Circulation Disclosure: Total Circulation May Vary. Publisher retains the right to adjust circulation based on a number of factors including but not limited to: print and digital distribution by mail, email, and website for industry tradeshows, educational events, including nonpaid bulk copies and/or digital access provided to events, clients and educational institutions. ISSN number 2372-8396
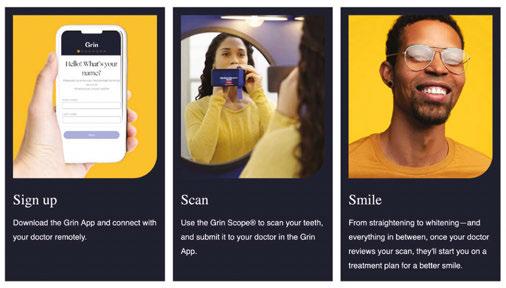
Ramp up your aligner practice
Orthodontists everywhere are looking for ways to “ramp up” their practices with new technologies and services. If you’re one of these doctors, take a deeper look at the products you’re using. I have tried several aligner options over the past 8 years to move my practice to the next level, and reduce workflow-related stress. I also was looking for control and flexibility for effective aligner planning and educational opportunities that would improve treatment planning with minimal investment.
Software: When choosing an aligner brand, finding one that simplifies the user experience is essential. One way of doing this is through the use of CBCT and software. Since the arrival of an effective software program, I have spent minimal time approving cases and can use 3D controls that allow me to change attachment size, shape, and location within a few minutes. I can make these changes without requiring another revision by the technician, and I can have the design team closely follow my clinical preferences when making my adjustments. For efficient diagnosis and patient education, the aligner workflow allows for multiple setups (and can be requested at no extra charge).
Attachments: Let’s face it, consistent placement of attachments can be tricky, so many of us assign the aligner bonding appointment to our best and most proven assistants.1 For exceptional results, we need a template with defined attachment wells that are easy to fill. Most importantly, one should be able to see any voids in the well, which prevents voids in the final attachment. The template should give me the confidence to assign bonding appointments to any assistant in the office, which significantly improves our efficiency.
Materials: The fact is that not all aligner materials are equal. For aligners, you want the best fit to enable treatment predictability and engaging of attachments, and for expansion movements and final stages of treatment, rigidity is imperative. Of course, patients appreciate stain resistance for optimal esthetics during the treatment process.
I have chosen Spark™ Clear Aligners for all of the above reasons. From RealTime Approver software and Spark Attachment Template to workflow and TruGen™ and TruGenXR™ materials, this aligner brand has reduced workflow-related stress and provided increased profitability. I also appreciate how this aligner treatment gives the doctor the control and flexibility to make the treatment effective, and it offers incentives with its educational tracks that will improve treatment planning with minimal investment.
1. The regulations regarding the delegation of tasks vary by local jurisdiction. Please follow your local regulations when delegating tasks.
*** The opinions expressed are those of Dr. Coreil as a paid consultant to Ormco. Ormco is a medical device manufacturer and does not dispense medical advice. Clinicians should use their own professional judgment in treating their patients. Individual patient results may vary.
Mark N. Coreil, DDS, is a board-certified orthodontist, researcher, and inventor. He is an Associate Professor of Clinical Orthodontics at the Louisiana State University School of Dentistry and has been actively involved as an orthodontist on the New Orleans Children’s Hospital Cleft and Craniofacial Team for over 25 years. Dr. Coreil graduated from Louisiana State University School of Dentistry in 1986 and completed his orthodontic specialty training at LSU in 1988. He completed the Roth/Williams Advanced Clinical Program in 1993 and has lectured both nationally and internationally for the past 30 years. His professional interests include esthetics, biomechanics, digital workflow, and 3D printing. Dr Coreil consults with numerous orthodontic manufacturers and technology companies.
In the driver’s seat
Dr. Andrew Sarpotdar explains how Spark™ Clear Aligners provides a cutting-edge tool that puts control back into the hands of orthodontists
Dr. Jacquee Schieck avoided orthognathic surgery for this high school patient
X. Phan and Agnieszka Klucinska illustrate a system for treating patients with lifestyle, occupational, and condition-
Cover image of Dr. Sarpotdar courtesy of Ormco.
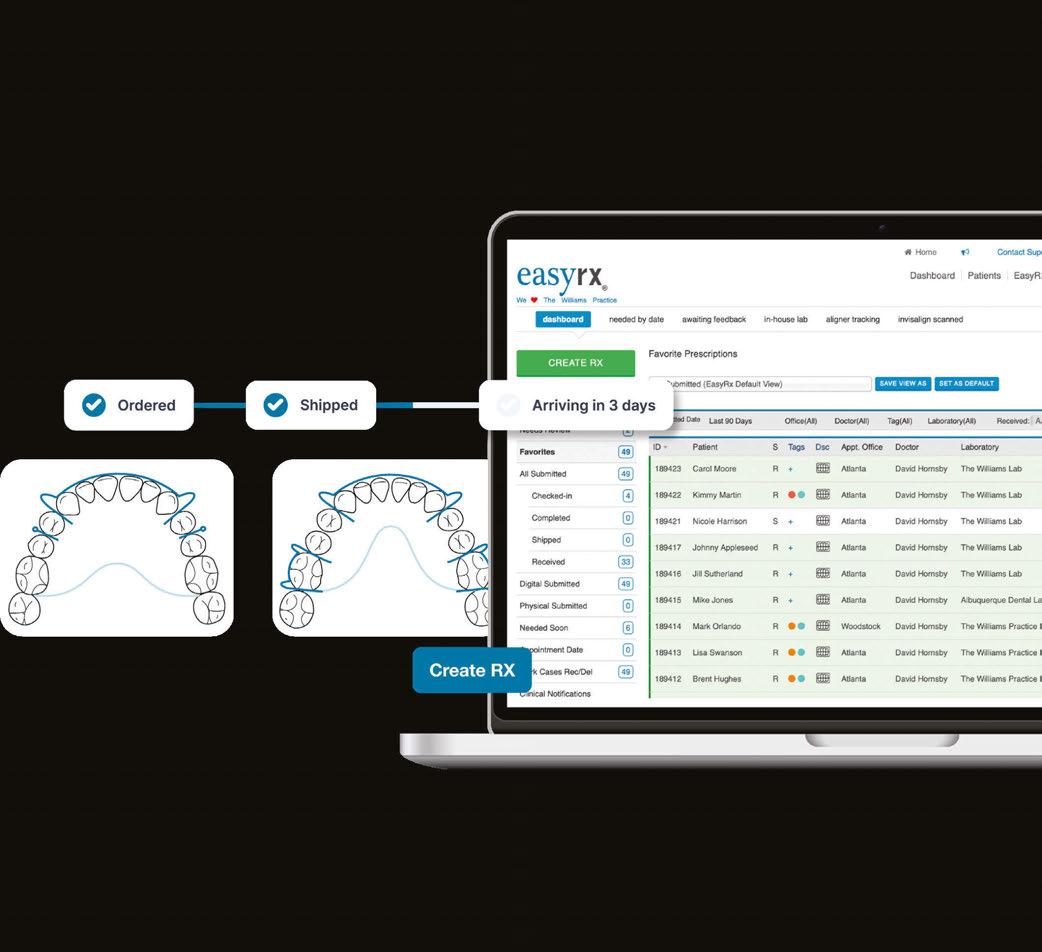
Never lose a patient appliance again
EasyRx gives you one easy-to-manage digital workflow to submit, manage, and track your lab prescriptions so patients get their appliances on time, every time.
CONTINUING EDUCATION
Perspectives on orthodontic retention
Dr. Dustin S. Burleson discusses the importance of following up on orthodontic treatment 24
PRACTICE DEVELOPMENT Is your practice transactional or transformational?
Digital technology impacts orthodontic results
Dr. David Alpan reviews digital options that can
JoAn Majors discusses the importance of creating a human connection ................................... 36 GOING
Thomas Terronez offers some guidance on keeping your practice data safe from cyberattacks ............................... 38
Dr. Ryann Christensen discusses how DentalMonitoring has transformed her practice 40
My Rx for summer
How many times have you written prescriptions for your patients? Even after they leave your office, you strive to ease their pain, head off their infections, and get them back to healthy lives. I’m not a dentist, but I have played one for almost 20 years now! So, for this summer issue, it’s my turn to write a prescription — to encourage ongoing mental and physical health for our dedicated readers.
My Rx for a productive and rejuvenating summer
Vitamin D: Take some time to get out in the sun and soak up the relaxing rays! Change out of your scrubs and breathe some fresh air — and don’t forget your hat and sunscreen. You will return to work revitalized and ready to tackle any patient.
Lisa Moler Founder/Publisher, MedMark Media
Get moving: Even if you don’t have time to get to the beach or take a longer vacation, exercise is one of the best ways to relieve tension and clear your mind. The CDC recommends 150 minutes of moderate-intensity physical activity per week. You don’t even need to join a gym — a daily walk will keep that blood flowing. Breaking the time up into 30 minutes a day for 5 days is very doable and can become a healthy habit.
Give your mind some thought: Every day, take some time for mindful thought or meditation. It doesn’t have to be the same time every day, or even done in the same way. Just pick a comfortable spot, close your eyes, breathe deeply, and focus on your breathing. Picture the beach, a mountain trail, or any spot that brings you peace. Taking a few minutes can reduce stress, ease frustration, and open the door to serenity. Read, watch television, or listen to music: Having a way to unwind first thing in the morning or before bed can calm your mind and body.
Eat healthy, but give yourself a treat: We all know the drill — eat healthy fruits, vegetables and grains, go big on the protein and low on fats and sugars. But, as with all things under heaven, there is a time for ice cream and cake too (in moderation).
Build a trusted team, in and out of the office: Having support people to boost you when you are sad and laugh with you when you are happy can make life a warmer, more welcoming place.
Forgive yourself! One of my main mantras throughout this journey of life is to give yourself a break. Everyone makes mistakes, and no matter what some people think, no one is perfect. Every mistake is an opportunity to learn from and grow.
Keep learning: Whether you are in the office or on vacation, take MedMark specialty publications with you! Keep learning new concepts so when you return to work, you can expand your patients’ options for care.
In our Cover Story, Dr. Andrew Sarpotdar encourages orthodontists to hone their skills, evaluate their choices, and find the ones that work best for their practices and patients. He chooses Spark Clear Aligners™ for control, flexibility and effective treatment. Our CE by Dr. David Alpan reviews the digital technologies that can bring more efficiency, accuracy, and precision to diagnosis and treatment. The CE by Dr. Dustin S. Burleson provides insight on retention after orthodontic treatment. He discusses scientific principles that influence tooth movement and stability and how to get patients invested in their posttreatment care.
Even if your summer is busy with patients, there are plenty of ways to keep a healthy outlook on life. Journalist Charles Bowden once said, “Summertime is always the best of what might be.” Try a few of my Rx recommendations, and you will feel that endless summer in your hearts and minds for all future seasons.
To your best success,
Lisa Moler
Published by
Publisher Lisa Moler lmoler@medmarkmedia.com
Managing Editor Mali Schantz-Feld, MA, CDE mali@medmarkmedia.com Tel: (727) 515-5118
National Account Manager Adrienne Good agood@medmarkmedia.com Tel: (623) 340-4373
Social Media Manager Felicia Vaughn felicia@medmarkmedia.com
Digital Marketing & Sales Administrator Sharif Rod sharif@medmarkmedia.com
Website Support Eileen Kane webmaster@medmarkmedia.com
MedMark, LLC 15720 N. Greenway-Hayden Loop #9 Scottsdale, AZ 85260 Tel: (480) 621-8955
Toll-free: (866) 579-9496 www.medmarkmedia.com
www.orthopracticeus.com
Subscription Rate 1 year (4 issues) $149 https://orthopracticeus.com/subscribe/
In the driver’s seat
Dr. Andrew Sarpotdar explains how Spark™ Clear Aligners provides a cuttingedge tool that puts control back into the hands of orthodontists
Alittle over a decade ago, I proudly defended my master’s thesis on clear aligner utilization in modern orthodontic practice to a room full of residents at Columbia University. It thus came as no surprise when, upon graduating, I immediately invited the local aligner representative to on-board the orthodontic team at my first job in group practice. I was stoked; aligners were the cutting edge of orthodontic treatment, and I was one of a handful of providers versed in using them. While case selection was limited, this modality opened up a whole new value proposition for patients averse to metal, and I, a freshly minted and hopelessly indebted young orthodontist, was the tip of the spear. After a brief presentation and a mediocre boxed lunch, I was dismayed to watch as my representative enrolled every referring dentist at my practice into their certification program, undermining my value and compromising a referral source I was desperately dependent on. Of course, back then, stories like this were becoming commonplace. There was only one viable option for aligner therapy, and orthodontists had to compromise beyond aloof representatives trying to cut us out of the picture. Competition drives innovation, and without it, aligners were little more than a costly novelty reserved for the simplest of cases or those willing to settle for “straight-ER.”
