Identification and treatment of orofacial muscle alignment to maximize teeth, palatal structure, and optimal airway development
Nicole Cavalea, MS
Tooth modification and occlusal equilibration
Dr. Gregori M. Kurtzman
Dr. Isaak Yelizar
DIGITALLY POWERED CLINICAL EXCELLENCE
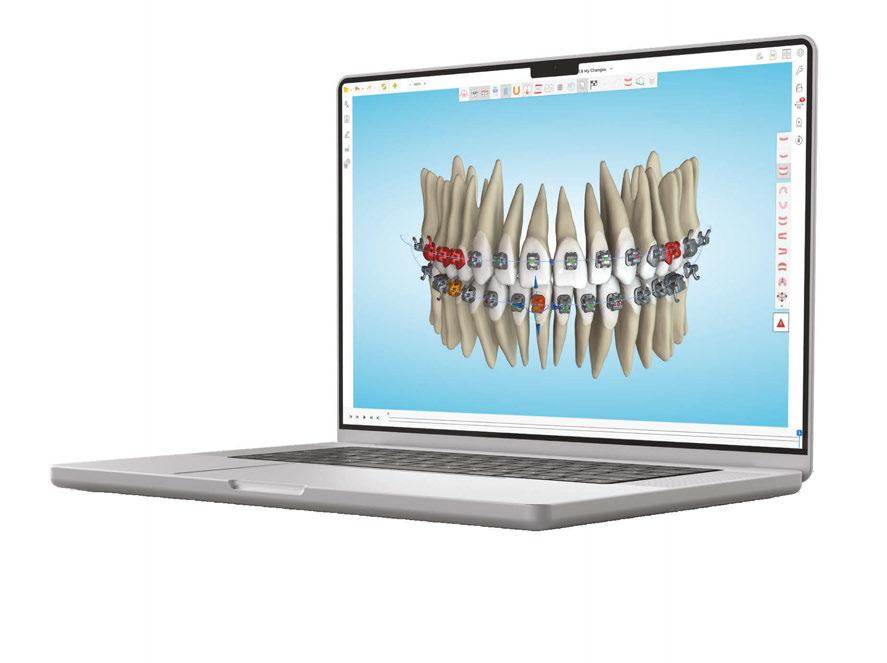
Streamline your practice efficiency with Ormco Digital Bonding, Powered by Spark Technology. Ormco Digital Bonding allows doctors to achieve customized bracket positioning by combining the best-in-class Damon Ultima™ brackets and the powerful Spark Approver Software.
EXPERIENCE ORMCO’S NEWEST INNOVATION
With Ormco Digital Bonding, we’ve leveraged our premiere orthodontic technologies to provide orthodontists with even greater flexibility and more treatment options.
One Case Submission Portal
One Easy-To-Use Software Platform
Damon Ultima™ Brackets
Explore Ormco Digital Bonding! go-orm.co/odb-orthopractice
Fall 2024 n Volume 15 Number 3
Editorial Advisors
Lisa Alvetro, DDS, MSD
Daniel Bills, DMD, MS
Robert E. Binder, DMD
S. Jay Bowman, DMD, MSD
Stanley Braun, DDS, MME, FACD
Gary P. Brigham, DDS, MSD
George J. Cisneros, DMD, MMSc
Jason B. Cope, DDS, PhD
Bradford N. Edgren, DDS, MS, FACD
Eric R. Gheewalla, DMD, BS
Dan Grauer, DDS, Morth, MS
Mark G. Hans, DDS, MSD
William (Bill) Harrell, Jr, DMD
John L. Hayes, DMD, MBA
Laurence Jerrold, DDS, JD, ABO
Marc S. Lemchen, DDS
Edward Y. Lin, DDS, MS
Thomas J. Marcel, DDS
Mark W. McDonough, DMD
Randall C. Moles, DDS, MS
Elliott M. Moskowitz, DDS, MSd, CDE
Rohit C.L. Sachdeva, BDS, M.dentSc
Gerald S. Samson, DDS
Margherita Santoro, DDS
Shalin R. Shah, DMD
Lou Shuman, DMD, CAGS
Scott A. Soderquist, DDS, MS
John Voudouris (Hon) DDS, DOrth, MScD
Neil M. Warshawsky, DDS, MS, PC
John White, DDS, MSD
Larry W. White, DDS, MSD, FACD
CE Quality Assurance Board
Bradford N. Edgren, DDS, MS, FACD
Fred Stewart Feld, DMD
Gregori M. Kurtzman, DDS, MAGD, FPFA, FACD, FADI, DICOI, DADIA
Circulation Disclosure: Total Circulation May Vary. Publisher retains the right to adjust circulation based on a number of factors including but not limited to: print and digital distribution by mail, email, and website for industry tradeshows, educational events, including nonpaid bulk copies and/or digital access provided to events, clients and educational institutions. ISSN number 2372-8396
An advanced approach to streamline complex cases
Thank you for this opportunity to share my success with a new approach to treating complex cases. As a preface, let me tell you a little about my personal journey and my philosophy for changing lives through simple and efficient orthodontic treatment.
Growing up, I had no access to proper dental care and was always self-conscious about my poorly aligned teeth. Later, as my teeth began to straighten with orthodontics, I became more outgoing and smiled more. My new smile increased my confidence and self-esteem. I went from a reserved, insecure 13-year-old to a confident young man.
This experience informed my career choice to go into dentistry. Working with patients to enhance their appearance is akin to creating art, which I had always loved, but drilling, filling, and surgery did not intrigue me. Had I gone a non-dental route, I’d have probably chosen architecture, but I fell in love with orthodontics which, like architecture, combines art and engineering. Empowering patients, boosting their confidence, and transforming their lives through radiant new smiles are the reasons my team and I go to work each day. One of the most gratifying aspects is figuring out the direct route to achieving an esthetically pleasing smile, no matter how challenging the case. My approach to orthodontics is “Less is more.” I follow Leonardo da Vinci’s maxim, “Simplicity is the ultimate sophistication.”
When I was introduced to Angel Aligner™ with their integrated angelButton™, I decided to challenge the claims of its ability to handle complex cases with minimal intervention. The cases presented in this editorial demonstrate how this appliance has revolutionized my approach to treating the wide range of complex cases we see in everyday practice and why it has become my exclusive aligner brand. With it, orthodontists now have an appliance that creates consistently predictable, beautiful finishes that can change people’s lives with simplicity and ease. I hope you see its benefits as well.
Respectfully yours,
Isaak Yelizar, DDS
Isaak Yelizar, DDS, a Board-certified orthodontist, received his dental degree from NYU College of Dentistry, where he was inducted into the Omicron Kappa Upsilon National Dental Honor Society. After a general practice residency at New York Methodist Hospital, he completed the orthodontic residency program at St. Barnabas Hospital, Bronx, New York. His practice, SimpliBraces, is located in Queens and Farmingdale, New York. Dr. Yelizar lectures nationally on technological advances in the field, inspiring clinicians to use their skills to transform patients’ lives through simple, effective orthodontic treatment.
Disclosure: Dr. Yelizar is a paid consultant for Angel Aligner.
Isaak Yelizar, DDS
Complex cases simplified with the angelButton™
Dr. Isaak Yelizar describes treatment with Angel Aligner™
CLINICAL
An OMD assessment with TMD muscle pain: a case study
Judith Dember-Paige, BSOHP, COM®, discusses how transformation sometimes takes years, but it’s worth the effort
Lisa Moler, Founder/CEO, MedMark Media............................... 6
ORTHO PERSPECTIVE
The science of stability: tooth modification and occlusal equilibration in orthodontics: a 2-part series
In part 1, Dr. Gregori M. Kurtzman discusses interproximal contouring techniques and considerations 14
CONTINUING EDUCATION
Identification and treatment of orofacial muscle alignment to maximize teeth, palatal structure, and optimal airway development Nicole Cavalea, MS, discusses the essential role of comprehensive management of oral dysfunction to restore proper function and structure........................................... 18
Cover image of Dr. Yelizar courtesy of Angel Aligner
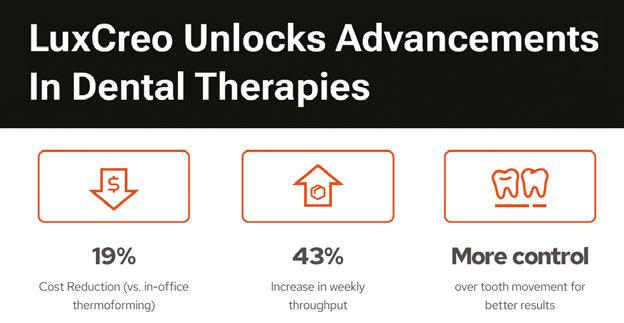
•The LuxCreo workflow makes clear aligner production more efficient, intuitive, and successful.
•Accurate, same-day clear aligners onsite.
•Reduce labor, overhead, and lead time.
LuxCreo is the first to reCeive US FDA ClASS II CleArAnCe for direCt 3d printed CLEAR ALIGNER produCtion.
“By
changing nothing, nothing changes.”
Change is hard — some days it feels like fate is not satisfied with any stable situation that makes us comfortable and secure. Sure, no one can dispute the serenity of “business as usual” in the midst of ever-changing world issues, politics, and everyday craziness. Instead of losing sleep or stomach lining over change, let’s consider the positive aspects of being open to expanding our comfort zones, living in the moment, and having a mindset of “faith over fear.” As the title quote from Tony Robbins suggests, you have to build up some momentum in order to actually get somewhere. Let’s hear from some successful and inspirational people on how change can bring positive movement to our lives.
Lisa Moler Founder/Publisher, MedMark Media
Neurologist and psychologist Viktor E. Frankl said, “When we are no longer able to change a situation, we are challenged to change ourselves.” Some people just need a bigger push to get moving. Taking the easy route and sticking with “the familiar” is only possible until the stress of the known outweighs the fear of the unknown. So, sticking with only the activities or mindsets that are within your safety zone will eventually leave you watching others who have the ambition and confidence to move forward. You don’t want to look around in a few years and see your friends and peers busy and fulfilled with new possibilities that can change your community or your world. There is a lot of competition out there, and being a pioneer or game changer may be a challenge at first, but will head off the future frustration of a stagnating life.
Actress Sarah Parish noted, “Living with fear stops us from taking risks, and if you don’t go out on the branch, you’re never going to get the best fruit.” Overcoming fear of making the wrong decision or failing can feel daunting. But, there are a lot of ways to build your confidence, such as talking to friends, mentors, experts, attending conferences, reading MedMark publications, and listening to those who bring you inspiration. There will be learning curves and maybe even some speed bumps, but most times, innovation will lead to new and exciting ways to grow.
Our fall issue is filled with innovation and information to create productive change. In our Cover Story, Dr. Isaak Yelizar talks about being an early adopter of Angel Aligner, which he describes as a game-changer and “an effective new approach to treating a wide range of case types.” In his CE, Dr. Steven Olmos delves into pediatric obstructive sleep apnea, its causes, symptoms, and potential treatments. In her CE, Nicole Cavalea explores how myofunctional disorders, tongue posture, mouth breathing, and tongue tie can impact patients’ overall health, and how a multidisciplinary approach to treatment can improve orofacial development. In his Orthodontic Perspective, Dr. Gregori Kurtzman starts his 2-part series on tooth modification and occlusal equilibration by addressing crowding, diastema, and other dental irregularities using interproximal recontouring products from SS White.
World famous performer Robin Williams said, “No matter what people tell you, words and ideas can change the world.” Don’t leave your success to chance. Change your ideas into action. Innovation will create a happier you, family, and work life. When you embrace change, the benefits will spread throughout your world!
To your best success,
Lisa Moler
Published by
Publisher Lisa Moler lmoler@medmarkmedia.com
Managing Editor Mali Schantz-Feld, MA, CDE mali@medmarkmedia.com Tel: (727) 515-5118
National Account Manager Adrienne Good agood@medmarkmedia.com Tel: (623) 340-4373
Social Media Manager Felicia Vaughn felicia@medmarkmedia.com
Digital Marketing & Sales Administrator Sharif Rod sharif@medmarkmedia.com
Website Support Eileen Kane webmaster@medmarkmedia.com
MedMark, LLC 15720 N. Greenway-Hayden Loop #9 Scottsdale, AZ 85260 Tel: (480) 621-8955
Toll-free: (866) 579-9496 www.medmarkmedia.com
www.orthopracticeus.com
Subscription Rate 1 year (4 issues) $149 https://orthopracticeus.com/subscribe/
MY BEST ORTHODONTIC EXPERIENCE.
Complex cases simplified with the angelButton™
Dr. Isaak Yelizar describes treatment with Angel Aligner™
Like many of you, my first experience employing aligners was with the leading brand. Since then, I’ve had considerable involvement with various aligner systems and am always open to exploring new options, driven by Leonardo da Vinci’s maxim, “Simplicity is the ultimate sophistication.”
As an early adopter, any new offering I consider must demonstrate a distinct advantage over current techniques to simplify the complex case management issues we encounter in daily practice. When I was introduced to Angel Aligner, it was explicitly the angelButton that intrigued me.
Angel Aligner with integrated angelButtons have transformed my approach to demanding cases. The angelButtons can be positioned on four to eight points on any tooth (Figure 1). With traditional hooks and bonded buttons, multidirectional movement is limited, and force is concentrated on the specific tooth to which the elastic is engaged.
The flexibility in positioning angelButtons creates an entirely new force dynamic for controlling the direction of tooth movement. Moreover, elastics can be attached to apply force to a single tooth, a quadrant, or an entire arch. Distributed anchorage is a significant advantage in treating any number of case types. It is particularly important in treating excessive gingival display through full-arch impaction.
