keeping their mouths closed
d. their use of facial exercises
3. ________ wrote that there is a “role of lip posture as an etiologic factor in the formation of a malocclusion” and that orthodontic treatment “may not be stable if the interlabial gap is large.”
a. Kingsley
b. Burstone
c. Angle
d. Farrar
4. __________ noted an “increased vertical movement of the natural dentition” adjacent to dental implants especially in the long-faced patient.
a. Op Heij
b. Burstone
c. Angle
d. Proffitt
5. In a large meta-analysis, downward-backward growth of the maxillofacial complex with narrow maxillas and dental crossbites were noted in mouth-breathing children.
a. True
b. False
6. ________ showed an association of lip forces, lingual inclination of the anterior teeth, and arch misalignment.
a. Angle
b. Yomo Ohno
c. Op Heij
d. Catlin
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://orthopracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://orthopracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 370
Date Published: March 28, 2024
Expiration Date: March 28, 2027
7. Dr. Ricketts concurs stating that lip incompetence “frequently results in a very unpleasant appearance of the lips and _______, and it actually is a source of embarrassment to many patients.”
a. the illusion of a weak chin
b. the illusion of a double chin
c. pronounced nasolabial folds
d. thicker lips
8. If the lips are separated in the anteroposterior or vertical dimension, then there is muscle strain to close in function.
a. True
b. False
9. Lip incompetence is not only associated with _______ but it also affects the neck with related spinal curvatures such as kyphosis, lordosis, as well as pelvic tilt.
a. improved facial esthetics
b. plump lips
c. unhealthy facial development
d. wrinkle reduction
10. Sleep-disordered breathing and obstructive sleep apnea are more prevalent in children with ________.
a. interlabial gap
b. mentalis strain
c. mouth breathing
d. all of the above
To provide feedback on CE, please email us at education@medmarkmedia.com
Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
Clinical implementation of AI systems in orthodontics
Drs. Aaron Glick, John Garza, Nisha Manila, and Jennifer Chang discuss the pros and cons of AI in orthodontic and general dental practice
Introduction
Although artificial intelligence (AI) has been integrated in daily life, most are not aware that it has become an integral part of many aspects of modern life over the past decades given the increased computing power, digitization of data, advances
Aaron Glick, DDS, works in healthcare innovation and is on faculty at the University of Texas Health Science Center at Houston School of Dentistry and Sam Houston State University College of Osteopathic Medicine. He is a Diplomate of the ABDSM, faculty member of the AADSM Mastery Program, and holds fellowship credentials with Academy of General Dentistry and International Congress of Oral Implantology. He enjoys all technologies and has a background in software programming for neuroscience research at Brandeis University and Harvard University using 3D modeling, AI, and fMRI technologies. Dr. Glick has been published in medical and dental journals and lectures nationally on dental sleep medicine and digital/software technologies.
John Garza, DDS, MSD, is a board-certified orthodontist practicing in the Houston, Texas area. Dr. Garza received his DDS, AEGD certificate, orthodontics certificate, and Master’s degree fromThe University of Texas School of Dentistry. He has taught in the Restorative and Prosthodontics Department as well as the Orthodontics Department at UT as a clinical assistant professor in both clinical and didactic courses. Additionally, Dr. Garza has enjoyed serving on research committees for several Master’s degree candidates in the Orthodontic department at UT. Dr. Garza is currently active in organized dentistry in orthodontics at the state level.
Nisha Manila BDS, PhD, is an Associate Professor and Director of Oral and Maxillofacial Radiology at California Northstate University College of Dental Medicine. With a dental degree from India, and a Ph.D. in Oral Radiation Oncology from Tokyo Medical and Dental University, Japan, she completed Oral and Maxillofacial Radiology training at Texas A&M University. Dr. Manila is a fellow of the American College of Dentists, and her research interests include applications of AI in dentistry, CBCT imaging, and advanced diagnostic imaging modalities. Dr. Manila is an active member of several professional organizations.
Jennifer Chang DDS, MSD, is an assistant professor and program director in the Department of Periodontics at The University of Texas School of Dentistry at Houston. She completed her Doctor of Dental Surgery degree and 2 years of general practice residency in Taiwan. She obtained her Master of Science in Dentistry degree in periodontics from Indiana University School of Dentistry. Dr. Chang is a board-certified Diplomate in Periodontology and Dental Implant Surgery. She maintains a part-time practice at the school’s faculty group practice and in the greater Houston area. Her clinical and research interests focus on improving treatment options for periodontal/peri-implant disease.
Educational aims and objectives
This self-instructional course for dentists aims to identify how artificial intelligence (AI) works, as well as its advantages and disadvantages in the orthodontic and general dental practice.
Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions by taking the quiz online at orthopracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
• Define AI and the evolving types of AI.
• Identify the basics of how the data is used in a clinical way by interacting with AI-enabled systems and machines.
• Recognize how AI systems are being used to improve aspects of the orthodontic process. Realize some of the issues that need to be addressed to ensure patient safety, clinical success, and to safeguard the practice from legal complications. 2 CE CREDITS
in algorithm, and improvements in accuracy. In fact, when a group of Americans were surveyed, over half were not able to identify that AI powered wearable fitness trackers, automated chatbots, product recommendations, security cameras that identify unrecognized people, music playlist recommendations, and email services identifying spam messages.1 In dentistry, some of these same AI systems, such as chatbots, have been integrated for general office support and software automations. Other AI systems that are more dental-specific have also been used for approximately a decade. These include systems that automatically identify dental landmarks in CBCT,2 maxillary/mandibular segmentation from radiographic images,3 and digital reconstruction of tooth surfaces.4
Some examples of more current AI systems in dentistry are decision support systems to aid clinicians in the diagnosis of caries and periodontal conditions, AI-enabled robotic surgeries, and creation of AI-generated dental restorations/appliances.5 Since AI is a tool, it can be used in multiple applications within the dental field; as the algorithms advance in accessibility and accuracy, the amount of products with embedded AI will likely increase (Table 1). Therefore, it is important as a dental practitioner to understand the tools used, particularly if they can have a direct or indirect effect on patients.