The choice is clear
Today, we are fortunate to have options for clear aligner therapy that have evolved far beyond the limitations of the past and provide orthodontists with the power and responsibility to choose wisely for their patients and practices. The best option will be one that is, first and foremost, effective. After trying several brands over the years, I have chosen Spark™ Clear Aligners, which gives the doctor all of the control and flexibility to make the treatment effective. In my opinion, predictable movement occurs first from the quality of the setup. While this is largely in the hands of the clinician, I have found the robust staging algorithm and superb communication within the Spark platform to make my life easier in this regard. The ability to integrate CBCT root imaging (with root collision alert feature) with setups is a recent development that also adds an exciting new dimension to my cases.
Andrew Sarpotdar, DDS, MS, is a board-certified orthodontist in private practice with his wife, Dr. Jenny Sun, in the greater Phoenix area. He attended dental school at UCLA before earning his master’s degree in orthodontics from Columbia University in 2013. He is co-founder of the Orthodontic Pearls Facebook group and its corresponding annual meeting, the Mother of Pearls Conference. He sits on the editorial board of Orthotown Magazine and writes a column on practice management for the PCSO Bulletin.
Disclosure: Dr. Sarpotdar is a paid Knowledge Expert for Ormco.
Furthermore, Spark offers enticing incentives with its educational tracks that will greatly improve your treatment planning with minimal investment. At the core of Spark’s effectiveness is its TruGEN™ aligner material. Aligners made from TruGEN have been shown to induce sustained force retention over a longer period than the leading aligner brand and have 19% greater contact with tooth surface area.1 For extra stubborn movements, try ordering the stiffer TruGEN XR™ for your refinements. After all, you wouldn’t treat your braces patients with only a NiTi wire, so why limit yourself to one type of plastic for every movement? Since using Spark, I have watched cases treated to near perfection that I wouldn’t have dreamed of treating with aligners when I first graduated.
Treatment must be effective, but the real value of aligners over other modalities comes from their enhanced patient experience. This is one of my favorite and most obvious advantages of Spark Clear Aligners. Run your finger over the scalloped edges, and you’ll be impressed with the smoothness of the finish. Spark Aligners are polished and scalloped to minimize irregularity and discomfort. Ever get a “clear” aligner back from the lab only to have it look like a topographical map of the Rockies? I haven’t
Figure 1: Drs. Andrew Sarpotdar and his wife, Dr. Jenny Sun, in front of their flagship private practice in Surprise, Arizona
seen this in years, thanks to a manufacturing process that minimizes the appearance of striations and other imperfections, resulting in greater transparency that my patients appreciate. I always warn my patients that aligner clarity is a privilege, not a right. To maintain it, there are rules like brushing after meals and not eating or drinking anything with their aligners in. Experience has taught me that I’m either a bad motivator, or my patients salivate coffee because I was often horrified by the amber coloration previous aligners would develop (“spontaneously,” according to my patients). This staining has greatly diminished after switching to Spark since TruGEN is designed to retain this coloration less than other aligner materials.
Setting up for success
Success with your Spark treatment begins with setting your clinical preferences on your office portal, greatly increasing your submission and revision process efficiency.
For example, in most cases, I optimize for smile arc, keeping the laterals 0.5 mm above the centrals and the canines 0.5 mm above the laterals. I also include instructions to fully develop upper and lower arch forms simultaneously before initiating vertical incisor movements. Your preferences will be inherently subjective, but the point is to have them written beforehand to preclude typing them specifically for every case. Submitting cases should be delegated to clinical assistants to the extent possible.2 In my office, we use dry-erase diagnosis sheets that I can quickly fill out chairside and correspond to the submission portal. Once a setup is returned, it is advisable to use digital diagnostic features such as Bolton discrepancy, grid overlay, and tooth movement table to plan your final tooth position. Be
sure to overengineer certain movements like incisor intrusion for a deep bite (I’ll often set the final overbite at 0 mm in these cases, like using a reverse Curve of Spee wire with braces). I hide attachments during this process to focus only on getting
Figure 2: Dr. Sarpotdar playing with his dog, Chief, whom he brings to the office as an emotional support dog for his patients
Figure 3: Dr. Sarpotdar removes adhesive from his patient’s teeth following successful orthodontic treatment
Figure 4: Dr. Sarpotdar stands at his front desk with his queue of Spark Aligners and ODB cases ready to be delivered
the optimal final tooth position. I will often resubmit the setup at this point before assessing the staging of the tooth movement. There are entire courses on staging, but the basic principle to remember is that aligners only push on teeth. This is especially important to consider with extrusive movements, for which an attachment is not a suitable replacement for good mechanics. Speaking of attachments, auxiliaries such as these are the final step in my case submissions only after I know where the teeth are moving and how they will get there. The algorithm will suggest attachments for you, but this is not a replacement for your clinical judgment and expertise.
Depending on the case’s complexity, you may need one or more refinements for completion, so be mindful of this when selecting your product (I use Spark Advanced for most of my cases since there is no limit to number of aligners or refinements). When a patient returns for a refinement, my clinical team starts by taking new photos and radiographs if necessary. They floss all contacts and note any loose or open ones. I perform a clinical exam and dictate specific corrections that need to be made, and then we scan and resubmit the case. I will rarely remove attachments at this time as I will often use them in the following setup, or I can have them removed digitally should I choose to do so. We repeat this process until the case is complete, at which time we remove attachments and, now with Spark On-Demand, the doctor can
order AOA retainers directly from the Spark Dtx portal. Our patients continue wearing their last tray at nighttime only until the retainers arrive, at which time they are happily dismissed!
Case 1: Deep bite, severe crowding
A 40-year-old patient’s concern was crowded incisors following a relapse of treatment completed as a child. The clinical exam showed a constricted/omega-shaped maxillary arch with retroclined central incisors and moderate crowding of the mandibular incisors with a severe Curve of Spee and corresponding deep bite.
Deep bite cases are some of the more challenging ones to treat with clear aligners.
I began, as I always do, with the development/expansion of the maxillary arch and simultaneous uprighting of the mandibular posterior teeth. Expansion creates a reciprocal movement of retraction/retroclination for incisors, so it was necessary to counter this effect by inducing constricting force on the patient’s second molars during case setup (this is often favorable since second molar teeth tend to be overexpanded naturally due to minimal muscle tone buccal to this region). Constriction of second molars coincides with premolar expansion and proclination of both upper and lower incisors during the first phase of tooth movement, during which alignment is mostly achieved. This is
Figure 5: Dr. Sarpotdar works on a Spark setup
Figure 6: Case 1 initial photos
Figure 7: Case 1 initial (left) and final (right) photos showing correction of retroclined incisors
Figure 8: Case 1 final photos
followed by intrusion and retraction of the lower incisors with lingual root torque during the second phase.
The patient received 25 aligners initially and was able to wear them to completion with no tracking issues. At a pace of one aligner per week, the patient returned for a refinement at the 25-week mark with a near-perfect alignment but with minor loose contacts. I also felt he could benefit from additional arch development/expansion, so I programmed this into his following setup, which came to 13 stages. Unfortunately, due to a mix-up on our end, his case did not get submitted right away, meaning we would not get his aligners back in time for his appointment. To resolve this, we exported the first three upper and lower .stl files from his setup (a nice feature of the Spark system) and printed the models in-house so treatment wouldn’t be delayed. Once the remaining aligners were received from Spark, he picked them up from our front desk and proceeded with trays 4-13, after which his treatment was deemed complete. Total time was 15 months from scan to retainer.
Case 2: Deep bite, mild crowding, ectopic cuspid, posterior crossbite
The patient was a 27-year-old male whose main concerns were crowding and poor smile esthetics. The clinical exam also revealed he had a maxillary left second bicuspid in lingual crossbite, a deep overbite due to an excessive Curve of Spee, and an ectopic/under-erupted maxillary left cuspid.
Like the previous case, we started the patient’s treatment with simultaneous premolar expansion, second molar constriction, and proclination of incisors, followed by retrusion and retraction of lower incisors to the final position. One additional challenge was the UL5 crossbite; however, this was treated out quite predictably, with some compensatory buccal root torque
during expansion. This was greatly aided by the distal anchorage of the UL6 and UL7, which made this a predictable movement. The real challenge in this case was the ectopic UL3. My initial setup failed to stage this tooth’s extrusion properly and relied too heavily on a gingivally beveled attachment for anchorage.
The attachment was rotated at 45 degrees from the occlusal plane to attempt simultaneous mesial in rotation and extrusion; however, only the former movement was successful. During my second refinement, 29 weeks after initial delivery, I programmed visible space mesial and distal to this tooth, then staged it to procline with buccal movement while maintaining its current vertical position. This was followed by simultaneous retraction, retroclination, and extrusion, which proved far more successful but didn’t get me to my final position. In this case, a third refinement was necessary, repeating the same protocol and obtaining an excellent outcome. The total time in treatment was 21 months.
In conclusion
Now is an exciting time to delve into the world of digital orthodontics. As competition increases in the clear aligner market, so do our options and the efficacy of those options. I encourage you to hone your skills, evaluate the choices, and find the ones that will work the best for your practice and your patients. The path to a bright future has never been clearer.
REFERENCES
1. Data on file with Ormco Corporation.
2. The regulations regarding delegation of tasks vary by local jurisdiction. Please follow your local regulations when delegating tasks.
** The opinions expressed are those of Dr. Sarpotdar as a paid consultant to Ormco. Ormco is a medical device manufacturer and does not dispense medical advice. Clinicians should use their own professional judgment in treating their patients. Individual patient results may vary.
Figure 9: Case 2 initial photos
Figure 10: Case 2 final photos
Digital treatment planning and precision orthodontic appliances
Dr. Jacquee Schieck avoided orthognathic surgery for this high school patient
Introduction
Orthodontists are trained in moving teeth and improving jaw imbalances, and along with our licenses, we are also granted the responsibility and gift of impacting a patient’s occlusion and also their self-esteem and confidence. One of the reasons I chose to become an orthodontist is due to the transformative power of a smile. I experienced this for myself as a teenager and am grateful to be able to provide it for others in my daily clinical work.
In my practice, I use the best technology available to me to provide planned, customized, and efficient treatments for my patients. Because of digital orthodontics, I can easily visualize the expected outcomes for more predictable treatment planning, motivate and educate my patients for best compliance, and achieve more efficient treatment times due to the customization of the appliance prescriptions. The impact of digital practice has been so significant that I now provide only custom, digitally-planned treatment options to all my patients. I do this by utilizing aligners, 3D-printed banded appliances, and 3D-printed custom braces.
This case report details the orthodontic journey of a 15-yearold patient, Grant, who presented to my office with what seemed like a straightforward request: to be able to smile with confidence during his high school years. However, he and his parents came to me after having had two previous consultations where he was told that orthognathic surgery was his only treatment option, and for best results, he would need to wait until all growth was completed. While I agree this may have been his most ideal option, and explained this to the family, I also believed we could use digital treatment planning and precision orthodontic appliances to achieve a significantly improved result for him during these formative years. With Grant, and all patients, I strive to understand their personal goals and to customize a plan that reaches or exceeds those goals for them.
Jacquee Schieck, DDS, MS, is a board-certified orthodontist with over 14 years of private practice experience. She graduated from the University of Missouri-Kansas City (UMKC) School of Dentistry and obtained her Master’s degree and a specialty certificate from the University of Minnesota. Her research has been published in the American Journal of Orthodontics and Dentofacial Orthopedics, and she previously served as adjunct associate professor of orthodontics at the University of Minnesota. In 2014, Dr. Schieck opened a de novo practice in Northfield, Minnesota, Schieck Orthodontics, where she resides with her husband and four children. Outside of work and family, she has a passion for music and is the bassist and vocalist for the all-orthodontist band, Relapse!
Patient background and initial presentation
Grant presented to my office as a healthy, well-adjusted teenager with ongoing concerns about his pronounced overjet which was causing difficulty with chewing, speech, and esthetics. He was a severe Class II vertical skeletal pattern, with vertical maxillary excess and a steep mandibular plane angle. His maxillary incisors were excessively proclined, resulting in severely increased overjet and mentalis strain. A maxillary transverse deficiency with a tapered arch form was also noted. Both arches
Figure 1: Initial images
were crowded, and the mandibular anterior tissue was thin with inadequate oral hygiene likely exacerbated by increased mouth breathing from the lip incompetence at rest.
Due to his obtuse nasolabial angle, tapered arch form, and mild crowding, upper premolar extraction to camouflage the Class II malocclusion was not considered. I did seek to reduce the lower third of his face as well as reduce the vertical excess of his maxilla and felt that posterior intrusion of the maxillary teeth was indicated to allow autorotation of the mandible and assist in reduction of the overbite and overjet.
