Using innovation to create a dental home for all children
Dr. E. LaRee Johnson
Five indicators of sleep disordered breathing

Dr. David E. McCarty
Conservative approach of fortuitously found odontoma in a child with severe autism
Dr. Gabriela Aurora Asensi
Tips to improve patient experience with laser technology
Dr. Jenny Jackson

FOR A BRIGHTER
INNOVATING
PROMOTING EXCELLENCE IN PEDIATRIC DENTISTRY Airway & Orthodontics n Watch for Our Spring 2024 Issue Fall 2023 Vol 1 No 2 pediatricdentalpractice.com
FUTURE
pulpdent.com/activademo
MERGING RESTORATIVE AND PREVENTIVE DENTISTRY



ACTIVA™ KIDS is an esthetic, BioACTIVE resin restorative that stimulates apatite formation and the natural remineralization process with release and recharge of calcium, phosphate and fluoride. It is an opaque white shade ideally suited for pediatric dentistry. Scan the QR code to schedule an in-person or virtual demo today.

 Photos courtesy of Dr. Leon Katz
Photos courtesy of Dr. Leon Katz
Pediatrics — an ever-evolving specialty
Welcome to the fall issue of Pediatric Dental Practice US! This is the second issue of a publication dedicated to bringing our profession new, cutting-edge treatment modalities so that we can not only be informed but also offer the very best to our patients. While it is always going to be important to know which sealant material performs better than another, the readership of this journal wants to dive deeper! It was such an honor to take part in the inaugural issue. Looking at the editorial themes of this issue — Airway, Orthodontics, Technology and Trends, Anesthesia and Sedation, Practice and Patient Management, and Behavioral Disorders — it’s going to be another exciting offering.
It’s been almost 10 years since the inaugural issue of The Journal of Dental Sleep Medicine and less than 100 years since Dr. Pierre Robin definitively made the connection between underdeveloped jaws and tongue obstruction as a cause of breathing challenges during sleep.1 Much has happened in our understanding as well as our ability to treat this debilitating condition. I believe we will see even more innovations, particularly in non-invasive laser applications and cranial-friendly approaches with
A Native Houstonian, Amy L. Luedemann, DDS, has been a board certified pediatric dentist since 2007. She has been a thought leader and innovator in her field for more than a decade. Dr. Luedemann’s clinic, Kidstown Dental, was the third clinic in the United States to have an interdisciplinary clinic on site to help infants with oral restrictions, including an osteopath for guided releases and IBCLCs for functional support. For “older” kids, she has brought in-house myofunctional therapy, PT, Integrative Chiropractors, SLPs, and a host of different types of providers depending on patient needs to support the most challenging patients. It is Dr. Luedemann’s passion for healing and transformation in a team setting with outside-the-box solutions that have drawn Functional Medicine MDs, Pediatric Neurologists, PTs, OTs, DCs, DOs, SLPs, ENTs, Midwives, Doulas, Neural Movement Specialists, Functional Nutritionists, and DDSs to join her Interdisciplinary Study Club that has met for almost 10 years in her office. This group of amazing, dedicated providers have met monthly for years to study and collaborate on best practices in the littlest of patients and have worked to set standards in the Greater Houston area and beyond. She has practiced “no-shot” laser pediatric dentistry since 2009. She has been transforming little lives with the ALF appliance since 2015, and in recent years has been one of the first providers to innovate new appliances that are helping 0-3 year old children with sleep apnea. Her appliance designs are based on osteopathic principles and are proving to be very powerful. If you ask “Dr. Amy” what her passions are, she will say that learning, innovating, and collaborating are passions of hers but that teaching others and sharing knowledge is when she feels she is living her purpose the most! In her time away from work, she enjoys traveling with her family and friends, reading, biohacking, and long scenic walks.

the foundation being a whole body approach to sleep-disordered breathing and sleep apnea in the coming decade. It is clear now that suffering patients need more than simply structural or medicinal solutions, and our profession is starting younger and looking deeper to help heal our little patients.
Speaking of looking deeper and offering more powerful solutions, you won’t want to miss the technology and trends section of this issue. The first medical-grade laser was introduced in 1963, and the first dental laser (a 1064 Nd YAG) was marketed to dentists in 1989.2 Boy, have we come a long way! Lasers are now successfully used for addiction, trigger points, healing, esthetics, trauma, PTSD, Alzheimer’s, Parkinson’s, Stroke, Bell’s Palsy, and now there is early and promising work being done to activate local stem cells and the nervous system to reverse dental infections. Search almost any diagnosis on PubMed, and you will be surprised at how lasers have made advances in so many areas of medicine and dentistry. And in this journal specifically, you can expect to receive a steady stream of the options available to us, within our scope of practice, to help treat and benefit our patients.
Almost I can’t comment on everything in this short introduction, but if you are a reader who wants to see beyond old and outdated approaches to ever-evolving challenges our patients are facing, you have the right publication in your hand. Please stay connected with us, and share the innovations and successes of your own practice and your experiences as we push forward into a new paradigm in pediatric dentistry!
REFERENCES
1. Robin P. A fall of the base of the tongue considered as a new cause of nasopharyngeal respiratory impairment: Pierre Robin sequence, a translation. 1923. Plast Reconstr Surg. 1994 May;93(6):1301-1303.
2. Parker, S. Introduction, history of lasers and laser light production. Br Dent J. 2007; 202:21–31.

1 pediatricdentalpractice.com Volume 1 Number 2 INTRODUCTION © MedMark, LLC 2023. All rights reserved. The publisher’s written consent must be obtained before any part of this publication may be reproduced in any form whatsoever, including photocopies and information retrieval systems. While every care has been taken in the preparation of this magazine, the publisher cannot be held responsible for the accuracy of the information printed herein, or in any consequence arising from it. The views expressed herein are those of the author(s) and not necessarily the opinion of either Pediatric Dental Practice US or the publisher.
Amy L. Luedemann, DDS
PD
It is clear now that suffering patients need more than simply structural or medicinal solutions, and our profession is starting younger and looking deeper to help heal our little patients.”
Using innovation to create a dental home for all children
Carolina Pediatric Dentistry finds the formula to deliver state-of-theart treatment to patients from diverse socioeconomic backgrounds

Cover image of Dr. E. LaRee Johnson courtesy of NuSmile.
CLINICAL
The five finger approach to sleep-wake complaints


Dr. David E. McCarty offers a collaborative patient-centered problem-solving tool for a complex world
“Smart” restorative materials in
Fred Berk discusses materials that behave more dynamically
2 Pediatric Dental Practice US Volume 1 Number 2 TABLE OF CONTENTS
PUBLISHER’S PERSPECTIVE Staying informed and safe Lisa Moler,
MedMark Media............................... 6 CLINICAL The missing link in pediatric sleepbreathing treatments Dr. Paulo Soares explores a myofunctional orthodontic treatment protocol for correcting sleep-disordered breathing ......................................................... 16 Conservative approach of fortuitously
odontoma
Dr. Gabriela
Asensi discusses treatment of a
needs patient .............................. 20
Founder/CEO,
found
in a child with severe autism
Aurora
special
PRODUCT PROFILE
........................................................ 23 8 11 COVER STORY
dentistry
The Next Step of Your Career Starts Here
D4C Dental Brands is the nation’s largest dental support organization focused exclusively on pediatric dentistry and orthodontics. Our approach is centered around nurturing growing smiles, exceptional clinical quality, and helping our patients develop healthy habits for life.


Start the next chapter of your career today by joining a likeminded network of clinical entrepreneurs, visionaries, and industry leaders. Your future begins here.

PRACTICE TRANSITIONS CAREER OPPORTUNITIES
d4cdentalbrands.com
Connect with our team today to learn more.
Pediatric Dentistry
Orthodontics
Supporting
and
Published by
Publisher
Lisa Moler lmoler@medmarkmedia.com
Managing Editor Mali Schantz-Feld, MA, CDE mali@medmarkmedia.com
Tel: (727) 515-5118
National Account Manager
Adrienne Good agood@medmarkmedia.com
Tel: (623) 340-4373
Sales Assistant & Client Services
Melissa Minnick melissa@medmarkmedia.com
Creative Director/Production Manager

Amanda Culver amanda@medmarkmedia.com
Marketing & Digital Strategy Amzi Koury amzi@medmarkmedia.com
eMedia Coordinator
Michelle Britzius emedia@medmarkmedia.com
Social Media Manager April Gutierrez socialmedia@medmarkmedia.com
Digital Marketing Assistant Hana Kahn support@medmarkmedia.com
Website Support Eileen Kane webmaster@medmarkmedia.com
MedMark, LLC
15720 N. Greenway-Hayden Loop #9 Scottsdale, AZ 85260
Tel: (480) 621-8955
Toll-free: (866) 579-9496
www.medmarkmedia.com
www.pediatricdentalpractice.com


4 Pediatric Dental Practice US Volume 1 Number 2 TABLE OF CONTENTS PRACTICE DEVELOPMENT Leveraging AI in pediatric dental marketing: from social media to SEO Scott Childress discusses spreading the word about your practice with AI.............................. 26 PEDIATRIC PERSPECTIVE Pediatric sleep issues last a lifetime; join the movement ASAP Dr. Michelle Weddle discusses how clinicians can play a large role in improving the lives of children with pediatric sleep disorders .......................................... 28 TECHNOLOGY This is not a drill: tips to improve patient experience with laser technology Dr. Jenny Jackson discusses the positive effects of using laser technology in her pediatric practice.............................................. 30 24
PLANS
Mary Bourke discusses the importance of optimizing children’s orofacial growth, development, and function
GROWING
Functional chewing and nasal breathing Dr.







































PRR & small Class 1 procedures are faster & easier using Beautifil KIds SA, bioactive self-adhesive flowable composite! are SNBKP-0823 Resin Tag Infiltration Beautifil Kids SA Dentin > Ideal handling for precision placement > High bond strength for reliable adhesion > Therapeutic bioactive Giomer Technology > Indicated for PRR and small Class I > Great for restless pediatric patients > Two shades, primary and permanent Bioactive Self-Adhesive Nano-Hybrid Flowable ELIMINATED THE TECHNIQUE SENSITIVE BONDING STEP! New! Beautifil Kids SA is great for the management of caries in restless children! New! Visit shofu.com Call 800.827.4638 Shofu Dental Corporation San Marcos CA 92078 1Gordan VV, Mondragon E, Watson RE, et al. A clinical evaluation of a self-etching primer and a giomer restorative material: Results at eight years. JADA. 2007;138(5):621-627. 3Asahi University School of Dentistry. *One product sample per of ce. While supplies last. See for yourself Get a FREE sample! Scan code or call Anti-Bacterial Protection Prevents Secondary Decay* Acid Neutralization Up to 30% Savings Over Other Brands 38-Year independent clinical study recorded 100% retention rate, no secondary caries, failures, or postoperative sensitivity. Minimal bacterial colonization Bioactive Giomer Technology** Conventional Composites Shukan C. Kanuga, DDS Mounika Falemban, DMD Advanced bacterial colonization Greatly reduce secondary decay using Shofu’s clinically proven bioactive Giomer Restoratives! 1
Staying informed and safe
Recently, I saw a movie called “The Sound of Freedom,” the story of Tim Ballard, a federal agent who quits his job with the Department of Homeland Security to start his own independent team to rescue child trafficking victims. One of the movie’s executive producers is Tony Robbins. Tony has been a mentor and inspiration to me. The movie was emotional and moving for me, watching (as Tony describes on his website), “the harrowing experiences faced by victims of human trafficking and the relentless dedication of those fighting to dismantle these dark criminal networks, which continue to enslave millions of children globally each year.”
Human trafficking is not just a movie. The U.S. Department of Homeland Security (DHS) notes, “Every year, millions of men, women, and children are trafficked worldwide — including right here in the United States. It can happen in any community, and victims can be any age, race, gender, or nationality.” Violence, manipulation, false promises of well-paying jobs, and even the promise of romantic relationships can lead to imprisonment of these innocent, frightened victims. DHS adds, “Language barriers, fear of their traffickers, and/or fear of law enforcement frequently keep victims from seeking help, making human trafficking a hidden crime.”
• Reasons why a victim may try to avoid being identified.
• Oral injuries that may indicate a trafficking victim.
• Resources for intervention specialists in human trafficking.
• What steps the clinician can take if the patient is identified as a trafficking victim.
The DHS says that in helping these victims, the healthcare professional also needs to pay careful attention to the safety of themselves and their teams. They warn, “Do not attempt to confront a suspected trafficker directly or alert a victim to any suspicions. It is up to law enforcement to investigate suspected cases of human trafficking.”
Lisa Moler Founder/Publisher, MedMark Media
At-risk victims may be hiding in plain sight. Dental professionals may not realize that patients who visit their offices may be impacted by this terrible crime. Because of signs and symptoms of human trafficking, dentists may be able to help a victim of human trafficking during the course of the dental visit. Several states mandate that dentists need a human trafficking continuing education course to renew their licenses. In these courses, dentists learn details such as:
• Work-settings that may employ trafficking victims.
• Physical and psychological clues that the patient may be being trafficked.
• Some key words that the victim or perpetrator may say to the dentist to avoid being identified as a trafficking situation.