With angelButtons, there is little need to bond buttons except perhaps when a specific tooth needs to be extruded or rotated. This precludes distortion that can occur with cutouts. Unlike hooks or bonded buttons, angelButtons maintain their original positions and shape and resist deformation and fracture. Compared with other aligners which are flexible and prone to deflection, Angel Aligner’s are constructed of three layers of a high-polymer material of a specific chemistry that resists deflec-
tion yet has an adaptability that hugs the teeth to move them efficiently to their planned positions.
The company has 20+ years of global experience with more than one million cases treated. Patient response to Angel Aligner has been overwhelmingly positive. Most comment about how clear and comfortable the aligners fit, even with elastics, and how quickly they see their smiles change.
The iOrtho™ treatment planning software offers all the benefits I’ve come to expect from a sophisticated treatment planning system. For those doctors with CBCT, the software accurately produces the 3D morphology of patients’ roots and alveolar bone (Figure 2). For traditional radiographic examinations, the system uses AI to create tracings and superimpositions to achieve the best possible tools to support diagnoses and treatment plans.
Many additional Angel Aligner features have proven effective in my practice, including traditional and precision attachments,
Figure 1: The integrated angelButton of Angel Aligner can be positioned on four to eight points on any tooth for 360° traction
Figure 2: iOrtho Software
Dr. Yelizar discusses how easily Angel Aligner will give this patient the smile she dreams about
pressure ridges, virtual roots, and a choice of trim lines. While virtual roots do not offer an identical bone-to-root relationship, they are an indispensable aid in determining the initial direction of tooth movement.
As for trim lines, we can choose between scalloped, high, or hybrid, which is a distinct advantage over other aligner systems. High trim lines are best suited in the posterior during distalization and intrusion. They also accommodate patients with short clinical crowns and those who prefer fewer attachments. Angel Aligner’s technicians are highly trained specialists so skilled that it usually takes only one or two revisions to approve my case setups.
As people worldwide seek to improve their appearance, a broad, attractive smile is often their priority. While orthodontic treatment can significantly improve one’s smile over a wide range of malocclusions, issues such as excessive gingival display usually necessitate orthognathic surgery with an involved orthodontic setup. Treatment using fixed appliances or aligners with TADs can preclude surgery but has historically required additional, intricate mechanics and considerable doctor involvement. With the advent of Angel Aligner, orthodontists now have an appliance that eliminates surgery for treatment of excessive gingival display, offering a simple orthodontic solution instead.
My experience with Angel Aligner began post-2023 AAO, so no complex cases are yet complete. Still, two such cases, including a gummy smile case, are close to finishing and showcase the benefits of this sophisticated aligner system.
Case 1
Patient A.M., age 28, presented with excessive gingival display she wished to correct (Figure 3). She lives in Boston and was willing to travel 3 hours each way to our practice in Queens,
New York. Multiple orthodontists near her home had prescribed surgical intervention for her case, but she had seen a gummy smile patient of mine treated nonsurgically and was excited about the prospects for herself (Instagram @NYCorthodontist).
Diagnosis
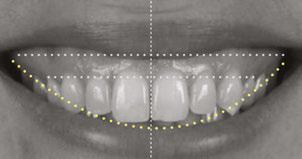
Mesocephalic in CL 1 occlusion with slight constriction in the posterior areas. The patient’s facial and cephalometric analysis appeared normal, and her facial thirds were well balanced. Looking closely at the Digital Smile Design Analysis (Figure 3), we can appreciate the excessive gingival display, ranging between 4 mm-6 mm in the posterior and 3 mm-4 mm in the anterior.
Treatment plan
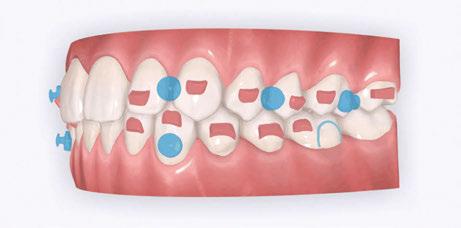
Maintain CL I occlusion. Develop the transverse relationships, eliminate the posterior negative root torques, and resolve the excessive gingival display via full-arch nonsurgical impaction. All vertical changes would be accomplished using only Angel Aligner, TADs, and elastics. Her maxillary lateral incisors may later require buildups to improve the Golden Proportion of the anterior teeth. My iOrtho software setup for maxillary intrusion was to place angelButtons (blue) between the U2s-3s, U4s-5s, and distal of the U6s (Figure 4).
My TAD placement protocol involved placing four TADs in the maxilla: two interradicular in the anterior and two infrazygomatic (IZC) in the posterior. The 2 mm x 12 mm IZC TADs were placed extra alveolar, so there was minimal risk for root impingement (Figure 5). Anteriorly, the 1.4 mm x 6 mm interradicular TADs were placed between the roots of the U2-3s, so greater care was required.
The biomechanics of impaction
Figure 6 demonstrates the typical iatrogenic side effects of full-arch maxillary impaction with TADs and elastics. Forces
Figure 3: Initial records with Digital Smile Design Analysis
Figure 4: My iOrtho virtual setup for Case 1. Note: This case was planned before virtual roots were available
Figure 5: Placement of IZC TADs in Case 1
Figure 6: The biomechanics of Intrusion: The iatrogenic labial crown torquing effect of maxillary intrusion
and moments are the key players in tooth movement. Forces are always “visible,” but moments must continually be “envisioned.” Elastics pull from TADs to bonded buttons creates both vertical and horizontal forces, which can lead to iatrogenic moments that cause labial crown torquing.
To manage this phenomenon, practitioners must employ additional mechanics. Some might choose to bond segmented wires occlusally and lingually; others might place additional TADs positioned labially and lingually for sling elastics worn over the occlusal surfaces. Since this was my first Angel Aligner gummy smile case, I designed and had fabricated a customized TAD-anchored palatal appliance to counter any unwanted crown torquing. Thankfully, this appliance did not need to be employed because of the integrated angelButtons and the inherent deflection-resistant properties of Angel Aligner.
Treatment progress
Doctor time in such cases is minimal: designing the setup and bonding the attachments. Other techniques to achieve full maxillary arch intrusion usually require monthly visits to reactivate the power chain to the TADs. Angel Aligner allowed us to send the patient home with all the aligners and elastics needed to manage the treatment herself. The patient would be seen every 8 weeks for close observation. With virtual monitoring, we would likely see such patients every 12 to 16 weeks.
Case progression (Figure 7)
Even at 4 months, treatment was already changing this young woman’s life. With exemplary patient compliance, there was a marked change in her smile architecture. Arch development had begun, and the buccal corridors were starting to fill in. At 10 months, the vertical changes in the posterior continue without any significant labial crown torquing of the posterior segments.
Case discussion
My question at the start of treatment was whether this demanding case could be treated only with Angel Aligner and TADs or if additional mechanics would be needed to preclude unwanted posterior labial crown torquing. Angel Aligner alone proved sufficient to deflect nearly all unwanted torquing.
Such transformative results not only change people’s lives but also inspire my continued passion for this profession. Angel Aligner and TADs give orthodontists an incredibly valuable
approach for treating patients with excessive gingival display and other complex issues. I hope this patient’s treatment motivates readers to see for themselves how these advanced techniques can achieve similar results for their patients, simply and effectively.
Case 2
Patient S.T., age 32, presented in the hope of creating a radiant smile and a functional bite. She had been dealing with dental problems all her life. Her X-rays exhibited multiple direct restorations as well as endodontic treatment. Due to the loss of her molars, her teeth had shifted considerably over the years. Her dentist recommended she see us to create a pleasing smile and to rehabilitate her occlusion for future prosthetic treatment (Figure 8).
Diagnosis
The patient’s occlusion was super CL I on the left and CL II on the right. Both arches showed slight constriction with lower anterior crowding. Her smile arc was canted, and both midlines were shifted in opposite directions. On cephalometric
Figure 7: Case 1 progress to date — 4 months (left) and 10 months (right)
Figure 8: Case 2 initial records
development, arch coordination, and mandibular labial crown torque control. Note how well her tissue responded to the slow, gradual changes with no gingival recession. This is simplicity.
Case discussion
analysis, her ANB was 5.84, and IMPA was 102.64, both representative of skeletal Class II with incisor proclination. There were two long-standing extraction sites into which the UR6 and UL6 (partial) had supraerupted. Her thin gingival mucosa posed a challenge in keeping the roots in the bone, so treatment had to be planned correctly and executed gradually to maintain her gingival architecture.
Treatment plan
Use Angel Aligner to sequentially distalize the UR and LL quadrants, correcting the AP relationship and obtaining midline coincidence (Figure 9). Intrude the supraerupted U6s to prepare the extraction sites below for implants. To preclude root resorption and fenestrations, careful attention would be paid to tooth movement velocity and the sequencing of those movements.
In the past, I would have used fixed appliances and TADs to treat this patient. I considered adding a TAD in the IZC area to intrude the supraerupted UR6, but I wanted to see what Angel Aligner alone could achieve.
Case progression
At 4 months, the maxillary right side had distalized with appreciable space created between the canine and first premolar (Figure 10). At 9 months, this patient has a wide, attractive smile emerging (Figure 11). We can also appreciate the transverse
This patient’s multiple dental and occlusal issues were resolved solely with Angel Aligner. Both U6s were intruded without needing TAD support or additional mechanics to preclude labial crown torquing. Angel Aligner proved more than adequate in displacing the UR6 vertically while simultaneously distalizing it into Class I (Figure 11). To be able to intrude and distalize simultaneously with no need for TAD-supported anchorage speaks to the exceptional capability of this appliance.
Many dental colleagues in my area would likely have either extracted the UR6 or performed a coronal hemisection in the hope of creating enough interocclusal space for the LR6 implant placement and restoration. Sharing this case with referring dental colleagues will demonstrate how orthodontics can create adequate space for implant sites while performing minimally invasive dentistry.
Conclusion
Angel Aligner with integrated angelButtons have given me an effective new approach to treating a wide range of case types. It is a game changer for simplifying complex cases, and I now consider it essential to my practice as my exclusive brand of aligners. I always prefer a simple treatment plan. Less is more. Angel Aligner supports my philosophy of creating consistently predictable, beautiful finishes that change people’s lives. I look forward to exploring all the benefits this remarkable appliance will continue to bring to my practice and my patients.
Figure 9: My iOrtho Case 2 setup demonstrates the plan to resolve her multiple dental issues and the distalization in each arch to free space for dental implants
Figure 10: My iOrtho Case 2 plan versus progress at 4 months
Figure 11: Case 2 at 9 Months — Progress to date
An OMD assessment with TMD muscle pain: a case study
Judith Dember-Paige, BSOHP, COM®, discusses how transformation sometimes takes years, but it’s worth the effort
Stan was referred to my office by a TMD specialist. His chief complaints were he could not chew or open his mouth without pain. It seemed the less he chewed, the more pain he experienced. As a result, an Orofacial Myofunctional Therapy (OMT) program was created to help support his muscles of the TMJ and craniofacial respiratory complex. He used his splint as instructed by his specialist. However, his anterior open bite widened, and his teeth became more misaligned over time.
TMD and orofacial muscle pain is a problem that can start small and grow in magnitude and dysfunction. Sometimes the pain may be associated with Orofacial Myofunctional Disorders (OMDs). Therapy may be needed to address the muscle pain that accompanies the dysfunction
Stan was a 28-year-old male in a lot of pain. He had just come from his TMJ specialist where he received an oral orthotic splint to relieve his discomfort. He told me it all started after a long dental appointment where he received a root canal and a new crown on the upper right. After this procedure, his jaws felt tight so he gave it a good stretch by opening very wide. He heard a rip and a crunch. Opening his mouth was never the same after that. He presented with a set of symptoms: TMD muscle pain, he could no longer chew his food without pain (food had to be the soft consistency of tofu), daytime clenching and night time grinding of
Judith Dember-Paige is a certified orofacial myologist, with 15 years in practice. Although retired from dental hygiene, she practiced for 35 years, and her license is current. Based in Westchester, New York, Judith now has a thriving practice specializing in both children and adults with orofacial myofunctional disorders. Beyond clinical practice, she is a respected lecturer/ writer among dental professionals and parent groups. She is an avid saltwater fisherwoman and loves camping. Her site is www.oromyologist.com.
his teeth. In addition, he had daily headaches and ear ringing. He could not open his mouth very wide without experiencing sharp pain. He took acetaminophen for his discomfort and zolpidem nightly to help him fall asleep easier.
Upon closer examination, there were contributing factors that led to his discomfort. Stan had been a stomach/face sleeper for years. He also bit his nails since childhood, had a smoking habit from his youth, and he was prone to ear infections. He had moderate tongue and buccal ties, obligate mouth breathing, aggravated by a deviated septum, narrow nares, low tongue resting posture, an anterior open bite, a lower jaw that deviated upon opening, and bouts of acid reflux.
An orofacial therapy program was created to allow his tongue to give better support and function to his oral structures, especially the TMJ joint. When the tongue rests in the palate, it removes the unwanted pressure off of the TMJ. As part of the course of his therapy, focus was made to reeducate his breathing to make his nose the primary way he breathes. Optimal breathing rate for an adult is slower than for a child. Good nasal breath-
ing during the day supports good nasal breathing during the night for optimal sleep.