Treatment goals and plan
At our initial consultation, I discussed treatment options at length with the family, advising that orthognathic surgery would provide the most ideal result as his dental malocclusion resulted from the disharmony in his skeletal relationships. However, for reasons mentioned above, we decided to proceed with non-surgical orthodontics to camouflage and modify this imbalance in his jaws and achieve as much improvement as possible during his remaining years of growth. We all knew that outcomes were uncertain, and orthognathic surgery was an option that would be left on the table to consider in the future, but I was optimistic we would be able to provide significant improvements for him in both esthetics and function by beginning treatment at this point in his development.
Primary goals for his treatment included reduction of overjet, coordination of arch forms, and alignment of both arches. Secondary goals included open-bite reduction, management of thin anterior gingiva and oral hygiene, improvement in lip competence, reduced mentalis strain, and a reduction in gingival display on smile.
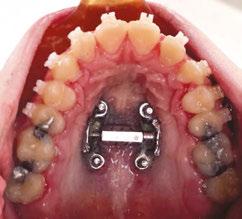
To achieve these goals, I planned a custom-designed miniscrew-anchored rapid palatal expander (MARPE) with precision 3D-printed fixed appliances (LightForce). Anchorage would be managed with Class II elastics and posterior TADs inserted into the maxillary posterior buccal cortical plate. I also proposed anterior TADs to reduce gingival display on smile, but the patient declined this option.
Treatment plan and progress
On April 22, 2022, I placed the custom MARPE using 4 palatal TADs. I placed the TADs myself during a routine office visit, with local anesthesia performed prior to the procedure at his general dentist’s office. The appliance was co-designed and printed by Partners Dental Studio in Minneapolis, Minnesota. The length of the TADs was determined by CBCT analysis to provide bicortical engagement, and the lumens of the appliance were printed to precisely guide the TADs to their desired location. We began turning the expander on the day of delivery.
A diastema was visible after the first few days of turning, and I discontinued expansion after approximately 6 mm of expansion had been achieved.
At this point, I took a new digital impression and provided the patient with a vacuum-formed retainer with a shade-matched
Figure 2: MARPE progress images
pontic to fill the diastema and retain tooth positions while I designed his LightForce appliances.
On June 28, 2022, we indirectly-bonded the LightForce braces to all available teeth using 3D-printed custom bonding jigs. Using these precision jigs in combination with the custom bracket prescription of the brackets allows me to predictably trust the appliances to begin moving the teeth in all three planes of space toward my planned goal from day one for increased efficiency and effectiveness.
The impact of digital practice has been so significant that I now provide only custom, digitallyplanned treatment options to all my patients.”
I placed a segmental arch wire in the maxillary arch (U22, U3-6 segments) to avoid extrusion of the anterior teeth and maintained the MARPE with bands on the U6s for anchorage.
The second archwire, an 18x18NT, was placed on July 20, 2022 with continued segmentation in the upper arch. At this point, we began full-time short Class II elastics (U4/L5 3/16”
3.5oz), and I also instructed Grant to resume turning of the MARPE to improve coordination with the lower arch as the mandibular posterior teeth had further decompensated.
After 6 months of treatment, I removed the bands and arms from the MARPE and maintained the TAD-supported screwbase of the expander for continued sutural stability after expansion. This allowed me to take a new digital impression of the teeth to fabricate custom brackets for the upper molars and continue with our intrusion mechanics. (As an aside, I now take only one digital impression and plan the custom molar tubes at the beginning of treatment for added efficiency. I also design my banded appliances with a buccal “window” to allow these custom tubes to be bonded at initial delivery along with the banded appliance.)
The custom molar tubes were bonded with individual printed IDB jigs at his next visit. I placed buccal TADs between the roots of the U5s and U6s, as close to the mucogingival junction as possible for maximum intrusion potential. I moved to a full-arch 18x18NT arch wire at this time and began activation of the TADs with power chain “slings” around the arch wires.
The slings were reactivated at regular intervals, until the TAD was contacting the arch wire. At that point, I stabilized the intrusion with steel ligatures from the TAD to the arch wires, while Class II mechanics with short elastics continued. This also provided anchorage support for the Class II mechanics.
The MARPE base was removed in February 2023, having been retained at least 6 months after the final turn. The buccal TADs were removed in October of 2023 after full Class II correction was achieved.
By this time, I had seen significant improvement in all areas of Grant’s occlusion, but I did discuss the option of replacing the buccal TADs and adding an anterior midline TAD to achieve further maxillary intrusion and reduction of gingival display. Grant ultimately decided he was satisfied with his results and declined this additional step.
After final Class II correction and stability were achieved, a digital impression was taken with brackets still in place to allow digital bracket removal and fabrication of retainers in advance. All appliances were removed and retainers delivered in March of 2024. He is currently retained with upper and lower Vivera retainers, worn nightly.
His total treatment time was 23 months, with 20 of those in full fixed appliances.
Treatment results
Both the family and I are thrilled with the result we were able to achieve for Grant. When comparing the predicted LightPlan side-by-side with his final photographs, you can appreciate the
power and accuracy of a customized plan and use of 3D-printed precision brackets.
By using the digital planning software and customized appliances, I was able to more predictably and efficiently treat Grant.
No detailing was performed in the arch wires — we finished this case using a 3-wire sequence, with the final wire being a 17x25NT in an .020 slot. Finishing cases in NiTi was not something I would have considered often prior to using LightForce. However, with the custom prescription, I can use lighter forces and provide a more comfortable and efficient treatment for my patients.
I am confident that because of our decision to intervene, we avoided a more complex and invasive orthognathic surgery and allowed Grant to have more years of self-confidence, improved health and well-being, and a functional occlusion.
We should always learn something from every case we treat, and I recommend reviewing your debanded cases to gain knowledge of areas to continue to improve. In Grant’s treatment plan, I wish I would have included more extrusion of the incisors to finish with an overcorrected overbite. I also would now consider a 19x25NT or TMA instead of 17x25 to achieve even more torque expression and arch form control. I can also see that combining some of the steps of treatment may have saved time overall, although due to the complexity and uncertainty of growth and cooperation, I am glad I decided to take each step of the treatment plan one at a time.
An appreciable reduction in the lower facial third and mentalis strain is noted on profile photos. I plan to continue to monitor Grant’s vertical growth and if we see his open bite returning, we can consider additional treatment in the future. This additional phase of treatment, if needed, will likely be minimal.
And although chin projection was not significantly impacted, we now have the option for a much less invasive surgical option to perform a chin implant at the time of wisdom tooth removal to encourage more chin projection and reduce the lower facial third.
Conclusion
Grant’s case is one example of how the power of precision appliances is significant when used in complex cases. I can trust that the bracket prescription is working with me to achieve my desired outcome, and my primary focus can be on managing clinical mechanics and anchorage. I was able to save months of treatment time by eliminating the detailing phase of treatment with a custom prescription and finished this case in NiTi wires.
It is also a helpful example of acknowledging that what may be considered “ideal” in a textbook may not be “ideal” for our patients. I am so honored that this family trusted me and my team to assist Grant in achieving his own goals, and that I was able to provide him with many years of improved function and esthetics.
Figure 4: LightPlan comparison
Figure 5: Final images
Robust. Intuitive. Efficient.
Empowering your team
Custom orthodontics redefines efficiency in practice
Staying ahead in orthodontics means adapting to innovations that enhance both patient care and operational efficiency.
For Dr. Melanie Wang of Dr. Melanie Orthodontics, the shift to KLOwen’s Full Custom Digital Solution was driven by a primary concern — efficiency.
Find out how she and her team implemented a custom digital approach to get practice growth without sacrificing time.
Why did you choose KLOwen Custom Orthodontics?
Dr. Wang: My reason for moving to the KLOwen Custom Digital Solution was my concern for efficiency. I started 2020 with a packed schedule and a new practice. I wanted growth without more clinical days, and I wanted to do it without bringing more stress on my team.
What were some of the challenges you had to overcome?
Dr. Wang: I know change can be hard — that my team might not like new tech for a couple of months, but I was committed to positive change.
Barbara: In conventional orthodontics, we were always stressed trying to give the patient a good experience and be efficient with their time. Moving from hand-placing brackets to indirect digital bonding (IDB) had a learning curve, but we jumped in and saw how efficient it was — way less stressful.
The most stressful appointment used to be the bonding day. Assistants would have patients prepped, and everyone would wait on the doctor. Now, the assistants do the bonding and have time to focus on the patient.
What do you love most about the KLOwen Custom Digital Solution?
Dr. Wang: We don’t want ortho appointments to be a burden to our patients. With a custom prescription and slot filling mechanics, where you position the teeth in KLOwen software is where they go biologically. It takes away the detailing appoint-
Dr. Melanie Wang has been practicing orthodontics for 17 years, and she is the owner of Dr. Melanie Orthodontics, where she has two locations in Rancho Santa Fe and San Diego, California.
Barbara Whitaker has been in orthodontics for over 20 years. She is a Registered Dental Assistant and the Lab Manager at Dr. Melanie Orthodontics.
ments at the end, so patients don’t have as many appointments along the way.
Barbara: I work with all the different types of software we use. I love how easy it is to upload the cases and review the digital setup in the KLOwen software. I submit our KLOwen custom cases, review the digital setup, and work with Dr. Wang on approvals.
Dr. Wang: She knows how to do it really well. So, she does a lot of setups for me. She finishes, and I maybe tweak it a little bit, but she gets the job done. It’s great to have her and for everything to not be waiting on me.
Barbara: Also, the KLOwen IDB trays are solid; you know they are in. The very first case we did, nothing came off which was great motivation for the team to keep going to learn more.
Dr. Wang: I remember doing a bonding during a time when we were very short-staffed. I was nervous because I hadn’t done a bonding in a long time. It worked seamlessly!
Barbara: The KLOwen team made it easy for me to learn, so I could train our team. With proper training, there wasn’t much of a learning curve for us. We rely on our Practice Development Specialist any time we feel like we may need a refresher or have questions.
What has been your biggest success since switching to the KLOwen Custom Digital Solution?
Dr. Wang: From 2019 to 2024, my practice has doubled, and I’m still working the same number of clinical days as before. I’m thrilled because it’s important for my team and me to have time outside of the practice to do things we love.
Barbara: We love having greater autonomy, efficiency, and not having to pull Dr. Wang in so many directions throughout the day. This custom treatment allows us to own the appointment and give more focus and attention to the patient, from start to finish.
This information was provided by KLOwen. OP
49%
Expanding orthodontic care: the role of OrthoFX NiTime Aligners
Loc X. Phan and Agnieszka Klucinska illustrate a system for treating patients with lifestyle, occupational, and condition-related challenges
Abstract
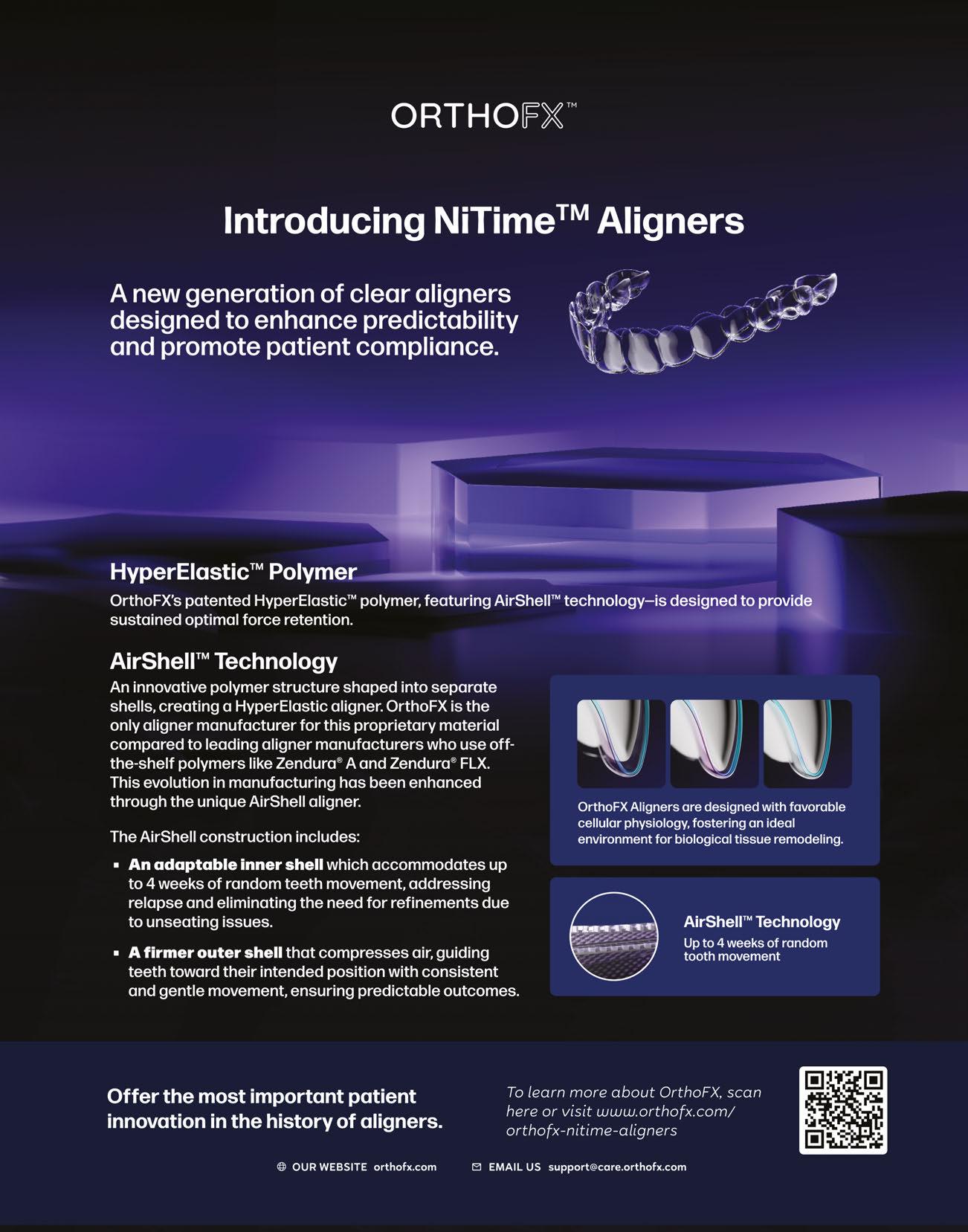
Orthodontic systems that use lower forces within the optimal range for moving teeth are commonly utilized in fixed appliance systems but have been unavailable in clear aligner therapy. OrthoFX has introduced the first aligner system employing light, sustained forces. The company has coined the term “HyperElastic” to describe its family of polymers, which offer a superior fit range and extended working range, facilitating comfortable and predictable tooth movement. The latest innovation from OrthoFX, NiTime Aligners, demonstrates even greater elasticity. By combining biologically friendly forces with enhanced fit capabilities, NiTime allows for reduced wear time. The comfort and convenience of the system improves patient compliance, further enhancing treatment predictability. Consequently, doctors can now treat patients who might have previously declined or postponed treatment, given the broad range of lifestyles and conditions suitable for NiTime Aligners.