Back to our fall issue, our Cover Story takes a look at California Pediatric Dentistry. Thanks to NuSmile, Dr. E. LaRee Johnson and her team are bringing effective, painless, and efficiency-enhancing innovation to patients from diverse socioeconomic backgrounds. Dr. David E. McCarty’s article gives a high-five to “The five finger approach to sleep-wake complaints,” a way of communicating the complex topic of sleep medicine to patients. In his article, Dr. Paulo Saores explores “The Missing Link in Pediatric Sleep Breathing Treatments” — the myofunctional orthodontic appliance protocol, a simple, scalable treatment approach.

In my Publisher’s Perspective column, I always share topics that are important to my growth not just as a publisher and entrepreneur, but also as a human being. Human trafficking is an outrageous and evil crime. Take a CE class on this topic to know warning signs and also to stay safe. Human trafficking “exists nationwide — in cities, suburbs, and rural towns — and possibly in your own community,” says DHS. Be aware, smart, and cautious — as you help patients to survive and thrive.
To your best success,
 Lisa Moler Founder/Publisher MedMark Media
Lisa Moler Founder/Publisher MedMark Media

6 Pediatric Dental Practice US Volume 1 Number 2 PUBLISHER PERSPECTIVE
Don’t Miss the Next Issue of Sign up for your free subscription at https://pediatricdentalpractice.com and opt-in to our enewsletter to stay informed between issues. INNOVATING FOR A PROMOTING EXCELLENCE IN PEDIATRIC DENTISTRY Airway&Orthodontics n WatchforOurSpring2024Issue Fall2023Vol No pediatricdentalpractice.com Fiveindicatorsofsleep disorderedbreathing Dr.DavidE.McCarty ofConservativeapproach odontomafortuitouslyfound in childwithsevereautism Dr.GabrielaAuroraAsensi Tipstoimprovepatient experiencewithlaser technology Dr.JennyJackson Using innovation to create a dental home for all children Dr.E.LaReeJohnson
Partner with Pediatric Dental Anesthesia Associates, the nation’s largest pediatric anesthesia practice for pediatric dentists.

• Board-certified physician anesthesiologists with extensive training and experience in pediatric anesthesia
• Unblemished safety record for over hundreds of thousands of patients
• Providing service in most states and hundreds of pediatric dental offices
For more information, visit PediatricSedation.com Connect at mgmt@pediatricsedation.com
• Child-friendly nursing staff trained in customer service
• Dedicated billing/scheduling team to support your staff
Read our patient reviews
Brooke Maryak, MD Pediatric Anesthesiologist
The highest standard of care when it matters most
Using innovation to create a dental home for all
children
Carolina Pediatric Dentistry finds the formula to deliver state-of-the-art treatment to patients from diverse socioeconomic backgrounds

Making a bold vision a reality
Dr. LaRee Johnson founded Carolina Pediatric Dentistry in 2002 with a vision of making the practice a dental home for all children. In 2015, Dr. Clark Morris partnered into the practice with an identical sentiment. Since then, Drs. Rosie Nguyen, Miranda Kalaskey, Taylor Windley, Jordan Reading, and Aïssatou Barry-Blocker have joined the practice to increase access to care for all children. “Our goal has always been to treat children regardless of the family’s income level,” said Dr. Johnson, “and we’re proud to say that our patients are just as likely to come from foster care as they are from highly affluent neighborhoods.” This practice routinely sees children who travel hours to receive treatment due to special healthcare needs, full-mouth zirconia crown restoration, or seeking access to care due to their type of insurance.
Dr. Johnson acknowledged that every pediatric dentist wants to serve all children; however, creating a fiscally-sound practice with this mission is another thing entirely. “Transforming this vision into a reality has required relentless commitment combined with an equally dedicated, trained, high-functioning team using innovative, affordable products that allow our practice to consistently provide positive clinical outcomes and operate at an exceptional level of efficiency,” she said.
E. LaRee Johnson, DDS, MS, FAAPD, was born in Southern California and migrated across the country for education. Ultimately, she landed in North Carolina where she and her husband have raised their children, and she has practiced fulltime since 1999. For Dr. Johnson, pediatric dentistry is the perfect combination of working with children and art (utilizing a medium of various dental materials to achieve a perfect esthetic result). Dr. Johnson believes all children deserve a dental home and has spent her career advocating for those with special health care needs and those with issues in access to care. Her practice is a dichotomy spanning underprivileged children to fee-for-service private pay and includes treatments such as full mouth dental rehabilitation with composite resins, BioFlx™, and zirconia (ZR) crowns. Dr. Johnson loves being a pediatric dentist and teaching others compassionate clinical excellence with efficiency.
Innovative technologies that boost efficiency — affordably!
Dr. Johnson apologized for being a few minutes late to her interview for this article, but she had a good excuse — she had just finished an emergency pulpotomy and zirconia crown procedure in which she was able to save the tooth of a 1-year-old.
An early adopter of innovative technologies throughout her dental career, Dr. Johnson said she relies on two new product lines from NuSmile. The first is NeoPUTTY®, a premixed MTA designed for pediatric use. Dr. Johnson also uses a combination of the SleeperOne and Soan (by Dentalhitec), a new line of local anesthetic digital delivery systems designed to be easy, convenient, and painless. “The condition of the tooth combined with a traumatized, wiggly 1-year-old’s intolerance for a dental procedure required swift treatment,” she said. “A pulpotomy was the only option. You can’t do a pulpectomy on a 1-year-old child with incomplete root formation. Conventional MTA would have taken longer to mix, but NeoPUTTY requires no mixing. The Dentalhitec devices allow for compassionate intraosseous

8 Pediatric Dental Practice US Volume 1 Number 2 COVER STORY
Diane Krueger and Dr. LaRee Johnson: An intersection of a shared mission for optimal and esthetic restorative care for all children
injections and subsequent immediate start of treatment, which made the child as comfortable as possible during the procedure.”
A special inspiration
NeoPUTTY, a bioceramic material, and the Dentalhitec devices come from the same manufacturer — NuSmile, a company primarily known for its esthetic pediatric crowns. Dr. Johnson has been an admirer of NuSmile and its Founder/CEO Diane Johnson Krueger since she started her pediatric dental residency as a 24-year-old. “I met Diane when I was a first-year resident, and it was immediately apparent just how seriously committed she was to serving children and pediatric dentists,” she recalled. “Her first product was the Signature pre-veneered crown, which revolutionized the way we restored primary anterior teeth. They can be placed quickly, they’re not as moisture-dependent or technique-sensitive as strip crowns, and they wear better. In fact, Signature crowns are still a go-to product in our practice, even though NuSmile’s zirconia crowns are my favorite.”
“When I founded NuSmile in 1991,” said Ms. Krueger, “I just wanted to make it possible for kids’ front teeth to be restored with something other than stainless-steel crowns. I never had silver teeth myself as a child, but I did have a fall that darkened one of my teeth. That made me very self-conscious and gave me some sense of how kids must feel with stainless-steel anterior crowns.”
Dr. Johnson says BioFlx™, NuSmile’s newest line of pediatric crowns, might be her favorite crown innovation yet. Made of medical grade polymer, BioFlx is the first flexible, durable, and esthetic pediatric crown. Doctors at Carolina Pediatric Dentistry can place a BioFlx crown in the same amount of time it takes to place a stainless-steel crown. Dr. Johnson is hopeful that dental insurance providers and Medicaid will eventually cover BioFlx to make it more affordable for all children. “I would love to
eliminate silver from children’s mouths,” she said. “All children deserve to have esthetic crowns.”
A shared passion for pediatric dentistry
“So many of the products we use as pediatric dentists are designed primarily for general dentists or other specialists,” said Dr. Johnson. She appreciates the fact that NuSmile is one of the few manufacturers that is truly focused on the unique needs of pediatric practitioners and patients. “I’ve been practicing for a long time, and I can’t think of another manufacturer that has ever asked my opinion about how their products could be improved. As a pediatric dentist, I really appreciate that.”
The feeling is mutual, according to NuSmile’s Founder and CEO. “I love pediatric dentistry and working with pediatric dentists,” said Ms. Krueger. “I love their demeanor, their commitment, their compassion, and what they do every day in their practices for their patients.”
According to Dr. Johnson, “Diane could have retired successfully following the launch of Signature crowns decades ago, but she didn’t. She keeps striving to bring us brilliant innovations that make life better for children, doctors, and their teams, and still manages to charge very reasonable prices for those innovations.”
Expanding the horizons of pediatric dentistry efficiency

Dr. Johnson is thrilled to see that NuSmile has recently expanded its flair for efficiency-enhancing innovation to the

9 pediatricdentalpractice.com Volume 1 Number 2 COVER STORY
Silvia Saucedo, RDH, about to deliver local anesthetic via the non-intimidating Soan device Painless intraosseous injection using a Dentalhitec device
The Dentalhitec devices allow for compassionate intraosseous injections and subsequent immediate start of treatment, which made the child as comfortable as possible during the procedure.”
world of local anesthetic devices. The company has just launched two local anesthetic digital delivery devices that Dr. Johnson has been testing, both part of Dentalhitec: the corded SleeperOne and the wireless Soan. “Both allow us to deliver local anesthesia in the kindest way possible by making it impossible to inject too fast and cause discomfort for our patients,” she said. “As providers, we all try to give our patients the most compassionate care possible; however, I’m confident that with conventional manual syringes, our injections often unintentionally deliver more than the one milliliter per minute (which is considered the most painless way to deliver local anesthetic). It is absolutely impossible to deliver local anesthetic too fast with the SleeperOne or the Soan.”
Dr. Johnson admires the two instruments’ designs, which are easy for dentists and hygienists to use and do not look scary to children. They also avoid another problem — after over 20 years of squeezing syringes, the thumb and forefinger on her right hand had developed ganglion cysts. Also, the thumb and forefinger on her right hand were significantly larger than the thumb and forefinger on her left hand due to chronic overuse inflammation. “But after 3 months of having the SleeperOne and Soan in our practice, the sizes of my ganglion cysts, right forefinger, and right thumb have decreased noticeably,” she said. “I feel I owe it to younger pediatric dentists who think they’re invincible to urge them to take care of their bodies by using ergonomically advanced products like the SleeperOne and Soan. And there’s another benefit — it’s much easier to interact with your patients using these devices — especially with the Soan’s ‘cruise’ setting that operates on its own with a simple tap of your foot,” avoiding the stress of squeezing and pressing and the risk of delivering anesthesia too rapidly with manual syringes.

Teaching about technique — and life
While Dr. Johnson has always been in full-time private practice, she has also had her hand in teaching at her alma mater, the University of North Carolina Adams School of Dentistry. She will begin soon as an adjunct faculty member at the East Carolina University School of Dental Medicine, and she also teaches at continuing education events sponsored by AAPD, other dental organizations, and NuSmile. She particularly enjoys showing her students 10-plus years of radiographic and photo follow-up on cases to illustrate best practices, as well as the cases she wishes she had done differently. “It’s especially gratifying to see students’ reactions when I show them how they can use one material in the pulpotomy instead of multiple or provide other insights that allow them to simplify a procedure while improving the outcome. I love teaching with a hands-on component; you can talk about something all day long, but until someone picks up a handpiece and utilizes a typodont, you can’t understand their knowledge gaps and technique barriers to success. It’s my favorite way to teach.”
According to Dr. Johnson, teaching needs to be about more than clinical procedures. “I also teach about the day-to-day aspects of running a practice, working in one, and maintaining a healthy work-life balance,” said the married mother of two young adults, Umstead 100-Mile Endurance Run Finisher, and three-time Ironman. “I’ll be forever grateful to the many outstanding teachers I had, and teaching others is a great way to pay that forward.”