When the tongue rests in the palate, it impacts facial development especially for children who are still growing. An adult, for example, like our friend Stan, the progress made is gradual but more likely to last a lifetime. Generally, therapy starts out once a week for about 2-3 months. Then therapy progresses to every other week for 2-3 months, and then changes to once a month for about 5 months for the rest of the year. The exercises are done a minimum of 2 times everyday. These exercises are designed to strengthen and tone the orofacial muscles, building brand new neuromuscular function. When the muscles of the face are well developed, it may favorably impact appearance and the overall integrity of the facial structures. The muscles of the face also include the tongue, lips, cheeks and neck. Although the therapy program is typically only a year, Stan really liked how good he felt and decided to continue with some of the exercises to this day. From the photos you can see how much the program has impacted his health and well-being.
During his therapy, there was a discussion about the possible benefits he may receive from having his jaws expanded, making more room for his tongue, then to be followed by a tongue and buccal frenums release. His intermolar width is 34 mm, and his intercanine width is 25 mm. I feel any expansion has a potential benefit.
After completing his course of myofunctional therapy, he was able to open his jaws with full range of motion and achieve his goal of being able to enjoy some of his favorite foods again. He was most excited about being able to bite into a juicy cheeseburger.
Stan has a very narrow external nasal valve and receives some benefit from using dilator nasal strips. There are a few more products on the market that may help make nasal breathing easier for him.
To document any initial assessment, the midpoint of therapy, and when therapy has ended, it is important to take detailed photos, videos, plus full measurements of the face and teeth. This makes it possible to compare results while showing that your therapy works based on the evidence you gathered before, during, and after treatment.
In conclusion, Stan was very proud of how hard he worked during his myofunctional therapy and urged me to share his exceptional results. OP
Figure 5
Figure 6: No room for his tongue
Figure 4: 7 years later on April 10, 2024. Anterior open bite closed a bit
Figure 2: Initial assessment on December 15, 2016 (top left). Later September 20, 2017, his anterior openbite widened (top right)
Figure 3: Milled orthotic splint
The science of stability: tooth modification and occlusal equilibration in orthodontics: a 2-part series
In part 1, Dr. Gregori M. Kurtzman discusses interproximal contouring techniques and considerations
Interproximal recontouring is a crucial component of orthodontic treatment that involves the careful reshaping of tooth surfaces where they touch. This procedure is essential for creating space for teeth movement, improving alignment, and enhancing overall smile esthetics.
Techniques for interproximal recontouring
Several techniques can be employed for interproximal recontouring, each suited to different clinical situations.
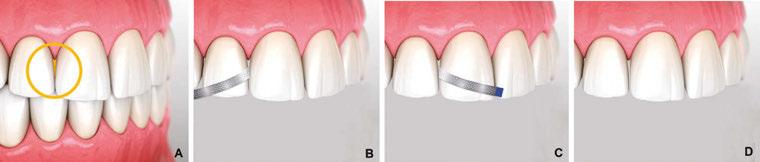
Diamond-coated disks
For cases where there is no overlapping of adjacent teeth, diamond-coated disks (Superflex, SS White, Lakewood, New Jersey) can be effectively used. These disks, available in single and double-sided options (Figure 5), are mounted on a slow-speed straight nose handpiece. To prevent accidental soft tissue injury, the use of a lip retractor is recommended. Due to the potential for soft tissue damage, the use of diamond-coated disks is primarily restricted to the anterior region (maxillary and mandibular).
When using a single-sided disk, the proximal surface of one tooth is modified first (Figure 6B), followed by the adjacent tooth after repositioning the handpiece 180 degrees (Figure 6C). For optimal results, the disk should be aligned parallel to the desired midline or vertical axis.
Diamond finishing strips
In cases involving crowding or the need for significant contact opening in posterior teeth, diamond finishing strips (Jazz Pro, SS White) are the preferred choice. These strips, available
Gregori M. Kurtzman, DDS, MAGD, FPFA, FACD, FIADFE, DICOI, DADIA, DIDIA, is in private general dental practice in Silver Spring, Maryland. He is a former Assistant Clinical Professor at University of Maryland in the department of Restorative Dentistry and Endodontics and a former AAID Implant Maxi-Course assistant program director at Howard University College of Dentistry. He has lectured internationally on the topics of restorative dentistry, endodontics and implant surgery, removable and fixed prosthetics, and periodontics. He has over 870 published articles, as well as several ebooks and textbook chapters. He can be reached at dr_kurtzman@ maryland-implants.com.
Figure 1
Figure 2
Figure 5
Figure 3 (left) and Figure 4 (right)
Final cleaning and polishing of teeth for a dazzling smile.
Debonding:
Removal of aligner buttons, brackets and wires (applicable to traditional braces).
SS White Dental understands the intricate relationship between orthodontics and restorative dentistry
Our precision orthodontic instruments are designed to complement your restorative treatments, ensuring optimal patient outcomes. Whether you're an orthodontist refining a complex bite or a restorative dentist preparing for aligner therapy, our tools provide the foundation for a seamless patient journey. Experience the difference of a truly collaborative approach to oral healthcare.
in coarse, medium, and fine grits (Figure 7), come in 4 mm and 2.5 mm widths to accommodate various clinical scenarios. The non-diamond coated center section of the strip allows for easy placement in tight contact areas.
To open a contact, the diamond abrasive surface of the strip is positioned at the tooth’s contact point. In posterior teeth, the strip is maintained parallel to the mesial or distal surface and gently pulled buccally and lingually to create a flat proximal surface. The strip is then reversed to modify the opposing proximal surface. To prevent food traps and facilitate subsequent orthodontic treatment, it is essential to avoid excessive reduction of the proximal contact area.
In the anterior region, where recontouring is aimed at correcting tooth width at the contact area, the strip is curved to follow the buccal-lingual curvature of the tooth (Figure 8B). The process is repeated on the adjacent tooth (Figure 8C).
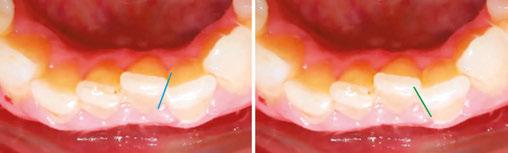
When dealing with severe crowding, especially in the mandibular anterior, it is crucial to orient the strip to match the tooth’s proximal orientation being modified (Figure 9). This ensures a natural appearance following orthodontic treatment.
Bur and high-speed handpiece
In cases of extreme crowding, initial tooth reduction may be necessary using a bur in a high-speed handpiece before employing diamond strips. Fine-pointed diamonds and carbides are suitable for this purpose (Figures 10 and 11). This technique helps restore natural curvature and prevents the creation of an undesirable flat proximal surface. A flat proximal surface can create an illusion of continuous teeth, while a curved surface imparts a more natural appearance.
Conclusion
Interproximal recontouring is a valuable adjunct to orthodontic treatment that significantly contributes to achieving optimal esthetic outcomes. By carefully selecting and applying appropriate techniques, clinicians can effectively address crowding, diastema, and other dental irregularities, resulting in improved tooth alignment, spacing, and overall facial harmony.
Acknowledgement: The author would like to thank Robert Wojciechowski for his assistance with creation of the illustrations in the article. This article was provided by SS White.
Figure 11
Figure 7
Figures 8A-8D
Figure 9
Figure 10
Figures 6A-6D
Identification and treatment of orofacial muscle alignment to maximize teeth, palatal structure, and optimal airway development
Nicole Cavalea, MS, discusses the essential role of comprehensive management of oral dysfunction to restore proper function and structure
Dentists, orthodontists, physicians, and otolaryngologists are often on the front line of identification of postural alterations such as tongue tie, low tongue tone, high narrow palatal structure, tonsil hypotrophy, dental wear, nasal patency, and open-mouth breathing patterns. The connection of orofacial muscle patterns and their impact on teeth, palatal structure, and optimal airway development has become increasingly important as research provides us with more information. Improper oral resting posture of the tongue and open mouth breathing patterns are known to contribute to narrowing of the dental and palatal arch, dysfunction of the temporomandibular joint, malocclusion, enlarged tonsils and adenoids, ultimately, negatively influencing the anatomy of the upper airway and contributing to sleep-disordered breathing.1
A short lingual frenulum (ankyloglossia) is a known factor in restricting tongue mobility and leads to abnormal development of the oral cavity, with clear impact on maxillary and mandibular growth. Morphological changes occur slowly during childhood, leading to a small upper airway that causes collapse of the upper airway during sleep and to the development of obstructive sleep apnea (OSA) later. Recognition and treatment early in life could avoid occurrence of the syndrome and its co-morbidities.2
Nicole Cavalea, MS, is the founder of Strategies for Success, a speech-language pathology practice and myofunctional therapy clinic in Los Gatos, California. She received her MS degree in Speech and Language Pathology from San Jose State University and has worked in the field of communication disorders for 20 years. Cavalea has extensive expertise working with children of all ages in the assessment, treatment, and management of speech and language disorders and myofunctional disorders.
After incorporating myofunctional techniques into her practice, she began noticing her clients improving with quicker and more precise results, leading her to further her training in myofunctional disorders and treatment, and attending multiple intensive training courses from the Academy of Orofacial Myofunctional Therapy. Her studies include an advanced course on breathing re-education, focusing on restoring adequate breathing in sleep apnea patients. Recently, Cavalea received her ambassador certificate after completing an extensive training course through The Breathe Institute, Sleep & Breathing and Tongue Tie Tone and Space. Cavalea has expanded her practice nationwide through telepractice and values and enjoys collaboration and co-treatment with multi-disciplinary teams across the country.
Educational aims and objectives
This self-instructional course for dentists aims to educate readers on the impact of tongue posture, mouth breathing, tongue tie, and myofunctional disorders on overall health, palatal structure, and airway development.
Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions by taking the quiz online at orthopracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can: Identify clinical signs of mouth breathing, tongue tie or low tone, dental wear, and narrow maxilla as risk factors for sleep disordered breathing (SDB).
• Realize how certain orofacial muscle patterns impact teeth, palatal structure, and optimal airway development.
• Realize effective current treatment protocols to address root-cause.
• Suggest treatment recommendations based on root-cause, as a multidisciplinary approach to improve orofacial development.
Other symptoms and long-term effects of improper orofacial muscle patterns due to tongue and lip tie include head, neck, and back tension and pain, TMJ pain, bruxism, speech impediments, and swallow and feeding dysfunction.
Recent studies explore the safety and efficacy of lingual frenuloplasty and myofunctional therapy for the treatment of ankyloglossia. Findings reveal that after tongue-tie releases paired with exercises to restore proper function of the tongue, most children experienced functional improvements in speech, feeding, and sleep. Overall, speech improved in 89%, solid feeding improved 83%, and sleep improved in 83% of patients.6
A study by Zaghi, et al., concluded that lingual frenuloplasty with myofunctional therapy is a safe and effective treatment for mouth breathing, snoring, clenching, and myofascial tension. In this study, there was an 87% improvement in quality of life through amelioration of mouth breathing (74.8%), snoring
Restricted mobility of the tongue may lead to dysfunctional compensations that may negatively affect nasal breathing and snoring due to low tongue posture.
OSA has become increasingly recognized as a notable heath concern in children given its impact on behavior, function, and quality of life. Statistically, 40% of children who suffer from SDB develop ADD, ADHD, and/or a learning disability. Additionally, if a child is diagnosed with SDB in the first 5 years of life and is left untreated, he/she is 60% more likely to require special needs education by age 8.
Children with sleep SDB were found to have lower tongue strength than healthy children (without SDB). Children with SDB exhibit tongue thrusting and abnormal swallow patterns (caused by nasal obstruction and a persistent mouth breathing posture), which may contribute to anterior open-bite clinical presentation.
Myofunctional therapy may be used as an effective treatment to integrate medical and surgical treatments for OSA and help to restore a normal resting posture of the tongue, appropriate oral, lingual, and facial muscle patterns, nasal breathing, normal lip posture, and a correct swallowing pattern.3
Traditionally, mouth breathing and airway obstruction have been considered a function of soft tissue hypertrophy (tonsil, adenoid, turbinate structures) because of an inflammatory cascade that secondarily obstructs the airway, indicating a progression from mouth breathing to obstructive sleep apnea and the implication on facial structure. This has led to medical or surgical treatment of adenotonsillar and/or inferior turbinate hypertrophy as a first-line approach in the standard of care for pediatric SDB.8
Palatal expansion (RPE) demonstrates considerable improvement related to adenoid or tonsil hypertrophy, maxillary or mandibular deficiency, and orthodontic or craniofacial abnormalities.