Introduction
Lower forces offer another well-known benefit — a more comfortable treatment experience for patients. While this advantage is certainly appreciated by patients using fixed appliances, it is critical in aligner treatment since aligners are removable. Increased comfort encourages patients to wear their aligners more consistently, thereby improving treatment predictability through enhanced compliance.
In orthodontics, it is widely recognized that systems using heavy forces to move teeth are less efficient. For example, Nitinol wires were introduced to provide light and continuous forces with considerable success. These types of force systems offer more predictable and efficient tooth movement by avoiding a cascade of side effects associated with high forces. With the benefits of these systems in mind, OrthoFX has developed a clear aligner system that employs optimal, sustained forces. While the properties of Nitinol wires are referred to as superelastic, OrthoFX aligners exhibit similar characteristics, which the company has termed “HyperElastic.” This term encompasses the new polymer’s ability to:
• Fit over multiple aligner stages
• Conform to the teeth as they move
• Sustain optimal forces for orthodontic tooth movements (OTMs) throughout the 1-week wear period
The latest innovation in the OrthoFX aligner family is NiTime, designed with even greater elasticity. (The name is a nod to Nitinol wires, whose properties this product is designed to mimic.) NiTime Aligners are the first aligners cleared by the FDA to provide a reduced wear time without extending the overall treatment duration. In a clinical study approved by the FDA as part of a 510(k) submission to change the indication for use, NiTime demonstrated that the appliance could achieve planned tooth movements with just 9-12 hours of continuous wear daily, compared to the 22-hour daily wear time required by all other aligners. With this reduced wear time, patient compliance is easier to achieve, further enhancing treatment predictability.
With the benefits of HyperElasticity combined with the reduced wear time requirement, practices are now attracting patients who previously did not consider orthodontics practical for their lifestyle or situation. Types of patients who may decline traditional options but are eligible for NiTime aligners include:
• Teens who do not want to take their aligners to school
• Adults with careers that require speaking or on-camera work
• Patients with dental conditions or special needs who cannot tolerate the discomfort of standard systems
• Athletes who play sports with mouthguards
Loc X. Phan is Vice President of Research & Development for OrthoFX, Fremont, California.
Agnieszka Klucinska is Vice President of Product and L&D OrthoFX, Fremont, California.
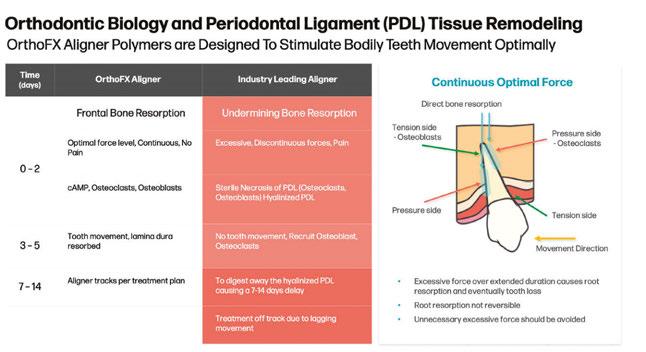
Figure 1: A comparison showing that OrthoFX uses a more biologically friendly approach
Optimal, sustained forces are more biologically friendly
To recognize how low forces move teeth more efficiently, it is helpful to review the bone remodeling process. The ideal forces for tooth movement are within the range of approximately 50.985 gf to 101.97 gf.1 However, industry-standard aligner systems traditionally use much higher forces as a compromise due to the intrinsic nature of the plastic. While forces above this level will move teeth, they have many negative side effects. First, the periodontal ligament (PDL) is compressed to the point that blood flow is cut off, resulting in cell death. The body then attempts to repair the damage, unfortunately also sweeping away the cells needed to build new bone as well as potentially resorbing the desired apical roots. Recovery time is required to complete this cleanup process and recruit the cells necessary to build new bone and support the tooth’s new position.
In contrast, OrthoFX aligners employ optimal, sustained forces that are more biologically friendly and therefore more efficient. See Figure 1 for a comparison of these two approaches.
NiTime Aligners use a new, patented construction
NiTime Aligners can produce optimal forces for tooth movement thanks to their new, patented construction. In contrast, standard aligners used by major brands are made from sheets of plastic that are fused together. Regardless of the number of layers, the physical property differences between the various pieces, or the order of their integration, they are still within the thermal plastic material classification.
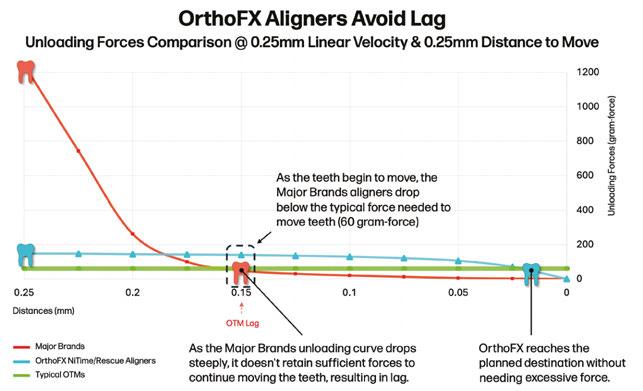
When thermal plastic experiences stress, it behaves as a viscoelastic material, meaning it can deform, yield, or even break when bent. Very little strain results in extreme levels of stress since thermal plastic stress and strain properties are logarithmically related. In aligner treatment, the plastic is repeatedly stressed as aligners are inserted and removed. Consequently, the performance of standard aligners declines over the course of wear, causing each stage of aligners to potentially fall short of achieving the planned movement. Any insufficient movement, known as lag, compounds each week until a refinement is required.
NiTime Aligners do not experience these limitations because they are not made from a single sheet or multiple sheets laminated into a single sheet. Instead, each aligner is composed of two shells with a cushion of air between them. As the teeth move, the NiTime aligners adapt closely to fit the teeth, and the air between the shells shifts to maintain optimal forces for tooth movement. By combining the benefits of “HyperElasticity” with improved patient compliance, lag is avoided (Figure 2).
Case examples
The following patients chose NiTime Aligner therapy due to specific circumstances that limited their options. With greater comfort and a reduced wear time, these patients were able to benefit from aligner treatment despite their lifestyle, occupational, and condition-related challenges.
Case 1 (Figure 3)
Contributing clinician: Dr. Neil Warshawsky, Illinois
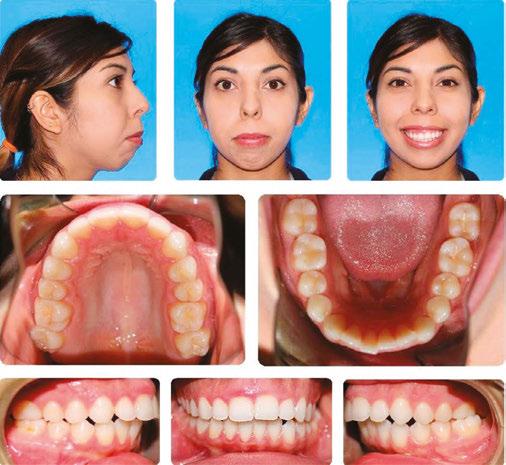
In the first case example, a 60-year-old patient, relapsed from prior orthodontic treatment, presented with an edge-to-edge bite, bilateral crossbite, and gingival recession. She had a periodontal consultation but decided to postpone surgery until after her son’s upcoming wedding. She requested a system that moves teeth more gently due to her periodontal concerns.
The doctor planned for expansion in the upper and lower arches with elastics on the first molars as well as enameloplasty for the upper-right incisor. The treatment objectives were achieved in 7 months with no worsening of her gingival recession. In addition to her periodontal status remaining stable, the patient’s primary goal of completing treatment in time for her son’s wedding was successfully met.
Figure 2: Comparison of unloading forces for NiTime versus major brands (conducted by an independent testing laboratory)
Figure 3: Case 1 initial records (left) and final records (right)
Case 2 (Figure 4)
Contributing clinician: Dr. Bill Dabney, Virginia
In this case, the patient is a 13-year-old with Down Syndrome and sleep apnea. NiTime appealed to the patient’s mother since she was very happy her daughter did not have to take her aligners to school. Mom did not want her daughter to have to keep up with her aligners and was afraid she would lose them. Mom was also very concerned about hygiene with braces.
The treatment plan is to close all spaces and extrude the incisors to close the open bite.
Case 3 (Figure 5)
Contributing clinician: Dr. Neil Warshawsky, Illinois
The next case example is a 33-year-old relapse patient who is a very busy plastic surgeon. She did not consider correcting her relapse until she heard about NiTime Aligners. She was 50% Class II and moderately crowded. The treatment plan was to level the lower occlusal plane and use Class II elastics for the right buccal segment to correct the tooth interdigitation as well as broaden the buccal segment and resolve crowding in the anterior teeth.
Case 4 (Figure 6)
Contributing clinician: Dr. Neil Warshawsky, Illinois
This 33-year-old patient was a Class I Div 2 malocclusion with a moderately deep overbite, moderate upper/ lower crowding, and retroclined incisors. She also had gingival recession on the lower canines and first premolars. She chose NiTime since she is a teacher and felt self-conscious about undergoing orthodontic treatment.
The treatment plan was to resolve her crowding through expansion with Class II elastics to procline the maxillary incisors and increase the overjet. The plan will also intrude the incisors and extrude the premolars to assist in the leveling of the case. Her treatment progress is shown at stage 28.
Case 5 (Figure 7)
Contributing clinician: Dr. John Conroy, Connecticut
The final case example is a 28-year-old patient who received orthodontic treatment initially at age 10, completing it at age 13 with braces, elastics, and springs, resulting in a Class 1 outcome. Lingual retainers were placed posttreatment; however they were broken during a dental cleaning years later. The patient returned with minor rotations of the lower incisors and excess overjet. The overjet was her chief complaint.
As treatment was about to begin, the patient learned she was pregnant and so refused attachments. Treatment was able to proceed due to the HyperElasticity of NiTime Aligners. Treatment results were: overjet improved, Class I maintained, and crowding corrected in 7 months (22 stages). The patient achieved a satisfactory outcome despite declining planned attachments.
Conclusion
OrthoFX NiTime Aligners stand out as the only clear aligner on the market FDA cleared for reduced wear time without any compromise to treatment duration. This milestone has enabled
doctors to provide treatment to patients who might otherwise postpone or avoid treatment due to discomfort or disruption to their job or lifestyle. Marketed as a “compliance-friendly” system, NiTime offers a unique solution for patients seeking more comfortable and convenient aligner treatment.
REFERENCE
1.
2019 Nov;156(5):582-592.
Theodorou CI, Kuijpers-Jagtman AM, Bronkhorst EM, Wagener FADTG. Optimal force magnitude for bodily orthodontic tooth movement with fixed appliances: A systematic review. Am J Orthod Dentofacial Orthop.