How AI works
AI is a broad term that generally refers to the ability for computers to perform tasks that typically require human intelligence (Figure 1); for example, viewing a dental X-ray and identifying interproximal caries. Machine learning (ML) refers to the mathematical approach to accomplish this perceived human intelligence. These algorithms are programmed to take information and “learn” from these datasets. Since there are alternative methods for artificial intelligence, machine learning is considered a subset of the approaches to achieve artificial intelligence. Multiple types of algorithms can be programmed by the user. In one approach, a convolutional neural network (CNN) can feed a large dataset to identify the features that are most salient in a classification task. For instance, with multiple pictures of apples or cats, the neural network would be a mathematical model used to make the binary decision on if the currently presented image should be classified as an apple or cat. The CNN approach is typically selected for image operations since this algorithm is optimized to process images based on the extraction of spatial features.
Depending on the task to be performed, there are multiple types of models that are specific to optimizing for the type of data or output intended. For instance, chatbots require a text-based approach with grammatical rules built into sequences of words. Therefore, language-specific models would be used for textbased tasks, typically called natural language processing (NLP).
Further into the black box
While most dentists today don’t consider building custom AI products, there are products that will democratize the use of AI through no-coding technologies.6 Whether coding the algorithms or not, understanding the basics of how the data is used to derive a clinical decision/outcome is important as dentists are increasingly interacting with AI-enabled systems and machines. When software manufacturers train an AI model, they require a large amount of data to process. In general, the full dataset is split into 3 distinct groups: 1) training set, 2) validation set, and 3) testing set (Figure 1). In a supervised model, a team of clinicians will label the full dataset. For instance, if the classification task is to automatically identify caries in bitewing radiographs, the clinician would identify areas of the radiographs with caries. These labeled radiographs serve as the “ground truth” for the algorithm. The bulk of the data is used in the training set to optimize the weights of the neural network identifying salient features of the categorized dataset. The model is then further optimized by using a validation dataset, where additional processes can improve the accuracy. The final step is to understand how accurate the fully trained AI model can perform on the similar dataset. Therefore, the testing dataset is then categorized by the trained model to provide an accuracy typically reported as a percentage of accurately categorized responses and Receiver Operating Characteristics (ROC) curve/area under the curve (AUC). The ROC curve and AUC offers additional details similar to the true positive rate and false positive rate. Ultimately, the large dataset is trained, and the same isolated dataset is used to assess the accuracy in a non-clinical setting.
Table 1: Multifaceted uses of AI in dentistry
Dental specialtyUse case
Endodontics
Implant dentistry
Oral surgery
Orthodontics and pediatric dentistry
Pathology
Periodontics
Prosthodontics and restorative dentistry
Radiology
Non-clinical
• Identify root morphology, minor apical foramen
• Diagnosis of apical lesion, root fracture
• Risk of peri-implant diseases
• Surgical procedures
• Identification of anatomic features
• Screening and classification of oral cancer
• Cephalometric analysis
• Treatment needs and outcome evaluation
• Vertebral growth assessment
• Analyze histologic slides and cytologic specimens
• Practice management (i.e., HR and insurance automations, financial projections, scheduling chatbots)
When building these algorithms, there are some additional key considerations as to how the algorithm uses data. In an oversimplification, an algorithm can be delineated as 1) super-
Figure 1: Visualization of the distinction between terminology for artificial intelligence (AI), machine learning (ML), and Convolutional Neural Networks (CNN)
vised/unsupervised or 2) static/continuous learning. Supervised learning is based on a clinician providing the algorithm with a ground truth for labelled data, similar to the previous example. Unsupervised learning is where the model learns without explicitly provided information to classify and can be accomplished through patterns within the data. Static learning algorithms are the traditional type of AI. However, some current algorithms are designed to update and improve themselves based on additional data acquired during use.
AI in orthodontics
AI is changing our daily lives and approaches to dentistry in general. In orthodontics, AI is being used for the following:
1. More rapid diagnosis through facial, radiographic, photographic, and intraoral scanning
2. Treatment planning for surgery/outcome prediction
3. Treatment progression through remote monitoring and treatment progression
AI is being used clinically as assistive technology that can assess various forms of diagnostic data to provide identification and decision-making support for orthodontics. For instance, automatic cephalometric analysis to identify anatomical landmarks in CBCT radiographs has been shown in one study to be up to 92% accurate.7 Additionally, automatic tooth position detection and tooth identification have been shown to have accuracies above 88%.8 Identification and automatic digital labelling can allow for a more rapid assessment and potential diagnosis. Further aiding in the decision-making process is determination of dental age based on radiographic indicators that has shown to be highly accurate at 94%.9 Other examples of a decision support system that could be used in orthodontics is an early-stage detection of osteoarthritis AI system trained using multiple patient-specific factors such as CBCT, biomolecular, and clinical features.10 Currently, AI analyses have been used to detect facial midline and asymmetries, yet has not shown to improve accuracies over traditional methods.11
Treatment planning in orthodontics can be aided by AI through decisions to extract, recommendations for orthognathic surgery, dentofacial complex predictions of outcome, and patient satisfaction in aligner therapy. In all cases, a well-functioning system can improve confidence for early-stage orthodontists, reduce overall treatment time, improve esthetic outcomes, and provide an improved patient experience. For instance, one study used patient, radiographic, and clinical data to construct an AI model to predict recommendations for extraction patterns and anchorage patterns.12 Predictive algorithms have also been developed to predict the posttreatment facial changes13 and patient experience with clear aligner therapy with indices of pain and anxiety.14 Other applications include prediction of C. difficile infections for major surgeries, selection of headgear, selection of fixed appliances, and optimizing the selection of patients for removable appliances.15
AI is being used during and posttreatment in orthodontics. Remote patient monitoring can utilize AI to track 3D tooth
movement during treatment with enough fidelity to reconstruct full 3D digital models.16 Use of remote patient monitoring can be done with the patient using their smartphone and can lead to increased patient compliance.17 In finalizing successful treatment, outcomes can be assessed using facial attractiveness models.18
A light in the black box
AI presents an exciting tool to simulate human intelligence to help dentists achieve a higher quality of life, better decision-making capability, and fewer postoperative complications.19 However, despite these advances, AI in dentistry is in its infancy. On the horizon are more autonomous systems that do not require human input at the clinical stage within the AI algorithm. While a good understanding of the basics of AI is useful, the actual processes of most algorithms and datasets are not transparent to clinicians. Accuracy, trust, data stewardship, and equity/sustainability are concerns that clinicians and AI software manufacturers need to address to ensure patient safety, clinical success, and safeguarding from legal complications.