According to research by Yoon, et al., RPE treatment can be considered as a valid and effective treatment option for pediatric OSA population with narrow high arch palate and adenotonsillar hypertrophy. According to this present study, compared to the control group, the expansion group experienced a statistically significant decrease in both adenoid and tonsil volume. For the expansion group, 90.0% and 97.5% of patients experienced significant reduction in adenoid and tonsil volume.4
In another study RPE treatment had a positive effect on children affected by chronic snoring and OSA, causing an increase in volume of the nasal cavity and nasopharynx, with expansion of the nasal osseous width and maxillary width. Enlarged maxillary width showed a direct correlation to increased airway volume, bringing functional improvement. The results show that the RME therapy can restore and improve a normal nasal airflow with disappearance of obstructive sleep breathing disorder.5
According to Zaghi, et al., current literature data indicate that this surgical approach is not often completely successful. This has encouraged a potential paradigm shift in the hypothesized progression of SDB in children. Guilleminault, et al., purport that orofacial dysfunction underlies structural dysmorphisms that lead to the onset of pediatric SDB.9,10 The Guilleminault musculoskeletal hypothesis purports that oral, nasal, maxillary, and mandibular structural variations, systematic inflammation, and/or postural maladaptation are often one of the inciting factors that predispose children to mouth-breathing.9 Concurrently, postural maladaptation (due to fascial, muscular, neurological, or craniosacral restrictions) may lead to functional variations that impact breathing, swallowing, and resting oral posture. The functional variations predispose to low tongue posture and dysfunctional chewing and swallowing patterns that lead to abnormal orofacial growth.8
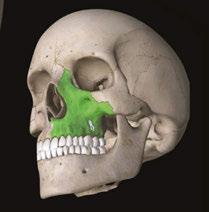
Figure 1: The. orofacial anatomy and its connection to airway development
Figure 2: Open-mouth breathing and snoring
Figure 3: Sleep-disordered breathing
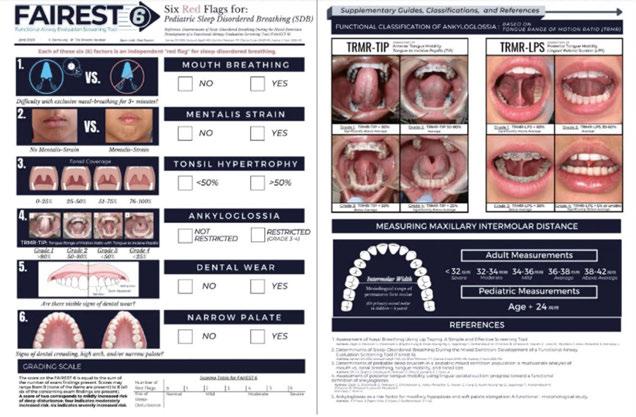
Figure 4: The Functional Airway Evaluation Screening Tool (FAIREST-6) is available at https://www.fairest.org/tools/ thanks to Dr. Soroush Zaghi and his colleagues
The Functional Airway Evaluation Screening Tool (FAIREST-6), developed by Zaghi, et al., has been determined to be concise and validated based on the current study results. These results state that because of the high incidence and burden of the consequences of untreated pediatric SDB, a team approach that recruits attention from multiple disciplines can optimize the likelihood of timely recognition and early intervention for children with SDB.8
There are several clinical findings that may be identified as pre-disposing factors to SDB in early childhood by pediatric dentists, orthodontist, ENTs, pediatricians, school nurses, and sleeplanguage pathologists (SLPs). These functional findings include swallowing/tongue thrust compensations, habitual mouth breathing when awake or asleep (screened by a functional breathing test, unable to breathe through the nose longer that 3 minutes), extraoral (the presence of mentalis strain), intraoral soft tissue (tonsil size-greater than 50-percent obstruction), restricted tongue mobility, intraoral hard tissue-dental wear, and narrow palate. Recent studies on the impact of tongue mobility on the mechanics of resting oral posture and swallow function suggest that such oral dysfunction may by a primary determination of malocclusion.8
Proper identification and assessment are the first step in optimal care and treatment of orofacial dysfunction and its impact on overall health, orofacial structure, sleep and airway development, speech development, swallow and feeding development.
Once identified, comprehensive management of the cycle of oral dysfunction to restore proper function and structure is essential. Some examples of structural restorations may include lingual or labial frenuloplasty (to allow for correct tongue and/or lip posture, and to correct open mouth breathing patterns), palatal expansion (to allow for improved volume of the nasopharynx cavity and airway), and surgical treatment of adenotonsillar or turbinate hypertrophy (to improve airway obstruction).
Functional treatment through orofacial myofunctional therapy is critical and intended to restore oral resting posture of the tongue and open-mouth breathing patterns to optimize the development of the dental and palatal arch, reduce malocclusions,
Figure 5: Tongue tie
optimize airway space to include reduction of the adenoids and tonsils, maximize temporomandibular joint function, establish correct feeding and swallowing patterns, and ultimately, influence the anatomy of the upper airway.
In conclusion, research indicates that the goal of optimal airway health requires comprehensive management of orofacial muscle patterns and their impact on postural alterations (tongue tie, low tongue tone, high narrow palatal structure, tonsil hypotrophy, dental wear, nasal patency, and open-mouth breathing patterns) and require identification and an integrated effort of the dentist, orthodontist, physician, otolaryngologist and myofunctional therapist.
REFERENCES
1. Yoon AJ, Zaghi S, Ha S, Law CS, Guilleminault C, Liu SY. Ankyloglossia as a risk factor for maxillary hypoplasia and soft palate elongation: A functional - morphological study. Orthod Craniofac Res. 2017 Nov;20(4):237-244.
2. Chien Y, Guilleminault C. 0442 Adult Short Lingual Frenulum And Obstructive Sleep Apnea; Sleep. April 2017;40(issue suppl 1):A164-A165.
3. Villa MP, Evangelisti M, Martella S, Barreto M, Del Pozzo M. Can myofunctional therapy increase tongue tone and reduce symptoms in children with sleep-disordered breathing? Sleep Breath. 2017 Dec;21(4):1025-1032.
4. Yoon A, Abdelwahab M, Bockow R, Vakili A, Lovell K, Chang I, Ganguly R, Liu SY, Kushida C, Hong C. Impact of rapid palatal expansion on the size of adenoids and tonsils in children. Sleep Med. 2022 Apr;92:96-102.
5. Pirelli P, Fiaschetti V, Fanucci E, Giancotti A, Condo’ R, Saccomanno S, Mampieri G. Cone beam CT evaluation of skeletal and nasomaxillary complex volume changes after rapid maxillary expansion in OSA children. Sleep Med. 2021 Oct;86:81-89.
6. Baxter R, Merkel-Walsh R, Baxter BS, Lashley A, Rendell NR. Functional Improvements of Speech, Feeding, and Sleep After Lingual Frenectomy Tongue-Tie Release: A Prospective Cohort Study. Clin Pediatr (Phila). 2020 Sep;59(9-10):885-892.
7. Zaghi S, Valcu-Pinkerton S, Jabara M, Norouz-Knutsen L, Govardhan C, Moeller J, Sinkus V, Thorsen RS, Downing V, Camacho M, Yoon A, Hang WM, Hockel B, Guilleminault C, Liu SY. Lingual frenuloplasty with myofunctional therapy: Exploring safety and efficacy in 348 cases. Laryngoscope Investig Otolaryngol. 2019 Aug 26;4(5):489-496.
8. Oh JS, Zaghi S, Peterson C, Law CS, Silva D, Yoon AJ. Determinants of Sleep-Disordered Breathing During the Mixed Dentition: Development of a Functional Airway Evaluation Screening Tool (FAIREST-6). Pediatr Dent. 2021 Jul 15;43(4):262-272.
9. Stupak HD, Park SY. Gravitational forces, negative pressure and facial structure in the genesis of airway dysfunction during sleep: a review of the paradigm. Sleep Med. 2018 Nov;51:125-132.
10. Guilleminault C, Huang YS. From oral facial dysfunction to dysmorphism and the onset of pediatric OSA. Sleep Med Rev. 2018 Aug;40:203-214.
Continuing Education Quiz
Identification and treatment of orofacial muscle alignment to maximize teeth, palatal structure, and optimal airway development CAVALEA
1. Improper oral resting posture of the tongue and open mouth breathing patterns are known to contribute to ________ and enlarged tonsils and adenoids, ultimately, negatively influencing the anatomy of the upper airway and contributing to sleep-disordered breathing.
a. narrowing of the dental and palatal arch
b. dysfunction of the temporomandibular joint
c. malocclusion
d. all of the above
2. __________ is a known factor in restricting tongue mobility and leads to abnormal development of the oral cavity, with clear impact on maxillary and mandibular growth.
a. Fuller lips
b. A short lingual frenulum (ankyloglossia)
c. Incipient caries
d. A metal crown
3. Morphological changes _________, leading to a small upper airway that causes collapse of the upper airway during sleep and to the development of obstructive sleep apnea (OSA) later.
a. don’t ever occur during childhood
b. occur quickly during childhood
c. occur slowly during childhood
d. seldom occur during childhood
4. Other symptoms and long-term effects of improper orofacial muscle patterns due to tongue and lip tie include head, neck, and back tension and pain, _______, and swallow and feeding dysfunction.
a. TMJ pain
b. bruxism
c. speech impediments
d. all of the above
5. A study by Zaghi, et al., concluded that after lingual frenuloplasty with myofunctional therapy, there was a/an _______ improvement in quality of life through amelioration of mouth breathing (74.8%), snoring (72.9%), clenching (91.0%), and/or myofascial tension (77.5%).
a. 56%
b. 63%
c. 87%
d. 95%
6. Statistically, ______ of children who suffer from SDB develop ADD, ADHD, and/or a learning disability.
a. 40%
b. 60%
c. 85%
d. 90%
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://orthopracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://orthopracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 430
Date Published: September 25, 2024
Expiration Date: September 25, 2027
2 CE CREDITS
7. Additionally, if a child is diagnosed with SDB in the first 5 years of life and is left untreated, he/she is _______ more likely to require special needs education by age 8.
a. 40%
b. 60%
c. 72%
d. 87%
8. Myofunctional therapy may be used as an effective treatment to integrate medical and surgical treatments for OSA and help to restore a normal resting posture of the tongue, appropriate oral, lingual, and facial muscle patterns, nasal breathing, normal lip posture, and a correct swallowing pattern.
a. True
b. False
9. According to research by Yoon, et al., RPE treatment can be considered as a valid and effective treatment option for pediatric OSA population with _______.
a. with narrow high arch palate
b. adenotonsillar hypertrophy
c. tongue tie
d. both a and b
10. The ________, developed by Zaghi, et al., has been determined to be concise and validated based on the current study results.
a. Epworth Sleepiness Scale
b. Functional Airway Evaluation Screening Tool (FAIREST-6)
c. Hypopnea Scale
d. Stanford Sleepiness Scale
To provide feedback on CE, please email us at education@medmarkmedia.com
Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
Screening and treating pediatric OSA
Dr.
Steven Olmos offers insights into how to approach a challenging sleep disorder
in children
The prevalence of pediatric obstructive sleep apnea (POSA) has increased from 3.3%-9.4% in studies published before 2014 to 12.8%-20.4% in studies published from 20162023. Habitual snoring prevalence ranges from 5.3%-34.5%.1 In comparison, adults diagnosed with OSA have a worldwide prevalence of 54%.2 The difference is likely due to lack of screening and availability of pediatric sleep physicians to make a diagnosis; however, the increase in numbers demonstrates that there is a greater awareness for these conditions.
There are similar associations of pathology in children and adults such as: cardiovascular and metabolic (Type 2 diabetes) disease, and obesity. The psychosocial pathology associated with OSA is less discussed. Untreated OSA impacts affective disorders such as depression and anxiety, and often leads to decline of cognitive functions or permanent brain damage.3 Adults with OSA in the U.S. have a relatively high prevalence of depressive symptoms, and the severity of OSA positively correlates with depressive symptoms.4 In children, sleep problems predict and are predicted by generalized anxiety/depression and oppositional defiant disorder.5 There is an increased risk for depression and withdrawn/depressed symptoms in children with OSA. Arterial oxygen desaturation nadir during sleep was strongly associated with depressive symptoms over time.6
Children treated with selective serotonin reuptake inhibitors (SSRIs) can result in delayed puberty.7 Attention-deficit/hyperactivity disorder (ADHD) is among the neurobehavioral sequelae associated with OSA. A study review found that children with OSA had a high rate of attentional deficits (95%), and up to 20%-30% of children with ADHD had OSA.8 ADHD and Autism Spectrum Disorder (ASD) in children are highly comorbid with prevalence rates of ADHD in ASD being 39.4% (ages 6-11) and 38% (ages 12-17).9 Both conditions are highly comorbid with
Steven Olmos, DDS, DABCP, DABCDSM, DABDSM, DAAPM, FAAOP, FAACP, FICCMO, FADI, FIAO, was in private practice for more than 40 years, with the last 30 years devoted to research and treatment of craniofacial pain and sleep-related breathing disorders. In 2023, he made the decision to retire from clinical practice to focus on advancing the fields of pain and sleep through research. He obtained his DDS from the University of Southern California School of Dentistry and is Board certified in both chronic pain and sleep-breathing disorders by the American Board of Craniofacial Pain, American Board of Dental Sleep Medicine, and American Board of Craniofacial Pain and Dental Sleep Medicine. Dr. Olmos is the founder of TMJ & Sleep Therapy Centres International, with over 70 licensed locations in seven countries dedicated exclusively to the diagnosis and treatment of craniofacial pain and sleep disorders. He continues to lead the field by continually publishing papers on the connection between pain, airway, and sleep disorders.
Disclosure: Dr. Olmos is the owner of Diamond Orthotic Lab. His course sponsors are BioResearch Inc. and Myofunctional Research Co. He has not received any remuneration for this article.
Educational aims and objectives
This self-instructional course for dentists aims to provide an overview of pediatric OSA, causes, symptoms, and treatments.
Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions by taking the quiz online at orthopracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
• Realize the prevalence of pediatric OSA and associated pathologies that can cause pediatric OSA.
• Identify some methods of screening for pediatric OSA.
• Realize the team of medical professionals that are needed for diagnosis of pediatric OSA.
• Identify possible treatments for pediatric OSA.