A dream come true
The dream of creating a practice that is truly a dental home for all children is both highly ambitious and very admirable. Fortunately for their patients, Carolina Pediatric Dentistry has clearly found the right formula, and the right partners, for success. PD

10 Pediatric Dental Practice US Volume 1 Number 2 COVER STORY
BioFlx medical grade polymer crowns: NuSmile again raises the bar for pedi atric dentistry!
High five! Happy child leaving after Dr. Johnson completed a half-mouth of restorative care in under 30 minutes utilizing Dentalhitec anesthesia, NeoPUTTY, and BioFlx crowns
The five finger approach to sleep-wake
complaints
Dr. David E. McCarty offers a collaborative patient-centered problem-solving tool for a complex world
The complexity of sleep apnea
Because it arises from multiple overlapping anatomic, physiologic, and functional deviations from optimum, with variable representation of obstructive versus central apnea processes, the entity known as “Sleep Apnea” is best characterized as a complex phenomenon1 for which there is no “one-size-fits-all” solution.2 What’s more, clinical management of breathing- and airway-related pathology requires navigation of countless non-apnea contributors to sleep-wake complaints, nesting the complexity of the breathing/airway issues within the complexity of a larger spectrum of sleep-provocative disease.
“Complex” environments differ from “complicated” ones by virtue of their unpredictability. For example, the cockpit of a 747 can be considered a “complicated” environment. Sure, there are scads of dials and knobs, but with the right training, you’d know just what to do to get a predicable result from that machine: you’d take off, you’d fly, and you’d land, and it would be predictable.
On the other hand, a “complex” environment involves variables that may be hidden to the problem-solvers, responses to therapy being less predictable. Compared to an aircraft cockpit, a “complex” environment is more like a Brazilian rainforest.3
Complicated environments tend to run efficiently with expert, top-down management styles. On the other hand, complex environments require a different mindset, one which is receptive to new information and intentionally collaborative.3
To explore this, let’s go to war…
Gen. Stanley McChrystal, Al Qaida in Iraq, and the Team of Teams
In his bestselling book Team of Teams, Stanley McChrystal (U.S. Army Gen, retired) describes his real-world approach to complexity and his successful strategy to harness true collaboration among America’s most elite strike forces: Navy SEALS, Army Rangers, Army Delta Force, and Air Force Special Tactics.4
Under McChrystal’s command, this consortium faced a devious and dangerous enemy called Al Qaida in Iraq in the early 2000s. In short, he found that these elite forces had difficulty merging their efforts at first — the squads seemed to compete with one another in the field and had trouble predicting one another’s
contingencies. Instead of enhancing one another’s efforts, squads often squabbled and defended their internal honor.
He described the phenomenon as feeling like the coach of a soccer team of exclusively world-class players, all of whom happened to play the game with blinders on.
McChrystal understood that he wouldn’t be able to command his way out of his predicament. He realized he needed to create an environment where collaboration would arise naturally. To do this, he introspectively asked what would make a good soccer team.
His answer included two elements:
1. Team-members needed to share an understanding of the playing field — what it looked like, what the rules were, and how things fit together — in other words, all players possessed a “shared consciousness” of the complexity of the situation.
2. Team-members had to experience “lateral connectivity” — a term which for McChrystal basically boiled down to a combination of “trust” and “empathetic connection.” Trust empowers an upfield player to kick the ball to an empty spot downfield, born of an empathetic bond with her teammate — whom she knows is fast enough to get there, and carries the shared consciousness that that’s where she’s expected to be.
To enhance team-wide shared-consciousness, McChrystal created an open-command-post mission control center, with planning stages open to all key members of the mission: even translators, drivers, and non-military governmental agencies like the CIA and FBI. As a leader, he was present, active, and available. Very few details were deemed “need to know.”
To enhance lateral connectivity, McChrystal instituted a crossteam embedding program — a SEAL would embed with the Rangers, for example, or a Delta would fly with Special Tactics.
Ultimately, McChrystal’s “Team of Teams” would go on to eliminate their most dangerous target, the charismatic radicalized leader of Al Qaida in Iraq, Abu Musab al-Zarqawi, a success McChrystal attributed to collaboration and field-empowered decision-making:
“At the core of the Task Force’s journey to adaptability lay a yin-and-yang symmetry of shared consciousness, achieved through strict, centralized forums for communication and extreme transparency, and empowered execution, which involved the decentralization of managerial authority.” 4
Complexity, collaboration, and Dave Snowden’s Cynefin Framework
Dave Snowden is a social scientist who specializes in making sense of complexity.5,6 He popularized the concept of collab-