Accuracy
The accuracy of an AI system is based on a predefined gold standard. Most clinical decision support tools are supervised algorithms and labeled by clinical dentists without histologic confirmation. Since the amount of data that is required to train the models is so large, it is impractical to build highly accurate datasets that are verified with high-quality standards. In fact, the sensitivity for dentists to detect interproximal caries in bitewings in dentin is low (.36),20 and provider agreement also is low (.4 kappa).21 Similar findings have been seen in other fields such as in periodontal conditions yet are task specific.22 While the quality of the dataset will likely not be transparent, the process for labeling the data as an important factor in the accuracy of the system could be stated by the manufacturer. Another issue that can affect AI is the imbalance of certain conditions like rare pathology that limit the number of instances for the algorithm to learn.
What is the clinical accuracy of these AI models? Is the trained dataset similar to your patient population or data in your EHR? Most report accuracies on the original dataset that was used, yet the true accuracies with different datasets or after clinicians have interacted with the AI system remain limited, and
Figure 2: Use of data with a supervised AI model
independent testing remains even more limited. In fact, some studies have shown that when AI presents incorrect information, clinicians are more likely to be misled by this recommendation which could result in poor patient outcomes.23,24 Should incorrect guidance be provided by the AI system and patient harm occurs, the current legal climate would hold the clinician liable.25 Additionally, when the AI system is accurate, there are concerns of other biases and trust.
Trust
In all cases, a well-functioning system can improve confidence for early-stage orthodontists, reduce overall treatment time, improve esthetic outcomes, and provide an improved patient experience.
A human-computer interaction exists between the dentist and AI system that can affect the perception of clinical information and ultimately treatment performance and decision. Trust is a well-studied concept that is affected by many factors with transparency, reliability, and tangibility as some of the commonly cited values that apply most to human-computer interaction.26 Transparency is inherent in trust, and AI systems can be built to be explainable. While most traditional forms of AI suffer from the “black box problem,” some offer detection strategies through computer vision,27 and others provide embeddings through natural language processing.28 Reliability offers a perception that the algorithm is making similar decisions in seemingly similar circumstances. For continuously learning algorithms, there is a potential risk that adaptive learning could introduce new errors and reduce reliable performance.29,30 Tangibility refers to the physical or virtual presence of the AI system and when it appears more real or anthropomorphic, which improves trust.31
Data stewardship
Machine learning sits at the intersection of big data and software algorithms. Given the need for large datasets to train models, the data stewardship in regulated industries, especially dentistry, is important. Dental offices handle private data on patients within their electronic health record system such as financial, demographic, disease state information, and other sensitive clinical information. With the digitization of records and equipment, the dental industry is a prime target for hackers and also lacks adequate knowledge about the prevention of these crimes.32 In fact, Henry Schein, a large distribution and software company with more than 23,000 employees and 1 million customers globally, halted operations due to a cyber security incident.33 Large, consolidated datasets with patient data are vulnerable to attacks. Additionally, generative AI that ingests data from multiple sources feeding back into the algorithm can pose a risk if patient data is used. For instance, divulging patient data on a generative AI platform to write patient notes more efficiently could put the dentist at risk of breaching HIPAA with patient data being used to continuously train the model. For example, Sarah Silverman is suing openAI and Meta over violations of her copyrighted book that surfaced when these platforms regurgitated substantial elements of her copyrighted materials.34
Equitability/sustainability
The equitable treatment of patients is an ethical value upheld by the American Dental Association where all treatment
decisions should be determined on the same basis as all other patients.35 As AI systems are built with human inputs, biases can be encoded into the model.36 In one example of this, Optum, a health service company, created an AI program to spot high-risk patients who should receive medical follow-up care. However, the follow-up care disproportionately identified white patients with 82% white and 18% black patients identified compared to an independent analysis finding that 53% white and 46% black patients should have been identified based on medical need. Before this error could be detected, the program had already been applied to 100 million patients.37 Additionally, the hardware that powers AI requires high energy and a large local ecological footprint.38 In fact, GPT3 took 1.287 gigawatt hours of electricity and 700,000 liters of clean freshwater.39
Implementation of AI systems
As manufacturers continue to release new and update current AI-embedded technologies, dentists should be aware of how these tools operate and can potentially change patient care. Many dentists are likely to already implement AI-embedded technologies without fully realizing it since AI is commonly used as a tool to accomplish a task or optimize tasks, and most backend systems are not transparent to the user.