2 CE CREDITS
sleep disorders and improve with treatment for sleep pathology.10 The American Academy of Pediatrics recently published guidelines for screening the increased risk of adolescent suicide. They did not include screening for sleep breathing disorders. Suicide is the second leading cause of death for 10-to-24 year olds in the U.S. Individuals with neurodevelopmental disorders, including attention-deficit/hyperactivity disorder, learning disabilities, and autism spectrum disorder, are at higher risk for suicide attempts.11 Almost one-third of children and adolescents with ASD who report suicidal thoughts are aged 8 years and younger.52
Screening
In screening for POSA, it is important to look at co-morbidities. Fatigue, anxiety, and depression are most related to excessive sleepiness secondary to OSA.12
A scoping review of the last 20 years on sleep bruxism in children predicts a possible prevalence of 15%-53%.13 Sleep bruxism (SB) occurring during non-rapid eye movement (NREM) sleep and increase in microarousals is the same for adults and children in mechanism. SB activity is secondary to microarousals, with higher activity in children than adults.14 SB has a common association with OSA.15 The American Academy of Sleep Medicine classifies sleep bruxism as a movement disorder in the same category as periodic limb movement (PLM) and restless leg syndrome (RLS). It is well known that children with ADHD have elevated PLM and increased risk of OSA.16 The prevalence of elevated PLM in children with ADHD varies with a range of 26%-64%.17-19 SB, PLM, and increased EEG arousals commonly concur during sleep in a time-linked manner.20 Children with elevated PLM have more awakenings and a decrease in rapid eye movement (REM) sleep.21,22
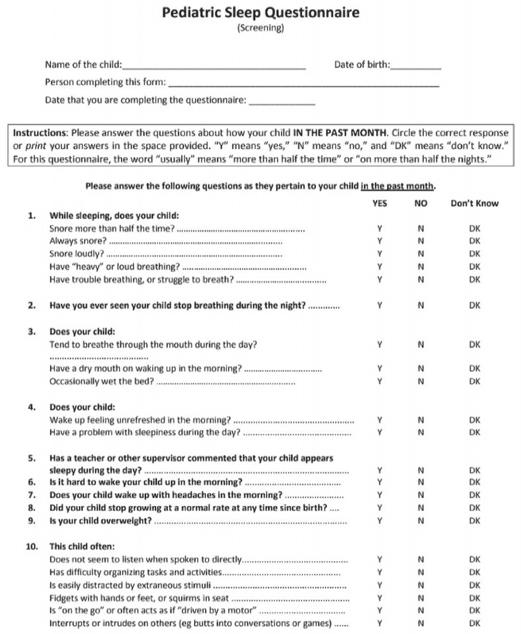
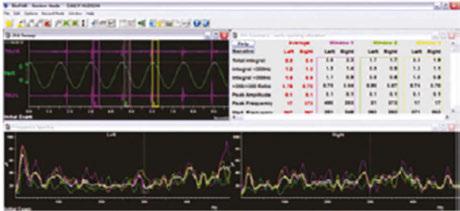
The validated Pediatric Sleep Questionnaire (PSQ) is the most utilized screening tool. It emphasizes snoring intensity and frequency, witnessed apnea, mouth breathing, daytime fatigue, bed wetting, morning headaches, low growth, and attention deficit symptoms (Figure 1).
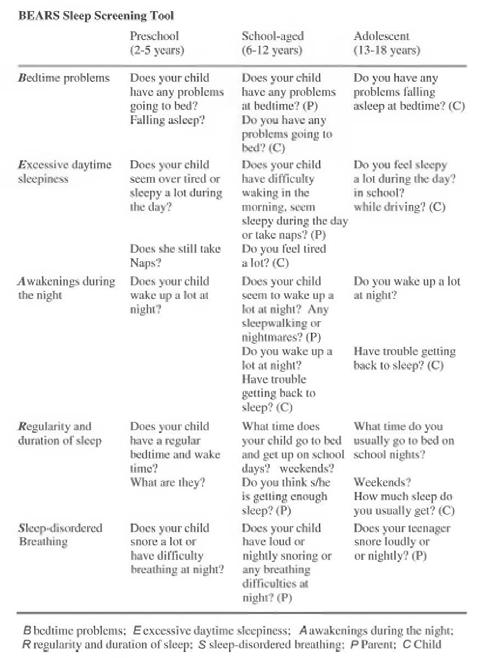
The BEARS Sleep Screening Tool developed by Judith Owens, MD (Director of Sleep Medicine, Center for Pediatric Sleep Disorders, Department of Neurology, Children’s Hospital Boston, Professor of Neurology Harvard University), divides symptoms of bedtime problems, excessive daytime sleepiness, awakenings during the night, regularity and duration of sleep, and sleep-disordered breathing by three age groups. The three age groups are around 2-5 years, 6-12 years, and 13-18 years (Figure 2).
A visual screening tool validation study has recently been concluded and submitted to the Journal of Evidence-Based Dental Practice. This study is the collaboration of this author and the principal investigator Judith Owens, MD, funded by a grant from the American Academy of Craniofacial Pain (AACP). This study looked at the risk factors for pediatric sleep-disordered breathing (SDB) and craniofacial features, validated using the PSQ and a 22-item parent reported measure for SDB risk in children. Subject characteristics included age, sex, race, and ethnicity. Various craniofacial features were evaluated, such as: retrognathic mandible, open mouth posture, convex profile, midface deficiency, flat cheeks, concave profile, dolichocephalic face, frontal asymmetry, forward head posture, and rolled shoulders. It also included intraoral evaluation of: crowding of teeth, crossbite, narrow vaulted palate, crowding of upper teeth, narrow
palate, open bite, tongue thrust, crowding of lower teeth, narrow lower jaw, tongue tie, and “heart”-shaped tip of tongue. Twelve data collection sites across the U.S. were sourced to demonstrate ease of use, reproducibility, and which conditions had highest correlation. It was found that the following conditions had the highest correlation in decreasing order: forward head posture, narrow vaulted palate, open bite, tongue thrust, tongue tie, and heart-shaped tongue.
Diagnosis
Only a physician can diagnose SDB for adults or children. The quantity and quality of diagnostic information needed to make a diagnosis is determined by the sleep specialist physician. The gold standard for the diagnosis of POSA is polysomnography (PSG); however, certain home sleep study (HST) units have been FDA-cleared. Interestingly, sleep specialty training covers both adults and children. The graduates decide their focus with the greater number treating adults, making the access to a pediatric diagnosis limited. The HST units that utilize chest and abdomen elevation belts, nasal airflow, temperature (thermistors), pulse oximetry, body position, and snoring are closest to the data collected by PSG. Many of the digital evaluation systems are based on algorithms a distance from PSG data collection. They may be used as screening tools, and their validation will be confirmed in future studies. Most diagnoses are focused on AHI>1 for POSA; however, hypercapnia is of equal concern in pediatric patients with SDB. Hypercapnia is an elevation of blood carbon dioxide secondary to abnormalities in the heart or lungs, such as
Figure 1: The validated Pediatric Sleep Questionnaire is the most utilized screening tool
Figure 2: BEARS Sleep Screening Tool
respiratory acidosis, altered acid-base balance, or inadequate ventilation of the alveoli. This demonstrates why flow limitation (respiratory distress) is important in the data collection. The diagnosis of hypercapnia is made when the end tidal carbon dioxide (ETCO2) exceeds 45 mmHg during sleep.23 Children are more likely than adults to suffer from hypercapnia when they sleep.24
Treatment
Deciding upon treatment goals will help determine a comprehensive and long-term treatment plan. The late seminal figure in pediatric sleep medicine, Dr. Christian Guilleminault, wrote that the ultimate treatment goal in POSA is “restoration of nasal breathing during wake and sleep.”25
The first line of treatment for POSA is usually tonsil/adenoid (T&A) surgery; however, numerous studies have demonstrated that it may not be as successful as once thought.26-32
The only study to follow children post-T&A surgery over a 3-year period (with systematic evaluation using PSG at 6, 12, 24, and 36 months) showed that there was a 75% relapse of SD after 6 months.33 A pilot study utilizing CO2 laser (Deka/Bio Research Inc., Figure 3) to shrink palatal and base of tongue tissue for incomplete responders of oral appliance therapy (OAT) for OSA is currently underway at the University of Alberta School of Dentistry, Edmonton, Canada, by the principal investigator Enoch T. Ng, DDS, PhD (Figure 3). He has published a case report on the effectiveness of photobiomodulation for pediatric hypertrophic tonsils.34 These devices may someday be FDA-cleared to shrink tonsils. The morbidity and mortality of T&A surgery could be replaced with dentists performing a simple and painless technique.
A second line treatment to treat POSA is positive airway pressure therapy (PAP), most often utilizing continuous positive airway pressure (CPAP). Midface deficiency and POSA are highly comorbid. This is demonstrated by the incidence of children with Down syndrome who have POSA after T&A surgery at 65%73%.35-38 CPAP use on children with POSA has been shown to prevent normal maxillary development and increase midface deficiency, thus making the patient more dependent on PAP.39 Maxillary development has been demonstrated to improve POSA
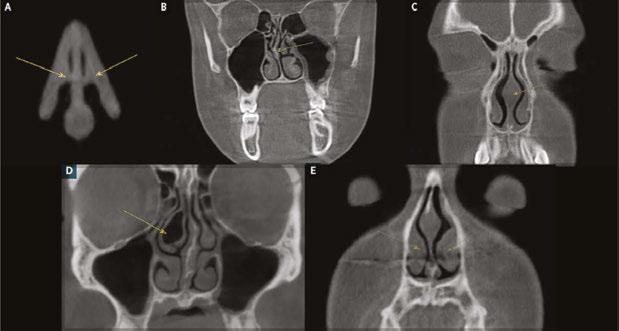
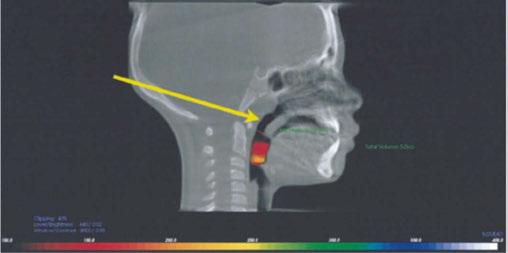
and nasal function by increasing volume.40,41 It has been shown that maxillary expansion can shrink T&A and increase the internal nasal valve (which is the first point of entry of air into the nose).42,43 Nasal valve compromise (narrowing of the internal nasal valve) has been found to result in a 7-times greater chance of TM joint capsulitis and facial and cervical myositis, via mouth breathing, when compared to other nasal obstructions (Figure 4).44
Protraction of the maxilla in combination with transverse development utilizing a Delaire’s mask for Class III patients with POSA has been shown to produce statistically significant increase in linear upper airway measurements and oropharyngeal and nasopharyngeal dimensions, improving airway patency and OSA (Figure 5).45 The problem with this technique is that it uses the frontal bone and the mandible as leverage, placing retractive forces on them. If the patient has articular disc displacement and or capsulitis (inflammation of the joint capsule), the retraction of the mandible can result in increased pathology. A proper screening of the TM joints via joint vibration analysis to measure soft and hard tissue vibrations during function (JVA BioResearch, Inc.), as well as a thorough clinical examination, will help to identify these patients (Figures 6 and 7).
Decompressing the TM joints with a removable lower appliance at a physiologic position (sibilant phoneme registration/ phonetic bite) has been shown to increase pharyngeal airway volume and decrease collapse. It also allows for stabilization of the TM joints, reducing pressure on the mandible without any pressure on the frontal bone.46,47 This Tandem Bow technique was explained in a previous case study titled, “Pediatric severe apnea/obesity/TMD/headache-Class III” in Orthodontic Practice US, May/June 2016, Volume 7, No. 3, pages 20-24. The 10-year-
Figure 3 (left): CO2 laser by Deka/Bio Research Inc. Figure 4 (middle): Nasal valve compromise. Figure 5 (right): Delaire’s mask
Figures 6 and 7: TM joint vibration analysis
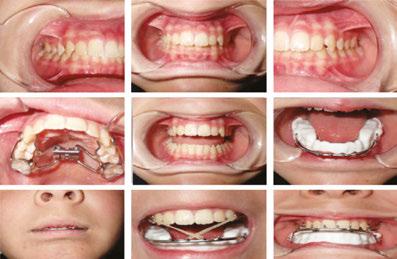
old patient who had been on CPAP for 5 years with an AHI of 118 was reduced to an AHI of 3 in 8 weeks and was able to discontinue her PAP therapy (Figure 8). Forward head posture corrections can be seen with decompression of the TM joints utilizing this technique (Figure 9). This technique is explained in Chapter 7 of Sleep Disorders in Pediatric Dentistry: Clinical Guide on Diagnosis and Management, edited by Dr. Edmund Liem, and published by Springer. Chapter 7 is authored by Dr. Edmund A. Lipskis, and titled, “Orthodontic and Dentofacial Orthopedic Treatment Strategies for Pediatric Sleep Disorders.” Advancing the entire maxilla is necessary to protract the palatine bones to increase the volume of the velopharynx (the narrowest part of the airway) (Figure 10).
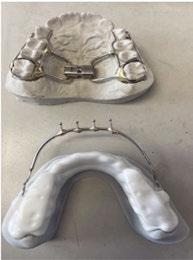
The lower appliance that receives the Tandem Bow is to be worn 12 hours per day and only removed to eat if necessary. Most children should sleep for 10 hours, so the device can be worn during sleep, an hour before bed and an hour after waking. The force of the elastics, worn for 12 hours per day (mostly while sleeping), should have approximately 200g per side in mixed dentition and 250-300g per side in permanent dentition (Figure 11).
When used on mixed dentition, there will be a need to place extra buccal retention on the lower deciduous molars for the “C” clasps (Figures 12 and 13).