Figure 4: Case 2 initial records
Figure 5: Case 3 initial records (left) and final records (right)
Figure 7: Case 5 initial records (left) and final records (right)
Figure 6: Case 4 progress (left) and facial comparison (right)
Perspectives on orthodontic retention
Dr. Dustin S. Burleson discusses the importance of following up on orthodontic treatment
Introduction
Orthodontic retention bridges the gap between the active phase of orthodontic treatment and the long-term stability of achieved results. There is a 35.22% overall failure rate¹ for bonded retainers, with an escalating trend observed in prolonged follow-up durations. This highlights the critical role retention plays in preserving orthodontic corrections and perhaps why so many orthodontists prescribe thermoformed retainers following orthodontic treatment.
The retention phase of orthodontic care aims to preserve the orthodontic correction achieved during active treatment. Its primary objective is to stabilize the dentition in its corrected position, facilitate occlusal settling, and mitigate the risk of relapse — a phenomenon in which teeth gradually revert to their pre-treatment alignment. Retention procedures are critical for both orthodontists and general practitioners (GPs) involved in post-treatment care.
Orthodontists rely on effective retention strategies to safeguard the time, effort, and resource investments made during active treatment. On the other hand, GPs contribute to the longterm success of orthodontic results by reinforcing the importance of compliance with retention protocols and promptly addressing any issues that might arise.
This article focuses on orthodontic retention, equipping orthodontists and GPs with essential knowledge and tools to optimize patient care and maintain a healthy and stable occlusion for each patient.
The science of retention
While the concept of orthodontic retention may seem straightforward, its efficacy depends on a thorough understanding of the underlying scientific principles that influence tooth movement and stability. Central to retention is the principle of tissue remodeling. This process involves the periodontal ligament and surrounding bone adapting to new tooth positions. This process is inherently influenced by biological factors such as:
• Bone density
• Gingival architecture
• Individual patient variability
Dustin S. Burleson, DDS, MBA, is a Board Certified Orthodontist and Adjunct Clinical Professor, UMKC School of Dentistry, Kansas City, Missouri. He is an Attending Orthodontist at the The Children’s Mercy Hospital, Kansas City, Missouri and an Associate Orthodontist at Corus Orthodontists in Seattle and Bellevue, Washington.
Disclosure: Dr. Burleson is a KOL for Retainer Club.
Educational aims and objectives
This self-instructional course for dentists aims to provide insight into the various aspects of orthodontic retention and why retention is an important part of orthodontic treatment.
Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions by taking the quiz online at orthopracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
• Identify the scientific principles that influence tooth movement and stability.
• Identify various types of orthodontic retainers.
• Realize the implications of hygienic care of retainers on oral health and some ways that retainers can be properly maintained.
• Realize some challenges of retainers.
• Realize the necessity to educate patients on the proper maintenance and care for retainers.
2 CE CREDITS
The stability of tooth position after treatment is determined by the principal fibers of the periodontal ligament and the supra-alveolar gingival fiber network. These fibers help maintain a balanced relationship between the teeth and the surrounding soft tissue.
Orthodontic treatment disrupts the periodontal ligament and the gingival fiber network, requiring these fibers to reorganize after removing the appliances.
The gingival fiber network consists of collagenous and elastic-like oxytalan fibers. While the collagenous fibers typically remodel in 4 to 6 months, the oxytalan fibers can take up to 6 years to fully reorganize.2 The slow remodeling of these supra-alveolar fibers, especially in initially rotated teeth, contributes to the risk of relapse after orthodontic treatment.
This extended timeline is why long-term, routine retainer use is critical. The retainers help maintain the new positions while the periodontal ligament and surrounding structures fully adjust and stabilize. Orthodontists typically recommend wearing retainers full-time for the first 3 to 6 months, followed by nighttime wear as advised, to ensure the teeth do not relapse into their original positions.
Moreover, the mechanical aspects of retention cannot be overlooked. Retainers serve as external forces counteracting teeth’s natural tendency to relapse into their original positions (Figures 1-4). Various retainer designs, ranging from traditional Hawley retainers to bonded lingual and thermoformed retain-
ers, exert different degrees of force and control on the teeth and periodontium. The significance of orthodontic retention cannot be overstated.
Retainer types
Hawley retainers are ideal for slight adjustments, as they exert gentle, passive forces to maintain the position of the teeth. An orthodontist can adjust the metal wire by applying light pressure if minor corrections are needed.
Bonded lingual retainers, also known as permanent retainers, provide constant contact to keep the teeth in place, preventing movement. This is especially important for maintaining the alignment of severe rotations or space closure, but without aftercare maintenance, relapse can occur due to the aforementioned risk of bond failure.
Thermoformed or clear plastic retainers offer full coverage of the teeth, maintaining their alignment with gentle, even pressure. They are especially good for preventing relapse and are often used as an ideal solution to retain tooth alignment and arch form.
Retention duration varies based on factors like the severity of the malocclusion and treatment method. Generally, orthodontists oversee retention for 12 to 24 months post-treatment.3 After this, they may expect GPs to monitor retention and subsequent dental changes. Clear communication between orthodontists and GPs is essential to ensure a smooth transition in retention responsibility and proper ongoing care.
Impact on patient health
Maintaining orthodontic results relies heavily on orthodontic retainers. However, their presence within the oral cavity can induce significant alterations in the oral ecosystem, potentially escalating the risk of various oral diseases.4 Fixed orthodontic appliances, including lingual bonded retainers, pose a unique challenge to oral hygiene. Their presence hinders the efficient removal of food particles and plaque, creating an environment conducive to bacterial growth and biofilm formation.
Bacterial colonization has many implications for oral health, including:
• Periodontal disease: Accumulation of bacterial biofilms on retainer surfaces can contribute to gingivitis and periodontitis, leading to gum inflammation and tissue damage.
• Halitosis: Bacterial growth in the oral cavity, including on retainer surfaces, can produce malodorous compounds, which contribute to halitosis or bad breath.
• Caries lesions: The presence of biofilms on retainers increases the risk of enamel demineralization and the formation of caries lesions, particularly in areas prone to plaque accumulation.
Clinical observations also confirm the presence of gingivitis and enamel decalcification around fixed appliances, manifesting as visible signs of inflammation and demineralization.5 Moreover, poor oral hygiene habits and past periodontal conditions contribute to the susceptibility to periodontal complications associated with orthodontic retainers. Therefore, orthodontic retention must go beyond a “set it and forget it” approach. It’s a continuous commitment, not just a one-time recommendation.
Care of retainers
Patients must be educated about the risk of orthodontic retainers serving as substrates for bacterial growth.6 The presence of irregularities on retainer surfaces (grooves and ridges) increases the likelihood of plaque biofilms forming. Additionally, microcracks and abrasions on thermoformed retainers, despite their promising results in controlling plaque index and gingival health, give bacteria a chance to grow. Patients in orthodontic retention should be educated on proper cleaning techniques and understand the significance of hygiene protocols to prevent the growth of bacterial biofilms.
One of the most efficient cleaning techniques is the daily use of a soft-bristled toothbrush combined with non-abrasive toothpaste. It’s important for patients to brush their retainers gently but thoroughly, ensuring all surfaces are cleaned, including the crevices where bacteria are likely to accumulate. In addition to manual brushing, soaking retainers in a non-alcoholic, antimicrobial solution can significantly reduce bacterial load. Solutions containing ingredients like chlorhexidine dissolve biofilms and kill
Figures 1-4: Patients seeking re-treatment due to unplanned tooth movement following fixed lingual retainer placement. Images courtesy of Leone and Vaughn Orthodontics, Seattle and Bellevue, Washington
bacteria more effectively than water alone.7 Soaking retainers daily or at least a few times a week in these solutions helps maintain a hygienic environment and prevents the build-up of odor-causing bacteria.
Challenges with fixed retainers
Fixed orthodontic retainers, while effective in maintaining tooth alignment, present unique challenges in terms of oral hygiene maintenance and bacterial adhesion. Unlike removable thermoformed retainers, fixed retainers cannot be easily removed for eating, drinking, or oral hygiene routines. This lack of accessibility creates an environment conducive to bacterial biofilm formation, posing several potential drawbacks.
The adhesion and growth of bacterial biofilms on fixed retainers can lead to various undesirable consequences like unpleasant odors, gingival inflammation, recession,8 and unplanned tooth movement. These can not only impact patient satisfaction but may also compromise compliance with retention protocols.
Moreover, bacterial biofilms on the retainer surface have broader implications for oral health. They can disrupt the existing oral microbiota and expose individuals to the conditions we’ve mentioned, further escalated by inconsistent oral hygiene practices and unhealthy diets.9 Fixed retainers may also interfere with oral hygiene practices and have the potential to for plaque and calculus. These complications highlight the importance of implementing preventive programs to minimize the adverse effects of orthodontic treatment.
Patient education on proper cleaning techniques, such as floss threaders and interdental brushes, is crucial for maintaining periodontal health. We advocate for a patient-centered approach that tailors treatment to individual needs. It’s essential to educate patients about the potential drawbacks associated with fixed lingual retainers.
Benefits of routine retainer replacement
Much like changing a toothbrush every 3 months to maintain oral hygiene, replacing removable or thermoformed retainers periodically is necessary because they endure significant wear. As they age, retainers may also become loose and prone to harboring bacteria, posing risks to oral health and compromising the effectiveness of orthodontic treatment.
Retainers should be replaced regularly for several reasons:
• Improved retention performance: A fresh retainer ensures optimal fit and function.
• Enhanced oral hygiene: Minimizes bacterial buildup on retainers, reducing the risk of oral diseases.
• Preservation of orthodontic investment: Protects treatment results by minimizing the potential for relapse and maintaining tooth alignment (Figures 5-10).
• Increased patient comfort: New retainers offer a better fit and feel, improving patient comfort, compliance, outcomes, and satisfaction.
Innovative retainer programs, such as Retainer Club, boost patient compliance and satisfaction. By partnering with orthodontists and GPs, Retainer Club offers a seamless solution for regular retainer replacement, providing patients with convenient access to online ordering and fast home delivery services. This approach not only streamlines the retainer replacement process but also empowers patients to prioritize their oral health while maximizing the value of their orthodontic investment.
Clinical recommendations
Orthodontists and GPs can benefit from practical guidelines for retainer selection and maintenance to optimize patient outcomes.
When choosing a retainer, consider:
• Patient compliance
• Treatment goals
• Individual anatomical factors
Removable retainers, such as thermoformed retainers, offer convenience and ease of use, particularly for patients with good compliance and mild retention needs. Alternatively, fixed retainers, including bonded lingual retainers or prefabricated retainers, may be more suitable for patients requiring greater retention or those prone to non-compliance.
Once a retainer is selected, proper maintenance is essential to ensure its effectiveness and longevity. Patients should be instructed on regular cleaning routines, including brushing the retainer with a soft toothbrush and mild soap or using specialized retainer cleaning solutions.
Figures 5-10: Removable retainer deterioration or non-compliance can result in relapse
Also, patients should also be advised to avoid exposing the retainer to extreme temperatures or excessive force. This can lead to damage or distortion of the appliance. For optimal results, educate patients about retainer retention and replacement. Highlighting the importance of retention boosts patient compliance; discussing neglect consequences, like bacterial buildup or retainer deterioration, reinforces protocol adherence. Promoting evidence-based practice will require orthodontists and GPs to stay up-to-date on the latest research findings and clinical guidelines regarding orthodontic retention. With this, practitioners can make informed decisions that prioritize patient safety and maximize treatment outcomes. Regular monitoring of fixed lingual retainers by orthodontists or general practitioners is crucial to ensure optimal dental health. Teeth can shift over time, retainers may break or become compromised, emphasizing the necessity for timely intervention to maintain the integrity of orthodontic treatment outcomes.
Conclusion
Orthodontic retention is a crucial part of orthodontic treatment, preserving the results obtained during active treatment. To mitigate the risks associated with retainer wear, clinicians must adopt proactive management strategies. This includes regular monitoring, timely replacement, and diligent maintenance to safeguard against potential complications such as bacterial buildup, retainer deterioration, gingival inflammation, periodontal recession, unplanned tooth movement, and relapse.
Patient education and engagement are central to successful orthodontic retention. Clinicians who inform patients about the benefits and potential consequences of regular maintenance are more likely to motivate and encourage patients to remain compliant. Encouraging patients to prioritize their oral health and follow recommended protocols is essential to promoting longterm orthodontic stability and oral health outcomes.
REFERENCES
1. Aye ST, Liu S, Byrne E, El-Angbawi A. The prevalence of the failure of fixed orthodontic bonded retainers: a systematic review and meta-analysis. Eur J Orthod. 2023 Nov 30;45(6):645-661.
2. Klineberg I, Eckert SE, eds. Functional occlusion in restorative dentistry and prosthodontics. Elsevier/Mosby; 2016.
3. Molyneaux C, Sandy JR, Ireland AJ. Orthodontic retention and the role of the general dental practitioner. Br Dent J. 2021 Jun;230(11):753-757. doi: 10.1038/s41415-021-28755. Epub 2021 Jun 11.
4. Levrini L, Novara F, Margherini S, Tenconi C, Raspanti M. Scanning electron microscopy analysis of the growth of dental plaque on the surfaces of removable orthodontic aligners after the use of different cleaning methods. Clin Cosmet Investig Dent. 2015 Dec 15;7:125-131.