In order to implement new technologies with AI into a dental office, technology acceptance and continual quality assurance should be a consideration. The primary factors for technology acceptance are perceived usefulness and perceived ease of use.40 Therefore, removing barriers to trust within the human-computer interaction can improve usage. Training with technology in a safe environment can build confidence and improve ease of use. Additionally, having a plan for continuous quality assurance with the use of AI can aid in patient safety given that the systems can change with updates or continuously learning models. AI behavior should be periodically monitored, and a set of well-defined metrics are needed to guide regularly scheduled testing.41
The U.S. government also functions to protect patients and dental offices’ implementation of AI through the FDA clearance process of software as a medical device. FDA has become increasingly more stringent on this type of software that predicts and identifies medical/dental conditions.42 As dentists expand their appetite for additional functionality of these software systems, there needs to be a balance between the regulatory burden and the ability to innovate.
Exciting future of AI in dentistry
With the digitization of dental records and radiographs, dentistry is an ideal profession to harness AI. Current applications
of AI are already being implemented to change the workflow of dental offices and patient care. Despite risks of inaccuracies, human-computer mistrust, data security concerns, and inequities in applications, it is easy to imagine overcoming these obstacles as the perceived future benefits outweigh the risks.43 Healthcare in general is expected to see an increase in venture investments as the value of AI in health is expected to grow from $4.9B in 2020 to $45.2B in 2026. Dentistry, however, is lacking in the amount and accuracy of data.44 To accelerate the advancement of AI, manufacturers need access to large, structured datasets that contain valid and reliable data. In fact, each of our practices holds valuable data that has the potential to improve the field.
REFERENCES
1. Kennedy B, Tyson A, Saks E. Public awareness of artificial intelligence in everyday activities. Pew Research Center. (Published February 15, 2023.) https://www.pewresearch.org/ science/2023/02/15/public-awareness-of-artificial-intelligence-in-everyday-activities/. (Accessed: November 24, 2023.)
2. Cheng E, Chen J, Yang J, Deng H, Wu Y, Megalooikonomou V, Gable B, Ling H. Automatic Dent-landmark detection in 3-D CBCT dental volumes. Annu Int Conf IEEE Eng Med Biol Soc. 2011;2011:6204-6207.
3. El-Bialy A. Towards a Complete Computer Dental Treatment System. 2008 Cairo International Biomedical Engineering Conference, Cairo, Egypt. 2008:1-8.
4. Sporring J., Hommelhoff Jensen K. Bayes Reconstruction of Missing Teeth. J Math Imaging Vis. 2008;31:245–254.
5. Chang J, Glick A. Clinical implementation of artificial intelligence systems. J Greater Houston Dent Soc. 2023; 94(2):18-19.
6. Sundberg L, Holmström J. Democratizing artificial intelligence: How no-code AI can leverage machine learning operations. Business Horizons. 2023;66(6):777-778.
7. Lee JH, Yu HJ, Kim MJ, Kim JW, Choi J. Automated cephalometric landmark detection with confidence regions using Bayesian convolutional neural networks. BMC Oral Health. 2020 Oct 7;20(1):270.
8. Chen CC, Wu YF, Aung LM, Lin JC, Ngo ST, Su JN, Lin YM, Chang WJ. Automatic recognition of teeth and periodontal bone loss measurement in digital radiographs using deep-learning artificial intelligence. J Dent Sci. 2023 Jul;18(3):1301-1309. doi: 10.1016/j. jds.2023.03.020. Epub 2023 Apr 10.
9. Guo YC, Han M, Chi Y, Long H, Zhang D, Yang J, Yang Y, Chen T, Du S. Accurate age classification using manual method and deep convolutional neural network based on orthopantomogram images. Int J Legal Med. 2021 Jul;135(4):1589-1597.
10. Bianchi J, de Oliveira Ruellas AC, Gonçalves JR, Paniagua B, Prieto JC, Styner M, Li T, Zhu H, Sugai J, Giannobile W, Benavides E, Soki F, Yatabe M, Ashman L, Walker D, Soroushmehr R, Najarian K, Cevidanes LHS. Osteoarthritis of the Temporomandibular Joint can be diagnosed earlier using biomarkers and machine learning. Sci Rep. 2020 May 15;10(1):8012.
11. Yurdakurban E, Duran GS, Görgülü S. Evaluation of an automated approach for facial midline detection and asymmetry assessment: A preliminary study. Orthod Craniofac Res. 2021 Dec;24 Suppl 2:84-91.
12. Li P, Kong D, Tang T, Su D, Yang P, Wang H, Zhao Z, Liu Y. Orthodontic Treatment Planning based on Artificial Neural Networks. Sci Rep. 2019 Feb 14;9(1):2037.
13. Park YS, Choi JH, Kim Y, Choi SH, Lee JH, Kim KH, Chung CJ. Deep Learning-Based Prediction of the 3D Postorthodontic Facial Changes. J Dent Res. 2022 Oct;101(11):1372-1379.
14. Xu L, Mei L, Lu R, Li Y, Li H, Li Y. Predicting patient experience of Invisalign treatment: An analysis using artificial neural network. Korean J Orthod. 2022 Jul 25;52(4):268-277.
15. Bichu YM, Hansa I, Bichu AY, Premjani P, Flores-Mir C, Vaid NR. Applications of artificial intelligence and machine learning in orthodontics: a scoping review. Prog Orthod. 2021 Jul 5;22(1):18.
16. Homsi K, Snider V, Kusnoto B, Atsawasuwan P, Viana G, Allareddy V, Gajendrareddy P, Elnagar MH. In-vivo evaluation of Artificial Intelligence Driven Remote Monitoring technology for tracking tooth movement and reconstruction of 3-dimensional digital models during orthodontic treatment. Am J Orthod Dentofacial Orthop. 2023 Nov;164(5):690-699.
17. Strunga M, Urban R, Surovková J, Thurzo A. Artificial Intelligence Systems Assisting in the Assessment of the Course and Retention of Orthodontic Treatment. Healthcare (Basel). 2023 Feb 25;11(5):683.
18. Kim BM, Kang BY, Kim HG, Baek SH. Prognosis prediction for Class III malocclusion treatment by feature wrapping method. Angle Orthod. 2009 Jul;79(4):683-691.