11 pediatricdentalpractice.com Volume 1 Number 2 CLINICAL
David E McCarty, MD, FAASM, is a Sleep Medicine clinician, author, cartoonist, and podcast creator/host. He is the co-author of Empowered Sleep Apnea: A Handbook for Patients and the People Who Care About Them, and the creator and co-host of Empowered Sleep Apnea: THE PODCAST.
orative decision-making in the business world and continues to consult for titans of industry.7 The following passage — taken from an essay Snowden wrote for Harvard Business Review in 2007 — observes breakthroughs when a leader is receptive to new information:
“Instructive patterns … emerge if the leader conducts experiments that are safe to fail. That is why, instead of attempting to impose a course of action, leaders must patiently allow the path forward to reveal itself. They need to probe first, then sense, then respond.”3
What Snowden describes here is essentially responsive listening, echoing the foundational ethos of patient-centered medicine. When he advises leaders to conduct “experiments that are safe to fail,” clinicians recall the scientific basis for the old-fashioned “N of 1” clinical treatment trial.8 Substitute “examine-diagnose-treat” for “probe-sense-respond,” and the parallel to patient-centered medicine is clear.
Complexity requires collaboration
Arguably, skillful navigation of complexity is the “art” of clinical practice. McChrystal’s wartime experience and Snowden’s work on complexity sense-making both suggest a method behind the “art,” with a receptive and collaborative posture at its foundation. It follows that providers best able to collaborate with their patients will be most successful navigating through medically complex terrain. The challenge we face is to communicate the complexity of the landscape of sleep medicine to our patients in an understandable and practically useable way.
The Five Finger Approach
The “Five Finger Approach” is a patient-centered collaborative clinical tool which organizes the complexity of problem-solving sleep-wake complaints into five functional and actionable domains:
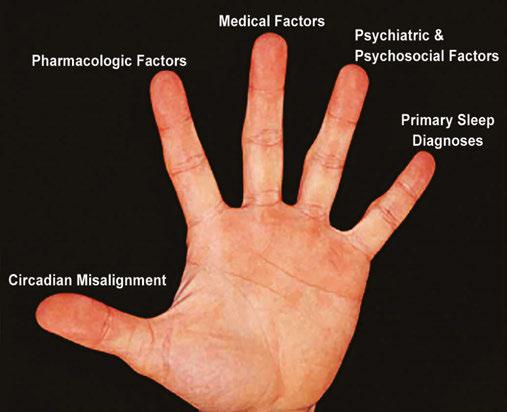
1. circadian misalignment
2. pharmacologic factors
3. medical factors
4. psychiatric/psychosocial factors
5. primary sleep medicine diagnoses.9
When used as a collaborative bedside tool, this framework helps patients participate in their own problem-solving by promoting a shared consciousness for the complexity that’s being deconstructed. When each domain is collaboratively explored by provider and patient, the partnership can identify actionable sources of suffering, discomfort, and dissatisfaction with the sleep-wake experience that otherwise would remain unseen and unaddressed.10
To properly explore the first two domains (circadian misalignment and pharmacologic factors), we’ll need to review some basic concepts of circadian neurobiology and clinical epidemiology.
First, let’s look at circadian misalignment.
Exploring circadian misalignment
The competing drives for “sleep” and “wake” can be summarized using a framework that’s called the Two Process Model of sleep-wake regulation.11 The two processes governing “sleep” and “wake” are called Process S (the “S” stands for a concept known as “sleep pressure”) and Process C (the “C” stands for “circadian”).
When the circadian drive to promote wakefulness is misaligned with the desired timeframe for sleep, the sleep-wake experience becomes problematic. It’s common for evening environmental variables to contribute to a delay in circadian sleep phase — creating a type of “social jet lag” which manifests as sleep-onset insomnia and morning grogginess.
The complexity of these topics can be easily shared with patients, as will be explained below.
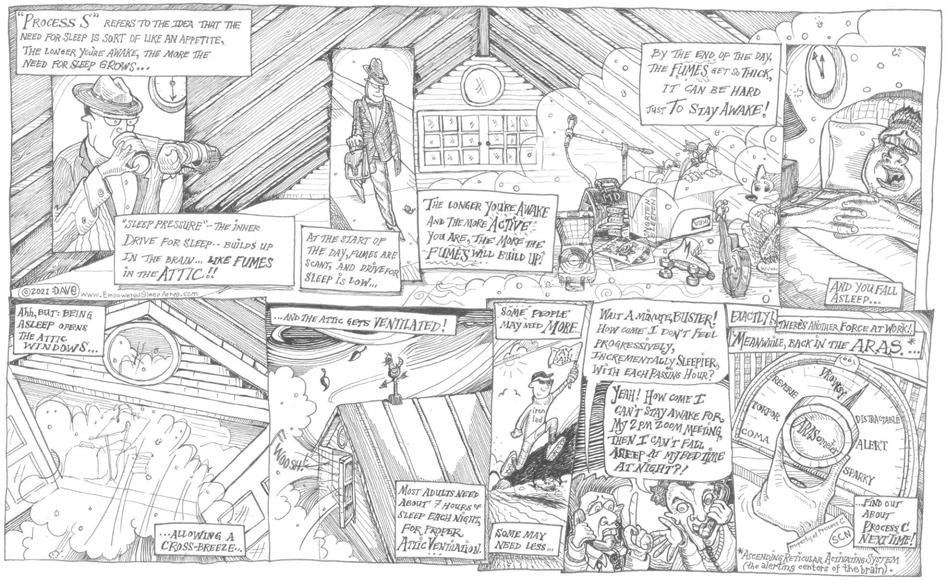
Process S: Fumes in the Attic
The concept of Process S can be easily explained by using the concept of “fumes in the attic.”12 The longer we’re awake, and the more active we are, the more “fumes” will build up in our “attic.” When “fumes” get too thick, we get sleepy, bleary-eyed, brainfogged. When we fall asleep, fumes clear out — it’s as if we’ve opened up all the windows in the attic to allow a cross-breeze to ventilate all those fumes away!
The cartoon on the next page illustrates the concept with a bit of whimsy.
Process C: Circadian Maintenance of Alertness
The deep brain neuronal structures keeping us awake are collectively referred to as the “Ascending Reticular Activating System” — “ARAS” for short. Stimulating these neurons makes us feel more awake. Damaging or blocking these neurons makes us feel sleepy, due to unopposed activity from Process S.
The neurons of the ARAS are programmed to fire at different levels, depending on the time of day, a process regulated by the seat of our circadian rhythm, the suprachiasmatic nucleus (SCN).13
Toward the end of the day, during roughly the 3 hours before our usual prolonged nocturnal sleep interval, the ARAS fires at high levels. This makes sense, because by the end of the day, there’s a lot of sleep pressure (i.e.: Process S, i.e.: “fumes”) hanging around. At that point, the ARAS must work hard to counterbalance the fumes, so it dials way up.13
This is the “second wind” our patients might recognize, in the early evening.
Researchers of circadian sleep biology have termed this timeframe in the circadian cycle the “forbidden zone” because
12 Pediatric Dental Practice US Volume 1 Number 2 CLINICAL
Figure 1A: Five Finger Approach (from McCarty 20109)
biologically, it’s difficult for one to sleep during this timeframe of robust ARAS activity.14 Delaying the “forbidden zone” contributes to “social jet lag” symptoms, like sleep-onset insomnia and morning grogginess.15
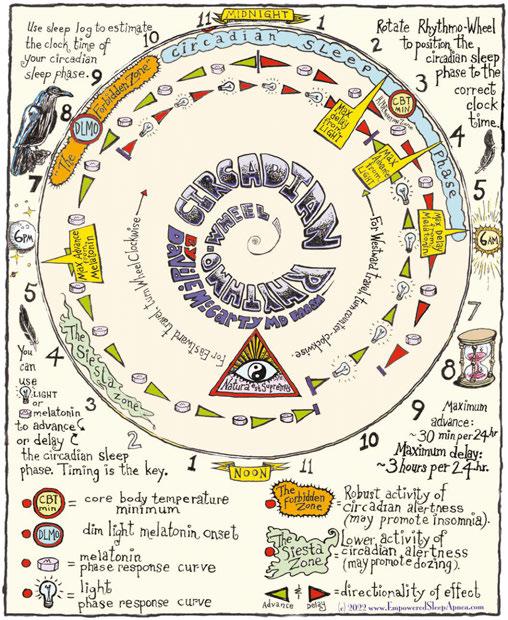
Teaching about circadian biology is enhanced with the use of visual aids, such as the interactive wheel shown in Figure 2.
Patients are often surprised to learn that common environmental variables in the timeframe of the “forbidden zone” — not just electric lights, but also social stimuli, such as eating, excitement, and exercise — all promote a subsequent delay in the sleep phase, thus compounding “social jet lag” misalignment symptoms.
Exploring pharmacologic factors
Prescription medications and social drugs (like nicotine, caffeine, alcohol, and, increasingly, marijuana) can have profound influences on sleep and wake. That’s why a diligent, non-judgmental pharmacologic review is essential in any investigation of an individual’s sleep-wake complaints.
How does one decide if a medication or drug is playing a role in a patient’s sleep-wake complaints? Evidence-based medicine pioneers, Sackett, et al., recommend a studied evaluation of whether there’s a repetitive signal in the published literature suggesting that the agent in question can cause the type of harm you’re worried about, coupled with a temporal sequence of exposure and outcome that makes sense for the narrative you’re dealing with.14
This bit of detective work is enhanced when patients understand the nature of the search and are deputized as active agents in the problem-solving process.10
A list of common pharmacologic factors affecting sleep-wake is listed in Table 1 on the following pages.
13 pediatricdentalpractice.com Volume 1 Number 2 CLINICAL
Figure 1B: “Fumes in the Attic” cartoon (from McCarty & Stothard 202212)
Figure 2: Circadian Rhythmo-Wheel (from McCarty & Stothard 202212). A bedside tool for teaching patients about circadian biology. The usual prolonged sleeping interval — the “circadian sleep phase” — is shown in blue (~10 p.m. to 6 a.m.). The “forbidden zone” is shown in orange (~7 p.m. to 10 p.m.). A free downloadable and interactive version of this tool is available at https://www.empoweredsleepapnea.com/circadian-rhythmo-wheel
Exploring the last three domains
The last three domains of the Five Finger Approach are
3. Medical Factors
4. Psychosocial/Psychiatric Factors
5. So-called “Primary Sleep Medicine diagnoses”
The final domain is the mental location to file our patient’s “known sleep diagnoses” and to question whether other common diagnostic labels might have been overlooked.
Strategically, these three domains are methodically addressed with the patient similarly to the first two, striving to engage Snowden’s mindful “probing” as a first step. In each setting, the process involves engaging the patient, probing collaboratively whether elements in that domain could be a factor contributing
Table 1: Common Pharmacologic Factors Affecting Sleep-Wake
Drug ClassCommon Examples – Generic Names (Trade Names)
Cardiovascular Drugs
Beta Blockers Metoprolol (Toprol XL) Labetalol
to their personal concerns, and then collaboratively exploring potential solutions.
What we’ve learned
1. Sleep Apnea — and the practice of Sleep Medicine — is not complicated, it’s complex! There’s a difference!
2. Complicated environments benefit from the efficiency of a top-down management style, run by an expert.
3. Complex environments benefit from collaborative decision-making responsive to unpredictability. This requires an approach of intentional probing and receptivity to change plans as new information arises.
4. Collaborative teamwork requires: 1. a shared consciousness
Effect on SLEEP and WAKE
Beta blockers promote insomnia and can disturb dreams. Disturbances in REM sleep can lead to nightmares or even to to the disquieting experience of dreaming while seemingly awake (hallucinations). Lipophilic beta blockers cross the blood-brain barrier more readily and are more likely to provoke sleep disturbances.
Note that beta blockers can also contribute to daytime WAKE-related symptoms of generalized lethargy and fatigue.
ACE inhibitors Lisinopril, Ramipril
Statins Atorvastatin, Rosuvastatin, Simvastatin
Mental Health Drugs
Selective serotonin reuptake inhibitors (SSRIs)
This drug class can increase airway irritability, leading to disruptive coughing that can disturb sleep. The upper airway irritability may worsen obstructive sleep apnea pathology.
Statins may provoke insomnia with or without causing muscle pain. If you get muscle pain with statins, this can also interfere with sleep.
Note that statin-induced muscle pain can also color the lens by which WAKE is viewed, leading to fatigue and poor exercise tolerance.
Fluoxetine, paroxetine, sertralineSSRIs contribute to “restless legs” symptoms (higher doses = worse effects).
SSRIs can also increase the likelihood of dream enactment behavior, which is another way of saying “moving around while you dream.” When dream enactment behavior happens for no good reason, it’s called REM Sleep Behavior disorder.
SSRIs can cause insomnia as an adverse effect (fluoxetine is famous for this). Alternatively, SSRIs can also cause WAKE-related symptoms of grogginess or sedation (paroxetine is famous for this).
Serotonin and Norepinephrine Reuptake Inhibitors
Norepinephrine and Dopamine Reuptake Inhibitors
Tricyclic antidepressants
CNS Stimulants
Venlafaxine, desvenlafaxine
Bupropion
All of the above that we just mentioned about SSRIs is true for this drug class. The norepinephrine reuptake inhibition is particularly provocative for insomnia, restless legs symptoms, and dream enactment behavior.
Think of this drug class as being an amplifier for the ARAS, and you’ll then understand why insomnia is one of the most common adverse sleep-related effects.
Bupropion is the only antidepressant that doesn’t provoke restless legs.
Amitriptyline, imipramine, protriptyline
Methylphenidate (Ritalin), amphetamine/dextroamphetamine (Adderall)
All tricyclics can provoke restless legs symptoms and signs (like periodic limb movements of sleep). They also can be sedating, and in seniors they can cause difficulty with memory, due to an anticholinergic side effect profile.
Stimulants are famous for causing sleep-onset insomnia. The longer-lasting the formulation, and the later it is taken in the day, the more likely it will be to interfere with transitioning to sleep.
14 Pediatric Dental Practice US Volume 1 Number 2 CLINICAL
Drug ClassCommon Examples – Generic Names (Trade Names)
Pulmonary / Rheumatology Drugs
Beta-2 Agonists Albuterol, salmeterol
Effect on SLEEP and WAKE
These inhalers tend to rev you up! Expect an increase to your pulse, and difficulty with getting to sleep, lasting for as long as the drug is active.
Corticosteroids Prednisone, methylprednisoloneCorticosteroids can cause many problems with your sleep. Difficulty getting to sleep, waking up too early, and abnormal dreams have all been described.
Anticonvulsant Drugs
Gabapentinoids Gabapentin, Pregabalin Drugs in this class are technically “anticonvulsants” but they’re mostly prescribed for reasons other than seizures. They are often used to manage chronic pain, headache syndromes, fibromyalgia, and symptoms of WED. They are sedating, in general, and can be considered “hypnotics” (sleeping pills). Of importance, these drugs can contribute to next-day sedation when dosed at bedtime!
Social Drugs
Nicotine Nicotine is not friendly to sleep, if used regularly. Pharmacologically, nicotine is a CNS stimulant, so it will interfere with sleep while the drug is active. The other side of the coin with nicotine is the physical and psychological discomfort that comes from withdrawal, which generally begins about an hour after the last dose, for heavy users. That sensation is also a potent stimulus for insomnia. Old-school smoking is particularly irritative to the upper airway and is likely to worsen obstructive pathology.
Alcohol Alcohol worsens the propensity for Sleep Apnea, particularly obstructive pathology. Though it may help you fall asleep faster, sleep worsens as your blood alcohol content drops, and second-half-of-night sleep is generally rocky and poor-quality. Alcohol hangover symptoms can confound interpretation of daytime neurobehavioral impairment.
Cannabis (THC) THC is the psychoactive component of marijuana. Depending on the strain, it may be activating or sedating. THC users may experience withdrawal symptoms of anxiety and insomnia, which can lead to a self-perpetuating problem.
Caffeine Caffeine can interfere with sleep for as long as the drug is in the system. Caffeine can mask daytime impairment symptoms, leading to a sudden “crash” in energy when the drug is metabolized away.
(adapted from McCarty & Stothard, 2022)
of the system’s complexity and 2. lateral connectivity (i.e., trust and empathetic connection) between team-members.
5. In a patient-centered clinical relationship, the patient is a member of the team.
6. “Root cause” complexity for sleep-wake complaints can be deconstructed with a “five-finger” collaborative exploratory tool: 1. circadian misalignment, 2. pharmacologic factors, 3. medical factors, 4. psychosocial/psychiatric factors, and 5. primary sleep medicine diagnoses.
7. Communicating and strategizing collaborative understanding of the first (circadian misalignment) and second (pharmacologic factors) domains requires a basic familiarity with simple concepts of sleep-wake/circadian biology and clinical epidemiology. These concepts are worthy of further study, as mastery improves the ability to characterize this complexity for our patients.
REFERENCES
1. McKeown P, O’Connor-Reina C, Plaza G. Breathing Re-Education and Phenotypes of Sleep Apnea: A Review. J Clin Med. 2021 Jan 26;10(3):471.
2. McCarty DE. There is No OSFA: How the Many Moving Parts of Sleep Apnea Demands Precision Medicine. Dental Sleep Practice. Spring 2023;10(1): 18-20.
3. Snowden DJ, Boone ME. A leader’s framework for decision making. A leader’s framework for decision making. Harv Bus Rev. 2007 Nov;85(11):68-76, 149.
4. McChrystal S, Collins T, Silverman D, Fussell C. 2015. Team of Teams: New Rules of Engage-
ment for a Complex World. New York: Portfolio/Penguin Books; 2015.
5. French S. Cynefin, statistics and decision analysis. Journal of the Operational Research Society. 2013. 64:4, 547-561.
6. Kurtz CF, Snowden DJ. The new dynamics of strategy: Sense-making in a complex and complicated world. IBM Systems Journal. 2003;42(3): 462-483.
7. Cognitive Edge Ltd & Cognitive Edge Pte. The Cynefin Company and The Cynefin Centre, Conwyll, Singapore, Wilmington. https://thecynefin.co/. Accessed June 13, 2023.
8. Sackett DL, Haynes RB, Tugwell P, Guyatt GH. N of 1 Trials: Selecting the Optimal Treatment with a Randomized Trial in an Individual Patient. In: Clinical Epidemiology: A Basic Science for Clinical Medicine (2nd Ed). Boston: Little Brown & Co.;1991:223-238.
9. McCarty DE. Beyond Ockham’s razor: redefining problem-solving in clinical sleep medicine using a “five-finger” approach. J Clin Sleep Med. 2010 Jun 15;6(3):292-296.
10. McCarty DE. Sometimes, You’re the One. OR: The Story about How the Five Finger Approach Found a Problem That Had Never Been Described and How it Changed Wendy’s Life. In: Dave’s Notes the official blog of Empowered Sleep Apnea: Published online November 18, 2022. Accessed August 1, 2023. https://www.empoweredsleepapnea.com/daves-notes/ sometimes-youre-the-one.
11. Borbély AA, Daan S, Wirz-Justice A, Deboer T. The two-process model of sleep regulation: a reappraisal. J Sleep Res. 2016 Apr;25(2):131-143.
12. McCarty DE, Stothard E. Empowered Sleep Apnea: A Handbook for Patients and the People Who Care About Them. Pennsaukin Township, NJ: BookBaby Press;2022.
13. Gabehart RJ, Van Dongen HPA. Circadian Rhythms in Sleepiness, Alertness, and Performance. IN: Kryger, Roth, Dement, eds. Principles & Practice of Sleep Medicine, 6th Ed. Elsevier Press, 2017:388-395.
14. Strogatz SH, Kronauer RE, Czeisler CA. Circadian pacemaker interferes with sleep onset at specific times each day: role in insomnia. Am J Physiol. 1987 Jul;253(1 Pt 2):R172-178.
15. Stothard ER, McHill AW, Depner CM, Birks BR, Moehlman TM, Ritchie HK, Guzzetti JR, Chinoy ED, LeBourgeois MK, Axelsson J, Wright KP Jr. Circadian Entrainment to the Natural Light-Dark Cycle across Seasons and the Weekend. Curr Biol. 2017 Feb 20;27(4):508-513.
16. Sackett DL, Haynes RB, Guyatt GH, Tugwell P. Deciding Whether Your Treatment Has Done Harm. IN: Clinical Epidemiology: A Basic Science for Clinical Medicine (2nd Ed). Boston: Little Brown & Co.;1991: 283-304.
15 pediatricdentalpractice.com Volume 1 Number 2 CLINICAL PD Table 1 Continued
The missing link in pediatric sleepbreathing treatments

Dr. Paulo Soares explores a myofunctional orthodontic treatment protocol for correcting sleep-disordered breathing