5. Pandey V, Chandra S, Dilip Kumar HP, Gupta A, Bhandari PP, Rathod P. Impact of dental neglect score on oral health among patients receiving fixed orthodontic treatment: A cross-sectional study. J Int Soc Prev Community Dent. 2016 Mar-Apr;6(2):120-124.
6. Rouzi M, Zhang X, Jiang Q, Long H, Lai W, Li X. Impact of Clear Aligners on Oral Health and Oral Microbiome During Orthodontic Treatment. Int Dent J. 2023 Oct;73(5):603-611.
7. Kiatwarawut K, Kuvatanasuchati J, Thaweboon B, Sirisoontorn I. Comparison of Various Antimicrobial Agents for Thermoplastic Polymeric Retainers. Polymers (Basel). 2022 Sep 8;14(18):3753.
8. McInnes N, Carty O. Gingival recession with fixed retainer. Br Dent J. 2021 Jul;231(1):4.
9. Lyros I, Tsolakis IA, Maroulakos MP, Fora E, Lykogeorgos T, Dalampira M, Tsolakis AI. Orthodontic Retainers-A Critical Review. Children (Basel). 2023 Jan 28;10(2):230.
Continuing Education Quiz
Perspectives on orthodontic retention
BURLESON
1. There is a _____ overall failure rate for bonded retainers, with an escalating trend observed in prolonged follow-up durations.
a. 35.22%
b. 45.24%
c. 62.45%
d. 70.42%
2. The primary objective(s) of retention is/are to _______.
a. stabilize the dentition in its corrected position
b. facilitate occlusal settling
c. mitigate the risk of relapse
d. all of the above
3. The stability of tooth position after treatment is determined by the principal fibers of the periodontal ligament and the supra-alveolar gingival fiber network.
a. True
b. False
4. While the collagenous fibers typically remodel in 4 to 6 months, the oxytalan fibers can take up to _________ to fully reorganize.
a. 1 year
b. 2 years
c. 6 years
d. 10 years
5. _____ are ideal for slight adjustments, as they exert gentle, passive forces to maintain the position of the teeth.
a. Bonded lingual retainers
b. Hawley retainers
c. Clear plastic retainers
d. Permanent retainers
6. Generally, orthodontists oversee retention for __________ months post-treatment.
a. 2-6 months
b. 6-8 months
c. 12 to 24 months
d. 36 to 48 months
7. In addition to manual brushing, soaking retainers in _______ can significantly reduce bacterial load.
a. a non-alcoholic, antimicrobial solution
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://orthopracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://orthopracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 370
Date Published: July 2, 2024
Expiration Date: July 2, 2027
b. alcohol
c. spring water
d. essential oil
8. The adhesion and growth of bacterial biofilms on fixed retainers can lead to various undesirable consequences like ________ and unplanned tooth movement.
a. unpleasant odors
b. gingival inflammation
c. recession
d. all of the above
9. Retainers should be replaced regularly for _______ and increased patient comfort.
a. improved retention performance
b. enhanced oral hygiene
c. preservation of orthodontic investment
d. all of the above
10. To mitigate the risks associated with retainer wear, clinicians must adopt proactive management strategies. This includes regular monitoring, timely replacement, and diligent maintenance to safeguard against potential complications such as bacterial buildup, retainer deterioration, gingival inflammation, periodontal recession, unplanned tooth movement, and relapse.
a. True
b. False
Large Practice Sales
Brings Multiple Bidders For
The Highest Value in IDSO Partnerships
“I was about to sign an offer I had in hand for $8 million from an IDSO I really liked. Chip convinced me to go through the LPS process to see my other options. LPS delivered nine bidders and the $8 million became $11 million from the same group!”
-Dr. T.S., Tennesee
“So glad I met you guys. You changed my life. My partner is great and I am still amazed how you achieved 3.9x collections for my practice.”
-Dr. S.L, Indiana
“I never could have achieved this value or completed this deal without you.Thank you for everything.”
-Dr. J.N., Maryland Achieved 12.2x EBITDA in 2023
Digital technology impacts orthodontic results
Dr. David Alpan reviews digital options that can benefit the orthodontic practice
Introduction
In the past, orthodontics did not require any digital technology to achieve straight teeth. Rudimentary treatments for crowding and palatal expanders can be traced back to 17th and 18th century Europe. Innovative dentists, such as Pierre Fauchard and Christophe-Franchois Delabarre, helped set the groundwork for orthodontics.1-4 Orthodontic history dates back over 200 years, and Edward Angle became the father of modern orthodontics in 1892. However, the concepts of proper treatment planning to the face, airway, and TMJ, incorporating complex restorative and retention plans was not even a consideration during those pioneering times. The ability to accomplish the goal without harming the patient was most important.
How long will it take for us to change how we use modern orthodontics? Would you walk far if you could drive? Would you write letters if you could get on the phone to talk? How many of us are still using Windows XP? How many of us do not have a computer involved in our treatment planning? As all technology needs updates, wouldn’t orthodontic delivery of care need updates? Digital technology has improved patients’ orthodontic treatment experience and results.19
For contemporary orthodontists, incorporating orthodontic digital technology can transform the experience for the doctor and outcome for the patient.19 Innovative technology assists the practitioner with making improved decisions — creating more efficiency, accuracy, and precision in overall diagnosis and treatment plans.5-7,19
Educational aims and objectives
This self-instructional course for dentists aims to provide insight into the reasons for incorporating digital technology into orthodontic practice.
Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions by taking the quiz online at orthopracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
• Realize how digital technology can lead to 3D diagnostic set-ups.
• Identify how 3D imaging can help to coordinate treatment, especially for patients who need restorative and orthognathic treatment.
• Realize how 3D imaging can help with patient motivation and communication.
• Identify how cone beam computed tomography (CBCT) imaging can help with diagnosis of airway, transpositions, supernumerary teeth, skeletal asymmetries, and pathology, and increases the scope of diagnosis and impacts treatment decisions.
• Gain insight into digital technology’s efficiencies such as reduced treatment time minimizing unwanted tooth movements, increased appointment intervals, virtual exams, virtual treatment, and retainer subscriptions — all requiring less visits.
3D imaging is now able to assist with developing incredible stable life-changing treatment outcomes that improve the overall health of the patient with less office visits and reduced treatment durations.13,15,19 Planning the end result in 3D prior to treatment saves time in the office and helps direct the treatment flow for the team and patients.19 Offering virtual exams and treatment opens the door to a higher level of customer service and convenience. Creating a retainer subscription program will improve retention and connection with our treated patients. Offering innovative technology differentiates the practice and helps create credibility.
David Alpan, DDS, MSD, earned his dental degree in 1996 and completed his orthodontic specialty certificate from UOP Arthur Dugoni School of Dentistry in 1998. He was awarded an MSD and wrote his Master’s thesis on the results of a TMJ research project. Dr. Alpan has multiple practice locations in Los Angeles where he currently treats patients. Alpan lectured for Invisalign from 1992-1998 at over 250 locations to over 10,000 doctors. He played an integral part of implementing the Invisalign system into the dental and orthodontic school curriculum. Dr. Alpan was an Ormco insider and helped 3M as a research panelist for many years. He was a KOL for AcceleDent® and Propel and has published several articles on accelerated orthodontics. As a Center of Excellence member for Incognito and a high-volume Insignia™ and now LightForce provider, he has incorporated several digital-based technologies into his digital workflow. Dr. Alpan is currently treating all his patients with Invisalign® or LightForce digital-based systems with airway and TMJ in mind. He can be reached at dalpan@aeortho.com.
3D imaging impacts treatment decisions
Orthodontic treatment planning is a multifactorial decision-making process that requires as much diagnostic information as possible.5-7 Orthodontic treatment planning considers age and stage of growth, which have a considerable influence on treatment decisions. The choices made can create very stable esthetic results or create unstable unattractive results. The more accurate and detailed data a practitioner has about the patients’
current condition, the more precise they can be with the treatment decisions.
Viewing patients’ anatomy utilizing the standard of care cephalometric, panoramic, periapical, and bitewing X-rays allows us see landmarks in two dimensions, which unfortunately causes us to misdiagnose what we cannot see. A 3-dimensional image is more diagnostic than our standard-of-care images. Utilizing 3D CBCT imaging in conjunction with 3D intraoral scanning leads to improved diagnosis and treatment planning of not only the teeth and occlusion, but also the TMJ and airway.
3D digital treatment planning affects my treatment duration and outcome (Figure 5). If we incorporate more data from digital records to our treatment plan at the onset, this leads to treatment decisions that can create a more stable result in less time. For example, surgical orthodontics with three-dimensional planning has reduced average surgical treatment time by over 12 months. Average treatment time across the world for orthognathic surgery patients is 30 months,8,10,11,12 and with digital technology, it can average 18 months (Figures 1-4).
With the advances of digital treatment planning such as Invisalign, LightForce, and surgical guides, reduced treatment times with the same or better results require less visits to the office. This is just one example of how digital technology impacts patients’ treatment results. The digital planning takes out many of the mid-treatment decisions like timing of IPR for tooth size discrepancies or coordinating arches for orthognathic cases prior to surgery.
With digital treatment planning, the clinician can measure the exact amount of interproximal reduction needed to reduce the tooth size discrepancy and complete it at the first or second appointment. Instead of realizing after leveling and aligning that the arches are not coordinated, with 3D treatment planning, the practitioner can coordinate the arches and level and align at the same time because the goal is created from the onset.
With the use of 3D simulation software, patients and doctors can verify multiple treatment plans and outcomes without ever having to touch the patient.9 Creating the best outcome and result can be challenging, but if the clinician can visualize those different results with a 3D digital plan prior to treatment, the best
Figure 1: Initial orthognathic surgery patient treated with AcceleDent and aligners with 3D digital set-ups
Figure 2: Final image. Total treatment time ortho and surgery was 15 months
Figure 3: Before-and-after frontal images of 15 months surgery case
Figure 4: Profile views of before and after
choice can be made without any guessing the outcome. In all orthodontic care, we must consider that compliance and biology can affect the best made plan, and our own clinical judgment will solve most complex problems. No matter if you have a CBCT machine or have a patient go to a lab, the images are more diagnostic and aid in treatment planning as more parameters can be used to make the best treatment decisions. How much do you care to know before making your final treatment decisions? Remember, your patients don’t care how much you know, just how much you care (Figure 9).
With the advent of 3D imaging, digital treatment plans can be fabricated to reduce unwanted tooth movements, especially round tripping.9 Utilizing 3D treatment planning software, the precise movement of teeth can be controlled in their timing and sequence, creating more efficiency in tooth movement. If you know where you are going, it is a lot easier to get there. With the use of 3D treatment planning tools from Invisalign or LightForce (Figure 8) as examples, patients are completing treatment within less overall time and requiring less visits to the office.13,14 I see better results from 3D treatment planning than traditional analog metal twin brackets, guiding the treatment at each appointment and praying for compliance. Digital technology will not take the place of tender loving care, but it will create more efficiencies and better outcomes. The experience for the patient and doctor is much different when both parties are working with a 3D plan agreed upon at the start.19
Now clinicians can offer a retainer subscription program via Align technology which automatically sets up a third-party to manage the transactions. This all starts with a 3D iTero™ scan which is stored for the future. A new retainer can be made from this stored data at any point without the doctor’s or team’s participation. This can lead to better retention and increased connectivity with our treated patients leading to more referrals. A retainer subscription program also leads to reduced time in the office for patients.
Airway is more important than occlusion and stability
The airway is more important for overall health than the occlusion or stability of the teeth. If orthodontic treatment deci-
sions were solely based on occlusion and stability, orthodontists would be making treatment decisions that are counterproductive for improving the airway. If the orthodontists’ decisions are solely made based on airway, occlusion and stability would not be as stable. Stability is based on many principles, but everyone agrees long-term retention is key. Other parameters that effect stability are upright teeth in bone, functional occlusion with no lateral interferences on excursions, centric stop for each tooth, and many other occlusal parameters.18
The use of 3D CBCT imaging (Figure 6) opened the door for orthodontists to screen and diagnose airway-related issues. Imaging led to measuring the volumetric space of the airway during growth as well as before and after orthodontic treatment. With the use of CBCT imaging, orthodontists can consider airway when treating patients. With this consideration, we can improve the bite, smile, and airway at the same time we have improved the overall health of the patient. The concept was first introduced to me by Sean Carlson and Juan-Carlos Quintero, but airway literature dates back nearly 100 years. The advent of CBCT imaging has given us a visual goal to increase the size and patency of airways as part of orthodontic treatment. Treatment planning to grow or change the airway while maintaining great occlusion and stable results is the ultimate goal of Airway Orthodontics. A very common airway centric treatment plan is to never prescribe extractions of premolars and typically involves more expansion treatments. During phase one treatment, the use of slow expansion has demonstrated the ability to enlarge the airway. Longterm growth analysis studies out of Stanford showed that airways grew up to age 30-35 and then began to shrink after age 35. As orthodontists, we can prevent airway-related issues with the use of 3D CBCT imaging to guide the proper treatment decisions to create patent airways and stable occlusion while creating an esthetic result.