19. Nguyen TT, Larrivée N, Lee A, Bilaniuk O, Durand R. Use of Artificial Intelligence in Dentistry: Current Clinical Trends and Research Advances. J Can Dent Assoc. 2021 May;87:l7.
20. Schwendicke F, Tzschoppe M, Paris S. Radiographic caries detection: A systematic review and meta-analysis. J Dent. 2015 Aug;43(8):924-933. Epub 2015 Feb 24. Erratum in: J Dent. 2021 Nov;114:103783.
21. Naitoh M, Yuasa H, Toyama M, Shiojima M, Nakamura M, Ushida M, Iida H, Hayashi M, Ariji E. Observer agreement in the detection of proximal caries with direct digital digital intraoral radiography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998 Jan;85(1):107-112.
22. Meusburger T, Wülk A, Kessler A, Heck K, Hickel R, Dujic H, Kühnisch J. The Detection of Dental Pathologies on Periapical Radiographs-Results from a Reliability Study. J Clin Med. 2023 Mar 13;12(6):2224.
23. Glick A, Clayton M, Angelov N, Chang J. Impact of explainable artificial intelligence assistance on clinical decision-making of novice dental clinicians. JAMIA Open. 2022 May 17;5(2):ooac031.
24. Gaube S, Suresh H, Raue M, Merritt A, Berkowitz SJ, Lermer E, Coughlin JF, Guttag JV, Colak E, Ghassemi M. Do as AI say: susceptibility in deployment of clinical decision-aids. NPJ Digit Med. 2021 Feb 19;4(1):31.
25. Maliha G, Gerke S, Cohen IG, Parikh RB. Artificial Intelligence and Liability in Medicine: Balancing Safety and Innovation. Milbank Q. 2021 Sep;99(3):629-647.
26. Glikson E, Williams Woolley A. Human trust in artificial intelligence: Review of empirical research. Academy of Management Annals. 2020;14.2: 627-660.
27. Meske C, Bunde E. “Transparency and trust in human-AI-interaction: The role of model-agnostic explanations in computer vision-based decision support.” Artificial Intelligence in HCI. First International Conference, AI-HCI 2020, Held as Part of the 22nd HCI International Conference, HCII 2020, Copenhagen, Denmark, July 19–24, 2020, Proceedings 22. Springer International Publishing, 2020.
28. Zini, JR, Awad M. On the explainability of natural language processing deep models. ACM Computing Surveys. 2022;55.5:1-31.
29. Vokinger KN, Feuerriegel S, Kesselheim AS. Continual learning in medical devices: FDA’s action plan and beyond. Lancet Digit Health. 2021 Jun;3(6):e337-e338.
30. Pianykh OS, Langs G, Dewey M, Enzmann DR, Herold CJ, Schoenberg SO, Brink JA. Continuous Learning AI in Radiology: Implementation Principles and Early Applications. Radiology. 2020 Oct;297(1):6-14.
31. Kim K, Bölling L, Haesler S, Bailenson, Bruder G, Welch G. Does a digital assistant need a body? The influence of visual embodiment and social behavior on the perception of intelligent virtual agents in AR. 2018 IEEE International Symposium on Mixed and Augmented Reality (ISMAR).
32. Melon E, Hernandez W. Cybersecurity in the dental healthcare sector: The need of knowledge for small practitioners. Issues in Information Systems. 2020;21(1):118-124.
33. Henry Schein. “Henry Schein provides information on cybersecurity incident.” [Press release]. Available at: https://investor.henryschein.com/news-releases/news-release-details/henry-schein-provides-information-cybersecurity-incident. (Accessed November 25, 2023).
34. Hayes, Carol Mullins, Generative Artificial Intelligence and Copyright: Both Sides of the Black Box (July 21, 2023). Available at SSRN: https://ssrn.com/abstract=4517799 or http:// dx.doi.org/10.2139/ssrn.4517799. Accessed January 4, 2024.
35. American Dental Association. Principles of Ethics & Code of Professional Conduct. https:// www.ada.org/-/media/project/ada-organization/ada/ada-org/files/about/ada_code_of_ ethics.pdf?rev=ba22edfdf1a646be9249fe2d870d7d31&hash=CCD76FCDC56D6F2CCBC46F1751F51B96. Accessed November 25, 2023.
36. Schönberger, Daniel. Artificial intelligence in healthcare: a critical analysis of the legal and ethical implications. International Journal of Law and Information Technology. 2019; 27(2):171-203.
37. Obermeyer Z, Powers B, Vogeli C, Mullainathan S. Dissecting racial bias in an algorithm used to manage the health of populations. Science. 2019 Oct 25;366(6464):447-453.
38. Kopka A, Grashof N. Artificial intelligence: Catalyst or barrier on the path to sustainability? Technological Forecasting and Social Change. 2022;175:121318.
39. Baxter K, Schlesinger Y. Managing the risks of generative AI. Harvard Business Review. https://hbr.org/2023/06/managing-the-risks-of-generative-ai. (Accessed November 11, 2023).
40. Alhashmi SFS, Alshurideh M, Al Kurdi B, Salloum S. “A systematic review of the factors affecting the artificial intelligence implementation in the health care sector.” Proceedings of the International Conference on Artificial Intelligence and Computer Vision (AICV2020). Springer International Publishing, 2020.
41. Mahadevaiah G, Rv P, Bermejo I, Jaffray D, Dekker A, Wee L. Artificial intelligence-based clinical decision support in modern medical physics: Selection, acceptance, commissioning, and quality assurance. Med Phys. 2020 Jun;47(5):e228-e235.
42. Harvey HB, Gowda V. How the FDA Regulates AI. Acad Radiol. 2020 Jan;27(1):58-61.
43. Tandon D, Rajawat J. Present and future of artificial intelligence in dentistry. J Oral Biol Craniofac Res. 2020 Oct-Dec;10(4):391-396.