The evolution of printed biofriendly materials produced by Diamond Orthotic Lab for removable orthopedic development and facial pain has greatly improved treatment (Figures 14 and 15). These appliances are made of Type 12 nylon and are thermally active, making them easy to adjust with either hot or cold water.
Myofunctional therapy for POSA has been shown to reduce AHI by 62%.48 This type of therapy is ideal primary treatment for 2- to 5-year-old patients exclusively. It is also utilized as a retentive therapy for post-orthopedic development. Myofunctional Research Co. (MRC) has a range of
products, including oral appliances (Myobrace®), lip and tongue strength exercise devices (myotalea®), and pharyngeal airway development (Myosa®) (Figures 16, 17, and 18).
Figure 8: Tandem Bow technique
Figure 9: Forward head posture corrections can be seen with decompression of the TM joints
Figure 10: Advancing the entire maxilla is necessary to protract the palatine bones to increase the volume of the velopharynx
Figure 11: Elastic force
Figure 12 and 13: Extra buccal retention on the lower deciduous molars for the “C” clasp
Figure 14 and 15: Printed biofriendly materials produced by Diamond Orthotic Lab for removable orthopedic development and facial pain
A new technique to North America, incorporating orthopedic development of the maxilla in combination with aligner therapy, is called Nuvola (BioMax). It was developed in Italy by Dr. Alessandro Carrafiello, an orthodontist/physician with remarkable treatment outcomes for both adults and children. Children as young as 5 can benefit from this treatment. This treatment utilizes a chewable oral device (Freedom appliance) that is used for only 30 minutes per day. The Freedom device comes in three types: regular, deep bite, and pediatric (Nuvola Jr). This device uses piezoelectric forces to develop the maxilla and mandible in combination with reinforced aligners, without the need for fixed appliances (Figure 19). It is tremendously easy to implement for practitioners and patients. Compliance is much higher than in previous treatments for malocclusion. There are currently no studies on how effective this treatment is for POSA; however, it looks promising.
Figures 16-18: Myofunctional Research Co. (MRC) has a range of products, including oral appliances (Myobrace), lip and tongue strength exercise devices (Myotalea), and pharyngeal airway development (Myosa)
Photobiomodulation (laser) treatment has been shown to accelerate orthodontic movement and reduce inflammation and pain from orthodontic therapy.49-51 Studies are being developed to combine laser therapy using NdYag (Deka/BioResearch Inc.) and MLS (BioResearch Inc.) and these outlined treatments for orthopedic and orthodontic movement, allowing shorter treatment times and maximum treatment outcomes (Figures 20 and 21). The future is now.
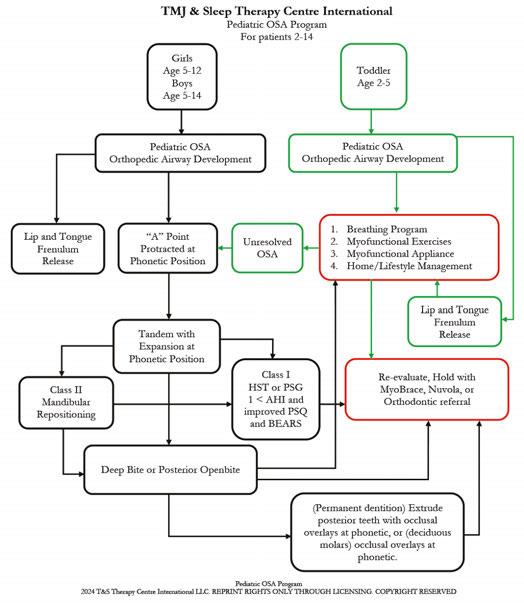
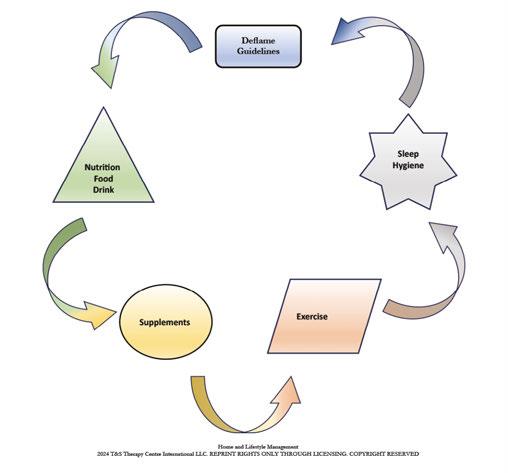
A proposed treatment outline for POSA might follow the timeline in Figure 22. A comprehensive treatment approach also includes home and lifestyle management (Figure 23).
Treating POSA has far greater effects than simply restoring restful sleep. The arguably more important effect may be in saving a child’s life. The psychosocial consequences illustrated in this article are rarely mentioned in the treatment of POSA and should motivate us to screen and treat patients as early as possible.
For training courses in the various methods outlined in this article, please visit our website www.tmjtherapycentre.com.
REFERENCES
1. Magnusdottir S, Hill EA. Prevalence of obstructive sleep apnea (OSA) among preschool aged children in the general population: A systematic review. Sleep Med Rev. 2024 Feb;73:101871.
2. de Araujo Dantas AB, Gonçalves FM, Martins AA, Alves GÂ, Stechman-Neto J, Corrêa CC, Santos RS, Nascimento WV, de Araujo CM, Taveira KVM. Worldwide prevalence and associated risk factors of obstructive sleep apnea: a meta-analysis and meta-regression. Sleep Breath. 2023 Dec;27(6):2083-2109.
3. Vanek J, Prasko J, Genzor S, Ociskova M, Kantor K, Holubova M, Slepecky M, Nesnidal V, Kolek A, Sova M. Obstructive sleep apnea, depression and cognitive impairment. Sleep Med. 2020 Aug;72:50-58.
4. Li M, Zou X, Lu H, Xin Y, et al. Association of sleep apnea and depressive symptoms among US adults: a cross-sectional study. BMC Public Health. 2023;23:427.
5. Shanahan L, Copeland WE, Angold A, Bondy CL, Costello EJ. Sleep problems predict and are predicted by generalized anxiety/depression and oppositional defiant disorder. J Am Acad Child Adolesc Psychiatry. 2014 May;53(5):550-558.
Figure 19: The Freedom device from Nuvola comes in three types: regular, deep bite, and pediatric (Nuvola Jr).
Figure 20 and 21: NdYag laser (left) from Deka/BioResearch Inc. and MLS laser (right) from BioResearch Inc.
Figure 22: Treatment outline for POSA
Figure 23: A comprehensive treatment approach also includes home and lifestyle management
6. Hodges E, Marcus CL, Kim JY, Xanthopoulos M, Shults J, Giordani B, Beebe DW, Rosen CL, Chervin RD, Mitchell RB, Katz ES, Gozal D, Redline S, Elden L, Arens R, Moore R, Taylor HG, Radcliffe J, Thomas NH. Depressive symptomatology in school-aged children with obstructive sleep apnea syndrome: incidence, demographic factors, and changes following a randomized controlled trial of adenotonsillectomy. Sleep. 2018 Dec 1;41(12):zsy180.
7. Alotoom OM, Marwaha R. Association Between SSRIS And Delayed Puberty In Children. Jour Amer Acad Child & Adolesc Psych. Oct 2023;62(10):S196.
8. Ivanov I, Miraglia B, Prodanova D, Newcorn, JH. Sleep Disordered Breathing and Risk for ADHD: Review of Supportive Evidence and Proposed Underlying Mechanisms. Journal of Attention Disorders. 2024;28(5):686-698.
9. Jones Piltz V, Halldner L, Markus J-F, Fridell A, Bolte S, Olsson NC. Symptom similarities and differences in social interaction between autistic children and adolescents with and without ADHD. Curr Psychol. 2024;43:3503-3513.
10. Berenguer C, Baixauli I, Rosa E, De Stasio S. Sleep problems in children with autism spectrum disorder and attention-deficit/hyperactivity disorder: A comparative study and effects on communication skills. Autism Res. 2024 Feb;17(2):355-365.
11. Hua LL, Lee J, Rahmandar MH, Sigel EJ; Committee On Adolescence; Council On Injury, Violence, And Poison Prevention. Suicide and Suicide Risk in Adolescents. Pediatrics. 2024 Jan 1;153(1):e2023064800.
12. Mjelle KES, Lehmann S, Saxvig IW, Gulati S, Bjorvatn B. Association of Excessive Sleepiness, Pathological Fatigue, Depression, and Anxiety With Different Severity Levels of Obstructive Sleep Apnea. Front Psychol. 2022 Mar 31;13:839408.
13. Huynh N, Fabbro CD. Sleep bruxism in children and adolescents-A scoping review. J Oral Rehabil. 2024 Jan;51(1):103-109.
14. Restrepo C, Lobbezoo F, Castrillon E, Svensson P, Santamaria A, Manfredini D. Correlations between sleep architecture and sleep-related masseter muscle activity in children with sleep bruxism. J Oral Rehabil. 2024 Jan;51(1):110-116.
15. American Academy of Sleep Medicine. In: International Classification of Sleep Disorders. Darien, IL: American Academy of Sleep Medicine;2014.
16. Youssef NA, Ege M, Angly SS, Strauss JL, Marx CE. Is obstructive sleep apnea associated with ADHD? Ann Clin Psychiatry. 2011 Aug;23(3):213-224.
17. Crabtree VM, Ivanenko A, O’Brien LM, Gozal D. Periodic limb movement disorder of sleep in children. J Sleep Res. 2003 Mar;12(1):73-81.
18. Chervin RD, Archbold KH, Dillon JE, Pituch KJ, Panahi P, Dahl RE, Guilleminault C. Associations between symptoms of inattention, hyperactivity, restless legs, and periodic leg movements. Sleep. 2002 Mar 15;25(2):213-218.
19. Picchietti DL, England SJ, Walters AS, Willis K, et al . Periodic limb movement disorder and restless legs syndrome in children with attention-deficit hyperactivity disorder. J Child Neurol. 1998;13(12):588-594.
20. van der Zaag J, Naeije M, Wicks DJ, Hamburger HL, Lobbezoo F. Time-linked concurrence of sleep bruxism, periodic limb movements, and EEG arousals in sleep bruxers and healthy controls. Clin Oral Investig. 2014;18(2):507-513.
21. Crabtree VM, Ivanenko A, O’Brien LM, Gozal D. Periodic limb movement disorder of sleep in children. J Sleep Res. 2003 Mar;12(1):73-81.
22. Gingras JL, Gaultney JF, Picchietti DL. Pediatric periodic limb movement disorder: sleep symptom and polysomnographic correlates compared to obstructive sleep apnea. J Clin Sleep Med. 2011 Dec 15;7(6):603-609A.
23. Almanza-Hurtado A, Polanco Guerra C, Martínez-Ávila MC, Borré-Naranjo D, Rodríguez-Yanez T, Dueñas-Castell C. Hypercapnia from Physiology to Practice. Int J Clin Pract. 2022 Sep 23;2022:2635616.
24. Kheirandish-Gozal L, Gozal D. Intranasal budesonide treatment for children with mild obstructive sleep apnea syndrome. Pediatrics. 2008 Jul;122(1):e149-155.
25. Guilleminault C, Sullivan SS. Towards Restoration of Continuous Nasal Breathing as the Ultimate Treatment Goal in Pediatric Obstructive Sleep Apnea. Enliven: Ped & Neonatal Bio. Sept 2014;1(1).
26. Guilleminault C, Partinen M, Praud JP, Quera-Salva MA, Powell N, Riley R. Morphometric facial changes and obstructive sleep apnea in adolescents. J Pediatr. 1989 Jun;114(6):997-999.
27. Tasker C, Crosby JH, Stradling JR. Evidence for persistence of upper airway narrowing during sleep, 12 years after adenotonsillectomy. Arch Dis Child. 2002 Jan;86(1):34-37.
28. Guilleminault C, Li K, Quo S, Inouye RN. A prospective study on the surgical outcomes of children with sleep-disordered breathing. Sleep. 2004 Feb 1;27(1):95-100.
29. Tauman R, Gulliver TE, Krishna J, Montgomery-Downs HE, O’Brien LM, Ivanenko A, Gozal D. Persistence of obstructive sleep apnea syndrome in children after adenotonsillectomy. J Pediatr. 2006 Dec;149(6):803-808.
30. Guilleminault C, Huang YS, Glamann C, Li K, Chan A. Adenotonsillectomy and obstructive sleep apnea in children: a prospective survey. Otolaryngol Head Neck Surg. 2007 Feb;136(2):169-75.
31. Amin R, Anthony L, Somers V, Fenchel M, McConnell K, Jefferies J, Willging P, Kalra M, Daniels S. Growth velocity predicts recurrence of sleep-disordered breathing 1 year after adenotonsillectomy. Am J Respir Crit Care Med. 2008 Mar 15;177(6):654-659.
32. Bhattacharjee R, Kheirandish-Gozal L, Spruyt K, Mitchell RB, Promchiarak J, Simakajornboon N, Kaditis AG, Splaingard D, Splaingard M, Brooks LJ, Marcus CL, Sin S, Arens R, Verhulst SL, Gozal D. Adenotonsillectomy outcomes in treatment of obstructive sleep apnea in children: a multicenter retrospective study. Am J Respir Crit Care Med. 2010 Sep 1;182(5):676-683.
33. Bonuck K, Freeman K, Chervin RD, Xu L. Sleep-disordered breathing in a population-based cohort: behavioral outcomes at 4 and 7 years. Pediatrics. 2012 Apr;129(4): e857-865.