There are numerous types of intraoral devices to treat Obstructive Sleep Apnea (OSA). All devices are designed to help reduce hypoxic events while sleeping. Unfortunately, these intraoral appliances can have negative long-term effects on the occlusion. With digital imaging technology, practitioners can visualize the airway in three dimensions to help aid in the decision to improve the airway or just focus on stable teeth results.
Patients who present with mild sleep apnea can be treated with dental expansion, but moderate to severe diagnosis of OSA are best treated with orthognathic surgical corrections to achieve the gold standard result.
Virtual exams/treatment improve communication via an app with AI & 24/7 virtual support
Increased communication improves the patient’s experience and orthodontic results. Utilizing a patient communication system to monitor and assist with treatment is the future. Grin® or others offer a patient communication tool which dramatically reduces the number of office visits because many of the questions or concerns are resolved virtually. This leads to less time for patients in the office. Not all the visits can be completed virtually, but
Figure 5 (left): iTero™ scanner to digitally scan teeth for 3D set ups and appliance fabrication. Figure 6 (right): i-CAT™ imaging machine for 3D CBCT X-ray images
8: LightForce delivers 3D-planned, fabricated, and fully customizable
with the use of Grin, we can track patients’ outcomes midway in treatment. So, we can be assured sooner or see the issues that need to be addressed earlier to avoid increased office visits and overall treatment time. Utilization of Grin Scopes and Grin AI have increased capacity and broadened the types of remote distant treatment that can be offered (Figure 7).
Conclusion
Offering more 3D digital diagnostic imaging — from teeth scanning, airway scanning, TMJ scans, three-dimensional toothpositioning diagnostic set ups, and root positioning — we can diagnose and treatment plan for ideal orthodontic outcomes with patent airways. Orthodontic treatment decisions do not have to compromise the patients’ airway or dental stability. As we create more patent airways, we also improve overall health. With increased patient communication using Grin AI and 24/7 support, we are finding decreased office visits and phone time. This allows treatment to progress on time with less difficulties for both patients and doctors. Utilizing 3D custom-designed aligners or braces with custom 3D-printed bases and prescription brackets, orthodontic end results are more comprehensive, stable, well balanced, and symmetric. Preparing restorative treatment options can be more accurate utilizing technology to image the occlusion, smile arc, and symmetry. Incorporating digital technology will shorten orthodontic treatment time, while improving overall outcomes, which are visible to the patient. Utilizing Grin AI helps to keep patients motivated and enthusiastic about treatment, leading to improved results. Happy, motivated, and compliant patients always have better outcomes, so start your digital journey now.
REFERENCES
1. Fleming PS. Orthodontic treatment planning: can we plan for stability? Br Dent J. 2021 Jun;230(11):717-721.
2. Hughes BO. Nature’s Plan and Orthodontics. Am J Orthod Oral Surg. 1945;31(7): 360-369.
3. Waldo CM. A Practical Approach to Problems of Orthodontics. Am J Orthod. 1953; 39(5):322-339.
4. Dewel DF. Serial extraction in orthodontics: indications, objectives, and treatment procedures. Am J Orthod.1954;40(12):906-926.
5. Larson BE. Cone-beam computed tomography is the imaging technique of choice for comprehensive orthodontic assessment. Am J Orthod Dentofacial Orthop. 2012
Figure 9: One-on-one communication showing graphically in 3D what treatment results, progress, and finish will look like
Apr;141(4):402, 404, 406 passim.
6. Dindaroğlu F, Yetkiner E. Cone Beam Computed Tomography in Orthodontics. Turk J Orthod. 2016 Mar;29(1):16-21.
7. Munaif V, Raghunath N, Jyothikiran H, Chandran N and Kabeer S. CBCT: A breakthrough in orthodontic diagnosis. Int J Appl Dent Sci. 2019;5(3): 360-365.
8. Paunonen J, Helminen M, Peltomäki T. Duration of orthognathic-surgical treatment. Acta Odontol Scand. 2017 Jul;75(5):372-375.
9. Sereewisai B, Chintavalakorn R, Santiwong P, Nakornnoi T, Neoh SP, Sipiyaruk K. The accuracy of virtual setup in simulating treatment outcomes in orthodontic practice: a systematic review. BDJ Open. 2023 Aug 28;9(1):41.
10. Luther F, Morris DO, Karnezi K. Orthodontic treatment following orthognathic surgery: how long does it take and why? A retrospective study. J Oral Maxillofac Surg. 2007 Oct;65(10):1969-1976.
11. Dowling PA, Espeland L, Krogstad O, Stenvik A, Kelly A. Duration of orthodontic treatment involving orthognathic surgery. Int J Adult Orthodon Orthognath Surg. 1999; 14(2):146-152.
12. Slavnic S, Marcusson A. Duration of orthodontic treatment in conjunction with orthognathic surgery. Swed Dent J. 2010;34(3):159-66.
13. Rossini G, Parrini S, Castroflorio T, Deregibus A, Debernardi CL. Efficacy of clear aligners in controlling orthodontic tooth movement: a systematic review. Angle Orthod. 2015 Sep;85(5):881-889.
14. Alpan D. A review of accelerated orthodontics. Orthodontic Practice US. 2016;7(5): 44-48.
15. Tweed CH. The Frankfort-mandibular plane angle in orthodontic diagnosis, classification, treatment planning, and prognosis. Am J Orthod Oral Surg. 1946 Apr;32:175-230.
16. Margolis HI. The axial inclination of the mandibular incisors. Am J Orthodontics Oral Surg. 1943;29(10):571-594.
17. Kesling HD. The philosophy of the tooth positioning appliance. Am J Orthod Oral Surg. 1945;31(6):297-304.
18. Howes AE. Case analysis and treatment planning based upon the relationship of the tooth material to its supporting bone. Am J Orthod. 1947 Aug;33(8):499-533.
19. Cunha TMAD, Barbosa IDS, Palma KK. Orthodontic digital workflow: devices and clinical applications. Dental Press J Orthod. 2021 Dec 15;26(6):e21spe6.
20. Keilig L, Fittgen A, Schneider H, Sifa R, Schwarze J, Bourauel C, Konermann A. Accuracy of Digital Orthodontic Treatment Planning: Assessing Aligner-Directed Tooth Movements and Exploring Inherent Intramaxillary Side Effects. J Clin Med. 2024 Apr 16;13(8):2298.
Figure 7: Grin 24/7 AI Patient support for tracking and monitoring treatment
Figure
braces
Continuing Education Quiz
Digital technology impacts orthodontic results
1. Orthodontic treatment planning considers _______, which have a considerable influence on treatment decisions.
a. age
b. stage of growth
c. patient’s gender
d. both a and b
2. Utilizing 3D CBCT imaging in conjunction with 3D intraoral scanning leads to improved diagnosis and treatment planning of not only the teeth and occlusion, but also the TMJ and airway.
a. True
b. False
3. Average treatment time across the world for orthognathic surgery patients is 30 months, and with digital technology, it can average
a. 9 months
b. 18 months
c. 24 months
d. 28 months
4. ________, the precise movement of teeth can be controlled in their timing and sequence, creating more efficiency in tooth movement.
a. Traditional analog treatment planning
b. Using 2D imaging
c. Utilizing 3D treatment planning software
d. Coordinating treatment with the GP
5. (Using a scan from an intraoral scanner) A new retainer can be made from this stored data at any point without the doctor’s or team’s participation.
a. True
b. False
6. Parameters that effect stability are ____________ and many other occlusal parameters.
a. upright teeth in bone
b. functional occlusion with no lateral interferences on excursions
c. centric stop for each tooth
d. all of the above
7. ________, practitioners can visualize the airway in three dimensions to help aid in the decision to help improve the airway or just focus on stable teeth results.
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://orthopracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://orthopracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 370
Date Published: July 2, 2024
Expiration Date: July 2, 2027
a. With traditional film imaging methods
b. With digital imaging technology
c. With an intraoral scanner
d. With digital photography
8. Patients who present with mild sleep apnea can be treated with dental expansion, but moderate to severe diagnosis of Obstructive Sleep Apnea (OSA) are best treated with ________ to achieve the gold standard result.
a. metal braces
b. clear aligners
c. orthognathic surgical corrections
d. mouth guards
9. “Grin” or others offer a patient communication tool which dramatically reduces the number of office visits because ___________.
a. many of the questions or concerns are resolved virtually
b. patients become reluctant to call the office
c. patients are intimidated by the doctor
d. patients like automated responses
10. Utilizing 3D custom-designed aligners or braces with custom 3Dprinted bases and prescription brackets, orthodontic end results are more ________ and symmetric.
a. comprehensive
b. stable
c. well balanced
d. all of the above
To provide feedback on CE, please email us at education@medmarkmedia.com Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
Is your practice transactional or transformational?
JoAn Majors discusses the importance of creating a human connection
It is easy with today’s advancements in efficiency and technology to provide orthodontic care and become transactional, if we are not careful. It is black and white with simple strategic outcomes. Although many times transformational care can include transforming one’s appearance, at least in our industry, it begins and ends differently. Let me ask you a question — how much of this is driven by human connection?
When we strive for the best possible patient (and parent) experience, we often overlook connection and curiosity when we focus on efficiency. For instance, when your potential new patient calls and asks (and we know they do) if you take “their plan” or if you “offer Invisalign” treatment, how does your team answer this? Do they take a posture of curiosity to learn more? Likely not, unless they have been trained in a proven system to do so. Do they feel skillful (and most do) by being factual and efficient with a yes-or-no answer because they know no difference? This is transactional behavior, not transformational. Sometimes they have been instructed to do so or most often not instructed at all. I’d like permission to dive deeper on this noteworthy behavior.
When I perform a seminar or a workshop for a group, I’ll often start with an exercise involving all attendees. In my experience and decades of research from the front of the room, I know that if team members “discover” a need on their own, adoption of the content or process then increases dramatically. The soft skills communication systems I might suggest are needed in the first place, will have more validity. (It’s their idea, if you will and
JoAn Majors, RDA, CSP, CVP, a trailblazer in team training, cofounded The Soft Skills Institute, a nationally recognized AGD PACE provider, with her dentist husband. Fondly referred to as the “verbal word surgeon,” she’s a content-creation specialist turning tough or technical conversations into scalable systems that produce stronger connections with curiosity. TSSI’s robust online library contains “snackable” training videos, giving teams actionable soft skills systems following her train the trainer workshops or seminars. Her writing and platform voice are similar, showcasing her master storytelling style. Published in 25 magazines and newsletters, she’s written five books. Her latest, Permission to Be Honest – Tough Talk on Soft Skills, is available on Amazon. JoAn’s happy place is inspiring teams to action with her signature “open arms” communication. JoAn is a Certified Speaking Professional (CSP), the highest earned designation in the speaking business by the National Speakers Association and achieved by less than 12% of professional speakers worldwide and only two clinical assistants. She holds the team training faculty position (the only non-dentist) for Misch Implant Institute, is a 2022 Industry Denobi Award Winner, and serves on the Advisory Board for Dental Entrepreneur Women (DeW). She is a member of AADOM/ASCA, ADIA, DSI, NSA, NSA Austin, and other organizations. For information, reach her at JoAn@JoAnMajors.com.
not mine.) It makes the following training much improved. When I conduct this exercise, it gets people up out of their chairs and moving around watching each other’s interaction. I’m also able to see the leaders emerge as I observe.
One of the four questions I use in the beginning, asks them to describe in three words or less what makes a five-star review in a professional setting. As the program progresses, and I offer a few other participation opportunities, I allow them to review and discuss in small groups so the learning increases. Around a midday break, I have a few participants come up and read off this large sticky note sheet with the answers from the early exercise about the five-star review. They do this reading each word aloud, and the audience will say together “soft skill” or “technical” as the descriptive words are read. It has been my experience doing this exercise with four significant questions that 80%-90% of the words used are, in fact, soft skills. Remember, they are reviewing their own research. They are now ready to truly lean in and work on these areas they themselves have pointed out to be primary for great service.
In today’s connection economy, the relationship is more important than ever. In a time when so much can be done digitally and often in fewer patient visits, each encounter should be intentional and well designed for the best possible patient experience. I worked in a busy orthodontic practice early in my career, and our doctor would walk through the multi-chair facility with “lite” interaction with the adult involved. Today with busy parents and people, many of the encounters are brief at most. Remembering that there’s a person attached to those teeth is critical to growth of the business. Marketing is much more sophisticated for both adults and children. Therefore, deciding what your practice will be known for is an important part of your success.
Doctor, deciding if you are known for the fee, the plan, the location, or the experience will help you learn if you’re more transactional or transformational in your communication. This also helps you lead your team in knowing what matters most for that shopper, referral source, or others calling or coming to your office. It will also help them understand their role in helping you create the environment that supports the type of practice you want to have. This is a critical piece of your planning and shouldn’t be left to chance.