44. Hassani H, Andi PA, Ghodsi A, Norouzi K, Komendantova N, Unger S. Shaping the future of smart dentistry: From Artificial Intelligence (AI) to Intelligence Augmentation (IA). IoT. 2021;2(3):510-523.
Continuing Education Quiz
Clinical implementation of AI systems in orthodontics
GLICK, ET AL.
1. AI is a broad term that generally refers to the ability for computers to perform tasks that typically require human intelligence; for example, viewing a dental X-ray and identifying interproximal caries.
a. True
b. False
2 ________ refers to the mathematical approach to accomplish this perceived human intelligence.
a. Neural learning
b. Machine learning
c. Database modeling
d. Natural Language Processing
3. __________ is based on a clinician providing the algorithm with a ground truth for labelled data.
a. A Receiver Operating Characteristic
b. The Convolutional Neural Network
c. Supervised learning
d. The Language-Specific Model
4. _________ is where the model learns without explicitly provided information to classify and can be accomplished through patterns within the data.
a. Unsupervised learning
b. Supervised learning
c. Neural Network Optimization
d. Predictive Outcome Recognition
5. In orthodontics, automatic cephalometric analysis to identify anatomical landmarks in CBCT radiographs has been shown in one study to be up to _______ accurate.
a. 76%
b. 88%
c. 92%
d. 98%
6. In orthodontics, automatic tooth position detection and tooth identification have been shown to have accuracies above ______.
a. 56%
b. 65%
c. 88%
d. 92%
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://orthopracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://orthopracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 010
Date Published: March 28, 2024
Expiration Date: March 28, 2027
7. Another issue that can affect AI is the imbalance of certain conditions like __________ that limit the number of instances for the algorithm to learn.
a. smaller dental offices
b. non-compliant patients
c. rare pathology
d. edentulous patients
8. For continuously learning algorithms, there is a potential risk that adaptive learning could _________.
a. introduce new errors
b. reduce reliable performance
c. produce unnatural language
d. both a and b
9. AI behavior should be periodically monitored, and a set of well-defined metrics are needed to guide regularly scheduled testing.
a. True
b. False
10. __________ has become increasingly more stringent on this type of software that predicts and identifies medical/dental conditions.
a. Food and Drug Administration (FDA)
b. Environmental Protection Agency (EPA)
c. Consumer Products Safety Commission (CPSC)
d. Occupational Safety and Health Administration (OSHA)
To provide feedback on CE, please email us at education@medmarkmedia.com Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
Important updates on Spark™ Aligners and Ultima™ Hooks
Spark™ Clear Aligner System
Spark’s advanced technology enables more sustained force retention and better surface contact with the tooth compared with the leading aligner brand.* The superior force retention and surface contact of the Spark aligner is due to its material choices and manufacturing technology. Spark Aligners are made with 80% better printing resolution and a more uniform surface texture than the leading aligner brand.*
Independent Dental Monitoring data confirms the advantages of Spark Aligners compared to other clear aligner brands in regards to refinements, treatment time, unseats, and damage during treatment.1
For example, Spark aligner treatments required an average of 23% less refinements compared to other clear aligner brands.
Plus, Spark’s Approver software – available on MAC, PC, and Web — is designed to give orthodontists start-to-finish control for more efficient and effective treatment planning. CBCT integration lets orthodontists import and visualize CBCT patient data, while posterior Bite Turbos can be added to address complex cases.*
Spark’s proprietary CBCT, TruRoot™, and Real Time Approval features
• Root visualization provided on all cases (not only on those submitted via CBCT)
• TruRoot™ provides the actual shape and positioning of the roots when doctors provide the CBCT scan. This provides accurate diagnostics of root movements while planning treatment.
• With the TruRoot CBCT Collision Alert System, you can predict and prevent collisions during treatment to help plan treatments with more precautions. This feature automatically detects and highlights areas on the root surfaces that are touching or penetrating cortical bone.
• Real Time Approval feature allows doctors to add, modify, or delete aligner features — as well as modify final tooth movement — without the need for change requests.
To learn more about Spark™ Clear Aligners, please visit https://ormco.com/spark.
The Damon Ultima™ System
The Damon Ultima™ System is the first true full expression* orthodontic system with a proprietary integrated wire and slot design that virtually eliminates play for faster and more precise finishing.* It provides orthodontists with earlier and precise control of rotation, angulation, and torque.* This unique and patented technology is designed to deliver the signature Damon™ Smile, resulting in full expression with lighter forces to treat in less time and to fully express your prescription with fewer wire bends.* With this system, 98.9% of cases were determined to have first-order rotations corrected with the first round-sided
rectangular wire, and full expression is achieved with the second.* After all rotations are corrected, the wire/bracket interface returns to a passive state while maintaining the desired rotational alignments throughout the remainder of treatment with the .0275” dimension wires.*
Enhanced torque control
Damon Ultima brackets deliver enhanced torque control when used with the procline and retrocline brackets.* The roundsided rectangular wire engages vertical contact points of the procline and retrocline slots to fully express the prescription.*
The Ultima™ Hook – Now available on both Ultima and Rectangular Wires
The Ultima Hook, the only re-positionable hook,2 is designed to save time for doctors who value performance and want to provide patients with healthier3 oral treatment and more comfortable experience.*
To learn more about the Damon Ultima System, please visit https://ormco.com/products/damon-ultima-system/ or https:// ormco.com/ultimahooks.
Join us at AAO Booth No. 2926 to learn more about how orthodontists like you are using Spark Aligners and Damon Ultima to achieve great finishes and beautiful smiles. Be sure to ask about our On-Site Promotions.
* Data on file.