Introduction
It is hard to turn a corner these days without hearing about mouth breathing and its effects on overall health. Aided by an increased exposure in pop culture and practitioner knowledge, patient awareness and demand for treatment continues to grow at a rapid pace. In response to this demand, practitioners have concluded that early treatment and prevention is best, but they continue to search for the best ways to help their patients.
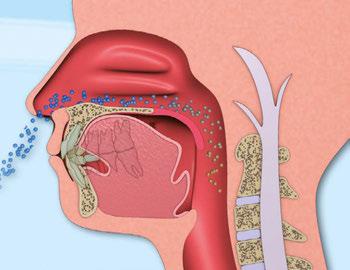
While physicians have traditionally treated breathing disorders, dentists and orthodontists are increasingly being called upon to assist in these efforts. Given the close relationship between the upper airway and the oral cavity, dentists play a crucial role in the treatment of breathing disorders,1 which have also been associated with dental conditions, such as caries and periodontal disease.2
Historical background
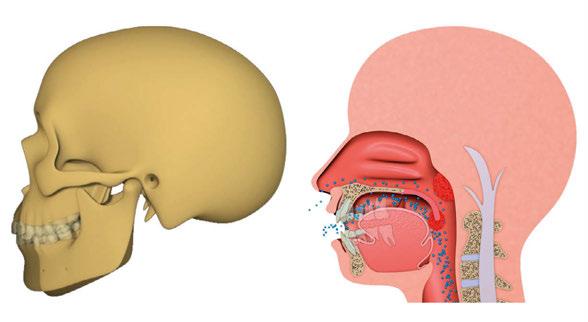
Optimum breathing patterns involve the mouth being closed, lips sealed, tongue resting in the palate, and gentle nasal breathing. In his 1907 textbook, the father of orthodontics Dr. Edward Angle stated, “Of all the various causes of malocclusion, mouth breathing is the most potent, constant, and varied in its results.”3 Angle understood that mouth breathing changed the function of the oral muscles (collectively known as myofunctional disorders), which changed the forces imparted on the teeth and jaws, leading to malocclusion.
In response to this idea, one of Angle’s students, Dr. Alfred Rogers, began implementing a series of oral exercises in the
Disclosure: Dr. Soares is a Myobrace Certified Provider and Educator.
16 Pediatric Dental Practice US Volume 1 Number 2 CLINICAL
Paulo Soares, DDS, MSD, is an orthodontist in Brazil. Dr. Soares graduated with his dental degree from the Universidade Federal de Sergipe, Brazil. He is a specialist in orthodontics and facial orthopedics with more than 15 years of experience in myofunctional and airway orthodontics. He is also a member of the Brazilian Dental Sleep Medicine Association (ABROS).
Mouth breathing creates dysfunctional forces on the craniofacial complex
1930s to correct this phenomenon, which was the birth of myofunctional therapy in orthodontics.4 As orthodontics became more focused on mechanics over biology, new bracket technology and better ways of straightening teeth dominated the discourse over the 20th century.5
Discovery of sleep-disordered breathing in children
Thanks to a series of discoveries in sleep medicine that occurred in the latter half of the 20th century, scientists began to understand that it is not just adults who suffer from Obstructive Sleep Apnea (OSA), but a new spectrum of breathing disorders called Sleep Disordered Breathing (SDB) became understood to affect children as well.
SDB includes (in order of severity) mouth breathing, snoring, Upper Airway Resistance Syndrome (UARS), and OSA6 and can affect patients from the first days of life. SDB is known to be linked to numerous mental and physical conditions in both children and adults. As with most medical conditions, prevention is better than cure, and this is what the father of sleep medicine Dr. Christian Guilleminault suggested when he advocated for early treatment and stated, “the only valid treatment goal is restoration of nasal breathing.”7
Integration of dentistry, orthodontics, and myofunctional therapy
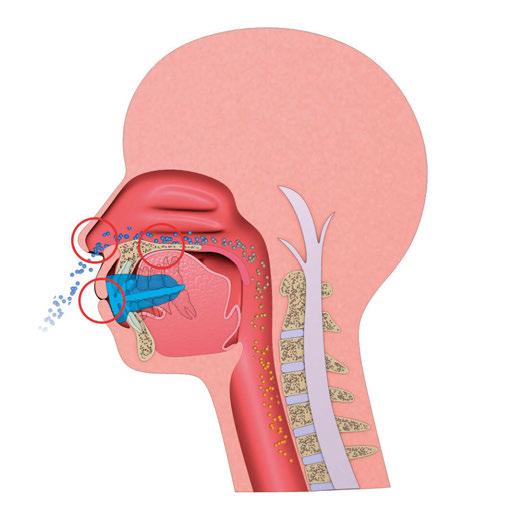
The research has led us to understand that there is an interplay of nasal obstructions or restrictions (e.g., allergic rhinitis or adenotonsillar hypertrophy), poor craniofacial development, and myofunctional disorders in the development of SDB, especially in non-obese patients. We also understand the cumulative damage imparted by SDB, which means the issue must be treated as soon as it is detected.8
The role of poor craniofacial development and myofunctional disorders in the development of SDB has led to the inclusion of dentistry, orthodontics, and myofunctional therapy in the treatment of breathing disorders (in cooperation with otolaryngology). In fact, the FDI World Dental Federation published a policy statement in 2018 urging dentists to be actively involved in treatment, more specifically “prevention of late-onset forms” of SDB.9
Challenges in current treatments
Unfortunately, the treatments proposed to address these breathing disorders and the restoration of nasal breathing have caused dissipation of enthusiasm among practitioners and patients. Positive Airway Pressure (PAP) therapy can be used, but it has been found to have adverse effects on facial development, potentially worsening breathing disorders in the long term.10
Orthodontic techniques have also been proposed, but their outcomes are unpredictable, unstable, and they may exacerbate myofunctional disorders.11 Surgical interventions are often a last resort due to their complexity, cost, and potential side effects, while research clearly shows that surgery is not the only answer.12,13 Parents and practitioners alike are also hesitant to explore surgical options unless absolutely necessary.
Resurgence of myofunctional therapy
In recent years, myofunctional therapy has experienced a resurgence as a non-invasive approach to correcting myofunctional disorders, improving SDB and promoting healthy craniofacial growth and development in patients. While the concept is sound, traditional myofunctional therapy suffers from issues of unpredictability, complexity, and lengthy treatment duration. This was the reason it originally fell out of favor, and unfortunately, the resurgence has done very little in the way of redesign or updates to this excellent intervention.
Poor patient compliance combined with the lack of a globally recognized and standardized programs have hindered its widespread success. To address these challenges, a structured, simple, and cost-effective rehabilitation protocol is necessary to meet the growing demand for treatment. Since our understanding of early treatment has improved, the need to apply this intervention to very young children means that the need to correct these deficiencies is even greater. Even if the treatment is not applicable to 100% of patients, even a modest reduction in the disease burden would still be worthwhile.
The myofunctional orthodontic appliance protocol
One potential solution that shows promise is the implementation of a myofunctional orthodontic appliance protocol. This approach involves the use of prefabricated myofunctional appliances as part of a simple and structured treatment plan. These appliances serve multiple functions, including promoting nasal breathing, developing dental arches, establishing correct habits, and aligning teeth. By combining non-invasive and cost-effective treatment methods, these appliances provide a way to correct poor habits associated with mouth breathing while improving orthodontic outcomes. Collaboration with medical practitioners is also integrated into the treatment protocols when necessary. Published studies have shown some potential for this technique, and as the openness of the profession to this novel approach improves, more high-quality studies are expected to arise.14
Sequential stages of treatment
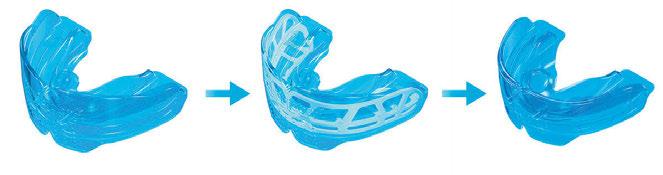
The myofunctional orthodontic appliance protocol typically consists of administering 3-4 appliances sequentially to progressively rehabilitate the patient. If we reflect on the cascade of
17 pediatricdentalpractice.com Volume 1 Number 2 CLINICAL
An interplay of airway obstructions, poor craniofacial development, and myofunctional disorder is implicated in SDB
events that cause these issues, we understand that mouth breathing precipitates poor oral habits, which alter the patient’s growth and development, and finally result in malocclusion.
In response, myofunctional orthodontic appliances address the problems in the order in which they occur. The initial stage concentrates on correcting breathing and myofunctional disorders, as these habits form the basis of treatment. The second stage focuses on developing dental arches while continuing to address breathing and myofunctional issues. The final stages aim to retain the arch form, align teeth, and assess the stability of habit correction. Each stage corrects a certain problem and sets the foundation for the next condition to be corrected in the cascade.
Benefits of myofunctional orthodontic treatment
The myofunctional orthodontic treatment protocol offers several advantages. The prefabricated nature of the appliances and their advanced features make treatment easy to learn and implement for practitioners. This allows for wider dissemination of the treatment to meet the demand for early intervention and prevention of mouth breathing and myofunctional disorders. Moreover, the simplicity and child-friendly approach of the protocols make it enjoyable for children to participate in habit correction. Accompanying digital and print resources further enhance the effectiveness of the treatment and improve compliance. Treatment delivery is a key part of the myofunctional orthodontic approach. Overall, the myofunctional orthodontic treatment protocol represents an exciting development in the fields of orthodontics, myofunctional therapy, and dental sleep medicine.
Conclusion
Prefabricated myofunctional appliances establish nasal breathing, correct myofunctional habits, and promote arch development for further functional correction
Myofunctional appliances employ a 3-stage approach to comprehensively rehabilitate patients with orthodontic, breathing, and myofunctional disorders
In conclusion, the treatment of pediatric sleep breathing disorders requires a comprehensive and proactive approach. The integration of dentistry, orthodontics, and myofunctional therapy has emerged as a vital part of addressing these issues. The myofunctional orthodontic appliance protocol offers a structured, simple, and cost-effective rehabilitation strategy that can be implemented on a large scale to meet the increasing demand for treatment. By focusing on early intervention and prevention, this protocol aims to restore nasal breathing, correct poor habits, and improve orthodontic outcomes in pediatric patients. While further research and refinement are needed, the myofunctional orthodontic approach holds great promise in bridging the gap in pediatric sleep breathing treatments and ensuring the long-term oral and overall health of children.
For more information on myofunctional orthodontics, visit www.myoresearch.com and start with the free online courses.
REFERENCES
1. Leibovitz S, Haviv Y, Sharav Y, Almoznino G, Aframian D, Zilberman U. Pediatric sleep-disordered breathing: Role of the dentist. Quintessence Int. 2017;48(8):639-645.
2. Ballikaya E, Guciz Dogan B, Onay O, Uzamis Tekcicek M. Oral health status of children with mouth breathing due to adenotonsillar hypertrophy. Int J Pediatr Otorhinolaryngol. 2018 Oct;113:11-15.
3. Angle E.H. Treatment of malocclusion of the teeth: Angle’s System. Philadelphia: S.S.
White Manufacturing Co.; 1907.
4. Rogers A. Evolution, development, and application of myofunctional therapy in orthodontics. Am J Orthod Oral Surg. 1939 Jan;25(1):1-19.
5. Ackerman JL. Was the destiny of orthodontics written in the stars? Am J Orthod Dentofacial Orthop. 2015 Mar;147(3):290-292.
6. Bonuck K, Freeman K, Chervin RD, Xu L. Sleep-disordered breathing in a population-based cohort: behavioral outcomes at 4 and 7 years. Pediatrics. 2012 Apr;129(4):e857-865.
7. Guilleminault C, Sullivan SS, Huang YS. Sleep-Disordered Breathing, Orofacial Growth, and Prevention of Obstructive Sleep Apnea. Sleep Med Clin. 2019 Mar;14(1):13-20.
8. Alison et al. Recent advances in paediatric sleep disordered breathing. Breathe 2022 18: 220151.
9. FDI World Dental Federation 2018. Dentistry and Sleep-Related Breathing Disorders. https://www.fdiworlddental.org/dentistry-and-sleep-related-breathing-disorders. Accessed August 2, 2023.
10. Roberts SD, Kapadia H, Greenlee G, Chen ML. Midfacial and Dental Changes Associated with Nasal Positive Airway Pressure in Children with Obstructive Sleep Apnea and Craniofacial Conditions. J Clin Sleep Med. 2016 Apr 15;12(4):469-475.
11. Barbosa DF, Bana LF, Michel MCB, Meira E Cruz M, Zancanella E, Machado Júnior AJ. Rapid maxillary expansion in pediatric patients with obstructive sleep apnea: an umbrella review. Braz J Otorhinolaryngol. 2023 May-Jun;89(3):494-502.
12. Huang YS, Guilleminault C, Lee LA, Lin CH, Hwang FM. Treatment outcomes of adenotonsillectomy for children with obstructive sleep apnea: a prospective longitudinal study. Sleep. 2014 Jan 1;37(1):71-76.
13. Guilleminault C, Li K, Quo S, Inouye RN. A prospective study on the surgical outcomes of children with sleep-disordered breathing. Sleep. 2004 Feb 1;27(1):95-100.
14. Ferreira FG. Novel Approaches for Class II Malocclusion Treatment using Myofunctional Orthodontics Therapy: A Systematic Review. Int J Dent Oral Sci. 2017;4(7):503-507.
18 Pediatric Dental Practice US Volume 1 Number 2 CLINICAL
PD


































































































