In my latest book, Permission to Be Honest, — Tough Talk on Soft Skills for Providers of Care & Their Teams, I offer many simple variations that can considerably change the outcomes of a current or no system. The simple practice of a telephone process that is based in transformational language and systems is specific and proven to onboard more new patients or shoppers than no system or one that isn’t measured. Here is an excerpt that I hope will make sense of what I am suggesting about the initial connection with your potential patients and those who are referred to as the gatekeeper in our practices.
“The gatekeeper sometimes limits a doctor’s potential success. In most cases this is not intentional, but it often occurs because, again, they don’t know what they don’t know. In some instances, they don’t know who they don’t know. Let me assure you this is not to place blame on anyone. However, it is to suggest that if you have no system in place, one is being created right now by default, period — one you have no knowledge of and no control over. Doctor, if this doesn’t cause concern for you as a new provider or a seasoned professional, it should.”
You are confident in the care and skills available to those who end up in the chair(s) in your practice. But if you are perfectly honest, do you ever wonder if your team can genuinely
convey the “value” of choosing your practice over others? It never surprises me to learn that many feel unsure about what is happening regarding those mystery callers. In other words, there is no system in place that is measured regularly to ensure that the team is connecting with curiosity and creating value for the care. Is the system that is in place there by default or intention?
Greeting or warm welcome?
In closing, I’d like to go back to the beginning. Frequently, I’ll ask a doctor if they know how their greeting and welcome for a new caller might go. Often, they look puzzled and share some version of, “Good morning, or thanks for calling, Amazing Smiles, Jessica speaking, how can I help?” What I’d like you to carry forward from this piece is simple and significant at the same time. Please read carefully. New callers make a judgment (I know it’s a strong word) about your care, based on the service first.
Most practices believe they welcome patients in their office with a greeting. Not true. Using a greeting and quickly answering the only question a caller knows to ask with yes, no, or a fee is not a warm welcome. It does not set you apart. It does set you up to be about the fee, the plan, or something besides the exceptional service. A warm welcome is intentional, believable, happens immediately following the caller’s question(s), and includes their name. It is personal! It feels and sounds quite different, and new callers know it’s great service immediately. They are engaged and connected at a completely different level because we have used their name and welcomed them before spouting fees, yes and no’s. This is transformational, not transactional.
P.S. If you’d like the paper on Greeting versus Warm Welcome, send me an email request, joan@joanmajors.com; I’m happy to help! OP
Orthodontic Practice US Webinars
LEARN about the lastest techniques and technology from industry leaders with our free live and archived educational webinars. Our online seminars are a convenient way to access great information and upskill. Check out our most recent webinars:
• Optimizing Orthodontic Treatment Workflow with Remote Monitoring and Dynamic Scheduling with host Dr. Mike Ragan
• Your Ultimate Orthodontic Workflow from Start to Finish with host Dr. Paul Trotter
• How a Digital Workflow and Remote Monitoring Made Me a “Better Version of Me” with host Dr. Joshua Adcox WATCH NOW at https://orthopracticeus.com/webinars/
Cybersecurity — a necessity, not a luxury
Thomas Terronez offers some guidance on keeping your practice data safe from cyberattacks
In today’s digital age, cybersecurity breaches are a major concern for businesses of all types and sizes — and your dental practice is no exception. The recent Change Healthcare breach was a wake-up call for the healthcare industry, proving that no organization is immune to cyberattacks. As a dental IT and cybersecurity expert with over 20 years in the trenches, I’ve seen firsthand the challenges practices face when it comes to protecting patient data. In this guide, I’ll dive deep into the specific risks targeting dental practices and share actionable strategies to strengthen your defenses.
Navigating the cybersecurity minefield
You might think your small practice is an unlikely target for hackers. Think again. Cybercriminals see dental offices as easy marks, thanks to your valuable patient data. Plus, the rise of high-tech dentistry has made practices even more reliant on IT systems, expanding your attack surface. The numbers don’t lie — cyberattacks on healthcare organizations, including dental practices, have skyrocketed in recent years. Ransomware, phishing scams, data breaches — the threats are real and growing.
Exposing your practice’s weak spots
• Weak security appliances: Outdated firewalls or bargain-basement security tools? They’re no match for today’s sophisticated cyber threats. Investing in strong perimeter defenses is non-negotiable.
So what makes dental practices so vulnerable? Here are some of the chinks in your armor:
• On-premise servers: Still relying on in-house servers? They’re a hacker’s dream if not properly secured and maintained. It’s like leaving your front door wide open.
• Elevated workstation settings: Your workstations need elevated security settings to run your practice management, EHR, and imaging software. Convenient, but risky if not configured correctly. One wrong move, and you’re exposed.
With over 20 years of experience in dental IT, Thomas Terronez is one of the nation’s renowned dental technology leaders. Thomas’ mission is to lead dental organizations through operational and scaling challenges by leveraging technology. He has a forward-thinking outlook and is solution-focused, which has led him to work with the top dental vendors on evolving and developing the technology infrastructure for the industry’s future. He is the founder and CEO of Medix Dental IT, the leading dental IT company focused on emerging and current dental organization needs. Presently, Thomas consults with dental groups, software companies, and DSOs across the country on technology strategy. Additionally, Thomas serves as an ongoing Business Scaling Mentor program at Stanford University, where he guides mentees on entrepreneurship and innovation.
• Insufficient staff training: Your team is your first line of defense — or your weakest link. Without proper cybersecurity training, they’re easy prey for social engineering attacks like phishing. And with most workstations having full server access, one slip-up can bring down the whole network.
• Small IT vendors: Local IT shops play a vital role in keeping your practice humming. But they may lack the specialized expertise to implement ironclad cybersecurity measures. Don’t confuse general IT support with the kind of in-depth security know-how you need.
Shoring up your defenses
Ready to bullet-proof your practice against cyber threats? Here’s your action plan:
• Embrace the Cloud: Making the leap to cloud-based software is a smart security move. Let the experts handle the heavy lifting while you reap the benefits of enhanced protection, from encryption to real-time monitoring. Just be sure to vet providers carefully.
• Invest in the best: When it comes to security tech, you get what you pay for. Spring for enterprise-grade firewalls from trusted names like Cisco, SonicWall, or Fortinet. Activate advanced threat protection to stay ahead of emerging dangers. Endpoint detection and response (EDR) solutions add an extra layer of defense.
• Train your team: Empower your staff to be your greatest security asset with regular cybersecurity training. From spotting phishing red flags to following data handling best practices, make security second nature for your whole team.
Cybercriminals see dental offices as easy marks, thanks to your valuable patient data.”
• Partner with pros: Join forces with an IT firm that specializes in the unique security needs of dental practices. They bring the deep expertise to tackle HIPAA compliance, data encryption, and more. You focus on patient care; they focus on keeping your data safe.
• Trust but verify: Regular security audits are like dental checkups for your network. They reveal hidden vulnerabilities and keep your defenses in fighting shape. Hire ethical hackers to really put your security through its paces.
• Back it up: Robust data backups are your lifeline in the face of threats like ransomware. Back up religiously to a secure offsite location, encrypt everything, and test your restore process regularly.
• Eyes on the prize: 24/7 security monitoring is like having a watchdog on patrol around the clock. Partner with a cybersecurity firm to keep tabs on your network, detect threats in real-time, and respond swiftly to minimize damage.
Cybersecurity is a never-ending battle, but with the right weapons in your arsenal, you can keep your practice safe and your patients’ trust intact. It takes commitment, vigilance, and ongoing effort, but it’s an investment in your practice’s future that you can’t afford to skrimp on. The cost of a breach — financial, legal, reputational — far outweighs the cost of prevention.
You’ve got enough on your plate keeping your patients smiling. Let the security experts help carry the load when it comes to locking down your data. Stay informed, stay alert, and keep putting your patients first — just don’t neglect the vital work of guarding their most sensitive information.
If you have any questions, need advice, or want to tighten up your practice’s cybersecurity game plan, I’m always ready to lend an ear and share some battle-tested wisdom. In this day and age, cybersecurity is a necessity, not a luxury. An ounce of prevention is worth a megabyte of cure. OP
DocTalk Dental
LEARN through our interactive and captivating DocTalk Dental live interview series. DocTalk Dental is your source for thought leader interviews in orthodontics. This series provides insightful and delightful conversations with top dental professionals. Each episode led by Lisa Moler, CEO and Founder of MedMark Media, takes a deep-dive into a different and intriguing area of dentistry.
• How To Leverage Your Dental Practice Real Estate
• Increasing Retention Revenue with an On-Demand Doorstep Delivery Retainer Program
• Dr. Mehdi Peikar, the Inventor of BRIUS
WATCH NOW at https://orthopracticeus.com/doctalk-dental/
The new standard of care
Dr. Ryann Christensen discusses how DentalMonitoring has transformed her practice
When I started using DentalMonitoring in my practice, I knew I had found a digital solution that could help solve many of the issues I was dealing with at Christensen Family Orthodontics in Fresno and Kingsburg, California. My busy practice was growing 19% year over year, which meant a busy, overbooked schedule. Also, I was working late nights and wanted to use office hours for ClinChecks and treatment planning.
The DentalMonitoring AI analyzes and notifies me and my team about what is happening to each patient after every scan. Using this information, I can closely observe treatment progress and keep the patient on track to complete treatment on time while often reducing in-person office visits. I have been able to leverage the clinical data from remote monitoring to create efficiency for myself and my team.
One of the immediate sources of relief from implementing DentalMonitoring has been in shifting many of the check visits and re-evaluations from in-office appointments to remote monitoring. With weekly remote monitoring, I have been able to identify the correct time to bring patients back into the office and shift some appointment intervals back.
Using
this information, I can closely observe treatment progress and keep the patient on track to complete treatment on time while often reducing in-person office visits.”
Weekly notifications from DentalMonitoring eliminate surprises in appointments and helps us to accurately prepare for every in-office appointment. This means that the CFO team can schedule precisely, knowing ahead of time if they will need to change a patient’s archwires or repair a debonded bracket instead of being surprised when the patient sits down in the practice chair. By eliminating surprises and reducing daily appointments, my team and I no longer need to stay late or work through lunch hours to catch up with the day’s work. Instead, we now have 2 hours a week dedicated to catching up with things that need to be done.
One of my goals was to find a true solution for oral hygiene compliance issues. It is disappointing to reach the end of treat-
Dr. Ryann Christensen is a highly skilled and compassionate orthodontist creating confidence-filled smiles in her hometown of Fresno, California. Dr. Christensen studied at the University of California, Los Angeles where she earned a Master of Science, a Doctorate of Dental Surgery, and a Certificate in Orthodontics. She is a proud member of the American Association of Orthodontists, American Dental Association, California Dental Association, and the FresnoMadera Dental Society.
ment and have a perfect bite and a perfect smile, but the patient has white spot lesions. When I only see patients in the office, there are only so many times I can encourage them to brush their teeth. But DentalMonitoring allows me to motivate patients to improve their oral health, without additional processes.
DentalMonitoring monitors the oral health of patients in weekly scans. When the AI observes an issue, it automatically messages the patient about the issue and encourages them to improve their brushing. The automated messaging system frees up me and my team, while still conveying the friendly tone that my patients expect when interacting with my practice.
I can open up the DentalMonitoring dashboard to see a patient changing their hygiene routine from week to week. I’m able to see evidence of the notifications working. Patients often have poor oral health scores because they aren’t used to brushing with braces, but as they receive regular reminders through the DentalMonitoring App, their oral health score improves. The exciting part is that much of this learning can now happen in between appointments, where before, the patient’s oral health wouldn’t be observed until they came to the office for a regularly scheduled appointment.
OP
This information was provided by DentalMonitoring.
BUY 100 CASES GET 80 CASES FREE (only 67¢ ea.)
+ 200 FREE MOLAR TUBES + 1 FREE CURING LIGHT!
Available in Mini & Standard Size twin bracket system
Integral Ball Hooks
Full Rotational Control Low Profile Design aesthetics + patient comfort
Vertical Scribe Line ensures precise positioning
Smooth Rounded Tie Wings + increased area for easy ligation
Compound Contour Base w/ built in torque
- Available in .018 or .022, Roth or MBT * & your choice of hooks
"I've been using the Allure Ortho Mini twin in my office for the better part of the last decade and I love it. I'm able to keep a low overhead without sacrificing quality. This is all wrapped up in Allure Ortho's exceptional customer service. You get great quality, great prices and service that is the best around. I highly recommend using this bracket."
--- Dr. David Harmon, Jr. | President of Middle Atlantic Society of Orthodontists (MASO) | Mitchellville, MD
- Highest quality German Stainless Steel
- Sharpest cutting & bending edges
- Long lasting, virtually maintenance free
- 100% corrosive resistant
BUY 8, GET 1 FREE (only $75 ea.)
- Lifetime warranty
BUY 12, GET 2 FREE (only $72 ea.) ONLY $85 ea.
T-CLASS pliers Our T-2000LS is the #1 Flush Cut on the Market!