1. When used with Dental Monitoring, based on a survey of 25,000 Dental Monitoring users.
2. Using the Ultima™ Hook Repositioning Instrument.
3. When used as a stop.
** Source article: https://www.mdpi.com/1198216
The results provided in this article are relating to the use of the DM Solution by Spark users and illustrate the benefits from the use of Spark aligners. These results which are aggregated data, excluding personal data, are from Dental Monitoring Analysis dated April 2023. DM specifically disclaims all implied warranties of merchantability, fitness for a particular purpose, and all warranties arising from course of dealing, usage, or trade practice.
This information was provided by Ormco. OP
5 ways to help your practice reduce credit card processing fees
Matt Rej offers tips on how to mitigate the costs of accepting credit cards
Credit cards are convenient for patients and medical practices alike. It’s easy for dentists and specialists to collect payments immediately following an appointment in a way that their patients prefer. This helps keep accounts receivables low and simplifies the medical billing process.
While there’s no debating the convenience of card payments, many practices overlook the credit card processing fees eating into their bottom lines. Dental and specialty practices pay upwards of $7,500 to $12,000 or more on processing fees alone. These costs are often accepted at face value and typically rise over time.
The vast majority of medical practices can save money on credit card processing without switching processors or changing anything. There are five proven ways to reduce processing fees that can potentially save dentists and specialists tens of thousands each year.
1. Audit your statements
Take a look at your last three credit card statements. Credit card processors are notorious for adding extra fees and inflating bills in the hopes that these charges go overlooked. Line items for terminal fees, AVS fees, PCI compliance fees, IRS reporting fees, terminal fees, and gateway fees are all examples of inflated markups that don’t need to be included on the bill. Identifying and removing these unnecessary charges can instantly save you $2,500 to $4,000 annually.
2. Assess your contract
Beyond the extra charges, look for any inconsistencies from one statement to the next. If the statements are confusing and deceptive, there’s a chance your processor is trying to bury other hidden markups on your statements. It’s suspicious if the fees aren’t presented in a way that’s clear, logical, and easy to understand.
Matt Rej is the managing partner of Merchant Cost Consulting and has been since 2017. Located in Boston, Massachusetts, MCC has been exposing the payments industry since 2016 to help bring transparency to business to ensure they are on the most competitive pricing applicable to their needs. The typical cost savings MCC achieves its clients ranges from 20%-60% on the total fees they currently pay, often without the hassle of making any changes to their current setup. Matt is proficient in Interchange Optimization, Pin Debit Card Routing, Payment Processor Service Markup analysis, and MCC Interchange categorization.
Review the merchant agreement that you signed to start accepting credit cards. It’s a little bit easier to negotiate fees if the contract is nearing its expiration date. Processors don’t want to lose your business. They make money every single time a card is swiped, dipped, or tapped at your practice. Leveraging your contract expiration is a highly effective way to lower your fees.
It’s also worth comparing your contract terms against the statements you’ve audited. Some processors breach contracts by increasing rates or adding fees that weren’t part of the initial agreement. If your processor breached those terms, you’re entitled to compensation in the form of a refund for those overages.
3. Negotiate and push back
There are three components of credit card processing: interchange, assessments, and markups. Interchange fees and assessments are imposed at the card network level by Visa, Mastercard, Discover, and American Express. These are non-negotiable rates that must be paid to the card brand each time one of those cards gets used as a payment. Markups are charged by the processor, and those rates are completely negotiable.
It’s easier to negotiate these rates if you’re on an “interchange plus” pricing plan. This means that you pay the card network’s
interchange “plus” the markups imposed by your processor. Everything other than the interchange fees and assessments can be negotiated. While processors are entitled to some fees for their role in facilitating the transaction, some of these markups are egregious and can often be cut in half.
4. Don’t switch processors
It’s a common misconception that switching processors will help save money on credit card processing. In reality, it’s usually more expensive. New processors will often ask to see what you’re currently paying and then undercut those rates to make their services seem more appealing. But then they inflate the processing rates by adding other markups to your statements. After a year or two, they’ll increase your rates, and you’ll end up paying more than you were with your old processor.
You’re much better off sticking with your current processor and just negotiating directly with them. If you aren’t getting anywhere in your negotiations, you can work directly with a merchant consultant to handle those conversations on your behalf. There’s no risk in going this route, as cost reduction firms aren’t compensated unless you save money.
5. Continue monitoring each statement
Even after you’ve successfully negotiated a reduction, you still need to make sure your statements have been adjusted appropriately. Unfortunately, many processors use deceptive tactics when dealing with merchants. So you can’t always take
While there’s no debating the convenience of card payments, many practices overlook the credit card processing fees eating into their bottom lines.
the word of a sales rep or customer service agent who promised a lower fee. Get everything in writing, and make sure those new rates are reflected on your next statement.
Furthermore, make sure that new hidden fees haven’t been added in place of the ones that were removed. Monthly monitoring is really the way to ensure that your negotiations have paid off, and it should be obvious that your total costs to process payments are lower. Rather than looking at just the fees, it’s often easier to calculate your “effective rate” as a more accurate representation of your average processing fees.1 This is a simple formula. Just divide the total amount that was deducted each month for processing by your total monthly sales. If this rate is higher or remains unchanged after your negotiations, then your processor is still doing something deceptive behind the scenes, and there’s more room to save money.
REFERENCE
1. O’Keefe C. Average Credit Card Processing Fees (2024). Merchant Cost Consulting. https://merchantcostconsulting.com/lower-credit-card-processing-fees/average-creditcard-merchant-fees/ (accessed January 16, 2024).