STRAIGHT TEETH THE NATURAL WAY MEETING PARENTS DEMAND FOR EARLY ORTHODONTIC TREATMENT THE FINAL EVOLUTION IN MYOFUNCTIONAL ORTHODONTICS Used by Dentists and Orthodontists in over 100 Countries Attend a seminar to learn more: www.myoresearch.com 866-550-4696 usa.courses@myoresearch.com ✔ Treat more children earlier ✔ Increase patient flow ✔ Improve efficiency by delegation ✔ Added financial benefits “The MyobraceSystem™ has packaged Habit Correction, Arch Expansion and Dental Alignment into one integrated system making orthodontics more effective with health benefits for the growing child.” Look for the ‘M’ shaped box.
Conservative approach of fortuitously found odontoma in a child with severe autism
Dr. Gabriela Aurora Asensi discusses treatment of a special needs

patient
Abstract
A case of an unexpectedly found compound odontoma discovered while treating a pediatric dental patient with autism during oral rehabilitation under general anesthesia is presented. This odontoma caused impaction of the right central maxillary incisor. This patient shows how an impacted maxillary central incisor with a completely formed root erupted into the mouth after removing its blocking odontoma which took 5 years to complete. Orthodontic extrusion was not achievable due to the patient’s inability to cooperate with orthodontic treatment. Subsequently orthodontic extrusion was not necessary. The conservative approach used with this patient shows how the teeth can erupt on their own. The patient illustrates how a conservative approach can pay off by giving patients with special needs and their caretakers hope when orthodontic treatment is not feasible because of special needs that preclude such treatment.
Introduction
Odontomas are defined as a benign tumor of odontogenic origin.1 They are basically classified into two types, complex and compound.2 Compound odontomas consist of small toothlike structures, and complex odontomas are a conglomeration of dentin, enamel, and cementum.3 Analysis has revealed that compound odontomas, the most common type,4 are usually diagnosed in the second decade of life.5 Their presence causes interferences in tooth eruption including impaction, delayed, and/or ectopic eruption.6 Normally, there is no potential for eruption when the impacted tooth has a completely formed root or when the homologous tooth has been erupted for at least 6 months with complete root formation.7 Orthodontic extrusion is a common way to erupt impacted teeth after odontoma removal if the root is completely formed.8 However, this might not be
Gabriela Aurora Asensi, DMD, MPH, CLC, received her first dental degree from Universidad Central de Venezuela. In 1996, she completed a general dentistry residency program at Miami Children’s Hospital becoming chief resident. In 2000, she also completed the joint residency program of Miami Children’s Hospital and University of Florida. She completed the Doctor of Dental Medicine (DMD) degree at Nova Southeastern University in 2003. Dr. Asensi also graduated from Florida International University (FIU) with a Master in Public Health in 2021. She is a pediatric dentist in private practice in Miami, Florida.
possible with autistic children. Although malocclusions occur more often in physically and/or mentally disabled children, the most severely handicapped patients are those least likely to receive orthodontic treatment due to their uncooperative behaviors.9 This patient shows how the removal of a fortuitously found odontoma in an autistic child treated under general anesthesia by a pediatric dentist allowed an impacted maxillary right central incisor to fully form a root and erupt into the mouth. This tooth found its way into the oral cavity but took 5 years to do so.
Description
An 8-year-old Hispanic male presented to our private practice in Miami, Florida with the chief complaint of a missing front tooth (Figure 1). Upon review of his medical history, the mother revealed that her son had Autism Spectrum Disorder and confirmed that his condition was severe. This patient did not take

20 Pediatric Dental Practice US Volume 1 Number 2 CLINICAL
Figure 1: Face of 8-year-old patient at initial consultation
BOYD’S PEDIATRIC DENTAL PRODUCTS ARE THE SOLUTIONS TO YOUR NEEDS

Customizable solutions for pediatric offices, ensuring a welcoming and organized environment that puts young patients and their families at ease. Trust in our longstanding dedication to creating spaces that prioritize both comfort and functionality.
Customize your perfect office today with Boyd.



SCAN FOR MORE INFO
PB4001
PEDIATRIC BENCH
BOOSTER SEAT
P3000LS TREATMENT CHAIR
any medications, was nonverbal, avoided eye contact with any staff member including the treating pediatric dentist, did not sit in the dental chair, and was constantly tapping his ears. No dental radiographs were obtained due to his uncooperative behavior. For the dental exam, the mother agreed and consented with placing him in a passive restraining device. With a limited visualization of his oral cavity, a mixed dentition was noted. The maxillary right permanent central incisor was absent. No significant pathology was found in his oral soft tissues. Dental caries was found on both primary and permanent molars. A decision was made to complete dental treatment using general anesthesia as a behavior management technique at the local children’s hospital.
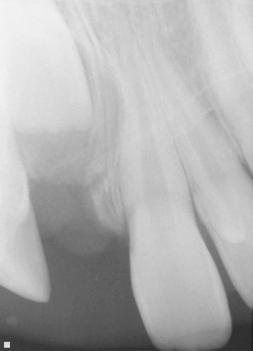
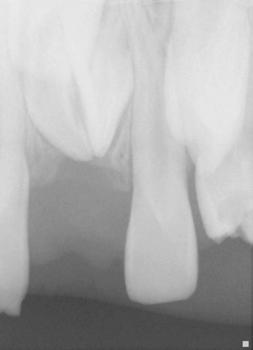
The following procedures were accomplished under general anesthesia on an outpatient basis — full mouth dental radiographs and a comprehensive oral exam. A complex odontoma was found to be the etiology of the noneruption of the maxillary right permanent central incisor (Figure 2). Since dental caries also was diagnosed, a full-mouth prophylaxis was completed. Dental caries was controlled, and teeth were restored. A 5 mm incision was made on the gingiva over the impacted maxillary right permanent central incisor, and two tooth-like structures were extracted from the right maxillary incisor area. A postoperative periapical radiograph was taken to confirm complete odontoma removal (Figure 3). Three interrupted sutures using 3-O chromic gut were placed.
At the postoperative consultation with the mother, we told her the tooth’s complete root formation might prevent its eruption. Orthodontic extrusion of the incisor was ruled out due to his behavior. A conservative approach with observation only was elected as treatment modality. This patient returned for follow-up appointments at ages 10, 11, 12, and 13. During all these visits, the maxillary right permanent central incisor had not erupted. At age 14, due to recurrent dental caries, the patient was taken to the local children’s hospital for dental rehabilitation again. During this second hospitalization, we noticed that the right maxillary central incisor was partially erupted into the oral cavity (Figure 4).
Discussion
It is well known that autism is a serious developmental disorder that impairs the ability to communicate and interact with others. Children with autism pose a challenge in terms of behavior management in the standard dental setting. Comprehensive orthodontic treatment offers clinicians even more of a challenge with these patients.
Every patient needs to be evaluated individually because a great deal of cooperation and time is required for orthodontic treatment. Parents need to understand that in severely autistic children, orthodontic treatment might not be a viable solution. Communication is paramount, and realistic expectations ought to be communicated with these children’s caretakers. This patient illustrates that a conservative approach consisting of odontoma removal was enough to allow eventual eruption of the incisor.
Conclusion
Pediatric dentists, by training and expectation are primarily therapists, but with this patient, minimal therapy produced a good outcome.
REFERNCES
1. Odontoma. Dorland’s Illustrated Medical Dictionary. Philadelphia: Elsevier Health Sciences; 2011:1313.
2. Satish V, Prabhadevi MC, Sharma R. Odontome: A Brief Overview. Int J Clin Pediatr Dent. 2011 Sep-Dec;4(3):177-185.
3. Katz RW. An analysis of compound and complex odontomas. ASDC J Dent Child. 1989 Nov-Dec;56(6):445-449.
4. Budnick SD. Compound and complex odontomas. Oral Surg Oral Med Oral Pathol. 1976 Oct;42(4):501-506.

5. Suri L, Gagari E, Vastardis H. Delayed tooth eruption: pathogenesis, diagnosis, and treatment. A literature review. Am J Orthod Dentofacial Orthop. 2004 Oct;126(4):432-445.
6. Kjær I. Mechanism of human tooth eruption: review article including a new theory for future studies on the eruption process. Scientifica (Cairo). 2014;2014:341905.
7. Kjær I. Mechanism of human tooth eruption: review article including a new theory for future studies on the eruption process. Scientifica (Cairo). 2014;2014:341905.
8. Chokron A, Reveret S, Salmon B, Vermelin L. Strategies for treating an impacted maxillary central incisor. Int Orthod. 2010 Jun;8(2):152-176.
9. Chaushu S, Becker A. Behaviour management needs for the orthodontic treatment of children with disabilities. Eur J Orthod. 2000 Apr;22(2):143-149.
22 Pediatric Dental Practice US Volume 1 Number 2 CLINICAL
Figures 2 and 3: 2. Periapical radiograph of involved area taken in the operatory during initial dental rehabilitation under general anesthesia (left). 3. Periapical radiograph of involved area taken in the operatory during initial dental rehabilitation under general anesthesia immediately after odontoma removal (right)
PD
Figure 4: Photograph of area at 14 years old during second rehabilitation under general anesthesia
“Smart” restorative materials in dentistry

Fred Berk discusses materials that behave more dynamically
In his visionary article “Smart Materials in Dentistry,” Professor John McCabe teaches that most traditional dental materials are hydrophobic and are designed to have a relatively “neutral” existence in the mouth. It is considered that if they are “passive” and do not react with the oral environment, they will be more stable, have greater durability, and cause neither harm nor injury. McCabe says this is an entirely negative approach and hides the possibility that positive gains can be achieved by using active (“smart”) materials that behave in a more dynamic fashion.
It is a fundamental principle of science that biochemistry only occurs in the presence of water, and only materials that have the capacity to transport water have the potential for dynamic behavior. Only moisture-friendly materials can release and recharge significant amounts of calcium, phosphate, and fluoride to support apatite formation and the natural remineralization process. Traditional dental composites are hydrophobic and do not have this capacity.
Resins that stimulate remineralization of damaged tooth structure represent both the holy grail and the future of dental restorative materials. Pulpdent’s development of the phosphate-rich, hydrophilic Embrace™ WetBond™ resin chemistry was the innovation that allowed for the development of dynamic esthetic composites. In addition, Pulpdent® overcame the brittleness of traditional composites by synthesizing a patented elastomeric resin molecule that provides fracture resistance to the cured resin.
In 2013, Pulpdent added glass ionomer to these novel chemistries and introduced ACTIVA™ BioACTIVE materials. This was a breakthrough that launched a new category of esthetic bioactive materials and a new conversation about the possibilities for “smart,” esthetic, restorative materials for dentistry. Pediatric dentists were among the early adopters of ACTIVA because they understood the need for restorative materials that helped developing teeth.
A true glass ionomer reaction requires a two-part material, and the next challenge was to create a one-part light-cure bioactive material. Pulpdent synthesized and patented a novel methacrylate-functionalized calcium phosphate molecule with highly-active remineralization properties. This is known as Crysta MCP technology and can be added to light-cure or dual-cure materials. Crysta has been incorporated in Pulpdent’s ACTIVA™
Presto stackable low-flow composite and Lime-Lite™ Enhanced light-cure cavity liner.
These “smart” materials play a dynamic role in the mouth and meet the challenge for moisture-friendly resin-based materials that are suitable for esthetic, durable, load-bearing applications.

Pulpdent is also applying these novel chemistries to other materials. Progress is being made for bonding agents with mineralization potential and antibacterial properties that discourage MMPs and extend the life expectancy of composite restorations, bioactive CAD/CAM blocks, resorbable bone cements that stimulate remineralization and are replaced by natural hard tissue, orthodontic adhesives, packable composites, pulp capping agents, and other applications.
These innovations transition dentistry from a passive, reactive repair model intended to do no harm to an active approach using dynamic materials that support the natural remineralization process and preventive dental care that is better for our patients.