34. Ng ET, Lagravere MO, David A. Photobiomodulation for pediatric hypertrophic tonsils: a clinical case report. Pediatr Med 2021;4:40. https://dx.doi.org/10.21037/pm-21-18.
35. Shott SR, Amin R, Chini B, Heubi C, Hotze S, Akers R. Obstructive sleep apnea: Should all children with Down syndrome be tested? Arch Otolaryngol Head Neck Surg. 2006 Apr;132(4):432-436.
36. Maris M, Verhulst S, Wojciechowski M, Van de Heyning P, Boudewyns A. Prevalence of Obstructive Sleep Apnea in Children with Down Syndrome. Sleep. 2016 Mar 1;39(3):699-704.
37. Hill CM, Evans HJ, Elphick H, Farquhar M, Pickering RM, Kingshott R, Martin J, Reynolds J, Joyce A, Rush C, Gavlak JC, Gringras P. Prevalence and predictors of obstructive sleep apnoea in young children with Down syndrome. Sleep Med. 2016 Nov-Dec;27-28:99-106.
38. Dyken ME, Lin-Dyken DC, Poulton S, Zimmerman MB, Sedars E. Prospective polysomnographic analysis of obstructive sleep apnea in down syndrome. Arch Pediatr Adolesc Med. 2003 Jul;157(7):655-660.
39. Roberts SD, Kapadia H, Greenlee G, Chen ML. Midfacial and Dental Changes Associated with Nasal Positive Airway Pressure in Children with Obstructive Sleep Apnea and Craniofacial Conditions. J Clin Sleep Med. 2016 Apr 15;12(4):469-475.
40. Cistulli PA, Palmisano RG, Poole MD. Treatment of obstructive sleep apnea syndrome by rapid maxillary expansion. Sleep. 1998 Dec 15;21(8):831-835.
41. Motro M, Schauseil M, Ludwig B, Zorkun B, Mainusch S, Ateş M, Küçükkeleş N, Korbmacher-Steiner H. Rapid-maxillary-expansion induced rhinological effects: a retrospective multicenter study. Eur Arch Otorhinolaryngol. 2016 Mar;273(3):679-87.
42. Yoon A, Abdelwahab M, Bockow R, Vakili A, Lovell K, Chang I, Ganguly R, Liu SY, Kushida C, Hong C. Impact of rapid palatal expansion on the size of adenoids and tonsils in children. Sleep Med. 2022 Apr;92:96-102.
43. Yoon A, Abdelwahab M, Liu S, Oh J, et al. Sleep and Breathing 2021;25:1019-1027.
44. Olmos SR. Nasal airway obstruction and orofacial pain: a multicenter retrospective analysis. Gen Dent. 2022 Nov-Dec;70(6):28-33.
45. Caruso S, Lisciotto E, Caruso S, Marino A, Fiasca F, Buttarazzi M, Sarzi Amadè D, Evangelisti M, Mattei A, Gatto R. Effects of Rapid Maxillary Expander and Delaire Mask Treatment on Airway Sagittal Dimensions in Pediatric Patients Affected by Class III Malocclusion and Obstructive Sleep Apnea Syndrome. Life (Basel). 2023 Mar 1;13(3):673.
46. Singh GD, Olmos S. Use of a sibilant phoneme registration protocol to prevent upper airway collapse in patients with TMD. Sleep Breath. 2007 Dec;11(4):209-216.
47. Olmos SR, Kritz-Silverstein D, Halligan W, Silverstein ST. The effect of condyle fossa relationships on head posture. Cranio. 2005 Jan;23(1):48-52.
48. Camacho M, Certal V, Abdullatif J, Zaghi S, Ruoff CM, Capasso R, Kushida CA. Myofunctional Therapy to Treat Obstructive Sleep Apnea: A Systematic Review and Meta-analysis. Sleep. 2015 May 1;38(5):669-675.
49. Cruz DR, Kohara EK, Ribeiro MS, Wetter NU. Effects of low-intensity laser therapy on the orthodontic movement velocity of human teeth: a preliminary study. Lasers Surg Med. 2004;35(2):117-120.
50. Doshi-Mehta G, Bhad-Patil WA. Efficacy of low-intensity laser therapy in reducing treatment time and orthodontic pain: a clinical investigation. Am J Orthod Dentofacial Orthop. 2012 Mar;141(3):289-297.
51. Qamruddin I, Alam MK, Mahroof V, Fida M, Khamis MF, Husein A. Effects of low-level laser irradiation on the rate of orthodontic tooth movement and associated pain with self-ligating brackets. Am J Orthod Dentofacial Orthop. 2017 Nov;152(5):622-630.
52. Schindel BJ, Baer Chen B, Wilcox HC, Marvin AR, Law JK, Lipkin PH. Suicidal thoughts and behaviors among children and adolescents with autism spectrum disorder. JAMA Pediatr. Published online April 1, 2004. doi:10.1001/jamapediatrics.2004.0207
Continuing Education Quiz
Screening and treating pediatric OSA OLMOS
1. The prevalence of pediatric obstructive sleep apnea (POSA) has increased from 3.3%-9.4% in studies published before 2014 to ________ in studies published from 2016-2023.
a. 12.8%-20.4%
b. 21.3%-30.1%
c. 34.3%-56.1%
d. 57.2%-66.8%
2. In comparison, adults diagnosed with OSA have a worldwide prevalence of _______.
a. 32%
b. 54%
c. 67%
d. 72%
3. There is ________ for depression and withdrawn/depressed symptoms in children with OSA.
a. an increased risk
b. no risk
c. no evidence of
d. no way to test
4. The validated Pediatric Sleep Questionnaire (PSQ) emphasizes snoring intensity and frequency, witnessed apnea, _______ morning headaches, low growth, and attention deficit symptoms.
a. mouth breathing
b. daytime fatigue
c. bed wetting
d. all of the above
5. _______ can diagnose SDB for adults or children.
a. Only a dentist
b. Only a myofunctional therapist
c. Only a physician
d. Only a sleep technician
6. The first line of treatment for pediatric OSA (POSA) is usually ______; however, numerous studies have demonstrated that it may not be as successful as once thought.
a. rapid palatal expansion
b. tonsil/adenoid (T&A) surgery
c. joint vibration
d. positive airway pressure
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://orthopracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://orthopracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 730
Date Published: September 25, 2024
Expiration Date: September 25, 2027
7. A second line treatment to treat POSA is ________.
a. tonsil/adenoid (T&A) surgery
b. photobiomodulation (laser) treatment
c. positive airway pressure therapy (PAP), most often utilizing continuous positive airway pressure (CPAP)
d. oral appliance
8. Decompressing the TM joints with a removable lower appliance at a physiologic position (sibilant phoneme registration/phonetic bite) has been shown to increase pharyngeal airway volume and decrease collapse.
a. True
b. False
9. Myofunctional therapy for POSA has been shown to reduce AHI by _______.
a. 35%
b. 46%
c. 62%
d. 76%
10. Myofuctional therapy for POSA is ideal primary treatment for ______ patients exclusively.
a. 2- to 5-year-old
b. 6- to 8-year old
c. 10-to 12-year old
d. 13- to 18-year old
To provide feedback on CE, please email us at education@medmarkmedia.com Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
Innovative same-day clear aligners and retainers
Leading dental professionals adopt LuxCreo’s 3DP solutions
LuxCreo engineered from scratch an end-toend 3D-printing system to solve the problems of directly printing clear orthodontic appliances, making the use easy and efficient for dental professionals to adopt in their clinic or laboratory. With a focus on delivering outstanding direct-print aligners in just 2 hours from the patient’s scan, LuxCreo engineered one-click design and nesting software, four integrated pieces of hardware, and its proprietary and FDA-cleared 4D Aligner resin.
Now, utilizing LuxCreo’s workflow, directly 3D-printed clear aligners are providing therapies that are challenging for thermoformed trays and are being delivered to patients within the same day at reduced cost to the practice.
Dr. Bill Layman, Clearwater, Florida
Bill Layman, DMD, is not just a cutting-edge orthodontist; he is a sharp businessman with a masters’ degree in Business Administration from the Wharton School. Marrying his clinical prowess with business training, Dr. Layman looks for ways to optimize his practice’s performance through adopting the best and most efficient technologies to deliver patient-centric care.
Focusing on the efficiency, workflow, and financial benefits of LuxCreo’s iLux Pro Dental aligner system (ILPD), Dr. Layman has done detailed time and cost studies in his office on two comparative workflows: 1) thermoforming aligners on 3D-printed models versus 2) LuxCreo’s direct-print 4D Aligners. His analysis shows that LuxCreo’s innovative 4D Aligner workflow saves a doctor in labor costs, material costs, and yield costs, to the tune of nearly 20% savings to the office. As an added financial and operational benefit, the LuxCreo direct-print workflow allows for an increase of more than 40% in weekly production of aligners in the office. The increase in weekly production with the same number of labor hours is due to the reduction in labor time it takes to create the aligners/retainers.
“For any orthodontist looking for an innovative advance in technology that also has a notable office savings advantage,” Dr. Layman suggests, “get the ILPD dental workflow for your office as soon as possible.”
Dr.
Neil Warshawsky, Chicago, Illinois
Neil Warshawsky, DDS, MS, has been making an impact in orthodontics for more than 30 years. In addition to his active orthodontic practice in Chicago, Dr. Warshawsky is an Associate
Professor of Orthodontics at the Craniofacial Center at the University of Illinois Health Center. He regularly lectures around the globe on a variety of orthodontic topics. Dr. Warshawsky focuses on utilizing innovative and disruptive dental technologies to help achieve his goal of improving orthodontics for everyone through his work. So, when he was able to adopt and implement the LuxCreo ILPD workflow and orthodontic resins in just a month’s time, he knew LuxCreo was the kind of technology he wanted to invest in for his practice and educational goals. “LuxCreo’s purpose in life is to help me, the orthodontist.”
Dr. Warshawsky has been particularly impressed with the 4D direct-print aligner workflow LuxCreo has created. The integration of automated design software, outstanding hardware designed for orthodontic cases, and proprietary, compliant printing resins allows Dr. Warshawsky to deliver unique clear aligners to his patients in just hours — aligners that can achieve things that traditional thermoformed aligners simply could not do for his patients.
4D Aligners have a superior fit that thermoform suck-downs simply cannot achieve, which means there is better control over torque forces in moving the teeth. It also requires the orthodontist to use less attachments on the tooth surface of the patient. That level of accurate fit, combined with the ability to design and print variable thickness trays, yields better control over movements and a better patient experience. As Dr. Warshawsky summarizes it, “With 4D Aligners, we can accomplish the treatment plan with less trays, less attachments, less refinements, and less visits. It is a better patient experience that also helps gets the orthodontist paid faster.”
LuxCreo’s 4D Aligners and its ILux Pro Dental printing system are a win-win for dental professionals and patients. This information was provided by LuxCreo. OP
www.luxcreo.com/industries/4d-aligner/
What’s got brackets, wires, and plaque all over?
Kristin Sheridan, RDH, explains how OrthoProtect’s key ingredients improve orthodontic patients’ oral health
There’s no riddle here; it’s your patients’ teeth. And honestly, this needs to be amended because patients with clear aligners also have plaque all over their teeth. Even when the appliances are removable, patients still struggle to clean their teeth properly. Our goal is to be able to provide the best overall outcome for ortho treatment, and a big part of that is getting patients on board with improving their home care. They already know that they are supposed to brush and floss, but rather than repeatedly educating them on this, have you ever discussed a therapeutic rinse that will have the ability to aid in remineralization and plaque reduction? There are a few key ingredients to look out for to help with this and improve orthodontic patient’s oral health.
Activated chlorine dioxide: Chlorine dioxide has a superior ability to break down the toughest microorganisms and biofilms, without corrosive action or negative impacts on the oral environment. It will not only break up the plaque, but also will also kill bacteria that causes decay and gum disease. It is safe and effective while being able to be used long term to help improve overall hygiene for patients. It is also effective against protozoa, viruses, and fungi and is considered more effective against microbes than many over-the-counter solutions.
Calcium lactate: In order to prevent cavities, you must reinforce the integrity of the enamel. This ingredient is a bioavailable form of calcium; it effectively contributes to the remineralization of tooth enamel, helping to repair early signs of tooth decay and strengthen teeth. Furthermore, calcium lactate
supports saliva’s protective functions by buffering oral acids and neutralizing pH levels.
Xylitol: Best known for its ability to reduce the growth of harmful decay-causing bacteria like streptococcus mutans, xylitol disrupts the bacteria’s ability to function because they are unable to metabolize this sugar alcohol. It also interferes with bacterial adhesion, helping to reduce plaque formation and lowering the risk of decay. Xylitol can also enhance remineralization of teeth when used in conjunction with calcium lactate, reinforcing the teeth’s strength against acids and bacteria. Additionally, it stimulates the production of saliva which naturally helps to wash away food particles. Since saliva naturally contains minerals, this also aids in the remineralization of teeth.
Poloxamer 407: Poloxamers enhance the effectiveness of other ingredients in solutions. They do this by reducing surface tension and increasing the “spreading and wetting properties” of products. This also creates a “slippery” surface that plaque has trouble building on, thereby minimizing the amount of plaque accumulation on tooth surfaces and brackets and wires.
Overall, each of these ingredients is special in some way. But Ortho Protect utilizes all these ingredients together to get the best outcomes with patients. It will help those who are in traditional bracket-and-wire appliances and those who are using clear aligners to improve their dental health.
No more riddles, just results.
This information was provided by OraCare.