Orthodontic Practice US Webinars
LEARN about the lastest techniques and technology from industry leaders with our free live and archived educational webinars. Our online seminars are a convenient way to access great information and upskill. Check out our most recent webinars:
• Optimizing Orthodontic Treatment Workflow with Remote Monitoring and Dynamic Scheduling with host Dr. Mike Ragan
• Your Ultimate Orthodontic Workflow from Start to Finish with host Dr. Paul Trotter
• How a Digital Workflow and Remote Monitoring Made Me a “Better Version of Me” with host Dr. Joshua Adcox
Freedom Day USA
Dr. Lou Shuman discusses how a lifetime of freedom can be repaid by giving a day for free
Every day, military men and women around the world are missing their families and risking their lives to protect our country. When they get back, despite their phenomenal service, they often quietly struggle to receive health and dental care. Eleven years ago, Dr. Robert Martino, CEO of Wilson Martino Dental, heard a touching testimonial about how much veterans endure to keep our country safe. He decided to show his appreciation in the best way he knew, by designating a day when his office would say thank you by providing free services to veterans. As the news spread about the incredible impact of his office’s day, the concept grew by leaps and bounds to become Freedom Day USA.
Over time, Freedom Day USA grew to having partners in every state with almost a million dollars in products and services donated. The concept was expanded so that non-dental businesses could partner with a dental team by donating door prizes or goods to be given at the dental office, or at their own location. Wendy Boyce, Vice President of Customer Relations for Wilson Martino Dental and Freedom Day USA National Director, notes that one local McDonald’s, whose franchise contains about 18 restaurants, gives veterans a free meal, as do Chick-fil-A and Honey Baked Ham. She says, “Our honored guests can eat hot dogs, and ice cream cones, all from our partner businesses for free. We have hair salons, manicure salons, a vision specialist and a chiropractor who provide services as well.”
Any company or practice, large or small, can help thank our military heroes. Vendors and large companies who support dental practices can extend an offer to a dental practice for free supplies or a service, such as one free lab fee. Boyce says, “We will communicate the offer to our participating dental providers, both local and national, and we connect them. Any company that provides Freedom Day USA support is included on our website, and all of the materials that we provide, as well as on our maps and social media.” She adds, “Many of our dental partners will print a flier to hand out to every patient who comes in the door that day with the names of companies who have partnered with them. That way participating companies get recognition for
Lou Shuman, DMD, CAGS, is the CEO of Cellerant Consulting Group, dentistry’s leading corporate incubator and accelerator bringing technologies into dentistry from all over the world. He is a venturer in-residence at Harvard’s i-Lab, co-founder of LightForce Orthodontics, founder of the Cellerant Best of Class Technology Awards, and just launched his third company, DSO Technology Solutions. He was selected in 2021 by Global Summits Institute as one of the World’s Top 100 Doctors.
whatever field they are in. If larger service or product providers want to offer services to dental offices, we can cultivate a flier offer that would go exclusively to Freedom Day dentists who are signed up for that year.”
Dr. Martino and his team realized that flexibility of scheduling would encourage more people to participate. Boyce explains, “The one-day restriction has been eliminated — businesses can
Veteran patient at Cosmetic Dentists of Houston
Dr. John Wilfong at Wilson Martino Dental of Buckhannon
choose whatever day of the week works for them, do the whole week, pick one day, half a day, or even book one appointment for a military person, veteran, or family member.” She adds, “Our goal is to convey that Freedom Day is easy. Whatever you can do supports our mission.”
Any company or practice, large or small, can help thank our military heroes.
When a veteran comes in to get their teeth cleaned on Freedom Day, which to most people is not a big deal, it can change their perception of how people feel about them. Boyce continues. “It says to them, ‘you are heroes, and you should be treated that way.’” Besides the self-esteem issues, veterans also face obstacles to receiving medical and dental care. “Many veterans may not be eligible for full benefits, and some local VAs have very long waits. That’s the beauty of Freedom Day — to address their pressing issues immediately and hopefully get someone to a healthier state and in a positive atmosphere,” Boyce says.
Freedom Day USA in October 2023 was a huge success. Boyce says, “We definitely consider ourselves bounced back from the COVID
years, and in a steady growth pattern.” The 2023 event had 431 participants, doubling from the year before. Of the total, 106 dental offices across the US joined the appreciation event.
Joining Freedom Day USA is free-of-charge, and the process is simple. Once an office signs up, they are sent a digital media kit, complete with information, a planning guide, flyers, templates, and anything needed to plan a successful event. The templates are in electronic format so the office’s specific information can be entered easily. An enewsletter gives tips and information on creating a memorable and fun event. “We tailor all of our marketing items to their specific date, no matter what date they choose,” says Boyce.
The official date for 2024 Freedom Day USA is Thursday, October 10. This year, as a gift for participating, every dental team that signs up will receive an official Freedom Day USA custom scrub top with a unique Freedom Day print. More scrub tops are available, but one will be provided for free. There is no cost for signing up and no requirements about treatment provided. Boyce notes, “Our only request is that it is not an if/then offer — meaning, if you buy this, we will give you that because a true thank you is given freely from the heart from your practice.”
After 2023 Freedom Day, heartwarming stories came streaming in. Mequon Smile Design in Wisconsin helped a veteran celebrate his 100th birthday with dental services and enthusiastic congratulations. Dr. Martino’s schedule, in his West Virginia office, was full with a waiting list. Boyce said, “We found some pretty serious health conditions that were identified through Freedom Day screenings, so we saved some lives.” In North Carolina, Ballantyne Dentistry extended their offer to a full makeover for a patient, who now looks amazing. Practices receive thank you cards, and they create photo albums. Boyce says that team spirit is important and inspiring. “It is more impactful than anyone realizes. It feels so good that the whole team is giving back in appreciation for what those brave men and women have done for us. And the veterans turn around and appreciate right back. It’s a wonderful day.”
For more information, visit www.freedomdayusa.org/.
Freedom Day became even more special when Mequon Smile Design in Wisconsin honored veteran Julian (pictured in the middle) on his 100th birthday and thanked him for his service
Veteran guest Daniel Hart at Wilson Martino Dental of Bridgeport