23 pediatricdentalpractice.com Volume 1 Number 2 PRODUCT PROFILE
This article was provided by Pulpdent®.
PD
Fred Berk is President of Pulpdent Corporation. Pulpdent is a family-owned dental research and manufacturing company founded by Dr. Harold Berk in 1947. It is located in Watertown, Massachusetts.
Figure 1: Special needs pediatric patient presents with rampant caries
Figure 2: Pulpal exposures after removal of caries and severely decalcified dentition
Figure 3: Completed case using Activa Bioactive restoratives. 10-week follow-up shows healed tissues. Case courtesy of Raymond Kimsey, DMD
Functional chewing and nasal breathing
Chewing is essential when it comes to stimulating neural pathways, chew reflexes, and developing the musculature to facilitate optimal facial tone and jaw growth. Processed mushy baby food, squeeze packs, pacifiers, bottles, and sippy cups all keep the suck reflex active when a baby should be developing their chewing pathways optimizing development on all levels. The natural growth forces generated from correct chewing make a big contribution to growing faces and maintaining ideal oral function for life.
The lack of fiber and over-processing of foods in today’s diet can lead to insufficient activation of the facial and peri-cranial muscles. As the saying goes, “stasis is the basis of disease” — chewing is essential to provide the necessary exercise that oxygenates and strengthens the muscles of the stomatognathic system. Just as humans require a mix of aerobic and strengthening exercises to maintain physical fitness, non-traumatic exercises are also crucial for the peri-cranial, facial, and neck muscles.
Chewing and jaw growth — it’s like assembling a tent!
Think of the face and jaw as a sturdy tent, supported by its poles and guy ropes. The guy ropes, in this case, are the muscles of the lips, face, and tongue. When these muscles have the right tension, the forces acting on our facial bones are well-balanced. This balance is crucial for proper bone growth, as the muscles pull on the bones to contribute to their development.
However, certain factors can disrupt this delicate balance in the face, such as pacifier use, thumb sucking, open-mouth breathing, and nasal obstruction. These disruptions can lead to incorrect growth forces and even result in issues like an open bite, as seen with thumb sucking.
It’s important to maintain the correct tension in these muscles, as they play a significant role in the development of the jaw, palate, and facial structures. By understanding and optimiz-
Mary Bourke, BSc, BAppSc, Chiropractor, has an expansive vision, as both a health professional with over 30 years of experience and as Myo Munchee CEO. She is dedicated to the young people of today and future generations, as well as to promoting the countless benefits of chewing, both within Australia and worldwide, with a deep passion and commitment. Dr. Bourke lives in Newcastle, NSW, Australia with her husband, three daughters, and dachshund, Alfie. She still chews a Munchee every day and spreads her time between Myo Munchee and a successful chiropractic practice.

ing these “length tension relationships,” we can ensure healthy growth and function.
The benefits of chewing are far reaching, and more are being discovered all the time. What we do know is:
• Chewing is involved in regulation and maintenance of bone growth.
• Chewing is the essential movement for optimal upper airway function to develop strength of the muscles involved in the complex process of swallowing.
• Chewing assists with Eustachian tube and sinus drainage.
• Chewing develops the strength of muscles to ensure strength and stability of the TM Joints.
• Chewing is involved in reducing stress and is known to be neuro-calmative.
• Chewing contributes to better cognition.
• Chewing allows for the breakdown and absorption of foods more efficiently.
Why start early?
In our busy world of such modern conveniences as pacifiers, baby capsules, and bottle-feeding, the lack of oral stimulation that babies are experiencing is becoming normalized. Without this crucial stimulation of the initial oral complex, children are sent along a trajectory of poor orofacial growth and function which can present in issues such as narrow palates, teeth crowding, and the huge cascade of health issues connected to mouth breathing. The movement essentials for optimal cranio-facial growth and function are sucking, swallowing, nasal breathing, and chewing. The earlier we can detect a developmental problem, the more likely we are able to shift the trajectory and get development back on track. Malocclusions can be predicted from as young as 6 months, and do not self-correct if left untreated.
Malocclusions are often the root cause for many issues including:

• speech and feeding
• dribbling and drooling
• ear infections
• mouth breathing
• sleep disturbance
• postural instability and weakness
When we have a patient in our clinic who is a baby or toddler, it is a fantastic opportunity to identify any dysfunctions, and correct and optimize the growth potential in front of us. Early detection and correction are essential to optimize growth potential and create a “good quality face.”
Without further ado — Let’s chew!
Head to myomunchee.com for more amazing resources.
24 Pediatric Dental Practice US Volume 1 Number 2 GROWING PLANS
Dr. Mary Bourke discusses the importance of optimizing children’s orofacial growth, development, and function
PD
With just 10 minutes of chewing per day, this amazingly powerful small device will help get facial function back on track!



Enhances:
Tone
Muscle strength
Co-ordination for better oral posture


Promotes:
Nasal breathing

Correct tongue posture
Reinforces correct swallow pattern
Use the code
PDM25
to receive 25% off our Sizing Kit - a fantastic way to get started on your Myo Munchee journey (expires Oct31, 2023)
For additional support please email our team at sales@myomunchee.com

JUNIOR TWEEN ADULT
MINI BEBE
Leveraging AI in pediatric dental marketing: from social media to SEO

Scott Childress discusses spreading the word about your practice with AI

The world is moving rapidly, and dental is no exception. Artificial Intelligence (AI) has shown promise in diagnostic imaging, caries detection, and diagnostic software. But did you know that AI can also be a powerful tool for pediatric dentists in digital marketing? From enhancing social media engagement to optimizing your website’s SEO, I’ve discovered that AI can revolutionize your pediatric dental practice marketing.
Social media content enhancement
Platforms like Instagram and Facebook can be vital channels to connect with parents and your local community. AI-powered tools can analyze engagement data, trends, and even audience sentiments to suggest what type of content will likely be the most engaging for your followers. We’ll often use tools like ChatGPT to help kick start ideas for posts or to suggest wording when we face writer’s block. Social media tools such as Canva have even started integrating AI directly into their dashboards for graphic creation. Whether it’s informative articles, interactive polls, or fun dental facts, AI can offer you content that resonates with your audience, thereby increasing engagement rates.
Localized, SEO-optimized website content
SEO (Search Engine Optimization) is crucial for online visibility. If your practice isn’t listed in the top 3 search results for your local area, you’re missing over 97% of all search traffic. To reach a local audience, localized, SEO-optimized content can be invaluable. AI tools can assist in keyword research and recommend local keywords that are likely to drive traffic to your website. For example, if you’re a pediatric dentist in Austin, AI can identify keywords like “best pediatric dentist in Austin” or “Austin children’s teeth care” that are being searched frequently. By incorporating these keywords in your website content, you significantly increase your chances of ranking higher in Google search results.
Moreover, AI can help you draft larger content, such as blog posts, more efficiently. There are several AI-based writing assistants that can generate a skeletal structure for your blog, which you can later refine and personalize, saving you time and effort.
A word of caution
While AI is a fantastic tool, it’s essential to remember that it isn’t perfect. When using AI for content generation, whether it’s social media posts or SEO-optimized blogs, you must take the time to refine and verify the content. Check for accuracy, particularly when discussing medical information, to ensure you provide your audience with reliable and trustworthy content. And you don’t want to use AI as your primary source for all your content — it still needs a human touch for the best results.
The integration of AI in your pediatric dental practice’s digital marketing strategies can be transformative. We’re finding new uses every day to help us do a fantastic job for our clients without increasing their costs or ours. AI is helping us efficiently engage parents on social media and is assisting our experts in optimizing website SEO, thereby improving Google rankings, and bringing in new patients for our clients. It’s not replacing humans (yet!), but is another great tool we can all take advantage of.
26 Pediatric Dental Practice US Volume 1 Number 2 PRACTICE DEVELOPMENT
We used AI to provide richer SEO when creating content for this new pediatric dental practice outside Chicago. The results have been phenomenal
PD
Scott Childress, CEO and co-founder Magnify Dental Marketing, is a digital marketing expert. He has directed web design, creative content development, local search, reputation management, and SEO assistance for over 1,000 pediatric dental practices and has lectured for dozens of dental groups including the AAPD.
Scott Childress and April Cunningham, founders, Magnify Dental Marketing
Pediatric sleep issues last a lifetime; join the movement ASAP
Dr. Michelle Weddle discusses how clinicians can play a large role in improving the lives of children with pediatric sleep disorders
“Michelle, you dentists don’t know what you can do for these kids. Medicine can diagnose this condition. They can manage and give the child allergy medications and CPAP. But you dentists can help treat it.”
Those memorable words were spoken to me by the late Dr. Christian Guilleminault in a private conversation. Treat is an ambitious word, but it’s also a goal we’re very comfortable with. Whether OSA or any of the conditions in the SRBD spectrum, we know the etiology is multifactorial. Because of that, treatment requires a multi-prong approach. It is idealistic at best and egotistic at worst to think that dentists can treat, to full resolution, every SRBD patient. But we know that in many cases we can make it better. Anecdotal feedback from other providers, patients, and their families can bring you to tears with the way some of the lives of these children have changed. Equally as important, this supposition is supported by a litany of medical and dental literature.
No one should deny a child airway therapy. And no one can deny dentistry’s vital role in the provision of pediatric airway therapies. From overt obstructive sleep apnea (OSA) to the milder conditions in the spectrum of sleep-related breathing disorders (SRBD), the literature is replete with evidence supporting the positive impact dentists can fulfill as part of a multi-disciplinary team delivering positive patient treatment outcomes that benefit their lifelong health trajectory.
In the adult sleep medicine field, we grasp the impact of oral appliance therapy in the life of a person. It affects every facet of their being — from their performance at work and familial relationships to their diets and medication profile.
With pediatric patients, the impact can be even more profound because of their ongoing development. Treated SRBD can
Dr. Michelle Weddle is a general dentist in private practice in NJ. She’s a graduate of the NYU College of Dentistry with a General Practice Residency certificate from Newark Beth Israel. She completed the mini-residency in dental sleep medicine at Tufts University and is a Diplomate of the American Board of Dental Sleep Medicine. Dr. Weddle studied at the Pankey Institute, The Dawson Center, and The Kois Center in her pursuit of acquiring higher education. Her general, sleep, and TMJ practices focus on the integration of oral health into whole body health. Her practice has a special focus on the management of airway issues in adults and children. Coming full circle, she served as a visiting faculty mentor for the Airway Prosthodontics Workshop at Spear Education. Dr. Weddle is a Fellow of the AGD and the ACD. She is a member of the American Academy of Oral Systemic Health, the AAPMD, the AADSM, and the IAO. She is a member of the AGD, the ADA, and the NJDA. Recently, she co-founded ASAP Pathway, a community of dentists learning to implement a collaborative, interdisciplinary model of pediatric airway management in private practice.