The Product You Never Knew You Needed
SureSmile ® Clear Aligners
A discreet treatment modality that addresses form and function
Clear aligners play an important role in the treatment of malocclusion. In the hands of a doctor, aligners can do more than improve esthetics by aligning the “social six” teeth patients associate with their smile. Clear aligners can effectively treat the entire mouth, correcting a broad array of malocclusions and potentially alleviating associated oral health issues to improve the patient’s health in a holistic fashion.
Clear aligner therapy also addresses a common patient concern about undergoing orthodontic treatment by allowing them to predictably achieve their desired outcome without the use of unsightly and uncomfortable brackets and wires.
Backed by Dentsply Sirona — a global leader in dental solutions with over 100 years of experience in oral healthcare — SureSmile Clear Aligners correct malocclusion in a deliberate, strategic, and holistic fashion. Expert technicians in the SureSmile® Digital Lab build customized setups and staging for clear aligners by applying more than 30 years of experience in orthodontic treatment planning to ensure doctors and their patients have an excellent treatment experience.
The SureSmile Digital Lab assesses all the forces being applied to each tooth throughout a clinician’s proposed treatment plan. SureSmile then uses that information to recommend the most efficient and least disruptive set of movements needed at each stage of the plan for a successful, predictable outcome. Synergistic movements require less force and often involve more movement of the crown.
Antagonistic movements require higher forces and are expressed over more aligners.1 When possible, we prefer to stage these combinations of movements independently.
Rooted in a deep understanding of orthodontic principles and propelled by state-of-the-art technologies, SureSmile empowers clinicians to treat the complexities of malocclusion with precision and compassion. From advanced software tools to seamless digital integration to high performance clear aligners, SureSmile is a trusted partner for doctors seeking to improve patients’ oral health and well-being. Our system acknowledges the systemic implications of malocclusion, underscoring its impact on overall health and quality of life.
For more information, download our White Paper by scanning the QR code or visiting https://www.dentsplysirona.com/ en-us/lp/suresmile-whitepaper.html.
REFERENCE
1. Cowley DP, Mah J, O’Toole, B. The effect of gingival-margin design on the retention of thermoformed aligners. J Clin Orthod. 2012;46(11):697-702. This information was provided by SureSmile. OP
Why the largest U.S. orthodontic practices have quietly partnered with IDSOs
Over the last 10 years, over 1,000 orthodontists have quietly partnered with Invisible Dental Support Organizations (IDSO). An IDSO becomes a doctor’s silent partner by buying 51% to 80% of a practice for cash up front at today’s low tax rates. Doctors remain as owners, with their brand, team, and full autonomy for years or decades. Practice performance can be enhanced with captive patient referral sources, and the upside in a doctor’s retained ownership can be far greater than competing alone.
IDSO partner practices benefit from the resources of a larger silent partner to reduce administrative burdens of banking, payroll, accounting, benefits administration, compliance, credentialing, tax, and legal. Doctors can also access 30% lower costs on supplies including clear aligners. And practices benefit from their partner’s professional, full-time recruiting and marketing teams.
While there are now almost 1,000 IDSOs and DSOs in the U.S., including 12+ ortho-only IDSOs, in the last 3 years, many new Dental Trifecta IDSOs have been created. They focus only on partnering with pedo, ortho, and OMS practices in the same regions. They are competing with the ortho only, pedo/ ortho, and multi-specialty IDSOs for great orthodontic practices nationally. In an LPS process, growing practices are achieving new record values, often with six or more eager, qualified bidders from which doctors can choose the right partner.
Tens of thousands of dental practices have quietly partnered with IDSOs over the last 35 years in all 50 U.S. states. Some may have only a few practice partners and others over 700. IDSO’s size gives them leverage in multiple areas including the cost of team benefits.
IDSOs are eager for growing orthodontic practices with at least $1.5 million in collections, and the younger the doctor, the more valuable the practice. In LPS’ $1.0 billion of completed
Chip Fichtner discusses how orthodontists can add liquidity and a strong growth partner to their practices OP
IDSO partnerships in the last 24 months, over $150 million have been for doctors in their 30s.
The IDSOs act as a doctor’s silent partner. Their goal is to support a practice, not to micromanage or homogenize it to meet some corporate standard. Doctors retain full autonomy, not just clinically, but also in how they hire, fire, and lead their teams. The owner doctor makes decisions, not the IDSO.
Ultimately, the IDSO can also provide doctors with a known exit strategy at retirement, years or decades in the future. Thousands of doctors have achieved dramatic increases in the value of their retained ownership over time. Some have exceeded 300%, 500%, and 1,000% or more when they selected the right IDSO partner.
Doctors today should understand the potential value of their practice in an IDSO partnership. Values achieved by LPS for orthodontic practices in the last 6 months have exceeded 3x collections and 10x EBITDA. Doctors who own their real estate also have two great options. They either gain an AAA credit tenant for decades, or, due to their new IDSO tenant, the value of the real estate increases in a sale to a Real Estate Investment Trust (REIT), now or in the future.
Chip Fichtner is co-founder of Large Practice Sales which completed over $1.0 billion of IDSO partnerships in 2022 and 2023. Over the last 40 years, he has built, bought, and sold public and private companies in a variety of industries, and has been featured in numerous media outlets. His tolerant wife of 34 years allows him to live on his airplane visiting clients every week.
To learn more about IDSOs and receive a confidential, no cost, no obligation practice valuation, doctors can contact Large Practice Sales by calling 844-405-0521, emailing ortho@largepracticesales.com, or by visiting www.LargePracticeSales.com.
This information was provided by Large Practice Sales.
Invisible Dental Support Organizations (IDSO)
become your silent partner by purchasing 51% to 80% of your practice for cash at today’s low tax rates
Silent Partners Buy Part of Your Practice - IDSOs purchase 51% to 80% of practices for cash now at low tax rates. Doctors retain ownership and have significant upside in the equity value. Some LPS orthodontic clients have achieved 3x to 7x equity returns over time.
Long-Term Wealth Building Partnership - Doctors continue to lead their practice with their brand, team and strategy for years or decades. Practices benefit from the resources of a larger, silent partner, but are not micromanaged or homogenized.
Six or More Choices in Partnership - LPS clients often have 6 to 10+ qualified bidders. LPS is the largest advisor in the U.S. which enables our clients to achieve record values that the little advisors cannot match.
√ Monetize 51%-80% of your practice value
√ Millions in cash now at low tax rates
√ Continue leading your practice
√ FULL AUTONOMY for years or decades
√ Gain the resources of a larger partner
√Grow faster, better and more profitably
√ Increase the value of your retained ownership
√ Choose the best offer from multiple bidders
√ No-cost, no-obligation practice valuation from the largest advisor to all specialties in the U.S.
844-734-8533
Your Value in Today’s Consolidation Frenzy - You should understand the value of your practice in an LPS-advised process. Doctors who deal directly with IDSOs often leave millions on the table and do not get to consider ALL of their options.
Large Practice Sales (LPS) is the largest transaction advisor to GP and specialty practices in the U.S. and has completed over $1 billion of Invisible Dental Support Organization (IDSO) partnerships in the last 24 months.
“I am ecstatic! You guys got me DOUBLE the best offer I could get on my own! Have any doctor call me and I’ll tell them you can’t go wrong with LPS. Use my name. I am referring all my friends.”
-T.J., DMD
Large Practice Sales Brings Multiple Bidders for the Highest Value In IDSO Partnerships
View the LPS Library of Webinars LargePracticeSales.com/webinars •IDSO: What’s Changed in 2024? •Wealth Building Strategy for Doctors of All Ages •Specialist Options Not Available to GPs
LightForce
Why personalization matters in orthodontics
Who is LightForce?
LightForce Orthodontics’ CEO and co-founder, Dr. Alfred Griffin III, has set a simple, yet powerful mission for the company: “To empower the experts to create the unique bite and smile that every patient deserves.”
It is little wonder then, that continually advancing orthodontic personalization is at the core of what LightForce does.
Why personalization matters
“We want to be the best at listening to orthodontists who use our technology.” Dr. Griffin attests.
The personalization of LightForce’s LightTray indirect bonding system is proof of that. By collecting data and listening to customer feedback, LightForce zeroed in on a clear correlation between the severity of crowding, spacing, tooth eruption, and debonds for certain teeth.
“By personalizing the IDB tray segment design in LightTrays, we’ve been able to improve the consistency of our bracket bond strength. This means fewer disruptions to patient care, and tooth movement is more direct.” Dr. Griffin explains.
According to Vice President of Product, Doran Robinson, the new LightTray innovations add another important degree of personalization in the bonding workflow.
“Historically, analog indirect bonding was challenged in determining how many teeth to include in the bonding tray. Some included full arches, and even LightForce included segments of four teeth. We learned through bracket reorder data that the real answer is that one size doesn’t fit all — it should depend on the patient’s unique clinical condition,” Robinson explains.
Analog brackets use a prescription based on averages from dental casts of a very small, non-diverse population (Andrews, LF. The six keys to normal occlusion. Am J Orthod. 1972;62(3);296309). Decades later, we’re still using the same brackets on every single person, and teeth take a less direct path as a result.
Unsurprisingly, this means orthodontists must spend a great amount of time compensating for a prescription that was never ideal to the patient to start with, ultimately yielding a final result that is still only “close enough” to the desired outcome.
“Even if a stock bracket had the ideal prescription, there’s so many factors that dilute the ability to express the prescription that is in that bracket, such as inaccurate positioning by a clinician and wire slot play,” Dr. Chris Bonebreak Jackson, LightForce’s Head of Clinical Affairs, explains.
All of those variables result in the need for bracket repositions or wire bends to achieve the desired outcome. Dr. Jackson also notes that the higher the forces that are applied to a tooth and the longer those forces are applied correlates with increased risk of root absorption (Roscoe, MG, Meira JB, Cattaneo PM. Association of orthodontic force system and root resorp-
tion: A systematic review. Am J Orthod Dentofacial Orthop. 2015;147(5):610-626), so multiple adjustments can actually be unhealthy for the patient.
Get to know the LightForce personalized platform
LightForce is a personalized end-to-end solution that seamlessly integrates into your practice, powered by 3D-printed custom brackets, advanced LightTray indirect bonding technology, and intuitive digital planning software. The three work in conjunction to ensure highly efficient delivery of the desired finish.
LightPlan
The proprietary digital planning software takes into account treatment planning principles and the doctor’s patient prescription to produce an ideal patient outcome, which can be easily modified by the orthodontist if needed.
LightBracket
LightForce’s 3D-printed brackets are personalized in significant aspects of the bracket (the base, the slot, and the positioning) to achieve the desired outcome using a straight wire.
LightTray
The LightTrays are digitally designed and 3D printed in a proprietary material to deliver the brackets to their intended position on the teeth. The unique, personalized design of each tray reduces the likelihood of bond failures or inaccurate bracket placement compared to a one-size-fits-all indirect bonding tray.
This information was provided by LightForce. OP
Gaidge 360 Consulting: Practice growth needs more than numbers
Transforming data into tangible practice growth
In business, data is king — but interpreting the data often requires expert insight. For one, the sheer volume of it can be overwhelming. Not to mention, discerning which metrics matter most and how to act on them can be time-consuming and challenging.
When it comes to breaking it all down, many orthodontic practices need a helping hand.
Fortunately, Gaidge 360 Consulting’s team of orthodontic consultants merge data-driven solutions with extensive industry knowledge. With their expert insight, practices can transform raw data into actionable strategies, leading to improved efficiency and growth.
Meet the Gaidge 360 Consulting Team
With a diverse group of seasoned orthodontic consultants, the Gaidge 360 Consulting team works closely with your practice to identify the best steps for growth and efficiency. Their collective experience and passion for orthodontic success ensure that your practice thrives.
Recently, the team welcomed Andrea Cook, adding valuable experience to their ranks. Andrea’s 20 years as a chairside assistant and her motivational training techniques energize clinical teams. Widely recognized for her clinical expertise, Andrea specializes in OSHA compliance training, sterilization systems design and management, and maximizing clinical efficiency through effective schedule design. Her experience includes working in multi-doctor practices and providing solutions for the daily challenges faced by orthodontic teams.
Altogether, the consultants’ collective knowledge and 100+ years combined experience in the orthodontic industry equip Gaidge 360 Consulting to guide practices in meeting every goal, no matter how big or small.
Personalized strategies to reach your growth goals
Every practice has different needs. For that reason, Gaidge 360 Consulting offers customized solutions designed to optimize every facet of your practice:
• Integrating new systems and technology to improve efficiency
• Streamlining billing processes and insurance management to boost profitability
• Clarifying job roles and providing team training to enhance performance and reduce stress
• Setting patient-focused goals to increase case acceptance and optimize schedules
• Conducting thorough reviews and creating actionable plans for effective branding and marketing
Importantly, Gaidge’s consultants also help you track and analyze crucial metrics such as production and collections, exams and starts, treatment efficiency, and more. These insights empower you to optimize your practice’s operations and improve patient care.
Your partner in simplifying orthodontic practice management
Navigating the complexities of data, practice operations, and team management in orthodontics can be daunting. But with experienced consultants by your side, it doesn’t have to be. Gaidge 360 Consultants combine advanced data analytics with hands-on expertise to help your practice thrive.
With their support, you can turn complex challenges into manageable strategies, ensuring sustained improvements and success in the ever-evolving field of orthodontics.
Reach out today to see how Gaidge’s consultants can help your practice achieve its goals.
OP
This information was provided by Gaidge 360 Consultants.
Tops’ complete ecosystem gives you the power, speed, and agility to move on to what’s next.
Personalized reminders, texts, and emails Fully-integrated payment processing Fast, reliable, and secure