have a pronounced positive impact while untreated SRBD can have a disproportionately deleterious impact on the following:
• IQ, brain development, and cognition
• Focus and school performance
• Breathing patterns and sports performance
• Behavior which can have implicit (attitudinal issues which affect peers, siblings, and parents) and explicit (juvenile crime, drug use) societal costs
• Accidents (auto, sports, etc.)
The effects are not only limited to the affected child. They ripple outward and may affect others in their sphere: parents, fellow students, siblings, and other caregivers. Additionally, the advent of COVID-19 underscored the importance of underlying health issues in a population.
Hopefully, I’ve convincingly established the fact that dentists can make a real difference. But who’s going to do it? Since we’re dealing with pediatrics, the most obvious choice is the pediatric dentist. But what about general dentists? What role does the orthodontist have? How about periodontists and oral surgeons? All these dentists have a role to play in the management of pediatric airway. Our study club sees all these specialties represented, and they each play unique, vital positions:
• General and Pediatric dentists: Screen, educate, triage, early treatment/management, referrals to specialists
• Orthodontists: Screen, educate, full management of growth guidance from childhood into adulthood
• Periodontists and Oral surgeons: Screen, performance of surgical assists in the orthodontic and growth guidance therapies, SFOT, TMJ support/therapies.
As a reader of Pediatric Dental Practice US, you are uniquely positioned to offer pediatric airway and sleep therapies. Consider the following:
• Many risk factors in airway and sleep conditions are genetic.
• Risk factors that are not genetic are functional, usually affected by the environment and diet, which these adults share with their children.
• Adult patients in this type of practice already understand the condition and are there to seek treatment.
• Trust and rapport have already been established between the patient (parent), dentist, and team.
Allow me to connect the dots here. All the points mentioned above mean that you and your practice can play a pivotal role in these kids’ lives. You are in the best position to add pediatric airway and sleep services to your practice.
Managing pediatric airway is firmly in our wheelhouse. This is very similar to the work dentists do daily. In dentistry, care is usually coordinated by the general or restorative dentist with
28 Pediatric Dental Practice US Volume 1 Number 2 PEDIATRIC PERSPECTIVE
referrals to many different specialists depending on the needs of the patients. We are masters of interdisciplinary treatment. In contrast, many outside the dental healthcare industry practice a multidisciplinary working model, which usually means that one specialty or branch does everything they can do for the patient, and then if there are still conditions that need to be addressed, the patient is referred to the next specialty for care of most (if not all) of the residual symptoms and issues. What’s the difference? Managing pediatric airway and sleep requires the interdisciplinary approach that dentists are very wellversed in. For growing kids, management is not a series of linear visits to one provider, then the next. It usually entails visits to multiple providers at the same time. Who will direct the care? Which providers will the child see and when? This IS in the dentist’s wheelhouse, and we are best suited to direct this care. You can have an incredible impact on these people’s lives. Will you heed the call?
Maybe you’re sold on the concept now. After sharing this information with my colleagues, they inevitably ask the subsequent three questions:
1. How do I learn to do this?
Compared to a decade ago, there are more places to get educated in pediatric airway. We’ve come a long way, but it is still deficient when compared to other continuing education topics like implants or even adult sleep medicine. Many of the education providers in pediatric dentistry are centered on a commercial product or singular technique. When looking for an education provider, it is important to get perspective from the clinical standpoint, e.g., dentists who have been using the product or practicing the technique. Ideally, these dentists are independent practitioners.
It’s also crucial to consider how we learn. While something may be resonant the first time, we only retain a miniscule amount of information upon first exposure. This is especially true of new concepts. Seek educational platforms that provide ongoing access to the educational materials. The information will be reinforced and take on different meaning as you get real-world experience.
2. Is it worth the investment?
Implementation is where the rubber of education meets the road of treatment on the path to the always desirable ROI. Attaining a significant ROI requires work from you and your dental team. This is definitely a team sport. You must have buy-in from the entire team — hygienists, assistants, administrative support, office manager, etc. Without them, you cannot productively do this. It can burn a lot of time and drive down production for the day if you don’t have efficient systems in place.
When considering implementing pediatric airway and sleep therapies in your practice, it is of paramount importance that you consider all the following:
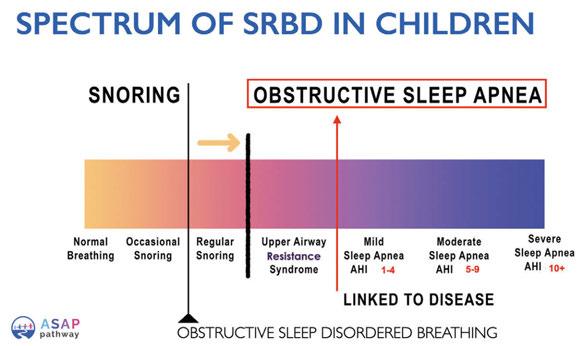
• Who are the team members who will help spearhead this in the practice? Do you have sufficient staff to do this without negatively affecting your general practice?
• How will the team be trained? Like every new product or procedure, successful implementation of pediatric airway and sleep depends on your team being engaged and knowledgeable about how these services fit in to the
other services that you offer in your practice. Have you allocated the budget and dedicated the time for this? What happens if there is staff turnover. How will new staff members be trained? How will offering this service fit into the existing flow of the practice?
• Do you have the support of an external team of healthcare providers to promote the team approach to managing these conditions?
3. Is it sustainable in my practice?
Incorporating any new procedure in the practice has challenges. To ensure the smoothest pathway to incorporate pediatric airway and sleep, you’ll need:
• Protocols tailored to how your practice operates.
• Cohesive dental team that understands the role of each person in the practice in the rationale for integrating this service into your existing services.
• Realistic financial arrangements that factor the cost to the practice regarding time, materials, and resources so that the practice stays financially viable while trying to incorporate these services.
• Support group of like-minded colleagues that have overcome the challenges you’ll face and exchange ideas, best practices, and share camaraderie.
Now what?
The field of pediatric airway and sleep is a rapidly growing field that has not yet reached its potential. There is an immense need for providers to help children and their families. It behooves the profession to increase awareness about how dentists can play a role in helping children with these issues through public awareness but also advocacy at the legislative level.
As with many procedures, the limitation for some patients to initiating treatment is financial constraints. Influencing third-party reimbursements for these conditions and services could go a long way in improving the health of the children affected. We are the frontline, the proverbial spearhead.
There is a lot of work to be done. Fortunately, there are many dentists. Kids need you. Their families need you. Society needs you. If you are interested in providing pediatric airway and sleep services (screening, early management, treatment, or advocacy), seek a comprehensive education platform focused on the subject ASAP. Join the movement. PD
29 pediatricdentalpractice.com Volume 1 Number 2 PEDIATRIC PERSPECTIVE
This is not a drill: tips to improve patient experience with laser technology
Dr. Jenny Jackson discusses the positive effects of using laser technology in her pediatric practice

Whether it’s a fear of needles, embarrassment over the state of their teeth, or worries about anesthesia, more than one-third of people in the United States have a fear of dental treatment, with about 12% reporting extreme fear.1 Meanwhile, only about 10% of people consider a visit to the dentist a relaxing experience. For some, even the sound of a drill is enough to make their heart race and their palms sweat.
Our patients are excited for anything we can do to make their visit more pleasant. Some of this will start before the patient ever gets into the chair, with a warm, welcoming team member answering the phone, or a beautiful, relaxing waiting room designed to put the family at ease. There are also many things you can do during appointments to reduce anxiety, minimize pain and discomfort, and improve outcomes and satisfaction.
Our dental practice specializes in pediatrics, which means we want to deliver positive experiences and outcomes for our young patients and their parents. Following are several methods we use that have helped us transform the dental experience for children of all ages, while turning parents into enthusiastic supporters of our office. In the process, we’ve grown our practice and improved our clinical outcomes.
1. Reduce the reliance on needles and numbing.
Fear of needles is one of the biggest factors driving dental anxiety. As many as two-thirds of children and a quarter of adults have a strong fear of needles, often due to previous negative experiences with injections.2 At our practice, we rarely use anesthesia. My Solea® All-Tissue Laser (Convergent Dental) allows me to complete fillings, stainless steel crowns, and even some minor extractions without injectable anesthetic. Incredibly, in the 3 years I have been using this laser, I can count on one hand the number of teeth I’ve had to anesthetize to restore.
Jenny Jackson, DMD, MPH, FAAPD, graduated as valedictorian with a degree in microbiology from North Carolina State University before attending the Harvard School of Dental Medicine where she was given the Silver Medal Award for overall excellence at the top of the class, as well as the Dean’s Community Service Award and was chosen to be a part of the HSDM/Forsyth Institute Research Academy. With a passion for helping children, Dr. Jackson opened her own practice in Asheville, North Carolina in 2007. She currently serves as Immediate past president of the NC Academy of Pediatric Dentistry, is an adjunct assistant professor at UNC Chapel Hill Dental School, and has volunteered extensively with the Asheville City Schools Head Start Program and teaching local GPR residents.
2. Reduce high-speed handpiece use and remove mental triggers
More than 20% of dental patients say they are afraid of dental drills, and even the sound of a drill is enough to induce anxiety in many patients. To exacerbate this, the vibrations of the high-speed handpiece can have a lifelong trigger effect on patients. Because I use the laser, the handpiece’s high pitch and vibrations are minimized during preps, plus we have more precise control, which allows us to do more from a procedural standpoint than I ever imagined. I’ve also found that patients get excited about laser technology. Their first experience with the laser is a transformative moment for many, as they realize that they can continue to receive excellent care without the noise and sensation of the drill. Hopefully my youngest patients will never have to experience traditional handpiece-only dentistry.
3. Work faster and reduce recovery time.
Beyond addressing patient fears, one of the biggest steps you can take to improve the experience of a dental visit is to get patients back to their day as soon as possible. Many parents may struggle to take time off work for checkups and procedures. With traditional methods, chair time may be longer because anesthetic or numbing is required. The Solea laser eliminates the need for numbing in most procedures, which allows our team to work faster and deliver excellent outcomes. Fillings can be done in a matter of minutes, and we can work in multiple quadrants during one visit, meaning fewer visits for patients. We can sometimes even work in treatment the same day as diagnosis; it really just boils down to our schedule. Since they don’t have to be numbed, patients and families can quickly get back to their days. The laser
30 Pediatric Dental Practice US Volume 1 Number 2 TECHNOLOGY
Disclosure: Dr. Jackson is a member of the Clinical Advisory Board for Convergent Dental, creator of the Solea All-Tissue Laser.
Dr. Jenny Jackson opened Asheville Pediatric Dentistry in 2007 with a goal of transforming the dental experience for young patients and their parents
SOLEA® ELEVATES THE PATIENT EXPERIENCE


Provide an experience that moves patients— and parents.
What if you could eliminate dental anxiety for even your smallest patients? And what if you could perform more same-day dentistry per visit, with children comfortably returning to school, sports, or camp?
That is what virtually anesthesia-free, blood-free, and pain-free procedures can do. Less blood, sweat and tears - more smiles, efficiency, and revenue for your practice.
Learn more at convergentdental.com/pediatric
©2023 by Convergent Dental. All rights reserved. Solea is a registered trademark of Convergent Dental.
also delivers an unexpected outcome: Patients who are asked about their experience with the laser often say it was fun!
4. Share more information to create engaged patients.


We all know that patients don’t want to be lectured about missed visits or poor oral health, and the last thing you want to do is to make patients feel badly about themselves. I’ve found that golden teaching moments often occur in the sharing of positive feedback about a patient’s oral health. A survey last year found that more than 86% of patients want their dentist to go beyond highlighting cavities and point out the condition of all of their teeth, even the ones in good health. Sharing positive messages like this can help patients feel like their oral health efforts are making a difference. At the same time, educating young patients and parents about the procedures you’re performing can make them feel more in control of their visit, which can help them relax. Knowing that you are using advanced technology to ensure the best outcomes can increase their satisfaction, encourage referrals for your practice, and may even inspire a young patient to pursue a career in dentistry.

5. Trusted relationships lead to practice growth.
Building trust with patients takes time. Once you’ve established trust, though, patients will look to you for as much of their dental care as possible. For example, because of the experience we’ve created for patients and parents, I’ve had the opportunity to use the laser for procedures like frenectomies, gingivectomies, and even exposing and bonding impacted canines, which I would have previously referred out. Our happy patients are spreading the word about their positive experiences. Partially because of the efficiency of laser dentistry, we were also able to regain our financial footage after the pandemic shutdowns in less than 1 year. Another result of this efficiency of incorporating the laser into our practice, we’ve seen an overall increase of 150% in practice production and a 50% increase in our daily operative average.
If adopting laser technology feels like a major step for your practice, I encourage you to think about the impact that laser technology can have on the patient experience. Not only does laser technology improve practice efficiency, which all patients appreciate, it can improve outcomes for young patients, while inspiring patients and parents to recommend your office to their friends. Since improving patient experience also allows you to expand your practice, the benefits can be even greater. At the center of it all is the heart and love that you get to put into what you do each day with greater ease and fluidity, with happier patients, a happier team, and less stress for all.
REFERENCES
1. Dentophobia. Cleveland Clinic website. https://my.clevelandclinic.org/health/diseases/22594-dentophobia-fear-of-dentists. Updated March 22, 2022. Accessed July 12, 2023.
2. Needle Fears and Phobia – Find Ways to Manage. Centers for Disease Control and Prevention website. https://www.cdc.gov/childrensmentalhealth/features/needlefears-and-phobia.html#:~:text=Estimates%20show%20that%20as%20many,have%20 strong%20fears%20around%20needles. Updated March 8, 2023. Accessed July 12, 2023.

3. Calladine H, Currie CC, Penlington C. A survey of patients’ concerns about visiting the dentist and how dentists can help. J Oral Rehabil. 2022 Apr;49(4):414-421.


32 Pediatric Dental Practice US Volume 1 Number 2 TECHNOLOGY
PD Connect. Be Seen. Grow. Succeed. | www.medmarkmedia.com READ the latest industry news and business RECEIVE news and event updates in your inbox by registering for our eNewsletter CONNECT with us on social media pediatricdentalpractice.com
Integrating laser dentistry into her practice has allowed Dr. Jackson to improve patient and parent satisfaction and enhance her practice outcomes



A Unique Approach to Saving Lives. www.nexusdentalsystems.com
A real pen grip enabling solid support points and maximum precision

2 injection modes (high/ low) efficiency for all your injections
Optimized with Effitec needles with patented scalpel bevel
SCHEDULE A Virtual Demo
Sterilizable containers reduce waste
Tissue resistance indicators Injection speed adapted in real time
Using SOAN in my practice relieved my hand muscles and boosted efficiency, allowing me more time for patient interaction and tasks.
DR. GERARDO MARTINEZ, DMD
Delaware Pediatric Dentistry


Cruise control Start the injection and let the Soan do the rest
nusmile.com
EFFECTIVE
CORDLESS
PAINLESS ,
&
DENTAL ANESTHESIA
